
Archived - Evaluation of the Federal Tobacco Control Strategy 2012-2013 to 2015-2016
Download the alternative format
(PDF format, 867 K, 96 pages)
Organization: Health Canada
Date published: 2017-06-13
Prepared by Office of Audit and Evaluation
Health Canada and the Public Health Agency of Canada
January 2017
Table of Contents
- Executive Summary
- Management Response and Action Plan
- 1.0 Evaluation Purpose
- 2.0 Program Description
- 3.0 Evaluation Description
- 4.0 Findings
- 4.1 Relevance: Issue #1 – Continued Need for the Program
- 4.2 Relevance: Issue #2 – Alignment with Government Priorities
- 4.3 Relevance: Issue #3 – Alignment with Federal Roles and Responsibilities
- 4.4 Performance: Issue #4 – Achievement of Expected Outcomes (Effectiveness)
- 4.5 Performance: Issue #5 – Demonstration of Economy and Efficiency
- 5. Conclusions
- Appendix 1 – Logic Model
- Appendix 2 – Summary of Findings
- Appendix 3 – Evaluation Description
- Appendix 4 – Case Studies
List of Tables
- Table 1. Initial Funding by Partner Department/Agency
- Table 2. Partner Department/Agency engaged in each activity area
- Table 3. Limitations and Mitigation Strategies
- Table 4. Rates of Non-Compliance with Selected Provisions of the Tobacco Act/Regulations and Number of Samples Analyzed – Manufacturing/Importing Sector, 2012-2013 to 2015-2016
- Table 5. Rates of Non-Compliance with Selected Provisions of the Tobacco Act/Regulations and Inspections Conducted – Retail Sector, 2012-2013 to 2015-2016
- Table 6. Reports Reviewed Deemed Incomplete and Letters of Deficiency Issued – Manufacturing/Importing Sector 2012-2013 to 2015-2016
- Table 7. RCMP Seizure Data on Contraband Tobacco
- Table 8. Canada Border Services Agency Seizure Data on Contraband Tobacco
- Table 9. Post-Event Surveys
- Table 10. Allocations and Expenditures
- Table 11. Leveraged funds for PHAC Federal Tobacco Control Stategy projects
List of Figures
- Figure 1: Smoking Prevalence Rates in Canada
- Figure 2: Smoking prevalence in youth and young adults, 2001, 2012, 2013
- Figure 3: Smoking Prevalence 1999-2013 – Current Smokers Age 15+
List of Acronyms
- AMPS
- Akwesasne Mohawk Police Service
- APS
- Aboriginal Peoples Survey
- CBSA
- Canada Border Services Agency
- CCDP
- Centre for Chronic Disease Prevention
- CIPR
- Cigarette Ignition Propensity Regulations
- COPD
- Chronic obstructive pulmonary disease
- CPAB
- Communications and Public Affairs Branch
- CRA
- Canada Revenue Agency
- CTADS
- Canadian Tobacco, Alcohol and Drugs Survey
- CTUMS
- Canadian Tobacco Use Monitoring Survey
- FCTC
- Framework Convention on Tobacco Control
- FDA
- Food and Drug Administration
- FNIC
- First Nations and Inuit Component
- FNIHB
- First Nations and Inuit Health Branch
- FTCS
- Federal Tobacco Control Strategy
- HECSB
- Healthy Environment and Consumer Safety Branch
- IHGP
- International Health Grants Program
- INSPIRE
- Implementing a National Smoking Cessation Program in Respiratory and Diabetes Education Clinics
- MANTRA
- Manitoba Tobacco Reduction Alliance
- MOA
- Memorandum of agreement
- OIA
- Office of International Affairs
- PAA
- Program Alignment Architecture
- PHAC
- Public Health Agency of Canada
- PPSC
- Public Prosecution Services Canada
- RCMP
- Royal Canadian Mounted Police
- RHS
- Regional Health Survey
- RORB
- Regulatory Operations and Regions Branch
- TCD
- Tobacco Control Directorate
- TCLC
- Tobacco Control Liaison Committee
- TCP
- Tobacco Control Program
- TDL
- Tobacco Dealer Licensees
- TEACH
- Training Enhancement in Applied Cessation Counselling and Health
- TFI
- Tobacco Free Initiative
- TPLR
- Tobacco Products Labelling Regulation (Cigarettes and Little Cigars)
- WHO
- World Health Organization
Executive Summary
This evaluation covered the Federal Tobacco Control Strategy (FTCS) for the period from 2012-13 to 2015-16. The evaluation was undertaken in fulfillment of the requirements of the Financial Administration Act and the Treasury Board of Canada's Policy on Evaluation (2009).
Evaluation Purpose and Scope
The purpose of the evaluation was to assess the relevance and performance of the FTCS. The evaluation covered the activities of the current federal partners (Health Canada, Public Safety Canada, the Royal Canadian Mounted Police, Canada Revenue Agency (CRA), Canada Border Services Agency, and the Public Health Agency of Canada (PHAC)). The time-limited funding provided to the Public Prosecution Service of Canada in 2012-13 was not covered by this evaluation.
Program Description
The FTCS is a comprehensive horizontal strategy involving a variety of partner departments and agencies across the federal government to address tobacco control. Health Canada, as the lead department, is in charge of the majority of FTCS activities, and as such is responsible for regulating tobacco products, conducting compliance monitoring and enforcement activities with respect to the Tobacco Act, developing policy, conducting research, assisting with the health of First Nations and Inuit peoples, providing litigation support, supporting the pan-Canadian quitline, and ensuring that FTCS activities are aligned with federal health priorities. PHAC's key responsibilities are finding innovative ways to help people stop smoking and the strategic management of international issues. Three organizations within the Public Safety portfolio (Public Safety, Royal Canadian Mounted Police, Canada Border Services Agency) are responsible for activities related to the contraband tobacco market and provide information to the Department of Finance. Finally, CRA's key activity is ensuring compliance with the Excise Act, 2001.
Conclusions – Relevance
Continued Need
Our analysis concludes that there continues to be a need for tobacco control across Canada. Although smoking prevalence has declined in Canada, the most recent data from the Canadian Tobacco, Alcohol and Drug Use Survey (CTADS) 2013 shows that the overall smoking prevalence was 14.6%. This means that in 2013 there were approximately 4.2 million Canadians aged 15 and older who smoke. Higher smoking rates are reported in both Inuit and First Nations communities (on-reserve). In 2010, 43% of adults living in First Nations communities were daily smokers and 13.7% were occasional smokers. Data from the 2012 Aboriginal Peoples Survey indicate that 54.1% of Canada's Inuit population aged 19 years and older smoke daily and 9.1% smoke occasionally. Tobacco use continues to have a health impact on Canadians, with tobacco smoking playing a causal role in over 10 different cancers, cardiovascular disease, stroke and chronic obstructive pulmonary disease. The economic burden of smoking in Canada was estimated at over $18 billion annually in 2013.
Alignment with Government Priorities
Tobacco control issues are aligned with the federal government's priority to protect the health and safety of Canadians. The Minister of Health's mandate letter (2015) specified tobacco control through plain packaging as one of the top priorities. Tobacco is a risk factor for chronic disease, and as such fits within the PHAC priority of "leadership on health promotion and disease prevention". CRA actively ensures that federal taxes on domestic tobacco products are paid. Public Safety portfolio partners in the FTCS monitor and assess the contraband tobacco market, as it aligns with their priorities to address organized crime and smuggling. As well, Canada has international commitments and obligations, particularly pursuant to the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC).
Alignment with Federal Roles and Responsibilities
A clear federal role pertaining to tobacco control has been established in existing legislation, namely the Tobacco Act and the Excise Act, 2001. There are also roles in tobacco control for other levels of government within their respective jurisdictional mandates. Input from key informants was consistent in noting that stronger federal leadership – particularly on regulatory matters – would serve to enhance uniformity and provide a consistent level of protection across Canada.
Conclusions – Performance
Achievement of Expected Outcomes (Effectiveness)
In general, the FTCS is making progress in achieving its expected outcomes. The overall decline in smoking prevalence has slowed down, but the downward trend in prevalence has continued. There was no prevalence target set for the 2012-2017 time period of the FTCS, so it is difficult to measure the success of the strategy in this regard.
Compliance with existing regulations and provisions of the Tobacco Act and the Excise Act, 2001 has increased. This has been accomplished through the continued and consistent monitoring from Health Canada and the CRA.
The support to enhance the quitline cessation services has resulted in an increase in the number of smokers receiving help to quit smoking. As well, early indications from projects addressing cessation show that they are on track for success. However, the reach of these projects remains limited.
Prevention has been addressed through provisions made under the Tobacco Act and its regulations, including prohibiting sales to youth, health-related labelling requirements, tobacco promotion restrictions and flavour restrictions. Stakeholders reported that prevention activities have been undertaken by other levels of government, creating a patchwork of efforts.
Young people have been protected from inducements to take up tobacco use through ongoing monitoring of promotions to youth as well as bans on flavours that may appeal to youth. While flavour restrictions on certain tobacco products have had success in decreasing youth usage, there are some areas of the tobacco environment where the federal government has not appeared as responsive, including the increasing popularity of vaping products.
With regards to contraband tobacco, FTCS efforts are focussed on monitoring and assessing the illicit market. Reported seizures of contraband tobacco products have decreased; however, seizure rates are variable over short time intervals and the reason behind these declines is unclear. There continues to be a demand for a better national understanding of the contraband tobacco market from both governmental and non-governmental sources.
The FTCS has conducted the activities it set out to do within the time period evaluated, and with the funding allocation provided to FTCS partners. Some key informants felt that these activities were not ambitious enough. However, Canada's activities align with the main articles of the WHO FCTC and provide a multi-sectoral national approach to tobacco control.
Demonstration of Economy and Efficiency
Many activities funded through the FTCS derived success through collaboration and partnerships. In particular, PHAC-funded projects leveraged funds using multi-sectoral partnership. However, further engagement of external organizations and other levels of government would be useful in advancing Canada's tobacco control goals.
FTCS funding was reduced by approximately 35% from the previous 5-year period. Reduced funding and a focus on economy negatively impacted operational efficiency in some areas. This is most apparent in the FTCS's research and surveillance capacity, in which the annual tobacco use survey was changed to a biennial survey covering multiple topics including alcohol and illicit drugs.
Inefficiencies were noted when considering differences among the province and territories for areas of federal interest. Stakeholders reported that provinces and territories developed patchwork legislation respecting emerging issues in the absence of action at the federal level, creating inequity for Canadians. Further, separate funding agreements for quitline service allowed for dissimilar levels of service resulting in confusion for service providers.
All federal partners were aware of their specific areas of responsibilities and did not report duplication of efforts. However, it was not readily apparent that there were linked activities taking place across several strategy partners and the level of engagement of the partners varied. Meetings of the Coordinating Committees were infrequent and concerns were noted regarding delays in approving common reports.
Recommendations
The findings from this evaluation of the Federal Tobacco Control Strategy have resulted in the following four recommendations.
Recommendation 1
Explore the setting of targets for the reduction of smoking prevalence rates, both for the general population and populations with higher prevalence rates.
The lack of a reduction target for smoking prevalence in the 2012-2017 FTCS was seen by stakeholders as an impediment in measuring the overall success of the program and in focussing the activities of the FTCS on a unified goal. Canada was successful in reaching the targets set in early versions of the FTCS, and has a current prevalence rate of 14.6%. The WHO voluntary target prevalence is 10.57% for Canadians aged 15 years or older by the year 2025, and based on projections Canada is on track to meet this. Other countries similar to Canada have set specific national tobacco reduction targets that are more ambitious.
There have never been targets set for groups within Canada with higher prevalence rates. These rates have not decreased as quickly as the overall prevalence rates, and may need more directed efforts. Given Health Canada's mandate for health services and benefits for First Nations and Inuit populations, as well as the federal government's overall commitment for a relationship with Indigenous peoples, engage First Nations and Inuit leadership and communities to establish targets that are relevant and appropriate may focus Strategy activities and help define the future direction of the Strategy.
Recommendation 2
Clearly identify and articulate the areas for federal leadership in tobacco control, particularly in light of the existing provincial, territorial and municipal actions.
Tobacco control requires concerted efforts from multiple levels of governments across jurisdictions. Moving forward with the FTCS, it will be important for the federal government, in consultation with stakeholders and other levels of government, to clearly identify and articulate the regulatory and policy areas for federal leadership. This will assist stakeholders and other levels of government in understanding their role in regard to tobacco control.
While there have been calls for more national action in regard to tobacco control, the partner departments will need to examine the areas and populations that may benefit most from these actions. Opportunities for these national actions could be explored within the Strategy where feasible.
Recommendation 3
Options for regulating new and emerging tobacco control issues should be explored.
The tobacco industry is innovative, and often legislation and regulation lags behind new developments. Stakeholders suggested that there is a need for consistent federal regulations, and enforcement of these regulations, to protect the health of Canadians, and in particular youth. Moving forward, the federal government should encourage responsiveness to emerging tobacco products and ensure that the appropriate regulatory framework is in place and communicated to both industry and the public.
As new and emerging issues arise and regulation is required to address them, it will be important to explore innovative funding approaches to address tobacco control. These funding approaches could be based on international models, such as the imposition of a 'tobacco levy'.
Recommendation 4
Examine the feasibility of integrated reporting on aspects related to contraband tobacco to facilitate Canada-wide analysis.
The continued existence of the contraband tobacco market undermines tobacco control efforts across Canada. Multiple federal departments and agencies independently monitor different dimensions of contraband tobacco, as do other levels of governments and law enforcement agencies in Canada. In addition to government efforts, industry-sponsored organizations have also attempted to assess the scope and nature of the contraband tobacco market, in particular how it relates to youth. While the monitoring of contraband tobacco is widespread, there is little consistency on what is reported. It is beneficial for departments and agencies to be able to provide a comprehensive and integrated overview of the tobacco market, including trends. Given that there are multiple departments and agencies involved, each with their own data collection systems and internal reporting requirements, the compilation of contraband data may pose a challenge. At this time, the feasibility for integrating reporting should be explored, and where possible, a streamlined approach to reporting should be undertaken.
Management Response and Action Plan
| Recommendations | Response | Action Plan | Deliverables | Expected Completion Date | Accountability | Resources |
|---|---|---|---|---|---|---|
| Recommendation as stated in the evaluation report | Identify whether program management agrees, agrees with conditions, or disagrees with the recommendation, and why | Identify what action(s) program management will take to address the recommendation | Identify key deliverables | Identify timeline for implementation of each deliverable | Identify Senior Management and Executive (DG and ADM level) accountable for the implementation of each deliverable | Describe the human and/or financial resources required to complete recommendation, including the source of resources (additional vs. existing budget) |
| The Strategy should explore the setting of targets for the reduction of smoking prevalence rates, both for the general population and populations with higher prevalence rates. | Agree | Targets will be set for the reduction of smoking prevalence rates in the context of work undertaken for a renewed approach to tobacco control in Canada. | Report on consultations with stakeholders. | May 2017 |
|
|
| Report on sex, gender-based and socioeconomic analysis of tobacco use in Canada. | January 2017 | |||||
| New targets set in the renewed approach to tobacco control. | April 2018 | |||||
| Identify the areas for federal leadership in light of the existing Provincial/Territorial and Municipal actions in the area of tobacco control. | Agree | The Directorate will proceed with an assessment of the current federal role in tobacco control and explore new areas of responsibility and partnership in the context of work undertaken for a renewed approach to tobacco control in Canada. | Report on consultations with stakeholders, including provinces, territories and municipalities. | May 2017 |
|
3 FTEs (existing resources) |
| Federal role delineated in the renewed approach to tobacco control. | April 2018 | |||||
| Explore options for regulating new and emerging tobacco control issues. | Agree | TCD will continue to develop a new vaping regime. | Introduction of the new legislation. | Nov 2016 |
|
2 FTEs (existing resources) |
| Coming into force of a new vaping regime. | TBD | |||||
| Examine the feasibility of integrating reporting on issues related to contraband tobacco to provide a Canada-wide picture. |
|
|
Inventory of what is currently being reported and how. | January 2017 |
|
|
| Inventory of existing reports regarding contraband tobacco. | January 2017 | |||||
| Gap analysis of reporting that exists and what is required. | February 2017 | |||||
| Recommendation on integration of reporting on contraband tobacco. | April 2017 |
1.0 Evaluation Purpose
The purpose of the evaluation was to assess the relevance and performance of the Federal Tobacco Control Strategy (FTCS) for the period of April 2012 to March 2016. The evaluation was undertaken in fulfillment of the Financial Administration Act and the Treasury Board of Canada's Policy on Evaluation (2009). The evaluation was conducted by the Health Canada and the Public Health Agency of Canada's Office of Audit and Evaluation in accordance with the Five-Year Evaluation Plan 2015-2016 to 2019-2020.
2.0 Program Description
2.1 Program Context
The FTCS is a horizontal initiative led by Health Canada in partnership with PHAC; Public Safety Canada; the Royal Canadian Mounted Police (RCMP); Canada Border Services Agency (CBSA); CRA; and the Public Prosecutions Service of Canada (PPSC). As the activities of the PPSC pertaining to tobacco control involved time-limited funding, they are not included in the scope of the evaluation.
The FTCS was introduced in 2001 as a 10-year, comprehensive, sustained and integrated strategy to achieve significant reductions in disease and death due to tobacco. It built on the progress made under the 1997 Tobacco Control Initiative and the 1994 Tobacco Demand Reduction Strategy. In Budget 2012, the FTCS was renewed for an additional five years (2012-2017) with a goal to preserve the gains of the past decade in continuing the downward trend of smoking prevalence, and to invest in new priorities, including populations with higher smoking rates.
As part of Budget 2012, the FTCS was streamlined and refocussed on new priorities. This included funding new targeted activities, such as the implementation of a pan-Canadian Quitline; a marketing campaign for young adults; First Nations and Inuit initiatives; and, tobacco cessation interventions to support chronic disease prevention. Broad-based contribution funding for non-governmental organizations and provinces and territories ended, as did retail inspections for tobacco sales-to-youth. The drugs, alcohol and annual tobacco surveillance tools were combined into a single biennial survey.
Throughout the evaluation report, tobacco refers to commercial tobacco use. Traditional or sacred tobacco use among First Nations is separate, and the FTCS respects and recognizes traditional forms and uses of tobacco within communities.
All forms of tobacco are regulated under the Tobacco Act. At the time of this report, this does not include e-cigarettes or vaping. Electronic cigarettes that contain nicotine or come with health claims fall within the scope of the Food and Drugs Act and require market authorization by Health Canada prior to being imported, advertised or sold. No vaping devices or electronic cigarettes or other vaping devices with nicotine have been authorized by Health Canada.
2.2 Program Profile
The FTCS is a comprehensive strategy involving a variety of partner departments and agencies across the federal government.
| Partner Department/Agency | Funding (in $000) | Percentage of total 5 year funding (%) |
|---|---|---|
| Health Canada – excluding FNIHB | 160.6 | 70.3 |
| Health Canada – First Nations and Inuit Health Branch | 22 | 9.6 |
| Public Health Agency of Canada – Health Promotion and Chronic Disease Prevention Branch | 10.25 | 4.54 |
| Public Health Agency of Canada – Office of International Affairs for the Health Portfolio | 1.25 | 0.5 |
| Public Safety | 3 | 1.3 |
| Royal Canadian Mounted Police | 8.5 | 3.7 |
| Canada Border Services Agency | 18.4 | 8.1 |
| Canada Revenue Agency | 4.5 | 2.0 |
| Source: Refocusing the FTCS. Financial data provided by the Office of the Chief Financial Officer | ||
The FTCS funded activities and role of each of the partners is described below.
Health Canada
Health Canada is the lead department for the FTCS and has multiple branches engaged in tobacco control activities.
The Healthy Environments and Consumer Safety Branch (HECSB) is responsible for the regulation of tobacco and promoting initiatives to reduce and prevent the harm caused by tobacco. Within this branch, the Tobacco Control Directorate (TCD) is responsible for activities such as developing policies on tobacco control, developing and maintaining international agreements on tobacco control, developing regulations under the Tobacco Act, monitoring industry compliance with the Act and its regulations and undertaking enforcement activities, surveying, monitoring and analyzing tobacco issues, and supporting the pan-Canadian Quitline. Administrative, financial, and strategic support is also provided to address Health Canada's obligations resulting from tobacco litigation. Compliance monitoring and enforcement activities are done in conjunction with the Regulatory Operations and Regions Branch (RORB).
The First Nations and Inuit Health Branch (FNIHB) works in partnership with First Nations, Inuit, provinces, territories and other government departments to improve health outcomes and to improve access to quality health programs and services that are responsive to the needs of First Nations and Inuit individuals, families, and communities. The FNIHB is responsible for a new initiative funded by the FTCS to assist a targeted number of on-reserve First Nations and Inuit communities to develop and implement evidence-based tobacco control projects and strategies that are holistic, culturally appropriate, and focussed on reducing non-traditional tobacco use. The approach is guided by best practices as identified by the World Health Organization Framework Convention on Tobacco Control (WHO FCTC). The approach is organized around the four pillars of leadership, health promotion, cessation, and research and evaluation.
The Communications and Public Affairs Branch (CPAB) ensures that communications and citizen engagement activities are coordinated and align with federal health priorities. CPAB is responsible for Break It Off, a tobacco cessation marketing campaign targeting young adult smokers.
Public Health Agency of Canada
The mission of PHAC focuses on promoting and protecting the health of Canadians. PHAC's role and responsibilities as part of the FTCS centre on supporting innovative ways to help people stop smoking. Through the tobacco stream of the Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease approach, PHAC has provided FTCS funding to organizations that have developed innovative ways to increase smoking cessation. All four of the projects that received funding during the reporting period focus on smoking cessation, including building health professional capacity in cessation training and delivery, integrating cessation into clinical settings and combining smoking cessation at the community level, with an established learn-to-run exercise program.
The Office of International Affairs for the Health Portfolio (OIA) is responsible for the strategic management of international issues within Health Canada and PHAC, and provides advice and support to the Minister of Health. OIA facilitates Canada's membership in the WHO FCTC and provides advice to advance Canada's engagement on international tobacco control issues. OIA pays Canada's voluntary assessed contribution to the WHO FCTC via the International Health Grants Program (IHGP) for the Health Portfolio.Footnote i
Public Safety Canada
Under the FTCS, Public Safety monitors contraband tobacco activity and related crime in support of evidence-based policy development, including information and policy advice to Finance Canada on the state of the contraband tobacco market. Public Safety administers a contribution agreement with the Mohawk Council of Akwesasne to enhance capacity for First Nations policing to develop and share intelligence related to criminal activities related to contraband tobacco. FTCS contributions also fund an analyst position within the department for tobacco control activities.
Royal Canadian Mounted Police
The RCMP is responsible for the enforcement of laws within Canada related to the international movement of goods and has within its investigative mandate the illicit manufacture, distribution, or possession of contraband tobacco. Under the FTCS, the RCMP is responsible for monitoring and assessing the illicit market by way of analyst positions to capture and share intelligence about tobacco seizures and investigations of illicit tobacco activities. Funding is also used to improve border security in order to better detect and monitor illegal border intrusions. The RCMP also prepares an annual report on the contraband tobacco market, including national seizures and related trends, which is submitted to the Department of Finance and Health Canada.
Canada Border Services Agency
CBSA and the RCMP carry out the enforcement of the Customs Act and the Excise Act, 2001, which are the main enforcement tools in countering the various aspects of the illicit tobacco trade. With regards to tobacco control, the CBSA is primarily concerned with goods imported into Canada and the possession of products not properly reported, and monitors the domestic and international contraband tobacco market. It prepares regular assessments of the contraband tobacco market for the Department of Finance.
Canada Revenue Agency
CRA's main activity is to ensure compliance with the Excise Act, 2001, which governs federal taxation of tobacco products and regulates activities involving the manufacture, possession and sale of tobacco products in Canada. The agency undertakes regular audits and regulatory reviews of the tobacco manufacturers and tobacco dealers licensed under the Act. Funding from the FTCS has been used to allow for more audits and regulatory reviews, which includes visiting the operating premises of licensees to examine books and records. The CRA also ensures that the stamping and marking requirements of the Act are met.
2.3 Program Narrative
The FTCS provides a comprehensive approach to address tobacco control and aligns with the direction provided by the WHO and the international guidelines developed under the WHO FCTC.
The long-term expected outcome for the FTCS is a reduction in smoking prevalence among Canadians. In previous iterations of the Strategy, specific targets were set. The original goal of the FTCS set in 2001 was to reduce the smoking prevalence from the 1999 level of 25% to 20%. This was achieved by 2006.
Four main activity areas contribute to the achievement of outcomes: policy and international commitments; research and surveillance; regulations and compliance; and community interventions (prevention and cessation efforts). Partner departments and agencies contribute to different activity areas as outlined in Table 2.
| Activity Area | Partner Department/Agency |
|---|---|
| Policy and International Commitments |
|
| Research and Surveillance |
|
| Regulations and Compliance |
|
| Community Interventions (prevention and cessation efforts) |
|
The immediate outputs and outcomes resulting from these activity areas are: compliance with the Tobacco Act and its regulations; implementation of prevention strategies; development of interventions/policies/regulations responsive to the tobacco environment, including the intensity of contraband market; and enhancement of the public awareness of the health hazards of using tobacco products.
Tobacco control regulations are found in both the Tobacco Act and the Excise Act, 2001. Prevention strategies are focussed on limiting the inducements for youth and others to begin smoking. However, mass media prevention campaigns have not been funded by the FTCS since 2009. Various interventions, policies and regulations have been implemented that support the overall objectives of the FTCS and address the contraband tobacco market.
The intermediate outcomes for the FTCS are: improved understanding of the contraband tobacco market in Canada; young persons and others protected from inducements to use tobacco products and the consequent dependence on them; an increase in cessation behaviors among Quitline users, First Nations and Inuit, young adult smokers, participants of PHAC-funded projects (including health care professionals and tobacco users in clinical and community settings), and the broader population. An improved understanding of the contraband tobacco market will assist the federal government in addressing the concerns raised by access to and availability of contraband tobacco and the impact on legitimate business. Preventing youth from starting to smoke has been a goal of the Strategy for many years. This helps reduce dependency, as well as the health risks, associated with smoking. Along with prevention, cessation is an important aspect of the Strategy. Current smokers require support from a variety of interventions to help users quit smoking and reduce the number of Canadians who smoke.
The intended reach for the Strategy is all Canadians. More recently there has also been a targeted focus on youth, and First Nations and Inuit communities.
The connection between these activity areas and the expected outcomes is depicted in the logic model (see Appendix 1). The evaluation assessed the degree to which the defined outputs and outcomes were being achieved over the evaluation time-frame.
2.4 Program Alignment and Resources
Within Health Canada, the activities of the FTCS are located under the Strategic Objective of "Health risks and benefits associated with food, products, substances, and environmental factors are appropriately managed and communicated to Canadians". The specific sub-program of the Program Alignment Architecture (PAA) is 2.5.1 Tobacco. Activities related to the First Nations and Inuit component align with the Healthy Living sub-sub-program, under sub-program 3.1.1: First Nations and Inuit Health Promotion and Disease Prevention.
From a horizontal perspective, the FTCS is also aligned with:
- Sub-program 1.2.3, Chronic (non-communicable) Disease and Injury Prevention(PHAC's PAA);
- Program 1.3, Countering Crime (Public Safety's PAA);
- Program 1.1, Police Operations (RCMP's PAA);
- Program 1.3, Risk Assessment and Security (CBSA's PAA); and
- Program: Collections, Compliance and Verification (CRA's PAA).
In total, the FTCS had a budget of $230 million over five years.
3.0 Evaluation Description
3.1 Evaluation Scope, Approach and Design
The scope of the evaluation covered the period from April 1, 2012 to March 31, 2016, and included all activities of the federal partners, except for the PPSC as these were time-limited activities completed in 2012-13.
The evaluation aligns with the Treasury Board of Canada's Policy on Evaluation (2009) and considered the five core issues under the two themes of relevance and performance, as shown in Appendix 2. Corresponding to each of the core issues, specific questions were developed based on program considerations and these guided the evaluation process.
An outcome-based evaluation approach was used for the conduct of the evaluation to assess the progress made towards the achievement of the expected outcomes, whether there were any unintended consequences, and what lessons were learned.
The Treasury Board's Policy on Evaluation (2009) also guided the identification of the evaluation design and data collection methods, so that the evaluation would meet the objectives and requirements of the policy. A non-experimental design was used based on the Evaluation Framework document, which detailed the evaluation strategy for this program and provided consistency in the collection of data to support the evaluation.
Data for the evaluation was collected using various methods, which included: a literature review, a document review, a financial data review, a performance data review, key informant interviews, three case studies, and a media scan. More specific details on the data collection and analysis methods used are detailed in Appendix 2. In addition, data were analyzed by triangulating information gathered from the different methods listed above. The use of multiple lines of evidence and triangulation were intended to increase the reliability and credibility of the evaluation findings and conclusions.
An Evaluation Working Group comprised of representatives from the FTCS partner departments and agencies and led by Health Canada's Office of Audit and Evaluation, guided the evaluation. These representatives assisted in the data collection, and validation of findings and conclusions.
3.2 Limitations and Mitigation Strategies
Most evaluations face constraints that may have implications for the validity and reliability of evaluation findings and conclusions. The following table outlines the limitations encountered during this evaluation. Also noted are the mitigation strategies put in place to ensure that the evaluation findings can be used with confidence to guide program planning and decision making.
| Limitation | Impact | Mitigation Strategy |
|---|---|---|
| Key informant interviews are retrospective in nature. | Interviews are retrospective in nature, providing recent perspective on past events. This can impact validity of assessing activities or results that may have changed over time. |
|
| Financial data structure is not linked to outputs or outcomes. | There is a limited ability to quantitatively assess efficiency and economy. | Used other lines of evidence, including key informant interviews and document reviews, to qualitatively assess efficiency and economy. |
| Most recent prevalence data from 2015 was not available. | Limits the ability to assess smoking prevalence trends for the timespan of the evaluation. | Used most recent data available (2013) which, when triangulated with other lines of evidence, provided the best possible information on smoking prevalence trends. |
4.0 Findings
4.1 Relevance: Issue #1 – Continued Need for the Program
Although smoking prevalence has decreased over time to the 2013 level of 14.6%, the health impacts of tobacco use indicates a continued need for tobacco control to further reductions, particularly among at-risk populations.
Smoking prevalence in Canada has either decreased or remained constant every year it has been measured between 1985 (35%) and 2013 (14.6%).Endnote 1 Although the prevalence is lower than before, there are still 4.2 million Canadians over the age of 15 who report smoking either daily or occasionally. Smoking has considerable health impacts on those who smoke and those who are exposed to smoke, as well as a negative economic impact on all of Canada.
Tobacco use plays a causal role in over 10 different cancers (e.g., lung, mouth, stomach, liver) and is the primary cause of chronic obstructive pulmonary disease (COPD) – an inflammatory disease where the lungs are obstructed, making it difficult to breathe.Endnote 2 Many people who continue to smoke will die from smoking-related diseases. It is estimated that 23% of all deaths in Canada, and specifically, 31% of cancer-related deaths in 2010 were attributable to tobacco.Endnote 3 The direct costs (i.e., hospital care, drugs, physicians and other health care professionals, health research and other health care expenditures) and indirect costs (i.e., short- and long-term disability and premature mortality) of smoking in 2012 was estimated to be $18.4 billion.Endnote 4
The 2013 CTADS and the 2014-15 Canadian Student Tobacco, Alcohol and Drugs Survey (CSTADS) provide the most recent data available in regard to smoking prevalence in the ten provinces. Neither include data from the three territories. Despite the prohibition on furnishing tobacco to youth found in the Tobacco Act, in 2014-15, 3.4% of students in grades six to 12 (approximately 87,000 students) were current cigarette smokers, with 1.6% smoking daily and 1.9% smoking occasionally. As well, results from the 2013 CTADS indicated that 6.3% of youth between the ages of 15 and 17 reported smoking daily (2.3%) or occasionally (4%). The smoking rate increases to 17.7% for youth between 18 and 19 years of age with 9.6% smoking daily and 8.1% smoking occasionally. It is the change from the younger group to those 18 to 19 years olds that experienced the largest increase for both daily and occasional smokers.
First Nations communities (on-reserve) have a higher smoking rate than the general population of Canada. The most recent comparable data available comes from the 2008-2010 Regional Health Survey (RHS), the 2012 Aboriginal Peoples Survey (APS), the 2009 Canadian Tobacco Use Monitoring Survey (CTUMS) and the 2013 CTADS. It should be noted that data from CTUMS and CTADS does not include the Yukon, Northwest Territories and Nunavut. These regions contain the highest proportion of Canadians who identify as Aboriginal.Endnote 5 The RHS reported that 43% of adults living in First Nations communities were daily smokers and 13.7% were occasional smokers. Younger adults (age 18 to 29) in First Nations communities, however, had the highest proportion of daily smokers (51.5%) and occasional smokers (15.9%). The APS reported that 52.2% of Canada's Inuit population aged 15 years and older smoke daily and 9.4% smoke occasionally. In contrast, the 2009 CTUMS reported that 14% of Canadians aged 15+ were daily smokers and 4% were occasional smokers.
From a health equity perspective, it is concerning that the prevalence rate for the rest of Canada is dropping by a greater degree than that of First Nations communities, as seen in Figure 1. Comparing RHS data from 2002-2003 and CTUMS data from 2002 to the data from 2009, the proportion of daily smokers from First Nations communities dropped from 46% to 43% while the proportion of daily smokers surveyed through CTUMS dropped from 18% to 14%.
Figure 1: Smoking Prevalence Rates in Canada
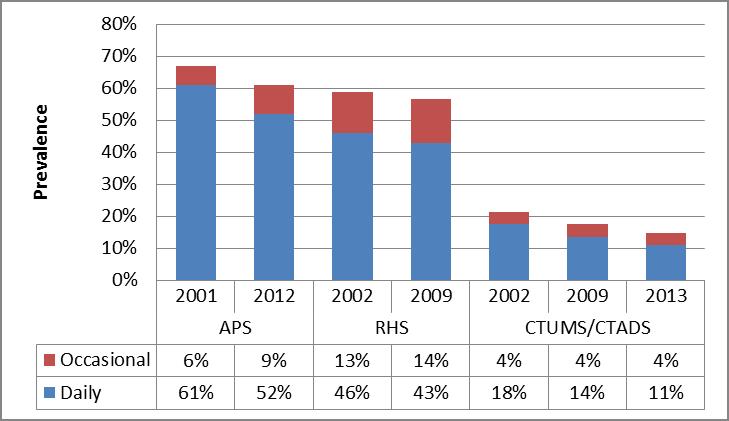
Figure 1 – Text description
This figure depicts a stacked bar graph showing the percentage of individuals who reported smoking daily and occasionally on the Aboriginal Peoples Survey (APS), the First Nations Regional Health Survey (RHS) and the Canadian Tobacco Use Monitoring Survey or Canadian Tobacco Alcohol and Drugs Survey (CTUMS/CTADS).
The following dates are listed along the x-axis: 2001 and 2012 for the APS, 2002 and 2009 for the RHS and 2002, 2009 and 2013 for the CTUMS/CTADS. The y-axis shows smoking prevalence in percentage with a scale from 0% to 80%.
The graph shows the following information for APS respondents. In 2001, 61% reported smoking daily and 6% reported smoking occasionally. In 2012, 52% reported smoking daily and 9% reported smoking occasionally.
The graph shows the following information for RHS respondents. In 2002, 46% reported smoking daily and 13% reported smoking occasionally. In 2009, 43% reported smoking daily and 14% reported smoking occasionally.
The graph shows the following information for CTUMS/CTADS respondents. In 2002, 18% reported smoking daily and 4% reported smoking occasionally. In 2009, 14% reported smoking daily and 4% reported smoking occasionally. In 2013, 11% reported smoking daily and 4% reported smoking occasionally.
Evidence suggests that individuals who stop smoking will improve their health, reduce their risk of chronic disease and increase their life expectancy.Endnote 6 Health Canada has compiled research on the benefits of quitting smoking. These include: within 8 hours of quitting, carbon dioxide levels in the blood return to normal; within 24 hours of quitting, the risk of heart attack is reduced; within 1 to 9 months of quitting, stronger lungs, improved breathing and less coughing occurs; after 1 year of quitting, the risk of coronary heart disease is reduced; and after 5 years of quitting, the risk of stroke is reduced to normal. It is estimated that smokers in Canada between the ages of 35 and 69 who died in 2010 lost an average of 24 years, and smokers over 69 years of age lost an average of 7 years of life.Endnote 7
Along with the health risks associated with tobacco, there are additional concerns related to contraband tobacco. Contraband tobacco has an impact on businesses (e.g., tobacco companies, convenience stores) who suffer the loss of sales of legal cigarettes, as well as a loss of revenue for the Government of Canada and the provinces and territories through taxation. Contraband tobacco is often sold in packaging that contravenes the Tobacco Act and does not provide health warning messages aimed at smokers and at rates that do not include all applicable taxes. The lower cost of contraband tobacco undermines the government approach to "…tax tobacco products at a high and sustainable level to discourage their consumption."Endnote 8 Contraband tobacco has also been linked to other illegal activities.Endnote 9
The general tobacco environment is fluid, with changes stemming from industry and public usage patterns. In addition to the ongoing activities the FTCS undertakes, it also has made efforts to anticipate and address future needs. These activities are necessary to be proactive, rather than reactive to change.
The FTCS has identified and addressed several anticipated needs. For example, PHAC's Grants and Contributions program, the Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease has provided funding to advance evidence-based, innovative projects that target tobacco cessation efforts, demonstrate measurable results and have the potential to be expanded across the country or to other target populations.
In addition, the Tobacco Control Program (TCP) has undertaken a national project-based planning approach to assess industry's business practices, identify areas of non-compliance and means to address changing industrial practices. The TCP has also initiated a program to identify and assess compliance of online retailers and the use of social media and smart phone applications for tobacco promotion.
One specific need identified for potential future involvement by the TCP and interviewees is the compliance and enforcement of vaping products. The TCP notes that in the future, it may be involved pan-regionally with compliance promotion activities and market intelligence gathering. However, at this point, vaping products do not fall under the purview of the FTCS.
The federal government has several on-going obligations related to tobacco control that they must continue to fulfill. Areas of core federal responsibility include the provision of health services and benefits to First Nations and Inuit populations, as well as addressing contraband and illicit trade. Surveillance, monitoring and enforcement of illicit tobacco activity are shared responsibilities between the federal agencies of the CBSA and the RCMP. The CBSA is responsible for all ports of entry and the RCMP is responsible for activity between the ports of entry and domestically. The federal government has a goal of achieving an increased level of health in Indigenous communities as outlined in the Federal Indian Health Policy (1979), and thus it is particularly concerned with the disproportionally high rate of smoking for First Nations and Inuit communities. The federal government is committed to providing financial resources to the provinces and territories to meet the additional demand for quitline services as a result of certain tobacco product packages featuring health warning messages that include a pan-Canadian Quitline phone number and web address as per the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars).
Finally, the federal government is obligated to undertake tobacco control activities as Party to the WHO FCTC, which Canada ratified in 2004. Countries that have ratified the WHO FCTC have committed to implementing strong tobacco control policies as a means of protecting the health of their populations. To advance the FCTC, the WHO has introduced a package of technical measures and resources to reflect and support the demand reduction provisions of the Framework. These measures include: monitoring tobacco use and prevention policies; protecting people from tobacco smoke; offering to help quit tobacco use; warning of the dangers to tobacco; enforcing bans on tobacco advertising, promotion, and sponsorship; maintaining effective tax rates on tobacco; and protecting public health policies from commercial and other vested interests of the tobacco industry. As Party to the WHO FCTC, Canada also participates in governing body meetings (i.e., Conferences of the Parties), reports biennially on compliance, and is a financial contributor through the Voluntary Assessed Contributions.
4.2 Relevance: Issue #2 – Alignment with Government Priorities
The objectives of the FTCS are aligned with the priorities of the FTCS federal partners and the broader federal government.
Since the renewal of the Federal Tobacco Control StrategyEndnote 10 in 2012, the strategy's objectives have been:
- preventing children and youth from starting to smoke;
- helping people to quit smoking;
- helping Canadians protect themselves from second-hand smoke; and,
- regulating the manufacture, sale, labeling and promotion of tobacco products by administering the Tobacco Act.
Federal budgets have included a focus on various aspects of tobacco control. For example:
- Budget 2014, Implementation of the RCMP Anti-Contraband Tobacco Force funded through internal reallocation.Endnote 11,Endnote 12,Endnote 13
- Budget 2014, Increase in tobacco rates to eliminate lower rate for domestic tobacco products for sale in duty free shop market.Endnote 14
- Budget 2013, Excise duty rate on "other manufactured tobacco" increased to be more consistent with the rate for cigarettes.Endnote 15
- Budget 2013, Enhancing the ability to combat contraband tobacco by providing funding to Public Safety for First Nations police services.Endnote 16
In 2015, the Prime Minister's Office's statement on National Non-Smoking Week noted the Government of Canada's commitment to "helping Canadians become and stay smoke-free" and that they are working with a range of partners to "educate Canadians about the dangers of smoking, help smokers quit, and discourage Canadians, especially young people, from starting to smoke".Endnote 17
The commitment to discourage Canadians from taking up smoking and to encourage smokers to quit was reinforced as a top priority in the Minister of Health Mandate Letter,Endnote 18 which instructed the Minister of Health to "introduce plain packaging requirements for tobacco products, similar to those in Australia and the United Kingdom." Further to this, the Minister of Health announced the launch of public consultations on tobacco plain packaging on May 31, 2016, which coincided with the WHO's World No Tobacco Day.Endnote 19,Endnote 20
One of the targets for the WHO's Sustainable Development Goals (Health) is to "strengthen the implementation of the WHO FCTC in all countries, as appropriate."Endnote 21 Meeting the goals of the FCTC and reporting to the Conference of the Parties have been key international commitments and obligations since Canada ratified the convention in 2004. Canada played a leadership role in the development of the Protocol on Illicit Trade in Tobacco Products in 2012 (the Protocol is not yet in force)Endnote 22 and in FCTC Guidelines for Implementation in 2014 (Articles 9 and 10 on the Regulation of Tobacco Products)Endnote 23 and recommendations (i.e., sustainable measures to strengthen the implementation of the Convention) developed under the FCTC.
Tobacco control related issues (e.g., plain packaging, health professional access to information, contraband tobacco, taxation) are a priority for all of the partner departments and agencies of the FTCS.
One of Health Canada's priorities is to "strengthen openness and transparency as modernization of health protection legislation, regulation and delivery continues"Endnote 24, and one of its strategic outcomes is that "health risks and benefits associated with food, products, substances, and environmental factors are appropriately managed and communicated to Canadians".Endnote 25 Health Canada also has Tobacco as one of the sub-programs in its PAA.
PHAC's strategic priority to provide "leadership on health promotion and disease prevention,"Endnote 26 is foundational to its focus on addressing risk factors, such as smoking, which have been shown to increase the potential for disease.Endnote 27 The Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease approach is captured under the Agency's Chronic (non-communicable) Disease and Injury sub-program. The multi-sectoral partnerships administer funding from sources including the FTCS and features population health approaches that address common risk and protective factors for chronic diseases, including smoking cessation. The multi-sectoral partnerships are based on the premise that no one sector alone can meaningfully address the causes of chronic disease, and that a wide range of partners are required to identify and generate sustainable solutions to improve the health of the population.Endnote 28
The CRA does not have a direct priority regarding tobacco; however, it is active in ensuring that taxes imposed on tobacco products under the Excise Act, 2001 are paid. The CRA also conducts compliance activities on domestic tobacco manufacturers, as per the Excise Tax Act, 2001Endnote 29 and works with stakeholders to ensure that tobacco control measures are effective.
Organizations within the Public Safety portfolio do not have priorities specific to tobacco, however, the Public Safety's strategic outcome is "A Safe and Resilient Canada"Endnote 30 which includes the sub-sub-program of Serious and Organized Crime. One of the foci of this sub-sub-program is contraband tobacco, a topic the former Minister of Public Safety raised in a number of news releases.Endnote 31,Endnote 32 As part of the Public Safety portfolio; the RCMP includes a focus on organized crime, as found in its organizational priority of Serious and Organized Crime,Endnote 33 and has an Anti-Contraband Force.Endnote 34 While the RCMP does not focus specifically on any commodity, the Federal Policing program targets organized crime groups and networks, which may be involved in the contraband tobacco market. Similarly, the CBSA priority of Secure the Border StrategicallyEndnote 35 includes a focus on the risk of contraband entering Canada. This risk is addressed by the CBSA's Intelligence sub-program which collects, analyses and shares intelligence with law enforcement partners, including intelligence on organized crime and smuggling.
4.3 Relevance: Issue #3 – Alignment with Federal Roles and Responsibilities
Tobacco control is a responsibility of the federal government, as well as other levels of government.
All levels of government play a role in tobacco control. The policy authority for the FTCS was renewed in 2012 for a period of five years (2012-2017), and aligns federal roles and responsibilities along four core functions: policy development and international commitments, research and surveillance, regulations and compliance, and community interventions (Appendix 1).
The FTCS funds activities that relate to the administration of the federal Tobacco Act, which emphasizes that "the health of Canadians needs to be protected in light of conclusive evidence implicating tobacco use in the incidence of numerous debilitating and fatal diseases." Among other considerations, this details a role for the federal government "to protect young persons and others from inducements to use tobacco products and the consequent dependence on them; to protect the health of young persons by restricting access to tobacco products; and, to enhance public awareness of the health hazards of using tobacco products."Endnote 36 The FTCS also funds activities that align with the federal Excise Act, 2001, which imposes federal excise duty on tobacco products and regulates the issuance of tobacco licenses to tobacco manufacturers and dealers; the stamping and marking of tobacco products; and, restrictions on the possession of tobacco products that are not stamped. In addition, the FTCS specifically funds the RCMP and CBSA to monitor the contraband tobacco products they seize as a result of exercising their role in enforcing federal laws, which is funded by monies outside of the FTCS.
At the international level, Canada is Party to the WHO FCTC.Endnote 37 The FTCS fully addresses Article 5 of the FCTC which mandates that "each Party shall develop, implement, periodically update and review comprehensive multi-sectoral national tobacco control strategies, plans and programmes in accordance with this Convention and the protocols to which it is a Party."Endnote 38 According to Health Canada's most current report to the Conference of the Parties on its implementation of the FCTC (April 2016), nearly all of the roles expected of Canada in controlling tobacco in a comprehensive manner have been implemented. However, a review of Health Canada's submitted reports shows that some specific FCTC-related expectations do remain unfulfilled. For example, a self-assessment revealed that Canada does not earmark any percentage of taxation income for funding the FTCS or tobacco control; does not prohibit the sales of tobacco products by minors; and does not prohibit the sale of tobacco products from vending machines.Endnote 39,Endnote 40 In support of Article 5.3, Health Canada's engagement with the tobacco industry is limited to instances where it is necessary to effectively regulate the industry and tobacco products. However, in a shadow report prepared by the Global Tobacco Forum, concerns were raised about the engagement of other departments, agencies or semi/quasi-public institutions with the tobacco industry. Instances of tobacco companies' donations to events and the inclusion of tobacco stocks into broader pension government of Canada do not align with the guideline recommendations of the FCTC.
Canada supports the Tobacco Free Initiative (TFI) under the Noncommunicable Diseases and Mental Health cluster of the WHO. The TFI strives to provide global policy leadership by encouraging mobilization at all levels of society. Canada has provided financial and technical expertise to activities carried out under this initiative.
Provincial, territorial and municipal governments continue to play an increasingly important role in advancing tobacco control. Stronger federal leadership would enhance uniformity and efficiency.
Provincial and municipal governments play an ever important role in advancing tobacco control.Endnote 41 All provinces and territories have tobacco control statutes in force, as well as strategies that vary in approach and focus to address smoking prevention, cessation, and to protect the public from the effects of second-hand smoke. Input from key informants was consistent in noting that stronger federal leadership – particularly on regulatory matters – would serve to enhance uniformity and provide a consistent level of protection across Canada. For example, some provincial health ministers, have noted that the lack of federal leadership on addressing menthol flavours in tobacco,Endnote 42,Endnote 43 and emerging issues such as vaping products, has led to a legislative patchwork of provincial actions. This was echoed by the majority of key informants. Since 2012, several provinces have passed and/or amended tobacco control laws to address matters that the federal government has not covered. The provinces of Alberta, New Brunswick, Nova Scotia, Québec and Ontario have amended their laws to add menthol to a list of banned flavours for tobacco products; meanwhile, British Columbia, Manitoba, Ontario, Québec, New Brunswick, Nova Scotia, and Prince Edward Island have started to address emerging issues like water pipes and vaping products. In some cases, the tobacco industry in Canada has taken issue with the provinces building upon gaps in federal legislation, and has filed lawsuits alleging in court documents that banning menthol in tobacco is outside a province's jurisdiction.Endnote 44,Endnote 45 In addition, the provinces continue to expand their legislative focus on defining smoke-free places to address matters related to second-hand smoke (e.g., patios, public housing and private motor vehicles with children present).
Provinces and Territories are also actively engaged in contraband tobacco issues. For over 30 years, the annual Interprovincial and Territorial Investigations Council Tobacco Workshop has brought together Provincial/Territorial and Federal partners involved in the enforcement of tobacco and tobacco products. The purpose of this workshop is to facilitate cooperation and the exchange of information necessary to combat contraband with a focus on interprovincial and international tax avoidance. The 2016 Workshop is co-hosted by the Ontario Ministry of Finance.
Building upon provincial legislationEndnote 46 and best practices,Endnote 47 municipalities in Ontario are attempting to further control tobacco and recover the cost of enforcement inspections through "Tobacco Retail Dealer's Permits". For example, the City of Ottawa administers a "Tobacco Vendor Licence" that is required for any business selling tobacco products, and the cost of this licence in 2016 is approximately $861 annually.Endnote 48 As one measure of impact, some merchants in Ottawa have publically noted that that the need for such a licence (as well as their increasing fees over time) is prompting them to reconsider the value of selling tobacco on their store shelves next to other alternatives.Endnote 49 Accordingly, the City of Ottawa has seen a significant reduction in the number of tobacco vendors, decreasing from approximately 800 in 2008 to 495 in 2016. The licensing fees collected by the City of Ottawa cannot yield any profits for the city, and are used to support the funding of necessary public health inspections, as well as to investigate tobacco control issues raised by the general public.
With funding from the Ontario Ministry of Health and Long-term Care, Canada's Non-Smokers Rights Association has developed and maintains a publically accessible database of smoke-free laws across Canada. A review of this database shows that between January 1, 2012 and April 30, 2016, approximately 115 municipalities across Canada passed and/or amended smoke-free restrictions at the local level. Furthermore, approximately 33% of these municipalities have passed and/or amended their by-laws to include a focus on vaping products.Endnote 50
4.4 Performance: Issue #4 – Achievement of Expected Outcomes (Effectiveness)
4.4.1 To what extent have the immediate outcomes been achieved?
Immediate outcome #1: Compliance with tobacco control regulations
Across Canada, the tobacco market has decreased its non-compliance with the provisions of both the Tobacco Act and the Excise Act, 2001. Continued and consistent monitoring from Health Canada and CRA has ensured low non-compliance.
The Tobacco Act regulates the manufacture, sale, labelling and promotion of tobacco products. Health Canada undertakes compliance promotion, compliance monitoring and enforcement in support of the Tobacco Act and its regulations. These compliance and enforcement activities address the manufacturing/importing sector, the retail sector and industry reporting. Overall, key informants felt that the constant and on-going monitoring was the main reason for the relatively low non-compliance rates with the Tobacco Act and its regulations.
In Canada, there are approximately 60 manufacturers and importers actively involved in the sale of tobacco products, with the majority located in Ontario and Quebec. For these manufacturers and importers the following measures are monitored for compliance:
- The cigarette ignition propensity standard, as set out in the Cigarette Ignition Propensity Regulations (CIPR);
- The prohibition on the use of certain additives in cigarettes, little cigars and blunt wraps, as per sections 5.1 and 5.2 of the Tobacco Act (Prohibited additives);
- The prohibition on promoting, by means of cigarette, little cigar and blunt wrap packaging, the presence of additives that cannot be in used in said products, as per section 23.1 of the Tobacco Act (Prohibition of Promotion of Banned Additives on Packaging);
- The minimum packaging requirements for cigarettes, little cigars and blunt wrapsFootnote ii, as per section 10.1 of the Tobacco Act (Minimum Packaging); and,
- The labelling requirements (specifically, health warnings, toxic emissions statements, and health information messages) as set out in the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) (TPLR).
- The reporting requirements (information on tobacco products including manufacturing procedures, sales, ingredients, research activities, emissions, constituents and promotional activities) as set out under the Tobacco Reporting Regulations.
Overall, the rate of non-compliance is very low, and there has been decreased non-compliance since 2012-13. The TPLR is the most recent regulation; it was adopted in September 2011. It was noted by internal key informants, that it generally takes two years for full compliance once new regulations come into force. In 2015-16, the compliance assessment of the Minimum Packaging regulations was targeted at little cigar packaging. The minimum packaging requirement for cigarettes has been in effect since 1997, and compliance was consistently at 100%.
| Provisions | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | ||||
|---|---|---|---|---|---|---|---|---|
| Number of Samples Analyzed | Non-Compliance Rate (%) | Number of Samples Analyzed | Non-Compliance Rate (%) | Number of Samples Analyzed | Non-Compliance Rate (%) | Number of Samples Analyzed | Non-Compliance Rate (%) | |
| Cigarette Ignition Propensity Regulations | 108 | 0% | 20 | 0% | 20 | 0% | 20 | 0% |
| Prohibited Additives | 60 | 0% | 318 | 0% | 197 | 0% | 100 | 0% |
| Prohibition of Promotion of Banned Additives on Packaging | 200 | 5% | 468 | 3% | 436 | 0% | 110 | 0% |
| Minimum Packaging | 200 | 5% | 262 | 3% | 247 | 0% | 79Table 4 note a | 0% |
| Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) | 211 | 35% | 488 | 21% | 457 | 9% | 382 | 4% |
Source: Annual Report on Compliance and Enforcement Activities (Tobacco Control) Table 4 notes
|
||||||||
In 2014-15, 20 warning letters were issued to manufacturers or importers. The most common reason for warning letters was alleged violations to labelling requirements. The increase in non-compliance with regards to promotion of banned additives on packaging is most likely due to the coming into force of new requirements for certain other types of cigars.
For retailers of tobacco products, Health Canada monitors the compliance with the following measures:
- Minimum packaging requirements;
- Prohibition of promotion of banned additives on packaging;
- Labelling requirements; and
- Prohibited promotional activities.
There are between 30,000 to 35,000 points of sale for tobacco products across Canada. Internal stakeholders noted that there are challenges with retail inspections in remote and rural areas, as the inspectors are based at the regional offices in urban centres. Inspections are conducted using a retail inspection model that incorporates several parameters, including number of retailers per region, relative distribution of urban versus rural retail locations, and a cyclical enforcement schedule of five to six years. In recent years, the number of inspections conducted at the retail level has declined. Some key informants reported concern that the current level of retail inspection coverage adequately covers the points of sale.
Monitoring of retailers on First Nations and Inuit communities is not consistently done across regions. However, inspectors are reaching out to retailers within First Nations and Inuit communities to increase awareness of, and compliance with, these regulations. Communities that are involved with the First Nations and Inuit component of the FTCS are supporting this through their own activities. Some communities are conducting their own monitoring activities and developing their own materials to support retailers in complying with the Tobacco Act. Details on inspections within First Nations and Inuit communities are not available at this time, and are not included in the calculation of compliance rates.
A retailer is identified as non-compliant if at least one case of non-compliance with a key measure is noted during an inspection. In 2014-15, enforcement actions included seizures at retail (216) and the issuing of warning letters (8). Letters may have made reference to a number of instances and/or type of non-compliance.
| Fiscal Year | Number of Inspections | Non-compliance Rate |
|---|---|---|
| 2012-13 | 9782 | 16% |
| 2013-14 | 7724 | 14% |
| 2014-15 | 6774 | 12% |
| 2015-16 | 6719 | 13% |
| Source: Annual Report on Compliance and Enforcement Activities (Tobacco Control) | ||
It is important to note that in fiscal year 2012-2013, Health Canada eliminated its retail inspections for the federal tobacco sales-to-youth provisions and financial support to 7 of the 10 provinces for similar activities. In a study published in 2014, Health Canada found that 85% of retailers refused to sell cigarettes to underage Canadians. This finding was statistically unchanged from 2009 (84%). Provincial key informants expressed disappointment that the federal government no longer conducts this inspection as it is a federal law. However, legal age for tobacco sales is also regulated at the provincial level. In 6 out of 10 provinces, the legal age is higher than the federal minimum age of 18.
The Tobacco Reporting Regulations requires tobacco manufacturers and importers to submit regular reports to the Minister of Health Canada that include sales data, manufacturing information, information on the ingredients used in their products, constituents and emissions information, as well as information on their research and promotional activities. The percentage of incomplete reports has declined since 2012-2013. In fiscal year 2015-2016, Health Canada reviewed 1485 reports from manufacturers and importers. Of the reports reviewed, 131 (8.8%) were determined to be incomplete, and a total of 58 letters of deficiency were issued. In a number of cases, one letter referred to more than one deficiency. Some cases are transferred to RORB for further enforcement actions.
| Fiscal Year | Number of reports reviewed | Number and Percentage of Reports Deemed Incomplete | Number of Letters of Deficiency sent |
|---|---|---|---|
| 2012-2013 | 1490 | 213 (14%) | 107 |
| 2013-2014 | 1186 | 139 (12%) | 108 |
| 2014-2015 | 1607 | 172 (11%) | 81 |
| 2015-2016 | 1485 | 131 (8.8%) | 58 |
| Source: Annual Report on Compliance and Enforcement Activities (Tobacco Control) | |||
Under the Excise Act, 2001, tobacco manufacturers and tobacco dealers are licensed by the CRA. Between 2012-13 and 2015-16 the number of tobacco manufacturer licensees across Canada has remained consistent at approximately 24. The number of tobacco dealer licensees (TDL) doubled from 5 TDL's in 2012-13 to 10 in 2015-16 and authorized premises for both tobacco manufacturers and dealers has increased from 45 to 48. CRA officials have unlimited and unannounced access to operating premises as a requirement of the tobacco license. CRA conducts both audits and regulatory reviews on an ongoing basis. In 2015-16, 13 audits and 208 regulatory reviews were completed with FTCS funding. This has maintained full coverage of licensees with an increased focus on specific regulations.
CRA conducts compliance activities on each tobacco licensee operating location numerous times a year (as a result of increased funding through the FTCS to the inspection program), and is permitted unfettered access as a condition of the license. There is a high rate of compliance amongst tobacco licensees with the provisions of the Excise Act, 2001. There were no reported instances of licenses being revoked between 2012-13 and 2015-16. Compliance activities have resulted in audit assessments and administrative penalties, but this has also declined from a high of 6 audit assessments totalling and $1.5 million in 2013-14. In 2015-16, compliance activities resulted in three audit assessments totaling $11,427. Frequent monitoring ensures that issues or concerns are caught and rectified quickly. Privacy provisions have limited the sharing of information on tobacco licensees between Health Canada and the CRA. This has not impacted the CRA inspections, but has created some barriers for Health Canada as the latter is not always aware of the status of tobacco licensees.
Tobacco sales create significant revenue for the federal government. Excise duty revenues from domestically manufactured tobacco products were $1.8B in 2014-15. This has increased by $300M since 2012-13, despite similar or lower actual sales. The increase was attributed to the increase in the rate of excise duty on cigarettes through Budget 2014.
Immediate outcome #2: Prevention strategies implemented
Prevention has been addressed through the Tobacco Act prohibiting sales to youth; prohibiting select additives; restricting tobacco promotion; and health warning labelling. Many stakeholders felt that prevention activities that have been undertaken by other levels of government have created a patchwork of efforts.
As most smokers begin smoking by age 19, the FTCS has focussed on the prevention of smoking initiation by youth.Endnote 51 Research has shown that it is more effective to prevent people from starting to smoke, rather than helping them to quit smoking, given the challenges with cessation and addiction.Endnote 52 This perspective was also supported by external stakeholders.
Specific prohibitions set out in the Tobacco Act and its regulations aim to prevent smoking initiation for youth by lessening the appeal of smoking. These include the restrictions of certain additives, such as flavours that make tobacco products more appealing to youth; the prohibition on the promotion of tobacco products that can be appealing to young persons, such as lifestyle advertising; the inclusion of pictorial health warnings that raise awareness of the risks of smoking; and, the prohibition on sales of tobacco products to young persons.
As mentioned previously, Health Canada no longer actively conducts retail inspections for the federal tobacco sales-to-youth provisions. A retail behavior study from 2014 showed that 85% of retailers refused to sell cigarettes to underage Canadians. In contrast, 34% of youth smokers who were too young to purchase cigarettes legally in their province of residence reported that they had purchased cigarettes from a regular legal source, such as a store.Endnote 53 Thirty-two percent of youth smokers obtained their cigarettes from a family member or friend.Endnote 54 Many key informants believe that youth begin smoking in their homes, and more prevention needs to be focussed on this area.
One of the six essential elements of the First Nations and Inuit component of the FTCS is prevention, which falls under the health promotion pillar. Under the essential element of prevention, communities are initiating activities with a strong focus on youth, including training youth as peer counsellors. Social marketing campaigns are aimed at preventing commercial tobacco use and misuse. Another common component of the prevention essential element is the support for smoke-free by-laws and the reduction of commercial tobacco use in homes (e.g., blue light competitions to identify smoke free spaces).
The majority of external stakeholders felt that the FTCS was not conducting any prevention strategies, and that the original iteration of the strategy (2001-2006) had been much more active in this regard. The prevention strategy examples provided by stakeholders were mass media focussed; they did not recognize the prevention efforts in regulations and legislation. It was felt that Canada was no longer a leader in national mass media prevention campaigns. The external stakeholders also felt that by limiting the prevention activities to regulations and legislation, there were no attempts to address the inequities in smoking prevalence across Canada. There was some concern that marginalized groups were not being impacted by prevention strategies. The original proposal for the marketing campaign within this round of the FTCS included youth prevention, along with cessation. However, due to limited funding, youth cessation became the sole objective of the campaign.
Other levels of governments have addressed smoking prevention through various strategies, such as the "Smoking, suffering, dying" awareness campaign in Quebec, and Smoke-Free Ontario. As these strategies are not consistent across the country, there is seen to be a patchwork of efforts that is causing inequity and inefficiencies.
Immediate outcome #3: Interventions/policies/regulations responsive to the tobacco environment including the intensity of contraband market
Partner departments and agencies, mainly Health Canada and Public Safety, have developed interventions, policies and regulations that are responsive to the tobacco environment. However, there are some areas of the tobacco environment, such as the increasing popularity of vaping products, where the federal government has not been as responsive as other levels of government to date.
Under the FTCS, Public Safety administers contribution funding to the Akwesasne Mohawk Police Service (AMPS) to undertake monitoring activities to determine the level of contraband activities in and around the Akwesasne Mohawk Territory. This territory straddles the borders of Ontario, Quebec and New York, and requires the cooperation and mutual support of multiple law enforcement agencies, at the local, regional, national and international levels. Over the period of this evaluation, the AMPS has continued to coordinate with multiple police services, and key informants recognized it as a best practice for law enforcement collaboration. Given the unique circumstances of its location, the AMPS has been asked to provide their expertise to other communities that require the integration of different levels of police servicing. AMPS's FTCS-funded activities have allowed the hiring of additional officers and increased resources to monitor and investigate contraband tobacco activities.
Over the past five years, the AMPS has seen a decrease in contraband seizures. However, key informants do not feel that there has been a decrease in contraband activities, as the mode of trafficking has shifted. There has been an increase in the trafficking of tobacco across water, rather than by land, due to the relocation of CBSA border inspections on Cornwall Island. The AMPS has limited capacity to conduct water-based activities.
Community leader involvement and awareness of the AMPS Joint Investigative Team (including members from other police services) activities were seen as beneficial to the continued success of the programs. Relationships developed through the FTCS-funded interventions have assisted in other areas of tobacco control. Overall, it is believed that these teams have worked well together and increased the visibility of efforts to be responsive to the contraband tobacco market in their jurisdiction.
The Tobacco Control Directorate has been responsive to the tobacco environment by developing and implementing internal policies, guidelines, procedures and tools to aid in the regulation of tobacco products and in the enforcement of provisions set out in the Tobacco Act and its regulations. Internal staff believe that their tools, policies and procedures were well documented and addressed all areas of the existing legislation and regulations.
There are other areas of the tobacco environment where stakeholders felt the government was not being responsive. The exclusion of menthol from the list of prohibited additives in the Cracking Down on Tobacco Marketing Aimed at Youth Act (2009) was mentioned by the majority of stakeholders as a gap in the legislation. There was also concern that the FTCS and Health Canada are not addressing vaping products. Vaping products in Canada are currently regulated under two acts. Vaping products containing nicotine or associated with a therapeutic claim are subject to the Food and Drugs Act and require authorization by Health Canada prior to sale based upon evidence of safety, efficacy and quality. As of September 2016, no vaping products have been authorized; nicotine-containing vaping products on the market are currently being sold illegally. Vaping products without nicotine and without therapeutic claims are legally available without authorization and are subject to the Canada Consumer Product Safety Act. However, stakeholders felt that there was not enough enforcement of current regulations and that the vaping products should be included under the activities of the Tobacco Control Directorate.
The Tobacco Control Directorate has undertaken researchEndnote 55 to better understand retailer behavior as it relates to youth access to vaping products (such as electronic cigarettes) and promotion. The research was conducted in 2015. Overall, 67% of retailers refused to sell electronic cigarette products to youth at retail locations across the country. The rate of refusal to sell was highest at grocery stores (77%), chain convenience stores (75%) and gas convenience stores (71%) and was the lowest when youth attempted to purchase at independent convenience stores (53%).Endnote 56 There are strict controls in Canada limiting tobacco display and tobacco access; these do not currently exist for vaping products. In 30% of the stores visited, there were internal store displays of vaping products, and in 6% of the stores, there was exterior advertising.
The federal government has not been as responsive to these issues as other jurisdictions, who have developed policies and legislation between 2012 and 2016 to address the existing gaps. Five provinces have enacted bans on the sale of menthol tobacco as of December 31, 2015. Some of these bans have been legally challenged by the tobacco industry. As of December 31, 2015, seven provinces have enacted legislation that addresses vaping products. These include prohibitions on vaping in shared public places, advertising and sales to youth.
Internationally, attention on tobacco control is moving towards alternative nicotine delivery devices (such as vaping products), which may transform the landscape. Canada lags behind the European Union and the United States for monitoring and control of these devices and other emerging tobacco products. Overall, stakeholders believe that the tobacco industry continues to be innovative and that the federal government needs to be more responsive, and timely, in addressing new and emerging issues.
Immediate outcome #4: Public awareness of the health hazards of using tobacco products is enhanced
Although health warning labels are effective in informing those that smoke about the health risks associated with tobacco use, there is a need to regularly rotate these messages.
The current set of health warning messages on packaging of cigarettes and little cigars have been in place since June 2012. The warning messages cover at least 75% of the front and back of packaging. These warning messages address some of the major risks associated with smoking and with second hand smoke, such as the risks of second-hand smoke exposure during pregnancy, as well as the risks to children's health.
A Health Canada survey in 2013 found that 79% of smokers looked at or read the health warning messages. This is an increase from 71% in 2012. In 2013, the majority of these smokers (86%) felt that the health warning messages provided important information, and 66% of smokers felt that the messages made smoking seem less attractive. This shows that, overall, the health warning messages have been effective in enhancing the awareness of current smokers on the risks associated with smoking. Research has shown that the labels need to change periodically in order to maintain effectiveness.Endnote 57 The WHO Article 11 Guidelines also support the frequent rotation of health warning messages, as the impact reduces over time. Canada has had the same labels since 2012.
While current smokers of cigarettes and little cigars reportEndnote 58 that health warning messages enhanced their awareness of the health hazards of using tobacco products, there is little available evidence of the awareness of non-smokers on the health hazards of using tobacco. The FTCS does not have any activities that are targeted at the awareness of current non-smokers.
4.4.2 To what extent have the intermediate outcomes been achieved?
Intermediate outcome #1: Improved understanding of the contraband tobacco market in Canada
Contraband tobacco jeopardizes public safety and undermines public health efforts to control tobacco in a comprehensive manner. While the RCMP, CBSA and Health Canada all independently monitor different dimensions of contraband tobacco, there continues to be a demand for a consolidated understanding the contraband tobacco market.
Contraband tobacco refers to any tobacco product that does not comply with federal and provincial laws, which can include matters related to: importation/exportation, marking, transportation, storage, manufacturing, stamping and the payment of duties and taxes. According to the RCMP there are four main sources of contraband tobacco in Canada: illegal manufacturers making unlicensed and unregulated products in Canada; counterfeit products entering the country often by way of sea containers or cross-border smuggling; tax-exempt diversions from First Nations communities; and, other illegal forms like the reselling of legal tobacco products obtained through theft.
Contraband tobacco is illegal, and it impacts public safety and public health. In a public safety context, the RCMP reports that organized crime groups are involved in the production, distribution, smuggling and trafficking of contraband tobacco.Endnote 59 Further, the threat of money laundering from illegal tobacco activities has been rated as very high, due to the sophistication level of organized crime groups involved in the trade. The central role played by organized crime in the contraband tobacco trade in Canada links this illegal activity with other kinds of crime; as most of the organized crime groups across the country involved in the illicit tobacco market are also active in other forms of criminality.Endnote 60 From a public health context, Health Canada reports that "smoking contraband cigarettes poses the same risk of harmful health effects as smoking legal cigarettes […] and contraband cigarettes are often sold in packaging that does not provide information required by current regulations, including: illustrated health warnings and toxic emissions information".Endnote 61 In presentations to the Standing Committee on Justice and Human Rights, the National Coalition Against Contraband Tobacco, as well as the Ontario Korean Businessmen's Association, further highlight that contraband tobacco has a negative impact on good government and public health controls, as its alleged availability in clear plastic bags on street corners undermines youth access restrictions that legitimate merchants uphold in accordance with the law.Endnote 62 In addition, contraband tobacco products can be purchased on the black market for much less than legitimate products that feature a stamp or tear tape indicating that the manufacturer has paid applicable taxes and duties, and the lower prices that result due to tax avoidance can undermine a leading theory of change that notes demand for tobacco best decreases as tobacco prices and taxes increase.Endnote 63,Endnote 64
Within the federal government, the RCMP, CBSA and Health Canada all independently monitor different dimensions of the contraband tobacco market. Monitoring efforts by Health Canada have focussed on surveying the purchasing patterns of people primarily between the ages of 15 to 24, and asking them to self-identify whether they have made efforts to purchase cigarettes at a cheaper cost. Among other questions,Endnote 65 CTADS asks people to self-identify whether they have purchased smuggled cigarettes, and/or cigarettes from a First Nations Reserve. According to the most current (2013) survey results available in the public domain, approximately 10% of Canadian smokers purchased illegal cigarettes from a First Nations Reserve, while two percent reported they purchased cigarettes that may have been smuggled.Endnote 66 The issue of tobacco as it relates to First Nations is complex, sensitive, and has many dimensions, including traditional vs commercial use and contraband tobacco.Endnote 67 According to the RCMP, in many cases organized crime networks operate in Aboriginal communities, often exploiting the politically sensitive relationship between those communities and various governments and enforcement agencies.Endnote 68 To address the contraband dimension in First Nations communities, the FTCS provides monies to Public Safety, who in turn allocates monies as a grant and contribution to the Akwesasne Partnership Initiative, which involves an effort by the AMPS. Key informants, as well as a recent Public Safety evaluation on the Akwesasne Partnership Initiative, note that funding has increased the capacity of the AMPS to perform intelligence-gathering activities and support other provincial, national and international law enforcement agencies on investigations and anti-contraband operations in the Akwesasne region. A key informant with the AMPS further notes that FTCS support over the past four years has been helpful in building collaborative networks to address organized crime elements, and at the same time support police work with aboriginal youth in guiding them away from a life of crime.
Monitoring efforts by the RCMP and CBSA have focussed on seizure rates, which result from their enforcement activities that are funded outside the FTCS. Monitoring data is independently reported to other federal departments, such as Finance Canada, who report using the data as one factor of consideration in the setting of tobacco taxation rates. Data on seizure rates, as well as the quantity of contraband goods seized, are highly variable over time. As shown in Table 7 and Table 8, while there is variation in how seizure data is recorded and presented by the RCMP and CBSA, the number of seizures recorded by both the RCMP and CBSA has shown a general downward trend between the years 2012 and 2015. The quantity of goods seized (in terms of weight or counts), however, does not necessarily follow a downward trend during the same period of time. Key informants have noted that this pattern may be attributed to the RCMP and CBSA refocusing their risk assessments and attentions on higher profile suspects and organized criminals, rather than specific commodities like tobacco.
| Seizure | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|
| # of seizures | 431 | 209 | 223 | 145 |
| # of cartons/bags of cigarettes seized | 356,000 | 101,000 | 94,000 | 24,700 |
| Quantity of fine-cut tobacco seized (kg) | 33,000 | 32,000 | 55,400 | 40,400 |
| Source: Compiled from RCMP FTCS Performance Reporting Templates | ||||
| Seizure* | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|
| # of seizures | 2,377 | 2,285 | 2,077 | 1,763 |
| Cigarettes (cartons) | 20,094 | 65,867 | 17,696 | 26,300 |
| Cigars (kg) | 138 | 143 | 777 | 1,953 |
| Manufactured tobacco (kg) | 148,378 | 221,903 | 71,392 | 50,331 |
| Other tobaccoTable 8 footnote a (kg) | 2,471 | 1,463 | 2,175 | 9,225 |
| The accuracy of the CBSA tobacco statistics is limited and depends on the consistent input by Border Services Officers when electronically recording seizures as well as the system's ability to record a consistent unit of measure | ||||
|
||||
| Source: Compiled from CBSA FTCS Performance Reporting Templates | ||||
All federal partners engaged in monitoring contraband tobacco felt that their roles were clear and the data they provide was useful. However, gaps do exist in the collating of contraband statistics across Canada. While not an express requirement of the FTCS to provide consolidated reporting, there continues to be a demand for Canada-wide aggregate data on the contraband tobacco market. For example, the Strategic Level Forum established in 2014 following a horizontal evaluation by Public Safety on Measures to Address Contraband Tobacco, has inferred that investments made in federal monitoring efforts conducted since 2012 have not been fully effective in achieving their intended outcomes. The Forum has expressed a need to improve understanding of the contraband tobacco market by conducting an environmental scan of the various federal efforts and their impact on the market."Endnote 69 The call for an environmental scan may stem in part from the observation that there is no integrated roll-up of all the contraband statistics collected by the federal government, or a comprehensive roll-up of the contraband statistics collected by other levels of governments and law enforcement agencies in Canada (e.g., Sûreté du Québec; Ontario Provincial Police).
In addition to government efforts, industry sponsored organizations (e.g., National Coalition Against Contraband Tobacco) have also attempted to specifically assess the contraband tobacco market as it relates to youth by analyzing the character of discarded cigarette butts on or near school campuses. While key informants recognize that industry-sponsored organizations have a self-serving bias to favour their economic interests over public-focussed considerations, all approaches to calculating clandestine activities are viewed to contain various methodological merits and limitations. For example, while the unobtrusive collection of discarded cigarette butts on campus grounds has the advantage of overcoming the potential under-estimation of contraband use that may occur when participants are asked to self-report an illegal behavior, there are some limitations to this approach. First, this approach estimates the proportion of cigarettes that are contraband, but not the proportion of individuals using contraband tobacco. Similarly, identification of contraband tobacco is restricted to what can be determined from visual inspection. Some forms of contraband tobacco (e.g., smuggled brand-name cigarettes and counterfeit cigarettes) cannot be readily identified through the process of examining discarded cigarette butts. Cigarette butts from First Nations tobacco products can be reliably identified, but are contraband only if the manufacture or sale of these cigarettes violates government regulations.Endnote 70 In sum, it warrants consideration that any attempt to monitor contraband tobacco in a strategic fashion be equally comprehensive and multi-disciplinary.
Intermediate outcome #2: Young persons protected from inducement to use tobacco products and the consequent dependence on them
Young people have been protected through ongoing monitoring of promotion to youth, as well as bans on flavours that may appeal to youth
As stated in Strong Foundation, Renewed Focus - An Overview of Canada's Federal Tobacco Control Strategy 2012-17, the FTCS continues to focus on preventing children and youth from starting to smoke. As part of this focus, emphasis is placed on limiting the tobacco industry's ability to market tobacco products to youth. In 2013, 11% of youth aged 15-19 and 18% of young adults aged 20-24 were current smokers (daily or occasional), compared to 22% of youth aged 15-19 and 32% of young adults aged 20-24 in 2001.Endnote 71 In 2014-15, 82% of Canadian students in grades 6-12 had never tried smoking.Endnote 72. This is an increase from 74% in 2010-11 and 76% in 2012-13.
Figure 2: Smoking prevalence in youth and young adults, 2001, 2012, 2013
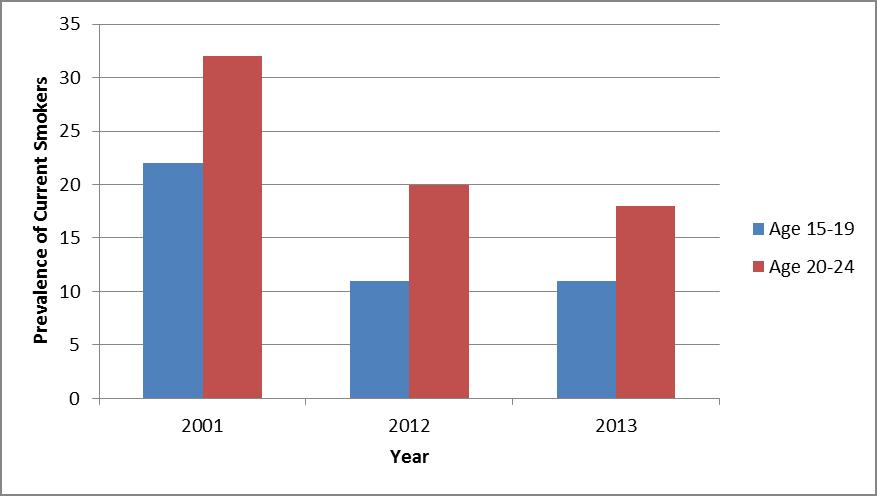
Figure 2 – Text description
This figure depicts a bar graph showing the percentage of individuals aged 15 to 19 and aged 20 to 24 who were smokers in the years 2001, 2012 and 2013.
The following dates are listed along the x-axis: 2001, 2012 and 2013. The y-axis shows the prevalence of current smokers in percentage with a scale from 0% to 35%.
The graph shows in 2001, 22% of those aged 15 to 19 smoked and 32% of those aged 20 to 24 smoked. In 2012, 11% of those aged 15 to 19 smoked and 20% of those aged 20 to 24 smoked. In 2013, 11% of those aged 15 to 19 smoked and 18% of those aged 20 to 24 smoked.
Source: Canadian Tobacco Use Monitoring Survey, 2012,Endnote 73 Canadian Tobacco Alcohol and Drugs Survey, 2013Endnote 74
Since the renewal of the FTCS in 2012, the federal government has implemented further legislation to help protect youth from inducements to use tobacco products. With the Cracking Down on Tobacco Marketing Aimed at Youth Act, which amended the Tobacco Act in 2009, Canada became the first country in the world to ban the use of certain additives in cigarettes, little cigars (weighing 1.4 grams or less), and blunt wraps. The prevalence of youth smoking of these tobacco products, decreased from 8% in 2009 to 4% in 2013.Endnote 75 The tobacco industry subsequently marketed cigar types that were heavier than 1.4 grams, effectively circumventing the flavour restrictions. On December 14, 2015, the Order Amending the Schedule to the Tobacco Act came into force, prohibiting the manufacture and sale of certain types of cigars (other cigars") that contain certain additives, such as flavours that appeal to youth. The packaging and sale of these products are also prohibited where their packaging suggests, including through illustrations, that they contain a prohibited additive.
Gaps in federal legislation were identified as a concern by some key informants, such as on the exemption on the use of mentholin tobacco products. Despite evidence that youth are more likely to startEndnote 76,Endnote 77 or continueEndnote 78,Endnote 79 smoking using mentholated tobacco products, as of September 2016 menthol remains exempt from the Tobacco Act. Many provinces and territories have implemented tobacco control legislation to fill these types of gaps in federal legislation and to try, in part, to prevent youth from starting smoking and to protect them from inducements to use tobacco products. Of students in grades 6-12 who had used any tobacco product in the past 30 days, 70% had used a flavoured product.Endnote 80
On April 29, 2016, the Minister of Health announced consultations on planned amendments to restrict the use of menthol in tobacco products. As stated in the news release, Despite success in reducing smoking rates among youth to a record low, recent data points to a spike in sales of menthol products and illustrates that youth smoke menthol cigarettes. This research supports restrictions on flavoured tobacco, including those with menthol, in order to reduce their appeal to youth". Endnote 81
Concerns were raised by internal key informants about how the tobacco industry bypasses regulations on promotions to youth through the use of internet-based promotions, including through social media (e.g., Facebook, YouTube). Health Canada began inspections of Canadian-based websites in 2015-16 to address this concern, but this can be difficult as promotions can disappear quickly from the internet, and some social media promotions are only available in private groups. Another challenge regarding the compliance and enforcement of online promotion of tobacco products is that the internet has changed beyond what could have been foreseen when the Tobacco Act came into force in 1997. At that time, for example, there were no online stores, nor social media, and as one key informant noted, the internet was seen as an extension of publications. The significant and frequent changes in the internet since 1997 make it challenging for legislation such as the Tobacco Act to keep pace.
While vaping and vaping products were not included in the 2012-17 FTCS, interviewees emphasized that it is now considered to be an important emerging issue in the area of tobacco control, particularly among youth. Vaping and vaping products are not regulated under the Tobacco Act. Key informants noted that the use of vaping products among youth has been associated with higher odds of smoking, that they do not discourage teenagers from smoking conventional cigarettes, and that they may encourage cigarette use,Endnote 82 and vice versa.Endnote 83 Exposure to advertisements for vaping products has been linked to higher odds of the use of these products among youth.Endnote 84 In addition, a recent study of grade nine students in the Niagara region of Ontario found that use of vaping products was common among the group studied. This study also found that many of the students used vaping products because they are seen as 'cool/fun/new'.Endnote 85
A Health Canada studyFootnote iii conducted in 2015 examined the willingness of retailers to sell vaping products to youth, and also looked at the placement, accessibility and promotion of vaping products in retail stores.Endnote 86 At the time of the study only a few provinces (i.e., New Brunswick, Nova Scotia) had restrictions on vaping products (e.g., accessibility, advertising). The study showed that 62% of retailers had vaping products placed within sight of the point of sale, but were inaccessible to the customer. Vaping products were out of sight in 19% of retail outlets, but 15% of the outlets visited had a self-service display at the point of sale. It was noted that the willingness of the retailer to sell vaping products to youth was higher when there was interior advertising (45%), promotions (18%) or exterior advertising (8%) present.
Water pipes (e.g., shisha, hookah) were another issue not included in the 2012-17 FTCS. Since the implementation of this strategy, some provinces have enacted legislation regarding water pipes. As mentioned by a number of key informants, the Tobacco Act does not address water pipes or the type of tobacco that goes into water pipes. It was also noted that water pipe use is on the rise in Canada, including among youth. Data from CTUMS and CTADS showed that in 2006, the first time the question was asked, 4% of Canadians age 15 and older reported having ever tried a water pipe", which increased to 8% in 2011, and 10% in 2012 and 2013. Less than 1% of Canadians reported using a water pipe in the past 30 days in 2011, the first year this question was asked, as well as in 2012 and 2013. However 3% of youth aged 15-19 and 4% of young adults also reported smoking a water pipe in the past 30 days in each of these years.Endnote 87,Endnote 88 While the prevalence of water pipe use is not as high as that of other tobacco and smoking products, this is an area that could deserve further attention.
Intermediate outcome #3: Increased cessation behavior among participants in FTCS-funded interventions
Since the renewal of the FTCS, funding has been provided through Health Canada and PHAC to a number of programs with the objective of increasing cessation behavior. The Pan-Canadian Quitline Initiative has resulted in an increase in the number of smokers receiving help to quit smoking. Some of the other initiatives receiving FTCS funding are aimed directly at the individual smoker, while others focus on training health care providers to assist their clients to quit smoking.
Quitline
A significant increase in the number of people calling quitlines in Canada was observed after the 2012 implementation of the pan-Canadian toll-free number that routes callers to their provincial or territorial quitline. A quarter of surveyed callers to the pan-Canadian Quitline reported having quit smoking or reduced their use of tobacco products.
A key feature of the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) Endnote 89 was the requirement for the display of a pan-Canadian toll-free quitline number and cessation web portal as part of the health warning messages and health information messages on packages. Callers to the pan-Canadian toll-free quitline number are redirected to the existing cessation services provided by the provinces and territories. In 2011-2012, Health Canada negotiated memoranda of agreement (MOAs) with each province and territory to reimburse jurisdictions for the cost associated with the increased service generated as a result of the new labelling regulations. According to the MOAs, provinces and territories committed to participate in an evaluation of this initiative. Five service providers cover all of the provinces and territories. Sykes Assistance Services provides quitline services to British Columbia, Northwest Territories and Nunavut. The Canadian Cancer Society covers Ontario, Manitoba, Saskatchewan, Nova Scotia, New Brunswick, Prince Edward Island and the Yukon. The remaining provinces are covered by provincial services or associations.
The Evaluation of the Pan-Canadian Toll-free Quitline InitiativeEndnote 90 examined the change resulting from the appearance of the pan-Canadian toll-free number on certain tobacco products starting in 2012. The evaluation found that the number of calls to Canadian quitlines increased significantly after the introduction of the toll-free number on packages of cigarettes and little cigars. There were 104,043 calls to Canadian quitlines in the three years after the introduction of the pan-Canadian toll-free number in 2012, compared to 61,157 calls to provincial quitlines in the three preceding years. The largest increase was in 2012, and has declined each year but remains higher than the baseline year of 2011. An initial increase in calls and decline to a level higher than the baseline was observed in other countries examined as part of the Evaluation of the Pan-Canadian Toll-free Quitline Initiative.
In Canada, the quitline users tend to more intense smokers, as measured by the number of cigarettes smoked daily, and the time to first cigarette. Almost 40% of quitline users smoked their first cigarette of the day within 5 minutes of waking up as compared to just over 20% of the comparable population of Canadian smokers.
As part of the evaluation, quitline clients were interviewed seven months and 18 months after initial contact. Out of the 5,366 respondents to the seven-month interview, 26% reported that they had been smoke-free for at least 30 days, and 29% reported having not smoked in the past seven days. These results are consistent with results from American quitline services and higher than the 30-day quit rates usually found in the general population. The evaluation also showed that those who had not quit smoking at time of the seven-month follow-up survey had changed their smoking behavior and 91% had taken actions towards quitting. At the seven-month follow-up, the percentage of heavy smokers decreased from 33% to 19%. In addition, the percentage of smokers who took their first cigarette within 5 minutes of waking decreased from 41% to 30%, which is an indicator of increased success in quitting smoking.Endnote 91Out of the 1,132 follow-up interviews at the 18-month follow-up survey,Footnote iv 79% of those who had quit smoking at the seven-month period remained smoke-free, and 64% of respondents had not smoked at all in the past 12 months. The evaluation determined that 15% of surveyed callers were able to remain smoke-free for a period of 12 months or more.
Data from the 2013 CTADS showed that 5.6% of smokers who had tried to quit in the past year, and those who had quit in the past two years, had used a telephone quitline. While not a large percentage, the results are comparable to those from the United States and other countries.Endnote 92 However, as discussed in the Evaluation of the Pan-Canadian Toll-free Quitline Initiative,Endnote 93 the demand for the quitline in Canada is not as high as in the United States of America. In Canada, the quitline was used by less than 1% of all smokers. In 2012, this was equal to 61 calls per 10,000 smokers. In the U.S., quitlines received 259 calls per 10,000 smokers in the same time period. There are many factors which may explain the increased reach, such as: most state run quitlines offer free cessation medication; overall spending on promotion and outreach is over 10 times more per smoker in the United States as compared to Canada; and the quitlines are a focal point for state-level tobacco control. The effectiveness of cessation counselling increase in association with cessation medication, and the combination of counselling and medication is seen as a standard in the FCTC. None of the Canadian quitlines provide free cessation medication, and no provinces require the use of the quitlines to access free or reduced cost cessation medications.
Break It Off campaign - Young Adult Smokers
The Break It Off campaign, an activity targeting young adult smokers and funded by the FTCS, found that approximately three-quarters of participants considered quitting.
According to the 2013 CTADS data, smoking prevalence among young adults aged 20-24 (18%) was higher compared to smoking prevalence in youth aged 15-19 (11%) and adults aged 25 and older (15%).Endnote 94 While this is a significant decrease from the smoking prevalence of 32% among young adults in 2001Endnote 95 it was still emphasized as a concerning trend in the 2012-17 FTCS.
A case study of the Break It Off campaign was conducted to examine its innovative approach to smoking cessation in greater detail. The Break It Off campaign was first launched by the Canadian Cancer Society in January 2012, with funding from Health Canada's previous iteration of the FTCS. This campaign was aimed at young adults aged 20-24, and piloted solutions to provide cessation support through digital and online services such as social media and a smartphone application. The project was then licenced by Health Canada and funded from April 2012 to March 2016.
A number of changes to the Break It Off campaign were made and presented in early 2014, as the program became a hybrid digital and in-person marketing campaign. The primary marketing tactic was in-person engagement events on university and college campuses and outdoor high traffic locations, to encouraging young adult smokers (aged 20-24) to participate in a dialogue on tobacco cessation while promoting the resources available on the website (breakitoff.ca) and the Break It Off mobile application.
The Break It Off campaign had two key outcomes: increased awareness of the health hazards of smoking and the benefits of quitting among target populations; and, changes in attitude toward quitting (such as increased motivation to quit) among those exposed to campaign materials.
Between January 2014 and March 2015, 92 events were held across Canada. 47,000 visits were made to the campaign website, and there were 1,335 downloads of the Break It Off application. From April 2015 to August 2015, another 41 events were held across Canada, with 57,848 interactions at these events, and 3,250 participants in the Break it Off video contest. There were also 22,238 visits to the Break it Off website, and 2,130 downloads of the application. Data on actual quit rates was not collected. The results from the post-event surveys showed that the majority of respondents agreed that the information received motivated them to consider quitting smoking (Table 9).
| Jan 2014-March 2015 | April-May 2015 | June-August 2015 | |
|---|---|---|---|
| Number of post-event surveys completed | 764 | 491 | 279 |
| Agreed that information at events motivated them to consider quitting | 73% | 78% | 75% |
| Agreed that information on website motivated them to consider quitting | 78% | 82% | 88% |
A number of social media outreach events were held to promote Break It Off, including a Twitter campaign (June 29 to August 2 2015), Google AdWords and YouTube pre-roll advertising (July 7 to August 2 2015), and a selfie-hashtag" contest on Instagram and Twitter in the summer of 2015. The Twitter campaign had over 1.4 million impressionsFootnote v and 8,000 clicks through 34 promoted Tweets, and there were over 575,000 impressions through the Google AdWords and YouTube promotions.
Among key informants interviewed, there was positive reaction to the in-person interactions, the stand-alone campaign website and the mobile application. However, the lack of social media marketing and outreach was criticized by some stakeholders. While the campaign initially conceived by the Canadian Cancer Society was primarily a social media campaign with broad engagement and reach to youth, this was not continued to the same extent with Health Canada. This was due to challenges related to government restrictions on social media. This reduction of social media engagement was believed to be a missed opportunity for Health Canada to deepen the reach of the campaign, and some key informants felt that an increased social media component to the campaign would have expanded the campaign's reach and impact.
PHAC project participants
Activities funded through PHAC's multi-sectoral partnership approach showed participants quitting or intending to quit.
The use of collaborative approaches in public health issues is useful in maximizing the resources and skills of the different partners.Endnote 96 While challenges can be expected when different organizations work together toward a common objective, research on other public- private partnerships, as well as interviews with key informants, identified many benefits, such as being able to reach a larger and more diverse target audience (individuals, organizations, sectors and communities); and through partnership agreements mechanisms, improved cross-sector engagement and accountability.Endnote 97
Since 2013, PHAC's Centre for Chronic Disease Prevention (CCDP) has invited organizations to submit applications for the funding of tobacco control projects if they meet the criteria of the Multi-Sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease initiative. This funding opportunity differs from others as it supports projects involving both public and private organizations and has a continuous intake, allowing for ongoing partnership and partner development. Importantly, it has a pay-for-performance model, whereby payments are tied to specified and agreed-upon measurable outputs and outcomes.Endnote 98 As of March 2016, there are four multi-sectoral projects which have received over $8 million FTCS funding through PHAC.
The Canadian Network for Respiratory Care (CNRC) received funding from PHAC for Enhancing the Capacity of Health care Professionals to Integrate Evidence-Based Smoking Cessation Interventions project. This project provides health care professionals with Certified Tobacco Educator training and certification in order to increase their capacity to provide clients with cessation information. Of the participating health care professionals surveyed, 88% (n=62) reported a change in tobacco cessation practice following their training and certification and another 92% (n=54) reported more successful quits (i.e., quit for longer periods of time) by their patients.
The Implementing a National Smoking Cessation Program in Respiratory and Diabetes Education Clinics (INSPIRE) project expands the Ottawa Model for Smoking Cessation into respiratory and diabetes education clinics across Canada. An early evaluation of the program found that 67% of participants (n=296) reported reductions in the number of cigarettes smoked at thirty days, 24% of participants (n= 231) reported being smoke-free at thirty days, and 18% reported being smoke-free at six months (n=138).
The Manitoba Tobacco Reduction Alliance (MANTRA; Building and Enhancing the Tobacco Cessation Capacity of Health Professional Interveners) developed a licenced program that trained front-line health practitioners in the Training Enhancement in Applied Cessation Counselling and Health (TEACH) program and expanded this program into cancer treatment centres in Manitoba. MANTRA partnered with a number of organizations, including the province of Manitoba, health care associations and foundations. Early results from this project reported that the short-term output of 20 health care professionals receiving facilitator training has been exceeded.
One of the evaluation case studies (see Appendix 4) examined the Run to Quit program, which aims to help participants stop smoking while learning to run, either through in-person clinics at Running Room locations, or online. The program was first conceived and developed by the Canadian Cancer Society who contacted the Running Room in order to bring together their expertise and resources. Run to Quit combines the Canadian Cancer Society's ten week cessation curriculum with the Running Room's Learn to Run curriculum.
The present Run to Quit program has three registration options: an in-store training program, an online training program, and the Commit to Quit, self-directed program. Both the in-store and online training programs are 10-weeks long and include a progressive training program on how to walk and/or run from a Running Room coach, guidance on how to quit smoking, as well as support calls from a Quit Coach from the participating provincial/territorial quitlines. The self-directed program has no registration fees, but does not include some of the services offered through the other options, such as coach support, and coupons for nicotine replacement therapy. All participants receive the Canadian Cancer Society self-help booklet, are guided to the telephone and web quitlines available to them, and can receive support and information through social media (Facebook, Twitter, and YouTube). All participants can qualify for prizesFootnote vi by completing the program, a 5km run/walk event, and proving they are smoke-free by a specified date, as assessed by cotinine testing.
The program launched in 2016, and the first in-store and virtual training programs, as well as the Break Free 5 km Run/Walk event was completed by July 2016. The program is expected to increase the number of Running Room locations holding the in-store training program to 50 locations in 10 provinces in 2017, and to all 110 (as of July 2015) Running Room locations by 2018. The first round of Run to Quit had a total of 1,079 participants online (virtual training, n=72; Commit to Quit, n=830) and at 21 Running Room locations (n=177). The number of registrants was significantly less than the target number of 5,775 registrations in 2016. A reason given for the lower than expected number of registrations in 2016 was the relatively short time between when the funding was approved and the launch of the program. The Run to Quit team has already conducted surveys with Run to Quit partners and with smokers who did not register for the programs to identify challenges and opportunities from the first year of the program in order to increase registrations in second and third years.
Partners in the Run to Quit initiative felt that there were advantages to the multi-sectoral approach, such as PHAC's involvement and official endorsement which increased the program's credibility, the increased ability to reach other potential partners, and that PHAC's funding allowed the Canadian Cancer Society and Running Room to bring attention to and implement the program across the country more easily. PHAC also benefited from the Run to Quit partnership, for example, the considerable positive media attention paid to the program resulted in an enhancement of the PHAC brand, including how it is able to be seen as a partner, not just the sole voice regarding public health.
While still in the initial stages, some funded projects through the First Nations and Inuit Component of the FTCS have had successes in increasing cessation behavior.Footnote vii
Cessation is one of the four pillars of tobacco control that were required to be addressed by projects to be funded by the First Nations and Inuit Component (FNIC) of the FTCS. Further detail on the FNIC is included in a detailed case study in Appendix 4. Although all successfully funded projects included activities under this pillar, the degree to which cessation was addressed varied by project and by community. Stakeholders described participation in cessation activities as variable depending on a community's stage of readiness for intervention. They noted that flexibility to choose which tobacco control pillar a community's activities are focussed on is important. Some communities (those with higher prevalence rates) may need to focus on prevention and educational awareness to denormalize tobacco use before there is an uptake in cessation activities. First Nations stakeholders also spoke to the importance of cessation activities clearly targeting commercial tobacco and ensuring traditional tobacco use is considered sacred.
FNIC-funded projects have undertaken a broad range of cessation activities including social- media campaigns, television commercials, cessation training and facilitating access to smoking cessation aids, tools and resources. The FNIC has also worked with local authorities to develop or enhance policies (e.g., adopting or increasing the number of smoke-free spaces in public areas) which decrease smoking prevalence. In 2015-16, the number of outdoor smoke-free spaces in participating communities tripled, and the number of indoor smoke-free spaces more than doubled from 2014-15.
Cessation components offered through the FNIC brought in many participants and increased participation in cessation activities. In the first full year of the FNIC, over 3000 people participated in a smoking cessation program or intervention and 35.7% of these participants completed the intervention. This was seen as moderately successful.Endnote 99 The First Nations Health Authority in British Columbia has also noted a 25% increase in the use of tobacco cessation aids funded through the supplementary health benefits from 2014-15 to 2015-16. Program representatives link this change to increased awareness in the availability of cessation aids through the tobacco control strategy.
4.4.3 To what extent has the longer term outcome been achieved?
Longer term outcome: Reduction in smoking prevalence among Canadians
Smoking prevalence continues to decline, however the decline has slowed in recent years. Canada remains comparable to other developed countries; however these countries have set ambitious future targets.
Smoking prevalence (daily and occasional use) in 2013 in Canada among those 15 and older is lower than the prevalence of many comparable developed countries. Canada's smoking prevalence was 14.6%, compared to 17% in New Zealand, 18% in the United States, and 20% in the United Kingdom (WHO Global Health Observatory data repository).Endnote 100Footnote viii
The prevalence of smokers (daily and occasional use) in Canada among those aged 15 and above has decreased from 25% in 1999 to 14.6% in 2013. While there has been a significant decrease in prevalence in the years since the FTCS was initiated, a number of key informants noted that the decrease has slowed in recent years. The previous FTCS had set a target of reducing smoking prevalence from 19% in 2006 to 12% by 2011, but the 2012- 2017 FTCS included no specific goal to reach in the five-year period. Some key informants mentioned the need for an end game, or a long-term target, and suggested that the target should be ambitious (e.g., 5% by 2035).
In 2013, under a United Nations mandate of reducing preventable premature mortality from non-communicable diseases, the World Health Assembly established a global voluntary tobacco use reduction target. This target was one of nine voluntary global targets agreed on as part of the WHO Global Monitoring Framework for Non-Communicable Diseases. It was endorsed, in 2014, at the Sixth Session of the Conference of the Parties to the WHO Framework Convention on Tobacco Control in Moscow. Using 2010 smoking prevalence levels as a baseline, WHO member states will attempt to reduce tobacco use by a relative 30%, by 2025, in their populations aged 15 years or older. For Canada, this target represents a reduction from 17% smoking prevalence in 2010 to 10.57% in 2025. An analysis of national survey data estimating country-level probabilities of achieving tobacco smoking targets has revealed that Canada is on track to achieve the targets both for men and for women. Endnote 101
Internationally, many countries have set targets that are more ambitious than the WHO's global reduction target. For example:
- The United States has an objective of reducing smoking by 40% from their 2008 baseline by 2020.Endnote 102
- Australia set a target of reducing the national smoking prevalence among adults to 10% or less, and to halve the adult smoking prevalence among Aboriginal and Torres Strait Islanders by 2018.Endnote 103
- New Zealand set a target of Smokefree 2025".Endnote 104
Several key informants discussed the difficulty of reducing smoking prevalence, as it is likely that a certain percentage of the general population will never be able to stop smoking. It was noted that it gets more expensive and more difficult to reduce smoking prevalence past a certain point, so there is a need to develop more innovative approaches to smoking cessation and prevention.
Figure 3: Smoking Prevalence 1999-2013 – Current Smokers Age 15+
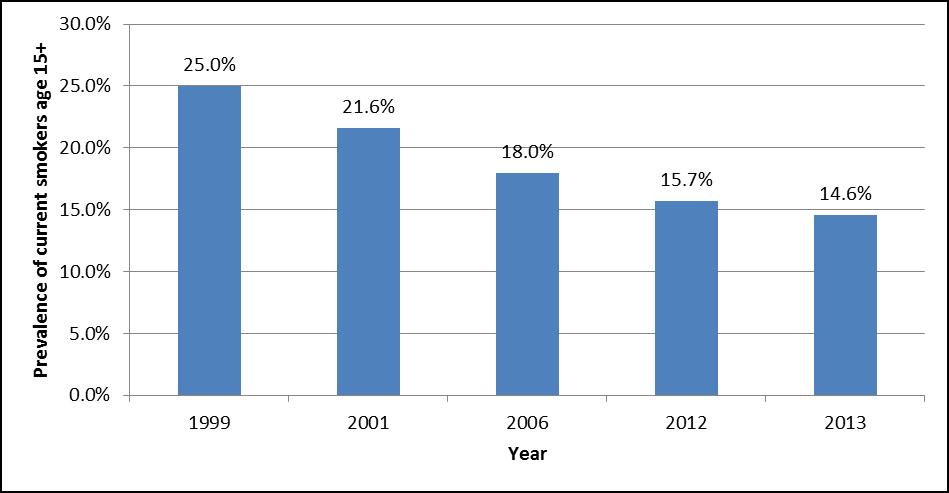
Figure 3 – Text description
This figure depicts a bar graph showing the percentage of individuals aged 15 and older who reported being smokers in the years 1999, 2001, 2006, 2012 and 2013.
The following dates are listed along the x-axis: 1999, 2001, 2006, 2012 and 2013. The y-axis shows the prevalence of current smokers in percentage with a scale from 0% to 30%.
The graph shows the following prevalence rates: 25% in 1999, 21.6% in 2001, 18% in 2006, 15.7% in 2012 and 14.6% in 2013.
Source: Canadian Tobacco Use Monitoring Survey, 1999, 2001, 2006, 2012, Canadian Tobacco Alcohol and Drugs Survey, 2013
Note: 'Current smokers' includes daily smokers and non-daily smokers (also known as occasional smokers)
The smoking rate for Canadian youth has decreased significantly since 2010-2011. The 2014-15 Canadian Student Tobacco, Alcohol and Drugs Survey indicated that youth in grades 6 to 12 were less likely to report being a current smoker (3%) in 2014-2015 than in 2012-13 (4%). This follows another significant decrease from 6% in 2010-11. A greater proportion of these youth also reported that they have never tried smoking (82% in 2014-2015 vs. 76% in 2012-13). Further, a significant decrease from 28% in 2012-13 to 23% in 2014-15 was also noted for these youth when considering if they had ever used any type of tobacco product.
4.5 Performance: Issue #5 – Demonstration of Economy and Efficiency
The Treasury Board of Canada's Policy on Evaluation (2009) and guidance document, Assessing Program Resource Utilization When Evaluating Federal Programs (2013), defines the demonstration of economy and efficiency as an assessment of resource utilization in relation to the production of outputs and progress toward expected outcomes. This assessment is based on the assumption that departments have standardized performance measurement systems and that financial systems link information about program costs to specific inputs, activities, outputs and expected results.
The data structure of the detailed financial information provided for the FTCS did not facilitate the assessment of whether program outputs were produced efficiently, or whether expected outcomes were produced economically. Specifically, the lack of output/outcome-specific costing data limited the ability to use cost-comparative approaches. In terms of assessing economy, challenges in tracking funding within the broader program envelope limited the assessment. Considering these issues, the evaluation provided observations on economy and efficiency based on findings from the literature review, key informant interviews and available relevant financial data.
Funding
The total allocation for the FTCS for the years 2012-2013 to 2016-2017 was $230 million. Given the focussed approach of the renewed strategy as part of Budget 2012, there was a decrease of $158.7 million in total allocation from the 2006-2007 to 2010-2011 iteration. At the end of 2012-2013, funding to the Public Prosecutions Service was eliminated to enhance compliance with the Excise Act, 2001 by using fine collections.
Across the strategy, there was $24.1 million in unused funding in the first three years. This lapsed funding represents 10% of the total allocated funds or 18% of the allocated funds that were expected to have been used to date. The full allocations and expenditures by federal partners are provided in Table 10. Notes from yearly reports provided to the Treasury Board Secretariat suggest that the lapsed funding is a result of the following: funds received late (Health Canada), delays in launching programs (Health Canada, PHAC), delays resulting from time required to negotiate with partners (PHAC), lower than anticipated funding requirements for litigation and the pan-Canadian quitline (Health Canada), and internal reallocation of resources to address contraband (RCMP). Public Safety exceeded their allocation during the first year of the new Strategy. Additional resources were spent in both salary and operational costs. This was not repeated in the other years.
For those areas within the Health Portfolio that received grants and contribution funding (Health Canada-FNIHB, PHAC-CCDP), there were no salary dollars or staff positions provided through the FTCS funding. This meant that the existing staff assumed the responsibilities of planning and administering new contribution funding. Internal stakeholders felt that with more dedicated resources, they would have been able to provide additional support to the funding recipients. Resources not funded by the FTCS have not been included in the expenditures.
| Year | Department | Planned Allocations ($M) | Expenditures ($M) | Variance ($M) | % Planned budget spent |
|---|---|---|---|---|---|
| 2012-2013 | Health CanadaTable 10 footnote a | 41.5 | 32.8 | -8.7 | 79% |
| PHAC | 1 | 0.5 | -0.5 | 50% | |
| Public Safety | 0.6 | 0.7 | 0.1 | 117% | |
| RCMP | 1.7 | 1.2 | -0.5 | 71% | |
| CBSA | 3.7 | 3.3 | -0.4 | 89% | |
| CRA | 0.9 | 0.9 | 0 | 100% | |
| 2013-2014 | Health Canada | 32.4 | 25.9 | -6.5 | 80% |
| PHAC | 2.4 | 1.5 | -0.9 | 63% | |
| Public Safety | 0.6 | 0.6 | 0 | 100% | |
| RCMP | 1.7 | 0.9 | -0.8 | 53% | |
| CBSA | 3.7 | 2.9 | -0.8 | 78% | |
| CRA | 0.9 | 0.9 | 0 | 100% | |
| 2014-2015 | Health Canada | 35.2 | 31.1 | -4.1 | 88% |
| PHAC | 2.4 | 1.4 | -1 | 58% | |
| Public Safety | 0.6 | 0.6 | 0 | 100% | |
| RCMP | 1.7 | 1.7 | 0 | 100% | |
| CBSA | 3.7 | 3.7 | 0 | 100% | |
| CRA | 0.9 | 0.9 | 0 | 100% | |
| Total for 1st 3 years | 135.6 | 111.5 | -24.1 | 82% | |
|
|||||
Observations on the Adequacy and Use of Performance Measurement Data
A performance measurement strategy exists for the programs within scope. The strategy is disaggregated by the components of the FTCS. All partner organizations report on performance results and highlights to Health Canada for inclusion in its Report on Plans and Priorities and Departmental Performance Reports and, ultimately, the Treasury Board Secretariat Horizontal Initiatives Database. The TCD prepares an annual report on performance that is shared with all federal partners and was used for this evaluation.
Previous iterations of the FTCS identified specific target reductions. There were five objectives of the FTCS to accomplish between 2001 and 2011: Reduce prevalence from 25% to 20%; reduce the number of cigarettes sold by 30%; increase retailer compliance to 80%; reduce the number of people exposed to second-hand smoke in public places; and, explore how to mandate changes to tobacco productsEndnote 105. Health Canada established revised objectives for the strategy from 2007 to 2011 to reflect significant progress in meeting the initial objectives. These objectives included: reducing smoking prevalence to 12% by 2011; reducing the youth smoking prevalence to 9%; increasing the number of adults who quit smoking by 1.5 million; reducing the prevalence of Canadians exposed to second-hand smoke to 20%; examining the next generation of tobacco control policy; contributing to the WHO FCTC; and, monitoring and assessing contraband tobacco activities and enhance compliance.Endnote 106
No targets were established for the 2012-2017 iteration of the FTCS. Rather, documents refer only to the activities that would be undertaken and two groups that would be the focus of these activities (i.e., on reserve First Nations and Inuit communities and young adults). This change was critiqued by stakeholders.
Observations on Efficiency
In 2012, the pan-Canadian Quitline toll-free number first appeared on tobacco product packages. The pan-Canadian Quitline initiative brings together cessation services from each province and territory, served by six independent service providers across Canada to one phone number and one web address that is displayed on tobacco product packages. An increase in the number of callers has allowed the quitlines to be more efficient in handling cases and referring clients to support services. When comparing the cost of the quitlines for the years 2009-2011 (pre-pan-Canadian quitline) and 2012-2014 (post-pan-Canadian quitline),Footnote ix there was a decrease in the average cost per client served: $771 per caller to $407 per caller and $2,964 per quitter to $1,566 per quitter.
However, it should be noted that after the initial increase, the number of callers has decreased every year since the pan-Canadian quitline was established. It is unclear what impact this may have on the continued efficiency of the quitlines.
One area of inefficiency noted by external stakeholders was the separate funding agreements made with each of the quitline service providers for each of the provinces and territories. This has led to confusion on the part of the service providers, such as the Canadian Cancer Society, as they must provide different levels of services depending on where the caller resides.
Partner organizations also noted that they had implemented measures to increase their own internal efficiencies. For instance, the TCD identified common measures for internal reporting with the aim of streamlining planning and reporting processes, thus reducing the burden on staff to track and report on different measures. Starting in 2011- 2012, CBSA streamlined its intelligence function by reducing the level of resources it devoted to the assessment and monitoring activities funded by the FTCS. This change better aligned the CBSA's resources to government priorities. In 2013-2014, CBSA trialled a new national project-based planning approach. Internal key informants found this approach to be useful and informative operationally and also a good opportunity to leverage efforts and resources across the country.
There were several instances in which key informants reported that concern for economyFootnote x reduced the effectiveness of the programming. Key stakeholders identified the merging of the annual Canadian Alcohol and Drug Use Monitoring Survey and the annual CTUMS to form the biennial CTADS as a less effective means to monitor tobacco use. It was reported that a significant amount of room for content related to tobacco was lost to allow room for new content on drugs and alcohol. This was suggested to be particularly concerning as new areas regarding tobacco control (e.g., vaping) were emerging and there was a competing need for new content regarding marijuana that further reduced the space available for tobacco-related questions.
Feedback with respect to the new CTADS survey suggested that the removed content was valued and seen as important by provinces and territories. The removed content provided a broader depth of understanding of the patterns of smoking and tobacco use.
Stakeholders further suggested that the move to CTADS created operational concerns regarding staff expertise, publication delays and timeliness. Staff were no longer able to be subject matter experts as when they were when focusing on one topic. The addition of drugs and alcohol was described as pulling staff too thin". Reports were also required to be approved through two different lenses – tobacco and drugs, which led to worries about delays. Stakeholders identified the biennial nature of CTADS to be an issue for tobacco-related data gathering for two reasons. First, the industry is perceived as fast-moving, and a two-year window does not allow the survey to be as responsive as needed. Second, it limits data available to assess the impact of policy changes.
Another area of inefficiency was seen with the development of separate yet similar legislation at the provincial and territorial level for areas of federal interest. Stakeholder interviewees suggested that it was necessary for the provinces and territories to develop legislation as little action was coming from the federal government with respect to emerging issues (e.g., flavoured tobacco, vaping products). It was noted that of the variety of legislation is not ideal as it is not comprehensive and uniform across the country, thereby creating inequity for Canadians. Furthermore, it was noted that the federally produced economic burden of tobacco use analysis has not been updated since 2006, which is based on 2002 data. Stakeholders from the provinces and territories indicated that this was a very useful document for policy decisions makers, but that it is increasingly difficult to use as it is outdated.
Despite new funding for marketing campaigns, stakeholders noted that mass media campaigns were absent from the 2012-2017 iteration of the FTCS. Previous mass media campaigns were viewed positively and in previous evaluations were noted to be effective at informing Canadians on the actions undertaken by the federal government. Stakeholders suggested that this was an important step in laying the groundwork for the tobacco control activities of external organizations and the provinces and territories. Certain stakeholders indicated that they were concerned that gains toward the denormalization of smoking and the increased knowledge of health concerns resulting from tobacco use would be lost without continued mass media campaigns.
Observations on Collaboration and Partnerships
As the area of tobacco control is a complex one, it requires partnership and collaboration. There have been instances of collaboration with many of the initiatives under the FTCS. In the area of contraband tobacco:
-
Public Safety works with the Akwesasne Partnership Initiative to support the Contraband Tobacco Enforcement Strategy. This has led to gains in addressing tobacco control, and key informants reported that without the partnership, the same impact would not have been achieved.
CBSA reports improved fraud and smuggling detection through coordinated intelligence and collaboration with international partners.
The Health Portfolio partners have also engaged in partnerships and collaboration. Some of the highlights of those collaborations are detailed below.
- Each of the communities funded by the First Nations and Inuit Component of the FTCS has engaged multiple partners, both within and outside the community. Some partners included schools, community elders and elder councils, educators, youth role models, nurses, and other health care service providers, Chiefs and Band Councils and community media.
- PHAC has been able to leverage partner support for tobacco-related activities through their Multi-sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease. Since 2012-2013, four projects have received funding. On average, projects were approved to receive $8.1 million from the PHAC, which leveraged almost $2.4 million in funding from partners and brought new partners with reach and influence to Canadians, including The Running Room, into the tobacco control arena.
| Project Title | Project Lead | PHAC Funding ($) | Partner Funding ($) | Total Funding ($) |
|---|---|---|---|---|
| Enhancing professional health care capacity to integrate | Canadian Network for Respiratory Care | 1,009,292 | 316,000 | 1,325,292 |
| National Smoking Cessation Program in Respiratory Clinics | University of Ottawa Heart Institute | 1,640,007 | 269,050 | 1,909,127 |
| MANTRA | Manitoba Tobacco Reduction Alliance | 450,000 | 150,000 | 600,000 |
| Run To Quit | Canadian Cancer Society | 4,997,757 | 1,665,939 | 6,663,696 |
| TOTAL (approved) | 8,097,056 | 2,400,989 | 10,498,115 | |
| Source: Financial information provided by PHAC | ||||
Observations on Governance
Within the Strategy, all partners were aware of their areas of responsibilities and did not believe that there was any duplication of efforts between the partners. Bilateral meetings between federal partners took place on issues of mutual interest. Within the Health Portfolio, there was some collaboration on activities, and key informants felt supported by the TCD when needed. For instance, PHAC reported engaging with the TCD during the review of project applications, and the TCD and CPAB collaborated on the Break it Off campaign. There was some coordination among the Public Safety portfolio partners, as there is a Strategic Level Forum on issues regarding contraband tobacco. This forum was not directly linked with FTCS activities, but did utilize the contraband monitoring information funded by the FTCS.
While there are two committees at the Director General level for governance of the FTCS (the Health Portfolio Director General FTCS Coordination Committee and the Interdepartmental Director General FTCS Coordination Committee), these committees have met infrequently. Many partners reported only engaging with the central coordinators of the FTCS regarding required reporting. There were also concerns with the delays for the approval of common reports, such as annual performance measurement reports. Horizontality of activities within the strategy partners was not readily apparent, and the level of engagement of the partners varied.
At the Federal/Provincial/Territorial level, the Tobacco Control Liaison Committee (TCLC) has been in place since 2000. The role of the TCLC has evolved; it is currently viewed by its members to be a forum for information sharing. According to key informants, the lack of in-person meetings has hampered the collaborative efforts of this committee.
Observations on the cost effectiveness of tobacco control measures
An econometric assessment of the FTCSEndnote 107 indicated that most changes in policy have had a significant and ongoing impact on the number of individuals consuming tobacco and amount of tobacco they consume. Though the econometric assessments on policy changes implemented during the previous iterations of the FTCS, the current FTCS continues to support and monitor these changes.
It was reported that since 1999, smoking rates have declined as tobacco-related policy (e.g., smoke-free places, smoking age, price increases) has been strengthened. This occurred for both youth (between the ages of 15 and 18) and adults. For youth, the adoption of the highest level of smoking bans in public places was associated with a five to six percentage point lower prevalence rate, and provinces with a higher legal smoking age had a four percentage point lower prevalence rate. The introduction on the Cracking Down on Tobacco Marketing Act in 2009 was associated with a 2 percentage point lower prevalence for youth.
The price of cigarettes was assessed by examining both an increase in the actual retail price of cigarettes and the amount of taxes applied to the cigarettes. For every 1% increase in price and in tax, there was a 0.43% and 0.34% (respectively) decrease in the youth prevalence rate and a 0.21% and 0.13% decrease in youth consumption. For adults, for every 1% percent increase in price and in tax, there was a 0.12% and 0.16% (respectively) decrease in prevalence rate and a 0.16% and 0.15% (respectively) decrease in consumption. The only examined policy change that was not associated with a change in either prevalence or consumption was display bans.
In addition to an improvement to the health of Canadians, there are significant health care costs that the government saves by undertaking tobacco control measures. It was estimated that for every individual that quits smoking, $8,533 will be averted in direct health care and short-term disability costs, and $413,000 will be averted in costs related to reducing the risk of premature deathEndnote 108. Recent well-being valuationFootnote xi analysis by PHAC has shown that the change from daily smoker to non-smoker results in the estimated equivalent value of $256 per week, and the change from occasional smoker to non-smoker results in an equivalent value of $63 per week.
The policies and programs that are part of the FTCS have been seen as cost-effective health measures internationally, and have been aligned with the WHO FCTC. While Canadian-specific information is not yet available, the European Respiratory Society (2013)Endnote 109 notes that smoking cessation interventions, whether pharmaceutical or through advice and counselling, are highly cost-effective health measures among existing smokers. They also note that smoking prevention policies such as promotion bans and high taxation play an invaluable role in preventing young people from taking up smoking: society will reap the benefits of these policies in future decades.
Health warnings on tobacco productsEndnote 110 have been recognized as a simple and cost- effective means to increase awareness of the health effects of smoking and to reduce tobacco use, as recognized in Article 11 Guidelines (Packaging and labelling of tobacco products) of the WHO FCTC. Canadian researchEndnote 111 also confirms the success of health warnings on tobacco packaging.
Observations on alternative approaches
Canada's tobacco control policies and the activities of the FTCS align with the direction provided by the WHO and the articles of the FCTC. However, as noted by external key informants, and as detailed in a document provided by external stakeholders as part of a budget consultation, there are options for more innovative funding mechanisms for Canadian tobacco control.
Many key informants noted that the high rates of excise taxes that are collected for tobacco products are not reflected in the funds available for tobacco control. The ear- marking of tobacco taxation income, through legislation, for funding tobacco control plans and strategies is supported by the WHO FCTC although they recognize the sovereign right of the Parties to determine and establish their taxation policies, and has been implemented by some countries.
The United States introduced the Family Smoking Prevention and Tobacco Act (Tobacco Control Act)Endnote 112 in 2009. This authorizes the U.S. Food and Drug Administration (FDA) to collect user fees from manufacturers and importers of tobacco products to fund the Center for Tobacco Products. The amount to be collected from the industry is set in advance based on an assessment of the Center's requirements for tobacco control activities. The user fees are allocated by market share percentage determined by data on sales submitted directly to the FDA by the companies under law. Within each class of tobacco products, the fees are then allocated among companies based on their share of the US market for that product class. The Tobacco Control Act gives the Secretary of the FDA the authority to assess and collect the fees on a quarterly basis.
Fees collected by the CTP are available until expended. This allows for long-term planning of complex research projects without the problem of lapsing funds. As per the Tobacco Control Act, fees can only be used for tobacco control activities, which are broadly defined and include product and population research, mass media campaigns, product assessment and review.
Other countries have also explored the options for a Tobacco Levy" or a direct tax on tobacco manufacturers and importers that would be apportioned to each company on the basis of their market share. For example, in 2016, Iceland reported that 0.9% of all tobacco tax collected is ear-marked for tobacco control and prevention,Endnote 113 and, in 2014, Poland reported that 0.5% of the excise duty on tobacco products goes to financing their tobacco control program.Endnote 114 Similarly, in the City of Ottawa, the cost of tobacco vendor licences were raised significantly, the proceeds from which fund public health inspections and the investigation of tobacco control issues. Some related recommendations by the Canadian Cancer Society included fees for product registration of all products and package variations, and performance-based incentives or penalties to be paid by tobacco manufacturers if tobacco prevalence targets are not achieved.
Comparing Canada with other countries, it was found that varying amounts of money are committed to tobacco control programs at the federal or national level. In 2014- 2015, approximately NZD 61.7 million (equivalent to USD 45.1 million) was spent in New Zealand for their Tobacco Control ProgrammeEndnote 115; in Australia, more than AUD 135 million (equivalent to USD 103 million) was to be spent on anti-smoking campaigns from 2009-2010 to 2015-2016Endnote 116; and in the United States, at the federal level, the 2016 budget for the Center for Tobacco Products was USD 635 millionEndnote 117 and an estimated USD 468 million was estimated to be spent by U.S. states in the 2016 fiscal year.Endnote 118 In 2014, the United States Centers for Disease Control recommended that the target for overall funding on tobacco control should be USD 7.41 to 10.53 on a per capita basis.Endnote 119 In 2016, only one state was within their recommended funding level.Endnote 120 The FTCS funding is equivalent to approximately USD 1 on a per capita annual basis. In contrast, the New Zealand Tobacco Control program spends, USD 10.1 per capitaFootnote xii. Australia spent USD 0.73 per capitaFootnote xiii on their anti-smoking campaigns, and the US federal spending was equivalent to USD 2 per capita in 2016.
Another option is the establishment of public-private partnerships, or multi-sectoral partnerships for tobacco control programs. PHAC has used the multi-sectoral partnership approach for its FTCS funded programs, such as the Run to Quit program. The Centers for Disease Control noted that the public-private partnerships in Colorado and Minnesota for quitline operations are considered best practices in tobacco control programs.Endnote 121 The quitline partnerships have the states' tobacco control programs working with private health plans to either reimburse the state quitline, or contract directly with a quitline vendor for the services. In Colorado's case, the Partnership Plan with the health plans offset the state's QuitLine costs by 12 to 14 percent."Endnote 122
5.0 Conclusions
5.1 Relevance Conclusions
5.1.1 Continued Need
Our analysis concludes that there continues to be a need for tobacco control across Canada. Although smoking prevalence has declined in Canada, the most recent data from the CTADS 2013 shows that the overall smoking prevalence was 14.6%. This means that in 2013 there were approximately 4.2 million Canadians aged 15 and older who smoke. Higher smoking rates are reported in both Inuit and First Nations communities (on-reserve). In 2010, 43% of adults living in First Nations communities were daily smokers and 13.7% were occasional smokers. Data from the 2012 Aboriginal Peoples Survey reported that 54.1% of Canada's Inuit population aged 19 years and older smoke daily and 9.1% smoke occasionally. Tobacco use continues to have a health impact on Canadians, with tobacco smoking playing a causal role in over 10 different cancers, cardiovascular disease, stroke and chronic obstructive pulmonary disease. As well, the economic burden of smoking in Canada was estimated at over $18 billion annually in 2013.
5.1.2 Alignment with Government Priorities
Tobacco control issues are aligned with the federal government's priority to protect the health and safety of Canadians. The Minister of Health's mandate letter (2015) specified tobacco control through plain packaging as one of the top priorities. Tobacco is a risk factor for chronic disease, and as such fits within the PHAC priority of leadership on health promotion and disease prevention". CRA actively ensures that federal taxes on domestic tobacco products are paid. Public Safety portfolio partners in the FTCS monitor and assess the contraband tobacco market, as it aligns with their priorities to address crime and smuggling. As well, Canada has international commitments and obligations, particularly pursuant to the WHO FCTC.
5.1.3 Alignment with Federal Roles and Responsibilities
A clear federal role pertaining to tobacco control has been established in the existing legislation, in particular the Tobacco Act and the Excise Act, 2001. There are also roles in tobacco control for other levels of government within their jurisdictional mandate. Input from key informants was consistent in noting that stronger federal leadership – particularly on regulatory matters - would serve to enhance uniformity and provide a consistent level of protection across Canada. While tobacco control is addressed by various jurisdictions and levels of government, efforts were seen to be complementary and not duplicative.
5.2 Performance Conclusions
5.2.1 Achievement of Expected Outcomes (Effectiveness)
In general, the FTCS is making progress in achieving its expected outcomes. The overall decline in smoking prevalence has slowed down, but the downward trend in prevalence has continued. There was no prevalence target set for the 2012-2017 time period of the FTCS, so it is difficult to measure the success of the strategy in this regard.
Compliance with existing regulations and provisions of the Tobacco Act and the Excise Act, 2001 has increased. This has been accomplished through the continued and consistent monitoring from Health Canada and the CRA.
The support to enhance the quitline cessation services has resulted in an increase in the number of smokers receiving help to quit smoking. As well, early indications from projects addressing cessation show that they are on track for success. However, the reach of these projects remains limited.
Prevention has been addressed through provisions made under the Tobacco Act and its regulations, including prohibiting sales to youth, health-related labelling requirements, tobacco promotion restrictions and flavour restrictions. Stakeholders reported that prevention activities have been undertaken by other levels of government, creating a patchwork of efforts.
Young people have been protected from inducements to take up tobacco use through ongoing monitoring of promotions to youth as well as bans on flavours that may appeal to youth. While flavour restrictions on certain tobacco products have had success in decreasing youth usage, there are some areas of the tobacco environment where the federal government has not appeared as responsive, including the increasing popularity of vaping products.
With regards to contraband tobacco, FTCS efforts are focussed on monitoring and assessing the illicit market. Reported seizures of contraband tobacco products have decreased; however, seizure rates are variable over short time intervals and the reason behind these declines is unclear. There continues to be a demand for a better national understanding of the contraband tobacco market from both governmental and non- governmental sources.
The FTCS has conducted the activities it set out to do within the time period evaluated, and with the funding allocation provided to FTCS partners. Some key informants felt that these activities were not ambitious enough. However, Canada's activities align with the main articles of the WHO FCTC and provide a multi-sectoral national approach to tobacco control.
Demonstration of Economy and Efficiency
Many activities funded through the FTCS derived success through collaboration and partnerships. In particular, PHAC-funded projects leveraged funds through multi- sectoral engagement. However, further engagement of external organizations and other levels of government would be useful in advancing Canada's tobacco control goals.
FTCS funding was reduced by approximately 35% from the previous 5-year period. Reduced funding and a focus on economy negatively impacted operational efficiency in some areas. This is most apparent in the FTCS's research and surveillance capacity, in which the annual tobacco use survey was changed to a biennial survey covering multiple topics including alcohol and illicit drugs.
Inefficiencies were noted when considering differences among the province and territories for areas of federal interest. Stakeholders reported that provinces and territories developed patchwork legislation respecting emerging issues in the absence of action at the federal level, creating inequity for Canadians. Further, separate funding agreements for quitline service allowed for dissimilar levels of service resulting in confusion for service providers.
All federal partners were aware of their specific areas of responsibilities and did not report duplication of efforts. However, it was not readily apparent that there were linked activities taking place across several strategy partners and the level of engagement of the partners varied. Meetings of the Coordinating Committees were infrequent and concerns were noted regarding delays in approving common reports.
5.3 Recommendations
The findings from this evaluation of the Federal Tobacco Control Strategy have resulted in the following four recommendations.
Recommendation 1
Explore the setting of targets for the reduction of smoking prevalence rates, both for the general population and populations with higher prevalence rates.
The lack of a reduction target for smoking prevalence in the 2012-2017 FTCS was seen by stakeholders as an impediment in measuring the overall success of the program and in focussing the activities of the FTCS on a unified goal. Canada was successful in reaching the targets set in early versions of the FTCS, and has a current prevalence rate of 14.6%. The WHO voluntary target prevalence is 10.57% for Canadians aged 15 years or older by the year 2025, and based on projections Canada is on track to meet this. Other countries similar to Canada have set specific national tobacco reduction targets that are more ambitious.
There have never been targets set for groups within Canada with higher prevalence rates. These rates have not decreased as quickly as the overall prevalence rates, and may need more directed efforts. Given Health Canada's mandate for health services and benefits for First Nations and Inuit populations, as well as the federal government's overall commitment for a relationship with Indigenous peoples, engage First Nations and Inuit leadership and communities to establish targets that are relevant and appropriate may focus Strategy activities and help define the future direction of the Strategy.
Recommendation 2
Clearly identify and articulate the areas for federal leadership in tobacco control, particularly in light of the existing provincial, territorial and municipal actions.
Tobacco control requires concerted efforts from multiple levels of governments across jurisdictions. Moving forward with the FTCS, it will be important for the federal government, in consultation with stakeholders and other levels of government, to clearly identify and articulate the regulatory and policy areas for federal leadership. This will assist stakeholders and other levels of government in understanding their role in regard to tobacco control.
While there have been calls for more national action in regard to tobacco control, the partner departments will need to examine the areas and populations that may benefit most from these actions. Opportunities for these national actions could be explored within the Strategy where feasible.
Recommendation 3
Options for regulating new and emerging tobacco control issues should be explored.
The tobacco industry is innovative, and often legislation and regulation lags behind new developments. Stakeholders suggested that there is a need for consistent federal regulations, and enforcement of these regulations, to protect the health of Canadians, and in particular youth. Moving forward, the federal government should encourage responsiveness to emerging tobacco products and ensure that the appropriate regulatory framework is in place and communicated to both industry and the public.
As new and emerging issues arise and regulation is required to address them, it will be important to explore innovative funding approaches to address tobacco control. These funding approaches could be based on international models, such as the imposition of a 'tobacco levy'.
Recommendation 4
Examine the feasibility of integrated reporting on aspects related to contraband tobacco to facilitate Canada-wide analysis
The continued existence of the contraband tobacco market undermines tobacco control efforts across Canada. Multiple federal departments and agencies independently monitor different dimensions of contraband tobacco, as do other levels of governments and law enforcement agencies in Canada. In addition to government efforts, industry- sponsored organizations have also attempted to assess the scope and nature of the contraband tobacco market, in particular how it relates to youth. While the monitoring of contraband tobacco is widespread, there is little consistency on what is reported. It is beneficial for departments and agencies to be able to provide a comprehensive and integrated overview of the tobacco market, including trends. Given that there are multiple departments and agencies involved, each with their own data collection systems and internal reporting requirements, the compilation of contraband data may pose a challenge. At this time, the feasibility for integrating reporting should be explored, and where possible, a streamlined approach to reporting should be undertaken.
Appendix 1 – Logic Model
Figure 4: Logic Model
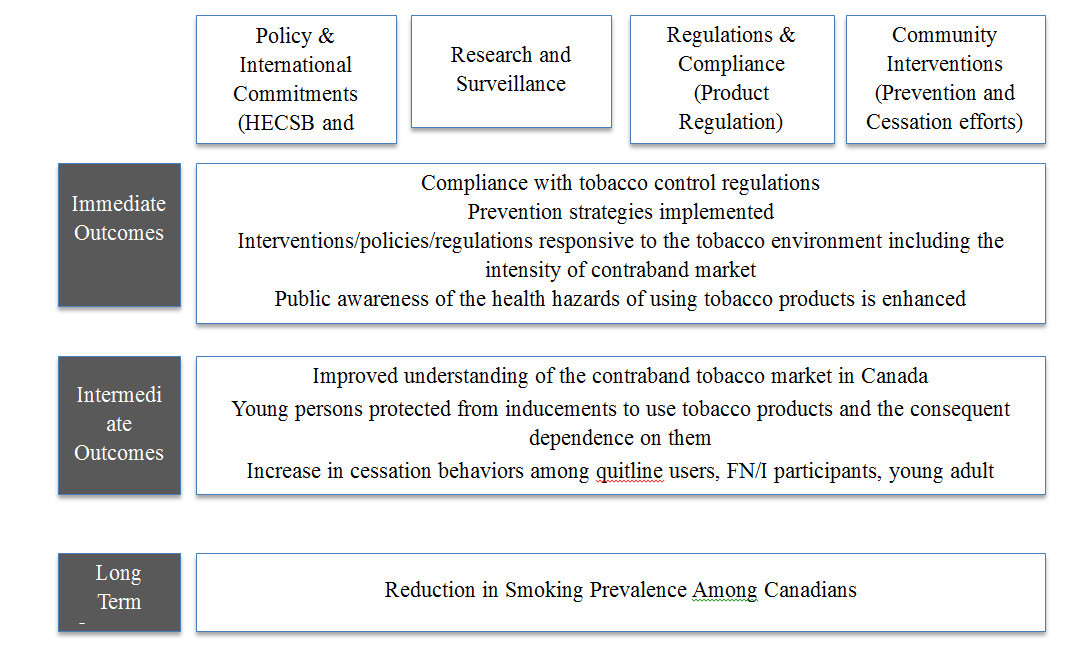
Figure 4 – Text description
Activities: Policy and international commitments (HECSB and partners departments), research and surveillance, regulations & compliance (product regulation), community interventions (prevention and cessation efforts)
The logic model identifies the Strategy's immediate outcomes as follows: compliance with tobacco control regulations, prevention strategies implemented, interventions and policies and regulations responsive to the tobacco environment including the intensity of contraband market, public awareness of the health hazards of using tobacco products is enhanced.
The logic model identifies the Strategy's intermediate outcomes as follows: improved understanding of the contraband tobacco market in Canada, young persons protected from inducements to use tobacco products and the consequent dependence on them, increase in cessation behaviors among quitline users, First Nations and Inuit participants, young adult smokers, PHAC projects participants and the broader population
Long-term outcome: Reduction in smoking prevalence among Canadians
Appendix 2 – Summary of Findings
Rating of Findings
Ratings have been provided to indicate the degree to which each evaluation issue and question have been addressed.
Relevance Rating Symbols and Significance:
A summary of Relevance ratings is presented in Table 1 below. A description of the Relevance Ratings Symbols and Significance can be found in the Legend.
| Evaluation Issue | Indicators | Overall Rating | Summary |
|---|---|---|---|
| Continued need for the program | |||
| What are the health and societal concerns contributing to the need for the FTCS, including activities of partner departments? Is the FTCS responsive to anticipated future needs? | Evidence of:
|
High | Although smoking prevalence has declined in Canada, the most recent data from the CTADS 2013 shows that the overall smoking prevalence was 14.6%. Higher smoking rates are reported in both Inuit and First Nations communities (on-reserve). In 2010, 43% of adults living in First Nations communities were daily smokers and 13.7% were occasional smokers. Data from the 2012 Aboriginal Peoples Survey reported that 54.1% of Canada's Inuit population aged 19 years and older smoke daily and 9.1% smoke occasionally. Tobacco use continues to have a health impact on Canadians, with tobacco smoking playing a causal role in over 10 different cancers, cardiovascular disease, stroke and chronic obstructive pulmonary disease. As well, the economic burden of smoking in Canada was estimated at over $18 billion annually in 2013. |
| Alignment with Federal Roles and Responsibilities | |||
| What are the federal roles relating to smoking and the control of tobacco products? |
|
High | A clear federal role pertaining to tobacco control has been established in existing legislation, namely the Tobacco Act and the Excise Act, 2001. There are also roles in tobacco control for other levels of government within their respective sphere of control. Input from key informants was consistent in noting that stronger federal leadership – particularly on regulatory matters - would serve to enhance uniformity and provide a consistent level of protection across Canada. |
| How have the Provinces/Territories (PT) and municipal roles related to tobacco smoking and the control of tobacco products changed since the last renewal of the FCTS? |
|
High | |
| Alignment with Government Priorities | |||
| What are the Government of Canada priorities relating to tobacco smoking and the control of tobacco products and how does the FTCS relate? |
|
High | Tobacco control issues are aligned with the federal government's priority to protect the health and safety of Canadians. The Minister of Health's mandate letter (2015) specified tobacco control through plain packaging as one of the top priorities. As well, Canada has international commitments and obligations, particularly pursuant to the WHO FCTC. |
| What are the departmental priorities and strategic outcomes relating to tobacco smoking and the control of tobacco products and how does the FTCS relate? |
|
High | Tobacco is a risk factor for chronic disease, and as such fits within the PHAC priority of leadership on health promotion and disease prevention". CRA actively ensures that federal taxes on domestic tobacco products are paid. Public Safety portfolio partners in the FTCS monitor and assess the contraband tobacco market, as it aligns with their priorities to address crime and smuggling. |
| Legend - Relevance Rating Symbols and Significance: High: There is a demonstrable need for program activities; there is a demonstrated link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program are clear. Partial: There is a partial need for program activities; there is some direct or indirect link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program are partially clear. Low: There is no demonstrable need for program activities; there is no clear link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program have not clearly been articulated. |
|||
Performance Rating Symbols and Significance:
A summary of Performance Ratings is presented in Table 2 below. A description of the Performance Ratings Symbols and Significance can be found in the Legend.
| Issues | Indicators | Overall Rating | Summary |
|---|---|---|---|
| Achievement of Expected Outcomes (Effectiveness) | |||
| To what extent has the immediate outcome, compliance with tobacco control regulations, been achieved? | Evidence of (performance data on) achievement of outputs and outcomes | Achieved | Overall non-compliance with the Tobacco Act and the Excise Act, 2001 as it relates to tobacco, is very low. Compliance with existing regulations and provisions of the Tobacco Act and the Excise Act, 2001 has increased over the period covered by the evaluation. This has been accomplished through the continued and consistent monitoring from Health Canada and the CRA. |
| To what extent has the immediate outcome Prevention strategies implemented, been achieved? | Number and nature of strategies implemented | Progress Made; Further Work Warranted | Prevention has been addressed through the Tobacco Act prohibiting sales to youth; prohibiting select additives; restricting tobacco promotion; and health warning labelling. Many stakeholders felt that prevention activities that have been undertaken by other levels of government have created a patchwork of efforts. |
| To what extent has the immediate outcome, Interventions/policies/regulations responsive to the tobacco environment including the intensity of contraband market, been achieved? |
|
Progress Made; Further Work Warranted | Partner departments and agencies, mainly Health Canada and Public Safety, have developed interventions, policies and regulations that are responsive to the tobacco environment. However, there are some areas of the tobacco environment, such as the increasing popularity of vaping products, where the federal government has not been as responsive as other levels of government to date. |
| To what extent has the immediate outcome, Public awareness of health hazards of using tobacco products is enhanced, been achieved? | Extent to which related outcomes and outputs delivered.
Extent to which 'health' or 'pregnancy/baby' is identified as the main reason to quit smoking (changes across time) Youth awareness of health risks associated with smoking (changes across time) |
Progress Made; Further Work Warranted | Health warning labels are effective in informing those that smoke about the health risks associated with tobacco use. In 2013 found that 79% of smokers looked at or read the health warning messages. This is an increase from 71% in 2012. In 2013, the majority of these smokers (86%) felt that the health warning messages provided important information, and 66% of smokers felt that the messages made smoking seem less attractive. There is little available evidence of the awareness of non-smokers on the health hazards of using tobacco. However, three- quarters of recent quitters cited health, as their main reason to quit smoking. |
| To what extent has the intermediate outcome, Improved understanding of the contraband tobacco market in Canada, been achieved? | Increased knowledge of:
Extent to which FTCS activities/outputs generate knowledge/awareness of the contraband tobacco market |
Progress Made; Further Work Warranted | With regards to contraband tobacco, FTCS efforts are focussed on monitoring and assessing the illicit market. Reported seizures of contraband tobacco products have decreased; however, seizure rates are variable over short time intervals and the reason behind these declines is unclear. There continues to be a demand for a better national understanding of the contraband tobacco market from both governmental and non- governmental sources. |
| To what extent has intermediate outcome, Young persons protected from inducement to use tobacco products and the consequent dependence on them, been achieved? |
|
Progress Made; Further Work Warranted | Young people have been protected from inducements to take up tobacco use through ongoing monitoring of promotions to youth as well as bans on flavours that may appeal to youth. While flavour restrictions on certain tobacco products have had success in decreasing youth usage, there are some areas of the tobacco environment where the federal government has not appeared as responsive, including the increasing popularity of vaping products. |
| To what extent has intermediate outcome, Increased cessation behavior among participants in FTCS funded interventions, been achieved? | Among FTCS projects funded (PHAC, FNIHB, Quitline) and general population:
|
Progress Made; Further Work Warranted | Early indications from projects addressing cessation show that they are on track for success. While the reach of these projects remains limited, the potential exists for reach to be expanded in the future. There was a significant increase in the number of people calling quitlines in Canada after the 2012 implementation of the pan-Canadian toll- free number that routes callers to their provincial or territorial quitline. A quarter of surveyed callers to the pan-Canadian Quitline reported having quit smoking or reduced their use of tobacco products. |
| What is the impact of the program on the Reduction in smoking prevalence among Canadians? |
|
Progress Made; Further Work Warranted | The overall decline in smoking prevalence has slowed down, but the downward trend in prevalence has continued. The smoking prevalence rate in Canada in 2013 was 14.6%. This is comparable to other developed countries. The smoking rate for Canadian youths has decreased significantly since 2010- 2011. The 2014-15 Canadian Student Tobacco, Alcohol and Drugs Survey indicated that youths in grades 6 to 12 were less likely to report being a current smoker (3%) in 2014- 2015 than in 2012-13 (4%). |
| Demonstration of Economy and Efficiency | |||
| Has the program undertaken its activities in the most efficient manner? Are there other programs that complement, overlap or duplicate the objectives of the FTCS? Are there alternative approaches to delivering this program? |
|
Progress Made; Further Work Warranted | Many activities funded through the FTCS derived success through collaboration and partnerships. In particular, PHAC-funded projects leveraged funds using multi-sectoral partnership. FTCS funding was reduced by approximately 35% from the previous 5-year. Reduced funding and a focus on economy negatively impacted operational efficiency in some areas. This is most apparent in the FTCS's research and surveillance capacity, in which the annual tobacco use survey was changed to a biennial survey covering multiple topics including alcohol and illicit drugs. All federal partners were aware of their specific areas of responsibilities and did not report duplication of efforts. However, it was not readily apparent that there were linked activities taking place across several strategy partners and the level of engagement of the partners varied. |
| Is there appropriate performance measurement in place? If so, is the information being used to inform senior management decision-makers? |
|
Achieved | A performance measurement strategy exists for the programs within scope. The strategy is disaggregated by the components of the FTCS. All partner organizations report on performance results and highlights to Health Canada for inclusion in its Report on Plans and Priorities and Departmental Performance Reports and, ultimately, the Treasury Board Secretariat Horizontal Initiatives Database. The TCD prepares an annual report on performance that is shared with all federal partners and was used for this evaluation. |
Appendix 3 – Evaluation Description
Evaluation Scope
This evaluation covered the Federal Tobacco Control Strategy (FTCS) for the period from 2012-13 to 2016-17. The evaluation was undertaken in fulfillment of the requirements of the Financial Administration Act and the Treasury Board of Canada's Policy on Evaluation (2009). The evaluation covered the activities of the current federal partners (Health Canada, Public Safety, the Royal Canadian Mounted Police, Canada Revenue Agency, Canada Border Services Agency, and the Public Health Agency of Canada). The time-limited funding provided to the Public Prosecution Services of Canada in 2012-13 was not covered by this evaluation.
Evaluation Issues
The specific evaluation questions used in this evaluation were based on the five core issues prescribed in the Treasury Board of Canada's Policy on Evaluation (2009).
These are noted in the table below. Corresponding to each of the core issues, evaluation questions were tailored to the program and guided the evaluation process.
| Core Issues | Evaluation Questions |
|---|---|
| Relevance | |
| Issue #1: Continued Need for Program | Assessment of the extent to which the program continues to address a demonstrable need and is responsive to the needs of Canadians
|
| Issue #2: Alignment with Government Priorities | Assessment of the linkages between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes
|
| Issue #3: Alignment with Federal Roles and Responsibilities | Assessment of the role and responsibilities for the federal government in delivering the program
|
| Performance (effectiveness, economy and efficiency) | |
| Issue #4: Achievement of Expected Outcomes (Effectiveness) | Assessment of progress toward expected outcomes (incl. immediate, intermediate and ultimate outcomes) with reference to performance targets and program reach, program design, including the linkage and contribution of outputs to outcomes
|
| Issue #5: Demonstration of Economy and Efficiency | Assessment of resource utilization in relation to the production of outputs and progress toward expected outcomes
|
Data Collection and Analysis Methods
Evaluators collected and analyzed data from multiple sources. Sources of information used in this evaluation included:
Document review – approximately 400 documents pertinent to the Federal Tobacco Control Strategy were reviewed for information regarding the relevance (priorities, roles and responsibilities) of the activities. Partner departments provided relevant documents regarding FTCS activities to the evaluation team.
Financial data review – a review of financial data from 2012-2013 to 2016-2017, including budgeted and actual expenditures for the partner organizations, was conducted.
Key informant interviews – Interviews were conducted with 65 stakeholders (internal stakeholders (n=37) (HC (n=17); PHAC (n=4); CRA (n=2); Public Safety (n=3); CBSA (n=2); RCMP (n=9) Footnote xiv); Provincial/Territorial stakeholders (n=10); external partners and key informants (n=18)). Interviews were, with a few exceptions, conducted by 2 evaluation team members, one with a primary responsibility for taking notes. Notes and transcripts were analysed with NVivo. Additional key informant interviews were conducted for the case studies.
Provincial, Territorial, and Municipal analysis – a review of tobacco control activities conducted by the provinces, territories, and municipalities (P/T/M) was carried out by scanning P/T/M government websites.
Literature review – a search for Canadian and international literature was conducted by a contracted firm. The literature review addressed key evaluation questions and examined how various tobacco control issues had changed since the initial launch of the FTCS in 2001. After examining documents to ensure relevance, 81 articles were reviewed.
Performance data review – a review of data on performance of cluster area activities between 2012-2013 and 2016-2017 (CTUMS, CTADS, project-level performance and evaluation reports).)
Case Study – three case studies were conducted on FTCS-funded programs: Break It Off (HC); Run to Quit (PHAC); and the First Nations and Inuit Component of the FTCS (HC). Case studies included interviews with key informants, document reviews, and financial data reviews, and addressed specific tobacco-related programs (e.g. tobacco cessation).
Media Scan – a media scan, which included social media, was conducted by Health Canada's Communications and Public Affairs Branch in order to examine the coverage of the Federal Tobacco Control Strategy between April 1 2015 and March 31 2016.
Data were analyzed by triangulating information gathered from the different sources and methods listed above. This included: systematic compilation, review and summarization of data to illustrate key findings; statistical analysis of quantitative data from databases; thematic analysis of qualitative data; and comparative analysis of data from disparate sources to validate summary findings.
Appendix 4 – Case Studies
- Case Study 1 – Run to Quit
- Case Study 2 – Break it Off
- Case Study 3 – First Nations and Inuit Component
Case Study 1 Run to Quit
Background
PHAC received Grants and Contributions funding through the Federal Tobacco Control Strategy (FTCS) to address tobacco use as a chronic disease risk factor. This funding was integrated into their larger chronic disease prevention approach and was used to develop and implement innovative tobacco interventions through the existing Multi- sectoral Partnerships to Promote Healthy Living and Prevent Chronic Disease Grants and Contributions program. PHAC is applying the Multi-sectoral Partnership approach to over 20 public health projects at this point in 2016.
The CCDP Multi-sectoral Partnership approach involved a number of key requirements that were different from other funding opportunities. Project ideas are solicited through a two-step continuous intake process which starts with the submission of project ideas via a Letter of Intent, which, if successful, could lead to an Invitation to Submit an Application for project funding. This ongoing process allows stakeholders to leverage new partnership opportunities and develop innovative project ideas while reducing the burden on applicants to complete project proposals which may not meet program requirements.
Projects are required to have matched funding, either through cash contributions, in- kind resources, or a combination of both from non-taxpayer-funded sources, as well as partnerships with non-governmental organizations (NGO). In addition, projects receive funding through a Pay for Performance approach, meaning that payments are tied to agreed-upon outputs and milestones.
Case Study Description
There were four projects that received funding from the FTCS through PHAC in the period between 2012 and 2016 (see Table 1): Run to Quit, Enhancing the Capacity of Health Care Professionals to Integrate Evidence-Based Smoking Cessation Interventions, INSPIRE, and Building and Enhancing the Cessation Capacity of Health Professional Interveners. In consultation with the program area, Run to Quit was selected as the subject of the case study for several reasons: it is receiving the most funding of the four tobacco cessation projects, it has a direct focus on smoking cessation, and it has gained media attention. The case study focussed on the implementation of the Run to Quit as a multi-sectoral partnership, and the early successes and lessons learned from the project.
| Project Title | Project Lead | PHAC Funding ($) | Partner Funding ($) | Total Funding ($) |
|---|---|---|---|---|
| Enhancing Professional Health care Capacity to Integrate Evidence-based Smoking Cessation Interventions | Canadian Network for Respiratory Care | 1,009,292 | 316,000 | 1,325,292 |
| National Smoking Cessation Program in Respiratory Clinics (INSPIRE) | University of Ottawa Heart Institute | 1,640,077 | 269,050 | 1,909,127 |
| Building and Enhancing the Cessation Capacity of Health Professional Interveners. | Manitoba Tobacco Reduction Alliance | 450,000 | 150,000 | 600,000 |
| Run To Quit | Canadian Cancer Society | 4,997,757 | 1,665,939 | 6,663,696 |
| TOTAL (approved) | 8,097,126 | 2,400,989 | 10,498,115 | |
The case study methodology included seven interviews with key informants (e.g. Canadian Cancer Society, PHAC, Running Room) and a document review. In addition, questions about Run to Quit were asked during interviews (n=9) with provincial and territorial stakeholders (n=10). There was limited performance measurement data available on the Run to Quit initiative, as funding began on August 1, 2015.
Run To Quit
Run to Quit is a program led by the Running Room that endeavors to help participants quit smoking while increasing physical activity. Participants take part in the Running Room's ten week Learn to Run program, with a specialized focus on how to quit smoking using the Canadian Cancer Society's (CCS) evidence-based resources. The present Run to Quit program has three registration options: an in-store training program, an online training program, and the Commit to Quit, self-directed program. Both the in- store and online training programs are 10-weeks long and include a progressive training program on how to walk and/or run from a Running Room coach, guidance on how to quit smoking, as well as support calls from a Quit Coach from the participating provincial/territorial Quit Lines. In the online program, participants receive walk/run coaching through weekly audio instruction, and cessation support via web or email. The self-directed program has no registration fees, but does not include some of the services offered through the other options, such as coach support, and coupons for nicotine replacement therapy. All participants receive the CCS self-help booklet, are guided to the telephone and web Quit Lines available to them, and can receive support and information through social media (Facebook, Twitter, and YouTube). All participants can qualify for prizesFootnote xv by completing the program, a 5km run/walk event, and being smoke-free by a specified date.
The program was first conceived and developed by the CCS based on existing research on the positive benefits of exercise on smoking cessation. Given the Running Room's Canadian expertise in walk/run programs for fitness the CCS contacted the company to aid in the program development. This led to the joint initiative, leveraging each organization's knowledge and experience, specifically, the CCS's cessation resources and expertise with the Running Room's Learn to Run curriculum. The CCS and the Running Room were sought by PHAC for program funding based on their established infrastructure, resources and experience, as well as their ongoing commitment to healthy living, including smoking cessation and promotion of physical activity, beyond the confines of the funding agreement.
Key discussions between the CCS and the Running Room regarding how to implement and test the program began in 2013. The pilot program took place in one store in Ottawa between April to June 2013, culminating in a 5km run on July 1 2013. Thirty-four participants were initially registered for the pilot, 24 attended the first session, and 14 completed the ten-week session. The pilot was evaluated by the University of Toronto, and included testing of the participants' carbon monoxide levels in order to confirm whether participants had abstained from smoking. Results of the evaluation showed that at the six month follow-up, 29% of participants had quit smoking for 30 days in the six months since the end of the program, and another 21% had not smoked for 8-weeks after the program. All participants reported increased physical activity at the six month follow-up.Endnote 123
These results were comparable to other cessation programs that include physical activity, such as the Ontario Quit & Get Fit program,Endnote 124 and those that provide nicotine replacement therapies, such as the BC Smoking Cessation Program.Endnote 125
The Quit & Get Fit program was implemented in 2010 by the Ontario Lung Association in partnership with GoodLife Fitness, and received funding from the Ontario Ministry of Health Promotion and Sport from 2010-2012.Endnote 126 Quit & Get Fit, similar to Run to Quit, incorporated physical activity under supervision of a personal trainer with smoking cessation support from a specially trained personal trainer. Results from Quit & Get Fit program in 2012 found that out of the 193 smokers who enrolled in the program 39.4% were smoke-free at the end of the program, and 22.3% were still smoke-free 3 months after the program. Average daily cigarette consumption had decreased among those who were still smoking, and both smokers and those who had quit smoking reported an increase in vigorous physical activity 3 months after the program.Endnote 127
The BC Smoking Cessation Program was launched in 2011, and offers eligible B.C. residents either a 12 week supply of non-prescription nicotine replacement therapy (NRT) gum or patch, or 12 weeks of prescription smoking cessation drugs. The evaluation of the program in 2015 found that out of the 3,001 respondents, 26.8% reported having quit smoking, 52% had remained smoke-free for more than 30 days after using the program, and 71% made at least one quit attempt where they stopped smoking for at least 24 hours.Endnote 128
Recent research on smoking cessation programs that incorporate exercise, with or without NRT products, found benefits to including physical activity as part of the overall cessation plan as smoking cessation rates did decrease.Endnote 129,Endnote 130 One study found that while the maintenance components helped maintain cessation at 14 weeks post- intervention, it was not as successful at later follow-ups, which raised the question of how to improve long-term cessation maintenance by participants.Endnote 131 Another study noted that additional telephone-delivered cessation sessions may help in longer-term maintenance of smoking cessation.Endnote 132
As the Run to Quit evaluation will follow up with participants a year after the program it may be possible to observe whether its approach will be more successful in helping participants remain smoke-free in the long-term. The project evaluation, led by Dr. Guy Faulkner at the University of British Columbia, is assessing smoking status and physical activity levels of participants in all three program options by self-report at the end of the 10-week program and again at six and twelve months. Carbon monoxide (CO) testing will be administered to all in-store participants throughout the 10-week clinic and saliva cotinine testing will be used to verify smoking cessation amongst the prize winners. A sample of in-store participants will have smoking status assessed by either CO monitoring or saliva cotinine at six and twelve months. . Additional data for the evaluation will be collected through a number of sources, including exit surveys with participants, interviews with Running Room staff, information from smokers' helplines, and direct observation of participating clinics.
The successful results of the pilot program motivated PHAC to contact the CCS and Running Room team to explore interest in a potential scale up of the pilot program. PHAC confirmed that Run to Quit met the criteria for the Multi-sectoral Partnership approach (i.e. tobacco cessation, physical activity, multi-sectoral partners) and supported the smoking cessation objectives of the FTCS.
The agreement between PHAC and the CCS commenced August 1, 2015, and will end on March 31, 2020. PHAC is providing approximately $5 million over five years to the CCS through a Pay for Performance approach where payments are tied to accomplishing outputs/outcomes that are specified in advance, jointly negotiated and measurable. As detailed in the contribution agreement, CCS (the recipient) will receive payment for the output achieved and is required to provide PHAC with an outline of the output achieved, a description of the performance, the date it was completed, and the actual expenditures incurred for that output.
Figure 5: Run to Quit Funding ($)
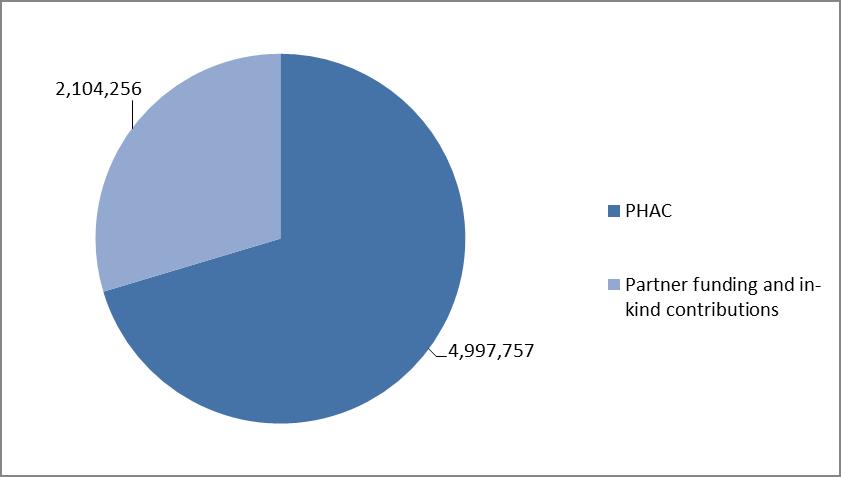
Figure 5 – Text description
This figure depicts a pie graph showing the amount of funding for the Run to Quit program contributed by PHAC and the amount of funding and in-kind contributions provided by partners.
The graph shows that PHAC contributed $2,104,256, which is approximately 30%, and partners contributed $4,997,757, which is approximately 70%.
The CCS will contribute $224,490 over the five-year period, provide their expertise in smoking cessation, along with resources such as their smoking cessation manual, individualized cessation support through the national and provincial Quit Lines, and provision of their smoking cessation curriculum to the Running Room clinic leaders and coaches. The Running Room has agreed to contribute $1.2 million over the five years, and is responsible for selecting the store locations for the Run to Quit clinics and the training of clinic leaders and Run to Quit coaches with assistance from the CCS. Additional funding and in-kind contributions come from private sector companies, including McNeil Consumer Health care.
The objectives of the funded project as listed in the project proposal and Appendix A of the contribution agreement are to address two key modifiable risk factors for chronic disease-tobacco use and physical inactivity. The ultimate goal is to help people engage in regular physical activity that will alone, or in combination with quitting smoking, reduce their risk of cancer, Type2 diabetes and cardiovascular disease.
The target population identified for the Run to Quit program consists of smokers in Canada who want to quit or are considering quitting smoking. While the FTCS identifies First Nations and Inuit communities and young adults as groups that should be the focus of FTCS activities, the Multi-sectoral Partnership funding program takes a population health approach, including multi-sectoral action and social innovation, with the goal of improving health for all population while reducing health inequalities among population groups, where necessary. As such, there was no requirement to address specific populations. However, the CCS noted that the identification of best practices and lessons learned could help adapt the program to reach more specific population groups, including those identified by the FTCS as requiring additional focus.
The Government of Canada announced the launch of the Run to Quit program on July 28, 2015.Endnote 133 Registration for the 2016 program was open from January 2016 until April 23, 2016 and the first in-store and virtual training programs, as well as the Break Free 5km Run/Walk event were completed by July 2016. The first round of Run to Quit had a total of 1,079 participants online (virtual training, n=72; Commit to Quit, n=830) and 177 participants at 21 Running Room locations, which was significantly less than the target number. The target number of registrations for 2016 was 5,775, which included 4,200 registrants for the free Commit to Quit self-guided online program, 525 registrants for the virtual training program, and 525 registrants for the In Store program. The Canadian Cancer Society chose these target numbers based on previous experience with another tobacco cessation program, Driven to Quit. The Running Room plans to hold the in- store training program in 50 locations in 10 provinces in 2017 with a rollout to all 110 (as of July 2015) Running Room locations by 2018, with higher target numbers each year.
A reason given for the lower than expected number of registrations in 2016 was the relatively short time between when the funding was approved and the launch of the program. Key informants interviewed noted that they expected the number of registrations to increase in coming years as they expand the program into more Running Room stores and as the program receives more attention.
Early successes
Run to Quit takes a partnership approach to tobacco cessation that leverages expertise, resources, public credibility and broad population reach from both traditional public health arenas and engaged private sector organizations. As such, all partners, including PHAC, are able to support a broad-based scale up of an evidence-based program, unique in Canada which combines effective smoking cessation and physical activity programming and outcomes.
Partners in the Run to Quit initiative felt that there were advantages to the multi-sectoral partnership approach. One advantage for the CCS and the Running Room was that PHAC's involvement increased the program's credibility because of PHAC's official endorsement, while another advantage was the increased ability to reach other potential partners for Run to Quit or other health related programs. The funding from PHAC was helpful in many ways, and allowed the Running Room and the CCS to bring attention to and implement the program across the country more easily. PHAC's previous experience with health-focussed programs helped guide the rolling out of Run to Quit, while allowing CCS and the Running Room to maintain control of administering the program. Meanwhile, the Multi-sectoral Partnership approach enabled sharing of information and greater access to audiences.
PHAC benefited from the Run to Quit partnership in a number of ways. While key informants stressed that the programs funded through the MSP approach are not only about the money, this non-traditional approach to funding programs allows for better leveraging of financial and non-financial resources. The Run to Quit program resulted in an enhancement of the PHAC brand, expanding perceptions of PHAC as a valuable partner rather than a promoter of public health. In addition, opportunities like Run to Quit allow PHAC to try new and innovative approaches to public health issues, which help reach and influence Canadians.
As described in the partnership literature,Endnote 134 there are challenges or risks involved with multi-sectoral partnerships, such as partners' motives and potential conflicts of interest; negative impacts on reputation, particularly for public or non-profit sectors; power imbalances between partner organizations; and the loss of autonomy, particularly for less powerful partners While challenges can be expected when different organizations work together toward a common objective, benefits can include sharing of knowledge and experience, increasing the reach of the organizations involved, and improving engagement and accountability through partnership agreements.
One of the successes of the Run to Quit program linked to FTCS outcomes is that over a thousand people in Canada registered for the program in order to attempt to quit smoking, which is one of the key goals of the FTCS. While the number of participants who quit smoking by the end of the first round of the program is not available at this time these numbers are being collected and follow-up surveys done by the University of British Columbia will discover how many participants remain smoke-free.
Another success linked to FTCS outcomes is that the integration of the lessons learned will expand the reach and possible impact of the Run to Quit program which would help more Canadians quit smoking, including those within FTCS target populations.
Lessons Learned
Partner Communication
The three partners identified a number of lessons learned including the need for innovative approaches to public health issues, such as smoking. There was a great deal of praise for PHAC and the relationships between it and the partners, particularly for the regular communication between PHAC and the CCS and the Running Room. The positive experience of this open communication channel, which occurs bi-weekly, has led PHAC to incorporate this into many of its other multi-sectoral partnership projects.
Prolonged Approval Process
The contribution agreement between PHAC and the CCS was signed in July 2015, after approximately two years of negotiation and proposal developments. PHAC, CCS, and the Running Room all acknowledged this to be a lengthy process, due in part to the funding process requiring a great deal of detailed information and multiple steps. As noted by PHAC, many promising interventions can still take considerable time to shape into a proposal ready for final approvals, especially with new and non-traditional partners, who have never developed a funding proposal or navigated Government templates and approval processes.
Low Registration
Surveys were conducted by the Run to Quit team with Run to Quit partners (i.e., Running Room, CCS, etc) and with smokers who did not register for the programs to identify challenges and opportunities from the first year of the program in order to increase registrations in second and third years. Some of the responses included holding the program more than once a year, changing images on the Run to Quit website that reflect their target demographic, particularly to attract smokers who do not perceive themselves as fit enough to do the program, and improving the website to make the registration process easier.
There was considerable positive media attention on the program, including on traditional (e.g. radio, tv) and social media (e.g. Twitter, Facebook). Results from the internal and external surveys conducted in 2016 are allowing the Run to Quit team to better target their audience so to be able to increase registrations. For example, in January 2017 the Run to Quit team will market the program to take advantage of New Year's resolutions as well as Smoke Free Week.
Intentional Partnering
The importance of partnering with respected organizations, such as the CCS, the Running Room, and PHAC, was noted, especially in partnering with organizations that have experience in organizing public events, have experience in running social media campaigns, and have a well-regarded brand and reputation. The CCS, for example, is careful about who to partner with, particularly in the case of for-profit organizations, because of the need to protect the CCS's reputation.
Adaptations
Some of the provincial and territorial key informants noted concerns with the Run to Quit program, such as charging a registration fee to participate in the program, which limits some peoples' access to the program. This view was echoed by certain Public Health Units and other groups. In response to concerns, the program is working to find solutions and to help promote the Commit to Quit stream. Provincial and territorial key informants raised concerns about various accessibility issues, such as regions where long winters may make it difficult to run outside, or in rural areas where there are fewer safe places to run. The Run to Quit team is working on more comprehensive packages for remote communities for years 2 and 3, although has noted that a number of remote and First Nations and Inuit communities have created their own groups and participated in the online and Commit to Quit programs. Other concerns raised related to the need for federally funded programs to focus on collaboration with existing provincial and territorial programs.
Conclusion
The Run to Quit program is aligned with the FTCS's objective of helping people quit smoking, as well as CCDP's mission to mobilize multi-sectoral, evidence-based action to promote healthy living and prevent chronic disease. The Run to Quit program may have the potential to be adapted to different communities, populations, and health issues, something the CCS and the Running Room expressed an interest in doing.
The CCS and the Running Room suggested that Run to Quit will continue past the end of the PHAC funding. Interviewees expressed interest in expanding the project into other areas of the country, as well as expanding the program into communities where there are no Running Room stores. As described in the annual report, rural communities have already used the online (free and paid) programs and created their own teams, which Run to Quit plans to learn from in order to reach similar communities in years 2 and 3. In addition, the Run to Quit partners described how the Run to Quit program could be broadened or adapted for different environments or to address other public health issues. The CCS and Running Room were already in communication with a First Nations community on how to come up with a model that would work well in a First Nations community.
The Run to Quit program is a particularly interesting example of how partnerships between private sector organizations, NGOs, and the federal government can develop and implement innovative public health programs. While there were some challenges encountered, primarily regarding the length of time involved in the funding and approval process, these were largely negated through the good communication and assistance provided by PHAC. On the whole, PHAC, the CCS, and the Running Room expressed that their experience implementing Run to Quit had been favourable, and incorporated into future programming to the benefit of the Multi-sectoral Partnership initiative.
Case Study 2: Break It Off
Background
In January 2012, the Canadian Cancer Society (CCS) launched Break It Off, a new digital campaign, funded by Health Canada to promote tobacco cessation in the six Smokers' Helpline partner provinces across Canada (SK, MB, ON, NB, NS, PEI). The initial Break It Off campaign had a budget of $514,712 CDN and ran from January to March 2012. The campaign used the metaphor of ending an unhealthy relationship to support Canadians in breaking up with smoking. Led by the CCS's free cessation service, Smokers' Helpline, the initiative piloted practical solutions to provide cessation support through social media and a dedicated micro-site and smartphone app, while also providing information regarding the development of future and existing smoking cessation services for 19 to 29 year-olds, who have the highest smoking prevalence in the country. Break It Off was subsequently licenced by Health Canada and funded for the four-year period of April 2012 – March 2016 (fiscal years 2012-13 to 2015-16).
Program Profile
After the initial CCS funding ended, Health Canada licensed Break It Off and included it as part of the Federal Tobacco Control Strategy. A collaborative agreement between Health Canada (HC) and CCS was signed in February 2013 and included joint activities such as Public Opinion Research (POR) participation and feedback as well as stakeholder engagement from 2013 through to 2017.When Health Canada licensed Break It Off, the focus shifted from a digital-only initiative to a hybrid digital and in- person marketing campaign. The initial year of the marketing campaign, 2012-13, focussed primarily on strategy development. POR was conducted on attitude and behaviors of young adults (aged 20-24) in February 2013. Results of the research were used to further shape the campaign, ensuring that the messaging, resources and methods of delivery resonated with young adult audiences.
During 2013-14, the campaign's second year, development continued and website adjustments, web content changes and development of a bilingual website were completed. Members of Health Canada's Young Adult Leadership Team were consulted on Campaign materials and approach. Website changes included the addition of a stakeholder resource section that housed downloadable web buttons and banners and sharable social media posts. The Break It Off mobile application was also adjusted and improved upon. Both the website and the mobile app changes were completed in time for the launch (Ministerial Event in Vancouver, BC) on January 20th, 2014. The primary marketing tactic was in-person engagement events on university and college campuses and outdoor high traffic locations in order to engage young adult smokers (aged 20-24) in a dialogue on tobacco cessation while promoting the resources available on breakitoff.ca, as well as the Break It Off mobile application. No advertising funds were approved by Privy Council Office (PCO) to further promote the campaign.
For 2014-15, the third year of the campaign, engagement events were repeated during a more temperate season (Fall) as well as during National Non-Smoking Week (January). The focus for this fiscal was to build an online community where young adult smokers could engage in conversation about quitting smoking and receive information about the engagement events. A Facebook events page was launched on the Healthy Canadians Facebook page to provide a digital platform for sharing and discussion.
Performance Assessment
Methodology
The case study used interviews, document and file review, including performance measurement, to examine the Break It Off campaign's achievement of its intended outcomes. Interviews were conducted with the following individuals:
- Health Canada – Communication and Public Affairs Branch (1)
- Canadian Cancer Society (1)
- Break It Off experiential marketing team lead (1)
- Health Canada – Young Adult Leadership Team (2)
Activities and Outputs
Performance measurement for Break It Off tracked the number of in-person engagement events, the number of interactions at the events, number and type of promotional materials distributed (flyers and branded mints), number of video contest participants, website and mobile app activity and social media outreach. The goal of the campaign activities and outputs was to make progress towards the intended outcomes of:
- Increased awareness of the health hazards of smoking and the benefits of quitting among target populations. (Immediate Outcome)
- Changes in attitude toward quitting (such as increased motivation to quit) among those exposed to campaign materials. (Intermediate Outcome)
Between January 2014 and March 2015, 92 events were held across Canada, which engaged over 126,000 young adults in a conversation about quitting smoking, resulting in 47,000 visits to the website BreakItOff.ca, with an average duration of 1:12 minutes. In addition, there were a total of 1,335 Break It Off app downloads (1,136 Apple, 199 Android, 68% English, and 32% French). The majority of key informants believed that, with the exception of the social media component, engagement activities were mostly undertaken as planned and were largely successful. Key informants from all groups highlighted the in-person interactions as an area of success. Most also highlighted the stand alone campaign website and mobile app as innovative and successful ways to target the young adults aged 20-24. By allowing the campaign to deviate from the common look and feel of federal government websites, key informants believed that it was more likely to resonate with the target age group. While overall, the website was thought to be positive, some noted that it could be friendlier to mobile devices and was occasionally slow to load.
The primary criticism key informants had of the Break It Off Campaign was the lack of social media marketing and outreach. While the initial campaign as conceived by the CCS was primarily a social media campaign with a broad engagement and reach with youth, the social media aspect was not continued with Health Canada. When Break It Off moved from the CCS to Health Canada, government approval was not granted for the social media aspect of the campaign to proceed as originally planned. The campaign did not have a stand-alone Facebook or Twitter account for use in engaging the target population. While a Facebook events page was created for Break it Off in- person engagements as part of the Healthy Canadians account, it is unclear whether the target age group was reached as Healthy Canadians is primarily directed to the parents of young families and not youth aged 20-24.
The lack of social media engagement was felt by interviewees from all areas to be a missed opportunity for Health Canada to deepen the reach of the campaign. It was noted, however, that the parameters for all outreach activities was extremely limited during the time period under review and some key informants expressed hope that recent changes may lead to a loosening of some of the restrictions on social media use by departments.
Outcomes
Data on a number of activities and outputs were collected to provide performance measurement information. The Break It Off campaign met its key performance indicators. In addition, the Communication and Public Affairs Branch had an annual results meeting where best practices and lessons learned for the past year were reviewed and integrated into upcoming Break It Off events.
As there are many factors that influence the campaign's two intended outcomes of increased awareness of the health hazards of smoking and the benefits of quitting, and changes in attitude toward quitting, it is not possible to draw a direct causal link between Break It Off activities and any desired changes in the target population. However, post- event surveys completed by 764 event participants indicate that:
- 73% of those who received information at the events agreed that it motivated them to consider quitting;
- 38% of those who attended the events also visited the website; and
- 78% of those who visited the website agreed that the web content motivated them to consider quitting.
While the post-event surveys indicated that respondents were motivated to consider quitting smoking after attending a Break It Off event, the number of respondents was only a small proportion of all individuals reached by campaign events and materials. In addition, no follow-up survey was conducted in the months following the event, so it is not possible to determine whether there was any behavior change among campaign participants. Future iterations of Break It Off should consider aligning survey questions with those asked as part of the Canadian Tobacco Use Monitoring Survey or the Youth Smoking Survey and adding a follow-up component to the survey in order to identify any behavior change among event participants.
Conclusions
Documents reviewed and performance measurement data collected show that campaign events and activities occurred largely as planned with little variation between years. There is data on web metrics, app downloads and the in-person events. Key informants stated that they believe progress was made towards the achievement of the Break It Off campaign's intended outcomes. While it is reasonable to infer that campaign activities had some impact, a lack of baseline data as well as the difficulty in demonstrating a direct causal impact of campaign activities means that it is not possible to state definitively that the intended outcomes were achieved.
The majority of key informants interviewed felt that in-person events were a success. However, the lack of a social media component to the campaign was cited as a disappointment. Interviewees thought that reach could have been much greater with dedicated campaign Facebook, Twitter, Snapchat, etc. accounts. Several stated that the lack of social media engagement was a missed opportunity for the campaign that should be addressed if it is to continue.
Case Study 3: First Nations and Inuit Component of the Federal Tobacco Control Strategy
Background
Smoking prevalence rates for First Nations and Inuit adults are significantly higher than the broader Canadian population and have not realised the same rate of decline. As part of the renewal of the Federal Tobacco Control Strategy (FTCS) in 2012, funding was provided to the FNIHB of Health Canada to support a targeted number of First Nations and Inuit communities in the development and implementation of comprehensive tobacco control projects and strategies.
The First Nations and Inuit Component of the FTCS (FNICFTCS) is based on the six key domains of the WHO FCTC. The FCTC outlines key strategic elements for successful tobacco control. These key elements are: prevention; cessation; education; protection; pricing; and research, surveillance and evaluation. The original Strategic Operating Review proposal to Cabinet for the FNICFTCS included all of these components.
Concerns were raised by both the Inuit Tapiriit Kanatami (ITK) and the Assembly of First Nations (AFN). ITK sought to ensure that an Inuit –specific perspective be incorporated in the initiative and that there would be adequate time to engage Inuit communities. The AFN did not support the first iteration of the FNICFTCS as it was concerned that the initiative would be limited to a number of communities and that projects would have to adhere to all elements of the FCTC. Specifically, the element of pricing and taxation was viewed as interfering with First Nations jurisdiction and self-governance. A revised approach was developed to allow greater freedom for communities to decide how to reduce access to and availability of tobacco products within communities and to allow for a greater distribution of projects across all regions. These modifications upheld the original intent of the original approach.
The projects selected for funding include a full range of interventions under the following four pillars: Leadership (protection, reducing access to tobacco products); Health Promotion (prevention, education); Cessation; and Research and Evaluation (data collection and monitoring). All projects engaged with a Community of Practice established through the National Aboriginal Diabetes Association (via a three year funding agreement with FNIHB) to develop common data collection tools and reporting templates. Projects were encouraged to share relevant resources, promising practices and strategies around a continuum of tobacco control and prevention efforts. The Community of Practice also facilitated communication between the participants and experts in research and evaluation and tobacco reduction/ cessation.
In total, sixteen projects across all regions were funded. Funding was also provided to the British Columbia First Nations Health Authority, and the Governments of Nunavut and the Northwest Territories to support/ supplement tobacco control efforts in these jurisdictions. Along with the community based projects, two research projects are underway to mine existing survey data to address the gaps in knowledge regarding smoking prevalence within First Nations and Inuit communities in Canada.
Case Study
The purpose of the case study was to explore the progress of the FNICFTCS in supporting the development and implementation of comprehensive tobacco control strategies for First Nations and Inuit communities. It supports the FTCS evaluation.
Case Study Methodology
The case study included a review of documents provided by the program area (i.e., project descriptions, project proposals, project presentations), review of the FNICFTCS Annual Outcome Report, interviews with FNIHB staff both at the national and regional level (n=6), and project representatives (n=5). As the case study data collection took place during natural disasters in Alberta, projects and representatives from that area were not contacted. Projects were selected for interviews to provide a cross-sample of projects of various sizes, funding amount and communities engaged.
Assessment
Roles and Relationships
Most regions are represented in the projects. Projects reach 350 communities south of 60° and 25 communities in Nunavut. There is broad coverage in many provinces with the majority of projects including multiple communities. For instance, the First Nations Health Authority in British Columbia served 201 communities in 2015-2016 and key informants from Quebec reported that 100% of communities were being supported by activities in the FNICFTCS. However, the level of involvement of the communities varied.
Project representatives reported the funding process was clearly explained, and the support provided by the FNIHB staff was appropriate. Key to this support was engagement at the federal level at a later point and allowing regional representatives to work directly with the communities to prepare the funding proposals. FNIHB staff indicated there was a high degree of capacity in the projects selected.
All projects reported they had strong community support for their activities. Regional representatives reported that engaging the communities at the beginning of the process was critical as it increases transparency and allows them to work in a true partnership." Community support was evidenced by the depth of engagement. Results of the two- year review of the FNICFTCS indicated projects partnered with a broad range of community supports including: nurses, addictions service providers, Chiefs and Band Councils, and community Elders, or Elder Councils. Significant increases in the number of community partnerships between the first and second years of the FNICFTCS were reported for 12 categories of community partners, including: federal/ provincial police, educators, health care providers, youth councils, business owners/retailers, schools, community media, daycares, bylaw officers, youth role models, recreation centres and Aboriginal Head Start programs. They also reported that they targeted populations in addictions treatment, school administrators and staff, chiefs and chiefs' councils and students.
Best Practices
Sharing information through Community of Practice
Collaboration amongst the projects, and in particular the Community of Practice, was identified as one of the major successes. Established by the National Aboriginal Diabetes Association through a three-year funding agreement with FNIHB, the Community of Practice supports project performance measurement and data collection activities, and oversees analysis and consolidation of outcome results into annual reports.
Interviewees reported that the inter-organization communication facilitated by the Community of Practice disseminated information regarding specific projects, promising practices and performance measurement strategies. The annual gathering hosted by the Community of Practice was viewed as an invaluable meeting to get a better understanding of the tobacco control environment for Indigenous communities and link these communities without the need to travel to locations that would otherwise be cost- prohibitive.
Resources can be shared
Projects benefitted from sharing resource material across organizations. Interviewees reported that program resources were obtained through provincial and other levels of government, past iterations of the FNICFTCS and Inuit Tapiriit Kanatami. Communities and individuals who had previously participated in the First Nations and Inuit Tobacco Control Strategy that ended in 2007-2008, were viewed as experts or champions and were relied upon for their experience. Further, interviewees reported that communities that had developed resource material for the FNICFTCS were offering this material to other communities, schools and other organizations interested in Indigenous-based programming.
Separating commercial tobacco from ceremonial tobacco
Interviewees reported that it was critical for projects to be able to build a model that differentiated between the traditional and commercial tobacco use and respected the ceremonial use while targeting the commercial use for intervention. It was reported that, initially, there was some pushback from communities that argued the World Health Organization's pillars, upon which the FNICFTCS is based, did not take into account the First Nations' perspective. However, interviewees noted that the programming was really working well" after the communities integrated their cultural beliefs into the program framework. It was also noted that this was not a concern for Inuit as tobacco does not have the same cultural significance.
Lessons Learned
Several lessons have been learned that will help further the FNICFTCS and overall tobacco control within communities.
Importance of traditional tobacco in First Nations communities
Tobacco control activities in First Nations communities should not only focus on commercial tobacco to the exclusion of ceremonial tobacco but also support awareness of issues surrounding ceremonial tobacco. Interviewees stressed the importance of developing respect and protection for traditional tobacco through increased awareness and knowledge of practices and sacred places. This would help First Nations communities distinguish between traditional and commercial tobacco, and help them better relate to the former. Access to traditional tobacco was identified as a related concern as it was perceived as often difficult to obtain and more expensive. This leads to the inappropriate use of commercial tobacco in traditional ceremonies. Future programming might consider addressing this need through education regarding the growing and cultivating of traditional tobacco and its use where it is feasible.
Different communities are at different stages
Flexibility in choosing specific pillars to focus on was reported to be an important feature for First Nations and Inuit communities establishing a FNICFTCS program. Although potential programs were to have submitted their plans to address all four required pillars, it was understood that communities could choose which area to emphasize. This allows programs to direct activities to the specific point at which the community required intervention. While some communities were in a position to begin adopting intervention practices, others were more in need of communication strategies to denormalize tobacco use. While the importance of a comprehensive approach was understood to be beneficial at the planning stage, the freedom to apply different strategies as per the needs of the community facilitated program adoption.
Sustainability
Concern was expressed by interviewees regarding the future of the FNICFTCS. Community stakeholders believed that the first iteration of the FNICFTCS, which began in 1997 (the First Nations and Inuit Tobacco Control Strategy), was successful with gains being made and momentum building. Thus, programs were disappointed when funding for the strategy ended in 2008-2009 and community representatives felt that the gains made during this period retreated. Interviewees reported that communities were hesitant to participate in the FNICFTCS as a result of the abrupt ending of the previous iteration. Programs indicated that it was difficult to obtain and retain staff as the stability of the positions was questioned. Difficulties in filling staff positions were identified as a cause for delays in program offerings.
Achievements
The FNICFTCS has four key-success indicators: increased smoke-free spaces, increased number of smoking related resolutions, decreased percentage of daily smokers and developing and sharing promising practices. Interviewees noted that measuring the impacts of the programming would be challenging as it has been estimated that it may take a generation to demonstrate changing attitudes and denormalization. Despite this concern, the 2015-2016 Annual Outcomes Report indicates that progress has been made on several fronts.
As measured against baseline data collected in 2014-2015, the number of smoke-free spaces has increased in 2015-2016 from 676 (466 indoor spaces, 210 outdoor spaces) to 1688 (1001 indoor, 687 outdoor). The average number of smoke-free spaces reported per project increased from 56 to 102. First Nations/ Band offices and schools were the types of spaces that were most frequently designated as smoke-free from 2014-2015 to 2015-2016.
In 2014-2015, one-third of projects reported that governing bodies in their area had passed smoking-related resolutions. This proportion increased to 67% in 2015-2016. Additionally, the number of smoking-related resolutions that these governing bodies passed increased. There had been 23 smoking-related resolutions passed in 2014-2015 and one year later, there had been 53 resolutions passed. Resolutions included designated smoke-free spaces, using tobacco-related revenues to fund health promotion activities, promoting smoke-free homes, expanding smoke-free perimeters surrounding buildings, and enforcing smoke-free spaces.
Seven projects reported smoking cessation activities directed toward one or more of the target groups were reported in 2015-2016. These projects estimated that 3197 individuals had started a smoking cessation program and that 1141 (36%) had already completed the program. Of those that had started the program 163 (5.1%) had reduced their levels of tobacco consumption and 52 had reported that they had quit smoking (1.6%).
More projects have begun undertaking activities to assess their performance such as collecting baseline data on smoking statistics, project monitoring and reporting. In 2014- 2015, 53% of projects had begun collecting cessation data using a population or community-level survey. In 2015-2016, this proportion increased to 73%. Further, a greater proportion of projects that were to collect smoking cessation data have started to collect their data (42% in 2015-2016 vs. 25% in 2014-2015) and more have now completed data collection (58% vs. 13%).
Conclusions
The FNICFTCS is an important element of the broader FTCS as it focuses on a segment of the Canadian population with higher prevalence rates. Interviews, documents and the Annual Outcome report indicate the FNICFTCS has had many successes in its first two years despite a limited timeframe to fully implement projects and collect outcome data. It should be expected that successes will accumulate as additional projects are fully implemented and others mature.
A community's ability to develop tobacco control activities specific to its needs has been an important feature of the FNICFTCS. The funded communities expressed support for this flexibility in programming and also in respecting traditional or sacred tobacco.
Funded projects also expressed support for connecting projects across the country through the Community of Practice. These connections have helped to develop a common reporting strategy that will facilitate measuring progress as the projects continue.