
Archived - Evaluation of the eHealth Infostructure Program 2011-2012 to 2015-2016
Download the alternative format
(PDF format, 1,098 K, 94 pages)
Organization: Health Canada
Date published: 2017-07-??
Prepared by Office of Audit and Evaluation
Health Canada and the Public Health Agency of Canada
March 2017
Table of Contents
- Executive Summary
- Management Response and Action Plan
- 1.0 Evaluation Purpose
- 2.0 Program Description
- 3.0 Evaluation Description
- 4.0 Findings
- 4.1 Relevance: Issue #1 – Continued Need for the Program
- 4.2 Relevance: Issue #2 – Alignment with Government Priorities
- 4.3 Relevance: Issue #3 – Alignment with Federal Roles and Responsibilities
- 4.4 Performance: Issue #4 – Achievement of Expected Outcomes (Effectiveness)
- 4.5 Performance: Issue #5 – Demonstration of Efficiency and Economy
- 5. Conclusions
- 6.0 Recommendations
- Appendix 1 – Logic Model: eHealth Infostructure Program (eHIP)
- Appendix 2 – Summary of Findings
- Appendix 3 – Evaluation Description
List of Tables
- Table 1. Limitations and mitigation strategies.
- Table 2. Broadband availability among First Nations Bands funded by the eHealth Infostructure Program for Internet connectivity as of March 2016.
- Table 3. Broadband availability amongst First Nations Bands funded by the eHealth Infostructure Program for Internet connectivity with nursing stations as of March 2016.202
- Table 4. Number of First Nations communities with Panorama Public Health Information System.
- Table 5. Number of First Nations communities with a non-Panorama Public Health Information System.
- Table 6. Number of First Nations communities with eHealth Infostructure Program-funded nursing stations with Panorama Public Health Information System.
- Table 7. Number of First Nations communities with eHealth Infostructure Program-funded nursing stations with a non-Panorama Public Health Information System.
- Table 8. Number of First Nations communities with access to Electronic Medical Records.
- Table 9. Number of First Nations communities with access to a provincial Electronic Health Records.
- Table 10. Number of First Nations communities with eHealth Infostructure Program-funded nursing stations with access to Electronic Medical Records.
- Table 11. Number of First Nations communities with eHealth Infostructure Program-funded nursing stations with access to a provincial Electronic Health Records.
- Table 12. Number of telehealth sites funded by the eHealth Infostructure Program in First Nations communities.
- Table 13. Number of telehealth sites funded by the eHealth Infostructure Program in First Nations communities with nursing stations.
- Table 14. Number of telehealth educational sessions.
- Table 15. Number of telehealth administrative sessions.
- Table 16. Number of telehealth clinical sessions.
- Table 17. Annual eHealth Infostructure Program budgets by fiscal year ($).
- Table 18. Annual eHealth Infostructure Program expenditures (actuals) by region by fiscal year ($).
- Table 19. Annual eHealth Infostructure Program expenditures (actuals) by financial code by fiscal year ($).
- Table 20. Cost avoidance of as a result of telehealth clinical sessions – Alberta, Saskatchewan, Manitoba and Ontario, 2015-2016.
- Table 21. Cost avoidance of medically necessary travel a result of telehealth clinical sessions – Alberta, Saskatchewan, Manitoba and Ontario, 2015-2016.
List of Figures
- Figure 1: eHealth components and elements.
- Figure 2: Top types of telehealth clinical sessions as reported by Keewaytinook Okimakanak eHealth Telemedicine Services for 2015-2016.
- Figure 3: Policy and regulation that could apply to remote monitoring solutions.
List of Acronyms
- AB
- Alberta
- ACES
- Alaska Clinical Engineering Services
- ACRRM
- Australian College of Rural and Remote Medicine
- ADMO
- Assistant Deputy Minister's Office
- AeHN
- Alaska eHealth Network
- AFHCAN
- Alaska Federal Health Care Access Network
- AFN
- Assembly of First Nations
- ANTHC
- Alaska Native Tribal Health Consortium
- BC
- British Columbia
- cEMR
- Community EMR
- CFOB
- Chief Financial Officer Branch – Health Canada
- CHIP
- Community Health and Immunization Program
- CSB
- Corporate Services Branch – Health Canada
- eHIP
- eHealth Infostructure Program
- EHR
- Electronic Health Record
- EMR
- Electronic Medical Record
- F/P/T
- Federal/Provincial/Territorial
- FNEC
- First Nations Education Council
- FNHSSM
- Nanaandawewigamig – First Nations Health and Social Secretariat of Manitoba
- FNIHB
- First Nations and Inuit Health Branch – Health Canada
- FNQLHSSC
- First Nations of Quebec and Labrador Health and Social Services Commission
- HCOM
- Health Co-Management
- HFCP
- Health Facilities and Capital Program
- HIE
- Health Information Exchange
- HISAP
- Health Infostructure Strategic Action Plan
- HQ
- Headquarters
- ICTs
- Information and Communications Technologies
- IMSD
- Information Management Services Directorate – Corporate Services Branch
- INAC
- Indigenous and Northern Affairs Canada
- Infoway
- Canada Health Infoway
- ISED
- Innovation, Science and Economic Development Canada
- ISP
- Internet Service Provider
- IT
- Information Technology
- ITK
- Inuit Tapiriit Kanatami
- KOeTS
- Keewaytinook Okimakanak eHealth Telemedicine Services
- KRG
- Kativik Regional Government
- LAN
- Local Area Network
- MATC
- Manitoba Adolescent Treatment Centre
- MB
- Manitoba
- mHealth
- Mobile Health
- MOP
- Management Operational Plan
- NB
- New Brunswick
- NIHB
- Non-Insured Health Benefits
- NITHA
- Northern Inter-Tribal Health Authority
- NL
- Newfoundland and Labrador
- NLCHI
- Newfoundland and Labrador Centre for Health Information
- NS
- Nova Scotia
- OCAP
- Ownership, Control, Access and Possession
- OHIP
- Ontario Health Insurance Plan
- ON
- Ontario
- OTN
- Ontario Telemedicine Network
- PCEHR
- Personally Controlled Electronic Health Record
- PDA
- Personal Digital Assistants
- PEI
- Prince Edward Island
- PHIS
- Public Health Information System
- QC
- Québec
- SK
- Saskatchewan
- SSC
- Shared Services Canada
- SUS
- Unified Health System
- TSAG
- Technical Services Advisory Group
Executive Summary
This evaluation covered the activities of Health Canada's eHealth Infostructure Program (eHIP) for the period from 2011-2012 to 2015-2016. The evaluation was required by Section 42.1 (1) of the Financial Administration Act (1985), according to which every department shall conduct a review, every five years, of the relevance and effectiveness of each ongoing program for which it is responsible. The Treasury Board of Canada's Policy on Results (2016) defines such a review as an evaluation.
Based on the evaluation findings, the Program continues to address a fundamental, demonstrable need and is well aligned with government priorities as well as federal roles and responsibilities. The Program has made considerable contributions to increase access to primary care delivery by First Nations communities and has exceeded many of its targets in the deployment of eHealth infostructure technologies and tools. It has enabled First Nations and health care providers to improve their skills and has partnered at multijurisdictional levels to effect the integration of health services. There remain many opportunities for improvement (e.g., in broadband connectivity, IT support, health facility readiness for eHealth technologies, local capacity and awareness, interoperable systems, telehealth utilization, and deployment of mobile health). Recommendations provided by the evaluation are geared towards supporting the Program in its continuing work in these areas.
Evaluation Purpose and Scope
The scope of the evaluation covered the period from April 1st, 2011 to March 31st, 2016 and included all the elements and eHealth components of the Program. The one area of exclusion was the assessment of any services transferred to the British Columbia First Nations Health Authority on July 2013 in accordance with the British Columbia Tripartite Framework Agreement on First Nation Health Governance and sub-agreements, which will be covered under a separate and forthcoming evaluation.
The evaluation was aligned with the Treasury Board of Canada's Policy on Results (2016) and considered core issues under the themes of relevance and performance. Corresponding to each of the core issues, specific questions were developed based on Program considerations and these guided the evaluation process. An outcome-based, non-experimental evaluation approach was used for the conduct of the evaluation to assess the progress made towards the achievement of the expected outcomes, whether there were any unintended consequences and what lessons were learnt.
Data for the evaluation was collected using various methods, which included a document and literature review, an administrative data review and analysis, key informant interviews, case studies, a review and analysis of eHealth approaches across international jurisdictions, and an examination of available financial data for the Program. Data was analyzed by triangulating information gathered through these different methods. The use of multiple lines of evidence and triangulation were intended as a way to increase the reliability and credibility of the evaluation findings and conclusions.
Program Description
eHIP, under the First Nations and Inuit Health Branch (FNIHB), works towards the modernization, transformation, improvement and sustainment of health care services in First Nations communities.Footnote i It supports and funds a combination of eHealth information, applications, technology and people to help provide First Nations with: optimal health services delivery; optimal health surveillance; effective health reporting, planning and decision making; and, integration/compatibility with other health services delivery systems. To carry out its mandate, eHIP functions in an environment that includes other federal partners, provinces, First Nations communities and regional organizations to achieve progress on the various dimensions of eHealth.
The implementation of eHIP is a shared responsibility between the national Program headquarters in Ottawa and six regional offices: the Atlantic region (including the provinces of Nova Scotia, Prince Edward Island, Newfoundland and Labrador and New Brunswick), Québec, Ontario, Manitoba, Saskatchewan and Alberta.
Conclusions - Relevance
Continued Need for the Program
The Program continues to address a demonstrable, fundamental need to improve the health status of First Nations. Specifically, the Program provides eHealth services to First Nations communities, reduces travel time and costs as well as displacement from family and community. By connecting patients with specialists for diagnostic examinations and follow ups, eHIP helps to narrow the gap in access to health care services for First Nations compared to the general population in the provinces. eHealth also allows for better continuity of care by facilitating information sharing between health care providers on- and off-reserve in support of better care assessment and decision making.
Alignment with Government Priorities
The Program is aligned with government priorities, which include keeping pace with technology and innovation, contributing to address health system challenges and system reform, and building relationships with Indigenous peoples. eHIP's objectives align with Health Canada's priorities and includes FNIHB's strategic objectives, namely, ensuring availability of, and access to, quality health services, supporting greater control of the health system by First Nations and Inuit, and supporting the improvement of First Nations health programs and services through improved integration, harmonization and alignment with federal/provincial/territorial (F/P/T) health systems.
Alignment with Federal Roles and Responsibilities
The Program is aligned with federal roles and responsibilities. While Health Canada has overall responsibility for the development and implementation of eHIP and ensuring that funding is appropriately allocated and spent according to established criteria and guidelines, FNIHB's role is to integrate F/P health systems for the benefit of First Nations, and to increase First Nations community health services capacity to address their own health needs.
Conclusions – Performance
Achievement of Expected Outcomes (Effectiveness)
Immediate outcomes
The evaluation found that First Nations communities and health care providers have access to eHealth technologies. For example, the Program has exceeded its target for broadband connectivity; however, while all eHIP funded First Nations Bands have Internet connectivity, the available bandwidth and connection reliability is variable. The Program has also exceeded its targets on Public Health Information Systems (PHIS) and Electronic Medical Record (EMR)/Electronic Health Record (EHR) implementation. Telehealth continues to grow but its uptake/utilization has been uneven across remote/isolated and isolated communities. Mobile Health (mHealth) appears promising and is in its developmental phase.
eHIP has enabled First Nations, FNIHB staff and health care providers to improve their skills and knowledge by providing opportunities through telehealth education and administrative sessions in various formats. Telehealth educational sessions offered to First Nations individuals and health care providers have allowed them to acquire information and knowledge on a number of health-related areas such as, diabetes education, drug awareness, population health, community health planning, health indicator development and measurement, public health surveillance, health information management, and training on new health equipment. Available information indicates the usefulness and efficiency of telehealth educational sessions among frontline health care workers, staff and communities.
The Program has engaged partners and stakeholders in collaborative, integrated planning of eHealth technologies by using a number of mechanisms for multi-party engagement. In terms of harmonization, eHIP is working with First Nations and F/P representatives in effecting the integration of health services by identifying opportunities and actively engaging in multi-jurisdictional partnerships.
Intermediate outcomes
First Nations and health care providers are using eHealth technologies for the delivery of health care services. Clinical telehealth sessions are delivered in many First Nations communities covering numerous topics. The Program has exceeded its target of providing clinical sessions via telehealth to First Nations communities. These sessions have covered a multitude of clinical specialties.
Opportunities exist for greater collaboration and integration with First Nations regional organizations, the federal family (i.e., Health Canada, Indigenous and Northern Affairs Canada – INAC, Innovation, Science and Economic Development Canada – (ISED)) as well as within Health Canada that could result in increased and more stable Internet connectivity and bandwidth thus further enabling clinical telehealth in remote/isolated and isolated First Nations communities. There is also an opportunity for addressing IT-related issues through a client-focused support approach that clearly defines the roles and responsibilities of all partners (i.e., eHIP, the Information Management Services Directorate – (IMSD) of Health Canada's Corporate Services Branch (CSB), and Shared Services Canada – (SSC)). This would support eHealth integration into primary and public health care delivery in First Nations communities.
Furthermore, developing standards and guidelines on network and connectivity/bandwidth requirements linked to each eHealth component would be advantageous as it would be the integrated planning and refurbishing of health facilities to accommodate eHealth and its components
Uptake of telehealth in some remote/isolated and isolated communities could be increased through promotion among First Nations individuals, families and communities as well as health care practitioners in addition to providing enhanced support on the ground (e.g., telehealth coordinators). Further support for mHealth by helping communities address challenges related to connectivity and communications security may aid technology adoption.
Interoperable eHealth technologies have been implemented in First Nations communities. PHIS and electronic records implementation have exceeded targets. Nonetheless, interoperable PHIS and electronic records are at different stages of implementation across provinces and First Nations communities. Despite progress, there is a need to resolve several legislative, jurisdictional and logistical issues that impede uptake in this area, none of which are in the sole purview of the Program. For example: lack of alignment between F/P privacy legislations affecting federal and First Nations nurses' access to patient information on provincial systems, adequate connectivity/bandwidth, proliferation of non-interoperable electronic records systems, clarification of responsibility for physician remuneration as a result of eHealth delivery, and provision of appropriate/ongoing funding.
Although an approach to EMR implementation has been developed by eHIP, interoperability with provincial systems remains a key challenge and largely outside the control of the Program. There is a need for greater collaboration to improve engagement and alignment between F/P governments and First Nations communities. A focus on the alignment of F/P privacy legislation together with the development of a common ground to spur collaboration between all parties would help overcome the barriers.
Strong partnerships with knowledgeable organizations around the principles of Ownership, Control, Access and Possession (OCAP), such as Canada Health Infoway (Infoway), may help to increase awareness and willingness to integrate health data among many remote/isolated and isolated First Nations communities; generally, these communities do not benefit from the leadership provided by strong First Nations regional organizations (e.g., communities in Southern Saskatchewan, those outside Keewaytinook Okimakanak eHealth Telemedicine Services – KOeTS in Ontario, and many in Atlantic Canada).
With respect to opportunities to increase the implementation efficiency of interoperable eHealth technologies, it would be desirable to arrive at commonly agreed F/P goals to assist First Nations in selecting solutions that address their needs while ensuring interoperability with provincial systems. In addition, a systematic, coordinated community assessment process to identify eHealth component readiness, community technical capacity (e.g., human resources), available/needed training and infrastructure would increase implementation success.
Long-term outcomes
Access to and quality of health care services has improved for First Nations individuals, families and communities over the past five years. Across the regions, eHealth components are being made available to federal and First Nations health care providers to enable the provision of timely access to health care services while allowing providers to engage with patients and improve the quality of care. Clinical telehealth is contributing towards improving access and enhancing the number of available health services in First Nations communities. Telehealth educational sessions are viewed as valuable for health care provider training and in health promotion and disease prevention in First Nations communities. While there are many examples to support increased access, quality and safety, there are opportunities to implement systematic surveying, analysis and reporting of user experience with the various eHealth components to allow for routine assessment of levels of satisfaction and identification of areas for improvement.
Planning, surveillance and reporting of health data in First Nations communities have also been enhanced as a result of eHealth, although there are further opportunities for improvement across communities, specifically in terms of the availability of qualified, dedicated personnel for data collection and regular analysis based on a core set of common indicators within and across regions.
Health care providers have access to and use provincial health information systems in First Nations communities. Where implemented, users see these systems as helpful in planning and in managing the health care of First Nations individuals, families and communities. For example, where deployed, nurses see immunization and vaccine inventory modules as enabling them to provide improved patient care. PHIS and electronic records are allowing for better case management, improved patient safety and informed decision-making by health care providers.
Demonstration of Efficiency and Economy
There is evidence to indicate that the Program's utilization of resources in relation to the production of outputs and progress toward expected outcomes is efficient and economical. Program goals are actively communicated while alignment between projects, eHealth components and regional needs and priorities are ensured.
Efficiency
Despite efforts to remain aligned, due to the rapidly changing eHealth context, it is challenging for eHIP to track regional status and overall national situation; hence, there is a need to conduct community and technology environmental scans on an ongoing basis to inform Program guidelines. Also, when decisions are made with respect to bandwidth or solutions for interoperability of systems between First Nations and provinces, regional and sub-regional contextual factors should be examined in order to attain a better fit for the communities. In this context, there may be a need to re-examine the Health Infostructure Strategic Action Plan (HISAP) to ensure it reflects a grassroots approach.
Currently, regions employ a variety of project plans and readiness assessment templates. While, in principle, a thorough assessment is being made through the use of ad hoc criteria, check lists and committees, opportunities exist for a more cohesive, planned approach to project assessment that would assist in greater efficiencies and economies of scale.
Economy
Program expenditures over the five years of the evaluation ranged between $22 and $25 million annually, with the exception being 2012-2013 when the highest expenditure of $30 million was incurred. Cost avoidance for the Program as a result of all telehealth clinical sessions delivered in four regions (for which data was available) in 2015-2016 was estimated at approximately $11.7 million. Cost avoidance as a result of those telehealth clinical sessions that would have been considered medically necessary by the Supplementary Health Benefits (Non-Insured Health Benefits) Program delivered in the same regions and during the same fiscal year was estimated at approximately $6.5 million.
Evidence suggests the need for a three- to five-year funding horizon to realize efficiencies from a longer-term implementation of the various technology-based eHealth components. Current year-to-year funding management may be creating efficiency gaps as a result of piecemeal, short term implementation (e.g., equipment purchased but not used). The longer-term plan should be based on a robust analysis of which communities would be supported first for basic needs like Internet connectivity and capacity training, and how the progression will be made with respect to eHIP component growth (e.g., electronic records, PHIS, telehealth and mHealth). The plan would also have room for funding innovation and for evergreening equipment.
Another aspect of planning and funding would involve engaging partners at multilateral tables to identify parallel funding sources (e.g., from other federal departments or provincial support). Examples include involvement of Infoway in some First Nations eHIP component implementation, use of the Health Services Integration Fund (HSIF), partnering with INAC to share connectivity with schools or fibre build, etc. This approach could be expanded to support innovation. There is also a need to develop a plan on how to address those communities that do not have a strong champion or regional leadership (such as the Technical Services Advisory Group – (TSAG), the Northern Inter-Tribal Health Authority – ( NITHA), the First Nations Health and Social Secretariat of Manitoba – (FNHSSM), the First Nations of Québec and Labrador Health and Social Services Commission – (FNQLHSSC), Atlantic Canada's First Nation Help Desk, and KOeTS) and may be falling behind on eHealth.
Performance measurement
Data collection and reporting has improved during the period of the evaluation, particularly in the last three years. Opportunities exist for consistent and timely data collection and reporting across all regions, communities and health facilities. Applying clear data definitions and focusing on Program-funded communities would help data quality.
There are many advantages to be realized by systematically collecting and analyzing performance data at timely intervals. It is understood that some communities, First Nations regional organizations and even regional Program offices may lack on the ground capacity to perform these activities. One of the key considerations in setting up a performance measurement system is to look at the feasibility of the required data given the capacity on the ground. The evaluation has suggested a number of indicators, some of which are already being used by the Program, around which data collection and analysis could be enhanced to lend support for future Program decisions, including funding needs.
Recommendations
The incremental work of the Program in the various eHealth areas has contributed to the achievement of its outcomes. While the Program has met or exceeded most of its key targets, the following recommendations identify areas where continuing work will help the Program further its work with a long term view towards deploying, maintaining and realizing the benefits of digital infrastructure for First Nations individuals, families and communities.
Recommendation 1. Enhance partnership, collaboration and integration with partners and stakeholders to continue to improve Internet connectivity to provide equitable access to underserved First Nations communities.
Broadband connectivity
Applying a coordinated and community-focused effort with Program partners and stakeholders, such as First Nations regional organizations, INAC, ISED, provincial governments and private industry, would allow eHIP to derive benefits from existing/planned activities, foster standardization in enabling appropriate bandwidth for eHealth components, and identify First Nations communities' broadband needs and available funding from various sources to address Internet connectivity challenges.
eHealth component requirements
Identifying and defining broadband requirements for eHealth components would allow the Program to ascertain service gaps. These requirements should be based on standardized technical guidelines for each eHealth component (e.g., electronic records, PHIS, telehealth) in alignment with provincial standards, if any. Assessing health facility readiness for eHealth based on these and other infrastructure requirements (e.g., plug-ins for telehealth equipment in emergency rooms, room acoustics/privacy considerations, Local Area Network and related equipment condition, etc.) would allow the Program to identify any needed enhancements.
Recommendation 2. Advance work with partners, to address IT- and health facility-related issues to enable health care practitioners (nurses) to integrate eHealth tools into primary and public health care delivery.
Roles and responsibilities for IT support and health facility infrastructure
Clarifying the roles and responsibilities of partners within and outside Health Canada (e.g., First Nations regional organizations, eHIP, the Health Facilities and Capital Program, IMSD, SSC), and establishing client-focused mechanisms to ensure that IT issues experienced by health care workers (e.g., nurses) are addressed in a timely manner, would help further eHealth adoption and integration into primary and public health care delivery. The current efforts between FNIHB and IMSD on improving IT support for FNIHB employees in remote/isolated and isolated communities should continue in order to address roles and responsibilities and, potentially, health facility infrastructure issues. In addition, the gap in IT infrastructure and support for transferred First Nation health facilities should be assessed periodically for sustained use of eHealth applications.
Recommendation 3. Work closely with provincial governments, federal partners (e.g., Infoway), First Nations regional organizations and communities to further integrate approaches to render electronic records and PHIS interoperable, effective and efficient by removing jurisdictional, legislative and logistical hurdles.
F/P privacy legislations
Collaboration among F/P partners should focus on identifying information sharing solutions to address issues surrounding federal and First Nations nurses and their access to patient data on provincially connected PHIS and electronic records. This is an area of high priority requiring resolution across most provinces.
Data sharing agreements
Successful implementation of data sharing agreements requires extensive engagement with First Nations, provincial and federal partners to address challenges with interoperable systems. Further engagement would help advance work on alignment with provincial systems and privacy issues as well as widespread integration of OCAP principles in data sharing agreements to ensure health data can be exchanged in a way that meets the needs of all parties. Resolving data privacy/sharing issues would not only contribute to the provision of seamless care on- and off-reserve but also to address issues related to health care practitioner billing.
F/P vision alignment
Defining a coordinated vision and partnership on eHealth systems with First Nations communities and provincial governments would help achieve commonly agreed goals for new technologies based on a common ground. This, in turn, would help establish realistic timelines for eHealth component implementation that would make optimal use of limited resources while ensuring implementation satisfaction.
Recommendation 4. Continue to engage First Nations communities to enhance knowledge, capacity and control over their health care service delivery and use of health data for evidence-based decision making.
Promotion
eHealth capacity and adoption would benefit from promoting best practices and success stories in the implementation of the various eHealth components (i.e., electronic records, PHIS, telehealth and mHealth). Further benefits would be accrued by sharing the positive results of partnerships with First Nations regional organizations such as FNHSSM, the First Nations of Quebec and Labrador Health and Social Services Commission, NITHA, TSAG, KOeTS and Atlantic Canada's First Nation Help Desk. First Nations communities with low awareness of eHIP or that lack a strong regional champion/leader may require support/encouragement to pool together and work with a First Nations regional organization to lead eHealth on their behalf.
Readiness assessments
In partnership with First Nations regional organizations and communities, developing and applying a systematic, coordinated, cohesive community assessment process to identify eHealth component readiness and community technical capacity (e.g., IT workers, data infrastructure staff, nursing staff, telehealth coordinators, data specialists) would help in identifying the required training and infrastructure to build capacity and successfully implement and maintain eHealth components.
Capacity development
Increasing the ground level capacity of health care practitioners and health facility staff on the use of eHealth tools may enhance primary and public health care delivery (e.g., continue to train nurses in the use of telehealth equipment). Moreover, continuing to grow the number of eHealth/telehealth coordinators would contribute to support and promote telehealth and other eHealth components (e.g., electronic records, PHIS and mHealth).
Collaborative strategy
Conducting regular community and technology environmental scans, within regional and sub-regional contexts, would help inform Program guidelines affecting all eHealth components. Reassessing HISAP in collaboration with First Nations communities and regional organizations would make it the product of a balanced, bottom-up (grassroots) and top-down process.
Recommendation 5. Improve performance data collection and analysis across regions and over time on key performance indicators by setting up a Program performance measurement system that takes into consideration the capacity on the ground.
Identifying key indicators, such as those reported by the evaluation, and establishing consistent definitions across regions and data collection entities would help improve data collection. Ensuring clarity of definitions and establishing a data reporting cycle would help accurate and regular analysis to inform timely decision-making.
Recommendation 6. Develop a long-term plan that is sufficiently flexible to accommodate technology innovation and a commensurate funding strategy for e-HIP.
Providing a long-term plan and funding view, in concert with technology-based projects, that fully supports all aspects of implementation and sustainability, including capacity, training and bandwidth, would contribute to the long-term vision of the Program. Part of this exercise should include identifying which communities would be supported first for basic needs like Internet connectivity and capacity training, and how the progression will be made with respect to eHIP component growth (e.g., electronic records, PHIS, telehealth, mHealth).
Incorporating innovation allocations would allow the plan to grow together with technology advancements, such as wireless connectivity, bandwidth and data security; technology development in mHealth and personal telehealth (e.g., via laptops and iPads); storage and streaming technologies for educational sessions; and, evergreening of equipment.
Management Response and Action Plan (or Management Response)
| Recommendations | Response | Action Plan | Deliverables | Expected Completion Date | Accountability | Resources |
|---|---|---|---|---|---|---|
| Recommendation as stated in the evaluation report | Identify whether program management agrees, agrees with conditions, or disagrees with the recommendation, and why | Identify what action(s) program management will take to address the recommendation | Identify key deliverables | Identify timeline for implementation of each deliverable | Identify Senior Management and Executive (DG and ADM level) accountable for the implementation of each deliverable | Describe the human and/or financial resources required to complete recommendation, including the source of resources (additional vs. existing budget) |
Recommendation 1 Enhance partnership, collaboration and integration with partners and stakeholders to continue to improve Internet connectivity to provide equitable access to underserved First Nations communities. |
Management agrees with the recommendation. | The eHealth Infostructure Program (eHIP) works together with its partners and stakeholders to improve broadband connectivity for First Nations communities. | 1.1 Site profiles for all in-scope facilities. | 1.1 September 2017 | Executive Director, CIAD, FNIHB | Existing budget |
|
In recognition of the importance of partnership, FNIHB has started the Connectivity for First Nation Health Facilities project to provide a clear understanding of connectivity needs for on-reserve health facilities in 6 regions (Atlantic, Quebec, Ontario, Manitoba, Saskatchewan and Alberta). The project links key partners, eHIP national office, eHIP regions, Internal Client Services and Transition Directorate, FNIHB, Health Facilities Program, FNIHB, Information Management and Systems Directorate, Corporate Services Branch (CSB), Real Property and Security Directorate, CSB, and Shared Services Canada. The project will identify current state connectivity by:
|
1.2 Connectivity Gaps Analysis Report. | 1.2 November 2017 | ||||
|
Recommendation 2 Advance work with partners, to address IT- and health facility-related issues to enable health care practitioners (nurses) to integrate eHealth tools into primary care delivery. |
Management agrees with the recommendation |
eHIP works with partners across Health Canada and Shared Services Canada toward greater collaboration with a view to improved delivery of primary care through the use of eHealth tools. Specifically, the program participates actively in the IT Support for FNIHB Nurses Working Group, led jointly by Information Management and Services Directorate, CSB, and Internal Client Services and Transition Directorate, FNIHB in support of incrementally addressing IT infrastructure and support for nurses working in remote and isolated locations where primary care services are provided by FNIHB employees. |
2.1 Development of model that will provide simpler service desk support to nurses. | 2.1 March 2018 |
Executive Director, CIAD, FNIHB Executive Director, ICST, FNIHB |
Existing budget |
|
Recommendation 3 Work closely with provincial governments, federal partners, (e.g., Infoway), First Nations regional organizations and communities to further integrate approaches to render electronic records and Public Health Information Systems interoperable, effective and efficient by removing jurisdictional, legislative and logistical hurdles. |
Management agrees with the recommendation | FNIHB has undertaken a region-by-region approach with provincial government partners, as appropriate, to identify information sharing solutions appropriate for the provincial context. Joint work on the development of action plans is in its early stages, and FNIHB will work together with provincial governments where there are willing partners. Resolving the information-sharing issues will translate to greater uptake of electronic medical records and public-health information systems. | 3.1 Joint action plans with provincial partners to address privacy issues. | 3.1 March 2019 |
Executive Director, CIAD, FNIHB Regional Executives, FNIHB |
Existing budget |
| eHIP regions are working with First Nations partners such as the Assembly of First Nations (AFN) and regional First Nations organizations to identify community-driven priorities and approaches , and with other partners, including Canada Health Infoway, in support of these priorities and approaches. | 3.2 Rollup of regional priorities regarding implementation of digital health technologies. | 3.2 March 2018 | ||||
|
Recommendation 4 Continue to engage First Nations communities to enhance knowledge, capacity and control over their health care service delivery and use of health data for evidence-based decision making. |
Management agrees with the recommendation |
FNIHB work with its national and regional First Nations partners to build capacity to support eHIP expansion in First Nations communities. As part of these efforts, eHIP will engage the Assembly of First Nations (AFN) and First Nations regional partners on expanding the existing readiness assessment tool used for eHealth project management. |
4.1 Revised readiness assessment tool, expanded in collaboration with AFN and regional First Nations organizations. | 4.1 September 2017 | Executive Director, CIAD, FNIHB | Existing budget |
|
The eHIP program already disseminates information about its work with the assistance of FNIHB regions and eHIP partners such as Indigenous and Northern Affairs Canada (INAC) and the Assembly of First Nations, and regional First Nations partners. The current approach for dissemination services across all the regions does not always leverage existing vehicles. FNIHB will develop a national marketing plan with First Nations to provide a clear sense of eHIP's role in support of improved health outcomes. The information included in the plan will flow from the Program's Health Infostructure Strategic Action Plan and Guidelines, overarching policy documents which set the strategic program policy framework and direction. |
4.2 National marketing plan for eHealth. | 4.2 March 2018 | ||||
|
Recommendation 5 Improve performance data collection and analysis across regions and over time on key performance indicators by setting up a Program performance measurement system that takes into consideration the capacity on the ground. |
Management agrees with the recommendation | Recognizing that the delivery of electronic services is not driven by the technology but rather the health services providers, Health Canada as a result has limited authority to standardize reporting protocol among partners. | 5.1 Criteria for standardized annual reporting on eHealth initiatives. | 5.1 March 2019 | Executive Director, CIAD, FNIHB | Existing budget |
|
The eHIP national office in collaboration with the regions and the First Nations Information Governance Centre, will explore the use of tools for annual reporting to improve data collection across the program. This would be achieved by:
|
5.2 Annual report based on new criteria. | 5.2 Fall 2019 | ||||
|
Recommendation 6 Develop a long-term plan that is sufficiently flexible to accommodate technology innovation and a commensurate funding strategy for eHIP. |
Management agrees with the recommendation |
The Program will continue to maintain current eHealth tools while looking ahead at sustainability of eHealth components and flexibility to adapt to new innovations in technology that are central to the work of the eHIP. eHIP will develop a five-year plan toward an enriched digital health infrastructure, based on the current Health Infostructure Strategic Action Plan and Guidelines. The plan will take into account these key factors, in alignment with the FNIHB Strategic Plan. |
6.1 Five-year plan to build on and sustain the digital health infrastructure for First Nations communities from 2018 to 2023. | 6.1 March 2018 | Executive Director, CIAD, FNIHB | Existing budget |
1.0 Evaluation Purpose
The purpose of the evaluation was to assess the relevance and performance of Health Canada's eHealth Infostructure Program (eHIP) for the period of 2011-2012 to 2015-2016.
The evaluation was required by Section 42.1 (1) of the Financial Administration Act (1985), according to which every department shall conduct a review, every five years, of the relevance and effectiveness of each ongoing program for which it is responsible. The Treasury Board of Canada's Policy on Results (2016) defines such a review as an evaluation. The evaluation has been conducted to inform "decision making, improvements, innovation and accountability"Footnote 126 by providing Health Canada's senior management, central agencies, Ministers, Parliamentarians and Canadians with a credible and neutral assessment of the ongoing relevance and performance (defined in terms of effectiveness, efficiency and economy) of eHIP.
2.0 Program Description
2.1 Program Context
In Canada, federal, provincial (F/P) and First Nation governments are focusing on ways to implement innovative information and communication technologies (ICTs) to modernize, transform and improve the way health services are delivered, contain costs and better manage health information for greater accountability and evidence-based decision making. eHealth Infostructure is the development and adoption of modern ICT systems for the purposes of defining, collecting, communicating, managing, disseminating and using data to enable better access, quality and productivity in the health and health care of First Nations.Footnote 36,Footnote 44
Within this context, eHIP works towards the modernization, transformation, improvement and sustainment of health care services in First Nations communities. It supports the combination of information, electronic health applications, technology and people with the intent to provide:Footnote 36
- Optimal health services delivery;
- Optimal health surveillance;
- Effective health reporting, planning and decision making; and,
- Integration/compatibility with other health services delivery systems.
The Program has evolved since the mid-1990s out of the need to align with First Nations' eHealth strategies, health plans and policy directions as well as the movement by provinces and the health industry towards increased use of ICTs to support health service delivery and public health surveillance.Footnote 36,Footnote 44
In April of 2010, Health Canada's First Nations and Inuit Health Branch (FNIHB) approved the Health Infostructure Strategic Action Plan (HISAP), which provides the road map for eHIP and FNIHB information/health information management activities and lays out a long-term strategic framework. HISAP is centred on four key goals:Footnote 36
- An Electronic Health Record (EHR) capacity and capability for all First Nations people by 2020;
- Seamless integration of First Nations infostructures with provincial EHR systems;
- Meaningful, standardized information for decision support available to First Nations, regions and FNIHB; and,
- Collaborative and sustainable partnerships between First Nations, provinces and the federal government.
Since eHIP's mandate is to develop the use of ICTs to support health service delivery in First Nations communities, it needs to function in an environment that includes First Nations communities and regional organizations, other federal partners and provinces, to achieve progress on the different parts of eHealth. This environment combined with technological developments, testing and acceptance by all partners and stakeholders requires long term planning in multiple phases. The current phase of eHealth is still on deploying suitable technologies to support health service delivery in First Nations.
2.2 Program Profile
The implementation of eHIP is a shared responsibility between the national Program headquarters (HQ) in Ottawa and six regional offices: the Atlantic region (ATL, including the provinces of Nova Scotia – (NS), Prince Edward Island – (PEI), Newfoundland and Labrador – (NL) and New Brunswick – (NB)), Québec (QC), Ontario (ON), Manitoba (MB), Saskatchewan (SK) and Alberta (AB).Footnote ii Program HQ sets the strategic Program policy framework and direction. Regional offices engage and work with First Nations regional organizations and communities in eHealth strategic planning, implementation and sustainment. The Program provides funding only to First Nations communities south of 60°.Footnote iii In order to achieve its mandate and goals, eHIP is focused on three principal areas of activity:Footnote 36
- Building the foundation elements that reflect the base requirements of eHIP, without which eHealth components will not operate;
- Implementing components that reflect the key application areas; and,
- Supportive services that provide good governance and management of eHIP.
According to the Program's Guidelines (2012), and as depicted in Figure 1, the Program's foundation elements include:Footnote 36
- Broadband connectivity to connect all on-reserve health facilities to either broadband or high speed Internet services, including connection of the health facility to a central broadband/Internet point within the community, maintenance of the connectivity and related costs.
- Capacity building in three main areas: human resources, infrastructure and governance, to assist with coordinating certain eHealth-related training for health care providers working in First Nations communities, community health workers as well as administrative and support staff.
- Information technology and operations to support the purchase and implementation of the Information Technology (IT) infrastructure, work with First Nations to harmonize community IT policy, support strategies and leverage approaches and resources for efficient community level IT services support, including coordination with other federal departments such as Indigenous and Northern Affairs Canada (INAC).
- Program/project management, planning and accountability, including the development, support and implementation of effective project management practices related to appropriate and effective resource and activity monitoring and control systems; risk management; change management; project reporting mechanisms; and, effective financial and project planning.
eHealth components include:Footnote 36
- Public Health Information Systems (PHIS), such as Panorama and other systems, through which FNIHB works to include or align national and regional public health surveillance systems for First Nations communities with those being implemented by the provinces.
- Electronic records, including Electronic Medical Records (EMRs), EHRs, client registries and other electronic systems that provide access to an individual's health information. EHRs are a secure and comprehensive electronic record of a person's critical health history that can be accessed by authorized health care providers in the community, province, and eventually across the country. An EMR provides physicians and their patient care team, including nurses and office support staff, with local electronic access to vital patient health information, decision support, billing and office administration tools. A client registry is a data repository that provides, according to Canada Health Infoway (Infoway) an "accurate patient identification to ensure the right health records are associated with the right patient."
- Telehealth to provide access to health care providers and patients to education and clinical sessions and to support community staff by enabling administrative sessions. This component includes the procurement of equipment, integration of the solution into regular service delivery, staff training, and facilitating change management.
- Mobile health (mHealth) or medical and public health practice supported by mobile devices (e.g., mobile phones, patient monitoring devices, Personal Digital Assistants – PDAs). mHealth applications include the use of mobile devices in collecting community and clinical health data, delivery of health care information to practitioners, researchers, and patients, real-time monitoring of patient vital signs and direct provision of care.
Supportive elements include the governance of the Program (strategic oversight, direction and guidance at both the national and regional levels) and partnerships with First Nations regional organizations and communities, other federal organizations, such as Infoway, other federal departments, such as INAC and Innovation, Science and Economic Development Canada (ISED), and provincial ministries of health to collaboratively plan, implement and advance the different Program foundation elements and eHealth components.Footnote 36
Figure 1. eHealth components and elements.
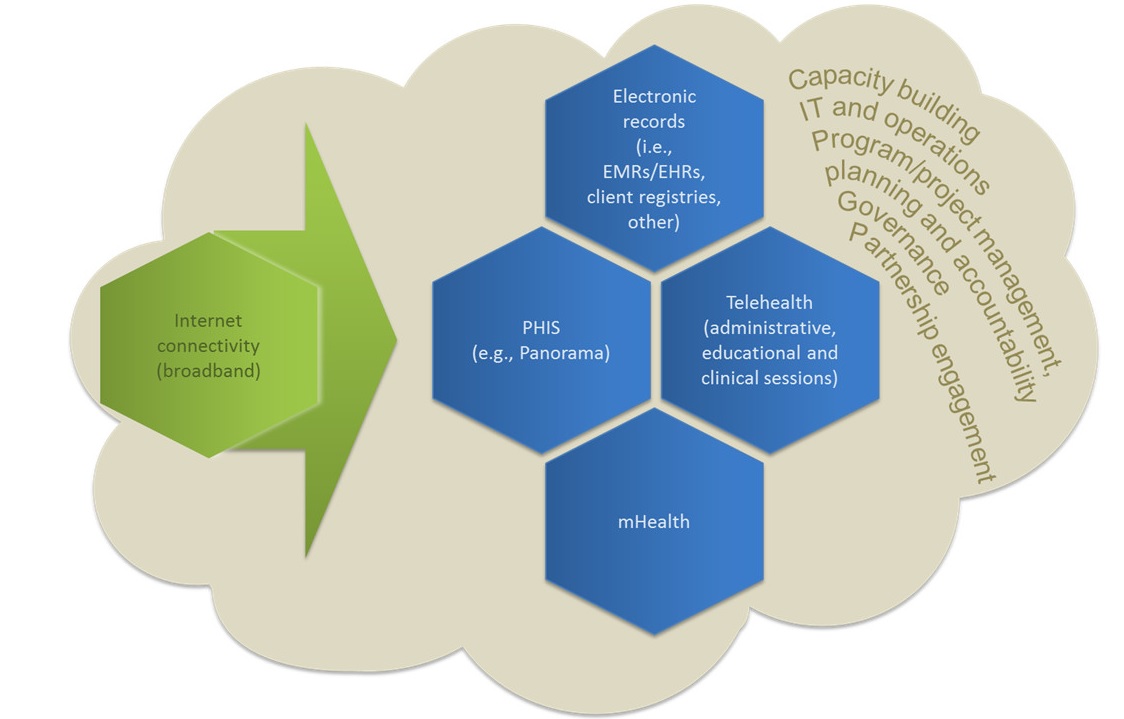
Figure 1: eHealth components and elements - Text Description
Figure 1 provides a visual overview of the key eHealth components and elements. The primary eHealth component given emphasis is internet connectivity (also referred to as broadband), followed by: Electronic Records (including electronic medical records, electronic health records, client registries); Public Health Information Systems (including Panorama); Telehealth (including administrative, educational and clinical telehealth sessions); and mobile health, which is also sometimes referred to as mHealth. The key elements of eHealth programming include: capacity building, information technology and operations; program and project management; planning and accountability; governance and partnership engagement.
2.3 Program Narrative
The objective of the Program is to improve access to quality health care services for First Nations individuals, families and communities through the use of eHealth technologies. In order to realize this objective, the Program's activities centre on four key areas, namely:
- Fund the deployment and maintenance of innovative technologies for the delivery of health care services;
- Provide First Nations, FNIHB staff and health care providers with support and capacity development to implement and maintain these innovative technologies;
- Engage stakeholders with a view to implementing and integrating eHealth technologies; and,
- Improve the availability of, and access to, quality data to better inform decision-making and priorities.
These activities lead to several outputs that are expected to contribute to the following immediate, intermediate and ultimate outcomes:
Immediate
- First Nations communities and health care providers have access to eHealth technologies;
- First Nations individuals, FNIHB staff and health care providers improve their skills/knowledge; and,
- Partners and stakeholders are engaged in collaborative, integrated planning of eHealth technologies.
Intermediate
- First Nations individuals and health care providers are using eHealth technologies for the delivery of health care services; and,
- Interoperable eHealth technologies are implemented in First Nations communities.
Ultimate
- Access, quality and safety of health care services are improved for First Nations individuals, families and communities; and,
- Health care providers have access to provincial health information systems.
The connection between the activity areas and expected outcomes is depicted in the logic model (see Appendix 1 ).Footnote iv The evaluation assessed the degree to which the defined outputs were being produced and outcomes were being achieved over the evaluation time frame.
2.4 Program Alignment and Resources
eHIP is part of Health Canada's Program Alignment Architecture under Strategic Outcome 3: First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status, Program 3.3: Health Infrastructure Support for First Nations and Inuit, Sub-Program 3.3.2: First Nations and Inuit Health System Transformation.
The Program's financial data for the years 2011-2012 through 2015-2016 are presented in Section 4.5 , Table 17, Table 18 and Table 19. The Program had expenditures of approximately $124 million over five years (2011-2012 to 2015-2016). In 2013, the Program received approximately $100 million from Treasury Board in additional funding over five years to maintain investments and expand eHIP to the remaining 25% of remote/isolated and isolated communities without telehealth (based on feasibility and readiness), and then to other communities. Funding was provided to sustain and increase the number of telehealth sites, sustain and increase connectivity, continue the roll out of PHIS, implement EMRs/EHRs, and support the implementation of mHealth technologies.
3.0 Evaluation Description
3.1 Evaluation Scope, Approach and Design
The scope of the evaluation covered the period from April 1st, 2011 to March 31st, 2016 and included all the elements and eHealth components of the Program. The one area of exclusion was the assessment of any services transferred to the British Columbia (BC) First Nations Health Authority on July 2013 in accordance with the British Columbia Tripartite Framework Agreement on First Nation Health Governance and sub-agreements, which will be covered under a separate and forthcoming evaluation.
The evaluation was aligned with the Treasury Board of Canada's Policy on Results (2016) and considered core issues under the themes of relevance and performance, as shown in Appendix 2. Corresponding to each of the core issues, specific questions were developed based on Program considerations and these guided the evaluation process.
An outcome-based evaluation approach was used for the conduct of the evaluation to assess the progress made towards the achievement of the expected outcomes, whether there were any unintended consequences and what lessons were learnt.
A non-experimental design was used based on the Evaluation Matrix developed during the planning phase of the evaluation, which detailed the evaluation strategy for this Program. The evaluation followed the Agreement for FNIHB Departmental Evaluations developed between the Assembly of First Nations (AFN), Inuit Tapiriit Kanatami (ITK), FNIHB and the Evaluation Directorate (now the Office of Audit and Evaluation), Health Canada and Public Health Agency of Canada, regarding the evaluation of FNIHB programming. This included consulting with AFN during the development of the evaluation methodology and providing AFN with the opportunity to review and comment on the instruments used in First Nations communities, the preliminary findings and the evaluation report. Consultation was not conducted with ITK as eHIP does not fund any communities north of 60°.
Data for the evaluation was collected using various methods, which included a document and literature review, an administrative data review and analysis, key informant interviews, case studies, a review and analysis of eHealth approaches across international jurisdictions, and an examination of available financial data for the Program. Details on the data collection and analysis methods are provided in Appendix 3. Data was analyzed by triangulating information gathered through these different methods. The use of multiple lines of evidence and triangulation were intended as a way to increase the reliability and credibility of the evaluation findings and conclusions.
For the purposes of the evaluation, the terms "partners" and "stakeholders" are used as follows: partners are organizations that assist in the implementation of the Program or that have parallel programs that deal with elements and eHealth components (e.g., provincial governments, federal organizations such as Infoway and departments such as INAC, National Indigenous Organizations such as AFN); stakeholders receive the benefits or the effects of the Program (i.e., health care providers, community health and administrative staff, etc.).
3.2 Limitations and Mitigation Strategies
Most evaluations face constraints that may have implications for the validity and reliability of evaluation findings and conclusions. Table 1 outlines the limitations encountered during the implementation of the selected methods for this evaluation. Also noted are the mitigation strategies put in place to ensure that the evaluation findings can be used with confidence to guide Program planning and decision making.
| Limitation | Impact | Mitigation strategy |
|---|---|---|
| Limitation | Impact | Mitigation strategy |
| A stakeholder survey of health facility personnel (including Health Directors, Programming Coordinators, nurses and physicians) could not be conducted as it was not possible to obtain a list with a sufficient number of contacts or sufficient contact information. | First hand perspectives of users of the different eHealth technologies were limited, in particular that of health care providers. | The approach to the key informant interviews was revised to gather additional information. The total number of interviews was also increased (from 16 to 40 interviews) to incorporate a larger number of stakeholders. Finally, the number of case studies was also increased (from four to seven) to obtain more detailed regional information. |
| The revised target of 40 interviews to compensate for the stakeholder survey was not achieved. | Limited; interviews with some partners and an additional expert could not be completed. | While the original approach was to use a combination of group and individual interviews, most individual interviews evolved into group interviews due to the multiple eHealth components explored and their inherent complexities (16 individual and 17 group interviews with 75 total participants). |
| The revised target of seven case studies (four site visits and three document reviews) was not achieved. | Limited; an in-depth look at one of the Program's regions was not conducted and an examination of a community not funded by the Program was not conducted. | Five case studies were conducted (four site visits and one document review). The five case studies covered five of the six Program regions. Additional efforts were made through the document and literature review to compensate. In the case of a community not funded by the Program to use as a point of comparison, additional comparison information was gathered through the review and analysis of international jurisdictions. |
| Performance data collected by the Program showed inconsistencies across years, regions and eHealth components. | Performance data reported in the tables shows a number of gaps. | Evaluators worked with Program representatives, both at HQ and the regions, to understand and validate the data analysis. The resulting data was completed and enhanced with information gathered through the document and literature review, key informant interviews and case studies. |
4.0 Findings
4.1 Relevance: Issue #1 – Continued Need for the Program
The Program continues to address a demonstrable need and is responding to the needs of its client population. The needs addressed by the Program are fundamental to improving the health status of First Nations.
The health status of First Nations individuals, families and communities, their access to health care service delivery, and the availability of related health data are behind that of the general Canadian population.Footnote 37 To address this inequity, there is a strong need to enable a First Nations health infostructure capability in line with those of the provinces.
eHIP, through its multipronged approach to increase social capital via connected networks of First Nations community-based health infostructures, aims at bridging this inequity. Many of the partners and stakeholders engaged through interviews and case studies acknowledged the needs addressed by the Program as being fundamental to improving the health status of First Nations. Specifically, the Program provides eHealth services to First Nations communities, reduces travel time and costs as well as displacement from family and community. eHIP helps to connect patients with specialists for diagnostic examinations and follow ups. eHealth also allows for better continuity of care by facilitating information sharing between health care providers on- and off-reserve in support of better care assessment and decision making.
4.2 Relevance: Issue #2 – Alignment with Government Priorities
The Program is aligned with government priorities. These include keeping pace with technology and innovation, contributing to address health system challenges and system reform, and building relationships with Indigenous peoples.
eHIP is aligned with the broader Government of Canada priority to "keep pace" with technology and to renew the relationship with Indigenous peoples. This priority has been highlighted in a number of previous Speeches from the Throne. In 2010, the Government of Canada committed to innovation and keeping pace with technology.Footnote 23 While not specific to eHealth, the 2015 Speech from the Throne underscored the Government's priority to renew relationships between Canada and Indigenous peoples based on co-operation and partnership.Footnote 108
The commitment to technology innovation and collaboration has also been highlighted in the Prime Minister's mandate letter to the Minister of Health in 2015 "advance pan-Canadian collaboration on health innovation to encourage the adoption of new digital health technology to improve access, increase efficiency and improve outcomes for patients".Footnote 35
The priority to "keep pace" with eHealth technology is also demonstrated through a variety of federal budget commitments, including Budget 2013, which allocated $99.8 million to eHIP over five years to maintain progress to date in implementing health technologies (e.g., telehealth/videoconferencing, EMRs, PHIS, broadband connectivity).Footnote 38 Furthermore, through the federal government has invested up to $500 million in Infoway to support continued work on EHRs for Canadians.Footnote 109 Funding was renewed in the 2013 budget to maintain existing investments and expand electronic health services in remote/isolated and isolated First Nation communities and other communities.Footnote 68,Footnote 84
eHIP is also aligned with the Government of Canada's aim to address some health system challenges and to assist in system reform. Through Infoway, the Government of Canada supports provincial and territorial efforts of implementing an interoperable EHR infrastructure (i.e., PHIS, EMRs) by providing funding, and collaboratively developing inter-jurisdictional standards, interoperability requirements and national strategies.Footnote 36
FNIHB has identified addressing eHealth infostructure as a key priority in many corporate planning documents over the past five years. Departmental Reports on Plans and Priorities (RPPs), within the scope of this evaluation, highlight how Health Canada works to support and sustain the use and adoption of appropriate health technologies that enable front line care providers to better deliver health services in First Nations and Inuit communities. RPPs also identify plans to support this priority by funding collaborative efforts with provinces on the expansion of eHealth technology, and through the expansion of telehealth sites, while continuing to support existing health centres with EMRs, and deploying Panorama.Footnote 83,Footnote 84,Footnote 85,Footnote 86 The plan to "improve the efficiency of health care delivery to First Nations and Inuit individuals, families, and communities through the use of eHealth technologies" is also emphasized.Footnote 87
eHIP's objectives align with Health Canada's priorities as outlined in its First Nations and Inuit Health Strategic Plan 2012, which includes ensuring access to quality health services as a key strategic goal for FNIHB. The First Nations and Inuit Health Strategic Plan 2012 sets out strategic objectives such as strengthening access, quality and safety of health services across the continuum of care for First Nations individuals,Footnote v families and communities.Footnote 45
Health Canada's HISAP identifies the following as FNIHB's strategic objectives: ensuring availability of, and access to, quality health services; supporting greater control of the health system by First Nations and Inuit; and, supporting the improvement of First Nations health programs and services through improved integration, harmonization and alignment with federal/provincial/territorial (F/P/T) health systems.Footnote 44
4.3 Relevance: Issue #3 – Alignment with Federal Roles and Responsibilities
The Program is well aligned with federal roles and responsibilities.
The Program is well aligned with federal roles and responsibilities. Improving the health of Indigenous people is a shared responsibility between F/P/T governments and Indigenous partners. The federal government's role in the provision or funding of health programs and services to First Nations and Inuit is based on policy and is consistent with the Indian Health Policy 1979, and subsequent departmental mission or mandate statements, rather than legislations or rights.Footnote 40,Footnote 45 The basis for the authority to provide or fund First Nations and Inuit health programs and services is found in the following: 1) section 4 of the Department of Health Act, which provides that the Minister of Health's powers include all matters over which Parliament has jurisdiction relating to the promotion and preservation of the health of the people of Canada not by law assigned to any other department, board or agency of the Government of Canada; 2) votes under the Appropriation Act which authorize Health Canada's spending on FNIHB's programs and services; and, 3) authority from Treasury Board for specific program activities.
Health Canada has overall responsibility for the development and implementation of eHIP and ensuring that funding is appropriately allocated and spent according to established criteria and guidelines.Footnote 36 FNIHB's role is to integrate F/P health systems for the benefit of First Nations, and to increase First Nations community health services capacity to address their own health needs.
4.4 Performance: Issue #4 – Achievement of Expected Outcomes (Effectiveness)
4.4.1 To what extent have the immediate outcomes been achieved?
Immediate outcome #1: First Nations communities and health care providers have access to eHealth technologies
The Program has exceeded its target for broadband connectivity; however, while all eHIP funded First Nations Bands have Internet connectivity, the available bandwidth and connection reliability is variable. The Program has also exceeded targets on PHIS and EMR/EHR implementation. Telehealth continues to grow but its uptake/utilization has been uneven across remote/isolated and isolated communities. mHealth appears promising and is in its developmental phase.
Level of Internet connectivity
For the purposes of eHIP, "connectivity" is defined as the ability of on-reserve health facilities to access the infrastructure required to send and receive health information (e.g., administrative, educational, clinical) using communication technologies (e.g., videoconferencing equipment connected to medical devices and software) and telecommunications services (e.g., broadband Internet). Program activities, therefore, include a focus on providing funding support to connect health facilities to a central broadband/Internet point within the community, which is further connected to external existing networks. Currently, First Nations Bands across the Program's regions have access to some degree of Internet connectivity. Table 2 shows the number of First Nations Bands that are supported by eHIP for connectivity charges. It should be noted that eHIP provides connectivity funding to First Nations communities who use telehealth. According to Program targets, 120 communities should have high-speed broadband connectivity by 2017-2018. Based on available data at the Band level, this target has been exceeded. 0 indicates the number First Nations Bands with nursing stations that receive support from eHIP for Internet connectivity.
| Region | Number of First Nations Bands funded by eHIP by bandwidth/technology | |||
|---|---|---|---|---|
| Satellite | < 5 Mbps | > 5 Mbps Total | Total | |
| Atlantic | - | - | 22 | 22 |
| Québec | 6 | 2 | 19 | 27 |
| Ontario | 1 | 6 | 18 | 25 |
| Manitoba | 1 | 24 | 14 | 39 |
| Saskatchewan | 1 | 6 | 2 | 9 |
| Alberta | - | 10 | 37 | 47 |
| Total | 9 | 48 | 112 | 169 |
|
||||
| Region | Number of First Nations Bands nursing stations funded eHIP by bandwidth/technology | |||
|---|---|---|---|---|
| Satellite | < 5 Mbps | > 5 Mbps Total | TotalFootnote vi | |
| Québec | 6 | 2 | 3 | 11 |
| Ontario | 1 | 5 | 12 | 18 |
| Manitoba | - | 17 | 5 | 22 |
| Saskatchewan | - | 1 | 1 | 2 |
| Alberta | - | 3 | - | 3 |
| Total | 7 | 28 | 21 | 56 |
|
||||
According to partners and stakeholders, in the last five years, broadband connectivity has improved considerably in some communities. Optimal connectivity appears to have been achieved in Alberta, where connectivity is not deemed an issue due to SuperNet's high speed, scalable connectivity. In Saskatchewan, the last mile project to improve bandwidth in rural and remote areas has been a success.Footnote 29 Fibre expansion has also been reported in the Atlantic Region, which is expected to have 29 out of 33 First Nation health centres connected to fibre by the end of 2017-2018. In Québec 30 communities have been working with the First Nations Education Council (FNEC) to enhance bandwidth for eHealth. Connectivity in eastern Ontario has been reported as a success, and the Northwestern Ontario Broadband Expansion Initiative between Bell Aliant and the F/P governments was an extensive project for the Nishnawbe Aski Nation (Internet parity for the northern First Nations).
The health facilities served by satellite communications in Ontario, Manitoba and Québec have less than optimal bandwidth and reliability (due to weather and power outages). In these cases, there is a pressing need to examine alternative technologies since C-band satellite will soon be obsolete. The Manitoba First Nations Technology Council (MFNTC) has announced plans for a project to connect all 63 communities by fibre in 10 years.Footnote 114
Access to/use of provincially integrated/interoperable Public Health Information Systems
PHIS involve secure databases that are accessible by authorized users to enter, extract and analyze health information. The information, typically at the individual level, such as immunization record, is used to better understand the health risks and status of communities as well as to plan interventions to address pressing issues. First Nations are mainly collaborating on implementing the immunization management and vaccine inventory modules of PanoramaFootnote vii or other provincially selected PHIS.
In general, progress to date on the implementation of PHIS has been achieved by prioritizing the implementation of the immunization management and vaccine inventory modules firstFootnote 19 in order to improve supply management, decrease wastage and accurately gauge coverage.Footnote 105 Nonetheless, each province, and First Nations communities within each province, is at different stages of implementation.Footnote 104 The number of First Nations communities that have implemented Panorama and a non-Panorama PHIS in the eHIP regions is shown in Table 4 and Table 5, respectively. According to Program targets, 24 communities should have implemented Panorama or an equivalent provincial integrated PHIS by the end of 2015-2016. Based on available data, this target has been exceeded.
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | - | - | 0 | 0 | 0 |
| Québec | - | 5 | 11 | 11 | 11 |
| Ontario | - | - | - | 0 | 0 |
| Manitoba | - | - | 0 | 1 | 1 |
| Saskatchewan | - | - | 0 | 25 | 25 |
| Alberta | - | - | 0 | 0 | 0 |
| Total | - | 5 | 11 | 37 | 37 |
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | - | - | 3 | 3 | 3 |
| Québec | - | - | 0 | 0 | 0 |
| Ontario | - | - | - | 0 | 0 |
| Manitoba | - | - | 0 | 0 | 0 |
| Saskatchewan | - | - | 11 | 0 | 0 |
| Alberta | - | - | 29 | 38 | 44 |
| Total | - | - | 43 | 41 | 47 |
Table 6 and Table 7 show the number of communities with nursing stations that have access to Panorama and non-Panorama PHIS, respectively.
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | - | - | N/A | N/A | N/A |
| Québec | - | - | 3 | 3 | 3 |
| Ontario | - | - | - | 0 | 0 |
| Manitoba | - | - | 0 | 0 | 0 |
| Saskatchewan | - | - | 0 | 6 | 6 |
| Alberta | - | - | 0 | 0 | 0 |
| Total | - | - | 3 | 9 | 9 |
| N/A = The Atlantic region does not have nursing stations. | |||||
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | - | - | N/A | N/A | N/A |
| Québec | - | - | 0 | 0 | 0 |
| Ontario | - | - | - | 0 | 0 |
| Manitoba | - | - | 0 | 0 | 0 |
| Saskatchewan | - | - | 6 | 0 | 0 |
| Alberta | - | - | 6 | 6 | 6 |
| Total | - | - | 12 | 6 | 6 |
| N/A = The Atlantic region does not have nursing stations. | |||||
In the Atlantic region, it has been difficult to achieve integration as each of the four provinces has moved towards different solutions. Newfoundland and Labrador has selected the Client Referral Management System (CRMS), Nova Scotia the Application for Notifiable Disease Surveillance (ANDS) system, New Brunswick the Client Service Delivery System (CSDS), and Prince Edward Island the IMS/immunization System. Provincial integration has been accomplished in two First Nations communities in Prince Edward Island and one in Newfoundland and Labrador.
In Québec, Panorama has been provincially deployed and is only used for vaccination; eHIP supports First Nations communities' Panorama implementation through the First Nations of Québec and Labrador Health and Social Services Commission (FNQLHSSC). Eleven communities have implemented Panorama's vaccination module, while other communities are waiting for a simplified version of Panorama. This lightweight version is being developed by the provincial government and deployment is planned for 2018. There is also a Health surveillance portal, sponsored by FNQLHSSC, which collects health data available from the communities.
In Ontario, the province has experienced delays in agreeing on a version of Panorama for First Nations communities. Originally, the plan was parallel First Nation and Public Health Unit implementation of Panorama with all parties entering immunization information into the provincial system. Recently, the province decided to place emphasis on supporting Public Health Unit immunization programs and is developing and testing a number of tools (Immunization Connects Ontario – ICON web tool, PEAR – Panorama Enhanced Analytic Reporting tool, Public Health Information Exchange – PHIX). Consequently, none of the First Nation initial subscribers (six First Nations and the Keewaytinook Okimakanak Tribal Council) have access to Panorama. Beyond these delays, work continues towards identifying Ownership, Control, Access and Possession (OCAP) compliant options for First Nations data disaggregation within provincial systems.
In Manitoba, only one community has implemented Panorama although there is readiness to implement it in all 63 communities as soon as challenges caused by differences between F/P privacy legislations are resolved. According to interviewees, negotiation of an information sharing agreement to allow federal employees to input and access information on a provincial system has set back implementation by two years. First Nations are waiting to finalize their own agreement with the province once the F/P issues are resolved.
In Saskatchewan, all 33 communities in the NITHA partnership have agreed to implement Panorama. A data sharing agreement is already in place, although some changes to the agreement are being initiated by the province regarding the trustee for the data. Federal nurses will not have access to Panorama unless they are included as part of the revised data sharing agreement. The 37 communities outside NITHA have not made progress in this regard.
Alberta has selected the Community Health and Immunization Program (CHIP) and First Nations (Alberta) Technical Services Advisory Group (TSAG) is working with the vendor to connect all First Nations communities. There is a real-time pilot of data exchange with the provincial immunization database on-reserve ahead of the off-reserve sites. It is built on the security platform of Alberta Netcare, which is available in 30 communities, and the provincial EHR. Three communities have data sharing agreements with the province to support real-time exchange, with others to follow suit.
Access to/use of a functional electronic record
For the purposes of this evaluation, 'functional electronic health record' refers to a number of data-sharing computer applications in which the health information of individuals may be recorded, stored, accessed by other authorized users, and combined with other records for analysis. Applications include EMRs, used to document an individual's interaction with a specific health care practitioner or facility, and EHRsFootnote viii, aimed at containing a portion of an individual's medical records from primary and hospital visits, including laboratory results, immunizations, prescriptions, etc., over time.Footnote 118 Numerous benefits from the use of these types of applications have been identified, such as:
- Improved data collection resulting in service improvement, including immunization coverage, reduction in medical errors and more efficient staff processes (EMR/EHR);Footnote 129
- Sharing of health information with the local health care provider from the wider provincial health system to ensure coordination of care for individuals in multiple facilities and avoid duplication of services,Footnote 8,Footnote 24,Footnote 47,Footnote 48,Footnote 127 especially in the case of rural and remote community residents (EHR);Footnote 60
- Evaluation of a clinic's work practices and outcomes (EMR);Footnote 24 and,
- Wider evaluation and planning of the allocation of health care resources as well as effectiveness of specific interventions (EMR).Footnote 24
EMRs/EHRs have been strongly promoted by Infoway as a means of improving the outcomes of provincial and territorial health systems. First Nations without a local EMR or access to a provincial EHR are as yet unable to realize the promised benefits, including information on health services provided off-reserve and the ability to keep track of their own First Nations health status information.Footnote 15
First Nations must often evaluate different EMR products to meet local information management needs that differ between communities given the level of local capacity to introduce and use such systems, the types of health and social services that need to be tracked,Footnote 47 and the need to share data with any provincial EHR system.Footnote 16,Footnote 17,Footnote 125 An approach to EMR implementation has been established by eHIP to define EMRs.
Table 8 provides the number of First Nations communities with access to an EMR and Table 9 provides the number of communities with access to a provincial EHR. At times, this could include a community EMR (cEMR, e.g., Mustimuhw), a viewer/EHR (e.g., Netcare in Alberta., eChart in Manitoba) or an information system for the management of clinical and administrative data for local community service centres (CLSCs) and certain hospital outpatient clinics as the I-CLSCs in Québec. In Ontario, the Giiwednong Health Link (GHL) project will provide an EMR to enhance the delivery of health care in its 14 member communities located along the north shore of Lake Huron and throughout Manitoulin Island. In addition, some communities have a client registry. It should be noted that data was not available for fiscal years 2011-2012 and 2012-2013. According to Program targets, there should have been 40 communities with interoperable EMRs/EHRs by 2015-2016. Based on available data, this target was exceeded.
| Region | Fiscal year | ||
|---|---|---|---|
| 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | 7 | 11 | 12 |
| Québec | 1 | 11 | 11 |
| Ontario | - | 2 | 12 |
| Manitoba | 2 | 2 | 2 |
| Saskatchewan | 12 | 12 | 12 |
| Alberta | 4 | 4 | 4 |
| Total | 26 | 42 | 53 |
| Region | Fiscal year | ||
|---|---|---|---|
| 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | 0 | 4 | 11 |
| Québec | 0 | 6 | 6 |
| Ontario | - | 0 | 0 |
| Manitoba | 35 | 36 | 44 |
| Saskatchewan | 0 | 0 | 0 |
| Alberta | 6 | 13 | 19 |
| Total | 41 | 59 | 80 |
Table 10 and Table 11 provide the number of communities with nursing stations that have access to an EMR and provincial EHR, respectively.
| Region | Fiscal year | ||
|---|---|---|---|
| 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | N/A | N/A | N/A |
| Québec | 0 | 6 | 6 |
| Ontario | - | 0 | 0 |
| Manitoba | 0 | 0 | 0 |
| Saskatchewan | 0 | 0 | 0 |
| Alberta | 0 | 1 | 2 |
| Total | 0 | 7 | 8 |
| N/A = The Atlantic region does not have nursing stations. | |||
| Region | Fiscal year | ||
|---|---|---|---|
| 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | N/A | N/A | N/A |
| Québec | 0 | 2 | 2 |
| Ontario | - | 0 | 0 |
| Manitoba | 20 | 20 | 21 |
| Saskatchewan | 0 | 0 | 0 |
| Alberta | 0 | 1 | 1 |
| Total | 20 | 23 | 24 |
| N/A = The Atlantic region does not have nursing stations. | |||
Mustimuhw, a cEMR tool, has been found valuable by various First Nations. More work is needed to address interoperability with provincial health repositories and with physician-oriented EMRs that have provincial approval and certification.
Telehealth
Telehealth is the use of ICTs to connect people to health care services at a distance. While delivering clinical sessions is the focus of telehealth, this component also enables the delivery of educational information/events (educational sessions) and supports health facility staff interactions (administrative sessions). Since 2010-2011, there have been a growing number of telehealth sites in First Nations communities.Footnote 43,Footnote 55,Footnote 57,Footnote 63,Footnote 72,Footnote 80,Footnote 89,Footnote 90,Footnote 91,Footnote 95,Footnote 107,Footnote 111 Telehealth, although deployed across Canada, has lower uptake/utilization in some small remote/isolated and isolated First Nations communities.
The number of telehealth sites in First Nations communities in those regions of relevance to the Program is provided in Table 12. Table 13 shows the number of communities with nursing stations that have access to telehealth. According to Program targets, there should have been 310 telehealth sites by 2014-2015.Footnote ix Based on available data, this target has not been met as there were 190 sites in 2014-2015 and 220 sites in 2015-2016.
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | 18 | 21 | 23 | 23 | 25 |
| Québec | - | - | 1 | 24 | 25 |
| Ontario | - | - | - | 26 | 26Footnote x |
| Manitoba | 23 | 30 | 36 | 45 | 47 |
| Saskatchewan | - | - | 3 | 5 | 37 |
| Alberta | 44 | 44 | 45 | 67 | 60 |
| Total | 85 | 95 | 108 | 190 | 220 |
| Region | Fiscal year | ||||
|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
| Atlantic | - | - | N/A | N/A | N/A |
| Québec | - | - | 1 | 11 | 12 |
| Ontario | - | - | - | 18 | 18 |
| Manitoba | - | - | 21 | 25 | 23 |
| Saskatchewan | - | - | 3 | 9 | - |
| Alberta | - | - | 12 | 14 | 13 |
| Total | - | - | 37 | 77 | 66 |
| N/A = The Atlantic region does not have nursing stations. | |||||
According to partners and stakeholders, telehealth has advanced to a great extent in the Atlantic region in the professional development (educational sessions) and clinical areas. In Ontario, Keewaytinook Okimakanak eHealth Telemedicine Services (KOeTS) and the Ontario Telemedicine Network (OTN) are partners in providing telehealth services to First Nations communities. These organizations provide administrative, educational and clinical sessions. In 2015-2016, KOeTS successfully delivered clinical sessions in a wide range of areas, e.g., addictions, endocrinology (including diabetes) and mental health (psychiatry and psychology). In Québec, there has been success with teleophthalmology but, according to Program representatives and stakeholders, additional effort is needed to address capacity, training and building a referral system for patients. In Manitoba, there is a very high demand for educational and clinical sessions as well as administrative sessions. MBTelehealth, the University of Manitoba College of Nursing and the Manitoba Adolescent Treatment Centre (MATC) partner in various activities. In Saskatchewan, according to interviewees, there has been an increase in the number of telehealth sites but data was not available from this region for 2015-2016 to confirm this observation. SaskTel's CommunityNet (CNet) is being upgraded to meet some of the additional bandwidth requirements. Telehealth coordinators are also just beginning to be employed to promote telehealth and increase utilization. Alberta is deemed to have no bandwidth issues, as it is connected to SuperNet, and is working with TSAG on increasing utilization and making physicians and community members more aware of telehealth. Alberta has had success with many clinical initiatives, including a telepharmacy project that allows for real-time drug prescription distribution in remote nursing stations. In general, clinical sessions have enhanced the delivery of care at a distance, thus enabling First Nations clients to receive specialized critical health care services without leaving their communities.
Mobile Health
mHealth is a term for medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, PDAs and other wireless devices. mHealth applications include the use of mobile devices in collecting community and clinical health data, delivery of health care information to practitioners, researchers, and patients, real-time monitoring of patient vital signs, and direct provision of care.
mHealth is in its developmental phase in many regions. It is being used for eHomecare (home care at a distance) applications in some First Nations communities in Alberta, Saskatchewan, Ontario and Québec (e.g., to deliver home care to chronically ill or aged patients). Many of these applications are pilots to identify solutions in wireless connectivity, data security and ease of use by visiting nurses and physicians. Some mHealth technology assessments are related to interoperability with EMRs/EHRs and PHIS at the community or provincial level.
eHomecare tools are needed for monitoring, education and data gathering in support of client care. In the case of monitoring and client care, tools are needed for contact assessmentsFootnote xi, community health assessments, mental health care, wound care, electronic service delivery reporting, electronic tracking of human resources, help desk, technical support, and patient monitoring. In particular, home and community care professionals need tools for using EMRs/EHRs.
Mobile devices, like iPads, are being used for client and patient education. eHomecare tools are needed for health care provider education and training in priority areas of chronic disease management, i.e., diabetes, chronic obstructive pulmonary disease, congestive heart failure, mental health and addictions.Footnote 42 The role of eHIP in promoting mHealth in First Nations communities could be significant. According to Program targets, there should be 50 communities with mHealth technologies by 2017-2018. During the period of the evaluation, mHealth implementation data was not available across the regions, except for some pilots described in the ensuing paragraphs.
The Atlantic region has conducted a number of mHealth pilots. Atlantic Canada's First Nation Help Desk has a technology that is advanced enough to allow handheld devices to join in videoconferencing via Polycom (RealPresence App). Nurses see value in connecting virtually with physicians or their offices when they are in a patient's home.
In Québec, mHealth has been used to track homecare in two communities. It has also been used to remotely undertake more rigorous follow-ups and monitoring of diabetic clients by an interdisciplinary team to optimize control of diabetes.Footnote 51
In Ontario, some First Nations communities are examining the feasibility of mobile units to triage patients before bringing them to a health facility. Similarly, a pilot is being conducted for the use of mHealth in emergency situations to lower response times. Education of homecare patients and the availability of apps for connecting patients to treatment centres are seen as important enablers of health care delivery to First Nations.
In Manitoba, Microsoft Surface tablets are available in some communities for home and community care workers to use during service calls to clients. A pilot was also planned to demonstrate the benefits of using mobile technology for facilitating communication among health care providers, coordinating services (e.g., referrals and scheduling), managing services (administration of staff activity), educating patients and staff, and collecting diagnostic information or images. The intent was to examine how wireless technology directly improves service delivery.Footnote 50
Saskatchewan has also conducted an iPad pilot. Recently, the region engaged in and supported the "Know Your Status" mHealth pilot project aimed at transitioning a paper based case management system to a secure, mobile electronic application. This was a nationally driven initiative implemented at the Spiritwood Health Centre.Footnote 92 The region has also shown interest in exploring the support of doc-in-a-boxFootnote xii with interested physicians that work in the area of Hepatitis C and HIV/AIDS.Footnote 91
In the Alberta region, some First Nations communities can access telehealth sessions from a laptop, iPad, a tablet or smartphone. The use of mobile videoconferencing has expanded in the last two years and it has the potential to grow even more for administrative, educational and clinical purposes. The technology has also offered another method for health care providers to deliver secure services to First Nation health facilities. It has allowed health directors and various Health Co-Management (HCOM)Footnote xiii members the ability to connect remotely to meetings with other members. The region has enabled 80 people (clinicians, health directors, senior management) with mHealth.Footnote 73,Footnote 74
Immediate outcome #2: First Nations individuals, FNIHB staff and health care providers improve their skills/knowledge
The Program has supported efforts to enhance the knowledge and skills of First Nations individuals, FNIHB staff and health care providers. Opportunities have been provided through telehealth education and administrative sessions in various formats. Available information indicates the usefulness and efficiency of telehealth educational sessions among frontline health care workers, staff and communities.
Telehealth – educational and administrative sessions
Opportunities to enhance the knowledge and skills of First Nations individuals, FNIHB staff and health care providers have been offered by eHIP. The numbers of educational and administrative sessions are shown in Table 14 and Table 15, respectively. In the case of Manitoba, the decline was due to a reclassification from educational to clinical sessions as well as the reduction in the number of sessions by one provider.
| Fiscal year | Regions | Total | |||||
|---|---|---|---|---|---|---|---|
| Atlantic | Québec | Ontario | Manitoba | Saskatchewan | Alberta | ||
| 2011-2012 | 228 | - | 133 | 1,255 | - | 647 | 2,263 |
| 2012-2013 | 349 | - | 160 | 1,967 | - | 1,274 | 3,750 |
| 2013-2014 | 232 | - | 334 | 1,767 | 34 | 346 | 2,713 |
| 2014-2015 | 220 | - | 434 | 1,142 | 79 | 747 | 2,622 |
| 2015-2016 | 161 | - | 459 | 724 | 96 | 746 | 2,186 |
| Total | 1,190 | - | 1,520 | 6,855 | 209 | 3,760 | 13,534 |
| Fiscal year | Regions | Total | |||||
|---|---|---|---|---|---|---|---|
| Atlantic | Québec | Ontario | Manitoba | Saskatchewan | Alberta | ||
| 2011-2012 | - | - | - | 495 | - | - | 495 |
| 2012-2013 | - | - | 92 | 645 | - | - | 737 |
| 2013-2014 | - | - | 91 | 775 | 43 | - | 909 |
| 2014-2015 | 31 | - | 140 | 598 | 208 | 802 | 1,779 |
| 2015-2016 | 28 | - | 140 | 783 | 69 | 573 | 1,593 |
| Total | 59 | - | 463 | 3,296 | 320 | 1,375 | 5,513 |
Educational and administrative sessions have been delivered through various modalities, such as videoconferencing (telehealth educational sessions) as well as formal training, orientation sessions and workshops. Telehealth educational sessions offered to First Nations individuals and health care providers have allowed them to acquire information and knowledge on a number of health related areas (e.g., diabetes education, drug awareness, population health, community health planning, health indicator development and measurement, public health surveillance, health information management) and training on new health equipment.Footnote 38,Footnote 39,Footnote 46
In the case of health care providers, this training may not have been available otherwise if travelling was required, especially due to primary care nursing budget constraints.Footnote 38 Telehealth educational sessions have supported health promotion and disease prevention efforts by providing patients with information about their condition and on how to manage and improve it.Footnote 38 In addition, education and training play an important role in building community capacity as eHealth initiatives move from the developmental to the operational stage.
Participant satisfaction with training opportunities for skill development
Educational sessions are provided 1) to patients and their families on diverse health topics for individuals to manage their health, and 2) to health care providers on training and continuing education. While some surveys have been conducted on patient and provider experience with telehealth clinical sessions, this has not been the case with administrative and educational sessions. In some cases, limited information has been collected (e.g., KOeTS, MBTelehealth). According to the 2013-2014 KOeTS Annual Report, telehealth technology as a training vehicle has been praised by community members for making previously difficult or impossible-to-access programs available, and making personal and professional development financially affordable by eliminating some of the economic and social costs linked to leaving home for training on extended periods of time.Footnote 100 These results tie in with a benefits evaluation survey undertaken by MBTelehealth: while responses were limited, participants believed that telehealth offered increased education and communication, and had provided additional access to educational events that staff would not have otherwise been able to attend due to time and cost limitations.Footnote 110 Based on limited information gathered through interviews and case studies conducted for the evaluation, the extent of satisfaction with telehealth educational sessions was above average (3.5 on a five-point scale; N = 6).
Immediate outcome #3: Partners and stakeholders are engaged in collaborative, integrated planning of eHealth technologies
The Program uses a number of mechanisms for multi-party engagement and to further collaborative integrated planning of eHealth. In terms of harmonization, eHIP is working with First Nations and F/P representatives in effecting the integration of health services by identifying opportunities and actively engaging in multi-jurisdictional partnerships.
Mechanisms to foster engagement and collaboration
Partnership is a key success driver of eHealth in First Nations communities. This partnership is made possible through a variety of mechanisms for engagement, such as regular weekly meetings, information forums, working groups, steering committees and advisory bodies.Footnote 75,Footnote 79 Often, discussions and information sharing take place with multiple parties including eHIP regional representation, First Nations regional organizations, First Nations Health Directors, the provinces, and other participants like Internet Service Providers (ISPs), vendors, universities and associations. Regional Program offices engage with stakeholders, such as FNQLHSSC, Atlantic Canada's First Nation Help Desk, the Membertou Data Centre, TSAG, Nanaandawewigamig – First Nations Health and Social Secretariat of Manitoba (FNHSSM) and KOeTS who, in turn, work directly with the communities in the delivery of clinical care, education and health services via telehealth and other components.Footnote 27,Footnote 90 At the national level, eHIP also participates in key multilateral exchanges with other federal partners (e.g., INAC) as well as within and outside FNIHB within Health Canada.
Collaborative plans, agreements and activities
In addition to providing and supporting a variety of enabling platforms for First Nations' involvement in information sharing and decision making, strides have been made in the area of collaborative, integrated planning of eHealth. eHIP is making progress in continuing to identify and advance shared priorities with First Nations, other federal departments, provinces and other partners through culturally-appropriate, collaborative planning and coordinated initiatives to improve health outcomes.
Some examples of the methods used for this collaborative planning include planning committees, setting terms of reference for partnerships, establishing service agreements and contribution agreements, etc. Generally, the various collaborative plans and strategies emphasize telehealth, PHIS (Panorama) and EMRs/EHRs.
Regions vary in the extent to which they engage in partnering with First Nations communities, First Nations regional organizations and provincial bodies. Manitoba has been particularly active with varying levels of partnership (with provincial and federal governments and First Nations regional organizations), such as the Manitoba First Nations Regional Telehealth Partnership.Footnote 1,Footnote 9,Footnote 32,Footnote 44,Footnote 68,Footnote 82
The Saskatchewan region coordinates efforts on multiple Program components (e.g., telehealth, connectivity and training) but particularly on PHIS (Panorama).Footnote 81 It engages First Nations communities as well as provincial and other partners (e.g., Athabasca Health Authority to provide access to provincial EMRs and Saskatchewan Ministry of Health).Footnote 68,Footnote 92
The Ontario region continues to promote and support active participation in trilateral tables such as the Trilateral First Nations Senior Health Officials Committee (TFNHSOC) and the Keewatin (Northern) Senior Trilateral Health Table. There are also other initiatives such as the F/P/Pikangikum Working Group, the Sioux Lookout Four Party Agreement, and the Weeneebayko Area Health Integration Framework Agreement.Footnote 58
Québec's Regional Infostructure Advisory Committee includes representatives from First Nations regional organizations, communities, eHIP, INAC and the province to support partnerships and joint planning of eHealth.Footnote 90 The region works closely with FNQLHSSC on general eHealth planning, specific projects, training and utilization of telehealth, and shares information with communities through the Québec First Nation Health Directors' Network.Footnote 90,Footnote 56
The Atlantic region's collaborative relationship with Atlantic Canada's First Nation Help Desk, the Membertou Data Centre, Tui'kn and the Newfoundland and Labrador Centre for Health Information (NLCHI) enables the Program to work on several projects delivered to First Nation communities. From the collaboration with NLCHI, Health Information Management projects have been used for knowledge translation and created "Fast Fact" pamphlets and posters that provided a broad overview of health status.Footnote 46
The Alberta region works collaboratively with provincial organizations (Alberta Health Services) and First Nations regional organizations (e.g., TSAG and the Alberta First Nations Information Governance Centre) to enhance the delivery of eHealth services consistent with HCOM.
Harmonization efforts and extent of harmonization
eHIP is working with partners and stakeholders in effecting the integration of health services. The Program is collaborating with federal partners, like INAC and Infoway, and is engaged in multilateral harmonization efforts with First Nations regional organizations, provincial governments, eHealth agencies (e.g., eHealth Saskatchewan, Manitoba eHealth) and regional health authorities.
Harmonization efforts at the provincial level have been identified as instrumental to the advancement of eHealth in First Nations communities. Manitoba's Regional Telehealth partnership is an example of multi-jurisdictional collaboration, whereby provinces, FNIHB and FNHSSM work together with MBTelehealth to deliver eHealth services to First Nations communities.Footnote 77,Footnote 82 The regional office and FNHSSM also collaborate with Manitoba eHealth on province-wide initiatives to First Nations communities (e.g., eChart and Panorama).Footnote 82
Multi-jurisdictional collaboration is also found in the Atlantic provinces' Community Health Technology Plans. The Atlantic First Nations Health Partnership is an example of integrated health governance in the Atlantic region.
The Québec regional office has worked with local authorities to facilitate the deployment of Panorama in First Nations communities according to the timeline and process set out by the local provincial authorities. In addition, the I-CLSC system, which is complementary to EMRs and is interoperable with provincial computer systems, has been implemented in several communities. These are examples of multi-jurisdictional collaboration of eHealth services with First Nations communities involving FNQLHSSC.Footnote 78,Footnote 33
In Ontario, there are several efforts to work closely with the province and First Nations. A Knowledge Management Advisory Group (KMAG) was established to "provide technical and policy direction related to health information and surveillance and future First Nation immunization information management systems".Footnote 25 While there have been difficulties in aligning eHIP and provincial priorities, as the province redefines its eHealth strategy, progress has been achieved recently in the area of EMRs, PHIS (Panorama) and telehealth. KOeTS works directly with First Nations Health Authorities, communities and health care providers to improve the level of collaboration and coordination of health services access.Footnote 100 For example, KOeTS is part of the Virtual Mental Health and Addictions Working Group (VMHAWG) that is piloting a service model in four remote communities.
Tri-partite partnerships are an effective method of harmonizing strategies and efforts for telehealth in First Nations communities. Alberta's Regional Telehealth Partnership has been maintained since 2005 in its role of managing and deploying telehealth in First Nations communities.Footnote 80 Alberta's telehealth is delivered by four key partners: eHIP, TSAG, province and other providers (e.g., SuperNet), and First Nations communities. This has enabled access to a larger pool of eHealth resources for the benefit of communities. A tripartite Memorandum of Understanding on First Nations Health and Well-Being in Saskatchewan was signed between the Federation of Saskatchewan Indian Nations, the Government of Canada and the Government of Saskatchewan with several goals, including to adapt and better integrate health and wellness programs of all jurisdictions by eliminating duplication, closing gaps and improving the coordination and efficacy of the health care systems.Footnote 44
Innovative and integrated health governance relationships are being maintained/established between the Program and its regions, communities, provincial governments, federal and other relevant partners.Footnote 44 Advisory bodies play a role in ensuring the harmonization of eHealth. For example, the Regional Infostructure Advisory Committee in Québec includes representatives of three First Nations organizations, eHIP's regional office, INAC and the province. This body serves as a key communication mechanism that fosters alignment between regional partners on eHealth activities.Footnote 90
4.4.2 To what extent have the intermediate outcomes been achieved?
Intermediate outcome #1: First Nations individuals and health care providers are using eHealth technologies for the delivery of health care services
Clinical telehealth sessions are delivered in many First Nations communities covering numerous topics. The Program has exceeded its target of providing clinical sessions via telehealth to First Nations communities. These sessions have covered a multitude of clinical specialties. Greater collaboration and integration across the federal family (i.e., Health Canada, INAC, ISED) as well as within Health Canada could result in increased and more stable Internet connectivity and bandwidth. Uptake/utilization of telehealth in some remote/isolated and isolated communities could be increased through promotion among First Nations individuals, families and communities as well as health care practitioners in addition to providing enhanced support on the ground (e.g., telehealth coordinators). Further support for mHealth by helping communities address challenges related to connectivity and communications security may aid technology adoption.
Telehealth – clinical sessions
Telehealth clinical sessions facilitate access to health care services while enhancing the number of health care services available to First Nations communities. Table 16 provides an overview of the number of clinical sessions being delivered in the regions. According to Program targets, there should have been 8,160 clinical sessions delivered in First Nations communities by 2016-2017. Based on available data, this target has been exceeded.
| Fiscal year | Regions | Total | |||||
|---|---|---|---|---|---|---|---|
| Atlantic | Québec | Ontario | Manitoba | Saskatchewan | Alberta | ||
| 2011-2012 | 24 | - | 2,421 | 1,664 | - | 771 | 4,880 |
| 2012-2013 | 26 | - | 2,538 | 2,329 | - | 1,542 | 6,435 |
| 2013-2014 | 28 | - | 2,852 | 3,082 | 14 | 2,272 | 8,248 |
| 2014-2015 | 27 | - | 2,782 | 3,556 | 85 | 4,140 | 10,590 |
| 2015-2016 | 91 | - | 3,205 | 3,708 | 98 | 3,287 | 10,389 |
| Total | 196 | - | 13,798 | 14,339 | 197 | 12,012 | 40,542 |
Nationally, clinical sessions have been provided in various specialties, e.g., respirology, psychology (e.g., youth suicide), mental health, addictions consultations, speech language pathology, oncology, teledentistry, endocrinology, dietitian, general practitioner.Footnote 77,Footnote 38,Footnote 78 Nonetheless, the type/topic of clinical sessions delivered is tracked regularly only in two regions (i.e., Ontario and Manitoba). The most consistent reporting has been kept by KOeTS, although classification of specialty areas varies from year to year making trend observations difficult. Figure 2 provides a breakdown of the top sessions representing over 75% of all sessions delivered by KOeTS in 2015-2016.Footnote 101
Figure 2. Top types of telehealth clinical sessions as reported by Keewaytinook Okimakanak eHealth Telemedicine Services for 2015-2016.
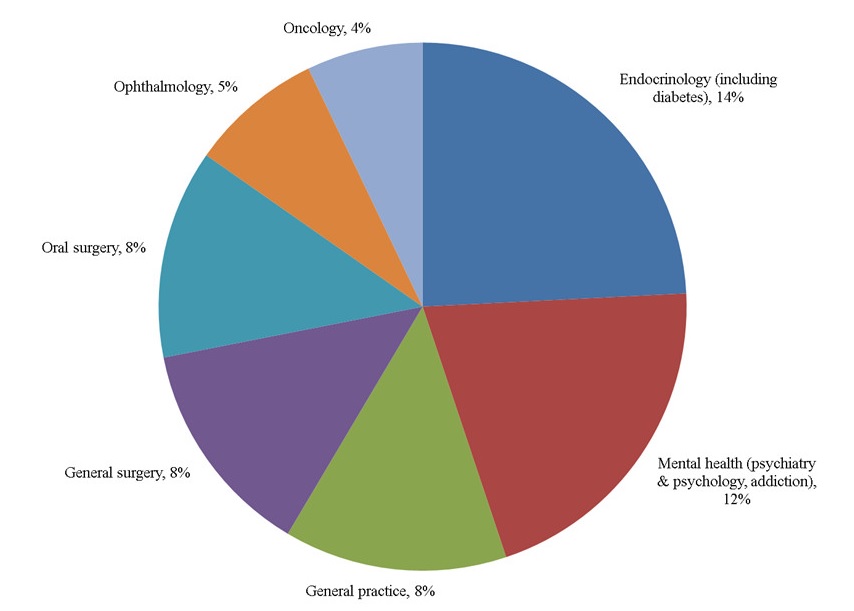
Figure 2: Top types of telehealth clinical sessions as reported by Keewaytinook Okimakanak eHealth Telemedicine Services for 2015-2016 - Text Description
A pie chart provides a breakdown of the top seven types of clinical sessions delivered via telehealth, as reported by Keewaytinook Okimakanak eHealth Telemedicine Services for the 2015-2016 fiscal year. The most popular clinical session involves endocrinology (including diabetes topics) at 14%; followed by mental health (including psychiatry, psychology, and additions topics) at 12%; general practice at 8%; general surgery at 8%; oral surgery at 8%; ophthalmology at 5%; and oncology at 4%.
According to partners and stakeholders, the following trends were evident across the different Program regions:
- In the Atlantic region, telehealth clinical sessions are conducted for cardiac wellness, telepsychiatry, diabetes, follow-up care for heart disease, cancer care, mental health and addictions. Despite growth within the region, the delivery of telehealth clinical sessions is deemed low as there may not be a driving need for telehealth given the proximity of many First Nations communities to urban centres. Also, there is a shortage of telehealth coordinators to schedule and organize the sessions, follow-up on appointments and promote the service.
- In Québec, telemental health and teleophthalmology have been successfully implemented. The retinopathy project is in place in 24 communities across Québec. FNEC, FNQLHSSC, and FNIHB are partners.
- In Ontario, KOeTS, using the OTN scheduler, has undertaken a variety of clinical sessions beyond those identified in the previous figure, such as wound care, infectious diseases, urology, pre- and post-general surgery assessments, pre-dental surgery assessments, dermatology, specialist consultations, radiology and homecare.
- In Manitoba, clinical sessions are enabled by MBTelehealth with involvement from the province, FNHSSM, Alcoholic Anonymous, and MATC. Examples of clinical specialties include cancer care, dermatology, foot care, orthopedics, mental health, wound care and speech therapy. MATC offers a provincial program that uses telehealth equipment funded by eHIP to improve service delivery to remote/isolated and isolated areas in Manitoba.Footnote 38
- In Saskatchewan, clinical sessions are being offered for rehabilitation, cardiac health, infectious diseases, oncology, nephrology, diabetes management, nutrition and meal planning. Delivery of clinical sessions in Saskatchewan was reported as low due to a lack of on the ground capacity, e.g., telehealth coordinators, and issues related to physician remuneration.
- In Alberta, while the number of clinical sessions exceeded the number of administrative and educational sessions, there was variability in utilization across the communities. TSAG continues to work with communities to retain or identify providers.
While there are not many surveys of client or provider satisfaction with clinical sessions, some data is available from MBTelehealth and KOeTS.Footnote 99,Footnote 100,Footnote 101,Footnote 97,Footnote 98,Footnote 110 Sometimes, forms are filled out (e.g., following delivery such as mental health sessions) and not tallied or contain too many open-ended responses to provide meaningful information, particularly if the response rate is low.
KOeTS conducted several patient satisfaction surveys during the evaluation period; however, response rates are too small to make conclusions. This being said, surveys show high respondent satisfaction with telehealth events and emphasize their additional benefits (e.g., increasing understanding and knowledge of health concerns). KOeTS also conducted surveys, interviews and regular meetings with key service providers to address service quality issues. These sources identify high satisfaction with the quality of service provided by telehealth. Finally, KOeTS also conducted surveys with other community stakeholders (e.g., Chief and Council members, Health Directors, community nurses and other community members); results show a high level of community buy in.Footnote 99,Footnote 100,Footnote 101,Footnote 97,Footnote 98
Opportunities to improve the delivery of health care services
Internet connectivity
As stated earlier, Internet connectivity is the backbone to all eHIP components like PHIS, electronic records and telehealth. All connectivity partners and stakeholders, including First Nations regional organizations, ISED, INAC, provinces and ISPs, are faced with the challenge of bringing sustainable, reliable and affordable connectivity to those remote/isolated and isolated communities hardest to reach (due to location, terrain), such as Natuashish in Newfoundland and Labrador, Fort Severn in northern Ontario and northern Manitoba. Communities with no access to a fibre optic network rely on satellite communications, which can be unreliable in inclement weather, are often expensive due to saturated payloads and are technically complex to operate. Moreover, remote/isolated and isolated communities tend to be charged higher connectivity rates by ISPs, which becomes a price barrier for some communities. Combined with limited budgets, this plays a key role in communities not being able to procure the necessary bandwidth, although it may be available. At this time, there does not appear to be an optimal technology to provide these communities with the necessary level of broadband access at an affordable price.
Currently, different mandates between ISED, INAC and FNIHBFootnote xiv, have not been conducive to integrated planning with a focus on First Nations communities that need broadband access for health care delivery. This is also the case of provincial government plans, which may bring fibre network infrastructure close to First Nations communities without extending the last mile to them. There are opportunities for eHIP to support First Nations led connectivity initiatives and to strengthen its partnership role with INAC, ISED and provincial governments, specifically in the area of planning and providing the necessary broadband connectivity to health facilities based on minimum eHealth requirements. Partners and stakeholders identified several challenges in the area of broadband connectivity, which could be broadly classified into: 1) providing connectivity with bandwidth that can sustain telehealth delivery in remote/isolated and isolated communities that experience power outages; 2) finding, where possible, more reliable and scalable communications technology alternatives to the current C-band satellite coverage; 3) enhancing and upgrading the fibre optics networks to sustain telehealth, PHIS and EMR/EHR solutions through appropriate bandwidth availability; and, 4) providing health facilities with dedicated bandwidth that is not consumed by the community for other purposes.
Dedicated bandwidth for health facilities is necessary, especially for roll out of EMR in communities. Community bandwidth consumption tends to reach peak levels (people use more when they have more), which impacts eHealth components since available community bandwidth tends to be shared with health facilities (i.e., no dedicated bandwidth for health facilities). The challenge is to ensure that the health facility has the necessary bandwidth for telehealth, EMR and PHIS.
Health facility infrastructure also has an impact on bandwidth. The roles and responsibilities of eHIP, Health Canada's Health Facilities and Capital Program (HFCP), the Information Management Services Directorate (IMSD) of Health Canada's Corporate Services Branch (CSB), Public Services and Procurement Canada and Shared Services Canada (SSC) are unclear to those working in the delivery of health care to First Nations. Identifying which organization is responsible for providing software/hardware support, training on new software, upgrading cable and network equipment, etc., was perceived as causing disruptions to eHealth services.Footnote 31,Footnote 128 Partners and stakeholders provided specific examples of situations where support is needed: resetting a router after a power outage; helping connect a nurse's computer to the health facility Local Area Network (LAN); ensuring that telehealth equipment can be used (connected) in emergency rooms; and, determining the minimum bandwidth requirements in health facilities to ensure telehealth, EMRs/EHRs and PHIS can function free of connectivity failures. Although some of these issues may not directly relate to eHIP's functions, they present obstacles to eHealth delivery.
The role of HFCP in making sure that health facilities have the necessary "behind the wall" wiring and suitable outlets is complicated as most health facilities are owned by First Nations and HFCP involvement only occurs at the planning/design stage (new builds, renovations, expansions). Engineering and architectural issues related to suitable room sizes for telehealth session delivery, appropriate acoustic standards and privacy, broad hallways to roll telehealth equipment, and availability of connections for telehealth equipment in emergency rooms could be met through strengthened collaboration between eHIP, HFCP and First Nations during the planning phase. Space suitability challenges can be experienced when new service delivery models are incorporated into legacy infrastructure. Support to retrofit legacy infrastructure for the roll-out of eHealth could be prioritized in regional plans. There is a need to examine the issues faced by health facilities and arrive at multiparty solutions that reflect a holistic, grassroots perspective.
With respect to the Program's administrative data, there is a need for a national assessment of the amount of broadband used by health facilities, which is necessary to determine if the level of connectivity is adequate to sustain eHealth activities. There is a need for clear guidelines or standards in place defining bandwidth requirements to support the various eHealth components. In addition, an assessment of the amount of broadband used by health facilities versus what is technically available at the First Nation community headend would be helpful in identifying areas with potential room for connectivity upgrades.
Finally, there is a need for standard definitions of terminology in the "field of connectivity that is clear, technically accurate, and consistently used" so that all partners understand their level of commitment and expectations ahead of project commencement in a multi-stakeholder environment.Footnote 93
Telehealth – educational and administrative sessions
Regions are delivering educational and administrative sessions. The potential uptake of these sessions could be improved by resolving issues related to insufficient bandwidth, unreliable connectivity and access.Footnote 39,Footnote 127 The number of educational sessions delivered through telehealth in some regions (e.g., Atl.) have decreased in some years due to these issues.Footnote 39 In addition, clinical sessions are given priority over other sessions, in terms of bandwidth and equipment availability, which at times results in an educational event being cancelled without notice causing frustration to session providers and recipients.Footnote 127 While clinical sessions should continue to have priority, dedicated bandwidth at the health facility together with better coordination and technology options (e.g., CODEC unitsFootnote xv) may alleviate this issue.
Availability of trained and knowledgeable human resources also impacts the delivery and availability of both educational and administrative sessions.Footnote 127,Footnote 76 In many small communities, where IT support is lacking, telehealth coordinators could provide basic troubleshooting related to equipment failure and connectivity issues. According to partners and stakeholders, the critical factor needed for the success of these types of sessions is the selection and training of telehealth coordinators, who may have to multitask between equipment handling, resetting routers in case of power outages, promoting sessions with community members and professionals, finding suitable providers to deliver sessions and partners, and offering translation services prior and during some sessions.
Other areas to be addressed for higher uptake and value of educational sessions is the availability of culturally appropriate information, e.g., for nutritional courses, and sufficient numbers of content providers. In some regions, the relationship with the provincial eHealth partner does not address joint delivery and dissemination of health related information for training and education. In other instances, linking up to a provincial partner like OTN may not be possible due to additional costs for the community (e.g., purchasing educational material or membership). An assessment of health facility staff educational requirements and needs would also help improve uptake.
Telehealth – clinical sessions
The uptake of clinical sessions could be improved by addressing key areas of concern, e.g., limited connectivity (bandwidth) in remote/isolated and isolated communities,Footnote 81,Footnote 71,Footnote 72,Footnote 89,Footnote 92,Footnote 99 cancellations and patient no-showsFootnote 81,Footnote 99 as well as sufficient and sustained funding for maintenance costs, costs for evergreening of equipment, etc.Footnote 76,Footnote 46,Footnote 55,Footnote 59,Footnote 72,Footnote 88 Health facility staff changes or turnover, lack of training for nurses in handling telehealth equipment, inadequate and timely IT support as well as a lack of resources and capacity development opportunities in First Nations communities are also seen as major deterrents.Footnote 61,Footnote 62,Footnote 72,Footnote 103 Other impediments include inadequate space and privacy for session delivery specifically in older facilities (which includes absence of a dedicated room and space for hardware), lack of cooperation from physicians who are not inclined to participate in telehealth due to remuneration concerns or familiarity with technology, and absence of telehealth coordinators.
Based on the feedback obtained through interviews and case studies, there is a strong need to promote telehealth. Currently, awareness of telehealth, its use and benefits is low in some communities, specifically those that do not have telehealth coordinators. Some communities have the equipment but do not seem to take advantage of it because there is no capacity on the ground to operate it, and some physicians are not familiar with incorporating telehealth into their practice, thus needing encouragement and training. Other factors also impact session delivery, for example: bad weather and power outages; physician access to and availability of patient provincial health insurance numbers (e.g., the Ontario Health Insurance Plan – OHIP); onerous requirements for doctors to fill multiple forms (e.g., in the case of telepsychology) leading to long wait times; availability of language translation/interpretation; and, availability of transportation for patients to attend sessions, especially for the elderly. Feedback obtained during the evaluation also suggests that the uptake of telehealth clinical sessions is very high in areas where there is a designated organization or telehealth coordinators to promote it, e.g., KOeTS, TSAG and MBTelehealth.
Mobile Health
As mentioned before, mHealth is in its developmental phase in many regions. While there is considerable potential for the uptake of mHealth, the availability and reliability of cellular connectivity as well as security of data communications are challenges that need to be addressed. Health care providers in First Nation communities need a secure way to share a patient's health information (text, images) with other health care providers for consultation purposes. A solution is needed that is both sufficiently secure and convenient to use to ensure adoption by end users. While the use of mobile devices is convenient, security requirements and practices that prevent privacy breaches are needed.Footnote 70
Figure 3 from Infoway shows the different policies and regulations that may be necessary to ensure that mHealth is secure and reliable.Footnote 21
Figure 3. Policy and regulation that could apply to remote monitoring solutions.
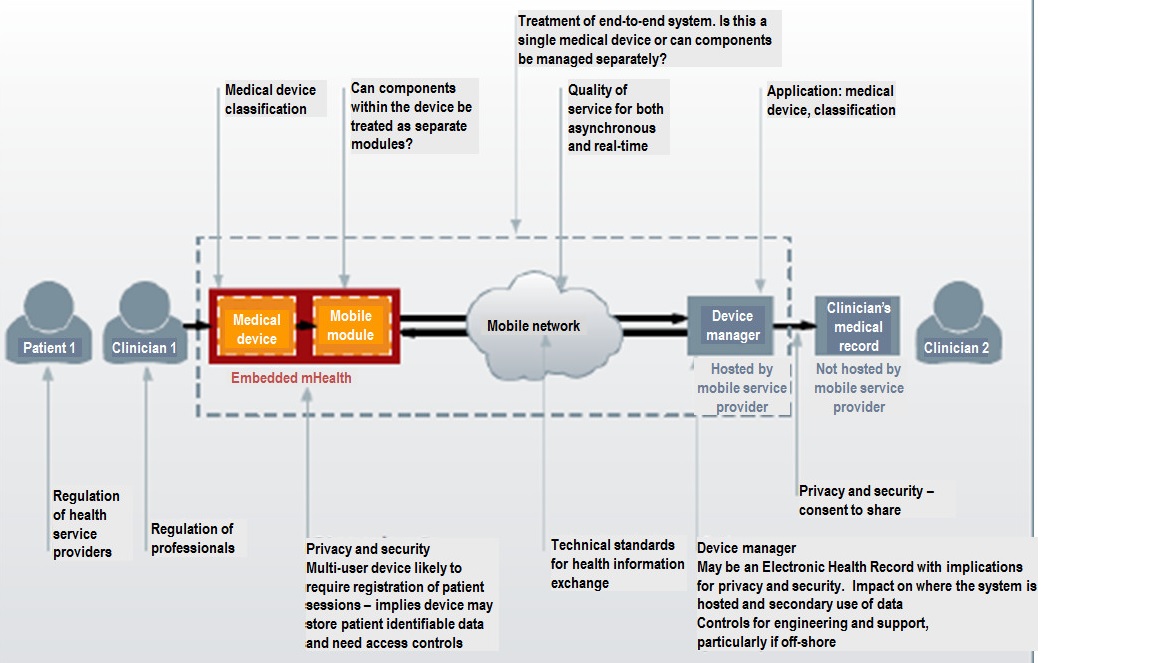
Figure 3: Policy and regulation that could apply to remote monitoring solutions - Text Description
Figure 3, A diagram created by Canada Health Infoway shows the different policies and regulations that may be necessary to ensure that mobile Health (also referred to as mHealth) is secure and reliable. For example, the regulation of health service providers has an impact on patients; the regulation of professionals has an impact on clinicians; and the process of sharing a clinician's medical record with other clinicians not hosted by mobile service providers has privacy and security impacts in terms of whether there is consent to share. Within the overall treatment of the end-to-end system, key considerations include whether a single medical device is involved, or whether components can be managed separately? The diagram further emphasizes that two key components are embedded in mHealth: the medical device and the mobile module. Connections between medical devices and mobile modules are impacted by medical device classifications and whether components within the device can be treated as separate modules; Connections between medical devices and mobile modules are also impacted by privacy and security matters, whereby a multi-user device is likely to require registration of patient sessions, which implies a device may store patient identifiable data and need access controls. Next, technical standards for health information exchanges, as well as the quality of service for both asynchronous and real-time impacts mobile networks. The device manager, hosted by a mobile service provider, may be an Electronic Health Record with implications for privacy and security and thereby have an impact on where the system is hosted and secondary use of data; including controls for engineering and support, particularly if off-shore.
According to Infoway, implementing mHealth would include:
- Defining a process to certify multiple vendors who would provide the different parts of the system.
- Developing and implementing a systematic assessment process to determine if the mHealth solution or component in question is considered a medical device and, therefore, subject to regulations and licensing.
- Licensing of the remote monitoring device (Health Canada) and possibly the mobile app.
- Establishing a privacy and security due diligence process to ensure the security and privacy of data throughout the various components of the mHealth solution.
Intermediate outcome #2: Interoperable eHealth technologies are implemented in First Nations communities
PHIS and electronic records implementations have exceeded targets. Progress is impeded due to the need to address various issues, none of which are in the sole purview of the Program, such as alignment of F/P privacy legislations, available connectivity/bandwidth, proliferation of non-interoperable electronic records systems, responsibility for physician remuneration as a result of eHealth delivery, and appropriate/ongoing funding.
Interoperable Public Health Information Systems
Interoperable PHIS are at different stages of implementation across provinces and First Nations communities. Interoperability is a key issue facing First Nations communities that need to link their client information system to the provincial system.
According to partners and stakeholders, there are several issues regarding data sharing agreements, data privacy, governance and ownership, as well as lack of F/P common ground to spur collaborative efforts that are impeding a more timely progress in this area. Of major concern to federal nurses, in provinces such as Manitoba, Ontario and Saskatchewan, is their inability to access provincial records in PHIS given differences between F/P privacy legislations. First Nations nurses face a similar challenge when their communities are not acknowledged as custodians of health information by provincial governments. There are also issues of capacity at the community level to implement, use and maintain the systems that hinder progress.
Interoperable electronic records
As discussed earlier, although an approach to EMR implementation has been developed by eHIP,Footnote 68 interoperability with provincial systems remains a key challenge and largely outside the control of the Program. In the case of EHRs, in many provinces, federal nurses are unable to access provincial patient electronic health records due to a lack of alignment between F/P privacy legislations, an issue that is currently being investigated according to Program representatives. Similarly, provincial governments may not recognize First Nations communities as custodians of health information. At the community level, there are challenges related to connectivity (broadband, bandwidth) and local capacity to implement, use and maintain systems. Electronic records implementation is also impacted by ongoing funding needs (for licensing, staff training, system maintenance), and the proliferation of different systems from different vendors.
Opportunities to improve the implementation of interoperable Public Health Information Systems and electronic records
Many of the areas requiring attention in the implementation of interoperable PHIS are similar to those in the implementation of electronic records. An area that needs considerable bolstering is the strength of partnerships. There are numerous logistical, jurisdictional and financial challenges that partners and stakeholders must work through in order to have a collaborative and effective engagement. Regions are at varying stages in finding viable solutions to these challenges but there is a need for greater collaboration to improve engagement and alignment between F/P governments and First Nations communities.Footnote 31,Footnote 44,Footnote 128
One of the key challenges faced in this area is the lack of alignment between F/P jurisdictions on privacy legislation that makes it difficult for federal nurses to access records/data on provincial data systems as part of health care service delivery to First Nations. Currently, in most provinces, federal nurses have no access rights to patient data on provincially operated PHIS or EHRs. This is an issue of high priority that needs resolution.
A unified vision and a partnership process that are client focused are necessary to bring eHealth to First Nations. In order to increase implementation efficiency in PHIS and electronic records interoperable with provincial PHIS and EHRs, it would be desirable to arrive at commonly agreed F/P goals for new technologies. In addition, a systematic, coordinated community assessment process to identify eHealth component readiness, community technical capacity (e.g., human resources), available/needed training and infrastructure would increase implementation success. At times, communities devote considerable effort to implement a solution that may not be the best fit for the province. An example of the need to keep in close contact with provincial decisions on EMRs/EHRs is illustrated by the recent decision by the province of Québec to implement Cristal-Net EHR across health facilities. FNQLHSSC is waiting to sign an agreement with the province before it moves ahead with implementing an EMR interoperable with Cristal-Net EHR.
With respect to partnership with First Nations, harmonization is progressing, especially in communities that have strong leadership organizations like TSAG, NITHA, FNHSSM, KOeTS, FNQLHSSC and Atlantic Canada's First Nation Help Desk. Many communities in the south of Saskatchewan, several communities outside KOeTS in Ontario, and communities in the Atlantic region, except for those that have a health data sharing agreement with the province as in Nova Scotia, would benefit from partnerships leading to harmonization. Nonetheless, even for communities with First Nations regional organizations showing leadership, the progress to ensure interoperability with provincial systems is difficult. Data governance and ownership issues delay the process and often First Nations regional organizations are unclear on the provincial lead in charge of interoperability. Through data sharing agreements, e.g., Saskatchewan, work is progressing on the issue of identifying OCAP compliant options for First Nations data disaggregation within provincial systems but it will take time to resolve. This issue, when resolved, will increase acceptance of eHealth among health care practitioners and help with their remuneration when delivering telehealth services.
4.4.3 To what extent have the longer term outcomes been achieved?
Longer term outcome # 1: Access, quality and safety of health care services are improved for First Nations individuals, families and communities
Based on available evidence, access to and quality of health care services has improved for First Nations individuals, families and communities over the past five years. According to information analyzed for the evaluation, planning, surveillance and reporting of health data in First Nations communities have also been enhanced as a result of eHealth, although there are further opportunities for improvement across communities.
Access, quality and safety
Progress on the immediate and intermediate outcomes shows that eHealth components, such as telehealth, are contributing to improve access and enhance the number of available health services in First Nations communities.Footnote 6,Footnote 10,Footnote 27,Footnote 34,Footnote 43,Footnote 48,Footnote 49,Footnote 55,Footnote 57,Footnote 62,Footnote 66,Footnote 71,Footnote 72,Footnote 75,Footnote 76,Footnote 77,Footnote 82,Footnote 90,Footnote 92,Footnote 100,Footnote 102,Footnote 103,Footnote 106,Footnote 107,Footnote 112,Footnote 127 Many of these eHealth components are in place across First Nations communities enabling and improving the quality of care.Footnote 44,Footnote 49,Footnote 57,Footnote 63,Footnote 66,Footnote 69,Footnote 71,Footnote 72,Footnote 75,Footnote 95,Footnote 96,Footnote 103,Footnote 107,Footnote 122 Across the regions, eHealth components are being made available to federal and First Nations health care providers and used to provide timely access to health care services while allowing providers to engage with patients.Footnote 2,Footnote 6,Footnote 10,Footnote 52,Footnote 69,Footnote 95,Footnote 96,Footnote 100
Examples provided by partners and stakeholders during case studies conducted for the evaluation identified several success stories related to eHealth component implementation:
- Telehealth equipment (moved by nurses into the emergency room) enabled an off-site doctor to work with nurses in an unexpected baby delivery.
- Two infants were born with assistance via telehealth while a community was surrounded by forest fires, which impeded travel out of the community.
- A seriously injured individual was able to receive ongoing care during a period of several months (consultations with two physicians) until full recovery without leaving the community.
- Patients (adults and children) were able to access a nurse clinician in an urban centre for tuberculosis screening without having to leave their community.
- Two individuals at risk of suicide received expert support.
- A culturally sensitive health care professional (psychiatrist) in an urban centre was able to interact and provide services to patients in remote/isolated and isolated communities.
- A family wanting to visit a relative in long-term hospital care, and for whom multiple trips would have been financially prohibitive, was able to use televisitation, a type of telehealth session, to conduct virtual visits.
- Elders have "televisited" for an hour with each other at the end of monthly educational sessions on topics of interest, turning what would have been a once-every-two-year trip into more regular engagement.
- Elders were able to attend educational tele-sessions/demonstration sessions on nutrition and how to eat better.
- Educational sessions have been delivered to multiple communities at once, leading to a high level of interaction.
Stakeholders found telehealth particularly valuable because a patient could see a doctor, regardless of ailment, without the interruptions that travel would cause in the patient's family or work life. Children and youth can receive comprehensive multi-system support and gain access to other services that would not be otherwise available.Footnote 38 Clinical sessions that support First Nations patients in a culturally appropriate and sensitive manner tend to have greater uptake by community members.Footnote 44,Footnote 48 Allowing family members to be present during the delivery of clinical sessions is believed by health care staff to be an important factor in encouraging patients to attend sessions. Health care staff members also believe that more patients receive treatment when they know that telehealth can be used to interact with a doctor instead of having to travel outside the community.Footnote 48 Key to this success is patient availability, equipment availability and transportation (to the telehealth site) as well as the role of telehealth/clinical coordinators. Without eHealth, many clinical sessions may not have occurred if patients had to travel for several hours for assessment, screening, follow-up, etc.Footnote 38,Footnote 44
Patients, physicians and the health care system are also benefiting from the integration of EMRs into clinical practice. To some degree, electronic records are allowing for better case management, patient safety and informed decision-making by health care providers.Footnote 34,Footnote 127
While the above examples provide evidence to increased access, quality and safety, the implementation of systematic surveying, analysis and reporting of user experience with the various eHealth components (e.g., PHIS, EMRs/EHRs) would allow for routine assessment of levels of satisfaction and identification of areas for improvement.
Planning, surveillance and reporting of health data
Based on available evidence, it appears that planning, surveillance and reporting of health data in First Nations communities has been enhanced as a result of the implementation of eHealth components, although there are significant opportunities for improvement across communities. For example, the Atlantic region has developed a number of Atlantic First Nations Health Status documents and reports.Footnote 55 There has also been increased participation of First Nations communities and regional organizations in health system planning and development (e.g., FNHSSM).Footnote 6
Regarding enhanced surveillance, funding provided to Manitoba First Nations communities has allowed them to upgrade both infrastructure and equipment and to collaborate with the province in the deployment of eChart and Panorama.Footnote 62 The Mustimuhw cEMR compiles mandatory information for the Community Based Reporting Template. In Saskatchewan, the Public Health Data Sharing Agreement between NITHA, the province and regional health authorities was expanded to include Panorama.Footnote 72 eHealth is enhancing the reporting capacity of First Nations communities by enabling tracking tools and increasing accessibility to information.
While planning, surveillance and reporting have improved, partners and stakeholders indicated that often a large number of indicators are collected but are not always analyzed and reported to make them useful for decision making. This was attributed to lack of capacity and dedicated staff to conduct the necessary data analysis. Also, there is no consistency as new studies and pilots take place, which take away the focus on what has been done so far.
Longer term outcome # 2: Health care providers have access to provincial health information systems
There has been considerable advance in PHIS and in EMRs/EHRs. Where implemented, users see these systems as helpful in planning and in managing the health care of First Nations individuals, families and communities.
There has considerable advance in PHIS and in EMRs/EHRs, with implementation having to adapt to provincial decisions and community data sharing agreements. Currently, some communities have access, others are waiting for data sharing agreements and provincially-approved versions, and yet others are not onboard. Where implemented, users see these systems as helpful in planning and in managing the health care of First Nations individuals, families and communities. Where immunization and vaccine inventory modules have been deployed, nurses see these modules as enabling them to provide improved patient care.
4.5 Performance: Issue #5 – Demonstration of Efficiency and Economy
Based on an assessment of available data, there is evidence to indicate that the Program's utilization of resources in relation to the production of outputs and progress toward expected outcomes is efficient and economical. Program goals are actively communicated while alignment between projects, eHealth components and regional needs and priorities are ensured. Nonetheless, given the rapidly changing environment, it is challenging for eHIP to track regional status and overall national situation. Cost avoidance as a result of all telehealth clinical session delivered in four regions in 2015-2016 was approximately $11.7 million.
The Treasury Board of Canada's guidance document Assessing Program Resource Utilization When Evaluating Federal Programs (2013) defines the demonstration of efficiency and economy as an assessment of resource utilization in relation to the production of outputs and progress toward expected outcomes. This assessment is based on the assumption that departments have standardized performance measurement systems and that financial systems link information about Program costs to specific inputs, activities, outputs and expected results.
This section of the report provides observations on efficiency and economy based on findings distilled from the available financial data provided by the Chief Financial Officer Branch (CFOB) of Health Canada supported by the results from document and literature review, key informant interviews, case studies and administrative data analysis. In addition, the findings below provide observations on the adequacy and use of performance measurement information.
4.5.1 Observations on Efficiency
Alignment between projects, components and regional needs
The Program uses a number of guidance documents to communicate its goals and ensure alignment between projects, eHealth components and regional needs, including the Program's Guidelines, HISAP and the Approach to Implementing EMRs 2016. The Program also employs a number of management tools to keep track of this alignment, including annual regional plans, regional year-end reviews and Management Operational Plans (MOPs). Regional priorities are discussed with partners in trilateral or multilateral tables. In addition, First Nations regional organizations, such as FNQLHSSC, KOeTS, FNHSSM, NITHA, Atlantic Canada's First Nation Help Desk and TSAG, bring strategic ideas/plans to these tables. The link between projects, components and regional needs is, thus, effected using both top-down and bottom-up (grassroots) approaches.
Calls for proposals are made in line with the strategic goals and objectives of eHIP. Project alignment is evaluated on a regular basis as is adherence to plans and budgets, for example:
- HCOM in Alberta performs gap analyses on TSAG's submission to identify regional priorities that may be missed, e.g., promotion of Alberta Netcare to nurses as a priority to view EHRs.
- In Manitoba, eHIP is part of the regional working committees on eChart, telehealth and EMR with FNHSSM and provincial representatives.
- In Ontario, KOeTS and the Kenora office of the Canadian Medical Association work with eHIP to address regional demand for mental health services and promote integrated telehealth videoconferencing activities.
- In Québec, eHIP works with FNQLHSSC. The regional infostructure action plan for First Nations helps ensure continued relevance and alignment with regional goals. This plan was developed in cooperation with First Nations and will remain in effect until 2017. The plan sets out a five-to-ten-year vision. An operational action plan is prepared annually based on the overall vision.
- Atlantic Canada's First Nation Help Desk is involved in bringing local community projects to assess their fit with eHIP's goals.
- In northern Saskatchewan, NITHA coordinates the operational plan with First Nations.
Due to the rapidly changing eHealth context, there is a need to conduct community and technology environmental scans on an ongoing basis to inform Program guidelines. Also, when decisions are made with respect to bandwidth or solutions for interoperability of systems between First Nations and provinces, regional and sub-regional contexts should be examined in order to attain a better fit for the communities. In this context, partners and stakeholders identified a need to re-examine HISAP to ensure it reflects a grassroots approach.
Community technical readiness assessments
Regional Program offices and First Nations regional organizations use a number of tools to assess projects. Nonetheless, although there is a national readiness assessment tool,Footnote 54 the approach to assess community readiness for the different eHealth components does not appear to be standardized. One example of community readiness assessment examined by evaluators was provided by KOeTS. In this case, needs are assessed based on a community profile, community willingness to adopt eHealth and availability in terms of connectivity, health facility characteristics (e.g., space for telehealth equipment, extent of modern technical wiring) and community technical capacity. Technical assessment teams involve First Nations regional organizations, Health Directors, nurses, provincial eHealth partners, ISPs, IT specialists and eHIP staff. When a community has been assessed, an application is submitted to eHIP, which then proceeds with its project assessment. Projects that meet identified needs and priorities may then be included in the MOP.
In some regions, First Nations regional organizations, such as KOeTS, FNQLHSSC, FNHSSM, TSAG, Atlantic Canada's First Nation Help Desk and NITHA, work closely with other partners and stakeholders to identify needs and priorities at the community level. In these cases, First Nations regional organizations act as community representatives assisting communities with their proposals. Criteria used for assessing proposals are usually stated in the call for proposal and could range from community capacity, types of needs assessments completed, alignment with regional/provincial/community priorities and needs, demonstrated value for money, care for the environment, etc. The review criteria vary across regions and projects, for example an equipment evergreening project would have different criteria compared to a project piloting a registry, or proposing a telehealth site.
Since each region, and each First Nations community within a region, is at a different state of maturity, the above process makes it challenging for eHIP to track regional status and overall national situation. First Nations community involvement in decision-making is also challenging when there is no First Nations regional organization leading the way: communities that do not have the know-how, capacity or "a champion" are not able to surface their ideas to eHIP.
4.5.2 Observations on Economy
Planning and funding
Two years of Program budget data were provided for the evaluation and are presented in Table 17. Budgets for these years include BC and could not be broken down by region.
| Fund | Fiscal year | Total | |||||
|---|---|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |||
| 301 | Salaries | N/A | N/A | N/A | 4,860,294 | 5,941,164 | 10,801,458 |
| 310 | Operation | N/A | N/A | N/A | 6,976,298 | 6,940,080 | 13,916,378 |
| 312 | Minor Capital | N/A | N/A | N/A | - | - | - |
| 326 | Contribution | N/A | N/A | N/A | 12,935,369 | 12,838,916 | 25,774,285 |
| Total | N/A | N/A | N/A | $24,771,961 | 25,720,160 | 50,492,121 | |
|
Source: CFOB. Information for fiscal years 2011-2012, 2012-2013 and 2013-2014 was not available at Program level. |
|||||||
Table 18 provides the Program's annual expenditures. Program expenditures have ranged between $22 and $25 million annually, with the exception being 2012-2013 when the highest expenditure of $30 million was incurred. While the variance between budgets and expenditures could not be examined for all years, it is noted that the Program lapsed funds in the two years for which budget data was available (i.e., 2014-2015 and 2015-2016).
Table 19 provides a breakdown of Program expenditures by financial code. It should be noted that financial codes for eHIP are well aligned with eHealth components, namely connectivity, EMRs/EHRs, PHIS, telehealth and mHealth as well as capacity building. According to this table, one may note the following:
- A steady decrease in eHealth infostructure policy development and Program oversight from $7.2 million in 2011-2012 to $5.2 million in 2015-2016.
- A steady increase in capacity building/education and training from $0.3 million in 2011-2012 to $0.7 million in 2015-2016.
- An increase in EMRs/EHRs from $0.8 million in 2014-2015 to $2.6 million in 2015-2016.
- An increase in telehealth deployment from $1.6 million in 2011-2012 to $4.5 million in 2014-2015.
- A decrease in telehealth maintenance from $6.8 million in 2012-2013 to $1.5 million in 2014-2015.
- A decrease in PHIS deployment with a peak of $7.8 million in 2012-2013 to $3.2 million in 2015-2016.
- A high for connectivity and IT deployment of $1.9 million in 2011-2012 and a low of $0.9 million in 2015-2016.
- A high for connectivity and IT maintenance of $3.5 million in both 2013-2014 and 2015-2016 and a low of $1.6 million in 2012-2013.
- A high for emerging technologies of $2.4 million in 2013-2014 and a low of $0.5 million in 2011-2012.
| Fiscal year | Fund | Region | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ATL | QC | ON | MB | SK | AB | Northern | HQ | ||||
| 2011-2012 | 301 | Salaries | 693,624 | 871,805 | 337,093 | 432,340 | 551,323 | 1,563,958 | 0 | 682,418 | 5,132,561 |
| 307 | Non-Controllable Salary | 76,987 | 23,456 | 21,876 | 50,350 | 35,042 | 48,892 | 0 | 133,783 | 390,386 | |
| 310 | Operation | 899,793 | 80,978 | 708,337 | 1,061,625 | 827,691 | 159,718 | 0 | 1,322,511 | 5,060,653 | |
| 326 | Contribution | 1,108,653 | 1,016,917 | 5,164,746 | 1,493,850 | 1,493,736 | 2,262,626 | 0 | 252,000 | 12,792,528 | |
| Sub-total | 2,779,057 | 1,993,156 | 6,232,052 | 3,038,165 | 2,907,792 | 4,035,194 | 0 | 2,390,712 | 23,376,128 | ||
| 2012-2013 | 301 | Salaries | 663,235 | 837,583 | 167,371 | 598,502 | 582,628 | 1,518,428 | 0 | 696,464 | 5,064,211 |
| 307 | Non-Controllable Salary | 38,301 | 34,204 | 16,104 | 27,286 | 69,659 | 130,042 | 0 | 45,231 | 360,827 | |
| 310 | Operation | 417,940 | 43,545 | 1,472,229 | 2,375,881 | 1,141,398 | 58,188 | 0 | 796,598 | 6,305,779 | |
| 326 | Contribution | 1,112,448 | 733,843 | 3,816,147 | 2,023,829 | 7,035,212 | 3,177,880 | 0 | 135,500 | 18,034,859 | |
| Sub-total | 2,231,924 | 1,649,175 | 5,471,851 | 5,025,498 | 8,828,897 | 4,884,538 | 0 | 1,673,793 | 29,765,676 | ||
| 2013-2014 | 301 | Salaries | 498,492 | 828,890 | 106,975 | 656,913 | 589,347 | 1,214,658 | 0 | 688,541 | 4,583,816 |
| 302 | Student Salary | 0 | 5,608 | 0 | 0 | 0 | 0 | 0 | 0 | 5,608 | |
| 307 | Non-Controllable Salary | 0 | 22,029 | 4,389 | 12,931 | 0 | 107,491 | 0 | 98,397 | 245,237 | |
| 310 | Operation | 61,604 | 158,900 | 1,134,907 | 1,022,515 | 1,094,409 | 37,056 | 0 | 327,505 | 3,836,896 | |
| 326 | Contribution | 1,147,678 | 1,627,371 | 4,854,937 | 2,485,993 | 1,624,663 | 3,824,572 | 0 | 129,500 | 15,694,714 | |
| Sub-total | 1,707,774 | 2,642,798 | 6,101,208 | 4,178,352 | 3,308,419 | 5,183,777 | 0 | 1,243,943 | 24,366,271 | ||
| 2014-2015 | 301 | Salaries | 704,150 | 912,867 | 418,255 | 619,172 | 594,831 | 1,135,099 | 96,083 | 598,371 | 5,078,828 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2,984 | 2,984 | |
| 307 | Non-Controllable Salary | 2,357 | 38,783 | 3,030 | 3 | 14,812 | 36,556 | 2,602 | 15,279 | 113,422 | |
| 310 | Operation | 64,984 | 160,597 | 28,563 | 996,643 | 1,031,622 | 91,972 | 26,200 | 258,127 | 2,658,708 | |
| 312 | Minor Capital | 0 | 49,198 | 0 | 0 | 0 | 0 | 0 | 0 | 49,198 | |
| 326 | Contribution | 1,267,515 | 2,586,777 | 3,265,973 | 2,182,380 | 1,626,345 | 2,724,607 | 0 | 170,000 | 13,823,597 | |
| Sub-total | 2,039,006 | 3,748,222 | 3,715,821 | 3,798,198 | 3,267,610 | 3,988,234 | 124,885 | 1,044,761 | 21,726,737 | ||
| 2015-2016 | 301 | Salaries | 643,366 | 834,914 | 400,709 | 739,026 | 596,082 | 581,570 | 98,608 | 612,375 | 4,506,650 |
| 302 | Student Salary | 0 | 175 | 0 | 0 | 0 | 674 | 0 | 3,925 | 4,774 | |
| 307 | Non-Controllable Salary | 4,384 | 42,565 | 610 | 8,227 | 63,063 | 41,599 | 352 | 16,222 | 177,022 | |
| 310 | Operation | 172,177 | 153,484 | 50,031 | 1,187,418 | 754,257 | 26,567 | 17,194 | 217,847 | 2,578,975 | |
| 326 | Contribution | 1,266,379 | 2,539,684 | 4,928,011 | 2,986,921 | 1,762,989 | 3,623,599 | 0 | 170,000 | 17,277,583 | |
| Sub-total | 2,086,305 | 3,570,822 | 5,379,361 | 4,921,593 | 3,176,392 | 4,274,009 | 116,154 | 1,020,369 | 24,545,004 | ||
| Total | 10,844,066 | 13,604,173 | 26,900,293 | 20,961,806 | 21,489,110 | 22,365,752 | 241,039 | 7,373,578 | 123,779,816 | ||
| Source: CFOB. | |||||||||||
| Program financial code | Fund | Fiscal year | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |||||
| KP00 | e-Health Infostructure - Policy Development & Program Oversight | 301 | Salaries | 2,661,198 | 2,356,345 | 1,993,103 | 2,600,163 | 2,725,154 | 12,335,963 |
| 302 | Student Salary | 0 | 0 | 5,608 | 2,984 | 4,774 | 13,366 | ||
| 307 | Non-Controllable Salary | 259,157 | 147,829 | 140,628 | 53,653 | 77,436 | 678,703 | ||
| 310 | Operation | 961,472 | 644,589 | 519,944 | 609,032 | 405,303 | 3,140,340 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 49,198 | 0 | 49,198 | ||
| 326 | Contribution | 3,341,057 | 3,598,869 | 3,352,469 | 2,597,277 | 2,015,443 | 14,905,115 | ||
| Sub-total | 7,222,884Table 19 footnote a | 6,747,632 | 6,011,752 | 5,912,307 | 5,228,109Table 19 footnote b | 31,122,684 | |||
| KP05 | Electronic Medical/Health Records | 301 | Salaries | 0 | 0 | 0 | 0 | 118,728 | 118,728 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 310 | Operation | 0 | 0 | 0 | 17,657 | 69,410 | 87,067 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 0 | 0 | 0 | 800,984 | 2,447,566 | 3,248,550 | ||
| Sub-total | 0 | 0 | 0 | 818,641Table 19 footnote b | 2,635,703Table 19 footnote a | 3,454,344 | |||
| KP10 | Capacity Building/Education and Training | 301 | Salaries | 134,715 | 164,386 | 137,576 | 169,920 | 39,868 | 646,465 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 0 | 20,966 | 0 | 0 | 0 | 20,966 | ||
| 310 | Operation | 22,709 | 75,825 | 24,209 | 14,054 | 12,185 | 148,982 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 183,246 | 140,746 | 274,456 | 327,950 | 678,861 | 1,605,259 | ||
| Sub-total | 340,670Table 19 footnote b | 401,923 | 436,241 | 511,924 | 730,914Table 19 footnote a | 2,421,672 | |||
| KP20 | Public Health Surveillance Systems | 301 | Salaries | 1,126,295 | 930,168 | 849,456 | 679,038 | 512,708 | 4,097,665 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 39,988 | 68,861 | 647 | 26,527 | 71,529 | 207,552 | ||
| 310 | Operation | 2,997,804 | 4,522,819 | 2,242,562 | 1,016,240 | 870,532 | 11,649,957 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 1,226,307 | 2,240,791 | 1,204,769 | 1,659,269 | 1,773,421 | 8,104,557 | ||
| Sub-total | 5,390,394 | 7,762,639Table 19 footnote a | 4,297,434 | 3,381,074 | 3,228,190Table 19 footnote b | 24,059,731 | |||
| KP30 | Telehealth - Deployment | 301 | Salaries | 263,432 | 175,920 | 256,207 | 282,925 | 82,374 | 1,060,858 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 0 | 47,095 | 21,760 | 19,352 | 0 | 88,207 | ||
| 310 | Operation | 522,791 | 300,065 | 236,685 | 366,266 | 490,191 | 1,915,998 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 818,520 | 3,668,998 | 3,741,383 | 3,855,541 | 3,131,631 | 15,216,073 | ||
| Sub-total | 1,604,743Table 19 footnote b | 4,192,078 | 4,256,035 | 4,524,084Table 19 footnote a | 3,704,196 | 18,281,136 | |||
| KP31 | Telehealth - Maintenance | 301 | Salaries | 170,822 | 141,440 | 151,934 | 160,985 | 133,493 | 758,674 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 30,748 | 5,599 | 8,017 | 0 | 1,563 | 45,927 | ||
| 310 | Operation | 319,255 | 379,217 | 439,090 | 348,196 | 437,375 | 1,923,133 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 4,215,983 | 6,253,577 | 1,071,022 | 990,119 | 1,999,468 | 14,530,169 | ||
| Sub-total | 4,736,808 | 6,779,833Table 19 footnote a | 1,670,063 | 1,499,300Table 19 footnote b | 2,571,900 | 17,257,904 | |||
| KP40 | Connectivity & IT Deployment | 301 | Salaries | 239,232 | 819,609 | 756,511 | 784,044 | 53,136 | 2,652,532 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 20,100 | 50,314 | 61,901 | 6,851 | 0 | 139,166 | ||
| 310 | Operation | 30,341 | 11,743 | 6,225 | 5,562 | 263 | 54,134 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 1,636,850 | 441,637 | 953,740 | 791,974 | 823,139 | 4,647,340 | ||
| Sub-total | 1,926,523Table 19 footnote a | 1,323,303 | 1,778,377 | 1,588,431 | 876,538Table 19 footnote b | 7,493,172 | |||
| KP41 | Connectivity & IT Maintenance | 301 | Salaries | 199,603 | 75,667 | 74,316 | 69,854 | 420,384 | 839,824 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 6,163 | 10,701 | 0 | 7,039 | 26,222 | 50,125 | ||
| 310 | Operation | 194,290 | 173,805 | 147,693 | 105,662 | 128,437 | 749,887 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 1,238,958 | 1,342,340 | 3,264,212 | 2,600,188 | 2,907,573 | 11,353,271 | ||
| Sub-total | 1,639,014 | 1,602,513Table 19 footnote b | 3,486,221Table 19 footnote a | 2,782,743 | 3,482,615Table 19 footnote a | 12,993,106 | |||
| KP50 | Emerging Technologies | 301 | Salaries | 337,264 | 400,676 | 364,713 | 331,899 | 420,806 | 1,855,358 |
| 302 | Student Salary | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 307 | Non-Controllable Salary | 34,230 | 9,462 | 12,284 | 0 | 273 | 56,249 | ||
| 310 | Operation | 11,991 | 197,716 | 220,488 | 176,039 | 165,280 | 771,514 | ||
| 312 | Minor Capital | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 326 | Contribution | 131,607 | 347,901 | 1,832,663 | 200,295 | 1,500,481 | 4,012,947 | ||
| Sub-total | 515,092Table 19 footnote b | 955,755 | 2,430,148Table 19 footnote a | 708,233 | 2,086,840 | 6,696,068 | |||
| Total | 23,376,128 | 29,765,676 | 24,366,271 | 21,726,737 | 24,545,004 | 123,779,816 | |||
| Source: CFOB. | |||||||||
|
|||||||||
The annual planning process used by eHIP, which results in funds being transferred to the regional offices, changed during the evaluation period. Previously, regional allocation decisions were made on the basis of a national eHealth budget amount distributed amongst the regions by HQ based on Program plan proposals submitted by each regional office. More recently, Program allocations have been integrated within the overall MOP process for all regional FNIHB programs under the direction of FNIHB's Assistant Deputy Minister's Office (ADMO). Funding decisions are limited to a one-year window. According to Program representatives and stakeholders, eHIP's annual funding request process is focussed on what is needed for the coming fiscal year; hence, it does not factor in a sustainable funding view for the Program over three-to-five years to respond to technology evolution and increasing costs (e.g., connectivity costs, licensing fees, training, equipment replacement and evergreening and new technology, such as mHealth).
Regions submit an annual MOP without full knowledge of available funding. The Program's funding is considered within the context of all funds available to the region for all health services. Consequently, funding for required Program activities and advancements may be eliminated from the MOP due to other regional priorities. As the MOP is approved and funding revised, projects may need to be reduced or eliminated. The MOP is then reconfigured to first cover all existing fixed expenses (e.g., connectivity costs) and the remainder is then split among those projects that could still be carried out. The lack of a long-term planning horizon creates an uncertain environment for the development of annual MOPs at the regional level.
In order to compensate for limited funding, some regions have received funding from other sources (e.g., other FNIHB programs, pressure funding and special allocation) or cash managed to keep projects going; examples include: receiving funding from the Children's Oral Health Initiative (COHI) for a teledentistry project, using PHIS funds (Panorama) to replace telehealth equipment, or using nursing funding to meet connectivity costs. It is noted that not all the regions have the budgetary flexibility or room for such adjustments.
To address the above issues, planning of sufficient funding to sustain technology projects that typically require a three- to five-year horizon to deliver results may be required. Considerations could include provisions for funding towards: ongoing project costs; indexed costs for fixed expenses (e.g., connectivity); expenditures for evergreening of equipment; allocation for licensing fees, training and capacity building); and, technology innovations, such as mHealth. A medium- and long-term vision on a regional and national basis across all eHealth components would be of more benefit to evolving and maintaining a technology-based Program since annual MOPs are not intended to provide this type of vision.
Cost avoidance
In order to assess economy, the evaluation followed the approach used by the Program in its two previous ministerial reports to Treasury Board: Year One Report (2014) and Year Two Report (2015) reports,Footnote 38,Footnote 39 that estimated cost avoidance as a result of clinical sessions delivered via telehealth. Cost avoidance should be understood as the equivalent travel cost that would have been incurred if a patient had actually travelled instead of attending a telehealth session. It is not an actual "cost savings" to FNIHB since telehealth has operational costs for connectivity, equipment and coordination of services. As such, a net gain may be much smaller. Table 20 presents the total cost avoidance as a result of all telehealth clinical sessions delivered in four regions in 2015-2016 as approximately $11.7 million. A number of assumptions have been made to arrive at an estimate of total cost avoidance:
- The estimated average cost per trip reported in the Year Two Report, being the latest information available from the Program, has been used to estimate the equivalent travel value. As a result, estimated equivalent travel values are only provided for those regions also included in the Year Two Report.
- The impact of escorts has been factored into the estimated average cost per trip for all regions except Ontario. At the time of the Year Two Report, the Ontario region made the assumption that the total number of escorts would be the total number of minor children attending clinical sessions, which translated into 35% of clinical sessions. This modifying factor has been used to estimate the equivalent travel value for Ontario.
- Cost avoidance of as a result of telehealth clinical sessions – Alberta, Saskatchewan, Manitoba and Ontario, 2015-2016.
| Region | Number of telehealth clinical sessions | Estimated number of escorts | Estimated average cost per trip ($) | Estimated equivalent travel value ($) |
|---|---|---|---|---|
| Alberta | 3,287 | N/A | 690 | 2,268,030 |
| Saskatchewan | 98 | N/A | 475 | 46,550 |
| Manitoba | 3,708 | N/A | 955 | 3,541,140 |
| Ontario | 3,205 | 1,122 | 1,350 | 5,841,450 |
| Total | - | - | - | 11,697,170 |
Table 21 provides the cost avoidance as a result of those telehealth clinical sessions that would have been considered medically necessary by the Supplementary Health Benefits (Non-Insured Health Benefits) Program or NIHB Program. The cost avoidance as a result of clinical sessions delivered in the same four regions was approximately $6.5 million. While the previous suppositions also apply to this table, additional assumptions have been made to arrive at an estimate of cost avoidance as a result of NIHB-eligible sessions:
- The NIHB Program determines clinical consult eligibility using detailed medical transportation criteria. According to eHIP representatives, a prudent standard for all regions is an assumption of 50% of sessions deemed medically necessary and, thus, resulting in necessary travel, although this percentage may have some regional variations. It should be noted that actual travel never took place.
- The most recent KOeTS Annual Report (2016),Footnote 101, estimated the number of medically necessary sessions at 1,945.
| Region | Number of telehealth clinical sessions | Percentage of telehealth clinical sessions considered NIHB-eligible | Number of eligible telehealth clinical sessions | Estimated number of escorts | Estimated average cost per trip ($) | Estimated equivalent travel value ($) |
|---|---|---|---|---|---|---|
| Alberta | 3,287 | 50% | 1,644 | N/A | 690 | 1,134,360 |
| Saskatchewan | 98 | 50% | 49 | N/A | 475 | 23,275 |
| Manitoba | 3,708 | 50% | 1,854 | N/A | 955 | 1,770,570 |
| Ontario | 3,205 | N/A | 1,945 | 681 | 1,350 | 3,545,100 |
| Total | - | - | - | - | - | 6,473,305 |
A similar report for educational sessions is not provided since it was not possible to determine, based on the available data, which sessions would have required in-person attendance, which sessions would have still been offered if telehealth were not available, and the recipients of the sessions (i.e., individuals/patients vs. health care providers). As such, the overall cost avoidance of telehealth, beyond clinical sessions, may be higher.
4.5.3 Observations on the Adequacy and Use of Performance Measurement Data
eHIP collects data on a number of variables linked to the different Program components. As evidenced by the tables provided in this report, data collection and reporting has improved during the period of the evaluation, particularly in the last three years. Program representatives acknowledged that much more needs to be accomplished in a systematic manner since the focus has been mostly on the implementation of eHIP components. First Nations regional organizations also indicated that, while more data is now being collected at the community level, there are opportunities for more systematic planning of which indicators are needed, who should collect them and how. It is noted, based on interviews, that data collection requirements are associated with developing on ground capacity and systems.
Data collection for the Program is a three-stage process: 1) data is collected by different stakeholders and in different formats at the community level; 2) data is then sent to the regional Program office that consolidates this information; and, 3) this data is then provided by the Program regional offices to headquarters through Regional Year-End Reviews. An examination of this process, review of the data gathered by the Program, and the resulting analysis needed to produce the tables for this report identified a number of areas requiring attention:
- There is a need for consistent and timely data reporting across all regions, which impacts data analysis and Program reporting. For example, in terms of consistency, some regions collect data on number of sessions, others do not; some regions collect data on types of session, others do not. Similarly, with respect to timeliness, Regional Year-End Review submission deadlines, which used to be before the end of the second quarter in the following fiscal year, are now being extended into the third and fourth quarters.
- Currently, definitions for data collected are not clearly established across regions. Hence, there is a lack of clarity on what a specific data set represents. For example, should a specific implementation be recorded as an EMR, EHR or PHIS (beyond Panorama)? What is a telehealth site vs. a telehealth end-point? Similarly, there is a need for consistent use of health facility definitions, as described by FNIHB, since INAC definitions have been used in some regions.
- There is a need to clearly identify what is funded by the Program. While it is advantageous to have the overall eHealth view, from the perspective of the Program and the evaluation, it is more important to know the status of those communities and eHealth components funded by the Program.
In order to enable a proper assessment of progress in the achievement of the Program outcomes, it is important to address the above issues. It is also important to revisit the indicators being tracked in order to determine what is necessary. Based on an examination of the indicators tracked by the Program and its stated outcomes, the following indicators should be tracked at a minimum:
- Level of broadband connectivity in use at the health facility (technology, bandwidth);
- Number of telehealth sites;
- Number of sessions by type (administrative, educational and clinical);
- Number of attendees by session type;
- Number of cancellations by session type;
- Number of educational sessions by area (e.g., nutrition, diabetes management);
- Number of clinical sessions by specialty (e.g., teledermatology, teleophthalmology);
- Access to PHIS (Panorama and others: specify tool); interoperable or not with provincial systems;
- Access to EMRs (specify tool); interoperable or not with provincial/community EHRs; and,
- Access to EHRs (specify tool); community or provincial.
These indicators should be tracked by the following overall classification:
- By funded community (i.e., those communities receiving funds either directly by the Program or through a funding agreement with a First Nations regional organization or First Nations Band);
- By type of community (i.e., remote/isolated, isolated, semi-isolated and non-isolated); and,
- By health facility type (i.e., nursing station, health centre, health station, health office, National Native Alcohol and Drug Abuse Program treatment centre and hospital).
It would also be advantageous to collect survey data on level of satisfaction with educational and clinical telehealth sessions. Surveying recipients of educational sessions (in particular health facility staff and health care providers) would allow the identification of gaps and ways to address them related to available training. The 2015 Canadian Telehealth Assessment identified this gap and, going forward, has identified the desire for more satisfaction surveys completed so that input from the direct beneficiaries can be collected and analyzed. With respect to clinical sessions, surveying health care provider experiences would allow the Program to identify difficulties that, for example, nurses and physicians face while delivering health care via telehealth. By addressing these difficulties, related to technology or lack of diagnostic equipment at the telehealth site, it would be possible to improve the patient/health care provider relationship as well as the willingness of health care providers to use telehealth technology.
It is hoped that these concrete suggestions will be actioned in the context of the current government-wide focus on Performance Information Profiles (PIPs).
5.0 Conclusions
The following sections distill the findings presented in the report and provide a way forward while recognizing the complexities inherent in an environment with multiple partners and stakeholders. While the relevance conclusions are specific to the Program, conclusions on performance reflect the complex multi-jurisdictional challenges. In addition, the conclusions also provide information on relevant international practices that may serve as examples.
5.1 Relevance Conclusions
5.1.1 Continued Need
The Program continues to address a demonstrable need and is responding to the needs of its client population. The needs addressed by the Program are fundamental to improving the health status of First Nations.
The Program provides eHealth services (directly or on a transferred basis) to First Nations communities, reduces travel time and costs as well as displacement from family and community. It has increased access to opportunities and skills development for providers, empowered patients with choices pertaining to their health care, and enhanced information for health promotion and disease prevention.
There is a continued need for the Program to work with partners to expand and upgrade broadband connectivity and telehealth, continue to enable interoperability of complex health systems that can work across multiple jurisdictions, and continue to enhance First Nations knowledge, capacity and control over how their data is collected, shared and analyzed as well as to increase their involvement in evidence-based decision making with respect to health care service delivery.
5.1.2 Alignment with Government Priorities
The Program is aligned with government priorities. These include keeping pace with technology and innovation, contributing to address health system challenges and system reform, and building relationships with Indigenous peoples.
eHIP is aligned with broader Government of Canada priorities as well as departmental and branch strategic objectives. HISAP continues to be relevant but more effort should be made to increase the participation and input of First Nations to make HISAP the product of a balanced bottom-up (grassroots) and top-down process.
5.1.3 Alignment with Federal Roles and Responsibilities
The Program is well aligned with federal roles and responsibilities.
At both the regional and HQ level, eHIP has strengthened its partnership role but needs to bolster this capability further to make the complex systems interoperable, effective and efficient. A stronger focus is needed on building partnerships to continue to integrate F/P health services and to increase First Nations communities' health services capacity to address their own health needs.
5.2 Performance Conclusions
5.2.1 Achievement of Expected Outcomes (Effectiveness)
The Program has exceeded its target for broadband connectivity; however, while all eHIP funded First Nations Bands have Internet connectivity, the available bandwidth and connection reliability is variable. The Program has also exceeded targets on PHIS and EMR/EHR implementation. Telehealth continues to grow: on one hand, administrative and educational sessions have provided opportunities for collaboration as well as knowledge and skill development; on the other hand, the large number of clinical sessions, exceeding targets, has provided access to a multitude of specialties. mHealth appears promising and is in its developmental phase; further support for this area may aid technology adoption.
While the Program is helping to bridge some of the inequities linked to health care service access and related data, there is a need for the Program to continue to work towards achieving all of its stated objectives across all First Nations communities. Ways forward are explored in each of the following sub-sections.
Internet connectivity
There is a need to continue supporting broadband connectivity in First Nations communities since this component is key to the deployment of eHealth tools.Footnote 49,Footnote 76,Footnote 77,Footnote 79,Footnote 88 A coordinated and community-focused effort with Program partners and stakeholders, such as First Nations, INAC and ISED, to identify First Nations communities' broadband needs and available funding (e.g., from the Program and other government sources) would serve to address current connectivity challenges. This approach would allow communities and partners to more efficiently extend connectivity to underserved areas while enhancing services where only basic connectivity is available.
Connectivity access also becomes more economical when demand from neighbouring communities is pooled via partnerships. For example, K-Net has worked with Treaty 9 communities and is looking to partner with Treaty 3 communities to realize economies of scale. The Northern Indigenous Community Satellite Network (NICSN) is a cooperative of K-Net in Ontario, Broadband Communications North (BCN) in Manitoba, and the Kativik Regional Government (KRG) in Québec, and, thus, has more buying power. Atlantic Canada's First Nation Help Desk and the Membertou Data Centre have followed a community aggregate model (Health centre, Band Office, School) to implement fibre connectivity in health facilities in the Atlantic region. In Alberta, TSAG manages Internet connectivity for 45 health facilities achieving economies of scale. Similar pools of communities could be formed in other regions, e.g., southern Saskatchewan.
Developing an IT client-focused support approach, by clearly defining the roles and responsibilities of all partners (i.e., eHIP, IMSD and SSC), would help tackle IT support problems that affect the delivery of eHealth in First Nations communities (e.g., nurse support, LAN reliability, etc.).
Above all, developing standards and guidelines on network and connectivity/bandwidth requirements linked to each eHealth component would be extremely advantageous. According to the Program's Connectivity Status in First Nation Communities, all health information technologies, such as PHIS, EMRs and various telehealth activities, need different bandwidth requirements, hence connectivity levels should be assessed based on health facilities and their specific requirements.Footnote 67 These standards and guidelines could then be shared with health facility planners to ensure that immediate, medium and long-term community eHealth requirements are considered at the planning stage.
Public Health Information Systems
For work on PHIS to continue to advance, the partners involved need to share a common vision, which should include the following elements:
- Integration of OCAP principles in data sharing agreements to ensure health data can be exchanged in a way that meets the needs of all parties.Footnote 127,Footnote 7
- Promotion to increase awareness of the benefits of PHIS through First Nations regional organizations (e.g., FNQLHSSC, FNHSSM, NITHA, TSAG, KOeTS, Atlantic Canada's First Nation Help Desk) and at the community level in communities that are not yet part of similar organizations.
- Encouragement of communities to work with First Nations regional organizations to lead advocacy on data governance and ownership as well as integration with provincial systems.Footnote 7,Footnote 6
- Dissemination of examples of PHIS progress in communities that have adopted PHIS to encourage others to adopt similar approaches.
- Assessment of local community capacity and readiness as well as training in implementing, using and maintaining PHIS.
- Identification of federal partners that could take leadership roles in addressing PHIS implementation challenges, for example: eHIP-Infoway on alignment with provincial systems and privacy issues; eHIP-ISED-INAC on obtaining and maintaining the necessary connectivity levels.
- Collaboration among F/P partners to identify information sharing solutions to address legislative issues surrounding federal and First Nations nurses access to provincial health systems/health information.
- Identification of OCAP compliant options for First Nations data disaggregation within provincial systems to ensure seamless on-reserve/off-reserve care for First Nations individuals while protecting their privacy.
- Provision of a long-term funding strategy to ensure PHIS is fully supported on all aspects of implementation, including capacity, training, maintenance and bandwidth.
The above would be comparable with some international best practices. For example, ANTHC's Immunization program works with statewide Tribal health partners to coordinate and advocate for the needs of Tribal immunization programs, and educate Tribal staff on immunization recommendations and vaccine-preventable disease. The Alaska Native Epidemiology Center, part of ANTHC, aggregates data from various systems to contribute to the wellness of Alaska Native people by monitoring and reporting on health data, providing technical assistance and supporting initiatives that promote health. The system has compiled data on a range of health indicators. This data provides an overview of the health status of the Alaska Native population.Footnote 5
Electronic records
In terms of EMRs/EHRs, it is essential to provide continued support for First Nations communities to meet standards for data management and privacy needed for provincial integration. First Nations communities are faced with the task of selecting an EMR that meets the needs of the community, local physicians and nurses, and be interoperable with provincial systems. To do this, First Nations communities should be informed about the benefits of EMRs and how these benefits can be realized while protecting First Nations communities' privacy and data ownership. Where there are community EMRs that are suited to meet local need, interoperability solutions should be encouraged through collaboration with the province.
Locally-held client registries can be used as a way for First Nations to assume ownership and control over health information of community members (according to OCAP principles) and serve as a basis for information-sharing agreements with provincial ministries of healthFootnote 8,Footnote 26 while protecting the privacy of individuals.Footnote 41
For successful implementation, change management processes should address issues of data privacy, security and managementFootnote 127 via strategies such as staff engagement and training at the local health facility.Footnote 20 Supportive and sustained engagement with regional health authorities to promote interoperability with regional EHR systems is vital.Footnote 17 Applications that are found to have worked well in one region and been adopted in others, as is the case with the Mustimuhw, should continue to be promoted for adoption in other regions.Footnote 17,Footnote 47,Footnote 10,Footnote 16
International best practices indicate that sustained funding is crucial for the development of EHRs and it is usually obtained from a variety of sources. For example, in Alaska, ANTHC receives funding from a number of government agencies including the Bureau of Indian Affairs and the Center for Disease Control for the various initiatives it oversees. The Alaska eHealth Network (AeHN) also received funding from the FCC, US Department of Health and Human Services, the State of Alaska as well as the Alaska Federal Health Care Partnership.Footnote 123 Additional funding is provided through grants and other government sources for specific eHealth initiatives (e.g., infrastructure based grants) or initiatives targeted for specific communities.
Interoperability initiatives are also in place to enable data exchange as in the case of the Health Information Exchange (HIE) initiative in Alaska and Kanta, the national system for patient health information in Finland. Partnership is a key ingredient in these interoperability initiatives. In Australia, eHealth NSW, a dedicated organization within New South Wales Health, partners with the local health district, specialty health networks and agencies to implement statewide programs, support local innovation and ensure eHealth project alignment with community needs. Under eHealth NSW, the Rural eHealth Program is focused on improving the way that tools and resources are managed and delivered to clinicians, staff and patients. Its priorities include:Footnote 117
- Strengthening eHealth operational and strategic governance;
- Providing sustainable and ongoing change management and training; and,
- Providing secure, reliable and highly available information and communication infrastructure
In many best practices from international jurisdictions, privacy is a key attribute, for example:
- In Alaska, access to EHRs is regulated under the Meaningful Use legislation of the Centers for Medicare and Medicaid Services. Personal health information can only be used for patient care or insurance claim functions. AeHN has a comprehensive privacy training program for all employees who use eHealth systems to ensure the protection of patient data that is stored in the HIE, telehealth equipment and networks.Footnote 124,Footnote 3
- The Australian government has established policies and controls to protect against privacy and security risks and breaches. These included the release of the Personally Controlled Electronic Health Record (PCEHR) Rules in 2012, which outlined access and control of personal health data,Footnote 14 and policies for underage or intellectually impaired individuals who would require an "authorized representative" to help control their records.Footnote 28 Further, individuals have control over their "My Health Record" (MyHR), the new name of the PCEHR, to allow/restrict access of health care providers as they wish.
- In Finland, the Decree on National EHR System Services specifies EHR regulatory requirements. These laws are broad in scope to help ensure data protection and privacy. They include: health data record keeping, requirements on the institution that hosts EHRs, interoperability of data requirements, consent, liability, secondary use and archiving duration, access and authentication, etc.Footnote 113
Telehealth – educational and administrative sessions
A number of factors should be addressed to support progress on educational and administrative sessions: sufficient bandwidth to ensure the quality and reliability of session delivery, sufficient numbers of telehealth coordinators to schedule and promote events, and sufficient and sustainable funding to support on ground capacity, equipment purchase/evergreening, and partnerships for content and material. There is also a need to diversify delivery by moving from specialized, videoconferencing rooms to personal computing, e.g., laptops, iPads or cellphones. This would be further supported by archiving events and making them available online for later access by community members and health care providers, allowing events to be streamed, and having session post-editing capabilities.
International best practices indicate that education on health topics is beneficial and can be successfully deployed. For example, in Brazil, the National Telehealth Network Program is a national initiative that seeks to improve the quality of primary care in the public health system, known as the Unified Health System (SUS), integrating education and health services through information technology tools. The program, along with the Telemedicine University Network, is focused on telemedicine in remote and rural areas. SUS has established its own online "open university" for continuing professional development across all health care professions. These programs are highly utilized, particularly for health care professionals in rural and underserved regions. Educational sessions connect health care providers and family health teams in smaller communities with up-to-date resources to improve care and access. In Australia, the Australian College of Rural and Remote Medicine (ACRRM) uses the Rural and Remote Medical Education Online (RRMEO) solution to host web-based online training and education to support local general practitioners. These online learning modules provide general practitioners with access to online communities of practice and help these practitioners stay up-to-date on medical practice.Footnote 12,Footnote 13
Telehealth – clinical sessions
Key factors affecting progress on the delivery of clinical sessions include: addressing bandwidth and connectivity issues, including power outages; ensuring sufficient numbers of telehealth coordinators are available to enable session delivery; and, promoting telehealth among First Nations individuals and health care practitioners. Local IT support to manage networking equipment and respond to IT issues (e.g., resetting routers after a power outage) would enhance delivery and reliability. Training nurses in the use of telehealth equipment so it can be fully integrated into primary and public health care delivery would be particularly advantageous (e.g., use for emergencies and after-hours care). Addressing the challenges posed with respect to protecting the identity of First Nations individuals while at the same time allowing seamless care on-reserve/off-reserve would help health care practitioners in service delivery and billing.
International best practices in this area offer valuable insight with respect to partnerships and mechanisms for clinician adoption and participation. With respect to partnerships, the Alaska Federal Health Care Access Network (AFHCAN) has been a key leader in driving telehealth programs through a spoke and hub delivery model. ANTHC manages the maintenance of electronic equipment, including telemedicine devices, through its biomedical engineering arm: Alaska Clinical Engineering Services (ACES). ACES also provides design and support consultation for biomedical systems and teleradiology services, including facility planning, safety surveys and equipment purchasing.
The mechanism for clinician adoption and participation in Alaska was to pass House Bill 281 to allow physicians to provide patient consultations, make diagnoses, and prescribe drugs over the phone. Senate Bill 74 further expanded telehealth services by allowing Alaska-licensed physicians to provide telehealth services from outside of the state. Alaska reimburses telemedicine services involving synchronous technology as well as store-and-forward and remote patient monitoring in some capacity. The state also covers home telemedicine, including telerehabilitative services within the home health benefit. In Australia, ACRRM is a strong advocate for clinician engagement and adoption. Under the Department of Health, the Medicare Benefits Schedule provides reimbursement for telemedicine consultations with physicians, nurse practitioners, midwives and Aboriginal health workers. Such rebates are only available to patients living outside of major cities in rural or remote areas, residential aged care facilities and Aboriginal Medical Services. The patient and remote specialist must be at least 15 km apart.Footnote 116,Footnote 115
Mobile Health
The benefits of mHealth with respect to accessibility of health care for patients in remote/isolated and isolated areas and for those unable to leave their homes, namely the chronically ill and aged patients, are recognizedFootnote 121,Footnote 22,Footnote 21 as is its educational value.Footnote 27 Key factors in continuing mHealth development are wireless connectivity (bandwidth, reliability), availability of commercial cellular networks and network security together with advancement in technology aimed at home care monitoring.Footnote 65 Providing appropriate training to health care practitioners on mHealth devices and developing remuneration models, as with telehealth clinical sessions, are also key elements. As the acceptance of mHealth among patients increases, and clinicians realize its potential to deliver health services remotely, there may be increasing funding demands to improve connectivity, data exchange, administration and training of health care practitioners.
Since applications are not mature, decisions would have to rely on technological assessments and trials.
There are examples from a number of countries that have specified adherence to mHealth guidelines, architecture, standards and certification programs when acquiring mHealth solutions. These countries include Denmark, Singapore and the United Kingdom. In Alaska, AFHCAN added Vidyo'sFootnote xvi, visual communications and collaboration capabilities to enable high-definition videoconferences on mobile devices. The devices have to comply with the Health Insurance Portability and Accountability Act (HIPAA). Australia has developed "ibobbly," a suicide prevention app for Aboriginals aged 18 to 35 in Western Australia. It is rooted in acceptance and commitment therapies and uses mindfulness and value-based action strategies. Once downloaded, the app does not require a continuous Internet connection. With regard to privacy, in addition to general privacy regulations around personal health information, there are also rules specifically around the types of information that can be collected through mobile apps and devices and how this information must be treated. Examples of information that falls under such legislation include photographs, IP addresses and other unique device identifiers, contact lists, voice and facial recognition, and location information.Footnote 119
The Program uses a number of mechanisms for multi-party engagement and to further collaborative integrated planning of eHealth. In terms of harmonization, eHIP is working with First Nations and F/P representatives in effecting the integration of health services by identifying opportunities and actively engaging in multi-jurisdictional partnerships.
Collaborative, integrated planning
While there have been improvements in partnerships, information sharing and coordination, there is a need for additional concerted efforts by all partners to meet the implementation goals of an eHealth component be it broadband connectivity, interoperable EMRs/EHRs or PHIS, or telehealth for educational and clinical purposes.
Clearly establishing roles, responsibilities and priorities between eHIP, IMSD and SSC may contribute to IT issues being addressed. FNIHB is working with IMSD on a project led by joint steering committees on improving IT support to FNIHB employees in remote/isolated and isolated communities.Footnote 64 It is also important to have standards and guidelines regarding responsibility for data communications, LAN operation and support (including associated equipment such as routers), etc.
Greater collaboration between eHIP and HFCP could help improve planning of new construction, renovation and expansion projects to ensure support for eHealth technologies.
ISED and INAC are key partners in enabling appropriate bandwidth and connectivity for all First Nations' broadband needs, including eHealth. A new ISED project is focused at the institutional instead of household level. This is an opportunity for eHIP to support First Nations communities and regional organizations to engage ISED and INAC to ensure that communities apply for the needed broadband connectivity. eHIP can provide insights into health facility bandwidth requirements to deliver the different components (e.g., telehealth, EMRs and PHIS). It is expected that strong proposals led by First Nations, First Nations regional organizations, provinces, municipalities and ISPs will be instrumental to securing the connectivity that is needed for eHealth. Provincial counterparts also have a role to play. There is an interdepartmental working group on broadband connectivity, which may serve as the venue for arriving at a strategy to support the work of First Nations, ISED, INAC, provinces and ISPs on addressing connectivity.Footnote 53
With respect to areas that have no fibre option, the viability of high throughput satellites could be considered with a focus on solutions serving multiple communities to benefit from economies of scale. This would require partnerships with K-Net, KRG, etc., to submit joint proposals to ISED for connectivity.
Partners like Infoway could play a stronger role. Currently, Infoway works with provinces to enable eHealth in an advisory capacity. The role of Infoway could be formalized so that it can directly interact with First Nations communities to advance eHealth. Infoway could then be used to promote interoperability of First Nations' systems with provincial EHRs and PHIS.
Seamless health care delivery requires seamless information sharing across jurisdictions (e.g., First Nations, federal, provincial) that incorporates OCAP principles. The experience and resources of Infoway linked to privacy issues could assist the process of interoperability, which is currently caught in the middle of provincial reluctance as well as governance, and privacy issues on the side of First Nations.
The partnership with provinces will require particular strengths from eHIP to find common ground, to work on solutions that suit both parties, and to time eHealth component implementation to best manage limited resources and ensure implementation satisfaction. In the case of the Atlantic region, there is a need for strong partnership models given that each province is at a different stage in its relationship with First Nations. Across provinces, there is a need to provide seamless health care delivery between provincially funded off-reserve health services and on-reserve health services while at the same time protecting the privacy of First Nations individuals.
With respect to engagement and partnership with First Nations, best practices should be made available so that all communities can benefit. Success stories in establishing agreements, as in the case of NITHA or Nova Scotia, could be examined to find key and common points. The experience of First Nations regional organizations such as FNHSSM, FNQLHSSC, NITHA, TSAG, KOeTS and Atlantic Canada's First Nation Help Desk could be communicated so that all communities can benefit from these lessons learnt. A case in point for best practices is the Tui'kn partnership between First Nations communities, Health Canada, the province of Nova Scotia, academia and industry to develop the Unama'ki Client Registry. Another example is work between the Kenora Chiefs Advisory, Infoway, Health Canada, the province and the North West Local Health Integration Network to implement and eventually link a client registry in seven First Nation communities to the provincial client registry.Footnote 120 In order to share these best practices, there is a need for a formal communications strategy between First Nations and eHIP. In increasing community participation and engagement, regions could potentially benefit from the provincial communication strategy plans as well as community engagement packages adapted into a culturally acceptable content and format.
Finally, there is a need to assess community capacity and capabilities in a systematic manner to identify opportunities for enhancement/development (IT workers, data infrastructure staff, nursing staff, telehealth coordinators, data specialists, EMR/EHR and PHIS trained staff) with an emphasis on capacity at the ground level to improve eHealth delivery and staff retention.
Examples of capacity building exist in British Columbia (e.g., teleophthalmology project specialized training, job shadowing, continuing education).Footnote 18 In terms of international best practices, capacity development is integrated in eHealth delivery in Brazil as part of the National Program of Access to Technical Education and Employment (PRONATEC) for rural dwellers and indigenous people in the less prosperous north and northeast of the country. In Alaska, AeHN oversees the Alaska Regional Extension Center, which provides EMR implementation support services to providers, including EMR readiness assessment, vendor selection, workflow redesign, training, and IT support.Footnote 4 In Australia, ACRRM provides general practitioners with access to online communities of practice and helps these practitioners stay up-to-date on medical practice through learning modules.Footnote 11,Footnote 13 In Finland eHealth capacity building, education regarding privacy, data security, patient security, procedures and radiation safety is provided. Web-based training for personnel is available in 100% of central hospitals, 92% of health care centres and over half of private service providers' offices.Footnote 30 Increasingly, pre-service training in eHealth is being provided to health sciences students.Footnote 130
5.2.2 Demonstration of Efficiency and Economy
Based on assessment of available data, there is evidence to indicate that the Program's utilization of resources in relation to the production of outputs and progress toward expected outcomes is efficient and economical. Program goals are actively communicated while alignment between projects, eHealth components and regional needs and priorities are ensured. Nonetheless, given the rapidly changing environment, it is challenging for eHIP to track regional status and overall national situation. Cost avoidance as a result of all telehealth clinical session delivered in four regions in 2015-2016 was approximately $ $11.7 million.
From a "desired state" perspective, there are opportunities for improved efficiency through greater utilization of some telehealth sites by promoting awareness and building capacity (e.g., continuing to train nurses in telehealth equipment use, providing adequate IT support, using telehealth coordinators). A renewal of HISAP may yield additional efficiencies with a bottom-up (grassroots) followed by a top-down strategic planning exercise, a cohesive approach to community and project readiness assessments, and a longer term funding view for planning technology-based projects. Benefits evaluation indicates that the Program has contributed towards cost avoidance as a result of clinical sessions delivered via telehealth. Although not quantified, similar cost avoidance stems from the delivery of educational sessions. Ways forward are explored in each of the following sub-sections.
Alignment between projects, components and regional needs
Due to the rapidly changing contexts for eHIP, there is a need to increase environmental scans on an ongoing basis to inform Program guidelines. In this context, there is a need to revisit HISAP with a grassroots approach and make it more current. Also, when decisions are made with respect to bandwidth or solutions for interoperability of systems between First Nations and provinces, regional and sub-regional contexts should be examined in order to attain a better fit for the communities.
Community technical readiness assessments
Currently, regions employ a variety of project plans and readiness assessment templates. While, in principle, a thorough assessment is being made through the use of ad hoc criteria check lists and committees, a more cohesive, planned approach to project assessment would assist in greater efficiencies and economies of scale. Although regional and community variations are to be allowed and recognized, a systematic approach across regions would ensure that projects are classified and assessed using appropriate templates that can provide a regional and national perspective. For example: a basic technical readiness assessment for communities that do not have access to eHealth; a readiness assessment for projects adding on new eHealth components to a community; and, a technology assessment for projects relating to innovation to achieve improved economy, efficiency or better quality of service. Project assessment would be more systematic if templates were developed for these assessments based on the eHealth Infostructure Readiness Assessment ToolFootnote 54 and other check lists and tools that regions are currently using. This systematic approach would enhance the equity of access to eHealth among all First Nations communities.
Planning and Funding
The lack of a three to five-year funding horizon lowers the efficiencies that could occur with a longer term plan for implementation of the various eHealth components. For example, telehealth equipment may be made available in a community but it may be underutilized or not used due to a lack of funding to support telehealth coordinators, or to provide adequate IT support, or to provide the necessary training. In such instances, the potential benefits accruing from the technology are not being realized. Examples identified during the evaluation (e.g., telehealth equipment and x-ray machines not being used) indicate the need for a longer funding planning horizon, and the development of strategic plans that cover all aspects for each component, such as technology and connectivity assessments, IT support for new equipment implementation, capacity development, training and maintenance.
The long-term plan would be based on a robust analysis of which communities should be addressed first for basic needs like connectivity, capacity training and telehealth, and how the progression will be made with respect to eHIP component growth, e.g., PHIS and EMRs/EHRs. The plan should also have room for funding innovation and for evergreening equipment.
Another aspect of planning and funding would involve engaging partners at multilateral tables to identify parallel funding sources (e.g., from other federal departments or provinces). Examples include involvement of Infoway in some First Nations eHIP component implementation, use of the Health Services Integration Fund (HSIF), partnering with INAC to share connectivity with schools or fibre build, etc. This approach could be expanded to support innovation.
There is also a need to develop a plan on how to address those communities that do not have a strong champion or regional leadership (such as TSAG, NITHA, FNHSSM, KOeTS, FNQLHSSC and Atlantic Canada's First Nation Help Desk) and may be falling behind on eHealth.
Adequacy and use of performance measurement data
There are many advantages to be realized by systematically collecting and analyzing data at timely intervals. It is understood that some communities, First Nations regional organizations and regional Program offices may lack on the ground capacity to perform these activities. Nonetheless, if decisions on eHealth components are to be made on strong underlying evidence, then an approach to funding tied to demonstration of results in as rigorous a fashion as possible may be needed. One of the key considerations in setting up a performance measurement system is to look at the feasibility of the required data given the capacity on the ground. The evaluation has suggested a number of indicators, some of which are already being used by the Program, around which data collection and analysis should be enhanced to lend support for future Program decisions, including funding needs.
6.0 Recommendations
The incremental work of the Program in the various eHealth areas has contributed to the achievement of its outcomes. While the Program has met or exceeded most of its key targets, the following recommendations identify areas where continuing work will help the Program further its work with a long term view towards deploying, maintaining and realizing the benefits of digital infrastructure for First Nations individuals, families and communities.
Recommendation 1. Enhance partnership, collaboration and integration with partners and stakeholders to continue to improve Internet connectivity to provide equitable access to underserved First Nations communities.
Broadband connectivity
Applying a coordinated and community-focused effort with Program partners and stakeholders, such as First Nations regional organizations, INAC, ISED, provincial governments and private industry, would allow eHIP to derive benefits from existing/planned activities, foster standardization in enabling appropriate bandwidth for eHealth components, and identify First Nations communities' broadband needs and available funding from various sources to address Internet connectivity challenges.
eHealth component requirements
Identifying and defining broadband requirements for eHealth components would allow the Program to ascertain service gaps. These requirements should be based on standardized technical guidelines for each eHealth component (e.g., electronic records, PHIS, telehealth) in alignment with provincial standards, if any. Assessing health facility readiness for eHealth based on these and other infrastructure requirements (e.g., plug-ins for telehealth equipment in emergency rooms, room acoustics/privacy considerations, LAN and related equipment condition, etc.) would allow the Program to identify any needed enhancements.
Recommendation 2. Advance work with partners, to address IT- and health facility-related issues to enable health care practitioners (nurses) to integrate eHealth tools into primary and public health care delivery.
Roles and responsibilities for IT support and health facility infrastructure
Clarifying the roles and responsibilities of partners within and outside Health Canada (e.g., First Nations regional organizations, eHIP, HFCP, IMSD, SSC), and establishing client-focused mechanisms to ensure that IT issues experienced by health care workers (e.g., nurses) are addressed in a timely manner, would help further eHealth adoption and integration into primary and public health care delivery. The current efforts between FNIHB and IMSD on improving IT support for FNIHB employees in remote/isolated and isolated communities should continue in order to address roles and responsibilities and, potentially, health facility infrastructure issues. In addition, the gap in IT infrastructure and support for transferred First Nation health facilities should be assessed periodically for sustained use of eHealth applications.
Recommendation 3. Work closely with provincial governments, federal partners (e.g., Infoway), First Nations regional organizations and communities to further integrate approaches to render electronic records and PHIS interoperable, effective and efficient by removing jurisdictional, legislative and logistical hurdles.
F/P privacy legislations
Collaboration among F/P partners should focus on identifying information sharing solutions to address issues surrounding federal and First Nations nurses and their access to patient data on provincially connected PHIS and electronic records. This is an area of high priority requiring resolution across most provinces.
Data sharing agreements
Successful implementation of data sharing agreements requires extensive engagement with First Nations, provincial and federal partners to address challenges with interoperable systems. Further engagement would help advance work on alignment with provincial systems and privacy issues as well as widespread integration of OCAP principles in data sharing agreements to ensure health data can be exchanged in a way that meets the needs of all parties. Resolving data privacy/sharing issues would not only contribute to the provision of seamless care on- and off-reserve but also to address issues related to health care practitioner billing.
F/P vision alignment
Defining a coordinated vision and partnership on eHealth systems with First Nations communities and provincial governments would help achieve commonly agreed goals for new technologies based on a common ground. This, in turn, would help establish realistic timelines for eHealth component implementation that would make optimal use of limited resources while ensuring implementation satisfaction.
Recommendation 4. Continue to engage First Nations communities to enhance knowledge, capacity and control over their health care service delivery and use of health data for evidence-based decision making.
Promotion
eHealth capacity and adoption would benefit from promoting best practices and success stories in the implementation of the various eHealth components (i.e., electronic records, PHIS, telehealth and mHealth). Further benefits would be accrued by sharing the positive results of partnerships with First Nations regional organizations such as FNHSSM, FNQLHSSC, NITHA, TSAG, KOeTS and Atlantic Canada's First Nation Help Desk. First Nations communities with low awareness of eHIP or that lack a strong regional champion/leader may require support/encouragement to pool together and work with a First Nations regional organization to lead eHealth on their behalf.
Readiness assessments
In partnership with First Nations regional organizations and communities, developing and applying a systematic, coordinated, cohesive community assessment process to identify eHealth component readiness and community technical capacity (e.g., IT workers, data infrastructure staff, nursing staff, telehealth coordinators, data specialists) would help in identifying the required training and infrastructure to build capacity and successfully implement and maintain eHealth components.
Capacity development
Increasing the ground level capacity of health care practitioners and health facility staff on the use of eHealth tools may enhance primary and public health care delivery (e.g., continue to train nurses in the use of telehealth equipment). Moreover, continuing to grow the number of eHealth/telehealth coordinators would contribute to support and promote telehealth and other eHealth components (e.g., electronic records, PHIS and mHealth).
Collaborative strategy
Conducting regular community and technology environmental scans, within regional and sub-regional contexts, would help inform Program guidelines affecting all eHealth components. Reassessing HISAP in collaboration with First Nations communities and regional organizations would make it the product of a balanced, bottom-up (grassroots) and top-down process.
Recommendation 5. Improve performance data collection and analysis across regions and over time on key performance indicators by setting up a Program performance measurement system that takes into consideration the capacity on the ground.
Identifying key indicators, such as those reported by the evaluation, and establishing consistent definitions across regions and data collection entities would help improve data collection. Ensuring clarity of definitions and establishing a data reporting cycle would help accurate and regular analysis to inform timely decision-making.
Recommendation 6. Develop a long-term plan that is sufficiently flexible to accommodate technology innovation and a commensurate funding strategy for eHIP.
Providing a long-term plan and funding view, in concert with technology-based projects, that fully supports all aspects of implementation and sustainability, including capacity, training and bandwidth, would contribute to the long-term vision of the Program. Part of this exercise should include identifying which communities would be supported first for basic needs like Internet connectivity and capacity training, and how the progression will be made with respect to eHIP component growth (e.g., electronic records, PHIS, telehealth, mHealth).
Incorporating innovation allocations would allow the plan to grow together with technology advancements, such as wireless connectivity, bandwidth and data security; technology development in mHealth and personal telehealth (e.g., via laptops and iPads); storage and streaming technologies for educational sessions; and, evergreening of equipment.
Appendix 1: Logic Model: eHealth Infostructure Program (eHIP)
Figure 4. Logic Model: eHealth Infostructure Program (eHIP)
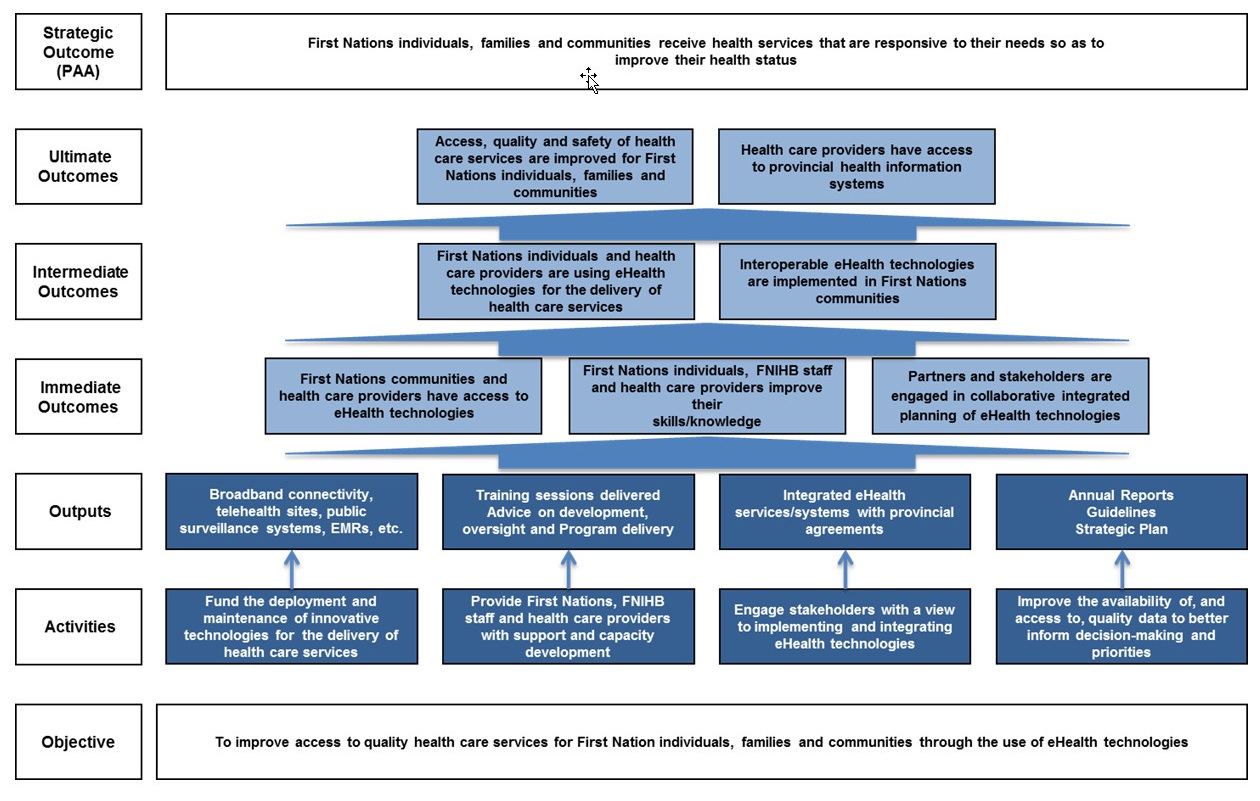
Figure 4: Logic Model: eHealth Infostructure Program (eHIP) - Text Description
Image four outlines the program's logic model. The objective of the program is to improve access to quality health care services for First Nation individuals, families, and communities through the use of eHealth technologies. To accomplish this, the program has four main activities. The first activity is the fund the deployment and maintenance of innovative technologies for delivery of health care services. The second is to provide First Nations, First Nations Staff, and health care providers with support and capacity development. The third is to engage stakeholders with a view to implementing and integrating eHealth technologies, and the fourth is to improve the availability of, and access to, quality data to better inform decision-making and priorities. Altogether, these four activities each are intended to produce four unique outcomes. The first outcome is broadband connectivity, telehealth sites, public surveillance systems, electronic medical records. The second outcome is training sessions delivered, as well as advice on development, oversight and program delivery. The third outcome is integrated eHealth services/systems with provincial agreements and the fourth outcome is Annual Reports, Guidelines and a Strategic Plan. From all of these outcomes, three immediate outcomes are sought: First Nations communities and health care providers have access to eHealth Technologies; First Nations individuals, First Nations Inuit Health Branch staff and health care providers improve their skills and knowledge; and, partners and stakeholders are engaged in collaborative integrated planning of eHealth technologies. Altogether, these outcomes are intended to lead to two intermediate outcomes: First Nations individuals and health care providers are using eHealth technologies for the delivery of health care services; second; interoperable eHealth technologies are implemented in First Nations Communities. The ultimate outcome of the program is that access, quality and safety of health care services are improved for First Nations individuals, families and communities; and that Health Care providers have access to provincial health information systems. The overall strategic outcome of this programming is that First Nations individuals, families, and communities receive health services that are responsive to their needs so as to improve their health status.
Appendix 2: Summary of Findings
Rating of Findings
Ratings have been provided to indicate the degree to which each evaluation issue and question have been addressed.
Relevance rating symbols and significance
A summary of relevance ratings is presented in Table 1 below together with a description of the ratings in the footnote to the table.
| Evaluation Issue | Indicators | Overall rating | Summary |
|---|---|---|---|
| Continued need for Program | |||
|
Does the Program continue to address a demonstrable need? Is the Program responsive to the needs of its client population? |
|
High | The eHealth Infostructure Program (eHIP) continues to address a demonstrable need and is responding to the needs of its client population. The needs addressed by the Program are fundamental to improving the health status of First Nations. |
| Alignment with government priorities | |||
|
Is the Program aligned with federal government priorities? Is the Program aligned with departmental strategic outcomes? |
|
High | The Program is aligned with government priorities. These include keeping pace with technology and innovation, contributing to address health system challenges and system reform, and building relationships with Indigenous peoples. |
| Alignment with federal roles and responsibilities | |||
| Is the Program aligned with federal roles and responsibilities? |
|
High | The Program is well aligned with federal roles and responsibilities. |
|
Overall rating: High: There is a demonstrable need for program activities; there is a demonstrated link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program are clear. Partial: There is a partial need for program activities; there is some direct or indirect link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program are partially clear. Low: There is no demonstrable need for program activities; there is no clear link between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes; role and responsibilities for the federal government in delivering the program have not clearly been articulated. |
|||
Performance rating symbols and significance
A summary of performance ratings is presented in Table 2 below together with a description of the ratings in the footnote to the table.
| Issues | Indicators | Overall rating | Summary |
|---|---|---|---|
| Achievement of expected outcomes (effectiveness) | |||
| To what extent have the immediate outcomes been achieved? | |||
| First Nations communities and health care providers have access to eHealth technologies |
|
Achieved. | The Program has exceeded its target for broadband connectivity; however, while all eHIP funded First Nations Bands have Internet connectivity, the available bandwidth and connection reliability is variable. The Program has also exceeded targets on Public Health Information Systems (PHIS) and on EMR/EHR implementation. Telehealth continues to grow but its uptake/utilization has been uneven across remote/isolated and isolated communities. Mobile health (mHealth) appears promising and is in its developmental phase. |
| First Nations individuals, FNIHB staff and health care providers improve their skills/knowledge |
|
Achieved. | The Program has supported efforts to enhance the knowledge and skills of First Nations individuals, First Nations and Inuit Branch (FNIHB) staff and health care providers. Opportunities have been provided through telehealth education and administrative sessions in various formats. Available information indicates the usefulness and efficiency of telehealth educational sessions among frontline health care workers, staff and communities. |
| Partners and stakeholders are engaged in collaborative, integrated planning of eHealth technologies |
|
Achieved. | The Program uses a number of mechanisms for multi-party engagement and to further collaborative integrated planning of eHealth. In terms of harmonization, eHIP is working with First Nations and federal/provincial (F/P) representatives in effecting the integration of health services by identifying opportunities and actively engaging in multi-jurisdictional partnerships. |
| To what extent have the intermediate outcomes been achieved? | |||
| First Nations individuals and health care providers are using eHealth technologies for the delivery of health care services |
|
Progress made; further work warranted. | Clinical telehealth sessions are delivered in many First Nations communities covering numerous topics. The Program has exceeded its target of providing clinical sessions via telehealth to First Nations communities. These sessions have covered a multitude of clinical specialties. Greater collaboration and integration across the federal family (i.e., Health Canada; Indigenous and Northern Affairs Canada; Innovation, Science and Economic Development Canada) as well as within Health Canada could result in increased and more stable Internet connectivity and bandwidth. Uptake/utilization of telehealth in some remote/isolated and isolated communities could be increased through promotion among First Nations individuals, families and communities as well as health care practitioners in addition to providing enhanced support on the ground (e.g., telehealth coordinators). Further support for mHealth by helping communities address challenges related to connectivity and communications security may aid technology adoption. |
| Interoperable eHealth technologies are implemented in First Nations communities |
|
Progress made; further work warranted. | PHIS and electronic records implementations have exceeded targets. Progress is impeded due to the need to address various issues, none of which are in the sole purview of the Program, such as alignment of F/P privacy legislations, available connectivity/bandwidth, proliferation of non-interoperable electronic records systems, responsibility for physician remuneration as a result of eHealth delivery, and appropriate/ongoing funding. |
| To what extent have the ultimate outcomes been achieved? | |||
| Access, quality and safety of health care services are improved for First Nations individuals, families and communities |
|
Achieved. | Based on available evidence, access to and quality of health care services has improved for First Nations individuals, families and communities over the past five years. According to information analyzed for the evaluation, planning, surveillance and reporting of health data in First Nations communities have also been enhanced as a result of eHealth, although there are further opportunities for improvement across communities. |
| Health care providers have access to provincial health information systems |
|
Progress made; further work warranted. | There has been considerable advance in PHIS and in EMRs/EHRs. Where implemented, users see these systems as helpful in planning and in managing the health care of First Nations individuals, families and communities. |
| Demonstration of efficiency and economy | |||
|
Is the Program using its existing resources optimally? Has the Program produced its outputs and achieved its outcomes in the most economical manner? How and in what ways can economy and/or sustainability be improved? Is performance data collected and used for decision-making? |
|
Progress made; further work warranted. | Based on assessment of available data, there is evidence to indicate that the Program's utilization of resources in relation to the production of outputs and progress toward expected outcomes is efficient and economical. Program goals are actively communicated while alignment between projects, eHealth components and regional needs and priorities are ensured. Nonetheless, given the rapidly changing environment, it is challenging for eHIP to track regional status and overall national situation. Cost avoidance as a result of all telehealth clinical session delivered in four regions in 2015-2016 was approximately $11.7 million. |
|
Overall rating: Achieved: The intended outcomes or goals have been achieved or met. Progress made; further work warranted: Considerable progress has been made to meet the intended outcomes or goals, but attention is still needed. Little progress; priority for attention: Little progress has been made to meet the intended outcomes or goals and attention is needed on a priority basis. |
|||
Appendix 3: Evaluation Description
Evaluation Scope
The scope of the evaluation included all the activities and services delivered by the eHealth Infostructure Program's (eHIP) national headquarters and regional offices. eHIP is managed at the national level by the Capacity, Infrastructure and Accountability Division (CIAD) of the First Nations and Inuit Health Branch (FNIHB) under Health Canada. The scope of the evaluation did not include any of the services provided by British Columbia's (BC) First Nations Health Authority in accordance with the BC Tripartite Health Agreement and sub-agreements. The period covered by the evaluation included activities from April 2011 to March 2016. Data collection, analysis and reporting activities spanned the period from June 2016 to March 2017.
Evaluation Issues
The specific questions used in this evaluation were based on five core issues. These are noted in the table below. Corresponding to each of the core issues, evaluation questions were tailored to the program and guided the evaluation process.
| Core issues | Evaluation questions |
|---|---|
| Relevance | |
| Issue #1: Continued need for Program | Assessment of the extent to which the Program continues to address a demonstrable need and is responsive to the needs of Canadians.
|
| Issue #2: Alignment with government priorities | Assessment of the linkages between program objectives and (i) federal government priorities and (ii) departmental strategic outcomes.
|
| Issue #3: Alignment with federal roles and responsibilities | Assessment of the role and responsibilities for the federal government in delivering the program.
|
| Performance (effectiveness, efficiency and economy) | |
| Issue #4: Achievement of expected outcomes (effectiveness) | Assessment of progress toward expected outcomes (including immediate, intermediate and ultimate outcomes) with reference to performance targets and program reach, program design, including the linkage and contribution of outputs to outcomes.
|
| Issue #5: Demonstration of efficiency and economy | Assessment of resource utilization in relation to the production of outputs and progress toward expected outcomes.
|
Data Collection and Analysis Methods
The evaluation methodology was based on multiple lines of evidence. It included a literature/document review, key informant interviews, case studies and a review and analysis of eHealth approaches across international jurisdictions. Data was analyzed by triangulating information gathered through each of these methods. This included:
- A systematic compilation, review and summarization of data to illustrate key findings.
- The compilation of quantitative data obtained from the Program's annual reports into a database. This was followed by analysis and validation with Program representatives.
- A thematic analysis of qualitative data.
A summary of the data collection methodology and its intended contribution to the evaluation process is provided in the following sub-sections.
Literature/document review
Method details:
- Review of documents, files and databases (including administrative and financial data) provided by the Program and identified during the evaluation through other methods (e.g., key informant interviews) together with an ongoing environmental scan of online sources.
- Over 500 documents reviewed.
Sources:
- Scientific journals; grey literature; official government documents; public opinion research reports; previous performance, evaluation and audit reports; policy documents; budget and expenditure information; performance measurement data reports; annual progress reports; and, administrative records specific to the evaluation questions.
Intended use:
- Provide background information on the history and objectives of the Program as well as progress towards the achievement of intended outcomes; key source of qualitative and quantitative information; provide insights into any important shifts/changes that have occurred during the life of the Program.
Key informant interviews
Method details:
- Guided individual and group interviews conducted in-person and/or via telephone.
- Interview guides tailored to the different target audiences.
- Thirty-three interviews conducted.
Target:
- Program representatives (headquarters and regional offices): one individual interview and seven group interviews (32 participants in total).
- Program partners (e.g., Health Canada's Corporate Services Branch, Innovation, Science and Economic Development Canada, Canada Health Infoway, Indigenous and Northern Affairs Canada, etc.): seven individual interviews, three group interviews (18 participants in total), and one refusal.
- Program stakeholders (e.g., First Nations regional organizations, First Nations Health Directors, other FNIHB programming, etc.): seven individual interviews and seven group interviews (24 participants in total).
- eHealth experts: one individual interview.
Intended use:
- Assist in further understanding the information gathered from other lines of evidence and provide additional context.
Case Studies
Method details:
- Combination of focus groups (site visits) and document review. Case studies were conducted in five of the six Program regions (Atlantic, Ontario, Manitoba, Saskatchewan and Alberta) covering all eHealth components (i.e., broadband connectivity, electronic records, Public Health Information Systems – PHIS, telehealth and mobile health – mHealth) and focussed on identifying challenges and best practices or innovative approaches.
- All eHealth components were addressed with a particular focus on identifying challenges, solutions and best practices.
- Case study selection was based on community type (e.g., remote/isolated, isolated, etc.), and regional focus/progress linked to the various eHealth components. Potential communities were validated with Program representatives on relevance.
- Four of the five case studies included site visits. These site visits consisted of two or more focus groups conducted with policy decision-makers (e.g., First Nations Band and regional organization representatives) and operational staff (e.g., health facility personnel such as nurses, telehealth coordinators, etc.).
- One case study was a document review.
- Two focus group guides were developed to address the two main audiences.
Sources:
- Program documentation, data available from each of the selected communities, discussions with representatives through focus groups.
Intended use:
- Assess and document the impact of eHealth technologies, identify barriers and best practices as well as success factors in the implementation of said technologies.
Review and analysis of eHealth approaches across international jurisdictions
Method details:
- Targeted literature/document review, environmental scan of online sources, and interviews with knowledgeable individuals on each of the selected jurisdictions for review.
- Four international jurisdictions were selected (Brazil, the USA in particular Alaska, Australia in particular New South Wales, and Finland) for review based on a number of criteria such as availability of information on key eHealth components (e.g., broadband connectivity, electronic medical and health records, public health surveillance systems, telehealth;), need to address Aboriginal populations or populations in remote locations, etc.
Sources:
- Data publicly available on each of the selected jurisdictions and interviews with experts on these jurisdictions.
Intended use:
- An exercise to review and analyze eHealth approaches in four international jurisdictions to identify lessons learnt that would be applicable to the Canadian context.
Endnotes
- Endnote 1
-
A. (2011). Terms of Reference - Manitoba First Nations Regional Telehealth Partnership, August 23, 2011 DRAFT - V2.2.
- Endnote 2
-
A. (2016). Meeting Package for May 18, 2016 - HD/NIC.
- Endnote 3
-
Alaska eHealth Network. (2012, June 29). Security Awareness and Training Procedure. Retrieved from http://www.ak-ehealth.org/wp-content/uploads/2.214-Security-Awareness-and-Training-Procedure.pdf
- Endnote 4
-
Alaska eHealth Network. (2016). Regional Extension Center (REC). Retrieved from http://www.ak-ehealth.org/regional-extension-center-rec/
- Endnote 5
-
Alaska Native Tribal Health Consortium. (2015). Overview. Retrieved from http://anthc.org/who-we-are/overview/
- Endnote 6
-
AMC eHealth Unit. (2014). AMC eHealth Update, July 2014.
- Endnote 7
-
AMC eHealth Unit. (2015). AMC eHealth Update, 2015-01, 1-6.
- Endnote 8
-
Assembly of First Nations. (2012). AFN – First Nations eHealth Strategy Framework, Draft.
- Endnote 9
-
Assembly of Manitoba Chiefs Secretariat. (2012). Manitoba First Nations eHealth Long Term Strategy - A 10 Year Plan for Action 2012-2022.
- Endnote 10
-
Assembly of Manitoba Chiefs, Manitoba eHealth, & Health Canada. (2014). eHealth Overview.
- Endnote 11
-
Australian College of Rural and Remote Medicine. (2012). ACRRM Telehealth latest news & updates. Retrieved from http://www.ehealth.acrrm.org.au/acrrm-telehealth-latest-news-updates
- Endnote 12
-
Australian College of Rural and Remote Medicine. (2015). Overview of training with the College. Retrieved from http://www.acrrm.org.au/training-towards-fellowship/overview-of-training-with-the-college
- Endnote 13
-
Australian College of Rural and Remote Medicine. (2015). Regional telecommunications independent review 2015.
- Endnote 14
-
Australian Government. (2012). PCEHR Rules 2012. Federal Register of Legislation. Retrieved from https://www.legislation.gov.au/Details/F2012L01703
- Endnote 15
-
Battcock, A. (2015). Enhanced access to provincial public health information systems for First Nations in Atlantic Canada project - Mushuau First Nation (Natuashish) report.
- Endnote 16
-
Battcock, A. (2016). Enhanced access to provincial public health information systems for First Nations in Atlantic Canada project - Abegweit report (DRAFT).
- Endnote 17
-
Battcock, A. (2016). Enhanced access to provincial public health information systems for First Nations in Atlantic Canada project - Eel Ground (Natoaganeg) report.
- Endnote 18
-
British Columbia Ministry of Health Services. (2011). Evaluating the Benefits, Telehealth – TeleOphthalmology Inter Tribal Health Authority and the Ministry of Health Services.
- Endnote 19
-
British Columbia Ministry of Health. (2013). Panorama Vaccine Inventory Module, Benefits Evaluation Report.
- Endnote 20
-
Canada Health Infoway. (2009). Experiences from the forefront of EMR use, 20 Canadian physician case studies.
- Endnote 21
-
Canada Health Infoway. (2014). Mobile Health Computing Between Clinicians and Patients.
- Endnote 22
-
Canada Health Infoway. (2016). Understanding the Current State of Patient-Provided Digital Health Information (Know Me)
- Endnote 23
-
Canada. (2010). Speech from the Throne to open the Third Session of the Fortieth Parliament of Canada.
- Endnote 24
-
Canadian Institute for Health Information and Canada Health Infoway. (2013). Better Information for Improved Health: A Vision for Health System Use of Data in Canada.
- Endnote 25
-
Chiefs of Ontario. (2013). Knowledge Management. Retrieved from http://health.chiefs-of-ontario.org/node/592
- Endnote 26
-
COACH. (2012). First Nations and the Jurisdictions eHealth Convergence Forum Summary Report.
- Endnote 27
-
COACH: Canada's Health Informatics Association. (2015). 2015 Canadian Telehealth Report.
- Endnote 28
-
Council for Intellectual Disability. (n.d.). My Health Record - opt out trials. Retrieved from http://www.nswcid.org.au/blog/my-health-record-opt-out-trials.html
- Endnote 29
-
Federation of Canadian Municipalities. (2014). Broadband Access in Rural Canada: The role of connectivity in building vibrant communities.
- Endnote 30
-
FinnTelemedicum and National Institute for Health and Welfare. (2015). E-health and e-welfare of Finland: Check point. THL. Retrieved October 17, 2016, from https://www.julkari.fi/bitstream/handle/10024/129709/URN_ISBN_978-952-302-563-9.pdf?sequence=1
- Endnote 31
-
First Nations and Inuit Health Information System. (2016). ADM Oversight of FNIHB IP Projects (presentation).
- Endnote 32
-
First Nations Health and Social Secretariat of Manitoba. (n.d.). eHealth Unit, Narrative Year-End Report, Manitoba First Nations, eHealth - Panorama, April 1, 2014 - March 31, 2015.
- Endnote 33
-
First Nations of Quebec and Labrador Health and Social Services Commission. (2014). 2013-2014 Annual report.
- Endnote 34
-
Gartner Consulting Inc. (2013). British Columbia eHealth Benefits Estimates: Executive Overview.
- Endnote 35
-
Government of Canada. (2015). Prime Minister's mandate letter to the Minister of Health.
- Endnote 36
-
Health Canada, First Nations & Inuit Health Branch. (2012). Guidelines for the FNIHB eHealth Infostructure Program (eHIP).
- Endnote 37
-
Health Canada, First Nations & Inuit Health Branch. (2012). Health Infostructure Strategic Action Plan.
- Endnote 38
-
Health Canada, First Nations & Inuit Health Branch. (2014). Report on enhanced monitoring of the impact of eHealth investments in first nation communities.
- Endnote 39
-
Health Canada, First Nations & Inuit Health Branch. (2015). Second Annual Report on enhanced monitoring of the impact of eHealth investments in first nation communities, draft.
- Endnote 40
-
Health Canada. (2005). Health Programs and Services Mapping.
- Endnote 41
-
Health Canada. (2012). A First Nation Community Guide to Privacy.
- Endnote 42
-
Health Canada. (2012). Business Case for eHealth Infostructure Program Funding Renewal - Transforming Community Health Services Delivery, Health Information Management, Program Reporting and Accountability, Draft.
- Endnote 43
-
Health Canada. (2012). E-Health Solutions Unit, First Nation and Inuit Health, Ontario, Regional Year-End Review 2011/2012.
- Endnote 44
-
Health Canada. (2012). First Nations and Inuit eHealth Infostructure Program (eHIP) Evaluation.
- Endnote 45
-
Health Canada. (2012). First Nations and Inuit Health Strategic Plan: A shared path to improved health.
- Endnote 46
-
Health Canada. (2012). First Nations and Inuit Health, Health Information Analysis & eHealth Solutions - Atlantic Region, Regional Year End Review 2011-2012 Final.
- Endnote 47
-
Health Canada. (2012). Project Charter - Federal Nursing Stations Electronic Medical Record Pilot.
- Endnote 48
-
Health Canada. (2012). Recognizing Strengths – Building for the Future, Primary Health Care Service Delivery Models in Remote and Isolated First Nation Communities, Final Report and Recommendations.
- Endnote 49
-
Health Canada. (2013). eHealth Infostructure Program, First Nations and Inuit Health Branch, Alberta, Regional eHealth Program Plan 2013-2014.
- Endnote 50
-
Health Canada. (2013). eHealth Infostructure Program, First Nations and Inuit Health Branch, Manitoba Region, Regional eHealth Program Plan Proposal 2013-2014.
- Endnote 51
-
Health Canada. (2013). eHealth Infostructure Program, First Nations and Inuit Health Branch, Quebec Region, Regional eHealth Program Plan Proposal 2013-2014.
- Endnote 52
-
Health Canada. (2013). First Nations and Inuit Health, Health Information Analysis & eHealth Solutions - Atlantic Region, Regional Year End Review 2012-2013 Final.
- Endnote 53
-
Health Canada. (2013). FNIHB (Health Canada) eHealth Departmental Broadband Connectivity Advisory Committee, Terms of Reference.
- Endnote 54
-
Health Canada. (2014). eHealth Infostructure Readiness Assessment Tool.
- Endnote 55
-
Health Canada. (2014). First Nations and Inuit Health, Health Information Analysis & eHealth Solutions - Atlantic Region, Regional Year End Review 2013-2014 Final.
- Endnote 56
-
Health Canada. (2014). Quebec Region, eHealth Program Plan 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 57
-
Health Canada. (2015). Alberta Region, eHealth Program Plan 2015/2016, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 58
-
Health Canada. (2015). Chiefs of Ontario Annual Health Forum, February 24, 25 and 26, 2015.
- Endnote 59
-
Health Canada. (2015). Draft Contribution Audit Report, For Contribution Agreements: For (Funding Arrangement) SK1100039 between Health Canada Saskatchewan and Fishing Lake First Nation.
- Endnote 60
-
Health Canada. (2015). Internal Service Agreement Between First Nations and Inuit Health Branch (FNIHB) - Manitoba Region eHealth Solutions Unit (eHSU) and Corporate Service Branch (CSB) - Information Management Services Directorate (IMSD) IT Service Delivery Division - Distributed Computing Services (DCS) Central - Manitoba, May 4, 2015, for the Provision of: Coordination of eHealth Infostructure and IM/IT Support Services.
- Endnote 61
-
Health Canada. (2015). Manitoba Region, eHealth Program Plan 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 62
-
Health Canada. (2015). Manitoba Region, eHealth Year-End Review 2013/2014, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 63
-
Health Canada. (2015). Ontario, eHealth Program Plan 2015/2016, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 64
-
Health Canada. (2015). Project Charter - Improving IT Support to FNIHB Employees in Nursing Stations & Health Centres, Version: Final Version 6.1.
- Endnote 65
-
Health Canada. (2015). Unleashing Innovation: Excellent Health care for Canada, Report of the Advisory Panel on Health care Innovation.
- Endnote 66
-
Health Canada. (2016). Atlantic Region Name, Year-End Review - DRAFT 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 67
-
Health Canada. (2016). Connectivity Status in First Nation Communities - Draft v4.
- Endnote 68
-
Health Canada. (2016). First Nations and Inuit Health Branch's Approach to Implementing Electronic Medical Records.
- Endnote 69
-
Health Canada. (2016). Manitoba Region, eHealth Program Plan 2015/2016, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 70
-
Health Canada. (2016). Manitoba Region, eHealth Program Plan 2016/2017, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 71
-
Health Canada. (2016). Manitoba Region, Year-End Review 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 72
-
Health Canada. (2016). Saskatchewan Region, Year-End Review 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 73
-
Health Canada. (n.d.). Alberta Region, eHealth Program Plan 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 74
-
Health Canada. (n.d.). Alberta Region, Year-End Review 2013/2014, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 75
-
Health Canada. (n.d.). Alberta Region, Year-End Review 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 76
-
Health Canada. (n.d.). eHealth Infostructure Program, First Nations and Inuit Health Branch, Alberta Region, Regional Year-End Review 2012/2013.
- Endnote 77
-
Health Canada. (n.d.). eHealth Infostructure Program, First Nations and Inuit Health Branch, Manitoba Region, Regional Year-End Review 2012/2013.
- Endnote 78
-
Health Canada. (n.d.). eHealth Infostructure Program, First Nations and Inuit Health Branch, Quebec Region, Regional Year-End Review 2012/2013.
- Endnote 79
-
Health Canada. (n.d.). eHealth Infostructure Program, First Nations and Inuit Health Branch, Saskatchewan, Regional Year-End Review 2012/2013.
- Endnote 80
-
Health Canada. (n.d.). e-Health Solutions Unit, First Nation and Inuit Health Branch, Alberta Region, Regional Year-End Review 2011/2012.
- Endnote 81
-
Health Canada. (n.d.). e-Health Solutions Unit, First Nation and Inuit Health Branch, Saskatchewan Region, Regional Year-End Review 2011/2012.
- Endnote 82
-
Health Canada. (n.d.). eHealth Solutions Unit, First Nation and Inuit Health Branch, Manitoba Region, Year-End Review 2011/2012.
- Endnote 83
-
Health Canada. (n.d.). Health Canada 2011-2012 Report on Plans and Priorities.
- Endnote 84
-
Health Canada. (n.d.). Health Canada 2012-2013 Report on Plans and Priorities.
- Endnote 85
-
Health Canada. (n.d.). Health Canada 2013-2014 Report on Plans and Priorities.
- Endnote 86
-
Health Canada. (n.d.). Health Canada 2014-2015 Report on Plans and Priorities.
- Endnote 87
-
Health Canada. (n.d.). Health Canada 2015-2016 Report on Plans and Priorities.
- Endnote 88
-
Health Canada. (n.d.). Ontario, Year-End Review 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 89
-
Health Canada. (n.d.). Quebec Region, Year-End Review 2013/2014, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 90
-
Health Canada. (n.d.). Quebec Region, Year-End Review 2014/2015, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 91
-
Health Canada. (n.d.). Saskatchewan Region, eHealth Program Plan 2015/2016, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 92
-
Health Canada. (n.d.). Saskatchewan Region, Year-End Review 2013/2014, eHealth Infostructure Program, First Nations and Inuit Health Branch.
- Endnote 93
-
Indigenous and Northern Affairs Canada. (2012). Data Methodology and Connectivity Glossary of Terms. Retrieved from http://www.aadnc-aandc.gc.ca/eng/1343671152692/1343671215545#chp1
- Endnote 94
-
Industry Canada. (2016). First Nations Connectivity Dataset - MFN.3.0.
- Endnote 95
-
JRAssociates. (2012). Accessibility, Acceptance & Financial Impact, an evaluation of KOeHealth Telemedicine Services - Performance Metrics: 2007-08 to 2011-12.
- Endnote 96
-
Keewaytinook Okimakanak Tele-Mushkiki. (n.d.). KO Telemedicine.
- Endnote 97
-
KO eHealth Telemedicine. (2012). 2011 – 2012 Annual Activity Report, June 30, 2012.
- Endnote 98
-
KO eHealth Telemedicine. (2015). Annual Report by KOeHealth Telemedicine Services (KOeTS) compiled for: First Nation and Inuit Health, Ontario Region.
- Endnote 99
-
KOeHealth Telemedicine Services. (2013). Annual Report by KOeHealth Telemedicine Services (KOeTS) compiled for: First Nation and Inuit Health, Ontario Region.
- Endnote 100
-
KOeHealth Telemedicine Services. (2014). Annual Report by KOeHealth Telemedicine Services (KOeTS): 2013-2014 compiled for: First Nation and Inuit Health, Ontario Region.
- Endnote 101
-
KOeHealth Telemedicine Services. (2016). Annual Report by KOeHealth Telemedicine Services (KOeTS) compiled for: First Nation and Inuit Health, Ontario Region.
- Endnote 102
-
Manitoba Adolescent Treatment Centre. (n.d.). MATC Rural & Northern Telehealth Service - Service Description.
- Endnote 103
-
Manitoba Adolescent Treatment Centre. (n.d.). TeleMental Health Programming for Remote First Nations Communities.
- Endnote 104
-
Manitoba eHealth. (2014). Panorama Bulletin, Issue #3, May 2014.
- Endnote 105
-
Manitoba eHealth. (2014). Panorama Bulletin, Issue #4, October 2014.
- Endnote 106
-
Manitoba eHealth. (2015). eHealth Advisory Partnership - Manitoba eHealth Update.
- Endnote 107
-
Manitoba eHealth. (n.d.). First Nations and Inuit Health Activity Report - Fiscal Year 2014/2015 ending March 31, 2015.
- Endnote 108
-
Manitoba Health. (2015). Letter to Manitoba Panorama Steering Committee members, October 22, 2015.
- Endnote 109
-
Manitoba Health. (2016). Panorama Project FNIHB Report, Reporting Period: 04/01/2015 - 03/31/2016.
- Endnote 110
-
MBTelehealth, & Manitoba eHealth. (2011). MBTelehealth Benefit Evaluation Report.
- Endnote 111
-
MBTelehealth. (n.d.). First Nations and Inuit Health Branch (FNIHB) MBTelehealth Utilization Report, 2014 - 2015 Fiscal Year: April 1, 2014 - March 31, 2015.
- Endnote 112
-
MBTelehealth. (n.d.). First Nations and Inuit Health Branch (FNIHB) MBTelehealth Utilization Report, 2015 - 2016 Fiscal Year: April 1, 2015 - March 31, 2016.
- Endnote 113
-
Mikkola, E., & Puustinen, M. (2014, March 3). Overview of the national laws on electronic health records in the EU Member States - National report for Finland. Brussels, Belgium.
- Endnote 114
-
Nanaandawewigamig - First Nations Health and Social Secretariat of Manitoba. (2016). Building the Manitoba First Nations network of the future initiative. Presentation to First Nations Health Managers Association "Celebrating and Sharing our Inherent Knowledge in Health Leadership and Management", November 17, 2016, Vancouver, BC.
- Endnote 115
-
National Rural Health Alliance Inc. (2013, August). eHealth and Telehealth in Rural and Remote Australia. Retrieved from http://ruralhealth.org.au/sites/default/files/publications/nrha-factsheet-ehealth.pdf
- Endnote 116
-
National Rural Health Alliance. (2013). Connectivity for rural and remote health. Retrieved from http://ruralhealth.org.au/sites/default/files/publications/nrha-factsheet-connectivity.pdf
- Endnote 117
-
NSW Government. (n.d.). Rural eHealth Strategy. Retrieved from eHealth NSW: http://www.ehealth.nsw.gov.au/programs/clinical/rural
- Endnote 118
-
Office of the Auditor General of Canada. (2010). Electronic Health Records in Canada.
- Endnote 119
-
Office of the Australian Information Commissioner. (2014). Mobile privacy: a better practice guide for mobile app developers. Retrieved from https://www.oaic.gov.au/agencies-and-organisations/guides/guide-for-mobile-app-developers
- Endnote 120
-
Ontario Local Health Integration Network. (2013). eHealth Services Plan 2013-2016: Building an Integrated eHealth Framework.
- Endnote 121
-
Parliament of Canada. (2013). Technological Innovation in Health Care - Report of the Standing Committee on Health.
- Endnote 122
-
Paterson, G.I., Shaw, N., Grant, A.M., Delisle, E., Leonard, K., Mitchell Corley, S., McCarrey, M., Pascal, B., and Kraetschmer, N. (2011). Cross-Canada EMR Case Studies: Analysis of Physicians' Perspectives on Benefits and Barriers. Electronic Journal of Health Informatics.
- Endnote 123
-
Sherry, P. (2009). Deploying a Health Information Exchange for Alaskans. Alaska eHealth Network.
- Endnote 124
-
State of Alaska. (2016). Meaningful use. Retrieved from Alaska Department of Health and Social Services: http://dhss.alaska.gov/HIT/Meaningfuluse/Pages/Default.aspx
- Endnote 125
-
The Barrington Consulting Group Inc. (2013). Atlantic Policy Congress of First Nations Chiefs Secretariat - Fit / Gap Analysis of Electronic Medical Records Systems in Nova Scotia First Nations Communities.
- Endnote 126
-
Treasury Board of Canada. (2016). Policy on Results.
- Endnote 127
-
University of British Columbia & University of Calgary. (2013). eHealth Evaluation, Phase 2: National Report.
- Endnote 128
-
University of British Columbia. (2014). "Connected, Informed, Healthier": Health care Human Factors in Remote and Isolated First Nations Nursing Stations.
- Endnote 129
-
World Health Organization. (2012). Management of patient information: Trends and challenges in Member States.
- Endnote 130
-
World Health Organization. (2016). Atlas of eHealth country profiles: The use of eHealth in support of universal health coverage. Geneva: WHO Document Production Services. Retrieved October 17, 2016, from http://apps.who.int/iris/bitstream/10665/204523/1/9789241565219_eng.pdf
Footnotes
- Footnote i
-
Although the Program's strategic direction is applicable to Inuit communities (i.e., in the identification of the components of infostructure), eHIP is focused on First Nation reserves from a funding and delivery perspective.
- Footnote ii
-
The scope of the evaluation excludes the British Columbia region and communities north of 60°as explained under Evaluation Scope, Approach and Design.
- Footnote iii
-
Although the Program's strategic direction is applicable to Inuit communities (i.e., in the identification of the components of infostructure), eHIP is focused on First Nation reserves from a funding and delivery perspective.
- Footnote iv
-
To obtain a copy of the logic model graphic please use the following e-mail "Evaluation Reports HC - Rapports Evaluation@hc-sc.gc.ca".
- Footnote v
-
eHIP's mandate applies to Indigenous communities south of 60°. The Inuit communities that fall into this category, in Québec and in the Atlantic provinces, do not receive federal funding.
- Footnote vi
-
There are at least 12 other nursing stations that are not funded by eHIP for broadband connectivity.
- Footnote vii
-
Panorama is a PHIS developed by IBM Canada on behalf of the provinces and territories for implementation across Canada. Panorama has seven modules: communicable disease case management, immunization management, outbreak management, notification management, vaccine inventory, family health and work management.
- Footnote viii
-
EHRs are typically composed of several types of databases networked together. Components usually include: i) a client registry list of all patients with identifying information; ii) a provider registry of health care professionals authorized to use the system; iii) a diagnostic imaging system for storage and distribution of medical images such as X-rays, MRIs etc.; iv) a drug information system for storage and access to an individual's prescription history; and, v) a laboratory information system for storage and access to medical lab test results.Footnote 128
- Footnote ix
-
The Program target of 310 telehealth sites by 2014-2015 includes the following:
- 66 projected sites for British Columbia, which is now out of scope as the British Columbia First Nations Health Authority, under the British Columbia Tripartite Framework Agreement on First Nation Health Governance, signed on October 1st, 2013; and,
- 44 projected sites for Ontario that included provincially funded sites.
- Footnote x
-
In Ontario the OTN provides services to additional telehealth sites, not included in the table, that are funded by the province and not eHIP.
- Footnote xi
-
A brief standardized clinical assessment designed to inform home care intake from community or hospital.
- Footnote xii
-
Doc-in-a-box is a portable device that uses a mobile phone connection to establish a high resolution, two-way video link between a doctor, say at his/her office, and patients and health care practitioners at diverse locations (e.g., a patient's home, at the scene of an accident, etc.). Peripherals can also be used to gather and deliver health data.
- Footnote xiii
-
HCOM is an advocacy group that represents First Nations communities in Alberta. Advocacy is conducted in six categories handled by six sub-committees: mental health & addictions, governance & capital, prevention programs, Non-Insured Health Benefits, public health, and children & youth.
- Footnote xiv
-
ISED has a household connectivity mandate; INAC has a community welfare mandate; and, FNIHB has the health mandate for First Nations.
- Footnote xv
-
Encoders/decoders with some form of video/audio compression.
- Footnote xvi
-
A platform for high definition videoconferencing.