
Social Isolation among Older Adults during the Pandemic
From: Federal/Provincial/Territorial Ministers responsible for Seniors Forum
On this page
- List of abbreviations
- List of figures
- List of tables
- Participating governments
- Acknowledgments
- Executive summary
- 1. Introduction
- 2. Literature review
- 3. What was learned from this review
- 4. Conclusion
- Annexes
- References
Alternate formats

Social Isolation among Older Adults during the Pandemic[PDF - 2.6 KB]
Large print, braille, MP3 (audio), e-text and DAISY formats are available on demand by ordering online or calling 1 800 O-Canada (1-800-622-6232). If you use a teletypewriter (TTY), call 1-800-926-9105.
List of abbreviations
- AFC
- Age-Friendly Cities
- AWIC
- Aging Well in Communities
- BC
- British Columbia
- BH
- Better at Home
- CAA
- Canadian Automobile Association
- CBSS
- Community-based seniors sector
- CFHI
- Canadian Foundation for Healthcare Improvement
- CIHI
- Canadian Institute for Health Information
- CIHR
- Canadian Institutes of Health Research
- CIP
- Community Initiatives Program
- CLSA
- Canadian Longitudinal Study on Aging
- COVID-19
- Coronavirus
- CTM
- Choose to Move
- DIA
- Dialogues in Action
- ESCC
- Edmonton Seniors Coordinating Council
- ECSF
- Emergency Community Support Fund
- EPIC
- Eldercare Project in Cowichan
- FAF
- Fresh Air Fun
- FPT
- Federal, Provincial and Territorial
- H2O
- Hand over Hand Network
- HIGI
- H2O Intergenerational Group Interactions
- HIMI
- H2O Intergenerational Mentorship Interactions
- HIPI
- H2O Intergenerational Paired Interactions
- INESSS
- Institut national d’excellence en santé et services sociaux
- INSPQ
- Institut National de santé publique du Québec
- LGBTQ2
- Lesbian, Gay, Bisexual, Transgender, Queer, Two-Spirit
- LTC
- Long-term care
- MASC
- Manitoba Association of Senior Centres
- NCCIH
- National Collaborating Centre for Indigenous Health
- NCCMT
- National Collaborating Centre for Methods and Tools
- NHSP
- New Horizons for Seniors Program
- NS
- Nova Scotia
- OACAO
- Older Adults’ Centres Association of Ontario
- OCSA
- Ontario Community Support Association
- OWSEP
- Older Winnipeggers Social Engagement Project
- PEGASIS
- Pan Edmonton Group Addressing Social Isolation in Seniors
- PEI
- Prince Edward Island
- PEIANC
- PEI Association for Newcomers to Canada
- PHAC
- Public Health Agency of Canada
- PPE
- Personal Protective Equipment
- SAGE
- Student Association for Geriatric Empowerment
- SAIL
- Seniors Abuse and Information Line
- SALC
- Seniors Active Living Centre
- SCWW
- Senior Centre Without Walls
- SSIPP
- Student-Senior Isolation Prevention Partnership
- SSSC
- Safe Seniors, Strong Communities
- TAPS
- Therapeutic Activation Program for Seniors
- TIP-OA
- Telehealth Intervention Program for Older Adults
- UK
- United Kingdom
- US
- United States of America
- UWLM
- United Way of the Lower Mainland
- WHO
- World Health Organization
List of tables
- Table 1: COVID-19 cases and deaths by age group
- Table 2: Loneliness patterns by age and sex, baseline (2011 to 2015), follow-up one (2015 to 2018), and during pandemic (2020), CLSA
- Table 3: Depression patterns by age and sex, baseline (2011 to 2015), follow-up one (2015 to 2018), and during pandemic (2020), CLSA
- Table 4: Befriending programs
- Table 5: Telephone outreach and help or information lines
- Table 6: Health promotion and wellness programs
- Table 7: Practical assistance programs
- Table 8: Technology training and donation programs
- Table 9: Senior Centre Without Walls programs
- Table 10: Other remote programs
- Table 11: Mechanisms to support learning and collaboration
- Table 12: Interventions to address social isolation in long-term care
- Table 13: Governmental grant programs and funding
Participating governments
- Government of Ontario
- Government of Québec*
- Government of Nova Scotia
- Government of New Brunswick
- Government of Manitoba
- Government of British Columbia
- Government of Prince Edward Island
- Government of Saskatchewan
- Government of Alberta
- Government of Newfoundland and Labrador
- Government of Northwest Territories
- Government of Yukon
- Government of Nunavut
- Government of Canada
*Québec contributes to the Federal, Provincial and Territorial Seniors Forum by sharing expertise, information and best practices. However, it does not subscribe to, or take part in, integrated federal, provincial, and territorial approaches to seniors. The Government of Québec intends to fully assume its responsibilities for seniors in Québec.
The views expressed in this report may not reflect the official position of a particular jurisdiction.
Acknowledgments
Prepared by Andrew V. Wister and Laura Kadowaki, Gerontology Research Centre, Simon Fraser University for the Federal, Provincial and Territorial (FPT) Forum of Ministers Responsible for Seniors.
The authors wish to acknowledge that the tabular data in this report were based on the data and biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation. The CLSA data were drawn from prior analyses by the lead author that were part of approved CLSA projects, as well as data drawn from the CLSA COVID-19 Survey Dashboard available on the CLSA web site. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland.
Executive summary
In this section
Introduction
The new Coronavirus (COVID-19) is a highly contagious disease that was discovered near the end of 2019. COVID-19 has been conceptualized as a “gero-pandemic,” defined as a disease that has spread globally with heightened significance and negative consequences for older populations (Wister & Speechley, 2020). Older people are particularly vulnerable to the harmful health impacts of COVID-19, as well as social isolation and loneliness as a result of public health measures to reduce transmission of the disease (for example, physical and social distancing measures, closure of community spaces).
This report investigates how the COVID-19 pandemic has affected older Canadians, focusing on social isolation and loneliness. Social Isolation is defined as “a lack in quantity and quality of social contacts” and “involves few social contacts and few social roles, as well as the absence of mutually rewarding relationships” (Keefe et al., 2006, p.1). Loneliness is “defined as a distressing feeling that accompanies the perception that one’s social needs are not being met by the quantity or especially the quality of one’s social relationships” (Hawkley & Cacioppo, 2010, p.1). While social isolation and loneliness can have both common and unique features, we use the term social isolation in this report to designate both terms except where distinct patterns require attention. To inform the report, a comprehensive search of academic and grey literature was conducted, including promising practices aimed at reducing social isolation. This was supplemented with new data from the Canadian Longitudinal Study on Aging (CLSA). The World Health Organization’s Age-Friendly Cities Framework was used as a guiding model for the review.
In Canada, data from the CLSA reveals striking increases in feelings of loneliness from the first results of the study (2011 to 2015) to COVID-19 (April to December 2020). It is estimated that there is a 67% increase in loneliness for women aged 65 to 74, and 37% for those aged 75 to 84. Smaller increases are observed for men, where there is a 45% relative rise for men aged 65 to 74 and 33% for the oldest group.
Literature review: challenges faced by older adults during the pandemic related to social isolation
Social isolation and vulnerable sub-populations of older adults
The literature identifies sub-populations of older adults who may be particularly vulnerable to social isolation during the COVID-19 pandemic, including: rural, remote, and Northern communities; LGBTQ2 older adults; ethnic minority and immigrant older adults; Indigenous peoples; people living with dementia; caregivers; and low-income older adults. The pandemic has exacerbated pre-existing inequities in health, access to health care, employment, and other areas for older Canadians. However, sources of resilience were also identified; for example, some First Nations communities have drawn upon traditional practices and culture to protect their elders (that is encouraging return to the land, governance of community entry).
Social isolation and community-dwelling older adults
Findings on the challenges faced by community-dwelling older adults as well as examples of interventions to address social isolation are organized in the report according to the 8 domains of the Age-Friendly Cities Framework.
- Respect and social inclusion: experts have expressed concerns about the intensifying of ageist views, intergenerational tensions, and aging-related social problems (such as elder abuse) during the pandemic (Ayalon, 2020; Makaroun et al., 2021). Befriending and other intergenerational programs have sought to create connections between older and younger generations
- Housing: older adults living alone and in social housing have been identified as at-risk groups during the pandemic (Emerson, 2020; Pirrie & Agarwal, 2021). Older adults living in non-institutional congregate living settings (such as assisted living, retirement communities) share similar vulnerabilities to long-term care (LTC) residents, but live in a setting guided by social models of care and with higher levels of autonomy (Zimmerman et al., 2020)
- Community support and health services: significant disruptions have occurred to community support and health services. While remote delivery was already being used for some services prior to the pandemic (for example, caregiver support programs), others have transitioned to new models of delivery. With support from government funding, practical assistance programs have been initiated or significantly scaled up in response to high levels of demand. In some jurisdictions, governments have taken a role in coordinating large-scale responses to the pandemic and supporting community agencies
- Transportation: data suggests transit use by older adults has declined during the pandemic (Palm et al., 2020a; 2020b). On the other hand, there has been a scaling up of volunteer driver services and delivery programs in many communities to support isolated older adults. However, some communities have reported shortages of volunteer drivers resulting in gaps in service (such as CBC News, 2021; Weldon, 2020)
- Communication and information: while data suggests over two-thirds of older Canadians use the internet (Davidson & Schimmele, 2019), certain segments of the population (such as low-income older adults; people living in rural, northern, and Indigenous communities; the very old; and older adults with physical disabilities or cognitive impairments) may encounter challenges in access and use. To overcome this “digital divide,” programs that provide training and access to digital technologies are being implemented or expanded across Canada. Telephone help and information lines and telephone outreach programs have also been initiated or enhanced for older adults who prefer low-tech interventions
- Social participation: the pandemic has disrupted the operations of community and recreation organizations, and many have switched to remote delivery of programs. The Senior Centre Without Walls model that offers telephone or virtual programs has been adopted by organizations in many jurisdictions. However, securing adequate funding to support their operations has been a challenge for some non-profit and community organizations (for example, Coordinated Pandemic Response Steering Committee, 2020)
- Civic participation and employment: for some older adults, work and volunteering are important sources of social connection. Older workers in Canada have been negatively impacted by workplace closures and growing unemployment rates during the pandemic (CLSA, 2021; Statistics Canada, 2021). Declining participation of older volunteers has also been observed, with COVID-related health concerns a contributing factor (Volunteer Canada, 2020; CLSA, 2021)
- Outdoor spaces and buildings: outdoor spaces can provide lower-risk locations to safely socialize and engage in physical activities. Strategies are needed to maximize the availability of outdoor community spaces and ensure that they are “COVID-19” age-friendly in design (INSPQ, 2020). Strategies are also needed so older adults can safely return to indoor spaces (such as providing hand sanitizer, smaller groups) (OACAO, 2020)
Social isolation among older adults residing in long-term care facilities
In LTC settings, concerns about social isolation have centred around how to safely facilitate family visits and offer social activities. Methods to support in-person visits during the pandemic have included: window visits, physically distanced outdoor visits, in-person visits in special rooms or containers with barriers in place, and physically distanced in-person visits in residents’ rooms or common areas. Technology (for example, telephone and video calls) can provide safe alternatives for staying connected to family members and friends but cannot replace face-to-face contact. Facilitating resident-family connections (whether they be in-person or virtual) requires a significant amount of time and effort from already overburdened staff. Ickert et al. (2020) estimate that a LTC home with 100 residents would require a minimum of 2 full-time and 1 part-time staff to provide most residents with a once-a-week visit with family for 30 minutes.
What was learned from this review
The following are key takeaway messages based on an analysis of what was learned:
- older Canadians are a heterogeneous population, and programs should be tailored to meet linguistic and cultural needs and delivered via a range of mechanisms (such as in-person, telephone, virtual, letter, etc.)
- a digital divide exists and there are sub-populations at risk of being further excluded during the pandemic as a result. Ensuring all Canadians have access to low-cost home internet and free internet in public spaces should be a priority
- intergenerational programs not only provide social benefits for older adults and younger people, but also have been shown to be effective at reducing ageism
- the development of partnerships that leverage the expertise and resources of stakeholders has contributed to the success of interventions
- government policies on LTC (for example, design of facilities, visitor policies, staffing levels) have a significant impact on the health and social lives of LTC residents. Policies should be reviewed with a focus on how they can balance disease mitigation and social connection needs
- in LTC facilities, adequate staff support is an essential enabler for visitation with families and caregivers (in-person or virtually), social activities, and coordinating with external organizations offering programs
- moving forward, ensuring the sustainability of successful interventions is a key issue. Many of the interventions being offered by community and non-profit organizations are supported by short-term funding, and sustainable funding sources are needed
The findings from this report highlight how federal, provincial, and territorial governments can influence the development of social isolation initiatives through their funding, large-scale coordination, knowledge sharing, and policy-making. Community and non-profit organizations were identified as being at the forefront of outreach and delivering services to vulnerable older adults. Businesses and academic institutions can also add their resources and expertise to interventions to support isolated older adults.
While there were limited formal evaluations of interventions to reduce the social isolation of older adults, anecdotal evidence and pre-pandemic evaluations suggest potential benefits of the following promising practices:
- Befriending programs: a small number of studies and anecdotal evidence suggest participation benefits both older adults and volunteers
- Telephone outreach programs and information lines: one pre-pandemic study has linked telephone outreach and help or information lines to reductions in social isolation. Anecdotal evidence suggests high call volumes during the pandemic
- Health promotion and wellness programs: pre-pandemic there was an emerging body of evidence supporting the provision of online caregiver support programs. Evidence of the effectiveness of other types of health promotion and wellness programs at reducing social isolation has been found, though these effects have been observed based on in-person versions of the programs
- Practical assistance programs: 2 pre-pandemic studies have linked the receipt of practical assistance (meal delivery) with reduced levels of loneliness. Anecdotal evidence suggests high rates of demand for these services
- Technology donation and training programs: anecdotal evidence suggests these programs have been successful at training older adults to use digital technology. A key enabler for their success is providing access to free internet
- Senior Centre Without Walls: to date, there have been 2 small evaluations of the Senior Centre Without Walls (SCWW) model, both of which reported reduced loneliness due to participation. Anecdotal evidence suggests consistent participation by older adults in SCWW and other virtual programs and positive feedback by participants
1. Introduction
In this section
1.1 COVID-19 and Canadian older adults – a “Gero-Pandemic”
The new Coronavirus (COVID-19) is a highly contagious disease that was discovered near the end of 2019. COVID-19 has resulted in unprecedented high levels of disease and mortality, especially among vulnerable populations (Liu et al., 2020; Renu et al., 2020). The rapid spread of the disease has produced a global pandemic that has created new challenges for public health, continuing and long-term care (LTC) systems, community support organizations, businesses and the economy, families, and individuals. COVID-19 has been conceptualized as a “gero-pandemic,” defined as a disease that has spread globally with heightened significance and harmful consequences for older populations (Wister & Speechley, 2020).
As of the second week of April 2021, COVID-19 cases surpassed 1 million in Canada and reached almost 135 million cases worldwide. The number of deaths passed the 23,000 mark in Canada and has exceeded 2.9 million globally (Government of Canada, 2020a). One in 5 positive cases are among persons 60 years of age and older, and about 96% of deaths are among this age group (consult table 1). Furthermore, more than two-thirds of all deaths are occurring in LTC facilities or congregate and assisted living environments (Government of Canada, 2020a). Due to the impacts of COVID-19 on LTC facilities, almost 70% of older Canadians have reported their opinion has changed on whether they would place themselves or a loved one in LTC (National Institute on Ageing, 2020). Yet, those living in the community also face risk of infection, and the effects of the pandemic response (Cohen & Tavares, 2020).
| Age group | 0 to 19 | 20 to 29 | 30 to 39 | 40 to 49 | 50 to 59 | 60 to 69 | 70 to 79 | 80 and over |
|---|---|---|---|---|---|---|---|---|
| % of COVID-19 cases | 17.7% | 18.8% | 16.1% | 14.7% | 13.3% | 8.4% | 4.7% | 6.3% |
| % of COVID-19 deaths | 0.0% | 0.2% | 0.4% | 0.9% | 2.8% | 8.0% | 19.4% | 68.3% |
Source: Data from Government of Canada (2020a), current as of April 9, 2021.
To stop the spread of COVID-19, federal, provincial, and territorial governments have implemented various public health measures such as recommendations to engage in physical and social distancing; closure of non-essential businesses and public spaces; implementation of lockdowns and stay at home orders; mask mandates; travel restrictions; and restrictions on visitors to LTC facilities. While these measures have resulted in some successes in reducing transmission of COVID-19, they have also led to significant changes to the lives of Canadians. Concerns have been raised about the potential negative impacts the prolonged periods of physical and social distancing and reduced social interactions will have on Canadians, with specific attention paid to impacts on older adults (for example, Morrow-Howell et al., 2020; Smith et al., 2020).
While age has become a major focal point in the pandemic (Morrow-Howell et al. 2020; Shahid et al., 2020), there are also other aspects that result in increased vulnerabilities to COVID-19 and the negative impacts of physical and social distancing policies. There is increased risk when age is coupled with pre-existing vulnerabilities such as:
- mental health conditions or lowered psychological well-being (Alonzi et al., 2020; Barber & Kim, 2020)
- physical health conditions (for example, cardiovascular disease, cancer, diabetes, obesity, and chronic obstructive pulmonary disease) (Mauvais-Jarvis, 2020; Mitra et al., 2020)
- the presence of 2 or more chronic illnesses (Wister, 2021a; 2021b)
- marginalization due to poverty; sexual orientation; race, ethnicity, or culture; immigration status; rural and remote environment; or other vulnerabilities (Wister, 2021a; 2021b)
While much research has focused on vulnerabilities to COVID-19, it is important to also recognize strengths and factors that contribute to individual, family, and community resilience. For example, some Indigenous reserve communities have utilized strong community connections and leadership to support pandemic mitigation strategies even though health care resources tend to be weaker (National Collaborating Centre for Methods and Tools & National Collaborating Centre for Indigenous Health [NCCMT & NCCIH], 2020). Finally, it is also important to understand the broader social structures and environmental contexts in which these risk factors occur (Morrow-Howell et al., 2020). For example, in LTC settings, policies on visitation and funding for pandemic responses can influence individual level experiences and risks (Andrew et al., 2020). These organizational strengths and weaknesses can also be assessed using system resilience factors, for instance, the preparation, recovery, and adaptation levels of LTC during pandemic adversity (Klasa et al., 2021a; 2021b).
1.2 Purpose of report
The purpose of this report is to investigate how the COVID-19 pandemic has impacted older Canadians, focusing on impacts related to social isolation. This report a) reviews academic and grey literature on social isolation during the COVID-19 pandemic; b) assesses promising policies and programs that are reducing the social isolation of older Canadians during the pandemic; and c) summarizes the lessons learned, promising practices, and potential roles for governmental and non-governmental actors. The focus of the report is social isolation as it relates to aging in community; however, the report also includes a section examining social isolation in LTC settings.
This review summarizes the key literature on the pandemic to date; however, due to the scarcity of COVID-19 literature it was not possible to explore all topics in depth. The literature in this report is current up until the first week of April 2021. Due to the recentness of the pandemic, a range of academic and grey area data and information sources were considered, including lower level anecdotal and non-experimental evidence (such as case reports, news articles, expert opinion articles, program reports), since it was recognized there would be limited higher level experimental and review evidence. When evaluation data on programs and policies were not available, anecdotal evidence was considered as well as relevant pre-pandemic evidence from evaluations of similar style interventions. A data request was also made to the Canadian Longitudinal Study (CLSA) to access their COVID-19 study data pertaining to social isolation and loneliness.Footnote 1
The literature review begins by exploring unique considerations relevant to social isolation and certain sub-populations of older adults that may be particularly vulnerable during the pandemic. Next, the literature on the impacts of the pandemic on community-dwelling older adults is reviewed as it relates to social isolation. Finally, considerations for residents of LTC facilities specific to social isolation are discussed. Annexes 2 to 10 provide Canadian examples of the types of interventions discussed in the literature review. The annexes describe a range of programs that represent the diversity of communities, organizations, and pandemic responses in Canada. It is important to acknowledge that the annexes provide only a sampling of the many valuable programs being implemented to assist older Canadians during the pandemic.
The Age-Friendly Cities (AFC) frameworkFootnote 2 is used as an organizing framework for this report. The AFC framework is an initiative of the World Health Organization (WHO, 2007) that was developed in 2006 based on consultations held in 33 cities around the world (see figure 1 for a visual depiction of the 8 domains of age-friendly cities).Footnote 3

Figure 1 - Text version
The WHO’s Age-Friendly City framework consists of 8 domains:
- respect and social inclusion
- housing
- community support and health services
- transportation
- communication and information
- social participation
- civic participation and employment
- outdoor spaces and buildings
The Public Health Agency of Canada (PHAC) describes an age-friendly community as follows:
“in an age-friendly community, the policies, services and structures related to the physical and social environment are designed to help seniors ‘age actively.’ In other words, the community is set up to help seniors live safely, enjoy good health and stay involved”
(PHAC, 2016).
PHAC (2011) states that age-friendly communities support older adults by:
- recognizing the range of capacities and resources of older adults
- respecting the decision-making of older adults
- anticipating and flexibly responding to age-related needs
- supporting vulnerable older adults
- promoting the inclusion of older adults in all areas of community life
1.3 Social isolation and loneliness
1.3.1 Risk factors and consequences of social isolation among older adults
Social isolation is commonly defined as “a lack in quantity and quality of social contacts” and “involves few social contacts and few social roles, as well as the absence of mutually rewarding relationships” (Keefe et al., 2006, p.1). A closely related concept to social isolation is loneliness “defined as a distressing feeling that accompanies the perception that one’s social needs are not being met by the quantity or especially the quality of one’s social relationships” (Hawkley & Cacioppo, 2010, p.1). The key distinction between social isolation and loneliness is that social isolation refers to the objective level of social connections, whereas loneliness reflects the perception of being disconnected from others (Courtin & Knapp, 2015). While these 2 concepts often overlap, there can be unique associations; for instance, some older adults may not feel lonely even if they have low levels of social connectedness, and some people who seemingly have many social contacts feel lonely. For the purpose of this report, the term social isolation is used to refer to both the objective (for example, actual levels of personal connectedness) and subjective (such as feelings of loneliness) experiences of older adults, but where necessary differentiations between social isolation and loneliness are made to reflect distinct dimensions.
Social isolation is a common public health concern among community-dwelling older adults, especially during the COVID-19 pandemic due to the risk of infection, the seriousness of the illness, and mitigation approaches including physical and social distancing (Shahid et al., 2020). Box 1 lists the negative health impacts social isolation is associated with for older adults. Older individuals experiencing social isolation have been shown to have lower access to health care services and lower health care utilization (Newall et al., 2015). Overall, given the wide-ranging impacts of social isolation on mortality, health, and quality of life, social isolation has received increasing attention in public health literature and gerontology literature, amid policy concerns around population ageing (Burholt et al., 2020; Courtin & Knapp, 2017; Fakoya et al., 2020; Leigh-Hunt et al., 2017).
Box 1: Negative impacts of social isolation among older adults
- Reduced happiness, life satisfaction, and psychological well-being
- Increased anxiety, distress, and depression
- Poorer physical health
- Reduced engagement in healthy behaviours
- Higher mortality
Sources: Golden et al. (2009); Leigh-Hunt et al. (2017); Wister et al. (2019)
Those who experience various forms of vulnerability and marginalization in society are particularly at risk. Box 2 outlines risk factors and groups associated with social isolation. Taken together, the vulnerabilities experienced by older adults and significant negative impacts of social isolation have led to the development and implementation of many programs and services aimed at reducing social isolation (and loneliness), with many new or retrofitted approaches necessary during the pandemic. The program evaluation literature in this area even pre-pandemic has not been developed to the level required for meta-evaluation or meta-analyses (analyses that combine the results of multiple studies). Evaluation of the success of programs during the pandemic requires assessment of a range of lower-level anecdotal and non-experimental evidence.
Box 2: Risk factors and groups associated with social isolation
- Advanced age
- Living alone
- Low income or poverty
- Lack of affordable housing and shelter and care options
- Widowhood
- Episodic or lifelong physical and mental health issues (including Alzheimer’s disease or other dementias, frailty, sensory loss, or multiple chronic illnesses)
- Loss of sense of community
- Challenges relating to technology use (access to WiFi, costs, literacy, comfort)
- People living in rural or remote areas
- Immigrant or ethnic older adults – especially visible minorities
- Indigenous elders
- Lesbian, gay, bisexual, or transgender seniors
- Caregivers with a heavy burden
Sources: De Jong Gierveld et al. (2015); Kirkland et al. (2015); National Seniors Council (2014a; 2014b; 2016); Newall et al. (2015); Wister et al. (2018)
1.3.2 The prevalence of social isolation during the pandemic
In order to estimate the increase in social isolation during the pandemic, we use unique data drawn from 3 separate waves of the CLSA: Baseline data (collected 2011 to 2015); Follow-up One data (collected 2015 to 2018); and data from the recent CLSA COVID-19 Study (collected April to December, 2020).Footnote 4 At the Baseline and Follow-up One time periods, feelings of loneliness are almost identical. Based on these data, it is estimated that, pre-pandemic, approximately 20% of older adults experienced loneliness some of the time or greater, and that about 10% experienced chronic or intense levels that are associated with negative health and well-being outcomes (Wister et al., 2018).
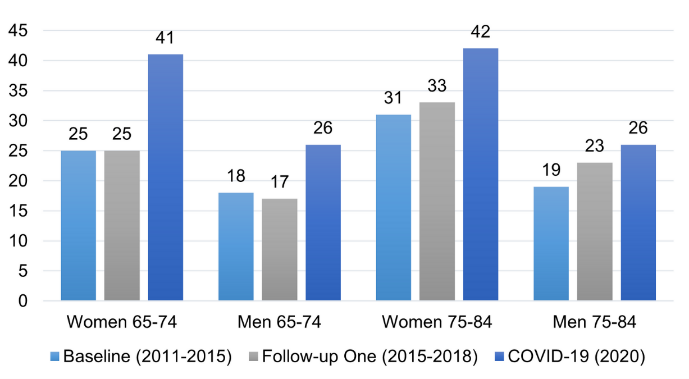
Turning to the CLSA COVID-19 Study, the rates increase significantly. Among older women aged 65 to 74 and 75 to 84, rates of loneliness are 41% and 42% respectively. For men, the rates also increased, but are lower than for women. Among men aged 65 to 74 and 75 to 84, 26% feel lonely at least some of the time. The increase in feelings of loneliness between the Baseline and COVID-19 (2020) time periods are striking. There is a 67% increase in loneliness for women aged 65 to 74, and 37% for those aged 75 to 84. Smaller increases are observed for men, where there is a 45% relative rise for men aged 65 to 74 and 33% for the oldest group (see Figure 2). The lower rates of loneliness among men, especially the oldest age group, may be indicative of stronger supports for this group, given that they are more likely to be partnered. Please see figure 3 for additional Canadian findings on the impacts of the pandemic from the CLSA.
Loneliness patterns by age and sex, CLSA
Loneliness Data Source: original analysis of CLSA Baseline, Follow-up one, and COVID-19 study data by authors.
Figure 2 - Text version
The Canadian Longitudinal Study on Aging surveyed older adults regarding if they felt lonely at least some of the time across 3 different time periods. The results of the CLSA are available in the following table:
| Age cohort | Baseline (2011 to 2015) | Follow-up one (2015 to 2018) | COVID-19 (2020) |
|---|---|---|---|
| Women 65 to 74 | 25 | 25 | 41 |
| Men 65 to 74 | 18 | 17 | 26 |
| Women 75 to 84 | 31 | 33 | 42 |
| Men 75 to 84 | 19 | 23 | 26 |
The rate of increase in loneliness over the course of the survey was:
- 67% for women aged 65 to 74
- 45% for men aged 65 to 74
- 37% for women aged 75 to 84
- 33% for men aged 75 to 84
The absolute percentage increase in loneliness among older adults ranged from 6% to 17%.
Note: absolute and rate of increases in loneliness were measured as changes from baseline to COVID-19.
CLSA COVID-19 study findings

Depression Data Source: Original analysis of CLSA Baseline, Follow-up one, and COVID-19 study data by authors.
Source for all other data: CLSA COVID-19 Study Dashboard.
Figure 3 - Text version
The Canadian Longitudinal Study on Aging report surveyed older adults regarding if they felt depressed. Full results of the CLSA are available in the following table:
| Age cohort | Baseline (2011 to 2015) | Follow-up one (2015 to 2018) | COVID-19 (2020) |
|---|---|---|---|
| Women 65 to 74 | 19 | 19 | 23 |
| Men 65 to 74 | 12 | 12 | 14 |
| Women 75 to 84 | 21 | 23 | 23 |
| Men 75 to 84 | 12 | 16 | 13 |
From baseline to COVID-19, relative increases in rates of depression were between 8% and 21% depending on the age group and gender. Depression rose more among the 65 to 74 age group than the 75 to 84 group.
Other CLSA COVID-19 study findings are provided below.
- Caregiving: about 12% of persons aged 50 and over had problems providing caregiving to others
- Anxiety: rates of anxiety (mild, moderate, and severe) ranged from around 8% up to 25%, with higher rates among persons aged 65 to 74, especially women
- Family connection: about two thirds of women over the age of 65 felt separated from their family, compared to slightly over half of the men that age
- Access to supplies: among all age and gender groups, about 13% experienced difficulty obtaining necessary food and supplies
- Income: among all age and gender groups, 17% had a loss of income, with higher rates among older men
- Access to health care: among all age and gender groups, about 22% felt they were unable to access healthcare
Additional survey findings
The results of additional surveys also suggest older Canadians are experiencing high rates of social isolation during the pandemic:
- Gutman et al. (2021) surveyed Canadians aged 55 and up and they found 51% of respondents felt lonely some or most of the time (55% of women and 37% of men) and 57% felt isolated some or most of the time (60% of women and 46% of men). Women were more likely than men to follow social distancing guidelines most of the time, report changes in social support levels, and experience negative emotions
- a survey conducted by the National Institute on Ageing (2020) reported that 40% of Canadians aged 55 and up have experienced a lack of social connections and companionship during the pandemic
- a survey of retired teachers in Ontario (Savage et al., 2021) reported 43% of respondents felt lonely at least some of the time. Gender (female), living alone, being a caregiver, and being in fair or poor health were associated with increased odds of feeling lonely
Findings from the United States (US) also suggest increasing levels of loneliness during the pandemic. Several longitudinal studies have found patterns of increased loneliness experienced by older adults (Kotwal et al., 2020; Krendl & Perry, 2021; Luchetti et al., 2020). Generally, levels of loneliness tended to level off or decrease as the pandemic progressed; however, for some loneliness levels persisted or worsened (Kotwal et al., 2020; Luchetti et al., 2020). Kotwal et al. (2020) note that older adults experiencing worsening loneliness often report a lack of social support, difficulties accessing or using social technology, and challenges coping emotionally. On the other hand, those who experience little negative impact on loneliness report using technology, positive coping strategies, and access to municipal and community services.
Social isolation during the pandemic has been linked to negative outcomes for older adults such as depression (Krendl & Perry, 2021; Robb et al., 2020), sleep problems (Grossman et al., 2021), and anxiety (Robb et al., 2020). Feeling stressed or alone is associated with non-adherence with physical distancing recommendations (Coroiu et al., 2020). Experts have also expressed concern that physical distancing and isolation will lead to increased incidences of suicide among the elderly, and suggest interventions targeting social isolation can play a role in suicide prevention (Sheffler et al., 2021; Wand et al., 2020). Pandemic restrictions have also been associated with increased sedentary behaviour and decreased levels of exercise for older adults (Gutman et al., 2021; Richardson et al., 2020).
2. Literature review: challenges faced by older adults during the pandemic related to social isolation
In this section
2.1 Social isolation and vulnerable sub-populations of older adults
2.1.1 People living with dementia
The COVID-19 pandemic has exacerbated the vulnerabilities of people living with dementia. Sources of care and social support have been reduced due to lockdown measures (for example, closure of health and community services, diversion of resources and efforts towards the pandemic, restrictions on contact with family and friends) (Alonso-Lana et al., 2020; Roach et al., 2020). People living with dementia may find it difficult to understand and comply with physical distancing and lockdown measures. Increases in neuropsychiatric symptoms (such as agitation, anxiety, depression) have been observed during the pandemic (Manca et al., 2020; Rainero et al., 2021; Roach et al., 2020). For example, an Italian survey of caregivers of people living with dementia found 55% reported declining cognitive functions of care recipients and 52% worsening of behavioural symptoms (Rainero et al., 2021). Furthermore, 69% of residents in LTC have dementia (Canadian Institute for Health Information [CIHI], 2018), and as described previously the majority of COVID-19 deaths have taken place in LTC.
2.1.2 Ethnic minority and immigrant older adults
Analysis of neighbourhood mortality rates by Statistics Canada (2020a) suggests that COVID-19 infection rates are 3 times higher in ethnically diverse neighbourhoods and mortality rates are 2 times higher. Survey data from Statistics Canada (2020a) also suggests minority group members are experiencing higher unemployment rates and greater financial challenges due to COVID-19 compared to the general population. People of Asian visible minority groups have reported experiencing increased harassment and discrimination (Statistics Canada, 2020a). The pandemic has worsened the already existing disparities in health and access to services for ethnic minority and immigrant groups in Canada (Wang et al., 2019). Researchers from the US suggest that the social networks of minority groups are more likely to be disrupted by the pandemic (for example, higher COVID-19 mortality rates, disruptions to religious and cultural activities, less likely to use technology) (Gauthier et al., 2020).
To help ensure equity, it has been suggested that social isolation interventions should be developed with vulnerable and minority groups (Dassieu & Sourial, 2021). For example, participation at places of worship and religious activities are particularly important for some ethnic minority groups and should be incorporated into pandemic interventions (Chatters et al., 2020; Gauthier et al. 2020; Giwa et al., 2020). Religious organizations can work with their community members to offer remote outreach, support, and services to older adults (Chatters et al., 2020).
2.1.3 Rural, remote, and northern communities
Older adults living in rural and remote communities face unique circumstances that present additional pressures during the pandemic: limited access to health care services; housing that is overcrowded, older or of poor quality; communities that are facing economic insecurity; less access to technology and high-speed internet services; and limited infrastructure to assist with daily tasks (for example, grocery shopping, transportation) (Henning-Smith, 2020). These circumstances pose challenges for pandemic responses and also mean these communities may face greater challenges when recovering from the pandemic (Henning-Smith, 2020). Furthermore, activities and services for older adults in rural areas are often offered by small seniors clubs and groups with limited funds and resources. For example, on Prince Edward Island, logistical challenges such as regular meeting spaces being unavailable or too small for social distancing and being unable to afford to heat buildings without fundraising gatherings create challenges for in-person activities, while at the same time lack of access to digital infrastructure make virtual activities impractical in many areas. Some groups have adapted by, for example, decreasing the size of activities and not serving food in order to safely hold activities in-person (personal communication, P.E.I. Senior Citizens' Federation).
However, the more tight-knit nature of rural communities is a strength, and older Canadians living in rural communities report higher levels of social support than urban residents (Frank, 2020). For example, in Clarenville, Newfoundland, the town and local groups and organizations have taken steps to support the community during the pandemic such as: organizing physically distanced hikes, creating an outdoor skating rink and sliding area, offering free grocery delivery, and running a free pancake breakfast each week (with takeout options) (personal communication).
While Northern communities have seen limited cases of COVID-19 for most of the pandemic, the lack of health care infrastructure makes them particularly vulnerable to the impacts of outbreaks if they occur. Older adults living in Northern communities face similar circumstances as those described above for rural and remote communities, but also may face additional concerns such as food insecurity, fragile supply chains, access to water for handwashing and cleaning, housing shortages and overcrowding, and high rates of tuberculosis (Arctic Council, 2020; Fryer & Collier, 2020; Inuit Tapiriit Kanatami, 2020).
2.1.4 Indigenous peoples
Pre-existing vulnerabilities such as geographic isolation, lack of access to medical and community care, and high rates of chronic conditions make COVID-19 a disease of particular concern for Indigenous communities in Canada (Statistics Canada, 2020b). In response to the pandemic, many Indigenous people are drawing upon traditional practices and culture and taking steps to protect their elders and communities. For some Indigenous peoples, isolation of the community or family groups is a traditional practice that has been used in the past to safeguard the wellbeing of the community. Rules on community entry, self-isolation trailers, and family groups returning to the land are examples of ways Indigenous peoples have responded to the pandemic (Banning, 2020; NCCMT & NCCIH, 2020).
The pandemic has had a significant impact on cultural activities since it has not been possible to hold large cultural gatherings and elders are not able to participate in regular intergenerational and cultural activities (Assembly of First Nations, 2020). It is important to acknowledge that past bans on Indigenous cultural and spiritual ceremonies were a source of trauma for Indigenous peoples (First Nations Health Authority, 2020). During the pandemic, the First Nations Health Authority (2020) has suggested embracing alternative or adapted cultural activities such as: spending more time on the land; connecting to the Creator; modifying ceremonies or cultural practices so they follow COVID-19 guidelines or holding them with only your household; and providing bagged lunches rather than shared meals at small events. It has also been suggested that sustained COVID-19 funding should be provided to encourage participation in on the land activities and continued connection to culture (Assembly of First Nations, 2020).
As we move into the vaccine phase of the pandemic response, resistance to mainstream health care may pose a challenge in some Indigenous communities due to historical negative experiences (Funnell, 2021). Indigenous communities have been prioritized in the vaccine roll-out, and many communities have relied on key opinion leaders and elders in the community to support vaccine compliance and uptake.
2.1.5 LGBTQ2
Lack of social support and isolation, past traumas and experiences of discrimination, and disparities in health and access to health services contribute to an increased level of vulnerability for LGBTQ2 older adults during the pandemic (Jen et al., 2020). However, past experiences living through the HIV and AIDS pandemic are a potential source of resilience, with lesbian, gay, and bisexual older adults reporting feeling prepared and more ready to act during the COVID-19 pandemic as a result of their past experiences (Gutman et al., 2021).
Based on survey data collected during the pandemic, Gutman et al. (2021) found no differences in reported levels of loneliness between lesbian, gay, and bisexual and heterosexual Canadians aged 55 and up; however, lesbian, gay, and bisexual Canadians reported worse mental health (such as depression, anxiety, and sadness) than the general population. They also were more likely to have no one to turn to if they needed help, suggesting an increased need for practical help during the pandemic.
2.1.6 Caregivers
The pandemic has increased the pressures being placed on informal caregivers in Canada (for example, providing more hours of care, decreased social support, difficulties accessing health care services) (Anderson & Parmar, 2020; Ontario Caregiver Organization, 2020). A survey of Ontario caregivers found 43% often feel isolated and lonely, while a survey in Alberta found 86% of caregivers have experienced loneliness since the pandemic began (Anderson & Parmar, 2020; Ontario Caregiver Organization, 2020). Analysis of data from a large study in the United Kingdom (UK) found that higher levels of loneliness during the pandemic resulted in a 4 times higher risk of depression for caregivers (Gallagher & Wetherell, 2020).
2.1.7 Low-income older adults
As many services and programs transition to virtual modes of delivery during the pandemic, low-income older adults are particularly at risk of isolation as they may not be able to afford access to digital technology and high-speed internet (Conroy et al., 2020). Data from Statistics Canada shows only a little over half of low-income Canadians use the internet (Davidson & Schimmele, 2019), creating a “digital divide” (a term referring to the divide in uptake and access to digital technology). Low-income older adults also report having less social support available than other older adults (Frank, 2020).
2.2 Social isolation and community-dwelling older adults
2.2.1 Respect and social inclusionFootnote 5
Ageism and the risks of treating older adults as a homogeneous group
During the pandemic, both positive (for example, community initiatives to support older adults, building social connections) and negative (for example, ageism, discrimination in the healthcare system) responses towards older adults emerged (Monahan et al., 2020). Positive responses promote intergenerational solidarity and positive views about aging, while negative responses can cause immediate harm (such as neglect of older adults in LTC) and also have potential long-term impacts on attitudes towards aging (Monahan et al., 2020). Ageism can increase feelings of loneliness and social isolation among older adults and is a risk factor for lower number and quality of social relationships (WHO, 2021). During the pandemic, negative self-perceptions of aging have been associated with loneliness and psychological distress (Losada-Baltar et al., 2021). Ageism has also been associated with higher levels of anxiety during the pandemic (Bergman et al., 2020a).
Experts state that the portrayal of older adults as a homogeneous, vulnerable group during the pandemic has intensified ageist views and intergenerational tensions (for example, Ayalon, 2020; Fraser et al., 2020; Meisner, 2020; Wister & Speechley, 2020). COVID-19 has been presented as primarily a problem for older adults, rather than a shared societal challenge (Ayalon, 2020; Fraser et al., 2020). An experiment conducted by Yildirim (2020) highlights the negative effects of such messaging. Participants who viewed a video framing the pandemic as primarily a risk to older adults were more likely to perceive the pandemic as posing little risk to themselves and were more likely to favour saving the economy over human lives.
New forms of age segregation, but intergenerational connections are emerging
The pandemic has also increased age segregation within communities, with few opportunities for older adults to safely interact with younger generations (Burke, 2020). A report from the UK highlights the challenges intergenerational programs are facing during the pandemic: the closure of intergenerational spaces, the digital divide, challenges adapting programs to the digital world, and narratives about conflicts between generations (InCommon & Clarion Futures, 2020).
Intergenerational activities have been recommended as a means to reduce feelings of social isolation (Day et al., 2020; Jopling, 2020). Intergenerational contact and friendships can also protect against ageism (WHO, 2021). As highlighted in the annexes, many programs to reduce social isolation among older adults during the pandemic have intergenerational components. Befriending programs in particular have sought to forge connections between older and younger generations (consult Annex 2). While there has been limited evaluation of the intergenerational programs implemented during the pandemic, recent systematic reviews suggest potential benefits for loneliness and social isolation though the evidence to-date is quite limited (Peters et al., 2021; Zhong et al., 2020). It is also encouraging that there have been many grassroots initiatives and expressions of intergenerational solidarity during the pandemic (Burke, 2020; Fraser et al., 2020; Morrow-Howell, 2020). The pandemic has also motivated families to make greater and more sustained efforts to stay in contact and connect with each other (Hwang et al., 2020; Morrow-Howell, 2020).
Concerns that the pandemic is increasing vulnerabilities to elder abuse
Social isolation is a key risk factor for elder abuse (Pillemer et al., 2016). Experts have expressed concerns that circumstances during the pandemic such as physical distancing, closures of sources of social support, the increased dependency of older adults, pressures on caregivers, financial uncertainty, and escalating ageism will increase the risks of elder abuse (Elman et al., 2020; Han & Mosqueda, 2020; Makaroun et al., 2021). Organizations in the US that support elder abuse victims have adapted to the pandemic by offering remote services and conducting telephone outreach to vulnerable older adults (Elman et al., 2020). D’cruz and Banerjee (2020) have advocated for the development of helplines for elder abuse reporting, information provision, and emotional support. In Canada, helplines and telephone programs provide older adults with a range of information and supports, including information on elder abuse (consult Annex 3).
2.2.2 Housing
Older adults living alone are particularly at risk
Research suggests that older adults living alone are more likely to experience increased loneliness during the pandemic (Emerson, 2020; Savage et al., 2021). Data from Statistics Canada shows older adults living alone are less likely to have social support available (Frank, 2020), suggesting a greater need for practical help. Analysis of survey data by Fingerman et al. (2020) suggests that during the pandemic US older adults living alone primarily have relied on increased contact with friends. While Fingerman et al. (2020) found in-person contact had a positive effect on older adults living alone, speaking on the telephone resulted in negative effects, possibly because it made older adults more aware of their isolation. More research is needed to better understand these patterns.
Risks in social housing settings
Low-income older adults living in social housing (many of whom live alone) have also been identified as a vulnerable group during the pandemic (Archambault et al., 2020; Pirrie & Agarwal, 2021). However, social housing settings provide the opportunity to reach many vulnerable older adults with interventions (consult annexes for examples). Some of the recommendations for supporting older adults in social housing include identifying high-risk buildings and populations; delivering food and essential supplies; developing communication systems to keep residents informed; ensuring safety protocols for common areas; providing safe opportunities for social activities; and ensuring access to the internet (Archambault, 2020; Pirrie & Agarwal, 2021).
Risks in non-institutional congregate living settings
While less policy attention has been paid to non-institutional congregate living settings (for example, assisted living, continuing care retirement communities, independent living communities) than LTC, many of the residents are vulnerable to COVID-19 and there are limited regulations and guidance for their safety (Coe & van Houtven, 2020; Zimmerman et al., 2020). A large British Columbia (BC) survey found that 57% of assisted living residents were confined to their room at some point during the pandemic (Office of the Seniors Advocate British Columbia, 2020) (consult section 2.3.1 for description of the negative impacts of isolation in LTC or assisted living settings). These types of housing operate based on social models of care, and residents are used to high levels of autonomy, regular excursions outside of the facility, and frequent social interactions. As a result, COVID-19 restrictions may be particularly challenging for residents to adapt to (Zimmerman et al., 2020). Experts suggest non-institutional congregate living settings can help residents to stay connected by offering scheduled times to use shared technology, organizing virtual group activities, providing one-on-one support, and involving residents in decision-making about COVID-19 restrictions (Gray-Miceli et al., 2020; Hill et al., 2020; Zimmerman et al., 2020).
2.2.3 Community support and health services
Community support and health services are adjusting to the pandemic
As a result of the pandemic, disruptions have occurred to regular community support and health care services, cutting off older adults from important sources of social support (Meisner et al., 2020; Morrow-Howell, 2020). For example, in a survey of Alberta caregivers 48% reported reductions in publicly subsidized home care services due to the pandemic (Anderson & Parmar, 2020). Home care workers can be an important source of social interaction for older adults, and prior to the pandemic, research has found unmet home care needs are associated with higher levels of loneliness (Kadowaki et al., 2015).
Many community and health organizations have been quick to transition services to virtual and telephone models, though these are not workable alternatives for all older adults. Lam et al. (2020) estimate that in the US 38% of older adults are unready for video-based visits (primarily due to physical disabilities and technological challenges) while 20% are unready for telephone visits (primarily due to physical disabilities). PHAC (2020) recommends both digital and low-tech telephone health care appointments be made available. Some evidence-based health promotion interventions have also transitioned to remote delivery (consult Annex 4). While programs such as Choose to Move and Minds in Motion have not been assessed in the remote format, previous evaluations suggest they positively impact loneliness and mental wellbeing (Franke et al., 2021; Regan et al., 2017). For some older adults, home visits by health professionals may also be appropriate to provide health care services, as well as to initiate health promotion initiatives (Carr et al., 2020; Day et al., 2020).
Social prescribing programs as an emerging practice
In recent years, social prescribing programs where health professionals refer patients to community navigators who assist them to access community supports and services have been an emerging trend to reduce social isolation. In Ontario, a pilot of social prescribing programs at 11 community health centres conducted over 2018 to 2019 found 49% of clients reported decreases in loneliness (Alliance for Healthier Communities, 2020). As described in Annex 4, during the pandemic social prescribing programs have been used to connect vulnerable older adults with needed services and social supports.
Importance of mental health supports during the pandemic
Mental health support for older adults and their caregivers is crucial during the pandemic. In Canada, many mental health and caregiver organizations have been able to move their services online and offer telehealth, online support groups, and peer-based counselling (Flint et al., 2020) (consult Annex 4 for examples). Prior to the pandemic providing caregiver supports online was an emerging practice, and a review of these programs found feeling less alone was a benefit of participation (Armstrong & Alliance, 2019). For some older adults, loneliness may be psychologically-based, in which case one-on-one counselling, meditation, cognitive behavioural interventions, and other psychosocial interventions are needed (Conroy et al., 2020; Van Orden et al., 2020). It also has been suggested that health professionals can assist older adults to develop “Connection Plans” to plan how they can maintain social contact (Van Orden et al., 2020). Mental health is an especially challenging barrier for older adults who have lost a loved one to COVID-19 since it intensifies other problems. Virtual funerals, remote support from hospice workers and volunteers, and peer support or friendly telephone calls are suggested to help older adults to cope with their loss and reduce feelings of loneliness (Carr et al., 2020).
High levels of demand for practical assistance
Practical assistance is an important need for vulnerable older adults, who may feel unsafe going out in the community or be cut off from regular sources of social support. During the pandemic, the New Horizons for Seniors Program (NHSP) and Emergency Community Support Fund (ECSF) have both provided substantial funding to community agencies to provide services to support vulnerable older adults (for example, grocery delivery, outreach to address social isolation) (United Way Centraide Canada, 2020a; 2021). The Province of British Columbia and the City of Edmonton are 2 regions where large-scale coordinated responses were implemented to meet the needs of older adults (consult Annex 5 for more details). In British Columbia, Safe Seniors, Strong Communities provides older adults across the province with access to check-ins, grocery shopping, meal delivery, and prescription delivery (Hannah, 2020). In Edmonton, a coordinated pandemic response focusing on 3 areas (food and transportation, outreach and friendly checks-ins, and psychosocial support) was implemented to identify gaps, develop or expand needed programs, and facilitate referrals between organizations (Coordinated Pandemic Response Steering Committee, 2020).
Programs providing practical assistance often include social components. For example, volunteers delivering meals or groceries can provide friendly conversation and information to isolated older adults. Although the evidence is limited, findings from 2 pre-pandemic US studies suggest that meals on wheel style programs can be effective at reducing loneliness among older adults (Thomas et al., 2016; Wright et al., 2015). Practical assistance programs can also help older adults to care for their pets (for example, buying pet food, walking dogs) who provide an important form of companionship for isolated older adults (Rauktis & Hoy-Gerlach, 2020). Practical assistance programs have made various adaptations to their procedures and operations in order to continue to safely provide services during the pandemic.
2.2.4 Transportation
Declining use of public transportation services during the pandemic
While many activities have moved online during the pandemic, it is still essential that older adults have options available for travelling outside of the home to meet their daily and social needs. However, at advanced ages, many older adults do not drive and public transportation, volunteer driver programs, and ridesharing options all carry a degree of COVID-19 risk (DeLange Martinez et al., 2020).
Surveys conducted in the early months of the pandemic with frequent transit users found 55% of older adult transit users in Toronto and 54% in Vancouver stopped using transit during the pandemic (Palm et al., 2020a; 2020b). Research from the Older Adults’ Centres Association of Ontario (OACAO) suggests only 37% of transit users would feel comfortable using public transportation to travel to an older adult centre during the pandemic (OACAO, 2020).
Municipal and community transportation programs
In the US, some municipalities have implemented shuttle services especially for older adults with enhanced safety measures as an alternative to public transportation (DeLange Martinez et al., 2020). Numerous volunteer driver programs for older adults are continuing to operate in Canada during the pandemic, but some are struggling with volunteer recruitment as they often rely heavily on older adult volunteers (for example, CBC News, 2021; Weldon, 2020). Some transportation programs have also implemented or enhanced grocery and meal delivery programs to assist older adults who are choosing to isolate themselves at home, as described in the previous section (consult Annex 5).
2.2.5 Communication and information
Growing internet and digital technology use by Canadian older adults
Internet use by older Canadians has been steadily increasing over time. Statistics Canada reports that use of the internet by older adults increased from 32% to 68% over 2007 to 2016; however, there is a significant age gradient as less than half of those aged 80 and up use the internet (Davidson & Schimmele, 2019). Data collected during the pandemic suggests older adults are continuing to become more comfortable with digital technology, although an age gradient remains:
- a poll of Canadian older adults found that 88% use the internet daily, 65% own a smartphone, and 72% feel confident using technology. Increases in the use of video calls, social media, online activities, and food delivery services were reported due to the pandemic (AgeWell NCE., 2020a)
- according to CLSA (2021) data, 83% of older adults isolating at home used the telephone to stay in contact during the pandemic, 48% video calls, and 44% social media. Significant age gradients existed for the use of video calls and social media, with those aged 85 and up the least likely to use them (for example, 64% of people 65 to 74 used video calls compared to 31% of those 85 and up)
With the growing use of digital technology by older Canadians, video calls and social media have been incorporated into interventions to reduce social isolation. Video call technologies (for example, Facebook Messenger, Zoom, etc.) can be used both to connect with family and friends, as well as to participate in group meetings and activities (AgeWell NCE., 2020b; Conroy et al., 2020). Social media sites can be used to maintain and build social networks (Conroy et al., 2020). Reviews of the impacts of digital technology use on older adults suggest it has positive impacts on components of social isolation (such as increasing contact with family, intergenerational relationships), but evidence of the impacts on loneliness has been less consistent (Chen & Schulz, 2016; Damant et al., 2017; Ibarra et al., 2020). The associations specifically between social media and social isolation are unclear, as Hajek and König (2020) reviewed the small amount of literature on this topic and found only 1 study reported reductions in social isolation scores for older adults. There are also many resources available on the internet that can help to connect older adults to needed services and supports (for example, the Islanders Helping Islanders Volunteer Services Directory on PEI, Volunteer NS in Nova Scotia).
Barriers and facilitators of digital technology adoption
Benoit-Dubé et al. (2020) and Gorenko et al. (2021) have highlighted potential barriers and facilitators of digital technology adoption for older adults during the pandemic:
- perceived benefits of using the technology
- access to and affordability of the technology
- attitudes, self-confidence, and knowledge about using technology
- whether the technology is suitable for people experiencing physical and cognitive declines
- whether assistance is available from others (for example, family, staff, technical support) to use the technology
In a survey of municipal, community, and health organizations in Ontario, the most common barriers for technology use by older adults that organizations reported were limited access to the internet, lack of knowledge on the use of technology, and the need for assistance with setting up technology (Ontario Age-Friendly Communities Outreach Program, 2021a).
A digital divide continues to exist in Canada
While the majority of older Canadians use digital technology, researchers have identified segments of the population who are less likely to use or have access to high-speed internet and digital technology. These populations include low-income older adults (Conroy et al., 2020; Davidson & Schimmele, 2019); people living in rural, northern, and Indigenous communities (Conroy et al., 2020; Ryerson Leadership Lab, 2021); and older adults with physical disabilities or cognitive impairments that present challenges for using technology (Lam et al., 2020; Lee & Miller, 2020). For people without access to home internet, public spaces such as libraries and community centres are often used to access the internet, but many of these have been closed during the pandemic (Ryerson Leadership Lab, 2021). Furthermore, digital technology options may not be well suited to meet the needs of older adults who are unfamiliar with digital technology, have lower literacy levels, or are from linguistic minority groups (Hebblethwaite et al., 2020).
Digital technology training and access are needed to overcome the digital divide
To overcome the digital divide, there is a need for digital technology education and training programs for older adults, as well as access to low-cost technology and high-speed internet services (Conroy et al., 2020; Day et al., 2020; Science and Technology for Aging Research, 2019; Sixsmith, 2020; Son et al., 2020). In the US, to ensure equity in access to digital technology, some communities have developed digital inclusion plans (for example, offering low-cost internet and affordable devices, providing tech support in multiple languages) (DeLange Martinez et al., 2020). Programs that provide training and access to digital technologies are being implemented or expanded in Canada (consult Annex 6). In Nova Scotia, prior to the pandemic, the government provided funding for internet and digital literacy pilots for community-dwelling older adults, including programs targeting Indigenous and African Nova Scotian communities. An evaluation of a pre-pandemic tablet training program for older adults in Ontario found the program improved attitudes towards technology and use, but no changes for loneliness or social isolation were observed (Neil-Sztramko et al., 2020). However, the results of the study were likely hampered by its small sample size. During the pandemic, a study by Rolandi et al. (2020) in Italy found older adults who had completed a social networking course prior to the pandemic were less likely to report feeling left out, though no differences in loneliness were observed.
With increasing digital technology use, it is vital to ensure that older adults are aware of potential technology-related frauds and scams. In the US, older adults are increasingly being targeted with tech support, text messaging, and internet service scams (Payne, 2020). It is also important to educate older adults about the importance of examining the quality and accuracy of online information since Statistics Canada data shows people aged 55 and up are the most likely to share COVID-19 misinformation online (Garneau & Zossou, 2021).
Low-tech interventions remain important for reaching isolated older adults
For some older adults, low-tech telephone-based interventions may be the most practical and appropriate options (for example, if the older adult prefers not to use computers, lacks access to high-speed internet, etc.) (Conroy et al., 2020). A review of the pre-pandemic literature found social activities, educational sessions, and befriending programs can be successfully conducted over the telephone (Gorenko et al., 2021).
Many telephone help and information lines have received enhanced funding during the pandemic due to high call volumes. For example, funding from the federal government has expanded 211 telephone information and referral services to all jurisdictions in Canada (United Way Centraide Canada., 2020b). Telephone lines and telephone outreach programs can provide friendly conversation and play an essential role in connecting older adults to organizations offering services to reduce social isolation (consult Annex 3). Pre-pandemic, interviews with staff and users of a seniors helpline in the UK revealed that older adults often called the helpline to seek friendly conversation and alleviate loneliness (Preston & Moore, 2019). During the pandemic, reported benefits of telephone outreach programs in the US have included positive emotions and connecting older adults to needed services (Office et al., 2020; Rorai & Perry, 2020). Telephone outreach programs also provide volunteer opportunities for older adults, as they can be trained virtually to become telephone volunteers (Lee et al., 2021). Institut national de santé publique du Québec [INSPQ] (2020) notes that in addition to the telephone, additional creative methods should be employed to reach isolated older adults (for example, providing information in the mail, working with health professionals and essential services to coordinate outreach).
2.2.6 Social participation
There has been a shift to remote modes of social participation
The COVID-19 pandemic has disrupted the operations of senior centres, fitness centres, libraries, restaurants, and many other places older adults go to participate socially. While some of these places have been able to remain open with safety precautions in place, older adults may still feel uncomfortable visiting them. Many organizations have switched to the remote delivery of services and programs (consult Annex 7). Examples of activities that can be offered remotely include book clubs, discussion groups, social games, creative arts, group health promotion initiatives, lectures, and virtual tours and cultural opportunities (Day et al., 2020; Hebblethwaite et al., 2020; INSPQ, 2020; Son et al., 2020).
Evaluations of virtual programs for older adults conducted prior to the pandemic suggest that they can reduce social isolation (Botner, 2018; Gorenko et al., 2021). The OACAO (2020) conducted a province-wide survey of participants at older adult centres and found 35% were now participating in virtual programming. For those who did not participate in virtual programs, the main reasons were lack of interest (52%) and discomfort with using the technology (32%). Cohen-Mansfield et al. (2021) conducted a telephone survey of older Israelis on their participation in Zoom activities during the pandemic. They identified physical activity, social interaction, and relief from boredom and loneliness as the central factors influencing participation. Key factors leading to non-participation included awareness, technological difficulties, and convenience of program times and dates.
Rapid spread of the Senior Centre Without Walls model
Senior Centre Without Walls (SCWW) is a model of offering remote programs (either by telephone or virtually) that has been widely adopted by community and non-profit organizations in Canada during the pandemic (consult Annex 7 for examples). The first SCWW in Canada was launched in Manitoba in 2009 by the organization A & O: Support Services for Older Adults and provided isolated older adults with access to telephone-based social and educational activities. A process evaluation of the program found that it was successful in reaching isolated older adults and participants felt more connected and less lonely (Newall & Menec, 2015). The SCWW at Edmonton Southside Primary Care Network (no date) is another pre-pandemic SCWW, and a pre- and post-evaluation of the program found statistically significant declines in loneliness scores (for high users of the program) and declines in anxiety and depression scores. Over half of participants also reported making new friends due to the program. Prior to the pandemic, the Government of Alberta provided a grant to the Edmonton Southside Primary Care Network to work with other communities to expand the SCWW model in the province. The Government of Ontario has provided $467,500 to the OACAO to disburse as micro-grants to support the development of SCWW programs during the pandemic.
Befriending programs are an emerging trend
Befriending programs have commonly been implemented by community members and non-governmental organizations to reduce the social isolation of older adults during the pandemic (consult Annex 2). In befriending programs, volunteers regularly engage in friendly visits with older adults (most programs have switched to remote visiting). An evaluation of a 6-week program implemented in the US during the pandemic found both students and older adults reported benefits and 66% of pairs continued to stay in contact after the program ended (Joosten-Hagye et al., 2020). Previously, in an evaluation of a UK telephone befriending program older adults reported the alleviation of loneliness and isolation as an outcome of participation (Cattan et al., 2011).
Encouraging physical activity during the pandemic
Due to the evidence linking higher levels of physical activity with better immune system function, reduced opportunities to participate in physical activities during the pandemic is an important concern (Damiot et al., 2020; Scartoni et al., 2020). Gutman et al. (2021) found that 37% of Canadians 55 and up reported declining levels of exercise during the pandemic. While there are various exercise videos available online, recreation staff can also offer online classes to provide opportunities for social connections (Son et al., 2020). Older women particularly would benefit from online classes, since past research suggests they prefer to exercise in social settings (Gutman et al., 2021). It has also been suggested that the feel of community can be created for people participating in individual physical activities, for example, by setting group goals or holding friendly competitions (Son et al., 2020; Hwang et al., 2020). Consult Annex 4 for examples of remote and outdoor physical activities during the pandemic.
Community and non-profit organizations are facing challenges adapting to the pandemic
While community and non-profit organizations are continuing to offer many programs and services to reduce the social isolation of older adults, there have been challenges adapting to the pandemic. While many programs and services can be retrofitted for remote delivery, organizations must repurpose staff and secure funds to adapt programs (Smith et al., 2020; Xie et al., 2020). The OACAO (2020) survey found that older adult centres are facing unique challenges during the pandemic, including: reduced revenue from membership and activity fees; access to liability insurance; the costs of implementing needed safety measures; the need for guidelines for high-risk programs; and overcoming the digital divide, and developing virtual programs of interest to their members. In Edmonton, interviews with Coordinated Pandemic Response members revealed that, while the pandemic has resulted in many new partnerships and successful transitions to virtual programming, for some organizations it has also resulted in funding shortages and staff layoffs (Coordinated Pandemic Response Steering Committee, 2020). In BC, interviews with members of the community-based seniors services sector uncovered strengths of the sector that have enabled effective responses to the pandemic, such as: familiarity with the needs of older adults in their community, the ability to deliver responsive and tailored programming, and strong relationships and partnerships. However, challenges for the sector have also emerged, including: staff burnout, a heavy reliance on volunteers, and concerns about the sustainability of funding for the future (United Way of the Lower Mainland [UWLM] & Dialogues in Action [DIA], 2021). In some jurisdictions, online platforms have supported knowledge exchange and learning among community and non-profit organizations about effective interventions and adapting services to the pandemic (consult Annex 8).
2.2.7 Civic participation and employment
Older workers have experienced disruptions to their employment
For older workers, employment can provide important opportunities for social interaction. CLSA (2021) data from older workers shows that 21% of their workplaces were completely closed during the pandemic, while 49% were partially closed. Over the course of the pandemic, the unemployment rate for workers aged 55 and up has increased from 4.5% to 7.9% (in comparison, the unemployment rate for core aged workers 25 to 54 is 7.0%) (Statistics Canada, 2021). Experiences from prior recessions suggest that unemployed older adults will experience more difficulties re-entering the workforce when the pandemic ends (Morrow-Howell, 2020). Key considerations related to older workers include: capacity of older adults to telework; health and safety concerns; providing accommodations for workers at high risk of COVID-19; and potential discrimination in hiring and layoff practices (Monahan et al., 2020; Morrow-Howell, 2020).
Declining engagement by many older volunteers during the pandemic
In 2018, approximately 4.6 million Canadian volunteers were Baby Boomers or older, and these volunteer cohorts provided the most hours on average (Hahmann et al., 2020). While some organizations have scaled up their volunteer activities during the pandemic, others have experienced disruptions to their volunteer operations (Volunteer Canada, 2020; UWLM & DIA, 2021). Declines in volunteer engagement for some organizations have occurred due to age and health-related concerns, the discontinuation of programs, and the shift to remote models of volunteering. A survey by Volunteer Canada (2020) found that currently 26% of active and 41% of inactive volunteers are aged 65 and up. Additionally, the CLSA (2021) found 72% of participants reported a decrease in their regular number of volunteer hours per week.
Organizations need to adjust volunteering opportunities for older adults
Volunteering has been suggested as a means for older adults to maintain social connections during the pandemic as well as potentially help other older adults (Wu, 2020). Sin et al. (2020) studied Canadian and American adults during the pandemic and found that older adults who volunteered formally exhibited higher levels of positive emotions and social satisfaction. A key challenge for volunteer managers is how to safely support older adults to return to volunteering (for example, additional training, supervision to ensure safety protocols are followed) (Grotz et al., 2020). Alternative volunteering opportunities can be offered to older adults such as telephone support, writing for local newspapers, and engaging in skills-based activities at home (like sewing masks) (DeLange Martinez et al., 2020; Son et al., 2020). Another challenge is how organizations can support volunteers who are inactive due to the pandemic (Grotz et al., 2020). Volunteer organizations have attempted to address some of these pandemic-related challenges. For example, to support the non-profit sector and volunteerism during the COVID-19 pandemic, Volunteer Alberta has produced resources on volunteering during COVID-19, virtual volunteer engagement, fundraising, and financial assistance.
2.2.8 Outdoor spaces and buildings
Steps are being taken to facilitate participation in outdoor activities
During the pandemic, outdoor activities have been recommended as a way for older adults to continue to engage in physical activities and interact socially at a safe distance (for example, DeLange Martinez et al., 2020; Hwang et al., 2020). In Canada, 82% of older adults report they have a park close to their home, though in the early stages of the pandemic many parks were closed by governments (Dewis, 2020). While the outdoors is a safer place for activities, older adults may still feel uncomfortable as many people do not wear masks outside (DeLange Martinez et al., 2020). To decrease the risk of COVID-19 transmission, the Government of Canada (2020b) has recommended that dedicated times be provided for older adults to access parks or participate in outdoor activities. Age-friendly communities, walkable neighbourhoods, and shared community spaces can also create spaces for friendly interactions while safely maintaining physical distancing (DeLange Martinez et al., 2020; INSPQ, 2020). For example, communities can seek to maximize the availability of outdoor green and community spaces by reorganizing streets to increase the room for pedestrians and cyclists (INSPQ, 2020).
Preparing for the eventual re-opening of buildings and public spaces
Many community and recreation spaces have closed during the pandemic, although with the development of COVID-19 vaccines it will likely be possible to re-open some buildings in the near future. In the OACAO (2020) survey the most common strategies older adults suggested for the safe re-opening of older adult centres were: providing hand sanitizer, requiring the use of masks, running classes of less than 10 people, daily COVID-19 screenings, and reducing building capacity. Older adults identified fitness programs as the number one type of program that should be prioritized in re-openings.
2.3 Social isolation among older adults residing in long-term care facilities
This section focuses specifically on issues related to social isolation in LTC facilities, although it is important to acknowledge that the pandemic has exposed a range of longstanding systemic issues within LTC (for example, see Estabrooks et al., 2020; Long-Term Care and Covid-19 Task Force, 2020). While beyond the scope of this report, many of these systemic issues (for example, staffing levels and mix, financing) have implications for the ability of the LTC sector to support social connections for residents during a pandemic.
2.3.1 Negative impacts of restrictions on visitors and socialization in LTC
In LTC facilities, social connection has been linked to positive mental health outcomes such as less depression, more verbal expressions, and better mood and emotions (Bethell et al., 2020). Survey data suggests Canadian LTC residents have experienced significant negative impacts due to pandemic restrictions. In BC, over the time period in which the strictest LTC visitor restrictions were in place, 61% of family members reported they believed the condition of their loved one worsened significantly (Office of the Seniors Advocate British Columbia, 2020). In an Alberta survey of LTC residents, 75% reported experiencing stress, anxiety, or depression due to being unable to visit with loved ones (Health Quality Council of Alberta, 2021). During the pandemic, having fewer contacts with friends and family has been associated with higher rates of depression in Canadian LTC homes (CIHI, 2021).
Residents who do not speak English or French are particularly vulnerable to experiencing social isolation, as they rely heavily on family, visitors, and other residents who speak their language for companionship and to communicate with staff (Shippee et al., 2020).
2.3.2 Visitor restrictions and policies
LTC visitor restrictions have been implemented in most jurisdictions
LTC residents tend to be complex patients with pre-existing conditions that place them at higher risk of serious COVID-19 disease complications and death. In the initial periods of the pandemic, most jurisdictions enacted visitor policies that tightly restricted the ability of caregivers, family, friends, and others (for example, volunteers, paid companions, entertainers) to visit older adults residing in LTC facilities. There have been variations, for instance, some jurisdictions allowed for 1 or more essential or designated visitors, but usually the essential or designated visitor was a family caregiver who was involved in providing care to the resident. Exceptions were also sometimes made for compassionate care visitors. (Consult Stall et al., 2020 for an overview of policies from July 2020).Footnote 6 Footnote 7
It is acknowledged that, while restricting visitors to LTC has a significant role to play in preventing COVID-19 transmission, policies have been critiqued. These critiques entail: being too strict, unclear and poorly communicated, failing to acknowledge the important role of family members as care partners, and being implemented with little input from residents and family or friend visitors (for example, Office of the Seniors Advocate British Columbia, 2020; Tupper et al., 2020). Based on a review of the visitor policies of the 13 provinces and territories and consultation with experts, family caregivers, and visitors, Stall et al. (2020) propose the following core principles for visitor policies:
- policies must differentiate between “family caregivers” and general visitors
- restrictions must balance the risks of COVID-19 with the risks of social isolation
- policies should not be “one-size-fits all” and must prioritize equity, flexibility, and compassion
- LTC facilities must provide regular, transparent, accessible, and evidence-based communication and direction about visitor policies
- data on the re-opening of LTC to visitors should be collected and reported; and
- mechanisms should be established for feedback and rapid appeals
In-person visitation options during the pandemic
A survey by Wammes et al. (2020) in the Netherlands on COVID-19 visitation policies has revealed family members are most satisfied with in-person visits that take place outdoors or indoor visits with physical distancing protocols or barriers. In a BC survey, family members and residents expressed preferences for 2 or more visitors being allowed to visit in-person with physical distancing for 1-hour-long visits a few times a week (Office of the Seniors Advocate British Columbia, 2020). Strong infection prevention and control precautions (for example, screening, testing as appropriate, contact tracing systems, personal protective equipment) are essential for any in-person visits to LTC homes (Bergman et al., 2020b). Common methods to facilitate in-person visits during the pandemic are described below.
- Window visits involve residents and visitors interacting through the windows of the facility; these require conveniently placed windows and a method for communication (such as telephone or whiteboard) (Ickert et al., 2020)
- Physically distanced visits can take place outdoors. Some LTC facilities have purchased tents to protect residents and visitors from the sun and rain (Ickert et al., 2020). However, in Canada snow and cold weather make outdoor visits impractical for significant portions of the year
- In-person visits also may take place in special facilities or rooms where physical barriers (like plexiglass) have been set up. In Manitoba, the Provincial Government committed $17.9 million to build 90 visitation shelters in fall 2020 (consult Annex 9)
- In some cases, LTC facilities may allow in-person visits in residents’ rooms or common areas. In older LTC facilities in Canada, the lack of common areas and frequency of rooms that house multiple residents create challenges for both infection control and facilitating in-person visits (Estabrooks et al., 2020)
In the Netherlands, a study was conducted evaluating the impacts of a policy to allow visitors (1 per resident) back into LTC homes. The study found the visits were very positively received by stakeholders, visitors generally complied with guidelines, and 4 weeks post-introduction there were no new COVID-19 infections (Verbeek et al., 2020).
In order to support the development of promising practices in LTC during the pandemic (including family visitation practices), the Canadian Foundation for Healthcare Improvement (2020) has funded research teams across Canada to participate in the LTC+: Acting on Pandemic Learning Together initiative.
Remote visitation options during the pandemic
Technology (for example, telephone, social media, and video calls) can provide safe alternatives for staying connected to family members and friends. However, there is limited evidence on the effectiveness of these methods for reducing social isolation among LTC residents. A systematic review of pre-pandemic literature by Noone et al. (2020) concluded that video calls had little to no effect on loneliness, depression, or quality of life for LTC residents. There was a small reduction in depression at 1-year follow-up. Under COVID-19 circumstances, it is possible that video and telephone calls may have a greater positive impact on the well-being of residents given the lack of other options for social contact. A study conducted at 7 LTC homes in New Brunswick comparing resident assessment data from 2017 and 2020 during the pandemic found that the proportion of residents with depression decreased from 19.9% to 11.5%. There was little change in the levels of resident social contact and engagement except for in-person visits. The authors suggest that the social isolation interventions implemented (for example, government providing iPads to facilitate video calls, window and outdoor visits, and hiring students to visit with older adults) may have been effective at mitigating the negative influence of the pandemic on certain outcomes (McArthur et al., 2021).
There are key limitations to the implementation and use of technologies in LTC facilities. Challenges related to the use of video calls include the availability of digital devices, older buildings having no WiFi or internet infrastructure, knowledge and ability of residents and family members, and reliance on staff to set-up video calls (Ickert et al., 2020). To overcome the digital divide, some jurisdictions (for example, New Brunswick, Nova Scotia, PEI) have supplied digital devices to LTC facilities (see Annex 9). Challenges also exist with telephone use in LTC facilities; a recent BC survey reported only 41% of LTC residents had a personal telephone and over 85% required help using the phone (Office of the Seniors Advocate British Columbia, 2020). International research on preferences for, and satisfaction with, telephone versus video calls during the pandemic has produced mixed results (Monin et al., 2020; Sacco et al., 2020; Wammes et al., 2020). Yet, “low tech” options may be more easily distributed, especially in areas in which WiFi is not available, or residents are not acquainted with the use of “high tech” options, such as iPads or Zoom, etc.
A rapid review by Institut national d'excellence en santé et services sociaux [INESSS] emphasizes the importance of also supporting caregivers and family members remotely, as they may experience significant distress due to being separated from their loved ones. For example, it is suggested that regular emails or telephone messages about the status of the LTC home should be shared. A primary contact should also be established who can provide regular updates about the wellbeing of residents to caregivers and family members (INESSS, 2020).
Staff support is essential for facilitating in-person or virtual visits
Facilitating resident-family connections (whether they be in-person or virtual) requires a significant amount of time, effort, and increases in disease risk from overburdened staff. Staff are needed to provide regular updates to family members about their loved ones and visitation protocols; schedule visits; set-up technology; train residents and family on technology use; clean and disinfect technology and other items after visits; and accompany residents to locations for in-person visits (Ickert et al., 2020; Verbeek et al., 2020; Wammes et al., 2020). Ickert et al. (2020) estimate that in a LTC home with 100 residents, a minimum of 2 full-time and 1 part-time staff would be required to provide most residents with a once-a-week visit with family for 30 minutes.
2.3.3 Recreation and social activities
Creative approaches have been required to adapt LTC recreation programs
During the pandemic there have been significant disruptions to regular recreational programming, and group-style activities have had to be cancelled or adapted to meet disease protocol policies. Thus, many residents may be confined to their rooms at times during the pandemic (for example, in BC 30% of residents have reported being confined to their room at some point) (Office of the Seniors Advocate British Columbia, 2020). Recreation therapists have adopted creative approaches for programming such as small group activities, hallway bingo, pen pal programs, and virtual entertainment (for example, Bridgepoint Active Healthcare, 2020; Kennedy, 2020). In LTC facilities, recreation staff have also taken a lead role in keeping residents connected with family members; unfortunately, this sometimes leads to less time available to devote to recreational activities (Ickert et al., 2020; McArthur et al., 2020).
A scoping review by Bethell et al. (2020) of pre-pandemic literature identified a variety of recreational activities that have been demonstrated to promote social connection for LTC residents: creative expression programs, exercise, religious and cultural practices, gardening, pet therapy (real or robotic), using technology to communicate, laughter therapy, and reminiscent therapy. Bethell et al. (2020) suggest that such activities can be adapted to COVID-19 circumstances and used as strategies for promoting social connection.
External groups have been offering support to LTC residents
Befriending programs and one-on-one volunteer visits provide important social contact for residents; however, pandemic restrictions have disrupted these programs. Some programs have pivoted to providing virtual or telephone visits, and new programs have been established in response to the pandemic (consult Annex 9). Feedback from staff and volunteers suggests that residents enjoy connecting with volunteers remotely (Fearn et al., 2021; van Dyck et al., 2020). Fearn et al. (2021) make the following key recommendations about remote befriending programs:
- assign a staff member to assist with coordination and scheduling
- ensure technology access and provide set-up assistance for residents
- provide volunteers with training on how to communicate with people with hearing or cognitive impairments
- provide headphones for residents with hearing impairments
- if possible arrange a face-to-face visit or video call for the first visit
- exchange short bios between the residents and volunteers
3. What was learned from this review
In this section
3.1 Lessons learned about supporting older adults during the pandemic
3.1.1 Technology and bridging the digital divide
The pandemic has accelerated the adoption of internet use and digital technologies by older Canadians and the organizations that serve them. There are certain segments of the older adult population who are less likely to be able to adopt these new technologies and as a result of this digital divide are at risk of being further excluded during the pandemic. To address gaps in access, programs have been developed to provide or loan digital devices to older adults and provide training on how to use them. Partnerships with businesses are particularly valuable to support these types of programs due to the costs associated with providing access to digital technology and the internet and the need for technical expertise when setting up or managing devices. An important priority for the future should be ensuring that all Canadians have access to low-cost internet in their home regardless of where they live and free internet in public spaces. While most activities are expected to return to in-person delivery after the pandemic, the trend of increasing digitization will only continue to accelerate in the future.
3.1.2 Diversity of delivery and programming needs
Older Canadians are a heterogeneous population, and as highlighted in section 2.1 sub-populations experience a range of different circumstances that make them particularly vulnerable to social isolation during the pandemic. There is a need for programs that are tailored to meet the linguistic and cultural needs of different population groups and provide safe and inclusive spaces for participation. Programs have been developed to meet the needs of diverse groups such as Inuit elders, LGBTQ2 older adults, and immigrant and visible minority older adults (consult annexes 2 to 7). Interventions also should be delivered via a range of mechanisms (for example, in-person, telephone, virtual, letter, etc.) in response to individual preferences and the pandemic context of different regions.
Based on a literature review and environmental scan of programs to address social isolation, the Ontario Age-Friendly Communities Outreach Program (2021) provides the following tips for developing targeted programs:
- ground the program in a theoretical model
- engage older adults prior to starting a program to recognize the unique needs of the target population
- reach out to organizations serving your target population
- consider the potential impacts of personal (such as ethnicity, comfort with technology, sexual orientation) and environmental factors (for example, access to transportation, available government funding)
- for generic programs, consider how specific sub-populations can be engaged
As well, continually reassessing these components will help ensure the program is responding to the needs of the target population and optimize implementation of the program.
3.1.3 Combatting ageism and supporting intergenerational connections
While the pandemic has worsened ageist views and behaviours, there also have been positive expressions of intergenerational solidarity. Notably, many of the outreach and befriending programs described in the annexes have been initiated by university students. Such programs can provide benefits not only for older adults but also for students who have seen significant disruptions to their schooling and social lives. Literature reviews of pre-pandemic initiatives to reduce ageism have found intergenerational programs are also one of the most effective types of interventions for reducing ageism towards older people (Burnes et al., 2019; WHO, 2021).
3.1.4 Building partnerships to support isolated older adults
The challenges faced by isolated older adults are complex and cross-cutting, and supports may be required from multiple sectors. Many of the interventions profiled in the annexes represent partnerships between multiple stakeholders (such as government, local community organizations, academic institutions, private sector) that leverage the expertise and resources of each partner. For example, in Manitoba the 311 Food Security Line delivers food hampers to isolated older adults through a partnership between A & O (operates the 311 line), Manitoba Harvest (provides the food hampers), and CAA (delivers the hampers). Partnerships have also been used to deliver large-scale coordinated responses at the provincial and municipal levels as described in section 2.2.3. Governmental organizations often play an essential role in partnerships by acting as funding or coordinating partners (consult Annex 10 for examples of governmental funding opportunities). In a survey of community-based seniors’ services in BC, 80% reported that partnerships enhanced the effectiveness of their pandemic responses (UWLM & DIA, 2021). Partnerships can be supported by capacity-building (leadership and networking skills); creating a culture of collaboration and leveraging existing partnerships; encouraging inter-sectoral partnerships (for example, community-based, health care, municipal, etc.); and supporting small communities to network regionally and provincially (UWLM & DIA, 2021).
3.1.5 Capacity of LTC staff to support resident social connections
As described in section 2.3, LTC facilities have adopted a range of approaches to allow residents to visit with family and caregivers during the pandemic (for example, remote visits, window visits, outdoor visits, in-person visits with physical distancing or barriers). The type of visits utilized have depended on government policy and circumstances specific to the facility. Regardless of what form visits take, some staff support is required to facilitate the visits (such as screening visitors, setting up technology). Staff also are required to provide social activities for residents and to coordinate with external organizations offering programs (like befriending programs). Adequate staff support and training are essential enablers for facilitating resident social connections during the pandemic.
3.1.6 Sustainability of pandemic interventions
Numerous interventions to reduce the social isolation of older adults have been implemented by community and non-profit organizations during the pandemic. However, as described in section 2.2.6, the pandemic has led to financial struggles for some non-profit and community organizations. Many of the programs profiled in the annexes are being supported by short-term grants and funding. This raises the question as to how these programs can continue to be supported as the pandemic winds down and transitions into the next phase. There will undoubtedly continue to be isolated and homebound older adults who require support, and the abrupt stoppage of pandemic programs may exacerbate feelings of loneliness and isolation unless these are adapted to a new context. Consideration should be given to providing non-profit and community organizations with long-term grants or sustainable operational funding to support successful programs and services.
3.2 Promising practices
Based on this review of the literature, it appears that few interventions to reduce the social isolation of older adults during the pandemic have been the subject of formal evaluation research to date. A contributing factor to the lack of research is the lag of time between research being conducted and the publication of results. However, many of these interventions are adaptations or enhancements of long-standing program models and practices. Pre-pandemic programs have been the subject of a greater degree of evaluation, though the evaluation research is still underdeveloped as many community organizations lack the capacity to formally evaluate their programs. At this time, the success of interventions is primarily being judged based on a wide range of often incomplete evidence (for example, anecdotal information, demand from older adults, feedback from participants, initial study results) or based on evaluations of pre-pandemic programs. Further research should be conducted on the impacts of transitioning programs to remote delivery. Below some of the promising practices identified in this literature review are summarized.
3.2.1 Befriending programs
Description: volunteers are matched with an older adult to whom they provide regular support and companionship. Meetings may take place in-person or remotely. Some befriending schemes incorporate additional components such as creative arts projects, social groups, information and referral, and meal deliveries.
Examples: 2 examples are the Student-Senior Isolation Prevention Partnership (operates at 12 universities across Canada and pairs older adults with a health care student) and Art of the Conversation (an artist is paired with an older adult and creates a piece of art inspired by them). See Annexes 2 and 9 for more examples.
Evidence of impacts: a small number of studies suggest that there are benefits from these programs during the pandemic. Anecdotal evidence suggests participation helps both older adults and volunteers. Befriending programs have also been implemented in LTC facilities, though there has been limited evaluation in this setting.
3.2.2 Telephone outreach programs and information lines
Description: in telephone outreach programs, staff or volunteers call isolated older adults to conduct check-ins, offer support, and make referrals to needed services. There are also telephone help and information lines that older adults can call seeking help or information (for example, mental health support, referral to needed services).
Examples: an example of a telephone outreach program is the Red Cross’ Friendly Calls programs that provides routine safety checks to isolated individuals living in the Atlantic provinces. An example of a telephone information line is 211 which provides callers with information and assistance navigating government and community-based health and social services. The Government of Canada provided time-limited funding in 2020 to expand 211 telephone services to reach all Canadians. See Annex 3 for more examples.
Evidence of impacts: a pre-pandemic study linked telephone outreach and help or information lines to reductions in social isolation among older adults. During the pandemic, anecdotal evidence demonstrates that these services have experienced significant increases in call volumes.
3.2.3 Health promotion and wellness programs
Description: caregiver support programs, physical activity programs, and socialization and wellness programs for vulnerable older adults have begun transitioning to online, over the telephone, and outdoor modes of delivery during the pandemic. Programs are usually delivered by trained staff to support older adults in multiple areas.
Examples: caregiver support organizations such as Family Caregivers of BC, Caregivers Alberta, and Ontario Caregiver Organization have begun offering online caregiver support groups during the pandemic. Other examples of health promotion and wellness program are Choose to Move (evidence-based program that motivates older adults to become more physically active through one-on-one and group support; during the pandemic the program has pivoted to operating over phone and Zoom) and social prescribing programs (described in 2.2.3). See Annex 4 for more examples.
Evidence of impacts: pre-pandemic, there was an emerging body of evidence supporting the provision of online caregiver support programs. Other remote health promotion and wellness programs were uncommon, so it is unclear what the longer-term impacts of transitioning to remote delivery will be. However, evidence from the in-person versions of certain health promotion programs (for example, social prescribing, Minds in Motion, Choose to Move) suggest the potential to reduce loneliness and social isolation.
3.2.4 Practical assistance programs
Description: vulnerable older adults and people who are self-isolating can contact practical assistance programs to receive services such as meal delivery, grocery shopping, and transportation. Services usually are delivered by volunteers. Delivery of meals and food is a core component of many programs, with food serving as an avenue for engaging in other forms of outreach (for example, friendly conversation, delivery of letters and cards, provision of information, referral to other programs, etc.).
Examples: grants from the NHSP have been used to fund practical assistance programs across Canada. Most programs are multi-service, with grocery supports and social isolation outreach being the most offered services. Annex 5 provides additional examples of practical assistance programs, focusing on examples that incorporate social connection components or are a part of multi-service outreach interventions.
Evidence of impacts: 2 pre-pandemic studies have linked the receipt of practical assistance (meal delivery) with reduced levels of loneliness. Anecdotal evidence suggests high rates of demand for these services.
3.2.5 Technology donation and training programs
Description: to promote internet and digital technology access, tablets and iPads have been donated to older adults living in the community and LTC facilities. Programs have also been implemented to train community-dwelling older adults on how to use digital technologies, thus opening the door to them using email, video calls, and social media and participating in virtual programs. A key enabler for the success of these programs has been providing access to free internet.
Examples: an example of a technology program for community-dwelling older adults is the Vaughan Community Health Centre’s program that loans low-income older adults tablets and provides them with technology training and access to a technology helpline. In LTC facilities, digital technologies have been donated to facilitate virtual visits with family as described in section 2.3.2. See Annexes 6 and 9 for more examples.
Evidence of impacts: pre-pandemic evidence suggests digital technology access and training positively impact components of social isolation, though associations with loneliness are less clear. Anecdotal evidence suggests that these programs have successfully trained older adults on how to use digital technologies. There is limited evidence on the effectiveness of virtual visits for older adults residing in LTC, though a study from New Brunswick suggests it may be an effective component of strategies to reduce social isolation in LTC facilities during the pandemic.
3.2.6 Senior Centre Without Walls (SCWW)
Description: senior centres, community centres, and other organizations offering programs to older adults quickly began to transition their programs to telephone or virtual delivery during the pandemic and pre-existing SCWW have scaled up their services. Examples of types of programs offered include discussion groups, art classes, exercise classes, lectures, and games. The Edmonton Southside Primary Care Network (2020) has developed a useful toolkit for the development of SCWW programs.
Examples: examples of SCWW style programs include Yet Keen Seniors’ Day Centre’s virtual programs (offers Cantonese and Mandarin telephone and Zoom programs) and Rainbow Circle (weekly Zoom group for LGBTQ2S seniors). See Annex 7 for more examples.
Evidence of impacts: to date, there has been limited evaluation of the SCWW model, though 2 pre-pandemic evaluations have reported reductions in loneliness due to participation. Anecdotal evidence suggests consistent participation by older adults in SCWW and other virtual programs and positive feedback.
3.3 Potential roles for governmental and non-governmental organizations
3.3.1 Governmental roles
Funding to support interventions: many of the intervention examples in this report have been supported by funding from the federal, provincial, or territorial governments (see Annex 10). At the federal level, the NHSP and ECSF have provided essential support to numerous community and non-profit organizations during the pandemic. At the provincial level, in addition to pandemic-specific funding, grants and funding programs support initiatives in many areas that impact the lives of isolated older adults (for example, the Community Transportation Assistance Program in Nova Scotia; Seniors Active Living Centre Program in Ontario). In LTC facilities, governments have provided funding for the purchase of digital technology and construction of visitor centres. These findings highlight how federal, provincial, and territorial governments can influence the development and sustainability of social isolation initiatives through their funding powers.
Coordinating responses and knowledge sharing: in some cases, provincial or municipal governments have worked with stakeholders to facilitate large-scale coordinated responses during the pandemic as described in section 2.2.3. To develop comprehensive and coordinated supports for older adults, governments can leverage their ability to bring together multiple stakeholders and sectors. Federal, provincial and territorial governments have also supported the development of online knowledge sharing and mobilization platforms (see Annex 8), and governments can play a role in encouraging stakeholders to engage in collaboration and knowledge sharing.
Policy-making: policies at all levels of government (for example, age-friendly community strategies, support for caregivers, LTC visitor policies, design of LTC facilities) have impacted pandemic responses to reduce social isolation among older adults. LTC policies are particularly influential given the almost complete dependency of residents on these facilities for care and comfort. Within LTC, policies pertaining to minimum room size and other physical design features that promote healthy aging need to be re-examined against the unique risks posed by a pandemic, especially since there will likely be others in the future. For example, innovative designs could be considered, such as small cluster housing and facilities where each resident has their own room and clustered into small groups within a building or into multiple smaller buildings could be considered (Regnier, 2018). Policies on visitors to LTC facilities during the pandemic must also be carefully examined, to balance the need to protect residents and staff with the right of residents to spend time with their loved ones. The adequacy of current policies on LTC staffing levels and requirements also should be considered.
3.3.2 Non-governmental roles
Community and non-profit organizations: a broad range of non-profit and community organizations (such as senior centres, multipurpose non-profits, community health centres, grassroots volunteer groups, ethno-specific and cultural organizations) have been at the forefront of delivering services to support older adults during the pandemic. Due to their connections with the community and on-the-ground knowledge, these organizations are well poised to engage with and deliver services to isolated and vulnerable older adults in the community. Community and non-profit organizations should consider how to adapt their programs and services to the next phases of the pandemic and eventually post-pandemic life. Particular attention needs to be paid to supporting marginalized groups of older adults within the community. To prevent unnecessary ‘reinventing of the wheel’, community and non-profit organizations can engage in collaboration and knowledge sharing to share pandemic lessons.
Schools and academic institutions: even before the pandemic, there was a lack of research evaluating the success of interventions to reduce social isolation among older adults, and to-date, there have been few evaluations of interventions implemented during the pandemic. Many of the organizations implementing interventions (like non-profit and community organizations) have limited expertise and resources for conducting rigorous evaluations of their programs. Partnerships among academics, non-profit and community organizations, and the private sector have the potential to build capacity to evaluate the effects of promising interventions. Schools and academic institutions can also support student-led initiatives by providing small seed grants to get initiatives started, offering credits for participation in service initiatives, and recognizing student initiatives and achievements.
Businesses: during the pandemic, some businesses have donated their expertise and resources to support interventions to reduce social isolation among older adults. In particular, businesses can play pivotal roles in supporting practical assistance programs (for example, donations of food and meals from restaurants and grocery stores) and technology training and donation programs (such as donating technology, helping to set up technology).
4. Conclusion
Data from the CLSA reveals significant increases in levels of loneliness among older Canadians during the COVID-19 pandemic. To address the negative impacts caused by the pandemic, effective interventions to reduce social isolation among older adult populations are required. Using the AFC framework as a guide, this report has reviewed evidence and key considerations on interventions to reduce the social isolation of older adults during the pandemic.
Key findings of the report include:
- interventions to reduce the social isolation of older adults have involved a range of stakeholders, and many successful interventions have relied on leveraging the expertise and resources of multiple partners (for example, government, community and non-profit organizations, academic institutions, private sector)
- the review identified the need to address sources of marginalization, vulnerability and exclusion among older adults, including bridging the digital divide, tailoring interventions to meet the needs of linguistic and cultural groups, and combatting ageism
- the LTC environment presents unique challenges for social isolation interventions, and the systemic issues of staffing levels and capacity were identified as having implications for supporting social connections for residents
- moving forward, the sustainability of successful interventions is an important consideration, as many interventions are currently being supported by short-term or emergency funding
- potential roles identified for governmental organizations in efforts to reduce social isolation among older adults include funding, supporting coordinated responses and knowledge sharing, and policy-making
- for non-governmental organizations, community and non-profit organizations were identified as being at the forefront of delivering services to support isolated older adults. Additionally, potential roles were identified for businesses and academic institutions and schools
While there is limited evaluative evidence on the impacts of specific types of interventions to reduce the social isolation of older adults during the pandemic, a spectrum of research findings and grey area evidence exists, including extensive pre-pandemic literature that can be applied. Through an examination of this evidence, 6 promising practices were identified: befriending programs; telephone outreach and information line programs; remote health promotion and wellness programs; practical assistance programs; technology donation and training programs; and SCWW.
Moving forward, it is important to build upon the progress that has been made in supporting isolated older adults during the COVID-19 pandemic. While some challenges identified in this review will be diminished in what will become our post-pandemic world, others will continue to persist and may become intensified (for example, digital divide, need for culturally and linguistically appropriate programming). The lessons learned during the COVID-19 pandemic should be applied to the eventual post-pandemic circumstances, including:
- adapting and continuing to fund successful and promising interventions
- addressing causes of marginalization and supporting vulnerable populations
- encouraging intergenerational connections
- supporting partnership building
- ensuring reform to LTC to support the social and well-being needs of residents
Annexes
In this section
- Annex 1. Report methodology
- Annex 2. Examples of befriending programs for community-dwelling older adults
- Annex 3. Examples of telephone outreach programs, and help or information lines for community-dwelling older adults
- Annex 4. Examples of health promotion and wellness programs for community-dwelling older adults
- Annex 5. Examples of practical assistance programs for community-dwelling older adults
- Annex 6. Examples of technology training and donation programs for community-dwelling older adults
- Annex 7. Examples of Senior Centre Without Walls (SCWW) and other telephone or virtual activity and social programs for community-dwelling older adults
- Annex 8. Examples of mechanisms to support learning and collaboration during the pandemic
- Annex 9. Examples of interventions to address the social isolation of older adults living in long-term care facilities
- Annex 10. Governmental grant programs and funding to support the implementation of interventions to address the social isolation of older adults during the pandemic
Annex 1. Report methodology
Both English and French language literature are included in this review. Data collection was conducted over January-March 2021 and relied on a 4-pronged approach.
- Academic literature search: a search of academic databases was conducted using the EbscoHost search engine. Keywords utilized in the search include “older adults” (and appropriate synonyms) and “COVID-19” (and appropriate synonyms) paired with additional keywords such as “social isolation,” “social participation,” “loneliness,” and “technology,” among others
- Grey literature search: grey literature (for example, reports, news articles, briefings, etc.) was located via: Google searches; searching the websites of relevant non-governmental organizations, research groups, and governmental organizations; reviewing reference lists; and connecting with experts and service providers
- Provincial and territorial points of contact: provincial and territorial contacts advised the project team on relevant interventions within their jurisdiction
- Analysis of CLSA Data: a data request was submitted to the CLSA to access their COVID-19 study data pertaining to social isolation and loneliness. We present original CLSA data using Baseline data (collected 2011 to 2015; n=51,338); Follow-up One data (collected 2015 to 2018; n=44,817); and data from the recent CLSA COVID-19 Study (collected April to December, 2020; n=28,559). Currently, the COVID-19 survey data cannot be linked to other CLSA waves; therefore, we use the surveys as individual samples capturing patterns pre-pandemic and during the pandemic. Table 2 presents the full data on percentages of CLSA participants feeling lonely, using the identical measure derived from the single loneliness item comprising the CES-D depression scale. Those participants who report being lonely some of the time, occasionally, or all of the time are deemed to be lonely (compared to rarely or none of the time). Table 3 presents the full data on the prevalence of depression based on the CES-D 10 scale, and the 10+ cut point
Table 2: Loneliness patterns by age and sex, baseline (2011 to 2015), follow-up one (2015 to 2018)b, and during pandemic (2020)c, CLSA
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Lonely at least some of the timea d |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Lonely at least some of the timeb d |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84e |
|---|---|---|
| Lonely at least some of the timec d |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Absolute percentage increase in loneliness |
|
|
| Rate of increase in loneliness |
|
|
a Data drawn from Wister et al. (2018).
b Generated from Follow-up One CLSA data by authors.
c Generated from the CLSA COVID-19 Study, CLSA Data Centre, McGill University.
d Includes: All of the time, Occasionally, and Some of the time responses – compared to rarely or none of the time.
e Only includes these ages to compare to baseline and follow-up ages.
Note: all percentages were calculated to 2 decimal places before being rounded. The numbers used to calculate the absolute and relative increases in loneliness included 2 decimal places, and then the final results were rounded.
Table 3: Depression patterns by age and sex, baseline (2011 to 2015), follow-up one (2015 to 2018), and during pandemic (2020), CLSA
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Depresseda b |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Depresseda b |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84d |
|---|---|---|
| Depresseda c |
|
|
| Status | Ages 65 to 74 | Ages 75 to 84 |
|---|---|---|
| Absolute percentage increase in depression |
|
|
| Rate of increase in depression |
|
|
- a Scores of 10+ on CES-D.
- b Generated from Follow-up One CLSA data by authors.
- c Generated from the CLSA COVID-19 Study, CLSA Data Centre, McGill University.
- d Only includes these ages to compare to baseline and follow-up ages.
Note: all percentages were calculated to 2 decimal places before being rounded. The numbers used to calculate the absolute and relative increases in depression included 2decimal places, and then the final results were rounded.
Annex 2. Examples of befriending programs for community-dwelling older adults
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Student-Senior Isolation Prevention Partnership (SSIPP)a –Canada |
12 SSIPP university chapters | SSIPP was developed in 2019 by students at the University of Toronto and during the pandemic was re-launched as a virtual and telephone program. Isolated older adults are referred to the program by health care professionals and are paired with a health care student. Students make weekly calls to the older adult and provide friendly conversation and information about community resources and COVID-19. The program at the University of Toronto has over 270 volunteers. SSIPP has now expanded to 12 university campuses. |
Friendly Visitor Programb –Prince Edward Island |
PEI Senior Citizens’ Federation; Department of Social Development and Housing (funder) | This service provides friendship and companionship to Island older adults who may be at risk of becoming socially isolated. Volunteers must be 50 and up and are carefully screened and matched with older adults. As a result of the pandemic, the program transitioned from in-person to telephone visits. The telephone was the only feasible option for visits as many participants live in small apartments and only one participant in the program has internet access. The program is in the process of hiring a coordinator and plans to expand telephone visits, as well as hopefully restart in-person visits in the summer. |
Keep in Touchc d –Lethbridge, Alberta |
Volunteer Lethbridge | Keep in Touch is a new program intended to reduce isolation, loneliness and disconnectedness amongst older adults and vulnerable community members in Lethbridge. The program connects individuals for social interaction with regular, friendly conversations through a weekly telephone support system. The program aims to build relationships that ease loneliness and provide support during stressful times due to a pandemic that has hit older adults particularly hard. The program has paired about 60 older adults with volunteers. A similar program has been launched by the Community Foundation of Southeastern Alberta. |
Phone Pal Programe –Edmonton, Alberta |
Strathcona Place Society | The Phone Pal Program pairs older adults with youthful volunteers and like-minded peers who can lift their spirits, build resiliency, and strengthen their ability to cope during the pandemic. The phone calls also provide an outlet through which older adults can share concerns or issues which, depending on severity, may be referred to the Outreach Department for resolution. |
Community Connectsf g –New Brunswick |
Mount Allison University and Nursing Homes Without Walls | Community Connects was initiated during the pandemic and pairs university students with isolated older adults. Originally students and older adults met for lunch once a week, but due to changes in COVID-19 restrictions connections are now being made remotely. The program has also partnered with Open Sky Co-Op to drop off food for the older adults. Both students and older adults have provided positive feedback about the program. While originally an 8-week program, due to popular demand the program has continued to operate. |
Intergenerational Initiativeh –Chilliwack, British Columbia |
Compassionate Neighbourhood Health Partners Society | The program pairs up high school students with older adults in the community. Students are expected to make one 30-minute call to their older adult partner each week, and the program runs from January to March 2021. To date, the program has matched 53 older adults with students. Positive feedback has been received on the program from older adults, as well as from students who are able to accrue volunteer hours needed for high school graduation. |
| H2O Intergenerational Paired Interaction (HIPI)b –Ontario |
Hand Over Hand (H2O) Network | The H2O Network seeks to build a bridge between older and younger people and facilitate mutually beneficial interactions. During the pandemic, their programs transitioned to online delivery. H2O Intergenerational Paired Interactions (HIPI) pairs younger people with older adults for conversations via video or phone. H2O Intergenerational Group Interactions (HIGI) is a weekly group where older adults and younger people can meet. Finally, the H2O Intergenerational Mentorship Interactions (HIMI) facilitates mentorship sessions between older adults and younger people. There are about 7 pairs currently in HIPI, 30 to 40 people who participate in HIGI, and 3 mentors who mentor small groups of students in HIMI. Testimonials from both younger and older people suggest the relationships they build through the programs are valuable. |
Art of Conversationi –Fort McMurray, Alberta |
Arts Council Wood Buffalo and St. Aidan's Society | While originally Art of Conversation was intended to be a collaborative group project that would produce a mural, during the pandemic the program pivoted to matching individual artists with older adults. The artists connect with and get to know the older adult, and then create a piece of art inspired by them. The program paired 35 artists with older adults and some pairs continued to remain in contact after the project ended. Suncor has provided funding to continue the project for another year. |
Au bout du filj –Montreal, Quebec |
Les Petits Frères | Au bout du fil (On the Line) is a program for Quebec older adults aged 75 and up who are experiencing isolation. The program offers participants 2 phone calls by volunteers per week. For Christmas, special outreach was conducted including sending out advent calendars and gift and treat boxes; distributing letters and crafts from children at partner schools; and providing on Christmas day a special pre-recorded phone message by Béatrice Picard (famous actress). The organization has provided support to 1,542 older adults. |
Telehealth Intervention Program for Older Adults (TIP-OA)k –Montreal, Quebec |
Jewish General Hospital and McGill University | In this program, volunteers make weekly friendly phone calls to older adults to check in, form connections, provide information about COVID-19 and connect clients to community resources as needed. As of October 2020, 150 volunteers had been trained and 305 older adults have been reached. A protocol is in place for evaluating the initiative. TIP-OA has been designed by staff from the Jewish General Hospital and McGill University and modelled after successful telehealth interventions. |
Un brin de lecturel –Quebec |
Les Amis de BAnQ | Isolated older adults can register to have volunteers from the national library and archives of Quebec (BAnQ) call them for 15-minute reading sessions once a week. Older adults are matched with a volunteer who will call them once a week and read excerpts from books or other written works. |
- a Parsons, C. (2020, April 16). 'We care and are here for them': U of T students help seniors cope with distancing during COVID-19. U of T News.
- b Information provided through personal communication with organization.
- c Campbell, Q. (2020, December 28). ‘Keep In Touch’ program helping seniors in Lethbridge deal with isolation. Global News.
- d Dahlman, R. (2020, September 14). Keep in Touch Program will help southern Alberta. Prairie Post.
- e Healthy Aging CORE Alberta. (2020). Phone Pal Program.
- f Lyall, L. (2021, February 9). University students pair with N.B. seniors to ease loneliness of pandemic. CTV News.
- g Weldon, T. (2020, September 20). Struck by loneliness of seniors in pandemic, N.B. student pairs them with peers. CBC News.
- h Bathe, A. (2021, February 28). 99-year-old and high school student find unlikely friendship. CBC News.
- i Malbeuf, J. (2021, January 2). Seniors and artists team up for Fort McMurray art project. CBC News.
- j Les Petits Frères. (2020). Au bout du fil.
- k Dikaios, E., Sekhon, H., Allard, A., Vacaflor, B., Goodman, A., Dwyer, E., Lavin-Gonzalez, P., Mahdanian, A., Park, H., Walsh, C., Sasi, N., Nazar, R., Gruber, J., Su, C. L., Hanganu, C., Royal, I., Schiavetto, A., Cinalioglu, K., Rigas, C., Launay, C., … Bukhari, S. N. (2020). Connecting during COVID-19: A protocol of a volunteer-based telehealth program for supporting older adults' health. Frontiers in Psychiatry, 11, 598356.
- l Les Amis de BAnQ. (n.d.). Un brin de lecture.
Annex 3. Examples of telephone outreach programs, and help or information lines for community-dwelling older adults
Table 5: Telephone outreach, and help or information lines
| Intervention | Organizations | Description and outcomes |
|---|---|---|
No Islander Alonea –Prince Edward Island |
Hospice PEI, in partnership with United Way of PEI; NHSP (funder) | No Islander Alone was launched as a COVID-19 response to assist isolated older adults. Hospice PEI’s specially trained volunteers provided wellness checks and emotional support by phone on a weekly basis to approximately 50 Island older adults. The program was time-limited, and eventually service responsibilities were transferred to the Red Cross. |
Friendly Callsa –New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island |
Red Cross; Bell Let’s Talk (funder) | In the summer of 2020, the Canadian Red Cross launched a new Friendly Calls Program for residents aged 18 and up of the Atlantic provinces. The Friendly Calls Program provides regular, pre-scheduled calls to individuals who are feeling isolated due to the pandemic. The service is provided as a routine safety check and to reduce loneliness. In some cases, staff and volunteers will connect callers with resources available to them in their community to further assist. The program has been funded by Bell Let’s Talk, for up to 1 year. |
Talk2NICEb –Ontario |
National Initiative for the Care of the Elderly | The National Initiative for the Care of the Elderly initiated Talk2NICE in March 2020 in response to the pandemic. It is a free, over-the-phone outreach support service to connect older adults with social workers and social work students. The aim of the program is to provide much-needed support during and after the enforced isolation, as part of the current response to COVID-19, the recovery, and an adjustment to a new normal in the community and in institutional settings, such as LTC. Approximately 500 older adults have connected to the program. These older adults receive ongoing friendly check-ins over the phone to help decrease feelings of isolation and loneliness, with the aim of improving their mental well-being. |
Maintaining Community Connectionsc –Toronto, Ontario |
Harbourfront Centre | Harbourfront Centre, a non-profit cultural centre, had over 480 volunteers pre-pandemic but had to halt their programs when the pandemic hit. Many volunteers were older adults who reported missing the social aspects of volunteering. A check-in program was initiated where experienced volunteers would telephone, video call, or email other isolated volunteers. The centre also began to host zoom workshops for their volunteers. Over 190 volunteers have now been re-engaged or reconnected through remote programs. |
Caring Hearts Connectiona –Stony Plain and Parkland County, Alberta |
Stony Plain Family and Community Support Services | In response to COVID-19, Stony Plain Family and Community Support Services is launching Caring Hearts Connectors to take calls and connect residents to community resources including wellness check-ins. It is hoped that this connection will reduce social isolation, ensure all residents are supported, and help to provide information to residents on how to have their basic needs met through this difficult time. |
Algoma Seniors Telephone Outreach Programd –Sault Ste Marie, Ontario |
Sault Area Hospital | The Algoma Seniors Telephone Outreach Program began in May 2020 and has 31 participants. Volunteers make weekly wellness check calls to participants. To date, volunteers have put in over 260 hours of telephone calls. Older adults have provided positive feedback on the community connections created by the program. |
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Seniors Safety Linea –Ontario |
Elder Abuse Prevention Ontario; Government of Ontario (funder) | The Seniors Safety Line offers 24 hours a day, 7 days a week free information, referrals and support in over 150 languages for older adults experiencing abuse. In 2020 to 2021 the Government of Ontario provided an additional investment of up to $130,000 to hire and train more operators to address the higher call volumes generated by the COVID-19 pandemic. |
A Friendly Voicee –Ontario |
Rural Ottawa South Support Services; Trillium Foundation (funder) | A Friendly Voice is a telephone hotline for older adults. The line is staffed by volunteers 7 days a week from 8 am to 12 am. Volunteers can provide friendly conversation and referrals to community resources. The program is funded by a 3-year grant from The Trillium Foundation. |
Seniors Telephone Linea –Nova Scotia |
Nova Scotia Department of Seniors | The Nova Scotia Department of Seniors provides a toll-free seniors’ telephone line to respond to individual inquiries for information on various government services. Inquiries have increased during the pandemic. The Department also responds to email requests. |
Seniors Toll Free Information Linea –Prince Edward Island |
PEI Department of Social Development and Housing | The PEI Department of Social Development and Housing administers a toll-free seniors telephone line to provide support and information on government programs and services. The Department experienced an increase in inquiries during the pandemic. The Department also has a seniors email address which is monitored and responded to on a daily basis. |
Toronto Seniors Helplinef –Toronto, Ontario |
WoodGreen Community Services | The helpline is staffed with trained social workers 365 days a year. Older adults who call can receive information, assistance with mental health, and practical help. In the first 8 months of 2020 the helpline received over 22,000 calls. There has been a large increase in older adults calling for mental health support. |
Information and Referral Linea –Newfoundland and Labrador |
SeniorsNL | SeniorsNL operates a provincial information and referral service. Regular reports from SeniorsNL indicate strong and consistent usage of this service from all regions of the province. |
Mobile Crisis Centresa –Saskatchewan |
Multiple organizations across Saskatchewan | 6 mobile crisis centres are located across Saskatchewan and operate 24 hours a day, 7 days a week. Their helplines provide counselling, support, information, and referral services for those who need help. |
The CHANNAL Warm Linea –Newfoundland and Labrador |
CHANNAL | The Warm Line is a province-wide non-emergency, non-crisis telephone support and referral service. People with lived experience receive training to operate the service. |
Joy4All Programg –Alberta |
Ever Active Schools | Joy4All is a free positive message hotline that was launched in April 2020. The hotline was created by Calgary high school students to connect with isolated older adults. Callers can call the hotline and hear recorded jokes, poems, and messages of positivity. New content is regularly created for the hotline by volunteers. In its first week, the hotline received over 1,800 calls. |
Seniors Abuse and Information Line (SAIL)b –British Columbia |
Seniors First BC; BC Ministry of Health (funder) | SAIL is a province-wide confidential telephone line that provides a safe place for older adults, and those who care about them, to talk to a trained intake worker about abuse or mistreatment and receive information and support about issues that impact the health and well being of an older adult. In 2020, there was an increase in the number of calls to the line and a greater need for emotional support (not only related to elder abuse, but also for general mental health and access to basic needs). The majority of the elder abuse calls identified emotional or psychological abuse, followed by financial abuse. In the abuse calls the majority identified the abuser as a family member and most were living with the older adult. |
First Link –Canadah |
Alzheimer’s Societies across Canada | First Link programs connect people living with dementia to local health services and resources. First Link programs can be accessed through referrals by health professionals or calling the local First Link program. |
- a Information provided by provincial or territorial contact.
- b Information from personal communication with organization.
- c Volunteer Toronto. (2020). Case Study: Maintaining Community.
- d Sault Area Hospital. (n.d). Algoma Seniors Telephone Outreach Program. Sault Area Hospital.
- e Szperling, P. (2020, March 26). A Friendly Voice is available for seniors alone and wanting to chat to someone. CTV News.
- f Ireland, N. (2020, December 24). Call volumes soar at seniors helpline as COVID-19 plunges more people into isolation. CBC News.
- g Dawson, C. (2020, April 20). Students launch a hotline with jokes, stories and support for isolated seniors. CNN.
- h Alzheimer Society of Canada. (n.d.). First Link. Alzheimer Society of Canada.
211 Programs (Canada-wide)Footnote 8
211 is a free, confidential, 24 hours a day, 7 days a week service that provides Canadians with information, referral, and assistance navigating government and community-based health and social services. The Government of Canada provided time-limited funding in 2020 to United Way Centraide Canada to expand 211 telephone services to reach all Canadians. 211 was already operating in British Columbia, Alberta, Saskatchewan, Ontario, Nova Scotia, Prince Edward Island, and most of Quebec and this new investment has allowed 211 to expand telephone services to Yukon, Northwest Territories, Nunavut, Manitoba, New Brunswick, Newfoundland and Labrador and further into Quebec. As of the first week of April, the new Manitoba, New Brunswick, and Newfoundland and Labrador programs have received over 15,377 calls. For the pre-existing 211 programs, funding is provided from provincial, municipal, and other sources. Examples of pre-existing programs include Ontario 211 (Funder - Government of Ontario), 211 Nova Scotia (Funder – Government of Nova Scotia), and bc211 (Funders - Province of British Columbia, the United Way, and the City of Vancouver).
Below are 211 needs data compiled by United Way Centraide Canada with source data provided by 211 service providers and aggregated at the national level by United Way. The data compares volumes of needs identified when Canadians contacted 211 for help from 2019/20 to 2020/21 (note: 2019/20 baseline data does not include the expansion regions as they were not yet operational). In the early stages of the pandemic (April 2020) there were significant spikes in food-related requests in particular (for example, increase of 12,213% for food outlets as shown in the graph below, 2,045% for emergency food, and 602% for meals). There also have been consistent increased levels of demand for mental health assessment (crisis interventions), warmlines (mental health helplines focusing on early intervention), and information on income assistance during the pandemic.
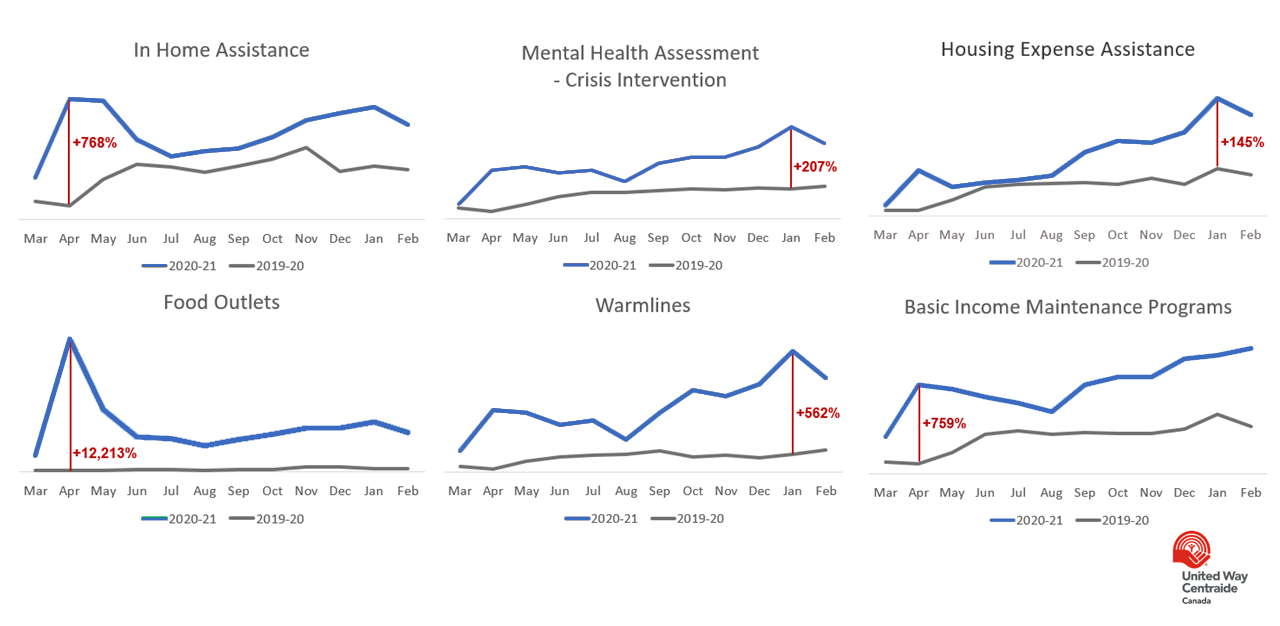
Source: United Way Centraide Canada
Figure 4 - Text version
The United Way Centraide provided the following data from the calls they received in 2019 to 2021.
- In April 2020, calls to the 211 service for in home assistance increased by 768% compared to the previous year
- In January 2021, calls to the 211 service for mental health assessments for crisis intervention increased by 207% compared to the previous year
- In January 2021, calls to the 211 service for housing expense assistance increased by 145% compared to the previous year
- In April 2020, calls to the 211 service for food outlets increased by 12,213% compared to the previous year
- In January 2021, calls to the 211 service for warmlines (mental health helplines focusing on early intervention) increased by 562% compared to the previous year
- In April 2020, calls to the 211 service for basic income maintenance services increased by 759% compared to the previous year
The following are samples provided by United Way Centraide Canada of 211 calls made by older adults to bc211:
- looking for someone to come in and help him get ready to move as he is selling his home and downsizing because he is 87 years old and has no family here to help him
- had a fall, dealing with pain and needs physio. Also needing help with transportation and other supports because of reduced mobility
- caller having cancer surgery later in the month and is feeling down and wants someone to talk to
- service provider has a senior client who is depressed due to isolation, looking for a number to call. Also wondering when they can access the vaccine
- caller wanted to know where to call to find out info about vaccine plan as she doesn't have computer access
Annex 4. Examples of health promotion and wellness programs for community-dwelling older adults
Table 6: Health promotion and wellness programs
| Intervention | Organizations | Description and outcomes |
|---|---|---|
BC’s Virtual Caregiver Support Groupa –British Columbia |
Family Caregivers of British Columbia | Family Caregivers of British Columbia runs a virtual support group twice a month for family caregivers. In addition, once a month they run a caregiver support group specifically for men. The online support groups were developed specifically in response to the COVID-19 pandemic and total attendance over the fiscal year 2020 to 2021 was approximately 593. The organization also operates a Caregiver Support Line and there were an estimated 1,592 calls by the end of March for the fiscal year 2020 to 2021. This is a 76% increase over the last fiscal year. |
Caregiver Support Communityb –Alberta |
Caregivers Alberta | In response to the evolving COVID-19 situation, Caregivers Alberta has had added new Online Caregiver Support Community groups. The Caregiver Support Community is a virtual program that aims to empower caregivers' well-being by providing a supportive space to connect with other caregivers, have open conversations about the ups and downs of caregiving, and learn about topics relevant to caregivers. This group is led by a trained facilitator who is there to help guide caregivers with education and support. The Government of Alberta has provided $3 million in funding to Caregivers Alberta to help expand support programs and resources for family and friend caregivers providing care at home or in the community. This funding will ensure caregivers have access to the supports they need to maintain their well-being during the pandemic and into the future. |
Online Support Groupc –Ontario |
Ontario Caregiver Organization | Ontario Caregiver Organization has launched online support groups for caregivers during the pandemic. Support groups are available 3 days a week. Currently, 2 of the 3 programs are full. |
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Well Connectedb –Alberta |
Caregivers Alberta and ElderCare Edmonton | Well Connected is a community-based, virtual day program. Groups are facilitated by therapeutic recreation specialists. Benefits of participating in the programs include enjoying therapeutic recreation in an at-home setting; remaining connected to the community; engaging the body, mind and spirit through a wide range of topics; and promoting activity and supporting independence well-being. |
Senior Connectb –Calgary, Alberta |
Calgary Seniors’ Resource Society | Senior Connect provides an urgent same-day social work response for older adults identified as being at-risk or in crisis and is available outside regular hours. |
| Fresh Air Funa | PEI Association for Newcomers to Canada (PEIANC) | Fresh Air Fun (FAF) is an intergenerational program developed in response to the pandemic. Previously, PEIANC hosted Friday Friendship Hour, a weekly get-together that provided newcomers opportunities for socialization and was attended by a significant number of newcomers aged 50 or over. During the pandemic, Friday Friendship Hour went through several evolutions and has now become FAF. FAF provides the opportunity to participate in fun and safe outdoor activities and events. The program runs about once a week and is scheduled based on the weather. A group of regulars attend almost every week, plus drop-ins. If needed, PEIANC provides a taxi voucher to and from the rural locations. Participants have provided feedback on the positive impacts of the program on their mental wellbeing. |
Integrated Community-based Programs for Older Adults with Higher Needsa b –British Columbia |
Managed by United Way of Lower Mainland; Government of BC (funder) | These programs are a part of demonstration project (running until March 31, 2022) that existed prior to the pandemic. The programs target homebound, at risk, and isolated seniors who are unable to access service on their own. There are 3 streams of demonstration projects. The one most aligned with reducing isolation of seniors is the Therapeutic Activation Program for Seniors (TAPS). TAPS supports isolated seniors who are experiencing barriers in accessing community resources. Programs include proactive outreach through daily or weekly telephone calls to participants, transportation to and from the program, a nutritious meal, and exercise, education, or recreational activities tailored to the needs of different individuals within the program. To ensure safe delivery of the program to participants during COVID-19, the delivery model shifted (for example, delivery of meals rather than in-person group meals; offering outdoors, physically distanced, or remote social programs and activities; one-on-one check-ins) while still striving to meet original program objectives around reducing isolation. The other 2 project streams are social prescribing programs (had just begun launching in early 2020 and have prioritized supporting Safe Seniors, Strong Communities during the pandemic) and caregiver support programs (most have been offering remote supports during the pandemic). |
Social Prescribingd –Ontario |
Alliance for Healthier Communities | From 2018 to 2019, the Alliance for Healthier Communities piloted social prescribing programs at 11 community health centres. While these programs target vulnerable people of all ages, over half of clients are aged 61 and over. During the COVID-19 pandemic, the social prescribing programs have continued to support clients by, for example, offering telephone or virtual appointments and working with cultural and arts organizations to offer online experiences for clients. The evaluation of the 11 pilot projects found 49% of participants reported decreased levels of loneliness. |
Jardinons nos balcons!e –Quebec |
CISSS de Chaudière-Appalaches | The project was launched in summer 2020 and provided 1,000 older adults living in social and community housing in the Chaudière-Appalaches region with supplies to create small gardens on their balconies. The intention of the project is to promote mental wellbeing and reduce isolation. The program is led by CISSS de Chaudière-Appalaches and supported by multiple regional and local partners. |
Connection in Actionf –Halton, Ontario |
Links2Care | The Connection in Action initiative supports older adults aged 55 and over across the Halton region who may be experiencing social isolation. The program is an initiative of the Community Safety and Well-Being in Halton plan. Older adults can be referred to a Connections Specialist who will work with them over the phone or in-person to access resources and services in their community. |
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Active Living Programb –Clarenville, Newfoundland and Labrador |
Eastern Health | The Active Living program is continuing with programming for older adults, via Zoom. This includes limited mobility fitness, yoga, chair yoga, and aerobics. There is a weekly calendar of events for which people can sign up. |
Choose to Moveb g –British Columbia (province-wide) |
Active Aging Society | Choose to Move (CTM) is a 12-week evidence-based health promotion program to increase physical activity and decrease social isolation in older adults. The program targets low active older adults, aged 65 and over, who spend less than 150 minutes for moderate to vigorous physical activity per week. Prior to pandemic, the CTM program ran in person. As soon as the pandemic started, Active Aging Society recognized that seniors confined to their homes are at even greater risk from the impacts of social isolation and decreased mobility. They were able to quickly pivot to provide service by phone and Zoom through Choose to Move at Home (CTM@Home). As of December 1, 2020, 55 CTM@Home programs had been offered through 21 delivery partners with 30 trained activity coaches. Active Aging Society anticipates that by the end of their current winter session, they will have run 74 programs and had over 600 participants in CTM@Home. As CTM@Home delivers the same CTM intervention, just virtually instead of in person, Active Aging Society anticipates similar outcomes. Anecdotally, they have consistently heard through their delivery partners about the positive impact the program is having on seniors’ social and physical health. The original program’s impact on loneliness has been published in a journal article. |
Minds in Motionh i –Canada |
Alzheimer’s Societies across Canada | Minds in Motion is an exercise and social program for people with early-stage dementia and their caregivers. The program is offered by multiple Alzheimer’s Societies across Canada. While originally offered in-person, during the pandemic programs have been pivoting to online delivery. An evaluation of the in-person program reported statistically significant improvements in mental well-being as a result of participation. |
- a Information from personal communication with organization.
- b Information provided by Provincial or Territorial contact.
- c Ontario Caregiver Organization. (n.d.). Online caregiver support group.
- d Alliance for Healthier Communities. (2020). Rx: Community – Social prescribing in Ontario, final report.
- e Centre intégré de santé et de services sociaux de Chaudière-Appalaches. (2020, June 22). « Jardinons nos balcons! » : un projet mobilisateur pour les aînés [Press release].
- f Links2Care. (2020). Connection in Action Halton Initiative.
- g Franke, T., Sims-Gould, J., Nettlefold, L., Ottoni, C., & McKay, H. A. (2021). "It makes me feel not so alone": features of the Choose to Move physical activity intervention that reduce loneliness in older adults. BMC Public Health, 21(1), 312.
- h See the websites of various Alzheimer Societies across Canada for information on online Minds in Motions.
- i Regan, K., White, F., Harvey, D., & Middleton, L.E. (2019). Effects of an exercise and mental activity program for people with dementia and their care partners. Journal of Aging and Physical Activity, 27(2), 276–283.
Annex 5. Examples of practical assistance programs for community-dwelling older adults
| Intervention | Organizations | Description and outcomes |
|---|---|---|
New Horizons for Seniors Program (NHSP) Grantsa –Canada |
Managed by United Way Centraide Canada network; NHSP (funder) | A total of $9 million in funding from the NHSP was dispersed in April 2020 to 876 community agencies to provide essential services to support vulnerable older adults during the pandemic. The funding was managed by the United Way Centraide Canada network. A total of 1.3 million interventions were offered to support 703,339 vulnerable older adults across Canada. The most commonly offered services were food and grocery supports (69%), social isolation outreach (57%), hygiene and cleaning supports and supplies (35%), mental health supports (27%), and capacity-building to ramp up new services (27%). Four-fifths of programs offered more than 1 type of service. |
Safe Seniors, Strong Communities (SSSC)b c –British Columbia (province-wide) |
Managed by United Way of Lower Mainland; Government of BC (funder) | Safe Seniors, Strong Communities (SSSC) was launched on March 26, 2020, in response to the COVID-19 pandemic. It was developed collaboratively by the Ministry of Health, the United Way of the Lower Mainland, Office of the Seniors Advocate British Columbia, and bc211. The program targets community-based older adults whose regular support network has been disrupted by the pandemic, or whose need for support has increased as they self-isolate. SSSC uses a hub and spoke model that leverages UWLM’s pre-existing networks. 24 of UWLM’s Better at Home programs serve as community hubs for SSSC and over 140 local referral agencies (existing UWLM funded programs that were asked to divert funding and staff to support SSSC) and spoke agencies (non-funded UWLM programs that the hub agencies have strong relationships with) are involved in providing services. bc211 was expanded beyond the Lower Mainland so older adults and volunteers anywhere in BC can now call 211 and be directed to a hub and connected with local services. The program uses local volunteers to provide non-medical supports, including virtual wellness checks to reduce social isolation. Other supports include grocery shopping and delivery, meal prep (pre-made drop-offs or in-home support), prescription drop-off and medication pick up, transportation, laundry etc. Delivery services also provide opportunities for informal wellness checks and the delivery of special items (such as cards, holiday deliveries). As of September 30, 2020, 15,502 seniors and 10,405 volunteers have registered with the program. A total of 351,661 services were delivered to the seniors including 179,970 virtual check-ins and wellness visits to reduce social isolation. |
The Seniors Lunch Programd –Golden, British Columbia |
Community Response Network and Golden Community Resources Society | The Seniors Lunch Program was launched in April 2020. Volunteers deliver soup and extras (such as food, books, masks) to vulnerable older adults in the Golden area. Lunch recipients are also provided with information about wellness and elder abuse and connected to local services. In return for receiving the soup, participants in the program are asked to call 5 other older adults in the community to check-in and connect with them. The program assists 75 to 90 older adults each week. |
Meal Delivery Programe –Vancouver, British Columbia |
Whole Way House Society | Whole Way House Society has partnered with local cooking schools and restaurants to provide meal delivery to older residents in 18 non-profit housing buildings across Vancouver. Staff and over 50 volunteers assist with delivering the meals. When volunteers drop off the meals they also provide friendly conversation and inquire if there are any supports the older adults need. The program provides meals to over 600 low-income older adults and vulnerable residents. Program staff report that older adults are very appreciative of the meals, and the care and human connection that accompanies them. |
Mobile Seniors Outreachf –Abbotsford, British Columbia |
Archway Community Services | Archway Community Services launched the Mobile Seniors Outreach program to provide practical help and social support to isolated older adults. Older adults are provided with assistance with practical tasks (like grocery shopping, tech support) as well as friendly phone chats if they have been identified as vulnerable to loneliness. The program is run by 1 staff member and 10 volunteers. |
Coordinated Pandemic Responseg –Edmonton, Alberta |
Edmonton Seniors Coordinating Council, City of Edmonton, and SAGE Seniors | To ensure an effective response to the pandemic in Edmonton, 3 programmatic task groups (food and transportation, outreach and friendly checks-ins, and psychosocial support) were formed consisting of a lead agency, an ESCC representative, a government representative, and content experts. The task forces worked to identify gaps, develop or expand needed programs, and facilitate referrals and information sharing between organizations. From March to November 2020: 7,740 rides and deliveries were provided by Drive Happiness; 9 senior serving organizations offered friendly phone calls to over 7,000 older adults; and 5 seniors organizations began offering new online programming. |
Seniors Social Support Programsh –Calgary, Alberta |
Calgary Seniors’ Resource Society | To adapt to COVID-19 and respond to emerging needs, Calgary Seniors’ Resource Society has developed modified social support programs delivered by volunteers. Volunteer programs include: Practical Kindness (provides urgent one-time support), Caring Companion, Essential Transportation, Pet Assist, Friendly Check-in, and Volunteer Drop Offs. To ensure all seniors in need can access services during the pandemic, eligibility requirements have been reduced, program access streamlined, and the volunteer process has been fast-tracked. |
Ontario Community Support Programi –Ontario |
Ontario Community Support Association (OCSA); Government of Ontario (funder) | The Ontario Community Support Program was continued, with a total investment of $16 million over 2 years to connect people with disabilities, low-income seniors and others with underlying medical conditions who are self-isolating at home with meals, medicines, and other essentials. Older adults and their caregivers can access the program’s services both online and through Ontario211. Those without Internet access, or who require service in a language other than English or French can dial 211 or 1-877-330-3213 (toll-free). TTY service is also available. Between April 21, 2020 and September 30, 2020, over 40,000 low-income seniors and people with disabilities received over 457,000 deliveries of meals, over 48,000 food hampers and almost 29,000 essentials. |
Letters of Positivity Campaignc –West Elgin, Ontario |
West Elgin Community Health Centre | West Elgin Community Health Centre operates a Meals on Wheels program that delivers meals 3 days a week. Local kindergarten to Grade 6 students were recruited to create messages and pictures to be included with the Meals on Wheels deliveries. The program operated from April until the end of the 2020 school year and a new letter was sent out with every meal delivery. Since then, staff have continued to arrange one-off special deliveries to accompany the meal deliveries (like Bear Hug crafts, positive-tea cards and valentine notes). In June 2020 about 30 older adults were receiving deliveries from the program. Older adults, teachers and children provided positive feedback about the program. |
Provincial Food Delivery Networki –Nova Scotia |
Employment Support and Income Assistance and Feed NS | Employment Support and Income Assistance and Feed NS partnered to design a provincial food delivery network to alleviate food insecurity for the most vulnerable Nova Scotians impacted by COVID-19. Pilot testing is currently underway in Dartmouth and Sydney. Funding has also been provided to Feed Nova Scotia to provide food to vulnerable Nova Scotians in response to reductions in donations and challenges in accessing food locally. |
Emergency Food Bankj –Newfoundland and Labrador |
Connections for Seniors | Connections for Seniors offers a range of services to empower older adults to overcome barriers to safe and affordable housing and provide support services that help reduce risks to well-being and promote quality of life. Emergency Food Bank, a food bank and delivery service for older adults, has seen a significant increase in demand during the pandemic. |
Food Bank and Salvation Armyi –Prince Edward Island |
Food Bank Association and Salvation Army of PEI; Government of PEI (funder) | The PEI Government provided funding to the PEI Food Bank Association to support increased demands from Islanders, including older adults, during the pandemic. Funding support was also provided to the Salvation Army for its home heating and food programs. |
| Compassion Fundh | Managed by United Way | With support from the Government of PEI, private sector and individuals, United Way’s Compassion Fund supported organizations serving marginalized community members to provide front line services to mitigate and address negative impacts of the pandemic. Services included provision of food, safe transportation, medication, and social and mental health supports. |
311 Food Security Linec –Winnipeg, Manitoba |
A & O: Support Services for Older Adults | The 311 Food Security Line connects isolated older adults with a range of resources available from A & O, such as grocery delivery and referrals to social programs. A & O partners with Manitoba Harvest (provides food hampers) and CAA (delivers hampers) to deliver food to isolated older adults. For the period of April 1, 2020 to December 9, 2020, A & O arranged 790 food hampers. Demand for hampers is increasing, and since December 2020 hamper deliveries have nearly doubled (1,562 food hampers delivered in total from April 1, 2020 to February 25, 2021). From April 1, 2020 to February 25, 2021 the Food Security line has worked with approximately 923 new clients, and at this time 608 client files remain open. A & O is a part of the larger Older Winnipeggers Social Engagement Project (OWSEP) that is funded by a NHSP grant. |
Better at Homec i –British Columbia |
Managed by United Way of Lower Mainland; Government of BC (funder) | Better at Home (BH) is a program that existed prior to the pandemic. The network and expertise of BH agencies were instrumental in the expedited development and implementation of the Safe Seniors, Strong Communities program (this was in addition to continuing to provide services to regular BH clients). BH is a community-based program that uses both contractors and volunteers to provide seniors with access to simple, non-medical home support services, including friendly visiting to reduce social isolation, to help them stay independent in their own homes and connected to their communities for as long as possible. Services offered by Better at Home include light housekeeping, light yard work, snow shoveling, grocery shopping, minor home repairs, and transportation to appointments. During the early stages of the pandemic some services temporarily ceased (like housekeeping and transportation) due to safety concerns, but later with sufficient PPE, appropriate policies, and in compliance with health mandates, programs were able to re-open these services as appropriate. As of March 31, 2021, there are 81 core BH program sites operating in communities across BC, serving over 260 communities, 4 of which are on First Nations reserves. |
Friendly Neighbour Hotlinek –Toronto, Ontario |
University Health Network’s OpenLab | Older adults living in low-income housing in Toronto can call the hotline and be connected with a volunteer who will deliver groceries or other essential supplies to them. The hotline is available Monday to Friday and can offer service in 180 languages. Since the hotline first launched in March 2020, over 1,500 people have volunteered (there are 700 active volunteers as of March 2021). As of March 2021, volunteers are also doing door-to-door outreach in some Toronto Community Housing buildings. |
Senior Safety Programs and Community Linksi –Nova Scotia |
NS Department of Seniors | The Department of Seniors to-date has allocated $470,000 ($240,000 from Department of Energy) to Senior Safety Programs and Community Links to help vulnerable older adults. Funding supports an increase in the number of hours these programs can provide direct time and support to individual vulnerable older adults. In addition, funding has gone to a range of supports facilitated by these programs such as: delivery of medications; purchase and delivery of groceries, frozen meals; purchase and delivery of reusable face masks; community-based transportation fares to get to medical appointments, grocery stores, etc.; keeping older adults physically active – develop and share online home exercises; and facilitated group support and psychoeducational sessions via Zoom. An additional $376,000 was invested in the program in the second wave of the pandemic. |
Brampton Seniors Support Task Forcel –Brampton, Ontario |
City of Brampton | In response to the COVID-19 pandemic the City of Brampton set up the Seniors Support Task Force. The Seniors Support Task Force connects older adults to needed services. The task force also offered grocery delivery and payment (City would pay for the groceries and invoice the older adults if they were unable to pay online themselves) directly in the early stages of the pandemic (now being offered through referrals to other organizations). The task force is working on setting up a pet food service. The City is also offering free virtual workshops and activities and weekly call-in chats for older adults. |
Collaboration for the Food Security of Isolated Seniors in North Vancouverm –North Vancouver, British Columbia |
Silver Harbour Seniors’ Activity Centre (with collaborating partners) | Prior to the pandemic Silver Harbour Seniors’ Activity Centre offered in-person lunches at their centre. During the pandemic, in collaboration with other organizations in North Vancouver, Silver Harbour redesigned their food services by pivoting their transportation service to deliver food and working with partners to identify vulnerable older adults in the community and 4 subsidized housing facilities who would benefit from meal deliveries. In addition to meals, additional items such as information and kindness cards were added to the deliveries. Over April to September 2020 nearly 450 meals were delivered each week. The program was supported by funding from local businesses and foundations, including NHSP and Safe Seniors, Strong Communities funding. |
Eldercare Project in Cowichan (EPIC)m –Cowichan, British Columbia |
Volunteer Cowichan, Cowichan Seniors Community Foundation, and Hiye’ye Lelum Society | During the pandemic, Volunteer Cowichan, Cowichan Seniors Community Foundation, and Hiye’ye Lelum Society worked together to develop a coordinated response that would meet the needs of older adults in Cowichan, including providing culturally appropriate care to elders from the Cowichan Tribes. A volunteer coordinator was hired to organize volunteers to offer grocery shopping, delivery, and friendly phone call services. Volunteers were also coordinated to make over 5,000 masks which were distributed to community members. A respected Elder of the Cowichan tribes was recruited to promote mask wearing. |
- a United Way Centraide Canada. (2020a, November 17). New Horizons for Seniors Program – United Way Centraide Grant results [Press Release].
- b Hannah, J. (2020). A Report on “Safe Seniors, Strong Communities”. United Way of the Lower Mainland.
- c Information provided through personal communication with organization.
- d Healthy Aging CORE British Columbia. (2020). Golden Seniors Table - The Seniors Lunch Program.
- e Healthy Aging CORE British Columbia. (2020). Whole Way House Society – Meal Delivery Program.
- f Healthy Aging CORE British Columbia. (2020). Archway Community Services - Mobile Seniors Outreach Program.
- g Coordinated Pandemic Response Steering Committee. (2020). Coordinated Pandemic Response for Edmonton Senior Service Community.
- h Calgary Seniors’ Resource Society. (n.d.). Seniors Social Supports.
- i Information provided by Provincial or Territorial contact.
- j Walsh, A. (2021, February 8). Many N.L. seniors can't afford to eat, let alone choose healthy food, say advocates. CBC News.
- k University Health Network’s OpenLab. (n.d.). Friendly Neighbour Hotline.
- l City of Brampton. (2021). Seniors Support Task Force.
- m United Way of the Lower Mainland & Dialogues in Action. (2021). Rising to the Challenge: How BC's CBSS agencies stepped up during Covid-19. United Way of the Lower Mainland.
Annex 6. Examples of technology training and donation programs for community-dwelling older adults
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Social Inclusion and Digital Literacya –Winnipeg, Manitoba |
South Winnipeg Seniors’ Resource Council | The Social Inclusion and Digital Literacy program provides isolated older adults with digital technology training and access to the internet and an iPad for 6 months. After the 6 month period, the older adults will have the option of purchasing the iPad at a reduced cost. The program is funded by the ECSF. |
Digital Learning Pilot Programs: ITECH Packagesb c –British Columbia |
United Way of the Lower Mainland (funding partner) | Community agencies can apply to receive ITECH Packages (up to 5 devices, 12 months of data, technical support, and access to a curated resource library) to distribute devices to isolated older adults. The program will run from April 2021 to March 2022. The ITECH program will provide 100 tablets total to community agencies and agencies will be able to decide whether to loan or gift the tablets. The tablets will come pre-loaded with relevant apps and be set up by Best Buy’s Geek Squad, and ongoing technical support will be available from the Geek Squad. HelpAge Canada is the digital literacy partner on the project and will provide resources and mentoring to community agencies on topics such as digital learning plans and safety and security. |
Tablets for Loan for Seniors Projectc –Vaughan, Ontario |
Vaughan Community Health Centre; Human Endeavour (technology partner) | Vaughan Community Health Centre has moved many of their programs online during the pandemic and offers virtual programs Monday to Friday (for example, dance, social groups, and brain training). About 9 to 14 older adults regularly participate in each program. Vaughan Community Health Centre has loaned 23 tablets to low-income isolated older adults and provides them with data so they can stay connected and participate in virtual programming. Training was provided on how to use the tablets. A technology helpline operates Monday to Friday to assist the older adults and the helpline staff are able to remotely access the tablets to easily provide support. Vaughan Community Health Centre has partnered with the non-profit Human Endeavour who manage the helpline and data. The tablets have been on loan since the summer and the program is funded by a NHSP grant that will last until March 2021. Older adults have provided positive feedback on the program and use the tablets to stay connected with community. |
Notebook Projectc –Winnipeg, Manitoba |
Manitoba Association of Senior Centres (MASC) | The Notebook Project is a part of the larger Older Winnipeggers Social Engagement Project (OWSEP) program that is supported by NHSP funding. MASC partnered with Fort Garry Rotary Villa, a low-income housing building for older adults, to provide digital devices and training to residents. The training program covers topics such as how to use the digital devices and cyber safety. The Villa has on-site staff who are able to provide the training to small socially distanced groups of residents. The availability of WiFi within the building was a key enabler for the project. |
Tech Savvy Empowered Older Womend –North York, Ontario |
North York Women’s Centre | North York Women’s Centre has provided tablets and computer training to 53 older women who live alone so they can access virtual programs. Individualized in-home training was provided over the summer until the women became comfortable using the tablets. The Centre also pays for data for women who do not have internet plans (60% of participants). A virtual drop-in activity session is held every Friday on Zoom that about half of the women participate in. The program is supported by multiple sources of funding, including a grant from United Way’s Local Love Fund. |
Cyber-Seniorse f –Ontario |
Cyber-Seniors | Cyber-Seniors develops and disseminates resources that enable community organizations to provide tech-training for older adults using an intergenerational model. Youth are provided with lessons and learning activities to train them to act as digital mentors, and older adults gain access to effective technology training and intergenerational communities that keep them socially connected and engaged. The Niagara chapter has begun several new initiatives to support older adults during the pandemic: offering online activities (for example, yoga, tech training webinars); providing low-income older adults with access to technology, Wi-Fi, and training; and helping older adults to participate in remote volunteering opportunities. |
CanConnectg –British Columbia |
CanAssist | CanAssist, at the University of Victoria, is an organization that develops innovative technologies and programs improving the independence and quality of life of people living with disabilities. CanAssist has developed a wide variety of technologies that can assist older adults to communicate and use technology during the pandemic. CanAssist is currently piloting the CanConnect Device (CanConnect and the Custom Case) – allowing people with a wide range of barriers (conditions associated with aging, such as dementia and frailty, cognitive and physical disabilities) to communicate easily and securely with family, friends, caregivers and clinicians in real-time video over the Internet. The development of the device is supported by the Province of BC as a part of the CanStayHome Initiative. |
Empowering Seniors Through Technology projecth –Nova Scotia |
Nova Scotia Community Technology Network; Nova Scotia Department of Communities, Culture, and Heritage (funder) | Through the provincial initiative Shift, the Nova Scotia Department of Communities, Culture, and Heritage received $50,000 per year to undertake community internet and digital literacy pilots for community-dwelling older adults across the province. The funds were directed to the Community Technology Network to engage in this work. An additional $20,000 was leveraged from the Department’s Diversity and Community Capacity Fund to support 4 pilots in culturally diverse and traditionally marginalized communities (Mi’kmaq and African Nova Scotian communities). The Community Technology Network provided training to over 900 older adults across the province (with many returning for additional sessions) before sites were closed due to the pandemic. Almost all respondents to the exit survey said the program gave them skills and knowledge they could use to stay better connected to family members, be more socially active, and the knowledge they needed to be comfortable going online and shopping online. They also indicated that they wished more training was available. |
- a Strachan, S. (2020, August 7). iPad program to reduce seniors’ isolation. Winnipeg Free Press.
- b Healthy Aging CORE British Columbia. (2020). Active Aging + & Digital Learning Pilot info session recording & slides.
- c Information provided through personal communication with organization.
- d Palamarchuk, A. (2020, December 9). Tech-savvy program helps North York seniors get 'connected'. Toronto News.
- e Cyber-Seniors. (2021). About Cyber-Seniors.
- f Singh, S. (2021, February 26). Online webinars and programming connect Niagara seniors to digital world. Niagara This Week.
- g CanAssist. (2020). CanConnect device pilot. Healthy Aging CORE British Columbia.
- h Information provided by Provincial or Territorial contact.
Annex 7. Examples of Senior Centre Without Walls (SCWW) and other telephone or virtual activity and social programs for community-dwelling older adults
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Seniors Centres without Wallsa –Kelowna, British Columbia |
Seniors Outreach and Resource Centre | SCWW was launched in Fall 2020 and provides a variety of social programs (for example, Bingo, live music, mindfulness) over the telephone and Zoom to isolated older adults in the Central Okanagan area. The program is being run by a practicum student and volunteers. Participants have provided feedback on how the programs have positively impacted their lives and improved their social connectedness. |
Seniors’ Centres Without Wallsb –Surrey, British Columbia |
Surrey Intercultural Seniors Social Inclusion Partnership | The SCWW program provides free telephone-based activities (for example, recreational activities, discussions, wellness talks) to isolated older adults. The program was in the planning stages in early 2020, and as a result of the pandemic the scope of the program was significantly scaled up. In its first 3 weeks of operation, 40 older adults registered to participate. |
Virtual Programsc –Ottawa, Ontario |
Yet Keen Seniors’ Day Centre | The Yet Keen Seniors’ Day Centre serves primarily Cantonese and Mandarin speaking older adults. Beginning in mid-April 2020 the centre began transitioning programs to remote delivery (Zoom or telephone). The centre offers remote programs such as Tai Chi, line dance, English classes and health and wellness talks. Most programs are offered in Cantonese or Mandarin. About 60 of the centre’s members are now on Zoom and about 30 use telephone programs. Around 20 or more people consistently attend classes such as Tai Chi and line dance each week. |
Senior Centre Without Wallsd e –Manitoba |
A & O: Support Services for Older Adults | The first SCWW in Canada was launched in Manitoba in 2009 by the organization A & O and provides isolated older adults with access to telephone-based social and educational activities. A process evaluation of the program found that it was successful in reaching its target audience of isolated older adults and participants reported feeling more connected and less lonely. Programs were already very well attended prior to the pandemic, and attendance has increased during the pandemic. Individual registrations in programs increased from 1,847 in January to March 2020, to 2,281 in October to December. |
Senior Centre Without Wallsd f –Edmonton, Alberta |
Edmonton Southside Primary Care Network | The Edmonton Southside Primary Care Network SCWW was operating pre-COVID-19. The initial development of the program was supported by a NHSP grant as a part of the Pan Edmonton Group Addressing Social Isolation in Seniors (PEGASIS) project. A pre and post-intervention evaluation of the program found statistically significant decreases in loneliness scores (for high users of the program) and anxiety and depression scores. Over half of participants also reported making new friends from the program. During the past year, the number of participants actively using the SCWW program has increased by about 3-fold, and in response the SCWW has tripled their programming to accommodate the new participants. |
Virtual Programsg –Edmonton, Alberta |
Multiple organizations in Edmonton | In Edmonton, in addition to the already operating SCWW from the Edmonton Southside Primary Care Network, during the pandemic the Edmonton Seniors Centre, Westend Seniors Activity Centre, Shaama Centre, MWSA, and Strathcona Place have begun offering virtual programs. Almost 6,600 online programming offerings have been made available from these organizations. |
Seniors' Centres Without Walls Micro-Grant Programh –Ontario |
Government of Ontario (funder); OACAO | In September 2020, the Government of Ontario invested $467,500 in the OACAO to administer a new Seniors' Centres Without Walls Micro-Grant program, and other capacity-building initiatives. The purpose of these grants is to support seniors' organizations in helping older adults to stay connected to their communities through telephone-based social and educational programs. |
Digital Learning Pilot Programs: Active Aging Plus (AA+) Grantsi –British Columbia |
United Way of the Lower Mainland (funder) | Active Aging Plus (AA+) Grants provide funding to community agencies to develop or adapt Active Aging programs to be delivered virtually. The grants prioritize agencies serving Indigenous persons, rural and remote communities, and other underserved groups. A total of 30 grants are available. |
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Rainbow Circlej –Toronto, Ontario |
Sunshine Centres for Seniors | Rainbow Circle was introduced during the pandemic and is a weekly Zoom group that provides LGBTQ2S seniors with a chance to chat and connect. Participation in the Rainbow Circle program has rivalled past in-person programs. Due to the success of the program an additional social program, Rainbow Tea and Talk, was developed. |
Virtual Community Gatheringsk –Ottawa, Ontario |
Inuuqatigiit Centre for Children, Youth and Families | The Inuuqatigiit Centre for Children, Youth and Families provided laptops and training on their use to Inuit elders during the pandemic. Since November 2020, they have been hosting weekly community gatherings on Zoom where elders can sing, pray, share stories, and check up on each other in Inuktitut. The gatherings include 30 participants from Ottawa and nearby communities. The Centre also provides additional supports to elders such as materials for sewing and traditional activities, country food, and phone top-ups to connect with family back home. The program is supported by funding from the Federal Government and United Way. |
No Limits Community Connectionsh –Alberta |
Black Canadian Women in Action | The program aims to help visible minority seniors aged 55 and over increase their mental, social, and emotional well-being during the pandemic with virtually engaging activities that also promote inclusion and community. Every week, seniors virtually meet with their matched volunteer mentor to socialize and troubleshoot basic technology and internet questions. Through an online platform, a technology expert and wellness professionals lead weekly workshops that help support seniors’ wellness, as well as enhance their proficiency with technology, the internet, and social media. |
Studio Without Wallsl –Saskatchewan |
University of Regina | Studio Without Walls is a telephone-based arts program that pairs older adults with professional artists. The artists provide older adults with advice over the phone on various creative arts (such as painting, writing). The program targets older adults living in rural areas, though all older adults are welcome to participate. Interviews are currently being conducted with participants as a part of a larger research project. |
StoryShare For Seniorsm –Calgary, Alberta |
Storytelling Alberta and Calgary Seniors Resource Society | The StoryShare program connects older adults with volunteer storytellers via telephone or video call. Volunteers are able to speak English, French, Spanish, Dutch and Urdu. StoryShare offers 3 free program options:
|
Confinés, ensemble!n –Quebec |
School of Public Health of the University of Montreal and Center for Public Health Research | Confinés, ensemble! is a project that invites seniors to take photos of their confinement during COVID-19 and then participate in weekly online meetings with other older adults to discuss their experiences. The project targets older adults who are living alone, living in a seniors residence, or a member of the LGBTQ community. The photos have now been developed into a virtual exhibition. |
- a Healthy Aging CORE British Columbia. (2020). Seniors Centre Without Walls (Seniors Outreach and Resource Centre).
- b Healthy Aging CORE British Columbia. (2020). Senior Centre Without Walls.
- c Alliance for Healthier Communities. (2020, July 29). Virtual care forum lunch & learn: Creating safe & accessible online spaces for marginalized older adults [Webinar]. Alliance for Healthier Communities.
- d Information provided through personal communication with organization.
- e Newall, N. E., & Menec, V. H. (2015). Targeting socially isolated older adults: A process evaluation of the senior centre without walls social and educational program. Journal of Applied Gerontology, 34(8), 958–976.
- f Edmonton Southside Primary Care Network. (n.d.). Project Highlights (Data from July 2016-April 2019). Edmonton Southside Primary Care Network.
- g Coordinated Pandemic Response Steering Committee. (2020). Coordinated Pandemic Response for Edmonton Senior Service Community.
- h Information provided by Provincial or Territorial contact.
- i Healthy Aging CORE British Columbia. (2020). Active Aging + & Digital Learning Pilot info session recording & slides.
- j Sunshine Centres for Seniors. (2020). Introducing Rainbow Tea and Talk, a new program for LGBTQ+ seniors!.
- k Hwang, P. (2021, February 12). Ottawa-area Inuit elders gather online to beat pandemic blues. CBC News.
- l Atter, H. (2021, February 8). 'Studio without Walls' connects older adults to artists over the phone. CBC News.
- m Lizee, T. (2021, February 22). Calgary outreach program connects with seniors virtually, records ‘legacy stories’. Global News.
- n Confinés, ensemble!. (2021). Le projet.
Annex 8. Examples of mechanisms to support learning and collaboration during the pandemic
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Healthy Aging CORE British Columbiaa –British Columbia |
United Way of the Lower Mainland; BC Ministry of Health and Employment and Social Development Canada (funding partners) | Healthy Aging CORE is an online virtual network that brings together community-based seniors’ services and other stakeholders to learn, share and collaborate. It was launched in February 2019. CORE was developed primarily with funding support from the BC Ministry of Health with some additional funding from the federal government through Employment and Social Development Canada. There are now almost 1,900 members who have joined CORE. CORE supports knowledge sharing through webinars, communities of practice, discussions groups, and a twice-monthly newsletter with over 1,200 subscribers. During the pandemic, the newsletter increased to weekly distribution, with alternate weeks focused on sharing COVID-19 related research, learnings, and educational opportunities. The CORE platform has also been used to manage and coordinate initiatives such as Safe Seniors, Strong Communities and the Digital Learning Pilot Projects during the pandemic. |
Healthy Aging CORE Albertab –Alberta |
United Way of Calgary and Area (backbone organization and fiscal agent); Government of Alberta, Alberta Health Services, Alberta Blue Cross, and the federal government (funding partners) | With volunteer leadership from 6 community organizations, the United Way of Calgary and Area acts as the backbone organization and fiscal agent for this project. The CORE Alberta website launched in May 2020 to provide information, resources, and training opportunities for Community-based seniors sector (CBSS) and allied agencies and individuals and to make it easier for these groups to communicate, coordinate, and collaborate during the COVID-19 pandemic and beyond. A Social Connection, Wellness and Mental Health discussion group focuses on developing solutions to help older adults maintain their social connections to others and maintain positive mental health. Since May 2020, the website has attracted over 560 members and hosted 14 discussion forums and learning events with over 870 participants. Follow-up surveys to the events indicate 85 per cent of participants find the events useful to their work. The CBSS initiative and CORE Alberta also offer a bi-weekly newsletter, which has over 850 subscribers. |
Info Centre - COVID-19 Resourcesb –Alberta |
Volunteer Alberta | Volunteer Alberta is equipping the non-profit sector to thrive and supporting volunteerism during the COVID-19 pandemic. Information includes volunteering during COVID, virtual volunteer engagement, fundraising, and financial assistance. |
Age-Friendly Community Outreach Programb –Ontario |
Age-Friendly Ontario; Government of Ontario (funder) | In 2020 to 2021, Ontario provided $165,000 to the Age-Friendly Community Outreach Program to support the development of more inclusive, accessible environments for older adults in communities across Ontario through outreach promotion and knowledge exchange. In response to the pandemic, this program supports social inclusion and healthy living for older adults through the creation of a new Community of Interest on Social Isolation and Loneliness that shares strategies to support isolated older adults through regular newsletters. Webinars related to COVID-19 issues (for example, isolation, financial security, and vulnerable populations) are also offered through the program. The Community of Interest on Social Isolation and Loneliness has nearly 200 participants. |
Community Transportation Networkb –Nova Scotia |
Nova Scotia Community Transportation Network Nova Scotia Department of Communities, Culture and Heritage (funder) |
The Community Transportation Network advocates for accessible transportation and helps support community-based transportation services. The network provides an opportunity for providers to share information, build the network, and help government enact policies that support growth. An important focus of the network is addressing transportation issues faced by socially isolated older adults. |
- a Information provided through personal communication with organization.
- b Information provided by Provincial or Territorial contact.
Annex 9. Examples of interventions to address the social isolation of older adults living in long-term care facilities
Table 12: Interventions to address social isolation in long-term care
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Shipping Container Visiting Spacea –New Westminster, British Columbia |
Queen's Park Care Centre | A shipping container has been converted into a furnished, heated visiting area with separate sections for residents and their family members, joined by a plexiglass window. Family members can book times to visit their loved ones. This project was funded by a $25,000 grant from the government. |
All-Season Visitation Sheltersb –Manitoba |
Government of Manitoba | The provincial government committed $17.9 million to build 90 shelters for personal care homes across Manitoba. The shelters can accommodate 1 resident and up to 5 visitors, with enhanced ventilation and cleaning. An enclosed link connects the shelter to the care home, and there is a separate entrance for visitors. |
Tablet Provision Programc –New Brunswick |
Government of New Brunswick | The provincial government provided each LTC facility with 1 tablet for every 10 residents (480 tablets total) to keep residents connected with family. Tablets also have applications to facilitate virtual care provision. The technology company BrunNet Inc. is responsible for providing the tablets and technical support. |
iPad Donationsd –Nova Scotia |
Government of Nova Scotia | The provincial government provided funding for the purchase of iPads for nursing homes to support connection with families. |
Tablets for Seniorsd –Prince Edward Island |
Government of PEI | The provincial government contributed funding and partnered with the Community Foundation of PEI to provide tablets to LTC and community care facilities across PEI to address social isolation of older adults during pandemic visitor restrictions. |
Project Joye –Alberta |
Project Joy | Project Joy was initiated during the pandemic and collects old tablets and smartphones to donate to older adults living in LTC facilities. The project has donation locations in Edmonton, Calgary, Red Deer, and Lethbridge. RJ Systems, a local technology company, assists with the setup, refurbishment, and management of the devices. Each device can be used by about 5 to 8 older adults, and to date over 1,000 older adults have been assisted. |
| LTC+ Initiatived | Canadian Foundation for Healthcare Improvement | The federal government provided $6.4 million over 2 years, starting in 2020 to 2021, to the Health Canada-funded Canadian Foundation for Healthcare Improvement (CFHI) to expand its LTC+ initiative. This initiative supports pandemic preparedness in LTC facilities and seniors residences with coaching and seed funding to help address gaps in infection prevention and control, and one of the areas of focus is the presence of family and essential care partners (caregivers). As well, CFHI released a checklist for essential care partners (ECPs) for safely re-entering LTC homes during COVID-19. This work builds on CFHI’s LTC + Initiative. |
| Intervention | Organizations | Description and outcomes |
|---|---|---|
Creative Connectionf –Canada-wide |
Creative Connection | Creative Connection was initiated by students from Western University during the pandemic. The program is operating at 16 institutions across Canada. It pairs student performers with residents in LTC homes, retirement homes and hospitals for virtual live musical and art performances and conversation. Sessions can be delivered 1-on-1 or as small group concerts. The program has over 170 volunteers and has connected with over 750 residents. Staff and residents have provided positive feedback about the musical performances. |
Companion Callsg –Toronto, Ontario |
Student Association for Geriatric Empowerment (SAGE) | SAGE was established by students at the University of Toronto and was developed to support LTC workers and residents. In the Companion Calls program, student volunteers make telephone or video calls to residents in LTC. SAGE has also provided other supports to LTC homes including letters, cards, and gardening supplies. |
- a CBC News. (2021, February 2). Shipping container gives care home residents and their families a new way to visit. CBC News.
- b Gerwing, M. (2020, September 15). Manitoba unveils all-season visitation shelters for care homes. CTV News.
- c Government of New Brunswick. (2020, April 22). Nursing homes provided with iPads; no new cases today [Press Release].
- d Information provided by Provincial or Territorial contact.
- e Poignant, G. (2021, February 6). Tech-savvy charity connects seniors with loved ones. St. Albert Today.
- f Mackay, C. (2020, December 7). Music sparks virtual connections with the community’s most vulnerable. Western News.
- g McNeely, S. (2020, August 20). COVID-19: After studying elder care, U of T students form group to support seniors and front-line staff. U of T News.
Annex 10. Governmental grant programs and funding to support the implementation of interventions to address the social isolation of older adults during the pandemic
| Grant program | Governmental organization | Grant description |
|---|---|---|
| Community Transportation Assistance Program | Nova Scotia Department of Communities, Culture and Heritage | Municipalities and non-profit organizations can apply for funding from the Community Transportation Assistance Program to cover a portion of the operating costs of a community-based, inclusive transportation service. Inclusive transportation services are community-based public transportation systems in rural Nova Scotia aimed at improving transportation options to Nova Scotians who need transportation to and from medical appointments, education, and recreation opportunities. Supporting community transportation providers is a key priority of Shift: Nova Scotia’s Action Plan for an Aging Population. |
| Age-Friendly Communities Grant | Nova Scotia Department of Seniors | The Age-Friendly Communities Grant program is an ongoing program offered by the Department of Seniors. One of the goals of the program is to help overcome the social isolation of older adults, and help them stay active, healthy, and engaged in their communities. Examples of funded initiatives of Nova Scotia’s Age-Friendly Communities Grant |
| PlanH Community Connectedness Grants (2020/21) | BC Healthy Communities Society (which manages PlanH on behalf of the BC Ministry of Health) | For 2020 to 2021, one of the PlanH Healthy Communities grant program streams focuses on Community Connectedness. These grants support communities as they take multi-sectoral action to explore, learn, and innovate, enhancing community cohesion and sense of belonging. While not specific to older adults, this grant stream fosters connection to others within community, even during public health emergencies that call for people to be physically apart in order to combat the negative long-term health outcomes of loneliness and isolation. The grants were awarded to 15 recipient communities, including 4 First Nation communities and 1 Métis Society. As the initiatives supported by these grants roll out, there will be a better understanding of their impacts. BC Healthy Communities conducts an evaluation with each of the recipient communities. |
| BC Age-Friendly Communities (AFC) grant program | BC Ministry of Health | The AFC grants and capacity-building supports are made available to local governments (for example, municipalities, regional districts, First Nations) to promote age-friendly public health by fostering physical and social environments to assist older adults as they age. To date, 397 grants have been issued to promote age-friendly community initiatives to across BC. |
| Emergency Funding | Government of Alberta | The funding ($30 million) targets charities, not-for-profits and civil society organizations. Successful grant recipients are providing services to address the social well-being of those most affected by COVID-19 and the measures implemented to limit the spread of the virus. Programs or services provided include mental health, emotional support, access to information and supports, outreach, technology, and social isolation. |
| Community Initiatives Program Operating grant | Government of Alberta | The Community Initiatives Program (CIP) provides funding for organizations (non-profit and charitable organizations) that create opportunities for Albertans to engage with and help develop their communities. This one-time intake prioritized small and medium-sized organizations that focus on food security, shelter, and housing, and addictions and mental health supports so they can continue to care for vulnerable Albertans. Increased funding ($8 million) has been provided to this program. |
| Increased mental health supports | Government of Alberta | The program provides funding ($53 million) to charitable organizations, non-profits, faith organizations, and small community groups to implement more online, phone and in-person mental health and addiction recovery support to make it easier for Albertans to access services from anywhere in Alberta during and after the COVID-19 pandemic. |
| Aging Well in Communities (AWIC) grant program | Government of Alberta | The grants help non-profit and charitable organizations provide supports to seniors to help them remain independent and participate in their communities. The 2018 to 2019 call for proposals provided up to a maximum of $100,000 per project, for up to a 3-year term. In early 2020, AWIC grant recipients were offered flexibility as they adapt their services in response to the pandemic, including addressing the social isolation of seniors. |
| Inclusive Community Grants Program | Government of Ontario | On November 9, 2020, Ontario launched a new Inclusive Community Grants program to provide grants of up to $60,000 for local initiatives designed to create more age-friendly and inclusive communities for older adults and people with disabilities. This is an investment of $3.5 million over 2 years in local governments and community organizations. |
| Seniors Community Grants Program | Government of Ontario | The 2020 to 2021 Seniors Community Grant Program is providing over $4 million to support local community organizations in addressing issues faced by older adults, including social isolation. Since 2018, Seniors Community Grants will have supported almost 700 local community programs in Ontario. |
| Seniors Active Living Centre Program | Government of Ontario | To help combat social isolation during COVID-19, Ontario invested an additional $3.1 million in 2021 to 2022 for a total of $17.2 million in the Seniors Active Living Centre (SALC) Program. Ontario provides support to almost 300 SALC programs across the province, which provide social connections and programing to older adults. During COVID-19, SALC operators stopped in-person programming but many shifted to offering virtual supports, including working with the Older Adult Centres’ Association of Ontario (OACAO) to expand use of the SCWW model. |
| Seniors Secretariat Grant Program | Government of PEI | Seniors groups may apply on annual basis for funding of up to $5,000 to implement projects designed to address social isolation, among other criteria. In recent years, the Program has seen a growth in interest. |
| Seniors’ Social Inclusion Initiative | Government of Newfoundland and Labrador | The Seniors’ Social Inclusion Initiative provides support to 50 plus clubs, other seniors’ organizations and other organizations that support seniors. Unincorporated groups receive up to $1,000 and incorporated groups up to $2,000 to support social engagement of older adults. Reports from funded groups indicate an increase in social engagement. The program has been responsive to the changing COVID situation by allowing groups to reprofile funds (for example instead of outings and gatherings, groups are providing PPE and healthy food hampers). |
Note: all information provided by provincial or territorial contacts in February or March 2021.
References
AgeWell NCE. (2020a). COVID-19 has significantly increased the use of many technologies among older Canadians: poll.
https://agewell-nce.ca/archives/10884
Age-Well NCE. (2020b). Living under Covid-19 restrictions: The experiences of older adults and caregivers.
https://agewell-nce.ca/wp-content/uploads/OACAC_Living_under_COVID-19_restrictions_June2020.pdf
Alliance for Healthier Communities. (2020). Rx: community – Social prescribing in Ontario, final report.
https://cdn.ymaws.com/aohc.site-ym.com/resource/group/e0802d2e-298a-4d86-8af5-21156f9c057f/rxcommunity_final_report_mar.pdf
Alonso-Lana, S., Marquié, M., Ruiz, A., & Boada, M. (2020). Cognitive and neuropsychiatric manifestations of COVID-19 and effects on elderly individuals with dementia. Frontiers in Aging Neuroscience, 12, 588872.
https://doi.org/10.3389/fnagi.2020.588872
Alonzi, S., La Torre, A., & Silverstein, M. W. (2020). The psychological impact of pre-existing mental and physical health conditions during the COVID-19 pandemic. Psychological Trauma, 12(S1), S236–S238.
Anderson, S., & Parmar, J. (2020). A tale of two solitudes experienced by Alberta family caregivers during the COVID-19 pandemic. University of Alberta.
https://corealberta.ca/resources/alberta-family-caregivers-impacts-covid-19-pandemic
Andrew, M., Searle, S. D., McElhaney, J. E., McNeil, S. A., Clarke, B., Rockwood, K., & Kelvin, D. J. (2020). COVID-19, frailty and long-term care: Implications for policy and practice. Journal of Infection in Developing Countries, 14(5), 428–432.
https://doi.org/10.3855/jidc.13003
Archambault, D., Sanford, C., & Perry, T. (2020). Detroit’s efforts to meet the needs of seniors: Macro responses to a crisis. Journal of Gerontological Social Work, 63(6/7), 706–708.
Arctic Council. (2020). Covid-19 in the Arctic: Briefing document for senior Arctic officials.
https://oaarchive.arctic-council.org/bitstream/handle/11374/2473/COVID-19-in-the-Arctic-Briefing-to-SAOs_For-Public-Release.pdf?sequence=3&isAllowed=y
Armstrong, M. J. & Alliance, S. (2019). Virtual support groups for informal caregivers of individuals with dementia. Alzheimer Disease & Associated Disorders, 33(4), 362–369.
https://doi.org/10.1097/WAD.0000000000000349
Assembly of First Nations. (2020). A new path forward: AFN COVID-19 discussion paper – Summary for input.
https://www.afn.ca/wp-content/uploads/2020/12/20_11_16_DRAFT-Discussion-Paper_Summary-Document.pdf
Ayalon, L. (2020). There is nothing new under the sun: Ageism and intergenerational tension in the age of the COVID-19 outbreak. International Psychogeriatrics, 32(10), 1221–1224.
https://doi.org/10.1017/S1041610220000575
Banning, J. (2020). How Indigenous people are coping with COVID-19. Canadian Medical Association Journal, 192(27), E787–E788.
https://doi.org/10.1503/cmaj.1095879
Barber, S. J., & Kim, H. (2021). COVID-19 worries and behavior changes in older and younger men and women. The Journals of Gerontology, Series B, Psychological Sciences and Social Sciences, 76(2), 17–23.
https://doi.org/10.1093/geronb/gbaa068
Benoit-Dubé, L., Jean, E. K., Aguilar, M. A., Zuniga, A.-M., Bier, N., Couture, M., Lussier, M., Lajoie, X., & Belchior, P. (2020). What facilitates the acceptance of technology to promote social participation in later life? A systematic review. Disability and Rehabilitation. Assistive Technology, 1–11.
https://doi.org/10.1080/17483107.2020.1844320
Bergman, Y. S., Cohen-Fridel, S., Shrira, A., Bodner, E., & Palgi, Y. (2020a). Covid-19 health worries and anxiety symptoms among older adults: The moderating role of ageism. International Psychogeriatrics.
https://doi.org/10.1017/S1041610220001258
Bergman, C., Stall, N. M., Haimowitz, D., Aronson, L., Lynn, J., Steinberg, K., & Wasserman, M. (2020b). Recommendations for welcoming back nursing home visitors during the COVID-19 pandemic: Results of a delphi panel. Journal of the American Medical Directors Association, 21(12), 1759–1766.
Bethell, J., Aelick, K., Babineau, J., Bretzlaff, M., Edwards, C., Gibson, J.-L., Hewitt Colborne, D., Iaboni, A., Lender, D., Schon, D., & McGilton, K. S. (2020). Social connection in long-term care homes: A scoping review of published research on the mental health impacts and potential strategies during COVID-19. Journal of the American Medical Directors Association.
https://doi.org/10.1016/j.jamda.2020.11.025
Botner, E. (2018). Impact of a virtual learning program on social isolation for older adults. Therapeutic Recreation Journal, 52(2), 126–139.
Bridgepoint Active Healthcare. (2020, April 21). Distancing but still social – Therapeutic recreation during COVID-19. Sinai Health.
https://www.sinaihealth.ca/news/distancing-but-still-social-therapeutic-recreation-during-covid-19/
Burholt, V., Winter, B., Aartsen, M., Constantinou, C., Dahlberg, L., Feliciano, V., De Jong Gierveld, J., Van Regenmortel, S., Waldegrave, C., & Working Group on Exclusion from Social Relations, part of the COST-financed Research Network ‘Reducing Old-Age Exclusion: Collaborations in Research and Policy’ (ROSENet). (2019). A critical review and development of a conceptual model of exclusion from social relations for older people. European Journal of Ageing, 17(1), 3–19.
https://doi.org/10.1007/s10433-019-00506-0
Burke, S. (2020). Stronger together? Intergenerational connection and Covid-19. Quality in Ageing & Older Adults, 21(4), 253–259.
https://doi.org/10.1108/QAOA-07-2020-0033
Burnes, D., Sheppard, C., Henderson, C. R., Jr, Wassel, M., Cope, R., Barber, C., & Pillemer, K. (2019). Interventions to reduce ageism against older adults: A systematic review and meta-analysis. American Journal of Public Health, 109(8), e1–e9.
https://doi.org/10.2105/AJPH.2019.305123
Canadian Foundation for Healthcare Improvement. (2020). LTC+: Acting on pandemic learning together.
https://www.cfhi-fcass.ca/what-we-do/enhance-capacity-and-capability/ltc-acting-on-pandemic-learning-together
Canadian Institute for Health Information. (2018). Dementia in long-term care.
https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-long-term-care
Canadian Institute for Health Information. (2021). The impact of COVID-19 on long-term care in Canada: Focus on the first 6 months.
https://www.cihi.ca/sites/default/files/document/impact-covid-19-long-term-care-canada-first-6-months-report-en.pdf
Canadian Longitudinal Study on Aging. (2021). COVID-19 study data dashboard.
https://www.clsa-elcv.ca/covid-study-results
Carr, D., Boerner, K., & Moorman, S. (2020). Bereavement in the time of coronavirus: Unprecedented challenges demand novel interventions. Journal of Aging & Social Policy, 32(4–5), 425–431.
https://doi.org/10.1080/08959420.2020.1764320
Cattan, M., Kime, N., & Bagnall, A‐M. (2011). The use of telephone befriending in low level support for socially isolated older people – an evaluation. Health & Social Care in the Community, 19(2), 198–206.
https://doi.org/10.1111/j.1365-2524.2010.00967.x
CBC News. (2021, February 2). Calgary group recruiting volunteers to drive seniors to appointments. CBC News.
https://www.cbc.ca/news/canada/calgary/senior-transportation-volunteer-vaccine-1.5896936
Chatters, L. M., Taylor, H. O., & Taylor, R. J. (2020). Older black Americans during COVID-19: Race and age double jeopardy. Health Education & Behavior, 47(6), 855–860.
https://doi.org/10.1177/1090198120965513
Chen, Y. R., & Schulz, P. J. (2016). The effect of information communication technology interventions on reducing social isolation in the elderly: A systematic review. Journal of Medical Internet Research, 18(1), e18.
https://doi.org/10.2196/jmir.4596
Coe, N. B., & Van Houtven, C. H. (2020). Living arrangements of older adults and COVID‐19 risk: It is not just nursing homes. Journal of the American Geriatrics Society, 68(7), 1398–1399.
https://doi.org/10.1111/jgs.16529
Cohen, M., & Tavares, J. (2020). Who are the most at-risk older adults in the COVID-19 era? It’s not just those in nursing homes. Journal of Aging and Social Policy, 32(4–5), 380–386.
https://doi.org/10.1080/08959420.2020.1764310
Cohen-Mansfield, J., Muff, A., Meschiany, G., & Lev-Ari, S. (2021). Adequacy of web-based activities as a substitute for in-person activities for older persons during the COVID-19 pandemic: Survey study. Journal of Medical Internet Research, 23(1), e25848.
https://doi.org/10.2196/25848
Conroy, K. M., Krishnan, S., Mittelstaedt, S., & Patel, S. S. (2020). Technological advancements to address elderly loneliness: Practical considerations and community resilience implications for COVID-19 pandemic. Working with Older People: Community Care Policy & Practice, 24(4), 257–264.
https://doi.org/10.1108/WWOP-07-2020-0036
Coordinated Pandemic Response Steering Committee. (2020). Coordinated pandemic response for Edmonton senior service community.
https://www.seniorscouncil.net/uploads/files/Edmonton-Senior-Serving-Pandemic-Response-Report-FINAL.pdf
Coroiu, A., Moran, C., Campbell, T., & Geller, A. C. (2020). Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS ONE, 15(10), 1–20.
https://doi.org/10.1371/journal.pone.0239795
Courtin, E., & Knapp, M. (2017). Social isolation, loneliness and health in old age: A scoping review. Health & Social Care in the Community, 25(3), 799–812.
https://doi.org/10.1111/hsc.12311
Damant, J., Knapp, M., Freddolino, P., & Lombard, D. (2017). Effects of digital engagement on the quality of life of older people. Health & Social Care in the Community, 25(6), 1679–1703.
https://doi.org/10.1111/hsc.12335
Damiot, A., Pinto, A. J., Turner, J. E., & Gualano, B. (2020). Immunological implications of physical inactivity among older adults during the COVID-19 pandemic. Gerontology, 66(5), 431–438.
Dassieu, L., & Sourial, N. (2021). Tailoring interventions for social isolation among older persons during the COVID-19 pandemic: Challenges and pathways to healthcare equity. International Journal for Equity in Health, 20(1), 1–4.
Davidson, J., & Schimmele, C. (2019). Evolving internet use among Canadian seniors. Statistics Canada.
https://www150.statcan.gc.ca/n1/pub/11f0019m/11f0019m2019015-eng.htm
Day, P., Gould, J., & Hazelby, G. (2020). A public health approach to social isolation in the elderly. Journal of Community Nursing, 34(3), 54–59.
D’cruz, M., & Banerjee, D. (2020). “An invisible human rights crisis”: The marginalization of older adults during the COVID-19 pandemic—An advocacy review. Psychiatry Research, 292.
De Jong Gierveld, J., Keating, N., & Fast, J. E. (2015). Determinants of loneliness among older adults in Canada. Canadian Journal on Aging, 34(2), 125–136.
https://doi.org/10.1017/S0714980815000070
DeLange Martinez, P., Nakayama, C., & Young, H. M. (2020). Age-friendly cities during a global pandemic. Journal of Gerontological Nursing, 46(12), 7–13.
https://doi.org/10.3928/00989134-20201106-02
Dewis, G. (2020). Access and use of parks and green spaces: The potential impact of COVID-19 on Canadian households. Statistics Canada.
https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00031-eng.htm
Edmonton Southside Primary Care Network. (n.d.). Project Highlights (Data from July 2016-April 2019). Edmonton Southside Primary Care Network.
Edmonton Southside Primary Care Network. (2020). Seniors' centre without walls toolkit.
https://corealberta.ca/programs/seniors-centre-without-walls-program
Elman, A., Breckman, R., Clark, S., Gottesman, E., Rachmuth, L., Reiff, M., Callahan, J., Russell, L. A., Curtis, M., Solomon, J., Lok, D., Sirey, J. A., Lachs, M. S., Czaja, S., Pillemer, K., & Rosen, T. (2020). Effects of the COVID-19 outbreak on elder mistreatment and response in New York City: Initial lessons. Journal of Applied Gerontology, 39(7), 690–699.
Emerson, K. G. (2020). Coping with being cooped up: social distancing during COVID-19 among 60+ in the United States. Pan American Journal of Public Health, 44(e81).
https://doi.org/10.26633/RPSP.2020.81
Estabrooks, C.A., Straus, S., Flood, C.M., Keefe, J., Armstrong, P., Donner, G., Boscart, V., Ducharme, F., Silvius, J., & Wolfson, M. (2020). Restoring trust: COVID-19 and the future of long-term care. Royal Society of Canada.
Fakoya, O. A., McCorry, N. K., & Donnelly, M. (2020). Loneliness and social isolation interventions for older adults: A scoping review of reviews. BMC Public Health, 20(1), 1-14.
Fearn, M., Harper, R., Major, G., Bhar, S., Bryant, C., Dow, B., Dunt, D., Mnatzaganian, G., O’Connor, D., Ratcliffe, J., Samuel, S., Bagnall, A. M., & Doyle, C. (2021). Befriending older adults in nursing homes: Volunteer perceptions of switching to remote befriending in the covid-19 era. Clinical Gerontologist: The Journal of Aging and Mental Health.
https://doi.org/10.1080/07317115.2020.1868646
First Nations Health Authority. (2020). Fewer faces, wide-open spaces: A guide to gatherings and events during Covid-19.
https://www.fnha.ca/Documents/FNHA-Fewer-Faces-Wide-Open-Spaces-A-Guide-to-Gatherings-and-Events-During-COVID-19.pdf
Fingerman, K. L., Ng, Y. T., Zhang, S., Britt, K., Colera, G., Birditt, K. S., & Charles, S. T. (2020). Living alone during COVID-19: Social contact and emotional well-being among older adults. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences.
https://doi.org/10.1093/geronb/gbaa200
Flint, A. J., Bingham, K. S., & Iaboni, A. (2020). Effect of COVID-19 on the mental health care of older people in Canada. International Psychogeriatrics, 32(10), 1113–1116.
https://doi.org/10.1017/S1041610220000708
Frank, K. (2020). COVID-19 and social support for seniors: Do seniors have people they can depend on during difficult times? Statistics Canada.
https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00007-eng.htm
Franke, T., Sims-Gould, J., Nettlefold, L., Ottoni, C., & McKay, H. A. (2021). "It makes me feel not so alone": Features of the Choose to Move physical activity intervention that reduce loneliness in older adults. BMC Public Health, 21(1), 312.
https://doi.org/10.1186/s12889-021-10363-1
Fraser, S., Lagacé, M., Bongué, B., Ndeye, N., Guyot, J., Bechard, L., Garcia, L., Taler, V., Group, C. S. I. and S. W., Adam, S., Beaulieu, M., Bergeron, C. D., Boudjemadi, V., Desmette, D., Donizzetti, A. R., Éthier, S., Garon, S., Gillis, M., Levasseur, M., & Lortie-lussier, M. (2020). Ageism and COVID-19: What does our society’s response say about us? Age & Ageing, 49(5), 692–695.
https://doi.org/10.1093/ageing/afaa097
Fryer, S., & Collier, B. (2020, May 26). Inuit Nunangat and COVID-19. Library of Parliament.
https://hillnotes.ca/2020/05/26/inuit-nunangat-and-covid-19/
Funnell, S. (2021, January 12). Vaccine hesitancy and First Nations, Inuit and Métis populations – Potential implications during COVID-19 [Webinar]. National Collaborating Centre for Infectious Disease.
https://nccid.ca/webcast/vaccine-hesitancy-and-first-nations-inuit-and-metis-populations-during-covid-19/
Gallagher, S., & Wetherell, M. A. (2020). Risk of depression in family caregivers: Unintended consequence of COVID-19. BJPsych Open, 6(6), e119.
https://doi.org/10.1192/bjo.2020.99
Garneau, K., & Zossou, C. (2021). Misinformation during the COVID-19 pandemic. Statistics Canada.
https://www150.statcan.gc.ca/n1/pub/45-28-0001/2021001/article/00003-eng.htm
Gauthier, G. R., Smith, J. A., García, C., Garcia, M. A., & Thomas, P. A. (2021). Exacerbating inequalities: Social networks, racial/ethnic disparities, and the COVID-19 pandemic in the United States. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 76(3), e88–e92.
https://doi.org/10.1093/geronb/gbaa117
Giwa, S., Mullings, D. V., & Karki, K. K. (2020). Virtual social work care with older black adults: A culturally relevant technology-based intervention to reduce social isolation and loneliness in a time of pandemic. Journal of Gerontological Social Work, 63(6-7), 679–681.
https://doi.org/10.1080/01634372.2020.1800885
Golden, J., Conroy, R. M., Bruce, I., Denihan, A., Greene, E., Kirby, M., & Lawlor, B. A. (2009). Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. International Journal of Geriatric Psychiatry, 24(7), 694–700.
https://doi.org/10.1002/gps.2181
Gorenko, J. A., Moran, C., Flynn, M., Dobson, K., & Konnert, C. (2021). Social isolation and psychological distress among older adults related to COVID-19: A narrative review of remotely-delivered interventions and recommendations. Journal of Applied Gerontology, 40(1), 3–13.
https://doi.org/10.1177/0733464820958550
Government of Canada. (2020a). Coronavirus disease (COVID-19). Retrieved April 12, 2021 from
https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19.html
Government of Canada. (2020b). Risk mitigation tool for outdoor recreation spaces and activities operating during the COVID-19 pandemic. Retrieved February 28, 2021 from
https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/risk-mitigation-tool-outdoor-recreation-spaces-activities-operating-covid-19.html
Gray-Miceli, D., Bouchaud, M., Mitchell, A. B., DiDonato, S., & Siegal, J. (2020). Caught off guard by Covid-19: Now what?. Geriatric Nursing, 41(6), 1020–1024.
https://doi.org/10.1016/j.gerinurse.2020.10.009
Grossman, E. S., Hoffman, Y. S. G., Palgi, Y., & Shrira, A. (2021). COVID-19 related loneliness and sleep problems in older adults: Worries and resilience as potential moderators. Personality & Individual Differences, 168.
Grotz, J., Dyson, S., & Birt, L. (2020). Pandemic policy making: The health and wellbeing effects of the cessation of volunteering on older adults during the COVID-19 pandemic. Quality in Ageing & Older Adults, 21(4), 261–269.
https://doi.org/10.1108/QAOA-07-2020-0032
Gutman, G., de Vries, B., Beringer, R., Daudt, H., & Gill, P. (2021). COVID-19 experiences and Advance Care Planning (ACP) among Older Canadians: Influence of age, gender and sexual orientation. SFU Gerontology Research Centre.
http://www.sfu.ca/lgbteol.html
Hahmann, T., du Plessis, V., & Fournier-Savard, P. (2020). Volunteering in Canada: Challenges and opportunities during the COVID-19 pandemic. Statistics Canada.
https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00037-eng.htm
Hajek, A., & König, H.-H. (2020). Social isolation and loneliness of older adults in times of the COVID-19 pandemic: Can use of online social media sites and video chats assist in mitigating social isolation and loneliness?Gerontology, 1–3.
https://doi.org/10.1159/000512793
Han, S. D., & Mosqueda, L. (2020). Elder abuse in the COVID-19 era. Journal of the American Geriatrics Society, 68(7), 1386–1387.
https://doi.org/10.1111/jgs.16496
Hannah, J. (2020). A report on “Safe Seniors, Strong Communities”. United Way of the Lower Mainland.
https://bc.healthyagingcore.ca/resources/report-safe-seniors-strong-communities-6-month-summary-march-27-september-30-2020
Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Annals of Behavioral Medicine, 40(2), 218–227.
https://doi.org/10.1007/s12160-010-9210-8
Health Quality Council of Alberta. (2021). Residents’ perceptions and lived experiences during the COVID-19 pandemic report.
https://hqca.ca/covid-19-continuing-care
Hebblethwaite, S., Young, L., & Martin Rubio, T. (2020). Pandemic precarity: Aging and social engagement. Leisure Sciences.
https://doi.org/10.1080/01490400.2020.1773998
Henning-Smith C. (2020). The unique impact of COVID-19 on older adults in rural areas. Journal of Aging & Social Policy, 32(4-5), 396–402.
https://doi.org/10.1080/08959420.2020.1770036
Hill, P. L., Lewis, N. A., & Burrow, A. L. (2020). Purpose after retirement during COVID-19: Trying to find direction in retirement communities. American Journal of Geriatric Psychiatry, 28(7), 788–789.
https://doi.org/10.1016/j.jagp.2020.04.019
Hwang, T.-J., Rabheru, K., Peisah, C., Reichman, W., & Ikeda, M. (2020). Loneliness and social isolation during the COVID-19 pandemic. International Psychogeriatrics, 32(10), 1217–1220.
https://doi.org/10.1017/S1041610220000988
Ibarra, F., Baez, M., Cernuzzi, L., & Casati, F. (2020). A systematic review on technology-supported interventions to improve old-age social wellbeing: Loneliness, social isolation, and connectedness. Journal of Healthcare Engineering, 2020, 2036842.
https://doi.org/10.1155/2020/2036842
Ickert, C., Rozak, H., Masek, J., Eigner, K., & Schaefer, S. (2020). Maintaining resident social connections during COVID-19: Considerations for long-term care. Gerontology & Geriatric Medicine, 6, 2333721420962669.
https://doi.org/10.1177/2333721420962669
InCommon and Clarion Futures. (2020). Sustaining intergenerational connections at a time of crisis.
https://corealberta.ca/resources/sustaining-intergenerational-connections-time-crisis
Institut national d'excellence en santé et services sociaux. (2020). COVID-19 et la socialisation à distance entre les personnes hébergées et les proches aidants en contexte d’interdiction de visite.
https://www.inesss.qc.ca/en/covid-19/services-sociaux/socialisation-a-distance-personnes-hebergees-et-proches-aidants.html
Inuit Tapiriit Kanatami. (2020). The potential impacts of COVID-19 on Inuit Nunangat.
https://www.itk.ca/the-potential-impacts-of-covid-19-on-inuit-nunangat/
Institut national de santé publique du Québec. (2020). Lutter contre l’isolement social et la solitude des personnes aînées en contexte de pandémie.
https://www.inspq.qc.ca/sites/default/files/publications/3033-isolement-social-solitude-aines-pandemie-covid19.pdf
Jen, S., Stewart, D., & Woody, I. (2020). Serving LGBTQ+/SGL elders during the novel Corona Virus (COVID-19) pandemic: Striving for justice, recognizing resilience. Journal of Gerontological Social Work, 63(6/7), 607–610.
https://doi.org/10.1080/01634372.2020.1793255
Joosten-Hagye, D., Katz, A., Sivers-Teixeira, T., & Yonshiro-Cho, J. (2020). Age-friendly student senior connection: students' experience in an interprofessional pilot program to combat loneliness and isolation among older adults during the COVID-19 pandemic. Journal of Interprofessional Care, 34(5), 668–671.
https://doi.org/10.1080/13561820.2020.1822308
Jopling, K. (2020). Promising approaches revisited: Effective action on loneliness in later life. Campaign to End Loneliness.
https://www.campaigntoendloneliness.org/promising-approaches-revisited/
Kadowaki, L., Wister, A. V., & Chappell, N. L. (2015). Influence of home care on life satisfaction, loneliness, and perceived life stress. Canadian Journal on Aging, 34(1), 75–89.
https://doi.org/10.1017/S0714980814000488
Keefe, J., Andrew, M., Fancey, P., & Hall, M. (2006). Final report: A profile of social isolation in Canada. Submitted to the Chair of the F/P/T Working Group on Social Isolation.
Kennedy, T. (2020, May 29). Recreation therapy gets creative. Alberta Health Services.
https://www.albertahealthservices.ca/news/features/2020/Page15505.aspx
Kirkland, S. A., Griffith, L. E., Menec, V., Wister, A., Payette, H., Wolfson, C., & Raina, P. S. (2015). Mining a unique Canadian resource: The Canadian Longitudinal Study on Aging. Canadian Journal on Aging, 34(3), 366–377.
https://doi.org/10.1017/S071498081500029X
Klasa, K., Galaitsi, S., Trump, B., & Linkov, I. (2021a). Science and practice of resilience: Disaster systems applications to aging model development. In A. Wister & T. Cosco, (Eds.), Resilience and Aging: Emerging Science and Future Possibilities. Springer.
Klasa, K., Galaitsi, S., Wister, A., & Linkov, I. (2021b). System models for resilience in gerontology: Application to the COVID-19 pandemic. BMC Geriatrics.
Kotwal, A. A., Holt-Lunstad, J., Newmark, R. L., Cenzer, I., Smith, A. K., Covinsky, K. E., Escueta, D. P., Lee, J. M., & Perissinotto, C. M. (2021). Social Isolation and Loneliness Among San Francisco Bay Area Older Adults During the COVID-19 Shelter-in-Place Orders. Journal of the American Geriatrics Society, 69(1), 20–29.
https://doi.org/10.1111/jgs.16865
Krendl, A. C., & Perry, B. L. (2020). The impact of sheltering-in-place during the COVID-19 pandemic on older adults’ social and mental well-being. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences.
https://doi.org/10.1093/geronb/gbaa110
Lam, K., Lu, A. D., Shi, Y., & Covinsky, K. E. (2020). Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Internal Medicine, 180(10), 1389–1391.
https://doi.org/10.1001/jamainternmed.2020.2671
Lee, K., Fields, N. L., Cassidy, J., & Feinhals, G. (2021). Process and outcomes of telephone reassurance program training for older adult volunteers. Educational Gerontology, 47(1), 36–45.
Lee, H., & Miller, V. J. (2020). The disproportionate impact of COVID-19 on minority groups: A social justice concern. Journal of Gerontological Social Work, 63(6/7), 580–584.
Leigh-Hunt, N., Bagguley, D., Turner, V., Turnbull, N., Valtorta, N., & Caan, W. (2017). An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health, 152, 157–171.
https://doi.org/10.1016/j.puhe.2017.07.035
Liu, Y., Gayle, A., Wilder-Smith, A., & Rocklöv, J. (2020). The reproductive number of COVID-19 is higher compared to SARS coronavirus. Journal of Travel Medicine, 27(2), taaa021.
https://doi.org/10.1093/jtm/taaa021
Long-Term Care and Covid-19 Task Force. (2020). Long-term care and Covid-19: Report of a special task force prepared for the Chief Science Advisor of Canada. Office of the Chief Science Advisor of Canada.
https://www.ic.gc.ca/eic/site/063.nsf/eng/h_98049.html
Losada-Baltar, A., Jiménez-Gonzalo, L., Gallego-Alberto, L., Pedroso-Chaparro, M. D. S., Fernandes-Pires, J., & Márquez-González, M. (2021). “We are staying at home.” Association of self-perceptions of aging, personal and family resources, and loneliness with psychological distress during the lock-down period of COVID-19. Journals of Gerontology, Series B, Psychological Sciences and Social Sciences, 76(2), e10–e16.
https://doi.org/10.1093/geronb/gbaa048
Luchetti, M., Lee, J. H., Aschwanden, D., Sesker, A., Strickhouser, J. E., Terracciano, A., & Sutin, A. R. (2020). The trajectory of loneliness in response to COVID-19. American Psychologist, 75(7), 897–908.
https://doi.org/10.1037/amp0000690
Makaroun, L. K., Beach, S., Rosen, T., & Rosland, A. M. (2021). Changes in Elder Abuse Risk Factors Reported by Caregivers of Older Adults during the COVID-19 Pandemic. Journal of the American Geriatrics Society, 69(3), 602–603.
https://doi.org/10.1111/jgs.17009
Manca, R., De Marco, M., & Venneri, A. (2020). The impact of COVID-19 infection and enforced prolonged social isolation on neuropsychiatric symptoms in older adults with and without dementia: A review. Frontiers in Psychiatry, 11, 585540.
https://doi.org/10.3389/fpsyt.2020.585540
Marston, H. R., & van Hoof, J. (2019). "Who doesn't think about technology when designing urban environments for older people?" A case study approach to a proposed extension of the WHO's age-friendly cities model. International Journal of Environmental Research and Public Health, 16(19), 3525.
https://doi.org/10.3390/ijerph16193525
Mauvais-Jarvis, F. (2020). Aging, male sex, obesity, and metabolic inflammation create the perfect storm for COVID-19. Diabetes, 69(9), 1857–1863.
McArthur, C., Saari, M., Heckman, G. A., Wellens, N., Weir, J., Hebert, P., Turcotte, L., Jbilou, J., & Hirdes, J. P. (2021). Evaluating the effect of COVID-19 pandemic lockdown on long-term care residents’ mental health: A data-driven approach in New Brunswick. Journal of the American Medical Directors Association, 22(1), 187–192.
https://doi.org/10.1016/j.jamda.2020.10.028
Meisner, B. A. (2020). Are you ok, boomer? Intensification of ageism and intergenerational tensions on social media amid covid-19. Leisure Sciences.
https://doi.org/10.1080/01490400.2020.1773983
Meisner, B. A., Boscart, V., Gaudreau, P., Stolee, P., Ebert, P., Heyer, M., Kadowaki, L., Kelly, C., Levasseur, M., Massie, A. S., Menec, V., Middleton, L., Sheiban Taucar, L., Thornton, W. L., Tong, C., van den Hoonaard, D. K., & Wilson, K. (2020). Interdisciplinary and collaborative approaches needed to determine impact of COVID-19 on older adults and aging: CAG/ACG and CJA / RCV Joint Statement. Canadian Journal on Aging, 39(3), 333–343.
Menec, V. H., Means, R., Keating, N., Parkhurst, G., & Eales, J. (2011). Conceptualizing age-friendly communities. Canadian Journal on Aging, 30(3), 479-493.
Mitra, A.R., Fergusson, N.A., Lloyd-Smith, E., Wormsbecker, A., Foster, D., Karpov, A., Crowe, S., Haljan, G., Chittock, D.R., Kanji, H.D., Sekhon, M.S., & Griesdale, D. (2020). Baseline characteristics and outcomes of patients with COVID-19 admitted to intensive care units in Vancouver, Canada: a case series. Canadian Medical Association Journal, 192(26), E694–E701.
https://doi.org/10.1503/cmaj.200794
Monahan, C., Macdonald, J., Lytle, A., Apriceno, M., & Levy, S. R. (2020). COVID-19 and ageism: How positive and negative responses impact older adults and society. American Psychologist, 75(7), 887–896.
https://doi.org/10.1037/amp0000699
Monin, J. K., Ali, T., Syed, S., Piechota, A., Lepore, M., Mourgues, C., Gaugler, J. E., Marottoli, R., & David, D. (2020a). Family communication in long-term care during a pandemic: Lessons for enhancing emotional experiences. The American Journal of Geriatric Psychiatry.
https://doi.org/10.1016/j.jagp.2020.09.008
Morrow-Howell, N., Galucia, N., & Swinford, E. (2020). Recovering from the COVID-19 pandemic: A focus on older adults. Journal of Aging & Social Policy, 32(4/5), 526–535.
https://doi.org/10.1080/08959420.2020.1759758
National Collaborating Centre for Methods and Tools & National Collaborating Centre for Indigenous Health. (2020). Rapid review: What factors may help protect Indigenous peoples and communities in Canada and internationally from the Covid-19 pandemic and its impacts?
National Institute on Ageing. (2020). Pandemic perspectives on ageing in Canada in light of COVID-19: Findings from a National Institute on Ageing/ TELUS Health national survey.
https://static1.squarespace.com/static/5c2fa7b03917eed9b5a436d8/t/5f85fe24729f041f154f5668/1602616868871/PandemicPerspectives+oct13.pdf
National Seniors Council. (2014a). Report on the social isolation of seniors.
https://www.canada.ca/en/national-seniors-council/programs/publications-reports/2014/social-isolation-seniors.html
National Seniors Council. (2014b). Scoping review of the literature: Social isolation of seniors.
https://www.canada.ca/en/national-seniors-council/programs/publications-reports/2014/scoping-social-isolation.html
National Seniors Council. (2016). Who’s at risk and what can be done about it? A review of the literature on the social isolation of different groups of seniors.
https://www.canada.ca/en/national-seniors-council/programs/publications-reports/2017/review-social-isolation-seniors.html
Neil-Sztramko, S. E., Coletta, G., Dobbins, M., & Marr, S. (2020). Impact of the AGE-ON tablet training program on social isolation, loneliness, and attitudes toward technology in older adults: Single-group pre-post study. JMIR Aging, 3(1), e18398.
https://doi.org/10.2196/18398
Newall, N., McArthur, J., & Menec, V. H. (2015). A longitudinal examination of social participation, loneliness, and use of physician and hospital services. Journal of Aging and Health, 27(3), 500–518.
https://doi.org/10.1177/0898264314552420
Newall, N. E., & Menec, V. H. (2015). Targeting socially isolated older adults: A process evaluation of the senior centre without walls social and educational program. Journal of Applied Gerontology, 34(8), 958–976.
https://doi.org/10.1177/0733464813510063
Noone, C., McSharry, J., Smalle, M., Burns, A., Dwan, K., Devane, D., & Morrissey, E. C. (2020). Video calls for reducing social isolation and loneliness in older people: A rapid review. The Cochrane Database of Systematic Reviews, 5, CD013632.
https://doi.org/10.1002/14651858.CD013632
Office, E. E., Rodenstein, M. S., Merchant, T. S., Pendergrast, T. R., & Lindquist, L. A. (2020). Reducing social isolation of seniors during COVID-19 through medical student telephone contact. Journal of the American Medical Directors Association, 21(7), 948–950.
https://doi.org/10.1016/j.jamda.2020.06.003
Office of the Seniors Advocate British Columbia. (2020). Staying apart to stay safe: The impact of visit restrictions on long-term care and assisted living survey.
https://www.seniorsadvocatebc.ca/osa-reports/staying-apart-to-stay-safe-survey/
Older Adult Centres’ Association of Ontario. (2020). The OACAO COVID-19 re-opening survey: Perspectives of centre participants. Provincial report.
Ontario Age-Friendly Communities Outreach Program. (2021a, March). How are organizations using technology to mitigate social isolation and loneliness, and increase social participation among older adults? Community of Interest on Social Isolation & Loneliness Newsletter.
https://mcusercontent.com/fa3447764d8d1381928e407da/files/e53f46d6-b940-471c-aaa9-d4ffea5e1c94/issue_7_attachment.02.pdf
Ontario Age-Friendly Communities Outreach Program. (2021b). Building connections: Promising practices to reduce older adult social isolation for age-friendly community initiatives.
https://sagelink.ca/wp-content/uploads/2021/04/Building-Connections-April-2021.pdf
Ontario Caregiver Organization. (2020). 3rd annual spotlight on Ontario’s caregivers Covid-19 edition.
https://ontariocaregiver.ca/wp-content/uploads/2020/12/OCO-Spotlight-report-English-Dec10.pdf
Palm, M., Allen, J., Widener, M., Zhang, Y., Farber, S., & Howell, N. (2020a). Preliminary results from the public transit and COVID-19 survey.
https://uttri.utoronto.ca/files/2020/05/Preliminary-Report-on-the-Public-Transit-and.pdf
Palm, M., Farber, S., Allen, J., Zhang, Y., Widner, M., & Howell, N. (2020b). Public transit and COVID-19 survey: Results from the City of Vancouver.
https://mobilizingjustice.ca/transit-%26-covid-19-survey
Payne, B. K. (2020). Criminals work from home during pandemics too: A public health approach to respond to fraud and crimes against those 50 and above. American Journal of Criminal Justice, 45(4), 563–577.
Peters, R., Ee, N., Ward, S. A., Kenning, G., Radford, K., Goldwater, M., Dodge, H. H., Lewis, E., Xu, Y., Kudrna, G., Hamilton, M., Peters, J., Anstey, K. J., Lautenschlager, N. T., Fitzgerald, A., & Rockwood, K. (2021). Intergenerational programmes bringing together community dwelling non-familial older adults and children: A systematic review. Archives of Gerontology and Geriatrics, 94, 104356.
https://doi.org/10.1016/j.archger.2021.104356
Pillemer, K., Burnes, D., Riffin, C., & Lachs, M. S. (2016). Elder abuse: Global situation, risk factors, and prevention strategies. The Gerontologist, 56(Suppl. 2), S194–S205.
https://doi.org/10.1093/geront/gnw004
Pirrie, M., & Agarwal, G. (2021). Older adults living in social housing in Canada: The next COVID-19 hotspot? Canadian Journal of Public Health, 112(1), 4–7.
https://doi.org/10.17269/s41997-020-00462-8
Preston, C., & Moore, S. (2019). Ringing the changes: The role of telephone communication in a helpline and befriending service targeting loneliness in older people. Ageing and Society, 39(7), 1528–1551.
https://doi.org/10.1017/S0144686X18000120
Public Health Agency of Canada. (2011). On the Road to Age-Friendly Communities (Brochure).
https://www.canada.ca/en/public-health/services/health-promotion/aging-seniors/publications/publications-general-public/on-road-friendly-communities-brochure.html
Public Health Agency of Canada. (2016). Age-Friendly Communities.
https://www.canada.ca/en/public-health/services/health-promotion/aging-seniors/friendly-communities.html
Public Health Agency of Canada. (2020). From risk to resilience: An equity approach to COVID-19. Public Health Agency of Canada.
Rainero, I., Bruni, A. C., Marra, C., Cagnin, A., Bonanni, L., Cupidi, C., Laganà, V., Rubino, E., Vacca, A., Di Lorenzo, R., Provero, P., Isella, V., Vanacore, N., Agosta, F., Appollonio, I., Caffarra, P., Bussè, C., Sambati, R., Quaranta, D., Guglielmi, V., … SINdem COVID-19 Study Group (2021). The impact of COVID-19 quarantine on patients with dementia and family caregivers: A nation-wide survey. Frontiers in Aging Neuroscience, 12, 625781.
https://doi.org/10.3389/fnagi.2020.625781
Rauktis, M. E., & Hoy-Gerlach, J. (2020). Animal (non-human) companionship for adults aging in place during COVID-19: A critical support, a source of concern and potential for social work responses. Journal of Gerontological Social Work, 63(6/7), 702–705.
https://doi.org/10.1080/01634372.2020.1766631
Regan, K., White, F., Harvey, D., & Middleton, L.E. (2019). Effects of an exercise and mental activity program for people with dementia and their care partners. Journal of Aging and Physical Activity, 27(2), 276–283.
https://doi.org/10.1123/japa.2017-0300
Regnier, V. (2018). Housing design for an increasingly older population: Redefining assisted living for the mentally and physically frail. John Wiley & Sons, Inc.
Renu, K., Prasanna, P., & Valsala Gopalakrishnan, A. (2020). Coronaviruses pathogenesis, comorbidities and multi-organ damage: A review. Life Sciences, 255, 117839
Richardson, D. L., Duncan, M. J., Clarke, N. D., Myers, T. D., & Tallis, J. (2020). The influence of COVID-19 measures in the United Kingdom on physical activity levels, perceived physical function and mood in older adults: A survey-based observational study. Journal of Sports Sciences, 1–13.
https://doi.org/10.1080/02640414.2020.1850984
Roach, P., Zwiers, A., Cox, E., Fischer, K., Charlton, A., Josephson, C. B., Patten, S. B., Seitz, D., Ismail, Z., & Smith, E. E. (2020). Understanding the impact of the COVID-19 pandemic on well-being and virtual care for people living with dementia and care partners living in the community. Dementia, 1471301220977639.
https://doi.org/10.1177/1471301220977639
Robb, C. E., de Jager, C. A., Ahmadi-Abhari, S., Giannakopoulou, P., Udeh-Momoh, C., McKeand, J., Price, G., Car, J., Majeed, A., Ward, H., & Middleton, L. (2020). Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: A survey of older adults in London, UK. Frontiers in Psychiatry, 11, 591120.
https://doi.org/10.3389/fpsyt.2020.591120
Rolandi, E., Vaccaro, R., Abbondanza, S., Casanova, G., Pettinato, L., Colombo, M., & Guaita, A. (2020). Loneliness and social engagement in older adults based in Lombardy during the COVID-19 lockdown: The long-term effects of a course on social networking sites use. International Journal of Environmental Research and Public Health, 17(21).
https://doi.org/10.3390/ijerph17217912
Rorai, V., & Perry, T. E. (2020). An innovative telephone outreach program to seniors in Detroit, a city facing dire consequences of COVID-19. Journal of Gerontological Social Work, 63(6/7), 713–716.
https://doi.org/10.1080/01634372.2020.1793254
Ryerson Leadership Lab. (2021). Overcoming digital divides: Workshop series.
https://www.ryersonleadlab.com/framing-paper
Sacco, G., Lléonart, S., Simon, R., Noublanche, F., & Annweiler, C. (2020). Communication technology preferences of hospitalized and institutionalized frail older adults during COVID-19 confinement: Cross-sectional survey study. JMIR MHealth and UHealth, 8(9), e21845.
https://doi.org/10.2196/21845
Savage, R. D., Wu, W., Li, J., Lawson, A., Bronskill, S. E., Chamberlain, S. A., Grieve, J., Gruneir, A., Reppas-Rindlisbacher, C., Stall, N. M., & Rochon, P. A. (2021). Loneliness among older adults in the community during COVID-19: A cross-sectional survey in Canada. BMJ Open, 11(4), e044517.
https://doi.org/10.1136/bmjopen-2020-044517
Scartoni, F. R., Sant’Ana, L. de O., Murillo-Rodriguez, E., Yamamoto, T., Imperatori, C., Budde, H., Vianna, J. M., & Machado, S. (2020). Physical exercise and immune system in the elderly: Implications and importance in COVID-19 pandemic period. Frontiers in Psychology, 11, 593903.
https://doi.org/10.3389/fpsyg.2020.593903
Science and Technology for Aging Research. (2019). Key issues in aging in the 21st century. STAR Institute, Simon Fraser University.
Shahid, Z., Kalayanamitra, R., McClafferty, B., Kepko, D., Ramgobin, D., Patel, R., Aggarwal, C. S., Vunnam, R., Sahu, N., Bhatt, D., Jones, K., Golamari, R., & Jain, R. (2020). COVID-19 and older adults: What we know. Journal of the American Geriatrics Society, 68(5), 926–929.
https://doi.org/10.1111/jgs.16472
Sheffler, J. L., Joiner, T. E., & Sachs-Ericsson, N. J. (2021). The Interpersonal and Psychological Impacts of COVID-19 on Risk for Late-Life Suicide. The Gerontologist, 61(1), 23–29.
https://doi.org/10.1093/geront/gnaa103
Shippee, T. P., Akosionu, O., Ng, W., Woodhouse, M., Duan, Y., Thao, M. S., & Bowblis, J. R. (2020). COVID-19 pandemic: Exacerbating racial/ethnic disparities in long-term services and supports. Journal of Aging & Social Policy, 32(4/5), 323–333.
https://doi.org/10.1080/08959420.2020.1772004
Sin, N. L., Klaiber, P., Wen, J. H., & DeLongis, A. (2020). Helping amid the pandemic: Daily affective and social implications of COVID-19-related prosocial activities. The Gerontologist.
https://doi.org/10.1093/geront/gnaa140
Sixsmith, A. (2020). COVID-19 and AgeTech. Quality in Ageing & Older Adults, 21(4), 247–252.
https://doi.org/10.1108/QAOA-07-2020-0029
Smith, M. L., Steinman, L. E., & Casey, E. A. (2020). Combatting social isolation among older adults in a time of physical distancing: The COVID-19 social connectivity paradox. Frontiers in Public Health, 8, 403.
https://doi.org/10.3389/fpubh.2020.00403
Son, J. S., Nimrod, G., West, S. T., Janke, M. C., Liechty, T., & Naar, J. J. (2020). Promoting older adults’ physical activity and social well-being during Covid-19. Leisure Sciences.
https://doi.org/10.1080/01490400.2020.1774015
Stall, N. M., Johnstone, J., McGeer, A. J., Dhuper, M., Dunning, J., & Sinha, S. K. (2020). Finding the right balance: An evidence-informed guidance document to support the re-opening of Canadian nursing homes to family caregivers and visitors during the Coronavirus disease 2019 pandemic. Journal of the American Medical Directors Association, 21(10), 1365.
https://doi.org/10.1016/j.jamda.2020.07.038
Statistics Canada. (2020a). Impacts on immigrants and people designated as visible minorities.
https://www150.statcan.gc.ca/n1/pub/11-631-x/2020004/s6-eng.htm
Statistics Canada. (2020b). Impacts on Indigenous Peoples.
https://www150.statcan.gc.ca/n1/pub/11-631-x/2020004/s7-eng.htm
Statistics Canada. (2021). Labour Force Survey, December 2020.
https://www150.statcan.gc.ca/n1/daily-quotidien/210108/dq210108a-eng.htm
The Standing Senate Committee on Social Affairs, Science and Technology. (2013). In from the margins, part II: Reducing barriers to social inclusion and social cohesion. Report of the Standing Senate Committee on Social Affairs, Science and Technology.
https://sencanada.ca/content/sen/Committee/411/soci/rep/rep26jun13-e.pdf
Thomas, K. S., Akobundu, U., & Dosa, D. (2016). More than a meal? A randomized control trial comparing the effects of home-delivered meals programs on participants' feelings of loneliness. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 71(6), 1049–1058.
https://doi.org/10.1093/geronb/gbv111
Tupper, S. M., Ward, H., & Parmar, J. (2020). Family presence in long-term care during the COVID-19 pandemic: Call to action for policy, practice, and research. Canadian Geriatrics Journal, 23(4), 335–339.
https://doi.org/10.5770/cgj.23.476
United Way Centraide Canada. (2020a, November 17). New Horizons for Seniors Program – United Way Centraide Grant results [Press Release].
https://www.unitedway.ca/blog/new-horizons-for-seniors-report/
United Way Centraide Canada. (2020b, October 15). 211 service goes nationwide with funding from the Government of Canada [Press Release].
https://www.unitedway.ca/blog/211-service-goes-nationwide-with-funding-from-the-government-of-canada/
United Way Centraide Canada. (2021, January 14). Emergency community support fund: Investment update [Press Release].
https://www.unitedway.ca/blog/emergency-community-support-fund-grant-results/
United Way of the Lower Mainland & Dialogues in Action. (2021). Rising to the Challenge: How BC's CBSS agencies stepped up during Covid-19. United Way of the Lower Mainland.
https://bc.healthyagingcore.ca/resources/report-and-executive-summary-rising-challenge-how-bcs-cbss-agencies-stepped-during-covid
Van Dyck, L. I., Wilkins, K. M., Ouellet, J., Ouellet, G. M., & Conroy, M. L. (2020). Combating heightened social isolation of nursing home elders: The telephone outreach in the COVID-19 outbreak program. The American Journal of Geriatric Psychiatry, 28(9), 989–992.
https://doi.org/10.1016/j.jagp.2020.05.026
Van Orden, K. A., Bower, E., Lutz, J., Silva, C., Gallegos, A. M., Podgorski, C. A., Santos, E. J., & Conwell, Y. (2020). Strategies to promote social connections among older adults during “social distancing” restrictions. The American Journal of Geriatric Psychiatry.
https://doi.org/10.1016/j.jagp.2020.05.004
Verbeek, H., Gerritsen, D. L., Backhaus, R., de Boer, B. S., Koopmans, R. T. C. M., & Hamers, J. P. H. (2020). Allowing visitors back in the nursing home during the COVID-19 Crisis: A Dutch national study into first experiences and impact on well-being. Journal of the American Medical Directors Association, 21(7), 900–904.
https://doi.org/10.1016/j.jamda.2020.06.020
Volunteer Canada. (2020). The volunteering lens of Covid-19: Fall 2020 survey.
https://volunteer.ca/index.php?MenuItemID=433
Wand, A. P. F., Zhong, B.-L., Chiu, H. F. K., Draper, B., & De Leo, D. (2020). COVID-19: The implications for suicide in older adults. International Psychogeriatrics, 32(10), 1225–1230.
https://doi.org/10.1017/S1041610220000770
Wang, L., Guruge, S., & Montana, G. (2019). Older immigrants' access to primary health care in Canada: A scoping review. Canadian Journal on Aging, 38(2), 193–209.
https://doi.org/10.1017/S0714980818000648
Wammes, J. D., Kolk, Ms., Daisy, van den Besselaar, M., Judith H., MacNeil-Vroomen, P., Janet L., Buurman-van Es, R., Bianca M., & van Rijn, P., Marjon. (2020). Evaluating perspectives of relatives of nursing home residents on the nursing home visiting restrictions during the COVID-19 crisis: A Dutch cross-sectional survey study. Journal of the American Medical Directors Association, 21(12), 1746–1746.
Weldon, T. (2020, May 25). Charity that provides affordable rides desperate for volunteers. CBC News.
https://www.cbc.ca/news/canada/new-brunswick/rural-urban-rides-westmorland-albert-affordable-transportation-1.5580887
Wister, A.V. (2021a). Health promotion and aging during a pandemic: Risk, resilience and COVID-19. In I. Rootman, P. Edwards, M. Levasseur & F. Grunberg (Eds.), Health of Older Adults: The Canadian Experience. Canadian Scholars Press Inc.
Wister, A.V. (2021b). Precarious aging: COVID-19 risk, resilience and response. In B. Trump & I. Linkov (Eds.), COVID: Risk and Resilience. Springer.
Wister, A.V., Menec, V., & Mugford, G. (2018). Loneliness, social isolation and social engagement. In P. Raina, C. Wolfson, S. Kirkland, & L. Griffith (Eds.), The Canadian Longitudinal Study on Aging (CLSA) Report on Health and Aging in Canada: Findings from Baseline Data Collection 2010-2015 (pp.56-73). Public Health Agency of Canada.
Wister, A., Cosco, T., Mitchell, B., Menec, V., & Fyffe, I. (2019). Development and concurrent validity of a composite social isolation index for older adults using the CLSA. Canadian Journal on Aging, 38(2), 180–192.
https://doi.org/10.1017/S0714980818000612
Wister, A., & Speechley, M. (2020). COVID-19: Pandemic risk, resilience, and possibilities for aging research. Canadian Journal on Aging, 39(3), 344-347.
World Health Organization. (2007). Global age-friendly cities: A guide.
http://www.who.int/ageing/publications/ Global_age_friendly_cities_Guide_English.pdf
World Health Organization. (2021). Global report on ageism. World Health Organization.
https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/combatting-ageism/global-report-on-ageism
Wright, L., Vance, L., Sudduth, C., & Epps, J. B. (2015). The impact of a home-delivered meal program on nutritional risk, dietary intake, food security, loneliness, and social well-being. Journal of Nutrition in Gerontology and Geriatrics, 34(2), 218–227.
https://doi.org/10.1080/21551197.2015.1022681
Wu, B. (2020). Social isolation and loneliness among older adults in the context of COVID-19: A global challenge. Global Health Research and Policy, 5, 27.
https://doi.org/10.1186/s41256-020-00154-3
Xie, B., Charness, N., Fingerman, K., Kaye, J., Kim, M. T., & Khurshid, A. (2020). When going digital becomes a necessity: ensuring older adults’ needs for information, services, and social inclusion during COVID-19. Journal of Aging & Social Policy, 32(4–5), 460–470.
https://doi.org/10.1080/08959420.2020.1771237
Yildirim, U. (2020). Disparate impact pandemic framing decreases public concern for health consequences. PloS One, 15(12), e0243599.
https://doi.org/10.1371/journal.pone.0243599
Zhong, S., Lee, C., Foster, M. J., & Bian, J. (2020). Intergenerational communities: A systematic literature review of intergenerational interactions and older adults' health-related outcomes. Social Science & Medicine, 264, 113374.
https://doi.org/10.1016/j.socscimed.2020.113374
Zimmerman, S., Sloane, P. D., Katz, P. R., Kunze, M., O’Neil, K., & Resnick, B. (2020). The need to include assisted living in responding to the COVID-19 pandemic. Journal of the American Medical Directors Association, 21(5), 572–575.