
Supplementary Information (Tables)

Download the entire report
(PDF format, 1.08 MB, 56 pages)
Organization: Public Health Agency of Canada
Date published: 2016-11-21
Related Topics
Table of Contents
- Departmental Sustainable Development Strategy
- 1. Overview of the Federal Government's Approach to Sustainable Development
- 2. Themes I to III: Department- and Agency-Led Targets
- 3. Themes I to III: Implementation Strategies
- 4. Theme IV: Targets and Implementation Strategies
- 5. Additional Departmental Sustainable Development Activities and Initiatives
- 6. Sustainable Development Management System
- 7. Strategic Environmental Assessment
- Details on Transfer Payment Programs of $5 Million or More
- Aboriginal Head Start in Urban and Northern Communities (AHSUNC)
- Assessed Contribution to the Pan American Health Organization (ACPAHO)
- Canada Prenatal Nutrition Program (CPNP)
- Canadian Diabetes Strategy (CDS)
- Community Action Program for Children (CAPC)
- Federal Initiative to Address HIV/AIDS in Canada (FI)
- Healthy Living Fund (HLF)
- Innovation Strategy
- National Collaborating Centres for Public Health (NCCPH)
- Horizontal Initiatives
- Internal Audits and Evaluations
- Response to Parliamentary Committees and External Audits
- Status Report on Projects Operating with Specific Treasury Board Approval
Departmental Sustainable Development Strategy
1. Overview of the Federal Government's Approach to Sustainable Development
The Federal Sustainable Development Strategy (FSDS) 2013–16 presents the Government of Canada's sustainable development activities, as required by the Federal Sustainable Development Act. In keeping with the objectives of the Act to make environmental decision making more transparent and accountable to Parliament, the Agency supports the implementation of the FSDS through the activities in this supplementary information table.
This Departmental Sustainable Development Strategy presents the results for Theme I — Addressing Climate Change and Air Quality and Theme IV — Shrinking the Environmental Footprint — Beginning with Government.
2. Themes I to III: Department and Agency-led Targets
| FSDS Goal | FSDS Performance Indicator | FSDS Target | FSDS Performance Status |
|---|---|---|---|
| Not applicable (N/A) | N/A | N/A | N/A |
3. Themes I to III: Implementation Strategies
FSDS Theme I: Addressing Climate Change and Air Quality
Linkages to the Program Alignment Architecture (PAA): 1.2.1.3 Sub-Sub-Program: Food-borne, Environmental and Zoonotic Infectious Diseases
FSDS Goal 1 — Climate Change: In order to mitigate the effects of climate change, reduce greenhouse gas emission levels and adapt to unavoidable impacts.
FSDS Target 1.2 — Climate Change Adaptation: Facilitate reduced vulnerability of individuals, communities, regions and economic sectors to the impacts of climate change through the development and provision of information and tools.
FSDS Implementation Strategy led by PHAC: 1.2.2 Sub-Program: Conditions for Healthy Living. Work with domestic and international stakeholders to reduce infectious disease risks and public health threats related to climate change by increasing public health capacity and expertise through targeted research, modelling and cost-benefit analysis.
| CAA Program | Expected Results | Performance Indicators | 2015–16 Performance Summary |
|---|---|---|---|
2011–16: PPHSACC Program |
Increased collaboration on climate change adaptation. |
Number of collaborations with organizations. |
Met
|
|
Targeted communities and sectors recognize the need for adaptation |
Number of presentations requested on public health and environmental change. |
Met
Presentations: (eight)
Planned Presentations (abstracts submitted) (two):
Workshops/Meeting:
|
|
Targeted communities and sectors are aware of relevant adaptation measures. |
Number of science-based decision-making tools disseminated. |
Met
One communications product made available:
|
|
|
Number of reports disseminated. |
Met
Report and Information Requests (nine):
|
|
|
Number of publications disseminated. |
Met
Books:
|
|
Adaptation measures have been identified to address risks and opportunities arising from climate change. |
Number of stakeholders / organizations that identify the need to develop adaptation plans/strategies to address their needs. |
Met
|
PHAC seeks to reduce the vulnerability of individuals, communities, and regions to climate change impacts which have the potential to adversely affect the health of Canada's population. Through the PPHSACC Program, PHAC fosters engagement and capacity building with federal/provincial/territorial and regional stakeholders as well as international public health organizations. The Program aims to reduce infectious disease emergence, and address the risk associated with climate change through enhancing evidence-based information. Key activities include conducting risk assessments; and developing, validating and refining practical adaptation strategies and tools. CAA Planned Spending for 2015–16: $1,100,000 CAA Actual Expenditures for 2015–16: $1,008,973 |
|||
4. Theme IV: Targets and Implementation Strategies
Goal 7: Waste and Asset Management
Target 7.1: Real Property Environmental Performance
As of April 1, 2014, and pursuant to departmental Real Property Sustainability Frameworks, an industry-recognized level of high environmental performance will be achieved in Government of Canada (GoC) real property projects and operations.
Scope and Context
The Agency is custodian of three laboratories totalling 20,900 m² and is a tenant in 66,600 m² of leased space that accommodates 2,143 employees in 63 locations.
PHAC and HC worked jointly to transform their individual Green Buildings Strategic Frameworks into a shared Real Property Sustainability Framework. Greening practices outlined in the Framework are applied to all temperature controlled office and laboratory spaces over 1,000 m² where benchmark information is available.
Link to the Organization’s Program
Internal Services
Performance Measurement
Expected Result
An industry-recognized level of high environmental performance will be achieved in GoC real property projects and operations.
| Performance indicator | Performance level achieved |
|---|---|
Real Property Sustainability Framework in place to improve the management of energy, waste and water in departmental real property assets by March 31, 2015. |
March 26, 2015 |
Total number of existing Crown-owned buildings (over 1,000 m² ) and new lease or lease renewal projects (over 1,000 m² ) where the Crown is the major lessee, assessed for environmental performance using an industry-recognized assessment tool, and total associated floor space (m² ). |
0 Crown-owned buildings |
0 New lease or lease renewal projects |
|
Assessment tool used: |
|
Total number of existing Crown-owned buildings, new construction, build-to-lease projects, and major renovation projects achieving an industry-recognized level of high environmental performance, and associated floor space m² ). |
0 Crown-owned buildings |
0 New construction projects |
|
0 Build-to-lease projects |
|
0 Major renovation projects |
|
Number of fit-up and refit projects achieving an industry-recognized level of high-environmental performance. |
0 fit-up and refit projects |
Implementation strategy element or best practice |
Performance level achieved |
7.1.1.1. Achieve a level of performance that meets or exceeds the custodian's current commitment(s) to sustainable buildings using industry-recognized assessment and verification tool(s) |
Achieved |
7.1.1.3. Develop plans to address environmental performance assessment recommendations for existing Crown owned buildings. |
Achieved |
7.1.1.4. Manage the collection, diversion and disposal of workplace waste in Crown-owned buildings in an environmentally responsible manner. |
Achieved |
7.1.1.5. Manage construction, renovation and demolition waste in Crown-owned buildings in an environmentally responsible manner. |
Achieved |
| Implementation Strategy Element or Best Practice | Performance level achieved |
| 7.1.1.1. Achieve a level of performance that meets or exceeds the custodian's current commitment(s) to sustainable buildings using industry-recognized assessment and verification tool(s) | Achieved |
| 7.1.1.3. Develop plans to address environmental performance assessment recommendations for existing Crown owned buildings. | Achieved |
| 7.1.1.4. Manage the collection, diversion and disposal of workplace waste in Crown-owned buildings in an environmentally responsible manner. | Achieved |
| 7.1.1.5. Manage construction, renovation and demolition waste in Crown-owned buildings in an environmentally responsible manner. | Achieved |
Target 7.2: Green Procurement
As of April 1, 2014, the Government of Canada will continue to take action to embed environmental considerations into public procurement, in accordance with the federal Policy on Green Procurement.
Scope and Context
PHAC has continued to focus on greening its procurement of office supplies, information technology (IT) hardware, and office equipment. The scope of each target area is outlined below:
- Office Supplies: Excludes purchases using acquisition cards;
- IT Hardware: Includes automatic data processing equipment (e.g. computers) and excludes laboratory, field equipment and purchases using acquisition cards; and
- Office Equipment: Includes all printers, faxes, scanners, multi-functional devices and photocopiers and excludes laboratory, field equipment, and purchases using acquisition cards.
PHAC relies on HC’s procurement and materiel management specialists in order to fulfill these functions.
Link to the Organization’s Program
Program: Internal Services
Sub-Program: Asset Management Services
Performance Measurement
Expected Result
Environmentally responsible acquisition, use and disposal of goods and services.
| Performance indicator | Performance level achieved |
|---|---|
| Departmental approach to further the implementation of the Policy on Green Procurement in place as of April 1, 2014. | Yes, March 31, 2014 |
| Number and percentage of procurement and/or materiel management specialists who have completed the Canada School of Public Service Green Procurement course (C215) or equivalent, in fiscal year 2015–16. | 3 100% |
| Number and percentage of managers and functional heads of procurement and materiel whose performance evaluation includes support and contribution toward green procurement, in fiscal year 2015–16. | 1 100% |
Departmental green procurement target
By March 31, 2017, 90% of IT hardware purchases will include criteria to reduce the environmental impact associated with the production, acquisition, use and/or disposal of the equipment.
| Performance indicator | Performance level achieved |
|---|---|
| Volume of IT hardware purchases that meet the target objective relative to the total dollar value of all IT hardware purchases in the year in question. | 100% |
Departmental green procurement target
By March 31, 2017, 80% of office supply purchases will include criteria to reduce the environmental impact associated with the production, acquisition, use and/or disposal of the supplies.
| Performance indicator | Performance level achieved |
|---|---|
| Volume of office supply purchases that meet the target objective relative to the total dollar value of all office supply purchases in the year in question. | 89.5% |
Departmental green procurement target
By March 31, 2017, 90% of purchases of office equipment (printers, faxes, scanners and photocopiers) will have one or more environmental features.
| Performance indicator | Performance Target (RPP) |
|---|---|
| Volume of office equipment purchases that meet the target objective relative to the total dollar value of all purchases for office equipment in the year in question | 96.8% |
| Implementation strategy element or best practice | Performance level achieved |
|---|---|
| 7.2.1.5. Leverage common use procurement instruments where available and feasible | Achieved |
Target 7.3: Sustainable Workplace Operations
As of April 1, 2015, the GoC will update and adopt policies and practices to improve the sustainability of its workplace operations.
Scope and Context
PHAC has over 2,143 employees located in 63 locations across Canada. Although some unique situations exist, the majority of PHAC workplaces are offices, boardrooms, and cafeterias containing typical office equipment: computers, telephones, printers, and photocopiers.
PHAC and HC, through a shared consultative Sustainable Workplace Operations Working Group, developed an Approach to Sustainable Workplace Operations which outlines the commitment of both organizations to improve the sustainability of workplaces across the country.
Link to the Organization’s Program
Internal Services
Performance Measurement
Expected Result
Departmental workplace operations have a reduced environmental impact.
| Performance indicator | Performance level achieved |
|---|---|
| An approach to maintain or improve the sustainability of the departmental workplace is in place as of March 31, 2015. | December 16, 2014 |
| Implementation strategy element or best practice | Performance level achieved |
| 7.3.1.1. Engage employees in greening government operations practices. | Achieved |
| 7.3.1.3. Maintain or improve existing approaches to sustainable workplace practices (i.e., printer ratios, paper usage, and green meetings) | Achieved |
| 7.3.1.6. Dispose of e-waste in an environmentally sound and secure manner. | Achieved |
Goal 8: Water Management
Target 8.1: Water Management
As of April 1, 2014, the GoC will take further action to improve water management within its real property portfolio.
Scope and Context
PHAC is custodian of three laboratories totalling 20,900 m² and a tenant in 66,600 m² of leased space that accommodates approximately 2,143 employees in 63 locations.
Through the implementation of a Real Property Sustainability Framework, PHAC has defined its approach to sustainable water management within its real property portfolio.
Link to the Organization’s Program
Program: Internal Services
Sub-Program: Asset Management Services
Performance Measurement
Expected Result
Water is managed sustainably in Government of Canada real property operations.
| Performance indicator | Performance level achieved |
|---|---|
| Approach to improving water management included in Real Property Sustainability Framework by March 31, 2015 | March 26, 2015 |
| Amount and percentage of floor space in buildings over 1,000 m² that includes water metering, in 2015–16 (where feasible). | 20,900 m² existing Crown-owned 100% |
| 0 m² new Crown and built-to-lease 0% |
|
| 0 m² major renovations 0% |
|
| 60,400 m² leases 100% |
|
| Implementation strategy element or best practice | Performance level achieved |
| 8.1.1.1. Conserve potable water. | Achieved |
| Best Practice 8.1.3. Analyze the water consumption data collected to determine steps to improve water management in Crown-owned assets. |
Achieved |
5. Additional Departmental Sustainable Development Activities and Initiatives
Not applicable.
6. Sustainable Development Management System
The purpose of the FSDS is to make environmental decision making more transparent and accountable to Parliament. Sustainable development (SD) is one of the lens through which PHAC undertakes its business and delivers on its core vision of healthy Canadians and communities in a healthier world in order to derive added benefits or to avoid or mitigate negative impacts on human health for both present and future generations.
PHAC’s SD vision is guided by the following principles:
- Strengthen Canada’s capacity to protect and improve the health of Canadians;
- Build an effective public health system that enables Canadians to achieve better health and well-being in their daily lives; and
- Reduce health disparities between the most advantaged and disadvantaged Canadians.
The PHAC Assistant Deputy Minister Sustainable Development Champion (Champion) provided leadership to sustain integrated consideration of environmental impacts in decision making. The Champion led the processes and mechanisms to develop PHAC’s DSDS and to report on its implementation. The Champion oversaw the renewal and implementation of PHAC’s Strategic Environmental Assessment (SEA) policy suite, and SEA attestation process. The Champion communicated the PHAC SEA policy to employees and management to reinforce the importance of SEA as a risk assessment tool to inform decision-making.
PHAC’s SD planning, reporting and consideration of Canada’s environmental goals and targets under the FSDS are linked with the federal government’s core expenditure planning and reporting systems. PHAC reported on its SD commitments and progress against these commitments through the DSDS in the Supplementary Information Tables of the Report on Plans and Priorities and the Departmental Performance Report.
PHAC contributed to the federal approach to SD, FSDS 2016–19 renewal and 2015 Progress Report on 2013–16 FSDS through its ongoing participation in interdepartmental committees and related processes.
7. Strategic Environmental Assessment
During the 2015–16 reporting cycle, PHAC considered the environmental effects of initiatives subject to the Cabinet Directive on the Environmental Assessment of Policy, Plan and Program Proposals, as part of its decision making processes. As PHAC did not develop any initiatives that required a SEA, no related public statements were produced.
In 2015, PHAC undertook targeted initiatives to strengthen its SEA capacity and proposal coverage, including the renewal of its SEA Policy, Operational Guidance, SEA Preliminary Scan Form and other supporting materials. PHAC also launched classroom training on the SEA process and requirements, and refreshed the PHAC sustainable development intranet page to include renewed SEA materials.
In 2015–16, PHAC applied the SEA process to all PHAC-led TB Submissions (4) and Ministerial Recommendations (3). PHAC completed the SEA process for three additional proposals which had undergone a SEA preliminary scan in 2014–15, by securing the SD Champion SEA attestation. There were no PHAC-led Memorandum to Cabinet undertaken during the 2015–16 reporting cycle.
With the launch of the new PHAC Policy on SEA in December 2015, PHAC also applied the SEA process to 80% (4) of the warranted proposals, including: (1) Regulatory Submission and (3) other strategic proposals. Of the warranted Memoranda to the Minister, PHAC applied the SEA process to 100%, of which all five were identified as exempt as the proposals were previously assessed.
The impact of proposals on achieving the 2013–16 FSDS goals and targets were taken into account. Of the proposals subject to PHAC’s SEA process, three PHAC-led proposals were found to potentially contribute directly or indirectly to two of the four 2013–16 FSDS themes: two proposals concluded that they would contribute to Theme I “Addressing Climate Change and Air Quality’, Goal 1 “Climate Change”, Target 1.2 “Climate Change Adaptation”; and one proposal would contribute to Theme II: “Maintaining Water Quality and Availability”.Details on Transfer Payment Programs of $5 Million or More
Aboriginal Head Start in Urban and Northern Communities (AHSUNC)
General Information
| Name of transfer payment program | AHSUNC (Voted) |
|---|---|
Start date |
1995–96 |
End date |
Ongoing |
Fiscal year for terms and conditions |
2009–10 |
Strategic outcome |
Protecting Canadians and empowering them to improve their health |
Link to the Organization’s Program 1.2 Program Health Promotion and Disease Prevention; 1.2.2 Sub-Program Conditions for Healthy Living; and 1.2.2.1 Sub-Program Healthy Child Development |
|
Description Objective: Provide Aboriginal preschool children in urban and northern settings with a positive sense of themselves, a desire for learning, and opportunities to develop fully and successfully as young people. Why this Transfer Payment Program (TPP) is Necessary: Aboriginal children are at higher risk for poor developmental and health outcomes than non-Aboriginal children. Considerable evidence supports the mitigating role of community-based early childhood development programs in the lives of children facing similar risks. Intervention Method: Funded projects must incorporate the six core program components (health promotion, nutrition, education, Aboriginal culture, parental involvement and social support) into their program design. Within the context of this pan-Canadian consistency, sites are locally tailored to the needs and assets within their communities. Repayable Contributions: No. |
|
Results achieved The AHSUNC program supported community organizations in providing services to approximately 4,600 children at 133 sites across the country, which represents approximately 4% of eligible Aboriginal children zero to six years of age living off-reserve. The AHSUNC program celebrated its 20th Anniversary in 2015. A national event was held at the University of British Columbia that hosted 52 AHSUNC youth graduates from across the country and resulted in a Reflections Paper, video and analysis of the positive impact of culturally-appropriate early childhood programming. In addition, the AHSUNC Strategic Fund contributed to the development of an outdoor curriculum, “Take It Outside”, piloted by the Under One Sky site in New Brunswick. The pilot places a strong emphasis on child health and wellbeing in a holistic sense, with a focus on teaching language and culture through engagement with the natural world. AHSUNC continued the delivery of an accredited community-based applied Inuit early childhood diploma/certificate program by Nunavut Arctic College that included the use of technology to enhance learning. PHAC found that the AHSUNC programming has led to positive changes in family practices. This was evidenced through data collected in May 2015 with the implementation of a parent survey. The results demonstrated that 84% of parents/caregivers reported feeling more positive in their role as a parent; 87% reported doing more things with their child to help him or her learn; 80% reported making time to read to their child more often; and, 82% of parents/ caregivers reported using ideas they had learned in the program to help them as a parent. Other evidence from the parent survey pointed to improvements in school readiness of program participants. More specifically, 93% of survey respondents reported that their child was more prepared to start school; 89% report that their child was better able to express him/herself; 88% report their child was more interested in being read stories, or looking at books; and 84% reported that the program had helped improve the health and well-being of their child(ren). In addition, the AHSUNC program demonstrated sustainability through leveraging multi-sectoral collaborations at AHSUNC sites. In 2015–16, 77% of AHSUNC sites leveraged multi-sectoral collaborations. |
|
Comments on variances: Actual spending was more than planned primarily due to additional ongoing funding secured for the Aboriginal Head Start Strategic Fund during the reporting period. |
|
Audits completed or planned |
Not applicable (N/A) |
Evaluations completed or planned |
Evaluation of the Aboriginal Head Start in Urban and Northern Communities Program at the Public Health Agency of Canada (2012) Next planned evaluation: 2016–17 |
Engagement of applicants and recipients: Recipients are engaged through targeted solicitations. Funded recipients deliver comprehensive, culturally appropriate, locally controlled and designed early childhood development programs for Aboriginal pre-school children and their families living in urban and northern communities across Canada. They also support knowledge development and exchange at the community, provincial/territorial (P/T), and national levels through training, meeting and exchange opportunities. |
|
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 32,666,837 | 32,994,509 | 29,134,000 | 33,828,782 | 33,676,570 | 4,542,570 |
| Total other types of transfer payments | ||||||
| Total program | 32,666,837 | 32,994,509 | 29,134,000 | 33,828,782 | 33,676,570 | 4,542,570 |
Assessed Contribution to the Pan American Health Organization (ACPAHO)
| Name of transfer payment program | ACPAHO (Voted) | |
|---|---|---|
Start date |
July 2008 |
|
End date |
Ongoing |
|
Fiscal year for terms and conditions |
2013–14 |
|
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
|
Link to the Organization’s Program 1.1 Program Public Health Infrastructure; and 1.1.2 Sub-Program Public Health Information and Networks |
||
Description Objective: Comply with Canada’s obligation, as a Member State of the Pan American Health Organization (PAHO), to provide funding for the Organization to advance its public health work in the Americas. The program also allows Canada to advance global health and foreign policy priorities and contribute to the security of the Americas region to protect the health of Canadians. Intervention Methods: As a member of PAHO, Canada is able to protect the health of Canadians and advance Canada’s health priorities through:
Repayable Contributions: No. |
||
Results achieved ACPAHO has met its primary objective of complying with Canada’s obligation to provide funding for the Organization to advance its public health work while allowing Canada to advance global health and foreign policy priorities and contribute to the security of the Americas region to protect the health of Canadians. PAHO plays an important role in providing a forum for addressing public health issues of common interest across Member States. PAHO’s mission is to “lead strategic collaborative efforts among member states and other partners to promote equity in health, to combat disease, and to improve the quality of and lengthen the lives of the peoples of the Americas”. As a Member State and partner, Canada’s support to PAHO helped advance its work by:
Canada's contributions to PAHO support the implementation of PAHO’s Strategic Plan (2014-2019). Through its implementation, and a 15-year consolidated effort, the Americas became the world’s first Region to eliminate rubella and congenital rubella syndrome. This is an historic milestone for public health. Canada has been active in refining the assessment and monitoring components of the PAHO Strategic Plan over the last year. In particular, Canada played a leadership role advising the PAHO secretariat on the development of a framework that will be used to guide the allocation of resources to various program areas. As well, PAHO adopted the Health-Adjusted Life Expectancy (originally developed in Canada) as one of the most significant impact indicators for the Plan. Canada’s support for PAHO contributes to our efforts to enhance global health security by strengthening public health infrastructure in the region, establishing mechanisms to share information, facilitate surveillance and strengthen capacities for response to public health emergencies of international concern. PAHO’s convening role during outbreaks and pandemics is critical to quickly address and mitigate public health events of importance in the region. PAHO supported the response to the rapid spread of Zika virus in the Region of the Americas. The Organization activated the Incident Management System to better respond to the needs of the Member States and communicate more effectively with them. As a Member State of PAHO, Canada participates in governing body meetings and provides contributions to fund the Organization. As the second largest contributor of assessed contributions to PAHO in calendar year 2015, Canada continues to advocate for accountability and transparent management of the Organization’s budget. In September 2015, Canada concluded a successful three-year term on PAHO’s Executive Committee. Representation on the Executive Committee provided Canada an opportunity to streamline agendas for governing body meetings to enhance efficiency and effectiveness of the Organization. In addition, the Executive Committee membership has provided a constructive forum to strengthen Canada’s bilateral and multilateral relations in the region. Through its membership on the Executive Committee, Canada strategically advanced its priorities for engagement with PAHO, fostered a stronger relationship with the Organization and raised its profile in the region. At the PAHO Directing Council in September 2015, Canada hosted a side-event on “Multi-sectoral Partnerships for Healthy Living and Chronic Disease Prevention” with Argentina. The event was well-attended and raised Canada’s profile as a leader on innovative initiatives for multi-sectoral policy implementation for non-communicable diseases. In 2015, Canada played a leadership role developing the PAHO Strategy and Plan of Action on Strengthening the Health System to Address Violence against Women. Canada provided financial support ($20,000) towards its development, contributed to early drafts, and co-chaired regional consultations on the Strategy. By adopting the Strategy and Plan of Action, PAHO Member States recognized that violence against women is a public health and human rights problem, and pledged to ensure that their health systems fulfill their responsibilities to prevent and respond to such violence. PAHO Strategy served as a main input to the WHO-led Canada responded to 28 requests for technical support, helping to build capacity in the region through sharing of best practices and expertise. Canada also worked with and supported WHO/PAHO Collaborating Centres (27 are located in Canada and six are within the Health Portfolio). As a Member State of PAHO, Canada has access to funding to support projects of common interest through the Canada-PAHO Biennial Work Plan. The following five projects were completed jointly by PAHO and the Health Portfolio in late 2015: Supporting the development of regulatory capacity for medicines and other health technologies in the Americas -USD $100,000: Activities contributed to the development of regional regulatory capacity in the area of medicines and other health technologies, and to regulatory convergence in the region. The regional approach facilitated the sharing of similar experiences and challenges between countries based on their level of development and needs. Formal training course for health officials on the development and implementation of tobacco product regulations in the area of product attractiveness reduction – USD $90,295: Activities contributed to capacity building for tobacco product regulation in the region. 10 countries participated in the piloting of technical capacity building workshop. The workshop materials were adapted and made available as an online course on tobacco control. Factsheets on tobacco industry interference and information required from the industry were produced and translated and distributed to all countries in the Region. Promoting mental health in indigenous populations –USD $49,945: Activities provided an opportunity for participants from Chile, Argentina, Brazil and Nunavut to exchange and discuss experiences, best practices and topics of common interest in the area of mental health in indigenous populations, including links between traditional medicine and formal health services. Proficiency program for serotyping of Haemophilus influenza and molecular characterization of Haemophilus influenza strains in PAHO countries – USD $75,497: Activities contributed to improving the capacity of four National Reference Laboratories (Brazil, Chile, Colombia and Panama) for Haemophilus influenza serotyping. The quality control program indicated that in addition to improved serotyping, the surveillance data obtained on invasive Haemophilus influenza disease obtained from the PAHO Reference Laboratories were of good quality and reliable, thereby enhancing surveillance and detection capabilities in the region. Support to the implementation of surveillance of water quality in health institutions in Haiti – USD $34,789: Activities contributed to the establishment of a water quality monitoring system for health institutions in 20 hospitals and health centres in Haiti. To ensure sustainability of the project, technical training was provided to officials on sampling, reporting, data gathering and database management. The system produces weekly reports and has enhanced the surveillance and detection of water-borne disease, including cholera. |
||
Comments on variances: Canada’s annual assessed contribution for PAHO is calculated in US dollars and disbursed in Canadian funds. Variances from planned versus actual spending is related to the currency exchange rate between the US dollar and the Canadian dollar. |
||
Audits completed or planned |
N/A |
|
Evaluations completed or planned |
Last completed evaluation: 2013–14 |
|
Engagement of applicants and recipients: As a member of PAHO, Canada sits on the Directing Council as a voting member, thereby influencing the direction of the PAHO’s work as well as the use of its budgets. |
||
| Program: Public Health Infrastructure | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 13,298,807 | 14,334,724 | 12,500,000 | 14,818,529 | 14,622,256 | 2,122,256 |
| Total other types of transfer payments | ||||||
| Total program | 13,298,807 | 14,334,724 | 12,500,000 | 14,818,529 | 14,622,256 | 2,122,256 |
Canada Prenatal Nutrition Program (CPNP)
| Name of transfer payment program | CPNP (Voted) | |
|---|---|---|
Start date |
1994–95 |
|
End date |
Ongoing |
|
Fiscal year for terms and conditions |
2009–10 |
|
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
|
Link to the Organization’s Program 1.2 Program Health Promotion and Disease Prevention; 1.2.2 Sub-Program Conditions for Healthy Living; and 1.2.2.1 Sub-Sub-Program Healthy Child Development |
||
Description Objectives: Mitigate health inequalities for pregnant women and infants, improve maternal-infant health, increase the rates of healthy birth weights, as well as promote and support breastfeeding. The TPP also seeks to promote the creation of partnerships within communities and strengthen community capacity to increase support for vulnerable pregnant women and new mothers. Why this TPP is Necessary: Evidence shows that maternal nutrition, as well as the level of social and emotional support provided to a mother and her child, can affect both prenatal and infant health, as well as longer-term physical, cognitive and emotional functioning in adulthood.Footnote 1 This program raises stakeholder awareness and supports a coherent, evidence-based response to the needs of vulnerable children and families on a local and national scale. It also supports knowledge development and exchange on promising public health practices related to maternal-infant health for vulnerable families, community-based organizations and practitioners. Intervention Methods: Programming delivered across the country includes: nutrition counselling; provision of prenatal vitamins, food and food coupons; parenting classes; social supports; and education on prenatal health, infant care, child development, and healthy living. Repayable Contributions: No. |
||
Results achieved CPNP provided services to over 48,000Footnote 2 participants including pregnant women, post natal women and parents and caregivers.Footnote 3 The CPNP contributed to building knowledge and skills of parents and caregivers, which support maternal, child and family health. Data collected via a survey in May 2015 points to these gains. For example, as a result of coming to the program, 86% of survey respondents reported having a better understanding of the effects of drinking alcohol during pregnancy on their baby; 92% of respondents reported knowing more about the importance of breastfeeding; 83% of survey respondents reported being better able to cope with stress; and 85% reported making healthier food choices. In addition, the CPNP has been able to demonstrate sustainability through leveraging collaborations and funding sources. Overall, 88% of projects were able to leverage multi-sectoral collaborations and 64% were able to leverage funds from other sources. |
||
Comments on variances: N/A |
||
Audits completed or planned |
||
Evaluations completed or planned |
||
Engagement of applicants and recipients: CPNP funding recipients play an important role in responding to their participants’ needs. Recipient organizations are engaged through monitoring and program support in areas that include program delivery and knowledge development and exchange. |
||
Performance information (dollars)
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 27,845,909 | 26,757,290 | 27,189,000 | 27,089,211 | 26,990,094 | (198,906) |
| Total other types of transfer payments | ||||||
| Total program | 27,845,909 | 26,757,290 | 27,189,000 | 27,089,21 | 26,990,094 | (198,906) |
Canadian Diabetes Strategy (CDSFootnote 4)
| Name of transfer payment program | CDS (Voted) |
|---|---|
Start date |
2005–06 |
End date |
Ongoing |
Fiscal year for terms and conditions |
2009–10 |
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
Link to the Organization’s Program 1.2 Program Health Promotion and Disease Prevention; and 1.2.3 Sub-Program Chronic (non-communicable) Disease and Injury Prevention |
|
Description Objectives: Promote multi-sectoral partnerships and innovative approaches focused on promoting healthy active living, thereby reducing the risk of developing a chronic disease as the incidence of type 2 diabetes rises due to an increasingly inactive and overweight Canadian population. Why this TPP is Necessary: Type 2 diabetes is one of the fastest growing diseases in Canada with more than 60,000 new cases yearly. It is estimated that two million Canadians have diabetes and one-third of them are unware that they have the disease. The risk factors for type 2 diabetes are becoming more common. Intervention Methods: This TPP supports federal leadership by facilitating multi-sectoral partnerships between governments, non-governmental organizations, and the private sector to ensure that resources are deployed to maximum effect. Repayable Contributions: No. |
|
Results achieved PHAC continued to seek out, test and implement preventative interventions aimed at addressing common risk factors for chronic disease, and to employ various funding arrangements and partnership models, including pay-for-performance models that tie payment to tangible outcomes. A total of nine projects received funding under the CDS in 2015–16, using the multi-sectoral partnerships approach to promote healthy living and prevent chronic disease. This includes the three examples below that will assess short-, medium-, and long-term changes in knowledge, attitudes, skills, and behaviour related to diabetes prevention and healthy lifestyles. First, the Build on Kids' Success (BOKS) project is in year two of a five-year partnership between PHAC, Reebok Canada, the Canadian Football League and the Propel Centre for Population Health Impact to implement this before school physical activity program. Since launching in September 2014, over 213 schools have enrolled, representing a 47% attainment of the five year recruitment goal of 450 schools overall. BOKS is currently running in 10 provinces, with the support of 589 volunteer trainers. Given the strong evidence base for the BOKS program in the United States, and the opportunity to implement in Canada for the first time, a rigorous evaluation approach is being conducted by the Propel Centre for Population Health Impact. Data is being collected throughout the intervention and compared over time to examine the impact of the program on students in grades three through six. The evaluation will measure whether the BOKS program leads to increases in physical activity, self-confidence and mental health outcomes, as well school attendance and engagement. Early results on physical activity outcomes reveal that BOKS students take more steps per day than non-BOKS students, including on weekends while at home. Second, the UPnGO with ParticipACTION project (in its first year of implementation) is a partnership between PHAC, ParticipACTION, Public Inc., the British Columbia (BC) Ministry of Health, the Ontario Trillium Foundation and AstraZeneca. UpnGo will test an innovative workplace wellness program that nudges and rewards Canadians for sitting less and moving more in their workplace. Inspired by Dr. Mike Evans' internet video, 23 and ½ hours,the program is designed to help sedentary Canadian adults to incorporate 30 minutes of daily walking into their day. UPnGO with ParticipACTION is one of PHAC’s flagship "walking" initiatives, which uses an innovative digital platform and app to support employees to increase steps and reduce sitting time through weekly challenges, interactive tools such as prompts and notifications, incentives, social connectedness and on-site events. UPnGOwas piloted in five BC workplaces, including TELUS, the City of Richmond, the University of British Columbia, Providence Healthcare and AutoTRADER, and evaluation results are being compiled to inform further implementation in other provinces across Canada. And third, Phase 1 of the Play for Prevention Program, a partnership between PHAC, Right to Play (RTP) and Maple Leaf Sports and Entertainment, which enabled the adaptation of RTP’s Play program for urban Aboriginal communities, was completed in March 2016. This diabetes prevention program tailored to unique community needs has reached over 2000 Aboriginal youth and community mentors. A total of 13 urban Aboriginal communities received programming which addressed the gap in diabetes prevention among Indigenous youth by focussing on education, awareness and the promotion of healthy and active living. In addition to the weekly program activities, 63% of children and youth reported participating in other programs, sports, and activities in their community and 58% of children and youth reported becoming more physically active since the program started. The program also demonstrated that 56% of the youth participants actively promoted healthy behaviours in their community by encouraging friends and family to eat healthy and be more active, while 38% demonstrated a desire to sustain their own healthy behaviours beyond the program and set specific goals to increase physical activity and/or healthy eating. Beginning in April 2016, Play for Prevention Phase 2 expands into Manitoba, Alberta and British Columbia allowing the program to reach an additional 1,000 Aboriginal children and youth per year, for a total of 3,500 children over five years. |
|
Comments on variances: Actual spending was less than planned spending primarily due to a reallocation of funds to other PHAC priorities. |
|
Audits completed or planned |
2010 Internal Audit of Chronic Disease Prevention and Control; |
Evaluations completed or planned |
Integrated Strategy on Healthy Living and Chronic Disease: Formative Evaluation of Diabetes Community-Based Programming (2009) |
Engagement of applicants and recipients: Funding opportunities are made available through the Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease, which engages multiple sectors of society to leverage knowledge, expertise, reach and resources, to work towards the common shared goal of producing better health outcomes for Canadians. |
|
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | 1,227,000 | (1,227,000) | ||||
| Total contributions | 2,707,592 | 4,228,159 | 5,051,000 | 4,529,258 | 3,600,377 | (1,450,623) |
| Total other types of transfer payments | ||||||
| Total program | 2,707,592 | 4,228,159 | 6,278,000 | 4,529,258 | 3,600,377 | (2,677,623) |
Community Action Program for Children (CAPC)
| Name of transfer payment program | CAPC (Voted) |
|---|---|
Start date |
1993–94 |
End date |
Ongoing |
Fiscal year for terms and conditions |
2009–10 |
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
Link to the Organization’s Program 1.2 Program Health Promotion and Disease Prevention; 1.2.2 Sub-Program Conditions for Healthy Living; and 1.2.2.1 Sub-Sub-Program Healthy Child Development |
|
Description Objectives: Fund community-based groups and coalitions to develop and deliver comprehensive, culturally appropriate early intervention and prevention programs to mitigate health inequalities and promote the health and development of children aged 0 to six years and their families facing conditions of risk. The TPP also seeks to promote the creation of partnerships within communities and to strengthen community capacity to increase support for vulnerable children and their families. Why this TPP is Necessary: Compelling evidence shows that risk factors affecting the health and development of children can be mitigated over the life course by investing in early intervention services that address the needs of the whole family.Footnote 5 Intervention Method: Programming across the country may include education on health, nutrition, early childhood development, parenting, healthy living and social supports. Repayable Contributions: No. |
|
Results achieved CAPC provided services to over 226,500 participants. The CAPC program contributed to building knowledge and skills of parents and caregivers, which support maternal, child and family health. Data collected via survey in May 2015 pointed to these gains. For example: 86% of survey respondents reported the program had helped to improve their parenting skills; 85% of respondents reported knowing more about how to keep their child healthy as a result of program participation; 83% of respondents reported their child is better able to express him/herself as a result of program participation; and, 82% of respondents reported their child recognizes more colours, or shapes, or letters, or numbers, as a result of program participation. The CAPC demonstrated sustainability through leveraging collaborations and funding sources. Overall, 87% of CAPC projects were able to leverage multi-sectoral collaborations and 73% were able to leverage funds from other sources. Additional evidence collected in May 2015 showed that 87% of survey respondents reported having a better relationship with their child, and that 91% reported doing more things with their child to help him or her learn, as a result of coming to the CAPC program. In 2015–16, PHAC updated the Nobody’s Perfect parenting program resources for use by vulnerable parents and facilitators, and invested in facilitator training events across Canada, including dissemination of parent kits. PHAC, in collaboration with the Department of Justice, revised the What’s Wrong with Spanking brochure to help parents guide their child's behaviour in a positive way. |
|
Comments on variances: Actual spending was more than planned spending primarily due to an internal reallocation of funds to support priorities such as Infant Mental Health and Nobody’s perfect. |
|
Audits completed or planned |
|
Evaluations completed or planned |
|
Engagement of applicants and recipients: CAPC funding recipients play an important role in responding to their participants’ needs. Recipient organizations are engaged though monitoring and program support in areas that include program delivery and sharing program learnings and practices. |
|
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 56,365,887 | 54,874,998 | 53,400,000 | 57,230,175 | 57,216,454 | 3,816,454 |
| Total other types of transfer payments | ||||||
| Total program | 56,365,887 | 54,874,998 | 53,400,000 | 57,230,175 | 57,216,454 | 3,816,454 |
Federal Initiative to Address HIV/AIDS in Canada (FI)
| Name of transfer payment program | FI (Voted) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Start date |
January 2005 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
End date |
Ongoing |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Fiscal year for terms and conditions |
2009–10 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Link to the Organization's Program 1.2 Program Health Promotion and Disease Prevention; 1.2.1 Sub-Program Infectious Disease Prevention and Control; 1.2.2 Sub-Program Conditions for Healthy Living; 1.2.1.2 Sub-Sub-Program Infectious and Communicable Diseases; and 1.2.2.2 Sub-Sub-Program Health Communities |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Description Objectives: Prevent and control HIV and associated sexually transmitted and blood-borne infections (STBBIs); facilitate access to testing, diagnosis, treatment, and information on prevention; and enhance the use of evidence, and knowledge about effective interventions. Why this TPP is Necessary: The FI Evaluation indicated that HIV/AIDS remains a persistent public health issue for Canada that disproportionately affects vulnerable populations. While the rate of infection of HIV/AIDS has stabilized, new cases continue to be diagnosed. As such, prevention efforts are still needed as well as greater emphasis on increasing access to testing, diagnosis, and treatment. Intervention Methods: In addition to facilitating access to testing, diagnosis, treatment, and information on prevention methods, the FI also supports and strengthens multi-sector partnerships to address the determinants of health. It supports collaborative efforts to address factors which can increase the transmission and acquisition of HIV. This includes sexually transmitted infections and co-infection issues with other infectious diseases (e.g., Hepatitis C and Tuberculosis). People living with and vulnerable to HIV/AIDS are active partners in FI policies and programs. Repayable Contributions: No. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Results achieved Transfers payments made under the Federal Initiative and the Hepatitis C Prevention Support and Research Program, which are jointly administered, enable 131 national and community-based organizations to implement 159 projects to develop and conduct activities to prevent and control HIV and Hepatitis C, and in support of global targets such as the UNAIDS 90-90-90 targets as well as the World Health Organization's Hepatitis C targets. In 2015–16 projects were able to demonstrate clear results for Canadians. To improve frontline capacity, 27 organizations worked with service providers and community-based organizations to strengthen their practices and improve the quality of services offered to individuals at risk for and living with HIV and AIDS. Over 1,400 not-for-profit front-line service providers/elders, more than 1,300 public health professionals, and nearly 1,200 clinical care providers benefitted from activities at conferences, health fairs, and educational events. 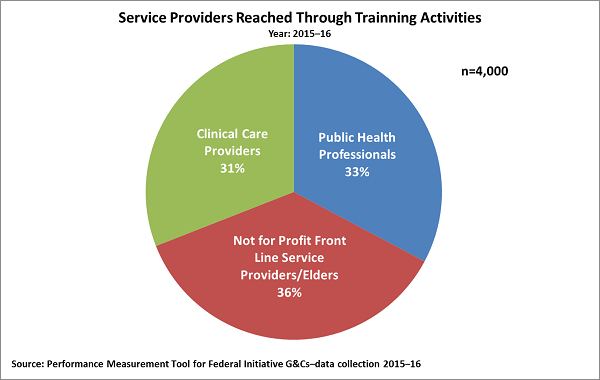
Service Providers Reached Through Training Activities, Year: 2015–16 - Text description
Source: Performance Measurement Tool for Federal Initiative - G&Cs - data collection 2015–16 To ensure front-line organizations use reliable and up-to-date knowledge and evidence in their work with key populations, the HIV and Hepatitis C knowledge broker distributed more than 607,000 copies of HIV and Hepatitis C resources. Of these, more than 61,000 copies of PHAC's booklet entitled "STI: Sexually Transmitted Infections" and 52,000 copies of "HIV Basic Facts" were distributed. Because one's health is affected by social and economic factors, the physical environment, and individual behaviors, known as the determinants of health, 95% of projects engaged in 3,800 formal partnership agreements to address determinants of health as part of HIV and Hepatitis C project activities. To help work toward the 90-90-90 and WHO Hepatitis C targets, PHAC funded organizations that worked with 292,000 individuals belonging to priority populations through community outreach programs, educational activities, referral services, etc.Footnote 6 This included reaching more than 102,000 youth, nearly 37,400 people living with HIV, Hepatitis C, and/or other related STBBIs and over 43,000 people who use drugs. Projects also reached 31,000 individuals identified as being gay, two-spirit, bisexual, or other men who have sex with men as well as more than 3,000 individuals identified as trans-sexual of which nearly 1,200 were trans-men. When age information was provided, approximately half (158,000 individuals) could be identified by their age. 60% were individuals below the age of 29. Among the more than 32,000 indigenous peoples reached there were nearly 19,500 First Nations individuals, more than 5,300 Metis individuals, and over 1,500 Inuit individuals reached. 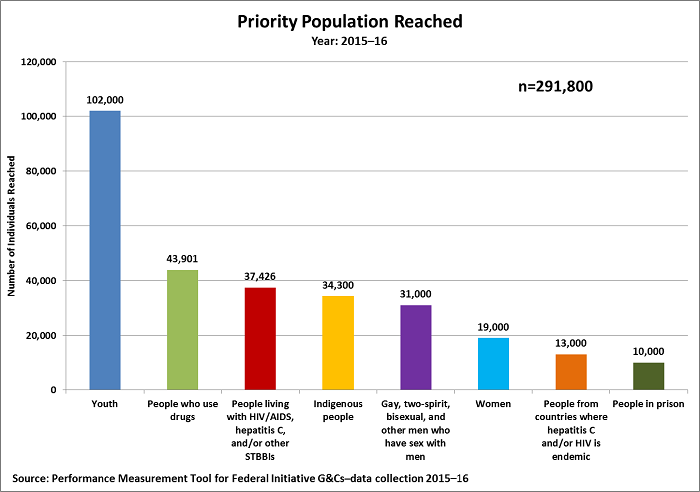
Priority Population Reached, Year: 2015–16 - Text description
Source: Performance Measurement Tool for Federal Initiative G&Cs – data collection 2015–16 To increase the adoption of personal behaviors that prevent the transmission of HIV, Hepatitis C, and related STBBI's, organizations worked with 108,000 individuals from priority populations to increase their knowledge of HIV, Hepatitis C and other STBBI risk factors. 77% of respondents surveyed felt they had improved their awareness of risk factors. In an effort to help manage and mitigate risk factors organizations worked to improve individual capacities (skills, competencies, and abilities) which could include things such as getting tested, complying with treatment, negotiating condom use with sexual partners, or using clean needles. 49,000 individuals were reached and 92% of individuals surveyed indicated they had improved their ability to manage their health. Following organization efforts to promote the uptake of behavior that can reduce transmission, 79% of individuals surveyed indicated intention to adopt healthy sexual behavior that may reduce transmission. 72% indicated intention to adopt practices other than health sexual behavior that may reduce transmission. 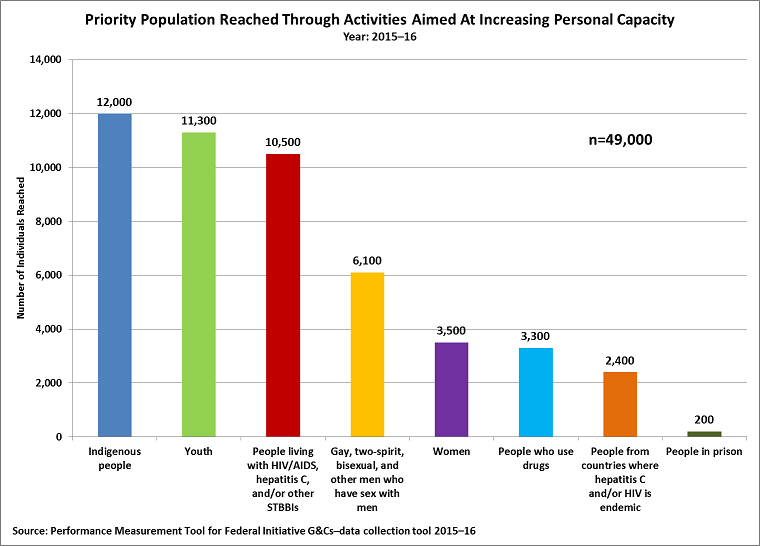
Priority Population Reached Through Activities Aimed At Increasing Personal Capacity, Year: 2015–16 - Text description
Source: Performance Measurement Tool for Federal Initiative G&Cs - data collection tool 2015–16 To promote the 90-90-90 targets and the WHO Hepatitis C targets, organizations undertook activities to improve the access of priority populations to prevention and control services. 72% of individuals surveyed indicated that they had increased access to care, treatment, and support. Because access to service often begins with improving awareness of priority populations, projects engaged 164,000 people through targeted campaigns in order to encourage individuals, specifically at-risk populations, to thinking about potential risk factors and health concerns, and to learn more about HIV, Hepatitis C, and other STBBIs. 
Estimated Priority Populations Reached Through Activities Aimed at Improving Awareness, Year: 2015–16 - Text description
Source: Performance Measurement Tool for Federal Initiative - G&Cs - data collection 2015–16 Projects have increasingly made use of social media technology to further their goals. To help individuals identify their risks and to find local services available for testing, treatment, and support, two organizations collaborated in order to develop smart phone applications. One of these applications was downloaded nearly 2,400 times in 2015–16 and been translated to other languages and made available in Europe. To reduce barriers faced by individuals that may limit access to services such as stigma surrounding HIV, Hepatitis C and/or other STBBIs, organizations worked to improve knowledge of HIV, Hepatitis C, and other STBBI related stigma. More than 56,000 individuals participated in activities with this goal in mind and a survey among 20% of these participants indicated that 70% felt they had improved their knowledge of stigma. Improving knowledge of stigma helps individuals to develop the self-confidence to seek out assistance from medical practitioners. Following project activities, 72%, of those surveyed reported improved confidence to speak with health care providers about STBBI risk behaviours. In addition to working with priority populations, organizations also worked with service providers to improve their practices regarding stigma. For example over 5,700 service providers received training on HIV, Hepatitis C, and other STBBI related stigma and of the 64% who were surveyed following the training, 87% indicated that they had improved their awareness of stigma related issues and 92% reported changing their practices. By improving their practices, service providers can make clients/ patients feel safer and more comfortable to disclose their risk behaviors or other risk factors and thus decrease barriers to accessing services like testing and treatment. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comments on variances: N/A |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Audits completed or planned |
Completed 2014–15 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Evaluations completed or planned |
Last Completed evaluation: 2013–14 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Engagement of applicants and recipients: Senior PHAC officials engaged with national non-governmental organizations to discuss the development of the new HIV/AIDS and Hepatitis C Community Action Fund which will be implemented in 2017. PHAC officials continued to engage in activities with community-based organizations to promote knowledge exchange and to support the development of regionally specific approaches to HIV/AIDS, including webinars, face-to-face meetings, and multi-stakeholder workshops. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | 175,000 | 7,430,000 | 126,938 | 125,000 | (7,305,000) | |
| Total contributions | 23,772,078 | 22,708,436 | 15,631,758 | 22,911,669 | 22,894,206 | 7,262,448 |
| Total other types of transfer payments | ||||||
| Total program | 23,772,078 | 22,883,436 | 23,061,758 | 23,038,607 | 23,019,206 | (42,552) |
Healthy Living Fund (HLF)
| Name of transfer payment program | HLF (Voted) | |
|---|---|---|
| Start date | June 2005 | |
| End date | Ongoing | |
| Fiscal year for terms and conditions | 2013–14 | |
| Strategic Outcome | Protecting Canadians and empowering them to improve their health. | |
Link to the Organization's Program 1.2 Program Health Promotion and Disease Prevention; and 1.2.3 Sub-Program Chronic (non-communicable) Disease and Injury Prevention |
||
Description Objective: Support multi-sectoral partnerships and innovative approaches focused on promoting healthy active lifestyles, thereby reducing the risk of chronic disease. Why this TPP is Necessary: Complex public health challenges defy single solution approaches that are developed in isolation. By engaging multiple sectors of society, partners can leverage knowledge, expertise, reach and resources, allowing each to do what it does best, in working towards the common shared goal of producing better health outcomes for Canadians. Intervention Method: The TPP engages and provides funding to multiple sectors and builds partnerships between governments, non-governmental organizations and other sectors, including the private sector. Repayable Contributions: No. |
||
Results achieved Under the Multi-Sectoral Partnership Approach to Healthy Living and Chronic Disease Prevention initiative, PHAC continues to invest approximately $20,000,000 per year in projects that focus on addressing common risk factors, such as unhealthy eating, physical inactivity, and smoking, to prevent chronic disease. As part of this approach, a total of nine projects received funding under the HLF in 2015–16 to test and implement innovative preventative interventions aimed at addressing common risk factors for chronic disease. PHAC has launched innovative incentive-based models as a means to encourage Canadians to make sustained healthy living choices. This approach is characterized by using financial instruments as policy levers; harnessing technology to improve access, reach and measurement/reporting of results; and engaging Canadians across all sectors of society. Key examples in 2015–16 include: In March 2016, PHAC launched Carrot Rewards, Canada's first wellness reward app. The initiative, valued at $5,000,000 over five years, represents a unique partnership between PHAC, the BC Ministry of Health, the private sector partner, Social Change Rewards and non-governmental organizations such as the Heart and Stroke Foundation, the Canadian Diabetes Association, YMCA Canada, and the BC Healthy Living Alliance. Carrot Rewards, first launched in British Columbia, invited British Columbians to install the Carrot app on their mobile devices which rewards them with popular loyalty points, such as Aeroplan, Petro-Points, Scene and More Rewards, for doing so. The app offers points for referring friends and family, creating new opportunities to connect with Canadians, and for taking healthy actions such as completing a heart health quiz, learning about and making healthy eating choices, or visiting a local YMCA. Since the launch, the app has been generating a very positive response, with user acquisition progressing steadily and rapidly. The app acquired over 55,000 users two months following the launch and over 750,000 actions have been completed to date. Carrot Rewards is being launched soon in Newfoundland and is anticipated to expand to interested provinces and territories. The APPLE Schools Project focuses on strategies to improve physical activity, mental wellbeing and healthy eating. This project builds on work beginning in 2008 in 10 APPLE Schools that demonstrated that students consumed more fruits and vegetables (10%), reduced their calorie intake, and were nearly 40% less likely to be obese than other students in Alberta. PHAC funding, beginning in April 2016, will support the next phase of implementation of the APPLE Schools model in vulnerable and remote regions of Alberta, Manitoba and the Northwest Territories. APPLE Schools is delivered in partnership with PHAC and new partners in the resource industry and charitable sector, including Canadian Natural Resources Limited, Pembina Pipeline, Allan P. Markin and the Joyce Foundation, and is supported by the Joint Consortium for School Health and the governments of Alberta, Manitoba and the Northwest Territories. The impact of this project on APPLE School students, staff, and parents will be assessed through a rigorous evaluation protocol designed and implemented by the School of Public Health at the University of Alberta. Dietary intake, physical activity levels, body weights, food security and socioeconomic background will be measured through a combination of surveys and time-stamped pedometers at baseline and again in Year 2 and Year 4 in all participating Grade 5 students. The Trottibus Walking School Bus project, submitted by the Canadian Cancer Society – Quebec Division (CCS-QD), was selected in 2015 by Canadians as the winning submission under The Play Exchange. The Play Exchange was launched as a national challenge to Canadians to submit their innovative ideas for inspiring Canadians to lead healthier and more active lives. The Trottibus Walking School Bus is a pedestrian bus service that provides elementary school children with a safe, fun and active way to get to school. The objective of the project is to support children to engage in regular physical activity by walking to school, leading to a lifetime healthy habits, as well as reduced incidence of unhealthy weights and chronic disease. Over three years (2015 to 2018), CCS-QD is receiving up to $1,000,000 from PHAC to expand the Trottibus Walking School Bus to more than 300 Quebec primary schools, reaching up to 9,000 participants, and informing over 135,000 students and their families of the benefits of physical activity and active transport. The initiative will also be piloted in other provinces such as Ontario. To date, the Trottibus Walking School Bus has successfully reached over 1,950 elementary school children who engage in regular physical activity by walking to school. Of significant note, more than 40% of children who currently participate in the Trottibus Walking School Bus did not previously use active transport to get to school. Setting the groundwork for active living at a young age is key to a lifetime of healthy habits. A good example of a project announced in previous years that continues to show effective engagement and results in 2015–16 is the Air Miles–YMCA Physical Activity Project. This partnership between Loyalty One and YMCA Canada is meant to encourage physical activity through the use of incentives. Since the project launch in April 2013, registered YMCA members who visited the YMCA in 15 locations in Ontario, Alberta and New Brunswick received Air Miles Reward Miles for reaching pre-defined physical activity milestones. Year-over-year comparisons showed that over 60% of active YMCA members in participating locations visited the YMCA at least one more time each week compared to the same time the previous year. Further, YMCA members enrolled in the project visited the YMCA 17.3% more frequently than YMCA members not enrolled in the project. Since launch, 101,042 participants registered for the program, far exceeding the original target of 25,000. During its third and final year, the program has been testing the effects on physical activity levels when Air Miles Reward Miles are reduced or removed, for which results are expected in summer 2016. |
||
Comments on variances: Actual spending was less than planned spending primarily due to a longer than anticipated timeframe for the launch of the wellness application. Additionally, funding was reallocated to other Agency priorities. |
||
Audits completed or planned |
2009 (completed) |
|
Evaluations completed or planned |
Evaluation of the Public Health Agency of Canada's Chronic Disease Prevention Activities 2009–2010 to 2014–2015 |
|
Engagement of applicants and recipients: Funding opportunities are made available through the Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease, which engages multiple sectors of society to leverage knowledge, expertise, reach and resources, to work toward the common shared goal of producing better health outcomes for Canadians. |
||
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 5,677,386 | 7,051,788 | 5,388,000 | 5,387,183 | 4,732,395 | (655,605) |
| Total other types of transfer payments | ||||||
| Total program | 5,677,386 | 7,051,788 | 5,388,000 | 5,387,183 | 4,732,395 | (655,605) |
Innovation Strategy (IS)
| Name of transfer payment program | IS (Voted) | |
|---|---|---|
| Start date | 2009–10 | |
| End date | Ongoing | |
| Fiscal year for terms and conditions | 2009–10 | |
| Strategic Outcome | Protecting Canadians and empowering them to improve their health. | |
Link to the Organization’s Program 1.2 Program Health Promotion and Disease Prevention; 1.2.2 Sub-Program Conditions for Healthy Living; and 1.2.2.2 Sub-Sub-Program Healthy Communities |
||
Description Objectives: Support the development, adaptation, implementation, and evaluation of promising, innovative population health interventions and initiatives across various settings and populations in Canada using an intervention research approach. In addition, use the systematic collection of results and outcomes of these interventions to promote their use more widely. Why this TPP is Necessary: There is little evidence available for use by decision-makers on effective public health interventions. Also, data are lacking that show how a successful, pilot intervention moves past the experimental stage and into the expanded, replicated, adapted, and sustained stages. The program funds applied research to generate knowledge about policy and program interventions that impact health at the population level. Intervention Method: The TPP supports activities in two areas:
Repayable Contributions: No. |
||
Results achieved In 2015, under the IS, nine interventions to promote mental health and well-being completed Phase 2, reaching over 280,000 individuals at risk. All funded projects demonstrated changes in health outcomes, risk factors or protective factors. This included improved mental health or well-being, coping strategies, emotional control, resilience and social skills (attitude, reflection, dealing with conflict). Of the nine mental health and wellbeing projects, four were selected to receive Phase 3 funding, to scale up their interventions in order to reach more people and achieve sustainable system change. The IS also completed the second year of its Phase 2 funding to 11 achieving healthier weights interventions. Phase 2 is a four year funding period that will end in 2017–18. In 2015–16, the achieving healthier weights interventions reached over 33,000 individuals at risk and 64% of the projects (seven out of 11) reported changes in health outcomes, risk factors or protective factors. Reported changes included increased fruit and vegetable consumption; improved physical activity; increased consumption of wild foods; increased cooking skills; and, perceived improvements in mental health and physical health. The Phase 3 funding for the IS is currently underway and aims to increase the reach and impacts of successful interventions to benefit more people and foster sustainable policy and program development. Traditionally, IS projects have demonstrated the development of new or sustained partnerships that have supported the delivery of interventions by leveraging expertise and resources from across a range of sectors, including health, education, agriculture and industry. For example, in 2014–15, the most recent year for which data is available, approximately 624 partnerships were developed, of which 45% were sustained three years or more (60% of partnerships for Mental Health projects and 35% for Healthy Weights projects). 65% of IS projects leveraged over $4,800,000 in additional funding, and over $1,000,000 in in-kind support. Leveraged funds accounted for approximately 35% of total PHAC project funding for IS projects, with in-kind support accounting for approximately 10% of total PHAC project funding. As projects move into Phase 3, the scale up phase, the development of such strong intersectoral partnerships are critical to the long-term sustainability of population health IS interventions. Additionally, in collaboration with key partners and stakeholders, IS projects have developed knowledge products and provided examples of how their knowledge have been used to inform policy, programs or practice. For example, in the last reporting cycle, IS projects developed over 1,000 knowledge products, reaching over 338,970 stakeholders. A total of 50% of stakeholders participating in knowledge use surveys indicated that they used knowledge generated by IS projects in their work. |
||
Comments on variances: Actual spending was more than planned spending primarily due to an internal reallocation of funds to support priorities such as Dementia Friends Canada and Active and Safe Play: Concussions. |
||
Audits completed or planned |
N/A |
|
Evaluations completed or planned |
Population Health Fund Evaluation 2008 Final Report; Next planned evaluation: 2019–20 |
|
Engagement of applicants and recipients: Open and targeted calls for proposals are utilized to solicit proposals from potential applicants. Various approaches are used to engage applicants and optimize the quality of submitted proposals, including those to develop information events, tools and resources. The IS places a high priority on and supports the systematic collection of learnings and the sharing of this information between funded recipients, PHAC, and other partners to influence future program and policy design. |
||
| Program: Health Promotion and Disease Prevention | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | 99,866 | 7,370,000 | 806,000 | 805,998 | (6,564,002) | |
| Total contributions | 10,371,935 | 9,060,034 | 2,877,000 | 11,001,939 | 10,652,475 | 7,775,475 |
| Total other types of transfer payments | ||||||
| Total program | 10,371,935 | 9,159,900 | 10,247,000 | 11,807,939 | 11,458,473 | 1,211,473 |
National Collaborating Centres for Public Health (NCCPH)
| Name of transfer payment program | NCCPH (Voted) | |
|---|---|---|
Start date |
2004–05 |
|
End date |
Ongoing |
|
Fiscal year for terms and conditions |
2012–13 |
|
Strategic Outcome |
Protecting Canadians and empowering them to improve their health. |
|
Link to the Organization’s Program 1.1 Program Public Health Infrastructure; and 1.1.2 Sub-Program Public Health Information and Networks |
||
Description Objective: Promote the use of knowledge for evidence-informed decision making by public health practitioners and policy-makers across Canada. The National Collaborating Centres (NCCs) synthesize, translate, and share knowledge to make it useful and accessible to policymakers, program managers, and practitioners. |
||
Results achieved The NCCPH increased public health capacity at multiple levels of the public health system using a variety of methods ranging from online training, workshops, outreach programs, and networking events to broadly disseminate a wide array of knowledge products. During 2015–16 the NCCPH increased the development and dissemination of knowledge translation products and activities by producing and providing over 1900 new products and activities consisting of evidence reviews, published materials, videos, workshops, webinars, online courses and conference presentations which supported practitioners and decision makers in applying new knowledge in their environments. Visits to the NCCPH websites to access knowledge products and activities also increased significantly with a total of 421,206 unique visitors. In addition, the NCCPH undertook 311 knowledge-related needs and gaps identification activities to provide knowledge brokers with the resources and structures required to strengthen evidence informed decision making. The NCCPH also engaged and maintained over 350 partnerships and collaborative activities with Health Portfolio partners, provincial/territorial (P/T) government departments, public health practitioners, and other external organizations to develop evidence-based interventions to reduce health risks. These collaborations were augmented with NCC knowledge exchange tools, resources, and expertise to facilitate and increase public health outreach. |
||
Comments on variances: Actual spending was more than planned spending primarily due to additional funding for the development of Ebola related tools, training and guidance for first responder and other emergency and care workers. |
||
Audits completed or planned |
N/A |
|
Evaluations completed or planned |
Last Completed Evaluation: 2014–15 |
|
Engagement of applicants and recipients: Contribution Agreements for all six National Collaborating Centres were in place for 2015–2016 with funding until March 31, 2020. |
||
| Program: Public Health Infrastructure | ||||||
|---|---|---|---|---|---|---|
| Type of Transfer Payment | 2013–14 Actual spending | 2014–15 Actual spending | 2015–16 Planned spending | 2015–16 Total authorities available for use | 2015–16 Actual spending (authorities used) | Variance (2015–16 actual minus 2015–16 planned) |
| Total grants | ||||||
| Total contributions | 8,740,589 | 6,169,000 | 5,842,000 | 6,498,455 | 6,430,239 | 588,239 |
| Total other types of transfer payments | ||||||
| Total program | 8,740,589 | 6,169,000 | 5,842,000 | 6,498,455 | 6,430,239 | 588,239 |
Horizontal Initiatives
Federal Initiative to Address HIV/AIDS in Canada (FI)
| Name of horizontal initiative | FI |
|---|---|
Name of lead department |
Public Health Agency of Canada (PHAC) |
| Federal partner organizations | Health Canada (HC), Canadian Institutes of Health Research (CIHR), and Correctional Service of Canada (CSC) |
Non-federal and non-governmental partners |
Not applicable (N/A) |
Start date of the horizontal initiative |
January 13, 2005 |
End date of the horizontal initiative |
Ongoing |
Total federal funding allocated (start to end date) (dollars) |
Ongoing |
Funding contributed by non-federal and non-governmental partners (dollars) |
N/A |
Description of the horizontal initiative (HI) Objectives:
Why this HI is Necessary:
Intervention Methods: Government of Canada partners are responsible for:
Partners develop multi-sector partnerships and collaborative efforts to address factors which can increase the transmission and acquisition of HIV. This includes sexually transmitted infections (STIs) and co-infection issues with other infectious diseases (e.g., Hepatitis C and tuberculosis). People living with and vulnerable to HIV/AIDS are active partners in FI policies and programs. |
|
Shared outcomesFootnote 7 First-level outcomes:
Second-level outcomes:
Ultimate outcomes:
|
|
Governance structures
|
|
Performance Highlights
|
|
Comments on variances: N/A |
|
Results achieved by non-federal and non-governmental partners |
N/A |
Contact information Marsha Hay-Snyder |
|
| Federal organizations | Link to organization’s programs | Contributing programs and activities | Total allocation (from start date to end date) (dollars) |
2015–16 (dollars) | |||
|---|---|---|---|---|---|---|---|
| Planned spending | Actual spending | Expected results | Actual results against targets | ||||
| PHAC | Public Health Infrastructure | Public Health Laboratory Systems | Ongoing | 5,056,959 | 5,049,033 | ER 1.1 ER 1.2 ER 1.3 |
AR 1.1 AR 1.2 AR 1.3 |
| Health Promotion and Disease Prevention | Infectious and Communicable Diseases | Ongoing | 2,434,753 | 2,326,809 | ER 1.1 ER 1.2 |
AR 1.1 AR 1.2 |
|
| Healthy Communities | Ongoing | 32,611,714 | 31,714,268 | ER 1.1 ER 1.2 ER 1.3 |
AR 1.1 AR 1.2 AR 1.3 |
||
| HC | First Nations and Inuit Primary Health Care | Sexually Transmitted and Blood Borne Infections -HIV/AIDS | Ongoing | 4,515,000 | 4,515,000 | ER 2.1 | AR 2.1 |
| CIHR | Horizontal Health Research Initiatives | Health and Health Service Advances | Ongoing | 21,700,000 | 21,700,000 | ER 3.1 ER 3.2 |
AR 3.1 AR 3.2 |
| CSC | Custody | Institutional Health Services | Ongoing | 4,187,261 | 4,895,830 | ER 4.1 ER 4.2 |
AR 4.1 AR 4.2 |
| Total for all federal organizations | Ongoing | 70,505,687 | 70,200,939 | N/A | |||
Expected and actual results achieved for 2015–16:
ER 1.1: Public health decisions and interventions are supported by laboratory reference service testing and the identification of new and existing HIV strains in Canada which directs attention to HIV outbreaks. Use of laboratory-generated knowledge is increased and laboratory research expertise and knowledge platforms are further consolidated, to develop a hub for global leadership in HIV research and viral diagnostics, outbreak response, and genetic linkages to risk of disease.
AR 1.1: In an effort to improve the accuracy and timeliness of HIV testing in Canada, PHAC laboratories upgraded their medical laboratory accreditation. This promotes quality assurance practices among Canadian HIV testing labs by providing expertise to internal and external labs.
To foster the quality of HIV point-of-care testing for HIV viral load and early infant diagnosis to increase capacity in response to help meet the UNAIDS 90/90/90 targets, PHAC also provided quality assurance programs for markers (physiological characteristics) of successful HIV care and treatment. These quality assurance programs were provided to over 40 laboratories across Canada and over 1400 internationally through its Quality Assessment and Standardization for Immunological measures program. This has resulted in a demonstrable increase in the quality of HIV testing within Canada and around the world.
Using digital polymerase chain reaction (PCR) expertise, PHAC developed and currently provides the only HIV-2 viral load assay in Canada. PHAC also participates in the Early Pediatric Initiation - Canadian Child Cure Cohort Study using digital PCR to examine treatment and “cure” phenotype.
In 2015, PHAC was re-accredited as a WHO specialized global drug resistance (DR) laboratory in the WHO/HIVResNet network. In this capacity, PHAC has developed a series of Next Generation Sequencing (NGS)-based HIV DR assays, which both reduce the cost of HIV DR surveillance and significantly improve the sensitivity of the analysis. In addition, PHAC has developed a web-accessible NGS DR analysis system referred to as HyDRA, suitable for handling the massive amounts of sequence data generated by NGS. Technology transfer was provided to several laboratories (Brazil, Chile, Mexico and Puerto Rico) and assistance also extended to a WHO ResNet laboratory in Africa (Uganda).
ER 1.2: Provinces and territories are engaged through the Public Health Network to increase pan-Canadian understanding of trends and factors associated with HIV and AIDS and related communicable diseases, through enhanced biological-behavioral surveillance, and using this surveillance to guide best practices in prevention and control efforts. 13 chapters of the STIs Guidelines will be reviewed and five chapters of the HIV/AIDS Epi Updates publications will be revised.
AR 1.2: PHAC supported the application of knowledge in public health practice through monitoring activities which enhanced the understanding of the HIV epidemic at local, provincial and national levels, and informed HIV prevention and control strategies addressing the needs of vulnerable populations at risk for HIV in Canada.
PHAC monitored the prevalence of HIV, hepatitis C, other related STBBIs and associated risk behaviors among people born in countries where HIV is endemic in partnership with local health authorities, community groups and academia. Extensive environmental scans were conducted to identify best practices towards the redevelopment of biological and behavioural surveillance activities among key populations in Canada. The findings were presented in the report were behaviors among people born in countries where HIV is endemic.
To improve Canada’s ability to monitor the HIV care cascade (testing and diagnosis, linkage/enrollment to care, retention in care, treatment and viral suppression) as per the UNAIDS 90-90-90 targets, PHAC worked with PT representatives on common surveillance indicator definitions. This will also help to monitor how people at risk for or living with HIV in Canada are engaged across the HIV care cascade spectrum.
As part of the GoC commitment to meeting the 90-90-90 targets for HIV, PHAC updated the Canadian Guidelines on the Sexually Transmitted Infections mobile application to encourage health professionals to offer an HIV test to individuals who disclose certain risk behaviors at the time of their patient interaction.
PHAC collaborated with global partners to promote the use of its modelling tool to improve how estimates of HIV incidence, prevalence and proportion of undiagnosed cases are calculated. Canada is one of a few countries able to produce such estimates on a regular basis and to show historical trends along with the estimates for the current year. The tool was endorsed by the UNAIDS Reference Group and as a result will be incorporated in the UNAIDS Spectrum software for global HIV estimation used by other governments domestically and internationally, as well as academia and researchers.
To ensure more appropriate treatment for people living with HIV, PHAC worked with six provinces to monitor HIV drug resistance in Canada through the Canadian HIV Strain and Drug Resistance Surveillance Program.
To equip public health and healthcare professionals with the latest evidence to help improve the health care for people living with HIV and AIDS, PHAC published two systematic reviews on the management of early syphilis among HIV co-infected persons and on the impact of antiviral therapy for the herpes virus in the HIV positive population.
PHAC also published an overview of recent evidence on barriers and facilitators to HIV testing in the Canada Communicable Disease Report.
ER 1.3: Public health and community capacity is enhanced to prevent and control HIV and AIDS and related communicable diseases, through integrated approaches to HIV and AIDS, related communicable diseases and health factors; renewed stakeholder engagement; targeted information products for key populations; training and knowledge exchange; and global engagement.
AR 1.3: The Ministerial Advisory Committee on the Federal Initiative (MAC-FI) to Address HIV/AIDS membership was renewed with the appointment of nine members and two ex-officio representatives and saw its mandate expanded to include Hepatitis C and other STBBIs. The mandate of the National Aboriginal Council on HIV/AIDS was also expanded to include other STBBIs and the membership was renewed with the appointment of ten members and two ex-officio representatives. Both committees were actively engaged in informing the development of the new HIV and Hepatitis C Community Action Fund and the facilitation of Council work on priorities related to the prevention and control of HIV and other STBBIs.
Working on issues such as eliminating stigma and discrimination in health care settings, PHAC worked with UNAIDS under the UNAIDS-Health Portfolio Arrangement for 2014–2019, and PHAC influenced the development of global policy documents and strategies, including the UNAIDS Strategy for 2016–2021. PHAC also provided input into the draft World Health Organization global health sector strategies for HIV/AIDS, Hepatitis C and sexually transmitted infections. PHAC forged bilateral relationships with key partners to support the development of public health and community capacity, including the development of indicators for the HIV care cascade.
The consistent provision of evidence-based, strategic and timely program policy advice supported a coherent PHAC and Government of Canada response to HIV, Hepatitis C and other STBBIs.
ER 2.1: Complete the development of a national framework that provides strategic direction to HC’s STBBIs programming to reduce the incidence, prevalence and burden of STBBIs in First Nations on reserve in partnership with key stakeholders such as First Nations’ leaders; federal organizations such as CSC; provincial partners; experts; and health care workers.
AR 2.1: To contribute in reducing the incidence, prevalence and burden of STBBIs in priority populations, Health Canada and the Assembly of First Nations (AFN) worked collaboratively to conduct twelve engagement sessions with the AFN National Public Health Experts Advisory Committee, Aboriginal People with HIV/AIDS, the National Aboriginal Council on HIV/AIDS, the Ministerial Advisory Council on the FI, and a broad range of partners and stakeholders. These sessions informed the development of a draft framework on STBBIs for First Nations on-reserve. The first draft of the Framework has been completed and circulated to stakeholders for feedback. Completion of the Framework is postponed to fiscal year 2017–18 to allow for greater engagement of First Nations Communities, including First Nation youth, and provincial and regional partners.
ER 3.1: Scientific knowledge about the nature of HIV/AIDS and ways to address the disease is created and research capacity built across priority areas including co-morbid health conditions in people living with HIV and the search for an HIV cure.
AR 3.1: Four team grants, funded through the CIHR HIV/AIDS Research Initiative, focused on HIV co-morbidities, specifically HIV and Aging; and HIV, Mental Health and Neurological Conditions, continued research efforts in 2015–16. A team, focused on the determinants of increased risk of cardio-vascular diseases in HIV-infected individuals, enrolled 500 individuals in a cohort study and secured funding for an additional four sub-studies relating to atherosclerosis. A second team, created a new academic community including investigators from many disciplines to address the understanding and treating brain health in people with HIV.
To strengthen collaboration and focus on the identification and scale-up of effective interventions, as identified in the 2013–14 Federal Initiative Evaluation, the CIHR HIV/AIDS Research Initiative partnered with Health Canada (First Nations and Inuit Health Branch), Corrections Services Canada and PHAC to support nine grants to address Implementation Science related to getting evidence into practice for HIV. The first grantees of the multi-phase Initiative were funded with one year grants totaling over $1,300,000 for adaptation grants intended to support the establishment of multi-sectoral HIV teams with related Hepatitis C and other STBBI research, including those where Indigenous populations are affected.
The CIHR HIV/AIDS Clinical Trial network which is a major investment of this initiative ($4,600,000), submitted their first annual report under the renewed funding arrangement with an increased focus on knowledge translation and emphasis on tackling increasing rates of infection in Saskatchewan. The CIHR Canadian HIV Trials Network hosted its first External Advisory Committee meeting in the fall of 2015. The CTN continues to contribute to improving health outcomes for people living with HIV and the development of new HIV researchers.
CIHR continued to fund the CIHR Canadian HIV Observational Cohort Collaboration (CANOC), with investigators in five provinces. CANOC has the largest Canadian database of HIV-positive individuals on highly active antiretroviral therapy, representing over 10,000 people. In 2015–16, the CANOC collaboration expanded to a site in Saskatchewan. In 2015–16 CANOC released new findings that the overall life expectancy of people living with HIV who have initiated antiretroviral therapy is 65 years of age.
The CIHR Centre for Research Evidence into Action for Community Health (REACH), with investigators in nine provinces aims to address the factors that contribute to risk and poor health and improve access to effective evidence-based interventions for people most affected by HIV and other STBBIs and hepatitis C. Researchers associated with REACH received funding to scale-up the MOBILISE! project, a community-based research project in Montréal that seeks to analyze and improve access to combination prevention strategies for men that have sex with men. The research team will work towards the implementation of this project in Vancouver, Toronto, and Ottawa. Using ethnographic methods and a participatory approach, the MOBILISE! research team will map services provided by community organizations, community health centres, medical clinics and other public and private agencies.
HIV positive Aboriginal women, in partnership with Canadian Aboriginal AIDS Network and the University of Victoria, received $1,200,000 in funding from CIHR to develop a culturally-grounded and strength-based intervention for HIV positive Aboriginal Women. Visioning Health II builds on the results of Visioning Health I: an arts-informed and community-based participatory research project that engaged HIV positive Aboriginal Women as co-researchers to explore their experience of ‘health’, rather than illness, and the supporting role culture and gender plays. Findings from this study revealed that health for HIV positive Aboriginal women is holistic, relational, and fundamentally about ‘feeling connected’. The study found that the process of participating in this project was, in itself, health enhancing. Visioning Health II will enable the research to expand to seven sites across Canada to better reflect the diversity of Aboriginal communities and to co-create new knowledge on the meaning of health for HIV positive Aboriginal women that resists the pan-Aboriginal approach typically taken when describing, exploring and addressing their experiences.
To promote the development of new knowledge and facilitate the exchange and uptake of this knowledge, CIHR launched and funded a diverse range of HIV research including: Community-based Research Catalyst and Operating grants (general and Indigenous stream); travel awards - to support participation in national and international conferences and the dissemination of research results; and Planning and Dissemination grants - to ensure researchers, practitioners, policy makers and community members have the chance to come together to plan research projects and to share research results.
In the last year, PHAC has developed new scientific knowledge on topics ranging from improving HIV testing techniques to determining how host mucosal and genetic factors affect susceptibility to HIV transmission, to the role of co-morbidities such as Hepatitis C and Mycobacterium tuberculosis in driving HIV disease. This body of published work is changing the global understanding of HIV diagnostics, microbicide and vaccine development, and HIV cure approaches.
ER 3.2: Coordination of a strategic research agenda is fostered through the initiation of a new strategic plan for 2015–20; the creation and maintenance of partnerships; and research programs focused on key populations and interventions to enhance the prevention of HIV and other STBBIs.
AR 3.2: Following a broad national consultation which engaged a large number of researchers, public health professionals, community-based organizations, people living with HIV/AIDS and other interested stakeholders, CIHR developed an updated Strategic Plan for its HIV/AIDS Research Initiative. The new plan outlines future strategic directions and priorities for research funding from 2015 to 2020. The first funding call aligned with this new strategic plan was the launch of a new Biomedical/Clinical Innovative grants program.
CIHR continued to support the Canadian Initiative for HIV Cure Research, a research collaboration focused on studying HIV persistence and developing strategies towards a functional HIV Cure. This scientific program is supported by CIHR, the Canadian Foundation for AIDS Research (CANFAR) and the International AIDS Society. Dr. Éric Cohen, Team Leader for CanCURE, published a study in the scientific journal PLOS Pathogens showing how an HIV protein known as "Vpu" tricks the immune system by using its own regulatory process to evade the host’s first line of defence. This discovery paves the way towards future therapeutic strategies for an HIV Cure.
In 2015–16 CanCURE produced an educational bilingual video to engage people with HIV and the broader Canadian public in CanCURE's research towards cure(s) for HIV.
CIHR played a significant role in the 2015 International AIDS Society Conference on HIV Pathogenesis, Treatment and Prevention and contributed to the Government of Canada efforts to showcase Canadian researchers in partnership with the CTN and CANFAR through a Canadian research booth.
To strengthen the range of research and communication skills for new and mid-career investigators, CIHR hosted five workshops with the Canadian Association for HIV Research. Two hundred investigators from cities from the east to west coast participated. In addition CIHR partnered with the Canadian Association for HIV Research on a Café Scientifique on Pre-Exposure Prophylaxis.
A short-term catalyst grant created a new interdisciplinary team with an interest in Pre-Exposure Prophylaxis research and HIV prevention efforts. This team developed a preliminary understanding of the issues relevant to (PrEP) rollout among gay, bisexual and other men who have sex with men (MSM). The findings underscore the importance of broader efforts to raise awareness about how MSM can assess their own HIV risk in order to maximize the clinical and public health potential or Pre-Exposure Prophylaxis. This team has gone on to receive funding for several related research grants in this area from the Ontario HIV Treatment Network, the CIHR, and the CIHR Canadian HIV Trials Network, among others.
ER 4.1: Enhanced understanding of the prevalence of HIV/AIDS, other STBBIs and other communicable diseases which facilitates prevention of new infections is achieved through comprehensive screening and assessment of offenders in federal penitentiaries.
AR 4.1: CSC continues to employ an integrated approach to screening and testing for blood-borne and sexually transmitted infections. Screening protocols for HIV comply with the national standards. Almost all (95%) new admissions were offered an assessment for blood-borne and sexually transmitted infections on admission to a federal institution. CSC has undertaken a review of HIV prevention program options and ways to evaluate the effectiveness and impact on reducing transmission among inmates while incarcerated. Consistent with the notion of treatment as prevention to prevent transmission, 91% of inmates known to have HIV infection were on anti-retroviral therapy in 2015–16.
ER 4.2: Offenders have increased knowledge and awareness of the nature of HIV/AIDS, other STBBIs and other communicable diseases and ways to address these diseases and associated chronic conditions as a result of educational activities and information materials which are informed by health surveillance. Particular emphasis will be placed on reducing stigma which may impede offender access to prevention, diagnosis, treatment, care and support.
AR 4.2: CSC continues to collect HIV and other STBBI testing data in order to track prevalence and to understand transmission while incarcerated. CSC has expanded enhanced surveillance to include treatment and viral suppression in order to contribute to the Government of Canada response to the UNAIDS 90-90-90 HIV care cascade targets. The Reception Awareness Program (RAP) is a voluntary program that provides information on infectious diseases and encourages health behaviors and practices. RAP participation continues to be below target.
Health promotion and access to inmate peer support workers in CSC institutions (including culturally competent Aboriginal peer support workers) continues to be an important part of the HIV prevention program. HIV continues to be the focus of awareness materials each December in support of World AIDS Day. Understanding HIV-related stigma and the role CSC can play to minimize stigma is the focus of a research proposal launched in 2015–16.
CSC participated in several external conferences and continues to meet with stakeholder and P/T colleagues on issues related to infectious disease and mental health among incarcerated populations. CSC participated as a federal partner with CIHR on HIV implementation science granting opportunities and entered into a Memorandum of Understanding with CIHR to advance research in HIV and other STBBIs in incarcerated populations.
Canadian HIV Vaccine Initiative (CHVI)
| Name of horizontal initiative | CHVI |
|---|---|
Name of lead department |
PHAC |
Federal partner organizations |
HC; Innovation, Science and Economic Development Canada (ISED); Global Affairs Canada (GAC); and CIHR |
Non-federal and non-governmental partners |
Non-governmental stakeholders, including research institutions and not-for-profit community organizations |
Start date of the horizontal initiative |
February 20, 2007 |
End date of the horizontal initiative |
March 31, 2017 |
Total federal funding allocated (start to end date) (dollars) |
$111,000,000 |
Funding contributed by non-federal and non-governmental partners (dollars) |
N/A |
Description of the horizontal initiative Objectives:
Why this HI is Necessary: Intervention Method: |
|
Shared outcomes Immediate (one–three years) Outcomes:
Intermediate Outcomes:
Long-term Outcome |
|
Governance structures
|
|
Performance highlights
|
|
Comments on variances: N/A |
|
Results achieved by non-federal and non-governmental partners |
N/A |
Contact information Marc-André Gaudreau |
|
Federal Organizations |
Link to Organization's Program |
Contributing programs and activities |
Total allocation (from start date to end date) (dollars)Footnote k |
2015–16 (dollars) |
|||
|---|---|---|---|---|---|---|---|
Planned spending |
Actual spending |
Expected results |
Actual results against targets |
||||
PHAC |
Health Promotion and Disease Prevention |
Healthy Communities |
18,000,000 |
1,231,978 |
1,049,142 |
||
HC |
Internal Services |
Governance and Management Support Services |
1,000,000 |
0 |
0 |
||
Health Products |
Regulatory Capacity Building Program for HIV Vaccines |
4,000,000 |
1,042,000 |
941,130 |
|||
ISED |
Commerciali-zation and Research and Development Capacity in Targeted Canadian Industries |
Industrial Research Assistance Program's Canadian HIV Technology Development Component |
13,000,000 |
2,500,000 |
2,314,831 |
||
GAC |
Global Engagement and Strategic Policy |
International Development Assistance Program |
60,000,000 |
2,400,000 |
2,400,000 |
||
CIHR |
Health and Health Services Advances |
Institute Strategic Advances – HIV/AIDS |
15,000,000 |
1,660,000 |
1,788,599 |
||
Total for all federal organizations |
111,000,000 |
8,833,978 |
8,493,702 |
N/A |
|||
|
|||||||
Expected and actual results achieved for 2015–16:
ER 1.1: Continue to support domestic and international efforts related to the research and development of an HIV vaccine.
AR 1.1: PHAC supported and participated in national and international meetings of researchers, funders, policy makers, community stakeholders and advocates from around the world to ensure greater joint planning, opportunities for collaboration, the identification of priorities for future HIV vaccine research, increasing research capacity, and community awareness.
ER 1.2: Support the continued work of the Alliance Coordinating Office (ACO) to establish a strong and vibrant network of HIV vaccine researchers and other vaccine researchers both in Canada and internationally.
AR 1.2: In an effort to promote collaboration, information exchange and increase awareness, the ACO delivered presentations, including 5 webinars to diverse national and international stakeholders to discuss scientific advances and gaps in HIV vaccine research. PHAC supported the maintenance of a virtual community.
To help support the next generation of HIV vaccine researchers and raise the priority of vaccine research training nationally, the ACO collaborated with partner organizations to coordinate priority training opportunities for New and Early Career Investigators which resulted in four workshops and four scholarships. To further define and advance research and development tools PHAC collaborated with global HIV vaccine stakeholders.
The ACO hosted a satellite at the International AIDS Society Conference in Vancouver in July 2015, entitled “Mucosal Immunology Research in Canada: Collaborative Contributions to the Field”.
ER 1.3: Enable effective communications, strategic planning, coordination, reporting and evaluation within the Government of Canada.
AR 1.3: PHAC continued to lead and coordinate CHVI Partner meetings. The meetings were successful in ensuring effective communications among Partners, and enabling the development of sound policy advice on CHVI related issues based on Partner direction and feedback.
PHAC was the focal point for implementing CHVI’s horizontal performance measurement strategy. That included collecting performance information and reporting on results achieved for parliamentarians as well as internally to enable strategic planning, priority-setting, and decision-making. PHAC also coordinated and submitted a response to the annual global HIV prevention research investment report.
ER 1.4: Lead interdepartmental activities related to determining the future of the CHVI.
AR 1.4: To guide future Government of Canada approaches to addressing HIV/AIDS prevention and treatment, including vaccine research, PHAC engaged its CHVI federal partners to document the partnerships and collaborations created as a result of CHVI investments to-date. A draft report was developed and is planned to be released in 2016–17.
ER 2.1: Increased regulatory convergence and exchange of domestic and international best practices, policies and protocols related to the regulation of vaccines, with a focus on HIV/AIDS vaccines.
AR 2.1: In collaboration with the WHO, HC delivered regulatory training in two PAHO countries (Chile and Trinidad & Tobago), sponsored 11 participants from 11 countries for the Chile workshop, and 13 participants from 6 countries for the Trinidad & Tobago workshop.
HC ensured that CHVI activities remain relevant, creative and innovative in the Canadian and global HIV vaccine research landscape by providing valuable opportunities to connect with stakeholders in the HIV research community to explore new avenues for regulatory capacity building; and ensuring that the CHVI regulatory capacity building program is complementary to existing initiatives, HC presented a poster entitled “Regulatory Capacity Building under the Canadian HIV Vaccine Initiative: Addressing Challenges of Developing National Regulatory Authorities”, at the Canadian Association for HIV/AIDS Research Conference outlining their process and lessons learned
HC also supported the WHO to transition the African Vaccines Regulatory Forum virtual platform to the WHO. In addition, a pilot platform was set up with Ghana, Uganda, Cameroon & Sierra Leone.
ER 2.2: Increased regulatory readiness and strengthened capacity of regulatory authorities in LMICs in the area of vaccine products and clinical trials through training and the establishment of a mentorship program.
AR 2.2: To promote regulatory readiness and strengthen regulatory authority capacity, HC sponsored 29 participants from 29 countries from Africa, Latin America, Asia and Eastern Europe to participate in HC’s Health Products and Food Branch-International Regulatory Forum.
The forum has become internationally recognized among peers for the quality of its content and presenters.
ER 3.1: New and innovative technologies for prevention, treatment and diagnosis of HIV in pre-commercial development are advanced at small-and medium-sized enterprises operating in Canada.
AR 3.1: Continued advancement in the development of new and innovative technologies for the prevention, treatment and diagnosis of HIV, CHVI continued funding of 12 Canadian HIV Technology Development contribution agreements with SMEs.
ER 4.1: In collaboration with CIHR, CHVI increased capacity and greater involvement and collaboration amongst researchers working in HIV vaccine discovery and social research in Canada and in Low and Middle Income Countries (LMIC)s.
AR 4.1: A vaccine research project partnered with GAC, and led by Robert Lorway at the University of Manitoba, focused on the socio-cultural aspects of implementing HIV vaccine programs among MSM and female sex workers in Asia and Africa. The Vaccine Acceptability among Stigmatized Populations (VASP) Team developed a research program with selected communities of MSM and female sex workers at three culturally contrasting sites: in Sichuan Province, China; in Karnataka State, India; and in the District of Nairobi, Kenya.
Investigators report that this study adds to the limited body of literature focusing on future HIV vaccine acceptability in LMICs and highlights some of the several complexities surrounding vaccine acceptability and uptake among key populations in Karnataka, India. The findings reveal a lack of awareness of clinical trials among frontline health service provider participants, suggesting an important area for capacity building and staff development before viable and ethical clinical trials can be set up in the region.
In Kenya, the study argues that unpacking Willingness to Participate in relation to culturally specific legacies of medical research in low- and middle- income countries is not only fundamental to the public health objective of developing a safe, efficacious vaccine but also integral to informing the ethical considerations associated with HIV vaccine dissemination within those very communities whose members will have served as trial participants.
In China, three graduate MSc students in Sichuan University completed their thesis using VASP data. These findings have been translated and findings are currently being prepared for publication.
As part of a $17,000,000 partnership project supported by Global Affairs Canada, CIHR continued to administer funding for five large teams of Canadian and LMIC researchers. Over the past year, these research teams have continued to do capacity-building and collaboration activities amongst researchers working in HIV vaccine discovery and social research in Canada and in LMICs. For example, in 2015–16, graduate students have progressed on the analyses of data concerning vaccine acceptability among stigmatized populations. Their findings are currently being written into peer-reviewed publications.
ER 4.2 : Enhanced knowledge of communities, health care workers, and Ministry of Health staff in LMICs on the prevention of mother-to-child transmission of HIV and maternal, newborn, and child health issues.AR 4.2 : GAC supported the INSPIRE Project, managed by the WHO in Zimbabwe, Malawi and Nigeria ($20,000,000 in 2010–15 with a no-cost extension to March 2017) and the ACCLAIM Project, managed by the Elizabeth Glaser Pediatric AIDS Foundation in Zimbabwe, Swaziland and Uganda ($10,000,000 in 2012–16).
The INSPIRE project trained 614 health care workers across six projects to strengthen their skills in good clinical practices, viral load testing, tracking of missing patients, quality documentation, epidemiology, implementation research science, and Prevention of Mother-To-Child Transmission (PMTCT) program delivery. A total of 3,935 health care workers were trained since the study’s inception. 5,119 pregnant women with HIV were enrolled across the six projects.
The INSPIRE Nigeria Partners Meeting was convened by WHO Nigeria Country Office to share INSPIRE Nigeria projects’ “early learning” with international and national partner organizations, academic institutions, and Medical Office of Health representatives.
The International Conference on AIDS and STIs in Africa was held in Harare, Zimbabwe (December 2015). Two INSPIRE project presentations (Zimbabwe and Malawi) and one poster session (Nigeria) were accepted for the approximately 200 people that attended the PMTCT INSPIRE satellite sessions.
In the ACCLAIM project, implementation concluded for all community interventions in all three countries in September 2015. The activities were focused on finalising the implementation of Community Action Plans, community days and peer group interventions.
Community Leaders completed 1,123 community dialogues in 2015–16, bringing the cumulative project total to 12,088 meetings (Zimbabwe, 3,687; Swaziland 1,792; Uganda, 6,609). Six community days were conducted (Swaziland 3; Uganda 3) with a total of 122 completed community days across all three countries since being of the project. In total, 104 peer facilitators were trained. There was high participant retention within the peer group sessions where 92% of male and 88% of female participants completed all four peer group sessions.
In relation to PMTCT outcomes, ACCLAIM clusters reported an increase of 37% from baseline of HIV-exposed infants receiving antiretroviral medications at birth; an increase in antenatal care attendance before 20 weeks of 43% over baseline; and an increase in the percentage of women delivering in health facilities by 33% from baseline.
ER 5.1: Continued knowledge creation and strengthened HIV vaccine research capacity.
AR 5.1: CIHR and its partners continued to fund HIV vaccine research, with several projects completing their grants and reporting significant findings.
Michel Tremblay at Université Laval concluded a study of HIV-1 virus-like particles. These findings demonstrated that HIV-1-based virus-like particles could be used in vaccine strategies aimed at preventing HIV-1 infection.
In partnership with the BMGF, CIHR supported three research projects focused on Mucosal Immunology relevant for HIV Vaccine Research and Development. Combined these three projects supported 28 trainees in 2015–16.
One of the researcher-leads, Dr. Kaushic based at McMaster University, has recently published in the high impact journal, PLoS Pathogens, demonstrating that the genital mucosa has a unique microenvironment whereby estradiol (known to confer protection against HIV and other sexually transmitted infections) enhances CD4+ T cell anti-viral immunity.
Dr. Adam Burgener, Research Scientist with the National Laboratory for HIV Immunology, PHAC, began leading an international team comprised of experts in mucosal immunology, mathematics, proteomics, epidemiology, clinical infectious diseases, and the microbiome. This team utilized techniques, and mathematical modeling, to be able to best predict HIV infection outcome, and their relationship to hormones and hormonal contraceptives. This may uncover valuable targets for HIV-1 prevention and will represent the first study of its kind to incorporate these tools to understand HIV acquisition
To explore novel aspects of HIV susceptibility and approaches to HIV mucosal vaccine development, a collaborative research team brought together HIV immunologists, vaccinologists, and clinical trials experts from longstanding Toronto-Kenya and Toronto-Uganda collaborations, microbial ecologists and community experts. Dr. Rupert Kaul, based at University of Toronto, built on previous research on HIV acquisition in the foreskin, to develop new ways to prevent HIV, and undertook preclinical development of a nanovaccine against HIV.
ER 5.2: Enhanced linkages amongst researchers, stakeholders, and funders.
AR 5.2: CIHR hosted a vaccine workshop, which included 36 participants, linking CIHR funded vaccine researchers, the CHVI Alliance Coordinating Office, GAC and the International AIDS Vaccine Initiative.
The workshop reviewed current investments in vaccine research for HIV through CIHR, conducted a comparative analysis of vaccines and other biomedical prevention strategies, and identify priority areas for future potential investments in HIV vaccine research in Canada. The workshop was guided by a steering committee comprised of HIV research experts and stakeholders.
In addition to supporting research through the CHVI, CIHR supported an additional $3,600,000 in HIV Vaccine Research projects.Internal Audits and Evaluations
Internal Audits Completed in 2015–16
Complete Audit Reports are available online.
| Title of Internal Audit | Internal Audit Type | Completion Date |
|---|---|---|
| Audit of Shared Accountability in Interdepartmental Service Arrangements | Governance, Risk Management, Internal Controls | August 2015 |
| Audit of Key Financial Controls – Year 2 | Internal Controls | April 2015 |
| Audit of Key Financial Controls – Year 3 | Internal Controls | November 2015 |
| Audit of Maternal and Child Health Programs | Governance, Risk Management, Internal Controls | January 2016 |
Audit of the Project Management Framework |
Governance, Risk Management, Internal Controls | April 2015 |
Audit of Risk Management Framework |
Governance, Risk Management, Internal Controls | April 2015 |
| Audit of Procurement and Contracting | Governance, Risk Management, Internal Controls | July 2015 |
Evaluations in Progress or Completed in 2015–16
Complete Evaluation Reports are available online.
| Title of the Evaluation | Status | Deputy head approval date | Link to Organization’s Program |
|---|---|---|---|
| Evaluation of Travel Health and Border Security | Completed | July 2015 |
|
| Evaluation of Tuberculosis Activities | Completed | August 2015 | 1.2 Health Promotion and Disease Prevention |
| Evaluation of Non-Enteric Zoonotic Infectious Disease Activities | Completed | March 2016 | 1.2 Health Promotion and Disease Prevention |
| Evaluation of Community Action Program for Children, the Canadian Prenatal Nutrition Program and Associated Activities | Completed | March 2016 | 1.2 Health Promotion and Disease Prevention |
Response to Parliamentary Committees and External Audits
| Response to parliamentary committees |
|---|
Standing Committee on Justice and Human Rights On May 8, 2015, the Report of the Standing Committee on Justice and Human Rights entitled Study of the Subject Matter of Bill C-583; An Act to amend the Criminal Code (fetal alcohol spectrum disorder) was tabled in the House of Commons. The Report summarizes the testimony and briefs, presents the Committee’s findings, and includes seven recommendations that identifies where the federal government could take further action to address fetal alcohol spectrum disorder (FASD). The Government Response to the Report was tabled in the House of Commons on June 19, 2015. The response highlights the Government’s key activities related to FASD and demonstrates the Government’s commitment to working with Provinces, Territories and stakeholders to address FASD-related issues among vulnerable populations, including support to those suffering from FASD and their families, and those along the criminal justice continuum. The Government supports the spirit of the Report’s recommendations. The response consists of a letter to the Chair of the Committee that addresses each of the recommendations and outlines key federal positions and activities on FASD. |
Response to the Auditor General (including to the Commissioner of the Environment and Sustainable Development) |
Office of the Auditor General – Audit of Federal Anti-Microbial Resistance (AMR) Prevention and Control Objective: To determine whether PHAC and HC fulfilled key responsibilities to mitigate the public health risks posed by the emergence and spread of antimicrobial resistance in Canada. |
Response to external audits conducted by the Public Service Commission of Canada or the Office of the Commissioner of Official Languages |
Office of the Procurement Ombudsman – Review of government-wide procurement practices regarding standing offers and supply arrangements Objective: The objective of this review was to determine whether departmental contracts issued against standing offers and supply arrangements were consistent with applicable sections of the Treasury Board Contracting Policy, the Financial Administration Act and regulations made under it, and support the principles of fairness, openness and transparency. Objective: To examine the framework in place that governs the use of portable electronic storage devices, with the objective of contributing to enhancing privacy protections. |
Status Report on Projects Operating with Specific Treasury Board Approval
| Project Name and Project Phase | Original estimated Total Cost (dollars) | Revised Estimated Total Cost (dollars) | Actual total cost (dollars) |
2015–16 (dollars) | Expected date of close-out | |||
|---|---|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total authorities | Actual Spending | |||||
| 1.3.3 Sub-Program Biosecurity | ||||||||
| Human Pathogens and Toxins Biosafety/Biosecurity Program | 12,394,200 | 12,394,200 | 12,200,228 | 0 | 1,897,472 | 1,897,472 | 1,517,187 | 2016 |
| Single Window | 5,090,000 | 5,090,000 | 2,086,835 | 1,006,560 | 1,006,560 | 1,006,560 | 576,824 | 2017 |
Footnotes
Page details
- Date modified: