
How Healthy are Canadians?
A trend analysis of the health of Canadians from a healthy living and chronic disease perspective
Table of Contents
- Executive Summary
- Introduction
- Main Findings
- International Comparisons
- Conclusions
- Methodological Notes
- Contributors
- References
Executive Summary
Good health is a major resource for social, economic and personal development and an important dimension of quality of life. Healthy, productive citizens reduce the burden on the health care system and contribute to a strong economy.
In general, Canada is a healthy nation. Over the past several decades the overall mortality rate and life expectancy have improved considerably, and in general, Canada compares well with the other developed nations. Nevertheless, Canada continues to face significant public health challenges in preventing chronic diseases. Major chronic diseases, including cardiovascular diseases (CVDs), cancer, chronic respiratory diseases (CRDs) and diabetes are the cause of 65% of all deaths in Canada each year and are the leading causes of death globally. In addition, depression and anxiety disorders are respectively, the second and eighth leading causes of years of life lost due to disability globally.
This Trend Analysis examines the last ten to fifteen years of available data investigating key risk factors, major chronic diseases and mood and anxiety disorders as well as overall life expectancy and asks the central question: How healthy are Canadians?
The Good News - Canadians are Living Longer
- Both life expectancy (LE) and health-adjusted life expectancy (HALE)Footnote a in Canada have been steadily increasing in the past decade, and the gap between men and women has been narrowing.
- Overall mortality and premature mortality rates, particularly for CVDs, continue to decrease at a steady rate.
- The declining incidence ratesFootnote b for CVDs and chronic obstructive pulmonary disease (COPD) are linked to the major decrease in smoking rates in Canada across all age groups. Smoking rates have continued to decline in the past decade, especially among Canadian youth aged 15-24.
- Canada ranks among the top and middle third performers among Organisation for Economic Co-operation and Development (OECD) member states for most indicators.
Areas of Concern
Health implications for an ageing population
- Nearly one in six Canadians (5.8 million) are 65 years or older, and this age group is growing four times faster than overall population.
- More than one in five Canadian adults live with one of the following chronic diseases: CVD, cancer, CRD or diabetes.
- One in 25 Canadian adults aged 20 years and older reported having a mood and anxiety disorder and at least one of the four major chronic diseases.
- The prevalence ratesFootnote c for CVDs and CRDs have increased since 2000, reflecting that more Canadians are living with those diseases every year.
- In 2011/12, an estimated 2.3 million of Canadians were living with ischemic heart disease, almost 2 million were living with COPD, and about 700,000 were living with the effects of a stroke.
- Cancer is the leading cause of death. As of 2009, over 800,000 Canadians had been diagnosed with cancer within the previous 10 years, and nearly 90% of all newly diagnosed cancers were in Canadians 50 years or older.
- In addition, inequalities in chronic disease prevalence across subgroups of Canadians exist.
Canada's persistently high prevalence of preventable chronic disease risk factors
- Approximately four in five Canadian adults have at least one modifiable risk factor for chronic disease (self-reported tobacco smoking, physical inactivity, unhealthy eating and harmful use of alcohol).
- Physical inactivity, sedentary behaviours and obesity rates remain high, especially among children and youth.
- In fact, more than 90% of Canadian children are not meeting current physical activity guidelines in Canada.
- Canada ranks amongst the worst of OECD countries for adult obesity rates.
The impact of type 2 diabetes rates
- About 2.7 million Canadians are now living with diabetes (types 1 and 2 combinedFootnote d). Diabetes has seen the second highest annual percent increase since 2000/01 among all diseases studied.
- The increase in diabetes prevalence rates is likely attributable to the high rates of obesity and overweight in the Canadian population as well as the ageing of the Canadian population.Footnote 1
- The number of prevalent cases for diagnosed diabetes is projected to be over four million people by 2020.Footnote 2
Although trends show a major decrease in mortality in Canada, they also point to an increasing overall burden of disease. While Canadians are living longer, it is important that they live longer in good health. This trend report provides key information to help inform policy and programmatic decisions in health promotion and chronic disease prevention.
Introduction
There are many ways of looking at the health of a population. A focus on healthy living, chronic diseases and related risk factors—mainly cardiovascular diseases (CVDs), cancers, chronic respiratory diseases (CRDs) and diabetes—offers a perspective that is particularly relevant to public health as these conditions represent the leading causes of death and could largely be prevented. Most premature deaths are linked to common risk factors, namely tobacco smoking, unhealthy eating, physical inactivity and harmful use of alcohol. Addressing these risk factors and enhancing the management of these chronic diseases and conditions formed the basis of the World Health Organization's (WHO) Global Action Plan for the Prevention and Control of Noncommunicable Diseases (NCDs) 2013-2020.Footnote 3.
In Canada, four in five Canadian adults have at least one modifiable risk factor, and one in five live with at least one of the following major chronic diseases: CVD, cancer, CRD and diabetes. Two-thirds of all deaths each year are caused by these major chronic diseases. In addition, mood and anxiety disorders are also common among Canadians and account for the leading cause of disability for working age adults. These four chronic diseases, along with mood and anxiety disorders, account for about one third of direct health-care expenditures in Canada.Footnote 4,Footnote e.
This report from the Public Health Agency of Canada (PHAC) seeks to determine the level of health of Canadians. To do so, we looked at whether progress on main health indicators has been achieved in the last 10 to 15 years.
This report is structured primarily around the four major "physical" chronic diseases included in the WHO Global Plan of Action, four risk factors (smoking tobacco, physical inactivity, unhealthy eating and harmful use of alcohol) and two risk conditions (obesity and hypertension). To these we have added mood and anxiety disorders (measured by use of health services) because of their major impact on the working age population. Multi-morbidity (i.e. two or more of the four major "physical" chronic diseases co-existing, and mood and anxiety disorders co-morbid with one of the four major "physical" chronic diseases), a relatively common phenomena among the elderly, has also been examined. Moreover, several key international health indicators are included: infant/neonatal mortality, premature mortality, life expectancy (LE) and health-adjusted life expectancy (HALE). Finally, since those living with chronic diseases are particularly affected by influenza infections, the report also provides information on influenza immunization coverage. See Table 1 for an overview.
When feasible, this report focuses on Canadian prevalence and incidence trends—from 2000 to the latest year of data available—and presents further comparisons by sex, age group and geography (i.e. provinces and territories). A few selected international indicators were examined to compare the health of Canadians relative to other nations and are contextualized in the reporting of the Organisation for Economic Co-operation and Development (OECD).
Note: An examination of other major chronic diseases such as musculoskeletal conditions and neurodegenerative conditions as well as developmental disorders is outside the scope of this report. While these conditions contribute significantly to population morbidity and mortality, they have been explored in other reports. For more information on these conditions, please see:
| Areas of focus | Health indicators |
|---|---|
| Risk Behaviours |
|
| Risk Conditions |
|
| Chronic Diseases |
|
| Chronic Disease Multi Morbidity |
|
| Other Health Indicators |
|
Technical note: Crude prevalence and incidence rates are usually reported except when comparing trends over time and rates among the provinces and territories where age-standardized rates are used. Age-standardization takes into account the differences in population age structure (e.g. the distribution of the population by age groups). Therefore, the crude and age-standardized rates will likely differ slightly. The 2011 Canadian standard population was used for age standardization in this report. While age-standardized rates allow for comparisons, they are artificial rates based on a static population.
Main Findings
Risk Behaviours
Smoking
More than one in six (17.9%, or over 5 million) Canadians aged 12 and over report smoking on a daily or occasional basis (2014, CCHS).
Tobacco smoking is related to a large number of chronic diseases and conditions, including CRDs, CVDs and many types of cancer. It has been associated with negative impacts on nearly every organ of the body and a reduction in overall health. While Canada has seen a considerable decrease in smoking rates in the last few decades, smoking is still the leading risk factor for preventable death.Footnote 5,Footnote 6.
Trend - Since 2001, there has been a significant decrease in the age-standardized rate (ASR) of daily or occasional smokers, from 25.1% ASR in 2001 to 17.8% ASR in 2014, representing a 2.1% annual decrease.
The proportion of daily or occasional smokers has declined in all age groups, but has declined the most in younger age groups (12-19 and 20-34).
Smoking in 2014 by
Sex - In 2014, a greater proportion of males were daily or occasional smokers than females: 21.1% vs. 14.8% (statistically significant difference).
Age - 7.8% of youth (12-19 years old) reported daily or occasional smoking. Rates were highest among young adults aged 20-34 years (24.3%). Among adults aged 35-64 years smoking rates are stable at around 20%. The proportion of older adults who report daily or occasional smoking is significantly lower: 10.5% among those aged 65-79 and 4.6% among those aged 80 years and older.
Geography - British Columbia has the lowest age-standardized rate (14.4%) ASR, while the proportion of daily or occasional smokers in Newfoundland and Labrador, Prince Edward Island, Nova Scotia, New Brunswick, Yukon, the Northwest Territories and Nunavut were all at least 20% greater than the national average. The difference is most pronounced in the Northwest Territories and Nunavut, with the proportion of daily or occasional smokers nearly double in the Northwest Territories and more than three times that of the Canadian average in Nunavut.
Image 1: Prevalence of Smoking
Image 1: Prevalence of Smoking - Text Description
- 17.9% (2014)
- Over 5 million Canadians aged 12+
- Trend (2001-2014) Decreasing - 2.1% Annual Change
- Woman to man ratio: 0.7 : 1
- 1/4 of adults aged 20-34 smoke
Physical inactivity
More than three quarters (77.8%, or 20.1 million) of Canadian adults 18 and over and 90.7% of children and youth aged 5-17 years are not meeting the Canadian Physical Activity Guidelines (2012-13, CHMS).
Physical inactivity has been identified as an important public health concern for Canadians of all ages. It has been identified by the WHO as the fourth leading risk factor for global mortality and linked to a number of chronic diseases, including CVDs, cancer and diabetes.Footnote 7.
It is recommended that children and youth engage in moderate-to-vigorous physical activity for at least 60 minutes each day. For adults, the recommendation is for 150 minutes of moderate-to-vigorous physical activity each week, in bouts of 10 minutes or more.Footnote 8.
Trends - There has been no significant change in the proportion of children not obtaining 60 minutes per day of moderate-to-vigorous physical activity since 2007-2009 when data from accelerometers were examined (90.9% ASR in 2012-13). The pedometer data used to track federal/provincial/territorial physical activity targets over the last decade (2005-2015) have shown no change in the proportion of children and youth meeting recommendations, but have demonstrated a small and statistically significant decrease in the mean number of steps taken [CANPLAY].
The proportion of adults not meeting the guidelines based on accelerometer data has not changed significantly in recent years: 82.9% ASR (2007-09), 86.6% ASR (2009-11) and 78.2% ASR (2012-13). Based on self-reported data over the last decade (2005-2015), there was a small but statistically significant increase in the proportion of adults who reported being active or moderately active [CCHS].
Physical Inactivity in 2012-2013 by
Sex - A significantly greater proportion of girls (94.1%) than boys (86.9%) do not meet the level of activity recommended by the guidelines. The proportion of men and women who do not obtain enough physical activity to meet the guidelines does not differ significantly: 76.5% for men and 79.1% for women.
Age - In general, adherence to the guidelines diminishes with age. The most recent data show that the proportion of 5-11 year olds who do not meet the guidelines is 86.5%, while it climbs to 94.4% for 12-17 year olds. In adults, adherence to the guidelines diminishes with age. A greater proportion of younger adults (aged 18-34) achieve the recommended amount of moderate-to-vigorous physical activity when compared to older adults. More than four in five adults aged 35 or older are inactive: 82.0% for 35-49 year olds, 83.3% for 50-64 year olds and 88.2% for adults aged 65 years and over.
Image 2: Prevalence of Physical Inactivity
Image 2: Prevalence of Physical Inactivity - Text Description
- 90.7% of children and youth (2012-13)
- Over 4.5 million Canadians aged 5-17
- 77.8% of adults (2012-13)
- 20.1 million Canadians aged 18+
- Trend (2007-2013) Stable
- Girl to boy ratio: 1.1 : 1
- Woman to man ratio: 1 : 1
- 75% of adults 35+ are inactive
Sedentary behaviour
Half (51.8%, or 2.54 million) of children and youth (5-17 years) fail to meet the Canadian Sedentary Behaviour Guidelines (2012-13, CHMS).
Sedentary behaviour is a relatively new public health issue. Sedentary behaviours, which are generally characterized by long periods of sitting, such as watching TV, playing passive video games and using a computer, have been associated with health risks, including obesity and decreased fitness. There is strong evidence that this association is independent of physical activity. The Canadian Society for Exercise Physiology, with the support of PHAC, released Canada's first evidence-based sedentary behaviour guidelines in 2011.Footnote 9 These guidelines recommend limiting recreational screen time to no more than two hours per day for children and youth.
In 2012-2013, 51.8% of children and youth aged 5-17 failed to meet the Canadian Sedentary Behaviour Guidelines. The trend is stable since 2007-2009 with 48.7% not meeting the guidelines in 2007-2009 and 49.6% in 2009-2011. At present, long-term-trend data are not available for this specific indicator. Similarly, since 2007, the amount of time children spend engaged in sedentary activity has remained stable at approximately 8.5 hours per day.
Sedentary Behaviour in 2012-2013 by
Sex - In 2012-2013, 49.8% of the girls and 53.8% of the boys were not meeting the Guidelines. This difference was not statistically significant though.
Age - Younger children spend less time being sedentary than older children and youth: 7.4 hours/day among children aged 5-9 years compared to 8.8 hours/day among those aged10-14 years and 9.5 hours/day among those aged 15-17 years. With rapidly changing technology, increasing internet usage and the popularity of social media, developing consistent measures to monitor trends in sedentary behaviour can be expected to be a public health focus for the short-to-medium term in Canada.
Image 3: Prevalence of Sedentary Behaviour

Image 3: Prevalence of Sedentary Behaviour - Text Description
- 51.8% of kids and youth (2012-13)
- Over 2.54 million Canadians aged 5-17
- Trend (2007-2013) Stable
- Girl to boy ratio: 0.9 : 1
- Lowest in 5-9 years old: 7.4 hours/day
- Highest in youth 15-17 years:
- 9.5 hours/day
Unhealthy eating
More than half (60.3%, or 17.1 million) of Canadians aged 12 years and older consume fruits and vegetables less than five times per day (2014, CCHS).
Fruits and vegetables are important components of a healthy diet. Fruit and vegetable consumption as part of the daily diet may reduce the risk of CVDs and certain types of cancer and lower the risk of all-cause mortality, particularly cardiovascular mortality.Footnote 10,Footnote 11 Canada's Food Guide recommends consuming at least 7 to 10 servings of vegetables and fruits per day for adults and 4 to 8 for children and youth.Footnote 12 We report those who do not achieve the threshold of consuming fruits and vegetables five or more times per dayFootnote f, as a measure of "unhealthy eating."Footnote 13
Trend - In 2001, 62.0% ASR of Canadians aged 12 years and older consumed fruits and vegetables less than five times per day. This number dropped to a low of 54.3% ASR in 2009 and has increased since then to the current rate of 60.2% ASR (2014) (age-standardized rates). While there was an annual decrease of 1.4% between 2001 and 2009, this was unfortunately followed by a 1.8% annual increase from 2009 to 2014.
Unhealthy Eating in 2014 by
Sex - Significantly more men than women consume fruits and vegetables less than five times per day (67.6% vs. 53.3%).
Age - Unhealthy eating varies across age groups: from 56.4% in youth aged 12-19 to 63.6% in people aged 50-64, followed by a decline in the older age groups.
Geography - The proportion of Canadians eating fruits and vegetables less than five times a day exceeded the national average by more than 20% in Newfoundland and Labrador and Nunavut, with a rate of 74.1% ASR and 76.6% ASR respectively.
Image 4: Prevalence of Unhealthy Eating

Image 4: Prevalence of Unhealthy Eating - Text Description
- 60.3% (2012-13)
- 17.1 million Canadians aged 12+
- Trend (2001-2014) Stable
- Woman to man ratio: 0.8 : 1
- Highest in adults aged 50-64
Harmful use of alcohol
One in six (15.7%) Canadians aged 15 and over exceed the Low-Risk Drinking Guidelines (2013, CADUMS).
More than one in six (17.9%, or over 5.2 million) Canadians aged 12 and over report heavy drinking on at least one occasion per month in the past year (2014, CCHS).
Canada's Low-Risk Alcohol Drinking Guidelines were developed in 2011 to help Canadians moderate their alcohol consumption and reduce immediate and long-term alcohol-related harms. Immediate health risks are associated with "binge" or heavy drinking, which is characterized by the consumption of four or more drinks for women and five or more drinks for men on a single occasion. Long-term excessive alcohol consumption has been associated with an increased risk of chronic disease, including chronic liver disease, certain cancers, CVDs and premature death.Footnote 14.
Trends - Between 2001 and 2014, the age-standardized proportion of Canadians who reported heavy drinking increased from 14.9% ASR to 17.9% ASR, representing an annual increase of 1.4%.Footnote g
Heavy Drinking (2014) and Adherence to Low-risk Drinking Guidelines (2013) by
Sex - The proportion of males that reported exceeding the low-risk alcohol drinking guidelines for chronic drinking is higher compared to females (18.8% vs. 12.7%); this difference is even greater for heavy drinking in males compared to females (22.6% vs. 13.3%).
Age - The prevalence rates of Canadians exceeding the low-risk drinking guidelines vary from a high of 21.8% in 25-34 year olds to a low of 11.4% in those aged 50 and over. These differences are statistically significant. Similarly, rates of heavy drinking are highest among young adults, aged 20-34 (30.6 %), and decline with age.
Geography - There were no differences greater than 20% of the national average in the age- standardized prevalence rate of adherence to the low-risk guidelines among the provinces (the territories were not included in the CADUMS). However, compared to the national average (17.9% ASR), a greater proportion of individuals in Nova Scotia, New Brunswick, Newfoundland and Labrador, Yukon and the Northwest Territories reported heavy drinking: 21.4%, 22.6%, 26.1%, 26.5% and 29.3% ASR, respectively. The rate from Nunavut is unavailable.
Image 5: Prevalence of Heavy Drinking
Image 5: Prevalence of Heavy Drinking - Text Description
- 17.9% (2014)
- Over 5.2 million Canadians aged 12+
- Trend (2001-2014) Increasing
- +1.4% Annual Change
- Woman to man ratio: 0.6 : 1
- Highest in young adults aged 20-34
Comparing risk behaviours and conditions
Figure 1 below outlines the age-standardized prevalence trends for key risk behaviours and conditions in Canada. A further breakdown of the trends by age group is provided in Figure 2, while Figure 3 presents the distribution by number of modifiable risk behaviours.
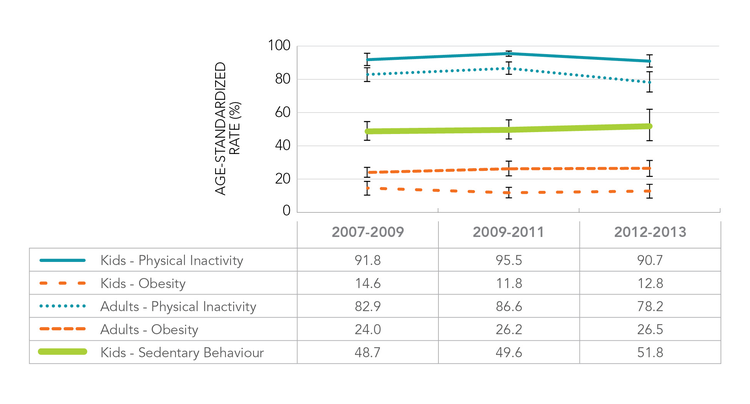
Figure 1. Age-standardized prevalence (%) trends in sedentary behaviour, physical inactivity and obesity among Canadian kids (aged 5-17) and adults (18+), Canada (2007-2009 to 2012-2013)
Source: Canadian Health Measures Survey (2007-2009 to 2012-2013)
Figure 1. Age-standardized prevalence (%) trends in sedentary behaviour, physical inactivity and obesity among Canadian kids (aged 5-17) and adults (18+), Canada (2007-2009 to 2012-2013) - Text Description
Figure 1 is presented as a time series line graph. It shows age-standardized prevalence trends over a period of 7 years for selected risk behaviours and conditions among Canadian kids (aged 5-17) and adults (aged 18 and over). Using measured and self-reported data from three cycles of the Canadian Health Measures Survey (2007-2009; 2009-2011; and 2012-2013); age-standardized prevalence (as a percentage) was calculated and presented for physical inactivity and obesity in both kids and adults, and for sedentary behaviour in kids only.
Looking at time trends over the three cycles presented in the Figure 1 table below, there have been no significant changes in the proportion of inactive kids, or inactive adults. The age-standardized prevalence of physical inactivity is higher among kids when compared to adults in every year studied.
In terms of age-standardized obesity prevalence, no significant changes have been observed in kids or adults over time either. According to the data from 2012-2013, the proportion of obese Canadian adults is roughly double (26.5%) that of Canadian kids (12.8%). The level of sedentary behaviour among kids was stable, around 50%, over the 7 year period.
| Year | |||
|---|---|---|---|
| 2007-2009 | 2009-2011 | 2012-2013 | |
| Kids - Physical Inactivity | 91.8 | 95.5 | 90.7 |
| Adults - Physical Inactivity | 82.9 | 86.6 | 78.2 |
| Kids - Obesity | 14.6 | 11.8 | 12.8 |
| Adults - Obesity | 24.0 | 26.2 | 26.5 |
| Kids - Sedentary Behaviour | 48.7 | 49.6 | 51.8 |
| Source: Canadian Health Measures Survey (2007-2009 to 2012-2013) | |||
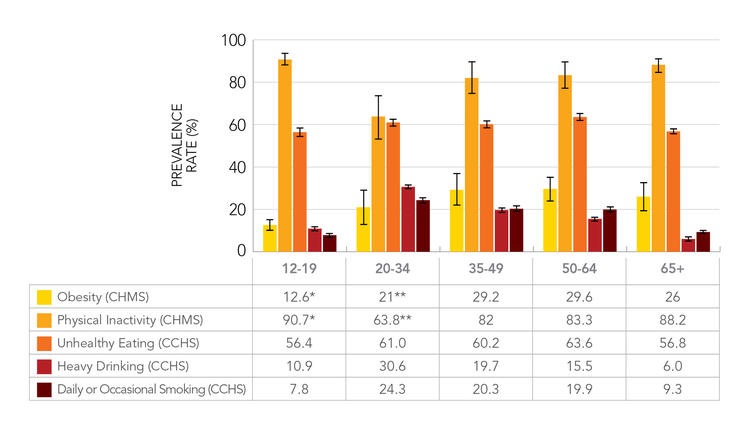
Figure 2. Prevalence (%) of obesity, physical inactivity, unhealthy eating, heavy drinking and smoking among Canadians, by age group, Canada (CHMS 2012-2013, CCHS 2014)
Sources: Canadian Health Measures Survey (2012-2013), Canadian Community Health Survey (2014)
Note: * 5-17 years old - ** 18-34 years old. Obesity rate for 18-34 age group should be interpreted with caution, give a coefficient of variation between 16.6% and 33.3%.
Figure 2. Prevalence (%) of obesity, physical inactivity, unhealthy eating, heavy drinking and smoking among Canadians, by age group, Canada (CHMS 2012-2013, CCHS 2014) - Text Description
Figure 2 is presented as a multi-series vertical bar graph. It shows prevalence of obesity, physical inactivity, unhealthy eating, heavy drinking and daily or occasional smoking broken down by age group, among Canadians aged 5 and up. Using measured and self-reported data from the latest cycles of the Canadian Health Measures Survey (2012-2013) and the Canadian Community Health Survey (2014), age group specific prevalence (as a percentage) was calculated and presented for the four selected risk behaviours and one risk condition.
Data for Figure 2 are presented in the table below. Note: The symbols "*" and "**" indicate where age groups differ from those noted in the column heading. The obesity rate for the 18-34 age group should be interpreted with caution, given a coefficient of variation between 16.6% and 33.3%.
The prevalence of both physical inactivity and unhealthy eating is consistently higher across all age groups in comparison to the other four behaviour/condition prevalence estimates. With the exception of the age group representing young adults (aged 18-34); prevalence estimates for physical inactivity for all other life-course age groups were above 80%. Additionally, observed estimates for the proportion of unhealthy eating across all age groups were over 55%.
The prevalence of heavy drinking and daily or occasional smoking was highest among younger adults aged 20-34 (30.6% and 24.3% respectively). The prevalence of heavy drinking was lowest among older adults aged 65 and older (6.0%). Prevalence estimates for physical inactivity were highest among children aged 5-17 (90.7%) and lowest in young adults aged 18-34 (63.8%). In terms of unhealthy eating, prevalence estimates ranged from 56.4% in children and youth aged 12-19 to 63.6% in adults aged 45-64.
| Risk Behaviours and Conditions | Age | ||||
|---|---|---|---|---|---|
| 12-19 | 20-34 | 35-49 | 50-64 | 65+ | |
| Obesity (CHMS) | 12.6Figure 2 Table 1 footnote * | 21Figure 2 Table 1 footnote ** | 29.2 | 29.6 | 26 |
| Physical Inactivity (CHMS) | 90.7Figure 2 Table 1 footnote * | 63.8Figure 2 Table 1 footnote ** | 82 | 83.3 | 88.2 |
| Unhealthy Eating (CCHS) | 56.4 | 61.0 | 60.2 | 63.6 | 56.8 |
| Heavy Drinking (CCHS) | 10.9 | 30.6 | 19.7 | 15.5 | 6.0 |
| Daily or Occasional Smoking (CCHS) | 7.8 | 24.3 | 20.3 | 19.9 | 9.3 |
|
Sources: Canadian Health Measures Survey (2012-2013), Canadian Community Health Survey (2014)
|
|||||
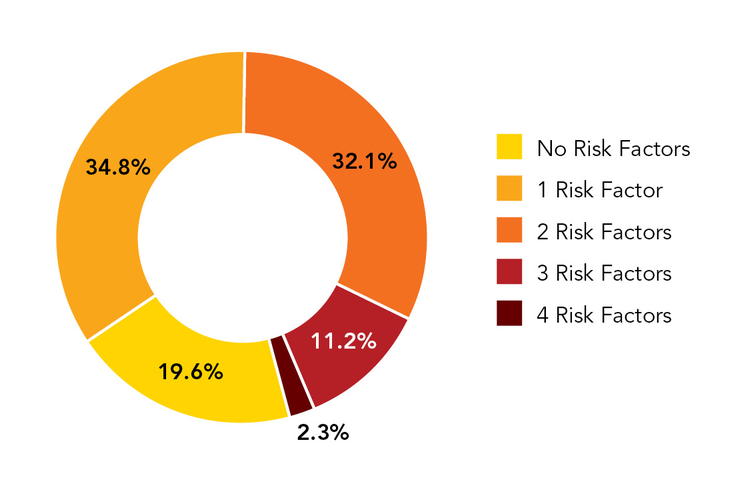
In 2014, while 80.4% of Canadians aged 20 years and older reported at least one of the four main risk factors, 2.3% reported all four. Overall rates among females were statistically lower (77.4%) than in males (83.7%). Interestingly, the proportion of those reporting at least one risk factor decreased with age: from 84.4% among the 20-34 age group to 68.8% among those 80 and over.
Figure 3. Proportion of the Canadian population 20+ years of age with zero to four of the main modifiable risk behaviours,Figure 3 - Footnote * Canada (2014)
- Figure 3 - Footnote *
-
Risk factors include self-reported
- heavy drinking,
- smoking (daily or occasional),
- physical inactivity (self-reported),
- consumption of fruits and vegetables less than five times per day
Source: Canadian Community Health Survey (2014)
Figure 3. Proportion of the Canadian population 20+ years of age with zero to four of the main modifiable risk behaviours, Canada (2014) - Text Description
Figure 3 is presented as a doughnut chart. It shows the proportion of Canadians aged 20 years and older with none of the four main modifiable risk behaviours, up to those with four of them. The major modifiable risk behaviours include: heavy drinking, smoking (daily or occasional), physical inactivity and unhealthy eating.
The Figure 3 table below contains self-reported data collected through the 2014 Canadian Community Health Survey. Among Canadians aged 20 and older, less than 20% reported having none of the four main risk behaviours. The majority - over two-thirds, of those with a risk behaviour associated with chronic disease had either one risk behaviour (34.8%) or two (32.1%). Finally, about 13.5% of the population reported having as many as three or four of the main modifiable risk factors.
| Number of risk behaviours | Proportion (%) |
|---|---|
| No Risk Factors | 19.6 |
| 1 Risk Factor | 34.8 |
| 2 Risk Factors | 32.1 |
| 3 Risk Factors | 11.2 |
| 4 Risk Factors | 2.3 |
| Sources: Canadian Community Health Survey (2014) | |
Risk Conditions
Obesity
One in four adults (26.4%), one in six youth aged 12-17 (16.5%) and one in eleven children aged 5-11 (8.8%) are obese (CHMS, 2012-13).
Obese individuals are at an increased risk of certain chronic conditions including hypertension, type 2 diabetes, CVDs, some cancers and even premature death.Footnote 15 In addition, excess body weight can also affect quality of life, educational attainment and learning potential.Footnote 16 Moreover, the strongest predictor of being obese as an adult is being obese as a child.Footnote 17 Obesity rates have dramatically increased in the last few decades, while only 13.8% of adults and 6.3% of children and youth were obese in 1978-79.Footnote 18,Footnote 19,Footnote 20
Trends - No statistically significant differences in the age-standardized prevalence of obesity among Canadian adults have been observed since 2007-09: 24.0% ASR in 2007-09, 26.2% ASR in 2009-11 and 26.5% ASR in 2012-13. The obesity rate for children and youth reached a peak in 2007-09, with 14.8% ASR of them affected. Since then, no statistically significant changes have been observed.
Obesity in 2012-2013 by
Sex - Rates among men (26.5%) and women (26.2%) are similar. Among children and youth aged 5-17 years, boys (14.7%) have a higher rate of obesity than girls (10.3%). However, the difference is not statistically significant.
Age - In adults, rates were highest in the 35-49 and the 50-64 age groups, with 29.2% and 29.6% of them being obese, respectively.
Image 6: Prevalence of Obesity
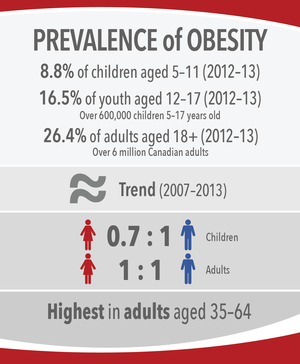
Image 6: Prevalence of Obesity - Text Description
- 8.8% of children aged 5-11 (2012-13)
- 16.5% of youth aged 12-17 (2012-13)
- Over 600,000 children 5-17 years old
- 26.4% of adults aged 18+ (2012-13)
- Over 6 million Canadian adults
- Trend (2007-2013) Stable
- Girl to boy ratio: 0.7 : 1
- Woman to man ratio: 1 : 1 Adults
- Highest in adults aged 35-64
Hypertension
About 6.9 million (24.9%) Canadians aged 20 years and older are living with diagnosed hypertension (2011/12, CCDSS).
Globally, high blood pressure or hypertension is one of the most important risk factors for death and disability.Footnote 21 When the blood pressure is consistently high for long periods of time, it leads to damaged arteries and decreased blood flow to affected organs. Left untreated and uncontrolled, it can cause heart attacks, stroke, heart failure, dementia, renal failure and blindness.Footnote 22 With about 68% of Canadians having their blood pressure controlled, mainly due to the increased use of medications, Canada has the world's highest reported national blood pressure control rate.Footnote 23,Footnote 24 However, high rates of sedentary behaviours, obesity and sodium consumptionFootnote 25 are likely to further contribute to the hypertension burden.
Trends - The age-standardized prevalence of diagnosed hypertension has increased from 18.0% ASR in 2000/01 to 24.4% ASR in 2011/12. This represents an average annual increase of 2.8%.
The age-standardized incidence of diagnosed hypertension decreased from 2,563 per 100,000 ASR in 2000/01 to 1,867 per 100,000 ASR in 2011/12. This represents an average annual decrease of 2.6%.
Hypertension in 2011/12 by
Sex - Prevalence rates were similar in females (25.6%) and in males (24.2%).
Age - In 2011/12, the prevalence of diagnosed hypertension increased with increasing age, with over 70% of adults aged 65 years and older being affected.
Geography - In 2011/12, while the highest age-standardized prevalence rate was seen in Newfoundland and Labrador (31.1% ASR), the lowest prevalence was observed in the Northwest Territories (22.0% ASR).
Image 7: Prevalence of Hypertension
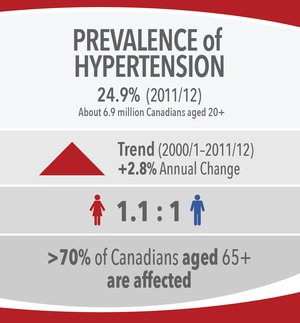
Image 7: Prevalence of Hypertension - Text Description
- 24.9% (2011/12)
- About 6.9 million Canadians aged 20+
- Trend (2000/1-2011/12) Increasing
- +2.8% Annual Change
- Woman to man ratio: 1.1 : 1
- >70% of Canadians aged 65+ are affected
Chronic Diseases
Cardiovascular Diseases
Ischemic heart disease (IHD)
About 2.3 million (8.4%) Canadians aged 20 years and older are living with diagnosed ischemic heart disease (2011/12, CCDSS).
In Canada, heart disease is the second leading cause of death,Footnote 26 after cancer, and a leading cause of hospitalization.Footnote 27 Ischemic heart disease is a chronic condition in which the heart muscle is damaged or works inefficiently because of the absence or relative deficiency of its blood supply. Moreover, IHD is the number one cause of years of life lost (YLLs) due to premature mortality and the second leading cause of disability-adjusted life years (DALYs) lost in 2013.Footnote 28.
Trends - Over time, the age-standardized prevalence of diagnosed IHD increased from 7.2% ASR in 2000/01 to 8.3% ASR in 2006/07, and has stayed stable since then, with a slight decrease in 2011/12 to 8.1% ASR. This represents an average annual increase of 1.0%.
The age-standardized incidence of diagnosed ischemic heart disease decreased from 1,244 per 100,000 ASR in 2000/01 to 709 per 100,000 ASR in 2011/12. This represents an average annual decrease of 5.1%.
IHD in 2011/12 by
Sex - 9.8% men over the age of 20 were living with a diagnosed IHD, while 7.1% women 20 years and older were living with the same condition.
Age - IHD prevalence increased with age, while males had higher rates than females in all age groups. Overall, more than a quarter of Canadians aged 65 years and older had been diagnosed with IHD.
Geography - In 2011/12, New Brunswick had the highest age-standardized prevalence rate of IHD (9.4% ASR) and Nunavut the lowest (4.6% ASR).
Image 8: Prevalence of IHD
Image 8: Prevalence of IHD - Text Description
- 8.4% (2011/12)
- About 2.3 million Canadians aged 20+
- Trend (2000/1-2006/7) Increasing
- +1.0% Annual Change
- Trend (2006/7-2011/12) Stable
- Woman to man ratio: 0.7 : 1
- 2/3 of IHD cases are aged 65+
Stroke
About 700,000 (2.7%) Canadians aged 20 years and older are living with diagnosed strokeFootnote h (2011/12, CCDSS).
Stroke, also called cerebrovascular disease, is a sudden loss of brain function that occurs when blood flow supplying oxygen to a part of the brain is interrupted.
In Canada, stroke is the third leading cause of death, after cancer and heart disease.Footnote 29 Stroke is the fourth leading cause of years of life lost due to premature mortality and the tenth largest contributor to disability adjusted life years (DALYs)Footnote i, in 2013.Footnote 30 Although hospitalizations and deaths due to stroke have steadily declined over the past few decades, the absolute number of individuals living with the effects of a stroke is increasing.Footnote 31 Moreover, studies have shown that the burden is increasing among younger adults, with the proportion of all strokes in those aged less than 55 years old increasing over time and mean age of stroke decreasing.Footnote 32,Footnote 33 As a result, the burden of stroke is likely to increase even further.
Trends - The age-standardized prevalence of diagnosed stroke has been increasing from 2.3% ASR in 2003/04 to 2.5% ASR in 2011/12. This represents an average annual increase of 1.0%.
The age-standardized incidence of diagnosed stroke decreased from 383 per 100,000 ASR in 2003/04 to 305 per 100,000 ASR in 2011/12. This represents an average annual decrease of 2.6%.
Stroke in 2011/12 by
Sex - Males and females were equally affected (2.7%).
Age - The prevalence of diagnosed stroke increased with increasing age, with about 10% of adults aged 65 years and older being affected.
Geography - While the highest prevalence was observed in Prince Edward Island (3.0%), the lowest prevalence was in Newfoundland and Labrador (2.1%).
Image 9: Prevalence of Stroke
Image 9: Prevalence of Stroke - Text Description
- 2.7% (2011/12)
- About 700,000 Canadians aged 20+
- Trend (2003/4-2011/12) Increasing
- +1.0% Annual Change
- Woman to man ratio: 1 : 1
- 1/3 of cases are aged 80+
Cancer
Over 800,000 (2.4%) Canadians have been diagnosed with cancer in the past 10 years and are still alive (2009, CCR).
Cancer is not just one disease, but a large group of almost 100 diseases. Its two main characteristics are uncontrolled growth of the cells in the human body and the ability of these cells to migrate from the original site and spread to distant sites. Although major advances in cancer treatment and survival occurred in the last few decades, cancer has been the leading cause of death in Canada since 2006. In 2009, over 800,000 (2.4%) Canadians had been diagnosed with cancer in the previous 10 years. Prostate, breast and colorectal cancers account for over half of all prevalent cases in Canada. Approximately two in five Canadians are expected to be diagnosed with cancer in Canada in their lifetime, and one in four will die from cancer.Footnote 34.
Trends - The age-standardized 10-year cancer prevalence rate increased from 2.3% ASR in 2002 to 2.5% ASR in 2009, with an annual percent change of +1.1%.
The age-standardized incidence rate of cancer was 528 per 100,000 ASR in 2000 and 507 per 100,000 ASR in 2013, with an annual percent decrease of -0.3% per year.
Cancer in 2009 (for 10-year prevalence) and in 2013 (for incidence) by
Sex - In 2009, 10-year prevalence in men (2.45%) was higher than that of women (2.40%). This difference is due to the higher incidence rate of cancer in men compared to women. In 2013, the number of men who received a diagnosis of cancer was 91,900 (incidence rate: 559/100,000) and the number of women was 88,600 (incidence rate: 472/100,000).
Age - In 2009, the 10-year prevalence was 11.2% in people 80 years of age and older, 9.5% in those 65-79, 3.7% in those 50-64, 1.1% in those 35-49, 0.3% in those 20-34 and 0.1% in those 0-19. In 2010, nearly 90% of all newly diagnosed cancers were in Canadians over the age of 50, and 40% in those over the age of 70.
Geography - In general, cancer incidence rates are higher in eastern Canada and lower in western
Canada. In 2013, the lowest incidence rate ASR was observed in Yukon (397/100,000).
Image 10: 10-Year Prevalence of Cancer
Image 10: 10-Year Prevalence of Cancer - Text Description
- 2.4% (2009)
- Over 800,000 Canadians
- Trend (2002-2009) Increasing
- +1.1% Annual Change
- Woman to man ratio: 1 : 1
- 90% diagnosed in adults ≥50
Chronic respiratory diseases
Chronic obstructive pulmonary disease (COPD)
More than 1.9 million (9.6%) Canadians aged 35 and older are living with COPD (2011/12, CCDSS).
COPD is a chronic and progressive condition characterized by gradual airway obstruction, shortness of breath, cough and sputum production. Cigarette smoking is the main cause of COPD.Footnote 35 Quitting smoking has been associated with improved lung function, reduced chronic cough and airway mucus production, and decreased mortality from COPD.Footnote 36 COPD is the seventh leading cause of years of life lost due to premature mortality and the ninth largest contributor to DALYs in 2013.Footnote 37.
Trends - The age-standardized prevalence of diagnosed COPD increased from 7.0% ASR in 2000/01 to 9.4% ASR in 2011/12. This represents an annual increase of 2.5%.
The age-standardized incidence of diagnosed COPD decreased from 1202 per 100,000 ASR in 2000/01 to 915 per 100,000 ASR in 2011/12. This represents an annual decrease of 1.8%.
COPD in 2011/12 by
Sex - The prevalence rates of COPD were very similar for males (9.6%) and females (9.5%) aged 35 and older.
Age - The prevalence rates steadily increased from 2.8% in the 35-49 age group to 25.4% in the 80 and older age group.
Geography - The age-standardized prevalence of COPD among adults 35 years and older ranged from 8.4% ASR in Prince Edward Island to 23.3% ASR in Nunavut. Nova Scotia and the three territories all had rates that were more than 20% higher than the Canadian rate.
Image 11: Prevalence of COPD
Image 11: Prevalence of COPD - Text Description
- 9.6% (2011/12)
- Over 1.9 million Canadians aged 35+
- Trend (2000/1-2011/12) Increasing
- +2.5% Annual Change
- Woman to man ratio: 1 : 1
- >1/3 of cases are aged 50-64
Asthma
About 3.8 million (10.7%) Canadians aged one year and older are living with physician-diagnosed asthma, representing 9.5% of adults aged 20 and older and 15.3% of children aged 1-19 (2011/12, CCDSS).
Asthma is a chronic condition characterized by cough, shortness of breath, chest tightness and wheezing. Asthma symptoms and attacks usually occur after exercise, exposure to allergens or irritants, or viral respiratory infections.Footnote 38 Despite the increase in adherence to appropriate care strategies and awareness of asthma attack triggers, two out of three Canadians with active asthma do not have good control of their condition.Footnote 39 Asthma is the tenth leading cause of years lived with disability (YLDs) in 2013.Footnote 40
Trends - The age-standardized prevalence of diagnosed asthma among those aged one and older increased from 6.5% ASR in 2000/01 to 10.8% ASR in 2011/12. This represents an annual increase of 4.4%.
However, the age-standardized incidence of diagnosed asthma among those aged one and older decreased from 905 per 100,000 ASR in 2000/01 to 499 per 100,000 ASR in 2011/12. This represents an annual decrease of 5.0%.
Asthma in 2011/12 by
Sex - The prevalence of asthma was 11.3% among females and 10.2% among males.
Age - The prevalence rates for diagnosed asthma were highest in the 1-19 (15.3%) and 20-34 (11.4%) age groups after which they declined until age 65 where they began increasing again. The rate among those aged 80 and older was 10.3%.
Geography - The age-standardized prevalence of diagnosed asthma among those aged one and older ranged from 3.8% ASR in Nunavut to 12.1% ASR in Ontario. The three territories all had rates more than 20% lower than the Canadian rate.
Image 12: Prevalence of Asthma
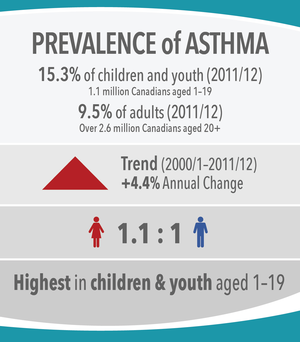
Image 12: Prevalence of Asthma - Text Description
- 15.3% of children and youth (2011/12)
- 1.1 million Canadians aged 1-19
- 9.5% of adults (2011/12)
- Over 2.6 million Canadians aged 20+
- Trend (2000/1-2011/12) Increasing
- +4.4% Annual Change
- Girl to boy ratio: 1.1 : 1
- Highest in children & youth aged 1-19
Diabetes
More than 2.7 million (7.7%) Canadians aged one year and older are living with diagnosed diabetes (type 1 and 2 combinedFootnote j), representing 9.8% of adults aged 20 years and older and 0.3% of children aged 1-19 (2011/12, CCDSS).
Diabetes is a chronic disease that occurs when the body is either unable to sufficiently produce or properly use insulin. Diabetes can lead to many complications, including cardiovascular disease, vision loss/blindness, kidney failure, nerve damage, problems with pregnancy, oral disease and depression.Footnote 41 Worldwide, it is the tenth leading cause of years of life lost to premature death.Footnote 42
Trends - Overall, the age-standardized prevalence of diagnosed diabetes in Canada increased from 4.8% ASR in 2000/01 to 7.6% ASR in 2011/12, with an average annual increase of 4.2%.
Overall, the age-standardized incidence rate of diagnosed diabetes in Canada rose from 660 per 100,000 ASR in 2000/01 to a high of 761 per 100,000 ASR in 2006/07, with an average annual increase of 2.2%, and dropped thereafter to 662 per 100,000 in 2011/12, representing an average annual decrease of 2.2%.
Diabetes in 2011/12 by
Sex - 7.2% of females and 8.3% of males aged one year and older were living with diagnosed diabetes (type 1 and type 2 combined) in Canada.
Age - The prevalence rates for diagnosed diabetes increased by age group, starting at 0.3% for those aged 1-19, rising slowly to 4.5% among those 35-49, and then climbing more steeply, with the highest rates being among those in the 65-79 (24.6%) and 80 and older (26.1%) age groups.
Geography - Although the provincial and territorial age-standardized prevalence rates of diabetes ranged from a low of 6.5% ASR in Nunavut to a high of 8.9% ASR in Yukon, they did not differ by more than 20% from the national average.
Image 13: Prevalence of Diabetes
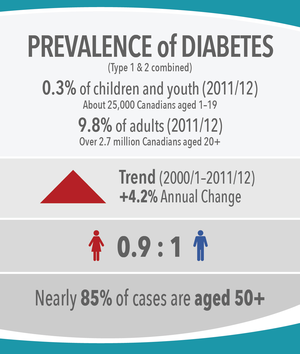
Image 13: Prevalence of Diabetes - Text Description
- (Type 1 & 2 combined)
- 0.3% of children and youth (2011/12)
- About 25,000 Canadians aged 1-19
- 9.8% of adults (2011/12)
- Over 2.7 million Canadians aged 20+
- Trend (2000/1-2011/12) Increasing
- +4.2% Annual Change
- Woman to man ratio: 0.9 : 1
- Nearly 85% of cases are aged 50+
Mood and anxiety disorders (health services use)
Over 3.5 million (or 10%) Canadians aged one year and older use health servicesFootnote k for mood and anxiety disorders annually (2011/12, CCDSS).
Mood disorders are characterized by the lowering or elevation of a person's mood, while anxiety disorders are characterized by excessive and persistent feelings of apprehension, worry and even fear. Mood and anxiety disorders are the most common types of mental illnesses in Canada, accounting for three quarters of Canadians who use health services for a mental illness.Footnote 43 They have the potential to impact every aspect of an individual's life, including relationships, education, work, and community involvement. According to the 2010 Global Burden of Disease Study, in Canada, major depressive disorder was ranked as the second leading cause of years of life lost due to disability, and anxiety disorders were ranked the eighth leading cause.Footnote 44
Trend - The age-standardized annual prevalence of the use of health services for mood and anxiety disorders among Canadians aged one year and older remained relatively stable over the surveillance period, ranging from 11.0% ASR in 2000/01 to 10.0% ASR in 2011/12, with an average annual percent change of -1%.
Use of Mental Health Services 2011/12 by
Sex - The annual prevalence of those using health services for mood and anxiety disorders was higher among females (2.2 million or 12.6%) compared to males (1.3 million or 7.5%).
Age - Approximately 257,000 (or 3.4%) Canadian children and youth (1-19 years) used health services for mood and anxiety disorders. In the same year, approximately 3.3 million Canadian adults (20+ years) used health services for mood and anxiety disorders. Among adults, rates were highest among those between the ages of 35 and 64 and decreased slightly over the surveillance period with increasing age.
Geography - In 2011/12, the age-standardized annual prevalence of the use of health services for mood and anxiety disorders was highest in Nova Scotia (12.0% ASR) and lowest in Nunavut (5.1% ASR). Newfoundland and Labrador, Quebec, the Northwest Territories and Nunavut all had rates more than 20% lower than the Canadian average.
Image 14: Annual Prevalence of Health Services Use for Mood and Anxiety Disorders
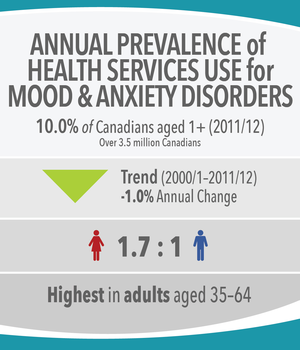
Image 14: Annual Prevalence of Health Services Use for Mood and Anxiety Disorders - Text Description
- 10.0% of Canadians aged 1+ (2011/12)
- Over 3.5 million Canadians
- Trend (2000/1-2011/12) Decreasing
- -1.0% Annual Change
- Woman to man ratio: 1.7 : 1
- Highest in adults aged 35-64
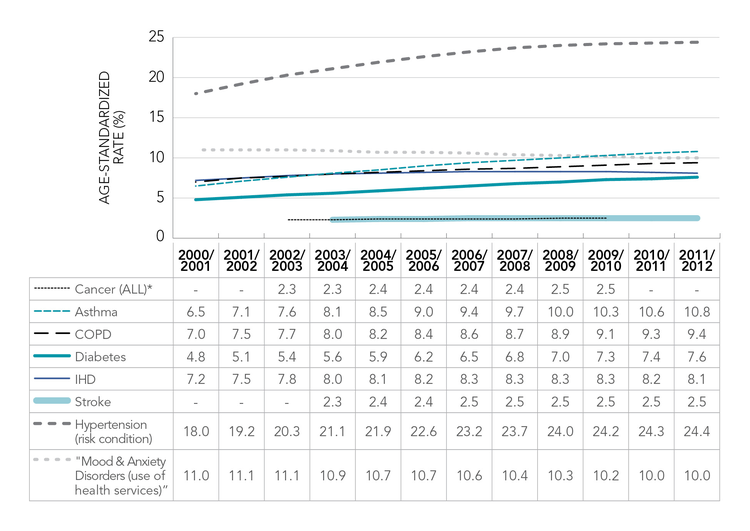
Comparing diseases and risk conditions
Figure 4 outlines the age-standardized prevalence trends for major chronic diseases and conditions in Canada. A further breakdown by age group is provided in Figure 5.
Figure 4. Age-standardized prevalence (%) trends in major chronic diseases and risk conditions among Canadians 1 year and older, Canada (2000/01 to 2011/12)Figure 4 - Footnote *
Sources: Canadian Cancer Registry 2000-2010, Canadian Chronic Disease Surveillance System FY 2000/01-2011/12.
- Figure 4 - Footnote *
-
Cancer data are presented by calendar year; all other data are presented by fiscal year.
Figure 4. Age-standardized prevalence (%) trends in major chronic diseases and risk conditions among Canadians 1 year and older, Canada (2000/01 to 2011/12) - Text Description
Figure 4 is presented as a time series line graph. It shows age-standardized prevalence trends over a 12-year period for seven chronic diseases and one risk condition among Canadians. Annual age-standardized prevalence estimates have been calculated as percentages for each fiscal year between 2000/01 and 2011/12, except for cancer, where annual prevalence estimates reflect calendar years. The seven chronic conditions include: all types of cancers combined; asthma; chronic obstructive pulmonary disease (COPD); diabetes; ischemic heart disease (IHD); stroke; and mood and anxiety disorders (where prevalence represents the use of health services). The prevalence of hypertension, a chronic risk condition, is also presented in this figure.
Among the major chronic diseases and risk conditions, the prevalence of hypertension was the highest (24.4% in 2011/12), while those for all cancers and stroke were the lowest (2.5% in 2009/10 and 2.5% in 2011/12 respectively).
With respect to trends over the 12-year period, the age-standardized prevalence increased annually for stroke (1.0%), all cancers (1.1%), COPD (2.5%), hypertension (2.8%), diabetes (4.2%) and asthma (4.4%), while rates decreased for health services use for mood and anxiety disorders (-1.0%). Age-standardized prevalence for IHD indicated an increasing annual trend up to 2006/7, followed by a stabilization period and slight decrease in the last two years of surveillance, accounting for an overall 1.0% annual increase.
The Figure 4 table below provides the age-standardized annual prevalence in percentages by year for the major chronic diseases and conditions noted above:
| Year | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2000/ 2001 | 2001/ 2002 | 2002/ 2003 | 2003/ 2004 | 2004/ 2005 | 2005/ 2006 | 2006/ 2007 | 2007/ 2008 | 2008/ 2009 | 2009/ 2010 | 2010/ 2011 | 2011/ 2012 | |
| Cancer (ALL ages)* | 2.3 | 2.3 | 2.4 | 2.4 | 2.4 | 2.4 | 2.5 | 2.5 | ||||
| Asthma (ages 1+) | 6.5 | 7.1 | 7.6 | 8.1 | 8.5 | 9.0 | 9.4 | 9.7 | 10.0 | 10.3 | 10.6 | 10.8 |
| COPD (ages 40+) | 7.0 | 7.5 | 7.7 | 8.0 | 8.2 | 8.4 | 8.6 | 8.7 | 8.9 | 9.1 | 9.3 | 9.4 |
| Diabetes (ages 1+) | 4.8 | 5.1 | 5.4 | 5.6 | 5.9 | 6.2 | 6.5 | 6.8 | 7.0 | 7.3 | 7.4 | 7.6 |
| IHD (ages 20+) | 7.2 | 7.5 | 7.8 | 8.0 | 8.1 | 8.2 | 8.3 | 8.3 | 8.3 | 8.3 | 8.2 | 8.1 |
| Stroke (ages 20+) | 2.3 | 2.4 | 2.4 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | |||
| Hypertension (ages 20+) (risk condition) | 18.0 | 19.2 | 20.3 | 21.1 | 21.9 | 22.6 | 23.2 | 23.7 | 24.0 | 24.2 | 24.3 | 24.4 |
| Mood & Anxiety Disorders (ages 1+) (use of health services) | 11.01 | 11.07 | 11.06 | 10.91 | 10.73 | 10.74 | 10.59 | 10.41 | 10.26 | 10.16 | 10.03 | 10.04 |
| Sources: Canadian Cancer Registry 2000-2010, Canadian Chronic Disease Surveillance System fiscal years 2000/01-2011/12. | ||||||||||||
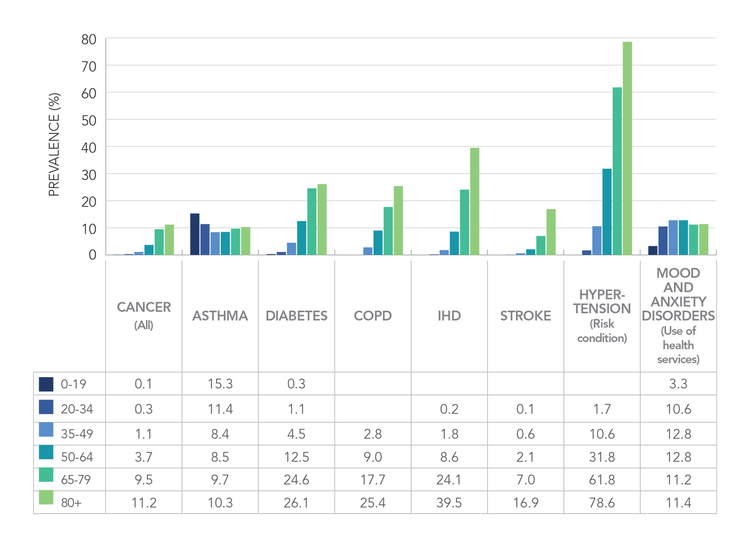
Figure 5. Prevalence (%) of major chronic diseases and risk conditions in Canadians, by age group, Canada (2011/12)Figure 5 - Footnote *
Source: Canadian Cancer Registry, Chronic Disease and Injury Indicator Framework (2015 update), Canadian Chronic Disease Surveillance System.
- Figure 5 - Footnote *
-
Cancer data are presented by calendar year (2009); all other data are presented by fiscal year (2011/12).
Figure 5. Prevalence (%) of major chronic diseases and risk conditions in Canadians, by age group, Canada (2011/12) - Text Description
Figure 5 is presented as a multi-series vertical bar graph. It shows the prevalence (in percentages) of major diagnosed chronic diseases and conditions in Canadians, by age group, for the fiscal year 2011/12, and in the case of all cancers combined, for the 2009 calendar year. The seven chronic conditions include: all types of cancers combined; asthma; diabetes; chronic obstructive pulmonary disease (COPD); ischemic heart disease (IHD); stroke; and mood and anxiety disorders (where prevalence represents the use of health services). The prevalence of hypertension, a chronic risk condition, is also presented in this figure.
According to Figure 5 and the data table below, prevalence estimates for six of the major chronic diseases and conditions (all cancers, COPD, diabetes, IHD, stroke and hypertension) increased with age. The most notable rise was seen in hypertension - going from 1.7% in Canadians 20-34 years of age to 78.6% in Canadians aged 80 years and over. The life-course prevalence of asthma and health services use for mood and anxiety disorders did not follow similar increasing patterns with age. Instead, for asthma, the age groups with the highest prevalence included children and youth aged 0-19 years old (15.3%) and young adults aged 20-34 years old (11.4%). For mood and anxiety disorders, the prevalence of health services use was highest among Canadians adults aged 35-64 (12.8%).
The Figure 5 data table below provides the most current crude annual prevalence in percentages for the major chronic diseases and conditions noted above, by life-course age groupings:
| Chronic Diseases and Risk Conditions | Age | |||||
|---|---|---|---|---|---|---|
| 0-19 | 20-34 | 35-49 | 50-64 | 65-79 | 80+ | |
| Cancer (all) | 0.1 | 0.3 | 1.1 | 3.7 | 9.5 | 11.2 |
| Asthma | 15.3 | 11.4 | 8.4 | 8.5 | 9.7 | 10.3 |
| Diabetes | 0.3 | 1.1 | 4.5 | 12.5 | 24.6 | 26.1 |
| COPD | 2.8 | 9.0 | 17.7 | 25.4 | ||
| IHD | 0.2 | 1.8 | 8.6 | 24.1 | 39.5 | |
| Stroke | 0.1 | 0.6 | 2.1 | 7.0 | 16.9 | |
| Hypertension (risk condition) | 1.7 | 10.6 | 31.8 | 61.8 | 78.6 | |
| Mood and Anxiety Disorders (use of health services) |
3.3 | 10.6 | 12.8 | 12.8 | 11.2 | 11.4 |
| Source: Canadian Cancer Registry, Chronic Disease and Injury Indicator Framework (2015 update), Canadian Chronic Disease Surveillance System. | ||||||
Chronic Disease Multi-Morbidity
Multi-morbidityFootnote l
More than one in 30 (3.6% or over 975,000) Canadian adults aged 20 years and older and nearly one in eight (11.7%) of Canadians aged 65 and older have at least two of the four major chronic diseases—CVD, cancer, CRD and diabetes (2014, CCHS).
The recognition that people may have two or more chronic diseases or conditions concurrently, referred to as multi-morbidity, adds another layer of complexity to prevention and management. These individuals are at a greater risk of adverse health outcomes and have increased health care needs.Footnote 45,Footnote 46.
Trend - Among Canadians aged 65 and over, prevalence rates have slightly increased in the last decade from 10.7% ASR (2005) to 11.9% ASR (2014), representing an annual percent increase of 1.5%.
Multi-morbidities among the four major chronic diseases in 2014
Sex - Females aged 65 and older had significantly higher rates (13.1%) than males (10.3%).
Age - Among Canadian adults aged 20 years and older, 3.6% have at least two of the four major "physical" chronic diseases. This proportion increases dramatically with age, ranging from 0.3% in those aged 20-34 and 0.9% in those aged 35-49, to 3.7% in those aged 50-64, 11.0% in those aged 65-79 and up to 13.9% in those aged 80 and over.
Geography - The highest age-standardized prevalence rates among Canadians 65 and over were in Yukon (14.7% ASR) and Alberta (14.4% ASR), and the lowest rates in British Columbia (9.5% ASR) and Manitoba (8.8% ASR). All these rates differ by at least 20% from the Canadian rate.
See Figure 6 for the distribution by number of diseases.
Image 15: Prevalence of Multi-Morbidity
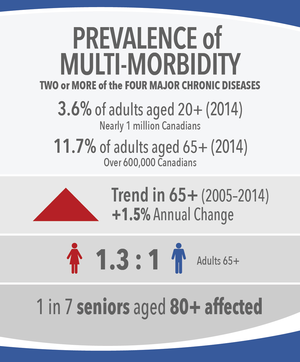
Image 15: Prevalence of Multi-Morbidity - Text Description
- Two or more of the four major chronic diseases
- 3.6% of adults aged 20+ (2014)
- Nearly 1 million Canadians
- 11.7% of adults aged 65+ (2014)
- Over 600,000 Canadians
- Trend in 65+ (2005-2014) Increasing
- +1.5% Annual Change
- Woman to man ratio: 1.3 : 1
- 1 in 7 seniors aged 80+ affected
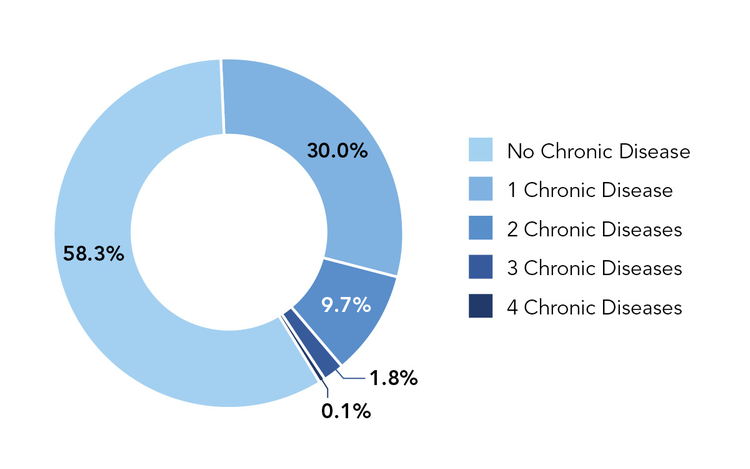
Figure 6. Proportion of Canadians aged 65 and older with zero to four self-reported major chronic diseases (cancer, CVD, CRD, diabetes), Canada (2014)
Source: Canadian Community Health Survey, 2014
Figure 6. Proportion of Canadians aged 65 and older with zero to four self-reported major chronic diseases (cancer, CVD, CRD, diabetes), Canada (2014) - Text Description
Figure 6 is presented as a doughnut chart. It shows the proportion of Canadians aged 65 and older with none of the four major chronic diseases, up to those with four of them. The major chronic diseases include: cardiovascular diseases (CVD), cancer, chronic respiratory diseases (CRD), and diabetes.
The Figure 6 table below contains self-reported data collected through the 2014 Canadian Community Health Survey. Among Canadians aged 65 and older, nearly 60% (58.3%) reported having none of the four major chronic diseases. While 30% reported living with one and nearly 10% (9.7%) were living with two major chronic diseases. Less than 1% of those aged 65 and over reported living with up to four major chronic diseases (0.1%).
| Number of Major Chronic Diseases (cancer, CVD, CRD, diabetes) | Proportion % | Population Number (rounded to 100) |
|---|---|---|
| None | 58.3 | 3100900 |
| 1 | 30.0 | 1595300 |
| 2 | 9.7 | 515600 |
| 3 | 1.8 | 94900 |
| 4 | 0.1 | 3600 |
| Source: Canadian Community Health Survey (2014). | ||
Mood and anxiety disorders co-morbidity with at least one of the four major chronic diseases
One in 25 (4.0 %) Canadian adults aged 20 years and older have a mood and anxiety disorder co-morbid with at least one of the four major chronic diseases (2014, CCHS).
Mood and anxiety disorders frequently coexist with other chronic diseases or conditions. Many associations have been observed, although these remain poorly understood. The early onset of depressive and anxiety disorders has been shown to be associated with an increased risk of developing heart disease, asthma, arthritis, chronic back pain and chronic headaches in adult life.Footnote 47 Furthermore, mood and anxiety disorders can lead to unhealthy behaviours that increase the risk of developing or exacerbating other chronic diseases or conditions.Footnote 48,Footnote 49 On the other hand, depressive and anxiety disorders may result from the burden of living with a chronic disease or condition.Footnote 50,Footnote 51,Footnote 52
Trend - There was a significant increase in the prevalence Canadian adults with a mood and anxiety disorder and co-morbid chronic disease(s), from 2.7% ASR in 2005 to 3.9% ASR in 2014, corresponding to an annual percent increase of 3.8%.
Mood and anxiety disorder co-morbidity in 2014 by
Sex - Females aged 20 and older have significantly higher rates than males (4.8% vs. 3.1%).
Age - The prevalence ranged from a low of 2.4% in the 20-34 years old to a high of 5.8% in the 50-64 age group.
Geography - The highest age-standardized prevalence rates were seen in Nova Scotia (5.7% ASR) and New Brunswick (5.3% ASR), and the lowest in British Columbia (3.2% ASR), Saskatchewan (3.0% ASR) and Manitoba (2.3% ASR). Those rates were at least 20% different from the national average. Note: Rates from the three territories could not be included due to extreme variability of estimates.
Other Health Indicators
Influenza immunization
About half (48.2%) of Canadians with a chronic disease receive the recommended annual influenza vaccine (2014, CCHS).
The elderly and those with chronic diseases are at high risk from complications and death due to influenza infection.Footnote 53,Footnote 54 Moreover, influenza infection may trigger an exacerbation and deterioration of their pre-existing conditions, particularly for CRDs (COPD and asthma) and CVDs (e.g. heart failure and IHD).Footnote 55 Therefore, annual vaccination is the cornerstone of influenza prevention and acts as primary and secondary prevention for these individuals.
Trends - The influenza vaccination rate among those with one of the four major chronic diseases has fluctuated over the last decade, with a high of 51.7% in 2005 and a low of 40.6% in 2010.
Influenza immunization in 2014 by
Sex - While the vaccination rate for females with a chronic disease (50.0%) was slightly higher than that of males (46.8%) the difference was not statistically significant.
Age - The immunization rate among individuals with a chronic disease generally increased with age from 23.0% in those aged 20-34 years to a high of 66.5% in those aged 65-79 years. More than a quarter of the children and youth (12-19 years old) with a chronic disease had been vaccinated.
Geography - The rates ranged from 39.4% ASR in Manitoba to a high of 62.5% ASR in Nova Scotia. Only Nova Scotia had a rate at least 20% higher than national average.
Image 16: Influenza Immunization Rate
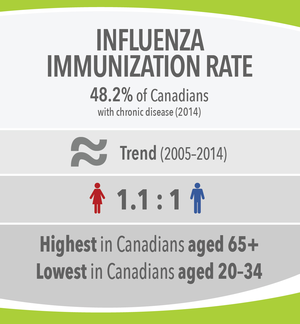
Image 16: Influenza Immunization Rate - Text Description
- 48.2% of Canadians with chronic disease (2014)
- Trend (2005-2014) Stable
- Woman to man ratio: 1.1 : 1
- Highest in Canadians aged 65+
- Lowest in Canadians aged 20-34
Neonatal and infant mortality
While the infant mortality rate among live births ≥500 g is 3.9 per 1,000 live births, the neonatal death rate is 2.6 per 1,000 live births (2010, Vital Statistics).
The infant mortality rate is a key population health indicator and receives widespread public attention since it reflects economic development, social equity and health care services within a population.Footnote 56,Footnote 57.
Infant mortality rateFootnote m is defined as the number of deaths of live-born babies in the first year after birth per 1,000 live births, while neonatal deaths include only those occurring within 28 days of birth.Footnote 58 The leading causes of infant death in Canada are prematurity, congenital anomalies and asphyxia.
Trends - The infant mortality rate of live births ≥500 g declined from 4.2 per 1,000 live births in 2000 to 3.9 per 1,000 live births in 2010. The annual percent decrease was 0.8%. The neonatal death rates remained stable at 2.6 per 1,000 live births, with slight fluctuations between 2000 and 2010.
Neonatal and Infant Mortality in 2010 by
Sex - The infant mortality rate was 4.4 per 1,000 live births for males and 3.3 per 1,000 live births for females, and the neonatal mortality rate was 3.0 per 1,000 live births for males and 2.2 per 1,000 live births for females. Infant mortality is higher in boys than girls in most parts of the world due to genetic and biological makeup, and boys in general are more susceptible to disease and premature death.Footnote 59
Geography - Between 2001 and 2010, the infant mortality rates ranged from 2.6 per 1,000 live births in Prince Edward Island and 3.2 in Nova Scotia to 5.1 in the Yukon, 5.5 in Manitoba, 5.6 in Saskatchewan,
6.2 in the Northwest Territories and 12.2 per 1,000 live births in Nunavut, which represents more than three times the Canadian average. The neonatal mortality rates also varied widely from 1.8 per 1,000 live births in Nova Scotia and 1.9 in Prince Edward Island to 3.3 in Saskatchewan, 3.5 in Manitoba and the Northwest Territories and 5.1 per 1,000 live births in Nunavut. All these rates differ by at least 20% from the national average.
Image 17: Neonatal and Infant Mortality Rates
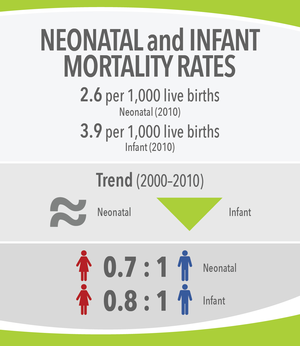
Image 17: Neonatal and Infant Mortality Rates - Text Description
- 2.6 per 1,000 live births
- Neonatal (2010)
- 3.9 per 1,000 live births
- Infant (2010)
- Trend (2000-2010)
- Neonatal - stable Infant - decreasing
- Neonatal girl to boy ratio: 0.7 : 1
- Infant girl to boy ratio: 0.8 : 1
Premature mortality
Ten percent (10.7%) of 30-year-old Canadians are expected to die before their 70th birthday from either a cardiovascular disease, cancer, diabetes, or chronic respiratory disease, assuming current mortality rates (2012, Vital Statistics).
In Canada, as in the other developed countries, the majority of deaths occur in the older population. Consequently, the usual mortality measures reflect mainly the outcomes of the diseases occurring among the elderly. On the other hand, premature mortality refers to deaths that occur at a younger age than expected and, therefore, reflect the potential for avoidable deaths.
Following the 2011 Political Declaration of the UN High Level Meeting on the Prevention and Control of NCDs, the member states of the World Health Assembly agreed to adopt a global target of a 25% reduction in premature mortalityFootnote n from cardiovascular diseases, cancer, diabetes and chronic respiratory diseases by 2025.Footnote 60.
Trends - An important decrease in premature mortality from the four main NCDs was observed, with a drop from 14.3% (2000) to 10.7% (2012). This accounts for an annual percent decrease of -2.5%. The downward trend was mainly due to the decrease of premature mortality from cardiovascular diseases and from cancer.
Premature Mortality in 2012 by
Sex - The probability of dying between ages 30-69 from any of the 4 main chronic diseases was higher in males (12.7%) than in females (8.8%). This was also true for each of these diseases, particularly for cardiovascular diseases which were 2.5 times more likely for males compared to females.
Geography - The population of Nunavut had a rate more than two times greater than the Canadian average. This territory displayed very high premature mortality for chronic respiratory diseases (8X) and cancer (2X). In addition, the Northwest Territories, Yukon and Newfoundland and Labrador presented a risk of premature mortality at least 20% higher than for Canada as a whole.
Image 18: Premature Mortality
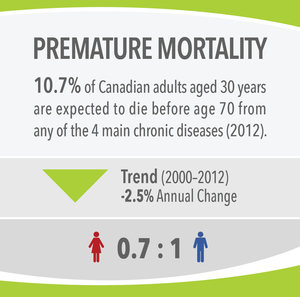
Image 18: Premature Mortality - Text Description
- 10.7% of Canadian adults aged 30 years are expected to die before age 70 from any of the 4 main chronic diseases (2012).
- Trend (2000-2012) Decreasing
- -2.5% Annual Change
- Woman to man ratio: 0.7 : 1
Life expectancy and health-adjusted life expectancy
Life expectancy (LE) at birth is 83.0 years in Canada (2010/11-2012/13, CCDSS).
Health-adjusted life expectancy (HALE), which reflects the number of years lived in "full health," is 72.6 years at birth (2008/09-2010/11 CCDSS, CCHS 2009).
LE is one of the most commonly used measures for international health comparisons. It describes the overall health status of a population and is defined as the average number of years a person of a certain age would be expected to live given current mortality rates.Footnote 61
HALE is the average number of years that a person is expected to live in full health.Footnote 62,Footnote 63 HALE is increasingly endorsed and used internationally for monitoring the impact of public health. In 2014, HALE was adopted by the Pan American Health Organization (PAHO) as the highest level impact indicator for their region-wide 2014-2019 Strategic Plan.
Trends - Both LE and HALE in Canada have been steadily increasing in the past decade, with a drop in the disparity between males and females. Most of the increase in HALE is due to the decrease in mortality.
From 1999/2000-2001/02 to 2010/11-2012/13, LE at birth increased at a rate of 2.8 months per calendar year. From 2000/01 to 2010/11, HALE has increased by 2.0 months per calendar year.
LE (in 2009/10-2011/12) and HALE (IN 2008/09-2010/11) by
Sex - Females currently have a LE at birth of 85.2 years and males of 80.8 years in Canada.
When taking health-related quality of life into consideration, females have a HALE at birth of 73.7 years and males 71.4 years.
Geography - None of the provinces and territories had a LE or HALE which differed by more than 20% from the Canadian average. However, LE ranged from a low of 76.3 years in Nunavut and the Northwest Territories to a high of 83.7 in British Columbia. Similarly, Nunavut, the Northwest Territories and Yukon had the lowest HALE (66.4 years), while Quebec had the highest (73.9 years).
See Figure 7 for HALE by province and territory.
Image 19: LE and HALE
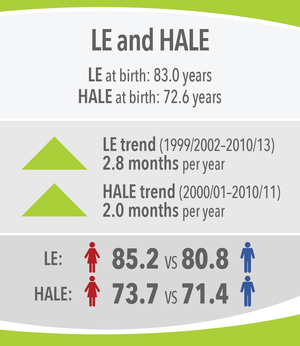
Image 19: LE and HALE - Text Description
- LE at birth: 83.0 years
- HALE at birth: 72.6 years
- LE trend (1999/2002-2010/13) Increasing
- 2.8 months per year
- HALE trend (2000/01-2010/11) Increasing
- 2.0 months per year
- LE Woman to man ratio: 85.2 : 80.8
- HALE Woman to man ratio: 73.7 : 71.4
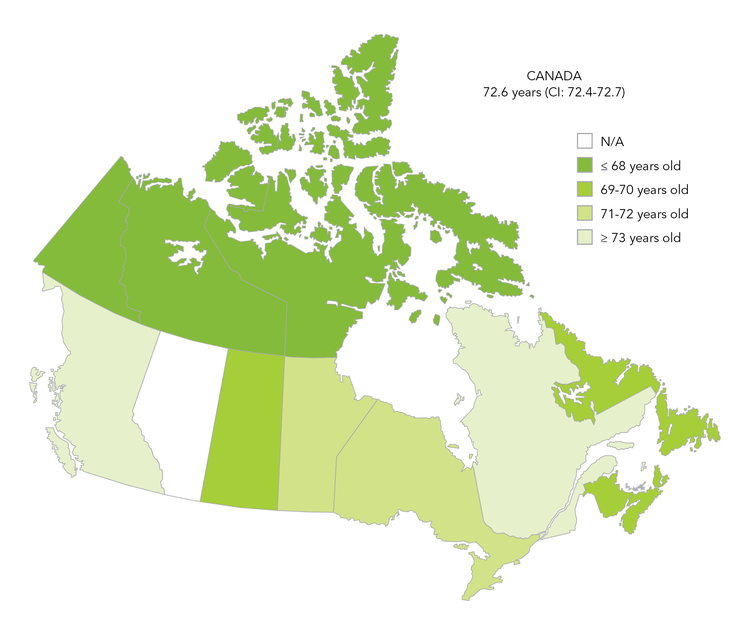
Figure 7. Health-adjusted life expectancy (HALE) by province and territory, CanadaFigure 7 - Footnote * (2008/09-2010/11)
Source: Canadian Chronic Disease Surveillance System and CCHS
- Figure 7 - Footnote *
-
Data do not include Alberta.
Figure 7. Health-adjusted life expectancy (HALE) by province and territory, Canada (2008/09-2010/11) - Text Description
Figure 7 is presented as a colour-coded map of Canada with a legend. It shows health-adjusted life expectancy (HALE), by province and territory across Canada for the fiscal years 2008/9 to 2010/11 combined. The legend is colour-coded in a gradient from deep green to white where: dark green represents a HALE of 68 years of age and under; medium green represents a HALE of 69-70 years of age; light green represents a HALE of 71-72 years of age; lightest green represents a HALE of 73 years of age and older; and white indicates that no data was available.
HALE is a measure of the average number of years that an individual is expected to live in a healthy state. The higher the number is (age in years), the more positive the result. According to the Figure 7 table below, the overall HALE for Canadians calculated for the period above was close to age 73 (72.6 years of age). Compared to this, three provinces-Prince Edward Island, British Columbia, and Quebec- had a higher HALE result ranging from 73 to just under 74 years of age. The other provinces and territories had lower values ranging from roughly 66 years of age for the combined territories to just over 72 years of age for Ontario. Alberta data were not available. For the combined fiscal years between 2008/9 and 2010/11, health-adjusted life expectancy was highest in Quebec at nearly 74 years of age, and lowest in the three Territories combined at about 66 years of age.
| Province/Territory | Age |
|---|---|
| NT YT NU (combined) | 66.4 |
| NS | 69.9 |
| NL | 70.1 |
| SK | 70.7 |
| NB | 70.8 |
| MB | 71.1 |
| AB | - |
| ON | 72.2 |
| PE | 73.0 |
| BC | 73.4 |
| QC | 73.9 |
| Canada | 72.6 |
| Sources: Canadian Chronic Disease Surveillance System (CCDSS) and Canadian Community Health Survey | |
International Comparisons
Canada ranks among the top and middle third performers among OECD member states for all indicators studied except adult obesity, cancer incidence and infant mortality (2015, OECD).
In its most recent report, Health at a Glance 2015: OECD Indicators, Canada's performance across a range of population health and health care system performance indicators is presented in comparison to the other 33 member countries of the OECD. Data were not always available for all 34 member countries, yet where data were available, the performance of as many as ten additional OECD partner countries was also presented. However, the following comparisons only include OECD member countries.Footnote 64
It should be noted that the indicators used in the OECD report are often different from those in our report mainly due to data availability across the 34 OECD countries. In these comparisons, Canada's performance varies across indicator categories.
| Canada (%) | OECD Average (%) | |||
|---|---|---|---|---|
| Top third | Daily tobacco smoking (aged 15+ years) | 6th out of 34 | 14.9 | 19.7 |
| Alcohol consumption - alcohol sales (aged 15+ years) | 11th out of 34 | 8 litres per capita | 8.8 litres per capita | |
Healthy eating (adults)
|
6th out of 29 9th out of 29 |
69.4 74.0 |
60.4 65.6 |
|
| Middle 3rd | Overweight and obesity - based on Physical Measures Survey
|
21st out of 29 25th out of 29 |
25.0 24.0 |
24.3 22.1 |
| Bottom third | Obesity in adults - BMI > 30 (aged 18+ years) |
29th out of 34 | 25.8 | 18.9 |
| Canada (Per 100,000 Population) |
OECD Average (Per 100,000 Population) |
|||
|---|---|---|---|---|
| Top 3rd | Mortality from cerebrovascular disease | 2nd out of 34 | 38 deaths | 65.8 deaths |
| Type 2 diabetes - hospital admission rate (aged 15+ years) | 10th out of 32 | 95.3 admissions | 149.8 admissions | |
| Middle 3rd | Mortality from ischemic heart disease (IHD) | 17th out of 34 | 95 deaths | 117.4 deaths |
| Bottom 3rd | Cancer incidence | 24th out of 32 | 295.7 cases | 270.5 cases |
| Canada | OECD Average | |||
|---|---|---|---|---|
| Middle 3rd | Life expectancy | 13th out of 34 | 81.5 yearsTable 4 footnote * | 80.5 |
| Bottom 3rd | Infant mortality | 28th out of 34 | 4.8 deaths per 100,000Footnote o live births | 3.8 deaths per 100,000 live births |
|
||||
Note: Caution must be used when interpreting Canada's relative NCD performance relative to other countries with different demographic profiles, as age represents a significant risk factor in its own right, and only mortality rates have been age-standardized across reporting countries
Conclusions
This examination of key risk factors, major chronic diseases and overall life expectancy illustrates a mixed picture of the health of Canadians.
Canadians are living longer than ever before, and the life expectancy gap is closing between men and women. Nearly one in six Canadians (5.8 million) are 65 years or older, and this age group is growing four times faster than the overall population.Footnote 65 Furthermore, rates of smoking continue to decrease in Canada, and mortality from major chronic conditions (especially that related to CVDs, CRDs and certain cancers) has also declined.
By contrast, the high rates of physical inactivity, sedentary behaviours and obesity rates, especially among Canada's children and youth, are a major concern. While Canadians are living longer, it is important that they live longer in good health.
Most chronic diseases are preventable. The WHO estimates that at least 80% of heart disease, stroke and diabetes and 40% of all cancers are preventable.Footnote 66 Central to the prevention of chronic disease are a few key risk factors. The current overweight and obesity rates in Canada must be tackled, particularly in children, youth and young adult populations. Canadian youth are now being diagnosed with conditions and diseases, like hypertension and type 2 diabetes, which were previously seen only in adults and are most likely a result of increased obesity. Diabetes overall is a major public health concern, as the prevalence rate has significantly risen over the past decade.
The higher prevalence of health service use for mood and anxiety disorders observed among working age adults (30-64 years old) may relate in part to the specific or unique challenges that these subpopulations often face, including work-related stress and the challenges of balancing work and personal/family life.Footnote 67.
Canadians must also become more active. Physical activity not only helps individuals manage weight, but it also independently increases sensitivity to insulin, reduces risk for CVDs and some cancers, and improves overall well-being.
Individual (e.g. lifestyle behaviours), community (e.g. built environment) and population (e.g. policy) level interventions are all critical to addressing these public health challenges. Evidence-based interventions and the identification and replication of best practices to prevent chronic disease and promote healthy living remain an important function of PHAC.
Surveillance is a core public health function. An examination of these trends illustrates the importance for continued surveillance and the need to identify new opportunities to assess and track the health of Canadians to inform health policies and practices.
Methodological Notes
The majority of data presented in this report are available from the Chronic Disease and Injury Indicator Framework (CDIIF) and the Chronic Disease Infobase Online Data Cubes.
- Crude rates for Canada and provinces/territories were calculated after random rounding counts to the nearest 10. Age-standardized rates were calculated using non-rounded counts. Prevalence counts for Canada, provinces and territories and life-course age groups were rounded to the nearest 100.
- The 2011 Canadian standard population was used for the calculation of age-standardized rates.
- All differences highlighted in this report between national and provincial/territorial averages were ≥ 20% from the Canadian average unless otherwise noted.
- Trends in incidence rates may reflect true change in population health status, but may also be a function of a change in data collection methods, coding/classification systems, clinical practices, billing methods, etc.
Depending on the data sources, the reporting year is either based on calendar year or fiscal year. For example, 2011/12 denotes a fiscal year whereas 2011-12 denotes two calendar years.
The data sources for chronic disease estimates included:
- The Canadian Chronic Disease Surveillance System (CCDSS) for physician-diagnosed disease prevalence, use of health services for mood and anxiety and incidence derived from physician billing and hospitalization records. Provincial and territorial data were contributed to the CCDSS as of November 2015. The opinions, results and conclusions reported in this paper are those of the authors. No endorsement by the provinces/territories is intended or should be inferred. The CCDSS currently covers fiscal years 1995/96 to 2011/12.
- The Canadian Cancer Registry (CCR): 1992 to 2009.
- The Canadian Community Health Survey (CCHS) for self-reported multi-morbidity, mood and anxiety disorders comorbidity, CVDs (heart disease and stroke), cancer, CRDs (asthma and COPD), diabetes and mood and anxiety disorders. Data from the CCHS were available for the years 2003, 2005, 2007 and 2008-2014.
The data sources for risk behaviour and risk condition estimates included:
- Canadian Health Measures Survey (CHMS) for physical activity, sedentary behaviour and obesity. Data from three cycles of the CHMS are available: 2007-09, 2009-11 and 2012-13.
- The Canadian Community Health Survey (CCHS) for unhealthy eating, smoking and alcohol (heavy drinking), as well as for the calculation of prevalence of self-reported chronic diseases. Data from the CCHS were available for the years 2003, 2005, 2007, 2008-2014.
- The Canadian Tobacco, Alcohol and Drug Survey (CTADS) and Canadian Alcohol and Other Drug Use Monitoring Survey (CADUMS) for alcohol (low-risk drinking guidelines). Data from these surveys cover the years 2005 to 2013.
Contributors (in alphabetical order)
- Jay Barber
- Sharon Bartholomew
- Marisol Betancourt
- Bernard Choi
- Paromita Deb-Rinker
- Alain Demers
- Ragen Lane Halley
- Lidia Loukine
- Wei Luo
- Louise McRae
- Siobhan O'Donnell
- Jay Onysko
- Bob McDougall
- Louise Pelletier (Lead)
- Neel Rancourt
- Deepa Rao
- Karen C Roberts
- Cynthia Robitaille
- Annie J Stewart
- Ming Su
- Wendy Thompson
- Chris Waters
- Peter Walsh
- Xiaoquan Yao
- Dianne Zakaria