
Fifth Annual Report on Medical Assistance in Dying in Canada, 2023

Download in PDF format
(1.2 MB, 82 pages)
Organization: Health Canada
Date published: 2024-12-11
Cat.: H22-1/6E-PDF
ISBN: 2563-3643
Pub.: 240657
On February 1, 2025, the following sections were edited for clarity and accuracy:
- Highlights: Added counts to the paragraph on disability.
- Section 3.6: Revised two of the x-axis labels in Figure 3.6a to "inadequate pain control or concern about it" and "inadequate control of other symptoms or concern about it" (previously "inadequate pain control" and "inadequate control of other symptoms", respectively).
- Section 5.1: Revised the duration categories in Table 5.1b to "Less than one year" and "One year or more" (previously "Less than one month" and "One month or more", respectively).
Table of contents
- Highlights
- Minister's message
- 1 Introduction and overview of MAID data
- 2 MAID requests and outcomes
- 2.1 MAID requests and outcomes
- 2.2 MAID provisions
- 2.3 Requests not resulting in MAID
- Table 2.3a: Reasons for ineligibility reported in cases where a MAID request was determined to be ineligible
- Table 2.3b: Reasons for withdrawal of MAID Request in cases where a person withdrew their request
- Table 2.3c: Reasons for natural death before MAID could be provided, and median days between MAID request and death
- 3 MAID assessments: grievous and irremediable medical conditions
- 3.1 Most common serious and incurable illnesses
- 3.2 Frailty and chronic pain
- 3.3 Dementia
- 3.4 Length of time living with a serious and incurable illness, disease or disability
- 3.5 Advanced state of irreversible decline in capability
- 3.6 Nature of suffering
- 3.7 Determination of the MAID request as voluntary
- 4 Socio-demographic considerations, access and inequality
- 4.1 Importance and challenges of collecting data on identity
- 4.2 MAID by racial, ethnic or cultural group
- 4.3 Indigenous people who received MAID
- 4.4 Persons with disabilities who received MAID
- 4.5 Socio-economic and community analyses
- Figure 4.5a: Neighbourhood income quintiles, by track, compared to all 2023 deaths in Canada
- Figure 4.5b: Neighbourhood marginalization quintiles, by track, compared to all 2023 deaths in Canada
- Figure 4.5c: Percentage of MAID recipients who lived in urban areas, by track, and all 2023 deaths from urban areas
- Figure 4.5d: Percentage of MAID recipients who lived in remote areas by province, compared to the population of Canada
- 5 Social supports and use of health services
- 6 MAID providers and delivery
- 7 Conclusion
- Appendix A: MAID eligibility criteria, safeguards and reporting requirements
- Appendix B: Methodology and limitations
- Appendix C: Indigenous engagement on MAID
- Appendix D: Profile of MAID by jurisdiction
- Table D.1: Outcomes of MAID requests made in 2023, by province or territory
- Table D.2: Medical conditions reported by MAID recipients, by province
- Table D.3: Profile of MAID recipients, by province
- Table D.4: Median and average age of MAID recipients, by province
- Table D.5: Place of residence of persons who received MAID, by province
- Table D.6: Disability support services and palliative care services received by MAID recipients, by province
- Table D.7: Unique practitioners and provisions, by province
- Table D.8: Location of MAID provision, by province
- Figure D.1: Canadian index of multiple deprivation, by province
- Appendix E: MAID requests, eligibility, and procedural requirements
- Figure E.1: Index of remoteness quintiles in Canada
- Table E.1: Outcomes of previous MAID requests from MAID recipients, by track
- Table E.2: From whom did the practitioner receive the request for MAID, by track
- Table E.3: Specialty of MAID providers, by track
- Table E.4: Type of facility where palliative care was received
- Table E.5: Type of palliative care services received
Highlights
The Fifth Annual Report on Medical Assistance in Dying (MAID) in Canada provides a summary of MAID requests, assessments and provisions for the 2023 calendar year. This information is provided to Health Canada by physicians, nurse practitioners, preliminary assessors, pharmacists and pharmacy technicians directly or via provinces and territories. The Fifth Annual Report is the first report to present data collected under the amended Regulations for the Monitoring of Medical Assistance in Dying, which came into force on January 1, 2023. These data include new information on who requests MAID, what health and other support services are offered and, where possible, how assessments are informed. Given that this was the first year collecting these additional variables, including self-identification measures such as race, Indigenous identity, and disability, there are some important data limitations to consider, including: an inability to present trends over time, some missing data, and limited quality and reliability of some measures. Nevertheless, the report provides important insight into who requests and receives MAID, and how and where it is delivered.
What is MAID?
Medical assistance in dying (MAID) is a health service that allows someone who is found to be eligible to receive assistance from a medical practitioner to end their life. The Criminal Code sets out strict eligibility criteria to determine who can receive MAID, and robust safeguards to ensure that MAID is safely provided. MAID is only available to persons who freely choose it and only under very specific circumstances and rules. To be eligible for MAID, an individual must:
- be at least 18 years old and mentally competent
- have a grievous and irremediable medical condition, specifically:
- have a serious illness, disease or disability;
- be in an advanced state of decline that cannot be reversed; and
- experience unbearable physical or mental suffering from the illness, disease, disability or state of decline that cannot be relieved under conditions that the person considers acceptable
- make a voluntary request for MAID
- give informed consent to receive MAID
- be eligible for health services funded by province or territory, or the federal government
In addition, there are a number of safeguards that must be met before MAID can be administered. Where an individual's death is not "reasonably foreseeable", additional safeguards have been put in place.
While the number of MAID provisions increased in 2023, the rate of growth was halved over previous years. (See Section 2)
- This report details 19,660 reports of MAID requests that Health Canada received in 2023. There were 15,343 people who received MAID; the remaining cases were requests for that did not result in MAID (2,906 died before receiving MAID, 915 individuals were deemed ineligible and 496 individuals withdrew their request).
- The number of MAID provisions in 2023 represents an increase of 15.8% over 2022. This represents a slowing over previous years (2019 to 2022) which had an average growth rate of approximately 31%.
- It is not yet possible to make reliable conclusions about whether or not these findings represent a stabilization of growth rates over the longer term. An increased awareness of MAID within the care continuum, population aging and the associated patterns of illness or disease, personal beliefs and societal acceptance, as well as the availability of practitioners who provide MAID may all influence the rate of provisions.
For every five individuals who received MAID, another individual was not able to access this health service before their death. (See Section 2)
- In 2023, 2,906 individuals who requested MAID died before their request for MAID could be fulfilled.
The vast majority of MAID provisions (95.9%; n=14,721) were for individuals in Track 1; 4.1% (n=622) of MAID provisions were for individuals in Track 2. (See Section 2)
- This report provides insights into the circumstances of people receiving MAID under two separate "tracks":
- Those in "Track 1" who met the eligibility criteria set out above and were assessed as having a natural death that was "reasonably foreseeable."
- Those in "Track 2" who met the eligibility criteria set out above and were assessed as having a natural death that was not "reasonably foreseeable."
- There are important and expected differences between these two groups.
Consistent with findings from previous years, those who received MAID under Track 1 were older, and more likely to have cancer as an underlying medical condition. (See Section 3)
- The median age was 77.7 years and 59.7% were over 75 years of age.
- 51.6% were men and 48.4% were women.
- Cancer was the most frequently reported underlying medical condition, cited in 64.1% of cases.
Those receiving MAID under Track 2 predominantly women, slightly younger, and lived with their illness for a much longer period of time. (See Section 3)
- The median age was 75.0 years and 50.2% were over 75 years of age.
- 58.5% were women and 41.5% were men. This is consistent with overall population health trends where women experience long-term chronic illness, which can cause enduring suffering but would not typically make a person's death reasonably foreseeable.
- Lived longer with a serious and incurable condition than those in Track 1: 31.8% of people receiving MAID under Track 2 lived with a serious and incurable illness, disease or disability for more than 10 years, compared to 7.7% of those under Track 1.
- Neurological conditions and "other" conditions (such as diabetes, frailty, autoimmune conditions, chronic pain) were the most commonly cited underlying medical conditions.
The number of people deemed ineligible is proportionally much higher for Track 2 than for Track 1. (See Section 2)
- Although Track 2 provisions represent 4.1% of MAID cases, they represent 26.9% of ineligible requests.
This report includes, for the first time, data on the racial, ethnic or cultural identity of MAID recipients. (See Section 4)
- A total of 9,619 people of the 15,343 who received MAID responded to this question, the vast majority of whom (95.8%) identified as Caucasian (White). The second most commonly reported racial, ethnic or cultural identity was East Asian (1.8%).
- 80 people who received MAID identified as First Nations, 36 identified as Métis and 23 identified as both First Nations and Métis. The vast majority of people identifying as Indigenous who received MAID received it under Track 1 (fewer than five people identifying as Indigenous received MAID under Track 2).
Two-thirds of individuals who received MAID provided information on disability. (See Section 4)
- Of the 10,581 people who responded to questions on disability, 3,633 self-identified as having a disability.
- 33.5% (3,423) of Track 1 respondents self-identified as having a disability compared to 58.3% (210) of Track 2 respondents.
- For Track 1, the share of people who self-reported having a disability increases with age.
- For Track 2, the largest proportion of people reporting a disability were in the 65 to 74 age group; the share of people reporting a disability gradually declines among the older age groups.
- The most frequently reported disabilities were mobility- and pain-related.
- Proportionally more women than men reported having a disability, which aligns with disability trends among the general population of Canada.
- These findings should be interpreted with caution, however, given varying interpretations regarding what constitutes a "disability". Health Canada is working with provinces, territories and health care professionals to improve data consistency going forward.
Health Canada conducted analyses to better understand the characteristics of the communities that MAID recipients lived in. (See Section 4)
- These analyses suggest, at a high level, that people who receive MAID do not disproportionately come from lower-income or disadvantaged communities. Findings indicate that MAID recipients live in neighbourhoods across the income and marginalization spectrum as well as in urban, rural and remote communities.
- These analyses are based on neighbourhood-level measures and do not speak to the situation of the MAID recipients themselves. As such, they should be interpreted with caution.
Most MAID recipients who required either palliative care or disability support services received these services. (See Section 5)
- 75.0% received palliative care; 76.9% of people who received MAID under Track 1 received palliative care, compared to 29.6% of people who received MAID under Track 2.
- 2.8% required, but did not receive, palliative care services; of these individuals, 80.5% confirmed that services were accessible to them.
- 33.8% received disability support services; 33.1% of people who received MAID under Track 1 received disability support services, compared to 49.4% of people under Track 2.
- 2.8% required, but did not receive, disability support services; of these individuals, 36.6% confirmed that services were accessible to them.
MAID appears to be becoming an area of focused expertise for some practitioners. (See Section 6)
- There were 2,200 unique MAID practitioners in 2023. The majority (94.5%) were physicians, while 5.5% were nurse practitioners.
- A group of 89 practitioners were responsible for 35.1% of all Track 1 and 28.6% of all Track 2 cases respectively.
- In 73.2% of Track 2 cases, the two practitioners performing the assessment were able to complete it without seeking additional expertise. In the remaining cases, practitioners sought a third assessor to provide additional expertise in the condition causing the person's suffering to help determine if a person was eligible for MAID. When a third assessor was required, the most commonly cited specialties were neurology, pain management, geriatric medicine, and psychiatry.
Note to readers: Data collected with respect to MAID requests and provisions are not the same as the data collected about deaths that occur in Canada (i.e., vital statistics). As such, they should not be directly compared to one another.
| Vital Statistics | MAID Data | |
|---|---|---|
| Who submits the report | Medical practitioner, nurse practitioner, coroner, or medical examiner, | MAID assessors and providers, i.e., medical practitioners or nurse practitioners |
| What do they report | An underlying cause of death, and optional, multiple contributing cases of death, classified according to the World Health Organization "International Statistical Classification of Diseases and Related Health Problems". | The medical condition(s) that are causing a person's suffering and are the basis for the person's MAID request as well as any comorbidities. These are not differentiated from one another. |
| Who summarizes the data and shares with Canadians | Statistics Canada | Health Canada |
| What guides reporting | Provincial and territorial Vital Statistics Acts (or equivalent legislation) | Regulations for the Monitoring of Medical Assistance in Dying |
Minister's message
I am pleased to present Health Canada's Fifth Annual Report on Medical Assistance in Dying in Canada (2023). This report represents the ongoing collaboration among federal, provincial and territorial governments and health care professionals to provide a comprehensive picture of the provision of medical assistance in dying (MAID) in Canada.
This year's annual report is the first to include data collected under the amended Regulations for the Monitoring of Medical Assistance in Dying which came into force on January 1, 2023. These regulations include updated reporting requirements to provide a more comprehensive and inclusive picture of who requests MAID, what health and other support services are offered and, where possible, how assessments are informed.
Over the past year, the Government of Canada continued to support several initiatives related to fostering dialogue and ensuring the safe and consistent delivery of MAID, including:
- The Canadian MAID Curriculum, developed by the Canadian Association of MAID Assessors and Providers in consultation with experts from across the country, is the first comprehensive, bilingual, nationally accredited, evidence-based educational program supporting the practice of MAID in Canada.
- The Model Practice Standard for MAID and the companion Advice to the Profession document to help practitioners align their practice with clear guidance and assist health professional regulatory authorities to ensure the protection of the public in the context of complex MAID cases.
- Engagement with Indigenous partners, including Indigenous-led engagement projects, an online questionnaire, and a series of knowledge exchange roundtables to hear the perspectives of First Nations, Inuit and Métis Peoples on MAID.
Further, the Government is supporting research on MAID to inform future policy development and support best practice. For example, through the Canadian Institutes of Health Research, we are funding research to better understand care for persons applying for and/or receiving MAID when death is not reasonably foreseeable (Track 2). This knowledge will be shared throughout the project to support high-quality care for patients, their family members and loved ones. We are also supporting research on models of MAID delivery and oversight to identify best practices for the review of complex cases and continuous quality assurance.
Most recently, the Government has launched a national conversation to hear the perspectives of Canadians on advance requests for MAID. This national conversation will engage with patients, provincial and territorial governments, providers, stakeholders, Indigenous Peoples, and the public on advance requests for MAID.
The additional data presented in this latest annual report will contribute to informed discussions on MAID, especially in the context of the national conversation.
The Government of Canada is committed to ensuring that Canada's federal legal framework for MAID reflects the needs of Canadians, protects those who may be vulnerable, and supports autonomy and freedom of choice.
The Honourable Mark Holland, P.C., M.P.
Minister of Health
1 Introduction and overview of MAID data
1.1 Introduction
MAID involves a number of competing interests and values. On the one hand is the autonomy of individuals to make decisions about their health care, including end-of-life care; on the other is the protection of individuals who may be vulnerable. With this Fifth Annual Report, Health Canada endeavours to contribute to greater insight and understanding of MAID to support the ongoing public dialogue on these issues.
This report provides the most current summary of MAID assessment and provision in Canada. It presents data reported for the 2023 calendar year, and is the first report to present a year of data collected under the amended Regulations for the Monitoring of Medical Assistance in Dying which came into force on January 1, 2023.
In 2021, in response to jurisprudence that found that the requirements for MAID were unconstitutional as being too restrictive, the Criminal Code was amended to create two separate "tracks" for MAID. Under both tracks, individuals must meet the minimum eligibility requirements before being able to be considered for MAID:
- Track 1: Refers to a request for MAID made by a person who meets the eligibility requirements set out in the Criminal Code and whose natural death is "reasonably foreseeable"
- Track 2: Refers to a request for MAID made by a person who meets the eligibility requirement set out in the Criminal Code and whose natural death is not "reasonably foreseeable"
Requests from individuals assessed as Track 2 are subject to additional safeguards, including a minimum 90 day assessment period from the day on which the first assessment begins to provision of MAID. Where someone's death is not reasonably foreseeable, the Criminal Code requires that the person be informed of available and appropriate means to relieve their suffering, including counselling services, mental health and disability support services, community services, and palliative care, and be offered consultations with professionals who provide those services. Additionally, the person and their practitioners must have discussed reasonable and available means to relieve the person's suffering and agree that the person has seriously considered those means.
Appendix A provides further information on the eligibility criteria for MAID, the safeguards for Tracks 1 and 2, and the reporting requirements.
As of 2023, physicians and nurse practitioners (referred to as "practitioners" throughout this report) who receive a request for or administer MAID are obligated to report on several new or modified reporting requirements. These data will help to give a better understanding of who requests MAID, what health and other support services are offered and, where possible, how assessments are informed.
This year's report marks a departure from previous years both because of the additional information reported and the analyses undertaken. This is part of a broader commitment to address questions related to safeguards, socio-economic status, access to services and supports, and other factors in the context of MAID.
Health Canada is grateful for the partnership and collaboration among federal, provincial, and territorial levels of government, MAID practitioners and pharmacists, Indigenous partners and key stakeholders which has permitted the collection and validation of the data and analysis contained in this report.
1.2 Complexity involved in MAID assessment
As highlighted previously, under the current legislation, there are two separate "tracks" for MAID, based on whether or not a person's natural death is reasonably foreseeable. For MAID requests falling under Track 2 (natural death is not reasonably foreseeable), assessing eligibility can be considerably more complex. For instance, these applicants can have long and complicated health care histories, requiring significant time on the part of assessors to work closely with the person to fully understand their condition, care trajectory and potential alternatives to alleviate suffering.Footnote 1 This involves, for instance, obtaining "collateral history" (through discussions with people who know and interact with the person such as those within the person's social circle and past or current treating clinicians); gathering and reviewing past medical records (sometimes from multiple practitioners, regions and institutions); consulting practitioners with expertise in the person's condition to elaborate on therapeutic options, seeking diagnostic clarification, or evaluating the adequacy of past treatments; and navigating available services and supports.Footnote 2Footnote 3 Making a decision regarding a person's eligibility for MAID based on this information requires astute clinical judgement.
Recognizing the complexities involved in MAID assessment and the importance of practitioner guidance, Health Canada has supported the development of two key resources for MAID assessors and providers and health professional regulatory authorities:
- The Canadian MAID Curriculum,Footnote 4developed by the Canadian Association of MAID Assessors and Providers, is the first nationally accredited, bilingual MAID education program available to licensed physicians and nurse practitioners across the country.
- The Model Practice Standard for MAIDFootnote 5and the companion Advice to the ProfessionFootnote 6 document to help practitioners align their practice with clear guidance and assist health professional regulatory authorities to ensure the protection of the public in the context of complex MAID cases.
1.3 Overview of MAID data
To protect confidentiality, Health Canada does not present findings when there are fewer than five cases due to the risk that an individual or small groups of individuals could be identified (for instance, if reviewed in conjunction with other publicly available data, such as those presented within this report or at the provincial/territorial level). Datapoints representing more than five cases may also be suppressed if they would have otherwise provided enough information to calculate the number of cases in another suppressed group. Data that are suppressed for confidentiality purposes are notated with an "X" throughout the report.
The regulations that came into force in January 2023 introduced several new reporting requirements for health care practitioners, who are required to collect data on new and updated questions.
As 2023 was the first year of the new and expanded data collection, there are some important limitations to note:
- The ability to present trends over time is limited for some variables: given that several reporting requirements and questions have been updated, there are instances where data collected in 2023 are not fully comparable with the data collected in previous years.
- There are some missing data for new variables due to time delays for provinces, territories and practitioners to transition to the new data collection requirements.
- The quality and reliability of the self-identification data (race, Indigenous identity, and disability) is limited due to variation in data collection approaches, inconsistency in interpretation of variables and potential reluctance on part of the person to self-identify.
Health Canada has established a dedicated working group made up of federal, provincial and territorial officials committed to improving data collection, consistency and quality going forward. Practitioners are becoming more familiar with reporting requirements and as of September 2023, all provincial and territorial reporting forms are up to date and in use. With this, Health Canada expects the quality of data to continue to improve in subsequent years.
More details with respect to the methodology and limitations are outlined in Appendix B.
2 MAID requests and outcomes
2.1 MAID requests and outcomes
This report details 19,660 reports of MAID requests that Health Canada received in 2023. There were 15,343 people who received MAID; the remaining cases were requests for MAID that did not result in MAID being provided (2,906 died before receiving MAID, 915 individuals were deemed ineligible and 496 individuals withdrew their request).
In previous years, reporting obligations for practitioners were based solely on written requests for MAID. This did not capture:
- verbal requests, or requests received by a health care professional other than a nurse practitioner or physician that did not result in a MAID provision.
- written requests initially received by a nurse working within a care coordination service, which were never forwarded to a physician or nurse practitioner due to an initial assessment of ineligibility.
These gaps made the data related to the total number of requests an unreliable indicator of the overall interest in MAID across Canada.
Under the amended MAID monitoring regulations, reporting requirements may be triggered by any intentional and deliberate request for MAID (verbal or in writing), including those received by preliminary assessors.Footnote 7 This approach is expected to better capture more subtle demonstrations of interest in MAID.
Given that the amended regulations only came into effect on January 1, 2023, and there have been some delays in implementation of the new data collection requirements, the total number of MAID requests for 2023 is likely an underrepresentation of requests for MAID across Canada. Data reliability will improve in future years with new tools and supports now in place for provinces, territories and practitioners.
This report details 19,660 reports of MAID requests and provisions that Health Canada received in 2023. As outlined in Table 2.1a, a total of 15,343 people were provided MAID; the remaining cases were requests for MAID that did not result in MAID provision (2,906 died before receiving MAID, 915 individuals were deemed ineligible and 496 individuals withdrew their request). Note that it is possible that a person is included in these groups more than once (for example, a person could request MAID, withdraw and then apply again and receive it, or make several requests for MAID which are all each deemed ineligible). Only MAID requests that were made in 2023 and resolved in 2023 were included in this report ("resolved" is defined as a request that is withdrawn or the individual requesting is found to be ineligible, or has died).
Not included in the above counts are: (a) five MAID provisions that are excluded from the total count and subsequent analysis as they are missing information on key variables and follow-up and validation with provinces and territories was not complete prior to analysis being undertaken; (b) MAID requests that were initiated in 2022 or earlier and resolved in 2023 (see above); and (c) MAID requests resolved in 2022 or earlier and submitted late in 2023.
Comparisons between the four groups listed in Table 2.1a should be made with caution because the inclusion criteria for MAID provisions and MAID requests in this analysis differ. Further, the same person could be included multiple times in these counts. As such, the percentage that each group represents of the total number of reports is not presented; Health Canada recommends instead that data users focus on the ratios between the groups. For example, for every 17 times that MAID was provided, there was one person who requested MAID and was deemed ineligible (i.e., 15,343/915= 16.7).
| Requests or provisions | All cases | Track 1 | Track 2 | Did not assess track | |||
|---|---|---|---|---|---|---|---|
| Count | Count | Percent (%) | Count | Percent (%) | Count | Percent (%) | |
| MAID provisions in 2023 | 15,343 | 14,721 | 95.9 | 622 | 4.1 | - | - |
| Requests made in 2023 where individual was deemed ineligible in 2023 | 915 | 416 | 45.5 | 246 | 26.9 | 253 | 27.7 |
| Requests made in 2023 where individual died of another cause in 2023 | 2,906 | 2,617 | 90.1 | 37 | 1.3 | 252 | 8.7 |
| Requests made in 2023 that were withdrawn in 2023 | 496 | 303 | 61.1 | 88 | 17.7 | 105 | 21.2 |
| Total | 19,660 | - | - | - | - | - | - |
2.2 MAID provisions
The vast majority of MAID provisions (95.9%) were for individuals in Track 1; 4.1% of MAID provisions were for individuals in Track 2. The median age of MAID recipients was 77.6 years.
As noted above, MAID was provided to 15,343 individuals in 2023, representing an increase of 15.8% over 2022. This represents half of the growth rate from previous years: there was a 32.6% increase from 2020 and 2021, and a 31.2% increase from 2021 to 2022. Based on previous reports, there were 44,958 MAID provisions since its legalization in 2016 to 2022, which brings the total number of MAID provisions in Canada to 60,301.
In 2023, 95.9% of MAID cases (n=14,721) were individuals whose death was reasonably foreseeable (Track 1) and 4.1% (n=622) were individuals whose death was not reasonably foreseeable (Track 2). To compare to previous years, between 2021 and 2022, the number of Track 2 MAID provisions doubled (from 223 provisions in 2021 to 463 provisions in 2022).Footnote 8 The increase between 2022 and 2023 was comparatively smaller, with 34% more Track 2 MAID cases reported. The proportion of Track 1 MAID cases across different jurisdictions is provided in Table D.3 (Appendix D).
It is not yet possible to make reliable conclusions about whether or not these findings represent a stabilization of the number of annual MAID provisions over the longer term. An increased awareness of MAID within the care continuum, population aging and the associated patterns of illness or disease, personal beliefs and societal acceptance, as well as the availability of practitioners who provide MAID (see Section 6.1) may all influence the number of provisions. MAID, particularly MAID outside the context of a reasonably foreseeable natural death, is still a relatively new health care service in Canada and assessments take far longer than the required 90 days, sometimes taking many months. It will take several more years before trends related to overall demand can be conclusively identified.
In 2023, 4.7% of Canadians who died received MAID.Footnote 9 This number may change with final counts from Statistics Canada.
It is important to note that because MAID is not considered a cause of death by the World Health Organization, the number of MAID provisions should not be compared to cause of death statistics in Canada to assess prevalence of MAID or to rank MAID as a cause of death (see Appendix B for more detail).
As stated by the World Health Organization, a "cause of death" is the disease or injury that initiated the train of events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury.Footnote 10 MAID, by contrast, is a health service provided as part of end-of-life or complex care, which a person can access in very limited circumstances (i.e., if they meet the strict eligibility criteria outlined in the legislation, including having a "grievous and irremediable medical condition," described in greater detail in Section 3.1). For example, if a person suffering from advanced cancer chooses to receive MAID to alleviate their suffering at the end of their life, the cause of death extracted from their death certificate for the purposes of vital statistics will be cancer.
Consistent with previous years, the majority of MAID provisions occurred in Quebec (36.5%), Ontario (30.3%) and British Columbia (18.0%) in 2023, with these three provinces accounting for nearly 85% of all MAID provisions (Table 2.2a). The number of MAID provisions increased in most jurisdictions, except for Prince Edward Island where the number remained the same as in 2022, and in the Yukon and Newfoundland and Labrador where the number decreased.
MAID was administered by a practitioner in nearly all cases. In 2023, MAID was self-administered in fewer than five instances. While self-administration of MAID is permitted in all jurisdictions in Canada (except for Quebec), very few people have chosen this option since 2016.
| Province or territory | MAID provisions | |
|---|---|---|
| Count | Percent (%) | |
| N.L. | 72 | 0.5 |
| P.E.I. | 44 | 0.3 |
| N.S. | 359 | 2.3 |
| N.B. | 299 | 1.9 |
| Que. | 5,601 | 36.5 |
| Ont. | 4,644 | 30.3 |
| Man. | 227 | 1.5 |
| Sask. | 344 | 2.2 |
| Alta. | 977 | 6.4 |
| B.C. | 2,759 | 18.0 |
| Y.T.Table 2.2a Footnote a | X | X |
| N.W.T.Table 2.2a Footnote a | X | X |
| Nvt. | 0 | 0.0 |
| Total | - | 100% |
|
||
Age
In 2023, the median age of MAID recipients was 77.6 years. The median age of Track 1 and Track 2 MAID recipients was 77.7 years and 75.0 years respectively. The average age of MAID recipients has been increasing slightly from year to year, from 75.2 in 2019 to 77.0 in 2022.Footnote 11 The average age of MAID recipients across different jurisdictions is provided in Table D.4 (Appendix D).
Figure 2.2a depicts the proportion of individuals receiving MAID across the age groups under Tracks 1 and 2. The 75 to 84 age group was most cited. As expected, a greater percentage of MAID Track 1 recipients were 75 years or older (59.7%) compared to Track 2 (50.2%), while a greater percentage of Track 2 MAID recipients were under 64 years of age (23.5%) compared to Track 1 (13.8%).
Figure 2.2a: MAID provisions, by track and age category, as a percentage of provisions within each track

Figure 2.2a: Text description
| Age group | Track 1 (%) | Track 2 (%) |
|---|---|---|
| 18 to 44 | 1.1 | 4.0 |
| 45 to 54 | 2.4 | 7.2 |
| 55 to 64 | 10.4 | 12.2 |
| 65 to 74 | 26.4 | 26.4 |
| 75 to 84 | 32.5 | 29.4 |
| 85 and older | 27.3 | 20.7 |
Figure 2.2b provides a breakdown of MAID provisions by sex and track. Slightly more men (51.2%) than women (48.8%) received MAID, similar to 2022. However, breaking these findings down further by track demonstrates that while more men received MAID under Track 1 (men 51.6% vs. women 48.4%), more women received MAID under Track 2 (women 58.5% vs. men 41.5%). A breakdown of MAID provisions by sex by jurisdiction is provided in Table D.3 (Appendix D).
These findings are consistent with overall population health trends. Women are more likely to experience long-term chronic conditions, such as osteoarthritis, osteoporosis, dementia, asthma and rheumatoid arthritis.Footnote 12Footnote 13 While such conditions can cause enduring suffering, they would not typically make a person's death reasonably foreseeable. In contrast, men experience higher rates of heart disease and the most severe forms of cancer, which have a higher mortality burden.Footnote 14
Figure 2.2b: MAID provisions, by track and sex, as a percentage of provisions within each track

Figure 2.2b: Text description
| Track | Female (%) | Male (%) |
|---|---|---|
| Track 1 | 48.4 | 51.6 |
| Track 2 | 58.5 | 41.5 |
| Combined | 48.8 | 51.2 |
2.3 Requests not resulting in MAID
Request was determined to be ineligible
Although Track 2 provisions represent 4.1% of MAID cases, they represent 26.9% of total ineligible requests.
A MAID request is reported as "ineligible" if a practitioner or preliminary assessor has determined that the person did not meet one or more of the eligibility criteria outlined in the legislation, without necessarily having assessed all the criteria. In 2023, 915 individuals who requested MAID were determined to ineligible for the procedure. Additionally, it is possible that this finding is an underrepresentation of ineligible requests given that not all practitioners and MAID care coordination systems had transitioned to the updated MAID reporting requirements at the beginning of 2023. Given that reporting is now triggered by a written or verbal request, as discussed in Section 2.1, one could expect to see a higher number of MAID cases determined to be ineligible in 2023 (and in future years) compared to previous years.
Among the 915 individuals determined to be ineligible for MAID, 45.5% were assessed as Track 1 and 26.9% were assessed as Track 2. The remaining 27.7% had not been assessed as either Track 1 or Track 2. It is worth noting that, although Track 2 provisions represent 4.1% of MAID cases, they represent 26.9% of ineligible requests.
Table 2.3a outlines the reasons why people were found ineligible for MAID, based on the legislative criteria. The most common reason for a request being determined to be ineligible was due to the person being assessed as incapable of making decisions with respect to their health. Other common reasons were that the person was determined as not: being in an advanced state of irreversible decline; experiencing intolerable suffering; or having a serious and incurable illness, disease or disability.
| Practitioner indicated "no" to the following eligibility requirements | Responses, count |
|---|---|
| Was the person capable of making decisions with respect to their health? | 320 |
| Was the person in an advanced state of irreversible decline in capability? | 273 |
| Did the person's illness, disease or disability, or their state of decline cause them enduring physical or psychological suffering that was intolerable to them and could not be relieved under conditions that they considered acceptable? | 261 |
| Did the person have a serious and incurable illness, disease or disability? | 234 |
| Did the person give informed consent to receive MAID after having been informed of the means that are available to relieve their suffering, including palliative care? | 206 |
| Did the person make a voluntary request for MAID that, in particular, was not made as a result of external pressure? | 41 |
| Was the person eligible for health service funded by a government in Canada? | 12 |
| Was the person at least 18 years of age?Table 2.3a Footnote a | X |
|
|
Request was withdrawn
A person can withdraw during the MAID assessment or after completion of the assessment. In 2023, 496 individuals withdrew their request for MAID, of whom 61.1% (n=303) were assessed as Track 1 and 17.7% (n=88) were assessed as Track 2. The remaining (21.2%, n=105) individuals were not yet assessed as either Track 1 or Track 2. The federal reporting requirements require practitioners to declare if an individual withdrew their request immediately before giving consent and receiving MAID. There were 36 people who withdrew their request at this time. If considered as a percentage of all withdrawals within the track, 11.2% of Track 1, and 2.3% of Track 2 withdrawals happened immediately before a scheduled MAID provision.
Under the federal monitoring regime for MAID, practitioners must provide the reason(s) why a person is withdrawing their request for MAID. These reasons are outlined in Table 2.3b. The most common reasons for withdrawing a MAID request were that the person changed their mind upon learning additional information about MAID, "other", and that the person accepted other available means to relieve their suffering. Among those accepting other available means to relieve their suffering, the means that were most often pursued were pharmacological, non-pharmacological (e.g., neuro stimulation, electroconvulsive therapy) and counselling.
| Reason a person withdrew their request for MAID | Responses, count |
|---|---|
| Upon learning additional information about MAID, the person decided it was not a path they wish to pursue | 177 |
| The person accepted means to relieve their suffering | 140 |
| Individuals who the person considers important in their lives (religious leaders, family, caregivers, or professionals) do not support MAID | 30 |
| Meeting the needs of a transfer and/or consultation were too cumbersome for the person | 6 |
| Other | 189 |
| Unknown | 30 |
Died of another cause
In 2023, 2,906 individuals who requested MAID died prior to receiving it. When practitioners report this outcome, they must provide, if known, at least one reason why the person died a natural death before they were able to receive MAID. Table 2.3c outlines these reasons, along with the frequency and median number of days between a MAID request and the individual's death. Individuals who died before they had selected a date for receiving MAID had the longest median time between request and death (32 days). All other groups had a median time of less than 24 days between request and death, for the following reasons: the referral was made too late; no assessor or provider was readily available; assessments were not completed; the person was eligible but died before the scheduled MAID provision; the person lost capacity before the waiver of final consent was completed; or operational issues. These findings bring into focus how even modest delays can interfere with a person's ability to receive MAID.
| Reason for natural death before MAID could be provided | Days between request and death, median | Frequency of responses, count |
|---|---|---|
| Person never chose a date to proceed with MAID provision | 32 | 795 |
| Operational issues (i.e., could not be moved to a facility that allowed MAID, medication shortages, bed shortages, health care personnel unavailable)
|
24 | 24 |
| Person was found eligible but died before scheduled MAID provision | 16 | 864 |
| Other | 15 | 145 |
| Loss of capacity to consent without a waiver of final consent being completed | 13 | 84 |
| Person died before both assessments were completed | 7 | 503 |
| No assessor/provider available/willing | 6 | 19 |
| Person was referred or requested MAID too late (i.e. referral time was too short) | 4 | 319 |
| Lack of pharmacy willing to provide MAID medicationsTable 2.3c Footnote a | X | X |
|
||
A breakdown of requests not resulting in MAID by jurisdiction is provided in Table D.1 (Appendix D).
3 MAID assessments: grievous and irremediable medical conditions
3.1 Most common serious and incurable illnesses
Cancer was the most common medical condition among people who received MAID under Track 1; neurological and "other" conditions were the most frequently cited among people who received MAID under Track 2.
In order to be eligible for MAID (both Tracks 1 and 2), a person must have a "grievous and irremediable medical condition". This criterion is met only when assessors are of the opinion that:
- the person has a serious and incurable illness, disease, or disability;
- the person is in an advanced state of irreversible decline in capability; and
- the illness, disease, or disability or that state of decline causes the person enduring physical or psychological suffering that is intolerable to the person and cannot be relieved under conditions that the person considers acceptable.
The nature and severity of the medical condition(s) a person experiences will have a significant bearing on a practitioner's judgement regarding whether or not each of the three elements of the "grievous and irremediable medical condition" eligibility criterion apply. Eligibility is always assessed on an individual basis and takes all relevant circumstances into account.
For each MAID request, a practitioner must report on the specific serious and incurable illness that is the cause of the individual's suffering. However, individuals requesting MAID very often suffer from more than one serious and incurable medical condition (see Section 3.4). This can create a challenge for reporting as practitioners must consider all of the requester's circumstances, and singling out only one medical condition may not reflect the seriousness of the person's condition and the suffering they experience.
For this reason, practitioners may – and often do – select more than one medical condition, and do not rank them in order of most significant impact on the individual's health. The broad categories provided to practitioners for MAID reporting purposes are cancer, neurological conditions, respiratory diseases, cardiovascular conditions, organ failure and "other" conditions (practitioners can select more than one). The conditions provided for the "other" conditions category include: diabetes, frailty, autoimmune conditions, chronic pain and mental disorders, but practitioners sometimes listed other conditions such as joint bone and muscle issues, hearing and visual issues and various internal diseases in the write-in fields. Note that within the broad categories, practitioners can select multiple specific conditions.
For those who received MAID under Track 1, cancer was the most frequently cited medical condition (n=9,435), followed by "other" conditions (n=3,918), then cardiovascular conditions, such as congestive heart failure, atrial fibrillation or vasculopathy (n=2,416). For Track 2, the most frequently indicated medical condition were neurological conditions (n=349) and "other" conditions (n=343).
The full list of reported conditions, and the percentage reported among men and women, is provided in Figure 3.1a. When reports for each medical condition are compared by sex under Track 1, proportionally more men than women were reported under each medical condition; the exception is the "other" conditions category, where a greater number of women were reported than men. Under Track 2, there were more women than men reported with each medical condition.
Figure 3.1a: Medical condition by track and sex, as a percentage of those within each track reporting the medical condition
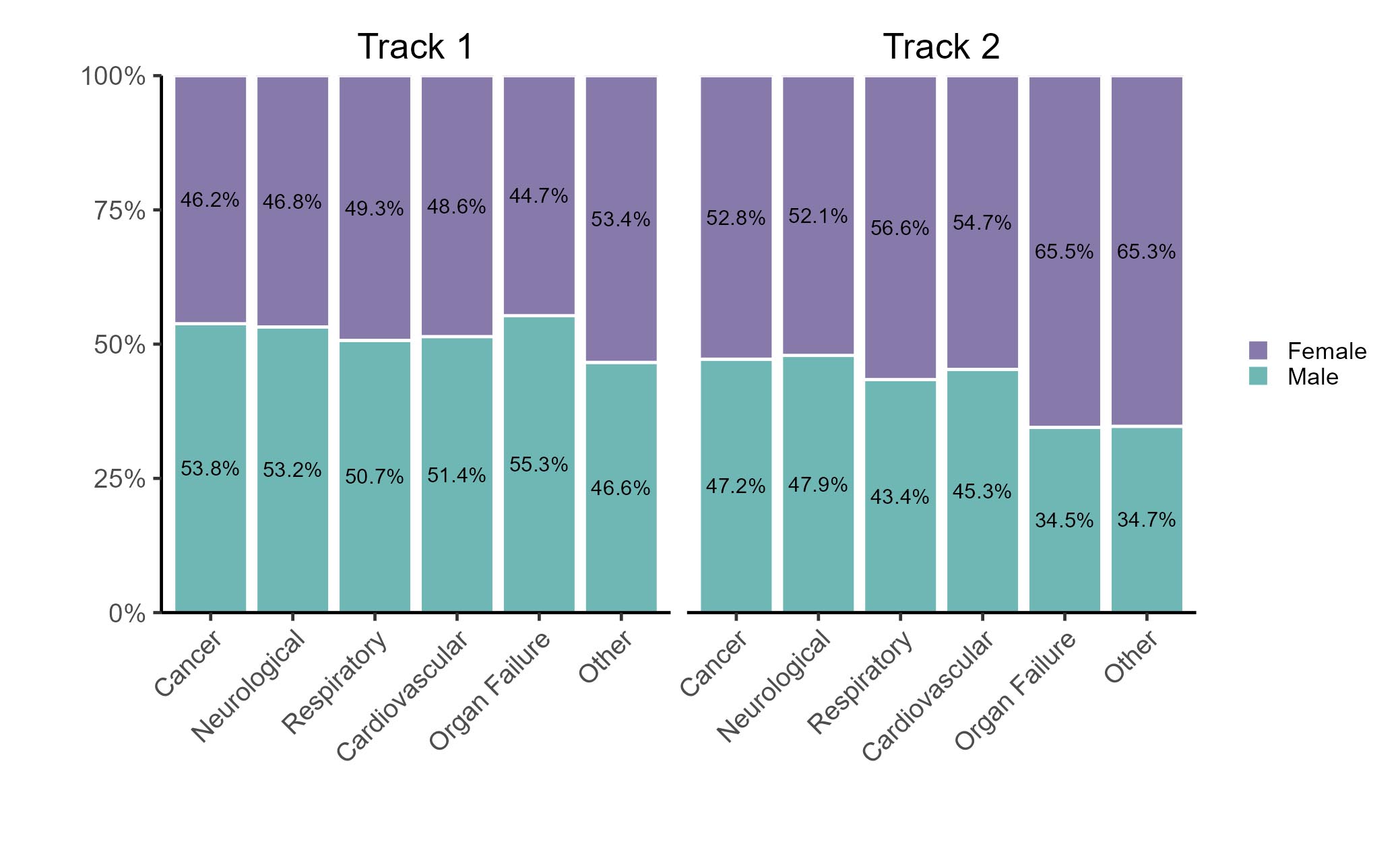
Figure 3.1a: Text description
| Medical condition | Track 1 | Track 2 | ||
|---|---|---|---|---|
| Male (%) | Female (%) | Male (%) | Female (%) | |
| Cancer | 53.8 | 46.2 | 47.2 | 52.8 |
| Neurological | 53.2 | 46.8 | 47.9 | 52.1 |
| Respiratory | 50.7 | 49.3 | 43.4 | 56.6 |
| cardiovascular | 51.4 | 48.6 | 45.3 | 54.7 |
| Organ failure | 55.3 | 44.7 | 34.5 | 65.5 |
| Other | 46.6 | 53.4 | 34.7 | 65.3 |
Cancer-related illness was the most frequently cited medical condition among people of nearly all age groups who received MAID in 2023. The exception is those 85 years or older for whom "other" conditions were the most frequently cited. Figure 3.1b depicts the age distribution of people reporting each underlying medical condition. For cardiovascular conditions, "other" conditions and organ failure, the largest age group was people aged 85 years or older. For cancer, neurological conditions and respiratory disease, the largest age group was 75 to 84 year olds. People receiving MAID that were reported as having cancer and neurological conditions were younger (i.e., a larger percentage of these individuals were aged 18 to 54 and 55 to 64) compared to those reporting the other conditions.
Figure 3.1b: Medical condition by age group, as a percentage of those reporting each medical condition
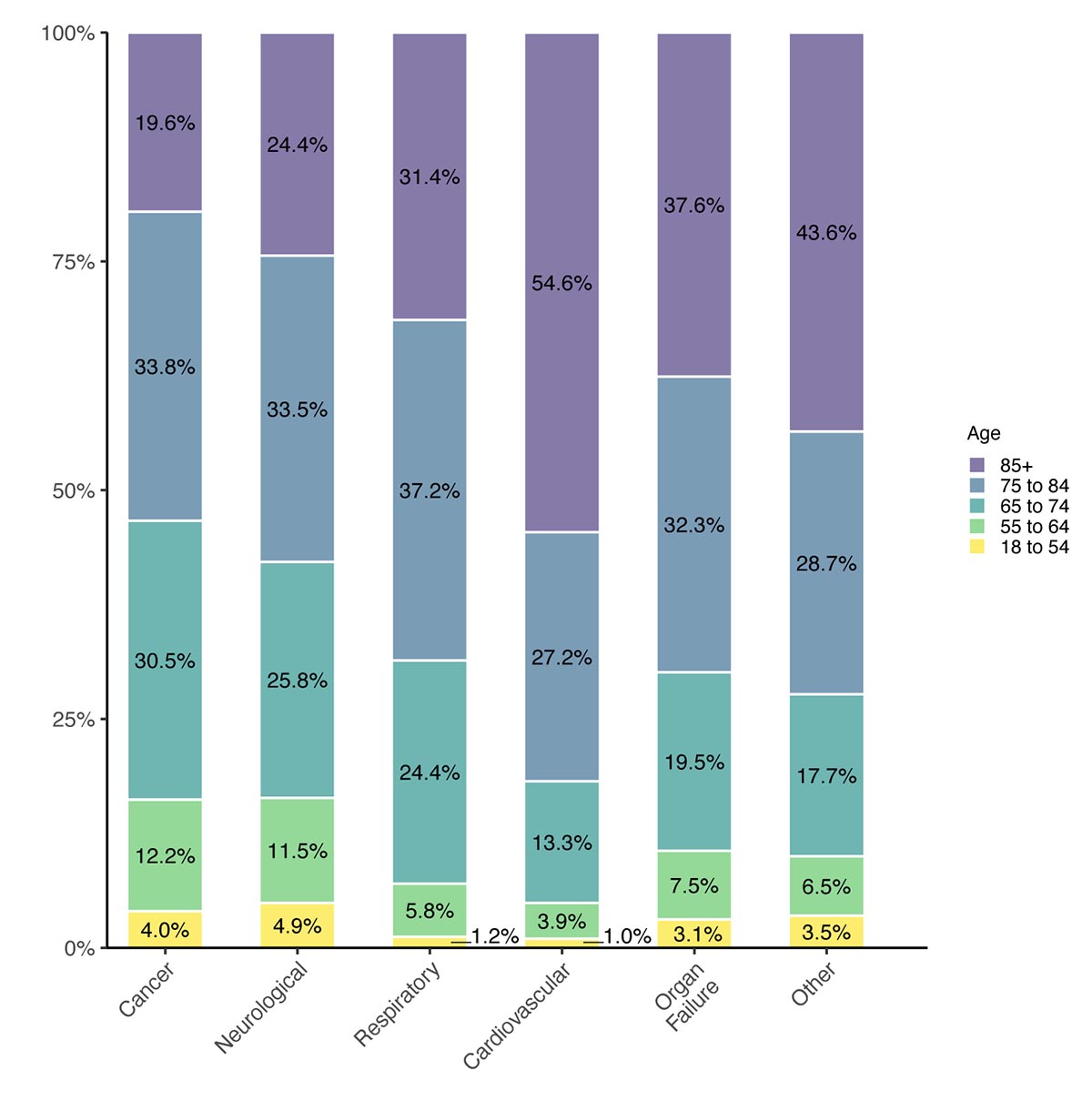
Figure 3.1b: Text description
| Medical condition | Age group | ||||
|---|---|---|---|---|---|
| 18 to 54 (%) | 55 to 64 (%) | 65 to 74 (%) | 75 to 84 (%) | 85 and older (%) | |
| Cancer | 4.0 | 12.2 | 30.5 | 33.8 | 19.6 |
| Neurological | 4.9 | 11.5 | 25.8 | 33.5 | 24.4 |
| Respiratory | 1.2 | 5.8 | 24.4 | 37.2 | 31.4 |
| cardiovascular | 1.0 | 3.9 | 13.3 | 27.2 | 54.6 |
| Organ failure | 3.1 | 7.5 | 19.5 | 32.3 | 37.6 |
| Other | 3.5 | 6.5 | 17.7 | 28.7 | 43.6 |
Among MAID recipients with cancer, the most frequently specified types were lung, colorectal, hematological, and pancreatic cancer. Among MAID recipients with neurological conditions, the most frequently specified conditions were Parkinson's disease, Amyotrophic Lateral Sclerosis (ALS or, Lou Gehrig's disease), dementia and multiple sclerosis. As noted previously, practitioners can report more than one medical condition (e.g., both cancer and a neurological condition). Within each medical condition, they can also report more than one type per individual (e.g., both lung cancer and breast cancer).
Table D.2 (Appendix D) provides an overview of the medical conditions among MAID recipients, broken down by sex, MAID track, and province.
3.2 Frailty and chronic pain
Frailty and chronic pain are known sources of enduring and intolerable suffering. Indeed, frailty and chronic pain were the most frequently reported medical conditions among MAID recipients with medical conditions categorized as "other". While there is no doubt both are serious medical conditions, they are complex and vary greatly from person to person, which can pose challenges for MAID assessors.
Frailty
Frailty is a common clinical diagnosis in older adults that puts them at increased risk for poor health outcomes including falls, hospitalization, and mortality.Footnote 15 Frailty may include loss of muscle mass and strength, cognitive impairment, fatigue or exhaustion, weakness, and reduced tolerance to medical interventions, leading to poor health outcomes. People who are frail are less resilient, having a reduced ability to recover from a stressor or illness. The Canadian Frailty Network reports that over 1.5 million Canadians over the age of 65 are "medically frail".Footnote 16 A research study published by Statistics Canada in 2021 found that older adults who were frail were more than three times as likely to die as those who were not frail (25% vs. 7%).Footnote 17 While frailty is often chronic, progressive, and associated with shortened survival, some individuals may be able to improve their frail status.Footnote 18 Physicians have reported challenges in MAID assessments for frail individuals, given the dynamic nature of frailty and ambiguities in the interpretation of the eligibility criteria as they relate to frailty.Footnote 19
Table 3.2a provides a breakdown of MAID cases where frailty was reported by age, sex and track. Frailty was reported as a medical condition for 1,392 MAID recipients (1,319 Track 1 MAID cases and 73 Track 2 MAID cases), and it was the sole medical condition in 92 of these cases. In all cases where frailty was the sole medical condition, the individual was over the age of 75, with the majority being aged 85 years or older (86.6%) and female (72.9%). The vast majority of people for whom frailty was reported as the sole medical condition received MAID under Track 1. Consistent with research on frailty in Canada,Footnote 20 frailty was more commonly reported among women than men in the context of MAID. Among MAID recipients reported as having frailty, the other most commonly reported medical conditions were cardiovascular conditions, cancer, and neurological conditions.
| Prevalence of frailty among MAID recipients | Track 1, count | Track 2, count |
|---|---|---|
| All people indicating frailty as a medical condition | 1,319 | 73 |
| Characteristics of those with frailty | Track 1, percent (%) | Track 2, percent (%) |
| 18 to 74 | ||
| Male | 4.8 | 12.3 |
| Female | 4.7 | 16.4 |
| 75 to 84 | ||
| Male | 9.3 | 11.0 |
| Female | 11.9 | 11.0 |
| 85 and older | ||
| Male | 22.3 | 13.7 |
| Female | 47.1 | 35.6 |
| Total | 100% | 100% |
Chronic pain
Similar to frailty, chronic pain is recognized as a potentially debilitating illness. The World Health Organization now recognizes chronic pain as a disease, rather than only an outcome of something else.Footnote 21 Chronic pain is generally understood as pain lasting three months or longer and may result from an underlying disease or treatment (i.e., cancer treatment, rheumatoid arthritis) or have no identifiable cause (i.e., fibromyalgia).Footnote 22 Individuals with chronic pain:
- May experience fluctuations in pain severity.Footnote 23
- Often encounter challenges related to the availability and accessibility of treatment such as long wait times, limited access to services in rural and remote areas and financial barriers to accessing certain services, such as psychological support and physiotherapy.Footnote 24
- Often have a co-morbid psychiatric condition, such as major depressive disorder.Footnote 25
These factors can create challenges in the context of a MAID eligibility assessment.
Table 3.2b provides a breakdown of MAID cases where chronic pain was reported by age, sex and track. As shown in the table, chronic pain was reported in 767 Track 1 MAID cases and 166 Track 2 MAID cases, for a total of 933 cases. Chronic pain was the sole medical condition in 23 of these cases. In the absence of additional information, it is unclear what the cause of the individual's pain was, and how it would contribute to an assessment of whether they were in Track 1 or Track 2. Consistent with research on chronic pain in Canada,Footnote 26 chronic pain was more commonly reported among women than men in the context of MAID. It was most commonly reported among women aged 85 years or older who received MAID under Track 1. Among MAID recipients reported as having chronic pain, the other most commonly reported medical conditions were cancer, cardiovascular conditions, and respiratory diseases.
| Prevalence of chronic pain among MAID provisions | Track 1, count | Track 2, count |
|---|---|---|
| All people indicating chronic pain as a medical condition | 767 | 166 |
| Characteristics of those with chronic pain | Track 1, percent (%) | Track 2, percent (%) |
| 18 to 64 | ||
| Male | 5.2 | 12.6 |
| Female | 4.4 | 18.6 |
| 65 to 74 | ||
| Male | 8.1 | 9.0 |
| Female | 6.9 | 13.2 |
| 75 to 84 | ||
| Male | 10.6 | 6.6 |
| Female | 13.6 | 18.0 |
| 85 and older | ||
| Male | 15.6 | 5.4 |
| Female | 35.6 | 16.8 |
| Total | 100% | 100% |
3.3 Dementia
Dementia is an umbrella term used to describe a set of symptoms affecting brain function that are caused by neurodegenerative and vascular diseases or injuries.Footnote 27 It is characterized by a decline in cognitive abilities and can also affect mood and behaviour.Footnote 28 A person with dementia may request and receive MAID as long as they meet the eligibility criteria.
In contrast, people suffering exclusively from mental illness are not currently eligible for MAID through the temporary exclusion in the Criminal Code which is slated for repeal in March 2027. This exclusion applies to conditions primarily within the domain of psychiatry which raise concerns related to suicidality and challenges associated with assessing capacity and determining irremediability; it does not apply to dementia.Footnote 29
MAID eligibility assessment for people with dementia involves complex considerations. The Canadian Association of MAID Assessors and Providers has developed guidance for practitioners to help them assess if a person with dementia requesting MAID is in "an advanced state of irreversible decline in capability", can provide informed consent and has a reasonably foreseeable natural death.Footnote 30 According to the guidance document, an individual may be in "an advanced state of irreversible decline in capability," if the loss of capacity is believed to be imminent.Footnote 31 Additionally clinicians can assess the capacity of a person to consent to MAID with the aid of available empirical tools; they are advised to systematically document their findings regarding the ability of the person to communicate choice, understand the relevant information, appreciate the consequences of the decision and reason about the alternatives.Footnote 32
Dementia was reported as a medical condition in 241 people who received MAID in 2023. Of these, slightly less than half (n=106) were reported as having dementia as the sole medical condition. Table 3.3a provides a breakdown of these cases by sex and track. In the majority (76.4%) of these cases, the person received MAID under Track 1; the remainder (23.6%) received MAID under Track 2.
| Track 1 | Track 2 | |||
|---|---|---|---|---|
| Count | Percent (%) | Count | Percent (%) | |
| Male | 45 | 42.5 | 11 | 10.4 |
| Female | 36 | 34.0 | 14 | 13.2 |
| Total | 81 | 76.4% | 25 | 23.6% |
3.4 Length of time living with a serious and incurable illness, disease or disability
People who received MAID under Track 2 lived with a serious and incurable condition for a much longer period of time than those who received MAID under Track 1.
Practitioners are required to report how long the person requesting MAID has had a serious and incurable illness, disease or disability.
Table 3.4a outlines the length of time MAID recipients lived with a serious and incurable illness, disease or disability, broken down by track. People receiving MAID under Track 2 tended to live with a serious and incurable condition for a longer period of time than those receiving MAID under Track 1: 31.8% of people receiving MAID under Track 2 lived with a serious and incurable illness, disease or disability for more than 10 years, compared to 7.7% of those under Track 1. In contrast, 4.4% of people receiving MAID under Track 2 lived with a serious and incurable illness, disease or disability for less than one year, compared to 41.4% of those under Track 1.
Length of time with serious incurable illness |
Track 1, percent (%) |
Track 2, percent (%) |
|---|---|---|
| Less than 1 year | 41.4 | 4.4 |
| Between 1 and less than 5 years | 33.5 | 36.0 |
| Between 5 and less than 10 years | 9.5 | 18.9 |
| More than 10 years | 7.7 | 31.8 |
| Do not know | 7.9 | 8.9 |
| Total | 100% | 100% |
In addition, many MAID recipients lived with more than one serious and incurable medical condition for a significant duration of time. Among MAID recipients in both Tracks 1 and 2 who were living with a serious and incurable medical condition for less than one year, 72.9% had one medical condition, 17.4% had two medical conditions and the remaining 9.7% had three or more medical conditions.Footnote 33 For those living with a serious and incurable medical condition for more than one year, 66.6% had one medical condition and 20.5% had two medical conditions and the remaining 12.9% had three or more medical conditions.
3.5 Advanced state of irreversible decline in capability
The second element of the "grievous and irremediable medical condition" eligibility criterion is that the person is in "an advanced state of irreversible decline in capability". This is understood to mean that the reduction in the person's ability to undertake activities that are meaningful to them is severe and cannot be improved through reasonable interventions.Footnote 34 This loss of capability may be sudden, gradual, ongoing, or stable.Footnote 35
The most frequently cited indicator of irreversible decline in capability reported by practitioners was an inability of the person to do most or all activities of daily living (e.g., feeding, bathing and toileting oneself), or instrumental activities of daily living (e.g., managing finances, meal preparation, managing medications). This was followed by persistent significant fatigue or weakness, and chronic pain. It is important to note that practitioners often reported more than one reason for a person being in an irreversible state of decline. For example, in more than half of MAID cases, practitioners reported that the person was both incapable of performing activities of daily living and experienced significant fatigue.
3.6 Nature of suffering
The third element of the "grievous and irremediable medical condition" eligibility criterion is that the person is experiencing "enduring physical or psychological suffering that is intolerable to them and that cannot be relieved under conditions that they consider acceptable."
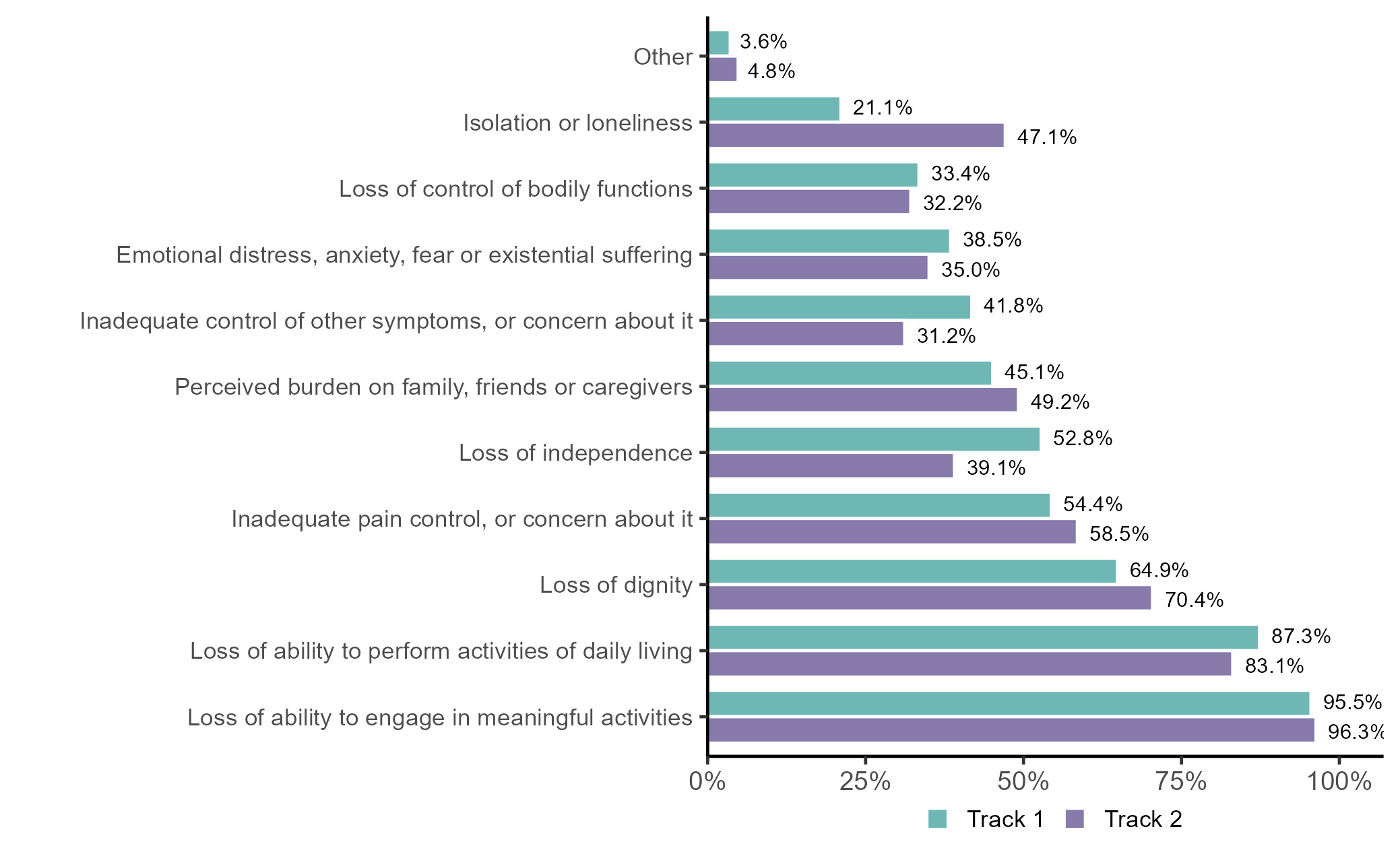
Figure 3.6a outlines the sources of suffering related to the person's medical condition that were reported by practitioners. As shown in the figure, loss of ability to engage in meaningful activities was the most commonly reported source of suffering among MAID recipients in both Tracks 1 and 2. This finding is consistent with previous years. Track 1 recipients were more likely to report loss of ability to perform activities of daily living, loss of independence and inadequate control of other symptoms than Track 2 recipients. In contrast, Track 2 recipients were more likely to report loss of dignity, inadequate pain control, and isolation or loneliness than Track 1 recipients. As discussed in Section 3.2, chronic pain was sometimes reported as one of the medical conditions for which a person received MAID (and less frequently, as the sole condition). Pain is also prevalent in patients with cancer and at the end stages of chronic and progressive disease.Footnote 36 In almost every instance, practitioners reported more than one source of suffering related to the person's medical condition. Practitioners most commonly reported five sources of suffering.
Figure 3.6a: Reported nature of suffering, by trackFigure 3.6a Footnote a
- Figure 3.6a Footnote a
-
More than one option could be selected. Totals will exceed 100%.
Figure 3.6a: Text description
| Type of suffering | Track 1 (%) | Track 2 (%) |
|---|---|---|
| Loss of ability to engage in meaningful activities | 95.5 | 96.3 |
| Loss of ability to perform activities of daily living | 87.3 | 83.1 |
| Loss of dignity | 64.9 | 70.4 |
| Inadequate pain control, or concern about it | 54.4 | 58.5 |
| Loss of independence | 52.8 | 39.1 |
| Perceived burden on family, friends and caregivers | 45.1 | 49.2 |
| Inadequate control of other symptoms, or concern about it | 41.8 | 31.2 |
| Emotional distress, anxiety, fear or existential suffering | 38.5 | 35.0 |
| Loss of control of bodily functions | 33.4 | 32.2 |
| Isolation or loneliness | 21.1 | 47.1 |
| Other | 3.6 | 4.8 |
3.7 Determination of the MAID request as voluntary
The federal legislation stipulates that an individual's request for MAID must be voluntary and not made as a result of external pressure. As part of their reporting obligations when providing MAID, practitioners are required to specify how they formed the opinion that the individual's MAID request was voluntary. Results for 2023 are consistent with findings from previous years.
In virtually all cases where MAID was provided, practitioners reported that they had consulted directly with the person to determine the voluntariness of the request for MAID. Other commonly stated approaches for confirming this opinion include consultation with family members or friends, review of the person's medical records, and consultation with other health or social service professionals. A full list is provided in Table 3.7a.
| Indication that MAID request was voluntary | Responses, count |
|---|---|
| Consultation with person | 15,248 |
| Consultation with family members or friends | 9,947 |
| Person's medical records | 8,257 |
| Consultations with other health or social service professionals | 6,221 |
| Knowledge of person from prior consultations or treatments for reasons other than MAID | 2,062 |
| Other | 45 |
4 Socio-demographic considerations, access and inequality
4.1 Importance and challenges of collecting data on identity
In 2021, the Criminal Code was amended to allow expanded data collection on MAID to include information respecting race, Indigenous identity and disability. The purpose of this data collection is to help determine the presence of individual or systemic inequity or disadvantage in the context of the delivery of MAID. As a result, the Regulations for the Monitoring of MAID were amended to align with these legislative changes (along with several additional/modified reporting requirements as outlined in Appendix A).
Health Canada's guidance document for practitioners and preliminary assessors is aligned with the current MAID monitoring regulations. This document clarifies that the data elements on race, Indigenous identity and disability are "self-identification" questions and must reflect how the person identifies themselves.Footnote 37 Responses do not reflect legal status or registration in the case of Indigenous identity and they should not be a health care professional's interpretation based on the appearance or other characteristics of the person, which could skew the data. The person must also consent to the collection of this information.
It is recognized that an individual's willingness to self-identify during the MAID assessment process, or any clinical encounter, depends on many factors. The person could have concerns about how this information may be used and how it could impact the services they are offered. Experiences of racism and discrimination could also deter a person from self-identifying. For instance, Indigenous Peoples frequently report experiences of anti-Indigenous racism in the health care system, resulting in an erosion of trust.Footnote 38
Given this, practitioners and preliminary assessors are encouraged to provide open and transparent information to the person about the purpose of collecting these data (i.e., to better understand the characteristics of people seeking MAID and help to determine if there are any groups or populations that are disproportionately impacted in the context of MAID). They are also encouraged to clarify that providing the information is voluntary and that refusal to answer questions will not affect the person's care or MAID assessment.
Data collection on identity in 2023
As mentioned in Section 1.3, given that 2023 was the first year of data collection under the amended MAID monitoring regulations, there are data limitations of note. These should be kept in mind when reviewing the sections below, particularly in regards to the quality and reliability of the self-identification data.
Provinces and territories have also taken different approaches to the collection of this information. In some jurisdictions, including British Columbia, the Northwest Territories, and Alberta, this information is collected through patient request forms. In provinces such as Saskatchewan and Manitoba, it is collected through care coordination services. In remaining jurisdictions, it is up to individual practitioners to ask the requester if they wish to self-identify.
The varied approach to how these important and sensitive questions are asked has led to inconsistent results across provinces and territories, and concerns about the quality of the data collected. For example, in jurisdictions where the information must be collected by the provider, practitioners have reported being reluctant to ask this series of questions (even though a person can choose not to self-identify). This reluctancy stems from concerns regarding the impact on the clinical relationship or the potential to create distrust. In jurisdictions that have used a patient request form or in care coordination systems, definitions for terms (such as disability) are not always provided leading to inconsistent responses and response rates across provinces and territories. Health Canada has published the data collected, wherever possible, in the interests of transparency, but acknowledges that analyses of these data are limited.
As mentioned in Section 1.3, Health Canada has established a dedicated working group made up of federal, provincial and territorial officials committed to improving data collection, consistency and quality going forward. More details regarding data limitations are provided in Appendix B.
4.2 MAID by racial, ethnic or cultural group
In the context of a MAID request, preliminary assessors or practitioners are instructed to ask the person to indicate to which racial, ethnic or cultural group they belong. The racial, ethnic or cultural group categories are based on guidance from the Canadian Institute of Health InformationFootnote 39 and consistent with the Statistics Canada "visible minority" identity question in the Census, 2021.Footnote 40 Individuals who identify with multiple groups or mixed groups can select more than one of the listed categories, or may choose to provide specific details under the "specify other race category".Footnote 41
A total of 9,619 people of the 15,343 who received MAID responded to this question, the vast majority of whom (95.8%) identified as Caucasian (White).Footnote 42 The second most commonly reported racial, ethnic or cultural identity was East Asian (1.8%). Given both the data limitations (noted in Section 4.1), and the relative homogeneity of the responses provided, it is not possible to undertake more meaningful analysis with respect to potential differences with respect to the provision of MAID according to racial or ethnic identity. The proportion of MAID recipients identifying as Caucasian (White) across different jurisdictions is provided in Table D.3 (Appendix D).
4.3 Indigenous people who received MAID
First Nations, Inuit and Métis Peoples have diverse views on MAID. This was demonstrated during Parliamentary discussions of former Bill C-7. During these discussions, some expressed concerns that Indigenous Peoples, and others who may experience social inequality, could request and receive MAID in the absence of adequate health and social supports.Footnote 43Footnote 44Footnote 45 Others, however, noted that making an informed decision about MAID, in the context of a trusting relationship with health care practitioners, can be an important means of exercising self-determination.Footnote 46 More recent discussions with Indigenous Peoples also reflect that views on MAID are rich and varied (see text box).
Since 2022, Health Canada has been partnering with Indigenous organizations and governments who are leading community engagement and building organizational policy capacity on MAID and broader end-of-life care issues. In addition, from February to April 2024, Health Canada did a series of in-person and virtual national knowledge exchange roundtables with Indigenous Peoples. The following are some quotes from those discussions:
"Could we have a place for the end of life journey with MAID that would integrate our traditional values?"
"Culturally appropriate protocol should follow after the fact and is of great importance to Indigenous peoples. Knowing that these protocols are going to follow my passing can or will allow for me to help make this kind of decision."
"MAID is something that is really new to us and our older generation are still against it. In my community there are people who are Christian and that would not be allowed in that context and then there are people who follow traditional ways and it is something where there are many mixed feelings about it in our community"
More details regarding the engagement process are outlined in Appendix C.
In the context of a MAID request, preliminary assessors or practitioners are instructed to ask the person to indicate if they belong to one of the three constitutionally recognized groups of Indigenous Peoples: First Nations, Inuit and Métis, or choose more than one option, if applicable in their case.
In 2023, 80 people who received MAID identified as First Nations, 36 identified as Métis and 23 identified as both First Nations and Métis. Fewer than five individuals identifying as Inuit received MAID. Fewer than five people identifying as First Nations, Inuit or Métis received MAID under Track 2 (i.e., natural death was not reasonably foreseeable). The most commonly reported underlying medical conditions among Indigenous people who received MAID mirror those of the overall population of people in Canada who received MAID (see Section 3.1). In light of concerns regarding the quality of these data outlined previously, and the need to ensure the data are used and interpreted responsibly, Health Canada is not undertaking additional analysis of these data at this time.
Health Canada has begun having conversations with Indigenous partners regarding the collection and appropriate use of data on Indigenous identity in the context of MAID. Health Canada will share this feedback with provinces and territories and work with them to better understand the current processes in place for asking about Indigenous identity and identify opportunities for improvement. As well, Health Canada will continue to build relationships and engage with Indigenous rights-holders, governments and organizations to inform policy, practice and guidance for health professionals on MAID data collection.
Recognizing the limitations of the 2023 data on Indigenous identity, and the importance of Indigenous data sovereignty, the data on Indigenous identity will not be shared with outside researchers without further discussions with Indigenous partners.
4.4 Persons with disabilities who received MAID
Persons with disabilities are valued members of Canadian society. The disability community continues to be concerned about the influence of socioeconomic barriers faced by persons with disabilities. Reducing these barriers to inclusion will require collective effort by all levels of government. Through initiatives such as the Disability Inclusion Action Plan,Footnote 47 Canada is working to achieve the full and meaningful participation of persons with disabilities. It is recognized, however, that persons with disabilities continue to experience social and economic exclusion and discrimination when accessing health care services due to longstanding systemic inequities.
Against this backdrop, MAID (particularly MAID under Track 2 when death is not reasonably foreseeable) is a sensitive topic in the disability community. Some have expressed concerns about the potential impacts of the current legislation on broader societal beliefs regarding the value of the lives of persons with disabilitiesFootnote 48 and the risk of people requesting MAID in the absence of adequate supports.Footnote 49 It is important to note that having a disability in and of itself does not automatically make one eligible for MAID; one must meet the legislative eligibility criteria (listed previously in Section 3.1). Several enhanced safeguards are in place for individuals under Track 2 to provide additional protections.
Health Canada will continue to engage with persons with disabilities to better understand their views on MAID and its implementation.
In the context of a MAID request, preliminary assessors or practitioners are instructed to ask the person to indicate if they have a disability. If the person requests a further explanation as to what is meant by the term "disability", health care professionals are encouraged to describe this as "a functional limitation in any one of the following ten areas, which cannot be corrected with the use of aids: seeing, hearing, mobility, flexibility, dexterity, pain-related, learning, developmental, mental health related or memory."Footnote 50
As noted in Section 1.3 there are some concerns regarding the quality and reliability of these data, given that: some jurisdictions did not collect this information for the first part of 2023; there was variation in how this question was asked (i.e., sometimes the practitioner asked the question and sometimes the question was included in an old data collection form); and the definition of "disability" was not always provided. Despite these limitations, responses to the follow up questions among those who did self-identify were relatively consistent, thereby allowing for further analysis on key questions.
Table 4.4a outlines the number of people receiving MAID who self-reported having a disability and their distribution by track, sex, age and requirement for disability support services (An analysis of access to palliative care and disability support services in presented later in Section 5.1). Of the 10,581 people who responded to this series of questions, 3,633 self-identified as having a disability: 33.5% of Track 1 respondents self-identified as having a disability compared to 58.3% of Track 2 respondents. Proportionally more women than men reported having a disability which aligns with disability trends among the general population of Canada.Footnote 51
For Track 1, the share of people who self-reported having a disability increases with age. For Track 2, the largest proportion of people reporting a disability were in the 65 to 74 age group; the share gradually declines among the older age groups. Practitioners have noted some confusion regarding what constitutes a disability among Track 1 recipients who are near end of life and have limited quality of life. The difference between the two tracks and how they require and access disability support services reflects this, with the proportion of respondents who reported having a disability and requiring disability support services being higher in Track 2 (75.7%) than in Track 1 (68.4%). Table D.3 (Appendix D) provides a breakdown of those identifying as having a disability by track across jurisdictions.
| Track 1 | Track 2 | |||
|---|---|---|---|---|
| Prevalence of disability among people who received MAID | ||||
| Count | Count | |||
| Self-reported having a disability | 3,423 | 210 | ||
| Total respondents to the self-identified disability questionTable 4.4a Footnote a | 10,221 | 360 | ||
| Percent (%) | Percent (%) | |||
| Percentage of people reporting a disability, out of respondentsTable 4.4a Footnote a | 33.5 | 58.3 | ||
| Characteristics of those self-identifying as having a disability | ||||
| Count | Percent (%) | Count | Percent (%) | |
| Sex | ||||
| Male | 1,669 | 48.8 | 95 | 45.2 |
| Female | 1,754 | 51.2 | 115 | 54.8 |
| Age | ||||
| 18 to 44 | 45 | 1.3 | 10 | 4.8 |
| 45 to 54 | 82 | 2.4 | 19 | 9.0 |
| 55 to 64 | 349 | 10.2 | 31 | 14.8 |
| 65 to 74 | 768 | 22.4 | 59 | 28.1 |
| 75 to 84 | 1,009 | 29.5 | 54 | 25.7 |
| 85 and older | 1,169 | 34.2 | 37 | 17.6 |
| Required disability support services | ||||
| Yes | 2,342 | 68.4 | 159 | 75.7 |
| No | 646 | 18.9 | 34 | 16.2 |
| Do not know | 435 | 12.7 | 17 | 8.1 |
|
||||
Figure 4.4a outlines the types and frequency of reported disabilities among MAID recipients who self-identified as having a disability. The most frequently reported disabilities were mobility (reported by 2,903 people) and pain-related (reported by 1,840 people).
Figure 4.4a: Frequency of reporting each type of disability among those who self-reported having a disability
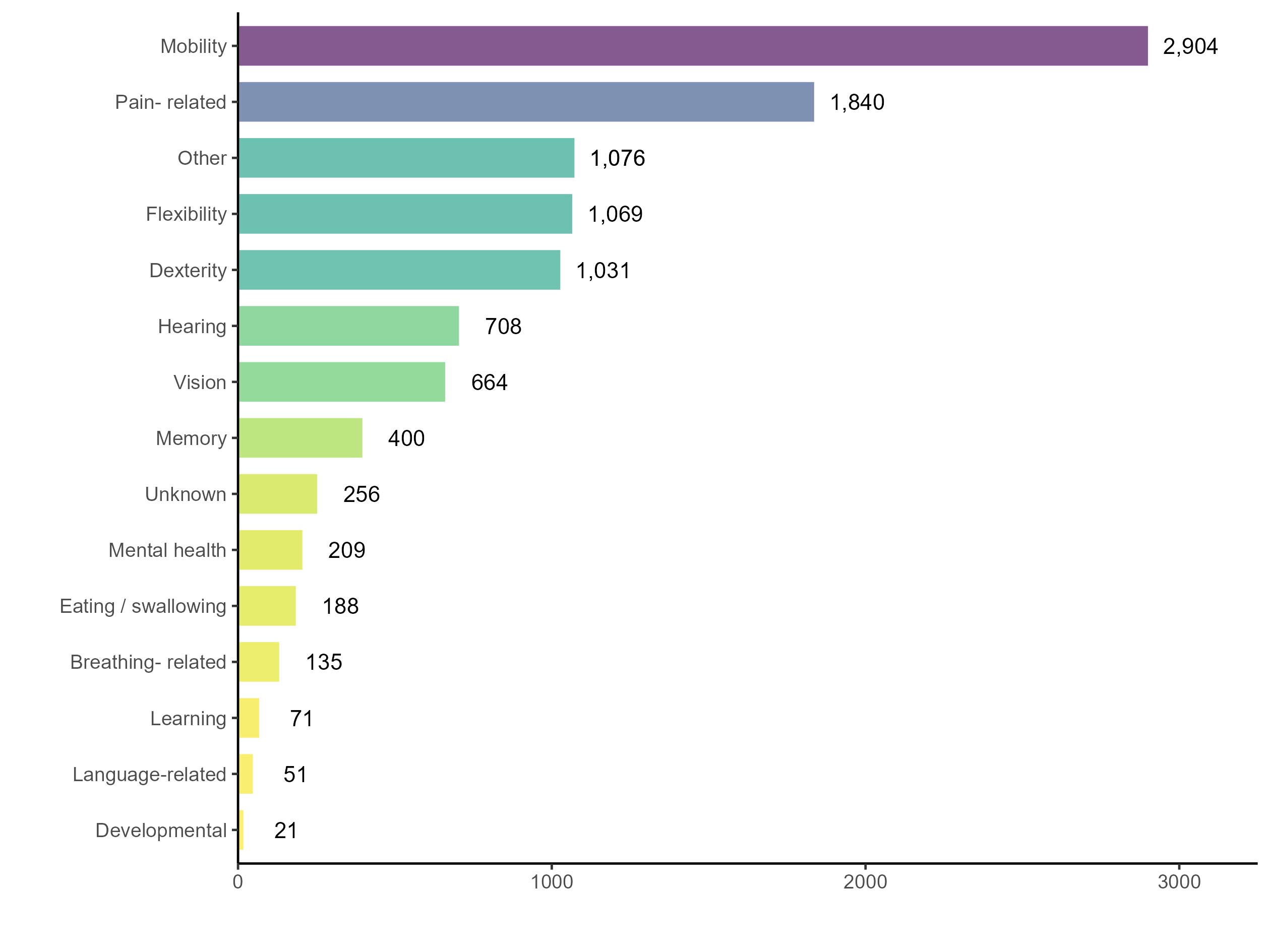
Figure 4.4a: Text description
| Type of disability | Frequency |
|---|---|
| Mobility | 2,904 |
| Pain-related | 1,840 |
| Other | 1,076 |
| Flexibility | 1,069 |
| Dexterity | 1,031 |
| Hearing | 708 |
| Vision | 664 |
| Memory | 400 |
| Unknown | 256 |
| Mental health | 209 |
| Eating and swallowing | 188 |
| Breathing related | 135 |
| Learning | 71 |
| Language-related | 51 |
| Developmental | 21 |
Time spent with a disability over the lifespan was calculated by dividing years reported with a disability by age at the time that MAID was provided. People receiving MAID under Track 1 who reported having a disability were found to have lived with a disability for 11.0% of their lifespan, on average. This same group under Track 2 was found to have lived with a disability for 20.3% of their lifespan, on average.
Table 4.4b outlines the medical conditions reported by persons who self-reported having a disability. In Track 1, the most frequently specified medical conditions among persons self-reporting as having a disability were cancer (45.6%) and "other" medical condition (46.2%). When assessing persons who self-report as having a disability within Track 2, the most frequently specified medical conditions were neurological conditions (56.7%) and "other" medical conditions (62.9%).
| Track 1Table 4.4b Footnote a | Track 2Table 4.4b Footnote a | |||
|---|---|---|---|---|
| Count | Percent (%) | Count | Percent (%) | |
| Cancer | 1561 | 45.6 | 10 | 4.8 |
| Neurological condition | 854 | 24.9 | 119 | 56.7 |
| Cardiovascular condition | 853 | 24.9 | 30 | 14.3 |
| Respiratory disease | 665 | 19.4 | 21 | 10.0 |
| Organ failure | 402 | 11.7 | 8 | 3.8 |
| Other conditions | 1582 | 46.2 | 132 | 62.9 |
| Total | 3423 | - | 210 | - |
|
||||
4.5 Socio-economic and community analyses
Health Canada conducted analyses to better understand the circumstances of people receiving MAID. These analyses suggest, at a high level, that people who receive MAID do not disproportionately come from lower-income or disadvantaged communities. Findings indicate that MAID recipients live in neighbourhoods across the income and marginalization spectrum as well as in urban, rural and remote communities.
Some people in Canada have raised concerns about how social inequality and uneven access to health and social services might influence MAID requests.Footnote 52Footnote 53 Others suggest that practitioners could have a biases or concerns about providing MAID to someone who may be seen as "vulnerable" that could lead them to refuse a legitimate request.Footnote 54 Health Canada has conducted analyses to better understand the circumstances of people receiving MAID, including:
- Socio-economic analyses using neighbourhood-level income measures; and
- Analyses of proximity to health and social services using geographic measures.
Neighbourhood-level measures were used to infer individual-level characteristics of MAID recipients, as the MAID monitoring questionnaire does not collect this type of information. It is possible that people are miscategorized into income or marginalization quintiles by these measures, however, these are the best approximations that are available at this time.
These analyses suggest, at a high level, that people who receive MAID do not live in uniquely marginalized neighbourhoods, nor do they live in areas with poor access to health care services, compared to reference groups. There are, however, some key differences of note within the population of people who received MAID:
- Proportionally more women than men were in the lowest income neighbourhoods (this was the case in both Tracks 1 and 2).
- Track 2 recipients are more likely than Track 1 recipients to live in neighbourhoods that are considered "unstable" (i.e., more renters, more apartment buildings, more people living alone, more people that moved recently, and fewer people that are married or common-law) according to the Statistics Canada measure of residential instability.
- Track 2 recipients are more likely than Track 1 recipients to live in urban areas. All MAID recipients were more likely to live in urban areas than the reference population (all deaths in 2023).
More details on these analyses are provided in the subsequent paragraphs and the methodology is detailed in Appendix B.
Socio-economic analyses
Some have expressed concerns that people who are economically vulnerable (i.e., without financial means to live comfortably) may seek MAID. To assess this, Health Canada analyzed MAID data using measures of neighbourhood income and marginalization.
Firstly, data on MAID recipients was linked to a neighbourhood-level measure of income from Statistics Canada, using the residential postal code collected as part of MAID monitoringFootnote 55 and compared to all deaths reported in Canada in 2023Footnote 56 (Figure 4.5a). Findings indicate that the reference population (all deaths in Canada) has a proportionally lower income at the neighbourhood level compared to both Tracks 1 and 2. This suggests that those who receive MAID are not overly represented in lower income neighbourhoods.
When comparing neighbourhood income among MAID recipients by sex the findings suggest that women receiving MAID live in lower income neighbourhoods compared to men receiving MAID. This was the case under both Tracks 1 and 2.
To date, research on the socio-economic status of MAID recipients has focused primarily on MAID in the context of a reasonably foreseeable natural death. The findings of this research have been mixed, with some studies finding that people receiving MAID had higher levels of educational attainment and were of a higher socioeconomic status,Footnote 57Footnote 58Footnote 59 whereas others have found that while a higher number of individuals with comparatively lower socioeconomic status requested MAID, the number of individuals who received MAID was evenly distributed across income groups.Footnote 60
Figure 4.5a: Neighbourhood income quintiles, by track, compared to all 2023 deaths in Canada

Figure 4.5a: Text description
| Track | Sex | Income quintiles | ||||
|---|---|---|---|---|---|---|
| 1 (lowest) | 2 | 3 | 4 | 5 (highest) | ||
| Track 1 | Male (%) | 22.5 | 21.5 | 19.5 | 18.0 | 18.6 |
| Female (%) | 25.6 | 21.3 | 18.9 | 17.1 | 17.1 | |
| All (%) | 24.0 | 21.4 | 19.2 | 17.5 | 17.8 | |
| Track 2 | Male (%) | 26.1 | 18.6 | 18.1 | 18.6 | 18.6 |
| Female (%) | 29.9 | 18.6 | 18.3 | 19.3 | 13.8 | |
| All (%) | 28.3 | 18.6 | 18.2 | 19.0 | 15.8 | |
| All deaths in 2023 | All (%) | 28.0 | 21.9 | 18.7 | 16.7 | 14.8 |
Secondly, Health Canada used Statistics Canada's measures for quantifying neighbourhood marginalizationFootnote 61 to provide further insight on the socio-economic circumstances of MAID recipients. These measures assess: (1) residential instability (e.g., how many residents are renters), (2) situational vulnerability (e.g., how many residents do not have a high school diploma), and (3) economic dependency (e.g., how many residents are youth or seniors). The measures are designed so that the Canadian population is classified into one of five groups, with 20% of the population included in each group. For this analysis, the reference category used was all 2023 deaths in Canada.Footnote 62 Track 1 and Track 2 were considered separately as particular concerns have been expressed regarding the economic vulnerability of people whose natural death is deemed not foreseeable.
The findings suggest, at a high level, that people who receive MAID do not disproportionately come from lower-income or disadvantaged communities. Track 1 recipients lived in less or similarly marginalized neighbourhoods, by all three measures, compared to the reference group (Figure 4.5b). Track 2 recipients followed a similar pattern, living in less marginalized neighbourhoods than the reference group on the measures of "economic dependency" and "situational vulnerability". However, on the measure of "residential instability" as defined by Statistics Canada, there are higher percentages of Track 2 recipients than Track 1 recipients and the reference category. While this does not speak to the situation of the MAID recipients themselves, it means that Track 2 recipients are more likely to live in neighbourhoods with more renters, more apartment buildings, more people living alone, more people that moved recently, and fewer people that are married or common-law. These results are comparable to a study done by the Chief Coroner of Ontario on 2023 MAID provisions in that province, which found that 48.3% of Track 2 recipients fell into the lowest residential instability quintile, compared to 34.3% of Track 1 recipients.Footnote 63
Figure 4.5b: Neighbourhood marginalization quintiles, by track, compared to all 2023 deaths in Canada
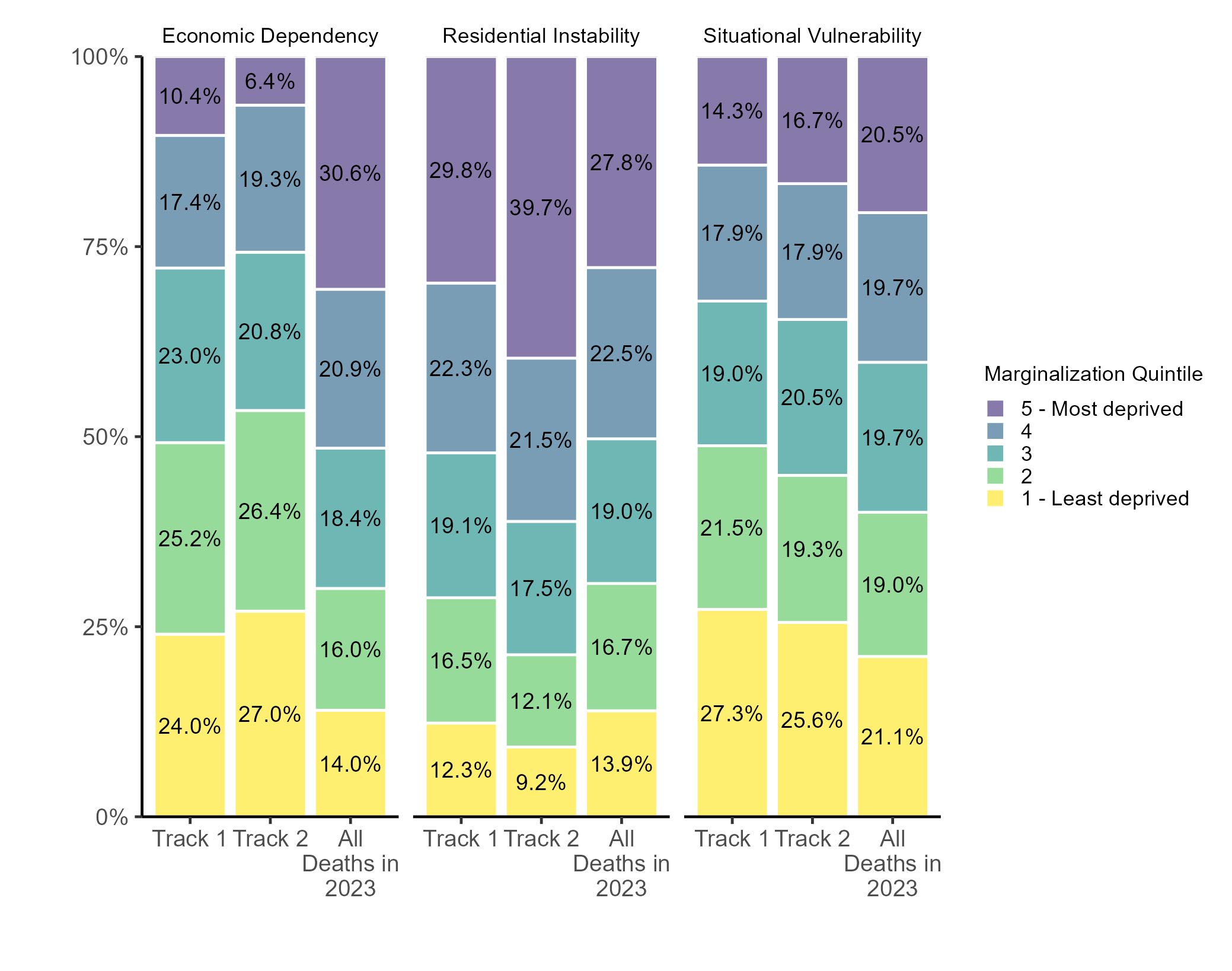
Figure 4.5b: Text description
| Marginalization | Track | Marginalization quintiles | ||||
|---|---|---|---|---|---|---|
| 1 (least deprived) | 2 | 3 | 4 | 5 (most deprived) | ||
| Economic dependency | Track 1(%) | 24.0 | 25.2 | 23.0 | 17.4 | 10.4 |
| Track 2 (%) | 27.0 | 26.4 | 20.8 | 19.3 | 6.4 | |
| All deaths in 2023 (%) | 14.0 | 16.0 | 18.4 | 20.9 | 30.6 | |
| Residential instability | Track 1(%) | 12.3 | 16.5 | 19.1 | 22.3 | 29.8 |
| Track 2 (%) | 9.2 | 12.1 | 17.5 | 21.5 | 39.7 | |
| All deaths in 2023 (%) | 13.9 | 16.7 | 19.0 | 22.5 | 27.8 | |
| Situational vulnerability | Track 1(%) | 27.3 | 21.5 | 19.0 | 17.9 | 14.3 |
| Track 2 (%) | 25.6 | 19.3 | 20.5 | 17.9 | 16.7 | |
| All deaths in 2023 (%) | 21.1 | 19.0 | 19.7 | 19.7 | 20.5 | |
Analyses of proximity to health and social services
Concerns have been raised that people living in an underserved community could be driven to request MAID because they are unable to access needed treatments and supports.Footnote 64 At the same time, there are concerns that accessing MAID in an underserved community may be difficult due to a lack of willing or qualified providers, particularly when specialized assessments are required.
To gain insight on proximity to health and social services among MAID recipients, Health Canada conducted an analysis of MAID provisions by urban and rural communities by attaching the measure of Population Centre and Rural Area Type from Statistics CanadaFootnote 65 to the postal code collected during MAID monitoring (i.e., the postal code on a person's health card) and then compared to all deaths reported in Canada in 2023.Footnote 66 People who received MAID were more likely to live in urban areas (80.2% of Track 1, 84.4% of Track 2) compared to all deaths reported in Canada in 2023 (76.9%) (Figure 4.5c). Track 2 MAID recipients, were most likely to live in urban areas which may reflect a greater need to live near health and community services.
Figure 4.5c: Percentage of MAID recipients who lived in urban areas, by track, and all 2023 deaths from urban areasFootnote 67

Figure 4.5c: Text description
| Track | Urban population (%) |
|---|---|
| Track 1 | 80.2 |
| Track 2 | 84.4 |
| All deaths in 2023 | 76.9 |
This analysis was supplemented with an examination of place of residence and remoteness, using the remoteness measure from Statistics Canada, as it represents accessibility to health care services and supports that promote health.Footnote 68Footnote 69 When comparing residential remoteness of MAID recipients across different jurisdictions to the general population (from population counts included in the remoteness data file), the differences are not stark (Figure 4.5d), indicating that MAID recipients are not necessarily seeking MAID because of a remote location and a related lack of accessibility to health care services or services that promote health.
The findings of this analysis align with those of previous annual reports, which have consistently shown that the majority of people needing and wanting access to palliative care and disability supports have received it.Footnote 70Footnote 71Footnote 72Footnote 73 These findings were further supported by a study of Ontario data that found that, in the majority of cases, palliative care providers were involved in the person's care at the time they requested MAID.Footnote 74 Future analysis will compare MAID provisions to all deaths across Canada by remoteness.
Figure 4.5d: Percentage of MAID recipients who lived in remote areas by province, compared to the population of Canada

Figure 4.5d: Text description
| Province | Remote population (%) | |
|---|---|---|
| MAID recipients | Population of Canada | |
| N.L. | 48.8 | 40.9 |
| P.E.I. | 9.8 | 14.2 |
| N.S. | 8.8 | 11.5 |
| N.B. | 23.0 | 22.8 |
| Que. | 3.7 | 3.5 |
| Ont. | 2.6 | 1.5 |
| Man. | 9.5 | 12.1 |
| Sask. | 17.9 | 19.0 |
| Alta. | 4.1 | 4.9 |
| B.C. | 8.1 | 7.4 |
5 Social supports and use of health services
5.1 Palliative care and disability support services
75.0% of MAID recipients accessed palliative care services; those who required but did not receive palliative care services typically had access to them.
Information about access to palliative care and disability supports is important to ensure that MAID is not being sought because of a lack of options for end-of-life-care or support services.
Table 5.1a outlines the requirement for, and duration and accessibility of, palliative care services among people who received MAID. Consistent with findings in previous years, MAID practitioners reported that the majority of MAID recipients in 2023 (75.0%) had accessed palliative care. Most people who received MAID under Track 1 received palliative care (76.9%, or n=11,326) while a smaller number of people receiving MAID under Track 2 received these services (29.6%, or n=184). As shown in the table, the largest group comprised those who received palliative care for a period of one month or more. In six cases, palliative care was required but was not accessible to the person.
A systematic review and meta-analysis looking at duration of palliative care before death in international routine practice found that the median duration from initiation of palliative care to death was 18.9 days.Footnote 75 The findings presented below show that the duration of palliative care among MAID recipients often exceeds this median.
| Requirement for, and receipt of, palliative care services | Number of persons | Percentage of all MAID provisions (%) | Duration or accessibility of palliative care | Number of persons | Percentage of all MAID provision (%) |
|---|---|---|---|---|---|
| Required and received | 11,510 | 75.0 | Duration of palliative care for those who received it | ||
| Less than one month | 4,792 | 31.2 | |||
| One month or more | 5,712 | 37.2 | |||
| Unknown length | 1,006 | 6.6 | |||
| Required, did not receive | 431 | 2.8 | Accessibility of palliative care for those who did not receive it | ||
| Care was not accessible | 6 | < 0.1 | |||
| Care was accessible | 347 | 2.3 | |||
| Unknown if care was accessible | 78 | 0.5 | |||
| Other | 3,402 | 22.2 | Unknown if required | 1,139 | 7.4 |
| Did not require care | 2,263 | 14.7 | |||
| Total | 15,343 | 100% | 15,343 | 100% | |
Table 5.1b outlines the requirement for, and duration and accessibility of, disability support services among people who received MAID. As shown in the table, 33.8% of individuals who received MAID were reported by the MAID practitioner as having required and received disability support services, a decrease from 36.8% in 2022. Of the 5,181 people who received disability support services, 4,874 were assessed as Track 1 and 307 were assessed as Track 2. The largest group comprised those who received disability support services for a period of less than one year. In a small number of cases (n=5) disability support services were required but were not accessible to the person.
| Requirement for, and receipt of, disability support services | Number of persons | Percentage of all MAID provisions (%) | Duration or accessibility of disability support | Number of persons | Percentage of all MAID provisions (%) |
|---|---|---|---|---|---|
| Required and received | 5,181 | 33.8 | Duration of disability support services for those who received them | ||
| Less than one year | 2,570 | 16.8 | |||
| One year or more | 1,669 | 10.9 | |||
| Unknown length | 942 | 6.1 | |||
| Required, did not receive | 432 | 2.8 | Accessibility of disability support services for those who did not receive them | ||
| Care was not accessible | 5 | < 0.1 | |||
| Care was accessible | 158 | 1.0 | |||
| Unknown if care was accessible | 269 | 1.8 | |||
| Other | 9,730 | 63.4 | Unknown if required | 3,104 | 20.2 |
| Did not require care | 6,626 | 43.2 | |||
| Total | 15,343 | 100% | 15,343 | 100% | |
Information on the need and provision of palliative care and disability support services, by province is presented in Table D.6 (Appendix D).
Table 5.1c outlines the disability support services received by MAID recipients under Tracks 1 and 2. For those receiving MAID under either Track 1 or 2, the most commonly received disability supports were mobility aids, physical support (including support from personal support workers, occupational therapists, physiotherapists, nurses, etc.) and safety aids.
| Type of disability support service | Track 1, count | Track 2, count |
|---|---|---|
| Mobility aids | 3,269 | 180 |
| Physical support, e.g., personal support worker, occupational therapist | 2,584 | 140 |
| Safety aids | 2,220 | 117 |
| Visibility aids | 529 | 31 |
| Mental health or social support | 360 | 50 |
| Other | 308 | 18 |
| Income support | 243 | 43 |
| Dependent on life sustaining treatmentsTable 5.1a Footnote a | 119 | X |
| Meal preparation and housekeepingTable 5.1a Footnote a | 11 | X |
|
||
5.2 Place of residence and living arrangement
Social isolation and loneliness are shown to have a serious impact on physical and mental health, quality of life, and longevity.Footnote 76 Information on the usual place of residence and living arrangement is collected to provide insight into the presence of social isolation among people who received MAID. Information related to a person's living arrangement is sought only in instances when the person identified their usual place of residence as a private residence.Footnote 77
Table 5.2a outlines the place of residence and living arrangement of MAID recipients as a percentage by track.Footnote 78 As shown in the table, most MAID recipients reported living in a private residence with family or alone in a private residence. The percentage of people receiving MAID under Track 1 living with family (45.9%) was higher that than of those living alone (30.2%). For those receiving MAID under Track 2, however, the percentage of people living alone (35.7%) was slightly higher than the percentage of people living with family (32.8%). A breakdown of place of residence by jurisdiction is provided in Table D.5 (Appendix D).
| Place of residence | Living arrangement of those living in private residences | Track 1, percent (%) | Track 2, percent (%) |
|---|---|---|---|
| Private residenceTable 5.2a Footnote a | Living alone | 30.2 | 35.7 |
| Living with family (partner, children, parents) | 45.9 | 32.8 | |
| Living with non-relatives | 1.4 | 1.3 | |
| Living with relatives | 2.3 | 1.8 | |
| Do not know | 3.9 | 3.4 | |
| Residential care facilityTable 5.2a Footnote b | - | 6.1 | 12.9 |
| Palliative care facilityTable 5.2a Footnote c | - | 3.9 | 1.0 |
| InstitutionTable 5.2a Footnote d | - | 2.0 | 4.4 |
| Other, no fixed address | - | 4.3 | 6.7 |
| Total | 100% | 100% | |
|
|||
5.3 Means to relieve suffering
For all Track 2 MAID cases, the legislation requires that the practitioner "ensure that the person has been informed of the means available to relieve their suffering, including, where appropriate, counselling services, mental health and disability support services, community services and palliative care and has been offered consultations with relevant professionals who provide those services or that care." In 2023, the most common means that were offered and discussed were pharmacological, followed by health care services, including palliative care and disability support services.
For individuals being assessed under Track 2 to be found eligible to receive MAID, a practitioner must be satisfied that the person has given serious consideration to reasonably available means to relieve their suffering. Table 5.3a outlines the ways that practitioners reported having formed this opinion, with the most common responses being: consulting with the person, reviewing their medical records, and consulting other health care professionals. Depending on the complexity of the person's circumstances, the practitioner may reach out to friends and family or other experts, in addition to consulting the person and their medical records.
| Activity | Responses, count |
|---|---|
| Consultation with person | 386 |
| Review of medical records | 287 |
| Consultation with professional care / medical providers | 233 |
| Consultation with family/friends | 229 |
| Accepted/attempted multiple treatments appropriate for the condition | 213 |
| Receptive to discussion on available means to relieve suffering | 192 |
| Previous knowledge of person | 66 |
| Other | 19 |
6 MAID providers and delivery
6.1 MAID practitioners
A group of 89 practitioners was responsible for 35.1% of all Track 1 and 28.6% of all Track 2 cases respectively, suggesting that MAID is becoming an area of focused expertise for some.
There were 2,200 unique MAID practitioners in 2023, the majority (94.5%) of whom were physicians, while 5.5% were nurse practitioners. Involvement in MAID can be emotionally challenging, politically contentious and require significant time and clinical judgement. The sections above demonstrate the complexity of cases and some of the challenges in assessment, requiring clinical guidance and specific training.
Interest in MAID has been growing as more Canadians become aware of it, fueling concerns across the country that demand for MAID may outstrip the supply of willing and available providers.Footnote 79 Based on previous annual reports, it is apparent that the increase in unique practitioners has not kept pace with the increase in MAID provisions: in 2019, there were 5,631 MAID provisions and 1,271 unique practitioners who provided MAID; in 2023, there were 15,343 MAID provisions and 2,200 unique MAID practitioners. While the number of MAID provisions in 2023 was nearly three times that of 2019, the number of unique practitioners in 2023 has not quite doubled.
However, there is evidence that suggests that access to MAID does not necessarily require a one-to-one increase in practitioners because a relatively small number of practitioners are taking on a larger share of the case load. Of all MAID practitioners in 2023, 807 (36.8%) provided MAID once, 1023 (46.7%) provided MAID two to ten times, 187 (8.5%) provided 11-20 times, 85 (3.9%) provided 21-30 times, and 89 (4.1%) provided 31 or more times. It is worth considering MAID practitioners within the context of case load and how this case load varies by MAID track. Although practitioners providing MAID only one time represents 36.8% of MAID practitioners, this group accounts for the provision of only 5.1% of Track 1 and 9.6% of Track 2 cases (Figure 6.1a). Conversely, the 4.1% of MAID practitioners who provided MAID 31 or more times were responsible for 35.1% of all Track 1 and 28.6% of all Track 2 cases respectively. It appears that MAID is becoming an area of focused expertise for some. Practitioners who performed MAID 11 or more times in 2023 oversaw 66.4% of Track 1 cases and 58.4% of Track 2 cases.
A breakdown of unique practitioners and provisions, by jurisdiction is presented in Table D.7 (Appendix D).
Figure 6.1a: MAID practitioners, by case load and track

Figure 6.1a: Text description
| Number of procedures | Track 1 (%) | Track 2 (%) |
|---|---|---|
| 1 | 5.1 | 9.6 |
| 2 to 10 | 28.5 | 32.0 |
| 11 to 20 | 17.6 | 16.1 |
| 21 to 30 | 13.7 | 13.7 |
| 31 or more | 35.1 | 28.6 |
For all Track 2 cases, the law requires at least one of the two practitioners assessing eligibility to have expertise in the condition that causes the person's suffering. If neither of the practitioners have that expertise, they must seek a third assessor that does.
In 73.2% of Track 2 cases, at least one of the two practitioners had expertise in the condition causing the person's suffering and were able to complete the assessment themselves. In the remaining cases, these practitioners sought additional expertise in the condition causing the person's suffering to help assess eligibility for MAID. Table 6.1a provides a list of practitioner specialties among those undertaking Track 2 MAID assessments. As outlined in the table, pain management, geriatric medicine, general internal medicine, and neurology were the most frequently cited specialties among the first or second assessors. When a third practitioner was required to assess the person requesting MAID, the most cited specialties were neurology, pain management, geriatric medicine and psychiatry. Practitioners could select more than one specialty.
| Medical specialty | First or second assessing practitioner,Table 6.1a Footnote a percent (%) | Third opinion required,Table 6.1a Footnote a percent (%) |
|---|---|---|
| Pain management | 21.8 | 17.0 |
| Geriatric medicine | 12.8 | 12.3 |
| General internal medicineTable 6.1a Footnote b | 11.8 | X |
| Neurology | 12.1 | 29.2 |
| Psychiatry | 5.2 | 11.3 |
| NephrologyTable 6.1a Footnote b | 0.0 | X |
| CardiologyTable 6.1a Footnote b | X | 0.0 |
| Respiratory medicineTable 6.1a Footnote b | X | X |
| Other specialty | 54.3 | 38.7 |
|
||
It is noteworthy that psychiatry was also often called upon to provide a specialized opinion or assessment of the person's condition. Although MAID where a mental illness is the sole underlying medical condition is not currently permitted under the law, there are a range of other conditions where psychiatry may be engaged. For example, some autoimmune disorders, cardiovascular diseases, Huntington's disease, and Parkinson's disease have been linked to either a higher prevalence of mental disorder as a comorbidity, or the presentation of psychiatric symptoms.Footnote 80 As discussed in Section 3.3, dementia was identified as a sole medical condition in 25 Track 2 cases. In these cases, psychiatry or geriatric psychiatry may also be engaged.
Beyond the legislative requirements, practitioners also consult with other health care professionals during MAID assessment. In 2023, practitioners consulted other health care professionals in 26.0% of Track 1 and 48.9% of Track 2 assessments. The fact that additional consultations were done in twice as many Track 2 cases highlights the additional complexities involved with these assessments and the need to undertake due diligence to fully understand the person's condition.
6.2 Timing of MAID
Data on the timing of MAID provides important insights into the experiences of people receiving MAID and highlights the important balance that must be struck between the need to ensure adequate time for reflection and respond to urgent medical circumstances.
For individuals assessed as Track 1, there is no minimum specified period of time that must pass between completion of the eligibility assessment and MAID provision. In 2023, the median number of days between the MAID request and MAID provision for individuals under Track 1 was 13 days. This finding suggests that most people under Track 1, where natural death is reasonably foreseeable, received MAID quickly once the they were deemed eligible.
For individuals assessed as Track 2, the legislation requires practitioners to ensure there are at least 90 clear days between the date the first assessment began and the day on which MAID is provided. This safeguard aims to respond to the additional challenges and concerns that may arise in the context of these MAID assessments, including whether the suffering is caused by factors other than the medical condition, and whether there are ways of addressing the suffering other than MAID. It also serves to help ensure that enough time is devoted to exploring all the relevant aspects of the person's situation, including whether there are treatments or services that could help reduce the person's suffering, such as counselling services, mental health and disability support services, community services and palliative care.Footnote 81
The 90 clear day requirement for Track 2 can be waived if both assessors are of the opinion that the loss of the person's capacity to provide consent to receive MAID is imminent. The requirement for at least 90 clear days between the beginning of first assessment and MAID provision was waived for 28 individuals in 2023.
Practitioners are required to report the length of time required to complete the entire assessment process for Track 2. In 2023, the assessment process took between 90 to 365 days for the majority of individuals under Track 2 (n=281), less than 90 days for 97 individuals and more than a year for 28 individuals. Even if the practitioner's assessment takes less than 90 days, the individual cannot receive MAID until the end of the legislated 90 day assessment period (unless this period is waived as stated above).
Waiver of final consent
In 2021, the Criminal Code was amended to allow for the waiver of the requirement to provide consent immediately before receiving MAID in very limited circumstances (known as "Audrey's amendment"), specifically:
- The person's natural death is reasonably foreseeable (Track 1); and,
- While they had decision making capacity:
- They were assessed and approved to receive MAID;
- They were advised by the practitioner that they were at risk of losing capacity to provide final consent;
A waiver of final consent is a written arrangement made by the individual with their practitioner that identifies a chosen date to receive MAID and provides consent in advance of that date, should the individual no longer have capacity to consent at that time. While confirmation of consent is not required at the moment of administration in such cases, the waiver of final consent agreement becomes invalid if the person, after having lost decision-making capacity, demonstrates refusal or resistance to the administration of MAID.
In 2018, Audrey Parker, a 57-year old Halifax woman diagnosed with cancer which had spread to her brain, called on lawmakers to amend the legislation to allow people who had been found eligible for MAID to waive the final consent requirement in the law.
Ms. Parker had hoped to spend one last Christmas with family and friends. However, she chose to receive MAID earlier than she wanted out of concern that the cancer in her brain, or the medications needed to ease her suffering, would impact her ability to consent and make her ineligible for MAID at a later date.
Her case elicited overwhelming support across the country, leading to a change in the law permitting the waiver of final consent for persons whose natural death is reasonably foreseeable.
In 2023, there were 594 reported instances of individuals who received MAID under a waiver of final consent arrangement due to a loss of capacity. In cases where MAID was provided under a waiver of final consent, the most common speciality of the practitioner involved was family medicine (73.6%), followed by palliative care (13.1%) and anaesthesiology (5.1%).
6.3 Location of MAID
In 2023, private residences (37.8%) continued to be the primary setting for the administration of MAID, followed by hospitals (32.7%). This trend holds when Track 1 and Track 2 are considered separately. The next largest group of provisions took place in palliative care facilities (21.8%), the vast majority of which were Track 1. The remaining 7.7% of provisions took place in a variety of settings such as residential care facilities, funeral homes and community-based settings.
In some instances, people are required to transfer locations prior to receiving MAID. In 2023, a total of 884 people were transferred to another location for the provision of MAID, representing 5.8% of total MAID cases.Footnote 82 When submitting a MAID report, practitioners can select multiple reasons why a person was transferred. The most selected reason was that the person requested to transfer to an alternate location (n=429) followed by the need to comply with the policies of the facility where the person was located (n=352). Other less common reasons had to with the ability of the provider to secure privileges at the facility where the person was located or the availability, capacity or comfort of practitioners within the facility where the person was located.
Institutional objection to MAID resulting in patient transfers is a fraught issue. Since the legalization of MAID in 2016, several faith-based hospitals, long-term care facilities and hospices in Canada have enacted policies to prohibit MAID from taking place on their premises. Table 6.3a outlines the percentage of MAID provisions that involved a transfer as well as the percentage of MAID transfers indicating that one of the reasons for the transfer was due to institutional policies, by province. As shown in the table, a relatively high proportion of transfers were done in accordance with institutional policies in Alberta (85.7%) and Manitoba (70.0%), while in Quebec, only 9.0% of transfers were done for this reason. Quebec passed legislation last year amending its Act respecting end-of-life care to specify, in particular, that "palliative care hospices may not exclude medical aid in dying from the care they offer,"Footnote 83 which may impact the incidence of patient transfers in that jurisdiction in future years.
| Province | MAID provisions within the province that involved a transfer, percent (%) | MAID transfers within the province due to policies of the facility where the person was located, percent (%) |
|---|---|---|
| N.L.Table 6.3a Footnote a | 13.9 | X |
| P.E.I.Table 6.3a Footnote a | X | X |
| N.S.Table 6.3a Footnote a | 3.3 | X |
| N.B.Table 6.3a Footnote a | 10.7 | 28.1 |
| Que. | 2.6 | 9.0 |
| Ont. | 8.0 | 42.9 |
| Man. | 13.2 | 70.0 |
| Sask. | 9.6 | 45.5 |
| Alta. | 9.3 | 85.7 |
| B.C. | 5.6 | 34.2 |
|
||
7 Conclusion
This Fifth Annual Report is made possible through the collaborative effort among federal, provincial, and territorial governments and health care professionals to provide and report on MAID in Canada. With the new and expanded data collection, this report has been able to present for the first time a deeper understanding of who is accessing MAID under Track 1 and Track 2, including information on how they self-identify and their social and economic circumstances. Through this analysis, Health Canada endeavours to bring information and nuance to difficult and sometimes polarized conversations about deeply personal decisions.
Health Canada will continue to seek new ways to better understand and enrich the analysis of these data, including through its engagement with people in Canada, including persons with lived experience, persons with disabilities and health care professionals, as well as First Nations, Inuit and Métis governments, organizations and rights-holders, to inform MAID policy and practitioner guidance. Health Canada will also explore opportunities for more advanced analysis in the future that could be made possible with record linkage to administrative datasets hosted by Statistics Canada. The program will continue its work with provinces, territories and practitioners to continuously improve data collection, consistency and quality, especially as it relates to self-identification.
The data presented demonstrates the complexity of MAID assessment in many situations, especially with regard to frailty, chronic pain, and dementia. This information underlines the importance of complex assessment training and practice guidelines – work that Health Canada continues to help support through organizations such as the Canadian Association of MAID Assessors and Providers, along with health care professionals, health professional regulatory authorities, provinces and territories.
Data collection on MAID is essential for better understanding who is receiving MAID and at what stage in their journey of life. The Government of Canada will continue its work to help ensure that the framework for MAID in Canada is safe, reflects the needs of people in Canada, protects those who may be vulnerable, and supports autonomy and freedom of choice.
Lastly, it is hoped that the analysis presented in this report is able to animate the research community to delve deeper into the MAID data available through the Statistics Canada Research Data Centres for more insights into the context of MAID delivery in our communities and health systems.
Appendix A: MAID eligibility criteria, safeguards and reporting requirements
| Eligibility criteria | Safeguards | |
|---|---|---|
| Natural death is reasonably foreseeable (Track 1) | Natural death is not reasonably foreseeable (Track 2) | |
|
|
|
| Modified reporting requirements | Collection of additional data elements |
|---|---|
|
|
Appendix B: Methodology and limitations
Methodological notes
The MAID monitoring regulations require physicians, nurse practitioners, preliminary assessors, pharmacists and pharmacy technicians to provide information related to requests for, and the provision of, MAID. These individuals must report to Health Canada in one of two ways:
- Directly to Health Canada via a secure web-based collection portal: Newfoundland and Labrador, Prince Edward Island, Nova Scotia, New Brunswick, Ontario (requests not resulting in provision of MAID, as well as reports from pharmacists/pharmacy technicians), Manitoba, and Yukon.
- Through a designated provincial or territorial body which in turn submits the data quarterly to Health Canada: Quebec, Ontario (requests resulting in provision of MAID), Saskatchewan, Alberta, British Columbia, Northwest Territories, and Nunavut.
The data collected by Health Canada undergoes a series of processing steps including cleaning, verification, validation and, where necessary, a follow up with a designated provincial or territorial body or practitioner to ensure quality, accuracy and completeness. In cases where socio-demographic groups had counts that required suppression to ensure confidentiality, Health Canada created aggregate groups that ensured that these MAID provisions were included in the analysis but that a person could not be identified.
Provinces and territories were consulted during the preparation of the report and had the opportunity to provide comments. For all years, the number of MAID provisions are counted in the calendar year in which MAID was provided. For all other requests which did not result in MAID being provided (i.e., ineligibility, withdrawal of request, or individual died prior to MAID), the request is counted in the calendar year in which the request was received by the practitioner.
There has been a simplification of the methodology in 2023 where the number of MAID provisions in Canada is counted solely based on the formal cases submitted as part of 2023 submissions, rather than including additional MAID provisions counted by the jurisdictions but not yet reported to Health Canada in the overall count. The 2023 total of 15,343 MAID provisions is directly comparable to the 13,102 MAID provisions formally reported in the Fourth Annual Report (2022 data).
The presentation of this year's report focuses on areas of interest to stakeholders, provinces, territories and Indigenous partners. New monitoring questions enable disaggregated data analysis by Indigenous identity and race, in addition to age, sex, and MAID track. This report does not include analysis by gender, although this information was collected in addition to sex, as this variable requires further assessment of disclosure risk. Measures of socio-economic status were attached to the MAID data in order to explore how this varies within this population and how it compares to the Canadian population. The postal code collected as part of MAID monitoring was used along with the Postal Code Conversion File +, which attached census geography to the data file and enabled linkage to the Canadian Index of Multiple Deprivation. These results may be relevant to help provide insight into differences in how MAID is accessed by different groups.
Data limitations
The new reporting requirements mandated under the amended MAID monitoring regulations expanded the information being collected on all requests for MAID. The Fifth Annual Report presents the first year of data collected under these regulations. This being the transitional year, the data/analysis presented in the report needs to be considered in light of some limitations:
- Delay in uptake of new data collection forms: Most provinces and territories were not able to revise their data collection forms by the time the new regulations came into force on January 1, 2023, resulting in missing data on all the new variables for the first several months of 2023. Further, lack of awareness among many practitioners that new reporting requirements were in place also led to some missing data.
- Assessments crossing calendar year: Often the assessment and provision of MAID spans over several months. There are cases where the assessment of eligibility was started/completed prior to January 1, 2023, (in the calendar year 2022), but MAID was administered in 2023 with a subsequent report submission. Most of these cases would have missing data for the new variables introduced in 2023, as this information was not collected at the time of assessment back in 2022 and could not be retrieved from individual's medical records.
- Variation in data collection approaches and interpretation of the new variables: The approach to collect data on self-identification parameters is not standardized across jurisdictions, making meaningful comparisons across jurisdictions challenging. Given the complexity around some variables, there is a lack of consistency in interpretation by individuals (in responding to self-identity parameters) and practitioners (around the details of some eligibility and safeguard parameters).
- Reluctance of practitioners to ask and requesters to disclose the self-identity parameters: There has been some reported reluctance on the part of practitioners to request this information (even though a person can choose not to self-identify), due to concerns about the impact this may have on the clinical relationship. Also, requesters may choose not to self-identify, due to concerns about how this could impact how they are treated when interacting with the health care system.
Health Canada has worked with provinces and territories to address some of the above issues where possible and is continuing to work with them to improve data consistency and quality going forward.
Marginalization analysis
The marginalization analysis was completed by first using the Postal Code Conversion File + to attach census geographies to the MAID data file, then attaching the Canadian Index of Multiple Deprivation, merging by standardized Canadian geographic variables. The Canadian Index of Multiple Deprivation is an area-based index that uses census data to devise four dimensions of deprivation and marginalization. These dimensions are residential instability (tendency of neighbourhood inhabitants to fluctuate over time, comprised of the following measures: proportion of dwellings that are apartment buildings, proportion of dwellings that are owned, proportion of persons living alone, proportion of the population who moved within the past five years, and the proportion of the population that is married or common-law), situational vulnerability (variations in socio-demographic conditions in the areas of housing and education, while taking into account other demographic characteristics, comprised of the following measures: proportion of population that identifies as Indigenous, proportion of dwellings needing major repairs, and proportion of population aged 25-64 without a high school diploma), economic dependency (the reliance on the workforce, or a dependence on sources of income other than employment income, comprised of the following measures: proportion of population aged 65 and older, proportion of population participating in labour force (aged 15 and older), ratio of employment to population, dependency ratio (population aged 0-14 and 65 and older divided by the population aged 15-64), and proportion of population receiving government transfer payments) and ethno-cultural composition (people who identify as visible minorities or are immigrants, comprised of the following measures: proportion of population who self-identify as visible minority, proportion of population that is foreign born, proportion of population with no knowledge of either official language, proportion of population who are recent immigrants).Footnote 85 The latter dimension was omitted from the analysis given that:
- Self-reported data on racial, ethnic or cultural identity are already collected as part of MAID monitoring.
- These data suggest that the population of MAID recipients is relatively homogenous (the vast majority self-identified as Caucasian, or White), which limits the validity of this dimension as a measure of marginalization.
Within each dimension, scores are assigned a quintile value of 1 though 5, which represents the least to most deprived respectively.
A comparison of MAID data and vital statistics data
All deaths in Canada are registered by the provincial or territorial vital statistics registry within the province or territory where the death occurred. The death registration form consists of personal information, supplied to the funeral director by an informant, and the medical certificate of cause of death, completed by a medical practitioner, coroner or medical examiner.Footnote 86 The provincial and territorial vital statistics registries then submit data from deaths registered in their jurisdiction to Statistics Canada who releases official mortality statistics. All of the information that appears on the medical certificate of cause of death is coded and the underlying cause of death is determined. The underlying cause of death is defined as (a) the disease or injury which initiated the train of events leading directly to death, or (b) the circumstances of the accident or violence which produced the fatal injury.Footnote 87 In accordance with international standards and practices, Statistics Canada has always coded causes of death according to the World Health Organization's International Classification of Diseases and Related Health Problems (ICD) and is currently using the 10th revision.Footnote 88 Using the rules outlined in ICD-10, a singular underlying cause of death is determined, which is used to tabulate mortality statistics by Statistics Canada. There is no code for MAID in the ICD. Death certificates for individuals who received MAID are coded to the condition that led the decedent to avail themselves of MAID.
Conversely, under the federal MAID monitoring program, information on all requests for and provisions of MAID is collected by Health Canada in accordance with the Regulations of the Monitoring of Medical Assistance in Dying. All physicians and nurse practitioners report to Health Canada either directly via a secure web-based collection portal or through a designated provincial or territorial body which in turn submits the data quarterly to Health Canada. All intentional requests leading to a reportable outcome (MAID provision, finding of ineligibility, person withdrawing their request and person dying from a reason other than MAID) need to be reported.
The MAID monitoring questionnaire requires practitioners and assessors to provide details of the serious and incurable medical condition which is causing intolerable suffering and leading the person to seek and/or receive MAID. Note that more than one medical condition can be specified and there is no hierarchy to differentiate between the 'sole condition' and 'other condition(s)/co-morbidities'.
Appendix C: Indigenous engagement on MAID
During Parliamentary debates and public discussions of former Bill C-7, the Government of Canada received criticism on the part of some Indigenous partners, Parliamentarians and advocacy groups for not adequately engaging Indigenous Peoples in the development of the legislation. This criticism has continued following the passage of former Bill C-7, most notably during meetings of the Special Joint Committee on Medical Assistance in Dying (AMAD), which was established to conduct a statutory review of Canada's legislation on MAID.
The second report of AMAD, tabled in February 2023, included a recommendation that "Health Canada provide updates to the House of Commons Standing Committee on Indigenous and Northern Affairs and the Standing Senate Committee on Indigenous Peoples on its engagement with First Nations, Inuit and Métis on the subject of MAID."Footnote 89 The first report was submitted in March 2024.
Health Canada recognizes the need to build positive and collaborative relationships with Indigenous Peoples, while respecting their priorities and timelines. In this respect, Health Canada is providing over $3 million in funding to nine Indigenous partners over three years (2022 to 2025) to lead community engagement on continuing care and MAID as follows:
- Les Femmes Michif Otipemisiwak received funding to engage Métis women and Two Spirit, LGBTQI+ Métis on MAID where a mental disorder is the sole underlying medical condition.
- The Native Women's Association of Canada received funding to engage Indigenous women, two-spirit, transgender, and gender-diverse people on MAID.
- The National Association of Friendship Centres received funding to engage Friendship Centres and Provincial/Territorial Associations from across the country on MAID and palliative care.
- The Six Nations of the Grand River received funding to engage on MAID and advanced care planning using a two-eyed seeing approach to integrate Haudenosaunee and Western understandings of end-of-life care.
- The Congress of Aboriginal Peoples received funding to engage off-reserve and non-status Indigenous Peoples on palliative care and MAID through a two-eyed seeing approach, supported a national discussion on MAID where a mental disorder is the sole underlying medical condition and did journey mapping on MAID and palliative care resources.
- The Métis National Council received funding to work with their Governing Members to engage Métis citizens on palliative care.
- The Mawi Ta'mk Society received funding to work with the Wabanaki Council on Disability to conduct community engagement on end-of-life care, including palliative care and MAID, using Ancestral traditional knowledge and perspectives.
- The Métis Nation British Columbia received funding to host regional gatherings with Métis Elders and seniors to discuss advanced care planning and MAID.
- The Manitoba Métis Federation received funding to engage Red River Métis citizens on MAID through an advisory group, focus groups and interviews, and to disseminate the resulting knowledge to Métis citizens, policymakers and other stakeholders.
In addition to Indigenous-led engagement, Health Canada has supported a series of engagement activities on MAID and broader end-of-life care issues, to hear from First Nations (with and without status), Inuit and Métis, including Indigenous people living in urban settings and/or off-reserve, Two-Spirit, LGBTQI+ and gender diverse Indigenous people, and Indigenous people with disabilities. These include:
- Launching an online engagement survey aimed at gathering the views and perspectives of Indigenous Peoples on MAID (this survey ran from August 2023 to June 2024).
- Working with Mahihkan Management Inc., an Indigenous-owned firm, to facilitate a series of in-person and virtual national dialogue sessions with Indigenous Peoples to hear their views, experiences and recommendations on MAID (these took place across Canada between February and April 2024).
- Working with Saint Elizabeth Health's First Nation Inuit and Métis program to conduct a three-day knowledge exchange forum in February 2024 entitled Advancing Indigenous Policy and Practice: Supporting the Journey Home When Seriously Ill.
Through its engagement work, Health Canada has endeavoured to provide culturally-safer avenues for First Nations, Inuit and Métis people to share their perspectives on MAID and end-of-life care. It is recognized that barriers still exist for many Indigenous people who may wish to participate in these discussions and that the views of First Nations, Inuit and Métis people on these issues are rich and varied. As such, the findings are not to be taken as representing the views of First Nations, Inuit or Métis Peoples as a whole. This engagement work represents just one small step on the broader reconciliation journey.
Appendix D: Profile of MAID by jurisdiction
Table D.1 shows outcomes of MAID requests, broken down by province and territory. Quebec has the greatest number of withdrawals and persons found ineligible. British Columbia has the highest number of deaths due to another cause before MAID could be provided. MAID requests that do not result in MAID are most common in Quebec and British Columbia, where MAID provisions are also most common (as shown in Table 2.3a).
| Province or territory | Request made and withdrawn in 2023, count | Requests made in 2023 that were deemed ineligible in 2023, count | Requests made in 2023 where the person died of another cause in 2023, count |
|---|---|---|---|
| N.L.Table D.1 Footnote a | X | 7 | 14 |
| P.E.I.Table D.1 Footnote a | 0 | X | 9 |
| N.S.Table D.1 Footnote a | X | X | 53 |
| N.B.Table D.1 Footnote a | X | 8 | 41 |
Que. |
266 | 415 | 881 |
Ont. |
90 | 143 | 751 |
Man. |
15 | 36 | 119 |
Sask. |
67 | 83 | 100 |
Alta. |
27 | 83 | 364 |
B.C. |
24 | 136 | 565 |
| Y.T.Table D.1 Footnote a | X | X | X |
| N.W.T.Table D.1 Footnote a | 0 | 0 | X |
| Nvt. | 0 | 0 | 0 |
|
|||
Table D.2 provides an overview of the medical conditions reported for MAID recipients, by province. Practitioners could indicate more than one medical condition per person. Cancer was the most frequently reported medical condition across all provinces.
| Province | Cancer, count | Neurological conditions, count | Respiratory disease, count | Cardiovascular conditions, count | Organ failure, count | Other conditions, count |
|---|---|---|---|---|---|---|
| N.L.Table D.2 Footnote a | 50 | 7 | 8 | X | X | 8 |
| P.E.I.Table D.2 Footnote a | 32 | X | 6 | X | X | X |
| N.S. | 213 | 51 | 34 | 54 | 26 | 73 |
| N.B. | 194 | 38 | 27 | 29 | 15 | 45 |
| Que. | 3,590 | 770 | 756 | 678 | 476 | 1,080 |
| Ont. | 2,785 | 675 | 713 | 903 | 327 | 1,024 |
| Man.Table D.2 Footnote a | 139 | 31 | 22 | 30 | X | 37 |
| Sask. | 244 | 52 | 74 | 94 | 34 | 149 |
| Alta. | 618 | 151 | 141 | 164 | 85 | 343 |
| B.C. | 1,596 | 504 | 504 | 540 | 330 | 1,496 |
|
||||||
Table D.3 provides a profile of MAID recipients, broken down by province. Across all provinces, Track 1 represents the vast majority of MAID provisions. In Newfoundland and Labrador, Prince Edward Island, Nova Scotia, New Brunswick, Quebec, Ontario, and Alberta there were more women receiving MAID than men. In Manitoba, Saskatchewan, and British Columbia, there were more men receiving MAID. Across all provinces, nearly all MAID recipients were Caucasian (White). The rates at which persons receiving MAID self-reported having a disability varied widely across provinces, even when split by Track. For Track 1 the rate was as low as 12.8% in Alberta to 82.7% for Saskatchewan, and for Track 2, as low as 7.7% in Alberta, and 81.0% in New Brunswick. In most provinces, Track 2 consistently had a higher proportion of provisions that reported a disability compared to Track 1, with the exception of Alberta.
| Province | Track 1 provisions, percent (%) | Female, percent (%) | Caucasian, percent (%) | Reporting having a disability, Track 1, percent (%) | Reporting having a disability, Track 2, percent (%) |
|---|---|---|---|---|---|
| N.L.Table D.3 Footnote a | X | 47.2 | 100.0 | 58.3 | X |
| P.E.I.Table D.3 Footnote a | X | 47.7 | 97.7 | 37.5 | X |
| N.S. | 97.5 | 45.1 | 99.0 | 43.5 | 66.7 |
| N.B. | 93.0 | 44.8 | 99.0 | 23.4 | 81.0 |
| Que. | 94.1 | 47.2 | 98.9 | 14.2 | 53.7 |
| Ont. | 97.5 | 49.6 | 94.7 | 24.3 | 62.9 |
| Man.Table D.3 Footnote a | X | 51.5 | 94.0 | 33.1 | X |
| Sask.Table D.3 Footnote a | X | 52.6 | 97.0 | 82.7 | X |
| Alta. | 94.2 | 48.2 | 98.0 | 12.8 | 7.7 |
| B.C. | 97.2 | 51.3 | 94.7 | 59.4 | 64.3 |
|
|||||
Table D.4 presents the average and median ages of MAID recipients, broken down by track and province. Average and median age for all MAID provisions and Track 1 cases were highest in British Columbia, Manitoba and Ontario respectively. Average age for Track 2 was highest in Ontario, Quebec and New Brunswick and median age was highest in British Columbia and Ontario.
| Province | All MAID provisions | Track 1 | Track 2 | |||
|---|---|---|---|---|---|---|
| Median | Average | Median | Average | Median | Average | |
| N.L.Table D.4 Footnote a | 72.0 | 71.4 | 72.1 | 71.8 | X | X |
| P.E.I.Table D.4 Footnote a | 75.5 | 72.3 | 75.4 | 71.8 | X | X |
| N.S. | 76.5 | 75.5 | 76.6 | 75.6 | 76.5 | 69.5 |
| N.B. | 74.0 | 73.5 | 74.3 | 73.7 | 74.0 | 71.4 |
| Que. | 77.0 | 76.6 | 77.0 | 76.6 | 77.0 | 75.4 |
| Ont. | 78.6 | 77.8 | 78.7 | 77.9 | 78.6 | 73.9 |
| Man.Table D.4 Footnote a | 78.9 | 78.1 | 79.0 | 78.3 | X | X |
| Sask.Table D.4 Footnote a | 75.4 | 75.6 | 75.6 | 75.7 | X | X |
| Alta. | 76.4 | 75.2 | 76.7 | 75.7 | 76.4 | 68.2 |
| B.C. | 79.1 | 78.3 | 79.4 | 78.6 | 79.1 | 69.4 |
|
||||||
Table D.5 shows place of residence of persons who received MAID, broken down by province. Private residences (including long-term care facilities) were the most frequently reported location in every province.
| Province | Hospital,Table D.5 Footnote a count | Palliative care facility,Table D.5 Footnote b count | Residential care facility,Table D.5 Footnote c count | Private residence,Table D.5 Footnote d count | Other,Table D.5 Footnote e count |
|---|---|---|---|---|---|
| N.L.Table D.5 Footnote f | X | X | 9 | 52 | 0 |
| P.E.I.Table D.5 Footnote f | 7 | X | X | 33 | X |
| N.S.Table D.5 Footnote f | 12 | X | 20 | 314 | X |
| N.B. | 32 | 34 | 14 | 217 | 24 |
| Que. | 57 | 79 | 81 | 1,521 | 17 |
| Ont. | 43 | 107 | 251 | 4,226 | 0 |
| Man. | 18 | 12 | 16 | 181 | 18 |
| Sask. | 12 | 12 | 39 | 263 | 33 |
| Alta. | 7 | 80 | 127 | 625 | 425 |
| B.C. | 23 | 85 | 162 | 1,991 | 0 |
|
|||||
Table D.6 contains information on the need and provision of both disability and palliative care support services, by province. Saskatchewan, British Columbia, and Ontario has the highest proportion of MAID recipients who required and received disability support services. Prince Edward Island, Quebec, and Ontario had the highest proportion of MAID recipients that required and received palliative care support services. Alberta had the highest number of persons who required, but did not receive, palliative care services. However, these findings must be compared to those presented in Table 5.1b, which shows that most people who required but did not receive palliative care services had access to them
| Province | Required and received, percent (%) | Required but did not receive, percent (%) | Unknown or did not require, percent (%) |
|---|---|---|---|
| Disability support services | |||
| N.L.Table D.6 Footnote a | X | X | 63.9 |
| P.E.I. | 22.7 | 0.0 | 77.3 |
| N.S.Table D.6 Footnote a | X | X | 75.2 |
| N.B.Table D.6 Footnote a | X | X | 87.0 |
| Que. | 12.8 | 0.4 | 86.7 |
| Ont. | 47.5 | 0.9 | 51.6 |
| Man. | 19.8 | 0.0 | 80.2 |
| Sask. | 65.1 | 3.5 | 31.4 |
| Alta. | 38.4 | 1.7 | 59.9 |
| B.C. | 52.3 | 2.4 | 45.4 |
| Palliative care services | |||
| N.L.Table D.6 Footnote a | 76.4 | X | X |
| P.E.I.Table D.6 Footnote a | 84.1 | X | X |
| N.S.Table D.6 Footnote a | 55.7 | X | X |
| N.B.Table D.6 Footnote a | 71.9 | X | X |
| Que. | 79.9 | 0.3 | 19.7 |
| Ont. | 78.8 | 1.0 | 20.2 |
| Man.Table D.6 Footnote a | 70.0 | X | X |
| Sask. | 61.0 | 4.9 | 34.0 |
| Alta. | 69.8 | 16.2 | 14.0 |
| B.C. | 65.2 | 3.8 | 30.9 |
|
|||
Table D.7contains information on both the number of unique MAID practitioners and their case load, by province. Quebec had more unique practitioners than all other provinces combined. In Quebec and Manitoba, all unique MAID practitioners were physicians (i.e., none were nurse practitioners). However, under the Act Respecting End-of-Life Care, specialized nurse practitioners were authorized to administer MAID as of December 7, 2023, meaning that this finding for Quebec may change in subsequent years. Quebec had the highest proportion of practitioners who provided MAID only once. British Columbia had the highest proportion of practitioners who provided MAID 11 or more times.
| Province | Unique practitioners, count | Unique practitioners that are physicians, percent (%) | Practitioners performing 1 provision, percent (%) | Practitioners performing 2 to 10 provisions, percent (%) | Practitioners performing 11 or more provisions, percent (%) |
|---|---|---|---|---|---|
| N.L.Table D.7 Footnote a | 34 | X | 50 | 50 | 0 |
| P.E.I.Table D.7 Footnote a | 11 | X | X | 63.6 | X |
| N.S.Table D.7 Footnote a | 61 | 77.1 | X | 57.4 | X |
| N.B.Table D.7 Footnote a | 43 | X | 39.5 | 37.2 | 23.3 |
| Que. | 1,197 | 100.0 | 47.0 | 43.3 | 9.7 |
| Ont. | 472 | 89.8 | 24.2 | 52.7 | 23.0 |
| Man.Table D.7 Footnote a | 20 | 100.0 | X | 40.0 | X |
| Sask. | 42 | 76.2 | 19.0 | 66.7 | 14.3 |
| Alta. | 118 | 86.4 | 22.9 | 49.1 | 28.0 |
| B.C. | 199 | 86.4 | 18.6 | 44.2 | 37.2 |
|
|||||
Table D.8 provides an overview of the location of MAID provisions, by province. The highest reported location of provision was in hospital (excluding palliative care beds or units), across provinces.
| Province | Hospital,Table D.8 Footnote a count | Palliative care facility,Table D.8 Footnote b count | Residential care facility,Table D.8 Footnote c count | Private residence,Table D.8 Footnote d count | Other,Table D.8 Footnote e count |
|---|---|---|---|---|---|
| N.L.Table D.8 Footnote f | 28 | 19 | 7 | 18 | X |
| P.E.I.Table D.8 Footnote f | 20 | X | 0 | 18 | X |
| N.S.Table D.8 Footnote f | 133 | 51 | 19 | 152 | X |
| N.B.Table D.8 Footnote f | 73 | 109 | 12 | 105 | X |
| Que. | 2,170 | 1,479 | 316 | 1,612 | 24 |
| Ont. | 1,315 | 825 | 198 | 2,208 | 98 |
| Man.Table D.8 Footnote f | 78 | 48 | X | 88 | X |
| Sask. | 142 | 39 | 34 | 119 | 10 |
| Alta. | 317 | 153 | 126 | 356 | 25 |
| B.C. | 743 | 608 | 216 | 1,115 | 79 |
|
|||||
Figure D.1 shows measures of neighbourhood marginalization among MAID recipients by province (measures of marginalization are explained in Section 4.5). When people who received MAID are a larger than expected share of people in the most marginalized quintile, it is by the measures of situational vulnerability and residential instability.
Figure D.1: Canadian index of multiple deprivation, by province

Figure D.1: Text description
| Province | Income quintile (%) | ||||
|---|---|---|---|---|---|
| 1 (least deprived) | 2 | 3 | 4 | 5 (most deprived) | |
| N.L. | 13.9 | 15.3 | 16.7 | 22.2 | 31.9 |
| P.E.I. | X | X | 25.0 | X | X |
| N.S. | 18.8 | 16.3 | 17.1 | 23.9 | 23.9 |
| N.B. | 12.6 | 18.4 | 16.7 | 24.9 | 27.3 |
| Que. | 20.3 | 20.7 | 21.9 | 21.0 | 16.0 |
| Ont. | 31.0 | 22.9 | 18.2 | 15.9 | 11.9 |
| Man. | 16.6 | 15.7 | 18.8 | 17.5 | 31.4 |
| Sask. | 21.5 | 19.2 | 18.9 | 18.9 | 21.5 |
| Alta. | 27.8 | 21.1 | 18.5 | 16.4 | 16.2 |
| B.C. | 39.5 | 22.5 | 15.4 | 13.5 | 9.1 |
| Province | Income quintile (%) | ||||
|---|---|---|---|---|---|
| 1 (least deprived) | 2 | 3 | 4 | 5 (most deprived) | |
| N.L. | 11.1 | 31.9 | 27.8 | 19.4 | 9.7 |
| P.E.I. | X | X | 18.2 | 22.7 | 29.5 |
| N.S. | 11.0 | 17.4 | 20.2 | 23.0 | 28.4 |
| N.B. | 9.9 | 24.2 | 22.2 | 19.1 | 24.6 |
| Que. | 8.0 | 13.1 | 17.3 | 22.5 | 39.2 |
| Ont. | 16.8 | 19.3 | 19.7 | 21.2 | 22.9 |
| Man. | 12.6 | 14.3 | 12.1 | 24.7 | 36.3 |
| Sask. | 17.7 | 14.2 | 19.8 | 27.7 | 20.6 |
| Alta. | 19.0 | 18.1 | 18.9 | 21.1 | 22.9 |
| B.C. | 10.4 | 16.0 | 21.1 | 23.7 | 28.9 |
| Province | Income quintile (%) | ||||
|---|---|---|---|---|---|
| 1 (least deprived) | 2 | 3 | 4 | 5 (most deprived) | |
| N.L. | 59.7 | 29.2 | X | X | X |
| P.E.I. | 29.5 | 25.0 | 27.3 | X | X |
| N.S. | 43.0 | 30.9 | 15.2 | 9.3 | 1.7 |
| N.B. | 51.9 | 30.4 | 11.6 | X | X |
| Que. | 42.0 | 25.2 | 16.4 | 12.0 | 4.3 |
| Ont. | 11.0 | 26.7 | 26.4 | 21.3 | 14.6 |
| Man. | 14.8 | 19.3 | 31.4 | 19.7 | 14.8 |
| Sask. | 34.2 | 22.4 | 20.1 | 18.9 | 4.4 |
| Alta. | 12.5 | 23.1 | 26.8 | 25.4 | 12.3 |
| B.C. | 7.3 | 23.0 | 30.8 | 21.9 | 16.9 |
Appendix E: MAID requests, eligibility, and procedural requirements
Figure E.1 is a map of the Index of Remoteness, which was incorporated into the analysis of MAID, and how it is distributed across Canada.Footnote 90 Areas around large urban centres are classified as easily accessible, or accessible. Remote or very remote areas tend to be in northern parts of the country.
Figure E.1: Index of remoteness quintiles in Canada

Figure E.1: Text description
A map of Canada, with areas presented as belonging to 1 of 6 categories according to ease of access to MAID:
- Easily accessible
- Accessible
- Less accessible
- Remote
- Very remote
- No assigned value
Table E.1 shows the outcomes of previous MAID requests among MAID recipients, by track. As a proportion of MAID provisions, there were more past requests made by people receiving MAID through Track 2, and the outcome of the past request being "assessed and found ineligible" was more likely compared to Track 1.
| Outcome of the previous MAID request | Track 1, count | Track 2, count |
|---|---|---|
| Assessed and found ineligible | 55 | 17 |
| Assessed and found eligible but person withdrew requestTable E.1 Footnote a | 26 | X |
| Assessed and found eligible but considerable time elapsed since the assessmentTable E.1 Footnote a | 33 | X |
| Request not actionedTable E.1 Footnote a | 50 | X |
| OtherTable E.1 Footnote a | 20 | X |
| Person did not follow through with a full assessmentTable E.1 Footnote a | 31 | X |
| Unable to find provider | 12 | 0 |
| Total | 227 | 27 |
|
||
Table E.2 shows where practitioners received the request for MAID, by track. In most cases, practitioners received requests from the person directly, from another practitioner or preliminary assessor, or from a care coordination service.
| Where practitioner received the request | Track 1, count | Track 2, count |
|---|---|---|
| Person directly | 3,495 | 162 |
| Another practitioner or preliminary assessor | 3,312 | 117 |
| Care coordination service | 7,317 | 319 |
| Another third person | 270 | 15 |
| Social worker | 111 | 7 |
| Family memberTable E.2 Footnote a | 108 | X |
| Health care setting (including palliative care, patient charts, and clinics)Table E.2 Footnote a | 108 | X |
|
||
Table E.3 shows the primary area of specialty of physicians who provided MAID, by track. As shown in the table, the majority of physicians work within the speciality of family medicine, followed by palliative medicine and anesthesiology across both tracks.
| Physician's primary area of specialty | Track 1,Table E.3 Footnote a percent (%) | Track 2,Table E.3 Footnote a percent (%) |
|---|---|---|
| Family medicine | 64.0 | 69.5 |
| Palliative medicine | 12.6 | 8.2 |
| Anesthesiology | 11.6 | 6.8 |
| Internal medicine | 3.1 | 2.0 |
| Critical care and emergency medicine | 2.5 | 4.3 |
| OncologyTable E.3 Footnote b | 1.2 | X |
| OtherTable E.3 Footnote b | 0.7 | X |
| Surgery | 4.3 | 7.3 |
|
||
Table E.4 reports on the type of facility where palliative care was received among MAID recipients. Home-based palliative care was the most frequency reported setting, followed by hospital based inpatient care.
| Type of facility where palliative care received | Responses, count |
|---|---|
| Home-based | 4,936 |
| Hospital based inpatient | 3,379 |
| Hospital based palliative | 795 |
| Hospital-based outpatient or medical clinic / ambulatory service | 799 |
| Hospice care | 769 |
| Long term care facility | 177 |
| Other | 333 |
Table E.5 describes the type of palliative care services received among MAID recipients. Palliative care for pain and symptom management was the most frequency reported service, followed by personal support services, psychosocial care, and palliative chemotherapy.
| Type of palliative care services received | Responses, count |
|---|---|
| Pain symptom management | 7,741 |
| Personal support services | 3,658 |
| Psychosocial care and or counselling | 1,563 |
| Palliative chemotherapy | 1,110 |
| Palliative radiation therapy | 968 |
| Spiritual care and or counselling | 838 |
| Occupational therapy | 730 |
| Physiotherapy | 566 |
| Other | 524 |
| Volunteer services | 367 |
| Do not know | 378 |
| Dependent on life sustaining treatment | 125 |
| Nutritional | 51 |
| End of life care | 21 |
| Surgery | 16 |
| Speech language pathology | 15 |
| Equipment | 11 |
- Footnote 1
-
Pesut, Barbara, Sally Thorne, Kenneth Chambaere, Margaret Hall, and Catharine J. Schiller. "The Evolving Complexities of MAID Care in Canada from a Nursing Perspective." Global Qualitative Nursing Research 11, (2024): https://doi.org/10.1177/23333936241228233
- Footnote 2
-
Pesut, "The Evolving Complexities of MAID Care in Canada from a Nursing Perspective."
- Footnote 3
-
Health Canada. "Advice to the Profession: Medical Assistance in Dying (MAID)." Ottawa, ON: Government of Canada, 2023. https://www.canada.ca/en/health-canada/services/publications/health-system-services/advice-profession-medical-assistance-dying.html
- Footnote 4
-
Canadian Association of MAiD Assessors and Providers. "Canadian MAiD Curriculum." Victoria, BC: CAMAP, 2024. https://camapcanada.ca/curriculum/
- Footnote 5
-
Health Canada. "Model Practice Standard for Medical Assistance in Dying (MAID)." Ottawa, ON: Government of Canada, 2023. https://www.canada.ca/en/health-canada/services/publications/health-system-services/model-practice-standard-medical-assistance-dying.html
- Footnote 6
-
Health Canada, "Advice to the Profession: Medical Assistance in Dying (MAID)."
- Footnote 7
-
In some provinces and territories, health professionals other than physicians and nurse practitioners are involved in triaging MAID requests by collecting information about the person requesting MAID, which may inform a determination of ineligibility. A preliminary assessor may include any regulated professional in a care team, a care coordination service, or other relevant settings. Under the regulations, these "preliminary assessors" are only required to report a determination of ineligibility and have no other obligations under the regulations. The legislation provides for only physicians and nurse practitioners to be able to confirm a person's eligibility for the purposes of receiving MAID.
- Footnote 8
-
Health Canada. "Fourth annual report on Medical Assistance in Dying in Canada, 2022." Ottawa, ON: Government of Canada, 2023. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2022.html
- Footnote 9
-
Statistics Canada. "Deaths, 2023." Ottawa, ON: Government of Canada, 2024. https://www150.statcan.gc.ca/n1/daily-quotidien/241204/dq241204a-eng.htm
- Footnote 10
-
World Health Organization. "International Statistical Classification of Diseases and Health Related Problems, 10th Revision, Sixth Edition, Volume 2." Geneva, Switzerland: 2019. https://icd.who.int/browse10/Content/statichtml/ICD10Volume2_en_2019.pdf
- Footnote 11
-
Health Canada, "Fourth annual report on Medical Assistance in Dying in Canada 2022."
- Footnote 12
-
Statistics Canada. "Health of Canadians." Ottawa, ON: Government of Canada, 2023. https://www150.statcan.gc.ca/n1/pub/82-570-x/2023001/section1-eng.htm
- Footnote 13
-
Public Health Agency of Canada. "Common chronic diseases in women compared to men." Ottawa, ON: Government of Canada, 2021. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/common-chronic-diseases-women-compared-men-aged-65-years-older.html
- Footnote 14
-
Luy, Marc, and Yuka Minagawa. "Gender gaps--Life expectancy and proportion of life in poor health." Ottawa, ON: Statistics Canada Health Reports 25, no. 12 (2014): 12-19. https://www150.statcan.gc.ca/n1/pub/82-003-x/2014012/article/14127-eng.htm
- Footnote 15
-
Xue, Qian-Li. "The frailty syndrome: definition and natural history." Clinics in geriatric medicine 27, no. 1 (2011): 1-15. https://doi.org/10.1016/j.cger.2010.08.009
- Footnote 16
-
Canadian Frailty Network. "Frailty Matters." Ottawa, ON. 2024. https://www.cfn-nce.ca/frailty-matters/#1574890408921-bde36ff7-f581
- Footnote 17
-
Gilmour, Heather, and Pamela L. Ramage-Morin. "Association of frailty and pre-frailty with increased risk of mortality among older Canadians." Health Rep 32, no. 4 (2021): 15-26. https://www.doi.org/10.25318/82-003-x202100400002-eng
- Footnote 18
-
Government of British Columbia. "Frailty in Older Adults - Early Identification and Management." Vancouver, BC. 2023. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/frailty
- Footnote 19
-
Engelhart, Sarah, Nathan M. Stall, and Kieran L. Quinn. "Considerations for assessing frail older adults requesting medical assistance in dying." CMAJ 194, no. 2 (2022): E51-E53. https://doi.org/10.1503/cmaj.210729.
- Footnote 20
-
Gilmour, Heather, and Pamela L. Ramage-Morin. "Association of frailty and pre-frailty with increased risk of mortality among older Canadians." Health Reports 32, no. 4 (2021): 15-26. https://www.doi.org/10.25318/82-003-x202100400002-eng
- Footnote 21
-
Government of Canada. "About chronic pain." Ottawa, ON. 2023. https://www.canada.ca/en/public-health/services/diseases/chronic-pain/about-chronic-pain.html
- Footnote 22
-
Government of Canada, "About Chronic Pain."
- Footnote 23
-
Chhabra, Gaurav. "Chronic pain syndromes." London, UK: BMJ Best Practice. 2023. https://bestpractice.bmj.com/topics/en-us/694
- Footnote 24
-
Health Canada. "Best Brains Exchange report: Treatment of chronic pain and complex concurrent mental health and substance use conditions." Ottawa, ON: Government of Canada, 2023. https://www.canada.ca/en/health-canada/services/publications/healthy-living/best-brains-exchange-report-2023.html
- Footnote 25
-
Johnston, Keira J. A. and Laura M. Huckins. "Chronic Pain and Psychiatric Conditions." Complex Psychiatry 9, no. 1-4 (2023): 24–43. https://doi.org/10.1159/000527041
- Footnote 26
-
Schopflocher, Donald, Paul Taenzer, and Roman Jovey. "The prevalence of chronic pain in Canada." Pain Research & Management: The Journal of the Canadian Pain Society 16, no. 6 (2011): 445. https://doi.org/10.1155/2011/876306
- Footnote 27
-
Public Health Agency of Canada. "A Dementia Strategy for Canada: Together We Aspire." Ottawa, ON: Government of Canada, 2019. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/dementia-strategy.html
- Footnote 28
-
Public Health Agency of Canada, "A Dementia Strategy for Canada: Together We Aspire."
- Footnote 29
-
Department of Justice. "Legislative Background: Bill C-7: Government of Canada's Legislative Response to the Superior Court of Quebec Truchon Decision." Ottawa, ON: Government of Canada, 2021. https://www.justice.gc.ca/eng/csj-sjc/pl/ad-am/c7/index.html
- Footnote 30
-
Canadian Association of MAiD Assessors and Providers. "Medical Assistance in Dying (MAiD) in Dementia." 2024. https://camapcanada.ca/wp-content/uploads/2022/02/Assessing-MAiD-in-Dementia-FINAL-Formatted.pdf
- Footnote 31
-
Canadian Association of MAiD Assessors and Providers. "Medical Assistance in Dying (MAiD) in Dementia."
- Footnote 32
-
Canadian Association of MAiD Assessors and Providers. "Medical Assistance in Dying (MAiD) in Dementia."
- Footnote 33
-
In this analysis, a medical condition was considered to be: cancer, neurological condition, cardiovascular condition, respiratory disease, organ failure, or "other" condition. Multiple specific conditions within each broad category were not counted.
- Footnote 34
-
Health Canada, "Advice to the Profession: Medical Assistance in Dying (MAID)."
- Footnote 35
-
Government of Canada. "Medical Assistance in Dying: Implementing the Framework." Ottawa, ON: 2024. https://www.canada.ca/en/health-canada/services/health-services-benefits/medical-assistance-dying/implementing-framework.html
- Footnote 36
-
Lowey, Susan E. "Management of Severe Pain in Terminally Ill Patients at Home: An Evidence-Based Strategy." Home Healthcare Now 38, no. 1 (2020): 8–15. https://doi.org/10.1097/NHH.0000000000000826
- Footnote 37
-
Health Canada. "Guidance Document: Reporting Requirements under the Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying." Ottawa, ON: Government of Canada, 2022. https://www.canada.ca/en/health-canada/services/publications/health-system-services/guidance-document-reporting-requirements-under-regulations-amending-regulations-monitoring-medical-assistance-dying.html
- Footnote 38
-
Turpel-Lafond, Mary Ellen, and Harmony Johnson. "In Plain Sight: Addressing Indigenous-Specific Racism and Discrimination in B.C. Health Care." Victoria, BC: Government of British Columbia, 2020. https://doi.org/10.14288/bcs.vi209.195283
- Footnote 39
-
Canadian Institute for Health Information. "Guidance on the Use of Standards for Race-Based and Indigenous Identity Data Collection and Health Reporting in Canada." Ottawa, ON. 2022. https://www.cihi.ca/sites/default/files/document/guidance-and-standards-for-race-based-and-indigenous-identity-data-en.pdf
- Footnote 40
-
Health Canada. "Guidance Document: Reporting Requirements under the Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying."
- Footnote 41
-
Health Canada. "Guidance Document: Reporting Requirements under the Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying."
- Footnote 42
-
95.7% of Track 1 respondents identified as Caucasian (White); 97.8% of Track 2 respondents identified as Caucasian (White)
- Footnote 43
-
Standing Senate Committee on Legal and Constitutional Affairs. "Evidence." Ottawa, ON: Senate of Canada, February 3, 2021. https://sencanada.ca/en/Content/Sen/Committee/432/LCJC/12EV-55130-E
- Footnote 44
-
Standing Senate Committee on Legal and Constitutional Affairs. "Evidence." Ottawa, ON: Senate of Canada, February 2, 2021. https://sencanada.ca/en/Content/Sen/Committee/432/LCJC/11MN-55129-E
- Footnote 45
-
Standing Senate Committee on Legal and Constitutional Affairs. "Evidence." Ottawa, ON: Senate of Canada, November 26, 2020. https://sencanada.ca/en/Content/Sen/Committee/432/LCJC/05MN-55075-E
- Footnote 46
-
Standing Senate Committee on Legal and Constitutional Affairs. "Evidence." Ottawa, ON: Senate of Canada, November 26, 2020. https://sencanada.ca/en/Content/Sen/Committee/432/LCJC/05MN-55075-E
- Footnote 47
-
Employment and Social Development Canada. "Canada's Disability Inclusion Action Plan, 2022." Ottawa, ON: Government of Canada. 2022. https://www.canada.ca/en/employment-social-development/programs/disability-inclusion-action-plan/action-plan-2022.html
- Footnote 48
-
Jonas-Sébastien Beaudry. "Bill C-7, assisted dying and "lives not worth living," Policy Options, December 14, 2020, https://policyoptions.irpp.org/magazines/december-2020/bill-c-7-assisted-dying-and-lives-not-worth-living/
- Footnote 49
-
Leyland Cecco. "Are Canadians being driven to assisted suicide by poverty or healthcare crisis?" The Guardian, May 11, 2022, https://www.theguardian.com/world/2022/may/11/canada-cases-right-to-die-laws.
- Footnote 50
-
Health Canada. "Guidance Document: Reporting Requirements under the Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying."
- Footnote 51
-
Statistics Canada. "New data on disability in Canada, 2022." Ottawa, ON: Government of Canada. 2023. https://www150.statcan.gc.ca/n1/pub/11-627-m/11-627-m2023063-eng.htm
- Footnote 52
-
Gabrielle Peters. "Dying for the right to live," Maclean's, November 12, 2020, https://macleans.ca/society/dying-for-the-right-to-live/
- Footnote 53
-
Ramona Coelho. "Barriers to care persist but access to MAiD keeps expanding: Ramona Coelho for Inside Policy," MacDonald-Laurier Institute, February 21, 2024, https://macdonaldlaurier.ca/maid-keeps-expanding-ramona-coelho-for-inside-policy/
- Footnote 54
-
Lazin, Sarah J. and Jennifer A. Chandler. "Two Views of Vulnerability in the Evolution of Canada's Medical Assistance in Dying Law." Cambridge Quarterly of Healthcare Ethics 32, no. 1 (2023): 105–117. https://doi.org/10.1017/s0963180121000943
- Footnote 55
-
Postal CodeOM Conversion File Plus (PCCF+), area-based after-tax neighbourhood income quintile.
- Footnote 56
-
Analysis performed by Statistics Canada for Health Canada.
- Footnote 57
-
Redelmeier, Donald A., Kelvin Ng, Deva Thiruchelvam, and Eldar Shafir. "Association of socioeconomic status with medical assistance in dying: a case–control analysis." BMJ open 11, no. 5 (2021). http://dx.doi.org/10. 1136/bmjopen-2020-043547
- Footnote 58
-
Downar, James, Robert A. Fowler, Roxanne Halko, Larkin Davenport Huyer, Andrea D. Hill, and Jennifer L. Gibson. "Early experience with medical assistance in dying in Ontario, Canada: a cohort study." CMAJ 192, no. 8 (2020): E173-E181. DOI: https://doi.org/10.1503/cmaj.200016
- Footnote 59
-
Trudel, Pierre, Marie-Hélène Quesnel-Olivo, Mathieu Blais, and Nicolas Dupre. "Describing and Comparing ALS Patients who Request Medical Assistance in Dying with Patients Dying Directly of the Disease (P5-6.005)." In Neurology 102, no. 17 supplement 1 (2024). https://doi.org/10.1212/WNL.0000000000204855
- Footnote 60
-
Tran, Manny, Kimia Honarmand, Robert Sibbald, Fran Priestap, Simon Oczkowski, and Ian M. Ball. "Socioeconomic Status and medical assistance in dying: a regional descriptive study." Journal of Palliative Care 37, no. 3 (2022): 359-365. https://doi.org/10.1177/08258597211053088
- Footnote 61
-
Statistics Canada. "The Canadian Index of Multiple Deprivation (CIMD)." Ottawa, ON: Government of Canada. 2019. https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&Id=1186297.
- Footnote 62
-
Extracted on request by Statistics Canada
- Footnote 63
-
Chief Coroner of Ontario. "Lessons Learned from the Coroner." Presentation at Canadian Association of MAiD Assessors and Providers Conference. Ottawa, ON, May 3, 2023.
- Footnote 64
-
Special Joint Committee on Medical Assistance in Dying. "Medical Assistance in Dying in Canada: Choices for Canadians." Ottawa, ON: Government of Canada, 2023. https://www.parl.ca/Content/Committee/441/AMAD/Reports/RP12234766/amadrp02/amadrp02-e.pdf
- Footnote 65
-
Statistics Canada. "Postal CodeOM Conversion File Plus (PCCF+) Version 8A, Reference Guide." Ottawa, ON, Government of Canada, December 2024. https://www150.statcan.gc.ca/n1/en/catalogue/82F0086X
- Footnote 66
-
Analysis performed by Statistics Canada for Health Canada.
- Footnote 67
-
Analysis performed by Statistics Canada for Health Canada.
- Footnote 68
-
Alasia, Alessandro, Frederic Bedard, Julie Belanger, Eric Guimond, and Christopher Penney. "Measuring Remoteness and Accessibility - A Set of Indices for Canadian Communities." Ottawa, ON: Statistics Canada, May 9, 2017. https://www.publications.gc.ca/collections/collection_2017/statcan/18-001-x/18-001-x2017002-eng.pdf
- Footnote 69
-
Statistics Canada. "Index of Remoteness." Ottawa, ON: Government of Canada, 2023. https://www150.statcan.gc.ca/n1/pub/17-26-0001/172600012020001-eng.htm
- Footnote 70
-
Health Canada, "Fourth Annual Report on Medical Assistance in Dying in Canada 2022."
- Footnote 71
-
Health Canada. "Third Annual Report on Medical Assistance in Dying in Canada 2021." Ottawa, ON: Government of Canada, 2022. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2021.html
- Footnote 72
-
Health Canada. "Second Annual Report on Medical Assistance in Dying in Canada 2020." Ottawa, ON: Government of Canada, 2021. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2020.html
- Footnote 73
-
Health Canada. "First Annual Report on Medical Assistance in Dying in Canada 2019." Ottawa, ON: Government of Canada, 2020. https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2019.html
- Footnote 74
-
Downar, James, Robert A. Fowler, Roxanne Halko, Larkin Davenport Huyer, Andrea D. Hill, and Jennifer L. Gibson. "Early experience with medical assistance in dying in Ontario, Canada: a cohort study."
- Footnote 75
-
Jordan, Roberta I., Matthew J. Allsop, Yousuf ElMokhallalati, Catriona E. Jackson, Helen L. Edwards, Emma J. Chapman, Luc Deliens, and Michael I. Bennett. "Duration of palliative care before death in international routine practice: a systematic review and meta-analysis." BMC medicine 18 (2020): 1-25. https://doi.org/10.1186%2Fs12916-020-01829-x
- Footnote 76
-
World Health Organization. "Social Isolation and Loneliness." 2024. https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/social-isolation-and-loneliness
- Footnote 77
-
Health Canada. "Guidance Document: Reporting Requirements under the Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying."
- Footnote 78
-
In ten instances, practitioners did not know the person's usual living arrangements.
- Footnote 79
-
Frolic, Andrea and Allyson Oliphant. "Introducing Medical Assistance in Dying in Canada: Lessons on Pragmatic Ethics and the Implementation of a Morally Contested Practice." HEC Forum 34, no. 4 (2022): 307–319. https://doi.org/10.1007/s10730-022-09495-7
- Footnote 80
-
Mental Health Commission of Canada. "Towards Better Mental and Physical Health: Preventing and Managing Concurrent Mental and Physical Conditions: A Scoping and Rapid Realist Review." Ottawa, ON, 2021. https://mentalhealthcommission.ca/resource/preventing-and-managing-concurrent-mental-and-physical-conditions/
- Footnote 81
-
Department of Justice. "Legislative Background: Bill C-7: Government of Canada's Legislative Response to the Superior Court of Quebec Truchon Decision."
- Footnote 82
-
During a transfer for MAID, there is a possibility that a patient may lose capacity to consent or die before they can receive MAID. As such, the number of reported patient transfers may not fully represent the number of MAID requesters that underwent a transfer.
- Footnote 83
-
Government of Quebec. "Bill 11: An Act to Amend the Act Respecting End-of-Life Care and Other Legislative Provisions." Quebec, QC: Government of Quebec, 2023. https://www.assnat.qc.ca/en/travaux-parlementaires/projets-loi/projet-loi-11-43-1.html
- Footnote 84
-
This date was amended from March 17, 2024 by the former Bill C-62: An Act to amend An Act to amend the Criminal Code (medical assistance in dying), No. 2.
- Footnote 85
-
Statistics Canada. "The Canadian Index of Multiple Deprivation (CIMD)." Ottawa, ON: Government of Canada, 2019. https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5274
- Footnote 86
-
Statistics Canada. "Canadian Vital Statistics – Death Database." Ottawa, ON: Government of Canada, 2024. https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=3233
- Footnote 87
-
World Health Organization. "Cause of Death". Geneva, Switzerland: 2024. . https://www.who.int/standards/classifications/classification-of-diseases/cause-of-death
- Footnote 88
-
World Health Organization. "International Statistical Classification of Diseases and Health Related Problems, 10th Revision, Sixth Edition, Volume 2." Geneva, Switzerland: 2019. https://icd.who.int/browse10/Content/statichtml/ICD10Volume2_en_2019.pdf
- Footnote 89
-
Special Joint Committee on Medical Assistance in Dying. "Medical Assistance in Dying in Canada: Choices for Canadians."
- Footnote 90
-
Statistics Canada. "Index of Remoteness."