
Updated guidance on influenza vaccination during pregnancy

Download in PDF format
(1.76 MB, 81 pages)
Organization: Public Health Agency of Canada
Date published: 2023-12-18
On this page
- Preamble
- Summary of information contained in this statement
- Introduction
- Methods
- Epidemiology
- Vaccine
- Ethics, equity, feasibility and acceptability considerations
- Discussion
- Recommendations
- Research priorities
- Surveillance priorities
- Tables
- List of abbreviations
- Acknowledgements
- Appendix A: Review update methods
- Appendix B: Prisma flow diagram for review update
- References
Preamble
The National Advisory Committee on Immunization (NACI) is an External Advisory Body that provides the Public Health Agency of Canada (PHAC) with independent, ongoing and timely medical, scientific, and public health advice in response to questions from PHAC relating to immunization.
In addition to burden of disease and vaccine characteristics, PHAC has expanded the mandate of NACI to include the systematic consideration of programmatic factors in developing evidence-based recommendations to facilitate timely decision-making for publicly funded vaccine programs at provincial and territorial levels.
The additional factors to be systematically considered by NACI include: economics, ethics, equity, feasibility, and acceptability. Not all NACI Statements will require in-depth analyses of all programmatic factors. While systematic consideration of programmatic factors will be conducted using evidence-informed tools to identify distinct issues that could impact decision-making for recommendation development, only distinct issues identified as being specific to the vaccine or vaccine-preventable disease will be included.
This statement contains NACI's independent advice and recommendations, which are based upon the best current available scientific knowledge.
This document is being disseminated for information purposes. People administering the vaccine should also be aware of the contents of the relevant product monograph. Recommendations for use and other information set out herein may differ from that set out in the product monographs of the Canadian manufacturers of the vaccines. Manufacturer(s) have sought approval of the vaccines and provided evidence as to its safety and efficacy only when it is used in accordance with the product monographs. NACI members and liaison members conduct themselves within the context of PHAC's Policy on Conflict of Interest, including yearly declaration of potential conflict of interest.
Summary of information contained in this statement
The following highlights key information for immunization providers. Please refer to the remainder of the statement for details.
What
Seasonal influenza infection is a respiratory illness that can lead to serious complications and adverse outcomes, particularly for pregnant individuals, the developing fetus, and infants under 6 months old. Influenza vaccination is safe and the best way to prevent infection in both pregnant people and infants under 6 months old. Pregnant individuals are prioritized to receive influenza vaccines because of the increased risks of severe disease during pregnancy; despite this, influenza vaccination uptake among this group remains suboptimal.
The following recommendations for influenza vaccination in pregnancy supplement NACI's overarching recommendations for influenza vaccination, which are available in the NACI seasonal influenza vaccine statement. NACI recommends that individuals at any stage of pregnancy should receive an age-appropriate inactivated unadjuvanted (IIV) or recombinant influenza vaccine (RIV) each influenza season.
Who
This supplemental statement provides an evidence summary on the safety and vaccine effectiveness (VE) of influenza vaccination in pregnant individuals, and the benefits and risks to the developing fetus and infants under 6 months of age.
How
IIV or RIV should be offered annually, at any gestational age, during pregnancy. Influenza vaccination may be given at the same time as, or at any time before or after administration of another vaccine, including the COVID-19 or pertussis vaccine.
Why
Pregnant people, their fetuses, and infants are at high risk of complications from influenza; therefore, annual influenza vaccination during pregnancy is strongly recommended. Influenza vaccination during pregnancy has consistently been shown to be safe and is supported by numerous studies, moreover vaccination has been shown to reduce the morbidity and mortality associated with influenza infection. Additionally, since influenza-related outcomes experienced during pregnancy can negatively impact the development of the fetus, vaccination of the pregnant person helps protect the fetus. Furthermore, passive transfer of antibodies from vaccination during pregnancy protects newborns during their first months of life when they are at high risk of complications from influenza infection, and too young to be immunized. Overall, the evidence supports the safety and VEs of influenza vaccines during pregnancy.
Introduction
Background on influenza vaccines, immunization programs and recommendations during pregnancy in Canada
Prior to the COVID-19 pandemic, influenza viruses caused approximately 40,000 laboratory-confirmed influenza (LCI) cases, 12,200 hospitalizations, and 3,500 deaths among Canadians each yearFootnote 1Footnote 2Footnote 3. As such, NACI recommends that influenza vaccine should be offered annually to anyone 6 months of age and older who does not have a contraindication to the vaccine. NACI has also identified groups at higher risk of influenza complications for whom influenza vaccination is particularly recommended (Strong NACI recommendation).
NACI has identified pregnant individuals as one of the high-risk groups for whom influenza immunization is particularly important. Because of pregnancy-related changes in anatomy and the immune and cardiovascular systems, pregnant individuals are at higher risk for severe influenza disease and related complications such as pneumonia, hospitalization, and death compared to non-pregnant individualsFootnote 4Footnote 5Footnote 6. Influenza infection during pregnancy not only affects pregnant persons, but can also impact the developing fetus, and increases the risk of late-stage pregnancy loss, still birth, low birth weight and pre-term birthFootnote 6Footnote 7. Therefore, immunizing pregnant persons against influenza is strongly recommended to protect both them and their infants from severe disease, especially as infants under 6 months of age are not eligible for influenza vaccination.
The NACI recommendations for the use of influenza vaccines in pregnancy and breastfeeding have evolved over time. Prior to 2007, NACI encouraged all pregnant people to be vaccinated against influenza but did not identify pregnant people without comorbidities as a priority group for vaccination programs. In 2007, NACI revised its recommendation to identify all pregnant individuals as a group for whom influenza vaccine is particularly recommended by nature of being at high-risk of influenza-related complications. NACI now also highlights that influenza vaccination in pregnancy protects both pregnant individuals and their newborn infants with passive immunity via transplacentally-transferred antibodies from the pregnant person up to the time infants can receive the vaccine themselves.
Despite pregnant people being prioritized to receive influenza vaccines because of the increased risks of severe disease, vaccine uptake remains lower compared to the non-pregnant population. Further, a disproportionate burden of disease and low uptake is observed among populations who are pregnant and racialized, Indigenous, younger, and/or have lower household incomeFootnote 8Footnote 9Footnote 10Footnote 11.
More literature continues to be published on the safety, efficacy, and effectiveness of influenza vaccines in pregnancy. The need for this NACI Supplemental Statement on the use of influenza vaccines during pregnancy was triggered by a study identifying a potential risk of increased early spontaneous abortion in pregnant people who received influenza vaccines in 2010 and 2011Footnote 12. Since then, several studies have been published finding no association of influenza vaccines administered during pregnancy and adverse outcomes in pregnant persons or infantsFootnote 13Footnote 14Footnote 15Footnote 16. NACI has taken this opportunity to review the safety, efficacy, and effectiveness of influenza vaccine in pregnancy. Moreover, this statement aims to synthesize the key information and evidence to support provincial and territorial vaccine programs and primary care providers in offering influenza vaccine to pregnant individuals.
The beneficial effects of immunization during pregnancy for the fetus as well as the newborn infant have been well documented. Vaccination during pregnancy has consistently been shown to be safe and protects the pregnant individual from vaccine-preventable diseases that may otherwise be acquired and transmitted to the fetus or infant. In addition, protective concentrations of antibodies are transferred to the fetus transplacentally, which usually results in infant protection from infection in the first few months of life. For information on the benefits and safety of recommended vaccines during pregnancy and breastfeeding, refer to the immunization in pregnancy and breastfeeding chapter in the Canadian Immunization Guide (CIG).
Guidance objective
The following advisory committee statement on influenza vaccination in pregnancy supplements NACI's overarching recommendations for influenza vaccination, which are available in the NACI seasonal influenza vaccine statement. The objective of this supplemental statement is to provide updated guidance on the use of influenza vaccination during pregnancy. The statement describes the disproportionate risk of morbidity and mortality for pregnant individuals and infants under 6 months old who acquire influenza compared to the general population; reviews the available evidence on the efficacy, effectiveness, and safety of influenza vaccination during pregnancy; and explores the EEFA considerations of immunizing pregnant people against influenza. Based on this body of evidence, the supplemental statement reaffirms the safety and importance of influenza vaccination during pregnancy.
Breastfeeding
It is recognized that pregnant and breastfeeding individuals are closely overlapping populations; however, there are differences in the considerations of vaccination for each. The purpose of this supplemental statement is to examine influenza vaccination in pregnancy specifically, given an identified possible concern regarding its safety. Therefore, this supplemental statement does not examine the safety and effectiveness of influenza vaccination during breastfeeding.
As stated in the NACI Seasonal Influenza Vaccine Statement, annual influenza vaccination is recommended during breastfeeding, and either non-live influenza vaccines or live attenuated influenza vaccine (LAIV) can be administered to breastfeeding individuals. There have been no identified safety signals for influenza vaccination in breastfeeding, and no hypothesized biological mechanism for a safety issue with currently authorized products. For more information on this topic, please see the aforementioned Statement and CIG chapter on immunization in pregnancy and breastfeeding.
A note on language
NACI recognizes that not all people giving birth or breastfeeding will identify as women or mothers. Much of the research available currently refers only to "women" when discussing pregnancy. When citing research, NACI refers to the language used in the study. In these cases, "woman" refers to someone who was assigned female at birth and "maternal" is used to identify the person who is pregnant or postpartum. For the purposes of this statement, the terms "woman", "women", and "maternal" should be considered to also apply to those individuals who do not specifically identify as female gender but are the parent gestating the fetus or breastfeeding/chestfeeding the infant.
Methods
In brief, the broad stages in the preparation of a NACI statement are:
- Knowledge synthesis: retrieval and summary of literature, assessment of the quality of the evidence (summarized in Table 1. Summary of evidence).
- Synthesis of the body of evidence: benefits (efficacy and effectiveness) and potential harms (safety), considering the quality of the synthesized evidence and, where applicable, the magnitude of effects observed across the studies.
- Use of a published, peer-reviewed framework and evidence-informed tools to ensure that issues related to EEFA are systematically assessed and integrated into the guidanceFootnote 17. Completion of health economic analyses as needed.
- Use of the evidence to inform recommendations.
Further information on NACI's process and procedures is available elsewhere.
To meet the objectives of this statement, a de novo systematic review (SR) was conducted to gather evidence to inform NACI's recommendations regarding the use of influenza vaccines during pregnancy. The methodology was specified a priori in a written protocolFootnote 18. The review protocol and knowledge synthesis were developed and performed in collaboration with the Methods and Applications Group for Indirect Comparisons (MAGIC) through the Drug Safety and Effectiveness Network (DSEN) and supervised by the NACI Influenza Working Group (IWG). An update to the literature search was completed by the NACI Secretariat in conjunction with a librarian from the Health Library of Health Canada and PHAC. A health economic analysis was not conducted as it was not deemed necessary for this statement. The evidence and proposed recommendations were presented to NACI for deliberation on April 27, 2023, and approved following a thorough review of the evidence. Relevant considerations, rationale for specific decisions, and knowledge gaps are described in the following sections.
For a comprehensive description of the review methods, including details on the study eligibility, literature search, study selection, data collection and statistical methods, please refer to Wolfe et al. (2020)Footnote 18. Methods related to the review update completed by the NACI Secretariat are reported in Appendix A.
The policy question addressed in this statement is: Should pregnancy (regardless of gestational age) continue to be listed as one of the risk categories for priority influenza vaccination?
To meet the objective of this statement, other informal literature reviews were conducted as needed to gather data and information including:
- Epidemiology and estimated burden of influenza illness among pregnant persons and infants under 6 months of age;
- An environmental scan of recommendations and considerations for use of influenza vaccines during pregnancy in Canadian provinces and territories and in other high-income countries.
To develop comprehensive and appropriate immunization program recommendations, NACI considers several factors. In addition to critically appraising evidence on burden of disease and vaccine characteristics such as safety, efficacy, immunogenicity and effectiveness, NACI applies the EEFA framework with accompanying evidence-informed tools (Ethics Integrated Filters, Equity Matrix, Feasibility Matrix, Acceptability Matrix) to systematically consider these programmatic factors for the development of clear, comprehensive, appropriate recommendations for timely and transparent decision-makingFootnote 19. For details on the development and application of NACI's EEFA Framework and aforementioned evidence-informed tools, please see Ismail et al. (2020)Footnote 19.
Epidemiology
Estimated burden of influenza among pregnant persons
Pregnant individuals are more susceptible to severe influenza illness throughout pregnancy, notably in the third trimesterFootnote 20Footnote 21Footnote 22Footnote 23Footnote 24. A 2019 meta-analysis (MA) on seasonal and pandemic (H1N1) influenza found that pregnant persons had a 7-times higher risk of influenza-associated hospital admission compared to non-pregnant persons (odds ratio [OR]=6.80; 95% confidence interval [CI]: 6.02-7.68), but were not at higher risk for intensive care unit (ICU) admission or deathFootnote 22. During the 2009 H1N1 pandemic however, a SR demonstrated that pregnant persons had a greater risk of influenza-related hospitalization, ICU admission, and death compared to non-pregnant personsFootnote 25. Particularly, the median relative risk of influenza infection was 6.8 (range 3.5-25.3) compared to the general population.
Estimated impact of influenza on perinatal outcomes
Influenza infection during pregnancy can result in serious perinatal outcomes. A 2021 meta-analysis of worldwide studies on seasonal and pandemic (H1N1) influenza reported that pregnant individuals had a 3-times higher risk of stillbirth following influenza infection (risk ratio [RR]=3.62; 95% CI: 1.60 to 8.20)Footnote 26. Studies from Australia, India, Peru, and Thailand also discovered a significant link between seasonal influenza infection during pregnancy to lower birth weight and late pregnancy lossFootnote 6Footnote 27. Moreover, a 2017 SR reported limited, mixed evidence when evaluating the risk of adverse birth outcomes, including preterm birth, small-for-gestational-age (SGA) birth, or fetal death, in individuals with clinical influenza disease or LCI infection during pregnancy compared to those without influenzaFootnote 28. Although a small subgroup of higher-quality studies reported an association between pandemic H1N1 influenza (pH1N1) disease and preterm birth (with RRs ranging from 2.4 to 4.0 for severe disease) and fetal death (RR of 1.9 for mild-to-moderate disease and 4.2 for severe disease), no firm conclusions about the magnitude of the association can be drawn at this time based on these limited data.
Estimated burden of influenza among infants under 6 months of age
Young infants are particularly vulnerable to influenza infection and its complications due to their underdeveloped immune systems and ineligibility for the influenza vaccine. Influenza is a leading cause of respiratory infection among children under age 1 year and causes approximately 280,000 respiratory hospitalizations globally in those under 6 months old each year (95% CI: 150,000 to 344,000)Footnote 7Footnote 29Footnote 30Footnote 31. In 2018, hospital admissions and in-hospital deaths due to seasonal influenza in children under 5 years of age occurred disproportionately in infants under 6 months old (23% and 36%, respectively) and predominantly in low and lower-middle-income countriesFootnote 32. In Canada, a national active surveillance study of pediatric influenza admissions revealed that infants under 6 months old accounted for 13.5% of children under 16 years of age admitted for influenza during 2010-2011 to 2020-2021, emphasizing the significant burden of influenza and its associated complications for this age groupFootnote 33. Furthermore US surveillance data from 2004-2012 reported that infants under 3 months of age were 40% more likely while those aged 3-6 months were 45% more likely to be admitted to the ICU with LCI compared to infants aged 6-12 months (OR=1.40; 95% CI: 1.04 to 1.88 and OR=1.45; 95% CI: 1.03 to 2.04, respectively)Footnote 29. The influenza-associated mortality rate was estimated at 0.66 (95% CI: 0.53 to 0.82)Footnote 34. During the 2009 H1N1 pandemic, a U.S. study reported a LCI hospitalization rate of 20.2 per 10,000 infants under 6 months of ageFootnote 35.
Influenza vaccination coverage among pregnant persons in Canada
In Canada, influenza vaccination coverage in pregnancy increased from 45.0% in 2019 to 52.7% in 2021Footnote 36. However, coverage varied by province/territory; in 2021, Nova Scotia had the highest vaccination rate (82.5%) and Quebec had the lowest (44.2%). Overall, vaccination coverage increased in all jurisdictions from 2019 to 2021, except Saskatchewan (64.9% to 64.8%, respectively) and the Northwest Territories (84.8% to 71.7%, respectively). Vaccination coverage also varied by Indigenous status and income. The gap in influenza vaccination coverage between Indigenous pregnant people and non-Indigenous pregnant people increased in 2021 (vaccination coverage of 28% vs. 54% respectively) compared with 2019 (vaccination coverage of 35% vs. 46% respectively)Footnote 36. As well, those in lower income groups (household income under $80,000) had lower vaccination rates against influenza relative to those in the highest household income groupFootnote 36.
Vaccine
Concurrent administration with other vaccines
Influenza vaccines may be administered concurrently with (i.e., same day), or at any time before or after, other vaccines recommended during pregnancy. Current evidence suggests that administering recommended vaccines concurrently during pregnancy is safe, despite the potential increase in local and systemic adverse reactions, including fever. There is no evidence to support adverse pregnancy sequelae from fever related to vaccine reactogenicity. A cohort study conducted in Australia involving 1,851 participants who received both IIV3 and tetanus toxoid, reduced diphtheria toxoid and reduced acellular pertussis (Tdap) vaccines concurrently during pregnancy found a low incidence of adverse events (AEs), providing support for the safety of concurrent vaccine administration during pregnancyFootnote 37. Other studies have similarly reported no significant safety concerns with concurrent administration of these vaccines during pregnancyFootnote 38Footnote 39.
Efficacy and effectiveness
The DSEN SR assessed the effect of seasonal influenza vaccination during pregnancy against influenza-related infection and hospitalization in pregnant persons and/or their infants using findings from 4 randomized controlled trials (RCTs)Footnote 40Footnote 41Footnote 42Footnote 43 and 2 observational studiesFootnote 44Footnote 45. Additional observational studies (n=6) were identified from the updated literature search reporting data on influenza VE in pregnant persons and/or their infants up to 6 months of ageFootnote 46Footnote 47Footnote 48Footnote 49Footnote 50Footnote 51.
Benefits to the pregnant person: Vaccine efficacy/effectiveness outcomes
Summary of study characteristics
Overall, 4 studies reported data on LCI and 3 reported data on hospitalization due to LCI infection during pregnancy or up to 6 months post-partum. Among those, 3 RCTs compared the efficacy of seasonal influenza vaccination during pregnancy to placebo (n=2)Footnote 40Footnote 41 or active comparator (n=1; meningococcal quadrivalent vaccine, Menactra®, Sanofi)Footnote 42 against LCI from enrollment to 6 months post-partum. In the 3 RCTs, the occurrence of LCI among 5,089 people receiving IIV was compared to 4,985 people randomized to the placebo or active comparator group. One (1) prospective cohort study identified from the updated literature search evaluated the effectiveness of seasonal IIV4 compared to no influenza vaccination during pregnancy against LCIFootnote 46. One (1) study identified from the DSEN SR that used a test-negative study design evaluated the VE of seasonal influenza vaccination amongst pregnant persons hospitalized for acute respiratory or febrile illness against LCI infectionFootnote 44. One (1) prospective cohort study, 1 prospective case-control study and 1 test-negative study design identified from the updated literature search evaluated the effectiveness of seasonal influenza vaccination during pregnancy on LCI hospitalization in pregnant personsFootnote 47Footnote 48Footnote 52.
Summary of vaccine efficacy/effectiveness
A MA of the 3 RCTs suggested that seasonal influenza vaccination during pregnancy reduces the risk of lab-confirmed influenza infection in pregnant persons prior to delivery and up to 6 months post-partum (pooled VE=50%; 95% CI: 22 to 68%, I2=49.22%). The results suggest that the benefit of seasonal influenza vaccination was similar from delivery to 6 months post-partum (pooled VE=57%, 95% CI: 14 to 78%, I2=35.88%) compared to the period between enrollment and delivery (pooled VE=54%, 95% CI: -48 to 86%, I2=72.28%). One (1) prospective cohort study conducted during the 2019-2020 influenza season in Greece also found a protective effect of seasonal IIV4 against LCI infection in pregnant persons (adjusted VE [aVE]=43.5%, 95% CI: 28.4 to 55.6%)Footnote 46.
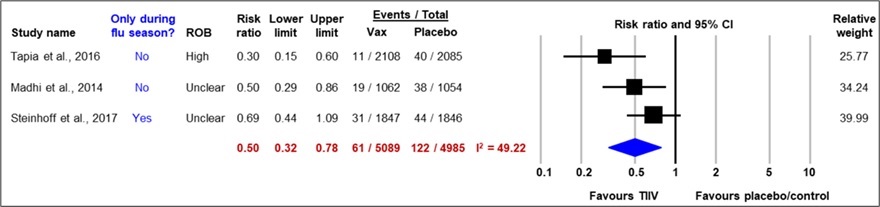
Figure 1: Text description
Figure 1 depicts a forest plot showing results of a random-effects meta-analysis reporting the risk of maternal lab-confirmed influenza from enrolment to six months post-partum comparing trivalent inactivated seasonal influenza vaccines (TIIV) to a placebo or active comparator. The leftmost column lists the three included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: whether the study period was limited to the influenza season or not, the study's risk of bias, the point estimate of the risk ratio, the lower and upper bounds of the confidence interval (CI), and the number of individuals having the outcome of interest (events) over the sample size of the intervention (TIIV) and over the sample size of the comparison group (placebo/control). The x-axis representing the risk ratio estimates and 95% CI ranges from 0.1 to 10. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour TIIV (on the left) and the placebo/control (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The blue diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 1.
| Author, year | Only during flu season? | Risk of bias | Risk ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size | Placebo/control events | Placebo/control sample size | Relative weight |
|---|---|---|---|---|---|---|---|---|---|---|
| Tapia et al., 2016 | No | High | 0.30 | 0.15 | 0.60 | 11 | 2108 | 40 | 2085 | 25.77 |
| Madhi et al., 2014 | No | Unclear | 0.50 | 0.29 | 0.86 | 19 | 1062 | 38 | 1054 | 34.24 |
| Steinhoff et al., 2017 | Yes | Unclear | 0.69 | 0.44 | 1.09 | 31 | 1847 | 44 | 1846 | 39.99 |
| Statistical model | Risk ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size | Placebo/control events | Placebo/control sample size | Heterogeneity, I2 |
|---|---|---|---|---|---|---|---|---|
| Random effect model | 0.50 | 0.32 | 0.78 | 61 | 5089 | 122 | 4985 | 49.22 |
A MA of 2 test-negative studies suggested that seasonal influenza vaccination during pregnancy reduces the risk of hospitalization due to lab-confirmed influenza in pregnant persons prior to delivery and up to 42 days post-partum (pooled aVE=42%, 95% CI: 19 to 58%, I2=0%)Footnote 44Footnote 47.

Figure 2: Text description
Figure 2 depicts a forest plot showing results of a random-effects meta-analysis of studies using a test-negative study design reporting the risk of maternal lab-confirmed influenza hospitalization during pregnancy or 42 days post-partum among those vaccinated with inactivated influenza vaccines (IIV) compared to unvaccinated individuals during pregnancy. The leftmost column lists the two included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: the log odds ratio (OR), the standard error (SE), the sample size of the intervention (IIV) and the comparison group (unvaccinated), the relative weight of the study, and the odds ratio with its corresponding 95% confidence interval (CI). The x-axis representing the odds ratio estimates and 95% CI ranges from 0.01 to 100. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour IIV (on the left) and no vaccine (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a red box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The black diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 2.
| Author, year | Log[Odds Ratio] | SE | IIV sample size | Unvaccinated sample size |
Weight | OR [95% CI] |
|---|---|---|---|---|---|---|
| Nunes, 2022 | -0.633 | 0.3357 | 148 | 253 | 25.1% | 0.53 [0.28, 1.03] |
| Thompson, 2019 | -0.5108 | 0.1943 | 169 | 821 | 74.9% | 0.60 [0.41, 0.88] |
| Statistical model | TIIV sample size | Placebo sample size | Weight | OR [95% CI] | Heterogeneity, Tau2, Chi2, df (p-value), I2 | Test for overall effect, Z (p-value) |
|---|---|---|---|---|---|---|
| Random effect model | 317 | 1074 | 100.0% | 0.58 [0.42, 0,81] | 0.00; 0.10; 1 (P=0.75); 0% | 3.22 (P=0.001) |
One (1) prospective cohort study reported VE of 38% (95% CI: 14 to 55%) against LCI hospitalization during pregnancy or up to 2 days after deliveryFootnote 48.
Together, these studies suggest that seasonal influenza vaccination during pregnancy reduces the risk of LCI infection and hospitalization due to LCI during pregnancy and up to 6 months post-partum.
Infant benefits: Vaccine efficacy/effectiveness outcomes
Summary of study characteristics
Overall, 7 studies reported data on LCI infection. Among those, 4 RCTs compared the efficacy of IIV to placebo (n=2)Footnote 40Footnote 53 or active comparators (n=2; pneumococcalFootnote 43 or meningococcal vaccineFootnote 42) during pregnancy against LCI infection in infants up to 6 months of age. Three (3) cohort studies identified from the updated literature search compared the effectiveness of seasonal influenza vaccination during pregnancy against LCI infection in infants up to 6 months of ageFootnote 46Footnote 49Footnote 50.
A total of 5 studies (3 test-negative studies, including 1 identified from the DSEN SRFootnote 45Footnote 47Footnote 51, and 2 cohort studiesFootnote 49Footnote 50 reported data on the effectiveness of influenza vaccination during pregnancy on hospitalization due to LCI infection in infants up to 6 months of age.
Summary of vaccine efficacy/effectiveness
A MA of the 4 RCTs demonstrated a protective effect of seasonal influenza vaccination during pregnancy against LCI infection in infants up to 6 months of age (pooled VE=37%, 95% CI: 22 to 49%, I2=0.00%). Results from the RCTs suggest that the greatest effect of seasonal influenza vaccination during pregnancy against LCI infection in infants was found from birth up to 2 months of age (pooled VE0 to <2 months=61%, 95% CI: 17 to 81%, I2=39.57%), following which the protective effect of vaccination during pregnancy waned as infant age increased (pooled VE2 to <4 months=42%, 95% CI: -13 to 70%, I2=59.67% and pooled VE4 to <6 months=24%, 95% CI: -3 to 44%, I2=0.00), a biologically plausible finding due to the waning of the effects of passive transfer of antibodies in neonates.
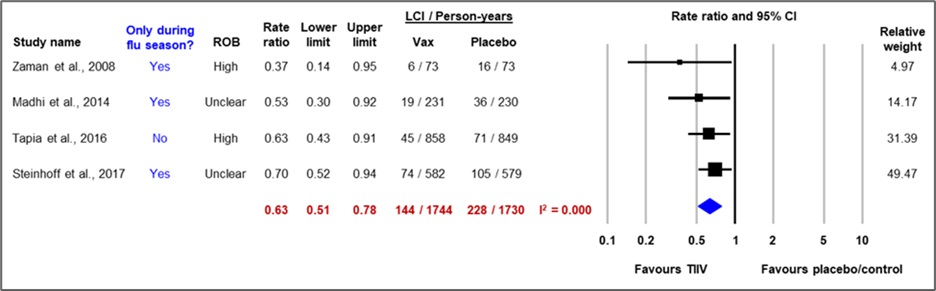
Figure 3: Text description
Figure 3 depicts a forest plot showing results of a random-effects meta-analysis of randomized controlled trials reporting the risk of infant lab-confirmed influenza among infants born to pregnant persons vaccinated against influenza or receiving a placebo or active control during pregnancy. The leftmost column lists the four included studies, which are each identified by the first author's name and the publication year. Next, to the right, the following information is presented: whether the study period was limited to the influenza season or not, the study's risk of bias, the point estimate of the rate ratio, the lower and upper bounds of the confidence interval (CI), and the number of individuals having the outcome of interest (events) over the sample size in person-years of the intervention (TIIV; trivalent inactivated influenza vaccine) and over the sample size in person-years of the comparison group (placebo/control). The x-axis representing the rate ratio estimates and 95% CI ranges from 0.1 to 10. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour TIIV (on the left) and the placebo/control (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The blue diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 3.
| Author, year | Only during flu season? | Risk of bias | Rate ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size (person-year) | Placebo/control events | Placebo/control sample size (person-year) | Relative weight |
|---|---|---|---|---|---|---|---|---|---|---|
| Zaman et al., 2008 | Yes | High | 0.37 | 0.14 | 0.95 | 6 | 73 | 16 | 73 | 4.97 |
| Madhi et al., 2014 | Yes | Unclear | 0.53 | 0.30 | 0.92 | 19 | 231 | 36 | 230 | 14.17 |
| Tapia et al., 2016 | No | High | 0.63 | 0.43 | 0.91 | 45 | 858 | 71 | 849 | 31.39 |
| Steinhoff et al., 2017 | Yes | Unclear | 0.70 | 0.52 | 0.94 | 74 | 582 | 105 | 579 | 49.47 |
| Statistical model | Rate ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size | Placebo/control events | Placebo/control sample size | Heterogeneity, I2 |
|---|---|---|---|---|---|---|---|---|
| Random effect model | 0.63 | 0.51 | 0.78 | 144 | 1744 | 228 | 1730 | 0.000 |
A MA of the 3 cohort studies demonstrated a protective effect of seasonal influenza vaccination during pregnancy against LCI infection in infants up to 6 months of age (pooled aVE=41%, 95% CI: 23 to 55%, I2=17%)Footnote 46Footnote 49Footnote 50.
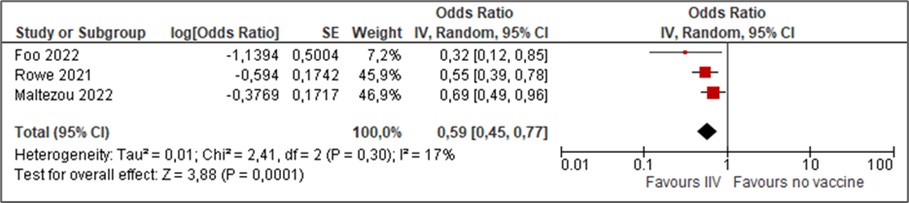
Figure 4: Text description
Figure 4 depicts a forest plot showing results of a random-effects meta-analysis of cohort studies reporting the risk of infant lab-confirmed influenza among infants born to pregnant persons vaccinated and unvaccinated against influenza during pregnancy. The leftmost column lists the three included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: the log odds ratio (OR), the standard error (SE), the relative weight of the study, and the odds ratio with its corresponding 95% confidence interval (CI). The x-axis representing the odds ratio estimates and 95% CI ranges from 0.01 to 100. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour influenza vaccine (on the left) and no vaccine (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a red box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The black diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 4.
| Author, year | Log[Odds Ratio] | SE | Weight | OR [95% CI] |
|---|---|---|---|---|
| Foo 2022 | -1.1394 | 0.5004 | 7.2% | 0.32 [0.12, 0.85] |
| Rowe 2021 | -0.594 | 0.1742 | 45.9% | 0.55 [0.39, 0.78] |
| Maltezou 2022 | -0.3769 | 0.1717 | 46.9% | 0.69 [0.49, 0.96] |
| Statistical model | Weight | OR [95% CI] | Heterogeneity, Tau2, Chi2, df (p-value), I2 |
Test for overall effect, Z (p-value) |
|---|---|---|---|---|
| Random effect model | 100.0% | 0.59 [0.45, 0.77] | 0.01; 2.41; 2 (P=0.30); 17% | 3.88 (P=0.0001) |
A MA of the 3 test-negative studies demonstrated a protective effect of seasonal influenza vaccination during pregnancy against hospitalization due to LCI infection in infants up to 6 months of age (pooled aVE=42%, 95% CI: 16 to 59%, I2=71%)Footnote 45Footnote 47Footnote 51. Two (2) cohort studies reported data on hospitalization due to LCI infection in infants up to 6 months of age, but only one demonstrated a significant protective effect of influenza vaccination during pregnancy (aVE, 95% CI: 62%, 9 to 84%Footnote 49, and 21%, 95% CI: -18 to 47%Footnote 50).
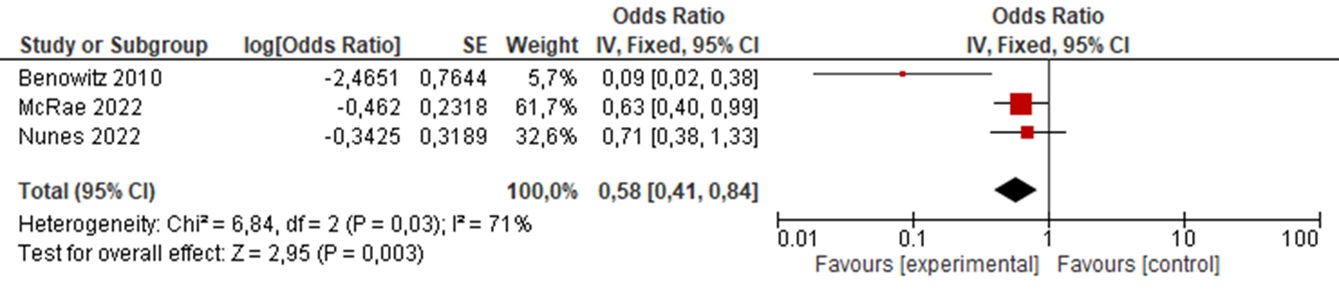
Figure 5: Text description
Figure 5 depicts a forest plot showing results of a fixed-effects meta-analysis of studies using a test-negative study design reporting the risk of lab-confirmed influenza hospitalization in infants up to six months of age born to pregnant persons vaccinated or unvaccinated against influenza during pregnancy. The leftmost column lists the three included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: the log odds ratio (OR), the standard error (SE), the relative weight of the study, and the odds ratio with its corresponding 95% confidence interval (CI). The x-axis representing the odds ratio estimates and 95% CI ranges from 0.01 to 100. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour influenza vaccine (on the left) and no vaccine (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a red box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The black diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 5.
| Author, year | Log[Odds Ratio] | SE | Weight | OR [95% CI] |
|---|---|---|---|---|
| Benowitz 2010 | -2.4651 | 0.7644 | 5.7% | 0.09 [0.02, 0.38] |
| McRae 2022 | -0.462 | 0.2318 | 61.7% | 0.63 [0.40, 0.99] |
| Nunes 2022 | -0.3425 | 0.3189 | 32.6% | 0.71 [0.38, 1.33] |
| Statistical model | Weight | OR [95% CI] | Heterogeneity, Chi2, df (p-value), I2 |
Test for overall effect, Z (p-value) |
|---|---|---|---|---|
| Fixed effect model | 100.0% | 0.58 [0.41, 0.84] | 6.84; 2 (P=0.03); 71% | 2.95 (P=0.003) |
Together, these studies suggest that seasonal influenza vaccination during pregnancy reduces the risk of LCI infection and hospitalizations due to LCI infection in infants up to 6 months of age.
Vaccine safety
Summary of study characteristics
The DSEN SR on the safety of influenza vaccination during pregnancy evaluated non-obstetric serious adverse events (SAE) in pregnant persons related to the administration of seasonal influenza vaccination during pregnancy using findings from 3 RCTs and 3 cohort studies. Additionally, the SR included 4 RCTs and 24 observational studies, including 20 cohort and 4 case-control studies, addressing other safety and/or pregnancy/birth related outcomes (i.e., infant death, spontaneous abortion, stillbirth, preterm birth, SGA, low birth weight and congenital anomalies). Outcomes of seasonal influenza vaccination were compared with those for other vaccines (e.g., meningococcal, or pneumococcal vaccines), placebo or no vaccination.
Eleven (11) additional observational studies were identified from the updated literature search evaluating non-obstetric SAEs/AEs and other safety and/or pregnancy/birth outcomes (i.e., spontaneous abortion, stillbirth, preterm birth, SGA, low birth weight and congenital anomalies) related to the administration of influenza vaccine during pregnancy. Of those, 3 were single-arm cohort studies and one was a case series derived from registries of AEs of interest. These study designs were not included in the DSEN SR, but were included in the updated literature search to capture studies reporting data on the safety of administration during pregnancy of more recently licensed influenza vaccines that are based upon new different technologies, including quadrivalent mammalian cell culture-based vaccines (e.g., IIV4c; Flucelvax® Quad) and RIV (e.g., quadrivalent recombinant influenza vaccines [RIV4]; Supemtek™), given the limited published peer-reviewed evidence on these vaccines.
Summary of vaccine safety
Harms to the pregnant person: Non-obstetric serious adverse events in pregnant people
Serious systemic reactions within 7 days of vaccination
Two (2) RCTs evaluated the risk of severe systemic reactions within 7 days of seasonal influenza vaccination in pregnant people. One (1) RCT conducted in South Africa by Madhi et al. (2014) found 27 of 181 people who received trivalent IIV (IIV3) (14.9%) and 19 of 172 who received a saline placebo (11.0%) experienced at least one severe systemic reaction, which included severe weakness/tiredness, headache, fever, joint pain, and muscle pain, within 7 days of vaccine administrationFootnote 41. A larger RCT conducted in Mali by Tapia et al. (2016) found that 2 of 2,105 women who received IIV3 (0.1%) and none of the 2,082 people who received meningococcal vaccine (0.0%) experienced a severe systemic adverse reaction within 7 days of vaccine administrationFootnote 42; the 2 severe reactions included febrile sensation and headache, and it was unclear whether those 2 events occurred in the same participant. No significant difference in the frequency of severe systemic reactions within 7 days of seasonal influenza vaccination was observed within each individual study (RR=1.35, 95% CI: 0.78 to 2.34Footnote 41, and RR= 4.95, 95% CI: 0.24 to 102.95Footnote 42); pooled estimates were not calculated given the substantial differences in the risks of SAEs in the intervention groups of the 2 studies and the control groups. There were likely unknown differences in outcomes definitions or other sources of heterogeneity.
Other serious non-obstetric adverse events
Two (2) RCTs, 6 cohort studies and 1 case-series reported data on other non-obstetric SAEs. One (1) RCT conducted by Madhi et al. (2014) found no difference in the occurrence of non-obstetric SAEs that were possibly or probably related to influenza vaccination within 30 days of vaccination administration (1 in 1,062 IIV3 and 0 in 1,054 saline placebo recipients; RR=2.98, 95% CI: 0.12 to 73.01)Footnote 41. Another RCT conducted by Zaman et al. (2008) reported data on peripartum hospitalizations due to non-obstetric causes, with no apparent difference between IIV3 and pneumococcal vaccine recipients (1 event in 159 IIV3 and 2 events in 157 pneumococcal vaccine recipients; RR=0.49, 95% CI: 0.05 to 5.39)Footnote 43.
Five (5) cohort studies reported non-obstetric SAEs either within 42 days of vaccination or within an unknown time period. In an American study, Munoz et al. (2005) found 2 hospitalization events unrelated to pregnancy in 225 vaccinated pregnant persons and 3 in 826 unvaccinated pregnant persons within 42 days of intervention, with none related to vaccination (RR=2.45, 95% CI: 0.41 to 14.56)Footnote 54. The cause of hospitalization included influenza illness with emesis and migraine headache in the vaccinated group, and influenza with emesis, appendicitis, and calculus ureter-stent replacement in the unvaccinated group. Finally, 4 cohort studies did not report any SAEs after the administration of IIV4 (Fluzone® Quadrivalent)Footnote 55, IIV4-cc (Flucelvax® Quad)Footnote 56 and IIV3 during pregnancyFootnote 57Footnote 58.
Guillain-Barré syndrome
One (1) cohort study and 1 case-series reported data on Guillain-Barré syndrome following seasonal influenza vaccination during pregnancy. Within 42 days of intervention, Nordin et al. (2013) identified no inpatient cases of Guillain-Barré syndrome in 75,906 vaccinated pregnant persons and 1 case in 147,992 unvaccinated pregnant persons in the USA (RR=0.65, 95% CI: 0.03 to 15.95)Footnote 59. One (1) case series identified from the updated literature search reported 1 case (n=239) of Guillain-Barré syndrome that occurred 5 days after IIV4 administration during the third trimester of pregnancy in a 29-year-old woman. The woman gave birth to a healthy baby while recovering and has fully recoveredFootnote 60.
These studies suggest that pregnant persons vaccinated with seasonal influenza vaccines during pregnancy appear to experience the same rates of non-obstetric serious AEs as non-pregnant persons vaccinated with seasonal influenza vaccines, pregnant persons vaccinated with pneumococcal or meningococcal vaccines, as well as unvaccinated pregnant persons.
Infant harms: Infant death from 0 to 6 months of age
Four (4) RCTs compared the effect of seasonal influenza vaccination to placebo (n=2)Footnote 40Footnote 41 or active comparators (n=2; meningococcal quadrivalent vaccineFootnote 42 or 23-valent pneumococcal vaccineFootnote 43) during pregnancy on infant death up to 6 months of age. All RCTs were conducted in low-to-middle-income countries, and the control group infant death risk ranged from 1.1% and 2.8%. A MA of these RCTs did not demonstrate an association between seasonal influenza vaccination during pregnancy and infant death (pooled RR=1.14, 95% CI: 0.86 to 1.50, I2=9.33).
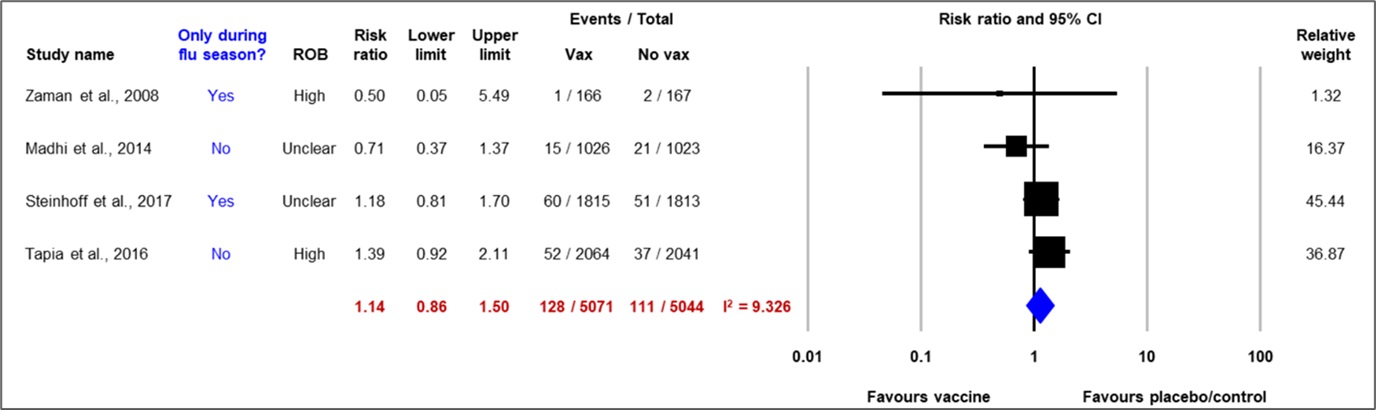
Figure 6: Text description
Figure 6 depicts a forest plot showing results of a random-effects meta-analysis of randomized controlled trials reporting the risk of infant death up to six months of age among infants born to pregnant persons vaccinated or unvaccinated against influenza during pregnancy. The leftmost column lists the four included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: whether the study period was limited to the influenza season or not, the study's risk of bias, the point estimate of the risk ratio, the lower and upper bounds of the confidence interval (CI), and the number of individuals having the outcome of interest (events) over the sample size of the intervention (influenza vaccine) and over the sample size of the comparison group (placebo/control). The x-axis representing the rate ratio estimates and 95% CI ranges from 0.01 to 100. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour influenza vaccine (on the left) and placebo/control (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The blue diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 6.
| Author, year | Only during flu season? | Risk of bias | Risk ratio | Lower bound of the CI | Upper bound of the CI | IIV events | IIV sample size | Placebo/control events | Placebo/control sample size | Relative weight |
|---|---|---|---|---|---|---|---|---|---|---|
| Zaman et al., 2008 | Yes | High | 0.50 | 0.05 | 5.49 | 1 | 166 | 2 | 167 | 1.32 |
| Madhi et al., 2014 | No | Unclear | 0.71 | 0.37 | 1.37 | 15 | 1026 | 21 | 1023 | 16.37 |
| Steinhoff et al., 2017 | Yes | Unclear | 1.18 | 0.81 | 1.70 | 60 | 1815 | 51 | 1813 | 45.44 |
| Tapia et al., 2016 | No | High | 1.39 | 0.92 | 2.11 | 52 | 2064 | 37 | 2041 | 36.87 |
| Statistical model | Risk ratio | Lower bound of the CI | Upper bound of the CI | IIV events | IIV sample size | Placebo/control events | Placebo/control sample size | Heterogeneity, I2 |
|---|---|---|---|---|---|---|---|---|
| Random effect model | 1.14 | 0.86 | 1.50 | 128 | 5071 | 111 | 5044 | 9.326 |
No infant death was reported from a prospective cohort study conducted in Japan among infants diagnosed with fever from 0 to 6 months of age born from vaccinated and unvaccinated pregnant people (0/36 IIV3 and 0/47 unvaccinated)Footnote 61.
These studies suggest that seasonal influenza vaccination during pregnancy is not associated with infant death up to 6 months of age.
Infant harms: Spontaneous abortion
Three (3) cohort studies and 3 observational studies evaluated the effect of IIV during pregnancy on spontaneous abortion (SAB) under 20 and 22 weeks gestational age. Two (2) prospective cohort studies were included in a MA and no association between IIV and SAB was demonstrated (pooled adjusted hazard ratio [aHR]=0.77, 95% CI: 0.31 to 1.89, I2=37.51%)Footnote 62Footnote 63. A third prospective cohort study conducted in Japan found the same risk of SAB under 22 gestational weeks (0.4%) among unvaccinated and vaccinated pregnant people (first-trimester vaccination)Footnote 64.

Figure 7: Text description
Figure 7 depicts a forest plot showing results of a random-effects meta-analysis of cohort studies reporting the risk of spontaneous abortion among pregnant persons vaccinated and unvaccinated against seasonal influenza during pregnancy. The leftmost column lists the two included studies, each identified by the first author's name and the publication year. Next, to the right, the following information is presented: the exposure time, the country where the study was conducted, whether the study period was limited to influenza season or not, the study's risk of bias, the point estimate of the hazard ratio, the lower and upper bounds of the confidence interval (CI), and the number of individuals having the outcome of interest (events) over the sample size of the intervention (TIIV; trivalent inactivated influenza vaccine) and over the sample size of the comparison group (no vaccine). The x-axis representing the risk ratio estimates and 95% confidence interval (CI) ranges from 0.1 to 10. The vertical line of 'no effect' appears at the value of 1 and separates the outcomes that favour TIIV (on the left) and no vaccine (on the right). Each horizontal line of the forest plot represents an individual study with the results plotted as a box and the 95% CI of the result displayed as the line. The size of the box surrounding each estimate represents the relative weight of that study in producing the pooled result. The blue diamond shows the pooled result when the individual studies are combined together and averaged. The horizontal points of the diamond are the limit of the 95% CI of the combined point estimate.
The following information is depicted in Figure 7.
| Author, year | Exposure time | Country | Only during flu season? | Risk of bias | Hazard ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size | No vaccine events | No vaccine sample size | Relative weight |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chambers et al., 2016 | Week 1-20 | USA | No | 7 | 1.09 | 0.49 | 2.41 | 11 | 380 | 15 | 267 | 63.18 |
| Mohammed et al., 2020 | Week 9-16 up to 20 | Australia | No | 7 | 0.42 | 0.12 | 1.46 | 3 | 603 | 31 | 650 | 36.82 |
| Statistical model | Hazard ratio | Lower bound of the CI | Upper bound of the CI | TIIV events | TIIV sample size | no vaccine events | No vaccine sample size | Heterogeneity, I2 |
|---|---|---|---|---|---|---|---|---|
| Random effect model | 0.77 | 0.31 | 1.89 | 14 | 983 | 46 | 917 | 37.51 |
Two (2) retrospective case-control studies conducted by the same set of investigators in the US assessed the association between SAB and vaccination within 28 days prior to SAB. The first study was conducted over 2 consecutive influenza seasons following the 2009 H1N1 pandemicFootnote 12. The authors observed an increased risk of SAB following IIV only in the first post-pandemic season (2010-2011 adjusted odds ratio [aOR] = 3.70, 95% CI: 1.40 to 9.40) but not the second (2011-2012 aOR=1.40, 95% CI: 0.60 to 3.30). Post-hoc analyses of 2010-2011 data found that people who had been previously vaccinated in the 2009-2010 season with the H1N1 pandemic vaccine were at increased risk of SAB following IIV in the 2010-2011 season, which was not observed in those not vaccinated with the H1N1 pandemic vaccine in 2009-2010 but vaccinated with IIV in 2010-2011.
The second study conducted over 3 consecutive influenza seasons (i.e., 2012-2013, 2013-2014 and 2014-2015) by Donahue, et al. (2019) sought to confirm the association observed between SAB and history of influenza vaccinationFootnote 65. No association was found between seasonal influenza vaccination during pregnancy and SAB within 28 days of vaccination (aOR = 0.80, 95% CI: 0.60 to 1.10), including among people vaccinated in the previous season. The authors state that the association of prior season vaccination found in the initial study may have been a spurious result due to residual confounding or random error, or it may have been due to differences in the time periods of the 2 studies. One (1) cohort study identified from the updated literature search conducted in the US over the 2008-2009 to 2013-2014 influenza seasons did not find an association between the history of pandemic H1N1 containing influenza vaccination and spontaneous abortion within 28 days of vaccination (aHR=1.19, 95% CI: 0.97 to 1.46)Footnote 66.
Three (3) additional single-arm cohort studies and 1 case series identified from the updated literature search reported data on SAB in persons vaccinated with IIV during pregnancy. The 1 case-series study described SABs after vaccine exposure that were reported from several countries to the Fluzone® Quadrivalent (IIV4, Sanofi) Pregnancy Registry from 2013 to 2019. Four (4) SABs were captured by the pregnancy registry; however, the frequency of neonatal adverse outcomes presented in the study are consistent across the literature and do not exceed the expected rates in the general population. One (1) cohort study described SABs identified among IIV-exposed pregnancies that were reported to the US registry or through GSK worldwide safety database. From the US registries, 3 spontaneous abortions were reported from 115 pregnancies. From the 3 SABs reported, there were 2 SABs in which exposure occurred during the first trimester, and 1 for which the date of exposure was unknown. From the worldwide database, 26 out of 676 reports of influenza vaccine exposure during pregnancy resulted in SABs; however, there was no information on exposure timing. SABs originate during the first and second trimesters of pregnancy (i.e., at risk periods), therefore, exposures occurring in the third trimester are not likely to be causally associated. Two (2) prospective cohort studies that were conducted to fulfill a post-marketing commitment to the US Food and Drug Administration (FDA) evaluated the safety of IIV4 (Afluria® Quadrivalent) and IIV4-cc (Flucelvax® Quadrivalent) administrated during pregnancy. The studies reported 2.5 and 1.9% SABs after administration of IIV4 and IIV4-cc during the first trimester of pregnancy, respectively, which was not increased when compared to the rate in the general US population. Overall, from the 3 single-arm cohort studies and the case series study, no safety signals were identified among pregnant persons exposed to IIV.
One cohort study did not observe a significant association between immunization with a pandemic H1N1-containing influenza vaccine prior to 21 6/7 weeks' gestation and spontaneous abortion, regardless of the vaccine received in the prior influenza season (i.e., pandemic H1N1-containing influenza vaccine or non-pandemic-H1N1-containing influenza vaccine)Footnote 66.
Together, these studies suggest that seasonal influenza vaccination during pregnancy does not appear to be associated with an increased risk of spontaneous abortion.
Infant harms: Other birth outcomes
No safety issues were identified regarding the administration of seasonal influenza vaccines during pregnancy, with respect to other adverse birth outcomes including stillbirth (≥18-22 gestational weeks or ≥500g); preterm birth; SGA; low birth weight; and congenital anomalies identified at birth or up to 6 months of age. Evidence was derived from both RCTs and observational studies, including case-control studies and cohort studies. Limited published peer-reviewed evidence regarding the safety of administration during pregnancy of more recently licensed influenza vaccines that are based upon new different technologies, including mammalian IIV-cc (e.g., IIV4-cc; Flucelvax® Quad) and RIV (e.g., RIV4; Supemtek™) was identified. Details on other adverse birth outcomes are available in Table 1. Summary of evidence.
Ethics, equity, feasibility and acceptability considerations
Ethics considerations
NACI evaluated the following ethical considerations when making its recommendations: promoting well-being and minimizing risk of harm; maintaining trust; respect for persons and fostering autonomy; and promoting justice and equity. NACI also identified the ethical imperative to protect the public's health and the health of the most vulnerable. NACI addressed the identified ethical considerations throughout the vaccine guidance development process and these considerations have been incorporated into the recommendations.
Equity considerations
No distinct inequities that may arise because of the recommendations were identified. However, the following intersectional factors described in NACI's EEFA framework were considered: pre-existing conditions; social factors; place of residence; and access to healthcare.
Pregnant individuals and individuals with chronic health conditions are identified among the groups at greater risk of influenza-related complications or hospitalizationFootnote 1. Racialized people and Indigenous people may also be at increased risk for severe influenza disease due to a variety of intersecting factors, including underlying medical conditions and potentially decreased access to healthcare resources. Canadians with low household incomes, unstable or crowded housing, and individuals living in remote or rural areas may face increased exposure to influenza and challenges accessing healthcareFootnote 36. Gender-diverse pregnant people are more likely to face discrimination or poor treatment in medical settings and may be more reluctant to seek healthcare. Individuals such as international students and newcomers to Canada may face language barriers in accessing healthcare.
Feasibility considerations
Based on the feasibility matrix NACI completed as part of its EEFA analysis, there were no distinct, significant issues identified for feasibility with respect to resource and integration implications that could impact decision making for this recommendation since this is an existing immunization program. Recommendations that allow vaccination at all gestational stages of pregnancy would reduce feasibility barriers in vaccination programs.
Acceptability considerations
NACI evaluated the following acceptability considerations when making its recommendations: individual beliefs; values and knowledge; socio-demographic factors; and systemic factors. Refusing vaccination during pregnancy is common globally, resulting in a low vaccine coverage rateFootnote 70. Low vaccine uptake in pregnant individuals has been partly attributed to vaccine hesitancy, which is complex and multidimensional and can be influenced by individual, logistical, cultural, and sociologic factors.
A pregnant individual's beliefs, values, and knowledge about seasonal influenza and vaccination affect the acceptance of vaccination during pregnancyFootnote 70Footnote 71. Individuals who believe the vaccines to be safe and effective and individuals who perceive themselves to be at risk of seasonal influenza and have the desire to protect others against the virus are more likely to pursue vaccinationFootnote 70Footnote 71Footnote 72Footnote 73. Conversely, pregnant individuals are less likely to pursue vaccination if they have anti-vaccination beliefs and concerns regarding the effects of vaccination on the health of the individual and fetus, and limited knowledge regarding the risks of influenza and the benefits of vaccination during pregnancyFootnote 70Footnote 71Footnote 73. In the 2021 Canadian Survey on Vaccination During Pregnancy Study (SVP), 51% of participants responded that their reason for not getting the influenza vaccine during pregnancy was "not wanting to be vaccinated during pregnancy"Footnote 36. Furthermore, evidence from Okoli et al. (2021) suggests a potential vulnerability of multiparous women with respect to the uptake of preventive careFootnote 74, as they may assume that their current pregnancy will be uneventful because previous pregnancies were uneventful and may become complacent about vaccination. These data suggest that programs designed to enhance pregnant individuals' information and vaccine literacy may promote greater seasonal influenza vaccine acceptance during pregnancyFootnote 74. Additionally, it is important to note that in 2021, the SVP reported a significant increase (53%) in influenza vaccination among pregnant individuals since the 2019 survey (45%)Footnote 36.
Systemic factors contribute to the acceptability of seasonal influenza vaccination among pregnant individuals. Systems and policies or delivery models that promote universal access to vaccines are most effective at improving uptake and coverage in the Canadian contextFootnote 72. Healthcare providers also play an important role in offering the influenza vaccine and positively influencing pregnant individuals' perceptions of seasonal influenza vaccinationFootnote 70Footnote 71Footnote 73Footnote 75Footnote 76. Increased access to trusted healthcare providers who inform pregnant individuals of the benefits and recommendations of seasonal influenza vaccination during pregnancy is associated with increased acceptabilityFootnote 77. Qiu et al. (2021)'s internationally sourced SR findings suggest that a healthcare provider's recommendation was a main facilitator of vaccine acceptability among pregnant individuals, and its absence was the main barrier reported among unvaccinated womenFootnote 78. Blanchard-Rohner et al. (2012) found in their Switzerland based study that most past-partum people neither recalled being recommended vaccination nor informed about the risks of influenza during pregnancyFootnote 79. Evidence from the SVP study (2021) supports these conclusions in the Canadian context with the proportion of women vaccinated against influenza during pregnancy being substantially higher among women who received a recommendation to be vaccinated (70%), compared to those who did not receive a recommendation to be vaccinated (14%)Footnote 36. Providers' knowledge and beliefs about the influenza vaccine, their experiences supporting pregnant individuals, as well as their workload and time constraints, affect their practices in advocating for the influenza vaccine during pregnancyFootnote 80. These findings suggest that improved access to healthcare providers who are well informed and can communicate the importance of seasonal influenza during pregnancy is the most likely way to increase vaccine acceptability.
Impact of COVID-19 pandemic on vaccination during pregnancy
The COVID-19 pandemic has affected the acceptability of vaccination and seasonal influenza vaccination. The Childhood National Immunization Coverage Survey (CNICS) collects information on national immunization coverage for vaccines administered to children and pregnant individuals. Data from the CNICS released in December 2022 showed the proportion of pregnant people who were more inclined to get vaccinated as a result of the pandemic varied across provinces and territories, from a low of 9% (Quebec) to a high of 32% (Yukon). Survey results also showed that the pandemic increased intent to receive vaccination among racialized groups; for example, a significantly higher proportion of Filipino Canadians (39%) and South Asian Canadians (26%) were more inclined to get vaccinated as a result of the pandemic relative to non-Indigenous and non-racialized people (14%)Footnote 81.
Furthermore, the SVP study (2021) identified systematic barriers to receiving vaccinations in Canada in the context of the COVID-19 pandemic. This survey (2021) found that 11% of the pregnant individuals surveyed reported that they encountered an obstacle or delayed vaccination during the COVID-19 pandemic. Of those, 73% reported limited appointment availability, 40% were concerned about being exposed to COVID-19, 25% reported a lack of walk-in options, and 12% received recommendations from a doctor or local public health authority to delay vaccinationFootnote 36.
Discussion
The present SR and MA examined current literature on the use of influenza vaccines during pregnancy. Findings from this review suggest that influenza vaccination during pregnancy is effective in reducing the risk of LCI infection and hospitalization in both pregnant individuals and their infants up to 6 months post-partum. Overall, the evidence from this review indicates that seasonal influenza vaccine efficacy and effectiveness in pregnant individuals appear to be comparable to the general population of healthy adults and consistent with VE point estimates reported in a previous MA by Osterholm, et al. (2012)Footnote 82.
The evidence also suggests that influenza vaccination during pregnancy does not increase the risk of non-obstetric SAEs in pregnant persons; infant death; spontaneous abortion; stillbirth; pre-term birth; small for gestational age; low birth weight; and congenital anomalies. In fact, some studies suggested a protective effect of influenza vaccination for stillbirthFootnote 83Footnote 84Footnote 85 and low birth weightFootnote 63Footnote 86Footnote 87Footnote 88Footnote 89.
The SR and MA findings are in accordance with other reviews that have been undertaken to evaluate the efficacy/effectiveness of influenza vaccination during pregnancyFootnote 15Footnote 16Footnote 90. By comparison, the SR and MA by Quach et al. (2020) reported similar protective effects of seasonal influenza vaccine against LCI in pregnant persons (RR=0.15, 95% CI: 0.06 to 0.36 and OR=0.37, 95% CI: 0.23 to 0.61)Footnote 16. Moreover, Nunes et al. (2017) and Jarvis et al. (2020) consistently reported similar protective effects, with meta-analyses demonstrating a reduction in the risk of LCI in infants born to the vaccinated parent (RR=0.52, 95% CI: 0.41 to 0.67Footnote 90 and RR=0.66, 95% CI: 0.50 to 0.85Footnote 15). Minor differences in the pooled results from the findings of the present review may be attributed to variations in the study inclusion criteria, MA methods and other factors.
The findings of this SR are also consistent with previous reviews that investigated the safety of influenza vaccines administered during pregnancy and found no significant association with increased safety riskFootnote 13Footnote 14Footnote 15Footnote 16Footnote 90Footnote 91. Particularly, Minozzi et al. (2022) and Hansen et al. (2021) reported pooled estimates that support the present review's findings, demonstrating a lack of association between the influenza vaccine and infant death (RR=1.24, 95% CI: 0.96 to 1.60Footnote 13 and RR=1.11, 95% CI: 0.87 to 1.41)Footnote 14. Furthermore, current evidence suggests that there are no adverse early childhood health outcomes associated with influenza immunization during pregnancyFootnote 92Footnote 93Footnote 94.
Despite similarities in the estimates of efficacy and effectiveness of influenza vaccines during pregnancy, limitations in the included studies in this review should be noted. Firstly, adjustment for confounding was not consistently conducted in the observational studies, nor was accounting for immortal time bias for time-dependent outcomes. With respect to study design, there was high variability in the outcome definitions and the time points for some outcomes. Furthermore, it was unclear if some RCT outcomes could be generalized to the Canadian context. Finally, assumptions were made regarding equivalence of effect estimates and for VE estimates, as the concordance of influenza vaccine strains with circulating strains was not considered.
Beyond the scope of this review, a wide range of additional influenza vaccine efficacy/effectiveness and safety outcomes regarding influenza vaccination during pregnancy have been systematically explored in the literature. For example, Jarvis et al. (2020) and Quach et al. (2020) assessed influenza vaccine efficacy/effectiveness during pregnancy by investigating the incidence of influenza-like illness (ILI) and other respiratory illnessesFootnote 15Footnote 16. Conversely, Hansen et al. (2021) assessed seasonal influenza vaccine safety by reporting on non-influenza infectious AEs, all-cause mortality, and mortality from presumed infectious causesFootnote 14, whereas Jarvis et al. (2020) reported long-term respiratory conditions (asthma)Footnote 15.
Studies considering the impact of timing of influenza vaccination on protection of the pregnant individual and fetus/newborn are limited. A 2019 SR and MA on optimal timing on influenza vaccination during pregnancy found that individuals vaccinated later during pregnancy had a greater immune response to vaccination and increased antibody transfer to the fetusFootnote 95. However, prioritizing vaccination during a later gestational age could leave the pregnant person vulnerable to influenza infection for a significant proportion of the pregnancy and may be challenging to implement programmatically.
NACI will continue to monitor the evidence base and will update its guidance as needed.
Recommendations
Following the review of available evidence summarized above, as well as the assessment of EFFA considerations with the EEFA Framework, the following section outlines the evidence-informed recommendations made by NACI regarding influenza vaccination in pregnancy. NACI will continue to carefully monitor the scientific developments related to influenza vaccines, as well as ongoing vaccine pharmacovigilance, and will update its recommendations as required. Additional information on the strength of NACI recommendations is available in Table 4.
The following recommendation for influenza vaccination in pregnancy supplements NACI's overarching recommendations for influenza vaccination, which are available in the NACI seasonal influenza vaccine statement. The overarching NACI recommendation for influenza vaccination is that an age-appropriate influenza vaccine should be offered annually to anyone 6 months of age and older (Strong NACI Recommendation), noting product-specific contraindications.
1. NACI recommends that influenza vaccine should be offered to pregnant individuals. Recommended products include: IIV-SD, IIV-cc, and RIV. (Strong NACI Recommendation)
- There has been no identified safety signal regarding the use of RIV during pregnancy although published clinical data are limited.
- There has been no identified safety signal regarding the use of LAIV in pregnancy, although there are more data on the safety of other influenza vaccine products in pregnancy. There is also evidence that IIV has higher efficacy than LAIV in healthy adults. Note that vaccination with LAIV during pregnancy should not be considered a reason to terminate pregnancy.
- The only adjuvanted vaccine in Canada for the 2023/2024 influenza season is the adjuvanted inactivated trivalent influenza vaccine (IIV3-Adj), which is authorized for infants 6 to 23 months (Fluad Pediatric®) and adults 65 years and older (Fluad®). There has been no identified safety signal regarding adjuvanted influenza vaccines in pregnancy; however, IIV3-Adj is not authorized for people of reproductive age.
- The only high-dose vaccine in Canada for the 2023/2024 influenza season is the high-dose inactivated quadrivalent influenza vaccine IIV4-HD (Fluzone® High-Dose Quadrivalent) which is authorized for adults 65 years and older. There has been no identified safety signal regarding high-dose influenza vaccines in pregnancy, however, IIV4-HD is not authorized for people of reproductive age.
Summary of evidence and rationale:
- The safety of influenza vaccination during pregnancy is consistently supported by numerous studies, including clinical trials and observational studies, and routine pharmacovigilance data from safety reporting systems.
- Published data, including currently available studies of fetal death, spontaneous abortion, and congenital malformations, do not report unexpected or concerning patterns. The evidence reaffirms that seasonal influenza vaccination during pregnancy does not appear to be associated with significant safety issues with respect to adverse birth outcomes or maternal non-obstetric SAEs.
- Published data continue to demonstrate the efficacy/effectiveness of influenza vaccination during pregnancy for protection against LCI infection and to help mitigate the severity of influenza infection.
- The efficacy/effectiveness of seasonal influenza vaccination in pregnant individuals is comparable to the general adult population.
- Studies have demonstrated that infants receive protection from maternal antibodies as a result of influenza vaccination during pregnancy, and their results suggest that seasonal vaccination during pregnancy reduces the risk of LCI infections and LCI hospitalizations in infants up to 6 months of age.
2. NACI recommends that influenza vaccination should be offered at any stage of pregnancy (i.e., in any trimester). (Strong NACI recommendation)
- If an individual's pregnancy extends over 2 influenza seasons, that person may receive 2 doses of influenza vaccine (i.e., one dose in each season, during the course of the pregnancy).
Summary of evidence and rationale:
- There is insufficient evidence to establish the optimal timing of influenza vaccination for maternal or fetal/newborn outcomes.
- Prioritizing vaccination during a specific gestational stage may lead to programmatic challenges and missed vaccination opportunities.
3. NACI recommends the inclusion of all pregnant individuals, at any stage of pregnancy, among those who are particularly recommended to receive influenza vaccination. (Strong NACI recommendation)
Summary of evidence and rationale:
- The evidence consistently shows an association between pregnancy and increased disease severity with influenza infection. This includes hospitalization, admission to the ICU, invasive mechanical ventilation, and maternal mortality.
- There is also a higher risk of adverse neonatal outcomes (e.g., premature delivery, low birth weight, NICU admission) with influenza infection during pregnancy.
- The risks for preterm delivery, low birth weight and admission to the NICU increase with disease severity in the pregnant person.
- Infants under 6 months are at increased risk of hospitalization due to influenza infection compared to children from other ages. However, influenza vaccine is not effective in infants under 6 months; therefore, passive immunization of fetuses through transplacentally transmitted anti-influenza antibodies is currently the best available prevention strategy.
- Despite the increased risks of severe disease there is a suboptimal uptake of influenza vaccination during pregnancy in Canada, with only approximately 53% of pregnant individuals receiving the vaccine in 2021.
- Among pregnant people, there is a disproportionate burden of disease and low vaccine uptake among those who are racialized, Indigenous, younger, low-income, and/or living in rural settings.
4. NACI reiterates its recommendation that influenza vaccination may be given at the same time as, or at any time before or after administration of another vaccine, including COVID-19 or pertussis vaccine. (Strong NACI recommendation)
- Every appropriate opportunity to immunize during pregnancy, with any immunization for which the pregnant person is eligible, should be taken.
Summary of evidence and rationale:
- No known safety signal for concurrent administration of influenza with another vaccine during pregnancy has been identified.
- Administration of multiple vaccines at the same visit is a strategy for increasing immunization uptake.
Research priorities
- Study the longer-term outcomes of infants and children exposed to influenza infection in-utero.
- Research on seasonal influenza illness and vaccination rates among pregnant individuals and infants outside of a 2009 H1N1 pandemic context, particularly during/following the COVID-19-pandemic.
- Collect national-level influenza surveillance data for pregnant individuals and infants under 6 months of age in Canada will help to better define the burden of disease for pregnant people and infants.
- Study the longer-term outcomes for children born to individuals vaccinated during pregnancy.
- Collect additional safety data for newer vaccine technologies, including cell culture and RIV.
- Study the timing of influenza immunization in pregnant individuals with respect to duration or waning of protection against infection and severe disease.
- Examine vaccine confidence and acceptability among pregnant individuals in Canada, especially among racialized groups.
- Investigate range and complex interplay of factors that influence acceptability of influenza immunization in general and for high-risk groups (including pregnant individuals).
- Study the COVID-19 pandemic's potential ongoing impact on vaccine hesitancy and maternal vaccine uptake.
- Learn more about patient, provider, and system-level barriers to vaccination in pregnancy in Canada, including:
- Policy and structural factors;
- Patients' knowledge, understanding and beliefs about influenza vaccination during pregnancy, especially given the heterogeneity of Canada's population (i.e., differences in socioeconomic and cultural backgrounds and differences in trust in the medical system).
Surveillance priorities
Ongoing and systematic data collection, analysis, interpretation, and timely dissemination is fundamental to planning, implementation, evaluation, and evidence-based decision-making. To support such efforts, NACI encourages ongoing surveillance and continued expansion of surveillance details in the epidemiology of influenza in Canada.
Overall, there is a gap in knowledge on the impact of seasonal influenza among pregnant persons and perinatal/postnatal outcomes in Canada and worldwide. To date, most epidemiological studies have focused on the 2009 H1N1 pandemic in certain high-income countries (e.g., US) and report inconsistent findings on the association between influenza illness and adverse perinatal outcomes. There is also a shortage of studies conducted after the COVID-19 pandemic, beginning in late 2019/early 2020. Therefore, more updated surveillance on seasonal influenza among pregnant persons and young infants in low, medium, and high-income countries, including Canada, is needed to better understand the burden of disease and develop targeted vaccine campaigns for these high-risk groups.
In Canada, FluWatch, the national surveillance system, monitors the spread of influenza and ILI by province/territory and age group, but does not specify pregnancy status. Therefore, initiatives are needed to collect influenza information (e.g., ILI incidence, viral strain, hospitalization) from pregnant persons to inform appropriate public health efforts such as targeted vaccination campaigns and education.
Tables
| Study | Outcome | Vaccine | Study design | Participants (n/N) | Summary of key findings | Summary | |
|---|---|---|---|---|---|---|---|
| Level of evidence | Quality | ||||||
| Vaccine efficacy | |||||||
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the Canadian Institutes of Health Research (CIHR) and the Drug Safety and Effectiveness Network (DSEN) |
Lab-confirmed influenza (LCI) assessed by RT-PCR during pregnancy and up to 6 months post-partum |
IIV3 (Vaxigrip®, Sanofi) Placebo Active control: |
RCTsFootnote 40Footnote 41Footnote 42 Countries: Follow-up: One RCT was restricted to the 2011-2012 and 2012-2013 influenza seasonsFootnote 40 Funding: |
Pregnant persons (n=10,074) IIV3: n=5,089 (50.5%) Placebo or active control: n=4,985 (49.5%) |
The MA included 3 RCTs The pooled vaccine efficacy was 50% (95% CI: 22 to 68%), I2=49.22% |
Level I |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Laboratory-confirmed influenza (LCI) assessed by RT-PCR in infant up to 6 months of age |
IIV3 (Vaxigrip®, Sanofi and Fluarix, GSK) Placebo Active control: |
RCTsFootnote 40Footnote 41Footnote 42Footnote 43 Countries: Follow up: One RCT was restricted to the 2011-2012 and 2012-2013 influenza seasonsFootnote 40 Funding: |
Infants up to 6 months of age (n=3,474) IIV3: n=1,744 (50.2%) Placebo or active control: n=1,730 (49.8%) |
The MA included 4 RCTS The pooled vaccine efficacy was 37% (95% CI: 22 to 49%), I2=0.00% |
Level I |
Fair |
| Vaccine effectiveness | |||||||
Maltezou HC, Stavros S, Asimakopoulos G et al. Effectiveness of maternal vaccination with quadrivalent inactivated influenza vaccine in pregnant women and their infants in 2019-2020. 2022Footnote 46 Funded by Sanofi |
Lab-confirmed influenza assessed by RT-PCR during pregnancy |
IIV4 (VaxigripTetra®, Sanofi) |
Prospective cohort study Country: Follow up: Funding: |
Pregnant persons 18 to 45 years of age (n=636) IIV4: n=406 (63.8%) Unvaccinated: n=230 (36.2%) |
The aVE was 43.5% (95% CI: 28.4 to 55.6%) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN And study identified from the update literature search: Funded by the National Institute for Communicable Diseases of the National Health Laboratory Service; the US Centers for Disease Control and Prevention; and the Bill and Melinda Gates Foundation |
Hospitalization due to LCI assessed by RT-PCR during pregnancy or up to 42 days post-partum |
IIV (Seasonal influenza vaccine) |
TND studies (Thompson 2019 and Nunes 2022)Footnote 44Footnote 47 Countries: Follow up: Funding: |
Pregnant persons (n=1,391) IIV: n=317 (22.8%) Unvaccinated: n=1,074 (77.2%) |
The MA included 2 TND studies The pooled aVE was 42% (95% CI: 19 to 59%), I2=0.00% |
Level II-2 |
Good |
Vousden N, Bunch K, Knight M et al. Incidence, risk factors and impact of seasonal influenza in pregnancy: A national cohort study. 2021Footnote 48 Funded by the National Institute for Health Research (NIHR) |
Hospitalization due to LCI assessed by virological testing at any stage of pregnancy or up to 2 days after delivery |
IIV (Seasonal influenza vaccine) |
Prospective cohort study Country: Follow up: Funding: |
Individuals hospitalized at any stage of pregnancy or up to 2 days after delivery (n=1,099) IIV: n=320 (29.1%) Unvaccinated: n=466 (42.4%) Unknown/missing: n=313 (28.5%) |
The VE was 38% (95% CI: 14 to 55%) |
Level II-2 |
Fair |
Studies identified from the update literature search: Funded by Sanofi Foo D, Sarna M, Pereira G et al. Longitudinal, population-based cohort study of prenatal influenza vaccination and influenza infection in childhood. 2022Footnote 49 Funded by the National Health and Medical Research Council, Curtin University Graduate Research School, Wesfarmers Centre of Vaccines and Infectious Disease Rowe SL, Leder K, Perrett KP, et al. Maternal Vaccination and Infant Influenza and Pertussis. 2021Footnote 50 Funded by the Victoria State Government Department of Health in Australia as part of routine vaccine program evaluation |
LCI in infants up to 6 months of age |
IIV (Seasonal influenza vaccine) |
Cohort studiesFootnote 46Footnote 49Footnote 50 Countries: Follow up: Not restricted to influenza season (n=2) between 2012 and 2017 Funding: |
Infants up to 6 months of age (n=296,611) Infants born to vaccinated gestational parent: n=100,042 (33.7%) Infants born to unvaccinated gestational parent: n=196,569 (66.3%) |
The MA included 3 cohort studies The pooled VE was 41% (95% CI: 23 to 55), I2=17% |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN And studies identified from the update literature search: Funded by the National Institute for Communicable Diseases of the National Health Laboratory Service; the US Centers for Disease Control and Prevention; and the Bill and Melinda Gates Foundation McRae J, Blyth CC, Cheng AC et al. Preventing severe influenza in Australian infants: Maternal influenza vaccine effectiveness in the PAEDS-FluCAN networks using the test-negative design. 2022Footnote 51 Funded by the National Health and Medical Research Council, Australian Government Department of Health, and Departments of Health in NSW, Victoria, Queensland, South Australia, Western Australia, and the Northern Territory |
Hospitalization due to LCI infection in infants up to 6 months of age |
IIV (Seasonal influenza vaccine) |
TND studies (Benowitz 2010, McRae 2022, and Nunes 2022)Footnote 45Footnote 47Footnote 51 Countries: Follow up: Funding: |
Infants up to 6 months of age (n=1,702) Infants born to vaccinated gestational parent: n=612 (36.0%) Infants born to unvaccinated gestational parent: n=1,090 (64.0%) |
The MA included 3 TND studies The pooled aVE was 42% (95% CI: 16 to 59%), I2=71% |
Level II-2 |
Fair |
Foo D, Sarna M, Pereira G et al. Longitudinal, population-based cohort study of prenatal influenza vaccination and influenza infection in childhood. 2022Footnote 49 Funded by the National Health and Medical Research Council, Curtin University Graduate Research School, Wesfarmers Centre of Vaccines and Infectious Disease |
Hospitalization due to LCI in infants up to 6 months of age |
IIV (Seasonal influenza vaccine) |
Retrospective, population-based cohort study Country: Follow up: Funding: |
Singleton, live-born infants (n=124,760) Infants born to vaccinated gestational parent: n=14,396 (11.5%) Infants born to unvaccinated gestational parent: n=110,364 (88.5%) |
The aVE was 62% (95% CI: 9 to 84%) |
Level II-2 |
Good |
Rowe SL, Leder K, Perrett KP, et al. Maternal Vaccination and Infant Influenza and Pertussis. 2021Footnote 50 Funded by the Victoria State Government Department of Health in Australia as part of routine vaccine program evaluation |
Hospitalization due to LCI in infants up to 6 months of age |
IIV (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Infants up to 6 months of age (n=185,404) Infants born to vaccinated gestational parent: n=85,365 (46.0%) Infants born to unvaccinated gestational parent: n=86,012 (46.4%) Infants born to gestational parents with missing/unknown vaccination status: n=14,027 (7.6%) |
The aVE was 20.85% (95% CI: -17.74 to 46.79%) in infant under 6 months of age The aVE was 34.37% (95% CI: -14.83 to 62.49%) in infant under 2 months of age, and the aVE was 4.00% (95% CI: -66.75 to 44.73%) in infants 2 months to under 6 months of age |
Level II-2 |
Fair |
| Safety | |||||||
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: severe systemic reactions within 7 days of intervention |
IIV3 (Vaxigrip®, Sanofi) Placebo Active control: Meningococcal quadrivalent vaccine (Menactra®, Sanofi) |
2 RCTsFootnote 41Footnote 42 Countries: Follow up: Funding: |
Pregnant individuals (n=4,540) IIV3: n=2,286 (50.3%) Placebo: n=172 (3.8%) Active control: n=2,082 (45.9%) |
No discernible difference between groups in either included RCT Tapia et al., 2016: 2 of 2,105 vaccinated and 0 of 2,082 controlFootnote 42 Madhi et al., 2014: 27 of 181 vaccinated and 19 of 172 control (p=0.36)Footnote 41 |
Level I |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: peripartum hospitalization |
IIV3 (Fluarix, GSK) Active control: Pneumococcal vaccine, 23-valent (Pneumovax® 23, Merck) |
RCTFootnote 43 Country: Follow up: Funding: |
Pregnant individuals (n=316) IIV3: n=159 (50.3%) Active control: n=157 (49.7%) |
Single RCT found no apparent difference in risk between IIV3 (1 event/159) and active control (2 events/157) |
Level I |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: events possibly or probably related to vaccination within 30 days of intervention |
IIV3 (Vaxigrip®, Sanofi) Placebo |
RCTFootnote 41 Country: Follow up: Funding: |
Pregnant individuals (n=2,116) IIV3: n=1,062 (50.2%) Placebo: n=1,054 (49.8%) |
Single RCT found no apparent difference in risk between IIV3 (1/1,062) and placebo (0/1,054) groups |
Level I |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: events unrelated to pregnancy causing hospitalization within 42 days of vaccine administration |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort studyFootnote 54 Country: Follow up: Funding: |
Pregnant persons in the second or third trimester of gestation (n=1,051) IIV3: n=225 (21.4%) Unvaccinated: n=826 (78.6%) |
A single cohort study found no apparent difference in risk between IIV3 (2/225) and unvaccinated pregnant individuals (3/826) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: inpatient Guillain-Barré syndrome within 42 days |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort studyFootnote 59 Country: Follow up: Funding: |
Pregnant persons in the first trimester of gestation (n=223,898) IIV3: n=75,906 (33.9%) Unvaccinated: n=147,992 (66.1%) |
A single cohort study found no significant difference between IIV3 vaccinated (0/75,906) and unvaccinated (1/147,992) pregnant persons (p=0.34) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Non-obstetric SAEs in pregnant persons: no defined and time of follow-up not reported |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort studyFootnote 58 Country: Follow up: Funding: |
Pregnant persons (n=346) IIV3: n=288 (83.2%) Unvaccinated: n=58 (16.8%) |
No events found in a single cohort study of 288 IIV3 vaccinated and 58 unvaccinated pregnant persons |
Level II-2 |
Fair |
Ledlie S, Gandhi-Banga S, Shrestha et al. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. 2022Footnote 60 Funded by Sanofi |
Non-obstetric AEs in pregnant persons: Guillain-Barré syndrome |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Retrospective and prospective case series, multicenters Countries: Follow up: Between 2013/08 and 2019/09 Funding: |
Individuals of reproductive age who were exposed to IIV4 during pregnancy or within 30 days of their last menstrual period (n=239) Trimester of exposure, n (%): |
One (0.4%) case of Guillain-Barré syndrome occurred within 5 days of vaccination in a 29-year-old female who recovered and gave birth to a healthy baby while recovering |
Level III |
Poor Reporting bias High rate of loss to follow up (80%) |
Carreras JJ, Lluch JA, Taboada JA, et al. Adverse events in pregnant women with the tetravalent influenza vaccine obtained from cell cultures. 2022Footnote 56 Funded by Seqirus |
Non-obstetric AEs in pregnant persons at any time after vaccine administration |
IIV4-cc (Flucelvax® Quad, Seqirus) |
Retrospective cohort study, multicenter Country: Follow up: Funding: |
Individuals 18 to 64 years old vaccinated with IIV4-cc (n=244,731) Pregnant individuals: N=24,870 (10.2%) Non-pregnant individuals: N=219,861 (89.8%) |
The rate of AEs per 100,000 doses administered was 4.0 and 5.9 in pregnant and non-pregnant individuals, respectively No serious AE were reported among pregnant individuals |
Level II-2 |
Poor Reporting bias Inconsistency in the quality of data Limited data provided on AE and timing following vaccine administration |
Betancourt-Cravioto M, Cervantes-Powell P, Tapia-Conyer R et al. Improved post-marketing safety surveillance of quadrivalent inactivated influenza vaccine in Mexico using a computerized, SMS-based follow-up system. 2022Footnote 55 Funded by Sanofi |
Non-obstetric AEs in pregnant persons within 42 days of vaccine administration |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Prospective cohort study, multicenter Country: Follow up: Funding: |
Individuals 6 months and older who received a routine influenza vaccine at study centers (n=2,013) Pregnant individuals: n=18 (0.9%) |
One (5.6%) pregnant individual reported a non-serious AE (i.e., AE did not require a medical visit) |
Level II-2 |
Poor Small sample size Reporting bias No information on AE reported, including severity and duration |
Vanni T, Thomé BdC, Oliveira MMM, et al. Active pharmacovigilance of the seasonal trivalent influenza vaccine produced by Instituto Butantan: A prospective cohort study of five target groups. 2021Footnote 57 Funded by the Butantan Foundation |
Non-obstetric AEs in pregnant persons within 42 days of vaccine administration |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort study, multicenter Country: Follow up: Funding: |
Individuals 6 months of age and older who received a routine influenza vaccine at study centers (n=942) Pregnant individuals: n=108 (11.5%) |
82 (75.9%) pregnant individuals had an AE 78 (72.2%) pregnant individuals had an adverse reaction (i.e., any AE with a reasonable causal relationship with the vaccine, according to "Uppsala Monitoring Centre" of the World Health Organization UMC-WHO) No SAE was reporting in pregnant |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Infant death up to 6 months of age |
IIV3 (Seasonal influenza vaccine: Vaxigrip®, Sanofi; n=3, Fluarix, GSK; n=1) Placebo (n=2) Active control: Meningococcal quadrivalent vaccine (n=1, Menactra®, Sanofi) or Pneumococcal vaccine, 23-valent (n=1, Pneumovax® 23, Merck) |
4 RCTs (Zaman 2006, Madhi 2014, Tapia 2016, Steinhoff 2017)Footnote 40Footnote 41Footnote 42Footnote 43 Countries: Follow up: Funding: |
Infants up to 6 months of age (n=10,115) IIV3: n=5,071 (50.1%) Placebo or active control: n=5,044 (49.9%) |
The MA included 4 RCTs The pooled risk ratio was 1.14 (95% CI: 0.86 to 1.50), I2=9.33% |
Level I |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Infant death up to 6 months of age |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 61 Country: Follow up: Funding: |
Infants diagnosed with fever (n=83) Infants born to vaccinated gestational parent: n=36 (43.4%) Infants born to unvaccinated gestational parent: n=47 (56.6%) |
No Infant death was reported among infants born to vaccinated and unvaccinated gestational parent |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Spontaneous abortion (<20 gestational weeks) |
IIV (Seasonal influenza vaccine) |
2 cohort studiesFootnote 62Footnote 63 Countries: Follow up: Funding: |
Pregnant persons (n=1,900) II V: n=983 (51.7%) Unvaccinated: n=917 (48.3%) |
The MA included 2 cohort studies The pooled aHR was 0.77 (95% CI: 0.31 to 1.89), I2=37.51% |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Spontaneous abortion (<22 gestational weeks) |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 64 Country: Follow up: Funding: Non-industry |
Individuals in their first trimester of pregnancy (n=2,826) IIV3: n=1,121 (39.7%) Unvaccinated: n=1,705 (60.3%) |
A single cohort study reported raw data with the same risk in both exposed and unexposed groups (0.4% and 0.4%, respectively) |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Spontaneous abortion (<20 gestational weeks) within 28 days of vaccine administration |
IIV3 (Seasonal influenza vaccine) |
Retrospective case-control study)Footnote 65 Country: Follow up: Funding: |
Pregnant individuals between 18- and 44-year-old vaccinated against influenza (n=970) |
The aOR was 3.70 (95% CI: 1.40 to 9.40) in 2010/2011 and 1.40 (95% CI: 0.60 to 3.30) in 2011/2012 Post-hoc analyses of 2010/2011 data: |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Spontaneous abortion (<20 gestational weeks) within 28 days of vaccine administration |
IIV3 (Seasonal influenza vaccine) |
Retrospective case-control studyFootnote 65 Country: Follow up: Funding: |
Pregnant individuals between 18- and 44-year-old (n=2,472) Vaccinated in the previous season: n=1,254 (50.3%) Not vaccinated in the previous season: n=1,218 (49.3%) |
Overall, the aOR was 0.80 (95% CI: 0.60 to 1.10) The aOR was 0.9 (95% CI: 0.6 to 1.5) in those vaccinated in the previous season and 0.7 (95% CI: 0.4 to 1.1) in those not vaccinated in the previous season |
Level II-2 |
Good |
Romano CJ, Hall C, Khodr ZG, et al. History of pandemic H1N1-containing influenza vaccination and risk of spontaneous abortion and birth defects. 2021Footnote 66 Funded by the Defense Health Agency Immunization Healthcare Division and the U.S. Navy Bureau of Medicine and Surgery |
Spontaneous abortion (<22 gestational weeks) within 28 days of vaccine administration |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Pregnant individuals 17 years and older (n=26,264) Exposed to a pH1N1-containing vaccine in the season prior to pregnancy: n=21,736 (82.8%) Exposed to non-pH1N1-containing vaccine in the season prior to pregnancy: n=4,528 (17.2%) |
The aHR was 1.19 (95% CI: 0.97 to 1.46) |
Level II-2 |
Good |
Robinson C, Oberye J, Van Boxmeer J et al. A prospective cohort study on pregnancy outcomes of persons immunized with a seasonal quadrivalent inactivated influenza vaccine during pregnancy. 2022Footnote 68 Funded by Seqirus Inc |
Spontaneous abortion (<20 gestational weeks) |
IIV4 (Afluria® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4 at any time during pregnancy (n=483) Trimester of exposure: Vaccinated <20 gestational weeks: n=160 (33.1%) |
4 events (2.5%, 95% CI: 0.7 to 6.3%) were reported among those vaccinated at under 20 gestational weeks (n=160) |
Level III |
Fair |
Robinson C, Van Boxmeer J, Tilson H, et al. Outcomes in pregnant persons immunized with a cell-based quadrivalent inactivated influenza vaccine: A prospective observational cohort study. 2022Footnote 69 Funded by Seqirus Inc |
Spontaneous abortion (<20 gestational weeks) |
IIV4-cc (Flucelvax® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4-cc at any time during pregnancy (n=665) Trimester of exposure: Vaccinated <20 gestational weeks: n=211 (31.7%) |
4 events (1.9%, 95% CI: 0.5 to 4.8%) were reported among those vaccinated at under 20 gestational weeks (n=211) |
Level III |
Fair |
Ledlie S, Gandhi-Banga S, Shrestha et al. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. 2022Footnote 60 Funded by Sanofi |
Spontaneous abortion |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Retrospective and prospective case series, multicenters Countries: Follow up: Funding: |
Individuals of reproductive age who were exposed to IIV4 during pregnancy or within 30 days of their last menstrual period (n=239) Trimester of exposure, n (%): |
4 events (6.4%, 95% CI: 2.08 to 15.90%) were reported |
Level III |
Poor Reporting bias High rate of loss to follow up (80%) |
Nwoji U. Seasonal influenza vaccine exposure in pregnancy: 5-year results from a pregnancy registry. 2022Footnote 67 Funded by GlaxoSmithKline Biologicals SA |
Spontaneous abortion (<22 gestational weeks) |
IIV3 (Fluarix and FluLaval, GSK) or IIV4 (Fluarix Quadrivalent and FluLaval Quadrivalent, GSK) |
Prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated during pregnancy or within 28 days preceding conception (n=507) Trimester of exposure, n (%): Lost to follow up: n=359 (70.8%) |
3 events (2.6%) were reported 2 occurred among those vaccinated during the first trimester of pregnancy and one had unknown trimester of exposure |
Level III |
Poor Reporting bias High rate of loss to follow up (70.8%) |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort studyFootnote 83 Country: Follow up: Funding: |
Pregnant individuals (n=58,008) IIV3: n= 5,076 (8.8%) Unvaccinated: n= 52,932 (91.2%) |
The aHR was 0.49 (95% CI: 0.29 to 0.83) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV (Seasonal influenza vaccine) |
Retrospective case-control studyFootnote 96 Country: Follow up: Founding: |
Pregnant persons (n=12,109) II V: n=1,736 (14.3%) Unvaccinated: n=10,373 (85.7%) |
The aOR was 0.95 (95% CI: 0.79 to 1.14) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV (Seasonal influenza vaccine) |
Retrospective cohort studyFootnote 97 Country: Follow up: Funding: |
Individuals in their first trimester of pregnancy (n=11,955) IIV: n=2,391 (20.0%) Unvaccinated: n=9,564 (80.0%) |
The adjusted risk ratio (aRR) was 1.18 (95% CI: 0.64 to 2.18) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 62 Countries: United States Follow up: Funding: |
Pregnant individuals (n=1,707) IIV: n=1,240 (72.6%) Unvaccinated: n=467 (27.4%) |
The risk ratio was 0.38 (95% CI: 0.05 to 2.92) In analysis restricting to vaccination during the first trimester of pregnancy, the risk ratio was 0.98 (95% CI: 0.13 to 7.50) |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 84 Country: Follow up: Funding: |
Pregnant persons (n=85,783) IIV3: n=8,864 (10.3%) Unvaccinated: n=76,919 (89.7%) |
The risk ratio was 0.60 (95% CI: 0.41 to 86) In analysis restricting to vaccination during the first trimester of pregnancy, the risk ratio was 2.54 (95% CI: 0.36 to 18.01) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 64 Country: Follow up: Funding: |
Pregnant individuals (n=10,330) IIV3: n=3,943 (38.2%) Unvaccinated: n=6,387 (61.8%) |
The risk ratio was 0.44 (95% CI: 0.12 to 1.58) In analysis restricting to the first trimester of pregnancy, the risk ratio was 0.30 (95% CI: 0.01 to 6.33) |
Level II-2 |
Fair |
Giles ML, Davey MA, Wallace EM. Associations Between Maternal Immunisation and Reduced Rates of Preterm Birth and Stillbirth: A Population Based Retrospective Cohort Study. Frontiers in Immunology. 2021Footnote 85 Funding: Not reported |
Stillbirth |
IIV (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Pregnant persons with singleton pregnancies >28 gestational weeks (n=269,493) IIV: n=138,698 (51.5%) Unvaccinated: n=112,155 (41.6%) Not reported/unknown: n=18,640 (6.9%) |
The aRR was 0.25 (95% CI: 0.20 to 0.31) |
Level II-2 |
Fair |
Robinson C, Oberye J, van Boxmeer J, et al. A Prospective Cohort Study on Pregnancy Outcomes of Persons Immunized with a Seasonal Quadrivalent Inactivated Influenza Vaccine during Pregnancy. Vaccines. 2022Footnote 68 Funded by Seqirus Inc |
Stillbirth (≥20 gestational weeks or ≥500g) |
IIV4 (Afluria® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4 at any time during pregnancy (n=483) Trimester of exposure: |
2 (0.4%, 95% CI: 0.1 to 1.5%) events were reported One occurred in an individual vaccinated during the first trimester and one in an individual vaccinated during the second trimester of pregnancy |
Level III |
Fair |
Robinson C, Van Boxmeer J, Tilson H, et al. Outcomes in Pregnant Persons Immunized with a Cell-Based Quadrivalent Inactivated Influenza Vaccine: A Prospective Observational Cohort Study. Vaccines. 2022Footnote 69 Funded by Seqirus Inc |
Stillbirth (≥20 gestational weeks or ≥500g) |
IIV4-cc (Flucelvax® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4-cc at any time during pregnancy (n=665) Trimester of exposure: |
No event was reported |
Level III |
Fair |
Nwoji U. Seasonal influenza vaccine exposure in pregnancy: 5-year results from a pregnancy registry. Hum Vaccin Immunother. 2022Footnote 67 Funded by GlaxoSmithKline Biologicals SA |
Stillbirth (≥18-22 gestational weeks or ≥500g) |
IIV3 (Fluarix and FluLaval, GSK) or IIV4 (Fluarix Quadrivalent and FluLaval Quadrivalent, GSK) |
Prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated during pregnancy or within 28 days preceding conception (n=507) Trimester of exposure, n (%): Lost to follow up: n=359 (70.8%) |
One (0.9%) event was reported among an individual vaccinated during the first trimester of pregnancy Causal association with vaccination was ruled out |
Level III |
Poor Reporting bias High rate of loss to follow up (70.8%) |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Pre-term birth (<37 completed gestational weeks) |
IIV3 (Seasonal influenza vaccine) |
Fifteen cohort studies Countries: Follow up: Funding: Non-industry (n=10), non-industry and insurance (n=2), mixed (n=1), no funding (n=1), and not reported (n=1) |
Studies that accounted for immortal time bias (n=152,476) IIV3: n=66,749 (43.8%) Unvaccinated: n=85,727 (56.2%) Studies that did not account for immortal time bias (n=151,032) IIV3: n=67,558 (44.7%) Unvaccinated: n=83,474 (55.3%) When influenza vaccination during the first trimester of pregnancy was considered (n=47,211) IIV3: n=19,135 (40.5%) Unvaccinated: n=28,076 (59.5%) |
The MA included 6 cohort studies that accounted for immortal time bias The pooled aHR was 1.09 (95% CI: 0.89 to 1.33), I2=28.18% for studies that accounted for immortal time bias The MA included ten cohort studies that did not account for immortal time bias The pooled aRR was 0.86 (95% CI: 0.76 to 0.97), I2=71.15% for studies that did not account for immortal time bias A MA included six cohort studies restricted to vaccination during the first trimester of pregnancy The pooled aHR was 1.05 (95% CI: 0.92 to 1.20), I2=30.46% for studies restricted to vaccination during the first trimester of pregnancy |
Level II-2 |
Good |
Duque J, Howe AS, Azziz-Baumgartner et al. Multi-decade national cohort identifies adverse pregnancy and birth outcomes associated with acute respiratory illness hospitalisations during the influenza season. 2022Footnote 87 Funding: not reported |
Preterm birth (<37 weeks of gestation) |
IIV (Seasonal influenza vaccine) |
Retrospective cohort Country: Follow up: Funding: |
Individuals between 15 and 49 years of age who were pregnant (n=822,391) Vaccinated pregnant persons with preterm birth between 2010 and 2018: n=3,895 (6.1%) Unvaccinated pregnant persons with preterm birth between 2010 and 2018: n=29,825 (8.0%) |
The aHR was 0.79 (95% CI: 0.77 to 0.82) |
Level II-2 |
Good |
Giles ML, Davey M and Wallace EM. Associations between maternal immunisation and reduced rates of preterm birth and stillbirth: A population based retrospective cohort study. 2021Footnote 85 Funding not reported |
Preterm birth (<37 weeks of gestation) |
IIV (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Pregnant persons with singleton pregnancies >28 gestational weeks (n=269,493) IIV: n=138,698 (51.5%) Unvaccinated: n=112,155 (41.6%) Not reported/unknown: n=18,640 (6.9%) |
The aRR was 0.69 (95% CI: 0.66 to 0.72) |
Level II-2 |
Fair |
Robinson C, Oberye J, van Boxmeer J, et al. A Prospective Cohort Study on Pregnancy Outcomes of Persons Immunized with a Seasonal Quadrivalent Inactivated Influenza Vaccine during Pregnancy. Vaccines. 2022Footnote 68 Funded by Seqirus Inc |
Preterm birth (<37 weeks of gestation) |
IIV4 (Afluria® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4 at any time during pregnancy (n=483) Trimester of exposure: |
Overall, 31 (7.2%) events were reported Events by trimester of exposure, n (%): |
Level III |
Fair |
Robinson C, Van Boxmeer J, Tilson H, et al. Outcomes in Pregnant Persons Immunized with a Cell-Based Quadrivalent Inactivated Influenza Vaccine: A Prospective Observational Cohort Study. Vaccines. 2022Footnote 69 Funded by Seqirus Inc |
Preterm birth (<37 weeks of gestation) |
IIV4-cc (Flucelvax® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4-cc at any time during pregnancy (n=665) Trimester of exposure: |
Overall, 52 (9.2%) events were reported Events by trimester of exposure, n (%): |
Level III |
Fair |
Ledlie S, Gandhi-Banga S, Shrestha et al. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. 2022Footnote 60 Funded by Sanofi |
Preterm birth (<37 weeks of gestation) |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Retrospective and prospective case series, multicenters Countries: Follow up: Between 2013/08 and 2019/09 Funding: |
Individuals of reproductive age who were exposed to IIV4 during pregnancy or within 30 days of their last menstrual period (n=239) Trimester of exposure, n (%): |
One (6.67%) event was reported among reports with known neonatal outcomes (n=15) |
Level III |
Poor Reporting bias High rate of loss to follow up (80%) |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN And study identified in update literature search: Funding not reported |
Small-for-gestational-age birth |
IIV (Seasonal influenza vaccine) |
12 cohort studies Countries: Follow up: Not restricted to influenza season between 2004 and 2017 (n=10) Funding: |
Pregnant persons (n=548,277) IIV: n=271,045 (n=49.4%) Unvaccinated: n=277,232 (50.6%) |
The MA included 12 cohort studies The pooled aRR was 0.97 (95% CI: 0.90 to 1.04), I2=71% |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN And study identified in update literature search: Funding not reported |
Low birth weight (<2,500 g) |
IIV (Seasonal influenza vaccine) |
3 cohort studiesFootnote 63Footnote 86Footnote 87 Countries: Follow up: Funding: |
Pregnant persons (n=168,633) IIV: n=68,039 (40.3%) Unvaccinated: n=100,594 (59.7%) |
The MA included 3 cohort studies The pooled aHR was 0.89 (95% CI: 0.83 to 0.96), I2=37% |
Level II-2 |
Good |
Robinson C, Oberye J, van Boxmeer J, et al. A Prospective Cohort Study on Pregnancy Outcomes of Persons Immunized with a Seasonal Quadrivalent Inactivated Influenza Vaccine during Pregnancy. Vaccines. 2022Footnote 68 Funded by Seqirus Inc |
Low birth weight (<2,500 g) |
IIV4 (Afluria® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4 at any time during pregnancy (n=483) Trimester of exposure: |
Overall, 25 (5.4%) events occurred Events by trimester of exposure, n (%): |
Level III |
Fair |
Robinson C, Van Boxmeer J, Tilson H, et al. Outcomes in Pregnant Persons Immunized with a Cell-Based Quadrivalent Inactivated Influenza Vaccine: A Prospective Observational Cohort Study. Vaccines. 2022Footnote 69 Funded by Seqirus Inc |
Low birth weight (<2,500 g) |
IIV4-cc (Flucelvax® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4-cc at any time during pregnancy (n=665) Trimester of exposure: |
Overall, 37 (5.8%) events occurred Events by trimester of exposure, n (%): |
Level III |
Fair |
Ledlie S, Gandhi-Banga S, Shrestha et al. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. 2022Footnote 60 Funded by Sanofi |
Low birth weight (<2,500 g) |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Retrospective and prospective case series, multicenters Countries: Follow up: Funding: |
Individuals of reproductive age who were exposed to IIV4 during pregnancy or within 30 days of their last menstrual period (n=239) Trimester of exposure, n (%): |
2 (10.0%) events were reported among reports with known neonatal outcomes (n=30) |
Level III |
Poor Reporting bias High rate of loss to follow up (80%) |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Congenital anomalies identified at birth |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 63 Country: Follow up: Funding: |
Pregnant persons (n=1,207) IIV3 during the first trimester of pregnancy: n=141 (11.7%) Unvaccinated: n=1,066 (88.3%) |
The aRR was 0.33 (95% CI: 0.04 to 2.73) |
Level II-2 |
Good |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Congenital anomalies identified at birth |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 84 Country: Follow up: Funding: |
Pregnant persons (n=77,366) IIV3 during the first trimester of pregnancy: n=447 (0.6%) Unvaccinated during the first trimester of pregnancy: n=76,919 (99.4) |
The OR was 0.67 (95% CI: 0.36 to 1.25) |
Level II-2 |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Congenital anomalies identified at birth |
IIV3 (Seasonal influenza vaccine) |
Prospective cohort studyFootnote 64 Country: Follow up: Funding: |
Pregnant persons (n=2,826) IIV3 during the first trimester of pregnancy: n=1,121 (39.7%) Unvaccinated: n=1,705 (60.3%) |
Single cohort study reported no significant difference between infants born to gestational parent vaccinated with IIV3 in the first trimester (33/1,121) and unvaccinated gestational parents (55/1,705); p=0.67 |
Level II-2 |
Fair |
Robinson C, Oberye J, van Boxmeer J, et al. A Prospective Cohort Study on Pregnancy Outcomes of Persons Immunized with a Seasonal Quadrivalent Inactivated Influenza Vaccine during Pregnancy. Vaccines. 2022Footnote 68 Funded by Seqirus Inc |
Congenital anomalies identified at birth |
IIV4 (Afluria® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4 at any time during pregnancy (n=483) Trimester of exposure: |
2 (1.2%) cases of major congenital malformation were identified among infant born to parent that received IIV4 vaccine during the first trimester of pregnancy |
Level III |
Fair |
Robinson C, Van Boxmeer J, Tilson H, et al. Outcomes in Pregnant Persons Immunized with a Cell-Based Quadrivalent Inactivated Influenza Vaccine: A Prospective Observational Cohort Study. Vaccines. 2022Footnote 18 Funded by Seqirus Inc |
Congenital anomalies identified at birth |
IIV4-cc (Flucelvax® Quadrivalent, Seqirus) |
Single-arm prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated with IIV4-cc at any time during pregnancy (n=665) Trimester of exposure: |
One live-born infant (0.6%) with major congenital malformation was born to an individual that received IIV4-cc during the first trimester of pregnancy and the reported birth defect had a known cause other than exposure to the study vaccine |
Level III |
Fair |
Wolfe D, Garritty C, Hamel C, et al. Safety and effectiveness of influenza vaccine during pregnancy – a systematic review. 2022Footnote 18 Funded by the CIHR and the DSEN |
Congenital anomalies identified from birth up to 6 months of age |
IIV (Seasonal influenza vaccine) |
Retrospective case-control studyFootnote 98 Country: Follow up: Funding: |
Pregnant persons (n=4,277) IIV during the first trimester of pregnancy: n=711 (16.6%) Unvaccinated: n=3,566 (83.4%) |
The aOR was 1.01 (95% CI: 0.85 to 1.21) |
Level II-2 |
Fair |
Romano CJ, Hall C, Khodr ZG, et al. History of pandemic H1N1-containing influenza vaccination and risk of spontaneous abortion and birth defects. 2021Footnote 66 Funding: Defense Health Agency Immunization Healthcare Division and the U.S. Navy Bureau of Medicine and Surgery |
Congenital anomalies identified from birth up to 6 months of age |
IIV3 (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Pregnant individuals 17 years and older (n=26,264) Exposed to a pH1N1-containing vaccine in the season prior to pregnancy: n=21,736 (82.8%) Exposed to non-pH1N1-containing vaccine in the season prior to pregnancy: n=4,528 (17.2%) |
The aHR was 1.05 (95% CI: 0.83 to 1.34) |
Level II-2 |
Good |
Sarna M, Pereira GF, Foo D et al. The risk of major structural birth defects associated with seasonal influenza vaccination during pregnancy: a population-based cohort studyFootnote 99 Funded by Curtin University of Technology; National Health and Medical Research Council; Norges Forskningsrad; Telethon Kids Institute, Department of Health |
Congenital anomalies identified from birth up to 6 months of age |
IIV (Seasonal influenza vaccine) |
Retrospective cohort study Country: Follow up: Funding: |
Pregnant persons (113,936) IIV during the first trimester of pregnancy: n=2,811 (2.5%) Unvaccinated: n=111,125 (97.5%) |
Weighted prevalence ratio up to one month of birth was 0.98 (95% CI: 0.68 to 1.43) |
Level II-2 |
Good |
Nwoji U. Seasonal influenza vaccine exposure in pregnancy: 5-year results from a pregnancy registry. Hum Vaccin Immunother. 2022Footnote 67 Funded by GlaxoSmithKline Biologicals SA |
Congenital anomalies identified from birth up to 6 months of age |
IIV3 (Fluarix and FluLaval, GSK) or IIV4 (Fluarix Quadrivalent and FluLaval Quadrivalent, GSK) |
Prospective cohort study Country: Follow up: Funding: |
Individuals vaccinated during pregnancy or within 28 days preceding conception (n=507) Trimester of exposure, n (%): Lost to follow up: n=359 (70.8%) |
Among those with known pregnancy outcome (n=115), 3 (2.6%) events were deemed unlikely to be causally associated with IIV and one (0.9%) event had insufficient information to assess causality |
Level III |
Poor Reporting bias High rate of loss to follow up (70.8%) |
Ledlie S, Gandhi-Banga S, Shrestha et al. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. 2022Footnote 60 Funded by Sanofi |
Congenital anomalies identified from birth up to 6 months of age |
IIV4 (Fluzone® Quadrivalent; Sanofi) |
Retrospective and prospective case series, multicenters Countries: Follow up: Between 2013/08 and 2019/09 Funding: |
Individuals of reproductive age who were exposed to IIV4 during pregnancy or within 30 days of their last menstrual period (n=239) Trimester of exposure, n (%): |
One event was reported among those vaccinated during the first trimester of pregnancy with known neonatal outcomes |
Level III |
Poor Reporting bias High rate of loss to follow up (80%) |
Abbreviation: |
|||||||
| Level | Description |
|---|---|
| I | A randomized controlled trial. |
| II-1 | A controlled trial without randomization. |
| II-2 | A cohort or case-control analytic studies, preferably from more than one centre or research group using clinical outcome measures of vaccine efficacy. |
| II-3 | A multiple time series with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin treatment in the 1940s) could also be regarded as this type of evidence. |
| III | Clinical experience, descriptive study or case report, or report of expert committees. |
| Quality rating | Description |
|---|---|
| Good | A study (including meta-analyses or systematic reviews) that meets all design- specific criteriaTable 3 Footnote a well. |
| Fair | A study (including meta-analyses or systematic reviews) that does not meet (or it is not clear that it meets) at least one design-specific criterion* but has no known "fatal flaw". |
| Poor | A study (including meta-analyses or systematic reviews) that has at least one design-specificTable 3 Footnote a "fatal flaw", or an accumulation of lesser flaws to the extent that the results of the study are not deemed able to inform recommendations. |
|
|
| Strong | Discretionary | |
|---|---|---|
| Wording | "should/should not be offered" | "may/may not be offered" |
| Rationale | Known/anticipated advantages outweigh known/anticipated disadvantages ("should"), or Known/Anticipated disadvantages outweigh known/anticipated advantages ("should not") |
Known/anticipated advantages are closely balanced with known/anticipated disadvantages, or uncertainty in the evidence of advantages and disadvantages exists |
| Implications | A strong recommendation applies to most populations/individuals and should be followed unless a clear and compelling rationale for an alternative approach is present. | A discretionary recommendation may be offered for some populations/individuals in some circumstances. Alternative approaches may be reasonable. |
List of abbreviations
- AE
- Adverse event
- aHR
- Adjusted hazard ratio
- aOR
- Adjusted odds ratio
- aRR
- Adjusted risk ratio
- aVE
- Adjusted vaccine effectiveness
- CI
- Confidence interval
- CIG
- Canadian Immunization Guide
- CIHR
- Canadian Institutes of Health Research
- CNICS
- Childhood National Immunization Coverage Survey
- DSEN
- Drug Safety and Effectiveness Network
- EEFA
- Ethics, equity, feasibility, and acceptability
- FDA
- Food and Drug Administration (United States)
- GRADE
- Grading of Recommendations, Assessment, Development, and Evaluation
- HA
- Hemagglutinin
- HI
- Hemagglutination inhibition
- HR
- Hazard ratio
- ICU
- Intensive care unit
- IIV
- Inactivated influenza vaccine
- IIV3
- Trivalent inactivated influenza vaccine
- IIV4
- Quadrivalent inactivated influenza vaccine
- IIV4-cc
- Cell-culture based quadrivalent inactivated influenza vaccine
- IIV4-SD
- Standard-dose quadrivalent inactivated influenza vaccine
- IIV-Adj
- Adjuvanted inactivated influenza vaccine
- IIV-HD
- High-dose inactivated influenza vaccine
- IIV-SD
- Standard-dose inactivated influenza vaccine
- ILI
- Influenza-like illness
- IM
- Intramuscular
- IRR
- Incidence rate ratio
- IWG
- Influenza Working Group
- LAIV
- Live attenuated influenza vaccine (egg based)
- LBW
- Low birthweight
- LCI
- Laboratory-confirmed influenza
- MA
- Meta-analysis
- NA
- Neuraminidase
- NACI
- National Advisory Committee on Immunization
- NOC
- Notice of Compliance
- NOS
- Newcastle Ottawa Scale
- OR
- Odds ratio
- PHAC
- Public Health Agency of Canada
- RCT
- Randomized controlled trial
- RIV
- Recombinant influenza vaccine
- RIV4
- Quadrivalent recombinant influenza vaccine
- RoB
- Risk of bias
- RR
- Risk ratio
- RT-PCR
- Reverse transcription polymerase chain reaction
- rVE
- Relative vaccine efficacy
- SAB
- Spontaneous abortion
- SAE
- Serious Adverse Event
- SGA
- Small for Gestational Age
- SR
- Systematic Review
- SVP
- Canadian Survey on Vaccination During Pregnancy Study
- Tdap
- Tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis
- US
- United States
- VAERS
- Vaccine Adverse Event Reporting System (US)
- VE
- Vaccine effectiveness
- WHO
- World Health Organization
Acknowledgements
This statement was prepared by: P Doyon-Plourde, A Sinilaite, W Siu and J Papenburg, on behalf of the NACI Influenza Working Group and was approved by NACI.
NACI gratefully acknowledges the contribution of: F Crane, R Garno, A Gil, K Gusic, SH Lim, B Pe Benito, S Pierre, C Tremblay, R Yorke, M Tunis, C Williams, and M Xi.
NACI Influenza Working Group
Members: J Papenburg (Chair), P De Wals, D Fell, I Gemmill, R Harrison, J Langley, A McGeer, and D Moore.
Former members: D Fell
Liaison representatives: L Grohskopf (Centers for Disease Control and Prevention [CDC], United States).
Ex-officio representatives: L Lee (Centre for Immunization and Respiratory Infectious Diseases [CIRID], PHAC), K Daly (First Nations and Inuit Health Branch [FNIHB], Indigenous Services Canada [ISC]), B Warshawsky (Vice President's Office, Infectious Disease Prevention and Control Branch [IDPCB]), and M Russell (Biologics and Genetic Therapies Directorate [BGTD], Health Canada [HC]).
External experts (topic of pregnancy and breastfeeding): T Bogler, I Boucoiran, K Campbell, E Castillo, and D Money.
NACI
S Deeks (Chair), R Harrison (Vice-Chair), M Andrew, J Bettinger, N Brousseau, H Decaluwe, P De Wals, E Dubé, V Dubey, K Hildebrand, K Klein, M O'Driscoll, J Papenburg, A Pham-Huy, B Sander, and S Wilson.
Liaison Representatives: L Bill/M Nowgesic (Canadian Indigenous Nurses Association), LM Bucci (Canadian Public Health Association), S Buchan (Canadian Association for Immunization Research and Evaluation), E Castillo (Society of Obstetricians and Gynaecologists of Canada), J Comeau (Association of Medical Microbiology and Infectious Disease Canada), M Lavoie (Council of Chief Medical Officers of Health), J MacNeil (Centers for Disease Control and Prevention, United States), D Moore (Canadian Paediatric Society), M Naus (Canadian Immunization Committee), M Osmack (Indigenous Physicians Association of Canada), J Potter (College of Family Physicians of Canada), and A Ung (Canadian Pharmacists Association).
Former Liaison Representatives: N Dayneka, and J Emili
Ex-Officio Representatives: V Beswick-Escanlar (National Defence and the Canadian Armed Forces), E Henry (Centre for Immunization and Respiratory Infectious Diseases [CIRID], Public Health Agency of Canada [PHAC]), M Lacroix (Public Health Ethics Consultative Group, PHAC), P Fandja (Marketed Health Products Directorate, Health Canada), M Su (COVID-19 Epidemiology and Surveillance, PHAC), S Ogunnaike-Cooke (CIRID, PHAC), C Pham (Biologic and Radiopharmaceutical Drugs Directorate, Health Canada), M Routledge (National Microbiology Laboratory, PHAC) and T Wong (First Nations and Inuit Health Branch, Indigenous Services Canada).
Appendix A: Review update methods
The methods related to the review update completed by the NACI Secretariat were generally aligned with those used by Wolfe et al. (2020)Footnote 18.
Review questions
The following research questions were addressed:
Research question 1: Are influenza vaccines safe for pregnant persons and their newborn infants if received any time during pregnancy?
Research question 2: Are influenza vaccines effective for preventing influenza and its complications for pregnant persons and their newborn infants if received at any time during pregnancy?
Study eligibility criteria
Eligibility criteria defining studies for inclusions were the same as those used by Wolfe et al. (2020) apart from the inclusion of single-arm cohort studies and studies based on databases of voluntary reporting or surveillance of AEs (Table 5)Footnote 18. These studies were included in the review update completed by the NACI Secretariat to capture evidence on more recently licensed influenza vaccines that are based upon new different technologies, including quadrivalent mammalian cell culture-based vaccines and RIV.
| Inclusion criteria | Exclusion criteria | |
|---|---|---|
| Population | Pregnant women and their unborn and newborn infants under 6 months of age | Women vaccinated preconception or post-partum |
| Interventions | Seasonal and pandemic influenza vaccines of any valency that were indicated for adults | Vaccines contraindicated during pregnancy (e.g., live-attenuated vaccines) |
| Comparators | Placebo, no influenza vaccine, active comparators (e.g., other influenza vaccine, meningococcal or pneumococcal vaccines) | No comparator or vaccines contraindicated during pregnancy |
| Outcomes | Dichotomous measures of the following outcomes: Maternal
Infant
Birth outcomes
|
|
| Study designs | RCTs, prospective and retrospective cohort studies, case-control and test-negative studies, nested designs, single-arm cohort studies, studies based on databases of voluntary reporting or surveillance of adverse events | Systematic reviews, narrative reviews, case reports, abstracts |
| Language | English and French language publications only | Other languages |
Literature search
The updated search strategy was developed in collaboration with librarian from the Health Library of Health Canada and PHAC (search strategy available upon request). Separate strategies were performed for RCTs and observational studies. The RCT search was performed in Ovid MEDLINE® ALL, Embase, and the Cochrane Central Register of Controlled Trials. The observational studies were identified using Ovid MEDLINE® ALL and Embase. All searches were performed on January 13, 2023. Searches were restricted to articles published in English and French. Articles retrieved in the Health Library of Health Canada and PHAC literature searches were loaded into RefWorks (ProQuest LLC, Ann Arbor, MI), and uploaded to DistillerSR (Evidence Partners, Ottawa, Canada).
Study selection process
Two (2) reviewers independently screened titles and abstracts for study eligibility. The full texts of studies identified in the first phase of screening were assessed independently by 2 reviewers for inclusion in the SR. Screening conflicts were resolved by discussion or arbitration by a third reviewer.
Data extraction
A data extraction form was developed for this SR. The extraction process was piloted independently by 2 reviewers to assess quality and consistency of data collection. Data were extracted by one reviewer and verified by a second. Study authors were contacted by email to obtain additional data or confirm data when necessary.
The following data were extracted from each report: study design, population characteristics definition of intervention and comparator, outcome definition, statistical analyses, and key findings.
Risk of bias assessment
Following data extraction, 2 reviewers independently assessed the risk of bias (RoB) at the outcome level using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) or adaptations of the Newcastle-Ottawa Scale (NOS) for cohort and case-control studies as described by Wolfe et al. (2020)Footnote 18. Disagreements were resolved by discussion or arbitration by a third reviewer.
Synthesis and statistical methods
Data were combined with Wolfe et al. (2020) findings by outcome to evaluate the availability of quantitative evidence, as well as the feasibility and appropriateness of meta-analysisFootnote 18.
Meta-analyses were conducted when 2 or more study reported evidence that was not clinically heterogenous as described by Wolfe et al. (2020)Footnote 18. Briefly, random effect models were used, and statistical heterogeneity was assessed using the I2 statistic, with a threshold of 50% or higher suggesting potentially important heterogeneity. Forest plots were used to present meta-analyses. Evidence was summarized narratively when meta-analysis was deemed inappropriate. All analyses were conducted using the Review Manager software (Version 5.4)Footnote 100.
Appendix B: Prisma flow diagram for review update
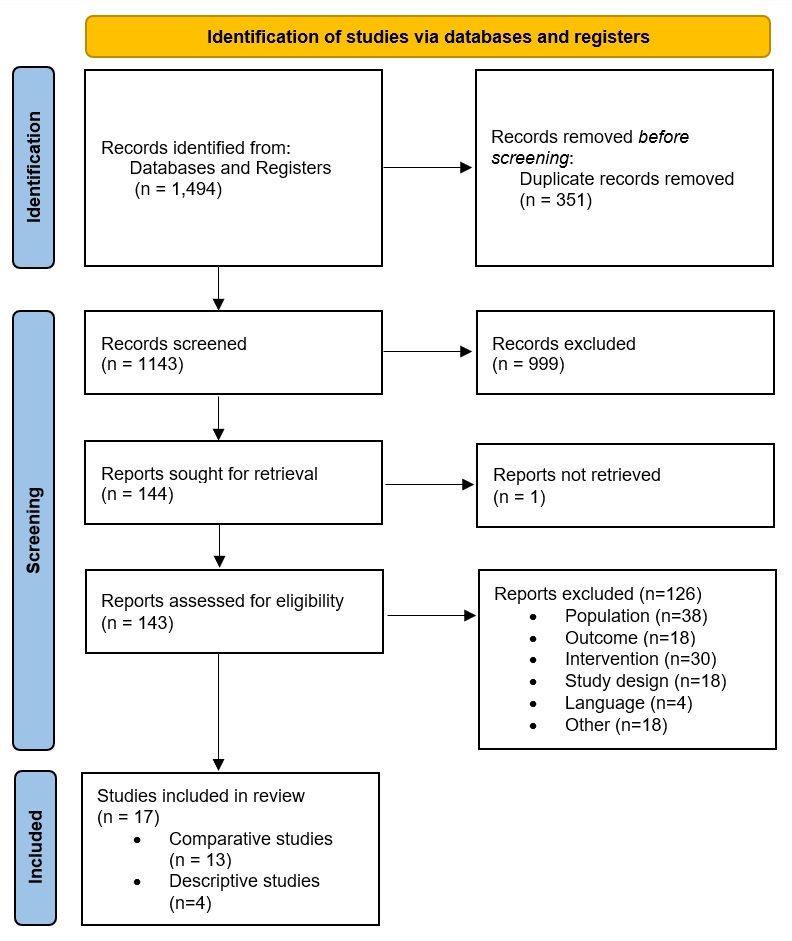
Appendix B: Text description
The PRISMA flow diagram describes the process by which studies or records were identified and selected via databases and registers. The process is broken down into three stages: Identification, Screening and Included.
Stage 1: Identification
- There were 1,494 records identified through database and register searching, 351 duplicate records were removed before screening.
Stage 2: Screening
- 1,143 records were screened. Of these 999 records were excluded, with a remainder of 144 full texts. One full text was not retrieved and was excluded.
- A total of 143 full texts were assessed for eligibility. Of these, 126 articles were excluded. The reasons for their exclusion are as follows: 38 articles did not focus on the relevant population of interest, 18 articles did not report outcomes of interest, 30 articles did not involve relevant interventions, 18 articles were not conducted with the desired study design, 4 articles were in languages that were not accessible for review, and 4 articles were excluded for various other reasons.
Stage 3: Included
- 17 articles were included in the review. Of those, 13 were comparative studies, and 4 were descriptive studies.
References
- Footnote 1
-
National Advisory Committee on Immunization (NACI). Statement on Seasonal Influenza Vaccine for 2023–2024 [Internet]. Ottawa (ON): Public Health Agency of Canada; 2023 May 31 [cited 2023 Aug 16]. Available from: https://www.canada.ca/en/public-health/services/publications/vaccines-immunization/national-advisory-committee-immunization-statement-seasonal-influenza-vaccine-2023-2024.html.
- Footnote 2
-
Schanzer DL, McGeer A, Morris K. Statistical estimates of respiratory admissions attributable to seasonal and pandemic influenza for Canada. Influenza Other Respir Viruses. 2013 Sep;7(5):799-808. https://doi.org/10.1111/irv.12011.
- Footnote 3
-
Schanzer DL, Sevenhuysen C, Winchester B, Mersereau T. Estimating influenza deaths in Canada, 1992-2009. PLoS One. 2013 Nov 27;8(11):e80481. https://doi.org/10.1371/journal.pone.0080481.
- Footnote 4
-
Public Health Agency of Canada. Flu (influenza): For health professionals [Internet]. Ottawa (ON): Government of Canada; 2023 Mar 03 [cited 2023 May 25]. Available from: https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html.
- Footnote 5
-
Influenza (Seasonal) [Internet]. Geneva (CH): World Health Organization; 2023 Jan 12 [cited 2023 May 25]. Available from: https://www.who.int/en/news-room/fact-sheets/detail/influenza-(seasonal).
- Footnote 6
-
Dawood FS, Kittikraisak W, Patel A, Rentz Hunt D, Suntarattiwong P, Wesley MG, et al. Incidence of influenza during pregnancy and association with pregnancy and perinatal outcomes in three middle-income countries: a multisite prospective longitudinal cohort study. The Lancet Infectious Diseases. 2021 Jan;21(1):97-106. https://doi.org/10.1016/S1473-3099(20)30592-2.
- Footnote 7
-
MacDonald NE, McDonald JC. The benefits of influenza vaccine in pregnancy for the fetus and the infant younger than six months of age. Paediatr Child Health. 2014 Nov;19(9):121.
- Footnote 8
-
Rolland-Harris E, Vachon J, Kropp R, Frood J, Morris K, Pelletier L, et al. Hospitalization of pregnant women with pandemic A(H1N1) 2009 influenza in Canada. Epidemiol Infect. 2012 Jul;140(7):1316-27. https://doi.org/10.1017/S0950268811001737.
- Footnote 9
-
Corbeau M, Mulliez A, Chenaf C, Eschalier B, Lesens O, Vorilhon P. Trends of influenza vaccination coverage in pregnant women: a ten-year analysis from a French healthcare database. Sci Rep. 2022 May 03;12(1):7153. https://doi.org/10.1038/s41598-022-11308-3.
- Footnote 10
-
Woodcock T, Novov V, Skirrow H, Butler J, Lovett D, Adeleke Y, et al. Characteristics associated with influenza vaccination uptake in pregnancy: a retrospective cohort study. Br J Gen Pract. 2023 Jan 26;73(727):e148-55. https://doi.org/10.3399/BJGP.2022.0078.
- Footnote 11
-
Arnold LD, Luong L, Rebmann T, Chang JJ. Racial disparities in U.S. maternal influenza vaccine uptake: Results from analysis of Pregnancy Risk Assessment Monitoring System (PRAMS) data, 2012-2015. Vaccine. 2019 Apr 24;37(18):2520-6. https://doi.org/10.1016/j.vaccine.2019.02.014.
- Footnote 12
-
Donahue JG, Kieke BA, King JP, DeStefano F, Mascola MA, Irving SA, et al. Association of spontaneous abortion with receipt of inactivated influenza vaccine containing H1N1pdm09 in 2010-11 and 2011-12. Vaccine. 2017 Sep 25;35(40):5314-22. https://doi.org/10.1016/j.vaccine.2017.06.069.
- Footnote 13
-
Minozzi S, Lytras T, Gianola S, Gonzalez-Lorenzo M, Castellini G, Galli C, et al. Comparative efficacy, and safety of vaccines to prevent seasonal influenza: A systematic review and network meta-analysis. eClinicalMedicine. 2022 Mar 24;46:101331. https://doi.org/10.1016/j.eclinm.2022.101331.
- Footnote 14
-
Hansen KP, Benn CS, Aamand T, Buus M, da Silva I, Aaby P, et al. Does Influenza Vaccination during Pregnancy Have Effects on Non-Influenza Infectious Morbidity? A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Vaccines. 2021 Dec 08;9(12):1452. https://doi.org/10.3390/vaccines9121452.
- Footnote 15
-
Jarvis JR, Dorey RB, Warricker FDM, Alwan NA, Jones CE. The effectiveness of influenza vaccination in pregnancy in relation to child health outcomes: Systematic review and meta-analysis. Vaccine. 2020 Feb 11;38(7):1601-13. https://doi.org/10.1016/j.vaccine.2019.12.056.
- Footnote 16
-
Quach THT, Mallis NA, Cordero JF. Influenza Vaccine Efficacy and Effectiveness in Pregnant Women: Systematic Review and Meta-analysis. Matern Child Health J. 2020 Feb;24(2):229-40. https://doi.org/10.1007/s10995-019-02844-y.
- Footnote 17
-
National Advisory Committee on Immunization (NACI). National Advisory Committee on Immunization (NACI): Guidelines for the economic evaluation of vaccination programs in Canada [Internet]. Ottawa (ON): Public Health Agency of Canada; 2023 Aug 02 [cited 2023 Aug 19]. Available from: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/methods-process/incorporating-economic-evidence-federal-vaccine-recommendations/guidelines-evaluation-vaccination-programs-canada.html.
- Footnote 18
-
Wolfe D, Garritty C, Hamel C, Thavorn K, Skidmore B, Fell D, et al. Safety and effectiveness of influenza vaccine during pregnancy—a systematic review. OSF. 2022 Jun 30. https://doi.org/10.17605/OSF.IO/XEY2K.
- Footnote 19
-
Ismail SJ, Hardy K, Tunis MC, Young K, Sicard N, Quach C. A framework for the systematic consideration of ethics, equity, feasibility, and acceptability in vaccine program recommendations. Vaccine. 2020 Aug 10;38(36):5861,5876. doi: 10.1016/j.vaccine.2020.05.051. https://doi.org/S0264-410X(20)30696-4.
- Footnote 20
-
Meijer WJ, van Noortwijk AGA, Bruinse HW, Wensing AMJ. Influenza virus infection in pregnancy: a review. Acta obstetricia et gynecologica Scandinavica. 2015 Aug;94(8):797-819. https://doi.org/10.1111/aogs.12680.
- Footnote 21
-
Mertz D, Geraci J, Winkup J, Gessner BD, Ortiz JR, Loeb M. Pregnancy as a risk factor for severe outcomes from influenza virus infection: A systematic review and meta-analysis of observational studies. Vaccine. 2017 Jan 23;35(4):521-8. https://doi.org/10.1016/j.vaccine.2016.12.012.
- Footnote 22
-
Mertz D, Lo CK, Lytvyn L, Ortiz JR, Loeb M. Pregnancy as a risk factor for severe influenza infection: an individual participant data meta-analysis. BMC Infectious Diseases. 2019 Aug 02;19(1):683. https://doi.org/10.1186/s12879-019-4318-3.
- Footnote 23
-
Ohfuji S, Deguchi M, Tachibana D, Koyama M, Takagi T, Yoshioka T, et al. Estimating influenza disease burden among pregnant women: Application of self-control method. Vaccine. 2017 Aug 24;35(36):4811-6. https://doi.org/10.1016/j.vaccine.2017.07.006.
- Footnote 24
-
Sullivan SG, Price OH, Regan AK. Burden, effectiveness, and safety of influenza vaccines in elderly, paediatric and pregnant populations. Therapeutic Advances in Vaccines and Immunotherapy. 2019 Feb 07;7:2515135519826481. https://doi.org/10.1177/2515135519826481.
- Footnote 25
-
Mosby LG, BA, Rasmussen, Sonja A., MD, MS, Jamieson, Denise J., MD, MPH. 2009 pandemic influenza A (H1N1) in pregnancy: a systematic review of the literature. American journal of obstetrics and gynecology. 2011 Jul 01;205(1):10-8. https://doi.org/10.1016/j.ajog.2010.12.033.
- Footnote 26
-
Wang R, Yan W, Du M, Tao L, Liu J. The effect of influenza virus infection on pregnancy outcomes: A systematic review and meta-analysis of cohort studies. International Journal of Infectious Diseases. 2021 Apr;105:567-78. https://doi.org/10.1016/j.ijid.2021.02.095.
- Footnote 27
-
Regan AK, Moore HC, Sullivan SG, De Klerk N, Effler PV. Epidemiology of seasonal influenza infection in pregnant women and its impact on birth outcomes. Epidemiology and infection. 2017 Oct 01;145(14):2930-9. https://doi.org/10.1017/S0950268817001972.
- Footnote 28
-
Fell D, Savitz D, Kramer M, Gessner B, Katz M, Knight M, et al. Maternal influenza, and birth outcomes: systematic review of comparative studies. BJOG: an international journal of obstetrics and gynaecology. 2017 Jan;124(1):48-59. https://doi.org/10.1111/1471-0528.14143.
- Footnote 29
-
Chaves SS, Perez A, Farley MM, Miller L, Schaffner W, Lindegren ML, et al. The Burden of Influenza Hospitalizations in Infants From 2003 to 2012, United States. Pediatr Infect Dis J. 2014 Sep;33(9):912-9. https://doi.org/10.1097/INF.0000000000000321.
- Footnote 30
-
Shi T, McLean K, Campbell H, Nair H. Aetiological role of common respiratory viruses in acute lower respiratory infections in children under five years: A systematic review and meta–analysis. Journal of Global Health. 2015 Jun;5(1):010408. https://doi.org/10.7189/jogh.05.010408.
- Footnote 31
-
Lafond KE, Nair H, Rasooly MH, Valente F, Booy R, Rahman M, et al. Global Role and Burden of Influenza in Pediatric Respiratory Hospitalizations, 1982-2012: A Systematic Analysis. PLoS medicine. 2016 Mar 24;13(3):e1001977. https://doi.org/10.1371/journal.pmed.1001977.
- Footnote 32
-
Wang X, Li Y, O'Brien KL, Madhi SA, Widdowson M, Byass P, et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: a systematic review and modelling study. Lancet Glob Health. 2020 Apr;8(4):e497-510. https://doi.org/10.1016/S2214-109X(19)30545-5.
- Footnote 33
-
Schober T, Morris SK, Bettinger JA, Bancej C, Burton C, Foo C, et al. Outcomes of immunocompromised children hospitalized for Influenza, 2010-2021, the Canadian Immunization Monitoring Program Active (IMPACT). Clinical microbiology and infection. 2023 Jul;29(7):924-32. https://doi.org/10.1016/j.cmi.2023.04.001.
- Footnote 34
-
Shang M, Blanton L, Brammer L, Olsen SJ, Fry AM. Influenza-Associated Pediatric Deaths in the United States, 2010-2016. Pediatrics. 2018 Apr;141(4):e20172918. https://doi.org/10.1542/peds.2017-2918.
- Footnote 35
-
Fell DB, Johnson J, Mor Z, Katz MA, Skidmore B, Neuzil KM, et al. Incidence of laboratory-confirmed influenza disease among infants under 6 months of age: a systematic review. BMJ Open. 2017 Sep 01;7(9):e016526. https://doi.org/10.1136/bmjopen-2017-016526.
- Footnote 36
-
Public Health Agency of Canada. Results of the Survey on Vaccination during Pregnancy 2021 [Internet]. Ottawa (ON): Government of Canada; 2022 Dec 13 [cited 2022 May 25]. Available from: https://www.canada.ca/en/public-health/services/publications/vaccines-immunization/survey-vaccination-during-pregnancy-2021.html.
- Footnote 37
-
Regan AK, Tracey LE, Blyth CC, Richmond PC, Effler PV. A prospective cohort study assessing the reactogenicity of pertussis and influenza vaccines administered during pregnancy. Vaccine. 2016 Apr 29;34(20):2299-304. https://doi.org/10.1016/j.vaccine.2016.03.084.
- Footnote 38
-
Sukumaran L, McCarthy NL, Kharbanda EO, Weintraub ES, Vazquez-Benitez G, McNeil MM, et al. Safety of Tetanus Toxoid, Reduced Diphtheria Toxoid, and Acellular Pertussis and Influenza Vaccinations in Pregnancy. Obstet Gynecol. 2015 Nov;126(5):1069-74. https://doi.org/10.1097/AOG.0000000000001066.
- Footnote 39
-
Petousis-Harris H, Walls T, Watson D, Paynter J, Graham P, Turner N. Safety of Tdap vaccine in pregnant women: an observational study. BMJ Open. 2016 Apr 18;6(4):e010911. https://doi.org/10.1136/bmjopen-2015-010911.
- Footnote 40
-
Steinhoff MC, Katz J, Englund JA, Khatry SK, Shrestha L, Kuypers J, et al. Year-round influenza immunisation during pregnancy in Nepal: a phase 4, randomised, placebo-controlled trial. Lancet Infect Dis. 2017 Sep;17(9):981-9. https://doi.org/10.1016/S1473-3099(17)30252-9.
- Footnote 41
-
Madhi SA, Cutland CL, Kuwanda L, Weinberg A, Hugo A, Jones S, et al. Influenza vaccination of pregnant women and protection of their infants. N Engl J Med. 2014 Sep 04;371(10):918-31. https://doi.org/10.1056/NEJMoa1401480.
- Footnote 42
-
Tapia MD, Sow SO, Tamboura B, Tégueté I, Pasetti MF, Kodio M, et al. Maternal immunisation with trivalent inactivated influenza vaccine for prevention of influenza in infants in Mali: a prospective, active-controlled, observer-blind, randomised phase 4 trial. Lancet Infect Dis. 2016 Sep;16(9):1026-35. https://doi.org/10.1016/S1473-3099(16)30054-8.
- Footnote 43
-
Zaman K, Roy E, Arifeen SE, Rahman M, Raqib R, Wilson E, et al. Effectiveness of maternal influenza immunization in mothers and infants. N Engl J Med. 2008 Oct 09;359(15):1555-64. https://doi.org/10.1056/NEJMoa0708630.
- Footnote 44
-
Thompson MG, Kwong JC, Regan AK, Katz MA, Drews SJ, Azziz-Baumgartner E, et al. Influenza Vaccine Effectiveness in Preventing Influenza-associated Hospitalizations During Pregnancy: A Multi-country Retrospective Test Negative Design Study, 2010-2016. Clin Infect Dis. 2019 Apr 24;68(9):1444-53. https://doi.org/10.1093/cid/ciy737.
- Footnote 45
-
Benowitz I, Esposito DB, Gracey KD, Shapiro ED, Vázquez M. Influenza vaccine given to pregnant women reduces hospitalization due to influenza in their infants. Clin Infect Dis. 2010 Dec 15;51(12):1355-61. https://doi.org/10.1086/657309.
- Footnote 46
-
Maltezou HC, Stavros S, Asimakopoulos G, Pergialiotis V, Raftopoulos V, Talias MA, et al. Effectiveness of maternal vaccination with quadrivalent inactivated influenza vaccine in pregnant women and their infants in 2019-2020. Expert Rev Vaccines. 2022 Jul;21(7):983-92. https://doi.org/10.1080/14760584.2022.2013820.
- Footnote 47
-
Nunes MC, Walaza S, Meiring S, Zar HJ, Reubenson G, McMorrow M, et al. Effectiveness of Influenza Vaccination of Pregnant Women for Prevention of Maternal and Early Infant Influenza-Associated Hospitalizations in South Africa: A Prospective Test-Negative Study. Open Forum Infect Dis. 2022 Oct 19;9(11):ofac552. https://doi.org/10.1093/ofid/ofac552.
- Footnote 48
-
Vousden N, Bunch K, Knight M. Incidence, risk factors and impact of seasonal influenza in pregnancy: A national cohort study. PLoS One. 2021 Jan 15;16(1):e0244986. https://doi.org/10.1371/journal.pone.0244986.
- Footnote 49
-
Foo D, Sarna M, Pereira G, Moore HC, Regan AK. Longitudinal, population-based cohort study of prenatal influenza vaccination and influenza infection in childhood. Vaccine. 2022 Jan 28;40(4):656-65. https://doi.org/10.1016/j.vaccine.2021.11.084.
- Footnote 50
-
Rowe SL, Leder K, Perrett KP, Romero N, Nolan TM, Stephens N, et al. Maternal Vaccination and Infant Influenza and Pertussis. Pediatrics. 2021 Sep;148(3):e2021051076. https://doi.org/10.1542/peds.2021-051076.
- Footnote 51
-
McRae J, Blyth CC, Cheng AC, Quinn HE, Wood N, Macartney KK. Preventing severe influenza in Australian infants: Maternal influenza vaccine effectiveness in the PAEDS-FluCAN networks using the test-negative design. Vaccine. 2022 Apr 26;40(19):2761-71. https://doi.org/10.1016/j.vaccine.2022.03.042.
- Footnote 52
-
Drăgănescu AC, Miron VD, Streinu-Cercel A, Florea D, Vlaicu O, Bilaşco A, et al. Circulation of influenza A viruses among patients hospitalized for severe acute respiratory infection in a tertiary care hospital in Romania in the 2018/19 season: Results from an observational descriptive epidemiological study. Medicine (Baltimore). 2021 Dec 30;100(52):e28460. https://doi.org/10.1097/MD.0000000000028460.
- Footnote 53
-
Nunes MC, Cutland CL, Jones S, Hugo A, Madimabe R, Simões EAF, et al. Duration of Infant Protection Against Influenza Illness Conferred by Maternal Immunization: Secondary Analysis of a Randomized Clinical Trial. JAMA Pediatr. 2016 Sep 01;170(9):840-7. https://doi.org/10.1001/jamapediatrics.2016.0921.
- Footnote 54
-
Munoz FM, Greisinger AJ, Wehmanen OA, Mouzoon ME, Hoyle JC, Smith FA, et al. Safety of influenza vaccination during pregnancy. Am J Obstet Gynecol. 2005 Apr;192(4):1098-106. https://doi.org/10.1016/j.ajog.2004.12.019.
- Footnote 55
-
Betancourt-Cravioto M, Cervantes-Powell P, Tapia-Conyer R, Ledlie S, Gandhi-Banga S. Improved post-marketing safety surveillance of quadrivalent inactivated influenza vaccine in Mexico using a computerized, SMS-based follow-up system. Hum Vaccin Immunother. 2022 Dec 31;18(1):1935170. https://doi.org/10.1080/21645515.2021.1935170.
- Footnote 56
-
Carreras JJ, Lluch JA, Taboada JA, Pastor-Villalba E, Nartallo-Penas V, Díez-Domingo J. Adverse events in pregnant women with the tetravalent influenza vaccine obtained from cell cultures. Enferm Infecc Microbiol Clin (Engl Ed). 2022 Nov 28:S2529-4. https://doi.org/10.1016/j.eimce.2022.11.005.
- Footnote 57
-
Vanni T, Thomé BdC, Oliveira MMMd, Gattás VL, Salomão MdG, Koike ME, et al. Active pharmacovigilance of the seasonal trivalent influenza vaccine produced by Instituto Butantan: A prospective cohort study of five target groups. PLoS One. 2021 Feb 11;16(2):e0246540. https://doi.org/10.1371/journal.pone.0246540.
- Footnote 58
-
Singh M, Tanvir T, Nagoji D, Madan A, Gattem S, Singh H. Influenza vaccine: A viable option to protect pregnant women and infants from seasonal flu: A retrospective hospital-based study in India. Int J Clin Pract. 2019 Jul;73(7):e13361. https://doi.org/10.1111/ijcp.13361.
- Footnote 59
-
Nordin JD, Kharbanda EO, Benitez GV, Nichol K, Lipkind H, Naleway A, et al. Maternal safety of trivalent inactivated influenza vaccine in pregnant women. Obstet Gynecol. 2013 Mar;121(3):519-25. https://doi.org/10.1097/AOG.0b013e3182831b83.
- Footnote 60
-
Ledlie S, Gandhi-Banga S, Shrestha A, Mallett Moore T, Khromava A. Exposure to quadrivalent influenza vaccine during pregnancy: Results from a global pregnancy registry. Influenza Other Respir Viruses. 2022 Jan;16(1):90-100. https://doi.org/10.1111/irv.12897.
- Footnote 61
-
Sugimura T, Nagai T, Kobayashi H, Ozaki Y, Yamakawa R, Hirata R. Effectiveness of maternal influenza immunization in young infants in Japan. Pediatr Int. 2016 Aug;58(8):709-13. https://doi.org/10.1111/ped.12888.
- Footnote 62
-
Chambers CD, Johnson DL, Xu R, Luo YJ, Louik C, Mitchell AA, et al. Safety of the 2010-11, 2011-12, 2012-13, and 2013-14 seasonal influenza vaccines in pregnancy: Birth defects, spontaneous abortion, preterm delivery, and small for gestational age infants, a study from the cohort arm of VAMPSS. Vaccine. 2016 Aug 17;34(37):4443-9. https://doi.org/10.1016/j.vaccine.2016.06.054.
- Footnote 63
-
Mohammed H, Roberts CT, Grzeskowiak LE, Giles LC, Dekker GA, Marshall HS. Safety and protective effects of maternal influenza vaccination on pregnancy and birth outcomes: A prospective cohort study. EClinicalMedicine. 2020 Sep 09;26:100522. https://doi.org/10.1016/j.eclinm.2020.100522.
- Footnote 64
-
Ohfuji S, Deguchi M, Tachibana D, Koyama M, Takagi T, Yoshioka T, et al. Safety of influenza vaccination on adverse birth outcomes among pregnant women: A prospective cohort study in Japan. Int J Infect Dis. 2020 Apr;93:68-76. https://doi.org/10.1016/j.ijid.2020.01.033.
- Footnote 65
-
Donahue JG, Kieke BA, King JP, Mascola MA, Shimabukuro TT, DeStefano F, et al. Inactivated influenza vaccine and spontaneous abortion in the Vaccine Safety Datalink in 2012-13, 2013-14, and 2014-15. Vaccine. 2019 Oct 16;37(44):6673-81. https://doi.org/10.1016/j.vaccine.2019.09.035.
- Footnote 66
-
Romano CJ, Hall C, Khodr ZG, Bukowinski AT, Gumbs GR, Conlin AMS. History of pandemic H1N1-containing influenza vaccination and risk for spontaneous abortion and birth defects. Vaccine. 2021 Oct 22;39(44):6553-62. https://doi.org/10.1016/j.vaccine.2021.09.003.
- Footnote 67
-
Nwoji U. Seasonal influenza vaccine exposure in pregnancy: 5-year results from a pregnancy registry. Hum Vaccin Immunother. 2022 Dec 31;18(1):1932213. https://doi.org/10.1080/21645515.2021.1932213.
- Footnote 68
-
Robinson C, Oberye J, van Boxmeer J, Albano JD, Tilson H, Scialli A, et al. A Prospective Cohort Study on Pregnancy Outcomes of Persons Immunized with a Seasonal Quadrivalent Inactivated Influenza Vaccine during Pregnancy. Vaccines (Basel). 2022 Sep 21;10(10):1577. https://doi.org/10.3390/vaccines10101577.
- Footnote 69
-
Robinson C, Van Boxmeer J, Tilson H, Scialli A, Vanchiere JA, Ides E, et al. Outcomes in Pregnant Persons Immunized with a Cell-Based Quadrivalent Inactivated Influenza Vaccine: A Prospective Observational Cohort Study. Vaccines (Basel). 2022 Sep 23;10(10):1600. https://doi.org/10.3390/vaccines10101600.
- Footnote 70
-
Kilich E, Dada S, Francis MR, Tazare J, Chico RM, Paterson P, et al. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PloS one. 2020 Jul 09;15(7):e0234827. https://doi.org/10.1371/journal.pone.0234827.
- Footnote 71
-
Adeyanju GC, Engel E, Koch L, Ranzinger T, Shahid IBM, Head MG, et al. Determinants of influenza vaccine hesitancy among pregnant women in Europe: a systematic review. Eur J Med Res. 2021 Sep 28;26(1):116. https://doi.org/10.1186/s40001-021-00584-w.
- Footnote 72
-
Gates A, Gates M, Rahman S, Guitard S, MacGregor T, Pillay J, et al. A Systematic Review of Factors that Influence the Acceptability of Vaccines among Canadians. Vaccine. 2021 Jan 08;39(2):222-36. https://doi.org/10.1016/j.vaccine.2020.10.038.
- Footnote 73
-
Yuen CYS, Tarrant M. Determinants of uptake of influenza vaccination among pregnant women - a systematic review. Vaccine. 2014 Aug 06;32(36):4602-13. https://doi.org/10.1016/j.vaccine.2014.06.067.
- Footnote 74
-
Okoli GN, Reddy VK, Al‐Yousif Y, Neilson CJ, Mahmud SM, Abou‐Setta AM. Sociodemographic and health-related determinants of seasonal influenza vaccination in pregnancy: A systematic review and meta-analysis of the evidence since 2000. Acta Obstet Gynecol Scand. 2021 Jan 08;100(6):997-1009. https://doi.org/10.1111/aogs.14079.
- Footnote 75
-
Morales KF, Menning L, Lambach P. The faces of influenza vaccine recommendation: A Literature review of the determinants and barriers to health providers' recommendation of influenza vaccine in pregnancy. Vaccine. 2020 Jun 26;38(31):4805-15. https://doi.org/10.1016/j.vaccine.2020.04.033.
- Footnote 76
-
Frew PM, Randall LA, Malik F, Limaye RJ, Wilson A, O'Leary ST, et al. Clinician perspectives on strategies to improve patient maternal immunization acceptability in obstetrics and gynecology practice settings. Human vaccines and and immunotherapeutics. 2018 Feb 15;14(7):1548-57. https://doi.org/10.1080/21645515.2018.1425116.
- Footnote 77
-
Wong VWY, Lok KYW, Tarrant M. Interventions to increase the uptake of seasonal influenza vaccination among pregnant women: A systematic review. Vaccine. 2016 Jan 02;34(1):20-32. https://doi.org/10.1016/j.vaccine.2015.11.020.
- Footnote 78
-
Qiu X, Bailey H, Thorne C. Barriers and Facilitators Associated With Vaccine Acceptance and Uptake Among Pregnant Women in High Income Countries: A Mini-Review. Frontiers in immunology. 2021 Apr 26;12:626717. https://doi.org/10.3389/fimmu.2021.626717.
- Footnote 79
-
Blanchard-Rohner G, Meier S, Ryser J, Schaller D, Combescure C, Yudin MH, et al. Acceptability of maternal immunization against influenza: the critical role of obstetricians. The journal of maternal-fetal and and neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2012 Mar 16;25(9):1800-9. https://doi.org/10.3109/14767058.2012.663835.
- Footnote 80
-
Alhendyani F, Jolly K, Jones LL. Views, and experiences of maternal healthcare providers regarding influenza vaccine during pregnancy globally: A systematic review and qualitative evidence synthesis. PLOS ONE. 2022 Feb 10;17(2):e0263234. https://doi.org/10.1371/journal.pone.0263234.
- Footnote 81
-
Statistics Canada. Recommended vaccines received during pregnancy, 2021 [Internet]. Ottawa (ON): Government of Canada; 2022 Dec 13 [cited 2023 May 25]. Available from: https://www150.statcan.gc.ca/n1/daily-quotidien/221213/dq221213a-eng.htm.
- Footnote 82
-
Osterholm MT, Kelley NS, Sommer A, Belongia EA. Efficacy, and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet Infect Dis. 2012 Jan;12(1):36-44. https://doi.org/10.1016/S1473-3099(11)70295-X.
- Footnote 83
-
Regan AK, Moore HC, de Klerk N, Omer SB, Shellam G, Mak DB, et al. Seasonal Trivalent Influenza Vaccination During Pregnancy and the Incidence of Stillbirth: Population-Based Retrospective Cohort Study. Clin Infect Dis. 2016 May 15;62(10):1221-7. https://doi.org/10.1093/cid/ciw082.
- Footnote 84
-
Sheffield JS, Greer LG, Rogers VL, Roberts SW, Lytle H, McIntire DD, et al. Effect of influenza vaccination in the first trimester of pregnancy. Obstet Gynecol. 2012 Sep;120(3):532-7. https://doi.org/10.1097/AOG.0b013e318263a278.
- Footnote 85
-
Giles ML, Davey M, Wallace EM. Associations Between Maternal Immunisation and Reduced Rates of Preterm Birth and Stillbirth: A Population Based Retrospective Cohort Study. Front Immunol. 2021 Sep 07;12:704254. https://doi.org/10.3389/fimmu.2021.704254.
- Footnote 86
-
Zerbo O, Modaressi S, Chan B, Goddard K, Lewis N, Bok K, et al. No association between influenza vaccination during pregnancy and adverse birth outcomes. Vaccine. 2017 May 31;35(24):3186-90. https://doi.org/10.1016/j.vaccine.2017.04.074.
- Footnote 87
-
Duque J, Howe AS, Azziz-Baumgartner E, Petousis-Harris H. Multi-decade national cohort identifies adverse pregnancy and birth outcomes associated with acute respiratory illness hospitalisations during the influenza season. Influenza Other Respir Viruses. 2023 Jan;17(1):e13063. https://doi.org/10.1111/irv.13063.
- Footnote 88
-
Dodds L, MacDonald N, Scott J, Spencer A, Allen VM, McNeil S. The association between influenza vaccine in pregnancy and adverse neonatal outcomes. J Obstet Gynaecol Can. 2012 Aug;34(8):714-20. https://doi.org/10.1016/S1701-2163(16)35336-1.
- Footnote 89
-
Legge A, Dodds L, MacDonald NE, Scott J, McNeil S. Rates, and determinants of seasonal influenza vaccination in pregnancy and association with neonatal outcomes. CMAJ. 2014 Mar 04;186(4):157. https://doi.org/10.1503/cmaj.130499.
- Footnote 90
-
Nunes MC, Madhi SA. Influenza vaccination during pregnancy for prevention of influenza confirmed illness in the infants: A systematic review and meta-analysis. Human Vaccines and and Immunotherapeutics. 2018 Mar 04;14(3):758-66. https://doi.org/10.1080/21645515.2017.1345385.
- Footnote 91
-
Nunes MC, Aqil AR, Omer SB, Madhi SA. The Effects of Influenza Vaccination during Pregnancy on Birth Outcomes: A Systematic Review and Meta-Analysis. Am J Perinatol. 2016;33(11):1104-14. https://doi.org/10.1055/s-0036-1586101.
- Footnote 92
-
Foo DYP, Sarna M, Pereira G, Moore HC, Fell DB, Regan AK. Early Childhood Health Outcomes Following In Utero Exposure to Influenza Vaccines: A Systematic Review. Pediatrics. 2020 Aug;146(2):e20200375. https://doi.org/10.1542/peds.2020-0375.
- Footnote 93
-
Giles ML, Krishnaswamy S, Macartney K, Cheng A. The safety of inactivated influenza vaccines in pregnancy for birth outcomes: a systematic review. Hum Vaccin Immunother. 2019;15(3):687-99. https://doi.org/10.1080/21645515.2018.1540807.
- Footnote 94
-
Mehrabadi A, Dodds L, MacDonald NE, Top KA, Benchimol EI, Kwong JC, et al. Association of Maternal Influenza Vaccination During Pregnancy With Early Childhood Health Outcomes. JAMA: the journal of the American Medical Association. 2021 Jun 08;325(22):2285-93. https://doi.org/10.1001/jama.2021.6778.
- Footnote 95
-
Cuningham W, Geard N, Fielding JE, Braat S, Madhi SA, Nunes MC, et al. Optimal timing of influenza vaccine during pregnancy: A systematic review and meta‐analysis. Influenza and Other Respiratory Viruses. 2019 Sep;13(5):438-52. https://doi.org/10.1111/irv.12649.
- Footnote 96
-
Panagiotakopoulos L, McCarthy NL, Tepper NK, Kharbanda EO, Lipkind HS, Vazquez-Benitez G, et al. Evaluating the Association of Stillbirths After Maternal Vaccination in the Vaccine Safety Datalink. Obstet Gynecol. 2020 Dec;136(6):1086-94. https://doi.org/10.1097/AOG.0000000000004166.
- Footnote 97
-
Speake HA, Pereira G, Regan AK. Risk of adverse maternal and foetal outcomes associated with inactivated influenza vaccination in first trimester of pregnancy. Paediatr Perinat Epidemiol. 2021 Mar;35(2):196-205. https://doi.org/10.1111/ppe.12715.
- Footnote 98
-
Louik C, Kerr S, Van Bennekom CM, Chambers C, Jones KL, Schatz M, et al. Safety of the 2011-12, 2012-13, and 2013-14 seasonal influenza vaccines in pregnancy: Preterm delivery and specific malformations, a study from the case-control arm of VAMPSS. Vaccine. 2016 Aug 17;34(37):4450-9. https://doi.org/10.1016/j.vaccine.2016.06.078.
- Footnote 99
-
Sarna M, Pereira GF, Foo D, Baynam GS, Regan AK. The risk of major structural birth defects associated with seasonal influenza vaccination during pregnancy: A population-based cohort study. Birth Defects Res. 2022 Nov 15;114(19):1244-56. https://doi.org/10.1002/bdr2.2049.
- Footnote 100
-
The Cochrane Collaboration. Review Manager (RevMan). 2020;5.4.
Page details
- Date modified: