
Canada-Alberta Agreement to Work Together to Improve Health Care for Canadians (2023-24 to 2025-26)
Tables of contents
- Funding agreement
- Annex 1 - Common statement of principles on shared health priorities
- Annex 2 - Shared pan-Canadian interoperability roadmap
- Annex 3 - Headline common indicators
- Annex 4 - Action plan
Funding agreement
(the "Agreement")
BETWEEN:
HIS MAJESTY THE KING IN RIGHT OF CANADA (hereinafter referred to as "Canada" or "Government of Canada") as represented by the Minister of Health and the Minister of Mental Health and Addictions and Associate Minister of Health (herein referred to as "the federal Ministers")
- and -
HIS MAJESTY THE KING IN RIGHT OF ALBERTA(hereinafter referred to as "Alberta" or "Government of Alberta") as represented by the Minister of Health and the Minister of Mental Health and Addiction (herein referred to as "the provincial Ministers")
REFERRED to collectively as the "Parties", and individually as a "Party"
PREAMBLE
WHEREAS, on February 27, 2023 Canada and Alberta announced an overarching agreement in principle on Working Together to Improve Health Care for Canadians, supported by almost $200 billion over ten years in federal funding, including $46.2 billion in new funding to provinces and territories;
WHEREAS, Canada has also announced a 5 per cent Canada Health Transfer (CHT) guarantee for the next five years, starting in 2023-24, which will be provided through annual top-up payments as required. This is projected to provide approximately an additional $17 billion over 10 years in new support. The last top-up payment will be rolled into the CHT base at the end of the five years to ensure a permanent funding increase, providing certainty and sustainability to provinces and territories;
WHEREAS, Working Together to Improve Health Care for Canadians includes a federal commitment of $25 billion in bilateral funding to provinces and territories over ten years focused on four shared health priorities:
- expanding access to family health services, including in rural and remote areas;
- supporting our health workers and reducing backlogs;
- improving access to quality mental health, substance use, and addictions services; and
- modernizing health systems with health data and digital tools.
WHEREAS, in the area of mental health, substance use, and addictions services, Working Together to Improve Health Care for Canadians also includes a commitment by Canada and Alberta to continue to work to support collaboration on the Common Statement of Principles on Shared Health Priorities (hereinafter referred to as the "Common Statement", attached hereto as Annex 1), supported by the federal Budget 2017 investment of $5 billion over ten years;
WHEREAS, Alberta makes ongoing investments in health consistent with its broader responsibilities for delivering health care services to its residents and in supporting diversity, equity, and the needs of First Nations, Inuit and Métis; and underserved and/or disadvantaged populations, including, but not limited to official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians), and 2SLGBTQIA+;
WHEREAS, Canada authorized the federal Ministers to enter into agreements with the provinces and territories, for the purpose of identifying activities that provinces and territories will undertake in respect of the four shared health priorities, and for funding in this Agreement associated with the federal investment for mental health, substance use, and addictions services consistent with the Common Statement (and menu of actions outlined in Annex 1);
WHEREAS, the Government Organization Act authorizes the provincial Ministers to enter into agreements with the Government of Canada under which Canada undertakes to provide funding toward costs incurred by the Government of Alberta associated with the federal investment for four shared health priorities, and mental health, substance use and addictions services consistent with the Common Statement; and
NOW THEREFORE, this Agreement sets out the terms betweenCanada and Alberta as follows:
1.0 Key Principles and collaboration
The key principles and commitment to collaboration agreed to in Working Together to Improve Health Care for Canadians are outlined below.
1.1 Canada and Alberta acknowledge that this Agreement will mutually respect each government's jurisdiction, and be underpinned by key principles, including:
- A shared responsibility to uphold the Canada Health Act that strengthens public health care systems;
- Principles agreed to in the Common Statement (outlined in Annex 1);
- Reconciliation with Indigenous Peoples, including access to quality and culturally safe health services that is free from racism and discrimination anywhere in Canada, through seamless service delivery across jurisdictions and meaningful engagement and work with First Nations, Métis, and Inuit partners and governments; and
- Equity of access for underserved groups and individuals, including those in official language minority communities.
1.2 Canada and Alberta acknowledge the importance of supporting health data infrastructure, data collection and public reporting, and will work together to improve the collection, sharing and use of de-identified health information, respecting federal/provincial/territorial privacy legislation, to improve transparency on results and to help manage public health emergencies, and to ensure Canadians can access their own health information and benefit from it being shared between health workers across health settings. This includes:
- collecting and securely sharing high-quality, comparable information needed to improve services to Canadians, including disaggregated data on key common health indicators with the Canadian Institute for Health Information (CIHI);
- adopting common interoperability standards (both technical exchange and content of data), including the Shared pan-Canadian Interoperability Roadmap (outlined in Annex 2), to improve Canadians' access to their health information in a usable digital format and support the exchange and analysis of health data within and across Canada's health systems in a way that protects Canadians' privacy and ensures the ethical use of data to improve the health and lives of people;
- work to align provincial and territorial policies and legislative frameworks, where necessary and appropriate, to support secure patient access to health information, and stewardship of health information to support the public good, including improving health care quality, patient safety, privacy protection, system governance and oversight, planning and research;
- promoting health information as a public good by working with federal-provincial-territorial Ministers of Health to review and confirm overarching principles, which would affirm Canadians' ability to access their health information and have it follow them across all points of care. The existing Health Data Charter, as outlined in the Pan-Canadian Health Data Strategy would serve as the starting point for the discussion of these principles; and
- collecting and sharing available, public health data (e.g., vaccination data, testing data) with the Public Health Agency of Canada to support Canada's preparedness and response to public health events, building on commitments made as part of the Safe Restart Agreements.
1.3 Canada and Alberta acknowledge they will work with other provinces and territories to streamline foreign credential recognition for internationally-educated health professionals, and to advance labour mobility, starting with multi-jurisdictional recognition of health professional licences.
1.4 Canada and Alberta acknowledge a mutual intent to engage in a two-phased formal review process:
- Phase 1: This review will be done in 2026 by a joint committee of Federal, Provincial, and Territorial health and finance officials to assess results and determine next steps for bilateral agreements related to improvements to home and community care, mental health, substance use, and addiction services associated with the Common Statement and long-term care; and
- Phase 2: A formal five-year review of the healthcare plan outlined on February 7, 2023, recognizing the importance of long-term sustainability for provincial-territorial health systems. This review would consist of an assessment of both the bilateral agreements (herein) and the CHT investments (not included as part of this bilateral agreement). The review will be done by a joint committee of Federal, Provincial, and Territorial health and finance officials, commencing by March 31, 2027, and concluded by December 31, 2027, to consider results achieved thus far in the four shared health priority areas and will include:
- an assessment of progress-to-date on public reporting to Canadians using the common indicators;
- sharing of de-identified health information, and other health data commitments; and
- current and forward-looking Federal, Provincial, and Territorial investments to support this plan.
2.0 Objectives
2.1 Canada and Alberta agree that, with financial support from Canada, Alberta will continue to build and enhance health care systems towards achieving some or all of the objectives of:
- timely access to high-quality family health services, including in rural and remote areas;
- a sustainable, efficient and resilient health workforce that provides Canadians timely access to high-quality, effective, and safe health services;
- access to timely, equitable, and quality mental health, substance use, and addictions services to support Canadians' well-being; and
- access to a patient's own electronic health information that is shared between the health professionals they consult to improve safety and quality of care, and which informs Canadians on how the system is working.
2.2 Canada and Alberta agree that, with Budget 2017 financial support from Canada outlined in 5.2.2, Alberta will continue to work to improve access to mental health, substance use, and addictions services consistent with the Common Statement (and menu of actions outlined in Annex 1).
3.0 Action plan
3.1 Alberta set out in their Action Plan (attached as Annex 4) how the federal investment under this Agreement will be used, as well as details on targets and timeframes based on common headline indicators in priority areas where federal funds will be invested, as well as jurisdiction-specific indicators, for each of the initiatives.
3.2 Alberta will invest federal funding as part of the 2017 commitment for mental health, substance use, and addictions services provided through this Agreement in alignment with the menu of actions listed in the Common Statement.
3.3 Alberta will invest federal funding in some or all of the four shared health priority areas, without displacing existing planned spending in those areas.
3.4 In developing initiatives under this Agreement, Alberta agrees to implement the commitments in the Action Plan specific to the needs of First Nations, Inuit and Métis; and underserved and/or disadvantaged populations, including, but not limited to official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians), and 2SLGBTQIA+.
3.5 Alberta's approach to achieving objectives is set out in their three-year Action Plan (2023-24 to 2025-26), as set out in Annex 4.
4.0 Term of agreement
4.1 This Agreement comes into effect upon the date of the last signature of the Parties and will remain in effect until March 31, 2026 ("the Term"), unless terminated in accordance with section 11 of this Agreement. Funding provided under this Agreement will cover the period April 1, 2023 to March 31, 2026.
4.2 Renewal of Bilateral Agreements
4.2.1 Upon signing renewed bilateral agreements, Alberta will have access to the remainder of its share of the federal funding, subject to appropriation by Parliament, for:
- 2026-27, the allocation based on the federal commitment in Budget 2017 of $5 billion over ten years for mental health, substance use and addiction services; and
- 2026-27 to 2032-33, the allocation based on the federal commitment in Budget 2023 of $25 billion over ten years to support the Working Together to Improve Health Care for Canadians plan.
5.0 Financial provisions
5.1 The funding provided under this Agreement is in addition to and not in lieu of those that Canada currently provides under the CHT to support delivering health care services within the province.
5.2 Allocation to Alberta
5.2.1 In this Agreement, "Fiscal Year" means the period commencing on April 1 of any calendar year and terminating on March 31 of the immediately following calendar year.
5.2.2 Canada has designated the following maximum amounts to be transferred in total to all provinces and territories under this initiative based on the allocation method outlined in subsection 5.2.3 for the Term of this Agreement.
Working Together to Improve Health Care for Canadians
- $2.5 billion for the Fiscal Year beginning on April 1, 2023
- $2.5 billion for the Fiscal Year beginning on April 1, 2024
- $2.5 billion for the Fiscal Year beginning on April 1, 2025
Budget 2017 Mental Health, Substance Use, and Addictions Services
- $600 million for the Fiscal Year beginning on April 1, 2023
- $600 million for the Fiscal Year beginning on April 1, 2024
- $600 million for the Fiscal Year beginning on April 1, 2025
5.2.3 Allocation Method
- For the funding associated with Working Together to Improve Health Care for Canadians, annual funding will be allocated to provinces and territories on base ($5,000,000 if population is less than 100,000; $20,000,000 if population is between 100,000 and 500,000; and $50,000,000 if population is greater than 500,000) plus per capita basis. The final total amount to be paid to each jurisdiction will be calculated using the following formula: B + (F - ((N * 5,000,000) + (O * 20,000,000) + (S * 50,000,000)) x (K / L), where:
- B is the base amount allocated to each province or territory based on population ($5,000,000 if population is less than 100,000; $20,000,000 if population is between 100,000 and 500,000; and $50,000,000 if population is greater than 500,000), as determined using annual population estimates on July 1 st from Statistics Canada;
- F is the total annual funding amount available outlined under this program;
- N is the number of provinces and territories with a population less than 100,000, as determined using annual population estimates on July 1 st from Statistics Canada;
- O is the number of provinces and territories with a population between 100,000 and 500,000, as determined using annual population estimates on July 1 st from Statistics Canada;
- S is the number of provinces and territories with a population greater than 500,000, as determined using annual population estimates on July 1 st from Statistics Canada;
- K is the total population of Alberta, as determined using annual population estimates on July 1 st from Statistics Canada; and
- L is the total population of Canada, as determined using annual population estimates on July 1 st from Statistics Canada.
- For funds associated with Budget 2017 Mental Health, Substance Use, and Addictions Services, annual funding will be allocated to provinces and territories on a per capita basis. The per capita funding for each Fiscal Year, is calculated using the following formula: F x K/L, where:
- F is the annual total funding amount available under this program;
- K is the total population of Alberta, as determined using the annual population estimates on July 1st from Statistics Canada; and
- L is the total population of Canada, as determined using the annual population estimates on July 1st from Statistics Canada.
5.2.4 Subject to annual adjustment based on the formulas described in section 5.2.3, Alberta estimated share of the amounts will be:
| Fiscal Year | Working Together to Improve Health Care for Canadians Estimated amount to be paid to Alberta Footnote* (subject to annual adjustment) | Budget 2017 Mental Health, Substance Use, and Addictions Services Estimated amount to be paid to Alberta Footnote* (subject to annual adjustment) |
|---|---|---|
| 2023-2024 | $285,150,000 | $70,020,000 |
| 2024-2025 | $285,150,000 | $70,020,000 |
| 2025-2026 | $285,150,000 | $70,020,000 |
| * Table 1 Footnote Amount represent annual estimates based on Statistics Canada's July 1st, 2022, population estimates. | ||
5.3 Payment
5.3.1 Funding provided by Canada will be paid in semi-annual installments as follows:
- In 2023-2024, the first installment will be paid within approximately 30 business days of execution of this Agreement by the Parties. The second installment will be paid on or about November 15.
- Starting in 2024-2025, the first installment will be paid on or about April 15 of each Fiscal Year and the second installment will be paid on or about November 15 of each Fiscal Year.
- The first installment will be equal to 50% of the notional amount set out in section 5.2.4 as adjusted by section 5.2.3.
- The second installment will be equal to the balance of funding provided by Canada for the Fiscal Year as determined under sections 5.2.3 and 5.2.4.
- Canada will notify Alberta prior to the first payment of each Fiscal Year, of their notional amount. The notional amount will be based on the Statistics Canada quarterly preliminary population estimates on July 1 of the preceding Fiscal Year. Prior to the second payment, Canada will notify Alberta of the amount of the second installment as determined under sections 5.2.3 and 5.2.4.
- Canada shall withhold payments if Alberta has failed to provide reporting in accordance with 7.1.
- Canada shall withhold the second payment in 2023-24 if Alberta has failed to satisfy all reporting requirements associated with the preceding Canada - Alberta Home and Community Care and Mental Health and Addictions Services Funding Agreement 2022-23, specifically to:
- continue to participate in a Federal-Provincial-Territorial process to improve reporting on and provide data to CIHI for the 6 common indicators to measure pan-Canadian progress on improving access to mental health, substance use, and addictions services; and
- provide the annual financial statement, with attestation from Alberta's senior financial officers for Alberta Health and Alberta Mental Health and Addiction, of funding received the preceding Fiscal Year from Canada for mental health and addiction services under the Canada - Alberta Home and Community Care and Mental Health and Addictions Services Funding Agreement 2022-23 compared against the Expenditure Plan 2022-23, and noting any variances, between actual expenditures and the Expenditure Plan 2022-23.
- The sum of both installments constitutes a final payment and is not subject to any further payment once the second installment has been paid.
- Payment of Canada's funding for this Agreement is subject to an annual appropriation by the Parliament of Canada for this purpose.
5.4 Retaining funds
5.4.1 For Fiscal Years 2023-24 through 2024-25, upon request, Alberta may retain and carry forward to the next Fiscal Year up to 10 percent of funding that is in excess of the amount of the eligible costs actually incurred in a Fiscal Year and use the amount carried forward for expenditures on eligible areas of investment. Any request to retain and carry forward an amount exceeding 10 percent will be subject to discussion and mutual agreement in writing by the Parties' designated officials, at the Assistant Deputy Minister level (herein referred to as "Designated Officials"), and is subject to monitoring and reporting to Canada on the management and spending of the funds carried forward on a quarterly basis.
5.4.2 Any amount carried forward from one Fiscal Year to the next under this subsection is supplementary to the maximum amount payable to Alberta under subsection 5.2.4 of this Agreement in the next Fiscal Year.
5.4.3 Upon request, Alberta may retain and carry forward up to 10 percent of funding provided in the last Fiscal Year of this Agreement for eligible areas of investment, to be noted in the new agreement and subject to the terms and conditions of that new agreement. The new Action Plan will provide details on how any retained funds carried forward will be expended. Any request by Alberta to retain and carry forward an amount exceeding 10 percent will be subject to discussion and mutual agreement in writing by the Parties' Designated Officials, and is subject to monitoring and reporting to Canada on the management and spending of the funds carried forward on a quarterly basis.
5.5 Repayment of overpayment
5.5.1. In the event payments made exceed the amount to which Alberta is entitled under this Agreement, the amount of the excess is a debt due to Canada and, unless otherwise agreed to in writing by the Parties, Alberta shall repay the amount within sixty (60) calendar days of written notice from Canada.
5.6 Use of funds
5.6.1. The Parties agree that funds provided under this Agreement will only be used by Alberta in accordance with the initiatives outlined in Annex 4 (Action Plan).
5.7 Eligible expenditures
5.7.1. Eligible expenditures under this Agreement are the following:
- data development and collection to support reporting;
- information technology and health information infrastructure;
- capital and operating funding;
- salaries and benefits;
- training, professional development; and
- information and communications material related to programs.
6.0 Performance measurement
6.1 Alberta agrees to designate an official or official(s), for the duration of this Agreement to participate in a CIHI led Federal-Provincial-Territorial indicator process to:
- Refine the eight common headline indicators (outlined in Annex 3);
- Work to identify additional common indicators that are mutually agreed upon, including indicators focused on the health of Indigenous populations with acknowledgement of the role for Indigenous partners in this work;
- Improve reporting on common indicators to measure pan-Canadian progress on improving access to mental health, substance use, and addictions services, associated with the commitment in the Common Statement; and
- Share available disaggregated data with CIHI and work with CIHI to improve availability of disaggregated data for existing and new common indicators to enable reporting on progress for Indigenous peoples, First Nations, Inuit, Métis; and underserved and/or disadvantaged populations including, but not limited to, official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians), and 2SLGBTQIA+.
7.0 Reporting to Canadians
7.1 Funding conditions and reporting
7.1.1 By no later than October 1, in each Fiscal Year, in respect of the previous Fiscal Year, Alberta agrees to:
- Provide data and information annually to CIHI related to the new headline indicators set out in Annex 3, additional common indicators, in addition to the mental health, substance use, and addictions services indicators identified as part of commitment made in the Common Statement.
- Beginning in Fiscal Year 2024-25, report annually and publicly in an integrated manner to residents of Alberta on progress made on targets outlined in Annex 4 for headline indicators in the priority area(s) where federal funds are to be invested, and on jurisdiction-specific indicators for each of the initiatives tailored to their jurisdiction's needs and circumstances.
- Beginning in Fiscal Year 2024-25, provide to Canada an annual financial statement, with attestation from Alberta's senior financial officers for Alberta Health and Alberta Mental Health and Addiction, of funding received the preceding Fiscal Year from Canada under this Agreement or the Previous Agreement compared against the Action Plan, and noting any variances, between actual expenditures and the Action Plan:
- The revenue section of the statement shall show the amount received from Canada under this Agreement during the Fiscal Year;
- The total amount of funding used for each of the shared health priority areas that are supported by the federal funds;
- If applicable, the amount of any funding carried forward under section 5.4; and
- If applicable, the amount of overpayment that is to be repaid to Canada under section 5.5.
7.1.2 Alberta will provide quarterly reporting to Canada on the management and spending of the funds retained to the next Fiscal Year.
7.2 Audit
7.2.1 Alberta will ensure that expenditure information presented in the annual financial statement is, in accordance with Alberta's standard accounting practices, complete and accurate.
7.3 Evaluation
7.3.1 Responsibility for evaluation of programs rests with Alberta in accordance with its own evaluation policies and practices.
8.0 Communications
8.1 The Parties agree on the importance of communicating with citizens about the objectives of this Agreement in an open, transparent, effective and proactive manner through appropriate public information activities.
8.2 Each Party will receive the appropriate credit and visibility when investments financed through funds granted under this Agreement are announced to the public.
8.3 In the spirit of transparency and open government, Canada will make this Agreement, including any amendments, publicly available on a Government of Canada website.
8.4 Alberta will make publicly available, clearly identified on a Government of Alberta website, this Agreement, including any amendments.
8.5 Canada, with prior notice to Alberta, may incorporate all or any part of the data and information in 7.1, or any part of evaluation and audit reports made public by Alberta into any report that Canada may prepare for its own purposes, including any reports to the Parliament of Canada or reports that may be made public.
8.6 Canada reserves the right to conduct public communications, announcements, events, outreach and promotional activities about the Common Statement and this Agreement. Canada agrees to give Alberta 10 days advance notice and advance copies of public communications related to the Common Statement, this Agreement, and results of the investments of this Agreement.
8.7 Alberta reserves the right to conduct public communications, announcements, events, outreach and promotional activities about the Common Statement and this Agreement. Alberta agrees to give Canada 10 days advance notice and advance copies of public communications related to the Common Statement, this Agreement, and results of the investments of this Agreement.
8.8 Canada and Alberta agree to participate in a joint announcement upon signing of this Agreement.
8.9 Canada and Alberta agree to work together to identify mutually agreeable opportunities for joint announcements relating to programs funded under this Agreement.
9.0 Dispute resolution
9.1 The Parties are committed to working together and avoiding disputes through government-to-government information exchange, advance notice, early consultation, and discussion, clarification, and resolution of issues, as they arise.
9.2 If at any time a Party is of the opinion that the other Party has failed to comply with any of its obligations or undertakings under this Agreement or is in breach of any term or condition of the Agreement, that Party may notify the other Party in writing of the failure or breach. Upon such notice, the Parties will endeavour to resolve the issue in dispute bilaterally through their Designated Officials.
9.3 If a dispute cannot be resolved by Designated Officials, then the dispute will be referred to the Deputy Ministers of Canada and Alberta responsible for health and for mental health and addiction, and if it cannot be resolved by them, then the federal Ministers and the provincial Ministers shall endeavour to resolve the dispute.
10.0 Amendments to the agreement
10.1 The main text of this Agreement may be amended at any time by mutual consent of the Parties. Any amendments shall be in writing and signed, in the case of Canada, by the federal Ministers, and in the case of Alberta, by the provincial Ministers.
10.2 Annex 4 may be amended at any time by mutual consent of the Parties. Any amendments to Annex 4 shall be in writing and signed by each Party's Designated Official.
11.0 Termination
11.1 Either Party may terminate this Agreement at any time if the terms are not respected by giving at least 6 months written notice of intention to terminate.
11.2 As of the effective date of termination of this Agreement, Canada shall have no obligation to make any further payments.
11.3 Sections 1.0, and 8.0 of this Agreement survive for the period of the 10-year Working Together to Improve Health Care for Canadians plan.
11.4 Sections 5.4 and 7.0 of this Agreement survive the termination or expiration of this Agreement until reporting obligations are completed.
12.0 Notice
12.1 Any notice, information, or document provided for under this Agreement will be effectively given if delivered or sent by letter, email, postage or other charges prepaid. Any communication that is delivered will be deemed to have been received in delivery; and, except in periods of postal disruption, any communication mailed by post will be deemed to have been received eight calendar days after being mailed.
The address of the Designated Official for Canada shall be:
Assistant Deputy Minister, Strategic Policy Branch
Health Canada
70 Colombine Driveway
Brooke Claxton Building
Ottawa, Ontario
K1A 0K9
Email: jocelyne.voisin@hc-sc.gc.ca
The address of the Designated Officials for Alberta shall be:
Assistant Deputy Minister, Strategic Planning and Performance
19th Floor, ATB Place North Tower
10025 Jasper Avenue NW
Edmonton, AB
T5J 1S6
Email: kim.simmonds@gov.ab.ca
Assistant Deputy Minister,
Mental Health and Addiction
13th Floor, Telus House
10020 100 Street NW
Edmonton, AB
T5J 0N3
Email: chad.mitchell@gov.ab.ca
13.0 General
13.1 This Agreement, including Annexes, comprises the entire Agreement entered into by the Parties.
13.2 This Agreement shall be governed by and interpreted in accordance with the laws of Canada and Alberta.
13.3 No member of the House of Commons or of the Senate of Canada or of the Legislature of Alberta shall be admitted to any share or part of this Agreement, or to any benefit arising therefrom.
13.4 If for any reason a provision of this Agreement, that is not a fundamental term, is found by a court of competent jurisdiction to be or to have become invalid or unenforceable, in whole or in part, it will be severed and deleted from this Agreement, but all the other provisions of this Agreement will continue to be valid and enforceable.
13.5 This Agreement may be executed in counterparts, in which case (i) the counterparts together shall constitute one agreement, and (ii) communication of execution by fax transmission or emailed in PDF shall constitute good delivery. Electronic signature(s) may be accepted as originals so long as the source of the transmission can be reasonably connected to the signatory.
IN WITNESS WHEREOF the Parties have executed this Agreement through duly authorized representatives.
SIGNED on behalf of Canada by the Minister of Health this 20th day of December, 2023
The Honourable Mark Holland, Minister of Health
SIGNED on behalf of Canada by the Minister of Mental Health and Addictions and Associate Minister of Health this 20th day of December, 2023
The Honourable Ya'ara Saks, Minister of Mental Health and Addictions and Associate Minister of Health
SIGNED on behalf of Alberta by the Minister of Health this 19th day of December, 2023
The Honourable Adriana LaGrange, Minister of Health
SIGNED on behalf of Alberta by the Minister of Health and Addiction
The Honourable Dan Williams, Minister of Mental Health and Addiction this 19th day of December, 2023
Approved pursuant to Alberta's Government Organization Act:
Intergovernmental Relations, Executive Council
Annex 1 - Common Statement of Principles on Shared Health Priorities
Common Statement of Principles on Shared Health Priorities
Annex 2 - Shared pan-Canadian interoperability roadmap
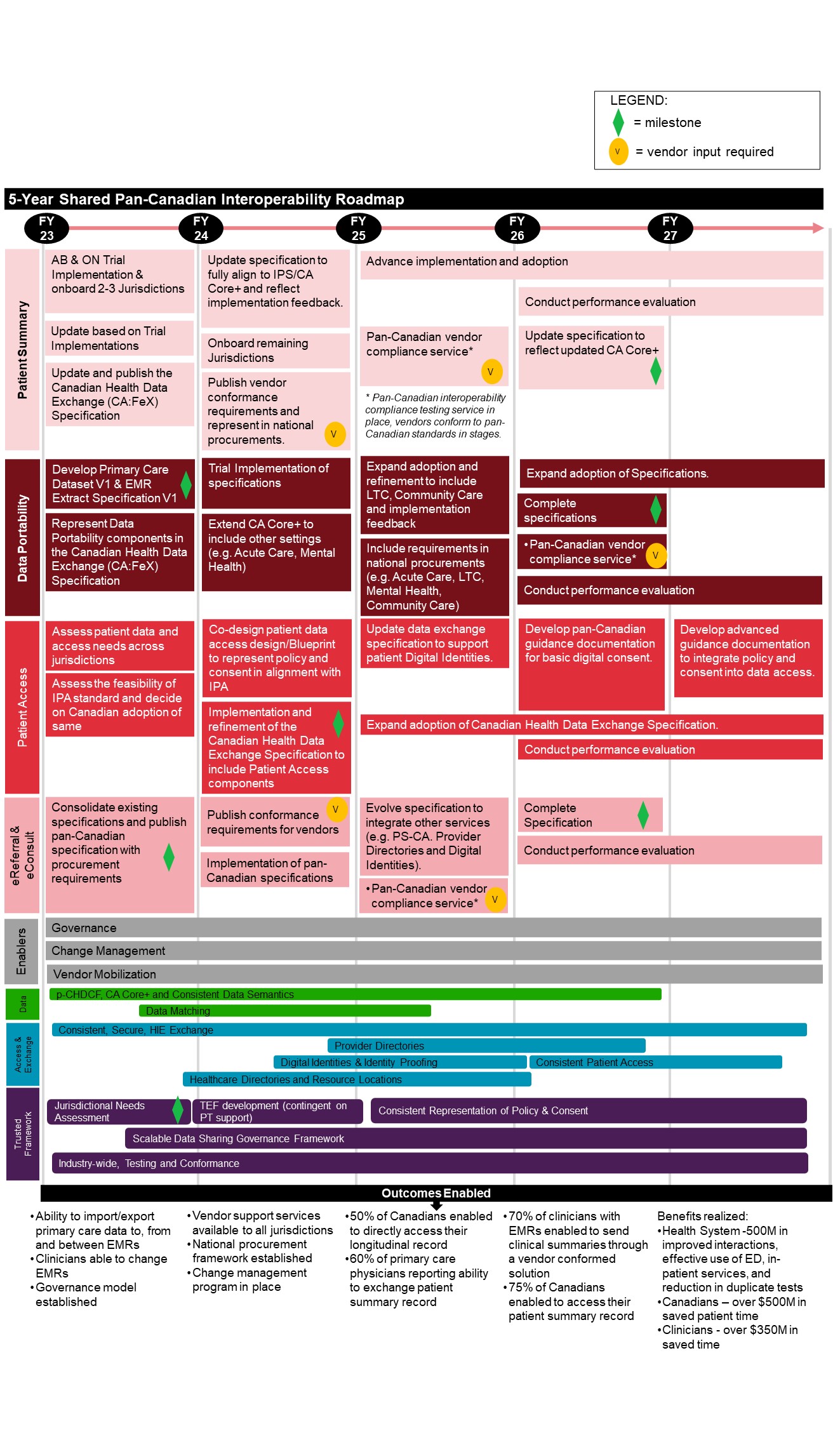
Figure 1 - Text description
5-Year Shared Pan-Canadian Interoperability Roadmap
The Roadmap outlines 8 categories of activities planned for fiscal years 2023 to 2027, followed by anticipated outcomes enabled. Notes are also included throughout to highlight a "milestone", where "vendor input is required", and/or when an activity is "continued" across multiple fiscal years.
Patient Summary
- Fiscal Year 2023
- Alberta & Ontario Trial Implementation & onboard 2-3 Jurisdictions
- Update based on Trial Implementations
- Update and publish the Canadian Health Data Exchange (CA:FeX) Specification
- Fiscal Year 2024
- Update specification to fully align to IPS/CA Core+ and reflect implementation feedback
- Onboard remaining jurisdictions
- Publish vendor conformance requirements and represent in national procurements [vendor input required]
- Fiscal Year 2025
- Advance implementation and adoption
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Fiscal Year 2026
- Advance implementation and adoption [continued]
- Conduct performance evaluation
- Update specification to reflect updated CA Core+ [milestone]
- Fiscal Year 2027
- Advance implementation and adoption [continued]
- Conduct performance evaluation [continued]
Data Portability
- Fiscal Year 2023
- Develop Primary Care Dataset V1 & EMR Extract Specification V1 [milestone]
- Represent Data Portability components in the Canadian Health Data Exchange (CA:FeX) Specification
- Fiscal Year 2024
- Trial Implementation of specifications
- Extend CA Core+ to include other settings (e.g. Acute Care, Mental Health)
- Fiscal Year 2025
- Expand adoption and refinement to include LTC, Community Care and implementation feedback
- Include requirements in national procurements (e.g. Acute Care, LTC, Mental Health, Community Care)
- Fiscal Year 2026
- Expand adoption of Specifications
- Complete specifications [milestone]
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Conduct performance evaluation
- Fiscal Year 2027
- Expand adoption of Specifications [continued]
- Conduct performance evaluation [continued]
Patient Access
- Fiscal Year 2023
- Assess patient data and access needs across jurisdictions
- Assess the feasibility of IPA standard and decide on Canadian adoption of same
- Fiscal Year 2024
- Co-design patient data access design/Blueprint to represent policy and consent in alignment with IPA
- Implementation and refinement of the Canadian Health Data Exchange Specification to include Patient Access components [milestone]
- Fiscal Year 2025
- Update data exchange specification to support patient Digital Identities
- Expand adoption of Canadian Health Data Exchange Specification
- Fiscal Year 2026
- Develop pan-Canadian guidance documentation for basic digital consent
- Expand adoption of Canadian Health Data Exchange Specification [continued]
- Conduct performance evaluation
- Fiscal Year 2027
- Develop advanced guidance documentation to integrate policy and consent into data access
- Expand adoption of Canadian Health Data Exchange Specification [continued]
- Conduct performance evaluation [continued]
eReferral & eConsult
- Fiscal Year 2023
- Consolidate existing specifications and publish pan-Canadian specification with procurement requirements [milestone]
- Fiscal Year 2024
- Publish conformance requirements for vendors [vendor input required]
- Implementation of pan-Canadian specifications
- Fiscal Year 2025
- Evolve specification to integrate other services (e.g. PS-CA. Provider Directories and Digital Identities)
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Fiscal Year 2026
- Complete Specification [milestone]
- Conduct performance evaluation [continued]
- Fiscal Year 2027
- Conduct performance evaluation [continued]
Enablers
- Fiscal Years 2023 to 2027
- Governance
- Change Management
- Vendor Mobilization
Data
- Fiscal Year 2023
- p-CHDCF, CA Core+ and Consistent Data Semantics
- Data Matching
- Fiscal Year 2024
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Data Matching [continued]
- Fiscal Year 2025
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Data Matching [continued]
- Fiscal Year 2026
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Fiscal Year 2027
- N/A
Access & Exchange
- Fiscal Year 2023
- Consistent, Secure, HIE Exchange
- Healthcare Directories and Resource Locations
- Fiscal Year 2024
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories
- Digital Identities & Identity Proofing
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2025
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories [continued]
- Digital Identities & Identity Proofing [continued]
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2026
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories [continued]
- Digital Identities & Identity Proofing [continued]
- Consistent Patient Access
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2027
- Consistent, Secure, HIE Exchange [continued]
- Consistent Patient Access [continued]
Trusted Framework
- Fiscal Year 2023
- Jurisdictional Needs Assessment [milestone]
- Scalable Data Sharing Governance Framework
- Industry-wide, Testing and Conformance
- Fiscal Year 2024
- TEF development (contingent on PT support)
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2025
- Consistent Representation of Policy & Consent
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2026
- Consistent Representation of Policy & Consent [continued]
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2027
- Consistent Representation of Policy & Consent [continued]
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
Outcomes
- Ability to import/export primary care data to, from and between EMRs
- Clinicians able to change EMRs
- Governance model established
- Vendor support services available to all jurisdictions
- National procurement framework established
- Change management program in place
- 50% of Canadians enabled to directly access their longitudinal record
- 60% of primary care physicians reporting ability to exchange patient summary record
- 70% of clinicians with EMRs enabled to send clinical summaries through a vendor conformed solution
- 75% of Canadians enabled to access their patient summary record
- Benefits realized:
- Health System - $500M in improved interactions, effective use of ED, in-patient services, an reduction in duplicate tests
- Canadians - over $500M in saved patient time
- Clinicians - over $350M in saved time
Annex 3 - Headline common indicators
| Shared health priority area | Indicator |
|---|---|
| Family health services | Percentage of Canadians who report having access to a regular family health team, a family doctor or nurse practitioner, including in rural and remote areas |
| Health workers and backlogs | Size of COVID-19 surgery backlog |
| Net new family physicians, nurses, and nurse practitioners | |
| Mental health and substance use | Median wait times for community mental health and substance use services |
| Percentage of youth aged 12 to 25 with access to integrated youth services (IYS) for mental health and substance use | |
| Percentage of Canadians with a mental disorder who have an unmet mental health care need | |
| Modern health data system | Percentage of Canadians who can access their own comprehensive health record electronically |
| Percentage of family health service providers and other health professionals (e.g., pharmacists, specialists, etc.) who can share patient health information electronically |
Annex 4 - Action plan
1.0 Selection of shared health priorities, summary of context and current status
The Government of Alberta is committed to an accessible, integrated, accountable, high quality, person- centered and sustainable health system that emphasizes staying healthy and well, while also supporting equitable access to required care when needed. It is critical that the Government of Alberta's objectives are accomplished within the pillars of the Canada Health Act.
Top performing health systems are purposely organized around primary health care. Primary Health Care (PHC) is the main place people go for health or wellness advice and programs, treatment of a health issue or injury, and diagnosis and management of health conditions through every stage of life. In this context, PHC would include a broad spectrum of supports that addresses health conditions using a collaborative approach, including with Alberta Mental Health and Addiction to provide services in the primary care system. PHC coordinates between primary care and social and community care. Alberta is investing in opportunities to improve primary health care and working toward Alberta's vision for a primary health care system that supports Albertans to be as healthy as they can be. The strategic outcomes for this vision are access, integration, quality, Albertans as partners, and culturally safe and appropriate care.
An accessible, integrated, and high-quality primary health care system can be achieved through the collaborative practice of diverse teams working to their optimized scopes of practice and coordinating and communicating to support seamless transitions and continuity of care. This streamlined and accountable system would drive continuous improvement and have the flexibility to meet local needs and support Albertans to be meaningful partners in achieving their health and wellness goals. Several initiatives are under way to move toward this vision including investing in team-based primary health care, developing a sustainable primary health care governance structure, and the Health Workforce Strategy.
With an enhanced focus on primary health care and supporting improved access to culturally safe primary health care for Indigenous peoples, the province's overall health system will be less dependent on emergency care and hospitalizations and provide the care Albertans need when and where they need it. This focus on primary care will also bring about better health outcomes for Albertans.
Building on the excellent work of Alberta's doctors, nurses, and other health care providers, the health care system requires reform to address the needs of Albertans including Indigenous peoples. Alberta has made significant steps in addressing major health care challenges by increasing system capacity, recruiting more health care workers, and implementing changes to improve the system.
As part of this effort to drive system improvement, on November 8, 2023, the Alberta Government outlined the plans for a refocused health care delivery system. This refocused system will be a fully integrated health care delivery system that centers around four priority sectors: primary care, acute care, continuing care and mental health and addiction. A strengthened governance framework will enhance the oversight, delivery, coordination, and integration of services across these key areas.
Incremental funding provided specifically under the Working Together to Improve Health Care for Canadians (Working Together) plan will contribute to Albertans' immediate needs, as well as the overall health refocus agenda.
Areas of Action
This Action Plan supports the commitment to the bilateral agreement structure which includes an agreement to Key Principles to guide collaboration and a commitment to streamline foreign credential recognition and to advance labour mobility.
Initiatives described in this action plan represent incremental investments in areas that align with the four areas of shared priorities outlined in Working Together, which include:
- Expanding access to family health services, including in rural and remote areas;
- Reducing backlogs and supporting our health care workers;
- Improving access to quality mental health and substance use services; and
- Modernizing health systems with health data and digital tools.
Given the span of these shared priorities, as well as the interconnectivity of each area, integration will be a key focus for the Ministry of Health (Alberta Health) and the Ministry of Mental Health and Addiction as initiatives and programs are further developed and implemented.
The Action Plan is designed to ensure Alberta has maximum flexibility to adapt its approach to reflect the evolving needs of Albertans. Should Albertans provide new direction, the Government of Alberta will work with Health Canada under the terms of the agreement to pursue new, revised or enhanced initiatives that align with the shared priorities as necessary.
Priority 1: Expanding access to family health services, including rural and remote areas
Overview of current system
Alberta's vision is to build a PHC system that supports Albertans to be as healthy as they can be. Alberta recognizes the importance of ensuring that all Albertans have access to high-quality family health services that are integrated, comprehensive, collaborative, and person-centered when needed, including in rural and underserved communities.
Family physician clinics, which include comprehensive family medicine clinics and walk-in clinics, as well as other primary care settings like pharmacies, provide a significant portion of primary care services.
Most family physicians work in solo or group practices and bill Alberta Health on a fee-for-service basis.
Most of the primary care workforce is located in approximately 1,200 physician offices, which include physicians and other team members such as nurse practitioners, medical office assistants, and other allied health professionals (e.g., pharmacists, dieticians).
Key System Elements
Alberta has a strong foundation in PHC delivery, including a series of initiatives that have been implemented to help improve access to day-to-day health services.
Primary Care Networks (PCNs)
In 2003, Alberta Health, drawing on the federal Primary Health Care Transition Fund mandate, funded the creation of PCNs through joint ventures between a group of family physicians who form a non-profit corporation and Alberta Health Services (AHS), the provincial health authority. These partnerships support cross-disciplinary programming and help primary care providers in the network with planning and PHC transformation management support.
There are 39 PCNs funded through grants by Alberta Health. Physician membership is voluntary, and approximately 84 per cent of family physicians in Alberta are members of PCNs, associated with approximately 3.8 million Albertans.
In June 2017, a Ministerial Order established the PCN governance structure, which includes the Provincial PCN Committee and the five Zone PCN Committees. In September 2020, the Minister of Health signed a five-year Ministerial Order which continued the Provincial PCN Committee and five Zone PCN Committees. The governance structure's purpose is to advance provincial and government priorities and to advise the Minister on PCN governance and leadership issues; operational PCN policy; integration and alignment of health services between and across PCNs, AHS, and community organizations, including shared services; and a measurement and evaluation framework.
Primary Care Service Delivery Models
| Delivery model | Description |
|---|---|
| Physician clinics |
|
| Community Health Centres (CHCs) |
|
| Family Care Clinics (FCC) |
|
| Virtual Care Models |
|
Other key initiatives
| Initiative | Description |
|---|---|
| Indigenous Health Services |
|
| Nurse Practitioner Support Program |
|
| Community Information Integration / Central Patient Attachment Registry (CII/CPAR) |
|
| Alberta Find a Doctor tool |
|
| MyHealth Records Patient Portal |
|
Primary Care Spending
In Alberta, the primary components of primary care spending are physician compensation and funding for service delivery models and organizations such as PCNs, the PCN Nurse Practitioner Support Program, health services in community health centres, and AHS-operated family care clinics.
Alberta Health allocates over $2 billion per year for primary care services, which primarily covers physician compensation ($1.8 billion+) and PCNs (~$250 million).
Plans and priorities for the next three years
Top issues
- Reasonable access to a family doctor;
- Rural and remote access;
- Indigenous health; and
- Integrated models of care.
Key actions
Alberta continues to work toward the vision of a primary health care system that supports Albertans to be as healthy as they can be and is taking a multipronged approach with significant investments to move toward it, including:
- Team-based primary health care service delivery;
- Flexible delivery models that leverage alternative compensation mechanisms and a range of primary health care providers;
- An integrated approach to the prevention and management of chronic conditions and diseases,
- Continuity of care across the patient journey;
- A sustainable primary health care governance structure; and
- A comprehensive health workforce strategy.
The Modernizing Alberta's Primary Health Care System (MAPS) initiative was announced in September 2022 to identify early investment opportunities and long-term recommendations and a 5-10- year roadmap that can build on the many primary health care successes in Alberta. The MAPS recommendations have a particular focus on addressing challenges that Indigenous and rural Albertans face when trying to find a family doctor or other primary health care provider, and aim to ensure First Nations, Métis and Inuit peoples have access to high-quality, culturally safe care that is free of racism and respects their unique health care needs.
As part of Budget 2023, the government announced an investment of $125 million over three years to support implementation of the recommendations for early opportunities for investment from MAPS. These early investment opportunities are the actions reflected in this action plan, where funding under Working Together is incremental to Budget 2023 funding (i.e., Working Together funding is expanding on proposed programs for broader impact). In October 2023, Alberta announced it is moving forward on developing an implementation plan that includes recommendations in the final report to improve access to primary care for all Albertans.
To better support health outcomes for Indigenous peoples in Alberta, the Alberta government will act on the recommendations to build more meaningful connections with Indigenous leaders and communities to identify improvements that reflect the unique nature of their communities.
Notwithstanding the incremental federal funding, significantly more investment will be required to implement the early investment opportunities and to advance implementation of the longer-term strategy. It is critical that funding provided consider long-term sustainability (versus short term or one-time investments).
Priority 2: Reducing backlogs and supporting health care workers
Overview of current system
There is a critical shortage of health human resources in Alberta. This issue existed pre-pandemic but has worsened in recent years. A new Health Workforce Strategy has been developed to guide investments and actions to address this gap.
In 2019, Alberta introduced the Alberta Surgical Initiative to address the backlog and deal with those patients waiting outside of clinically appropriate wait times. Work has been ongoing to ramp up overall surgeries through better utilization of existing space, capital investment in new operating rooms and the increased use of chartered surgical facilities. More recently, Alberta is implementing a Health Care Action Plan to take more targeted and immediate action to address backlogs and wait times.
Key system elements
The main elements that are guiding work in this area include:
- Alberta's Health Care Action Plan identifies immediate government actions to build a better health care system that supports patients needing care while setting clear measurements for success.
- In Budget 2023, Alberta's government committed approximately $158 million towards a new Health Workforce Strategy to support rural physician recruitment and retention.
- Alberta's Health Workforce Strategy is built around five pillars:
- Retain and support- Provide a safe, engaging, and meaningful work environment to retain Alberta's health care workers.
- Attract- Recruit new workers from across Canada and the globe to build a sustainable workforce with the right skills.
- Grow- Create capacity to educate and train the workforce of the future.
- Strengthen- Implement collaborative, proactive and evidence-informed approaches to long- term workforce planning.
- Evolve- Design and implement new models of care and enabling tools to deliver more efficient, high-quality care.
- As part of Alberta's Budget 2021, the government released the CT and MRI Action Plan to address the backlog. The plan invested an additional $33 million, above existing CT/MRI funding, to support incremental scans in AHS facilities. Budget 2023 included an additional $12 million to support the plan and increase scans in AHS facilities.
$12 million to support the plan and increase scans in AHS facilities.
Plans and priorities for the next three years
Top issues
- Acute care system pressures (wait time and surgical backlog);
- Human Health Resources ; and
- Diagnostic and Imaging backlog (specifically CT/MRI).
Key actions
- Addressing acute care pressures under the Health Care Action Plan, with a focus on the following: Decrease emergency room wait times;
- Improve emergency medical services response times;
- Reduce wait times for surgeries; and,
- Empower frontline workers to deliver health care.
- Implementation of the Health Workforce Strategy which will build on current action to address labour shortages in the health care system including steps to streamline the recognition of foreign credentials for health care workers. Specific areas of focus include:
- Short-Term/Immediate: Utilization of Current Workforce (including scope of practice)
- Medium-Term: Immigration
- Long-Term: Training
- Implementation of the Health Workforce Strategy which will build on current action to address labour shortages in the health care system including steps to streamline the recognition of foreign credentials for health care workers. Specific areas of focus include:
- Waitlist for Diagnostic Imaging: Identify alternative delivery models and partnerships for publicly funded services to accelerate action to reduce the backlog.
Priority 3: Improving access to quality mental health and substance use services
Overview of current system
The Ministry of Mental Health and Addiction (MHA) is leading the Government of Alberta's efforts to develop a recovery-oriented system of care across the province in collaboration with partner ministries. A recovery-oriented system of care is a coordinated network of community-based services and supports that are person-centered and build on the strengths and resilience of individuals, families, and communities to achieve wellness and quality of life for those who are experiencing negative impacts related to mental health and substance use problems.
This approach focuses on treating mental health and addiction as interconnected health care and social issues, while also keeping communities safe. This is accomplished in part by ensuring Albertans have access to a coordinated continuum of supports, with multiple clear entry points to the type of support needed based on an individual's unique circumstance.
Albertans living with mental health and addiction challenges are supported in their pursuit of recovery through a holistic, integrated, recovery-oriented system of care including services that support prevention, early intervention, treatment, and recovery. In Alberta, the full range of addiction and mental health services, including prevention, promotion, early intervention, treatment, and recovery supports, are delivered in community settings (e.g., schools, community mental health clinics, supportive housing), specialized centres (e.g., addiction treatment centres, hospitals, specialized clinics) and standalone/acute psychiatric institutions.
Through the two previous Canada-Alberta Home and Community Care and Mental Health and Addiction Services Funding Agreement in support of the 2017 Common Statement of Principles on Shared Health Priorities (CSOP), Alberta utilized funding to support and improve access to pre-existing mental health and addiction programs and services. Specifically, funding provided:
- Additional support to enhance follow-up in the community and the provision of crisis support and outreach services to reduce acute and emergency care demand;
- The provision of community day programs and residential services for children and youth at risk for serious mental health or addiction issues; and
- Community addiction and mental health supports by adding intensive care options and increasing the range and type of specialized services offered across the province.
The shift towards a recovery-oriented system of care came following the 2022 final report recommendations from the Mental Health and Addictions Advisory Council (the Council) that was established in fall 2019. The Council was mandated to inform an approach to improve access to recovery-oriented MHA services and supports in Alberta.
Key system elements
The Ministry of Mental Health and Addiction holds responsibility for addiction and mental health system oversight and governance. This ensures services are being monitored and evaluated, and decisions related to systems planning are driven by evidence. The Ministry is also responsible for establishing safe and high-quality addiction and mental health related legislation, standards, and policies, which includes licensing service providers and monitoring compliance to protect Albertans.
Service providers, non-profit and for-profit, deliver a wide variety of MHA services to Albertans. They may be funded publicly such as through grants provided by the Government of Alberta, or funded through fee for service (clients, insurance companies).
The Mental Health Patient Advocate, who is responsible for responding to concerns raised to the Office of the Alberta Health Advocates regarding Albertans' navigation of the addiction and mental health system, and access to the appropriate resolution service to address concerns, including those specific to the Mental Health Act.
- More than $1 billion is spent annually on mental health and addiction services across government (approximately 80 per cent on clinical services and 20 per cent non-clinical and training/promotion). An additional $700 million is spent on physician billing for related services.
- Over the last four years, the Government of Alberta has expanded funding for mental health and addiction by over 62 per cent ($330 million) to drastically increase the amount of supports available for Albertans. An additional $155 million in capital was invested to increase treatment capacity.
Plans and priorities for the next three years
Top issues
- Addiction and Opioid Crisis
- Each day approximately 3-4 Albertans die of an opioid overdose, with higher proportions impacted by alcohol and other addictions.
- All programming previously funded by the Canada-Alberta Emergency Treatment Fund bilateral agreement has continued into the 2023-24 fiscal year.
- Child and Youth Mental Health
- Widespread concerns about worsening child and youth well-being stemming from the pandemic, including from social isolation, barriers to access existing services and increased waitlists.
- Efficacy of Performance Indicators and Outcome Measurement
- Current indicators do not effectively measure client outcomes but rather focus on outputs such as utilization. Current indicators do not support early response to emerging issues or discrete events like increased suicide or drug overdose. Nor do they drive the system towards supporting and measuring recovery or population wellness.
- Indicators and outcomes need to better include client experience to ensure the system is responsive to client need.
Key actions
- Expand access to recovery-oriented supports in the health, justice, and social sectors in collaboration with partner ministries to improve care for Albertans affected by addiction or mental health concerns.
- Enhance the capacity and capability to monitor and evaluate addiction and mental health outcomes across health, justice, and social systems to ensure evidence-based decision making.
- Establish new and optimize existing addiction treatment spaces and recovery communities across the province to support more Albertans in their pursuit of recovery.
- Expand efforts to ensure culturally appropriate addiction and mental health community supports are in place for First Nations, Métis, and Inuit peoples in Alberta.
- Ensure Albertans can access a continuum of recovery-oriented supports that meet their unique needs to improve their mental health.
- Expand the range of recovery-oriented services to support people living with a severe mental illness, with a focus on children and youth.
Priority 4: Modernizing health systems with health data and digital tools
Overview of current system
Alberta has a mature eHealth ecosystem that provides patients and providers with digital tools to access and manage health information. It includes Alberta Netcare, the provincial electronic health record (EHR); MyHealth Records, the provincial patient portal; Connect Care, the clinical information system underpinning AHS; as well as electronic medical records (EMRs) in physician offices and other point-of- care systems. It also includes supporting IT services and technologies for exchanging clinical information across the health system to support continuity of care, and for capturing this information for analysis, reporting and health system management.
Ministry of Health data administrative systems are key for surveillance and monitoring purposes to review trends and to use a data approach to inform policy decisions and support program development.
Key system elements
Modernization and expansion of the eHealth ecosystem is a key objective of Alberta's Provincial eHealth Strategy, a 10-year vision anchored on improving the patient's care journey. The goal of the strategy is to address current gaps and limitations in Alberta's eHealth services, particularly around primary care integration, and empower patients and providers with the correct information and tools for improved quality care delivery and better health outcomes. While the total annual spend on health IT systems is approximate $700 million, less than 5% of this total is directly focused on the initial work to implement the E-Health strategy. Incremental funding under Working Together will accelerate and enhance current planning.
- Previous federal funding was used to enhance Alberta's capacity to respond to the COVID-19 pandemic, such as increased capacity for virtual care and streamlines immunization services. Future incremental federal funding through the Working Together plan will build on this work to modernize foundational IT infrastructure to increase resiliency, and to enhance integration of Alberta's eHealth ecosystem.
- Future incremental federal funding through the Working Together plan represents an approximate additional 28 per cent of required costs for infrastructure and integration objectives.
Plans and priorities for the next three years
Top issues
- Patient access to their own data (electronic)
- Seamless flow of health data across care providers
Key actions
Over the next three years Alberta will focus on two key objectives for eHealth services.
- Modernizing eHealth infrastructure by making progress on the following actions:
- Implementing new provider portal, followed by the patient portal, that will expand access to health information and provide new digital tools for care providers;
- Replacing legacy administrative data repositories with a modern consolidated clinical data repository that supports improved data exchange capabilities;
- Expanding information sharing services to allow more seamless flow of clinical data between electronic health systems and the care providers they support; and,
- Continuing to roll out Connect Care across AHS facilities and services.
- Building new eHealth services that improve patient care by making progress on the following actions:
- Accelerating EMR interoperability by increasing the number of physicians linked to the CII service, implementing patient summary sharing, and developing a new EMR vendor strategy for the province;
- Beginning to implement closed-loop electronic referral and consult services in support of the Alberta Surgical Initiative; and
- Upgrading provincial data warehouse systems to improve the analysis and reporting of health information for quality improvement efforts. This includes further opportunities to support the availability of disaggregated data (e.g., sex, gender, age, Indigeneity) to better reflect the diversity of the province's population.
This work will be coordinated with other jurisdictions and federal health agencies where appropriate to align with the Pan-Canadian Interoperability Roadmap. These key actions will improve the breadth and depth of clinical information sharing across the province, both with the patient and between the members of their health team. To facilitate care, the collected data will be largely disaggregated, allowing information to be summarized to better support analysis and reporting efforts. EHealth modernization will also broaden information flow from Indigenous and First Nations reserves, and rural and remote areas of Alberta.
2.0 Description of initiatives supported by incremental funding
Priority 1: Expanding access to family health services, including rural and remote areas
Initiatives
1. Primary health care transformation - Modernizing Alberta's primary health care system
As part of the ongoing transformation of primary health care, Alberta Health convened advisory panels to identify immediate and long-term actions to strengthen PHC and to achieve a PHC- oriented health system that delivers the outcomes of access, integration, quality, Albertans as partners, and culturally safe and appropriate care. On October 18, 2023, the Alberta government announced it is beginning to move forward on the recommendations, which will be implemented through a phased approach.
To improve primary health care and increase Albertans' access to medical care they need, Alberta's government is acting immediately on recommendations to:
- Create a primary health care division within Alberta Health;
- Allocate funding to provide family doctors and nurse practitioners with support to help manage their increasing number of patients;
- Work with the Alberta Medical Association to create a task force to recommend a new
payment model for family physicians that encourages comprehensive primary care;
- Develop a memorandum of understanding with the Alberta Medical Association to collaborate on a transition to a new physician compensation model, modernize primary care governance and enable family doctors to spend more time with patients and less time on paperwork and immediately stabilize primary care;
- Expand online mental health services, allowing doctors to bill for virtual mental health checks and therapy, and compensate them for extra time spent with patients virtually;
- Ensure doctors get paid if patients cannot prove insurance coverage, reducing administrative burden; and
- Introduce a payment system to support nurse practitioners to open their own clinics, take on patients and offer services based on their scope of practice, training and expertise.
To strengthen health care and support better health outcomes for Indigenous peoples in Alberta, the Alberta government will act on recommendations, including:
- Creating an Indigenous health division within Alberta Health;
- Creating a fund for Indigenous communities to design and deliver innovative primary health care services and projects;
- Creating an Indigenous patient complaints investigator and Elders roster to investigate incidences of racism during the delivery of health care and provide culturally safe support to Indigenous patients through the patient complaint process; and
- Investing in a community-based Indigenous patient navigator program to support Indigenous peoples through their health care journey.
Incremental funding provided under Working Together will be used to bolster, expand and add to the following MAPS actions, divided between the Indigenous and non-Indigenous-specific initiatives.
1.1 Innovation funding supports for indigenous-led primary health care programs and supports
Funding and capacity support to establish a demonstration project partnership and explore opportunities for Indigenous health unit projects with First Nations, Metis Settlements, Otipemisiwak Métis Government, and other Indigenous health serving providers in Alberta to enhance access to primary health care in Indigenous communities, particularly in rural, remote, and isolated locations.
1.2 Support for First Nations and Métis communities, including the Metis settlements and the Otipemisiwak Métis Government, to establish information sharing agreements
This support will enable First Nations and Métis communities, including the Metis Settlements, and Otipemisiwak Métis Government to have access to their community's health data and information. This, includes funding for the communities to develop health human resource capacity at the community level, and infrastructure to improve the collection and use of health information and data.
1.3 Stimulus funding for team-based care
Providing funding for primary care providers to enable direct care (e.g., clinical services) and indirect care (e.g., administrative services) is expected to increase Albertans' access by increasing panel sizes, improving same day and after-hours availability, leveraging team members to their full scope of practice, and supporting continuity of care.
Identifying new and expanding existing solutions to provide comprehensive services to Albertans though innovative initiatives, is expected to enable improvements key areas, including the number of Albertans who are attached to a primary care provider and enable Albertans' voices to be heard.
The expected impacts are increasing access to primary care services (including after-hours and same-day appointments), with more Albertans having a regular primary care provider and improved continuity of care.
1.4 Integrated supports for underserved Albertans
Alberta Health is working to expand existing integrated health, community, and social services models that provide comprehensive services and outreach to people who face barriers to accessing health services (due to ethnicity, poverty, trauma, social isolation, addiction, mental illness, literacy and education, systemic racism and discrimination, lack of Alberta Health Care Coverage, and/or lack of appropriate housing).
Individuals within these populations typically live with multiple and complex physical, medical, mental, emotional, and social challenges which may be due to adverse childhood experiences, intergenerational trauma, and social determinants of health.
1.5 Virtual care program
Planning is underway to enable a virtual program to improve access, facilitate attachment of unattached patients, and provide additional supports to patient medical homes. This aims to improve access without compromising continuity of care, driving higher volumes of unnecessary visits and diagnostics, or contributing to poor patient outcomes.
Funding allocations will provide increased after-hours availability of appointments, and a decreased in time to the next available appointment. Additionally, there is the potential to reduce the use of emergency departments for health needs that can be effectively addressed with primary health care.
2. Virtual care codes
To ensure that complex patients have greater access to mental health services, Alberta has developed new virtual care codes for prolonged and complex mental health services. For example, this included streamlining the health service codes used for virtual psychiatric treatment by family physicians and pediatricians, and included new codes for virtual group and family therapy that will pay the same rate as in-person care. Funding will support provider payments under these new virtual care codes.
3. Primary care stabilization
Funding to physician practices to provide stabilization of the existing primary care system and reduce administrative burden facing primary care providers, with a focus on supporting family practice in community settings. This short-term bridge funding will be in place until longer-term funding arrangements are established.
This program seeks to improve access and attachment to primary care providers by alleviating current pressures that prevent practitioners from seeing patients. Support may include funding for panel management, quality improvement, advancing the patient medical home and supporting and evolving the workforce.
4. Community-based pilot programs
4.1 Prostate Cancer Centre Provincial Expansion - Pilot program
This mobile men's health clinic ("MAN VANTM") expands access to prostate-specific antigen blood testing used for early detection of prostate cancer for men aged 50-75 and offers mental health wellness checks and pre-habilitation before surgery. Currently operating in southern Alberta and Calgary, expansion of the MAN VAN TM services to northern Alberta and Edmonton will increase annual patient impact from 7,000 up to 30,000 and reach targeted rural, diverse ethnic groups, and Indigenous populations that need a point of entry to care. This program seeks to improve patient outcomes while reducing the cost of care to the health care system.
4.2 Cancer Care Community Treatment - Pilot program
This program seeks to test and assess the opportunities to deliver infusion therapy outside of the traditional acute facility settings where it is feasible to do so. This provides opportunities for addressing surge pressures, as well as meet growing overall demands for these therapies. The proposed patient pathway to be tested in a pilot is similar, however there are differences that make it more streamlined and comfortable as the patient would receive their therapy in a fit-for- purpose clinic with appropriate space, effective equipment and beneficial amenities to ensure comfort and privacy during their infusion. Opportunities to test additional community care models are also being explored.
4.3 Reducing the Burden on Alberta's Emergency Health Care System through Community-Based Education and Supports for People with Epilepsy - Pilot Program
The program seeks to improve health outcomes for people with epilepsy, while reducing costs to the health care system by reducing the non-medical burden of epilepsy on Alberta's overstressed emergency health care system. This pilot project will expand on existing evidence-based epilepsy education and support services to improve the lives of Southern Albertans diagnosed with epilepsy. Over three years, this program will support 3,300 people resulting in a reduction of 750 non-urgent visits to emergency rooms annually, and 1,200 epilepsy-related inpatient admissions over the course of the pilot.
4.4 Pulmonary Testing - Pilot Program
In Alberta, pulmonary function testing (PFT) labs are available in a small number of metropolitan areas. This program seeks to expand access to pulmonary function testing to improve health outcomes for Albertans living in rural and remote areas with lung conditions such as asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and lung cancer. A mobile PFT lab will provide regularly scheduled visits to rural and remote areas and "at your doorstep" service for patients with mobility issues. Mobile diagnostics enables earlier diagnosis and treatment and reduces medical inequity for rural and remote Albertans.
4.5 Diabetes Care - Pilot program
This program seeks to test and assess opportunities to use virtual platforms for chronic disease management, particularly diabetes prevention, care and management in alignment with the pending recommendations drafted by the Premier's Diabetes Working Group. Building on the strong evidence generated by the Virtual Diabetes Prevention Program conducted by the Diabetes, Obesity and Nutrition Strategic Clinical Network (with a company that is no longer operating), this program aims to demonstrate the scalable impact of virtual care for diabetes prevention and reversal. Leveraging an Alberta Type 2 Diabetes Model created by the Institute of Health Economics, the pilot or pilots will be designed to convincingly advance the evidence base with respect to the health and economic benefits of a scalable model of care that is already shown to improve patient outcomes and quality of life while reducing pressure in the health system. The proposed care methodology provides 24/7 patient interaction to optimize well-being, improve health outcomes and contain long-term system costs in a manner that respects constraints such as those related to health workforce availability, rural and remote care.
4.6 Heartway - Pilot Program
The Heartway Initiative is a collaboration with University Hospital Foundation and Novartis Pharmaceuticals Canada to introduce and implement innovative solutions, technologies, and care pathways to reduce the incidence and improve outcomes for Albertans with atherosclerotic cardiovascular disease (ASCVD).
Pilots aim to develop an evidence-based common approach to lipid optimization intervention in at risk patients through education, lifestyle modification and appropriate use of lipid lowering therapies.
An evaluation framework is being developed jointly by the Canadian VIGOUR Centre (University of Alberta) and the O'Brien Institute for Public Health (University of Calgary) to assess the clinical and operational outcomes of the pilot projects.
5. French services
Health-focused efforts are a key element of the Government of Alberta's French Policy 2023-28 Action Plan. Current initiatives include translation of select health care resources and funding for the Saint Thomas Community Health Centre (Centre de Santé Communautaire) through a clinical alternative relationship plan to expand its primary health care services to French-speaking Albertans. Further, the government is creating a comprehensive inventory of health care services that are available in French and promote these services to French communities. AHS continues to increase access to professional medical interpreters in French across all AHS sites. Increased access to educational health information in French continues to be updated as part of the inventory list of French resources.
Through Campus Saint-Jean at the University of Alberta, the Consortium national de Formation en Santé aims to improve access to social and health services for official language minority communities by increasing access to health training programs. Campus Saint-Jean offers three programs through its partnerships with the Consortium:
- Health Care Aide Program (HCA), offered by the Centre collegial de l'Alberta;
- Bilingual Bachelor of Science in Nursing program undergraduate program; and
- Certificate of Graduate Studies in Speech-Language Pathology in a Francophone Environment graduate program.
The following projects have been identified for implementation through a partnership with the Association canadienne-française de l'Alberta (ACFA) and the Réseau santé Alberta (RSA). Some elements will be explored in concert with the Ministry of Mental Health and Addictions and with funding under the Working Together plan. Additional programs will be added as the revised strategy is developed.
- Strategies to Develop the Active Offer and Demand for Health Care Services in French: Establish a permanent mechanism for collaboration between the Government of Alberta and stakeholder organizations within Alberta's Francophonie. This mechanism, which could take the form of a multi- stakeholder committee on French-language health, would help identify and implement the best strategies for developing the active offer of health care services in French.
- Expanding the Scope of Health Services in French in Edmonton, Calgary and Rural Regions: Identify the gaps of health care professionals and delivery of services in French. This evidence will be used to develop an overview of the needs for health care services in French across the province.
- TAO Tel-Aide in Alberta: Develop mental health services in French to address the gaps that Alberta's Francophonie has identified in this sector. Funding for TAO Tel-Aide would help preserve services already available. The helpline is offered directly and only in French.
- Supporting Health Care Professionals who want to Improve their French Language Skills: A pilot project to improve the French-language skills of health care professionals so that Alberta can implement the "Café de Paris" concept of creating an informal space that would allow employees to acquire or maintain basic French language skills.
6. Women's Health
Launched by the Royal Alexandra Hospital Foundation in 2020, the Alberta Women's Health Foundation (AWHF) is a pan-provincial women's health advocacy and fundraising brand that fills gaps in women's health research in partnership with the Women and Children's Health Research Institute (WCHRI), Lois Hole Hospital for Women, and other provincial and federal research organizations and women's health programs.
The Legacy Grant will enable AWHF to:
- Attract global women health innovators and researchers to the province;
- Advance women's health research within the province and place Alberta as a leading Canadian province in women's health research within the Canadian setting;
- Advance clinical care outcomes for women in Alberta;
- Leverage further funding from other sources of funding and investments including the Government of Canada, health industry and other sources;
- Leverage and increase its philanthropy and fund raising from private and corporate donors towards women's health research and innovation; and
- Accelerate awareness and advocacy of women's health.
Outcomes
The outcomes for Indigenous health focused initiatives are:
- First Nations, Métis and Inuit peoples have access to high quality health care services that are free of racism.
- First Nations, Métis and Inuit peoples are partners in the design and delivery of health care services.
Alberta Health will be looking to develop indicators that correspond to the above initiatives; however, work is still underway.
The outcomes for Alberta's Primary Health Care system are:
- Access: All Albertans have access to appropriate, high-quality PHC services when they need it, regardless of where they live in the province. Care options are flexible and reflect both individual and population health needs. Barriers to access are addressed, particularly those that affect populations living with complex health and social needs.
- Integration: Albertans receive PHC from a regular provider and team, with whom they have an ongoing care relationship. Albertans' health care is coordinated throughout the system by providers who collaborate across professions and specialties. Care transitions are smooth and timely; Albertans are supported as they move in and out of care and across providers and settings. PHC services are linked to social supports and community resources.
- Quality: PHC is effective, efficient, and safe. Treatments and interventions are based on current scientific knowledge and evidence-informed practice, use resources efficiently to achieve the desired outcomes, and eliminate or mitigate risk to those receiving service.
- Albertans as Partners: Whenever possible, Albertans are meaningful partners in achieving their health and wellness goals, with the support of a collaborative and interdisciplinary care team. Albertans have a positive care experience; care provided is respectful of individual health, social, mental, cultural, and spiritual needs.
- Culturally Safe and Appropriate Care: First Nations, Métis, and Inuit persons have access to high-quality, culturally safe care that is free of racism, and designed and delivered in a manner that meets their unique health care needs.
Priority 2: Reducing backlogs and supporting health care workers
Initiatives
7. Use of Community Providers for Public Diagnostic Imaging - Pilot Project
Expand the potential for "surge up" systems by providing time-limited funding to community providers to offer publicly funded (non-urgent) MRI and CTs to address the diagnostic imaging backlog and reduce the waitlist to within clinically appropriate wait times.
This approach builds on the model that has been used with AHS as part of the CT and MRI Action Plan (one-time incremental funding from Alberta Health to AHS to supplement baseline MRI and CT levels).
Funding under Working Together would be provided to community providers under contract by AHS to provide a targeted number of MRIs and CTs (no funding is currently provided to community providers for supplemental work). Capacity exists in the Edmonton Zone, including through MIC Medical Imaging, with additional capacity in Edmonton and Calgary Zones to be confirmed. Analysis by the Institute of Health Economics is also nearly complete to help determine the contracting strategy that will have the most positive impact on clinical outcomes and wait list reduction
This model would ensure alignment with the Canada Health Act as this is publicly funded and no patient would pay out of pocket for these services.
Outcomes
- Reduce the number of Albertans on the waitlist for MRI and CT scans.
- Minimize the number of Albertans waiting longer than clinically appropriate wait times for MRI and CT scans.
- Improve health outcomes and quality of life for Albertans by decreasing their wait times for MRI and CT scans.
Priority 3: Improving access to quality mental health and substance use services
Initiatives
8. Maintain mental health and addiction enhancements previously supported by the 2017 CSOP bilateral agreements
The aim of this initiative is to support and improve access to pre-existing mental health and addiction programs and services. Specifically, funding provided will enable continuation of support to:
8.1 Community-based addiction and mental health services
Enhance follow-up in the community, the provision of crisis support/outreach, and the provision of community addiction and mental health supports by adding intensive care options.
8.2 Mental health and addiction services for children and youth
Implement school-based clinical mental health teams in high priority communities across the province.
8.3 Specialized addiction and mental health services
Increase the range and type of specialized services offered across the province.
9. Mental health and addiction services for children and youth with serious mental health issues. Improve outcomes for children and youth at risk who are currently experiencing serious mental health and addiction issues by:
- Expanding community day programs and residential services; and
- Expanding access to clinical mental health services for underserved populations such as youth in corrections, youth in government care, and those accessing youth services.
Provincial funding supported existing baseline services, but there is a need to further expand these to increase access and meet demands for services. Federal incremental funding will support implementation of the additional programming referenced above, alongside additional supplementary provincial funding.
10. Increase addiction and mental health supports for adult populations (and those transitioning out of youth services or with complex needs) to have appropriate supports in place and to reduce wait times for services.
The aim of this initiative to enable Albertans to have access to high-quality, person-centered mental health and addiction programs and services by prioritizing the well-being of Albertans and their ability to access high-quality recovery-oriented addiction and mental health support based on their unique circumstances through:
Enhancing and expanding services for complex and high-risk emerging adults, including for those with cross-ministerial involvement (e.g., Ministries of Health, Children and Family Services, and Justice), those with a history of requiring involuntary confinement for safety, or a high risk of suicide, repeated suicide attempts and ideation, and youth transitioning out of government care and corrections. The Ministry of Mental Health and Addiction will continue to augment existing programs by:
- Enhancing recovery-oriented supports in urban areas with the greatest need to expand the province's response to the addiction crisis and provide more treatment options for Albertans;
- Establishing new and optimize existing addiction treatment spaces and recovery communities across the province to support more Albertans in their pursuit of recovery; and
- Expanding efforts to ensure culturally appropriate addiction and mental health community supports are in place for First Nations, Métis, and Inuit peoples in Alberta.
Provincial funding has supported existing baselines services, but there is a need to further expand these to increase access and meet demands for services. Federal incremental funding will support implementation of the additional programming, alongside additional supplementary provincial funding.
Outcomes
These initiatives will increase access to mental health supports for children and youth, particularly those with complex mental health or addiction needs, and help families in crisis. Children and youth across Alberta will have more opportunities to access community-based specialty treatment and improve their mental health. Importantly, there will also be more supports for youth with complex needs as they transition into adult services, which many people with lived experience say is a particularly challenging and important time to maintain effective care.
Furthermore, the health system will continue its transformation into a recovery-oriented system of care, where every person struggling with addiction and mental health challenges is supported in their pursuit of recovery, with impact reaching past the health care system and into more of society. This includes dramatically increasing access to mental health supports for children and youth throughout their communities, in specialty clinics, and in schools.
Since 2017, these initiatives have been supported by funding from the 2017 CSOP while also being supplemented with additional provincial funding. This model is expected to continue.
Priority 4: Modernizing health systems with health data and digital tools
Initiatives
11. Replace and expand Alberta Netcare repositories and provider portal
The aim of this initiative is to continue building the clinical value of the provincial EHR by expanding data contributions from community-based health care providers, enabling access across more members of the patient's care team, and increasing adoption of standardized data exchange technologies and standards across the health system. This will result in a more timely and comprehensive record of the care provided to Albertans.
12. Enhance and expand MyHealth Records patient portal
The aim of this initiative is to expand the ability of Albertans to digitally access their health information and securely interact with their care teams through MyHealth Records (MHR). It includes several projects occurring concurrently to empower patients and their families. MHR continues to evolve by adding additional data feeds and health information to empower patients in the management of their care. Potential enhancements include expansion of information available to Albertans by adding specialist referral status history, expanding diagnostic imaging results to include cardiology reports, and adding operative, investigative, and procedure reports. As of October 31, 2023, there are 1.6 million registered users.
13. Accelerate EMR interoperability
The aim of this initiative is to increase the number of family physicians, specialists and nurse practitioners who can share information electronically in a secure, standardized manner. This includes the ability to contribute patient summaries and other important clinical information to the provincial EHR and to receive information back from provincial systems through more integrated EMR software systems. This includes care providers in Indigenous communities (including First Nations reserves) in rural and remote regions of Alberta. This initiative will support continuity of care along the patient's health care journey.
14. Implement electronic referral services
The aim of this initiative is to enable the secure sharing of electronic referral and consult advice requests between providers and service organizations, as a first step to closed-loop orders. Alberta has implemented a province-wide central intake model for surgical services to ensure that patients receive necessary services with the shortest possible wait-times. Electronic referrals and e-consults will build upon this framework to eliminate manual data entry, improve referral quality, and expedite service delivery. It will also provide Alberta with more accurate and comprehensive information on surgical and referral wait times.
15. Upgrade provincial data warehouse systems
The aim of this initiative is to improve the provincial data analytics environment, and through that, improve the capability of the province to understand and report on health service delivery in Alberta. This includes development of new reporting services for primary care data and advancement of de- identification tools to protect the privacy of Albertans while furthering efforts to analyze and improve quality of care. It will also allow Alberta Health to share quality improvement reports back with care providers across the province through portal services.
Outcomes
These initiatives will improve Albertans' access to their health information and digital health services to empower them in the management of their own care; improve the breadth and depth of information available to providers at the point-of-care to enable them to deliver quality care to their patients; and support the secure exchange of health data across the health system and analysis of this data for health system management in a way that protects the privacy of Albertans.
Funding allocation
| Initiative | Incremental Investments ($M) | Total | ||
|---|---|---|---|---|
| 2023-24 | 2024-25 | 2025-26 | ||
| Expanding access to family health services (including rural and remote) | $48.7 | $249.2 | $241.1 | $539.0 |
| 1. Total MAPS Initiative (items 1.1-1.5) | $37.9 | $109.9 | $109.9 | $257.7 |
| 1.1 - Innovation funding supports for Indigenous-led Primary Health Care programs and supports | $2.1 | $1.7 | $1.7 | $5.5 |
| 1.2 - Information sharing agreements with First Nations and Metis Communities | $0.4 | $0.3 | $0.3 | $1.1 |
| 1.3 - Implement stimulus funding for team-based care | - | $79.1 | $79.1 | $158.1 |
| 1.4 - Expand integrated supports for vulnerable and underserved Albertans | $31.2 | $25.4 | $25.4 | $81.9 |
| 1.5 - Enhance access through a virtual care program | $4.2 | $3.4 | $3.4 | $11.1 |
| 2. Virtual care codes | $7.5 | $16.0 | $17.5 | $41.0 |
| 3. Primary care stabilization | - | $100.7 | $100.7 | $201.4 |
| 4. Community-based pilot projects | $2.9 | $9.6 | $6.0 | $18.5 |
| 5. French services program | $0.4 | $3.0 | $2.0 | $5.4 |
| 6. Women's health | - | $10.0 | $5.0 | $15.0 |
| Reducing backlogs and supporting health care workers | $15.0 | $15.0 | $15.0 | $45.0 |
| 7. Community diagnostic imaging providers | $15.0 | $15.0 | $15.0 | $45.0 |
| Improving access to mental health and substance use services | $141.0 | $142.0 | $143.0 | $426.0 |
| 8. Mental Health and Substance Use (2017 CSOP bilateral funding) (items 8.1-8.3) | $70.0 | $70.0 | $71.0 | $211.0 |
| 8.1 - Community-based addiction and mental health services | $8.8 | $8.8 | $9.1 | $26.7 |
| 8.2 - Mental health and addiction services for children and youth | $25.2 | $25.2 | $25.6 | $76.0 |
| 8.3 - Specialized addiction and mental health services | $36.0 | $36.0 | $36.3 | $108.3 |
| 9. Youth mental health and addiction treatment Capacity and integrated and community youth support programs (capital and operating) | $25.7 | $34.0 | $55.7 | $115.4 |
| 10. Adult addiction and mental health treatment and recovery community capacity (capital and operating) | $45.3 | $38.0 | $16.3 | $99.6 |
| Modernizing health systems with health data and digital tools | - | $16.0 | $43.0 | $59.0 |
| 11. Replace and expand Alberta Netcare Repositories and Provider Portal | - | $5.0 | $10.0 | $15.0 |
| 12. Enhance and expand MyHealth Records Patient Portal | - | - | $5.0 | $5.0 |
| 13. Accelerate EMR interoperability | - | $2.0 | $2.0 | $4.0 |
| 14. Implement Electronic Referral Services | - | $4.0 | $6.0 | $10.0 |
| 15. Upgrade provincial data warehouse systems | - | $5.0 | $20.0 | $25.0 |
| Total spending | $205 | $422 | $442 | $1,069 |
| Federal funding available under Working Together* | $355 | $356 | $358 | $1,069 |
| Planned annual carry over | $150 | $84 | - | - |
|
Note: Some annual amounts may not appear to sum to three-year totals due to rounding. *Federal funding available based on notional estimates and subject to annual adjustment. |
||||
Reporting on results
| Indicator | Baseline | Target | Timeframe | |
|---|---|---|---|---|
| Expanding access to family health services (including rural and remote areas) | ||||
| Percentage of Albertans who report having access to a regular primary care providerFootnote 1 | 87.3 | 90 | 2026 | |
| Family Practice Sensitive Conditions (Percentage of ED visits deemed unnecessary/could be addressed in a family medicine physician's office)Footnote 2 | 20 | 17 | 2026 | |
| Percent Increase in Virtual Care Services by Family Medicine Providers2 | 2022 Total (6,811,847) | +15 | 2026 | |
| Reducing backlogs and supporting health care workers | ||||
| Size of COVID-19 surgery backlogFootnote 1 | -10% | 0% | 2024 | |
| Net new family physicians, nurses, and nurse practitioners per 10,000 populationFootnote 1 | Family Physicians | 12 | 12.6 | 2026 |
| Nurse Practitioners | 1 | 1.7 | 2026 | |
| Registered Nurses | 82 | 82.6 | 2026 | |
| Percent Increase in MRI/CT ScansFootnote 2 | 2022/23 Budgeted Scans (743,515) |
3% | 2026 | |
| Improving access to quality mental health and substance use services | ||||
| Median wait times for community mental health counsellingFootnote 1 (see below for Alberta wait time indicator) | N/AFootnote 3 | N/AFootnote 3 | N/AFootnote 3 | |
|
Number of youth aged 12-25 with access to integrated youth services for mental health and substance useFootnote 1 Note: Alberta is reporting the number of new specialized child and youth services available in schools and the number of new child and youth preventative programs available in schools. |
4 | 102 | 2026 | |
| Percentage of Albertans with a mental disorder who have an unmet mental health care needFootnote 1 | 8.7Footnote 4 | 7Footnote 4 | 2026 | |
| Median wait times for community mental health and substance use servicesFootnote 2 | 19 days (2022/23) |
17 days | 2026 | |
| First contact in the emergency department (Percentage of individuals seen at the emergency department for mental health and addiction-related reasons with no physician health services in previous two years)Footnote 2 | 24.9% (2021/22) |
20.8% | 2026 | |
| Albertans receiving care at an appropriate level (MHA specific) | Under development | Under development | Under development | |
| Recovery Capital scores of Albertan communities | Under development | Under development | Under development | |
| Recovery Capital Index (RCI) scores of Albertans accessing publicly funded addiction or mental health treatment and participating in the My Recovery Platform | Under development | Under development | Under development | |
| Modernizing health systems with health data and digital tools | ||||
| Percentage of Albertans who can access their own comprehensive health record electronicallyFootnote 1 | 47 | 50 | 2026 | |
| Percentage of family health service providers and other health professionals who can share patient health information electronicallyFootnote 1 | 30 | 40 | 2026 | |
| CPAR participation rates by family physiciansFootnote 2 | 25% | 30% | 2026 | |
|
||||
Page details
- Date modified: