
Influenza A(H5Nx) clade 2.3.4.4b virus and related future novel viruses: Pandemic risk scenario analysis

Download in PDF format
(768 KB, 9 pages)
Organization: Public Health Agency of Canada
Date published: 2023-07-27
Date of this assessment: March 31, 2023
On this page
- Disclaimer
- Goal
- Risk statement
- Key recommendations
- Method
- Conclusion
- Acknowledgments
- Figure 1. Poll results on current and most likely scenario in 1 year
- Figure 2. Progression of scenarios
- References
Disclaimer
This analysis was conducted by a multi-sectoral expert team. The qualitative and expert-opinion-based methodology is intended to be used in situations where policy decisions need to be made in the face of high uncertainty. The analysis was primarily informed by the team's collective professional knowledge. It is not intended as a literature review. The findings and conclusions represent the consensual, but not necessarily unanimous, opinions of the participants, and do not represent the views of the participants' respective organizations.
Goal
This report is the summarized analysis of the work conducted by a multi-sectoral expert team. Footnote 1 The aim was to analyze the public health risk associated with global emergence of a virus with pandemic potential from influenza A(H5Nx) Footnote 2 clade 2.3.4.4b in the next year (up to March 31, 2024). Key objectives of the analysis were to inform pandemic preparedness and monitoring and surveillance activities, and to identify knowledge gaps and research needs.
There has continued to be widespread and persistent transmission of this clade among wild and domestic birds, an increasing number of reported cases in non-human mammals, and sporadic avian-to-human zoonotic transmission globally. This evolving situation increases the possibility of viral evolution that might support transmission between humans. In order to assess that risk, a forward-looking analysis was required.
The majority of experts in a Canadian One Health multi-sectoral team, consisting of federal and provincial experts from human, animal, and ecosystem health sectors, agreed with the following key risk statement and proposed recommendations coming out of this analysis. The results of the expert poll, showing the diversity of opinions and uncertainty levels, is provided in Figure 1.
Risk statement
- The rising prevalence and expanding geographic distribution of influenza A(H5Nx) clade 2.3.4.4b in Canada and globally provide more frequent opportunities for mammalian infection and genetic changes in the virus that may favour mammalian adaptation.
- The current situation is one of widespread avian transmission with limited non-human mammal-to-mammal transmission with sporadic human infections, according to the majority of a Canadian multi-sectoral expert team.
- The most likely scenario for this time next year was considered one of sustained transmission in non-human mammals, which would provide increased possibilities for viral adaptation or reassortment potentially leading to transmission between humans.
- All scenarios were considered credible, but the worst-case scenario of sustained transmission between humans (pandemic) in the next year was considered less likely. Nonetheless, it could have significant human health, health system and other direct and indirect impacts on other sectors.
- There is a high level of uncertainty associated with these risk considerations.
Key recommendations
It is recommended that:
- One Health partners continue their planning and preparedness for a potential future pandemic. Coordination of planning among One Health partners is of great importance given the potential for ongoing viral activity in humans, animals and at the human-animal-ecosystem interface in all scenarios.
- Existing intersectoral groups set priorities for One Health surveillance to detect changes in the situation, and partners increase sharing of animal and human surveillance data. Surveillance of mammal-to-mammal transmission was identified as a priority for public health.
- Partners across sectors collaborate to address program, capacity and knowledge gaps, particularly those for current and most likely future scenarios.
- The Public Health Agency of Canada engage One Health partners in future assessments of risks to public health associated with current and future influenza A(H5Nx) strains, as was done in this scenario analysis.
Method
On February 17, 2023, the Centre for Integrated Risk Assessment at the Public Health Agency of Canada convened a Canadian One Health multi-sectoral team, consisting of federal and provincial experts from human, animal, and ecosystem health sectors, representing a variety of disciplines such as epidemiologists, virologists, wildlife biologists, veterinarians, and physicians. The integration of expert opinion from a multi-disciplinary, multi-sectoral team strengthened the analysis by contributing data, knowledge, and expertise, improving the validity of the analysis itself, and identifying early markers of change to enhance multi-sectoral action on recommendations.
Four hypothetical yet credible future scenarios over a 1-year period were developed to account for potential viral evolution and influenza pandemic.
Scenario 1: Avian transmission and limited Footnote 3 transmission in mammals (continued current situation)
Scenario 2: Sustained Footnote 4 transmission between non-human mammals
Scenario 3: Limited transmission between humans
Scenario 4: Sustained transmission between humans (pandemic)Footnote 5
All descriptions of avian, non-human mammal, or human transmission refer to either an influenza A (H5Nx) clade 2.3.4.4b virus, or a future novel virus that has adapted or reassorted from this clade.
The analysis provided a relative likelihood of these different scenarios in the face of high uncertainty. Rather than looking at current risk, scenario analysis broadens the thinking of experts toward future perspectives. Although it is possible that these scenarios may not unfold at all, or sequentially as presented, the intermediate scenarios signal an escalation in the situation and that additional actions and preventative activities should be considered. Each scenario was examined to capture assumptions, uncertainties, considerations affecting likelihood, potential impacts, monitoring activities, and evidence gaps.
A risk pathway was developed to illustrate the potential progression of steps to future scenarios (refer to Figure 2). Possible key monitoring and intervention activities along this pathway were identified from a One Health perspective to monitor and mitigate the public health risks.
Conclusion
Influenza viruses can adapt and reassort, but there is a high level of uncertainty regarding the likelihood and timing of virus evolution that would result in a virus better adapted to transmission among mammals or humans. Nonetheless, the rising prevalence and expanding geographic distribution of influenza A(H5Nx) clade 2.3.4.4b in Canada and globally provides more frequent opportunities for mammalian infection, mutational changes that may favour further mammalian adaptation, and co-infection with other influenza viruses that may lead to reassortment.
This analysis was strengthened by the integration of expert opinion from a multi-disciplinary, multi-sectoral team. The results underscore the importance of continued efforts to monitor the situation and prepare for a future worst-case scenario, as well as additional activities as needed for prevention, detection, preparedness, and response at the human-animal-ecosystem health interface. Moving forward, a One Health approach is recommended for setting joint priorities for surveillance and sharing of surveillance data, epidemiological investigation, risk assessment, and prevention, preparedness and response.
Experts highlighted the need for timely updates to public health guidance and risk communications should the situation change, a lesson learned from the COVID-19 pandemic. They recommend that important risk information from this analysis be used to inform planning for guidance and communications in future scenarios. The public health risk may change over time. If we shift from one scenario to another, continued vigilance, coordination and analysis by a multi-sectoral team is recommended.
Acknowledgments
The individuals listed, along with their affiliated agencies, are acknowledged for their contributions to this report.
Alberta Health and Alberta Agriculture and Irrigation: Hussein Keshwani
British Columbia Centre for Disease Control: Aamir Bharmal, Erin Fraser, Linda Hoang, Agatha Jassem, Shannon Russell, Inna Sekirov, Danuta Skowronski
British Columbia Ministry of Agriculture: Theresa Burns, Chelsea G. Himsworth
Cadham Provincial Laboratory (Manitoba): Paul Van Caeseele
Canadian Food Inspection Agency: Tamiru Alkie, Yohannes Berhane, Maud Carron, Caroline Dubé, Andrea Ellis, Logan Flockhart, Kathleen Hooper, Charles Nfon, Marc Sabourin, Primal Silva
Canadian Veterinary Medical Association: Mike Petrik
Environment and Climate Change Canada: Michael Brown, Brigitte Collins, Jolene Giacinti, Jack Hughes, Daniel Leclair, Hannah Lewis
Indigenous Services Canada: Kim Daly, Amole Khadilkar, Constantine Tikhonov, Maxime Trubnikov
Institut national de santé publique du Québec: Maude Bigras, Hugues Charest, Alejandra Irace-Cima
Manitoba Agriculture: Dale Douma
Ministère de l'Agriculture, des Pêcheries et de l'Alimentation du Québec: Isabelle Picard
Ministère de la santé et des services sociaux du Québec: Josée Dubuque, Colette Gaulin, Juliette Martin
Nova Scotia Health Authority: Todd Hatchette, Jason Leblanc
Ontario Ministry of Agriculture, Food and Rural Affairs: Paul Innes
Ontario Ministry of Health: Melissa Helferty
Parks Canada: Todd Shury
Prince Edward Island Chief Public Health Office: Karen Phillips
Public Health Agency of Canada: Rukshanda Ahmad, Sandra Radons Arneson, Nicole Atchessi, Dima Ayache, Christina Bancej, Nathalie Bastien, Philippe Belanger, Anna Bellos, Samuel Bonti-Ankomah, Natalie Bruce, Peter Buck, Sharon Calvin, Joyce Cheng, Taeyo Chestley, Lesley Doering, Victoria Edge, Catherine Elliott, Raquel Farias, Aamir Fazil, Manon Fleury, Vanessa Gabriele-Rivet, Eleni Galanis, Corey Green, Heather Hannah, Marianne Heisz, Kirsten Jacobsen, Emmanuelle Jean, Nina Jetha, Ram Kamineni, Mira Kelada-Antoun, Darwyn Kobasa, Irene Lambraki, Lisa Landry, Erin Leonard, Tiffany Locke, Janice Merhej, Rachel Milwid, Rhonda Mogk, Rashmi Narkar, Nicholas Ogden, Toju Ogunremi, Renee Parisien, Matthew Peake, Charlene Ranadheera, Barbara Raymond, Simran Sandhu, Jill Sciberras, Lisa Slywchuk, Ming Su, Clarence Tam, Francois-William Tremblay, Jan Trumble-Waddell, Matthew Tunis, Linda Vrbova, Lisa Waddell, Lindsay Whitmore
Public Health New Brunswick: Jackie Badcock, Carole Breau, Richard Garceau, Shelley Landsburg, Arifur Rahman
Public Health Ontario: Emily Karas, Richard Mather, Karam Ramotar
Sunnybrook Health Sciences Centre: Samira Mubareka
Figure 1 : Poll results on current and most likely scenario in 1 year
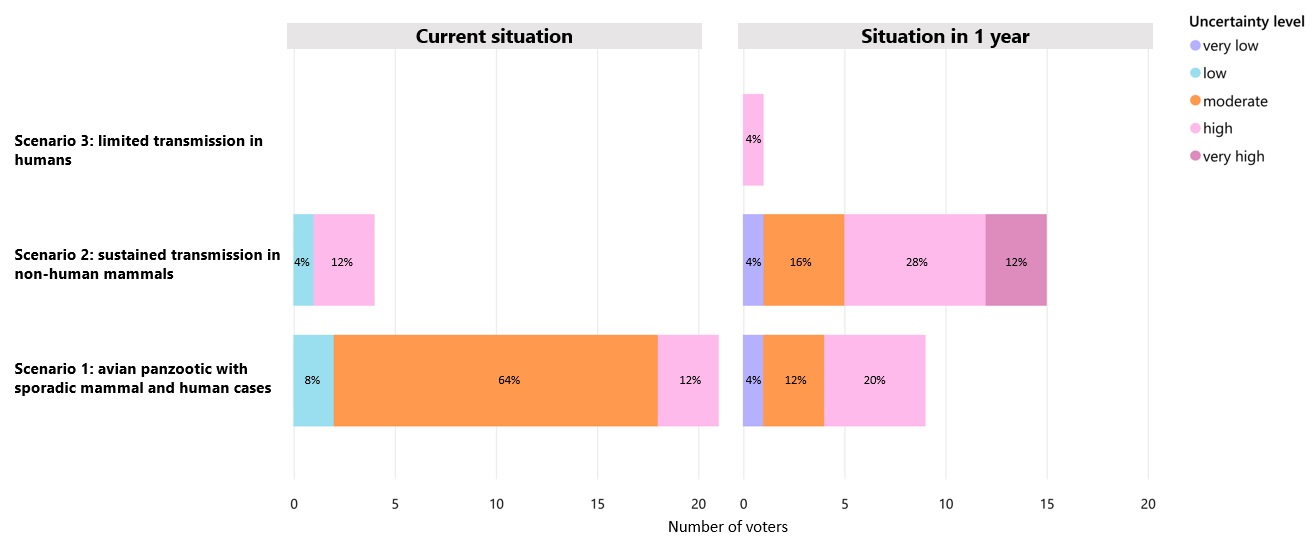
Figure 1: Text description
Current situation |
Situation after a year |
|---|---|
Scenario 1: Avian panzootic with sporadic mammal and human cases |
|
8% of responses (low uncertainty level) |
4% of responses (very low uncertainty level) |
64% of responses (moderate uncertainty level) |
12% of responses (moderate uncertainty level) |
12% (high uncertainty level) |
20% of responses (high uncertainty level) |
Scenario 2: Sustained transmission in non-human mammals |
|
4% of responses (low level of uncertainty) |
4% of responses (very low uncertainty level) |
12% of responses (high uncertainty level) |
16% of responses (moderate uncertainty level) |
NA |
28% of responses (high uncertainty level) |
NA |
12% of responses (very high uncertainty level) |
Scenario 3: Limited transmission in humans |
|
NA |
4% of responses (high uncertainty level) |
NA |
NA |
Multi-sectoral Expert Team members' responses to the questions: "What scenario are we currently in and what is the level of uncertainty?" (left panel) and "What is the most likely scenario at this time next year and what is the level of uncertainty?" (right panel).
- Scenario 1 (avian panzootic with sporadic mammal and human cases) was thought to be the most likely current scenario (84% of responses). A minority thought Scenario 2 (sustained transmission in non-human mammals) was already occurring (16%). Most respondents viewed the associated uncertainty as moderate or high, with only 12% of respondents considering uncertainty to be low.
- Scenario 2 (sustained transmission in non-human mammals) was thought to be the most likely situation at this time next year by 60% of respondents, followed by Scenario 1 (avian panzootic with sporadic mammal and human cases) [36%] and Scenario 3 (sustained avian or mammalian transmission with limited transmission in humans) [4%]. Most respondents viewed the associated uncertainty as moderate to very high, with only 8% of respondents considering uncertainty to be very low.
These poll results are from the multi-sectoral expert team. They reflect which scenario we are currently in, and the most likely scenario in a year. Bars represent the number (and percentage) of responses, colours indicate the level of uncertainty in individuals' response. No experts voted for Scenario 4.
Figure 2 : Progression of scenarios
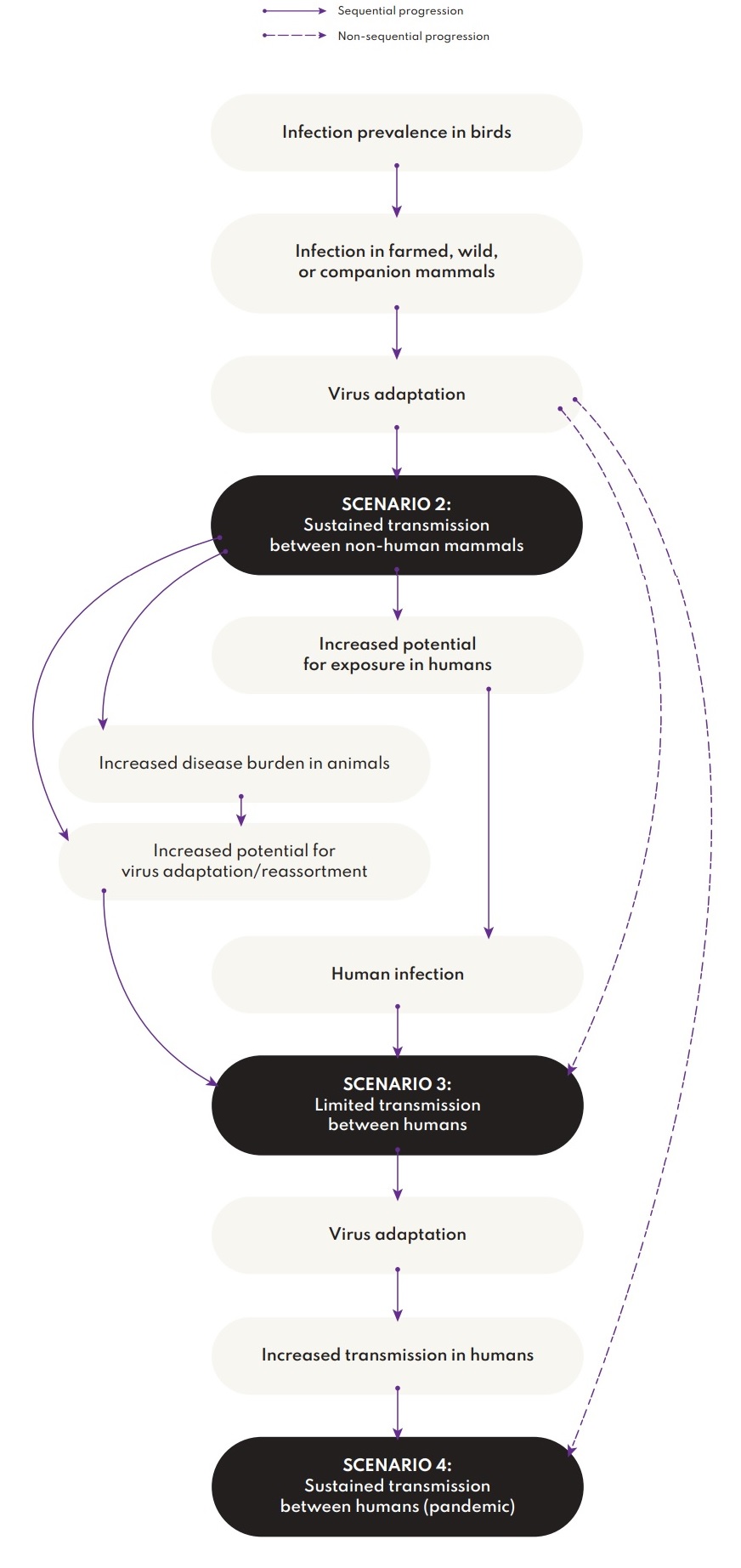
Figure 2: Text description
The diagram shows scenario progression from infection prevalence in birds to sustained transmission between non-human mammals (Scenario 2), through an avian or mammalian panzootic with limited transmission between humans (Scenario 3), towards a pandemic caused by an influenza A(H5Nx) clade 2.3.4.4b virus (Scenario 4).
- Drivers that increase the likelihood of Scenario 2 are infection prevalence in birds, progressing to infection in farmed, wild or companion mammals, progressing to virus adaptation that leads to sustained transmission between non-human mammals. Virus adaptation in animals could also lead directly to limited transmission between humans, or to sustained transmission between humans.
- Scenario 2 leads to increased potential for exposure in humans, resulting in human infection and leading to limited transmission between humans (Scenario 3). Scenario 2 also leads to increased disease burden in animals, increased potential for virus adaptation or reassortment that could lead to limited transmission between humans.
- Scenario 3 could lead to further virus adaptation resulting in increased transmission in humans, which could lead to sustained transmission between humans (Scenario 4).
This simplified progression of scenarios illustrates the potential progression of steps to future scenarios. Infection in birds can lead to infection in mammals and subsequent virus adaptation to mammals. Sustained transmission may then occur in non-human mammals (Scenario 2), or virus adaptation could lead directly to scenarios 3 or 4.
References
- Footnote 1
-
Pandemic Risk Scenario Analysis: Influenza A(H5Nx) clade 2.3.4.4b virus and related future novel viruses, Public Health Agency of Canada report, unpublished.
- Footnote 2
-
This analysis is focused on clade 2.3.4.4b, which includes H5N1 and other H5Nx viruses, and the potential future H5Nx viruses originating from this clade.
- Footnote 3
-
Limited: virus infects an individual or a few people/animals in clusters who are in close contact with each other, such as in a family or a marine mammal setting but does not spread further.
- Footnote 4
-
Sustained: virus transmits easily from one person/animal to the next and then further onward.
- Footnote 5
-
Pandemic as defined in World Health Organization. Pandemic influenza preparedness (PIP) framework. https://www.who.int/initiatives/pandemic-influenza-preparedness-framework. Accessed April 6, 2023