
ARCHIVED - X-Ray Equipment in Medical Diagnosis Part A: Recommended Safety Procedures for Installation and Use - Safety Code 20A
1999
ISBN: 0-0-662-29034-8
Cat. No.: H46-2/00-65E
Notice to reader: We have archived Safety Code 20A, published in 1999. For updated guidance, please refer to Safety procedures for the installation, use and control of X-ray equipment in large medical facilities (Safety Code 35) (2024).
Correction notice: Please note that in Appendix 2, Figure 2 of Safety Code 20A, the unit of measure for concrete on the horizontal axis should be centimetres and not millimetres.
Table of Contents
- Explanatory notes
- Acknowledgements
- 1. Introduction
- 2. Scope and principal aims of the Code
- 3. Responsibility and personnel
- 4. Building and installation requirements
- 5. Radiation protection surveys
- 6. Equipment specifications
- 7. Darkroom and film processing
- 8. Procedures to reduce dose to x-ray personnel
- 8.1 General recommendations
- 8.2 Recommendations for operation of radiographic units
- 8.3 Recommendations for operation of fluoroscopic units
- 8.4 Recommendations for operation of mobile units
- 8.5 Recommendations for operation of photofluorographic units
- 8.6 Recommendations for special radiological procedures
- 9. Procedures for minimizing dose to patients
- 10. Guidelines for reduction of gonad dose
Appendices
- Appendix I Maximum permissible dose of ionizing radiation to operators and other occupationally exposed personnel
- Appendix ll Shielding guides for diagnostic x-ray installations
- Appendix lll
- Appendix lV Shielding guides for storage of radiographic film
- Appendix V Agencies responsible for radiation safety of medical x-ray installations
- Appendix Vl Radiation measurement units - International (SI) System
- Bibliography
Explanatory notes
This document is one of a series of Safety Codes prepared by the Radiation Protection Bureau to set out requirements for the safe use of radiation emitting devices. Included in this Code are sections for the specific guidance of the radiologist, the physician, the operator and the medical or health physicist concerned with safety procedures, equipment performance and protection surveys.
The safety procedures, equipment and installation guidelines detailed in this Code are primarily for the instruction and guidance of persons employed in Federal Public Service Departments and Agencies, as well as those coming under the jurisdiction of the Canada Labour Code. This Safety Code is also intended to assist other users of equipment that produces x-rays for general patient diagnosis. However, it should be noted that facilities under provincial jurisdiction may be subject to requirements specified under provincial statutes. The authorities listed in Appendix V should be contacted for details of the regulatory requirements of individual Provinces.
This Code supersedes Safety Code RPB-SC-4, entitled "X-Rays in Medical, Dental and Paramedical Diagnostic Radiology -Recommended Installation and Safety Procedures", and it is intended to complement x-ray equipment design, construction and performance standards promulgated under the Radiation Emitting Devices Act.
The words "must" and "should" in this Code have been chosen with purpose. The word "must" indicates a recommendation that is essential to meet the currently accepted standards of protection, while "should" indicates an advisory recommendation that is highly desirable and that is to be implemented where applicable.
In a field in which technology is advancing rapidly and where unexpected and unique problems continually occur the Code cannot cover all possible situations. Blind adherence to rules cannot substitute for the exercise of sound judgment, so the recommendations may need to be modified in unusual circumstances, but only upon the advice of experts with recognized competence in radiation protection. This Code will be reviewed and revised periodically and a particular requirement may be reconsidered at any time if it becomes necessary to cover an unforeseen situation. Interpretation or elaboration on any point can be obtained by contacting the Radiation Protection Bureau, Health Canada, Ottawa, Ontario, K1A 1C1.
This Code reflects the results of the work of many individuals, and was compiled and drafted by Dr. W.M. Zuk in cooperation with Mr. A. Tod, and Mr. M.H. Repacholi.
Acknowledgements:
The various draft versions of this Safety Code were reviewed and commented on by a number of regulatory authorities and professional and manufacturers' associations. The contributions of the following organizations and associations to the Code are gratefully acknowledged:
- Federal/Provincial Subcommittee on Radiation Surveillance
- Bureau of Radiological Health, U.S. Department of Health and Human Services
- Bureau of Medical Devices, Health Canada
- Medical Services Branch, Health Canada
- Canadian Association of Physicists
- Canadian Association of Radiologists
- Canadian Association of Medical Radiation Technologists
- Canadian Association of Manufacturers of Medical Devices
Acknowledgement is gratefully made to Mr. J. Gordon for preparation of the graphs in Appendix II. Appreciation is also expressed to Mr. P. Dvorak, Mr. J. Cairnie and Dr. P.J. Waight for their advice during the preparation of the Code.
1. Introduction
Diagnostic x-rays are an essential part of present day medical practice. In North America, over 60% of the population with access to modern medical care undergo radiological procedures each year. Over half of all important decisions for the welfare of patients are based on radiological procedures. The diagnostic x-ray is thus one of the most valuable tools used in modern health care.
Although individual doses are usually small, in total exposure, diagnostic x-rays account for the major portion of man-made radiation exposure to the general population. However, with well-designed, installed and maintained x-ray equipment, and through use of proper procedures by trained operators, unnecessary exposure to patients can be reduced significantly, with no decrease in the value of medical information derived. To the extent that patient exposure is reduced, there is, in general, a decrease in the exposure of machine operators and other health care personnel.
The need for radiation protection exists because exposure to ionizing radiation can result in deleterious effects that manifest themselves not only in the exposed individual but in his descendants as well. These effects are called somatic and genetic effects, respectively. Somatic effects are characterized by observable changes occurring in the body organs of the individual exposed. These changes may appear within a time frame of a few hours to many years, depending on the amount and duration of exposure of the individual. Genetic effects are an equal cause for concern at the lower doses used in diagnostic radiology. Although the radiation doses may be small and appear to cause no observable damage, the probability of chromosomal damage in the germ cells, with the consequence of mutations giving rise to genetic defects, can make such doses significant when considered for a very large population.
There are four main aspects of the problem to be considered. Firstly, radiological procedures should be based on a demonstrated medical need. Secondly, when radiological procedures are required, it is essential that patients be protected from excessive radiation during the exposure. Thirdly, it is necessary that personnel in radiology departments be protected from excessive exposure to radiation in the course of their work. Finally, personnel in the vicinity of radiology facilities and the general public require adequate protection.
While for radiation workers and the general public maximum permissible levels of exposure have been defined, no specific levels have been recommended for patients undergoing diagnostic x-ray procedures. For patients the risk involved in the exposure must always be weighed against the medical requirement for accurate diagnosis. However, there must always be a conscious effort to reduce patient exposures to the lowest practical levels and to eliminate "unnecessary" exposures.
2. Scope and Principal Aims of the Code
This Safety Code is concerned with the protection of all individuals who may be exposed to radiation emitted by x-ray equipment used in the practice of medical diagnostic radiology.
2.1 Principal aims
The principal aims of this Code are:
- to minimize patient exposure in medical diagnostic radiology;
- to ensure adequate protection of personnel operating or using x-ray equipment; and
- to ensure adequate protection of the general public in the vicinity of areas where diagnostic procedures are in progress.
2.2 Scope
To assist personnel in achieving these objectives, this Safety Code:
- specifies minimum standards of safe design, construction and performance for diagnostic x-ray equipment;
- presents recommended practices for minimizing patient and operator exposures and ensuring that diagnostic x-ray equipment is used in a safe manner;
- supplies information and methods for calculating or otherwise determining the effectiveness and adequacy of shielding in attenuating primary and scattered radiation; and
- sets out the relative responsibilities of the owner, responsible user, operator and other personnel.
3. Responsibility and personnel
3.1 Responsibility
The owner is ultimately responsible for the radiation safety of a diagnostic x-ray facility. It is the responsibility of the owner to ensure that the equipment provided for the responsible user and operators, and the facilities in which such equipment is installed and used, meet all applicable radiation safety standards.
The owner may delegate this responsibility to staff. How this responsibility is delegated will depend upon the size of the staff and on the amount of x-ray equipment owned. In any event, one or more persons must be designated to carry out the roles described below. For small institutions some of the duties listed under 3.1 (b) and 3.1 (c) may be assumed by suitable consulting bodies.
a. Responsible User
There must be at least one person designated as the responsible user to undertake responsibility for:
- ensuring that the equipment is maintained properly and functions correctly;
- ensuring that the equipment is used and maintained only by competent personnel;
- ensuring that the equipment is used correctly;
- establishing safe operating procedures for the equipment and ensuring that operating staff are adequately instructed in them;
- promulgating rules of radiation safety and ensuring that staff are made aware of them;
- investigating any high x-ray exposures received by personnel;
- ensuring that radiation levels outside controlled areas are below the maximum permissible limits given in Appendix I; and
- ensuring that the Radiation Protection (Safety) Officer and all operators receive, or at least have access to, a copy of this Safety Code.
b. Radiation Protection (Safety) Officer
There should be a "Safety Officer" (preferably a medical or health physicist) to act as advisor on all radiation protection aspects, both during the initial stages of construction of the facility and installation of the equipment, and during subsequent operations.
The Safety Officer should have responsibility for:
- ensuring that the installation complies with all applicable regulatory requirements;
- "certifying" the safety of an installation at the time of planing and/or construction;
- the establishment of safe working conditions according to the recommendations of this Safety Code and the statutory requirements of Federal or Provincial legislation, where applicable;
- ensuring that established safety procedures are being followed and reporting any non-compliances to the Responsible User;
- reviewing the safety procedures periodically and updating them to ensure optimum patient and operator safety;
- instructing personnel in proper radiation protection practices;
- carrying out routine checks of equipment and facility safety features and radiation surveys;
- ensuring that appropriate radiation survey instruments are available, serviceable and properly calibrated;
- keeping records of radiation surveys, including summaries of corrective measures recommended and/or instituted;
- organizing participation, where necessary, in a personnel radiation monitoring service, such as that provided by the Radiation Protection Bureau, Ottawa, Ontario, K1A 1C1;
- declaring who is to be considered as an occupationally exposed person (i.e., all operators of x-ray equipment, together with persons (e.g., nurses) who routinely participate in radiological procedures and others likely to receive a radiation dose in excess of 1/20th of the maximum permissible specified);
- keeping records of occupational exposures received by personnel;
- investigating each known or suspected case of excessive or abnormal exposure to determine the cause and to take remedial steps to prevent its recurrence;
- assuring that all safety devices recommended by this Code are functioning and that appropriate warning signs are properly located; and
- ensuring that operators understand the contents of this Code.
3.2 X-ray equipment operators
All operators should be certified according to a recognized standard, such as that of the Canadian Association of Medical Radiation Technologists, and must possess qualifications required by any relevant Federal and Provincial regulations or statutes.
All operators must:
- be aware of the contents of this Safety Code;
- be aware of the radiation hazards associated with their work and that they have a duty to protect their patients, themselves and others;
- have a thorough understanding of their profession, of safe working methods and of special techniques;
- through conscientious use of proper techniques and procedures, strive to eliminate or reduce to lowest practical values all patient exposures; and
- be 18 years of age or older.
A female operator should be encouraged to notify her employer if she believes herself to be pregnant, in order that appropriate steps may be taken to ensure that her work duties during the remainder of the pregnancy are compatible with accepted maximum radiation exposure, as set out in Appendix I.
3.3 Students or operators-in-training
All operators in training and inexperienced personnel must work only under the direct supervision of a qualified operator.
It must be noted that persons starting work at an age less than 18 years must not receive an annual dose equivalent exceeding 1 mSv (see Appendix I).
4. Building and Installation Arrangements
4.1 Design criteria
In the planning of any medical x-ray facility account must be taken of the expected maximum workload of the equipment, of use factors of the barriers and of occupancy factors for areas adjacent to the facility. Allowance should be made for possible future changes in any one or all of these parameters, such as increased operating kilovoltage and workload, or modifications in techniques that may require ancillary equipment and an increase in the degree of occupancy of surrounding areas.
Certain basic principles must be observed when determining the shielding requirements for a room used routinely for diagnostic radiology, including fluoroscopy and special procedures. These are as follows:
- The radiation levels in controlled areas that are occupied routinely by radiation workers only, must be such that no radiation worker is occupationally exposed to more than 20 mSv per year.
- The radiation levels in uncontrolled areas must be such that no person can receive more than 1 mSv per year.
In general, radiation levels in the immediate vicinity of x-ray equipment are such that the above limits would be exceeded even at very low workloads. Reduction in radiation intensity can be accomplished by a suitable combination of distance from the sources of radiation and physical shielding barriers, provided that radiation workers or the general public are restricted from all areas in which the respective maximum permissible dose could be exceeded.
The shielding required to reduce radiation levels to within the acceptable limits may be computed on the basis of distance, maximum tube potential (kilovoltage), workload (W), use factor (U) and occupancy factor (T), as described in Appendix II. To ensure that the radiation levels are always below acceptable limits the maximum possible workload should be used in the calculations. Also, due consideration should be given to possible future increases in use and occupancy factors and x-ray tube potential.
Other areas where x-ray equipment is used less frequently, such as operating theatres, recovery rooms, emergency wards, etc., may require special consideration. However, the same basic principales of distance, time, and shielding still apply in determining the protection needs.
4.2 General recommendations
Protection of operating personnel and others working in the vicinity of x-ray equipment should be achieved by:
- ensuring that diagnostic radiological rooms are designed to provide adequate working space to allow for ease of patient movement;
- ensuring that the useful beam is always directed towards adequately shielded areas. Particular attention must be paid to adequacy of shielding for chest radiography using wall-mounted cassette holders;
- absorbing the useful beam and scatatered radiation as close as possible to the patient or scatterer;
- shielding, where necessary, floors, walls, ceilings and doors on the basis of maximum expected x-ray tube potentials (kilo-voltages), workloads (output), use and occupancy factors;
- constructing shielding to form an unbroken barrier. Care should be taken in the use of shielding materials, especially lead, which must be adequately supported to prevent "creeping";
- providing a control booth for the protection of the operator. The control booth, and the viewing window in the booth, must have shielding properties such that no operator is occupationally exposed to more than 20 mSv per year. Mobile protective screens must not be considered adequate as a control booth for radiographic rooms containing stationary x-ray equipment;
- locating the control booth, whenever possible, such that the radiation has to be scattered at least twice before entering the booth. In installations where the useful beam may be directed towards the booth, the shielding of the booth must be that of a primary barrier;
- positioning control booths so that, during an exposure, no one can enter the radiographic room without the knowledge of the operator;
- use of warning signs, which must be posted on all entrance doors of each radiographic room. The warning signs must incorporate the x-radiation warning symbol specified in Appendix III and should incorporate the words "Unauthorized Entry Prohibited";
- arranging for the final plans of the installation to be reviewed by the appropriate responsible government agencies. For installations under federal jurisdiction, the responsible agency is the Radiation Protection Bureau of Health Canada. For installations under provincial jurisdiction the responsible agencies are listed in Appendix V. The dimensions of the shielding and the materials used must be indicated on the plans. The plans must also show the positions of all windows, doors, pipes and louvres that may affect the protection requirements. Adjacent rooms, as well as rooms above and below, must also be noted;
- considering mobile x-ray equipment used routinely in one location as a fixed installation and shielding the installation accordingly;
- shielding an installation containing photofluorographic x-ray equipment such that all personnel in the vicinity of the equipment are adequately protected, during routine use, without the necessity for protective clothing.
5. Radiation Protection Surveys
A radiation protection survey of a facility is intended to demonstrate not only that the x-ray equipment itself functions properly and according to applicable standards but also that the equipment is installed in a safe environment and is used in a way which provides maximum radiation safety for patients and operators. It is important, therefore, that x-ray facilities be surveyed at regular intervals.
5.1 General procedures
Routine operation of any new installation should be deferred until a complete survey has been made by a qualified expert and the installation has been declared to be in compliance with pertinent government installation and use regulations. A survey must also be carried out after any change in an existing installation, which might produce a radiation hazard, such as alterations to protective barriers, replacement of x-ray equipment with equipment operating at higher potentials or changes in operating procedures.
It is particularly advantageous to make visual inspections during construction of a new facility, to ensure compliance with specifications and to identify faulty material or workmanship, since deficiencies can be remedied more economically at this stage than later. Such inspections should include determination of thickness of lead and/or concrete thickness and density, degree of overlap between lead sheets or between lead and other barriers, as well as thickness and density of leaded glass used in viewing windows.
Details on survey procedures and measurements to be carried out for specific types of x-ray equipment and facilities are presented in Diagnostic X-Ray Equipment Compliance and Facility Survey (H46-2/94-184E). This Code also contains examples of appropriate survey forms and recommendations on information to be included in survey reports.
The results of the survey and conclusions drawn by the qualified expert must be submitted to the owner or responsible user in the form of a written report. All such written reports must be retained by the owner or responsible user.
5.2 Survey report
The survey report must present, in a clear systematic way, details and results of the measurements carried out, as well as the conclusions drawn and recommendations made by the surveyor. In the report for an existing installation attention must be drawn to any unusual findings with respect to the equipment itself, the installation or operating procedures, which could affect the safety of patients, operators or other persons in the vicinity of the x-ray facility.
The survey report must include at least the following:
- a sketch of the facility, showing the locations of the x-ray equipment and control booth within the facility as well as the nature and occupancy of the areas adjoining the facility;
- identification of the x-ray equipment (i.e., name of the manufacturer, model designation and serial number of the generator, control, x-ray tube assembly, x-ray table, etc., as applicable). The date, or at least approximate date, of manufacture should be included;
- the method of support of the x-ray tube assembly (i.e., floor-to-ceiling tube stand, ceiling suspended over-table tube, etc.);
- observations on the operational condition (both electrical and mechanical) of the x-ray equipment at the time of the survey. Particular attention should be drawn to any conditions which could lead to future malfunctioning of the equipment;
- the actual or estimated total workload of the facility, as well as the workload apportioned into the various useful beam directions and procedures used, etc.;
- results of radiation measurements carried out both inside and outside the controlled area under "typical" and "worst case" operating conditions. The locations at which the measurements have been made must be indicated on the sketch of the facility;
- an assessment of the condition of lead aprons, gloves, gonad shields, mobile lead screens and other protective devices;
- an estimate of potential exposures to personnel working in or around the facility;
- an assessment of radiological techniques from the point of view of radiation safety. Attention must be drawn to any practices which are or could be detrimental to the patient or to personnel working in the facility. Recommendations of improved or safer techniques should be made in such cases;
- a summary of typical technique factors used and a measurement of the total filtration in the useful beam;
- recommendations regarding the need for a follow-up survey. The survey report should also include the results of investigations of any unusually high exposures from previous personnel dosimetry reports and recommend whether other persons should be included in the personnel dosimetry service.
6. Equipment Specifications
6.1 New x-ray equipment
All new medical x-ray equipment and accessories for such equipment, sold in Canada, must conform to the requirements of the Radiation Emitting Devices Act and the Food and Drugs Act. The requirements are specified in the Radiation Emitting Devices Regulations and the Medical Devices Regulations promulgated under these two Acts respectively. The former regulations specify standards of design, construction and performance, with respect to radiation safety, and are mandatory requirements for new equipment only. The latter regulations encompass all safety considerations and the question of efficacy for all medical x-ray equipment, both old and new. It is the responsibility of the manufacturer or distributor to ensure that the equipment conforms to the requirements of the regulations.
The Radiation Emitting Devices Regulations in effect for medical x-ray equipment, at the time of printing of this Safety Code, include those for dental x-ray equipment, photofluorographic x-ray equipment, and diagnostic x-ray equipment. The specific requirements of the latter two regulations are reproduced in Appendix III of this Code.
The regulations may be amended, from time-to-time, to keep abreast of changing technology in the field. Information on the applicability and currency of the Radiation Emitting Devices Regulations and details of any promulgated amendments may be obtained by contacting the Radiation Protection Bureau, Health Canada, Ottawa, Ontario, K1A 1C1. Similar information on the Medical Devices Regulations may be obtained by contacting the Medical Devices Bureau, Health Canada, Ottawa, Ontario, K1A 1B6.
6.2 Existing x-ray equipment
Whenever possible, and to the extent that it is practical, existing x-ray equipment should be upgraded to incorporate as many as possible of the safety and performance features required of new x-ray equipment. It should be noted that replacements for any component or subassembly of an x-ray machine, for which a design, construction or performance standard has been specified in the Radiation Emitting Devices Regulations applicable to that class of machine, as required to comply with the standards in effect at the time of replacement.
To ensure maximum protection for patients and staff, all existing x-ray equipment must at least meet certain basic requirements. These are itemized in the remainder of these sections.
6.2.1 General requirements
- Warning Signs - The x-ray control panel must bear a permanent and conspicuous sign warning that hazardous x-radiation is emitted when the equipment is in operation and prohibiting unauthorized use.
- Markings - All controls, meters, lights and other indicators relevant to the operation of the equipment must be readily discernible and clearly labelled or marked as to function.
- Indicator Lights - There must be readily discernible, separate indicators on the control panel that respectively indicate:
- when the control panel is energized and the machine is ready to produce x-rays, and
- when x-rays are produced. When more than one x-ray tube is controlled by one control panel, there must be clear and visible indication, at or near the tube housing and on the control panel, of which tube is connected and ready to be energized.
- Focal Spot - The location of the focal spot must be clearly and accurately marked on the tube housing.
- Filtration - The external surface of the x-ray tube housing must bear a permanent mark or label which sets out the minimum permanent inherent filtration in the useful beam, expressed as millimetres of aluminum equivalent at a specified peak tube potential. The total permanent filtration in the useful beam must be equivalent to at least the following thicknesses of aluminum:
- 0.5 millimetre of aluminum, for machines designed to operate with x-ray tube potentials below 50 kilovolts peak;
- 1.5 millimetres of aluminum, for machines designed to operate with x-ray tube potentials from 50 kilovolts peak to 70 kilovolts peak, and
- 2.5 millimetres of aluminum, for machines designed to operate with x-ray tube potentials above 70 kilovolts peak;
- Mechanical Stability - The x-ray tube must be securely fixed and correctly aligned within the tube housing. Also, the tube housing must maintain its required exposure position or movement without excessive drift or vibration during operation. The x-ray tube housing must be supported by mechanical means. It must not be hand-held during operation.
- Exposure Control - There must be an exposure switch, timer, or other device to initiate and terminate x-ray production. This control must automatically terminate the exposure after a preset time, product of current and time, or exposure has elapsed. Where an exposure switch is provided, the exposure switch must:
- require continuous pressure by the operator to produce x-rays (i.e., "dead man" type);
- if in the form of a footswitch, be so constructed that if overturned inadvertent exposures do not result;
- be so located that convenient operation outside of a shielded area is not possible, (except for exposure switches used in conjunction with mobile x-ray equipment, with spot film devices, in fluoroscopy and with certain special procedures), and
- for mobile x-ray equipment, be equipped with a cable at least three metres long.
- Indication of Technique Factors - For x-ray machines having adjustable technique factors, the control panel must incorporate electrical meters or other indicators that enable determination of the x-ray tube potential (kilovolts), tube current (milliamperes) and time (seconds), or combinations of these. For equipment having non-adjustable technique factors, permanent marks or labels may be used to indicate these parameters. The actual peak kilovoltage should correspond to the selected or indicated value to within 5% of the selected or indicated value. The millammeter should be accurate to within 5% of the full scale reading and be temperature compensated for normal operating conditions.
- X-Ray Tube Shielding - The x-ray tube must be enclosed in a shielded housing. The shielding of the housing must be such that, at each rating specified by the manufacturer for that tube, the leakage radiation, measured at a distance of one metre in any direction from the focal spot of the x-ray tube, does not exceed 0.1% of the exposure rate at the same distance along the central axis of the useful beam.
For radiographic equipment designed specifically for mammography, the leakage radiation, measured at a distance of 5 cm from the housing and averaged over a detect ion area of 100 square centimetres, must not exceed two milliroent gen per hour (516 nC/kg per hour).
6.2.2 Stationary general purpose radiographic equipment
- Collimation - The x-ray tube housing must be equipped with an adjustable collimator which provides stepless adjustment of the size of the x-ray field and which must provide the same degree of shielding towards leakage radiation as is required of the tube housing. The collimator should incorporate means to indicate the size of the x-ray field at the image receptor. if in the form of a light localizer, it should give an average illumination of at least 100 lux at 100 cm or the maximum target-to-image receptor distance, whichever is less.
- Filtration - The filters must be permanently and securely mounted to the x-ray port of the tube housing or beam limiting device, or both.
- Timer Accuracy - The timer or exposure control must be such that:
- it can be set to control exposures as short as 1/60 second or 5 milliampere-seconds, whichever is greater, and
- at each setting it is accurate to 1/60 second or 7% of that setting, whichever is greater.
- Reproducibility - For any given combination of x-ray tube potential (kVp), tube current (mA) and exposure time (seconds) in excess of 0.1 second, or selected radiation exposure to the image receptor (milliroentgen or coulomb/kg) the coefficient of variation C, given by
where
Xi = ith exposure measurement
= mean value of the exposure measurements
n = number of exposure measurements;
of any 10 consecutive radiation measurements, taken at the same source-to-detector distance within a time period of one hour and with the line voltage for each measurement within 1% of the mean value for all of the measurements, must not be greater than 0.05. Furthermore, each of the 10 radiation exposures measured must be within 15% of the mean value of the 10 measurements. - Linearity - For any fixed value of x-ray tube potential (in kVp), within the range of values specified for the equipment, the average ratios of exposure (in milliroentgen or coulomb/kg) to tube current-exposure time product (in milliampere-seconds) at any two consecutive tube current settings must not differ by more than 0.10 times their sum.
That is,
where
X1 and X2 are the average mR/mAs values based on 10 exposures at each of two consecutive x-ray tube current settings. - Line Voltage Compensator - The equipment must be equipped with means to compensate for variations in x-ray tube potential caused by line voltage fluctuations. By these means it must be possible to set and maintain the peak tube potential (kVp), prior to initiation of an exposure, to within 5% of the selected value, for a line voltage variation of ± 7% of its nominal value.
- Current Stabilization - The equipment should be provided with a tube current stabilizer to maintain preset current to within ± 5% of the required value for exposures of 1/5 second or more.
Changes in tube potential should not result in a variation of tube current greater than ± 5%.
6.2.3 Mobile radiographic equipment
The requirements given in sections 6.2.2 (1) to (7) inclusive, apply. Additional requirements for mobile radiographic equipment are as follows:
- Target-to-Skin Distance - The equipment must be equipped with means to prevent operation at target-to-skin distances of less than 30 centimetres.
- Exposure Control - The exposure switch must be of the dead-man type and must be provided with a cable at least 3 metres long. A "coiled-type" cable is the most practical for this purpose.
- Capacitor Discharge Equipment - Capacitor discharge type mobile equipment must be equipped with:
- a safety shutter or other means to prevent emission of x-radiation from the exit port of the x-ray tube housing assembly when the exposure switch or timer is not activated;
- a warning light, or other visual indicator, to indicate that the high potential capacitor is charged;
- an electrical meter, or other indicator, to indicate the state of charge of the high potential capacitor, and
- means to enable the high potential capacitor to be discharged to a residual potential difference of less than 30 volts, without the production of x-radiation.
6.2.4 Fluoroscopic equipment
- Collimation - The x-ray tube housing must be equipped with an adjustable collimator which provides stepless adjustment of the size of the x-ray field and which must provide the same degree of shielding towards leakage radiation as is required of the tube housing. The maximum size of x-ray field permitted by the collimator should not be larger than the useful area of the input phosphor on the image intensifier. The useful beam should be centred on the input phosphor and the beam margins should be tangential to the area being viewed. Where a larger area is required for spot films an interlock or other positive means must prevent the use of the fluoroscopic mode unless the conditions of this paragraph are met.
- Direct Beam Absorbers - A primary protective barrier must be permanently incorporated into the equipment to intercept the entire cross section of the direct beam, for all possible target-to-image receptor distances. The barrier must be so installed that its removal from the useful beam causes automatic termination of the exposure. The lead equivalent thickness of the primary protective barrier must be at least 2 mm for machines capable of operating up to 100 kVp. For each additional kilovolt of operating tube potential an additional 0.01 mm lead equivalent is required.
- Image Intensification - All fluoroscopic x-ray machines must be equipped with an image intensification system. On a mobile fluoroscopic machine the image intensifier must either be an integral part of the equipment or be interlocked in such a way that its removal prevents x-rays from being produced. The image intensification system must be adequately shielded so that neither the useful beam nor the scattered radiation from the intensifier will produce significant exposure to the operator or other personnel. The shielding must be such that the exposure rate to an object having a cross-sectional area of 100 cm2, with no linear dimension greater than 20 cm, of x-radiation due to transmission of the useful beam through or scattering from the window of the fluoroscopic imaging assembly, does not exceed 2 milliroentgen per hour (516 nC/kg/h) at 10 centimetres behind the plane of the image receptor, for each roentgen per minute of entrance exposure rate.
- Target-to-Skin Distance - Fixed fluoroscopic equipment must incorporate means to limit the target-to-skin distance to not less than 38 centimetres. In the case of a fluoroscopic machine designed for special applications that would be impossible at the above minimum distance, provision may be made for operation at shorter target -to-skin distances; but in no case must this distance be less than 20 centimetres.
- Material Between Patient and Image Receptor - The aluminum equivalent of the table top must not be greater than 1 mm when measured at 100 kVp.
- Exposure Switch - The fluoroscopic exposure switch must be of a dead-man type.
- Timer - There must be a cumulative timing device, activated by the fluoroscopic exposure switch, which requires manual resetting. This timer must have a maximum setting not exceeding 5 minutes. Whenever a preset time has been reached, it must give a clearly audible signal.
- Indication of TubePotential and Current - Electrical meters or other visual indicators must be provided to enable continuous monitoring by the operator of tube potential and current during fluoroscopy.
- Entrance Exposure Rate - At the shortest target-to-skin distance specified for the equipment, the entrance exposure rate must not exceed 10 roentgen (2.58 mC/kg) per minute for any combination of tube current and potential. With modern equipment most fluoroscopy can and should be carried out with exposure rates of less than 5 roentgen (1.29 mC/kg) per minute.
- Bucky Slot Shielding - Shielding must be provided with the equipment to cover the Bucky Slot. This should provide the equivalent protection of at least 0.5 mm of lead at 100 kVp.
- Table Shielding - The side of the fluoroscopic table should have an equivalent thickness of at least 0.5 mm of lead at 100 kVp to restrict scattered radiation passing through it.
- Operator Shielding - To protect the operator from radiation scattered above the table-top, there should be a lead rubber apron of dimensions not less than 45.7 cm × 45.7 cm (18" × 18") The material must have a lead equivalent of not less than 0.5 mm at 100 kVp and the apron must be attached to the lower edge of the fluoroscopic screen when the latter is vertical and to the side when the screen is horizontal. The apron may consist of several overlapping parts. In the absence of such a protective apron a retractable lead shield must be incorporated in the equipment to project at least 15 cm above the table when in use. It must be mounted on the front side of the table and have a lead-equivalent thickness of at least 0.5 mm at 100 kVp.
6.2.5 Photofluorographic equipment
- Collimation - The equipment must be permanently fitted with a collimator which must confine the beam to the area of the fluorescent screen. The beam must not be greater than 35 cm × 43 cm (14" × 17") at the screen surface, regardless of the target-to-skin distance.
- Beam Alignment - The photofluorographic camera and x-ray tube must be coupled together so that the direct beam always centres on the mid-point of the screen.
- Gonad Shield - The lower edge of the beam-defining device should be curved to prevent irradiation of the female gonads.
- Maximum Entrance Exposure - The entrance exposure to a patient must not exceed 200 milliroentgen and should not exceed 100 milliroentgen (25.8 microcoulomb/kg) per film.
6.3 Protective clothing
6.3.1 Protective body aprons
Protective body aprons used for radiographic or fluoroscopic examinations with peak x-ray tube potentials of up to 150 kVp must provide attenuation equivalent to at least 0.5 mm of lead. The lead equivalent thickness of the material used must be permanently and legibly marked on the apron.
6.3.2 Gonad shields
Contact-type gonad shields used for routine diagnostic radiology must have a lead equivalent thickness of at least 0.25 mm and should have a lead equivalent thickness of 0.5 mm at 150 kVp. Contact-type gonad shields must be of sufficient size and shape to exclude the gonads completely from primary beam irradiation.
6.3.3 Protective gloves
Protective gloves used in fluoroscopy must provide attenuation equivalent to at least 0.25 mm of lead at 150 kVp. This protection must be provided throughout the glove, including fingers and wrist.
6.4 Film cassettes
The proper amount of filtration placed in the useful beam between the x-ray tube and the patient reduces exposure to the patient. However, any material placed between the patient and the radiographic film has the effect of increasing patient exposure. With this in mind, the front panel of the film cassette must not exceed an aluminum equivalence thickness of 1.0 mm and should not exceed an aluminum equivalence thickness of 0.5 mm.
Film cassettes must be completely light-tight. As soon as the material used for achieving light-tightness becomes worn and light leakage occurs, either the material or the cassette should be replaced.
It is also important to have good film-screen contact; therefore screens should be cleaned regularly and their contact with the film checked.
7. Darkroom and Film Processing
The x-ray exposure necessary to produce a radiography of satisfactory diagnostic quality, commensurate with minimum exposure to the patient, depends not only on the exposure technique and film-screen combination employed but also on the handling and processing of the film. These require a good darkroom and proper developing techniques.
7.1 Darkroom
Most modern x-ray departments use automatic film processors for film development. Nevertheless, good darkrooms are still an essential requirement whether they be used for manual processing of films or for loading automatic film processors. While specific details may vary from installation to installation all darkrooms should include certain basic features:
- The room must be completely light-tight.
- If adjacent to a radiography room, the darkroom must be adequately shielded to ensure that exposure of personnel and film to x-radiation does not occur.
- The darkroom should be designed to incorporate a lockable door, double doors or a blackened maze entrance to ensure light tightness when undeveloped films are being handled.
- A warning light should be located outside the darkroom, at the entrance, to indicate when the room is in use.
- Safelights fitted with bulbs of correct intensity must be provided above the work areas within the darkroom. The safelights must have filters appropriate to the specifications of the film used and must be positioned at the proper distances from work areas.
7.2 Film processing
Improper or careless processing of exposed radiographic films can cause films of poor diagnostic quality and consequently the chance of wrong diagnosis or requests for repeat exposures. To achieve full development of a film which has been exposed, using correct radiographic technique factors, the film must be processed in chemically fresh developer, at proper temperature and for sufficient time to ensure that the silver in exposed silver halide crystals in the film emulsion is completely reduced. If this is not done the blackening of the film will not be optimum and the tendency will be to increase radiation exposure to achieve proper image density.
To ensure proper processing of films certain basic recommendations should be followed:
- Manufacturers' recommendations with respect to strength of solutions, temperature and time must be followed to ensure optimum development.
- Developing solutions should be replenished as necessary and should be changed regularly, as required.
- Developing solutions should be monitored regularly. Even unused developer deteriorates with time. Developer should not be used when it becomes necessary to develop significantly longer than the recommended times in order to obtain optimum film density.
7.3 Film storage
Unexposed radiographic films must be stored in such manner that they are shielded from stray radiation. Storage should be provided such that no film receives more than 0.2 milliroentgen of stray radiation before use. The amount of shielding required will depend on the storage time and on the workload of the facility. It can be determined from the table in Appendix IV.
Films should be stored on end in a cool, dry area.
8. Procedures to Reduce Dose to X-Ray Personnel
The guidelines and procedures outlined in this section are primarily directed toward occupational health protection. However, adherence to these will also, in many instances, provide protection to visitors and other individuals in the vicinity of an x-ray facility. The safe work practices and procedures for using various types of x-ray equipment should be regarded as a minimum, to be augmented with additional requirements, when warranted, to cover special circumstances in particular facilities.
To achieve optimum safety, radiologists and radiographers must make every reasonable effort to keep exposures to themselves and to other personnel as far below the limits specified in Appendix I as reasonably achievable.
8.1 General recommendations
- An x-ray room must not be used for more than one radiological investigation simultaneously.
- Except for those persons whose presence is essential, no person must be in the x-ray room when the exposure is carried out.
- Personnel must at all times keep as far away from the useful beam as is practicable. Exposure of personnel to the useful beam must never be allowed unless the beam is adequately attenuated by the patient and by protective clothing or screens.
- All personnel must take full advantage of the protective devices available.
- Operators should remain inside the control booth or behind protective screens when making an x-ray exposure. In cases where there are reasons that make this impractical, protective clothing must be worn.
- When there is a need to support children or weak patients, holding devices should be used. If parents, escorts or other personnel are called to assist, they must be provided with protective aprons and gloves, and be positioned so as to avoid the useful beam. No one person should regularly perform these duties.
- When a lead equivalent protective apron is worn, the personnel dosimeter must be worn under the apron. If extremities are likely to be exposed to significantly higher doses, additional extremity monitors should be worn.
- All operators of x-ray equipment, together with personnel (e.g.nurses) who routinely participate in radiological procedures, and others likely to receive a radiation dose in excess of 1/20th of the maximum permissible specified in Appendix I, must wear personnel dosimeters.
- All entrance doors to an x-ray room, including patient cubicle and preparation room doors, should be kept closed while a patient is in the room.
- X-ray machines which are energized and ready to produce radiation must not be left unattended.
- Where radiation doses in excess of 5% of the maximum permissible specified in Appendix I are being received regularly by any one person, appropriate remedial steps must be taken to improve techniques and protective measures.
- X-ray equipment must only be operated by, or under the direct supervision of, qualified individuals. (See sections 3.2 and 3.3).
- An x-ray housing must not be held by hand during operation.
8.2 Recommendations for operation of radiographic units
- The x-ray exposure should, as a general rule, be controlled from the control panel located inside the control booth or behind a shielded wall. In the case of special techniques where the operator is required to control the exposure while at the side of the patient, appropriate protective clothing must be worn.
- The operator must have a clear view of the patient during every exposure and be able to communicate with the patient and/or attendants without leaving the control booth.
- Cassettes must never be held by hand during an exposure.
8.3 Recommendations for operation of fluoroscopic units
- All persons, with the possible exception of the patient, required to be in the room during a fluoroscopic procedure should wear protective aprons. Lead shields or curtains mounted on the fluoroscopic unit must not be considered a sufficient substitute for the wearing of protective clothing.
- Protective gauntlets should be worn by the radiologist during palpation in every fluoroscopic examination. During fluoros-copy, palpation with the hand should be kept to a minimum.
- During fluoroscopy and spotfilm operation associated with fluoroscopic operation, where personnel are required to be at the side of the patient, appropriate protective clothing must be worn by these personnel.
- All fluoroscopic examinations should be carried out as rapidly as possible and with minimum dose-rates and x-ray field sizes.
- Direct-viewing fluoroscopy must not be carried out; image-intensified fluoroscopy must be used.
8.4 Recommendations for operation of mobile units
- Mobile units must be used only if the condition of the patient is such as to make it inadvisable for the examination to be carried out with a stationary unit in the main x-ray department.
- During operation, the primary beam should be directed from occupied areas if at all possible, and every effort must be made to ensure that this beam does not irradiate any other persons in the vicinity of the patient.
- The operator must stand at least 3 metres from the x-ray tube and out of the direct beam.
- The operator must be shielded when exposures are made.
- In a capacitor discharge unit after an x-ray exposure has been made there is a residual charge left in the capacitors. This residual charge can give rise to a "dark current" and result in x-ray emission even though the exposure switch is not activated. Therefore, the residual charge must be fully discharged before the unit is left unattended.
8.5 Recommendations for operation of photofluorographic units
Photofluorographic x-ray machines in general can give significantly higher patient doses than conventional diagnostic machines, therefore their use is severely restricted in Canada. When, subject to the guidelines outlined in section 9.4, the use of such units is justified, the following recommendations apply:
- Only the operator and the patient should be in the room or vehicle in which the unit is installed when an exposure is made.
- When a photofluorographic unit is mounted in a vehicle appropriate steps must be taken to ensure that persons awaiting examination and personnel are protected from exposure to x-radiation. Such persons should be kept well clear of the vehicle when exposures are being made.
8.6 Recommendations for special radiological procedures
- Cystoscopic radiography, Hystero-salpingography, Needle Biopsies of the Lung, Transhepatic Needle Cholangiography, Pancreatography, and other similar procedures. In these procedures the radiologist and other personnel in the vicinity of the patient can be subjected to appreciable scattered radiation from the patient when the x-ray beam is on. Therefore, the radiologist and other personnel should wear protective glasses and clothing and should remain as far away from the patient as practicable, unless adequate scatter shields can be incorporated into the x-ray equipment. The protective devices (e.g., shielded panels, leaded drapes, extended collimator cones, etc.) provided with the x-ray equipment should be used whenever they do not interfere unduly with the diagnostic procedures. The smallest x-ray field consistent with the procedure should be used.
- Angiography. Angiography is potentially one of the sources of greatest exposure to personnel in diagnostic radiology, since it requires the presence of a considerable number of personnel close to the patient and involves fluoroscopy for extended periods of time and multiple radiographic exposures. For such procedures all personnel must be aware of the radiation hazards involved and make every effort to adhere to the recommendations below:
- Full use must be made of the protective devices provided with x-ray equipment (e.g., shielded panels, leaded drapes, bucky slot covers, etc.).
- All personnel must wear protective clothing and personnel dosimeters. Protective glasses should also be worn.
- All personnel who are not required to be immediately adjacent to the patient during the procedure must stand back as far as possible from the patient and, if at all possible, should stand behind a protective shield.
- Where indicated and feasible, special shields in addition to the protective devices provided with the machine should be used.
9. Procedures for Minimizing Dose to Patients
The largest single contributor of man-made radiation exposure to the population is medical diagnostic radiology. In total exposure, medical use of x-rays accounts for more than 90% of the total man-made radiation exposure to the general population. It is generally agreed by experts in the scientific community that medical x-ray exposure can be reduced substantially with no decrease in the value of medical information derived.
To accomplish this reduction, it is essential that patients not be subjected to unnecessary radiological examinations and, when radiological procedures are required, it is essential that patients be protected from excessive exposures during the examination.
The recommendations and procedures for the protection of the patient outlined in this section are directed toward the physician, the radiologist and the operator. They are intended to provide guidelines for elimination of unnecessary radiological procedures and for minimizing exposures to patients when radiological examinations are indicated. Included also are recommended upper limits on patient exposures for certain common radiographic examinations.
9.1 Guidelines for the prescription of diagnostic x-ray examinations
The medical practitioner is in a unique position to reduce unnecessary radiation exposure to the patient by ensuring that all examinations are clinically justified. The practitioner can achieve this by adhering, as much as possible, to certain basic recommendations. These are as follows:
- The prescription of an x-ray examination of a patient should only be based on a clinical evaluation of the patient and should be for the purpose of obtaining diagnostic information.
- Routine or screening examinations, such as for preemployment physical examinations, tuberculosis screening, mass mam-mographic screening, etc., in which there is no prior clinical evaluation of the patient, should not be prescribed.
- It should be determined whether there have been any previous x-ray examinations which would make further examination unnecessary, or allow for the ordering of an abbreviated examination. Relevant previous radiographs or reports should be examined along with a clinical evaluation of the patient.
- When a patient is transferred from one physician or hospital to another any relevant radiographs or reports should accompany the patient and should be reviewed by the consulting physician.
- When prescribing a radiological examination, the physician should specify precisely the clinical indications and information required.
- The number of radiographic views, required in an examination, should be kept to the minimum practicable, consistent with the clinical objectives of the examination.
- In prescribing x-ray examinations of pregnant or possibly pregnant women, full consideration should be taken of the consequences of foetal exposure.
- If a radiograph contains the required information, repeat exposures should not be prescribed simply because the radiograph may not be of the "best" diagnostic quality.
- Specialized studies should be undertaken only by, or in close collaboration with, a qualified radiologist.
- Medical practitioners should not operate x-ray equipment, or be responsible for the use of such equipment.
- A patient's clinical records should include details of x-ray examinations carried out.
9.2 Guidelines for radiography of pregnant women
Radiography of the pelvic area of a woman known to be pregnant simultaneously irradiates the patient's gonads and the whole body of the foetus. Irradiation of the unborn foetus increases the infant's risk of somatic effects and also increases the risk of genetic effects in subsequent offspring. Therefore, every effort should be made to avoid unnecessary irradiation of any woman known to be, or who might be pregnant. This is particularly important during the earliest stages of pregnancy when the potential for radiation damage of the rapidly dividing tissues is the greatest. Clearly, however, in spite of the possibility of radiation damage, if a radiological examination is required for the diagnosis or management of an urgent medical problem it must be done, irrespective of whether the patient may or may not be pregnant.
The following recommendations apply to x-ray examinations involving pregnant or potentially pregnant women:
- Radiography of the pelvic area in women of child-bearing age should be undertaken in the ten-day period following the onset of menstruation, since the risk of pregnancy is very small during this period.
- Only essential investigations should be taken in the case of pregnant or suspected pregnant women. Elective radiography of the abdominal and pelvic area in pregnant women must be avoided. ("Elective" is taken to mean an examination of the abdomen and pelvis which does not contribute to the diagnosis or treatment of a women in relation to her immediate illness.)
- Pregnant women or women who may be pregnant must not be accepted for chest photofluorographic (mass radiographic) examinations.
- When radiography of the pelvic area or abdomen is required, the exposure must be kept to the absolute minimum necessary and full use must be made of gonadal shielding and other protective shielding if the clinical objectives of the exmaination will not be compromised.
- If a radiographic examination of the foetus is required the prone position should be used. This has the effect of shielding the foetus from the softer x-rays and hence reducing the foetal dose.
- Radiography should not be used for the determination of abnormal presentations of the foetus, or for placenta localizations. Other techniques such as ultrasonography are better suited for this purpose.
- Radiography of the chest, extremities, etc., of a pregnant woman, for valid clinical reasons, should only be carried out using a well-collimated x-ray beam and with proper regard for shielding of the abdominal area.
9.3 Guidelines for radiographic examination of the breast (Mammography)
For mammographic x-ray equipment see "Radiation Protection in Mammography".
9.4 Radiological chest screening
- The use of mass radiological screening should only be considered in areas of high incidence of tuberculosis or in special population groups who may be particularly susceptible to lung disease. Selection of population groups for x-ray screening should be based upon the probability of discovering a significant number of cases of cardiopulmonary disease and on the availability of full follow-up facilities for individuals requiring treatment.
- Mass x-ray screening of the general population for tuberculosis and other chest diseases must not be carried out.
- Routine hospital admission chest x-rays should only be taken in identified high risk groups.
- Chest x-rays should not be required as a routine part of a pre-employment medical check-up or for admission to educational institutions.
- Since photofluorographic x-ray machines require a higher level of x-ray exposure than do convential radiographic machines to produce a film and since the yield of significant information is low, photofluorographic x-ray machines must not be used for chest examinations in place of conventional machines, and should not be used for mass screening when conventional machines are available.
9.5 Guidelines for carrying out x-ray examinations
Next to elimination of unnecessary x-ray examinations, the most significant factor in reducing patient exposure is ensuring that a necessary examination is performed with good technique. It is possible, for example, to obtain a series of diagnostically-acceptable radiographs and have the patient exposure vary widely because of choice of technique factors used. It is the responsibility of the operator and radiologist to be aware of this and to know how to carry out a prescribed examination with the lowest possible exposure to the patient.
The recommendations that follow are intended to provide guidance to the operator and radiologist in exercising their responsibility towards reduction of patient exposure.
9.5.1 General recommendations
- The operator must not perform any examination which has not been prescribed by a physician responsible for the patient.
- The exposure of the patient must be kept to the lowest practicable value, consistent with clinical objectives and without loss of essential diagnostic information. To achieve this, techniques appropriate to the equipment available should be used.
- Particular care, consistent with the recommendations of Section 9.2, must be taken when radiological examinations of pregnant or potentially pregnant women are carried out.
- The x-ray beam must be well-collimated to restrict it as much as is practicable to the area of diagnostic interest.
- The x-ray beam size must be limited to the size of the image receptor or smaller.
- The x-ray beam should not be directed towards the gonads unless it is absolutely essential, in which case gonad shielding must be used whenever the value of the examination is not impaired by such use. Guidelines on the use of gonal shielding are given in section 10 of this Code.
- Shielding should be used where appropriate and practicable to limit the exposure of body tissues. It is particularly important that special effort to be made to protect the blood-forming organs, gonads and thyroids of children.
- The target-to-skin distance should be as great as possible, consistent with good radiographic technique.
- For very young children, special devices should be employed to restrict movement.
- Full details of the radiological procedures carried out should be noted on the patient's clinical records.
9.5.2 Recommendations for radiographic procedures
- The edges of the x-ray beam should be seen on all x-ray films to ensure that no more than the desired area has been irradiated. The film size used should be as small as possible, consistent with the diagnostic objectives of the examination.
- Screen-type film should not be used for non-screen techniques because it is less sensitive to direct x-radiation than non-screen film.
- The fastest film or intensifying screen-film combination, consistent with diagnostically-acceptable results, should be used. When highest definition is not required a high-speed film-screen combination should be used. X-ray intensifying screens made from rare earth phosphors should be used where appropriate. Exposure reductions in excess of 50%, compared to conventional calcium tungstate systems, are possible using the rare earth-type intersifying screens and the films developed for use with such screens. These reductions result from greater x-ray absorption and increased conversion efficiencies of the new phosphors - the rare earth systems have a conversion efficiency of x-rays to light of 15-20%, compared to approximately 5% for calcium tungstate systems.
- To ensure that patient exposure is kept to a minimum, consistent with image quality, full advantage should be taken of a combination of techniques, such as:
- use of an antiscatter grid or air gap between the patient and the image receptor;
- use of the optimum focus-to-film distance appropriate to the examination;
- use of the highest kilovoltage which produces films of good quality;
- use of automatic exposure control devices designed to keep all exposures and repeat exposures to a minimum.
- The radiographer should see the films after processing in order to verify that the techniques being used are producing diagnostic quality films and that the x-ray equipment is functioning correctly.
- To avoid the necessity of retakes, it is particularly important before taking a long series of films that a single preliminary film of the series should be taken and processed to verify correctness of settings.
- While maximum permissible levels of exposure have been defined for radiation workers and the general population, no specific permissible levels have been recommended, to date, for patients undergoing diagnostic x-ray procedures. For patients the risk involved in the exposure must always be weighed against the medical requirement for accurate diagnosis. However, from data obtained in the Nationwide Evaluation of X-Ray Trends (N.E.X.T.) program, it is now feasible to recommend upper limits on patient skin entrance exposure, for routine, non-specialty, radiographic examinations. For a reference patient, having the anthropometrical characteristics shown in Table 1, the skin entrance exposure (without backscatter) should not exceed the values indicated in Table 2.
| Body Part | Thickness (cm) |
|---|---|
| Head (lateral) | 15 |
| Neck (A/P) | 13 |
| Chest (P/A) | 23 |
| Abdomen (A/P) | 23 |
| Foot (D/P) | 8 |
| Examination (Projection) | ESE (mR) |
|---|---|
| Chest (P/A) | 20 |
| Skull (Lateral) | 170 |
| Abdomen (A/P) | 450 |
| Cervical Spine (A/P) | 120 |
| Thoracic Spine (A/P) | 400 |
| Full Spine (A/P) | 250 |
| Lumbo-Sacral Spine (A/P) | 500 |
| Retrograde Pyelogram (A/P) | 500 |
| Feet (D/P) | 200 |
Note: In practice, it should be feasible to have actual skin entrance exposures substantially lower than these limits.
9.5.3 Recommendations for fluoroscopic procedures
- In view of the relatively high exposure that results from fluoros-copy, such procedures should only be carried out when an equivalent result cannot be obtained from radiography. Fluoros-copy must not be used as a substitute for radiography.
- Flurorscopy must only be carried out by, or under immediate supervision of, a radiologist or physician properly trained in fluoroscopic procedures.
- All fluoroscopic procedures should be carried out as rapidly as possible with the smallest practical x-ray field sizes.
- The exposure rate used in fluoroscopy should be as low as possible and must not exceed 10 roentgens (2.58 mC/kg) per minute at the position where the central axis of the x-ray beam enters the patient. With modern equipment, most fluoroscopic procedures can be readily carried out with exposure rates of less than 5 roentgens (1.29 mC/kg) per minute.
- Image intensification must be used in order to reduce patient exposure. Image intensifiers can significantly reduce both exposure rate and exposure time. However, the operator must monitor the x-ray tube current and voltage on equipment with automatic brightness control, since both can rise to high values without the knowledge of the operator, particularly if the gain of the intensifier is decreased.
- Television monitoring should be used in conjunction with the image intensifier.
- Mobile fluoroscopic equipment should only be used for examinations where it is impractical to transfer patients to a permanent fluoroscopic installation.
- Cinefluorography produces the highest patient doses in diagnostic radiology because the x-ray tube currents and potentials used are generally higher than those used in fluoroscopy. Therefore, this technique should not be used unless significant medical benefit is expected.
9.5.4 Recommendations for photofluorographic procedures
- The x-ray beam must be restricted to the area of the fluorescent screen and should be limited to the minimum size consistent with clinical requirements.
- Appropriate steps must be taken to exclude or shield the gonads from the direct beam.
- The performance of the equipment must be monitored routinely. Special emphasis should be placed on the speed of the optical systems used. These should be as fast as possible and should be replaced when noticeable deterioration in performance occurs.
9.5.5 Recommendations for mammography
For mammographic x-ray equipment see Safety Code 33 "Radiation Protection in Mammography".
9.5.6 Recommendations for special procedures
- Significant exposure to the patient's eyes can result during neurological examinations, such as carotid angiography. In projections where it does not interfere with the diagnostic information sought, eye shielding should be used.
- During cardiac catheterization and angiography significant exposure of the patient's thyroid gland can occur. Therefore, appropriate shielding should be used whenever possible.
10. Guidelines for Reduction of Gonad Dose
Ionizing radiation has the ability to produce gene mutations and chromosome aberrations in cells. When such effects occur in reproductive cells, undesirable mutations may be transmitted to subsequent generations. These genetic effects, once imparted to the genetic pool of a population, may take generations to be eliminated.
Medical x-ray diagnosis is, at present, the major contributor of gonadal radiation exposure to the population. By reducing the gonad dose to individual patients one can, in fact, make a significant contribution toward the reduction of the genetically significant dose to the population.
It is generally presumed that there is no threshold dose below which genetic effects cannot occur. Therefore, it is important that even small radiation exposures to be gonadal areas of patients be avoided, unless such exposures can be shown to be medically necessary.
10.1 Recommendations for reducing gonad dose to the patient
Radiologists and radiographers must pay special attention to four factors that are important for reducing gonad dose to the patient:
- Correct collimation of the x-ray beam. - It is not sufficient merely to limit the beam to the size of the image receptor. Care should be taken to further restrict the beam to the region of the patient's body that is of diagnostic interest. Irradiation of any part of the body outside that region contributes nothing to the objective of the examination and only increases dose both to the body and the gonads.
- Gonad shielding. - Appropriate use of specific area gonad shielding is strongly advised when:
- the gonads, of necessity, lie within, or are in close proximity to, the primary x-ray beam;
- the patient has reasonable reproductive potential; and
- clinical objectives will not be compromised.
- Appropriate selection of technique factors. - An appropriate selection of tube voltage, current and filtration is particularly important for diagnostic procedures in which the gonads lie within or near the primary x-ray beam. For example, in fluoros-copy, use of higher tube voltage and filtration and lower tube current will almost always reduce the gonad dose.
- Sensitivity of imaging systems. - The gonad dose is inversely proportional to the sensitivity of the imaging system. Thus, doubling the sensitivity halves the gonad dose; conversely, halving the sensitivity doubles the gonad dose. It is, therefore, very important to maintain the sensitivity of the imaging system at its optimum value and to be alert for any significant deterioration.
10.2 Recommendations for reducing gonad dose to operators
Adherence to the safe use procedures specified in Section 8 of this Safety Code will ensure that gonad dose to radiologists and radiographers is kept to the minimum practicable.
Appendix I - Recommended Dose Limits of Ionizing Radiation
For the purpose of radiation protection, individuals may be classified in one of two categories: those exposed to radiation from man-made sources during their work (radiation workers), and others. The recommended dose limits are given for both categories in the following table. These dose limits are based on the latest recommendations of the International Commission on Radiological Protection (ICRP) as specified in ICRP Publication 60.
It must be noted that the dose limits for radiation workers apply only to irradiation resulting directly from their occupation and do not include radiation exposure from other sources, such as medical diagnosis and background radiation.
| Applicable Body Organ or Tissue | Radiation Workers | Others |
|---|---|---|
| Whole body | 20 mSv | 1 mSv |
| Lens of the eye | 150 mSv | 15 mSv |
| Skin | 500 mSv | 50 mSv |
| Hands | 500 mSv | 50 mSv |
| All other organs | 500 mSv | 50 mSv |
- It is emphasized that any irradiation may involve some degree of risk and the levels suggested in this Appendix are maximum recommended values. All doses should be kept as low as reasonably achievable and any unnecessary radiation exposure must be avoided.
- ICRP does not recommend discrimination in the dose limits between men and women of reproductive capacity, if the dose is received at an approximately regular rate.
- For occupationally exposed women, once pregnancy has been declared, the foetus should be protected from x-ray exposure by applying a dose limit of 2 mSv to the surface of the woman's abdomen for the remainder of the pregnancy. For women who are also occupationally exposed to nuclear activities or substances, the Atomic Energy Control Board recommends an effective dose limit of 4 mSv for the remainder of the pregnancy from all the above sources.
- For technologists-in-training and students, the recommended dose limits for members of the public should apply.
- ICRP does not recommend different limits for individual organs. For occupationally exposed workers, ICRP believes that deterministic effects will be prevented by applying an equivalent dose limit of 500 mSv in a year to all tissues except the lens of the eye, for which it recommends a limit of 150 mSv in a year.
- For the skin, the equivalent dose is averaged over its whole area. In situations where deterministic effects are possible, the recommended equivalent dose limit for the skin is 500 mSv and is averaged over areas of no more than 1 cm2. This limit applies to the skin of the face and the hands.
- ICRP limits allow, in special circumstances, a higher value of dose than is allowed in a one year period, as long as the average dose over a five year period is not greater than the annual limit. This higher value is 50 mSv for occupationally exposed personnel. However, in mammography, there is no circumstance where such provision should apply.
- Some provincial jurisdictions may have recommended dose limits for some workers. Consultation with the proper agency may be required to determine the recommended dose limits in effect in a particular jurisdiction.
Appendix II - Shielding Guides for Diagnostic X-Ray Installations
To determine the shielding necessary for a diagnostic x-ray installation certain preliminary information is essential. The required thickness of shielding can be calculated using the formulae contained in this Appendix, in conjunction with Figures 1 to 3. In both instances answers to the following questions are required:
- What is the distance between the nearest point of the area to be shielded and the mean operational position of the x-ray tube?
- Is the area to be designated as a controlled or uncontrolled area, i.e. will the area be occupied by radiation workers (subject to the limit of 20 mSv per year) or non-radiation workers (subject to the limit of 1 mSv per year)?
- What will be/is the occupancy factor (T) of the area? The occupancy factor is defined as the time an area is normally occupied, expressed as a fraction of the working week. (If not accurately known, use Table 1).
- Will the intervening shield between the x-ray tube and the occupied area act as a primary or secondary protective barrier, i.e. will the barrier be required to attenuate the direct useful beam or stray (leakage and scattered) radiation only?
- What will the use factor (U) of the required protective barrier? The use factor is defined as the fraction of the operational time during which the useful beam will be/is directed at the barrier or area under consideration. (If not accurately known, use Table 2).
- What will be/is the workload (W) of the x-ray unit? The workload indicates the operational time of an x-ray machine expressed in terms of milliampere-minutes per week.
- What will be/is the maximum and average operating tube potential, and output?
The occupancy factors given in this table are for use as a guide in planning shielding for facilities where actual occupancy factor data are not available.
Table 1. Occupancy Factors
- T = 1 (Full occupancy)
- Control space, offices, nurses' stations, corridors and waiting spaces large enough to hold desks, wards and patients' rooms, darkrooms, workrooms and shops, rest rooms and lounge rooms routinely used by occupationally exposed personnel, living quarters, children's play areas, and occupied space in adjoining buildings.
- T = 1/4 (Partial occupancy)
- Corridors too narrow for desks, utility rooms, rest rooms and lounge rooms not used routinely by occupationally exposed personnel, elevators using operators, unattended parking lots, patients' dressing rooms.
- T = 1/16 (Occasional occupancy)
- Closets too small for future occupancy, toilets not used routinely by occupationally exposed personnel, stairways, automatic elevators, sidewalks, streets.
The use factors given in this table are for use as a guide in planning shielding for facilities where actual use factor data are not available.
Table 2. Use Factors for Primary Protective Barriers

- U = 1 (Full use)
- Floors of radiation rooms, walls containing avertical cassette holder; any other walls, doors orceiling areas routinely exposed to the useful beam.
- U = 1/4 (Partial use)
- Doors and wall areas of radiation rooms notroutinely exposed to the useful beam.
- U = 1/16 (Occasional use)
- Ceiling areas of radiation rooms not routinelyexposed to the useful beam.
Note: The use factor for secondary protective barriers is always taken to be 1

| Daily Patient Load |
Workload mA-min/week | |||
|---|---|---|---|---|
| #100 kVp |
125 kVp | 150 kVp | ||
| Chest (36 cm × 43 cm) (14" × 17") |
60 | 150 | - | - |
| Cystoscopy | 8 | 600 | - | - |
| Fluoroscop y includingspot filming | 24 | 1500 | 600 | 300 |
| Fluoroscopy withoutspot filming | 24 | 1000 | 400 | 200 |
| Fluoroscopy withimage intensificationincluding spot filming | 24 | 750 | 300 | 150 |
| General Radiography | 24 | 1000 | 400 | 200 |
| Special Procedures | 8 | 700 | 280 | 140 |
| Tube Potential |
Attenuation Material | |||
|---|---|---|---|---|
| Lead (mm) | Concrete (cm) | |||
| kVp | HVL | TVL | HVL | TVL |
| 50 | 0.06 | 0.17 | 0.43 | 1.5 |
| 70 | 0.17 | 0.52 | 0.84 | 2.8 |
| 85 | 0.22 | 0.43 | 1.25 | 4.5 |
| 100 | 0.27 | 0.88 | 1.60 | 5.3 |
| 125 | 0.28 | 0.93 | 2.00 | 6.6 |
| 150 | 0.30 | 0.99 | 2.24 | 7.4 |
| 200 | 0.52 | 1.70 | 2.50 | 8.4 |
| 250 | 0.88 | 2.90 | 2.80 | 9.4 |
| 300 | 1.47 | 4.80 | 3.10 | 10.4 |
| Thickness | Weight in Pounds for 1 Square Foot Section | ||
|---|---|---|---|
| Inches | Millimetre Equivalent |
Nominal Weight |
Actual Weight |
| 1/64 | 0.40 | 1 | 0.92 |
| 3/128 | 0.60 | 1 1/2 | 1.38 |
| 1/32 | 0.79 | 2 | 1.85 |
| 5/128 | 1.00 | 2.1/2 | 2.31 |
| 3/64 | 1.19 | 3 | 2.76 |
| 7/128 | 1.39 | 3 1/2 | 3.22 |
| - | 1.50 | - | 3.48 |
| 1/16 | 1.58 | 4 | 3.69 |
| 5/64 | 1.98 | 5 | 4.60 |
| 3/32 | 2.38 | 6 | 5.53 |
| - | 2.50 | - | 5.80 |
| - | 3.00 | - | 6.98 |
| 1/8 | 3.17 | 8 | 7.38 |
| 5/32 | 3.97 | 10 | 9.22 |
| 3/16 | 4.76 | 12 | 11.06 |
| 7/32 | 5.55 | 14 | 12.90 |
| 1/4 | 6.35 | 16 | 14.75 |
| 1/3 | 8.47 | 20 | 19.66 |
| 2/5 | 10.76 | 24 | 23.60 |
| 1/2 | 12.70 | 30 | 29.50 |
| 2/3 | 16.93 | 40 | 39.33 |
| 1 | 25.40 | 60 | 59.00 |
Notes:
- The density of commercially rolled lead is 11.36g.cm-3
- The commercial tolerances are ± 0.005 inches for lead up to 7/128 and ± 1/32 heavier sheets.
- Lead sheet less than 1/32 inch thick is frequently more expensive than heavier sheet in cost of material and cost of installation.
Figure 1. Attenuation in lead of x-rays generated at 50 to 300 kVp.
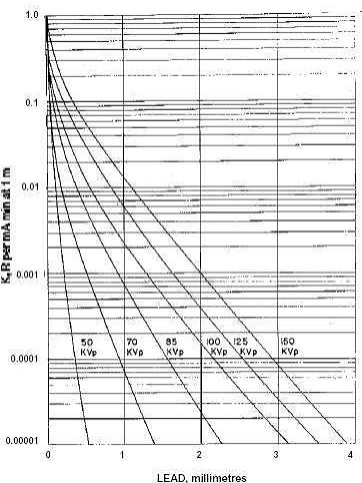
Figure 1. Attenuation in lead of x-rays generated at 50 to 300 kVp. (continued)
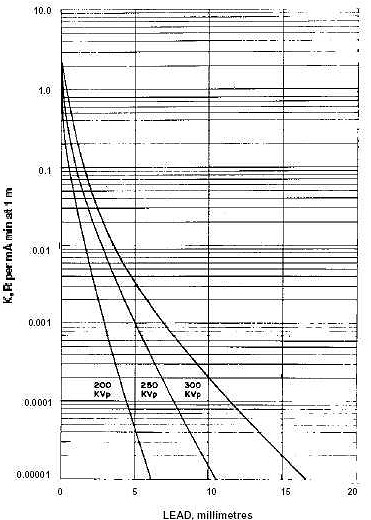
Figure 2. Attenuation in concrete of x-rays generated at 50 to 300 kVp.
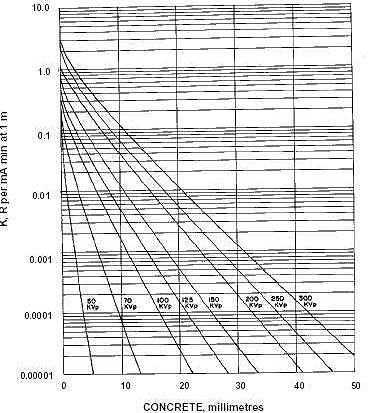
Formulae for calculation of shielding requirements
The thickness of shielding required can be calculated using the formulae given below. This method requires knowing the Workload W, in mA-min. per week, the Use Factor U, the occupancy factor T and the distance d, in metre, from the source to the occupied area. Typical values of T, U and W are given in Tables 1 to 3 respectively.
This method involves computation of an average value for the exposure per unit workload at unit distance, K, (in R/mA-min at 1 metre) and then using the curves shown in Figures 1 and 2 and to determine the thickness of lead or concrete required to reduce radiation levels to the required value.
1. Primary protective barriers
For primary protective barriers the value of K can be computed from the following equation:

where:
- P = maximum permissible weekly exposure rate expressed in R/week. or controlled areas P= 0.04 R/week; for uncontrolled areas P=0.002 R/week.
- d = distance in metres from the target to the primary area.
- W = workload in mA-min/week.
- U = use factor.
- T = occupancy factor.
- K = exposure per unit workload at unit distance, in R/mA-min at 1 metre.
Example: Determine the thickness of primary barrier required to protect a controlled area 3 metres from the target of a 150 kVp diagnostic unit having a weekly workload of 2000 mA-min. The wall has a use factor of 1 and the occupancy factor of the area beyond the wall is 1.
For this case,
- P = 0.1 R
- d = 3m
- W = 2000 mA-min.
- U = 1
- T = 1
Using equation (1),
The 150 kVp curves of Figures 1 and 2, respectively show that the required barrier thickness is 2.3 mm of lead or 20.5 cm of concrete.
2. Secondary protective barriers
Secondary protective barriers are required to provide shielding against both leakage and scattered radiation. Since these two types of radiation are of different qualities, it is necessary to determine the barrier thickness requirements for each separately. If the computed barrier thicknesses for leakage and scatter radiations are about the same, one half-value layer should be added to the larger one to obtain the total secondary barrier thickness. If the computed leakage and scattering thicknesses differ by at least three half-value layers, the larger of the two will be adequate.
2.1 Barrier against leakage radiation
To determine the barrier thickness required to protect against leakage radiation it is necessary to calculate the transmission factor, B, required to reduce the weekly exposure to P. For a diagnostic-type tube housing, where the maximum allowable leakage from the housing is 0.1 roentgen in an hour, the transmission factor is given by the following formula:

Figure 3. Relation between the transmission Factor B and the number of half-value layers, N, or tenth-value layers, n.
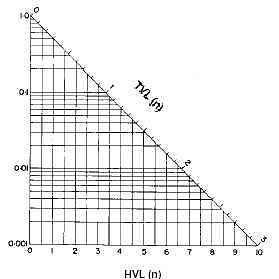
where:
- P = maximum permissible weekly exposure rate, expressed in R/week. For controlled areas P = 0.04 R/week; for uncontrolled areas P = 0.002 R/week.
- d = distance in metres from the tube housing to the secondary barrier.
- I = tube current in milliamperes.
- W = workload in mA-min/week.
- T = occupancy factor.
Having calculated the transmission factor, B, the barrier thickness, as a number of half-value layers, N, or tenth-value layers, n, can be determined from Figure 3. The required barrier thickness in mm of lead or cm of concrete can be obtained from Table 4, for the appropriate energy.
Example: Determine the thickness of barrier required to protect a controlled area 2 metres from the housing of a 200 kVp diagnostic unit having a weekly workload of 2000 mA-min. Assume that the tube operates at 5 mA and that the area in question has an occupancy factor of 1. For this case,
- P = 0.1 R
- d = 2 m
- W = 2000 mA-min
- T = 1
- I = 5 mA
Using equation (2),

From Figure 3, a transmission 0.6 corresponds to 0.13 TVL's or 0.7 HVL's. From Table 4 the HVL for 200 kVp is 0.52 mm lead or 2.5 cm concrete. Thus the required barrier thickness for protection against leakage radiation is
- (0.7 × 0.52) = 0.36 mm lead
- (0.7 × 2.5) = 1.75 cm concrete
2.2 Barrier against scatter radiation
Scattered radiation has a much lower exposure rate than that of the incident beam and usually is of lower energy. However, for x-ray machines operating below 500 kVp it is usually assumed that the scattered x-rays have the same barrier penetrating capability as the primary beam. For x-rays generated at kVp's of less than 500 kV, the value for K can be determined from the formula -

where:
- K = exposure per unit workload at 1 metre, expressed in R per mA-min at 1 m.
- P = maximum permissible exposure rate, expressed in R/week. For controlled areas P = 0.04 R/week. For uncontrolled areas, P = 0.002 R/week.
- d = distance in metres from the target to the scatterer.
- D = distance in metres from the scatterer to the secondary barrier.
- a = ratio of scattered to incident exposure (Tabulated in Table 6).
- W = workload in mA-min/week.
- T = occupancy factor.
- F = field area in cm2.
Having computed K from formula (3), the curves shown in Figures 1 and 2 are then used to determine the thickness of lead or concrete required in the same way as for the primary barrier.
If the barrier thickness for leakage and for scattered radiation differ by at least 1 TVL, the thicker of them will be adequate. If they differ by less than 1 TVL, 1 HVL should be added to the thicker one to obtain the required total secondary barrier thickness.
| Tube Potential KvP |
Scattering Angle (from Central Axis of Beam) | |||||
|---|---|---|---|---|---|---|
| 30° | 45° | 60° | 90° | 120° | 135° | |
| 50 | 0.0005 | 0.0002 | 0.00025 | 0.00035 | 0.0008 | 0.0010 |
| 70 | 0.00065 | 0.00035 | 0.00035 | 0.0005 | 0.0010 | 0.0013 |
| 85 | 0.0012 | 0.0007 | 0.0007 | 0.0009 | 0.0015 | 0.0017 |
| 100 | 0.0015 | 0.0012 | 0.0012 | 0.0013 | 0.0020 | 0.0022 |
| 125 | 0.0018 | 0.0015 | 0.0015 | 0.0015 | 0.0023 | 0.0025 |
| 150 | 0.0020 | 0.0016 | 0.0016 | 0.0016 | 0.0024 | 0.0026 |
| 200 | 0.0024 | 0.0020 | 0.0019 | 0.0019 | 0.0027 | 0.0028 |
| 250 | 0.0025 | 0.0021 | 0.0019 | 0.0019 | 0.0027 | 0.0028 |
| 300 | 0.0026 | 0.0022 | 0.0020 | 0.0019 | 0.0026 | 0.0028 |
Appendix IIIFootnote 1
A. Radiation emitting devices regulations for photofluorographic x-ray equipment
The Radiation Emitting Devices Regulations establishing standards of design, construction and functioning for photo-fluorographic x-ray equipment were passed by Governor-in-Council on November 3, 1977, and were published in the Canada Gazette Part II of November 23, 1977. These Regulations define photo-fluorographic equipment as "being x-ray generating appliances designed primarily for the examination of human cheses and the recording photographically in reduced size of the image produced on a fluoroscent screen."
The specific requirements of the Regulations are reproduced below.
"PART VI"
Photofluorographic x-ray equipment
Interpretation
1. In this Part, "attenuation" means a decrease in radiation intensity caused by absorption and scattering in a medium;
"coefficient of variation" means the ratio of the standard deviation to the mean value of a series of exposure measurements calculated by using the following equation:
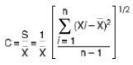
where
- C = coefficient of variation
- Xi = ith exposure measurement
- X = mean value of the exposure measurements
- n = number of exposure measurements;
"collimator" means a device or mechanism that limits the shape and size of the useful beam;
"effective focal spot" means the projection of the focal spot on the plane that is perpendicular to the x-ray beam axis and that passes through the centre of the focal spot;
"filter" means material placed in the useful beam to attenuate preferentially the lower energy radiations;
"focal spot" means the section at which the anode of an x-ray tube intercepts the electron beam;
"leakage radiation" means all radiation, except the useful beam, coming from within the housing of an energized x-ray generating tube;
"useful beam" means the radiation passing through the aperture, cone or collimator of the housing of an X-ray generating tube.
Standards of Design
2. Photofluorographic x-ray equipment shall be designed in such a way that all controls, meters, lights or other indicators are readily discernible and clearly labelled to indicate their function.
3. Photofluorographic x-ray equipment shall be designed to include the following safety features:
- on the control panel, the x-radiation warning sign described in section 6;
- a warning sign that:
- is in clear view of and readily discernible by the operator,
- is permanently affixed to the x-ray control panel,
- indicates the possibility of hazardous radiation emission when the equipment is in operation, and
- prohibits unauthorized use;
- electrical meters or other indicators that:
- are in clear view of the operator,
- are permanently affixed to the x-ray control panel, and
- show
- the preset operating kilovoltage of the equipment when used in the phototiming mode,
- the preset operating kilovoltage and milliamperage of the equipment when not used in the phototiming mode, and
- for battery-operated equipment, the state of charge of the battery;
- separate aural or visual indicators on the control panel that:
- are clearly discernible by the operator, and
- indicate when the x-ray machine is powered and when x-rays are being produced;
- where more than one x-ray tube is controlled by one control panel, it shall not be possible to energize more than one x-ray tube at the same time and there shall be:
- at each x-ray tube housing, a visible indicator that indicates when the tube is connected and ready to be energized,
- at the control panel, a visible indicator that indicates which tube is connected and ready to be energized, and
- at the normal position of the operator, visible indicators that provide the information required by subparagraph 3(c)(iii);
- an exposure switch on the control panel of a kind that requires continuous pressure by the operator to complete the circuit;
- a timer so designed that:
- when the production of x-rays is automatically terminated after a preset time interval:
- the preset time interval is clearly indicated,
- an exposure cannot be initiated with the timer set to zero or in the OFF position, and
- the minimum exposure time is not greater than 1/60 second,
- when the production of x-rays is automatically terminated after the integrated radiation exposure to a photocell or similar component behind the fluorescent screen is measured, there is incorporated in the timer's electrical circuitry:
- an aural or visual indicator that indicates clearly to the operator when the phototimer has failed to terminate the exposure, and
- a back-up or safety timer, with a maximum setting of one second, that will terminate the exposure in the event of phototimer failure, and
- when the production of x-rays is automatically terminated after a preset milliampere-second interval, the minimum milliampere-second interval is no greater than 1 milliampere-second;
- when the production of x-rays is automatically terminated after a preset time interval:
- a collimator that renders the machine inoperative if a part of the useful beam at the plane of the fluorescent screen extends beyond the useful portion of the fluorescent screen, and
- where the photofluorographic x-ray equipment is designed for a variable image receptor size and the target to fluorescent screen distance is variable:
- the collimator shall be adjustable, and give a rectangular be am,
- the alignment of the centre of the useful beam with the centre of the fluorescent screen shall be within 2 per cent of the target to the fluorescent screen distance,
- there shall be an apron (providing attenuation equivalent to 0.25 millimetre lead for a 100 kilovolts (peak) x-ray beam of half value layer 2.7 millimetres of aluminum) on a bracket attached to the bottom of the fluorescent screen mounting that can be swiveled into place to protect the patient's gonad area from the useful beam,
- means shall be provided to ensure that the axis of the x-ray beam can only be perpendicular to the plane of the fluorescent screen, and
- a light beam generator shall be incorporated into the collimator assembly:
- that visually defined the outline of the useful
beam, and - that does not permit a misalignment of the visually defined field with the x-ray field along either
the length or width of the x-ray field to exceed 2 per cent of the target to fluorescent screen distance, and
- that visually defined the outline of the useful
- where the photofluorographic x-ray equipment is designed for a constant image receptor size and the target to fluorescent screen distance is fixed:
- there shall be a shaped lower leaf or an apron on a bracket as described in clause 3(h)(i)(C) designed to protect the patient's gonad area from the useful beam,
- the alignment of the centre of the useful beam with the centre of the fluorescent screen shall be within 2 per cent of the target to fluorescent screen distance, and
- means shall be provided to ensure that the axis of the x-ray beam can only be perpendicular to the plane of the fluorescent screen;
- where the photofluorographic x-ray equipment is designed for a variable image receptor size and the target to fluorescent screen distance is variable:
- a filter that:
- is securely installed in the path of the useful beam, and
- provides attenuation, including inherent filtration, at least equivalent to that afforded by 2.5 millimetres of aluminum at 100 kilovolts (peak);
- a readily visible mark on the x-ray tube housing indicating, to within 2 millimetres, the location on the tube housing of the projection, at right angles to the beam axis, of the position of the focal spot on the target;
- an effective focal spot size of not greater than 1.5 square millimetres for units designed to operate at not more than 150 kilovolts (peak);
- a lock, on the x-ray machine control panel, of a type that requires the insertion of a key before x-rays can be produced and the removal thereof causes termination of the production of x-rays;
- an appliance or other means that:
- ensure that the machine is not able to be operated if the target to fluorescent screen distance is less than 100 centimetres, and
- clearly indicate the target to fluorescent screen distance to within 2 per cent;
- means that allow data to be recorded automatically on to each film;
- an interlock on the film holder mechanism that:
- prevents more than one film exposure being recorded without resetting, and
- prevents the same film frame receiving more than one exposure;
- means that prevent the use of films of size smaller than 70 millimetres × 70 millimetres; and
- on or near the power-input socket,a statement of power requirements at the maximum line current and, for battery operated units, a statement of charge-use frequency.
Standards of Construction
4. (1) Photofluorographic x-ray equipment shall be constructed in such a way that:
- the x-ray tube is securely fixed and correctly aligned within the tube housing;
- the x-ray tube head maintains its exposure position without drift, tipping or vibration during operation;
- the equipment, under normal conditions of use, functions in accordance with the standards described in section 5 for as long as the x-ray machine has its original components or replacement components recommended by the manufacturer;
- where there is provision for insertion of a grid, there is a holder containing a label that indicates the grid ratio of the grid used;
- mirrors, lenses or other optical components within the camera hood are securely fastened so that optical misalignment cannot occur with normal use;
- the camera hood, containing the whole optical system, does not admit light that can fog the film;
- any material between the film side of the fluorescent screen and the first optical component does not reduce the light intensity or alter the spectrum of the light emitted from the fluorescent screen;
- the front panel at the camera hood, located between the patient and the fluorescent screen, has less than 0.5 millimetre aluminum equivalence measured with an x-ray beam of potential 100 kilovolts (peak) with a half value layer of 2.7 millimetres of aluminum;
- the device bears a replaceable label mounted on the camera hood in clear view of the operator, indicating the type and date of insertion of the fluorescent screen; and
- when the recommended schedule of maintenance for the device is followed, the device will function in accordance with section 5 for the normal lifetime of the device.
(2) Photofluorographic x-ray equipment shall bear, on the tube housing and on the control panel, a permanent mark or label that:
- is clearly visible; and
- carries, with reference to the x-ray machine and x-ray tube, the name of the manufacturer, the model number, the serial number and the date and place of manufacture.
Standards of Functioning
5. Photofluorographic x-ray equipment when fully assembled for use shall function under normal conditions of use in such a way that:
- it is not possible to preset the filovoltage below 70 kilovolts (peak);
- the preset kilovoltage of the x-ray tube is maintained or is adjustable to within 3 kilovolts when the line voltage supply varies by plus or minus 10 per cent of its nominal value;
- for any combination of kilovoltage, current and time, the coefficient of variation of any ten consecutive radiation exposures, taken at the same distance within a time period of one hour, is not greter than 0.05;
- the entrance exposure to a sheet of 99.9 per cent pure copper of dimensions 45 centimetres × 45 centimetres × 1.41 millimetres, placed oveer the front panel, and phototimed with the exposure taken at 85 kilovolts (peak), does not exceed 50 milliroentgens per exposure to obtain at the centre of the film an optical density above gross fog of not less than 0.5;
- at any fixed kilovoltage, the average ratios of milliroentgen exposure to milliampere-seconds obtained at any two consecutive tube current settings do not differ by more than 0.10 times their sum, namely,
where and are the average milliroentgen per milliampere-second values obtained at each of two consecutive tube current settings;
- the leakage radiation from the x-ray tube assembly, when the machine is operated at any kilovoltage and current within the rating of the x-ray tube, is such that the average exposure rate of x-rays to any object having a 100 square centimetre cross-section and centred at 1 metre from the focal spot of the x-ray tube does not exceed 100 milliroentgens in one hour; and
- emission of ionizing radiation by any component other than the x-ray tube assembly, when the machine is operated at any kilo-voltage and current within the rating of the x-ray tube, is such that the average exposure rate of x-rays to any object having a 10 square centimetre cross-section and centred at 5 centimetres from any accessible surface of the device does not exceed 2.5 milliroentgens per hour.
Warning Sign
6. The x-radiation warning sign referred to in section 3 of this Part is a sign that:
- is shown in two contrasting colours;
- is clearly visible and identifiable from a distance of 1 metre;
- has no outer dimensions less than 2 centimetres;
- bears the words "CAUTION X-RAYS" and "ATTENTION RAYONS X"; and
- is designed in accordance with the following diagram:
B. Radiation emitting devices regulations for diagnostic x-ray equipment
The Radiation Emitting Devices Regulations establishing standards of design, construction and functioning for diagnostic x-ray equipment were passed by Governor-in-Council on December 18, 1980, and were published in the Canada Gazette Part II of January 14, 1981. These Regulations define diagnostic x-ray equipment as:
"being x-ray machines designed primarily for the examination of humans but excluding dental x-ray equipment, photofluoro-graphic chest x-ray equipment, radiation therapy simulators and computer assisted tomographic equipment."
The specific requirements of the Regulations are reproduced below.
"PART XII"
Diagnostic x-ray equipment
Interpretation
1. In this Part,
- "aluminum equivalent", in respect of a material under specified conditions, means the thickness of aluminum (Aluminum Association type 1100 alloy) that, under those conditions, affords the same attenuation, as that material;
- "attenuation" means a decrease in radiation intensity caused by absorption and scattering in a medium;
- "automatic exposure control" means a device that automatically controls one or more technique factors to obtain a required amount of radiation;
- "beam limiting device" means a device that restricts the dimensions of the useful beam;
- "coefficient of variation" means the ratio of the standard deviation to the mean value of a series of measurements calculated by using the following equation:
where- X = ith measurement
- = mean value of the measurements
- S = estimated standard deviation
- n = number of measurements
- c = the coefficient of variation;
- "control panel" means those parts of the x-ray control having switches, knobs push buttons or other controls necessary for manually setting the technique factors;
- "field emission equipment" means equipment that has an x-ray tube in which electron emission from the cathode is due solely to the actin of an electric field;
- "filter" means material placed in the useful beam to preferentially attenuate certain parts of the x-ray spectrum;
- "fluoroscopic imaging assembly" means the assembly of components comprising the device in which x-ray photons produce a fluoroscopic image and includes, as appropriate, the image receptor, image intensifier, equipment housings, interlocks and shielding;
- "general purpose radiographic x-ray machine" means any radiographic x-ray machine other than a machine designed for radiographic examinations of specific anatomical regions;
- "half-value layer" or "(HVL)" means the thickness of specified material that attenuates the beam of radiation to such an extent that the exposure rate is reduced to one-half of its original value;
- "image receptor" means a device that converts incident x-radiation into a visible image or into a form that can be made into a visible image by further transformation;
- "lead equivalent" in respect of a material under specified conditions, means the thickness of lead that, under those conditions, affords the same attenuation as that material;
- "leakage radiation" means any radiation: other than the useful beam, coming from within the tube housing assembly while the exposure switch or timer is activated, or produced when the exposure switch or timer is not activated;
- "light field" means the area of light in the plane of the image receptor that is directly outlined by the beam limiting device, the perimeter of which is the locus of points at which the illumination is one-fourth of the maximum in the plane of the image receptor;
- "mobile equipment" means transportable equipment designed to be moved from one location to another, between periods of use, on its own wheels or similar means of support;
- "stationary equipment" means equipment that is permanently installed in one location;
- "technique factors" means the conditions of operation of the diagnostic x-ray equipment and includes the peak tube potential inkilovolts, the tube current in milliamperes, the exposure time in seconds, the exposure in milliroentgen or combinations of those measurements;
- "tube housing assembly" means the x-ray tube housing with the x-ray tube installed;
- "useful beam" means the x-radiation passing through the tube housing port and the aperture of the beam limiting device when the exposure switch or timer is activated;
- "x-ray field" means the area of the intersection of the useful beam and any one of the set of planes parallel to and including the plane of the image receptor, the perimeter of which is the locus of points at which the exposure rate is one-fourth of the maximum in the intersection.
Standards of design and construction
General Requirements
2. Every diagnostic x-ray machine shall be designed and constructed in such a manner that when installed and maintained in accordance with the instructions referred to in paragraph 3(a), it functions in accordance with section 19 for as long as the device has its original components or has replacement components recommended by the manufacturer.
3. Every diagnostic x-ray machine shall be equipped with:
- installation and maintenance instructions supplied by the manufacturer of the device that, if followed by trained and experienced persons, will enable the device to comply with the requirements of these Regulations; and
- the following written information from the manufacturer with respect to the device:
- the maximum power requirements or maximum line current;
- the nominal focal spot size of the x-ray tube target and the method of its determination;
- adequate instructions for assembly and installation, including specification as to adequate line voltage and line impedance; and
- where the machine is battery-powered, the minimum state of charge necessary for operation.
4. Every diagnostic x-ray machine shall bear:
- on the external surface of the main x-ray control panel:
- a warning sign that
- includes a statement prohibiting unauthorized use, and
- indicates tht hazardous radiation emission is produced when the device is in operation;
- the x-radiation warning sign described in section 20;
- a readily discernible and clearly visible permanent mark or label that sets out with respect to the x-ray control and x-ray generator combination
- the name of the manufacturer,
- the model designation,
- the serial number,
- the date of manufacture, and
- the country of manufacture;
- a warning sign that
- on the external surface of the x-ray tube housing, a readily discernible and clearly visible permanent mark or label that sets out:
- with respect to the x-ray tube,
- the name of the manufacturer,
- the model designation,
- the serial number,
- the date of installation of the tube in the housing, and
- the country of manufacture; and
- with respect to the x-ray tube housing assembly, the minimum permanent filtration in the useful beam provided by the assembly, expressed as millimetres of aluminum equivalent at a specified peak tube potential;
- with respect to the x-ray tube,
- on the external surface of the x-ray tube housing:
- a permanent mark or marks that define or indicate to within ± 4 millimetres
- the location of the focal spot, in the case of single focus x-ray tubes, and
- the location of the point midway between the centres of the two focal spots, in the case of double focus x-ray tubes, and
- permanent marks or labels that indicate clearly the anode and cathode terminals; and
- a permanent mark or marks that define or indicate to within ± 4 millimetres
- on the external surface of any beam limiting device that adds filtration to the useful beam, a permanent mark or label that sets out, with respect to the beam limiting device, the total permanent filtration, expressed in millimetres of aluminum equivalence at a specified peak tube potential.
5. (1) Every diagnostic x-ray machine shall be designed and constructed in such a manner that:
- all marks, labels and signs required by these Regulations are securely fixed to the device and clearly visible;
- all controls, meters, lights or other indicators required by these Regulations are readily discernible and clearly labelled or marked as to function;
- the x-ray tube is securely fixed and correctly aligned within the tube housing;
- the x-ray tube housing maintains its required exposure position or movement without excessive drift or vibration during operation;
- where more than one x-ray tube is controlled by one control panel, except in the case of a diagnostic x-ray machine specifically designed for two-tube techniques,
- it shall not be possible to energize more than one x-ray tube at the same time, and
- there shall be
- on or near each tube housing, so as to be clearly visible to the operator, a visible indication when that x-ray tube is connected and ready to be energized, and
- at the control panel, a visible indication of which x-ray tube is connected and ready to be energized.
(2) Every diagnostic x-ray machine shall be designed and constructed to include:
- means to compensate for variations in x-ray tube potential caused by line voltage fluctuations, such that the device complies with the standard of functioning prescribed by subparagraph 19(b)(ii);
- either
- a visible or audible indicator that warns the operatoror
- a device that prevents x-rays from being produced when the variation in line voltage exceeds the limits prescribed by subparagraph 19(b)(ii);
- a control panel having the following safety features:
- separate warning lights, in clear view of the operaor, that respectively indicate
- when the control panel is energized and the device is ready to produce x-rays, and
- when x-rays are produced,
- where the device has adjustable technique factors, electrical meters or other indicators that enable the following factors, or any combination thereof, to be determined before the irradiation is initiated, that is to say,
- operating tube potential, in kilovolts,
- tube current, in milliamperes,
- the irradiation time, in seconds,
- where the device has non-adjustable technique factors, permanently affixed marks or labels, or electrical meters or other indicators that enable, at specified target-to-image receptor distances, the following factors, or any combination thereof, to be determined before the irradiation is initiated, that is to say.
- operating tube potential, in kilovolts,
- tube current, in milliamperes, and
- the irradiation time, in seconds, and
- where the device is battery-powered, a visual indicator that shows whether the battery is adequately charged for proper operation;
- separate warning lights, in clear view of the operaor, that respectively indicate
- an exposure switch, timer, or other mechanism to initiate and terminate the irradiation;
- an audible signal to indicate termination of an irradiation;
- radiation filters that:
- are permanently fixed to the exit port of the x-ray tube housing, or beam limiting device or both, and
- for a given x-ray tube potential, result in a half-value layer of the useful beam that is not less than the values given in or obtained by linear interpolation or extrapolation of the table to this section:
- keyed filter interlock switches or other positive means to ensure that necessary added filtration is in place in any tube housing assembly that:
- has permanent inherent filtration of 0.5 millimetre or less aluminum equivalence, and
- is designed to be operated with added filtration; and
- where the device is designed to move under remote control around or across a patient, provision for an emergency stop switch, the activation of which immediately terminates both the motion of the machine and the production of x-rays.
6. (1) An exposure switch provided with a diagnostic x-ray machine:
- shall be designed so that it requires continuous pressure by the operator to produce x-rays;
- where it is a footswitch, shall be so constructed that an unintended exposure does not occur if the switch is overturned;
- shall be located so that it cannot be conveniently operated outside a shielded area, except in the case of an exposure switch used in conjunction with mobile x-ray equipment, with spot-film devices, in fluoroscopy or in special procedures; and
- where it is part of a mobile machine, shall be equipped with a cable at least 3 metres long.
(2) A radiographic timing device provided with a diagnostic x-ray machine shall be designed so that:
- it terminates an irradiation on completion of any one of the following:
- a preset time interval,
- a preset product of current and time, (mAs), or
- a preset number of pulses;
- it permits the operator to terminate the irradiation at any time;
- it automatically resets to its original position or zero at the termination of the irradiation; and
- when it is at the zero or OFF position, an irradiation cannot be initiated.
(3) Permanent diaphragms, cones or other beam limiting devices provided with a diagnostic x-ray machine, as permitted by these Regulations, to collimate the useful beam shall afford the same degree of shielding as that required of the tube housing assembly.
Radiographic Machines
7. Every radiographic machine equipped with an automatic exposure control shall:
- be designed to include, on the control panel, a clear indication as to when the automatic exposure control mode of operation has been selected;
- where the x-ray tube operating potential is 50 kilovolts peak or greater, be designed and constructed to have minimum exposure time capability:
- in the case of a field emission machine rated for pulsed operation, equal to or less than the time interval equivalent of two pulses, or
- in the case of all other machines, equal to or less than 1/60 second or the time interval required to deliver 5 milliampere-seconds, whichever is the greater;
- be equipped with a means for ensuring that:
- where the x-ray tube potential is less than 50 kilovolts peak, the product of the x-ray tube current and the exposure time does not exceed 2000 milliampere-seconds per exposure,
- where the x-ray tube potential is 50 kilovolts peak or more,
- the product of the x-ray tube current and the exposure time does not exceed 600 milliampere-seconds, or
- the product of the peak x-ray tube potential, current and exposure time does not exceed 60 kilowatt-seconds per exposure;
- be equipped with a back-up timer having a maximum setting:
- in the case of a tomographic machine, of 10.0 seconds, and
- in the case of any other machine, of 3.0 seconds; and
- be designed:
- to include, on the control panel, a visible light indicator that will warn the operator, and
- to require manual resetting of the machine before another automatically timed exposure can be made, when termination of an automatically timed exposure occurs because the limits specified in paragraph (c) or (d) have been reached.
8. (1) Every stationary general purpose radiographic x-ray machine shall be designed and constructed to include:
- an x-ray beam limiting device that meets the requirements of sub-sections (2) and (3);
- a light localizer that visually defines the outline of the x-ray beam and that, at a distance of 100 centimetres, or at the maximum target-to-image receptor distance, whichever is less, gives an average illumination of not less than 100 lux;
- an adjustable light beam diaphragm or other mechanism that, when the axis of the x-ray beam is perpendicular to the plane of the image receptor, visually defines the outline of the x-ray field in accordance with the following requirements:
- misalignment of the visually defined field, with respect to the x-ray field, along either the length or width of the x-ray field shall not exceed 2 per cent of the target-to-image receptor distance, and
- the size of the x-ray field in the plane of the image receptor shall be indicated at selected distances and the indicated dimensions shall be accurate to within 2 per cent of the target-to-image receptor distance;
- a means that indicates when the axis of the useful x-ray beam is perpendicular to the plane of the image receptor;
- a means that enables the alignment of the centres of the x-ray field and the image receptor to within 2 per cent of the target to image receptor distance.
(2) An x-ray beam limiting device referred to in paragraph (1)(a) shall:
- provide for stepless adjustment of the size that does not exceed 5 centimetres by 5 centimetres at a target-to-image receptor distance of 100 centimetres;
- with the central axis of the useful x-ray beam perpendicular to the plane of the image receptor and with the image receptor inserted in a cassette tray or permanently mounted vertical cassette holder, either:
- provide, within 5 seconds of insertion of the image receptor, automatic adjustment of the x-ray field in the plane of the image receptor to
- the dimensions of the image receptor, or
- the dimensions of a preselected portion of the image receptor, where means are provided to preselect portions of the image receptor, or
- prevent x-ray production until the beam limiting device is manually adjusted so that the size of the useful beam in the plane of the image receptor is no greater than the image receptor size, with sufficient accuracy to ensure that the x-ray field does not exceed, in width or in length, the image receptor or the preselected portion of the image receptor, as the case may be, by more than 3 per cent of the target-to-image receptor distance and that the sume of the width and length of the x-ray field does not exceed the sum of the width and length of the image receptor or the preselected portion of the image receptor, as applicable, by more than 4 per cent; and
- provide, within 5 seconds of insertion of the image receptor, automatic adjustment of the x-ray field in the plane of the image receptor to
- include a means that allows the operator to adjust the dimensions of the x-ray field at the image receptor to smaller than those of the image receptor.
(3) Where a stationary general purpose radiographic x-ray machine equipped with positive beam limitation referred to in subsection (2), is equipped with means to enable the operator to bypass or override positive beam limitation in the event of system failure or in order to perform procedures that cannot be carried out in the positive beam limitation mode, such means shall:
- be activated by a key switch of a type that either prevents removal of the key while the bypass or override is in effect or causes automatic return of the equipment to the positive beam limitation mode of operation, when the key is removed;
- automatically reset to the positive beam limitation mode of operation after each time the image receptor is changed; and
- include a clearly visible and readily discernible warning light that indicates when the positive beam limitation bypass or override is in effect.
9. Every mobile radiographic x-ray machine shall be designed and constructed to include:
- an x-ray beam limiting device that provides stepless adjustment of the size of the x-ray field and a minimum field size that does not exceed 5 centimetres by 5 centimetres at a target-to-image receptor distance of 100 centimetres;
- a light localizer that visually defines the outline of the x-ray beam that, at a distance of 100 centimetres, or at the maximum target-to-image receptor distance,whichever is the lesser, shall give an average illumination of not less than 100 lux; and
- an adjustable light beam diaphragm or other mechanism that when the axis of the x-ray beam is perpendicular to the plane of the image receptor visually defines the outline of the x-ray field in accordance with the following requirements:
- misalignment of the visually defined field, with respect to the x-ray field, along either the length or width of the x-ray field, does not exceed 2 per cent of the target-to-image receptor distance, and
- the size of the x-ray field in the plane of the image receptor shall be indicated at selected distances and the indicated dimensions shall be accurate to within 2 per cent of the target-to-image receptor distance of 100 centimetres.
10. Every radiographic x-ray machine designed for use with only one size of image receptor and at a fixed target-to-image receptor distance shall be designed and constructed to include an x-ray beam limiting device that ensures that:
- the centre of the x-ray field is aligned with the centre of image receptor to within 2 per cent of the target-to-image receptor distance; and
- the x-ray field in the plane of the image receptor does not extend beyond any edge of the image receptor.
11. (1) Every radiographic x-ray machine designed specifically for mammography shall be designed and constructed to include:
- an x-ray beam limiting device that limits the size of the useful beam so that, at any target-to-image receptor distance specified for the machine, the x-ray field in the plane of the image receptor
- does not exceed the edge of the image receptor next to the chest wall of the patient by more than 2 per cent of the target-to-image receptor distance, and
- does not extend beyond any other edge of the image receptor; and
- an image receptor supporting device with sufficient shielding to ensure that the device complies with the standard of functioning prescribed by paragraph 19(e).
(2) Where a radiographic x-ray machine designed specifically for mammography is equipped with a removable fixed-aperture beam limiting device, the device shall bear on its external surface clearly visible permanent markings stating:
- the image receptor size; and
- the target-to-image receptor distance for which the device is designed.
12. Every general purpose radiographic x-ray machine equipped with special attachments for mammography shall be designed and constructed in such a manner that when the attachments are in service, the machine meets the requirements of section 11.
13. Every radiographic x-ray machine equipped with a spot-film device shall be designed and constructed to include positive field limitation between the x-ray beam perpendicular to the plane of the image receptor,
- the size of the x-ray field in the plane of the film is automatically adjusted to the size of that portion of the film that has been selected on the spot-film selector, except where that field size is smaller than that of the selected portion of the film;
- where the initial x-ray field size in the plane of the film is less than or equal to the selected portion of the film, field limitation is accomplished manually; and
- misalignment of the edges of the x-ray field with that portion of the film that has been selected on the spot-film selector, along the length or the width, does not exceed 3 per cent of the target-to-image receptor distance, and the sum of the misalignment along any two orthogonal dimensions does not exceed 4 per cent of the target-to-image receptor distance.
14. Every radiographic x-ray machine, other than a machine described in sections 8 to 13, shall be designed and constructed to include an x-ray beam limiting device so that, when the axis of the useful beam is perpendicular to the plane of the image receptor,
- the centre of the x-ray field is aligned with the centre of the image receptor to within 2 per cent of the target-to-image receptor distance; and
- the edges of the x-ray field do not extend beyond the corresponding edges of the image receptor by more than 2 per cent of the target-to-image receptor distance.
Fluoroscopic Machines
15. Every fluoroscopic x-ray machine shall be designed and constructed to include:
- an image intensification system that:
- includes a shielded protective barrier and shielding so that
- the entire cross section of the useful beam is intercepted within the protective barrier for any target-to-image distance;
- the useful beam and scattered radiation from the image intensifier are sufficiently attenuated before reaching the fluoroscopist;
- the fluoroscopy x-ray tube is not capable of producing x-rays unless the shielding is in place to intercept the useful beam, and
- the attenuation of the x-radiation transmitted through or scattered from the entrance window of the assembly is sufficient to ensure compliance with the standard of functioning prescribed by paragraph 19(k), and
- on a mobile machine is an integral part of the equipment or is interlocked in such a manner that its removal prevents x-rays from being produced,
- includes a shielded protective barrier and shielding so that
- a shield of at least 0.25 millimetres lead equivalent at 100 kilovolts peak, such as overlapping protective drapes, hinged or sliding panels, or other shielding to intercept scattered radiation that would otherwise reach the fluoroscopist;
- where it is stationary equipment, means to prevent the x-ray tube fromproducing x-rays unless there is an image receptor inplace to intercept the x-ray beam;
- that exposure switch to control x-ray production of a type that:
- requires continuous pressure by the operator for the entire period of any exposure, and
- during the recording of serial fluoroscopic images enables the operator to terminate the series at any time;
- an audible signal that:
- indicates completion of any preset time of use up to a maximum of 5 minutes, and
- whenever x-rays are produced after the preset time of use has expired, continues to sound until the timer is reset;
- positive field limitation so that, with the beam axis perpendicular to the plane of the image receptor, the misalignment of the edges of the x-ray field, with respect to the visible portion of the image receptor, along any dimension of the x-ray field in the plane of the image receptor, does not exceed 3 per cent of the target-to-image receptor distance and the sum of the excess length and the excess width does not exceed 4 per cent of the target-to-image receptor distance, and for rectangular x-ray fields used with circular image receptors, the error in alignment shall be determined along the length and width dimensions of the x-ray field that pass through the centre of the visible area of the image receptor.
- electrical meters orother visual indicators, on the control panel that provide a continuous indication of x-ray tube potential (in kilovolts) and current (in milliamperes); and
- means to limit the target-to-skin distance to not less than
- 30 centimetres, in the case of mobile machines,
- 38 centimetres, in the case of stationary machines,and
- 20 centimetres in the case of an image-intensified machine designed for special applications that would be impossible at the minimum target-to-skin distances specified in sub-paragraphs (i) and (ii).
16. Every fluoroscopic x-ray machine designed specifically for cinefluorography shall be equipped with electrical meters or other visual indicators on the control panel that provide a continuous indication of x-ray tube potential (in kilovolts) and current (in milliamperes).
17. Where an optional high level control is provided ina fluoroscopic x-ray machine, the control shall require:
- special means to activate it;
- continuous manual activation by the fluoroscopist for its operation; and
- a continuous signal audible to the fluoroscopist to indicate that the high level control is being employed.
Limits on Material Between Patient and Image Receptor
18. (1) Subject to subsections (2) and (3), the aluminum equivalent of each of the items listed in column I of the table to this section that is used between the patient and the image receptor in any diagnostic x-ray equipment shall not exceed the limits shown therefor in column II of the table, as determined using an x-ray beam having a potential of 100 kilovolts peak and a half-value layer of 2.7 millimetres of aluminum.
(2) The total aluminum equivalent of all the material, other than the screen and its associated mechanical support panel or grids, that is present between the patient and the image receptor shall not exceed 3.5 millimetres.
(3) Commencing one year from the date of the coming into force of these Regulations, the total aluminum equivalent of all the material, other than the screen or grids, that is present between the patient and the image receptor shall not exceed 3.5 millimetres.
| Column I Item |
Column II Aluminium Equivalence (millimetres) |
|---|---|
| Front panel(s) of cassette holder (total of all) | 1.0 |
| Front panel(s) of film changer (total of all) | 1.0 |
| Stationary table top | 1.0 |
| Movable tabel top (including stationary sub-top) | 1.5 |
| Cradle | 2.0 |
Standards of Functioning
19. Every diagnostic x-ray machine when fully assembled for use shall function under normal conditions of use in such a manner that:
- for any given combination of x-ray tube potential (in kilovolts peak), tube current (in milliamperes), exposure time (in seconds) of not less than 0.1 second, or for selected radiation exposure to the image receptor (in milliroentgen)
- the coefficient of variation of any ten consecutive radiation exposure measurements, taken at the same source-to-detector distance within a time period of one hour, is no greater than 0.05, and
- each of the ten radiation exposures measured is within 15 per cent of the mean value of the ten measurements, when the line voltage for each measurement is within plus or minus 1 per cent of the mean value for all of the measurements,
- for any selected setting of the peak x-ray tube potential:
- the actual peak kilovoltage corresponds to the selected value to within plus or minus 5 per cent of the selected value, and
- for a line voltage variation of plus or minus 7 per cent of its nominal value, the peak kilovoltage, prior to initiation of an exposure, is capable of being maintained to within plus or minus 5 per cent of the selected value.
- the radiographic timer or automatic exposure control:
- can be set to control irradiations as short as 1/60 second or 5 milliampere-seconds, whichever is greater;
- at each setting is accurate to 1/60 second or 7 per cent of that setting, whichever is greater, and
- at each setting complies with the reproducibility requirements of paragraph (a);
- for any fixed indicated value of x-ray tube potential (in kilovolts peak), within the range of values of operating tube potential specified for the equipment, the average ratios of exposure (in milliroentgen) to the product of the tube current and exposure time (in milliampere-seconds) obtained at any two consecutive tube current settings do not differ by more than 0.10 times their sum, that is, to say
where and are the average mR/mAs values obtained at each of two consecutive tube current settings. - the transmission of the primary x-ray beam through the mam-mographic image receptor support device referred to in paragraph 11(1)(b) results, with the equipment operated:
- in the mammographic mode;
- at the minimum target-to-image receptor distance for which it is designed, and
- at the maximum rated peak x-ray tube potential and maximum rated tube current-exposure time product for that peak tube potential, in a radiation exposure, averaged over a detection area of 100 square centimetres, with no linear dimension greater than 20 centimetres and centred at 5 centimetres from any accessible surface beyond the plane of the support device, that does not exceed 0.1 milliroentgen for each activation of the x-ray tube;
- where it is a fluoroscopic x-ray machine
- without automatic exposure rate control, at the shortest target-to-skin distance specified for the equipment, no combination of x-ray tube potential and current results in an entrance exposure rate, where the centre of the useful beam enters the patient, of greater than
- 5 roentgen per minute except during recording of fluoroscopic images, or
- where an optional high level control is provided, 10 roentgen per minute with the high level control activated,
- with automatic exposure rate control, at the shortest target-to-skin distance specified for the equipment, no combination of x-ray tube potential and current results in an entrance exposure rate, where the centre of the useful beam enters the patient, of greater than
- 10 roentgen per minute except during recording of fluoroscopic images, or
- where an optional high level control is provided, 5 roentgen per minute unless the high level control is activated;
- without automatic exposure rate control, at the shortest target-to-skin distance specified for the equipment, no combination of x-ray tube potential and current results in an entrance exposure rate, where the centre of the useful beam enters the patient, of greater than
- subject to paragraph (h), the exposure rate fromleakage radiation averaged over a detection area of 100 square centimetres with no linear dimensions greater than 20 centimetres and located at a distance of 1 metre in any direction from the focal spot of the x-ray tube does not exceed 0.1 per cent of the exposure rate at the same distance along the central axis of the useful beam;
- where it is a radiographic x-ray machine designed specifically for mammography, the exposure rate from leakage radiation averaged over a detection area of 100 square centimetres with no linear dimensions greater than 20 centimetres, located at 5 centimetres from any point on the external surface of the x-ray tube housing does not exceed 2 milliroentgen per hour;
- where there is a possibility of a high voltage appearing across the x-ray tube without the exposure control or timer activated, the emission of x-radiation from the x-ray tube, with the beam limiting device fully open, does not result in an exposure rate, averaged over a detection area of 100 square centimetres and centred at 5 centimetres from any accessible external surface of the x-ray tube housing, in excess of 2 milliroentgen per hour;
- emission of ionizing radiation by any component other than the x-ray tube housing assembly, when the x-ray tube is operated at its maximum rated tube potential and current, does not result in an exposure rate averaged over a detection area of 100 square centimetres with no linear dimension greater than 20 centimetres and centred at 5 centimetres from any accessible surface of the component, that exceeds 2 milliroentgen per hour, when averaged over a period of 1 hour; and
- when it is used for fluoroscopy, the exposure rate, averaged over a detection area of 100 square centimetres with no linear dimension greater than 20 centimetres, of x-radiation due to transmission of the useful beam through or scattering from the window of the fluoroscopic imaging assembly, does not exceed 2 milli-roentgen per hour at 10 centimetres behind the plane of the image receptor, for each roentgen per minute of entrance exposure rate.
Warning Sign Specifications
20. The x-radiation warning sign referred to in section 4 of this Part is a sign that:
- is shown in two contrasting colours;
- is clearly visible and identifiable from a distance of 1 metre;
- has no outer dimensions less than 2 centimetres;
- bears the words "CAUTION X-RAYS" and "ATTENTION RAYONS X"; and
- is designed in accordance with the following diagram:
Appendix IV - Shielding Guides for Storage of Radiographic Film
To reduce the radiation level to the film to 0.2 mR for weekly workloads of:
- 1000 mA-min at 100 kVp
- 400 mA-min at 125 kVp
- 200 mA-min at 150 kVp
| Storage Time | 7ft (2.1m) | 10ft. (3.1m) | 14ft (4.3m) | 20ft. (6.1m) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lead | Con- crete |
Lead | Con- crete |
Lead | Con- crete |
Lead | Con- crete |
|||||
| mm | in | in | mm | in | in | mm | in | in | mm | in | in | |
| For primary barriers | ||||||||||||
| 1 hour | 2.0 | 3/32 | 6.1 | 1.8 | 1/16 | 5.4 | 1.5 | 1/16 | 4.8 | 1.3 | 1/16 | 4.1 |
| 1 day | 2.7 | 3/32 | 8.0 | 2.5 | 3/32 | 7.4 | 2.2 | 3/32 | 6.7 | 2.0 | 3/32 | 6.0 |
| 1 week | 3.4 | 1/8 | 9.6 | 3.1 | 1/8 | 8.9 | 2.8 | 1/8 | 8.2 | 2.6 | 3/32 | 7.6 |
| 1 month | 3.8 | 5/32 | 10.9 | 3.6 | 5/32 | 10.2 | 3.3 | 1/8 | 9.6 | 3.1 | 1/8 | 8.9 |
| For secondary barriers | ||||||||||||
| 1 hour | 0.3 | - | 1.1 | 0.2 | - | 0.6 | - | - | - | - | - | - |
| 1 day | 0.9 | 1/32 | 2.9 | 0.7 | 1/32 | 2.3 | 0.5 | - | 1.7 | 0.3 | - | 1.1 |
| 1 week | 1.4 | 1/16 | 4.4 | 1.2 | 1/16 | 3.7 | 1.0 | 1/32 | 3.1 | 0.7 | 1/32 | 2.4 |
| 1 month | 1.9 | 1/16 | 5.7 | 1.6 | 1/16 | 5.0 | 1.4 | 1/16 | 4.4 | 1.2 | 1/16 | 3.7 |
Appendix V - Agencies Responsible for Radiation Safety of Medical X-Ray Installations
Alberta
Director
Radiation Health Branch
Occupational Health and Safety Division
Workers' Health, Safety & Compensation
2nd Floor, Oxbridge Place
9820-106th Street
Edmonton, Alberta
T5K 2J6
British Columbia
Worker's Compensation Board of British Columbia
P.O. Box 5350
Stn Terminal
Vancouver, British Columbia
V5Z 1E2
Manitoba
Head
Physics Department
Radiation Protection Section
Manitoba Cancer Treatment & Research Foundation
700 Bannatyne Avenue
Winnipeg, Manitoba
R3E 0V9
New Brunswick
Senior Radiation Physicist
New Brunswick Department of Health
P.O Box 6000
Fredericton, New Brunswick
E3B 5H1
Newfoundland
Director
Radiation Protection Officer
Division of Occupational Health and Safety
Department of Labour and Manpower
Beothuck Building, Crosbie Place
St. John's, Newfoundland
A1C 5T7
Northwest Territories
Chief
Health Programs and Standards
Department of Health
Government of the Northwest Territories
Yellowknife, N.W.T.
X1A 2N1
Nova Scotia
Radiation Health Officer
Department of Health
7th Floor, Joseph Howe Building
P.O. Box 488
Halifax, Nova Scotia
B3J 2R8
Ontario
Chief X-Ray
Inspection Service Ontario
Ministry of Health
7 Overlea Boulevard,
3rd Floor
Toronto, Ontario
M4H 1A8
Prince Edward Island
Chairman
Hospital Services Commission of Prince Edward Island
P.O. Box 4500
Charlottetown, P.E.I.
C1A 7P4
Québec
Responsable de la radioprotection
Service de l'agrément des laboratoires privés
Ministère des affaires sociales
1075, chemin Ste-Foy
Québec, Québec
G1S 2M1
Appendix VI Radiation Measurement Units-International (SI) System
EXPOSURE
The COULOMB/KILOGRAM (C/kg) replaces the ROENTGEN (R) as the unit of exposure. The relationship between the two units is as follows:
1 C/kg ~ 3876 R
1 R ~ 258 µ C/kg
1 mC/kg ~ 3876 mR
1 mR ~ 258 nC/kg
Note:
- m = milli = 10-3;
- µ = micro = 10-6;
- n = nano = 10-9
ABSORBED DOSE
The GRAY (Gy) replaces the RAD (rad) as the unit of absorbed dose. The relationship between the two units is as follows:
1 Gy = 100 rad
1 rad = 10 mGy
1 mGy = 100 mrad
1 mrad = 10 µGy
DOSE EQUIVALENT
The SIEVERT (Sv) replaces the REM (rem) as the unit of DOSE EQUIVALENT. The relationship between the two units is as follows:
1 Sv = 100 rem
1 rem = 10 mSv
1 mSv = 100 mrem
1 mrem = 10 µSv
Bibliography
Further details on the topics covered in this Safety Code may be obtained from the references listed below.
- "Protection of the Patient in X-Ray Diagnosis", ICRP Publication 16, (1969).
- "Recommendations of the International Commission on Radiological Protection", ICRP Publication 26, Annals of the ICRP, Volume 1, No. 3, (1977).
- "Structural Shielding Design and Evaluation For Medical Use of X-Rays and Gamma Rays of Energies up to 10 MeV", National Council on Radiation Protection and Measurements, NCRP Report No. 49, (1976).
- "Medical Radiation Exposure of Pregnant and Potentially Pregnant Women", National Council on Radiation Protection and Measurements, NCRP Report No. 54, (1977).
- "The Effects on Populations of Exposure to Low Levels of Ionizing Radiation", National Academy of Sciences, National Research Council, Washington, D.C. (1972).