
Highlights from the 2015–2016 Children’s Programs Performance Measurement Tool: AHSUNC
Download the alternative format
(PDF format, 1.73 MB, 1 page)
Organization:
Public Health Agency of Canada
Date published: March 2018
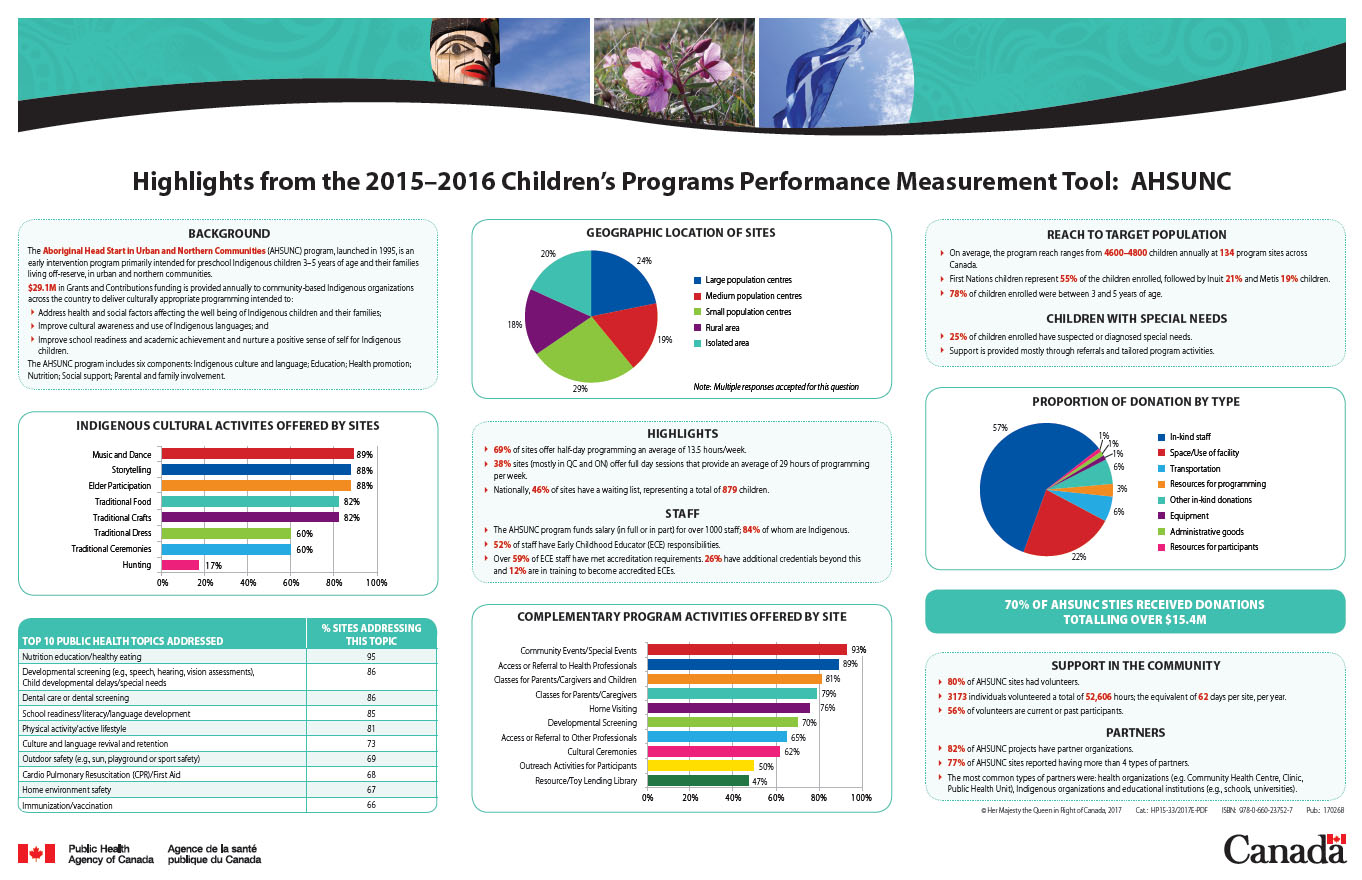
The infographic displays nine figures and graphs to describe various highlights from the 2015–2016 Children’s Programs Performance Measurement Tool (CPPMT) where it pertains to the Aboriginal Head Start in Urban and Northern Communities (AHSUNC) program. From top to bottom, left to right, these are:
Figure 1: Background
The Aboriginal Head Start in Urban and Northern Communities (AHSUNC) program, launched in 1995, is an early intervention program primarily intended for preschool Indigenous children 3-5 years of age and their families living off-reserve, in urban and northern communities.
$29.1M in Grants and Contributions funding is provided annually to community-based Indigenous organizations across the country to deliver culturally appropriate programming intended to:
- Address health and social factors affecting the well- being of Indigenous children and their families;
- Improve cultural awareness and use of Indigenous languages; and
- Improve school readiness and academic achievement and nurture a positive sense of self for Indigenous children.
The AHSUNC program includes six components: Indigenous culture and language; Education; Health promotion; Nutrition; Social support; Parental and family involvement.
Figure 2: Geographical locations of AHSUNC sites across the country
AHSUNC sites are located across the country in communities of varying sizes: large population centres, medium population centres, small population centres, rural areas, and isolated areas. The percentage of AHSUNC sites located in each of these areas is as follows:
- Large population centres: 24%
- Medium population centres: 19%
- Small population centres: 29%
- Rural areas: 18%
- Isolated areas: 29%
Figure 3: AHSUNC’s reach to target populations and children with special needs
Reach to Target Population
- 4,600 children and their families participate in the program every year, at one of the 134 program sites across Canada.
- First Nations children represent 55% of the children enrolled followed by Inuit 21% and Metis 19%.
- 78% of children enrolled were between 3 and 5 years of age.
Children with Special Needs
- 25% of children enrolled have suspected or diagnosed special needs.
- Support is provided mostly through referrals and tailored program activities.
Figure 4: Indigenous cultural activities offered by site
AHSUNC sites incorporate a number of Indigenous cultural activities into their day to day programming. Some examples of these activities are reported in the Children’s Programs Performance Measurement Tool (CPPMT) and the percentages of AHSUNC sites offering these activities are as follows:
- Music and Dance: 89%
- Storytelling: 88%
- Elder Participation: 88%
- Traditional Food: 82%
- Traditional Crafts: 82%
- Traditional Dress: 60%
- Traditional Ceremonies: 60%
- Hunting: 17%
Figure 5: Information on site highlights and staff
Highlights
- 69% of sites offer half-day programming an average of 13.5 hours/week.
- 38% sites (mostly in QC and ON) offer full day sessions that provide an average of 29 hours of programming per week.
- Nationally, 46% of sites have a waiting list, representing a total of 879 children.
Staff
- The AHSUNC program funds salary (in full or in part) for over 1,000 staff, 84% of whom are Indigenous.
- 52% of staff have Early Childhood Educator (ECE) responsibilities.
- Over 59% of ECE staff have met accreditation requirements. 26% have additional credentials beyond this and 12% are in training to become accredited ECEs.
Figure 6: Proportion of donation by type
AHSUNC sites often receive donations to support their activities; the key types of donations and the percentage of sites receiving these donations is as follows:
- In-kind staff: 57%
- Space or use of facility: 22%
- Transportation: 6%
- Resources for programming: 3%
- Other in-kind donations: 6%
- Equipment: 1%
- Administrative goods: 1%
- Resources for participants: 1%
70% of AHSUNC sites received donations totalling over $15.4 million.
Figure 7: The top ten public health topics being addressed by AHSUNC sites
The AHSUNC program addresses public health topics. The top ten public health topics addressed, and the percentage of sites addressing each, is as follows:
- Nutritional education/healthy eating: 95%
- Developmental screening (e.g. speech, hearing, vision assessment, child developmental delays/special needs: 86%
- Dental Care or dental screening: 86%
- School readiness/literacy/language development: 85%
- Physical activity/active lifestyle: 81%
- Culture and language revival and retention: 73%
- Outdoor safety (sun, playground or sport safety): 69%
- Cardio Pulmonary Resuscitation (CPR)/ First Aid: 68%
- Home environment safety: 67%
- Immunization/ vaccination: 66%
Figure 8: Complementary program activities offered by sites
Many AHSUNC sites offer complementary program activities. The main activities and the percentage of sites offering these are as follows:
- Community Events or special events: 93%
- Access or referral to Health Professionals: 89%
- Classes for parents or caregivers and children: 81%
- Classes for Parents or Caregivers: 79%
- Home Visiting: 76%
- Developmental Screening:70%
- Access of referral to other Professionals: 65%
- Cultural Ceremonies: 62%
- Outreach Activities for Participants: 50%
- Resource or Toy Lending Library: 47%
Figure 9: Support in the community and partners
Support in the community
- 80% of AHSUNC sites had volunteers.
- 3,173 individuals volunteered a total of 52,606 hours; the equivalent of 62 days per site, per year.
- 56% of volunteers are current or past participants.
Partners
- 82% of AHUSNC projects have partner organizations.
- 77% of AHSUNC sites reported having more than 4 types of partners.
- The most common types of partners were: health organizations (e.g. Community Health Centre, Clinic, and Public Health Unit), Indigenous organizations, and educational institutions (e.g., schools, universities).