
Federal Tobacco Control Strategy 2001-2011- Horizontal Evaluation
Final Report
June 2012
Table of Contents
- Management Response and Action Plan
- Executive Summary
- 1.0 Introduction
- 2.0 Background on tobacco control in Canada
- 3.0 Federal Tobacco Control Strategy
- 3.1 FTCS Governance
- 3.2 FTCS Budget History
- 3.3 FTCS Activities
- 4.0 The FTCS Evaluation
- 5.0 Evaluation Findings - Relevance
- 6.0 Evaluation Findings - Performance
- 6.1 Overall and Youth Prevalence
- 6.1.1 Smoking Prevalence Trends
- 6.1.2 Overall Prevalence
- 6.1.3 Youth Prevalence
- 6.1.4 Overall and Youth Prevalence Summary
- 6.2 Second-Hand Smoke Exposure
- 6.2.1 Recent Trends
- 6.2.2 Second-Hand Smoke Summary
- 6.3 World Health Organization (WHO) - the Framework Convention on Tobacco Control (FCTC)
- 6.4 The Next Generation of Tobacco Control Policy
- 6.5 Monitor and Assess Contraband Tobacco Activities and Enhance Compliance
- 6.6 Efficiency and Economy
- 6.1 Overall and Youth Prevalence
- 7.0 Conclusions and Recommendations
- Appendix A -- Profile of Grant and Contribution Projects
- Appendix B -- Estimated Average Smoking-attributable Mortality by Difference Underlying Causes
Management Response and Action Plan
The Federal Tobacco Control Strategy (FTCS) was launched in 2001 and was designed as a comprehensive, integrated and sustained approach to achieving reductions in tobacco usage led by Health Canada, in partnership with Public Safety Canada, Royal Canadian Mounted Police, Canada Border Services Agency, Canada Revenue Agency, and the Public Prosecutions Service of Canada.
This ten-year summative evaluation is the fourth evaluation of federal tobacco control efforts. It follows on the evaluations of the Tobacco Demand Reduction Strategy (TDRS - 1994-1997), the Tobacco Control Initiative (TCI - 1997-2001) and the mid-term evaluation of the FTCS (2001-2006).
Policy authority for the FTCS expired March 31, 2012. The Government of Canada is currently exploring new approaches to tobacco control. As such, the findings of this evaluation will be used to inform policy development on the future federal role in tobacco control.
Health Canada has reviewed the evaluation and generally agrees with the findings of the evaluation, however the Controlled Substances and Tobacco Directorate has expressed concerns about the manner in which the Tobacco Products Information Regulations (TPIR) are characterized, and potentially confusing assertions concerning health warning messages in relation to smoking cessation. The Management Action Plan outlines some actions that Health Canada will take in collaboration with other Federal Partner Departments, and makes general observations with regard to how the TPIR are characterized.
- CBSA Management Response:
The CBSA generally agrees with the findings of the evaluation. The CBSA will continue to work with Health Canada and federal partners to address tobacco control - Public Safety Canada Response:
Public Safety Canada accepts the findings of the evaluation report and supports its recommendations. Public Safety Canada will support Health Canada in implementing its management action plan, where applicable. - Royal Canadian Mounted Police Response:
The Royal Canadian Mounted Police (RCMP) accepts the findings of the evaluation report and supports its recommendations. The RCMP will support Health Canada in implementing its management action plan, where applicable. - Canada Revenue Agency Response:
The CRA generally agrees with the findings of the evaluation and will continue to work with Health Canada and federal partners to address tobacco control. - Public Prosecution Service of Canada Response:
The Public Prosecution Service of Canada generally agrees with the findings of the evaluation and will continue to work with Health Canada and federal partners to address tobacco control where applicable.
| Recommendations | Response & Action | Deliverables | Responsible Manager | Timelines |
|---|---|---|---|---|
| Streamline tobacco activities to focus on administering the Tobacco Act, which contains the Cracking Down on Tobacco Marketing Aimed at Youth Act, and maintaining a leadership role through research and surveillance activities to inform policy and regulation as well as guide the direction of collaborative efforts to deliver a comprehensive and integrated national tobacco control strategy. | HC, in collaboration with the FTCS federal partner departments, are committed to implementing measures to reduce smoking rates and protect the health of Canadians.
The recommendation will be taken into consideration in the policy development process. |
Announcement of new tobacco program
Approval and implementation of a new tobacco program |
Director General of the Controlled Substance and Tobacco Directorate (CSTD), Healthy Environments and Consumer Safety Branch (HECSB), Health Canada (HC) | June 2013 |
| Identify best/promising practices among the G&C projects and ensure this information is shared with relevant partners. | Management agrees with the need to glean as much learning as possible from the G&C projects that were implemented under the FTCS and to share these learnings with stakeholders and partners.
HC will conduct a review of all grants and contributions projects funded under the FTCS to identify promising practices and lessons learned. HC will share the findings from this review with stakeholders and partners. |
Completion of the review of grants and contributions funded projects to identify promising practices and lessons learned. | Director General of the Controlled Substance and Tobacco Directorate (CSTD), Healthy Environments and Consumer Safety Branch (HECSB), Health Canada (HC) | March 2014 |
| Develop a systematic approach to performance measurement concentrating on linking the performance data to the logic model and performance indicators to guide the evaluation and reporting processes. | Management agrees with the need for a strong performance strategy to monitor and report on results, and to provide management with regular information for oversight and to ensure achievement of established objectives, outcomes and activities.
A performance measurement strategy will be developed aligning policy directions and outcomes to the future federal role of tobacco control. Implementation of the performance measurement including collection of identified indicators. |
Performance Measurement Strategy that is approved by Treasury Board Secretariat. | Director General, CSTD, HCSB, HC | October 2013 |
| An evaluation framework will be developed, building on the program performance measurement plan with input from the federal partners. | Evaluation Framework that meets TBS standards | Head of Evaluation, Director General, Evaluation Directorate PHAC | One year after program approval - December 2013 |
General Observations
The Federal Tobacco Control Strategy Horizontal Evaluation is intended to measure the objectives of the FTCS as a whole. One of the stated objectives is smoking cessation.
The Controlled Substances and Tobacco Directorate (CSTD) is concerned that the report could be interpreted to suggest that the purpose of tobacco product package labels (required pursuant to the Tobacco Products Information Regulations - TPIR) pertains to smoking cessation.
The TPIR were made under the authority of the Tobacco Act. One of the purposes of this Act, as indicated in its section 4, is to enhance public awareness of the health hazards of using tobacco products. This same objective was mentioned in the regulatory impact analysis statement for the TPIR, published in the July 19, 2000 issue of the Canada Gazette, Part II. However, the report as drafted makes potentially confusing assertions concerning health warning messages in relation to smoking cessation.
In order to ensure that these issues are accurately addressed in future evaluations, CSTD staff will work collaboratively with the Evaluation Directorate to increase awareness and understanding of the Tobacco Act, the TPIR and other regulations.
Acronyms
- ADMO
- Assistant Deputy Minister's Office
- AMPS
- Akwesasne Mohawk Police Service
- BI
- Business Intelligence
- CAMH
- Centre for Addiction and Mental Health
- CBSA
- Canada Border Services Agency
- CCAT
- Canadian Coalition for Action on Tobacco
- CEPA
- Canadian Environmental Protection Act
- CRA
- Canada Revenue Agency
- CSTD
- Controlled Substances and Tobacco Directorate
- CTUMS
- Canadian Tobacco Use Monitoring Survey
- DTIP
- Drugs and Tobacco Initiatives Program
- FCTC
- Framework Convention on Tobacco Control
- FNIHB
- First Nations and Inuit Health Branch
- FNITCS
- First Nations and Inuit Tobacco Control Strategy
- FTCS
- Federal Tobacco Control Strategy
- G&C
- Grant and Contribution
- GST
- Goods and Services Tax
- GTA
- Greater Toronto Area
- HC
- Health Canada
- HECSB
- Healthy Environments and Consumer Safety Branch
- HRSDC
- Human Resources and Skills Development Canada
- HWMs
- Health Warning Messages
- IAD
- International Affairs Directorate
- MACTC
- Ministerial Advisory Committee on Tobacco
- NAO
- National Aboriginal Organizations
- NAPS
- National Action Plan on Smuggling
- NFFE
- Niagara Falls Fort Erie
- NFRP
- National Fine Recovery Program
- NGOs
- Non-Government Organizations
- NSRTU
- National Strategy to Reduce Tobacco Use
- OPSP
- Office of Policy and Strategic Planning
- ORC
- Office of Regulations and Compliance
- OTRSE
- Office of Tobacco Research, Surveillance and Evaluation
- PAA
- Program Activity Architecture
- PS
- Public Safety Canada
- PPSC
- Public Prosecution Service of Canada
- PST
- Provincial Sales Tax
- P/Ts
- Provinces and Territories
- RAPB
- Regions and Programs Branch
- RCMP
- Royal Canadian Mounted Police
- RMAF
- Results-based Management and Accountability Framework
- SAF
- Smoking Attributable Fraction
- SAM
- Smoking-Attributable Morbidity
- SAMMEC
- Smoking-Attributable Morbidity, Mortality and Economic Costs
- SEP
- Safe Environments Program
- TCI
- Tobacco Control Initiative
- TCIMS
- Tobacco Control Information Monitoring System
- TCLC
- Tobacco Control Liaison Committee
- TCLC-WG
- Tobacco Control Liaison Committee Working Group
- TDRS
- Tobacco Demand Reduction Strategy
- TPCA
- Tobacco Products Control Act
- TPCR
- Tobacco Products Control Regulations
- TPIR
- Tobacco Products Information Regulations
- TRR
- Tobacco Reporting Regulations
- WHPSP
- Workplace Health & Public Safety Program
- YPLL
- Years of Potential Life Loss
- YSS
- Youth Smoking Survey
Executive Summary
This evaluation is intended to assess progress made towards the Federal Tobacco Control Strategy's (FTCS) objectives from 2001-2011 with a particular focus on the second half of the FTCS (2007-2011). It examines relevance and performance in order to fulfill accountability requirements outlined in the Government of Canada Policy on Evaluation. The evaluation has also attempted to take into account not only the external factors associated with outcome results but also the complex interactions of contributions from different levels of government where possible.
The FTCS was introduced as a ten-year strategy (2001-2011) intended to reduce tobacco-related disease and death in Canada. The FTCS was designed to be a comprehensive, integrated and sustained tobacco control program based on international best practices, with a focus on building upon previous federal initiatives to reduce tobacco demand.
A key component of Health Canada's (HC) tobacco control effort is the enforcement of the Tobacco Act adopted in 1997, and a range of regulations. The focus of the Tobacco Act is to regulate manufacturing, sale, labelling and promotion of tobacco products in Canada. It aims to protect all Canadians, with a particular focus on youth, from the health consequences of tobacco use.
A number of regulations have been made pursuant to the Tobacco Act, including the Tobacco Products Information Regulations (TPIR) that came into force in 2000, and the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) that replaced for cigarettes and little cigars the TPIR requirements in 2011. Both require graphic health warning messages on tobacco products packaging. Tobacco products labelling is a key component of the federal's government efforts to inform Canadians on the health risks of tobacco use and the health benefits of quitting.
In 2001, almost $560M was allocated over for the first five years of the FTCS to engage in tobacco control activities including: mass media; development and enforcement of regulations pursuant to the Tobacco Act; research and surveillance; national co-ordination of tobacco control efforts; collaboration with federal partners to monitor contraband tobacco; support for First Nations and Inuit tobacco reduction programs; and funding various activities through Grants and Contributions (G&Cs).
The Terms and Conditions for the FTCS were renewed in 2007. While the monies for federal partners remained the same at approximately $16M annually, a much smaller amount than previous years was allocated to HC's tobacco control activities (approx. $57M annually). Therefore, the total allocation for the second phase of the FTCS was $285M for HC and $80M to federal partners over five years.
The 2006 FTCS summative evaluation noted that almost all of the objectives set in 2001 were met or exceeded by 2005. However, there were limitations in the extent to which this success could be attributed to the FTCS. In the context of having achieved its initial objectives, objectives for the FTCS were revised for its second phase and an overarching goal of reducing Canadian smoking prevalence from 19% to 12% by 2011 was set as a stretch target. Objectives for the FTCS in 2001 and revised specific objectives for the second phase of the FTCS are summarized as follows:
| Phase 1 - 2001 | Phase 2 - 2007 |
|---|---|
| Reduce smoking prevalence to 20% from 25% in 1999 | Reduce overall smoking prevalence from 19% (2006) to 12% by 2011 |
| Reduce the number of cigarettes sold by 30% | Reduce the prevalence of smoking among youth from 15% to 9% |
| Increase retailer compliance regarding youth access to sales from 69% to 80% | Increase the number of adults (including young adults) who quit smoking by 1.5 M |
| Reduce the number of people exposed to environmental tobacco smoke in enclosed public spaces | Reduce the prevalence of Canadians exposed to daily second-hand smoke from 28% to 20% |
| Explore how to mandate changes to tobacco products to reduce hazards to health | Examine the next generation of tobacco control policy in Canada |
| Contribute to the global implementation of the World Health Organization (WHO) - Framework Convention on Tobacco Control (FCTC) | |
| Monitor and assess contraband tobacco activities and enhance compliance |
The FTCS terms and conditions were renewed in 2007, at which time, HC's functions with respect to surveillance, research, regulations, and compliance remained similar to those described in 2001. However, emphasis on compliance shifted from retailers to manufacturers, and intelligence gathering with respect to the industry. Policy functions also remained similar, but additional focus was placed on international activities and examining the next generation of tobacco control, via the inclusion of objectives reflecting these activities. Mass media was not identified as part of the FTCS in 2007.
Governance
HC was responsible for the overall management and implementation of the FTCS. The Controlled Substances and Tobacco Directorate (CSTD) within the Healthy Environments and Consumer Safety Branch (HECSB) of HC was the lead directorate. It relied on other areas within the Department which either provided direct control over various aspects of the FTCS or provided support and expertise.
Between 2008 and 2010 two major changes in the governance structure were undertaken - the creation of the Regions and Programs Branch (RAPB) and the merging of the tobacco and controlled substances programs. The creation of RAPB resulted in the transfer of all functions related to G&Cs as well as other program delivery components to the Drugs and Tobacco Initiatives Program (DTIP) within this Branch. Compliance and enforcement activities related to the Tobacco Act in the regions were also transferred to RAPB. Other FTCS activities continued under HECSB.
The objective concerning contraband tobacco as well as the objective with respect to the World Health Organization - Framework Convention on Tobacco Control (WHO-FCTC) relies on many federal departments including Royal Canadian Mounted Police (RCMP), Canada Border Services Agency (CBSA), Public Safety Canada (PS), Department of Justice (DoJ), Department of Foreign Trade and International Development (DFAIT), Public Prosecution Service of Canada (PPSC) and the Canada Revenue Agency (CRA) as well as Health Canada.
The FTCS places a strong emphasis on partnerships between the federal government and other levels of government. Given that tobacco control is a multi-jurisdictional activity, collaboration is necessary not only with other levels of government but also with many non-government organizations to achieve common goals.
Evaluation Scope and Methodology
The evaluation examined the Government of Canada's core evaluation issues of relevance and performance. The relevance assessment focused on questions related to the continued need for the FTCS, the Strategy's alignment with federal roles and responsibilities as well as alignment with government priorities. Performance was evaluated by examining the achievement of the FTCS objectives and an analysis yielding estimated returns on investment (ROIs).
The methodology for this evaluation of the ten-year FTCS (2001-2011) used multiple lines of evidence including a literature and document review, econometric modeling, secondary data analysis, key informant interviews and a stakeholder survey. It also used both the process and impact evaluations previously conducted to assess the Grant & Contribution (G&C) Program component of the FTCS. These methods were employed to provide quantitative and qualitative data and confirm findings where appropriate. In addition, data collected over the course of the evaluation process was validated through informal interviews with FTCS program personnel.
Evaluation Findings
Relevance
Smoking prevalence rates in Canada have declined significantly over the past decade and are among the lowest in developed countries. There has also been an increased involvement of the provinces and territories in tobacco control. By 2007, all provinces had Acts which enhanced what was once only federal legislation concerning tobacco control. In addition, provincial and territorial expenditures on tobacco control strategies have more than doubled since 2001.
Nonetheless, there still seems to be a perceived need among stakeholders for continued efforts on the part of the federal government to sustain work on tobacco control. Stakeholders believe that the main role for the federal government is a leadership role responsible for coordination at the national and international level which would include developing national frameworks, legislation and regulations.
Despite the fact that current federal priorities do not highlight tobacco control as a main federal focus, the Government of Canada still has the responsibility to administer the Tobacco Act (amended in 2009 as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act) and its regulations.
Performance
Overall smoking rates, which have been steadily declining since the 1960s, continued to decline since the introduction of the FTCS in 2001. According to the Canadian Tobacco Use Monitoring Survey (CTUMS), overall smoking rates, which include daily and occasional smokers, declined from 21.7% in 2001 to 16.7% in 2010. However, the stretch target of a reduction in overall smoking prevalence to 12% by 2011 was not met. That said, the current daily smoking prevalence rate is 13% and is the lowest of comparable countries. In addition to reaching a new low for adult prevalence, the target of a 9% prevalence rate in the youth population was achieved; however, there has not been a statistically significant change since 2007. Nevertheless, even with these reduced prevalence rates, the rate of decline has slowed considerably since 2007.
The FTCS made a small contribution to the decline in smoking prevalence through its labelling and youth access regulations as well as its support to implement provincial second-hand smoke bans. Even though retailer and manufacturer compliance was reported as high, making statements about the contribution of other FTCS regulations to the declining smoking rates was difficult due to the limitations of the econometric model and the conflicting findings from other lines of evidence. According to the econometric modelling conducted as part of this evaluation, external influences outside of the FTCS (i.e., level of education achieved, followed by provincial and excise tax) were found to be the most significant predictors of both smoking participation and consumption. Retail display bans as well as the legal age in which cigarettes can be purchased were also predictors of smoking participation.
Although some of the contribution cessation projects demonstrated high quit rates in the impact evaluation of G&C projects, due to the limited participation in and reach of these interventions combined with very limited outcome data, generalizations about the effectiveness of these projects in reducing prevalence were not possible. However, other G&C projects that focused on knowledge application were able to demonstrate some influence with respect to policy/legislation development as evidenced by the implementation of provincial second-hand smoke bans, pan-Canadian quitlines and the Canadian Action Network for the Advanced Dissemination and Adoption of Practice informed Tobacco Treatment (CAN-ADAPTT) smoking cessation guidelines. In addition, funded projects related to policy and knowledge exchange were able to support and inform policy at federal, provincial and organizational levels.
The objective of reducing second-hand smoke exposure to Canadians was achieved. HC promoted smoke-free environments through its contribution funding, mass media campaigns as well as its leadership role in the implementation of smoking bans via both informational and monetary resources. The implementation of second-hand smoke bans across most provinces is an illustration of how the federal government can influence change.
Through the FTCS, HC, along with its other partner departments, assisted with fulfilling Canada's commitment to participate in the WHO-FCTC by being a contributor to the development of the FCTC and providing technical advice on both the original Articles and ongoing support for their global implementation. This participation in the FCTC illustrated that international leadership is being provided by the Government of Canada.
Over the course of the FTCS, research and surveillance activities appeared to be active functions and used to inform the development of legislation, regulations and various policies and positions. Furthermore, G&C projects as well as work with stakeholders were important to the advancement of the next generation of tobacco control policy, both federally and provincially.
Knowledge generation and translation was a predominant characteristic of the FTCS. Investments were made to ensure the continued generation of knowledge that will assist with developing additional policy work in the future. Overall, it appeared that knowledge generation and its subsequent application helped to regulate tobacco in Canada, educated jurisdictions in Canada on emerging issues as well as guided the direction of collaborative efforts in tobacco control.
PS, CBSA and RCMP used FTCS funding to monitor and assess contraband tobacco activities which may have contributed to the significant increase in the volume of seizures observed between 2001 and 2009. Also, the evaluation found that there was an increased capacity through additional staffing to conduct intelligence analysis. Given that the objective was to simply monitor and assess the market to inform tax policy, the volume of seizures does indicate that monitoring activity has taken place and information in the form of intelligence reports and departmental meetings was provided to Finance Canada to inform tax policy. CRA demonstrated compliance-related activity through the increased number of audits and reviews while the PPSC demonstrated such activity through increases in fine recoveries, both with increased staffing. How this impacted the availability of legal or illegal tobacco products could not be determined.
The estimated total annual expected economic benefit of all tobacco control measures in place in Canada is $1.8B. The analysis revealed that if the FTCS made a contribution of approximately 5% to reduction in smoking prevalence, then the annual ROI (i.e., return on investment) would be estimated at $17M. On the other hand, if the FTCS contribution was assumed to be higher than 5%, the ROI would also be higher.
Conclusions and Recommendations
While the duration of the FTCS (2001-2011) has seen large declines in smoking prevalence, between 2007 and 2010 prevalence remained relatively stable. The overall prevalence objective for Phase 2 was a stretch target set at 12% in light of the early accomplishment of the original objectives in Phase 1 of the FTCS. Nonetheless, this goal of reducing prevalence to 12% was not met. However the target of reducing youth smoking prevalence to 9% was met.
Overall, the FTCS contributed to the decline in smoking prevalence through its labelling and youth access regulations as well as its support to implement provincial second-hand smoke bans. However, lines of evidence suggested that external measures not funded by the FTCS, such as level of education achieved and taxation, were the main contributors to changes in prevalence with provincially-legislated retail display bans and legal age for purchasing tobacco products following.
Most large-scale environmental changes (i.e., tax and second-hand smoke bans) were implemented between 2001 and 2007 and since that time there was little change in the Canadian tobacco control environment. Changes made by the provinces in tobacco control during this period included restrictions on point of sale advertising via provincial retail display bans, province-wide second-hand smoke bans and provincial smoke-free vehicle legislation. With the increase in action from provinces and territories, many tobacco control issues are now addressed at a provincial/territorial level, and prevention or cessation programming is increasingly conducted at this level.
The only major changes at the federal level were the passage of the Cracking Down on Tobacco Marketing Aimed at Youth Act that amended the Tobacco Act in 2009 and the new health-related labels prescribed under the new Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) made in 2011. The impact of these amendments to the Tobacco Act on prevalence could not be assessed in this evaluation as these amendments did not come into effect until late 2009 for some provisions and mid-2010 for others.
The evaluation illustrated compliance with Tobacco Act and its regulations was stable and high, while smokers' participation in cessation programming provided by G&C projects participating in the G&C Impact Evaluation was limited. Additionally, the data available was not able to determine the overall impact of the cessation projects funded by the G&C projects on prevalence - not surprisingly seeing as many of the cessation projects were aimed at vulnerable populations and were only intended to contribute to a reduction in smoking prevalence rates. Evidence from this evaluation and the stabilizing of prevalence rates, indicates that smoking cessation success in the current smoker population will be limited unless G&C projects are able to improve project participation and reach.
Other G&C projects that focussed on knowledge application demonstrated some influence in providing information which was applied to policy/legislation development. In addition, funded projects related to policy and knowledge exchange were able to support and inform policy at the federal, provincial and organizational levels.
Federal leadership was evident throughout the evaluation including HC's role in the WHO-FCTC, the implementation of second-hand smoke bans, the research and surveillance available on smoking in Canada, the research conducted to facilitate the provincial retail display bans, as well as the Cracking Down on Tobacco Marketing Aimed at Youth Act that amended the Tobacco Act. Continued leadership in tobacco control requires continued investment in research and surveillance to identify emerging tobacco issues and to be able to respond to them through stakeholder relations or policy activities.
The objective related to contraband tobacco was to simply monitor and assess the market and to enhance compliance in order to inform policy. Therefore, the increased volume of seizures indicated that monitoring contraband tobacco had taken place and the increased number of audits and regulatory reviews as well as fines recovered indicated that there has been enhanced compliance-related activity.
Considering the findings and conclusions of the evaluation and the current tobacco control environment, the FTCS, as it is presently structured, may need to be streamlined. Nonetheless, there still seems to be a need for sustained efforts on the part of the federal government in tobacco control not only to administer the Tobacco Act and its regulations but also to provide a leadership role responsible for coordination at the national and international level. In order to deliver a comprehensive and integrated national tobacco control strategy, identified as a best practice, the strategic approach of combining federal regulations, policy development, research and surveillance as well as supporting provincial and international tobacco control efforts is necessary.
The evaluation approach for the FTCS used sophisticated simulation modeling as one line of evidence in order to provide quantitative performance data which was intended to be corroborated by a performance measurement system that would provide both qualitative and further quantitative data. However, as mentioned in the methodology section of this report, the performance measurement system was not implemented for various reasons. During the evaluation report writing process, it became evident that data gaps existed. Therefore, an ad-hoc internal document review was performed to try to capture retrospective qualitative data to fill these gaps. Although a substantial amount of information was captured through the internal document review process, there were still some areas where triangulation with multiple lines of evidence was impossible. It also became evident that the FTCS has an abundance of performance data; however, it is not well organized/tracked according to the program outcomes and associated performance indicators. Lastly, other lines of evidence (such as the econometric modelling and literature review) concentrated on tobacco control in Canada more broadly (which would include activities initiated by P/Ts, NGOs and municipalities) instead of specifically on the activities of the FTCS which are the responsibility of the federal government.
Therefore the recommendations stemming from the evaluation are to, under the leadership of HC:
- Streamline tobacco activities to focus on administering the Tobacco Act (as amended as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act) and its regulations, and maintaining a leadership role through research and surveillance activities to inform policy and regulation, as well as guide the direction of collaborative efforts to deliver a comprehensive and integrated national tobacco control strategy.
- Identify best/promising practices amongst the G&C projects and ensure this information is shared with relevant partners.
- Develop a systematic approach to performance measurement, concentrating on linking the performance data to the logic model and performance indicators to guide the evaluation and reporting processes.
1.0 Introduction
A commitment was made for Health Canada (HC) to conduct an evaluation of the Federal Tobacco Control Strategy (FTCS) in fiscal year 2010-2011 and to return to Cabinet by the Fall of 2011 to present a path forward for tobacco control using the evaluation results as one line of evidence to inform the Cabinet process. This evaluation is in keeping with the 2009 Government of Canada's Policy on Evaluation by examining all five core issues falling under relevance and performance. Additionally, this report addresses FTCS activities and accomplishments between 2001 and 2011, but with a particular focus on 2007-2010, as a summative evaluation of the Strategy was completed in 2006. Overall conclusions and recommendations are presented in the final section of this report.
2.0 Background on Tobacco Control in Canada
The Federal Tobacco Control Strategy (referred to as either the FTCS or the Strategy throughout the report) was announced in 2001 as a comprehensive tobacco strategy, led by HC, to reduce disease and death due to tobacco use. This Strategy followed a lengthy history of tobacco control activities undertaken by the federal government since the 1960s.
The types of tobacco activities, including interventions by the Government of Canada over different time periods, went through a gradual shift from tobacco-related (mostly research) activities to tobacco control interventions, which became more comprehensive over time. Publicly visible intervention measures began with public education (1963-1964) which later evolved into health promotion or 'social marketing' programming (1980s to 2000s), combined with initially voluntary restrictions on some commercial activities by tobacco companies. These negotiated changes to marketing activities, began briefly in 1971-1972 under the threat of proposed legislation, eventuated in a more concerted policy development process beginning in the early 1980s that culminated in the enactment of the former Tobacco Products Control Act, S.C. 1988 c.20.
The strategic approach combining legislation, regulation and health promotion began in 1986 with the National Strategy to Reduce Tobacco Use (NSRTU roughly 1986-1993), which obtained its funds from internal reallocation from the drug program. This was the first tobacco strategy and was followed by: the Tobacco Demand Reduction Strategy (1994-1997), the Tobacco Control Initiative (1997-2001) which was announced concurrently with the Anti-Smuggling Initiative, then the FTCS (2001-2011).
The Tobacco Demand Reduction Strategy (TDRS) was part of the National Action Plan on Smuggling (NAPS) launched by the federal government on February 8, 1994. The timing of this initiative was designed to correspond to a series of tobacco taxation roll-backs, prompted by increasing prevalence of contraband tobacco. The Strategy was to last until March 31, 1997, and its objective was, through programs, public education and enforcement, to minimize the anticipated negative impact of tax cuts on the consumption of tobacco products, particularly in those groups most likely to initiate or increase tobacco use as a result of lower prices. HC was assigned the responsibility for implementing the Strategy. A total of $104M was spent under the TDRS over the three-year period.
The Tobacco Control Initiative (TCI) was introduced by the federal government in 1997-1998 with a budget of $50M. These resources were allocated over five years ending in March 2002 for work related to regulations and compliance. An ongoing funding stream of $10M per year was added in 1998-1999 for a public education component. A policy case was subsequently made to incorporate the ongoing stream of funding into the Federal Tobacco Control Strategy (FTCS), which replaced the TCI in 2001.
The FTCS covers the majority of tobacco control activities undertaken by the federal government, but is not representative of all of the activities which affect the use, impact or availability of tobacco products. The following departments undertake activities that are not funded through FTCS but are related to tobacco:
- Department of Finance is responsible for taxation of tobacco products;
- Human Resources and Skills Development Canada (HRSDC) holds the Non-Smokers Health Act;
- Public Health Agency of Canada conducts some healthy living interventions that may include prevention and cessation messages; and
- Agriculture Canada addresses the farming of tobacco and runs a program to help farmers transition from growing tobacco.
3.0 Federal Tobacco Control Strategy
Following the TCI, the FTCS was introduced as a ten-year strategy (2001-2011, and extended one year) intended to reduce tobacco-related disease and death in Canada. The FTCS was designed to be a comprehensive, integrated and sustained tobacco control program based on international best practices, with a focus on building upon the work of previous federal initiatives.
A key component of HC's tobacco control effort is the enforcement of the Tobacco Act adopted in 1997, and a range of regulations. The focus of the Tobacco Act is to regulate manufacturing, sale, labelling and promotion of tobacco products in Canada. It aims to protect all Canadians, with a particular focus on youth, from the health consequences of tobacco use.
A number of regulations have been made pursuant to the Tobacco Act, including the Tobacco Products Information Regulations (TPIR) that came into force in 2000, and the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) that replaced for cigarettes and little cigars the TPIR requirements in 2011. Both require graphic health warning messages on tobacco products packaging. Tobacco products labelling is a key component of the federal's government efforts to inform Canadians on the health risks of tobacco use and the health benefits of quitting.
It is worth noting that in 2007, the Supreme Court of Canada in Canada (Attorney General) v. JTI-Macdonald Corp., [2007] 2 S.C.R. 610, concluded that both the Tobacco Act and the TPIR were constitutional in their entirety.
The government's rationale for increasing its investments in tobacco control was based on the need for comprehensive action to address the diversity of complex issues associated with tobacco use. Evidence from California's Tobacco Control Program and research by the Center for Disease Control in the United States, noted that independent actions, even when well funded, do not work or have little benefit, especially over the long term.
In 2001, almost $560M was allocated for the first five years of the FTCS to engage in tobacco control activities including: mass media; development and enforcement of regulations pursuant to the Tobacco Act; research and surveillance; national co-ordination of tobacco control efforts; collaboration with federal partners to monitor the problem of contraband; support for First Nations and Inuit tobacco reduction programs; and funding various activities through G&Cs.
The FTCS terms and conditions were renewed in 2007 and while the monies for federal partners remained the same at approximately $16M annually, a much smaller amount from previous years was allocated to HC's tobacco control activities ($57M annually). Therefore, the total allocation for the second phase of the FTCS was approximately $285M for HC and $80M to federal partners.
The first formal evaluation of the FTCS, conducted in 2006, noted that almost all of the objectives set in 2001 were met or exceeded by 2005. However, there were limitations in the extent to which this success could be attributed to the FTCS. In the context of having achieved its initial objectives, objectives for the FTCS were revised for the second phase of the FTCS and an overarching goal of reducing Canadian smoking prevalence from 19% to 12% by 2011 was set as a stretch target. Objectives for the FTCS in 2001 and revised specific objectives for the second phase of the FTCS are summarized in the table below:
| Phase 1 - 2001 | Phase 2 - 2007 |
|---|---|
| Reduce smoking prevalence to 20% from 25% in 1999 | Reduce overall smoking prevalence from 19% (2006) to 12% by 2011 |
| Reduce the number of cigarettes sold by 30% | Reduce the prevalence of smoking among youth from 15% to 9% |
| Increase retailer compliance regarding youth access to sales from 69% to 80% | Increase the number of adults (including young adults) who quit smoking by 1.5 M |
| Reduce the number of people exposed to environmental tobacco smoke in enclosed public spaces | Reduce the prevalence of Canadians exposed to daily second-hand smoke from 28% to 20% |
| Explore how to mandate changes to tobacco products to reduce hazards to health | Examine the next generation of tobacco control policy in Canada |
| Contribute to the global implementation of the World Health Organization (WHO) - Framework Convention on Tobacco Control (FCTC) | |
| Monitor and assess contraband tobacco activities and enhance compliance |
The FTCS terms and conditions were renewed in 2007, at which time HC's functions with respect to surveillance, research, legislation and regulations, and compliance remained similar to those in 2001. However, emphasis in compliance shifted from retailers to manufacturers, and intelligence gathering with respect to the industry. Policy functions also remained similar, but additional focus was placed on international activities and examining the next generation of tobacco control, via the inclusion of objectives reflecting these activities. Mass media was not identified as part of the FTCS in 2007.
Although raising awareness about the health risks associated with tobacco is still a goal for the government, the 2007 Strategy indicated that prevention, cessation and education interventions should be aimed at changing smoking behaviours and determining what interventions are effective in impacting behaviour change. Another important change in activity and funding was the cancellation of the First Nations and Inuit Tobacco Control Strategy. Further, while not explicitly stated, defence of the Tobacco Act against litigation emerged as a funding pressure.
3.1 FTCS Governance
Health Canada
HC was the lead department in the FTCS and was responsible for the overall management and implementation of the Strategy. There were two Branches within HC that had direct responsibility for the Tobacco Control Strategy; however, they may have relied on other areas within the department for support and expertise in areas of potential overlap. The Controlled Substances and Tobacco Directorate (CSTD) within the HECSB was the lead area within HC.
When the FTCS terms and conditions were renewed in 2007, governance structures had largely remained stable within HC. Functions and offices were very similar to those in place in 2001, but after 2007, more substantial change was seen in HC. Between 2008 and 2010 two major changes in the governance structure were undertaken - the creation of the Regions and Programs Branch (RAPB) and the merging of the tobacco and controlled substances programs.
The creation of RAPB resulted in the transfer of all functions related to G&Cs as well as other program delivery components to the Drugs and Tobacco Initiatives Program (DTIP) with this Branch. Compliance and enforcement activities related to the Tobacco Act in the regions were also transferred to RAPB. Other FTCS activities continued under the HECSB. FTCS functions were further divided within RAPB, with the G&C activities located in the Programs Directorate, and compliance and enforcement activities in the Regions. HECSB retained governance of compliance and enforcement with RAPB regional delivery of the regional component.
Following the reorganization of HECSB and RAPB, HC made a decision to amalgamate the HC functions that were part of Canada Drug Strategy, and later the National Anti-Drug Strategy with those of the FTCS. In 2009 a new organization was thus created, titled the Controlled Substances and Tobacco Directorate (CSTD). Previously the "Tobacco Control Directorate" was responsible for leading Health Canada's activities, and it was this Directorate that was merged with the Directorate responsible for controlled substances. With these organizational changes the FTCS remained under the Program Activity Architecture (PAA) of "Substance Use and Abuse" and "Tobacco" sub-activity.
The Office of Regulations and Compliance (ORC) of CSTD was responsible for monitoring the compliance and enforcement activities related to the Tobacco Act and undertook the modification of existing or development of new regulations under the Act. Also some enforcement activities related to the Tobacco Act were transferred from ORC to the Regions group within RAPB.
Partnership under the FTCS was demonstrated through strong linkages not only across federal departments but also between the Government of Canada and provincial, territorial and municipal governments. The Strategy was further strengthened through close collaboration with the private and voluntary sectors and, internationally, with the world community. This approach recognizes that responsibility for tobacco control is shared and that tobacco use remains a significant and ongoing health challenge that requires sustained commitment of resources and attention from all tobacco control partners.
Within HC, there were a number of other partners that supported the FTCS besides CSTD of HECSB and the RAPB in order to continue tobacco control efforts in Aboriginal communities, in the international world, and with provinces and territories. This coordinated effort requires involvement from the following partners:
First Nations Inuit Health Branch (FNIHB)
HECSB and RAPB worked with FNIHB on an ongoing basis in order to ensure coordination and consistency of HC's tobacco control activities. With the cancellation of the First Nations and Inuit Tobacco Control Strategy in 2006, some G&C projects targeted on-reserve First Nations and Inuit living in Inuit communities. RAPB continued to work closely with FNIHB as well as First Nations and Inuit health organizations to identify priorities in support of tobacco programming.
International Affairs Directorate (IAD)
CSTD and RAPB worked with the International Affairs Directorate of HC to develop Canada's contributions to international tobacco control initiatives - e.g. the World Health Organization (WHO) and the Framework Convention on Tobacco Control (FCTC).
Tobacco Control Liaison Committee (TCLC)
The Director General of the CSTD was the co-chair of the TCLC. The Tobacco Control Liaison Committee was a group of federal/provincial/territorial government representatives that met twice a year to fulfill the following mandates:
- Provide a forum for collaboration between federal, provincial and territorial governments on elements of the New Directions for Tobacco Control in Canada - A National Strategy;
- Develop and monitor progress on a work plan for joint action related to elements of the Strategy;
- Bring forward issues of importance and provide advice to the Advisory Committee on Population Health and Health Security (ACPHHS), which advises the Conference of Deputy Ministers of Health;
- Integrate tobacco control within the broader population and public health agenda, territorially, provincially and nationally; and
- Facilitate continued collaboration with non-governmental organizations active in tobacco control.
Ministerial Advisory Council on Tobacco Control (MACTC)
The MACTC was active beginning in 2001, but had not met since the fall of 2005. The Council provided advice on the strategies, policies, mechanisms and activities required for the effective implementation of the FTCS and for federal support to the National Strategy endorsed by the federal, provincial and territorial Ministers of Health as well as Non-Government Organizations. The Council also monitored and evaluated tobacco control activities undertaken in Canada and in other jurisdictions.
Other Federal Partners
The objective of monitoring and assessing the contraband market and enhanced compliance relied on other federal departments. The monitoring and assessment of the contraband tobacco activities was the responsibility of the Royal Canadian Mounted Police (RCMP), Canada Border Services Agency (CBSA) and Public Safety Canada (PS); whereas the enhanced compliance aspect of this objective was the responsibility of the Public Prosecution Service of Canada (PPSC) and Canada Revenue Agency (CRA).
Other Jurisdictions
The FTCS placed a strong emphasis on partnerships between the federal government and other levels of government. Given that tobacco control is a multi-jurisdictional activity, collaboration is necessary not only with other levels of government but also with many non-government organizations to achieve common goals.
3.2 FTCS Budget History
In 2001, the FTCS had funding of almost $560M for the first five years. Steady funding of approximately $16M annually was allocated to federal partners for contraband surveillance and monitoring, while the annual budget for HC ramped up from $54.5M a year to $99.2M by 2004-2005. Additionally, $10M in ongoing funding from the previous Tobacco Control Initiative was provided.
In 2007, while the monies for federal partners remained the same at approximately $16M annually, a much smaller amount from previous years ($57M annually) was allocated to HC's tobacco control activities. Therefore, the total allocation for the second phase of the FTCS was approximately $285M for HC and $80M to federal partners.
Health Canada Allocation
The reduction in FTCS monies for HC during the second half of the FTCS was primarily the result of major permanent reductions, and the decision to discontinue the First Nations and Inuit Tobacco Control Strategy as part of the 2006 Expenditure Review (see table below).
| Funds | Total |
|---|---|
| TCI Total | $10,000,000 |
| FTCS Total for HC | $99,800,000 |
| Total For Health Canada | $109,800,000 |
| CEPA | $-13,000,000 |
| PCO Advertising Fund | $-16,488,217 |
| FNIHB reduction | $-12,278,000 |
| Government Reallocations | $-8,224,706 |
| HC Reallocations | $-3,821,570 |
| Collective Agreement Funding | $1,488,483 |
| Technical ARLU Adjustments | $118,721 |
| EBP ARLU Adjustments | $-272,411 |
| Total Remainder for Health Canada | $57,322,300 |
This decrease in funding reduced the HC allocation under the FTCS to approximately $57M annually. Since 2007-2008, HC's FTCS funding experienced further departmental reallocations ($0.2M) and government reductions ($3.3M), resulting in a funding level of $53M by 2011. Other large deductions, transfers and lapses also occurred.
In the first year of the FTCS, there was a $4.3M transfer to the First Nations and Inuit Health Branch (FNIHB). In the second year there was a $3.1M transfer to the Safe Environments Program's Water Bureau re-allocation (SEP), an $8.7M lapse in the third year, and a $12.7M branch reallocation in the fourth. Each year major transfers, deductions or lapses occurred and this is not limited to the early years of the FTCS. There were several elections/prorogation that created delays in funding approvals particularly in the second phase of the Strategy causing lapses to occur. In 2008-2009 $6.3M was transferred to FNIHB and $2.5M lapsed in 2009-2010.
In addition to lapses and transfers, a significant proportion of funding was required to support corporate costs. For example, in 2009-2010 "Corporate Branches" were allocated $3.8M, $1M was identified as supporting "Enterprise IT", $0.8M was transferred to cover a series of "Corporate Reductions". An annual permanent reduction of $2.8M was applied to the FTCS to support Branch-level function.
These corporate and departmental deductions of $8.5M impacted the amount of funding available for direct tobacco control activities. Spending on tobacco control activities for 2010-2011 totalled less than $45M, including litigation at $6.3M.
It should be noted that in the second half of the FTCS, litigation emerged as a funding pressure. The Government of Canada was named as a third party by tobacco companies in several court cases, and a number of other cases were identified as potential future risks, thus an Office for Tobacco Litigation Support was created as part of the CSTD. Financial support for litigation activities was initially taken from unspent G&C dollars - a delay in approval for the FTCS terms and conditions in 2007-2008 resulted in a significant surplus of funds that fiscal year. Funding to address litigation costs was approved in 2008-2009, but it was noted that additional funds, of approximately $3M per year would be provided from the FTCS budget to support litigation. In years where litigation costs exceeded this funding allocation and the $3M from the FTCS, additional funds were redirected from the FTCS. For example, in 2010-2011 approximately $6.1M in litigation funding was supported by the FTCS.
Federal Partners Funding
The approximately $16M allocation to federal partners for contraband-related activities did not change in Phase 2 of the FTCS, and was allocated as follows:
| Federal Partners | Allocation |
|---|---|
| PS | $610,000 |
| PPSC | $1,988,000 |
| CRA | $888,910 |
| CBSA | $10,560,800 |
| RCMP | $1,723,480 |
| Total | $15,771,190 |
| Note: There is a small discrepancy in the above numbers and those reported by PPSC | |
FTCS funds allocated to federal partners were identified for enhancing compliance with the federal tobacco tax legislation as well as monitoring and surveillance, but these departments conduct additional activities with respect to tobacco. FTCS allocated dollars are used in combination with departmentally held funds to undertake comprehensive activities related to contraband tobacco and ensure that legal tobacco market complies with federal tobacco tax laws.
3.3 FTCS Activities
Activities in Phase 2 of the Strategy were similar to those undertaken since 2001, with notable exceptions of the removal of mass media, and support for the First Nations and Inuit Health Branch (FNIHB). It was noted that the focus of the Strategy would be to concentrate efforts on developing and testing cessation and prevention techniques and approaches and from retail compliance to industry/manufacturer level compliance and enforcement. The various FTCS activities are described in the following sections.
The Tobacco Act and Associated Regulations
Adopted in 1997, the federal Tobacco Act regulates the manufacture, sale, labelling and promotion of tobacco products in Canada. The Tobacco Act aims to protect all Canadians with a particular emphasis on youth from the health consequences of tobacco use.
Section 4 of the Tobacco Act defines the purpose of the Act which serves:
- To protect the health of Canadians in light of conclusive evidence implicating tobacco use in the incidence of numerous debilitating and fatal diseases;
- To protect young persons and others from inducements to use tobacco products and the consequent dependence on them;
- To protect the health of young persons by restricting access to tobacco products; and
- To enhance public awareness of the health hazards of using tobacco products.
The Tobacco Act also imposes restrictions and prohibitions and provides authorities to regulate in key areas to support the established purposes:
Tobacco Products, including standards and information reporting
The Tobacco Reporting Regulations (TRR), adopted in June 2000, require manufacturers and importers to submit to the Minister of Health detailed reports on their tobacco products, including information on product composition and their emissions, information on sales, product packaging, research projects undertaken by or on behalf of a manufacturer, among other information.
Prohibition on sales to youth
The Tobacco Act prohibits the sale of tobacco products to persons less than 18 years of age and requires retailers of tobacco products to post signs that inform the public that providing tobacco products to young persons is prohibited by law. The Tobacco (Access) Regulations specify the place, manner, form and content of signs to be posted in retail outlets. The regulations also set out the documentation that may be used to verify the age of the person purchasing tobacco products.
Health-Related Labelling of tobacco products (except for cigarettes and little cigars), including Health Warning Messages
The Tobacco Products Information Regulations (TPIR) made in 2000 under the authority of the Tobacco Act provide the requirements for the health warning messages, health information messages and toxic emissions information that must be displayed on every packages of various tobacco products (except for cigarettes and little cigars since 2011). These health-related labels were made to increase awareness of the health hazards and health effects associated with tobacco use.
Health-Related Labelling of Cigarettes and Little Cigars, including Health Warning Messages
The Tobacco Products Labelling Regulations (Cigarettes and Little Cigars), made in 2011, replace the labelling requirements for cigarettes and little cigars that were previously enshrined in the Tobacco Products Information Regulations (TPIR) by new messages that are more memorable, noticeable and engaging. These Regulations also include a pan-Canadian toll-free quitline number and cessation Website portal to be displayed on all health warning messages and on some health information messages. These Regulations build on the achievements of the TPIR while aiming to improve its overall effectiveness. However, they were not examined as part of this evaluation as they have only come into effect recently and therefore effectiveness cannot be assessed.
Promotion, Prohibited Terms
The Promotion of Tobacco Products and Accessories Regulations (Prohibited Terms), made in 2011, prohibit the use of the terms "light" and "mild", and variations thereof, from various tobacco products, their packaging, promotions, retail displays, as well as from tobacco accessories. Again, given that this regulation was put into place in 2011, it will not be examined as part of this evaluation.
Promotion, including at retail and other forms of promotion
Advertising tobacco products is permitted under the Tobacco Act only if it is "information" or "brand-preference" advertising that is in a publication provided by mail and addressed to an adult or in signs in a place where young persons are not permitted by law. In this regard, the restrictions on promotion of tobacco products are aimed at limiting exposure of individuals and youth to tobacco advertising, strictly restricting "lifestyle" or "appealing to young persons" type of advertising. With some exceptions, foreign publications and broadcasts are exempt from these restrictions to disseminate promotion that is prohibited by the Tobacco Act.
Seizure of tobacco products
The Tobacco Act contains enforcement powers that can be employed by designated inspectors. Where an inspector seizes a tobacco product or other product, its owner may apply to a court for a restoration of the seized product. The restoration procedure under the Tobacco Act is outlined in the Seizure and Restoration Regulations.
As part of the FTCS, the Office of Regulations and Compliance (ORC) was responsible for managing compliance and enforcement activities related to the Tobacco Act and its regulations, undertaking some compliance and enforcement actions, as well as developing new regulations or updating existing regulations under the Act. Also some enforcement activities related to the Tobacco Act were transferred from ORC to the Regions group within RAPB.
Research
The Office of Tobacco Research, Surveillance and Evaluation (OTRSE) in HECSB was directly linked to the functional activity area of Research and Policy Development. Most of the work done in this Office contributed to the objective of examining the future of tobacco control. The major activities of OTRSE were divided across three portfolios: surveillance, evaluation and research, and business intelligence.
Surveillance (CTUMS, YSS)
OTRSE undertook a number of monitoring and surveillance activities in support of the FTCS which included surveillance of the smoking behaviour of Canadians, retailer compliance with youth access regulations, and public opinions. More specifically, surveillance activities include (while not being limited to) the annual Canadian Tobacco Monitoring Survey (CTUMS) and the bi-annual Youth Smoking Survey (YSS) (more detail is provided in the methodology section under secondary data analysis).
Evaluation and Research (Bio-Monitoring)
The OTRSE conducted scientific research related to smoking and tobacco to support the development of regulations, policies and programs, and the dissemination of information. The bulk of this work involved bio-monitoring projects as well as additional research related to tobacco product science.
Business Intelligence
As per Phase 2 of the Strategy, the OTRSE established a Business Intelligence (BI) unit in November 2008. The primary focus of the unit was to ensure a thorough analysis of information submitted by the industry to HC.
Policy
The Office of Policy and Strategic Planning (OPSP), HECSB led the policy development for the FTCS and was identified as the Office of Primary Interest for the Government of Canada planning and reporting requirements for the FTCS. Between 2007 and 2010, the main functions of the tobacco policy group involved: policy development, international work on the Framework Convention on Tobacco Control (FCTC), and stakeholders relations.
Policy Development
The key activities of OPSP since 2007 have been the development of the amendments to the Tobacco Act as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act; support for the renewal of the Health Warning Messages (the new Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) made in 2011); the evaluation of the Federal Tobacco Control Strategy; and the development of options for the future federal role in tobacco control.
International Activities on the Framework Convention on Tobacco Control (FCTC)
The FCTC is an international tobacco control instrument under the World Health Organization (WHO) which was developed in response to the globalization of the tobacco epidemic and asserts the importance of demand reduction strategies as well as supply issues. A number of federal partners and other departments were involved in the interdepartmental coordination and preparation of negotiating positions, including: Public Safety Canada, the Royal Canadian Mounted Police, Canada Border Services Agency, and Canada Revenue Agency. HC was involved given the health focus of the FCTC and concern over the public health impact of contraband tobacco products.
Stakeholder Relations
HC had many partners under the FTCS, including federal partners, provinces and territories, and non-governmental organizations. HC was responsible for managing relationships with these groups and chairing a number of working groups held as part of the FTCS.
Programming
G&Cs
G&Cs under the FTCS were funding mechanisms through which the federal government supported non-government organizations and other levels of government in conducting tobacco control activities.
Under the FTCS, funding for G&C projects was available under three broad categories:
- Knowledge Development Projects - smaller projects aimed at researching, designing and testing a service where the focus of the evaluation was on measuring project outcomes.
- Knowledge Application Projects - the majority of G&C funded projects were expected to be Knowledge Application Projects. The objective of these projects was to change the smoking behaviour of Canadians by increasing the number of people who quit or try to quit smoking, reducing the number of people who start smoking, and increasing action on second-hand smoke.
- Knowledge Transfer Projects - the focus of these projects was to accelerate the transfer and adoption of the service by other government or non-governmental organizations that are better positioned to impact behaviour.
Appendix A is a summary of the G&C projects that were funded by the FTCS. Many of these projects focused on "knowledge application", in particular smoking cessation. Consistent with the emphasis on cessation, 72% of the projects targeted smokers. Of that smoker community, many projects targeted sub-groups identified as vulnerable populations such as, mental health clients, youth and the Aboriginal community (both on and off reserve). Projects also targeted other populations, such as: health practitioners (36% of projects); the tobacco control community, e.g., policy makers, researchers, (22%); non-smokers (18%); or other groups (e.g., families, employers) (12%). Twenty-eight percent of the contribution projects had a client group consisting of aboriginal on-reserve and 26% of funding allocated was for aboriginal off-reserve groups. Projects were rolled out to experiment with different or new interventions or test techniques on new target groups.
Public Education
RAPB provided a comprehensive range of information and resources on tobacco use, cessation, prevention and protection to various audiences such as youth, adults, workplaces, pregnant women as well as the First Nations and Inuit population.
Contraband Tobacco
Activities related to the FTCS objective concerning the monitoring and assessment of contraband tobacco were the responsibility of several partner departments - i.e. Public Safety Canada (PS); Canada Border Services Agency (CBSA); and Royal Canadian Mounted Police (RCMP). Whereas the Public Prosecution Service of Canada (PPSC) and Canada Revenue Agency (CRA) were responsible for enhancing compliance to ensure that the legal tobacco market complies with federal tobacco tax laws thereby ensuring that there is no diversion to the contraband market. FTCS funding was used to increase departments' capacity, mainly through increased staffing to conduct intelligence analysis and inform policy-makers.
National Mass Media
In 2001, resources were sought for mass media in the amounts of $30M in 2001-2002, $40M in 2002-2003 and 2003-2004, and $50 M annually thereafter. These amounts were reduced significantly and during the second half of the FTCS (2007 to 2011), mass media campaigns were discontinued. To date, national mass media campaigns have utilized a budget of $100.8M for media, research and production purposes since fiscal 2001-2002. Additionally, a regional mass media contribution funding program was in place in 2001 and then reallocated by 2007.
First Nations Tobacco Control Program
In addition to the main objectives of the first half of the FTCS (2001-2006), a major focus of the FTCS was to target First Nations on-reserve communities south of 60°, and Inuit and all First Nations communities north of 60° where smoking prevalence was high. The First Nations Tobacco Control Program was discontinued by HC in 2007.
4.0 The FTCS Evaluation
4.1 Purpose of the Evaluation, Scope and Considerations
This evaluation planned to assess progress made towards the FTCS objectives. It addressed the core issues of relevance and performance in order to fulfill accountability requirements outlined in the Government of Canada Policy on Evaluation. The evaluation questions related to the core issues of relevance and performance are outlined in the table below.
A previous evaluation of the FTCS was conducted in 2006. Therefore, this current evaluation examined the ten years of the Strategy from 2001-2011 but had a specific focus on the second half of the FTCS (2007-2011). The evaluation also attempted to take into account not only the external factors associated with outcome results but also the complex interactions, of or contributions from, different levels of government where possible. Additionally, the evaluation was intended to be used as one line of evidence in the program renewal process.
| Evaluation Issue | Evaluation Questions |
|---|---|
| Relevance | |
| Is there a continued need for the FTCS? | |
| Are the FTCS activities and objectives aligned with the federal roles and responsibilities? | |
| Is the FTCS aligned with government priorities? | |
| Performance | |
| Effectiveness | To what extent has the FTCS been able to meet its objectives? |
| Which activities have had the greatest impact? | |
| Efficiency and Economy | What are the economic impact of smoking and the benefits of reducing smoking? |
| What is the return on investment for the FTCS? | |
Evaluation Approach
The Results-based Management and Accountability Framework (RMAF) developed in 2007, called for a four step evaluation approach intended to provide an analysis of relevance and performance.
The 2007 RMAF also referred to the development of a model which was expected to be used to determine value for money. This would have provided decision makers with precise quantitative estimates on long-term health and economic benefits directly attributable to the FTCS. Two research streams were necessary to support the simulation:
- An econometric model was required to examine the impact of various social, demographic and economic variables as well as the impact of various interventions which could be or not funded under the FTCS. Additional details will be provided later on in the methods section; and
- A micro level analysis of the effectiveness of the FTCS interventions (including FTCS G&C funded projects and legislation/regulations) was also required to support the simulation approach.
Cumulatively the results from these two streams were needed to assess with more accuracy the effectiveness of the FTCS. Limited progress in addressing existing data gaps prevented the population-level simulation modelling from providing the precise quantitative estimates on long-term health and economic benefits directly attributable to the FTCS that were hoped to be achieved.
To address the evaluation questions identified in the RMAF as well as support the evaluation core issues as required under the current Government of Canada Policy on Evaluation, the current evaluation strategy focused primarily on macro-level econometric and population-level modeling, supported by micro-level data from evaluation reports of Grant and Contribution projects, public opinion research and interviews with key stakeholders as well as validation interviews.
4.2 Methodology
This section describes the methods used in the evaluation of the FTCS (2001-2011). Multiple lines of evidence including a literature and document review, econometric modeling, secondary data analysis, key informant interviews and a stakeholder survey were employed to provide quantitative and qualitative data and confirm findings where appropriate. In addition, data collected over the course of the evaluation process was validated through informal interviews with FTCS Program personnel. The following is a description of the key lines of evidence.
Econometric Modeling
The purpose of the Econometric Modeling study was to provide an econometric analysis of the impact of tobacco control policies in Canada on smoking prevalence and quantity smoked. The model assessed the impact of both federal (FTCS and non-FTCS policy tools) and provincial, territorial and municipal interventions including: taxes on tobacco products (Department of Finance); second-hand smoke bans (P/Ts); retail display bans (P/Ts); retailer compliance with bans on sales to minors (FTCS); health warning messages (FTCS); legal age for smoking (FTCS and P/Ts); HC tobacco control expenditures. In addition to tobacco control policy variables, the model also included demographic variables (e.g., level of education, income, marital status).
Following Gagné and Gagné and TeddsFootnote 1, a two-part model using CTUMS data was selected for the analysis and modeling. This two-part model consisted of estimating:
- participation was defined as the probability that an individual smokes; and
- consumption was defined as the number of cigarettes a smoker smokes in a given period of time.
Separate participation and consumption (for smokers) estimates were generated for youth, for adults, and for workers, with youth being defined as those who have not reached legal age for smoking in their province.
This two part model is an easily implementable model that has been used in previous researchFootnote 2 and that does not rely on exclusion restrictions to adjust for potential selection bias because the consumption equation focuses on smokers rather than on the whole population.Footnote 3
For both youth and adults, estimates were generated for three different models which will later in the report be referred to as:
- Model I – Includes observations from 1999 to 2009. This model does not control for provinces and time, therefore unlike Model II, this model does not account for the influence of unobserved variables.
- Model II – Controls are included for provinces and time so this model accounts for unobserved heterogeneity however, it is more likely to represent short- rather than long-term effects, which is problematic in the context of an addiction.
- Model III – Same as Model I but only includes observations for 2001 to 2009. As for Model I, this model does not account for the influence of unobserved variables.
Review of Documents
A number of documents were reviewed to provide background information on the FTCS activities, the governance structure as well as contribute to the evaluation findings sections on relevance and performance. This included internal documents such as government documents, annual reports, internal memos and the 2006 summative evaluation of the FTCS. Additional documents were reviewed as part of efforts to assess FTCS relevance. These documents included major government priority setting documents: Speeches from the Throne and the Budgets (including the Budget Speeches and Budget Plans). Additionally, a review of communications from the Prime Minister of Canada was conducted.
Process Evaluation of Grant and Contribution Projects (2011)
Results from the 2011 Process Evaluation of G&C Projects were used as a line of evidence in the current evaluation of the FTCS. The process evaluation was conducted to examine G&C project roll-out, challenges and barriers, progress accomplished and lessons learned. Expected results as described in project proposals and Quarterly Progress Reports for all G&C projects funded by the FTCS were analyzed and summarized. Based on a review of the expected results and descriptions of the projects, the contribution projects were organized according to seven categories or project clusters: Helplines, Ottawa Model, Counselling, Policy and Knowledge Exchange, Training, Workplace-based, and School-based. Analysing projects by cluster facilitated the identification of lessons learned, best practices and challenges specific to each cluster of projects. The process evaluation examined the key objectives, activities and planned outputs; the financial status; the partnerships; the successes; and the challenges and barriers associated with the 104 G&C funded projects. The conduct of the process evaluation entailed a detailed content analysis of project proposals, project progress reports and final project reports completed by March 2011.
Impact Evaluation of Grant and Contribution Projects (2010)
This study was intended to evaluate the effectiveness of a sample of G&C projects launched by FTCS for fiscal years 2007-2008 to 2009-2010 that could be evaluated through an experimental design (i.e., through the use of a comparison group) which proved not to be possible and thus, a quasi-experimental design was implemented instead. The number of participants (n= 655 of 1051 at baseline) were drawn from a total of 17 funded projects. Because the number of participants in projects was much lower than expected, a census survey of project participants consenting to the Impact Evaluation, was conducted (not a sample as originally envisioned). This also explains why an experimental design approach could not be implemented for the 2010 Impact Evaluation of G&C Projects.
The design of the survey instruments was based on the objectives of the impact evaluation, and drew heavily from existing questionnaires on tobacco behaviour (e.g., CTUMS). The baseline survey was designed to be administered primarily by interviewers over the telephone and was approximately 20 minutes in length. The survey was re-administered to each participant at 3-months, 6-months and 12-months after completion of the baseline survey. The questionnaireFootnote 4 addressed issues such as:
- smoking history (e.g., age started smoking);
- current smoking behaviour (e.g., smoking behaviour in last seven days, last 30 days);
- household smoking restrictions;
- prior quit attempts;
- project participation (e.g., source of awareness of the project, level of commitment, type of intervention, steps to prepare); and
- socio-demographic information (e.g., language, education, marital status, health status).
The majority of survey interviews were completed using telephone administration; however, a small number of surveys were completed on-line or via pencil and paper. While there are methodological implications to using such a mixed mode approach to data collection, the vast majority of interviews were completed by telephone. As well, given the need to ensure as many participants in each project completed the survey, it was decided that the need for a larger number of completed surveys outweighed the methodological issues related to mixed mode of data collection.
Smoking-Attributable Morbidity, Mortality and Economic Costs (SAMMEC)
The Smoking-Attributable Morbidity, Mortality and Economic Costs (SAMMEC) software modules were used to estimate Smoking-Attributable Morbidity (SAM), smoking-attributable Years of Potential Life Loss (YPLL), and productivity losses attributed to diseases caused by smoking in the efficiency and economy section of the report.
Stakeholder Survey
HC contracted an on-line survey of tobacco control stakeholders, including both non-governmental organizations which have received funding from the FTCS for tobacco control activities and those that did not as well as tobacco industry stakeholders. The stakeholders' survey was used to update the information obtained in 2006 through public opinion research, which could not be repeated for this evaluation. The survey instrument was designed in close consultation with HC to address all pertinent issues, which included:
- continued need for tobacco control efforts in Canada;
- continued need for a federal strategy in tobacco control, and the appropriate focus for the federal government in tobacco control;
- perceived impacts of the FTCS, as well as overall strengths and weaknesses of the FTCS;
- shifts in provincial and federal roles and responsibilities in the area of tobacco control;
- outcomes and impacts of FCTS funding to stakeholders; and
- information sources utilized and gaps in information pertaining to tobacco control.
A total of 521 stakeholders, identified by HC were sent the on-line survey, with a response rate of 40%. 64% of respondents had received funding from the FTCS. It should be noted that findings of this survey may reflect the vested interests of many of the stakeholders.
Key Informant Interviews
As follow-up to the stakeholder survey, a total of 19 key informant interviews were completed in October 2010. The 19 were selected via a purposive sampling strategy: a number of individuals who had provided more elaborate comments were included; individuals representing key stakeholder organizations; and, individuals representing small, medium and large organizations were selected. The purpose of the key informant interviews was to obtain more detailed feedback on the issues addressed in the survey, as well as to contribute to the analysis of survey findings. Interviews were conducted using an interview guide and semi-structured questions.
Literature Review
A literature review was conducted in 2010 using Canadian and international studies on tobacco and government documents. The literature reviewed behavioural measures, mass media, health warning messages on cigarette packages, retailer compliance with regulations and cigarette promotion regulations. A search was conducted using the Cochrane Database and PubMed for articles presenting findings from quantitative evaluations of specify program interventions (e.g., smoking cessation helplines). All relevant articles were then reviewed on the basis of methodology for inclusion. Included articles were summarized and synthesized for each of the intervention types included.
Secondary Data Analysis
The main secondary source of data for this evaluation was the CTUMS, which is designed to monitor trends in smoking prevalence in Canada. CTUMS is a repeated cross-sectional survey with a nationally representative sample that collects data on smoking prevalence, cigarette consumption, cessation behaviour, as well as socio-demographic information including age, sex, marital status and education. Persons aged 15 years and over who live in Canada are the target population for CTUMS, and residents of the Yukon, Northwest Territories and Nunavut and full-time residents of institutions are excluded. Over 20,000 observations are collected per year, with the number of observations usually spread equally among the 10 Canadian provinces, half of the observations collected from individuals aged 15 to 24, and the other half from individuals aged 25 and over. Respondents are selected through a list of working telephone numbers and a systematic sample of numbers drawn within each sampling stratum for the survey (Microdata user guide: CTUMS cycle 1, February - June 2005).
The Youth Smoking Survey (YSS), funded by HC, was created to study the factors that increase and diminish the likelihood of tobacco use among youth. Initially this survey covered students in grades 5 through 9 as well as their parents, but the age groups changed in later versions of the survey, including students up to grade 12, and not including parents. In addition to collecting data on prevalence, the YSS also provides details on the attitudes and behaviours related to youth smoking such as: experimentation; purchasing behaviour and sources of cigarettes; awareness of health risks of smoking; recollection and opinions regarding health warning messages; experience with alcohol and drugs and the social demographic factors associated with smoking behaviour. The YSS was first administered in 1994 and was repeated in 2002, 2004-2005, 2006-2007, and most recently in 2008-2009.
4.3 Limitations
Other lines of evidence originally planned were not implemented due to policies around polling Canadians as well as funding and staffing resource restrictions. These include surveys other than the stakeholder survey (i.e., the exposure survey; the national public opinion survey on Canadian attitudes toward smoking), the case studies; and the performance monitoring system designed to capture detailed operational inputs.Furthermore, some methods that were implemented experienced data challenges, including the 2010 Impact Evaluation of G&C Projects which could not be implemented as planned. As the G&C program unfolded, far fewer projects were funded than originally anticipated and only a small sub-set of these were found to be appropriate for the impact evaluation. Due to the limited initial sample size and attrition of the sample over the four measurement periods, the impact analysis was based on a relatively small number of cases, presenting challenges to conducting project-based or intervention-based analysis to determine effectiveness.
In addition, it should be noted that the projects that were included in the 2010 Impact Evaluation of G&C Projects were very heterogeneous in terms of their client target (e.g., students, seniors, hospital patients, mental health/addictions patients) and nature of their intervention (e.g., peer counselling, webcasts, and clinician interventions). The bivariate analysis (e.g., by the socio-demographic characteristics of participants, type of intervention) were, therefore, difficult to interpret without the ability to control for an array of influencing variables. Again, the paucity of supporting micro-level results of projects and interventions inhibited the ability to attribute progress on many FTCS objectives to FTCS activities.
This means that the data available for the FTCS evaluation with the several lines of evidence will provide a reasonable picture of tobacco control measures within Canada and what types of activities seem to work better than others. However, attribution issues remain due to the many influences on prevalence rates and the multitude of players involved in the area of tobacco control – not to mention that many of the micro-level lines of evidence, besides the evaluations of projects supported by contribution funding, were not implemented to support and ground the higher macro-level data with respect to the Strategy specifically.
In order to mitigate these attribution challenges that became apparent throughout the evaluation process, a number of different strategies were employed. Firstly, due to the lack of a performance data system, performance data was retrieved via a manual review of annual reports and internal documents to provide some micro-level evidence of what the FTCS has accomplished with respect to its outcomes. Secondly, the FTCS evaluation attempted to perform a quantitative analysis using the econometric model to determine the feasibility of establishing a logit regression model to develop coefficients capable of providing estimates on contribution of the FTCS to the overall accomplishments of tobacco control in Canada. As the limitations of the approach became clear, this work was modified and a more crude return on investment analysis was included in the report. Lastly, due to the lack of a comparison group in the 2010 Impact Evaluation of G&C Projects, as well as the bivariate nature of some of these funded projects, a quasi-experimental design was used instead of an experimental design as mentioned previously. In addition, informal validation interviews were conducted to confirm preliminary findings and conclusions.
5.0 Evaluation Findings Relevance
The Evaluation Findings section of the report has been organized by core issue (i.e., relevance and performance). The findings are presented according to each Phase 2 objective and a summary is provided at the end of each section.
5.1 Continued Need for the FTCS
The survey of stakeholders indicated that the majority of stakeholders agreed that Canada has experienced considerable success in the area of tobacco control over the past 10 years (77%), that smoking rates have declined and that awareness of the health hazards of smoking and second-hand smoke is high (74%). Based on 2010 CTUMS data, the smoking prevalence rates have declined over the years of the Strategy, but the decline has slowed and even "reached a plateau" over the last five years.
Follow-up interviews conducted with key informants suggested that stakeholders seemed to perceive that involvement and focus of the federal government on tobacco control has slowed in the past few years. Many key stakeholders interviewed pointed to a perceived reduction in the level of commitment and effort, monetary investment, as well as the scope of federal government activities in tobacco control. Despite this perception from stakeholders, the sentiment that there is a need for continued tobacco control efforts in Canada was high with 87% of respondents agreeing that there is still a need for tobacco control in Canada. A majority of stakeholders (72%) also believed that tobacco control continues to be an important priority for Canadians.
Stakeholders surveyed were asked to rate the extent to which there continues to be a need for efforts in specific areas related to tobacco control:
- Reducing the number of youth who smoke received the highest rating in terms of the continued need for involvement (88%). This was also identified as the highest priority for continued efforts in the 2006 survey done as part of the evaluation. However, the youth prevalence rate noted in the CTUMS (9%) suggested that youth prevalence has reached a new low in Canada in 2010.
- Increasing the number of smokers who quit smoking was also perceived as an area where there is a high need for continued effort (82%). Similar to the situation observed for youth, the overall smoking rate noted in the CTUMS for the population aged over 15 years old (17%) suggested that overall smoking rates have reached a new low in 2010.
- Over 7 in 10 stakeholders perceived a high need for continued efforts in terms of regulating the sale of tobacco (73%), reducing contraband tobacco (71%), and regulating the manufacture of tobacco (70%).
The survey also asked stakeholders about the priorities of the FTCS and while over half the stakeholders surveyed agreed that the priorities of the FTCS are appropriate as is, 45% identified additional priorities they felt could be a focus of the Strategy. Additional priorities identified included a focus on the Aboriginal population, addressing industry marketing tactics, and addressing other at-risk populations.
From a review of documents, it is clear that what was once mainly a federal role on tobacco control has now expanded to include provincial/territorial control measures. With this increased action from provinces and territories, many tobacco control issues are now addressed at a provincial/territorial level, and prevention or cessation programming is increasingly conducted at this level. Provinces and territories have also introduced a number of legislative and regulatory measures, such as retail display bans, smoking bans in cars, smoking bans in public places, and increasing the minimum age of purchase.
Tobacco stakeholders were also asked their opinion about the impact on tobacco control in Canada should the FTCS not be renewed. Seventy-nine percent of stakeholders (n = 126) having received funding under the Strategy believed that the impact would be high. Perceptions of stakeholders not having received funding under the Strategy (n = 37) were more evenly distributed, but still one third of them considered that the impact would be moderate or high. It should also be noted that while overall 69% of stakeholders consider the impact of not renewing the FTCS would be high, only 23% mentioned it would result in an increase of smoking prevalence.
Many stakeholder interviewees noted that they were worried that the federal government believes that "tobacco is done". Interviewees unanimously agreed that the rate of smoking was still too high and that Canada cannot afford to stop working to decrease prevalence even though the daily smoking rate for the Canadian population aged 15 or older was at 13% (CTUMS, 2010), which was the lowest of comparable countries. However, there are still some vulnerable populations who are experiencing higher than average prevalence rates, such as, the Aboriginal population.
5.2 Alignment with Federal Roles and Responsibilities
The 2006 Public Opinion Survey suggested that there were areas where the federal government had a clearer mandate than other levels of government or other partners. At the time, Canadians placed their strongest support behind federal responsibility in the areas of legislation and regulation of both the manufacturing and sale of tobacco products, as well as anti-smuggling. Canadians most often cast the role of the federal government as equal partner with provinces and non-governmental organizations, with about one in four favouring the federal government in a leadership role. Cessation, prevention of youth uptake and second-hand smoke were areas where the role of any single organization was less clear. In these cases, Canadians were more often seeing a coordinated approach, involving many partners, and no clear consensus on one leader.
According to the survey of tobacco stakeholders conducted in 2010, 45% of them believed that the need for a federal government role is about the same as 10 years ago and 46% believed such a need is higher than 10 years ago, despite the fact that prevalence has drastically reduced over the last 10 years. It should be noted that stakeholders having received FTCS funding in the past are more apt to perceive the need of federal tobacco control as high (94%), or perceive the need to have remained the same (52%). Those who have never received funding are more apt to see the need as lower than 10 years ago.
As part of the survey, stakeholders were asked to indicate what level of responsibility they believe would be most useful or appropriate for the federal and provincial/territorial governments to play in a number of tobacco control areas or priorities. Results of this survey suggested that the federal government should be assigned the greatest responsibility for international leadership and participation in global forums as well as facilitating agreements (between levels of government and other organizations) on tobacco control (86% versus 14% for P/Ts).
Stakeholders also indicated that the bulk of responsibility for implementation of legislation and regulation should be the federal government role (75%). The other strong federal roles that were identified were addressing issues related to contraband tobacco (73%), tobacco research and dissemination (69%) and mass media campaigns (65%).
The enforcement of tobacco control legislation and regulations was seen to be more evenly split between the federal and other organizations with 54% of stakeholders assigning the responsibility to the federal government. Results are similar for the responsibilities of funding of other jurisdictions and organizations for cessation activities (58% assigned it to the federal government) as well as for public education activities (49% assigned it to the federal government). Not to mention the prevailing legacy of the continued partnership and shared responsibility between all levels of government as well as other national organizations with respect to tobacco control. Nonetheless, it still remains that 74% of responding stakeholders believed the primary responsibility should reside with the federal government.
Key informants were then asked more specifically about what they understood as the necessary continued role of the Government of Canada. Stakeholders described this role along a number of key themes:
- national role - coordination, bridging gaps, ensuring consistency, showcasing a commitment;
- setting the framework, targets, and strategy - creating a plan for others to follow;
- tackling the supply side - legislation and regulations, contraband, "fighting the industry";
- coordinating information and roles, best practices - fostering networks, meetings, consultation, discussion, and transparency;
- innovation, creativity, new ideas, generating discussion; and
- working closely with other stakeholders - engaging the provinces and territories.
5.3 Alignment with Government Priorities
The review of federal government documents, found that despite having received consistent funding throughout the 1990s and 2000s, tobacco control has not been identified in current government documentation (Speeches from the Throne, Budgets, etc.) as a major government priority in key government priority setting documents since the late 1990s.
Since 1996 "tobacco" and "smoking" have only been mentioned in two Speeches from the Throne; in 1997 and in 2001. The 1997 Throne Speech identified tobacco control as a pressing health need, along with the Canadian breast cancer initiative and the national HIV-AIDS strategy. This speech announced that resources for the Tobacco Demand Reduction Strategy would be doubled, with a "focus on community-based programs to prevent young Canadians from starting to smoke and to encourage smokers to quit".
In 2001, tobacco was mentioned as part of a section of the Throne Speech that identified a number of community-based health promotion and disease prevention measures, noting that the government would strengthen efforts to "reduce tobacco consumption". However, the Budget Plan references to tobacco and smoking were almost exclusively in terms of taxation of tobacco products.
The 2000 and 2001 Budget Plans included line items noting that monies will be provided to a tobacco control strategy, but no further commentary was provided. The 2005 and 2008 Budget Plans were the only ones that mentioned tobacco or smoking and provided additional details about these as a health-related priority. These Budget Plans explicitly linked taxation with smoking cessation and prevention. Budget Updates similarly focused on taxation with reference to tobacco and smoking.
In Phase 2 of the FTCS, communications from the office of the Prime Minister referenced tobacco control on only two occasions which related to the amendments to the Tobacco Act in 2009 as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act.
5.4 Relevance Summary
The FTCS, as it is currently structured, may need to be streamlined given the current tobacco control environment. Prevalence rates in Canada have declined significantly over the past and are among the lowest in developed countries. However, there are some sub-populations that are still experiencing higher prevalence rates such as the Aboriginal community. Also, there has been an increased involvement of the provinces and territories in tobacco control. By 2007, all provinces had Acts that enhanced what was once solely federal legislation concerning tobacco control, and P/T expenditures on provincial/territorial tobacco control strategies have more than doubled since 2001.
Nonetheless, there still seems to be a perceived need among stakeholders for continued efforts on the part of the federal government to continue work on tobacco control. Stakeholders believe that the main role for the federal government is a leadership role responsible for coordination at the national and international level, which would include developing national frameworks, legislation and regulations.
Despite the fact that current federal priorities do not highlight tobacco control as a main federal focus, the Government of Canada still has the responsibility to administer the Tobacco Act, (amended in 2009 as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act), and its various regulations.
6.0 Evaluation Findings - Performance
6.1 Overall and Youth Prevalence
6.1.1 Smoking Prevalence Trends
Over the past four decades the smoking prevalence rate has been steadily declining across all demographic groups. In 1965, 49.5% of Canadians aged 15 and older were smoking either everyday or occasionally. While smoking rates declined between the 1960s and 1970s, smoking rates began to fall more sharply in the mid 1970s. Between 1975 and 1985, smoking rates fell from 45.5% to 34%. Rates continued to decline through the 1980s and 1990s. Between 1991 and 2001 overall smoking rates declined from 31% to 21.7% with much of this decline occurring in the later portion of the decade.
The Figure 1 illustrates the steadily declining smoking prevalence rate.
Figure 1: Smoking rates in Canada (Ages 15+), 1965-2000
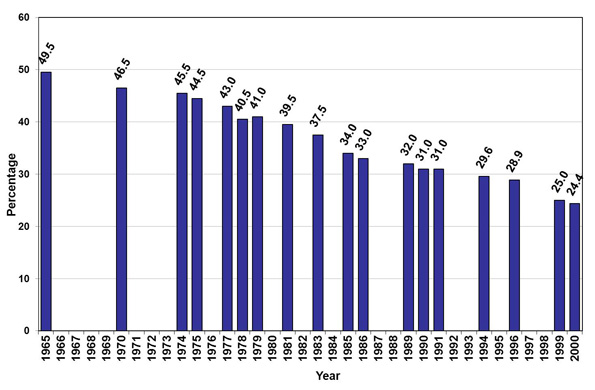
Text description - Figure 1: Smoking rates in Canada (Ages 15+), 1965-2000
Figure 1 is a bar graph that illustrates the smoking prevalence rates among Canadians aged 15 and older from the year 1965 to 2000. The smoking prevalence rate in 1965 was 49.5% and decreased steadily over the years to 24.4% in the year 2000.
- 1965 = 49.5;
- 1970 = 46.5;
- 1974 = 45.5;
- 1975 = 44.5;
- 1977 = 43.0;
- 1978 = 40.5;
- 1979 = 41.0;
- 1981 = 39.5;
- 1983 = 37.5;
- 1985 = 34.0;
- 1986 = 33.0;
- 1989 = 32.0;
- 1990 = 31.0;
- 1991 = 31.0;
- 1994 = 29.6;
- 1996 = 28.9;
- 1999 = 25.0;
- 2000 = 24.4
Smoking rates among youth aged 15-19 have also generally declined since rising through much of 1990s. Between 1991 and 1997 youth rates rose from 22.6% to 29.1%, however smoking rates among youth aged 15-19 have since declined to 22.5% in 2001.
Although smoking among those aged 20-24 is higher than for those in the 15-19 age group, smoking rates have also been declining steadily. Between 1985 and 2001, smoking in this age group declined from 42.7% to 32.1%.
6.1.2 Overall Prevalence
This section presents evaluation findings for the prevalence objectives established for the FTCS in both Phases and as it pertains to the overall population - i.e. 15 years and older. These objectives were:
For Phase 1 of FTCS (2001-2006):
- reduce smoking prevalence to 20% from 25% in 1999; and
- reduce the number of cigarettes sold by 30%.
For Phase 2 for the FTCS (2007-2011):
- reduce overall smoking prevalence from 19% to 12% by 2011; and
- increase the number of adults (including young adults) who quit smoking by 1.5M.
It should be noted, the prevalence objectives have been streamlined to facilitate reporting in this report. First, the overall prevalence objectives for the first and second phases were 'combined' given the modification of the target in Phase 2. In other words, the objective reported was a reduction in overall smoking prevalence from 25% (in 1999) to 12% (by 2011).
Second, the objective stated in 2007, reduce overall smoking prevalence from 19% to 12% by 2011, and the one objective pertaining to the number of former smokers are actually the same objective; the former being expressed as a rate and the latter being expressed as the absolute number of former smokers required to reach the 12% prevalence rate.
Finally, the refocusing of the FTCS objectives that took place in 2007 resulted in the removal of the objective pertaining to the number of cigarettes sold. In this context, this objective was not reported on as part of this evaluation report.
Recent Trends
The overall smoking rate, which has been steadily declining since the 1960s, has continued to decline since the introduction of the FTCS in 2001. Furthermore, the overall smoking rate (which includes daily and occasional smokers) has declined from 21.7% to 18.6% between 2001 and 2006, indicating the target established for the first phase was met.
In the subsequent years, the overall smoking rate further declined to 16.7% by 2010 (which means that there are still approximately 4.7M Canadians who continue to smoke). However, much of the 5% decline observed between 2001 and 2010 occurred in the early 2000s. By 2005, the overall smoking rate reached 18.7%; a decline of 3 percentage points since 2001. While in 2010, the overall smoking rate reached 16.7%; a decline of 2 percentage points since 2005. Over 62% of the overall reduction in smoking since 2001 occurred by 2005.
The daily smoking rate has declined to 13% in 2010, which is lowest prevalence rate of comparable countries. The daily smoking population consists of "hard core" smokers, those who have smoked at least 100 cigarettes and have no intentions of quitting, and regular smokers, those who would like to quit and have tried at least once in their life. Occasional smokers (those who do not smoke daily and may go weeks without smoking a cigarette) have remained fairly stable and comprise approximately 4% of the smoker population. As the daily smoking rate has decreased, occasional smoking has grown as a proportion of the current smokers. Occasional smoking has not changed significantly as a proportion of the overall population, indicating a possible shift from daily to occasional smoking.
As noted earlier, one of the new objectives for the second phase of the Strategy was to increase the number of former smokers by 1.5M, which was the number of quits necessary to reach a 12% national prevalence rate. A former smoker is defined as someone who has smoked at least 100 cigarettes in a life time but currently does not smoke. According to 2010 CTUMS data, the number of former smokers aged 15 and over in Canada increased by approximately 1.3M between 1999 and 2010, but there has been no statistically significant change in the number of former smokers between 2007 and 2010. The point-specific estimate indicates a decrease in the number of former smokers by approximately 0.16M between 2005 and 2010 (which falls within the margin of error).
Of the current smoking population, the majority has tried to quit smoking at some time in their lives. The percentage of current smokers who have made at least one 24 hour quit attempt in the past year was 47% in 2010. This percentage remained surprisingly consistent from year to year. Also, the evaluation noted that the successful quit rates are usually around 3-5% of the smoker population.Footnote 5 Even with the large number of smokers who have attempted, or have intentions to quit, few are successful. These figures reinforce the difficulty of quitting smoking.
Although the overall smoking prevalence rates have decreased significantly over the last decade, there are still some vulnerable populations who are experiencing higher than average prevalence rates. One of these populations to note is the aboriginal community.
Contribution of FTCS activities
This section speaks to the effectiveness of a number of different tobacco control interventions supporting the FTCS that have been assessed through econometric modelling, literature reviews and public opinion research.
Regulations
The FTCS activities expected to have had the greatest impact on a reduction of overall smoking prevalence were the regulations associated with the Tobacco Act - i.e., prohibition on sales to youth, labelling of tobacco products (including health warning messages) as well as promotion, including at retail and other forms of promotion. It should be noted that the mechanism as to how regulations impact smoking behaviour is not known at this point; whether it influences smoking cessation or prevention or both. Also, the amendments to the Tobacco Act made in 2009 as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act and the new Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) made in 2011 can only influence future smoking prevalence rates as most of the implementation of its measures was only initiated recently.
Prohibition on sales to youth
Compliance and enforcement activities related to this prohibition and related requirements set out in the Tobacco (Access) Regulations were undertaken at the retail level by federal inspectors in some provinces (Saskatchewan and Alberta), and by provincial inspectors in others, by way of Memorandum of Agreement between federal and provincial governments.
Tracking national retailer compliance was done via two means - Tobacco Control Information Monitoring System (TCIMS) data, and the Evaluation of Retailers' Behaviour towards Certain Youth Access-to-Tobacco Restrictions (retailer survey). Both methods had some limitations. The retailer survey was rolled out every year to a limited number of cities (approximately 30 cities) across the nation, and therefore was only a sample of the nation. Also, data concerning the retailer survey was only available to 2009 due to its recent cancellation. The TCIMS database was populated mainly by federal inspectors because it was only voluntary for provincial inspectors, therefore gaps exist in the completeness of the data.
Nonetheless, retailer compliance had always been reported as high. Based on the retailer survey, compliances ranged from a low of 67.7% in 2003 to a high of 85.9% in 2008. In 2009 the retailer compliance rate was 84% according to the survey. Information contained in TCIMS and data collected from provinces demonstrated an even higher compliance rate.
The youth population was captured under both objectives - i.e. overall prevalence (15 and older) and youth prevalence (15-17). The prohibition on sales to youth was designed to reduce the availability of tobacco products, particularly to children and youth. It was based on the rational that restraints on access decrease the likelihood that some young persons experimenting with smoking will become regular smokers and emphasize their dangerous nature. For the purpose of this evaluation, this prohibition was expected to impact youth prevalence which was then expected to impact overall prevalence. In this context, findings on prohibiting sales to youth are relevant under both objectives but will be discussed under the youth prevalence section.
Labelling of tobacco products
The compliance and enforcement work with respect to Health Warning Messages (HWMs) and Health Information was usually done via inspections at the manufacturing level as the bulk of this work occurred at the time of manufacturing. Compliance and enforcement activities conducted with respect to the Tobacco Products Information Regulations (TPIR) were generally conducted by federal inspectors. Data from the 2009-2010 fiscal year indicated a 98% compliance with these regulations.
Regular public opinion research (POR) studies to examine the public's responses to the TPIR were also conducted from 2000 to 2007. These studies investigated: the number of times people looked at the messages, responses to the messages, awareness of health effects of smoking and the credibility of the messaging.
These studies found that awareness of the health harms of smoking and the specific harms depicted in the messages was consistently high. Also, while the explicit aim of HWMs was to increase awareness of health harms, the last POR study, in 2007, noted that:
- 57% of adult smokers believed the health warning messages were effective in getting them to smoke less around others;
- 52% said that the messages increased their desire to quit smoking; and
- 43% said that these messages have been effective in getting them to try to quit smoking and in getting them to smoke less (40%).
Each wave of the survey/study asked smokers and potential quitters (smokers seriously thinking about quitting smoking) whether they felt that HWMs were effective in getting them to try to quit. The results demonstrated that there had been little change in the effectiveness of HWMs to increase cessation rates among smokers, and that respondents were fairly evenly divided in their assessment of whether the messages were effective in getting them to try to quit smoking.
As this survey was not longitudinal, there was no way to track changes in individual behaviour, or to attribute quitting behaviour to the messages. However the studies did ask about smoking and cessation behaviour. Despite favourable responses about the effectiveness of HWMs in encouraging smokers to try to quit smoking, these surveys showed no significant change in the number of quit attempts made. In the 2007 survey, the proportion of smokers who reported having stopped smoking for at least 24 hours once in the past year was unchanged from the November-December 2000 baseline survey. This would suggest that smokers were not making more quit attempts following the implementation of this regulation.
The literature review, which was conducted as part of this evaluation, examined randomized controlled trials and the effect of cigarette package warnings on smoking cessation or prevalence. No studies with randomized controlled trials were found. As a result, the parameters of the literature review were broadened to include non-controlled trials. The findings of the literature review indicated that while the measures of effectiveness varied in the different studies, they were nonetheless reporting positive findings on the effectiveness of health warning messages, with smokers retrospectively attributing some changes in smoking behaviour to these messages. These findings were only aggregate measures and therefore identifying sub-groups (youth, females, etc...) of the populations was impossible. Although the findings were consistently positive, it was difficult to provide a reliable attribution of impact.
Another point of interest for research related to HWMs was the exploration as to whether these messages "wear out". While findings of various studies gauging the potential "wearing out" of health warning messages appeared not to be consistent, a study done in 2007 as part of the International Tobacco Control Policy Evaluation Survey (ITC Project) found that changing the format of the warnings increases the impact. However, there has been a general decline in reactions to warnings in Canada since implementation. The authors hypothesized that this finding "would suggest that there may be health promoting advantages in changing the health warnings from time to time, but failure to do so will not negate all the beneficial effects".Footnote 6 This is in line with findings from the public opinion survey conducted in 2007Footnote 7 which found that more than 54% of the respondents felt HWMs were worth re-reading, but 66% described them as worn out and having lost their effectiveness.
Further, the findings from econometric modelling conducted as part of this evaluation suggested that HWMs had an initial small effect on adult smoking participation (uptake), but that this effect diminished over time to a point where no effect was seen by 2009. HWMs were also found not to have a significant impact on consumption (number of cigarettes smoked) by the adult population.
Promotion, including at retail and other forms of promotion
Compliance dealing with promotion was generally high. Based on the 2009 retailer survey, the compliance rate was over 95%. Tobacco Act sections dealing with false promotion, testimonials/endorsements and sales promotion also found a 99% compliance rate.
Measurement of the direct impact of these legislative measures in Canada was conducted at the time of their implementation in the early years of tobacco control. Given that tobacco promotion and advertising have been restricted in Canada for many years, the impact, meaning the change in people's behaviour due to these advertising bans, over the past 10 years would be difficult to ascertain.
Systematic searches, conducted as part of the literature review, found no relevant studies published in the last decade that examined the effect of measures prohibiting and/or limiting cigarette/tobacco promotion and advertising on smoking prevalence or quit rates even when search parameters were enlarged to include uncontrolled studies.
Despite the adoption of measures prohibiting and/or limiting advertising by any person; the breadth of jurisdictions taking up these restrictions; and/or the duration in which these restrictions have been in place, there was still no recent evidence concerning the effectiveness of this type of measures on smoking prevalence or quit rates.
Leadership
The Government of Canada, through the FTCS, played an active role in the development of both provincial and federal restrictions on tobacco sales and promotion in Canada, including at retail. The Tobacco Act prohibits promotion in general except as authorized by the Act or its regulations. For example, the Act allows the display of tobacco products at retail under subsection 30 (1)). Several provinces have taken the initiative to ban retail displays of tobacco products, reducing the potential for youth to be exposed to tobacco marketing efforts. This also removes tobacco products from the view of those who are trying to quit smoking, potentially making it easier for them to successfully quit.
The FTCS supported the idea of retail display bans by conducting research on international retail environments, by conducting and analyzing retailer surveys as well as surveys of the general population about their knowledge and attitudes concerning retail advertising. Given that tobacco promotion in the retail environment has been a shared jurisdiction, governments at all levels were involved in identifying acceptable solutions. The Government of Canada, through the FTCS, continued to work with all levels of government to promote federal and provincial tobacco restrictions.
The federal government had also influenced the implementation of provincial second-hand smoke bans by providing contribution funding (seed money) in the early stages of second-hand smoke bans to municipalities, by promoting these bans through public education as well as by developing informational resources to support municipalities in implementing the bans (e.g., "how to" toolkits). This is discussed in more detail in the Second-Hand Smoke Exposure section of this report.
Grants and Contributions
According to Phase 2 of the FTCS, Grant and Contribution projects funded under the FTCS were to focus on knowledge development, application and transfer and to move away from raising awareness about the health harms of tobacco use. It also was to concentrate on funding projects that develop and test cessation and prevention techniques to ascertain best practices and transfer this knowledge to stakeholders.
Appendix A provides a profile of G&C projects funded by the FTCS. Based on this data, most contribution agreements (92%) were multi-year agreements and were distributed across the country. With respect to objectives of the funded projects, the majority of G&C projects (representing both 67% of projects and of dollars allocated) address the cessation objective. Far fewer - 5% and 3% respectively - had a primary focus on prevention or protection. About 1 in 10 projects addressed other objectives such as "next generation" projects, which addressed forward-looking or more strategic issues in implementing future tobacco control policies and programs (9%) or projects that embodied multiple objectives (11%), with a smaller proportion related to the Framework Convention on Tobacco Control (FCTC) (5%).
Because projects' objectives and activities may have reflected more than one project type (knowledge development or application or transfer), a "multiple response" indicator allowing more than one type descriptor was createdFootnote 8. The projects were further coded by primary type of project. Knowledge application projects - interventions with the objective of changing the behaviour of smokers - represented the most common type of project (50% of projects were categorized as application projects, representing 45% of dollars allocated). Knowledge development (research/design of a service or resource) and knowledge transfer (encourage adoption of successful projects/best practices/strategies by other governments or NGOs) projects were represented equally - 25% of projects respectively. The latter type - knowledge transfer projects - represented a proportionately higher allocation of FTCS contribution funding (39% compared to 16% for knowledge development projects).
The "knowledge application" projects, meaning interventions that targeted changing smoking behaviour, were intended to have a strong assessment component in order to test these interventions so that best practices could be identified and shared with stakeholders. However, only a small portion of these projects were able to provide outcome data that could relate to the interventions' effectiveness. Therefore the identification of rigorously evaluated practices was limited.
Many of these projects also experienced low participation, as captured by participant profiles and as indicated as problematic in the 2010 Impact Evaluation of G&C Projects. Additionally, many projects that delivered direct smoking interventions experienced a decline in participation as the intervention progressed - furthering the low participation rate. Notably, there were two projects that identified no participation in the impact evaluation.
The projects included in the 2010 Impact Evaluation of G&C Projects did have some success with relatively high quit rates. Quit rates were calculated in a number of ways to try to control for non-response biases as well as potential positive bias for self-reported behaviours by smokers.
Other assessments of cessation programs addressed these potential response biases by inputting a response for non-responders. For this evaluation, the method used was the "intention to treat" method that applied a 5% spontaneous quit rate to the non-respondent groupFootnote 9 given it was the one appearing to provide the most reasonable/credible estimate of quit rate. Applying a 5% spontaneous quit rate to non-responders demonstrated an estimated quit rate of 27% at 3 months, 19% at 6 months, and 13% at 12 months.
Although high quit rates were reported by contribution projects in the 2010 Impact Evaluation of G&C Projects, participation in this evaluation was limited by the nature of the participating populations (i.e., vulnerable populations) as well as the implementation of the evaluation design. Vulnerable populations create an interesting dilemma for evaluation studies because getting consent can be problematic (adult/guardian consent is required for mental health patients and youth). Also doing follow-up measurements of those with no fixed address or no telephone skills can be difficult. As for the impact evaluation design, only a small sample of projects (n=17 of a possible 98) were selected for participation in the evaluation due to the type of activity funded, the target group involved, the stage of implementation of the project and the ability of the project to have results-based data, making it impossible to make any generalized conclusions about the overall impact of the contribution projects on prevalence.
Given the low participant reach for projects in the impact evaluation, the projects funded through contributions did not generate a significant impact on national prevalence rates. However, many projects targeted vulnerable groups who were difficult to reach and were known to have low participation in organized programming. Furthermore, the G&C funding program was designed to "contribute to" a change in overall prevalence as opposed to create a direct impact on prevalence as indicated by the Terms and Conditions of the Program.
On the other hand, a few of the projects that funded cessation activities experienced success beyond high quit rates. For example, The Canadian Action Network for the Advanced Dissemination and Adoption of Practice informed Tobacco Treatment (CAN-ADAPTT), was a project led by the Centre for Addiction and Mental Health (CAMH). The project established a national practice based research network to facilitate research and knowledge exchange to inform the development of a dynamic set of cessation guidelines for use in clinical practice and population based strategies within Canada. This project produced a dynamic set of smoking cessation guidelines derived from practitioner informed research that are grounded in and intended to improve practice. It also actively disseminated these practice based recommendations and supported the training of practitioners in their implementation.
Another example was the "Ottawa Model" project, which was a smoking cessation intervention that targeted smokers who were admitted into the hospital as inpatients. The project's goal was to screen all patients for tobacco use and for all identified smokers to be offered support with smoking cessation. The University of Ottawa Heart Institute's evaluation of their Ottawa Model showed that since 2006 over 32,000 smokers had been reached, and by 2009 nearly 90 health care settings (including 65 hospitals) had been engaged in the systematic treatment of smokers. Ottawa Model hospitals have observed an average improvement of 11.1% in long-term cessation rates, resulting in nearly 10,000 quitters. The "Ottawa Model" type projects (n = 5) established important partnerships with internal hospital partners who were critical to the successful implementation of the project (e.g., patient care, health records) by initiating the initial screening of patients and triggering the intervention.
Partnerships were noted in both the 2010 Impact Evaluation and 2011 Process Evaluation of G&C Projects as a necessary component of any successful project, particularly those projects targeting vulnerable groups. Training and professional development of counsellors and others involved in project delivery are also frequently identified as project successes. There is evidence that these projects continued their professional development efforts as well as efforts to maintain partnerships through knowledge exchange sessions and resource sharing (e.g., Crossroads Treatment Centre in BC with Interior Health in British Columbia, Richmond Addictions Services with CAMH, Saskatchewan projects targeted to Aboriginal residents with the PACT pharmacy-based project, among others).
Environmental Influences
The environmental influences described below refer to demographic and/or socio-demographic variables that can influence smoking rates as well as interventions that were not included/funded through the FTCS. These findings stem from the econometric modelling conducted as part of this evaluation.
Demographic and Socio-economic Characteristics
The econometric modelling suggested demographic and socio-economic characteristics influenced both participation and consumption. For adults, participation and consumption increased with age. Consumption also increased with smoking duration, with smokers smoking 2.4 more cigarettes per week, for each additional year of smoking. Males were more likely to smoke, with a participation rate 3.9 percentage points higher than for females, and male smokers smoked 19-20 more cigarettes per week than female smokers. The presence of children deterred both participation and consumption. Participation declined by 1.3 percentage points with the presence of children and consumption was lower by 5 cigarettes per week. Participation declined by over 8 percentage points for married respondents and consumption was lower by 6-7 cigarettes per week.
Level of Education
Level of education achieved was the most significant predictor of both participation and consumption. Consumption also decreased substantially with progressive increases in education.
Policies, legislation and regulations that have been implemented and enforced primarily by other federal departments or other levels of government were also tested as part of the econometric model. The following are the findings associated with these analyzes.
Provincial and excise taxes (excluding sales taxes)
The impacts of tax on participation and consumption were statistically significant in Model I and IIIFootnote 10, but not in Model II. Based on Model I estimates, predicted prevalence in a region with the lowest observed taxes ($13.78 per carton) would be 10 percentage points higher than in a region with the highest taxes ($52.64) and weekly consumption for smokers would be lower by 12 cigarettes. Tax that was restricted to tobacco products had a greater impact on prevalence rates because it increased the price of tobacco relative to other products. Whereas, GST and PST were not expected to have the same impact as they apply to all goods and their effect on the demand for tobacco is less certain.
Retail display bans
According to the econometric model, retail display bans did not impact smoking participation in the adult population. This finding was confirmed by a study conducted in IcelandFootnote 11.
Provincial smoking bans
For adults, the gold standard smokingFootnote 12 bans did not have an impact on participation but predicted lower consumption in Models I and III. The silver standard smoking bans predicted lowered participation in all models, but no impact on consumption. The bronze standard smoking bans predicted lower participation in all models and lower consumption in Models I and III.
Provincial workplace bans
This legislation predicted a small but significant decrease in consumption in Models I and III, but no impact on participation. It should be noted that there was significant overlap between workplace bans and public place bans. Also, workplace bans should have an impact on workers, but less so on non-workers, yet these results included all adult respondents, regardless of their employment status. Additional models were estimated for workers only using CTUMS data for workers from 2003 and later. However, a number of issues were found in testing this variable. For that reason, none of the Models could have effectively and reliably measured the singular effect of a workplace bans on smoking. Model II estimates of workplace bans were likely biased downward while estimates obtained with Model I were likely biased upward.
In this context, the econometric analysis suggested that the real impact of workplace smoking bans was expected to be somewhere between the estimates in Model I and Model II. A study conducted a systematic review for the effect of smoke-free workplaces on smoking behaviour.Footnote 13 It concluded that totally smoke-free workplaces were associated with reductions in prevalence of 3.8% and that smokers in these workplaces smoked 3.1 fewer cigarettes than smokers in other workplaces. These estimates were considerably lower than Model I estimates. A number of the studies selected by Fichtenberg and Glantz could only have identified short-term impacts. According to the econometric report, Model I estimates were more likely to represent long-term impacts.
6.1.3 Youth Prevalence
The second FTCS objective for 2007-2011 was to reduce the prevalence of Canadian youth (ages 15-17) who smoke from 15% to 9%. It should be noted though that while this target identified a reduction in youth smoking prevalence from 15% to 9%, smoking rates for this age group had not been as high as 15% since 2003.
Recent Trends
Prevention was identified as a component of the FTCS as youth were seen as a driver for increasing overall smoking prevalence. When prevalence is broken down by age, a large increase in smoking is seen before the age of 30, and as uptake in younger age groups drops, so does prevalence.
While declines in smoking prevalence between 2001 and 2010 were seen across all age groups, the decline was particularly pronounced among youth and young adults. Smoking rates for the 15-17 years old declined from 18.4% to 10.9% between 2001 and 2006 and further declined to 9% during the second phase of the FTCS. While the target identified in the program objectives of FTCS has been met, the change (decline) in youth smoking between 2007 and 2010 was a reduction of two percentage points, from 10.4% to 8.9%.
Contribution of FTCS activities
As previously noted, the "overall prevalence" objective referred to the Canadian population aged 15 and older, the "youth prevalence" objective dealt with youth aged 15-17. Therefore the findings found in this section present some overlap with some of the content found previously under the overall prevalence objective.
Regulations
Prohibition on sales to youth
Literature reviews were conducted and measures related to youth access were included in the econometric model in order to assess the impact of FTCS youth access restrictions on youth smoking prevalence. One of these literature reviews found six studies that had explored the effect of retailer compliance on smoking prevalence among adolescents: four of the six studies included were controlled trials; three of which were randomized or had a control conditionFootnote 14. All of these studies found that high retailer compliance with restrictions on youth access to tobacco had some positive effect on reduced levels of smoking prevalence and thus may have potentially contributed to reducing smoking prevalence among adolescents.
Another literature review, conducted in conjunction with the econometric model, found a different result. The youth access literature reviewed in this case was relatively consistent in finding little positive impact of youth access laws and their enforcement on youth smoking prevalence. These results found that while active enforcement was needed for compliance by retailer, it was unclear that higher compliance reduced youth smoking. Authors even questioned whether it is cost-efficient to spend tobacco control dollars on youth access laws and their enforcement.
The econometric modelling further suggested that the retailer compliance rates did not seem to have the desired impact on youth smoking participation or consumption between the years 1999 and 2009. However, the variable used in the modelling process may not have been particularly robust as it represented a provincial average and there could be considerable variation in compliance rates within provinces. According to the econometric model, the mean weekly consumption of cigarettes was lower by 14 cigarettes in Model I and by 19 in Model II, which could be interpreted as the difference in weekly consumption between a region/area where there was no enforcement of restrictions on sales to minors compared to full enforcement of restrictions.
Lastly, it appears that most youth were able to obtain cigarettes through social sources relatively easily. In 2001, 26.4% of 15-17 year olds reported that they received their cigarettes (for free) from a social source, but by 2007 this rate had risen to 43%. While the proportion of youth reporting having received their cigarettes from a social source has decreased to 32.1% in 2009, such data suggests that a significant proportion of the youth population acquires cigarettes through social sources. Therefore, there was a possibility of a relationship between the availability of cigarettes from social sources and the effectiveness of youth access restrictions. However, it had not been tested to date.
Labelling of tobacco products
The econometric model indicated that there was a depressing effect of HWMs on participation (smoking uptake) that increased over time for youth. This means that warning messages were effective in reducing smoking in youth. This effect became stronger over time. Under Model I of the econometric model, cigarette HWMs predicted a decline in youth participation of 2.1%, but an increase in consumption (the quantity smoked) by young smokers of 7 cigarettes per week. Under Model II, HWMs effect on youth participation was associated with an increase in consumption of 10 cigarettes per week. These findings suggested that HWMs had been increasingly successful at postponing smoking uptake in youth and remain successful over time but did not have the desired impact in reducing consumption of cigarettes by the youth population. However, as individuals age and the population becomes more accustomed to the warnings, the effects diminish.
As noted in findings pertaining to the overall prevalence objective, findings from public opinion surveys suggested that most youth and adult smokers said the messages made smoking less attractive. Almost all Canadians reported having seen the current health warnings, though less than one-half of smokers said they read them every day. Only 7% of youth smokers aged 12 to 18 years said they never look at the messages.
As mentioned in the previous section, findings concerning HWMs seemed to have had a positive effect on encouraging smokers to try to quit smoking but did not translate into a significant change in the number of quit attempts made. Findings stemming from the literature review reported positive findings on the effectiveness of HWMs, with smokers retrospectively attributing some changes in smoking behaviour to these messages. More details on these findings can be found in the labelling section under the overall prevalence objective.
Grants and Contributions
The 2011 Process Evaluation of G&C Projects in Phase 2 of the FTCS identified 31 projects that included youth or young adults as a target in either smoking cessation or smoking prevention interventions. These projects represented a total dollar value of $8.6M and 29% of the G&C expenditures.
Youth projects, identified in the 2011 Process Evaluation, included "quit to win" challenges to encourage Aboriginal youth to quit smoking or stay smoke-free by implementing structured challenges that incorporated concrete group activities. Engagement of the youth population was high with many of them staying smoke-free during the challenge. However, it is unknown whether these youth remained smoke-free beyond the duration of the projects. Some projects used group counseling techniques to encourage peer cessation (e.g., Young Adults and Tobacco use in PEI - Phase 2, School-Based and Residential Youth Caring Facility Approach). Other projects promoted prevention interventions to elementary school-aged children using technology (e.g., tobacco trivia games) to increase awareness of the hazards of smoking.
The sample of projects included in the 2010 Impact Evaluation of the G&C Projects examined only one project aimed at youth prevention that was amenable for the impact evaluation. Although, the projects discussed earlier under the overall prevalence section did not explicitly exclude youth, the project participant profiles collected as part of the impact evaluation indicated that there was very limited participation from those aged 15-17. Given the 2011 process evaluation focused on implementation and the 2010 impact evaluation included only one youth project (with no participants falling under the youth category of age 15-17 who also participated in the evaluation), outcome-based information was very limited and the effectiveness of these projects on youth prevalence was unknown.
Environmental Influences
The environmental influences described below refer to demographic and/or socio-demographic variables that can influence youth smoking rates as well as to interventions that were not included or funded through the FTCS. These findings stemmed from the econometric modelling.
Demographic and Socio-economic Characteristics
These findings suggested that smoking participation increased with age (among youth aged 15-19). According to Model I results, 16 year olds had a participation rate that was 4.6 percentage points higher than that of 15 year olds, 17 year olds had a participation rate that was 9.0 percentage points higher than that of 15 year olds, and so on. Similarly, weekly consumption also increased with age. Compared to 15 year olds, 16 year olds smoked four more cigarettes per week, 17 year olds smoked 9 more cigarettes per week, and 18 year olds smoked 8 more cigarettes per week.
Participation was lower by 6.1 percentage points for those who did not speak primarily English or French at home. Participation was lower in higher income provinces, but per capita income did not influence consumption.
Although males were equally likely to smoke as females, male smokers smoked 8 cigarettes more per week than female smokers. Those who spoke neither French nor English at home smoked 20 fewer cigarettes per week than those who spoke either French or English at home. Consumption also increased with smoking duration, even after controlling for age, with youth smoking 7 more cigarettes per week per year since the day they started. To illustrate the compounded impact of age and duration, a 17 year old smoker who started smoking at age 15 was predicted to smoke 23.5 more cigarettes per week than a 15 year old that just started smoking.
Policies, legislation and regulations that have been implemented and enforced primarily by other federal departments or other levels of government were also tested as part of the econometric model. The following are the findings associated with these analyzes.
Provincial and excise taxes (excludes sales taxes)
Youth participation and consumption both declined with provincial and excise taxes on tobacco. Based on the estimates from Model I, an increase in average real taxes from $20.81 (February 1999) to $39.66 (December 2009) on a carton of cigarettesFootnote 15, resulted in a decline in youth smoking prevalence of 4.6 percentage points and a decline in weekly consumption of 5.3 cigarettesFootnote 16. The impact of taxation on participation and consumption suggested that taxation can be very helpful in reducing youth smoking.
Provincial smoking bans
According to Model I, youth participation and consumption were responsive to smoking bansFootnote 17. For instance, implementing a gold standard ban was expected to reduce youth participation by 4.8 percentage points and youth consumption by 8 cigarettes per week according to Model I. The silver standard ban effect on participation was not statistically significant. However, a silver ban predicted a decline in weekly consumption by smokers of 18 cigarettes. The bronze ban had no impact.
Retail display bans
As the majority of avenues for the promotion of tobacco products had been closed through legislation, display of tobacco products at retail was one of the only remaining advertising arenas for tobacco companies. However, due to provincial legislation, retail displays bans of tobacco merchandise (commonly referred to as "powerwalls") and other counter-top displays became regulated in order to stop the advertising of tobacco in common retail locations such as convenience stores and gas stations. It was thought that this advertising contributed to the perception that tobacco products were just like any other consumer product and countered the message that they are harmful to health. These provincial retail display bans were somewhat effective in lowering smoking participation in the youth population (but not so in the adult population) according to the econometric model.
Legal age
The legal age to purchase a tobacco product under the Tobacco Act is 18 years old. However, several provinces increased the legal age for smoking to 19 in an effort to further reduce smoking prevalence. The econometric model demonstrated that an earlier legal age for smoking predicted a higher participation rate of 4.9 percentage points, but had no impact on the consumption of smokers, which was reasonable as the duration variable already accounted for the impact of an earlier smoking start in the consumption model.
6.1.4 Overall and Youth Prevalence Summary
Overall, prevalence rates declined over the past 10 years to a point where, in 2010, Canada reached a new low for both adult and youth populations. Since 2007, the rate of decline slowed considerably. The stretch target of a reduction in overall smoking prevalence to 12% by 2011 was not met. However, the target of a 9% prevalence rate in the youth population was achieved.
Certain FTCS-related activities contributed to these declining rates, namely the health warning messages and provincial smoke bans. Even though retailer and manufacturer compliance with tobacco control legislative and regulatory measures had been reported as high, making statements about the contribution of the FTCS to the declining smoking rates was difficult due to the limitations of the econometric model and the conflicting findings from other lines of evidence.
According to the econometric modelling conducted as part of this evaluation, external influences (outside of the FTCS) were found to be the most significant predictors of both smoking participation and consumption, mainly level of education followed by provincial and excise tax; followed by provincially-legislated retail display bans and legal age to purchase tobacco products.
Although the G&C projects demonstrated high quit rates in the 2010 Impact Evaluation of G&C Projects, due to the limited participation in, and reach of, these interventions combined with very limited outcome data, generalizations about the effectiveness of these projects were not possible. However, some successes were highlighted, such as the "Ottawa Model" project and the CAN-ADAPTT cessation guidelines.
6.2 Second-Hand Smoke Exposure
Over the past ten years, reducing the prevalence of Canadians exposed daily to second-hand smoke had been a key objective of the FTCS. This section reviews the recent trends in daily exposure to second-hand smoke as well as the role and objectives of the FTCS in reducing exposure to second-hand smoke.
In Canada, protection for the public from second-hand smoke exposure was achieved through a combination of activities including legislation implemented primarily by provinces that restricts where people can smoke as well as through efforts around public education and social marketing campaigns aimed at raising public awareness of the dangers of second-hand smoke. These campaigns also had the objective of promoting support for policies and regulations concerning smoke-free spaces.
6.2.1 Recent Trends
The objective from the second phase of the FTCS was to reduce the prevalence of Canadians exposed daily to second-hand smoke from 28% to 20%. Based on a closer examination of CTUMS data, in 2005, 26.5% of Canadians reported being exposed either every day or almost every day to second-hand smoke. According to this measure, daily exposure to second-hand smoke was not measured by CTUMS as being as high as 28% in the period from 2005-2010 (see table below).
Fewer Canadians reported exposure to second-hand smoke in 2010 than in 2005. Between 2005 and 2010 the proportion of Canadians who reported being exposed to second-hand smoke either every day or almost every day fell from 26.5% to 20%.
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | |
|---|---|---|---|---|---|---|
| Every Day | 13.6 | 11.9 | 11.7 | 10.4 | 10.1 | 9.9 |
| Almost Every Day | 13 | 12.9 | 12.3 | 11.3 | 10.9 | 10.5 |
| Either Every Day or Almost Every Day | 26.5 | 24.8 | 24 | 21.6 | 20.9 | 20.4 |
Contribution of FTCS activities
HC contributed to informing Canadians of the dangers of second-hand smoke as well as promoting smoke-free environments and behaviour in public places and in private domains, particularly around children. FTCS funded activities related to second-hand smoke included:
- providing contribution funding for the implementation of local smoking bans;
- funding of capacity building, public education, and social marketing activities through G&Cs; and
- mass media campaigns.
Grants and Contributions
Since 2001, HC funded a total of 72 contribution projects worth approximately $14M with objectives aimed at increasing knowledge and awareness regarding the dangers of second-hand smoke. An additional 13 contribution projects, worth approximately $3.7M, identified addressing second-hand smoke issues as one of their multiple objectives. In total 85 projects worth $17.7M were directed at protecting Canadians from exposure to second-hand smoke.
The majority of contribution projects aimed at second-hand smoke (n=55) were approved prior to 2006 (and prior to the second-hand smoke bans being implemented provincially) and represented the bulk of total expenditure on second-hand smoke protection (approximately $11.4M). Activities funded by these projects included: social marketing, public education, research and policy development and capacity building. Many of these activities focused on raising the awareness on the dangers of second-hand smoke, promoting smoke-free public places, workplaces and schools as well as private places, such as homes and vehicles particularly in the presence of children.
Eighteen projects worth $5.4M were aimed generally at knowledge exchange and raising awareness of the dangers second-hand smoke covering a variety of topics. Sixteen projects worth approximately $3.9M were aimed at increasing awareness of the dangers of second-hand smoke to children and promoting smoke-free private places such as homes and vehicles. Many of these projects were targeted at parents, particularly mothers including pregnant women as well as the community in general. Most of these projects involved the production of media campaigns and media material such as print, radio and television messaging. An additional 8 projects worth $1.7M were aimed at youth with the goal of educating youth on the dangers of second-hand smoke and empowering youth in advocating for smoke-free spaces. Six projects (worth $3.4M) focussed on workplace-based smoke-free spaces aimed at educating employees and employers.
The development and implementation of second-hand smoke bans in both public places and workplaces was also a focus of early contribution projects. Eleven projects, worth $2.5M, were funded to promote the need for smoke-free legislation in order to educate the public as well as to facilitate the passage of second-hand smoke bans in municipalities.
One project in particular, the "Smoke-Free Public Places: You Can Get There" offered hands-on, easy-to-use resources to help municipalities and communities through the various stages of planning, implementing and evaluating non-smoking by-laws and policies in public places in their community. This "toolkit" was pilot-tested through the Federation of Canadian Municipalities (FCM). Results of the pilot-testing were used to develop and modify the toolkit to make it a valuable resource to implement many smoke-free bylaws in Canada and were then endorsed internationally as a best practice by the World Health Organization.
In addition, approximately $11M of contribution funding was provided to provinces and territories as project initiation money for the implementation of local smoking bans in public places. This influx of money and the promotion and public education around the need for second-hand smoke bans, along with the "how to toolkit" for municipalities, was FTCS's contribution in facilitating the implementation of second-hand smoking bans.
Since 2007, the projects that focused primarily on second-hand smoke were worth $1.2M. By this time, a majority of the Canadian population was protected by comprehensive municipal and provincial second-hand smoke bans in public places, and these projects reflected a corresponding shift in emphasis. The largest expenditure related to second-hand smoke during this period was a project worth $1.1M, which funded the Non-Smokers' Rights Association to conduct research, knowledge exchange and policy development.
Other projects worth approximately $181K were aimed at increasing support for public smoking restrictions (Northwest Territories) or to inform the public on amendments made to public smoking legislation (Nova Scotia).
The focus of the majority of other second-hand smoke projects were a follow-up on previous projects or campaigns and often related to smoke-free private places, with an emphasis on second-hand smoke and children. Many of these projects were targeted at parents as well as pregnant women including First Nations communities.
The 2010 Impact Evaluation on G&C Projects included two projects whose objectives were to reduce exposure to second-hand smoke. About one-third (43%) of participants in second-hand smoke projects were exposed to second-hand smoke every day or almost everyday in the month previous to the baseline survey. One in five (18%) were exposed to second-hand smoke at least weekly. 19% had relatively little exposure (at least once in the past month). Frequency of exposure to second-hand smoke appeared to have decreased over time - 34% and 36% of participants in second-hand smoke projects indicated being exposed everyday or nearly everyday at the 3- and 6-month measurement periods (a decrease of 9 and 11 percentage points respectively from the baseline). At the 12-month measure, only 23% of project participants indicated this level of second-hand smoke exposure (a 20 percentage point decrease). Second-hand smoke exposure in homes decreased consistently and substantially over the study period (a decrease of 33 percentage points between baseline and 12-month survey).
Mass Media
As part of the FTCS, HC funded three major national mass media campaigns aimed at raising awareness about the health risks of exposure to second-hand smoke among non-smokers, particularly in the workplace as well to youth and children. These mass media campaigns included three television campaigns as well as radio scripts and print media and cost a total of $22.7M. All three of these campaigns were evaluated as part of the 2006 FTCS summative evaluation; however, the data was inconclusive and no impact could be attributable to FTCS.
The first of the mass media campaigns focused on diseases related to second-hand smoke. It targeted youth and encouraged them to protect their family and friends as well as themselves from the effects of second-hand smoke. This campaign consisted of one television advertisement, the "Couch". The television ad was aired over two time periods between November 12, 2002 and February 9, 2003. This campaign also included a brochure and a series of posters which providing further information regarding the dangers of second-hand smoke. Evaluative analysis intended to measure the impacts of this campaign on reducing exposure to second-hand smoke was inconclusive due to a lack of suitable data. The total cost of this campaign was $7.2M.
The second campaign addressed in the workplace. For this campaign HC worked with Physicians for a Smoke-Free Canada to produce a mass media campaign sharing the personal story of Heather Crowe, a non-smoker who was diagnosed with lung cancer following many years of work as a waitress in smoky restaurants. The advertisements were designed to target a broad audience of adult Canadians aged 20-55 (smokers and non-smokers), in addition to opinion leaders (at the community/municipality level), decision makers, business labour and union leaders, physicians and media.
Public opinion research associated with this "Heather Crowe" campaign identified a range of more indirect objectives including: "to gain support from the media, decision makers, and to mobilize all Canadians whether smokers or non-smokers on the need for continued federal action on the harmful effects of second-hand smoke". Additionally, the associated research suggested that the campaign was designed to contribute to the overall first phase FTCS objective "of reducing the number of people involuntarily exposed to environmental tobacco smoke".
Evaluative analysis found that there was no significant difference in the support for smoking bans for all public places or smoke-free environments between those who recalled the advertisement and those who did not, regardless of smoking status. However, those who recalled the advertisement were significantly more likely to report that they felt comfortable asking an employer to implement or expand a smoking policy in the workplace than those who did not recall the advertisement. This finding was tied to an objective of the campaign to mobilize Canadians on the need for action against exposure to second-hand smoke in the workplace. The total cost of this campaign was $5.7M.
The third mass media campaign focused on the dangers of second-hand smoke in the home, particularly to children. The campaign was designed to target parents between the ages of 20 and 54, and consisted of three separate television advertisements. The portion of the smoke-free homes campaign that included all three advertisements cost a total of $13.1M. The impact of these advertisements was evaluated using public opinion research. Analysis of the first two advertisements found no conclusive evidence of a positive impact on the implementation of household smoking restrictions, while analysis of the third advertisement suggested it was able to "influence its target audience in the intended way."
Environmental Influences
Legislation and regulations that restrict smoking in public places, in workplaces or in the presence of children became increasingly prominent in the last ten years, and today almost all Canadians live in a jurisdiction where smoking is prohibited in all public places including restaurants, bars, and workplaces.
Provincial Legislation
Since 2001, the proportion of Canadians protected by smoking bans (either municipal or provincial) had increased from 6.5%, representing an estimated 2M Canadians and complete coverage in all provinces as of 2009. Since 2005, a number of provinces have implemented province-wide smoking bans in public places such as restaurants, bars and taverns, thus increasing the level of protection to cover an estimated 24.4M Canadians in 2006 and 25.4M in 2007.
The first public smoking bans in Canada were initially enacted at the municipal level (assisted by the FTCS funding and toolkits mentioned previously) and coverage of smoking bans increased as more municipalities across the country passed by-laws that restricted smoking in public places. Eventually, as popular support for public smoking bans grew, provinces began enacting province-wide 100% smoke-free public places legislation:
- Manitoba (Non-Smokers' Health Protection Act) and New Brunswick (Smoke-Free Places Act) passed legislation in 2004, which prohibited smoking in virtually all enclosed workplaces;
- in 2005, Saskatchewan introduced The Tobacco Control and Newfoundland and Labrador the Smoke-Free Environment Act;
- in 2006, Nova Scotia (Smoke-Free Places Act), Ontario (Smoke-Free Ontario Act) and Quebec (The Tobacco Act) enacted province-wide 100% smoke-free public places legislation bringing the proportion of Canadians protected by such legislation to over 80%;
- in 2007, Alberta amended its Smoke-Free Places Act prohibiting smoking in virtually all workplaces including bars and restaurants effective January 1, 2008;
- also in 2008, British Columbia enacted its Tobacco Control Act; and
- in 2009 Prince Edward Island enacted its Smoke-Free Places Act which provided province-wide 100% smoke-free workplaces and workplaces.
Legislation in the Northwest Territories (Tobacco Control Act, 2006) prohibits smoking in almost all public places while in Yukon (Smoke-Free Places Act, 2008) anti-smoking legislation is somewhat stronger, prohibiting smoking in all enclosed public places and workplaces and also provides strong protection in outdoor public spaces, such as bar and restaurant patios and entrances. Nunavut's Tobacco Control Act 2004 prohibits smoking in all enclosed public places that are also workplaces; however, it exempts restaurants and bars.
By 2006, 80% of Canadians were protected by comprehensive smoking bans in all public places, and by 2008 it was nearing 100%. Additionally, provisions to these regulations, including bans on smoking in some outdoor spaces, such as patios, were implemented in some jurisdictions.
As protection from second-hand smoke in public places became widespread in Canada, smoke-free policies began to expand beyond public places in many provinces into private spaces. For example, since 2007, eight provinces passed legislation that prohibits smoking in vehicles when children are present:
- Nova Scotia (2007);
- Yukon Territory (2008);
- Ontario (2008);
- British Columbia (2008);
- New Brunswick (2009);
- Prince Edward Island (2009);
- Manitoba (2009); and
- Saskatchewan (2010).
Federal Legislation
Federally, the Minister of Labour was responsible for the Non-Smokers' Health Act (NSHA) and the corresponding regulations, which governed exposure to second-hand smoke in federally regulated workplaces (such as the banking and telecommunications sectors; marine, air and rail transport). The Labour Program of Human Resources and Social Development Canada administered the NSHA, which dated back to 1985.
In November 2007, the Non-Smokers' Health Regulations were revised, enhancing protection from second-hand smoke for workers by largely eliminating Designated Smoking Rooms and Designated Smoking Areas in federally-regulated workplaces, such as the Canadian Broadcasting Corporation and Canada Post. HC was consulted and provided input during the process of revising the Regulations.
6.2.2 Second-Hand Smoke Summary
The objective of reducing second-hand smoke exposure to Canadians was achieved. The FTCS may have contributed to informing Canadians of the dangers of second-hand smoke through mass media campaigns and the provision of contribution funding. Data problems made it difficult to determine the actual impact of the contribution projects and the mass media campaigns on the FTCS objective.
Nonetheless, HC promoted smoke-free environments through its leadership role in the implementation of local smoking bans via both informational and monetary resources. The implementation of second-hand smoke bans across provinces and territories is an illustration how the federal government can influence change.
6.3 World Health Organization (WHO) - the Framework Convention on Tobacco Control (FCTC)
Another objective of Phase 2 of the FTCS was identified as contributing to the global implementation of the WHO-FCTC, the WHO's first public health treaty. The following information was taken from a review of internal documents and validated with key program staff.
6.3.1 Overview of the WHO-FCTC
The WHO-FCTC was the first international treaty negotiated under the auspices of the WHO. It was adopted by the World Health Assembly in May 2003 and entered into force in February 2005. It had since become one of the most rapidly and widely embraced treaties in the United Nations' history, with 174 Parties having ratified the treaty as of June 2011.
The FCTC was developed in response to the globalization of the tobacco epidemic. The spread of the tobacco epidemic was facilitated thorough a variety of complex factors including cross-border effects; global marketing; transnational tobacco advertising; the international movement of contraband and illicit tobacco products; and direct foreign investment. The FCTC represented a shift in developing a regulatory strategy to address addictive substances by including the importance of demand reduction as well as supply issues.
6.3.2 Canada's Commitment to Tobacco Control
Canada participated in each Conference of the Parties (COP), the governing body of the WHO-FCTC, and provided expertise and experience for the implementation of the FCTC to other countries. Canada was one of the original 40 Parties to ratify the treaty. Once ratified, Canada became bound to implement the treaty's provisions. The FCTC supported and affirmed Canada's federal, provincial and territorial tobacco control efforts by reflecting Canadian tobacco control initiatives in its obligations. The Convention further supported Canada's efforts by grounding Canadian tobacco control legislation in international best practice. This helped establish international norms, useful in defending domestic legislation. Canada was active in the negotiations of the FCTC that took place between October 2000 and February 2003, in Geneva. Many of the FCTC provisions were closely modeled on Canadian law or regulations, and at ratification of the treaty, Canada was in compliance with many of the provisions of the treaty.
6.3.3 The FTCS' Contribution to Canada's Commitment
Recognizing that Canada was in compliance with the majority of the WHO-FCTC treaty obligations upon ratification in 2005, only a small number of changes to domestic polices, legislation and regulations were undertaken to ensure compliance. Regulations were developed, and subsequently updated under the Tobacco Act that ensured further restrictions be placed on tobacco advertising and promotion to youth, and changes were also implemented increasing the size of health warning messages on tobacco products.
Additionally, policy and regulatory action was taken to ensure that the Non-Smokers' Health Act was compliant with the effective protection from second-hand smoke. Through extensive collaboration with Canada's provinces and territories, comprehensive provincial and territorial legislation was developed to protect Canadians from second-hand smoke.
FTCS funded HC's involvement in the FCTC, which allowed HC to participate in the COP sessions. The COP established an intergovernmental process for the development of guidelines for the implementation of different provisions of the Convention. Guidelines for the implementation of several articles were adopted by the COP. Work on additional guidelines was undertaken by working groups established by the COP. Some examples of the work done through the intergovernmental process are:
- the development of guidelines on Articles 9, 10 and 11 of the Convention supporting the regulation of the contents of tobacco products, the regulation of tobacco product disclosures and the packaging and labelling of tobacco products for which Canada was a key facilitator;
- the development of guidelines on Article 12 and 14 of the Convention supporting education and demand reduction measures, where Canada's representation on this working group was comprised of representatives of HC and a provincial representative; and
- the ongoing negotiations of an international protocol to eliminate the illicit trade in tobacco products, where Canada's delegation is led by Public Safety Canada with membership from the RCMP, CBSA, HC, Canada Revenue Agency, the Department of Justice and the Department of Foreign Affairs and International Trade.
As part of the FTCS, funding for international tobacco work was also available through two mechanisms: (1) contributions in support of the FTCS, and (2) the International Health Grants Program (IHGP).
A small portion of the FTCS contribution funding program was targeted towards the global implementation of the WHO-FCTC. The FTCS contribution funding program provided funding to domestic organizations to help achieve this objective. Since 2007, a total of $1.1M was spent on international work under this funding program. The following types of activities were supported in developing countries in Central and South America, Africa, India and the Middle East:
- knowledge brokering and technical assistance;
- education, communication, training and public awareness; and
- policy research, surveillance and exchange of information and best practices.
Through the IHGP, HC supported global efforts on tobacco control thereby fulfilling its international commitments and obligations under the WHO-FCTC to support the implementation of the treaty. The program allowed HC to not only support global action on tobacco control, but also to broaden international knowledge of Canada's approach to prevention and control. In 2007-2008, the overall IHGP budget was $16.4M, including $835K for international tobacco-related activities. As of 2009-2010, Strategic Review permanently reduced the overall IHGP budget, including the tobacco allocation, by $895K to $15.5M.
Priorities for international grants were jointly determined by the RAPB, HECSB and the International Affairs Directorate (IAD). IHGP provided grants for initiatives related to international tobacco control including research (i.e., pictorial health warnings), and capacity building (i.e., training, policy development, legal frameworks, and advocacy). The eligible recipients for program-based projects under the IHGP program were international and Canadian not-for-profit organizations and institutions, including domestic and international organizations working in tobacco control. The program allowed recipients to conduct research and advocacy activities with the aim of supporting policy and program development for tobacco control, particularly in developing countries.
Funds from the IHGP were also used to pay Canada's biennial Voluntary Assessed Contribution (VAC) to support the implementation of the treaty. As a Party to the WHO-FCTC, this was HC's key priority under IHGP. The VAC fluctuated based on US currency rates (approximately $400K). As such, if additional funds were available after payment of the VAC, funding was used to support priorities identified by the COPs to the FCTC and contained in HC's International Health Strategy. The following types of activities were supported in developing countries in Central and South America, Africa, and Asia:
- education, communication, training and public awareness; and
- policy research, product regulation, surveillance and exchange of information and best practices.
6.3.4 WHO-FCTC Summary
Through the FTCS, HC, along with its other partner departments, assisted with fulfilling Canada's commitment to participate in the FCTC by being a contributor to the development of the FCTC and providing technical advice on both the original Articles and ongoing support for their global implementation.
Not only does this participation in the FCTC illustrate that international leadership was being provided by the Government of Canada, and it also provided a mechanism for possible knowledge uptake that may be used to assist the federal government with its national leadership role on tobacco control in Canada.
6.4 The Next Generation of Tobacco Control Policy
The fourth objective of the FTCS was to examine the next generation of tobacco control policy. The following information came from a review of Annual Performance Reports, internal documents, including the 2011 Process Evaluation of G&C Projects funded by the FTCS and stakeholder opinions.
6.4.1 Overview of FTCS Contribution to the Next Generation of Tobacco Control Policy
HC examined and informed the next generation of tobacco control policy through various mechanisms: (1) research activities like the analysis of business intelligence, and laboratory analysis of novel tobacco products, (2) surveillance using the Canadian Tobacco Monitoring Survey (CTUMS) and the Youth Smoking Survey (YSS), (3) G&C funding for projects related to policy and knowledge exchange, and (4) work with stakeholders. Additionally, research and federal funding were used over the last five years to generate information for future policy work. The following sections elaborate on all of these efforts.
Research - Product Regulation, Business Intelligence and the Development of New Legislative and Regulatory Measures
FTCS product regulation activities included the formation of the Business Intelligence (BI) Unit. Because there were no requirements for pre-market assessments of tobacco products, policy with respect to novel products had to be created post-market. BI allowed HC to not only address new or modified tobacco products before use of these products becomes widespread in Canada, but also it allowed for informed action to be taken early with respect to emerging issues. This action may include legislative or regulatory change, and can be seen as contributing to the next generation of tobacco control.
The primary focus of the BI Unit was articulated as ensuring a thorough analysis of information submitted by the industry to HC and this information was to be used by the BI Network to identify needs and establish priority projects. The BI Unit developed numerous reports on tobacco trends, including sales, buying patterns and advertising. These reports were used in decision making and have fed into policy decisions, such as the development, for example, of amendments to the Tobacco Act as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act.
The Cracking Down on Tobacco Marketing Aimed at Youth Act, previously known as Bill C-32 received Royal Assent on October 8, 2009. These amendments to the Act were aimed to protect children and youth from tobacco industry marketing practices that encourage them to use tobacco products. It was anticipated that these amendments to the Tobacco Act would contribute to the prevention activities of the FTCS and decrease smoking prevalence among youth.
Research - Laboratory Analyses and Nicotine Policy Development
Through the BI Unit, HC undertook monitoring activities with respect to Novel Tobacco Products on an on-going basis and performed laboratory analyses on different Novel Tobacco Products. These analyses not only allowed HC to compare the novel tobacco products with more established products and any associated marketing claims, but they also facilitated work on nicotine policy development between 2007 and 2010.
Surveillance and Policy Development
The effectiveness of policies and programs requires accurate knowledge of Canadian demographic trends in tobacco use. Given the nature of tobacco use is complex and dynamic, ongoing and systematic surveillance was required to assist with policy and program development. The two surveys used by FTCS to facilitate this work were the CTUMS and the YSS.
The CTUMS provided HC with timely, reliable and continual data on tobacco use and related issues and was designed to monitor trends in smoking prevalence among all persons aged 15 and older living in Canada (excluding those living full-time in institutions, as well as territorial residents). The main objective of the YSS was to collect smoking prevalence data nationally for students.
Over the course of FTCS, CTUMS data was used in virtually all policy documents, including policy related to the Cracking Down on Tobacco Marketing Aimed at Youth Act that amended the Tobacco Act, pan-Canadian toll free number to support quitlines, e-cigarettes, snus and bio-monitoring. The YSS was also used as a data source for policy related to the Cracking Down on Tobacco Marketing Aimed at Youth Act.
Grant and Contribution Funding for Policy and Knowledge Exchange Projects
The work carried out during the second phase of the FTCS (2007-2011) by approximately 20 Policy and Knowledge exchange projects funded through HC's G&C program served to support the general body of knowledge available concerning tobacco control. As the information generated by these projects came from civil society, collectively it provided insight into the diffuse ideas that existed on any given tobacco control issue in the public sphere. Consequently, information that was produced and disseminated by the funding recipients, served to inform HC policy analysis with the diverse range of perspectives. With this information, the federal government was better prepared to make and support its decisions. Tobacco Control policy decisions were made taking into account the information and perspectives of civil society. There was, therefore, a value to the outputs produced by the projects, which was independent of whether or not they directly resulted in a given decision. Some examples of how these projects supported and informed federal policy and regulations are provided below.
With HC contribution funding the Student's Commission of Canada supported the Youth Action Committee (YAC) to strengthen the involvement of youth in the FTCS. HC consulted the YAC in 2009 as a youth audience focus group, in addition to other audiences, where draft HWMs were presented. Feedback was received from the various focus groups, including the YAC group. HC considered all of the feedback and implemented some of the recommendations by changing some of the HWMs. HC met with the YAC in 2010 to show the committee how the draft messages had been changed based on the all of the input. The messages are now in official regulations for tobacco product labelling.
HC funding provided to support provincial/territorial quitlines also supported the federal tobacco product labelling regulations. Beginning in 2002, FTCS funding contributed to (along with other forms of promotion not necessarily funded federally) the implementation and then promotion and evaluation of provincial quitlines in Manitoba, Saskatchewan, New Brunswick, Prince Edward Island, Newfoundland & Labrador and Nova Scotia. Provinces now provide funding for quitline operations.
More recently, FTCS O&M funds supported the implementation and promotion of telephone quitlines in the Yukon, Northwest Territories and Nunavut. This investment in provincial/ territorial quitline service capacity and infrastructure provided support for negotiations with provinces and territories on the establishment of the pan-Canadian Quitline initiative. The pan-Canadian Quitline initiative was a federal/provincial/territorial initiative where two toll-free telephone numbers seamlessly redirected callers to provincial/territorial quitline services. The pan-Canadian Quitline initiative was linked to the recent regulations on tobacco labelling. These Regulations were a registered in September 2011, and as of June 19, 2012 all cigarette and little cigar packaging sold in Canada will promote the pan-Canadian Quitline telephone number as part of the renewed Health Warning Messages.
Not only has G&C funding supported federal policy, but this funding also supported provincial and organizational policy. Several examples of these results are described.
HC provided funding to the Ontario Tobacco Research Unit to develop an on-line course on tobacco prevention, cessation, second-hand smoke and evaluation. The course was integrated into the Province of Ontario's funding policy where it became a requirement that all health authority staff working in tobacco control take this training before receiving funding from the province. This course was also a prerequisite for the intensive smoking cessation counselling certificate training offered by the Centre for Addiction and Mental Health across Canada.
With contribution funding, at the regional health authority level in British Columbia, the Interior Health Authority created a policy where treating tobacco dependence became a "standard of care" and was integrated into all clinical settings in the health authority, across disciplines. Important milestones in implementing this policy were met including: standardizing tracking questions used on paper and electronic records as well as moving from a perception that tobacco was a public health department issue to a multidisciplinary, cross health authority issue.
HC contribution funding supported organizational policy at the University of British Columbia - Okanagan Campus by enabling the university to pass and implement a policy limiting smoking on campus to designated smoking areas. The university set a goal of 70% usage of designated areas during the HC funding period and was able to achieve an overall campus usage rate of 70.9%. A further component of the policy implementation included training all health and wellness clinicians on campus (both nurses and counsellors) in tobacco cessation support to reinforce the campus policy.
Also in British Columbia, a Residential Treatment Centre implemented an organizational policy that incorporated tobacco cessation awareness as a standard component of its youth treatment services. In addition, the treatment centre implemented a smoke free policy for staff, prohibiting smoking on centre property for all staff.
In addition, contribution funding received from HC supported organizational policy in the Atlantic Canada trucking industry. The purpose of this project was to reduce tobacco usage in the trucking sector. Some trucking carriers made it policy to distribute the project tool kits, developed through contribution funding, to smoking employees upon employment. Carriers were also incorporating the use of videos produced through this project to educate management as well as to motivate employees to quit smoking. The project ultimately created resources that the trucking industry adopted and planned to continue to implement as part of their daily human resource practices and policies.
Work with Stakeholders and Policy Development
To examine the next generation of tobacco control policy, engagement of stakeholders was seen to be integral. Stakeholder consultation was done on emerging issues, and stakeholders viewed national coordination as one of the strengths of the FTCS. They indicated that the Strategy facilitated coordination and sharing across initiatives and provinces, and that the ability to set national goals and to encourage collaboration towards common goals had contributed to successes in tobacco control. A few examples of stakeholder consultation and engagement are described.
In response to the Ministerial Advisory Committee on Tobacco Control's position that banning retail tobacco product displays is a positive strategy that should be encouraged in order to ensure youth are not targeted by these displays, in 2006-2007, HC undertook consultation with retailers and distributors, the tobacco industry, non-governmental organizations, governmental organizations and the general public on regulating the display and promotion of tobacco and tobacco-related products. These consultations helped to inform positions on retail displays and HC's continued work with the provinces to promote federal and provincial retail restrictions.
HC also worked to increase the awareness of retailers about their responsibilities under both federal and provincial legislation pertaining to the sales of tobacco to minors as well as the general public on the main goals of the FTCS. The FTCS utilized three information initiatives to engage stakeholders: (1) information kits were either mailed directly to the retailer or indirectly through their respective industrial or retailer's association, (2) a number of media venues were used to communicate the main thrust of the FTCS to retailers and the general public regarding promotion legislative and regulatory restrictions, and (3) a toll-free line was established to answer questions from the general public and retailers.
These consultations on retail displays, the retailer education on legislative responsibilities, the toll-free telephone line, and work with the provinces was HC's contribution to prohibiting sales to minors and promotion in Canada, including the implementation of provincial retail display bans.
Three other venues were also identified as forums where discussions and consultations concerning the next generation of tobacco control policy took place: the Tobacco Control Liaison Committee, the Canadian Coalition for Action on Tobacco and the Interdepartmental Director General Committee on the WHO Framework Convention on Tobacco Control. HC was responsible for managing relationships with these groups and chairing a number of working groups held as part of the FTCS.
Research and Federal Funding Activities and Future Policy Development
Research and contribution funding were used over the last five years to generate information for future policy work. A few examples of this proactive production of knowledge are outlined below.
Human biomonitoring of environmental chemicals is the measurement of a chemical or its components in blood, urine and other tissues. It indicates how much of a chemical is present in a person and collection of this data, especially on a national scale, can be used as a starting point for future monitoring and research. Data on biomonitoring should assist with improving the understanding of chemical exposure in people. Two major projects were launched under the FTCS to conduct biomonitoring work, which were intended to eventually help with the development of policies to protect the health of Canadians.
The first biomonitoring project was the Canadian Health Measures Survey (CHMS) carried out by Statistics Canada. In partnership with HC's Safe Environments Programme, HC entered into a Memorandum of Understanding with Statistics Canada in 2006-2007 to conduct the survey. It was hoped that the survey might add to an understanding of tobacco-related illnesses and the extent to which many diseases may be undiagnosed among Canadians as well as provide scientific data to support and accelerate the development of policies and regulations. HC was one of many collaborators on this project, supporting the collection of smoking information and exposure to second-hand smoke; and the collection and analysis of biological samples for cotinine (a metabolite of nicotine). Launched in 2007-2008, this ongoing survey collected information on residents 6 to 79 years of age.
The second project, the Maternal-Infant Research on Environmental Chemicals (MIREC) Study, was a complementary to the CHMS. The MIREC Study was conducted in partnership with the Safe Environments Programme (SEP), HC. In 2008-2009 OTRSE entered into an Internal Letter of Agreement with the SEP for this study, which collects long-term, biomarker data from mothers and children. Overall, the results of this research were expected to strengthen health risk assessments (including promotion of breastfeeding) and to support measures to reduce release of contaminants into the environment, and limit exposure of the general population.
Funding was made available to support projects that aimed to build capacity and share knowledge in Canada on tobacco product-related applied, social and regulatory sciences. The primary focus was on activities with the potential to contribute significantly to tobacco product science knowledge and tobacco product legislative and regulatory efforts in Canada. An example of one of these funded projects was the Health Behaviour Research Laboratory of the University of Waterloo. This project received funding to conduct original evaluation work on the tobacco product chemistry information that was previously released by Heath Canada and to disseminate findings of the research.
The primary outcome of the University of Waterloo project was to prepare an evaluation report to be submitted to a peer-reviewed journal in the area of public health/tobacco control to provide an opportunity to educate the broader tobacco control community about the nature of contents and emissions and their relation to measures of exposure and risk. The dissemination efforts were expected to facilitate knowledge transfer and uptake within key stakeholders groups (i.e. researchers, regulators, and civil society) as well as between these groups. The findings from the published report illustrated important differences in product chemistry between domestically manufactured cigarettes and imported US blended cigarettes. The report also provided important benchmarks for making historical and international comparisons across brands on key constituents that may be used for future policy recommendations in the area of tobacco product legislation and regulations.
6.4.2 Next Generation of Tobacco Control Policy Summary
Over the course of the FTCS, research and surveillance activities appeared to be active functions and were used to inform the development of legislation, regulations and various policies and positions. Furthermore, G&C projects as well as work with stakeholders were important to the advancement of the next generation of tobacco control policy, both federally and provincially.
Knowledge generation was a predominant characteristic of the FTCS. In general, FTCS activities linked to research, surveillance, federal funding and work with stakeholders were regularly used to inform the next generation of tobacco control through the development of legislation, regulations, policies and positions. In addition, investments were made to ensure the continued generation of knowledge that will assist with developing additional policy work in the future. Overall, it appeared that knowledge generation and translation helped to regulate tobacco in Canada, educated jurisdictions in Canada on emerging issues as well as guided the direction of collaborative efforts in tobacco control.
6.5 Monitor and Assess Contraband Tobacco Activities and Enhance Compliance
The sixth objective of the FTCS was to monitor and assess contraband tobacco activities and enhance compliance. Unlike some of the other objectives, no specific target was set for this objective. This section reports on results of the partner department activities as they relate to the FTCS and the contraband objective.
6.5.1 Overview of Contraband Tobacco
According to the document and literature review conducted, the contraband tobacco market surfaced as a significant concern in the 1990s when higher taxes were imposed to deter individuals from taking up or continuing smoking. Since 2001, the largest quantity of illicit tobacco found in Canada originated from manufacturers on Aboriginal reserves located on both sides of the Canada-United States border. Depending on the source referenced, the market share of contraband tobacco was estimated to be approximately 30% - 32%. This market share suggests that in 2008, illicit cigarettes sales were at $13B, representing approximately $2.4B in lost federal and provincial tax revenues. It should be noted that the size of the contraband tobacco market was difficult to assess given its "underground" nature, and therefore these figures were only estimates.
Given that taxation was identified as an effective measure to reduce smoking prevalence and that contraband tobacco could undermine the achievement of this objective, the Government of Canada, through the FTCS, provided funding to departments to enhance activities in the area of contraband tobacco. The following section outlines the activities of the partner departments responsible for monitoring and assessing contraband tobacco activities and enhancing compliance.
Monitoring of the tobacco industry and tobacco sales falls under the Tobacco Act and tobacco products that are not properly stamped and do not follow the tax regulations are illegal under the Excise Act, 2001. Therefore, taxation is one of the distinguishing elements between contraband and legal tobacco. Contraband has been defined as tobacco products which do not comply with federal or provincial laws that control or tax tobacco products. Increases in sales of contraband tobacco appear to be an unintended impact of tobacco taxation policies, which are administered by the Department of Finance and provincial governments.
Contraband tobacco interdiction was not included in the FTCS. However, federal partners were funded through the FTCS to monitor and assess contraband tobacco products and enhance compliance with the federal tobacco tax legislation. There was no funding under the FTCS for activities related to enforcement of contraband tobacco, including activities such as search and seizure of contraband tobacco products. Activities within the FTCS related to contraband tobacco products were focused on monitoring and assessing contraband activities with the intent of providing analysis for informing tax policy.
The partner departments and agencies that worked collaboratively to monitor and assess contraband tobacco activities were Public Safety Canada (PS), Canada Border Services Agency (CBSA), and the Royal Canadian Mounted Police (RCMP); while Public Prosecution Service of Canada (PPSC) and Canada Revenue Agency (CRA) worked to enhance compliance with the Excise Act, 2001.
6.5.2 Partner Department Activities
Public Safety Canada (PS)
PS provided policy advice and support to the Minister of Public Safety in the area of policing and law enforcement with respect to the Government of Canada's tobacco control initiatives, and evaluated the impacts of these initiatives on tobacco smuggling activities. Also, PS chaired the Task Force on Illicit Tobacco Products, which was comprised of departments and agencies involved in tackling illicit tobacco, including the RCMP, CBSA, CRA, Finance Canada and Agriculture and Agri-Food Canada, Department of Justice, Health Canada and Indian and Northern Affairs Canada. The mandate of the task force was to identify concrete measures that would disrupt and reduce the trade in contraband tobacco.
As part of the FTCS, PS administered contribution fundingFootnote 18 to the Akwesasne Mohawk Police Service (AMPS) to undertake, in cooperation with the RCMP, CBSA and CRA, monitoring activitiesFootnote 19 in an effort to determine the level of contraband tobacco activities in and around the Akwesasne Mohawk Territory. This territory straddles the Canada-United States and Ontario-Quebec-New York State borders, which requires law enforcement agencies to work together. The territory was identified as a transit point for illicit tobacco. The proportion of cartons seized by the Cornwall and Valleyfield detachments combined declined from 48% in 2004 to 34% in 2009 and increased again to 53% of total national seizures (includes RCMP and CBSA) of tobacco cartons (including unmarked bags of cigarettes) in 2010.
A team within the AMPS, the Joint Investigation Team (JIT)Footnote 20, reported that it was able to increase its surveillance and monitoring of tobacco smuggling in Akwesasne Mohawk Territory, and it actively participated in operations that led to seizures, including tobacco. Although seizures are normally used as an indication of enforcement activities (which are not funded through the FTCS), they were used here to provide some indication (a proxy measure) of the potential influence monitoring activities may have had on enforcement activities that took place over the course of the FTCS.
As illustrated in the table below, carton seizures increased from 102,000 cartons in 2004 to 533,000 in 2010. Given the tobacco seizures for the Central St. Lawrence Valley detachment represented a significant proportion of RCMP seizures nationally - from 28% in 2006 to 53% in 2010 - these results, in conjunction with Akwesasne jurisdictional and geographic particularities, suggested that increased monitoring and surveillance activities conducted on the Akwesasne Mohawk Territory may have contributed to the improvement of law enforcement partners' capacity to disrupt and/or control contraband activities, and reduced or mitigated the increase in the availability of contraband cigarettes in Canada.
| Year | Cartons/Unmarked bags of cigarettes | Fine cut tobacco (kg) | ||
|---|---|---|---|---|
| Cornwall/Valleyfield detachments | National Tobacco Seizures | Cornwall/Valleyfield detachments | National Tobacco Seizures | |
| 2004 | 102,000 (47.6%) |
214,166 | 420 (3.7%) |
11,241 |
| 2005 | 232,000 (45.9%) |
504,895 | 460 (2.9%) |
15,983 |
| 2006 | 240,000 (28.0%) |
856,095 | 545 (1.0%) |
53,747 |
| 2007 | 233,000 (26.0%) |
894,754 | 38,000 (84.7%) |
44,848 |
| 2008 | 465,000 (41.0%) |
1,132,300 | 58,000 (81.5%) |
71,140 |
| 2009 | 393,000 (33.6%) |
1,170,195 | 17,700 (39.5%) |
44,826 |
| 2010 | 533,000 (53.0%) |
1,006,286 | 36,000 (46.3%) |
77,773 |
| National statistics above are based on seizure information provided by CBSA and RCMP. Annual breakdown of national statistics by agency is provided on later on in the report. | ||||
The AMPS continued to improve its ability to detect, target and investigate organized crime offences and organizations, through the leveraging of resources from the various organizations (e.g., the Cornwall Community Police Service, the Ontario Provincial Police, the St. Regis Tribal Police), and through the ongoing sharing of information and intelligence with law enforcement partners, in Canada and the United States. All enforcement actions/seizures related to tobacco and other contraband were reported through the RCMP-led Cornwall Regional Task Force and then compiled into RCMP reports.
In addition, training related to organized crime and cross-border criminal activities in this region (i.e., the smuggling of all contraband, including tobacco) was provided to AMPS/JIT members, which was partly funded through the AMPS contribution agreement. The AMPS reported that this training contributed to enhancing members' knowledge and understanding of organized crime issues and law enforcement tools.
Canada Border Services Agency (CBSA)
Monitoring and assessment activities by CBSA relied on intelligence to assess trends in activity in order to predict threats that were contrary to customs enforcement objectives, and assisted in the development of effective counter-measures. The intelligence capabilities of CBSA were augmented with funding from the FTCS to provide resources to monitor and assess the level of contraband tobacco activity in Canada, and to provide an objective overview of the contraband tobacco market.
Initially, funding provided by the FTCS to CBSA was used for salary dollars for officers and analysts allocated to all regions across the country and at CBSA headquarters. CBSA was responsible for the collection of data and for monthly and annual assessments of the nature and extent of contraband tobacco activity at the border. The assessments included an analysis of domestic tobacco production and sales, monitoring of imports and exports, collection of intelligence information from a wide variety of sources. Resources were divided between Intelligence Officers and Intelligence Analysts and were allocated according to the amount and/or threat of contraband tobacco in each region.
Funding was provided for a portion of the FTEs at CBSA headquarters, in the Borders Intelligence Division and in the Analysis and Assessment Division. This headquarters component coordinated and monitored inter-regional and international operations, provided strategic intelligence, training, developed new policy and procedures, and monitored the use of tobacco resources.
Subsequent intelligence analysis of information gathered since 2001 resulted in the production of monthly and annual assessments by CBSA and the RCMP for the purpose of informing policy-makers, including the Department of Finance from a tax policy perspective, mainly through the Interdepartmental Working Group on Tobacco Enforcement, which included participation of the three departments. This group, chaired by the Department of Finance, was the vehicle used to share information pertaining to contraband tobacco and federal enforcement efforts aimed at combating tobacco contraband activities.
Royal Canadian Mounted Police (RCMP)
The RCMP, specifically the Customs and Excise Program, was responsible for the enforcement of laws within Canada in relation to the international movement of goods along the uncontrolled border (between ports of entry). In addition, the illicit manufacture, distribution or possession of contraband tobacco products fell within its investigative mandate. As it related to the FTCS, the RCMP collected, analyzed and distributed strategic intelligence in order to provide ongoing monitoring of contraband tobacco issues.
With the funding obtained from the FTCS, the RCMP created seven tobacco analyst positions, which were strategically deployed in the Atlantic, Central, Northwest and Pacific regions and two housed within RCMP national headquarters. These regional analysts, through key partnerships with various law enforcement agencies as well as provincial and regulatory government and non-government organizations, captured and shared intelligence associated to tobacco seizures, investigations and other illicit tobacco activities. Information gathered permitted the analysts to paint a regional picture of the status of illicit tobacco activities, seizure levels, trends and criminal networks. Reports developed from the four regions were collected and analyzed at the national level in an effort to develop more in-depth study reports and draw further intelligence and information. These reports were then shared with a host of stakeholders who relied on the information to support their own initiatives or brief their respective senior management.
The FTCS also provided funding to the RCMP to offset specific technical support and undertake covert monitoring of suspected illegal cross-border intrusions associated with the illicit tobacco trade. The five technical support FTEs assisted various Customs & Excise units through the deployment of a variety of electronic surveillance devices along the Canada-US border which supported complex investigations. Investigators relied heavily on this technology in the fight against well-orchestrated organized crime networks that targeted the shear vastness of the shared border to move illicit tobacco products. Sensing and monitoring equipment acted as a force multiplier by tracking clandestine tracked activities on a continuous basis which permitted investigators to be more strategically focussed during their enforcement activities along the border.
RCMP and CBSA
Measuring the impact of the FTCS contribution to the RCMP and CBSA monitoring of contraband tobacco activities was done using contraband tobacco investigations leading to volume of seizures as a readily available proxy measure to provide illustration of the potential influence of monitoring activities. However, because the exact size of the contraband tobacco market or its fluctuations was not known, the absolute volume of seizures was not a precise measure of improvement, deterioration or stagnancy of the market.
It should be noted that federal taxes increased in 2001 followed by increases in provincial tobacco taxes, which varied considerably in terms of magnitude. Also, according to the document and literature review, contraband tobacco seizures appeared to follow changes in taxation within about three years, due to the time for the black market to re-organize itself; and/or the time necessary for the enforcement law to adjust with the expansion of the illicit trade. This information should be considered when examining the table below.
RCMP seizures, after having gone from 29,000 cartons in 2001 to 120,000 cartons in 2004, increased steadily thereafter (see table below). As pertains to CBSA, data suggested that the rise in seizure volumes at ports of entry was not as linear as was the case for the RCMP.
| Year | RCMP | CBSA | Totals | RCMP | CBSA | Totals |
|---|---|---|---|---|---|---|
| Cigarettes Cartons | Fine-Cut Tobacco (kg) | |||||
| 2001 | 29,000 | 26,292 | 55,292 | n/a | 127 | 127 |
| 2002 | 39,800 | 34,068 | 73,868 | n/a | 276 | 276 |
| 2003 | 59,300 | 339,296 | 398,596 | n/a | 718 | 718 |
| 2004 | 120,000 | 94,166 | 214,166 | 11,000 | 241 | 11,241 |
| 2005 | 369,000 | 135,895 | 504,895 | 14,000 | 1,983 | 15,983 |
| 2006 | 472,300 | 383,795 | 856,095 | 4,000 | 49,747 | 53,747 |
| 2007 | 626,000 | 268,754 | 894,754 | 28,000 | 16,848 | 44,848 |
| 2008 | 965,000 | 167,300 | 1,132,300 | 69,000 | 2,140 | 71,140 |
| 2009 | 975,000 | 195,195 | 1,170,195 | 34,000 | 10,826 | 44,826 |
| 2010 | 782,000 | 224,286 | 1,006,286 | 43,000 | 34,773 | 77,773 |
| Total 2001-2010 | 4,437,400 | 1,869,047 | 6,306,447 | 203,000 | 117,679 | 320,679 |
| Sources: National statistics above are based on seizure information provided by CBSA and RCMP | ||||||
Overall, total number of contraband tobacco seizures in Canada by RCMP and CBSA combined have increased from 2001-2009 with a small decline in 2010.
Public Prosecution Service of Canada (PPSC)
The National Fine Recovery Program (NFRP) of the PPSC contributed to the FTCS objective to "monitor and assess contraband activities and enhance compliance" by working to increase compliance with the Excise Act 2001. The program was nationally implemented in 2002 with the mandate to enforce sentencing by recovering outstanding fines ordered against individuals and companies convicted for any federal offence, including tobacco-related offences such as contraband tobacco, illegal sale of tobacco products and tobacco sales to minors.
The NFRP consisted of 19 FTEs who were located in eight PPSC regional offices (Vancouver, Edmonton, Saskatoon, Winnipeg, Toronto, Ottawa, Montreal and Halifax), and collected outstanding federal fines in 10 provincial jurisdictionsFootnote 22. The NFRP funding was established entirely through the FTCS, and was fixed annually at $1.988M.
The NFRP regional Fine Recovery Units (FRUs) in these locations collectively compiled and maintained an inventory of federal fines that had been imposed by criminal courts across CanadaFootnote 23. As previously mentioned, the NFRP pursued all categories of outstanding federal fines in addition to tobacco-related fines. The relative importance of each fine category within the inventory over the period stemming from 2001-2002 to 2009-2010, is shown in the table below.
Tobacco smuggling and contraband fines represented a relatively small number of inventoried fines throughout the measurement period. In addition, their relative proportion consistently decreased, from a high of 7.9% in 2001-2002 to a low of 3.2% in 2009-2010 as shown in the table below. The decline in the proportion of tobacco-related fines in the inventory can be attributed, at least in part, to the priority given to recovering these fines by NFRP.
| 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | |
|---|---|---|---|---|---|---|---|---|---|
| Tobacco Smuggling/ Contraband | 1,099 (7.9%) |
1,119 (6.9%) |
1,118 (6.4%) |
933 (5.2%) |
902 (4.9%) |
808 (4.2%) |
758 (3.8%) |
716 (3.4%) |
662 (3.2%) |
| Other Tobacco Offences | 83 (0.6%) |
87 (0.5%) |
88 (0.5%) |
87 (0.5%) |
91 (0.5%) |
96 (0.5%) |
98 (0.5%) |
102 (0.5%) |
95 (0.4%) |
| Drug Offences | 5,684 (40.8%) |
7,470 (45.9%) |
8,345 (47.8%) |
9,091 (50.5%) |
9,642 (51.9%) |
10,239 (52.8%) |
10,824 (53.6%) |
11,594 (54.9%) |
11,515 (56.0%) |
| Employment Insurance | 810 (5.8%) |
821 (5.0%) |
830 (4.8%) |
855 (4.8%) |
862 (4.6%) |
868 (4.5%) |
866 (4.3%) |
843 (4.0%) |
802 (4.0%) |
| Fisheries | 2,320 (16.7%) |
2,693 (16.6%) |
2,815 (16.1%) |
2,858 (15.9%) |
2,788 (15.0%) |
2,835 (14.6%) |
2,888 (14.3%) |
2,881 (13.6%) |
2,755 (13.0%) |
| Taxes/GST | 2,681 (19.3%) |
2,759 (17.0%) |
2,891 (16.6%) |
2,802 (15.6%) |
2,927 (15.8%) |
3,115 (16.1%) |
3,213 (15.9%) |
3,301 (15.6%) |
3,102 (15.0%) |
| Other OffencesTable 1 footnote 1 | 1,250 (9.0%) |
1,320 (8.1%) |
1,369 (7.8%) |
1,373 (7.6%) |
1,367 (7.4%) |
1,432 (7.4%) |
1,551 (7.7%) |
1,683 (8%) |
1,706 (8.3%) |
| Total non-tobacco related offencesTable 1 footnote 2 | 12,745 (91.5%) |
15,063 (92.6%) |
16,250 (93.1%) |
16,979 (94.3%) |
17,586 (94.6%) |
18,489 (95.3%) |
19,342 (95.7%) |
20,302 (96.1%) |
19,880 (96.4%) |
| Total Number of Fines | 13 927 (100%)Table 1 footnote 2 |
16,269 (100%) |
17,456 (100%) |
17,999 (100%) |
18,579 (100%) |
19,393 (100%) |
20,198 (100%) |
21,120 (100%) |
20,637 (100%) |
Table 1 footnotes
|
|||||||||
The table below tracks the size and value of the NFRP fine inventory, as well as the amounts recovered and left outstanding over the nine-year evaluation period.
| Fiscal Year | Dollar Value | ||||
|---|---|---|---|---|---|
| (Number of fines in inventory) | Value of Fines in InventoryTable 2 footnote 1 | Value of Amounts RecoveredTable 2 footnote 2 | Value / % of Tobacco-related Compared to Total Amounts Recovered | Value of Outstanding AmountsTable 2 footnote 2 | |
| 2001-2002 | 13,927 | $117,977,600 | $5,336,900 | $286,399 5% |
$39,561,300 |
| 2002-2003 | 16,269 | $125,826,500 | $5,687,600 | $471,011 8% |
$46,893,200 |
| 2003-2004 | 17,456 | $126,735,200 | $11,613,300 | $437,916 4% |
$53,496,300 |
| 2004-2005 | 17,999 | $125,432,600 | $5,734,400 | $524,345 9% |
$60,199,700 |
| 2005-2006 | 18,579 | $128,312,500 | $10,904,800 | $368,246 3% |
$66,289,200 |
| 2006-2007 | 19,393 | $122,129,500 | $4,610,400 | $363,987 8% |
$76,738,600 |
| 2007-2008 | 20,198 | $129,573,100 | $5,298,900 | $360,169 7% |
$87,413,200 |
| 2008-2009Table 2 footnote 3 | 21,120 | $145,579,200 | $5,188,700 | $540,811 10% |
$106,736,700 |
| 2009-2010 | 20,637 | $140,940,000 | $6,269,600 | $373,655 6% |
$112,145,800 |
Table 2 footnotes
|
|||||
Although not limited to fines imposed for tobacco-related offences, a total of $60.6M in federal fines was recovered as a result of NFRP interventions during the evaluation period. This excluded over $9M in outstanding fines collected by the Quebec pilot fine recovery project from 1998 to 2001, prior to FTCS funding. As shown above, the number and percentage of inventoried tobacco smuggling and contraband fines consistently decreased over the time period from 7.9% to 3.2%. In contrast, the amounts recovered for tobacco-related offences varied from year to year, generally representing between 5% and 10% of amounts recovered for all types of fines. Such variations are less a reflection of NFRP activities than of the fine amounts imposed by the courts.
Canada Revenue Agency (CRA)
By ensuring compliance with Canada's tobacco tax laws, the CRA supported the regulatory framework for the control of tobacco. Further, the CRA ensured the collection of the tax (duty) imposed on tobacco products in support of the government policy of imposing a high level of taxation on tobacco products, which contributed to the objective of reducing tobacco consumption.
FTCS funding provided for an increased number of audits and regulatory reviews. These additional activities ensured the correct reporting and remitting of duty as well as compliance with the controls on the manufacture, possession, and sale of tobacco products in Canada.
Audits entailed the detailed examination and evaluation of books and records, their supporting documentation, and underlying internal controls to ensure compliance with the financial requirements, including assessment and payment of duties, under the Excise Act, 2001. Regulatory reviews verified that licensees control their tobacco and tobacco products, including exports, in accordance with the requirements of Excise Act, 2001. As well, the CRA ensured that the stamping and marking requirements of Excise Act, 2001 were met.
FTCS funding was used to enhance the CRA systems to address legislative changes dealing with export activities. This ensured that persons involved in the legal tobacco industry were correctly identified and monitored to make certain that they met the reporting requirements of the law, including the payment of excise duty and that there were no overpayments of refund amounts.
These audits, regulatory reviews and administrative control activities enhanced compliance by supporting the regulatory framework for the control of tobacco and the government's policy on taxation of tobacco products.
| Fiscal Period | Excise Duty collected on tobacco products |
|---|---|
| 2004-2005 | $2.97B |
| 2005-2006 | $2.69BFootnote 25 |
| 2006-2007 | $1.60B |
| 2007-2008 | $1.43B |
| 2008-2009 | $1.29B |
| 2009-2010 | $1.37B |
| Fiscal Period | Regulatory Reviews | Audits |
|---|---|---|
| 2004-2005 | 29 | 18 |
| 2005-2006 | 97 | 16 |
| 2006-2007 | 177 | 22 |
| 2007-2008 | 202 | 23 |
| 2008-2009 | 176 | 19 |
| 2009-2010 | 149 | 17 |
6.5.3 Contraband Tobacco Summary
PS, CBSA and RCMP used FTCS funding to monitor and assess contraband tobacco activities which may have contributed to the significant increase in the volume of seizures observed between 2001 and 2009. Also, the evaluation found that there was an increase in capacity through additional staffing to conduct intelligence analysis to inform policy makers.
Given that the objective was to simply monitor and assess the market to inform tax policy, the volume of seizures did indicate that monitoring points had taken place.
CRA demonstrated compliance-related activity through the increased number of audits and regulatory reviews attributed to increased staffing. The PPSC was able to demonstrate an increase in the number of the fines recovered through enhanced recovery processes such as GST/HST and income tax set offs. How these activities impacted the availability of legal or illegal tobacco products was not known.
6.6 Efficiency and Economy
6.6.1 Context
The FTCS's evaluation plan included two types of analyses that were conducted to provide some estimates on the economic impact and benefits of reducing smoking prevalence. The first set of analyses involved several steps to estimate the economic impact and benefits:
- estimating the impact of smoking on mortality [i.e., Smoking-Attributable Mortality (SAM)];
- estimating the Years of Potential Life Lost (YPLL);
- combining SAM estimates with YPLL to determine the productivity loss averted (i.e., net economic productivity savings);
- using SAM, YPLL, and productivity loss averted to determine the impact on economic cost savings;
- smoking-attributable healthcare expenditures were determined by applying the smoking-attributable fraction of expenditure (SAF) to the total healthcare costs;
- impact on healthcare costs were then converted to an annual net healthcare savings estimate; and
- using the net healthcare system estimated benefit combined with the net productivity loss averted (cost savings) to generate an estimated total economic benefitFootnote 26.
The data from the last set of analyzes (i.e., estimated total economic benefit) was then used in a second set of analyzes that attempted to demonstrate a type of 'cost-benefit'Footnote 27 assessment. That is, a theoretical correlation with modeled benefits from statistical data and specific activities of the FTCS, with the intention of identifying a crude estimate of the net benefit expressed as a return on investment (ROI)Footnote 28.
6.6.2 Analysis 1 -- Estimating the Economic Impact of Smoking and Benefits of Reductions in Smoking Prevalence
Various Estimated Economic Impacts and Benefits
Smoking tobacco products and exposure to second-hand smoke are associated with illnesses and premature deaths from chronic diseases. Smoking is the primary causal factor for various cancers, chronic obstructive pulmonary disease (COPD), and early cardiovascular diseases (CVDsFootnote 29). Beyond the health consequences and related productivity losses, smoking also imposes higher healthcare expenditures to individuals, employers and healthcare systemFootnote 30.
To understand the economic impact caused by smoking, the Smoking-Attributable Morbidity, Mortality and Economic Costs (SAMMEC) software module developed by the Center for Disease Control and Prevention (CDC)Footnote 31 in the United States (US) was utilized. This software provided estimates for Smoking Attributable Mortality (SAM) and Years of Potential Life Loss (YPLL) due to the reduction in average life expectancy (premature mortality). Estimates of SAM and YPLL were then used, with additional economic data to estimate productivity losses attributed to deaths caused by smoking related diseases as well as smoking-attributable healthcare costs.
Economic benefit estimates, including productivity loss averted, annual net healthcare savings and total economic benefit were also generated, providing an indication of the potential economic benefit of reductions in smoking prevalence that were most likely influenced by wide-ranging tobacco control efforts.
Methodology for Various Estimated Economic Impacts and Benefits
As mentioned in the methodology section, SAMMEC software modules were used to estimate SAM, YPLL, productivity losses attributed to diseases caused by smoking, productivity loss averted and healthcare expenditures. SAMMEC methodology is a cross-sectional approach for these estimates, and is a useful method for approximating the aggregate economic burden of smoking to a society at one point in time.Footnote 32
For theses analyses, determining sex- and age-specific smoking-attributable deaths were calculated by multiplying the total number of deaths for smoking-related disease categories by estimates of the Smoking-Attributable Fraction (SAF) of preventable deaths. The attributable fractions provided estimates of the public health burden of each risk factor and the relative importance of risk factors for multi-factorial diseases.
The SAMMEC web-application did not allow users to enter the Canadian population-specific relative risks (RRs) of mortality for current smokers and former smokers compared to those who never smoked. Therefore, default RRs of mortality were used that were obtained from a study by American Cancer Society's Cancer Prevention Study (CPS-II) to compute smoking-attributable fractions of mortalities (SAFs). Relative risks of mortality used by the Centre for Substance Abuse (CCSA)Footnote 33 were not the same as that of CPS-II RRs resulting in small variations in smoking-attributable mortalities by various underlying causes of deaths. For adults, SAFs were derived using sex- and age-specific relative risk (RR) estimates from the American Cancer Society's Cancer Prevention Study-II (CPS-II) for current and former smokers for each cause of death.
Sex- and age-specific (35-64 years and >65 years) current and former cigarette smoking prevalence estimates from Canadian Tobacco Monitoring Survey (CTUMS) were used to calculate SAM. Smoking-attributable YPLL and productivity losses were estimated by multiplying sex- and age-specific SAM by remaining life expectancy at the time of death and lifetime potential earnings data. Smoking-attributable residential fire-related deaths, lung cancer and heart disease deaths attributable to exposure to second-hand smoke and smoking-attributable neonatal deaths were not included (assumed constant) in the SAM, YPLL and productivity loss estimates.
The Canadian Socio-Economic Information Management System (CANSIM) was the source of data on smoking-related mortalities and their underlying causes (ICD-10). CANSIM mortality data from 2000 to 2005 were used to estimate the average smoking-attributable mortality by different underlying causes of disease and deaths (see Appendix B).
Additional Data Required for Estimated Economic Impacts and Benefits
Smoking prevalence among adults aged 35 years and over was used to determine smoking-attributable mortality (see table below). Canada-specific smoking prevalence data from 1999 to 2008 (current smokers, former smokers and those who never smoked) were obtained from CTUMS and demographic data including life expectancy were obtained from Statistics Canada.
| Gender | Age Group (Years) |
1999 | 2008 | ||
|---|---|---|---|---|---|
| Current | Former | Current | Former | ||
| Male | 35-64 | 27.60 | 33.30 | 20.48 | 36.40 |
| 65 + | 12.90 | 54.00 | 8.47 | 60.72 | |
| Female | 35-64 | 23.10 | 26.30 | 17.42 | 29.98 |
| 65 + | 11.00 | 30.60 | 7.10 | 32.38 | |
| Overall | 15 + | 25.2 | 25.3 | 17.9 | 28.7 |
| Note: Smoking rates are organized by age group and gender to make the data compatible with SAMMEC application. | |||||
Estimated Smoking-Attributable Mortality (SAM)
Differences in estimated SAM between 1999 and 2008 were the result of the change in the proportion of current smokers, former smokers and people who never smoked in the Canadian population. Sex- and age-specific smoking prevalence were also considered in the estimates. The objective of this analysis was to estimate the change in SAM over time. The SAMMEC application was used to approximate an annual SAM in year 1999 and in year 2008Footnote 34.
Using SAMMEC, it was estimated that a total of 35,392 Canadians died from tobacco use in 1999. By 2008, the number of smoking related deaths had declined by 1,990 to 33,402, which is a decline of 5.6%. Thus, the results from this analysis show that there has been a decline in average annual SAM from 1999 to 2008. This decline in SAM is attributed to the changes in the proportion of current and former smokers over the past decades.
Estimated Years of Potential Life Loss (YPLL)
Cigarette smoking reduces life expectancies by increasing the mortality risks. The YPLL were estimated taking into consideration SAM, age distribution at the time of deaths and gender-specific life expectancies of Canadians. The decline in SAM from 1999 to 2008 saved approximately 26,431 YPLL per year.
Estimated Productivity Loss Averted
Measurement of productivity lossesFootnote 35 based on YPLL represents the present value of future earnings from paid labour and the value of future household production that would have been lost because of premature SAMs. Labour productivity data were taken from Industry Canada to estimate productivity loss averted. Using a conservative approach to the value of life-year-saved, the analysis indicated that the average annual labour productivity loss averted from the saved lives as a result of wide-ranging tobacco control efforts was estimated to be $388M, which translates into $14,687 per life year savedFootnote 36.
Estimated Smoking-Attributable Healthcare Costs Between 1999 and 2009
In order to estimate the smoking-attributable healthcare expenditures, 1999 to 2009 healthcare expenditure data published by the Canadian Institute for Health Information (CIHI) were used. Healthcare expenditure data were adjusted taking into account a few factors. Smoking related illnesses were minimal among youths below 15 years of age (16.6% of the Canadian population). Similarly, dental and vision care related costs (9-10% of total healthcare expenditures) were excluded from the smoking-attributable costs estimates. After adjustments for these confounding factors and inflation in the total healthcare expenditures, smoking-attributable healthcare expenditures were estimated. The healthcare expenditures included in this analysis were:
- costs of hospitalization,
- costs of outpatient visits,
- costs of prescription drugs, and
- costs for other services (e.g., nursing home care).
Smoking-attributable healthcare expenditures were assumed to impact healthcare costs immediately, with changes in smoking status calculated as the excess of the personal healthcare costs of smokers and former smokers compared to those who have never smoked. Analyses revealed that smoking-attributable healthcare expenditures have increased from $5.5M in 1999 to $8.9M in 2009.
From these analyses it was evident that even though there were decreases in smoking prevalence in Canada between 1999 and 2009, smoking-attributable expenditures increased during the same period. It was suggested in the literature that this increase was due to the fact that newer and improved medical treatments were availableFootnote 37 and because of the higher growth rate in per capita total healthcare expenditures.Footnote 38
Estimated Annual Net Healthcare Savings
In order to determine an estimated savings to the healthcare system due to the declining prevalence rate, the per-smoker healthcare costs were calculated and then multiplied by the number of former smokers between 1999 and 2009. The per-smoker healthcare costs were $1,219Footnote 39, and there were, in 2009, 1.2M more former smokers in Canada since 1999 based on CTUMS data. This suggests that, as a crude estimate, the reduction in smoking rates since 1999 resulted in an annual savings to the healthcare system of $1.46B.
Estimated Total Annual Economic Benefit
The estimated total economic benefit was generated by adding the annual net healthcare savings of $1.46B and the annual net productivity loss averted estimate of $388M. This calculation resulted in an estimated annual total economic benefit of $1.8B. This estimated annual total economic benefit stemmed from the declining smoking prevalence rates that most likely had been influenced by wide-ranging tobacco control efforts.
6.6.3 Analysis 2 -- Estimating a Potential Annual Economic Benefit of the FTCS
Methodology for Estimating a Potential Annual Return on Investment (ROI)
A theory-based approach to evaluation can assist in demonstrating how an expected or intended outcome (impact and/or benefit) is supported by observing actual change (results) and a comparison with a validated or substantiated theory of changeFootnote 40. The need to utilize a theory-based approach is often the case when there is an absence of a specific and quantifiable evaluative design, a lack of baseline and/or trend data, or specific performance measures that can be validated as directly attributable to the results of an evaluation. The theory of change that needs to be generated in a theory-based approach provides a framework in which data and information that is gathered can be reported against to demonstrate progress and/or achievement of the expected results.
For the purpose of this evaluation, a theory-based approach was used with the ROI analysis to examine the possible economic benefit of specific activities under the FTCS that contributed to the reduction in smoking prevalence. That is, the ROI analysis was correlated to the following theory of change: investments to decrease smoking prevalence translate into a net economic benefit in terms of savings to the healthcare system and net productivity loss averted (net economic productivity savings)Footnote 41.
Estimated Potential Annual Return on Investment (ROI) in 2008
The ROI analysis was challenged by the fact that it required use of a precise numerical estimate of the contribution of FTCS activities on the declining smoking prevalence. Unfortunately, it was not possible to quantify the exact contribution of the FTCS to the decline in smoking prevalence.
However, multiple results of the econometric modelling indicated that the contribution of certain FTCS activities were positive (i.e., are above zero). More specifically, the econometric modelling found that some regulatory activities under the FTCS contributed to the declining prevalence rate, with most analyses demonstrating small contributions. Even though the contribution estimates were very crude, each run of the model suggested that the FTCS contribution was somewhere under 10%.
With the acknowledgement that specific legislative and regulatory activities of the FTCS had a small contribution to the declining prevalence rate, a potential return on investment was generated by speculating the estimated numerical contribution the FTCS, presumably under 10%. Production of the economic return estimate also required knowing: (1) FTCS funding allocations (i.e., $73M in 2008), (2) the productivity loss averted (i.e., $388M in 2008), and (3) the estimated total annual economic benefit (i.e., $1.8B).
| Total expected economic benefits | Percent contribution of FTCS to benefits accrued | Actual accrued benefits based on percentage estimate (column 2) | FTCS allocated investment | Return on investment (ROI) |
|---|---|---|---|---|
| $1,8B | 5 % | $90M | $73M | $17M |
| $1,8B | $10 % | $180M | $73M | $107M |
| $1,8B | 15 % | $270M | $73M | $197M |
| $1,8B | 20 % | $360M | $73M | $287M |
6.6.4 Efficiency and Economy Summary
The estimated total annual expected economic benefit of all tobacco control measures in place in Canada was $1.8B. If the FTCS made a contribution of approximately 5% to reduction in smoking prevalence, then the annual return on investment was estimated at $17M. If the FTCS contribution was assumed to be higher than 5%, then the estimated ROI would also be higher as indicated by the table above.
7.0 Conclusions and Recommendations
While the duration of the FTCS (2001-2011) has seen large declines in smoking prevalence, between 2007 and 2010 prevalence remained relatively stable. The overall prevalence objective for Phase 2 was a stretch target set at 12% in light of the early accomplishment of the original objectives in Phase 1 of the FTCS. Nonetheless, this goal of reducing prevalence to 12% was not met. However the target of reducing youth smoking prevalence to 9% was met.
Overall, the FTCS contributed to the decline in smoking prevalence through its labelling requirements and youth access restrictions as well as its support to implement provincial second-hand smoke bans. However, lines of evidence suggested that external measures not funded by the FTCS, such as level of education achieved and taxation, were the main contributors to changes in prevalence with provincially-legislated retail display bans and legal age for smoking following.
Most large-scale environmental changes (i.e., tax and second-hand smoke bans) were implemented between 2001 and 2007 and since that time there was little change in the Canadian tobacco control environment. Changes made by the provinces in tobacco control during this period included restrictions on point of sale advertising via provincial retail display bans, province-wide second-hand smoke bans and provincial smoke-free vehicle legislation. With the increase in action from provinces and territories, many tobacco control issues are now addressed at a provincial/territorial level, and prevention or cessation programming is increasingly conducted at this level.
The only major change at the federal level was the passage of the Cracking Down on Tobacco Marketing Aimed at Youth Act that amended the Tobacco Act in 2009. The impact of these amendments on prevalencecould not be assessed in this evaluation as some amendmentsdid not come into effect until late 2009 and mid-2010 for others.
The evaluation illustrated compliance with Tobacco Act restrictions and regulations was stable and high, while smokers' participation in cessation programming provided by G&C projects participating in the G&C Impact Evaluation was limited. Additionally, the data available was not able to determine the overall impact of the cessation projects funded by the G&C projects on prevalence - not surprisingly seeing as many of the cessation projects were aimed at vulnerable populations and were only intended to contribute to a reduction in smoking prevalence rates. Evidence from this evaluation and the stabilizing of prevalence rates, indicates that smoking cessation success in the current smoker population will be limited unless G&C projects are able to improve project participation and reach.
Other G&C projects that focussed on knowledge application demonstrated some influence in providing information which was applied to policy/legislation development. In addition, funded projects related to policy and knowledge exchange were able to support and inform policy at the federal, provincial and organizational levels.
Federal leadership was evident throughout the evaluation including HC's role in the WHO-FCTC, the implementation of second-hand smoke bans, the research and surveillance available on smoking in Canada, the research conducted to facilitate the provincial retail display bans, as well as the recent amendments to the Tobacco Act as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act. Continued leadership in tobacco control requires continued investment in research and surveillance to identify emerging tobacco issues and to be able to respond to them through stakeholder relations or policy activities.
The objective related to contraband tobacco was to simply monitor and assess the market and to enhance compliance in order to inform policy. Therefore, the increased volume of seizures indicated that monitoring contraband tobacco had taken place and the increased number of audits and regulatory reviews as well as fines recovered indicated that there has been enhanced compliance-related activity.
Considering the findings and conclusions of the evaluation and the current tobacco control environment, the FTCS, as it is presently structured, may need to be streamlined. Nonetheless, there still seems to be a need for sustained efforts on the part of the federal government in tobacco control not only to administer the Tobacco Act but also to provide a leadership role responsible for coordination at the national and international level. In order to deliver a comprehensive and integrated national tobacco control strategy, identified as a best practice, the strategic approach of combining federal legislation and regulations, policy development, research and surveillance as well as supporting provincial and international tobacco control efforts is necessary.
The evaluation approach for the FTCS used sophisticated simulation modeling as one line of evidence in order to provide quantitative performance data which was intended to be corroborated by a performance measurement system that would provide both qualitative and further quantitative data. However, as mentioned in the methodology section of this report, the performance measurement system was not implemented for various reasons. During the evaluation report writing process, it became evident that data gaps existed. Therefore, an ad-hoc internal document review was performed to try to capture retrospective qualitative data to fill these gaps. Although a substantial amount of information was captured through the internal document review process, there were still some areas where triangulation with multiple lines of evidence was impossible. It also became evident that the FTCS has an abundance of performance data; however, it is not well organized/tracked according to the program outcomes and associated performance indicators. Lastly, other lines of evidence (such as the econometric modelling and literature review) concentrated on tobacco control in Canada more broadly (which would include activities initiated by P/Ts, NGOs and municipalities) instead of specifically on the activities of the FTCS which are the responsibility of the federal government.
Therefore the recommendations stemming from the evaluation are to, under the leadership of HC:
- Streamline tobacco activities to focus on administering the Tobacco Act (as amended as part of the Cracking Down on Tobacco Marketing Aimed at Youth Act) and its regulations, and maintaining a leadership role through research and surveillance activities to inform policy and regulations, as well as guide the direction of collaborative efforts to deliver a comprehensive and integrated national tobacco control strategy.
- Identify best/promising practices amongst the G&C projects and ensure this information is shared with relevant partners.
- Develop a systematic approach to performance measurement, concentrating on linking the performance data to the logic model and performance indicators to guide the evaluation and reporting processes.
Appendix A -- Profile of Grant and Contribution Projects
| Profile Variable | Number of Projects (n=104) | Percentage (n=104) | Total $ Value (n=104) | % Dollar Value (n=104) |
|---|---|---|---|---|
| Agreement Duration | ||||
| Single-year | 8 | 8% | $1,511,570 | 3% |
| Multi-year | 96 | 92% | $45,011,665 | 97% |
| 13-18 months | 13 | 12% | $5,603,209 | 12% |
| 19-24 months | 32 | 31% | $9,309,430 | 20% |
| 25-30 months | 21 | 20% | $11,906,002 | 26% |
| 31-36 months | 12 | 11% | $4,628,258 | 10% |
| 37-42 months | 7 | 7% | $3,364,086 | 7% |
| 43-48 months | 11 | 11% | $10,200,679 | 22% |
| Region | ||||
| NCR | 32 | 31% | $25,296,332 | 54% |
| Northern Region | 3 | 3% | $916,212 | 2% |
| BC | 12 | 11% | $3,140,983 | 7% |
| Alberta | 5 | 5% | $2,184,663 | 5% |
| Saskatchewan-Manitoba | 13 | 12% | $3,358,356 | 7% |
| Ontario | 13 | 12% | $4,100,991 | 9% |
| Quebec | 11 | 11% | $3,287,723 | 7% |
| Atlantic | 15 | 14% | $4,237,974 | 9% |
| Value | ||||
| <$50K | 3 | 3% | $131,587 | 0% |
| $50K-$99K | 6 | 6% | $424,348 | 1% |
| $100K-$249K | 37 | 35% | $6,640,245 | 14% |
| $250K-$500K | 34 | 33% | $13,178,263 | 28% |
| +$500K | 24 | 23% | $26,148,791 | 56% |
| Average | $447,339 | |||
| Component | ||||
| Cessation | 70 | 67% | $30,977,066 | 67% |
| Prevention | 5 | 5% | $1,278,545 | 3% |
| Protection | 3 | 3% | $1,159,580 | 3% |
| FCTC | 5 | 5% | $3,236,290 | 7% |
| Next Generation | 9 | 9% | $6,033,289 | 13% |
| Comprehensive (multi-component) | 12 | 11% | $3,838,464 | 8% |
| Type (Primary) | ||||
| Knowledge development (research/design of a service or resource) | 26 | 25% | $7,282,318 | 16% |
| Knowledge application (interventions with the objective of changing the smoking behaviour) | 52 | 50% | $20,835,461 | 45% |
| Knowledge transfer (encourage adoption of successful projects/best practices/strategies by other governments or NGOs) | 26 | 25% | $18,405,455 | 39% |
| Type (Including primary and secondary, multiple response) | ||||
| Knowledge development (research/design of a service or resource) | 54 | 52% | $21,899,445 | 47% |
| Knowledge application (interventions with the objective of changing the smoking behaviour) | 68 | 66% | $25,782,520 | 55% |
| Knowledge transfer (encourage adoption of successful projects/best practices/strategies by other governments or NGOs) | 52 | 51% | $25,937,627 | 56% |
| Target Group (multiple response) | ||||
| Smokers | 74 | 72% | $26,519,287 | 57% |
| Non-smokers | 19 | 18% | $5,473,282 | 12% |
| Health practitioners | 37 | 36% | $23,944,494 | 52% |
| Tobacco control community (policy makers, decision makers, researchers) | 23 | 22% | $15,483,651 | 33% |
| Other (children, young women) | 12 | 12% | $6,192,466 | 13% |
| Client Group (multiple response) | ||||
| Youth/students | 31 | 38% | $8,670,201 | 29% |
| Aboriginal - on-reserve | 27 | 33% | $8,127,075 | 28% |
| Aboriginal - off-reserve | 24 | 30% | $7,538,579 | 26% |
| Pregnant women/parents/families | 12 | 15% | $4,328,584 | 15% |
| Employees (sector-specific) | 13 | 16% | $4,724,410 | 16% |
| Health consumers (e.g., acute care patients, outpatient) | 7 | 9% | $7,520,937 | 26% |
| Mental health, addictions/substance abuse | 8 | 10% | $2,141,637 | 7% |
| None/all smokers | 18 | 22% | $6,243,295 | 21% |
| Other (e.g., prison inmates) | 6 | 7% | $2,085,734 | 7% |
| Key Activity/Outputs (primary) | ||||
| Consultations/research/policy/strategy/best practice development/conferences/workshops | 13 | 13% | $883,868 | 21% |
| Curricula development/ professional development/clinical practice guidelines/learning opportunities | 11 | 11% | $5,368,202 | 12% |
| Product/resource development/dissemination (e.g., tool kits, cessation materials) | 20 | 19% | $6,194,681 | 13% |
| Intervention/cessation program delivery (e.g., counselling, quitlines) | 46 | 44% | $18,659,518 | 41% |
| Awareness-raising/promotion | 9 | 9% | $2,553,198 | 6% |
| Other (utilization of quitlines) | 4 | 4% | $3,374,173 | 7% |
| Key Activity/Outputs (multiple response) | ||||
| Consultations/research/strategy/best practice development/conferences/workshops | 37 | 36% | $20,467,504 | 44% |
| Curricula development/clinical practice guidelines/learning opportunities/ professional development | 22 | 22% | $16,340,719 | 35% |
| Resource development/dissemination (e.g., tool kits, cessation materials) | 51 | 50% | $16,556,015 | 36% |
| Intervention/cessation program delivery (e.g., counselling, quitlines) | 62 | 61% | $22,540,961 | 49% |
| Awareness-raising/promotion | 59 | 58% | $23,493,811 | 51% |
| Other (e.g., development of network) | 13 | 13% | $9,575,057 | 21% |
| Source: Health Canada Proposal Tracking Form (July 31, 2011) | ||||
Appendix B -- Estimated Average Smoking-attributable Mortality by Difference Underlying Causes
| Disease Category | Deaths by Age Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 35-39 | 40-44 | 45-49 | 50-54 | 55-59 | 60-64 | 65-69 | 70-74 | 75-79 | 80-84 | 85+ | All (>=35) | |
| Lip, oral cavity, pharynx | 7 | 16 | 36 | 66 | 83 | 102 | 100 | 106 | 83 | 61 | 24 | 684 |
| Esophagus | 8 | 19 | 40 | 71 | 112 | 140 | 145 | 182 | 171 | 115 | 39 | 1,042 |
| Stomach | 11 | 20 | 38 | 61 | 83 | 107 | 148 | 192 | 187 | 168 | 72 | 1,087 |
| Pancreas | 7 | 26 | 47 | 98 | 152 | 192 | 234 | 272 | 271 | 197 | 78 | 1,574 |
| Larynx | 0 | 3 | 12 | 22 | 36 | 53 | 417 | 502 | 442 | 268 | 238 | 1,993 |
| Trachea, lung, bronchus | 22 | 88 | 232 | 460 | 813 | 1,187 | 1,513 | 1,916 | 1,856 | 1,270 | 392 | 9,749 |
| Cervix uteri | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Kidney and renal pelvis | 5 | 15 | 39 | 57 | 87 | 97 | 110 | 137 | 132 | 101 | 45 | 825 |
| Urinary bladder | 1 | 5 | 16 | 25 | 48 | 76 | 103 | 178 | 209 | 210 | 115 | 986 |
| Acute myeloid leukemia | 16 | 30 | 32 | 41 | 68 | 97 | 137 | 201 | 220 | 190 | 84 | 1,116 |
| Ischemic heart disease | 2 | 3 | 5 | 6 | 7 | 11 | 14 | 20 | 25 | 25 | 12 | 130 |
| Other heart disease | 97 | 271 | 549 | 886 | 1,246 | 1,561 | 2,018 | 2,869 | 3,608 | 3,801 | 2,487 | 19,393 |
| Cerebrovascular disease | 51 | 78 | 107 | 162 | 220 | 253 | 345 | 533 | 743 | 912 | 784 | 4,188 |
| Atherosclerosis | 22 | 51 | 76 | 124 | 176 | 250 | 401 | 718 | 1,094 | 1,337 | 942 | 5,191 |
| Aortic aneurysm | 0 | 2 | 5 | 13 | 18 | 28 | 44 | 57 | 91 | 110 | 102 | 470 |
| Other arterial disease | 7 | 12 | 24 | 35 | 62 | 101 | 167 | 257 | 329 | 324 | 179 | 1,497 |
| Pneumonia, influenza | 9 | 25 | 27 | 42 | 53 | 63 | 95 | 171 | 300 | 461 | 507 | 1,753 |
| Bronchitis, emphysema | 1 | 1 | 2 | 4 | 9 | 14 | 25 | 42 | 55 | 48 | 26 | 227 |
| Chronic airway obstruction | 2 | 6 | 14 | 36 | 83 | 169 | 331 | 657 | 994 | 1,138 | 706 | 4,136 |
| Total (male) | 268 | 671 | 1,301 | 2,209 | 3,356 | 4,501 | 6,347 | 9,010 | 10,810 | 736 | 6,832 | 56,041 |
| Disease Category | Deaths by Age Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 35-39 | 40-44 | 45-49 | 50-54 | 55-59 | 60-64 | 65-69 | 70-74 | 75-79 | 80-84 | 85+ | All (>=35) | |
| Lip, oral cavity, pharynx | 5 | 5 | 12 | 17 | 24 | 27 | 42 | 42 | 51 | 49 | 29 | 303 |
| Esophagus | 1 | 4 | 6 | 11 | 21 | 27 | 40 | 50 | 63 | 66 | 39 | 328 |
| Stomach | 7 | 17 | 28 | 32 | 37 | 49 | 62 | 92 | 125 | 126 | 85 | 660 |
| Pancreas | 7 | 17 | 35 | 61 | 103 | 126 | 181 | 236 | 320 | 297 | 167 | 1,550 |
| Larynx | 0 | 1 | 3 | 3 | 6 | 10 | 14 | 13 | 16 | 11 | 4 | 81 |
| Trachea, lung, bronchus | 30 | 118 | 274 | 421 | 615 | 808 | 983 | 1,184 | 1,216 | 879 | 328 | 6,856 |
| Cervix uteri | 22 | 34 | 43 | 43 | 37 | 29 | 27 | 30 | 30 | 34 | 15 | 344 |
| Kidney and renal pelvis | 4 | 6 | 12 | 27 | 40 | 42 | 50 | 77 | 86 | 84 | 48 | 476 |
| Urinary bladder | 1 | 3 | 8 | 10 | 15 | 23 | 32 | 51 | 79 | 95 | 76 | 393 |
| Acute myeloid leukemia | 12 | 18 | 27 | 31 | 37 | 61 | 81 | 113 | 140 | 157 | 105 | 782 |
| Ischemic heart disease | 1 | 4 | 6 | 8 | 11 | 17 | 27 | 41 | 53 | 56 | 39 | 263 |
| Other heart disease | 22 | 62 | 110 | 188 | 317 | 476 | 785 | 1,407 | 2,414 | 3,538 | 4,407 | 13,726 |
| Cerebrovascular disease | 23 | 41 | 60 | 74 | 104 | 146 | 218 | 406 | 707 | 1,136 | 1,702 | 4,617 |
| Atherosclerosis | 25 | 49 | 74 | 103 | 131 | 181 | 290 | 566 | 1,085 | 1,800 | 2,238 | 6,542 |
| Aortic aneurysm | 0 | 1 | 2 | 2 | 6 | 9 | 19 | 37 | 67 | 121 | 236 | 500 |
| Other arterial disease | 3 | 6 | 10 | 14 | 22 | 38 | 71 | 124 | 205 | 271 | 253 | 1,017 |
| Pneumonia, influenza | 10 | 13 | 18 | 22 | 32 | 46 | 66 | 129 | 261 | 480 | 907 | 1,984 |
| Bronchitis, emphysema | 0 | 1 | 1 | 3 | 6 | 10 | 17 | 28 | 35 | 35 | 29 | 165 |
| Chronic airway obstruction | 1 | 6 | 12 | 28 | 78 | 153 | 275 | 502 | 740 | 890 | 692 | 3,377 |
| Total (female) | 174 | 406 | 741 | 1,098 | 1,642 | 2,278 | 3,280 | 5,128 | 7,693 | 10,125 | 11,399 | 43,964 |
Page details
- Date modified: