
Extreme Heat Events Guidelines: Technical Guide for Health Care Workers

2011
ISBN: 978-1-100-18172-1
Cat. No.: H128-1/11-642E
HC Pub.: 110055
Acknowledgements
Health Canada gratefully acknowledges the contribution of the following people in reviewing chapters.
Health Canada recognizes the particular efforts of Jean-Christophe Blachère PhD and Pierre Gosselin MD, from the Institut national de santé publique du Québec (INSPQ) in co-authoring Chapter 4, Heat Risk Factors Associated with Medications.
Health Professionals Information and Training Advisory Committee
- Geoffrey Dover PhD
- Paul Eagan MD
- Richard Gould MD
- Joan Hayes RPh, BScPharm
- Glen P. Kenny PhD
- Kieran Moore MD
- David Mowat MD
- Sonya Nobbe ND
- Lori Payne
- Pammla Petrucka RN, PhD
External Reviewers
- Sheri Armstrong RN, BScN, MS
- Sandra Brioux RN, BA
- Janet Chee RN, BScN, MN
- Audrey Danaher RN, MSc
- Katie Dilworth MHSc, RN, CCHN(C)
- James Ducharme MD, CM, FRCP(C), DABEM
- Doris Grinspun RN, MSN, PhD, O.ONT.
- Stephanie Gower PhD
- Laura Hanson RN, BN, MN
- Kathryn Hardill BScN, RN(EC)
- Brenda Jacklitsh MS
- Carol Mee RN, BScN, MEd
- Robert Milling LLB, LLM
- Lynn Anne Mulrooney RN, MPH, PhD
- Daniel Rainham PhD
- Brent Ruddock RPh, BScPharm
- Howard Shapiro MD MSc FRCP(C)
- Carol M. Stephenson PhD
- Althea Stewart-Pyne RN, BN, MHSc
- Jill Skinner
- Tim Takaro MD, MPH, MS
- Pamela VanBelle, RN, BScN, MN
Heat Alert and Response Systems Pilot Reviewers
- Ada Bennett MD
- Neil Gamey RN, PCP
- Stephan Hamel MSc
- Lori Jones RN, BScN
- Tom P. McCormack
- Robert Munro
- Toni Morris-Oswald PhD, BSW, MNRM
- Karina Richters
- Adrian Robertson MD
- Brent Roussin MD, LLB, MPH(C), CCFP
- Sally Shurvell
Heat Alert and Response Systems Advisory Committee
- Quentin Chiotti PhD
- Patty Gorr
- Jane MacDonald RN, MHSc
- Franziska Matthies PhD
- Bettina Menne MD, PhD
- Scott Sheridan PhD
Table of Contents
- Acknowledgements
- List of Abbreviations
- Executive Summary
- 1. Introduction
- 2. Physiology and Pathology of Heat Illness
- 3. Risk Factors Associated with Heat-Related Illness and Death
- 4. Heat Risk Factors Associated with Medications
- 5. Heat-Related Illnesses
- 6. Questions and Answers: Preventing Heat-Related Illnesses
- 7. Extreme Heat Summary Advice for Medical Officers of Health and Public Health Staff
- 7.1 Extreme Heat Events and Heat-Related Illnesses
- 7.2 Individual and Community Risk Factors
- 7.3 Effective Prevention Measures to Advise the Public to Adapt to the Heat
- 7.4 Messages Developed for Communication with the Public
- 7.5 Mid- to Long-Term Public Health Planning: Prevention for Municipal Planners
- 8. Disaster Preparedness for Health Care Services
- 9. Conclusions and Future Directions
- Glossary
- Appendix A: Guideline Development Methods
- Appendix B: Fact Sheets for Health Care Workers
- Appendix C: Heat Resilient Canadians and Communities
- Appendix D: Heat-Health Fact Sheets
- References
List of Abbreviations
- ACGIH®
- American Conference of Governmental Industrial Hygienists
- ACh
- Acetylcholine
- ADH
- Antidiuretic Hormone
- ALT
- Alanine Aminotransaminase
- AQI
- Air Quality Index
- AQHI
- Air Quality Health Index
- AST/SGOT
- Aspartate Aminotransferase/ Serum Glutamic-Oxaloacetic Transaminase
- ATP
- Adenosine Tri-Phosphate
- °C
- Degree(s) Celsius
- CI95
- 95% Confidence Interval
- CNF
- Canadian Nutrient File
- CNS
- Central Nervous System
- COPD
- Chronic Obstructive Pulmonary Disease
- CPK
- Creatine Phosphokinase
- DIC
- Disseminated Intravascular Coagulation
- EHE
- Extreme Heat Event
- °F
- Degree(s) Fahrenheit
- GHG
- Greenhouse Gas
- HPIT
- Health Professional Intervention/ Information and Training
- HSP
- Heat Shock Protein
- ICD
- International Classification of Disease
- IPCC
- Intergovernmental Panel on Climate Change
- kcal
- Kilocalorie
- kJ/hr
- Kilojoules per hour
- mEq/L
- Milliequivalents of solute per litre of solution
- MODS
- Multi-Organ Dysfunction Syndrome
- OR
- Odds Ratio
- PM
- Particulate Matter
- RR
- Relative Risk
- RH
- Relative Humidity
- SRES
- Special Report on Emissions Scenarios
- SSRI
- Selective Serotonin Re-uptake Inhibitor
- SGPT
- Serum Glutamic-Pyruvic Transaminase
- Twb
- Natural Wet-Bulb Thermometer
- Tg
- Globe Thermometer
- Tdb
- Dry-Bulb Thermometer
- TLV®
- Threshold Limit Value
- UHI
- Urban Heat Island
- UV
- Ultraviolet
- WBGT
- Wet-Bulb Globe Temperature
- WHO
- World Health Organization
- W
- Watts
- VO2 max
- Maximum Volume of Oxygen over time
- VOC
- Volatile Organic Compound
Executive Summary
Extreme heat events (EHEs), more commonly known as heat waves,Reference a have affected health and resulted in a significant number of preventable deaths in recent years. Notably, in the summer of 2003, Europe experienced 70,000 deaths as a result of the extreme heat.Reference 1 Experts believe that climate change will significantly impact the frequency, duration and intensity of EHEs, resulting in an increased incidence of heat-related illness and fatality in Canada. For example, in the absence of effective mitigation and adaptation measures in Toronto, Windsor, London and Winnipeg, the number of days with a maximum temperature of 30°C is projected to double by 2021-2040 and more than triple by 2081-2100, likely resulting in further heat-related mortality.Reference 2 Reference 3 As a result, decision makers need to make a concerted effort to address and adapt to these increased risks in order to protect populations considered at risk. The goal of the Health Canada Heat Resiliency Project is to facilitate these adaptations in particular at a local and regional level. The information within the Guidelines has been written with the goal that health care workers can adapt it for the needs of the populations they serve.
Health care worker involvement is needed at all levels in Canada to make decisions concerning adaptation and planning for EHEs. This challenge requires integrating input from multiple disciplines into both short-term and long-term planning. The Guidelines are comprised of this Technical Guide of heat-health information and targeted Fact Sheets (for Acute Care, Community Care, and Facilities Preparation) as well as a brief User Guide which provides policy guidance for health organizations.
The Guidelines are designed to provide a broad overview for health care workers and to facilitate linkages on common concerns and solutions regarding extreme heat. The Technical Guide provides current national and international research in a format designed to promote translation of global imperatives into evidence-based adaptations. The targeted Fact Sheets are each one double-sided page intended to be both brief and sufficient for most busy health care providers. These Fact Sheets groupings were developed to address the needs of several disciplines within each topic. The User Guide was developed as a synthesis of the key actions for organizations and institutions to take when promoting adaptation. Together, this suite of products was developed and designed to meet the various needs of health care workers in both addressing and preventing heat illnesses through education and health promotion.
The target audience for this suite of products is health care workersReference b including, but not limited to:
- medical officers of health
- public health practitioners
- medical physicians
- medical helpline workers
- nurse practitioners
- nurses
- naturopathy practitioners
- 911 dispatchers
- chiropractors
- paramedics
- midwives
- dieticians
- home care workers
- pharmacists
- respiratory therapists
- occupational therapists
- physiotherapists
- athletic therapists
- personal trainers
- personal support workers
- community support workers
- traditional and indigenous healers
- workplace health and safety personnel
In addition, the target audience includes the staff and managers of public health organizations and the various health facilities including, but not limited to, hospitals, retirement homes and longterm care facilities.
The research related to EHEs has identified several approaches to aid in the prevention of, and response to, heat-related illness. One of the main gaps identified by this research is the lack of education and training material for health care workers regarding EHEs. Filling this gap would benefit not only the health care worker, but also would improve the knowledge transfer to those at greatest risk. The majority of heat stroke cases and heat-related illnesses are preventable through behavioural changes to manage the risks related to EHEs.Reference 4 The Guidelines are designed to address these issues by providing evidence-based information for effective public health action by health care workers (see Summary below).
Describing the Issue
- Heat and the changing nature of EHEs (Chapter 1)
- Critical challenges for health care workers during EHEs (Chapter 1)
- Key definitions (Glossary and list of abbreviations)
Assessing Individuals
- Human physiology of heat (Chapter 2)
- Populations at risk (Chapter 3)
- Medications that increase the risk of heat illness (Chapter 4)
Interventions
- Interventions to address heat-related illnesses (Chapter 5)
- Strategies to prevent heat-related illnesses and mortality (Chapter 6)
EHE Preparedness
A central problem is that many heat stroke victims die before contact is ever made with a health care worker.Reference 5 The challenge is therefore to help at-risk patients and clients (reviewed in Chapters 2-4) and their direct caregivers become aware of prevention options for heat-related illness (reviewed in Chapter 6); have the ability to recognize early signs and symptoms of heat illness (reviewed in Chapters 5, 7); to understand and implement at-home therapeutic interventions for heat illness (reviewed in Chapters 5, 7); and to recognize when to consult with a health care worker or to call an ambulance (reviewed in Chapters 5, 7, 8). To succeed, two main actions must be taken:
- Health care workers need to contribute to community efforts aimed at educating at-risk groups on heat-health risks and develop tailored prevention strategies prior to the annual spring-summer heat season; and
- During an EHE, health care workers need to assist members of at-risk groups to adopt preventive actions in their daily routines.
Community care can play a pivotal role in the prevention of heat illnesses. Several studies have analyzed EHEs and populations most at risk. Among the identified key risk factors for death in an EHE are physical and social isolation (i.e. confinement to bed, low level of independence, inability to care for oneself, and not leaving the house). It is likely that many health care providers have regular contact with people at risk and this essential resource group should be engaged to help prevent heat illnesses and mortality by raising awareness of heat-health risks and effective prevention options. However, the most at-risk people are those that are isolated and do not receive much assistance or services, despite their need for support. Strategic community engagement and social contact is needed to reach out to isolated people. Engagement of health care workers is needed to initiate discussion with patients/clients of possible risk factors and simple protective actions to prevent heat-related illnesses. Health care workers can play an important role in changing a person's perceptions of the risks associated with heat as most people do not believe that they are at risk. Effective prevention is dependent on the recognition of risk as this is the first step to altering behaviour and adopting protective actionsReference c
The key messages to protect oneself from heat illnesses and deaths are to: "Stay Cool, Stay Hydrated and Rest when Necessary." Despite this, heat illnesses during EHEs remain a problem.Reference 5-Reference 8 To address EHEs effectively public health challenges need to be outlined.
The Guidelines are written to enable health care workers to become more effective in establishing preventative action by providing them with action-focussed information and the analysis of the risk factors that make vulnerable population groups susceptible to the negative impacts of EHEs. Information on effective diagnostic methods and interventions is provided to address the risks to health associated with extreme heat, including interventions most appropriate for vulnerable populations. Ultimately it is the responsibility of employers and curricula developers to decide whether to integrate the Guidelines into education and training of staff, workers and new graduates. The Chapters, as outlined in the Guidelines can be used as educational objectives to facilitate their use as an educational tool for health care worker teaching and professional development. Commitment to, and availability of, education and training are needed to ensure that all staff, regardless of profession, are given the opportunity to update their knowledge base so that they can implement the Guidelines' recommendations.
As always, health care workers should use their professional judgement and tailor the Guidelines to their patients when applying the recommendations. Patients and their caregivers should be informed about their risk for heat illness and should be involved in shared decision-making discussions regarding strategies to prevent heat illness. An integrated approach to preventing heat illnesses requires all members of an interdisciplinary team to be engaged and active.
1. Introduction
Key Terms: heat-related illnesses, excess death, acclimatization, adaptation, extreme heat event, urban heat island, built environment, emission scenario
Summary Points:
- Heat and especially extreme heat can cause a range of heat-related illnesses and exacerbate certain chronic conditions.
- The definition of extreme heat events can differ and exposure to heat is affected by several factors including the urban heat island effect and building characteristics of residences.
- The intensity, duration and frequency of extreme heat events are projected to increase. Therefore, additional prevention and response plans will be required by many professionals including health care workers.
1.1 Heat Illnesses in Canada
Heat illness may be viewed as a continuum of disease relating to the body's inability to cope with heat. It includes minor problems, such as heat edema (swelling), heat rash, and heat cramps, as well as more severe illnesses such as heat syncope (fainting), heat exhaustion and, the most serious of these, heat stroke.
There are two forms of heat stroke: exertional and classic heat stroke, both of which are medical emergencies. Exertional heat stroke generally occurs in individuals who engage in strenuous physical activity for a prolonged period of time in a hot environment. Classic heat stroke more commonly affects sedentary older individuals, people who are chronically ill, and young children. Both types of heat stroke are associated with high morbidity and mortality, especially when body cooling is delayed.Reference 9

Both seasonal heat and extreme heat events (EHEs) pose a health risk to Canadians. The analysis of mortality curves relative to temperature indicates that relative death rates can begin to rise even at daily average temperature s as low as 20°C (Figure 1.1).Reference 10 Reference 11 A review of heat threshold mortality curves in 64 locations in six continents indicates the temperature at which a rise in relative deaths is seen is related to the acclimatization of the population.Reference 12 This means that in regions where high temperatures are typical, the health risk to the population occurs at higher temperatures than in more temperate regions. It also means that extreme heat early in the spring is a greater risk than late in the summer when the population has acclimatized to the regional weather.Reference 12 During EHEs air conditioning is highly protective in averting illness and its use should be encouraged for at-risk populations.Reference 13 Communicating the importance of heat considerations remains a challenge, particularly since the ideal temperature at which to set indoor temperature depends on an individual's health and thermal comfort. For health care facilities, recommendations for summer indoor temperature may be outlined in occupational health and facility management guidelines.
Figure 1.1: The relationship between temperature and mortality in seven Canadian cities.
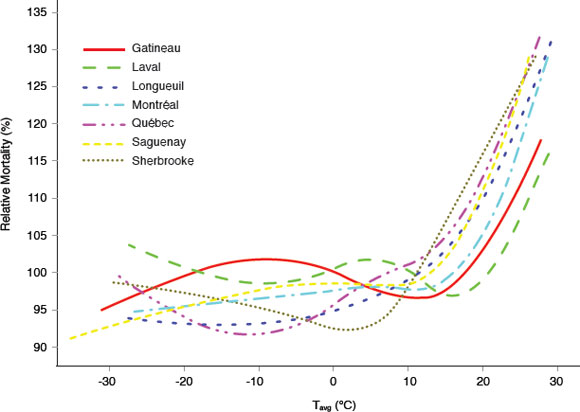
Text description
A graph illustrating the relationships between relative mortality (expressed in percentage) and the average daily temperature in seven cities in Quebec, which include Gatineau, Laval, Longueuil, Montreal, Quebec, Saguenay and Sherbrooke. This graph demonstrates a sharp increase in the percentage of relative mortality at an average daily temperature between 15 and 20 degrees Celcius. However one city, Sherbrooke, shows a sharp increase in the percentage of relative mortality at daily average temperatures of only 5 degrees Celcius. In contrast, there is no increase in relative mortality at colder temperatures, down to negative 30 degrees Celcius.
Currently the relative mortality in relation to average daily temperatures has been evaluated in several cities in Quebec. As the temperature increases above the threshold so does the percent relative mortality.Reference 10Reference 11 Further investigations are ongoing to assess threshold temperatures in other Canadian cities.
In addition to the heat illnesses described above, EHEs can also aggravate a pre-existing condition that is sensitive to the heat. These illnesses are usually a result of increased strain on the cardiopulmonary system resulting from a reduced body water volume and/or other thermoregulatory factors that strain the heart and may contribute to a heart attack.Reference 14 In addition to cardiac disease, co-morbidity has been reported with pulmonary conditions,Reference 15 renal illnesses,Reference 16 and neurological diseases.Reference 15 These pre-existing conditions are significant risk factors for heat-related illnesses and mortality.
Any one of the heat-related illnesses may occur alone or in combination with other heat illnesess or other chronic illness symptoms. In Canada, heat-related illnesses are likely under-reported by patients/clients and by health care workers.Reference 17 As a result, the relative impact of heat on the health of Canadians is under-reported and therefore under-recognized.
1.2 Extreme Heat Events in Canada
The precise definition of an EHE varies, but always refers to unusually hot temperature and/or high Humidex readings as compared to the typical regional average for that season. EHEs are not new to Canada. Between 1900 and 2005, five major EHEs occurred in Canada - from Ontario to the Atlantic Ocean (1912), Western and Central Canada (1936), Toronto region (1953), Halifax region (1963), Prairie Provinces and Central and Southern Ontario (1988) - causing over 1,200 deaths and many heat-related illnesses.Reference 18 To protect the public, Environment Canada issues Heat and Humidex Advisories when temperatures are expected to reach or exceed 30°C/ 86°F and/or the Humidex value (a combination of humidity and temperature) is expected to reach or exceed 40 on the Humidex scale of perceived temperature.Reference 19 Environment Canada defines a heat wave as "a period with more than three consecutive days of maximum temperatures at or above 32°C/ 90°F."
Defining when an EHE is a risk to human health remains a challenge due, in part, to both individual and region-specific factors. Regional differences include, among others, mean temperature, population acclimatization, and both individual and community-level risk factors. These compounding factors result in populations in certain regions being at higher risk at lower temperatures compared with other communities.
Figure 1.2: The relationship between temperature and the built environment.
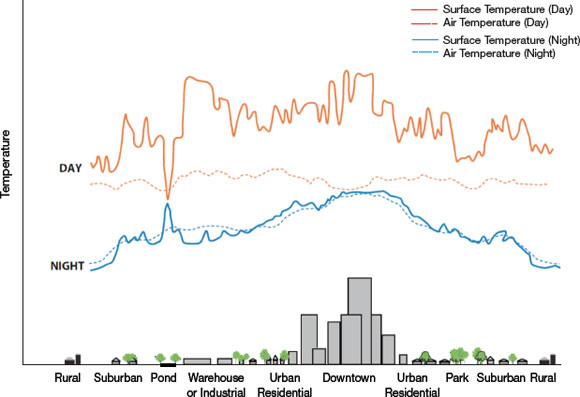
Text description
This figure illustrates day- and nighttime surface and air temperatures across various types of built environments, including rural, suburban, pond, park, warehouse or industrial, urban residential, and downtown environments. This figure shows a large increase in daytime surface temperatures in the industrial and downtown environments. Smaller increases in daytime surface temperatures are also seen in the suburban and urban residential environments. In contrast, the daytime air temperatures remain constant in all environment types. The nighttime surface temperatures show a similar pattern as the daytime surface temperatures, with a larger increase in the downtown and smaller increases in urban residential environments. The night time air temperatures mirror the night time surface temperatures.
In built environments with little green space the temperature is increased during both the day and the night, resulting in the urban heat island (UHI) effect.Reference 26Reference 27
These risk factors are further compounded by variables that affect exposure to heat itself. From a population standpoint, the environmental exposure to heat differs significantly among urban, suburban and rural environments. This is in part due to the increased thermal load from the urban heat island (UHI) effect,Reference 20 Reference 22 an effect that is dependent on city design. Canadian cities are built to withstand cold and retain heat. The cumulative effect of heat absorption by urban surfaces correlates to the absorptivity, density and emissivity of the built environment (e.g. asphalt and concrete) and leads to the UHI effect. These materials continue to radiate heat even as the air temperature is dropping (e.g. due to evening). This can lead to a difference of several degrees between urban and rural areas in the same region, as shown in Figure 1.2. Depending on local design suburban areas can also have a significant UHI effect. It is important to note that the environmental health risk of heat is not only due to high daytime temperatures, but also due to high nighttime temperatures, which prevent an evening reprieve from the heat.Reference 23Reference 3 This is particularly important when there are three or more sequential days of high daytime air temperature and/or humidity combined with high evening air temperature and/or humidity.Reference 24 The difference in the surface temperature of urban parks and industrial areas is largest in the daytime due to the cooling effect of the vegetation. The temperature difference between the urban and the rural environment is largest in the evening and demonstrates a relationship between night temperature and the density of the built environment.Reference 25 This is of particular interest because nighttime temperature is predicted to have the greatest differential increase as a result of climate change.
To address the health risks associated with heat, many municipalities have developed communityspecific criteria for issuing a heat alertReference 28Reference 29 because multiple region-specific variables need to be considered when developing a heat alert and response system.Reference 30 Many municipal planners have also initiated adaptive behaviours to reduce heat stress. These adaptations can include alterations to infrastructure designed to minimize the UHI effect and through strategic municipal planning which create more urban green space.Reference 31 Reference e
1.3 Projected Increase in Extreme Heat Events in Canada
The 4th Intergovernmental Panel on Climate Change (IPCC) (2007),Reference 32 Natural Resources Canada (2008)Reference 33 and Health C anada (2008)Reference 30 conclude that many regions in Canada will very likely face EHEs of increasing intensity, duration and frequency. EHEs will have an impact on the health of Canadians in the absence of effective prevention, emergency planning, and other adaptations. For example, in Toronto, Windsor, London and Winnipeg, the number of hot days is projected to double by 2021-2040 and more than triple by 2081-2100 (Figure 1.3) likely resulting in further heat-related mortalityReference 2Reference 3 in the absence of effective adaptations.
Figure 1.3: Current and projected number of days exceeding 30°C (86ºF) for Canadian cities
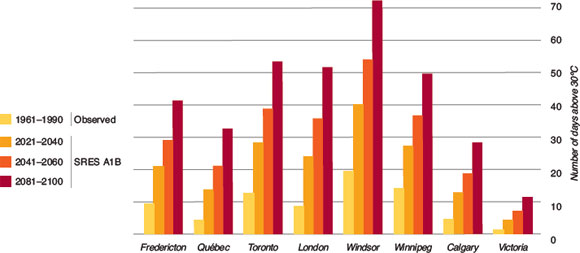
Text description
This graph illustrates the observed and expected number of days above 30ºC (86°F) for Fredericton, Quebec, Toronto, London, Windsor, Winnipeg, Calgary and Victoria. The expected increases are based on modelling from the Special Report on Emissions Scenarios (SRES) using the Intergovernmental Panel on Climate Change conservative emissions scenario (A1B). The highest increase in the number of hot days is seen in Windsor, Ontario with an increase from the observed 18 hot days in 1961 to 1990 to 40 days from 2021 to 2040, 54 hot days from 2041 to 2060 and 72 hot days from 2081 to 2100. Toronto, London and Winnipeg had similar increases from their respective observed values of 12, 8 and 15 hot days to 28, 24 and 27 hot days from 2021 to 2040, 39, 35 and 37 hot days from 2041 to 2060, and 53, 52 and 49 hot days from 2081 to 2100. Fredericton shows an increase from the observed 8 hot days to 21, 28 and 41 hot days in each of the respective time periods. Quebec and Calgary show similar expected values each with 5 observed hot days and 13, 21 and 32 hot days for Quebec, and 12, 18 and 28 expected hot days from Calgary in each time period. Victoria had the least amount of observed and expected hot days. Observed showed only 2 hot days, and increases to 4, 6 and 12 hot days for the time periods of 2021 to 2040, 2041 to 2060 and 2061 to 2080, respectively.
Climate modelling indicates Canadian cities will see an increase in the number of hot days (with a temperature high of 30°C) in the future as compared to the observed number of hot days between 1961 and 1990.Reference 2Reference 3 Temperature projections depicted for selected Canadian cities were analyzed using the Special Report on Emissions Scenarios (SRES) using the Intergovernmental Panel on Climate Change (IPCC) conservative emissions scenario (A1B)Reference 34. The number of hot days for each city is based on the observed temperature data between 1961 and 1990, and projected for 2021-2040, 2041-2060 and 2081-2100.
The projected increase in frequency, intensity and duration of EHEs places the population in many Canadian cities at particular risk, since many cities are not prepared for, nor well adapted to, such events.Reference 30Reference 32 Health care workers play a key role in patient/client education and are influential community leaders. They need effective tools to assist them in helping their clients adapt to the risks and avoid heat-related illnesses. The Guidelines will help prepare health care workers provide this guidance. This is needed to provide public health strategies with accurate regional and national information regarding the relative heat-health risks. Health care workers and communities can prepare for EHEs by providing information on heat and health to support prevention of heat-related illnesses.
2. Physiology and Pathology of Heat Illness
Key Terms: hypothalamus, heat balance, thermoregulation, heat dissipation, evaporative cooling, acclimatization, Wet-Bulb Globe Temperature Index
Summary Points:
- Sweating alone does not release heat from the body; it is the evaporation of sweat from the surface of the skin that enables cooling. Evaporative cooling is the only physiological response that always results in heat loss and never in heat gain.
- During exercise in hot conditions the heart has to continue to pump blood to the working muscles while simultaneously increasing blood flow to the skin. This puts an additional burden on the heart.
- The body contains a finite number of sweat glands. When exposed to heat stress the increase in sweat production can be due to an increase in the amount of sweat produced from each gland and/ or an increase in the number of active sweat glands.
- The process of acclimatization or gradual tolerance of repeated exposure to heat, results in physiological adaptations which improve the ability to dissipate excess body heat.
2.1 Temperature Regulation

Adopting good behaviour when out in the heat is a good way to help regulate temperature.
To fully understand the human physiological response to heat stress, it is important to be familiar with the body's ability to thermoregulate and the mechanisms used to deal with excess heat. Humans are able to maintain a relatively constant core temperature of approximately 37°C despite changes in the external environment and fluctuations in internal heat production. The body must be able to protect internal organs from thermal changes which take place outside the body as well as to release the extra heat, that is produced internally, to the environment. Within a temperature range of 25°C to 27°C, known as the critical air temperature,Reference 35 an unclothed person can maintain core temperature by balancing heat production with heat loss. This heat balance is achieved by matching heat gained with heat
lost through autonomic mechanisms such as the sweating response. However, outside this temperature range people are able to adjust their body temperature through behavioural mechanisms (such as moving into the shade).
The body produces heat internally by metabolizing the food that we consume and absorb through the intestines. The cells then use this food in the form of glucose for energy. The production and utilization of adenosine tri-phosphate (ATP) releases energy in the form of heat, which is then used to maintain core temperature. Additionally, physical exertion, specifically muscle contractions, also increases the amount of heat produced within the body. Short bursts of muscle contractions in any single muscle can release up to 100 times its normal resting amount of heat. For the most part, the body generates more heat than is required to maintain core temperature and therefore the excess heat must be eliminated from the body. This is achieved by transferring the heat produced within the body to the skin surface through the circulatory system and through internal contact of tissues. This transfer of heat is based on a temperature gradient and occurs by conduction within the tissue from the core to the skin surface. Only when the heat reaches the surface of the skin can it be released to the environment through four mechanisms which include:
Conduction: Refers to the bi-directional transfer of heat between two surfaces of differing temperatures through direct physical contact. This includes both external conduction (contact of the skin with cooler objects) and internal conduction (contact of tissues inside the body, which is important in heat distribution to the surface of the skin).
Convection: Refers to the bi-directional transfer of heat through contact with air or water molecules across the skin. The transfer of heat from the surface of the skin by air helps carry heat away from the body. It should be noted however that heat must first be conducted to the skin surface and then to the air and only after this is the heat finally carried away. In hot weather conditions when the air temperature is higher than skin temperature heat will be gained from the environment, by convection (skin temperature is normally around 35°C, but can vary between 20°C and 40°C without harm to the bodyReference 36).
Radiation: Refers to the bi-directional transfer of infrared waves emitted from one object and absorbed by another. A person can radiate heat to cooler objects, and absorb heat from warmer objects. As a means of heat gain from the sun, the efficacy of radiation depends on the angle of the sun, the season, the presence of clouds (or other shading factors), as well as clothing (degree of insulation and reflectance). Radiant heat could be generated by a number of sources such as direct sunlight, ovens, hot asphalt and buildings that absorb sunlight during the day and radiate it back to cooler objects or to the environment even after the sunset. The radiant heat from these sources contributes to the amount of heat to which people are exposed. The body may also radiate heat to assist in cooling itself.
Evaporation: Refers to the evaporation of water from the skin (in the form of sweat) or from the respiratory passages (through breathing). Evaporation is unidirectional and will always result in body heat loss and never in heat gain. At high ambient temperatures, evaporation of sweat is the most important thermoregulatory mechanism. In fact, when the air temperature is higher than skin temperature, sweating is the only avenue for heat loss and is responsible for approximately 90% of it.Reference 37 Wind speed or air movement will also increase evaporative cooling. However, if the surrounding air is near-saturated with water (during periods of high humidity) and ambient temperature is higher than skin temperature, evaporation will not be as efficient or can be inhibited altogether. Sweating alone does not release heat from the body; it is the evaporation of sweat that enables cooling. During times of high heat and humidity, an increase in the body's thermal load (heat strain) may occur which leads to an increase in body temperature and susceptibility to various heat illnesses.
Figure 2.1: Temperature regulation.
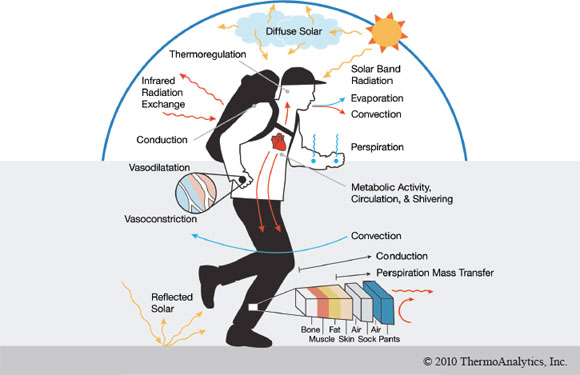
Text description
Figure demonstrates the avenues for heat transfer in a human. Heat is generated by the body through metabolic activity, circulation and shivering. The heat is then circulated throughout the body from the heart, which causes vasodilation in the extremities. This heat is lost to the environment through convection, evaporation (from the mouth) and perspiration (from the evaporation of water from the surface of the skin). Infrared radiation exchange causes heat to be absorbed and lost by the body, whereas solar band radiation and reflected solar from the sun only causes a person to absorb heat. Convection from the air can allow for heat to be lost from the body. Conduction of heat through the several layers of the body and clothing (from inner to outer layers: bone, muscle, fat, skin, air, sock, air, pants) can also release heat. Perpiration mass transfer only occurs from the clothing to the environment.
This diagram demonstrates the heat generated by internal processes (metabolism and muscle contraction) and the avenues of heat transfer to the surrounding environment (evaporation, radiation, conduction, convection).
Under normal physiologic conditions, core temperature is controlled by the hypothalamus, by linking the nervous system to the endocrine system through the pituitary gland. The hypothalamus acts like an internal thermostat with a set-point (approximately 37°C) control that monitors the body's core temperature. Deviations from this set-point will initiate heat loss or heat production mechanisms as appropriate. However, small, normal variations also occur in core temperature without any increases in blood flow or sweating. The sensation of external heat is picked up by peripheral thermosensors located on the surface of the skin and in the muscles and central (more sensitive) thermosensors located in the brain which transmit information regarding core temperature to the preoptic-anterior hypothalamus.Reference 38Reference 39 The hypothalamus then processes the incoming information into a series of appropriate and widespread physiological responses such as initiating the sweating response and increasing blood flow.Reference 40 Under circumstances where changes in sweating and skin blood flow cannot facilitate an adequate rate of heat loss (e.g. intense physical activity in hot, humid conditions and/or impairment of normal thermoregulatory function), the body's core temperature will continue to rise.
The direct impact of heat on the individual is further complicated by many physiological as well as external factors. For example, body fat can affect thermal regulation in several important ways. Firstly, body fat can impair heat transfer to the skin reducing the rate at which the body can cool itself. Secondly, when exposed to the same amount of heat stress, the temperature of adipose tissue will increase more quickly than in leaner tissues resulting in a rapid temperature rise due to their different heat capacities.Reference 41 Predisposing health factors, such as certain chronic illnesses, medications or previous heat illness can impact the body's ability to sense heat, to regulate its temperature or to maintain an appropriate level of hydration. People who have adjusted to heat (acclimatized) through improved thermoregulation and repeated exposure to high summer temperatures can be more tolerant to hot weather and experience less heat illnesses. However, it should be noted that many people may not be able to acclimatize to heat without putting themselves at risk; these vulnerable groups will be discussed in detail in this chapter.
2.2 Environmental Parameters Affecting Heat Balance
2.2.1 Description of the Environmental Parameters Comprising Heat
Exposure to a hot environment is the primary risk factor for developing a heat-related illness. When a person is in direct contact with high levels of heat, whether it be outdoors or indoors, in proximity to a heat source such as an oven, or in a hot room with inadequate ventilation and air flow, their susceptibility to heat-related illness increases. Heat is considered to be the energy transferred from one body or system to another through thermal contact. However, there is a common misconception regarding the type of environmental conditions that increase a person's vulnerability in such situations. Heat is more than just temperature. In fact, four environmental parameters constitute heat, specifically, ambient temperature, radiant solar load, humidity and air velocity. It is a combination of these factors that provides an accurate indication of a person's level of heat stress. These four parameters are described in Box 2.1.
Box 2.1: Environmental Factors Comprising Heat
Ambient temperature refers to the common measurement of how hot or cold it is outdoors. Temperature is usually measured by a thermometer in degrees Celsius or degrees Fahrenheit. For accurate measurements, the thermometer should be shielded from the sun (i.e. the temperature reported is what it would be in the shade).
Radiant load is the transfer of heat from a heated surface. The most common form of radiant heat transfer is the transfer of heat from the sun to the earth through electromagnetic rays (infrared heat rays). This energy from the sun can be absorbed or reflected by various surfaces including buildings and/or people. Generally dark-coloured surfaces (such as parking lots and building roofs) absorb more radiant heat from the sun than light-coloured surfaces which have a tendency to reflect the sun's solar radiation.
Humidity is the amount of water vapour in the air. Absolute humidity is the quantity of water in a particular volume of air (grams per cubic meter). Relative humidity is an indication of how many grams of water can be held in the air at a given temperature, and is therefore relative to ambient temperature. Humidity is an important factor when considering the dissipation of heat from the body. In conditions with high humidity the evaporation of sweat from the skin surface is impeded. When humidity is combined with high ambient temperatures, it can contribute significantly to heat stress.
There are several common ways to quantify the effects of humidity, including "apparent temperature" metrics such as the Humidex. Humidex is an absolute number combining the effects of both relative humidity and temperature and its value is reported on a scale of perceived thermal comfort. For example, Humidex is often used as an indicator for how hot 'it feels' outside.
Air velocity refers to the speed at which air moves. The extent of air movement is usually measured with an anemometer and reported in kilometres per hour or miles per hour. Air velocity is critical for enhancing the evaporation of sweat from the skin and can have a large effect on cooling. Alternatively, if relative humidity is near 90-100% and ambient temperature is greater than skin temperature, the body may gain heat through convection.
The combination of these four factors is the most physiologically relevant way to assess the environmental variables of heat that contribute to heat stress and each factor plays a different role in the burden of heat felt by an individual.
2.2.2 Assessing Environmental Conditions

Figure 2.2: Measurement of the parameters comprising the Wet-Bulb Globe Temperature (WBGT) Index by military personnel.
From left to right, the sensors are the dry-bulb thermometer (Tdb), natural wet-bulb (Twb) and the globe thermometer (Tg ), which are incorporated by algorithm to represent the WGBT.
The most widely used index of heat-related health risk is the Wet-Bulb Globe Temperature (WBGT). The WBGT Index is a heat-stress indicator that considers the effects of temperature, humidity, radiant heat and wind speed. The WBGT Index was invented, evaluated and first used during the 1950s to control heat illness in training camps of the United States Army and Marine Corps. It was then adopte d for the prevention of heat illness during sporting activities and in workplace settings. Many organizations use the WGBT Index including most occupational health authorities, sports associations such as The National Athletic Trainer's Association, and in national (UK, China, Japan, USA, Australia etc.), regional (European) and international (ISO) standardsReference 42 since it is the most inclusive heat-stress indicator currently available. The WBGT incorporates a consideration of all four environmental factors comprising "heat" listed above, expressed as a composite single figure.
The WBGT index is easily calculated from the readings of three different thermometers; a natural wet-bulb (Twb), a globe thermometer (Tg), and a dry-bulb thermometer (Tdb). The WBGT responds to all four elements of the thermal environment, but not necessarily in the same way as the human body, due to differences in size and shape. The basic idea of WBGT is:
- Twb represents the cooling effect of the evaporation of perspiration from the skin and is affected by both humidity and wind speed
- Tdb represents the ambient temperature
- Tg responds to the environmental heat load (radiation from the sun)
Specifically, radiant heat will warm Tg to some level above Tdb, while wind will cool it towards Tdb. Consequently Twb measures the combined effect of radiant heat, air temperature, and wind speed. Evaporation cools Twb; the amount of cooling being increased by low humidity and by wind, while radiant heat warms it.
It should be noted that the principal shortcoming of the WBGT Index is that it only assesses environmental parameters. Personal characteristics such as variations in the insulative properties of clothing, or individual physiological parameters such as metabolic heat production are only incorporated through simple correction factors for broadly generalized groups.Reference 43
For the workplace, and most healthy workers, there are WBGT scales that indicate the upper limit of exposure (Table 2.1), thereby protecting the individual from heat-related illnesses. Currently, many Canadian occupational health and safety regulators as well as private companies have adopted the American Conference of Governmental Industrial Hygienists' Threshold Limit Values (TLV®s) as a heat-stress screening criterion. TLV®s refer to the level of heat stress that all workers may be repeatedly exposed to, day after day, without adverse effects (based on WBGT values). These scales are based on the concept that nearly all acclimatized, fully clothed workers, with adequate hydration should be able to function effectively under the given conditions without a substantial rise in core body temperature.Reference 44 The Action Limit values are applied to the general population of workers. However, the thresholds need to be modified to address specific needs of most people.
Table 2.1: Threshold Limit Values (TLV ®s) and Action Limit Values and their associated Wet-Bulb Globe Temperature (WBGT) criteria for light, moderate, heavy and very heavy work loads.
Work below the Action Limit is presumptively acceptable stress for any healthy worker, whereas the TLV® is the maximum allowable limit.Reference 45
Obtaining WBGT background information may be problematic for some health care workers as they are unaware of its location, however it is easily accessed onlineReference 46. Although widely used in athletic and occupational settings, the WBGT Index is not applied in many other types of facilities since a WBGT measuring instrument is not always readily available. In addition, the general public is not often aware of its applications.
2.3 General Physiological Changes
2.3.1 Heat Loss through Circulatory Changes
The initial response to heat stress is to increase the conductance of heat from the body core by increasing blood flow to the skin. This allows more heat to pass from the body's internal organs (gastrointestional system, liver and kidneys) to the body's outer shell, namely the muscles and the skin. This movement of heat outward occurs as a result of increased cardiac output, as well as peripheral skin vasodilation.Reference 35Reference 39Reference 47 An internal temperature rise of less than 1°C (in some instances a rise less than 0.2°C) in circulating blood is enough to stimulate an increase in blood flow to the skin for heat dissipation.Reference 39Reference 48Reference 49
The large variations in blood flow to the skin can account for as much as 30% of total cardiac output and can impede the delivery of blood and nutrients to other organs, contributing to a host of other problems often seen in heat-related illness.Reference 4 In addition to redirecting blood flow, the excessive damage of cells due to the onset of heat stroke triggers the blood clotting cascade by damaging the epithelial cells to which platelets adhere, causing coagulation abnormalities and microthrombus obstructions.Reference 47Reference 51
It is important to know that there are limits to the cardiovascular capacity of the body to thermoregulate, especially when exercising in the heat. If a person is working in a hot environment, the load on the heart is much greater than normal. The circulatory system has to continue to transport blood to the working muscle and concurrently increase blood flow to the skin in order to transport the excess heat to the skin surface.Reference 52 At some point, the heart can no longer compensate for the increased demands of endurance activity and the need to dissipate heat.
In non-exertional instances, cardiac output, muscle blood flow and stroke volume may remain constant or decrease slightly, which may result in a gradual upward drift in heart rate.Reference 53 If dehydration occurs (typically above 2-3% of total body weight loss), muscle blood flow may decrease, sweat production will decrease and electrolyte loss may occur. In addition, the release of aldosterone (which increases the rate of re-absorption of sodium in the sweat gland) and antidiuretic hormone (ADH) increase, which can lead to an expansion in plasma volume.Reference 54
2.3.2 Heat Loss through Sweat Production
Figure 2.3: The ions found in sweat and their relative proportions. When a person secretes large amounts of sweat, a large amount of these ions can be lost.

The release of heat from the surface of the skin is most readily accomplished through the production and evaporation of sweat, and is therefore extremely important in human thermoregulation. The evaporation of water from the body occurs in several different ways, but each avenue releases a different amount of heat, some more efficiently than others. The least efficient mechanisms include heat loss through the mucous membranes of the mouth, nose and respiratory passages as well as passive diffusion through the skin. The body's most efficient heat loss mechanism occurs through the evaporation of sweat.
It is the evaporation of sweat that contributes significantly to heat loss, and the amount of heat loss depends on two factors:
- the amount and rate of sweat production by sweat glands, and
- the rate at which sweat is evaporated from the surface of the skin.
This second factor is affected by the ability of the ambient environment to remove the sweat from the skin.Reference 55 If the surrounding environment is hot and dry, sweat can be evaporated easily and heat loss will be limited by the rate of sweat production. This increase in sweat production can be due to an increase in the density of active sweat glands, an increase in the amount of sweat produced per gland, or a combination of both.Reference 56 If the air is hot, humid and still, then the release of heat is dependent on the ability of the environment to remove (or evaporate) the sweat, which in such conditions is considerably difficult to do. With high humidity the evaporation of sweat is greatly decreased despite elevated sweat rates. Individual variations in the density and activity of sweat glands exist, as well sweating differences from one region of the body to another.Reference 7 Specifically, the sweating rate of the trunk is generally greater than that of the limbs. This is important when choosing clothing as the areas of the body which produce the greatest amount of sweat are often most covered by clothing.
Figure 2.4: Typical eccrine sweat gland.

Text description
This drawing demonstrates all the components of a human sweat gland. Deep in the dermis, a coiled sweat gland is innervated by sympathetic nerves that release acetylcholine. A duct emerges from the coiled section and runs upwards towards the surface of the skin. This duct passes through the various layers of the skin. A droplet of sweat has been released at the mouth of the sweat duct and sits at surface of the skin.
The sweat gland is innervated by cholinergic sympathetic nerve fibres and consists of two portions: a coiled section in which a precursor secretion is produced, and a duct leading to the surface of the skin where a droplet of sweat can be deposited on the surface of the skin for evaporation.
The body contains a finite number of eccrine glands (also known as sweat glands) that are distributed throughout the surface of the body. A sweat gland is a tubular structure that consists of two parts; a deep coiled gland section that secretes sweat and a duct section that leads to the skin surface.Reference 36 Sweat glands are solely innervated by the sympathetic nervous system, therefore for these glands to secrete sweat they must be stimulated by a nerve impulse. The volume of sweat that is secreted is proportional to the frequency of these efferent nerve impulses. When a cholinergic sympathetic nerve fibre (i.e. those that release acetylcholine) is stimulated, a complex exchange of electrolytes is activated and a precursor secretion is produced. The components of this precursor are altered as it travels through the coiled section and up into the sweat gland duct. The duct portion of the gland is involved in the re-absorption of sodium and chloride ions, usually at very low rates. When sweating increases, the re-absorption of the sodium and chloride remains the same, releasing more ions into the sweat at the surface of the skin. The end result is an increase in electrolyte loss.Reference 36
The circulation of heated blood stimulates the sweating response in the hypothalamus by causing the release of acetylcholine (ACh) from cholinergic sympathetic fibres in the skin that innervate sweat glands.Reference 39 Reference 49 In addition, the sensation of thirst may not be sufficient to stimulate fluid replacement of all lost body water, and dehydration and electrolyte loss may result.Reference 35Reference 49 A decrease in plasma volume follows, which increases the viscosity of the blood putting further strain on the heart.Reference 37
2.4 Heat Acclimatization
Acclimatization refers to the physiological adaptations in response to repeated exposures to a hot/dry or a hot/humid environment and can have a dramatic effect on a person's ability to tolerate these types of conditions. Acclimatization occurs when these adaptations take place in a natural environment, whereas acclimation occurs in an artificial environment such as in a controlled environmental chamber.
The physiological adaptations of acclimatization sometimes include changes in core and skin temperatures and oxygen consumption but usually include changes in sweat production, heart rate and salt conservation by the sweat glands and kidneys. Other physiological changes include increases in central blood volume, aerobic metabolic rate and reductions in muscle lactate levels and glycogen utilization; however the full impact of these effects remains unclear.Reference 58Reference 62 The cardiovascular changes generally occur first with rapid increases in plasma volume within the first one to four daysReference 35; whereas the changes in sweat rate generally take longer (up to 10 days). The key outcomes of heat acclimatization areReference 45:
- Increased heat loss via evaporative and dry heat transfer avenues
- Lower skin and core temperatures
- Increased sweat production and changes in the distribution of sweat on the surface of the body
- Sweat becomes more dilute
- Blood flow to the skin is reduced, therefore more blood available to muscles
- Blood volume increases
- Lowered heart rate
2.4.1 Process of Achieving Heat Acclimatization
The process of acclimatization or gradual tolerance of repeated exposure to increasing temperatures, results in physiological adaptations which improve the ability to dissipate excess body heat. This process is not instantaneous; it involves many changes and can take up to two weeks before someone can withstand heat that was previously considered intolerable.Reference 37Reference 45 Heat acclimatization is best achieved by exercising for 60 to 90 minutes in the heat, each day, for 9 to 14 days to be considered heat acclimatized,Reference 45 however most of the classical signs of acclimatization and a decrease in body heat content can be achieved by passive, short daily periods of exposure to heat as long as core temperature is elevated.Reference 63Reference 64 Generally, during the first day of heat acclimatization the discomfort is very noticeable, however with each succeeding day, the symptoms gradually decrease. Progressively, the individual is able to perform with a reduced level of thermal strain. Heat acclimatization to hot, dry conditions and hot, humid conditions produces slightly different responses: yet, the overall protection is thought to be the same.Reference 65 However, loss of these protective effects has been shown to occur more quickly when a person has undergone initial acclimatization in a hot, humid environment.Reference 66Reference 67

Workers that are exposed to high heat levels, either indoor or outdoor, can acclimatize to increase their protection from developing a heat-related illness.
These changes help individuals adjust to hot environmental conditions associated with extreme heat. The most rapid and substantial changes in temperature regulation appear to occur during the first week of the acclimatization process, and can account for up to 80% of the entire improvement.Reference 68Reference 69 It should be noted however that some people have an enhanced ability to acclimatize compared to others. Although the physiological responses to acclimatization are similar between different people, the degree of response is highly variableReference 68 and should be taken into consideration. This can be particularly important for vulnerable populations described later in this chapter.
Acclimatization to EHEs is much more difficult, as EHEs are usually short-term periods of high heat levels, not allowing enough time for acclimatization to occur.
2.4.2 Changes in the Sweating Mechanism
During acclimatization the sweating mechanism is altered in two ways. Firstly, the sweat glands themselves are able to produce more dilute sweat than in an unacclimatized person, and secondly the onset of sweating is much earlier (Figure 2.5). The core temperature required to activate sweating can be decreased by as much as 0.5°C.Reference 63Reference 70 It is postulated that this may be in part due to an increase in the sensitivity of the sweat gland itself to nerve impulses and/or to each molecule of acetylcholine,Reference 71 or an increase in the number of nerve impulses received from the temperature receptors in the skin. It should also be noted that in an acclimatized person regional variations exist in the distribution of sweat on the surface of the skin, and that there is a shift of sweat distribution from the trunk towards the limbs.Reference 72 This is beneficial in that it provides a greater surface area for the evaporation of sweat; however, these changes in distribution can also increase the amount of sweat which drips from the body and does not contribute to body heat loss but wastes body water content.
Figure 2.5: Changes in sweat rate and average rectal temperature between an acclimatized and an unacclimatized person.Reference 71
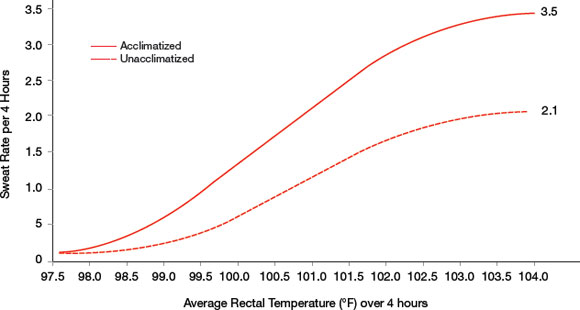
Text description
This graph illustrates an increase in sweat rate with an increase in average rectal temperature in degrees Farenheit over a four hour period in humans, starting with a base sweat rate of 0. Beginning with no sweat production at a rectal temperature of 97.5 degrees Farenheit, an acclimatized person can increase their sweat rate to 3.5 litres after four hours as their rectal temperature increases to 104 degrees Farenheit. An unacclimatized person can reach the same rectal temperature and only increases their sweat rate to 2.1 litres after four hours. The increase in sweat rate for an acclimatized person at all rectal temperatures is consistently above that of an unacclimatized person for the four hour period, beginning at 98 degrees Farenheit.
Figure 2.5: Changes in sweat rate and average rectal temperature between an acclimatized and an unacclimatized person.
At similar temperatures, sweat rate increases much more quickly in an acclimatized person than in someone who is not acclimatized. (Adapted from Reference 71)
2.4.3 Changes in Blood Flow
Similar to the changes in sweat rate during acclimatization, changes in blood flow are also apparent and contribute to heat loss through a decrease in the threshold core temperature which triggers the onset of blood redistribution to the skin. Resting pulse rate and pulse rate relative to blood flow have also been found to be lower following acclimatization.Reference 63 As outlined previously, with the increase in sweat production during acclimatization and the greater sensitivity of the sweat glands, there is a greater capacity to dissipate heat by evaporative cooling. With acclimatization, heart rate and blood flow can also be kept within acceptable physiological limits with increased exertion in the heat, which leads to greater endurance when undergoing activity or work hot conditions.
When a person is not acclimatized, increased strain on the cardiovascular system is expected when exposed to extreme heat, because the body is trying to properly maintain adequate blood flow and must increase cardiac output (total blood pumped through the heart) accordingly. Blood volume decreases which in turn initiates both a reduction in stroke volume (volume of blood pumped in each heart beat) and an increase in heart rate. If a person has undergone adequate acclimatization then an expansion of plasma volume occurs which causes an increase in total blood volume through an influx of protein and other molecules from interstitial spaces.Reference 73 Both heart rate and stroke volume decreaseReference 63 allowing cardiac output and arterial blood pressure to be maintained.
2.4.4 Fluid Balance
When sweat production is increased during exposure to hot conditions, there is the potential to cause a significant amount of sodium and chloride ion loss, as well as a reduction in water volume. The concentration of electrolytes is critical for the movement of fluid between intracellular and extracellular compartments and for maintaining membrane electrochemical potentials.Reference 58Reference 74 Acclimatization has been found to reduce sodium loss by increasing the re-absorptive ability of the eccrine sweat gland duct.Reference 75 In turn, people who are acclimatized have more dilute sweat and consequently more sodium and chloride ions in extracellular spaces. The mechanism of increased re-absorption is unknown however it is thought to involve increases in the secretion of the hormone aldosterone which increases the activity of the sodium channels in the sweat gland duct.Reference 75
2.4.5 Loss of Acclimatization
Tolerance to heat can begin to disappear after only a few days or weeks in the absence of exposure, and varies substantially between individuals.Reference 45 The first adaptations to be lost are those that are developed first, which include the changes in heart rate and other cardiovascular adjustments.Reference 76 The exact amount of time it takes until the benefits are lost is variable and depends on the conditions in which a person reached heat acclimatization. Research has found that a person is only slightly less efficient two to three weeks after acclimatizationReference 68 with virtually no loss for at least a week.Reference 77Reference 78 For the most part, acclimatization to heat appears to decrease after about three weeks without exposure. Interestingly, it has been shown that the loss of acclimatization occurs more quickly following adaptation to a hot, humid environment (34ºC, 91% RH) relative to a hot, dry environment (49ºC, 20% RH).Reference 66Reference 67 Although air conditioning use has been criticized for disrupting the acclimatization process, the effect of regular periods of cold exposure, such as with air conditioning, has not been found to affect the maintenance of heat acclimatization.Reference 79 Conversely, excessive use of air conditioning (occurring in people who travel from an air-conditioned house, to an air-conditioned car and workplace) may limit a person's ability to acclimatize since exposure to the heat is limited.
2.5 Physiological Challenges in At-Risk Populations
2.5.1 Heat Stress in Older Adults
As people age, physiological changes occur that interfere with the body's ability to deal with extreme heat. For example, the ability to maintain normal body core temperature is decreased. This may be attributed to several factors including decreased sweat rate, decreased blood flow to the skin and extremities (needed for heat dissipation) as well as a reduction in cardiac output.Reference 41Reference 45
With aging, even if physically active, a person's maximal capacity to transport and utilize oxygen during exercise (often referred to, and measured as aerobic capacity or cardiorespiratory fitness, i.e. VO2 max) is reduced by approximately 10% per decade, beginning in their 20s or 30s.Reference 80 Older adults must work much harder for a given activity level, and therefore produce more metabolic heat than their younger counterparts. For example, simply walking up stairs requires much more exertion for an active older adult, subsequently producing much more internal metabolic heat, than for someone who is 10 years younger. These differences can be unfavourable during hot ambient conditions, as this additional heat must be dissipated and heat dissipation is compromised in older adults.

Athletic trainer provides advice to older
clients about their heat/health risk
Evidence also suggests that older adults have a greater decrease in plasma volume than a younger adult during heat exposure.Reference 81 For those with diminished cardiovascular function, the combination of the redistribution of blood flow to the skin and the subsequent loss of fluids and salts through sweat can be enough to burden the heart, which can ultimately fail to maintain adequate cardiac output.Reference 82 It is for this reason that for people who succumb to heat illness the cause of death is often coded as "heart failure". Even in active, healthy older adults the sensation of thirst is decreased which can lead to further dehydration during hot weather.Reference 83 Older adults may also have lower overall fitness, increased body fat, and reduced lean body mass, which have been associated with compromised heat-sensing and heat-dissipating mechanisms.Reference 41
Older Adults
- Reduced sweating ability
- Decreased plasma volume
- Reduced cardiac output
- Decreased blood flow to skin and extremities
- Lower fitness, increased body fat, reduced lean body mass
- Reduced thirst sensation leading to increased susceptibility to chronic dehydration
- Increased susceptibility to chronic dehydration
Children
- Lower physical intensity but often more active overall
- Faster heat gain from the environment if air temperature is greater than skin temperature, due to greater surface-area-to-body weight ratio
- Reduced sweating ability
- Inability to increase cardiac output
- Dependence on caregivers for awareness and recognition of the impact of heat
Pregnant Women and Fetus Development
- Heat can act as a teratogen during specific stages of fetus development
- Disruption of mitochondrial structure and function
- Disruption of serotonin levels
- Effects on heat shock proteins during embryonic development
Physically Active
- Increased metabolic heat production
- Pooling of blood in the cutaneous circulation
- Insufficient fluid replenishment and blood volume loss due to insufficient fluid replenishment and profuse sweating
2.5.2 Heat Stress in Children
Historically, children have been regarded as a heat-vulnerable group due to a greater incidence of heat-related mortality and a perceived reduced efficiency to thermoregulate in comparison to adults under the same heat-stress conditions.Reference 50Reference 84Reference 85 These comparative results have largely been based on studies in which children and adults performed activities at matching exercise intensities. However it has been recently demonstrated that, when metabolic heat production during exercise is normalized to exercise intensity, these physiological differences between children and adults disappear.Reference 86Reference 87 This is important as children rarely exercise at the same intensity as adults and accordingly, a child has a lower physical intensity (proportional to body size) during regular activities.Reference 86 This suggests that the previous assumption that children are less tolerant to exercise in heat than adults, is not correct. Therefore, the increased risk formerly identified in children may not be due to the differences in metabolic and muscular heat production. Nevertheless, it is obvious that physiological differences do exist between children and adults and in general children are very active, which can impact the child's ability to tolerate heat.
Children have a higher body-surface-area-to-mass ratio, which not only allows for more efficient heat dissipation under cooler conditions, but also causes children to absorb much more heat from a hot environment.Reference 50Reference 88 Therefore, during hot, humid conditions when the child's body relies more on dry heat loss and less on evaporative cooling, the highly exposed surface area may greatly increase their heat burden.Reference 84Reference 87 It has been demonstrated that the sweating capacity of children is lower than in adults and that the temperature at which children begin to sweat is higher.Reference 89 The evaporation of sweat is the fundamental means of heat dissipation during EHEs and may become a thermoregulatory liability for children in such conditions. On the other hand, a low sweat rate and decreased sweat electrolyte concentration may also lessen a child's susceptibility to dehydration. Therefore, it is thought that children may be at a higher risk of increasing core temperatures during extremely hot environmental conditions; however, these circumstances have not been investigated as requisite information is limited, for ethical reasons.
Compared with adults, children have a greater increase in blood flow to the skin during exercise in high heat conditions. As a result, a greater proportion of their cardiac output is diverted to the periphery.Reference 87 Additionally, in comparison to adults, children also have a lower cardiac output. Coupled with a lower blood volume, a large strain can be put on a child's circulatory system.Reference 84Reference 87 Therefore in conditions of extreme heat the ability to exercise intensely and the ability to thermoregulate may be compromised in children.Reference 59

Epidemiological evidence has also demonstrated that children appear to be at an increased risk of morbidity and mortality when subjected to extreme environmental conditions.Reference 90 Reference 92 Although the reasons for this remain unclear, it may be due to lack of caregiver understanding and knowledge, lack of judgement in avoiding heat illness (i.e. staying out of the sun) or pre-existing chronic illnesses, especially those affecting hydration status and thermoregulation.Reference 88 Children (especially infants and toddlers) are reliant on caregivers to be aware of the environmental surroundings during EHEs and make changes accordingly, such as increasing fluid intake, dressing for the weather, moving to a cooler environment, and reducing activity. Caregiver reasoning will also influence a small child's response to increased heat, therefore it is imperative to ensure that education and messaging be repeated.
2.5.3 Heat Stress during Pregnancy
The teratogenic effects of heat in mammals have been widely studied for decades, however, the consequences of hyperthermia during human pregnancy remains unclear. The objective of this section is to briefly outline some of the effects that may result from an increase in core temperature in women during the various stages of pregnancy. It should be noted, however, that heat only acts as a teratogen when exposure occurs during certain susceptible stages of development of the fetus and that the extent of knowledge regarding these vulnerable stages is minimal. The critical threshold temperature ranges from approximately 2 to 2.5°C above the normal body core temperature.Reference 93
Increases in core temperature during the third week of human pregnancy have been linked to anencephaly (a serious fetal disorder where the neural tube, the precursor to the central nervous system, fails to close and the brain does not develop properly).Reference 94 Elevated temperatures have also been linked to other fetal and newborn malformations.Reference 93 An association has been noted between maternal hyperthermia during the first five months of pregnancy and congenital malformations such as the occurrence of microphthalmia (abnormally small eyes).Reference 95 Other physiological disruptions of the fetus resulting from increased core temperature during pregnancy include disruption of mitochondrial structure and function,Reference 96 disruption of serotonin levels,Reference 97 effects on heat shock proteins during embryonic development,Reference 98 and central nervous system developmental abnormalities.Reference 99
Less is known regarding the effects of increased heat on the mother, and her ability to properly thermoregulate. During moderate heat stress induced by exercise, maternal thermoregulation mechanisms appear to dissipate heat effectively by both the metabolically active mother and fetus.Reference 10 Women have been shown to have efficient mechanisms to dissipate heat, which may contribute to their ability to adjust their cardiovascular mechanisms to preserve plasma volume during heat stress. This is thought to help maintain optimal feto-maternal heat transfer and dissipation by having plasma volume available for other purposes.Reference 100
Although research into these areas is inconclusive, women who are pregnant should avoid unnecessary exposure to extreme heat from extreme weather or hot tubs, saunas or steam rooms. If such exposure is unavoidable, a woman who is pregnant should exercise all options to remain cool in order to prevent the elevation of core temperature.
2.5.4 Heat Stress in the Physically Active
Two forms of heat stroke exist: exertional heat stroke and classic heat stroke. Exertional heat stroke occurs mainly in healthy individuals participating in strenuous physical exertion, usually in a hot environment for a prolonged period of time. Exertional heat stroke is most commonly seen in athletes and some occupations where the potential for heat illness is higher due to increased metabolism and/or increased heat exposure (which requires a greater amount of heat to be dissipated from the body). Classic (non-exertional) heat stroke affects mainly older adults, the chronically ill and young children during prolonged exposure to certain environmental conditions such as high ambient temperatures and humidity.
In athletes and workers, acute circulatory failure has been found in 20-65% of exertional heat stroke cases and is thought to be due to the pooling of blood into the cutaneous circulation, insufficient fluid replenishment resulting in blood volume loss from profuse sweating, and shock.Reference 101 In addition, kidney failure is more often seen in exertional heat stroke than in classic heat stroke.Reference 102
Athletes are often required to wear protective athletic gear when participating in practices or games in the heat. Along with the aforementioned physiological risks, heat dissipation is often further impeded by the insulative effects of the athletic gear required for certain group sports.Reference 45 Many exertional heat stroke deaths in young athletes have been documented in high intensity and competitive contact sports such as football.
2.5.5 Heat Stress in the Workplace
The problems associated with heat stress and occupational safety are twofold. Firstly, the risk of developing a heat-related illness can be increased if a person is working under environmental conditions in which they are exposed to high heat levels and they are unable to dissipate the excess heat. The second is the physical discomfort and mental status changes that may increase the potential for accidents and injuries. Heat stress has been shown to impair mental function, alertness, motor control and contributes to muscle fatigue leading to decreases in physical performance.Reference 103Reference 104 In addition, with increased core body temperature a person becomes more irritable, angry and can have other emotional states which may cause workers to overlook safety procedures, or have decreased attention when performing hazardous tasks thus increasing the likelihood of an accident.Reference 105
To date, heat stress in the workplace has been extensively covered in the literature and the resources available are well developed and provide widespread information relevant for occupational health and safety purposes. In addition, each province and territory has its own occupational health and safety regulations and workers are encouraged to become familiar with the information that is relevant to their place of employment. The intent of the Guidelines is not to replace existing valuable resources regarding occupational heat stress, but to synthesize existing research and provide clarity for those who would not have access to such material. It is for this reason that the Guidelines will not discuss heat stress in the context of the workplace. Please refer to your workplace guidelines.
For further information, the following resources are available:
- ACGIH Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices, available online.Reference 46
- Further resources for occupational heat stress are listed in Table 2.2. It should be noted however, that the documents provided are not necessarily endorsed by Health Canada.
| Organization | Resource | |
|---|---|---|
| Canada | Canadian Centre for Occupational Health and Safety | www.ccohs.ca |
| Ontario | Health and Safety Ontario | Heat Stress Kit: www.csao.org/t.tools/t6.news/heat_stress.cfm |
| Ontario Ministry of Labour | Health and Safety Guidelines: www.labour.gov.on.ca/english/hs/pdf/gl_heat.pdf |
|
| Workplace Safety and Insurance Board | Prevent Heat Stress: www.wsib.on.ca/files/Content/PreventionHSGuide/HeatStressGuide.pdf | |
| Quebec | Government of Quebec | Regulation Respecting Occupational Health and Safety: www2.publicationsduquebec.gouv.qc.ca/ dynamicSearch/telecharge.php? type=3&file=/S_2_1/S2_1R19_01_A.HTM |
| Direction du Santé Publique | Prévention en pratique médicale: www.santepub-mtl.qc.ca/Publication/ pdfppm/ppmjune04.pdf |
|
| Manitoba | Government of Manitoba | The Workplace Safety And Health Act: http://web2.gov.mb.ca/laws/regs/pdf/ w210-217.06.pdf |
| Guidelines for Thermal Stress: http://safemanitoba.com/uploads/ guidelines/thermalstress.pdf |
||
| Workers Compensation Board of Manitoba | Worker Discomfort in Increased Temperatures: http://safemanitoba.com/ worker_discomfort_in_increased_ temperatures_bulletin_133.aspx |
|
| Alberta | Alberta Employment and Immigration | Best Practice Working Safely in the Heat and Cold: http://employment.alberta.ca/documents/WHS/ WHS-PUB_gs006.pdf |
| Saskatchewan | Government of Saskatchewan, Occupational Health and Safety Division | Working Under Hot Conditions: www.labour.gov.sk.ca/hotconditions/ |
| British Columbia | WorkSafe BC | OHS Guidelines: www2.worksafebc.com/Publications/OHSRegulation/ GuidelinePart7.asp#SectionNumber:G7.27(1) |
| Preventing Heat Stress at Work: www.worksafebc.com/publications/health_and_safety/ by_topic/assets/pdf/heat_stress.pdf |
||
| Newfoundland | The Law Society of Newfoundland and Labrador | Occupational Health and Safety Regulations: www.canlii.org/nl/laws/regu/1996r.1165/20080818/ whole.html#10_ |
| New Brunswick | Government of New Brunswick | Occupational Health and Safety Act: www.gnb.ca/0062/regs/91-191.htm |
| WorkSafe NB | Risk Alert and Working Outdoors: www.worksafenb.ca/docs/Sun.pdf |
|
| Nova Scotia | Government of Nova Scotia | Heat Stress: www.gov.ns.ca/lwd/healthandsafety/heatstress.asp |
| Workplace Health, Safety and Compensation Commission | Hazard of Heat: www.whscc.nf.ca/Prev_HealthAndSafety InformationSheets.whscc |
|
| Prince Edward Island | Workers Compensation Board | Guide to Prevention of Heat Stress at Work: www.wcb.pe.ca/photos/original/wcb_heat_stress.pdf |
| Prevention Update: www.wcb.pe.ca/photos/original/wcb_sn_sfty_ pu.pdf |
||
| Yukon, North West Territories and Nunavut | Government of Yukon | Government of Yukon: www.gov.yk.ca/legislation/regs/oic1986_164D.pdf |
| Yukon Workers' Compensation Health and Safety Board | Yukon Occupational Health Regulations: www.wcb.yk.ca/Media/documents/ Occupational_Health_Regs.pdf |
3. Risk Factors Associated with Heat-Related Illness and Death
Key Terms: pre-existing illness, morbidity, heat-vulnerable groups, social isolation, socio-economic status, protective factors, relative risk, odds ratio
Summary Points:
- Many of the risk factors identified as increasing the susceptibility to heat-related illness and death are interrelated.
- Often people are at risk for more than one reason.
- Most risk factors fall into one of two categories: physiological or socio-economic.
- Some pre-existing conditions are exacerbated by exposure to heat, and increase a person's vulnerability to heat-related illness.
- Protective factors also exist which are thought to decrease the risk of developing a heat-related illness.
3.1 Risk Factors Associated with Mortality During Extreme Heat Events
Understanding the risk factors associated with an increased likelihood of heat morbidity (illness) and mortality (death) is important in order to advise patients and caregivers who may be unaware or unconcerned about the potential dangers of extreme heat. However, identifying the interactions between these risk factors is complex. Individuals may have physiological or socio-economic conditions that increase their likelihood of developing a heat-related illness (and not because of their failure to take appropriate actions). People may not adapt their behaviours during extreme heat, even if they are informed of the risks, perhaps because they are simply unaware that they are considered vulnerable. In addition, due to a person's socio-economic reality, many of the best options for protection from extreme heat are not always feasible. There is very little knowledge regarding the interactive effects on individuals who possess multiple risk factors. To this end, individuals should be advised to take, when possible, necessary precautions to protect themselves and those in their care from heat stroke and other heat-related illnesses.
Figure 3.1: Risk factors associated with exposure to heat.
Text description
A Venn diagram, with three overlapping circles, demonstrates three risk factors associated with increased susceptibility to heat-related illnesses: having a chronic illness, taking certain medications and living alone. When two of these risk factors overlap, they are at a higher risk, and where all three risk factors overlap a person is at the highest risk.
A schematic representation of some of the most prominent risk factors identified in the literature. An individual who has a chronic illness, is socially isolated and is on various medications is at increased risk of developing a heat-related illness. Individuals who experience two of these conditions are at further risk and those with all three are at highest risk.
The following risk factors have been identified in the literature as increasing the susceptibility to heat-related death.
These risk factors have been selected through a systematic approach based on several criteria which include: how often the risk factors were identified, how often they were studied, the extent to which they increase a person's risk of succumbing to a heat-related illness (odds ratio and relative risk) and an evaluation of the quality of the study from which they are cited (Appendix A).
Many of these risk factors interact with one another and those who experience heat illness or death are likely to have more than one of the characteristics listed below. For example, those who utilize health care aides (e.g. personal care attendants) and various at-home services likely have decreased mobility and in turn are more socially isolated than individuals who are more mobile and able to leave the home to carry out daily activities without assistance. In addition, people may also be taking medications that put them at risk for heat-related illness and the combination can be more than additive. Due to the cumulative effects of these risks and the difficulty in addressing them separately, the identified risk factors have been divided into generalized categories. This concept is described more broadly in Figure 3.1.
If a patient or client does not have one of the more specific risk factors but falls into the larger generalized group, such as compromised mental status, social isolation, individual living circumstances or lower socio-economic status, a health care worker should use proper judgement and caution the individual of the potential risk if they believe it to be of concern during extreme heat events (EHEs) by orienting the individual to protective behaviours.
3.1.1 Physiological Factors
Some pre-existing conditions increase a person's risk for developing heat-related illnesses due to the physiological factors that result in a compromised heat tolerance. These risk factors are listed below:
- Cardiovascular conditions
- Pulmonary conditions
- Renal illness or failure
- Neurological disease
- Age
- Hypertension
- Diabetes
- Malnutrition
Cardiovascular Illness

During EHEs the number of hospital admissions does not adequately reflect the actual increases in mortality due to heat. This is likely due to the fact that many victims die before they can achieve, or seek, access to medical attention. Cardiovascular deaths often occur rapidly in hot conditions, prior to the involvement of medical attention, resulting in fatal outcomes in a short period of time and in isolated (non-clinical) places.Reference 14Reference 106Reference 107
For those with cardiovascular-related illnesses, the decreased capacity of the heart to pump blood throughout the body can be detrimental when extreme heat is involved. The body regulates its temperature through increased blood flow which brings body heat to the skin surface to promote cooling. Anyone with pre-existing cardiovascular illnesses (such as those affecting the cardiac muscle) would have compromised cardiac function, and therefore decreased ability to dissipate heat.Reference 108
Temperature regulation may also correlate with changes in systemic vascular resistance and circulating catecholamines (stress hormones), blood platelets, red and white cells, blood viscosity, plasma cholesterol, and blood pressure. A heart in poor condition may not be able to cope with these changes and consequently may fail.Reference 14Reference 109Reference 110
Additionally, it has been shown that increases in airborne particulate matter (PM) and ozone (O3), which often coincide with EHEs, can have a direct effect on the heart and have been associated with death from cardiopulmonary disease, circulatory disease, and ischemic heart disease.Reference 111Reference 112
Pulmonary Conditions

The direct mechanisms through which high temperatures increase the risk of hospitalization for pulmonary illnesses remain unclear.Reference 14 However, air pollution is frequently worse during an EHE, and because hot weather and air pollution often coincide, it is difficult to separate the two effects.Reference 113 Increases in certain air pollutants can be associated with EHEs, and these may further aggravate respiratory diseases, such as asthma.Reference 114 Increased death during extreme heat has been associated with airway and systemic inflammation, hyperventilation and consequently dynamic hyperinflation (resistance to air flow where the lungs may not have enough time to empty before the next inhalation), pulmonary vascular resistance and chronic obstructive pulmonary disease (COPD).Reference 14Reference 115Reference 116 It is also important to note the role of pollutants on chronic respiratory illnesses during high temperatures. Air pollutants, especially ozone (O3), (the most damaging pollutant in terms of air quality for some locationsReference 117) may be implicated. Ozone often increases with high temperatures and sunshine levels and therefore hot, sunny days are generally associated with higher local production of O3 levels which may aggravate respiratory illnesses.Reference 116
Renal Illness or Failure
The role of the kidneys is to regulate electrolyte concentrations, maintain acid-base balance and control blood pressure; therefore, it is not surprising that renal disorders were found to be frequently associated with increased risk of heat illness and death (80% of the time).Reference 23Reference 118Reference 121 In addition, dehydration, which is frequently associated with heat illness, compromises renal physiology by reducing glomerular filtration rate (the volume of liquid filtered by the kidney) and renal plasma flow (volume of plasma supplied to the kidney). It has also been suggested that extreme hyperthermia may directly cause death of renal tubular cells and contribute to acute renal failure.Reference 122 Kidney stones are linked to dehydration and therefore extreme heat also contributes to their prevalence.Reference 123
Secondary hypertension (elevated blood pressure associated with another condition, in this case kidney disease) is found in more than 80% of seniors suffering from chronic kidney disease, further elevating a person's risk of developing a heat-related illness.Reference 13 The increased risks associated with hypertension (impaired circulation, taking medications) are often in individuals with renal disorders. Increased hospital admissions for renal illness, many of which are of older adults, can be expected during an EHE.Reference 16Reference 124
Neurological Disease
There are more than 600 types of neurological diseases, which include degenerative diseases such as Parkinson's and Alzheimer's, seizure disorders such as epilepsy, genetic disorders such as Huntington's and muscular dystrophy, and infections such as meningitis. These neurological diseases compromise the body's nervous system and are known to affect motor system capabilities. The symptoms associated with neurological diseases (muscle coordination and muscle weakness, paralysis, pain and confusion) are often found in older adults suffering from chronic illnesses who are unable to adequately care for themselves.Reference 125Reference 126 Therefore many of these diseases coincide with other risk factors due to decreased mobility such as confinement to bed and need for health aides.
Some of these conditions also have a higher prevalence in older adults. The medications used to treat such conditions, of particular note, medications for Parkinson's disease and for depression, can interfere with the physiological response to temperature extremes. Medication effectiveness can also be compromised above certain temperatures, increasing the risk of heat-related effects on health.Reference 48Reference 127Reference 129
Age
Studies have shown that older adults are among the most affected by extreme heat due to a decreased ability to sense heat and adapt behaviour appropriately, consequently decreasing their ability to physiologically maintain core temperature. Sensing and addressing dehydration is also an issue in an older age group.Reference 13Reference 41 Age is correlated with the increased presence of chronic illnessReference 130 which adds an additional burden on older adults during EHEs.
Whereas morphologically and physically children should be more at risk, this is not supported in the epidemiological literature with extreme heat and so the risks associated with children are not included in this chapter. (For a more detailed explanation of the physiological challenges of thermoregulation associated with older and younger age see Chapter 2).
Hypertension
Hypertension is frequently linked with cardiovascular illness and renal illness and so can exacerbate other pre-existing conditions (listed above). Individuals diagnosed with hypertension experience similar risks as those with a compromised cardiovascular system during extreme heat. High blood pressure is characterized by a reduction in blood flow, usually due to partially blocked arteries and reduces the ability of the body to thermoregulate. Individuals with hypertension often exhibit elevated peripheral resistance and a variety of circulatory changes such as hypotrophy of vascular smooth muscle (loss of muscle) as well as vascular rarefaction (decrease in density of blood vessels) which could lead to the impairment of blood flow control to the skin. Many medications prescribed for hypertension can also exacerbate the effects of extreme heat (see Chapter 4).Reference 41Reference 130
Diabetes
In-patient admissions of individuals with diabetes have been found to be 30% higher than those of the general population during EHEs.Reference 132 However, the physiological mechanism associated with this increase in risk is unclear. Additionally, current research has not differentiated between the risk associated with Type I, Type II, or gestational diabetes. The increased risk is thought to be caused by decreased sweat production due to impaired central mechanisms associated with heat sensitivity in the hypothalamus, the reduced ability of blood vessels in the skin to dilate and dissipate heat as well as other vascular impairments.Reference 41Reference 132 The sensitivity of peripheral heat sensors is also decreased leading to inadequate behavioural changes during hot weather. Diabetics also have a high incidence of co-morbid conditions such as cardiovascular disease, renal disease and neurological impairment, which increase the risk of developing a heat-related illness. Diabetic patients should be cautioned regarding an elevated susceptibility to becoming dehydrated if they have poor glucose control or uncontrolled hyperglycaemia.Reference 133
It is especially important to be aware of the proper storage of insulin during EHEs. Studies have shown that insulin vials stored at 32°C can lose 14-18% of their potency after 28 days, compromising the reduction of blood glucose levels.Reference 134 Although it is unlikely that an EHE would have such duration, many storage areas can retain heat for longer periods of time. In addition, even short exposures to high temperatures may reduce insulin potency.
Malnutrition
Malnutrition encompasses many conditions where there is an improper balance between what an individual eats and what is required to maintain health. This includes a reduced intake of nutrients (anorexia, bulimia), dietary excess or an imbalance of basic nutrients such as protein, carbohydrates and fat, or improper absorption of nutrients. The identification of malnutrition as a risk during EHEs can be attributed to several factors. First, the proportion of patients/clients in long-term care who are malnourished can be anywhere between 23% and 46%.Reference 135 This can further worsen the ability of older adults to properly thermoregulate due to compromised health. In addition, it is well known that the residents of these facilities are primarily on regimented diets. For older adults living independently and outside facility care homes, the incidence of malnutrition may be much greater due to either a lack of nutritional awareness or reduced resources, which may increase the risk of developing a heat-related illness. In addition, malnutrition has been found to be linked with increased age, cardiovascular illness and respiratory diseases,Reference 135 and is often a consequence of low income, further intensifying the problem.
It should be noted that homeless people do not always have access to complete meals or potable water and are subsequently susceptible to malnourishment. These individuals should also be considered at increased risk.
3.1.2 Compromised Mental Status
In the literature, compromised mental status refers to mental conditions that affect a person's cognitive awareness. More specifically our definition includes:
- Symptoms of depression
- Taking antidepressants
- Other mental health concerns or psychiatric illnesses
- Taking neuroleptics (antipsychotics)
The likelihood of succumbing to a heat-related illness during an EHE has been shown to be twice as high in hospitalized patients suffering from mental and behavioural disorders in comparison to non-hospitalized people with psychiatric illness, and four times higher than the general public.Reference 136 It has also been suggested that mental illness increases the risk of heat-related illness in younger individuals.Reference 125

There are several overlapping reasons that may be responsible for this increased risk. Firstly, from a physiological perspective, the neurotransmitters for thermoregulation are involved in schizophrenia and depressive disorders.Reference 136Reference 137 Psychotropic medication use can also alter the body's ability to thermoregulate by affecting the parasympathetic pathwayReference 16. Other risks include increased agitation, decreased cognitive awareness and decreased coping mechanisms which may lead to the neglect of protective behaviours and the dismissal of precautionary advice during extreme heat.Reference 16Reference 136
Secondly, this increased risk may be compounded by the hospital's inability to manage EHEs due to an absence of a heat-emergency plan or inadequate emergency preparedness, an absence of (or limited) air conditioning, or lack of patient and caregiver education and knowledge regarding the risks of heat. In addition, most people who suffer from mental illness are not hospitalized or closely monitored, therefore awareness of protective behaviour is fundamental in these vulnerable groups.
Medications for several mental health disorders exacerbate the effects of heat by affecting several physiological mechanisms including changes in the:
- Hypothalamus and the body temperature set-pointReference 138
- Sweat rateReference 139Reference 140
- Renal function or general body dehydrationReference 141
- Susceptibility to radiant heat and UV exposureReference 142Reference 144
3.1.3 Social Isolation
Social isolation is largely identified in the literature as a prominent risk factor during EHEs and public health interventions often have difficulty reaching these vulnerable groups. These individuals include those who:
- Live alone
- Do not have regular visitors
- Do not leave home
Evidence that exists in the literature demonstrates that the extent of an individual's community integration and social network involvement is related to individual health status.Reference 145 As such, people who are isolated may be at increased risk of mortality from multiple causes (e.g. chronic illness, socio-economic status and isolation).Reference 146 In addition, a lack of social networks has been associated with increases in unhealthy behaviour, such as alcohol over-consumption,Reference 145 which can contribute to dehydration and impaired judgement.
Living alone was found to greatly increase the likelihood of dying during an EHE in population-based studies in both the United States and Europe.Reference 13Reference 147 During the 1995 heat wave in Chicago, the Public Administration Office experienced their busiest week ever managing the estates of unclaimed decedents. Among these victims, 170 people remained unspoken for until an aggressive campaign was started to seek out relatives with missing family members.Reference 5 These issues could have been greatly reduced if the victims had visitors who were willing to check-in on a regular basis during times of extreme heat. In France, during the 2003 EHE, 92% of the victims were living alone.Reference 147 Living alone is also a particular risk when combined with chronic conditions and other socio-economic factors such as low income, reduced access to transportation and lack of air conditioning in the home.Reference 148
Not leaving the home, even though the residence is uncomfortably hot and cooler options are available elsewhere, extends exposure to heat unnecessarily. The increase in mortality among individuals who do not leave home during an EHE may be due to their inability or unwillingness to visit areas with air conditioning or that have cooler temperatures, as well as feeling unwelcome in these areas. Visiting air-conditioned places during EHEs is associated with reduced risk of death.Reference 13Reference 41Reference 149
3.1.4 Individual's Living Circumstances
Although hazardous living conditions can incorporate many different circumstances, there are several instances that are related to a person's housing and lifestyle that can lead to a higher risk of heat-related illness. Specifically, these have been identified as:
- Confinement to bed
- Need for health aide, home nurse or home services
- Living on the top floor of a building
The living circumstances listed above which are most prominently identified in the literature as those that increase susceptibility to heat-related death are often related and indicative of individuals who suffer from a chronic illness. For example, one of the strongest contributors to increased susceptibility in extreme heat is confinement to bed. This is symptomatic of late stages of chronic diseases such as cancer, diseases relating to bones and joints, respiratory diseases and cardiovascular diseases. Individuals who used at-home services such as personal care or nursing aides, or delivery services (such as meals-on-wheels), were found to have a mortality rate approximately six times higher than people who did not need such assistance.Reference 149

In addition, the inability to care for oneself has been associated with a fivefold increase in the relative risk of developing heat strokeReference 13Reference 150 because voluntary hydration and effective cooling are likely limited and dependent on the caregiver. A need for assistance is also suggestive of home confinement which may then lead to social isolation; two other significant risk factors of heat-related death identified in the literature. From a prevention perspective, it is important to consider that many of these vulnerable groups have developed relationships with a health care provider, presenting an opportunity for health care workers to increase a patient's awareness of the dangers of heat.
Living on the top floor of a building, when combined with poor socio-economic status and a lack of air conditioning, was found to be a risk factor in 75% of the studies in which these building characteristics were studied.Reference 23Reference 121Reference 125Reference 146Reference 149 Multiple stairs can be an impediment to venturing outside, especially for those with limited mobility.Reference 151 Living on the top floor may also be an increased risk because, in the absence of air conditioning, the top floor can be much hotter than the ground level.Reference 23 The nature of the characteristics of the buildings can also be detrimental. Buildings that are located in urban centres may be more prone to high indoor temperatures as compared to buildings located in more rural settings, due to the urban heat island effect. Heat levels would likely be most extreme at the top of the building.
3.1.5 Lower Socio-Economic Status
There are many factors associated with low socioeconomic status that increase the risk of developing a heat-related illness. These can include low income, lower levels of education, reduced access to transportation, occupation of a single room, lack of air conditioning and ventilation in the home, and/or failure to use existing or available cooling processes due to the lack of money among such groups.Reference 115Reference 121Reference 125Reference 146 Marginalized people, although aware of their increased risk, may also feel unwelcome in many cooling centres and public air-conditioned places and are therefore reluctant to visit. During the 1995 Chicago heat wave, it was well documented that many people living in unsafe neighbourhoods succumbed to the extremely hot conditions because they refused to open windows or leave their homes due to fear of being harmed or robbed.Reference 5 Due to the large differences in quantifying socio-economic status, the associated risk factors for such groups are also difficult to determine. Health care workers should bear in mind patient socio-economic factors when implementing intervention options.
Recent investigations in Canada regarding linkages between socio-economic status and extreme city surface temperatures have been explored. These studies have found that areas of the community which are considered as 'high' on the deprivation index,Reference 153Reference 154 indicative of low material and socio-economic status, often correspond to areas with high urban surface temperatures. The deprivation index is based on an individual's disadvantage relative to the local community and takes into account various indicators including housing, education, employment, personal revenue, marital status, family structure and social ties.Reference 153Reference 154 These disadvantages are demonstrated in Montreal (Figure 3.2) where the neighbourhoods with high deprivation (Figure 3.2.A), represented in purple, also correspond to the neighbourhoods that have high surface temperatures (Figure 3.2.B). Areas with a high proportion of these vulnerable groups are often located in close proximity to large scale commercial and industrial areas, which are found to have the most severe UHI effects characterized by large buildings and parking lots with dark surfaces.Reference 155
Figure 3.2: Calculated deprivation index (meterial and socio-economic status) and corresponding surface temperatures in Montreal, Que.
Areas considered to be socially disadvantaged (A: purple) often correspond with high surface temperatures (B).
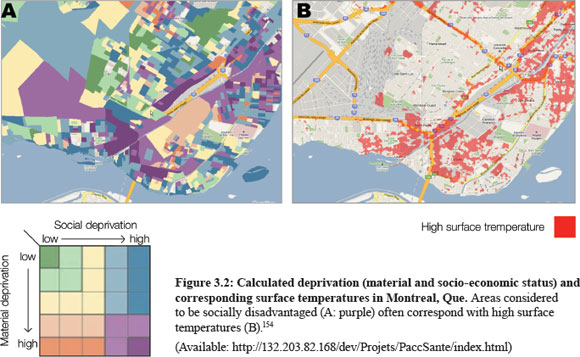
Text description
This figure shows two corresponding maps of Montreal Island, Quebec: a) one with a mapped social-deprivation index and b) one with mapped high surface temperatures. The most deprived areas (material and social deprivation) match up with the areas with the highest surface temperatures, namely areas such as Montreal West (Saint Pierre and LaSalle) and the South West of Montreal (Ville-Emard and Verdun).
Box 3.1: Heat as a Risk Factor for the Homeless
The definition of homelessness includes individuals who sleep in shelters, as well as the individuals who sleep outdoors, often referred to as "absolute homelessness". Although homelessness is not usually reflected in the literature, due to the presence of many other health conditions in this population as well as unique socio-economic factors, people who are homeless are at increased risk of heat-related illness and death.

Compromised Health
Many of the risk factors identified in the literature to increase a person's susceptibility to heat-related illness and death are found to be more common in individuals who are homeless. For example, chronic diseases are often more prevalent due to delays in seeking care, non-adherence to therapy and cognitive impairment.Reference 152 Medical conditions such as diabetes, high cholesterol and hypertension, also tend to be less controlled among the homeless. Respiratory disease, cardiac disease, mental illness and substance abuse are also more widely reported in homeless populations.Reference 152
Decreased Access to Services
People who live in shelters and outdoors are automatically at a higher risk of heat-related illness and death due to increased exposure to the environmental conditions. Often these people inhabit areas of the urban core, which also subjects them to the urban heat island effect. In addition, many do not have access to air conditioning; have limited or no transportation to local shelters and community services, which restricts their ability to seek helpReference 5; have limited options for hydration; must carry around belongings, which causes increased physical burden; and have a high probability of social isolation, an independent risk factor in itself. Although many cities are beginning to address these issues (for example the City of Toronto distributes transit tokens to the homeless so that they can reach cooling centres), outreach to this vulnerable population remains a challenge for community services.
3.1.6 Other Risk Factors
Several other risk factors have been investigated in the literature, but the extent of their impact is unclear. Nonetheless, an individual with several of these risk factors may be at increased risk of heat-related illness or death during an EHE. The risk factors listed below have been reported in the literature and found to significantly increase heat-related risk in at least one instance. These are listed to raise health care worker awareness, but will not be discussed in detail.
Risks Related to Building Characteristics
- Lives in building with flat, dark roof
- Occupies a single room
- Building of residence located in city
- Building of residence has more than two stories
- No shower or bath present in home
- No ventilation present in home
Risks Related to Individual Behaviour
- Decreases showers/baths during extreme heat
- Consumes less than 1L liquid/day
- Tries to conserve electric energy use by not using air conditioner during extreme heat (economic or environmental reasons)
Risks Related to Health
- Unable to care for oneself
- Pre-existing cerebrovascular illness
- Decreased ability to maintain daily activities
- Chronic illness (in addition to cardiovascular, renal, neurologic and respiratory)
- On antipyretics
- Cancer
- Dementia or other memory problems
- Musculoskeletal disorders
3.2 Factors Associated with Heat Morbidity
The additional factors listed below are known to increase the susceptibility to heat-related illness, especially in those who already have any of the risk factors outlined in Section 3.1.
- Obesity
- Alcoholism
- Dehydration
- Sunburn
- History of heat stroke/illness
- Use of certain medications
- Lack of or improper acclimatization
Obesity
It has been found that the occurrence of heat stroke is more than three times as likely in individuals who are obese and overweight than those with average body weight.Reference 41 This is thought to be due to a decreased thermal sensitivity, a decreased capacity to dissipate heat due to a decreased blood flow, and greater insulation. In addition, an increase in the cost of metabolic activities is thought to exist, which increases metabolic heat production at a faster rate than in people with a smaller body mass index.Reference 41
Alcoholism
People suffering from alcoholism may increase their chances of developing a heat-related illness. For the most part, excessive and chronic alcohol consumption can drastically alter an individual's awareness and perception, which may lead to inadequate protective behaviour when subjected to increased heat stress. For example, a study showed that alcohol was found to decrease the reaction time taken to reduce exposure to radiant heat.Reference 156
Studies have also found that at certain ambient temperatures (specifically those between 34ºC and 37ºC) consumption of alcohol raised the core temperatures of mammalsReference 157 and suggested that at any given dose of ethanol, the effect of ethanol on body temperature was dependent on the temperature of the surrounding environment. In addition, general findings in people suffering from alcohol withdrawal include the elevation of core temperature.
Dehydration
For people who exercise, work, or even walk long distances outdoors in hot conditions, it is important that water is consumed prior to the commencement of any activity to prevent dehydration. Research has found that water intake during exertion does not adequately replace body water losses.Reference 58 In addition, individuals who live outdoors should also be conscious of the need to consume water before feeling thirsty during extreme heat. The loss of water and salts increases core temperature in both temperate and hot environments and the magnitude of the core temperature elevation can range from 0.23 -1ºC for every percentage of body weight loss.Reference 58 Dry and evaporative heat loss are also compromised when a person is dehydrated. It is therefore important that individuals remain properly hydrated during extreme heat to prevent heat illness.
Sunburn

Many sunburns occur every year
when people do not use the proper protection when spending time outdoors
Although sunburn is sometimes classified as a heat-related illness in itself, it is also a risk factor for more serious heat-related illnesses and therefore its inclusion is critical when describing the exacerbation of these conditions. Sunburns and the subsequent damage to the skin (from as little as one hour of midday exposure) have been shown to affect the body's ability to properly thermoregulate. Not only is the sweating response compromised due to the inhibition of actual sweat production and the release of sweat from the gland, but the damage to the dermal vasculature and the sweat glands themselves is thought to last more than three weeks following sunburn onset.Reference 158 This is important when considering the body's ability to dissipate heat during exposure to heat stress, as the primary mechanism to cool off is from the evaporation of sweat from the surface of the skin. Perceptual responses during exercise, such as perceived exertion and thermal sensation, have also been found to be elevated in those suffering from mild sunburn.Reference 159 Further resources on protecting family and friends from sunburn can be accessed online on the Health Canada website.Reference 160
History of Heat Illness

Individuals who have a previously developed heat illness are at an increased disadvantage if exposure to heat stress is recurrent, and are more susceptible to exacerbating the conditions of the existing heat illness. For example, a study subjected healthy, heat-acclimatized men to heat and work stress tests seven days following the development of miliaria rubra (heat rash). Although no damage was visible on the skin surface, at the onset of exercise there was significant absence of the sweating response which decreased the men's ability to withstand the heat.Reference 159 This decrease in sweat led to heat exhaustion in many of the subjects.
Although some research has been done regarding the return of athletes to training following episodes of exertional heat stroke, very few general recommendations are available. This is due to limited scientifically valid criteria to assess recovery from exertional heat stroke, and inadequate scientifically valid criteria to predict who may be predisposed to a subsequent heat injury after experiencing exertional heat stroke.Reference 161 Most of this insufficient information is due to lack of understanding regarding the individual underlying factors that contributed to the initial heat illness episode, as well as initiation and effectiveness of treatment. For this reason most organizations recommend return to play after the resolution of any abnormal clinical symptoms and to gradually increase physical activity and exposure to heat stress.Reference 162 For non-athletes who have previously developed a heat illness the same principles should apply, however the cause of the initial episode should be identified and prevented in the future.
Medication Use
It has been stated several times in The Guidelines that many types of medications exacerbate the potential of developing heat-related illness and that the effectiveness of the medication can also be compromised. This term could include prescribed, over-the-counter and recreational drugs, and is explained in detail in Chapter 4.
Lack of or Improper Acclimatization
The physiological changes associated with acclimatization happen gradually, and can take up to fourteen days before someone is considered 'acclimatized'. In addition, if the acclimatization process is interrupted or not continual during this time, these physiological adaptations can be lost very quickly. Therefore a dangerous aspect of improper acclimatization is the individual's perception of being protected, which may lessen their adoption of protective behaviour during hot conditions.
3.3 Protective Factors
Many factors have been investigated in the literature to determine which activities or behaviours can be undertaken during EHEs to reduce an individual's susceptibility.Reference 121Reference 125Reference 146Reference 149Reference 150Reference 163 Although these protective factors have not been studied as extensively as those that cause harm, there has been considerable progress in helping to recognize and quantify such heat defensive activities.
Highly Protective Factors
- Participating in non-exertional group activities
- Has air conditioning in home
- Increasing time in air conditioning (visited places with air conditioning, etc.)
Protective Factors
- Taking showers/baths
- Friends in city, or received phone call during EHE
The protective factors that will be presented here outline the importance of two key activities that should be considered during EHEs: time spent in air-conditioned places and increasing socialization with others. The highly protective factors listed above were found to be the most prominent and highly ranked protective factors in the literature. The protective factors have been identified as possessing protective characteristics, but were not reported as frequently or consistently.
3.3.1 Participated in Non-Exertional Group Activities
The importance of increased socialization through participation in non-exertional activities is clearly defined in the literature and can greatly increase a person's chance of survival during an EHE. For example, increased socialization may lead to the encouragement to consume adequate supplies of water, or take other appropriate actions to prevent the development of a heat-related illness. In addition, socialization may increase awareness among friends/family that a person feels ill, and may provide more opportunities for the person to seek advice. The ability to participate in social activities may also be an indication of overall health status, suggesting that a person is in good health and capable of interacting outside the home and generally better able to tolerate the heat.
3.3.2 Access to, and Increased Time Spent in, a Cool Environment or Air Conditioning

Spending time in an air-conditioned environment, even for a short period of time, allows for direct relief from the heat. This may be sufficient to allow the body to cool off enough to minimize the likelihood of a heat-related illness. If air conditioning is not available in the home, it is recommended that a person leaves (if capable) to seek out a public place in which air conditioning is accessible, such as a library. The protective benefit of a brief amount of time spent in a cool place was demonstrated in a study in which it was found that individuals who lived in apartment buildings with access to air conditioning in the lobby had a lower risk of mortality.Reference 149 However, there is no information to date regarding the requisite amount of time to spend in a cool environment to reduce relative risk of heat-related illness and death.Reference 101 The general guide to stay in an air-conditioned environment until cool and refreshed is helpful. This is also the concept behind taking frequent cool showers and/or baths, which has also been found in several studies to have a protective effect against the heat.Reference 121Reference 125Reference 146
3.3.3 Socialization
Increasing or maintaining social activities is also important during an EHE as well as recognizing signs of heat strain during these visits. The Chicago heat wave showed that even though people were seen or spoken to one day, they had succumbed to the heat prior to the following day's visit,Reference 125 which emphasizes the importance of multiple visits a day, if possible. In some cases, it was even noted that signs of heat-related illness were present and no protective action was taken. It is therefore important that family, neighbours and health care workers who regularly check-in with vulnerable people during EHEs are familiar with the signs and symptoms associated with heat-related illnesses. This knowledge will help visitors recognize when someone may be at increased risk or in danger, as a person can succumb to the heat in just one day. For individuals who live alone, increasing social activities is valuable to allow for the recognition of problems by others. Regular contact may help alleviate any apprehension or embarrassment in asking for help during extreme heat if required, or can help the person move to a safer environment.
4. Heat Risk Factors Associated with Medications
Key Terms: antihypertensive, antidepressant, antipsychotic/neuroleptic, anti-Parkinson's agent, anxiolytic, anticholinergic effects, hidrosis, hypohidrosis, diuretic, hyponatremia, odds ratio, confidence interval, polypharmacy.
Summary Points:
- Various drugs/medications are known to interfere with the body's thermoregulatory mechanisms, predisposing the consumer to heat illnesses.
- It is critical that this drug/heat interactive information be disseminated to those who prescribe, dispense and use these drugs, as this relationship appears to be under-recognized to these groups.
- Understanding the various mechanisms by which medications alter the body's thermoregulatory response is important in anticipating heat-related risk factors.
- The relationship between drugs, heat exposure and morbidity has been demonstrated by epidemiological research.
4.1 Drug Use and Heat
It is well-established, as outlined below, that the use of certain drugs (which includes diverse medications) leads to an increased risk of the consumer/patient experiencing a heat-related illness.
In an effort to communicate this, various groups have published lists of drugs that are thought to increase the risk of developing a heat illness. For example, in 1999, as a result of coroner investigation into two deaths, the Ontario Chief Coroner's Office published a list of 47 drugs that could increase their consumers' health risk.Reference 164 Such lists have been published in a number of review articles.Reference 165Reference 166
Sources such as the Compendium of Pharmaceuticals and Specialties (CPS)Reference 138 also alert the reader that: "Phenothiazines affect thermoregulation. Use chlorpromazine with caution in patients who may be exposed to extreme heat or cold. Anticholinergic drugs such as antihistamines, anti-Parkinson's agents, atropine, monoamise inhibitors and tricyclic antidepressants may have additive anticholinergic effects when administered with chlorpromazine. Concomitant use of these drugs may increase the predisposition of patients treated with phenothiazines to heat stroke." More broadly: for olanzapine "Disruption of the body's ability to reduce core temperature has been attributed to antipsychotic agents. Appropriate care is advised when prescribing ZYPREXA for patients who will be experiencing conditions which may contribute to an elevation of core temperature" (e.g. exercising strenuously, exposure to extreme heat, receiving concomitant medication with anticholinergic activity, or being subject to dehydration).Reference 138
The French Health Products Agency's document Clarification Concerning the Good Use of Drugs in the Event of a Heat WaveReference 167 states clearly that its summary of the potentially detrimental human health effects of a drug, combined with heat exposure, is based uniquely on the mechanism of action of the drug. That is, as opposed to an epidemiological study of the use of the drug in a population that gives not only potential effects, but the actual clinical consequences of the administration of the medication during extreme heat.
The French Health Products Agency's list was put together as a consequence of the extreme heat events in Europe in 2003 which caused over 70,000 excess deaths.Reference 1 This same catastrophic occurrence also enabled various studies to be conducted in the wake of the episode, which highlighted the potentially harmful effects of certain drugs during extreme heat events (EHEs). This chapter systematically examines the bulk of the currently available scientific data on this topic.
This chapter focuses on classic heat stroke as a consequence of drug use in the presence of extreme environmental heat. However, drug use can also increase the risk of developing exertional heat stroke. In either case, heat stroke is a medical emergency and requires immediate intervention. Milder forms of heat-related illnesses can also be precipitated by some drugs. Despite this, health care workers are often uninformed about the potential risks associated with the use of certain drugs in extreme heat.Reference 168 This is not surprising, as documented reports of drugs contributing to weather-related heat illnesses are rarely discussed in the scientific literature.Reference 49
The intent of this chapter is to highlight that the use of many types of drugs can predispose an individual to heat-related illness, and to alert health care workers of the need to be vigilant in this respect.
4.2 Effects of Drugs on Body Thermal Regulation
Drugs can interfere with natural thermoregulatory mechanisms, as mediated through the:
- Hypothalamus, and the body temperature set-point
- Heat perception, leading to behavioural change (avoidance)
- Changes in cardiac output
- Changes in peripheral vasodilation
- Changes in sweat rate
- Changes due to renal function, body hydration and/or electrolyte status generally
Prescribing drugs is a challenging process, especially for patients taking multiple drugs. It is critical for clinicians to be aware that many drug classes can be hazardous when taken during EHEs. This risk should be taken into account when choosing the appropriate treatment regimen and in giving advice to the patient, especially in groups at high risk of hyperthermia and heat stroke, such as workers in hot environments, athletes, seniors and people with chronic diseases.
Although it is clear that users of certain drugs are at significantly greater risk of developing serious heat-related illnesses, it is difficult to quantify this risk. It should be noted that there is no straightforward relationship between the consumption of a drug and a resultant hyperthermic state. First of all, heat stroke may occur in those who are not on any medications.Reference 169 Secondly, there are various drugs that can induce a hyperthermic state in the absence of extreme environmental heat or exercise.Reference 170Reference 171
4.3 Polypharmacy Case Studies

The following case studies outline some of the reports from the literature of patients on multiple drugs who experienced heat stroke. They show how difficult it is to formulate a scientific opinion on the subject of which drug to implicate in the heat stroke, or whether to attribute it to an interaction between several.
Alternatively, the heat stroke episode could be due to a physiological condition that predisposed the particular patient to heat hypersensitivity (e.g. poor hydration), and may not be associated with the drug(s) in question. In addition, these case studies illustrate various time courses associated with cases of heat stroke.
- Two men died of heat stroke. One was on pimozide and clomipramine, the other on zuclopenthixol, dexetimide, droperidol, promethazine and propranolol. These drugs have both anticholinergic and antidopaminergic effects; the latter can increase the core body temperature set-point,Reference 172 therefore core body temperature will be much higher before heat dissipating mechansisms are initiated.
- A man taking fluoxetine (Prozac) and lithium carbonate was working under hot, dry conditions. He became hyperthermic and lost consciousness for five days; a year later, the cerebellar effects were still apparent. The influence of lithium was considered likely to be minor, given the relative half-lives of the two drugs. Fluoxetine is a selective serotonin reuptake inhibitor (SSRI); these drugs increase hypothalamic serotonin levels which in turn increase cholinergic heat-production pathways and inhibit dopaminergic heat-loss pathways.Reference 173
- A person taking benzhexol, chlorpromazine and zuclopenthixol decanoate who was working in the sun was hospitalized twice: once for heat stroke and once for heat exhaustion.Reference 174
- A man taking chlorpromazine and benztropine mesylate collapsed under hot outdoor conditions. During the diagnostic workup process, he was found to be hyperthermic (rectal temperature 42.9°C) and, despite intensive intervention, died 16 hours after admission.Reference 175
- A man taking zuclopenthixol, quetiapine and benztropine who was working in the heat lost consciousness. His rectal temperature was 42.2°C. He died the next morning.Reference 176
- An 11-year-old girl who was taking two amphetamines (phentermine and propylhexedrine hydrochloride) for weight loss as well as a diuretic (bumetanide), but with last dose taken three days earlier, went on a four km hike with 107 classmates, while the air temperature was 34°C. She collapsed and became delirious, ultimately losing consciousness. Although she was in hospital within 45 minutes (body temperature 42°C), cooling methods had been applied in the interim, and numerous therapeutic interventions were performed in the two hospitals she was admitted to, she died some 19 hours after her initial collapse. None of the other children on the hike suffered any significant heat-related illnesses. Her death was attributed to the peripheral vasoconstrictive and endogenous heat-producing effects of the two amphetamines she was taking. Given the half-life and time of the last dose of the diuretic, it is not believed to have contributed to her death.Reference 177
These case reports provide an idea of the difficulty of attributing cause to one drug or another, a physiological or pathophysiological predisposition in the patient, environmental overexposure to heat, or interactions among all of these factors. Unlike the case reports, the publications in the next section focus only on epidemiological or human experimental studies.
4.4 Drugs Implicated in Heat-Related Illnesses
Systematic reviews are currently under way in Canada to improve heat exposure risk assessment for five groupings of prescribed drugs that affect the: central nervous system; cardiovascular and renal systems; hormonal system; gastrointestinal system; and musculoskeletal and immune systems. The reviews are being conducted by Institut national de santé publique du Québec (INSPQ) and the Faculty of Pharmacy of the University of Montreal. The results will be published by grouping in 2011. At the time of writing, only the report on central nervous system drugs is available; the report on cardiovascular drugs is being prepared.Reference 178Reference 179 These two drug classes appear to pose the greatest potential risk during EHEs. The main conclusions of the reports are summarized below.
4.4.1 Central Nervous System Drugs
Antipsychotics (Neuroleptics)
It was found that, of 1405 patients admitted to the emergency department at a hospital in Bordeaux, France (during the August 2003 EHE), 4% were diagnosed with heat stroke or hyperthermia.Reference 180 Of these cases, multivariate analysis showed that, compared to community controls (not admitted, but who were taking at least one drug, most commonly psychotropic), their odds ratios (OR) (and 95% confidence intervals, CI95Reference f of being treated independently with the drugs listed as in Table 4.1 Reference 180:
| Drug Type | Odds Ratio | 95% Confidence Interval |
|---|---|---|
| Anticholinergic | 6.0 | 1.8-19.6 |
| Antipsychotics | 4.6 | 1.9-11.2 |
| Anxiolytics | 2.4 | 1.3-4.4 |
Note: The anticholinergics mentioned will be discussed below in the section on anti-Parkinson's agents.
For individuals on neuroleptics, the odds of death due to heat stroke during an EHE were also found to be elevated in three other studies, with OR 1.90 (CI951.3-2.8)Reference 13; OR 1.4 (CI95 0.7-2.6)Reference 121; and OR 1.20 (CI95 1.12-1.29).Reference 181 In addition, a laboratory stress test on schizophrenics performed in a 40°C room showed that rectal temperature in individuals on haloperidol or fluphenazine was higher than in normal subjects.Reference 182
Antidepressants
In a case-control study that considered deaths that occurred just prior to (Aug. 1-4) and during (Aug. 5-13) the 2003 French EHE, univariate analysis showed that individuals from 70 to 100 years of age who died during the EHE used antidepressants more frequently than the controls (OR 1.75, CI95 1.62-1.90), with tricyclic antidepressants featuring most prominently (OR 2.2, CI95 1.80-2.69).Reference 183
Similarly, they found that all of the antipsychotics except for thioxanthenes were more frequently used in the cases than in the controls (OR 2.19, CI95 1.96-2.45). A report on the 2003 French EHE states that individuals on antidepressants faced a significant risk of death at the peak of the EHE as opposed to the non-EHE period in August (OR 1.24, CI95 1.17-1.32).Reference 181 Another report on the EHE, issued by the Institut de veille sanitaire, states that antidepressants were significantly associated with death during the EHE (OR 4.13, CI95 1.41-12.10).Reference 146
Selective Serotonin Reuptake Inhibitors (SSRIs)
Hyponatremia is a side effect of SSRIs and can be dangerous for patients taking these drugs during an EHE. A sizeable number of studies have established a link between hyponatremia and SSRIs,Reference 184 Reference 186 and some show that the concomitant use of diuretics considerably increase the odds ratio for hyponatremia (OR 13.5, CI95 1.8-101),Reference 187 (OR 11.2, CI95 2.2-58.1).Reference 188
Lithium
A number of studies show that the concentration of lithium salts in the blood varies with the season, being lower in winter and higher in summer.Reference 189Reference 190 The authors suggest that dehydration affects lithium concentrations in plasma. Elevated blood lithium levels can reach a toxic threshold that is dangerous to the patient. A retrospective study on adverse reactions associated with lithium showed that 11.5% of lithium poisonings requiring hospitalization were due to summer heat exposure and consequent dehydration.Reference 191 Hydrate with water rather than an electrolyte solution to minimize potential hypernatremic complications.
Antiepileptics
Topiramate is a drug used to treat refractory epilepsy and is more commonly prescribed for children than for adults. Two prospective studies showed that 11% of children on topiramate developed hypohidrosis (decreased sweating)Reference 139 and 19% of patients reported severe hyperthermia during the summer.Reference 140 An experimental study in children and adults showed that 69% of patients on topiramate reported hypohidrosis.Reference 192 The authors of this article concluded that the risk of taking topiramate during extreme heat should not be underestimated. Studies on antiepileptics other than topiramate also show that hyponatremia is a side effect requiring close monitoring.Reference 193Reference 196
Anti-Alzheimer's agents
Cholinesterase inhibitors, which are used in treating Alzheimer's disease, do not figure very prominently in the literature on the implication of drugs during EHEs, but they do have side effects that need to be monitored during EHEs. In the first three weeks of the initial treatment phase, the most common side effects are diarrhea and vomiting, with OR 1.91 (CI95 1.59-2.30) for diarrhea and 4.82 (CI95 3.91-5.94) for vomiting.Reference 197 Diarrhea and vomiting can lead to severe dehydration at any time of year, but in summer, the risks of beginning such treatment are even greater. Multiple prospective studies show that dehydration is a serious side effect that can affect 1.5%Reference 198 to 3.1%Reference 199 of the study population. The appearance of vomiting and diarrhea symptoms is also dose-dependent.Reference 200
Anti-Parkinson's agents

The potential risk of taking an anti-Parkinson's agent during extreme heat is very difficult to assess, because the disease itself is a significant mortality factor during long EHEs (OR 9.20, CI95 2.09-40.59).Reference 146 However, some studies have established odds ratios for the use of anti-Parkinson's agents during extreme heat.
For example, one publication makes an association between hospital admissions and anticholinergics (OR 6.0, CI951.8-19.6)Reference 180; the only anticholinergics in this study were anti-Parkinson's agentsReference 201. In addition, two reports issued by the Institut national de veille sanitaire stated that the drugs significantly associated with deaths during the 2003 French EHE were anti-Parkinson's agents: OR 6.02 (CI95 0.72-50.37) for older adults living in their own homes,Reference 146 and OR 2.2 (CI95 0.8-6.4) for older adults living in care facilities.Reference 121
4.4.2 Cardiovascular Drugs
Diuretics
Univariate analysis of 345 people admitted with heat stroke in France in August 2003 showed that the use of diuretics, but not anxiolytics, antidepressants or alcohol, led to a significantly increased risk of death during that period.Reference 141 During an EHE, it was observed that 30.1% of hospitalized patients were on diuretics, and that 68.7% of those who subsequently died were long-term users of antihypertensives (primarily diuretics).Reference 202 The authors concluded that the use of antihypertensives during EHEs should be optimized as much as possible. In the 1993 Adelaide EHE 36% of persons hospitalized for heat stroke were taking diureticsReference 203. The most common side effect of diuretics was found to be hyponatremia, which, according to the studies, affects 30%Reference 204 to 43%Reference 205 of people hospitalized during EHEs.
Antiarrhythmics

The most commonly cited side effect of antiarrhythmics and cardiotonics is vomiting and can affect 20% of patients.Reference 206 With nitrate vasodilators, vomiting can affect 24% of the study population,Reference 207 and ACE-II inhibitors can affect 7% of the population.Reference 208 With ACE-II inhibitors, hyponatremia is also a side effect: OR 12.2 (CI95 1.26-21.2).Reference 209 These side effects increase the risk of dehydration during EHEs.
Calcium channel blockers
The side effects of calcium channel blockers should also be monitored during the summer months. Diarrhea is the most frequently cited side effect,Reference 210Reference 212 and more rarely, hot flashes associated with sweating.Reference 213
Table 4.2: Hazardous Drugs and Recommendations Reference 179
Whether a patient should drink water, or the electrolyte solution described in the footnote below, should be as indicated by the prescribing primary care provider. One important cause of hyponatremia during EHEs is the over-consumption of water, as experienced in France's second EHE in 2006. The appearance of symptoms should lead to the notification of the pharmacist/physician, who will decide on the appropriate course of action.
| Drug Class | Side Effects to Monitor | General Recommendations | Specific Recommendations |
|---|---|---|---|
| Antipsychotics/ Neuroleptics |
|
|
No specific recommendations |
| Antidepressants |
|
|
Especially in individuals taking selective serotonin reuptake inhibitors. |
| Lithium |
|
|
Avoid electrolyte solutions due to the risk of hypernatremia |
| Antiepileptics |
|
|
Topiramate: watch for hyperthermia and heat intolerance. Oxcarbazepine and carbamazepine: take precautions against hyponatremia and hyperhydration. |
Anti-Alzheimer's agents (Cholinesterase inhibitors) |
|
|
Side effects during initial treatment phase. Carefully monitor patients who are starting the medication in the summer. |
| Anti-Parkinson's agents |
|
|
No specific recommendations |
| Diuretics |
|
|
No specific recommendations |
| Antiarrhythmics and cardiotonics |
|
|
No specific recommendations |
| Nitrate vasodilators |
|
|
No specific recommendations |
| ACE-II inhibitors |
|
|
No specific recommendations |
| Calcium channel blockers |
|
|
No specific recommendations |
Adapted fromReference 179
4.5 Conclusions
The reviewed studies have demonstrated that there is an increased risk, during EHEs, linked either directly or indirectly with the consumption of certain drugs. However, note that there may be omissions from this list, if a drug has not been adequately studied and/or reported on, and/or as may be described in the systematic groupings of the body systems to follow.
This list should allow health care workers to improve the focus of their surveillance. Anyone taking a drug listed in Summary Table 4.2, for example, should consult their prescribing medical care provider before summer begins and find out about the potential risks the drug may pose during an EHE. The care provider should advise, and also subsequently intervene as necessary.
These recommendations will also help patients manage their own heat-related behaviour and fluid intake according to the type of drug they are taking, as advised by their physician. These are complex decisions, because it should always be borne in mind that there are risks associated with changing treatment in progress for an underlying disease; accordingly, minimization of heat exposure would be the best course of action for those patients on these medications.
It would be recommended for health professional schools to ensure that the potential adverse relationship between heat and certain drugs is part of their curriculum. There is a need for the health team (doctors, nurses, pharmacists, etc.) and consumers to be made aware of the effects that various drugs can have in the face of extreme heat exposure.
5. Heat-Related Illnesses
Key Terms: heat edema, miliaria rubra, heat cramps, heat syncope, hyponatremia in endurance athletes, heat exhaustion, exertional heat stroke, classic heat stroke, ice-water bath, multi-organ dysfunction syndrome, mental status
Summary Points:
- Heat illnesses are thought to be under-recognized and under-reported and this affects the transfer of prevention information to patients and populations at risk.
- Heat stroke is a medical emergency requiring rapid cooling of the body and the involvement of emergency medical services.
- Ice-water baths are the fastest way to cool the body and are the most effective treatment for exertional heat stroke.
- Hyponatremia has recently been described in ultraendurance athletes (e.g. marathoners) especially during competitions in the high heat as a syndrome attributed to excessive consumption of water.
5.1 Heat-Related Illnesses
Studies have shown a clear relationship between increases in morbidity, mortality and increasing ambient temperature, above a "threshold" value, which varies from place to place.Reference 13Reference 23Reference 41 Due to the projected increase in climate extremes and the number of extreme heat events (EHEs), an increase in heat-related illnesses is expected. It is therefore important that both health care workers and patients are familiar with the signs and symptoms of heat stress, because prevention and early recognition are crucial for patient survival and recovery. Primary prevention of heat-related illness is described in detail in the next chapter and will require more public education at workplaces, schools, churches, retirement homes and community centers. Prevention is the best method for addressing EHEs as effective prevention will reduce the number of people who suffer from the adverse effects of heat.

EHEs have been associated with marked short-term increases in mortality, with reported excess mortality ranging from 4% to 142%.Reference 208Reference 214 This increase in mortality is sometimes associated with a lag time of one to three days following peak ambient temperature.Reference 24Reference 215 Despite the hypothesis that increased mortality may be due to a culling effect, the evidence indicates that only a small proportion of excess deaths represents short-term mortality displacement.Reference 215 Of the excess deaths occurring during EHEs few are actually reported as being directly attributable to the effects of excess heat. This may be in part the result of insufficient recognition and reporting of heat-related illnesses and in part the result of the heat exacerbating pre-existing illnesses (e.g. cardiovascular, renal and respiratory diseases, and diseases of the nervous system) which are recognized as the primary illness without identifying heat as a factor. In addition, heat can aggravate other upstream health determinants such as those related to socio-economics and social isolation (refer to Chapter 3). These pre-existing conditions and determinants may be the only conditions noted and reported by the health care worker involved. An effort to report heat as a factor in these cases is necessary to improve recognition and monitoring of heat-related illnesses in Canada. To help address upstream health determinants it is important to ensure coordination with social networks and community care services to ensure that those most isolated are receiving the support they need (especially when they are discharged from a care facility).
The effect of extreme heat on population morbidity is rarely investigated following EHEs. Observations regarding patient care received during an EHE differ in some respects. Some report hospital admissions increase during EHEsReference 1Reference 14Reference 16Reference 208Reference 217 while others report that people die quickly during an EHE before they are able to reach hospital or medical help.Reference 5 To address either of these scenarios, pre-heat event planning and sharing of prevention information is required. In particular, studies of patients admitted to hospitals during EHEs for treatment of heat stroke have shown that this illness is associated with poor short- and long-term outcomes.Reference 218 These outcomes are directly related to a delay in cooling the patient.
The number of heat illnesses and deaths in Canada is not known, as they are often reported as another pre-existing illness without including heat as a factor. A number of direct heat-related illnesses can result from exposure to heat and range from self-containing and mild to severe and life-threatening.Reference 219 Below is a series of heat illnesses which describes the signs and symptoms, predisposing factors, the physiological basis, prevention options and first aid and treatment of these conditions.
5.2 Heat Illnesses
5.2.1 Heat Edema
Heat edema refers to temporary peripheral swelling, most common in the extremities, which occurs when a person is exposed to heat.
Signs and symptoms: Marked peripheral vasodilation and sweating, decreased plasma volume, increased aldosterone production, sodium and water retention, transitory edema (hands and feet).Reference 220
Predisposing factors: This swelling generally occurs due to heat or working in hot environments and may be most prevalent in an unacclimatized person.
Physiological basis: The exact physiological basis is not known but probably includes vasodilation and extravascular fluid shifts.
Prevention: Both heat acclimatization and reduced activity are needed. For those with chronic conditions that limit acclimatization, avoiding exposure to the heat is often most effective.Reference 221
First aid and treatment: The condition is self-limiting. Gentle movement and/or elevation of legs may help to reduce swelling. Generally the heat edema resolves after the first few days of exposure either due to the removal of heat exposure or as the person becomes acclimatized to constant heat.
5.2.2 Miliaria Rubra (Heat Rashes)
Miliaria Rubra are tiny spots on the skin and are the result of inflammation caused when sweat glands are plugged.
Signs and symptoms: Profuse tiny raised red vesicles (blister-like) on affected areas causing prickling sensation during heat exposure. The patient will present with the complaint of an itchy rash.
Predisposing factors: The primary factors are the unrelieved exposure to humid heat and prolonged skin contact with sweat.
Physiological basis: The plugging of sweat gland ducts with the retention of sweat and an inflammatory reaction. The condition occurs when sweat gland pores become blocked with keratin (occluded ducts) and infiltrate into the surrounding dermis. These obstructed ducts may rupture, with subsequent development of vesicles in the deeper layers of the skin. A secondary staphylococcal infection may develop. Miliarial skin cannot fully participate in thermoregulatory sweating; therefore, the risk of developing a more severe heat illness is increased in proportion to the amount of skin surface involved.
Prevention: Provide cool dry sleeping quarters to allow skin to dry between exposures. Prevention includes keeping the skin clean and dry, wearing clean, loose-fitting clothes; and avoiding talc and creams which clog pores.
First aid and treatment: Mild drying lotions and skin cleanliness are important to prevent infection. Cooling and drying of affected skin, avoiding conditions that induce sweating, controlling infection and relieving pruritis (itch) is recommended. Treatment is handled with chlorhexidine lotion or cream with or without salicyclic acid or with low-dose topical corticosteroids. For diffuse pustular rash, systemic antibiotics may be prescribed.
5.2.3 Heat Cramps
Heat cramps are characterized by sharp, painful spasm of skeletal muscles including the muscles of the extremities and abdomen and can last anywhere between a few minutes to hours.
Signs and symptoms: Muscular tightening and spasm are present during or after intense prolonged exercise in the heat and can range from relatively mild to extremely painful. Lower limb muscles are involved most commonly, but any muscles may be affected, including the abdominals, intercostals and arm muscles. Smooth, cardiac, and diaphragm muscles may be involved, but the cramps are usually isolated to one area. The cramp in an individual muscle is usually preceded by a palpable or visible spasm and lasts approximately two to three minutes. The cramp produces a hard lump in the muscle. Clinically, body core temperature is normal and there is rarely evidence of dehydration. Signs of heat exhaustion, exertional hyponatremia, or heat stroke should be evaluated, before confirming an isolated diagnosis of heat cramps.Reference 222
Predisposing factors: Includes heavy sweating during vigorous activity in the heat; drinking large volumes of water, and the lack of acclimatization. Heat cramps may be seen in physically fit and unfit individuals. Cramps tend to be recurrent and may be precipitated by vigorous use of affected muscles or ongoing negative mineral balance.
Physiological basis: The exact cause of heat cramps is not known. In general, the physiological basis is thought to be due to the loss of salt through the sweat; sometimes this is accompanied by water (hypotonic) intake further diluting electrolytes causing muscles to spasm.Reference 223 It is postulated that intracellular calcium is increased by a reduction in the sodium gradient across the cell membrane favouring accumulation in the cell. The increased intracellular calcium accumulation is then thought to stimulate actin-myosin interactions causing the muscle contraction.
Prevention: Eating nutritious meals with adequate salt intake is recommended (particularly for individuals trying to acclimatize to intense physical activity in the heat).Reference 224 Heat cramps usually affect unacclimatized persons who are doing an unusual amount of activity in a high heat environment. The intensity of physical activity may need to be re-evaluated. An attempt should be made to determine the reason for the heat cramp episode so that appropriate advice can be given to avoid future episodes. Maintaining hydration before and during activity and drinking beverages that contain sodium or electrolytes may be beneficial.Reference 225
First aid and treatment: The immediate goal of treatment is the relief of the cramp, not the replacement of electrolyte losses. Rest and cooling down, massage, and stretching of affected muscles is usually effective. Salty liquids by mouth and by intravenous (IV) infusions have been reported to resolve cramps rapidly although the mechanism of action is unclear.Reference 223Reference 226Reference 227 No significant complications have been reported from heat cramps except muscle soreness and perhaps local muscle injury.Reference 222 An episode of heat cramps does not imply any predisposition to heat injury. Extremely painful cramps may require more aggressive therapy and may be a warning sign of impending heat exhaustion. Heat cramps are benign; however, if the condition does not resolve in a timely manner with the above treatment, the care provider should consider checking creatine phosphokinase (CPK) to rule out exertional rhabdomyolysis (muscle breakdown).Reference 226 Persistent cramps may also reflect other mineral deficiencies; evaluate potassium, calcium and magnesium levels.
- Most Canadians consume too much salt. Many consume more than the Health Canada recommended daily intake (1500 mg/day of sodium) and a large number consume more than the daily intake which will lead to health problems (the tolerable upper intake level 2300 mg/day).Reference 228 The average Canadian consumes 3092 mg/day of sodium.Reference 229
- Many of the heat illnesses described in this Chapter are caused by electrolyte or salt deficiencies. However, it should be noted that low dietary sodium is very rarely a concern for Canadians and nutritional analysis for the individual should be completed before proceeding with a recommendation to increase dietary salt consumption (Refer to Canada's Food Guide for dietary guidanceReference 230).
5.2.4 Heat Syncope (Heat Fainting)
Heat syncope is heat-induced dizziness and fainting which can be caused by a temporary, insufficient flow of blood to the brain while a person is standing, due to a "pooling" of the blood in the legs.
Signs and symptoms: Symptoms range from light-headedness, dizziness, tunnel vision, pale/sweaty skin, decreased pulse rate to loss of consciousness. Syncope or light-headedness can also be seen at the end of an endurance race, or following unusual physical effort in the heat. Core temperature may not be elevated unless fainting follows exercise and the skin may be cool and moist.Reference 231
Diagnostic criteria: Brief fainting, normal body core temperature, rapid recovery with rest (usually lying supine with elevated legs).
Predisposing factors: Heat syncope often, but not always, occurs during prolonged standing or abrupt standing following vigorous activity and is often associated with hot weather environments. Other factors include exposure to high heat and/or humidity, lack of acclimatization to heat, unacclimatized exertion, ending strenuous exercise without a cool-down, and/or dehydration. The same phenomenon may occur when going from a cold environment (such as a cold bath) to a hot sauna or hot tub.
Physiological basis: The person is maximally vasodilated when activity is stopped and the blood pools in the peripheral veins. The pooling of blood in dilated vessels of the skin and the lower parts of body results in temporary circulatory failure. Consequently the heart has too little venous return to pump an adequate supply to the brain. Leg muscles can act as venous pumps contributing to venous return, but situations when legs are not used as venous pumps such as attempts to stand still (e.g. military or church) or abrupt halting of strenuous activity can contribute to difficulty in circulating blood to the brain. The decreased blood flow to the brain causes fainting.
Prevention: Acclimatize to the heat. At least upon initial exposure to heat, reduce the intensity of physical activity with intermittent rest to assist venous return to the heart when activity is stopped. Avoid unaccustomed activity in the heat. Get up slowly after breaks in the heat, avoid excessive stationary periods and sudden stationary periods after strenuous activity.
First aid and treatment: Rest in sitting, recumbent or supine position; recovery is prompt and complete. Complications are rare. The person will benefit from a period of rest lying down in a cool place with slightly elevated legs. The drinking of cold water while sitting comfortably is recommended when the person is ready. Complete recovery of stable blood pressure and heart rate may take an hour or two. A complete history has to be obtained to rule out other causes of fainting, including a more severe heat illness or a medical diagnosis unrelated to heat. Heat syncope occurring after more than five days of (exertional) heat exposure may indicate dehydration or heat exhaustion. Syncope occurring during or after work in the heat may indicate heat exhaustion or exertional heat illness both of which should be considered.
5.2.5 Hyponatremia
Hyponatremia has recently been described in ultraendurance athletes (e.g. marathonersReference 232) especially in high heat as a syndrome attributed to excessive hypotonic fluid consumption.Reference 233Reference 234 This phenomenon is also present in other groups such as older adults.Reference 204 Hyponatremia can be associated with taking certain medications during EHEs (see Chapter 4).
Signs and symptoms: Symptoms of mild cases include malaise, fatigue, dilute urine, lethargy, nausea, vomiting, confusion and muscle cramps; severe cases include, hyponatremic exercise-associated collapse, may involve seizures, psychosis and coma. In severe cases the condition can be lethal.Reference 235
Diagnostic criteria: For heat-related hyponatremia the sodium levels are <130 mEq/L and rectal temperature is <40°C (104°F).236
Predisposing factors: Lengthy physical activity on successive days, accompanied by excessive fluid replacement and excessive sweat loss replaced with water.Reference 232Reference 237
Physiological basis: Hyponatremia is classified as a complication of low plasma sodium levelsReference 232 by disrupting the osmotic balance across the blood brain barrier resulting in a rapid influx of water to the brain.Reference 129 Perspiration may contribute to hyponatremia through the loss of electrolytes in sweat. A range of 10-30% of the incidence of this disease is associated with decreased sodium.Reference 238 Although overconsumption of fluids is not the only risk factor associated with hyponatremia (disorders that suppress the release of antidiuretic hormone will cause impairment of renal water excretion), the primary cause is over-hydration.Reference 233Reference 235Reference 239

Prevention: Education about appropriately replacing fluid losses, based on individual sweat rate (not to exceed 500-1000 mL/hr), particularly for endurance athletes, is needed. When replacing large fluid losses, hypotonic sodium/carbohydrate solutions and sports drinks may be better than water.Reference 240 Eating healthy balanced meals is beneficial to ensure adequate dietary electrolytes and minerals.Reference 230
First aid and treatment: In mild cases, fluid restriction alone usually leads to adequate diuresis and resolution. More intensive treatment is needed for severe cases, which should be transferred to an emergency facility. Severe hyponatremia is a medical emergency and requires immediate medical treatment based on the underlying cause and severity of symptoms.Reference 238Reference 241
5.2.6 Heat Exhaustion
Heat exhaustion is the most common form of heat-related illness and is not associated with evidence of organ damage. It occurs when the body cannot sustain the necessary level of cardiac output to meet the combined demands of skin blood flow for thermoregulation and blood flow for the metabolic requirements of exercising skeletal muscle and vital organs. The subsequent insufficient blood flow to the periphery impairs thermoregulation.
Signs and symptoms: Symptoms are often vague, and patients may not realize that heat is the cause. Symptoms may include heavy sweating, fatigue, weakness, dizziness, giddiness, headache, diarrhea, malaise, nausea, and sometimes vomiting. Skin may be clammy and moist (sweating may be profuse), complexion may be pale, muddy or flushed; there may be rapid pulse and low blood pressure.Reference 242Reference 243 Mental status is typically normal, unlike in heat stroke and is no worse than mild confusion, agitation and lack of coordination. If the patient is incoherent or unconscious, evaluate as possible heat stroke. The body core temperature is usually normal and, if elevated, usually does not reach or exceed 40°C.Reference 48 Heat exhaustion may or may not be accompanied by heat cramps and/or heat syncope. Inability to continue work or exercise in heat is typical. If due to water restriction then the urine volume is small and highly concentrated; if due to salt restriction then urine is less concentrated. Two heat exhaustion patterns are described and are usually overlapping:
1. Sodium depletion
- Develops over several days, but onset of symptoms is acute.
- Symptoms include fatigue, profound weakness, light-headedness, sweating, muscle cramps, occasionally headache, nausea, vomiting and/or diarrhea.
- Signs include normal or moderately elevated temperature, increased pulse, sometimes blood pressure is decreased. Normal mental status; heat syncope is rare.
2. Water depletion
- Symptoms include thirst, headache, mild anxiety, muscle weakness, generalized fatigue, lack of neuromuscular coordination.
- Signs include high fever (but <40°C), decreased skin elasticity, increased pulse, blood pressure is decreased. Mental status includes some confusion and agitation. The sweating mechanism is intact, but may be reduced because of hypernatremia.
Diagnostic criteria: The diagnosis of heat exhaustion versus more severe classic or exertional heat stroke is important due to the difference in treatment and prognosis. The diagnosis of heat exhaustion in those with severe symptoms is primarily a diagnosis of exclusion (i.e. unable to maintain activity, rectal temperature <40°C (104°F), minimal or no central nervous system dysfunction). Heat stroke should be the working diagnosis in anyone who has been exposed to extreme heat and has an alteration in mental status. Any loss of consciousness and any mental status changes need to be documented. Such patients need to be evaluated for potential exertional or classic heat stroke. Mental status can be determined with questions regarding name, location, date, personal identifiers (e.g. social insurance number, address, phone number) (See Box 5.3). Be conscious of individuals who have mild symptoms but do not improve, or even worsen, with initial management or those who have severe symptoms. When in doubt send patients to the nearest hospital for additional laboratory assessment. Measuring the aspartate transaminase, and alanine transaminase levels can help to point to a more severe heat injury.
Predisposing factors: Exposure to high heat and humidity, sustained exertion in heat, lack of acclimatization and/or low fluid intake or low dietary salt intake.
Physiological basis: Heat exhaustion is an illness characterized by body fluid volume depletion resulting from an inadequate replacement of water and/or electrolytes lost during exposure to a hot environment, particularly through sweating.Reference 244 There is failure of the cardiovascular response to meet workload demands due to circulatory strain from competing demands for blood flow to the skin and to active muscles. This may be caused by dehydration from deficiency of water resulting in a decrease in circulating blood volume. Sodium depletion heat exhaustion is caused by the lack of acclimatization and excess loss of electrolytes due to sweating. Water depletion heat exhaustion is caused by the lack of hydration when exposed to the heat.

Prevention: Have drinking water available at all times and take frequent breaks during periods of high activity. Acclimatize workers or athletes slowly to the heat by increasing physical activity demands over five to ten days.Reference 246 During appointment time discuss Fact Sheets (for older adults, physically active, and/or young children) with patients/clients and their families.
First aid and treatment: Management is directed to correcting the two pathogenic components of the illness: excessive cardiovascular demand and water/electrolyte depletion. The load on the heart is reduced by rest and cooling. Water/electrolyte depletion is corrected by administering oral (or IV) fluids. Heat exhaustion victims should improve rapidly with rest, cooling, and rehydration; those who do not improve or get worse need to be moved to the next higher level of medical care and evaluated for heat stroke. Treatment should begin immediately to prevent progression to a more severe heat injury. If untreated, heat exhaustion can lead to heat stroke and death.Reference 245 Heat exhaustion itself has no chronic harmful effects. Activity can resume the following day if the patient is well, and medical evaluation is normal,Reference 247 however the patient should not overexert and re-exposure should be gradual.
People with heat exhaustion retain the ability to cool spontaneously if removed from the heat. Rapid cooling techniques are usually not necessary, but heavy clothing should be removed and gentle cooling (time in a cool environment, cold compresses and fanning) are needed. Aiding in active cooling however, does reduce the circulatory demand on the heart and prevents body core temperature from continuing to rise. Active cooling is of particular importance when body core temperature is below 40°C but above 38.5°C.
Rehydrate orally, but use IV rehydration if nausea or vomiting is present. Rapid administration of moderate amounts of normal saline may be necessary if significant tissue hypoperfusion is evident. Older patients and patients with moderate to severe symptoms should receive a workup and should be considered for hospital admission. Measure serum sodium; if markedly elevated hydrate cautiously to avoid inducing cerebral edema. Patients with water-depleted heat exhaustion are hypernatremic and it is therefore necessary to hydrate slowly (2 mEq/L per hour) as slow hydration prevents iatrogenic cerebral edema.Reference 246Reference 248
Rectal temperature should be monitored frequently (every 15 minutes) to ensure that core temperature is returning to normal levels. Although it is convenient to measure temperature in the mouth, or the ear canal, medical personnel should not use these temperatures in the evaluation or management of heat illnesses due to their monitoring inaccuracies of core temperature. Hyperventilation may cause oral temperature to be ~3°C (~5°F) lower than rectal temperature in heat stroke, and the temperature of the external auditory canal or tympanic membrane has been observed to be as much as ~5°C (~9°F) below rectal temperature in collapsed runners. The measurement of core body temperature is most accurately assessed by rectal thermometer.Reference 249-Reference 251
| Terms in bold are key diagnostic factors | ||
| Heat Exhaustion | Heat Stroke | |
|---|---|---|
| Temperature |
|
|
| Neurological |
|
Mental status changes:
|
| Cardiac |
|
|
| Skin |
|
|
| Other |
|
|
| Outcome | If left untreated, in the presence of ongoing heat exposure, heat exhaustion can worsen and become heat stroke. | In later stages, pulmonary edema, hepatic failure, renal failure, rhabdomyolysis (muscle fibre breakdown), death |
Adapted fromReference 9
5.2.7 Heat Stroke
Heat stroke is a medical emergency. Signs of heat stroke include body core temperature greater than 40°C, and complete or partial loss of consciousness. Lack of sweating is not an accurate sign of heat stress as there are two types of heat stroke with distinct symptoms:
- Classic heat stroke is accompanied by little or no sweating with dry and hot skin. It usually occurs in children, persons who are chronically ill and older adults who have been exposed to excessive environmental heat.
- Exertional heat stroke is increased body temperature due to the combination of environmental heat and strenuous activity, usually with the presence of profuse sweating.
Classic heat stroke and exertional heat stroke are different and can require different treatment interventions which need to be assessed for each patient. These conditions affect different patient groups with very different illness prevention needs. In both cases the likelihood of organ and neurological damage from heat stroke is very high.Reference 252
Signs and symptoms: Symptoms include body core temperature over 40°C and altered mental status. Central nervous system dysfunction is indicated by changes in mental status ranging from confusion to delirium, seizures and coma.Reference 48Reference 101 General malaise, weakness, rapid pulse and rapid breathing are common even when the patient is supine. In classic heat stroke, the skin is hot and dry indicating a challenge to the hypothalamus. In exertional heat stroke, sweating is relatively common. In both, the core temperature is above 40°C and is not spontaneously reversible as thermoregulatory impairment prevents control of elevated core temperature without external cooling. Even in patients who retain the ability to sweat, heat stroke progresses to cardiovascular and central nervous system collapse in the absence of prompt cooling.Reference 253
Diagnostic criteria: The primary criteria are rectal temperature >40°C (104°F) and central nervous system dysfunction.Reference 101 Ideally, core temperature of the patient is taken with a rectal thermometer. Oral, tympanic membrane and aural canal temperature do not correlate well with core temperature in heat-injured patients. Practically, in many cases, cooling commences when heat injury is suspected and may preceed clinical diagnosis. Because of this, core temperature may not be at its peak when the measurement is taken; this delay should be considered when diagnosing. A conservative approach is recommended if the patient presents with a lower than peak core temperature when cooling measures have already been initiated. The clinical onset of heat stroke may be confirmed with alteration of neurological function, often a sudden loss of consciousness, but also including irritability, bizarre behaviour, combativeness or hallucinations. Virtually any neurological abnormality may be present and should be assessed (see Section 5.3).101
Predisposing factors: Such factors include sustained physical exertion in high heat and/or high humidity (e.g. sports, military, occupation) with minimum rest and rehydration breaks. Predisposing factors include dehydration and chronic cardiovascular disease and others as outlined in Chapter 3 on risk factors. Onset can be rapid, but often on the second or third day of heat exposure, particularly when sleeping in hot conditions because the body does not have the opportunity to cool off. Athletic or occupational gear (such as football pads) and uniforms can further add to heat strain due to their thermal insulation.254
Physiological basis: The partial or complete failure of the sweat mechanism leads to loss of evaporative cooling and an uncontrolled rise in body core temperature. Protein degradation occurs due to the high body core temperature and leads to organ dysfunction and failure. The high cellular strain, including interference with cellular membranes and large production of heat shock proteins (HSPs),Reference 255 leads to apoptosis (cell death).Reference 48
Prevention: Prevention of heat stroke includes reducing exposure to extreme heat, adequate fluid intake during strenuous activity, and avoiding strenuous activity during peak hours of hot, humid weather. Extra precaution related to restricting strenuous activity with certain medications is needed during the extreme heat (see Chapter 4 for a list of medications). Plan daily tasks based on health status, physical fitness and acclimatization of the individual.Reference 9 Monitor endurance during sustained work in extreme heat and rest frequently.Reference 253 In some cases, such as before commencing demanding work in the extreme heat, medical screening is recommended.Reference 256

First aid and treatment: The primary goal in treatment is the rapid reduction of body core temperature (0.15-0.30°Reference 257 High body core temperature can lead to protein denaturing and organ failure and the duration of high body core temperature should be limited as much as possible.Reference 258 Hospitalization will be required to monitor for complications. Potential complications include the following: heart failure, cardiovascular collapse, hepatic failure, disseminated intravascular coagulation (DIC), rhabdomyolysis, cerebral edema, pulmonary edema, and myoglobinemia with renal failure.Reference 202 Especially in patients with heat stroke, a specialized emergency or intensive care facility is necessary for airway management, oxygenation (with or without respirator), careful fluid and electrolyte administration, circulatory support, and cardiac, hemodynamic and laboratory monitoring.Reference 48Reference 101Reference 251Reference 259
Treatment is Rapid External Cooling
Ice-water baths are effective for treatment of exertional heat stroke in athletes and workers.Reference 9Reference 258 The key to this treatment is to ensure that the core portion of the body is submerged, accompanied by regular monitoring of vital signs and body core temperature.Reference 101 However, ice-water baths are effective in only 50% of cases of classic heat stroke.Reference 101 Alternative cooling methods best suited for classic heat stroke are unknown. At a minimum, supporting evaporative cooling can be achieved by removing the patient from external sources of heat (in the outdoors this means moving to a cooler space and off of cement/asphalt surfaces), removing excessive clothing, and applying water to the entire skin surface, and fanning vigorously.Reference 260
Antipyretics have not been demonstrated to be effective in the cooling treatment of heat stroke patients.Reference 101Reference 261 Pharmaceutical treatment (e.g. Dantrolene) in heat management is not as effective as cooling the body directly.Reference 262Reference 263 The treatment of surrounding issues related to maintaining airway, breathing and circulation, as well as balancing osmolarity and renal function (cardiac arrhythmias, rhabdomyolysis, serum chemistry abnormalities, disseminated intravascular coagulation) is required. But the primary goal must be to cool quickly (see Figure 5.1).
Figure 5.1: Cooling curves for early and late intervention.
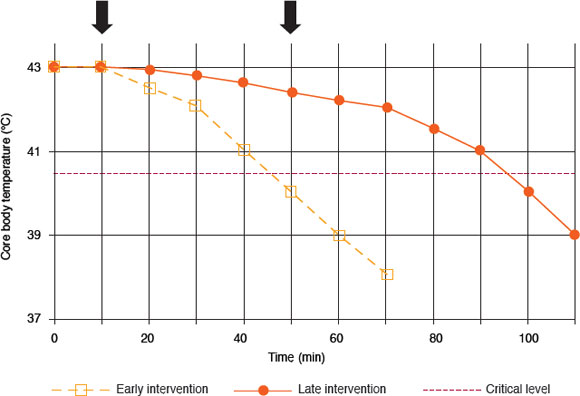
Text description
This graph illustrates the decreases in core body temperature in degrees Celcius when cooling intervention is started early (10 minutes) in comparison to late intervention (50 minutes). If early intervention is initiated, the core body temperatures drops back to normal levels after 70 minutes, whereas if intervention is initiated late, after 110 minutes, the body is still not back in normal core temperature range. The critical level is shown at 39.75 degrees Celcius. Early intervention allows the core body temperature to reach below this critical level after 45 minutes, whereas it takes at least 95 minutes for core body temperature to be below this critical level if cooling intervention is initiated late.
If cooling intervention is initiated late (closed circles) body core temperature takes much longer to decrease and the likelihood of recovery from heat illness decreases. Alternatively, if cooling intervention is initiated early (open squares) the body core temperature decreases to normal levels sooner. The two arrows mark the commencement of cooling at 10 minutes for early intervention and 50 minutes for late intervention.Reference 9
Outside a care facility (e.g. in the field), external cooling should begin immediately with the availability of trained staff and supplies. Options depend on the situation at hand. First, stop exercise, move to shade or air-conditioned shelter, and elevate legs. Cool immediately through ice-water immersion or alternate protocol if immersion cannot take place (recognizing that other cooling options are inferior). Either, wet the patient down and use a fan to speed evaporation, or remove excessive clothing and pack the patient with ice (less effective method of cooling, but may be the only option in the field). Transport to hospital as soon as possible.Reference 246
The risk of permanent organ damage and death increases with time elapsed between core temperature elevation and initiation of cooling therapy.Reference 264 When applying external cooling, monitoring core body temperature is important to avoid overcooling (see Box 5.2).
Hydration Considerations During Treatment

It is important to note that dehydration may be limited during heat stroke, as opposed to heat exhaustion, and that overzealous fluid administration may produce pulmonary edema (especially in older adults). This may be further compounded by the predisposition of heat stroke patients to circulatory failure.Reference 251 In more serious cases intravenous hydration may be necessary, although monitoring of serum sodium levels is important to prevent cerebral edema. Fluid resuscitation is important but should be closely monitored, and renal function may need to be protected.Reference 246
Decreased renal function can also be a risk; some recommend monitoring urine output (50-100 mL/hour) to ensure adequate renal function (if dysfunctional can be supported with diuretics).Reference 276 average of one litre (0.5-2.5 L) of crystalloids titrated to central venous pressure (3 to 8 cm H2O) can be administered to obtain normalized hydration state.Reference 101Reference 277
Invasive techniques including iced saline perinatal lavage, rectal/bladder and gastric lavage to cool quickly, by bypassing the outer shell, have inherent risks and their usefulness is debatable.Reference 101Reference 266Reference 278
Athletes may or may not be dehydrated. During exercise poorly-conditioned athletes lose less fluid (1-2 litres) but more sodium (65 mEq per L/hour) compared to highly-conditioned athletes (3-4 liters; 5 mEq per L/hour).Reference 279 The highly-conditioned athlete may excessively dilute electrolyte concentrations by consuming excessive amounts of water despite their decreased loss of salt.Reference 279
At high core temperatures (>40°C) intracellular proteins and membranes denature, with the brain cells being particularly susceptible.Reference 265 The duration of heat stress is the determining factor in survival and delayed cooling increases mortality.Reference 266 The rapid cooling of the body is therefore the priority for improved survival in heat stroke patients and the rate of cooling in patients should be monitored by rectal temperature every 15 minutes to ensure cooling effectiveness. The body can be cooled through conduction (e.g. ice water), convection (e.g. cold air), radiation (e.g. body radiating heat), and evaporation (e.g. evaporation of sweat or sprayed mist). These methods are not all equally effective. Water has a substantially greater capacity to accept thermal energy than air; in addition the rate of energy transfer is greater in water than air.
The fastest means to cool the hyperthermic patients is through cold-water (2-4°C) immersion.Reference 267Reference 268 Most research available addresses exertional heat stroke (e.g. sports, military and manual labour) and this research supports the use of ice-water baths.Reference 101Reference 257 Importantly, ice-water baths can be initiated quickly on site without electricity and are currently recommended for first-aid planning at many athletic events (e.g. football, marathons).Reference 9
In Bouchama et al.Reference 101 a review of these studies of ice water submersion is outlined for cooling and hemodynamic management of heat stroke until more evidence-based data are generated. This may be inconvenient and unsafe in many environments so research has tried to outline some alternatives (that although less efficient are better than no action). Using cold water to cool any part of the body is better than doing nothing and, as a minimal intervention will improve comfort; cooling over the largest area, with fanning, greatly improves cooling efficiency.Reference 269 Reference 271
Evaporative cooling essentially simulates the evaporation of sweat by wetting the patient's skin and encouraging increased evaporation with fanning. The most effective evaporative cooling technique is with warm water mist (to avoid vasoconstriction) and fanning in a body cooling unit described by Weiner and Khogali.Reference 272 Of particular note for facilities with the infrastructure to set up these body cooling units, is that it can facilitate other medical interventions and supportive measures (e.g. monitoring vital signs, performing cardiopulmonary resuscitation).Reference 273 This method is not associated with convulsions and has an efficient cooling rate.Reference 272Reference 274
There appears to be geographical divide in the recommendation of evaporative cooling.Reference 275 This may reflect average humidity levels in hot months in certain areas, since high humidity reduces the rate of evaporation and thus slows the cooling potential, while in areas of high heat, low humidity promotes evaporative cooling.
In classic heat stroke there is much less information available particularly regarding frail or vulnerable patients (e.g. young children, older adults, and people with one or more chronic conditions). Further research into the use of cooling methods in classic heat stroke is needed.Reference 101 Given the needs of many victims of classic heat stroke the currently available resultsReference 272Reference 274 suggest evaporative cooling is worth recommending.Reference 246Reference 260Reference 275
The cooling end-point needs to be identified when treating heat stroke patients with any cooling method to avoid the risk of hypothermia. The cooling treatment cut-off point varies throughout the literatureReference 101 with an average range of 38-38.5°C.Reference 246Reference 275
Heat Stroke Complications
Complications can include muscle breakdown (exertional rhabdomyolysis), which often occurs with exertional heat stroke and increases the risk of renal failure. Also, multiple electrolyte and metabolic abnormalities are observed including hyperkalemia or hypokalemia, hypernatremia or hypocalcemia, hyperphosphatemia, hypoglycaemia, lactic acidosis and uremia.Reference 48 Complications may extend to all major organ systems (see Table 5.2) leading to multi-organ dysfunction syndrome (MODS).Reference 279
| Cardiovascular | Hematologic |
|---|---|
|
|
| Central Nervous System | Musculoskeletal |
|
|
| Gastrointestinal | Pulmonary |
|
|
| Renal | |
|
|
5.3 Differences in Mental Status for Heat Stroke and Heat Exhaustion
One of the main differences between heat exhaustion and heat stroke is the changes in the central nervous system, and thus a patient's mental state. As core temperature rises, the most prominent observations of mental status change include delirium, hallucinations, impairment of consciousness, ultimately leading to coma.Reference 280
People with psychiatric illness and those over 75 years are at increased risk for heat illness in part due to their medications, their limited ability for self-care and/or social isolationReference 163 and are among the most likely to die of heat stroke during an EHE. They also present unique challenges and require particular care to assess a change in mental status in the extreme heat. Awareness among health care workers regarding this increased risk is needed.Reference 283
Careful assessment of the patient's mental status will ensure proper diagnosis. An example of a mini-mental assessment for monitoring the level of consciousness in any patient with compromised neurological function can be found in Box 5.3. Depending on the institution and patient population the Glasgow coma scale, the AVPU scale (Alert, Voice, Pain, Unresponsive) or other may be more relevant.Reference 281 The following questions in Box 5.3 may help in assessing a patient's mental status.
Current orientation to person, place and time:
- What is your name? Who are you? What are you doing here?
- What is the year? Season? Month? Day of the week? Date?
- Where are you? What country? Province? City? Building?
Orientation to past event:
- What was your last address and phone number before coming to this site?
- Could you concentrate normally and fully at the time of illness?
- Were you confused about anything while ill?
Examples of patient responses to past events indicating confusion:
- "I just wasn't all there, thinking was fuzzy."
- "I was getting dumb."
- "I don't know where I was, I couldn't answer questions."
- "I was having trouble doing simple math."
- "I was disoriented, couldn't remember where I was."
- "I couldn't think clearly, couldn't concentrate."
- "I couldn't keep a thought in my head, forgot instructions."
- "I don't remember if I went out or not, things became confused."
Adapted fromReference 280Reference 282
6. Questions and Answers: Preventing Heat-Related Illnesses
Key Terms: prevention, hydration status, clothing properties, caffeine consumption, humidity, evaporative cooling, acclimatization
Summary Points:
- During an extreme heat event it is important to drink water before feeling thirsty. By the time a person feels thirst, they have lost about 2% body water and dehydration has already begun.
- For the general public, there are minimal advantages to drinking sports drinks during extreme heat and it is recommended that water be consumed instead.
- To permit adequate ventilation and promote evaporative cooling and dry heat exchange, clothing worn during extreme heat should be loose-fitting, light-coloured and made of breathable fabric.
- The rate at which sweat is evaporated from the skin is related to the moisture content (humidity) of the surrounding air, and is a function of the air flow.
6.1 Preventing Heat-Related Morbidity and Mortality
Heat-related morbidity and mortality are largely preventable through knowledge, education and adaptive behavioural actions. The amount of lead time in forecasts of extreme heat events (EHEs) is now helping public health officials and the public to prepare for dangerous heat conditions. Today, health care workers are in a unique position to ensure the safety of their patients and/or clients by promoting adequate preparation for EHEs through direct personal communication. The education of patients, workers and athletes regarding effective prevention of heat-related illness can help them avoid potentially serious health problems when exposed to extreme heat.
The understanding of which groups are heat-vulnerable, the associated risk factors and the barriers to action are important for health care workers providing advice regarding proper preventative actions. Several common questions and responses regarding the prevention of heat-related illness are listed below. Each question is accompanied by an appropriate response that can be conveyed by health care workers during consultations, front-line supervisors at the workplace or coaches during practice. For further information regarding the development and modification of heat-health communication strategies for EHEs please refer to Health Canada's Communicating the Health Risks of Extreme Heat Events: Toolkit for Public Health and Emergency Management Officials.Reference 284
Question 1: What is the importance of individual hydration status during an extreme heat event?
Response:

Dehydration impairs the body's ability to maintain optimal core temperature. Many messages to the public which recommend the appropriate quantity and frequency of water consumption during extreme heat can be confusing for the average person since many different suggestions exist.Reference 285 Therefore, during extreme heat, health care workers should encourage the consumption of water before the sensation of thirst, since once thirst is perceived a person is already suffering from mild dehydration (Box 6.1).
Box 6.1: Progression of Dehydration by Percent of Total Body Weight Loss
1%
Already classified as mild dehydration and characterized by reduced blood volume and compromised cardiovascular capacity
2%
Dehydration is well establishedReference 9 and is classified by marked thirstReference 35
4%
Dry mouth and throatReference 35
5%
Shown to impair work abilitiesReference 290
6-8%
Loss of saliva production, speech becomes difficult and large increases in heart rateReference 35
10%
12%
Mental incapacitationReference 35
No longer able to swallow, and cannot recover without medical assistanceReference 35
The body and its many organs depend on water to maintain membrane ion gradients in cells needed for electrical activity and to support normal cell function. Changes in ion and electrolyte concentrations can interrupt cardiac muscle contractions, cause muscle spasms,Reference 286 gastro-intestinal disturbances and lead to problems with the normal functioning of muscles and nerve cells.Reference 42 Older adults are more at risk of dehydration since their perception of thirst is much lower than that in younger adults, and they have a reduced ability to conserve water and electrolytes in their kidneys when the body is in water deficit.Reference 74 Also, some older adults restrict fluid consumption due to continence considerations.
Although drinking water should be encouraged, it is also important to avoid overconsumption of water as it could result in over-hydration (hyponatremia).Reference 287Reference 288 Hyponatremia is classified as a complication of low plasma sodium levelsReference 232 due to the disruption of the osmotic balance across the blood brain barrier resulting in a rapid influx of water to the brainReference 129 and may lead to health complications and even death.Reference 235 Although uncommon in the general population, studies have shown that hyponatremia can be present in 15%-18% of patients in chronic care facilities, and to a lesser extent in nursing homes, often due to the impairment of water metabolism associated with many chronic diseases.Reference 289 In addition, some endurance athletes are also more prone to drinking copious amounts of water prior to an event. When faced with these vulnerable groups, health care workers should emphasize the risk of consuming very large amounts of water in a short period of time. In the case of endurance athletes, sports drinks may be more appropriate.
In areas where drinking water is thought to be unsafe (e.g. when travelling abroad) health care workers should encourage travellers to boil their drinking water or use water purification or filtration methods prior to consumption. Chlorine-or iodine-based compounds are most widely used for water disinfection. An activated carbon filter may also be used to remove excess taste and odour caused by these agents.Reference 291
Question 2: Should one cease consumption of caffeine during extreme heat?
Response:

Studies have found that habitual consumers of caffeine (approximately one to six 250 mL cups of brewed coffee per day) can develop a tolerance to caffeine which reduces its diuretic effects.Reference 292 Reference 294 Alternatively, those who do not regularly consume caffeine, will experience diuretic effects if large amounts of caffeine are consumed.Reference 294 Studies have also been conducted on the effects of acute caffeine consumption and none suggested impairments in heat tolerance or physical performance following ingestion if hydration is maintained.Reference 292Reference 295 Reference 298
Cautioning patients/clients who regularly consume caffeine to abstain from drinking coffee, tea or soda is not well supported by the literature and should not be advised. However, it is recommended not to increase regular consumption of caffeinated beverages during EHEs.
Question 3: Should alcoholic beverages be avoided during extreme heat?
Response:

The absolute need to avoid alcohol during EHEs is a common recommendation by public health personnel. Health care workers should be cautious when informing patients/clients regarding the effects of alcohol consumption on heat tolerance. Investigation into the effects of alcohol consumption is limited; however, studies have found some diuretic effects which vary according to the alcohol content of the drink.Reference 299- Reference 301 For example, it has been found that for every 1 g of alcohol consumed 10 mL of additional urine was excreted.Reference 299Reference 300 (A standard drink in North America is 350 mL beer, 147 mL of wine or 44 mL spirits, each containing 13.7 g of alcohol).Reference 302
Advice should distinguish between the acceptable moderate intake of beverages with a low alcohol-to-water content (such as beer) and the inappropriate consumption of 'hard' alcohol (such as spirits).Reference 299Reference 300
Health care workers should also discourage excessive or chronic consumption of any type of alcohol. Excessive consumption of alcohol is known to impair judgement and may contribute to poor decision-making, leading to inadequate prevention and protection during extreme heat. Epidemiological studies have found correlations between alcohol consumption and heat-related mortality during EHEs in both Europe and North America,Reference 150Reference 303 however the amount of alcohol consumption is not described.
In addition, alcohol has been shown to cause significant decreases in systolic blood pressure when consumed during exposure to extreme heatReference 304 and may be dangerous for people with certain conditions such as cardiovascular disease or hypertension. Alcohol also has many adverse side effects in combination with certain medications, which should be made aware to the client or patient.
Question 4: Is it better to drink water or sports drinks during hot weather?
Response:

Increased consumption of water is recommended, without the need for supplementary sports or energy drinks during hot weather conditions. Some studies have demonstrated increased voluntary fluid intake with beverages containing carbohydrates and electrolytesReference 305- Reference 307 which may be due to enhanced flavouring.Reference 308 Therefore health care workers may recommend the dilution of sport drinks (or better yet, natural fruit juices) with water to encourage drinking by improving the taste. In addition, discussing the nutritional requirements of patients/clients and discouraging consumption of regular sport drinks in people with certain conditions such as diabetes (due to high sugar content), impaired kidney function and on low-calorie diets is recommended,Reference 309 as people with these conditions are often on regimented diets that have exclusive and controlled restrictions. For people who are on fixed budgets, sports drinks may also be an unnecessary cost and will not provide an added health benefit.
Some studies have found detrimental effects of sports drinks by linking carbohydrate intake with elevated core temperature due to increased work and power output.Reference 310- Reference 312 In contrast, recent studies have not shown any alterations in core temperature, heart rate, fluid retention, plasma volume, urine volume, sweat loss, serum sodium concentrations and thirst in individuals who consumed carbohydrate and/or electrolyte solutions as compared to water.Reference 285Reference 313- Reference 315 Ongoing research continues to study the effects of sports-drinks on measurable health outputs.
Question 5: What should I eat during an extreme heat event?
Response:

In addition to drinking water during hot weather, individuals should maintain a proper and well-balanced diet whenever possible. Up to 65% of a person's average daily water intake is through the ingestion of food. Health care workers should recommend that people continue to eat well during hot weather, but may encourage the consumption of foods with high water content such as raw fruits and vegetables. In addition, to avoid the added radiant heat, it is suggested that individuals consume meals that do not require the use of an oven during EHEs.
It is especially important for vulnerable groups (such as older adults) to continue eating as usual since they often already have a tendency to consume less. The type of food ingested, such as foods containing sodium, may also influence water absorption and retentionReference 316 and so caution should be taken to reduce the intake of high sodium foods. Although different foods may contain large amounts of water, the consumption of food cannot accelerate the recovery of the body's water stores if a person is already dehydratedReference 317Reference 318 therefore it is important to maintain proper hydration throughout the day during extreme heat.
Information regarding the nutrient content of most foods can be accessed through the Canadian Nutrient File (CNF)Reference 319. Examples of common foods and their water content are listed in Table 6.1.
| High Water Content | Low Water Content | ||
|---|---|---|---|
| Food | Water Content | Food | Water Content |
| Iceberg lettuce, raw | 95.6 % | Steak, lean, cooked | 50.8 % |
| Cucumber with peel, raw | 95.2 % | Pizza, with toppings | 46.7 % |
| Watermelon | 91.4 % | Bread, wheat | 36.4 % |
| Pink Grapefruit, raw | 88.0 % | Commercial cookies | 5.3 % |
| Squash, cooked | 82.9 % | Cereal, Cheerios | 3.5 % |
| Pasta and meatballs | 75.4 % | Peanuts, roasted | 1.7 % |
Question 6: How does my choice of clothing affect my ability to sustain extreme heat?
Response:

Clothing properties and the composition of the material should be considered when dressing during conditions of high heat and humidity. Clothing should be light-coloured to decrease heat absorption, permeable to allow for water vapour to move through and help with evaporative cooling, have adequate ventilation to allow for air movement through the fabric and/or through openings such as cuffs and collars, and have low insulative effects to permit dry heat exchange.Reference 320- Reference 322 A good example of appropriate clothing would be light-coloured, loose-fitting, cotton clothes.
Polyester should be avoided whenever possible as it does not allow for air or water to pass through. Studies comparing the thermal properties of polyester and cotton on thermophysiological responses found rectal temperature, pulse rate and sweating rates to be significantly higher in subjects wearing polyester clothing as compared to the rates in those wearing similar cotton clothing.Reference 323Reference 324 Many sports fabrics are designed to increase air permeability,Reference 325Reference 320 however many of these clothes are expensive and it is difficult to assess the benefits associated with such fabrics as research is limited.
If the skin is unprotected, exposure to solar radiation (which includes ultraviolet, visible and infrared radiation) can result in sunburn which is not only painful but decreases sweating efficiency.Reference 159 Short-sleeved shirts and shorts are suitable to wear during the heat to allow for the evaporation of sweat, but it is important that all exposed skin is covered with sunscreen. The use of hats for protection from solar radiation is essential, but individuals must also keep in mind that headgear worn in hot and humid weather should not impede evaporative heat loss. Basic scientific principles, as well as traditional designs in hot climates, indicate that hats that are worn to protect against the sun should be:
- Wide-brimmed - peaked baseball caps offer good protection to the nose, but are ineffective in protecting other areas of the face, including the ears and back of the neck. Hats with a wide brim (at least 7.5 cm) are necessary in order to provide adequate ultraviolet protection.Reference 327Reference 328 It has also been found that radiant heat gain is proportional to the amount of surface area exposed to the heat source.Reference 329
- Well-ventilated - ventilation is practical in enhancing both convective and evaporative heat loss from the body and decreasing the physiological burden in a hot environment.Reference 330
Although light-coloured material is generally recommended, a recent study comparing two baseball-style caps (white and black) found no effect of cap colour on heat transfer.Reference 329 Therefore until further information is available, health care workers should not necessarily advise against the use of dark-coloured headgear, but simply to advocate wearing a properly ventilated hat with a brim of at least 7.5 cm. An umbrella can also be used to avoid the sun as it does not interfere with evaporative cooling and provides lots of shade.
Question 7: Should I reduce my activity levels during extremely hot weather?
Response:

Encouraging patients to reduce strenuous activity during periods of extreme heat, and to plan physical activities for cooler parts of the day is recommended. Individuals may also choose to exercise in an air-conditioned place, or a cooler outdoor location such as a tree-shaded area away from high traffic to avoid high levels of air pollution. Pollution levels tend to be higher on hot days; the Air Quality Health Index (AQHI)Reference 331 can be used to determine the air quality in a person's neighbourhood.
Although the primary focus of most research pertains to exertional heat illness and involves athletes, military personnel and workers in physically demanding jobs, the recommendation of avoiding strenuous activities for the general public is sensible. Information is lacking regarding tolerable activity levels in many vulnerable people, and so patients and clients should be aware of the signs and symptoms of heat-related illness to properly self-assess their risk in hot weather and minimize physical activities accordingly. It is therefore the role of the health care worker to ensure patients are informed of these signs and symptoms as well as the appropriate actions to take (for more details see Chapter 7).
Those who organize sporting events, such as round-robin tournaments, outdoor sports leagues and marathons, should take precautions and modify rules and equipment appropriately when these events take place during extreme heat. Many sports organizations have adopted a protocol for hot conditions such as increasing scheduled water breaks, using umbrellas on sidelines, incorporating heat acclimatization into practices in the summer, having an emergency plan, equipment modifications for practice in hot weather, etc. Many examples of these types of protocols are available online. It is important that adults, caregivers and teachers take special precautions when scheduling outdoor activities for children and youth during extreme heat, and limit the intensity and duration of any exercise. The use of a buddy system is also encouraged to help monitor for early signs of heat strain.
Studies have found an association between the risk of exertional heat illness and high outdoor heat levels for the day of, as well as the days preceding, the onset of heat-related illness.Reference 332- Reference 335 However, there are no demonstrated heat levels without some risks.Reference 335 It should be noted that the hottest part of the day varies across North America, and depending on a person's location, their body could gain heat from various sources, such as from direct sunlight during the day or from pavement and buildings even after the sun sets.Reference 336 In addition, individual physiological characteristics such as age, weight distribution and physical fitness can influence a person's susceptibility to heat. Individuals must use prior knowledge and best judgement to identify safe conditions for activities, based on the combined effects of environmental conditions and a person's health and physical condition, degree of acclimatization to heat, and clothing.Reference 335 For workers, specific guidelines termed Threshold Limit Values (TLV®s)Reference 44 are available (see Chapter 2).
Question 8: Should I use air conditioning (or evaporative coolersh) during extreme heat events?
Response:

Air conditioning has been shown to be one of the most protective factors for preventing heat-related illness and death.Reference 13Reference 125Reference 146Reference 149Reference 150Reference 163 Reviews have analyzed several epidemiological studies which have demonstrated that the use of air conditioning during an EHE has a considerable protective effect against heat-related deathReference 13Reference 41 and up to an 80% reduction in the incidence of heat-related illness.Reference 149 On the other hand, scientific evidence regarding the amount of time necessary to spend in an air-conditioned environment to maximize its protective effect is lacking, since it is variable and based on individual characteristics. It is almost impossible to give standardized recommendations due to the variations in a person's perception of feeling hot and the physiological characteristics that may increase their risk in the heat (obesity, age, chronic diseases, etc.). It is for these reasons that a person's self-assessment of heat strain is a helpful guide, and if feeling heat-stressed an individual should remain in an air-conditioned or cool environment until normal core temperature range is attained, or until feeling refreshed. If access to an air-conditioned environment is not possible, efforts to increase ventilation can also reduce temperature (see Question 10).
If someone does not have access to air conditioning at home, visiting a public air-conditioned place, community pool or spray pad, or even a tree-shaded area are reasonable alternatives.Reference 327Reference 337 Visiting public places is also a more energy efficient alternative. Additionally, cool showers and baths can also be recommended, but health care workers should be aware that older adults and children need to be cautious of injuries, such as from slips and falls.Reference 338Reference 339
h Evaporative coolers are similar to air conditioners but cool the air (which then flows indoors) by the evaporation of water and not with the use of refrigerants. These types of coolers are most efficient in hot, dry climates where humidity levels are low.
Question 9: How does humidity affect me during extreme heat?
Response:

Water absorbs a great deal of heat when it evaporates and the evaporation of water from the surface of the skin can remove large amounts of body heat. The evaporation of sweat from the skin cools the skin surface thereby cooling the blood perfusing the skin which is then recirculated back to the central core region. As ambient temperatures rise, the body becomes increasingly dependent on evaporative cooling. Above skin temperature (34-36°C) convection and radiation no longer contribute significantly to heat loss. A rise in humidity reduces the ability and rate of water evaporation from the skin due to the saturation of water in the air, which can result in further fluid loss as the body continues to produce sweat despite the inability of it to evaporate. Due to this continual production of sweat it is important to keep drinking water to maintain hydration.
The rate at which sweat is evaporated from the skin is proportional to the moisture content (humidity) of the surrounding air. When temperatures are below 30°C, evaporative heat loss (through breathing and perspiration) accounts for approximately 25% of total heat loss. In hot environments, 90% of heat loss is through evaporation;Reference 37 however, when the air is near-saturated with water, evaporation is impeded. If excessive sweating continues without evaporation, skin drips with sweat resulting in dehydration as wet skin does not have a beneficial heat-loss effect if the water is not vaporized.
Question 10: Should I use a fan to promote cooling when it is hot?
Response:

There are many instances in which a fan can be beneficial during extreme heat. These instances can be separated into two types: environmental advantages and physiological advantages. In addition, there may be instances when fan use is not recommended.
Fans with Environmental Advantages:
Ceiling Fans: When set in reverse (often clockwise) ceiling fans can help move hot air from the ground up towards the ceiling and out windows. This can reduce the temperature closer to the ground in a particular room. When set at regular settings (often counter-clockwise), a ceiling fan can help with evaporative cooling by increasing air movement over the body if someone is resting directly beneath it.
Window Fans: A fan placed in the window can help draw in fresh, cooler air from the outside and lower the temperature inside a room. This is especially useful at night when temperatures are generally lower outdoors.
Fans which Promote Physiological Advantages:
Air is cooler than skin temperature (34-36ºC): When the air temperature is cooler than a person's skin temperature, sitting in the direct path of the fan's air flow can help with convective heat loss in addition to evaporative heat loss. To further cool down, a bowl of ice can be placed in front of the fan which will blow colder air on a person, increasing the temperature gradient between the person and the surrounding air, to increase convective heat loss even more.
Air is warmer than skin temperatures (above 36ºC): When the air temperature is higher than a person's skin temperature, sitting in the direct path of the fan's air flow can help with evaporative heat loss only if someone is sweating, or misting themselves with water. Otherwise, the hot air can warm a person through convection.
When Not to Use a Fan:
Fan use can be counter-productive when the evaporation of sweat from the surface of the skin is compromised, which occurs during times of high heat and humidity, or due to certain medications: therefore, during these instances use of a fan should be discouraged. During extreme heat, temperatures inside can be much hotter than the temperature outside, and so re-circulating extremely hot air can be dangerous. It is also possible that some older fans have poor air flow and are not as efficient. In addition, some fans radiate heat when turned on which may increase the temperature of the surrounding air.
To date, very little physiological research on vulnerable populations has studied the use of fans during periods of high heat and humidity, and so it is therefore difficult to properly assess the associated risks and benefits. Epidemiological studies have also found varying results. Some studies have found no associations between use of electric fans and the onset of heat stroke,Reference 125Reference 149Reference 150 whereas in other cases fan use has been found to be slightly protective.Reference 13 Proper ventilation in the home has also been associated with having a protective effect.Reference 13Reference 23
Question 11: Should I cool myself by misting my body with water?
Response:

Misting in dry environments can contribute to short-term cooling through conduction from the cool mist as well as through the evaporation of water off the surface of the skin. As with the use of fans, when the air becomes near-saturated with water, the effects of misting or damping the surface of the skin are negligible if the water cannot be evaporated. If one decides to mist or dampen the surface of the skin, cool or cold water is necessary to elicit a protective effect through conductive cooling. Unfortunately, studies are limited to research in animals, and so the points discussed here are based on the scientific principles of evaporative heat loss.
Question 12: Why should I acclimatize? How would I do this?
Response:

Humans successfully inhabit many hot climates due to the body's ability to acclimatize. Acclimatization refers to the gradual physiological changes that improve a person's tolerance to heat and allows for a reduction in the detrimental effects of heat strain when exposed to heat stress. Heat acclimatization is best achieved by exercising for 60 to 90 minutes in the heat, each day, for 9 to 14 days.Reference 45 However, most of the classic signs of acclimatization and a decrease in body heat content can be achieved by passive, short daily periods of exposure to heat, as long as core temperature is elevated.Reference 63Reference 64 Heat acclimatization is also particularly important in the spring period (if possible) prior to the arrival of hot ambient conditions.
Health care workers should note that active acclimatization is recommended for people who are in general good health and who are physically active, and may not be suitable for some older adults, people with cardiovascular, respiratory or other chronic illnesses, and young children. Limited research exists regarding the tolerance of these heat-vulnerable groups to acclimatization. It should also be noted that one is only considered to be acclimatized up to the level of heat experienced during the acclimatization process; for example, if someone acclimatizes to temperatures at 30ºC, then they will mainly reduce their risk of developing heat-related illnesses when exposed to temperatures at 30ºC or below.
Acclimatization can be difficult in the Canadian climate as EHEs are generally short in duration and sufficient time may not become available to be adequately protected. However, some changes can be seen in the first one to four days.Reference 35 Generally during the first day of heat acclimatization the discomfort is very noticeable, however with each succeeding day the symptoms gradually decrease. Progressively, the individual is able to perform the required tasks with a reduced level of thermal strain. Although the physiological responses to acclimatization are similar between different people, the degree of response is highly variableReference 68 and should be taken into consideration (see Chapter 2). The onset and benefits of acclimatization for most people begin early, but these effects can also be lost quickly if exposure is discontinued. If a week or two passes without exposure, re-acclimatization would be needed and may take four to seven days.Reference 45
Question 13: Why are parked cars dangerous for people and pets during extreme heat?
Response:

Insist that patients/clients do not leave those in their care in a parked vehicle for any amount of time during hot weather, even if the windows are left open by a small amount. Temperatures inside a vehicle can rise dramatically in short periods of time, even without sun exposure.
Every year children and pets left unattended in motor vehicles during conditions of extreme heat die due to heat-related effects. In addition to these deaths, it is estimated that hundreds of children experience heat-related illness annually from being left inside motor vehicles.Reference 341 With the increase in stress, lack of sleep and having to multi-task in today's society, many people are consumed with things to do and are unaware that a child is still in the back seat. Many resources and tricks exist nowadays to help someone remember a child in the back seat of a car, some include:
- Putting something you'll need like your cell phone, handbag, employee ID or briefcase on the floor of the back seat.
- Getting in the habit of always opening the back door of your vehicle every time you reach your destination.
- Keeping a large stuffed animal in the child's car seat when it's not occupied. When the child is placed in the seat, put the stuffed animal in the front passenger seat.
Studies have shown that on days with high radiant load, even when the ambient temperature is relatively low, the interior temperature of a vehicle can significantly increase in a short period of time. For example, on days when ambient temperature is 23°C, the internal temperature of the vehicle has been shown to reach approximately 50°C within 60 minutes. Opening the window by a small amount does not reduce a vehicle's internal temperature or the rate of temperature increase.Reference 341
Question 14: What long-term prevention strategies can be used at home to decrease a person's risk of developing a heat-related illness in the future?
Response:

It may be in the interest of the health care worker to approach the subject of long-term prevention with a patient or client, as heat-health risks are expected to become more prevalent due to the projected increase in the duration, intensity and frequency of EHEs. There are several different actions the public can take to protect themselves and their family at home. These include:
- Planting plants and trees around the home which not only creates shade, but can also reduce greenhouse gases and remove air pollution, which in turn improves air quality
- Installing awnings and outdoor shutters to create shade and keep heat out
- Using light-coloured materials for covering external surfaces
- Using building materials that are designed to decrease heat retention (by having the ability to reflect heat)
- Installing an air conditioner in at least one room
- Increasing vapour barrier and insulation of the building envelope (to limit unwanted air exchange)
Outdoor heat, especially in urban environments, can potentially be lowered by reducing the amount of radiant energy from the sun that is absorbed by buildings. Increasing the vegetation around the home can accomplish this by providing direct shade to structures and dark surfaces such as asphalt.Reference 342 Awnings and shutters have a similar effect, by reducing the amount of heat that enters the home. Outdoor shutters are thought to be more beneficial than curtains since they are able to keep the heat outdoors, whereas curtains have a tendency to trap heat indoors, between the curtain and the window.
Solar-reflective surfaces, which maintain low surface temperatures in sunlight, can also reduce a building's energy use for cooling. These low surface temperatures (and a decrease in energy costs) can be achieved for an individual building by increasing its albedo (the amount of sunlight that is reflected).Reference 343 Increasing a structure's albedo can subsequently help with cooling, which can translate into increased protection of the people living or working inside or around the building. There are many materials that have a high solar-reflectance which are currently available. For example, walls can be covered with white coatings such as paint and siding, and roofs can be finished with white gravel, or with reflective shingles or tiles.
Box 6.2 Summary Recommendations for Prevention of Heat Strain
- There are home strategies that a person can use to decrease exposure to extreme heat in the long- and short-term.
- Encourage the consumption of water before the sensation of thirst, since once thirst is perceived a person is already suffering from mild dehydration.
- The consumption of caffeine should not be prohibited if the person is a regular consumer. However, a person should not increase caffeine intake during extreme heat.
- Excessive or chronic consumption of any type of alcohol should be discouraged. Beverages with low alcohol-to-water ratio (such as beer) are acceptable to drink during extreme heat with moderate intake. However, hard alcohol (such as spirits) should be avoided.
- Recommend increased consumption of water during extreme heat, without the need for supplementary sports or energy drinks, especially for children and individuals on regimented diets.
- Individuals should continue to eat during extreme heat, but may be advised to consume foods with higher water content (such as fruits and vegetables). The use of an oven should be discouraged (stove top and microwave are good alternatives).
- Light-coloured, loose-fitting, breathable clothing should be worn when it is hot out. Light-weight cotton is a good option. If shorts and T-shirts are worn, a person must use sunscreen on all exposed skin. A ventilated hat with a brim of at least 7.5 cm is the best option to protect the face.
- Encourage patients to reduce strenuous activity during periods of extreme heat, and to plan physical activities for cooler parts of the day. If this is not possible, individuals can exercise in an air-conditioned environment, in outdoor areas that are cooler such as a tree-shaded area or swimming in cool water, or increase the frequency of rest and water breaks.
- Encourage spending at least some time in an air-conditioned place. If this is not possible, cool showers or baths are a reasonable alternative.
- Discourage leaving anyone in a parked car for any amount of time, even if the windows are left open by a small amount.
- Misting cool water on the skin in dry environments can contribute to heat loss especially when complemented with fanning. In humid environments misting is less useful due to the decreased evaporation of water from the surface of the skin.
- Heat acclimatization is best achieved by exercising for 60 to 90 minutes in the heat, each day, for 9 to 14 days. However, most of the classic signs of acclimatization and decreased body heat can be achieved by passive, short daily periods of exposure to heat, as long as core temperature is elevated.
7. Extreme Heat Summary Advice for Medical Officers of Health and Public Health Staff
Key Terms: heat alerts, Humidex, recognizing heat-related illnesses, individual risk factors, community risk factors, co-benefits, public messages, long-term planning
Summary Points:
- Both individual and community factors affect heat exposure and the resulting physiological effects. Raising awareness about these factors helps to ensure that those most at risk receive the information they need to prevent heat-related illnesses.
- Effective prevention requires behavioural change to reduce exposure, help the body thermoregulate and encourage your community to adapt.
- Long-term public health planning can help address urban heat islands and enable local resilience to the heat. This requires among other things, engagement between public health personnel and municipal planners and builders.
7.1 Extreme Heat Events and Heat-Related Illnesses

Extreme heat events (EHEs) and heat alerts are currently based on regional guidelines and local needs.Reference i Heat illnesses can be described as direct if they are caused by exposure to heat or indirect if they are caused by both a pre-existing condition and exposure to the heat. The goal for treatment of heat illness is to cool the body. Early cooling of the body can prevent the long-term consequences of heat stroke and can even save lives.
7.2 Individual and Community Risk Factors
Although every individual reacts differently to heat stress, from a community perspective there are many individual and group settings to consider which are at particular risk with exposure to heat. Specific groups have been identified as being more vulnerable to heat stress:
- Older adultsReference 344
- Young childrenReference 50Reference 86Reference 87
- Socially isolated (low income, homeless, living alone, confined to bed)Reference 13
- Occupational groupsReference 345 (outdoor workers, miners, workers in commercial kitchens)
- People exercising vigorously outdoorsReference 346 (long-distance running, football)
- Tourists (large outdoor gatherings, long exposure to heat in areas with reduced access to drinking water)Reference 347Reference 348
Certain pre-existing chronic conditions put individuals at risk. These conditions affect the body's ability to thermoregulate, putting the individual at increased risk to develop a heat illness. In addition, heat itself can exacerbate these pre-existing conditions. Conditions which increase the risk of illness or death in extreme heat:
- Cardiovascular illness (hypertension, coronary artery disease, heart conduction disorders)Reference 107
- Mental illness (dementia, depression, schizophrenia, Alzheimer's)Reference 183Reference 349
- Mental and behavioural disordersReference 157Reference 350 (due to psychoactive substance use, alcoholism)
- Neurological diseaseReference 351 (Parkinson's disease)
- Pulmonary conditionsReference 352 (chronic obstructive pulmonary disease, bronchitis)
- Renal illness or failureReference 16 (renal failure)
- Metabolic conditions (diabetes,Reference 133 obesityReference 353)
Some pre-existing conditions can also affect the body's ability to thermoregulate; in some cases the medications prescribed to treat the pre-existing condition affect the ability to thermoregulate and increase the health risks from extreme heat. Medications that put individuals at increased risk for heat illnesses and the mechanism by which they do so are outlined in Table 7.1.

As indirect heat illnesses arise due to a pre-existing condition in combination with exposure to heat, it is very important to recognize and identify heat as a factor in illness or death. Recognizing and recording heat as a contributing factor to illness in case charts will lead to improved monitoring of heat-related illnesses and consequently a better assessment of prevalence in the community. In addition to this research, community-based vulnerability assessments may provide greater insight into the most prevalant risks in your community. Health Canada has developed Adapting to Extreme Heat Events: Guidelines for Assessing Health VulnerabilityReference 356 which can be used to assess your community's heat-health risk.

People who are not acclimatized to heat stress or who live in specific types of housing (e.g. higher floors without air conditioning) are at greater risk of illness or death from heat stress.Reference 23Reference 121Reference 125Reference 146Reference 149 Certain community characteristics can influence their residents' heat-related health risks, such as:
- Maximum daytime and minimum nighttime temperature trends experienced in the community (especially when there are several days in a row).Reference 23Reference 24
- Magnitude of urban heat island effect (e.g. high-density areas of asphalt and concrete with little vegetation).Reference 21Reference 357
- Number and nature of outdoor events that occur in the summer (e.g. large outdoor tournaments or festivals, marathons).Reference 358
- Percentage of population that work outdoors or in occupations with high heat exposure (e.g. farmers, construction workers).Reference 359- Reference 361
- Common materials used in building structures (e.g. types of roofs, shutters on windows, screen doors, efficient ventilation).Reference 25
- Number and location of outdoor cooling areas (e.g. swimming pools, beaches, splash pads, shaded park areas).Reference 8Reference 362
- Availability and access to air conditioning in public buildings and homes (e.g. libraries, malls, nursing homes, daycares, hospitals).Reference 13
- Number and location of health care facilities without air conditioning (retirement and care facilities, hospitals, clinics).Reference 13
| Medication | Mechanism |
|---|---|
| Antiadrenergics and β-Blockers (e.g. Atenolol, Metoprolol) |
Can decrease cardiac output, and therefore shunting of warm blood from body core to periphery, limiting cooling. |
| Anticholinergics (e.g. Scopolamine) |
Can prevent sweat glands from functioning properly (i.e. inhibit rate of sweating and therefore rate of cooling). |
| Antidepressants (e.g. Prozac, Zoloft, other SSRIs) |
Many have anticholinergic properties (see above) and some can raise the brain's thermal set-point decreasing centrally induced thermoregulation. SSRIs can increase the risk of hyponatremia. |
| Antihistamines (e.g. Brompheniramine) |
Can inhibit the sweating mechanism |
| Anti-Parkinson's agents (e.g. Benztropine, Levodopa, Trihexyphenidyl) |
Can inhibit the sweating mechanism |
| Antipsychotics (e.g. Olanzapine) |
Can inhibit the sweating mechanism. Can induce a hyperthermic syndrome (neuroleptic malignant syndrome) on their own, which would be compounded by the effects of heat. |
| Sympathomimetics (e.g. Pseudoephedrine) |
Can prevent dilation of the blood vessels in the skin of the periphery (hands, feet, face) reducing the ability to dissipate heat by convection. |
| Diuretics (e.g. Lasix) |
Can lead to dehydration and hyponatremia is a common side effect |
| Several drug classes (e.g. Cholinesterase inhibitors, antiarrhythmics, calcium blockers) |
Can provoke diarrhea and/or vomiting, leading to dehydration |
Adapted from Reference 354Reference 355
Key Actions to Address Risk Factors in the Community
- Help the public to assess their risk (and the risk of those they care for).
- Discuss preventive actions that could be taken to reduce risk before and during EHEs.
- Educate and increase awareness of the risk factors, signs and symptoms, and treatment for heat-related illnesses.
Public Health Interventions
Examples of public health interventions targeted towards at-risk and homeless individuals are listed below. Health care providers should be encouraged to do some or all of the following:

- Create a list of vulnerable clients (due to social isolation, psychiatric illness, poor housing quality, etc.) and ensure there is a plan in place to check on those individuals daily during EHEs. Special attention should be paid to those without an alternate daily source of personal care or home care. Setting up a tracking mechanism to ensure that at-risk individuals are checked on regularly can be critical to prevent heat stroke and other heat-related illnesses.
- Public health staff can lobby, advocate and work with municipal shelter and housing staff to develop emergency plans for homeless shelters. Few of these facilities are air-conditioned or have adequate number of showers, although they shelter people with multiple risk factors for heat-related illness (chronic illness, medications, social isolation, etc.).
- Conduct education with local drop-in centers and shelters regarding the risks their homeless or at-risk clients face during EHEs. Advocate that those agencies having air conditioning extend hours during EHEs and have "low threshold" behavioural requirements for attendees.
- Public health and/or local primary health care providers should work together, with appropriate municipal authorities, to create innovative community outreach models.
- Public health departments should ensure, that those municipalities with high numbers of homeless and other vulnerable people living in poor quality housing, open emergency cooling centers during EHEs.
7.3 Effective Prevention Measures to Advise the Public to Adapt to the Heat
Heat-related illnesses are largely preventable through behavioural adaptations because heatstress conditions are predictable. However, because heat stroke has a fast onset and poor survival rate,Reference 128Reference 202 promotion and prevention efforts must begin when high temperatures are forecast rather than when they arrive.
The prevention measures to address key questions from the public regarding hydration, use of hats, clothing and fans, physical activity in the heat, and cooling optionsReference 363Reference 364 are outlined in Section 7.4. In addition, three summary handouts for the public have been prepared, specifically for older adults, the physically active, and those who care for young children (see Appendix D). The key information for health care workers has been summarized for three broad target audiences including Acute Care, Community Care and Health Facility Preparation (see Appendix B). These Fact Sheets are available as pads of tear away sheets to promote easy distribution. This information should be brought forward to the public and health care workers in the spring, before the hot weather is about to hit and prevention efforts should continue though to the fall.

For effective prevention of heat illnesses and to stimulate behavioural change, information needs to be presented in an appropriate context. This may require additional tailoring for certain audiences and is encouraged for effective communication. Health care workers can play a key role in health promotion, especially when effectively conveying the need for behavioural change. When communicating directly with the public, the distribution of Fact Sheets is most effective when combined with a verbal discussion with emphasis on the individual's specific needs.
7.4 Messages Developed for Communication with the Public
These messages were developed and discussed extensively in Health Canada's Communicating the Health Risks of Extreme Heat Events: Toolkit for Public Health and Emergency Management Officials.Reference 284 Please refer to the Toolkit for advice about timing of messages (i.e. before or during EHEs) and the modes of tailoring and channels for disseminating the messages for your target groups of interest (e.g. different ages, gender specific, ethnic and culturally specific, language specific). The Toolkit provides advice to convey succinctly in communication pieces (such as a news release or interview). Lastly, the Toolkit provides information on evaluating the importance of messages and effectiveness of the various interventions. Below is a focussed summary of the messages developed for communication with the general public.
A. Raise awareness regarding heat as a health risk
Message 1:
Heat illnesses are preventable.
Message 2:

While extreme heat can put everyone at risk from heat illnesses, health risks are greatest for:
- older adults;
- infants and young children;
- people with chronic illnesses, such as breathing difficulties, heart conditions, or psychiatric illnesses;
- people who work in the heat;
- people who exercise in the heat;
- homeless people; and
- low-income earners.
Message 3:

If you are taking medication or have a health condition, ask your primary care provider if it increases your health risk in the heat and follow their recommendations.
B. Educate the public about the signs and symptoms of heat-related illnesses
Message 4:

Heat illnesses include heat stroke, heat exhaustion, heat fainting, heat edema (swelling of hands, feet and ankles), heat rash and heat cramps (muscle cramps).
Watch for symptoms of heat illness, which include:
- dizziness or fainting;
- nausea or vomiting;
- headache;
- rapid breathing and heartbeat;
- extreme thirst; and
- decreased urination with unusually dark yellow urine.
If you experience any of these symptoms during extreme heat, immediately move to a cool place and drink liquids. Water is best.
Message 5:

Heat stroke is a medical emergency! Call 911 or your local emergency number immediately if you are caring for someone, such as a neighbour, who has a high body temperature and is either unconscious, confused or has stopped sweating.
While waiting for help, cool the person right away by:
- moving them to a cool place, if you can;
- applying cold water to large areas of the skin or clothing; and
- fanning the person as much as possible.
C. Educate the public regarding protective measures
Message 6:

Frequently visit neighbours, friends and older family members, especially those who are chronically ill, to make sure that they are cool and hydrated.
Message 7:

Drink plenty of cool liquids, especially water, before you feel thirsty to decrease your risk of dehydration. Thirst is not a good indicator of dehydration.
Message 8:

Reschedule or plan outdoor activities during cooler parts of the day.
Message 9:

Wear loose-fitting, light-coloured clothing made of breathable fabric.
Message 10:

Never leave people or pets in your care inside a parked vehicle or in direct sunlight.
Message 11:

Take a break from the heat by spending a few hours in a cool spot. It could be a tree-shaded area, swimming facility or an air-conditioned place, such as a public building, shopping mall, grocery store, place of worship or public library.
Message 12:

Take cool showers or baths until you feel refreshed.
Message 13:

Prepare meals that don't need to be cooked in your oven.
Message 14:

Block sun out by closing awnings, curtains or blinds during the day.
Message 15:

Avoid sun exposure. Shade yourself by wearing a wide-brimmed, breathable hat or using an umbrella.
Public Health Interventions: Communication of a Heat Alert and Response System
In emergencies, public health agencies and officials often take a role in organizing and monitoring community response. Key roles for public health can include:

- Coordinating and distributing heat information to community agencies working with vulnerable groups, both within the government and non governmental sectors.
- Acting as the agency which evaluates the impact of heat on the health of the community.
- Coordinating the response and help in the development of heat response triggers and alerts.
To create or improve your Heat Alert and Response Plan refer to Health Canada's Heat Alert and Response Systems to Protect Health: Best Practices Guidebook. The public health roles with regards to the planning, response and recovery from EHEs are outlined in this document. Public health can use a heat advisory system to communicate the increasing risk to human health posed by weather conditions.
Some of the possible communication and outreach opportunities are listed below:
- Distribute informative educational materials on how to stay cool and how to identify and guard against heat-induced illnesses like heat stroke.
- Distribute heat and health awareness information to front-line city, police, home support and health and housing outreach workers for distribution to the public and in particular vulnerable seniors, the homeless and people with marginal housing.
- Develop a broad public awareness campaign to help the public understand and use appropriate heat-coping strategies.
- Identify public spaces, water sources and locations where people can find shade and socialize in cooler spaces.
- Provide portable water stations during summer outdoor events, races, festivals etc.
7.5 Mid- to Long-Term Public Health Planning: Prevention for Municipal Planners
The measures required to protect health are not only behavioural change by either the person at risk or individuals in their support circle, but also long-term environmental change. There is an increasing need for public health officials to engage with municipal planners and builders.Reference 365Reference 366
Both of these groups would benefit from sharing knowledge regarding the built environment and human health. In particular, these groups need to work together to develop plans, policies and processes for reducing the carbon footprint and the urban heat island contributions of municipal buildings and urban areas. These measures will help to reduce the present impact of heat, and will enable the adaptation of the local area to heat. These modifications can involve using different building materials (e.g. reduce concrete and asphalt while increasing vegetation) and changing behaviour (e.g. increasing access to water fountains in parks).
In addition there are mid-term strategies that could be implemented at the community level to help address the upstream determinants of health. This is needed since some of the behavioural strategies identified here would be very difficult for someone with a low income to implement. For example, taking a bath or shower until refreshed is difficult if you have shared bathroom facilities, as in a rooming house or shelter. Shorter-term, community level interventions might include, among others:

- Organizing to check in on people who otherwise do not have support (such as in a low-income building).
- Ensuring that cooling centres are very accessible, welcoming to those who use drugs or have mental health issues, within a short walking distance of, or within subsidized housing buildings themselves.
- Provide access to air conditioners at low cost.
- Provide reduced cost or free public transportation so that people who rely on food banks, shelters or meal programs (often at a great distance) can reduce physical activity in the hottest times of day while still being able to meet their basic needs.
The current research regarding the upstream determinants of health, the built environment and health outcomes indicate several co-benefits to coordinating efforts in this respect.Reference 367Reference 368 Addressing environmental risk factors broadly is an effective way to manage a range of public health risks.
8. Disaster Preparedness for Health Care Services
Key Terms: ACGIH®, TLV®, Wet-Bulb Globe Temperature, heat risks, facilities preparation, emergency plan, strategic planning, surge capacity
Summary Points:
- Extreme heat events should be included in health institutions' and organizations' disaster preparedness plans.
- The response to extreme heat events is similar to most other disasters with a few exceptions, notably the protocol for calling a state of emergency.
- Both long-term solutions and emergency (short-term) actions are required to adequately address extreme heat events.
8.1 Managing Extreme Heat Events
Heat has a significant impact on human health, and is an important factor when planning emergency management needs. However, it is not always considered in natural-disaster planning.Reference 369 The goal of this chapter is to provide the information needed to integrate extreme heat considerations into health care institutions, organizations and current facility emergency plans. Included are some suggested practices for heat emergencies and for activating response systems. However, these are only a representative model prepared for consideration. Local needs should be considered to determine the most appropriate response in your area.
One of the most significant differences between an extreme heat event (EHE) and other natural disasters is that it usually causes much less infrastructure damage than other emergencies. It is critical to note that despite the decreased infrastructure damage the negative impacts on health can be much greater than other natural disasters.Reference 1 In addition to the other risk factors outlined in Chapter 3, EHEs present a unique scenario for health care workers and emergency management workers. Heat is therefore sometimes termed the "silent killer" because it may not be noticed early enough and therefore the activation of the all-hazards plan may be delayed.Reference 370
Like many risks, defining heat risks in absolute terms is very difficult. The climate, social structure and urban landscape all have to be considered to assess the regional risk. The individual risk is based on unique physical or behavioural vulnerabilities as well as degrees of acclimatization. In addition, seasonal, regional and acclimatization variability, rather than heat intensity, is thought to be the most important factor defining human sensitivity to heat.Reference 371 In areas where high heat exposure is consistent, the population adapts to heat and is less sensitive to extremes. On the other hand, temperate areas are at greater risk for higher mortality among local people during an EHE due to their lack of acclimatization to the heat, especially early in the heat season.
An emergency plan developed for heat, while similar to most other emergencies, does vary in key ways. To begin integrating heat into an all-hazards emergency plan these exemptions and priorities need to be identified. Previous EHEs have highlighted some central needs regarding heat-health management and are outlined further in this chapter.
8.2 Heat-Related Death May Occur at Home Alone
A unique problem for health care workers is that many victims of heat-related illnesses die at home before consulting with a health care worker.Reference 5 Addressing this problem requires:
- Increased awareness of heat-related illnesses among at-risk patients/clients and members of their support networks
- The recognition of early signs and symptoms of heat illnesses
- The recognition of when to consult with a health care worker. In particular patients and caregivers need to know when to call a nurse for more information (e.g. telehealth nurses are available in many areas 24 hours/day), when to call an ambulance, or when to simply administer a home remedy.Reference 372Reference 373
To facilitate building this awareness and recognition two key actions from health care providers are needed:
- Health care workers need to educate at-risk groups on heat-health risks and develop tailored prevention tactics before the annual heat season; and
- Health care workers need to assist at-risk groups and the institutions that serve them to adopt preventive actions in their daily routine.

In some cases, a home care provider may be the only health care worker to have contact with the patient before the onset of heat-related illness and therefore can play a strategic role in preventing a negative outcome. The key element for health care provider organizations in order to prepare for the summer season and heat emergencies is to increase communication with staff and clients/patients regarding effective prevention of heat illnesses. To address this issue, Appendix B of this document contains separate Fact Sheets for distribution to the health care provider. Targeted step brochures to distribute to the clients and patients have been prepared and are available for order (see Appendix D).
Heat-emergency plans intended to help in-patients and at-home clients should include:
- time for health care providers to help the patient stay cool (and educate on self-care) during a scheduled visit;
- a response plan to address the situation when there is no answer at the door for an expected visit and;
- an outline of the process to increase the frequency of checking in on vulnerable groups by phone or ideally in person during EHEs.
Health care workers are often unaware of which groups are at-risk for heat illnesses. This adversely affects the sharing of preventive information and needs to be addressed during emergency management training. Key questions to ask patients, to assess their individual risk, include inquiry regarding medications, chronic illness, occupation and other predisposing factors. Ensuring employee education regarding EHEs and their risks is essential if preventive strategies are to be effective.Reference 369
Additional heat-related illness prevention guidance is needed for patients/clients who are homeless, have reduced ability for self-care and are living alone with no scheduled social/home care despite their need.Reference 141Reference 374Reference 375 Reduced ability for self-care can occur for a variety of reasons including those of mental health, physical health or the extremes of age.Reference 374 The heat risk for some of these individuals is increased by reduced voluntary rehydration and fewer options to move to a cooler area. In many cases, there may be insufficient staff to address the increased demands from individuals with reduced self-care during EHEs. Planning for care options during periods of high demand can greatly facilitate response during an emergency.
8.3 Hospitals and Nursing Homes without Air Conditioning
Heat-related illnesses are more likely in hospitals and nursing homes without air conditioning. This fact highlights the need to revise patient management during the extreme heat in facilities without air conditioning regardless of the cause (either due to building design, or a black out). It should be noted that air conditioning is not needed for all care facilities. The ability to address the extreme heat, however, requires emergency preparation and management; in many cases, current plans merit improvement.

As with many natural disasters, EHEs can occur rapidly and the mortality rate can quickly overwhelm a facility's and community's capacity. This highlights only one of the many problems and lessons learned regarding emergency management during an EHE.Reference 109 For example, the "code orange" for hospital emergency management procedures can be considered a base to build on in preparation for an EHE, but requires additional heat considerations.Reference 376 An in-house plan will likely provide the groundwork for hospitals' and facilities' preparation for EHEs.Reference 14Reference 15Reference 377 The recommendations require consideration of rural, remote and urban settings; the operational needs of long-term care facilities, nursing homes, and personal care homes; as well as the physical infrastructure of the facility.
8.4 Emergency Preparedness
As with other emergencies, when dealing with heat emergencies the engagement and coordination of an interdisciplinary and intersectoral response team is required. Coordination among health care worker disciplines is no exception and outlining key roles and responsibilities as they apply in the work environment will enable an efficient response.Reference 369 This process of outlining the key issues can be viewed in layered stages of preparation:
- Identify your roles and responsibilities
- Know how to meet these responsibilities
- Keep up-to-date contact lists of key collaborators to help meet incoming needs

A major issue in dealing with heat and other disasters can be misinformation regarding certain roles and responsibilities, which can leave gaps unaddressed. The best approach to avoid this is for interdisciplinary and intersectoral planning to explicitly outline the roles of each team member, followed by coordination with managers and educators to ensure enough information and know-how is provided to fulfill the identified responsibilities. For interdisciplinary and intersectoral planning to occur, a common vocabulary is critical and often lacking (use plain language as much as possible).
Recommendations for health care facilities managers and staffReference 378:
- Have an integrated plan for EHEs. At a minimum, establish a policy and plan to deal with extreme temperatures and integrate it into your current emergency plan.
- Provide staff with up-to-date information/training regarding extreme heat emergency measures.
- Actively disseminate and discuss prevention and emergency guidelines
The emergency plan should be tailored to the needs of your facility. Key elements may be toReference 379:
- Ensure there is an administrative procedure to meet emergency/surge staff capacity needs.
- Keep older adults and the chronically ill cool and comfortable.
- Plan and implement emergency cooling options (air-conditioned rooms, fans, ice-water baths/showers).
- Consider the need for back-up generators, during possible power brown-outs/black-outs which can coincide with an EHE.
- Ensure that back-up generators available are inspected as part of the regular maintenance plan to address power brown-outs/black-outs.
- Revise emergency planning education and training (as needed) to provide staff with up-to-date heat-health risk information.
- Include a plan to manage employee heat exhaustion (e.g. air conditioning in the staff room, extra breaks, and accessibility of drinking water).
For building management of health care facilities some key elements to prepare for and address are to recognize when an EHE is in your region and to know your regional building-management guidelines. The monitoring of heat is directed by the various needs of the facility and client type. Typically regular monitoring with thermometers, thermohygrometers, or the Wet-Bulb Globe Temperature (WBGT) is done to ensure rooms are in a safe range for patients and workers.

Reducing heat stress in facilities can be done in several waysReference 354:
- Block direct sun: Use window awnings, shutters, thermal curtains/blinds, and outdoor umbrellas; plant trees.
- Control air flow: Increase ventilation, encourage cross breeze from open windows, use electric fans, increase insulation.
- Evaporative coolers: Effective in dry heat, but efficiency decreases with high humidity.
- Dehumidifiers: Effective in areas with high humidity, but give off heat.
- Electric fans: Effective in dry heat, but efficiency decreases with high humidity.
- Air conditioners: Effective during extreme heat, but decrease seasonal heat acclimatization with excessive use.
Considerations for the management of staff and supplies includeReference 378:

- Ensure staff is aware of signs and symptoms of heat illnesses such as dehydration, heat cramps, heat exhaustion, heat stroke (classic and exertional). Ensure staff is aware of and follow first-aid procedures and treatment appropriately.
- New staff orientation material could review heat-related illness issues and emergency responses.
- Protect staff from extreme heat; follow your emergency/surge procedure to ensure adequate capacity and ensure personnel are working within guidelines for work-rest cycles in the heat as outlined in your region and personal cooling options (see Table 2.2).
- Ensure appropriate cooling supplies are available for your patients and residents (e.g. cooling jackets, ice-water baths), and provide appropriate support to avoid injury.
- Provide a cool option or area, available for several hours each day (e.g. a designated cool room, cool showers, a fan, options for submerging hands/forearms or sponging with cool water).
- Keep medications cool (for room temperature storage below 26°C is typical).
- Ensure food is being stored and prepared with the extreme heat in mind (serve light meals, pay attention to correct storage and ensure spoiled food is discarded).
- Identify which rooms, if any, require evacuation due to extremely high temperature.
- Develop contingency and heat-emergency plans and educate your staff on these plans/interventions.
- Integrate heat information in training material for health care workers in work place emergency training and in annual reviews (e.g. as per organizations' WHIMS).
Patient needs will increase with the rising heat. Patient care management considerations could include:
- The review of the clinical management of patients and residents most at risk either due to reduced mobility, chronic illnesses (pulmonary, cardiovascular, renal), or certain medications.
- Increased frequency of patient/client visits especially to those at high risk.
- Advising staff to monitor closely for any early indicators of heat illnesses and to initiate appropriate treatment (e.g. check room temperature, patient temperature, monitor fluid intake and output, pulse rate, and blood pressure) .
- The consideration of indoor/outdoor temperatures when planning group activities.
Integrating heat-emergency considerations into regular emergency training and drills provide a good venue for staff to practice their skills. This will also help to ensure that appropriate supplies are maintained for priority tasks and that communication networks are functional. In particular, focussing on appropriate triage for older people, and increased monitoring of patients, clients and residents, including the consideration of fluid intake is needed. Coordination with other emergency responses is critical for effectiveness. Refer to Health Canada's Heat Alert and Response Systems to Protect Canadians: Best Practices Guidebook.Reference 380 The roles and responsibilities with regard to the planning, response and recovery from EHEs are described in this document.
8.5 Long-Term Planning

Understanding the risks of heat and how they relate to health is essential for health care workers, municipal planners, builders and regional legislators, to be able to protect public health and develop increased comprehensive community care for the future.Reference 26
Together public health professionals and planners can coordinate strategic initiatives to guide development plans for future buildingsReference 381 and renovations. The following factors should be considered in order to increase the resilience of their institutionsReference 354:
- Vegetation and trees to decrease greenhouse gases (GHG) and remove air pollutionReference 382
- Permeable surfaces (rather than asphalt for example) to reduce runoff from heavy rainfalls and the radiant heat load from the surface
- Geometrical configuration of the building (layout, height, type of roof)
- Location of the building (proximity to tree-shaded spaces, waterfronts)
- Orientation of the building (light and radiation considerations)
- Size and location of the windows (solar radiation, natural ventilation)
- Thermal properties of the building materials (ability to absorb/reflect heat, insulation, efficiency of ventilation/cooling system)
- Colour of external surfaces (light-coloured surfaces, reflective materials)

Key Actions for Capacity Building
- Outline strategies to address the effect of the built environment on human health.
- Coordinate public health professionals and planners to:
- Implement options to improve the effects of the built environment on health; and
- Develop plans, policies and processes to reduce the carbon footprint and the urban heat island contributions of your facility (e.g. use green space strategically to provide shade, consider alternate surfaces for parking lots and roofs
8.6 Conclusion

In summary, to best address EHEs and emergency planning for health care workers, the following objectives have been identified:
- Recognize the role the health sector plays in preparing for and responding to EHEs
- Raise awareness of heat-health risks
- Integrate heat into current emergency framework in your workplace
- Integrate heat information in training material for health care workers in work place emergency training
- Connect with your regional emergency groups and ensure they have a plan to address EHEs and determine how to coordinate your teams
There are challenges to each of these elements which are common among other emergencies and natural disasters. Learning from regional experiences in other natural disasters as well as EHEs in other regions can help address these challenges.
9. Conclusions and Future Directions
This document presents an up-to-date overview of the national and international literature regarding the health impacts of extreme heat. Although The Guidelines provide a recent amalgamation of various information sources, there continues to be many heat and health issues that need to be addressed. These challenges include expanding the practical information that is available for health care workers, increasing science-based research studies, recognizing the lack of current knowledge transfer into health care worker training and education, as well as acknowledging the need for clear management and injury prevention strategies regarding heat. Although occupational heat stress was outside the scope of this document, the need to educate employers and employees about the occupational health risks from heat remains an issue in many settings. These challenges will require health care worker engagement as well as leadership from key decision makers. For these challenges to be addressed future direction from these leaders is needed.
The main issue facing decision makers is that heat illness is underreported in both Canada and internationally. Although the number of excess deaths due to heat is reported and available in some regions, there is little consistency among this accessible information. Heat illnesses and death in Canada are often recorded as other co-morbidities, such as respiratory or cardiovascular illnesses and, as a result, the exact incidence and prevalence of heat-related illnesses is unknown.
As a result, it is important to consider incomplete health coding when planning curricula for health care worker education. In particular, those who record charts and reports need to be educated to facilitate increased awareness of the importance of recording heat as a factor when a patient presents with an observed illness.Reference 383 A broad spectrum of individuals who record health codes are included such as hospital health coders, coroners, nurse help-lines, and emergency medical service workers. To ensure efficiency, key guiding principles should be transferred such as the importance of specific probing questions related to heat. In particular, there is a need during extreme heat events (EHEs) to record the incidence of heat-related illness.Reference 17
In addition, mortality associated with EHEs has been reported to be greatest in urban areas, especially in those with high nighttime temperatures, high levels of air pollution and poor housing conditions. Some risk factors for heat-related illness, such as air pollution, are known, but merit further investigation to examine their combined effects on health during EHEs. High ambient temperatures can increase air pollutant concentrations of respiratory irritantsReference 384 such as ozone, carbon monoxide, nitrogen dioxide, and particulate matter.Reference 378 The collection of further scientific data regarding heat and air pollution-related mortality would enable the provision of better advice to protect patient health.Reference 385- Reference 391
A further challenge is the lack of randomized double-blind clinical trials assessing effective prevention and/or treatment options for heat illnesses. Randomized controlled trials in the case of heat illness are impractical and unethical; however other study designs (e.g. cohorts, case-control) may allow adequate assessments. In particular, the heat-health information regarding the best cooling alternative to ice-water baths for classic heat stroke patients remains controversial due to the lack of available information. In addition, the prevention and treatment needs are diverse in several patient populations. To address these diverse needs of the various patients requires qualitative assessments. The Guidelines are a synopsis of current primary literature, systematic reviews and meta-analyses of observational studies and present the best available approach to provide evidence-based recommendations for the health care provider. When guidance was deemed necessary by health care worker stakeholders on topics that had less evidentiary support, consensus was established through our advisory committee and further reviewed by various Canadian health care worker associations and public health institutions (see Appendix A).
Prevention of heat-related illnesses through behavioural adaptation and changes to the built environment are the most effective methods for addressing heat-related illnesses in the long term. The behavioural changes required are simple, cost effective and can be stated simply as "Stay Cool, Stay Hydrated and Rest when Necessary." The widespread communication of these messages from health care workers in addition to public health programs that facilitate their adoption will help to ensure those most vulnerable to EHEs receive the support they need. An effective method to address the added heat strain due to the built environment is to increase the available green spaces. The emphasis of future work should be to ensure these simple actions are taken by the public and community planners, and are specifically encouraged for the most vulnerable.
The research presented demonstrates that community health workers are key players in the prevention of heat-related illnesses through their work on the front lines with those considered most vulnerable. A remaining key challenge is to further the education of health care workers regarding EHEs so that they, in turn, can inform their patients, families and the general public. This will enable these groups to take action to mitigate their heat-health risks. This is required to aid in the dissemination of the information provided within the Guidelines as well as to ensure the adoption of the outlined practices.
Glossary
Acclimatization (Heat Acclimatization): The gradual exposure to increasing temperatures which results in physiological adaptations that can improve a person's tolerance to heat. The process of acclimatization is not instantaneous; it involves many physiological changes and can take up to several weeks before someone can work safely in heat that was previously considered intolerable.Reference 37Reference 45
Adaptation: Adjustment in natural or human systems in response to actual or expected effects of climate change and variability, which moderates harm or exploits beneficial opportunities.Reference 30
Advisories Warnings Watches (Weather): Environment Canada issues weather advisories, warnings and watches to inform people about current or developing weather systems. An advisory is a bulletin that informs people that actual or expected weather conditions may cause general inconvenience or concern, but do not pose a serious threat. A watch alerts people that conditions are favourable for the development of severe weather, while a warning tells them that severe or hazardous weather is occurring or highly probable.
Air Quality Index (AQI): The AQI is an indicator of air quality, based on air pollutants that have adverse effects on human health and the environment. The pollutants are ozone, fine particulate matter, nitrogen dioxide, carbon monoxide, sulphur dioxide and total reduced sulphur compounds. Several state-of-the-art air monitoring stations are operated by the provincial Ministry of the Environment and form the AQI network. The ministry takes real-time air quality data from its AQI monitoring sites to produce AQI readings for each location. The readings are reported to the public and news media hourly.
Air Quality Health Index (AQHI): The AQHI is a scale designed to help you understand what the air quality around you means to your health. It is a health protection tool that is designed to help you make decisions to protect your health by limiting short-term exposure to air pollution and adjusting your activity levels during increased levels of air pollution. It also provides advice on how you can improve the quality of the air you breathe. This index pays particular attention to people who are sensitive to air pollution and provides them with advice on how to protect their health during air quality levels associated with low, moderate, high and very high health risks.
Air Velocity: Air velocity refers to the speed at which air moves. The extent of air movement is usually measured with an anemometer and reported in kilometres per hour or miles per hour.
All-Hazards Approach: Ensures that disaster planning achieves its aims efficiently by collecting information on the full range of threats so subsequent risk management decisions can be made appropriately.Reference 30
Ambient Temperature: Ambient temperature refers to the common measurement of how hot or cold it is outdoors. Temperature is usually measured by a thermometer in degrees Celsius or degrees Fahrenheit. For accurate measurements, the thermometer should be shielded from the sun (i.e. the temperature reported is what it would be in the shade).
American Conference of Governmental Industrial Hygienists (ACGIH®): ACGIH® is a member based organization that advances occupational and environmental health. The organization has contributed substantially to the development and improvement of worker health protection. The organization is a professional society, not a government agency.Reference 45
Apparent Temperature (AT): The apparent temperature is an index which combines air temperature and humidity and is a measure of relative discomfort. It was developed by R.G. Steadman in 1979 and is based on physiological studies of evaporative skin cooling for various combinations of ambient temperature and humidity. The AT can also be extended to take wind and solar radiation into account as well, though generally this is not done.
Body Mass Index (BMI): The BMI is a ratio of a person's weight-to-height. Research studies in large groups of people have shown that the BMI can be classified into ranges associated with health risk. BMI is calculated using the formula: BMI = [weight in kilograms] / [(height in metres)Reference 2].
Carbon Dioxide (CO2): A naturally occurring gas, also a by-product of burning fossil fuels and biomass, as well as from land use changes and other industrial processes. It is the principal anthropogenic (man-made) greenhouse gas that affects the Earth's radiative balance. It is the reference gas against which other greenhouse gases are measured.Reference 44
Climate: Climate in a narrow sense is usually defined as the average weather, also defined in statistical terms as the mean and variability of relevant variables and over a period of time ranging from months to thousands or millions of years. The classical period for averaging these variables is 30 years, as defined by the World Meteorological Organization (WMO). Variables taken into account most often include air temperature, precipitation and wind. Climate in a wider sense is the state, including a statistical description, of the climate system.Reference 30
Climate Change: Climate change refers to a change in the state of the climate that can be identified (e.g. by using statistical tests) by changes in the mean and/or the variability of its properties, and that persists for an extended period, typically decades or longer. Climate change may be due to natural internal processes or external forcing, or to persistent anthropogenic changes in the composition of the atmosphere or in land use. Note that the United Nations Framework Convention on Climate Change (UNFCC), in its Article 1, makes a distinction between climate change attributable to human activities altering the atmospheric composition and climate variability attributable to natural causes.Reference 30
Climate Model: A numerical representation of the climate system based on the physical, chemical and biological properties of its components, their interactions and feedback processes, and accounting for all or some of its known properties. Coupled Atmosphere-Ocean General Circulation Models (AOGCMs) provide a representation of the climate system that is the most comprehensive currently available. Climate models are applied as a research tool to study and simulate the climate, and for operational purposes, including monthly, seasonal and interannual climate predictions.Reference 30
Climate Projection: A projection of the response of the climate system to emission or concentration scenarios of greenhouse gases and aerosols, or radiative forcing scenarios, often based upon simulations by climate models. The use of emission/concentration/radiative forcing scenarios and attendant assumptions about, for example, future socio-economic and technological developments that may or may not be realized introduce substantial uncertainty in climate projections and distinguish them from climate predictions.Reference 30
Climate Scenario: A plausible and often simplified representation of the future climate, based on an internally consistent set of climatological relationships and assumptions in radiative forcing, which has been constructed for explicit use in investigating the potential consequences of anthropogenic climate change, often serving as input to impact models. Climate projections are often the raw material for constructing climate scenarios, but climate scenarios usually require additional information, such as about the observed current climate. A climate change scenario is the difference between a climate scenario and the current climate.Reference 30
Climate Variability: Refers to the variations in the mean and other statistics (e.g. standard deviations, the occurrence of extremes) of the climate on all temporal and spatial scales beyond that of individual weather events. Variability may be due to natural internal processes within the climate system or to variations in natural or anthropogenic external forcing.Reference 30
Conduction: Refers to the bi-directional transfer of heat between two surfaces of differing temperatures through direct physical contact. This includes both external conduction (contact of the skin with cooler objects) and internal conduction (contact of tissues inside the body, which is important in heat distribution to the surface of the skin).
Confidence Interval: The width of the confidence interval gives us some idea about how uncertain we are about the unknown parameter (or the precision of the mean estimate). A very wide interval may indicate that more data should be collected before anything very definite can be said about the parameter. If independent samples are taken repeatedly from the same population, and a confidence interval calculated for each sample, then a certain percentage (confidence level) of the intervals will include the unknown population parameter. The CI95 represents the middle 95% of the distribution from the estimated mean.
Convection: Refers to the bi-directional transfer of heat through contact with air or water molecules across the skin. The transfer of heat from the surface of the skin by air helps carry heat away from the body. It should be noted however that heat must first be conducted to the skin surface and then to the air and only after this is the heat finally carried away. In hot weather conditions when the air temperature is higher than skin temperature (skin temperature is normally around 35°C, but can vary between 20°C and 40°C without harm to the bodyReference 36) heat will be gained from the environment, by convection.
Disaster: An event that exceeds the ability of the local community to cope with the harmful effects and requires extraordinary response and recovery measures.Reference 30
Disaster Mitigation: The prevention of natural hazards from becoming natural disasters. It includes policies and actions taken before or after a disaster to reduce the impacts on people and property, such as building public awareness and support; development of local and regional plans for land use to prevent inappropriate development in hazardous areas; and changing building codes and standards to protect people, property and infrastructure from extremes.Reference 30
Diurnal Temperature Range: The difference between the maximum and minimum temperature during a day.Reference 30
Emergency: Serious mishaps that involve more people, as victims and responders, than accidents, but do not overwhelm the community to the point of being a disaster.Reference 30
Emergency Mandate: Organizations with an emergency mandate consist of those with emergency relief services as part of their constitutional mission and/or their established tradition of community service delivery.Reference 30
Emergency Response: Actions taken in anticipation of, during and immediately after an emergency to ensure that its effects are minimized and that people affected are given immediate relief and support.Reference 30
Emission Scenario: A plausible representation of the future development of emissions of substances that are potentially radiatively active (e.g. greenhouse gases, aerosols), based on a coherent and internally consistent set of assumptions about driving forces (e.g. demographic and socio-economic development, technological change) and their key relationships. Concentration scenarios, derived from emission scenarios, are used as input to a climate model to compute climate projections. Since 1992, the IPCC has published two series of emission scenarios, most recently in the IPCC Special Report on Emission Scenarios.Reference 30
Extreme Event: An occurrence that can cause severe damage within a community, including property destruction, personal injury and death.Reference 30
Extreme Heat Event(s): Extreme Heat Events and Heat Alerts are described currently based on regional guidelines and local needs as a period of extreme heat for that location and seasonal time. There is no standard definition of an extreme heat event. The European heat research project defines a heat wave as a period where the maximum apparent and minimum temperatures are over the 90th percentile of the monthly distribution for at least two days.Reference 378 Environment Canada issues online Heat and Humidex advisories when temperatures are expected to reach or exceed 30°C and/or the Humidex value (a combination of relative humidity and temperature) is expected to reach or exceed 40 on the Humidex scale of perceived temperature.Reference 19 Environment Canada defines a heat wave as a period with more than three consecutive days of maximum temperatures at or above 32°C. A physiologically based definition identifies a period of high heat as the threshold and duration of which is associated with increased morbidity and mortality of a specific population.
Extreme Weather Events: An event that is rare within its statistical reference distribution at a particular place. Definitions of rare vary, but an extreme weather event would normally be as rare as or rarer than the 10th or 90th percentile. Examples of extreme weather events include floods and droughts.Reference 30
Evaporation: Refers to the evaporation of water from the skin (in the form of sweat) or from the respiratory passages (through breathing). Evaporation is unidirectional and will always result in body heat loss and never in heat gain. At high ambient temperatures, evaporation of sweat is the most important thermoregulatory mechanism. In fact, when the air temperature is higher than skin temperature, sweating is the only avenue for heat loss and is responsible for approximately 90% of heat loss.Reference 37 Wind speed or air movement will also increase evaporative cooling.
Greenhouse Effect: The process in which the absorption of infrared radiation by the atmosphere warms the Earth. In common parlance, the term greenhouse effect may be used to refer either to the natural greenhouse effect, due to naturally occurring greenhouse gases, or to the enhanced (anthropogenic) greenhouse effect, which results from gases emitted as a result of human activities.Reference 30
Greenhouse Gas (GHG): Gaseous constituents of the atmosphere, both natural and anthropogenic, that absorb and emit radiation at specific wavelengths within the spectrum of infrared radiation emitted by the Earth's surface, the atmosphere itself, and by clouds. Water vapour (H2O), carbon dioxide (CO2), nitrous oxide (N2O), methane (CH4) and ozone (O3) are the primary greenhouse gases in the Earth's atmosphere. A number of entirely human-made greenhouse gases exist in the atmosphere, such as the halocarbons and other chlorine- and brominecontaining substances.Reference 30
Ground-Level Ozone (O3): Ground-level (tropospheric) ozone is a colourless and highly irritating gas that forms just above the earth's surface when nitrogen oxides (NOx) and volatile organic compounds (VOCs) react in sunlight and stagnant air. Exposure to O3 has been linked to premature mortality and a range of morbidity health end-points such as hospital admissions and asthma symptom days, as well as negative impacts on vegetation and synthetic materials.Reference 30 (See also ozone).
Heat Strain: Heat strain is the work required by the body's overall physiological response resulting from heat stress and is dedicated to dissipating excess heat from the body.Reference 44 Generally speaking, heat strain can be looked at as being uncompensated heat stress. In the context of heat, illness occurs when a person is no longer able to physiologically maintain their core body temperature at its normal operating temperature of 37°C and the core temperature rises above this figure. Until there is a risk of heat strain, the heat stress amounts to a simple comfort issue.
Heat Stress: Heat stress is the overall heat burden on the body from the combination of the body heat generated while working, from environmental sources (air temperature, humidity, air movement, radiation from the sun or hot surfaces/sources) and clothing requirements. Heat stress on the body can lead to heat-related illnesses.Reference 44
Heat Island Effect: See Urban Heat Island (UHI) Effect.
Heat Wave: Heat wave is a commonly used term for extreme heat event. Since the most dangerous heat is sustained over time and does not fluctuate (as typically illustrated by a wave), the term extreme heat event is thought to most accurately describe a prolonged episode of hot environmental conditions. Environment Canada defines a heat wave as a period with more than three consecutive days of maximum temperatures at or above 32°C [90°F].
Humidex: Humidex is an absolute number combining the effects of both relative humidity and temperature and its value is reported on a scale of perceived thermal comfort. For example, Humidex is often used as an indicator for how hot it feels outside. Humidex values are intended to represent the effect that high humidity and high temperatures have on the human body. Comfort levels for Humidex readings are: 20-29 (comfortable), 30-39 (varying degrees of discomfort), 40-45 (almost everyone is uncomfortable), and +45 (many types of work and exercise should be restricted).Reference 30
Humidex Advisory: Advisories are issued by Environment Canada when temperatures are expected to reach or exceed 30°C and the Humidex values are expected to exceed 40.
Humidity: Humidity is the amount of water vapour in the air. Absolute humidity is the quantity of water in a particular volume of air (grams per cubic meter). Relative humidity is an indication of how many grams of water can be held in the air at a given temperature, and is therefore relative to ambient temperature. Humidity is an important factor when considering the dissipation of heat from the body. In conditions with high humidity the evaporation of sweat from the skin surface is impeded. When humidity is combined with high ambient temperatures, it can contribute significantly to heat stress. There are several common ways to quantify the effects of humidity, including apparent temperature and metrics such as the Humidex.
Hyperthermia: Elevated body core temperature.
Hyponatremia: Hyponatremia is classified as a complication of low plasma sodium levelsReference 232 by disrupting the osmotic balance across the blood brain barrier resulting in a rapid influx of water to the brain.Reference 129 Evidence points to fluid overload with dilutional hyperthermia and may include abnormal fluid retention leading to increased intracellular volume. Perspiration may contribute to hyponatremia through the loss of electrolytes in sweat. A range of 10-30% of the incidence of this disease is associated with decreased sodium. Although overconsumption of fluids is not the only risk factor associated with hyponatremia (disorders that suppress the release of antidiuretic hormone will cause impairment of renal water excretion), the primary cause is over-hydration.Reference 233- Reference 235Reference 239
Intergovernmental Panel on Climate Change (IPCC): A panel established by the World Meteorological Organization (WMO) and the United Nations Environment Programme (UNEP) in 1988 to assess scientific, technical and socio-economic information relevant for the understanding of climate change, its potential impacts and options for adaptation and mitigation. It has three working groups (climate science; vulnerability, impacts and adaptation; mitigation) and a task force on national greenhouse gas inventories.Reference 30
Infrared Radiation: Radiation emitted by the Earth's surface, the atmosphere, and clouds. It has a distinctive range of wavelengths longer than the wavelength of the red colour in the visible part of the spectrum - humans can sense it as heat.
Morbidity: Rate of occurrence of disease or other health disorder within a population, taking account of the age-specific morbidity rates. Health outcomes include chronic disease incidence/prevalence, rates of hospitalization, primary care consultations, disability days (i.e. days when absent from work) and prevalence of symptoms.Reference 30
Mortality: Rate of occurrence of death within a population within a specified time period; calculation of mortality takes account of age-specific death rates, and can thus yield measures of life expectancy and the extent of premature death.Reference 30
Odds Ratio: The odds ratio is a way of comparing whether the probability of a certain event is the same for two groups. An odds ratio of one implies that the event is equally likely in both groups. An odds ratio greater than one implies that the event is more likely while an odds ratio less than one implies that the event is less likely.
Ozone (O3): Ozone, the triatomic form of oxygen, is a gaseous atmospheric constituent. In the troposphere, it is created both naturally and by photochemical reactions involving gases resulting from human activities (photochemical smog). In high concentrations, tropospheric ozone can be harmful to a wide range of living organisms. Tropospheric ozone acts as a greenhouse gas. In the stratosphere, ozone is created by the interaction between solar ultraviolet (UV) radiation and molecular oxygen. Stratospheric ozone plays a decisive role in the stratospheric radiative balance. Depletion of the stratospheric ozone, due to chemical reactions that may be enhanced by climate change, results in an increased ground-level flux of UV-B radiation.Reference 30 (See also ground-level ozone.)
Particulate Matter (PM): Very small solid exhaust particles emitted during the combustion of fossil and biomass fuels. Particulates may consist of a wide variety of substances. Of greatest concern for health are particulates of less than or equal to 2.5 micrometres in diameter, usually designated as PM2.5.Reference 30
Radiant Load: Refers to the transfer of heat from a heated surface. The most common form of radiant heat transfer is the transfer of heat from the sun to the earth through electromagnetic rays (infrared heat rays). This energy from the sun can be absorbed or reflected by various surfaces including buildings and/or people. Generally dark-coloured surfaces (such as parking lots and building roofs) absorb more radiant heat from the sun than light-coloured surfaces which have a tendency to reflect the sun's solar radiation.
Relative Risk: A more direct measure than odds ratio comparing the probabilities in two groups is the relative risk, which is also known as the risk ratio. The relative risk is simply the ratio of the two conditional probabilities. Like the odds ratio, a relative risk equal to one implies that the the event is equally probable in both groups. A relative risk greater than one implies that the event is more likely in the first group. A relative risk less than one implies that the event is less likely in the first group.
Risk: Risk refers to the uncertainty and magnitude that surrounds future events and outcomes.Reference 30
Risk Management: Risk management is about making decisions involving uncertain future situations. Risk management is the systematic process - the practices and procedures - that an organization uses to manage the risks it faces. It is about setting a preferred course of action under uncertainty by identifying, assessing, understanding, acting on and communicating risk issues.Reference 30
Scenario: A plausible and often simplified description of how the future may develop based on a coherent and internally consistent set of assumptions about driving forces and key relationships. Scenarios may be derived from projections, but are often based on additional information from other sources, sometimes combined with a narrative storyline.Reference 30
SRES Scenarios: The storylines and associated population, Gross Domestic Product (GDP) and emission scenarios associated with the Special Report on Emissions Scenarios (SRES), and the resulting climate change and sea-level rise scenarios. Four families of socio-economic scenarios (A1, A2, B1 and B2) represent different world futures in two distinct dimensions: a focus on economic versus environmental concerns and global versus regional development patterns.Reference 30
Strenuous Exercise: Strenuous exercise is physical activity that exceeds 70% of a person's physical capacity.
Surge Capacity: Refers to a system's ability to rapidly expand beyond normal services to meet the increased demand for qualified personnel, and services in the event of large-scale emergencies or disasters.Reference 30
Sustainable Development: Development that meets the needs of the present without compromising the ability of future generations to meet their own needs.Reference 30
Teratogen: An agent or factor which causes malformation of an embryo.
Threshold Limit Values (TLV®): Threshold limit Values are developed as guidelines by the ACGIH® (see above) to assist in the control of health hazards. These recommendations and guidelines are intended for use in the practice of industrial hygiene, to be used by a person trained in this discipline. They are not developed for use as legal standards however, it is recognized that in certain circumstances individuals and organizations may wish to make use of these recommendations or guidelines as a supplement to their occupational safety and health programs.Reference 45
Traditional Knowledge: Various systems of knowledge, practice and belief gained through experience and culturally transmitted among members and generations of a community.Reference 30
Ultraviolet Radiation: Solar radiation within a certain wavelength, depending on the type of radiation (A, B or C). Ozone absorbs strongly in the UV-C range (<280 nm) and solar radiation in these wavelengths does not reach the Earth's surface. As the wavelength is increased through the UV-B range (280 nm to 315 nm) and into the UV-A range (315 nm to 400 nm) ozone absorption becomes weaker, until it is undetectable at about 340 nm allowing these wavelengths to reach the Earth's surface.Reference 30
United Nations Framework Convention on Climate Change (UNFCCC): Convention signed at United Nations Conference on Environment and Development in 1992. Governments that become Parties to the Convention agree to stabilize greenhouse gas concentrations in the atmosphere at a level that would prevent dangerous anthropogenic interference with the climate system.Reference 30
Urban Heat Island (UHI) Effect: The effect whereby a region within an urban area is characterized by ambient temperatures higher than those of the surrounding area because of the absorption of solar energy by materials like asphalt.Reference 30
Urbanization: Net rural-to-urban migration, resulting in an increasing percentage of the population in any nation or region living in settlements that are defined as urban centres, and the associated conversion of land from a natural state or managed natural state (e.g. agriculture) to cities.Reference 30
Vulnerability: Vulnerability is the susceptibility to harm. Vulnerability to climate change is the degree to which a system is susceptible to, or unable to cope with, adverse effects of climate change, including climate variability and extremes. Vulnerability to climate change is a function of the character, magnitude and rate of climate variation to which a system is exposed, its sensitivity and its adaptive capacity.Reference 30
Weather: Weather is the state of the atmosphere at a given time and place with regard to temperature, air pressure, humidity, wind, cloudiness and precipitation. The term weather is used mostly for conditions over short periods of time.Reference 30
Appendix A: Guideline Development Methods
Extreme Heat Events Guidelines: Technical Guide for Health Care Workers and Targeted Fact Sheets (the Guidelines for short) are the result of a broad literature review including peer-reviewed and grey literature, guidance from an inter-disciplinary expert advisory committee, as well as internal and external peer review processes.
A.1 Literature Review
The purpose of the literature review was to:
- Determine the ideal scope of the Guidelines
- Determine unresolved issues concerning heat-health vulnerabilities
- Collect sources of evidence to address priority topics and issues
- Identify and describe current heat-health information available to health care workers
In order to create the literature database, a systematic review of the peer reviewed heat literature was conducted to identify the primary references and to review available articles regarding heat and its relationship with various factors. PubMed and Scopus were searched for English and French language articles published (without publication date limitation) using the term "heat", in combination with Boolean searches for each topic. A comprehensive search was completed by both subject matter experts and a research librarian. Other citations were identified through PubMed's additional links service and from the reference lists of the articles. A search for existing practice guidelines related to heat illness was also undertaken. The websites and publications of public health departments, health care workers, health-related occupational associations, government, international agencies and relevant stakeholder organizations, were reviewed in addition to general information websites concerned with heat and disaster management. Articles and information were manually reviewed for relevance of the content for health care workers. The search was designed to collect a broad range of information available to health care workers regarding heat in order to set priorities for the Guidelines. Summarizing heat studies is challenging and there is no formal guidance on how to best review the current evidence base. To assist in this process, the literature review was complemented by direct communication with numerous experts in the field in order to ensure the inclusion of the most current, accurate and relevant information. Both qualitative and quantitative information was gathered. A reviewing strategy for these documents was defined based on the key issues identified. Given the goal of the review for clinical application, the literature was prioritized with an emphasis on meta-analyses, systematic reviews, and classic synthesis/summary reviews.
A.1.1 Risk Factors Literature Assessment Methods
A.1.1.1 Study Selection
The primary literature for risk factor analysis included in the Guidelines was selected based on the four following criteria:
- The study was related to the health effects of extreme heat in human populations.
- The study was peer-reviewed through a journal review process, or by a series of experts.
- The study was primary literature (no reviews or meta-analyses were included).
- The calculations for the risk factors (ORs, RRs, observed or expected deaths) included 95% confidence intervals.
A.1.1.2 Data Extraction and Study Appraisal
Fifteen epidemiological studies relating to the topic of heat-health were selected for inclusion in the risk factor analysis. Data was extracted from the studies by two independent reviewers (CS and KB) using a predefined data extraction form and each study was ranked based on various criteria. Any differences in study appraisal were resolved by communication between the reviewers.
None of the fifteen studies were rated less than satisfactory and as a result all studies that were not considered either excellent, very good, or good, were excluded from analysis for the risk assessment (n=1). However, due to the lack of studies investigating protective factors, all 15 studies were included in the analysis for protective factors.
To determine the relative significance of the risk factors associated with mortality during extreme heat events, the following methods were used:
- If the risk factors and associated confidence intervals from the selected studies were statistically significant, the odds ratios (ORs) or relative risks (RRs) were extracted for inclusion in analysis. For studies that provided statistical significance for observed, expected or excess deaths, RRs were calculated based on the methods of Kenny et al.Reference 41
- All subsequent ORs or RRs (used interchangeably) for each individual study were sorted based on greatest risk (largest number).
- To determine the individual importance and prevalence of each risk, the risk factors were ranked based on:
- the amount of risk
- the number of times a risk factor was found to be statistically significant
- the number of times a risk factor was reported or investigated
The methods to determine the factors considered most protective were undertaken with the same approach, with the exception that the greatest risk was interchanged with the greatest protective effect.
Final inclusion of risk and protective factors was based on expert input, and consideration of the study population's geographical location and cultural norms.
A.2 Inter-Disciplinary Expert Advisory Committee
HPIT Advisory Committee
- Geoffrey Dover PhD
Assistant Professor, Department of Exercise, Concordia University - Paul Eagan MD
Major, Department of National Defence - Richard Gould MD
Medical Officer of Health, Annapolis Valley District Health Authority - Joan Hayes RPh, BScPharm
Pharmacist, private practice - Glen P. Kenny PhD
Professor, Faculty of Health Sciences, University of Ottawa - Kieran Moore MD
Emergency Room Physician and Associate Professor, Queen's University - David Mowat MD
Medical Officer of Health, Peel Region - Sonya Nobbe ND
Naturopathic Doctor, private practice - Lori Payne
Director, Communications and Development Ontario, Community Support Association (OCSA) and Director, Personal Support Network of Ontario (PSNO) - Pammla Petrucka RN, PhD
Associate Professor, University of Saskatchewan
The purpose of convening the Inter-Disciplinary Expert Advisory Committee (comprised of key experts and stakeholders) was to:
- Define the key questions to be addressed in the Guidelines
- Discuss how to best meet the needs of health care workers
- Identify key challenges and bridging solutions for interdisciplinary documents
- Outline a dissemination strategy to best reach health care workers including endorsement and integration into current education programs
An advisory committee with representatives from at least 12 health care worker disciplines was formed and chaired by Health Canada. The Health Professional Intervention/Information and Training (HPIT) Advisory Committee was formed to assist in the development of the Guidelines. Three HPIT Advisory Committee meetings were held to prioritize the key issues, to discuss knowledge gaps, to establish priorities and to review written drafts of the Guidelines.
The meetings provided an opportunity to collect expert opinions and review the needs of Canadian health care workers while assessing several dissemination strategies. A product description and rationale was prepared alongside a detailed annotated Table of Contents which were reviewed prior to development of the Guidelines. The information and priorities collected were amalgamated and reviewed by heat experts, and key stakeholders.
A.3 External and Internal Peer-Review Process of the Guidelines
The Guidelines were subject to an external and internal peer-review process to:
- Synthesize results into a scientific report
- Prepare the Guidelines in an efficient format for health care workers
- Peer-review the Guidelines by key experts and stakeholders
The Guidelines were developed and reviewed by Health Canada. They were prepared to appeal to a wide range of health care workers and to facilitate the knowledge translation from peer-reviewed journal articles to clinical practice applications. Referencing is extensive to allow for experts to have easy access to the details of the scientific studies and reports used to compile the Guidelines.
The draft Guidelines were peer-reviewed by key experts and stakeholders including health and climate change partners, health care workers, and heat specialists. Several health disciplines were engaged for review to ensure practical use and relevance for a broad spectrum of health care workers.
The first step in the projects development was an all day stakeholders' workshop to discuss and prioritize the overall needs for development of heat-health products and messaging for the public and health professionals. This workshop addressed many of the initial assessment needs for the heat-health products. Table A.1 contains the list of participants.
Considerations of format and content were addressed to ensure the relevance of the print publication of the Guidelines to meet the needs of health care workers. The publication was further complemented with input from Health Canada and the Public Health Agency of Canada. In addition, the Guidelines were sent for review to health care worker associations, and distributed to Canadian non-governmental organizations. This input was then considered and revisions were made accordingly. The reviewers and their affiliations are listed in the following section.
| Participant | Organization |
|---|---|
| Health – Clinical | |
| Della Faulkner, RN, PhD | Nurse Consultant, Public Policy, Canadian Nurses' Association |
| Jill Skinner | A/Associate Director Office for Public Health, Canadian Medical Association |
| Sandra Hirst, RN, PhD | Professor, University of Calgary, Canadian Gerontological Nurses' Association, National Seniors Council |
| Maurice Lanteigne | Project Manager, Canadian Lung Association |
| Sue Sullivan | Project Manager, Canadian Public Health Association |
| Health – Community Service Providers | |
| Jane MacDonald, RN, MHSc | Vice President, Public Affairs and Community Engagement, Victorian Order of Nurses |
| Cam Manson | Chief Steward, Community Care Access Centre, Champlain Region |
| Emergency Preparedness | |
| Don Shopshire | National Office, Canadian Red Cross |
| Suzanne Carrier | Field Officer, Emergency Management Ontario |
| First Responders | |
| Bill Alexander | National Coordinator, Disaster Services, St. John's Ambulance |
| Occupational Health and Safety | |
| Lorraine Davison, MSc, MEng (Teleconference) | Manager, Chemical Services, Canadian Centre for Occupational Health and Safety |
| Children and Youth | |
| Kelly Nolan, PhD | Canadian Paediatric Society |
| Faith-Based Groups | |
| Perry Rowe | Executive Director, Salvation Army |
| Aboriginal and First Nations | |
| Stuart Wuttke | Environmental Stewardship Unit, Assembly of First Nations |
| NCR Community Groups | |
| Mary Wiggin | Executive Director, Ottawa Community Coalition for Literacy |
| Health Portfolio Partners | |
| Catherine Huang, MA | Policy Analyst, Office of Vulnerable Populations, HC |
Diane McClymont Peace Erin Myers |
First Nations & Inuit Health Branch, HC Manager, Climate Change and Health Environmental Research Officer, Climate Change and Health |
| Jane Swan | Liaison Officer, Division of Aging & Seniors, PHAC |
| Stephen Parker | Program Coordinator, Centre for Foodborne, Environmental and Zoonotic Infectious Diseases, PHAC |
| Partner Communities | |
Stephanie Gower, PhD Carol Mee, RN, BScN, MEd
|
Toronto Public Health Research Consultant, Healthy Public Policy Supervisor Environmental Information and Education, Healthy Public Policy Manager, Healthy Environments Directorate |
| Shelley Hudson, RN | Ottawa Public Health |
External Reviewers
The external reviewers were selected based on their expertise and scope of knowledge and are listed below:
- Sheri Armstrong RN, BScN, MS
Public Health Nurse, Regional Municipality of Waterloo, Public Health - Sandra Brioux RN, BA
President, Telepractice Nursing Interest Group, Registered Nurses' Association of Ontario - Janet Chee RN, BScN, MN
Senior Program Manager, International Affairs, Best Practice Guidelines Program Registered Nurses' Association of Ontario - Audrey Danaher RN, MSc
Professional Practice (Public Health), Community Health Nurses' Initiatives Group - Katie Dilworth MHSc, RN, CCHN(C)
President, Community Health Nurses' Initiatives Group, Registered Nurses' Association of Ontario - James Ducharme MD, CM, FRCP(C), DABEM
Clinical Professor, Division of Emergency Medicine, McMaster University Invited reviewer on behalf of the Royal College of Physician and Surgeons of Canada - Stephanie Gower PhD
Research Consultant, Healthy Public Policy, Toronto Public Health - Doris Grinspun RN, MSN, PhD, O.ONT.
Executive Director, Registered Nurses' Association of Ontario - Laura Hanson RN, BN, MN
Community Health Nurse - Kathryn Hardill BScN, RN(EC)
Primary Health Care Nurse Practitioner, Bancroft Medical Clinic - Brenda Jacklitsh MS
Epidemiologist, National Institute for Occupational Safety and Health - Carol Mee RN, BScN, MEd
Supervisor, Environmental Information and Education, Healthy Public Policy, Toronto Public Health - Robert Milling LLB, LLM
Director, Health and Nursing Policy, Registered Nurses' Association of Ontario - Lynn Anne Mulrooney RN, MPH, PhD
Senior Policy Analyst, Registered Nurses' Association of Ontario - Daniel Rainham PhD
Chair in Sustainability and Environmental Health, Dalhousie University Research Associate, Atlantic Health Promotion Research Centre - Brent Ruddock RPh, BScPharm
Senior Pharmacist, Drug Information Research Center, Ontario Pharmacists' Association - Howard Shapiro MD, MSc, FRCP(C)
Associate Medical Officer of Health, Healthy Environments, Toronto Public Health - Jill Skinner
A/Associate Director, Office for Public Health, Canadian Medical Association - Carol M. Stephenson PhD
Chief, Training Research Branch, National Institute for Occupational Safety and Health - Althea Stewart-Pyne RN, BN, MHSc
Program Manager, International Affairs, Best Practice Guidelines Program, Registered Nurses' Association of Ontario - Tim Takaro MD, MPH, MS
Associate Professor, Associate Dean for Research, Faculty of Health Sciences, Simon Fraser University - Pamela VanBelle, RN, BScN, MN
Program Manager, International Affairs, Best Practice Guidelines Program, Registered Nurses' Association of Ontario
Heat Alert and Response Systems Advisory Committee Reviewers
The Heat Alert and Response System Advisory Committee was formed with national and international participants to input into the development of the broader Health Canada Heat Resiliency Project. Some members reviewed the Guidelines and are listed below:
- Quentin Chiotti PhD
Air Program Director and Senior Scientist at Pollution Probe - Patty Gorr
Policy Analyst, Division of Aging and Seniors, Public Health Agency of Canada - Jane MacDonald RN, MHSc
Vice President, Public Affairs and Community Engagement, Victoria Order of Nurses - Franziska Matthies PhD
Technical Officer, Climate Change, Green Health Services and Sustainable Development, WHO Regional Office for Europe - Bettina Menne MD, PhD
Programme Manager (a.i.), Climate Change, Green Health Services and Sustainable Development, WHO Regional Office for Europe - Scott Sheridan PhD
Editor-in-Chief, International Journal of Biometeorology, Associate Professor and Graduate Coordinator, Department of Geography, Kent State University
Heat Alert and Response Systems Pilot Reviewers
A component of the Health Canada Heat Resiliency Project is the development of Heat Alert and Response Systems in four Canadian communities. The Guidelines were sent to each community for their review and input was received from the list of participants that they selected:
- Ada Bennett MD
Emergency response coordinator, Winnipeg Regional Health Authority - Neil Gamey RN, PCP
EMS Manager of Operations, Assiniboine Regional Health Authority - Stephan Hamel MSc
Fredericton Pilot Regional Coordinator (Fact Sheets only) - Lori Jones RN, BScN
Coordinator, Facility Program Standards, Assiniboine Regional Health Authority - Tom P. McCormack
Regional Director, Disaster Management Program, Winnipeg Regional Health Authority - Robert Munro
Disaster Management Specialist, Manitoba Health, Office of Disaster Management - Toni Morris-Oswald PhD, BSW, MNRM
Manitoba Health, Office of Disaster Management - Karina Richters
Pilot Coordinator Windsor (Fact Sheets only) - Adrian Robertson MD
Provincial Medical Director of EMS, Manitoba Health, RCPS(C) specialist in Emergency Medicine and Critical Care - Brent Roussin MD, LLB, MPH(C), CCFP
Community Medicine Resident, Winnipeg Regional Health Authority - Sally Shurvell
Assiniboine Regional Health Authority Pilot Regional Coordinator (Fact Sheets only)
Government Reviewers
The invitation for a horizontal government review was extended to many partners and below is a list of those who participated:
- Alan Abelsohn MBChB, CCFP, FCFP
Physician Epidemiologist, Air Quality Health Index Section, Healthy Environments Consumer Safety Branch, Health Canada - Marc Berthiaume MD, CCFP
Director, Marketed Pharmaceuticals and Medical Devices Bureau, Marketed Health Products Directorate, Health Canada - Manon D. Fleury MSc
Biostatistician/Epidemiologist, Environmental Issues Division, Public Health Agency of Canada - Mark Lysyshyn MD, MPH, FRCP(C)
Medical Epidemiologist, Public Health Agency of Canada - Diane McClymont Peace
Manager, Climate Change and Health Office, First Nations and Inuit Health Branch, Health Canada - Nick Previsich PhD
Director, Environmental Issues Division, Public Health Agency of Canada - Susan Robertson MD
Senior Advisor, Office of Risk Management, Healthy Environments and Consumer Safety Branch, Health Canada
Appendix B: Fact Sheets for Health Care Workers
- Acute Care During Extreme Heat
Recommendations and Information for Health Care Workers - Community Care During Extreme Heat
Heat Illness: Prevention and Preliminary Care - Health Facilities Preparation for Extreme Heat
Recommendations for Retirement and Care Facility Managers
Appendix C: Health Canada's Heat Resiliency Publications

Heat Alert and Response Systems to Protect Health: Best Practices Guidebook - outlines best practices implemented in Canada and other countries and discusses steps that communities can take to mitigate heat-health risks and promote heat resiliency among Canadians.

Communicating the Health Risks of Extreme Heat Events: Toolkit for Public Health and Emergency Management Officials - identifies best communication practices, challenges faced by heat-vulnerable people, and scientifically informed public heat-health messages and explanations. In addition, it provides communication strategies to follow when developing heat-health communication campaigns.
Audience-Specific Public Heat-Health Brochures - use consistent and scientifically informed heat-health messages, tailored to the needs of heat-vulnerable groups. The audiences are older adults, the physically active, and parents with young children.
Extreme Heat Events Guidelines: Technical Guide for Health Care Workers - is an evidence-based technical guide for health care workers that provides information on recognizing, treating and preventing extreme heat-related illnesses. The Guidelines include: health promotion and injury prevention for vulnerable individuals; risk assessment of individuals for health practitioners; identification of heat illness signs and symptoms; and clinical recommendations to reduce health risks.

Extreme Heat Events Guidelines: User Guide for Health Policy Makers - is a summary document containing key figures and content from the technical guide to provide policy guidance to health care organisations and institutions.

Fact Sheets for Health Care Workers - provide health care workers with information to enhance their understanding of vulnerability to extreme heat, and their ability to identify effective preventions and mitigation measures. The targeted fact sheets have been developed for three distinct audiences: Acute Care, Community Care and Facilities Preparation.

Adapting to Extreme Heat Events: Guidelines for Assessing Health Vulnerability - provides guidance for conducting heat-health vulnerability and adaptation assessments as a means to better understand vulnerabilities and stimulate action to reduce individual and community vulnerability.
For more information please contact Climatinfo@hc-sc.gc.ca
Appendix D: Heat-Health Fact Sheets
- Older Adults
Protect yourself from the dangers of very hot weather
It's way too hot! - Physically Active
Protect yourself from the dangers of extreme heat
You're active in the heat! You're at risk! - Young Children
Protect your child from the dangers of extreme heat
Keep children cool!