
Streamlined IME Panel Member Guide
- An introduction to the streamlined immigration medical examination process
- Section 1: general guide for panel members
- Your work as a panel member
- Ethical conduct and conflicts of interest
- Administrative instructions
- Quality assurance, incidents and complaints
- The Streamlined Immigration Medical Examination
- General information about the Streamlined IME
- How do I determine what examinations are required for clients undergoing a Streamlined IME?
- Verifying an applicant’s identity and preventing fraud
- Required documents
- If an applicant does not have approved identification
- If you have an identity concern
- Client Declaration and Notice
- Medical Report – Client Biodata and Summary - Streamlined (IMM 1020)
- Upfront Medical Report – Client Biodata and Summary (IMM 1017B Upfront)
- Medical Report (514 Medical examination)
- Resettlement Needs Assessment (Exam 948 in eMedical)
- Pregnant Client – X-Ray Deferred (IMM 5733)
- Additional forms for the Streamlined IME
- Additional information for submitting IME forms
- Panel members who work in Canada
- The Interim Federal Health Program (IFHP)
- Section 2: supplementary information
- Instructions for completing paper-based streamlined IMES
- General information about the Streamlined IME
- How do I determine what examinations are required?
- Verifying an applicant’s identity
- If you have an identity concern
- Required documents
- If an applicant does not have approved identification
- Client Consent and Declaration
- Medical Report: Client Biodata and Summary - Streamlined (IMM 1020)
- Excessive demand exempt (EDE) applicants
- Non-EDE applicants
- Refugee overseas applicants
- Upfront Medical – Client Biodata and Summary (IMM 1017B Upfront)
- Medical Report (IMM 5420)
- Resettlement Needs Assessment (IMM 5544)
- Pregnant Client – X-Ray Deferred (IMM 5733)
- Additional Forms for paper-based IMEs
- Additional information for submitting forms
- Legislation related to the immigration medical examination
- The Immigration and Refugee Protection Act
- The Privacy Act
- The Access to Information Act
- Acronyms, initialisms and definitions
- Instructions for completing paper-based streamlined IMES
- Section 3: Appendices
An Introduction to the Streamlined Immigration Medical Examination Process
A program administered by IRCC
Immigration, Refugees, and Citizenship Canada’s (IRCC) Migration Health Branch administers and delivers Canada’s medical screening program for people who want to visit or immigrate to Canada.
If someone applies to stay in Canada, they need to meet a set of criteria, including medical standards for admissibility. To be considered admissible, an applicant must not create a danger to public health or public safety, and must not create excessive demand on Canada’s healthcare or social services.
IRCC has developed a Streamlined IME, a lighter-touch health screening exam compared to the ‘standard’ IME. The Streamlined IME has been developed to support operational needs and to improve client service for applicants who meet certain eligibility criteria.
Who needs an IME?
Many criteria go into the decision about whether someone coming to Canada needs an IME, including how long they plan to stay, their type of visa application and where they have lived or travelled. In most situations, migration officers determine who requires an IME before the applicant sees a panel physician.
In the context of the Streamlined IME, applicants who meet certain eligibility criteria will be issued instructions to undergo a Streamlined IME by an IRCC Migration Officer. Clients are instructed to let their panel physician know if they were issued a Streamlined IME upon booking their appointment. Please ensure to check the client’s file in eMedical to verify the type of IME they are required to undergo.
What this guide tells you
This guide provides comprehensive information about the Streamlined IME for panel members, including:
- the general responsibilities of your work, including your ethical and professional responsibilities
- how to conduct a Streamlined IME, including what examinations to do, the forms you will need, and how to administrate the paperwork
- how to use the Interim Federal Health Program (medical insurance)
- a reminder about the legislation that applies to conducting Streamlined IMEs
Leveraging eMedical
As with the ‘standard’ IME, panel members will be responsible for completing and transmitting Streamlined IMEs using eMedical. The ‘standard’ and Streamlined IME differ in eMedical, as the Streamlined IME has fewer health screening requirements. In eMedical, the Streamlined IME will be referred to as module 514, while the ‘standard’ IME will continue to be module 501.
Panel members will not need to decide which clients receive a ‘standard’ or Streamlined IME. IRCC will make that decision and it will be communicated to panel members via eMedical and on the Medical Report – Client Biodata and Summary – Streamlined (IMM 1020) form.
A small number of panel members do not have access to eMedical. Those who work with a paper-based system will find key information about how to conduct a Streamlined IME in Part 2 of this guide.
Check back for new information
The processes for medically screening immigrants, and the immigration process itself, are subject to change. IRCC will update this guide as needed, and the updates will override the text they replace. Your RMO will also send you new information as it becomes available.
Please consult our list of acronyms, initialisms and definitions for clarification as you read this guide.
Visit IRCC’s website for more information on Canada’s immigration program.
Section 1: General guide for panel members
Your work as a panel member
For information about becoming a panel member, getting your unique identifier and login, designation, eMedical user identification, and detailed responsibilities to be carried out by panel members, please consult the information in the Canadian Panel Member Guide to Immigration Medical Examinations 2020.
A summary of your responsibilities
Panel members are authorized to perform Streamlined IMEs, arrange for certain testing if authorized by an RMO, and complete IME forms. You do not have the authority to assess or determine whether the medical conditions of applicants are grounds for health admissibility to Canada. More specifically, you may not give applicants an opinion on their medical admissibility. That decision rests with Canadian migration officers.
Panel members performing Streamlined IMEs should ensure that they meet IRCC’s performance service standards and that there are no conflicts of interest in providing services. You are also required to help prevent fraud and abuse of Canada’s immigration laws, submit to performance evaluations, follow proper procedures for absences, and use English or French in your communications with IRCC.
For all applicants, the Canadian Streamlined IME will include an examination by a panel member and a medical assessment by IRCC. Sometimes, applicants can be asked to undergo further medical evaluation to ensure compliance with Canada’s Immigration and Refugee Protection Regulations.
The assessment of whether or not a client is admissible on health grounds is largely based on findings reported in the Streamlined IME, but it can include information unknown to panel members.
In parallel to the Immigration Medical Examination process, panel members are to provide appropriate and timely advice to the client when they discover a serious medical condition not known to the client. In doing so, panel members are to uphold professional and ethical standards by referring the client back to their usual treating physician or to an appropriate specialist upon request.
Here are your general responsibilities, organized according to your role in the IME process.
All panel members
As a panel member, you must do the following:
- Stay familiar with the latest version of this guide and all associated administrative and IME instructions.
- Follow instructions about verifying the applicant’s identity.
- Hold valid professional registration and licensing issued by local or national regulatory authorities and ensure your RMO has a copy, along with an official translation in either English or French, if it is not in one of Canada’s official languages.
- Maintain valid professional registration and licensing throughout the relationship with IRCC. If your license or other certification expires, it is your responsibility to send updated documents to your RMO promptly. If you fail to do so, you could be removed from the Panel Network.
- Keep all immigration medical information in your possession confidential and store it securely.
- Ensure that the fees you charge for immigration medical services fairly represent the services you perform, and that they comply with local guidelines or those of a medical association or group.
- Ensure that a list of fees and charges for the IME and related expenses is either posted in your clinic, office or website, or emailed to applicants before their examination:
- The list should include fees for required radiological and laboratory investigations, postage or courier charges, and other services.
- Any special fees for groups or large families should also be listed.
- Copies should be available for applicants on request.
- All applicants should receive a receipt for services.
- Ensure that all panel clinic staff members who you supervise are aware of the requirements and standards for the IME and its procedures, and that they understand your role and obligations.
- Always offer to have a chaperone present for an IME. If a chaperone is declined, this should be documented.
- Ensure that individual and clinic contact information is up to date. eMedical users must keep their contact information updated in the system and also alert their RMO when they make changes. Those who use paper-based forms must inform their RMO of changes in contact information.
- Ensure high-quality work by all professionals involved in conducting IMEs, including staff members and specialist consultants.
Panel physicians
As a panel physician you must do the following:
- Get the applicant’s consent and declaration by having them fill out IRCC’s Client Consent and Declaration Form.
- Follow your country’s public health regulations for notifying authorities when you discover a public health concern, such as active tuberculosis, untreated syphilis, human immunodeficiency virus (HIV) or acute viral hepatitis.
- Conduct a complete, age-appropriate IME according to instructions provided in this guide as well as in IRCC’s technical instructions (TIs) You will find links for each TI in Appendix IV.
- Coordinate all the IME results and the IME report to be submitted to the RMO, including chest x-rays, as well as reports from other consultants and specialists when required by your RMO.
- Inform your RMO as soon as possible when you suspect fraud, misrepresentation or non-compliance.
- You must ensure that the laboratory you use:
- is aware of the requirements and standards for the Canadian IME
- is registered and licensed by a local or national regulatory authority, and can provide proof of that when the RMO requests
- has appropriate quality control procedures in place
- follows instructions for verifying the applicant’s identity
- complies with administrative requirements
- completes the Laboratory Requisition and Report section of the Medical Report (IMM 5420 accurately
- prevents fraudulent substitution
Chief radiologists
As a chief radiologist, you must do the following:
- Monitor the performance of all nominated radiologists and their staff, and work with IRCC to resolve cases or issues of concern related to nominated radiologists. (A nominated radiologist is a licensed radiologist nominated by the chief radiologist to perform, grade and submit chest x-rays for Canada’s IMEs.)
- Ensure that every nominated radiologist undertaking Canadian immigration radiological examinations is qualified as a specialist in radiology, that their license is valid, and that they are registered to work in the country where they practice.
- Provide your RMO with the names, dates of birth, genders and unique email addresses of each of your nominated radiologists.
- Add your nominated radiologists to the clinic profile in eMedical and notify IRCC of these changes so that we can grant them access to submit Canadian cases.
- Supervise all nominated radiologists – including ensuring accuracy and quality control of the Chest X-Ray Requisition section of the Medical Report (IMM 5420).
- Ensure that all nominated radiologists complete IRCC’s training regime.
- Ensure that radiological examinations are conducted at the agreed site(s).
- Implement and monitor the procedures for checking the identity of applicants.
- Circulate any communications from RMOs and IRCC to nominated radiologists and their staff.
- Advise IRCC of any anticipated interruption of service and any change related to the list of nominated radiologists. This includes absences, changes to staff, clinic contact details, capabilities and other working arrangements that could affect service.
- Ensure that nominated radiologists conduct chest x-rays (routine posterior-anterior view for applicants 11 years old and older) according to the instructions laid out in this guide – and that they adhere to all procedures in this guide.
- Ensure the quality and integrity of the IME process as it relates to radiology.
Nominated radiologists
Nominated radiologists are panel members who have been nominated by the chief radiologist at their clinic to help conduct IMEs. Your chief will have verified that you are a specialist in radiology, that your license is valid and that you are registered to work in the country where you practice. Your personal information will have been transmitted to your RMO to obtain a unique identifier, or “P” number for you to use.
As a nominated radiologist, you are responsible for managing your caseload and submitting chest x-rays for IMEs in a timely manner.
Chief and nominated radiologists
Both of these groups must do the following:
- Conduct chest x-rays (routine posterior-anterior view only for applicants 11 years old and older) according to the instructions laid out in this guide.
- Ensure that the associated panel physician is informed without delay of all chest x-rays where there is a high suspicion of active pulmonary tuberculosis.
- Follow all procedures laid out in this guide.
Using eMedical
eMedical is a web-based system used by IRCC for electronically recording and transmitting IMEs. eMedical is also used by the Australian Department of Home Affairs, Immigration New Zealand, and the United States Centers for Disease Control and Prevention. It is available around the globe with a few exceptions; therefore, all panel members must submit IME results via eMedical whenever possible.
In rare cases where a panel member is unable to use eMedical (no internet signal, no computer available due to crisis, etc.), your RMO will consider allowing you to submit paper-based IME results. (Paper-based clinics, please see our special set of instructions.)
Where eMedical is available, all panel members must:
- complete and submit all IMEs and related documents through the eMedical system
- maintain and keep a secure eMedical account, including user ID, password, and secret questions and answers, that you do not share with anyone in your clinic
- ensure all clinic staff who enter data into eMedical have their own account information
- ensure that your personal and business information in the system is updated and accurate at all times
- notify your RMO immediately if your password becomes known by an unauthorized person
- take all reasonable steps to guarantee the security of applicants’ personal information in eMedical
- ensure that applicants’ personal information contained in eMedical is treated in a manner consistent with Canadian privacy laws – including, but not limited to, protecting collected information against loss and unauthorized access, use, modification, disclosure and other misuse
- ensure all panel clinic staff under your supervision are aware of and abide by the requirements and standards for completing IMEs in the eMedical system
Performance guidelines and expected timelines
IRCC’s service standards for Streamlined IME activities do not differ from the service standards associated with the ‘standard’ IME. However, your RMO may reach out to you to book an applicant’s appointment and submit their IME without delay if their situation is deemed urgent. These cases should be prioritized where possible.
Panel physicians are expected to perform roughly 80 percent of these activities within the timelines set out in the table below. If you are unable to meet these standards, you should notify your RMO. You may be asked to provide a justification for the delay. These standards also apply to when you are forwarding material you receive after the original IME is complete.
| Activities | Time frame (in calendar days) |
|---|---|
| Appointment with panel physician | 10 days |
| Appointment with panel physician in cases where the applicant is furthered | 10 days |
| Obtain lab results | 7 days after date of the exam |
| Obtain x-ray results | 7 days after date of the exam |
| Submission of the IME to RMO by the panel physician | 10 days of date of the exam |
| Responding to correspondence from RMO | 48 hours |
| Forwarding inactive immigration medical files to the RMO | Paper-based: 8 week old IMEs eMedical users: Files are auto deleted after 365 days of inactivity |
| Notifying the responsible RMO of any change in practice location or contact information | At least 14 days before the change takes place |
| Notifying the responsible RMO of any absence of 7 days or more | At least 14 days’ notice, (preferably by email) |
| Being available for provision of performance and technical information related to the IME process (e.g. quality assurance visits, annual audits) | 7 days’ notice |
If you are not available for IME activities
If you plan to be unavailable for IMEs for more than seven calendar days, you must inform your RMO. Here are the rules that apply to your absences:
- Enter leave dates directly into your eMedical profile.
- If possible, tell your RMO when you will depart from work and when you will return. This is important information for applicants to know.
- If a locum tenens will replace you while you are away, tell your RMO at least 14 days in advance, preferably by email. This will enable your RMO to approve your recommended replacement and activate their eMedical account. For more information, see our section below on using a locum tenens.
- If you are identified as “on leave” in eMedical, you cannot submit IMEs. Your locum tenens can complete IMEs on your behalf.
- If you have extended or repeated unreported absences, your status as a panel member may be revoked.
Please note that you are required to keep your contact information updated in the system.
Using a locum tenens
As panel member, you may ask your RMO to approve a locum tenens for your clinic if:
- you will be absent from your clinic for longer than seven days
- your clinic is experiencing a high volume of requests for IMEs and does not have the capacity to meet IRCC’s service guidelines
Here is the process for requesting a locum tenens:
- Contact your RMO to get approval. (Your RMO can consider your request before you send documentation.)
- Send your RMO the name and contact information for the locum tenens you want, as well as a copy of the locum’s medical registration and licence.
- Send your RMO a statement from your proposed locum saying that they have read this guide and agree with the standards and requirements it defines. Note that before you recommend a particular physician or radiologist as your locum tenens, you must be satisfied that they have the qualifications and experience to perform IMEs, and that they understand the reporting procedures and are aware of any updates issued by eMedical or IRCC’s Migration Health Branch.
If your RMO approves the request, it will send you a written response by letter or email. You can then tell your locum that they have been authorized.
You must give your RMO at least 14 days’ notice, preferably by email, for every period of time where the locum will be acting on your behalf, or where a locum is required to temporarily increase capacity in the clinic. This gives the RMO time to activate the locum’s eMedical account. You also need to specify an end date for the locum.
- IRCC will provide your locum tenens with a unique identifier.
- The locum will get their own password for eMedical. You must not share your password with the locum.
- The system will be updated with appropriate information about your locum, and their eMedical account will have a specific end date that aligns with the dates approved by your RMO.
- If you are terminated by IRCC, this will automatically cancel prior approvals for your locums.
Referring applicants to consultants and specialists
For the Streamlined IME, Panel physicians should only refer applicants to a specialist when requested by an RMO. Panel physicians must ensure that any consultants or specialists they refer applicants to are registered, certified or licensed by national regulatory bodies. All consultants and specialists must also be aware of IRCC’s requirements for the IME, particularly about verifying the applicant’s identity.
All consultants and specialists must send reports directly to the applicant’s panel physician. They must not send reports to panel physicians through the applicant. Consultants, specialists and facilities that provide supplemental tests need to understand that the request for additional information is for a medical evaluation for Canadian immigration purposes – and not intended for therapeutic purposes or to establish medical fitness to fly
If you relocate your practice
If you become a panel member and relocate your practice, you must tell your RMO because your designation is related to where you work. If you relocate, you may lose your designation as a panel physician. Once IRCC has assessed its requirements in your new location, it will let you know whether it needs you as a panel member there. You will have an opportunity to respond.
As a panel member, you must ensure IRCC has up-to-date documentation throughout the relationship. If your license or other certification expires, you must send the updated documents to IRCC. If you fail to do so you could be removed from the IME network.
Ethical conduct and conflicts of interest
As a panel member, you are expected always to conduct yourself ethically. When you conduct an IME for an applicant, you must carry out your professional obligations with competence, integrity and loyalty – the same way you do with all your patients.
You must also ensure that the people you employ and associate with in your practice meet these requirements. In conducting IMEs, you must:
- be courteous and respectful towards all applicants
- be mindful of applicants’ time, dignity, privacy and cultural practices
- display integrity in professional practice, particularly in relation to conflicts of interest
Here are some of the more specific ways in which you are expected to behave:
- Do not behave in a manner where you appear to be acting in a biased way because of a personal interest. You are expected to show professional behaviour and perform your IME-related activities in keeping with the principles of proper ethical medical practice and IRCC policy.
- Provide appropriate and timely advice to an applicant when you discover a significant medical concern they either did not know about or did not fully understand. In such a situation, you must inform the applicant of the concern and, with their consent, refer them to an appropriate clinician.
- Perform the duties of your practice impartially, uninfluenced by fear or favour.
- Avoid situations where your private, financial or other interests might reasonably be thought to conflict with conducting IMEs for applicants.
- An example where a conflict of interest could arise is if there is a working relationship between your clinic and an immigration consulting firm, where you accept their referrals to conduct IMEs and, in return, you refer your clients to them.
If the following issues or events arise, you must notify your RMO as soon as possible:
- You are suspended or come under investigation by your medical regulatory authority.
- You learn that you have been accused of malpractice or improper behaviour, even if it has not yet been investigated.
- You discover inappropriate activity relative to the provision of IMEs by your clinic, office, laboratory, or radiology centre staff.
- You become aware that any associated panel member is under investigation for a criminal activity or has been charged with or convicted of a criminal offence.
IRCC reserves the right to suspend a panel member’s designation after an investigation has been completed by a medical or regulatory authority.
Equal rights for all applicants
The principle of equal rights applies to all applicants that a panel member encounters, regardless of their:
- race, national or ethnic origin, colour, religion
- gender or sexual orientation
- age, mental or physical disability
Canada protects the rights and privacy of an individual to identify in the gender of their choice and express their gender and sexual orientation freely. As a panel member, you are required to show the same respect and privacy for IRCC applicants.
This includes using proper gender pronouns and preferred names when addressing an applicant. Outside of IME procedures, you should never disclose an applicant’s medical information, including gender expression and sexual orientation.
Accommodating cultural and other needs
Some applicants may ask for special accommodation during the IME due to personal or cultural sensitivities. As good practice, you should routinely offer to have a chaperone present when you are examining a client. Patient consent is always necessary for a chaperone to be present.
Female applicants may be uncomfortable with a male examiner (and vice versa), in which case you should either offer to have a chaperone present during the examination or make alternate arrangements that preserve the integrity of the IME.
Preferably, the chaperone should be a trained health professional familiar with the examination so they can confirm it was appropriately conducted. If that is not possible, you can use non-medical staff. In some cases, it may be reasonable for you to suggest that the patient choose a person to bring to the examination.
Overall, you should accommodate personal and cultural sensitivities, while keeping in mind that IME standards must be respected. When you make an accommodation, record on the examination form the type of accommodation you provided and the roles other people played who may have been present during the IME.
Should you not be comfortable examining a client for any reason – due to a conflict of interest, dispute, religious reason, personal belief, etc. – it is your responsibility to tell the applicant and your RMO.
Using Canada’s official languages
English and French are the official languages of Canada and, as a panel member, you must be able to communicate verbally and in writing in at least one of them. You must also complete the IME in one of the official languages. Other things to keep in mind:
- Inform IRCC of your preferred official language for correspondence, as well as any other language you speak. You can tell us about your other languages in a drop-down list in your eMedical profile.
- You must choose your preferred official language for processing IMEs in eMedical.
- When you submit reports from specialists as part of an IME, you must do so in one of Canada’s official languages. If a specialist submits a report in another language, you must have it translated.
Employing a medical interpreter
When you perform an IME, you may find yourself examining an applicant who does not speak one of Canada’s official languages – or any language you speak. In these cases, you will need an interpreter.
IRCC recommends that applicants use the services of a professional interpreter. However, an interpreter can be a friend, a relative of the applicant or any other person. The person acting as an interpreter:
- should be at least 18 years old (the interpreter must be mature enough to understand and appreciate the importance of the proceedings and questions)
- should not have a citizenship application in progress
- must have sufficient knowledge of English or French to communicate with Immigration, Refugees and Citizenship Canada (IRCC) officials
- must be able to provide the required assistance
Administrative instructions
IRCC’s Migration Health Branch has put together this list of administrative instructions to guide you in various situations – from how to advertise your services to how to handle complaints from applicants.
Guidelines for managing records
All the forms, documents and results of investigations involved in completing IMEs are the property of IRCC once the IME is submitted. You can access the IME for 365 days after you submit it.
Panel members who perform IME-related activities must follow the procedures and guidelines here for copies and files as well as for original documents and information:
- Keep a paper or electronic copy of the original IME for at least two years – or for the minimum retention time for medical documents in your area of jurisdiction, whichever is longer.
Information you collect during the IME is for Canadian immigration medical purposes only. You may not use it for other purposes – including research, clinical studies or investigations – without IRCC’s consent. Direct your consent requests to the Integrated Medical processing network by:
Email: IRCC.MHBIMPN-RITDMDGMS.IRCC@cic.gc.ca
Mail:
Senior Director, Integrated Medical Processing Network
Migration Health Branch
Immigration, Refugees, and Citizenship Canada
250 Tremblay Road
Ottawa, ON K1G 5P4- Forward original documents and information related to an IME to your RMO electronically via eMedical.
- Save a full copy or a summary of the IME for your own records.
- Print a copy of the IME by clicking the “Print health Case” button at the bottom of the Health Case details window.
- Print out a full copy or a summary of the IME to give to the applicants or, in the case of children, their guardian – unless there is a strong reason to not do so. Examples include when there is information in the IME from a different client, or when releasing the information could reasonably lead to another person or entity being subject to significant inappropriate behaviour by the applicant.
- Applicants may request a copy or a summary of their IME at any time. You should provide the requested information as long as your office has retained it – unless there is a strong reason to not do so.
- Applicants who wish to have further access to IRCC’s review and assessment of their IME can do so by filing an access request.
Advertising your services
You may wish to advertise your IME services outside your clinic by using a website, or electronic or printed material. If you do this, the following rules apply:
- You may:
- include information about regular fees associated with both the ‘standard’ and Streamlined IME (including user and related fees), the services included in your fees, your clinic’s address and contact information
- provide links to Government of Canada websites
- You may not:
- post a summary of this information, as it changes frequently
- associate a Canadian flag with your website or advertisement
- use IRCC’s insignia in any way
- use the eMedical insignia or logo in any way.
How to communicate and where to send your questions
To learn more, please refer to this section in the Canadian Panel Member Guide to Immigration Medical Examinations 2020.
Charging and collecting fees for Streamlined IMEs
All applicants, except those eligible for the Interim Federal Health Program, are responsible for paying all fees and costs associated with their IME. These fees include the following:
- panel physician services
- radiological services
- consultations with specialists (if applicable)
- investigations and treatment – e.g. when referred for treatment of tuberculosis or syphilis (if applicable)
- costs related to sending medical documents to the RMO
You may also charge reasonable fees for:
- follow-up visits in the case of furtherances
- providing copies of the IME to the client upon request
- missed appointments in accordance with local standards of practice
- user fees – e.g. the IME clinic is in a hospital and the hospital charges the client a fee for using the facility
Rules associated with charging fees:
- You should only charge the applicant for the necessary services rendered under the appropriate type of IME. Clients should not be charged for all of the services of a ‘standard’ IME if they only received a Streamlined IME.
- All current user or additional fees must be included in the cost of your clinic’s IMEs wherever the cost is displayed or advertised.
- You should charge reasonable fees and either post a fees list in your clinic, office or website, or email your fees to the applicant before their examination.
- Applicants should receive an itemized receipt that clearly indicates the services for which you charged them and includes the applicant’s name, age and IME number.
- Your fees must reflect local conditions and service charges. Consequently, the fees for IMEs may vary from country to country and even within a country.
Quality assurance, incidents and complaints
Clear and transparent procedures for quality assurance, responding to complaints and resolving problems improve IRCC’s service to applicants and the overall integrity of the immigration medical program.
For more information, please consult this section in the Canadian Panel Member Guide to Immigration Medical Examinations 2020.
The Streamlined Immigration Medical Examination
This section provides panel members who use eMedical with information they need to complete the Streamlined IME and associated forms.
Panel members using a paper-based system should refer to our supplementary section in this guide. IRCC has redesigned certain IME paper forms to ensure they are consistent with eMedical Streamlined IMEs.
General information about the Streamlined IME
The Streamlined IME consists of a medical history questionnaire and age-specific chest x-ray. In certain cases, at the request of the RMO, additional tests may be required.
Usually, routine, age-specific tests include:
- chest x-ray (posterior-anterior view) – applicants age 11 and older
A medical examination includes any or all of the following:
- review of past medical history
- chest x-ray (posterior-anterior view) – applicants age 11 and older
A Streamlined immigration medical examination does not include, laboratory tests, diagnostic tests, urinalysis, syphilis testing, or HIV testing unless requested by an RMO.
Unless advised otherwise by the RMO, a physical examination is not required in the context of the Streamlined IME and a fortiori, breast, genital, gynecological or rectal examination are not conducted in the context of the IME. If the client has a history or there is a clinical suspicion of breast, genital, gynecological or colorectal malignancy, or any other significant condition, please make note of it in the medical history portion of the IME.
How do I determine what examinations are required for clients undergoing a Streamlined IME?
As the panel physician, you are never required to decide on a course of treatment or additional tests. Once you submit the applicant’s IME, a medical officer working with your RMO will decide if additional tests are required and notify you through eMedical. Alternatively, instructions may be provided by your RMO before eMedical prompts have been updated. Instructions from your RMO supersede any prompts from eMedical.
Verifying an applicant’s identity and preventing fraud
It is essential that you identify applicants throughout the IME process to ensure the person undergoing the IME is the same person applying for entry to Canada, and that there is no substitution at any time during the lifecycle of the IME. An applicant’s identity is confirmed through a process of verifying the applicant’s photographs and identity documents.
- You must take a live digital photograph of the client in your clinic and upload it to eMedical.
- Photographs must meet IRCC’s photographic specifications standards (PDF, 506 KB).
- The eMedical system will include the photograph on all requisitions and referrals (laboratory, radiology, specialists and others).
Required documents
The applicant must submit a passport or other identification document acceptable for the Canadian IME. IRCC strongly prefers that applicants submit passports. This includes new passports and passports expired for no more than a year.
Other approved identification documents include the following:
- national ID card (an original birth certificate is an acceptable national ID document for applicants under the age of consent only)
- driver’s licence (Canadian licences only)
- refugee travel document
- Red Cross travel document
- UN laissez-passer
- Seaman’s book
- Organization of American States travel document
- Refugee Protection Claimant Document
If an applicant does not have approved identification
If an applicant does not provide an approved identification document, they must provide an alternative form of identification. You should not turn such applicants away, and you should conduct the IME as long as the applicant presents some form of identification.
If the applicant provides identification that is not approved, you must report “identity concern” in the eMedical system.
Important: To ensure the integrity of the IME process, the applicant must use the same identity document for all components of the IME, including laboratory, radiology and specialist referrals. Please inform applicants accordingly.
If you have an identity concern
If you cannot confirm that the person who has arrived for an IME is the person on the ID documents being presented, you should report that as an ID concern. In all cases except upfront medicals, which are not offered for clients undergoing the Streamlined IME, biodata and information extracted from the applicant’s visa application will already appear in eMedical. You should compare this information with what the client attending the IME is presenting.
You should not report as an ID concern any minor differences in the eMedical information and the ID document such as misspelling of names, minor errors in date of birth or differences in validity dates.
If the applicant provides personal details that seem inconsistent with the information on the identity documents they submit, you must identify the concern in the eMedical system. For paper-based IMEs, report your concern on the IMM 1020: Medical Report – Client Biodata and Summary – Streamlined form.
Scan the identity document you are concerned about and attach a copy to the health case in the IME. You should then complete the IME according to customary procedures. The document will be submitted to IRCC once you have completed the IME.
IRCC will investigate your concern about the applicant’s identity.
Client Declaration and Notice
(See our sample Client Declaration and Notice form in Appendix II.)
Before undergoing an IME, all applicants must complete the Client Declaration and Notice form. A legal guardian or parent may provide and sign the declaration on behalf of the applicant if the applicant is under 16 years of age or is unable to complete and sign the declaration for reasons of incompetency (for example, if they have reduced mental capacity).
The Client Declaration and Notice form includes the following:
- a declaration stating that all information provided at the time of the IME is true and complete
- a notice stating that the IME information will be collected and temporarily stored in the eMedical system on segregated databases located in Australia
- a notice explaining that the collection, use and disclosure to IRCC of IME information follows Canada’s Immigration and Refugee Protection Act or protects the health and safety of Canadians
- a notice explaining the collection, storage, use and disclosure of vaccination information where the applicant has consented to the disclosure of this information to IRCC
Other important details:
- eMedical will automatically enter the applicant’s information on the Client Declaration and Notice form beforehand.
- You should print the form from eMedical and provide it to the applicant. The applicant must sign the copy of the Client Declaration and Notice provided in eMedical. Forms that have been altered or translated into another language are not acceptable.
- You or your staff should review the Client Declaration and Notice form with the applicant and answer any questions.
- The Client Declaration and Notice form is not a consent document and should not be construed as consent for the purpose of the IME or for vaccination.
- You must ensure to obtain client consent according to your country’s guidelines or legal requirements before performing medical tests and procedures required for the IME and before administering any vaccination, where applicable.
- You must ensure that the applicant understands and accepts that any relevant personal information collected during the IME process, including IME information and any vaccine-related information, when applicable, will be disclosed to IRCC.
- If an applicant does not complete the Client Declaration and Notice form, you cannot carry out the IME and you must notify your RMO.
- The applicant (or legal guardian/parent) must sign and date the Client Declaration and Notice form.
- You must scan and upload the form to eMedical.
- Tick the Client declaration check box in eMedical.
- You cannot submit the IME information in eMedical unless the Client Declaration and Notice form is attached.
Medical Report – Client Biodata and Summary - Streamlined (IMM 1020)
(See our sample IMM 1020 form in Appendix III.)
IRCC has implemented the Medical Report – Client Biodata and Summary - Streamlined (IMM 1020, for all immigration categories completing a Streamlined IME. This form displays information such as:
- client information (biodata)
- immigration information
- IMM type: excessive demand exempt (EDE), non-EDE, or refugee overseas (see below for an explanation)
- IME grading
- panel physician declaration
Excessive demand exempt (EDE) applicants
EDE applicants are people who cannot be deemed inadmissible on the grounds that they would place an excessive demand on publicly funded Canadian health and social services. EDE applicants include refugees, refugee claimants, individuals with protected person status, and certain clients in the family classes.
However, EDE clients are assessed for:
- danger to public health
- danger to public safety
Non-EDE applicants
Non-EDE applicants are assessed for:
- danger to public health
- danger to public safety
- excessive demand on publicly funded Canadian health and social services
Refugee overseas applicants
Refugee overseas applicants are automatically assessed as EDE. Panel physicians must complete and submit the Resettlement Needs Assessment Form (IMM 5544) for overseas refugees.
IRCC typically issues the Medical Report – Client Biodata and Summary - Streamlined (IMM 1020) form with the applicant’s information and immigration information sections completed.
Applicants who have been issued a Medical Report – Client Biodata and Summary - Streamlined (IMM 1020) must present the form to your clinic when they arrive for their IMEs. The form will include two applicant identifiers: IME number and UCI number. (Note: This form may not include a client photo).
- Clinic staff must search for the applicant’s health case in eMedical using the IME number. They may search using the applicant’s name and passport number, or UCI number or UMI number.
- Clinic staff should confirm the applicant’s identity by comparing the applicant’s information with the approved identity document.
- The clinic must take a digital photo of the applicant and upload it to eMedical to verify the applicant’s identity throughout the IME process.
- The panel members involved in the applicant’s IME then complete all components of the examination in the eMedical system.
Upfront Medical Report – Client Biodata and Summary (IMM 1017B Upfront)
Clients will not be able to ask for a Streamlined IME; it must be issued to them by IRCC. Panel physicians may not perform a Streamlined IME for clients who present to a clinic for an upfront medical exam. Panel physicians will be able to tell which clients are eligible for a Streamlined IME based on what is indicated on their IMM 1020 form in addition to what is indicated in eMedical for that client.
If you are completing an upfront exam for a client requiring a ‘standard’ IME, please consult this section in the Canadian Panel Member Guide to the Immigration Medical Exam.
Medical Report (514 Medical Examination)
You will use the applicant’s medical report to assess their medical condition. The medical report may be completed by clinic staff or the applicant, but you as the panel physician must review it to confirm the information.
Medical history questions
You must provide details along with all “Yes” answers to medical history questions – these details are specified in each of IRCC’s technical instructions.
You must either provide this information in the comments section or attach a report to the IME.
The following table lists additional requirements when the answers to medical report questions show abnormality – whether the IME is completed in eMedical or on paper. See IRCC’s technical instructions for more information.
Table: Medical history questions
| Question | Related TI | IMM type | Requirements if “yes” in eMedical |
|---|---|---|---|
| Tuberculosis (TB), treatment for tuberculosis | TIs related to screening for danger to public health | EDE and non-EDE clients | Please refer to Technical Instructions |
| Close household or work contact with tuberculosis (within last 5 years) | TIs related to screening for danger to public health | EDE and non-EDE clients | Please refer to Technical Instructions |
| Have you ever been arrested, hospitalized, or treated medically for (1) actions that caused harm or posed a high risk of being harmful to others or (2) substance use that had a harmful impact on yourself or others? | TIs related to screening for danger to public safety | EDE and non-EDE clients | Please refer to Technical Instructions |
| Does the client present a health condition listed in the Excessive Demand Technical Instructions? | TIs related to screening for excessive demand | non-EDE clients | Please refer to Technical Instructions |
| Was a chaperone offered? | - | EDE and non-EDE clients | Non applicable. A chaperone should be offered to everyone. |
| For female clients: a) Are you pregnant? | N/A | EDE and non-EDE clients | N/A |
| b) If yes, what is the expected date of delivery? | N/A | N/A | eMedical generates this Pregnancy Deferral Letter. |
| c) If yes, do you wish to defer your chest x-ray at this time? | N/A | N/A | N/A |
Chest X-Ray Requisition and Report
Routine posterior-anterior chest x-rays (CXRs) are mandatory for applicants 11 years of age or older. If a chest x-ray is required for a child less than 11 years old, an anteroposterior view is mandatory. A panel physician should request a CXR, regardless of age, if the medical questionnaire reveals a history of tuberculosis infection or treatment in applicants or their close contacts. All chest X-rays must be submitted in DICOM format. DICOM tag elements must state the client’s name, DOB, gender and the institution name.
The CXR must be examined for:
- general radiological findings
- evidence of active or inactive TB disease
The CXR must contain the following information:
- applicant’s name
- applicant’s date of birth
- applicant’s gender
- date of the chest x-ray
Applicants must bring their IME number, UMI number and UCI number with them to undergo their CXR. Panel radiology clinic staff will use these numbers or the applicant’s name and passport number to retrieve the applicant’s health case in eMedical.
If an applicant is pregnant for the CXR
There may be cases where an applicant is not pregnant for the IME, but is pregnant for the x-ray examination. If an applicant is pregnant and elects to proceed with the CXR examination with adequate pelvic lead shielding, there are no changes to the CXR procedures.
If the client chooses to defer her CXR because of pregnancy:
- IRCC is informed electronically by eMedical that the client is pregnant, along with her estimated date of delivery
- eMedical generates a pregnancy deferral letter with instructions for the client
- the IME is put on hold status until the chest x-ray has been completed
- the IME is submitted to IRCC along with the CXR results when they become available
Please note that in urgent processing contexts, RMOs may request that you follow different procedures.
CXR indicating active tuberculosis
When a panel radiologist indicates suspected active TB in the applicant’s CXR, they notify the panel physician. As the panel physician, you must do the following:
- Arrange immediately for the client to undergo sputum testing.
- For confirmed, active TB cases, notify the public health authorities according to the country’s or region’s public health guidelines and directives.
- Submit the health case in eMedical within the service standard, including all reports available. The RMO will instruct you if further examinations are required.
- Proceed with contact tracing as per the tuberculosis technical instructions for all family members or close contacts who are also IRCC clients
- Recommend that non-IRCC close contacts see their own physicians for screening
Panel Physicians should notify the RMO as soon as possible if IMEs have already been completed and submitted for family members who require contact tracing.
As a result of contact tracing, applicants discovered to have latent TB should be reviewed by a local TB specialist to determine if treatment is recommended.
See IRCC’s technical instructions for more information.
Radiology grading
Before submitting the CXR, the radiologist must provide a grading for the image.
- The system will automatically provide a radiology grade based on the reported findings.
- Grade A indicates that there is no evidence of TB or abnormalities suggestive of other significant diseases identified.
- Grade B indicates that there is evidence of TB or abnormalities suggestive of other significant diseases identified.
- If the system has provided an A grade and the radiologist believes that there is evidence of TB or abnormalities suggestive of other significant diseases, they may change the grade to B.
- If the system has provided a B grade, it cannot be changed to an A grade.
- No comments are permitted for A-grade CXRs.
- Comments are mandatory for B-grade CXRs.
Panel Radiologist Declaration
The radiologist declaration confirms the following:
- The client’s identity has been verified.
- The radiology report is an accurate record of the radiologist’s findings.
Important information:
- Panel radiologist declarations are provided electronically.
- Radiology support staff can declare on behalf of a panel radiologist.
Submitting CXRs
- Digital CXRs are uploaded to the eMedical system.
- The radiologist or authorized radiology support staff enter the general and special findings in the eMedical system.
- The CXR is graded in the eMedical system and submitted to the client’s IME.
- The panel physician’s clinic is notified that the CXR examination has been completed.
- The panel physician reviews the radiologist report and grading.
- Once all examinations are completed, the panel physician submits the IME to IRCC.
Resettlement Needs Assessment (Exam 948 in eMedical)
When an applicant is being processed as a refugee overseas, the migration office issues a Medical Report: Client Biodata and Summary - Streamlined (IMM 1020) with the IMM category of “refugee overseas”.
In such cases, the Resettlement Needs Assessment is included in the medical instructions sent to the applicant by a migration office as part of the IME.
The form is available electronically under section 948 in eMedical. Panel physicians must complete this section for all applicants in the refugee overseas category. Please note that, for privacy reasons, this form must only indicate the anticipated services for the applicant and not provide medical information or a diagnosis.
See IRCC’s technical instructions under Resettlement Needs Assessment for detailed instructions on how to complete the form.
Pregnant Client – X-Ray Deferred
If the client chooses to defer her chest x-ray (CXR) because of pregnancy, the following steps apply:
- eMedical informs IRCC electronically when a CXR is deferred. The health case is put on hold when an applicant is pregnant and chooses to defer her CXR.
- eMedical generates a CXR requisition and instructions, which are then provided to the applicant.
- eMedical generates a “Pregnancy Deferral Letter” with instructions for the applicant.
- The panel physician completes all other components of the IME, checks the box for “pregnancy” and submits the IME in eMedical. Migration officers can see the status of the IME in GCMS: “On HOLD pregnancy” until the CXR is completed.
- The IME will be submitted to IRCC along with the CXR results when they are available for assessment by the RMO.
Please note that in urgent processing contexts, RMOs may request that you follow different procedures.
Additional forms for the Streamlined IME
You must print out, sign and scan this form when promoted by eMedical.
- IMM 5734: Specialist’s Referral Form
Referrals may only be completed if requested by the RMO. The panel physician will send most referrals electronically. You may print the letter if the applicant requests a printer version, or for any other reason you wish.
Additional information for submitting IME forms
IME grading: Grade A or Grade B
Before you submit the IME, you must provide a grade for it. The system will automatically provide an IME grade based on your reported findings:
- Grade A indicates that there are no abnormal findings present and no significant abnormal history.
- Grade B indicates that there are significant abnormal findings present and/or an abnormal history.
- If the system has provided an A grade and you believe there are significant abnormal findings, you may change the grade to B.
- If the system has provided a B grade, you cannot change it to an A grade.
- No comments are permitted for A grade IMEs.
- Comments are mandatory for B grade IMEs.
Panel physician declaration
The panel physician’s declaration is provided electronically. It confirms the following:
- You have verified the applicant’s identity.
- The IME and medical report are an accurate record of your findings.
Furtherance process
RMOs may need more information to complete their medical assessment. They get this through the furtherance process. Furtherance might create additional costs for the applicant, including additional tests and specialist evaluation.
As the panel physician who did the original IME, you are responsible for the following:
- When requested by the RMO, refer the applicant for additional testing to another panel physician, or to an appropriate specialist for consultation. (You, not the applicant, are responsible for selecting the specialist.) The applicant’s previous medical records may be provided along with the additional reports requested by the RMO.
- Complete the furtherance requirements by reviewing the new medical results and ensuring they respond fully to the original furtherance request, then submitting the results to the RMO. If the new medical result does not respond fully to the original furtherance request, provide a written explanation as to why.
Here are the next steps of the process:
- The RMO issues a letter to the applicant with instructions to return to a panel physician for further investigations.
- The furtherance request is transferred to eMedical.
- You retrieve the furtherance request from eMedical by carrying out a search using the IME or UCI number indicated in the client’s letter.
- You complete the additional examination(s) or generate a referral letter with the information that will be sent to a specialist for the required investigation(s).
- You enter the information into eMedical and submit the information to IRCC.
Panel members who work in Canada
This section of the guide provides information, instructions and reference material for panel members operating in Canada. It does not apply to panel members who perform Canadian IMEs in other countries.
Providing primary care for IME applicants
If you are asked to provide treatment to an applicant or provide a medical opinion outside the IME, you should make sure the applicant understands the different duties and responsibilities of a third-party physician (i.e. a panel physician) versus a treating physician. For example, if you recommend a treatment that is not mandatory for immigration purposes, the applicant must understand this.
The provincial and territorial medical licensing authorities give doctors guidance on the difference between a treating and third-party physician. Applicants should also understand that any medical services not related to the IME or covered under the Interim Federal Health Program do not involve IRCC.
Providing services in Canada’s official languages
IRCC is committed to providing applicants in Canada with service in their preferred official language: English or French. If your clinic cannot provide service in the applicant’s official language of choice, you should refer them to the nearest panel physician who can. If no such physician exists nearby, you should ask the applicant to contact IRCC’s Call Centre at 1-888-242-2100, or consult IRCC’s website.
Protection of personal information
Several Canadian statutes protect people’s personal information. They include:
- the Privacy Act
- the Access to Information Act
- the Canadian Charter of Rights and Freedoms
- the Library and Archives Act
- the Personal Information Protection and Electronic Documents Act (PIPEDA)
- Various provincial and territorial privacy laws
As a panel physician, you must follow these laws when you collect, use, disclose, retain and dispose of people’s personal information. It is critical, for example, to collect and store personal information in a way that protects it from unauthorized disclosure.
The laws of other jurisdictions where information is collected may also apply to your treatment of applicants’ personal information.
To comply with legislation, the IME forms sometimes require applicants to consent to the disclosure of their personal health information to third parties.
Panel physicians in Canada can get advice from their professional organizations or regulating bodies on how to apply the Personal Information Protection and Electronic Documents Act (PIPEDA) and provincial or territorial privacy legislation, as well as how to properly manage personal information.
Refugee determination system in Canada
Refugee claimants – more appropriately called “asylum seekers” – are individuals who, after they arrive in Canada, make a formal claim to an IRCC or Canada Border Services Agency officer asking for Canada’s protection.
Under the Immigration and Refugee Protection Act (IRPA), all people seeking asylum must get an IME. They are referred for an IME when they make their claim. The IME forms and requirements for asylum seekers are the same as for other immigrants. They are given medical instructions and a list of panel physicians. They must undergo their IME within 30 days following their claim for asylum.
Immigrants are examined to identify medical conditions that might affect their admissibility to Canada under IRPA. Asylum seekers fall under the excessive demand exempt (EDE) category. This means they are examined primarily to identify conditions that might pose risks to public health and public safety; however, any additional services required by IRCC’s technical instructions may also be provided.
Asylum seekers who have been granted protected person status by the Canadian authorities are entitled to health care under the Interim Federal Health Program (IFHP) until they become eligible for provincial or territorial health care coverage. This means their first IME is covered. If they must undergo a second IME, it is not covered under the IFHP.
Your duty to report tuberculosis
Individuals whose IME shows they have inactive tuberculosis are placed under medical surveillance in Canada. The Public Health Liaison Unit (formerly known as the Medical Surveillance Unit) reports such cases to the appropriate provincial or territorial public health authorities.
However, as a panel physician, you are also required to notify the appropriate provincial or territorial public health authorities of such cases according to the laws of the province where you practice.
At no time should routine investigation or management of active or suspected active tuberculosis be deferred or delayed because of immigration medical activities. If you cannot contact an applicant suspected of having an active notifiable infectious disease such as tuberculosis, you should immediately inform the IRCC Migration Health Branch.
The Interim Federal Health Program (IFHP)
IFHP for panel members working in Canada
The IFHP provides limited, temporary coverage of health care benefits in Canada to groups not eligible for provincial or territorial health insurance, such as resettled refugees, refugee claimants, victims of human trafficking and individuals detained under the Immigration and Refugee Protection Act.
IFHP covers the costs of services and products to eligible beneficiaries in Canada as indicated in the IFHP benefit grids. It is important to note that, in Canada, the IFHP only covers the cost of one IME and related tests.
The IFHP’s claims administrator, Medavie Blue Cross, adjudicates and pays claims for the program.
Panel members must register with IFHP
A panel member or any service provider assisting with IME-related tests must register as an IFHP Provider and comply with the terms and conditions of Medavie Blue Cross.
Please refer to the IFHP Benefit Grid – IME and IME tests available on the Medavie Blue Cross website for more information on the services, diagnostic tests, and the maximum dollar amount.
Verifying IFHP eligibility
Eligibility documents
There are three types of documents that show that an individual may be eligible under IFHP in Canada. Individuals must show one of these documents to their health care provider at each visit:
- Refugee Protection Claimant Document (RPCD)
- Interim Federal Health Certificate (IFHC)
- Acknowledgement of Claim and Notice to Return for Interview letter (AOC)
Confirm eligibility with Medavie Blue Cross
Panel physicians must confirm with Medavie Blue Cross that the individual’s coverage is active before the examination is carried out. It is important to note that it takes two business days for the IFHP eligibility to be reflected in the Medavie Blue Cross system. However, beneficiaries are still eligible during this two-day period. When an IFHP client asks for your services within two business days of the date on the IFHP eligibility documents, you must:
- review the “effective date” on the eligibility document to confirm that it is within the two business-day period
- provide the services and delay submitting the invoice to Medavie Blue Cross until the coverage has been updated in their system
Additional information
Please see the IFHP Information Handbook for Health Care Professionals (PDF, 7 MB) for more information. The handbook is available on the Medavie Blue Cross website, where you can find the IFHP Benefit Grids and more information about the IFHP, including:
- prior approval procedures
- claim submission guidelines
- provider terms and conditions
- payment procedures
- important information on how to perform IMEs for refugee claimants in Canada
IFHP for panel members working overseas (pre-departure medical services)
On April 1, 2017, the IFHP was expanded to cover certain pre-departure medical services (PDMS) for Canada-bound resettled refugees before they come to Canada.
The claims administrator for the IFHP, Medavie Blue Cross, administers claims submitted by health care providers and secondary care providers such as hospitals, laboratories and specialists who have provided services to individuals eligible for PDMS. More information on PDMS is available on the Medavie Blue Cross website.
Groups and individuals eligible for PDMS
The following are eligible for PDMS:
- individuals identified for resettlement to Canada (i.e. government-assisted refugees)
- privately sponsored refugees
- blended visa office-referred refugees
- groups or individuals who have been specially designated by the Minister of IRCC
- certain people who are being resettled in Canada as a result of a public policy or on humanitarian and compassionate grounds as determined by the Minister of IRCC
Registering for PDMS
Panel members – whether or not they are affiliated with the International Organization for Migration (IOM) – should register with the IFHP through Medavie Blue Cross.
IOM-affiliated panel members must register with the IFHP; however, they will receive reimbursements for their services directly from IOM. They are not required to submit the claims for reimbursements to Medavie Blue Cross.
Non-IOM affiliated panel members are required to register with the IFHP and claim reimbursement for their services directly from Medavie Blue Cross.
To learn more about the registration process, see the IFHP Handbook for Pre-Departure Medical Services (PDMS) Providers (PDF, 5.1 MB).
PDMS coverage and benefits
The scope of the IFHP PDMS coverage is limited to:
- the cost of the Immigration Medical Examination (IME) and follow-up treatment for health conditions that would affect an individual’s medical admissibility to Canada (i.e. active tuberculosis and untreated syphilis)
- communicable disease prevention and control by providing vaccinations that are aligned with Canadian immunization guidelines
- medical support required during travel to Canada includes medical attendant and/or medical devices (e.g. oxygen, wheelchairs)
- management and control of communicable diseases in refugee camps
Please see the IFHP Benefit Grid for PDMS (PDF, 357 KB) for a list of eligible services and additional information.
Pre-departure vaccination services
Panel physicians affiliated with the International Organization for Migration (IOM), can provide certain vaccination services covered by the IFHP to eligible individuals. This service is voluntary and does not impact their application for resettlement to Canada.
Immunizations can be provided only in countries where the IOM has the capacity to deliver vaccinations.
The Immunization Manual (PDF, 1.5 MB) contains more information including:
- standard operating procedures
- vaccine administration and schedule
- consent form and vaccination documentation worksheet
Medical support in transit
The costs related to medical support in transit (medical attendant and/or medical devices) are covered by the IFHP. A prior approval request (PDF, 178 KB) must be sent to the IFHP Unit (IRCC.IFHP-PFSI.IRCC@cic.gc.ca) with the provider’s Regional Medical Office (RMO) in cc. The request must include clinical information and recommendations for medical support in transit with detailed medical services, devices or products required and expected cost.
If approved, an IFHP officer will sign and return Part 1 (administrative) of the form to the requestor. For more information or questions, please contact IRCC.IFHP-PFSI.IRCC@cic.gc.ca.
You can find the Medical Support in Transit Form (PDF, 226 KB) (prior approval request) on the web site of the IFHP Claims Administrator Medavie Blue Cross.
Outbreak response
When a communicable disease outbreak occurs in a refugee camp, the IFHP will reimburse services and products related to the following:
- diagnostic testing (rapid and serologic)
- post-exposure prophylaxis (vaccines and drug therapy)
- pre-departure health screening and personnel cost, including the cost of physician and nursing visits.
The costs related to the management and control of an outbreak are covered by the IFHP. A prior approval request must be sent to the RMO as soon as an outbreak is identified by the PP/IOM. Please note that the request will also be reviewed by the IFHP Unit to ensure compliance with the IFHP Policy. The request must include the following information:
Location and description
Provide a short description of population demographics and a description of the area/facility where the outbreak has occurred (i.e. camp, region, province, country, etc.)
Confirmation of an outbreak
Your description should include the following:
- epidemiological case definition
- case finding
- lab confirmation (if any)
- how the outbreak was initially reported and steps taken to confirm it
- how serious the outbreak is (potential for spread, mortality and complications)
- number of cases and particular groups at risk among those identified for resettlement to Canada
- how soon the individuals will be traveling to Canada
Ongoing action (capacity)
Provide a brief description of the current response and capacity, including the investigations done and control measures taken (human, medical, etc.)
Proposed response
What should be done to control this outbreak? Propose the control activities and supplies needed (medicines, materials) and the expected cost per individual, including:
- treatment of cases and carriers
- isolation of cases
- surveillance of suspects
- immunizations:
- Obtain all immunization records (consult IFHP Vaccination Documentation Worksheet (PDF, 321 KB), if available).
- Identify required vaccine(s) and number of doses.
- Confirm the vaccine cost per dose, including the administration cost.
- chemoprophylaxis
- personal protection
- environmental hygiene
- personal hygiene
- disinfection and sterilization
- pre-departure screening
- other
For claims-related instructions please consult the provider handbook.
Verifying IFHP eligibility for PDMS services
It is your responsibility as a panel physician to confirm an individual’s eligibility to the IFHP before services are rendered. This is an important aspect of protecting the integrity of the program.
Non-IOM affiliated providers must complete the following procedures:
- confirm that the individual has an IFHC
- confirm that the identity of the individual on the IFHC matches the individual in the identification document
- retain a photocopy of the individual’s IFHC in their records
IOM-affiliated providers will do the following procedures to confirm an individual’s eligibility:
- confirm that the individual’s name appears on the list received from IRCC visa offices
- confirm that the identity of the individual matches the individual in the identification document
- retain a copy of the list of eligible individuals received from IRCC visa offices
Important: If you have questions related to an individual’s eligibility, please contact Medavie Blue Cross at medavieworld@bellaliant.net including the individual’s UCI and the benefit code.
For more information, please see the PDMS provider handbook (PDF, 5.1 MB).
Claim submission guidelines for in-Canada or overseas services
You have up to six months after providing your services to submit invoices to either the IOM or Medavie Blue Cross. When you submit claims for IMEs and related tests, you must use current IFHP benefit codes, which you can find in IFHP Benefit Grid – IME and IME tests available on the Medavie Blue Cross website (for panel members working in Canada) or the Benefit Grid for PDMS (PDF, 357 KB) (for panel members working overseas).
Here are some key elements of IFHP’s fee policy:
- Your compensation is based on a fee-for-service model. The IFHP fee policy is to reimburse physicians according to usual and customary fee rates in place on the date of service or according to fee rates established by the IFHP.
- You must not collect from the client the difference between the total amount billed for the services and the amount to be reimbursed by Medavie Blue Cross, if any.
- The IFHP is not designated to reimburse beneficiaries directly. Do not directly charge patients covered by the IFHP. If a beneficiary pays you directly for services or products covered by the IFHP, they cannot be reimbursed.
- You may not refuse to provide IMEs for individuals covered by the IFHP. However, you may charge for missed appointments according to your local standards of practice. This charge will not be reimbursed under the IFHP.
- You must accept whatever method of payment an applicant wishes to use. In addition, the services you provide must not be influenced by whether the service is a covered benefit for the client.
Section 2: Supplementary Information
Instructions for completing paper-based Streamlined IMEs
This section provides panel members who use a paper-based system with information they need to complete the Streamlined IME and associated forms.
Panel members using eMedical should refer to The Streamlined Immigration Medical Examination section of this guide.
IME paper forms have been redesigned to ensure they are consistent with eMedical Streamlined IMEs.
General information about the streamlined IME
The IME consists of a medical history and age-specific chest x-ray.
Usually, routine, age-specific radiologic tests include:
- chest x-ray (posterior-anterior view) – applicants age 11 and older
A Streamlined medical examination includes any or all of the following:
- review of past medical history
- chest x-ray (posterior-anterior view) – applicants age 11 and older
- Resettlement Needs form for all categories of refugees
Panel members may request additional screening only when authorized by an RMO.
It also be necessary to screen applicants below the ages indicated. See IRCC’s technical instructions for more information.
How do I determine what examinations are required?
As the panel physician, you are never required to decide on a course of treatment or additional tests for an applicant. Your regional medical office (RMO) will contact you with the specifics of the applicant’s case and the medical examinations they require. You must follow the technical instructions for all tests and procedures.
Getting your unique identifier and login, contact information and absences, & managing paper records
To find information about getting your unique identifier and login, reporting contact information and absences, and general guidelines about managing paper records, please see the relevant sections in the Canadian Panel Member Guide to the Immigration Medical Examination.
Fees for Streamlined IMEs
If you are completing a paper-based Streamlined IME that must be mailed to the RMO, you should discuss the method and cost of sending the documents with the applicant beforehand.
Verifying an applicant’s identity
It is essential that you identify applicants throughout the IME process to ensure the person undergoing the IME is the same person applying for entry to Canada, and that there is no substitution at any time during the lifecycle of the IME. An applicant’s identity is confirmed through a process of verifying the applicant’s photographs and identity documents.
Obtain photos of the applicant
- The applicant must provide four recent photographs to the panel clinic.
- Photographs must meet IRCC’s photographic specifications standards (PDF, 506 KB).
- If the photographs do not meet the specifications, ask the applicant to provide new photographs before you complete the IME.
What to do with the photos:
- You must attach photos to the Medical Report – Client Biodata and Summary - Streamlined (IMM 1020) as well as on the “Chest X-Ray Requisition Report” sections of the IMM 5420: Medical Report form.
- When your clinic uses these photos, it must confirm that the photos are a true and recent likeness of the applicant being examined.
- You must signed the photograph on the top right corner with your panel physician’s ID.
If you have an identity concern
If you cannot confirm that the person who has arrived for an IME is the person on the ID documents being presented – or if the applicant provides personal details that seem inconsistent with the information on the identity documents they submit – you should report that as an ID concern.
Attach photocopies of the identification document in question to the IME and submit it to IRCC.
IRCC will investigate your concern about the applicant’s identity.
Required documents
The applicant must submit a passport or other identification document acceptable for the Canadian IME. IRCC strongly prefers that applicants submit passports. This includes new passports and passports expired for no more than a year.
Other approved identification documents include the following:
- national ID card (an original birth certificate is an acceptable national ID document for minors under the age of consent only)
- driver’s licence (Canadian licences only)
- refugee travel document
- Red Cross travel document
- UN laissez-passer
- Seaman’s book
- Organization of American States travel document
- Refugee Protection Claimant Document
If an applicant does not have approved identification
If an applicant does not provide an approved identification document, they must provide an alternative form of identification. You should not turn such applicants away, and should conduct the IME as long as the applicant presents some form of identification.
If the applicant provides identification that is not approved, or if you have doubts about the authenticity of the document presented, you must report your concern on the Medical Report – Client Biodata and Summary - Streamlined form (IMM 1020). A copy of the identity document of concern should be attached to the IME.
Important: To ensure the integrity of the IME process, the applicant must use the same identity document for all components of the IME, including radiology and specialist referrals. Please inform your clients accordingly.
Client Consent and Declaration
(See our sample Client Declaration and Notice form in Appendix II.)
Before undergoing an IME, all applicants must complete the Client Declaration and Notice form. A legal guardian or parent may provide and sign the declaration on behalf of the applicant if the applicant is under 16 years of age or is unable to complete and sign the declaration for reasons of incompetency (for example, if they have reduced mental capacity).
The Client Declaration and Notice form for paper-based IMEs includes the following:
- a declaration stating that all information provided at the time of the IME is true and complete
- a notice stating that the IME information will be collected and temporarily stored in the eMedical system on segregated databases located in Australia
- a notice explaining that the collection, use and disclosure to IRCC of IME information follows Canada’s Immigration and Refugee Protection Act or protects the health and safety of Canadians
- a notice explaining the collection, storage, use and disclosure of vaccination information where the applicant has consented to the disclosure of this information to IRCC
Other important details:
- The applicant must sign the copy of the Client Declaration and Notice provided by you or your staff. Forms that have been altered or translated into another language are not acceptable.
- You or your staff should review the Client Declaration and Notice form with the applicant and answer any questions.
- Clinic staff must attach the form and submit it along with the IME.
- The IME must not be submitted to your RMO without a completed Client Declaration and Notice form.
- The Client Declaration and Notice form is not a consent document and should not be construed as consent for the purpose of the IME or for vaccination.
- You must ensure to obtain client consent according to your country’s guidelines or legal requirements before performing medical tests and procedures required for the IME and before administering any vaccination, where applicable.
- You must ensure that the applicant understands and accepts that any relevant personal information collected during the IME process, including IME information and any vaccine-related information, when applicable, will be disclosed to IRCC.
- If an applicant does not complete the Client Declaration and Notice form, you cannot carry out the IME and you must notify your RMO.
- The applicant (or legal guardian/parent) must sign and date the Client Declaration and Notice form.
Medical Report: Client Biodata and Summary - Streamlined (IMM 1020)
(See our sample IMM 1020 form in Appendix III.)
IRCC has implemented the Medical Report – Client Biodata and Summary - Streamlined (IMM 1020), for all immigration categories. This form displays information such as:
- client information (biodata)
- immigration information
- IMM type: excessive demand exempt (EDE), non-EDE, refugee
- IME grading
- panel physician declaration
Excessive demand exempt (EDE) applicants
EDE applicants are people who cannot be deemed inadmissible on the grounds that they would place an excessive demand on publicly funded Canadian health and social services. EDE applicants include refugees, refugee claimants, individuals with protected person status, and certain clients in the family classes.
However, EDE clients are assessed for:
- danger to public health
- danger to public safety
Non-EDE applicants
Non-EDE applicants are assessed for:
- danger to public health
- danger to public safety
- excessive demand on publicly funded Canadian health and social services
Refugee overseas applicants
Refugee overseas applicants are automatically assessed as EDE. Panel physicians must complete and submit the Resettlement Needs Assessment Form (IMM 5544) for overseas refugees.
IRCC typically issues the Medical Report – Client Biodata and Summary - Streamlined (IMM 1020) form with the applicant’s information and immigration information sections completed.
Applicants who have been issued a Medical Report – Client Biodata and Summary - Streamlined (IMM 1020 must present the form to your clinic when they arrive for their IMEs. The form will include two applicant identifiers: IME number and UCI number. (Note: This form may not include a client photo).
Here are the steps you should take as a paper-based clinic:
- Confirm the applicant’s identity by comparing the applicant’s information with the approved identification document.
- Attach a recent applicant photo (provided by the applicant) to the Medical Report - Streamlined (IMM 1020).
- Complete and submit the Medical Report - Streamlined (IMM 1020) along with all other IME forms.
Upfront Medical – Client Biodata and Summary (IMM 1017B Upfront)
Clients will not be able to request a Streamlined IME unless it has been issued to them by IRCC. Panel physicians may not perform a Streamlined IME for clients who present to a clinic for an upfront medical exam.
Medical Report (IMM 5420)
You will use the applicant’s medical report to assess their medical condition. The medical report may be completed by clinic staff or the applicant, but you as the panel physician must review it to confirm the information.
Medical history questions
You must provide details along with all “Yes” answers to medical history questions – these details are specified in each of IRCC’s technical instructions.
You must either provide this information in the comments section or attach a report to the IME.
The following table lists additional requirements when the answers to medical report questions show abnormality – whether the IME is completed in eMedical or on paper. See IRCC’s technical instructions for more information.
| Question | Related TI | IMM type | Requirements if abnormal |
|---|---|---|---|
| Tuberculosis (TB), treatment for tuberculosis | TIs related to screening for danger to public health | EDE and non-EDE clients | Please refer to Technical Instructions |
| Close household or work contact with tuberculosis (within last 5 years) | TIs related to screening for danger to public health | EDE and non-EDE clients | Please refer to Technical Instructions |
| Have you ever been arrested, hospitalized, or treated medically for (1) actions that caused harm or posed a high risk of being harmful to others or (2) substance use that had a harmful impact on yourself or others? | TIs related to screening for danger to public safety | EDE and non-EDE clients | Please refer to Technical Instructions |
| Does the client present a health condition listed in the Excessive Demand Technical Instructions? | TIs related to screening for excessive demand | Non-EDE clients | Please refer to Technical Instructions |
| Was a chaperone offered? | - | EDE and non-EDE clients | Non applicable. A chaperone should be offered to everyone. |
| For female clients: a) Are you pregnant? | N/A | EDE and non-EDE clients | N/A |
| b) If yes, what is the expected date of delivery? | N/A | N/A | N/A |
| c) If yes, do you wish to defer your chest x-ray at this time? | N/A | N/A | Attach IMM 5733 Instructions for Pregnant Client – X-Ray Deferred |
Chest X-Ray Requisition and Report
Routine posterior-anterior chest x-rays (CXRs) are mandatory for applicants 11 years of age or older. A panel physician should request a CXR, regardless of age, if the medical questionnaire reveals a history of tuberculosis infection or treatment in applicants or their close contacts.
The CXR must be examined for:
- general radiological findings
- evidence of active or inactive TB disease
Information to include on the CXR
The panel physician must enter the applicant’s personal information on the chest x-ray (CXR) requisition form:
- surname
- given name
- date of birth
- IME or UMI number (if applicable)
- the applicant’s photograph must be attached to the CXR requisition form
If an applicant is pregnant for the CXR
There may be cases where an applicant is not pregnant for the IME, but is pregnant for the x-ray examination. If an applicant is pregnant and elects to proceed with the CXR examination with adequate pelvic lead shielding, there are no changes to the CXR procedures.
If the client chooses to defer her CXR because of pregnancy:
- The radiology clinic must notify the panel physician that the CXR has been deferred.
- The panel physician may complete the IME, except for the CXR.
- The IME is submitted only once the post-partum CXR is returned to the panel physician.
- See the sample Instructions for Pregnant Client − X-Ray Deferred (IMM 5733) form in Appendix III.
Please note that in urgent processing contexts, RMOs may request that you follow different procedures.
CXR indicating active tuberculosis
When a panel radiologist indicates suspected active TB in the applicant’s CXR, they notify the panel physician. As the panel physician, you must do the following:
- Arrange immediately for the client to undergo sputum testing.
- For confirmed, active TB cases, notify the public health authorities according to the country’s or region’s public health guidelines and directives.
- Submit by mail the IME within the service standard, including all reports available. The RMO will instruct you if further examinations are required.
- Proceed with contact tracing as per the tuberculosis technical instructions for all family members or close contacts who are also IRCC clients
- Recommend that non-IRCC close contacts see their own physicians for screening
As a result of contact tracing, applicants discovered to have latent TB should be reviewed by a local TB specialist to determine if treatment is recommended.
See IRCC’s technical instructions for more information about tuberculosis screening.
Radiology grading
Radiologists must provide a radiology grade based on their reported findings.
- Grade A indicates that there is no evidence of TB or abnormalities suggestive of other significant diseases identified.
- Grade B indicates that there is evidence of TB or abnormalities suggestive of other significant diseases identified.
- Comments should not be included for A-grade chest x-rays.
- Comments are mandatory for B-grade chest x-rays.
Panel Radiologist Declaration
Radiologist declarations are provided in writing on the radiology report and include the panel radiologist’s name, signature, number and the date of the CXR report.
Submitting CXRs
- The radiologist provides the general and special findings and grades the digital CXRs or film using the proper form.
- The radiologist or authorized radiology staff forward the CXRs and the report to the panel physician.
- The panel physician reviews the radiologist’s report and grading.
- Once all examinations are completed, the panel physician send the IME to IRCC.
Resettlement Needs Assessment (IMM 5544)
When an applicant is being processed as a refugee overseas, the migration office issues a Medical Report: Client Biodata and Summary - Streamlined (IMM 1020) with the IMM category of “refugee overseas”.
In such cases, the Resettlement Needs Assessment (IMM 5544) is included in the medical instructions sent to the applicant by a migration office as part of the IME.
As the panel physician, you must complete the Resettlement Needs Assessment IMM 5544 along with the IME and send them both.
Pregnant Client – X-Ray Deferred (IMM 5733)
If the client chooses to defer her Chest x-ray (CXR) because of pregnancy, the following steps apply:
- Complete the CXR requisition and give it to the applicant.
- Complete the Instructions for Pregnant Client – X-Ray Deferred (IMM 5733) and give it to the applicant. (The applicant may forward a copy of the IMM 5733 to the migration office as proof that the IME has been started and the CXR has been deferred because of pregnancy.)
- You may complete the IME, except for the CXR.
- Send the IME only once the post-partum CXR has been returned to you.
See the sample Instructions for Pregnant Client − X-Ray Deferred (IMM 5733) form in Appendix III.
Please note that in urgent processing contexts, RMOs may request that you follow different procedures.
Additional Forms for paper-based IMEs
- IMM 5734: Specialist’s Referral Form
Additional information for submitting forms
IME grading: Grade A or Grade B
Before you submit the IME, you must provide a grade for it based on your reported findings:
- Grade A indicates that there are no abnormal findings present and no significant abnormal history.
- Grade B indicates that there are significant abnormal findings present and/or an abnormal history.
- Comments cannot be included for A-grade IMEs.
- Comments are mandatory for B-grade IMEs.
Panel physician declaration
The panel physician’s declaration is provided in writing on the Medical Report - Streamlined (IMM 1020) and includes your name, signature, number and the date of the IME submission.
Furtherance process
RMOs may need more information to complete their medical assessment. They get this through the furtherance process. Furtherance might create additional costs for the applicant because the panel physician involved cannot be employed at the clinic where the initial IME was completed.
Here is what is involved in the furtherance process:
- The RMO issues a letter to the applicant with instructions to return to a panel physician for further investigations.
- The RMO provides the applicant with a sealed letter for the panel physician, which details the specific instructions for further investigations.
- As the panel physician, you either complete the additional examination(s) or refer the client to a specialist.
- Your referral letter must include the client’s biodata and photograph, and clearly indicate the investigations required by IRCC.
- Once all the required investigations have been completed, you return the reports to IRCC.
Note: If a furtherance is issued on paper it cannot be completed in eMedical.
Legislation related to the Immigration Medical Examination
Immigration is a shared federal/provincial responsibility. As a panel member, you should be aware of the following three pieces of legislation – in particular how they relate to the administration of IMEs, your responsibilities for protecting the personal information of applicants and how an applicant can be denied admission on health grounds.
The Immigration and Refugee Protection Act
The Immigration and Refugee Protection Act (IRPA) is a federal act. One of its objectives is to ensure that the movement of people into Canada contributes to the country’s cultural, social, and economic interests, and affirms its humanitarian commitments while protecting the health, safety and security of Canadians.
IRPA and its accompanying regulations set out the medical requirements for applicants who want to come to Canada as temporary or permanent residents. The legislation also sets out the grounds on which a person may be found to be inadmissible to Canada – including inadmissibility on health grounds.
A foreign national can be found inadmissible on health grounds if their medical condition:
- is likely to be a danger to public health
- is likely to be a danger to public safety
- might reasonably be expected to cause an excessive demand on health or social services
The Privacy Act
The purpose of this legislation is to protect the privacy of people’s personal information when it is collected, retained, used and disclosed by government, and provide individuals with the right to access their personal information.
Many aspects of the Privacy Act apply to your work as a panel member – in particular your responsibility to protect the information of the applicants you examine.
Take a closer look at the Privacy Act.
Collection of panel members’ personal information under IRPA
IRCC’s Migration Health Branch is responsible for administering the department’s medical screening program. This includes managing panel members who perform IMEs in Canada and abroad. As part of the medical screening program, the branch collects and creates personal information about panel members, including your:
- name
- business name
- provider type/specialty
- professional affiliation, licensing or certification
- contact information (address, postal code)
- languages spoken
- sex
- signature
- photograph
- evaluations performed by IRCC’s Migration Health Branch
- evaluations shared with Canada by the governments of Australia, New Zealand, the United Kingdom and the USA
The Access to Information Act
The Access to Information Act gives every Canadian citizen, permanent resident, individual or corporation in Canada the right to request access to records, in any format, held by a government institution, subject to certain exceptions.
Take a closer look at the Access to Information Act.
Find out how to request access to information or personal information.
It is not necessary for applicants to use these acts to get a copy of their own IME. As a panel physician, you are authorized to give them a copy if they ask.
Acronyms, Initialisms and Definitions
The following list provides definitions for acronyms and technical terms found in this guide:
- Biodata:
- Information that establishes each client’s identity
- IRCC:
- Immigration, Refugees, and Citizenship Canada
- Chief radiologist:
- Licensed radiologist designated by IRCC to perform, grade and submit chest x-rays for Canada’s immigration medical examinations (IMEs).
- Client:
- A foreign national seeking to enter or remain in Canada who may be required to submit to an IME (in accordance with the Immigration and Refugee Protection Act and its regulations).
- Clinic staff:
- Persons who are working in the panel member’s clinic and may be involved in the immigration medical examination process.
- CXR:
- Chest x-ray
- ED:
- Excessive demand – a type of demand placed by a client on Canadian health or social services.
- EDE:
- Excessive demand exempt refers to specified groups of IRCC clients who are not denied entry or permission to stay in Canada because their medical condition may create an excessive demand.
- eMedical:
- An online application that provides a paperless process for electronic recording, transmission and storage of immigration medical examination results.
- Furthered cases:
- Cases that require additional supplemental information.
- Guardian:
- A person who looks after and is legally responsible for someone who is unable to manage their own affairs, especially an incompetent or disabled person or a child.
- Guide:
- This guide is the standard reference for the orientation and training of panel members. All panel members must ensure that they remain familiar with it and with related departmental instructions, including interim changes and updates provided by IRCC.
- IFHP:
- Interim Federal Health Program – a program funded by IRCC that provides limited, temporary coverage of costs related to health screening and care for specific categories of people, including protected persons, refugee claimants (asylum seekers in Canada), rejected refugee claimants in Canada, certain persons detained under the Immigration and Refugee Protection Act and other specified groups.
- IGRA:
- Interferon gamma release assay. A blood test that is a screening test used to determine if a client has latent (inactive) tuberculosis.
- IMA:
- Immigration medical assessment – the medical opinion made by Migration Health Branch concerning an IRCC client’s health admissibility to Canada as defined under immigration legislation.
- IME (Standard):
- Immigration medical examination – the examination conducted by panel members. The results of these examinations are sent to IRCC regional medical offices via eMedical (or exceptionally by courier/post) who then provide an IMA.
- IME number:
- Immigration medical examination number – a unique number assigned to a specific IME.
- IMM 1020:
- A Streamlined IME form containing the client’s biodata, IME grading and panel physician declaration.
- IMM 5420:
- A Streamlined IME form containing the client’s medical history, chest x-ray requisition results and the client’s consent and declaration.
- IMM 5544:
- Supplemental medical and resettlement needs assessment form providing information on special accommodations a refugee may require to settle in Canada.
- IOM:
- The International Organization for Migration, an intergovernmental organization that became a related organization of the United Nations in 2016.
- IRCC:
- Immigration, Refugees, and Citizenship Canada. The Canadian federal government department that has primary responsibility for managing the entry into Canada of foreign nationals.
- IRPA and IRPR:
- Immigration and Refugee Protection Act and the Immigration and Refugee Protection Regulations (IRPR). Canadian legislation setting out the requirements for entry to Canada by foreign nationals. This legislation determines requirements to enter Canada including requirements for an IME. View the Act and regulations.
- locum tenens:
- Medical practitioners who replace panel physicians for a short period while they are on vacation, taking training or unable to provide service for other reasons.
- LTBI:
- Latent tuberculosis infection – sometimes referred to as ‘inactive tuberculosis’.
- Nominated radiologist:
- Licensed radiologist nominated by a chief radiologist located in the same radiology clinic to perform, grade and submit chest x-rays for Canada’s IMEs.
- Panel clinic:
- A clinic where designated physicians and/or radiologists conduct IMEs.
- Panel member:
- A general term that refers to a panel physician, panel radiologist or panel laboratories or specialists authorized by IRCC to perform IME related activities.
- Panel physician:
- A licensed medical doctor designated by IRCC to perform, grade and submit IMEs. Designated medical practitioner (DMP) was the previously used term.
- P number:
- A unique identifier given to specific panel members issued by IRCC’s Migration Health Branch.
- Protected person – In Canada:
- A person in Canada who according to Canada’s Immigration and Refugee Protection Act, is a person who has been determined to be either (a) a convention refugee or (b) a person in need of protection (including, for example, a person who is in danger of being tortured if deported from Canada).
- PTB:
- Pulmonary tuberculosis
- Radiologist:
- For IRCC purposes, this refers to both chief and nominated radiologists.
- Refugee overseas:
- A person overseas who has been determined to be a convention refugee or a person in similar circumstances. A convention refugee is a person who meets the refugee definition in the Geneva Convention signed in 1951 relating to the status of refugees and the protocol to that convention signed in New York in 1967.
- RMO:
- RMO stands for regional medical office. These offices contain IRCC employees who are responsible for providing Canadian immigration medical services in a specific region. In 2019, there were four RMOs, located in Ottawa, London, New Delhi and Manila.
- Streamlined IME:
- A lighter-touch health screening alternative to the ‘standard’ IME that relies on a simplified medical history questionnaire and chest x-ray, and when applicable, a Resettlement Needs Assessment.
- TB:
- Tuberculosis.
- TIs:
- Technical instructions – the instructions for completion of the IME.
- UCI:
- Unique client identifier. A unique number assigned to a client used for internal IRCC identification purposes.
- UMI:
- Unique medical identifier. A unique number used to associate to a specific upfront medical.
- Visa Officer:
- Any IRCC employee who under Canadian legislation has the delegated authority to make decisions/recommendations on visa issues. Previously the term visa officer referred to IRCC employees outside of Canada and migration officers referred to IRCC employees in Canada.
Section 3: Appendices
Appendix I: How to contact us
In Canada
For general inquiries about the Interim Federal Health Program (IFHP), please contact the IFHP team:
Migration Health Branch
Immigration, Refugees, Citizenship Canada
300 Slater Street, 7th Floor
Ottawa, ON K1A 1L1
Email: IRCC.IFHP-PFSI.IRCC@cic.gc.ca
To register as an Interim Federal Health Program service provider, and for inquiries about eligibility, benefits, claim requests or for general information, please contact the Medavie Blue Cross IFHP provider inquiry team:
IFHP Medavie Blue CrossTM
644 Main St., P.O. Box 6000
Moncton, NB E1C 0P9
Website: https://www.medaviebc.ca
Customer Service Centre: 1-888-614-1880
Email: CIC_Inquiry@medavie.bluecross.ca
Fax for inquiries: 506-867-4651
Fax for claims submissions: 506-867-3841
Send paper-based IME and other documents that cannot be uploaded to eMedical to:
Operations Directorate
Integrated Medical Processing Network Division
Migration Health Branch
Immigration, Refugees, Citizenship Canada
300 Slater Street, 7th Floor
Ottawa, ON K1A 1L1
eMedical systems support
For service in English
Contact the Australian Department of Home Affairs via the “Contact Us” tab in the eMedical system.
For service in French
Email IRCC at: IRCC.MHBeMedical-eMedicalDGMS.IRCC@cic.gc.ca
This email is monitored from 8 a.m. to 4 p.m., Canadian Eastern Time, Monday to Friday, excluding statutory holidays.
For critical incidents
Contact IT support immediately.
Telephone: +61-2-6264-0400
Email: ITSupport@homeaffairs.gov.au
Critical incidents include the following:
- total loss of the eMedical system (unexpected outages)
- loss of core functions (cases cannot be submitted, attachments cannot be uploaded)
Note: This service is provided by the Australian Department of Home Affairs 24 hours a day, seven days a week, in
English only.
For enquiries regarding medical clinical issues
Panel members should continue to direct all immigration medical exam-related enquiries to their regional medical office.
Regional medical offices
Your RMO is your point of contact for attaining your status as a panel member, submitting IME results and reports, and all other matters regarding your work as a panel physician or radiologist.
London
Overseas Regional Medical Office
Canadian High Commission
Canada House – Trafalgar Square
London SW1Y 5BJ
United Kingdom
Email: LDNPPMD@international.gc.ca
Manila
Overseas Regional Medical Office
Canadian Embassy
Level 7, Tower 2, RCBC Plaza
6819 Ayala Avenue
Makati City 0707
Philippines
Fax: +632-843-1103
Email: MANILMC-MD@international.gc.ca
New Delhi
Overseas Regional Medical Office
High Commission of Canada
7/8 Shantipath, Chanakyapuri
New Delhi 110021
India
Fax: +91-11-41782020
Email: Delhi-mc@international.gc.ca
Americas
Ottawa Regional Medical Office
Migration Health Branch
Immigration, Refugees, Citizenship Canada
300 Slater Street
Ottawa, ON Canada K1A 1L1
Fax: +1-613-941-2179
Email: IRCC.MHBPMInquiries-RenseignementsMPDGMS.IRCC@cic.gc.ca
Appendix II: Client Declaration and Notice
Appendix III: Forms
- IMM 1020: Medical Report – Client Biodata and Summary - Streamlined
- IMM 5420: Streamlined IME Medical Report
- IMM 5733: Instructions for Pregnant Client − X-Ray Deferred
- IMM 5734: Specialist’s Referral Form
IMM 1020: Medical Report – Client Biodata and Summary - Streamlined
IMM 5420 Streamlined IME Medical Report

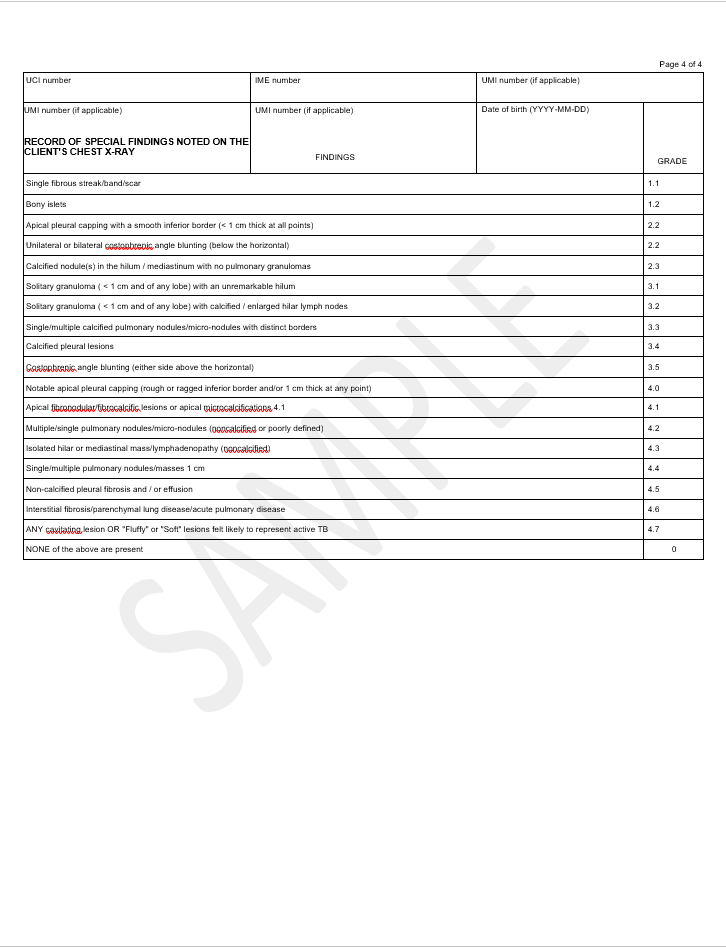
IMM 5733: Instructions for Pregnant Client − X-Ray Deferred
IMM 5733: Instructions for Pregnant Client − X-Ray Deferred (PDF, 2 MB)
IMM 5734: Specialist’s Referral Form
IMM 5734: Specialist’s Referral Form (PDF, 2 MB)
Appendix IV: List of immigration medical examination technical instructions
A) TIs related to process changes resulting from eMedical implementation
Any additional tests can only be performed if requested by an RMO. If an RMO instructs you to complete a test that is not normally part of the Streamlined IME, please consult the associated Technical Instructions in the Panel Member Guide for the ‘standard’ IME.
Resettlement needs assessment
Subject
Instructions for evaluating and reporting the resettlement needs of refugees overseas who have been selected for resettlement in Canada in the context of the Immigration Medical Examination (IME).
Goal/objective
These instructions are provided to ensure panel physicians (PPs) follow a consistent and appropriate process in the:
- assessment of the resettlement needs of refugees overseas
- proper completion of the section 948 resettlement needs
Instructions
Background
It is important that refugees with extensive medical and/or social needs are able to 1) travel to Canada efficiently and safely and 2) be able to settle into Canada with their medical and social needs being recognized and attended to quickly and effectively.
The section 948 in eMedical; resettlement needs has been created in order to capture vital information in support of proper resettlement from a medical perspective. For all overseas refugees selected for resettlement in Canada, section 948 in eMedical is mandatory. In countries where eMedical is not implemented, the Visa Office will issue the IMM 5544 form “Resettlement needs Assessment Form” together with the medical instructions. (IMM 1020 Medical report: client biodata and summary).
The table below provides information for the PP regarding eMedical and paper-based submission of the IMM 5544.
eMedical-enabled panel clinics
- Visa Office (VO) issues IMM 1020 with IMM category of refugee-overseas
- Section 948 is required to be filled out in eMedical and submitted along with the health case
- IMM 5544
Paper-based panel clinics
- Visa Office (VO) issues IMM 1020 with IMM category of refugee-overseas
- IMM 5544 is included in medical instructions sent to client by VO as part of the IME
- Panel physician will complete the IMM 5544 and submit it along with the paper-based IME
The resettlement needs section is used to provide additional information for three important purposes:
- to facilitate safe and efficient travel to Canada
- to maximize post-arrival settlement arrangements on arrival to Canada
- and to help in determining the destination city in Canada where the medical and social services required for the refugee are available
Completing the resettlement needs section
The Resettlement needs section is to be completed for every overseas refugee, even those without medical conditions or concern. Even a negative answer is important. When a refugee has no special travel requirements or settlement issues, the PPs must check the box following the statement “There are no special travel requirements or resettlement needs” (see figure below):

Text version
There are no special travel requirements or settlement issues.
If there are special travel or resettlement issues the PPs will complete, as appropriate, sections 1, 2, 3, 4 and 5.
The list below (indicative but not exhaustive) highlights some commonly encountered medical conditions which do not warrant the detailed filling in of the resettlement needs section:
- Hypertension, well controlled with medication
- Asthma, well controlled with medication
- Inactive pulmonary tuberculosis
- Syphilis, treated
- Epilepsy under good control
- Diabetes under good control without end organ complications
- Skin conditions/infections (psoriasis, fungal infections)
- Visual acuity deficit of equal or better than 6/15 when corrected
- Radiographic cardiomegaly without clinical manifestations or impairment
In order to preserve medical confidentiality, no personal medical information is to be placed on the resettlement needs section. Thus, the PPs must attempt to get across the basis of the medical problem and the special needs of the refugee without referring to a specific medical diagnosis. This applies as well for psychological assessment of the refugee client which is an important aspect in the evaluation of resettlement needs. This is very important to remember since the information on the resettlement needs section will be made available to people who are not medical professionals.
These 5 sections of the resettlement needs section are:
- Functional Assessment (physical and psychological),
- Special Travel Requirements,
- Post-arrival Service Requirements,
- Housing and Daily Activities or Assistance requirements, and
- Other Resettlement needs.
Section 1: Functional assessment
The functional assessment on the resettlement needs section is clear in identifying major problems that can impact on resettlement of the refugee in Canada (see figure below):

Text version: Section 1: Functional assessment
Functional assessment: Indicate Yes or No for every listed impairments: Hearing impairment (Partial or Complete); Vision impairment (Partial or Complete); Speech impairment (Partial or Complete); Cognitive impairment (Mild or Moderate or Severe); Mobility impairment (indicate the current mobility aid and the mobility aid required); Other impairment (provide details). Activity of daily living (Independent or Partial care or Total care; provide details).
Note: Please indicate complete when the impairment is complete, and partial when there is a partial impairment. Complete is not meant to indicate that the PP has completed their assessment, it is meant to indicate that the client is completely blind for example, in relation to a visual impairment.
If any of the above noted impairments is present the PPs must indicate “yes”. If they are not present the PPs must check “No”. Even when only one impairment is present, all other answers must be completed with a “No” response.
When there is a positive response to any of these functional assessment questions, the PPs must provide additional information about the impairment (That is, degree of impairment, use of/requirement for a mobility aid). The PPs must also indicate what level of Activities of Daily Living (ADL) the refugee is functioning at and must also add any details that would assist in understanding the degree to which a refugee might be dependent on others for care (for example: the requirement for assistance with feeding, bathing or toileting).
When “Other” functional impairment is marked, remarks are required from the PPs in order to provide information regarding what the problem is, without stating a medical diagnosis.
If the refugee is currently using, or requires, a mobility aid, the nature of that aid must be noted in the space “Current mobility aid” and if the refugee needs a different aid, this must be stated in the option marked: “Mobility aid required”. The most commonly used mobility aids are canes, walkers and wheelchairs.
Finally, if a person is using or would benefit from a mobility aid, the PPs must take this into account when completing section 4, “Housing Requirements” by adding a notation regarding the need for a single level dwelling and/or elevator access.
Section 2: Special travel requirements
The special travel requirements for the refugee to get to their final destination in Canada are listed on the Resettlement needs section (see figure below):

Text version: Section 2: Special travel requirements
- Special Travel Requirements: In the “Special travel requirements” section, select the applicable ones: None, Wheelchair, Stretcher, Medical escort required, Other. Provide details if necessary.
A “Wheelchair” must be indicated whenever the refugee is using or requires a mobility aid. An indication of the size/type of wheelchair required would be helpful. A wheelchair should also be indicated for persons with any medical condition limiting their ability to move quickly or safely when transferring between terminals at an airport. Often this would be the case for persons with mobility problems associated with osteoarthritis, amputation, or cerebral palsy. It should also be considered for persons with cardio-respiratory disorders such as angina, congestive heart failure, valvular heart disease, or chronic obstructive pulmonary disease (COPD).
Please note that request for a “Medical Escort” will be vetted by the Regional Medical Office (RMO) responsible for the refugee’s IME and by IRCC in Ottawa.
If the “Other” option is used, the PPs must provide the specific information in the “Details” section below the responses. Most commonly the option of “Other” will be used when the refugee should be accompanied by an adult family member or might need assistance in undertaking immigration formalities at the Port of Entry in Canada.
It is possible for more than one box to be completed in this section. For example a refugee with severe congestive heart failure might need both a wheelchair during the travel period as well as a medical escort.
Section 3: Post-arrival services required
This section of the resettlement needs Assessment is important as it indicates the actual social and/or medical services that the refugee will require in Canada. Please keep in mind that all refugees will be seen by general practitioners (GPs) in Canada within weeks of their arrival. We are asking PPs to note in this section any requirement for services that would be outside of the services provided by GPs. For example, common diabetes or hypertension are handled by GPs in Canada. Follow up for diabetes would therefore not represent a post-arrival service worth noting.
Social services available in Canada range from special education, speech therapy, occupational therapy, physiotherapy to vocational rehabilitation, attendant care. Social services can also include specialized housing services such as home care and long term care (these housing and care services would require an application to be made and would usually require an assessment by a health professional regarding the need and eligibility for the service). Medical services available in Canada run the full range of specialties and include operative and non-operative care for such medical conditions as cancer, renal failure, coronary artery disease, osteoarthritis, hepatitis and the human immunodeficiency virus (HIV).
In filling in the resettlement needs section, the post-arrival services requirements are either “no services required” or “Consultation with a health care professional required” (see figure below):

Text version: Section 3: Post-arrival services required
- Post-arrival services required. In the “Post-arrival services required” section of the Resettlement Needs section, the requirements are either “no services required” or “Consultation with a health care professional required”. If “Consultation with a health care professional required” is checked, indicate if it is Urgent (72 hrs); Specialized services, Within X weeks, Long term services or As required. Provide details if necessary.
When a consultation is required, the PPs must indicate how quickly that should take place (as shown in the figure above). Again, please keep in mind that post-arrival services worth noting are those provided outside the scope of what GPs would provide.
In deciding on the number of weeks that would be reasonable before the refugee should be seen by a specialist consultant, the PPs must keep in mind that a consultation with a specialist in Canada, can take several weeks and even months to set up. Thus, for a chronic, well controlled, medical condition, one should indicate “as required”.
Long standing conditions that require assessment for a special education class, vocational training, or rehabilitation can also usually be marked “as required”.
Conditions that might benefit from being seen by a specialist in a shorter period of time would be unstable angina or congestive heart failure, or newly diagnosed diabetes needing training of the use of insulin.
In general, almost any refugee requiring a medical escort to accompany them safely to Canada will require an “urgent” specialist assessment. This might include a case of severe COPD requiring oxygen for travel or for everyday use, or a case of severe valvular heart disease requiring stabilisation of secondary heart failure and an “urgent” assessment for consideration of valve replacement surgery. Individuals requiring an assessment for home care or long term residential care must also be marked “urgent”.
If there is any uncertainty with respect to the urgency or time-frame for an Applicant to be assessed by a medical specialist upon arrival to Canada, please contact your Regional Medical Office.
If the refugee’s visual impairment appears to be, or is most likely due to a simple refractive error (most often with younger clients) the best option would be recommendation to see an optometrist. If on the other hand, the visual problem could reasonably be due to cataracts or glaucoma (based on clinical findings or the age of the client) the best option would be referral to an ophthalmologist.
As stated earlier, the “Specialised Services” noted under “Consultation with a health care professional” can refer to needs for such varied social and medical services as:
- special education
- occupational therapy
- physiotherapy
- speech therapy
- vocational training
- lip reading or sign language training
- training for a blind person in navigating his home and community
Long term services can refer to such services as placement of the refugee in a long term care centre for someone who has had a stroke and is not (and will never be) independent in their activities of daily living
Section 4: Housing and daily activities/assistance requirements
The housing and daily activities/assistance requirements section offers the PPs four options for completion (see figure below):

Text version: Section 4: Housing and daily activities/assistance requirements
- Housing and daily activities/assistance requirements. The “housing and daily activities/assistance requirements” section offers the PPs four options for completion: Fully independent, no assistance required; Wheelchair access required; Home care/support services required (Periodically or Permanently); Specialized services required to accommodation functional impairments. Please specify the specialized services required.
The first two options are more or less self-explanatory. The PPs shall keep in mind that someone who does not currently use a wheelchair but who would benefit from one must have the “Wheelchair access required” response checked. This must correspond with a previous positive response regarding “Mobility impairment” in Section 1 of this form.
If the PPs consider that “Home care/support services” are required for a refugee to carry out daily activities in their own home, this must be checked as well as the anticipated frequency of that service. For example, attendant care (for example, nursing care) might be considered necessary for an elderly person who is not able to see well enough to count out daily medications or to give an insulin injection. This would be required daily and permanently. For someone requiring assistance with bathing, the visits by a home care nurse might only be once a week, in which case “periodic” must be checked.
Types of home care services available in Canada are “periodic” and “permanent” (see figure above).
The last option for the PP to consider under Housing and Daily Activities is “Specialized services required to accommodate functional impairments”. This could include long term care in a residential facility with 24-hour nurse staff. Normally this expensive form of residential care is limited to persons who cannot safely function with the more limited nursing services available through home care. Another specialized service might be home oxygen for a refugee with severe COPD.
Section 5: Other comments related to resettlement needs
This section must only be used when relevant details are needed and cannot be written in any of the above sections. Again under no circumstances should a medical diagnosis or information that leads to a medical diagnosis appear on the Resettlement needs section. The PPs must attempt to get across the basis of the medical problem and needs without referring to a specific medical diagnosis.
Once the Resettlement needs section is completed, PPs will submit the completed document electronically. PPs who works on paper IME will date and sign at the bottom of the form indicating their P number and the place where the form was completed.
Example: Section 948 Resettlement needs in eMedical
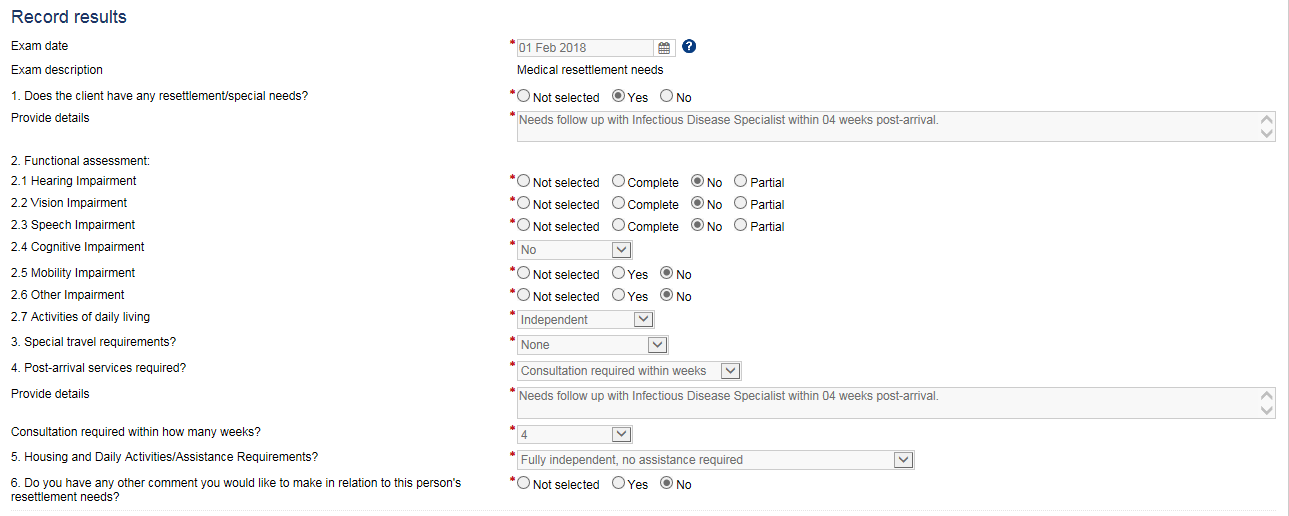
Text version: Section 948 Resettlement needs in eMedical
In eMedical, Section 948 Resettlement Needs, in the Record results section:
Select the exam date.
- Q1: Does the client have any resettlement/special needs? Select Yes and provide details.
- Q2: Functional assessment
- Q2.1 Hearing impairment (No, Partial or Complete)
- Q2.2 Vision impairment (No, Partial or Complete)
- Q2.3 Speech impairment (No, Partial or Complete)a
- Q2.4 Cognitive impairment (Mild or Moderate or Severe)
- Q2.5 Mobility impairment (indicate the current mobility aid and the mobility aid required)
- Q2.6 Other impairment (provide details).
- Q2.7 Activity of daily living (Independent or Partial care or Total care).
- Q3: Special travel requirements: Select the applicable one: None, Wheelchair, Stretcher, Medical escort required, Other.
- Q4: In the “Post-arrival services required” section, the requirements are either “No services required” or “Consultation with a health care professional required”. If “Consultation with a health care professional required” is checked, indicate if it is: Urgent (72 hrs); Specialized services, Within X weeks, Long term services or As required. Provide details if necessary. Indicate in how many weeks the consultation is required.
- Q5: In the “housing and daily activities/assistance requirements” section offers the PPs four options for completion: Fully independent, no assistance required; Wheelchair access required; Home care/support services required (Periodically or Permanently); Specialized services required to accommodation functional impairments.
- Q6: Do you have any other comment you would like to make in relation to this person’s resettlement needs? Select Yes or No.
Resettlement needs assessment form
B) TIs related to screening for danger to public health
Subject
For the purposes of the Streamlined immigration medical examination (IME), these screening instructions will focus on the detection of active pulmonary tuberculosis infections.
Goal/objective
This document provides guidelines, instructions and algorithms for the screening and diagnosis of active tuberculosis according to the latest Canadian Tuberculosis Standards2 and World Health Organization (WHO) guidelines on TB.3
These instructions are provided to ensure that panel physicians follow a consistent and appropriate process for the following:
- Identification of clients with active TB;
- Investigation of clients where there is clinical suspicion of active TB;
- Investigation of clients who are close contacts of an individual with active TB; and
- Completion and grading of an IME of a client with active TB.
Instructions
Particular attention must be paid to signs, symptoms and risk factors suggestive of active tuberculosis. Some of the strongest predictors of active TB include the country of origin, living conditions, recent contact with active TB and medical comorbidities (Appendix A)4. The following instructions apply to all clients who require a Streamlined IME:
- Screen all clients for tuberculosis during the review of medical history.
- Require a postero-anterior chest x-ray (CXR) for all clients ≥ 11 years of age.
- Require an antero-posterior and lateral CXR for all clients < 11 years of age who are a close contact of someone with active TB or are presenting with signs and symptoms suggestive of active TB.
- Perform the tuberculosis screening algorithm to detect TB.
IMEs for clients who have CXR lesions ≥ 4.1 and/or have symptoms of active TB should be graded B, specify active TB concern in the comments, indicate which additional tests are being completed (see information below), and promptly submitted in eMedical. Concurrently, panel member should undertake the following steps:
Note: Do not delay the IME submission while completing or awaiting results for the following tests.
601 - Sputum smears & cultures (x3): If available, molecular testing for Mycobacterium tuberculosis (MTB) based on nucleic acid amplification (NAAT) must be performed on the first specimen when all acid-fast bacilli (AFB) smears are negative OR on one of any specimen with a positive smear (Appendix B).
Contact Tracing
If a person infected with pulmonary tuberculosis is identified during the course of the IME, it is imperative to conduct contact tracing on the family members of the index case as soon as possible. Any client that meets the definition of a close contact (Appendix A) and requires an IME must undergo screening as outlined in the instructions.
For clients = 2 years of age, IGRA testing is required using one of the following two tests: QIAGEN QuantiFERON® for TB (or any iteration, such as QuantiFERON-TB Gold Plus) or Oxford Immunotec T-SPOT®.TB. For immigration purposes, an indeterminate, borderline, or weakly positive IGRA results should be reported as negative.
The tuberculin skin test (TST) can be used in place of IGRA only if both of the above mentioned 2 IGRA products are not licensed in the country of practice.
For clients < 2 years of age, a TST should be performed using purified protein derivative (PPD) administered intradermally by the Mantoux method. Preparations used should be equivalent to 5TU.
A TST positive result is a measured induration = 5mm read 48 to 72 hours after planting the PPD. Clients with documented positive PPD results should be reported as positive and PPs should proceed with the algorithm.
To note: an induration = 10 mm is clinically used for positive results. Panel Physicians should notify the RMO as soon as possible if IMEs have already been completed and submitted for family members who require contact tracing.
If additional tests, screening, or treatment is required, RMOs will notify you through the furtherance process.
Urgent processing
In an urgent processing context (such as in response to a humanitarian crisis), the RMO may reach out to you to provide modified instructions and request accelerated submissions of IMEs. In these instances, panel physicians should aim to submit the IMEs without delay. Where required and appropriate, RMOs will create a furtherance request for the outstanding information or additional tests.
Reporting Results to IRCC
When indicated, tuberculosis screening with sputum testing should be requested. If it is not possible to obtain sputum samples or if procedures require a specialist referral, submit file with a note indicating: “Applicant unable to produce sputum” or “Specialist referral required”. The RMO will provide further instructions.
Any previous chest x-rays or specialist reports available should be submitted with IME.
For results and reporting for contact tracing, go directly to the contact tracing algorithm below.
Grading and submission of files
All IMEs for clients with CXR lesions ≥ 4.1 or with active or symptoms of pulmonary TB, or where panel members are suspicious of active pulmonary TB must be graded B. All results and specialist reports must be attached to the file. General comments should be entered as per the algorithm.
All files are to be submitted within the 10-day client service standard.
Public Health Reporting
In parallel to the immigration medical examination process, panel physicians are to provide appropriate and timely advice to the client when they discover a medical condition not known to the client and follow the appropriate steps required in their jurisdiction. In doing so, they are to uphold their professional and ethical standards by referring the client back to their usual treating physician or to an appropriate specialist upon request.
Pulmonary Tuberculosis Screening Algorithm
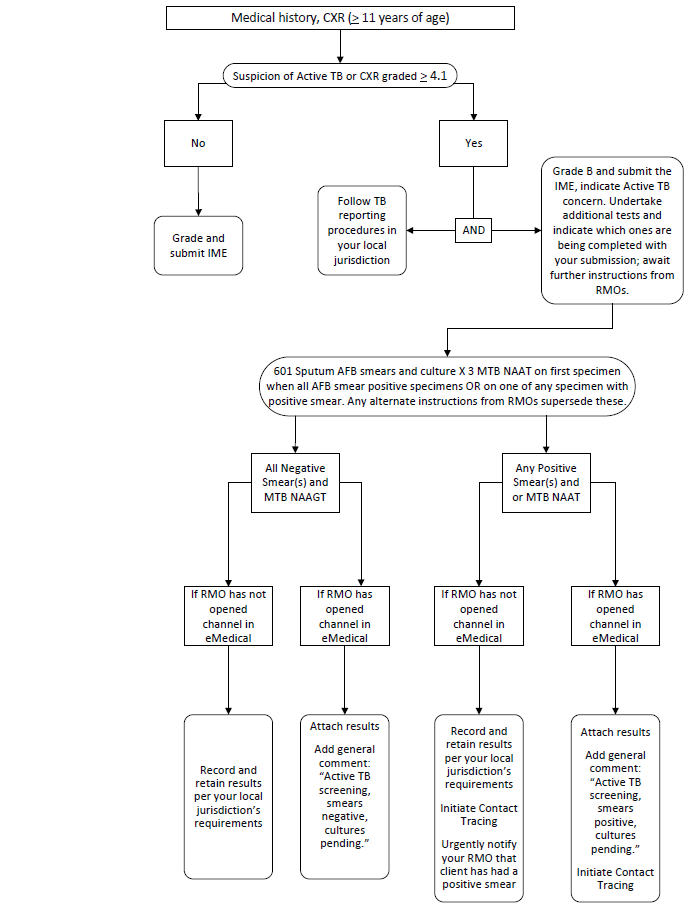
Text version: Pulmonary Tuberculosis Screening Algorithm
All clients are screened for TB during medical history taking, physical examination and CXR (= 11 years)
Active TB
Q1: Is there suspicion of Active TB and /or CXR graded = 4.1?
Yes: Grade B and submit the IME, indicate Active TB concern. Undertake additional tests and indicate which ones are being completed with your submission; await further instructions from RMOs.
and
Follow tuberculosis reporting procedures in your local jurisdiction.
No: Grade and Submit the IME.
Q2: 601 Sputum AFB smears and culture X 3 MTB NAAT on first specimen when all AFB smear positive specimens or on one of any specimen with positive smear. Any alternate instructions from RMOs supersede these.
All Negative Smear(s) and MTB NAAGT:
- If the RMO has not opened channel in eMedical: Record and retain results per your local jurisdiction’s requirements.
- If the RMO has opened a channel in eMedical: Attach results. Add general comment: “Active TB screening, smears negative, cultures pending.”
Any Positive Smear(s) and or MTB NAAT
- If the RMO has not opened channel in eMedical: Record and retain results per your local jurisdiction’s requirements. Initiate Contact Tracing. Urgently notify your RMO that client has had a positive smear.
- If the RMO has opened a channel in eMedical: Attach results. Add general comment: “Active TB screening, smears positive, cultures pending.” Initiate Contact Tracing.
Contact Tracing Algorithm

Text version: Contact Tracing Algorithm
Grade B and submit the IME, initiate contact tracing and undertake additional tests. As part of your IME submission, indicate “Close Contact with confirmed or suspected Active TB” and indicate which tests are being completed.
Clients require 950 – IGRA if ≥ 2 years of age or TST if the client is < 2 years AND clients < 11 years of age require a 502-AP CXR and 510-Lateral CXR.
Q1: All the results are negative (IGRA, TST <5mm, CXR < 4.1)
- If RMO has not opened channel in eMedical: Record or retain results per your local jurisdiction’s requirements.
- If RMO has opened channel: Attach results. Add general comment: “Contact tracing completed, all results negative.”
Q2: Any positive results (IGRA, TST ≥ 5mm, CXR ≥ 4.1)
- If RMO has not opened channel in eMedical: Record or retain results per your local jurisdiction’s requirements. Send urgent communication to your RMO indicating the positive result and Active TB concern, await further instructions from RMO.
- If RMO has opened channel: Attach results. Proceed with TB screening algorithm.
Appendix A – Predictors of Active Pulmonary Tuberculosis
Symptoms
- Persistent cough
- Fever
- Night sweats
- Anorexia
- Fatigue
Signs
- Bronchial breathing, rales or crepitation
- Weight loss
- Hemoptysis
- Fibrotic lesion on chest x-ray
Risk Factors
- Country of origin with high TB incidenceFootnote 15
- Medical conditions affecting Immune System
- Extra Pulmonary Disease
- HIV infectionFootnote 4
- MalnutritionFootnote 4
- Work environment with silica exposureFootnote 13
Definition of Close ContactFootnote 16
A TB close contact is an individual who has shared the same air space for a prolonged period of time with a person with infectious TB. The exact duration of exposure is traditionally at least 8 hours of cumulative exposure.
Examples of close contacts may include individuals:
- living in the same household
- sharing a confined workplace
- sharing sleeping quarters for at least one night
- living in residential institutions such as
- military barracks
- correctional institutions
- boarding schools
Appendix B – Sputum Collection/Induction
| Specimen | Comment |
|---|---|
| Spontaneous Sputum |
|
| Induced Sputum |
|
Technical Instruction for all specimen typesFootnote 14
- Collection in morning under direct supervision and at least 1 hour between specimen
- Distilled or filtered bottle only for rinsing mouth
- Collection container: sterile, single use, screw capped 20 to 50 ml centrifuge tube
- Centrifugation required before preparing smears
- Identification: each specimen identified with unique bar code/number, date/time, specimen information
- Requisition: clearly mark sputum spontaneous or induced
- Transport: same day delivery. If not possible to deliver immediately to laboratory, refrigerate (2-8°C) using a refrigerator or cooler with ice packs
Procedures to be performed in designated collection area by trained technician using protective equipment (adequate respiratory protection with N-95 mask and gloves).
Initial TB investigation consists of three sputum specimens to undergo smear microscopy for acid-fast bacilli (AFB) as well as culture for Mycobacteria at the M. tuberculosis complex level for all three specimens. When available, molecular testing for Mycobacterium tuberculosis (MTB) based on nucleic acid amplification (NAAT) should be performed on the first specimen when all AFB smears are negative OR on one of any specimen with a positive smearFootnote 2,Footnote 6. Note that this test is not accepted as a substitute for tuberculosis cultures, which are required in all cases where sputum is collected.
The 3 sputum specimens can be collected on the same day at least 1 hour apart. Preferably spontaneously produced deep cough sputum should be obtained. When not possible to obtain spontaneous sputum, it is recommended that sputum induction be performed.Footnote 2
Concentrated sputum smear microscopy using auramine stain with fluorescence microscopy is preferable, but Zielh-Neelsen or Kinyoun staining is acceptable.Footnote 2 Solid and liquid medium cultures are required for every specimen sent for smear microscopy.Footnote 7 Drug susceptibility test (DST) using phenotypic method should be performed for all first positive culture.Footnote 1
References
C) TIs related to screening for danger to public safety
Subject
These instructions have been developed to support the following medical history question in the Canadian Streamlined immigration medical examination (IME):
Have you ever been arrested, hospitalized, or treated medically for (1) actions that caused harm or posed a high risk of being harmful to others or (2) substance use that had a harmful impact on yourself or others?
Goal
These instructions will help ensure that panel physicians follow a consistent and appropriate process for:
- Identifying clients that meet the criteria described in the screening question;
- Recording key details about the client’s response where appropriate; and
- Completing and grading the IME.
Instructions
The panel physician’s role, through the aforementioned medical history question, is to help screen for conditions of public safety concern. A condition of public safety concern refers to a mental health condition in an individual, for which the examining physician is of the opinion that the person poses a risk to cause harm to others. To help ensure a consistent interpretation and application of the medical history question, the panel physician must consider the following in their examination of the client:
(1) Context
Clients identified with a condition of public safety concern may face different systemic responses and outcomes across jurisdictions, often due to differences in access to mental health services, policy, mental health literacy and awareness, as well as stigma and discrimination. Even within a single jurisdiction, different systemic responses may be observed across similar cases. Accordingly, panel physicians should consider that conditions of public safety concern could lead to various outcomes across clients, including: incarceration or other criminal justice consequences, hospitalization (including for extended periods of time), or medical treatment. For clients who indicate that they have been arrested or had interactions with the criminal justice system as a result of a condition of public safety concern, panel physicians must only enquire about, and record details on, information directly relevant to these instructions and the immigration medical examination screening requirements.
(2) Harmful behaviour
A harmful behavior is defined as an action associated with a condition or disorder that is causing or has caused any of the following: (a) serious psychological or physical injury to the individual or to others (e.g., a suicide attempt, child abuse, etc.); (b) a serious threat to health or safety (e.g., driving while intoxicated, verbally threatening to kill someone, etc.).
Disorders most commonly associated with harmful behavior include:
- Mood disorders that include major depression and bipolar disorders and can be associated with high rates of suicide and aggression.
- Anxiety disorders that include post-traumatic stress disorder, panic disorders, phobias, and may be associated with harmful behavior.
- Personality disorders that include antisocial, paranoid, and borderline personality disorders and can be associated with impulsive acts of violence.
- Sexual disorders that include paraphilia, which may lead to harmful behaviors like sexual assault, rape, etc.
- Schizophrenia and other psychotic disorders that can be associated with delusions, paranoia, suicide, and aggressive acts.
- Substance-related disorders that include substance dependence or abuse.
A current or past history of any of the following characteristics might also be associated with harmful behaviours and suggest that the individual could pose a danger to public safety:
- Delusional behaviour, or a diagnosis of schizophrenia or schizoaffective disorder
- Antisocial, violent, or impulsive behaviour (including impaired driving)
- Paranoid ideas or odd beliefs
- Homicidal or suicidal thoughts
- Substance use disorder
- Memory disturbance
- Psychological or physical trauma, including post-traumatic stress disorder (PTSD)
- Aberrant sexual disorders, such as pedophilia
As part of their examination of the client, where appropriate, the panel physician should seek to make a determination about whether the harmful behaviour may be related to an aforementioned health condition or disorder.
Occasionally, there are cases where harmful behavior may primarily occur due to the applicant’s environment (e.g., an abusive household or the applicant lives in a region in which they are persecuted). These cases should be carefully evaluated on a case-by-case basis and an exception to the above definition of harmful behavior may be made, depending on the circumstances.
Another exception that may be considered is when individuals with significant intellectual disability may exhibit behaviors such as hitting, biting, and head-banging, as a means of expressing frustration. However, careful evaluation must be made to ensure that such repetitive behaviors are not done with intent to harm.
To note: Many conditions listed above can be adequately managed through treatment and/or medication and will not result in an individual posing a danger to public safety. For example, anxiety disorders, personality troubles or mild mood disorders requiring no or minimal follow up and that have no impact on public safety are quite common. Panel physicians must therefore use their discretion, in combination with these instructions, to only report cases that are associated with a genuine concern that the individual has a condition of public safety concern.
(3) Substance Use
Substance use is different for everyone and can be viewed on a spectrum with varying stages of benefits and harms.
Higher-risk substance use is use that has a harmful and negative impact to a person, their family, friends and others. Examples include binge drinking, impaired driving, use of illegal drugs, increasing quantity used, increasing frequency of use, and combining multiple substances.
Substance use disorder is a medical condition that affects the brain and involves compulsive and continuous use despite negative impacts to a person, their family, friends and others. Substance use disorders are important to identify due to their association with antisocial and criminal behaviours, as well as their ability to induce mood disturbances and psychosis.
Substances of abuse may include, but are not limited to: alcohol, marijuana, opioids, cocaine, methamphetamine, benzodiazepines, prescription or over-the-counter medications.
For the purposes of the Streamlined immigration medical examination, panel physicians should only seek to identify clients with higher-risk substance use or above on the spectrum provided below.

Text version: Substance Use Spectrum
Non-use: Avoiding use of substances (abstinence).
Example: No drugs, tobacco or alcohol
Beneficial Use: Use that can have positive health, social, or spiritual effects.
Example: Tasking medication as prescribed, ceremonial/religious use of tobacco (such as smudging)
Lower-risk Use: Use that has minimal impact to a person, their family, friends, and others.
Example: Drinking alcohol following the low-risk alcohol guidelines, cannabis use according to the lower-risk cannabis use guidelines
Higher-risk Use: Use that has a harmful and negative impact to a person, their family, friends, and others.
Example: Use of illegal drugs, impaired driving, binge drinking, combining multiple substances, increasing frequency, increasing quantity
Addiction (Substance use disorder): A treatable medical condition that affects the brain and involves compulsive and continuous use despite negative impacts to a person, their family, friends and others.
Example: When someone cannot stop using drugs, tobacco or alcohol event if they want to
Grading, Recording Comments, and Submission of Files
All IMEs for clients who answer yes to the question ‘Have you ever been arrested, hospitalized, or treated medically for (1) actions that caused harm or posed a high risk of being harmful to others or (2) substance use that had a harmful impact on yourself or others?’ must be graded B.
Panel physicians must also record the following details in the appropriate eMedical comment box:
- Description of the behaviour and current symptoms;
- Details and history of the condition or disorder;
- Investigations and treatment completed at the time of the behaviour if not current (including medication, hospital admissions, out-patient visits etc.); and
- Evaluation of the behaviour(s) that could potentially be harmful to self or others.
Where available, provide any available reports (psychiatry, psychotherapy, social worker, etc.) as an attachment in your IME submission.
All files are to be submitted within the 10-day client service standard. In cases where report(s) are pending, submit the IME with a note indicating that additional medical information is pending. The Regional Medical Office will create a ‘furtherance request’ for the pending information as required.
Reporting
Panel physicians must not refer clients to specialists unless instructed by the Regional Medical Office. Submit the IME without delay and await further instructions from the Regional Medical Office.
In parallel to the Immigration Medical Examination process, panel physicians are to provide appropriate and timely advice to the client when they discover a serious medical condition not known to the client. In doing so, they are to uphold professional and ethical standards by referring the client back to their usual treating physician or to an appropriate specialist upon request.
D) TIs related to screening for excessive demand on health and social services
Subject
These instructions have been developed to support the following medical history question in the Canadian Streamlined immigration medical examination (IME):
“Does the client present a health condition listed in the Excessive Demand Technical Instructions?”
Goal
These instructions will help ensure that panel physicians follow a consistent and appropriate process for:
- Identifying clients with one or more of the listed health conditions below;
- Recording details about the health condition(s) before the Streamlined IME is submitted; and
- Completing and grading a Streamlined IME for clients with a listed health condition.
Instructions
Rationale
In Canada, health care is delivered through a publicly-funded health care system. Some treatments, therapies, and services that are needed to treat or manage certain health conditions can be costly, and for some conditions, in short supply. IRCC, through its immigration medical examination, is responsible for screening individuals who might reasonably cause an excessive demand on health or social services in Canada or who may displace Canadians on existing waitlists for certain treatments or procedures.
Screening and testing
As part of the medical history questionnaire, panel physicians should screen each client to confirm the presence of any of the health conditions listed below. If the client confirms the presence of a health condition, or if based on their assessment, panel physicians suspect the presence of one of the listed health conditions, additional details should be provided in the appropriate eMedical comment boxes (see each health condition below for more information).
Unless instructed otherwise by a Regional Medical Office (RMO), panel physicians should only provide information readily available from the client and should not request any additional testing, screening or referrals for the client for the purposes of their Streamlined immigration medical examination. Panel physicians should record and submit the Streamlined immigration medical examination without delay. If any additional screening or information is required, the RMO will create a furtherance request.
Health Conditions
Panel physicians should screen each client to confirm the presence of any of the health conditions listed in this section.
Please note that health conditions listed in these technical instructions may be updated in the future. Panel physicians should review this page on a regular basis to ensure they are screening for the appropriate health conditions.
Health Condition 1: chronic renal failure / chronic kidney disease
If a client responds ‘yes’ to the question “has a healthcare provider diagnosed you with ongoing (chronic) kidney disease?”, panel physicians must record as much of the following information in the ‘please specify’ comment box as possible:
- Date of diagnosis and current stage of disease if known
- Current management (e.g. medication, dialysis)
- Details about recent hospitalizations
- Impact on activities of daily living
- Anticipated future treatment needs
If a report from a treating physician or existing lab results are available, please include them as an attachment with the IME.
Health Condition 2: cancer (any type)
If a client responds ‘yes’ to the question “are you currently undergoing cancer treatment?”, panel physicians must record as much of the following information in the ‘please specify’ comment box as possible:
- Diagnosis (including cancer staging) and date of diagnosis
- Condition management (including treatment needs related to surgery, chemotherapy, radiation therapy, planned duration of treatment, and other medications)
- Current clinical status
If a report from a treating physician is available, please include it as an attachment with the IME.
Health Condition 3:Any health condition that requires the client to have routine and ongoing assistance with activities of daily living (e.g. bathing, feeding, dressing and toileting), such as:
- Senile dementia
- Cerebrovascular accident (stroke)
- Other debilitating conditions for which institutional care might be needed
If a client responds ‘yes’ to the question “do you require routine and ongoing assistance with activities of daily living such as bathing, feeding, dressing, and toileting?”, panel physicians must record as much of the following information in the ‘please specify’ comment box as possible:
- Diagnosis/differential diagnosis, and etiology if known
- Details about the duration, stability, and/or progression of symptoms
- Details about their ability to complete activities of daily living and live independently
- Level of assistance currently provided (e.g., at-home care, long-term care facility etc.)
- Recent medical/health care received (for example, hospitalization, specialist consultations)
If a report from a treating physician is available, please include it as an attachment with the IME.
Grading and submission of files
All Streamlined IMEs for clients who responded ‘yes’ to any of the health conditions listed above must be graded B.
All files are to be submitted within the 10 day client service standard. Where required, the RMO will create a furtherance request for outstanding information or additional screening.
Reporting
In parallel to the immigration medical examination process, panel physicians are to provide appropriate and timely advice to the client when they discover a medical condition not known to the client. In doing so, they are to uphold their professional and ethical standards by referring the client back to their usual treating physician or to an appropriate specialist upon request.