
Public Health Agency of Canada 2020-21 Departmental Results Report

Download in PDF format
(2.70 MB, 100 pages)
Organization: Public Health Agency of Canada
Date published: February 2022
ISSN: 2561-1410
Table of Contents
- From the Ministers
- Results at a glance
- Core Responsibilities Results: what we achieved
- Analysis of trends in spending and human resources
- Corporate information
- Supporting information on the program inventory
- Supplementary information tables
- Federal tax expenditures
- Organizational contact information
- Appendix: definitions
From the Ministers


The COVID-19 pandemic is one of the largest global crises we have faced in our lifetime. It has caused significant loss of life, mental distress, and social and economic instability. Yet, despite the tragedies and challenges, Canadians have consistently demonstrated resilience, creativity and compassion.
We have found new ways of working, new ways of connecting with family and friends, and new ways of celebrating successes and grieving loss. As the Minister of Health and Minister of Mental Health and Addictions and Associate Minister of Health, we want to take this moment to acknowledge and thank all Canadians and Indigenous Peoples for their significant and collective efforts in response to the pandemic.
We also want to share our deep appreciation for the dedication of our researchers, public health experts, healthcare workers, and public servants who have worked tirelessly in order to provide science-based advice and implement unprecedented measures to respond to this pandemic.
We would also like to thank our provincial and territorial colleagues and industry partners. From the outset of the pandemic it was clear that we needed a Team Canada approach in order to mount a successful response to this crisis.
The 2020–21 Departmental Results Report for the Public Health Agency of Canada (PHAC) outlines PHAC’s achievements over the past fiscal year. Working in an unpredictable and high-stakes environment, PHAC employees accomplished many remarkable achievements over the past year. As the location of the Immunization National Operations Center for the vaccination program, PHAC acted as the central hub for the largest immunization program in our history. PHAC worked closely with Public Services and Procurement Canada (PSPC) to secure and distribute one of the most diverse portfolios of vaccines in the world in order to achieve the ultimate goal of reducing hospitalizations and slowing the spread of COVID-19.
PHAC also worked with PSPC to secure and distribute millions of pieces of personal protective equipment and other supplies to provincial and territorial partners and partnered with provinces and territories to: facilitate national surveillance of COVID-19; develop testing methodologies and strengthen testing capacity across Canada; and develop and implement public health procedures for our international borders.
Communicating directly—and frequently—with Canadians has been crucial during this pandemic.
As our knowledge and understanding of the virus increased, PHAC diligently developed and revised public health measures and guidance to ensure that Canadians, governments and businesses had the tools and advice they needed to stay safe. Throughout the evolution of the pandemic, PHAC has demonstrated a readiness to shift direction and adjust strategy as the science evolved.
A notable challenge of COVID-19 has been that health inequities across Canada have worsened and become more apparent. As the Chief Public Health Officers’ 2020 Report outlined, the health impacts of COVID-19 have been worse for seniors, essential workers, racialized populations, people living with disabilities and women. Throughout the pandemic, PHAC has worked to ensure that equity was at the heart of their advice, in particular our vaccination programs, and that we continued to support community organizations serving our most vulnerable. For example, PHAC supported distress centres with increased funding during the pandemic to address the parallel pandemic of mental health problems, increasing substance use and the deadly toxic drug supply. We have supported municipalities to secure safe, voluntary isolation sites for those without access to a safe place to self-isolate as we continue to recognize the importance of health equity to the health security of the entire country.
Reflecting on the past year, we have faced many difficult decisions in an ever-changing environment. As this pandemic presents us with new challenges, PHAC will continue building on lessons learned in order to improve the Agency’s emergency management response and seize opportunities to strengthen public health in Canada.
We would like to once again acknowledge the dedication of PHAC’s employees for steering us through these extraordinary times. We take great pride in their commitment to protecting the health and safety of Canadians.
We would also like to reiterate our gratitude to Canadians and our provincial, territorial and Indigenous partners for their continued commitment and compassion. We will get through this together.
The Honourable Jean-Yves Duclos, P.C., M.P.
Minister of Health
The Honourable Carolyn Bennett M.D., P.C., M.P.
Minister of Mental Health and Addictions and Associate Minister of Health
PHAC acknowledges that this report was written on the traditional, unceded territory of the Algonquin Anishinabeg Nation.
Results at a glance
Spotlight on PHAC's COVID-19 response
On March 11, 2020, the World Health Organization declared COVID-19 a global pandemic. PHAC took center stage in leading the largest federal public health response in Canadian history, in collaboration with provinces, territories, Indigenous communities and other federal government departments. From the outset, PHAC recognized the need for a collective and integrated approach to responding to COVID-19 and the need to be flexible and agile in order to respond to evolving science. The Agency stood up and built on its emergency operations center to coordinate and execute pandemic response efforts, which included maintaining and leveraging effective partnerships and collaboration between federal departments and other jurisdictions. This coordination resulted in the identification of various priorities which were outlined in Canada's Federal/Provincial/Territorial Public Health Response Plan for Ongoing Management of COVID-19. Building on these priorities, PHAC coordinated its efforts around the following ten COVID-19 Priority Areas, ensuring that appropriate synergies were realized within and across these priorities.
Priority: Health system capacity
Purpose: Build public health system capacity, increasing the ability to address public health needs of the population.
The Federal Health Portfolio Operations Centre (HPOC), located within PHAC, served as the Health Portfolio's focal point for the coordination of COVID-19 pandemic response efforts through a dedicated network of public health emergency response specialists. HPOC's work included the mobilization of significant human and financial resources. In particular, to support PHAC's COVID-19 response, surge support was urgently needed to effectively implement COVID-19 public health measures. As such, PHAC undertook responsibility for:
- Activating the Federal/Provincial/Territorial governance structure (Jan 2020) as outlined under the Public Health Response Plan for Biological Events to facilitate the formal engagement and coordination on emerging issues that require a high level response;
- Expediting the hiring, training and deployment of new screening officers and quarantine officers to meet the rapidly growing public health demand;
- Repositioning some Environmental Health Officers from the field to land points of entry;
- Conducting site visits of government-authorized accommodations and temporary foreign worker accommodations to ensure that public health measures were being implemented at those sites;
- Providing required training to 852 Compliance Verification Officer trainees (i.e., 290 call centre staff and 562 on-site security officers), 320 public health officer trainees at our borders, comprised of Screening Officers, Clinical Screening Officers, Quarantine Officer and support officers;
- Ensuring that 32 of the 36 identified ports of entry had PHAC physical presence; and
- Maintaining a staff complement of between 49 and 120 PHAC employees on site at all times, with additional staff available to provide health and quarantine assessments and assistance by phone 24/7.
PHAC's compliance promotion and enforcement efforts contributed to supporting health system capacity. PHAC developed guidance and a training curriculum on the promotion and enforcement of the Quarantine Act, increased compliance and enforcement capacity and implemented a compliance verification protocol for travellers entering Canada. PHAC established an on-site compliance verification program to conduct on-site visits with travellers in quarantine and Canadians staying at voluntary isolation sites to verify and improve compliance with the Quarantine Act, which included contracting, training and designating more than 500 security firm officers. Between January 29, 2021 and March 31, 2021, this program completed 136,226 visits. This program also completed 950,000 live verification calls that were made between September 28, 2020 and March 31, 2021 and 804,981 automated calls that were made between December 17, 2020 and March 31, 2021.
PHAC increased engagement with the Royal Canadian Mounted Police and other police partners across Canada to support the verification and enforcement activities related to the Quarantine Act and its Emergency Orders, including the development and dissemination of a reference guide to support police officers in appropriately enforcing the Quarantine Act. In order to maintain air travel safety, the Agency established capacity to issue tickets under the Contraventions Act in 2021 to travellers who were not compliant with the mandatory testing requirements (i.e., failure to provide a pre-departure test; failure to go to a government-authorized accommodation (GAA) and/or designated quarantine facility when required and/or directed). Enforcement through ticketing was limited to the provinces and territories signatory to the Contraventions Act. PHAC worked with law enforcement partners in all provinces and territories to verify compliance with quarantine requirements. In total PHAC made 1,228,709 referrals to law enforcement in provinces and territories, including 54,088 high or urgent priority referrals.
In addition to bolstering federal resources, PHAC worked with Health Canada to establish the COVID-19 Public Health Rapid Surge Capacity initiative to assist provinces and territories in managing the impacts of COVID-19 outbreaks when their needs exceeded their capacity. This included support on outbreak management, testing and contact tracing, as well as the procurement of PPE, vaccine ancillary supplies, biomedical equipment and other medical supplies on their behalf.
Between April 2020 and March 2021, PHAC mobilized epidemiologists in response to 34 requests to provide COVID-19 related epidemiological surge support to British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec, New Brunswick, Newfoundland, Nunavut and Northwest Territories. In the same timeframe, in response to 97 requests, infection prevention and control personnel were deployed across British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec, Nova Scotia, and New Brunswick in various settings such as correctional services, designated quarantine sites and hospital networks. Further, PHAC placed a total of 24 Public Health Officers from the Canadian Public Health Service in the provinces and territories to support joint federal, provincial and territorial COVID-19 response efforts which included surveillance, the vaccine roll-out and providing evidence to inform public health actions.
PHAC has also been able to provide testing services across multiple jurisdictions through the National Microbiology Laboratory (NML). NML has five surge laboratories across Canada that have supported provinces and territories with COVID-19 testing. In addition, NML currently has two mobile laboratory trucks available for COVID-19 testing.
In September 2020, the Safe Voluntary Isolation Sites Program (SVISP) was launched, which aims to decrease community transmission of COVID-19 by providing space for individuals who are unable to safely self-isolate due to crowded housing conditions and/or resource constraints. The program is one of the COVID-19 surge supports for provinces and territories. Between September 2020 and March 2021, the Government of Canada funded isolation sites in 18 different communities across Canada.
Priority: Public health measures guidance
Purpose: Minimize transmission through timely provision of technical guidance and advice on public health measures, with a consistent pan-Canadian approach to implementing and lifting measures.
In consultation with federal, provincial and territorial partners, various government departments, Indigenous stakeholders, external stakeholders and public health experts, PHAC developed and revised technical guidance documents on different Public Health Measures (PHM) in response to evolving scientific evidence in order to mitigate the spread of COVID-19 at the individual level or in community settings. PHAC based this guidance on the best current scientific knowledge, expert opinions and established public health practices. This resulted in the development of and updates to 14 guidance products on the use of PHM to support a coordinated pan-Canadian approach.
For example, guidance on individual and community-based measures to mitigate the spread of COVID-19 and guidance on public health management of cases and contacts associated with COVID-19.
PHAC also developed, revised and maintained several web pages and awareness products to translate PHM technical guidance into practical advice for the general public and operators of different community settings aligned to rapidly evolving scientific evidence. This resulted in the development and updates of 5 risk mitigation tools for different community settings, as well as over 20 other web products, including awareness resources, to promote understanding and adherence to PHMs.
As part of its commitment to openness and transparency, PHAC integrated public health measures guidance into its communications with Canadians to increase awareness and improve public engagement. PHAC also supported the development of printable resources in many languages - on topics such as handwashing, making a mask, and how to isolate - so all Canadians can better understand and take steps to protect themselves and their families, and launched a national public education campaign that provided evidence-based information on COVID-19 that encouraged behaviours that protect individuals and our communities.
In addition to developing general guidance, PHAC provided sector specific guidance and risk mitigation advice, in particular with respect to border measures. This included developing COVID-19 guidance for airlines and air terminals in order to manage the safe operations of these services for essential travel and slow reopening. The Agency also reviewed 135 Risk Mitigation Plans in support of requests for National Interest Exemptions to Canada's border-closure measures.
PHAC supported the Canadian Centre for Occupational Health and Safety in developing and curating a COVID-19 Workplace Web Portal and sector-specific COVID-19 workplace guidance. This guidance portal supplemented supports from the provinces and territories to provide a consistent framework for businesses looking to adapt their operations to protect their employees and customers and adapt to local public health conditions. This portal was visited 115,000 times.
Did you know?
74% of viewers felt that public health measures featured in various Government of Canada ads motivated behaviour change.
PHAC was also responsible for developing outbreak protocols, guidance, risk assessments and capacity building at the federal level in response to COVID-19. This included the development of a COVID-19 Outbreak Response Protocol based on key guiding principles and operating procedures for the identification and response to COVID-19 outbreaks. In collaboration with provincial and territorial outbreak partners, PHAC contributed to developing a consolidated "Operational Guidance Collection" and "Evaluating COVID-19 disease transmission and public health measures in schools: Outbreak investigation guidance," technical guidance for epidemiological methods for investigating COVID-19 outbreaks in schools which provided access to various tools and guidance documents (e.g., questionnaires, outbreak definitions).
Priority: Communications and outreach
Purpose: Engage and mobilize Canadians to make decisions and adopt behaviours that support pandemic control.
Clear and transparent communications with Canadians about the pandemic continues to be essential to maintaining trust and encouraging the adoption of behaviours that reduce the spread and severe outcomes of COVID-19. Despite a continuously changing environment and evolving science, PHAC committed to providing real-time information through frequent public updates and the provision of crucial public health guidance. For instance, PHAC delivered:
- An average of 3 news conferences weekly with the Chief Public Health Officer (CPHO);
- Daily statements and timely announcements by the CPHO;
- 7,600 media responses;
- Messaging and communications products to support the dissemination of information on epidemiology, public health measures, modelling, vaccines, testing and therapeutics;
- Public education and advertising campaigns promoting public health measures, including the ArriveCAN app;
- 8,512 social media account posts from the CPHO;
- 19,512 social media account posts from PHAC's Healthy Canadians account;
- 448,690 COVID information line queries and 58,670 ArriveCAN toll free calls received and responded to; and
- 80,246 Government Authorized Accommodations toll free calls answered.
Did you know?
PHAC partnered with Environment and Climate Change Canada to include a link from their WeatherCAN app to COVIDTrends. Since the launch of COVIDTrends, there have been 1,590,333 visits, and 89% of them came via the WeatherCAN link. COVIDTrends is a tool that provides summary data about COVID-19 in a particular area. When searching by municipality (city, town), or by the first 3 characters of a postal code, data from the associated health region will appear. Between its launch on September 28, 2020 and March 31, 2021, COVIDTrends received 798,672 visits with an average of 4,317 visits per day. There were 394,985 visitors to COVIDTrends during this time period.
PHAC worked closely with provinces, territories and other stakeholders to inform Canadians of public health measures, to help reduce the spread and importation of COVID-19 and the importance of vaccination against COVID-19 as a preventative measure. To raise awareness of public health guidance and recommendations among Canadians during the pandemic, PHAC developed numerous reference documents such as infographics, videos and fact sheets in over thirty languages.
PHAC used innovative communications methods to provide critical COVID-19 information to Canadians, which included developing and launching an online Virtual Assistant tool on Canada.ca that kept 1.28 million users [(55,800 email subscribers)] informed when new COVID-19 topics or updates were added to the site. To complement paid digital advertising, PHAC produced organic social media, publishing over 11,000 messages on, or related to, COVID-19, which resulted in 728 million impressions and 4.4 million visits to Canada.ca's web content. In addition, PHAC answered 490,839 calls to the dedicated COVID-19 toll-free information line, 19,491 calls to the general toll-free information line and provided interpretation services to over 175 callers. PHAC expanded the Canada.ca/coronavirus website to include a horizontal whole-of-government approach, enabling greater access for Canadians seeking COVID-19 related information, including vaccination and financial programs from a single site (e.g., 10,130,939 web visits to health-themed content on Canada.ca/coronavirus).
To encourage vaccine uptake among Canadians and dispel vaccine misinformation, PHAC launched an educational awareness campaign to increase public access to reliable, accurate and timely information about vaccines. PHAC's educational awareness campaign had 39,023,310 impressions and 708,341 click-throughs. Recognizing that Government is not always the "go to" source for information, PHAC also launched a Call for Proposals to fund community organizations to provide information on vaccines. It is anticipated that projects funded through this call for proposals will begin in summer 2021.
PHAC also launched a multi-faceted and multi-departmental communications campaign to provide travellers with guidance on COVID-19 testing and quarantine requirements prior to and upon arrival at air and land points of entry. In addition to promoting this campaign on websites and social media, PHAC produced and distributed 50 communications products, which included travel health notices, handouts, digital posters and infographics.
Priority: Borders and quarantine
Purpose: Protecting the health and safety of Canadians through safe, responsible and compassionate management of the shared border with the United States and other ports of entry facilitating international travel into Canada.
In 2020-21, PHAC sustained and evolved robust border measures to reduce the importation and spread of COVID-19 and variants of concerns in Canada. Throughout the year, PHAC developed and operationalized 38 Emergency Orders in Council (OIC) under the Quarantine Act to prohibit entry into Canada and require mandatory quarantine, isolation and other obligations. PHAC also ensured that necessary public health screening(s)/quarantine requirements and coordination were aligned with new OICs (e.g., pre-departure testing).
In partnership with Transport Canada, PHAC was able to monitor and assess country by country epidemiological situations. This collaboration enabled the Agency to take timely action in limiting the risk of importation by imposing various measures such as Notices to Airmen (NOTAM) when needed. PHAC also collaborated with Transport Canada on the air industry's voluntary suspension of flights to sun destinations and funneling international arrivals through four main airports (Vancouver, Calgary, Toronto and Montreal).
Working in partnership with key departments and agencies, PHAC planned and implemented a range of evidence-based adjustments to border measures that aimed to mitigate public health risks. These adjustments were planned and implemented while continuing to facilitate essential cross-border trade, movement of essential workers, family reunification and entry for compassionate reasons. PHAC also worked with other federal departments and provinces and territories to facilitate essential cross-border activities by persons in geographically remote areas and the safe entry of international students. It is important to note that these borders measures were made possible through an enduring and extremely collaborative partnership with the Canada Border Services Agency (CBSA) and their front line Border Services Officers who were Canada's first line of defence and service to returning Canadians and international travellers.
Effectively protecting Canada's borders meant efficiently collaborating with partners and stakeholders. Working with other government departments, PHAC initiated the development of a high-level framework for Canada's COVID-19 Border Strategy to support economic/social reopening through a gradual and phased approach to easing border measures that was accompanied by measures to mitigate importation of COVID-19 and public health risks. The Agency was further informed through its use of indicators, which allowed PHAC to monitor and assess whether to pause or proceed to the next phase. PHAC also coordinated with its Legal Services on a number of COVID-19 travel health, border measures and quarantine judicial reviews filed against the Crown and Government of Canada.
PHAC undertook and supported multi-pronged approaches to ensure that measures were available to support the mandatory quarantine of incoming travelers. This included the establishment and management of 13 designated federal quarantine facilities at nine locations across Canada and the use of two provincial/territorial sites in Manitoba and Yukon to lodge 5,075 travellers between October 1, 2020 and March 31, 2021. PHAC also established 59 privately managed government-authorized accommodations near the Calgary, Vancouver, Toronto and Montreal international airports.
In April 2020, PHAC and CBSA launched ArriveCAN to facilitate the collection of relevant data for international travellers arriving into Canada by land, air, or marine vessel. This mandatory, integrated digital tool collects information from incoming travellers to Canada and is available as a mobile app or by signing in online. Traveller data submitted in ArriveCAN-including information on contact and travel details, travel history, pre-entry COVID test results and proof of COVID-19 vaccination-is critical in managing Canada's health security and to inform reporting on key border data measures. By leveraging ArriveCAN on digital platforms, the use of the paper form is reduced, which reduces points of contact and enables timelier sharing of essential public health information to the provinces and territories. The ArriveCAN app was used by over 85% of travellers arriving by air and almost 20% of travellers arriving by land, including essential workers. A Quarantine Case Management System was also developed to further modernize the way traveller information was collected and actioned, supporting tracking, monitoring and reporting in real-time.
PHAC also established a national testing perimeter that included the capability to provide genetic sequencing of positive cases for the detection of variants of concern with the assistance of the Canadian Red Cross:
- Effective February 22, 2021, self-swab test kits were handed out to travellers at 112 land Ports of Entry (PoE) for at-home testing and on-site testing operations began at five high-volume land PoE;
- On March 4, 2021, an additional 11 high-volume land PoE began on-site testing operations; and
- Between March 5, 2021 and March 31, 2021 more than 23,000 tests were completed at air and land borders.
PHAC also worked with key federal government partners to establish four alternate testing protocols in March 2021 with the provinces of Manitoba, New Brunswick, Nova Scotia and Prince Edward Island to support the administration of testing by provincial health authorities for temporary foreign workers in the agriculture, agri-food and seafood sectors destined for these provinces.
Priority: Testing and contact tracing
Purpose: Testing and contact tracing capacity is sufficient to control transmission rates and to ensure chains of transmission are disrupted, supporting the safe lifting of restrictive public health measures.
Throughout 2020-21, PHAC remained at the forefront of providing federal testing support services, including working with PSPC to procure testing supplies and equipment to meet the demand for COVID-19 testing nationwide (i.e., provincial, territorial, northern, remote and isolated communities). The Agency delivered upwards of $1 billion dollars in supplies, equipment and services to governments and labs across the country over the course of the year. This included securing on-going testing supplies (e.g., reagents, plastics and swabs) to increase national supply levels and meet Canada's COVID-19 testing needs. Notably, through the Northern, Remote and Isolated (NRI) Initiative, PHAC contributed to reducing health inequities by increasing access to diagnostic testing through:
- The establishment of 234 NRI testing sites across Canada;
- The deployment of 419 testing devices;
- The delivery of 110 training sessions; and
- The distribution of 65,000 GeneXpert COVID tests and 40,000 ID Now COVID tests to NRI Communities.
Working in partnership with Environment and Climate Change Canada, the Canadian Food Inspection Agency and the Department of Fisheries and Oceans Canada, PHAC established five surge laboratories to provide accredited COVID-19 testing across the country (locations). These sites provided additional support for provinces and territories as well as for border testing. As a result of these efforts:
- 150 staff have been trained remotely;
- 4 robotic systems have been implemented to increase testing throughout; and
- Just under 100,000 tests were performed by March 31, 2021, including more than 25,000 land borders tests.
At the beginning of the pandemic, there was no centralized tool available to collect data on COVID-19 testing at the national level. In order to scale up testing capacity quickly and efficiently distribute supplies to address rapidly changing disease dynamics, a national picture of testing in Canada was needed. PHAC established a System for Analysis of Laboratory Tests (SALT) to capture COVID-19 testing data from all provincial public health laboratories to summarize provincial testing data and provide the total COVID-19 tests conducted in Canada. Developed by the Canadian Network for Public Health Intelligence (CNPHI) in partnership with the Canadian Public Health Laboratory Network, SALT leveraged CNPHI's online platform to collect the testing data from across the country and allow epidemiologists and decision makers to visualize and analyze the data. The data collected from provincial partners was shared in the form of reports with public health stakeholders and was used to inform decision making about testing strategies and procurement.
PHAC's NML not only developed the original protocol for testing for COVID-19 in Canada, but also demonstrated national leadership through the provision of COVID-19 guidance on various testing technologies, including the use of rapid antigen tests, indications for screening and testing and repeated Polymerase Chain Reaction (PCR) testing in previously COVID-19 positive individuals. This included working with private sector companies to validate methodologies and doing quality assurance on testing products as they were delivered in order to ensure that products being shipped to provinces and territories were ready to use.
As the federal government and other public health partners rapidly scaled up their contact tracing workforce, in October 2020 and in partnership with Health Canada, PHAC released a series of free online learning modules to support COVID-19 contact tracing efforts across the country. Since then, over 10,000 registrants have enrolled online to access the courses.
Priority: Vulnerable populations and community support
Purpose: Support populations most at-risk from COVID-19 in taking action to reduce their risks.
In addition to public health guidance and equity based vaccine allocation, PHAC developed and implemented the Safe Voluntary Isolation Sites Program to support the most vulnerable in being able to take action to protect themselves and their families. The Safe Voluntary Isolation Program contributed to reducing the risks of spreading the virus among household contacts, both in Canada's densely populated urban centres, as well as in locations where people are faced with crowded housing and resource constraints. PHAC provided $100 million in funding over two years which helped to establish a total of 24 voluntary isolation sites across 18 communities in Ontario and Saskatchewan by March 31, 2021.
Mindful that the risks presented by the pandemic are not restricted to physical health, PHAC also worked with Health Canada to provide expertise and advice on establishing virtual mental health and substance use supports and services for Canadians during the pandemic. Specifically, the Wellness Together Canada (WTC) portal provides free and confidential online mental health and substance use supports accessible 24/7 to individuals across Canada in both official languages. Through the portal, individuals have immediate access to a range of supports that include assessments, self-guided programming, peer-support and counselling. WTC has essentially eliminated wait times for clients and, as a virtual tool, provides access to all Canadians regardless of their location.
As call volumes and service demands at local, regional and national distress centres across Canada significantly increased during the COVID-19 pandemic, PHAC urgently mobilized support to expand the capacity and enhance the viability of eligible distress centres by:
- Investing $7.5 million in the Kids Help Phone-to address the surge in demand for mental health support for children and youth; and
- Providing $9.275 million in funding to 587 distress centres across Canada, including organizations that provide crisis support for specific populations such as seniors, Indigenous communities, LGBTQI2S+ populations and racially and linguistically diverse communities.
Did you know?
To better support young people during the pandemic, the Kids Help Phone provided young people with immediate access to mental health support over the phone and via text.
PHAC has also leveraged data to continue to drive progress in policy and programming to improve the health and well-being of vulnerable populations. For example, the Pan-Canadian Health Inequalities Reporting Initiative developed methodology to combine census data with COVID-19 deaths. Results are available by sex, income, ethno-cultural concentration, urban geography, dwelling type and size, and living arrangement. The results have been summarized and released in a "Social inequalities in COVID-19 deaths in Canada" report on the Government of Canada's COVID data trends web page. The underlying analysis helped facilitate the inclusion of identity factors into policy and program development, notably through a targeted approach to the promotion and distribution of COVID-19 vaccines to minimize mortality and severe health outcomes for the most at-risk populations.
Did you know?
The Chief Public Health Officer's annual report for 2020 focused on equity and health, examining why some groups, such as seniors, workers who provide essential services, racialized populations, people living with disabilities, and women, faced greater risk of contracting COVID-19 and greater risk of experiencing the social and economic impacts of the pandemic. The report underscored the influence of social policies, such as employment conditions (level of income and access to sick leave benefits) safe and affordable housing and access to high quality social and health services, have on health and well-being. This points to the need to align social and economic policy and public health actions to strengthen our pandemic efforts and support health equity.
Priority: Personal Protective Equipment (PPE), medical equipment, and national emergency strategic stockpile
Purpose: The National Emergency Strategic Stockpile has sufficient supply of PPE and other medical supplies and equipment to meet provincial and territorial needs.
The novel nature of COVID-19 and global spread of the virus drove unparalleled demand for medical supplies, which initially resulted in an extraordinary global shortage of key medical equipment and supplies. The role of the National Emergency Strategic Stockpile (NESS) is to provide surge capacity to provinces and territories at their request when their own supplies are not sufficient, and it is the sole provider of certain vaccines or antidotes required for rare public health emergencies. The NESS contains medical supplies (e.g., PPE) and equipment (e.g. ventilators); pharmaceuticals; and social service supplies (e.g., beds, blankets). While the NESS has long held supplies for requested surge supports to respond to public health emergencies, it was not designed to be a primary supplier of medical supplies in an emergency.
To support the needs of Canada's frontline healthcare response, PHAC, in coordination with other federal government departments, provinces and territories, took aggressive and unprecedented action to address these challenges, including significant bulk procurement of key medical supplies on behalf of provinces and territories.
In April 2020, the Allocation of Scare Resources - COVID-19 Interim Response Strategy was endorsed by federal, provincial, and territorial Ministers of Health, which formalized how supplies received under bulk procurement would be allocated. The proactive allocation of scarce resources allocated 80% of purchased products to the provinces and territories proportionate to respective populations, 18% to the NESS, and 2% allocated to Indigenous Services Canada for Indigenous peoples.
Since the start of the pandemic, PHAC acquired over 3.5 billion units of PPE, medical equipment and supplies, distributed over 892 million units to provinces and territories and responded to 99 Requests for Assistance for urgent needs from provinces and territories. PHAC also established an eight week supply of five key PPE commodities, including N95 respirators, surgical masks, face shield, gowns, and nitrile gloves. The NESS stockpile of biomedical equipment, such as ventilators and high flow nasal oxygen devices, necessary to support and monitor hospitalized patients with respiratory distress caused by COVID-19 was also significantly expanded.
To accommodate the tremendous volume of medical supplies and equipment, PHAC expanded the number of sites from eight federally managed warehouses to 19 warehouses. This represented an increase of approximately 167,000 square meters of dedicated storage capacity through temporary warehousing and third-party logistics solutions to manage and efficiently deliver the exceptional volume of health assets. In addition, PHAC rapidly established capacity to undertake robust quality assurance processes to ensure that medical supplies and equipment distributed by PHAC met appropriate performance standards.
As part of the strategy to address shortages, PHAC worked closely with Innovation, Science and Economic Development (ISED) and PSPC to engage a diverse set of new suppliers and manufacturers both internationally and through the Government of Canada's domestic "Call to Action" to increase domestic production of needed PPE and medical equipment. PSPC streamlined procurement processes and strategies to facilitate the timely awarding of contracts and over 300 contracts were issued for medical supplies and equipment. The Call to Action, launched on March 20, 2020, successfully met its objective to mobilize domestic industry to produce medical supplies and equipment at a time when global supply was highly uncertain and limited.
The Office of the Auditor General (OAG) undertook a performance audit on the Government of Canada's ability to meet the needs of provinces and territories, and the healthcare sector, for PPE and medical devices to respond to the COVID-19 pandemic. The audit period covered January 2020 through to August 31, 2020. The OAG report was made public on May 26, 2021.
Overall, the OAG found that PHAC helped to meet the needs of provincial and territorial governments for PPE and medical devices during the pandemic. The report does however highlight that as a result of long-standing unaddressed problems with the systems and practices in place to manage the NESS, PHAC was not as prepared as it could have been to respond to the needs of provinces and territories for PPE and medical devices.
PHAC has committed to addressing the recommendations from the OAG within one year of the end of the COVID-19 pandemic.
Priority: Vaccines and other medical countermeasures
Purpose: Canadians are protected from COVID-19 as quickly as possible through the development, acquisition, delivery and administration of vaccines and therapeutics, with priority placed on high risk populations.
In partnership with the provinces, territories and Indigenous communities, the Government of Canada is continuing to successfully roll out Canada's COVID-19 immunization campaign, the largest in the country's history. To provide Canadians with access to safe and effective vaccines to protect against COVID-19, PHAC established the Vaccine Roll-out Task Force (VRTF) to deliver on an ambitious plan through a principled and evidence-informed approach that puts protecting the health and safety of Canadians first.
From the outset, PHAC worked with relevant partners to identify the most promising vaccines and therapeutics. In partnership with Innovation, Science and Economic Development, the Health Portfolio set up a Vaccine Task Force (VTF) comprised of Canadian experts from relevant fields to advise the government about which vaccines had the most promise.
Using expert advice from the VTF, PHAC provided recommendations for a diversified vaccine portfolio and the VRTF worked closely with Public Services and Procurement Canada (PSPC) to negotiate and finalize Advance Purchase Agreements (APAs) with vaccine manufacturers to secure early access to a range of COVID-19 vaccine options for Canadians. Overall, Canada has secured access to up to 409 million COVID-19 vaccine doses under these APAs, enough to vaccinate all eligible persons in Canada who want a vaccine.
In addition to procuring vaccines for Canadians, PHAC also contributed to international efforts to ensure global access to COVID-19-related health interventions. This included supporting international mechanisms, such as the COVAX Facility, to secure and redistribute vaccines to the global community to help facilitate equitable access and reduce global spread. PHAC also supported Health Canada in procuring COVID-19 vaccines through the COVAX Facility, a global pooled procurement mechanism and assisted with the initial planning of Canada's ongoing COVID-19 vaccine procurement needs for 2022 and the years following.
PHAC provided public health expertise and worked with the broader vaccination community to facilitate a consistent and equitable approach to developing vaccine administration plans. This included supporting the development of public health plans for vaccination and ensuring Canada's readiness to receive and distribute vaccines and related supplies.
To support smooth delivery and effective deployment of vaccines, the VRTF developed a federal, provincial and territorial allocation framework. As part of these allocation discussions, the VRTF worked in close collaboration with federal, provincial and territorial governments, Indigenous stakeholders (including National Indigenous Organizations and Indigenous regional health authorities), and other key stakeholders to ensure the prioritization of vulnerable populations for early vaccine rollout in the context of limited supply. These populations included the elderly, residents and staff of congregate living arrangements (e.g., care facilities), front line health care workers, people in living or working conditions with elevated risk for infection or disproportionate consequences and Indigenous populations.
As part of the preparatory work for the deployment of vaccines, PHAC also supported the development and publication of vaccine guidance documents by the National Advisory Committee on Immunization (NACI) on the prioritization of vulnerable populations for early vaccination in the context of limited COVID-19 vaccine supply. PHAC also actively monitored, collected and synthesized relevant evidence in order to support NACI in making its decisions to develop new or updated guidance, as evidence on the vaccines and COVID-19 evolved, and as Health Canada authorized COVID-19 vaccines for use in Canada.
In addition to the allocation framework and guidance, PHAC, in collaboration with Health Canada and Statistics Canada, developed and launched a forecasting dashboard for COVID-19 vaccines, enabling federal jurisdictions, provinces and territories to forecast expected supply of vaccines against administration scenarios.
PHAC also developed an IT system called VaccineConnect to enable a fully connected federal, provincial and territorial digital ecosystem that enhances the Agency's ability to address its nationwide mandate to manage distribution and reporting. VaccineConnect utilizes three core modules: Intelligent Supply Chain, which processes vaccine orders and tracks inventory and logistics in near real-time; Immunization Information System, which analyzes and reports national immunization, effectiveness, safety and coverage levels; and Immunization Program Management, which manages end-to- end vaccine program execution. VaccineConnect addresses the immediate and urgent need to manage COVID-19 vaccination distribution and administration and will remain a critical tool in the management of other vaccination programs.
In order to address potential supply chain gaps and to have contingencies available, PHAC engaged with Canada's private sector to deliver a broad range of end-to-end logistics and support services to assist provinces and territories in the management of COVID-19 vaccines, notably the introduction of ultra-low temperature and frozen vaccines. PHAC engaged the services of Innomar Strategies and FedEx Express Canada to provide logistics support. Innomar's warehouses, which are equipped to store complex pharmaceutical products including those with cold chain requirements, provide a safe and secure storage option for central management of the vaccines as they arrive into Canada, supports provinces and territories in managing their portfolio of vaccines with varying storage and handling requirements. Innomar also provides specialist services to ensure that shipments of vaccines across Canada and to Canadian's and their families serving overseas - from single vials to entire pallets - are packaged to allow for strict temperature-control, validated by monitoring system to protect the vaccine shipments.
These temperature-sensitive vaccines are then shipped through the FedEx Express Canada network with consistent reporting on the condition of the vaccine, to monitor critical data including temperature, location and light exposure to help ensure the integrity and security of the vaccines. Additionally PHAC procured and distributed 600 fridges and freezers to bolster the national capacity to store the vaccines in the jurisdictions, and developed a standing offer for equipment including dry ice to safely ship, store and administer enough vaccine to ensure access for all Canadians. PHAC also worked with the Canadian Armed Forces and Transport Canada to build contingencies for COVID-19 vaccine delivery to remote and isolated communities, ensuring risks of delayed or non-delivery were mitigated.
From planning to purchase to delivery, PHAC supported provinces, territories and indigenous communities in laying the groundwork for successful deployment of COVID-19 vaccinations. First doses were shipped in December 2020, less than a year after the pandemic was declared by the WHO. By the end of March 2021, over 7.4 million vaccine doses had been ordered and safely shipped and delivered to federal, provincial and territorial stakeholders for administration.
Following initial deployment, PHAC worked with federal, provincial, territorial and Indigenous co-planning stakeholders to determine additional supply requirements and worked with PSPC to ensure the procurement and distribution of supplies to vaccination clinics across Canada. A notable milestone achieved in March 2021 was the initial delivery of ancillary supplies (i.e. syringes, personal protective equipment, alcohol swabs etc.) in sufficient quantity to administer doses of COVID-19 vaccines to all eligible individuals in Canada.
Did you know?
The National Advisory Committee on Immunization (NACI) published 20 technical vaccine guidance statements and statement updates in 2020-21 to support Canada's COVID-19 vaccine rollout. For comparison, prior to the COVID-19 pandemic, NACI would publish approximately four statements/statement updates annually. NACI also made unprecedented efforts to communicate its findings and recommendations, participating in numerous Parliamentary Committee meetings and media appearances in 2020-21.
PHAC also supported jurisdictions through bilateral engagements to monitor supply chain capacity and capability, ensuring jurisdictions received the necessary equipment and training to effectively execute their administration plans. Working with federal, provincial and territorial stakeholders, PHAC launched the Vaccine Implementation Community of Practice, providing stakeholders weekly opportunities for in-depth engagement on distribution.
PHAC provided Healthcare Provider (HCP) training and education, including vaccine-related instructional webinars, to prepare for the expansion of clinics so that traditional and non-traditional vaccinators in the provinces and territories could begin vaccinating the general population in Canada. This ensured accurate training was provided to administer authorized vaccines. PHAC also produced the first iteration of Canada's COVID-19 vaccine tool kit for HCPs in 2020-21, in consultation with HCP associations and other organizations, providing convenient online access to COVID-19 vaccine fact sheets, webinars and other tools to promote COVID-19 vaccine administration, confidence and uptake.
Alongside Health Canada, PHAC also played a role in setting up COVID-19 vaccine surveillance to carefully monitor vaccine coverage, safety and effectiveness. The Agency provided support and coordination with provinces and territories for the early detection, assessment and reporting of adverse events following immunization, including the identification and investigation of potential safety signals requiring possible regulatory or public health action. PHAC launched and maintained daily public reports on the number of doses administered and weekly public reports on vaccine coverage and any reported side effects following COVID-19 vaccination in Canada.
The Agency worked to develop the Vaccine Injury Support Program (VISP) to provide a no-fault financial support mechanism for people in Canada, in the rare instance where they are seriously and permanently injured as a result of receiving a vaccine authorized for use and administered in Canada on or after December 8, 2020. To ensure this resource was in place for Canadians as the majority of the population became eligible for vaccination, PHAC launched an open solicitation to identify a third-party administrator for the program and established a federal, provincial and territorial committee on the VISP to promote collaboration and the timely exchange of information related to implementation.
As is part of the Agency's core mandate for all vaccination campaigns, PHAC monitored vaccine coverage and factors that influenced the uptake of vaccines. Key initiatives included the development of provincial and territorial vaccine coverage surveys to provide estimates of vaccination coverage for key populations across Canada, including information on knowledge, attitudes and beliefs about vaccination. PHAC also coordinated with Indigenous Services Canada on increased reporting of Indigenous-specific data to better understand vaccine acceptance and uptake among Indigenous communities. Further, in 2020-21, PHAC leveraged its existing Immunization Partnership Fund to bolster COVID-19 vaccine confidence and uptake, amending existing funding agreements, responding to direct solicitations and launching a public open solicitation for new projects to better orient funded efforts towards Canada's COVID-19 vaccine rollout.
PHAC also supported vaccine effectiveness studies in collaboration with the COVID-19 Immunity Task Force's Vaccine Surveillance Reference Group and with provinces and territories to assess protection in population subgroups.
Priority: Surveillance, data, modelling, and research
Purpose: Collect and analyse the information needed to inform evidence-based decisions. The Government of Canada mobilizes industry, innovation and research continuously to respond to COVID-19 and significant findings arising from these research efforts are provided to decision-makers in a useful and timely way.
Enabling the collection of accurate and real-time data to support decision making in emergency situations is critical. To support COVID-19 surveillance and response initiatives, PHAC revised its data infrastructure to eliminate data redundancy and inconsistency, streamline data acquisition from provinces and territories, and facilitate timely access to data. These improvements provided for a single, authoritative, point of reference for data partners and intelligence gathering initiatives across the Health Portfolio.
To better understand the effectiveness of public health measures in response to the COVID-19 pandemic, PHAC supported data collection efforts by:
- Implementing new protocols and accelerated data collection to track the incidence of COVID-19 hospitalizations, COVID-19 in children with pre-existing conditions and emerging inflammatory syndromes related to COVID-19 infections.
- Playing a leadership and coordination role in the collection of data and the development of research on critical questions related to the wider health impacts of COVID-19 in collaboration with Health Canada, the Canadian Institutes of Health Research, Statistics Canada and the Canadian Institute for Health Information; and
- Increasing data collection about COVID-19 impacts on vulnerable populations (e.g., based on ethnicity, gender and socio-economic status).
PHAC also used anonymous and aggregated mobility data to better understand the movement of populations during the COVID-19 pandemic, to gain insight into the effectiveness of provincial stay-at-home orders including volume of visits to points of interest (i.e., grocery stores and pharmacies). PHAC also worked in collaboration with the Canadian Primary Care Sentinel Surveillance Network to explore leveraging primary care electronic medical records to address public health surveillance gaps, including those related to COVID-19 surveillance.
PHAC also received additional funding for the development of key data collection platforms through the Agency's Safe Restart Agreements. The goal was to gain a better understanding of the societal impacts of COVID-19. Some examples of the results achieved include the following:
- PHAC supported the Canadian Longitudinal Study on Aging in launching a COVID-19 Questionnaire Study, which collected data from participants on a weekly/bi-weekly and monthly basis over a period of 9 months to understand the epidemiology of COVID-19 among older adults living in Canada. The data collected has included information on COVID-19 symptoms and status, risk factors, healthcare use, health behaviours and psychosocial and economic consequences of the pandemic;
- The CANCOVID-PREG, a pan-Canadian surveillance project that aims to better our understanding of COVID-19 in pregnancy was initiated. Data collected will help to inform recommendations for the management and care of pregnant people and their infants during the pandemic; and
- The Cancer in Young People in Canada surveillance and research program revised its protocol to begin monitoring COVID-19 infection as a complication in children and youth receiving cancer treatment to gain a better understanding of the pandemic's impact on this vulnerable population. In addition, this Program is also closely monitoring the incidence rate of childhood cancers to determine whether delays in health care-seeking and/or reduced access to diagnostic procedures may be contributing to a delay in diagnosing childhood cancer.
In October 2020, PHAC established the Corporate Data and Surveillance Branch (CDSB) to focus on corporate data oversight; coordinate surveillance, data management and innovation efforts; lead engagement with strategic partners to gather and deploy public health intelligence; and advance knowledge translation so that data can be used effectively by decision makers. Within its first year, CDSB led the development of the Data Management Pillar of the COVID-19 Testing Strategy, providing a roadmap for the Government of Canada's efforts in collectively and strategically addressing data and systems gaps in Canada's COVID-19 Response. In addition, CDSB successfully launched the pan-Canadian Health Data Strategy which aims to:
- Address critical data and knowledge gaps in support of responding to the COVID-19 pandemic; and
- Address long-standing health data gaps and provide recommendations on the collection, sharing and use of health data for the benefit of Canadians.
This strategy leveraged external expertise and partnerships with the provinces and territories to identify areas for improved data sharing in the short, medium and long term. The goal of the strategy is to address not only current data issues in the context of the COVID-19 pandemic, but also to lay the foundation for improved use of data during future emergencies.
Much of PHAC's work on surveillance supported provinces, territories and the federal government in making informed decisions. For example, PHAC developed daily, weekly and monthly reports on COVID-19 to support informed decision-making that were distributed to the public and other internal and external stakeholders.
To ensure guidance, communications and decisions were factual and evidence based, PHAC coordinated quantitative and qualitative reviews on the rapidly produced publications and supported succinct synthesis, where possible. Evidence summaries were shared in response to inquiries, disseminated to public health partners and decision makers and made available to the public via the Canada.ca/coronavirus site.
To predict when and where the virus was likely to emerge or re-emerge, PHAC developed models and made predictions to contribute to the efforts aimed at protecting the health of Canadians. PHAC's COVID-19 modelling work was guided by data and mathematical modelling, highlighting the importance of detecting and isolating COVID-19 cases in guiding public health action. As PHAC learned more about the virus, the Agency updated its models accordingly. In 2020-21, PHAC shared 14 public models with Canadians, with provinces, territories and Canadians. PHAC's modelling also supported the following activities:
- The development of public health guidance and best practices for managing outbreaks;
- The development of new and revised guidance on public health measures in response to emerging scientific evidence; and
- Strengthened collaboration between PHAC, the Natural Sciences and Engineering Research Council of Canada, the academic community and stakeholders in the establishment of networks of specialists across the country in modelling infectious diseases, which were applied to public needs associated with emerging infectious diseases and pandemics such as COVID-19.
To gain a better understanding of potential population-level immunity, PHAC supported the Government of Canada's COVID-19 Immunity Task Force in administering the Serosurveillance and Research Program that enabled serological studies that contributed to the discovery of the rate of COVID-19 transmission in Canada and among vulnerable populations. The Program also delivered a clear and comprehensive pan-Canadian Serosurveillance Strategy that aligned researchers across Canada to generate evidence to inform Public Health pandemic decision-making and management. This work was able to move forward as a result of a partnership with McGill University who acted as host of the CITF secretariat function, and as well as through engagements with the leading academic institutions, blood banks and non-governmental organizations in Canada.
Through the Serosurveillance and Research Program, PHAC provided $104 million in funding to 54 projects and an additional $55 million in funding is available to projects pending approval. This program also published 30 papers, including pre-print.
Did you know?
The number of reported COVID-19 cases among Canadians in 2020-21 was likely lower than the actual number of infections. To adjust for the disparity between reported cases and actual cases, PHAC applied serological surveillance to determine the extent of COVID-19 infections among Canadians and inform Public Health decisions.
PHAC advanced the following activities related to data collection on immunity including:
- The degree and duration of immunity arising from infection and the risk of reinfections;
- How best to measure immunity linked to COVID-19 using diverse tests (e.g., venipuncture, finger-prick, nasopharyngeal, other);
- Data modeling of aggregate reporting of seroprevalence findings in Canada and globally through support for the creation of SeroTracker;
- Establishment of bio-banking for storage of blood samples so they can be accessed to answer new questions as understanding of the immunology of COVID-19 advances; and
- Establishment of studies to monitor immunity and vaccine efficiency and safety.
To facilitate the early detection of COVID-19 outbreaks, PHAC deployed innovations in wastewater surveillance. PHAC scientists were instrumental in quickly establishing complex laboratory tests and pilot studies across Canada. Working closely with other federal agencies, such as Statistics Canada, Environment and Climate Change Canada, Indigenous Services Canada and Correctional Service Canada, as well as with several provincial and academic partners, PHAC:
- Conducted COVID-19 wastewater surveillance at 15 sites in five major cities: Vancouver, Edmonton, Toronto, Montreal and Halifax;
- Initiated wastewater surveillance in seven northern, remote and/or isolated communities and five additional sites in First Nations communities; and
- Undertook a pilot surveillance study at two correctional institutes which could serve as a model for closed communities.
To facilitate increased coverage of testing across all regions, PHAC developed a deployable test to detect COVID-19 in wastewater samples and is currently collaborating with the Canadian Water Network to deliver a COVID-19 wastewater surveillance initiative in select communities as an alternative way for monitoring the prevalence of COVID-19 in the community.
NML researchers also investigated the COVID-19 virus to understand how it transmits and survives in the environment. In total, 20 studies were undertaken, contributing to:
- PHAC's understanding of the factors that contribute to severe disease;
- The identification of targets for therapeutic intervention; and
- The identification of early indicators of potential severe disease progression.
Leveraging their knowledge from the creation of in-house vaccines and the completion of over 50 studies on COVID-19 vaccine candidates, NML scientists continue to work with their global peers, including those in academia, to solicit input on research into the development of new and improved vaccines for COVID-19 in the upcoming years. This includes studies on the effectiveness of future vaccines for newly emergent variants of COVID-19.
Priority: Resource management and organizational well-being
Purpose: PHAC has the tools and resources required to support an effective pandemic response, while protecting employee well-being.
Sustaining a heightened emergency response posture for an extended period of time has a direct and serious impact of the health and well-being of an organization. Public health experts in particular have been working around the clock to share their knowledge and provide expert advice in a high-stress and continuously changing environment. While some staff can cycle through the organization to provide relief, it is more challenging to provide relief to healthcare workers and public health specialists. Providing support to all staff and ensuring appropriate human resources are available is critical to sustaining an effective emergency response.
To position the Agency to respond to the COVID-19 pandemic, PHAC underwent significant organizational changes, including:
- Organizational reviews to identify human resource gaps and new resource requirements to better support the COVID-19 response;
- A functional realignment project which included the implementation of new branches, new senior management positions and expanded roles and responsibilities (e.g., surveillance, laboratories, emergency management and horizontal operations and coordination); and
- Hiring for new skills and surge capacity.
PHAC leveraged assignments, secondments, actings and deployments from other Government of Canada departments and agencies to rapidly fill positions and skills gaps. PHAC also introduced a corporate staffing strategy that supported the use of collective staffing processes and specialized staffing processes for public health professionals (e.g., nurses and epidemiologists). In 2020-21, PHAC added 564 new Full-Time Equivalents (FTEs), of which 254 Footnote 1 FTE's were scientists and tech experts, enabling a continued COVID-19 response and delivery on its mandate.
PHAC also continued work to create a workplace culture that supports psychological health and safety, inclusivity and respect. Organizational well-being has taken on greater prominence during the pandemic and is necessary not only to have a healthy workplace, but also to be able to serve Canadians effectively. Recognizing this, PHAC:
- Launched a mental health events calendar-a "one-stop-shop" access point for employees to mental health training, events and webinars;
- Launched two employee check-in surveys;
- Embedded 16 mental health councillors within teams impacted by operational stress during the pandemic; and
- Encouraged employee engagement through listening sessions and Voices of Mental Health; and Implemented the Mental Health and Wellness in the Workplace Strategy.
PHAC's COVID-19 response timeline
January 2020
- Activation of the Federal/Provincial/ Territorial governance structure to facilitate the formal engagement and coordination of all levels of government on emerging issues; and
- PHAC's NML detects the first case of SARS-CoV-2.
March 2020
World Health Organization declares COVID-19 a global pandemic.
May 2020
PHAC's Chief Public Health Officer has participated in a total of 76 briefings since January 2020 to update Canadians on COVID-19.
June 2020
PHAC launches COVID-19 modelling scenarios to estimate how many new cases and deaths we might see in the coming week and how the epidemic might unfold over the coming months based on:
- how the virus behaves; and,
- the potential impact of public health measures.
July 2020
PHAC establishes a System for Analysis of Laboratory Tests (SALT) to capture COVID-19 testing data from all provincial public health laboratories to enable reporting to collect provincial testing data and provide the total COVID-19 tests conducted in Canada.
September 2020
- Launch of the Safe Voluntary Isolation Sites Program's initial pilot site.
- First meeting of the Waste Water Federal Advisory Committee to support wastewater surveillance of COVID-19.
November 2020
PHAC launches ArriveCAN to facilitate the collection of relevant border data from air, land, and marine point of entries to inform reporting on key border data measures.
December 2020
PHAC's Vaccine Rollout Task Force develops a federal, provincial, and territorial allocation framework that prioritizes COVID-19 vaccines for vulnerable populations.
January 2021
- Working with the Canadian Armed Forces and Transport Canada to build vaccine delivery capacity; and
- Over 1 million doses of the Pfizer and Moderna COVID-19 vaccines delivered across Canada.
March 2021
Delivery of supplies (e.g., needles, syringes, alcohol pads) in sufficient quantity to administer doses of COVID-19 vaccines to all eligible individuals in Canada.
| Core responsibility | Spotlight on PHAC's COVID-19 priorities |
|---|---|
| 1. Health Promotion and Chronic Disease Prevention |
|
| 2. Infectious Disease Prevention and Control |
|
| 3. Health Security |
|
| Internal Services |
|
In support of the pandemic response, PHAC identified the 10 COVID-19 priority areas outlined above in the Spotlight on PHAC's COVID-19 Response. The following crosswalk connects the Spotlight on PHAC's COVID-19 Priorities with the Agency's Core Responsibilities to identify the expected results and outcomes expressed in PHAC's Departmental Results Framework.
Core responsibilities results: what we achieved
1. Health Promotion and Chronic Disease Prevention
Description
Promote the health and well-being of Canadians of all ages by conducting surveillance and public health research and supporting community-based projects which address the root causes of health inequalities and the common risk and protective factors that are important to promoting better health and preventing chronic disease.
Results
The Departmental Results are:
-
Canadians have improved physical and mental health.
-
Canadians have improved health behaviours.
-
Chronic diseases are prevented.
Result 1.1: Canadians have improved physical and mental health
Improve monitoring and reporting on health inequalities
Through the Pan-Canadian Health Inequalities Reporting Initiative (HIRI), PHAC continues to strengthen monitoring, reporting and action on health inequalities in Canada in collaboration with the Pan-Canadian Public Health Network, Statistics Canada and other partners.
Immediately following the emergence of the COVID-19 pandemic in Canada in spring 2020, PHAC redirected HIRI resources and capacity towards supporting PHAC's pandemic response through rapid assessments and syntheses of COVID-19-related health inequalities data and emerging evidence. Working with its data partners, PHAC also explored the development of new HIRI indicators and methodologies to monitor and report on social inequalities as a direct and indirect impact of the pandemic and mapping culturally responsive and equity-focused data practices and methods.
Did you know?
Some people with experiences of violence can be triggered by incidental physical contact or loud noises.
Projects funded through PHAC's family and gender-based violence investments use a trauma- and violence-informed approach to create physically and emotionally safe environments for participants that support positive physical and mental health outcomes. This approach is based on an understanding of the impact of trauma and violence on survivors' lives and behaviors, and informs all project components - from program design to research and evaluation methods.
For example, as part of their trauma- and violence-informed approach, the Boys and Girls Clubs of Canada's Bounce Back League feature a "Zone" away from the field of play where participants can cool down, refocus, check-in, strategize, reset, or self-regulate; and Coaches of the Shape Your Life non-contact boxing program give participants options for engagement, and seek permission before touching participants to support technique.
PHAC continued to make progress on the Health Inequalities Data Tool through the development of new indicators, population groups and knowledge resources in support of reducing health inequities in chronic diseases and their common behavioural and social risk factors.
Improve the well-being for Canadians affected by autism spectrum disorder
Budget 2018 announced $20 million over five years to PHAC, for two new initiatives to support the needs of Canadians living with autism spectrum disorder, herein after autism, and their families.
PHAC invested $9.1 million in community-based projects that support innovative program models, help reduce stigma, and support the integration of health, social and educational programs to better serve the complex needs of families. This included funding ten community-based projects through the Autism Spectrum Disorder Strategic (ASD) Fund, that provide safe and inclusive spaces (Les Grands Ballet Canadiens de Montréal), resources to support adults and adolescents’ ability to cope with stress(ors) (York University’s Autism Mental Health Promotion Project) and opportunities to develop the life skills needed to navigate healthy relationships (Autism Nova Scotia Society).
PHAC also invested $10.9 million in the creation of an Autism and/or Intellectual Disabilities Knowledge Exchange Network (AIDE) to help connect people with autism and their families to information, resources, employment opportunities and local programming. For example, AIDE developed and launched a COVID-19 resource hub compiled of information and resources to support individuals and their families.
In collaboration with provinces, territories and stakeholders PHAC is committed to improving the health and well-being of children and adults with ASD, including supporting parents and caregivers by working towards the creation of a National Autism Strategy. In 2020-21, PHAC announced an investment of $1.46 million for the Canadian Academy of Health Sciences to lead consultations for the development of the National Autism Strategy.
Prevent family and gender-based violence
Family violence and gender-based violence are serious public health issues with impacts on individuals, families and communities.
The impacts of these types of violence can persist throughout peoples' lives and can affect future generations. Through the Supporting the Health of Survivors of Family Violence Investment the Health of Survivors of Family Violence Investment and the Preventing Gender-Based Violence: The Health Perspective Investment (part of Canada's Strategy to Prevent and Address Gender-Based Violence), PHAC invested $15 million in projects that aimed at identifying effective ways to prevent and address violence, improve health outcomes for survivors and equip health and allied professionals to recognize and respond safely and effectively to these types of violence.
Funded projects delivered and tested diverse approaches to prevent and address family and gender-based violence, including:
- Support for parents and young children exposed to family violence;
- Culturally relevant programming for Indigenous communities;
- Trauma-informed sports and recreation programming; and
- Youth-led initiatives to prevent teen/youth dating violence.
The Family Violence Knowledge Hub and the Youth Dating Violence Community of Practice are examples of projects delivering and evaluating health promotion interventions designed to improve health outcomes for survivors of family violence. In response to COVID-19, projects paused, adapted, or pivoted activities as required.
Capacity-building projects engage a wide range of professionals, including public health promoters, social workers, physicians, midwives, volunteer coaches, researchers and policy makers. This ensures that projects are equipping professionals with the skills and resources required to address the needs of survivors and those at risk of experiencing family or gender-based violence.
Support the mental health of children, youth and their caregivers
Through the Mental Health Promotion Innovation Fund (MHP-IF), PHAC funded projects that reached over 17,000 children, youth and caregivers across a variety of communities including Indigenous, newcomers and immigrants and transgender groups.
PHAC also supported projects in adapting interventions in response to the evolving COVID-19 context. This included shifting methods to allow for the rapid deployment of virtual interventions among other innovative ways to continue offering support for the mental health of children, youth and caregivers.
Did you know?
The MHP-IF also supported a Knowledge Development and Exchange Hub (KDE Hub) to build awareness on the funded projects and strengthen meaningful connections to advance the mental health promotion for children and youth in Canada.
Support the mental health and well-being of Black Canadians
As part of a new initiative on Promoting Health Equity: Mental Health for Black Canadians Fund, PHAC partnered with community-based organizations, researchers and other Black communities to generate new evidence on culturally focused programs and interventions that address mental health and its determinants for Black Canadians. PHAC also published a "Snapshot on Social Determinants and Inequities in Health for Black Canadians" and established sixteen partnerships and funding agreements. PHAC continued supporting multi-year projects that aim to improve the mental health of Black Canadians, including the following examples:
- Aspire for Higher Elite Basketball
Developed a mental health education curriculum in consultation with mental health professionals, education professionals, child welfare organizations and other partners and organizations. This project secured funding for the next 12 months to move into their implementation phase, which includes an after school program to educate Black youth about mental health using an anti-Black racism lens. - TAIBU Community Health Centre
The IMARA project recruited youth of diverse gender, age, sexual orientation, ethnicity and locations across the Greater Toronto Area as peer leaders to facilitate and deliver 14 virtual mental health awareness and capacity building sessions. The peer leaders worked alongside of a Black mental health professional, to deliver content on themes such as Mental Health 101, Africentric Model Development, Anti- Black Racism and Trauma and Resilience. The virtual nature of these sessions reduced a number of barriers for youth from diverse communities to participate, while respecting confidentiality and privacy. - Head and Hands
The Storytelling, Training, Advocacy and Youth drop-in (STAY) project launched a playlist activity pilot in fall 2020 as part of the storytelling component to promote their project. The project also launched their advocacy activities through the development of "Know Your Rights" cards, which were distributed to youth as a resource to ensure that when they interact with police they understand what the police are and are not allowed to ask of them.
Did you know?
Results from the first survey on COVID-19 and mental health indicated that:
- 6% of participants screened positive for PTSD (i.e., reported moderate to severe symptoms of PTSD);
- Female participants (8%) were twice as likely as male participants (4%) to screen positive for PTSD; and
- Female participants between the ages of 18 and 34 (12%) and frontline workers (i.e., First Responders, nurses, and doctors) (10%) had the highest incidence of screening positive for PTSD.
Implement the Federal Framework on Posttraumatic Stress Disorder
Understanding Posttraumatic Stress Disorder (PTSD), its prevalence in Canada and helping people get effective help early, has been an urgent priority for PHAC in recent years. The urgency of this work has been reinforced by the pandemic as Canadians—in particular essential workers and First Responders—live and work in an environment of increased risks to their personal safety which makes them more susceptible to trauma and PTSD. The disproportionate stressors facing frontline workers and First Responders informed PHAC’s collaboration with partners and stakeholders to develop and implement the Federal Framework on Posttraumatic Stress Disorder.
To advance the effectiveness of the delivery of services and support to Canadians, during and after the pandemic, PHAC collaborated with Statistics Canada to undertake the Survey on COVID-19 and Mental Health to collect data to assess the impacts of COVID-19 on the mental health and well-being of Canadians in the fall and spring of 2020-21. This survey included questions on the concern of violence, substance harm, mental health and mental illness, among other topics. Results are now available on PHAC's website: Symptoms of anxiety and depression during the COVID-19 pandemic and Symptoms of posttraumatic stress disorder (PTSD) during the COVID-19 pandemic.
The survey on Stressful Events and Mental Health is another survey PHAC worked with Statistics Canada to develop and data collection is currently underway. This survey is more specific to PTSD and results are expected in fall 2021.
Support the Federal Framework for Suicide Prevention
As the federal department responsible for the Federal Framework for Suicide Prevention, PHAC supports the coordination and collaboration efforts for the prevention of suicide, enabling the sharing of information and complementing the important work already underway by others in the sector. In December 2020, PHAC published the Federal Framework for Suicide Prevention - Progress Report, which provides an update on federal activities related to suicide prevention between 2018 and 2020. PHAC continues to focus on reducing stigma and raising awareness, connecting people, information and resources and advancing knowledge and evidence to better understand suicide and inform prevention, treatment and recovery strategies.
Did you know?
During the development of the Federal Framework for Suicide Prevention, stakeholders identified the need for alignment in research, sharing of information and knowledge translation. As a result, PHAC is working with the Mental Health Commission of Canada partners to develop the Shared Canadian Research and Knowledge Translation Agenda for suicide and its prevention. This initiative was informed by researchers, suicide prevention experts and other stakeholders and will inform priorities for research and knowledge translation.
In 2020, PHAC announced funding of $21 million over five years for the Centre for Addiction and Mental Health (CAMH) to implement a pan-Canadian suicide prevention service in partnership with the Canadian Mental Health Association and Crisis Services Canada. The service is currently available 24/7 by voice in English and French, with text messaging to be available by March 31, 2022 and online chat by March 31, 2023. This multi-modal functionality is crucial to reducing barriers to access crisis services so that all Canadians can find the support they need. From April 2020 to March 2021, there were 1,818 active rescues (an active rescue involves collaboration with emergency services to help someone in crisis).
As the COVID-19 pandemic continues to put a strain on the mental well-being of Canadians, PHAC is committed to advancing continuous, collective and collaborative efforts that work towards a Canada where suicide is prevented and everyone lives with hope and resilience.
Efforts to prevent dementia and improve the quality of life of those impacted by dementia
Launched in 2018, PHAC's Dementia Community Investment (DCI) funds community-based projects seeking to optimize the wellbeing of people living with dementia as well as family/ friend caregivers by increasing knowledge about dementia and its risk and protective factors. In fall 2020, PHAC launched a second open solicitation for projects and initiatives that address the objectives and priorities of the DCI in the context of COVID-19.
Did you know?
As of March 2021, PHAC's DCI has supported 18 community-based projects seeking to optimize the wellbeing of people living with dementia, including family/friend caregivers and sharing knowledge on dementia and its risk factors.
As of March 2021, PHAC funded 189 projects that aim to increase knowledge about dementia and/or improve the quality of life of those impacted by dementia. To further support the objectives of the DCI, PHAC funded Schlegel-UW Research Institute for Aging Foundation to implement a knowledge hub that facilitates a community of practice for the DCI projects and disseminates program findings and best practices to the dementia policy and program community across Canada.
Through the Dementia Strategic Fund (DSF), a national public education and awareness campaign is being developed and is expected to launch in September 2021. Media resources (e.g., articles, radio and video spots) focusing on reducing dementia stigma and risk reduction were developed; between January 2021 and March 2021 these media resources produced approximately 2.9 million impressions across Canada.
The DSF is funding a project led by the Native Women's Association of Canada which was launched in June 2020 and focuses on building capacity to undertake awareness raising on stigma. Additionally, the project proposals for the open funding opportunity, DSF: Awareness Raising Initiatives, were reviewed. Recommended projects on how to prevent or delay onset, reduce stigma-including stigmatizing behaviours-and encourage and/or support communities to be more dementia-inclusive are expected to launch in 2021.
Phases I and II of the Dementia Guidelines and Best Practices Initiative were launched in 2020-21. Phase I engaged an expert panel to assess the quality of existing dementia guidance and identify gaps. Phase II engaged dementia guidance users to better understand use and uptake, including barriers to obtaining or using dementia guidance. The results of these projects will inform future activities that support improved access to and use of, dementia guidance.
Result 1.2: Canadians have improved health behaviours
Support Canada's response to the opioid crisis and emerging drug threats
Canada’s struggles with historic rates of fatal and non-fatal drug overdoses have been exacerbated by the COVID-19 pandemic, as persons experience increasing feelings of isolation, stress and anxiety, and the availability or accessibility of services for people who use drugs is limited by pandemic response measures. To better understand and respond to Canada’s opioid overdose crisis, we need to continue to work with our partners across Canada to mitigate the devastating impacts on communities and families. PHAC is committed to a collaborative, compassionate and evidence-based approach to the opioid overdose crisis.
Work undertaken in 2020-21 by the Agency included conducting studies and publishing reports that improve our understanding of the overdose crisis on a national level. For example, PHAC developed a simulation model of opioid-related deaths that provides information on the number of these deaths that might occur during the COVID-19 outbreak in 2020 and 2021. While models can't predict what will happen, they can help governments and Canadians understand what might happen in certain scenarios, helping us to plan and act to achieve the best possible outcome. Two versions of this model were released, in October and December 2020, and were updated to reflect recent surveillance data on opioid overdoses and future potential scenarios. The model released in December 2020 indicated that, under some scenarios, the opioid overdose crisis may resurge or surpass levels seen at the height of the opioid overdose crisis in late 2018. This was observed in surveillance data released in December 2020 and March 2021.
In support of the Government of Canada’s efforts to reduce substance-related harms, PHAC continued to fund five projects that mobilize existing evidence to improve access and reduce barriers to care for people who use drugs. This included $3.6 million to projects under the Supporting Pathways to Care for People Who Use Drugs program.
Did you know?
In the six months following the implementation of public health measures to reduce the spread of COVID-19 (April to September 2020), Canada recorded 3,351 apparent opioid toxicity deaths, representing a 74% increase in comparison to six months prior (October 2019 to March 2020 - 1,923 deaths). In response, PHAC strengthened its surveillance activities to raise awareness about the rate and the context in which such harms occur, particularly during the COVID-19 pandemic in Canada.
PHAC also engaged with partners and stakeholders to mobilize knowledge on upstream approaches to the prevention of substance use and related harms in youth. This included engaging with communities to build capacity and support evidence-informed interventions that help enhance youth resilience and prevent substance-related harms. PHAC also supported the development of a resource for school communities that encourages the adoption of evidence-based, comprehensive strategies to reduce substance-related harms among youth: Blueprint for Action: Preventing substance-related harms among youth through a Comprehensive School Health approach.
In partnership with Health Canada and the United States, as part of the Canada/U.S. Action Plan on Opioids, PHAC facilitated the exchange of knowledge and expertise on issues such as stigma and prevention.
In partnership with the Health Portfolio, PHAC expanded the national quarterly update beyond opioid-related harms to capture harms due to other substances such as methamphetamine and cocaine to better characterize the role of polysubstance use in substance-related overdoses and deaths. The March 2021 release includes data on deaths, hospitalizations and Emergency Medical Services responses involving opioids and/or stimulants between January 2016 and September 2020. In addition, the impact of the COVID-19 pandemic on trends of opioid-related harms continued to be reflected in the March update. This is the second national-level release that demonstrated the severe impact of COVID-19 on Canada's overdose crisis, the first occurring in December 2020.
Address the rapid rise of vaping
As youth vaping continues to rise, PHAC is taking action to address it. While youth smoking is at its lowest level in decades, vaping is putting a new generation of Canadians at risk of nicotine addiction and the other harms caused by vaping. To support the reduction of harms from the use of vaping, tobacco and cannabis, PHAC is:
- Supporting the Chief Public Health Officer as a leading voice on public health in Canada and developing tailored public education resources on substance use for various target audiences such as school communities, older adults and postsecondary students;
- Supporting research and analysis on vaping, cannabis and tobacco use among students in Canada as part of the eighth cycle of the Health Behaviour in School Age Children study, to identify the protective factors that might lower the incidence of youth vaping;
- Supporting the Canadian Paediatric Society in the development of Vaping: A clinician's guide to counselling youth and parents; and
- Collaborating with the Canadian Paediatric Surveillance Program on three studies on the short term impacts of vaping-related harms among children and youth; and
- Leading the federal response to the emergence of vaping-associated lung illness (VALI) through a Canadian outbreak investigation with collaboration from partners involved in the Council of Chief Medical Officers of Health (CCMOH) Federal-Provincial-Territorial VALI Task group, in order to inform public health action and education initiatives:
- A total of 20 VALI cases were reported in this outbreak since 2019 (no deaths), and no common cause was identified among them. Although reporting of VALI cases have decreased, the Agency is transitioning from response to the implementation of further surveillance to continue monitoring vaping-related harms and VALI cases in Canada.
Support tobacco cessation and prevention for Canadians
Tobacco use is the leading preventable cause of disease and premature death in Canada. PHAC continued to support 8 projects that focused on tobacco cessation and prevention in target populations such as LGBTQI2S+ youth and young adults through the Healthy Living and Chronic Disease Prevention—Multi-Sectoral Partnerships (MSP) program. For example, the University of Toronto's All Together Now! project engaged LGBTQI2S+ youth and young adults to assist in the development of its content messaging, resources and services.
One part of the engagement was via an online survey which included questions on smoking, vaping, mental and physical health, connection to LGBTQI2S+ communities and perceived stigma. A second part of the engagement was the hosting of a series of virtual focus groups with representatives from a range of age groups, genders and sexual orientations. Findings of the focus groups indicate that stress, mental health and social connection form the major themes contributing to smoking among LGBTQI2S+ young adults. As a direct result of this engagement, the need for culturally appropriate and a diverse array of services addressing root causes of smoking-including mental health and stress management-have been identified as important components of tobacco prevention and cessation efforts.
Did you know?
In January 2021, federal, provincial, and territorial ministers responsible for sport, physical activity and recreation endorsed a recommendation to establish an annual concussion awareness week starting in September 2021.
Support a pan-Canadian concussion strategy
PHAC continued work with Canadian Heritage (Sport Canada) to implement the shared commitment of developing a pan-Canadian concussion strategy to raise awareness of concussion treatment for parents, coaches and athletes. PHAC focused on the surveillance of concussions and other traumatic brain injuries to learn more about the incidence, prevalence and sport and recreational activities where these types of injuries are most likely to occur. PHAC also partnered with Statistics Canada to initiate a Rapid Response Survey on Head Injuries/ Concussions and published Injury in Review, 2020 Edition: Spotlight on Traumatic Brain Injuries Across the Life Course. In addition, PHAC worked to promote education and awareness resources for parents, schools and sport stakeholders that support Canadians in their return to school, sport and daily activities post-concussion and other concussion treatment resources for medical and health professionals.
Support early positive development and stronger beginnings for Canadians
In response to the challenges that COVID-19 created for Indigenous Early Learning and Child Care, PHAC provided $8.8 million in emergency funding to preserve the availability of culturally relevant programming at 85 Aboriginal Head Start in Urban and Northern Communities (AHSUNC) projects across Canada to ensure their safe reopening in adherence with provincial and local public health guidelines.
PHAC continued to invest in maternal and child health for key populations facing vulnerable conditions, including supporting positive early development and stronger beginnings for Canadians. Projects funded under the Community Action Program for Children, Canada Prenatal Nutrition Program and Healthy Early Years program continued to successfully implement a range of programming and activities for pregnant individuals, young children and families facing health inequities by adapting and adjusting projects to be delivered in new ways during the pandemic. This included shifting to virtual programming where possible, focusing on providing essential care need items and one-on- one socially distanced supports, as well as doing what was possible to address acute food insecurity needs.
In addition to these measures for supporting positive early development and health, PHAC published a number of resources related to perinatal and early child health, including:
- Two new breastfeeding resources for Canadians; and
- A new joint statement on traumatic head injury due to child maltreatment.
PHAC also published a range of maternal child and youth health surveillance products on topics that included:
- Perinatal Health Indicators;
- Childhood cancer incidence and survival rates; and
- The prevalence of developmental disorders.
Encourage healthy living and physical activity
PHAC launched the Healthy Canadians and Communities Fund (HCCF) to replace the Healthy Living and Chronic Disease Prevention - Multi-Sectoral Partnerships (MSP) program in support of interventions that address the behavioural risk factors (i.e., physical inactivity, unhealthy eating and tobacco use) for chronic diseases by creating physical and social environments that support Canadians in achieving healthy living and physical activity. The HCCF's first solicitation invited Design Phase applications that seek to determine the needs of priority populations to develop multi-sectoral partnerships and to design an intervention that has potential to enable health behaviour change(s).
Did you know?
PHAC supported ParticipACTION's Let's Get Moving initiative that aimed to increase Canadians participation in daily physical activity through the ParticipACTION app in 2020-21, launching challenges such as the Great Big Move and True North. As of March, 2021 the ParticipACTION app has reached over 180,000 users. Among the app users with at least 8 weeks of physical activity data, 35% had an increase of at least 10 minutes of moderate to vigorous physical activity.
Working within the framework A Common Vision for Increasing Physical Activity and Reducing Sedentary Living in Canada: Let's Get Moving, PHAC continued to fund non-governmental Champions projects that support the common vision of a Canada where all Canadians move more and sit less, more often. These Champions support: Cultural Norms, Spaces and Places, Public Engagement, Partnerships, Leadership and Learning and Progress.
PHAC released the first ever 24-Hour Movement Guidelines for Adults to increase awareness among Canadians on what a healthy 24 hours should look like when it comes to physical activity, sedentary behaviours and sleep. The guidelines feature recommendations for ages 18-64 and 65 and older and were developed in collaboration with the Canadian Society for Exercise Physiology, Queen's University, ParticipACTION and a network of researchers and stakeholders from across Canada.
Did you know?
As of March 2021, PHAC investments in the 8 significant projects below came to an end. Tremendous impact and insights have been achieved based on strong multi-sectoral partnerships (for descriptions see hyperlinks and scroll down for results). Although PHAC investment has ended, some of these project partnerships continue to thrive.
The Apple School Foundation
Transforming Healthy School Communities developed school action plans to encourage healthy eating and physical activity among children.
Boys and Girls Clubs of Canada
Kid Food Nation combined a community-based food literacy and skills intervention, an annual national recipe contest and event to help develop healthy eating practical knowledge and experiences in children/youth and their families.
Canada's National Ballet School
Sharing Dance developed dance programming for children, youth and seniors across Canada through community settings and care facilities.
Capsana
Activezvotre santé / Activate your health supported individuals in the workplace, especially women to improve their lifestyle choices in eating habits and physical activity.
Childhood Obesity Foundation
Aim2Be A Healthy Lifestyle App for Canadian Families developed a gamified healthy lifestyle application for youth and their families designed to help families adopt healthy behaviours.
Heart and Stroke Foundation of Canada
ACTIVATE community-based lifestyle modification program increased awareness of high blood pressure and CVD risk among participants 40 years and over to improve their ability to effectively manage their modifiable risk factors through online tools and referrals to community resources.
Right to Play Canada
Right to Play addressed diabetes prevention in urban First Nations, Inuit and Métis populations by raising awareness and promoting healthy living; promoting leadership skills among Aboriginal youth; providing culturally appropriate tools and resources; and promoting community development and sustainability.
St. James Town Family Literacy Services
Healthy Living in St. James Town helped newcomers in their efforts to assess and address their risks of diabetes, cancer and heart health through community based health promotion and disease prevention activities and events.
Promote healthy built environments
PHAC partnered with the Canadian Institute for Health Research to create a joint funding opportunity in support of the Healthy Cities Implementation Science Team Grants, which aims to improve urban Canadians' built environments to improve population health and well-being. This funding opportunity was made public in March 2021 with a formal launch taking place in May 2021.
PHAC also continued to support the University of Alberta's Housing Health project, an initiative aimed at designing housing communities in such a way that encourages physical activity, healthy eating and a sense of community belonging. This initiatives involves working in partnership with close to 200 community stakeholders with representation from various sectors to incorporate active design features into the housing sites.
Result 1.3: Chronic diseases are prevented
Promote healthy weights at home, at school and in the community
PHAC continues to support efforts to reduce childhood obesity as outlined in Curbing Childhood Obesity: A Federal, Provincial and Territorial Framework for Action to Promote Healthy Weights by promoting healthy weights at home, at school and in the community. For example, PHAC supported:
- Alliance Health's Healthy Kids Initiative, a 12-week program that supports children and youth who are overweight to realize measureable changes in health outcomes through increased physical activity, healthy eating and social supports. A total of 2,290 children/youth completed the program and test results showed significant improvements in aerobic fitness and mental health well-being;
- The Childhood Obesity Foundation's mobile app for youth called Aim2Be. The app engaged youth and their families through interactive content and personalised coaching to adopt lifelong healthy behaviours in four areas - healthy eating, physical activity, screen time and sleep. The teens who used the Aim2Be app reported improved self-efficacy and motivation to adopt healthy behaviours, decreased screen time use and juice intake, as well as an increase in the consumption of fruits and vegetables. Parents themselves also reported an increase in their fruit and vegetable intake and a decrease in their sugar-sweetened beverages; and
- Western University's Hockey Fans in Training which aims to increase physical activity and healthy eating behaviours among middle-aged, overweight and obese men at risk of chronic disease. Over 640 men enrolled in the program in communities across Canada.
Help Canadians prevent diabetes
In collaboration with LMC Prevention Ltd., PHAC continued to fund the Canadian Diabetes Prevention Program, a 12-month lifestyle intervention program aimed at reducing the risk of Type 2 diabetes through behaviour changes and weight loss. A total of 724 participants have enrolled in the program. Preliminary findings from the first cohort of participants who completed the program showed overall improvement in a number of measures of Type 2 diabetes risks such as blood glucose, blood pressure and weight.
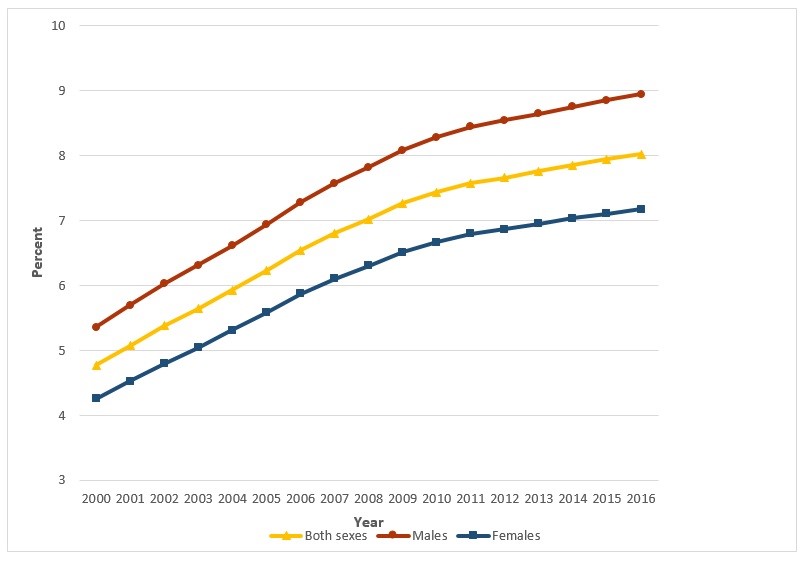
Source: Public Health Agency of Canada - Health Promotion and Chronic Disease Branch Canadian Chronic Disease Surveillance System data files provided by provinces and territories, as of August 2019 (data up to 2016-17).
- Footnote *
-
- Nunavut data excluded before 2005-06;
- Yukon data excluded before 2010-11;
- Nova Scotia data among individuals aged 1-19 are excluded;
- Saskatchewan data were not available for 2016-17.
Figure 1 - Text description
This graph depicts the age-standardized prevalence rate of diabetes in Canada as a percentage of the population who is age 1 and older and breaks down into 3 lines depicting both sexes, males and females presenting information between the years 2000 and 2016.
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Both sexes | 4.77 | 5.07 | 5.38 | 5.64 | 5.92 | 6.22 | 6.54 | 6.8 | 7.02 | 7.26 | 7.43 | 7.57 | 7.66 | 7.76 | 7.85 | 7.94 | 8.02 |
| Males | 5.35 | 5.69 | 6.02 | 6.31 | 6.61 | 6.93 | 7.28 | 7.57 | 7.82 | 8.08 | 8.28 | 8.44 | 8.54 | 8.64 | 8.75 | 8.85 | 8.94 |
| Females | 4.25 | 4.52 | 4.79 | 5.04 | 5.31 | 5.58 | 5.87 | 6.1 | 6.3 | 6.51 | 6.66 | 6.79 | 6.86 | 6.95 | 7.03 | 7.1 | 7.17 |
Sex and Gender-based Analysis Plus
PHAC continued to advance gender equality through the integration of a Sex and Gender- based Analysis Plus (SGBA Plus) lens in all aspects of its work, such as providing advice on Canada's COVID-19 response and advising Canadians on COVID-19 related guidance. More than 175 documents were reviewed in order to incorporate SGBA Plus, diversity, inclusion and health equity considerations.
The Agency also continued to incorporate an SGBA Plus perspective into its various funding programs such as PHAC's Autism Spectrum Disorder Strategic Fund and Healthy Canadians and Communities Fund.
Data continued to be a focus for SGBA Plus considerations, as evidenced by the Pan-Canadian Health Inequalities Reporting Initiative which developed estimates of COVID-19 mortality for specific populations, meaningful to health equity, using provisional COVID-19 deaths in a vital statistics database (January - July/August 2020) integrated with 2016 Census data. This allowed for results to be aggregated by sex, income, ethno-cultural concentration, urban geography, dwelling type and size and living arrangement. Results will be available in June 2021 on the Government of Canada's COVID-19 data trends page.
Innovation and experimentation
PHAC used innovative approaches to help tackle complex issues. One example was the Vaccine Community Innovation Challenge, launched in March 2021. This program uses an innovative prize/challenge model in order to support community-driven information campaigns to promote confidence in vaccination against COVID-19 and continued compliance with public health measures. The program offers supportive messaging from trusted community voices to communities experiencing health and social inequities and/or those who are disproportionately impacted by COVID-19. The messaging is targeted, informed and culturally sensitive.
PHAC took a new approach to funding programs through the new Healthy Canadians and Communities Fund, formerly known as the Healthy Living and Chronic Disease Prevention - Multi-sectoral Partnerships Program. Launched in March 2021, the Healthy Canadians and Communities Fund continued the work started under the MSP program by leveraging outcomes-based funding models through a social finance strategy as part of the evaluations of all projects. As identified in the 2020 Evaluation of the Multi-Sectoral Partnerships Program, the Program was perceived as a leader among those within the Government of Canada who use experimental program design and apply innovative funding models.
PHAC also experimented with the application of Artificial Intelligence (AI) to collect anonymous data on the prevalence of suicide-related verbalization and associated risk and protective factors on publicly available social media. The goal of this pilot project was to determine if AI can produce more timely data on suicide-related behaviours. A summary report of the results will be published in 2021.
In collaboration with the RADIUS Health Promotion Lab at Simon Fraser University, PHAC supported innovative approaches in public health through the creation and incubation of innovative new models, ventures, partnerships and health system intervention. The lab funded projects that aim to build the organizational capacity of social enterprises to find new solutions to complex problems. Using an equity-based framework, the Lab addressed risk factors for chronic disease through dialogue and action.
To further the study of behaviours that cause chronic disease, PHAC worked with the Healthy Futures project offered by LEAP Social Ventures (LEAP). The project supports and scales breakthrough social ventures by way of incubator/accelerator programs. The social ventures are developing innovative solutions to help Canadians move more, sit less, eat better and quit smoking. The project provides the ventures with guidance, expert advice and resources with an aim to grow and expand, reach and impact. As project operating results and outcomes are reported, PHAC will use them to inform future decision-making.
In collaboration with Western University, PHAC supported the use of a base + premium payment funding model with the Hockey Fans in Training (Hockey FIT) to cover all eligible project expenditures, as well as premium payments contingent on the project achieving pre- determined health outcomes. Premium payments are focused on project reach and significant changes in the health of participants.
To further the study of behaviours that cause chronic disease, PHAC worked with offered by LEAP Social Ventures (LEAP). The project supports and scales breakthrough social ventures by way of incubator/accelerator programs. The social ventures are developing innovative solutions to help Canadians move more, sit less, eat better and quit smoking. The project provides the ventures with guidance, expert advice and resources with an aim to grow and expand reach and impact. As project operating results and outcomes are reported, PHAC will use them to inform future decision-making.
2030 Agenda for Sustainable Development
PHAC contributed to supporting global targets related to chronic disease prevention, including supporting Health Canada with tobacco cessation, increased physical activity and healthy eating in order to prevent chronic disease including diabetes, cancer and cardiovascular disease.
In alignment with the United Nations Sustainable Development Goal (SDG) 3: Ensure healthy lives and promote well-being for all at all ages, the United Nations General Assembly declared 2021-2030-the Decade of Healthy Ageing. The decade promotes four areas of action:
- Changing how we think, feel and act towards age and aging;
- Ensuring that communities foster the abilities of older people;
- Delivering person-centred integrated care and primary health services that are responsive to older people; and
- Providing access to long-term care for older people who need it.
PHAC is leading Canada's plan to support and advance the Decade of Healthy Ageing through the uptake and implementation of age-friendly communities across Canada.
| Departmental results | Performance indicators | Target | Date to achieve target | 2018-19 Actual results |
2019-20 Actual results |
2020-21 Actual results |
|---|---|---|---|---|---|---|
Canadians have improved physical and mental health |
% of low-income children in very good or excellent health |
At least 80% |
Mar. 31, 2025 |
84.1% |
84.1% |
84.1% |
% of population who have high psychological well-being |
At least 75% |
Mar. 31, 2025 |
75% |
75% |
75% |
|
Canadians have improved health behaviours |
% increase in average minutes/day of physical activity among adults |
At least 20% (30 min/day) |
Mar. 31, 2025 |
-4% 24 min/day |
+4% 26 min/day |
+4% 26 min/day |
% increase in average minutes/day of physical activity among children/youth |
At least 10% (64 min/day) |
Mar. 31, 2025 |
+9% 63 min/day |
+9% 63 min/day |
+9% 63 min/day |
|
Chronic diseases are prevented |
% increase in years lived in good health by seniors |
At least 4% (HALE at age 65 = 17.0 years) |
Mar. 31, 2022 |
1% 16.6 years (CCDSS 2013-14 to 2015-16) |
1% 15 years |
1% 15 years (Statistics Canada 2010-2012 to 2015-17) |
Rate of new diabetes cases among Canadians |
At most 6.2 Cases per 1,000 age 1 and older |
Mar. 31, 2025 |
6.1 cases per 1,000 age 1 and older (CCDSS 2015-16) | 6.2 cases per 1,000 age 1 and older (CCDSS 2016-17) |
6.2 cases per 1,000 age 1 and older (CCDSS 2016-17) | |
% of adults who are obese |
At most 28% |
Mar. 31, 2025 |
27% |
24% |
24% |
|
% of children and youth who are obese |
At most 13% |
Mar. 31, 2025 |
11% |
10% |
10% |
|
Legend: CCDSS - Canadian Chronic Disease Surveillance System; |
||||||
| 2020-21 Main Estimates |
2020-21 Planned spending |
2020-21 Total authorities available for use |
2020-21 Actual spending (authorities used) |
2020-21 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 280,813,789 | 280,813,789 | 406,594,486 | 291,289,487 | 10,475,698 |
| Variance between Actual spending and Planned spending is explained in the section "Analysis of trends in spending and human resources." | ||||
| 2020-21 Planned full-time equivalents |
2020-21 Actual full-time equivalents |
2020-21 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 550 | 542 | (8) |
| Variance between Actual full-time equivalents and Planned full-time equivalents is explained in the section "Analysis of trends in spending and human resources." | ||
Financial, human resources and performance information for PHAC’s Program Inventory is available in GC InfoBase.
2. Infectious Disease Prevention and Control
Description
Protect Canadians from infectious diseases by predicting, detecting, assessing and responding to outbreaks and new threats; and contribute to the prevention, control and reduction of the spread of infectious diseases among Canadians.
Results
The Departmental Results are:
- Infectious diseases are prevented and controlled.
- Infectious disease outbreaks and threats are prepared for and responded to effectively.
To make progress towards achieving these results, PHAC focused its 2020-21 efforts on key initiatives and activities that provide Canadians and public health stakeholders with the science, data, information and resources to prevent infectious diseases and reduce harms when these diseases occur.
Result 2.1: Infectious diseases are prevented and controlled
Increase vaccination rates
Vaccinations are one of the most effective public health strategies for protecting populations against infectious disease threats. In 2020-21, PHAC continued its core efforts to increase vaccination rates in Canada while responding to the COVID-19 pandemic. For example, PHAC's annual seasonal influenza campaign was delivered in 2020 as planned to promote influenza vaccine uptake, contributing to historically low seasonal influenza incidence rates in Canada.
Seasonal influenza presents an ongoing disease burden in Canada during the fall and winter months. The burden of severe illness from influenza is substantially higher for adults aged 65 years and older compared to younger adults. To help protect this population during the 2020-21 influenza season when both COVID-19 and influenza were co-circulating, PHAC secured 316,000 doses of Fluzone® High-Dose Quadrivalent influenza vaccine to ensure one dose for every long-term care resident aged 65 or older in Canada.
In addition to the purchase of the High-Dose influenza vaccine in 2020, PHAC also created a reserve of more than 1.8M doses of various standard-dose influenza vaccines. This reserve provided surge supply for PT programs in anticipation of significant demand increases for influenza vaccines, with approximately 1.7M doses ordered by PTs for use in their 2020-21 influenza programs.
In total, nearly 17 million influenza vaccine doses were made available by PHAC for public vaccination programs in Canada for the 2020-21 influenza season.
Through the Immunization Partnership Fund (IPF), PHAC invested in capacity-building projects that aimed to increase vaccine acceptance and uptake among Canadians. This included launching mass campaigns to increase vaccine-related awareness among Canadians and build information-sharing networks to support PHAC's epidemiological, public health and medical expertise and capacity. PHAC also directed IPF solicitation and funding towards vulnerable populations and others disproportionately impacted by COVID-19. This included directed solicitations and amendments to existing projects and launching an open call for solicitations that yielded 228 letters of interest.
PHAC supported provincial and territorial governments' decision-making on vaccination programs through NACI's expert guidance on the use of vaccines, including COVID-19 vaccines. PHAC also continued to implement NACI's expanded mandate, including the application of Economics and the Ethics, Equity, Feasibility and Acceptability (EEFA) Framework to relevant NACI guidance statements. This broader range of evidence and analysis from NACI will further empower provinces and territories to make informed decisions about optimal publicly funded immunization programs suited to their unique population and subpopulations.
The goal of Canada’s COVID-19 immunization response is to enable as many Canadians as possible to be immunized as quickly as possible against COVID-19, while ensuring that high risk populations were prioritized. In November 2020, NACI released guidance on key populations for early COVID-19 immunization to inform planning for the efficient, effective, and equitable allocation of COVID-19, when there was a limited initial vaccine supply. NACI’s Stage 1 recommendation for prioritization included:
- Residents and staff of congregate living settings that provide care for seniors;
- Adults 70 years of age and older, beginning with adults 80 years of age and older, then decreasing the age limit by 5-year increments to age 70 years as supply becomes available;
- Health care workers (including all those who work in health care settings and personal support workers whose work involves direct contact with patients); and
- Adults in Indigenous communities where infection can have disproportionate consequences.
In an effort to respond to the disproportional consequences COVID-19 could have in northern, remote and Indigenous communities, federal, provincial and territorial deputy ministers of Health agreed to provide the Moderna vaccine to all of the territories and to remote and isolated Indigenous communities in sufficient quantities to vaccinate 75% of their population 18 years of age and over.
In March 2021, NACI further recommended that jurisdictions should maximize the number of individuals benefiting from the first dose of vaccine by extending the second dose of COVID-19 vaccine up to four months after the first. The prioritization of key populations and extending intervals between first and second doses helped Canada protect the most vulnerable against the worst outcomes of COVID-19 and move more rapidly to offering vaccines to the general population.
To support the principles of transparency, fairness and equity espoused in Canada's COVID-19 Immunization Plan, the VRTF developed an allocation framework, informed through close engagement with FPT stakeholders across Canada and regular ongoing engagements through the Canadian Immunization Committee (CIC) and the Scientific Advisor Committee (SAC). Due to limited initial vaccine supply availability, FPT governments worked together to develop a clear and transparent process for the allocation of vaccines across jurisdictions , informed by expert advice from public health, scientific and medical experts, including NACI and provincial immunization committees.
This effort resulted:
- In over 5.82 million doses of COVID-19 vaccines being administered by March 27, 2021, representing 11.9% of the total population with at least one dose.
- 73.2% of seniors aged >80 vaccinated with one dose and 9.3% fully vaccinated.
- 33.1% of seniors aged 70-79 vaccinated with one dose and 1.8% fully vaccinated.
- 64.4% of adults in territories vaccinated with one dose and 33.9% fully vaccinated.
- Indigenous Services Canada also reported 246,675 doses had been administered in First Nations, Inuit and territorial communities.
Support clean growth and action on climate change
PHAC continued to support the delivery of the Pan-Canadian Framework on Clean Growth and Climate Change through the implementation of the Infectious Disease and Climate Change Program. The Infectious Disease and Climate Change Program addresses the impacts of climate change on human health by building and increasing access to infectious diseases evidence-bases and developing and disseminating education resources. The Agency continued to invest in projects to mobilize community capacity, support local action and equip health professionals, communities and Canadians with the ability to protect themselves from climate-driven infectious diseases. Since launching the Infectious Disease and Climate Change Fund (IDCCF) in 2017, PHAC has invested in 32 projects that support surveillance and monitoring activities, health professional education and public awareness activities, including several with First Nations and high-risk populations (e.g., children, youth and pregnant people). PHAC also continued work with the Métis National Council and Governing Members to deliver on the dedicated Métis Nation funding to advance action on climate change and health, as committed in Budget 2017.
PHAC worked closely with provinces, territories, non-government organizations, academia, health professionals and others to increase knowledge on climate-driven infectious diseases, associated health risks and measures to protect public health. This included the development of risk communications, education and awareness building resources (videos, infographics), developing and sharing of risk maps and annual surveillance reports, disease forecasting tools and knowledge synthesis on ways to prevent and control identified infectious disease risks. As part of this work, PHAC continued to prioritize non- enteric emerging/re-emerging zoonotic diseases by evaluating multiple conflicting criteria in decision making and by applying a 'one health' lens that incorporates climate impacts. As priority diseases are identified, resources for health professionals will continue to be developed.
Minimize the impact of antimicrobial resistance
Antimicrobial resistance (AMR) places a significant financial burden on the Canadian healthcare system, costing approximately $1.4 billion a year in 2018. If resistance rates to first-line antimicrobials increase to 40% by 2050, it is estimated that the cumulative costs of AMR to the healthcare system will approach $120 billion. Likewise, AMR has had a sizable negative impact on the economy, having reduced Canada's GDP by an estimated $2 billion in 2018. By 2050, if resistance rates remain at 26% or gradually increased to 40%, the economy could lose between $13 and $21 billion per year.
During the pandemic, PHAC published the most up to date analysis of AMR and antimicrobial use (AMU) across Canada in the Canadian Antimicrobial Resistance Surveillance System Report (CARSS). Tracking AMR and AMU from animals, food, the community and hospitals enriches the understanding of AMR across the One Health Spectrum. PHAC also published the Canada Communicable Disease Report, a bilingual, open-access, peer reviewed journal on the prevention and control of emerging and persistent infectious diseases.
In collaboration with the Canadian Integrated Program for Antimicrobial Resistance Surveillance (CIPARS), PHAC posted a suite of communication products on the CIPARS website and supported the presentation of results from the integrated surveillance of AMU and AMR in 2019.
Ongoing AMR monitoring in enteric bacteria from animals, food and people was temporarily scaled back due to the Canada-wide reallocation of public health resources to the COVID-19 response. Despite this resource reallocation towards the COVID response, AMR remains a priority public health concern. Sample collection, laboratory analysis, epidemiological analysis and reporting were conducted when possible while adhering to COVID-19 public health measures. It is anticipated that the scientific learnings, advancements in data sharing and public health capacity built during the pandemic (e.g. wastewater surveillance, lab testing capacity) will provide valuable lessons, learnings, platforms and relationships that can be leveraged to reinvigorate progress on AMR in a post COVID-19 environment.
During the pandemic, PHAC continued to provide support to the Global Health Security Agenda's Action Package on AMR, the Transatlantic Task Force on AMR and the Codex ad hoc Intergovernmental Taskforce on AMR.
Prevent Lyme disease and other tick-borne diseases
PHAC launched an educational campaign aimed at increasing Canadians' awareness of Lyme disease and how to protect against tick bites. The campaign targeted parents of kids ages 0-14 living in higher risk areas, as well as outdoor enthusiasts of all ages. The campaign featured:
- Ads on Facebook, Instagram and various news websites that were also accessible on mobile devices;
- Printed educational and awareness products such as " How to properly remove a tick " wallet cards and " Top 10 Tick Hiding Spots on Your Body " posters;
- The Children's Travelling Tick Exhibit displayed for two months (July-September) at the Museum of Nature and Sciences in Sherbrooke, Québec (scaled back due to COVID-19); and
- In partnership with PHAC, Mark's/Canadian Tire Corporation made a version of PHAC's "Enjoy the Outdoors without a Tick" postcard available at all 380 Mark's retail stores across Canada.
To inform future awareness activities and enhance knowledge sharing, PHAC invested in 15 external projects that aim to enhance surveillance and monitoring activities, increase education and expertise and develop baseline data on the spread and risks of Lyme disease.
In addition, the first edition of the Lyme disease surveillance annual report (2018) was released in February 2021.
Reduce the health impact of sexually transmitted and blood-borne infections
To inform funding priorities and identify culturally-responsive public health actions, PHAC engaged Indigenous partners, community-based organizations and people with lived experience to enable the develop and launch the HIV and Hepatitis C Community Action Fund and the Harm Reduction Fund solicitations.
PHAC continued to monitor and report on the national rates of infection and treatment of HIV, Hepatitis C and other Sexually Transmitted and Blood-borne Infections (STBBI), including syphilis, chlamydia and gonorrhea:
- Published the Report and infographic on Estimates of HIV Incidence, Prevalence and Canada's Progress Towards Meeting the HIV 90-90-90 Targets;
- Published an infographic on national estimates of HCV incidence and prevalence;
- As part of the FPT Syphilis Outbreak Investigation Coordination Committee, published an infographic on national rates of reported syphilis, including congenital syphilis;
- Published the 2018 Canadian Notifiable Disease Surveillance System data on 60 nationally notifiable diseases;
- Published annual HIV surveillance results through a report and infographic; and
- PHAC updated STBBI guidance for health professionals to promote routine offers for testing and to reduce the use of stigmatizing language. PHAC also developed resources to raise awareness among providers following Health Canada's approval of an HIV self-test for use in Canada.
As recommended in the 2019 reports Evaluation of Viral Hepatitis and Sexually Transmitted Infection Activities and the Horizontal Evaluation of the Federal Initiative to Address HIV/AIDS in Canada, PHAC continued work to develop indicators and targets to measure progress against the Pan-Canadian STBBI Framework for Action, in collaboration with provincial, territorial and Indigenous partners. The finalization of the Indicators framework has been limited by federal/ provincial/territorial public health capacity to participate in indicator/target development due to the COVID-19 pandemic and will be restarted in 2021-22 as the pandemic allows.
Result 2.2: Infectious disease outbreaks and threats are prepared for and responded to effectively
Enhance laboratory capacity and laboratory modernization
In response to COVID-19, PHAC worked to enhance laboratory capacity and laboratory modernization. Most notably, PHAC focused on increasing access to diagnostic testing for areas of greatest need, such as remote communities.
Further work to enhance laboratory capacity is evidenced by PHAC's National Microbiology Lab's (NML) collection, sequencing and analysis of Canadian COVID-19 genome sequences for nationwide surveillance, outbreak investigation and response to:
- Establish genetic sequencing capacity to sequence COVID-19 positive samples from incoming travellers to determine if a variant of concern was present; and
- Bolster provincial public health laboratory capacity to implement genomics through the deployment of Genomics Liaison Technical Officers to provincial public health laboratories in areas of greatest need to provide the technical capacity for genomic sequencing to increase processing and reduce turnaround time. The resulting sequence data will feed into national and international data sharing arrangements via the Canadian Public Health Laboratory Network.
While the majority of effort was focused on the COVID-19 response, PHAC continued to provide laboratory capacity, leadership and services for priority pathogens including vector-borne diseases (e.g. Lyme disease), foodborne illness, sexually transmitted and blood borne infections and pathogens with epidemic/pandemic or outbreak potential (e.g. Ebola).
Reduce the incidence of tuberculosis in Canada
As part of the effort to reduce the incidence of tuberculosis (TB) in Canada, PHAC continued collaborative work with federal, provincial, territorial and Indigenous partners to improve national surveillance of active TB disease and TB drug resistance. The goal of this collaborative initiative is to inform, guide and evaluate anti-TB public health actions. This project work started with the production of a detailed 2008-2018 surveillance report, followed by informal engagement with primary provincial and territorial partners. Depending on the availability of resources, this project is anticipated to be completed within the next two to three years.
One of PHAC's commitments was to evaluate the impact of enhanced testing for latent TB infection among a cohort of high-risk migrants. Contracting issues, in addition to global travel restrictions and the limited processing of medical exams abroad, have led to significant delays in PHAC and Immigration, Refugees and Citizenship Canada's efforts to complete the evaluation in collaboration with provincial public health authorities. However, PHAC has continued to support Inuit-led TB elimination efforts in Canada's northern communities by contributing public health expertise and building diagnostic capacity.
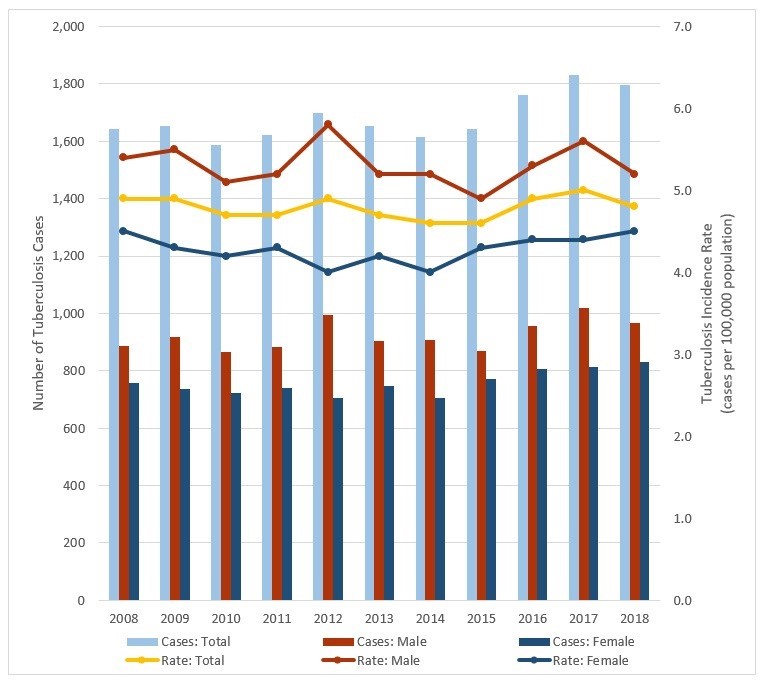
Source: Public Health Agency of Canada – Infectious Diseases Programs Branch
Figure 2 - Text description
This graph depicts the incidence rate of active tuberculosis in Canada between 2008 and 2018 and illustrates the cases and the rate for females, males and the total of both.
| Cases/Rate | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases: Total | 1,642 | 1,654 | 1,586 | 1,621 | 1,700 | 1,654 | 1,616 | 1,643 | 1,763 | 1,831 | 1,797 |
| Rate: Total | 4.9 | 4.9 | 4.7 | 4.7 | 4.9 | 4.7 | 4.6 | 4.6 | 4.9 | 5 | 4.8 |
| Cases: Male | 886 | 917 | 865 | 882 | 994 | 903 | 909 | 870 | 955 | 1019 | 965 |
| Rate: Male | 5.4 | 5.5 | 5.1 | 5.2 | 5.8 | 5.2 | 5.2 | 4.9 | 5.3 | 5.6 | 5.2 |
| Cases: Female | 756 | 737 | 721 | 739 | 706 | 748 | 706 | 773 | 808 | 812 | 831 |
| Rate: Female | 4.5 | 4.3 | 4.2 | 4.3 | 4 | 4.2 | 4 | 4.3 | 4.4 | 4.4 | 4.5 |
Reduce impact of foodborne illness outbreaks
PHAC continued to support the collection and reporting by the National Enteric Surveillance Program on the national incidence of foodborne pathogens. Working in collaboration with provincial public health laboratories, represented by the Canadian Public Health Laboratory Network, PHAC analysed submissions and reported the findings on a weekly basis to these laboratories and to other stakeholders such as federal and provincial/territorial epidemiologists, researchers and public health professionals.
PHAC continued to facilitate FoodNet Canada, a multi-partner initiative that supports activities that will reduce the burden of enteric disease through comprehensive sentinel site surveillance, implemented through local health units and provincial public health laboratories. As such, PHAC facilitated:
- FoodNet Canada/ Canadian Integrated Program for Antimicrobial Resistance Surveillance's results on pathogen levels found on retail meat products that were provided to federally inspected establishments; and
- The FoodNet Canada tables and figures report that provides the annual results of the Agency's surveillance activities conducted in 2019.
In 2019, there was a significant national decrease in the human incidence rate for Salmonella Enteritidis (overall decrease of 33%, from 2017-2019 inclusive) observed and communicated to stakeholders through PHAC foodborne disease surveillance programs. This suggests that collective efforts and multiple interventions including food safety and public health awareness initiatives may have contributed to the decrease in occurrence of S. Enteritidis infections.
PHAC continues to work collaboratively with international, federal and provincial/territorial partners, to detect and respond to multi- jurisdictional foodborne illness outbreaks in a timely manner, including responding to a number of outbreaks from various pathogens and food sources.
Maintain vigilance for existing and emerging respiratory disease threats
PHAC maintained timely detection and response to various respiratory infectious disease outbreaks based on epidemiological analysis, risk assessments and surveillance assessments which contributed to the identification and control of new respiratory infectious disease threats. For example, PHAC responded to multiple emerging respiratory pathogen events, such as H1N1v and H1N2v (Swine Influenza) in Manitoba and H1N2v in Alberta. To ensure situational awareness of emerging respiratory pathogens, PHAC conducted weekly analysis of human emerging respiratory pathogens reported internationally and domestically, summarized in an Event Bulletin.
PHAC quickly developed new and enhanced surveillance initiatives in response to COVID-19. This included pivoting the FluWatchers program for COVID-19 syndromic surveillance, with an increase in participation of 10,000 new participants. When COVID-19 vaccines were rolled out in Canada, FluWatchers was further able to add a question on immunization status.
Through the creation of the Outbreak Response Unit for COVID-19, PHAC has increased the Agency's capabilities to respond to future respiratory infectious disease outbreaks and provide outbreak response coordination to the provinces and territories.
Sex and Gender-based Analysis Plus
PHAC continued its efforts to advance the implementation of an SGBA Plus lens into research and surveillance areas, where infectious agents may affect sexes differently and/or where sex/gender could influence the risk of infection. PHAC also continued to explore new approaches to ensure equitable access to testing across geographic regions, cultures and other factors (i.e., including, but not limited to, sex and gender).
PHAC supported several initiatives focused on vulnerable populations, remote communities and areas in which a particular population was disproportionately affected by an infectious disease. Using an SGBA Plus lens, PHAC analysed sex, age and other identifying factors to inform program responses in 2020-21, including:
- Determining the levels and trends in COVID-19 infection through seroprevalence assessments across age groups, risk groups and occupational and geographical hotspots in Canada;
- Working extensively with provincial and territorial partners to improve the national COVID-19 case report form and allow for the collection of information such as race, occupation and other social-economic variables at the national level;
- Addressing issues of variable risk factors among women, men and gender-diverse people (e.g., to provide equitable access to the program or service) when designing interventions that address the needs of diverse populations; and
- Conducting surveys on the impact of COVID-19 among key populations (e.g., African, Caribbean and Black Canadians; people who use drugs; and Indigenous peoples) to inform the development of guidance and public health practices.
PHAC supported a cohesive and historic COVID-19 vaccine rollout across Canada with SGBA+ considerations integrated into all stages of Canada's COVID-19 Immunization Program to better identify health inequities across Canada's diverse populations. The vaccine program is intended to benefit all Canadians equitably and from the beginning therefore, PHAC followed NACI's guidance to identify priority populations, which included age-group, sex and key populations (e.g., seniors 80 years of age or older, healthcare workers, long-term care and other congregate living residents and populations in remote and isolated communities). As well, since January 2021, PHAC has been posting pan-Canadian data on vaccine coverage on a weekly basis. PHAC has also closely monitored the safety and effectiveness of approved COVID-19 vaccines though an SGBA Plus lens.
When collecting information on the impact of COVID-19 on access to and delivery of Sexually Transmitted and Blood-Borne Infection (STBBI) prevention, testing, treatment services and harm reduction services among Canada's vulnerable populations (e.g., people from African, Caribbean and Black (ACB) communities, Indigenous peoples (on and off reserve) and people who use drugs), PHAC applied an SGBA Plus lens.
Innovation and experimentation
Building on the success of previous experimentation initiatives, the National Microbiology Lab (NML) evaluated the feasibility of using dried blood spots (DBS) for sample collection for COVID-19 testing. DBS allows for easier collection (it does not require a medical professional) and transportation (there are no temperature stability limitations) making it an ideal method to reach remote or underserviced areas or increase participation in research studies. The NML engaged with public health partners involved in the COVID-19 Immunity Task Force to provide support and guidance on the use of DBS for large-scale studies of immunity in Canada and targeted populations (e.g., long-term care homes, correctional facilities, education workers). In 2020-21, PHAC securely transmitted over 75,000 genomes and associated metadata to the Canadian COVID Genomics Network (CanCOGeN) National Database and provided real-time electronic requisition and reporting of over 150,000 border testing samples and associated sequence data in support of the Federal Border Testing program.
In support of cross-jurisdictional collaboration, PHAC began experimenting with digital technology to develop a proof-of-concept platform to inform future developments of data infrastructure for other surveillance programs (i.e. beyond COVID-19). This platform- National COVID-19 Public Health Surveillance Platform and Portal -aims to improve the collection, management and sharing of data with provinces and territories through access to centralized and interoperable public health data within an analytical environment supported by modern agile tools and appropriate confidentiality and security controls.
Vaccinations - interactive portal for the Canadian Immunization Guide
Through the Innovative Solutions Canada Program (ISC), PHAC continued to experiment with Canadian businesses to create an interactive portal assisted by artificial intelligence for the Canadian Immunization Guide. This tool aims to address gaps in knowledge and beliefs and will make it easier for health-care providers and the general public to find answers to their vaccine- relevant questions based on the expert and evidence-based guidance of the NACI.
Foodborne Illnesses - an interactive approach to sharing surveillance data
To improve accessibility to PHAC's surveillance data for multiple purposes, audiences and end users, the Agency continued experimenting with new interactive ways of providing data on foodborne illnesses to stakeholders and senior management in an expedited manner. The scope of this work was temporarily expanded to include COVID-19 as part of PHAC's public health response. This initiative would also provide greater flexibility in customizing analysis requirements based on needs.
2030 Agenda for Sustainable Development
PHAC continued to support Canada's efforts to implement the United Nations' 2030 Agenda for Sustainable Development and contribute towards global targets under SDG 3: "Good Health and Well-Being." PHAC supported this goal through initiatives aimed at increasing vaccination rates, reducing health impacts of Sexually Transmitted and Blood-Borne Infections (STBBI) and enhancing laboratory capacity through modernization. These initiatives continue to support global targets related to reducing the rates/occurrences of tuberculosis and hepatitis, the management of national and global health risks and vaccine research and development.
As part of Canada's efforts to take action to address SDG 13: "Climate Action," PHAC continued to support the Pan-Canadian Framework on Clean Growth and Climate Change, Canada's plan to meet its Paris Agreement commitments, stimulate Canada's economy and build climate resilience across the country, specifically as it relates to the priorities to protect and improve human health and well-being. PHAC also supported government-wide efforts to implement Canada's strengthened climate plan: A Healthy Environment and a Healthy Economy, to create jobs and support people, communities and the planet.
By increasing access to infectious disease evidence-bases and developing and disseminating educational and awareness raising resources, PHAC continued to address the impacts of climate change on human health.
| Departmental results | Performance indicators | Target | Date to achieve target | 2018-19 Actual results |
2019-20 Actual results |
2020-21 Actual results |
|---|---|---|---|---|---|---|
Infectious diseases are prevented and controlled |
% of 2 year old children who have received all recommended vaccinations |
At least 95% |
Dec. 31, 2025 |
Data is collected bi-annually |
68% |
Data is collected bi-annually |
Proportion of national vaccination coverage goals met for children by 2 years of age |
Exactly 7 Footnote 1 |
Dec. 31, 2025 |
Data is collected bi-annually |
0/7 |
Data is collected bi-annually |
|
Rate per 100,000 of new diagnosed cases of Human Immunodeficiency Virus (HIV) Footnote 2 |
0.6 Cases per 100,000 population |
Dec. 31, 2030 |
6.5 Cases per 100,000 (2017) |
6.9 Cases per 100,000 (2018) |
5.6 Cases per 100,000 (2019) |
|
Rate of a key antimicrobial resistant infection identified among people in hospitals |
At most 0.7 cases per 1,000 patient admissions Footnote 3 Footnote 4 |
June 30, 2025 |
0.78 cases per 1,000 patient admissions (2018) |
0.82 cases per 1,000 patient admissions (2019) |
Expected date of data availability is Fall 2021 |
|
Infectious disease outbreaks and threats are prepared for and responded to effectively |
% of foodborne illness outbreaks responded to within 24 hours of notification |
At least 90% Footnote 5 |
Mar. 31, 2022 |
91% |
98% |
93% |
% of new pathogens of international concern that Canada has the capacity to accurately test for |
At least 90% |
Mar. 31, 2022 |
100% (2018) |
100% (2019) |
100% (2020) |
|
Footnotes
|
||||||
| 2020-21 Main Estimates |
2020-21 Planned spending |
2020-21 Total authorities available for use |
2020-21 Actual spending (authorities used) |
2020-21 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 210,906,872 | 210,906,872 | 12,877,517,135 | 3,794,133,883 | 3,583,227,011 |
Variance between Actual spending and Planned spending is explained in the section "Analysis of trends in spending and human resources." |
||||
| 2020-21 Planned full-time equivalents |
2020-21 Actual full-time equivalents |
2020-21 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 1,073 | 1,149 | 76 |
| Variance between Actual full-time equivalents and Planned part-time equivalents is explained in the section "Analysis of trends in spending and human resources." | ||
Financial, human resources and performance information for PHAC’s Program Inventory is available in GC InfoBase.
3. Health Security
Description
Prepare for and respond to public health events and emergencies; address health and safety risks associated with the use of pathogens and toxins; and address travel-related public health risks.
Results
The Departmental Results are:
- Public health events and emergencies are prepared for and responded to effectively.
- Public health risks associated with the use of pathogens and toxins are reduced.
- Public health risks associated with travel are reduced.
Result 3.1: Public health events and emergencies are prepared for and responded to effectively.
Strengthen Canada's public health emergency preparedness and response system
To further position PHAC as a trusted leader in public health emergency management, PHAC established a new Emergency Management Branch (EMB) as a Health Portfolio resource for the prevention and mitigation of, preparedness for, response to and recovery from emergencies. EMB provides 24/7 support, coordination, resources, information and expertise to all Health Portfolio programs to help identify, develop, test and implement public health emergency management measures. EMB continues to develop a sustainable support structure that enables a scalable, timely and coordinated response to and recovery from, the on-going COVID-19 pandemic, as well as future public health events and emergencies with a view to minimize negative impacts to the health and safety of Canadians.
The Federal Health Portfolio Operations Centre (HPOC) is the Health Portfolio's focal point for the coordination of response activities related to public health emergencies. Through the establishment of a COVID-19 Public Health Rapid Surge Capacity initiative, PHAC served as a single window for provinces and territories to coordinate surge support for their COVID-19 responses, under eight fields: Public Health Rapid Response Team; Outbreak Management; COVID-19 Patient Testing; Laboratory Services; Laboratory Equipment; Contact Tracing; Safe Voluntary Isolation Sites; and Human Resources Recruitment. This initiative resulted in a more efficient identification and deployment of supports to meet federal/provincial/territorial needs.
Since January 15, 2020, COVID-19 pandemic response efforts have been managed through a dedicated network of public health emergency response specialists. PHAC mobilized significant human and financial resources to enable:
- Timely, relevant and credible communications with Canadians;
- Access to safe and effective vaccines to protect against COVID-19;
- Rapid procurement and distribution to safe and effective COVID-19 therapeutics;
- Border measures to reduce the risk of COVID-19 importation;
- Increasing the remote support capacity for health and quarantine assessments 24/7 to address border demands during peak periods or where traveller volumes do not warrant on-site presence;
- Compliance promotion and enforcement of the Quarantine Act;
- The establishment of designated quarantine facilities and government-authorized accommodations;
- Federal testing support;
- The establishment of the COVID-19 Public Health Rapid Surge Capacity initiative;
- COVID-19 research and surveillance (e.g., serological surveillance and research, innovations in wastewater surveillance);
- COVID-19 information, data and guidance (e.g., improve data availability and analysis, understanding the societal impacts, supporting informed decision-making, mathematical modelling);
- Public health guidance on COVID-19 infection prevention and control (e.g., community-level support, support for distress centres); and
- Procurement and distribution of Personal Protective Equipment (PPE), vaccine ancillary supplies, other medical equipment (including biomedical equipment), drugs and supplies.
PHAC invested approximately $4.1 billion in the procurement and distribution of PPE, medical equipment, therapeutics and other supplies in support of Canada's COVID-19 response. This required robust quality assurance processes to assess the safety and quality of purchased supplies and equipment.
PHAC supported the ongoing placement of 24 Public Health Officers (e.g., Epidemiologists and Nurses) to support provinces and territories in advancing shared federal, provincial and territorial public health priorities (e.g., substance-related harms, Sexually Transmitted and Blood-Borne Infections (STBBI), Tuberculosis). PHAC hired and placed an additional 12 Public Health Officers to address pressing needs related to COVID-19 response across Canada. In addition, PHAC's COVID-19 response mobilized 28 nurses (Quarantine Officers) to support repatriation sites at Trenton and Cornwall and another 15 nurses at the airports.
Furthermore, PHAC supported 40 requests for assistance coming from provinces, territories, and federal partners needing surge epidemiological support for COVID-19 response and other public health threats. These requests for assistance resulted in the mobilization of 45 epidemiologists, which is more than double the average number of yearly mobilizations pre-pandemic.
To better situate Canada's response to emerging or re-emerging infectious diseases and related challenges, PHAC further integrated with the Security and Intelligence (S&I) community. In the context of COVID-19, PHAC engaged in ad hoc structures alongside key S&I departments and partners to prepare and protect the vaccine rollout in Canada and share intelligence to inform Canada's pandemic response.
To test PHAC's response capacity and capability, the Agency conducted simulated public health exercises, including for example, the development of interdepartmental public health emergency exercises related to a simulated vaccine roll-out and a simulated international outbreak of Ebola. PHAC also initiated a robust exercise program, in collaboration with the Public Health Infrastructure Steering Committee of the pan- Canadian Health Network, with the aim of testing Canada's response to a pandemic influenza outbreak. This exercise program was ultimately put on hold due to the COVID-19 pandemic.
Did you know?
PHAC's National Emergency Strategic Stockpile (NESS) managed the movement of approximately 3.5 billion units of PPE, medical equipment, and supplies, through an expanded warehousing and logistics infrastructure?
PHAC's NESS also responded to 99 requests for assistance from provinces and territories and managed the deployment of vaccine ancillary supplies, and other medical equipment and supplies to provinces and territories in support of the COVID-19 vaccine rollout.
This past year has proved the importance of remaining prepared for any type and scale of health emergency. PHAC has continued to work with other government departments and agencies, as well as Indigenous, international and domestic partners to strengthen the Agency's capacity to prepare for and respond to public health events and emergencies. This included securing long-term funding to maintain and enhance the stockpile of medical countermeasures in the National Emergency Strategic Stockpile (NESS) to respond to chemical, biological and radiological, or nuclear events.
Result 3.2: Public health risks associated with the use of pathogens and toxins are reduced
Strengthen regulatory oversight of Canadian laboratories and promote compliance
Pathogens and toxins pose a risk to Canadians because of their ability to cause disease or death. These agents are used in a wide range of Canadian sectors for many different purposes including: teaching and research at universities, disease diagnosis at hospitals and public health facilities and vaccine development in the pharmaceutical industry.
PHAC regulates the use of human and terrestrial animal pathogens and toxins to protect the health and safety of the public. Program components are designed to prevent both the accidental release of these agents from a laboratory, including by way of an infected worker and deliberate release by way of an act of terrorism or other criminal activity.
In response to COVID-19 pandemic, PHAC cancelled all planned on-site inspections and in consultation with domestic and international regulatory counterparts, strengthened regulatory oversight by developing the capacity and capability to conduct virtual inspections. In total, PHAC conducted 6 virtual inspections and a further 26 oversight activities to assess compliance of Canadian laboratories with regulatory requirements.
PHAC also adapted internal policies and procedures to streamline licensing and security clearance processes in light of the pandemic while implementing strategies to manage higher than normal application volumes. In total, the Agency issued 679 Pathogen and Toxin licences and a further 47 Human Pathogen and Toxins Act security clearances.
PHAC also provided critical scientific and regulatory guidance to Canadian laboratories on the novel pathogen SARS-CoV-2-the virus that causes COVID-19-including:
- Issuing biweekly updates of PHAC's SARS- CoV-2 pathogen risk assessment to maintain an accurate risk group classification as new information on the virus became available;
- Publishing two updates to PHAC's Biosafety Advisory for SARS-CoV-2 to support local risk assessments and assist clinical, diagnostic and research laboratories in implementing proper biosafety procedures to handle samples that may contain SARS- CoV-2; and
- Developing a set of frequently asked questions on working with samples of SARS-CoV-2 to help facilities navigate the regulatory requirements for the safe handling of a novel pathogen.
Notably, the Agency published a guideline on Biosafety in the Elementary, Intermediate and Secondary School Classroom to help keep students, teachers, personnel and the community safe.
Given PHAC's continued engagement in COVID-19 response efforts, the 5-year review of the 2015 Human Pathogens and Toxins Regulatory framework, originally planned for 2020-21, has been postponed with a new target completion date of March 2022. Preliminary work undertaken in 2020-21 includes stakeholder consultations and the collection of external expert recommendations to enhance the effectiveness of the regulatory framework.
Advance global health priorities in biosafety and biosecurity
PHAC supported the implementation of the International Health Regulations by influencing high impact programs and policies to build sustainable international health security capacity. The Agency collaborated with international partners in the Global Health Security Agenda Action Package Prevent-3 on Biosafety and Biosecurity to draft a joint statement highlighting that safety and security should remain key considerations as countries rapidly bolster their laboratory and disease surveillance surge capacities in response to COVID-19. PHAC also maintained attendance at GHSA and Global Partnership Working Group meetings, taking opportunities to promote PHAC products such as the Analytical Approach, a tool to strengthen global biosafety and biosecurity.
PHAC secured re-designation as a World Health Organization (WHO) Collaborating Centre for Biosafety and Biosecurity for a 4-year term, demonstrating its ongoing support for the WHO.
PHAC also continued to support global efforts to effectively contain poliovirus. As Canada's national authority for containment, PHAC ensured Canada met its international commitments for global polio eradication. PHAC:
- Submitted Canada's 2019 Annual Polio Eradication and 2020 Polio Containment reports to the Pan American Health Organization;
- Actioned and implemented the Regional Certification Commission 2019 recommendations, including risk mitigation strategies in accordance with the WHO poliovirus potentially infectious material (PIM) guidance risk-classification; and
- Met Canada's international commitments under World Health Assembly Resolution 71.16 by continuing work in reducing the number of facilities intending to retain poliovirus infectious or potentially infectious material through targeted outreach.
PHAC struck an Intelligence Coordination Working Group for Communications with the Biosecurity program Regulated Parties (RP) to coordinate and share unclassified information with the research community. Members include security and intelligence partners from other government departments. The working group collaborated on two RP reported suspicious incidents, two alerts issued to RPs and Chief Medical Officers of Health and a newsletter article issued to regulated and interested parties.
PHAC also participated in the G7 Experts' Meeting on Strengthening Laboratory Biorisk Management. This meeting explored how the G7 can advance evidence-based and transparent laboratory biorisk management practices. Expert participants developed 11 recommendations to advance by harnessing and amplifying ongoing work, especially with respect to multilateral collaboration and scientific exchanges.
PHAC shared information in the ongoing work of the independent expert group convened by the United Kingdom, as chair of the G7, which reviewed supply for key sectors, including health, the identification of emerging risks, common vulnerability indicators and methodologies and development of forecasting exercises and crisis simulations on supply chain disruptions.
Result 3.3: Public health risks associated with travel are reduced
Improve Canadian's knowledge of travel-related public health risks
Management of Canada's Points of Entry (PoE) was critical in detecting and preventing COVID-19 and its variants from entering the country. As a result of border measures introduced by PHAC and other government departments and agencies for management of the COVID-19 pandemic, total monthly travellers entering Canada declined from 4.6 million in March 2020, to 1.0 million in March 2021 (Statistics Canada, Table 24-10-0041-01, International travellers entering or returning to Canada, by type of transport). This decrease, together with quarantine and screening measures for travellers, significantly mitigated the risk of importing cases of COVID-19. To help achieve this, PHAC increased the number of Public Health Officers to 188 at Canada's four main international airports. PHAC also increased the number of Public Health Officers present at 16 land PoE to 132 daily. To reduce the likelihood of COVID-19 entering the country without detection, PHAC established a national testing perimeter which included the capability to provide genetic sequencing of positive cases for detection of variants of concern.
PHAC played an important role in communicating with Canadians on travel-related public health risks. Using the Government of Canada's travel.gc.ca website and social media, PHAC increased awareness among travellers of Canada's border measures and traveller obligations. PHAC also leveraged industry partners such as air carriers to promote Canada's requirements to air travellers.
PHAC also developed a framework that analyzed the risks associated with easing border measures, ensuring ongoing discussion with other government departments and provincial/ territorial stakeholders as new measures were considered and/or existing measures eased.
Manage travel-related public health risks on passenger conveyances and at the border
To minimize the introduction and spread of COVID-19 and its variants into Canada, PHAC worked with other government departments, provincial and territorial counterparts and private sector stakeholders and partners to develop robust policy proposals and to implement measures to manage public health risks associated with travellers entering Canada's international borders. For example, PHAC worked closely with Immigration, Refugees and Citizenship Canada, Global Affairs Canada and the provinces and territories on a process for designated learning institutions to confirm their readiness to safely receive international students; consequently, the Orders in Council prohibiting entry into Canada under the Quarantine Act were amended in October 2020 to allow the entry of students to attend a list of institutions.
PHAC worked with other government departments to plan and implement processes to gradually ease border restrictions under certain conditions for key cohorts, including to support greater family reunification, entry for compassionate reasons and the safe and gradual entry of some international students.
PHAC also monitored international public health events while working with the travel industry and federal, provincial and international partners to prepare for, identify and respond to health events, as required. PHAC also increased internal and external stakeholder engagement, which has been key in PHAC's COVID-19 response and overall decision making. As such, PHAC:
- Sustained the Agency's international engagement to ensure the PHAC pandemic response is coordinated with key partner countries and multilateral institutions like the World Health Organization;
- Strengthened partnerships with provinces and territories, including
through:
- Engagement and consultation on proposed border measures and compliance and enforcement referrals; and
- Development of mechanisms to ensure that post-secondary institutions were prepared to support incoming international students and had COVID-19 readiness plans in place.
- Worked with federal partners to facilitate the entry, testing and quarantine of Temporary Foreign Workers in Canada, who work in the agriculture, agri-food, fish and seafood sector
- Worked with industry and service providers to implement border measures, such as testing, designated quarantine facilities, government-authorized accommodations and compliance verification and enforcement, to manage public health risks; and
- Focused efforts on areas of greatest risk to public health by conducting potable water, food and sanitation inspections of aircraft, ferries, trains and cruise ships and their ancillary services. For example:
- PHAC inspected 91 conveyances and their ancillary services for compliance with potable water, food safety and sanitation. Conveyances and ancillary services included 57 ferries; 7 aircraft; 2 trains; 14 flight kitchens; 4 supply depots; 4 aircraft terminals; and 3 marine terminals. For the period of April 1, 2020, to March 31, 2021, 100% of inspected passenger transportation operators were in compliance.
Sex and Gender-based Analysis Plus
When procuring PPE for the healthcare sector, PHAC's National Emergency Strategic Stockpile purchased a wide range of products in various sizes that will fit the majority of healthcare workers regardless of gender. Research had indicated a roughly even split between women and men in non-healthcare sectors that require PPE, and that there are higher numbers of women in the healthcare sector compared to other sexes and genders. While this information omits non-binary individuals, it indicated the wide range of product sizes required.
PHAC's Biosecurity Program measures its impact on a broader scale that includes all Canadians and devises its implementation strategy accordingly. For example, the program considered specific health risks to particular populations (e.g., sex, gender, children, elderly, etc.) in the development of a Pathogen Risk Assessment and Pathogen Safety Data Sheets, enabling stakeholders to perform their duties effectively.
New border measures implemented were subject to on-going assessment for potential disparate impacts based on both biological differences (sex-based, ability-based, age-based) and socio-cultural differences (gender-based, geographical location-based, language- and literacy-based, etc.). Where actual or potential disparate impacts were identified, mitigations were developed and implemented; for example:
- In April 2020, the Mandatory Isolation Order in Council was amended to clarify that medical care professionals entering Canada cannot provide direct care to the most vulnerable population of persons over age 65; and
- In June 2020, the Mandatory Isolation Order in Council was further amended to provide exemptions for persons living in transborder communities, in particular the Mohawk Community of Akwesasne.
PHAC additionally focused exemptions from border measures to mitigate disparate impacts when possible, including to government-authorized accommodations (GAA), by applying an SGBA Plus lens for: age, gender, ability/ dependency, geographical location and social, cultural, or economic status; for example:
- In February 2021, the Quarantine Isolation and Other Obligations Order in Council was amended to provide an exemption for unaccompanied minors from the stay in (GAA) pending receipt of a negative on-arrival test; and
- In March 2021, the Quarantine Isolation and Other Obligations Order in Council was further amended to provide an exemption for dependent adults from the stay in GAA pending receipt of a negative on-arrival test.
Innovation and experimentation
Due to physical distancing requirements, public health measures and limited domestic travel across provincial borders, PHAC's Biosecurity inspection program was temporarily paused. In order to reinstate regulatory inspections under the Human Pathogens and Toxins Act and Regulations amid the ongoing restrictions, the program explored the development of a virtual approach to conduct inspections which was successfully implemented. Four pilot virtual inspections of containment level 2 laboratories were conducted, consisting of two small single room laboratories and two larger multi-suite labs. For the duration of the pandemic, amid ongoing restrictions, PHAC will continue to undertake virtual inspections for all planned inspections. In a post-pandemic environment, this approach to inspections will provide the ability to conduct (some) oversight function remotely, resulting in the potential for cost savings, including a significant reduction in travel costs and/or expanded program reach.
2030 Agenda for Sustainable Development
PHAC supports the United Nations 2030 Agenda and Sustainable Development Goal 3: Ensure healthy lives and promote well- being for all at all ages, by providing countries with technical assistance and tools to meet commitments under the International Health Regulations and enhancing global development of biosafety and biosecurity oversight frameworks. Specifically, PHAC:
- Participated on an ongoing basis in fora with multiple international partners to share knowledge and expertise. This included support for the WHO, the Global Health Security Agenda and the Global Partnership against the Spread of Weapons and Materials of Mass Destruction, among others. These engagements provided PHAC with opportunities to promote Canadian resources and best practices, share information and learn about activities and initiatives being undertaken by other countries, demonstrating Canada's interest in and commitment to building international biosecurity capacity; and
- The International Experts Groups of Biosafety and Biosecurity Regulators, of which PHAC is a member and secretariat, promoted the launch of its free mobile application "Compendium of International Biosafety and Biosecurity Oversight Systems for Human and Animal Pathogens and Toxins" among its international stakeholders. The app serves as a capacity- building reference tool by comparing and contrasting the different regulatory aspects of its member countries, which can be used to simplify the development and implementation of biosafety and biosecurity oversight, enabling measures for good health and well-being in partner countries.
| Departmental results | Performance indicators | Target | Date to achieve target | 2018-19 Actual results |
2019-20 Actual results |
2020-21 Actual results |
|---|---|---|---|---|---|---|
Public health events and emergencies are prepare for and responded to effectively |
Canada's readiness to respond to public health events and emergencies as addressed independently by the World Health Organization |
4 (Rating out of 5) |
Jun. 30, 2023 |
4.5 |
4.5 |
4.5 |
% of provincial and territorial requests for assistance responded to within negotiated timelines |
Exactly 100% |
Mar. 31, 2022 |
100% |
100% |
100% |
|
Public health risks associated with the use of pathogens and toxins are reduced |
% compliance issues in Canadian laboratories successfully responded to within established timelines |
At least 85% |
Mar. 31, 2022 |
88% |
98% |
100% |
Public health risks associated with travel are reduced |
Canada's capacity for effective public health response at designated points of entry into Canada |
4 (Rating out of 5) |
Mar. 31, 2023 |
5 |
5 |
5 |
% of inspected passenger transportation operators that meet public health requirements |
95% |
Mar. 31, 2022 |
94% |
96% |
100% |
| 2020-21 Main Estimates |
2020-21 Planned spending |
2020-21 Total authorities available for use |
2020-21 Actual spending (authorities used) |
2020-21 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 51,775,030 | 51,775,030 | 7,435,379,211 | 4,459,284,771 | 4,407,509,741 |
Variance between Actual spending and Planned spending is explained in the section "Analysis of trends in spending and human resources section." |
||||
| 2020-21 Planned full-time equivalents |
2020-21 Actual full-time equivalents |
2020-21 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 389 | 743 | 354 |
| Variance between Actual full-time equivalents and Planned full-time equivalents is explained in the section "Analysis of trends in spending and human resources section." | ||
Financial, human resources and performance information for PHAC’s Program Inventory is available in GC InfoBase.
Internal Services
Description
Internal Services are those groups of related activities and resources that the federal government considers to be services in support of Programs and/or required to meet corporate obligations of an organization. Internal Services refers to the activities and resources of the 10 distinct services that support Program delivery in the organization, regardless of the Internal Services delivery model in a department. These services are:
- Management and Oversight Services
- Communications Services
- Legal Services
- Human Resources Management Services
- Financial Management Services
- Information Management Services
- Information Technology Services
- Real Property Management Services
- Materiel Management Services
- Acquisition Management Services
Results
PHAC focused on advancing the following results:
- Building a healthy, diverse and inclusive workforce; and
- Modernizing the workplace to enable a safe and productive workforce with access to modern tools and facilities.
To make progress towards achieving these results, PHAC focused its efforts on key initiatives and activities that mitigate the impact of COVID-19 on how the Agency works. PHAC worked to support employees in their adaptation to remote work, ensuring the availability of mental health supports, increasing awareness on the importance of diversity and inclusion in the Agency and realigning the organization to deliver critical programming and services throughout the pandemic.
See the Spotlight on PHAC's COVID-19 Response for additional information on the work behind the scenes as the Agency ramped up human and financial resources, increased communications and engagement with Canadians beyond anything it had done in the past and delivered meaningful and impactful awareness campaigns.
Results highlights
Building surge capacity
As PHAC has been addressing the COVID-19 pandemic, management of human resources has become a crucial aspect of the Agency's ability to support Canadians. This year, PHAC became responsible for various new taskforces, such as those for borders and quarantine, as well as the vaccine roll out, which has further cemented the importance of adaptive human resource management.
Over that time, from the initial period of "surge," the Agency used flexible staffing processes and internal rotations to ensure PHAC was securing timely access to PPE. As the impacts and implications of COVID-19 continued to evolve, efforts began to shift towards building the capacities necessary to tackle the growing implications and challenges that COVID-19 would bring, such as increased physical presence at the border, increased testing capacity, a vaccine roll out plan and the establishment of quarantine facilities. PHAC worked quickly to build surge capacity, adding 1,464 new full-time equivalents between 2020 and 2021, to tackle short-term emergencies and due to this, the Agency needed to greatly consider the well-being of the organization itself. Moving forward, maintaining organizational well-being remains vital to the development of the Agency and its ability to respond to future emergencies.
Organizational well-being
As the need for pandemic response activities spanned the entire fiscal year and continues to be required for a yet to be determined period going forward, it is crucial that PHAC bolsters its organizational well-being and sustains the long-term health and well-being of each of its employees. Recognizing the acute need to ensure the well-being of PHAC and Health Canada employees in order to continue supporting the well-being of all Canadians, the Corporate Services Branch's Employee Assistance Services (EAS) enhanced its services and delivery in the following ways:
- The creation of the COVID-19 Mental Health Response (CMHR) Unit to
support the acute mental health-related needs of PHAC employees. The Unit
serves three main functions:
- Proactive outreach: to senior management to address pressing health-related needs at the individual, team and organizational levels;
- Research: best practices and preferred mental health interventions; and
- Assessment, Advice and Service Coordination: to propose holistic mental health interventions that include internal and external resources.
The 2020 Public Service Employee Survey Results revealed that during the COVID-19 pandemic, 87% of PHAC respondents believed the Agency has effectively communicated the mental health services and resources available to them. Despite this, only 63% of PHAC respondents believed senior managers in the agency have taken adequate steps to support the mental health of employees during pandemic. While PHAC effectively promoted and communicated mental health services available to employees, there is still work to be done to encourage a healthy work-life balance at all levels of the organization.
In alignment with Bill C-65, PHAC enhanced measures for the prevention of harassment and violence, including launching the Policy and Directive on Workplace Health and Violence Prevention and implementing mandatory training for all employees, continuing to build a safe and inclusive workplace.
PHAC also worked with the community of persons with disabilities to encourage their success as public servants by creating a one stop Workplace Wellness Service Centre to support employees and managers with implementing accommodations. This simplified the process to ensure employees have the tools and supports they need to do their job. The success of this program was recognized as it was nominated by the Office of Public Service Accessibility for an International Innovation Award.
Functional realignment
The Agency has grown significantly this year through the framework of PHAC's Re-alignment project that has taken the organization from 3 branches to 8 in order to tackle the pandemic on a global scale, while increasing organizational effectiveness and resiliency. The growth and increase of various Health programs aimed to ensure that new or redesigned programs were able to support the increased responsibilities PHAC has to Canadians during the pandemic.
Diversity and inclusion
PHAC continued to foster a diverse and inclusive workforce by inviting employees to come together virtually to celebrate the achievements of various communities and to raise awareness of ongoing challenges and bias faced by community members. PHAC celebrated its 15th annual Diversity and Inclusion Week with the theme of "Creating a Barrier-Free Workplace," launching tools and resources to help employees and their teams foster a more diverse and inclusive workplace. PHAC also encouraged employees to join networks related to diversity and inclusion that engage senior management to create actions that will bring positive change, address representativeness and measureable progress towards a more diverse and inclusive workplace that is free from bias and discrimination. In the 2020 Public Service Employee Survey Results, it was revealed that 84% of PHAC respondents felt that the people who they work with value their ideas and opinions and 85% believed that overall, the Agency treats them with respect. The Agency is committed to fully implementing all aspects of the Clerk's Call to Action on Diversity and Inclusion, issued in January 2021.
Employment equity
As shown in the graphs below, PHAC's representation of visible minorities and women in the organization surpasses the Labour Market Availability of both groups. The Agency still has room for improvement in achieving employment equity for Indigenous peoples and persons with disabilities. PHAC is continuing to build partnerships with educational institutions across Canada to promote and market opportunities to Indigenous communities as well as persons with disabilities. To assist managers in their recruitment efforts, PHAC promoted an Inclusive Recruitment Guide and improved the Unconscious Bias training already in place, which will be made mandatory for all managers at PHAC by 2022.

Source: Public Health Agency of Canada – Corporate Services Branch
Figure 3 - Text description
| Visible Minorities | Indigenous People | Women | Persons with Disabilities | |
|---|---|---|---|---|
| Representation | 21.6% | 2.8% | 69.3% | 4.4% |
| LMA 2012 | 19.5% | 3.7% | 63.6% | 4.1% |
| LMA 2017 | N/A | N/A | N/A | 8.2% |
Note: Under the Employment Equity Act, PHAC strives to meet representation levels, based on estimated workforce availability, for the four employment equity designated groups: women, Aboriginal peoples, persons with disabilities and members of visible minorities. Labour Market Availability (LMA) figures for visible minorities, Indigenous Peoples and Women are based on the 2016 Census. LMA figures for Persons with disabilities are based on the 2012 or 2017 Canadian Survey on Disability (CSD). Between 2012 and 2017, the CSD was changed to incorporate a broader set of disabilities; however, the self-id process was not modified to reflect these changes. Therefore, users are able to compare representation to either LMA.
Improve access to modern tools and facilities
COVID-19 brought fundamental change to the way we work. In 2020-21, PHAC employees were asked to work remotely whenever and wherever possible, while also being heavily relied on to ensure continued critical government operations and services were provided to Canadians. Working with Shared Services Canada to support its employees, PHAC:
- Upgraded the network infrastructure to deliver modern digital tools that are accessible by design, contribute to enhanced productivity and support employees in working collaboratively;
- Stabilized infrastructure such as bandwidth and Virtual Private Network (VPN) capabilities for reliable remote access to the corporate network;
- Enabled the use of Protected B materials on authorized public cloud(s); and
- Equipped employees with mobile, accessible and digital tools such as Microsoft Office 365 that enable employee collaboration through chat, video and audio calling across their Government of Canada desktops and mobile devices.
This transition allowed PHAC employees to continue to deliver the same high-quality of service to Canadians, while they were also working remotely.
PHAC established funding and prepared an annual Information Management/Information Technology (IT) plan to become a leader in the delivery of modern, digitally enabled programs and services including data analytics, sound governance, stable and reliable digital infrastructure, open communications such as Open Government and service orientation. At the same time, PHAC reviewed its IT assets and established a multi-year IT asset management modernization plan, tailored to meet security and accessibility needs, while continuing to seamlessly provide services to Canadians.
As PHAC employees continued to adapt to working remotely in 2020-21, the Agency supported employees in increasing their awareness of the importance of safeguarding information and assets through a suite of online tools and resources (e.g., Procedures for reporting a security incident). PHAC established a virtual ergonomic assessment program, which completed 171 virtual assessments. This helped employees with their home workspaces and provided ergonomic services, guidance and tools to optimize the ergonomic adjustment of remote workspaces.
Based on an analysis of the Agency's pre-existing physical spaces, PHAC expanded the National Emergency Strategic Stockpile's (NESS) warehouse footprint to over 167,000 square meters. This expansion of infrastructure permitted the Agency to address supply chain challenges for key medical supplies and equipment needed to support the COVID-19 response.
Sex and Gender-based Analysis Plus
PHAC is continuing efforts to integrate SGBA Plus into daily operations, planning and training for employees. SGBA Plus also forms part of the planning strategy required for PHAC marketing campaigns. For example, in the following marketing campaigns, a SGBA Plus lens was applied to the target audience selection, media strategy, creative development and key messages:
- Seasonal flu: Based on various data points for each identified audience (adults aged 65 years and older, parents of children under 5 years of age and pregnant people), the campaign had a slight skew to women as they are often the primary healthcare decision makers within a family;
- Childhood vaccination: As with the Seasonal flu campaign, women are often the primary healthcare decision makers within the family. Women tended to have a lower level of trust in vaccinations however, they also tend to be social network power users who seek out and share health advice with others. In the case of childhood vaccination, advertising was skewed towards women and mothers; and
- COVID-19 vaccination uptake: From a health equity approach, PHAC targeted racialized and minority communities through partnerships with other government departments and community leaders, as well as through targeted advertising placements to reach these communities.
Innovation and experimentation
PHAC initiated a pilot project that provided internal business support services through a centralized reporting model. The initiative included the provision of administrative support services for Human Resources (HR), finance, contracting and procurement and planning and reporting services. Based on the success of this pilot project, this initiative will be expanded in the future to include other branches across the Agency. By delivering internal business support services through a centralized model, PHAC benefited from the added-value of increasing efficiencies (e.g., by streamlining and developing standardized operating procedures) and building a culture of knowledge sharing.
In consultation with the Persons with Disabilities Network and Health Canada, PHAC shared the results and lessons learned from the Agency's Accessible and Inclusive Meeting Spaces pilot project. Examples of lessons learned include:
- Leveraging unbiased third-party consultants to identify client requirements as opposed to suppliers;
- The need for more flexibility in controls for volume and lighting; and
- Improved setup for cables and device management.
PHAC currently has an Accessible and Inclusive Meeting Space and has begun planning for up to two more.
| 2020-21 Main Estimates |
2020-21 Planned spending |
2020-21 Total authorities available for use |
2020-21 Actual spending (authorities used) |
2020-21 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 98,331,024 | 98,331,024 | 326,418,488 | 213,051,491 | 114,720,467 |
Variance between Actual spending and Planned spending is explained in the section "Analysis of trends in spending and human resources section." |
||||
| 2020-21 Planned full-time equivalents |
2020-21 Actual full-time equivalents |
2020-21 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 655 | 426 | (229) |
Variance between Actual full-time equivalents and Planned full-time equivalents is explained in the section "Analysis of trends in spending and human resources section." |
||
Financial, human resources and performance information for PHAC’s Program Inventory is available in GC InfoBase.
Analysis of trends in spending and human resources
Actual expenditures
The following graph presents planned (voted and statutory spending) over time.
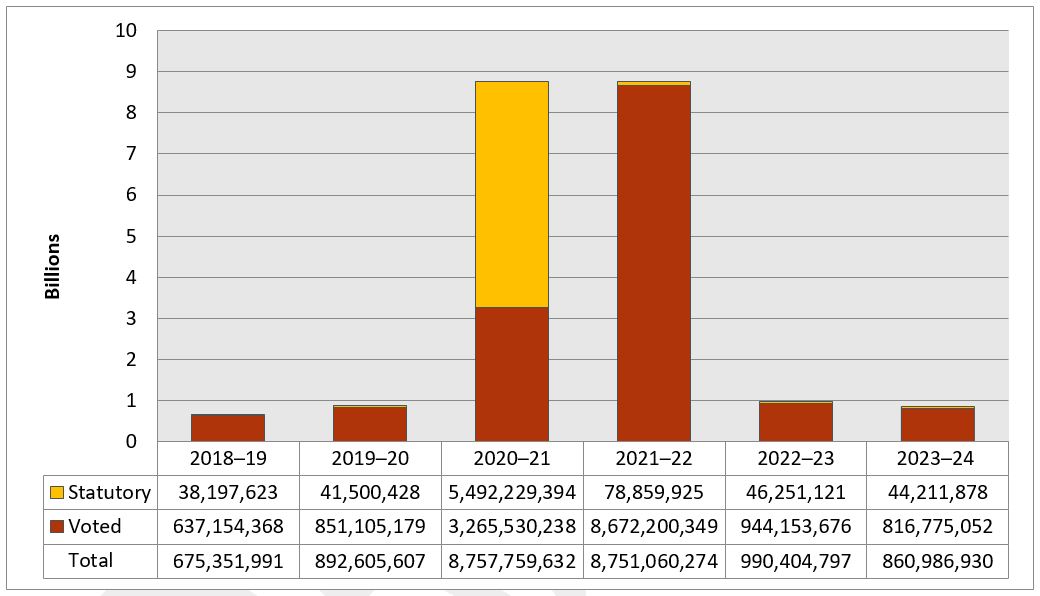
Source: Public Health Agency of Canada – Office of the Chief Financial Officer
Figure 4 - Text description
The departmental spending trend graph shows statutory and voted spending in billions of dollars for fiscal years 2018-19 to 2023-24.
| Fiscal Year | Total | Voted | Statutory |
|---|---|---|---|
2018-19 |
675,351,991 |
637,154,368 |
38,197,623 |
2019-20 |
892,605,607 |
851,105,179 |
41,500,428 |
2020-21 |
8,757,759,632 |
3,265,530,238 |
5,492,229,394 |
2021-22 |
8,751,060,274 |
8,672,200,349 |
78,859,925 |
2022-23 |
990,404,797 |
944,153,676 |
46,251,121 |
2023-24 |
860,986,930 |
816,775,052 |
44,211,878 |
The substantial increase in spending for 2020-21 is due to the Agency's response to COVID-19, notably for the following initiatives: the acquisition of PPE and medical equipment; medical research and vaccine developments; border and travel health and isolation sites and personnel related to surge capacity for the Agency.
The significant increase in statutory spending for 2020-21 relates to the enactment of the Public Health Events of National Concern Payments Act. This act was rescinded on December 31, 2020, resulting in a reduction of statutory funding for fiscal years 2021-22 and onward.
Planned spending in 2021-22 includes the Agency's permanent funding and significant temporary funding for several COVID-19 related measures such as medical research and vaccine developments, medical countermeasures, border and travel health and isolation sites, personal protective equipment Safe Restart and Innovative research and testing technologies and personnel related to surge capacity for the Agency. Planned spending decreases in 2022-23 and 2023-24 as the majority of this temporary COVID-19 funding sunsets in 2021-22.
| Core responsibilities and Internal Services | 2020-21 Main Estimates |
2020-21 Planned spending |
2021-22 Planned spending |
2022-23 Planned spending |
2020-21 Total authorities available for use |
2018-19 Actual spending (authorities used) |
2019-20 Actual spending (authorities used) |
2020-21 Actual spending (authorities used) |
|---|---|---|---|---|---|---|---|---|
Health Promotion and Chronic Disease Prevention |
280,813,789 |
280,813,789 |
340,398,576 |
272,594,458 |
406,594,486 |
318,391,163 |
273,405,685 |
291,289,487 |
Infectious Disease Prevention and Control |
210,906,872 |
210,906,872 |
6,027,645,406 |
272,038,876 |
12,877,517,135 |
199,658,422 |
257,498,145 |
3,794,133,883 |
Health Security |
51,775,030 |
51,775,030 |
2,138,514,806 |
342,315,260 |
7,435,379,211 |
55,577,234 |
248,500,491 |
4,459,284,771 |
Subtotal |
543,495,691 |
543,495,691 |
8,506,558,788 |
886,948,594 |
20,719,490,832 |
573,626,819 |
779,404,321 |
8,544,708,141 |
Internal Services |
98,331,024 |
98,331,024 |
244,501,486 |
103,456,203 |
326,418,488 |
101,725,172 |
113,201,286 |
213,051,491 |
Total |
641,826,715 |
641,826,715 |
8,751,060,274 |
990,404,797 |
21,045,909,320 |
675,351,991 |
892,605,607 |
8,757,759,632 |
PHAC's increase in spending from 2019-20 to 2020-21 is primarily due to the Agency's response to the COVID-19 pandemic. Increased spending was noted for the acquisition of PPE and medical equipment; medical research and vaccine developments; border and travel health and isolation sites; surge capacity for the Agency; Serosurveillance Consortium; lab facilities; and mental health.
| Core responsibilities and Internal Services | 2020-21 Actual gross spending |
2020-21 Actual revenues netted against expenditures |
2020-21 Actual net spending (authorities used) |
|---|---|---|---|
Health Promotion and Chronic Disease Prevention |
291,289,487 |
N/A | 291,289,487 |
Infectious Disease Prevention and Control |
3,794,133,883 |
N/A | 3,794,133,883 |
Health Security |
4,459,995,414 |
(710,643) |
4,459,284,771 |
Subtotal |
8,545,418,784 |
(710,643) |
8,544,708,141 |
Internal Services |
213,051,491 |
N/A | 213,051,491 |
Total |
8,758,470,275 |
(710,643) |
8,757,759,632 |
Actual human resources
| Core responsibilities and Internal Services | 2018-19 Actual full-time equivalents |
2019-20 Actual full-time equivalents |
2020-21 Planned full-time equivalents |
2020-21 Actual full-time equivalents |
2021-22 Planned full-time equivalents |
2022-23 Planned full-time equivalents |
|---|---|---|---|---|---|---|
Health Promotion and Chronic Disease Prevention |
476 |
524 |
550 |
542 |
581 |
533 |
Infectious Disease Prevention and Control |
982 |
1,054 |
1,073 |
1,149 |
2,134 |
1,262 |
Health Security |
354 |
385 |
389 |
743 |
1,253 |
475 |
Subtotal |
1,812 |
1,963 |
2,012 |
2,434 |
3,968 |
2,270 |
Internal Services |
322 |
333 |
655 |
426 |
1,027 |
654 |
Total |
2,134 |
2,296 |
2,667 |
2,860 |
4,995 |
2,924 |
* Internal Services planned full-time equivalents updated in comparison to 2021-22 Departmental Plan. |
||||||
PHAC's actual full-time equivalents increased by 564 from 2019-20 to 2020-21 primarily due to operations in support of the Agency's increased activities during the pandemic. This included additional staff to support critical Agency operations such as the acquisition and management of PPE and vaccine countermeasures, the management of border and travel health and isolation sites, testing and internal services to support the rapid growth of the Agency. Trending beyond 2021-22 to 2023-24, time limited investments are planned to sunset to reflect the temporary nature of COVID-19 funding.
Expenditures by vote
For information on the Public Health Agency of Canada's organizational voted and statutory expenditures, consult the Public Accounts of Canada 2020-2021.
Government of Canada spending and activities
Information on the alignment of the Public Health Agency of Canada's spending with the Government of Canada's spending and activities is available in GC InfoBase.
Financial statements and financial statements highlights
PHAC's financial statements (unaudited) for the year ended March 31, 2021, are available on the departmental website.
| Financial information | 2020-21 Planned results |
2020-21 Actual results |
2019-20 Actual results (restated)Footnote * |
Difference (2020-21 Actual results minus 2020-21 Planned results) |
Difference (2020-21 Actual results minus 2019-20 Actual results) |
|---|---|---|---|---|---|
Total expenses |
678,815,784 |
3,687,827,930 |
713,580,851 |
3,009,012,146 |
2,974,247,079 |
Total revenues |
14,123,867 |
22,277,818 |
13,101,200 |
8,153,951 |
9,176,618 |
Net cost of operations before government funding and transfers |
664,691,917 |
3,665,550,112 |
700,479,651 |
3,000,858,195 |
2,965,070,461 |
|
|||||
2020-21 Departmental Plan - Future-Oriented Statement of Operations
Total expenses for the Agency increased by $3.01 billion over planned results primarily due the Agency's response to the COVID-19 pandemic for the following initiatives:
- The purchase and use/distribution to Provinces and Territories of personal protective equipment, medical supplies and vaccine countermeasures;
- Salaries and employee benefits due to the increase of full-time equivalents to support the Agency's COVID-19 operations;
- The management of border and travel health and isolation sites; and
- Professional services such as advertising campaigns and storage.
The increase is offset by increased revenues over the previous year and over the planned results primarily due to gains on foreign exchange valuations for COVID‑19 purchases of personal protective equipment and vaccine countermeasures.
| Financial information | 2020-21 | 2019-20 (Restated)Footnote * |
Difference (2020-21 minus 2019-20) |
|---|---|---|---|
Total net liabilities |
894,450,072 |
191,168,218 |
703,281,854 |
Total net financial assets |
859,480,476 |
165,968,350 |
693,512,126 |
Departmental net debt |
34,969,596 |
25,199,868 |
9,769,728 |
Total non-financial assets |
5,516,146,336 |
415,813,011 |
5,100,333,325 |
Departmental net financial position |
5,481,176,740 |
390,613,143 |
5,090,563,597 |
|
|||
The Departmental net financial position increased significantly over the previous year primarily due to increases for inventory holdings such as personal protective equipment and medical supplies, prepaid expenses and tangible capital assets related to the Agency's operations in response to COVID-19.

Source: Public Health Agency of Canada – Office of the Chief Financial Officer
Figure 5 - Text description
This pie chart presents the net liabilities, as percentages over the previous fiscal year's total, differentiated by the type of liability.
| Liability type | Net percentages over the previous fiscal year's total |
|---|---|
| Accounts payable and accrued liabilities | 96% |
| Vacation pay and compensatory leave | 3% |
| Employee future benefits | 1% |
| Other liabilities | 0% |
| Deferred revenue | 0% |
Total net liabilities were $894,450,072, an increase of $703,281,854 (368%) over the previous year's total. The increase is primarily due to an increase in ongoing payables for the purchases of personal protective equipment, vaccine countermeasures, laboratory equipment and testing materials processed at the end of the year which accounted for $694,897,905 (99%) of the variance year over year.
Of the total liabilities:
- Accounts payable and accrued liabilities represented $857,634,945 (96%);
- Vacation pay and compensatory leave represented $26,371,887 (3%);
- Employee future benefits represented $8,693,522 (1%);
- Other liabilities represented $1,748,109 (0%); and
- Deferred revenue represented $1,609 (0%).
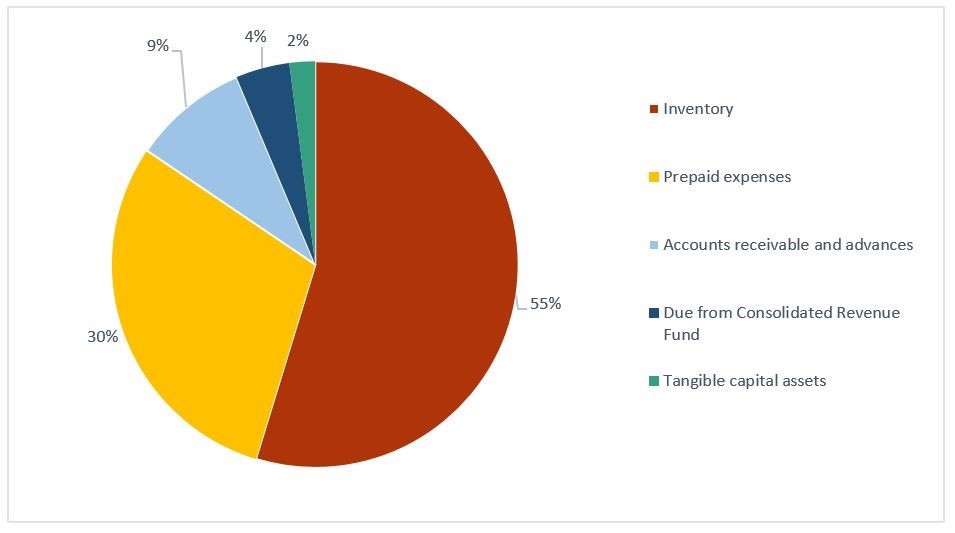
Source: Public Health Agency of Canada – Office of the Chief Financial Officer
Figure 6 - Text description
This pie chart presents assets, as percentages over the previous fiscal year's total, differentiated by asset type.
| Asset type | Percentages over the previous fiscal year's total |
|---|---|
| Inventory | 55% |
| Prepaid expenses | 30% |
| Accounts receivable and advances | 9% |
| Due from Consolidated Revenue Fund | 4% |
| Tangible capital assets | 2% |
Total assets were $6,375,626,813, an increase of $5,793,845,452 (996%) over the restated previous year's total of $581,781,361. This increase in assets is also reflected in the significant year-to-year variance of the Agency's net financial position. The variance is primarily due to an increase in inventory $3,370,517,850 (58%) and prepaid expenses $1,686,954,574 (29%) related to the acquisition of the personal protective equipment, medical and laboratory equipment, laboratory supplies, medical countermeasures and testing devices. The Agency's accounts receivable and advances increased by $566,163,989 (2,840%) primarily due to the timing of receipt for an outstanding receivable due for GST.
Of the total assets:
- Inventory represented $3,488,542,540 (55%);
- Prepaid expenses represented $1,897,045,622 (30%);
- Accounts receivable represented $586,097,740 (9%);
- Due to Consolidated Revenue fund represented $273,382,737 (4%); and
- Tangible capital assets represented $130,558,174 (2%).
Corporate information
Organizational profile
Appropriate minister: The Honourable Jean Yves Duclos, P.C., M.P. Minister of Health, and the Honourable Carolyn Bennett, M.D., P.C., M.P. Minister of Mental Health and Addictions and Associate Minister of Health
Institutional head: Dr. Harpreet S. Kochhar, President
Ministerial portfolio: Health
Enabling instruments: Public Health Agency of Canada Act, Department of Health Act, Emergency Management Act, Quarantine Act, Human Pathogens and Toxins Act, Health of Animals Act, Federal Framework on Lyme Disease Act and the Federal Framework for Suicide Prevention Act.
Year of incorporation / commencement: 2004
Other: In June 2012, the Deputy Heads of Health Canada and the Public Health Agency of Canada signed a Shared Services Partnership Framework Agreement. Under this agreement, each organization retains responsibility for a different set of internal services and corporate functions. These include: human resources; real property; information management / information technology; security; internal financial services; communications; emergency management; international affairs; internal audit services; and evaluation services.
Raison d'être, mandate and role: who we are and what we do
"Raison d'être, mandate and role: who we are and what we do" is available on PHAC's website.
For more information on the Agency's organizational mandate letter commitments, see the Minister's mandate letter and supplementary mandate letter.
Operating context
PHAC operates in an ever evolving environment. This year, PHAC significantly augmented its efforts to keep Canadians healthy and safe from emerging threats - a core element of PHAC's mandate. COVID-19 has highlighted the importance of PHAC's role in the centre of the federal pandemic response.
Drivers such as social determinants of health, climate change and advancements in technology impact the health of Canadians and set the tone for PHAC's response. In collaboration with provinces, territories and other federal government departments, this year PHAC led the largest public health response in Canadian history. Initial efforts centered on short-term emergency response, though as COVID-19 continued to affect our daily lives, the Agency pivoted to account for the long-term implications of the pandemic. As was the case with the securement of PPE and the bolstering of the National Emergency Strategic Stockpile. PHAC expanded capacities to improve supply chain for the future. As well, PHAC's vaccine and testing and surveillance rollout centered on Canada's most vulnerable populations in the beginning, such as the elderly and those in rural areas. The Agency promoted vaccination and encouraged public health measures to protect the population at- large. Additionally, PHAC collaborated with other government departments to ensure compliance with border and quarantine measures and provide public health guidance in order to prevent misinformation and protect Canadians.
Given the dynamic and evolving nature of public health events, PHAC must continue to have the capacity to prevent, prepare for and respond quickly to public health events and emergencies. Increasingly, public health events tend to be complex, with far-reaching causes and consequences and have undefined timelines, potentially requiring urgent action and a long- term response, as evidenced by the COVID-19 pandemic and Canada's ongoing opioid crisis. PHAC will continue to adapt its resources (such as human resources, skill sets), tools, processes and partnerships to maintain the capacity to rapidly and effectively prevent, detect and respond to emerging global and domestic public health events. The ability to proactively recognize key risks to health and contributing factors and to be prepared with the appropriate resources and supports to respond effectively, may positively influence the ability of PHAC's programs to achieve positive results for Canadians.
Timely and reliable data and knowledge are essential for developing sound policies, ensuring effective programming that delivers results to Canadians, delivering accurate information to Canadians and supporting overall government priorities (e.g., Sex and Gender-based Analysis Plus (SGBA Plus), Sustainable Development Goals and Innovation and Experimentation). In addition, strengthening surveillance, collection and access to national data supports evidence-based decision-making.
As this year has shown, global supply chains and rapid international transportation systems move goods and people across borders and with this movement comes the risk that a health threat emerging from somewhere in the world could quickly reach Canada without immediate detection. Similarly, climate change presents a range of risks, from poor air quality to the spread of vector-borne diseases, such as Lyme disease. Additionally, the amount of misinformation found online including through social media is a direct contributor to the growing global and domestic concern of vaccine hesitancy, which may lead to increasing rates of vaccine-preventable diseases among Canadians.
Although Canada is one of the healthiest countries in the world, health inequalities persist. While the life expectancy at birth for Canadian men and women is above international benchmarks at 79.9 years (men) and 84 years (women), not all experience the same health status. Certain populations (such as Northern, rural and remote communities, low-income families, children living in conditions of risk, Indigenous Peoples, unemployed or underemployed adults, older adults and LGBTQI2S+) continue to experience poorer health outcomes than the average Canadian. The COVID-19 pandemic reminds us that there is increased risk among these populations.
Canada will continue to face some persistent public health challenges in the coming years. As the population lives longer, chronic diseases (e.g., diabetes, dementia) have become more common. For example, the prevalence of diabetes is increasing by 3.3% per year. Depression, anxiety and posttraumatic stress disorder continue to be of concern, with approximately 11 people dying by suicide every day in Canada. Harms and deaths associated with the problematic use of alcohol and other substances (e.g., opioids, vaping products) are significant public health challenges.
While the current response to COVID-19 continues to focus on immediate crisis measures and re-opening segments of the economy and society in the shorter term, the pandemic will have long-lasting impacts that will shape policy measures for many years. Building a more resilient public health system will need to be part of a broader and coordinated set of longer-term government initiatives. The multi-jurisdictional nature of public health also creates a diverse collaboration, coordination and engagement environment. Public health is a shared responsibility in Canada, with coordination between the federal, provincial, territorial and municipal governments. By improving our understanding of the priorities, activities and concerns of partners and stakeholders, PHAC will be better able to adapt its programs (including those supported through grants and contributions) to respond to the diverse public health needs across Canada. PHAC's commitment to accountability, openness and results will help promote important multi-sectoral collaborations and the solutions needed to help improve the health of Canadians.
For more information on PHAC's results achieved, see the Results: what we achieved section of this report.
Reporting framework
PHAC's Departmental Results Framework and Program Inventory of record for 2020-21 are shown below.
Core responsibility 1: Health Promotion and Chronic Disease Prevention
Result 1.1 Canadians have improved physical and mental health
- Indicator: % of low-income children in very good or excellent health
- Indicator: % of population who have high psychological well-being
Result 1.2 Canadians have improved health behaviours
- Indicator: % increase in average minutes/day of physical activity among adults
- Indicator: % increase in average minutes/day of physical activity among children/youth
Result 1.3 Chronic diseases are prevented
- Indicator: % increase in years lived in good health by seniors
- Indicator: Rate of new diabetes cases among Canadians
- Indicator: % of adults who are obese
- Indicator: % of children and youth who are obese
Program Inventory
- Program: Health Promotion
- Program: Chronic Disease Prevention
- Program: Evidence for Health Promotion, and Chronic Disease and Injury Prevention
Core responsibility 2: Infectious Disease Prevention and Control
Results 2.1 Infectious diseases are prevented and controlled
- Indicator: % of 2 year old children who have received all recommended vaccinations
- Indicator: Proportion of national vaccination coverage goals met for children by 2 years of age
- Indicator: Rate per 100,000 of new diagnosed cases of Human Immunodeficiency Virus (HIV)
- Indicator: Rate of a key antimicrobial resistant infection identified among people in hospitals
Result 2.2 Infectious disease outbreaks and threats are prepared for and responded to
- Indicator: % of foodborne illness outbreaks responded to within 24 hours of notification
- Indicator: % of new pathogens of international concern that Canada has the capacity to accurately test for
Program Inventory
- Program: Laboratory Science Leadership and Services
- Program: Communicable Diseases and Infection Control
- Program: Vaccination
- Program: Foodborne and Zoonotic Diseases
Core responsibility 3: Health Security
Result 3.1 Public health events and emergencies are prepared for and responded to effectively
- Indicator: Canada's readiness to respond to public health events and emergencies as assessed independently by the World Health Organization
- Indicator: % of provincial and territorial requests for assistance responded to within negotiated timelines
Result 3.2 Public health risks associated with the use of pathogens and toxins are reduced
- Indicator: % of compliance issues in Canadian laboratories successfully responded to within established timelines
Result 3.3 Public health risks associated with travel are reduced
- Indicator: Canada's capacity for effective public health response at designated points of entry into Canada
- Indicator: % of inspected passenger transportation operators that meet public health requirements
Program inventory
- Program: Emergency Preparedness and Response
- Program: Biosecurity
- Program: Border and Travel Health
Internal Services
- Management and Oversight Services
- Communications Services
- Legal Services
- Human Resources Management Services
- Financial Management Services
- Information Management Services
- Information Technology Services
- Real Property Management Services
- Materiel Management Services
- Acquisition Management Services
Supporting information on the program inventory
Financial, human resources and performance information for the Public Health Agency of Canada's Program Inventory is available in GC InfoBase.
Supplementary information tables
The following supplementary information tables are available on PHAC's website:
Federal tax expenditures
The tax system can be used to achieve public policy objectives through the application of special measures such as low tax rates, exemptions, deductions, deferrals and credits. The Department of Finance Canada publishes cost estimates and projections for these measures each year in the Report on Federal Tax Expenditures. This report also provides detailed background information on tax expenditures, including descriptions, objectives, historical information and references to related federal spending programs as well as evaluations and GBA+ of tax expenditures.
Organizational contact information
Rouben Khatchadourian
Vice-President, Strategic Policy Branch
Public Health Agency of Canada
130 Colonnade Road
Ottawa, ON K1A 0K9
Telephone: 343-542-6434
Email: Rouben.Khatchadourian@phac-aspc.gc.ca
Appendix: definitions
- appropriation
- Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
- budgetary expenditures
- Operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
- core responsibility
- An enduring function or role performed by a department. The intentions of the department with respect to a core responsibility are reflected in one or more related departmental results that the department seeks to contribute to or influence.
- Departmental Plan
- A report on the plans and expected performance of an appropriated department over a 3-year period. Departmental Plans are usually tabled in Parliament each spring.
- departmental priority
- A plan or project that a department has chosen to focus and report on during the planning period. Priorities represent the things that are most important or what must be done first to support the achievement of the desired departmental results.
- departmental result
- A consequence or outcome that a department seeks to achieve. A departmental result is often outside departments' immediate control, but it should be influenced by program-level outcomes.
- departmental result indicator
- A quantitative measure of progress on a departmental result.
- departmental results framework
- A framework that connects the department's core responsibilities to its departmental results and departmental result indicators.
- Departmental Results Report
- A report on a department's actual accomplishments against the plans, priorities and expected results set out in the corresponding Departmental Plan.
- experimentation
- The conducting of activities that seek to first explore, then test and compare the effects and impacts of policies and interventions in order to inform evidence-based decision-making, and improve outcomes for Canadians, by learning what works, for whom and in what circumstances. Experimentation is related to, but distinct from innovation (the trying of new things), because it involves a rigorous comparison of results. For example, using a new website to communicate with Canadians can be an innovation; systematically testing the new website against existing outreach tools or an old website to see which one leads to more engagement, is experimentation.
- full-time equivalent
- A measure of the extent to which an employee represents a full person-year charge against a departmental budget. For a particular position, the full-time equivalent figure is the ratio of number of hours the person actually works divided by the standard number of hours set out in the person's collective agreement.
- government-wide priorities
- For the purpose of the 2020-21 Departmental Results Report, those high-level themes outlining the government's agenda in the 2019 Speech from the Throne, namely: Fighting climate change; Strengthening the Middle Class; Walking the road of reconciliation; Keeping Canadians safe and healthy; and Positioning Canada for success in an uncertain world.
- horizontal initiative
- An initiative where two or more federal organizations are given funding to pursue a shared outcome, often linked to a government priority.
- non-budgetary expenditures
- Net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
- performance
- What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve, and how well lessons learned have been identified.
- performance indicator
- A qualitative or quantitative means of measuring an output or outcome, with the intention of gauging the performance of an organization, program, policy or initiative respecting expected results.
- performance reporting
- The process of communicating evidence-based performance information. Performance reporting supports decision making, accountability and transparency.
- plan
- The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally, a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead to the expected result.
- planned spending
- For Departmental Plans and Departmental Results Reports, planned spending refers to those amounts presented in Main Estimates.
A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their Departmental Plans and Departmental Results Reports. - program
- Individual or groups of services, activities or combinations thereof that are managed together within the department and focus on a specific set of outputs, outcomes or service levels.
- program inventory
- Identifies all the department's programs and describes how resources are organized to contribute to the department's core responsibilities and results.
- result
- A consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead they are within the area of the organization's influence.
- Sex and Gender-Based Analysis Plus (GBA Plus)
- An analytical process used to assess how diverse groups of women, men and gender-diverse people experience policies, programs and services based on multiple factors including race ethnicity, religion, age, and mental or physical disability.
- statutory expenditures
- Expenditures that Parliament has approved through legislation other than appropriation acts. The legislation sets out the purpose of the expenditures and the terms and conditions under which they may be made.
- target
- A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
- voted expenditures
- Expenditures that Parliament approves annually through an appropriation act. The vote wording becomes the governing conditions under which these expenditures may be made.
Footnote
- Footnote 1
-
283 physical employees which are equivalent to 254 full-time equivalents.
Page details
- Date modified: