
Stakeholder consultation on personal production of cannabis for medical purposes: Public health and safety factors
Introduction
Health Canada developed the Draft Guidance on Personal Production of Cannabis for Medical Purposes to support applicants and registered persons and promote understanding of the program requirements among other stakeholders. It also set out proposed factors that Health Canada may consider in refusing or revoking a registration on public health and public safety grounds.
Health Canada conducted a 60-day public consultation from March 8 to May 7, 2021 on the Draft Guidance on Personal Production of Cannabis for Medical Purposes. Stakeholders were invited to review the guidance document and respond to questions relating to the following proposed factors that may be considered by Health Canada when refusing to issue or revoking a registration on public health and public safety grounds:
- Amount of daily authorized cannabis by the health care practitioner and information to support the amount authorized
- Non-compliance or history of non-compliance with the Cannabis Act and Regulations by the registered or designated person, including the relevant circumstances
- Criminal activity and / or diversion of cannabis
- Heath care practitioner is or has been involved with criminal activities or has been subject to disciplinary review or action by a licensing authority in relation to their prescribing practices with cannabis or controlled substances
Stakeholders were also invited to suggest additional factors for consideration in assessing public health and public safety grounds as they relate to refusing or revoking a registration, as well as provide any additional comments on aspects of the draft guidance document unrelated to the factors for consideration.
This report summarizes the feedback received during the consultation period, focusing largely on those responses that could strengthen and clarify the draft guidance document.
Who provided feedback
A total of 677 responses were receivedFootnote 1. Sixty-five (65) percent of respondents provided their feedback using the online questionnaire and the remaining 35% provided their feedback by email. Those who provided email submissions provided very little demographic information and were removed from the demographic data totals so as not to bias the final results.
The majority of responses came from Ontario (48%) and British Columbia (18%). Most respondents in British Columbia identified as patients (that is, registered persons) authorized to access cannabis for medical purposes, while those in Ontario were almost evenly split between registered persons and non-registered persons.

Figure 1 - Text description
Figure 2 shows a pie graph of the proportion of questionnaire respondents by province or territory. The proportions are Ontario 48%, British Columbia 18%, Quebec 9%, Manitoba 7%, Alberta 7%, New Brunswick 3%, Nova Scotia 3%, Saskatchewan 3%, Newfoundland 1%, less than 1 percent in each of Northwest Territories, Nunavut and Prince Edward Island.
Most responses (85%) were from individuals. Organizations that responded included municipalities, police services, provinces and territories, businesses, health care associations or organizations, non-governmental organizations, advocacy organizations and lobby groups, and Indigenous groups and organizations.
Sixty-two percent (62%) of individual respondents were authorized to access cannabis for medical purposes.
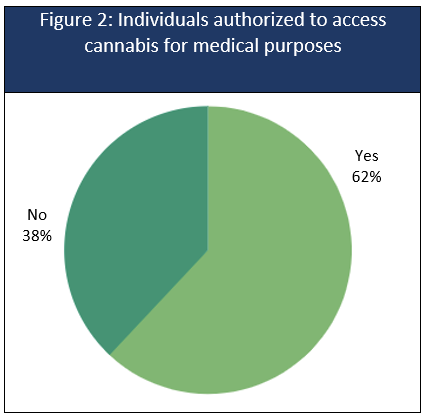
Figure 2 - Text description
Figure 2 shows a pie graph of individual respondents who were authorized by their health care practitioners to access cannabis for medical purposes. 62% were authorized and 38% were not authorized.
Of the respondents who were authorized by their health care practitioner to access cannabis for medical purposes, 82% were registered to produce cannabis for their own medical purposes or designated someone to produce in on their behalf. Some respondents selected multiple options.
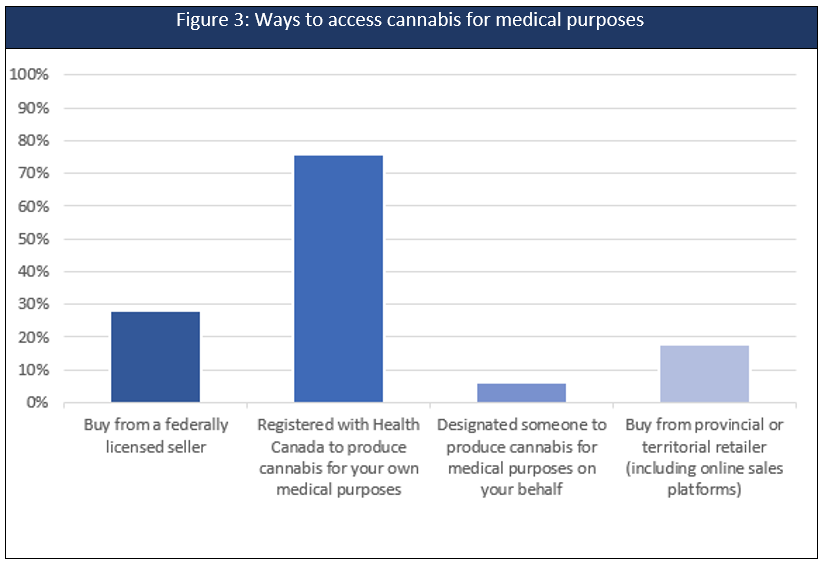
Figure 3 - Text description
Figure 3 shows a bar graph of respondents who were authorized by their health care practitioner to access cannabis for medical purposes and the ways they accessed cannabis: 28% bought cannabis from a federally licensed seller; 76% were registered with Health Canada to produce cannabis for their own medical purposes; 6% designated someone to produce cannabis for medical purposes on their behalf; and, 18% bought cannabis from a provincial or territorial retailer (including online sales platforms).
What we heard
Respondents were asked to indicate whether each of the four proposed factors for refusing or revoking a registration were clear ("yes or no"). They were then given an opportunity to explain ("please explain") and to provide additional comments on the factor.
Overall, a strong majority of respondents (70% or more) indicated that the factors were clear. Most respondents who felt that the factors were clear did not provide further feedback on the factor.
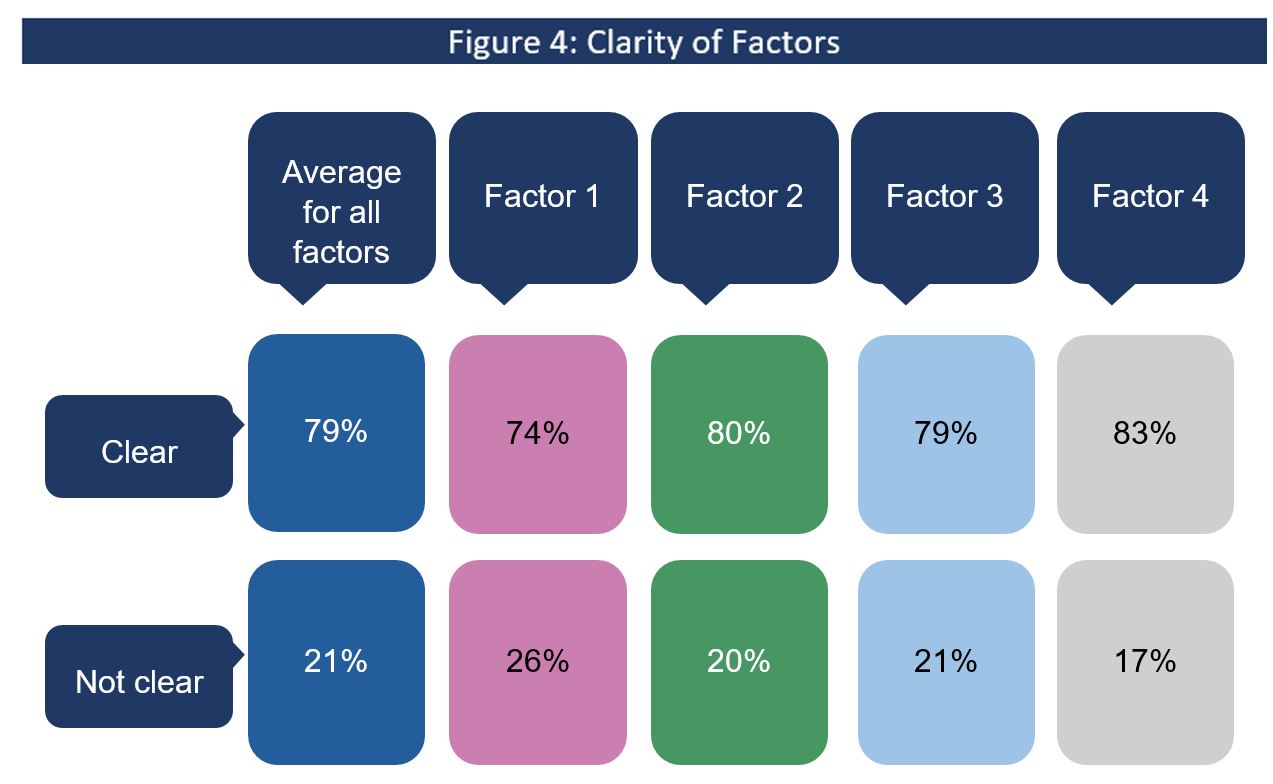
Figure 4 - Text description
Figure 4 shows the proportion of respondents who said that each of the four factors in the guidance document were clear or not clear.
Average: 79% clear, 21% not clear
Factor 1: 74% clear, 26% not clear
Factor 2: 80% clear, 20% not clear
Factor 3: 79% clear, 21% not clear
Factor 4: 83% clear, 17% not clear
The remaining data analysis focused on the small number of respondents (30% or less) who commented that the factors for refusing or revoking a registration were not clear, along with an even smaller proportion who said that the factors were clear and provided additional comments.
In reviewing the report, the following terms apply to describe the feedback received from the small number of respondents who provided comments:
Most: more than 50% of respondents who provided an answer to this question
Some: 10 to 49% of the respondents who provided an answer to this question
Few: less than 10% of the respondents who provided an answer to this question
Factor 1: Amount of daily authorized cannabis by the health care practitioner and information to support the amount authorized
- Is the authorized daily amount of cannabis supported by credible clinical evidence and/or published treatment guidelines?
- Is the amount of daily authorized cannabis considered reasonable, after taking into account the route of administration and potential for product loss from processing activities?
Seventy-four percent (74%) of respondents said that this proposed factor was clear and as one person said, simply, "Factor 1 makes sense - quantity and justification seem relevant here."
Twenty-six percent (26%) of respondents said the factor was not clear. Among those who provided additional explanation and comments, a few respondents commented that they wanted more definition, detail or specificity on the "information" required to support the authorized amount.
Some respondents also expressed concern that Health Canada may not use a transparent approach regarding how the information to support the authorized amount is used. They also asked whether the "information" described in the factor was meant to be provided by the registered person or by the health care practitioner. For example, one person said,
"It is not clear what amount might be considered to raise a red flag, nor is it clear whether the 'information' to support the amount is information provided by the patient or information provided by the medical practitioner."
Respondents also identified contextual issues that were important when considering the authorized amount, such as the potency of the cannabis, route of administration, tolerance to cannabis, nature of the illness, and the cost to the registered person. A few respondents also raised concerns with the formula used to calculate a registered person's maximum number of plants.
Some respondents shared concerns that this factor did not include considerations around differences in growing choices and conditions. These included a limited growing season, registered persons' desires to only grow for a limited time during the year, and crop failure due to weather, among other conditions. Two respondents said,
"Keep in mind some patients grow their medicine seasonally and not year round. Not to be confused with diversion or criminal activity."
"Many patients only grow 1 or 2 cycles per year. The way the system is set up, and in order for them to be able to store enough cannabis for an entire year, they need higher daily amounts."
Factor 2: Non-compliance or history of non-compliance with the Cannabis Act and Regulations by the registered or designated person, including the relevant circumstances
- What is the overall history of non-compliance, including the number, nature and severity of previous instances of non-compliance? How much time has elapsed since the last non-compliance, and how has the person responded to previous non-compliance?
- Are the registered or designated person growing, or have they grown, more than the amount authorized by the registration?
- Are the registered or designated person taking, or have they taken, reasonable steps to ensure the security of the cannabis in their possession?
- Is someone other than the designated or registered person tending, or has someone other than them tended, to the cannabis plants?
- Is the registered person "selling or renting", or has the registered person "sold or rented", their registration?
- Is there, or has there been, an apparent, intentional effort on the part of the registered or designated person to circumvent the Act or Regulations such as obstruction of Health Canada inspectors?
Eighty percent (80%) of respondents said that this proposed factor was clear.
Respondents who said it was not clear indicated they would like further clarity on the severity and frequency of non-compliance or history of non-compliance leading to a review or revocation of an authorization. As one respondent stated,
"It isn't clear how many non-compliance events are required before a license [sic] review is required."
Factor 3: Criminal activity and / or diversion of cannabis
- Is the production site linked, or has it been linked, to the diversion of cannabis, a controlled substance or a precursor, or to criminal activities?
- Are the registered or designated person, the owner of the production site or an individual with another direct link to the site or operation involved in the diversion of cannabis, a controlled substance or a precursor, or have they been involved in or do they contribute or have they contributed to such diversion?
- Is the production site linked, or has it been linked, to organized crime? Are the registered or designated person, the owner of the production site or an individual with another direct link to the site or operation associated with organized crime or have they been associated with organized crime?
Seventy-nine percent (79%) of respondents said that the factor was clear.
Those respondents who said that the factor was not clear indicated that more precise definitions were needed for the terms "diversion and "criminal activity". For example, several respondents did not know what 'diversion' meant, including what activities would be considered diversion of cannabis for medical purposes.
Comments included:
"Too ambiguous and will just lead to legal cases and costs to the public."
"Does diversion include non-intentional diversion…?"
Some respondents also wanted more precision around the nature of the criminal activity that was referenced in this factor. There were questions around whether the criminal activity included any criminal offence, or whether it was specific to cannabis-related crimes. Two comments were:
"It seems prejudiced to indicated (sic) that any criminal record could result in being denied a personal production license (sic). I think the criminal activity needs to be more thoroughly defined. Will this be any criminal activity related to black-market cannabis or broader? Rehabilitated individuals or those who have paid their debt shouldn't be penalized for previous errors in judgement. So it would be better to define the criminal activities that will likely get your request denied."
"Criminal activity is very broad, as is, it could include shoplifting, etc. Could be more specific i.e. 'criminal activity relating to cannabis.'"
A related comment focused on the timing, in particular, whether the criminal activity included being charged with growing cannabis before the Cannabis Act came into force.
Factor 4: Heath care practitioner is or has been involved with criminal activities or has been subject to disciplinary review or action by a licensing authority in relation to their prescribing practices with cannabis or controlled substances
- Has a provincial licensing authority investigated or disciplined the health care practitioner in relation to their prescribing practices with cannabis or other controlled substances?
- Is or has the health care practitioner been involved in or contributed to activities prohibited by or conducted in contravention of the Cannabis Act or the Controlled Dugs and Substances Act?
- Is or has the health care practitioner been a member of a criminal organization as defined in subsection 467.1(1) of the Criminal Code, or is or has been involved in, or contributes or has contributed to, the activities of such an organization?
Eighty-three percent (83%) of respondents said that this proposed factor was clear. As one person commented,
"A Physicians (sic) may not have any past history with criminal activities or a professional review. If they do, then this factor is well described."
When asked for any additional comments, a few respondents specified that this factor was "broad" without any other detail or comment.
A few respondents felt that the wording could benefit from clarity about the nature of criminal activities and/or activities that a health care practitioner would have been involved in. Some comments were:
"How are you defining criminal activities?"
"Again "criminal activities" is very broad... should be specific to cannabis."
A few respondents felt that this factor could discourage health care practitioners from being willing to authorize cannabis for medical use, or discourage them from authorizing a greater amount of cannabis if needed.
Additional factors that could be considered in assessing public health and public safety concerns as it relates to refusing or revoking a registration for personal and designated production of cannabis for medical purposes
The additional factors suggested for consideration included regulation of health care practitioners, odour control, and limiting the location of sites where cannabis is grown. These factors are outside of Health Canada's responsibility (notably, regulation of health care practitioners) or are beyond the scope of the guidance document and would require regulatory changes to enact (for example, odour and location of the site where cannabis is grown).
Comments on aspects of the draft Guidance on Personal Production of Cannabis for Medical Purposes document, unrelated to the factors for consideration
Many of the comments received during the consultation were unrelated to the content of the guidance document. This included more general feedback on the Medical Access Program and the Cannabis Act and its Regulations, including some proposed regulatory changes. They also focused on specific issues with the administration of the access to cannabis for medical purposes program and the impacts of the program on stakeholders or their communities. Stakeholder comments and concerns are summarized in the remainder of the report.
Concerns regarding continued access to cannabis for medical purposes
Some stakeholders perceived that the guidance document was intended to limit access to the cannabis for medical purposes program, and to require registered persons to buy from licence holders.
Some stakeholders also expressed concern that the factors themselves and/or the guidance document would discourage health care practitioners from prescribing, which would then impact a registered person's ability to obtain an authorization. One person noted:
"It is significant to note that patient needs for a high daily gram count do exist, and patients cannot afford to obtain such volumes from Standard Cultivators/Licensed Producers or dispensaries as the costs of procurement are onerous. It is therefore dangerous to scare health care practitioners away from authorizing high daily gram counts, as it may well imperil critical instances where patients require access to such volumes of cannabis."
A few respondents expressed concerns about the affordability of medical cannabis, and suggested that high prices from commercial licence holders are creating demand for illicit cannabis. They argued that this contributes to the prevalence of large-scale medical production sites, some of which may be fueling the illicit cannabis market. As one respondent noted:
"If the recreational market was better and more competitive we wouldn't be having this issue."
There were a few suggestions to subsidize the cost of buying medical cannabis from federally licensed sellers, or to cover medical cannabis under insurance plans.
A few respondents also mentioned the high cost of becoming a commercial licence holder. They suggested that some growers, who would otherwise join the legal market, continue to sell illicit cannabis under the guise of a medical registration due to the high cost and burden of becoming a commercial licence holder. They argued that it should be easier for large-scale personal and designated producers to convert their operations into federally licensed micro-cultivators, so that they can sell their excess cannabis as legal "craft" products.
Concerns related to authorizations
Under the Cannabis Regulations, health care practitioners set authorized amounts for their registered persons in grams per day, with no maximum amount.
Some respondents raised concerns regarding the high amounts authorized by health care practitioners, leaving the program vulnerable to misuse which would result in greater controls being imposed on legitimate program participants.
Some respondents wanted to see limits placed on the amounts that health care practitioners can authorize, limits on the number of plants that can be permitted per site, restrictions on the number of registrations per site, and even a definition of "production site" that would preclude a large number of registrations on a site by subdividing sites or "address splitting". Examples of these comments are:
"There should be no more than four plants allowed per person per household regardless of how many people live in the home and how many licenses (sic) are available."
"Having a set number of plants that can be grown at one residence would be helpful to deter the criminal element. People are pooling their medical licenses (sic) together to grow an unlimited number of plants at one location."
"Without a medical report from a physician for extenuating medical circumstances, no prescription should be above 30 grams per day."
A few respondents had a desire to see authorizations provided in measures other than grams per day, or to use canopy size rather than plant count to determine the amount that can be grown.
"For medical purposes it's the number of mg of THC and CBD that is meaningful, not the number of grams of dried cannabis."
Impact on stakeholders' homes, communities and crime
Some respondents were concerned about odour, light pollution, and about the involvement of criminals in communities diverting cannabis to the black market. The following quote is an example of this:
" Fix it. The neighbourhoods that are being impacted by this problem are suffering. The odours, the noise, the lighting, the safety issues - that is not fair."
Accountability, through enforcement by relevant authorities, was a priority among some respondents who participated in this consultation. Comments also included a desire for stronger penalties for registered persons found to be non-compliant or with a history of non-compliance. One comment stated:
"Health Canada has failed to ensure that diversion from designated growers do (sic) not occur. It is unclear from this document that Health Canada will put into place any actions that would detect criminal activity/diversion, only that action will be taken once known."
In the context of these concerns, comments focused on frequency of inspections and the roles and responsibilities of key stakeholders such as provincial and municipal bodies.
Inspections
Some respondents emphasized the importance of Health Canada conducting inspections, and indicated that these inspections rarely occurred. Some suggested mandated yearly or bi-yearly inspections. Comments included:
"But until Health Canada actually starts inspecting and verifying the ACMPRFootnote 2 facilities, the diversion to the black market will continue."
"… Health Canada consider the following actions: Proactively inspect designated production facilities for criminal activity and/or diversion of cannabis, [and] Inspect designated production facilities upon expiry of the registration to ensure there is no further cannabis production."
"Once any municipal or criminal infraction is suspected, federal inspection should immediately take place and should any irregularity be found, immediate suspension of the licenses (sic), and seizure of all inventory should occur."
Roles and responsibilities
Health Canada shares responsibility for enforcement of the Cannabis Regulations with law enforcement. Different levels of government and health care practitioner licensing bodies also have a role in maintaining public safety with respect to cannabis. Some comments focused on roles of other governing bodies and actions they should take.
A few suggestions included mandating Electrical Safety Authority inspections and household audits:
"The safety of the public is paramount. Electrical Safety Authority [ESA] inspections should be mandated at each cannabis grow location regardless of the number of plants. Ongoing, yearly inspections by ESA and the City Permitting department need to be mandated to ensure safety."
Other suggestions included "authorizing" local law enforcement to inspect grow-ops to determine and prevent criminal activity and diversion to the illicit market. For example:
"We would suggest that local law enforcement be given inspection power by Health Canada to ensure that licensees are complying and the operation is not criminal."
"If someone carries a license (sic) to produce over a certain amount (more than say 25 plants) the police agency of jurisdiction should be notified and given permission to inspect the location to ensure compliance. If police are not granted reasonable access to the location, police can notify Health Canada and the license (sic) should be revoked."
A few respondents noted that provincial and territorial regulatory bodies needed to better exercise their responsibility to educate, investigate or discipline health care practitioners in relation to their prescribing practices. Some comments expressed concern that trafficking was taking place as a result of inappropriate prescribing (for example, "pay per plant" prescriptions), and that some are authorizing amounts of cannabis that are unsupported by scientific evidence. Some suggestions were made that health care practitioners in these scenarios should have their licences removed.
"Health care practitioners are extremely helpful, however there are many circumstances of doctors charging for prescriptions or not completing examinations, which affects all patients. However this is not something that should be controlled by Health Canada and should be overseen by the College of Medicine."
There was also a desire for regulatory bodies to educate health care practitioners on the evidence base for cannabis dosing. One comment was,
"Health care practitioners haven't had the associated education to begin to know what 'amount' would help."
Conclusion
Health Canada wishes to thank all stakeholders who included their comments in this consultation. The relevant data from this consultation helped shape the final guidance document on the access to cannabis for medical purposes program, and on the provisions related to refusing or revoking a registration to produce cannabis for medical purposes under the Cannabis Regulations.
Footnotes
- Footnote 1
-
Where respondents preferred not to provide a response, these “prefer not to say” frequencies were not reported.
- Footnote 2
-
Access to Cannabis for Medical Purposes Regulations (ACMPR). The ACMPR were replaced by the Cannabis Regulations.