
Planning for a Sustainable Future: Health Canada's 2011-2014 Sustainable Development Strategy - Performance Report for 2011-12
June 2012
Internet Component
This Internet component linked from Health Canada's 2011-12 Departmental Performance Report is intended to supplement Health Canada's performance against the 2011-2014 Departmental Sustainable Development Strategy.
Health Canada
Table of Contents
- Executive Summary
- Introduction
- 1. The 2012 Federal Sustainable Development Strategy Progress Report and Health Canada's 2011-12 Sustainable Development Strategy Performance Report
- 2. Health Canada and Sustainable Development
- 3. Health Canada's Decision-Making and Sustainable Development Practices
- 4. Health Canada's Departmental Sustainable Development Strategy: An Overview of Progress
- 5. Conclusion
- 6. Report Overview
- Annex A: Climate Change
- Annex B: Air Quality
- Annex C: Water
- Annex D: Chemicals Management
- Annex E: Shrinking the Environmental Footprint of Government
- Annex F: Health Canada Clean Air Agenda - Clean Air Regulatory Agenda Theme Performance Report (2011-12)
- Annex G: Health Canada Clean Air Agenda - Adaptation Theme Performance Report (2011-12)
Executive Summary
This is Health Canada's first Departmental Sustainable Development Strategy (DSDS) Performance Report. It accounts for performance against commitments made in Health Canada's first DSDS, and complements both Health Canada's Departmental Performance Report (DPR) and the 2012 Federal Sustainable Development Strategy (FSDS) Progress Report.
Health Canada is reporting on 32 implementation strategies, in three of the four FSDS thematic areas:
- Theme 1: Addressing Climate Change and Air Quality;
- Theme 2: Maintaining Water Quality and Availability; and
- Theme 4: Shrinking the Environmental Footprint of Government [also known as Greening Government Operations (GGO)].
As part of Theme 1, Addressing Climate Change and Air Quality, Health Canada committed to 12 implementation strategies aimed at advancing knowledge and communications about health risks to Canadians regarding climate change and indoor and outdoor air pollutants. Included in these strategies are initiatives to demand improved performance through the development of guidelines, regulations for industrial emissions, chemicals management requirements for key pollutants and risk management measures to address harmful substances.

As part of Theme 2, Addressing Water Quality and Availability, Health Canada committed to nine implementation strategies. These include updating and developing federal guidance and guidelines on water quality and providing provinces and territories and the international community with information concerning water quality. Some of this work was undertaken in collaboration with provinces and territories. Health Canada also committed to advancing knowledge and information concerning the management of chemicals to protect health with respect to water quality. Work also aimed at increasing the percentage of First Nations communities with acceptable water and wastewater facility risk ratings. Health Canada helps increase capacity among First Nations to put in place guidelines and risk management measures for improving drinking water and wastewater management.
Finally, as part of Theme 4, Shrinking the Environmental Footprint of Government, Health Canada identified 11 distinct targets to support reducing the Department's environmental footprint. Federal government departmental operations impact on the environment. Impacts from operations range from the energy used to heat and cool buildings; to run vehicle fleets; to use and dispose of goods and services; and to deliver programs to Canadians.
Introduction
The Federal Sustainable Development Act (FSDA) requires that any Minister whose department/agency is named in Schedule 1 of the Financial Administration Act prepare a Departmental Sustainable Development Strategy (DSDS).
Health Canada's first DSDS was published in June 2011. This Performance Report is intended to demonstrate the progress Health Canada has made in meeting the objectives outlined in the first DSDS.
1. The 2012 FSDS Progress Report and Health Canada's 2011-12 SDS Performance Report
The information provided in this DSDS Performance Report is supported by the 2012 FSDS Progress Report prepared by Environment Canada, as well as by Health Canada's 2011-12 Departmental Performance Report (DPR). State of the environment indicators presented in DPRs, and the 2012 FSDS Progress Report demonstrate the Government of Canada's progress towards environmental sustainability goals and targets.
This DSDS Performance Report outlines Health Canada's FSDS implementation strategies and corresponding performance information applicable over the immediate and intermediate timeframes. Generally, progress toward a broad outcome is not always directly attributable to any one factor such as a government program or policy, however, the link between the broad outcome and government actions can be demonstrated, documented and made transparent. Moving from the implementation strategy performance measure to the state of the environment measure (indicator), the direct attribution to any one factor is reduced - nonetheless, links between Health Canada's programs and policies and broad health outcomes remain.
2. Health Canada and Sustainable Development

The fundamental link between human health and sustainable development was a principle in the preamble of the Rio Declaration on Environment and Development adopted at the United Nations Conference on Environment and Development in Rio de Janeiro in 1992. It states that "human beings are at the centre of concern for sustainable development. They are entitled to a healthy and productive life in harmony with nature".
Consistent with these concepts, Health Canada is committed to supporting and contributing to the FSDS by delivering on its vision:
Health Canada is committed to improving the lives of all of Canada's people and to making this country's population among the healthiest in the world as measured by longevity, lifestyle and effective use of the public health care system.
Implicit in this vision is the recognition that social, economic and environmental conditions play an important role in determining the state of human health, for both present and future generations, as reflected in Figure 1.
Figure 1: Relationship of social, economic and environmental conditions and the state of human health
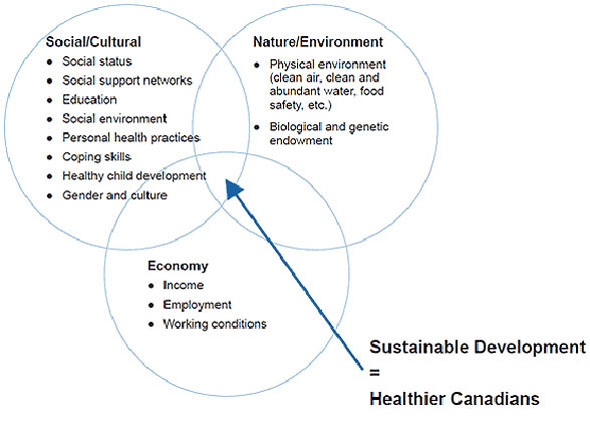
Text description
Chart shows the three pillars of sustainable development and how they work together to contribute to healthier Canadians. The first pillar is social/cultural, which includes social status, social support networks, education, social environment, personal health practices, coping skills, healthy child development, and gender and culture. The second pillar is nature/environment, which includes physical environment (clean air, clean and abundant water, food safety etc.) and biological and genetic endowment. Finally, the third pillar is the economy, which includes income, employment and working conditions.
3. Health Canada's Decision-Making and Sustainable Development Practices
Health Canada integrates sustainable development in its policies and operations through:
3.1 Internal Management Structure on Sustainable Development
Accountabilities related to sustainable development are being articulated in Health Canada's Sustainable Development Policy that is under development. It will define the responsibilities of leaders so that priority sustainable development objectives are integrated into planning and decision-making processes of policies, plans and programs.
Decisions about sustainable development, and how such decisions are applied to Health Canada's mandate, are brought to Health Canada's senior executive level committees for consideration and approval.
The Department provides training to support employees in the consideration of sustainable development principles through the application of analytical tools and resources. The objective of such training is aimed at promoting effective policy and planning decision-making that takes into account the social, environmental and economic factors, inherent to sustainable development.
Health Canada contributes to the federal approach to sustainable development by participating in standing and ad hoc interdepartmental working groups and committees.
3.2 Integration with Health Canada's expenditure, planning and reporting processes
As part of the Government of Canada's reporting on FSDS, Health Canada has integrated its DSDS achievements in its DPR and this document, which together form Health Canada's DSDS Performance Report.
The implementation strategies which Health Canada leads or supports under the FSDS are fully integrated into the Department's Management Resources and Results Structure.
As a basis for reporting, Health Canada measures and monitors its progress against FSDS commitments as follows:
- Goals and Targets
At the government-wide level, under the FSDS, various environmental performance measures, otherwise known as indicators, have been established to assess progress against the FSDS goals and targets. These are presented in the FSDS. Some indicators that address the goals and targets for Themes 1, 2 and 3 (air and climate change, water and nature), have been developed by the Canadian Environmental Sustainability Indicators initiative, with additional indicators coming from affected federal departments. Health Canada has identified specific indicators for some of its targets within the FSDS. - Implementation Strategies
Implementation strategies are generally more detailed and departmentally focused. As a result, specific Health Canada departmental performance measures are used to monitor Health Canada's progress, as outlined in this DSDS Performance Report. - Greening Government Operations
This theme, theme 4, has government-wide targets. Health Canada has established implementation strategies and the means for assessing progress at the departmental level. The GGO performance results are published in supplementary tables of Health Canada's DPR.
3.3 Application of Analytical Tools and Techniques
Successful integration of sustainable development into policies, plans and programs is supported by the use of analytical tools and management practices that consider, compare and incorporate environmental, social and economic objectives with the aim of preserving similar benefits for future generations.
The tools most commonly identified and used to inform decision-making and to manage risks pertaining to policy, plan and program implementation include: cost-benefit analysis; public surveys; workshops; risk assessment; advisory committees; and literature and case analysis. Risk management is embedded into Health Canada's evidence-based decision-making processes and provides reasonable assurance that policy objectives and desired outcomes will be achieved. Health Canada makes use of Treasury Board's Integrated Risk Management Framework and the Decision-making Framework for Identifying, Assessing, and Managing Health Risks. These frameworks promote a broad perspective to risk assessment and management and take into account feedback from interested and affected parties.
The precautionary principle is inherent to evidence-based decision-making and is identified in the preambles of two pieces of legislation and in the body of another for which Health Canada has regulatory responsibilities: the Canada Consumer Product Safety Act, the Canadian Environmental Protection Act, 1999 and the Pest Control Products Act.
3.3.3 Strategic Environmental Assessment: An Analytical Tool for Assessing Environmental and Associated Effects
In accordance with The Cabinet Directive on the Environmental Assessment of Policy, Plan and Program Proposals, Health Canada's policies, plans and programs destined for ministerial or Cabinet approval, and whose implementation may have important environmental effects, either positive or negative, require a SEA. The Guidelines for Implementing the Cabinet Directive on the Environmental Assessment of Policy, Plan and Program Proposals were revised in October 2010 and reflect the requirement to apply FSDS goals and targets when undertaking SEAs. As a means of supporting these revised guidelines, Health Canada has:
- Revised and received senior management approval of departmental SEA Policy;
- Developed departmental guidance and tools to support the implementation of Health Canada's SEA Policy; and
- Delivered two SEA training sessions based on the updated policy, tools and guidance.
Health Canada monitors departmental compliance with the SEA Policy. A tiered risk assessment process is applied to ensure a level of assessment commensurate with the potential environmental and associated risk(s) posed from implementing the policy, plan or program. Health Canada has committed to achieving a 95% compliance rate with applying the Policy. The first half of 2011-12 was dedicated to putting in place an effective monitoring and tracking mechanism. Data collected during the last two quarters confirmed that Health Canada has met this target.
In 2011-12, one SEA (detailed assessment) was undertaken by Health Canada as part of the development of the second phase of the Chemicals Management Plan (CMP). The SEA confirmed that the CMP supports three goals in the FSDS under the themes associated with air, water and nature, as follows:
- Minimizing the threat to air quality so that the air Canadians breathe is clean and supports healthy ecosystems;
- Protecting and enhancing the quality of the water so that it is clean, safe and secure for all Canadians and supports healthy ecosystems; and
- Maintaining productive and resilient ecosystems with the capacity to recover and adapt; and protecting areas in ways that leave them unimpaired for present and future generations.
The Public Statement of the Strategic Environmental Assessment of the Chemicals Management Plan identifies positive environmental effects resulting from implementation of the Plan and briefly outlines measures taken to enhance these positive effects.
4. Health Canada's Sustainable Development Strategy: An Overview of Progress

Health Canada's DSDS Performance Report demonstrates the link between its programs and activities and the following three thematic areas identified in the 2012 FSDS Progress Report:
- Addressing Climate Change and Air Quality;
- Maintaining Water Quality and Availability; and
- Shrinking the Environmental Footprint of Government.
Consistent with its vision, Health Canada made contributions to the identified themes of the FSDS by addressing environmental risks to human health and by endeavouring to shrink its environmental footprint.
Health Canada's contribution to the FSDS goals, targets and implementation strategies were achieved as part of its regular business. Sections 4.1 to 4.3 provide an overview of the achievements made by Health Canada. Refer to Annexes A-E for more detailed information on these achievements and how they link to corresponding FSDS implementation strategies.
4.1 FSDS Theme 1: Addressing Climate Change and Air Quality

Health Canada's work addressing climate change and air quality are outlined in Annexes A: Climate Change; and B: Air Quality, and D: Chemicals Management. Although some hazardous contaminants in the air, such as lead, have declined in recent years, others remain and continue to be problematic. As an industrialized country, Canada contributes to the release of a variety of air pollutants. As well, a significant level of air pollution in certain areas of Canada can be directly attributed to United States industrial sources. Additionally, some Canadian industrial facilities contribute to air pollution in the United States. The human health effects of poor air quality are far reaching, but principally, affect the body's respiratory and cardiovascular systems. They also increase the risk of certain types of cancer. Climate change also affects the health and well-being of Canadians by increasing risks associated with such issues as extreme heat events, respiratory and cardiovascular illnesses, natural hazards, water and food borne contamination, vector borne and zoonotic diseases, and certain cancers.
Health Canada has undertaken scientific research, risk assessments, monitoring and reporting of climate change impacts and air quality factors that affect human health. This information has supported actions to reduce health risks by all levels of government. These actions include developing new regulations, policies and tools to reduce Canadians' exposure to air pollution, and to help Canadians adapt to the potential negative effects of climate change.
With respect to climate change (Annex A: Climate Change), Health Canada has worked to increase the knowledge about how changing climatic conditions affect human health and has applied this knowledge to support regulatory program development and public awareness campaigns. This knowledge also was used to develop tools, guidelines and programs to help Canadians adapt to, and protect themselves from climate change. With respect to air quality, Health Canada made strides in addressing both indoor and outdoor air quality for such substances as ozone, particulate matter, indoor radon and mould (Annex B: Air Quality), existing and new chemical substances under the Chemicals Management Plan (Annex D: Chemicals Management). Indoor and outdoor air quality guidelines and standards were developed in order to provide a health-basis for risk management measures to protect human health. Fuels and emission management technologies were also assessed for potential adverse effects. Air health research and assessments support the development of a new national framework to manage air quality, in collaboration with Environment Canada, and provinces and territories.
In addition, Health Canada communicated air pollution health risks to Canadians through the Air Quality Health Index and targeted outreach campaigns such as Hazardcheck: Hazards in Your Home. Health Canada consistently collaborates with other international and federal government departments to support international agreements for reducing health risks. Such international initiatives include the Canada-United States Air Quality Agreement (1991), and the Gothenburg Protocol under the UN Economic Commission for Europe Convention on Long-range Transboundary Air Pollution.
Further, air quality and climate change adaptation activities also support Health Canada's sustainable development goals and targets as part of the Clean Air Agenda (CAA), as described in Annexes F and G.
4.2 FSDS Theme 2: Maintaining Water Quality and Availability

Access to clean, safe and secure water is crucial for the health of Canadians. Health Canada, as outlined in Annex C: Water, has continued to help protect Canadians through the development of health-based drinking water guidelines. Health exposure and risk assessments were completed to develop these water quality guidelines and standards so that risk management measures are put in place to protect human health. These guidelines are used by the provinces and territories as a basis for establishing their own enforceable requirements for drinking water quality. Health Canada has also developed guidance on drinking water quality for provinces, territories and federal departments/agencies, as well as guidelines for recreational water quality.
Health Canada collaborated with First Nations communities and other federal departments in order to enhance First Nations communities' capacity to protect their public health through monitoring of drinking water quality and wastewater disposal, and providing First Nations with communications products and tools to enhance public awareness and knowledge about environmental health. There also has been an increased percentage of First Nations communities with acceptable water and wastewater facility risk ratings.
In addition, Health Canada worked with Environment Canada to reduce health risks to Canadians posed by harmful substances. As identified in Annex D: Chemicals Management, under the Chemicals Management Plan Health Canada continued to assess priority existing substances and new chemical substances for which Environment Canada has been notified by industry of their intended manufacture, use or import.
4.3 FSDS Theme 4: Shrinking the Environmental Footprint of Government

In Health Canada's 2011-2014 DSDS, the Department committed to implementing a number of initiatives in support of the federal effort to minimize the government's environmental footprint. Health Canada made progress in implementing Greening Government Operations in the area of buildings, information technology, management of electronic and electrical equipment, execution of meetings, and printing management.
Annex E: Shrinking the Environmental Footprint of Government, provides additional information on how Health Canada supports the Greening of Government Operations. It includes the three-year federal commitments and provides a brief overview of Health Canada's 2011-12 performance highlights with a link to detailed performance tables.
5. Conclusion
Health Canada's first DSDS Performance Report under the 2011-2014 FSDS demonstrates its dedication to sustainable development through delivering results aimed toward the achievement of its core vision. Namely, Health Canada has committed:
To improving the lives of all of Canada's people and to making this country's population among the healthiest in the world as measured by longevity, lifestyle and effective use of the public health care system.
Going forward, Health Canada will continue to assess its progress and seek ways to improve on integrating the three pillars of sustainable development - environmental, social, and economic.
6. Report Overview
In support of the FSDS themes, Health Canada has organized its implementation strategies by program in recognition that some implementation strategies support more than one theme (i.e. the Chemicals Management Plan).

Theme One: Addressing Climate Change and Air Quality is supported by the following programs:

- Climate Change (Annex A)
- Air Quality (Annex B); and
- Target 2.1 - Air Pollutants, and
- Target 2.2 - Indoor Air Quality
- Chemicals Management (Annex D)
- Target 2.3 - Chemicals Management
Theme Two: Maintaining Water Quality and Availability is supported by the following program:

- Water (Annex C)
- Target 3.10 - Drinking Water Quality
- Target 3.11 - Drinking Water Quality
- Chemicals Management (Annex D)
- Target 3.12 - Chemicals Management
Theme Four: Greening Government Operations is supported by the Department's Internal Services.

- Shrinking the Environmental Footprint of the Government (Annex E)
- Targets 8.1-8.11
The Targets and associated Implementation Strategies information for Themes One and Two have been organized as follows:
- Brief description of Health Canada's activities under FSDS Target
- Link to Health Canada's Program Activity Architecture
- Relationship between the FSDS Target and the Implementation Strategy
- Description of the Implementation Strategy and the activities undertaken by Health Canada to support it
- Achievements Supporting FSDS Goals, including links to the Clean Air Agenda (CAA), where applicable.
Theme Four information provided in this Report includes a description of the FSDS implementation strategies and key 2011-12 performance highlights. A link to Health Canada's 2011-12 DPR and the Greening Government Operations Supplementary Information Tables has been provided.
Clean Air Agenda
- Clean Air Regulatory Agenda Theme (Annex F)
- Adaptation Theme (Annex G)
Annex A: Climate Change
Goal 1: Climate Change: Reduce greenhouse gas emission levels to mitigate the severity and unavoidable impacts of climate change.
1.1 Target: Climate Change Mitigation
Health Canada's Climate Change and Health program assists public health and emergency management decision makers to address the health impacts of climate change through the identification of risks and vulnerabilities to water quality, and from extreme weather events such as heat waves.
Climate change and health activities support FSDS implementation strategies under the following theme:
- Theme 1 - Addressing Climate Change and Air Quality
Link to Health Canada's Program Activity Architecture
Theme 1 - Addressing Climate Change and Air Quality, Target 1.1 - Climate Change Mitigation relates to Health Canada's Program Activity Architecture as follows:
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating.
- Program Activity 2.3: Environmental Risks to Health
- Program Sub Activity 2.3.1: Climate Change
| Theme | FSDS Target | Implementation Strategy |
|---|---|---|
| 1 | 2.1 Reduce air pollutants in order to maintain or improve air quality across the country and achieve the emission targets which are currently under development, in consultation with provinces, territories and stakeholders. |
2.1.2 Undertake scientific research and reporting in support of regulatory and other programs delivered, including data analysis, inventory development, monitoring, modeling and assessment of the effectiveness of efforts as well as research on options, costs and benefits including economic and social and technology assessments. (Environment Canada, Health Canada, National Research Council of Canada) |
| 2.1.3 Communicate outdoor air pollution health risks to Canadians through the Air Quality Health Index (AQHI): Continue development of the AQHI and support implementation into additional census metropolitan areas (CMAs). The AQHI provides current and forecast air quality information and advice on health risks in order to assist Canadians in making decisions on how to reduce their level of exposure. (Health Canada, Environment Canada) |
||
| 2.1.8 Continue to work collaboratively with provinces and territories to develop and implement a coherent approach to managing air quality, including national ambient air quality standards and national industrial emissions requirements for key pollutants. (Environment Canada, Health Canada) |
||
| 2.1.31 Work with the United States to reduce transboundary emissions under the Canada-United States Air Quality Agreement. (Environment Canada, Health Canada) |
||
| 2.1.35 Participate in negotiations for revisions of the Gothenburg Protocol under the United Nations Economic Commission for Europe (UNECE) Convention on Long-range Transboundary Air Pollution (LRTAP). (Environment Canada, Health Canada) |
Description of Implementation Strategy
This implementation strategy does not relate directly to Climate Change Mitigation. By preparing Canadians for extreme heat events, Health Canada is strengthening Canada's adaptive capacity to reduce the health impacts of our changing climate. While Health Canada's Heat Alert Response Systems (HARS) support adaptation to the unavoidable impacts of climate change, they do not contribute to reducing greenhouse gas emissions.
Climate change is expected to increase the risks to human health in a number of areas including air and water quality, extreme weather events, and infectious diseases. The extent of these effects depends on how quickly our climate changes, and on how well we adapt to the new environmental conditions and risks to health.
Extreme heat poses a growing risk to the health and well-being of Canadians as climate change is expected to produce a greater intensity, frequency and duration of extreme heat events. Public health and emergency management officials in several Canadian communities are already taking actions to reduce their vulnerability to heat-health risks. Communities and individuals are seeking information about the most effective ways to protect themselves, their families and those most at risk.
Achievements Supporting FSDS Goals
The Climate Change and Health program provided guidance and expert advice to public health and emergency management professionals in the development of HARS, as well as training tools for health professionals to reduce the vulnerability of communities to extreme heat.
More specifically, Health Canada successfully implemented pilot HARS in four Canadian communities; produced a set of Guidelines for Health Care Professionals for Extreme Heat Events; developed a series of targeted factsheets and brochures on reducing the health risks from extreme heat; and released a toolkit to communicate health risks associated with extreme heat events. In spring 2012, Health Canada released a Best Practices Guide in Developing HARS.
| Implementation Strategies | Performance Indicators | Program Performance Targets | Program Performance Status | CAA Theme Link |
|---|---|---|---|---|
| 1.1.5 | Increased application of heat alert and response systems by Canadian communities. | By 2013, up to three new communities have implemented heat alert and response systems (HARS). | On Schedule: Targeted engagement in several at risk communities in Southern B.C., and Saskatchewan, Southwestern Ontario and New Brunswick to either support the development of a new HARS or strengthen existing components of an established system. |
Adaptation/Heat Alert and Response Systems |
Annex B: Air Quality
Goal 2: Air Pollution: Minimize the threats to air quality so that the air Canadians breathe is clean and supports healthy ecosystems.
Under Goal 2, Health Canada supports two FSDS Targets, 2.1 Air Pollutants, and 2.2 Indoor Air Quality.
2.1 - Target: Air Pollutants
As a means of addressing outdoor air quality risks to human health, Health Canada's Air Quality program conducts research and assessments on the impacts of outdoor air pollutants on human health to support the development of regulations, standards, guidelines and other risk management actions.
Health Canada's activities under Target 2.1 support FSDS implementation strategies under the following theme:
- Theme 1 - Addressing Climate Change and Air Quality
Link to Health Canada's Program Activity
Theme 1 - Addressing Climate Change and Air Quality, Target 2.1 - Air Pollutants relates to Health Canada's Program Activity Architecture as follows:
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating.
- Program Activity 2.3: Environmental Risks to Health
- Program Sub Activity 2.3.2: Air Quality
| Theme | FSDS Target | Implementation Strategy |
|---|---|---|
| 1 | 2.1 Reduce air pollutants in order to maintain or improve air quality across the country and achieve the emission targets which are currently under development, in consultation with provinces, territories and stakeholders. |
2.1.2 Undertake scientific research and reporting in support of regulatory and other programs delivered, including data analysis, inventory development, monitoring, modeling and assessment of the effectiveness of efforts as well as research on options, costs and benefits including economic and social and technology assessments. (Environment Canada, Health Canada, National Research Council of Canada) |
| 2.1.3 Communicate outdoor air pollution health risks to Canadians through the Air Quality Health Index (AQHI): Continue development of the AQHI and support implementation into additional census metropolitan areas (CMAs). The AQHI provides current and forecast air quality information and advice on health risks in order to assist Canadians in making decisions on how to reduce their level of exposure. (Health Canada, Environment Canada) |
||
| 2.1.8 Continue to work collaboratively with provinces and territories to develop and implement a coherent approach to managing air quality, including national ambient air quality standards and national industrial emissions requirements for key pollutants. (Environment Canada, Health Canada) |
||
| 2.1.31 Work with the United States to reduce transboundary emissions under the Canada-United States Air Quality Agreement. (Environment Canada, Health Canada) |
||
| 2.1.35 Participate in negotiations for revisions of the Gothenburg Protocol under the United Nations Economic Commission for Europe (UNECE) Convention on Long-range Transboundary Air Pollution (LRTAP). (Environment Canada, Health Canada) |
Descriptions of Implementation Strategies
This activity supports improvements to air quality and associated human health risks through research and assessment of the health risks posed by substances Canadians may be exposed to from ambient air and by supporting the development of ambient air quality standards.
Under the Clean Air Regulatory Agenda (CARA), Health Canada plays an important role in improving ambient air quality and protecting the health of Canadians through a broad range of activities. Research studies are conducted to determine what substances Canadians may be exposed to from ambient air. Health risk assessments on these and other substances are carried out in order to develop ambient air quality standards that are used by public health professionals and regulators to better manage air quality. Conventional fuels and their alternatives, as well as fuel emission management technologies, are assessed for any potential adverse health impacts from their use or introduction into the Canadian marketplace. Economic research supports the development of cost-benefit analyses for proposed government options to control air pollution sources.
Through the development and implementation of the AQHI, Health Canada provides Canadians with a tool to assess their potential risk associated with air pollution in real time on a daily basis and advice on how Canadians can reduce their exposure to air pollution.
The AQHI is a tool designed to help Canadians make decisions to protect their health by limiting short-term exposure to air pollution and adjusting their activity levels during increased levels of air pollution. It also provides advice on how Canadians can improve the quality of the air they breathe. This tool has been developed by Health Canada and Environment Canada, in collaboration with the provinces and key health and environment stakeholders.
This Index pays particular attention to people who are sensitive to air pollution and provides them with advice on how to protect their health during air quality levels associated with low, moderate, high and very high health risks.
This activity ensures a coherent approach to managing air quality through Health Canada's provision of research, assessments and guidelines to provinces and territories. Health Canada's assessment of the potential adverse impacts of conventional fuels and their alternatives and fuel emission management technologies, as well as our cost-benefit analyses for proposed government options to control air pollution sources support the development of national industrial and transportation emissions requirements for key pollutants.
Health Canada, along with Environment Canada, worked with the provinces and territories and other key stakeholders, to develop a national framework to manage air quality including developing new health-driven Canadian ambient air quality standards, local air zone management and emissions requirements for major industrial sectors. Health Canada research and assessments provide the health basis and guidance for developing actions to reduce the health risks from outdoor air pollutants. Economic research supports the development of cost-benefit analyses for proposed government options to control air pollution sources.
A significant level of air pollution in certain areas of Canada can be directly attributed to United States industrial sources. Additionally, some Canadian industrial facilities contribute to air pollution in the United States. This implementation strategy relates to the FSDS target of providing a forum in which shared air quality strategies can be addressed and agreements to reduce emissions can be reached.
The Canada-United States Air Quality Agreement was signed by Canada and the United States in 1991, to address transboundary air pollution leading to acid rain. Both countries agreed to reduce emissions of sulphur dioxide and nitrogen oxides, the primary precursors to acid rain, and to work together on acid rain related scientific and technical cooperation.
In 2003, Canada and the United States signed on to the Border Air Quality Strategy to build on the success of the 1991 Canada-United States Air Quality Agreement which saw reductions in acid rain in the 1990s and today is reducing transboundary air pollutants. Health Canada is collaborating with its partners (US Environmental Protection Agency, other federal departments, provincial and municipal governments, industry and business interests, non-government organizations, health professionals and academics) to identify and assess the negative impacts of transboundary air pollution on human health and contribute to the development of a framework for coordinated air shed management.
Under the Clean Air Regulatory Agenda, Health Canada is involved in the development of a comprehensive air quality system which will lead to reductions in industrial air emissions and provide the basis for negotiating a Particulate Matter Annex to the Canada-United States Air Quality Agreement.
In addition, Health Canada conducts health science assessments in support of regulations to reduce air pollutant emissions from industrial sectors; and coordinated science activities under Sub-committee 2 of the Canada-United States Air Quality Agreement.
The Convention on LRTAP was signed in 1979 to address major environmental problems in the UNECE region through scientific collaboration and policy negotiations. The Gothenburg Protocol was added to the Convention in 1999.
Health Canada, as a member of the UNECE LRTAP Health Effects Task Group, continues to provide advice and guidance into World Health Organization and European Union air quality initiatives, including the Gothenburg Protocol.
The Gothenburg Protocol will set emission ceilings for 2020 for four pollutants: sulphur, nitrogen oxides, volatile organic compounds and ammonia. These ceilings were negotiated on the basis of scientific assessments of pollution effects and abatement options. Some discussions are underway to incorporate black carbon (in the context of particulate matter) into the protocol. Other LRTAP protocols include persistent organic pollutants and heavy metals.
Additionally, Health Canada is a member of the Working Group on Strategies and Review under the UNECE LRTAP Convention.
These venues provide an opportunity for an international exchange on current science and new developments which assists Canada in positioning regulatory initiatives.
Target 2.1 Achievements Supporting FSDS Goals
The Air Quality program's 2011-12 research and assessment activities provided the health basis and guidance for actions to reduce the health risks from outdoor air pollutants, including supporting the development of a new national framework to manage air quality, new ambient air quality standards, and expansion of the AQHI.
| Implementation Strategies | Performance Indicators | Program Performance Targets | Program Performance Status | CAA Theme Link |
|---|---|---|---|---|
| 2.1.2 | Trend data shows improvements in air quality and health benefits. | Baseline for air quality and health benefit improvements to be set in 2013-14. Following that, air quality and health benefit improvements will be reported every three years, by percentage change over the period. | On Schedule: An air health indicator (AHI) has been developed for ozone and for fine particulate matter, showing trends in cardiorespiratory mortality due to exposure to each of these air pollutants in the Canadian population. Air health indicators for ozone and fine particulate matter were released publicly in July 2011 through the Canadian Environmental Sustainability Indicators (CESI) website). Subsequent work focused on updating the mortality data for ozone and fine particulate matter, and acquiring and analyzing data to develop a morbidity-based AHI is underway. The AHI also provides some of the input to inform the Air Quality Health Index (AQHI) and the Air Quality Benefits Assessment Tool (AQBAT). |
Clean Air Regulatory Agenda (CARA) - Science Integration, Accountability and Benefits of Action |
| Date to achieve target: March 31, 2014 | ||||
| 2.1.2 2.1.8 2.1.31 |
Number of planned regulations, standards and guidelines developed in support of risk management strategies, leading to improvements in air quality. | Complete particulate matter and ozone ambient air quality standards to drive emission reduction and assess effectiveness of regulatory framework. | On Schedule: Particulate Matter (PM) and ozone Canadian Ambient Air Quality Standards and management threshold levels were developed by a multi-stakeholder working group co-chaired by Health Canada; (approval by Canadian Council of Ministers of the Environment (CCME) anticipated for 2012). |
CARA - Atmospheric Pollutant Policy |
| Date to achieve target: March 31, 2012 | ||||
| 2.1.2 | Number of assessments and studies in support of standards and guidelines by product type (assessment, study). | Complete two draft substance assessments and three sector-based assessments of air pollutants in support of regulations, standards and guidelines for ambient air. | On Schedule: Canadian Smog Science Assessment Highlights and Key Messages published (co-authored by HC and EC); draft risk assessments for carbon monoxide (CO) and coarse particulate matter were completed and internally reviewed; risk assessments for sulphur dioxide and nitrogen dioxide were initiated; population exposure assessments were initiated for seven industrial sectors. |
CARA - Atmospheric Research, Monitoring and Modeling CARA - Health and Environmental Impacts of Atmospheric Pollutants |
| 2.1.2 | Complete one health impact assessment of a selected fuel or greenhouse gas mitigation technology to support policy and risk management actions. | Completed: Completed the biodiesel health risk assessment for publication in Canada Gazette Part I (CGI) in 2012-13 and supported the human health cost-benefit analysis for the Reduction of Carbon Dioxide Emissions from Coal-Fired Generation of Electricity Regulations published in CGI in August 2011. |
CARA - Health and Environmental Impacts of Atmospheric Pollutants | |
| 2.1.2 | Complete three research studies and three exposure studies, to provide information on health effects of air pollutants, as well as exposure and source data for indoor and outdoor contaminants. | Completed: Data analysis phase was completed for an intervention study to determine health benefits from indoor air cleaners in a First Nation. Continued to publish results from multi-year exposure studies conducted in homes in Halifax, Edmonton and Ottawa (apartments). Data collection phase was completed for: (1) pilot study of school transportation and air quality; (2) monitoring to assess the impact of base metal and aluminum smelting on local air quality in BC; (3) monitoring to assess exposure of pregnant women to naphthalene; (4) monitoring of exposure to air pollution and respiratory and cardiovascular health in asthmatic children (Montreal); and (5) follow up study of the impacts of a wood stove change out program in BC. |
CARA - Health and Environmental Impacts of Atmospheric Pollutants | |
| 2.1.2 | Knowledge generated as needed on health impacts of air pollution using the Air Quality Benefit Assessment Tool. | Air Quality Benefit Assessment Tool is successful in providing information on benefits of proposed air quality management options in support of objectives, standards and regulations. | Completed and ongoing: The AQBAT was successfully used to generate estimates of health benefits valuation associated with regulatory and non-regulatory activities for controlling emissions of pollutants that would result in improved air quality and for addressing climate change. These include the proposed Coal-fired electricity generation regulation (analysis completed) and the illustrative Base Level Industrial Emission Requirements (BLIERS) (ongoing). |
CARA - Science Integration Accountability and Benefits of Action |
| Date to achieve target: March 31, 2012 | ||||
| 2.1.2 2.1.8 |
Number of knowledge transfer activities (e.g. citations, workshops, posters, peer reviewed publications, etc.) by: area of focus (water, air, climate change); and target group. | Seven air quality knowledge transfer activities and provision of advice on a yearly basis for air quality. | Completed: CARA research projects produced seven peer-reviewed publications, five conference presentations and 14 knowledge transfer activities that included client meetings, reports and the provision of research advice. |
CARA -Science Integration, Accountability and Benefits of Action; CARA - Data Collection and Reporting for Atmospheric Pollutants |
| Date to achieve target: March 31, 2012 | ||||
| 2.1.3 | Percent increase in the number of Canadians with access to the AQHI. | 10% increase per year based on baseline of approximately 50% coverage in 2010-11. | On Schedule: The AQHI is now available in all 10 provinces in 65 locations. Approximately 60% of Canadians now have access to the AQHI. Contact has been established with both the Yukon and NWT to discuss implementation of the AQHI in Northern communities. |
CARA - Data Collection and Reporting of Atmospheric Pollutants |
| Date to achieve target: 80% coverage by 2014-15 | ||||
| 2.1.8 | Trends in air quality-related health outcomes. | Baseline for air quality and health benefit improvements to be set in 2013-14. Following that, health outcomes and changes in benefits from actions to improve air quality will be reported every three years, by percentage change over the period. | On Schedule: An air health indicator (AHI) has been developed for ozone and for fine particulate matter, showing trends in cardiorespiratory mortality due to exposure to each of these air pollutants in the Canadian population. Air health indicators for ozone and fine particulate matter were released publicly in July 2011 (posted on the Canadian Environmental Sustainability Indicators (CESI) website). Subsequent work focused on updating the mortality data for ozone and fine particulate matter, and acquiring and analyzing data to develop a morbidity-based AHI. The AHI also provides some of the input to inform the Air Quality Health Index (AQHI) and the Air Quality Benefits Assessment Tool (AQBAT). The latter is a computer simulation tool designed to estimate the human health and welfare benefits or damages associated with changes in Canada's ambient air quality. |
CARA - Science Integration Accountability and Benefits of Action |
| Date to achieve target: March 31, 2014 | ||||
| 2.1.35 | Participate in meetings of LRTAP working groups and provide advice, as needed, to LRTAP Protocol science assessment process for pollutant emissions. | Participate in consideration of emission level for black carbon component of particulate matter. | Completed and ongoing: Health Canada participated in the Health Effect Task Group under the Protocol to discuss development of a health risk assessment for black carbon and potential management options. Provided input to an inter-departmental committee on an amendment to include black carbon in the Gothenburg Protocol and to update the Protocol in relation to persistent organic pollutants and heavy metals. |
N/A |
| Date to achieve target: March 31, 2015 (to be confirmed) |
2.2 - Target: Indoor Air Quality
Another aspect of Health Canada's Air Quality program deals with indoor air quality. Health Canada research and assessment activities support nation-wide outreach to improve air quality in residential and federal buildings. Health Canada scientists assess the exposure of Canadians to indoor air pollution; investigate the health effects of air pollution through research studies; review scientific studies on the health effects of air pollution to assess health risks. Health Canada also leads in the development of standards and guidelines to reduce health risks, usually in collaboration with other federal departments and/or with provincial and territorial governments. Finally, it informs the Canadian public, including First Nations communities about health risks from indoor air pollution such as radon and mould and provides recommendations on how to reduce these risks.
Health Canada's activities under the indoor air quality target supports FSDS implementation strategies under the following theme:
- Theme 1 - Addressing Climate Change and Air Quality
Link to Health Canada's Program Activity Architecture
Theme 1 - Addressing Climate Change and Air Quality, Target 2.2 - Indoor Air Quality relates to Health Canada's Program Activity Architecture as follows:
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating.
- Program Activity 2.3: Environmental Risks to Health
- Program Sub Activity 2.3.2: Air Quality
- Program Activity 2.6: Radiation Protection
Strategic Outcome 3: First Nations and Inuit communities and individuals received health services and benefits that are responsive to their needs so as to improve their health status.
- Program Activity 3.1: First Nations and Inuit Primary Health Care
- Program Sub Activity 3.1.2: First Nations and Inuit Public Health Protection
- Program Sub Sub Activity 3.1.2.2: First Nations and Inuit Environmental Health
| Theme | FSDS Target | Implementation Strategy |
|---|---|---|
| 1 | 2.2 Help protect the health of Canadians by assessing indoor air pollutants and developing guidelines and other tools to better manage indoor air quality. |
2.2.1 Conduct exposure and risk assessments and source identification studies to support guideline development on priority indoor air contaminants. (Health Canada) |
| 2.2.2 Create a database of indoor radon concentrations, map areas of high radon potential in Canada, test for radon in federal buildings in high-risk and radon-prone areas. The strategy includes a radon awareness program. (Health Canada) |
||
| 2.2.3 Implement the health promotion campaign on mould as part of the National Strategy to Address Mould in First Nations Communities. (Health Canada) |
Descriptions of Implementation Strategies
This activity develops guidelines and standards to better manage indoor air quality and provides advice for public health professionals and Canadians on how exposure to air pollutants can be reduced.
Health Canada plays an important role in improving indoor air quality and protecting the health of Canadians through a broad range of activities. Research studies are conducted to determine what substances Canadians may be exposed to in their homes or other indoor environments. Health risk assessments on these and other substances are carried out in order to develop indoor air quality guidelines that are used by public health professionals and regulators to better manage air quality. Communications products are developed for the general public and public health professionals and include recommended actions aimed at improving indoor air quality.
Testing for radon in federal buildings, raising public awareness of risks and health impacts and disseminating information to mitigate the risk of radon exposure are activities undertaken that support improved indoor air quality.
Testing for radon in federal buildings, raising public awareness of risks and health impacts and disseminating information to mitigate the risk of radon exposure are activities undertaken that support improved indoor air quality.
- Development of a radon potential map of Canada. Using geology, aerial surveys and fieldwork to identify levels of natural radiation in targeted areas, the Department will map areas of high radon potential in Canada. This component is expected to lead to increased knowledge of risks, health impacts and mitigation strategies related to radon.
- Testing of radon in federal buildings located in high risk radon-prone areas. By testing for radon in approximately 10,000 federal sites located in known and/or potentially high-risk radon areas, it is expected there will be increased knowledge of risks, health impacts and mitigation strategies related to radon.
- Radon education and awareness program. Through the design, implementation and coordination of a broad-based public awareness and education campaign, the Department aims to improve public awareness of health risks and causes of elevated radon, and inform Canadians of strategies to reduce their risk. The Health Canada radon awareness program focuses on raising awareness of radon and the potential health risks from exposure, as well as encouraging Canadians to test their homes and to reduce radon levels, if necessary.
In addition, a database of indoor radon concentrations will be developed and will be updated as new information is acquired from residential surveys, radon measurement service providers and members of the public. This information is important to perform validation of models used to produce a radon potential map.
Informing First Nations communities of the health risks associated with mould supports the confidence of First Nations residents to take action towards preventing or remediating mould in their homes.
Clean air is essential to good health and this is especially true for indoor air. Health Canada considers mould growth in residential buildings to be a potential health hazard. People living in buildings where mould grows are more likely to suffer from health problems, especially symptoms such as coughing, wheezing, and headaches. Asthmatics are especially at risk as mould may trigger asthma attacks. People respond to mould in different ways depending on the amount of exposure and the person's overall health. While this issue can impact the health of all Canadians, Health Canada has a specific role with respect to First Nations communities.
First Nations residents who are better informed about mould are able to take appropriate actions to prevent mould growth, remediate as needed, and minimize the potential risks to their health and that of their family members.
A report, titled " Quantitative Research on Indoor Air Quality and Mould in First Nations Households" (2007) concluded that 57% of First Nations community members knew something about mould. Only 33% of those with mould could suggest any way of removing it and even less (20%) could suggest methods for preventing mould growth in their home.
In order to enhance public awareness and knowledge of mould issues and increase the confidence of First Nations residents in their ability to do simple actions to prevent, or remediate mould in their homes, Health Canada develops and distributes mould communication products as part of the health promotion campaign on mould.
Achievements Supporting FSDS Goals
Health Canada increased awareness of indoor health risks to the Canadian public including First Nations communities. Health risk assessments, research studies and data analyses were conducted for a number of priority indoor contaminants. An additional 2,000 federal buildings underwent testing and assessment for radon. There has been an increase in the percentage of radon-related communications products being accessed through print, and electronic sources with the expected outcome of a more informed Canadian public.
| Implementation Strategies | Performance Indicators | Program Performance Targets | Program Performance Status | CAA Theme Link |
|---|---|---|---|---|
| FSDS Target 2.2 as reported in Health Canada's 2011-12 Departmental Performance Report Help protect the health of Canadians by assessing indoor air pollutants and developing guidelines and other tools to better manage indoor air quality. (Health Canada) |
Performance Status Risk assessments were conducted and new Residential Indoor Air Quality Guidelines were developed for priority indoor pollutants toluene and fine particulate matter (PM), including recommendations on how to reduce exposure and protect health. The final Residential Indoor Air Quality Guideline for toluene was issued, and the proposed PM2.5 guideline was published for public comment in the Canada Gazette, Part I. Indoor air quality was also a primary focus of Health Canada's Hazardcheck outreach campaign. |
|||
| 2.2.1 | Number of planned regulations, standards and guidelines developed in support of risk management strategies, leading to improvements in air quality. | Publish at least two indoor air guidelines in Canada Gazette, Part 1 (CGI) for consultation. | On Schedule: Final Residential Indoor Air Quality Guideline for Toluene was published in CGI; Proposed PM2.5 guideline was published in CGI for public comment. |
CARA — IAQ Management - Biological and Chemical Contaminants |
| Number of planned risk management strategies incorporated in building codes, and communicated through targeted information products, thereby reducing risk to health. | Develop at least two communication products to inform Canadians. | Indoor air quality was a primary focus of Health Canada's Hazardcheck outreach campaign, which included videos, quizzes, and retail engagements. New public fact sheets on indoor air pollutants were developed and added to Health Canada's Indoor Air Quality and the It's Your Health websites. | ||
| Date to achieve target: March 31, 2012 | ||||
| Number of assessments and studies in support of standards and guidelines by: product type (assessment, study). | Conduct screening assessments of indoor air contaminants to identify priorities for full assessments. | On Schedule: Developed a new methodology to more rapidly assess the risks of volatile organic compounds (VOCs) found in indoor air. Health risk assessment for benzene, naphthalene and Legionella were finalized, following internal and external peer review. |
||
| Complete two draft assessments in support of guidelines and other risk management strategies for indoor air. | Two draft risk assessments for carbon monoxide (CO) and coarse particulate matter were completed and internally reviewed; risk assessments for sulphur dioxide and nitrogen dioxide were initiated; population exposure assessments were initiated for seven industrial sectors. Canadian Smog Science Assessment Highlights and Key Messages were published (co-authored by HC and EC). | |||
| Complete one research study and one exposure study to provide information on health effects of air pollutants, as well as exposure and source data for indoor contaminants. | Continued to publish results from multi-year exposure studies conducted in homes in Halifax, Edmonton and Ottawa (apartments). | |||
| Date to achieve target: March 31, 2012 | ||||
| 2.2.2 | Number of federal buildings tested for radon by 2011-12. | 2,000 federal buildings. | On Schedule: Radon detectors were deployed in 2,000 federal buildings during 2011-12. Detectors for approximately 1,600 buildings have been received by the National Radon Laboratory and analysis is ongoing. The detectors for the remaining 400 buildings are in the field as the tests are still underway and will be collected by the individual departments at the end of the three month testing period. |
CARA - IAQ Management - Radioactive Contaminants |
| Number of hits on Health Canada radon web page Number of public inquiries Number of downloads of Radon: A Guide for Canadian Homeowners |
10% increase in hits and downloads over each previous year. | On Schedule: Radon web activity and public inquiries for Health Canada increased (5-10%) in 2011-12. |
||
| Number of brochures and fact sheets ordered. | Radon brochure distribution increased by approximately 15% in 2011-12. | |||
| Percent of data inputted into database. | 100% of data received inputted by end of fiscal year. | On Schedule: 100% of data received or generated for the National Radon Program has been inputted into the database of indoor radon results. |
||
| Number of field soil measurement projects completed in major population centres in 2011-12. | One field soil measurement project completed in three communities in BC. | No Longer Applicable: The field soil measurement deliverable was cancelled early in 2011-12 since funding for the project was received too late to allow the field work to be completed. Soil radon gas measurements can only be performed during a short window of opportunity when the weather conditions are appropriate. Health Canada rectified the data shortfall by using data from the 2011 Cross-Canada Radon Survey and from the indoor radon concentrations database. A methodology for mapping areas of high radon potential in Canada will be developed and made available to provinces and territories for their use in mapping radon potential in their jurisdictions. As a result, the field soil measurements are no longer required. |
||
| Number of provinces mapped for radon potential. | Validated map of southern Ontario completed by 2011-12. | Behind Schedule: Although Natural Resources Canada (NRCan) partners have drafted a map of southern Ontario, the project is behind schedule as they must still complete their investigation of the appropriate weighting of the geological data layers to produce the best correlation with the indoor radon data. This is needed to ensure the best quality map. The work is being performed by NRCan as expertise in the field of geochemistry and geology is essential. |
||
| Number of documents completed on mapping radon potential areas. | Protocol for mapping radon potential using numerous data parameters and process for validation completed by 2011-12. | Behind Schedule: This target is tied to the mapping protocol described in the previous target. Given that NRCan partners are currently evaluating which parameters give the best correlation with the indoor radon data from southern Ontario, the mapping methodology cannot be completed and published at this time. |
||
| Date to achieve target: Ongoing (data to be assessed on an annual basis). | ||||
| 2.2.3 | Health Canada, working the Canada Mortgage and Housing Corporation (CMHC) and Aboriginal Affairs and Northern Development Canada (AANDC), is in the process of developing an evaluation plan as part of the National Strategy to Address Mould in First Nations Communities. | On Schedule: Health Canada, in collaboration with the CMHC and AANDC, has developed a Performance Measurement and Accountability Framework as a part of the National Strategy to Address Mould in First Nations Communities. |
N/A | |
Annex C: Water
Goal 3: Water Quality: Protect and enhance the quality of water so that it is clean, safe and secure for all Canadians and supports healthy ecosystems.
3.10 - Target: Drinking Water Quality
Health Canada works with First Nations communities with the aim of ensuring that drinking water quality monitoring programs are in place in their communities. The review, interpretation and dissemination of water test results as well as the sharing of information products with First Nations communities are aimed at increasing the capacity and confidence of First Nations residents concerning the safety of their water supply.
Drinking water quality activities support FSDS implementation strategies under the following theme:
- Theme 2 - Maintaining Water Quality and Availability
Link to Health Canada's Program Activity Architecture
As First Nations Water and Wastewater Action Plan funding was originally only available until 2011-12, the implementation strategy did not extend for the entire three years of the FSDS. Budget 2012 has since identified an extension of this programming until March 31, 2014
Theme 2 - Maintaining Water Quality and Availability, Target 3.10 - Drinking Water Quality relates to Health Canada's Program Activity Architecture as follows:
Strategic Outcome 3: First Nations and Inuit communities and individuals received health services and benefits that are responsive to their needs so as to improve their health status.
- Program Activity 3.1: First Nations and Inuit Primary Health Care
- Program Sub Activity 3.1.2: First Nations and Inuit Public Health Protection
- Program Sub Sub Activity 3.1.2.2: First Nations and Inuit Environmental Health
| Theme | FSDS Target | FSDS Target |
|---|---|---|
| 2 | 3.10 Increase the percentage of First Nations communities with acceptable water and wastewater facility risk ratings by 2013. (Health Canada and Aboriginal Affairs and Northern Development Canada) |
3.10.3 - Work with First Nations communities to increase the frequency of testing drinking water quality. (Health Canada) |
3.10.6 - Continue to enhance capacity to monitor drinking water quality in First Nations communities to protect public health:
|
||
| 3.10.8 - Continue to provide First Nations with communications products to enhance public awareness and knowledge as well as increase the confidence of First Nations residents about the safety of their drinking water supply. (Health Canada) |
Descriptions of Implementation Strategies
There is an indirect relationship between this implementation strategy and the target. Over time, by working with First Nations communities to identify challenges with meeting recommended testing frequencies, and to implement appropriate actions, Health Canada will increase the frequency of drinking water quality testing at tap. Regular testing of drinking water quality offers timely identification of potential problems with drinking water quality, minimizing potential risks to public health and therefore contributes to increasing the percentage of First Nations communities with acceptable water and wastewater facility ratings by 2013.
Health Canada assists First Nations communities in establishing drinking water quality monitoring programs. This includes: verification monitoring of the overall quality of drinking water at tap, and reviewing, interpreting and disseminating results to First Nations; providing advice, guidance and recommendations for First Nations communities about drinking water safety and safe disposal of onsite domestic sewage; and reviewing water and wastewater infrastructure project proposals from a public health perspective.
Health Canada aims to ensure that drinking water quality in First Nations communities is tested as per the GCDWQ. The latest edition of the GCDWQ set out the basic parameters all drinking water systems should strive to achieve in order to deliver clean, safe and reliable drinking water at tap. Although the overall frequency of drinking water quality testing as per the GCDWQ in First Nations distribution systems has increased over the last few years, not all distribution systems are tested at the frequencies recommended in the GCDWQ.
In order to increase the frequency of drinking water quality testing, Health Canada continues to work with First Nations communities to identify challenges with meeting recommended testing frequencies and implementing appropriate actions.
3.10.6 - Continue to enhance capacity to monitor drinking water quality in First Nations communities to protect public health:
3.10.6.1 - Support all First Nations communities in ensuring access to a trained Community-Based Water Monitor (CBWM) or Environmental Health Officer (EHO). (Health Canada)
3.10.6.2 - Support all First Nations communities in monitoring drinking water quality as per the Guidelines for Canadian Drinking Water Quality (GCDWQ). (Health Canada)
There is an indirect relationship between this implementation strategy and the target. Over time, by continuing to enhance capacity to monitor drinking water quality in First Nations communities, Health Canada will increase the frequency of drinking water quality testing at tap. Regular testing of drinking water quality offers timely identification of potential problems with drinking water quality, minimizing potential risks to public health and therefore contributing to increasing the percentage of First Nations communities with acceptable water and wastewater facility ratings by 2013.
In First Nations communities, EHOs and CBWMs share responsibility for drinking water quality monitoring at tap as per the GCDWQ. EHOs monitor drinking water quality for bacteriological, chemical, physical and radiological parameters, interpret drinking water quality results, disseminate results to First Nations authorities and maintain quality assurance. CBWMs are First Nations community members trained by an EHO. They are responsible for monitoring bacteriological water quality and disseminating results.
Capacity to monitor drinking water quality as per the GCDWQ in First Nations communities is supported by Health Canada through the provision of funding to Chief and Council for drinking water monitoring through the CBWM program, and training of CBWMs to monitor the drinking water for potential bacteriological contamination as a final check on the overall safety of the drinking water at tap. EHOs and CBWMs are the primary service providers with respect to drinking water quality monitoring, and it is therefore important to provide them with the support necessary to perform their duties effectively to better protect the public health of First Nations residents.
There is an indirect relationship between this implementation strategy and the target. Over time, by continuing to provide First Nations with drinking water-related communications products, Health Canada will strive to enhance public awareness and knowledge, as well as increase the confidence of First Nations residents, about the safety of their drinking water supply. Greater awareness of water quality testing procedures and frequency, acceptable levels of contaminants in tap water and tap water quality enables residents to better understand and prioritize the implementation of protective measures (such as drinking water advisories). This will reduce potential risks to public health and therefore will contribute to increasing the percentage of First Nations communities with acceptable water and wastewater facility risk ratings by 2013.
Due to the complexities of water quality issues, and because public health is at stake, it is critical for First Nations residents to have access to appropriate information regarding drinking water quality issues. First Nations residents are better informed about their water quality, roles and responsibilities of key players, and day-to-day actions that they can take to protect the health of their family members and to minimize risk to their health.
In addition, the results of Public Opinion Research that was commissioned in 2009 showed that just over 75% of First Nations respondents feel that information on water quality testing procedures, testing frequency, and acceptable levels of contaminants in tap water and tap water quality would help them feel more confident about the quality of their drinking water.
In order to enhance public awareness and knowledge of water quality issues, as well as increase the confidence of First Nations residents about the safety of their drinking water supply, Health Canada develops and distributes drinking water-related communication products aimed at First Nations communities.
Achievements Supporting FSDS Goals
Health Canada issued four communications products to support public health and to prevent drinking water contamination in First Nations communities.
| Implementation Strategies | Performance Indicators | Program Performance Indicators | Program Performance Status |
|---|---|---|---|
| FSDS Target 3.10 as reported in Health Canada's 2011-12 Departmental Performance Report Increase the percentage of First Nations communities with acceptable water and wastewater facility risk ratings by 2013. (Health Canada and Aboriginal Affairs and Northern Development Canada) |
* Per the 2012 Annual Performance Inspection results (June 29, 2012), compared to data on the same systems from the National Assessment results (July 11, 2011)Footnote 1 : Water systems:
|
||
| 3.10.3 3.10.6.2 |
Percent of distribution systems meeting the testing frequency recommended in the GCDWQ. | By March 2012, a 5% increase from 2010-11 levels in the number of distribution systems with five or more connections that meet the testing frequency recommended in the GCDWQ. | Behind Schedule: In March 2012, 58% of distributions systems met the weekly testing frequency recommended in the GCDWQ which is the same level as in 2010-11. Despite the fact that the compliance rate remained the same as last year, there is an overall trend toward greater compliance. The current compliance rate is 32% higher than the 44% compliance rate in 2009-10. |
| 3.10.6.1 | Percent of First Nations communities that have access to a trained CBWM or an EHO. | By March 2012, all First Nations communities will have access to a trained CBWM or EHO. | Behind Schedule: By March 2012, 97% of First Nation communities had access to a trained CBWM or an EHO. |
| 3.10.8 | Number of communications products developed for First Nations on how to protect public health and prevent drinking water contamination in First Nations communities. | By March 2012, four communication products will be developed and distributed to First Nations residents. | Completed: Health Canada published and distributed the following products: 1) Guidance for Designing, Installing, Maintaining and Decommissioning Drinking Water Cisterns in First Nations Communities South of 60°; 2) Guidance on Trucked Drinking Water Delivery in First Nations Communities South of 60°; 3) Is this water safe to drink? Poster; and 4) Door Hanger for residents served by cisterns. |
* Aboriginal Affairs and Northern Development Canada provides the data for this performance indicator. |
|||
3.11 - Target: Drinking Water Quality
Health Canada's Water Quality program, in collaboration with partners and stakeholders, develops and promotes of the application of water quality guidelines and guidance (including guidance values), as well as strategies and tools, in support of safe of Canadian drinking water.
Drinking water quality activities support FSDS implementation strategies under the following theme:
- Theme 2 - Maintaining Water Quality and Availability
Link to Health Canada's Program Activity Architecture
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating.
- Program Activity 2.3: Environmental Risks to Health
- Program Sub Activity 2.3.3: Water Quality
| Theme | FSDS Target | Implementation Strategy |
|---|---|---|
| 2 | 3.11 Help protect the health of Canadians by developing health-based water guidelines. (Health Canada) |
3.11.2 Update "Guidance for providing safe drinking water in areas of federal jurisdiction." (Health Canada) |
| 3.11.7 Develop up to five guidelines and guidance on water quality (i.e. drinking water, recreational water and water re-use) in collaboration with provinces/territories, supported by technical documents, as a basis for their regulatory requirements. (Health Canada) |
||
| 3.11.10 Support provinces and territories and internationally by sharing and disseminating scientific risk assessments on drinking water contaminants. (Health Canada) |
Descriptions of Implementation Strategies
Health Canada provides scientific guidance and advice so that federal departments can meet their responsibilities for providing safe drinking water in a manner that is based on the multi-barrier approach and health-based water quality guidelines.
The development and updating of guidance documents for federal departments that have responsibilities for producing and/or providing safe drinking water in areas of federal jurisdiction includes federal lands (e.g. national parks), federal facilities (e.g. military bases) and First Nations communities. The document is produced by the Interdepartmental Working Group on Drinking Water, for which Health Canada provides the scientific secretariat. Health Canada provides scientific guidance and expertise for the document, which is updated regularly and is founded on a multi-barrier approach to providing safe drinking water. It incorporates the Guidelines for Canadian Drinking Water Quality as the minimum standard for safe drinking water.
Health Canada develops guidelines that are based on health risk assessments in collaboration with provinces and territories so that specific challenges to each region are addressed.
The GCDWQ are used by all provinces and territories as the basis for establishing their regulatory requirements for drinking water quality. Guidelines for recreational water quality, and for household reclaimed water, are also developed, and collaboration is undertaken on standards for drinking water materials. Work is done in close collaboration with partners and stakeholders, research related to drinking water is directed and supported by this activity, and partnerships are forged with stakeholders to address key challenges to drinking water safety, including small community drinking water supplies.
Health Canada provides scientific risk assessments of the impact of drinking water contaminants on human health in support of developing GCDWQ.
The development of health risk assessments for microbiological and chemical contaminants supports the development of guidelines for drinking water quality. These assessments are used by all provinces and territories as the basis for establishing their regulatory requirements for drinking water quality.
Achievements Supporting FSDS Goals
Planned 2011-12 water quality program activities were completed successfully, including guideline/guidance document approvals, the continued development and rollout of two tools/strategies to help identify threats to the safety of drinking water, and implementation of strategies to reduce these risks such as through a remote monitoring guidance document and the expansion of the Canadian Network of Public Health Intelligence's secure real-time alert system for drinking water advisories.
| Implementation Strategies | Performance Indicators | Program Performance Targets | Program Performance Status |
|---|---|---|---|
| FSDS Target 3.11 as reported in Health Canada's 2011-12 Departmental Performance Report Help protect the health of Canadians by developing health-based water guidelines (Health Canada). |
|||
| 3.11.2 3.11.7 3.11.10 |
Number of water quality guidelines/guidance documents approved by federal/provincial/territorial committees by product type (guideline, guidance document). | Five guidelines/guidance documents approved by federal/provincial/territory committees annually. | Behind Schedule: Four guidelines/guidance documents have been approved by the F/P/T Committee on Health and Environment: Protozoa (guidelines), E. coli (guidelines), Total Coliform (guidelines); and Heterotrophic Plate Count (guidance). |
| Date to achieve target: March 31, 2012 | |||
Annex D: Chemicals Management
2.3 and 3.12 - Target: Chemicals Management
Working collaboratively with Environment Canada under the Chemicals Management Plan (CMP), Health Canada assesses chemical substances for potential human health risks and develops risk management measures to protect Canadians from those substances determined harmful to human health.
Health Canada's chemicals management program contributes to the FSDS in supporting improvements in human health through its activities aimed at reducing threats to the health of Canadians from harmful chemical substances.
CMP supports FSDS implementation strategies under the following two themes:
- Theme 1 - Addressing Climate Change and Air Quality
- Theme 2 - Maintaining Water Quality and Availability
Link to Health Canada's Program Activity Architecture
Theme 1 - Addressing Climate Change and Air Quality and Theme 2 - Maintaining Water Quality and Availability, Target 2.3 and 3.12 - Chemicals Management relates to Health Canada's Program Activity Architecture as follows:
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating.
- Program Activity 2.3: Environmental Risks to Health
- Program Sub Activity 2.3.4: Health Impacts of Chemicals
| Theme | FSDS Target | Implementation Strategy |
|---|---|---|
| 1 and 2 | 2.3 and 3.12 Reduce risks to Canadians and impacts on the environment posed by harmful substances as a result of decreased environmental concentrations and human exposure to such substances. |
2.3.4 and 3.12 Assess 100% of existing commercial substances as identified under the Chemicals Management Plan for risks to human health and/or the environment (100% of total of 4300 by 2020). (Environment Canada, Health Canada) |
| 2.3.5 and 3.12.5 Assess 100% of new substances, for which Environment Canada has been notified by industry of their intended manufacture or import, to determine if they are suspected of being toxic within the timelines in the regulation or established services standards. (Environment Canada, Health Canada) |
||
| 2.3.8 and 3.12.7 Ensure at least one risk management measure is in place within the legally mandated timeframes for 100% of substances added to the List of Toxic Substances. (Environment Canada, Health Canada) |
Descriptions of Implementation Strategies
Through these FSDS implementation strategies below, Health Canada programs cooperate with Environment Canada under the Canadian Environmental Protection Act, 1999 to support FSDS goals through the assessment and management of the potential risks posed by existing substances produced, imported or used in Canada.
Health Canada activities include risk assessments of existing (post-market) substances and developing risk management strategies, policies and regulations for substances determined as harmful to human health, as a complement to Environment Canada's review of environmental impacts. These activities reduce the health risks to Canadians posed by substances by identifying those that may be harmful and taking appropriate steps to reduce this risk.
Health Canada is in the process of assessing existing substances as priorities identified under the CMP, both to determine whether they are harmful to human health due to their inherent properties, and the level of exposure to the Canadian public. Health Canada's research on the nature of existing substances and Canadians' exposure to them support the scientifically grounded, risk-based approach used to assess the impact of chemical substances on Canadians' health and to guide risk management or regulatory actions for substances determined to be harmful to human health.
Health Canada activities include assessing and managing potential health risks associated with new (pre-market) substances, including products of biotechnology. For new substances in Food and Drugs Act regulated products, the Department also assesses potential harm to the environment. These activities reduce the health risks to Canadians posed by substances by identifying those that may be harmful and taking appropriate steps to reduce this risk.
Health Canada also assesses substances and products of biotechnology that are new to the Canadian market both to determine whether they are harmful to human health due to their inherent properties and the level of exposure to the Canadian public. Health Canada's research on the nature of new commercial substances and the products of biotechnology and Canadians' exposure to them support a scientifically grounded, risk-based approach used to assess the impact of chemical substances on Canadian health and to guide risk management or regulatory actions for substances determined to be harmful to human health.
Under the Canadian Environmental Protection Act, 1999, the Department in cooperation with Environment Canada, develops and implements risk management strategies, policies and regulations to manage the potential risks posed by substances that are assessed to be harmful to human health. This implementation strategy relates to the FSDS targets by ensuring that timely risk management measures are put in place to mitigate human exposure and reduce the risk to Canadians posed by harmful substances.
It is directly through the risk management actions above that Health Canada contributes to decreases in environmental concentrations and human exposure to harmful substances.
Achievements Supporting FSDS Goals
Overall, the planned 2011-12 chemicals assessment and management activities under the CMP were completed on target and within timelines.
The CMP's 2011-12 achievements contributing to FSDS goals include:
- Approximately 97% of the existing substance assessments planned within 2011-12 were completed and published. This includes final screening assessment reports for:
- 22 substances in Batches 1, 6, 8, and 11 of the “Challenge” component of Phase 1 of the CMP;
- 30 substances under the Petroleum Sector Stream Approach; and
- aniline, hexabromocyclododecane and quinoline.
- Five draft screening assessment reports for which conclusions under CEPA 1999 were proposed for 601 substances (rapid screening, 1,2-dibromoethane, 1,1-dichloroethene, 53 high hazard substances and triclosan), and
- Three draft human health State of the Science reports (lead, long-chain chlorinated alkanes and decabromodiphenyl ether)
Further, 100% of the notifications received concerning substances newly produced, imported or used in Canada were assessed within legislated timelines and service standards. This included 305 chemicals and polymers, 38 substances in Food and Drug Act products, 17 products of biotechnology and 6 nanomaterials.
Finally, risk management strategies were published for 100% of substances assessed to be harmful to human health within mandated timeframes. These strategies outlined the risk management instrument(s) proposed to address the health risks associated with those substances, such as regulatory measures or restrictions on significant new activities involving these substances.
| Implementation Strategies | Performance Indicators | Program Performance Targets | Program Performance Status |
|---|---|---|---|
| FSDS Target 2.3 and 3.12 as reported in Health Canada's Departmental 2011-12 Performance Report Reduce risks to Canadians and impacts on the environment posed by harmful substances as a result of decreased environmental concentrations and human exposure to such substances. (Environment Canada and Health Canada) |
|||
| 2.3.4 2.3.5 3.12.4 3.12.5 |
Level of exposure to substances of concern. | To be established based on baseline to be set after release of cycle 1 in 2010. | Behind Schedule: Baseline levels for Substances of Concern will be set in 2012-13 based on data released in 2011-12, which was collected in Cycle 1 of the Canadian Health Measures Survey (CHMS). |
| * Canadian releases of selected controlled substances | * Compared to 1990, mercury emissions to air in 2010 had decreased by 87 percent (30.3 tonnes). Since 2005, there has been a decline in hexavalent chromium emissions to air. [Air and Climate Indicators] * From 2007-2010, levels of polybrominated diphenyl ethers (PBDEs) in fish and sediments were below the Federal Environmental Quality Guidelines within the majority of drainage regions in Canada. Exceedances occurred mainly for pentaBDEs in fish in most drainage regions and for tetraBDE, pentaBDE and decaBDE in fish and sediment samples within 4 of 13 sampled drainage regions. [Environmental Indicators] * The amount of mercury, cadmium and lead released to water was lower in 2010 than in 2003. [Release of Toxic Substances to Water] |
||
| Date to achieve target: March 31, 2012 | |||
| 2.3.4 3.12.4 |
Percent of targets/service standards met for existing substances; for 'In Commerce List' substances; and for new substances by: type of regulatory action taken; and result of regulatory action. | 100% of targeted substances, 2011, ongoing. | On Schedule: In 2011-12 the 'In Commerce List (ICL)' activity engaged in Phases 1 and 2 of the planned nomination process, identifying candidate substances for inclusion on the ICL. The Revised ICL will be published in Canada Gazette Part I in Fall 2012. The ICL substance nomination processes have been completed as targeted in the 2011-12 plans. |
| Date to achieve target: March 31, 2012 | |||
| 2.3.4 3.12.4 |
Efficiency of key Regulatory System Services: Number and percent of existing substances under the Chemicals Management Plan assessed for risk to human health within targets set. |
100% of substances assessed within targeted/regulated timelines. | Behind Schedule: Approximately 97% of assessments planned within 2011-12 were published according to planned timelines. This included 22 Challenge assessment reports and final screening assessment reports produced. Four screening assessment reports under the Petroleum Stream approach published. Three final screening assessment reports and three draft human State of the Science reports published in the Canada Gazette Part I. |
| Date to achieve target: March 31, 2012 | |||
| 2.3.4 3.12.4 2.3.8 3.12.7 |
Percent of substances assessed to be harmful to human health for which at least one risk management instrument was developed within mandated timeframes. | 100% of substances assessed to be harmful to human health have at least one risk management instrument developed within mandated timeframes. | On Schedule: Risk management strategies were published for 100% of substances assessed to be harmful to human health within mandated timeframes. |
| Date to achieve target: February 2012 | |||
| 2.3.4 3.12.4 |
Report on level of exposure in humans of substances of concern by substance. | CMHS report published every three years (next report to be published in 2013). | Behind Schedule: CHMS Cycle 1 data released. Determination of Cycle 1 list of Substances of Concern completed and related exposure data analysis for baseline setting is ongoing. Anticipate setting of baselines for Substances of Concern in July 2012. |
| 2.3.5 3.12.5 |
Efficiency of key Regulatory System Services: Number and percent new substances for which Health Canada has been notified by industry of their manufacture or import that are assessed within regulated timelines or established service standards to determine if they are suspected of being harmful to human health or the environment. |
100% of substances assessed within targeted/regulated timelines. | On Schedule: 100% of New Substances notifications received were assessed within legislated timelines or service standards. This included 305 chemicals and polymers, 38 substances in Food and Drug Act products, 17 products of biotechnology and 6 nanomaterials. |
| Date to achieve target: March 31, 2012 | |||
| * Environment Canada provides the data for this performance indicator. | |||
Annex E: Shrinking the Environmental Footprint of Government
The following is the list of Greening Government Operations targets of the FSDS.
- Theme 4 Greening Government Operations (GGO)
Minimize the environmental footprint of government operations
- 8.1 Target: As of April 1, 2012, and pursuant to departmental strategic frameworks, new construction and build-to-lease projects and major renovation projects will achieve an industry-recognized level of high environmental performance.
- 8.2 Target: As of April 1, 2012, and pursuant to departmental strategic frameworks, existing crown buildings over 1000 m², will be assessed for environmental performance using an industry-recognized assessment tool.
- 8.3 Target: As of April 1, 2012, and pursuant to departmental strategic frameworks, new lease or lease renewal projects over 1000 m², where the Crown is the major lessee, will be assessed for environmental performance using an industry-recognized assessment tool.
- 8.4 Target: As of April 1, 2012, and pursuant to departmental strategic frameworks, fit-up and refit projects will achieve an industry-recognized level of high environmental performance.
- 8.5 Target: The Government of Canada will take action now to reduce levels of greenhouse gas emissions from its operations, to match the national target of 17% below 2005 by 2020.
- 8.6 Target: By March 31, 2014, each department will reuse or recycle all surplus electronic and electrical equipment (EEE) in an environmentally sound and secure manner.
- 8.7 Target: By March 31, 2013, each department will achieve an 8:1 average ratio of office employees to printing units. Departments will apply target where building occupancy levels, security considerations, and space configuration allow.
- 8.8 Target: By March 31, 2014, each department will reduce internal paper consumption per office employee by 20%. Each department will establish a baseline between 2005-06 and 2011-12, and applicable scope.
- 8.9 Target: By March 31, 2012, each department will adopt a guide for greening meetings.
- 8.10 Target: As of April 1, 2011, each department will establish at least three SMART green procurement targets to reduce environmental impacts.
- 8.11 Target: As of April 1, 2011, each department will establish SMART targets for training, employee performance evaluations, and management processes and controls, as they pertain to procurement decision-making.
In 2011-12, the Department made progress in a number of areas. The following highlight the Department's key GGO achievements:
- As per Target 8.1 - 8.4, Health Canada developed and put into effect a Green Buildings Strategic Framework for the four green building targets;
- As per Target 8.6, Health Canada implemented a Plan for Managing Surplus Electronic and Electrical Equipment;
- As per Target 8.7, Health Canada established a baseline inventory of printing units and developed a Printing Unit Policy as part of the strategy to reduce the ratio of employees to printing units;
- As per Target 8.9, the Department adopted and implemented a Green Meeting Guide; and
- As per Target 8.10 Health Canada increased the percentage of environmentally friendly information technology hardware purchases to 88% from baseline of 29% in 2009-10.
A link to the performance details of Health Canada's GGO achievements is available in the Departmental Performance Report.
Annex F: Health Canada Clean Air Agenda (CAA) — Clean Air Regulatory Agenda (CARA) Theme Performance Report (2011-12)
Health Canada Report on Activities under the CARA 2011-12
Protecting the health and environment of Canadians is a key Government priority. Emissions of greenhouse gases (GHGs) and air pollutants threaten the health of Canadians, degrade the environment, contribute to climate change and smog and adversely affect the economy. CARA provides the coordinated framework for Government efforts to reduce GHGs and air pollutant emissions. Collectively, the work undertaken as part of CARA cuts across several Government departments - Environment Canada, Health Canada and the National Research Council. Health Canada's role is to provide leadership and expertise on actions to address the health impacts of air pollutants.
With respect to air quality, the Government is working in collaboration with the provinces and territories to implement a new national Air Quality Management System (AQMS) in order to further minimize threats to Canadians and their environment from pollution. This system is intended to include new health-driven Canadians ambient air quality standards, local air zone management and emissions requirements for major industrial sectors and for mobile sources.
CARA also supports the related scientific, modelling, monitoring, reporting and economic analysis necessary for policy and regulatory development and to ensure that the measures taken are based on sound science and achieve their intended effects.
Under CARA, Health Canada will continue to take action to improve indoor air quality, including promoting awareness of the need to test for radon in homes, and promote positive behavioural change among Canadians to reduce their exposure to air pollutants by extending the Air Quality Health Index (AQHI).
The following report provides a summary of Health Canada's CARA program and achievements for 2011-12. A link to the financial information on planned and actual expenditures under the CARA theme for 2011-12 is available on Health Canada's Sustainable Development website.
CARA 1.1 - ATMOSPHERIC RESEARCH, MONITORING AND MODELLING
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
A key objective of CARA is to establish a new national framework for managing air quality called the AQMS. It is being developed collaboratively between federal, provincial and territorial jurisdictions. The AQMS will include new Canadian Ambient Air Quality Standards (CAAQS), local and regional air quality management and requirements for key sources of industrial emissions for mobile sources.
To support the AQMS, Health Canada will use a multi-pollutant approach to assess the health risks posed by the range of pollutants emitted by individual industrial sectors. This information will be used to inform the development of more efficient sector specific emissions regulations and non-regulatory actions by federal/provincial and territorial jurisdictions. It will also inform decision-making at all levels related to the sector management of multi-pollutant emissions and support industry in optimizing their efforts to reduce air pollutants.
Health Canada expected achievements:
- Conduct exposure and health risks assessments from selected industrial sectors;
- Conduct studies on health effects of emissions from selected industrial sectors, including laboratory toxicology research; and
- Provide federal/provincial jurisdictions and industry with information regarding multi-pollutant health impacts.
Program Achievement / Performance Summary
Multi-pollutant risk assessments were initiated for six industrial sectors (aluminium, pulp and paper, cement, coal-fired electricity, iron and steel, and base metal smelting). Data was collected on the type of pollutants being released from each sector and computer models were used to estimate the levels to which people would be exposed at different distances and directions from the point of release. This is the first stage in assessing the health risks in a multi-pollutant risk assessment. Research to support assessment of the health risks from industrial emissions included: a study on the acute cardiovascular and respiratory effects of air pollution from steel plant emissions of air pollution in Sault Ste. Marie; a study on the acute cardiovascular and respiratory effects of air pollution from petroleum refinery emissions in Montreal; monitoring to assess the impact of base metal and aluminium smelting on local air quality in BC; and land-use regression models to predict daily air pollutant data.
Program Lessons Learned
A sector-based approach is challenging from a technical and scientific point of view due to the complexity of assessing the impacts of multiple pollutants at once. A focus on clearly explaining objectives, and ongoing communication and transparency in all aspects of work is essential to achieving the cooperation and sharing of information necessary for success.
CARA 1.2 - HEALTH AND ENVIRONMENTAL IMPACTS OF AIR POLLUTANTS
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
The transportation sector is a major contributor to air pollution, particularly in urban areas, and has been clearly linked to negative health outcomes in the general population. Health Canada will conduct health risk assessments and health-benefit studies of new fuels, technologies and transportation-related policies and will also conduct research on health impacts of pollutant emissions from transportation. These activities support the establishment of effective and efficient transportation and fuel regulations and management strategies to reduce emissions of GHGs and air pollutants from regulated sectors while maintaining competitiveness in those sectors.
Health Canada expected achievements:
- Conduct health risk assessments and health-benefit studies in support of the development of regulations related to transportation;
- Conduct exposure study on emissions from transportation; and
- Conduct studies on toxicity, including laboratory toxicology research, and health effects of transportation emissions.
Program Achievement / Performance Summary
Health Canada completed a biodiesel health risk assessment which was used to inform recent renewable fuels regulations. The department evaluated the co-benefits associated with new greenhouse gas regulations (e.g. heavy-duty trucks and coal-fired generation of electricity) in reducing emissions of air pollutants (i.e. non-greenhouse gas emissions) and the associated health impacts. The department also contributed to the health impact analysis of a marine emissions control area regulation through assessing proposed changes in fuel quality and emission controls.
A multi-year study to assess the impact of marine emissions on population exposure to air pollution in Halifax was initiated. Other research to support transportation risk assessment included: a study on childhood exposure to traffic related air pollution and asthma development in Toronto; and a pilot study on controlled exposure to diesel emission and the effects on cognitive function. Research was also conducted to analyze population exposure to traffic in Ontario cities and the effect on mortality. In addition, data on where and how Canadians spend their time were processed for 3000 participants in the Canadian Human Activity Pattern Survey 2. This survey provides information necessary to accurately estimate exposure to pollutants and associated health risks.
Program Lessons Learned
The early engagement of stakeholders and partners is essential to ensuring efficient and effective support of the regulatory development process.
CARA 1.3 - Science Integration, Accountability and Benefits of Action
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
Health Canada currently makes extensive use of economic valuation estimates in supporting the development of air quality and other regulations. However, the scientific understanding of the health impacts of environmental pollution is rapidly changing, with new impacts being discovered such as those on birth outcome and childhood development. Research to identify and quantify the relationship between air pollution and negative health impacts will be carried out to better predict the health benefits from improved air quality. These actions will assist in the development of more effective and efficient regulations and air quality strategies that better reflect the health and social impacts of air quality on Canadians, while maintaining competitiveness in those sectors. Scientific and economic research will also be used to update analytical tools such as the Air Quality Benefits Assessment Tool (AQBAT), which is used to monetize the health and economic impacts of changes in air quality.
Health Canada expected achievements:
- Conduct research to identify and quantify the socio-economic impacts of air pollution exposure;
- Improved analytical tools to assess the impact of current, or proposed air quality strategies and regulations (e.g. AQBAT); and
- Conduct health benefit analysis of ongoing and planned air quality regulatory or policy actions, as required.
Program Achievement / Performance Summary
The AQBAT, which is used to monetize the health and economic impacts of changes in air quality, was successfully used to generate estimates of health benefits valuation associated with regulatory and non-regulatory activities for controlling emissions of pollutants that would result in improved air quality and for addressing climate change. These include the coal-fired electricity generation regulation and the illustrative Base Level Industrial Emission Requirements. Research was completed to analyze adverse pregnancy outcomes and effects on non-cardiovascular and non-respiratory parameters related to air pollution.
Program Lessons Learned
By working closely with regulatory partners, health benefits assessments can be initiated early and can help guide policy development.
CARA 2.2 - DATA COLLECTION AND REPORTING FOR ATMOSPHERIC POLLUTANTS - AIR QUALITY HEALTH INDEX (AQHI) PROGRAM
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
Canada is an international leader by being the first country to have developed an index to communicate the health risks associated with a mixture of air pollutants and to provide air quality forecasts with protective health advice to reduce that risk. Health-based communication tools such as the AQHI are vital given that regulatory action alone cannot completely eliminate the health risks from air pollution. The AQHI is now available to 17 million Canadians and has fully replaced the older air quality indices in six provinces. With renewal funds, Health Canada and Environment Canada will expand the AQHI to additional communities, promote the index widely in order to gain acceptance and understanding, and ensure that the science underpinning the index is kept current.
Health Canada expected achievements:
- Agreement with provincial and public health programs to support local and regional implementation and to promote the AQHI to the general population and vulnerable groups;
- Marketing partnerships and targeted outreach to promote AQHI; and
- Targeted research to study the associations between the AQHI and health outcomes.
The objectives of this program are to implement a national, health-based communications tool for current and forecasted local air quality and to increase Canadians' knowledge of actions to take to protect their health and to reduce pollution.
Program Achievement / Performance Summary
The AQHI is now available in all 10 provinces in 65 locations, including nine communities in Alberta. Approximately 60% of Canadians now have access to the AQHI. Contact has been established with both the Yukon and NWT to discuss implementation of the AQHI in Northern communities. A media partnership with The Weather Network to promote the AQHI will be renewed for an additional four years. A "Train the Trainer" program has been developed in partnership with the College of Family Physicians of Canada to train health professionals to become ambassadors of the AQHI and promote the Index to their peers. An online course has also been developed in partnership with the University of British Columbia, to teach health professionals about the AQHI, among other air-health related issues. Research was conducted to analyze the associations between AQHI and emergency room visits for stroke.
Program Lessons Learned
Successful implementation of this program requires collaboration between provincial and local governments and non-governmental organizations that may have regional interests to consider. Collaboration is enhanced by employing flexible mechanisms to address regional differences and issues.
CARA 3.2 - ATMOSPHERIC POLLUTANT POLICY
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
A key element of the AQMS is the establishment of new Canadian Ambient Air Quality Standards (CAAQS) for targeted air pollutants that will drive the management of source emissions to improve health and environmental benefits. Health-based risk assessments of air pollutants will be used to develop CAAQS for Particulate Matter (PM) and Ozone (O3) and for additional priority pollutants such as Nitrogen Dioxide (NO2), Sulphur Dioxide (SO2) and carbon monoxide (CO). This program seeks to develop CAAQS that are endorsed by all jurisdictions who in turn undertake adequate actions to ensure the standards are met.
Health Canada expected achievements:
- Complete draft health risk assessments for outdoor air pollutants to support and develop proposals for CAAQS; and
- Conduct exposure and health effects studies for air pollutants to support additional CAAQS development and review.
Program Achievement / Performance Summary
In collaboration with Environment Canada, provincial/territorial governments, industry and non-governmental stakeholders, Health Canada developed proposed health-based CAAQS for PM and Ozone. An associated management system was developed that calls for increasingly stringent actions as pollutant levels approach the standard. The proposed CAAQS and management system will now go forward for consideration by the Canadian Council of Ministers of the Environment. The development of the CAAQS was strongly influenced by the Canadian Smog Science Assessment Highlights and Key Messages that was published by Environment Canada and Health Canada. Health risk assessments were initiated for other air pollutants (e.g. CO, SO2, NO2) to guide future development of new CAAQS.
Research was also conducted to improve understanding of the health impacts of outdoor air pollutants including, and analysis of the Canadian population's long-term exposure to criteria air pollutants and its impact on mortality and cancer incidence using the Canadian Census Cohort and income tax database.
Program Lessons Learned
The aim of the CAAQS is to drive continuous improvement in air quality and provide the basis for management of local air quality by provinces. In the longer-term, the CAAQS will be reviewed on a five-year cycle to decide if they should be made more stringent in an effort to drive further improvements in air quality and the associated health benefits.
CARA 5.1 - Indoor Air Quality Management - Radioactive Contaminants
Health Canada PAA 2.6.1 Radiation Protection
Program Description and Expected Achievements
In 2007, the federal government committed to develop a comprehensive agenda to address indoor air quality and health. A large number of air pollutants are found in Canadian homes, often at much higher levels than found outdoors. Poor indoor air quality is known to cause or exacerbate a wide range of health effects, such as asthma, allergies and other respiratory diseases, especially in sensitive populations such as children and those with pre-existing health conditions. Certain indoor pollutants are known or suspected carcinogens. Radon, which is a naturally occurring radioactive gas, is the second leading known cause of lung cancer, after smoking. Exposure to elevated levels of radon occurs primarily indoors and results in 1,900 deaths in Canada each year.
Further understanding of the health effects of indoor air contaminants, such as radon, is vital given that people spend 90% of their time indoors. People have significant individual control over their indoor air quality, through how a home is built or maintained, the products brought into the home and their activities indoors. Yet, they often lack the information needed to take steps to improve indoor air quality and protect their health.
Health Canada will focus on communicating solutions and developing resources to be made available to homeowners and builders with the intent to help Canadians reduce negative health impacts associated with indoor exposure to radioactive contaminants. The proposed activities will ensure the Government continues to build the comprehensive agenda required to address indoor air quality related to radioactive contaminants, and to improve the health of Canadians.
Health Canada expected achievements:
- Develop a communication plan and protocols to increase public awareness and education about radon;
- Strengthen Health Canada presence by making use of social media, conferences and events to disseminate information and distribute communication material;
- Develop a National Radon Awareness Campaign and continue with National Radon Program outreach activities;
- Coordinate testing of 2,000 federal buildings for radon to facilitate government compliance with the Canada Labour Code;
- Launch the Canadian Radon Certification Program; and
- Organize regional workshops and webinars to inform regional radiation specialists of the new certification.
Program Achievement / Performance Summary
Activities under Health Canada's communication plan included a proactive national media campaign, targeted stakeholder engagement, collaborative outreach programs, development of a radon web banner and use of social media such as tweets, attendance at home shows and stakeholder conferences across Canada. In addition, Health Canada's Radiation Protection Bureau hosted a web conference on radon reduction technologies, including information on related changes to the 2010 National Building Code.
Health Canada tested radon levels in approximately 2,000 high priority federal buildings in high-risk, radon-prone areas in 2011-12, and is currently on track towards meeting the target of testing 10,000 high priority buildings by the end of 2012-13. The Department also increased awareness of risks, health impacts and mitigation strategies related to indoor radon exposure. In support of the National Radon Awareness Campaign, radon brochure distribution increased by 15% and radon web activities and public inquiries increased between 5%-10% as compared to 2010-11. As part of the National Radon Program, all regions successfully engaged with stakeholder partners to deliver outreach activities, such as, community presentations and media events to encourage action to reduce radon exposure at home and at work. The department also published the Cross-Canada Survey of Radon Concentrations in Homes, which includes the results of a two-year study conducted by the Health Canada's National Radon Program.
Health Canada worked with the US-based National Environmental Health Association National Radon Proficiency Program (NEHA-NRPP) through a Memorandum of Understanding signed in the fall of 2011 to develop documentation, exams and training curricula needed to establish a new Canadian Radon Certification Program for radon professionals and analytical testing laboratories. Through presentations at the first annual CARST Conference, Health Canada communicated information on the new Program to national radon measurement and mitigation specialists and stakeholders.
Program Lessons Learned
Early engagement of other departments, provincial/territorial governments, and non-governmental organizations is important for implementing and coordinating public awareness and education outreach programs as well as ensuring efficient and effective support of the education and awareness activities.
CARA 5.2 - INDOOR AIR QUALITY MANAGEMENT - BIOLOGICAL AND CHEMICAL CONTAMINANTS
Health Canada PAA 2.3 Environmental Risks to Health
Program Description and Expected Achievements
Further understanding of the health impacts of exposure to indoor air contaminants is vital given that Canadians spend 90% of their time indoors. Individuals, with adequate knowledge and tools, can make substantial improvements to their indoor air quality. Program activities will support measures to reduce the health risks posed by indoor air contaminants, through the development of: guidelines and guidance documents; codes of practice; product standards; and communications products. The objective of these activities is to decrease risks to health. This objective is expected to be achieved through tools to improve indoor air quality, as well as promoting increased knowledge among individual Canadians, business and governments of the health risks posed by indoor air pollutants and the appropriate actions to reduce these risks.
Health Canada's expected achievements:
- Publication of residential indoor air quality guidelines for priority pollutants and technical documents addressing key indoor air sources or issues;
- Communications to raise awareness of health risks and to encourage adoption of risk management activities; and
- Assessment of interventions to improve indoor air quality and research on the exposure to and health impacts of indoor air pollutants.
Program Achievement / Performance Summary
Indoor air quality was a primary focus of Health Canada's Hazardcheck outreach campaign, which included videos, quizzes, and retail engagement events. A new Residential Indoor Air Quality Guideline for Toluene was issued and a proposed guideline for fine particulate matter (PM2.5) was published for public comment. A new methodology to more rapidly assess the health risks of volatile organic compounds found in indoor air was developed and health risk assessments for benzene, naphthalene and Legionella were finalized. An intervention study was conducted to determine health benefits from indoor air cleaners in a First Nations community. Health Canada also continued to publish results from a multi-year study on indoor air quality conducted in homes in Regina, Halifax, Edmonton and Ottawa (apartments).
Program Lessons Learned
Actions to address indoor air pollutants require support and cooperation from federal/provincial partners, industry stakeholders, NGOs and the general public. Ensuring early engagement of partners and stakeholders in the processes, including identification of priorities, and sharing of information, increases the success of any actions to improve indoor air quality.
Annex G: Health Canada Clean Air Agenda (CAA)
Adaptation Theme Performance Report (2011-12)
Health Canada Report on Activities under the CAA Adaptation Theme 2011-12
The Adaptation Theme supports critical complementary initiatives for adapting to the impacts of climate change. These initiatives seek to reduce risk to communities, infrastructure and the health and safety of Canadians, while also building capacity to adapt through planning and taking action.
Health Canada plans to address the health impacts of climate change by continuing to provide guidance and expert advice to public health and emergency management in development of heat alert and response systems, as well as training tools for health professionals to reduce the vulnerability of their community to extreme heat.
Health Canada also developed and delivers the Climate Change and Health Adaptation in Northern First Nations and Inuit Communities Program. The objectives of the program are to: (1) "Enable Northern First Nations and Inuit communities to identify and assess key vulnerabilities and health impacts related to climate change"; and (2) "Develop innovative and culturally sensitive human health risk management plans and tools to adapt to climate change".
ADAPTATION 1 - HEAT RESILIENCY PROGRAM
Health Canada PAA 2.3 Environmental Risks to health
Program Description and Expected Achievements
To support the Government's ongoing commitment to helping Canadians adapt to a changing climate and formulate guidance on adaptation measures to reduce potential risks to health and safety, Health Canada will enable individuals and communities to become resilient to extreme heat events by providing science-based information to health professionals, public health and emergency management institutions. Activities to support the delivery of this program include:
- Development of community-based heat alert and response systems in highly vulnerable regions and communities;
- Development and dissemination of health professional interventions and training, including guidance for healthcare workers on clinical diagnosis and interventions;
- Develop, in collaboration with key partners (i.e. Canadian Medical Association), accredited training materials for public health professionals;
- Guidelines and strategies for health professionals and emergency management on implementing Heat Alert and Response systems;
- Collaboration with key stakeholders and partners to assess and reduce vulnerabilities to extreme heat;
- Scientific research on health impacts of extreme heat to support evidence based decision-making.
Program Achievement / Performance Summary
The Heat Resiliency program achieved the following in 2011-12:
Increased awareness of risks (Intermediate Outcome)
- A series of webinars were held to inform public health and emergency management officials on research methods and best practices on adaptation to extreme heat; and
- Workshops on extreme heat and health were held in Toronto, Edmonton, Vancouver, and Montreal as well as collaborating with the Public Health Agency of Canada in its regional dialogues on climate change.
Increased availability/access to information and products (Immediate Outcome)
- Products were developed and released to support public health and emergency management decision-makers and health professionals address the health impacts of extreme heat. Three guidance documents were published:
- Clinical Guidelines for Health Care Workers;
- Heat-Health Communications Toolkit; and
- Guidelines for Conducting Vulnerability Assessments.
- The Best Practices Guide for developing heat alert and response systems (HARS) was completed but not released until early in the 2012-13 year.
- Produced, in partnership with The Weather Network and MétéoMédia, 14 vignettes (90 seconds in length) (7 English and 7 French) on heat and human health that were aired on both networks during summer 2011.
Tools, Processes, and Systems (Output)
- Successfully implemented pilot Heat Alert and Response Systems (HARS) in four Canadian communities (Fredericton, Windsor, Winnipeg, Assiniboine Regional Health Authority).
- Supported the expansion of the City of Windsor pilot HARS and the rest of Essex County, as well as the ongoing development of a province-wide HARS in Manitoba.
- Discussions were held with public health representatives in Saskatoon, Regina, Metro Vancouver and York Region about heat resiliency and the implementation of HARS.
Information, Decision-support tools and Training (Output)
- Initiated the development of heat and health accreditation course for health professionals.
Program Lessons Learned
Differences in the capacity of the four pilot communities resulted in each community progressing at different speeds during the development of their HARS. Cooperation with local public health and community/emergency social services was essential for the coordination of the HARS project.
ADAPTATION 2 - CLIMATE CHANGE AND HEALTH ADAPTATION PROGRAM IN NORTHERN FIRST NATIONS AND INUIT COMMUNITIES
Program Description and Expected Achievements
Health Canada's Program for Climate Change and Health Adaptation in Northern First Nations and Inuit Communities is unique among the adaptation programs in that it focuses on northern community adaptation and human health. Its purpose is to build capacity by funding community-based participatory research in cooperation with Aboriginal associations, academics, governments and agencies. This will enable communities to develop health-related adaptation plans and communication materials that will help in adaptation decision-making at the community, regional, national and circumpolar levels with respect to human health and a changing environment.
Since the launch of the Climate Change and Health Adaptation Program in 2008, Health Canada has funded 36 community-based projects across Canada's North that focus on relevant health issues caused by climate change. In addition, the program supported capacity-building workshops for northerners, as well as a Pan-Arctic Results workshop to bring communities together to showcase the results of their research.
Through these efforts, communities have increased their knowledge and understanding of the health effects related to climate change, and have developed local adaptation strategies. Examples include: numerous films and photo-voice products that engage youth and elders, which are available on the web; community-based ice monitoring, surveillance and communication networks; and information products on land, water and ice safety, drinking water and food security and safety, and traditional medicine.
The Climate Change and Health Adaptation Program has set a high standard with regard to program delivery and there is an expectation by Aboriginal organizations and northern communities to meet and exceed this standard. The program will continue to focus on building capacity, through various workshops, in order for northerners to gain the knowledge and experience needed to design, lead and implement community-driven climate change and health research projects. As well, the program will continue to promote the importance of this type of research both nationally and internationally, and continue to work with community partners to ensure that this program is continually meeting the needs of northern community members.
Program Achievement / Performance Summary
The Climate Change Program received Treasury Board approval in the Fall of 2011 and was not able to support any projects under the tight timelines. Therefore, the program transferred most of its grants and contributions to the 2012-13 funding year which the program felt would be more beneficial to the communities. The program achieved the following:
- Re-edited and distributed new 2012-13 Funding Application Guide;
- Released the Call for Proposals in October 2011;
- Worked with interested community members on proposal submission;
- Presented the program both nationally and internationally;
- Organized two Selection Committee meetings (a First Nations and an Inuit) to review proposals;
- Approved 15 community driven proposals for the 2012-13 funding year;
- Developed a website with the Institute for Circumpolar Health Research to share the results of community projects from 2008, Climate Telling; and
- Developed a Summary Report which will be distributed in the Fall of 2012.
Program Lessons Learned
The Climate Change and Health Adaptation Program, like any new program, has had its share of valuable lessons learned. The most valuable lesson of the last four years has been about how important it is to develop and maintain partnerships. This is a program for Northerners, and the program wishes to ensure that the final decisions on who receives funding should be decided by Northerners. Another valuable lesson is concerned with the essential aspect of engaging First Nations and Inuit at the community level in designing, evaluating and implementing climate change adaptation initiatives for their communities. For example, the First Nations and Inuit Selection Committee members have been essential in the success of the program. Not only do they provide essential expertise and advice while reviewing proposals, many of the members promote the program in their communities, in their region and abroad. The intention of the program is to support the many First Nations and Inuit voices in conducting climate change and health research.
The lessons learned have enabled many to gain knowledge and grow in a way to better meet the needs of Northerners in research. The program will continue to grow and will do so only with strong partnership, respect, and support.