
Canada-Saskatchewan Aging with Dignity funding agreement (2023-24 to 2027-28)
Tables of contents
- Funding agreement
- Annex 1 – Common statement of principles on shared health priorities
- Annex 2 – Shared pan-Canadian interoperability roadmap
- Annex 3 – Indicators: Access to home and community care
- Annex 4 – Action plan
Funding agreement
(the "Agreement")
Between:
His Majesty the King in right of Canada (hereinafter referred to as "Canada" or "Government of Canada") as represented by the Minister of Health (herein referred to as "the federal Minister")
- and -
His Majesty the King in right of Saskatchewan (hereinafter referred to as "Saskatchewan" or "Government of Saskatchewan") as represented by the Minister of Mental Health and Addictions, Seniors and Rural and Remote Health (herein referred to as "the provincial Minister")
Referred to collectively as the "Parties", and individually as a "Party"
Preamble
Whereas, on March 1, 2023, Canada and Saskatchewan announced an overarching agreement in principle on Working Together to Improve Health Care for Canadians, supported by almost $200 billion over ten years in federal funding, including $46.2 billion in new funding to provinces and territories, Canada and Saskatchewan acknowledged the importance of helping Canadians age closer to home;
Whereas, Canada has also announced a 5 per cent Canada Health Transfer (CHT) guarantee for the next five years, starting in 2023-24, which will be provided through annual top-up payments as required. This is projected to provide approximately an additional $17 billion over 10 years in new support. The last top-up payment will be rolled into the CHT base at the end of the five years to ensure a permanent funding increase, providing certainty and sustainability to provinces and territories;
Whereas, in the area of home and community care, Working Together to Improve Health Care for Canadians also includes a commitment by Canada and Saskatchewan to continue to work to support collaboration on the Common Statement of Principles on Shared Health Priorities (hereinafter referred to as the "Common Statement", attached hereto as Annex 1), supported by the federal Budget 2017 investment of $6 billion over ten years;
Whereas, this Agreement also provides financial support for long-term care as it relates to the Government of Canada's Budget 2021 investment of $3 billion over 5 years to support provinces and territories in keeping long-term care residents safe and improve their quality of life;
Whereas, Saskatchewan makes ongoing investments in health consistent with its broader responsibilities for delivering health care services to its residents and in supporting diversity, equity, and the needs of First Nations, Inuit and Métis; and underserved and/or disadvantaged populations, including, but not limited to official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians) and LGBTIQA2S+;
Whereas, Canada authorized the federal Minister to enter into agreements with the provinces and territories, for the purpose of identifying activities that provinces and territories will undertake in respect of long-term care, and for funding in this Agreement associated with the federal investment for home and community care consistent with the Common Statement (and menu of actions outlined in Annex 1);
Whereas, The Executive Government Administration Act authorized the provincial Minister agreements with the Government of Canada under which Canada undertakes to provide funding toward costs incurred by the Government of Saskatchewan associated with the federal investment for long-term care, and home and community care consistent with the Common Statement; and
Now therefore, this Agreement sets out the terms between Canada and Saskatchewan as follows:
1.0 Key principles and collaboration
The key principles and commitment to collaboration agreed to in Working Together to Improve Health Care for Canadians are outlined below.
1.1 Canada and Saskatchewan acknowledge that this Agreement will mutually respect each government's jurisdiction, and be underpinned by key principles, including:
- A shared responsibility to uphold the Canada Health Act that strengthens our public health care system;
- Principles agreed to in the Common Statement (outlined in Annex 1);
- Reconciliation with Indigenous Peoples, recognizing their right to fair and equal access to quality and culturally safe health services free from racism and discrimination anywhere in Canada, including through seamless service delivery across jurisdictions and meaningful engagement and work with Indigenous organizations and governments; and
- Equity of access for under-served groups and individuals, including those in official language minority communities.
1.2 Canada and Saskatchewan acknowledge the importance of supporting health data infrastructure, data collection and public reporting, and will work together to improve the collection, sharing and use of de-identified health information, respecting federal/provincial/territorial privacy legislation, to improve transparency on results and to help manage public health emergencies, and to ensure Canadians can access their own health information and benefit from it being shared between health workers across health settings. This includes:
- collecting and securely sharing high-quality, comparable information needed to improve services to Canadians, including disaggregated data on key common health indicators with the Canadian Institute for Health Information (CIHI);
- adopting common interoperability standards (both technical exchange and content of data), including the Shared pan-Canadian Interoperability Roadmap (outlined in Annex 2), to improve Canadians' access to their health information in a usable digital format and support the exchange and analysis of health data within and across Canada's health systems in a way that protects Canadians' privacy and ensures the ethical use of data to improve the health and lives of people;
- work to align provincial and territorial policies and legislative frameworks where necessary and appropriate to support secure patient access to health information, and stewardship of health information to support the public good, including improving care quality, patient safety, privacy protection, system governance and oversight, planning and research;
- promoting health information as a public good by working with federal-provincial-territorial Ministers of Health to review and confirm overarching principles, which would affirm Canadians' ability to access their health information and have it follow them across all points of care. The existing Health Data Charter, as outlined in the Pan-Canadian Health Data Strategy would serve as the starting point for the discussion of these principles; and
- collecting and sharing available public health data (e.g., vaccination data, testing data) with the Public Health Agency of Canada to support Canada's preparedness and response to public health events, building on commitments made as part of the Safe Restart Agreements.
1.3 Canada and Saskatchewan acknowledge they will work with other provinces and territories to streamline foreign credential recognition for internationally-educated health professionals, and to advance labour mobility, starting with multi-jurisdictional recognition of health professional licences.
1.4 Canada and Saskatchewan acknowledge a mutual intent to engage in a two-phased formal review process:
- Phase 1: This review will be done in 2026 by a joint committee of Federal, Provincial, and Territorial health and finance officials to assess results and determine next steps for bilateral agreements related to improvements to home and community care, mental health, substance use, and addiction services associated with the Common Statement and long-term care; and
- Phase 2: A formal five-year review of the healthcare plan outlined on February 7, 2023, recognizing the importance of long-term sustainability for provincial-territorial health systems. This review would consist of an assessment of both the bilateral agreements (herein) and the CHT investments (not included as part of this bilateral agreement). The review will be done by a joint committee of Federal, Provincial, and Territorial health and finance officials, commencing by March 31, 2027, and concluded by December 31, 2027, to consider results achieved thus far in the four shared health priority areas and will include:
- an assessment of progress-to-date on public reporting to Canadians using the common indicators;
- sharing of de-identified health information, and other health data commitments; and
- current and forward-looking Federal, Provincial, and Territorial investments to support this plan.
2.0 Objectives
2.1 Canada and Saskatchewan agree that, with financial support from Canada, Saskatchewan will continue to build and enhance health care systems towards achieving some or all of the objectives of:
- Improving access to home and community care services (listed in the Common Statement, attached as Annex 1); and
- Supporting workforce improvements for long-term care and standards, to keep long-term care residents safe and to improve their quality of life.
3.0 Action plan
3.1 Saskatchewan will set out in their Action Plan (attached as Annex 4) how the federal investment under this Agreement will be used, as well as details on targets and timeframes for each of the initiatives supported under the Agreement.
3.2 Saskatchewan will invest federal funding as part of the 2017 commitment for home and community care provided through this Agreement in alignment with the menu of actions listed in the Common Statement.
3.3 Saskatchewan will invest federal funding for long-term care provided through this Agreement to bolster efforts to support workforce improvements and standards by:
- Supporting activities/initiatives to achieve stability in the long-term care workforce, including through hiring and wage top-ups and/or improvements to workplace conditions (e.g., staff to patient ratios, hours of work); and
- Applying long-term care standards, with an emphasis on strengthened enforcement (e.g., enhanced inspection and enforcement capacity, quality and safety improvements to meet standards).
3.4 In developing initiatives under this Agreement, Saskatchewan agrees to implement measures that also respond to the needs of underserved and/or disadvantaged populations, including, but not limited to First Nations, Inuit and Métis, official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians), and LGBTIQA2S+.
3.5 Saskatchewan's approach to achieving home and community care and long-term care objectives is set out in their five-year Action Plan, as set out in Annex 4.
4.0 Term of agreement
4.1 This Agreement comes into effect upon the date of the last signature of the Parties and will remain in effect until March 31, 2028, unless terminated in accordance with section 12 of this Agreement. Funding provided under this Agreement will be for five years and will cover the period April 1, 2023 to March 31, 2028 ("the Term").
5.0 Financial provisions
5.1 The funding provided under this Agreement is in addition to and not in lieu of those that Canada currently provides under the CHT to support delivering health care services within the province.
5.2 Allocation to Saskatchewan
5.2.1 In this Agreement, "Fiscal Year" means the period commencing on April 1 of any calendar year and terminating on March 31 of the immediately following calendar year.
5.2.2 Canada has designated the following maximum amounts to be transferred in total to all provinces and territories under this initiative based on the allocation method outlined in subsection 5.2.3 for the Term of this Agreement.
Budget 2017 Home and Community Care
- $600 million for the Fiscal Year beginning on April 1, 2023
- $600 million for the Fiscal Year beginning on April 1, 2024
- $600 million for the Fiscal Year beginning on April 1, 2025
- $600 million for the Fiscal Year beginning on April 1, 2026
Budget 2021 Long-Term Care
- $600 million for the Fiscal Year beginning on April 1, 2023
- $600 million for the Fiscal Year beginning on April 1, 2024
- $600 million for the Fiscal Year beginning on April 1, 2025
- $600 million for the Fiscal Year beginning on April 1, 2026
- $600 million for the Fiscal Year beginning on April 1, 2027
- 5.2.3 Allocation Method
- For funds associated with Budget 2017 Home and Community Care committed by the federal government in 2017, annual funding will be allocated to provinces and territories on a per capita basis. The per capita funding for each Fiscal Year is calculated using the following formula: F x K/L, where:
- F is the annual total funding amount available under this program;
- K is the total population of Saskatchewan, as determined using the annual population estimates on July 1st from Statistics Canada; and
- L is the total population of Canada, as determined using the annual population estimates on July 1st from Statistics Canada.
- For funds associated with Budget 2021 Long-Term Care committed by the federal government in 2021, annual funding will be allocated to provinces and territories with a base amount of $1,200,000 and the remainder of the funding allocated on a per capita basis. The total amount to be paid will be calculated using the following formula: $1,200,000+(F-(N x 1,200,000)) x (K/L), where:
- F is the annual total funding amount available under this program;
- N is the number of jurisdictions (13) that will be provided the base funding of $1,200,000;
- K is the total population of Saskatchewan, as determined using the annual population estimates on July 1st from Statistics Canada; and
- L is the total population of Canada, as determined using the annual population estimates on July 1st from Statistics Canada.
- For funds associated with Budget 2017 Home and Community Care committed by the federal government in 2017, annual funding will be allocated to provinces and territories on a per capita basis. The per capita funding for each Fiscal Year is calculated using the following formula: F x K/L, where:
5.2.4 Subject to annual adjustment based on the formulas described in section 5.2.3, Saskatchewan estimated share of the amounts will be:
| Fiscal Year | Budget 2017 Home and Community Care Estimated amount to be paid to SaskatchewanTable 1 Footnote * (subject to annual adjustment) |
Budget 2021 Long-Term Care Estimated amount to be paid to SaskatchewanTable 1 Footnote * (subject to annual adjustment) |
|---|---|---|
| 2023-2024 | $18,415,000 | $19,130,000 |
| 2024-2025 | $18,415,000 | $19,130,000 |
| 2025-2026 | $18,415,000 | $19,130,000 |
| 2026-2027 | $18,415,000 | $19,130,000 |
| 2027-2028 | n/a | $19,130,000 |
|
||
5.3 Payment
5.3.1 Funding provided by Canada will be paid in semi-annual installments as follows:
- In 2023-24, the first installment will be paid within approximately 30 business days of execution of this Agreement by the Parties. The second installment will also be paid within approximately 30 business days of execution of this Agreement by the Parties, subject to 5.3.1.g.
- Starting in 2024-25, the first installment will be paid on or about April 15 of each Fiscal Year and the second installment will be paid on or about November 15 of each Fiscal Year.
- The first installment will be equal to 50% of the notional amount set out in section 5.2.4 as adjusted by section 5.2.3.
- The second installment will be equal to the balance of funding provided by Canada for the Fiscal Year as determined under sections 5.2.3 and 5.2.4.
- Canada will notify Saskatchewan prior to the first payment of each Fiscal Year, of their notional amount. The notional amount will be based on the Statistics Canada quarterly preliminary population estimates on July 1 of the preceding Fiscal Year. Prior to the second payment, Canada will notify Saskatchewan of the amount of the second installment as determined under sections 5.2.3 and 5.2.4.
- Canada shall withhold payments if Saskatchewan has failed to provide reporting in accordance with 8.1.
- Canada shall withhold the second payment in 2023-24 if Saskatchewan has failed to satisfy all reporting requirements associated with the preceding Canada – Saskatchewan Home and Community Care and Mental Health and Addictions Services Funding Agreement 2022-23, specifically to:
- continue to participate in a Federal-Provincial-Territorial process to improve reporting on and provide data to CIHI for the 6 common indicators (listed in Annex 3) to measure pan-Canadian progress on improving access to home and community care; and
- submit an annual financial statement, with attestation from the Ministry of Health's Executive Director - Financial Services Branch, of funding received the preceding Fiscal Year from Canada for home and community care under the Canada – Saskatchewan Home and Community Care and Mental Health and Addictions Services Funding Agreement 2022-23 compared against the Expenditure Plan, and noting any variances, between actual expenditures and the Expenditure Plan.
- The sum of both installments constitutes a final payment and is not subject to any further payment once the second installment has been paid.
- Payment of Canada's funding for this Agreement is subject to an annual appropriation by the Parliament of Canada for this purpose.
5.3.2 Where Saskatchewan will use cost-recovery agreements with one or more privately-owned for-profit facilities as an accountability measure and Saskatchewan has failed to put in place a cost-recovery agreement at the time it delivers funding to facilities, Canada shall deduct from the payment referred to in subsection 5.3.1(b) an amount equivalent to the amount of funding tied to the specific identified initiative in Annex 4 to be provided by Saskatchewan to those facilities with whom they do not have the required cost-recovery agreements in place.
5.4 Retaining funds
5.4.1 For Fiscal Years 2023-24 through 2026-27, upon request, Saskatchewan may retain and carry forward to the next Fiscal Year up to 10 percent of funding that is in excess of the amount of the eligible costs actually incurred in a Fiscal Year and use the amount carried forward for expenditures on eligible areas of investment. Any request to retain and carry forward an amount exceeding 10 percent will be subject to discussion and mutual agreement in writing by their designated officials, at the Assistant Deputy Minister level (herein referred to as "Designated Officials"), and is subject to monitoring and reporting to Canada on the management and spending of the funds carried forward on a quarterly basis.
5.4.2 For Fiscal Year 2027-28, Saskatchewan is not entitled to retain any amounts beyond March 31, 2028. Any amounts that remain unexpended at the end of that Fiscal Year are considered debts due to Canada and shall be repaid in accordance with section 5.5.2.
5.4.3 Any amount carried forward from one Fiscal Year to the next under this subsection is supplementary to the maximum amount payable to Saskatchewan under subsection 5.2.4 of this Agreement in the next Fiscal Year.
5.5 Repayment of overpayment
5.5.1 In the event payments made exceed the amount to which Saskatchewan is entitled under this Agreement, the amount of the excess is a debt due to Canada and, unless otherwise agreed to in writing by the Parties, Saskatchewan shall repay the amount within sixty (60) calendar days of written notice from Canada.
5.5.2 Funds not spent within the Term of the Agreement will be considered a debt due to Canada and Saskatchewan shall repay the amount within sixty (60) calendar days of written notice from Canada.
5.6 Use of funds
5.6.1 The Parties agree that funds provided under this Agreement will only be used by Saskatchewan in accordance with the initiatives outlined in Annex 4.
5.7 Eligible expenditures
5.7.1 Eligible expenditures under this Agreement are the following:
- data development and collection to support reporting;
- information technology and health information infrastructure;
- capital and operating funding;
- salaries and benefits;
- training, professional development; and
- information and communications material related to programs.
5.7.2 The Parties agree that the long-term care funding may be provided to:
- publicly-owned long-term care settings;
- privately-owned not-for-profit long-term care settings; and
- subject to section 6.0, privately-owned for-profit long-term care settings.
6.0 Accountability mechanisms for long-term care
6.1 Where federal funding is provided to privately-owned, for-profit facilities in accordance with this Agreement, Saskatchewan agrees to put in place the accountability mechanisms outlined in Annex 4.
6.2 Where Saskatchewan has cost-recovery agreements in place with one or more privately-owned for-profit facilities pursuant to subsection 6.1, Saskatchewan agrees to report on these in accordance with the requirements set out in subsection 8.1.1 and invest all funds recovered through those agreements in accordance with the terms of this Agreement and the initiatives outlined in Annex 4.
7.0 Performance measurement
7.1 Saskatchewan agrees to designate an official or official(s), for the duration of this Agreement to participate in a CIHI led Federal-Provincial-Territorial indicator process to:
- Improve reporting on common indicators to measure pan-Canadian progress on improving access to home and community care, associated with the commitment in the Common Statement;
- Work to develop new common indicators for long-term care that are mutually agreed upon; and
- Share available disaggregated data with CIHI and work with CIHI to improve availability of disaggregated data for existing and new common indicators to enable reporting on progress for underserved and/or disadvantaged populations including, but not limited to, Indigenous peoples, First Nations, Inuit, Métis, official language minority communities, rural and remote communities, children, racialized communities (including Black Canadians), and LGBTIQA2S+.
8.0 Reporting to Canadians
8.1 Funding conditions and reporting
8.1.1 By no later than October 1, in each fiscal year, with respect of the previous Fiscal Year, Saskatchewan agrees to:
- Provide data and information annually to CIHI related to the home and community care common indicators (listed in Annex 3) identified as part of the commitment made in the Common Statement, and, new common indicators on long-term care that are mutually agreed upon.
- Beginning in Fiscal Year 2024-25, report annually and publicly in an integrated manner to residents of Saskatchewan on progress made on targets outlined in Annex 4 (Action Plan).
- Beginning in Fiscal Year 2024-25, provide to Canada an annual financial statement, with attestation from the Ministry of Health's Executive Director - Financial Services Branch, of funding received the preceding Fiscal Year from Canada under this Agreement or the Previous Agreement compared against the Action Plan, and noting any variances, between actual expenditures and the Action Plan:
- The revenue section of the statement shall show the amount received from Canada under this Agreement during the Fiscal Year;
- The total amount of funding used for home and community care and long-term care;
- If applicable, the amount of any funding carried forward under section 5.4;
- If applicable, the amount of overpayment that is to be repaid to Canada under section 5.5; and
- With respect to the long-term care funding under this Agreement, where cost-recovery is used, the annual financial statement will also set out:
- The amount of the federal funding flowing to private, for-profit facilities; and
- The estimated amount of funds to be recovered under cost-recovery agreements, where applicable, and the priority areas where those funds will be reinvested.
8.1.2 Saskatchewan will provide quarterly reporting to Canada on the management and spending of the funds retained to the next Fiscal Year.
8.2 Audit
8.2.1 Saskatchewan will ensure that expenditure information presented in the annual financial statement is, in accordance with Saskatchewan's standard accounting practices, complete and accurate.
8.3 Evaluation
8.3.1 Responsibility for evaluation of programs rests with Saskatchewan in accordance with its own evaluation policies and practices.
9.0 Communications
9.1 The Parties agree on the importance of communicating with citizens about the objectives of this Agreement in an open, transparent, effective and proactive manner through appropriate public information activities.
9.2 Each Party will receive the appropriate credit and visibility when investments financed through funds granted under this Agreement are announced to the public.
9.3 In the spirit of transparency and open government, Canada will make this Agreement, including any amendments, publicly available on a Government of Canada website.
9.4 Saskatchewan will make publicly available, clearly identified on a Government of Saskatchewan website, this Agreement, including any amendments.
9.5 Canada, with prior notice to Saskatchewan, may incorporate all or any part of the data and information in 8.1, or any part of evaluation and audit reports made public by Saskatchewan into any report that Canada may prepare for its own purposes, including any reports to the Parliament of Canada or reports that may be made public.
9.6 Canada reserves the right to conduct public communications, announcements, events, outreach and promotional activities about the Common Statement and this Agreement. Canada agrees to give Saskatchewan 10 days advance notice and advance copies of public communications related to the Common Statement, this Agreement, and results of the investments of this Agreement.
9.7 Saskatchewan reserves the right to conduct public communications, announcements, events, outreach and promotional activities about the Common Statement and this Agreement. Saskatchewan agrees to give Canada 10 days advance notice and advance copies of public communications related to the Common Statement, this Agreement, and results of the investments of this Agreement.
9.8 Canada and Saskatchewan agree to participate in a joint announcement upon signing of this Agreement.
9.9 Canada and Saskatchewan agree to work together to identify mutually agreeable opportunities for joint announcements relating to programs funded under this Agreement.
10.0 Dispute resolution
10.1 The Parties are committed to working together and avoiding disputes through government-to-government information exchange, advance notice, early consultation, and discussion, clarification, and resolution of issues, as they arise.
10.2 If at any time a Party is of the opinion that the other Party has failed to comply with any of its obligations or undertakings under this Agreement or is in breach of any term or condition of the Agreement, that Party may notify the other Party in writing of the failure or breach. Upon such notice, the Parties will endeavour to resolve the issue in dispute bilaterally through their Designated Officials.
10.3 If a dispute cannot be resolved by Designated Officials, then the dispute will be referred to the Deputy Ministers of Canada and Saskatchewan responsible for health, and if it cannot be resolved by them, then the federal Minister(s) and the provincial Minister(s) shall endeavour to resolve the dispute.
11.0 Amendments to the agreement
11.1 The main text of this Agreement may be amended at any time by mutual consent of the Parties. Any amendments shall be in writing and signed, in the case of Canada, by the federal Minister(s), and in the case of Saskatchewan, by the provincial Minister(s).
11.2 Annex 4 may be amended at any time by mutual consent of the Parties. Any amendments to Annex 4 shall be in writing and signed by each Party's Designated Official.
12.0 Termination
12.1 Either Party may terminate this Agreement at any time if the terms are not respected by giving at least 6 months written notice of intention to terminate.
12.2 As of the effective date of termination of this Agreement, Canada shall have no obligation to make any further payments.
12.3 Sections 1.0 and 9.0 of this Agreement survive for the period of the 10-year Working Together to Improve Health Care for Canadians plan.
12.4 Sections 5.4 and 8.0 of this Agreement survive the termination or expiration of this Agreement until reporting obligations are completed.
13.0 Notice
13.1 Any notice, information, or document provided for under this Agreement will be effectively given if delivered or sent by letter, email, postage or other charges prepaid. Any communication that is delivered will be deemed to have been received on delivery; and, except in periods of postal disruption, any communication mailed by post will be deemed to have been received eight calendar days after being mailed.
The address of the Designated Official for Canada shall be:
Assistant Deputy Minister, Strategic Policy Branch
Health Canada
70 Colombine Driveway
Brooke Claxton Building
Ottawa, Ontario
K1A 0K9
Email: jocelyne.voisin@hc-sc.gc.ca
Or any replacement email provided by the federal Minister(s)
The address of the Designated Official for Saskatchewan shall be:
Assistant Deputy Minister
Ministry of Health
3475 Albert Street
T.C. Douglas Building
Regina, SK
S4S 6X6
Email: Norman.O'Neill@health.gov.sk.ca
Or any replacement e-mail provided by the provincial Minister.
14.0 General
14.1 This Agreement, including Annexes, comprises the entire Agreement entered into by the Parties.
14.2 This Agreement shall be governed by and interpreted in accordance with the laws of Canada and Saskatchewan.
14.3 No member of the House of Commons or of the Senate of Canada or of the Legislature of Saskatchewan shall be admitted to any share or part of this Agreement, or to any benefit arising therefrom.
14.4 If for any reason a provision of this Agreement, that is not a fundamental term, is found by a court of competent jurisdiction to be or to have become invalid or unenforceable, in whole or in part, it will be severed and deleted from this Agreement, but all the other provisions of this Agreement will continue to be valid and enforceable.
14.5 This Agreement may be executed in counterparts, in which case (i) the Parties have caused this Agreement to be duly signed by the undersigned authorized representatives in separate signature pages in accordance with the following signature process, which together shall constitute one agreement, and (ii) the Parties agree that facsimile signature(s) and signature(s) transmitted by PDF shall be treated as original signature(s). Electronic signature(s) may be accepted as originals so long as the source of the transmission can be reasonably connected to the signatory.
In witness whereof the Parties have executed this Agreement through duly authorized representatives.
Signed on behalf of Canada by the Minister of Health
The Honourable Mark Holland, Minister of Health
In witness whereof the Parties have executed this Agreement through duly authorized representatives.
Signed on behalf of Saskatchewan by the Minister of Mental Health and Addictions, Seniors and Rural and Remote Health
The Honourable Tim McLeod, Minister of Mental Health and Addictions, Seniors and Rural and Remote Health
Annex 1 – Common statement of principles on shared health priorities
Annex 1 – Common Statement of Principles on Shared Health Priorities
Common Statement of Principles on Shared Health Priorities
Annex 2 – Shared pan-Canadian interoperability roadmap
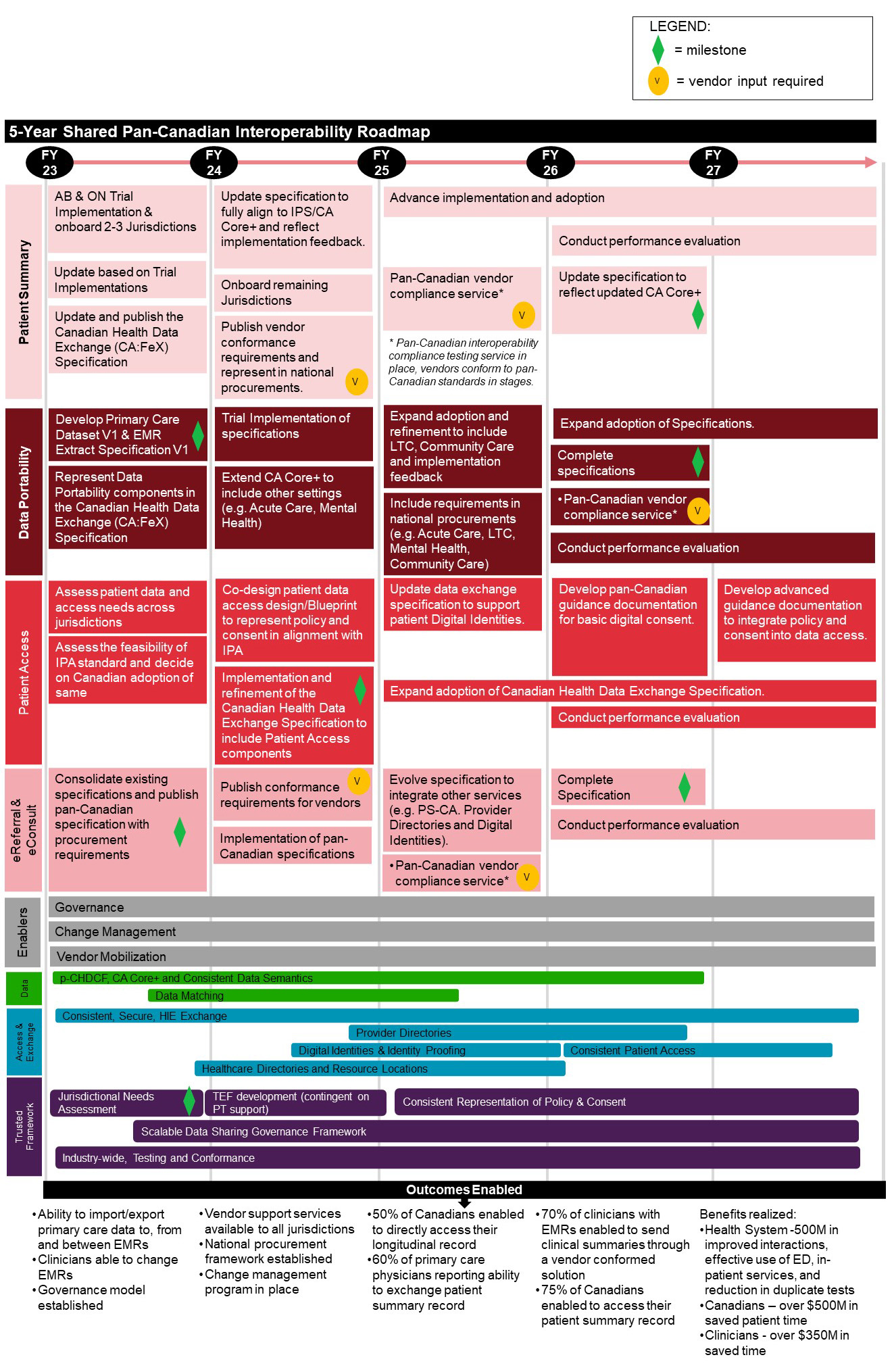
Figure 1: Text description
5-Year Shared Pan-Canadian Interoperability Roadmap
The Roadmap outlines 8 categories of activities planned for fiscal years 2023 to 2027, followed by anticipated outcomes enabled. Notes are also included throughout to highlight a "milestone", where "vendor input is required", and/or when an activity is "continued" across multiple fiscal years.
Patient Summary
- Fiscal Year 2023
- Alberta & Ontario Trial Implementation & onboard 2-3 Jurisdictions
- Update based on Trial Implementations
- Update and publish the Canadian Health Data Exchange (CA:FeX) Specification
- Fiscal Year 2024
- Update specification to fully align to IPS/CA Core+ and reflect implementation feedback
- Onboard remaining jurisdictions
- Publish vendor conformance requirements and represent in national procurements [vendor input required]
- Fiscal Year 2025
- Advance implementation and adoption
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Fiscal Year 2026
- Advance implementation and adoption [continued]
- Conduct performance evaluation
- Update specification to reflect updated CA Core+ [milestone]
- Fiscal Year 2027
- Advance implementation and adoption [continued]
- Conduct performance evaluation [continued]
Data Portability
- Fiscal Year 2023
- Develop Primary Care Dataset V1 & EMR Extract Specification V1 [milestone]
- Represent Data Portability components in the Canadian Health Data Exchange (CA:FeX) Specification
- Fiscal Year 2024
- Trial Implementation of specifications
- Extend CA Core+ to include other settings (e.g. Acute Care, Mental Health)
- Fiscal Year 2025
- Expand adoption and refinement to include LTC, Community Care and implementation feedback
- Include requirements in national procurements (e.g. Acute Care, LTC, Mental Health, Community Care)
- Fiscal Year 2026
- Expand adoption of Specifications
- Complete specifications [milestone]
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Conduct performance evaluation
- Fiscal Year 2027
- Expand adoption of Specifications [continued]
- Conduct performance evaluation [continued]
Patient Access
- Fiscal Year 2023
- Assess patient data and access needs across jurisdictions
- Assess the feasibility of IPA standard and decide on Canadian adoption of same
- Fiscal Year 2024
- Co-design patient data access design/Blueprint to represent policy and consent in alignment with IPA
- Implementation and refinement of the Canadian Health Data Exchange Specification to include Patient Access components [milestone]
- Fiscal Year 2025
- Update data exchange specification to support patient Digital Identities
- Expand adoption of Canadian Health Data Exchange Specification
- Fiscal Year 2026
- Develop pan-Canadian guidance documentation for basic digital consent
- Expand adoption of Canadian Health Data Exchange Specification [continued]
- Conduct performance evaluation
- Fiscal Year 2027
- Develop advanced guidance documentation to integrate policy and consent into data access
- Expand adoption of Canadian Health Data Exchange Specification [continued]
- Conduct performance evaluation [continued]
eReferral & eConsult
- Fiscal Year 2023
- Consolidate existing specifications and publish pan-Canadian specification with procurement requirements [milestone]
- Fiscal Year 2024
- Publish conformance requirements for vendors [vendor input required]
- Implementation of pan-Canadian specifications
- Fiscal Year 2025
- Evolve specification to integrate other services (e.g. PS-CA. Provider Directories and Digital Identities)
- Pan-Canadian vendor compliance service *(Pan-Canadian interoperability compliance testing service in place, vendors conform to pan-Canadian standards in stages.) [vendor input required]
- Fiscal Year 2026
- Complete Specification [milestone]
- Conduct performance evaluation [continued]
- Fiscal Year 2027
- Conduct performance evaluation [continued]
Enablers
- Fiscal Years 2023 to 2027
- Governance
- Change Management
- Vendor Mobilization
Data
- Fiscal Year 2023
- p-CHDCF, CA Core+ and Consistent Data Semantics
- Data Matching
- Fiscal Year 2024
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Data Matching [continued]
- Fiscal Year 2025
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Data Matching [continued]
- Fiscal Year 2026
- p-CHDCF, CA Core+ and Consistent Data Semantics [continued]
- Fiscal Year 2027
- N/A
Access & Exchange
- Fiscal Year 2023
- Consistent, Secure, HIE Exchange
- Healthcare Directories and Resource Locations
- Fiscal Year 2024
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories
- Digital Identities & Identity Proofing
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2025
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories [continued]
- Digital Identities & Identity Proofing [continued]
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2026
- Consistent, Secure, HIE Exchange [continued]
- Provider Directories [continued]
- Digital Identities & Identity Proofing [continued]
- Consistent Patient Access
- Healthcare Directories and Resource Locations [continued]
- Fiscal Year 2027
- Consistent, Secure, HIE Exchange [continued]
- Consistent Patient Access [continued]
Trusted Framework
- Fiscal Year 2023
- Jurisdictional Needs Assessment [milestone]
- Scalable Data Sharing Governance Framework
- Industry-wide, Testing and Conformance
- Fiscal Year 2024
- TEF development (contingent on PT support)
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2025
- Consistent Representation of Policy & Consent
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2026
- Consistent Representation of Policy & Consent [continued]
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
- Fiscal Year 2027
- Consistent Representation of Policy & Consent [continued]
- Scalable Data Sharing Governance Framework [continued]
- Industry-wide, Testing and Conformance [continued]
Outcomes
- Ability to import/export primary care data to, from and between EMRs
- Clinicians able to change EMRs
- Governance model established
- Vendor support services available to all jurisdictions
- National procurement framework established
- Change management program in place
- 50% of Canadians enabled to directly access their longitudinal record
- 60% of primary care physicians reporting ability to exchange patient summary record
- 70% of clinicians with EMRs enabled to send clinical summaries through a vendor conformed solution
- 75% of Canadians enabled to access their patient summary record
- Benefits realized:
- Health System – $500M in improved interactions, effective use of ED, in-patient services, an reduction in duplicate tests
- Canadians – over $500M in saved patient time
- Clinicians – over $350M in saved time
Annex 3 – Indicators: Access to home and community care
Indicator
- Death at home or in community (Percentage)
- Home care services helped the recipient stay at home (Percentage)
- Wait times for home care services (Median, in days)
- Caregiver distress (Percentage)
- New long-term care residents who potentially could have been cared for at home (Percentage)
- Hospital stay extended until home care services or supports ready (Median, in days)
Annex 4 – Action plan
Introduction
Saskatchewan's patient first approach recognizes the importance of meeting the needs of the individual. The priority of the provincial health system is to provide high quality health care for all its patients and families including, but not limited to, LGBTIQA2S+, rural and remote communities, official language minority communities, and First Nations and Métis populations. This means being sensitive to, and responding where possible, to the specific needs and challenges of different population groups.
Home and Community Care
Saskatchewan strives to keep citizens healthy and provide timely, appropriate health care to citizens in locations as close to home as possible. In most instances, citizens prefer to receive their health care at home, or in a community setting, and to avoid unnecessary acute care visits.
Efforts to preserve citizens' health, with preventative, robust primary health care delivered in the home or in the community are the foundations in an upstream approach to addressing hospital capacity issues.
Over the past decade, Saskatchewan has invested in programs to address home and community service gaps and strengthen primary home care services, including several pilot initiatives that aim to provide intermediate care for complex patients: Home First/Quick Response, Intermediate Care (formerly Seniors' House Calls), Community Paramedicine, and Connecting to Care.
Multidisciplinary home care teams currently deliver coordinated, comprehensive services in various settings that make the best use of global funding provided to the Saskatchewan Health Authority by effectively and efficiently serving those with the greatest needs. Despite efforts to offer equitable services across the province, there are ongoing challenges due to the vast geographic areas served.
Additionally, given Saskatchewan's aging population, there are challenges in providing home care services to clients with complex needs, and to those with needs that extend to after-hours and on weekends. These factors contribute to avoidable transfers into acute care settings and patient and caregiver distress.
For residents in and around Regina, Saskatoon, Prince Albert and North Battleford, Home First/Quick Response provides enhanced home care for intensive short-term needs to sustain seniors in their homes, facilitate appropriate discharge from acute care to community settings, and engage service providers to prevent admission to long term care facilities. Community Paramedicine uses Advanced Care Paramedics to provide medical care, treatment, and support to patients in their homes, including after-hours services, to stabilize patients, and eliminate the need to transfer to an acute care facility. Intermediate Care programs in Regina and Saskatoon provide vulnerable residents (often seniors) with complex medical needs with home- based physician or nurse practitioner visits and health care services using a team-based model. Connecting to Care, or Hotspotting, provides outreach and inter-disciplinary intensive case management services to Regina and Saskatoon clients with complex health needs who require a more individualized approach.
The Saskatchewan Health Authority has established health care networks to organize and integrate primary health services in the community, build capacity for community-based comprehensive care, and prevent overreliance on the hospital-based system. Networks contain interdisciplinary care teams intended to wrap services around clients to preserve health, promote independent living, prevent disease, and promote self-management of existing health conditions.
Based on a review of the evidence, provincial modelling, and outcomes from community care pilot programs, Saskatchewan is focusing on those areas where the predicted impact is greatest for shifting emphasis away from emergency- and hospital-based care and improving the connection and flow of patients into other care settings. Saskatchewan's Connected Care Strategy includes home, community, primary care, palliative, and acute care, and is focused on providing safe, seamless care for patients as they move from one care setting to another and ensuring that patients receive care in the setting that best matches their needs.
To date, the federal investment into the home, community, primary health care, and palliative elements of the Connected Care Strategy have complemented Saskatchewan's investment into hospital Accountable Care Units as well as build community capacity for patients whose needs can be better met outside of a hospital environment. Continued support will foster high quality transitions between hospitals and community-based services, including improved care coordination among team members and teams across care settings, improved medication safety, post-discharge symptom management, and outpatient follow-up and advance care planning.
Saskatchewan's population continues to show growth (an increase of 5% between October 2018 and October 2023Footnote 1) but the seniors population aged 65 years and older is growing at almost twice the rate of the general populationFootnote 2 and is predicted to almost double over the next 20 years.
The Government of Saskatchewan has emphasized the strategic importance of this work in ensuring Saskatchewan patients have sustainable access to the care they need when and where they need it.
Long-Term Care
Long-term care (LTC) is the provision of 24-hour, supervised institutional LTC services to individuals with heavy care needs that cannot be appropriately met through home- based/community services. Services may include day programs, adult night programs, respite, rehabilitative, convalescent and palliative care.
Saskatchewan has over 8,600 LTC beds in 151 LTC homes. All of the homes are operated by either the provincial health authority or non-profit organizations.
All LTC homes are required by legislation to comply with the Program Guidelines for Special Care Homes which are Saskatchewan's provincial standards for long term care. These guidelines set standards and policies for all facets of care and operations within care homes including administration and leadership, fees and charges, care, support services, safety, staffing and quality/reporting. They are substantially similar and, in some instances, completely aligned with national standards and those in other provinces and territories.
LTC homes are routinely inspected by the Ministry of Health to assess compliance with these provincial guidelines and best practices. Homes are required to remediate any deficiencies identified through the inspection and report remediation progress to the Ministry. In some cases, re-inspection occurs to ensure compliance.
In Saskatchewan, the cost of publicly funded LTC is heavily subsidized through funding provided by the Ministry of Health. Residents pay a monthly resident charge commensurate with their income. Those with limited income pay the lowest resident charge which is currently about $1,300 per month. This resident charge is provincially standardized which means that resident would pay the same charge regardless of the home in which they reside or the amount of care required.
Home and Community Care
The home and community care funding stream from the 2017 bilateral agreement, which is now part of the Aging with Dignity Action Plan, will continue to support community health centres and community health teams, and palliative care as detailed further.
Community Health Centres and Community Health Teams
In 2017-18 federal funding helped support a multi-year strategy to improve patient access to appropriate health care services in the community by shifting the delivery of care for non- emergent conditions away from hospitals. A key feature was the establishment of Community Health Centres in high-needs neighbourhoods in Regina and Saskatoon, bringing together teams of health providers to deliver both on-site and community/home-based services, with connections to broader primary care networks.
Both Regina and Saskatoon identified neighbourhoods with large senior populations with high prevalence of complex chronic conditions and high rates of hospital utilization.
In 2018-19, Regina established a Community Health Centre in its Central network which serves a population that is predominately low income and high needs. Approximately 16% are registered as Indigenous; this figure excludes non-status Indigenous and MétisFootnote 3. Similarly, Saskatoon introduced a multi-disciplinary community health team in 2018-19 that serves residents in six core neighbourhoods where residents are also predominately low-income and high needs. On average, 26% of residents of these neighbourhoods self-identify as IndigenousFootnote 4.
These community health centres operate with interdisciplinary teams, including nurses, nurse practitioners, pharmacists, physiotherapists, occupational, and mental health therapists, care assistants, case managers, navigation coordinators, health educators, social workers, addictions counselors, community paramedics, dieticians, Indigenous outreach cultural support workers, and ceremonial and Elder supports.
Additionally, Community Health Centres serve as physical hubs for co-located community health teams that provide health services and home visits in targeted communities and neighbourhoods. These Centres and teams are co-designed with family physicians and patients and families to meet the specific health care needs of the unique and diverse patient populations they serve.
Their focus is on improving and integrating access to primary health care and home- and community-based services as well as supporting a shift away from acute care, wherever it is appropriate to do so.
Additionally, Intermediate Care Services are provided to connect residents of certain LTC homes in Regina with care and services to prevent hospital admissions or readmissions.
Maturity of Health Networks and Connections to Patient Medical Homes
Announced in the 2023-24 budget, Saskatchewan invested in planning for strategic renewal in the area of primary care, hiring a consultant and forming a Provincial Oversight Committee to bring forward recommendations. One preliminary recommendation is to foster Patient Medical Homes (PMH) led by family physicians or nurse practitioners, and connect all citizens to such a "home" where they receive the majority of their primary care; and to integrate these PMHs into Health Networks operated by the Saskatchewan Health Authority.Footnote 5 These networks connect teams of health-care professionals and community partners to better meet the needs of the people they serve. Patients can be referred for the most appropriate care to meet their needs, whether it is delivered by a mental health counsellor, social worker, dietitian, physiotherapist, occupational therapist, pharmacist, or any other allied health professional.
Allied health professional care teams and support staff within each Health Network will provide supports to patients of the PMHs within the Network, ensuring interdisciplinary team huddles, case conferencing, shared care planning, patient rounding (includes patient in-person or on the phone), and warm handoffs between team members, and outreach and home care staff members, and hospital teams when patients are going into or returning home from hospital.
Complex patients will have longer appointments and access to members of the team to assist with preventative health and self-care. Outreach teams will supplement and integrate with primary home care services to provide enhanced home-based supports (e.g., rehabilitation, mental health, nutrition, medication management) to complex clients who require an additional level of support, thus reducing the burden on caregivers.
While focused work on maturing Health Networks Community Health Centres and teams will be supported by federal funds, this work merges with steps being taken across the province in urban and rural locations towards increased access to primary health care, team-based care, and improved transitions between hospital and community.
Saskatchewan's emergency, acute, and community health care systems often function independently of one another with no or few structured processes or accountabilities for transitions between care teams. This leaves patients and families to bridge the gaps and navigate the complex system on their own.
These investments align with the agreed upon A Common Statement of Principles on Shared Health Priorities by:
- spreading and scaling evidence-based models of home and community care that are more integrated and connected with primary health care;
- increasing support for caregivers; and,
- enhancing home care infrastructure, such as digital connectivity, remote monitoring, technology, and facilities for community-based service delivery.
Over the next four years, federal investment will contribute to:
Community Health Centres and Health Networks
- Expanding Community Health Centres as physical hubs for interdisciplinary community health teams (e.g. nurses, pharmacists, mental health therapists, community paramedics, etc.) that provide services and home visits in targeted indigenous, low income, and high needs communities and neighbourhoods;
- Maturing Health Networks and building interdisciplinary teams across the province – these networks will include physicians, nurses, therapists, social workers, and other providers, to deliver integrated care through clinic-based and home-based outreach services;
- Community Health Centres and Health Networks will be strategically located and tailor their services to meet the unique needs of each neighbourhood – this could include programs and services to address chronic care needs and other basic health services, including the expansion of operating hours, after-hours on-call and weekend coverage.
Intermediate care services for complex patients
- Outreach services (e.g., community paramedicine and home visits) for patients who are unable to get out of their homes (which may include individuals residing in long-term care homes) to seek services in traditional clinic settings.
Patient Medical Home Model Pilot
- Advancing the Patient Medical Home Model pilot, initiated in 2023, that sees community-based primary care providers create capacity to see more patients by utilizing a team-based approach to care that involves other supportive professionals (dietician, registered nurse, mental health counsellor).
Refugee Health Care Collaborative
- Supporting the Saskatoon Community Clinic (SCC) to operate the Refugee Engagement and Community Health (REACH) program. This program provides primary care to a cohort of patients with complex needs who would otherwise struggle to access timely care.
Palliative Care
In Saskatchewan, palliative care services continue to be provided through a variety of settings that include inpatient facilities, special-care homes, hospice, and community-based home care. The delivery of palliative care is focused on quality of life, maintenance of human dignity, and comfort for the terminally ill individual and their family, rather than cure.
Service provision can vary amongst communities. In urban centres, palliative care services are typically provided by palliative care teams and, in rural areas, palliative care services are provided by primary health care teams that include nurses and various other health care providers.
In September 2016, a provincial consultation reviewed the current state of palliative care services across the province and identified potential areas for improvement. Participants included representatives from the Ministry of Health, Saskatchewan Cancer Agency, former Regional Health Authorities, and community-based organizations, such as the Canadian Cancer Society, Sanctum, and AIDS Program South Saskatchewan. Three physicians who specialize in palliative care and four patient and family advocates were also in attendance.
Several improvement ideas emerged such as the enhanced use of nurse practitioners and paramedics, development of provincial palliative care standards, and the implementation of Learning Essential Approaches to Palliative Care and End-of-Life Care (LEAP) training. Following the consultation, a Palliative Care Working Group was established and developed recommendations to guide palliative care improvement work.
The palliative care enhancements were developed to align with these recommendations and A Common Statement of Principles on Shared Health Priorities by enhancing access to palliative and end-of-life care at home or in other facilities. As well, palliative care enhancements are in full alignment with the goals of the Connected Care Strategy to shift emphasis towards community-based care and ensure patients receive the care they need in the setting that best matches their needs. These funds will assist in further enhancing Saskatchewan's Palliative Care Program.
These enhancements continue to provide timely, appropriate, efficient and culturally sensitive palliative care services while taking into consideration the diverse needs of Saskatchewan people, including Indigenous populations while continuing efforts to accommodate the client's end-of-life care delivery preferences. 2020-21 data indicates that approximately 50.8% of deaths in Saskatchewan occurred at home or in the community (Canadian Institute for Health Information and Canadian Vital Statistics Death Database) compared to the Canadian average of 53.0%. Additional improvements in service delivery will benefit Saskatchewan citizens by ensuring they can die at home in the presence of loved ones when desired.
Key elements to be supported by the federal investment include:
Training for multidisciplinary teams
- Training for physicians, registered nurses (RNs), and nurse practitioners (NPs), continuing care assistants, and paramedics in end-of-life care.
Staffing for multidisciplinary teams
- Palliative Care Coordinator (RN) positions that support the multidisciplinary team with assessments, care planning, coordination of services, and provide clinical recommendations on pain and symptom management;
- Palliative care physicians who provide clinical recommendations on pain and symptom management and support a decrease in alternate level of care bed days during the final six weeks of life by managing patients' care outside the hospital setting; and,
- Nurse Practitioner (NP) positions which will lead integrated palliative care service teams in rural and remote areas to increase access to palliative care for patients who are typically underserved.
Delivery of palliative care services
- Operational funding for facilities providing hospice palliative care.
These investments align with the agreed upon A Common Statement of Principles on Shared Health Priorities by:
- spreading and scaling evidence-based models of home and community care that are more integrated and connected with primary health care;
- enhancing access to palliative and end-of-life care at home or in hospices; and,
- increasing support for caregivers.
| Home and community care Initiatives | 2023-24 | 2024-25 | 2025-26 | 2026-27 | Total |
|---|---|---|---|---|---|
| Community Health Centres (CHCs), Teams and Services | |||||
| Operations, including Community Health Centres and Health Networks | $8.0M | $8.0M | $8.0M | $8.0M | $32.0M |
| Community Outreach Teams | $2.5M | $2.5M | $2.5M | $2.5M | $10.0M |
| Patient Medical Home Model Pilot | $1.0M | $1.0M | $1.0M | $1.0M | $4.0M |
| Community Paramedicine | $.9M | $.9M | $.9M | $.9M | $3.6M |
| Intermediate Care Services in LTC | $.3M | $.3M | $.3M | $.3M | $1.2M |
| Refugee Health Care Collaborative | $.7M | $.7M | $.7M | $.7M | $2.8M |
| Sub-total | $13.4M | $13.4M | $13.4M | $13.4M | $53.7M |
| Palliative Care | |||||
| Training for multi-disciplinary teams | $.3M | $.3M | $.3M | $.3M | $1.2M |
| Positions for multi-disciplinary teams | $1.9M | $1.9M | $1.9M | $1.9M | $7.7M |
| Operations, including hospice facilities | $2.8M | $2.8M | $2.8M | $2.8M | $11.2M |
| Sub-total | $5.0M | $5.0M | $5.0M | $5.0M | $20.0M |
| Total | $18.4MTable a5.t1 Footnote * | $18.4M | $18.4M | $18.4M | $73.7MTable a5.t1 Footnote * |
|
|||||
Home and Community Care – Jurisdictional Performance Measures
Saskatchewan is responsible for the development of, and reporting on, performance measures related to the provincial health care system. On an annual basis the Ministry of Health is required to release a public business plan for the health system which includes specific performance measures; the measures are then reported in the Ministry's annual report.Footnote 6
For the purposes of the Aging with Dignity bilateral agreement, the following have been identified as jurisdictional specific performance measures.
Health Networks and Connecting Patient Medical Homes Performance Measure
- Reduce the rate of ambulatory care sensitive condition hospitalizations.
Baseline
- In 2022-2023 there were 417 per 100,000.
Target
- By March 31, 2026, 408 per 100,000, a 5% reduction.
Palliative Care Performance Measure
- Increase the number of home care services accessed by palliative care patients.
Baseline
- In 2022-23 there were 92,071 home care service units provided.
Target
- By March 31, 2027, increase the number of home care service units by 5%
Long-Term Care
Saskatchewan continues to support people remaining in their own homes and outside of LTC whenever possible. While the need for LTC will remain, our vision going forward is to ensure Saskatchewan has the community supports necessary to meet the evolving needs of the seniors of the future through improved home care or care in other non-traditional settings.
This shifting societal desire is not exclusively related to the impact of the COVID-19 pandemic in LTC. Since the pandemic, Saskatchewan has made efforts to improve LTC through improved ventilation, improved training in infection control and use of personal protective equipment and isolation techniques. Cleaning protocols, outbreak preparedness and outbreak management are all improving through regular quality and safety improvement processes.
The state of infrastructure of the LTC homes in the province varies widely. Saskatchewan is currently in the process of replacing many aged facilities and making improvements in others.
Saskatchewan has several means to assess the quality and safety of care in its LTC homes. Examples include:
- Satisfaction surveys are conducted on a regular basis with both residents of LTC and their families/supporters. Our most recent survey, conducted post-pandemic, demonstrates improvement in satisfaction for both residents and families. Residents overall satisfaction increased from 85% to 89% and families from 83% to 88%.
- Saskatchewan has established a process for the inspection of all publicly funded LTC homes in the province. The inspections assess the home's compliance with standards in the areas of care and other resident-centred work within the home. They assess the home's compliance with the province's Program Guidelines for Special Care Homes (Program Guidelines) and any related regulations and policies. Homes are required to remediate any deficiencies found in an inspection. All remediation work is led by the home, with remediation reports submitted to the Ministry through the Saskatchewan Health Authority.
- Residents of LTC are assessed quarterly to ensure their care plans are updated to reflect evolving needs. Those with rapidly changing needs are assessed more frequently. This is a requirement within the Program Guidelines for Special Care Homes. Data from the quarterly assessments informs a series of quality indicators (QI) measured and supported through the Canadian Institute for Health Information (CIHI). Overall Saskatchewan on those QIs monitored performs better than the national average in falls in the last 30 days and newly occurring pressure ulcers. Saskatchewan does not perform as well as the national average on daily physical restraints and antipsychotics without a diagnosis of psychosis.
- All LTC homes in Saskatchewan participate in Accreditation Canada's Qmentum LTC accreditation program. The LTC sector in Saskatchewan was most recently assessed in Fall 2022.
- Saskatchewan intends to use the LTC portion of the federal funding to support LTC homes in meeting provincial standards and the Program Guidelines for Special Care Homes, adding front line care staff to enhance quality and provision of care and resources targeted to the inspection of LTC homes.
Priority Area #1 – Improving Care
1. Enhancing Staff and Staff Training
Funds will support LTC homes to increase staff and other supports to enhance their ability to comply with Program Guidelines, best practice, standards of care and to meet the evolving complexity of care in LTC.
- This initiative will add front line care providers to improve access to care by individual residents. Most of these providers will be continuing care assistants (CCA). All LTC homes must ensure their care assistants (often called personal services workers in other provinces) are trained as continuing care assistants or that they become trained within two years of being hired. The educational program for this occupation is Saskatchewan based, delivered through our community college sector and its curriculum is regularly updated to meet the evolving needs of Saskatchewan LTC residents.
- While many of the new positions will be CCAs, depending on each LTC home's needs, some homes may choose to add registered nurse/registered psychiatric nurse, licensed practical nurse or nurse practitioner positions while others may have a desire for enhanced recreation therapy staff or environmental services personnel. All LTC team members contribute to the well-being and safety of LTC residents. We respect the value of all team members and support homes should non-nursing positions be required to meet resident need.
- Funds may also be used by LTC homes to enhance training and skill development to ensure staff have the skills and abilities to meet the complexity of care being seen in LTC.
2. Supporting Improvement
Federal funding will be used to support non-profit third party operated homes in order to bring these homes more in alignment with homes operated by the Saskatchewan Health Authority. These third parties are independent entities with independent boards. These homes will determine how best to allocate the funds, for example targeting specific providers, based on assessed needs of the residents. It is expected that there will be increases in the number of CCAs, nurses and recreation therapy services.
Priority Area #2 – Improving Inspections and Monitoring Compliance With Long-Term Care Standards
1. Enhancing Inspections and Follow-up
The Ministry conducts regular inspections of LTC homes to assess compliance with provincial standards and best practice. Homes are routinely inspected on a 3-year cycle with additional inspections within that period as required to ensure standards are met. In addition to on-site inspections, Ministry staff follow-up with homes as they remediate any deficiencies identified through the inspection process. This requires active engagement of Ministry staff through the Saskatchewan Health Authority to monitor progress, advise on processes and expectations, assess remediation efforts and verify when remediation is complete.
These federal funds will allow the Ministry to hire staff to support the inspection process including conducting inspections and monitoring follow-up and remediation. This will allow the Ministry to enhance the frequency of inspections and follow-up, specifically in those LTC homes where deficiencies are identified. The exact number of staff to be hired will be determined as further work is done on assessing need and existing capacity.
Inspecting publicly funded LTC homes provides the Government with a further indicator of LTC system performance. Currently, 58 (or 36%) of the LTC homes have been inspected over the last two years. Homes are required to remediate any deficiencies identified in an inspection. All remediation work is led by the home and the Saskatchewan Health Authority, with remediation reports being provided to the Ministry via the health authority.
| Long-Term Care Initiative | 2023-24 | 2024-25 | 2025-26 | 2026-27 | 2027-28 | Total |
|---|---|---|---|---|---|---|
| Priority Area 1 – Improving Care | ||||||
| Initiative 1 - Enhancing Staff and Staff TrainingTable a5.t2 Footnote * | $17.6M | $17.6M | $17.6M | $17.6M | $17.6M | $88.0M |
| Initiative 2 – Supporting Improvement | $1.0M | $1.0M | $1.0M | $1.0M | $1.0M | $5.0M |
| Subtotal | $18.6M | $18.6M | $18.6M | $18.6M | $18.6M | $93.0M |
| Priority Area 2 – Improving Inspections and Monitoring Compliance | ||||||
| Initiative 1 – Inspection Staff (salaries, benefits, inspection travel) | $.5M | $.5M | $.5M | $.5M | $.5M | $2.5M |
| Total | $19.1MTable a5.t2 Footnote * | $19.1M | $19.1M | $19.1M | $19.1M | $95.7MTable a5.t2 Footnote ** |
|
||||||
Accountability Measures in Place for Funds Directed to Private For-Profit Facilities
- Given there are currently no private for profit-homes operating in Saskatchewan, there will be no additional measures.
- Should Saskatchewan engage with the for-profit sector in the future, Saskatchewan will develop a cost-sharing model where any funding to be provided would be targeted and directed, through any contractual arrangement, to front line care providers.
Measuring and reporting on results
- Saskatchewan will continue to work with CIHI on the collection and reporting of LTC quality indicators and other information related to LTC.
- Saskatchewan will collaborate with CIHI and, as applicable, through its Shared Heath Indicators Council the development of new LTC indicators.
Long-Term Care – Jurisdictional Performance Measures
Saskatchewan is responsible for the development of, and reporting on, performance measures related to the provincial health care system. On an annual basis the Ministry of Health is required to release a public business plan for the health system which includes specific performance measures; the measures are then reported in the Ministry's annual report.Footnote 7
For the purposes of the Aging with Dignity bilateral agreement, the following have been identified as jurisdictional specific performance measures.
Improving Care in Long-Term Care (LTC) Facilities Performance Measure
- Increase the number of continuing care Aides (CCA) working in LTC homes.
Baseline
- In 2022-2023 there were 5,089 paid Full-Time Equivalents (FTEs).
Target
- By March 31, 2028, increase the number of paid FTEs by 100.
Inspections and Monitoring Compliance Performance Measure
- Increase the annual number of regularly scheduled inspections in LTC homes.
Baseline
- In 2022-23 there were 36 inspections done.
Target
- By March 31, 2028, increase the number of inspections to 50 per year.
| Initiative | Overall Funding Allocation | Total | ||||
|---|---|---|---|---|---|---|
| 2023-24 | 2024-25 | 2025-26 | 2026-27 | 2027-28 | ||
| Home and Community CareTable a5.t3 Footnote * | $18.4M | $18.4M | $18.4M | $18.4M | - | $73.7M |
| Long-term CareTable a5.t3 Footnote * | $19.1M | $19.1M | $19.1M | $19.1M | $19.1M | $95.7M |
|
||||||
Footnotes
- Footnote 1
-
http://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/Page.cfm?Lang=E&Geo1=PR&Code1=47&Geo2=&Code2=&Data=Count&SearchType=Begins&Sear chPR=01&B1=All
- Footnote 2
-
http://publications.gov.sk.ca/documents/15/100725-2016%20Census%20Age%20and%20Sex%20final.pdf
- Footnote 3
-
http://www12.statcan.gc.ca/census-recensement/2011/dp- pd/prof/details/page.cfm?Lang=E&Geo1=CSD&Code1=4706027&Geo2=PR&Code2=01&Data=Count&SearchText=Regina&SearchType=Begins&SearchPR=47&B1=All&Custom=&TABID=1
- Footnote 4
-
http://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/index.cfm?Lang=E
- Footnote 5
-
https://www.saskhealthauthority.ca/your-health/conditions-diseases-services/health-networks-team-based-care
- Footnote 6
-
https://saskatchewan.ca/government/government-structure/ministries/health#annual-reports
- Footnote 7
-
https://saskatchewan.ca/government/government-structure/ministries/health#annual-reports