
ARCHIVED - Audit of Chronic Disease Prevention and Control Program
For readers interested in the PDF version, the document is available for downloading or viewing:
Audit of Chronic Disease Prevention and Control Program (PDF document - 164 KB - 42 pages)
Approved by Chief Public Health Officer on January 12, 2011
Table of Contents
- Executive Summary
- Background
- About the Audit
- Audit Findings and Recommendations
- Conclusion
- Acknowledgments
- Appendix A: Audit Criteria
- Appendix B: Management Action Plan
- Appendix C: PHAC Chronic Disease Surveillance Systems
- Appendix D: List of Acronyms
Executive Summary
1. The overall objective of this audit was to assess the adequacy and effectiveness of the Management Control Framework for delivering the Chronic Disease Prevention and Control Program by the Centre for Chronic Disease Prevention and Control (CCDPC or the Centre), including the management of surveillance and knowledge development, as well as exchange and dissemination activities in collaboration with other delivery partners/stakeholders.
2. The audit examined key activities of the CCDPC in support of chronic disease prevention, management and control, in relation to the various program areas of focus (i.e. cancer, cardiovascular disease, diabetes, respiratory and neurological diseases). The audit scope included governance, strategic and operational planning, performance measurement, surveillance and knowledge development, exchange and dissemination activities, as well as grants and contributions management. The audit scope excluded the Health Promotion Programs (including the Healthy Living Fund) as these programs were subject to an internal audit in 2009-10. It also excluded the activities of the Health Surveillance and Epidemiology Division since this division was transferred to the CCDPC during the year.
3. In summary, the audit found that CCDPC needs to improve its internal processes related to planning, project management and performance measurement within the management control framework to increase the likelihood of achieving intended program results.
Governance
4. A governance structure to oversee execution and refinement of the Integrated Strategy on Healthy Living and Chronic Disease (ISHLCD or Integrated Strategy) has been established and roles and responsibilities have been defined, but challenges were encountered in implementing the governance structure. The focus of the ISHLCD coordination structure to date has been on sharing information with internal stakeholders related to the various program areas. This approach varies from a more structured program management approach focused on establishing and monitoring against detailed program implementation plans.
5. As part of the development of an ISHLCD risk-based management plan, the Branch Executive has committed to enhancing and implementing Healthy Living and Chronic Disease program governance.
Strategic and operational planning
6. Strategies have been defined in concept, and broad-based objectives have been established for each of the Centre’s core program disease areas of focus from the ISHLCD, as well as for more recent areas of focus (i.e. respiratory and neurological diseases).
7. The Centre has recently communicated updated strategic directions and priorities; however, it has not yet developed a comprehensive strategic plan, and the priorities and risks associated with the Centre’s various strategic initiatives have not yet been clearly articulated.
8. In addition, detailed implementation plans for ISHLCD Program and Functional Component areas need to be developed to guide program and functional activities. Effective processes for monitoring progress against planned program activities and within established resource levels also need to be developed.
9. Centre management was in the process of completing an assessment of the Centre’s priorities and programs funded under the ISHLCD, and also in identifying risks and opportunities in the context of current and emerging Branch objectives and pressures. This will likely provide the foundation from which the Centre’s management can develop a comprehensive Centre strategic plan.
Performance measurement
10. Clear measurement and reporting of performance is essential to sound management and to meeting expectations for accountability and transparency. The Centre has yet to develop, or implement a robust performance measurement system to support management decision making and accountability, although we understand that Performance Measurement Frameworks are intended to be finalized during the current fiscal year, and implemented in 2011-12.
Surveillance, knowledge development and exchange
11. The chronic disease surveillance activities are aligned to overall program objectives and priorities, and the Centre has a process in place to ensure that the information it collects is relevant, reliable and timely for decision making. The Centre has also analyzed and disseminated information to support chronic disease policies and programs. However, we noted areas for improvement related to planning, performance measurement, and timely reporting.
12. A governance structure was established for the Canadian Chronic Disease Surveillance System (CCDSS) to provide direction, advice and support to the Chronic Disease Surveillance Division. The Centre also has agreements on data sharing in place with all provinces, territories and a number of other data providers. The National Diabetes Surveillance System (NDSS) was expanded into the CCDSS to provide an integrated approach to the surveillance of other chronic diseases. However, there are still certain gaps, some of which are being addressed.
13. New strategic directions and priorities for the next three years were presented in November 2010 by the Centre’s management. These priorities have not yet been translated into a business plan that adequately describes how these priorities will be addressed in relation to other surveillance activities and to clearly identify what is expected, by when, and the resources that will be needed.
14. Delays in releasing some surveillance information need to be addressed. Performance indicators have been defined for the Surveillance Functional Component but targets and key indicators have not yet been identified. The plan is to have baseline performance data collected next year.
15. Knowledge development and exchange (KD&E) strategic directions and priorities have been defined. Program management was in the process of developing a strategic approach and plan, focused on putting effective interventions into practice, aimed at achieving its strategic directions.
Grants and contributions
16. While we noted improvements in the project approval process since our last internal audit involving grants and contributions (G&C) performed in 2009, the timing of the solicitation cycle and length of the approval process remain areas of concern. For example, the project review and approval process took an average of six months to complete for the files reviewed, which added to the administrative burden. Also, the Centre has not yet established an effective process for sharing the results and lessons learned (best practices) from its community-based programming with relevant functional or program areas in order to better inform program decisions and improve accountability.
Conclusion
17. We concluded that while progress has been realized in the area of surveillance and in grants and contributions relating to the Chronic Disease Prevention and Control Program, management’s attention is still required to:
- establish an integrated strategic plan for the overall program, and supporting business plans by key area (e.g. surveillance, knowledge development and exchange), and to implement a performance measurement system that will better support management decision making and reporting on results;
- establish a more structured program and project management approach to ensure that program execution activities are appropriately planned, resourced, monitored and reported; and
- review the timing of the G&C solicitation cycle in order to allow for more timely project approvals, and establish an effective process to share information and lessons learned on project results.
18. Effective planning, project management and monitoring of results is an essential contributor to achieving the objectives of the Chronic Disease Prevention and Control Program of reducing the burden of chronic disease in Canada.
Statement of Assurance
19. In my professional judgment as A/Chief Audit Executive, sufficient and appropriate audit procedures have been conducted and evidence gathered to support the accuracy of the audit conclusion provided and contained in this report. The audit conclusion is based on a comparison of the conditions, as they existed at the time, against pre-established audit criteria (see Appendix A) within the scope described herein.
A/Chief Audit Executive
Management Response
20. The Agency’s management agrees with our findings and recommendations and a Management Action Plan is presented in Appendix B.
Background
21. One of the Public Health Agency of Canada’s (PHAC or the Agency) key roles is to prevent and control chronic diseases and injuries. Since 2005, the Agency has been implementing the Integrated Strategy on Healthy Living and Chronic Disease (ISHLCD or Integrated Strategy), which represents a series of initiatives focused on health promotion and disease prevention. The ISHLCD was launched in October 2005 with $300 million in funding over five years (and $74.4 million ongoing). This Integrated Strategy represents a new way of working with a diversity of partners. With improved engagement, the Integrated Strategy is intended to positively influence individual and community capacity as well as the capacity of organizations and service providers. Enhanced capacity for action at various levels is expected to contribute to stronger public policies and more integrated, evidence-based and responsive health systems. The three inter-related pillars of the ISHLCD are:
- promoting health by addressing the conditions that lead to unhealthy eating, physical inactivity and unhealthy weights;
- preventing chronic disease through focused and integrated action on major chronic diseases and their risk factors; and
- supporting platforms for early detection and management of chronic disease.
22. The Agency’s efforts related to prevention and control of chronic disease have been undertaken in an environment where the burden of chronic disease is significant and growing. According to information provided by program management, research evidence demonstrates that chronic diseases are diminishing the quality of life of Canadians and their ability to enjoy long, productive lives; however public health interventions can effectively reduce rates of chronic disease.
23. To effectively support the response to these issues, the Agency continues to focus on building its capacity to:
- understand trends in chronic diseases and their determinants;
- build and apply a chronic disease “evidence base”;
- put effective chronic disease interventions into practice; and
- monitor and report performance.
24. The Centre for Chronic Disease Prevention and Control (CCDPC or the Centre) within the Agency provides strategic leadership in the development and implementation of integrated and disease-specific chronic disease prevention and control strategies. The Centre works with relevant stakeholders at national and international levels to ensure the development and execution of an integrated approach to chronic disease prevention and control. The Centre focuses its efforts in the following areas:
- Surveillance – supporting the development of integrated surveillance systems that inform chronic disease policy;
- Knowledge Development, Exchange and Dissemination – building and disseminating the evidence based on best practices, clinical practice guidelines and lessons learned to support chronic disease policies and programs;
- Science – synthesizing and disseminating scientific findings, modeling of the impacts of policy changes on risk factors and incidence, and demonstrating the economic impacts of interventions; and
- Policy and Program Development – supporting policies and disease-specific programs to develop a comprehensive approach to chronic disease prevention and control.
Organizational structure
25. As of September 2010, there were approximately 232 FTE positions within the CCDPC. Following a reorganization in 2010, the Centre has adopted the following structure.
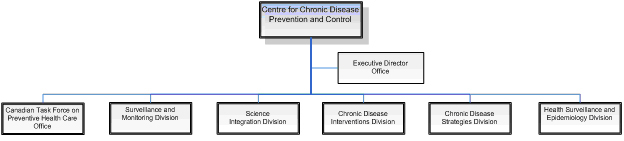
Text Equivalent
ARCHIVED - Organizational structure
This figure is an organizational chart of the Centre for Chronic Disease Prevention and Control. The following groups are part of the Centre: Executive Director Office, Canadian Task Force on Preventive Health Care Office, Surveillance and Monitoring Division, Science Integration Division, Chronic Disease Interventions Division, Chronic Disease Strategies Division, Health Surveillance and Epidemiology Division.
Financial Information
26. CCDPC represented approximately 83% of 2009-10 expenditures of the Chronic Disease Prevention and Control Program. In addition to CCDPC, there are other groups within the Agency that support these Program activities. Key contributors to these activities outside of CCDPC include the Agency Executive, Office of Public Health Practice, Centre for Infectious Disease Prevention and Control, and Regional Operations.
27. As outlined in Departmental Performance Reports, over the last two fiscal years, the total expenditures for the Chronic Disease Prevention and Control Program were $101 million compared to a total budget of $129 million. The main explanations provided by management for the under-spending of $28 million over the last two years were:
- the transfer of budget authorities to other program activities within PHAC ($17 million); and
- delays in finalizing or implementing collaborative arrangements for surveillance information, along with delays in staffing, and in the approval and solicitation process for transfer payments ($11 million).
About the Audit
Objectives
28. The objectives of this audit were:
- To assess the adequacy and effectiveness of the management control framework for delivering chronic disease programs;
- To assess the effectiveness of the Public Health Agency of Canada’s (PHAC or the Agency) management of surveillance, knowledge development, exchange and dissemination activities in collaboration with other delivery partners/stakeholders in delivering chronic disease programs; and
- To identify relevant opportunities for improvement.
Scope
29. The scope of this audit included an examination of key PHAC activities of the CCDPC in support of chronic disease prevention, management and control. Specifically, this audit addressed the following elements, related to the various program areas of focus (cancer, cardiovascular disease, diabetes, respiratory diseases, and neurological diseases):
- Governance
- Strategic planning, including partner relationships and stakeholder communication;
- Operational planning and management;
- Performance measurement;
- Surveillance;
- Knowledge development, exchange and dissemination (KD&E); and
- Grants and contributions (G&C).
30. The audit scope covered activities of the last two fiscal years, but also considered activities undertaken since implementation of the ISHLCD. We also considered regional operations relating to the administration of G&C for the diabetes program.
31. The audit scope excluded the Health Promotion Programs (including the Healthy Living Fund), as these programs were subject to an internal audit in 2009-10; and it also excluded the activities of the Health Surveillance and Epidemiology Division, since this division was transferred to the CCDPC during the year.
Approach and Methodology
32. This audit was conducted in accordance with the TB Policy on Internal Audit and the Institute of Internal Auditors’ (IIA) International Standards for the Professional Practice of Internal Auditing, except that no external assessment was performed to demonstrate that PHAC’s internal audit function complied with the IIA Standards and Code of Ethics. This audit was carried out in accordance with the Agency’s Risk-Based Audit Plan for fiscal year 2010-11. The audit was conducted from July to November 2010.
33. The audit included an assessment of processes, procedures and management practices related to the administration of chronic disease prevention, management and control programs. We reviewed the status of relevant actions taken by management in respect of chronic disease surveillance observations made in the Office of the Auditor General of Canada (OAG) follow-up audit in 2002 that was based on the recommendations made in Chapter 14 of their 1999 report, National Health Surveillance: Diseases and Injuries. We also reviewed management actions taken to date in relation to relevant evaluations conducted on components of the Integrated Strategy. The audit team conducted interviews with key PHAC personnel, reviewed key documents and processes, and conducted onsite visits at PHAC Headquarters, as well as two regional locations.
34. The audit criteria used were derived from the Framework of Core Management Controls and Audit Criteria produced by the Office of the Comptroller General (see appendix A).
Audit Findings and Recommendations
Governance
35. PHAC has one strategic outcome: healthier Canadians, reduced health disparities, and a stronger public health capacity.
36. In support of this outcome, the Chronic Disease Prevention and Control Program represents one area of focus. Working in cooperation with regional, provincial/territorial, national and international governments and stakeholders (including non-governmental organizations), this program provides national population health assessment and surveillance in relation to chronic diseases. It also provides and supports leadership and expertise in the development and implementation of pan-Canadian chronic disease prevention, control and management strategies.
37. Through this program, the Agency is expected to provide public health practitioners with data, analysis, web tools and technical advice that support policies, programs and public health interventions for chronic disease prevention. In addition, it is expected that public health decision/policy-makers and practitioners will be better informed about what works in the area of chronic disease prevention policies and programs to reduce the burden of chronic disease in Canada.
38. The ISHLCD provides a platform for executing against these expectations. It consists of integrated platforms and disease-specific strategies for diabetes, cancer and cardiovascular disease. It is composed of the following 14 Program Components and six Functional Components:
The ISHLCD Program Components are:
- Coordination, Monitoring and Evaluation;
- Healthy Living Fund;
- Intersectoral Healthy Living Network;
- Healthy Living Social Marketing;
- Healthy Living Knowledge Development and Exchange;
- Joint Consortium for School Health;
- Mental Health;
- Observatory of Best Practices;
- Demonstration Projects for Integrated Chronic Disease;
- International Collaborations;
- Enhanced Surveillance for Chronic Disease;
- Renewed Canadian Diabetes Strategy (non-Aboriginal element);
- Cancer; and
- Cardiovascular Disease.
The ISHLCD Functional Components are:
- Surveillance;
- Knowledge Development, Exchange & Dissemination;
- Community-Based Programming;
- Public Information;
- Leadership, Coordination and Strategic Policy Development; and
- Monitoring and Evaluation.
39. The primary work activities encompassed by the ISHLCD are delivered at PHAC jointly by the CCDPC, the Centre for Health Promotion (CHP) and the Communications Branch, which are located within PHAC’s national office, and the Agency’s regional offices.
40. ISHLCD Governance Structure. In delivering on program commitments related to the ISHLCD and other chronic disease programs (i.e. respiratory and neurological disease), we expected that the Centre had clearly defined governance structures in place to support delivery against program objectives.
41. We found that a governance structure to oversee execution and refinement of the ISHLCD had been established, and roles and responsibilities have been defined, but challenges have been encountered in implementing the governance structure.
42. A matrix organizational structure was used to coordinate the implementation of the ISHLCD by the following Agency functional groups:
- The CCDPC;
- The CHP;
- Communications Branch; and
- Agency Regional Offices.
43. This matrix organizational structure evolved through the first two years of the ISHLCD implementation. In 2007, the Agency established the following structure to guide, integrate and monitor program and functional activities.
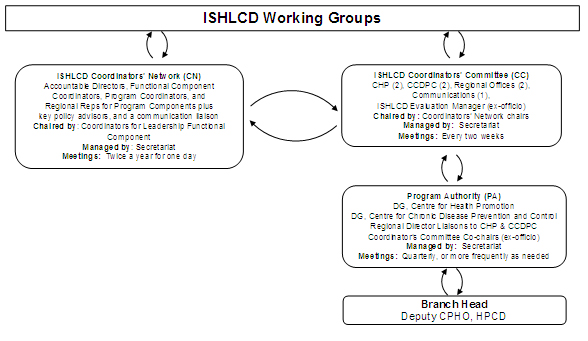
Text Equivalent
ARCHIVED - ISHLCD Working Groups
This figure is a pictorial description of the key components of the Integrated Strategy on Healthy Living and Chronic Disease (ISHLCD) Working Groups. There are four separate groups which interact with each other.
The first group is the ISHLCD Coordinators’ Network (CN). The network includes: Accountable Directors, Functional Component Coordinators, Program Coordinators, and Regional Reps for Program Components plus key policy advisors and a communication liaison. The network is chaired by the Coordinators for Leadership Functional Component. The network is managed by a Secretariat and meetings are held twice per year for one day.
The second group is the ISHLCD Coordinators’ Committee (CC) and has the following members: two representatives from CHP, two representatives from CCDPC, two representatives from Regional Offices, one representative from Communications and the ISHLCD Evaluation Manager as an ex-officio member. The Committee is chaired by the Coordinators’ Network chairs. The Committee is managed by a Secretariat and meetings are held every two weeks.
The third group is the Program Authority (PA). This group includes: (1) DG – Centre for Health Promotion, (2) DG – Centre for Chronic Disease Prevention and Control, (3) Regional Director Liaisons to CHP & CCDPC and (4) the Coordinator’s Committee Co-chairs (ex-officio). This group is managed by a Secretariat and meetings are held quarterly or more frequently as needed.
The fourth group is the Branch Head (Deputy CPHO, HPCD).
44. The adoption of this structure was supported by the definition of roles and responsibilities and establishment of expected meeting frequencies for each of the governance groups, including the Program Authority, the ISHLCD Coordinators Committee and the ISHLCD Coordinators Network. In addition, the governance structure included identification of an accountable Program/Functional Director, a Program/Functional Coordinator and a Regional Representative for each of the ISHLCD Program Components and Functional Components.
45. Despite these efforts, the second ISHLCD implementation review conducted in 2008 concluded that “although progress has been made in delivering activities and implementing the coordination mechanism for the ISHLCD, it is not clear to all staff that the coordinating structures and its accompanying tools have actually improved coordination.” It also states that “the matrix has by no means been fully operationalized and remains a somewhat theoretical construct for many staff.” This review found that the application of governance roles and responsibilities in practice was inconsistent and the tools for communicating and sharing information were not being effectively used.
46. We found that the above mentioned challenges continue to exist. The focus of the ISHLCD coordination structures to date has been on sharing information (e.g. accomplishments, future areas of focus, etc.) with internal stakeholders related to the various program areas. This approach varies from a more structured program management approach focused on not only sharing information, but also establishing and monitoring against detailed program implementation plans.
47.In 2010, CCDPC initiated a reorganization. This reorganization impacts the various roles and accountabilities defined in the ISHLCD coordination structure; however, these impacts have not yet been fully evaluated or addressed.
48. As part of the development of an ISHLCD risk-based management plan, the Branch Executive Committee has committed to enhancing and implementing Healthy Living and Chronic Disease program governance. A senior level working group has been established to carry out this work, which is chaired by the Director General, Centre for Chronic Disease Prevention and Control.
Recommendation
49. The Associate Assistant Deputy Minister, Health Promotion and Chronic Disease Prevention Branch, should ensure that proposed enhancements to program governance enable a more structured program management approach resulting in a more effective governance structure.
Strategic and Operational Planning
50. Strategic Planning. Since its initiation, the implementation of the ISHLCD has been impacted by the introduction of a number of key health initiatives including:
- In October, 2006, the Minister of Health announced a policy review for Diabetes. This review included the Renewed Canadian Diabetes Strategy (as part of ISHLCD) and was completed in 2008.
- In October, 2006, the Minister of Health announced funding, through the Agency, to develop a pan-Canadian strategy for heart health with the goal of reducing the growing burden and loss from cardiovascular disease in Canada. The Canadian Heart Health Strategy and Action Plan was delivered in February, 2009.
- In November, 2006 the Prime Minister announced the establishment of the Canadian Partnership Against Cancer (CPAC). The purpose of this new non-profit corporation was to implement the Canadian Strategy for Cancer Control. Budget 2006 committed new investments of $52 million per year to CPAC.
51. In addition, commencing in 2009-10, the Agency began receiving funding of $23.6 million for four years to take immediate and targeted action on lung and neurological diseases. While these initiatives are not considered to be part of the ISHLCD, they are consistent with the ISHLCD’s fundamental approach and are managed on behalf of the Agency by the CCDPC.
52. We expected that CCDPC had clearly defined and communicated its strategic directions and strategic objectives and that these were aligned with its mandate. We also expected that CCDPC had a process in place for making rational, evidence-based decisions for setting priorities and/or areas of action taking into consideration government priorities, identified risks and client/stakeholder needs.
53. A strategic plan is important in that it provides a clear explanation of how one or more strategic objectives are to be achieved by an organization or program. It typically outlines long-term objectives and details the specific strategies and programmatic goals that are to be pursued. Areas of risk are analyzed and specific strategies for overcoming those risks are adopted. The strategic planning process is typically iterative and maps a clear path between a present condition and a vision for the future. Revisiting the strategic plan to review accomplishments against documented objectives establishes a feedback loop that can influence future planning and decision making.
54. The Centre has not yet developed a comprehensive strategic plan, nor have the priority and risks associated with the Centre’s various strategic initiatives been clearly articulated.
55. Chronic Disease strategy definition. During this audit, we reviewed a variety of documents describing the strategic basis for the Centre’s key functions (e.g. surveillance, knowledge development, exchange and dissemination, etc.) and programs (e.g. diabetes, cancer, cardiovascular disease, etc.). Based on this review, we noted that strategies have been defined, in concept, and broad-based objectives have been established for each of the Centre’s core areas of focus from the ISHLCD, as well as for the focus areas of respiratory and neurological disease.
56. In addition, by way of reporting tools such as the Report on Plans and Priorities (RPP) Tracker, there is evidence that this strategic basis is aligned with and supports the broader agency mandate.
57. Alignment and Priority of Chronic Disease strategic initiatives. The Branch Strategic framework, completed in March 2010, includes strategic directions, priorities and key initiatives to which the Centre is a key contributor. In reviewing the Centre’s work activities/projects/initiatives as presented in various management tools (e.g. Integrated Operations Plan and Report on Plans and Priorities Tracker), there is evidence of alignment between the initiatives tracked in these tools and the Branch Strategic Framework. Less clear are those Centre initiatives or activities that are considered to be critical in support of ISHLCD strategic/program objectives. We further noted that the Centre has not yet adopted a formal process for identifying risks associated with the delivery of key initiatives, and developing monitoring and mitigation strategies to address those risks.
58. Centre management has recently implemented (April, 2010) a reorganization of functions, and also finalized (November, 2010) a document highlighting the strategic directions and priority areas of focus for the Centre over the next three years. Concurrently, an assessment is being undertaken to review priorities and programs, including those funded under the ISHLCD, and to identify risks and opportunities in the context of current and emerging Branch objectives/pressures. This ongoing review is expected to result in: the identification of flexibilities for investment in Branch priorities; to confirm application of ISHLCD authorities; and to consider reinvestment from other Branch programs. The initially planned completion date of November 30, 2010 has been extended into early 2011.
59. Completion of these management initiatives will likely provide the foundation from which the Centre’s management can develop a comprehensive Centre strategic plan.
60. Program monitoring and reporting. The Agency has undertaken several ISHLCD program reviews and evaluations in order to assess progress against meeting program objectives. These include:
- Two reviews conducted in 2007 and 2008 to examine early implementation progress;
- Four component program evaluations completed in 2009, including the:
- Surveillance Functional Component;
- Diabetes Community-Based Programming Functional Component;
- Knowledge Development, Exchange and Dissemination Functional Component; and
- Healthy Living Fund Program Component.
61. There was also a commitment to report to Cabinet within four years (of the 2005 launch) on progress in implementing the ISHLCD as well as to conduct an outcome program evaluation. This evaluation is now planned to be completed in 2013.
Strategic partner relationships and communication
62. Highlighted in the ISHLCD is the importance of the Agency working together with a diversity of partners in leveraging and organizing the resources of multiple partners in order to deliver on program commitments. As referenced in the ISHLCD: “Engaging the right internal and external stakeholders at the right time with the right intensity is a crucial initial outcome if the other desired results of the Strategy are to be achieved.”
63. In executing against this objective, the Centre must strike a balance between requirements that are externally imposed, such as the working relationships and the Agency’s role defined in the CPAC; as well as with areas where the Agency has more influence over the nature and extent of its strategic partnerships (e.g. partnerships developed in support of surveillance and knowledge development).
64. Within each of the chronic disease areas of focus (e.g. diabetes, cancer, etc.), there is evidence that the Centre has attempted to define and develop inventories of key stakeholders. However, the Centre, as part of a broader strategic view, has not defined at a sufficient level of detail what stakeholder groups the Centre’s engagement efforts need to be focused on; how these stakeholders will be engaged; and to what end. The Centre’s recent (November, 2010) Strategic Directions document highlights strategic partnerships as a key success factor. Our expectation is that the questions concerning issues such as: “what partnerships need to be developed?”; and “how to engage partners, develop partnerships and communicate with partners on an ongoing basis?”; as well as timing considerations of strategic partnerships would need to be addressed as part of a comprehensive Centre Strategic Plan, in order to build on the Centre’s efforts to develop and maintain successful partnerships with stakeholders.
65. Operational Planning. We expected that the organization had operational plans and objectives in place supporting the achievement of its strategic objectives, as well as processes and practices to ensure change initiatives are properly implemented.
66. We found that the Centre had not yet consistently developed detailed implementation plans for ISHLCD Program or Functional Component areas; nor had it developed effective processes for monitoring progress to ensure that planned program activities are completed on a timely basis within established resource levels. Consequently, it is difficult to assess whether progress reported against the various component areas are meeting management expectations or program commitments.
67.The intent of the matrix organizational structure was to implement the ISHLCD in such a manner that coordination and accountability run in two directions: across the 14 Program Components (e.g. the cancer program) as well as across six core public health functions common to the Program Components (e.g. surveillance).
68. The Agency management’s expectations related to operational planning and monitoring in a matrix management environment are unclear. On this point, the 2008 Implementation Review of the ISHLCD identifies a requirement for the development of “an integrated plan to set the course direction at a very detailed level.”
69. In place of detailed implementation plans, the Centre currently employs a variety of tools to communicate the Centre’s activities/initiatives and to monitor progress against such activities. These include:
- The Integrated Operational Planning (IOP) templates summarize planned and actual performance by program activity architecture categories and functional organization units;
- The RPP Tracker, a tool used by the Branch to report on the progress of activities in support of the established agency-wide Report on Plans and Priorities;
- ISHLCD program summaries, prepared in support of the annual ISHLCD Coordinators Network Working Session. These summaries, produced in 2007, 2008 and 2009, highlight accomplishments and summarize planned activities for each of the ISHLCD program areas; and
- The CCDPC workplanning database, an internally developed Lotus Notes database intended to provide users with a tool to define and monitor projects.
70. In relation to the tools currently used to plan, manage and monitor program activities, we noted some gaps:
- The IOP is not used in a meaningful manner by Centre management to guide program activities or assess/monitor progress. The current structure of the IOP does not intuitively support the planning, monitoring or reporting of ISHLCD program performance and progress of key initiatives.
- The Centre is committed to populate quarterly results using the RPP Tracker. Through a review of RPP Tracker updates, we noted that:
- The Tracker has not been updated on a consistent basis (there were three quarterly updates produced for 2009-10; but no quarterly update was yet available for 2010-11);
- The Tracker does not include baseline activity information or baseline timing targets to allow for an assessment of whether reported results achieved meet expectations.
71. Project and operational planning tools and processes. The Centre has commenced implementation of an operational planning methodology and supporting tool, but this capability has not yet been fully or consistently implemented across the Centre.
72. CCDPC has developed a Lotus Notes workplanning database that is intended to provide users with a tool to define information on specific projects, including project overview information, project accountabilities, key project activities and timing and summary financial information. Effective in 2010, the availability and use of this tool has been communicated to all CCDPC Divisions, along with the expectation that Divisions use this tool to plan and document project activities. Based on our review of the workplanning database and its content, we noted that this database has not yet been consistently adopted by all Divisions within the Centre to document and monitor project details. As this database is a relatively recent development for the Centre, there has been limited progress to date in developing standard project documentation requirements. Nor has the Centre committed resources to drive compliance to ensure that the Centre’s activities are appropriately captured in the database to support project monitoring and reporting.
73. The introduction of this database is a positive step towards supporting a more structured project management approach. Centre management attention is required to evaluate the degree to which the database supports management’s needs and to determine the required tasks and resources necessary to ensure full and consistent implementation.
Recommendations
74. The Director General, Centre for Chronic Disease Prevention and Control should:
- Complete the development of a comprehensive strategic plan to provide clear articulation of how the Centre’s strategic and program goals are to be achieved in terms of specific activities and initiatives undertaken by the Centre. This strategic plan should also identify key implementation risks and mitigation plans;
- Initiate a management process for periodically revisiting this strategic plan in order to review accomplishments against documented objectives, and to determine refinements required for future planning and decision making; and
- Implement a structured program and project management approach to ensure Centre program work activities are appropriately planned, resourced, monitored and reported on an ongoing and timely basis.
Performance Measurement
75. Clear measurement and reporting of performance is essential to sound management and to meeting expectations for accountability and transparency. A good performance measurement process and comprehensive performance indicators should provide an overview of the results achieved and allow an organization to report on performance, internally for decision making, and externally for accountability.
76. We expected that relevant information on results was gathered and used to make informed decisions, and for accountability purposes. We found that the Centre had yet to develop or implement a robust performance measurement system to support management decision making and accountability, although the CCDPC is currently in the final stages of defining Performance Measurement Frameworks (PMF) to address its key Functional areas. A PMF represents an objective basis for collecting information related to the intended results of a department and its programs. It sets out the strategic outcomes and expected results to be achieved, as well as specific outputs to be produced by its programs.
77. Within CCDPC, three PMFs are currently under development - Surveillance; Community-Based Programming; and Knowledge Development, Exchange and Dissemination. The basis for each PMF is a logic model that has been created for each of these functional areas. We noted that a wide variety of performance measures have been selected; however, key performance indicators, targets and the resources required to maintain this system have yet to be established. We understand that these PMFs are intended to be finalized during the current fiscal year, and then implemented in 2011-12.
78. Financial performance monitoring. The Treasury Board submission supporting the ISHLCD specifies funding levels for each of the program areas by year.
79. In an attempt to track actual expenditures by ISHLCD program area, the Agency defined a coding structure to support expenditure tracking by function (e.g. Surveillance, Knowledge Development and Exchange) and by program area (e.g. Diabetes program).
80. Based on our review of summary financial reports for CCDPC by chronic disease program area, the financial coding of salary and operating & maintenance expenditures by program area has not been consistently adhered to within the Centre. Accordingly, the Centre cannot accurately report on the extent of actual expenditures in comparison to planned expenditures as summarized by program area in the approved ISHLCD.
Recommendation
81. The Director General, Centre for Chronic Disease Prevention and Control, in consultation with the Chief Financial Officer, should:
- Complete the implementation of a performance measurement system to better support management decision making processes and accountability; and
- Implement a consistent process so that expenditures can be tracked and reported by program area.
Chronic Disease Surveillance
82. Health surveillance is a core public health function. It begins with the ongoing collection of information on disease, which is then integrated, analysed, and interpreted. The information produced is then disseminated in a variety of formats to those who need it so they can take appropriate action. In other words, surveillance should provide information on what happened, to what extent, to whom, as well as when and where.
83. One of the main priorities of PHAC is to increase capacity in the surveillance of chronic illnesses, including their risk factors and determinants in Canada. Increased capacity would help PHAC achieve one of its strategic results, which is to facilitate access to information and tools that are timely, reliable and evidence-based, and thereby help to provide informed decisions in the prevention of chronic diseases and the reduction of related risk factors.
84. In 2005, the Conference of Deputy Ministers of Health approved the report Enhancing Capacity for Surveillance of Chronic Disease Risk Factors and Determinants by the Advisory Committee on Population Health and Health Security’s Task Group. The recommended strategies from that report included the following:
- enhance the capacity to analyze, interpret, and use surveillance data;
- expand data sources to fill gaps in surveillance knowledge; and
- enhance collaboration, planning and evaluation for surveillance.
85. In 2005, the ISHLCD was announced and it provided much of the funding for chronic disease surveillance to enhance surveillance, as well as to address surveillance gaps (in areas such as asthma and arthritis). Other priority areas were identified in the lung and neurological disease initiatives announced by the Government in 2009.
86. Until 2005, PHAC had conducted surveillance on chronic diseases, but on a disease-specific basis, including the use of the National Diabetes Surveillance System (NDSS). In recent years, the Agency has worked to expand the scope of the NDSS to include an integrated approach to the surveillance of other chronic diseases. In 2009-10, the name of the NDSS was changed to the Canadian Chronic Disease Surveillance System (CCDSS).
87. The Chronic Disease Surveillance and Monitoring Division has an annual budget of about $16 million, along with 60 FTE.
88. We expected the chronic disease surveillance activities would be aligned to overall program objectives and priorities and that the Agency had a process in place to ensure the information it collects is relevant, reliable and timely for decision making. We also expected that the Agency had analyzed and disseminated the information needed to support its chronic disease policy and programs. We found that these expectations were met, but noted areas for improvement related to planning, performance measurement, and timely reporting.
89. Canadian Chronic Disease Surveillance System. Chronic disease information is collected from a number of sources, including disease registries, such as those for cancer; administrative data such as hospital records and provincial billing records for health services; morbidity and mortality data maintained by Statistics Canada; and the prevalence of chronic disease and risk factors from Statistics Canada surveys.
90. Once this information is collected, PHAC has a number of surveillance systems that integrate, analyze, and interpret disease-related information and then create and disseminate surveillance products based on that information.
91. We noted that PHAC has a governance structure in place for the CCDSS to provide direction, advice and support to the Chronic Disease Surveillance and Monitoring Division. This structure includes the Public Health Network Expert Group and Task Group; advisory committees on specific diseases (arthritis, chronic respiratory disease, cardiovascular disease, and mental illness were all established in 2006; diabetes was established in 2008; and neurological diseases established in 2009); the CCDSS Science Committee, CCDSS Technical Working Group and CCDSS disease-specific working groups.
92. Indicator Framework for the surveillance of chronic diseases. The purpose of a surveillance system is to collect data to inform decision making about policies, programs and services in order to improve the health status of the population. Thus, the selection of those indicators (what will be measured) for the surveillance system needs to be directly linked to the need for specific knowledge about the population.
93. The Chronic Disease Indicator Framework currently contains over 300 indicators from a broad range of data sources. However, this list is not up-to-date and data gaps exist. The Surveillance Division has a project underway to update and prioritize the list of indicator variables for use in a comprehensive and practical chronic disease surveillance system, as well as to produce annual external reporting.
94. Surveillance data sources. Since 2005, new data are collected, analysed and interpreted for the following priority conditions: cancer, diabetes, cardiovascular disease, chronic respiratory disease, arthritis and other bone and joint conditions, and mental illness. According to management, if the feasibility study currently underway determines that it is feasible, then collection of surveillance data on neurological conditions will begin following completion of the four year National Population Health Study on Neurological Conditions in 2012-13.
95. In 2008, the Public Health Network Task Group on Surveillance of Chronic Disease and Injury produced a plan that included NDSS expansion to other chronic diseases. We noted that PHAC expanded the NDSS into the CCDSS. The criteria for planning which diseases would be included in the CCDSS were identified as: their public health importance; their relationship to other diseases already in the system; as well as data quality and feasibility. There is a 17--step process in place to develop consensus recommendations for the expansion of the CCDSS; the implementation of these could take a few years before annual data for all major chronic diseases are collected.
96. Appendix C provides a status update on the degree of development of the surveillance systems as they pertain to various chronic diseases. As of November 2010, the CCDSS included new data on hypertension from provincial and territorial health administrative databases. Feasibility studies or work were underway to add data about mental illness, asthma and chronic obstructive pulmonary disease, heart, stroke, arthritis, osteoporosis and neurological disease conditions. As indicated in the following Table, there are still certain gaps, some of which are being addressed. Once the results of these feasibility studies are known, confirming what other chronic diseases can be included in the CCDSS, the Centre will be able to develop an overall plan with time frames to monitor and report on the development of all its related activities.
97. This fiscal year, a surveillance system for Cancer in Young People in Canada was implemented. Data collection contracts were established with the academic paediatric centres treating paediatric oncology patients. The purpose of this system is to collect data which will be used to establish a national, population based cancer surveillance system for children and youth that can be used by researchers to examine patterns of incidence, health care utilization, along with treatment and outcomes.
98. A pilot initiative conducted during 2008-09 and 2009-10 has been extended through a five year contribution agreement with the College of Family Physicians of Canada and nine collaborating practice-based research networks in six provinces. The objective of this initiative is to establish a national primary care sentinel surveillance system for chronic diseases using electronic medical records. Over 100 physicians participated during testing of collection of data on hypertension, osteoarthritis, diabetes, chronic obstructive pulmonary disease (COPD) and depression. The plan is to expand this initiative to include some 1,000 physicians over the next five years.
99. PHAC also has a project called Canadian Alliance for Regional Risk Factor Surveillance. In collaboration with public health stakeholders in Canada, PHAC created a network to collaborate and build capacity for regional/local area chronic disease risk factors surveillance that will be used for chronic disease prevention and control. It will facilitate the development and sustainability of local/regionally coordinated ongoing flexible data collection systems. This project is at an early stage.
100. The Branch Strategic Framework launched in March 2010 includes a number of priorities and key initiatives relating to surveillance. In addition, strategic directions and priorities for the CCDPC were presented in November 2010 by the Centre’s management. The priorities over the next three years related to understanding the trends in chronic diseases and their determinants are:
- continue to build the CCDSS;
- mobilize “real-time” data collection on chronic disease prevention priorities through the Canadian Primary Care Sentinel Surveillance Network;
- use information technology and strategic partnerships to increase access to and enhance the use of surveillance and monitoring information in decision making (i.e. utilization focused data systems);
- collaborate with the Infectious Disease Prevention and Control Branch on a cross-Agency Human Papilloma Virus Surveillance Program;
- complete the National Population Study on Neurological Conditions; and
- develop the national data system to support monitoring of childhood obesity.
101. The surveillance priorities identified in CCDPC Strategic Directions and through the Branch Strategic Framework need to be translated into a business plan that adequately describes how these priorities will be addressed in relation to other surveillance activities; and to clearly identify what is expected, by when, as well as the resources needed. This plan will ensure that progress against these priorities can be monitored and results reported for decision making and accountability purposes.
102. Surveillance data quality. PHAC has developed a new policy for the collection, use and dissemination of public health data. This policy became effective in June 2009. The policy objective, while ensuring compliance with relevant federal legislation and government and Agency policies, is to assist employees of the Agency:
- in the effective and efficient collection, use, and dissemination of accurate, timely, useful and relevant public health data for statistical or research purposes; and
- in identifying, assessing, resolving and mitigating risks inherent in these activities.
103. We noted that individual operating procedures for data collection and verification of quality are used, as well as agreements with data providers that cover some requirements of this policy. While we are not aware of any non-compliance with the policy, no review was made to ensure the new policy requirements were complied with.
104. Analysis, interpretation and dissemination of surveillance information. Surveillance includes analysis, interpretation of data and the dissemination of this information to public health planners and policy-makers for public health action.
105. Recently, comprehensive surveillance reports on Diabetes (2008), Heart Disease and Stroke (2009), Arthritis (2010), Hypertension (2010), as well as many reports on cancer were disseminated. Surveillance data is also made available on the Agency’s website. New Datacube software has been used to develop the Chronic Disease Infobase which was made available to Internet users in 2010. It allows users with Internet browsers easy, quick access to various aggregate health indicator data (such as risk factors and disease status) using various dimensions (such as geography, age group and gender).
106. We noted delays in releasing some surveillance information. For example, dissemination of the comprehensive surveillance report on arthritis was first planned for 2008-09. This report was released more than a year later in 2010. Delays and challenges were encountered in finalising the report on arthritis. We also noted delays in updating the information on the Agency’s website. At the time of our audit, the data available in the MAPS info-base was up to 2005. This was about two to three years behind the currently available data that could be posted. Management explained that a key cause for this delay was because of priority being given to the new Datacube application of the Chronic Disease Infobase. Since one of the main elements of this surveillance system is to provide ongoing and timely information on the health of the population, management needs to address these issues.
107. Follow-up to previous audit observations. In 2002, the Office of the Auditor General of Canada (OAG) did a follow-up audit to determine the progress made by Health Canada in addressing the observations and recommendations raised in Chapter 14 of the OAG’s 1999 Report, National Health Surveillance: Disease and Injuries.
108. They observed that limited progress was made towards resolving some of the weaknesses identified in the 1999 audit. More particular to chronic disease surveillance, the follow-up found that there were still some significant gaps in surveillance information for cardiovascular, musculoskeletal and chronic respiratory diseases, cancer (except for breast cancer), mental illness, and injuries. Furthermore, surveillance was also lacking for risk determinants and for impacts of interventions, screening, and treatment on health outcomes. This report also indicated a lack of agreements between Health Canada and the provinces and territories with respect to data sharing.
109. We did a follow-up of the OAG’s 2002 observations and recommendations, which had applied to all PHAC surveillance programs. With regard to CCDPC, we found that three of the six recommendations were implemented. Satisfactory progress was made on two additional recommendations (gaps in information collected in two cancer surveillance systems was one of those recommendations; the other recommendation involved addressing gaps in the surveillance of other chronic diseases). With respect to the other recommendation, we found that limited progress was made to address the lack of performance measurement and reporting results of Centre surveillance activities.
110. The Centre now has in place agreements on data sharing with all provinces, territories and other data providers. The NDSS was expanded into the CCDSS as indicated in paragraph 95. The Centre is now collecting provincial and territorial health data for hypertension, and plans are also in place to collect data for mental illness, asthma, heart disease and stroke, arthritis and neurological conditions. There is still no surveillance program on the impact of interventions on health outcomes, except for cancer and childhood cancer, and this has not been identified as a priority by the Center.
111. Performance indicators have been defined for the surveillance Functional Component but targets and key indicators have not yet been identified. The plan is to have baseline performance data collected in 2011-12.
112. As of May 2010, the CCDPC includes the Health Surveillance and Epidemiology Division (HSED). This Division focuses on surveillance activities related to intentional and unintentional injuries, developmental disorders, as well as infant/child and maternal health. While HSED was not included in the scope of the Chronic Disease Audit, it will be important to take the work of this Division into consideration when developing future strategic directions for surveillance.
Recommendation
113. The Director, Chronic Disease Surveillance and Monitoring Division should:
- develop and implement an integrated chronic disease surveillance business plan that reflects priorities, associated activities, timing and resources required in order to clearly identify what is expected, by when, and to ensure that progress against these priorities can be monitored and results reported for decision making and accountability purposes;
- update and prioritize the list of indicator variables as part of a comprehensive and practical chronic disease surveillance system, and to support annual reporting on chronic disease indicators in Canada; and
- define challenges, opportunities and plans for obtaining and disseminating more timely surveillance data.
Knowledge Development and Exchange
114. The ISHLCD calls for the development of a comprehensive system to:
- better inform and support public health decision-makers working in the areas of practice, policy and research; and
- address gaps in resources currently available with respect to the development and dissemination of best practices for chronic disease interventions.
115. The overall objective of knowledge development, exchange and dissemination (KD&E) is to enhance evidence-informed policy and practice decision making in chronic disease and healthy living programs. The activities associated with KD&E focus on identifying, generating, collecting, evaluating, sharing and supporting use of the knowledge required to inform policy and program decision making.
116. Following the recent reorganization of CCDPC, the Chronic Disease Interventions Division is the primary lead for KD&E initiatives and activities. The main activities of this division are:
- Chronic disease intervention research & knowledge exchange;
- Chronic disease prevention and control of best practices identification and dissemination;
- Development of interventions for health behavioural change for both members of the public and health care providers; and
- Development of health literacy approaches for CCDPC programming.
117. We expected that KD&E strategic directions, priorities and objectives were clearly defined and aligned to overall program objectives, and that the organization had operational plans aimed at achieving its strategic objectives in place. We found that these expectations had been partially met as strategic directions and priorities were defined. Program management was in the process of developing a strategic approach and plan, focused on putting effective interventions into practice, to fully address these expectations.
118. There are currently a number of initiatives and activities undertaken as part of the KD&E scope of work including: the Canadian Best Practices Initiative, the Canadian Task Force on Preventive Health Care and a number of disease-specific activities that focus on new knowledge development and synthesis, such as a quarterly scientific journal on Chronic Diseases in Canada.
119. Canadian Best Practices Initiative. The Canadian Best Practices Initiative (CBPI) consists of three components:
- An on-line portal to assist health promotion users in finding and applying evidence in their practice;
- Development of a knowledge exchange platform and capacity building activities to increase use of evidence, surveillance, science, and effective interventions content; and
- Monitoring the uptake, exchange and use of best practices in the Canadian context in order to be able to track their impact.
120. The CBPI was launched publicly in November of 2006. It contains:
- a catalogue of best practice systematic review sites;
- a searchable database of interventions; and
- resources to help users reach public health planning, chronic disease prevention and health promotion goals.
121. The purpose of the CBPI is to provide decision-makers with better access to published and unpublished information about proven and emerging "best" practices models, theories, methods, research evidence and practical experience.
122. The knowledge exchange platform also consolidates multiple sources of interventions, practices and resources for health promotion and chronic disease prevention that are recommended by experts across Canada and internationally.
123. Canadian Task Force on Preventive Health Care. This Task Force is an independent body consisting of fifteen primary care and prevention experts who recognize and support the need for evidence-informed preventive activities in primary care in Canada. The Task Force was first established in 1976 and disbanded in 2005; it was subsequently re-established in 2010.
124. The mandate of this Task Force is to develop and disseminate clinical practice guidelines for primary and preventive care, based on a systematic analysis of scientific evidence.
125. A Task Force Office within PHAC supports the work of this Task Force. A strategic plan is currently being developed. The Task Force met in early 2010 to establish topic priorities and have begun the guideline development process. Topics being worked on in 2010 include screening for breast cancer, hypertension, depression, diabetes and cervical cancer.
126. Status of KD&E strategic plan. The KD&E Functional Component of the Integrated Strategy was subject to a formative evaluation in 2008-09. Of note, this evaluation highlighted the need to define the “program theory of change” (i.e. strategy) and to clarify and develop related outputs and outcomes for KD&E initiatives. While management action on this item has been delayed as a result of the Centre’s reorganization, work has been initiated on the development of an overall KD&E strategic approach.
Recommendation
127. The Director, Chronic Disease Interventions Division, should develop and implement an integrated knowledge development, exchange and dissemination business plan that reflects priorities, associated activities, timing and resources required in order to clearly identify what is expected, by when, and to ensure that progress against priorities can be monitored and results reported for decision making and accountability purposes.
Grants and Contributions (G&C)
128. The Centre has utilized community-based programming as an instrument to deliver federal contributions to external partners. At the time of this audit, PHAC’s regional offices had active projects underway for the Canadian Diabetes Strategy. The Centre has active funding at the national level for projects in the following program areas:
- Canadian Breast Cancer Initiative;
- Cancer;
- Cardiovascular Disease;
- Enhanced Surveillance for Chronic Disease;
- Lung health; and
- Canadian Diabetes Strategy.
129. The Centre and regional offices had a total of 107 active chronic disease community-based projects for fiscal year 2009-10. Total expenditures for the chronic disease community-based programs are demonstrated in Table 1.
| National | FY 2009-10 |
|---|---|
| Contributions | $8,751,385 |
| Grants | $5,949,838 |
| Regions | FY 2009-10 |
| Contributions | $1,439,870 |
| Grants | $92,800 |
| Total | $16,233,893 |
130. We expected that the selection and approval process of transfer payments to recipients would be exercised with due diligence and that the results of community-based programming investments (i.e. G&C) would be monitored against objectives; shared and disseminated; and also serve to inform program decisions. A sample of 23 project files was selected for review to determine compliance with the terms and conditions of their respective programs.
131. Selection and Approval Process. The solicitation process is utilized to determine which community-based projects will be selected for funding. The main steps in this process include:
- determining the objectives and priorities;
- call for project proposals (open, targeted and directed);
- evaluating each project proposal; and
- obtaining necessary approvals.
132. We found improvements in PHAC’s project approval process since our internal audit involving G&C was performed in 2009. We noted the introduction of a “conference” approach to streamline the project approval process. While the length of this process has been reduced under the conference approach by bringing together a number of individuals whose approval is required, it remains an area of concern.
133. Timeliness of Grant and Contribution Funding. In our review of the recent contribution solicitation processes, we found that the timing of the solicitation process and delays in the Agency’s approval process have contributed to increased administrative requirements for the Agency and its recipients. In some cases these delays have affected the start date of projects, thus requiring recipients to modify their project work plans and budgets.
134. Two main factors contributing to this situation include:
- not beginning the solicitation process cycle early enough to ensure that project agreements are finalized in time to meet the intended project start date identified in the solicitation; and
- the project review and Agency approval process took, on average, six months to complete for the files reviewed.
135. Multi-Year Project Funding. We noted that the CCDPC is moving towards implementing a greater number of multi-year agreements. The move toward more multi-year funding reduces the administrative burden and uncertainty for recipients. It also allows the Agency to consider projects with a greater scope.
136. Project Risk Assessments. In a prior internal audit which examined project risk assessment tools, we had noted that the level of monitoring and reporting for projects was not always linked to the level of risk. The Agency has since introduced a new risk assessment tool, called the Agreement Recipient Risk Assessment Tool (ARRAT). The ARRAT requires that information be entered into the electronic tool and it assigns weighted values for several risk categories. The total score is then assessed against a corresponding scale of risk levels (low-medium-high). The ARRAT user guide provides guidelines on the level of monitoring/reporting that is required based on the assessed risk level of the project.
137. Sharing of Results and Lessons Learned. The ISHLCD states thatothe objectives of the G&C mechanism are not only to support community-based programming, but also to further support surveillance and KD&E activities.
138. The Agency requires that recipients submit a project evaluation at agreed-upon intervals. In some cases the recipient is required to perform an evaluation themselves; and in others the Agency requires the recipient to complete an Agency developed evaluation tool such as the Project Evaluation Reporting Tool.
139. We found that while the Centre has shared some results of community-based programs, it has not yet established an effective process for sharing the results and lessons learned (best practices) from its community-based programming with relevant functional or program areas in order to better inform program decisions and improve accountability.
Recommendation
140. The Director General, Centre for Chronic Disease Prevention and Control, should:
- Review the timing of the grant and contribution solicitation cycle in order to allow for more timely project approvals and reduced administrative burden; and
- Establish an effective process for sharing results and lessons learned from community-based programming.
Conclusion
141. We concluded that while progress has been realized in the area of surveillance and in grants and contributions relating to the Chronic Disease Prevention and Control Program, management’s attention is still required to:
- establish an integrated strategic plan for the overall program, and supporting business plans by key area (e.g. surveillance, knowledge development and exchange) and implement a performance measurement system to better support management decision making and reporting on results;
- establish a more structured program and project management approach to ensure that program execution activities are appropriately planned, resourced, monitored and reported; and
- review the timing of the grant and contribution solicitation cycle in order to allow for more timely project approvals and establish an effective process to share information and lessons learned on project results.
142. The lack of effective planning, project management and monitoring of results has limited management’s overall ability to measure the Centre’s progress in achieving the objectives of the Chronic Disease Prevention and Control Program of reducing the burden of chronic disease in Canada.
Acknowledgments
143. We wish to express ouruappreciation for the cooperation and assistance afforded to the audit team by management and staff during the course of this audit.
Appendix A: Audit Criteria
The audit criteria were derived from the Framework of Core Management Controls and Audit Criteria produced by the Office of the Comptroller General.
Criteria
Governance:
- The organization has clearly defined governance structures in place to support delivery against program objectives and incorporate all key program delivery partners
Strategic Planning:
- The organization has clearly defined and communicated strategic directions and strategic objectives, aligned with its mandate.
- The organization has a process in place for making rational, evidence based decisions for setting priorities and/or areas of action taking into consideration government priorities, identified risks and client/stakeholder needs.
Relationship Development & Coordination:
- Lines of communication exist between the organization, its clients and other external stakeholders to support timely, relevant and reliable information sharing.
- The organization leverages, where appropriate, collaborative opportunities in working with its partners to better achieve its objectives.
Operational planning and management:
- The organization has in place operational plans and objectives aimed at achieving its strategic objectives.
- The organization has processes and practices to ensure change initiatives are properly implemented
Performance Measurement:
- Relevant information on results is gathered and used to make informed decisions and for accountability purposes.
Program execution:
- Surveillance activities are aligned to overall program objectives and priorities and the Agency has a process in place to ensure that the information it collects is relevant, reliable and timely for decision making.
- The Agency has analyzed and disseminated the information needed to support chronic disease policy and programs.
- Knowledge development priorities are aligned to overall program objectives.
Grants & Contributions:
- Due diligence is exercised in selecting and approving recipients of transfer payments.
- Results of community based programming investments (i.e. G&C’s) are monitored against objectives and serve to inform program decisions.
Appendix B: Management Action Plan
| Recommendation | Management Action Plan | Officer of Prime Interest | Target Date |
|---|---|---|---|
| Governance | |||
| 49. The Associate Assistant Deputy Minister, Health Promotion and Chronic Disease Prevention Branch should ensure that proposed enhancements to program governance enable a more structured program management approach resulting in a more effective governance structure. | Agree. The Audit recognizes the complexities of matrix management of the Integrated Strategy on Healthy Living and Chronic Diseases (ISHLCD), while acknowledging that the Branch has put in place governance mechanisms. We agree that this governance structure is not fully effective and for that reason the Branch, led by CCDPC, is in the process of reviewing the ISHLCD. The Branch Executive Committee (BEC) will provide the governance oversight to ISHLCD and will consider the results of the ISHLCD review. This will include the development of terms of reference which will clearly articulate BEC's role and responsibility with regards to the ISHLCD as well as improved mechanisms for coordination and integration. |
AADM with DGs of HPCDPB | August 2011 |
| Strategic and Operational Planning | |||
74. The Director General, Centre for Chronic Disease Prevention and Control should:
|
Agree. The Audit Report notes the importance of a strategic plan in articulating the strategic objectives of an organization in guiding decision making and allocation of resources. The Centre has recently developed and communicated a strategic vision that provides the overarching framework for CCDPC. | DG–CCDPC | |
| To address this recommendation and build on the strategic vision document, Management will develop a 3 year Strategic Plan for CCDPC to identify priorities supported by activities along with associated risks to implementation and mitigation strategies. | DG-CCDPC | June 30, 2011 | |
| This will include initiating an outcome-based monitoring process for the Strategic Plan. This will inform any modifications to the Plan and associated allocation of resources. | DG-CCDPC | March 2012 | |
| The Strategic Plan will be operationalized through the Agency's Integrated Operational Planning process to plan, resource and monitor our planned business activities and report on them on a quarterly basis through the Branch Report on Plans and Priorities Tracking tool. Management will also conduct a lessons learned exercise following the pilot year (2010-11) of the implementation of the work-planning database to determine where enhancements can be made both in the tool and its adoption. | DG-CCDPC | September 2011 and ongoing | |
| Performance Measurement | |||
81. The Director General, Centre for Chronic Disease Prevention and Control, in consultation with the Chief Financial Officer, should:
|
Agree. We will build on the progress in developing outcome based Performance Measurement Frameworks (PMF) for functional components of the ISHLCD with a particular focus on implementation. These PMFs are in the final stages of completion (anticipated approval in January 2011). | ||
| Management will implement the completed PMFs to tell a functional and program performance story. At the Branch level a project has been initiated to integrate performance measurement practices into existing program management. This will be leveraged to create change towards a results-based environment. We will work closely with the Branch to align Centre performance measurement with Branch level expected results. | DG-CCDPC with Executive Director | September 2011 | |
| Further, we are initiating a Centre-wide needs assessment (anticipated to commence in January 2011) to inform the design of a system for capturing and reporting on performance information and implement a system based on the results. | DG-CCDPC and Executive Director | July 2011 and ongoing | |
| Agree. We acknowledge the importance of ensuring consistent practices in financial coding so that expenditures can be tracked and reported by function and program area. Work has been ongoing to improve financial monitoring in the Centre. We will work closely with PHAC Finance to ensure effective monitoring and reporting against the ISHLCD. CCDPC uses Functional Area Codes as created by PHAC Finance, to track expenditures by program and functional areas under the ISHLCD. Management will institute a semi-annual review of coding practice with Administrative Officers and rectify any inconsistencies. Findings of the reviews will be presented to the Centre Senior Management Committee. |
DG-CCDPC and Executive Director | January and August 2011 | |
| Chronic Disease Surveillance | |||
113. The Director, Chronic Disease Surveillance and Monitoring Division should:
|
Agree. We appreciate the value of strategic planning for surveillance as indicated through our support for the PHAC Surveillance Plan and the Branch Strategic Framework priorities related to surveillance. | ||
| The Centre has initiated a third-party expert Surveillance Review which will provide advice on potential measures to improve surveillance effectiveness in advancing chronic disease prevention in Canada. | Directors of CDSMD, HSED, SID | June 2011 | |
| Based on the Surveillance Review, Management will develop a CCDPC Surveillance Business Plan which will lay out a strategic approach for Surveillance and will guide decision making. This Business Plan will be aligned with the Centre Strategic Plan. | Directors of CDSMD, HSED, SID | December 2011 | |
| Work has been ongoing in CCDPC to update the Chronic Disease Indicator Framework and Management will ensure its completion and set a process for updating the Framework every three years. Delays in release of surveillance data are not fully in the control of CCDPC as we rely on the release of data from partners including Statistics Canada and the Canadian Institute for Health Information. |
Director of CDSMD | September 2011 and ongoing | |
| The issue of improving the promotion and timely dissemination of surveillance products will be addressed in the CCDPC Surveillance Business Plan. | Director of CDSMD | March 2012 | |
| Knowledge Development and Exchange | |||
| 127. The Director, Chronic Disease Interventions Division should develop and implement an integrated knowledge development, exchange and dissemination business plan that reflects priorities, associated activities, timing and resources required in order to clearly identify what is expected, by when and to ensure that progress against priorities can be monitored and results reported for decision making and accountability purposes. | Agree. With the re-organization of CCDPC, a primary focal point for knowledge development and exchange (KDE) has been identified, this was noted as progress in the Audit Report. With this development there is a need to identify priorities and an integrated approach for KDE across the Centre through the development of a KDE Business Plan. This will bring together the knowledge development, knowledge exchange and knowledge dissemination functions within the Centre with the goal of putting effective interventions into practice. The KDE Business Plan will be aligned with the CCDPC Strategic Plan. | Director of CDID | March 2012 |
| Grants and Contributions | |||
140. The Director General, Centre for Chronic Disease Prevention and Control, should:
|
Agree. The Audit Report recognizes overall improvements in the Agency's Grant and Contributions process, however there continue to be Agency-wide challenges with regards to the standard approvals timeline and timeliness of funding to recipients. We agree to take steps to ensure efficient processes for issues that are within our control. | ||
| As part of the annual operational planning cycle, in the Spring of each fiscal year the Centre will review solicitation plans for the following fiscal year, and will establish timelines for the identification of solicitation priorities, the actual solicitation, review of proposals and approvals. As well, we will continue to support and use the Centre Grants and Contributions Network, a community of practice, to build the Centre's Grants and Contributions capacity. | DG-CCDPC | May 2011 | |
| Agree. In accordance with the Branch Strategic Framework priority concerning synthesizing the learnings from investments in community capacity building, CCDPC will participate in a Branch-wide working group, led by Regional Operations, focused on sharing knowledge from grants and contributions programs. The Centre will commit to creating a mechanism to consider the results of the Branch working group to enhance sharing of results and lessons learned from community-based programming. The proposed way forward would be endorsed by the Centre Senior Management Committee. | DG-CCDPC | March 2012 | |
Appendix C: PHAC Chronic Disease Surveillance Systems
| Diseases | Surveillance Indicators | |||||
|---|---|---|---|---|---|---|
| Mortality | Incidence | Prevalence | Risk Factors | Determinants | Inequalities | |
| Status or Degree of development of chronic disease surveillance program: |
||||||
| Diabetes | 4 | 4 | 4 | 4 | 3 | 3 |
| CVD * | ||||||
| Heart disease | 4 | 4 | 4 | 4 | 3 | 3 |
| Hypertension | 4 | 4 | 4 | 4 | 3 | 3 |
| Stroke & AMI | 4 | 1 | n/a | 4 | 3 | 3 |
| Cancer ** | 4 | 4 | n/a | 0 | 0 | 0 |
| Musculoskeletal | ||||||
| Arthritis *** | 4 | 1 | 4 | 4 | 3 | 3 |
| Osteoporosis * | 4 | 1 | 3 | 2 | 2 | 2 |
| Mental Illness**** | 4 | 1 | 4 | 3 | 3 | 3 |
| Respiratory | ||||||
| COPD * & Asthma | 4 | 1 | 4 | 3 | 3 | 0 |
| Sleep Apnea | 4 | 0 | 3 | 4 | 2 | 1 |
| Neurological | ||||||
| Alzheimer’s* & Parkinson’s * | 4 | 0 | 1 | 1 | 1 | 1 |
| Obesity | n/a | 0 | 4 | 4 | 3 | 3 |
(Source: PHAC-Chronic Disease Surveillance and Monitoring Division)
Definition of Surveillance Indicators
Risk Factors
Appendix D: List of Acronyms
Page details
- Date modified: