
Page 9: Guidelines for Canadian Drinking Water Quality: Guideline Technical Document – Enteric Viruses
8.0 Risk assessment
The adoption of a risk-based approach, such as a multi-barrier approach, is essential to the effective management of drinking water systems (CCME, 2004). This approach should include assessment of the entire drinking water system, from the watershed/aquifer and intake through the treatment and distribution chain to the consumer, to assess potential impacts on drinking water quality and public health.
Current drinking water guidelines encourage the adoption of a multi-barrier approach to produce clean, safe and reliable drinking water. Numerous indicators, such as indicator microorganisms, turbidity and disinfectant residuals, are used as part of the multi-barrier approach to determine the quality of the treated drinking water. For example, E. coli and total coliforms are bacteriological indicators that are routinely used to verify the microbiological quality of drinking water. Although indicators are an important aspect of a multi-barrier approach, they do not provide any quantitative information on pathogens or the potential disease burden associated with drinking water of a given quality. It is important to note that even water of an acceptable quality carries some risk of illness, although it is extremely low.
QMRA is gaining acceptance as part of a multi-barrier approach. QMRA is a process that uses source water quality data, treatment barrier information and pathogen-specific characteristics to estimate the burden of disease associated with exposure to pathogenic microorganisms in a drinking water source. The benefit of using a QMRA approach is that assessments can be carried out by each water system to provide site-specific information:
- to understand how changes in the source water quality can impact the microbiological quality of the drinking water being produced;
- to look at the adequacy of existing control measures, given site-specific variations;
- to investigate potential improvements in microbiological drinking water quality with additional treatment barriers or optimization of existing treatment barriers; and
- to help establish limits for critical points in the treatment system.
Site-specific variations should include the potential impact of hazardous events, such as storms, contamination events or the failure of a treatment barrier. When interpreting the results from a QMRA, the following should be considered:
- The quality of the data obtained from a QMRA is dependent on the quality of the input data.
- There can be a high level of uncertainty associated with some data (e.g., source water quality data and pathogen removals by treatment systems).
- Assumptions are made in QMRA that may not accurately reflect the condition of the water system and/or individual exposure to pathogens at every point in time (see Section 8.3.4).
Because of these limitations, QMRA should not be used to try to estimate levels of illness in a population resulting from a particular water system. Rather, the disease burden estimates produced from a QMRA are useful for site-specific system evaluations as part of a multi-barrier approach to safe drinking water.
8.1 Health-based targets
Health-based targets are the "goal-posts" or "benchmarks" that have to be met to ensure the safety of drinking water. In Canada, microbiological hazards are commonly addressed by two forms of health-based targets: water quality targets and treatment goals. An example of a water quality target is the bacteriological guideline for E. coli, which sets a maximum acceptable concentration for this organism in drinking water. Treatment goals describe the reduction in risk to be provided by measures such as treatment processes aimed at reducing the viability or presence of pathogens. Treatment goals assist in the selection of treatment barriers and should be defined in relation to source water quality. They need to take into account not only normal operating conditions, but also the potential for variations in water quality and/or treatment performance. For example, short periods of poor source water quality following a storm or a decrease in treatment effectiveness due to a process failure may in fact embody most of the risk in a drinking water system (Gale, 2002; Medema et al., 2006). The wide array of microbiological pathogens makes it impractical to measure for all of the potential hazards; thus, treatment goals are generally framed in terms of categories of organisms (e.g., bacteria, viruses and protozoa) rather than individual pathogens. The health-based treatment goal for enteric viruses is a minimum 4-log reduction and/or inactivation of viruses. Many source waters will require a greater log reduction and/or inactivation to maintain an acceptable level of risk.
8.2 Acceptable levels of risk
The burden of disease estimates calculated during a risk assessment should be compared with a reference level of risk--that is, a level of risk that is deemed tolerable or acceptable. This comparison is needed to understand the public health implications of the disease burden estimate and to set health-based treatment goals.
Risk levels have been expressed in several ways. The World Health Organization's (WHO) Guidelines for Drinking-water Quality (WHO, 2004) use DALYs as a unit of measure for risk. The basic principle of the DALY is to calculate a value that considers both the probability of experiencing an illness or injury and the impact of the associated health effects (Murray and Lopez, 1996a; Havelaar and Melse, 2003). The WHO (2004) guidelines adopt 10−6 DALY/person per year as a health target. The Australian National Guidelines for Water Recycling (NRMMC-EPHC, 2006) also cite this target. In contrast, other agencies set acceptable microbial risk levels based on the risk of infection and do not consider the probability or severity of associated health outcomes. For example, the U.S. EPA has used a health-based target of an annual risk of infection of less than 1/10 000 persons (10−4) (Regli et al., 1991).
For comparison, the reference level of 10−6 DALY/person per year is approximately equivalent to an annual risk of illness for an individual of 1/1000 (10−3) for a diarrhoea-causing pathogen with a low fatality rate. For an illness with a more severe health outcome, such as cancer, 10−6 DALY/person per year is approximately equivalent to a lifetime additional risk of cancer over background of 10−5 (i.e., 1 excess case of cancer over background levels per 100 000 people ingesting 1.5 L of drinking-water per day containing the substance at the guideline value over a 70-year life span). QMRA is a useful tool in estimating whether a drinking water system can meet this health target, as current disease surveillance systems in developed nations such as Canada are not able to detect endemic illness at such a low level.
The risk assessment in this Guideline Technical Document estimates the disease burden in DALYs. There are several advantages to using this metric. DALYs take into account both the number of years lost due to mortality and the number of years lived with a disability (compared with the average healthy individual for the region) to determine the health impact associated with a single type of pathogenic organism. The use of DALYs also allows for comparison of health impacts between different pathogens and potentially between microbiological and some chemical hazards. Although no common health metric has been accepted internationally, DALYs have been used by numerous groups, and published, peer-reviewed information is available. The WHO (2004) reference level of 10−6 DALY/person per year is used in this risk assessment as an acceptable level of risk.
8.3 Quantitative microbial risk assessment approach
QMRA is an approach that uses mathematical modelling and relevant information from selected pathogens to derive disease burden estimates. QMRA follows a common approach in risk assessment, which includes four components: hazard identification, exposure assessment, dose-response assessment and risk characterization.
8.3.1 Hazard identification
The first step of QMRA is hazard identification, a qualitative process of identifying hazards to the drinking water system or to human health, such as microorganisms, toxins or chemicals. The enteric viruses of most concern as human health hazards in Canadian drinking water sources include noroviruses, rotaviruses, hepatitis viruses, enteroviruses and adenoviruses.
The presence and types of enteric viruses in a given drinking water source are variable. Therefore, it is important to identify all potential sources and events, regardless of whether they are under the control of the drinking water supplier, that could lead to enteric viruses being present at concentrations exceeding baseline levels, on a site-specific basis. Human faeces and, in some instances, urine are the main sources of enteric viruses, which may originate from point sources of pollution, such as municipal sewage discharges, or from non-point sources, such as septic systems. In addition to the potential sources of contamination, it is necessary to consider whether the presence of enteric viruses is continuous, is intermittent or has seasonal pollution patterns and how rare events, such as droughts or floods, will impact the enteric virus concentrations in the source water.
Although all enteric viruses of concern need to be identified, risk assessments do not usually consider each individual enteric virus. Instead, the risk assessment includes only specific enteric viruses (reference pathogens or, in this case, reference viruses) whose characteristics make them a good representative of all similar pathogenic viruses. It is assumed that if the reference virus is controlled, this would ensure control of all other similar viruses of concern. Ideally, a reference virus will represent a worst-case combination of high occurrence, high concentration and long survival time in source water, low removal and/or inactivation during treatment and a high pathogenicity for all age groups. Numerous enteric viruses have been considered as reference viruses, including adenoviruses, noroviruses, and rotaviruses. None of these viruses meet all of the characteristics of an ideal reference virus. Adenoviruses represent a worse-case for inactivation during treatment when using UV, however, they are less prevalent in the population than noroviruses or rotaviruses. Noroviruses, although they are a significant cause of viral gastroenteritis in all age groups, have no published dose-response model currently available. Rotaviruses are a common cause of infection in children, have the possibility of severe outcomes and a dose-response model is available, however, rotaviruses are more susceptible to treatment than some other enteric viruses. As no single virus has all the characteristics of an ideal reference virus, this risk assessment incorporates the key characteristics of rotavirus, with the CT values based on HAV and poliovirus (U.S. EPA, 1999) as the best currently available disinfection information for enteric viruses commonly found in surface water and groundwater sources.
8.3.2 Exposure assessment
Exposure assessments provide an estimate (with associated uncertainty) of the occurrence and level of a contaminant in a specified volume of water at the time of the exposure event (ingestion, inhalation and/or dermal absorption). The principal route of exposure considered in this risk assessment is consumption of drinking water. To determine exposure, the concentration of enteric viruses and the volume of water ingested need to be known or estimated. Exposure can be determined as a single dose of pathogens ingested by a consumer at one time or the total amount over several exposures (e.g., over a year).
Drinking water is not usually monitored for enteric viruses. Therefore, to determine exposure, the concentration of the reference virus in the source water needs to be measured or estimated. Measurements, as opposed to estimates, will result in the highest-quality risk assessment. Short-term peaks in virus concentration may increase disease risks considerably and even trigger outbreaks of waterborne disease; thus, seasonal variation and peak events such as storms should be included in the measurements or estimates. Once the source water concentrations are determined, treatment reductions are calculated to determine the concentration in the finished drinking water. This risk assessment assumes that any viruses that were not removed or inactivated during treatment are still capable of causing infection and illness.
For the volume of water ingested, it is important to consider only the unboiled amount of tap water consumed, as boiling the water inactivates pathogens and will overestimate exposure (Gale, 1996; Payment et al., 1997; WHO, 2004). In Canada, approximately 1.5 L of tap water are consumed per person per day. However, approximately 35% is consumed in the form of coffee or tea (Health and Welfare Canada, 1981). The elevated temperatures (boiling, or near boiling) used for making coffee and tea would inactivate any enteric pathogens present. Therefore, for estimating risk from pathogenic organisms, this risk assessment uses an average consumption of 1 L of water per person per day for determining exposure. This estimate is similar to consumption patterns in other developed nations (Westrell et al., 2006a; Mons et al., 2007). The WHO Guidelines for Drinking-water Quality also suggest using an estimate of 1 L for consumption of unboiled tap water (WHO, 2004).
8.3.3 Dose-response assessment
The dose-response assessment uses dose-response models to estimate the probability of infection and the risk of illness after exposure to the reference virus. The probability of infection (Pinfection) for this risk assessment is calculated using a dose-response model for rotavirus. The rotavirus dose-response data are well approximated by the beta-Poisson model (equation 1) (Haas et al., 1999):
Equation 1
Pinfection ~ 1 − (1 + d/β)−α
where:
- α
- = 0.265
- β
- = 0.4415
- d
- = estimated dose per day
The beta-Poisson model describes mathematically the distribution of the individual probabilities of any one organism to survive and start infection, where α and β are parameters describing the probability of infection. The approximation of the beta-Poisson model becomes poor, and therefore should not be used, at small values of β or when the estimated dose d is large. The α and β parameters are derived from dose-response studies of healthy volunteers and may not adequately represent effects on sensitive subgroups, such as immunocompromised persons, young children or the elderly (Ward et al., 1986). An individual's daily dose of organisms is estimated using the information from the exposure assessment. An individual's yearly probability of infection is estimated using equation 2. For this risk assessment, it is assumed that there is no secondary spread of infection.
Equation 2
Pinfection/year = 1 − (1 − Pinfection)365
Not all infected individuals will develop a clinical illness. The risk of illness per year for an individual is estimated using equation 3:
Equation 3
Risk of illness = Pinfection/year × S × I
where:
- Pinfection/year
- = the probability of infection per year obtained from equation 2
- S
- = the proportion of the population susceptible to infection
- I
- = the proportion of individuals that develop symptomatic illness after infection
The fraction of the population that is susceptible to infection and illness varies with the type of enteric virus being considered. For rotavirus, the population susceptible to infection is generally confined to young children. Based on Canadian data, this represents approximately 6% of the population (Ministry of Finance, 2003a,b). However, as this risk assessment uses rotavirus as a representative of all enteric viruses that may be present in drinking water, including those to which greater proportions or most of the population may be susceptible (e.g., norovirus), 100% of the population is assumed to be susceptible to infection. Not all infections result in symptomatic illness. Based on U.S. data, 88% of individuals will develop symptomatic illness after infection with rotavirus (Havelaar and Melse, 2003).
To translate the risk of illness per year for an individual to a disease burden per person, the DALY is used as a common"metric" that can to take into account diverse health outcomes. The key advantage of the DALY as a measure of public health is cited as its aggregate nature, combining life years lost (LYL) with years lived with disability (YLD) to calculate the disease burden. DALYs can be calculated as follows:
Equation 4
DALY = YLD + LYL
where:
- YLD
- = the sum of the [(outcome fraction) × (duration) × (severity weight)] for each health outcome contributing to morbidity
- LYL
- = [(life expectancy) - (age at death)] × severity weight
For rotavirus, the health effects vary in severity from mild diarrhoea to more severe diarrhoea and potentially death. The disease burden of gastroenteritis resulting from infection with rotavirus in drinking water is 8.46 DALYs/1000 cases (8.46 × 10−3 DALY/case) (Table 6).
| Health outcome | Outcome fractionTable 6 - Footnote a | Duration of illnessTable 6 - Footnote b | Severity weightTable 6 - Footnote c | DALYs/case | |
|---|---|---|---|---|---|
| Morbidity (YLD) |
Mild diarrhea |
0.50 |
0.01918 (7 days) |
0.067 | 6.43 × 10−4 |
| Bloody diarrhea | 0.49 | 0.01918 (7 days) |
0.39 | 3.67 × 10−3 | |
| Mortality (LYL) |
Death | 0.0001 | Life expectancyTable 6 - Footnote d; age at deathTable 6 - Footnote e |
1 | 4.15 × 10−3 |
| Disease burden | 8.46 × 10−3 | ||||
Using this disease burden (DALYs/case) and the risk of illness per year in an individual, the disease burden in DALYs/person per year can be estimated:
Equation 5
Disease burden (DALYs/person per year) = Risk of illness × Disease burden (DALYs/case)
where:
- Risk of illness
- = the value calculated from equation 3
- Disease burden (DALYs/case)
- = 8.46 × 10-3
8.3.4 Risk characterization
Risk characterization brings together the data collected or estimated on pathogen occurrence in source water, pathogen removal or inactivation through treatment barriers, consumption patterns to estimate exposure and pathogen dose-response relationships to estimate the burden of disease. Using this information, the potential disease burden associated with the specified drinking water system can be calculated. An example of a disease burden calculation is provided in Figure 1. This calculation has been presented as a point estimate; however, the calculation was done using a mathematical model that included probability functions with associated uncertainties (Appendix C). The calculated disease burden can then be compared with the acceptable risk level to determine if the drinking water being produced is of an acceptable quality. If the disease burden estimate associated with the drinking water does not meet the acceptable risk level, QMRA can then be used to calculate the level of treatment that would be required to meet the acceptable health risk target (10−6 DALY/person per year).
For example, as shown in Figure 1, when source waters have a mean concentration of approximately 1 rotavirus/100 L and the treatment plant consistently achieves at least a 4-log reduction in virus concentration, the burden of disease in the population would meet the reference level of 10−6 DALY/person per year (1 case/1000 people per year). A source water concentration of 1 rotavirus/100 L of water is relatively low. It generally represents groundwater sources and relatively pristine surface water sources. Many surface water sources will have virus concentrations on the range of 1-100 viruses/L of water (100-10 000/100 L). These levels require a much greater log reduction to meet the acceptable disease burden.
Figure 2 shows that a source water with a mean concentration of 10 rotaviruses/L of water (1000 rotaviruses/100 L of water) would require the treatment plant to consistently achieve at least a 7-log reduction in virus concentration to meet the acceptable reference level of risk. Consequently, the health-based treatment goal of a 4-log reduction of enteric viruses is a minimum requirement. A site-specific assessment should be done to determine what level of enteric virus reduction is needed for any given source water. Monitoring, as opposed to estimating, enteric virus concentrations in source water will result in the highest-quality risk assessment. However, if measurements are not possible, estimated concentrations may be based on perceived source water quality. Information obtained from sanitary surveys, vulnerability assessments, and information on other water quality parameters, such as indicator organisms, can be used to help estimate the risk and/or level of faecal contamination in the source water. It is important to consider, as part of the site-specific assessment, events that can significantly change source water quality, such as hazardous spills or storms. These will have an important impact on the treatment required, and including variations in source water quality will provide the best estimate of the risk in a system. Understanding and planning for the variations that occur in source water quality create a more robust system that can include safety margins. It is also important to take into consideration the level of uncertainty that is inherent in carrying out a QMRA to ensure that the treatment in place is producing water of an acceptable quality. A sensitivity analysis using a QMRA model such as the one described in Appendix C can also help identify critical control points and their limits.
Figure 1: Example of a risk assessment under specified conditions
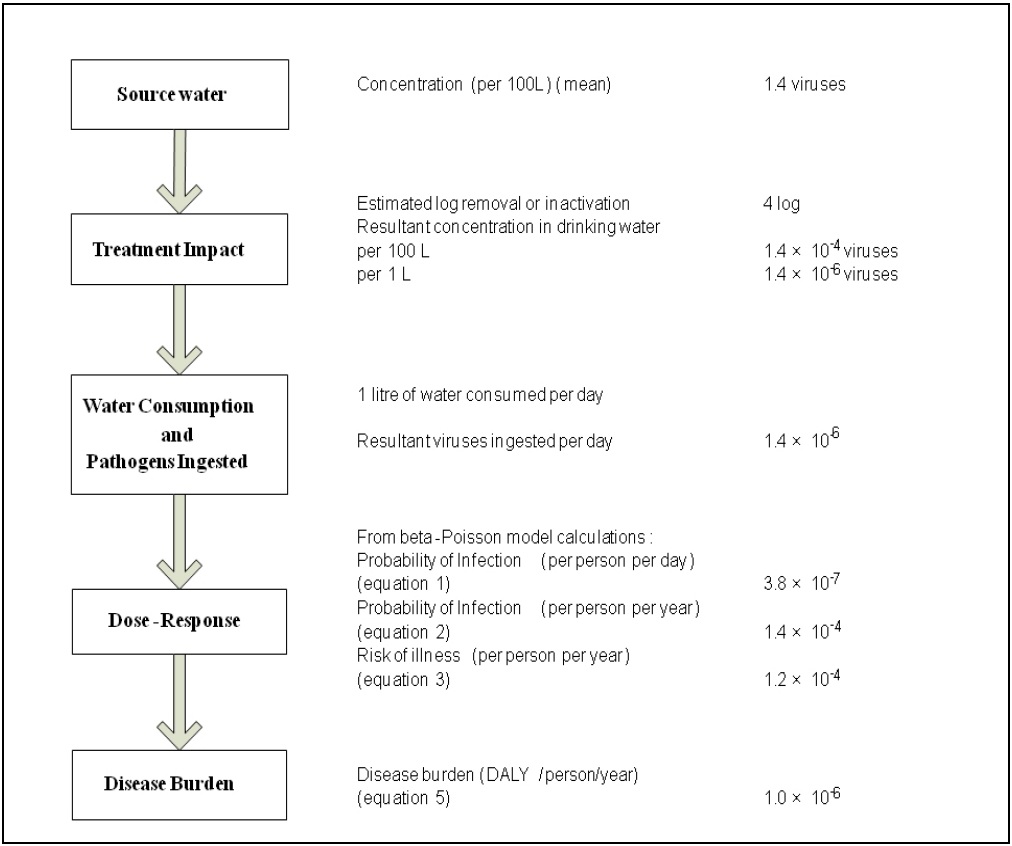
The calculation is presented as a point estimate; however, the calculation was done using a mathematical model that included probability functions with associated uncertainties.
Example of a risk assessment under specified conditions - Text equivalent
The steps in a quantitative microbial risk assessment for enteric viruses are presented as a flow chart along with an example risk assessment calculation. On the left side of the flowchart, in boxes, are the 5 steps; on the right side, parallel to each box, is the corresponding information from the example calculation. For step 1), source water, the example uses a mean concentration of 1.4 viruses per 100 litres of water. For step 2), treatment impact, the example calculation estimate for log removal or inactivation is 4 log and therefore the resultant concentration of viruses in drinking water would be 1.4x10-4 viruses per 100 litres, or 1.4x10-6 viruses per litre. For step 3), water consumption and pathogens ingested, the example calculation includes the assumption that 1 litre of water is consumed daily, therefore the number of viruses ingested per day would be 1.4x10-6. For step 4), dose-response, the information from step 3 and equations 1, 2 and 3 from the text, are used to calculate the probability of infection per person per day, the probability of infection per person per year, and the risk of illness per person per year which correspond to 3.8x10-7, 1.4x10-4, and 1.2x10-4, respectively. For step 5), disease burden, equation 5 from the text is used to calculate a disease burden, which for this example is 1.0x10-6 disability adjusted life years per person per year.
Figure 2: Treatment requirements to meet an acceptable level of risk of 10-6 DALY/person per year based on 1L consumption
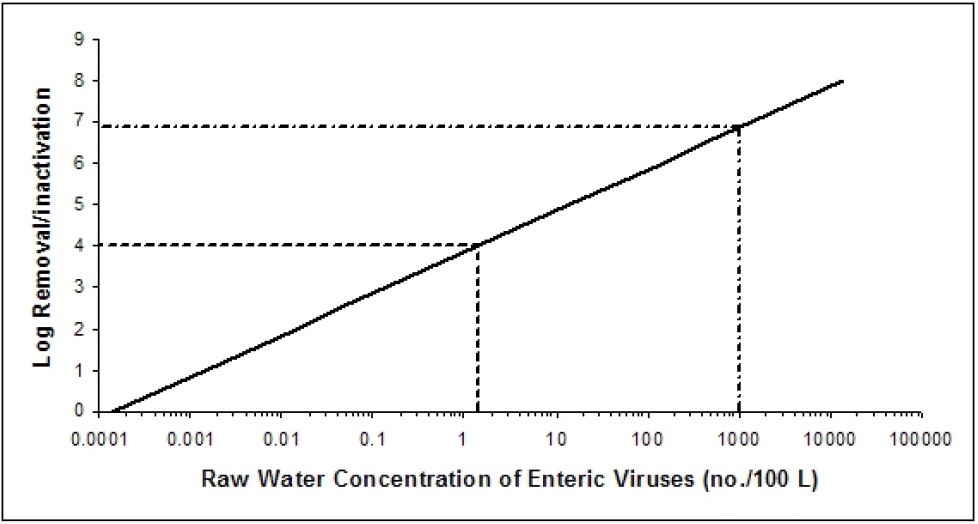
Treatment requirements to meet an acceptable level of risk of 10-6 DALY/person per year based on 1L consumption - Text equivalent
The level of treatment required to meet an acceptable level of risk based on 1 L consumption for enteric virus concentrations ranging from 0.0001 viruses per 100 litres to 10000 viruses per 100 litres in raw water is presented graphically. The x-axis of the graph is the raw water concentrations of enteric viruses per 100 litres using a log scale. The y-axis of the graph is the log removal using a linear scale. The relationship between the values on the x-axis and the values on the y-axis for the risk level of 10-6 DALY per person per year creates a diagonal line. Two examples of treatment requirements are illustrated on the graph using dotted lines. The first example draws a horizontal dotted line from the y-axis at approximately 4 log removal. This dotted line intersects the diagonal line at approximately 1 enteric virus per 100 litres of raw water. The second example draws a horizontal dotted line from the y-axis at approximately 7 log removal. This dotted line intersects the diagonal line at approximately 1000 enteric viruses per 100 litres of raw water.
8.4 International considerations
QMRA is increasingly being applied by international agencies and governments at all levels as the foundation for informed decision-making surrounding the health risks from pathogens in drinking water. WHO, the European Commission, the Netherlands, Australia and the United States have all made important advances in QMRA validation and methodology (Staatscourant, 2001; WHO, 2004; NRMMC-EPHC, 2006; Medema et al., 2006; U.S. EPA, 2006a,b). With the exception of the U.S. EPA, these agencies and governments have adopted an approach that takes full advantage of the potential of QMRA to inform the development of health targets (i.e., acceptable levels of risk or disease) and site-specific risk management (e.g., Water Safety Plans, as described in WHO, 2004). Building on the WHO work, the European Commission's Microrisk project has published an extensive guidance document that establishes methods and a strong science basis for QMRA of drinking water (Medema et al., 2006).
The Netherlands and the U.S. EPA provide two examples of QMRA-based regulatory approaches. In the Netherlands, consistent with the WHO approach, water suppliers must conduct a site-specific QMRA on all surface water supplies to determine if the system can meet a specified level of risk. Dutch authorities can also require a QMRA of vulnerable groundwater supplies. In contrast, recent regulatory activity in the United States has seen the U.S. EPA assess the health risks from waterborne pathogens through QMRA and apply this information to set nationwide obligatory treatment performance requirements (U.S. EPA, 2006a,b). In general, drinking water systems must achieve a 4-log removal or inactivation of enteric viruses to address risk from enteric viruses (U.S. EPA, 2006a). To address risk specifically from Cryptosporidium, drinking water systems must monitor their source water, calculate an average Cryptosporidium concentration and use those results to determine if their source is vulnerable to contamination and requires additional treatment. Water systems are classified into categories ("bins") based on whether they are filtered or unfiltered systems; these bins specify additional removal or inactivation requirements for Cryptosporidium spp. (U.S. EPA, 2006b).
Health Canada and the Federal-Provincial-Territorial Committee on Drinking Water have chosen the same approach as WHO (2004), providing QMRA-based performance targets as minimum requirements, but recommend the use of a site-specific QMRA as part of a multi-barrier source-to-tap approach. The QMRA approach offers a number of advantages, including 1) the ability to compare the risk from representative groups of pathogens (e.g., viruses, protozoa, bacteria) in an overall assessment; 2) the transparency of assumptions; 3) the potential to account for variability and uncertainty in estimates; 4) the removal of hidden safety factors (these can be applied as a conscious choice by regulatory authorities at the end of the process, if desired); 5) the site-specific identification of critical control points and limits through sensitivity analysis; and 6) the clear implications of system management on a public health outcome.
Page details
- Date modified: