
National safety monitoring of vaccines from CAEFISS, 2018-2019

 Download this article as a PDF (404 KB)
Download this article as a PDF (404 KB)Published by: The Public Health Agency of Canada
Issue: Volume 50-1/2, January/February 2024: Respiratory Syncytial Virus (RSV)
Date published: January/February 2024
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 50-1/2, January/February 2024: Respiratory Syncytial Virus (RSV)
Surveillance
National safety monitoring of vaccines from the Canadian Adverse Events Following Immunization Surveillance System (CAEFISS), 2018–2019
Maryem El Jaouhari1, Karin Johnson1, Helen Anyoti1, Yuhui Xu1, Charlotte Wells1, Ashley Weeks1, Allison Yeung1, Amanda Shaw1, Susanna Ogunnaike-Cooke1
Affiliation
1 Centre for Immunization Surveillance, Public Health Agency of Canada, Ottawa, ON
Correspondence
Suggested citation
El Jaouhari M, Johnson K, Anyoti H, Xu Y, Wells C, Weeks A, Yeung A, Shaw A, Ogunnaike-Cooke S. National safety monitoring of vaccines from the Canadian Adverse Events Following Immunization Surveillance System (CAEFISS), 2018–2019. Can Commun Dis Rep 2024;50(1/2):49–57. https://doi.org/10.14745/ccdr.v50i12a06
Keywords: vaccine safety, pharmacovigilance, adverse events following immunization
Abstract
Background: The Canadian Adverse Events Following Immunization Surveillance System (CAEFISS) is a comprehensive vaccine safety surveillance system that includes both passive and active surveillance of vaccines administered in Canada. This work presents a summary of adverse events following immunization (AEFI) nationally for 2018 and 2019.
Methods: Data extracted from CAEFISS included all AEFI reports received by the Public Health Agency of Canada by April 30, 2022, for vaccines marketed in Canada and administered between January 1, 2018, and December 31, 2019. Descriptive statistics were conducted on AEFI reports by type of surveillance program (i.e., active vs. passive), AEFIs, demographics, healthcare utilization, outcome, seriousness of adverse events and type of vaccine.
Results: Between 2018 and 2019, 5,875 AEFI reports were received from across Canada. The average annual AEFI reporting rate was 10.9/100,000 doses distributed in Canada for vaccines administered during 2018–2019 and was found to be inversely proportional to age. The majority of reports (91%) were non-serious events, involving vaccination site reactions, rash and allergic events. Overall, there were 511 serious adverse event reports during 2018–2019. Of the serious adverse event reports, the most common primary AEFIs were anaphylaxis followed by seizure. There were no unexpected vaccine safety issues identified or increases in frequency or severity of adverse events.
Conclusion: Canada's continuous monitoring of the safety of marketed vaccines during 2018–2019 did not identify any increase in the frequency or severity of AEFIs, previously unknown AEFIs, or areas that required further investigation or research.
Introduction
Vaccine safety surveillance is essential to detect any emerging issues or changes in the frequency of adverse events following immunization (AEFI). The Public Health Agency of Canada (PHAC) and Health Canada share the monitoring of the safety of vaccines in Canada.
The Canadian Adverse Events Following Immunization Surveillance System (CAEFISS) is a federal, provincial, and territorial (FPT) public health post-market vaccine safety surveillance system Footnote 1. The CAEFISS is managed by PHAC and is unique in that it includes both passive (spontaneous reports from FPTs) and active surveillance. The primary objectives of CAEFISS are to 1) continuously monitor the safety of marketed vaccines in Canada, 2) identify increases in the frequency or severity of previously identified vaccine-related reactions, 3) identify previously unknown AEFIs that could possibly be related to a vaccine, 4) identify areas that require further investigation and/or research and 5) provide timely information on AEFI reporting profiles for vaccines marketed in Canada, which could help inform immunization programs and guidelines Footnote 1.
In Canada, healthcare providers, manufacturers and the public each have a role to play in vaccine pharmacovigilance Footnote 2. Federal, provincial and territorial public health officials monitor vaccine safety through the Vaccine Vigilance Working Group (VVWG) of the Canadian Immunization Committee (CIC). The VVWG includes representatives from all FPT immunization programs across the country as well as Health Canada regulators and the Canadian Immunization Monitoring Program ACTive (IMPACT) surveillance system.
For more information about CAEFISS, IMPACT and VVWG, please refer to the Technical Annex, Supplemental material, for annual vaccine safety reports. In addition, a more comprehensive description of the roles and responsibilities for post-market pharmacovigilance can be found in the Canadian Immunization Guide and on the CAEFISS webpage Footnote 1Footnote 2. Details on provincial and territorial vaccination schedules can be found on the PHAC website Footnote 3. National reports on vaccine safety surveillance data have been published periodically using CAEFISS data Footnote 4Footnote 5Footnote 6Footnote 7Footnote 8Footnote 9Footnote 10Footnote 11Footnote 12Footnote 13Footnote 14Footnote 15.
The objectives of this report are to provide 1) a descriptive analysis of AEFI reports submitted to CAEFISS for vaccines administered in Canada in 2018–2019, 2) a descriptive review of healthcare utilization and outcome following an AEFI and 3) an analysis of serious adverse events (SAEs).
Methods
Definitions
An AEFI is defined as any untoward medical occurrence that follows immunization but that does not necessarily have a causal relationship with the administration of the vaccine. The adverse event may be a sign, symptom or defined illness Footnote 15.
A serious AEFI in CAEFISS is identified based on International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use as an event that results in death, is life-threatening, and requires inpatient hospitalization or prolongation of existing hospitalization, results in persistent or significant disability/incapacity or results in a congenital anomaly/birth defect. Any medical event which may not be immediately life-threatening but requires intervention to prevent one of the outcomes listed above may also be considered as serious Footnote 16.
Data sources
The CAEFISS combines reports from passive and active surveillance. Active surveillance is conducted by IMPACT, a network of 12 tertiary care paediatric hospitals across Canada that screens hospital admissions for specific AEFIs. Passive surveillance is initiated at the local public health level and relies on reporting of AEFIs by healthcare providers, vaccine recipients or their caregivers.
We searched CAEFISS for all AEFI reports received by April 30, 2022, with a date of vaccine administration between January 1, 2018, and December 31, 2019. The AEFI report forms used in Canada collect information on sex, age, vaccine administered, medical history, concomitant medications and adverse events experienced. In addition, historic AEFI reports with a date of vaccine administration between 2008 and 2017 were extracted from CAEFISS to assess trends over time. It should be noted that for one province/territory, not all AEFI reports were included due to technical issues with uploading the information onto the CAEFISS platform. The reports that were not included from this province/territory were of a small enough volume that this issue did not impact our confidence in the results.
Data analysis
Descriptive analyses were conducted for AEFI reports by year, type of surveillance (active vs. passive), primary reason for reporting, seriousness, healthcare utilization and outcome. Rates of AEFI were calculated using dose distributed data where possible. Sex and age-specific AEFI rates were calculated using population estimates as the denominator. Missing data were excluded from the calculations. All reports were medically reviewed and only reports with an outcome of death underwent causality assessment for this report. All analyses were conducted using SAS EG 7.1 and Microsoft Excel 2016.
Technical annex
The Technical Annex contains detailed methodological descriptions of the AEFI reporting process as well as the data extraction and analysis of the surveillance data. In addition, the annex includes information on AEFI surveillance definitions (i.e., primary AEFI, active and passive surveillance), how rates are reported, limitations of CAEFISS, information regarding vaccine abbreviations and marketed product/trade names, medical case review AEFI categories/subcategories and information on the severity classification for primary AEFIs in the medical case review.
Results
Our search identified a total of 5,875 AEFI reports between 2018 and 2019 in CAEFISS from 12 provinces and territories: 2,911 AEFI reports from 2018 and 2,964 AEFI reports from 2019. During this period, over 50 million vaccine doses were distributed. This represented an AEFI reporting rate of 11.5 per 100,000 doses distributed in 2018 and 2019. Over the preceding 11 years, the AEFI reporting rate decreased from 22.5 in 2008 to 11.2 per 100,000 doses distributed in 2019 (p<0.01) (Figure 1). The reduction in reporting occurred from the passive surveillance source, while the annual number of reports from active surveillance remained generally stable over time.
Figure 1: Total number of adverse events following immunization reports and reporting rate by reporting source, 2008–2019 (N=5,875)Figure 1 footnote a

Figure 1 - Text description
| Year | Passive system | Active system | Total | Doses distributed | AEFI reporting rate per 100,000 doses distributed |
|---|---|---|---|---|---|
| 2008 | 4,413 | 94 | 4,507 | 20,042,661 | 22.5 |
| 2009 | 3,846 | 116 | 3,962 | 21,650,423 | 18.3 |
| 2010 | 3,958 | 109 | 4,067 | 22,146,408 | 18.4 |
| 2011 | 3,801 | 114 | 3,915 | 23,743,216 | 16.5 |
| 2012 | 3,966 | 100 | 4,066 | 23,717,989 | 17.1 |
| 2013 | 3,356 | 101 | 3,457 | 21,979,521 | 15.7 |
| 2014 | 3,369 | 129 | 3,498 | 23,228,970 | 15.1 |
| 2015 | 3,292 | 108 | 3,400 | 24,762,130 | 13.7 |
| 2016 | 3,185 | 139 | 3,324 | 25,320,590 | 13.1 |
| 2017 | 3,193 | 127 | 3,320 | 23,452,909 | 14.2 |
| 2018 | 2,815 | 96 | 2,911 | 24,484,118 | 11.9 |
| 2019 | 2,856 | 108 | 2,964 | 26,395,876 | 11.2 |
Distribution of adverse events following immunization by age group
The median age of all cases reported in 2018–2019 at time of vaccination was 12 years (range: newborn to 100 years). The majority (55%) of AEFI reports were for children and adolescents under 18 years of age. Age-specific reporting rates were higher for younger age groups and lower for older age groups. Rates were highest for children younger than one year of age (123.9 per 100,000 population), followed by children one to younger than two years of age (123.6 per 100,000 population) (Figure 2). Among other age groups, the reporting rates were lower than 50 per 100,000 population.
Figure 2: Annual rate of adverse events following immunization by age group, 2008–2019 (N=5,814)Figure 2 footnote a
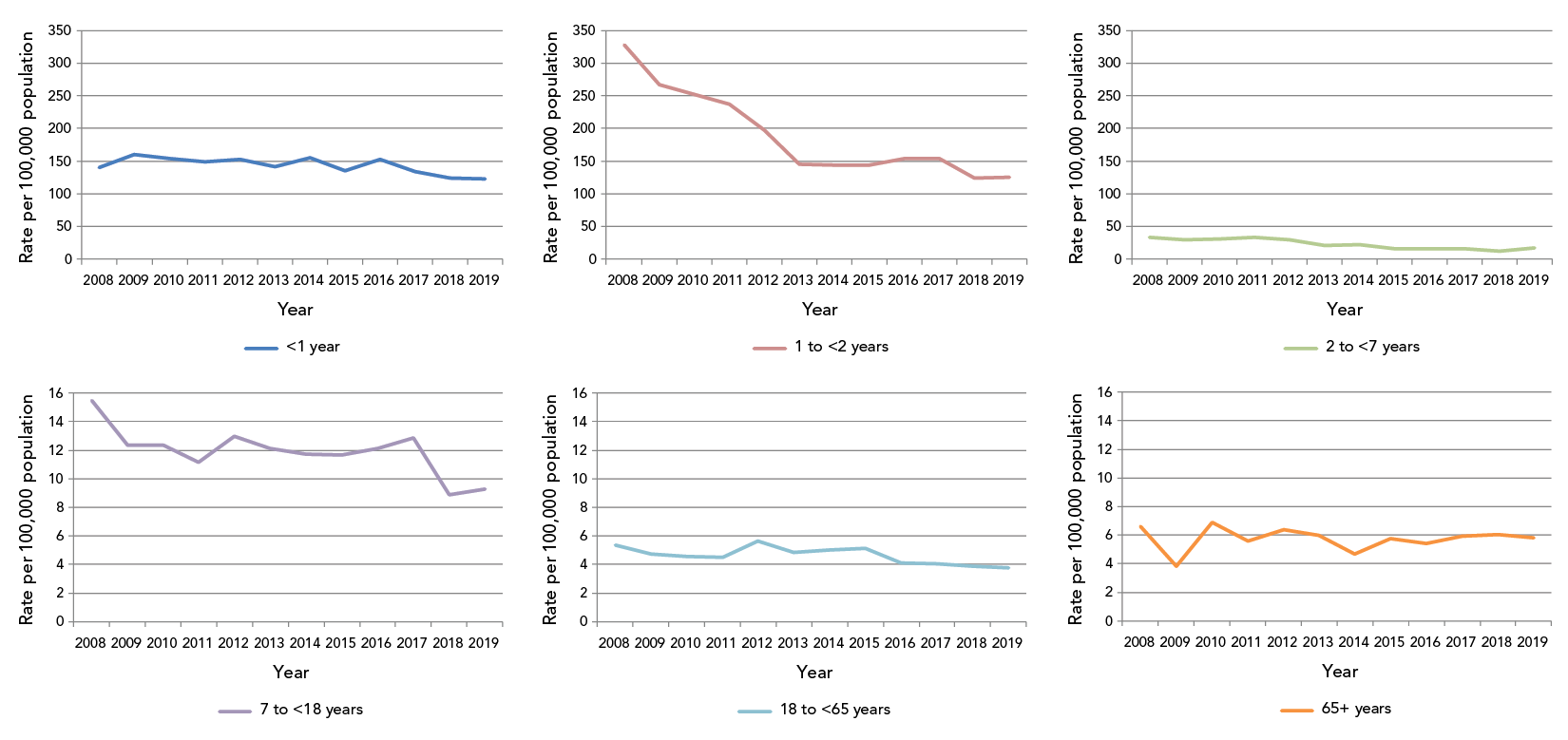
Figure 2 - Text description
| Age group | AEFI reporting rate per 100,000 population by year | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |
| <1 year | 140.8 | 160.7 | 154.3 | 148.5 | 153.3 | 141.7 | 154.8 | 135.0 | 152.7 | 134.3 | 123.9 | 122.8 |
| 1 to <2 years | 327.8 | 267.6 | 252.5 | 237.3 | 197.6 | 145.6 | 143.9 | 144.0 | 153.5 | 153.3 | 123.6 | 124.8 |
| 2 to <7 years | 33.8 | 30.2 | 31.3 | 33.2 | 29.5 | 20.9 | 22.2 | 16.3 | 16.0 | 16.3 | 12.0 | 17.0 |
| 7 to <18 years | 15.5 | 12.3 | 12.4 | 11.1 | 13.0 | 12.1 | 11.7 | 11.7 | 12.1 | 12.8 | 8.9 | 9.3 |
| 18 to <65 years | 5.3 | 4.8 | 4.6 | 4.5 | 5.7 | 4.9 | 5.0 | 5.1 | 4.1 | 4.1 | 3.9 | 3.8 |
| 65+ years | 6.6 | 3.8 | 6.9 | 5.6 | 6.4 | 6.0 | 4.7 | 5.8 | 5.4 | 5.9 | 6.1 | 5.8 |
Overall, between 2008 and 2019, decreases in AEFI reporting rates were seen in all age groups. The largest decrease (−62%) was seen in the 1 to <2 years age group, followed by the 2 to <7 years age group (−50%). The rate in the latter age group had slightly increased from 2018 to 2019 (+40%).
Distribution of adverse events following immunization by sex
Of the 5,875 reports, 60.5% were for females. As shown in Figure 3, there appears to be a slight male predominance of adverse events observed for children younger than seven years of age. Most age groups had relatively similar rates for males and females; however, within the age groups 18–64 years and 65 years and older the rate was higher for females.
Figure 3: Number and reporting rate of adverse events following immunization reports by age group and sex, 2018–2019 (N=5,814)Figure 3 footnote a
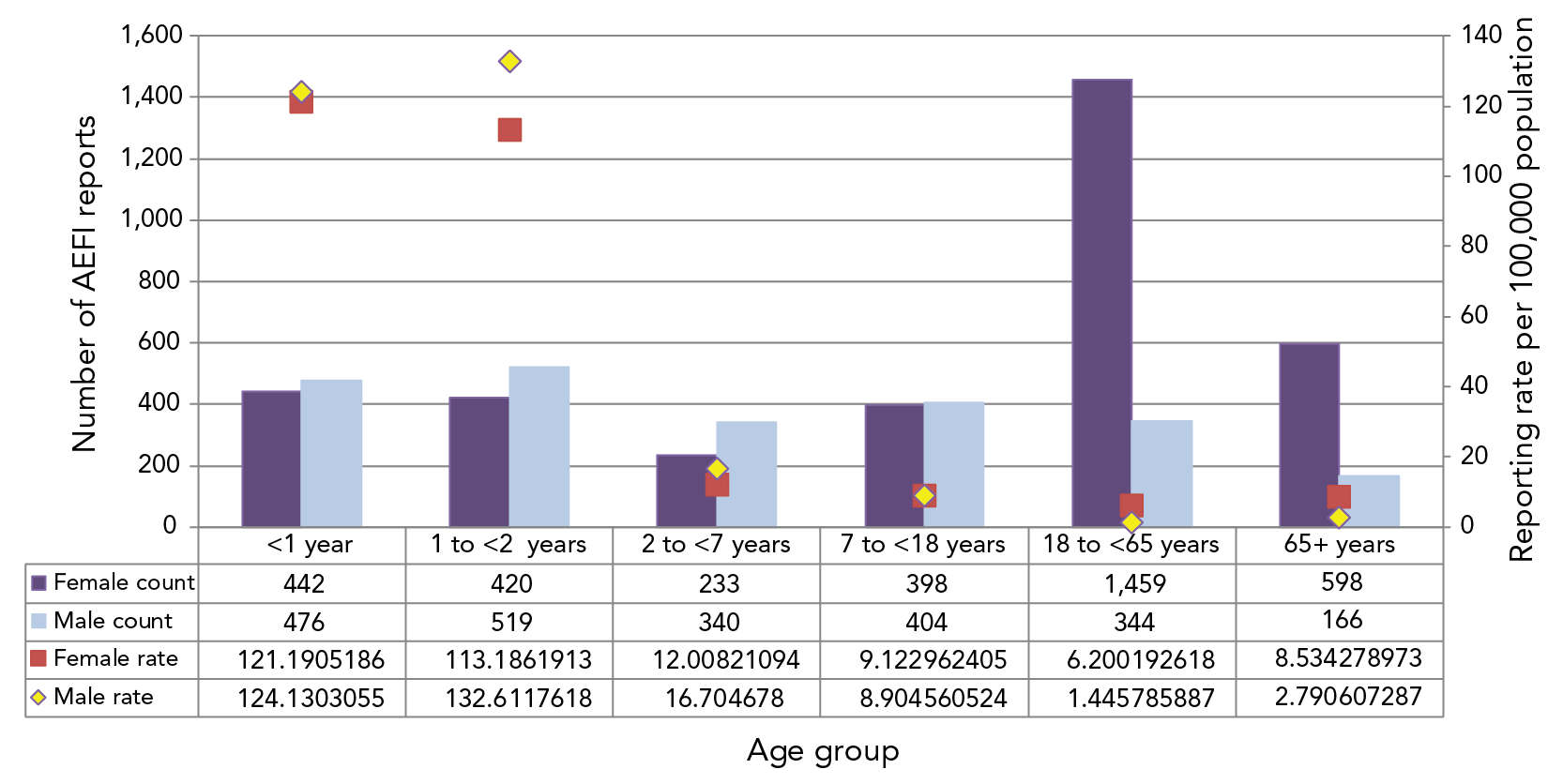
Figure 3 - Text description
| Age group | AEFI counts and reporting rate per 100,000 population by age group and sex | |||||
|---|---|---|---|---|---|---|
| Female count | Female population | Female rate | Male count | Male population | Male rate | |
| <1 year | 442 | 364,715 | 121.2 | 476 | 383,468 | 124.1 |
| 1 to <2 years | 420 | 371,070 | 113.2 | 519 | 391,368 | 132.6 |
| 2 to <7 years | 233 | 1,940,339 | 12.0 | 340 | 2,035,358 | 16.7 |
| 7 to <18 years | 398 | 4,362,618 | 9.1 | 404 | 4,537,001 | 8.9 |
| 18 to <65 years | 1,459 | 23,531,527 | 6.2 | 344 | 23,793,288 | 1.4 |
| 65+ years | 598 | 7,007,036 | 8.5 | 166 | 5,948,526 | 2.8 |
Primary reason for reporting adverse events following immunization
Table 1 provides a breakdown of reasons for submitting an AEFI report. The percentage of serious reports for each AEFI subcategory and the overall category is shown in the table. Vaccination site reactions were the most common primary AEFI reported (n=2,283, 40%) followed by allergic or allergic-like events (n=915, 16%) and rashes (n=653, 11%). These three categories combined represent 67% of all adverse event reports and 14% of all SAE reports submitted in 2018–2019. Figure 4 shows that the proportion of serious events was highest for the neurological event category (44%), followed by infection/syndrome/systemic symptoms (20%). Of note, only one report included vaccination errors, which was not a serious event. All AEFI reports were medically reviewed.
| Main reason for reporting | Detailed reason for reportingTable 1 footnote a | Number of reports | Serious reports (%) |
|---|---|---|---|
| Allergic or allergic-like events | Events managed as anaphylaxis | 101 | 100 |
| Oculo-respiratory syndrome | 61 | 0 | |
| Other allergic eventsTable 1 footnote b | 753 | 1 | |
| Total | 915 | 12 | |
| Infection/syndrome/systemic symptomsTable 1 footnote c | Fever only | 22 | 9 |
| Influenza-like illness | 13 | 0 | |
| Infection | 79 | 27 | |
| Rash with fever and/or other illness | 115 | 4 | |
| Syndromes | 39 | 82 | |
| Systemic | 75 | 12 | |
| Total | 343 | 20 | |
| Immunization anxiety | Other anxiety-relatedTable 1 footnote d | 9 | 0 |
| Presyncope | 12 | 8 | |
| Syncope | 37 | 3 | |
| Total | 58 | 3 | |
| Neurologic events | Aseptic meningitis | 5 | 100 |
| Ataxia/cerebellitisTable 1 footnote e | 3 | 67 | |
| Bell's palsy | 14 | 14 | |
| Encephalitis/acute disseminated encephalomyelitis/myelitis | 14 | 100 | |
| Guillain-Barré syndrome | 13 | 92 | |
| Other neurologic eventTable 1 footnote f | 64 | 30 | |
| Seizure | 223 | 43 | |
| Total | 336 | 44 | |
| Other | Arthralgia | 34 | 6 |
| Arthritis | 20 | 10 | |
| Gastrointestinal event | 452 | 7 | |
| Hypotonic-hyporesponsive episode | 48 | 31 | |
| Intussusception | 16 | 75 | |
| Other eventsTable 1 footnote g | 427 | 9 | |
| Paraesthesia/anaesthesia | 61 | 2 | |
| Parotitis | 8 | 0 | |
| Persistent crying | 37 | 0 | |
| Sudden unexpected/unexplained death syndrome | 2 | 100 | |
| Thrombocytopenia | 30 | 90 | |
| Vaccination failure | 1 | 100 | |
| Total | 1,136 | 11 | |
| Rash alone | Extent unknown | 36 | 0 |
| Generalized | 530 | 0 | |
| Localized | 87 | 0 | |
| Total | 653 | 0 | |
| Vaccination error | Total | 1 | 0 |
| Vaccination site reactions | Abscess | 21 | 19 |
| Cellulitis | 649 | 4 | |
| Extensive limb swellingTable 1 footnote h | 187 | 2 | |
| Other local reactionTable 1 footnote i | 1,291 | 1 | |
| Limb pain more than 7 days | 135 | 1 | |
| Total | 2,283 | 2 | |
Figure 4: Primary adverse events following immunization category by seriousness, 2018–2019 (N=5,726)Footnote aFootnote bFootnote c
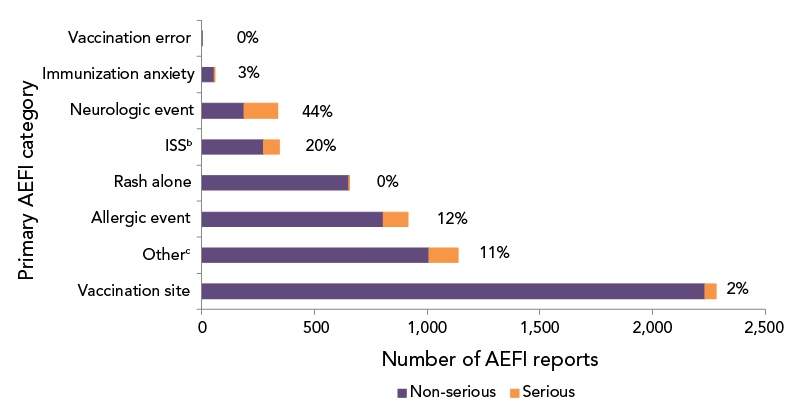
Figure 4 - Text description
| Primary AEFI | Number of non-serious reports | Number of serious reports | Percentage of serious reports |
|---|---|---|---|
| Vaccination site | 2,233 | 50 | 2 |
| Other | 1,008 | 129 | 11 |
| Allergic event | 805 | 110 | 12 |
| Rash alone | 652 | 1 | 0 |
| ISS | 274 | 69 | 20 |
| Neurologic event | 187 | 149 | 44 |
| Immunization anxiety | 56 | 2 | 3 |
| Vaccination error | 1 | 0 | 0 |
Figure 5 shows the distribution of AEFI by primary reason for reporting by age group. Vaccination site reactions represented the greatest number of AEFIs for all age groups except for children younger than one year of age. For children under the age of one, excluding the “other” event category, the most commonly reported AEFI was rash, followed by allergic event.
Figure 5: Distribution of primary adverse events following immunization reported by age group, 2018–2019 (N=5,726)Footnote aFootnote bFootnote c
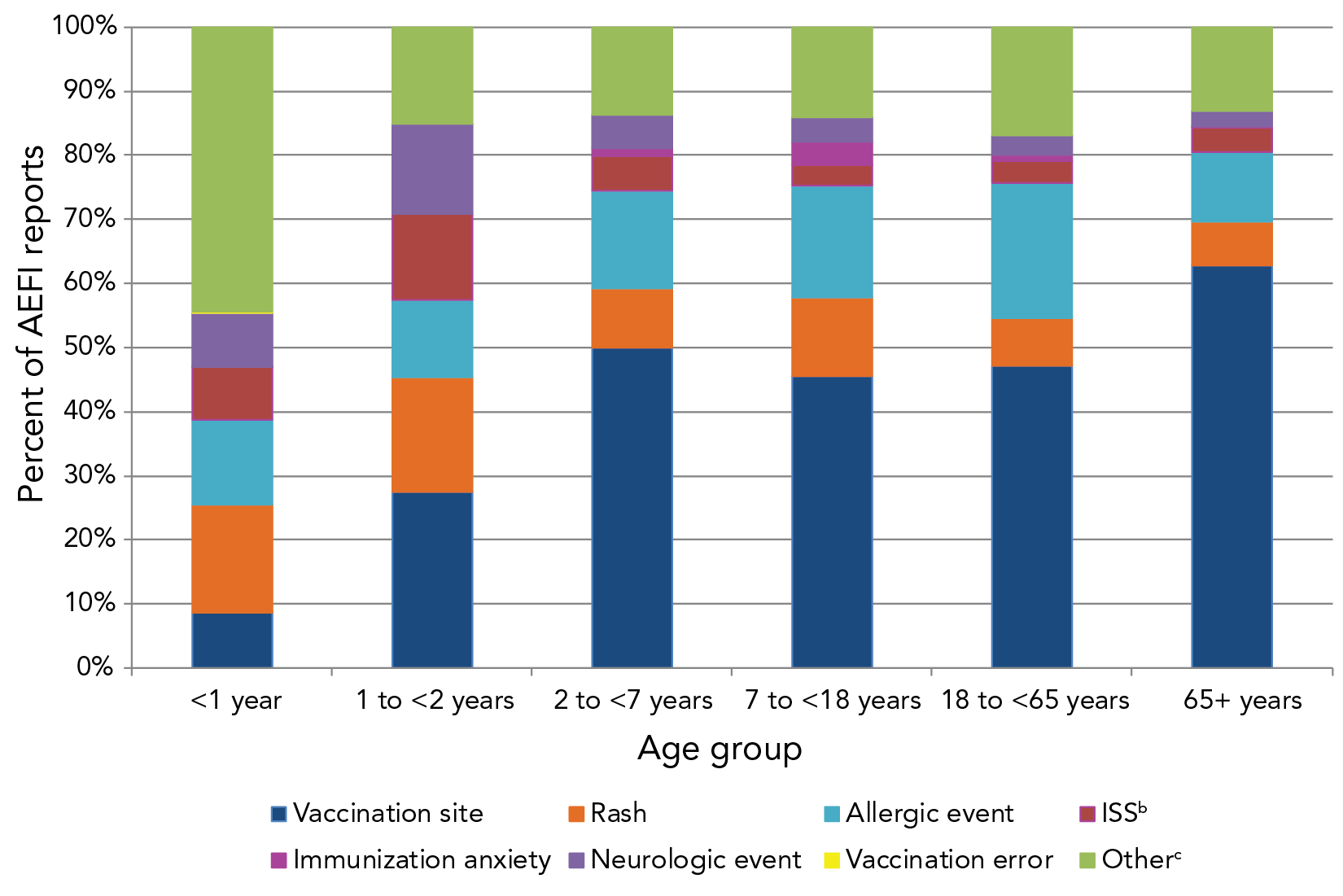
Figure 5 - Text description
| Primary AEFI | <1 year | 1 to <2 years | 2 to <7 years | 7 to <18 years | 18 to <65 years | 65+ years |
|---|---|---|---|---|---|---|
| Allergic event | 13.1 | 11.7 | 15.1 | 16.9 | 20.5 | 10.7 |
| ISS | 8.1 | 13.0 | 5.2 | 3.1 | 3.3 | 3.7 |
| Immunization anxiety | 0.1 | 0.0 | 1.2 | 3.5 | 1.1 | 0.3 |
| Neurologic event | 8.3 | 13.7 | 5.2 | 3.6 | 2.8 | 2.4 |
| Other | 44.0 | 14.7 | 13.3 | 13.6 | 16.4 | 12.7 |
| Rash | 16.8 | 17.4 | 9.0 | 11.8 | 7.2 | 6.5 |
| Vaccination error | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Vaccination site | 8.5 | 26.8 | 49.1 | 44.0 | 45.7 | 61.2 |
Serious adverse event reports
There were 511 SAE reports out of over 50 million vaccine doses distributed during the reporting period. This represents a reporting rate of 0.7/100,000 doses distributed and 9% of all AEFI reports for the 2018–2019 period. Figure 6 shows the distribution of SAE reports by reason for seriousness, with hospitalization (77%) and life-threatening events (19%) being the most common.
Figure 6: Classification of serious adverse event reports, 2018–2019Footnote a

Figure 6 - Text description
| Classification of serious adverse event reports, 2018–2019 | ||
|---|---|---|
| Severity | Frequency | Percent |
| Death | 10 | 2.0 |
| Hospitalization | 394 | 77.1 |
| Life–threatening | 95 | 18.6 |
| Prolonged hospitalization | 2 | 0.4 |
| Residual disability | 2 | 0.4 |
| Percentage of serious and non-serious reports, 2018–2019 | ||
| Non-serious | 5,364 | 91.3 |
| Serious | 511 | 8.7 |
The most frequently cited reason for reporting was events managed as anaphylaxis (n=101, 20%), followed by seizure (n=95, 18.6%). The majority (n=364, 71%) of SAE reports had fully recovered at the time of reporting. For those patients who had not fully recovered at the time of reporting, these reports were revised if updated information was received by CAEFISS from the reporting federal, provincial or territorial health authority. Other outcomes for SAE reports included fatal outcome (n=10, 2%) and permanent disability/incapacity (n=2, 0.4%). The majority of SAE reports were for children and adolescents younger than 18 years of age (n=397, 78%), with three quarters (75%) of these reported for children younger than two years of age.
All 10 reports of death underwent careful medical review, and none was considered to be related to the vaccines administered. There were seven deaths in children younger than five years of age; three of the deaths were considered to be a result of pre-existing medical conditions and another three were due to infections unrelated to vaccination. The seventh case had insufficient information, with the cause of death reported as unknown. Three deaths were reported in adults older than 70 years of age and were as a result of pre-existing medical conditions. There were two additional cases where outcome of persistent/significant disability were present at the time of reporting. No longer term outcome information was obtained on these cases.
Healthcare utilization
Table 2 shows the reported highest level of care sought following an AEFI. The most frequently reported was a non-urgent healthcare visit (43%). Most people with a reported AEFI (91%) did not require hospitalization. In 24% of the reports, no health care was sought, and these may have included self-reporting of milder AEFIs to public health units or healthcare providers.
| Highest level of care sought (N=5,489Table 2 footnote a) | n | %Table 2 footnote b | |
|---|---|---|---|
| Non-urgent visit | 2,369 | 43 | |
| None | 1,319 | 24 | |
| Emergency visit | 1,119 | 20 | |
| Required hospitalization | 405 | 7 | |
| Telephone advice from a health professional | 195 | 4 | |
| Resulted in prolongation of existing hospitalization | 1 | 0 | |
| Vaccination clinic | 1 | 0 | |
| UnknownTable 2 footnote c | 80 | 1 | |
Outcome
The outcome at time of reporting for all AEFI reports is shown in Table 3. Full recovery was indicated for 74% of the reports and 0.2% of reports reported death as an outcome.
| Outcome | Number of reports | Proportion of reports%Table 3 footnote b | |
|---|---|---|---|
| Fully recovered | 4,244 | 74 | |
| Not yet recovered | 1,222 | 21 | |
| UnknownTable 3 footnote c | 275 | 5 | |
| Permanent disability/incapacity | 2 | 0.0 | |
| Death | 10 | 0.2 | |
Discussion
In 2018–2019, the overall AEFI reporting rate was 11.5 per 100,000 doses distributed and represented a statistically significant decrease in reporting rates over the preceding 11 years. The decline in reporting rates over time may be due to increasing familiarity with expected side effects from vaccine over time (associated with reduced health care seeking for adverse events), under-reporting and changes in reporting requirements by jurisdictions over time. In comparison to the 2018 and 2019 Australian annual reporting rate of 16.9 and 14.9 per 100,000 population, respectively, the Canadian reporting rate is lower, which may in part be due to differences in case definitions used, immunization schedules, AEFI surveillance systems, reporting practices and population demographics Footnote 20Footnote 21. No vaccine safety issues or increases in frequency or severity of adverse events were identified by VVWG during the reporting period.
The majority of AEFI reports involved vaccines given to infants and young children younger than two years of age. This was expected, given that this age group receives many vaccines, both at a single visit and spaced closer together, leading to more opportunities for adverse events to be temporally associated with immunization and reported to a healthcare provider. For all age groups, a significant decrease in AEFI reporting occurred over the preceding 11 years, with the greatest decrease seen in the one to younger than two years old age group. A greater proportion of reports involved females; similar to other findings where female adults were found to consistently report more adverse events Footnote 6Footnote 13Footnote 14Footnote 22Footnote 23. The reported sex differences in AEFI counts and rates by age may also be explained in part by higher vaccine coverage in female adults Footnote 24. This is similar to other studies of sex-specific differences in AEFI reporting rates Footnote 20Footnote 21Footnote 22Footnote 23Footnote 25.
The majority of reported adverse events from approximately 50 million doses of vaccine distributed in Canada were non-serious vaccination site reactions, such as pain and redness, and allergic events, such as hypersensitivity and rash. In 2018–2019, 9% of AEFIs reported were SAEs. Comparing this to other countries that use the same definition for a SAE, this proportion is higher compared to that reported in New Zealand (3.5%) for the same time period Footnote 26 and is lower than that reported in Australia in 2018 and 2019 (16% and 12%) Footnote 20Footnote 21. It is also similar to previous years in Canada (8% and 9%) Footnote 6Footnote 14. The variations in proportions seen among different countries may be due in part to differences in methodology as stated previously.
The majority of reported SAEs occurred in children and adolescents, which may in part be explained by IMPACT, which actively searches for specific surveillance targets in children admitted to 12 paediatric tertiary care hospitals in Canada, resulting in a higher reporting rate in this age group Footnote 27Footnote 28Footnote 29. Immunization Monitoring Program ACTive contributed 6% of all AEFI reports and 50% of all serious reports in children under the age of 18 years, which is similar to the results reported in the 2013–2016 and 2017 reports for this age group. In all age categories, the proportion of SAEs was highest for the neurological event category, for which IMPACT specifically searches. No discernable trends were identified for the number of specific serious adverse events reported over the 2008–2019 time period. Regarding the most frequently cited reason for reporting among SAE reports for all age groups combined, the number and rate of reports of seizures have decreased from 0.45 to 0.19 per 100,000 doses distributed since 2016 and is below the expected frequency (very rare: less than 1/10,000 doses distributed) identified by the World Health Organization Footnote 30. The number and rate of reports of events managed as anaphylaxis have remained relatively stable since 2016 with an annual reporting rate of 0.20 per 100,000 doses distributed (two per million doses distributed), which is within the expected range of one to 10 episodes per million doses of vaccines administered Footnote 31. For both seizure reports and reports for events managed as anaphylaxis, the reports were distributed across multiple ages and vaccines with no lot-specific clusters. It should be noted that case definitions for events managed as anaphylaxis vary slightly by province and territory. In general, the definition of anaphylaxis is intentionally very sensitive to ensure that all potential cases of anaphylaxis are captured. At the time of reporting, the majority of individuals with SAEs had fully recovered. Of the 10 deaths reported over the two-year period, none were found to be related to the vaccines administered.
Limitations
Passive surveillance for AEFIs is subject to limitations such as under-reporting, lack of certainty regarding the diagnostic validity of a reported event, missing information regarding other potential causes such as pre-existing medical conditions or concomitant medications and differing AEFI reporting practices by jurisdictions within Canada. Passive surveillance detects temporal events; however, from the AEFIs described in this paper, causal inferences cannot be made since causality assessment was only conducted for reports that stated an outcome of death. Despite these limitations, passive surveillance is an essential tool for detecting potential vaccine safety signals, especially new or unusual adverse events too rare to assess during clinical trials. Seasonality was not analyzed as a potential variable in this report.
There are also limitations associated with active surveillance. Immunization Monitoring Program ACTive uses predetermined AEFI targets (such as seizure), which may limit its ability to identify new adverse reactions to immunizations. In addition, while IMPACT covers 90% of Canada's tertiary care pediatric beds and hospital admissions, its focus is on admitted paediatric cases, which means only the most serious cases are detected Footnote 29Footnote 30.
The number of doses administered in the population is not available at the national level; therefore, the denominator used in rate calculations was either doses distributed or population statistics. The use of doses distributed as the denominator can underestimate rates, as they do not take unused doses or wastage into account. Furthermore, doses distributed in one year may not be administered in that same year, further limiting the accuracy of the doses distributed denominator. Despite these limitations, a doses distributed-based denominator for rate calculations was used when possible in this report, as a population-based denominator assumes similar distribution of vaccine doses across population subgroups, and this may not be true in all cases.
Conclusion
There were no vaccine safety issues identified or increases in frequency or severity of expected adverse events in the CAEFISS data. The majority of reported AEFIs were expected and mild in nature and the overall proportion of serious adverse events were similar to previous years.
Authors' statement
- MEJ — Conceptualization, methodology, investigation, software, formal analysis, validation, writing–original draft, writing–review and editing
- KJ — Conceptualization, methodology, writing–original draft, writing–review and editing
- YX — Conceptualization, writing–review and editing, supervision
- CW — Writing–original draft, writing–review and editing, methodology, validation
- HA — Investigation, writing–original draft, writing–review and editing
- AW — Validation, writing–review and editing
- AY — Writing–review and editing
- AS — Writing–review and editing, supervision
- SO — Writing–review and editing, supervision
Competing interests
None.
Acknowledgments
This report would not be possible without the contribution of the public, healthcare providers, public health professionals, Immunization Monitoring Program ACTive (IMPACT) investigators and nurse monitors and Canadian Paediatric Society and local/regional and provincial/territorial public health authorities who submit reports to Canadian Adverse Events Following Immunization Surveillance System (CAEFISS), as well as the ongoing collaboration of the members of the Vaccine Vigilance Working Group. Furthermore, we would like to thank the members of this group, including the medical reviewers and coders in CAEFISS, for input and support in the development of this report. We would like to thank each individual who took the time to submit an adverse events following immunization report for their contribution to vaccine safety in Canada.
Funding
This work was funded by the Public Health Agency of Canada.
Supplemental material
These documents can be accessed on the Supplemental material file.

Page details
- Date modified: