
Guidance on planning for recovery following a nuclear or radiological emergency
(PDF Version, 708 Kb, 42 pages)
Health Canada is the federal department responsible for helping the people of Canada maintain and improve their health. Health Canada is committed to improving the lives of all of Canada's people and to making this country's population among the healthiest in the world as measured by longevity, lifestyle and effective use of the public health care system.
This guidance document is a product of ongoing collaboration between Health Canada, the Canadian Nuclear Safety Commission, Natural Resources Canada, the Department of National Defence/Canadian Armed Forces and Public Safety Canada.
Également disponible en français sous le titre :
Directives sur la planification du rétablissement à la suite d’une urgence nucléaire ou radiologique
To obtain additional information, please contact:
Health Canada
Address Locator 0900C2
Ottawa, ON K1A 0K9
Tel.: 613-957-2991
Toll free: 1-866-225-0709
Fax: 613-941-5366
TTY: 1-800-465-7735
E-mail: hc.publications-publications.sc@canada.ca
© Her Majesty the Queen in Right of Canada, as represented by the Minister of Health, 2020
Publication date: December 2020
This publication may be reproduced for personal or internal use only without permission provided the source is fully acknowledged.
Cat.: H129-109/2020E-PDF
ISBN: 978-0-660-36748-4
Pub.: 200307
Preface
This document provides guidance for decision makers on planning for recovery from nuclear and radiological emergencies. It does not include any regulations or requirements. Given that recovery from a nuclear or radiological emergency is a complex matter, the document is broadly scoped to provide high-level conceptual guidance to all levels of government and stakeholders with roles and responsibilities in nuclear emergency management.
This guidance document was developed through a partnership and ongoing collaboration between Health Canada, the Canadian Nuclear Safety Commission (CNSC), the Department of National Defence/Canadian Armed Forces (DND/CAF), Natural Resources Canada (NRCan) and Public Safety Canada (PSC). The guidance in this document is consistent with international best practices and the recommendations of the International Atomic Energy Agency (IAEA) and International Commission on Radiological Protection (ICRP).
Table of Contents
- Preface
- Table of Contents
- 1 Introduction
- 2 Exposure Situations
- 3 Transition to Recovery
- 4 Best Practices for Key Recovery Elements
- 4.1 Implementation of Protection Strategies for Recovery
- 4.2 Environmental and Food Chain Monitoring
- 4.3 Exposure Pathways and Dose Assessments
- 4.4 Health Monitoring
- 4.5 Epidemiological Studies
- 4.6 Management of Contamination
- 4.7 Remediation
- 4.8 Waste Management
- 4.9 Monetary Compensation
- 4.10 Communication
- 4.11 Protection of Workers
- 5 Establishing a New Normal
- Appendix: Abbreviations and Acronyms
- References
- Additional Information
Introduction
Nuclear Emergency Management in Canada
Emergency management in Canada is a shared responsibility, which relies on ongoing cooperation and communication between federal, provincial/territorial and municipal/regional governments. Provinces and territories are responsible for the health and safety of their populations and therefore have the authority to manage emergencies within their borders. Municipal or regional authorities, such as police, fire services and emergency medical services, provide the initial on-scene response. For emergencies that exceed municipal or regional response capacity, provincial and territorial authorities will provide strategic oversight, coordinate response actions among the organizations involved and implement public protective actions. If an emergency threatens to overwhelm the resources of any individual province or territory, the federal government will provide assistance upon request and is responsible for managing emergencies where it has primary jurisdiction (e.g., federally owned lands) in accordance with the Emergency Management Act Reference 1.
For large-scale emergencies requiring a national response, the federal government will coordinate a whole-of-government response in support of the affected provinces or territories. The mechanisms, roles and responsibilities for a coordinated Government of Canada (GC) response are described in the all-hazards Federal Emergency Response Plan (FERP) Reference 2. While the FERP outlines the all-hazards governance for any emergency requiring an integrated federal response, each federal department is responsible for developing plans to address specific hazards or events that impact their responsibilities, such as a nuclear or radiological emergency. These event-specific arrangements augment and integrate with the all-hazards governance described in the FERP.
In the event of a large-scale nuclear or radiological emergency in Canada, such as an accident at a Canadian nuclear power plant, a coordinated national response would be required due to the complexity, scale and technical nature of such an event. The federal government would mobilize to support the provincial/territorial authorities either upon request, in accordance with its regulatory role in the case of an emergency involving licensed sources or facilities Reference 3 Reference 4, or according to pre-established arrangements through the Federal Nuclear Emergency Plan (FNEP) Reference 5 and its provincial annexes. In the event of a nuclear emergency with transboundary consequences, the federal government would liaise with the international community and foreign diplomatic missions in Canada, and assist Canadians abroad.
The FNEP integrates with the emergency management structure established in the FERP and describes how federal scientific and technical resources would be coordinated as part of the overall GC response in support of provincial/territorial authorities. For instance, the FNEP would enable the federal government to assist in the technical assessment of the emergency, provide protective action recommendations to provincial/territorial authorities and support radiation monitoring activities, in addition to other nuclear emergency functions.
Canada’s Emergency Management Act requires organizations at all levels of government with nuclear emergency management roles and responsibilities to develop plans and arrangements spanning the four integrated functions of emergency management: prevention and mitigation, preparedness, response and recovery.
Therefore, the nuclear emergency management framework includes:
- Prevention and mitigation: actions taken to ensure that a nuclear emergency does not occur, or to reduce the likelihood of occurrence.
- Preparedness: actions taken in order to be ready to respond to, and manage the consequences of, a nuclear emergency (e.g., response procedures and plans, training and awareness, maintaining emergency facilities, exercises).
- Response: actions taken during a nuclear emergency to mitigate the magnitude of the hazard and manage its consequences to health, safety and the environment. Response actions may include shelter-in-place or evacuation, ingestion of potassium iodide (KI) tablets, worker protection, emergency medical assistance and emergency public communication, among others. A transition occurs between the response and recovery phases (referred to as the ‘transition phase’), whereby actions are taken to prepare for long-term recovery. Transition actions include adjusting response actions to fit the changing situation and implementing arrangements needed to terminate the emergency and commence recovery (e.g., coordinating the transfer of authority from response to recovery management organizations (see Section 3), implementing waste management plans, and populating databases for long-term medical monitoring).
- Recovery: short-term and long-term actions taken both on-site and off-site in order to restore the communities affected by the nuclear emergency to an acceptable level. Recovery actions include remediation, waste management, and long-term health and environmental monitoring, among others (see Section 4).
While Canada’s nuclear emergency management organizations have well-established roles, responsibilities, plans and procedures for the preparedness and response phases, the details of the transition, termination and recovery phase need to be elaborated and require further consideration and documentation at all levels of government. Municipalities in particular have a significant role to play in the recovery-phase decision-making process due to their direct involvement with affected individuals and communities.
This document provides best practices and key considerations to assist federal, provincial and municipal authorities in developing plans and arrangements for recovery following a nuclear or radiological emergency.
Definition of Nuclear or Radiological Emergency
A nuclear or radiological emergency is an emergency that has led to, or could lead to, the release of radioactive material, or exposures to uncontrolled sources of radiation, which pose, or could pose, a threat to health and safety, property, and the environment Reference 5 Reference 6. Henceforth, such an event will be referred to as a ‘nuclear emergency’ in this document.
Definition of Recovery
For the purpose of this document, recovery is defined as the actions taken following the emergency response to restore quality of life, social systems, economies, community infrastructure and the environment, while protecting the health of the affected populations.
The extent of the measures taken during recovery would be determined by the authority having jurisdiction, in consultation with the stakeholders affected by the emergency and its aftermath. Recovery efforts may begin during the response phase and their scope should be commensurate with the impact of the emergency on the surrounding population and environment.
Purpose
This document provides guidance for authorities and decision makers who are responsible for preparing and implementing plans for off-site recovery following a nuclear or radiological emergency.
Scope
The guidance provided in this document is for planning and executing off-site recovery operations following a nuclear or radiological emergency. ‘Off-site’ refers to the area outside the property boundary of a licensed nuclear facilityFootnote 1 or a Department of National Defence/Canadian Armed Forces (DND/CAF) authorization holderFootnote 2 Reference 5 Reference 7. Conversely, ‘on-site’ refers to the area inside those boundaries.
With respect to the application of recovery elements following a nuclear emergency, it is assumed in this document that a radioactive release has occurred and has resulted in levels of radiation above prescribed limits in the public domain (i.e., an area accessible to the public that is not under the direct control of a CNSC licensee or a DND/CAF authorization holder) where the consequences would require the implementation of a recovery plan.
The following topics are outside of the scope of this document:
- requirements and guidance for CNSC licensees for preparedness and nuclear emergency response, which are provided in Regulatory Document (REGDOC)-2.10.1, Nuclear Emergency Preparedness and Response Reference 3;
- licensee guidance for on-site recovery actions;
- requirements and guidance for DND/CAF authorized nuclear and radiological activities;
- security considerations associated with nuclear emergencies, given that these would have been managed before the initiation of the recovery phase;
- detailed arrangements for the management and coordination of the recovery phase of a nuclear emergency, which would be the responsibility of the authorities having jurisdiction (off-site) and licensees/authorization holders (on-site).
Alignment with International Standards, Requirements and Recommendations
Canada’s guidance for recovery after a nuclear or radiological emergency reflects international standards, requirements and recommendations, including those provided by the International Atomic Energy Agency (IAEA) and the International Commission on Radiological Protection (ICRP). Applying these best practices will contribute to worldwide harmonization of arrangements for preparedness, response and recovery from a nuclear emergency.
The IAEA establishes requirements for developing arrangements for the transition to recovery:
- Requirement 18 of IAEA General Safety Requirements (GSR) Part 7 Preparedness and Response for a Nuclear or Radiological Emergency Reference 10, states: “The government shall ensure that arrangements are in place and are implemented for the termination of a nuclear or radiological emergency, with account taken of the need for the resumption of social and economic activity.” Additional requirements and guidance for ensuring that appropriate arrangements are in place for the termination of the emergency are provided in sections 5.95 to 5.101 of IAEA GSR Part 7, and in IAEA General Safety Guide (GSG)-11 Arrangements for the Termination of a Nuclear or Radiological Emergency Reference 11.
- Requirement 46 of IAEA GSR Part 3 Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards Reference 12 states: “The government shall ensure that arrangements are in place and are implemented as appropriate for the transition from an emergency exposure situation to an existing exposure situation.”
The ICRP establishes best practices for transitioning from an emergency exposure situation to a new existing exposure situation, characterized by a change in management, from strategies mainly driven by urgency, to more decentralized strategies aimed at improving living conditions and by reducing exposures to as low as reasonably achievable (ALARA), taking into account social and economic factors. The complex circumstances must be managed with radiation protection considerations, but must also address health, environmental, economic, social, cultural, ethical, and political considerations Reference 13.
This guidance document for Canadian recovery actions following a nuclear emergency aims to promote alignment with these two IAEA requirements and ICRP best practices.
Key Concepts for Recovery Planning
Recovery planning is gaining the attention of the international nuclear emergency preparedness and response community in light of lessons learned from past nuclear emergencies. While Canada recognizes recovery as a key aspect of emergency management, there has been limited recovery planning in the preparedness phase. It is important to realize that some aspects of recovery can be initiated during the preparedness and response phases. Recovery planning therefore needs to occur in the preparedness phase and be included in response arrangements. In order to begin planning for recovery from a nuclear emergency, the concepts of existing exposure situations, reference levels and Recovery Management Organizations (RMOs) need to be introduced.
Section 2 describes the concept of exposure situations and introduces ‘existing exposure situation’ as part of the system of radiation protection for managing exposures in the recovery phase due to residual radioactive material in the environment. In order to help manage these exposures, the ICRP introduced reference levels applicable to existing exposure situations Reference 13 Reference 14. The selected reference level is a dose level used to help guide protective action decisions and the optimization of the protection strategy in order to reduce future doses. It is important to understand how the ICRP reference levels apply to existing exposure situations when planning for recovery.
Section 3 describes the transition from response to recovery, which is in part characterized by a shift in roles and responsibilities of the organizations involved. International guidance recommends that mechanisms be developed that allow for the coordinated transfer of authority from the organizations managing the response to the organizations managing the long-term recovery Reference 11. This would allow response organizations to return to normal operations and be ready to respond to future emergencies. To that effect, Section 3 describes the RMOs as a means to facilitate this transition and to establish roles, responsibilities and authorities for the management of recovery activities. Section 3 also discusses psychosocial consequences of nuclear emergencies and presents strategies for mitigating their impacts, many of which can be implemented prior to the recovery phase.
These concepts are foundational elements of recovery planning. They inform the development of the recovery phase protection strategy and would enable the successful implementation of the key recovery elements discussed in Section 4:
- Recovery phase protective actions (Section 4.1.1);
- Self-help actions (Section 4.1.2);
- Environmental and food chain monitoring (Section 4.2);
- Exposure pathways and dose assessments (Section 4.3);
- Health monitoring and epidemiological studies (Sections 4.4 and 4.5);
- Managing contamination and remediation (Sections 4.6 and 4.7);
- Waste management (Section 4.8);
- Monetary compensation (Section 4.9);
- Communication (Section 4.10);
- Worker protection (Section 4.11).
Recovery plans should include details of the recovery phase management structure, the roles and responsibilities of organizations involved in recovery activities, and arrangements for implementing protective actions and other recovery activities (see Section 4). Recovery plans should be designed for flexibility in their implementation, recognizing that the radiological situation would vary significantly depending on the nature of the emergency and the protection strategy would need to be adapted and adjusted as the radiological situation evolves.
All stakeholders should be consulted when planning for recovery, including municipal authorities, community leaders and members of the public. Indigenous peoples and communities should also be consulted in the planning process. These interested parties should be consulted early and often throughout the preparedness phase in order to establish trust, credibility and acceptance of recovery arrangements that address communities’ needs. This would facilitate continued dialogue and involvement of stakeholders in decision-making throughout the recovery phase, leading to more resilient and empowered communities. Resilient communities would be better prepared to withstand and mitigate the impacts of disasters and could more quickly reopen and restore businesses, workplaces and essential services required for the resumption of social and economic activity Reference 11 Reference 15.
By applying the guidance in this document with these concepts in mind, authorities having jurisdiction would be able to develop recovery plans that incorporate the key recovery elements discussed in Section 4.
Exposure Situations
The ICRP has proposed, and the IAEA has adopted, a framework for radiation protection that encompasses all exposure situations including planned, emergency and existing.
ICRP Publication 103, The 2007 Recommendations of the International Commission on Radiological Protection Reference 14, and IAEA GSR Part 7 Preparedness and Response for a Nuclear or Radiological Emergency Reference 10, outline the three exposure situations:
- Planned exposure situations involve the planned operation of a source (e.g., the operation of nuclear reactors) or planned activities that result in an exposure from a source (e.g., disposal of radioactive waste).
- Emergency exposure situations arise as a result of an accident, a malicious act or other unexpected event, and require prompt action in order to avoid or to reduce adverse consequences.
- Existing exposure situations already exist when a decision on control must be taken, including prolonged exposure situations after emergencies. These situations include exposure to natural background, exposure due to residual radioactive material that derive from past practices that were never subject to regulatory control, and exposure due to the residual radioactive material deriving from a nuclear emergency.
This approach allows the system of radiation protection to be applied to regulated activities such as the use of radioactive materials in industry or medicine as well as activities that would not normally be regulated, such as the use of lands where there is elevated natural background radiation. Consequently, nuclear emergency management authorities are able to adopt similar approaches for applying radiation protection measures to limit exposures, regardless of the exposure situation.
Notably, the principles of justification and optimization apply universally to all exposure situations Reference 14 Reference 16.
- The principle of justification is that any decision altering an exposure situation should do more good than harm. When applied, the decisions that aim to reduce exposure following a nuclear incident introduce additional constraints on individuals and communities in affected areas. The net benefit of the decisions must be positive, beyond simply the impact they have on the exposure to individuals.
- The principle of optimization aims at keeping individual exposures ALARA, taking into account economic, societal, and environmental factors. It aims to avoid unnecessary exposure, fair distribution of exposure among exposed individuals and treating people with respect.
In the context of nuclear emergency management, protective actions should first be justified and then optimized before being implemented for all exposure situations.
This document considers each of these three exposure situations, as follows:
- During the conduct of licensed activities, the exposure situation for a member of the public from these activities is considered a planned exposure situation.
- If a nuclear emergency occurs, then a member of the public may be exposed to radiation as a result, and this is considered an emergency exposure situation.
- Finally, as the nuclear emergency transitions from the response phase to the recovery phase, any additional exposure for a member of the public to radiation resulting from residual environmental contamination is considered an existing exposure situation.
Note: This document’s scope does not include potential exposure from recovery activities conducted under licenses issued under the NSCA Reference 8, such as contaminated waste disposal at licensed waste facilities. These activities are considered planned exposure situations.
For the management of planned and emergency exposure situations in Canada, there are regulations and license conditions that apply to CNSC licensees, whereas in the DND/CAF, there are orders and directives and authorization conditions that apply to DND/CAF authorization holders. These high-level documents specify dose limits that apply to persons working under a CNSC license (nuclear energy worker) or in accordance with a DND/CAF authorization (DND employees or CAF members). The dose limits are dependent on the specific exposure situation, with separate limits applicable to planned and emergency exposure situations.
The Radiation Protection Regulations (RPR) Reference 17 establishes dose limits for nuclear energy workers involved in planned exposure situations. In the event of a nuclear emergency, there are dose limits that apply to persons involved in the control of the nuclear emergency under the authority of the licensee. While the regulations specify dose limits to members of the public for planned exposure situations, such as the normal operation of a nuclear power plant, they do not specify dose limits for members of the public for the nuclear emergency or existing exposure situations. In order to manage exposure to members of the public and to off-site responders during the nuclear emergency and existing exposure situations, the ICRP reference levels are recommended. These reference levels are provided and explained in Section 2.1 and are consistent with recommendations in Health Canada’s document Generic Criteria and Operational Intervention Levels for Nuclear Emergency Planning and Response Reference 18.
In the DND/CAF, the Nuclear Safety Orders and Directives (NSOD) Reference 7 establishes dose limits for DND employees and CAF members where nuclear and radiological activities are conducted. The NSOD is consistent with the dose limits specified in the RPR and, along with DND/CAF authorizations, is based on the ICRP concept of planned and emergency exposure situations.
The following tools are used for managing exposure for the three exposure situations:
- Planned exposure situations: Regulatory dose limits in the RPR (applicable to all persons, excluding DND employees and CAF members) and dose limits in the NSOD (applicable to DND employees and CAF members only). The annual dose limit for a member of the public is 1 millisievert (mSv) in a planned exposure situation.
- Emergency exposure situations: Regulatory dose limits in the RPR for persons involved in the control of the emergency under the authority of the licensee and dose limits specified for off-site emergency workers in provincial response plans (applicable to persons involved in the control of the emergency); ICRP reference levels (applicable to all other persons, excluding DND employees and CAF members); dose limits in the NSOD (applicable to DND employees and CAF members only). The ICRP recommends establishing a reference level between 20-100mSv, acute or annual, for emergency exposure situations.
- Existing exposure situations: ICRP reference levels (applicable to all persons, except CAF members if deployed on operations). The ICRP recommends establishing a reference level between 1-20 mSv, acute or annual, for existing exposure situations.
The key elements to ensuring recovery following a nuclear emergency are outlined in Figure 1, which incorporates the concepts from updated international guidance on exposure situations Reference 12 Reference 14 and arrangements for the termination of a nuclear or radiological emergency Reference 11, along with regulatory dose limits Reference 17 and the dose reference levels recommended by the ICRP for the three exposure situations Reference 14.
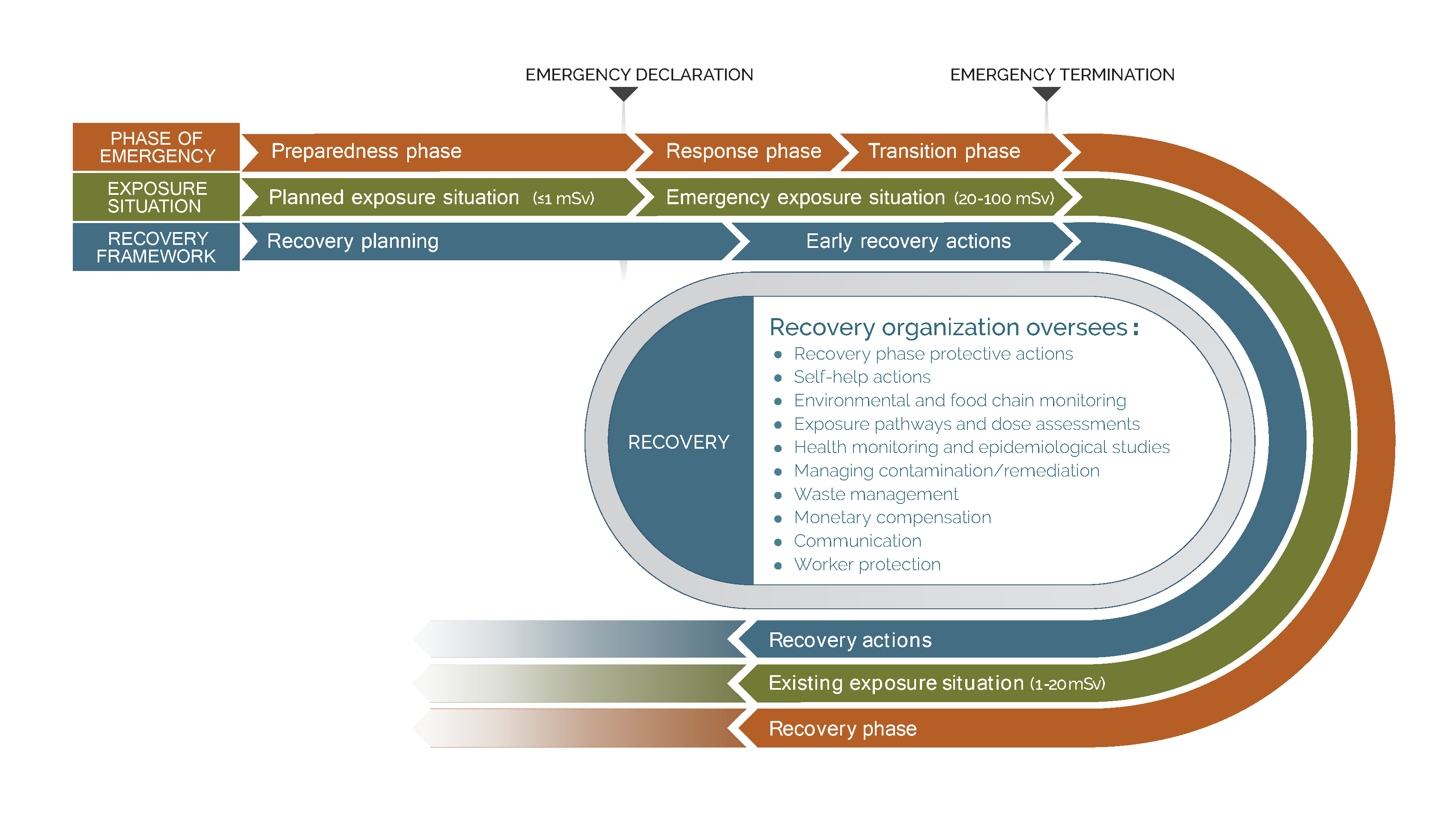
The interrelationship between the emergency phases, exposure situations and off-site recovery elements are depicted by the three lines in Figure 1:
- The orange line (outer line) depicts the progression of emergency phases from preparedness through to recovery. Importantly, the nuclear emergency would not be terminated off-site until the elements required for recovery (shown in the bulleted list in Figure 1) have been arranged. This concept is expressed in the IAEA document GSG-11, Arrangements for the Termination of a Nuclear or Radiological Emergency Reference 11, which describes how these arrangements are put in place during the transition phase.
- The green line (centre line) illustrates the progression from a planned exposure situation to an emergency exposure situation, and ultimately to an existing exposure situation – in relation to the emergency phases shown in the orange line. The exposure situations apply to members of the public in relation to the regulated source or activity that is involved in the nuclear emergency.
- The blue line (inner line) indicates when recovery elements should be planned for and implemented in relation to the nuclear emergency phases and the exposure situations. As shown in Figure 1, recovery planning should begin in the preparedness phase and early recovery actions should begin during the response phase in order to enable an effective transition to the recovery phase.
Recovery planning during the preparedness phase could include the development of preliminary waste management arrangements, such as the identification of suitable locations for temporary storage of radioactive waste arising from an emergency. Potential early recovery activities during the response phase could include populating databases with patients identified as requiring long-term medical follow-up, or developing more detailed remediation and waste management strategies once the radiological situation has been sufficiently characterized. It should be recognized that the implementation of early recovery actions may divert emergency response staff from their duties if dedicated recovery personnel are not available or if the RMO has not yet been activated. Response organizations should therefore establish rosters with a surplus of responders, or develop arrangements for surge capacity, during the preparedness phase in order to be able to implement early recovery actions without impacting the response
Reference Levels
The ICRP defines a reference level as “the level of residual dose or risk above which it is generally judged to be inappropriate to allow exposures to occur” and below which protective actions should be planned and optimized Reference 14. Reference levels are presented as a range or bands of exposure, to provide flexibility for decision makers. They are expressed in mSv and are applicable to doses received by members of the public after the implementation of protective actions. Table 1 presents the ICRP’s recommended reference levels.
| Reference level band(acute or per year) | Type of exposure situation |
|---|---|
| 20–100 mSv | Emergency exposure situations in which events with uncertain consequences require urgent protective actions, such as sheltering and evacuation, to be implemented to minimize the impacts of possible radiation exposures Reference 14 |
| 1–20 mSv | Existing exposure situations in which radioactivity is already present in the environment when protective action decisions are taken to reduce radiation exposures Reference 14; if doses are optimized below the reference level selected from within this band, it is safe to live in the contaminated area |
Doses within these reference levels should be optimized. Optimization in recovery would be a forward-looking, iterative process aimed at reducing future exposures; it should be seen as a ‘frame of mind’, in which people always question if the best has been done in the prevailing circumstances. Because the recovery process would be focused on the community, all key decisions should be centred on stakeholder involvement and consider technical and socio-economic factors.
Transition to Recovery
A transition from response to recovery could not take place until, at a minimum, the situation at the source had stabilized and there would no longer be a need to take additional urgent protective actions. As the situation moves from response to recovery, the decision-making process may become more complex. Roles and responsibilities would need to shift, and additional organizations would likely need to be involved.
As illustrated in Figure 1 (Section 2), recovery planning should begin in the preparedness phase. In order to enable an effective transition from response to recovery, authorities having jurisdiction should address the following recovery elements prior to an emergency:
- establishment of RMOs;
- pre-identification of goals of the recovery, such that action plans could be implemented expediently;
- identification of roles and responsibilities of the organizations involved in the recovery phase, to the extent practicable;
- a mechanism for a formal transfer of responsibilities to the RMOs that would take place during the transition phase.
The transition from the response phase (i.e., an emergency exposure situation) to the recovery phase (i.e., an existing exposure situation) would be characterized by a change in management and strategy. During the response phase, both management and strategy would be primarily driven by urgency, with potentially high levels of exposure and central decisions. During the recovery phase, strategies would be more decentralized, involve less urgency, and focus on improving living conditions and reducing exposures. Organizations that were active during the emergency response would be gradually or partially relieved of their duties so that they can return to a state of readiness for any future emergencies, and RMOs should be activated.
The function of the RMOs would be to coordinate and oversee the recovery activities listed in Figure 1. The RMOs should be led by the authority having jurisdiction and include representatives from organizations with the expertise or authority to implement the recovery activities relevant to the situation. Some of the same organizations involved in the response phase would remain active as members of the RMOs, such as environmental monitoring teams responsible for long-term assurance monitoring. However, since the recovery phase would be focused on a different set of activities and objectives compared to the response phase, the RMOs would include a number of new organizations not previously involved. Examples include organizations responsible for off-site waste management and remediation, as well as administering monetary compensation.
Recovery planning in the preparedness phase should include a formal mechanism for this transfer of authority, including arrangements to establish the composition of the RMOs and to enable their activation. Nuclear emergency management organizations should also develop arrangements to integrate the RMOs into their existing all-hazards emergency management organization structures, as well as those of other jurisdictions since recovery efforts would often require support from all levels of government.
For instance, a provincially-led RMO should have pre-defined arrangements to interface with the federal emergency management organizations described in the FERP and the FNEP, and vice versa.
In the case of severe accidents affecting large geographical areas, the transition from response to recovery may occur at different times for the contaminated areas Reference 11 Reference 12. This would require continual re-assessment of the situation, refinement of recovery plans and arrangements based on prevailing conditions and making recovery protective action decisions. Some areas may be ready to begin lifting or modifying protective actions and implementing recovery activities sooner than others based on variations in the prevailing conditions. In such situations, the RMOs should communicate to the public the reasons why different areas are transitioning to recovery at different times. Authorities should also inform the affected communities of the specific actions to take, when to take them and how the transition to recovery would impact their community Reference 11. Frequent and transparent communication would be important for maintaining trust and credibility with the public, particularly when messaging differs between geographical areas. The formal transition from response to recovery would be declared once the last affected area transitions.
Psychosocial Considerations
Emergencies can impact an individual’s psychological (i.e., mental or emotional) and social wellbeing, with each having an effect on the other. These interrelated impacts are referred to as psychosocial effects and can be observed at the individual, community and societal levels. Psychosocial effects can include fear, anxiety, feelings of loss of control, depression, and a sense of hopelessness and distress Reference 19 Reference 20. These effects result from social conditions (e.g., family separation, unemployment and disruption of social networks) and can impact mental health, leading to behavioral, emotional, and physiological consequences Reference 20. Psychosocial effects may be among the most significant and costly non-radiological impacts resulting from an accident Reference 21 Reference 22 Reference 23 Reference 24.
Following the large nuclear accidents at Chernobyl and Fukushima, the major health impacts observed were psychosocial in nature Reference 25 Reference 26. In the case of the Fukushima accident, the radiation doses of the affected population were much lower than those of the Chernobyl accident and, unlike Chernobyl, there were no deaths directly attributed to the exposure Reference 27. Given the observed prevalence of psychosocial impacts relative to radiological health impacts from these past nuclear accidents, it is imperative to consider psychosocial issues when making decisions about recovery phase protective actions.
The Chernobyl accident was not announced in a timely manner by the government of the former Ukrainian Republic of the Soviet Union, and the subsequent fear and anxiety stemming from the fallout was exacerbated by a loss of trust. The psychosocial consequences observed following Chernobyl are similar to those observed following atomic bombings and other nuclear accidents. However, findings related to Chernobyl are difficult to interpret and may be unique versus those of any other nuclear disaster, given that dispersion information was unavailable for years following the accident Reference 25.
The combination of the March 2011 earthquake, tsunami and nuclear accident at Fukushima led to psychosocial effects in the affected population in Fukushima Prefecture. These effects, which included depression and post-traumatic stress symptoms Reference 28 Reference 29, are common to most disasters and cannot be directly attributed to exposure Reference 30. The significant impact of the loss of lives and missing loved ones because of the earthquake and tsunami – in conjunction with other conditions such as evacuation, relocation, family separation, material and financial loss, along with fear and uncertainty related to exposure and its potential consequences – all contributed to increased mental distress Reference 31. There has also been a documented increase in mortality among the institutionalized elderly in the first year after the evacuation. This has been widely discussed as an example of how decisions based too narrowly on radiological concerns can result in harm due to non-radiological risks Reference 32.
The Japanese government instituted the Fukushima Health Management Survey to monitor the long-term health of the residents of the region, and to determine if long-term low-dose exposure from the Fukushima nuclear accident had an impact on health outcomes. The studies performed under this survey have underlined the need for more continuous observational studies, conducted over the long term, to understand the lasting mental health implications of the Fukushima nuclear accident. The results of many other studies conducted to date on the mental health consequences of the Fukushima nuclear accident (e.g., psychological, emotional and behavioral) indicate increased rates of psychological effects in the affected population, with higher prevalence compared to survivors of other disasters Reference 27.
Behavioural changes were also observed in the affected population in the years following the disaster, including increased alcohol and tobacco use and increased rates of suicide Reference 33. The prevalence of psychological issues was observed to be higher in vulnerable populations, including evacuees, mothers of young children and nuclear workers. These vulnerable groups were also subject to discrimination and stigmatization. Particular attention should be given to these groups when developing recovery arrangements for mental health and psychosocial support. These arrangements should include education and intervention measures, with a focus on adaptive behaviour Reference 33.
The World Health Organization Reference 31 indicated that psychosocial effects following nuclear or radiological accidents may be exacerbated for several reasons, namely:
- a fear of the unknown, since radiation cannot be seen, felt or heard;
- use of complex language to explain the magnitude of exposures and their potential effects;
- the high degree of uncertainty associated with some accidents;
- psychosocial effects being experienced in a geographical area beyond the region actually affected by radiological dispersion;
- a combination of some or all of the above factors, which may result in residents of affected areas feeling a sense of social stigma.
Mitigation of Psychosocial Effects
Recovery planning should consider not only the psychosocial impacts of the emergency itself, but also those of recovery phase protective actions and other recovery activities. Best practices to mitigate psychosocial effects during the response and recovery phases of a nuclear emergency should be developed during the preparedness phase and should be informed by the following key elements:
- Open communication lines: The severity and duration of psychosocial effects would likely be related to how the incident is perceived by the community. The provision of timely and accurate information on the amount of radiation released as a consequence of the nuclear emergency, its anticipated impacts and the subsequent emergency response and recovery phase protective actions taken by authorities should alleviate the community’s uncertainty and concern. Additionally, open lines of communication within and between family units, and amongst the broader community, would minimize conflict and uncertainty in the affected geography Reference 34.
- Access to educational resources: The provision of timely, clear, and easily accessible educational material to those impacted by nuclear emergencies would be fundamental to ensuring that negative psychosocial impacts are reduced when implementing necessary protective actions in the emergency response and recovery phases. Negative behavioural changes, such as increased alcohol and tobacco consumption and higher rates of suicide, were observed in affected populations of both the Chernobyl and Fukushima nuclear emergencies. Educational resources should address adaptive behaviour strategies and interventions Reference 33. In Fukushima, the broad deployment of an extensive thyroid screening survey was conducted with little education provided to the public on its purpose and in some cases, without the participants’ consent. This led to alarmist reactions among the participants who eventually had a limited understanding of the meaning of results, and much of the distress experienced in relation to the thyroid examination survey may have been minimized if an education and awareness campaign had been instituted. A study of the psychological issues related to the thyroid examinations in Fukushima and Chernobyl highlighted the impact of how decisions made about community health, communication about health issues and surveillance programs can contribute to a population’s concerns about health risks Reference 35. This information should be taken into account when decisions on emergency and recovery phase protective actions, including mental health care planning, are made.
- Training: Experience gained, and lessons learned, from nuclear accidents suggests that public support centres for the affected populations should be established as soon as possible following the accident. Local doctors, nurses, pharmacists, psychologists, experts from public universities and associations, and others in positions of trust and who have the respect of the community, including Indigenous leaders, should hold integral positions at these public support centres. Information that puts health hazards in perspective, along with proper training on effective approaches to risk communication, should be given to support centre workers and volunteers to enable them to provide appropriate public advice Reference 11.
- Empowerment of the public: Experience has shown that creating conditions and providing the means to encourage the direct involvement and empowerment of the affected population, such as holding community consultations, is effective in mitigating psychosocial impacts. Community consultations led by federal and/or provincial and local (e.g., municipal) authorities should be held to hear from the affected population as well as from local trusted professionals, including Indigenous leaders, on the challenges they face towards the long-term rehabilitation of living conditions. Consultations with local professionals and members of the public emphasize the human dimension of the situation, and therefore the particular importance of preserving the dignity of the population. Decisions on matters such as issuing, lifting or changing the status of protective actions should be community-driven Reference 36 Reference 37 Reference 38 Reference 39 Reference 40 – and most importantly, the outcomes of these decisions must do more good than harm Reference 41.
Without such consultations, decision-makers lack the perspective of affected communities in managing the recovery and may miss critical insight when making protective action decisions that do more good than harm. The public should also be given tools and training during recovery, such as dose and contamination monitors, to encourage self-help actions that promote community empowerment (further discussed in Section 4.1.2). - Minimization of time spent in temporary evacuation: Experience has shown that psychosocial impacts are reduced when disruption to evacuees is minimized; they are promptly informed of the decision for permanent relocation versus temporary relocation; the number of times they are to be relocated is limited; and they are allowed to return to their homes as soon as possible after a temporary evacuation. Given this, a balanced decision must be made when determining whether to allow residents to return home; projected doses cannot be considered in isolation of potential psychosocial impacts.
Establishing measures in advance to mitigate psychosocial impacts would contribute to the resiliency of communities and their ability to adapt to disruptions resulting from the emergency, the associated protective actions and the resulting ‘new normal’.
Best Practices for Key Recovery Elements
This section describes the following key recovery elements that are informed by international benchmarks, guidance, and lessons learned from experience with affected populations following nuclear (e.g., Chernobyl and Fukushima) and radiological (e.g., Goiânia) emergencies:
- Recovery phase protective actions (Section 4.1.1);
- Self-help actions (Section 4.1.2);
- Environmental and food chain monitoring (Section 4.2);
- Exposure pathways and dose assessments (Section 4.3);
- Health monitoring and epidemiological studies (Sections 4.4 and 4.5);
- Managing contamination and remediation (Sections 4.6 and 4.7);
- Waste management (Section 4.8);
- Monetary compensation (Section 4.9);
- Communication (Section 4.10);
- Worker protection (Section 4.11).
These key recovery elements are interdependent in achieving the overall recovery objectives and mitigating psychosocial effects. However, all recovery elements hinge on having a resilient infrastructure capable of sustaining its critical sectors. Critical Infrastructure, such as transportation networks, telecommunications, energy, utilities, food and agriculture, health, trade (open borders) and government, among others, are essential for enabling recovery actions.
The interrelationship between key recovery elements and critical infrastructure cannot be underestimated. As examples, it would be difficult to implement recovery protective actions and manage contamination, remediation and contaminated waste without the ability to move resources, including materials and workers. Health monitoring and epidemiological studies require a functioning health care system. Without telecommunications, it would be a significant challenge to implement an effective public communications plan, whereby the affected population could receive critical information on self-help and protective actions, as well as other key recovery activities. Therefore, strategies should be developed in the preparedness phase to restore critical activities and infrastructure (such as hospitals) in a timely manner following a nuclear emergency, despite the fact that many authorities may still be occupied with the nuclear emergency response. Since critical infrastructure restoration would be an early recovery action, the RMOs should be involved in the development of the critical infrastructure restoration strategy and should lead its implementation during the transition phase. These early recovery actions are necessary for enabling long-term recovery actions and the resumption of social and economic activities (e.g., workplaces and public services) in order to support normal living conditions in the affected areas Reference 11.
Implementation of Protection Strategies for Recovery
The overall objective of implementing a protection strategy for recovery would be to ensure that radiological exposures meet the reference levels and selected criteria within the reference bands, while considering the psychosocial impacts of any protective actions in order to achieve more good than harm.
Many factors can impact the protection strategy including timing, resources, waste management options, as well as social and ethical aspects. Input from stakeholders, as well as from Indigenous peoples and communities, should be sought during the development of the protection strategy.
A number of urgent and early protective actions may have been implemented during the response phase with the goal of reducing potentially harmful exposure. Such actions may include ingestion of KI tablets, sheltering, evacuation and temporary relocation. Protective actions implemented to control or reduce the ongoing effects of an emergency situation would need to be assessed and transitioned into the recovery phase and beyond. As time progresses, any actions taken during the nuclear emergency should be continuously examined to decide if changes are warranted. During the response phase, there would likely be an examination of protective actions taken, but such an examination also requires consideration during the recovery phase, depending on time frames involved. In some cases, protective actions such as access restrictions may need to be lifted or modified during the recovery phase. Other protective actions, such as restrictions on locally sourced food, milk and drinking water, or the reinforcement of protective works or containment structures, may need to be modified. Various government nuclear emergency response plans provide guidance on lifting the protective actions implemented during the response phase Reference 5 Reference 42 Reference 43.
Recovery protective actions may need to be taken to optimize doses below the desired reference level. Even if doses have been reduced below the reference level, consideration should be given to continuing these recovery protective actions if doses can be further lowered. The optimization principle Reference 13 must guide this decision, which should be a balanced consideration of potential dose savings, psychosocial impacts, and the economic costs of continuing to implement the actions.
In general, there are two types of actions that could be implemented during the recovery phase:
- Recovery phase protective actions: These are actions implemented or overseen by the RMOs, which, generally, cannot be implemented by individuals. (further discussed in Section 4.1.1).
- Self-help actions implemented by individuals: These are voluntary actions undertaken by individuals to manage their own exposure, i.e., external and internal exposure (further discussed in Section 4.1.2).
Responsibilities for implementing the recovery phase protection strategy should be established or considered at the preparedness stage. Such decisions should involve relevant response organizations as well as potentially impacted individuals and communities. The detailed recovery plans should be based on the specific nuclear emergency situation and, therefore, should be established by the RMOs either during the transition phase or recovery phase.
The following is a summary of key tasks that support the recovery strategy for public protection from radiation:
- a review of protective actions that have been put in place during the response phase to determine if these actions need to be modified or terminated;
- a review of the doses received by members of the public during the response phase, and identification of any required follow-up actions;
- an assessment of the current exposure situation, through environmental monitoring and exposure pathways modelling (where appropriate), and a prediction of the future exposure situation based on the results of this assessment;
- continuous reassessment of the exposure situation throughout the recovery phase; factors to consider include geographical area impacted, environmental and weather considerations, land-use considerations and the types and concentration of radionuclides present in the environment (see Section 4.2);
- identification and implementation of appropriate protective actions, based on the results of the assessment of the exposure situation compared to the selected reference level;
- reassessment of the appropriateness and effectiveness of the protective actions, alongside the reassessment of the exposure situation, and implementation of activities aimed at physically reducing radioactivity in the environment (e.g., decontamination, remediation, characterization and quantification of radioactive waste, and waste management);
- management of doses received by recovery workers who were involved in implementing the recovery phase protective actions and clean-up activities;
- management of doses received by emergency workers who were involved throughout the continuum of response and recovery actions.
A significant amount of monitoring and data collection would need to occur throughout the recovery phase in order to characterize the continuously changing radiological situation and support the key tasks described above. It is important to note that all monitoring activities would contribute to assurance monitoring for the population. Environmental and food chain monitoring would ensure that implemented protected actions are either lifted, or modified accordingly. Environmental monitoring activities would be prioritized in such a manner as to characterize the exposure of the most affected populations first. Characterization results would also inform the optimization of the protection strategy, including efforts to manage contamination, remediation, and waste. Dose monitoring of populations based on exposure pathway models should be corroborated with individual assessment results.
Recovery Phase Protective Actions
Recovery phase protective actions would be implemented by the RMOs in accordance with the protection strategy. These actions generally cannot be implemented by individuals and require government-level coordination. Characterizing the exposures of the affected population, which includes identifying the main exposure pathways and estimating doses (see Section 4.3), would help inform the selection of the most effective recovery protective actions by the RMOs in order to optimize doses below the reference level.
Recovery phase protective actions that could be implemented by the RMOs Reference 44 include the following:
- deciding if people can live in contaminated areas;
- decontaminating buildings, parks, and other public areas;
- remediating soil and vegetation;
- issuing controls on food consumption and providing clean food;
- introducing education and outreach programs, including programs for children;
- providing instruction and equipment to facilitate self-help actions (e.g., for dose measurements).
Recovery phase protective actions implemented by the RMOs may be institutional or engineered in nature Reference 45:
- An example of an institutional action is the placement of restrictions on ingesting locally produced food to avoid ingesting radionuclides.
- An example of an engineered action is the addition of a non-removable layer of pavement or cement, on streets or sidewalks, over gamma-emitting radionuclides. This would be done if the contamination was fixed in place and could not be easily removed.
RMOs should identify and delineate the borders of the contaminated area early on, and reassess and adjust these borders throughout the recovery phase. This delineation would enable the implementation of recovery phase protective actions, such as restrictions on food, and would also assist when communicating with the local population Reference 46. The delineation of the contaminated area would need to strike a careful balance between an excessive number of constraints on the area (potentially resulting in unnecessary remediation and inappropriate labelling of the area as unsafe) and inadequate protection or failure to address stakeholder concerns Reference 47.
Self-Help Actions
Self-help actions are actions undertaken by individuals to manage their own exposure, i.e., external and internal exposure. These actions also involve individuals self-monitoring and voluntarily adapting their way of life accordingly, as they see fit.
Experience has shown that the direct involvement of individuals, communities and local professionals in managing a recovery situation improves the process by empowering those impacted. Community consultations led by federal and/or provincial and municipal/regional authorities are an effective means for engaging and empowering individuals and communities in recovery decision-making. When RMOs facilitate the processes by which inhabitants define and apply their own protection strategies, not only are exposures reduced but adverse psychosocial impacts are also reduced Reference 13 Reference 45. The ICRP recognized the need to empower communities and individuals to make their own decisions concerning radiation protection and monitoring during recovery. The ICRP Fukushima Dialogues initiative put this concept into practice through a series of exchanges with citizens of affected areas, local governments and international experts that allowed all parties to share their perspectives. The structure of these meetings, the topics discussed and the outcomes were documented by the ICRP and provide a model for encouraging community empowerment during any future recovery efforts Reference 44.
Self-help actions require coordination, human resources support and the availability of experts to help the public interpret and understand radiological measurements. Authorities need to provide resources for effective education and information for self-help actions to be successfully implemented during recovery. In most cases, individuals would need to be trained in what to do, and the necessary infrastructure to assist them would need to be put in place (e.g., guidance materials and availability of equipment). The population should be given appropriate information to allow them to make informed decisions. Authorities should also facilitate opportunities for affected individuals to share lessons learned among themselves, as well as for communication between the affected population and relevant experts (e.g., health, radiation protection, agriculture authorities). Public information centres would be ideal locations for providing training and information on self-help actions, facilitating a forum for discussion, and serving as monitoring locations (e.g., a place to make monitoring equipment available for testing foods).
A challenge of self-help actions would be to balance the burden placed on the individuals (i.e., constant monitoring of foods eaten and places visited) against the benefits of empowerment to improve people’s control over their own exposure situations. As with all decisions in the recovery phase, a balanced approach – one that considers the optimization principle, economic consequences and psychosocial considerations – should be taken and involve input from stakeholders, as well as from Indigenous peoples and communities.
Examples of self-help protective actions include:
- monitoring ambient dose rates in living areas and work locations, to identify areas of higher dose rates, and adapting occupancy accordingly, where practical;
- measuring the presence of contamination in foods and modifying dietary habits;
- monitoring individual doses using personal dosimetry to provide additional information about opportunities to reduce exposures based on people’s daily habits.
Environmental and Food Chain Monitoring
The characteristics of the existing exposure situation would evolve during the recovery phase because of processes such as radiological decay, physical and chemical processes affecting the distribution of radionuclides in the environment, human activities that concentrate or dilute contamination in the environment, and changes to protective actions Reference 13. An environmental monitoring program that is adequate for the prevailing circumstances and flexible enough to accommodate changes to conditions should be established. Although environmental monitoring systems established for the response phase would also likely be relied upon in the recovery phase, there may be a need to enhance or modify current monitoring requirements to, for example, include monitoring of public infrastructure such as schools.
An environmental monitoring program in this context refers to the measurements of external dose rates in the environment and radionuclide activity concentrations in different substances (e.g., air, water, soil, vegetation, and food) Reference 48. The prioritization of monitoring populated areas and the prioritization of food chain monitoring would contribute to optimizing the protection strategy and would inform decisions about lifting or adapting protective actions. Environmental monitoring results should be made available with enough explanatory context to be easily understood by the general public Reference 46.
Various environmental monitoring programs already in place across Canada and around nuclear facilities are as follows:
- Health Canada has had a national environmental radioactivity monitoring program since 1959 and operates three distinct radiological networks composed of more than 100 detection and monitoring stations across the country. These are located in the vicinity of nuclear power plants, in all major population centres, and in the vicinity of ports visited by foreign naval nuclear-powered vessels.
- All Canadian nuclear power plants have environmental monitoring programs in place for their surrounding areas, in compliance with the conditions of the operating licences.
- Through independent sampling and analysis, the CNSC’s Independent Environmental Monitoring Program complements existing and ongoing activities conducted by the licensees to verify that public health and the environment around nuclear facilities are safe.
- The DND/CAF has an environmental radionuclide monitoring program in place for areas around the berthing locations of ports visited by foreign naval nuclear powered vessels to verify that the visits are not adversely impacting the marine environment.
- The Ontario Reactor Surveillance Program operates and maintains a radiological surveillance network to assess radiological concentrations around designated major nuclear facilities and selected natural background locations in the province. This program includes continuous surveillance of air and drinking water supply plants near nuclear facilities, and is supplemented by monitoring campaigns of precipitation, milk, recreational surface waters and foods.
- The Ontario Drinking Water Surveillance Program provides water quality information for selected municipal drinking water supply plants for scientific and research purposes through the monitoring of analytes including organic, inorganic and radiological parameters (i.e., tritium, gross alpha radiation and gross beta radiation).
The following are some specific objectives of monitoring the environment during recovery:
- to adapt or lift protective actions implemented during the response phase;
- to identify whether or not protective actions are required in areas where received doses are highest and approaching the reference level and in areas that are sources of food, milk and drinking water;
- to confirm that radiation levels are below the reference level in areas housing evacuated or temporarily relocated populations, as well as in areas where the population is expected to return (assurance monitoring);
- to identify areas in which remedial actions are justified or no longer required in radiological terms;
- to provide information for estimating actual or prospective doses to members of the public;
- to detect changes and evaluate long-term trends in environmental radiation levels as a result of the response and recovery efforts;
- to disseminate information to the public.
The environmental monitoring program should be informed by the radionuclides involved, the physical and chemical composition of the radioactive contamination, the substances containing the radionuclides, and practices relating to land and water use. The locations for measurement and sampling should be selected on a site-specific basis in such a way that the highest radiation doses can be assessed Reference 48.
As part of the development of an environmental monitoring program, the available resources for monitoring should be identified, including the following:
- organizations, expert bodies, local and national laboratories, private institutions, universities and research centres responsible for implementing the monitoring strategy;
- human resources and technical capabilities (including monitoring equipment and dose assessment tools);
- mechanisms for ensuring the comparability and consistency of measurements among organizations, as well as mechanisms to interpret these measurements, including training, quality management and inter-comparison exercises;
- an organization designated as responsible for the validation, recording and retention of monitoring results and assessments;
- a mechanism for incorporating monitoring results and assessments into decision-making processes.
In the transition phase, the monitoring strategy may be supported by decision-aiding tools such as models. Models can help adjust monitoring priorities to facilitate the effective and efficient use of available (but usually limited) resources and capabilities. The objective of using such tools and their limitations should be clearly communicated to all concerned parties and documented in the monitoring strategy. Decisions based on models alone should be considered interim until measurements can be collected from potentially affected areas Reference 11.
In the case of nuclear emergencies impacting the food supply, it would be particularly important to include sampling and analysis of food, milk and drinking water in the monitoring program. The monitoring program should be sufficiently robust to ensure compliance with any restrictions put in place, including the existing criteria for restricting contaminated food, milk and drinking water in the immediate aftermath of a nuclear emergency. For reference, see the operational intervention levels established in the Generic Criteria and Operational Intervention Levels for Nuclear Emergency Planning and Response Reference 18 and in the nuclear emergency response plans for New Brunswick and Ontario Reference 42 Reference 43. Additional criteria should be established to manage long-term contamination of the food supply from long-lived radionuclides Reference 47 and for the consumption of country foods that are not part of the managed commercial food supply chains. The criteria established by the Codex Alimentarius Commission may also need to be considered when monitoring food and food products for suitability for international trade Reference 49.
Exposure Pathways and Dose Assessments
In preparation for transitioning to recovery, a dose assessment should be conducted to inform the recovery phase protective actions imposed for the transition, as well as the initial choice of the reference level for the transition to an existing exposure situation. The dose assessment should be validated periodically after the initiation of the recovery phase as new monitoring data become available. Such dose assessments should be based on appropriate environmental monitoring data and a realistic pathways analysis. Exposure pathways are the routes by which radiation or radioactive materials can reach humans and cause exposure, resulting in a received dose.
The recovery phase would likely have different dose-related considerations than the response phase. For example, significant releases to the air from an accident at a nuclear power plant would not be expected to occur in the recovery phase; therefore, exposure to a radioactive plume released to the atmosphere (i.e., cloud shine) should no longer be a dominant exposure pathway. The remaining exposure pathways that may need to be considered in the recovery phase include, but are not limited to, the following:
- external exposure from radionuclides deposited on the ground (i.e., ground shine) and surfaces (i.e., rooftops);
- internal exposure from inhalation of re-suspended radionuclides;
- internal exposure from ingestion of contaminated food and drinking water.
With respect to exposure pathways, the pattern of deposition of radioactivity would likely be complex and the resulting exposure to individuals could vary greatly within a given area. Exposure pathways would depend on circumstances such as the types of land use and the habits of the directly affected people and communities. They may also be included in assessments to respond to concerns from the public. As such, additional pathways would need to be considered where appropriate. For example, ingestion of soil by children may need to be considered with regard to land use restrictions for parkland.
When transitioning to the recovery phase, preliminary dose assessments should be performed focusing on the doses that could be received in the future (i.e., in the existing exposure situation). Such dose assessment should be based on appropriate environmental monitoring and pathways analysis using realistic, as opposed to conservative, data. There would likely be a broad range of exposures; therefore, as information becomes available, internal dose assessments should be conducted for specific individuals, representative persons or portions of the population.
The following are examples of factors that may impact the dose assessment:
- the imposition or removal of restrictions on food;
- radioactive decay;
- completion of decontamination/remediation activities;
- radioisotope filtration through environmental mechanisms (e.g., leaching, migrations).
Individual monitoring campaigns may be useful in providing dose information for groups of persons or in specific locations where assessed doses may be high, or where there may be important sources of uncertainty in the assessed doses. Such campaigns may include measurements of external doses with dosimeters carried by individual members of the public for specified periods of time. In rare cases, they may include measurements of the quantities of radioactive substances in the body or in excreta, however these campaigns may be prohibitively complex or expensive.
These individual monitoring campaigns should include communication with various stakeholders throughout all stages of the study and support from the local residents would be essential for the data collection stage. Such studies would typically involve a small group of volunteers Reference 50. Individual monitoring studies may provide knowledge of realistic doses, help with the selection of dose mitigation strategies and address concerns from affected residents. Experience has shown, however, that it is important to prepare at the outset of the study to respond to questions and concerns from the public once the measurement results become available.
The combined use of data from individual measurements and modelling may be useful in dose assessment, in particular in the long-term following a nuclear emergency. Individual measurements are expensive and would be difficult to perform. Therefore, such measurements would usually be limited to a select part of the exposed population, with special attention to critical groups. However, participation in survey and monitoring programs should be voluntary so as to recognize the autonomy and dignity of the affected populations Reference 41.
In the recovery phase, dose assessment would be a continuous process whereby earlier dose assessments would be refined using available environmental monitoring data. This refinement may also include individual dosimetry results when available. This process would contribute to the continuous re-evaluation of the radiological situation, informing the justification and optimization of protective actions relating to food, milk and drinking water consumption, as well as the optimization of the reference level over time Reference 48.
Internal Dose Assessment
Internal dose assessment involves the estimation or measurement of radionuclides that enter the body, and calculation of the resulting radiation dose based on the contributions from the specific radionuclides.
There are a number of available methods and models for assessing internal doses based on environmental monitoring results as well as individual dosimetry measurements. These methods are complementary and serve to provide a more detailed picture of received and anticipated doses to individuals as well as the population.
In order to estimate the intake of radionuclides from the environmental monitoring results, transfer parameters are used to model how the contaminants enter the body. Canadian Standards Association (CSA) standards N288.1 Reference 51, N288.2 Reference 52 and IAEA Technical Report Series no. 479 Reference 53 provide transfer parameters and intake rates useful when completing a dose assessment.
Because of the variability in exposures to different individuals or portions of the population in the recovery phase, internal dose assessment in recovery should be based on pathways analysis. These dose assessments could be supplemented by specific individual monitoring studies that provide information on doses to defined portions of the population, rather than internal dose estimates for a large population. For internal doses from ingestion of long-lived radionuclides (e.g., tritium and caesium), adults consuming local food would usually be the most exposed population group.
For radionuclides where the dose assessment depends significantly on age because of their specific metabolic properties (e.g., strontium, radium and polonium), infants or children usually form the most exposed population group Reference 48. The dose assessment should consider realistic habits, the known pattern and extent of deposition of radionuclides in the environment, and the food consumed by the affected population. For instance, the population could be divided into groups based on geographical location or lifestyle habits to assist in tailoring the dose assessments. In some cases, direct individual dosimetry may be warranted or desired, and could be used for the dose assessment.
In regions where the inhabitants normally consume substantial amounts of locally sourced food products (e.g., game, freshwater fish, forest mushrooms and berries), it would be important to consider population-specific consumption rates. If environmental monitoring program data for food are unavailable or insufficient, the concentrations of radionuclides in food could be roughly estimated from data on soil deposition or water concentrations by using known coefficients of radionuclide transfer from soil or water to plants and animals. In areas that are significantly contaminated with radionuclides, or in areas with elevated rates of transfer of radionuclides from soil to biota, individual whole-body monitoring may be useful to determine the human body burden and to assess doses due to the internal exposure. Whole-body monitoring should be considered where appropriate monitoring equipment are available and for radionuclides that are readily detectable by such devices. This type of monitoring may not provide a comprehensive assessment of internal doses as it will not typically detect low energy gamma emitters and pure beta or alpha emitters. The results of individual measurements should be used for validation of the models applied for the purposes of internal dose assessment Reference 48.
In Canada, Health Canada, as well as some dosimetry services, perform internal monitoring using whole-body counting, bioassay and/or thyroid measurements (for exposures to radioiodine).
Special programs of monitoring may be undertaken for the validation of models. The most reliable method of validation of an ingestion model would be by comparing its predictions with internal dose assessments made on the basis of data from individual measurements of radionuclide contents in the human body performed by whole-body counting or by analyzing the concentrations of radionuclides in excreta Reference 48.
External Dose Assessment
The external dose to the population during the recovery phase may be estimated via environmental monitoring data as well as personal dosimetry. Care should be taken when relying on environmental monitoring data (i.e., ambient air monitoring) to estimate doses to the population. Experience from the Fukushima nuclear accident has shown that this method can significantly overestimate the dose to a population, and that dose values should be validated through other means, such as personal dosimetry, if practical Reference 50 Reference 54. Interviews may be used to refine estimations of typical occupancy times for living, working and rest areas Reference 48. Dose-rate measurement at various occupied locations, both outdoors and indoors, can be used to assess existing external doses. This could include an additional array of environmental dosimeters positioned throughout the contaminated areas. Additional external monitoring initiatives, such as vehicle based dose rate measurements, should be ongoing in order to assess doses further afield and to gauge the extent of the ground deposition. Dose rate maps could be produced from these data, which could in turn be used to communicate the current radiological situation to stakeholders and inform protective action decisions.
Health Monitoring
Following a nuclear emergency, the exposed population should receive some information regarding their levels of exposure (associated with the emergency exposure situation) and the potential related health risks. The population should also be made aware of psychosocial risk factors associated with the nuclear emergency.
During or prior to recovery, a health monitoring program should be established, along with the logistic, scientific and administrative resources needed for implementation Reference 46, to measure and monitor any health impacts that may arise among the individuals in the impacted population. The purpose of the health monitoring program would be to ensure that appropriate support and medical follow-up are provided to the affected population. Determining the level of health monitoring, support and medical follow-up required should be informed by medical professionals, input from stakeholders as well as Indigenous peoples and communities, and community-specific concerns.
Doses received during recovery (i.e., the existing exposure situation) would be expected to be low enough so as not to warrant medical follow-up. The doses referred to in this section are those that may have been incurred from the emergency exposure situation.
This health monitoring program should focus on:
- following up with individuals who may have received doses that resulted in, or could result in, significant deterministic effects (e.g., skin burns, cataracts) to provide appropriate medical attention;
- screening affected populations that may have an increased risk of developing cancer, so as to provide for early detection and diagnosis;
- screening affected populations that may have an increased risk for psychosocial impacts, so as to mitigate psychological health and social problems;
- developing a registry of individuals identified as requiring longer-term health monitoring (this list should be established during the response phase and should continue to be updated throughout the transition and recovery phases);
- offering medical, psychological and psychosocial support for affected individuals and populations.
Additionally, there would be a risk that screening populations for diseases associated with exposure, without strong justification for performing the monitoring, could have negative impacts on these populations. An example from the Fukushima nuclear accident is the widespread use of high-technology ultrasound to screen for thyroid diseases, which may have led to increased diagnoses of anomalies identified as potential thyroid cancers. The impact of undergoing further testing may have resulted in negative psychosocial consequences that outweighed the risk associated with the potential for thyroid cancer, which would be a slowly evolving and highly treatable condition.
The Fukushima nuclear accident also highlighted the importance of considering ethics during the design and implementation of health monitoring. The ICRP is considering the ethical foundations of a system of radiological protection, which include the core ethical values of dignity, beneficence/non-maleficence, justice and prudence. The following examples illustrate how these ethical values could be applied to health monitoring:
- dignity: respect the dignity of the individuals by obtaining prior consent;
- beneficence/non-maleficence: do more good than harm;
- justice: avoid social stigma;
- prudence: provide adequate information on the purpose of the monitoring, and the results.
Epidemiological Studies
Epidemiology is the study of the factors affecting the health and illness of populations and how disease is distributed. It serves as the foundation for public health and preventive medicine Reference 55. As described in a 2017 SHAMISEN Consortium report Reference 41, there are two main reasons to conduct epidemiological studies:
- they can be used as a surveillance tool to objectively evaluate the frequency of diseases and how this may change following an emergency;
- they can increase knowledge of the health effects of a nuclear emergency (not limited to radiation-induced effects).
Epidemiological studies evaluating the health of the population may also be conducted using individualized dose measurements and specific organ dose data to support long-term health monitoring following a nuclear emergency. This information differs from the effective dose data that would be generated by the dose assessment models used for protective action decision-making described in Section 4.3. Furthermore, additional data may need to be collected in order to link health-monitoring data with the affected population for the purpose of the epidemiological studies. The authority having jurisdiction would determine which data to collect. These data could include, but are not limited to, the following:
- date of birth;
- full name and name at birth, and any other surnames;
- sex;
- social insurance number;
- place of birth;
- place of residence;
- other radiation doses (e.g., medical diagnostics);
- health insurance number (used to link survey data);
- other health or lifestyle factors that may influence rates of diseases of interest;
- race;
- ethnicity;
- socioeconomic status;
- occupation;
- Indigenous status.
Participation in the health monitoring program and the use of personal data in the epidemiological study databases should be voluntary so as to recognize the autonomy and dignity of the affected populations Reference 41. It has been recognized that individuals may prefer to avoid the health monitoring programs due to perceptions of stigmatization associated with the monitoring programs and lack of self-determination.
Management of Contamination
Management of the contaminated environment could be carried out in many ways, and would depend on the prevailing conditions after the nuclear emergency. In general, effective management of the contamination may include minimization and isolation of the contaminated source material, decontamination to reduce and remove the potentially hazardous materials, and the management of waste.
It must be recognized that decontamination would only be part of the overall contamination management strategy, which could also include other types of activities such as imposing different land or commodity uses and restricting their use and export to other areas. Guidance based on experience from remediation of legacy sites, or sites contaminated by past practices, could provide insight into how to best manage contamination Reference 48.
The objectives of managing contamination are to Reference 45:
- allow any evacuated or relocated populations to return to their homes as soon as possible;
- allow anyone living in the area to resume living as normally as possible;
- allow the resumption of economic and social activities.
The management of contaminated areas, including decontamination and the management of waste, should begin as early as possible in the response phase (or the transition phase). Areas being managed for contamination should be clearly identified.
Although it would be preferred to remove contaminated materials and ship them to other locations for long-term management, practical considerations may cause nuclear emergency response authorities to decide to isolate the contaminated materials locally and to institute a management program to ensure safety. These institutional controls would need to be justified and supported in the recovery phase and beyond.
Remediation
Remediation involves removing contamination from the environment, thereby reducing it to an acceptably low level. Before remediation activities begin, the characteristics of the exposure situation should be well understood and responsible authorities would need to determine the level of contamination considered acceptable, as well as the amount of remediation required. One objective of setting an acceptable level of contamination would be to avoid unduly declaring low-level contaminated materials that do not pose a health risk as radioactive waste. The areas to be remediated should be prioritized based on those in which the population and critical infrastructure are to be reinstated, and according to which remediation efforts would be most effective in reducing individual exposures Reference 45 Reference 46.
A decision-making process to determine the methods used to remediate the environment would be required in order to ensure that the remediation strategy is justified and optimized. A justified and optimized strategy, which should be documented in a remediation plan, would help provide the best level of protection for the public and the environment, while accounting for social and economic factors. Some guidance on how to approach this decision-making process can be found in publications such as CSA Group or IAEA guidance on radiation monitoring for the protection of the public Reference 56 Reference 57 Reference 58. If radioactive material could not be physically removed from the environment, it may be appropriate to choose alternate options such as fixing it in place or covering it.
Remediation goals and criteria should be identified and set in terms of measurable quantities, and would need to be established based on an understanding of the following Reference 45 Reference 58 Reference 59:
- reference level chosen;
- predicted effectiveness of potential decontamination actions;
- area impacted (i.e., size, characteristics, location relative to the population);
- predicted use of the area (e.g., residential, recreational, agricultural);
- site-specific background levels of radioactivity (if known);
- impacts of the contamination and potential decontamination actions on human health and the environment;
- input from stakeholders, as well as Indigenous peoples and communities.
The method employed to remediate the environment would need to be selected in consideration of many of the same factors, including the following Reference 45 Reference 58 Reference 59:
- effectiveness of the action to protect human health and the environment over time;
- performance and costs of different technologies;
- effectiveness of the remediation action as the cleanup progresses;
- time to carry out the remediation;
- impacts on the local and regional economy;
- weather conditions and time of year;
- types of surfaces to be cleaned.
Setting remediation goals and implementing remediation strategies should be an iterative process. Remediation goals should be adjusted as experience is gained, and post-remediation management activities (e.g., monitoring, removal of area restrictions) should be implemented Reference 45 Reference 58.
Waste Management
Activities carried out in the recovery phase, particularly remediation of the environment, may result in a large amount of waste from varying sources and of different types. Some of the waste may contain high levels of radioactivity, especially if the waste was produced close to the nuclear emergency’s origin. Most of the waste could be expected to be only slightly contaminated, although potentially in large quantities Reference 45.
Early in the response phase, and during the transition phase, waste management may simply consist of storing waste in a dedicated area, if appropriate. Criteria would need to be established such that, once the resources become available, the waste could be sorted by the amount of radioactive material and the types of waste (e.g., solid, liquid or organic) based on an appropriate hazard assessment Reference 46 Reference 59. The hazard assessment should also consider the non-radiological properties of the waste (e.g., chemical, biological).
It may be possible to process the waste to reduce its quantity or to convert it into a more suitable form for disposal. Some processes that could be considered for waste reduction include: sorting, incinerating, filtering, distilling or solidifying liquids, and chemically treating liquids Reference 60. Dilution would generally not be considered acceptable since it would increase the volume of radioactive waste without reducing the inventory.
If the waste volumes are relatively small, then existing radioactive waste management facilities may have sufficient capacity to manage the waste. However, if a large amount of material is involved (which would be likely in a situation involving a more significant release), the capacity at these facilities may be exceeded. Lessons learned from the Fukushima and Goiânia accidents are that temporary storage facilities were required in order to allow time to establish more permanent solutions. New facilities could be constructed at the site where the release originated, elsewhere within the contaminated area, or away from the affected area altogether Reference 11. If the waste is to be relocated elsewhere, requirements for the acceptance and transportation of radioactive material should be considered. The final disposal strategy should consider the quantity and type of waste and the safety case of the final disposal facility. All waste sites would require appropriate controls, such as waste acceptance criteria, to protect public health and the environment from radioactivity. Highly radioactive materials would need more robust controls than slightly contaminated materials Reference 45. If the waste were to contain fissile materials, the potential for criticality would have to be calculated and managed.
As part of waste-management efforts, various disposal options may need to be considered. Waste disposal methods would generally be based on the principles of isolation and containment Reference 61:
- Isolation involves placing the waste in a location away from people’s homes and communities, and is typically appropriate for waste contaminated with long-lived radionuclides that cannot be removed.
- Containment includes those activities or structures designed to prevent the release of radioactive waste to the environment. Containment also protects the physical environment from the waste.
Any decision to manage wastes locally or in place should include strong justification, a long-term management and monitoring plan, and a commitment to maintaining the containment system(s) put in place. All waste management and disposal discussions would need to consider the long-term safety and institutional controls necessary to maintain public and environmental safety into the future Reference 62 Reference 63. There would need to be a commitment to monitoring and maintenance associated with future generations.
Waste generated as a result of off-site recovery activities (e.g., remediation of soil/vegetation, decontamination of buildings), including an accident’s effects that extend beyond borders, would need to be managed. Federal, provincial and territorial governments would need to coordinate the management of radioactive waste from a domestic emergency affecting multiple provinces/territories. In the event that off-site waste extends beyond national borders, the federal government would liaise with the international community and foreign diplomatic missions to Canada to support the management of waste in the affected country.
Monetary Compensation
The Nuclear Liability and Compensation Act (NLCA) Reference 64 establishes a compensation and liability regime in the unlikely event of a nuclear accident resulting in civil injury and damages.
Under the NLCA, operators of nuclear power plants and other lower-risk nuclear installations would be responsible to pay a specified amount for civil damages resulting from an accident, and must have insurance from an insurer approved by Natural Resources Canada (NRCan). In addition to the compensation amounts available under the NLCA, Canada is a Party to the Convention on Supplementary Compensation for Nuclear Damage, which would provide for predetermined supplementary funding from member countries based on a formula that considers economic and nuclear power capacity.
The NLCA would also provide for a special compensation system to accelerate efficient and equitable claim settlements to individuals and businesses. This streamlined claims settlement process would serve both to ensure claimants would be compensated in a timely manner, while also reducing the potential burden on the courts who may have limited capacity to administer a large number of claims. In the case where numerous claims may occur, the GC may determine that the public would be better served by the establishment of a special tribunal to administer claims. The NLCA elaborates the features and process of this special tribunal system.
Damages that could be compensated under the NLCA include:
- bodily injury;
- property damage;
- psychological trauma of a person who suffered bodily injury;
- environmental damage;
- economic loss as a result of bodily injury or damage to property;
- lost wages;
- costs related to preventive measures (such as evacuation costs).
The time period under the NLCA for submitting claims for the compensation of bodily injury is 30 years, while the time period for submitting claims for the compensation of other forms of damage is 10 years.
Communication
Throughout the recovery phase, increased levels of communication normally established at the outset of the accident and response phase should be maintained to address the uncertainties, the shift in priorities after the response phase and the new normal. The communication narrative would also provide an ongoing opportunity to proactively mitigate long-term psychosocial impacts within the community. As with all risk communications, it would be important to communicate with the public using terminology that is universally understood. Consistent, coordinated messages would need to come from credible sources and they should be communicated in a clear and simple manner, supported by facts and provided with appropriate context Reference 65.
A variety of tools and media should be used to communicate frequently with the public and other stakeholders, as well as Indigenous peoples and communities. The Government of Canada has adopted a “digital first” approach. In order to better connect with Canadians, government organizations are using the tools Canadians use, such as social media, video and the Web, as principal means of communications. This approach, balanced with the use of traditional communication methods whenever possible, such as television, print and radio, enables the Government to reach and engage with Canadians effectively and efficiently in the official language of their choice, regardless of where they reside.
Monitoring social media and other modes of communication would provide an awareness of any misinformation or rumours, and what is of interest to the public. It is essential to correct rumours and misinformation quickly. Consistent, ongoing messaging from authorities would help to avoid contradiction and confusion among members of the public.
A central communications strategy should be developed in the preparedness phase in order to reach those displaced by the accident and to maintain community engagement. This strategy should be coordinated amongst the various jurisdictions and levels of government involved, as well as with international partners and non-government organizations. Ongoing communication prior to a nuclear emergency would be crucial in building trust with community stakeholders, as well as Indigenous peoples and communities. Engaging the community prior to a nuclear emergency by partnering with community stakeholders and representatives would lead to an increased buy-in for public health research and eventual community self-sufficiency.
The public, other stakeholders and Indigenous peoples and communities would need to be informed and consulted regularly, and involved in decision-making. There must be clear communication as to the agencies, or groups of agencies, involved in recovery activities and their respective jurisdictions or responsibilities. This would enable the public to actively contribute to activities influencing their lives and to understand how the directions and procedures are relevant to their situation. Most individuals would be concerned about the potential health consequences, particularly for children, and the effects of the nuclear emergency on the environment. Decisions in the recovery phase would directly affect the daily lives of affected populations for an extended period. Direct engagement with the community would allow people to give feedback on their concerns and priorities, and allow authorities to respond directly, creating trust and transparency.
For affected populations, one effective method of communication would be to set up public reception and information centres to collect data and to provide support and information on topics such as exposure pathways and dose assessments. Educational programs on the health effects of radiation and the concept of risk presented in cooperation with educational institutions would improve public knowledge and understanding of the actions applied during the transition and recovery phases Reference 34. These types of centres would give the public an opportunity to share their experiences and receive direct responses to their questions Reference 44 Reference 46 and to have access to monitoring equipment to support self-help actions. It would also be important to use consistent and frequent communication to raise awareness about radiation protection measures within the community through the involvement of credible leaders, such as teachers, scientific professionals, association members and healthcare professionals. Local leaders could help reach the affected population, which would be an important first step in opening the dialogue.
Protection of Workers
In the recovery phase, there would be three distinct situations where workers may be occupationally exposed within the affected area:
- workers at a licensed facility in the affected area during the recovery phase (e.g., nuclear operator at a nuclear power plant);
- workers who would be tasked with conducting recovery actions under the direction of the RMO, referred to as “recovery workers” (e.g., workers with the duty of conducting soil remediation activities);
- workers who would not be tasked with recovery actions (e.g., workers in a fruit orchard), but who would be exposed because of their residence, work location and consumption of food within an affected area.
For each of these sets of workers, different dose limit considerations would apply:
- The radiation protection of on-site workers at the licensed facility and any other licensed facilities used to enable the recovery (e.g., licensed waste facilities) would be governed by the licensee’s protection programs. Exposure to these individuals as part of their occupation would be considered a planned exposure situation; this category would include workers at a nuclear power plant performing on-site recovery actions. The dose limits prescribed in the RPR Reference 17 would apply to these workers during the recovery phase and the ALARA principle would be required, taking economic and social factors into account.
- Exposure to off-site recovery workers would also be considered a planned exposure situation, however these workers would not be subject to the dose limits prescribed in the RPR. The protection of workers involved in implementing recovery activities under the direction of the RMOs would be managed through the implementation of similar protection programs with an all-hazards approach commensurate with the risks. It would be expected that occupational exposures to radiation for this group of workers would be planned, monitored and optimized such that they would remain below limits established by the RMO. As part of the safety programs, the RMO should provide information, training, protective equipment and dosimetry to workers.
- Doses received by workers not involved in recovery activities (e.g., workers in a fruit orchard), but who would be exposed post-emergency due to their residency, work location and consumption of food within an affected area, would be considered in the context of the reference levels for existing exposure situations. The RMO should provide public information, training and resources to help optimize the exposure to these workers below the reference level. Self-help actions may be used, for example, to limit time spent in areas with higher dose rates during the work day.
It is important to note that accounting for doses received by persons involved in the response to a nuclear emergency would be managed separately from those received by the same individuals during planned occupational exposures, which would include recovery efforts, or in existing exposure situations.
Similarly, a distinction should be made between doses that would be received by workers during recovery efforts as a consequence of their occupation (i.e., planned exposure situations) and those that would be received as a result of exposures due to environmental conditions resulting from the emergency (i.e., existing exposure situations). For instance, an on-site worker at a licensed facility, who would be subject to the dose limits in the RPR for the planned exposure situation, may also be living in the contaminated area and thus would receive additional dose from the existing exposure situation. Similarly, the off-site recovery workers under the direction of the RMO may also be subject to planned exposure situations due to their recovery work, as well as existing exposure situations should they also reside in the contaminated area. In this context, the doses received from the planned and existing exposure situations should be considered separately when comparing against the relevant limit or reference level.
Establishing a New Normal
It is recognized that following a nuclear emergency, it may not be possible for the affected areas to return to their original condition, and that a new normal would need to be established. This new normal may involve living in an existing exposure situation, where protective actions may have been implemented to reduce exposures.
If the desired reference levels could be achieved, then a protection strategy could be implemented to allow individuals to live in the affected areas. A protection strategy would further optimize the situation to maximize the margin of good over harm.
It would be equally important to account for psychosocial aspects when making decisions about returning a population to a new normal, as discussed in Section 3. The expected dose below the reference level should not be considered in isolation; the appropriate timing of the return of the population should also be considered. For example, the importance of psychosocial aspects was demonstrated through the results of the Fukushima Health Management SurveyFootnote 3 Reference 29, which revealed that some evacuees did not wish to return to their homes for reasons other than radiological concerns. These non-radiological concerns included poor access to medical services, the perception that the return of commercial facilities was unlikely, and the severe damage to old homes. The decision to return should therefore rest with the responsible RMOs in consultation with affected communities.
The new normal may be achieved by:
- establishing new routines, which may include self-help actions that allow for day-to-day life to resume such that impacts are minimized;
- living with some level of exposure that would be higher than pre-emergency conditions, but that would be within acceptable levels for human health;
- establishing communication and engagement with individuals and communities;
- periodic re-evaluation of the reference level throughout recovery as the exposure situation evolves.
It may sometimes be decided to abandon contaminated areas altogether and to resettle impacted individuals and communities to areas that were not directly affected by the nuclear emergency in a radiological sense. In this case, many of the activities described in Section 3.2 would not be applicable. It is important to note that there would be a high likelihood of psychological and social impacts associated with the nuclear emergency and resettlement, even in the absence of a radiological hazard. Decisions to resettle should only be made following extensive consultation and engagement with stakeholders, as well as Indigenous peoples and communities.
Communities and families would experience significant disruption to their daily lives, regardless of their new normal (e.g., returning home to an existing exposure situation vs. permanent relocation). This is why emergency management organizations should carefully plan for recovery during the preparedness phase in order to lessen this disruption in the event of a nuclear emergency. Consideration of the best practices in this document would help authorities to develop recovery plans and protection strategies that achieve the best outcome from a radiological health perspective, while accounting for social, economic and psychological factors. Consulting with and involving the public, other stakeholders, as well as Indigenous peoples and communities in the development of recovery plans, and communicating protective action decisions early and often, would contribute to community resilience and reduce longer-term psychosocial impacts.
Appendix: Abbreviations and Acronyms
- ALARA
- as low as reasonably achievable
- CNSC
- Canadian Nuclear Safety Commission
- CSA
- Canadian Standards Association
- DND/CAF
- Department of National Defence/Canadian Armed Forces
- FERP
- Federal Emergency Response Plan
- FNEP
- Federal Nuclear Emergency Plan
- GC
- Government of Canada
- GSG
- General Safety Guide (series of IAEA publications)
- GSR
- General Safety Requirements (series of IAEA publications)
- IAEA
- International Atomic Energy Agency
- ICRP
- International Commission on Radiological Protection
- mSv
- millisievert
- NLCA
- Nuclear Liability and Compensation Act
- NRCan
- Natural Resources Canada
- NSCA
- Nuclear Safety and Control Act
- NSOD
- Nuclear Safety Orders and Directives (DND/CAF document)
- PSC
- Public Safety Canada
- REGDOC
- Regulatory Document (series of CNSC documents)
- RMO
- Recovery Management Organization
- RPR
- Radiation Protection Regulations
References
- Reference 1
-
Emergency Management Act, S.C. 2007, c. 15.
- Reference 2
-
Public Safety Canada, Federal Emergency Response Plan, 2011.
- Reference 3
-
Canadian Nuclear Safety Commission, REGDOC-2.10.1, Nuclear Emergency Preparedness and Response, Version 2, 2016.
- Reference 4
-
Canadian Nuclear Safety Commission, Nuclear Emergency Response Plan – Master Plan, 2013.
- Reference 5
-
Health Canada, Federal Nuclear Emergency Plan Part 1: Master Plan (Fifth Edition), 2014.
- Reference 6
-
CSA Group, CSA N1600, General requirements for nuclear emergency management programs, 2016.
- Reference 7
-
Department of National Defence/Canadian Armed Forces, Defence Administrative Order and Directive 4002-0, Nuclear and Ionizing Radiation Safety Management, 2020.
- Reference 8
-
Nuclear Safety and Control Act, S.C. 1997, c. 9.
- Reference 9
-
Order-In-Council P.C. 2000-1421, DND Exclusion from the NSCA, 2000.
- Reference 10
-
International Atomic Energy Agency, IAEA Safety Standards Series No. GSR Part 7: Preparedness and Response for a Nuclear or Radiological Emergency, 2015.
- Reference 11
-
International Atomic Energy Agency, IAEA General Safety Guide No. GSG-11, Arrangements for the Termination of a Nuclear or Radiological Emergency, 2018.
- Reference 12
-
International Atomic Energy Agency, IAEA General Safety Requirements No. GSR Part 3, Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards, 2014.
- Reference 13
-
International Commission on Radiological Protection, Publication 146 Radiological Protection of People and the Environment in the Event of a Large Nuclear Accident. Ann ICRP 49(4). In press
- Reference 14
-
International Commission on Radiological Protection, The 2007 Recommendations of the International Commission on Radiological Protection, ICRP Publication 103: Ann. ICRP 37(2-4), 2007.
- Reference 15
-
Coleman, C. N, D. J. Blumenthal, C. A. Casto, et al. 2013. Recovery and Resilience After a Nuclear Power Plant Disaster: A Medical Decision Model for Managing an Effective, Timely, and Balanced Response. Disaster Med Public Health Preparedness 7(2):136-145.
- Reference 16
-
International Commission on Radiological Protection, Recommendations of the International Commission on Radiological Protection, ICRP Publication 26: Ann. ICRP 1 (3), 1977.
- Reference 17
-
Radiation Protection Regulations, SOR/2000-203.
- Reference 18
-
Health Canada, Generic Criteria and Operational Intervention Levels for Nuclear Emergency Planning and Response, 2018.
- Reference 19
-
Sorensen, J., J. Soderstrom, E. Copenhaver et al. Impacts of Hazardous Technology, the Psychosocial Effects of Restarting TMI–1. Albany: State University of New York Press, 1987.
- Reference 20
-
Inter-Agency Standing Committee (IASC). IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings. Geneva: IASC, 2007.
- Reference 21
-
Winston & Strawn LLP, The Price-Anderson Act and the Three Mile Island Accident. OECD/NEA Workshop. Nuclear Damages, Liability Issues, and Compensation Schemes. 2013.
- Reference 22
-
Ashley, S.F., G. J. Vaughan, W.J. Nuttall et al. 2017. Predicting the cost of the consequences of a large nuclear accident in the UK. Process Safety and Environmental Protection 112: 96–113.
- Reference 23
-
Laureto, J. J., J. M. Pearce. 2016. Nuclear Insurance Subsidies Cost from Post-Fukushima Accounting Based on Media Sources. Sustainability 8, 1301.
- Reference 24
-
Maeda, M., M. Oe, Y. Suzuki. 2018. Psychosocial effects of the Fukushima disaster and current tasks: Differences between natural and nuclear disasters. J. Natl. Inst. Public Health 67 (1): 50-58.
- Reference 25
-
International Atomic Energy Agency, Chernobyl’s Legacy: Health, Environmental and Socio-Economic Impacts and Recommendations to the Governments of Belarus, the Russian Federation and Ukraine. The Chernobyl Forum: 2003-2005, Second revised version. Vienna, 2006.
- Reference 26
-
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR), Sources Effects and Risks of Ionizing Radiation: UNSCEAR 2013 Report, Volume I. Report to the General Assembly, Scientific Annex A: Levels and effects of radiation exposure due to the nuclear accident after the 2011 great east-Japan earthquake and tsunami. Vienna, 2013.
- Reference 27
-
Shigemura J., T. Terayama, M. Kurosawa et al. 2020. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: a systematic review. Part 1: psychological consequences. CNS Spectrums.
- Reference 28
-
Normile, D. 2011. Newsmaker interview: Seiji Yasumura – Fukushima Begins 30-Year Odyssey in Radiation Health. Science. 333(6043): 684-85.
- Reference 29
-
Yasumura, S., M. Hosoya, S. Yamashita et al. 2012. Study protocol for the Fukushima Health Management Survey. J Epidemiol 22(5): 375-83.
- Reference 30
-
Ohtsuru, A., K. Tanigawa, A. Kumagai et al. 2015. Nuclear disasters and health: lessons learned, challenges, and proposals. Lancet 386(9992): 489-97.
- Reference 31
-
World Health Organization. Health risk assessment from the nuclear accident after the 2011 Great East Japan Earthquake and Tsunami based on a preliminary dose estimation, 2013.
- Reference 32
-
Yasumura, S. Evacuation effect on excess mortality among institutionalized elderly after the Fukushima Daiichi nuclear power plant accident. 2014. Fukushima J Med Sci 60(2): 192-95.
- Reference 33
-
Terayama, T., J. Shigemura, Y. Kobayashi et al. 2020. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: a systematic review. Part 2: emotional and behavioral consequences. CNS Spectrums.
- Reference 34
-
Canadian Nuclear Safety Commission, Study of Consequences of a Hypothetical Severe Nuclear Accident and Effectiveness of Mitigation Measures, 2015.
- Reference 35
-
Midorikawa et al. 2017. Psychosocial issues related to thyroid examination after a radiation disaster. Asia Pac J Public Health 29(25): 635-735.
- Reference 36
-
Barnes, G., J. Baxter, A. Litva et al. 2002. The Social and Psychological Impact of the Chemical Contamination Incident in Weston Village, UK: A Qualitative Analysis. Soc Sci Med 55: 2227‑41.
- Reference 37
-
Freudenburg, W. 1993. Risk and Recreancy: Weber, the Division of Labor, and the Rationality of Risk Perceptions. Soc Forces 71(4): 909-33.
- Reference 38
-
Freudenburg, W. 1997. Contamination, Corrosion and the Social Order: An Overview. Curr Sociol 45(3): 19-39.
- Reference 39
-
Gregory, R., and T. Satterfield. 2002. Beyond Perception: The Experience of Risk and Stigma in Community Contexts. Risk Anal 22(2): 347-58.
- Reference 40
-
J. Steven Picou, Brent K. Marshall, Duane A. Gill. 2004. Disaster, Litigation, and the Corrosive Community. Soc Forces 82 (4): 1493-1522.
- Reference 41
-
SHAMISEN Consortium, Recommendations and procedures for preparedness and health surveillance of populations affected by a radiation accident, 2017.
- Reference 42
-
Ministry of the Solicitor General, Provincial Nuclear Emergency Response Plan (PNERP) – Master Plan 2017, 2017.
- Reference 43
-
New Brunswick Department of Public Safety, Point Lepreau Nuclear Off-Site Emergency Plan, 2019.
- Reference 44
-
International Commission on Radiological Protection, ICRP Dialogue Initiative (2011-2015).
- Reference 45
-
United States Environmental Protection Agency, PAG Manual: Protective Action Guides and Planning Guidance for Radiological Incidents, 2017.
- Reference 46
-
Autorité de sûreté nucléaire, Comité Directeur pour la gestion de la phase post-accidentelle d’un accident nucléaire ou d’une situation d’urgence radiologique (CODIRPA), Éléments de doctrine pour la gestion post-accidentelle d’un accident nucléaire, 2012.
- Reference 47
-
National Council on Radiation Protection and Measurements, NCRP Report No. 175, Decision making for late-phase recovery from major nuclear or radiological incidents, 2014.
- Reference 48
-
International Atomic Energy Agency, IAEA Safety Standards Series No. RS-G-1.8, Environmental and Source Monitoring for Purposes of Radiation Protection, 2005.
- Reference 49
-
Codex Alimentarius Commission, Codex General Standard for Contaminants and Toxins in Foods, Schedule 1 – Radionuclides, 2010.
- Reference 50
-
W. Naito. “The Role of Individual Dosimetry for Affected Residents in Post Accident Recovery –From the Fukushima Experience.” ICRP 2017 Symposium presentation.
- Reference 51
-
CSA Group, CSA N288.1, Guidelines for calculating derived release limits for radioactive material in airborne and liquid effluents for normal operation of nuclear facilities, 2014.
- Reference 52
-
CSA Group, CSA N288.2, Guidelines for calculating the radiological consequences to the public of a release of airborne radioactive material for nuclear reactor accidents, 2014.
- Reference 53
-
International Atomic Energy Agency, Technical Report Series No. 479, Handbook of Parameter Values for the Prediction of Radionuclide Transfer to Wildlife, 2014.
- Reference 54
-
International Atomic Energy Agency, IAEA Safety Standards Series No. WS-R-3, Remediation of Areas Contaminated by Past Activities and Accidents, 2003.
- Reference 55
-
Canadian Nuclear Safety Commission (2014). Basic epidemiology concepts. Retrieved from http://www.nuclearsafety.gc.ca/eng/resources/health/health-studies/basic-epidemiology-concepts.cfm
- Reference 56
-
CSA Group, CSA N288.4-10, Environmental monitoring programs at Class 1 nuclear facilities and uranium mines and mills, 2015.
- Reference 57
-
International Atomic Energy Agency, Safety Reports Series No. 64, Programmes and Systems for Source and Environmental Radiation Monitoring, 2010.
- Reference 58
-
International Atomic Energy Agency, Safety Guide No. WS-G-3.1, Remediation Process for Areas Affected by Past Activities and Accidents, 2007.
- Reference 59
-
Nordic Guidelines and Recommendations, Protective Measures in the Early and Intermediate Phases of a Nuclear or Radiological Emergency, 2014.
- Reference 60
-
CSA Group, CSA N292.3-14, Management of low- and intermediate-level radioactive waste, 2014.
- Reference 61
-
International Atomic Energy Agency, IAEA Safety Standards Series No. SSR-5 Disposal of Radioactive Waste, 2011.
- Reference 62
-
International Atomic Energy Agency, IAEA Safety Standards Series No. SSG-23, The Safety Case and Safety Assessment for the Disposal of Radioactive Waste, 2012.
- Reference 63
-
United States Environmental Protection Agency, OSWER 9355.0-89, Institutional Controls: A Guide to Planning, Implementing, Maintaining, and Enforcing Institutional Controls at Contaminated Sites, 2012.
- Reference 64
-
Nuclear Liability and Compensation Act, S.C. 2015, c. 4, s. 120
- Reference 65
-
International Atomic Energy Agency, Report on International Symposium on Communicating Nuclear and Radiological Emergencies to the Public, 2018.
Additional Information
The following documents provide additional information that may be relevant and useful for understanding the guidance provided in this document:
- Australian Radiation Protection and Nuclear Safety Agency, Radiation Protection Series Publication No. 7, Recommendations: Intervention in Emergency Situations Involving Radiation Exposure, 2004.
- Canadian Nuclear Safety Commission, REGDOC-2.11.1, Waste Management, Volume II: Assessing the Long Term Safety of Radioactive Waste Management, 2018.
- Canadian Nuclear Safety Commission, REGDOC-3.6, Glossary of CNSC Terminology, 2016.
- Canadian Nuclear Safety Commission, Reference levels for nuclear emergency response and post-accident recovery, 2015.
- CSA Group, CSA N292.0, General principles for the management of radioactive waste and irradiated fuel, 2014.
- CSA Group, CSA N292.5, Guideline for the exemption or clearance from regulatory control of materials that contain, or potentially contain, nuclear substances, 2011.
- CSA Group, CSA N292.6, Long-term management of radioactive waste and irradiated fuel, 2018.
- Durham Emergency Management Office, Durham Region Risk-Specific Plan – Durham Nuclear Emergency Response Plan, 2016.
- Health Canada, Canadian Guide on Medical Management of Radiation Emergencies, 2015.
- International Atomic Energy Agency, IAEA Safety Glossary: Terminology Used in Nuclear Safety and Radiation Protection, 2018.
- International Atomic Energy Agency, Placing the Radiological Health Hazard in Perspective in an Emergency due to Severe Conditions at a Light Water Reactor, 2013.
- Municipality of Kincardine, Municipality of Kincardine Emergency Response Plan – Schedule “A” to BY-LAW No. 2006-009, 2016.
- Raskob, W., Gering, F., Lochard, J.et al. 2006. European Approach to Nuclear and Radiological Emergency Management and Rehabilitation Strategies. Nucl Eng Des 241(9): 3395-3402.
- United States Environmental Protection Agency, Manual of Protective Action Guides and Protective Actions for Nuclear Incidents, May 1992.
Footnotes
- Footnote 1
-
Under the Nuclear Safety and Control Act (NSCA) Reference 8, regulatory oversight of licensed nuclear facilities is the responsibility of the CNSC.
- Footnote 2
-
Under P.C. 2000-1421 DND Exclusion from the NSCA Reference 9, the DND/CAF are excluded from the NSCA and its regulations. Instead, regulatory oversight of DND/CAF authorization holders is the responsibility of DND’s Directorate of Nuclear Safety on behalf of the Assistant Deputy Minister (Infrastructure and Environment). For the purpose of this document, the DND/CAF authorization holders are the Commanders of the military establishments located at the three Canadian ports visited by foreign naval nuclear powered vessels.
- Footnote 3
-
The Fukushima Health Management Survey consisted of a basic survey and four detailed surveys: Thyroid Ultrasound Examination, Comprehensive Health Check, Mental Health and Lifestyle Survey, and Pregnancy and Birth Survey. The basic survey targeted a population of about 2.05 million people who had potentially been impacted by the events.