
Global Public Health Intelligence Network (GPHIN) Independent Review Panel Final Report
Download in PDF format
(9.38 MB, 82 pages)
Organization: Public Health Agency of Canada
Published: 2021-07-12
On this page
- Letter to the Minister of Health from the External Review Panel
- Introduction
- Chapter 1: GPHIN’s role and purpose
- Chapter 2: GPHIN’s organization and flow of information
- Chapter 3: GPHIN and technology
- Chapter 4: GPHIN’s future
- Conclusion
- Acknowledgements
- Abbreviations
- References
- Annex: Interim report for the review of the Global Public Health Intelligence Network
- Endnotes
Letter to the Minister of Health from the External Review Panel
May 28, 2021
The Honourable Patty Hajdu, PC, MP
Minister of Health
House of Commons
Ottawa, Ontario
K1A 0A6
Dear Minister Hajdu,
Please find attached the final report of the independent Global Public Health Intelligence Network (GPHIN) Review Panel.
These findings reflect six months of interviews, research and deliberations by the Panel. It builds on the initial findings of our interim report, dated February 26, 2021, and presents realistic and actionable recommendations we feel will make GPHIN fit for today’s purpose and that of tomorrow.
Since November 26, the Panel has met virtually 55 times. We conducted interviews with more than 55 individuals, including the GPHIN analysts, former and current PHAC employees, provincial officials, international partners, and technical experts from both the public and private sector (see Acknowledgements).
In addition to interviews conducted virtually, the Panel has reviewed information and documents from the Public Health Agency of Canada, and elsewhere, in line with key areas of inquiry. These have included reports, contracts, internal procedures and guidance, audits, presentations, and other foundational texts.
We hope the recommendations in this report will be useful to you, and that they provide a roadmap for positioning GPHIN – as well as the Government of Canada – as a leader in the rapidly evolving discipline of open-source, public health event-based surveillance, and help to inform future policy decisions around global public health surveillance.
Sincerely,
Margaret Bloodworth
Mylaine Breton
Dr. Paul Gully
Introduction
For citizens and the public sector alike, the COVID‑19 pandemic has helped reinforce the essential role of governments in public health. From public guidance on masks, personal hygiene and physical distancing, to the less obvious but critical public health surveillance that guides decisions and action, few Canadians have not been directly impacted by public health systems over the course of the last year.
Yet, most Canadians were unaware that on December 30, 2019, the Global Public Health Intelligence Network (GPHIN) detected a signal in an article published in the South China Morning Post about an outbreak of pneumonia. By January 1, thanks in part to this signal, both the President and Chief Public Health Officer (CPHO) of the Public Health Agency of Canada (PHAC) elevated the signal to senior tables across government. Canada’s response to what would become COVID‑19 had begun. In our interim report, we found the timing of detection of the signal to be commensurate with similar event-based surveillance (EBS) systems worldwide, and we saw no evidence that earlier detection by GPHIN would have been possible.
However, we also concluded that the system is not operating as clearly or smoothly as it should. At the time, we highlighted three key areas – mandate, governance, and information flows and technology – that we would be investigating further (see the full Interim report for the review of the Global Public Health Intelligence Network).
Since the February interim report, the Panel has continued to meet with experts, leaders and staff of PHAC to seek their views in these thematic areas and to invite their perspectives on how GPHIN should evolve in the future in order to remain relevant and effective.
This review has happened entirely within the federal government’s active and ongoing COVID‑19 response. We believe that this is an appropriate context for PHAC to position GPHIN in a way that reflects and captures the value it provides both domestically and internationally, and that recognizes the importance and potential of an open-source EBS system.
Our remit directs us to consider GPHIN first and foremost. However, for GPHIN to succeed, it must be situated within an environment that makes the best use of the intelligence it produces. Our recommendations, therefore, identify the enabling conditions within PHAC necessary for GPHIN to function effectively as part of an integrated public health surveillance system and be well connected to a coordinated, risk assessment function.
GPHIN must continue to partner, collaborate and evolve in order to take advantage of technological opportunities and ever-expanding sources of information. A recalibrated GPHIN will help PHAC continue to serve and protect all Canadians, while also meeting Canada’s international obligations as a trusted ally in the global public health surveillance community. It is our hope that the recommendations in this report serve as a roadmap to that future.
Chapter 1: GPHIN’s role and purpose
Protecting Canadians 24/7
GPHIN is an online early warning system that monitors global news sources in nine languages for potential public health risks happening anywhere in the world. It is an all-hazards system that identifies chemical, biological, radiological and nuclear public health threats, and constantly scans public open-source news in real time. It is considered a public health events-based surveillance (EBS) system, a type of surveillance that searches reports, stories, rumours and other sources of information for events that could be a serious risk to public health.
When it was created 25 years ago, GPHIN was groundbreaking. At that time, the sudden availability of massive amounts of open-source information through the Internet made real-time global EBS possible and allowed public health practitioners to have access to information faster than ever before.
While GPHIN’s original impetus arose out of a desire to protect Canadians, it quickly became a tool of global importance. Through the years, it has built a strong and trusted reputation for early detection of events such as the onset of the 2009 H1N1 pandemic, the development of Middle Eastern Respiratory Syndrome (MERS), and cases of Ebola virus disease. It is still regarded as one of the most important sources of early information related to outbreaks.
Much has changed in the intervening years. The volume of open-source information has grown exponentially, and the discipline of EBS has matured. Technology is quickly evolving, and the tools available to monitor and filter massive volumes of information are improving. And while one of GPHIN’s key strengths must continue through the exceptional human judgment built into its operations, the system itself needs to continue to be improved in order to remain effective. This chapter will consider GPHIN’s structure and functions in order to provide clear recommendations on its mandate within PHAC.
Mandating surveillance
The Public Health Agency of Canada Act, in its preamble, identifies the federal objective of undertaking public health measures, including surveillance and emergency preparedness and response. The preamble also embeds the goal of fostering collaboration in the field of public health domestically and internationally. And it includes the only specific reference within the Act itself to identifying and reducing public health risk factors.
Though its existence predates the Act, GPHIN has, since its earliest days, been in line with the legislated responsibilities of its organization. Yet, GPHIN is isolated from PHAC’s broader surveillance function. Unlike most surveillance activities, it is not linked directly to a specific disease or mode of transmission but resides within the Office of Situational Awareness, within PHAC’s Centre for Emergency Preparedness and Response.
Moreover, the Panel has observed that GPHIN is not well connected to the essential function of risk assessment, a critical step in early warning and response that builds on GPHIN’s detection, triage and initial verification of sources. The risk assessment function is what takes an initial signal and adds the situational context that describes how an event could affect a population and the corresponding public health measures that may be required. If GPHIN’s early signals are not being fully incorporated into the risk assessment continuum, then its intelligence is not being fully leveraged.
This is a problem for PHAC, and for GPHIN explicitly. It echoes concerns raised by the Auditor General’s Report 8: Pandemic Preparedness, Surveillance and Border Control Measures, which found that initial risk assessments did not consider the pandemic risk or its potential impact. PHAC’s risk assessment was found not to be sufficiently forward-looking, and Dr. Theresa Tam, the Chief Public Health Officer, has acknowledged that there is room to improve.
This requires careful consideration of the risk assessment function and the enabling governance structures within PHAC that can translate a signal into action. This function is an essential guidepost for GPHIN’s mandate. A longer discussion of risk assessment, and our related recommendations, will be provided in Chapter 2.
This is an opportune time for this critical rethink of these important functions and how GPHIN should fit within them. Just as surveillance and risk assessment needs and approaches have evolved, so too has the discipline of EBS.
A new way to serve
GPHIN’s primary function as an early signalling system is just one advantage of EBS. As the discipline has changed, new uses for these systems have been identified, and developing these other strengths presents a considerable opportunity for using global public health intelligence.
Leveraging these strengths will change GPHIN’s operations and have implications for PHAC’s surveillance function overall. If GPHIN is to be successful now and in the future, the first step is to acknowledge that EBS is a key part of PHAC’s overall surveillance regime through the articulation of a common, coordinated, agency-wide surveillance mandate. Only then can PHAC articulate a renewed mandate for GPHIN that enshrines the signalling function it already performs and anticipates how it will contribute to an overarching surveillance vision going forward.
The following section presents the history and context of public health surveillance at PHAC in order to guide its future work in establishing an overall mandate for surveillance and to better situate our recommendations for GPHIN within that ongoing work.
From vital statistics to vital intelligence: a brief history
Public health surveillance is defined as the ongoing, systemic use of routinely collected health data to guide public health action in a timely fashion.Footnote 1 Public health surveillance helps inform policies, programs and public health action intended to promote, protect and improve the health of Canadians.Footnote 2
This function has existed in Canada in some form for over a century. Responsibility for the collection and sharing of statistical information “relative to the social, economic and general activities and conditions of the population” was initially vested in the federal Statistics Act in 1918. The federal Department of Health, established a year later, would create its first national laboratory for public health and research in 1921. The department’s first Epidemiology Division was established in 1937.
In 1972, the Epidemiology Division was merged with the larger Canadian Communicable Disease Centre to form the Laboratory Centre for Disease Control. In 2000, Health Canada combined the Laboratory Centre for Disease Control with the Health Promotion and Programs Branch to create the new Population and Public Health Branch. PHAC assumed responsibility for this function upon its inception in 2004.
Defining public health surveillance
Though the collection and publication of health data have been enshrined in federal legislation for some time, the definition of public health surveillance has been more fluid. In 1968, the 21st World Health Assembly adopted the concept of population surveillance as “the systematic collection and use of epidemiologic information for the planning, implementation, and assessment of disease control.” The assembly also codified three distinct features of surveillance:
- the systematic collection of pertinent data,
- the orderly consolidation and evaluation of these data, and
- the prompt dissemination of results to those who need to know, particularly those in position to take action.Footnote 3
Definitions can vary across jurisdictions, but PHAC’s past and current ways of defining surveillance have drawn heavily from this international standard. PHAC’s definition, consistent with those of the US Centers for Disease Control and Prevention and the World Health Organization (WHO), emphasizes “public health action.”Footnote 3
Indicator-based surveillance and event-based surveillance
Indicator-based surveillance (IBS) involves the systematic collection, monitoring, analysis and interpretation of structured data, such as indicators produced by a number of well‑identified, mostly health‑based, formal sources,Footnote 4 and requires a high standard of data quality to be of use. The vast majority of the IBS that PHAC undertakes is domestically focused.
Event-based surveillance (EBS) is the type of surveillance that searches reports, stories, rumours and other sources of information for events that could be a serious risk to public health.Footnote 4 As a surveillance tool, IBS can be slower to detect signals, particularly in countries that might lack capacity.
GPHIN is PHAC’s main EBS system. The Canadian Network for Public Health Intelligence, which connects federal, provincial and territorial jurisdictions, has an event-based monitoring application called Knowledge Integration using Web-based Intelligence (KIWI). Recent research has suggested there is application for EBS as a tool for discipline-specific surveillance and national surveillance activities.Footnote 5
EBS and IBS are complementary, and both are considered important to global public health surveillance as well as early warning and response.
Public health surveillance at PHAC
The surveillance function at PHAC has been a core priority since its creation in 2004 and has been guided through the years by successive strategic plans that have sought to address governance, accountability, coordination, standards and evaluation.
PHAC’s first Surveillance Strategic Plan (PSSP1) was developed in 2007 at the request of the CPHO. PSSP1 led to the establishment of a formalized surveillance governance structure to ensure that mechanisms and processes were in place to analyze and communicate surveillance information, and to support public health policy development and decision-making.
PSSP1 provided an initial corporate vision for surveillance that recognized the need for coordinated approaches and for appropriate governance structures to guide surveillance.
PHAC’s second Surveillance Strategic Plan, issued in 2013 (PSSP2 2013-2016), advanced PHAC’s work in a few key areas. This plan re-emphasizes the pan-Canadian nature of surveillance and made explicit reference to public health intelligence:
[…] the starting point that leads to the production of accurate and timely public health intelligence on the health of the population and guides effective responses to emerging issues and public health challenges as well as facilitating public health planning and decision-making. As such, health surveillance is also central to our relationships with public health partners and stakeholders from coast to coast to coast, and internationally.Footnote 6
PSSP2 also acknowledged the shared responsibility for public health surveillance across Canada, making reference to the Blueprint for a Federated System for Public Health Surveillance. This report, prepared by the Pan-Canadian Public Health Network,Footnote 7 provided a vision and action plan intended to guide the development and implementation of an infrastructure for more effective collaboration.
The Blueprint acknowledged that risks to health “are not limited by political and geographic boundaries” and emphasized the need to work transnationally. The work was primarily focused on domestic surveillance systems, and on the need for standards and interoperability so that information could flow between jurisdictions.
The second surveillance strategic plan led to the development of a more formal PHAC surveillance governance structure, including the creation of the position of the Chief Health Surveillance Officer, reporting to the Branch Head of the Health Security Infrastructure Branch. The position of Chief Health Surveillance Officer was also responsible for reporting on surveillance activities to the PHAC Executive Committee, and for undertaking regular reviews of surveillance systems and activities for corporate decision-making.Footnote 8
PHAC drafted its most recent surveillance strategic plan in 2016. The Executive Committee approved the plan in principle in 2016, but the plan never received formal approval. However, a copy of the plan received by the Panel indicates some important initial direction. PSSP3 defines surveillance as:
the tracking and forecasting of any health event or health determinant through the ongoing collection of data, the integration, analysis and interpretation of those data into surveillance products, and the dissemination of those surveillance products to those who need to know, in order to undertake necessary actions or responses.Footnote 9
The third plan is also the first to acknowledge and include EBS, and GPHIN in particular, and states:
Stimulated by the renewal of the Global Public Health Intelligence Network (GPHIN), the PSSP3 has broadened the scope of surveillance to include event-based surveillance, which is defined by the World Health Organization as the organized and rapid capture of information about events that are a potential risk to public health.Footnote 9
This plan, like the ones before it, continued to emphasize the need for greater coordination, and it proposed new steps toward corporate models and governance structures for surveillance. The work was curtailed shortly after the plan was approved in principle. PHAC leadership, as well as documents reviewed by the Panel, has confirmed there has been no overall assessment of surveillance activities within PHAC since 2016, though individual systems might have been reviewed, in isolation, by certain program areas.
A 2020 internal surveillance audit indicates that one reason for this might have been the sunsetting of the Chief Health Surveillance Officer position, left vacant since 2017. The audit finds:
A governance structure was in place for oversight of surveillance activities from April 2017 to March 2019. However, key leadership responsibilities were not redistributed following the elimination of the [Chief Health Surveillance Officer] position. The lack of redistributed leadership responsibilities and the ineffectiveness of the [Surveillance Integration Team]Footnote 10 as a decision-making body reporting to senior management committees have impeded the implementation of measures articulated by the 2016 and 2013 strategic surveillance plans.Footnote 8
GPHIN itself is mentioned in a March 2018 internal audit of emergency preparedness and response.Footnote 11 The audit recognizes GPHIN’s contribution to early detection and response but noted that PHAC’s Centre for Emergency Preparedness and Response lacked information on how information on events is shared, particularly with senior management. It also highlighted the need for a more modern risk assessment model that better reflects PHAC’s capabilities. Both points will be addressed in the following chapter.
Surveillance at PHAC
Number of distinct surveillance systems: 82
Breakdown of surveillance systems:
- Emergency Management Branch: 1 (GPHIN)
- Infectious Disease Program Branch: 33
- Vaccine Rollout Task Force:Footnote 12 2
- National Microbiology Laboratory: 24
- Health Promotion and Chronic Disease Prevention Branch: 22
Number of strategic surveillance plans since 2007: 3
Last official review of all surveillance systems: 2016
Recalibrating GPHIN’s role in surveillance
PHAC’s detection of what would become COVID‑19 is the most recent example of GPHIN operating to detect early signals of a potential threat to public health. But that does not mean it is operating as well as it could, or that it currently has what it needs to ensure that EBS remains a key part of PHAC’s surveillance regime.
Currently, there are no clear and explicit mandates for overall surveillance and the role of individual systems such as GPHIN within those mandates. It is not always clear who is responsible for what in the flow of information, risk assessment and chain of decision-making.
The organization’s first task should therefore be to articulate a strong vision that fully acknowledges all surveillance activities, including GPHIN’s, and how they work together to meet PHAC’s overall surveillance objectives.
Recommendation
1.1 The Public Health Agency of Canada should articulate the Global Public Health Intelligence Network’s (GPHIN’s) role and mission in a way that takes into account its public health surveillance functions and contribution and positions it within the spectrum of surveillance activities of the Agency.
This overall mandate needs to respect the unique properties and needs of an EBS system while providing appropriate scope for some of the ways that GPHIN could evolve in the future, including its international contribution.
It should specifically set out how GPHIN will interact with the risk assessment function, with some care to consider the specific needs of an EBS, as opposed to that of more traditional, disease-specific assessment.
The mandate should reflect the fact that governments need a way to undertake forward-looking risk assessment. But it should also acknowledge that government alone may not have all the best tools or resources, and that partnerships and collaboration are an increasingly valuable way to address complex roles and functions for the common good.
The mandate should also take into account technological changes required to modernize surveillance approaches, including data strategies and technical infrastructure, and provide avenues for the continuous improvement of GPHIN, as opposed to a path that relies on incremental, uncoordinated system fixes made only as immediate need arises.
It is in considering this future that the Panel presents its second recommendation related to GPHIN’s mandate.
Recommendation
1.2 GPHIN’s operations should align and effectively link with the Public Health Agency of Canada’s overall surveillance and risk assessment approaches, and reflect whole-of-agency objectives related to those functions.
Just as surveillance and risk assessment needs and approaches have evolved, so too has the discipline of EBS changed. A critical next step for determining the future is to review in some detail how changes in EBS, evolving technology, and global mandates are creating new potential paths for GPHIN that build on its original design and purpose. The essential governance questions related to how these functions are organized will be the focus of Chapter 2.
GPHIN: a pioneer in event-based surveillance
GPHIN’s creation in the late 1990s was a product of multiple convergent factors, though the idea was formed in 1994, when pneumonic plague was identified in Surat, Gujarat, India, through television media broadcasts worldwide.
At that time, the sudden availability of massive amounts of open-source information through the Internet made global EBS possible and allowed public health practitioners to have access to information faster than ever before. Globalization, international trade and travel were rapidly expanding, and microbial threats could now spread more quickly and disperse more widely.
It was with these concerns in mind that the founders of GPHIN developed a public health surveillance system with a global scope. Although the initial impetus behind GPHIN’s creation was to protect Canadians, the GPHIN team quickly realized that the tool had value for the international public health community. One of the surest ways to protect Canadians from pandemics is to support the international community to identify and address events before they are out of control.
The prototype started as a partnership between Health Canada and the WHO in 1997 and was first deployed in 1999. It was limited to French and English articles and used websites, news wires and newspapers to monitor infectious diseases in humans. Without machine translation capabilities, GPHIN analysts translated foreign language articles manually into English before dissemination.
In 2002, GPHIN expanded to its second prototype phase, engaging Canadian private sector technology firm Alis Technologies Inc.Footnote 13 through a collaborative research agreement to improve the automated capacity and functions of Internet-based news monitoring. The scope of the prototype was also expanded to include all hazards. In addition to infectious diseases in humans, it could also search for animal diseases; threats related to food; radiation, chemical and nuclear events; and public health threats related to natural disasters.
In 2004, GPHIN evolved with the launch of an updated multilingual platform capable of machine learning and natural language processing. The new system was unveiled at the United Nations on November 17, 2004, by Canada’s Minister of Health, Ujjal Dosanjh, and PHAC’s first CPHO, Dr. David Butler-Jones.
“GPHIN represented a paradigm shift for infectious disease surveillance. […] The key to successful outbreak control was effective detection and response at the source.” (Dr. Stephen J. Corber, Area Manager of Disease Prevention and Control for the Pan American Health Organization of the WHO, November 17, 2004, UN Headquarters, New York.)
GPHIN is regarded as one of the most important sources of early information related to outbreaks, the signals of which are often informal and in local electronic news reports. In particular, GPHIN’s monitoring during the 2003 Severe Acute Respiratory Syndrome (SARS) outbreaks contributed to structural changes to the international rules governing global public health threats, known as the International Health Regulations (IHR).
GPHIN and the International Health Regulations (IHR)
The IHR lay out the international legal framework governing states’ public health capacity and response to public health events and emergencies. They are legally binding on 196 States Parties, including the 194 Member States of the WHO.
At the time of GPHIN’s creation, the existing IHR (1969) were limited in scope: notification by countries was limited to three diseases (cholera, plague and yellow fever), only official country notifications could be used by the WHO, and the document did not outline any formal international coordination mechanisms.Footnote 14 In 2003, in the midst of the SARS epidemic, the WHO set out to revise the IHR to address these limitations, resulting in the current IHR (2005).
Included in the new IHR (2005) were provisions requiring States Parties to “strengthen and maintain […] the capacity to detect, assess, notify and report events.” Whereas previously the WHO could use only official reporting to begin verification efforts, the IHR (2005) permit the WHO to use unofficial reports of public health events as a basis for requesting information or verification from a State Party.
GPHIN contributes directly to Canada’s obligationsFootnote 15 under the IHR (2005). In 2018, Canada secured the highest possible score for public health surveillance capacity under the WHO’s Joint External Evaluation of Canada’s IHR core capacities. As the mission report reads, “The cornerstone of the national public health early warning function is event‑based surveillance and relies on the GPHIN platform, which also constitutes the foundation of the public early warning function at the global level.”Footnote 16
Event-based surveillance systems worldwide
GPHIN was one of the first EBS systems developed and the first to combine automated and human analytical components.Footnote 17 It remains a key player in an international community of EBS systems and detection mechanisms.
The Panel heard how these systems are mutually reinforcing, and how they work in tandem to create an international public health surveillance ecosystem with redundancies and safety nets.Footnote 18 In surveillance, a system with a single point of failure risks missing a key signal. GPHIN is no longer one of the only systems; in its service of creating these necessary redundancies, however, its continued operation is valuable.
Existing EBS systems fall under three broad categories:
1. Moderated systems rely on human analysis to curate and assess sources.
The Program for Monitoring Emerging Diseases (ProMED) is one of the best known moderated systems. Launched in 1994 by the non-profit International Society for Infectious Diseases, ProMED’s volunteer team operates 24/7 in 32 countries and scans international media for reports of emerging or re-emerging infectious diseases without the aid of artificial intelligence or algorithms. Once ProMED’s moderators and experts have reviewed a signal, ProMED disseminates information to nearly 80,000 subscribers through its mailing list, as well as through social media platforms, smartphone apps and an RSSFootnote 19 feed.
2. Automated systems use algorithms to categorize and filter inputs before displaying them for public health professionals.
The Medical Information System (MediSys), founded in 2004 by the European Union, and HealthMap, founded in 2006 at the Boston Children’s Hospital, are both fully automated systems. Both systems incorporate a range of inputs: MediSys relies on the Europe Media Monitor, developed by the EU’s Joint Research Centre; HealthMap relies on ProMED, Google and Baidu news aggregation services, and official public health sources, among others. Inputs are then filtered through automated text-processing algorithms and overlaid on a map interface for user access.
3. Partially moderated systems combine automated and human components. While fully automated systems are cheaper and quicker than moderated systems, EBS researchers have pointed to the high signal-to-noise ratio and the correspondingly increased risk of false positives generated through the system.Footnote 18
GPHIN is a partially moderated system, combining the benefits of machine learning and algorithmic filtering processes with human analysis and judgment. GPHIN’s analysts collectively work in nine languages – Arabic, Chinese (traditional and simplified), English, French, Russian and Spanish (Portuguese and Farsi were added in 2008) – considered a significant advantage by most experts. The Panel heard that GPHIN is one of the best examples of this partially moderated system. This multi-staged filtering process brings the benefits of both approaches outlined above but is more expensive because of the human expertise required.
Outsourcing GPHIN?
A question the Panel has considered is that of outsourcing of all or parts of GPHIN’s operations or platform. There is a case to be made for outsourcing, if only because of government’s relatively poor track record in adopting new technologies.
However, the Panel believes that public health surveillance is a fundamental responsibility of government, and that PHAC in particular must retain the ability to collect and use all types of surveillance data in order to protect Canadians’ health. As such, we believe that GPHIN should not be outsourced in its entirety.
As EBS systems continue to emerge to meet new demand, one of the challenges facing PHAC is how to keep pace. There is no question that private sector companies are using and deploying vastly more powerful tools than ever before, and in some cases, the federal government is not equipped to do the same.
Even decisions to outsource a component of GPHIN, such as its platform, must carefully consider how PHAC will maintain oversight and control of decisions that affect GPHIN’s function and evolution. This is a lesson learned from past partnerships with private sector technology firms that GPHIN has worked with (see Chapter 3).
Government cannot expect to operate entirely alone, particularly when expertise and technology reside outside the public sector. PHAC should consider potential partnerships if it wishes to keep GPHIN at the leading edge of technology and methods. PHAC should be prepared to consider new models that address public good objectives while leveraging the ideas and abilities of academia and the private sector. It will be important when doing so to ensure that the appropriate degree of control and influence over the GPHIN platform is retained to ensure that the capacity within PHAC remains robust.
Recommendations
1.3 In recognition of the essential need and mandate for public health surveillance, GPHIN’s public health surveillance capacity should remain within the Public Health Agency of Canada.
1.4 The Public Health Agency of Canada should actively seek out partnerships and collaboration to leverage for the GPHIN platform more sophisticated technology and methodology used by different sectors, including academia and the private sector, while ensuring retention of key intellectual property and the ability to modify and improve the system in a timely manner.
An international cornerstone
Since its creation, GPHIN has demonstrated considerable international stewardship; it is trusted by the international stakeholders that anticipate receiving and using its products each day. In an era of growing distrust in public services, this value cannot be overstated.
Some of these relationships exist informally; after 25 years, GPHIN’s institutional memory is long, and its analysts are well connected to colleagues around the world who work in public health surveillance. Informal exchanges of information have been undertaken by analysts in the past, and these relationships have helped GPHIN build its international reputation.
GPHIN participates in international forums such as the Global Health Security Initiative (GHSI), a Group of Seven (G7) plus Mexico project launched in 2001 in Ottawa. The Initiative’s mandate is to undertake concerted global action to strengthen public health preparedness and response. One of the contributions of this important forum was the Early Alerting and Reporting project, intended to assess the feasibility and opportunity for pooling epidemic intelligence data from disparate systems, GPHIN among them. This collaboration contributed to the establishment of the WHO Epidemic Intelligence from Open Sources (EIOS) project in 2017.
The future of event-based surveillance systems
As the global community continues to develop and refine EBS methodology and systems, it is essential that PHAC continue to be involved and keep pace with technological, governance and systems innovation. The open-source public health surveillance system GPHIN interacts with the most is the WHO’s EIOS project, to which GPHIN contributes 20% of all input. But the Panel has heard that there are some limitations to this system due to silos that exist between various communities who participate, and limitations to how certain recipients could respond to different types of information.
The WHO is in the early stages of developing the Epidemic Big Data Resource and Analytics Innovation Network (EPI-BRAIN), an “innovative global platform that allows experts in data and public health to analyze large datasets for emergency preparedness and response.”Footnote 20 The Panel has been told that the WHO is in the process of planning and scoping the project. PHAC, and GPHIN, should continue to explore opportunities to collaborate and contribute to ongoing international research efforts: as EPI-BRAIN is in its infancy, PHAC is well placed to provide knowledge and expertise to its development and to benefit from its outputs in the future.
GPHIN’s potential contribution is not limited to the technical advice or processes it could provide; its contribution could include its algorithms, which dictate how the platform sorts and prioritizes inputs. These algorithms have already been shared with the WHO, and PHAC should consider how they could be of service to the post-COVID‑19 advancement of global public health surveillance. Chapter 3 considers the application of algorithms in greater detail.
Future international collaboration
Because of COVID‑19, the need for global epidemiological intelligence networking has never been clearer. The Independent Panel for Pandemic Preparedness and Response, established by the WHO, noted in its Second Report on Progress that while “the global pandemic alert system is not fit for purpose,” the WHO relies now more than ever on traditional news and social media reports about potential public health events of international concern.Footnote 21
The Independent Panel’s final report, issued on May 14, 2021, calls on the WHO to establish “a new global system for surveillance, based on full transparency by all parties, using state-of-the-art digital tools to connect information centres around the world.”Footnote 22 The report also pointed to a need for “consistent application of digital tools, including the incorporation of machine learning, together with fast-paced verification and audit functions.”
The United States issued a National Security Directive on January 21, 2021, that directs the establishment of a “National Center for Epidemic Forecasting and Outbreak Analytics and modernizing global early warning and trigger systems for scaling action to prevent, detect, respond to, and recover from emerging biological threats.”
And in early May, the WHO and the Federal Republic of Germany announced their intention to “establish a new global hub for pandemic and epidemic intelligence, data, surveillance and analytics innovation.”Footnote 23
Canada’s close ties to the US and the WHO, in addition to its existing EBS strengths, present a good opportunity for future alignment and collaboration. As the Independent Panel established by the WHO has observed, if global surveillance is to be effective, various EBS systems will need to interact. No single system will be able to catch all events, but collectively, well-integrated systems have a far greater chance of sharing information and intelligence to capture a clearer picture of an emerging event. GPHIN, as an established leader in this field, should position itself as a collaborator that can share its knowledge and expertise, and that can also learn about different approaches and new ideas being developed elsewhere.
Building on GPHIN’s international role
There is no question that GPHIN’s contribution to the WHO, and to global surveillance, is valuable. But whether this value has always been fully recognized by PHAC is less clear.
The Panel believes that GPHIN’s international contribution should remain a major focus. PHAC’s Global Health Security Framework highlights the need for coordinated engagement in international efforts in the areas of capacity-building, engagement and collaboration, and emergency management. GPHIN is ideally placed to contribute to achieving these objectives.
GPHIN analysts report that they do not feel as free as they once did to exchange information informally with counterparts around the world. A first step could simply be to encourage GPHIN analysts to build networks with professionals and share information more informally with their counterparts. Management should proactively support this. Although formal signals and collaborations need to be managed in order to properly assign accountability and resources, informal networks provide considerable benefits.
The Panel believes that GPHIN has done an admirable job in developing positive, mutually reinforcing international relationships based on the exchange of information, and that it should continue to do so. In the future, GPHIN’s analysts and leaders should consider how to make sure these partnerships and collaborations can help contribute to a strong public health intelligence community and, increasingly, harmonization across systems and frameworks, and to grow the team’s own learning and capacity in tandem.
Recommendations
1.5 GPHIN’s mandate should continue to reflect both the domestic and the international objectives of public health surveillance, including GPHIN’s international contribution.
1.6 The Public Health Agency of Canada’s international impact should be bolstered by reinforcing GPHIN’s existing international partnerships and by considering additional roles or contributions that GPHIN could make as an established leader in event-based surveillance.
The recommendations proposed thus far relate directly to GPHIN’s mandate and correspond to what the Panel believes its current and future role might be. We now turn to GPHIN itself, its products, its function and its position within PHAC.
GPHIN’s products and operations
The GPHIN system collects data from multiple open sources every day. The system automatically collects about 7,000 articles initially, about half of which are filtered out before analysts manually review the remaining 3,500.
The largest single source of information GPHIN collects is from a global news and monitoring service owned by Dow Jones & Company called Factiva, which accounts for 84% of all input, at a cost of $1.8 million every two years. Additional sources, including news aggregators, such as Google News, and social media are also monitored by analysts but are not automatically captured by the platform.
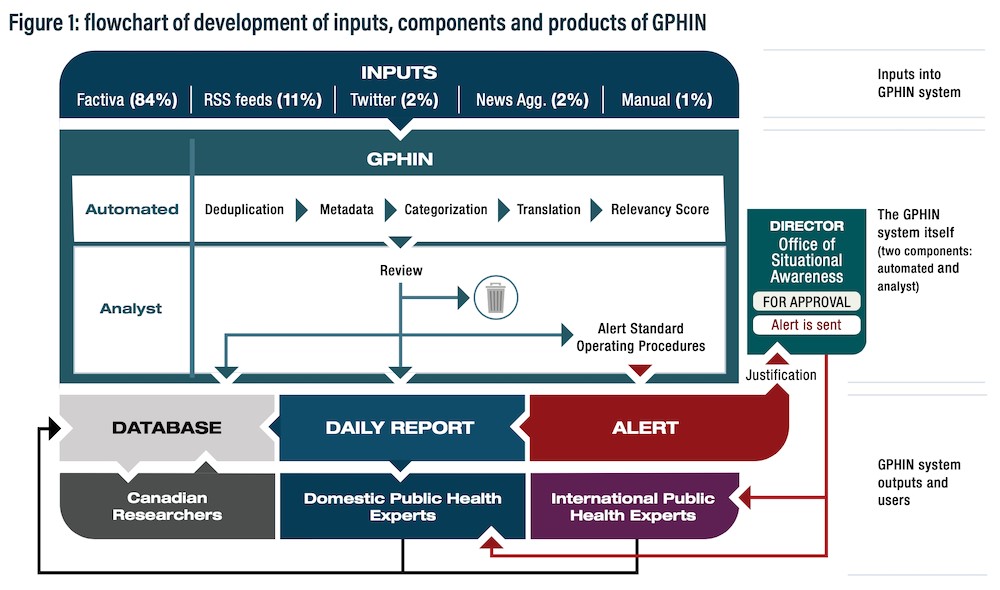
Figure 1 - Text description
Inputs into GPHIN’s system are made up of the Factiva news data which accounts for 84 percent of all input, followed by RSS feeds at 11 percent, Twitter at 2 percent, news aggregators at 2 percent, and other manual input at 1 percent.
The GPHIN system is made up of automated and analyst components. The automated component includes five phases: deduplication, metadata, categorization, translation, and relevancy scores.
The analyst component then reviews the automated work, and decides whether to issue an Alert, or whether to include an item in the database or daily report.
Alerts follow an approval process that involves verbal justification with the director of the Office of Situational Awareness, after which it is sent to international and domestic public health experts.
Daily reports are sent to domestic experts. Along with the international and domestic experts, Canadian researchers can also access the database.
GPHIN has always relied on a two‑step structure comprising automated processes and human analysis. A team of experienced, multilingual analysts with diverse backgrounds and geopolitical knowledge take initial automated output and manually filter and select news reports relevant to public health. Analysts continue to adjust and refine search algorithms and taxonomy to improve GPHIN’s monitoring over time.
The Panel has examined GPHIN’s historical expenditure data. GPHIN funding is included as one part of a larger cost centre within the Centre for Emergency Preparedness and Response, which required a manual review of expenditures to associate them with GPHIN activities. PHAC management, including its Chief Financial Officer, has isolated GPHIN’s funding from within this larger budget in order to estimate GPHIN’s expenditures and number of full-time equivalentsFootnote 24 since 2009-10. Table 1 provides these expenditures.
| Fiscal year | Full-time equivalents | Salary | Operations and maintenance (O&M) | Total estimated expenditures |
|---|---|---|---|---|
| 2009–10 | 15.1 | $1,291,073 | $1,007,095 | $2,298,168 |
| 2010–11 | 16.4 | $1,300,849 | $1,783,643 | $3,084,492 |
| 2011–12 | 16.3 | $1,248,081 | $1,393,077 | $2,641,158 |
| 2012–13 | 14.4 | $1,418,036 | $1,479,592 | $2,897,628 |
| 2013–14 | 15.1 | $1,357,937 | $1,232,544 | $2,590,481 |
| 2014–15 | 14.7 | $1,391,618 | $725,013 | $2,116,631 |
| 2015–16 | 12.8 | $1,114,407 | $2,944,232 | $4,058,639 |
| 2016–17 | 12.3 | $1,033,085 | $2,272,780 | $3,305,865 |
| 2017–18 | 11.5 | $1,086,272 | $2,018,983 | $3,105,255 |
| 2018–19 | 12.3 | $1,095,169 | $1,387,824 | $2,482,993 |
| 2019–20 | 10.9 | $1,066,122 | $1,730,278 | $2,796,400 |
| 2020–21 | 12.2 | $1,174,127 | $1,540,895 | $2,715,022 |
Of note, in 2012-13, two staff were lost due to the Deficit Reduction Action Plan initiative. PHAC has informed the Panel that since this reduction, staffing has fluctuated over time due to shifts in operational demands and employee leave. In 2014 and 2016, temporary positions were added to help respond to the Ebola virus disease surge. Employee leave can be offset by hiring temporary help, though these costs are considered an operating expense.
Also of note, O&M for 2014-15 does not include expenditures for newsfeeds and hosting the GPHIN platform (which are captured in other years), likely as a result of the lack of a dedicated cost centre for GPHIN. Newsfeeds and hosting costs typically range between $600,000 to $800,000 annually.
The costs directly related to salaries and the subscription to the Factiva account form the majority of GPHIN’s annual spending. GPHIN also received one-time funding of $7.9 million for the GPHIN Renewal Project in 2016, over and above its operating budget (see Chapter 3 for more information on the renewal).
In 2016, GPHIN’s platform was migrated from NStein’s private servers to those of National Research Council Canada, in part because of the high costs of annual hosting fees. This resulted in a one-time increase in O&M costs between 2015-16 and 2016-17.
The Panel has also been informed that GPHIN received an additional $830,000 in the 2020 Fall Economic Statement to support research, ongoing platform support, additional staff, and funding earmarked for international grants to the WHO EIOS project, which will be reflected in future year spending.
In the following sections, recommendations will include certain new functions, products or tools that will require additional investments, some of which could be significant. Any new tasks or functions will require the support of resources and time, and GPHIN analysts may require access to new skills and training. Fundamentally, analysts will need more time to dedicate to any new task assigned to them. The Panel will return to the needs of analysts in the following chapter.
The GPHIN Daily Report
Previously known as Situational Awareness Section Daily Reports, GPHIN’s Daily Reports capture the top articles of interest, organized into sections.Footnote 25 Articles with source links are briefly summarized in an email. Daily Reports are not sent to international recipients; they are sent only to domestic public health and government officials (just under 500 recipients), 91% of which are within the federal government (449 subscribers). About 9% of subscribers come from provincial and territorial governments (40 subscribers) and regional governmentsFootnote 26 (4 subscribers).
Of these federal government recipients, the majority reside within PHAC and the Health Portfolio, with 87% of subscribers.Footnote 27 The remaining 13% of subscribers are from other government departments. The Daily Report is issued every morning at 8:30 am, Eastern time.
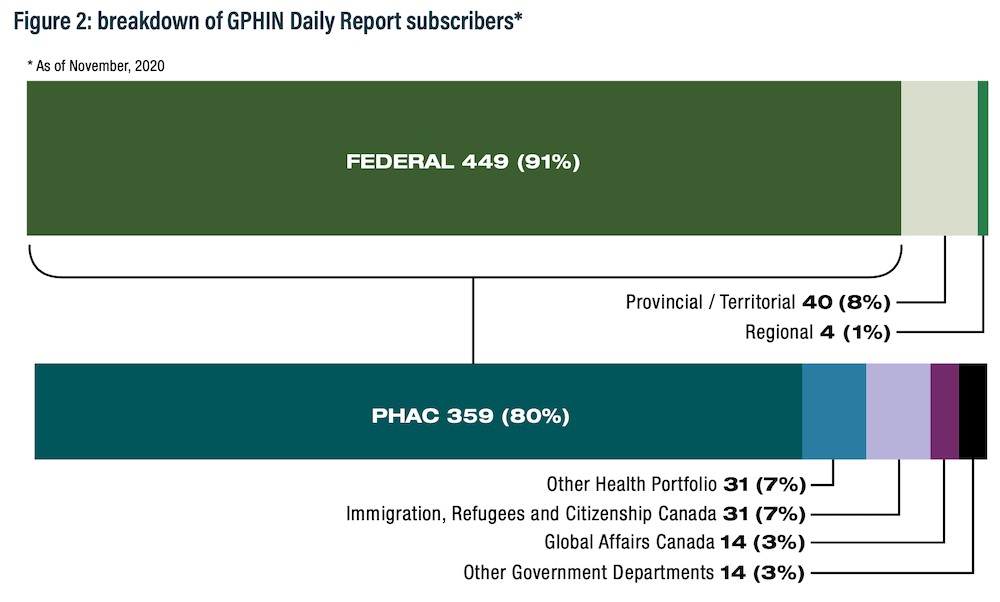
Figure 2 - Text description
Of the subscribers to the Daily Report:
- 449, or 91 percent, are from the federal government
- 40, or 8 percent, are from provincial and territorial governments
- 4, or 1 percent, are from regional governments
Of the 449 federal subscribers to the Daily Report:
- 359, or 80 percent, are from the Public Health Agency of Canada
- 31, or 7 percent, are from the Health Portfolio
- 31, or 7 percent, are from Immigration, Refugees and Citizenship Canada
- 14, or 3 percent, are from Global Affairs Canada
- 14, or 3 percent, are from other government departments
Numbers are as of November, 2020.
The Daily Report provides a regular channel through which to update and report on potential Alerts that might previously have been flagged. For example, if an Alert is issued on Monday but is found to have been a false positive by Thursday, the Daily Report would likely include articles that capture that outcome.
However, because international subscribers do not receive Daily Reports, they would not receive any further notification from GPHIN directly on the outcome of an Alert that later proves to be a false positive. International subscribers would either need to log into the GPHIN platform independently, provided they have the resources and knowledge, or consult other sources of information to confirm the development. Daily Reports were likely never envisioned for use by international recipients. But international recipients may benefit from a daily product that is more accessible than the GPHIN platform and that can send updates concerning Alerts straight to their inbox.
The Panel has learned that GPHIN is in the process of finalizing standard operating procedures specific to the Daily Reports. Equally important is the need to undertake regular review and evaluation of products and the procedures that guide them so that they continue to meet the needs of recipients. This practice builds on precedent: In 2019, an evaluation of user satisfaction regarding the Daily Reports, undertaken by the GPHIN team, found that they are widely and regularly read by recipients. Respondents reported that they use the Daily Reports for contextual awareness, as a starting point for further investigation, and as a component of their risk assessments. They also noted a number of adjustments that would improve the Daily Reports. Following this evaluation, enhancements to the product were made to better meet the needs of recipients.
In the future, regular and periodic evaluation of GPHIN’s outputs should be embedded in GPHIN’s operations, in step with PHAC-wide plans. This regular review will become even more essential as the surveillance function within PHAC becomes more defined and as risk assessment approaches are further developed.
As previously mentioned, PHAC has not undertaken a comprehensive review of its surveillance systems since 2016, though it has indicated it intends to do so once past the current COVID-19 crisis. The Panel would underscore the importance of this evaluation both as a function of GPHIN and as part of a fundamental corporate objective.
Recommendations
1.7 GPHIN should regularly evaluate the content, format, impact and reach of all its processes and products, and should use those evaluations to recalibrate its services according to its mandate.
1.8 Regular outreach with subscribers should be built into its operations, and input should guide the creation and regular evaluation of standard operating procedures for all products.
1.9 The Public Health Agency of Canada should consider whether the Daily Report or some similar product should be sent to international subscribers.
GPHIN Alerts
As we observed in our interim report, there has been considerable conflicting information and lack of clarity regarding the purpose and application of Alerts in the past. We noted that the terminology of “alert” does not seem to conform to the definition set out by the WHO’s guidance document, called Early Detection, Assessment and Response to Acute Public Health Events: Implementation of Early Warning and Response with a Focus on Event-Based Surveillance . The more rigorous definition of “alert,” according to this guidance, would be a public health event that a) has been verified, b) has been risk-assessed and c) requires intervention, including investigation, formal response or a communication. GPHIN Alerts are verified only in part, and according to this guidance, are more accurately called “signals.”
GPHIN’s use of the world “alert” predates any of these international definitions published by the WHO in 2014. Early warning and response guidance was developed well after GPHIN sent its first Alerts in the late 1990s. GPHIN’s use of the word “alert” might simply be based on precedent. In fact, a review of products issued by other EBS systems shows a high degree of variance in the terminology used to describe an alert or signal, including other terms such as “notification” and “post” and even “report.”
The Panel believes that it is the appropriate moment to reconsider the use of specific terms and words, including the word “alert,” which, according to the definitions set out in the WHO guidance, implies a degree of assessment that goes beyond GPHIN’s functions or the underlying intent of these early warning signals.
The initial line of inquiry on Alerts was a direct result of some senior management directly overseeing GPHIN who could not describe the purpose or audience for Alerts and may not have had a complete understanding of their intent. For instance, the Panel has heard on several occasions that some senior leaders were concerned about Alerts being interpreted as official Government of Canada positions on events happening internationally or that some Alerts may have been premature or unnecessary.
These are valid concerns to raise. But, in isolation, this confusion should not be the premise upon which PHAC alters its approach to international surveillance. Instead, the Panel believes that this example helps to underscore the importance of committing to regular review of terminology, standards and protocols for all products.
In the future, the ability to collaborate at the international level may benefit from the consistent use and application of terminology. PHAC and GPHIN have an opportunity to help bring a degree of international stewardship by showing a willingness to change its terminology proactively, in line with WHO guidance. The Panel also notes that the WHO guidelines are considered interim; if the post-COVID‑19 era brings new EBS systems online, it may be the right time to work together once again with international partners on the common terminology and attributes of international EBS.
Recommendation
1.10 The Public Health Agency of Canada and GPHIN should review their existing terminology and work with partners and subscribers on implementing useful standards, definitions and guidance for international EBS in the future.
The purpose of Alerts: signals for early warning
GPHIN Alerts are intended to flag to a recipient that there is a signal they may wish to take notice of or follow up on, guided by risk criteria set out in Annex 2 of the IHR (2005). An Alert consists of an email with a link to an article about an event occurring outside Canada. Alerts are intended as a tool for rapid dissemination of information on potential events of public health concern, for both domestic and international audiences. As of November 2020, 982 people receive Alerts, and more than half are international recipients. Of those international recipients, 10% are in the WHO in some capacity.
Note: six individuals have opted out of receiving Alerts.
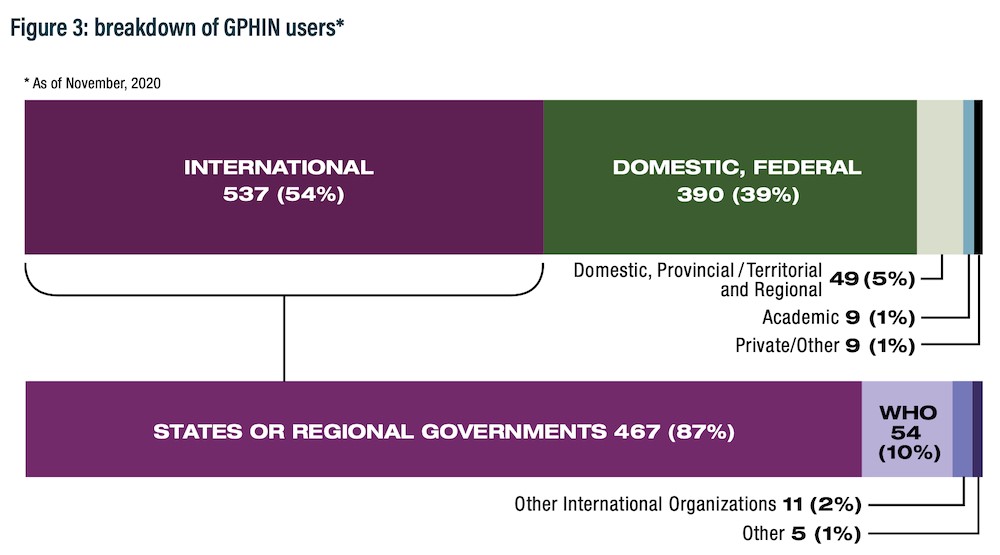
Figure 3 - Text description
Of the 994 subscribers who can access the platform:
- 537, or 54 percent, are international.
- 390, or 39 percent, are from the Canadian federal government.
- 49, or 5 percent, are from Canadian provincial, territorial or regional governments.
- 9, or 1 percent, are academics
- 9, or 1 percent, are private or other
Of the 537 subscribers who are international:
- 467, or 87 percent, are states or regional governments
- 54, or 10 percent, are from the WHO
- 11, or 2 percent, are from other international organizations
- 5, or 1 percent, are other
Numbers are as of November, 2020.
This rapid detection is very useful to both international and domestic recipients, as it singles out articles of particular interest quickly via email rather than requiring a subscriber to proactively log into the GPHIN platform. This is particularly true for international subscribers who do not receive Daily Reports. Such a signal can ensure that such events of interest are quickly addressed by those best placed to examine them further. This product should continue to be core to GPHIN’s operations.
GPHIN does not issue Alerts for domestic events. Provinces and territories are responsible for reporting to PHAC events that arise within Canada’s borders, drawing primarily on IBS. As the IHR National Focal Point for Canada, PHAC acts as a central hub for raising domestic events to the level of the international community. However, GPHIN can and does provide enhanced monitoring for domestic issues once identified, as it did for SARS and as it continues to do for COVID‑19.
Currently, the issuance of Alerts is guided by standard operating procedures (SOPs), implemented in October 2020. According to the SOPs, the decision to issue an Alert begins with a discussion among the GPHIN analysts on shift in consultation with the senior epidemiologist, based on an adapted version of the IHR (2005), as well as additional internal considerations, such as whether the source is credible and the size of the impacted population. A brief verbal justification is then submitted to the Director, Office of Situational Awareness, for approval before the Alert is issued electronically to domestic and international subscribers.
The introduction of these SOPs has helped to address the lack of clarity the Panel initially observed regarding who is responsible for what once the decision to issue an Alert is made. SOPs are procedurally useful, easy to understand, and detail who within the chain of command is responsible for what. These SOPs should set the standard for all future ones.
The existence of clear SOPs can also help avoid another scenario similar to that of early 2019, where changes to the level of approvals were poorly communicated and unclear. While the Panel has seen correspondence between analysts and their director referencing this change from that time period, no written directions were provided concerning appropriate steps to approve an Alert or when any new changes were expected to come into force.
Outside of future consideration of how terminology might be adjusted, the Panel believes that the underlying function of Alerts is appropriate and that the newly created procedures provide a far greater level of transparency about how this function is carried out. Now that these SOPs have set out clearly the purpose and procedures surrounding Alerts and have been in existence for almost a year, consideration should be given to whether the GPHIN manager would be an appropriate level of approval.
Recommendation
1.11 Early warning signals (Alerts) should remain a core function of GPHIN’s operations.
GPHIN and the early detection of COVID‑19
GPHIN initially detected signals of what would become the COVID‑19 pandemic on December 30, 2019, at 10:30 pm, Eastern time, by the GPHIN analyst on duty. The signal was distributed the following morning in the Daily Report for December 31, 2019, which cited an article published by Agence France‑Press and an article published by the South China Morning Post.
Both PHAC’s President, Tina Namiesniowski, and its Chief Public Health Officer Dr. Theresa Tam, took action upon receipt of the January 1 Special Report from GPHIN’s management shortly after 9 am. The President shared information with the Minister of Health’s office, as well as counterparts at the Privy Council Office, Global Affairs Canada and Public Safety Canada.
Canada’s response to COVID‑19 effectively began on the first day of 2020, in part due to event identification and notification of the initial signal by GPHIN staff. The Panel has seen no evidence suggesting that earlier identification by GPHIN of the outbreak would have been possible. Other systems, such as BlueDot and ProMed, identified the outbreak on the same day.
GPHIN analysts told the Panel that, following the first reports in late December, they undertook a retroactive review of the previous months of data to determine if they had failed to detect an event. Their internal assessment concluded that there was no earlier information available to them that would have led to an earlier signal. The Panel commends the analysts for this practice, as well as their diligence.
The GPHIN database
While the GPHIN database is not a product, it is nonetheless available to all subscribers and constitutes a resource of significant value. Of the 3,500 records analysts review on a given day, 1,000 to 1,500 will be published in the GPHIN database that can then be accessed by subscribers to undertake independent research and monitoring. (During COVID‑19, volumes have been higher – between 2,500 and 3,000 records a day.)
There are just under 1,000 database subscribers: 54% are international, with the remaining 46% comprising federal, provincial and territorial, regional, academic and private sector experts in Canada. While access to the database is limited to public health partners that “have the responsibility to monitor, respond to and or mitigate emerging public health threats,”Footnote 28 there is no charge to use it.
The database is also an important tool for specific international audiences such as the Pan American Health Organization, which does not receive Daily Reports. With these subscribers in mind, GPHIN does categorize articles of note for these specific audiences, through metatags (for example, Pan American Health Organization, vaping adverse effects). This categorization allows international subscribers to access a curated collection of articles of interest through the database directly, despite not receiving Daily Reports by email.
The Panel has heard that there is some interest in academia in being able to use GPHIN’s filtered data, but challenges persist related to interoperability between platforms, access and the stability of the platform itself (see Chapter 3).
The value of GPHIN’s underlying code
In addition to the data that GPHIN contains, there is also significant potential in its code base. The Panel has been told that this source of information is well suited to support the development of better artificial intelligence (AI) algorithms required to effectively manage an ever-growing volume of information. This is a contribution that GPHIN has made in the past, particularly to the international work led by the WHO. Overarching federal policies, including the Treasury Board Directive on Automated Decision-Making, are now helping to set the stage for the federal government’s use of AI, and capacity for managing and evaluating AI algorithms is growing. GPHIN can both contribute to this evolution and learn from it.
Managing and evaluating AI algorithms will require far better access to GPHIN’s code base as a start. Moreover, PHAC’s program areas may or may not be comfortable or aware of GPHIN’s capabilities, or how they could be adjusted to better capture specific events. Working with AI algorithms might also involve learning from other experts inside or outside government who work with AI algorithms extensively, and learning who can provide important input into their ongoing development and evolution. Recommendations related to the database and code are expanded upon in Chapter 3.
Making better use of GPHIN and event-based surveillance
Within PHAC
PHAC has struggled in the past with silos that limit interaction between teams and functions. One major potential for stronger intra-agency ties relates to a growing recognition of the application of EBS within program areas that have typically or traditionally relied on IBS.
GPHIN’s database is a useful resource for PHAC subject matter experts. While it was never intended to be an epidemiological database, the fact that it has captured, organized and filtered decades’ worth of public health articles effectively makes it a potential resource for historical research and study.
Moreover, as the discipline of EBS has matured, there has been growing recognition that over time the structured and systematic organization of data by analysts can be converted into indicator-based surveillance. Footnote 29 In fact, the Panel has heard that program areas are increasingly considering, and even building, small-scale event-based monitoring tools to complement their existing surveillance work.
GPHIN’s system can also be tailored to capture new terminology. In response to a new or evolving event, GPHIN analysts work with program counterparts on an ad hoc basis to develop and apply new search terms to the database so that program areas can complement their ongoing IBS with additional real-time monitoring from GPHIN. Some program areas may be unaware of GPHIN’s ability to incorporate key terminology and search terms that would allow the system to capture content specific to their area of focus.
This is an area where GPHIN’s analysts have much to contribute and could be used in a consulting capacity to guide methods and approaches. The Panel believes that program areas have much to gain from GPHIN and should be encouraged to seek analysts’ assistance and expertise. More formally, programs could be taking greater advantage of the GPHIN system by working with analysts on new terminology to guide GPHIN’s algorithms. In turn, the system can help these program areas incorporate EBS into area-specific, domestic surveillance.
Over time, there may be advantages to establishing a regular, cyclical review of terminology in consultation with program areas. This review could considerably expand the use of EBS across PHAC and complement the IBS surveillance underway in program areas. This shift cannot be driven by GPHIN alone and will require the full endorsement and active support of PHAC’s leadership.
Structural reform within PHAC is underway, including the development of a new corporate surveillance function. In this context, there are opportunities to reconsider and reset the informal links between existing and new branches.
Provinces and territories
GPHIN is not heavily used by provinces or territories. Provincial and territorial subscribers account for 5% of all users, though interest has grown since the start of the COVID-19 pandemic. About 40 provincial and territorial subscribers receive the GPHIN Daily Report. While PHAC works extensively with provinces and territories through many offices and channels, GPHIN’s direct interactions with those jurisdictions are informal.
Despite this, most of the experts consulted from the provinces recognized GPHIN’s role and benefits, and could recall having seen or used portions of its intelligence in the past. Several senior leaders were confident that analysis provided to them by their own teams had likely included input from GPHIN.
The Panel observes that provinces and territories could take greater advantage of GPHIN’s products and database, depending on their needs and capacity.
Expanding awareness and use
In late January, a presentation about GPHIN was made to members of the federal, provincial and territorial Logistics Advisory Committee. This kind of outreach is one way of promoting provincial and territorial awareness of GPHIN’s products and database, and making sure that other jurisdictions know that they can opt in to receiving them. This is one example where improved evaluation and outreach could inform any new potential products that respond to the unique needs of other jurisdictions.
For GPHIN to be useful at the provincial and territorial level, tailored support and capacity-building will be required. This recommendation builds upon the earlier observation that GPHIN analysts are well placed to offer training to others on how to use the platform and how to apply EBS data in their work.
The needs of each province and territory vary, and larger jurisdictions with robust surveillance capacity may not need GPHIN’s capacity, whereas smaller jurisdictions may not have the resources to undertake regular global surveillance alone. There is no one-size-fits-all approach, and access to GPHIN should not present an additional burden.
Recommendation
1.12 Provinces and territories in Canada should be proactively invited to access and use GPHIN products. GPHIN analysts should continue to provide tailored learning to help provinces and territories use the database, and interpret event-based surveillance, as needed.
Chapter 2: GPHIN’s organization and flow of information
For GPHIN products to be most effective, they must be incorporated into a risk assessment process that draws on the expertise of other teams within PHAC, gives the CPHO timely and value-added information, and permits them to advise the Minister of Health accordingly.
The Panel has reviewed whether the early detection of signals is leading to verification and a rapid risk assessment that can be used for decisions. We have found that current structures and processes are unclear.
For PHAC to deliver on its mandate, it should develop governance structures that promote coordination across surveillance functions and clearly assign accountability for risk assessment. GPHIN’s role and function must be situated within a context that connects it to the broader risk assessment cycle.
Our consideration of governance structures has included assessing whether GPHIN is currently in the right place within the organization in order to integrate more seamlessly with risk assessment. PHAC has already reorganized in the context of the COVID-19 pandemic, and it may look and operate quite differently in the near future. Therefore, recommendations will address the conditions required to optimize GPHIN’s role and function.
As GPHIN’s functions develop, the team should have access to additional training and support. For existing and future analysts, opportunities for skills enrichment, exchange and learning should be given new emphasis; institutional knowledge and experience serve as the starting point upon which to build.
Our scope with respect to the latter is not limited to the GPHIN team but also to the competencies required of its leadership, including higher management.
Finally, just as COVID‑19 has challenged PHAC to consider surveillance and public health intelligence, so too has the security and intelligence community become more engaged in public health objectives. At a governance level, this shift will require that PHAC clarify how it intends to manage new types of intelligence, and how this could affect decision-making, particularly in future emergency scenarios where public safety and public health mandates intersect.
Calculating the risk: how early warning results in action
In both IBS and EBS, a critical step in the use of surveillance products effectively lies in the ability to undertake timely risk assessment. Risk assessment is a systematic process for gathering, assessing and documenting information to assign a level of riskFootnote 30 so that decision-makers can take action and mitigate consequences of public health events.
Risk assessment is undertaken in many different parts of PHAC and in many different ways. There is no single risk assessment approach across PHAC; methods and standards have evolved according to sector and discipline.Footnote 30 The Panel has heard that some program areas have robust risk assessment procedures and investigate public health events regularly, whereas others may not have as much capacity or exposure.
This finding has been affirmed by the Auditor General of Canada, who recommended that “the Public Health Agency of Canada should strengthen its process to promote credible and timely risk assessments to guide public health responses to limit the spread of infectious diseases that can cause a pandemic, as set out in its pandemic response plans and guidance.”Footnote 31
PHAC has acknowledged this recommendation and has committed to review the risk assessment process, incorporating lessons from COVID‑19. PHAC also intends to engage both domestic and international partners, and stakeholders, as part of this review so that it is consistent and informed by other international risk assessment process reviews.Footnote 31
A review is also in line with Canada’s international obligations under the IHR (2005), which state that risk assessment capacity is an integral part of the prevention, surveillance and response system. Member States are, moreover, encouraged to apply a consistent, structured approach to the risk assessment of public health events.Footnote 30
This is an essential undertaking. Information presented to the Panel demonstrates that PHAC’s structures for risk assessment have diminished over time due to unclear accountability and internal changes that affected overall surveillance coordination.
In its interim report, the Panel identified risk assessment as an area for further investigation, based on initial impressions that there was an opportunity for GPHIN to better link to risk assessment so that early detection of signals can lead to decisions for action and response.
In service of this review, and with GPHIN as our central focus, the Panel has structured recommendations that address risk assessment in general. To do so, we revisit some of the lessons drawn from surveillance through the years and examine the clear consequences of letting overall coordination and governance tools erode and weaken. It is our hope that these recommendations provide useful parameters for thinking through this exercise.
The need for a central coordinating Risk Assessment Office
As PHAC begins the work of reviewing its risk assessment function, the Panel would urge it to consider some of the strengths of approaches taken previously that may still be appropriate.
The basis for these recommendations are guided by GPHIN’s needs and the nature of EBS. But they also draw from what we have heard directly from experts within PHAC who have noted ongoing confusion about how risks are assessed, how they are escalated, and who is responsible for escalation.
The Panel is convinced that risk assessment at PHAC requires accountable structures and that such accountability will not occur on its own. Currently, the responsibility for risk assessment appears to reside with the CPHO, though legislation is not clear on this point. Also, there is no dedicated team to coordinate assessments carried out across the many program areas.
Recommendations
2.1 The Chief Public Health Officer’s overall responsibility for risk assessment should be better supported by a dedicated Risk Assessment Office with a mandate to request, coordinate and produce the information required to undertake this role.
2.2 Consideration should be given to formally assigning responsibility for risk assessment to the Chief Public Health Officer in the Public Health Agency of Canada Act.
GPHIN and its role in risk assessment
GPHIN does not undertake risk assessment: it does not develop or recommend specific actions or policy responses. It provides early detection and initial verification of a potential event that may impact public health. While it is an essential part of the risk continuum, its main function is to signal events that could become significant.
GPHIN, as an all-hazards event-based system, would align with approaches recommended within emergency and disaster management response contexts, such as pandemic preparedness plans. As such, risk assessment in this report takes cues from the World Health Organization’s Rapid Risk Assessment of Acute Public Health Events guidebook, which is specific to public health risks from any type of hazard. According to this guidance, GPHIN’s main function lies in the detection of a potentially significant public health event – a surveillance function.
GPHIN’s analysts do apply an assessment to each item they flag – both stand-alone signals and items included in the Daily Reports – based on criteria set out in the IHR (2005). They validate the source; in open-source surveillance, not all articles are equal, and considering reputational as well as historic perspectives on reliable sources of reporting is among the analysts’ skills. Furthermore, standard operating procedures (SOPs) introduced in October 2020 clarify internal approval processes, roles and accountability for issuing Alerts.
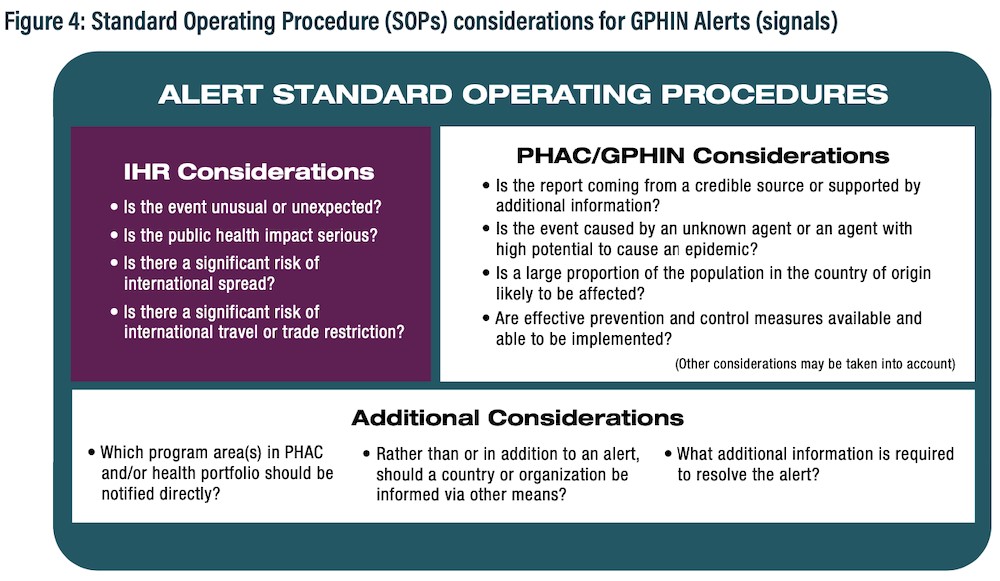
Figure 4 - Text description
The GPHIN Alert standard operating procedures involve answering the following questions to determine whether an alert should be issued:
Considerations under the International Health Regulations:
- Is the event unusual or unexpected?
- Is the public health impact serious?
- Is there a significant risk of international spread?
- Is there a significant risk of international travel or trade restriction?
Considerations related to the Public Health Agency of Canada and GPHIN:
- Is the report coming from a credible source or supported by additional information?
- Is the event caused by an unknown agent or an agent with high potential to cause an epidemic?
- Is a large proportion of the population in the country of origin likely to be affected?
- Are effective prevention and control measures available and able to be implemented?
- Other considerations may be taken into account.
Additional considerations:
- Which program areas in PHAC and/or health portfolio should be notified directly?
- Rather than or in addition to an alert, should a country or organization be informed via other means?
- What additional information is required to resolve the alert?
This initial assessment is valuable, even in cases where events may be resolved quickly or are prematurely signalled; false positives are an accepted outcome of EBS where it is important to be able to anticipate, predict and react quickly. The vast majority of experts confirm that a degree of redundancy is required, and that it is better to receive some signals that amount to nothing than to miss the signal that leads to the next pandemic.
Intelligence should be appropriately connected to teams and functions that can maximize its use and benefit. PHAC’s future risk assessment approach should take into consideration how GPHIN’s initial assessment should be connected to the larger risk continuum cycle and specifically to ensure that GPHIN’s signals are able to initiate the risk assessment that decision-makers require.
Thinking about GPHIN in the context of a continuum takes inspiration from the WHO’s guidance on early warning and response, but it is not novel. The 2008 May Report of the Auditor General of Canada on the surveillance of infectious diseases highlighted the need for integrated risk assessment. Notably, the initial response to this audit committed to the development of a Risk Assessment Framework by 2009.
Recommendation
2.3 GPHIN products should be part of an integrated risk assessment continuum that links its intelligence with the individuals that can undertake appropriate verification, risk assessment, coordination and action.
What follows is the Panel’s guidance on how best to establish this risk continuum and the supporting structures within PHAC that will allow GPHIN to connect into it.
GPHIN and the Risk Assessment Office
A persistent challenge that the Panel has noted is that GPHIN is somewhat isolated as a team and system. Because it is an all-hazards early detection system, it resides within PHAC’s Centre for Emergency Preparedness and Response rather than in a specific program area such as other surveillance teams.
GPHIN analysts provide initial signal detection and source verification for its products, but such actions do not constitute a full risk assessment. For that to transpire, signals must be rapidly validated by subject matter experts from other program areas. Ideally, signals also link to the modelling and forecasting expertise required to add the necessary context for a potential signal. In general, this type of collaboration does take place, and relationships between program experts and analysts have been mutually reinforcing.Footnote 32
One of the challenges of EBS, however, is that signals can sometimes require assessment by a number of experts from a variety of disciplines and areas. This challenge can be compounded by PHAC’s stovepipes. Without a regular daily cycle of surveillance and risk assessment, coordinated by a unit able to assign additional risk assessment capacity, GPHIN’s use as an early warning tool may be limited because information flows only one way and early verification is not as rapid or as coordinated as it needs to be.
Clear pathways need to exist between GPHIN’s analysts and those that can assess and action verifications if needed. GPHIN needs to be plugged into a daily risk assessment continuum so that its signals are assessed not just in isolation but as a continuous input on potential evolving public health events.
A Risk Assessment Office could provide an extremely valuable service. Work under this new office would focus primarily on the function and need to take a whole-of-agency approach to risk assessment. This approach would be taken in line with PHAC’s role in the prevention of disease and injuries and to support Canada’s readiness for potential health threats.
Though there are many ways to structure this office’s operations, a number of skills, levels of expertise and perspectives must be consolidated in order for the office to operate effectively.
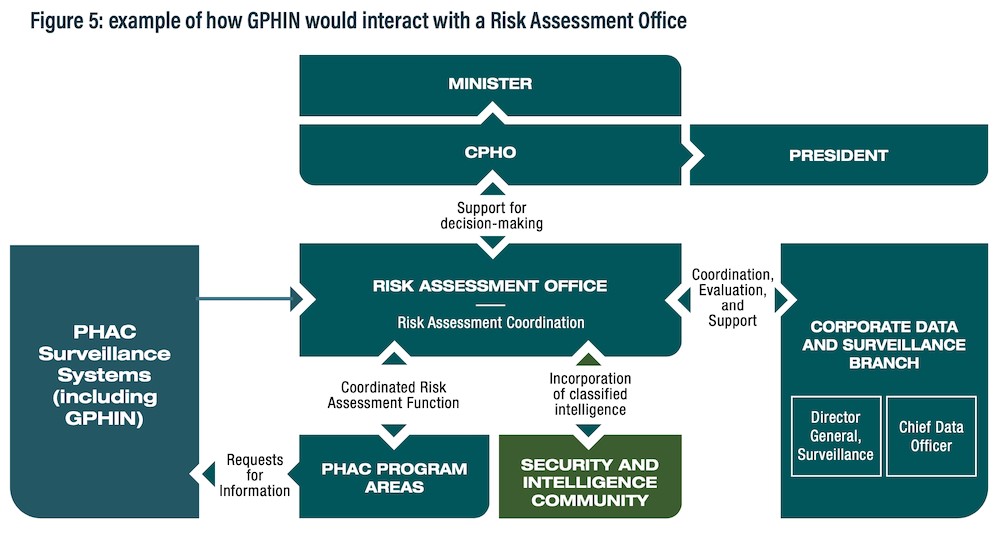
Figure 5 - Text description
Surveillance systems, including GPHIN, feed into the new Risk Assessment Office, which serves as a central hub for risk assessment coordination.
The Risk Assessment Office works with the security and intelligence community to incorporate classified intelligence into the Public Health Agency’s risk assessment processes.
The Risk Assessment Office also works with the Corporate Data and Surveillance Branch, which houses the office of the Chief Data Officer, as well as the new position of Director General, Surveillance.
The Risk Assessment Office plays a coordinated risk assessment function and supports program areas at the Public Health Agency. Program areas, in turn, can request additional information directly from the GPHIN system.
The Risk Assessment Office supports the Chief Public Health Officer in making decisions and determinations related to risk. The Chief Public Health Officer, in turn, supports and provides advice to the Minister and President.
The Risk Assessment Office should also be responsible for anticipating future needs, setting standards and protocols for risk assessment, and for negotiating and managing how risk assessments should evolve. These activities include linking experts within PHAC who have backgrounds in data visualization, modelling, forecasting, and other skills that might be drawn upon once a GPHIN signal has entered the risk continuum. The office will also ensure that it has strong links to the CPHO’s office, as well as that of PHAC’s President.
Recommendations
2.4 The Risk Assessment Office should coordinate and oversee risk assessment, based on all the necessary inputs for coherent risk assessment from across the Public Health Agency of Canada, of which GPHIN is one.
2.5 The Risk Assessment Office would be responsible for horizontal coordination of signal distribution, verification, risk assessment and required response.
Building links to national security
Improving PHAC’s integration with the security and intelligence community has been a consideration since before COVID‑19. Public health and security priorities have overlapped in the past, particularly in times of crisis, and PHAC maintains a presence at high-level national security decision-making tables.
The new Risk Assessment Office would be well placed to build capacity at PHAC to engage with the security and intelligence community, and to integrate classified flows of information into its decision-making where appropriate. The Risk Assessment Office should ensure it has a sufficient number of employees who have Top Secret security clearance in order to access the necessary classified information.
The Risk Assessment Office could also help establish stronger links in general to the national security community that can go beyond the strict exchange of intelligence. PHAC, and GPHIN in particular, may be able to benefit from how this community is building its own open-source surveillance capacity.
Closer integration of public health into national security policies is a significant undertaking. Culturally and historically, these two spheres have interacted only as necessary to respond to an immediate event or crisis. For that reason, the Risk Assessment Office should assume the lead in establishing this longer-term relationship on behalf of PHAC.
The lessons of COVID‑19 will set the stage for re-prioritized objectives that link public health and public safety, but integration is already underway. Intelligence organizations have developed stronger links to PHAC’s Health Portfolio Operations Centre’s operations throughout the response, and the Panel has heard multiple parties express a desire to continue to work more closely together.
At a higher level, the federal government must decide how to incorporate public health intelligence into national security priorities and what that will mean for ministers. Accountability, interoperability, and clear roles and mandate will once again be essential to setting the stage for a well-functioning, whole-of-government approach.
Closing the gaps
A centrally coordinated function mandated to oversee the entire risk assessment continuum can help support broader surveillance objectives, but it also represents an important evolution. As the lessons of the COVID‑19 response underscore the importance of planning for the next pandemic or widespread outbreak, one significant gap the new Risk Assessment Office will address relates specifically to diseases of unknown origin.
Responsibility for risk assessment is currently assigned to program areas based on disease or the mode of transmission of a given threat. If the nature of the disease or mode of transmission is not known, it is possible that it will not be tasked appropriately, and critical time can be lost in escalating to the appropriate levels.
Recommendation
2.6 The Risk Assessment Office should be able to fill existing gaps in risk assessment related to events where information is limited or the origin or means of spread are unknown.
This gap has been identified before. In the 2018 Evaluation of Emergency Preparedness and Response Activities prepared by the Office of Audit and Evaluation,Footnote 11 GPHIN is recognized for its contribution to early detection and response, but the report notes that the Centre for Emergency Preparedness and Response lacked information on how detection information about events is shared, particularly with senior management. It also highlighted the need for a more modern risk assessment model that better reflects PHAC’s capabilities.
Medical Officer on-Call (MOOC)
An instructive program from the recent past is the Medical Officer on-Call (MOOC) program, which used to provide rapid assessment of emerging risks, particularly when they arose outside normal working hours or across program areas, where a designated lead might not be assigned or available because the nature of the event or the disease is unknown.
When it existed, the MOOC program was able to elevate events according to defined response triggers and considerations. This type of rapid assessment on demand would clearly benefit from GPHIN’s design as an early warning system and address the existing gap between initial detection and full risk assessment.
A mutually reinforcing function
If a Risk Assessment Office can be structured and implemented in such a way that connects GPHN with the full continuum of risk assessment, then it seems both pertinent and possible to expand GPHIN’s functions accordingly so that subscribers of its products benefit directly from this new governance approach.
Earlier, the report outlined specific steps GPHIN could take now to guide its existing suite of outputs, with a view to providing the subscriber with clear information, based on established SOPs. We suggested that more regular outreach and evaluation by GPHIN would help clarify the needs of various subscribers.
Here, we add to that recommendation by proposing that GPHIN, with the support of a coordinated and central risk assessment function, could begin to insert additional disclosures and updates in its products or through its database.
The nature of this information would not be to provide formal risk assessment or advice. Rather, some additional clarity regarding the stages and status of a potential event could be of use, especially if provided on a timely basis.
For example, recipients are aware that an Alert is meant to flag a potential event. However, GPHIN does not currently provide updates on Alerts directly to recipients. Because verification of events is the responsibility of the WHO in the international context, and that of program areas domestically, GPHIN is not currently positioned to provide further context on whether verification has occurred with regard to an Alert and what the outcome might be after it has been issued.
It would be up to the Risk Assessment Office to be able to provide the relevant status updates, and to relate that information back to GPHIN in a manner that can be used for both the database and products. Correspondingly, if this value-added function is pursued, GPHIN will need to decide what manner of product could be used to reach its subscribers. Domestically, subscribers do have access to Daily Reports, and inclusion of risk assessment level or the evolution of an event could be a part of that daily product.
Internationally, the current option available is to include that information as part of the database through the use of metatags for subscribers. The Panel has already recommended that GPHIN consider whether international subscribers would benefit from a type of Daily Report.
Recommendation
2.7 With input from the new Risk Assessment Office, GPHIN’s products should clearly state the degree of analysis that has been applied where possible, particularly in the case of an evolving event.
A new home for GPHIN?
If GPHIN’s scope is to expand in the ways set out above, the Panel believes that there is sufficient rationale to re‑establish GPHIN in a context that can better support its functions now and in the future. The Panel is not convinced that GPHIN’s current position in PHAC’s organizational structure management is best placed to use GPHIN’s products or to decide how they should be used.
There are several reasons for this, including the fact that PHAC’s Centre for Emergency Preparedness and Response is primarily an operational branch and does not have surveillance expertise commensurate with other program areas. It has also been observed that there might not always have been a sufficiently high ratio of public health expertise in its management roles.
PHAC has already begun significant internal organizational change, reflective of the massive effort required to lead the COVID-19 pandemic response and the growth in staff numbers to match the capacity needs. As noted, organizational changes have included the creation of a new corporate surveillance team, which at a minimum will give GPHIN and PHAC a common point of reference for the surveillance function. But PHAC will no doubt continue to evolve as COVID‑19 lessons-learned exercises report back and new priorities in public health are set. As such, the Panel will not be prescriptive about the best fit for GPHIN at this time.
Wherever GPHIN resides, consideration of the operating context is essential. Based on our review, the Panel would propose the following recommendations.
Recommendations
2.8 There should be sufficient public health expertise in GPHIN’s management to fully understand event-based surveillance.
2.9 GPHIN should be well connected to risk assessment, and information should flow two ways between GPHIN analysts and the Risk Assessment Office.
2.10 GPHIN should be better linked to the broader surveillance capacity, and in particular, indicator-based surveillance systems, so that the benefits of event-based surveillance can be explored and leveraged.
The GPHIN analyst: skills for today and tomorrow
GPHIN analysts are talented, multidisciplinary experts. Several hold medical degrees from their country of origin. Collectively, they hold expertise in biology, computer science, medicine, nursing, engineering, chemistry, botany and toxicology. Team members can actively monitor nine different languages (English, French, Arabic, Chinese (traditional and simplified), Spanish, Portuguese, Russian and Farsi). The team works Monday to Friday between the hours of 6 am and midnight, and Sundays from 2 pm to midnight.
This capacity has enabled GPHIN analysts to apply an initial assessment on past signals and in their inclusion of articles for the Daily Report. They are able to weigh the merits of sources of information and prioritize them for key audiences from a public health lens. GPHIN has already fostered, and retained, a highly capable team.
A day in the life (today)
The first GPHIN shift of the day logs in at 6 am and picks up the work of their colleagues from the evening before. Analysts finalize the Daily Report, which is reviewed by the duty officer at 7 am and the senior epidemiologist at 7:30 am, before being sent to subscribers by 8:30 am.
Relevant information is reviewed at the Emergency Management Branch prep meeting ahead of the senior management daily meeting at 9:30 am; thereafter, the analysts turn to the preparation of the next Daily Report.
The morning shift hands their work off to their colleagues at 2 pm; the evening shift continues to collect and refine the next day’s report until midnight. Meanwhile, the GPHIN platform continues to process overnight, waiting for the analysts to return in the morning and begin again.
The production of the Daily Report is a time-consuming process that leaves little space for additional activities. Over the course of the day, analysts scan, sort and collate signals filtered through the GPHIN platform, checking machine translations for accuracy as needed.
Slow processing times and system instability complicate the work. Automating parts of the production of the Daily Report could spare analysts from the most repetitive tasks and free time for them to use their language skills and specializations in more detailed analysis. Previously, a technical advisor would have provided support and troubleshooting; currently, analysts must do the best they can with the tools at hand (see Chapter 3).
If an analyst picks up a signal of concern, the team has a brief conversation to check the signal according to protocols: if warranted, the signal is elevated to the Director, Office of Situational Awareness, with verbal justification, and an Alert is issued. The team conducts enhanced surveillance of issued Alerts but aren’t currently set up to send subsequent updates, corrections or clarifications as an event develops, beyond the domestic Daily Reports.
Recognized strengths
The starting point for future skills development lies in the past: two of GPHIN’s analysts have been on the team since before the launch at the United Nations in 2004. Finding ways to build a skills strategy that captures institutional knowledge will be fundamental to future success.
For example, the Panel was told that GPHIN’s analysts have become experts at working with the Factiva research tool, honed over years of first-hand experience. Not only can GPHIN analysts work efficiently with that source, but they also are best placed to make decisions about what to circulate, amounting to a comparative strength.
The Panel has also been told by many within and outside of PHAC that the range of language capacity among analysts is a strong advantage, especially among EBS systems. AI and natural language processing are advancing quickly, but there is no substitute for human judgment. And the ability to search in the language of origin to validate sources of information and understand the culture of the context in which the event occurred is a competence that should not be under-emphasized, especially in the near future.
Moreover, language ability is one of the reasons GPHIN’s algorithms are effective. Analysts’ ongoing ability to contribute new taxonomy to the GPHIN code base means that the system can evolve as new terms such as “COVID” appear.
The role of the technical advisor
One idea from the past that merits revisiting is having a technical advisor dedicated to the GPHIN team. This role was phased out in 2017. Formerly, this individual was embedded within the GPHIN team and acted as a facilitator between GPHIN analysts and the system itself, providing day-to-day support on any platform shortcomings.
More broadly, the technical advisor also provided a degree of technological stewardship for the system and could operate as the interface between the GPHIN team and the technological partners hosting, supporting or developing the system over time.
This report has already identified the potential of GPHIN’s database and how this platform might be recalibrated to support PHAC program areas and academics to a greater extent. GPHIN would be well served by a designated expert who could help oversee new applications of the database and make sure the GPHIN platform is not compromised or slowed as a result of any new uses. The Panel provides its formal recommendation on this matter in Chapter 3.
Hearing directly from GPHIN analysts
The Panel has consulted with GPHIN analysts and managers, both past and present, as part of this review. The extended GPHIN team (analysts, plus the senior epidemiologist, and students) were invited to share their thoughts through multiple facilitated interviews and also provided written comments to the Panel.
Their perspectives were an essential contribution to the review, particularly because of the long-serving nature of many analysts and the significant contribution several have made to the algorithms and taxonomy built into GPHIN’s code. Those who chose to participate were asked about GPHIN’s value, in their own words, and how their day-to-day work unfolds, as well as what they would like to spend more time on. They were also invited to identify the skills and experiences they would like to cultivate.
The Panel heard that the GPHIN system is not fully reliable and that issues with the platform detract from the time they have to apply to research and analysis, and this is a valid concern. It is also clear that there is a feeling that they have not been heard or recognized through subsequent past managerial reviews, and that their autonomy and needs have been compromised. There is also some question of how much priority has been placed on GPHIN’s platform in the context of ongoing server migration and some system upgrades that have not yet been uploaded (see Chapter 3 for a longer discussion).
The Panel would like to recognize the GPHIN team’s contribution to this review, and to express gratitude for their willingness to speak with us. With respect to the areas that analysts identified for future training, the Panel emphatically agrees that courses related to public health and epidemiology, alongside opportunities to engage with the public health intelligence and EBS communities, would be advantageous.
The Panel is also supportive of a desire to access assignments with other public health program areas, and sees additional value in micro-assignments within PHAC, to increase analysts’ exposure to the broader work of PHAC and to expand relationships and personal networks from within.
Retaining skilled employees should be a priority. But one critical objective will be to consider how GPHIN’s isolation has perhaps fostered a sense of disconnect between analysts and the work of PHAC. This is where the potential of assignment within PHAC offers a mutually reinforcing end. GPHIN analysts have a great deal to contribute to other program areas, especially as their contributions relate to the uses and applications of EBS.
Recommendations
2.11 GPHIN analysts should be supported in developing individual professional development plans that help map the skills and training they need to do their work to the best of their ability, now and into the future.
2.12 Professional development of current GPHIN analysts should be prioritized, with a view to expanding analysts’ skills and exposure to other parts of the organization or other relevant organizations.
Above all, the Panel would like to highlight that many of the recommendations related to new roles and functions for GPHIN will have an immediate impact on how analysts work. In the way work is currently structured, analysts do not have the time and resources that would be needed to commit to several of the new functions outlined to this point. Some things will have to change to allow GPHIN analysts to step into these new roles.
Reinforcing GPHIN
The Panel’s mandate calls for a comprehensive look at the future role of GPHIN in the context of EBS. It is clear that EBS must be one of the core functions that endures, and is reinforced, in the post-COVID‑19 world.
GPHIN was created when the Internet was still relatively new and EBS was still in its infancy. It has functioned admirably for 25 years. But to respond to public health intelligence needs in the future, GPHIN needs to evolve in both operations and technology.
The Panel’s recommendations on mandate, risk assessment and skills are interrelated and potentially consequential for the organization as a whole. There will be a significant need for strong change management to orient GPHIN toward the future.
There are multiple reasons for this. The management above GPHIN has experienced a high degree of turnover in the past five years. Through discussions with some of these past managers, the Panel has observed inconsistencies in how GPHIN’s products and core function are described.
Even when there may have been good reason for some proposed changes, GPHIN analysts themselves have at times been resistant to change. GPHIN analysts have indicated that their working context is misunderstood, yet this dynamic is more than a misunderstanding.
In particular, the decision in early 2019 to raise the approvals of Alerts to the Vice President caused significant distress for the team, particularly because management at the time provided no further direction on how this core function should be carried out.Footnote 33 Though SOPs were eventually developed that subsequently lowered approvals to a more appropriate level, and put in writing the approaches and protocols that addressed any outstanding concerns, the corrosive effect of this decision, and how it was carried out, is still apparent.
The Panel has already stated that GPHIN’s current operational environment may not be the best fit for several reasons. But the lessons learned from past changes and managerial approaches should also be taken into consideration by future managers and leadership that will inherit GPHIN’s considerable talent. Trust and mutual respect must be proactively fostered, and it is for management to create and build consensus around a common purpose.
Leadership of GPHIN in the near future will involve rebuilding trust. It will include helping analysts see themselves as part of the broader work of PHAC rather than being on the periphery looking outward. It will take ownership for some of the ways GPHIN analysts may have experienced changes thus far, acknowledge past difficulties, and assume ownership for things that can be done differently.
Elsewhere in government, the rise of open-source information, alongside dramatic changes in how humans engage with the Internet, has required some disciplines to respond rapidly to new sources of information, and to find ways to leverage technology on large and small scales in order to meet their objectives. Adaptation and continuous learning are essential. GPHIN should be calibrated similarly. But the solution will not be technology in isolation. In a moderated EBS system, the greatest strength is human analysis; in GPHIN, it is its analysts.
Planning for the future
GPHIN’s future, and the skills required of its analysts, will depend to a large extent on the technological platform and tools it is able to leverage. While some of GPHIN’s activities will likely continue to exist, the next generation of EBS, or the needs of potential new subscribers, could precipitate the need for skills not yet anticipated.
Attracting the next generation
GPHIN has long supported and contributed to academic research, and it regularly recruits students from public health, data and epidemiological backgrounds. This regular exchange of knowledge is extremely important, both to keep GPHIN’s methods and approaches modern, and to help provide first-hand experience to a new generation of public health professionals.
A greater emphasis on bringing in young students to train and learn directly from existing analysts could also be used as a tool for recruitment and to evaluate the skills and abilities that align well with GPHIN’s operations and functional needs.
The Panel has heard that right now in Ontario, the academic community has contributed to the provincial public health infrastructure, particularly as it relates to modelling. This also occurred during the 2009 H1N1 pandemic, when students from the University of Toronto were able to undertake scientific reviews to support higher-level analysis taking place within Public Health Ontario.
This is a smart and potentially useful idea for surge capacity when the next pandemic arrives. But the ease with which public sector interacts with academia could be improved, and giving students access and exposure to real-life surveillance skills should remain a priority.
Database trainers
If EBS capacity is expanded, there is also the potential that existing GPHIN experts might be well placed to offer training to others, both within PHAC, across Canadian jurisdictions and internationally. Such training is particularly relevant to GPHIN’s database, where untapped potential resides in the categorized research collected over years of GPHIN surveillance work. Using that database would benefit from pathfinding and instruction that draws on analysts’ expertise and experience.
Outreach and engagement
Another area worthwhile to emphasize is the ability to undertake proactive and productive engagement with people who read and use GPHIN’s products and to proactively outreach to new subscribers.
Right now, analysts’ roles may not allow for the time and space to work with researchers or policy areas on longer-term projects. But there appears to be both interest and demand from experts within PHAC and academia.
While the ability to collaborate requires underpinning arrangements or agreements in some cases, developing capacity for outreach and engagement is an appropriate role for GPHIN’s manager. A greater degree of emphasis on project management and engagement skills assigned to this role could expand the range of partners that GPHIN is able to work with.
Part of this exercise should also acknowledge that certain skills and competencies may not need to reside with the GPHIN analysts but rather could draw on skills elsewhere within PHAC. PHAC is undertaking steps that will bring advanced data analytics capacity under the banner of the Chief Data Officer. Where collaborative services such as this are available, GPHIN should be able to draw on those skills as needed.
The expanded functions proposed in this report should also invite a review of the existing responsibilities and levels of the team. The Panel has learned that the official levels of classification held by most analysts have remained static for over a decade. As the role and function evolve, PHAC leadership should re-evaluate the current levels to be sure they continue to reflect the experience and responsibilities analysts are contributing.
Recommendations
2.13 The Public Health Agency of Canada, GPHIN managers and analysts should work together to identify the appropriate skills and competencies for the future needs of GPHIN.
2.14 GPHIN should develop a recruitment strategy that maps the skills that could be required as new technology and techniques become available and that anticipates knowledge transfer between long-serving analysts and newcomers.
A vision of a day in the life (tomorrow)
The first GPHIN shift of the day logs in at 6 am and picks up the work of their colleagues from the evening before. Analysts finalize the Daily Report, which is reviewed by the duty officer at 7 am and the senior epidemiologist at 7:30 am, before being sent to subscribers by 8:30 am. The Daily Report now includes international recipients, who anticipate receiving these useful products from Canada each day.
But the news of the day contains an article of interest already, and the senior epidemiologist is already speaking with the Risk Assessment Office to activate support. Analysts are verifying the article, checking other local sources in the language of origin. The decision is made to escalate.
As the Risk Assessment Office coordinates with program areas and experts on a rapid basis to see if additional risk assessment input is readily available, GPHIN sends the signal to its entire stakeholder list. It will include a note that clarifies that the source has been validated and that PHAC’s risk continuum is engaged. Recipients will be reminded that subsequent updates will be part of the Daily Report and that they can log into the GPHIN database independently if they would like a closer look.
Another analyst will be looking at a story that requires more assessment and intelligence-gathering. Emails are sent to contacts within PHAC, the Government Operations Centre and internationally to assess whether there is other open-source information available to confirm or refute the importance of a story.
While this takes place, other GPHIN analysts are focused on the Daily Report. It’s still a major part of the day’s work, but through evaluation and discussion, as well as some useful information management and information technology (IM/IT) updates, the system runs more smoothly, and analysts have been able to reduce the amount of time needed to create it.
Elsewhere on the team, one analyst is spending the day with a PHAC program area that is curious about how EBS might help them with a domestic surveillance project. The analyst has a lot to contribute regarding how EBS works and is also helping experts learn to use the GPHIN platform so they can undertake their own research independently.
GPHIN’s manager is helping the latest PhD student onboard onto the team. The student has arrived from a post-secondary institution as part of a new partnership intended to share knowledge on AI and to work with GPHIN’s algorithms to see if they can make the AI better. This isn’t just a short assignment, and the relationship with the institution has been developed over a longer term to align with both PHAC’s research agenda and to facilitate continuous learning on both sides.
By mid-afternoon, the Risk Assessment Office has circled back to GPHIN to report on how the initial signal has been reviewed and interpreted. This time, the event raises enough concern to reach the CPHO, who is now aware and will be well placed to react quickly if the event evolves. GPHIN analysts include that information in the disclosure section of their Daily Report proactively; independent searching for additional articles that might inform the event continues.
Overnight, a bit of good news: articles appear that indicate the event has resolved as a false positive. GPHIN’s analysts include these articles in their Daily Report so that domestic and international recipients immediately know what has come from the signal of the day before. On arrival in the morning, the senior epidemiologist calls the Risk Assessment Office to report on the development, which ensures that this important information reaches the CPHO.
Chapter 3: GPHIN and technology
GPHIN was the result of visionary public servants who were able to understand and harness the unprecedented access to information offered by the Internet. While GPHIN at its onset was ahead of its time, regular renewal is essential to ensure that it can keep up with the pace of technological innovation; just as the skill set of analysts requires regular re-evaluation and support, so too does the GPHIN system itself.
The rapidly increasing volume and immediacy of media reports, the ubiquity of social media, and the emerging questions of trust and misinformation raise pressing questions that GPHIN, as well as media monitoring and public health surveillance teams across government, need to consider in order to adapt to accelerating shifts in the information technology landscape.
Over the Panel’s work, two points have become clear:
- in an age of technological dynamism, GPHIN cannot afford to remain static
- PHAC does not currently have the capacity to undertake this work alone
The use of new technologies is not an end in itself; technologies should be deployed to solve existing problems and gaps. Technology will not solve obstacles of authority or mandate, issues of governance, or enhance partnerships on its own. Future upgrades to GPHIN should involve clear problem definition undertaken in collaboration with subscribers inside and outside the federal government and the GPHIN team, proper knowledge of translation efforts, solid project management acumen, and strong communication between analysts and technical experts.
As a system that already deploys sophisticated technology in support of timely decision-making, GPHIN could be well positioned as a key technological success story of how the public service adapts to the information and technology landscape of the future.
GPHIN and technology: driven by partnerships
From its inception in 1997, GPHIN has been developed in partnership with other organizations.
The initial prototype was developed by Health Canada in partnership with the WHO. The development of GPHIN II was funded by Health Canada, the Nuclear Threat Initiative (led by philanthropist Ted Turner), and the WHO. At its formal launch at the United Nations in 2004, Ujjal Dosanjh, then Minister of Health, emphasized that GPHIN supports a strengthened network of international cooperation and communication.
From 2002 to 2016, the GPHIN system relied on public sector partnerships and private sector expertise and development. The initial collaborative research agreement established with Alis Technologies, Inc., a Canadian machine translation technology company, supported continued development of GPHIN’s machine language translation capabilities. In exchange for approximately $1 million of in-kind support, Alis Technologies was provided a licensing agreement to allow commercial use of the GPHIN platform in non-public health fields. When Alis Technologies declared bankruptcy in late 2003, the collaborative research agreement was transferred to NStein Technologies, another Canadian company familiar with the GPHIN system. NStein was given similar rights to commercialize the GPHIN system in other fields through a technology licence agreement in 2004.
Partnerships with the private sector were driven by the recognition that technological innovation inside government posed challenges that, at the time, were difficult to resolve. They were also driven out of need. In 2009, a proposal for PHAC’s Information Management and Information Technology Directorate to assume management of the GPHIN system was unsuccessful, as the directorate indicated it lacked the expertise and capacity to take responsibility for GPHIN at the time.
While private sector partnerships open new possibilities for technological innovation, they are not without their own obstacles. By 2010, NStein Technologies and its parent company, Open Text Corporation, owned the entire GPHIN system – both the technology and its underlying intellectual property. As a result, it became increasingly difficult and expensive to enhance the GPHIN system.
Through the GPHIN Renewal Project, undertaken in collaboration with National Research Council Canada (NRC) from 2015 to 2019, PHAC repatriated the GPHIN system and is now able to take a more active role in GPHIN’s technological development and stewardship.
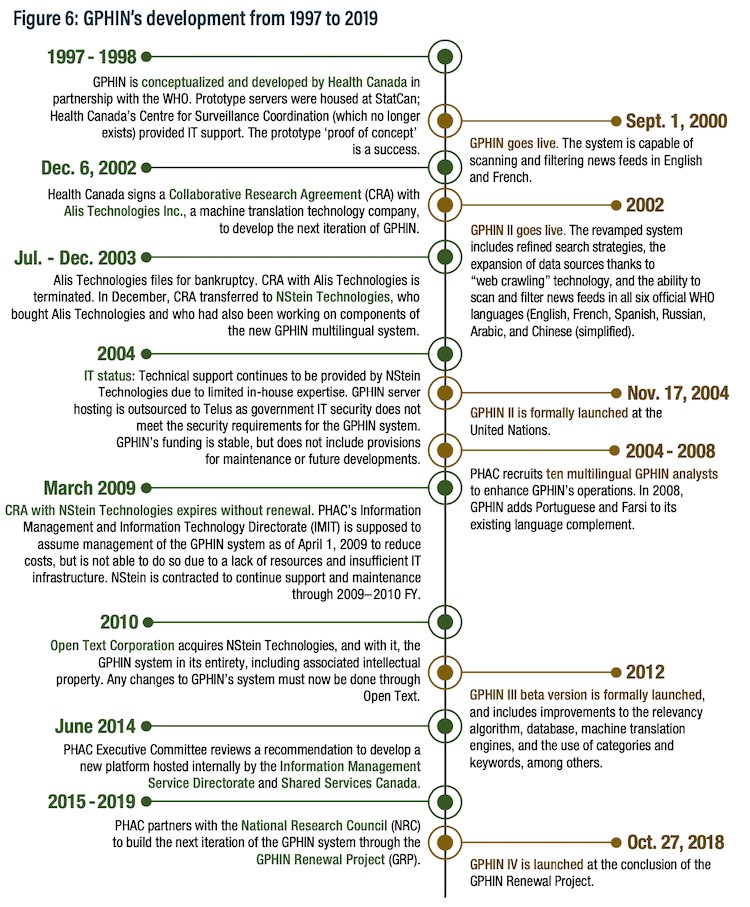
Figure 6 - Text description
GPHIN’s development
1997 to 1998: GPHIN is conceptualized and developed by Health Canada in partnership with the WHO. Prototype servers were housed at Statistics Canada; Health Canada’s Centre for Surveillance Coordination (which no longer exists) provided IT support. The prototype ‘proof of concept’ is a success.
September 1, 2000: GPHIN goes live. The system is capable of scanning and filtering news feeds in English and French.
December 6, 2002: Health Canada signs a Collaborative Research Agreement (CRA) with Alis Technologies Inc., a machine translation technology company, to develop the next iteration of GPHIN.
2002: GPHIN II goes live. The revamped system includes refined search strategies, the expansion of data sources thanks to “web crawling” technology, and the ability to scan and filter news feeds in all six official WHO languages (English, French, Spanish, Russian, Arabic, and Chinese (simplified).
July to December 2003: Alis Technologies files for bankruptcy. CRA with Alis Technologies is terminated. In December, CRA transferred to NStein Technologies, who bought Alis Technologies and who had also been working on components of the new GPHIN multilingual system.
2004: IT status: Technical support continues to be provided by NStein Technologies due to limited in-house expertise. GPHIN server hosting is outsourced to Telus as government IT security does not meet the security requirements for the GPHIN system. GPHIN’s funding is stable, but does not include provisions for maintenance or future developments.
November 17, 2004: GPHIN II is formally launched at the United Nations.
2004 to 2008: PHAC recruits ten multilingual GPHIN analysts to enhance GPHIN’s operations. In 2008, GPHIN adds Portuguese and Farsi to its existing language complement.
March 2009: CRA with NStein Technologies expires without renewal. PHAC’s Information Management and Information Technology Directorate (IMIT) is supposed to assume management of the GPHIN system as of April 1, 2009 to reduce costs, but is not able to do so due to a lack of resources and insufficient IT infrastructure. NStein is contracted to continue support and maintenance through fiscal year 2009 to 2010.
2010: Open Text Corporation acquires NStein Technologies, and with it, the GPHIN system in its entirety, including associated intellectual property. Any changes to GPHIN’s system must now be done through Open Text.
2012: GPHIN III beta version is formally launched, and includes improvements to the relevancy algorithm, database, machine translation engines, and the use of categories and keywords, among others.
June 2014: PHAC Executive Committee reviews a recommendation to develop a new platform hosted internally by the Information Management Service Directorate and Shared Services Canada.
2015 to 2019: PHAC partners with the National Research Council (NRC) to build the next iteration of the GPHIN system through the GPHIN Renewal Project (GRP).
October 27, 2018: GPHIN IV is launched at the conclusion of the GPHIN Renewal Project.
GPHIN Renewal Project
The GPHIN Renewal Project (GRP), the latest major GPHIN upgrade at a total cost of $7.9 million, consisted of two phases. After exploring various options, PHAC partnered with the NRC because of the latter’s suite of capabilities and because PHAC did not have the in-house information technology resources or capacity to undertake the upgrade alone.
Phase One, which began in January 2016, was driven by financial need. Due to the approaching Rio 2016 Summer Games and the GPHIN legacy system’s payment calendar, which required the annual hosting fee to NStein to be paid each June, PHAC required a replacement system to be produced quickly and at reasonable cost. This first phase would also bring the GPHIN system back under PHAC control and allow for easier access to the underlying code base, as at the time, changes to the GPHIN system had to be made through the private contractor, which was a costly and time-consuming process. The Panel heard that the NRC built and delivered this new replacement system on schedule and that Release 1 was celebrated as a success.
Phase Two of the GRP, which began in January 2017, involved the development and implementation of additional functions for the GPHIN system. While some GPHIN analysts expressed disappointment with the outcome of Phase Two, the Panel spoke to several PHAC and NRC managers, as well as technical experts, who stated that analysts had expectations for the GRP that exceeded the budget available for the project.
Throughout the Panel’s conversations, few issues provoked as much disagreement among participants as the process and outcome of the GRP. From one perspective, the project was a success. As the Panel noted in our interim report, the GRP was completed on time and under budget. Moreover, the GPHIN system was successfully repatriated under PHAC control and brought into compliance with existing Government of Canada IT policies and standards.
However, as the Panel also noted in our interim report, the GRP required re-scoping and additional governance mid-project to improve project management capacity. The Panel also heard that the use of an Interdepartmental Financial Agreement as the contracting mechanism did not allow for changes to the development path and provided PHAC with little recourse to refuse delivery or withhold payment.
PHAC has already conducted reviews into the GRP process and outcomes. The May 2018 Consulting Engagement of the GPHIN Renewal Project, prepared for the Vice President, Health Security Information Branch, found that:
there were insufficient project controls in place with respect to governance, risk management, and internal controls to oversee the GRP […] Release 1 of the project was relatively straightforward with a low level of project complexity. Release 2, which involved a much higher level of complexity of the project, was initiated in March 2017 […] the project continued to be managed in the same way as Release 1 and did not sufficiently incorporate project and change management practices to address the much higher complexity associated with Release 2.
The GRP Close-Out Report, in a similar vein, notes that, while the GRP objectives were met:
There were some challenges related to innovation in a government context, communication across disciplines and departments, governance and conflict resolution […] some of the cutting-edge and aspirational functionalities originally envisioned for the system were not realized in a way that fully met the hopes and expectations of some PHAC users. As well, the newest and most innovative features of the system, such as story-building, were difficult to evaluate because there was no baseline for comparison and no industry standard to determine what was technically possible.
What the Panel heard from GPHIN analysts, PHAC management, the NRC and technical experts who were working on the project at the time is largely consistent with the findings of these reviews, and the Panel is encouraged that PHAC, as well as those involved with the project, was able to identify pressure points and obstacles. The lessons learned from this project should be carefully incorporated into future GPHIN renewals.
The GRP is a lesson for technological innovation in the context of the public service. It demonstrates the need for a clear understanding of EBS, robust lines of communication between the GPHIN team and developers and technical experts, and strong project management to guide future GPHIN upgrades and renewals.
Technology: the way forward
As the Panel has stressed in the preceding chapters, the role of EBS systems in the early detection of COVID‑19 underscores the valuable role that GPHIN and similar systems play in the global public health surveillance ecosystem. Timely identification of signals paves the way for verification and risk assessment, the marshalling of necessary experts and resources to respond to a public health event, and both domestic and international coordination and mitigation efforts.
Going forward, the Panel believes it is essential that PHAC ensure that its EBS capacity remains up to date, efficient and forward-looking, both in terms of its technological capacity and human analysis (see Chapter 2). Achieving such EBS capacity will require concerted efforts and expertise, project management skills, knowledge translation capacity, and a clear understanding of how GPHIN fits into PHAC’s risk assessment continuum, as well as careful consideration of how partnership and collaboration with academia and the private sector can contribute to ensuring a future robust EBS capacity.
Inputs
The GPHIN platform currently draws on a number of sources. The majority (84%) of the system’s inputs come from Factiva, a global news and monitoring service offered by Dow Jones & Company. Analysts have created (and continue to refine) sets of complex logical queries that pull over 7,000 articles a day into the system. The other 16% of inputs come from Really Simple Syndication (RSS) feeds produced by both domestic and international public health entities, as well as news organizations not covered through Factiva (11%), Twitter accounts of key individuals and organizations (2%), news aggregator services such as Google News (2%), and other relevant sources manually identified by analysts (1%).
The analysts play an essential role in curating inputs, both through the manual identification of additional sources of inputs and through their extensive experience with Factiva. The Panel has learned how GPHIN analysts are experts at navigating Factiva’s system to adjust and react to changing flows of information, and that this expertise is a key asset. Further, the work done by both analysts and the platform to refine the raw inputs from Factiva is one of GPHIN’s more valuable contributions to the WHO’s EIOS system, and it is unlikely that at this time any other jurisdiction would be able to replace the existing expertise of the analysts in this respect.
A recurring theme in the Panel’s conversations was the rise of social media as a source of public health information. Integrating more social media data as inputs for the GPHIN system should be a key future consideration. One public health official noted that they rely on social media for information in addition to key EBS systems. Another explained to the Panel that international organizations are increasingly using Twitter and other platforms as a method of transmitting official information, even before more formal channels such as the WHO Event Information System. For example, the first official statement on the human-to-human transmissibility of COVID‑19 was a tweet by the WHO/Western Pacific Regional Office official account.
The GPHIN analysts have indicated the need to harness social media in future iterations of GPHIN, especially as early reports are increasingly found on social media platforms. For example, smartphones and Twitter data helped public health professionals identify an Ebola outbreak in West Africa three days before an official WHO announcement was made.Footnote 28 The Panel was also told that, currently, GPHIN lacks the technological capacity to comprehensively monitor open-source social media inputs. To do this, there are two main challenges that need to be addressed.
The first is the question of capacity. Currently, GPHIN analysts manually curate social media feeds and reports, which is both labour-intensive and time-consuming. As analysts are already working at capacity, further social media curation will need to be supported either through additional resources or through automation. Previously, a contractor had been engaged to develop a social media scraping tool; however, the Panel was told that these efforts were unsuccessful due in part to limitations imposed by Shared Services Canada policy and requirements, including limited access to websites locked behind firewalls.
The second challenge is the issue of social media sources themselves. A high signal-to-noise ratio increases the risks of both false positives and false negatives. Brief posts often do not contain sufficient context for analysis and assessment, and broad analysis of public sentiment or trends based on social media must be made judiciously because of the challenges of representativeness of the users of social media.Footnote 28
Issues of verification become even more vital when assessing a medium whose own governance structures struggle to address issues of authenticity, bot activity, and emerging technology such as “deep faking,” which is AI-generated audio or video that convincingly mimics actual recorded footage. These complex and continuously shifting trends require thoughtful and sustained analysis and engagement to be addressed, and the Panel encourages the GPHIN team to work with existing social media monitoring teams across government to learn and contribute to best practices.
PHAC is currently exploring additional methods of incorporating social media inputs into GPHIN and enhance its functionality as a health intelligence surveillance system through a research project partnership called Incorporating Advanced Data Analytics into a Health Intelligence Surveillance System. For this project, PHAC has partnered with Natural Resources Canada, McGill University, the Université du Québec à Montréal, and the Canadian Safety and Security Program;Footnote 34 it is funded both by the Canadian Safety and Security Program and in-kind contributions from the other partners. This project is developing three algorithms to better incorporate social media into EBS systems:
- an algorithm that uses social media and open-source media data to support forecasting of COVID‑19 in Canada
- an algorithm that conducts sentiment analysis, or the use of text analytics to infer social or emotional sentiments from a given sample, on COVID‑19 non-pharmaceutical interventions in Twitter data
- a neural network algorithm that can forecast weekly seasonal influenza activity in Canada
The Panel supports continued research and integration of social media functions into GPHIN in a manner that respects ethics guidelines and the privacy of Canadians as set out in government policy, and hopes that future R&D efforts related to surveillance systems and the integration of new sources of data will recognize the needs of GPHIN, as well as the EBS component of the Canadian Network for Public Health Intelligence, and will continue to collaborate with the GPHIN team. Further, when the results of research prove useful, they should be considered in future budgets and scoping of GPHIN.
The Panel has also learned how other public health surveillance and risk assessment processes are incorporating other data streams, such as flight and travel pattern data from the International Air Transport Association. PHAC’s Corporate Data and Surveillance Branch and the Office of the Chief Data Officer have told the Panel that they are working on a coordinated approach to agreements and procedures to procure and use additional sources of data. Going forward, PHAC should explore how, and to what extent, these data streams could complement the existing work of GPHIN analysts.
Recommendations
3.1 The GPHIN team should continue to explore incorporating further social media into its operations.
3.2 As GPHIN considers incorporation of additional social media, it should collaborate with other teams engaging in similar work to benefit from best practices and lessons learned.
3.3 The Public Health Agency of Canada should consider, on a regular basis, what other new sources of data could be usefully incorporated into GPHIN’s operations.
In the system
Once in the system, inputs are passed through GPHIN’s sophisticated algorithms. A duplicate detection algorithm clusters and flags near-identical articles to avoid the generation of multiple signals that stem from a single report. The system then generates metadata, or data describing the input in question, classifies the input according to the GPHIN system’s taxonomy, produces a machine-generated translation of non-English articles, and assigns each article a relevancy score based on keywords and GPHIN’s taxonomy that accounts for flexible language use (for example, reports of outbreaks of “Bieber Fever” occurring along a touring route would be identified and removed). High-scoring articles are automatically published into the GPHIN system, low-scoring articles are automatically trashed, and the remainder are passed to analysts for manual review. Through this process, the system pares down the approximately 7,000 inputs a day to roughly 3,500 outputs for analysts to review.
The Panel has heard differences of opinion as to the current state and responsiveness of the system. While it was suggested that the GRP significantly reduced analysts’ workloads, those closest to the system stated that the current system is unstable, often slow or unresponsive, and, on occasion, prone to crashes. The Panel heard about challenges stemming from an unreliable search function that has difficulty reproducing results, and a push function, used to save progress or publish articles, that often freezes and hampers analysts’ workflow. Some analysts also felt that the de-duplication function is currently insufficient and requires manual verification to avoid gaps in coverage, although this view was not universally shared.
Through conversations with the NRC, the Panel learned that the NRC has continued to make hundreds of bug fixes and improvements. The Panel also heard from the NRC that since fall 2018, PHAC has not migrated any of these fixes or improvements from the development server to the production server.
PHAC has confirmed that the current version of the GPHIN platform has been in use since fall 2018, and that no changes for GPHIN have been migrated due to plans to migrate the GPHIN platform from the NRC server.
While a migration from the NRC server to Shared Services Canada’s Enterprise Data Centre was originally part of the GRP, it was scoped out at the time due to the complexity involved, including issues in differences between test and production software environments, as well as security concerns expressed by Shared Services Canada. As a result, PHAC opted to migrate from the NRC to a cloud environment instead.
The subsequent planned March 2020 migration to the cloud was delayed as a result of the COVID‑19 pandemic. PHAC told the Panel that the migration would require GPHIN to be offline for approximately five business days, which would have hampered GPHIN’s contribution to the pandemic response. PHAC has assured the Panel that the full migration and upgrades will be complete before the end of March 2022, and that $400,000 has been allocated in the Fall Economic Statement 2020 to complete the migration.
The Panel recognizes the challenges posed by complex IT projects, especially on critical systems that support priority work. However, given that these issues predate the current pandemic, the Panel questions this rationale for delaying the implementation of all improvements for more than two years. The fact that these changes have not yet been implemented on the production server has made it difficult to assess the exact state of the current GPHIN system. As a result, the Panel recommends the following.
Recommendation
3.4 PHAC should work with National Research Council Canada to expedite the application of existing bug fixes to the GPHIN platform, and should ensure that, going forward, all bug fixes to the GPHIN platform are made in a timely manner.
The Panel also recognizes that PHAC’s IM/IT function is a shared service that formally resides at Health Canada. If PHAC wishes to become a truly technologically enabled organization capable of harnessing emerging technology and equipping its workforce with the appropriate tools and software, PHAC and Health Canada management should improve horizontal collaboration and prioritization efforts as it relates to GPHIN.
The Panel is heartened that the Office of the Chief Data Officer understands and has committed to addressing these challenges at the agency level, and hopes that senior management will champion this work as it progresses. This issue should also be addressed through the provision of additional dedicated technical support for GPHIN, particularly through the reinstated role of the technical advisor, as discussed below.
Data
Through the process described above, the GPHIN system generates a vast amount of filtered data for the analysts to review, label and assess. Once this happens, data are incorporated into GPHIN’s database, which is available to all GPHIN subscribers. The database is of particular importance for international subscribers, who access curated collections of articles created through the metadata and categorization features: as international subscribers do not currently receive Daily Reports, the database is their primary point of engagement with the GPHIN system.
In addition to its immediate uses in public health surveillance, the GPHIN database has the potential to be leveraged by researchers to guide both data-driven policy and future research in machine learning, natural language processing and text-based analytics. GPHIN data have been used previously to assess policy impacts: for example, the World Trade Organization worked with GPHIN during the H1N1 influenza to monitor the effect of trade bans.Footnote 28
While this work has often taken the form of situational awareness of ongoing public health events, the Panel believes that the use of GPHIN’s database to understand past events could support modelling efforts and more informed, data-driven decision-making in the future. Further, experts told the Panel that GPHIN’s valuable dataset could be used by researchers to drive innovation in machine-learning processes. For example, PHAC’s Incorporating Advanced Data Analytics into a Health Intelligence Surveillance System project, described above, will test its algorithms with data coming directly from GPHIN.
One expert noted that, in its current state, GPHIN is challenging for researchers to use. Canadian researchers cannot access the GPHIN system directly to extract required data, and front-end user access is insufficient for research purposes because the extraction of vast amounts of data grinds the entire GPHIN system to a halt.
The Panel recognizes the potential value of GPHIN’s filtered and labelled dataset to research. At the same time, the Panel also recognizes that GPHIN relies on input data from Dow Jones, which also sells database access to academic institutions. Opening GPHIN’s database to Canadian researchers will require, at minimum:
- confirmation with input sources that GPHIN is indeed capable of providing third-party access to its database
- an assessment of the resources required to retool GPHIN’s back end to facilitate data extraction and whether the benefits of an open database is worth the cost
- the development of clear guidelines for researchers on how to navigate GPHIN and PHAC’s bureaucratic and technological infrastructure
Recommendation
3.5 The Public Health Agency of Canada should examine what would be required to make GPHIN’s dataset available to researchers and explore what the benefits of this arrangement might be to both PHAC and academic institutions.
The Panel has also heard from experts who pointed to the valuable role of GPHIN’s database in training and refining the GPHIN platform’s algorithms. The Panel understands that GPHIN algorithms are trained and refined through a supervised learning process, which relies on an enormous quantity of labelled examples used to build a model capable of identifying patterns and predicting what labels an expert GPHIN analyst would apply to a given input.
The Panel learned that the most important element in building machine learning–driven systems is the quality of the data used to train the system itself, as the accuracy of the system depends on the accuracy and quality of the data it learns from. One expert told the Panel that the GPHIN analysts’ current approach to labelling data could benefit from clear documentation; improving the quality of the underlying data through a structured, standardized process will facilitate future training of the GPHIN’s algorithms.
Experts have told the Panel that while data-labelling is expensive and challenging, it is an essential step in improving the GPHIN’s system to quickly and efficiently filter data, a step that may not have been fully appreciated in the past: one expert noted that the GRP plan did not set aside sufficient time for data annotation. The Panel believes that consistently formatted data will be key to future renewals, and that, as such, ensuring the consistent quality of labelled data should be one of the GPHIN analysts’ responsibilities and be considered as the skills and workflow of the GPHIN analysts are reviewed. Time for data-labelling should be accounted for in the analysts’ schedules.
Recommendation
3.6 The GPHIN team should further develop and document a standard, structured data-labelling process to support future algorithm training and clarity of process.
The GPHIN database, as a valuable resource in itself, will require regular maintenance. Additionally, current and future PHAC-wide data stewardship efforts, especially the PHAC Data Strategy, should be mindful of GPHIN’s database and its needs. GPHIN’s dataset is unlike that of most IBS systems, which rely primarily on data related to disease, injury and health systems rather than media reports; nevertheless, it is important that the needs, uses and role of the GPHIN system be recognized by PHAC as it moves toward a data-enabled organization.
PHAC’s Data Strategy, launched in fall 2019, maps improvements to data infrastructure, science-based analytics and staff tools, among other implementation items. Given that all surveillance systems will have their own specific IM/IT requirements, and that the GPHIN system has, to date, existed somewhat apart from the PHAC’s broader surveillance and data agendas, the continued implementation of PHAC’s Data Strategy should take GPHIN’s needs into account, especially in the acquisition of new tools for data analytics and visualization.
The human dimension
GPHIN’s technology is only half of the GPHIN itself. Data require contextualization, assessment and the judgment of human analysts to ultimately determine whether a signal is of concern or not.
The Panel heard that the GPHIN analysts are the heart of the system. Experts explained that GPHIN’s value lies in its analysts: while the future of open-source surveillance is in AI and natural language processing, even the best AI will continue to require humans, both to train the system and to undertake the aggregation and analysis of system outputs. Analysts are also able to bring their knowledge of language, context and culture to bear on their work; this coupling of expert knowledge and human judgment cannot be automated.
The Panel has previously outlined its position on the skills required for analysts in Chapter 2. There are, however, additional considerations as part of GPHIN’s technological capacity.
First is the issue of how GPHIN analysts interact with the system itself. The GPHIN team previously included the position of an expert technical advisor who was familiar with the GPHIN system. The GPHIN analysts are not themselves technical experts. As such, the technical advisor provided support and advice to analysts and international GPHIN subscribers, addressed technical issues, and played a crucial knowledge translation function.
GPHIN’s last technical advisor left PHAC during the GRP in 2017 and was not replaced. This gap has been felt acutely by GPHIN analysts, who told the Panel that not only do they no longer have the in-house capacity to address and communicate issues with the platform, but also that they are now providing ad hoc technical troubleshooting for international subscribers, which they are not qualified to do.
Future upgrades will require careful balancing of system needs and the available resources. The Panel believes that, if possible, the next technical advisor should be someone who is familiar with both the technological underpinnings of the GPHIN system and broader organizational efforts to update and maintain PHAC’s IT infrastructure.
Recommendation
3.7 The Public Health Agency of Canada should restore the position of a dedicated GPHIN technical advisor as soon as possible to ensure that GPHIN receives necessary and timely technical support and advice.
Second, it will be important that the skills of GPHIN analysts are developed in tandem with any technological updates. The needs of GPHIN analysts and of subscribers to GPHIN products will point to areas where skills enhancement is needed. Technological tools are means to ends; as GPHIN incorporates new streams of information and new features, so too should analysts be supported in the development of additional expertise and skills essential for modern intelligence and surveillance work. Such expertise includes data analytics and visualization skills to support both increased analytical sophistication and the development of clear products to support decision-makers.
Recommendation
3.8 Technology changes to GPHIN’s system should not simply consider new tools such as artificial intelligence but also the human component of GPHIN’s system. Such tools may include training and development to ensure that analysts have the knowledge and skills required to interact with subject matter experts in data analytics and visualization, disinformation, and behavioural insights.
As discussed in Chapter 2, it will be important to explore the role that students play in the continued evolution of GPHIN’s skill sets. Regularly bringing students into the GPHIN team will not only assist ongoing recruitment and renewal but will be a key method of bringing new research and innovation to the system. Graduate students may wish to work directly with the GPHIN system and analysts as part of ongoing research. GPHIN already hosts some students. Such hosting should continue and be enhanced as well as supported and championed by PHAC. The expertise and energy of students are often overlooked assets of the public service, and the Panel supports additional efforts to integrate them into GPHIN’s work.
Outputs
Currently, GPHIN outputs are sent either in the body of an email or as a Microsoft Word document attachment. While it is an adequate method of sending information to subscribers, both analysts and experts suggested to the Panel that there are better methods of preparing and transmitting GPHIN products.
The Panel was told that current EBS systems struggle to package information for decision-makers. During the COVID‑19 pandemic, public health professionals have faced overwhelming demands on time, energy and resources. For example, the September 2020 Lessons Learned from PHAC’s COVID‑19 Response highlighted the CPHO’s extraordinary workload involving up to 20 hours a day, seven days a week. According to the report:
To bridge the gap and ensure that the CPHO was getting the information needed to help her fulfil her mandate, roles and responsibilities, she (and her office) had to take on additional work to integrate information from across the Agency in the development of CPHO-specific products.
This was often a vicious circle. The more she adapted the work herself to suit her communication style and the technical information required for the situation, the less time she had to provide feedback on what she needed.
While the CPHO is perhaps the highest-profile example of a key decision-maker running against the clock, she is by no means the only one. GPHIN outputs should not only be sensitive to the needs of decision-makers and other public health professionals; they should equally be attuned to the context in which they are received.
The medium is the message
The Panel heard from decision-makers and experts who insisted that the way information is presented is as important as the information itself. One participant stated that the most effective tools are useless if they cannot be easily understood or do not provide clear, useful advice to decision-makers.
Across government, a broad shift is underway to re-situate the consumer, not the producer, at the centre of product design. This shift involves not only thoughtful consideration of context, relevance and brevity; it also involves the use of new tools and formats that can lay out information and analysis in intuitive and engaging ways. In particular, data visualization is a key method of translating data for decision-making, as it makes abstract information easier to understand and shape into a narrative.
The Panel learned how other intelligence-producing organizations have begun to retool their own products to better support decision-makers through the use of placemats, dashboards and other forms of data visualization, and clear and consistent guidelines about (1) what the product’s intended purpose is, and (2) what consumers should do upon receipt.
PHAC is currently building capacity in this respect: the Corporate Data and Surveillance Branch has brought in data visualization experts who are now engaged across PHAC. The Panel believes that this is a vital capacity for both GPHIN and PHAC and should be championed and supported across the organization.
These efforts require cooperation between decision-makers and analysts. The former should clearly articulate their information needs; the latter should work to meet those needs and to present information in ways that are clear and readily understandable. In this way, GPHIN can better support effective and timely decision-making.
As noted in Chapter 1, the GPHIN team already engages in user satisfaction surveys and has made changes to its products as a result. To enhance its products further, PHAC should support the use of data visualization by GPHIN, either in the form of a dedicated data scientist resident at GPHIN or through collaboration with the office of the Chief Data Officer. Data visualization should support the GPHIN mandate as well as the specific needs of GPHIN subscribers; it is important that PHAC regularly reassess the needs of its subscribers so as to better respond to the shifting demands of decision-making contexts. Reassessment could result in alternate formats for the GPHIN products themselves, for example, by packaging a feed of relevant reports identified by GPHIN into an application programming interface, a set of functions that let applications access datasets and databases of other applications or systems.
The Panel is not prepared to recommend specific changes or improvements to the format of products themselves. However, the Panel believes that this is an avenue that deserves exploration as the technology that underlies the GPHIN system continues to be developed.
Future upgrades
As the Panel noted at the outset of this chapter, PHAC is not capable of developing and deploying sophisticated AI-driven technology entirely in-house. Continued partnerships across government, with academia and with the private sector, will play an important role in GPHIN’s future technological development.
The Panel was told that government as a whole is improving its ability to procure and deploy advanced technology. The Treasury Board Directive on Automated Decision-Making is a welcome step toward ensuring that decisions are data-driven, made responsibly, and in compliance with fairness and due process requirements. PHAC should remain abreast of the continued evolution of this directive.
There are currently only three government organizations capable of vetting AI algorithms: the Communications Security Establishment, NRC and Statistics Canada. The Panel encourages PHAC to collaborate with existing centres of expertise within government to understand the current state of surveillance technology as well as future possibilities.
Where collaboration within government is unfeasible or unwieldy, PHAC should be prepared to work with both academic partners and the private sector as needs dictate. Academic institutions are able to provide a depth of knowledge and research; private sector innovation can adjust rapidly to changing technology. Given the emerging conditions of the new intangible economy in which data and intellectual property play an increasingly important role in Canadian prosperity, every effort should be made to partner with Canadian universities and companies to support homegrown innovation efforts.
The Panel would observe that PHAC has a long research tradition and that science integration is a core responsibility vested in the Chief Science Officer. Research projects such as the ones noted above provide the scope and budgets for the research activity but typically do not include resources to operationalize any methodology. Clearly connecting research outputs to future system changes is an aspect of integration that may require strengthening in the future.
Further, links to the private sector will also be required in the future for the simple reason that there are now powerful privately owned public health event–based systems competing in the marketplace, which could significantly change how EBS is used in public and private sectors alike.
PHAC has partnered several times with one of these major private sector players, BlueDot,Footnote 35 and these various pilots have involved GPHIN’s participation. GPHIN did assist in a pilot project focused on International Air Transport Association flight data, which can be useful in assessing the potential spread of a virus by observing passenger flights in and out of event locations.
PHAC has also taken some positive steps in establishing the kind of mechanisms that allow groups within PHAC to partner more easily in order to leverage private sector expertise. For example, as a result of work undertaken by the Chief Data Officer, PHAC now has a central focal point for licences and distribution of BlueDot’s products.
While PHAC may not have the ability to deliver complex IT projects alone, it is essential that it develop the in-house capacity to engage with technical experts. Such development will involve both the ability to assess and evaluate technological needs and project outcomes, as well as robust technological literacy and knowledge translation functions to build links between practitioners and researchers, and to provide senior decision-makers and non-experts with clear process and project descriptions.
The Panel is encouraged by the early work of PHAC’s new Corporate Data and Surveillance Branch in this respect but emphasizes that this upskilling must be a whole-of-agency endeavour and not limited to a single program area or branch.
System and capacity
The rapid pace of technological progress will require GPHIN to re-evaluate its technological capacity at regular intervals to ensure that it remains fit for purpose. The above considerations address pieces of the GPHIN system but not the whole. What is clear to the Panel is that the current GPHIN system is not as easily alterable as it could be.
During the GRP, the technical advisor advocated for a modular GPHIN system, which allows individual components to be swapped in and out as resources and technological innovation permit, instead of requiring a complete rebuild to address specific features. Such a system also facilitates collaboration with subject matter experts on specific modules on a function-by-function basis, which would allow targeted improvements to the GPHIN system to be made as needed. These targeted improvements could be undertaken either with academic institutions or with private sector organizations with demonstrated expertise. They could also be supported through existing federal programs such as Innovative Solutions Canada, an innovation procurement program that issues outcome-focused challenges seeking novel solutions from the private sector.
This is not unproven technology: the WHO’s EIOS system is an example of a modular EBS system. The EIOS system is likewise supported through targeted collaboration with stakeholders and experts. For example, the EIOS team is currently collaborating with the Centre for Artificial Intelligence Research in Hong Kong on an abstractive summary module (abstractive summaries involve an algorithm that tries to understand and generate its own summary of a given text, as opposed to extractive summaries, which involve an algorithm identifying relevant phrases in a given text and collating them into a summary).
While this model may be more expensive in the short term, a modular GPHIN system will be agile, nimble and better equipped to leverage expertise to respond to changing information ecosystems and technological ceilings.
Recommendation
3.9 The next major upgrade to the GPHIN system should aim to develop an agile, modular GPHIN system that supports rapid innovation and collaboration.
Further, as the demands on EBS systems grow in the future, and as international partners such as the United States and the United Kingdom commit resources to develop other EBS and open-source surveillance systems, system interoperability will become a key piece of Canada’s multilateral cooperation. Future GPHIN upgrade projects should be mindful of existing and emerging EBS systems, and, where feasible, should aim to harmonize terminology, system requirements, and information-sharing practices. Public health surveillance is a global effort, and the Panel believes that GPHIN should continue to be an international leader in EBS.
Lessons learned
Equally important is the upgrade process itself. As previously noted, the GRP faced challenges of poor inter-organizational communication, a lack of appropriate governance structures and dispute resolution mechanisms, and unclear expectations and success metrics. Future upgrade projects should refer to both the Global Public Health Intelligence Network Platform Renewal Close-Out Report and the Office of Audit and Evaluation’s Consulting Engagement for the Global Public Health Intelligence Network Renewal Project – Final Report for VP HSIB to examine lessons learned.
Lessons learned from past upgrades
Going forward, the Panel suggests that upgrades and renewals take into account the following considerations:
Upgrades should not be undertaken for the sake of being “cutting edge” but instead should address a clearly defined problem or gap in GPHIN’s existing system. It is essential that problem definition should precede all technological upgrades, as without an articulation of the need being addressed, technical upgrades are unlikely to satisfy subscriber needs and will likely lack clear parameters for success.
When approaching future renewals, stakeholders may wish to use the following questions as a starting point:
- What are the current roles and responsibilities of the analysts?
- What can be done to improve or streamline those roles and responsibilities?
- What expertise cannot currently be mimicked by computers?
The problem definition should also be clearly shared with all relevant stakeholders, including analysts.
- The established and agreed-upon problem definition should then be transformed into a clear vision that is commensurate with existing resources, is well documented, has a rationale for how each additional component will enhance the GPHIN system or its output, and is accompanied by defined parameters for success that are agreed upon by all parties prior to the project’s start.
- Future upgrades should, from the outset, involve a formal governance structure that clarifies responsibilities, accountability and dispute resolution mechanisms that outline how the appropriate management levels will be engaged throughout the project.
- Once underway, there should be an open line of communication between the GPHIN team and the technical experts working on the system, especially as it relates to testing and training the GPHIN system.
- Both GPHIN management and analysts should have a clear understanding of any after-care arrangements for continued bug fixes and adjustments between major iterations. The navigation of this function would also be a key responsibility of the technical advisor, should they be reinstated.
For future upgrades, it will be important that both the GPHIN team and PHAC management understand how, and to what end, upgrades are undertaken.
Finally, through the Panel’s conversations with PHAC managers and experts, it became clear to the Panel that there is a lack of evaluation of PHAC’s disparate surveillance systems. Previous attempts to evaluate the performance of EBS and IBS systems appear to have relied primarily on self-assessments. In the aftermath of the COVID‑19 pandemic, public health functions across all levels of government will likely be grappling with the best way to deploy limited resources to address the biggest gaps and most pressing needs that have emerged in the last months. As such, understanding where, how, and to what end targeted interventions can most improve core functions of public health will be essential. The Panel understands that the future Director General of Surveillance will be working to bring clarity and oversight to the various surveillance functions across PHAC. The Panel therefore recommends the following.
Recommendation
3.10 As part of the Public Health Agency of Canada’s commitment to improve and harmonize its various complementary surveillance systems, the future Director General of Surveillance should develop a robust evaluation framework for public health surveillance systems to support ongoing prioritization and course correction.
Technological innovation in government requires dedication, perseverance, and a keen awareness of organizational priorities and limitations. While PHAC may not have the ability to deliver complex technological projects alone, it is well placed to use existing expertise and work with partners to do so. While this work will be challenging, it is essential to the long-term health of the GPHIN system.
GPHIN is a composite system: its operational component provides timely and relevant intelligence to decision-makers and public health professionals, and it is supported by its underlying technical component, which enables the early warning and analysis functions. Any future vision of GPHIN and all future upgrades should consider the interactions between these two key components. Without technological support, the analysts cannot succeed; without analyst expertise, the technology is blunt and undirected.
GPHIN is an important asset of PHAC and will continue to play a vital role in public health surveillance. The disorienting pace of technological change will only increase in the years to come. Shifts in information and communications technology, artificial intelligence and machine learning, and the domestic and international media ecosystem must be met head-on by a GPHIN that is capable of detecting threats to Canadians in whatever form they might become apparent, and that is capable of adjusting to and incorporating new contexts, sources of information and technological advances. The Panel firmly believes that this GPHIN is possible.
Chapter 4: GPHIN’s future
If there is an important lesson to draw at this critical point in Canada’s pandemic response, it is the one the Panel has heard repeatedly from the experts themselves: the best time to discuss pandemic preparedness is when it is most present in the minds of Canadians and of the governments who serve them. We strongly urge PHAC and its Minister to take advantage of the current alignment of political will and public opinion to build the interconnected and resilient public health surveillance system needed to protect Canadians in the future.
This report provides an initial blueprint for how GPHIN, and the important discipline of EBS, should contribute to PHAC’s overall mandate. It emphasizes the need for a clear vision for surveillance, and for how intelligence such as GPHIN’s plugs into a central, coordinated risk assessment continuum. Successfully orienting these two critical functions is the first step toward developing greater risk assessment capacity so that signals can translate into action as quickly as possible.
Because the question is not whether another pandemic will strike but when. Every day, Canada’s ability to respond and manage a pandemic is being tested and recast. But the measure of what Canadians have learned will be not only our response to the next pandemic but also how we will mitigate future threats through earlier detection and coordinated international action.
COVID‑19 has proven that global public health is a shared responsibility. There is no single entity, including GPHIN, that could or should undertake the significant task of global public health surveillance alone. Rather, the way forward must recognize that multiple surveillance systems working together stand the greatest chance of casting a net broad enough, and fine enough, to catch the next public health event of international concern.
Governments, the academic and private sectors, and public health interest groups and organizations will need to find new ways to partner and collaborate. Surveillance systems new and old must be linked and pathways cleared to exchange intelligence or information between organizations and jurisdictions.
Drawing on the recommendations and ideas presented in earlier chapters, our conclusion reiterates how GPHIN’s evolution, guided to date by partnerships and collaboration, will continue to depend on these strong relationships. From the actionable advice provided to date, we offer our parting vision of what GPHIN can become. And we urge PHAC, and its Minister, to make that vision real.
Learning to adapt
The Panel believes that GPHIN’s future will depend on partners to help elevate the impact and reach of their products and intelligence. The imperative to work with others needs to be built into the very foundation of a modern, technologically driven, 21st-century public health surveillance regime, not just in Canada but internationally. As the Independent Panel established by the WHO recommends in its report,Footnote 22 surveillance systems worldwide must be redesigned, “bringing together their detection functions – picking up signals of potential outbreaks – and their relay functions – ensuring that signals are verified and acted upon.” The Independent Panel’s report also states that both functions must happen “at near-instantaneous speed.”
The template for that future resides in the past: GPHIN has been built through partnerships and collaboration since its earliest days. Because of its ability to partner and collaborate, this small team has helped to reshape public health surveillance on a global scale, carving out a well-deserved reputation as a result. But what is required now is not simply reliance on a successful past but building and shaping a present ready to meet the challenges of the future.
Some of these partnerships and collaborations were also driven by necessity, particularly in relation to technology. In those instances, GPHIN has at times been able to sidestep government’s slower pace of technological adaptation. In later stages, GPHIN’s partnership with the NRC set the stage for the adaptation and evolution of systems that GPHIN created, and these systems are now being used in other government departments, such as the Canadian Food Inspection Agency.
Moreover, partnerships and collaboration are also useful approaches for accessing the knowledge and ideas of other sectors and players so that GPHIN itself can increase its capacity and reach. GPHIN must be calibrated to learn and discover the pathways to follow within the discipline of EBS, and to build on the strengths it already possesses.
This report has put forth recommendations that address some of the systemic issues limiting GPHIN’s function and operations. But the GPHIN of tomorrow should not aspire to merely fixing outstanding issues. GPHIN was a pioneer in the discipline of EBS and can continue to make a significant contribution to international public health surveillance. PHAC’s task in the years to come will include deciding what kind of contribution GPHIN can make, and how it must learn and evolve in order to provide it.
Recommendations linked to partnerships and collaboration
1.4 The Public Health Agency of Canada should actively seek out partnerships and collaboration to leverage for the GPHIN platform more sophisticated technology and methodology used by different sectors, including academia and the private sector, while ensuring retention of key intellectual property and the ability to modify and improve the system in a timely manner.
1.6 The Public Health Agency of Canada’s international impact should be bolstered by reinforcing GPHIN’s existing international partnerships and by considering additional roles or contributions that GPHIN could make as an established leader in EBS.
GPHIN’s future
One way to organize future partnerships and collaboration is to ground these opportunities in the underlying function of GPHIN: surveillance and contributing to risk assessment. As the Panel has recommended, one of the most important elements of the surveillance function is technology and the ability to continuously improve upon it. This is challenging for governments, whose procurement processes and legacy system management can take years to bring about even minor improvements from the perspective of the day-to-day work of the individual analyst.
The decision to proactively seek out access to technological tools and partners is consistent with GPHIN’s mandate and role. And while not every partnership and collaboration will necessarily result in major changes to GPHIN’s system, that network of expertise nonetheless becomes a new brick in GPHIN’s foundation and a stronger basis upon which to build.
With respect to its role in risk assessment, the Panel has outlined the importance of a deeper and more meaningful integration of GPHIN products into risk assessment functions. From this foundation, the Panel believes that GPHIN could continue to evolve and carry out the complementary and essential work of providing greater situational awareness, and of integrating early signals of potential concern more seamlessly into modelling and forecasts that support risk assessment capacity.
Conclusion
The Panel believes that approaching partnerships and collaboration with the surveillance function and risk assessment in mind will provide useful parameters for deciding which ones to pursue and where resources should be focused. But the success of this approach depends on PHAC’s and GPHIN’s ability to recalibrate their mandate and vision for the 21st century in the ways this report has set out.
Twenty-five years ago, the world needed a sentinel to keep its sights on the news of the Internet so that it could catch the earliest signal of a potential deadly threat. GPHIN has never been alone in these efforts. But in the future, the complexity and scale of the challenges of global public health surveillance will demand systems that can work together seamlessly in order to form the connective web that can filter and catch potential events before one becomes the next global crisis.
GPHIN’s success is not about returning to the past state but returning to the vision that inspired its creation. GPHIN, through its EBS role, has the potential to contribute to surveillance capacity that leads to proactive responses. This is the future we see for the discipline of EBS. Taking the necessary steps to enable GPHIN and ensure that it is well connected to the ecosystem of overall surveillance and risk assessment will allow Canadians to rest easier knowing that world-class tools are in place to scan the horizon for emerging public health threats.
Acknowledgements
The Panel is grateful for the support of a dedicated secretariat comprising Brian Pagan, John Ryan and Kym Shumsky. Their invaluable contributions included organizing Panel meetings, conducting research and facilitating the development of this report.
The Panel would like to recognize the individuals whose contributions and insights helped to shape the Panel’s deliberations and final report. Those who have granted us permission have been listed below.
Dr. Kahina Abdesselam
Senior Epidemiologist/Biostatistician
Public Health Agency of Canada
Dr. Horacio Arruda
National Director of Public Health and Assistant Deputy Minister
General Directorate of Public Health
Ministry of Health and Social Services
Government of Quebec
Ray Arthur
Director of the Global Disease Detection Operations Center
Center for Global Health
US Centers for Disease Control and Prevention
Abasse Asgaraly
Business Strategy Consultant
KMB Consulting Inc.
Dr. Christina Bancej
Manager, Centre for Immunization and Respiratory Infectious Diseases
Public Health Agency of Canada
Dr. Sylvie Briand
Director of the Global Infectious Hazard Preparedness
WHO Emergency Preparedness
John Brownstein
Chief Innovation Officer
Boston Children’s Hospital
Shelly Bruce
Chief
Communications Security Establishment
Dr. David Buckeridge
Professor, and Canada Research Chair in Health Informatics and Data Science
McGill University
Alixanderia Clymans
Director, Office of Situational Awareness
Public Health Agency of Canada
Dr. Natasha Crowcroft
Senior Technical Advisor – Measles and Rubella Control
World Health Organization
Alex Demarsh
Senior Director of Outbreak Science
BlueDot Inc.
Jean-François Duperré
Government Operations Centre
Public Safety Canada
Roger Ermuth
Assistant Comptroller General
Treasury Board of Canada Secretariat
Cindy Evans
A/Vice President, Emergency Management
Public Health Agency of Canada
Greg Fyffe
President
Canadian Association of Security and Intelligence Studies
Rev. Michael Garner
Priest and Epidemiologist
Anglican Church of Canada
Homeira Ghiasbeglou
Surveillance Analyst, GPHIN
Public Health Agency of Canada
Tracy Gibbons
Manager, UN and Global Health Security
Public Health Agency of Canada
Dr. Vivek Goel
Professor
Institute of Health Policy, Management and Evaluation
Dalla Lana
School of Public Health
University of Toronto
Gerardo Guerrero
Surveillance Analyst
Public Health Agency of Canada
Dr. Réka Gustafson
Deputy Provincial Health Officer
British Columbia Centre for Disease Control
Jim Harris
Director General, Strategic Engagement Branch
Shared Services Canada
Laurie Hunter
Director General, Centre for Emergency Preparedness and Response
Public Health Agency of Canada
Thomas Juneau
Associate Professor
University of Ottawa
Dr. Kamran Khan
Founder and CEO
BlueDot Inc.
Dr. Perry Kendall
Past Provincial Health Officer, 1999–2018
Province of British Columbia
James Knox
Knox Software Corporation
Rhonda Kropp
Vice-President, Corporate Data and Surveillance Branch
Public Health Agency of Canada
Dr. Joanne Liu
Panelist for the Independent Panel for Pandemic Preparedness and Response
Dr. Valerie Mann
Chief Population Health Epidemiologist
Population Health Branch
Ministry of Health
Government of Saskatchewan
Dr. Joel Martin
Acting Director General of the Digital Technologies Research Centre
National Research Council Canada
Abla Mawudeku
Former Chief, Situational Awareness Section
Public Health Agency of Canada
Marlène Mercier
Director, Department of Health Surveillance
Deputy Directorate General for the Protection of Public Health
Ministry of Health and Social Services
Government of Quebec
Dr. Pascal Michel
Chief Science Officer
Public Health Agency of Canada
Shamir Mukhi
Chief Engineer
Canadian Network for Public Health Intelligence
Public Health Agency of Canada
Tina Namiesniowski
Former President
Public Health Agency of Canada
Dr. Howard Njoo, MD, MHSc, FRCPC
Deputy Chief Public Health Officer and Interim Vice-President
Infectious Diseases Programs Branch
Public Health Agency of Canada
Tenzin Norzin
Epidemiologist/Biostatistician
Public Health Agency of Canada
Marcia Patricio
Surveillance Analyst, GPHIN
Public Health Agency of Canada
Dr. Barbara Raymond
Executive Medical Advisor
Public Health Agency of Canada
Svetlana Romanova
Surveillance Analyst, GPHIN
Public Health Agency of Canada
Dr. Ronald St. John
Co-Founder, Sitata.com
Iain Stewart
President
Public Health Agency of Canada
Dr. Theresa Tam, BMBS (UK), FRCPC
Chief Public Health Officer
Public Health Agency of Canada
Florence Tanguay
Manager, GPHIN
Public Health Agency of Canada
Patricia Thaine
Co-Founder and CEO
Private AI
Sally Thornton
Consultant
John Topping
Senior Director
Crown-Indigenous Relations and Northern Affairs Canada
Francisco Ucan-Marin
Surveillance Analyst, GPHIN
Public Health Agency of Canada
Anne-Marie Ugnat
Director General, Immunization Branch
Public Health Agency of Canada
Dr. Peter Uhthoff
Senior Medical Advisor and former Director, GPHIN
Public Health Agency of Canada
David Vigneault
Director
Canadian Security Intelligence Service
Dr. Denise Werker
Public Health and Preventive Medicine Consultant
Artur Wilczynski
Associate Deputy Chief SIGINT
Communications Security Establishment
Dr. David Williams
Chief Medical Officer of Health
Province of Ontario
Abdelhamid Zaghlool
Surveillance Analyst, GPHIN
Public Health Agency of Canada
Abbreviations
- CCMOH
- Council of Chief Medical Officers of Health
- COVID‑19
- coronavirus disease 2019
- CPHO
- Chief Public Health Officer
- EBS
- event‑based surveillance
- EIOS
- Epidemic Intelligence from Open Sources
- GPHIN
- Global Public Health Intelligence Network
- GPS
- Global Positioning System
- GRP
- GPHIN Renewal Project
- IBS
- indicator‑based surveillance
- IHR
- International Health Regulations
- IM/IT
- information management / information technology
- KIWI
- Knowledge Integration using Web-based Intelligence
- MediSys
- Medical Information System
- MERS
- Middle Eastern Respiratory Syndrome
- MOOC
- Medical Officer on-Call
- NRC
- National Research Council Canada
- O&M
- operations and maintenance
- PHAC
- Public Health Agency of Canada
- ProMED
- Program for Monitoring Emerging Diseases
- PSSP
- PHAC Surveillance Strategic Plan
- R&D
- research and development
- SARS
- Severe Acute Respiratory Syndrome
- SOPs
- standard operating procedures
- WHO
- World Health Organization
References
The following list is intended to support future Panel or review efforts into GPHIN, PHAC and public health surveillance. It is not an exhaustive list of references consulted by the Panel. Where possible, links have been provided.
GPHIN
- “Big Data and the Global Public Health Intelligence Network (GPHIN),” Canada Communicable Disease Report, Vol. 41-9, September 3, 2015 (Dion, M., AbdelMalik, P., Mawudeku, A.)
- “Global Public Health Surveillance Using Media Reports: Redesigning GPHIN,” Studies in Health Technology and Informatics, Vol. 270, 2020 (Carter, D., Stojanovic, M., Hachey, P., Fournier, K., Rodier, S., Wang, Y., De Bruijn, B.)
- “Risk assessment strategies for early detection and prediction of infectious disease outbreaks associated with climate change,” Canada Communicable Disease Report, 45(5), May 2, 2019 (Rees, E.E., Ng, V., Gachon, P., Mawudeku, A., McKenney, D., Pedlar, J., Yemshanov, D., Parmely, J., Knox, J.)
- Press Conference by Global Health Intelligence Network, United Nations (November 17, 2004)
- Saving Lives with News Coverage & Data: Public Health Agency of Canada and the Creation of the Global Public Health Intelligence Network, Dow Jones Factiva (PDF) (undated)
- “The Past, Present, and Future of Public Health Surveillance,” Scientifica, Vol. 2012, 2012 (Choi, Bernard C. K.)
GRP
- Close-Out Report: Global Public Health Intelligence Network (GPHIN) Platform Renewal (March 2019)
- Consulting Engagement for the Global Public Health Intelligence Network Renewal Project: Final Report for VP HSIB (May 2018)
- GPHIN Renewal Project (GRP) Technical Authority Exit Report (September 2017)
- GPHIN Renewal Project: Project Charter (March 2015)
Standard operating procedures and terms of reference
- COVID‑19 Foresight Group (CFG) Draft Terms of Reference (August 2020)
- Public Health Agency of Canada: Daily Update Committee Terms of Reference (undated)
- Public Health Daily Intelligence and Risk Assessment Meeting: Terms of Reference (Draft) (July 2013)
- Standard Operating Procedure (SOPs): GPHIN Alerts (September 2020)
PHAC and public health surveillance
- An Independent Assessment of Emergency Management Capacity and Relationship Readiness in the Public Health Agency of Canada (2020), prepared by Margaret Purdy Consulting, Inc.
- Audit of Surveillance Activities (Office of Audit and Evaluation, Health Canada and the Public Health Agency of Canada; September 2020)
- Blueprint for a Federated System for Public Health Surveillance in Canada: Vision and Action Plan (Pan-Canadian Public Health Network; 2016)
- Evaluation of Emergency Preparedness and Response Activities 2012-13 to 2016-17 (Office of Audit and Evaluation, Health Canada and the Public Health Agency of Canada; March 2018)
- Health Portfolio Strategic Emergency Management Plan (February 2012)
- Health Portfolio Strategic Emergency Management Plan 2.1 (March 2016)
- Joint External Evaluation of IHR Core Capacities of Canada: Mission Report (WHO; 2019)
- “KIWI: A technology for public health event monitoring and early warning signal detection,” Online Journal of Public Health Informatics, 8(3) (Mukhi, Shamir N.; December 28, 2016)
- Lessons Learned from the Public Health Agency of Canada’s COVID‑19 Response (Phase One) (PDF) (September 2020) and the Management Response and Action Plan (PDF) (September 2020)
- PHAC Surveillance Strategic Plan (1: 2007; 2: 2013; 3: 2016)
- Preparing PHAC for the Future: A Research Paper (October 2019), prepared by Dr. Perry Kendall and Dr. Richard Massé
- Public Health Agency of Canada’s Global Health Security Framework (October 2019)
- Report of the Auditor General of Canada to the House of Commons – Chapter 5: Surveillance of Infectious Diseases – Public Health Agency of Canada (PDF) (Office of the Auditor General of Canada; 2008)
- Report 8: Pandemic Preparedness, Surveillance, and Border Control Measures (Office of the Auditor General of Canada; 2021)
International
- Detect Earlier to Better Protect: Acute Public Health Events (PDF) (WHO; undated)
- Early Detection, Assessment and Response to Acute Public Health Events: Implementation of Early Warning and Response with a Focus on Event-Based Surveillance (WHO; 2014)
- Frequently Asked Questions About the International Health Regulations (2005) (PDF) (WHO; 2009)
- International Health Regulations (2005): Third Edition (WHO; 2005)
- National Security Directive on United States Global Leadership to Strengthen the International COVID‑19 Response and to Advance Global Health Security and Biological Preparedness (US; 2021)
- Rapid Risk Assessment of Acute Public Health Events (PDF) (WHO; 2012)
- Second Report on Progress (Independent Panel for Pandemic Preparedness and Response; 2021)
Annex: Interim report for the review of the Global Public Health Intelligence Network
Access the Interim report for the review of the Global Public Health Intelligence Network.
Endnotes
- Footnote 1
-
Health Promotion and Chronic Disease Prevention in Canada, “Retracing the history of the early development of national chronic disease surveillance in Canada and the major role of the Laboratory Centre for Disease Control (LCDC) from 1972 to 2000,” Vol. 35, No. 2, April 2015.
- Footnote 2
-
PHAC Surveillance Strategic Plan 3 (2016–2019).
- Footnote 3
-
Choi, Bernard C. K.: “The past, present, and future of public health surveillance,” Scientifica, Vol. 2012, October 23, 2012.
- Footnote 4
-
WHO: Early Detection, Assessment and Response to Acute Public Health Events: Implementation of Early Warning and Response with a Focus on Event-Based Surveillance, 2014.
- Footnote 5
-
Mukhi, Shamir N.: “KIWI: A technology for public health event monitoring and early warning signal detection,” Online Journal of Public Health Informatics, 8(3), December 28, 2016.
- Footnote 6
-
Pan-Canadian Public Health Network, Blueprint for a Federated System for Public Health Surveillance in Canada: Vision and Action Plan, 2016, p. 6.
- Footnote 7
-
The Pan-Canadian Public Health Network is a network of individuals across Canada from many sectors and levels of government who effectively work together to strengthen public health in Canada. It was created in 2005.
- Footnote 8
-
Office of Audit and Evaluation, Health Canada and the Public Health Agency of Canada: Audit of Surveillance Activities, September 2020.
- Footnote 9
-
PHAC Surveillance Strategic Plan 3, p. 1.
- Footnote 10
-
The Surveillance Integration Team, comprising surveillance experts from across PHAC, was once the forum for horizontal information exchange among programs and for issue management.
- Footnote 11
-
Office of Audit and Evaluation, Health Canada and the Public Health Agency of Canada: Evaluation of Emergency Preparedness and Response Activities 2012-13 to 2016-17, March 2018.
- Footnote 12
-
The Vaccine Rollout Task Force is a COVID-19 response mechanism and is not part of regular PHAC operations.
- Footnote 13
-
Alis Technologies Inc. filed for bankruptcy in 2003, but another Canadian firm, Nstein Technologies Inc., which had been involved in some of the prototyping, was able to continue the development work in the interim and entered into a new collaborative research agreement with GPHIN in 2004.
- Footnote 14
-
WHO: Frequently asked questions about the International Health Regulations (2005).
- Footnote 15
- Footnote 16
-
WHO: Joint External Evaluation of IHR Core Capacities of Canada: Mission Report, 2019.
- Footnote 17
-
ProMED predates GPHIN (1994) and is a moderated system without an algorithmic component.
- Footnote 18
-
Rees, E.E., Ng, V., Gachon, P., Mawudeku, A., McKenney, D., Pedlar, J., Yemshanov, D., Parmely, J., Knox, J.: “Risk assessment strategies for early detection and prediction of infectious disease outbreaks associated with climate change,” Canada Communicable Disease Report, 45(5), May 2, 2019.
- Footnote 19
-
Really Simple Syndication (RSS) is a web feed that allows users and applications to access updates to websites.
- Footnote 20
- Footnote 21
-
Independent Panel for Pandemic Preparedness and Response: Second Report on Progress (PDF), January 2021.
- Footnote 22
-
Independent Panel for Pandemic Preparedness and Response: COVID-19: Make it the Last Pandemic (PDF), 2021.
- Footnote 23
-
WHO: “WHO, Germany launch new global hub for pandemic and epidemic intelligence” (Press release: “The Hub, based in Berlin and working with partners around the world, will lead innovations in data analytics across the largest network of global data to predict, prevent, detect[,] prepare for and respond to pandemic and epidemic risks worldwide.”), May 5, 2021.
- Footnote 24
-
Full-time equivalents (FTEs) are a measure of the extent to which an employee represents a full person-year charge against a departmental budget.
- Footnote 25
-
Sections are as follows: The Highlight of the Day, a dedicated section on COVID-19 updates, domestic events, international events, and research, policies and guidelines.
- Footnote 26
-
Regional GPHIN subscribers refer to those who work in regional public health units, though they may be embedded within provincial and territorial health ministries.
- Footnote 27
-
The Health Portfolio comprises Health Canada, PHAC, the Canadian Institutes of Health Research, the Patented Medicine Prices Review Board and the Canadian Food Inspection Agency.
- Footnote 28
-
Dion, M., AbdelMalik, P., Mawudeku, A.: “Big Data and the Global Public Health Intelligence Network (GPHIN),” Canada Communicable Disease Report, Vol. 41-9, September 3, 2015.
- Footnote 29
-
WHO: Early Detection, Assessment and Response to Acute Public Health Events: Implementation of Early Warning and Response with a Focus on Event-Based Surveillance, 2014: “An example is the way in which the ad hoc EBS-detection of climatic events (e.g. heat or cold waves) could, over time, move toward a systematic collection and analysis of meteorological data with a definition of thresholds for human health, which then will pertain to IBS.”
- Footnote 30
-
WHO: Rapid Risk Assessment of Acute Public Health Events, 2012.
- Footnote 31
-
Office of the Auditor General of Canada: Report 8: Pandemic Preparedness, Surveillance, and Border Control Measures, 2021.
- Footnote 32
-
Program areas can help validate signals but can also help refine GPHIN’s algorithms so that the system can better capture articles of interest to program areas.
- Footnote 33
-
The Panel has not seen any documentation that could be considered formal direction on changing the Alert approval process. However, we have reviewed emails from early April 2019 that were exchanged among GPHIN analysts and managers that refer to the pending change and discuss how it might be implemented.
- Footnote 34
-
The Canadian Safety and Security Program is a federally funded program led by Defence Research and Development Canada’s Centre for Security Science, in partnership with Public Safety Canada.
- Footnote 35
-
BlueDot is a composite system that (1) organizes and structures inputs through an EBS system, (2) assesses the collected data and integrates it with other available datasets (for example, GPS and cellphone data, migration and flight data, climate records) to determine potential risk, and (3) produces tailored information products for clients. Because of its composite data streams, BlueDot is also able to incorporate IBS and EBS data in its risk assessments and communications. BlueDot is a privately owned, for-profit enterprise.
Page details
- Date modified: