
Human emerging respiratory pathogens bulletin: Issue 71, November 2022
Download the alternative format
(PDF format, 1.32 MB, 3 pages)
Organization: Public Health Agency of Canada
Published: 2022-12-13
Monthly situational analysis of emerging respiratory diseases affecting humans (data to November 30, 2022).
In this bulletin
- COVID-2019 update
- Avian influenza updates
- Swine influenza updates
- Middle East respiratory syndrome coronavirus (MERS-CoV) update
| Novel influenzaFootnote 1 | Cumulative Case CountFootnote 2 | Deaths | Case Fatality Rate %Footnote 3 |
|---|---|---|---|
| A(H7N9) | 1,568 | 615 | 39% |
| A(H5N1) | 886 | 463 | 52% |
| A(H5NX)Footnote 4 | 1 | 0 | 0% |
| A(H9N2) | 104 | 2 | 2% |
| A(H5N6) | 82 | 33 | 40% |
| A(H5N8) | 7 | 0 | 0% |
| A(H7N4) | 1 | 0 | 0% |
| A(H1N2)Footnote 5 | 2 | 0 | 0% |
| A(H10N3) | 2 | 0 | 0% |
| A(H3N8) | 2 | 0 | 0% |
| A(H3N2)v | 446 | 1 | <1% |
| A(H1N2)v | 46 | 0 | 0% |
| A(H1N1)v | 41 | 0 | 0% |
| A(H1NX)vFootnote 6 | 1 | 1 | 100% |
| Eurasian avian-like A(H1N1) | 10 | 0 | 0% |
| MERS-CoVFootnote 1 | Cumulative Case CountFootnote 2 | Deaths | Case Fatality Rate %Footnote 3 |
| Global Case CountsupFootnote 7 | 2,600 | 935 | 36% |
| Saudi ArabiasupFootnote 8 | 2,193 | 854 | 39% |
Footnotes
|
|||
COVID-19 update
On December 31, 2019, cases of a pneumonia of unknown etiology were reported in Wuhan, China. These cases have since been determined to be due to a novel coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19). On January 30, 2020, the World Health Organization (WHO) first declared the outbreak a Public Health Emergency of International Concern (PHEIC). On March 11, 2020, the WHO characterized the outbreak as a global pandemic. The WHO Director-General convened the International Health Regulations (IHR) Emergency Committee (EC) on COVID-19 thirteen (13) times through 2020 to 2022, continually assessing that COVID-19 constitutes a PHEIC.
The Public Health Agency of Canada is monitoring the situation closely.
Avian influenza updates
Avian influenza A(H9N2)
One (1) human case of avian influenza A(H9N2) was reported in November 2022 from China. The case was a 3-year-old male from Gansu Province. He experienced mild symptoms, was not hospitalized, and has recovered from illness. As of the time of reporting, none of the case's family members have reported symptoms of illness. Environmental samples all tested negative.
To date, 18 human cases of avian influenza A(H9N2) were reported worldwide in 2022. Since the emergence of this virus in the human population in 1998, 104 cases have been reported worldwide, with a case fatality rate (*CFR) of 2%. No cases have been reported in Canada.
*CFR: case fatality rate. Note that this rate is dependent on accurately reported deaths. For events with active cases, this value may be updated retrospectively as final disposition of the cases is known.
Avian influenza A(H5N6)
The most recent human case of avian influenza A(H5N6) was reported in October 2022 from China.
A total of 82 laboratory-confirmed human cases of avian influenza A(H5N6), including at least 33 deaths (CFR: 40%) have been reported globally since 2014. Since January 2021, 56 cases of avian influenza A(H5N6) have been reported globally (Figure 2); 55 A(H5N6) cases were reported from China and one (1) case was reported from Lao PDR (Figure 3). So far, 24 A(H5N6) human cases have been reported worldwide in 2022. No cases have been reported in Canadian residents.
Avian influenza A(H10N3)
The most recent human case of avian influenza A(H10N3) was reported in September 2022 from China.
Since the emergence of this virus in the human population in 2021, two (2) cases have been reported, both from China. The CFR is 0%; however, with only two human cases to date, the full spectrum of disease is highly uncertain.
Avian influenza A(H5N1)
One (1) human case of A(H5N1) was reported in November 2022 from Guangxi Province in China. The case was a 38-year-old female farmer who was hospitalized for severe pneumonia and later died. Prior to illness onset, she was exposed to backyard poultry and had slaughtered a sick chicken. Environmental samples were collected from the case's property and samples from her kitchen tested positive for H5. Genetic sequencing results are pending.
An ongoing A(H5N1) epizootic has impacted domestic poultry, wild birds, and some mammals throughout the Americas since introduced to Canada's east coast in November 2021 from migratory birds from Europe. There is little information about the spectrum of illness that could result from human infections with current A(H5N1) bird flu viruses. Five (5) human detections of A(H5N1) have been reported [U.K. (1), U.S. (1), Spain (2), China (1)] in 2022. The four (4) cases reported from U.K., U.S. and Spain were asymptomatic or mild. It is unknown if the virus strain related to this case from China is antigenically or genetically similar to the human, mammalian, and/or avian strains detected in Europe and the Americas. When available, genetic sequencing results will provide additional information on the spectrum of disease, a key element in the assessment of risk.
There have been 886 human cases of A(H5N1) reported globally since 1997, with a CFR of 52% (Figure 4). No domestically acquired A(H5N1) infections have ever been reported in Canada, although a significant number of A(H5N1) detections associated with the current 2021-2022 epizootic have been reported in domestic, backyard, wild bird populations, and other wild animal species across Canada. In 2014, Canada (Alberta) reported one single fatal case of A(H5N1) in a resident returning from travel in China.
Swine influenza updates
Swine origin influenza A(H1N2)v
The most recent human case of swine origin influenza A(H1N2)v was reported in October 2022 from the Netherlands.
A total of 46 A(H1N2)v cases have been reported globally since 2005, with a 0% case fatality rate. Seven (7) A(H1N2)v cases have been reported worldwide in 2022. Three (3) A(H1N2)v detections have been reported in Canadian residents since reporting began in 2005, and the latest case in Canada was reported in November 2021 from Manitoba.
Swine origin influenza A(H3N2)v
One (1) new human case of swine origin influenza A(H3N2)v was reported in November 2022 from New Mexico, United States. The case was <18 years of age, was not hospitalized and, as of the time of reporting, was recovering from their illness. The case was reportedly exposed to swine prior to illness onset. No human-to-human transmission of A(H3N2)v associated with this case has been identified.
Globally, 446 A(H3N2)v cases have been reported since 2005, with <1% case fatality rate. Five (5) A(H3N2)v cases have been reported worldwide in 2022. Two (2) A(H3N2)v detections have been reported in Canadian residents since reporting began in 2005, with the latest case reported in June 2021.
Swine origin influenza A(H1N1)v
The most recent human case of swine origin influenza A(H1N1)v was reported in October 2022 from Brazil.
Globally, 41 human cases of A(H1N1)v have been reported since 2005, with no associated fatalities. Four (4) A(H1N1)v cases have been reported worldwide in 2022. Two (2) A(H1N1)v detections have been reported in Canadian residents since reporting began in 2005, with the latest case reported in April 2021.
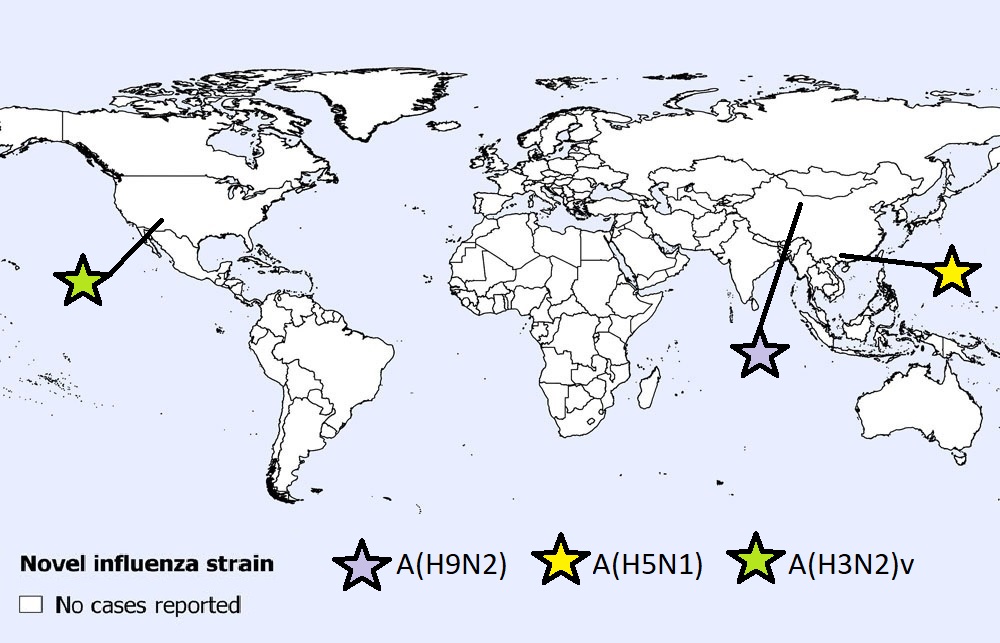
Figure 1 - Text description
One (1) A(H9N2) case was reported in China.
One (1) A(H5N1) case was reported in China.
One (1) A(H3N2)v case was reported in the United States.
Note: Map was prepared by the Centre for Immunization and Respiratory Infectious Diseases (CIRID) using data from the latest WHO Event Information Site (EIS) postings. This map reflects data available through these publications as of November 30, 2022.
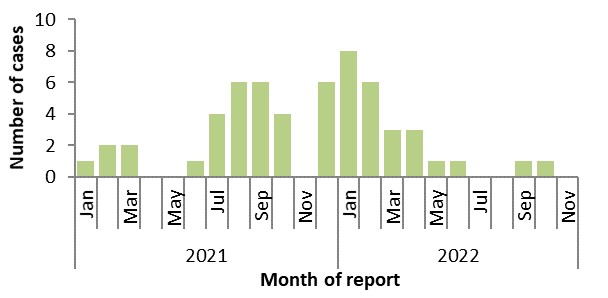
Figure 2 - Text description
| Year | Month | Cases |
|---|---|---|
| 2021 | Jan | 1 |
| Feb | 2 | |
| Mar | 2 | |
| Apr | 0 | |
| May | 0 | |
| June | 1 | |
| July | 4 | |
| Aug | 6 | |
| Sep | 6 | |
| Oct | 4 | |
| Nov | 0 | |
| Dec | 6 | |
| 2022 | Jan | 8 |
| Feb | 6 | |
| Mar | 3 | |
| Apr | 3 | |
| May | 1 | |
| June | 1 | |
| July | 0 | |
| August | 0 | |
| Sep | 1 | |
| Oct | 1 | |
| Nov | 0 |
Note: Graph was prepared by the Centre for Immunization and Respiratory Infectious Diseases (CIRID) using data from the WHO EIS postings and the Hong Kong Centre for Health Protection (CHP) press releases. This graph reflects data available as of November 30, 2022.
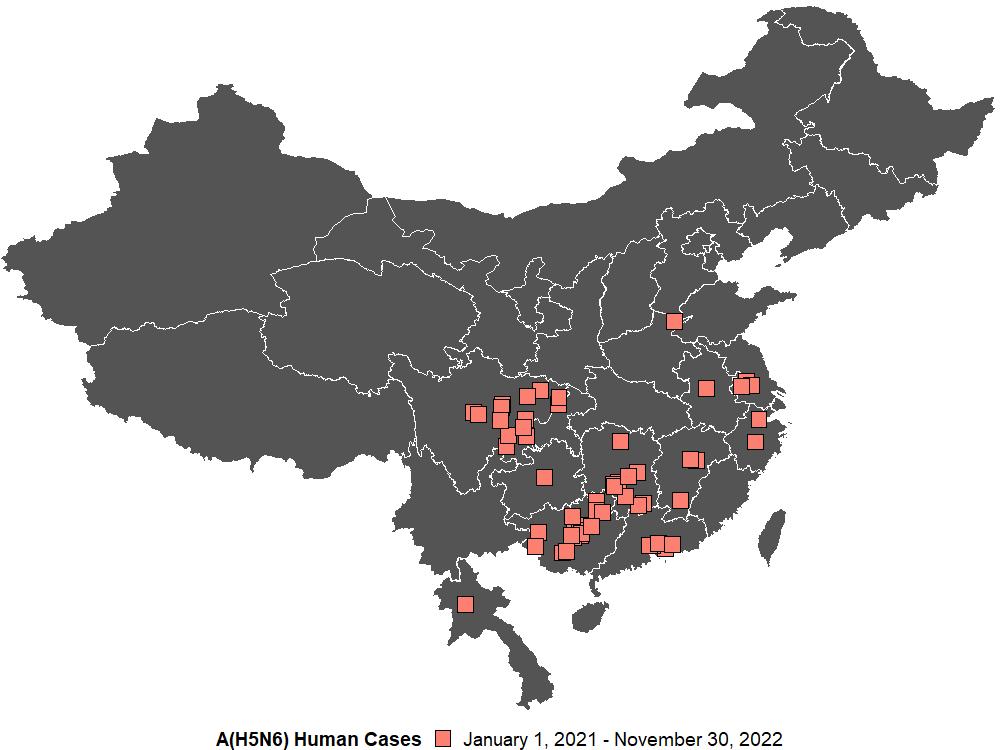
Figure 3 - Text description
Four cases were reported out of Yongzhou, Hunan Province, People's Republic of China.
Three cases were reported out of Guilin, Guangxi Zhuang Autonomous Region, People's Republic of China.
Three cases were reported out of Huizhou, Guangdong Province, People's Republic of China.
Three cases were reported out of Liuzhou, Guangxi Zhuang Autonomous Region, People's Republic of China.
Two cases were reported out of Baise, Guangxi Zhuang Autonomous Region, People's Republic of China.
Two cases were reported out of Chengdu, Sichuan Province, People's Republic of China.
Two cases were reported out of Chenzhou, Hunan Province, People's Republic of China.
Two cases were reported out of Dongguan, Guangdong Province, People's Republic of China.
Two cases were reported out of Guangxi Zhuang Autonomous Region, People's Republic of China.
Two cases were reported out of Hechi, Guangxi Zhuang Autonomous Region, People's Republic of China.
Two cases were reported out of Hengyang, Hunan Province, People's Republic of China.
Two cases were reported out of Sichuan Province, People's Republic of China.
Two cases were reported out of Tongnan District, Chongqing Municipality, People's Republic of China.
Two cases were reported out of Zhenjiang, Jiangsu Province, People's Republic of China.
One case was reported out of Anhui Province, People's Republic of China.
One case was reported out of Bazhong, Sichuan Province, People's Republic of China.
One case was reported out of Changde, Hunan Province, People's Republic of China.
One case was reported out of Deyang City, Sichuan Province, People's Republic of China.
One case was reported out of Fuzhou, Fujian Province, People's Republic of China.
One case was reported out of Ganzhou City, Jiangxi Province, People's Republic of China.
One case was reported out of Guizhou Province, People's Republic of China.
One case was reported out of Hangzhou, Zhejiang Province, People's Republic of China.
One case was reported out of Jiangxi Province, People's Republic of China.
One case was reported out of Kaijiang County, Sichuan Province, People's Republic of China.
One case was reported out of Laibin, Guangxi Zhuang Autonomous Region, People's Republic of China.
One case was reported out of Langzhong City, Sichuan Province, People's Republic of China.
One case was reported out of Luang Prabang Province, Lao People's Democratic Republic (the).
One case was reported out of Nanning, Guangxi Zhuang Autonomous Region, People's Republic of China.
One case was reported out of Puyang City, Henan Province, People's Republic of China.
One case was reported out of Xuanhan County, Sichuan Province, People's Republic of China.
One case was reported out of Yangzhou, Jiangsu Province, People's Republic of China.
One case was reported out of Yibin, Sichuan Province, People's Republic of China.
One case was reported out of Yongchuan District, Chongqing Municipality, People's Republic of China.
One case was reported out of Zhejiang Province, People's Republic of China.
One case was reported out of Zigong City, Sichuan Province, People's Republic of China.
One case was reported out of Nanning, Guangxi Province, People's Republic of China.
One case was reported out of Guangxi Zhuang Autonomous Region, People's Republic of China.
Note: Map was prepared by the Centre for Immunization and Respiratory Infectious Diseases (CIRID) using data from the WHO EIS postings and the Hong Kong Centre for Health Protection (CHP) press releases. This map reflects data available through these publications as of November 30, 2022.
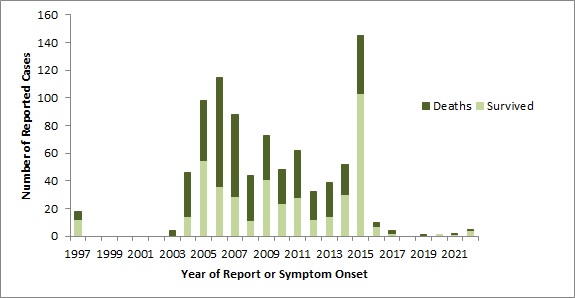
Figure 4 - Text description
| Year | Number of Cases | Deaths | Survived |
|---|---|---|---|
| 1997 | 18 | 6 | 12 |
| 1998 | 0 | 0 | 0 |
| 1999 | 0 | 0 | 0 |
| 2000 | 0 | 0 | 0 |
| 2001 | 0 | 0 | 0 |
| 2002 | 0 | 0 | 0 |
| 2003 | 4 | 4 | 0 |
| 2004 | 46 | 32 | 14 |
| 2005 | 98 | 43 | 55 |
| 2006 | 115 | 79 | 36 |
| 2007 | 88 | 59 | 29 |
| 2008 | 44 | 33 | 11 |
| 2009 | 73 | 32 | 41 |
| 2010 | 48 | 24 | 24 |
| 2011 | 62 | 34 | 28 |
| 2012 | 32 | 20 | 12 |
| 2013 | 39 | 25 | 14 |
| 2014 | 52 | 22 | 30 |
| 2015 | 145 | 42 | 103 |
| 2016 | 10 | 3 | 7 |
| 2017 | 4 | 2 | 2 |
| 2018 | 0 | 0 | 0 |
| 2019 | 1 | 1 | 0 |
| 2020 | 1 | 0 | 1 |
| 2021 | 2 | 1 | 1 |
| 2022 | 5 | 1 | 4 |
Note: Graph was prepared by the Centre for Immunization and Respiratory Infectious Diseases (CIRID) using data from the WHO EIS postings, the US CDC's Health Alert Network (HAN), and WHO cumulative case counts. This graph reflects data available as of November 30, 2022.
Middle East respiratory syndrome coronavirus (MERS-CoV) update
Four (4) new human cases of MERS-CoV were reported from Saudi Arabia. These cases occurred between December 2021 and September 2022. The cases ranged in age from 23 to 74, with a median age of 60.5 years. Most of the cases (3/4; 75%) were male. These four (4) cases were reported from three (3) different regions in Saudi Arabia: two (2) from Riyadh region, one (1) from Gassim region, and one (1) from Makkah Al Mukkarramah region. No epidemiological links between the two (2) reported cases in Riyadh region have been reported. All (4/4; 100%) of these cases were hospitalized and had reported various co-morbidities.
According to the WHO, 2,600 laboratory-confirmed cases of MERS-CoV, including 935 deaths, have been reported globally since reporting began in 2012 (CFR: 36%). Six (6) MERS-CoV cases have been reported worldwide to the WHO in 2022. No cases have been reported in Canada.