
Archived - Final Report: Audit of the Resolution Health Support Program, March 2016
Table of Contents
- Executive summary
- A - Introduction
- B - Findings, recommendations and management responses
- C - Conclusion
- Appendix A - Lines of enquiry and criteria
- Appendix B - Scorecard
- Appendix C - Resolution Health Support Program expenditures, by region
- Appendix D - Resolution Health Support Program services chart
- Appendix E - FNIHB organizational chart
- Appendix F - List of acronyms
Executive summary
The focus of the audit is the Indian Residential School Resolution Health Support Program (RHSP). In 2006, the government negotiated the Indian Residential Schools Settlement Agreement with First Nations and Inuit Communities. This agreement constitutes the largest out-of-court settlement in Canadian history. Health Canada is responsible for meeting Canada's legal obligation with respect to Mental Health and Emotional Health Support Services, one of the five components of the Settlement Agreement. The First Nations and Inuit Health Branch (FNIHB) is responsible for the management and delivery of these services. The RHSP delivers counselling through professional counsellors on a fee-for-service basis and provides emotional and cultural support through 124 contribution agreements.

(PDF format, 363 KB, 27 pages) Organization: Health Canada Type: [Publication Type] Published: 2016-03
The objective of this audit was to assess the management control framework in place to support the delivery of the RHSP and to provide assurance that the program is in compliance with the Treasury Board of Canada Policy on Transfer Payments. The audit was conducted in accordance with the Internal Auditing Standards for the Government of Canada and the International Standards for the Professional Practice of Internal Audit. Sufficient and appropriate procedures were performed and evidence gathered to support the audit conclusion.
Strategic direction is provided through FNIHB's Strategic Plan and Accountability Framework. The Accountability Framework describes the structure and process to support the relationship between headquarters and the regional offices. While the shared management and administrative accountability is documented at the branch level, the audit recommends that the RHSP develop terms of reference for its Regional Working Group, to document the mandate, roles and responsibilities and integrated service expectations.
Corporate risks are defined in Health Canada's annual Corporate Risk Profile and branch risks are identified and assessed annually in the branch risk registry. As part of the funding renewal exercise, program risks were identified and assessed and mitigating strategies were determined.
The RHSP has operational plans to manage its resources to support delivery. However, interviews, document reviews and data analyses indicate that there are discrepancies in the application of program eligibility criteria. The IRS Settlement Agreement, the funding agreement and the Program Framework clearly define client eligibility; however, a more liberal definition is applied by program officials. The audit recommends tracking and monitoring the approvals for professional counselling to persons other than students and family members and ensuring that the regions apply the eligibility criteria as defined. The RHSP's policies and guidance documents state that financial review and audit activities are conducted; however, the program was unable to provide a final version of a Provider Audit Framework or any evidence of a structured provider audit plan to be carried out by headquarters or the regions.
RHSP policies note that transportation benefits may be provided to help clients travel to the nearest appropriate cultural support provider or counsellor. It is further noted that if economical, the counsellor or cultural support provider can travel to the client's community. A travel data analysis was conducted for three regions and found that two regions use a cost-effective approach for making transportation decisions. The audit recommends communicating with the regions on expectations regarding the transportation guidelines, to support cost-effective decision-making and national program consistency for travel.
The RHSP uses an electronic system to capture data. It is planning to enhance the system to better meet regional needs and to integrate the Non-Insured Health Benefits (NIHB) Mental Health Benefit Program; the audit recommends that this work be finalized. As well, the RHSP recently completed an initial Privacy Impact Assessment on the system and noted the absence of a Personal Information Bank (PIB) on the Treasury Board of Canada Secretariat's Info Source, which provides information about the functions, programs, activities and related information holdings of government institutions subject to the Access to Information Act and the Privacy Act. A Personal Information Bank for the RHSP is currently being drafted and the audit recommends that it be finalized and posted on the Treasury Board of Canada's Info Source website.
The program was found to be compliant with the Financial Administration Act and the TB Policy on Transfer Payments. Minor exceptions were noted such as the absence of monthly activity reports.
A performance measurement strategy exists for the Mental Wellness programs, of which the RHSP is a component. While relevant performance data exists to support decision-making, current recipient reporting activities should be amended to decrease the reporting burden and capture activity-based data to assist program staff.
The audit makes three recommendations to further strengthen the existing management controls of the Resolution Health Support Program.
A. Introduction
1. Background
The Indian Residential Schools Settlement (IRS) Agreement, negotiated in 2006, is the largest out-of-court settlement in Canadian history. Health Canada (HC) is responsible for meeting Canada's legal obligation with respect to Mental Health and Emotional Health Support Services, the fifth component of the Settlement Agreement.
HC's Indian Residential Schools Resolution Health Support Program (RHSP) aims to ensure that the approximately 80,000 surviving former Indian Residential School students and their families have access to health support services, so that they may safely address the broad spectrum of mental wellness issues associated with their Indian Residential School experience. This fulfills the commitments made in the 2006 IRS Settlement Agreement, which includes professional counselling and cultural and emotional support.
The First Nations and Inuit Health Branch (FNIHB) is responsible for the management and delivery of the RHSP. The Program Alignment Architecture in Figure 1 shows where the program aligns within the strategic outcome for First Nations and Inuit primary health care and the associated funds at each level. HC spends an average of $55.5 million per year on the RHSP, with approximately 73% in transfer payments for emotional and cultural support, 23% for access to professional counselling and transportation services and 4% for salaries and wages (see Appendix C for a summary of program expenditures by region).
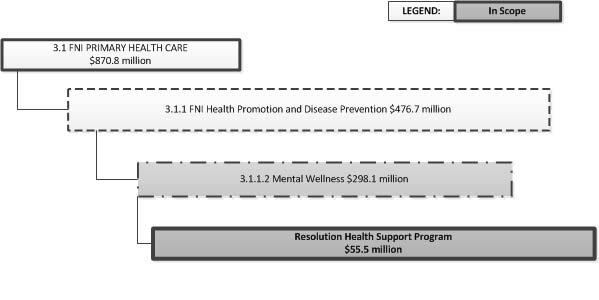
Figure 1 - Text Equivalent
Figure 1 outlines where the Resolution Health Support Program falls within the strategic outcome for First Nations and Inuit primary health care, as well as the associated funds at each level.
Program Alignment Architecture Component 3.1, First Nations and Inuit Primary Health Care, receives eight hundred and seventy point eight million dollars. Sub-component 3.1.1, First Nations and Inuit Health Promotion and Disease Prevention, receives four hundred and seventy-six point seven million dollars. Sub-sub-component 3.1.1.2, Mental Wellness, has a budget of two hundred and ninety-eight point one million dollars. The Resolution Health Support Program falls under sub-sub-component 3.1.1.2. Health Canada spends fifty-five point five million dollars per year on this program. The scope of this audit includes only the Resolution Health Support Program.
Program objectives
The objectives of the RHSP are to provide mental health, emotional and cultural supports throughout all stages of the Settlement Agreement process, including emotional and cultural services to those in attendance at Truth and Reconciliation Commission (TRC) events and Settlement Agreement commemoration events and during the Independent Assessment Process (IAP) (see Appendix D for a summary of the services). The program delivers emotional and cultural support through 124 contribution agreements to First Nations recipient organizations. Counselling is provided by clinical social workers and psychologists on a fee-for-service or per-diem basis. While the program is under the mental wellness program architecture (see Figure 1), the delivery model for counselling services and transportation is purposely similar to the model used by the Non-Insured Health Benefits (NIHB) Program. The NIHB Program delivers health-related goods and services that are not insured by provinces or territories or by other private insurance plans such as pharmacy and dental benefits.
The RHSP is designed to operate according to a number of guiding principles, such as national consistency and equitable access; non-judgmental, sensitive and compassionate service delivery; sustainable and fiscally responsible services, including transparent administrative processes supported by stakeholder input from First Nations and Inuit organizations.
Program eligibility
Eligible clients are those who attended Indian Residential Schools (IRS) or their family members. They include:
- former IRS students, regardless of their status (First Nations, Inuit, Métis, non-status, non-Aboriginal) or place of residence within Canada (on- or off-reserve), who have received or are eligible to receive Common Experience Payments (CEP);
- former IRS students who are resolving a claim against Canada through the Independent Assessment Process (IAP);
- former IRS students who are participating in Truth and Reconciliation Commission (TRC) or commemoration events.
In addition, in recognition for the intergenerational impacts that Indian Residential Schools had on families, RHSP services are also available to family members of former IRS students. Family members are defined as a spouse or partner; those raised by or raised in the household of a former IRS student; or any relation who has experienced effects of intergenerational trauma associated with a family member's time at an IRS.
Former students are provided with information on the program when they apply for the CEP and/or the IAP. HC reports that it has also widely disseminated information on how to access the services through community and friendship centre visits and direct mailings to communities. As well, HC has worked in partnership with the TRC, community organizations and other Settlement Agreement partners to ensure that an adequate number of support workers, cultural support providers and professional counsellors were available at all national and community TRC events and commemoration activities. Although the TRC has now completed its mandate, the RHSP's role will continue until all IRS Settlement Agreement activities have been completed.
Former students can access health support services from different points. Cultural and emotional supports can be accessed by contacting an RHSP contribution agreement recipient in the client's region. Clients may be put in touch with the appropriate service organization by contacting a known resolution health support worker (RHSW) or cultural support provider (CSP); the RHSP Regional Coordinator at the FNIHB regional office; or through a referral from the IRS Crisis Line.
Counselling services can be accessed by contacting the regional coordinator for the RHSP in the client's province or territory directly or through a third party (a family member, 24-hour National Crisis Line, lawyer, health support provider or community health worker).
Former students and their family members can choose the type of support they wish to receive: a professional counsellor, an RHSW or a CSP. The level and duration of the required services, including transportation, vary depending on each client's needs and circumstances.
Audit rationale
HC is expected to have designed a health support program that provides timely, quality services while being fiscally responsible. Given the delivery expectations of the RHSP, combined with the potential upcoming funding agreement, an audit of the management control framework was considered to be beneficial in providing assurance on the program's governance, risk management and internal controls. To date, the program has not been formally audited or evaluated internally.
2. Audit objectives
The objective of this audit was to assess the management control framework in place to support the delivery of the RHSP and to provide assurance that the program is in compliance with the Treasury Board of Canada Policy on Transfer Payments.
3. Audit scope
The scope of the audit includes financial and non-financial aspects of the program for the period from April 1, 2013 to December 31, 2015. Key management and accountability controls related to governance, risk, planning, information technology, privacy, service delivery and performance management were examined.
4. Audit approach
The audit was conducted at Health Canada's headquarters and in regional offices. The principal audit procedures included:
- a review and analysis of policy frameworks, planning documents, service delivery and performance-related documentation;
- interviews (in-person, by phone or video-conference) with key program personnel at headquarters and in the regional offices;
- on-site visits to the Northern, Alberta and Ontario regional offices for sampling and testing of transfer payments for compliance with the Financial Administration Act and the Policy on Transfer Payments.
5. Statement of conformance
In the professional judgment of the Chief Audit Executive, sufficient and appropriate procedures were performed and evidence gathered to support the accuracy of the audit conclusion. The audit findings and conclusion are based on a comparison of the conditions that existed as of the date of the audit, against established criteria that were agreed upon with management. Further, the evidence was gathered in accordance with the Internal Auditing Standards for the Government of Canada and the International Standards for the Professional Practice of Internal Auditing. The audit conforms to the Internal Auditing Standards for the Government of Canada, as supported by the results of the quality assurance and improvement program.
B - Findings, recommendations and management responses
1. Governance
1.1 Governance framework
Audit criterion: The First Nations and Inuit Health Branch (FNIHB) has an effective governance framework in place for achieving the objectives of the Resolution Health Support Program (RHSP).
Appropriately governing and managing programs is important in order to achieve public service effectiveness and efficiency. Governance structures and principles identify the distribution of roles and responsibilities among participants in an organization, including stakeholders, and the procedures for making and implementing sound decisions.
FNIHB developed an accountability framework in April 2012. The framework describes the structure and process to support the new accountability relationship between headquarters and the regional offices. It also explains how governance and oversight of the RHSP are informed through the ten-year strategic plan, the three-year branch work plan and the annual branch operational plans. Decision-making related to the RHSP mainly occurs through the Mental Wellness Cluster Leads' Forum and via regional teleconferences.
The Mental Wellness Cluster Leads' Forum within the Population Health and Wellness Division is guided by the branch's Strategic Plan, with the overall goal being to support greater First Nations and Inuit control of health programs and services. The main objective of the Forum is to provide general oversight and strategic planning advice to programs, in order to improve the access and quality of FNIHB-funded health programs and services in First Nations and Inuit communities. The audit obtained an up-to-date Terms of Reference and meeting minutes. The minutes reviewed showed that the RHSP is discussed, updates are provided to the Forum and decisions are made when required.
The Resolution Health Support Program Regional Working Group, which comprises participants from headquarters and the IRS Regional Coordinators, meets monthly via teleconference. This working group provides participants with an opportunity to discuss updates, changes or concerns related to the program. Interviews with headquarters and regional staff indicated that at times, there is an inconsistent understanding of the issues discussed; as well, it was noted that there are differing levels of communication of the issues within the regional offices. For example, RHSP staff in one of the regions audited was unaware of the availability of Mental Health Services Tracking System (MHSTS) ad hoc reporting, although this feature had been discussed regularly during working group meetings. Additionally, staff at headquarters confirmed that this region does not request MHSTS reports. The audit was able to obtain minutes of working group meetings, but noted that terms of reference have yet to be developed. The RHSP would benefit from developing terms of reference, which would provide an important overview the expectations for all participants.
The NIHB/IRS RHSP Regional Working Group was established in fiscal year 2015-16 to develop joint guidelines and tools. Meetings are held monthly between headquarters and the regional coordinators for both the NIHB Program and the RHSP.
In conclusion, FNIHB has an effective governance framework in place for achieving the objectives of the RHSP. However, the program would benefit from developing appropriate terms of reference for the RHSP Regional Working Group, to clarify its mandate and the obligations of committee members towards improving communications.
Recommendation 1
It is recommended that the Assistant Deputy Ministers, First Nations and Inuit Health Branch, develop Terms of Reference for the monthly Resolution Health Support Program - Regional Working Group.
Management response
Management agrees with the recommendation.
The First Nations and Inuit Health Branch (FNIHB) has an effective governance framework in place for achieving the objectives of the Indian Residential Schools Resolution Health Support Program (IRS RHSP), and the program will develop, as recommended, Terms of Reference for the monthly IRS RHSP Regional Working Group.
1.2 Roles and responsibilities
Audit criterion: The roles and responsibilities for the delivery of the RHSP are documented, clear and communicated.
Headquarters and regional staff share responsibility for the delivery of the RHSP; as such, it would be important to have clearly defined roles and responsibilities so that the program is delivered efficiently and effectively.
Headquarters is responsible for developing national policies to guide the administration of the program. It also provides advice and support to the regions, monitors regional health service delivery data and develops performance reporting tools and processes. Headquarters works with other Indian Residential School Settlement Agreement partners, such as Indigenous and Northern Affairs Canada, to address any concerns with the delivery of the agreement components.
The regions assist beneficiaries in accessing health support services. Regional staff also coordinates the delivery of counselling services and related transportation, as well as emotional and cultural support through contribution agreements with First Nations community organizations.
The audit noted that the organizational location of RHSP staff differs in each of three regions visited. Two of the regions deliver the program under one directorate, while one region divides the responsibilities under two directorates. Given the different organizational designs, terms of reference for the monthly Regional Working Group would minimize the risk that important program information and decisions are not communicated (see Recommendation 1).
In conclusion, roles and responsibilities for the delivery of the RHSP are documented, clear and understood.
2. Risk management
2.1 Risk management
Audit criterion: The risks associated with the delivery of the RHSP are identified, assessed and managed.
Risk management identifies potential negative events and takes steps to reduce the probability or lessen the impact of risks on the entity by identifying its strengths, weaknesses, opportunities and threats, along with mitigating strategies for each risk. Knowledge of the risks that the RHSP faces will give FNIHB additional options for dealing with potential problems before they arise.
Corporate risks are defined in Health Canada's 2015-2016 Corporate Risk Profile, while branch risks are identified in FNIHB's branch risk register 2015-16. FNIHB's risk register provides details on eight key risks, the sources of the risks, the existing controls and the impact, likelihood and manner in which the branch will respond to the risk. It also includes performance measures and the branch lead for each of the risk responses. Examples of risks identified include: sustainability of health services delivery; public health response; health human resources recruitment and retention; and management of grants and contributions.
In the most recent funding agreement, the branch notes the current risks and challenges. The document identified certain pressure points such as the following: program uptake may exceed current funding projections; the potential addition of institutions to the existing list of Indian Residential Schools; and insufficient human resource capacity. Management reports that these risks are being mitigated by entering into contribution agreements with recipients who have the flexibility to manage the workload and meet the demands within existing funding allocations.
The RHSP does not have a risk assessment exercise at either the Mental Wellness Cluster level or the program level. However, the NIHB Program performs an annual risk assessment to identify risks for its own mental health program. This risk exercise was reviewed in an internal audit conducted in 2014Footnote 1 and was found to be satisfactory. The NIHB Program and the RHSP provide some common services (for example, access to professional mental health counsellors) and there is some overlap in the client base; they cooperate through a joint working group, which meets monthly and has produced joint tools such as prior approval forms and the Guide to Mental Health Counselling Services. Examples of risks identified in the NIHB Program that apply to the RHSP include national consistency of mental health benefit coverage; inconsistency in application of provider registration policy; evolving scope of practice of mental health providers; and evolving industry practices. Management reports that these risks are being partially mitigated through the development and implementation of the 2015 NIHB-IRS Guide to Mental Health Counselling Services.In conclusion, risks are identified, assessed and managed at the branch level. The RHSP is also aware of its key program-specific risks, but would benefit from formally documenting and tracking these risks as a good management practice.
3. Internal controls
3.1 Operational management
Audit criterion: The RHSP has operational plans that demonstrate the use of its resources to support program delivery.
Operational plans are a key tool that supports a branch's strategic plan. The purpose of the operational plan is to provide management with a clear picture of the tasks and responsibilities in line with the goals and objectives contained within the strategic plan. This yearly exercise should present detailed information to direct people to perform the day-to-day tasks required in an organization. Consequently, it was expected that FNIHB would have developed plans and budgets, based on the objectives and expected results to be achieved, as well as the assignment of human and financial resources, including those from the branch's regional offices.
Operational planning
The FNIHB 2015-16 Operational Plan lists 13 deliverables related to the RHSP. These deliverables are linked to the branch strategic priorities and include quarterly milestones, expected results, performance indicators and planned resources required to accomplish the deliverables. An operational plan is also in place for the RHSP and is aligned with the FNIHB plan. The RHSP operational plan addresses key initiatives, deliverables and milestones. To support the delivery of the program, each regional office must develop its own operational plan for the delivery of counselling, transportation and contribution agreements and have the plan approved by headquarters. The audit reviewed the operational plans for all seven regions and found them to be similar in structure to the branch operational plan, with all deliverables linked to the branch strategic priorities and with the quarterly milestones, expected results, performance indicators and planned resources required to accomplish the deliverables.
Financial management
Funding to the regions for counselling, transportation and contribution agreements is reviewed annually by headquarters, based on regional needs expressed through their regional operational plan. At mid-year, the RHSP meets with each region to review progress on its plan and to adjust the financial resources as needed. Headquarters also reviews Management Variance Reports (MVR) provided by the Chief Financial Officer Branch. One region noted that due to the completion of the TRC hearings, the workload for RHSWs has diminished. Some of the recipients have taken the initiative to offer other activities to help the former IRS students and their families, while other recipients have not been as proactive, which has resulted in lapsed funds in 2014-15. The RHSP should assess the future role, activities and funding of the RHSWs in light of the completion of the TRC hearings.
Overall, the RHSP demonstrates the use of resources to support program delivery. Furthermore, the bi-annual financial review reallocates funding to those areas in the program where resources are most needed.
3.2 Service delivery and claims processing
Audit criterion: There is an effective suite of management controls, including information technology and privacy, for delivering services and managing service providers' claims.
The RHSP counselling and transportation benefits are delivered by psychologists and social workers enrolled through the NIHB Mental Health benefit. The RHSP does not enrol its own counsellors; rather, the NIHB Program manages the enrolment of providers on behalf of the RHSP, in keeping with the jointly developed criteria outlined in the 2015 NIHB-IRS Guide to Mental Health Counselling Services, ensuring that these providers maintain their good standing with their professional association and retain their professional insurance requirement. Currently, HC has enrolled 1,015 mental health professionals. In order to become an approved service provider, professionals must submit a request and attach documentation on their experience and qualifications, including proof of required education and registration with an appropriate professional college or association.
In early 2015, the NIHB Program and the RHSP jointly introduced a new Mental Health Counsellor Provider Agreement. The agreement sets out the terms and conditions for mental health counselling providers' eligibility criteria, responsibilities and the process to submit claims to Health Canada for services provided to eligible clients under the NIHB Program or the RHSP. The three regions visited reviewed and updated their provider lists by requesting that all service providers re-register with the RHSP and sign the agreement. The RHSP developed new forms and communications materials to guide the regions in the annual renewal of provider enrolments. This new process is planned to be implemented by June 2016.
Currently, the RHSP relies on a suite of management controls such as prior approval of the treatment plan, invoice processing, eligibility criteria, provider audits and policies to guide transportation.
Prior approval
Except for the automatic payment for the first two sessions, which allow providers to develop a treatment plan specific to the needs of the client, all other claims must receive prior approval in order to be paid. Twenty-nine client files were sampled in the Alberta, Northern and Ontario regions. They were reviewed for the presence of proper prior approval with adequate information to ensure that payments are within allowable maximums; to confirm the good standing of counsellors with their professional provincial bodies; to confirm attendance by the client; and to verify authorized signature approval. No issues were found.
Invoice processing
Invoices were sampled in each of the regions. The audit found that in one of the regions there was a delay of up to six months in the payment of its invoices, which caused suppliers such as hotels to refuse to further accommodate HC. During a site visit to the region, the auditors observed the manager approving an invoice from June in early December. Management noted that this delay was caused primarily by insufficient human resources in the region to support the claims processing. Management is currently staffing a position to support the claims processing unit.
Eligibility criteria
Eligibility criteria for the RHSP are documented in the IRS Settlement Agreement, the funding agreement and in the Program Framework. The eligibility criteria specifically state that the program's services are available to former IRS students and their family members (that is, spouse or partner, a person raised by or raised in the household of a former IRS students and any relation who has experienced effects of intergenerational trauma associated with an eligible family member's time at an IRS), as well as to any participants (such as counsellors) at a TRC meeting or commemoration event. Health Canada worked in partnership with the TRC, community organizations and other Settlement Agreement partners to ensure that an adequate number of support workers, cultural support providers and professional counsellors were available at all national and community TRC events and commemoration activities. However, interviews with headquarters and regional staff and a review of the contribution agreement schedules indicated that eligibility is verified against the former students' eligibility and not the actual person requesting the services. Management noted that this created situations where professional counselling services are extended to individuals other than students and family members and outside of TRC and commemoration events. The audit was unable to determine the extent of this practice, since the eligibility form does not have a category to track non-student/family approval for services. As such, the RHSP should track and monitor approvals for professional counselling services and clarify the definition of the eligibility criteria (see Recommendation 2).
Provider audits
The 2014 IRS RHSP Policy Framework and the 2015 NIHB-IRS Guide to Mental Health Counselling Services state that financial review and audit activities are conducted. The RHSP currently performs regional provider monitoring and has referred cases to the Office of Audit and Evaluation's Special Examinations Division for further examination when warranted. In its 2014-15 work plan, the program committed to developing a service provider audit framework. Provider audits will help detect excessive servicing, use or abuse by providers. Audit procedures generally entail a verification of services to ensure that payments are appropriate, thereby confirming that program funds are used appropriately to meet client requirements. Provider audits generally arise as a result of monitoring practices, such as the regional monitoring practices currently in place. At the completion of the audit fieldwork, the program had not yet finalized the provider framework or provided evidence of a structured provider audit plan by headquarters or the regions. A provider audit framework will promote and enable regional consistency, standardized processes and guidance, including sample selection, review of outliers and escalation measures, and will ensure that all clients receive appropriate care within available resources (see Recommendation 2).
Transportation
The 2012 IRS-RHSP Policy and Procedures notes that transportation benefits may be provided to help clients travel to the nearest appropriate cultural support provider or counsellor. The document further notes that if more economical, the counsellor or cultural support provider can travel to the client's community, in accordance with the NIHB Medical Transportation Policy (2005). The policy notes that medical transportation may be provided for clients to travel to see a traditional healer or, where economical, for a traditional healer to travel to the community. Overall, the transportation guidelines allow for flexibilities, within the regional context, to organize access to services in a cost-effective and equitable manner.
Of the three regions visited, the audit found that two regions applied cost-effective measures when making medical transportation decisions. The first region had 28 therapists on contract travelling to clients and had very few clients travelling to see therapists. This resulted in low travel costs - about five cents of transportation cost for every dollar of counselling expended. The second region used a cost-benefit analysis on a case-by-case basis to determine the best arrangement for counselling, resulting in approximately $1.85 of transportation cost for every dollar of counselling expended. Considering the geographical challenges in Region 2, it would be reasonable to expect this region to have higher transportation costs. However, due to its cost-benefit analysis, the region has been able to reduce transportation costs (see Table 1). The third region only transported clients to therapists, resulting in higher travel costs per counselling dollar.
| Region | Counselling | Transportation | Average cost of transportation per counselling dollar |
|---|---|---|---|
| Region 1 | $3,789,307.44 | $178,722.94 | $0.05 |
| Region 2 | $3,203,379.31 | $5,919,439.86 | $1.85 |
| Region 3 | $2,225,450.81 | $5,500,295.79 | $2.47 |
The RHSP should share the best practices from the regions that have applied a cost-effective lens and require all regions to operate in this manner. This approach will support the sustainable and fiscally responsible management of the program (see Recommendation 2).
Information technology
The Mental Health Services Tracking System (MHSTS) is a web-enabled, hosted database used by the RHSP to track mental health counselling and transportation costs associated with the program; it is also used for contribution agreement activity reporting. Headquarters described the current system as meeting the requirements, which mainly consist of central agency reporting. However, the regions indicated that this legacy system does not meet their operating needs. For example, the IT system does not track by travel authority; as well, a significant amount of relevant information is entered as notes, but reports cannot be produced based on notes. Furthermore, the regions cannot produce reports on their own data and must request reports from headquarters. As a work-around, each region has developed a spreadsheet to manage program delivery.
Management recognizes these limitations and has developed the business requirements for a Mental Health IT Modernization Project. This project's primary purpose is to integrate the Non-Insured Health Benefits (NIHB) mental health benefit into the IRS platform; however, the program is also taking this opportunity to address regional needs. A review of the latest version of the business requirements proposal confirms that regional concerns have been integrated. Management is aware of the benefits of system modernization. This system enhancement should help strengthen the monitoring activities and reduce the need for regions to use their own spreadsheets (see Recommendation 2).
Privacy
The audit reviewed the privacy and data protection for personal information collected, used, disclosed and retained, because the RHSP has access to and retains sensitive personal data, such as clients' personal information and information on mental health counselling sessions. Interviews with regional staff indicated that program staff is security and privacy conscious. They have locked cabinets to store sensitive information and work in secure office environments, with access limited by the use of access cards. A physical observation in the evening confirmed clean desks and the use of locked cabinets to store sensitive information.
In the latter half of 2015, the RHSP commissioned a Privacy Impact Assessment (PIA) for the MHSTS system. The PIA noted that FNIHB had not developed a Personal Information Bank (PIB) for the program and that such a failure constitutes a breach of subsection 10(1) of the Privacy Act and subsection 6.2.1 of the TBS Directive on Privacy Impact Assessment. The privacy notice on both the joint NIHB/RHSP prior approval form and confirmation of attendance sheet notes that "A Personal Information Bank is under development for NIHB and for IRS RHSP." As of February 2016, the program is developing a Personal Information Bank and is reviewing its Privacy Impact Assessment. The program is expecting to submit both the PIA and the PIB to the Treasury Board Secretariat later this year, for publication on TBS Info Source, which provides information about the functions, programs, activities and related information holdings of government institutions subject to the Access to Information Act and the Privacy Act (see Recommendation 2).
Overall, there is a suite of management controls to deliver counselling and transportation services; however, the controls could be more effective. The RHSP would benefit from upgrading the MHSTS to better meet the needs of the regional offices; from finalizing a personal information bank; and from developing and implementing a provider audit framework. The program could also benefit from the development of stronger guidelines on mental health transportation, to ensure greater consistency across regions and from a clarification of the eligibility criteria to better align with the program's Authority.
Recommendation 2
It is recommended that the Assistant Deputy Ministers, First Nations and Inuit Health Branch, strengthen the suite of management controls for service delivery and claims processing by:
- Developing and implementing a provider audit framework;
- Tracking and monitoring approvals for professional counselling for non-student/family members;
- Communicating with the regions on expectations of the transportation guidelines regarding cost-effectiveness;
- Finalizing the business requirement for the Mental Health IT Modernization Project; and
- Finalizing the personal information bank.
Management response
Management agrees with recommendation.
FNIHB will update the provider audit framework and finalize the business requirements for the Mental Health IT Modernization Project and the personal information bank submission.
Regarding the eligibility criteria, the program aims to ensure effective access to needed services. Its mandate is very precise about those to be supported during hearings or TRC events and follow-up counselling sessions. The program will further assess the number of individuals receiving counselling support who might not be eligible as former students, family members (defined as spouse/partner, those raised by or raised in the household of a former IRS student, and any relations who have experienced effects of intergenerational trauma associated with an eligible family member's time at an IRS), as well as TRC or Commemoration events participants.
The transportation guidelines allow for flexibilities within the regional context to organize services, taking into account cost-effectiveness, client needs, availability of services, provider availability to travel and privacy-related factors. The program will issue a reminder to all regions to ensure that continued attention is given to organizing supports in the most cost-effective, culturally appropriate and client-centred way.3.3 Transfer payments
Audit criterion: The RHSP has the tools to evaluate the recipients' capacity and resources to achieve program expectations. Risk-based recipient monitoring activities are conducted, including the review of recipient reporting, the receipt of deliverables before the release of payments and recipient audits.
Transfer payments represent a large part of the Government of Canada's spending and are one of the government's key instruments for furthering its broad policy objectives and priorities.
The government is committed to ensuring that transfer payments are managed in a manner that respects sound stewardship and the highest level of integrity, transparency and accountability. The government ensures that transfer payment programs are designed, delivered and managed in a manner that is fair, accessible and effective for all involved, including departments, applicants and recipients, all of whom have important contributions to make in achieving the objectives of the government and in furthering Canadian aims.
Contribution arrangements were established within a special purpose allotment for the Indian Residential Schools Resolution Health Support Program, under the Mental Health and Emotional Support Services component of the Indian Residential Schools Settlement Agreement. A set contribution approach is used, whereby the transfer payment is subject to performance conditions outlined in the funding agreement. Set contributions must be accounted for and are subject to audits. Interim and year-end reports are required and budgets are awarded annually. The regions monitor recipient activities, in compliance with the contribution agreements and the program terms and conditions. These activities include the provision of interim and year-end financial reports, annual work plans, recipient eligibility and monthly and quarterly activity reports.
While the contribution agreement states that activity reports are to be submitted quarterly, with a monthly breakdown of CSP and RHSW activities, the interpretation of the reporting requirement varied by recipient. Some recipients submitted quarterly reports only; others reported both monthly and quarterly. All recipients reported by CSP and RHSW separately, as required. While the expectation of monthly reports is articulated in the contribution agreement, the auditors were unable to determine the usefulness or the benefit of monthly versus quarterly reporting. Additionally, program staff expressed that the absence of narrative information in the activity reports, detailing the types of activities, lessened the value of the information as a tool to support program decision-making. Reducing the monthly reporting burden placed on recipients and enhancing the usefulness of the content of the reports are two aspects that program staff could explore.
In 2014-15, HC fully implemented Indian and Northern Affairs Canada's (now Indigenous and Northern Affairs Canada - INAC) risk management tool (the General Assessment) under the Grants and Contributions Information Management System (GCIMS). The internal processes for conducting joint assessments (for risk and default management) and the protocol for approvals between the two departments were enhanced, allowing for greater collaboration between the departments for common recipients. While risk assessments are shared, Health Canada is also able to use a departmental assessment based on internal reviews, if deemed appropriate.
The review of recipient work plans and interim and year-end reports is completed by regional staff. When warranted, accounts receivables are established for overpayments, while other sources of funding are explored for potential shortages.
Thirty recipient files were tested for compliance with the TB Policy on Transfer Payments and the TBS Directive on Transfer Payments, as well as for compliance with program terms and conditions and contribution agreement requirements. Results of the contribution agreements and reporting requirements testing were satisfactory, with minor exceptions such as the absence of monthly activity reports.
In conclusion, the RHSP was found to be compliant with the Financial Administration Act and the TB Policy on Transfer Payments.
3.4 Performance measurement
Audit criterion: Performance data exists and is utilized to support decision-making.
Performance information supports effective management and decision-making processes. Performance information also allows managers to monitor and assess the results of programs and the economy and efficiency of their management. Management can make informed decisions and take appropriate and timely actions, provide effective and relevant reporting and ensure that reliable and credible performance data is being collected to effectively support evaluation.
A performance measurement strategy framework (PMSF) exists for Health Canada's Mental Wellness Cluster, of which the RHSP forms a small part. The PMSF encompasses many other different aspects of mental wellness in addition to the RHSP. FNIHB has made a commitment to revising the PMSF by March 2016.
The information on the program is gathered mostly from the monthly or quarterly activity reports that recipients submit to regional offices, which detail the number of individual clients (former students and family members), the number of times each has used RHSW or CSP services, the client's sex, age cohort and status and the purpose of the interactions. The accuracy and consistency of the data reported could not be verified. The results of testing revealed inconsistent and in some cases incomplete activity reports. Although the current reporting structure to central agencies is annual, the reporting format requested of recipients is monthly. While the purpose of the activity reports was supposed to be for Treasury Board reporting, the contents of these reports were not included in the Treasury Board reports reviewed.
Additionally, in order to track clients and students in the manner requested by the activity reports, the recording of unique identifiers (for example, name or a unique number) would be required. It is unclear if recipients are tracking individual clients monthly, quarterly or annually (if at all). The consistency and accuracy of RHSP reporting could not be verified. The content of the activity reports is numeric, with a recipient comment area. In interviews with regional staff, the absence of narrative information, such as the types of activities, prevented the activity reports from being a useful source of information to inform program decision-making (see Section 3.3).
Until 2004, HC prepared biannual reports to Treasury Board through INAC. Reporting for 2015 will be an annual process; however, contribution agreement recipients are required to report monthly and quarterly by CSP and RHSW. This reporting requirement is inconsistently applied across all recipients. Some recipients are required to report both monthly and quarterly, while others report only quarterly. Of the staff interviewed, no one indicated a use for monthly reports; however, many spoke of the heavy workload involved for staff and recipients to respect the monthly and quarterly reporting requirements.
In conclusion, performance data exists to support decision-making; however, current recipient reporting activities could be amended to decrease the reporting burden and capture activity-based data to assist program staff.
Recommendation 3
It is recommended that the Assistant Deputy Ministers, First Nations and Inuit Health Branch, review the reporting requirements and the performance measurement strategy framework to ensure that data requested and received is clearly articulated, accurate, useful and informs decision-making.
Management response
Management agrees with the recommendation.
Health Canada's Mental Wellness Cluster performance measurement strategy framework, which includes the RHSP, will be updated by April 2016. The program currently captures performance data that is utilized to support decision-making. In alignment with the recommendation, the program will continue to review its reporting requirements to ensure that data collection supports decision-making, while balancing the need to reduce the reporting burden on contribution agreement recipients and program staff.
C- Conclusion
Overall, the management control framework for the delivery of mental and emotional health support services is appropriate. The Resolution Health Support Program (RHSP) is well-governed and risk-managed and has operational plans to support the use of its resources. Contribution agreements are risk-based and comply with the Financial Administration Act and the Treasury Board of Canada Policy on Transfer Payments.
The RHSP would benefit from enhancing its information technology system, finalizing a personal information bank and developing and implementing a provider audit framework. As well, the program should share the best transportation practices from the regions that have applied a cost-effective lens and require all regions to operate in this manner. As well, the RHSP should track and monitor approvals for professional counselling for other than students/family members and communicate to the regions the importance of applying the existing eligibility criteria. Finally, the RHSP should lessen the reporting burden on recipients and enhance information to assist with program decision-making.
The areas for improvement that have been noted in this audit report will collectively strengthen the effectiveness of the management controls for the Resolution Health Support Program.
Appendix A - Lines of enquiry and criteria
| Criteria title | Audit criteria |
|---|---|
| Line of enquiry 1: Governance | |
| 1.1 Governance frameworkAppendix A footnote 1 | The First Nations and Inuit Health Branch (FNIHB) has an effective governance framework in place for achieving the objectives of the Resolution Health Support Program (RHSP). |
| 1.2 Roles and responsibilitiesAppendix A footnote 1 | The roles and responsibilities for the delivery of the RHSP are documented, clear and communicated. |
| Line of enquiry 2: Risk management | |
| 2.1 Risk managementAppendix A footnote 1 | The risks associated with the delivery of the RHSP are identified, assessed and managed. |
| Line of enquiry 3: Internal controls | |
| 3.1 Operational managementAppendix A footnote 1 | The RHSP has operational plans that demonstrate the use of its resources to support program delivery. |
| 3.2 Service delivery and claims processingAppendix A footnote 1Appendix A footnote 2 | There is an effective suite of management controls, including information technology and privacy, for delivering services and managing service providers' claims. |
| 3.3 Transfer paymentsAppendix A footnote 3Appendix A footnote 4 | The RHSP has the tools to evaluate the recipients' capacity and resources to achieve program expectations. Risk-based recipient monitoring activities are conducted, including the review of recipient reporting, the receipt of deliverables before the release of payments and recipient audits. |
| 3.4 Performance measurementAppendix A footnote 1 | Performance data exists and is utilized to support decision-making. |
Appendix A footnotes
|
|
Appendix B - Scorecard
| Criterion | Rating | Conclusion | Rec # |
|---|---|---|---|
| Governance | |||
| 1.1 Governance framework | Needs minor improvement | FNIHB has an effective governance framework; however, the RHSP should develop terms of reference for its Regional Working Group. | 1 |
| 1.2 Roles and responsibilities | Needs minor improvement | Roles and responsibilities for the delivery of the RHSP are documented; however, formal terms of reference for the Regional Working Group will further clarify roles and responsibilities. | Refer to 1 |
| Risk Management | |||
| 2.1 Risk management | Needs minor improvement | Risks are identified, assessed and managed at the branch level. The RHSP is also aware of its key program-specific risks, but would benefit from formally documenting and tracking the effectiveness of the risk mitigating strategies. | |
| Internal Controls | |||
| 3.1 Operational management | Needs minor improvement | RHSP planning demonstrates the use of its resources to support program delivery. However, the program should assess the role and funding of resolution health support workers going forward. | |
| 3.2 Service delivery and claims processing | Needs moderate improvement | The RHSP should develop and implement a provider audit framework; finalize the personal information bank; communicate with the regions on expectations regarding the transportation guidelines; enhance the mental services tracking system; and track and monitor approvals for professional counselling for other than students/family members. | 2 |
| 3.3 Transfer payments | Satisfactory | Transfer payments are in compliance, recipients' capacity is assessed and monitoring activities and recipient audits are conducted. | |
| 3.4 Performance measurement | Needs moderate improvement | The performance measurement strategy should be reviewed to ensure that relevant performance data is collected to support decision-making. | 3 |
Appendix C - Resolution Health Support Program expenditures, by region
| FY 2014- 15 | Grants and Contributions | HC Service Delivery | Salaries and Wages | Total | % |
|---|---|---|---|---|---|
| Northern Region | $7,311,631.89 | $4,693,584.75 | $439,929.95 | $12,445,146.59 | 22.4% |
| Ontario Region | $4,966,654.00 | $4,002,416.38 | $289,548.03 | $9,258,618.41 | 16.7% |
| Alberta Region | $6,713,175.00 | $1,935,176.79 | $168,925.17 | $8,817,276.96 | 15.9% |
| Manitoba Region | $4,889,813.00 | $1,374,851.73 | $170,937.37 | $6,435,602.10 | 11.6% |
| Pacific RegionAppendix C footnote * | $6,400,000.00 | $7,681.74 | $6,407,681.74 | 11.5% | |
| Saskatchewan Region | $5,452,177.00 | $303,172.64 | $182,334.57 | $5,937,684.21 | 10.7% |
| Quebec Region | $3,332,027.00 | $181,149.79 | $213,893.03 | $3,727,069.82 | 6.7% |
| Atlantic Region | $1,329,075.00 | $249,677.00 | $115,650.18 | $1,694,402.18 | 3.0% |
| Headquarters | $124,200.00 | $15,444.98 | $699,542.20 | $839,187.18 | 1.5% |
| Grand Total | $40,518,752.89 | $12,763,155.80 | $2,280,760.50 | $55,562,669.19 | |
| 72.9% | 23.0% | 4.1% | |||
Appendix C footnotes
|
|||||
Appendix D - Resolution Health Support Program services chart
| Service | Delivered by | Administered by | Description |
|---|---|---|---|
Emotional Support |
Resolution Health Support Workers (RHSW) hired through community-based Aboriginal organizations |
Health Canada, through contribution agreements |
|
Cultural Support |
Cultural Support Providers (CSP) and Traditional Healers or Elders hired through community-based Aboriginal organizations |
Health Canada, through contribution agreements |
|
Individual Counselling |
Clinical social workers and psychologists registered with their specific regulatory body and with Health Canada and counsellors enrolled with Heath Canada |
Health Canada, using the IRS Policies and Procedures, as well as some NIHB guidelines, policies and procedures |
|
Group Counselling |
Clinical social workers and psychologists registered with their specific regulatory body and with Health Canada and counsellors enrolled with Heath Canada |
Health Canada, using the IRS Policies and Procedures, as well as some NIHB guidelines, policies and procedures |
|
Transportation |
IRS RHSP Regional Coordinators |
Health Canada, using the NIHB guidelines, policies and procedures |
|
| Source: Resolution Health Support Program Policy and Procedures, November 2012 | |||
Appendix E - FNIHB organizational chart
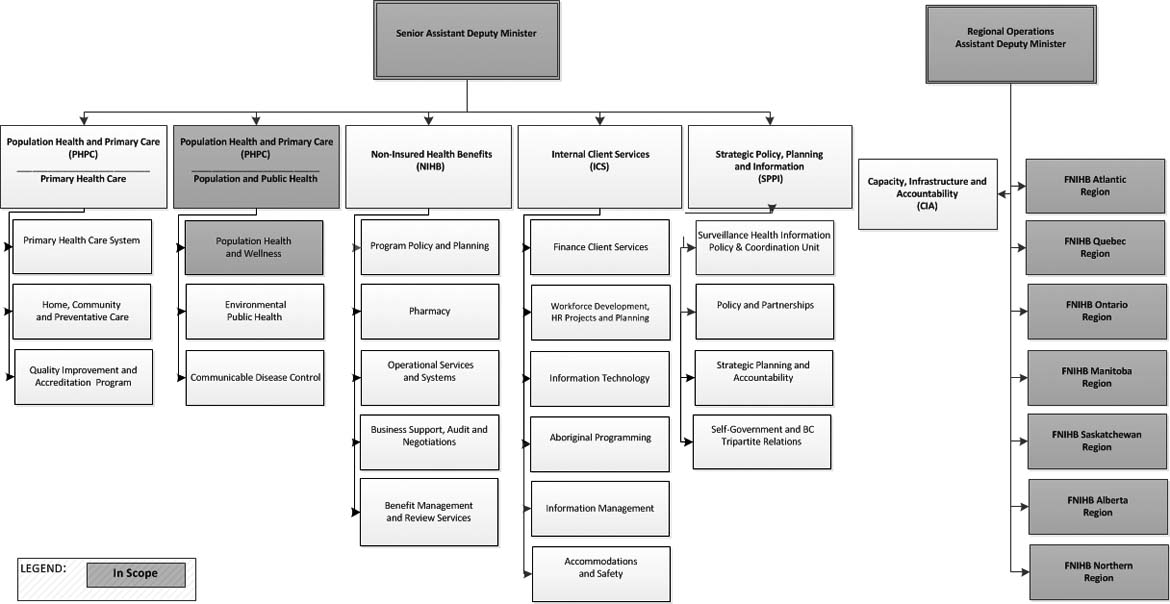
FNIHB Organizational Chart - Text Equivalent
Appendix E sets out the organizational structure for the First Nations and Inuit Health Branch, highlighting the areas that fall within the scope of this audit.
Five directorates report to the Senior Assistant Deputy Minister : Population Health and Primary Care - Primary Health Care; Population Health and Primary Care - Population and Public Health; Non-Insured Health Benefits; Internal Client Services; and Strategic Policy, Planning and Information.
Of these five directorates, only Population Health and Primary Care - Population and Public Health falls within the scope of this audit. Further, of the three areas that comprise this directorate, only Population Health and Wellness falls within the scope of this audit.
Regional Operations are under the direction of the Assistant Deputy Minister. Regional Operations comprises the seven First Nations and Inuit Health Branch regional offices: Atlantic Region; Quebec Region; Ontario Region; Manitoba Region; Saskatchewan Region; Alberta Region; and Northern Region. Each of these regional offices was included in the scope of this audit.
Source: FNIHB
Appendix F - List of acronyms
- CEP
- Common experience payments
- CSP
- Cultural support provider
- FNIHB
- First Nations and Inuit Health Branch
- HC
- Health Canada
- IAP
- Independent assessment process
- IRS
- Indian Residential School
- MHSTS
- Mental Health Services Tracking System
- NIHB
- Non-Insured Health Benefits
- PIA
- Privacy Impact Assessment
- PIB
- Personal Information Bank
- RHSP
- Resolution Health Support Program
- RHSW
- Resolution health support worker
- TB
- Treasury Board of Canada
- TBS
- Treasury Board of Canada Secretariat
- TRC
- Truth and Reconciliation Commission