
2022-23 Departmental Plan: Patented Medicine Prices Review Board
Catalogue no.: H79-11E-PDF
ISSN: 2371-7807
Patented Medicine Prices Review Board
The Honourable Jean-Yves Duclos
Minister of Health
Table of contents
- From the Acting Chairperson
- Plans at a glance
- Core responsibilities: planned results and resources, and key risks
- Internal services: planned results
- Planned spending and human resources
- Corporate information
- Supporting information on the program inventory
- Supplementary information tables
- Federal tax expenditures
- Organizational contact information
- Appendix: definitions
- Endnotes
From the Acting Chairperson
I am pleased to present the 2022-23 Departmental Plan for the Patented Medicine Prices Review Board (PMPRB).
The PMPRB is an independent quasi-judicial body established by Parliament in 1987 under the Patent Act (the “Act”). The PMPRB is a consumer protection agency with a dual regulatory and reporting mandate. Its regulatory mandate is to ensure that the prices of patented medicines sold in Canada are not excessive. Its reporting mandate is to provide stakeholders with pharmaceutical trends information to help them make informed choices.
For the better part of two years now, Canadians have endured the disruption and uncertainty occasioned by a once-in-a-century, global pandemic. COVID-19 has wreaked havoc with every aspect of our daily lives and spared no segment of society. Governments at the federal, provincial and territorial level have scrambled to mobilize resources and reprioritize their policies in order to meet the challenges posed by the pandemic and shield their populations from its most harmful effects. At the federal level, one of the policies that has taken a necessary backseat to COVID related priorities during this time has been the Government’s longstanding commitment to strengthen and modernize the PMPRB’s regulatory framework through amendments to the Patented Medicines Regulations. These amendments were originally slated to come into force in July of 2020. However, in order to avoid the imposition of a new administrative burden on the pharmaceutical industry in the midst of the pandemic, the Government has postponed their coming into force until, most recently, July of 2022.
While delaying the regulatory amendments is a perfectly reasonable course of action in the present circumstances, it has given rise to certain difficulties for the PMPRB in setting and meeting its yearly priorities. As mentioned in last year’s Departmental Plan, the PMPRB has been on a reform track for several years running. With the release of our new Guidelines in October of 2020, we anticipated turning the page on that chapter of our history and setting our sights on a new and different set of priorities. However, with the regulatory amendments now tentatively slated to come into force in July of 2022, and the possibility of further extension on the horizon depending on the evolving state of the pandemic, this leaves the PMPRB in somewhat of a holding pattern for the foreseeable future in terms of any priority setting with respect to this issue.
The upshot to the successive six-month deferrals in the coming into force of the regulatory amendments is that it has afforded PMPRB staff ample time to make the necessary changes to our online filing, standard operating procedures and data management systems and to provide patentees with the information and knowledge they need to comply with the new framework once it is up and operational. Accordingly, no further preparatory work is necessary on that front in order for the PMPRB to hit the ground running if and when the amendments come into force.
Notwithstanding the uncertain fate of the regulatory amendments in 2022-23, the PMPRB will continue to make productive use of whatever delay period is associated with their coming into force. This past year, the PMPRB conceived and consulted on a comprehensive Guidelines Monitoring and Evaluation Plan (GMEP). The purpose of the GMEP is to evaluate any changes in relevant trends following implementation of the new Guidelines and inform any future adjustments to ensure that they are working properly. It comprises four key areas of focus: prices, access, ecosystem and PMPRB processes. We anticipate further consultations with stakeholders in the coming year to assist us in identifying and quantifying the appropriate benchmarks to be used for comparison purposes before the implementation of the new regime.
As a member of the Health Portfolio, the PMPRB plays a role in advancing the broader objective of improving the health of Canadians through a responsible, accessible and sustainable health system. In the coming year, the PMPRB will continue to work in lockstep with our federal, provincial and territorial (F/P/T) health partners to align and optimize our respective processes. Likewise, under our National Prescription Drug Utilization Information System (NPDUIS) reporting mandate established by the Minister under s. 90 of the Act, we will continue to provide analytical support and expertise to our health partners, as appropriate, in our collective efforts to advance policy work on pan-Canadian initiatives to improve the pricing and reimbursement of pharmaceuticals in Canada, including the potential establishment of a Canadian drug agency, a national formulary and a rare disease drug strategy.
Given the opposition to the regulatory reforms from industry and some patient groups, the PMPRB has been mired in an unprecedented level of litigation of late, with multiple ongoing judicial reviews of the existing and amended legislation and the new Guidelines winding their way through the courts. We will continue to provide expertise and legal support to counsel for the Attorney General in their vigorous defence of the reforms. In that same vein, until such time as the new regulatory framework is in force, PMPRB staff will make the best use of the existing regulatory tools at its disposal in order to protect Canadians from excessive pricing in Canada in an era marked by a rapidly increasing number of extremely high cost drugs.
Finally, it should be noted that in November 2021, Dr. Mitchell Levine’s 5-year term as the PMPRB’s Chairperson came to an end. As Vice-Chair, it is my honour and privilege to serve as acting Chairperson until a duly appointed replacement for Dr. Levine may be found. Dr. Levine is not the only key member of our personnel to have recently left the PMPRB and we anticipate the possibility of further such departures in the coming year or two. Accordingly, as we move forward with measures to attract and retain talented and high performing people for positions of leadership within the organization, we will ensure that all our staffing and human resource processes uphold the principles of equity, diversity and inclusion and that our workplace is healthy, safe and reflective of the Canadian population we serve.
Mélanie Bourassa Forcier
Acting Chairperson
Plans at a glance
Priority 1 – Implement new pricing framework and begin evaluating its impact
In October 2020, the PMPRB issued new Guidelines. The Guidelines, which are non-binding, implement the amendments to the Patented Medicines Regulations, currently slated to come into force on July 1, 2022, and formalize the PMPRB’s move to a more risk-based approach to ensuring that prices of patented medicines are not excessive. To make the eventual transition to the PMPRB’s new regulatory framework as seamless as possible, the PMPRB will:
- continue its outreach strategy to raise awareness of the new Guidelines through webinars, information sessions and presentations, and guidance documents which will facilitate patentee compliance with the new filing requirements, comparator countries and excessive pricing factors;
- Continue to advance work under the Guidelines Monitoring and Evaluation Plan (GMEP) by identifying and quantifying the appropriate benchmarks to be used for comparison purposes before the implementation of the new regime.; and
- continue supporting the Attorney General of Canada in its defence against challenges to the amendments to the Patented Medicines Regulations and the new Guidelines.
Implementation of the PMPRB’s new Guidelines is the final step in a multi year effort to give effect to the Government of Canada’s 2017 commitment to improve access to prescription medications, lower drug prices and support appropriate prescribing
Priority 2 – Support the Government’s high-level priorities for the future of pharmaceutical management in Canada
This priority reflects ongoing work to better align and integrate the roles, responsibilities and processes of the various participants in the pan-Canadian pharmaceutical pricing and reimbursement system with a view to addressing concerns related to the price, accessibility and appropriate prescribing of medicines in Canada. These include the potential establishment of a Canadian Drug Agency, a national formulary and a rare disease drug strategy. To help advance the national conversation on these initiatives, the PMPRB will:
- Work with Federal/Provincial/Territory (F/P/T) health partners to align and optimize our respective processes in the context of its new regulatory framework and other recent or ongoing reforms that impact pricing and reimbursement;
- Provide analytical support and expertise to F/P/T health partners, as appropriate, in efforts to advance policy work in priority areas such as drugs for rare diseases, common formularies, and other pan-Canadian initiatives to improve the pricing and reimbursement of pharmaceuticals in Canada; and
- Focus reporting efforts on key areas for achieving greater savings for the Canadian health care systems in an era where very high-cost medicines pose an increasing threat to sustainability of public and private drug plans.
In the course of carrying out its regulatory and reporting mandate, the PMPRB has developed considerable policy and analytical capacity and is frequently used as a resource to support broader efforts by the federal Health Portfolio and pan-Canadian partners to foster a modern and sustainable health system. At a time of unprecedented change in the Canadian pharmaceutical ecosystem, the PMPRB will continue to leverage its resources and expertise to optimize its ability to protect consumers from excessive prices and maximize its value proposition to its F/P/T health partners and the health system as a whole.
For more information on the PMPRB’s plans, see the “Core responsibilities: planned results and resources, and key risks” section of this plan.
Core responsibilities: planned results and resources, and key risks
This section contains information on the department’s planned results and resources for each of its core responsibilities. It also contains information on key risks related to achieving those results.
Regulate Patented Medicine Prices
Description
The Patented Medicine Prices Review Board (PMPRB) regulates the prices of patented medicines by setting non-excessive price ceilings and taking enforcement action before the Board in the event of non-compliance.
Planning highlights
On October 23, 2020, the PMPRB published its new Guidelines. After successive six month delay periods, the amended Patented Medicines Regulations (the “Regulations”) are currently slated to come into force July 1, 2022. Together, these two instruments strengthen and modernize Canada’s pricing framework for patented medicines so that the PMPRB can continue to fulfill its statutory mandate to protect Canadian consumers from excessive prices in an era where high-cost medicines account for a rapidly growing share of public and private spending on pharmaceuticals. These reforms have the potential to save Canadians billions of dollars over the next decade.
The Guidelines explain the steps that will typically be taken by staff at the PMPRB in assessing whether a patented medicine appears to be priced excessively in Canada. The Guidelines also explain how the information patent-holding pharmaceutical companies must provide to the PMPRB pursuant to the Regulations is used to enable that assessment. 2022 will be the first year patentee data filings will be based on the amended Regulations. The PMPRB has worked hard to make the transition to the new filing requirements a smooth one.
To ensure the PMPRB’s new Guidelines are fair, functional and fit for their purpose, the PMPRB has developed a comprehensive GMEP to assess changes in trends following implementation of the new Guidelines and inform future adjustments as necessary to ensure they are working as intended.
As currently envisaged, the GMEP will focus on four key trendlines:
- Changes in prices - This will include both list and net prices, and their corresponding ceilings, as well as any changes in the prices of drugs not directly affected by the reforms.
- Changes in access - This will consider the access continuum, from the development of medicines (clinical trials), to medicine approval and availability, Health Technology Assessment (HTA), pan-Canadian Pharmaceutical Alliance (pCPA) negotiations and formulary listings.
- Changes in the ecosystem - This will focus on research, development and economic footprint, drug spending, and the supply chain.
- Changes in PMPRB processes - This will look at the operational aspects of the price assessment, scientific review of medicines, administrative burden in terms of compliance activities, and outreach activities (specifically the number of engagement activities the PMPRB is undertaking to assist patentees in understanding the Guidelines and their application).
Each area of focus will be monitored and evaluated by comparing trends prior to and post implementation of the PMPRB’s new regulatory framework. In 2022-23 the PMPRB will focus its efforts on finalizing the GMEP, consulting with the stakeholder community and generating baseline results which will serve as a benchmark against which to assess the impact of the new regulatory framework as well as identify key trends relevant for continued relevance of the PMPRB pricing guidelines. The trends under the new Guidelines will be monitored on an ongoing basis and compared against the established benchmarks starting in 2023-24.
The PMPRB’s Compliance Information Management System (“CIMS”) is a web-based database application used to assist the review and analysis of data filed by patentees. The PMPRB has made enhancements to CIMS so that it could accept and process the additional information patentees must provide under the new Regulations. In July 2022, when the PMPRB begins receiving data via the enhanced CIMS system, it will monitor and evaluate how well the system is functioning and make any necessary adjustments.
As directed by the Minister pursuant to s. 90 of the Act, under the National Prescription Drug Utilization Information System (NPDUIS) reporting mandate, the PMPRB provides decision makers with critical information and intelligence on price, utilization, and cost trends, so that Canada’s healthcare system has more comprehensive and accurate information on how medicines are being used and on sources of cost pressures.
The PMPRB supports and strengthens its NPDUIS engagement activities by regularly consulting with the NPDUIS Advisory Committee, participating in conferences and seminars, and organizing information sessions with interested stakeholders to share the results of the analytical studies. In 2022-23, NPDUIS plans to publish the results of several analyses as annual publications, report series, and chartbooks.
Gender-based analysis plus
The PMPRB recognizes that sex and gender differences, race, ethnicity, age and mental or physical disability are factors to consider in the accessibility, affordability and appropriate use of prescription medicines and medical devices. Differences in sex and gender+ roles, income and utilization of health care services can affect access to medicines and health insurance, prescribing patterns and medicine use and may have important repercussions for health and well-being.
Since the price of a patented medicine does not vary for the sex or gender+ of the user, the PMPRB’s price review process does not take explicit account of the diversity of user groups or their economic situation. Lower patented medicine prices, and associated savings for all payers, will benefit all populations directly through lower out of pocket costs and indirectly through health system reinvestments and improved access to better care. In addition, the very high-cost patented medicines, which will be the focus of the PMPRB’s new risk-based regulatory framework, often treat rare diseases that can impact certain minority ethnic groups disproportionately.
Experimentation
The PMPRB has not planned any experimentation. Over the past several years, the primary focus of the organization has been to reform and modernize its regulatory framework. To that end, it has conducted the most extensive and far reaching public consultations in its more than three decades long history. This process has been an all-hands-on deck effort. As the PMPRB switches gears from policy development of the new framework to its implementation, we will be experimenting, in a sense, with a newly reformed legal regime.
Key risk(s)
The PMPRB has identified five potential risks to the achievement of results for its Core Responsibility. The first risk is that coming into force of the amended Regulations will be further delayed because of the COVID-19 pandemic. The PMPRB has no control over the timing of coming into force as this is a decision of the Minister of Health and the Governor in Council. However, in the event of further delay, the PMPRB will continue to conduct price reviews under the old Guidelines and Regulations to achieve the best possible result for Canadians. It will also continue to focus its enforcement resources on cases that are most relevant to consumers.
The second risk is that implementation of the new regulatory framework mid year may cause confusion for patentees about what data to file and how and when that data will be used for ceiling price calculation and compliance purposes. To mitigate this risk, the PMPRB has implemented an outreach strategy so that patentees understand the new Guidelines and has developed tools to help them comply. In addition, under subsection 98(4) of the Act, the Board may provide advance guidance to a patentee on its price if there is enough information to do so.
The third risk is that the new regulatory framework may have unintended consequences on patient access to innovative new medicines or clinical trial activity in Canada. While the data does not support claims by opponents of the reforms that this is already happening, the PMPRB will implement a comprehensive plan for monitoring and evaluating their effect on price, access, research and development in Canada, and on the PMPRB’s processes so that corrective action can be taken quickly if warranted. However, the expectation and intent is that the cost savings achieved by public and private drug plans as a consequence of these reforms will enable public and private drug plans to pay for new, innovative medicines that might otherwise not be affordable given current budget constraints.
The fourth risk is that voluntary compliance with the PMPRB’s non-binding Guidelines may decline initially as patentees test the boundaries of the new regime. This may result in more investigations and potentially more hearings into the prices of patented medicines. Through Budget 2017, the PMPRB received additional funding to ensure it will have enough resources to implement the new framework and contend with any corresponding increase in contested pricing matters. The recently completed construction of the PMPRB’s own dedicated hearing facilities will ensure that it has the capacity to accommodate multiple parallel hearings, if necessary.
The final risk is that legal challenges to the amended Regulations and new Guidelines, to
s.79-103 of the Patent Act as a whole, and to certain pending PMPRB Board Orders (e.g., Soliris, Galderma) brought by patentees will result in court decisions that affect the work of the PMPRB. The PMPRB is working with the federal Attorney General to ensure that any such challenges are properly defended.
Planned results for the PMPRB
The following table shows, for Regulate Patented Medicine Prices, the planned results, the result indicators, the targets and the target dates for 2022–23, and the actual results for the three most recent fiscal years for which actual results are available.
| Departmental result | Departmental result indicator | Target | Date to achieve target | 2018–19 actual result | 2019–20 actual result | 2020–21 actual result |
|---|---|---|---|---|---|---|
Affordable patented medicine prices |
% of patented medicine prices in Canada are below the median of the PMPRB’s comparator countries |
50%(a) |
March 31, 2023 |
57.1% |
56.9% |
58.2%(b) |
% of patented medicine prices in Canada within the thresholds set out in the Guidelines |
95%(c) |
March 31, 2023 |
90.5% |
88.4%(d) |
86.3%(e) |
(a) This performance indicator was introduced in 2015-16. Operating under the premise that the PMPRB would continue to conduct its price reviews without significant changes in its regulatory framework, the PMPRB established a target of 50% of patented medicine prices being below the median price. Analysis in the PMPRB’s 2015 Annual Report indicated that the percentage of patented medicines priced below the median price of the PMPRB’s comparator countries was 51.8%, a decline from the previous two years. Based on these factors, it was determined that 50% would be a reasonable target.
(b) The 58.2% of patented medicine prices in Canada reported as being below the median international price includes a significant number of patented medicines being sold in fewer than five countries and therefore are not being compared to the actual median international price. Of the 1,272 patented medicines sold in Canada in 2020, only 746 were sold in five or more countries. Of this 746, only 353 patented medicines (47.3%) had a Canadian price below the median price. This is a significant difference from the reported 58.2%.
(c) This percentage, based on the number of price reviews completed by March 31 of the fiscal year referred to, is calculated as follows: the sum of the number of price reviews found to be within the Guidelines, plus the number of price reviews which did not trigger an investigation, plus the number of Voluntary Compliance Undertakings; divided by the number of patented medicines for which the price review was completed by March 31 of the fiscal year.
(d) Because of an adjustment to the calculation of the denominator this number does not match the number reported in the 2019-20 DRR.
(e) As of March 31, 2021, 54 patented medicines were still under review, and 166 were under investigation, two were the subject of a hearing and one was subject to a Stay Order.
The financial, human resources and performance information for the PMPRB’s program inventory is available on GC InfoBase.Footnote i
Planned budgetary spending for Regulate Patented Medicine Prices
The following table shows, for Regulate Patented Medicine Prices, budgetary spending for 2022–23, as well as planned spending for that year and for each of the next two fiscal years.
| 2022–23 budgetary spending (as indicated in Main Estimates) | 2022–23 planned spending | 2023–24 planned spending | 2024–25 planned spending |
|---|---|---|---|
13,870,473 |
13,870,473 |
13,870,473 |
13,870,473 |
Budgetary spending in 2022-23 and Planned spending for 2022-23 and beyond include funds for a Special Purpose Allotment (SPA) to conduct Public Hearings. The SPA can only be used to cover the costs of public hearings, such as external legal counsel and expert witnesses, etc. For purposes of forecasting Planned Spending, the PMPRB assumes that the entire SPA funding will be spent. This is because these expenditures are dependent on the number of hearings, and the length and complexity of the hearings held, which are difficult to predict. The amount of the SPA for 2022-23 and beyond is $4.5 million. Any unspent amount at the end of each fiscal year is returned to the Consolidated Revenue Fund.
Financial, human resources and performance information for the PMPRB’s program inventory is available on GC InfoBase.Footnote ii
Planned human resources for Regulate Patented Medicine Prices
The following table shows, in full‑time equivalents, the human resources the department will need to fulfill this core responsibility for 2022–23 and for each of the next two fiscal years.
| 2022–23 planned full-time equivalents | 2023–24 planned full-time equivalents | 2024–25 planned full-time equivalents |
|---|---|---|
| 60 | 60 | 60 |
Financial, human resources and performance information for the PMPRB’s program inventory is available on GC InfoBase.Footnote iii
Internal Services
Description
Internal services are the services that are provided within a department so that it can meet its corporate obligations and deliver its programs. There are 10 categories of internal services:
- management and oversight services
- communications services
- legal services
- human resources management services
- financial management services
- information management services
- information technology services
- real property management services
- materiel management services
- acquisition management services
Planning highlights
The PMPRB is committed to implementing the Clerk of the Privy Council’s call to action on anti-racism, equity, and inclusion; the PMPRB will work to complete action items for the Chairperson’s letter to the Clerk of the Privy CouncilFootnote iv in 2022-23. As part of the call to action, the PMPRB is on the Mentorship Plus Interdepartmental Working group for Small Departments and Agencies. Mentorship Plus is a new initiative co‑developed by members of employment equity (EE) and equity‑seeking groups to better support leadership development, with specific emphasis on supporting members of underrepresented groups who aspire to leadership and executive positions.
Planned budgetary spending for internal services
The following table shows, for internal services, budgetary spending for 2022–23, as well as planned spending for that year and for each of the next two fiscal years.
| 2022–23 budgetary spending (as indicated in Main Estimates) | 2022–23 planned spending | 2023–24 planned spending | 2024–25 planned spending |
|---|---|---|---|
| 3,132,740 | 3,132,740 | 3,132,740 | 3,132,740 |
Planned human resources for internal services
The following table shows, in full‑time equivalents, the human resources the department will need to carry out its internal services for 2022–23 and for each of the next two fiscal years.
| 2022–23 planned full-time equivalents | 2023–24 planned full-time equivalents | 2024–25 planned full-time equivalents |
|---|---|---|
| 24 | 24 | 24 |
Planned spending and human resources
This section provides an overview of the department’s planned spending and human resources for the next three fiscal years and compares planned spending for 2022–23 with actual spending for the current year and the previous year.
Planned spending
Departmental spending 2019–20 to 2024–25
The following graph presents planned spending (voted and statutory expenditures) over time.
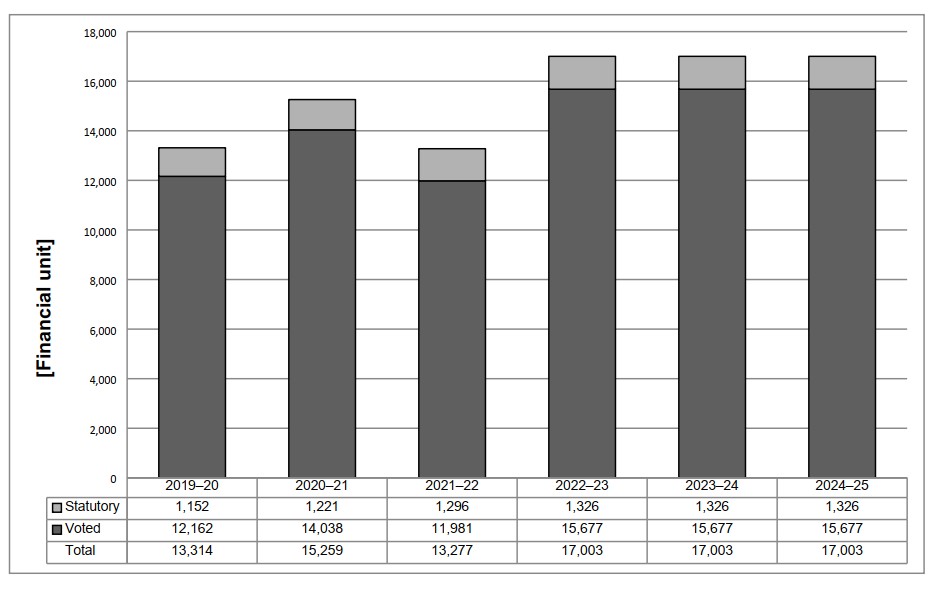
Long description
| 2019-20 | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 | |
|---|---|---|---|---|---|---|
| Statutory | 1,152 | 1,221 | 1,296 | 1,326 | 1,326 | 1,326 |
| Voted | 12,162 | 14,038 | 11,981 | 15,677 | 15,677 | 15,677 |
| Total | 13,314 | 15,259 | 13,277 | 17,003 | 17,003 | 17,003 |
As announced in Budget 2017, the PMPRB received additional funding for future years:
$5.7 million in 2019-20, $6.7 million in 2020-21, $7.7 million in 2021-22 and $5.7 million in 2022-23 and ongoing, including Employee Benefit Package (EBP) and increased funding for the Special Purpose Allotment (SPA).
Actual spending for 2020-21 is significantly higher than actual spending in 2019-20 because of increased funding and hiring of new staff to prepare for implementation of the new Guidelines, as well as expenses incurred for the construction of a hearing room. Planned spending for 2021-22 is lower than actual spending in 2020-21 because construction was completed, and no additional costs were incurred in 2021-22. Additionally, planned spending on the SPA is only $1 million, with a projected lapse of $5.2 million. Though total budget decreases in 2022-23 and beyond, planned spending is higher than 2021-22 as it is assumed the entirety of the SPA will be spent.
Budgetary planning summary for core responsibilities and internal services (dollars)
The following table shows information on spending for each of the PMPRB’s core responsibilities and for its internal services for 2022–23 and other relevant fiscal years.
| Core responsibilities and internal services | 2019–20 actual expenditures | 2020–21 actual expenditures | 2021–22 forecast spending | 2022–23 budgetary spending (as indicated in Main Estimates) | 2022–23 planned spending | 2023–24 planned spending | 2024–25 planned spending |
|---|---|---|---|---|---|---|---|
Regulate Patented Medicine Prices |
9,336,597 |
10,858,873 |
9,775,741 |
13,870,473 |
13,870,473 |
13,870,473 |
13,870,473 |
Subtotal |
9,336,597 |
10,858,873 |
9,775,741 |
13,870,473 |
13,870,473 |
13,870,473 |
13,870,473 |
Internal services |
4,042,060 |
4,400,210 |
3,501,893 |
3,132,740 |
3,132,740 |
3,132,740 |
3,132,740 |
Total |
13,313,880 |
15,259,083 |
13,277,634 |
17,003,213 |
17,003,213 |
17,003,213 |
17,003,213 |
The forecast spending for 2021-22 is based on actual spending and anticipated spending to year end, which does not anticipate full spending of the Special Purpose Allotment (SPA). At the time of preparing this report, forecasted spending of the SPA amounted to approximately $1.0 million of the $6.2 million allotted. This and an anticipated surplus of $1.1 million in Vote 1 spending account for the variance in 2021-22 forecast spending and 2022-23 planned spending.
For purposes of forecasting Planned Spending for 2022-23 and future years, the PMPRB assumes the entire SPA funding for hearings will be spent. This is because these expenditures are dependent on the number of hearings, and the length and complexity of the hearings held, which are difficult to predict. The amount of the SPA for 2022-23 and beyond is $4.5 million a reduction from the $6.2 million allotted in 2021-22. The SPA was reduced because the new Guidelines were originally expected to come into force in January 2019, and it was anticipated that, by 2022-23, Staff and patentees would have a better understanding of the how to apply the new Guidelines and there would be fewer contested pricing matters.
Planned human resources
The following table shows information on human resources, in full-time equivalents (FTEs), for each of the PMPRB’s core responsibilities and for its internal services for 2022–23 and the other relevant years.
Human resources planning summary for core responsibilities and internal services
| Core responsibilities and internal services | 2019–20 actual full‑time equivalents | 2020–21 actual full‑time equivalents | 2021–22 forecast full‑time equivalents | 2022–23 planned full‑time equivalents | 2023–24 planned full‑time equivalents | 2024–25 planned full‑time equivalents |
|---|---|---|---|---|---|---|
Regulate Patented Medicine Prices |
58 |
57 |
56 |
60 |
60 |
60 |
Subtotal |
58 |
57 |
56 |
60 |
60 |
60 |
Internal services |
21 |
23 |
24 |
24 |
24 |
24 |
Total |
79 |
80 |
80 |
84 |
84 |
84 |
The increase in planned FTEs for 2022-23 and beyond is a result of backfilling departures and hiring new staff to address the requirements of framework modernization.
Estimates by vote
Information on the PMPRB’s organizational appropriations is available in the 2022–23 Main Estimates.Footnote v
Future-oriented condensed statement of operations
The future‑oriented condensed statement of operations provides an overview of the PMPRB’s operations for 2021–22 to 2022–23.
The forecast and planned amounts in this statement of operations were prepared on an accrual basis. The forecast and planned amounts presented in other sections of the Departmental Plan were prepared on an expenditure basis. Amounts may therefore differ.
A more detailed future‑oriented statement of operationsFootnote vi and associated notes, including a reconciliation of the net cost of operations with the requested authorities, are available on the PMPRB’s website.
Future‑oriented condensed statement of operations for the year ending March 31, 2023 (dollars)
| Financial information | 2021–22 forecast results | 2022–23 planned results | Difference (2022–23 planned results minus 2021–22 forecast results) |
|---|---|---|---|
Total expenses |
14,760,508 |
18,668,777 |
3,908,269 |
Total revenues |
- |
- |
- |
Net cost of operations before government funding and transfers |
14,760,508 |
18,668,777 |
3,908,269 |
Note: The amounts included in this table differ from the information included in the other financial tables in this report because this table includes accrued information (e.g., amortization), as well as values for services provided to the PMPRB without charge.
The PMPRB is projecting $18.7M in expenses based on 2022-23 Main Estimates and accrued information. This amount does not include future supplementary estimates. It represents an increase of $3.9M from 2021-22 projections, primarily attributable to a lapse in SPA funding for hearings. The PMPRB assumes the entire SPA funding for hearings will be spent. This is because these expenditures are dependent on the number of hearings, and the length and complexity of the hearings held, which are difficult to predict.
The 2022-23 planned expenses by core responsibility are as follows:
- Regulate Patented Medicine Prices $15.1M; and,
- Internal Services $3.5M.
PMPRB receives most of its funding through annual Parliamentary appropriations.
Corporate information
Organizational profile
Appropriate minister(s): The Honourable Jean-Yves Duclos
Institutional head: Mélanie Bourassa Forcier, Acting Chairperson
Ministerial portfolio: Health Canada
Enabling instrument(s): Patent ActFootnote viiand Patented Medicines RegulationsFootnote viii
Year of incorporation / commencement: 1987
Other: The Minister of Health is responsible for the pharmaceutical provisions of the Patent Act set out in sections 79 to 103. Although the PMPRB is part of the Health Portfolio, because of its quasi-judicial responsibilities the PMPRB carries out its mandate at arm’s length from the Minister. It also operates independently of Health Canada, which approves drugs for safety, efficacy and quality; other Health Portfolio members, such as the Public Health Agency of Canada, the Canadian Institutes of Health Research and the Canadian Food Inspection Agency; and federal, provincial and territorial (F/P/T) public drug plans, which approve the listing of drugs for their respective formularies for reimbursement purposes; and the Common Drug Review, administered by the Canadian Agency for Drugs and Technologies in Health (CADTH), which recommends drugs that should qualify for reimbursement purposes by participating public drug plans.
Raison d’être, mandate and role: who we are and what we do
Information on the PMPRB’s raison d’être, mandate and role is available on the PMPRB’s websiteFootnote ix.
Information on the PMPRB’s mandate letter commitments is available in the Minister’s mandate letterFootnote x.
Operating context
Information on the operating context is available on the PMPRB’s website.Footnote xi
Reporting framework
The PMPRB’s approved departmental results framework and program inventory for 2022–23 are as follows.
| Departmental Results Framework | Core Responsibility: Regulate Patented Medicine Prices | Internal Services | |
| Departmental Result: Affordable drug medicine prices | Indicator 1: % of patented drug prices in Canada are below the median price of the PMPRB’s comparator countries | ||
| Indicator 2: % of patented drug prices in Canada within the threshold set out in the Guidelines | |||
| Program Inventory | Patented Medicine Price Regulation Program | ||
| Pharmaceutical Trends Program | |||
Supporting information on the program inventory
Supporting information on planned expenditures, human resources, and results related to the PMPRB’s program inventory is available on GC InfoBase.Footnote xii
Supplementary information tables
The following supplementary information tables are available on the PMPRB’s website:
Federal tax expenditures
The PMPRB’s Departmental Plan does not include information on tax expenditures.
Tax expenditures are the responsibility of the Minister of Finance. The Department of Finance Canada publishes cost estimates and projections for government‑wide tax expenditures each year in the Report on Federal Tax Expenditures.Footnote xv This report provides detailed information on tax expenditures, including objectives, historical background and references to related federal spending programs, as well as evaluations, research papers and gender-based analysis plus.
Organizational contact information
Mailing address
The Patented Medicine Prices Review Board
Box L40
Standard Life Centre
333 Laurier Avenue West
Suite 1400
Ottawa, Ontario K1P 1C1
Toll-free no,: 1-877-861-2350
TTY: (613) 288-9654
Fax: (613_ 288-9643
Email: PMPRB.Information-Renseignements.CEPMB@pmprb-cepmb.gc.ca
Website: https://www.canada.ca/en/patented-medicine-prices-review.htmlFootnote xvi
Appendix: definitions
appropriation (crédit)
Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
budgetary expenditures (dépenses budgétaires)
Operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
core responsibility (responsabilité essentielle)
An enduring function or role performed by a department. The intentions of the department with respect to a core responsibility are reflected in one or more related departmental results that the department seeks to contribute to or influence.
Departmental Plan (plan ministériel)
A document that sets out a department’s priorities, programs, expected results and associated resource requirements, covering a three‑year period beginning with the year indicated in the title of the report. Departmental Plans are tabled in Parliament each spring.
departmental result (résultat ministériel)
A change that a department seeks to influence. A departmental result is often outside departments’ immediate control, but it should be influenced by program-level outcomes.
departmental result indicator (indicateur de résultat ministériel)
A factor or variable that provides a valid and reliable means to measure or describe progress on a departmental result.
departmental results framework (cadre ministériel des résultats)
A framework that consists of the department’s core responsibilities, departmental results and departmental result indicators.
Departmental Results Report (rapport sur les résultats ministériels)
A report on a department’s actual performance in a fiscal year against its plans, priorities and expected results set out in its Departmental Plan for that year. Departmental Results Reports are usually tabled in Parliament each fall.
experimentation (expérimentation)
The conducting of activities that explore, test and compare the effects and impacts of policies and interventions in order to inform decision-making and improve outcomes for Canadians. Experimentation is related to, but distinct from, innovation. Innovation is the trying of something new; experimentation involves a rigorous comparison of results. For example, introducing a new mobile application to communicate with Canadians can be an innovation; systematically testing the new application and comparing it against an existing website or other tools to see which one reaches more people, is experimentation.
full‑time equivalent (équivalent temps plein)
A measure of the extent to which an employee represents a full person‑year charge against a departmental budget. Full‑time equivalents are calculated as a ratio of assigned hours of work to scheduled hours of work. Scheduled hours of work are set out in collective agreements.
gender-based analysis plus (GBA Plus) (analyse comparative entre les sexes plus [ACS Plus])
An analytical process used to assess how diverse groups of women, men and gender-diverse people experience policies, programs and services based on multiple factors including race, ethnicity, religion, age, and mental or physical disability.
government-wide priorities (priorités pangouvernementales)
For the purpose of the 2022–23 Departmental Plan, government-wide priorities are the high-level themes outlining the government’s agenda in the 2021 Speech from the Throne: protecting Canadians from COVID-19; helping Canadians through the pandemic; building back better – a resiliency agenda for the middle class; the Canada we’re fighting for.
horizontal initiative (initiative horizontale)
An initiative in which two or more federal organizations are given funding to pursue a shared outcome, often linked to a government priority.
non‑budgetary expenditures (dépenses non budgétaires)
Net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
performance (rendement)
What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve, and how well lessons learned have been identified.
plan (plan)
The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally, a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead up to the expected result.
planned spending (dépenses prévues)
For Departmental Plans and Departmental Results Reports, planned spending refers to those amounts presented in the Main Estimates.
A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their Departmental Plans and Departmental Results Reports.
program (programme)
Individual or groups of services, activities or combinations thereof that are managed together within a department and that focus on a specific set of outputs, outcomes or service levels.
program inventory (répertoire des programmes)
An inventory of a department’s programs that describes how resources are organized to carry out the department’s core responsibilities and achieve its planned results.
result (résultat)
An external consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead, they are within the area of the organization’s influence.
statutory expenditures (dépenses législatives)
Expenditures that Parliament has approved through legislation other than appropriation acts. The legislation sets out the purpose of the expenditures and the terms and conditions under which they may be made.
target (cible)
A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
voted expenditures (dépenses votées)
Expenditures that Parliament approves annually through an Appropriation Act. The vote wording becomes the governing conditions under which these expenditures may be made.