
Health Behaviour in School-aged Children: Trends Report 1990-2010
Table of Contents
- Foreword
- Chapter 1: Introduction
- Chapter 2: Mental Health
- Chapter 3: Home
- Chapter 4: School
- Chapter 5: Peers
- Chapter 6: Injury
- Chapter 7: Healthy Living
- Chapter 8: Healthy Weights
- Chapter 9: Substance Use and Related Risk Behaviours
- Chapter 10: Sexual Health
- Chapter 11: Bullying and Fighting Behaviour
- Chapter 12: International Trends
- Chapter 13: Summary Observations
PDF Document
15.73 Mb - 116 pages
Cat.: HP15-16/2013E-PDF
ISBN: 978-1-100-22318-6
Foreword
As the Deputy Chief Public Health Officer of Canada, I am pleased to present the Health Behaviour in School-aged Children: Trends Report 1990-2010. This report is based on the Canadian Health Behaviour in School-aged Children (HBSC) study, which is part of a cross-national, school-based survey conducted in collaboration with the World Health Organization.
The HBSC study is the only Canadian study that captures trends in health behaviours of youth 11 to 15 years of age. More specifically, it provides valuable information on young people's health indicators, such as mental health, eating habits, physical activity, injuries, bullying, and other health-risk behaviours. The report also identifies two decades worth of trends in youth health behaviours, including the impact of school, family, and other social factors affecting well-being.
Consistent with the Public Health Agency of Canada's mandate to promote the health of all Canadians, this report provides Canadians with timely and accurate information that can be used to inform program and policy development for our youth.
Thanks to the HBSC study, we have clear evidence that Canada is making progress on several health fronts. For example, I am encouraged to see that smoking rates among Canadian adolescents have gone down significantly over the past 20 years. In fact, we have one of the lowest weekly smoking rates among the 43 countries surveyed by the HBSC. That said, we still have work to do in areas like mental health and overweight/obesity, as our children and youth are reporting challenges that will require the collaboration of all sectors of our society to make a difference.
It is my hope that the HBSC Trends Report continues to serve as an important tool to monitor the risks and the protective factors that have an impact on the health of young Canadians. This report is a valuable source of data for comparing domestic and international trends. Reliable information is fundamental to our collective response to public health issues: this report provides an important research and surveillance resource for those working to improve the health behaviour of young Canadians and makes a unique contribution to our analysis of public health information.
Dr. Gregory Taylor,
Deputy Chief Public Health Officer
Public Health Agency of Canada
Chapter 1: Introduction
By Matthew King
Overview of the Report
This report presents trends in the health behaviours and attitudes of Canadian students over the six cycles of HBSC data collection from 1990 to 2010. The aim of this report is to provide timely and accurate information and to identify changes in the health behaviour of young Canadians that have occurred over the time period. It contributes towards building the evidence base for surveillance of health behaviours among youth 11 to 15 years of age. The report is intended to inform and influence health promotion and health education policy and initiatives at the provincial/territorial, federal and international levels and to increase our understanding of young people's health and well-being. The target audience for the report includes academics, researchers, health professionals, and public policy and advocacy professionals in the areas of health and education. Though national trends are the primary focus of the report, for selected items, data are presented on how young Canadian's health behaviours have changed over time relative to those in other HBSC countries. Chapter 2 presents data on a number of mental health measures, the focus of the National report for 2010. Chapters 3 through 5 examine the environments that impact the health of young people, home, school, and peers. Chapters 6 through 11 address broad topics that are priorities for the public health system in Canada: injury (Chapter 6), healthy living (Chapter 7), healthy weights (Chapter 8), substance use and related risk behaviours (Chapter 9), sexual health (Chapter 10), and bullying and fighting (Chapter 11). Each of Chapters 2 to 11 contain a set of trends figures on selected measures, a discussion of the changes evidenced over the course of the study, and some examples of particularly relevant federal and/or provincial/territorial policy initiatives and actions. Chapter 12 examines how Canadian results compare to other HBSC countries over the course of the study. The report concludes with a summary observations chapter.
Presentation of Findings
There are two types of figures presented in this report. Chapters 2 through 11 present national trends over time in the percentages of Grade 6, 8, and 10 boys and girls responding in a particular way on a number of measures. The findings are presented as percentages in line graph format, stratified by grade level. For clarity and following accepted precedents for policy-oriented audiences, we have intentionally chosen not to present confidence intervals and/or p-values, although these statistics are available upon request. The primary purpose of the descriptive analysis is to present major patterns and trends. Due to the large sample sizes involved, all differences in proportions of 4% or more can be considered to be statistically significant (p<0.05).
Figures are also presented to indicate where Canadian young people rank relative to students from other countries participating in the HBSC study. In keeping with international standards, when comparing Canadian students to those in other countries, 11, 13 and 15 year old age groups are used. Canadian students are categorized according to where they fit in the distribution of countries by quartiles over time. That is, for each age and gender group at each point in time, Canadian young people are identified as ranking in the bottom, second, third, or top quartile among countries. From this approach, we can consider whether Canadian young people have improved, remained the same, or responded more negatively relative to the other HBSC countries. This approach provides an opportunity to relate student health outcomes to policies, programs, interventions, and changing cultural norms across the HBSC network countries.
About the Health Behaviour in School-Aged Children (HBSC) Study
The Health Behaviour in School-Aged Children (HBSC) Study is a cross-national research study conducted in collaboration with the World Health Organization (WHO). The study involves health surveys conducted with students in classroom settings, with a focus on the early adolescent years (ages 11-15). HBSC is conducted every four years by participating countries following a common research protocol.
Internationally, the HBSC study was first initiated in 1982 by researchers from three European countries: England, Finland and Norway. Shortly thereafter the study was adopted by the WHO Regional Office for Europe as a WHO collaborative study. In 1983/84 the first HBSC survey administration took place in four countries. Canada's participation began with the third cycle of data collection in 1989/90 as one of 11 participating countries. The Canadian HBSC team headed by the Social Program Evaluation Group (SPEG) at Queen's University has since completed five more rounds of data collection, one every four years with the largest and most recent taking place in the 2009/10 school year. Since its inception, the project has expanded to become one of the largest research networks of its kind, encompassing 43 participating countries and regions across Europe and North America and over 350 researchers.
In its early years the HBSC network was a somewhat informal network of researchers sharing similar goals of gaining understanding into and monitoring young people's health behaviours and attitudes and factors that influence them. Over the course of the last 20 years, the HBSC network has out of necessity become a much more structured organization with formalized terms of reference and an extensive standardized international protocol to which all national research teams must adhere as members. The HBSC questionnaire has undergone continuous rigourous scientific review in the interests of optimizing item validity and reliability. Today the HBSC network brings together individuals from a wide range of backgrounds and perspectives with expertise in areas such as clinical medicine, epidemiology, human biology, paediatrics, pedagogy, psychology, public health, public policy, and sociology (HBSC, 2013).
HBSC Canada
HBSC Canada is the group responsible for the data source underlying this national report. The group consists of an academic team coordinated by the Social Program Evaluation Group at Queen's University at Kingston, as well as professional colleagues from the Public Health Agency of Canada (PHAC). It involves researchers, staff and students from Queen's, as well as McGill University in Montreal. The 2010 HBSC study was conducted with collaborative funding and support from the PHAC, as well as Health Canada. The study is undertaken with close input from the Joint Consortium for School Health (JCSH), as well as provincial and territorial policymakers in the health and education sectors.
The main purpose of the HBSC study in Canada is to inform and influence health promotion and health education policy and programs. Those researchers, policymakers, and research collaborators involved in HBSC aim to increase understanding of young people's health and well-being, and the factors that influence health. The HBSC team works with seven core objectives.
- To conduct national and international research on health behaviour, health and well-being, and the social contexts of school-aged children.
- To contribute new theoretical, conceptual, and methodological knowledge pertaining to these areas of research.
- To compare health experiences among young people in Canada with those in other HBSC member countries.
- To disseminate findings to the relevant audiences including researchers, health and education policymakers, health promotion practitioners, teachers, parents, and young people.
- To develop partnerships with other agencies that deal with adolescent health, to support health promotion efforts with populations of school-aged children.
- To inform policy making and program development.
- To contribute national expertise on health behaviour and on the social determinants of health in school-aged children.
Theory Underlying HBSC
HBSC researchers believe that young people's health should be considered in its broadest sense, encompassing physical, social, and emotional well-being. As per standard and widely accepted definitions, health is viewed as a resource for everyday living, and not just the absence of disease. HBSC researchers are intentional about considering positive aspects of health, as well as risk factors for future ill health and disease. This theoretical approach is informed by modern theories such as "assets-based approaches" to adolescent health research (Scales, 1999), in which factors that positively and negatively influence the health of youth populations are systematically examined.
In addition, HBSC research is almost always based upon population health thinking that focuses upon determinants of health, defined quite broadly (Health Canada, 1994). Among youth, these determinants include characteristics of home, school, peer group and neighbourhood settings, as well as socio-economic and behavioural influences. This theoretical approach suggests that health is influenced by the interaction of individual behaviours and environmental factors within these contexts.
HBSC Reports
The Canadian HBSC team has produced a major report that provides an overview of the national survey findings for each cycle of data collection except 1993/94: (1) The Health of Canada's Youth (1989/90) (King & Coles, 1992) presented Canada's data in an international context along with the data from the 10 other participating HBSC countries; (2) Trends in the Health of Canadian Youth (1997/98) (King et al., 1999) examined trends across the 1990, 1994, and 1998 data sets; (3) Young people in Canada: Their health and well-being (2001/2002) (Boyce, 2004) gave a general profile of the health of young Canadians and factors that influenced their health; (4) Healthy Settings for Young People in Canada (2005/06) (Boyce et al., 2008) related health outcomes to health contexts; (5) and The Health of Canada's Young People: A Mental Health Focus (2009/10) (Freeman et al., 2011) focused on mental health in young Canadians and related contextual factors, health behaviours, and health outcomes. For the 1993/94 data collection cycle the Canadian HBSC team redirected their dissemination focus to spearheading the first collaborative international HBSC report The Health of Youth: A Cross-National Survey (King et al., 1996).
Data Collection and Data Analysis
Sampling
In 2010, the HBSC Canada research team sampled students in Grades 6 to 10 from across the country. In each of the provinces, a systematic, two-stage cluster sample approach was used to select whole classes of students to participate in the study. A list of schools within school jurisdictions was created from which schools in the sample were selected. The numbers of classes in specific schools were estimated based on the grades in the school, the numbers of teachers, the total enrollment, and enrollment by grade, depending on the information available. Classes were given an approximately equal chance of being selected and were ordered on the sample lists according to school and school jurisdiction, community size, and community location within a province, and stratified by language of instruction and public/Roman Catholic designation. Classes were selected proportionally insofar as possible to match these characteristics. The specific classes selected in the sample schools were randomly selected by the school administrators using directions provided by the research team. The original sample of schools included an oversample to account for school jurisdictions declining to participate. Additionally, substitute schools and school jurisdictions were selected to replace those that declined to participate. The sampling methodology, with some minor adjusting based on the availability of specific information over time, has remained relatively constant since the first survey in 1989/90.
The 2010 sample does not include students from Prince Edward Island or New Brunswick. This nonparticipation has little impact on national estimates, due to their relatively small contribution to the national age-group population as a whole. In each of the other cycles of data collection all provinces and territories were represented in the data sets. Private and special schools including on-reserve schools were not included in the samples.
Within each of the three territories, the 2010 sample consisted of all eligible students in Grades 6 to 10. This sampling frame represented an attempt to obtain a census for the full student population, excluding private and special schools. In the earlier cycles of data collection, small numbers of classes from the territories were included in the samples so that students from the territories represented proportionately similar to the actual population.
The international HBSC network has since the beginning used age groupings as the basis for the international comparison (11-, 13-, and 15-year-olds). Under the 1990 and 1994 protocols, all countries sampled students from single grades (6, 8 and 10 in Canada) to match the target age groups as closely as possible. Starting in 1998 it was acknowledged that sampling from single grade groups to represent age groups, although practical from a cost perspective, was not optimum for best achieving representation of the three age groups. A compromise adopted in Canada and many other countries in 1998 resulted in a change in the sample from the three grades to a sample of Grades 6 through 10. Accordingly, comparisons of Canadian young people across the six cycles of data collection are presented for Grades 6, 8 and 10 students. In this report figures are also presented showing how Canadian young people's results rank in comparison to other HBSC countries and regions over time (Chapter 12). These data are presented by age group. Although the change in sampling methodology introduces a limitation for comparing Canadian students over time by age group, the fact that the age group samples at any one time are comparable across countries makes it valid to draw conclusions based on where Canada ranks internationally over the course of the study.
HBSC participating countries are required to contribute a national sample of 1500 students for each of the 3 age groups. Additionally, Canada has targeted a similar sized sample for each of the grades in the sample since 1998. The Canadian sample was increased to approximately 26,000 students in 2010. Past cycles averaged 7,000 to 10,000 students. The expansion was undertaken to achieve representative samples for 9 of Canada's 13 provinces and territories.
Table 1.1 provides sample sizes for each of the Canadian data sets referenced in this report. Due to some unavoidable conditions in the field during the administration of the 2002 sample, the data set corresponding to 2002 is somewhat smaller than in other years as well as being delayed in the time when it was administered in the school year. Generally, most of the data collection takes place during the winter months, while in 2002, more of the schools than usual completed the survey in the spring. The late administration can be expected to be a limitation when comparing results from 2002 to data from other years. Confidence intervals around the proportions presented for 2002 for Grade 8 and 10 students are larger than for other years due to the decreased sample size.
| Year of Survey | ||||||
|---|---|---|---|---|---|---|
| Grade/sex group | 1990 | 1994 | 1998 | 2002 | 2006 | 2010 |
| Grade 6 boys | 936 | 1115 | 1014 | 980 | 785 | 2552 |
| Grade 6 girls | 1003 | 1204 | 1089 | 1083 | 923 | 2551 |
| Grade 6 total | 1939 | 2329 | 2103 | 2063 | 1708 | 5103 |
| Grade 8 boys | 842 | 1113 | 1084 | 647 | 905 | 2595 |
| Grade 8 girls | 901 | 1235 | 1132 | 738 | 992 | 2662 |
| Grade 8 total | 1743 | 2348 | 2216 | 1385 | 1897 | 5257 |
| Grade 10 boys | 904 | 1122 | 1189 | 511 | 928 | 2448 |
| Grade 10 girls | 979 | 1205 | 1326 | 645 | 1045 | 2420 |
| Grade 10 total | 1883 | 2327 | 2515 | 1156 | 1973 | 4868 |
| Total (all grades) | 5565Table 1 - Footnote * | 7004Table 1 - Footnote * | 11243 | 7235 | 9715 | 26047 |
|
||||||
Text Equivalent - Table 1.1
Table 1.1 provides sample sizes for each of the Canadian data sets referenced in this report by grade, gender and year of survey. For survey cycle year 1990, the table shows a sample size of 936 Grade 6 boys and 1003 Grade 6 girls for a total 1939, for Grade 8, the table shows a sample size of 842 boys and 901 girls for a total of 1743 and for Grade 10, the table shows 904 boys and 979 girls for a total of 1883. The total sample size for all grades and sex groups for 1990 is 5565. For Survey cycle year 1994, the table shows a sample size of 1115 Grade 6 boys and 1204 Grade 6 girls for a total 2329, for Grade 8, the table shows 1113 boys and 1235 girls for a total of 2348 and for Grade 10, the table shows 1122 boys and 1205 girls for a total of 2327. The total sample size for all grades and sex groups for 1994 is 7004. For Survey cycle year 1998, the table shows a sample size of 1014 Grade 6 boys and 1089 Grade 6 girls for a total 2103, for Grade 8, the table shows 1084 boys and 1132 girls for a total of 2216 and for Grade 10, the table shows 1189 boys and 1326 girls for a total of 2515. The total sample size for all grades and sex groups for 1998 is 11243. For Survey cycle year 2002, the table shows a sample size of 980 Grade 6 boys and 1083 Grade 6 girls for a total 2063, for Grade 8, the table shows 647 boys and 738 girls for a total of 1385 and for Grade 10, the table shows 511 boys and 645 girls for a total of 1156. The total sample size for all grades and sex groups for 2002 is 7235. For Survey cycle year 2006, the table shows a sample size of 785 Grade 6 boys and 923 Grade 6 girls for a total 1708, for Grade 8, the table shows 905 boys and 992 girls for a total of 1897 and for Grade 10, the table shows 928 boys and 1045 girls for a total of 1973. The total sample size for all grades and sex groups for 2006 is 9715. For Survey cycle year 2010, the table shows a sample size of 2552 Grade 6 boys and 2551 Grade 6 girls for a total 5103, for Grade 8, the table shows 2595 boys and 2662 girls for a total of 5257 and for Grade 10, the table shows 2448 boys and 2420 girls for a total of 4868. The total sample size for all grades and sex groups for 2006 is 26047.
In the first two cycles of data collection, the sample consisted only of students in Grades 6, 8, and 10; in the last four cycles, Grades 6 through 10 inclusive were sampled.
Data Set Weighting
Due to the nature of the HBSC sampling approach, with oversamples in some provinces and an attempted census in the three Territories, results presented for the 2010 data set are weighted. Each province or territory data set is weighted within the national file, such that student responses from that jurisdiction contribute to the national results in proportion to the actual student population within the national grade group population. Effectively, provinces and territories that are over-represented in the student data file are given a weight of less than 1, while provinces that are under-represented in the data set are given a weight greater than 1.
Student Questionnaire
Student questionnaires are administered in classroom settings during one 45-70 minute session. In a very few instances, where students' level of literacy has been an issue, classes have used more than one class period to complete the survey. Survey items cover a wide range of topics related to health and health determinants.
In the most recent cycle of data collection, the survey instrument included a core set of approximately 120 mandatory items developed by the HBSC international network and used by all participating countries. The Canadian questionnaire included additional optional items agreed on in Canada by federal government partners, representatives of the Joint Consortium for School Health, and members of the core research team.
There are two versions of the Canadian questionnaire: one for Grades 6 to 8, and another for Grades 9 and 10. The questionnaire for the higher grades contains all the items found in the Grades 6 to 8 version, as well as additional items related to substance use and sexual health deemed appropriate only for older students. The questionnaire was made available in English, French and Inuktitut. Implicit or explicit consent procedures were followed, as per local school board customs.
The international network conducted a thorough review and reworking of the questionnaire leading up to the 2002 cycle of data collection. At this time, mandatory items and optional packages of items were standardized within the international protocol, as well as the guidelines for the formatting and submission of data files, sampling, and fieldwork. A number of changes were made to the survey, while, at the same time, many items were retained in the interest of maintaining the HBSC's capacity to have a monitoring function and examine trends over time. Since 2002, only minor changes have been made to the international protocol with respect to the items included in the survey.
For some items included in the current report, the question has remained the same over time while the response choices have been changed. Some items using Likert response choices ranging from "strongly agree" to "strongly disagree" to indicate agreement in 2002, 2006, and 2010 formerly employed the response choices "Yes," "No," and "Don't know" to indicate agreement.
References
- HBSC International Coordinating Centre Child & Adolescent Health Research Unit (2013). Health Behaviour in School-aged Children, a World Health Organization Collaborative Cross-National Survey.
- Health Canada (1994). Strategies for population health - investing in the health of Canadians, p. 106-108.
- Scales, P.C. (1999). Reducing risks and building developmental assets: Essential steps for promoting adolescent health. Journal of School Health, 69113-119.
Chapter 2: Mental Health
By Mary-Anne Reid
Why is Mental Health Important?
Positive mental well-being is rapidly becoming recognized as a significant contributor to a healthy and fulfilling life. For many, adolescence is a time of positive change, growth, learning, and trepidation. Children and youth who have greater social-emotional health experience greater overall success in life and have better abilities to overcome life's challenges. In addition, those who suffer from more mental health problems have more adjustment problems in the areas of health, school, self, and home (Buote, 2009).
In recognizing mental health as a major issue, there has been a shift to focus away from a deficit model (concerned solely with reducing mental illness) towards a more balanced perspective (Keyes, 2006). This approach considers both developmental contexts (e.g., parents, school) and the internal factors (e.g., confidence, competence) that contribute to adolescents' mental health and well-being (Benson & Scales, 2009). Fergus and Zimmerman (2005) link the idea that, with positive internal factors and developmental contexts, adolescents' ability to overcome exposure to difficult situations and cope with these difficult situations (i.e., resilience) is increased. When positive, these factors can, therefore, help youth develop in a constructive manner and can aid in the growth and maintenance of mental health.
In addition, poor mental health is often linked to other social issues. For example, the prevalence of conduct problems (e.g., arrested, skipped school) has been shown to decrease and psychosocial functioning (e.g., self-concept, school integration) to increase for adolescents as positive mental health is enhanced (Keyes, 2006).
With a better understanding of the impact mental health can have on adolescents' quality of life and the influence that positive adolescent mental health can have in a community (Waddell et al., 2005), there have been many initiatives in Canada that have aimed to explore this area. For example, the Mental Health Commission of Canada (MHCC) has made an effort to link with organizations around the nation to help instill change for individuals experiencing difficulty as a result of mental health issues (MHCC, 2012). Included in these initiatives is a focus group called the Child and Youth Advisory Committee, which is composed of individuals between the ages of 18 to 30 who have experienced living with mental health problems. The committee is currently working on dissemination of knowledge through various projects, such as The Evergreen Framework (Kutcher & McLuckie, 2010), which focuses on developing a national vision for youth mental health.
It is important to examine the mental health trends from the HBSC data to further understand the impacts that current initiatives are having on the mental health of Canadian youth or where initiatives may need to shift their focus. In recognizing the changes over time, we can adapt mental health strategies and initiatives to best help guide youth through this sensitive time.
What are We Examining in this Chapter?
For this chapter, the data are presented in three general categories: 1) emotional/psychological indicators; 2) psychosomatic indicators; and 3) behavioural indicators. The emotional/psychological category is further subdivided into indices of well-being (reflective of positive mental health) and indices of ill-being (reflective of a lack of positive mental health). We examine and discuss the measures within each of these categories in regards to Grade 6, Grade 8, and Grade 10 students, divided by gender for more detailed exploration. A brief overview of policy initiatives and government action related to mental health is also presented.
Emotional/Psychological Indicators
The emotional/psychological indicators of mental health were measured using eight items, which were then subcategorized into indices of well-being and indices of ill-being. Indices of well-being includes three items: 1) students who rate their life as 8 or higher on a 10 point scale, with 0 being the worst possible life and 10 being the best possible life; 2) students who agree or strongly agree to having confidence in themselves; and 3) students reporting 'good' or 'excellent' general health. Indices of ill-being include five items, three of which are measured as the percentage of students agreeing with a statement: 1) feeling lonely; 2) feeling hopeless; and 3) wishing they could change how they look. The other two items are measured by frequency: 1) feeling bad tempered or irritable more than once a week; and 2) feeling nervous once a week or more in the last six months.
Indices of Well-being
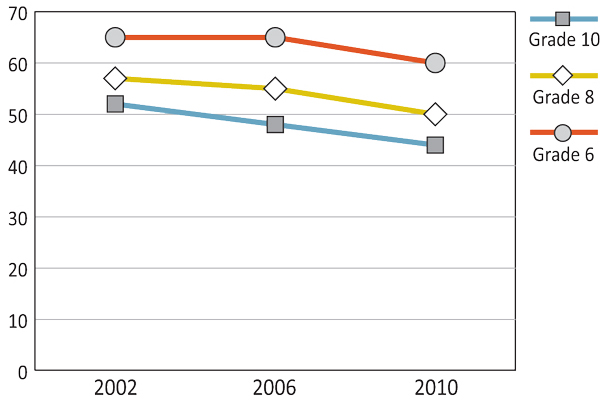
As shown in Figures 2.1 and 2.2, for both boys and girls in Canada there has been a decrease in the number of students ranking their life at 8 or higher on a 0-10 scale (0 as 'worst possible life' and 10 as 'best possible life'). For Grade 6 boys and Grade 10 girls the most significant decline happened between the 2002 and 2006 surveys, with the Grade 6 boys decreasing from 67% to 62% and Grade 10 girls decreasing from 52% to 48%. For Grade 8 boys and girls, the most significant decrease occurred between the 2006 and 2010 surveys, with boys dropping from 64% to 58% and girls from 55% to 50%. Grade 10 girls had the greatest change of an 8% decline from 2002 to 2010 in the ratings of 8 or higher for best possible life.
Figure 2.1: Boys who rate their life 8 or higher on a 0-10 scale with 0 = 'worst possible life' and 10 = 'best possible life' (%)

Text Equivalent - Figure 2.1
Figure 2.1 is a line graph that shows the percentage of boys who rate their life 8 or higher on a 0-10 scale with 0 being equal to the "worst possible life" and 10 being equal to the "best possible life" by grade and year of survey. The graph shows that among Grade 6 boys, 67% reported 8 or higher for best possible life in 2002, compared to 62% in 2006 and 62% in 2010. Among Grade 8 boys, 64% reported 8 or higher for best possible life in 2002, compared to 64% in 2006, and 58% in 2010. Among Grade 10 boys, 58% reported 8 or higher for best possible life in 2002, compared to 56% in 2006, and 55% in 2010.
Figure 2.2: Girls who rate their life 8 or higher on a 0-10 scale with 0 = 'worst possible life' and 10 = 'best possible life' (%)
Text Equivalent - Figure 2.2
Figure 2.2 is a line graph that shows the percentage of girls who rate their life 8 or higher on a 0-10 scale with 0 being equal to the "worst possible life" and 10 being equal to the "best possible life" by grade and year of survey. The graph shows that among Grade 6 girls, 65% reported 8 or higher for best possible life in 2002, compared to 65% in 2006 and 60% in 2010. Among Grade 8 girls, 57% reported 8 or higher for best possible life in 2002, compared to 55% in 2006, and 50% in 2010. Among Grade 10 girls, 52% reported 8 or higher for best possible life in 2002, compared to 48% in 2006, and 44% in 2010.
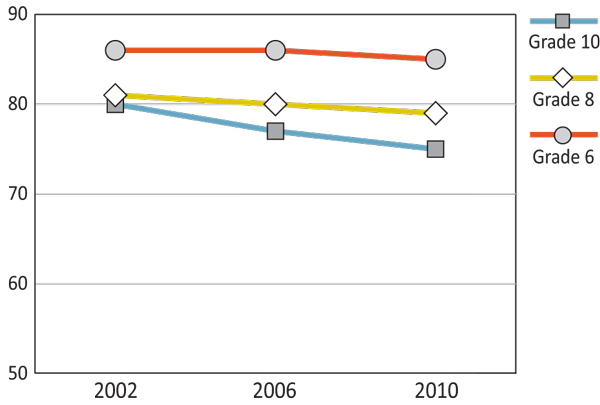
Since 2002, there has been a steady decline in the reported number of Canadian students agreeing to having confidence in themselves with the greatest decrease being for Grade 8 girls who decreased from 61% in 2002 to 53% in 2010 (Figures 2.3 and 2.4). Female adolescents tend to have lower confidence in themselves than male adolescents. As students get older, there are consistently more students agreeing to having less confidence in themselves with the most prominent group losing confidence being girls.
Figure 2.3: Boys who agree or strongly agree they have confidence in themselves (%)
Text Equivalent - Figure 2.3
Figure 2.3 is a line graph that shows the percentage of boys who agree or strongly agree they have confidence in themselves by grade and year of survey. The graph shows that among Grade 6 boys, 86% agree or strongly agree they have confidence in themselves in 2002, compared to 86% in 2006 and 85% in 2010. Among Grade 8 boys, 81% agree or strongly agree they have confidence in themselves in 2002, compared to 80% in 2006, and 79% in 2010. Among Grade 10 boys, 80% agree or strongly agree they have confidence in themselves in 2002, compared to 77% in 2006, and 75% in 2010.
Figure 2.4: Girls who agree or strongly agree they have confidence in themselves (%)
Text Equivalent - Figure 2.4
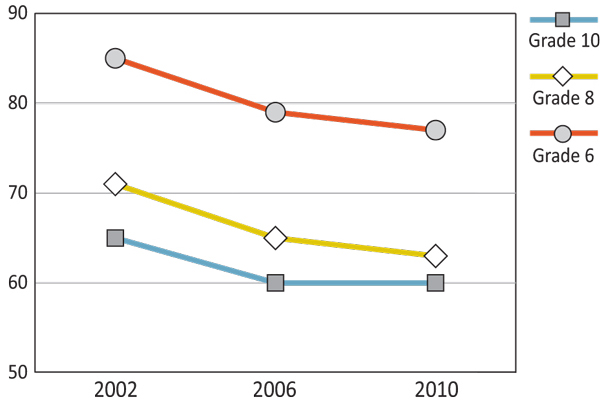
Figure 2.4 is a line graph that shows the percentage of girls who agree or strongly agree they have confidence in themselves by grade and year of survey. The graph shows that among Grade 6 girls, 85% agree or strongly agree they have confidence in themselves in 2002, compared to 79% in 2006 and 77% in 2010. Among Grade 8 girls, 71% agree or strongly agree they have confidence in themselves in 2002, compared to 65% in 2006, and 63% in 2010. Among Grade 10 girls, 65% agree or strongly agree they have confidence in themselves in 2002, compared to 60% in 2006, and 60% in 2010.
There has been a decrease in perspectives of 'good' or 'excellent' general health for Grade 10 boys from the 2006 to the 2010 survey (86% to 82%) and Grade 8 boys from the 2002 to the 2006 survey (89% to 86%). For both genders, Grade 6 students had the highest reported health with 88% or more students reporting 'good' or 'excellent' health (Figures 2.5 and 2.6). For Grade 6 girls, there was an increase in reported general health between the 2002 and 2010 surveys. In 2002, 88% of Grade 6 girls rated 'good' or 'excellent' general health increasing to 91% for the 2010 survey. Other than Grade 6 students, girls generally reported lower general health than boys.
Figure 2.5: Boys who report 'good' or 'excellent' general health (%)
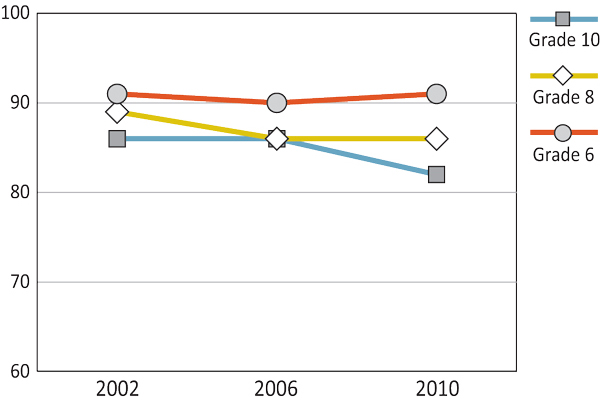
Text Equivalent - Figure 2.5
Figure 2.5 is a line graph that shows the percentage of boys who report "good" or excellent" general health by grade and year of survey. The graph shows that among Grade 6 boys, 91% report "good" or excellent" general health themselves in 2002, compared to 90% in 2006 and 91% in 2010. Among Grade 8 boys, 89% report "good" or "excellent" general health in 2002, compared to 86% in 2006, and 86% in 2010. Among Grade 10 boys, 86% report "good" or "excellent" general health in 2002, compared to 86% in 2006, and 82% in 2010.
Figure 2.6: Girls who report 'good' or 'excellent' general health (%)
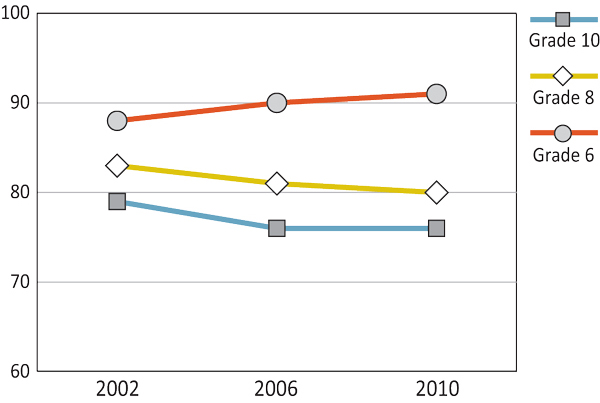
Text Equivalent - Figure 2.6
Figure 2.6 is a line graph that shows the percentage of girls who report "good" or excellent" general health by grade and year of survey. The graph shows that among Grade 6 girls, 88% report "good" or excellent" general health in 2002, compared to 90% in 2006 and 91% in 2010. Among Grade 8 girls, 83% report "good" or "excellent" general health in 2002, compared to 81% in 2006, and 80% in 2010. Among Grade 10 girls, 79% report "good" or "excellent" general health in 2002, compared to 76% in 2006, and 76% in 2010.
Indices of Ill-being
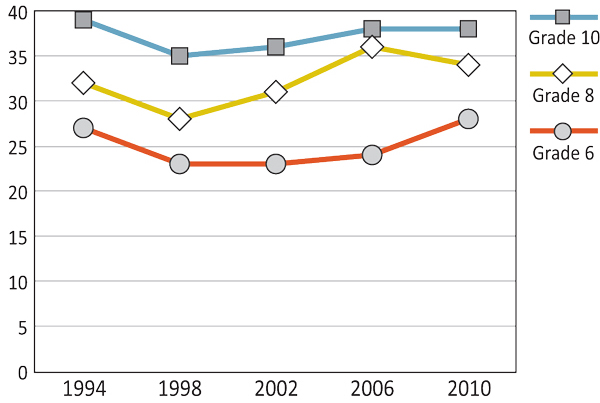
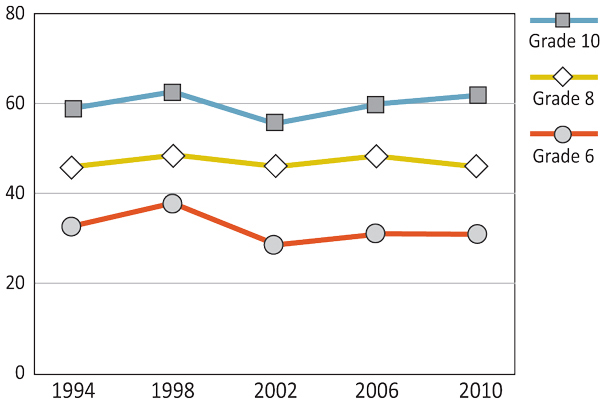
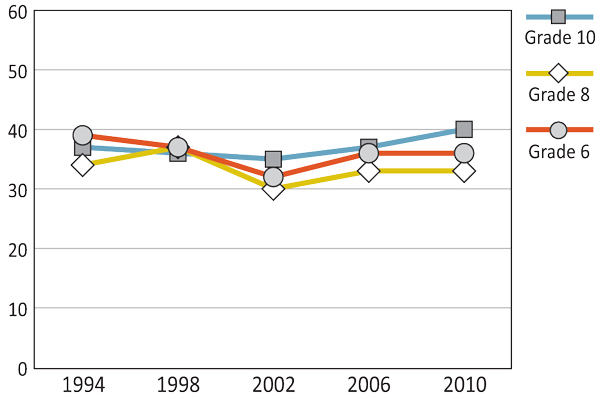
As illustrated in Figures 2.7 and 2.8, there has been a relatively steady decline in the number of students agreeing with the statement, 'I would change how I look if I could.' For Grade 8 and Grade 10 boys, this percentage increased between the 2006 and 2010 surveys. Across all grades and time points, girls agreed with the statement more often than boys.
Figure 2.7: Boys who agree with the statement, 'I would change how I look if I could.' (%)
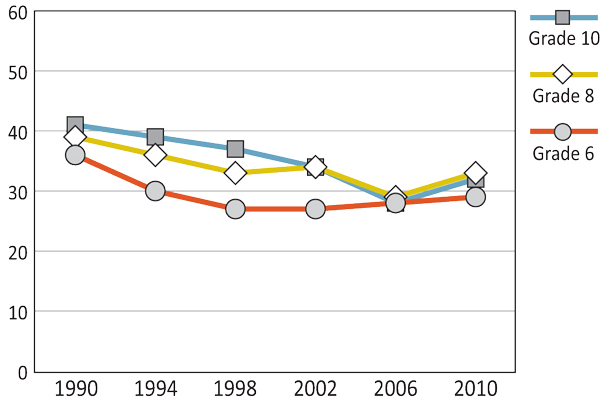
Text Equivalent - Figure 2.7
Figure 2.7 is a line graph that shows the percentage of boys who agree with the statement "I would change how I look if I could" by grade and year of survey. The graph shows that among Grade 6 boys, 36% agree with the statement "I would change how I look if I could" in 1990, compared to 30% in 1994, 27% in 1998, 27% in 2002, 28% in 2006 and 29% in 2010. Among Grade 8 boys, 39% agree with the statement "I would change how I look if I could" in 1990, compared to 36% in 1994, 33% in 1998, 34% in 2002, 29% in 2006 and 33% in 2010. Among Grade 10 boys, 41% agree with the statement "I would change how I look if I could" in 1990, compared to 39% in 1994, 37% in 1998, 34% in 2002, 28% in 2006 and 32% in 2010.
Figure 2.8: Girls who agree with the statement, 'I would change how I look if I could.' (%)
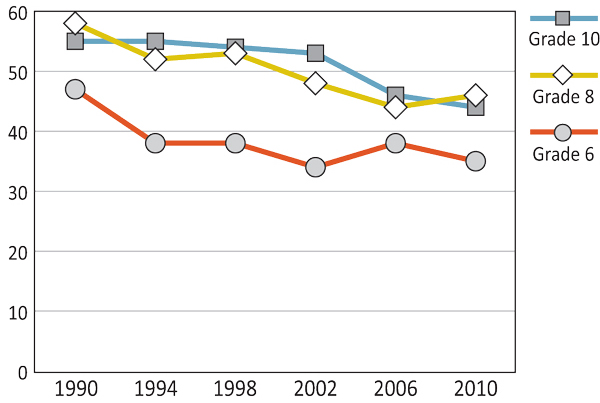
Text Equivalent - Figure 2.8
Figure 2.8 is a line graph that shows the percentage of girls who agree with the statement "I would change how I look if I could" by grade and year of survey. The graph shows that among Grade 6 girls, 47% agree with the statement "I would change how I look if I could" in 1990, compared to 38% in 1994, 38% in 1998, 34% in 2002, 38% in 2006 and 35% in 2010. Among Grade 8 girls, 58% agree with the statement "I would change how I look if I could" in 1990, compared to 52% in 1994, 53% in 1998, 48% in 2002, 44% in 2006 and 46% in 2010. Among Grade 10 girls, 55% agree with the statement "I would change how I look if I could" in 1990, compared to 55% in 1994, 54% in 1998, 53% in 2002, 46% in 2006 and 44% in 2010.
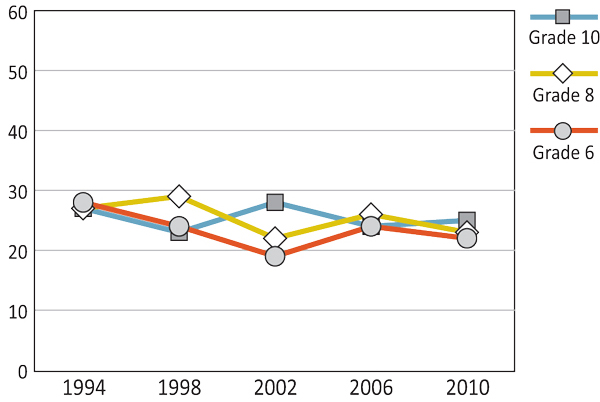
As shown in Figures 2.9 and 2.10, the reported levels of feeling depressed or low by young people varied little across survey years. Since 1994, Grade 8 and 10 girls' slightly increasing percentages of reported rates of feeling depressed or low exceeded boys' relatively stable levels. This gender gap in feeling depressed or low was not evident in Grade 6 students until the 2010 survey, when levels differed by 6% between boys and girls.
Figure 2.9: Boys who report feeling depressed or low at least once a month (%)

Text Equivalent - Figure 2.9
Figure 2.9 is a line graph that shows the percentage of students who report feeling depressed or low at least once a month, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 24% reported feeling depressed or low at least once a month in 1994, compared to 22% in 1998, 21% in 2002, 25% in 2006, and 22% in 2010. Among Grade 8 boys, 21% reported feeling depressed or low at least once a month in 1994, compared to 20% in 1998, 19% in 2002, 20% in 2006, and 19% in 2010. Among Grade 10 boys, 24% reported feeling depressed or low at least once a month in 1994, compared to 22% in 1998, 24% in 2002, 21% in 2006, and 23% in 2010.
Figure 2.10: Girls who report feeling depressed or low at least once a month (%)
Text Equivalent - Figure 2.10
Figure 2.10 is a line graph that shows the percentage of students who report feeling depressed or low at least once a month, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 26% reported feeling depressed or low at least once a month in 1994, compared to 22% in 1998, 22% in 2002, 23% in 2006, and 25% in 2010. Among Grade 8 girls, 32% reported feeling depressed or low at least once a month in 1994, compared to 29% in 1998, 32% in 2002, 38% in 2006, and 36% in 2010. Among Grade 10 girls, 39% reported feeling depressed or low at least once a month in 1994, compared to 35% in 1998, 36% in 2002, 38% in 2006, and 38% in 2010.
In Canada, the number of students who felt nervous once a week or more has decreased for boys and remained relatively steady for girls since the 1990s (Figures 2.11 and 2.12). More girls reported being nervous on a daily basis compared to boys. Grade 6, Grade 8, and Grade 10 boys decreased in reported daily nervousness, with the steepest decline occurring between the 1994 and 1998 surveys. Grade 6 girls declined consistently in feelings of nervousness between the 1994 and 2002 surveys, then increased again between the 2006 and 2010 surveys. Grade 10 girls increased in feeling nervous at least once a week or more between 2002 and 2006.
Figure 2.11: Boys who have felt nervous once a week or more in the past six months (%)
Text Equivalent - Figure 2.11
Figure 2.11 is a line graph that shows the percentage of boys who have felt nervous once a week or more in the past six months by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 34% felt nervous once a week or more in the past six months in 1994, compared to 29% in 1998, 28% in 2002, 30% in 2006, and 32% in 2010. Among Grade 8 boys, 39% felt nervous once a week or more in the past six months in 1994, compared to 30% in 1998, 28% in 2002, 33% in 2006, and 31% in 2010. Among Grade 10 boys, 43% felt nervous once a week or more in the past six months in 1994, compared to 35% in 1998, 35% in 2002, 36% in 2006, and 31% in 2010.
Figure 2.12: Girls who have felt nervous once a week or more in the past six months (%)

Text Equivalent - Figure 2.12
Figure 2.12 is a line graph that shows the percentage of girls who have felt nervous once a week or more in the past six months by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 41% felt nervous once a week or more in the past six months in 1994, compared to 36% in 1998, 32% in 2002, 32% in 2006, and 37% in 2010. Among Grade 8 girls, 46% felt nervous once a week or more in the past six months in 1994, compared to 39% in 1998, 41% in 2002, 42% in 2006, and 45% in 2010. Among Grade 10 girls, 48% felt nervous once a week or more in the past six months in 1994, compared to 45% in 1998, 41% in 2002, 48% in 2006, and 48% in 2010.
As shown in Figures 2.13 and 2.14, the percentage of young people feeling bad tempered or irritable has not changed substantially since the declining rates between the 1994 and 1998 surveys. For boys, regardless of grade, reporting of bad temper/irritability remained at a stable level throughout the last four survey cycles, while that of Grade 8 and 10 girls has increased slightly.
Figure 2.13: Boys who report feeling bad tempered or irritable more than once a week (%)
Text Equivalent - Figure 2.13
Figure 2.13 is a line graph that shows the percentage of students who report feeling bad tempered or irritable more than once a week, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 28% reported feeling bad tempered or irritable more than once a week in 1994, compared to 20% in 1998, 18% in 2002, 18% in 2006, and 15% in 2010. Among Grade 8 boys, 22% reported feeling bad tempered or irritable more than once a week in 1994, compared to 19% in 1998, 17% in 2002, 17% in 2006, and 16% in 2010. Among Grade 10 boys, 22% reported feeling bad tempered or irritable more than once a week in 1994, compared to 19% in 1998, 20% in 2002, 18% in 2006, and 17% in 2010.
Figure 2.14: Girls who report feeling bad tempered or irritable more than once a week (%)
Text Equivalent - Figure 2.14
Figure 2.14 is a line graph that shows the percentage of students who report feeling bad tempered or irritable more than once a week, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 27% reported feeling bad tempered or irritable more than once a week in 1994, compared to 20% in 1998, 17% in 2002, 17% in 2006, and 16% in 2010. Among Grade 8 girls, 27% reported feeling bad tempered or irritable more than once a week in 1994, compared to 21% in 1998, 22% in 2002, 22% in 2006, and 23% in 2010. Among Grade 10 girls, 27% reported feeling bad tempered or irritable more than once a week in 1994, compared to 23% in 1998, 22% in 2002, 24% in 2006, and 25% in 2010.
Overall, more female adolescents report feeling helpless than male adolescents in Canada (Figures 2.15 and 2.16). The percentage of Canadian students who reported often feeling helpless has increased for girls in Grade 6 and Grade 8, and boys in Grades 6 and Grade 10 since 2002. The number of boys in Grade 8 and girls in Grade 10 reporting feelings of helplessness remained similar from the 2002 to the 2010 survey. While there was negligible change for Grade 10 girls, they have consistently remained the highest reporters of feelings of helplessness since 2002, when the data were first collected.
Figure 2.15: Boys who often feel helpless (%)
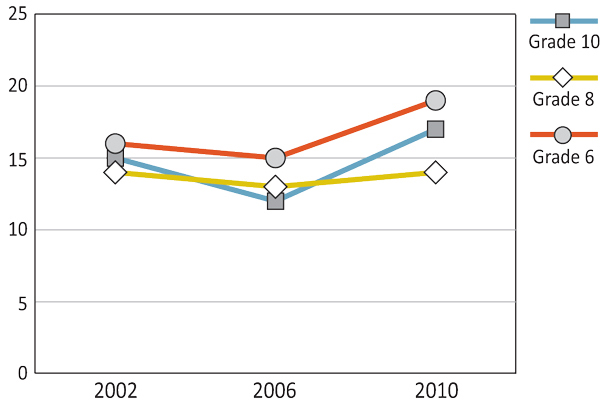
Text Equivalent - Figure 2.15
Figure 2.15 is a line graph that shows the percentage of boys who often feel helpless by grade and year of survey. The graph shows that among Grade 6 boys, 16% often feel helpless in 2002, compared to 15% in 2006 and 19% in 2010. Among Grade 8 boys, 14% often feel helpless in 2002, compared to 13% in 2006, and 14% in 2010. Among Grade 10 boys, 15% often feel helpless in 2002, compared to 12% in 2006, and 17% in 2010.
Figure 2.16: Girls who often feel helpless (%)

Text Equivalent - Figure 2.16
Figure 2.16 is a line graph that shows the percentage of girls who often feel helpless by grade and year of survey. The graph shows that among Grade 6 girls, 14% often feel helpless in 2002, compared to 15% in 2006 and 20% in 2010. Among Grade 8 girls, 17% often feel helpless in 2002, compared to 19% in 2006, and 22% in 2010. Among Grade 10 girls, 22% often feel helpless in 2002, compared to 20% in 2006, and 22% in 2010.
As illustrated in Figures 2.17 and 2.18, the percentage of students that reported often feeling lonely has remained consistent since 2002, with adolescent girls being more likely to agree to often feeling lonely when compared with adolescent boys. In contrast to the other groups, the number of Grade 6 girls reporting feelings of loneliness increased from 16% (2002) to 21% (2006) to 24% (2010). Grade 10 girls slightly increased their reporting of often feeling lonely between 2006 and 2010.
Figure 2.17: Boys who often feel lonely (%)
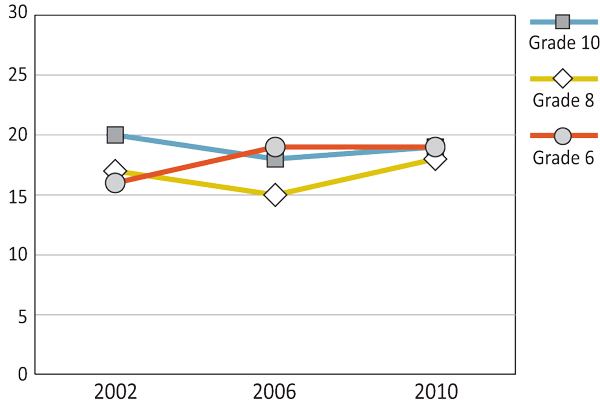
Text Equivalent - Figure 2.17
Figure 2.17 is a line graph that shows the percentage of boys who often feel lonely by grade and year of survey. The graph shows that among Grade 6 boys, 16% often feel helpless in 2002, compared to 19% in 2006 and 19% in 2010. Among Grade 8 boys, 17% often feel lonely in 2002, compared to 15% in 2006, and 18% in 2010. Among Grade 10 boys, 20% often feel lonely in 2002, compared to 18% in 2006, and 19% in 2010.
Figure 2.18: Girls who often feel lonely (%)
Text Equivalent - Figure 2.18
Figure 2.18 is a line graph that shows the percentage of girls who often feel lonely by grade and year of survey. The graph shows that among Grade 6 girls, 16% often feel helpless in 2002, compared to 21% in 2006 and 24% in 2010. Among Grade 8 girls, 22% often feel lonely in 2002, compared to 24% in 2006, and 23% in 2010. Among Grade 10 girls, 23% often feel lonely in 2002, compared to 22% in 2006, and 26% in 2010.
Psychosomatic Indicators
For psychosomatic indicators of mental health in Canadian students, there were four items measured. Three items asked about frequency per week in the previous six months (difficulty getting to sleep, having stomachaches, and having headaches), and one item looked at frequency in a one-month period (backaches). Items in this section include physical symptoms that may be reflective of overall mental health.
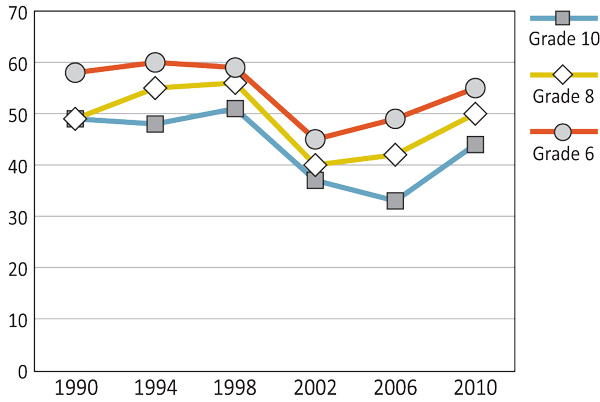
Throughout the survey years, the percentages of young people who reported backaches at least once a month increased with age and was typically highest in girls (Figures 2.19 and 2.20). This divergence between the genders was most apparent in Grade 10 students with an increasing differential between 2006 and 2010, as boys' levels decreased slightly from 53% to 49% while girls' levels remained relatively stable at 60% to 62%. Throughout survey cycles, Grade 8 students reported relatively stable rates of backaches, with higher proportions in girls. An exception to this gender gap in backaches was found in Grade 6 students where, aside from the 2006 survey when boys reported more backaches than girls, the rates of backaches were equal between the genders.
Figure 2.19: Boys who report having backaches at least once a month (%)
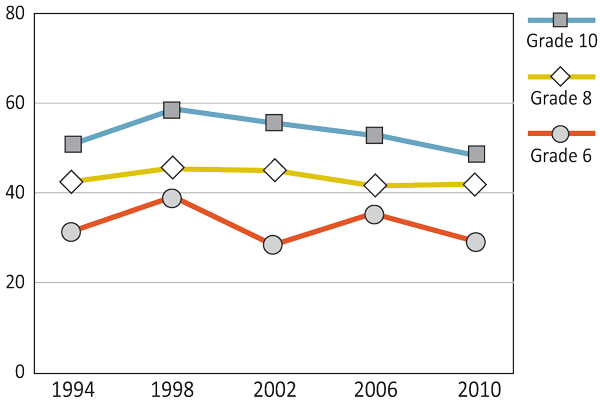
Text Equivalent - Figure 2.19
Figure 2.19 is a line graph that shows the percentage of students who report having backaches at least once a month, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 32% reported having backaches at least once a month in 1994, compared to 40% in 1998, 24% in 2002, 38% in 2006, and 30% in 2010. Among Grade 8 boys, 42% reported having backaches at least once a month in 1994, compared to 43% in 1998, 43% in 2002, 41% in 2006, and 41% in 2010. Among Grade 10 boys, 51% reported having backaches at least once a month in 1994, compared to 59% in 1998, 56% in 2002, 53% in 2006, and 49% in 2010.
Figure 2.20: Girls who report having backaches at least once a month (%)
Text Equivalent - Figure 2.20
Figure 2.20 is a line graph that shows the percentage of students who report having backaches at least once a month, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 37% reported having backaches at least once a month in 1994, compared to 39% in 1998, 29% in 2002, 31% in 2006, and 31% in 2010. Among Grade 8 girls, 43% reported having backaches at least once a month in 1994, compared to 44% in 1998, 43% in 2002, 44% in 2006, and 43% in 2010. Among Grade 10 girls, 59% reported having backaches at least once a month in 1994, compared to 62% in 1998, 56% in 2002, 60% in 2006, and 61% in 2010.
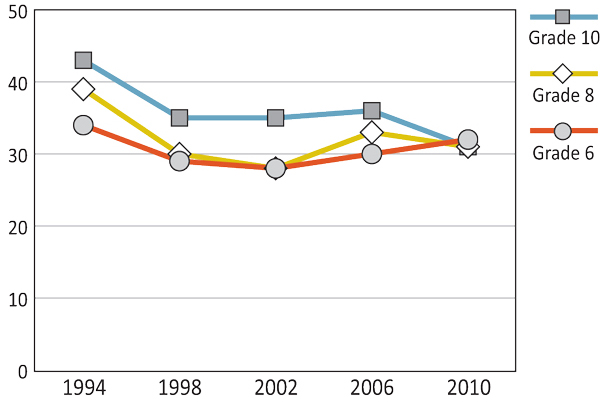
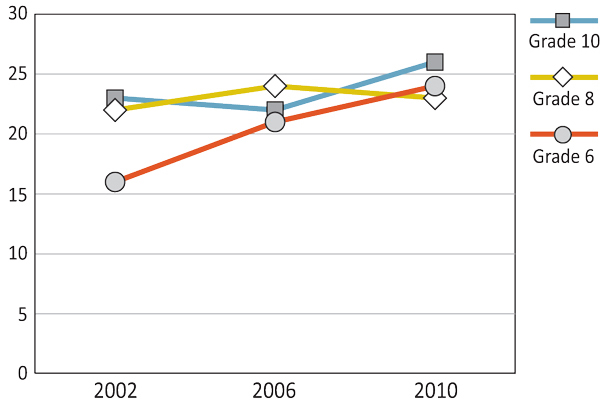
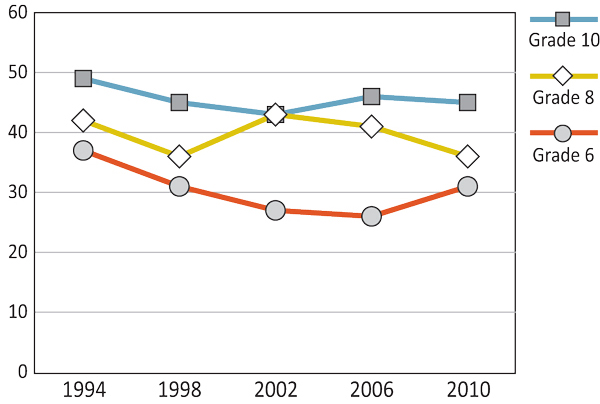
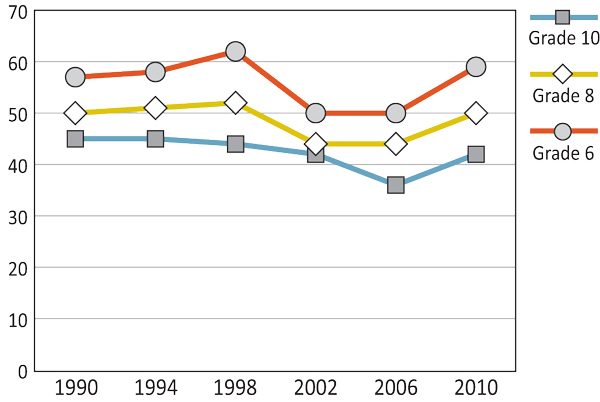
Consistent across grades and survey years, a greater number of female students than male students reported experiencing headaches at least once per week (Figures 2.21 and 2.22). The percentage of students reporting weekly headaches has decreased slightly for boys since the 1990s, while remaining relatively consistent with a slight decline for girls. For Grade 8 boys, the steepest decline of 7% in weekly headaches occurred between 1998 and 2002. For Grade 6 students, there was a steady decrease in the number of weekly headaches reported between 1994 and 2002, with a slight rise in the number of headaches for Grade 6 boys between 2002 and 2006. Grade 10 girls decreased in their reported headaches from 1994 to 2002 (from 49% to 43%) before increasing again back to 47% in 2010. This number is relatively higher than Grade 10 boys, who in their peak year (2002) had 28% reporting to have had headaches once or more per week in the last month.
Figure 2.21: Boys who report having headaches once a week or more in the past six months (%)
Text Equivalent - Figure 2.21
Figure 2.21 is a line graph that shows the percentage of boys who report having headaches once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 28% reported having headaches once a week or more in the past six months in 1994, compared to 24% in 1998, 19% in 2002, 24% in 2006, and 22% in 2010. Among Grade 8 boys, 27% reported having headaches once a week or more in the past six months in 1994, compared to 29% in 1998, 22% in 2002, 26% in 2006, and 23% in 2010. Among Grade 10 boys, 27% reported having headaches once a week or more in the past six months in 1994, compared to 23% in 1998, 28% in 2002, 24% in 2006, and 25% in 2010.
Figure 2.22: Girls who report having headaches once a week or more in the past six months (%)
Text Equivalent - Figure 2.22
Figure 2.22 is a line graph that shows the percentage of girls who report having headaches once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 37% reported having headaches once a week or more in the past six months in 1994, compared to 31% in 1998, 27% in 2002, 26% in 2006, and 29% in 2010. Among Grade 8 girls, 42% reported having headaches once a week or more in the past six months in 1994, compared to 36% in 1998, 43% in 2002, 41% in 2006, and 39% in 2010. Among Grade 10 girls, 49% reported having headaches once a week or more in the past six months in 1994, compared to 45% in 1998, 43% in 2002, 46% in 2006, and 47% in 2010.
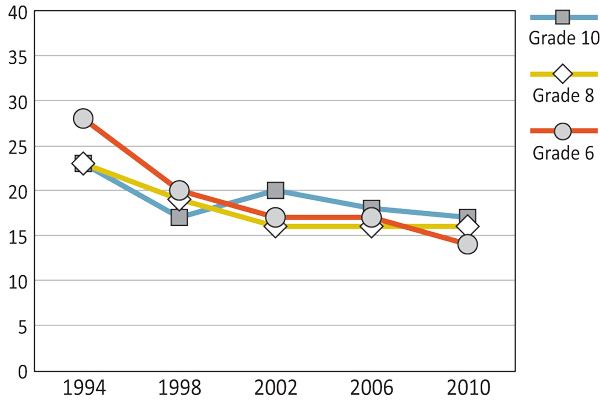
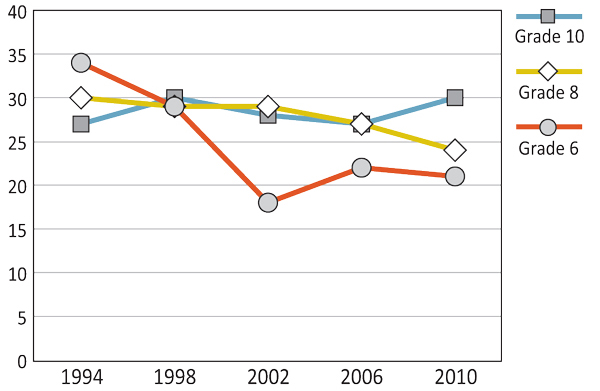
As shown in Figures 2.23 and 2.24, more female students reported experiencing stomach aches at least once a week in the past 6 months than male students. The number of students of both genders in Canada with daily stomach aches has decreased slightly since the 1990s, with the exception of Grade 10 students whose rates have remained relatively consistent. For Grade 6 students, the steepest decline in daily stomach aches occurred between the 1998 and 2002 surveys, with boys dropping from 19% to 13% and girls dropping from 29% to 18%. Grade 8 students decreased in the number of daily stomach aches from the 1994 to the 2010 survey by 6% for girls and 5% for boys.
Figure 2.23: Boys who report having stomach aches once a week or more in the past six months (%)

Text Equivalent - Figure 2.23
Figure 2.23 is a line graph that shows the percentage of boys who report having stomach aches once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 23% reported having stomach aches once a week or more in the past six months in 1994, compared to 19% in 1998, 13% in 2002, 16% in 2006, and 15% in 2010. Among Grade 8 boys, 18% reported having stomach aches once a week or more in the past six months in 1994, compared to 16% in 1998, 13% in 2002, 14% in 2006, and 13% in 2010. Among Grade 10 boys, 17% reported having stomach aches once a week or more in the past six months in 1994, compared to 17% in 1998, 20% in 2002, 17% in 2006, and 16% in 2010.
Figure 2.24: Girls who report having stomach aches once a week or more in the past six months (%)
Text Equivalent - Figure 2.24
Figure 2.24 is a line graph that shows the percentage of girls who report having stomach aches once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 34% reported having stomach aches once a week or more in the past six months in 1994, compared to 29% in 1998, 18% in 2002, 22% in 2006, and 21% in 2010. Among Grade 8 girls, 30% reported having stomach aches once a week or more in the past six months in 1994, compared to 29% in 1998, 29% in 2002, 27% in 2006, and 24% in 2010. Among Grade 10 girls, 27% reported having stomach aches once a week or more in the past six months in 1994, compared to 30% in 1998, 28% in 2002, 27% in 2006, and 30% in 2010.
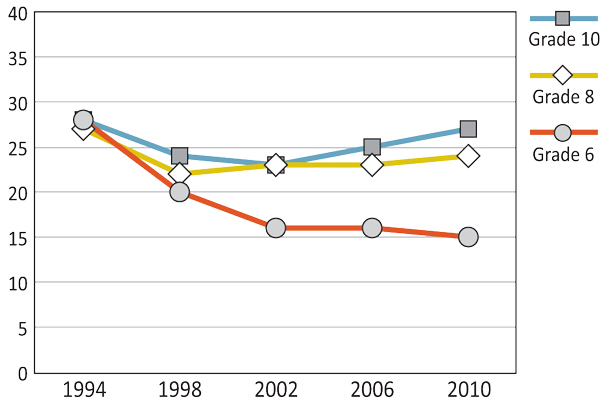
Overall, female students were more likely to report difficulties getting to sleep compared to male students (Figures 2.25 and 2.26), with the exception that both genders reported similar levels of difficulty getting to sleep in Grade 6. In Canada, difficulty getting to sleep once a week or more has been steadily increasing for Grade 10 girls since the 1990s. Grade 6 boys decreased in the number of individuals having difficulty getting to sleep from 1994 to 2002. Similarly, Grade 8 boys decreased in reported difficulty getting to sleep between the 1998 and 2002 surveys. Like the Grade 6 boys, Grade 6 girls decreased in the number of individuals having difficulty falling asleep between 1994 and 2002, but increased between the 2002 and 2010 surveys. Grade 8 girls followed a similar trend to Grade 10 girls in their increase in difficulty of falling asleep between the 2002 and 2010 surveys.
Figure 2.25: Boys who report having difficulty getting to sleep once a week or more in the past six months (%)
Text Equivalent - Figure 2.25
Figure 2.25 is a line graph that shows the percentage of boys who report having difficulty getting to sleep once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 39% reported having difficulty getting to sleep once a week or more in the past six months in 1994, compared to 37% in 1998, 32% in 2002, 36% in 2006, and 36% in 2010. Among Grade 8 boys, 34% reported having difficulty getting to sleep once a week or more in the past six months in 1994, compared to 37% in 1998, 30% in 2002, 33% in 2006, and 33% in 2010. Among Grade 10 boys, 37% reported having difficulty getting to sleep once a week or more in the past six months in 1994, compared to 36% in 1998, 35% in 2002, 37% in 2006, and 40% in 2010.
Figure 2.26: Girls who report having difficulty getting to sleep once a week or more in the past six months (%)
Text Equivalent - Figure 2.26
Figure 2.26 is a line graph that shows the percentage of girls who report having difficulty getting to sleep once a week or more in the past six months, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 44% reported having difficulty getting to sleep once a week or more in the past six months in 1994, compared to 38% in 1998, 33% in 2002, 36% in 2006, and 42% in 2010. Among Grade 8 girls, 42% reported difficulty getting to sleep once a week or more in the past six months in 1994, compared to 40% in 1998, 40% in 2002, 48% in 2006, and 46% in 2010. Among Grade 10 girls, 44% reported having difficulty getting to sleep once a week or more in the past six months in 1994, compared to 46% in 1998, 45% in 2002, 49% in 2006, and 51% in 2010.
Behavioural Indicators
Behavioural indicators of mental health in Canadian students were measured using three items that were based on the percentage of students agreeing to the statements: 1) 'I am often sorry for the things I do'; 2) 'I often feel left out of things'; and 3) 'I often have a hard time saying no'.
The number of students who agreed with the statement, 'I am often sorry for the things I do' has fluctuated across surveys (Figures 2.27 and 2.28). Younger students more consistently felt sorry for the things they did than older students. The lowest rates occurred in 2002 and 2006. Rates in 2010 were higher than the two previous surveys but still lower than surveys conducted in the 1990s.
Figure 2.27: Boys who agree with the statement, 'I am often sorry for the things I do.' (%)
Text Equivalent - Figure 2.27
Figure 2.27 is a line graph that shows the percentage of boys who agree with the statement, "I am often sorry for the things I do" by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 57% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 58% in 1994, 62% in 1998, 50% in 2002, 50% in 2006, and 59% in 2010. Among Grade 8 boys, 50% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 51% in 1994, 52% in 1998, 44% in 2002, 44% in 2006, and 50% in 2010. Among Grade 10 boys, 45% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 45% in 1994, 44% in 1998, 42% in 2002, 36% in 2006, and 42% in 2010.
Figure 2.28: Girls who agree with the statement, 'I am often sorry for the things I do.' (%)
Text Equivalent - Figure 2.28
Figure 2.28 is a line graph that shows the percentage of girls who agree with the statement, "I am often sorry for the things I do" by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 58% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 60% in 1994, 59% in 1998, 45% in 2002, 49% in 2006, and 55% in 2010. Among Grade 8 girls, 49% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 55% in 1994, 56% in 1998, 40% in 2002, 42% in 2006, and 50% in 2010. Among Grade 10 girls, 49% agree with the statement, "I am often sorry for the things I do" in 1990, compared to 48% in 1994, 51% in 1998, 37% in 2002, 33% in 2006, and 44% in 2010.
In 2002, the HBSC survey began to examine the percentage of students who agreed with the statement, 'I often feel left out of things.' Over the survey years, the percentage of Grade 8 and Grade 10 students reporting feelings of being left out have remained relatively stable, with a slight decrease in the 2006 survey year (Figures 2.29 and 2.30). In the most recent survey, 19% to 24% of Grade 8 and Grade 10 students reported feeling left out, with girls reporting slightly higher levels than boys.
Figure 2.29: Boys who agree with the statement, 'I often feel left out of things.' (%)
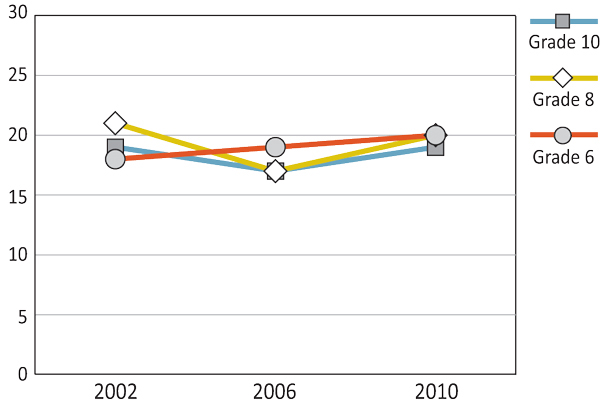
Text Equivalent - Figure 2.29
Figure 2.29 is a line graph that shows the percentage of boys who agree with the statement, "I often feel left out of things" by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 18% agree with the statement, "I often feel left out of things" in 2002, 19% in 2006, and 20% in 2010. Among Grade 8 boys, 21% agree with the statement, "I often feel left out of things" in 2002, 17% in 2006, and 20% in 2010. Among Grade 10 boys, 19% agree with the statement, "I often feel left out of things" in 2002, 17% in 2006, and 19% in 2010.
Figure 2.30: Girls who agree with the statement, 'I often feel left out of things.' (%)
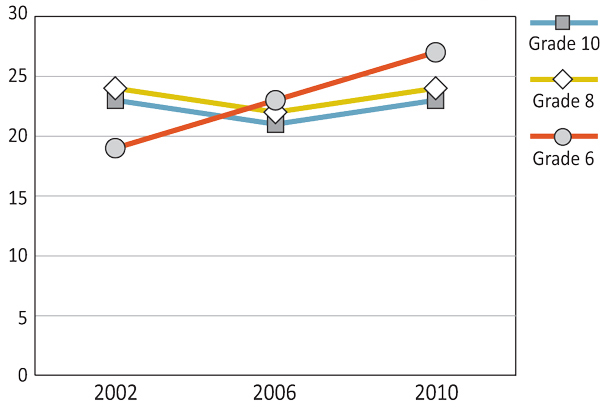
Text Equivalent - Figure 2.30
Figure 2.30 is a line graph that shows the percentage of girls who agree with the statement, "I often feel left out of things" by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 19% agree with the statement, "I often feel left out of things" in 2002, 23% in 2006, and 27% in 2010. Among Grade 8 girls, 24% agree with the statement, "I often feel left out of things" in 2002, 22% in 2006, and 24% in 2010. Among Grade 10 girls, 23% agree with the statement, "I often feel left out of things" in 2002, 21% in 2006, and 23% in 2010.
Throughout the survey years, the number of Grade 6 students reporting feelings of being left out has increased with time. Although this trend is evident for both genders, it is more pronounced for girls. Whereas Grade 6 boys displayed an increase of 2% over the three survey cycles, Grade 6 girls exhibited an increase of 8% in the same time span.
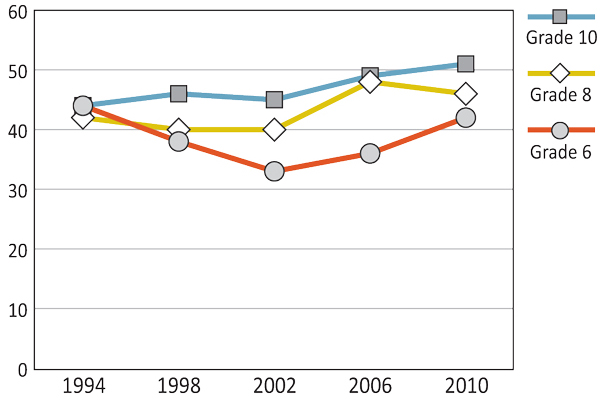
Students who reported agreeing with the statement 'I often have a hard time saying no' has followed a similar trend for both boys and girls in Canada (Figures 2.31 and 2.32). From 1990 to 1998, agreement with this statement increased slightly, before a sharp decrease between the 1998 and 2002 surveys. Since 2002, there has been another increase in the number of students agreeing to the statement. While both boys and girls follow a similar trend, girls report having more difficulty saying no than boys across the survey cycles.
Figure 2.31: Boys who agree with the statement, 'I often have a hard time saying no.' (%)
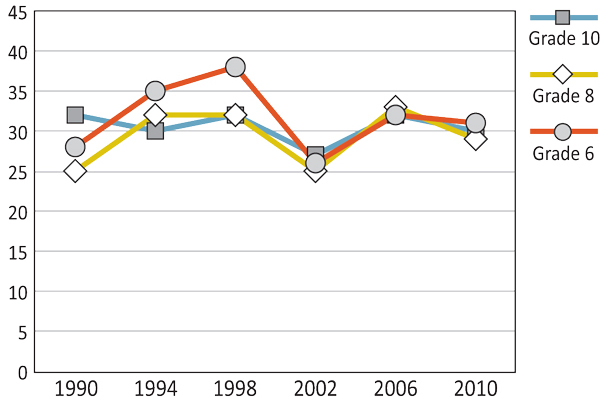
Text Equivalent - Figure 2.31
Figure 2.31 is a line graph that shows the percentage of boys who agree with the statement, "I often have a hard time saying no" by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 28% agree with the statement, "I often have a hard time saying no" in 1990, compared to 35% in 1994, 38% in 1998, 26% in 2002, 32% in 2006, and 31% in 2010. Among Grade 8 boys, 25% agree with the statement, "I often have a hard time saying no" in 1990, compared to 32% in 1994, 32% in 1998, 25% in 2002, 33% in 2006, and 29% in 2010. Among Grade 10 boys, 32% agree with the statement, "I often have a hard time saying no" in 1990, compared to 30% in 1994, 32% in 1998, 27% in 2002, 32% in 2006, and 30% in 2010.
Figure 2.32: Girls who agree with the statement, 'I often have a hard time saying no.' (%)
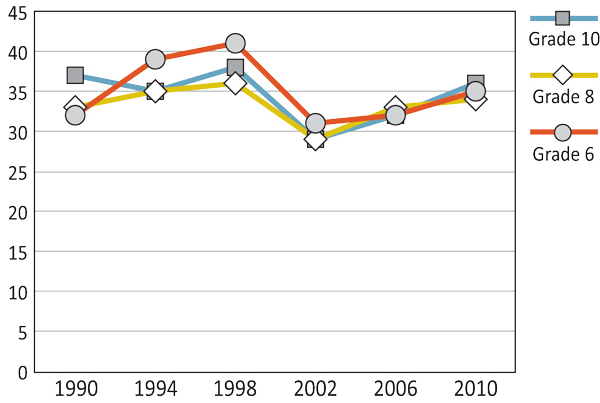
Text Equivalent - Figure 2.32
Figure 2.32 is a line graph that shows the percentage of girls who agree with the statement, "I often have a hard time saying no" by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 32% agree with the statement, "I often have a hard time saying no" in 1990, compared to 39% in 1994, 41% in 1998, 31% in 2002, 32% in 2006, and 35% in 2010. Among Grade 8 girls, 33% agree with the statement, "I often have a hard time saying no" in 1990, compared to 35% in 1994, 36% in 1998, 29% in 2002, 33% in 2006, and 34% in 2010. Among Grade 10 girls, 37% agree with the statement, "I often have a hard time saying no" in 1990, compared to 35% in 1994, 38% in 1998, 29% in 2002, 32% in 2006, and 36% in 2010.
In 2008, the growing awareness of and concern for mental health in Canada prompted the Standing Senate Committee on Social Affairs, Science and Technology to create the Mental Health Commission of Canada (MHCC). Among other initiatives (e.g., Changing Directions, Changing Lives: The Mental Health Strategy for Canada, 2012), the MHCC set forward in 2010 to develop a Mental Health Strategy for Canada that includes a framework, Evergreen, specifically for child and youth mental health. The aims are:
- to provide specific information relevant to children and youth for the Mental Health Strategy for Canada;
- to provide a framework of values and strategic directions to assist key authorities in their creation of policy and programming specific to the needs of children and youth; and
- to provide information to key stakeholders (e.g., young people, parents, professionals) on what needs to be done to address youth mental health across Canada as well as suggestions for how it could be implemented.
This framework includes specific initiatives (e.g., services and activities), which can be developed with the ultimate goal of maintaining population mental health and addressing mental disorders. The strategic directions are divided into four categories: 1) promotion; 2) prevention; 3) intervention and ongoing care; and 4) research and evaluation.
In addition, this past year, the Economic Action Plan 2012 for Canada proposed $5.2 million dollars for 2012-2013 to support the Canadian Depression Research and Intervention Network. This initiative was led by The Mood Disorders Society of Canada, together with MHCC, to connect some of Canada's most informed depression researchers. The goal was to have research focus on more effective diagnostic treatment tools, as well as on improving the lives of individuals lacking mental well-being.
(Government of Canada, 2012; Kutcher & McLuckie, 2010; Mental Health Commission of Canada, 2012)
As well as these national strategies, there are also individual provincial strategies that have foci targeting specific parts of the population. For example, in 1994 the Aboriginal Healing and Wellness Strategy was launched in Ontario (revised in 2010), which has a focus on promoting healthy Aboriginal communities through combining traditional and mainstream programs and services. Some examples of the aims of this strategy are:
- to continue to work in partnerships with the First Nations people to address the health and wellness of Aboriginal communities, both on and off reserves;
- to provide information and shelters for individuals experiencing mental illness and distress;
- to provide health care, health promotion, and health education.
(Ontario Ministry of Community and Social Services, 2010)
Another example of a provincial strategy is Creating Connections: Alberta's Addicition and Mental Health Strategy, which was published in 2011. The focus of this strategy is on community well-being as a means for increasing mental health (including youth) through an educative and comprehensive mental health system. There are five strategic directions that the document focuses on:
- Building healthy and resilient communities;
- Fostering the development of healthy children, youth, and families (including seniors);
- Enhancing community-based services, capacity, and supports;
- Addressing complex needs; and
- Enhancing assurance.
Goals for the Mental Health Framework include:
- providing accessible mental health supports;
- providing quality mental health services;
- providing mental health services in a sustainable fashion.
To implement the goals and strategic directions, the government of Alberta is engaging individuals involved with policy direction, as well as those with lived experiences. In addition, they are working on research dissemination through providing educational opportunities on mental health topics to the workforce and community members, while implementing funding and compensation frameworks for mental health initiatives.
(Government of Alberta, 2011)
Summary and Implications
The prevalence of reported well-being has been decreasing since the beginning of the survey cycles with other indices of mental health remaining relatively stable. Grade 8 and Grade 10 girls tend to report more negative feelings of mental health than boys of a similar age, while Grade 6 boys and girls are often similar, with more positive views of their mental health than the older students. These findings about well-being may reflect the increasing societal pressures on young people. The limited changes in other indices may suggest that there has not yet been enough time passed for some of the mental health youth initiatives to be fully integrated and disseminated. For example, the Evergreen Framework (Kutcher & McLuckie, 2010) that was developed to be a component of the Mental Health Strategy for Canada (MHCC, 2012) would not have been in place for long enough to affect change in the 2010 survey.
There are also some slightly more positive areas that should be acknowledged. For example, students reporting feelings of helplessness and feelings of loneliness have remained relatively low, with under 26% percent of individuals agreeing to these statements. Similarly, students in 2010 were less likely to report they wanted to change the way they looked.
In spite of measuring mental health in a variety of ways (i.e. psychosomatic, emotional/psychological, and behavioural), girls consistently reported more negative mental health across indices, with Grade 10 girls often being the most negative. The relatively negative reports for this group indicates the need for a specific focus on mental health promotion efforts as this group is also most at risk of developing lifelong mental illnesses. With the consistent differences between genders in indicators of mental health, targeting mental health initiatives by gender may be a productive strategy to affect change in this youth population. Perhaps the influences on boys and girls of these age groups are different, and mental health strategies need to reflect these differences in the way they work to promote mental health.
With the recent Economic Action Plan 2012 for Canada, which provides funding for mental health research, along with the continued efforts of provincial, territorial, and federal governments, Canada seems to have begun moving in an encouraging direction of helping youth develop and maintain positive mental health. As the trends with the HBSC surveys show, there are a relatively large number of youth who are struggling with mental health issues on a daily, weekly, and monthly basis. Efforts like the Evergreen Framework (Kutcher & McLuckie, 2010), which recognize the importance of individualizing mental health initiatives for youth well-being, will continue to lend credence to the importance of focusing these efforts to help impart change in the mental health of our youth across Canada.
References
- Benson, P.L., Scales, P.C. (2009). The definition and preliminary measurement of thriving in adolescence. Journal of Positive Psychology, 4, 85-104. doi:10.1080/17439760802399240
- Buote, D. (2009). Social-emotional health in middle childhood: What we know. Ottawa, ON: Public Health Agency of Canada.
- Fergus, S., Zimmerman, M.A. (2005). Adolescence resilience: A framework for understanding health development in the face of risk. Annual Review of Public Health, 26, 399-419.
- Government of Canada (2012). Budget plan 2012 .
- Keyes, C.L.M. (2006). Mental health in adolescence: Is America's youth flourishing? American Journal of Orthopsychiatry, 76, 395-402.
- Kutcher, S., Hampton, M.J., Wilson, J. (2010). Child and adolescent mental health policy and plans in Canada: An analytical review. Canadian Journal of Psychiatry, 55, 100-107.
- Kutcher, S., McLuckie, A. For the Child and Youth Advisory Committee, Mental Health Commission of Canada (2010). Evergreen: A child and youth mental health framework for Canada. Calgary, AB: Mental Health Commission of Canada.
- Mental Health Commission of Canada [MHCC] (2012). Changing directions, changing lives: The mental health strategy for Canada. Calgary, AB: Author.
- Ontario Ministry of Community and Social Services (2010). Goal of the Aboriginal Healing and Wellness Strategy .
- Waddell, C., McEwen, K., Shepherd, C.A., Offord, D.R., Hua, J.M. (2005). A public health strategy to improve the mental health of Canadian children. Canadian Journal of Psychiatry, 50, 226-233.
Chapter 3: Home
By Sean Cousins
What is the Home Setting?
Home and family, in context of this report, denote the parents or legal guardians of the students surveyed. The family is understood as a relationship of care between students and their guardians (mothers or fathers or their partners in the event such students do not live with their birth parents). Although the scope of the family may include siblings and other individuals in the home, these relationships are not captured in this report.
Why is the Home Setting Significant?
The family provides the first setting in which a child experiences a socializing context. Family acculturation influences youth well-being through its direct influence on children (Driscoll, Russell, & Crockett, 2008). Research examining the relation between parental styles and youth behaviours illustrates that positive parenting is a powerful predictor of child and adolescent adaptation in multiple domains (Shaffer, Suveg, Thomassin, & Bradbury, 2012).
In general, parental warmth and emotional support are strongly associated with indicators of childhood well-being (Brown, 2004). Moderate levels of parental control can be protective against harmful and delinquent behaviours among adolescents, such as substance abuse (Finkenauer, Engels, & Baumeister, 2010). Parents also have a significant impact on how youth feel about themselves. For example, children who feel loved and supported are happier and more confident (Gray & Steinberg, 1999; Wolfradt, Hempel, & Miles, 2003). Access to strong parental support is positively correlated with reduced delinquent behaviour, depression, and psychomatic symptoms for adolescents (Currie et al., 2008), thereby indicating the importance of having such support.
For some youth, adolescence can be a period of conflict in which bickering, squabbling, and arguments over everyday issues may characterize parent-adolescent relationships (Lerner & Steinberg, 2004). Although high levels of conflict during adolescence tend to be detrimental for adolescent development, relationships, and future adjustment (Laursen & Collins, 1994), some conflict in adolescence is a normative but temporary perturbation in transforming family relationships (Sessa & Steinberg, 1991; Smetana, Campione-Barr, & Metzger, 2006).
What are We Reporting in this Chapter?
In this chapter, we examine the extent to which Canadian adolescents felt trusted and understood by their parents, and their self-reported ease of communication with father and mother, arguments with parents, happiness of home life, degree of parental expectations for home and school, and thoughts of leaving home. The trends are divided into three categories: 1) parental understanding, trust, and ease of communication; 2) parental expectations and conflict; and 3) home life. Related policy and legislation are examined.
Parental Understanding, Trust, and Ease of Communication
From 1990 to 2002, the percentage of young people who indicated feeling understood by their parents steadily increased, with a substantial spike in the 2002 survey. As shown in Figures 3.1 and 3.2, these numbers have remained relatively stable since then.
Figure 3.1: Boys who report being understood by their parents (%)
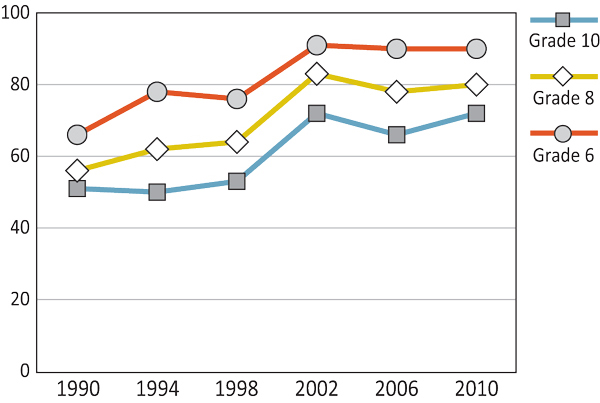
Text Equivalent - Figure 3.1
Figure 3.1 is a line graph that shows the percentage of boys who report being understood by their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 66% reported being understood by their parents in 1990, compared to 78% in 1994, 76% in 1998, 91% in 2002, 90% in 2006, and 90% in 2010. Among Grade 8 boys, 56% reported being understood by their parents in 1990, compared to 62% in 1994, 64% in 1998, 83% in 2002, 78% in 2006, and 80% in 2010. Among Grade 10 boys, 51% reported being understood by their parents in 1990, compared to 50% in 1994, 53% in 1998, 72% in 2002, 66% in 2006, and 72% in 2010.
Figure 3.2: Girls who report being understood by their parents (%)
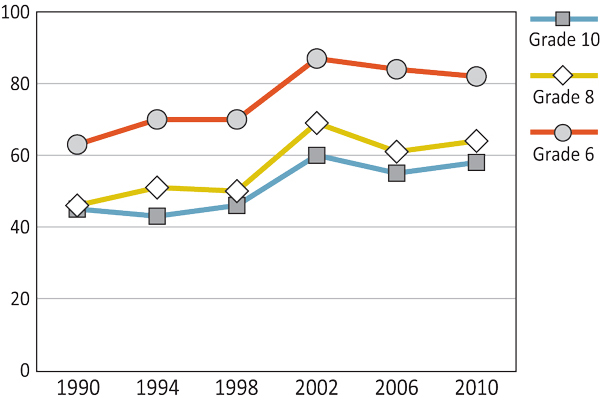
Text Equivalent - Figure 3.2
Figure 3.2 is a line graph that shows the percentage of girls who report being understood by their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 63% reported being understood by their parents in 1990, compared to 70% in 1994, 70% in 1998, 87% in 2002, 84% in 2006, and 82% in 2010. Among Grade 8 girls, 46% reported being understood by their parents in 1990, compared to 51% in 1994, 50% in 1998, 69% in 2002, 61% in 2006, and 64% in 2010. Among Grade 10 girls, 45% reported being understood by their parents in 1990, compared to 43% in 1994, 46% in 1998, 60% in 2002, 55% in 2006, and 58% in 2010.
Throughout the survey years, younger students felt more understood by their parents than older students. In the 2010 survey, whereas 82% of Grade 6 girls felt they were understood by their parents, only 58% of Grade 10 girls reported the same. Similarly, while 90% of Grade 6 boys indicated that they felt understood by their parents, only 71% of Grade 10 boys reported being understood. As well, there is a gender difference in young peoples' perception of being understood by their parents with boys consistently reporting higher rates than same-grade girls.
The percentage of boys and girls reporting parental trust were similar across the grades (Figures 3.3 and 3.4). Younger students consistently reported being trusted by their parents at higher rates than the older students. Like parental understanding, the most significant increase in parental trust occurred between 1998 and 2002 with numbers largely similar since then. The entire span of surveys shows a general slight positive trend in young people reporting feelings of parental trust.
Figure 3.3: Boys who report being trusted by their parents (%)
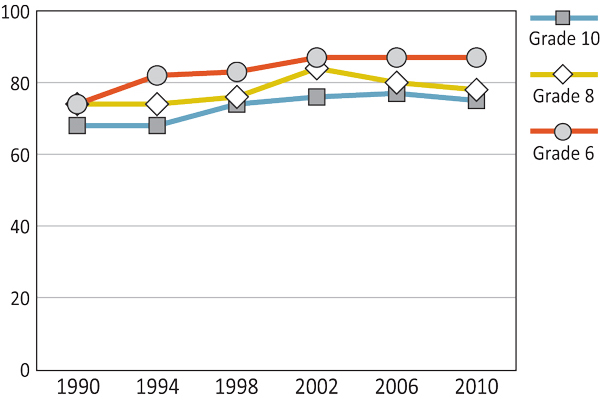
Text Equivalent - Figure 3.3
Figure 3.3 is a line graph that shows the percentage of boys who report being trusted by their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 74% reported being trusted by their parents in 1990, compared to 82% in 1994, 83% in 1998, 87% in 2002, 87% in 2006, and 87% in 2010. Among Grade 8 boys, 74% reported being trusted by their parents in 1990, compared to 74% in 1994, 76% in 1998, 84% in 2002, 80% in 2006, and 78% in 2010. Among Grade 10 boys, 68% reported being trusted by their parents in 1990, compared to 68% in 1994, 74% in 1998, 76% in 2002, 77% in 2006, and 75% in 2010.
Figure 3.4: Girls who report being trusted by their parents (%)

Text Equivalent - Figure 3.4
Figure 3.4 is a line graph that shows the percentage of girls who report being trusted by their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 79% reported being trusted by their parents in 1990, compared to 81% in 1994, 81% in 1998, 88% in 2002, 86% in 2006, and 86% in 2010. Among Grade 8 girls, 66% reported being trusted by their parents in 1990, compared to 70% in 1994, 71% in 1998, 78% in 2002, 75% in 2006, and 74% in 2010. Among Grade 10 girls, 62% reported being trusted by their parents in 1990, compared to 65% in 1994, 71% in 1998, 71% in 2002, 73% in 2006, and 73% in 2010.
Students were questioned about their ease of communication with their parents about things that concern them (Figures 3.5 through 3.8). Since 1990, students in all age groups have shown an overall increase in ease of communication with their mothers and fathers. Throughout the survey years, Grade 6 students consistently reported the highest levels of communication ease, with Grade 10 students reliably reporting the lowest levels. Overall, students were more likely to find it easier to talk to their mothers than their fathers about things that really bothered them, with this finding especially true of girls.
Figure 3.5: Boys who find it easy or very easy to talk to their father about things that bother them (%)
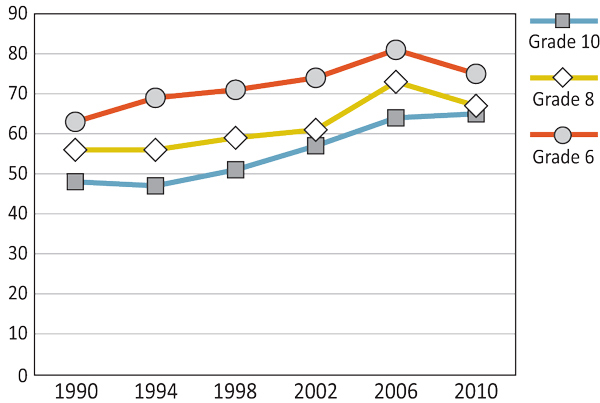
Text Equivalent - Figure 3.5
Figure 3.5 is a line graph that shows the percentage of boys who find it easy or very easy to talk to their father about things that bother them, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 63% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 69% in 1994, 71% in 1998, 74% in 2002, 81% in 2006, and 75% in 2010. Among Grade 8 boys, 56% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 56% in 1994, 59% in 1998, 61% in 2002, 73% in 2006, and 67% in 2010. Among Grade 10 boys, 48% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 47% in 1994, 51% in 1998, 57% in 2002, 64% in 2006, and 65% in 2010.
Figure 3.6: Girls who find it easy or very easy to talk to their father about things that bother them (%)
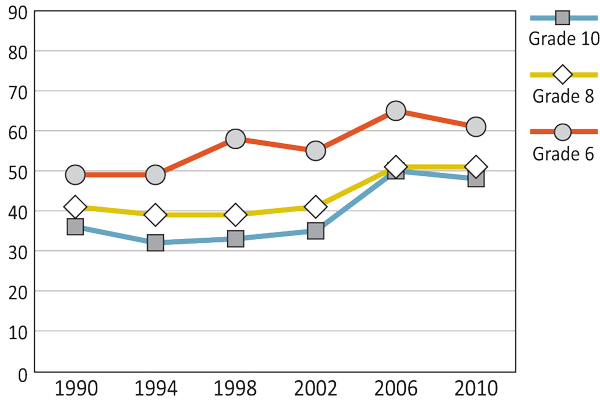
Text Equivalent - Figure 3.6
Figure 3.6 is a line graph that shows the percentage of girls who find it easy or very easy to talk to their father about things that bother them, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 49% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 49% in 1994, 58% in 1998, 55% in 2002, 65% in 2006, and 61% in 2010. Among Grade 8 girls, 41% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 39% in 1994, 39% in 1998, 41% in 2002, 51% in 2006, and 51% in 2010. Among Grade 10 girls, 36% find it easy or very easy to talk to their father about things that bother them in 1990, compared to 32% in 1994, 33% in 1998, 35% in 2002, 50% in 2006, and 48% in 2010.
Figure 3.7: Boys who find it easy or very easy to talk to their mother about things that bother them (%)
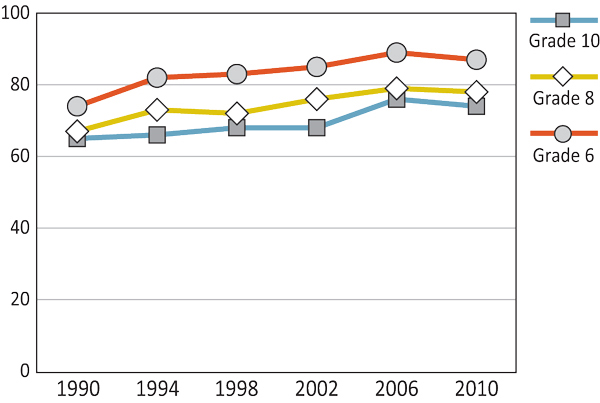
Text Equivalent - Figure 3.7
Figure 3.7 is a line graph that shows the percentage of boys who find it easy or very easy to talk to their mother about things that bother them, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 74% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 82% in 1994, 83% in 1998, 85% in 2002, 89% in 2006, and 87% in 2010. Among Grade 8 boys, 67% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 73% in 1994, 72% in 1998, 76% in 2002, 79% in 2006, and 78% in 2010. Among Grade 10 boys, 65% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 66% in 1994, 68% in 1998, 68% in 2002, 76% in 2006, and 74% in 2010.
Figure 3.8: Girls who find it easy or very easy to talk to their mother about things that bother them (%)

Text Equivalent - Figure 3.8
Figure 3.8 is a line graph that shows the percentage of girls who find it easy or very easy to talk to their mother about things that bother them, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 78% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 79% in 1994, 83% in 1998, 79% in 2002, 88% in 2006, and 86% in 2010. Among Grade 8 girls, 70% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 71% in 1994, 71% in 1998, 74% in 2002, 75% in 2006, and 75% in 2010. Among Grade 10 girls, 67% find it easy or very easy to talk to their mother about things that bother them in 1990, compared to 63% in 1994, 65% in 1998, 67% in 2002, 72% in 2006, and 74% in 2010.
Parental Expectations and Conflict
From 1990 to 2006, adolescent perceptions of their parental expectations remained relatively stable, as demonstrated in Figures 3.9 and 3.10. However, for all grade-gender combinations, perceptions of parental expectations increased between 2006 and 2010. While there is no clear pattern for gender with respect to parental expectations, Grade 6 students consistently indicate less often that their parents expect too much of them than do students in Grades 8 and 10.
Figure 3.9: Boys who think their parents expect too much of them at school (%)
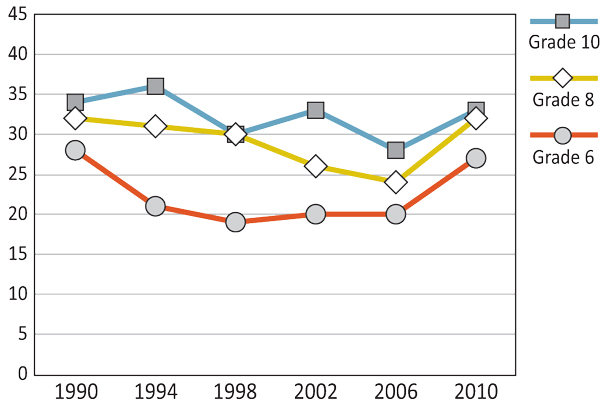
Text Equivalent - Figure 3.9
Figure 3.9 is a line graph that shows the percentage of boys who think their parents expect too much of them, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 28% reported that their parents expect too much of them in 1990, compared to 21% in 1994, 19% in 1998, 20% in 2002, 20% in 2006, and 27% in 2010. Among Grade 8 boys, 32% reported that their parents expect too much of them in 1990, compared to 31% in 1994, 30% in 1998, 26% in 2002, 24% in 2006, and 32% in 2010. Among Grade 10 boys, 34% reported that their parents expect too much of them in 1990, compared to 36% in 1994, 30% 1998, 33% in 2002, 28% in 2006, and 33% in 2010.
Figure 3.10: Girls who think their parents expect too much of them at school (%)
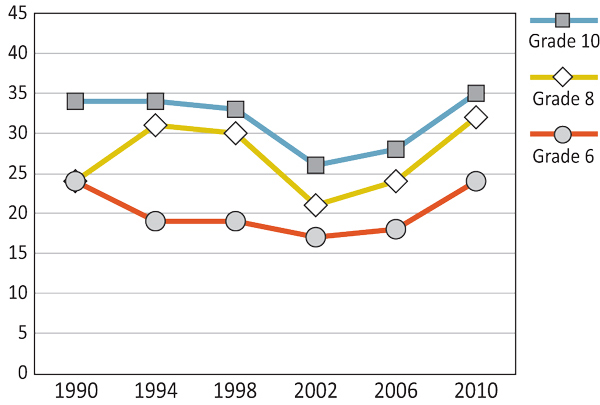
Text Equivalent - Figure 3.10
Figure 3.10 is a line graph that shows the percentage of girls who think their parents expect too much of them, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 24% reported that their parents expect too much of them in 1990, compared to 19% in 1994, 19% 1998, 17% in 2002, 18% in 2006, and 24% in 2010. Among Grade 8 girls, 24% reported that their parents expect too much of them in 1990, compared to 31% in 1994, 30% 1998, 21% in 2002, 24% in 2006, and 32% in 2010. Among Grade 10 girls, 34% reported that their parents expect too much of them in 1990, compared to 34% in 1994, 33% in 1998, 26% in 2002, 28% in 2006, and 35% in 2010.
Across the six survey cycles, Grade 10 girls consistently reported the highest percentages of conflict with their parents (Figures 3.11 and 3.12). For boys, regardless of age, arguing with parents has decreased slightly since 1990. No clear pattern can be seen for girls. Overall, older students, compared to younger students, reported higher rates of parental conflict, while girls in Grades 8 and 10 reported higher levels than boys in those grades.
Figure 3.11: Boys who report having a lot of arguments with their parents (%)

Text Equivalent - Figure 3.11
Figure 3.11 is a line graph that shows the percentage of boys who report having a lot of arguments with their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 26% reported arguing a lot with their parents in 1990, compared to 20% in 1994, 19% in 1998, 14% in 2002, 17% in 2006, and 17% in 2010. Among Grade 8 boys, 27% reported arguing a lot with their parents in 1990, compared to 24% in 1994, 26% in 1998, 20% in 2002, 20% in 2006, and 20% in 2010. Among Grade 10 boys, 30% reported arguing a lot with their parents in 1990, compared to 31% in 1994, 29% in 1998, 26% in 2002, 23% in 2006, and 23% in 2010.
Figure 3.12: Girls who report having a lot of arguments with their parents (%)
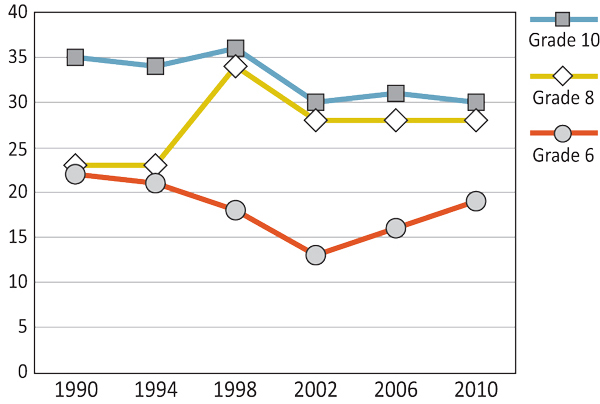
Text Equivalent - Figure 3.12
Figure 3.12 is a line graph that shows the percentage of girls who report having a lot of arguments with their parents, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 22% reported arguing a lot with their parents in 1990, compared to 21% in 1994, 18% in 1998, 15% in 2002, 17% in 2006, and 19% in 2010. Among Grade 8 girls, 22% reported arguing a lot with their parents in 1990, compared to 33% in 1994, 35% in 1998, 29% in 2002, 29% in 2006, and 29% in 2010. Among Grade 10 girls, 37% reported arguing a lot with their parents in 1990, compared to 36% in 1994, 38% in 1998, 31% in 2002, 33% in 2006, and 31% in 2010.
Home Life
Throughout the survey years, a high proportion of students reported that they had a happy home life, with Grade 6 students consistently reporting the highest rates (Figures 3.13 and 3.14). Although there is a marked decrease in having a happy home life as students got older, a majority of Grade 10 boys (75%) and Grade 10 girls (66%) reported positively on their home life in the 2010 survey year. Generally, boys were more likely to report having a happy home life compared to girls.
Figure 3.13: Boys who report having a happy home life (%)
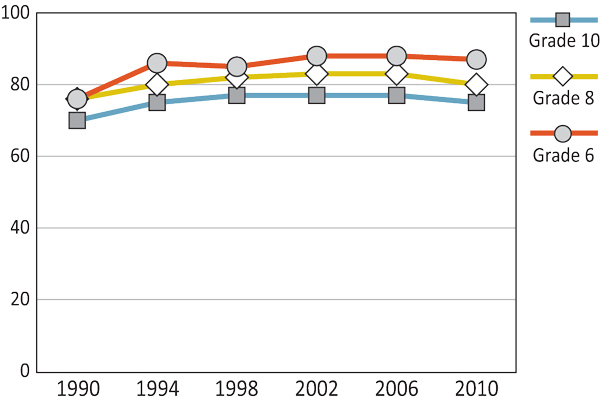
Text Equivalent - Figure 3.13
Figure 3.13 is a line graph that shows the percentage of boys who report having a happy home life, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 76% reported having a happy home life in 1990, compared to 86% in 1994, 85% in 1998, 88% in 2002, 88% in 2006, and 87% in 2010. Among Grade 8 boys, 76% reported having a happy home life in 1990, compared to 80% in 1994, 82% in 1998, 83% in 2002, 83% in 2006, and 80% in 2010. Among Grade 10 boys, 70% reported having a happy home life in 1990, compared to 75% in 1994, 77% in 1998, 77% in 2002, 77% in 2006, and 75% in 2010.
Figure 3.14: Girls who report having a happy home life (%)
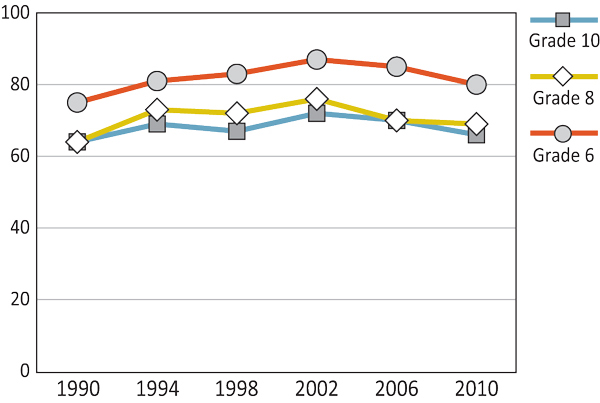
Text Equivalent - Figure 3.14
Figure 3.14 is a line graph that shows the percentage of girls who report having a happy home life, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 75% reported having a happy home life in 1990, compared to 81% in 1994, 83% in 1998, 87% in 2002, 85% in 2006, and 80% in 2010. Among Grade 8 girls, 64% reported having a happy home life in 1990, compared to 73% in 1994, 72% in 1998, 76% in 2002, 70% in 2006, and 69% in 2010. Among Grade 10 girls, 64% reported having a happy home life parents in 1990, compared to 69% in 1994, 67% in 1998, 72% in 2002, 70% in 2006, and 66% in 2010.
Since 1990, as seen in Figures 3.15 and 3.16, students across the grade levels have reported a decreasing desire to leave home with a marked decrease between the 1998 and 2002 surveys. Girls were much more likely to report that they would like to leave home than boys, particularly in higher grades. In 2010, for example, 36% of Grade 10 girls reported wanting to leave home at times, whereas 27% of Grade 10 boys reported the same.
Figure 3.15: Boys who agree with the statement, 'There are times I would like to leave home.' (%)
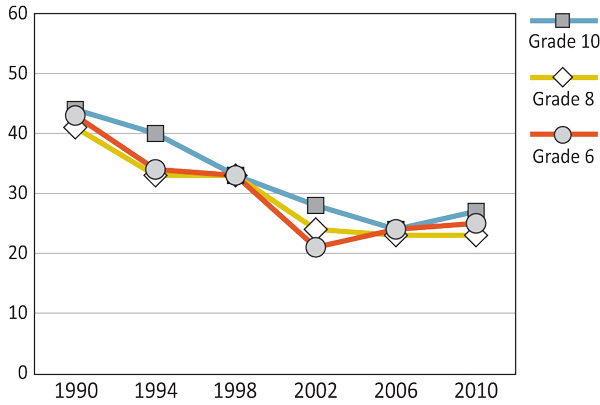
Text Equivalent - Figure 3.15
Figure 3.15 is a line graph that shows the percentage of boys who agree with the statement, “There are times I would like to leave home�, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 43% agree with the statement, “There are times I would like to leave home� in 1990, compared to 34% in 1994, 33% in 1998, 21% in 2002, 24% in 2006, and 25% in 2010. Among Grade 8 boys, 41% agree with the statement, “There are times I would like to leave home� in 1990, compared to 33% in 1994, 33% in 1998, 24% in 2002, 23% in 2006, and 23% in 2010. Among Grade 10 boys, 44% agree with the statement, “There are times I would like to leave home� in 1990, compared to 40% in 1994, 33% in 1998, 28% in 2002, 24% in 2006, and 27% in 2010.
Figure 3.16: Girls who agree with the statement, 'There are times I would like to leave home.' (%)

Text Equivalent - Figure 3.16
Figure 3.16 is a line graph that shows the percentage of girls who agree with the statement, “There are times I would like to leave home�, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 42% agree with the statement, “There are times I would like to leave home� in 1990, compared to 35% in 1994, 31% in 1998, 23% in 2002, 23% in 2006, and 28% in 2010. Among Grade 8 girls, 51% agree with the statement, “There are times I would like to leave home� in 1990, compared to 42% in 1994, 43% in 1998, 28% in 2002, 31% in 2006, and 34% in 2010. Among Grade 10 girls, 55% agree with the statement, “There are times I would like to leave home� in 1990, compared to 51% in 1994, 46% in 1998, 37% in 2002, 34% in 2006, and 36% in 2010.
The Employment Insurance Act (EIA), passed in 1996, sets out the basic framework of eligibility to receive entitlements for Parental Benefits. Individuals who are adopting a child or are caring for one or more newborn children may be entitled to receiving parental benefits.
Under the EI program, parental benefits are payable to one or both parents up to and including for 35 weeks. Parental benefits, therefore, provide a means of financial support that allows a parent(s) to be away from her/his work to care for the child.
(Service Canada, 2013)
Administered by the Canada Revenue Agency, the Canada Child Tax Benefit (CCTB) aims to help eligible Canadian families with the cost of raising children under the age of 18. This tax-free monthly payment may include the national child benefit supplement (NCBS) and the child disability benefit (CDB). The CDB is a monthly benefit providing financial assistance for families caring for children with mental or physical impairments. Additionally, the NCBS is a joint initiative of federal, provincial, and territorial governments, and First Nations. Families may also qualify for an additional provincial and territorial child benefit and credit program, such as:
- Alberta family employment tax credit
- BC family bonus
- New Brunswick child tax benefit
- Newfoundland and Labrador child benefit
- Northwest Territories child benefit
- Nova Scotia child benefit
- Nunavut child benefit
- Ontario child benefit
- Yukon child benefit
(Canada Revenue Agency, n.d.; 2008; 2013)
Summary and Implications
Since the 1990s, Canadian youth have reported stronger supportive ties to their parents. Feelings of being understood and trusted by their parents, as well as ease of communication with their mother and father, are four key indicators. These indicators represent such supportive ties to parents and suggest a partial picture of the mental health and well-being of youth across Canada.
Over the six survey cycles, a high proportion of Canadian youth felt they had a happy home life. While older students are less likely to report having a happy home life, the majority of students have reported positively on their home life since 1990. Generally, boys were more likely than girls to report having a happy home life. In contrast, Canadian youth have reported a decreasing desire to leave home, presenting rates in the most recent survey 14%-19% lower than the first survey year. Although there has been a decline in the number of youth who report wanting to leave home, overall girls have been more likely to feel this way than boys, particularly as they got older.
While the reports of parental expectations remained stable until the 2006 survey, during the last survey interval (2006-2010), Canadian youth across all grade levels reported between a 4%-9% increase in their feeling of parental pressure with respect to their schooling. This shift in perceived pressure from parents may be as a result of the changing context of school, where standardized testing plays a central role in monitoring student achievement, as well as shaping and guiding instruction, curriculum, and policy (Klinger, DeLuca, & Miller, 2008). This increasing trend indicates the need to continue efforts to mitigate or manage parental expectations.
Parental benefits in Canada may increase the quality of home life as the mother and/or father can directly bond and care for all their child(ren). The positive increase in students' feelings of being understood and trusted by parents, and the increasing ease of communication with parents, can be situated in a cultural context where the importance of parental care has been recognized by legislation. Aligning with these contributions, the Canadian Child Tax Benefit helps to alleviate the financial pressures placed on parents by providing eligible families with a tax-free monthly benefit payment. This reduction in financial pressure may further help to positively support the overall quality of home life for Canadian youth.
References
- Brown, J., & Mann, L. (1990). The relationship between family structure and process variables and adolescent decision making. Journal of Adolescence, 13, 25-37.
- Brown, S. (2004). Family structure and child well-being: The significance of parental cohabitation. Journal of Marriage and Family, 66, 351-367. doi:10.1111/j.1741-3737.2004.00025.
- Canada Revenue Agency (n.d.). National Child Benefits.
- Canada Revenue Agency (2008). National Child Benefit .
- Canada Revenue Agency (2013). Canada child tax benefit (CCTB).
- Driscoll, A., Russell, S., Crockett, L. (2008). Parenting styles and youth well-being across immigrant populations. Journal of Family Studies, 29, 185-209. doi:10.1177/0192513X07307843
- Finkenauer, C., Engels, R., Baumeister, R. (2010). Parenting behaviour and adolescent behavioural and emotional problems: the role of self-control. International Journal of Behavioural Development, 29, 58-69. doi: 10.1080/01650250444000333
- Gray, M.R., Steinberg, L. (1999). Unpacking authoritative parenting: Reassessing a multidimensional construct. Journal of Marriage and the Family, 61, 574-587.
- Klinger, D.A., DeLuca, C., Miller, T. (2008). The evolving culture of large-scale assessments in Canadian education. Canadian Journal of Educational Administration and Policy, 76(3), 1-34.
- Laursen, B., Collins, W.A. (1994). Interpersonal conflict during adolescence. Psychological Bulletin, 115, 197-209. doi:10.1037//0033-2909.115.2.197
- Lerner, R.M., Steinberg, L. (Eds.) 2004. Handbook of adolescent psychology (2nd ed.). Hoboken, NJ: Wiley.
- Moreno, C., Borup, I., del Carmen Grando-Alcón, M., Zaborskis, A., Dellago, L. (2008). Section 1: Social context. Family Culture. In C. Currie, S. Nic Gabhainn, E. Godeau, C. Roberts, R. Smith, … V. Barnekow (Eds.), Inequalities in young people's health: HBSC international report from the 2005/2006 survey. Health policy for children and adolescents, No 5 (pp. 21-28), WHO Regional Office for Europe, Copenhagen, Denmark.
- Service Canada (2013). Employment insurance maternity and parental benefits .
- Sessa, F.M., Steinberg, L. (1991). Family structure and the development of autonomy during adolescence. The Journal of Early Adolescence, 11, 38-55. doi:10.1177/0272431691111003
- Shaffer, A., Suveg, C., Thomassin, K., Bradbury, L. (2012). Emotion socialization in the context of family risks: Links to child emotion regulation. Journal of Child and Family Studies, 21, 917-924. doi:10.1007/s10826-011-9551-3
- Smetana, J.G., Campione-Barr, N., Metzger, A. (2006). Adolescent development in interpersonal and societal contexts. Annual Review of Psychology, 57, 255-284. doi:10.1146/annurev.psych.57.102904.190124
- Wolfradt, U., Hempel, S., Miles, J. (2003). Perceived parenting styles, depersonalization, anxiety and coping behaviour in adolescents. Personality and Individual Differences, 23, 521-532.
Chapter 4: School
By Sean Cousins
The Importance of the School Environment
The school is a setting in which many Canadian youth spend a majority of their scheduled time. During their time at school, youth experience a range of activities that shape their cognitive development, as well as influence perceptions of their physical and mental health. The school environment is strongly associated with how school-aged children perceive themselves in the context of their peers and with their teachers (Koth, Bradshaw, & Leaf, 2008), and the school environment, teachers, peers, and other adults can have a strong influence on individual children during important developmental stages (World Health Organization [WHO], 1999).
Positive health outcomes and behaviours of students are correlated with schools that promote vibrant and diverse learning experiences (Connop & King, 1999; Ma, 2007). Young people who feel welcomed in their school are much less likely to participate in activities that pose a significant risk to their mental health and emotional well-being (Suldo, McMahan, Chappel, & Loker, 2012). Young people require strong peer relations to develop healthy social experiences at school and positive behaviours in the context of their developing lives. However, when young people feel disconnected from their immediate school environment, they tend to form negative self-perceptions (King, Vidourek, Davis, & McLellan, 2002) and are more likely to participate in high-risk behaviours, such as substance abuse and unprotected sexual activities (Phillips-Howard et al., 2010; Roeser, Eccles, & Sameroff, 2000; Shochet, Dadds, Ham, & Montague, 2006).
What are We Reporting in this Chapter?
This chapter highlights results of previously administered surveys. For some survey items, we have trends that begin in 1990, while, for others, the item has only been on the survey since 2002. These results include several indicators of the school environment, including academic achievement, school climate, and interactions with peers and teachers. Trends are divided into three sections: 1) educational experiences; 2) support and belonging; and 3) students' beliefs about school.
Trends that emerge in the previous iterations of the HBSC survey and the specific educational policies in place can help us better understand how students' perceptions of school and learning are changing over time. They can provide a greater insight into a context that tends to be related to students' physical and mental health.
Educational Experiences
Since 1990, as shown in Figures 4.1 and 4.2, a majority of young people have reported that their teachers thought their school work was good or very good. Students in Grade 6 were the most likely to report positive teacher perceptions of their school work as compared to students in both Grade 8 and Grade 10. As an example, differences as large as 14% for boys and 12% for girls between Grade 6 and Grade 10 were found on this item in the 2010 survey cycle. Girls were also more likely to believe their teachers thought their school work was good or very good than boys across all grades and survey years.
Figure 4.1: Boys who report that teachers think their school work is good or very good (%)
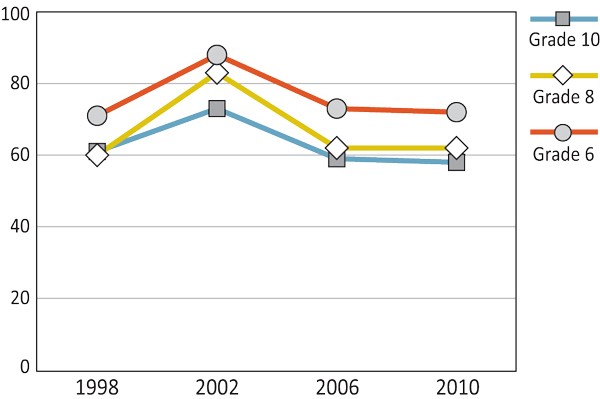
Text Equivalent - Figure 4.1
Figure 4.1 is a line graph that shows the percentage of boys who report that teachers think their school work is good or very good, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 71% reported that teachers think their school work is good or very good in 1998, compared to 88% in 2002, 73% in 2006, and 72% in 2010. Among Grade 8 boys, 60% reported that teachers think their school work is good or very good in 1998, compared to 83% in 2002, 62% in 2006, and 62% in 2010. Among Grade 10 boys, 61% reported that teachers think their school work is good or very good in 1998, 73% in 2002, compared to 59% in 2006, and 58% in 2010.
Figure 4.2: Girls who report that teachers think their school work is good or very good (%)
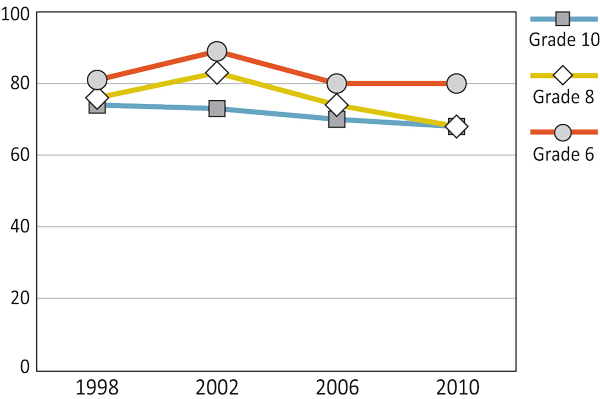
Text Equivalent - Figure 4.2
Figure 4.2 is a line graph that shows the percentage of girls report that teachers think their school work is good or very good, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 81% reported that teachers think their school work is good or very good in 1998, compared to 89% in 2002, 80% in 2006, and 80% in 2010. Among Grade 8 girls, 76% reported that teachers think their school work is good or very good in 1998, compared to 83% in 2002, 74% in 2006, and 68% in 2010. Among Grade 10 girls, 74% reported that teachers think their school work is good or very good in 1998, compared to 73% in 2002, 70% in 2006, and 68% in 2010.
While the majority of young people reported positive perceptions of their school work, they were much less likely to report that they liked school (Figures 4.3 and 4.4). Since 1990, less than half of young people reported liking school a lot. These numbers have generally remained stable over survey years. The students in Grade 6 were more likely to report they liked school as compared to students in either Grade 8 or Grade 10. The students in Grade 8 and Grade 10 tended to report similar levels of liking school. Girls reported higher levels of liking school a lot than boys.
Figure 4.3: Boys who like school a lot (%)
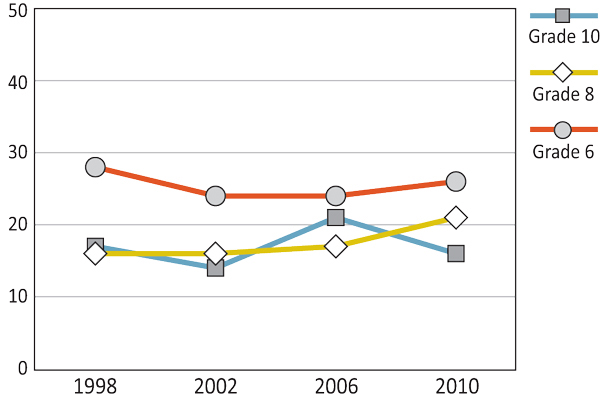
Text Equivalent - Figure 4.3
Figure 4.3 is a line graph that shows the percentage of boys who report that they like school a lot, by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 28% reported that they like school a lot in 1998, compared to 24% in 2002, 24% in 2006, and 26% in 2010. Among Grade 8 boys, 16% reported that they like school a lot in 1998, compared to 16% in 2002, 17% in 2006, and 21% in 2010. Among Grade 10 boys, 17% reported that they like school a lot in 1998, compared to 14% in 2002, 21% in 2006, and 16% in 2010.
Figure 4.4: Girls who like school a lot (%)
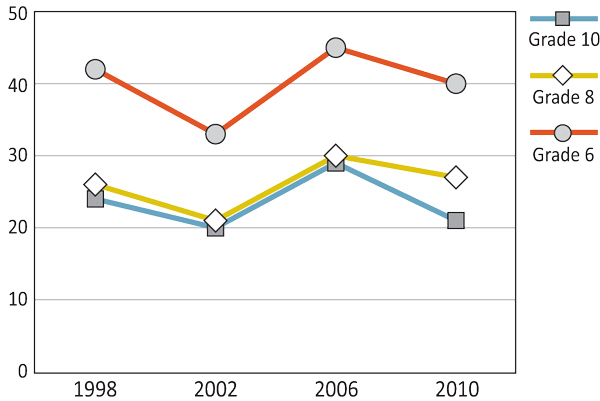
Text Equivalent - Figure 4.4
Figure 4.4 is a line graph that shows the percentage of girls who report that they like school a lot, by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 42% reported that they like school a lot in 1998, compared to 33% in 2002, 45% in 2006, and 40% in 2010. Among Grade 8 girls, 26% reported that they like school a lot in 1998, compared to 21% in 2002, 30% in 2006, and 27% in 2010. Among Grade 10 girls, 24% reported that they like school a lot in 1998, compared to 20% in 2002, 29% in 2006, and 21% in 2010.
Throughout the survey years of the HBSC study, a consistent portion of young people have reported feeling a lot of pressure because of school work (Figures 4.5 and 4.6). The proportions have remained stable over the years, with the lowest levels of school pressure being reported by boys and girls in Grade 6 and the highest levels being reported by girls in Grade 10. In the latest 2010 survey, young people in Grade 10 reported feeling pressured because of school work at rates 8% and 13% higher for boys and girls, respectively, compared to their Grade 6 counterparts.
Figure 4.5: Boys who feel a lot of pressure because of school work (%)
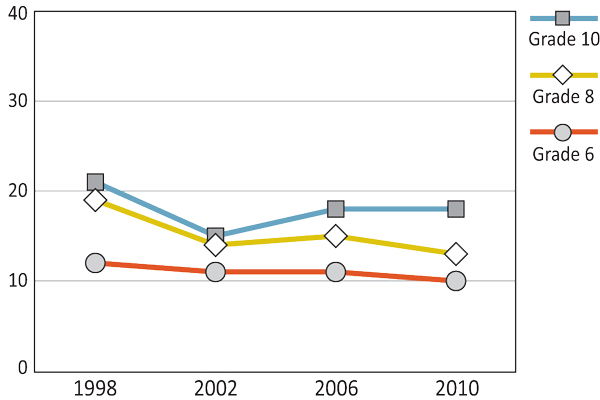
Text Equivalent - Figure 4.5
Figure 4.5 is a line graph that shows the percentage of boys who feel a lot of pressure because of school work, by grade, gender and year of survey. The graph shows that among Grade 6 boys, 12% of boys reported feeling a lot of pressure because of school work in 1998, compared to 11% in 2002, 11% in 2006, and 10% in 2010. Among Grade 8 boys, 19% reported feeling a lot of pressure because of school work in 1998, compared to 14% in 2002, 15% in 2006, and 13% in 2010. Among Grade 10 boys, 21% reported feeling a lot of pressure because of school work in 1998, compared to 15% in 2002, 18% in 2006, and 18% in 2010.
Figure 4.6: Girls who feel a lot of pressure because of school work (%)
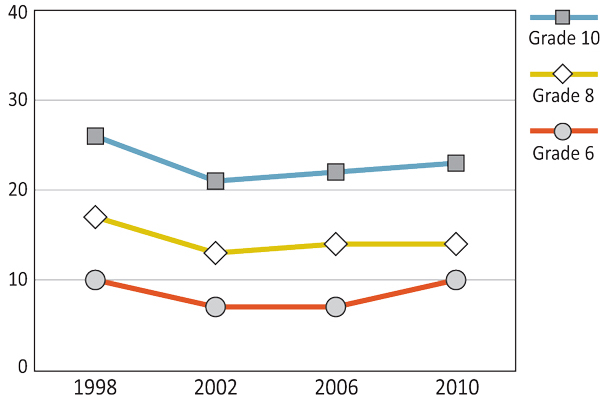
Text Equivalent - Figure 4.6
Figure 4.6 is a line graph that shows the percentage of girls who feel a lot of pressure because of school work, by grade, gender and year of survey. The graph shows that among Grade 6 girls, 10% reported feeling a lot of pressure because of school work in 1998, compared to 7% in 2002, 7% in 2006, and 10% in 2010. Among Grade 8 girls, 17% reported feeling a lot of pressure because of school work in 1998, compared to 13% in 2002, 14% in 2006, and 14% in 2010. Among Grade 10 girls, 26% report feeling a lot of pressure because of school work in 1998, compared to 21% in 2002, 22% in 2006, and 23% in 2010.
Support and Belonging
As shown in Figures 4.7 and 4.8, the majority of young people surveyed believe that other students accept them as they are. However, over the past three cycles of the HBSC in Canada (2002, 2006, and 2010), the proportion of young people who feel other students accept them has been declining, with the largest declines occurring in Grade 10 for boys and Grade 8 and 10 for girls. The decline for Grade 10 boys was 6% over this time period, while the drop for Grade 8 and Grade 10 girls was 8% and 5% respectively.
Figure 4.7: Boys who agree or strongly agree with the statement, 'Other students accept me as I am.' (%)
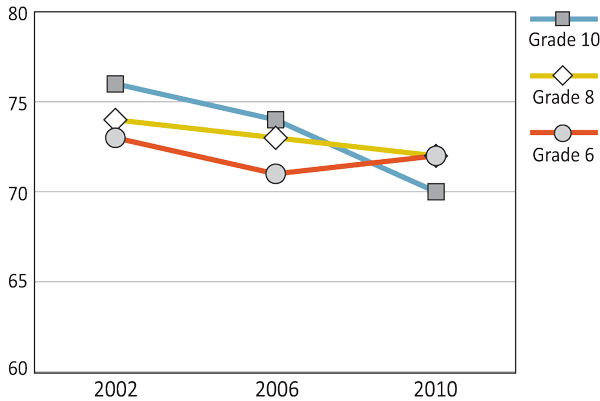
Text Equivalent - Figure 4.7
Figure 4.7 is a line graph that shows the percentage of boys who agree or strongly agree with the statement, “Other students accept me as I am.� by grade, gender and year of survey. The graph shows that among Grade 6 boys, 73% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 71% in 2006, and 72% in 2010. Among Grade 8 boys, 74% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 73% in 2006, and 72% in 2010. Among Grade 10 boys, 76% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 74% in 2006, and 70% in 2010.
Figure 4.8: Girls who agree or strongly agree with the statement, 'Other students accept me as I am.' (%)
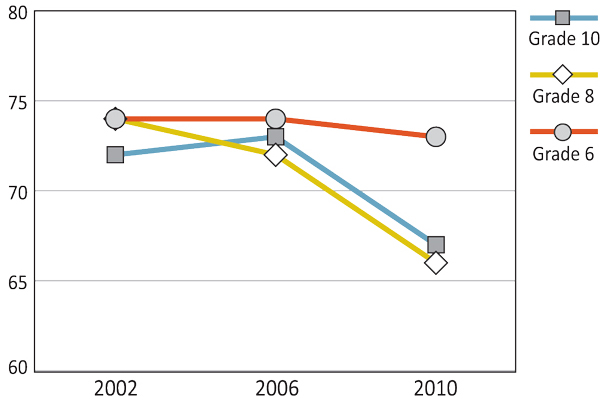
Text Equivalent - Figure 4.8
Figure 4.8 is a line graph that shows the percentage of girls who agree or strongly agree with the statement, “Other students accept me as I am.� by grade, gender and year of survey. The graph shows that among Grade 6 girls, 74% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 74% in 2006, and 73% in 2010. Among Grade 8 girls, 74% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 72% in 2006, and 66% in 2010. Among Grade 10 girls, 72% agree or strongly agree with the statement, “Other students accept me as I am.� in 2002, compared to 73% in 2006, and 67% in 2010.
The proportion of young people who feel they belong at school has tended to remain relatively constant over time for Grade 8 and 10 students (Figures 4.9 and 4.10). For Grade 6 students, this percentage has increased slightly over time. School belonging is largely unaffected by gender. Older students report lower levels of school belonging than do younger students.
Figure 4.9: Boys who agree or strongly agree with the statement, 'I feel like I belong at this school.' (%)

Text Equivalent - Figure 4.9
Figure 4.9 is a line graph shows the percentage of boys who agree or strongly agree with the statement, “I feel like I belong at this school.� by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 65% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 62% in 1998, 57% in 2002, 62% in 2006, and 71% in 2010. Among Grade 8 boys, 55% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 53% in 1998, 50% in 2002, 48% in 2006, and 61% in 2010. Among Grade 10 boys, 58% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 59% in 1998, 57% in 2002, 60% in 2006, and 57% in 2010.
Figure 4.10: Girls who agree or strongly agree with the statement, 'I feel like I belong at this school.' (%)
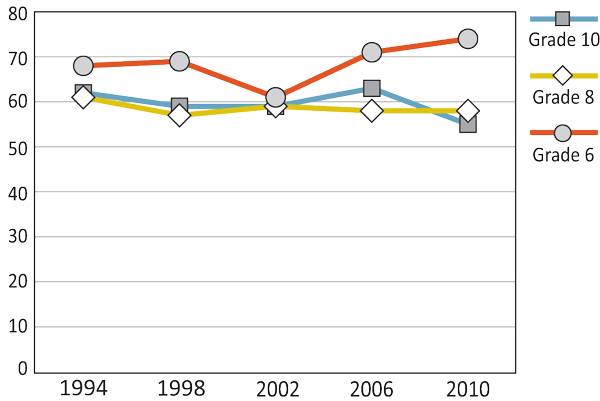
Text Equivalent - Figure 4.10
Figure 4.10 is a line graph shows the percentage of girls who agree or strongly agree with the statement, “I feel like I belong at this school.� by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 68% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 69% in 1998, 61% in 2002, 71% in 2006, and 74% in 2010. Among Grade 8 girls, 61% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 57% in 1998, 59% in 2002, 58% in 2006, and 58% in 2010. Among Grade 10 girls, 62% agree or strongly agree with the statement, “I feel like I belong at this school.� in 1994, compared to 59% in 1998, 59% in 2002, 63% in 2006, and 55% in 2010.
The majority of young people reported that students in their class(es) enjoyed being together (Figures 4.11 and 4.12). The percentage of agreement with the statement tended to be highest in 2002 when the surveys were generally administered later in the school year. Boys tended to be more likely to agree or strongly agree with the statement than girls.
Figure 4.11: Boys who agree or strongly agree with the statement, 'Students in my class(es) enjoy being together.' (%)
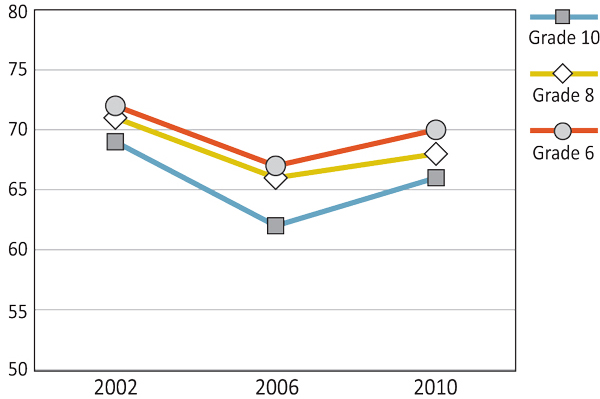
Text Equivalent - Figure 4.11
Figure 4.11 is a line graph shows the percentage of boys who agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 72% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, compared to 67% in 2002, and 70% in 2010. Among Grade 8 boys, 71% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, compared to 66% in 2006, and 68% in 2010. Among Grade 10 boys, 69% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, compared to 62% in 2006, and 66% in 2010.
Figure 4.12: Girls who agree or strongly agree with the statement, 'Students in my class(es) enjoy being together.' (%)
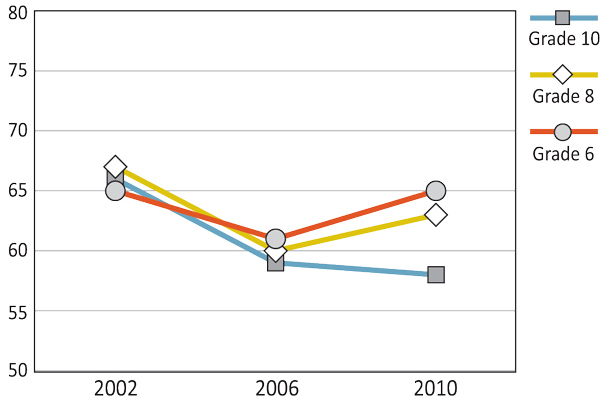
Text Equivalent - Figure 4.12
Figure 4.12 is a line graph shows the percentage of girls who agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 65% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, compared to 61% in 2006, and 65% in 2010. Among Grade 8 girls, 67% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, compared to 60% in 2006, and 63% in 2010. Among Grade 10 girls, 66% agree or strongly agree with the statement, “Students in my class(es) enjoy being together.� in 2002, 59% in 2006, and 58% in 2010.
Students' Beliefs about School
Figures 4.13 and 4.14 show the percentage of students who agree or strongly agree with the statement "our school is a nice place to be." There are minimal differences across time in student responses to this statement with the exception of lower agreement in 2002. Older students tend to agree with this statement less than do younger students. In Grade 6, girls are more likely to report their school is a nice place to be than boys, while there are minimal gender differences for Grade 10 students. Except for the most recent survey, there has been a tendency for Grade 8 girls to report their school as a nice place to be more than boys.
Figure 4.13: Boys who agree or strongly agree with the statement, 'Our school is a nice place to be.' (%)
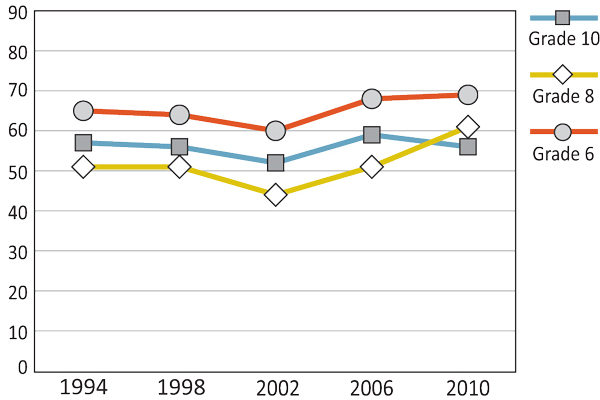
Text Equivalent - Figure 4.13
Figure 4.13 is a line graph that shows the percentage of boys who agree or strongly agree with the statement, “Our school is a nice place to be.� by grade, gender and year of survey. The graph shows that among Grade 6 boys, 65% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 64% in 1998, 60% in 2002, 68% in 2006, and 69% in 2010. Among Grade 8 boys, 51% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 51% in 1998, 44% in 2002, 51% in 2006, and 61% in 2010. Among Grade 10 boys, 57% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 56% in 1998, 52% in 2002, 59% in 2006, and 56% in 2010.
Figure 4.14: Girls who agree or strongly agree with the statement, 'Our school is a nice place to be.' (%)
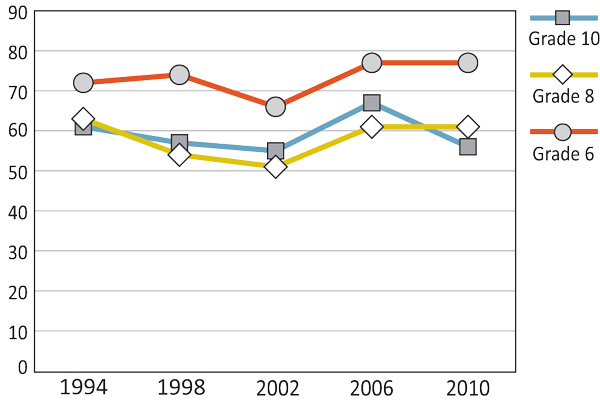
Text Equivalent - Figure 4.14
Figure 4.14 is a line graph that shows the percentage of girls who agree or strongly agree with the statement, “Our school is a nice place to be.� by grade, gender and year of survey. The graph shows that among Grade 6 girls, 72% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 74% in 1998, 66% in 2002, 77% in 2006, and 77% in 2010. Among Grade 8 girls, 63% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 54% in 1998, 51% in 2002, 61% in 2006, and 61% in 2010. Among Grade 10 girls, 61% agree or strongly agree with the statement, “Our school is a nice place to be.� in 1994, compared to 57% in 1998, 55% in 2002, 67% in 2006, and 56% in 2010.
The majority of Canadian adolescents surveyed think that their teachers treat them fairly (Figures 4.15 and 4.16). Grade 6 students tend to report the most positive perceptions of teacher fairness. In Grade 6, boys are less likely to report their teachers as treating them fairly than girls, while the reverse is true in Grade 10. There have been limited shifts in perceptions of teacher fairness across these four surveys.
Figure 4.15: Boys who agree or strongly agree with the statement, 'Our teachers treat us fairly.' (%)
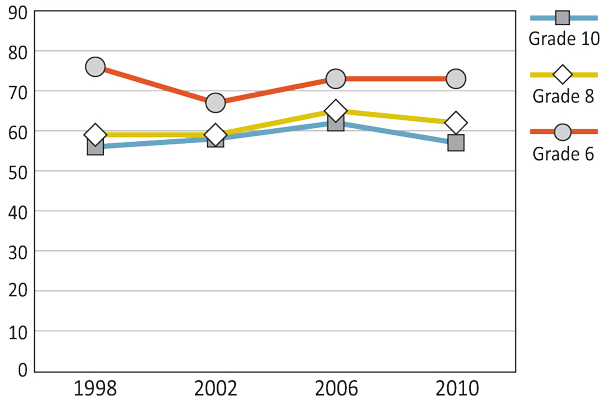
Text Equivalent - Figure 4.15
Figure 4.15 is a line graph that shows the percentage of boys who agree or strongly agree with the statement, “Our teachers treat us fairly.� by grade, gender, and year of survey. The graph shows that among Grade 6 boys, 76% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 67% in 2002, 73% in 2006, and 73% in 2010. Among Grade 8 boys, 59% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 59% in 2002, 65% in 2006, and 62% in 2010. Among Grade 10 boys, 56% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 58% in 2002, 62% in 2006, and 57% in 2010.
Figure 4.16: Girls who agree or strongly agree with the statement, 'Our teachers treat us fairly.' (%)
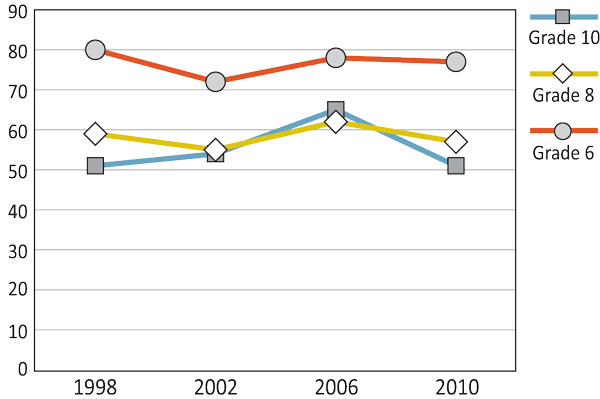
Text Equivalent - Figure 4.16
Figure 4.16 is a line graph that shows the percentage of girls who agree or strongly agree with the statement, “Our teachers treat us fairly.� by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 80% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 72% in 2002, 78% in 2006, and 77% in 2010. Among Grade 8 girls, 59% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 55% in 2002, 62% in 2006, and 57% in 2010. Among Grade 10 girls, 51% agree or strongly agree with the statement, “Our teachers treat us fairly.� in 1998, compared to 54% in 2002, 65% in 2006, and 51% in 2010.
Protecting the health and well-being of children and adolescents has been recognized as a national priority in Canada. In 2003, the Canadian Council of Ministers of the Environment called on the federal, provincial, and territorial governments to organize around issues relating to youth environmental health. Their call was based on evidence-based research that informed the drafting of a national framework designed to ensure special protection for children in publicly funded institutions. They stated that:
- Prevention of exposures is fundamental to protecting children's health;
- Best available science will play an integral role in the process of making decisions about children's environmental health;
- Children's vulnerabilities will be considered in developing environmental and health regulations, policies and standards; and
- Targeted environmental and health regulations, policies and standards may be required to protect children's health.
While it is reasonable to expect institutions to undertake efforts to reduce exposures to environmental hazards whenever and wherever possible, care-givers in day-cares, schools, and other educational settings in particular are held to a higher degree of responsibility because of their care for children, including vulnerable populations of children. School personnel, for example, are expected to minimize the risk of exposure to recognized hazards that would endanger the health and safety of the children and adolescents in their care. With a learning environment free of chemical, biological, and physical hazards, students can expect to have access to an education that is in keeping with the principles associated with environmental and workplace health.
(Health Canada, 2013)
Bully-victim problems, sexual harassment, and racial discrimination continue to be major public health concerns in Canada's elementary and secondary schools (Canadian Safe Schools Network, 2012). In the past decade, provincial and territorial governments across Canada have striven to develop positive and welcoming school cultures. However, the task to make optimal learning environments for youth in schools a reality remains an ongoing goal for educational stakeholders.
While safe schools legislation differs across Canada, such legislation incorporates a common framework for addressing the increased public concerns about youth violence in recent years. In 2008, British Columbia published Safe, Caring, and Orderly Schools, a guidebook that provides boards of education with provincial standards for codes of conduct, and identifies attributes of safe, caring, and orderly schools. In 2012, the National Assembly of Quebec passed similar legislation, specifically Bill 56, An Act to prevent and stop bullying in schools. This Act makes educational stakeholders and their partners responsible to see that their school provides a healthy and secure learning environment for every student to develop to his or her full potential, free from any form of bullying or violence. Similarly, in 2012, Nova Scotia introduced Private Member's Bill 28, otherwise known as An Act to Promote Safer, Inclusive and Peaceful Schools. While this Bill did not officially become law, it did address a vision for making possible objectives of promoting safer, more inclusive, and more peaceful schools across Nova Scotia.
(British Columbia Ministry of Education, 2008; Éducation, Loisir et Sport, Quebec, 2012; Nova Scotia Department of Education, 2012; Canadian Safe Schools Network, 2012)
Summary and Implications
The understanding of school found in the HBSC study over the survey years reveals one intriguing paradox. While the majority of Canadian young people school have reported not liking school a lot, these same young people have consistently reported being successful at school, and they have believed their teachers and peers supported them. Students' answers to the school items have remained fairly consistent over time with the exception of classmate acceptance, which has decreased. Grade 6 students generally saw their school experiences in a more positive light than Grade 10 students. Girls were more likely to report liking school a lot than boys, whereas boys were more in agreement with the statement that students enjoyed being together than girls. Other responses were largely gender-independent.
While the majority of Canadian youth report that the school is a positive place to be with positive social and learning interactions, there consistently has been a significant proportion of Canadian youth who have not reported such positive experiences. This group has been largest for Grades 8 and 10 students, the age at which many young people are in school environments where they begin to interact with different teachers and different students in various classrooms.
Given these findings, it is important that data representing the role of school in young people's lives continues to be examined and that the current initiatives to create healthy schools remain ongoing. These initiatives recognize the critical environment schools inhabit in the lives of adolescents.
References
- British Columbia Ministry of Education (2008). Safe, caring, and orderly schools: A guide.
- Canadian Safe Schools Network (2013). Our initiatives.
- Connop, H., King, A.J.C. (1999). Young women at risk. Toronto, Canada: University of Toronto Press.
- Éducation, Loisir et Sport, Quebec (2012). Projet de loi no. 56 (2012, chapitre 19): Loi visant à prévenir et à combattre l'intimidation et la violence à l'école.
- King, K., Vadourek, R., Davis, B., McLellan, W. (2002). Increasing self-esteem and school connectedness through multi-dimensional mentoring program. Journal of School Health, 72, 294-299.
- Koth, C.W., Bradshaw, C.P., Leaf, P.J. (2008). A multilevel study of predictors of student perceptions of school climate: The effect of classroom-level factors. Journal of Educational Psychology, 100, 96-104.
- Health Canada (2013). National strategic framework on children's environmental health.
- Ma, X. (2007). School experiences influence personal health and interpersonal relationships of adolescents: The Canadian case. School Effectiveness and School Improvement, 18, 209-240. doi:10.1080/09243450600909183
- Nova Scotia Department of Education (2012). Bill 28 (as introduced): Safer schools act.
- Phillips-Howard, P.A., Bellis, M.A., Briant, L.B., Jones, H. Downing, J., Kelly, I.E., Bird, T., Cook, P. A. (2010). Wellbeing, alcohol use and sexual activity in young teenagers: findings from a cross-sectional survey in school children in North West England. Substance Abuse Treatment, Prevention, and Policy, 5(27), 1-8. doi:10.1186/1747-597X-5-27
- Roeser R., Eccles, J.S., Sameroff, A.J. (2000). School as a context of early adolescents' academic and social-emotional development: A summary of research findings. The Elementary School Journal, 100, 443-71.
- Shochet, I.M., Dadds, M.R., Ham, D., Montague, R. (2006). School connectedness is an underemphasised parameter in adolescent mental health: Results of a community prediction study. Journal of Clinical Child and Adolescent Psychology, 35, 170-179.
- Suldo, S.M., McMahan, M.M., Chappel, A.M., Loker, T. (2012). Relationships between perceived school climate and adolescent mental health across genders. School Mental Health, 4, 69-80. doi:10.10007/s12310-012-9073-1
- World Health Organization [WHO] (1999). Improving health through schools: National and international strategies. Geneva, Switzerland: World Health Organization.
Chapter 5: Peers
By Heather Coe
Why are Peers Important?
Peers play an important role in the lives of adolescents. However, it is not just having friends that matters, but the quality of those relationships. The quality of friendships among youth has the potential to impact the lives of adolescents both positively and negatively (Hartup, 1996; Rusby, Forrester, Biglan, & Metzler, 2005). Peer support and high quality relationships among adolescents tend to have many positive outcomes, including social competence, altruism, and self-confidence (Hartup, 1996), as well as enjoyment and motivation for physical activity (Fitzgerald, Fitzgerald, & Aherne, 2012). In fact, high quality friendships buffer against adjustment problems, such as social anxiety (La Greca & Harrison, 2005) and drug use (Field et al., 2002). In addition, high quality friendships and peer interactions are associated with higher grade point average at school. Furthermore, high quality peer relationships positively influence the quality of other key relationships such as family (Field et al., 2002).
When compared to low support and low quality peer relationships, high quality relationships with a best friend or romantic partner are associated with greater overall well-being and lower levels of depression among youth (Field, Diego, & Sanders, 2002). In contrast, low quality relationships involving physical, verbal, and relational forms of peer victimization (e.g., hitting, name-calling, and social ostracism; Chen & Graham, 2012) are linked to higher levels of depression, anxiety, and loneliness, and lower self-esteem among youth (Graham & Juvonen, 1998; La Greca & Harrison, 2005). Furthermore, adolescents who are victimized by bullying are more likely to be rejected by their peers and less likely to have friends compared to youth who are not victimized (Juvonen, Graham, & Schuster, 2003). Moreover, victimized youth and adolescents involved in relationships with deviant peers may be more likely to engage in risky behaviours (such as skipping school, smoking cigarettes, drinking alcohol, and substance use) and may view the act of running away as a rational solution to family adversity (Chen, Adam, & Thrane, 2012; O'Brien, Albert, Chein, & Steinberg, 2011; Simons-Morton & Chen, 2006).
Given the salience and importance of peers in the lives and overall well-being of adolescents, it is important to examine peer interactions and relationships among Canadian youth. Understanding the nature and quality of peer relationships in Canadian youth should help promote proactive strategies for the development and maintenance of positive peer relationships.
What are We Examining in this Chapter?
In this chapter, we examine trends related to peer interactions and relationships among Canadian youth. These trends are divided into three categories: 1) interactions with friends; 2) ease of talking to friends; and 3) number of close friends. Some school based initiatives designed to promote healthy peer relationships are discussed.
In the HBSC surveys, reports on Grade 6, Grade 8, and Grade 10 student peer interactions were obtained. In particular, these reports provided an assessment of the percentage of students who spent four or five days a week with friends after school and the percentage of students who spent five or more nights a week with friends. In addition, the rates of young people who communicated with their friends by phone, text message, and email were assessed. Furthermore, students' ease of communication with friends of the opposite sex, friends of the same sex, and best friends are presented. Finally, trends related to the number of best friends are shown.
Interactions with Friends
The strongest pattern shown with respect to spending time with friends after school relates to the large difference between the results from 1994 and those from 2010 (see Figures 5.1 and 5.2). For boys, regardless of grade level, nearly one-half (45%-49%) reported spending four or five nights a week with their friends after school in 1994 compared to about one-third (32%-33%) in 2010. For girls, the numbers dropped from approximately one-third (32%-38%) in 1994 to around one-quarter (25%-26%) in 2010. For all groups except Grade 8 girls, spending time after school with friends was highest in 1994. For Grade 6 and Grade 8 students, it was lowest in 2010.
Figure 5.1: Boys who spend four or five days a week with friends right after school (%)

Text Equivalent - Figure 5.1
Figure 5.1 is a line graph that shows the percentage of boys who spend four or five days a week with friends right after school, by grade, gender and year of survey. The graph shows that among Grade 6 boys, 49% reported spending four or five days a week with friends right after school in 1994, compared to 37% in 1998, 44% in 2002, 43% in 2006, and 33% in 2010. Among Grade 8 boys, 45% reported spending four or five days a week with friends right after school in 1994, compared to 39% in 1998, 37% in 2002, 42% in 2006, and 33% in 2010. Among Grade 10 boys, 48% reported spending four or five days a week with friends right after school in 1994, compared to 38% in 1998, 37% in 2002, 31% in 2006, and 32% in 2010.
Figure 5.2: Girls who spend four or five days a week with friends right after school (%)
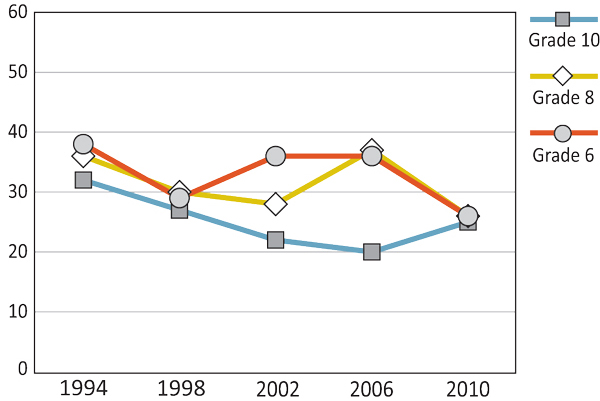
Text Equivalent - Figure 5.2
Figure 5.2 is a line graph that shows the percentage of girls who spend four or five days a week with friends right after school, by grade, gender and year of survey. The graph shows that among Grade 6 girls, 38% reported spending four or five days a week with friends right after school in 1994, compared to 29% in 1998, 36% in 2002, 36% in 2006, and 26% in 2010. Among Grade 8 girls, 36% reported spending four or five days a week with friends right after school in 1994, compared to 30% in 1998, 28% in 2002, 37% in 2006, and 26% in 2010. Among Grade 10 girls, 32% reported spending four or five days a week with friends right after school in 1994, compared with 27% in 1998, 22% in 2002, 20% in 2006, and 25% in 2010.
Figures 5.3 and 5.4 show that spending evenings with friends has a slightly different pattern than that of spending time with friends directly after school. Here the distinction is between the two surveys from the 1990s (1994 and 1998) and those conducted since 2000 (2002, 2006, 2010) with the percentages from the 1990s almost always exceeding the post-2000 numbers. There are limited grade and gender differences in spending evenings with friends.
Figure 5.3: Boys who spend five or more evenings a week with friends (%)
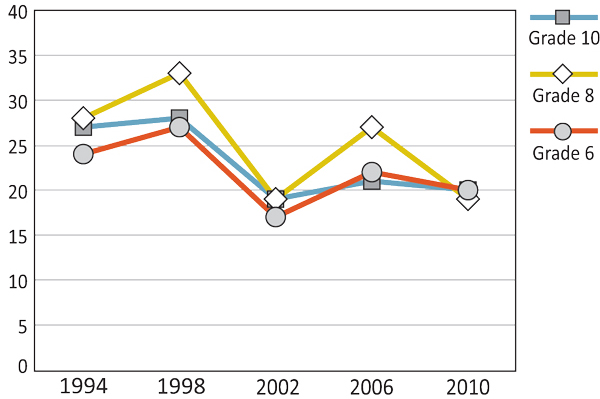
Text Equivalent - Figure 5.3
Figure 5.3 is a line graph that shows the percentage of boys who spend five or more evenings a week with friends, by grade, gender and year of survey. The graph shows that among Grade 6 boys, 24% reported spending five or more evenings a week with friends in 1994, compared to 27% in 1998, 17% in 2002, 22% in 2006, and 20% in 2010. Among Grade 8 boys, 28% reported spending five or more evenings a week with friends in 1994, compared to 33% in 1998, 19% in 2002, 27% in 2006, and 19% in 2010. Among Grade 10 boys, 27% reported spending five or more evenings a week with friends in 1994, compared to 28% in 1998, 19% in 2002, 21% in 2006, and 20% in 2010.
Figure 5.4: Girls who spend five or more evenings a week with friends (%)
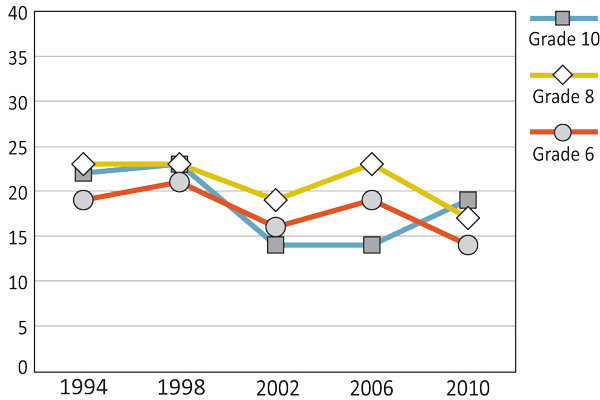
Text Equivalent - Figure 5.4
Figure 5.4 is a line graph that shows the percentage of girls who spend five or more evenings a week with friends, by grade, gender and year of survey. The graph shows that among Grade 6 girls, 19% reported spending five or more evenings a week with friends in 1994, compared to 21% in 1998, 16% in 2002, 19% in 2006, and 14% in 2010. Among Grade 8 girls, 23% reported spending five or more evenings a week with friends in 1994, compared to 23% in 1998, 19% in 2002, 23% in 2006, and 17% in 2010. Among Grade 10 girls, 22% reported spending five or more evenings a week with friends in 1994, compared to 23% in 1998, 14% in 2002, 14% in 2006, and 19% in 2010.
In 2002, the HBSC survey began to examine the percentage of students who talk on the phone, text, or email friends on a daily basis (Figures 5.5 and 5.6). Over the three survey years, girls have consistently displayed higher levels of digital communication across the grade levels than boys. In the 2010 survey, 65% of Grade 10 and 58% of Grade 8 girls reported talking on the phone, texting, or emailing friends daily. In the same survey year, 52% of Grade 10 and 39% of Grade 8 boys reported the same. Grade 6 girls and Grade 6 boys displayed the lowest levels of digital communication among Canadian youth, with 2010 survey reports of 32% and 23%, respectively.
Figure 5.5: Boys who talk on the phone, text, or email friends daily (%)
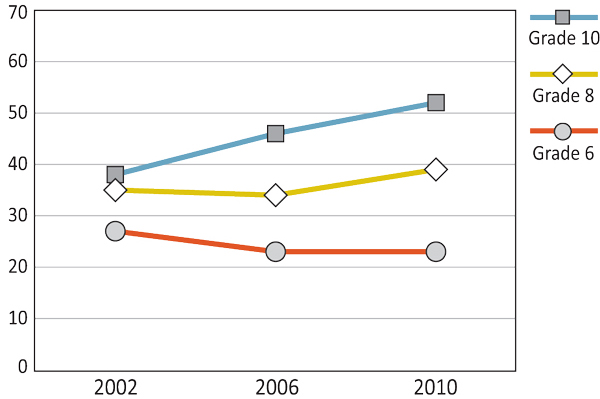
Text Equivalent - Figure 5.5
Figure 5.5 is a line graph that shows the percentage of boys who talk on the phone, text, or email friends daily by grade, gender and year of survey. The graph shows that among Grade 6 boys, 27% talk on the phone, text, or email friends daily in 2002, 23% in 2006, and 23% in 2010. Among Grade 8 boys, 35% talk on the phone, text, or email friends daily in 2002, 34% in 2006, and 39% in 2010. Among Grade 10 boys, 38% talk on the phone, text, or email friends daily in 2002, 46% in 2006, and 52% in 2010.
Figure 5.6: Girls who talk on the phone, text, or email friends daily (%)
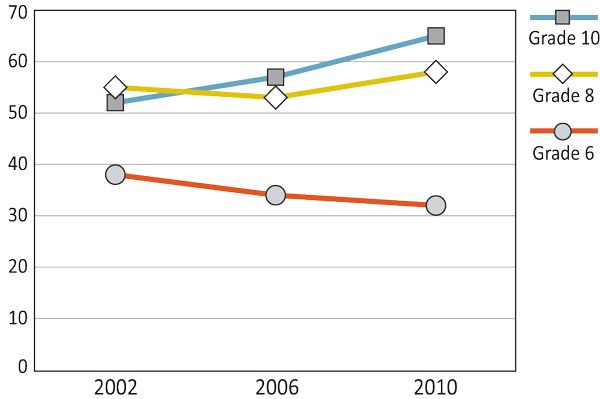
Text Equivalent - Figure 5.6
Figure 5.6 is a line graph that shows the percentage of girls who talk on the phone, text, or email friends daily by grade, gender and year of survey. The graph shows that among Grade 6 girls, 38% talk on the phone, text, or email friends daily in 2002, 34% in 2006, and 32% in 2010. Among Grade 8 girls, 55% talk on the phone, text, or email friends daily in 2002, 53% in 2006, and 58% in 2010. Among Grade 10 girls, 52% talk on the phone, text, or email friends daily in 2002, 57% in 2006, and 65% in 2010.
Ease of Talking to Friends
The percentage of students who find it easy to talk to friends of the opposite sex has remained relatively stable across the survey years (Figures 5.7 and 5.8). For both boys and girls, ease of talking to friends of the opposite sex increases with age. For example, in the 2010 surveys, 73% of Grade 10 students (both boys and girls) found it easy talking to friends of the opposite sex, whereas only 45% of Grade 6 boys and 37% of Grade 6 girls reported the same. Boys are more comfortable than girls in talking to friends of the opposite sex in Grade 6, but these gender differences disappear in Grades 8 and 10.
Figure 5.7: Boys who find it easy to talk to opposite sex friends (%)
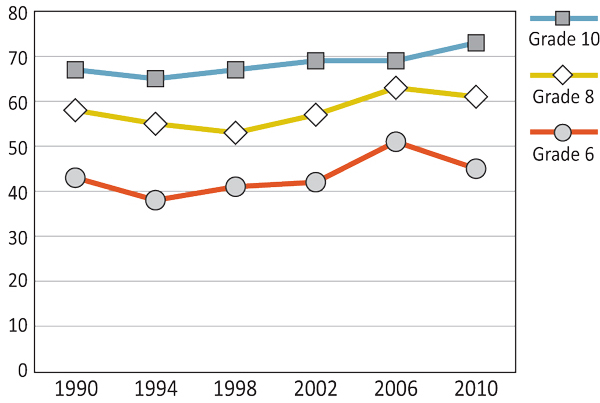
Text Equivalent - Figure 5.7
Figure 5.7 is a line graph that shows the percentage of boys who find it easy to talk to opposite sex friends by grade, gender and year of survey. The graph shows that among Grade 6 boys, 43% find it easy to talk to opposite sex friends in 1990, compared to 38% in 1994, 41% in 1998, 42% in 2002, 51% in 2006, and 45% in 2010. Among Grade 8 boys, 58% find it easy to talk to opposite sex friends in 1990, compared to 55% in 1994, 53% in 1998, 57% in 2002, 63% in 2006, and 61% in 2010. Among Grade 10 boys, 67% find it easy to talk to opposite sex friends in 1990, compared to 65% in 1994, 67% in 1998, 69% in 2002, 69% in 2006, and 73% in 2010.
Figure 5.8: Girls who find it easy to talk to opposite sex friends (%)
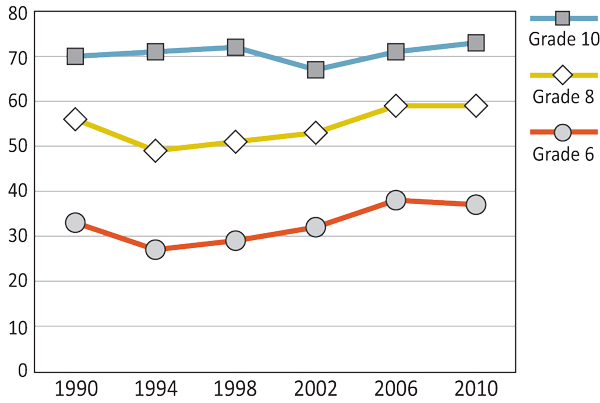
Text Equivalent - Figure 5.8
Figure 5.8 is a line graph that shows the percentage of girls who find it easy to talk to opposite sex friends by grade, gender and year of survey. The graph shows that among Grade 6 girls, 33% find it easy to talk to opposite sex friends in 1990, compared to 27% in 1994, 29% in 1998, 32% in 2002, 38% in 2006, and 37% in 2010. Among Grade 8 girls 56% find it easy to talk to opposite sex friends in 1990, compared to 49% in 1994, 51% in 1998, 53% in 2002, 59% in 2006, and 59% in 2010. Among Grade 10 girls, 70% find it easy to talk to opposite sex friends in 1990, compared to 71% in 1994, 72% in 1998, 67% in 2002, 71% in 2006, and 73% in 2010.
As illustrated in Figures 5.9 and 5.10, the percentage of students who find it easy to talk to friends of the same sex has decreased slightly over time. Grade 10 students typically display the highest levels of ease and Grade 6 students the lowest levels of ease, with girls displaying higher levels of ease than boys across all ag groups. For example, in the 2010 survey, 86% of Grade 10 girls reported ease in talking to friends of the same-sex, whereas only 75% of Grade 10 boys did so.
Figure 5.9: Boys who find it easy to talk to same sex friends (%)

Text Equivalent - Figure 5.9
Figure 5.9 is a line graph that shows the percentage of boys who find it easy to talk to same sex friends by grade, gender and year of survey. The graph shows that among Grade 6 boys, 76% find it easy to talk to same sex friends in 1990, compared to 69% in 1994, 65% in 1998, 69% in 2002, 73% in 2006, and 67% in 2010. Among Grade 8 boys, 80% find it easy to talk to same sex friends in 1990, compared to 74% in 1994, 65% in 1998, 69% in 2002, 73% in 2006, and 72% in 2010. Among Grade 10 boys, 81% find it easy to talk to same sex friends in 1990, compared to 78% in 1994, 77% in 1998, 74% in 2002, 73% in 2006, and 75% in 2010.
Figure 5.10: Girls who find it easy to talk to same sex friends (%)
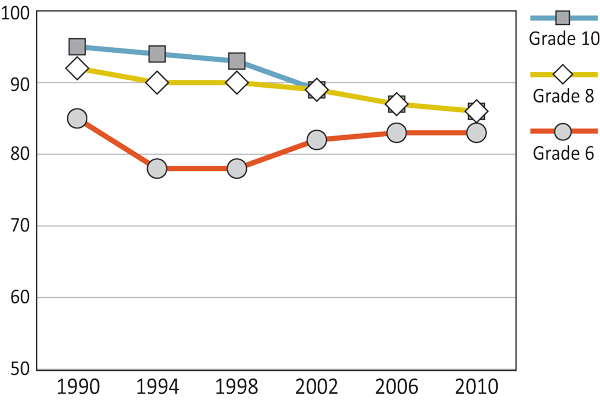
Text Equivalent - Figure 5.10
Figure 5.10 is a line graph that shows the percentage of girls who find it easy to talk to same sex friends by grade, gender and year of survey. The graph shows that among Grade 6 girls, 85% find it easy to talk to same sex friends in 1990, compared to 78% in 1994, 78% in 1998, 82% in 2002, 83% in 2006, and 83% in 2010. Among Grade 8 girls 92% find it easy to talk to same sex friends in 1990, compared to 90% in 1994, 90% in 1998, 89% in 2002, 87% in 2006, and 86% in 2010. Among Grade 10 girls, 95% find it easy to talk to same sex friends in 1990, compared to 94% in 1994, 93% in 1998, 89% in 2002, 87% in 2006, and 86% in 2010.
Ease of talking to one's best friend has remained stable over the three survey years examined (Figures 5.11 and 5.12). Girls consistently report higher levels of ease in talking to their best friend than do boys. Boys increase in their likelihood of finding it easy or very easy to talk to their best friend as they get older. The numbers for girls remain fairly consistent across the grades.
Figure 5.11: Boys who find it easy to talk to a best friend (%)
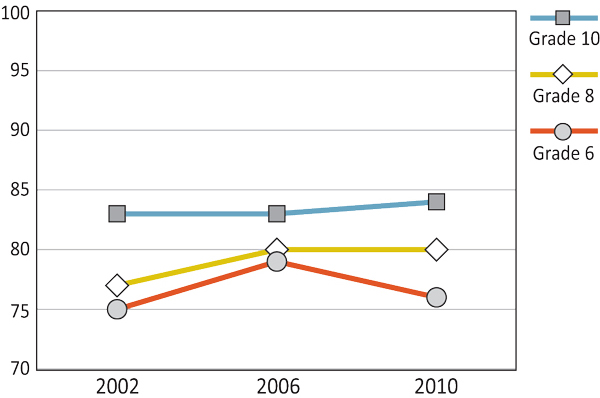
Text Equivalent - Figure 5.11
Figure 5.11 is a line graph that shows the percentage of boys who find it easy to talk to a best friend by grade, gender and year of survey. The graph shows that among Grade 6 boys, 75% find it easy to talk to a best friend in 2002, 79% in 2006, and 76% in 2010. Among Grade 8 boys, 77% find it easy to talk to a best friend in 2002, 80% in 2006, and 80% in 2010. Among Grade 10 boys, 83% find it easy to talk to a best friend in 2002, 83% in 2006, and 84% in 2010.
Figure 5.12: Girls who find it easy to talk to a best friend (%)

Text Equivalent - Figure 5.12
Figure 5.12 is a line graph that shows the percentage of girls who find it easy to talk to a best friend by grade, gender and year of survey. The graph shows that among Grade 6 girls, 85% find it easy to talk to a best friend in 2002, 89% in 2006, and 88% in 2010. Among Grade 8 girls, 91% find it easy to talk to a best friend in 2002, 90% in 2006, and 92% in 2010. Among Grade 10 girls, 92% find it easy to talk to a best friend in 2002, 91% in 2006, and 90% in 2010.
Number of Close Friends
Reports of having three or more close same sex friends have remained consistent across the three survey years reported (Figures 5.13 and 5.14). There are limited gender differences with respect to close same sex friends. Grade 10 students indicate they are less likely to have three or more close same sex friends than students in Grades 6 and 8. Overall, a large majority of students report having at least three close same sex friends.
Figure 5.13: Boys who have three or more close same sex friends (%)

Text Equivalent - Figure 5.13
Figure 5.13 is a line graph that shows the percentage of boys who have three or more close same sex friends by grade, gender and year of survey. The graph shows that among Grade 6 boys, 87% have three or more close same sex friends in 2002, 86% in 2006, and 86% in 2010. Among Grade 8 boys, 88% have three or more close same sex friends in 2002, 83% in 2006, and 86% in 2010. Among Grade 10 boys, 82% have three or more close same sex friends in 2002, 81% in 2006, and 79% in 2010.
Figure 5.14: Girls who have three or more close same sex friends (%)
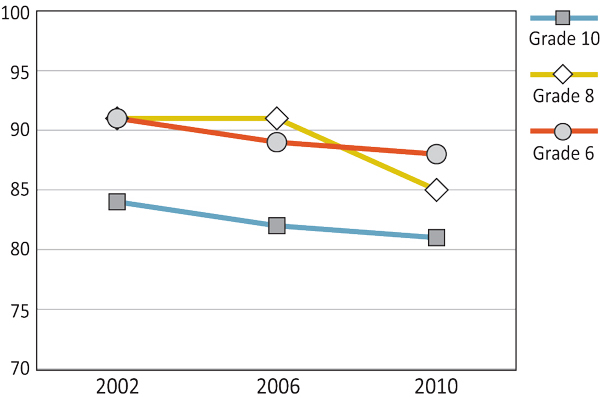
Text Equivalent - Figure 5.14
Figure 5.14 is a line graph that shows the percentage of girls who have three or more close same sex friends by grade, gender and year of survey. The graph shows that among Grade 6 girls, 91% have three or more close same sex friends in 2002, 89% in 2006, and 88% in 2010. Among Grade 8 girls, 91% have three or more close same sex friends in 2002, 91% in 2006, and 85% in 2010. Among Grade 10 girls, 84% have three or more close same sex friends in 2002, 82% in 2006, and 81% in 2010.
Student reports of having three or more close friends of the opposite-sex have stayed relatively consistent over the three survey years and across the grade levels (Figures 5.15 and 5.16). Grade 6 girls compared to boys in the same grade report more close opposite sex friends. There is no difference between boys and girls in Grade 8 and 10. Students are less likely to have three or more close opposite sex friends than they are to have three or more same sex friends.
Figure 5.15: Boys who have three or more close opposite sex friends (%)
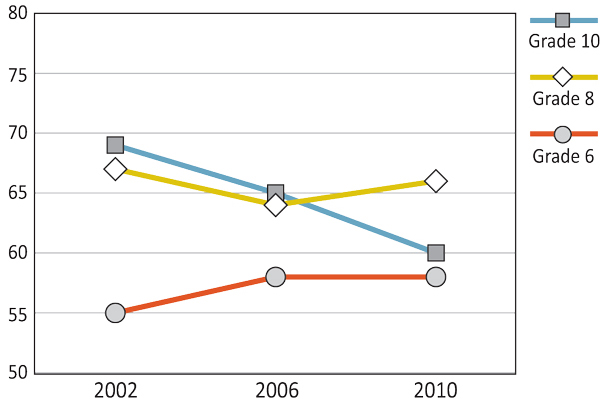
Text Equivalent - Figure 5.15
Figure 5.15 is a line graph that shows the percentage of boys who have three or more close opposite sex friends by grade, gender and year of survey. The graph shows that among Grade 6 boys, 55% have three or more close opposite sex friends in 2002, 58% in 2006, and 58% in 2010. Among Grade 8 boys, 67% have three or more close opposite sex friends in 2002, 64% in 2006, and 66% in 2010. Among Grade 10 boys, 69% have three or more close opposite sex friends in 2002, 65% in 2006, and 60% in 2010.
Figure 5.16: Girls who have three or more close opposite sex friends (%)
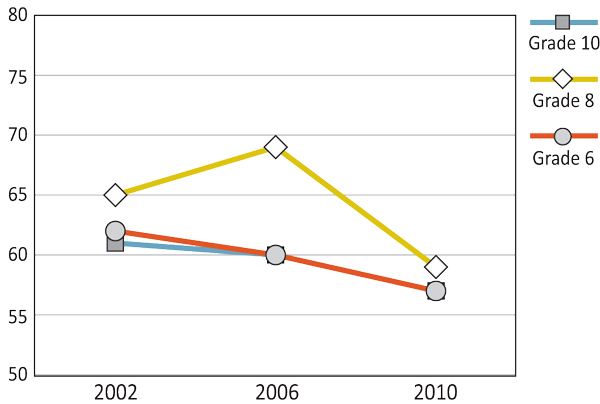
Text Equivalent - Figure 5.16
Figure 5.16 is a line graph that shows the percentage of girls who have three or more close opposite sex friends by grade, gender and year of survey. The graph shows that among Grade 6 girls, 62% have three or more close opposite sex friends in 2002, 60% in 2006, and 57% in 2010. Among Grade 8 girls, 65% have three or more close opposite sex friends in 2002, 69% in 2006, and 59% in 2010. Among Grade 10 girls, 61% have three or more close opposite sex friends in 2002, 60% in 2006, and 57% in 2010.
Within its Comprehensive School Health Framework, the Pan-Canadian Joint Consortium for School Health supports provinces and territories in the development of physically and emotionally healthy students. While encouraging learners to reach their full potential, this framework suggests that school health should be addressed in a planned, integrated, and holistic way. Also, within this framework, the social and physical environment is outlined as an important pillar to providing a strong foundation for comprehensive school health, emphasizing the importance of: the quality of the relationships among and between staff and students in the school; the emotional well-being of students; and relationships with families and the wider community.
In alignment with this framework, many provincial and territorial jurisdictions have implemented initiatives addressing peer relationships.
For example:
Healthy Schools
- Manitoba's school health initiative is designed to promote physical, emotional, and social health of students and school communities
- The province of Manitoba encourages the development of provincial health and wellness campaigns by providing funding to school to undertake projects that increase awareness of health issues and support school health.
- The most recent campaign to address peer relationships directly was the 'Healthy Relationships Campaign' in fall 2011. Throughout this campaign, schools engaged in various activities, including: school-wide relationship-building events; character education; goal setting (plans for longevity); and accessing resources.
Promoting a Positive School Climate
- Developed by the Ontario Ministry of Education as a tool to help schools encourage the development of healthy and respectful relationships among students and members of the school community.
- Promoting a Positive School Climate brings together ideas from various school initiatives that relate to relationships, including: character development; leadership development; and safe and healthy schools.
- Encourages students to be leaders and positive role models.
- Supports and reinforces positive behaviour. This support, in turn, provides students with opportunities to develop relationships that are free from discrimination, harassment, and racism.
(Joint Consortium for School Health, 2013; Ontario Ministry of Education, 2013; Province of Manitoba, 2012)
Summary and Implications
Across the survey years, the percentage of Canadian youth interacting with friends outside of school (after school and in the evening) has declined. The differences between the 1994 and 2010 surveys are particularly noticeable. The reduction in the percentage of youth reporting spending unstructured time with their peer is a possible area for concern. As the levels of peer interaction outside of school have declined, the percentage of Grade 8 and Grade 10 students engaged in digital communication with peers on a daily basis has increased, with girls consistently displaying the highest levels of digital peer interactions. In the most recent HBSC survey, Grade 10 girls displayed the highest levels of digital communication, with two-thirds reporting to talk on the phone, text, or email friends daily. The contrast between face-to-face and digital interaction supports the notion that the dynamics of peer relationships may be changing with time, moving from more direct forms of interactions to indirect. Such a shift may have implications for the psycho-social development of youth.
The number of close friends (only reported since 2002) and the ease of talking with these friends have remained relatively high and consistent across the survey years with a slight decline in ease of talking to close same sex friends. These statistics are encouraging and reveal that most adolescents have friends with whom they can communicate. The decline in ease of talking to close same sex friends mirrors the changing landscape of peer relationships, particularly evidenced in differences in time spent with friends in the 1994 versus the 2010 survey, and the move from more direct to less direct forms of communication.
As peer interactions and adolescent relationships continue to change with time, it is important that positive, high quality friendships are supported by the structures surrounding Canadian youth. Schools play an important role in the on-going social and emotional development of adolescents. In this respect, schools provide an ideal location for supporting healthy relationships among youth. Guided by greater understandings of the importance of schools promoting health, such as that seen in the Comprehensive School Health Framework, schools are beginning to implement projects and programming to encourage overall health and well-being among youth. If implemented effectively, these initiatives can encourage and support the development of positive peer relationships, which may, in turn, impact future HBSC findings.
References
- Chen, X., Adams, M., Thrane, L. (2012). Precursors of running away during adolescence: Do peers matter? Journal of Research on Adolescence, 22, 487-497. doi:10.1111/j.1532-7795.2012.00789.x
- Chen, X., Graham, S. (2012). Close relationships and attributions for peer victimization among late adolescents. Journal of Adolescence, 35, 1547-1556. doi:10.1016/j.adolescence.2012.06.003
- Crawford, A.M., Manassis, K. (2011). Anxiety, social skills, friendship quality, and peer victimization: An integrated model. Journal of Anxiety Disorders, 25, 924-931. doi:10.1016/j.janxdis.2011.05.005
- Field, T., Diego, M., Sanders, C. (2002). Adolescents' parent and peer relationships. Adolescence, 37, 121-130.
- Fitzgerald, A., Fitzgerald, N., Aherne, C. (2012). Do peers matter? A review of peer and/or friends' influence on physical activity among American adolescents. Journal of Adolescence, 35, 941-958. doi:10.1016/j.adolescence.2012.01.002
- Graham, S., Juvonen, J. (1998). Self-blame and peer victimization in middle school: An attributional analysis. Developmental Psychology, 34, 587-599.
- Hartup, W.W. (1996). The company they keep: Friendships and their developmental significance. Child Development, 67, 1-13.
- Juvonen, J., Graham, S., Schuster, M.A. (2003). Bullying among youth adolescents: The strong, the weak, and the troubled. Pediatrics, 112, 1231-1237.
- Joint Consortium for School Health [JCSH] (2013). Comprehensive school health framework.
- La Greca, A.M., Harrison, H.M. (2005). Adolescent peer relations, friendships, and romantic relationships: Do they predict social anxiety and depression? Journal of Clinical Child and Adolescent Psychology, 34, 49-61.
- O'Brien, L., Albert, D., Chein, J., Steinberg, L. (2011). Adolescents prefer more immediate rewards when in the presence of their peers. Journal of Research on Adolescence, 21, 747-753. doi:10.1111/j.1532-7795.2011.00738.x
- Ontario Ministry of Education (2013). Safe schools: Promoting a positive school climate.
- Province of Manitoba (2012). Healthy schools.
- Rubsy, J.C., Forrester, K.K., Biglan, A., Metzler, C.W. (2005). Relationships between peer harassment and adolescent problem behaviors. Journal of Early Adolescence, 25, 453-477. doi:10.1177/0272431605279837
- Simons-Morton, B., Chen, R.S. (2006). Over time relationships between early adolescent and peer substance use. Addictive Behaviors, 31, 1211-1223. doi:10.1016/j.addbeh.2005.09.006
- Waldrip, A.M., Malcolm, K.T., Jensen-Campbell, L.A. (2008). With a little help from your friends: The importance of high-quality friendships on early adolescent adjustment. Social Development, 17, 832-852. doi:10.1111/j.1467-9507.2008.00476.x
Chapter 6: Injury
By Ariel Pulver
Why is Injury an Important Issue?
Injury is a leading public health problem in Canada. Children and youth are disproportionately affected by injury compared with other groups, and it is the leading cause of death in such Canadian populations (Safe Kids Canada, 2006, 2011). Injury is costly in terms of direct health care costs as well as indirect costs and burdens placed on families, communities, and society. Injuries can result in substantial amounts of time lost for important developmental activities, such as extracurricular activities and time spent with friends, and can negatively impact school attendance (Hyman et al., 2007). Moreover, family members and others may be required to take time off from work and other duties to care for injured children and youth (Leitch, 2007).
The occurrence of injuries in young people is associated with a number of risk and protective factors. Examples include behaviours that predispose young people to risks, environmental factors that modify risks, use of protective equipment, and specific activities (Canadian Paediatric Society, 2012; Gropp, Janssen, & Pickett, 2013; Macpherson et al., 2002; Pickett, 2012). In that moderate amounts of risk-taking may be normative and perhaps inevitable, prevention strategies for young people need to recognize and manage their risks for injury (SMARTRISK online, n.d.). Another strategy to reduce injures involves optimizing environments to minimize risks (Centers for Disease Control, 2012).
Basic foundational information that describes patterns of injury occurrence is important for the planning of prevention strategies. Understanding time-related patterns in the occurrence of injury can be important. Changes in injury rates help to inform ongoing and innovative strategic planning and to identify new priority areas for management of this major public health issue.
What are We Reporting in this Chapter?
In this chapter we describe trends in injury over the years in Canadian young people by grade, gender, and year of survey (1994, 1998, 2002, 2006, and 2010). In the HBSC, "injury" is defined as any injury event reported in the last 12 months resulting in treatment by a doctor or nurse. One year is considered to be the time for which young people can accurately recall their injuries (Harel et al., 1994). Injuries that require significant medical treatment, including having to receive stitches, placement of a cast, or overnight admission in hospital, are considered to be "serious" injuries.
Injury trends are described further in three general sections of this chapter: 1) student injuries; 2) impact of injuries; and 3) where injuries occurred. Within these sections, we examine trends in the occurrence of various types of injuries: those requiring treatment from a doctor or nurse; students reporting multiple injuries in that time period according to the same definition; injuries resulting in five or more days lost from school or other usual activities; and locations where injuries occurred.
Student Injuries
The proportion of students reporting a medically treated injury in the past 12 months peaked in 2002 for both genders and across all grades, with higher percentages also reported in 2010 versus 1994 (Figures 6.1 and 6.2). Grade 6 students (both genders) consistently report the lowest rates of medically treated injury by grade. Boys report more injuries than girls in all grades.
Figure 6.1: Boys reporting one injury in the past 12 months requiring medical treatment by a doctor or nurse (%)

Text Equivalent - Figure 6.1
Figure 6.1 is a line graph that shows the percentage of boys who reported one injury in the past 12 months requiring medical treatment by a doctor or nurse by grade, gender, and year of survey. The graph shows that 34% of Grade 6 boys reported one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 38% in 1998, 55% in 2002, 44% in 2006, and 42% in 2010. Among Grade 8 boys, 42% reported one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 43% in 1998, 61% in 2002, 47% in 2006, and 47% in 2010. Among Grade 10 boys, 44% reported one injury in the past 12 months requiring medical treatment by a doctor or nurse activities in 1994, compared to 43% in 1998, 59% in 2002, 45% in 2006, and 46% in 2010.
Figure 6.2: Girls reporting one injury in the past 12 months requiring medical treatment by a doctor or nurse (%)
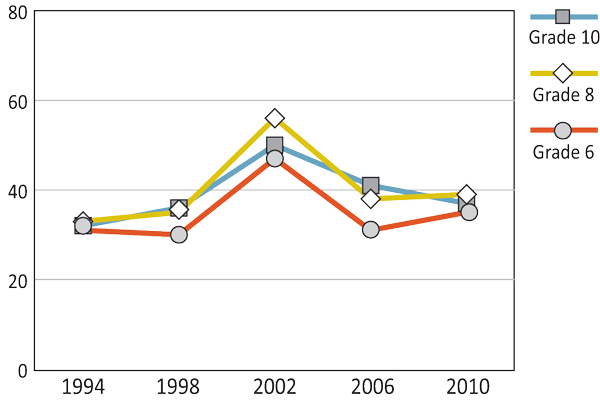
Text Equivalent - Figure 6.2
Figure 6.2 is a line graph that shows the percentage of girls who reported one injury in the past 12 months requiring medical treatment by a doctor or nurse by grade, gender, and year of survey. The graph shows that 31% of Grade 6 girls reported one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 30% in 1998, 47% in 2002, 31% in 2006, and 35% in 2010. Among Grade 8 girls, 33% reported one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 35% in 1998, 56% in 2002, 38% in 2006, and 39% in 2010. Among Grade 10 girls, 32% reported one injury in the past 12 months requiring medical treatment by a doctor or nurse activities in 1994, compared to 36% in 1998, 50% in 2002, 41% in 2006, and 37% in 2010.
As shown in Figures 6.3 and 6.4, the proportion of young people reporting multiple injury events has increased since the first survey cycle in 1994, with an uncharacteristic peak in the 2002 survey year, perhaps attributable to the change in survey methodology that year. In general, boys reported overall higher levels of multiple injury events requiring medical treatment than girls throughout the survey years, with Grade 10 boys reporting the highest rates of multiple injury events (26%) in the most recent cycle. Grade 6 students consistently present the lowest levels of multiple injury events. For example, in the most recent survey, 21% of Grade 6 boys and 16% of Grade 6 girls reported multiple injuries requiring medical treatment.
Figure 6.3: Boys reporting more than one injury in the past 12 months requiring medical treatment by a doctor or nurse (%)
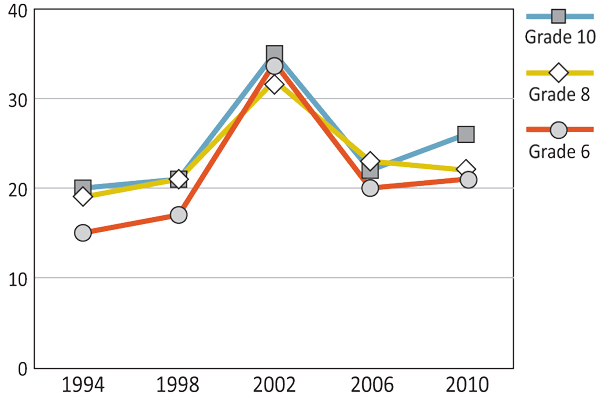
Text Equivalent - Figure 6.3
Figure 6.3 is a line graph that shows the percentage of boys who reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse by grade, gender, and year of survey. The graph shows that 15% of Grade 6 boys reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 17% in 1998, 34% in 2002, 20% in 2006, and 21% in 2010. Among Grade 8 boys, 19% reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 21% in 1998, 32% in 2002, 23% in 2006, and 22% in 2010. Among Grade 10 boys, 20% reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse activities in 1994, compared to 21% in 1998, 35% in 2002, 22% in 2006, and 26% in 2010.
Figure 6.4: Girls reporting more than one injury in the past 12 months requiring medical treatment by a doctor or nurse (%)
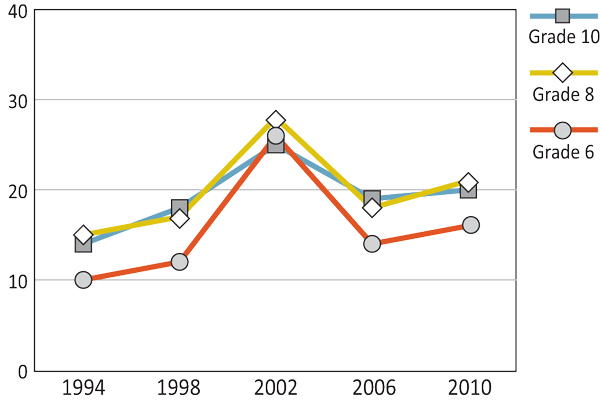
Text Equivalent - Figure 6.4
Figure 6.4 is a line graph that shows the percentage of girls who reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse by grade, gender, and year of survey. The graph shows that 10% of Grade 6 girls reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 12% in 1998, 26% in 2002, 14% in 2006, and 16% in 2010. Among Grade 8 girls, 15% reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse in 1994, compared to 17% in 1998, 28% in 2002, 18% in 2006, and 21% in 2010. Among Grade 10 girls, 14% reported more than one injury in the past 12 months requiring medical treatment by a doctor or nurse activities in 1994, compared to 18% in 1998, 25% in 2002, 19% in 2006, and 20% in 2010.
Impact of Injuries
With the exception of Grade 8 boys, the proportion of students in each grade and gender category who reported having missed five or more days of school or other activities due to an injury has increased since 1994 (Figures 6.5 and 6.6). Boys consistently reported missing school and other activities more frequently than girls in their grade. Moreover, the amount of time missed from these activities appears to increase with age.
Figure 6.5: Boys reporting injuries resulting in five or more days lost from school or usual activities (%)

Text Equivalent - Figure 6.5
Figure 6.5 is a line graph that shows the percentage of boys who reported injuries resulting in five or more days of lost from school or usual activities by grade, gender, and year of survey. The graph shows that 5% of Grade 6 boys reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 6% in 1998, 8% in 2002, 8% in 2006, and 6% in 2010. Among Grade 8 boys, 8% reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 7% in 1998, 9% in 2002, 8% in 2006, and 8% in 2010. Among Grade 10 boys, 9% reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 8% in 1998, 12% in 2002, 10% in 2006, and 10% in 2010.
Figure 6.6: Girls reporting injuries resulting in five or more days lost from school or usual activities (%)
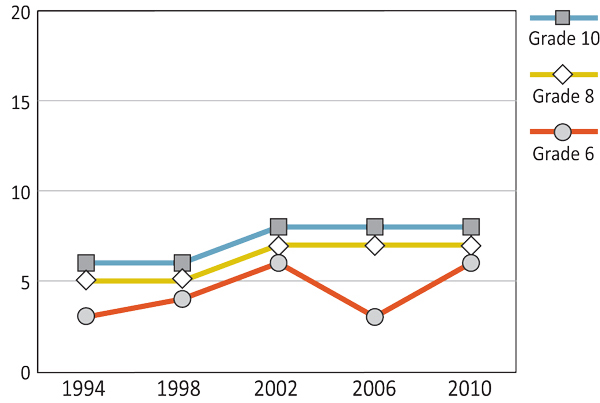
Text Equivalent - Figure 6.6
Figure 6.6 is a line graph that shows the percentage of girls who reported injuries resulting in five or more days of lost from school or usual activities by grade, gender, and year of survey. The graph shows that among Grade 6 girls, 3% reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 4% in 1998, 6% in 2002, 3% in 2006, and 6% in 2010. Among Grade 8 girls, 5% reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 5% in 1998, 7% in 2002, 7% in 2006, and 7% in 2010. Among Grade 10 girls, 6% reported injuries resulting in five or more days lost from school or usual activities in 1994, compared to 6% in 1998, 8% in 2002, 8% in 2006, and 8% in 2010.
The proportion of serious injury consistently remains highest for Grade 10 students, while youth in Grade 6 reported the lowest proportions injured. As with other injury events, injuries increased from 1994 to 2002, albeit slightly, before stabilizing or decreasing.
When all grades are considered together, reports of missing five or more days from school or usual activities due to injury remained fairly consistent over the years for both boys and girls. Despite the fact that injury remains a public health priority, the incidence of serious injury does not appear to have improved.
Where Injuries Occurred
Injuries most often occur at a sports facility or field, or at a home or yard. Over the survey cycles, reports of injuries occurring at a sports facility or field generally increased in the older grades (Figures 6.7 and 6.8). Among boys, youth in Grade 6 reported the lowest rates of injuries, which remained fairly consistent across survey cycles (24%-27%). Grade 8 boys remained in the middle, with rates reaching an all-time high of 39% in the most recent cycle. Grade 10 boys consistently reported the highest proportion of injuries occurring at a sports facility or field.
Figure 6.7: Boys - Proportion of the one most serious injury that occurred at a sports facility or field (%)
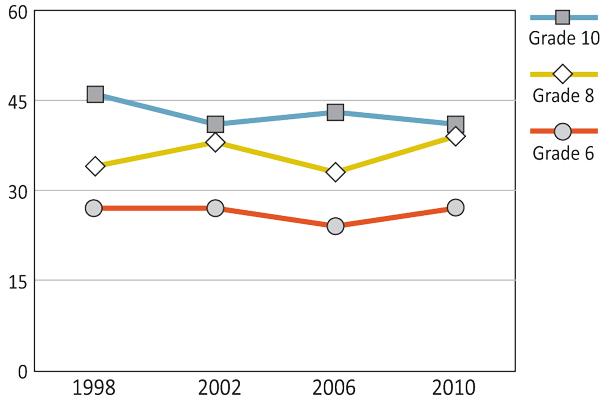
Text Equivalent - Figure 6.7
Figure 6.7 is a line graph that shows the percentage of boys who reported the proportion of the one most serious injury that occurred at a sports facility or field by grade, gender, and year of survey. The graph shows that 27% of Grade 6 boys reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, compared to 27% in 2002, 24% in 2006, and 27% in 2010. Among Grade 8 boys, 34% reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, compared to 38% in 2002, 33% in 2006, and 39% in 2010. Among Grade 10 boys, 46% reported more than one injury in the past 12 reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, compared to 41% in 2002, 43% in 2006, and 41% in 2010.
Figure 6.8: Girls - Proportion of the one most serious injury that occurred at a sports facility or field (%)
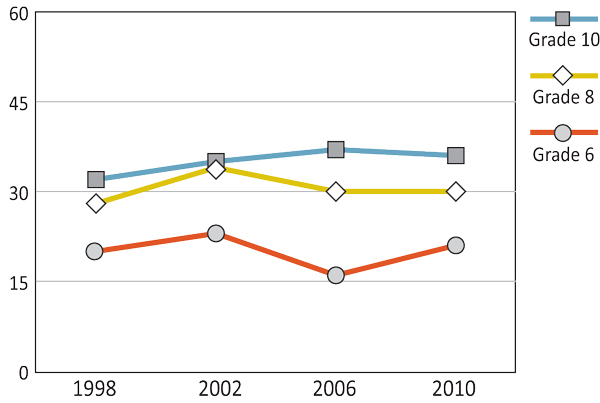
Text Equivalent - Figure 6.8
Figure 6.8 is a line graph that shows the percentage of girls who reported the proportion of the one most serious injury that occurred at a sports facility or field by grade, gender, and year of survey. The graph shows that 20% of Grade 6 girls reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, compared to 23% in 2002, 16% in 2006, and 21% in 2010. Among Grade 8 girls, 28% reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, 34% in 2002, 30% in 2006, and 30% in 2010. Among Grade 10 girls, 32% reported the proportion of the one most serious injury that occurred at a sports facility or field in 1998, compared to 35% in 2002, 37% in 2006, and 36% in 2010.
Regardless of survey year, Grade 6 girls reported the lowest proportions of injury occurring at a sports facility or field. Grade 10 girls have seen a slow, yet fairly consistent, increase in injuries occurring at a sports facility or field over the years.
For both boys and girls, it is apparent that, regardless of survey cycle, injuries that occur at home or in the yard represent a higher proportion of injuries among younger children than older children (Figures 6.9 and 6.10). For boys in Grade 6 and Grade 10, percentages remained consistent across survey cycles. These levels, however, decreased substantially from 25% to 19% between 2002 and 2006 for Grade 8 boys. For Grade 10 girls, the proportion of injuries occurring at home decreased from 1998 to 2010. In every survey cycle, Grade 10 boys had the lowest proportion of their injuries at home or yard.
Figure 6.9: Boys - Proportion of one most serious injury that occurred at a home or yard (%)
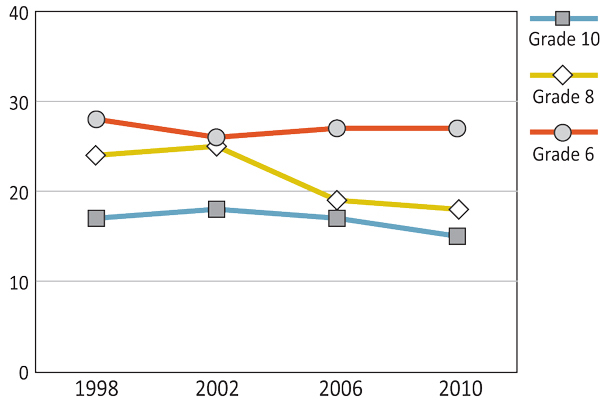
Text Equivalent - Figure 6.9
Figure 6.9 is a line graph that shows the percentage of boys reported the proportion of the one most serious injury that occurred at a home or yard by grade, gender, and year of survey. The graph shows that 28% of Grade 6 boys reported the proportion of the one most serious injury that occurred at a home or yard in 1998, compared to 26% in 2002, 27% in 2006, and 27% in 2010. Among Grade 8 boys, 24% reported the proportion of the one most serious injury that occurred at a home or yard in 1998, compared to 25% in 2002, 19% in 2006, and 18% in 2010. Among Grade 10 boys, 17% reported the proportion of the one most serious injury that occurred at a home or yard in 1998, compared to 18% in 2002, 17% in 2006, and 15% in 2010.
Figure 6.10: Girls - Proportion of one most serious injury that occurred at a home or yard (%)
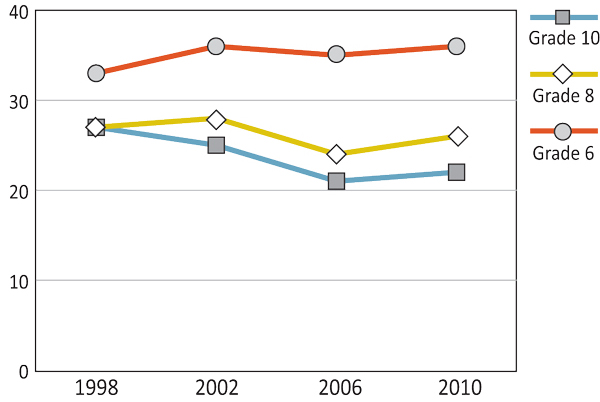
Text Equivalent - Figure 6.10
Figure 6.10 is a line graph that shows the percentage of girls who reported the proportion of the one most serious injury that occurred at a home or yard by grade, gender, and year of survey. The graph shows that 33% of Grade 6 girls reported the proportion of the one most serious injury that occurred at a home or yard in 1998, compared to 36% in 2002, 35% in 2006, and 36% in 2010. Among Grade 8 girls, 27% reported the proportion of the one most serious injury that occurred at a home or yard in 1998, 28% in 2002, 24% in 2006, and 26% in 2010. Among Grade 10 girls, 27% reported the proportion of the one most serious injury that occurred at a home or yard in 1998, compared to 25% in 2002, 21% in 2006, and 22% in 2010.
Child and youth injury prevention efforts are quite widespread in Canada. In fact, the Public Health Agency of Canada has identified injury to be one of its leading priority health issues (PHAC, 2009). There are injury prevention initiatives at national, provincial and community levels, as well as programs and policies targeted to schools, sports organizations, and parents. Generally, the public health approach to injury prevention involves the three E's--Education, Enforcement/legislation, and Engineering (Yanchar, Warda, & Fuselli, 2012). Education aims to increase knowledge, change attitudes and subsequently alter behaviours related to injury prevention. Enforcement involves developing and implementing legislation, safety regulations and policy to mitigate risks of injury. Engineering means designing and manufacturing safer products, environments, and effective protective equipment.
In 2012, following numerous calls for a national program, the Public Health Agency of Canada created the Active and Safe injury prevention program. The objective of this program is to reduce injuries sustained during sports and recreation for children and youth ages 0 to 19 years. It aims to increase awareness and understanding in sport and recreation safety practices among children, youth, families, and the community (including protective equipment use coupled with safety skills and training).
In recent history, there have been four leading national injury prevention groups: SMARTRISK; Safe Communities Canada; Safe Kids Canada; and ThinkFirst Canada. These groups have recently amalgamated to form one cohesive organization called Parachute, which is dedicated to preventing and reducing the risks of injury. These organizations conduct a variety of educational programs, and advocate for new policies and legislation to prevent injury (Yanchar, Warda, & Fuselli, 2012).
Consumer product injuries. Among youth, one potential source of injury occurring at home may be related to consumer products. To mitigate these risks, in 2010 Bill C-36: An Act respecting the safety of consumer products was implemented into law (Parachute, 2013). This bill covers safety legislation that suppliers must meet, as well as mandatory testing and recalls of dangerous products.
Playground equipment injuries. A second area for injury prevention in youth is on the playground. The Canadian Standards Association developed nationally recognized standards for children's play areas and equipment that specify design criteria to reduce the risk of injury. Schools that were upgraded to these standards showed a 49% decrease in injury (Howard et al., 2005).
Protective equipment. Head injuries are linked to low helmet use and, currently, only six provinces have helmet legislation in place, with only four having laws applying to all ages. Enforcing all-ages helmet legislation in each province and territory is recommended as a feasible solution to reduce risk of head injury in cycling (Macpherson et al., 2002). Similar calls have been made to encourage protective equipment use (helmets and wrist guards) while skiing and snowboarding (Warda & Yanchar, 2012)
Sports. Many youth get injured each year while playing sports. For example, body-checking is a common cause of injuries in youth ice hockey (Kukaswadia et al., 2010). Hockey Canada has mandated when body-checking may be introduced in minor hockey. The rules have changed a number of times over the past decade, and depending on the province, body-checking may be introduced as early as 9 years of age. Consensus has yet to be reached as to the most appropriate age to introduce body-checking.
All-terrain vehicles. Another risk for severe injury originates from the operation of ATVs. Currently, ATV laws vary by region and where they are being used (All-Terrain Vehicle Legislation Chart, 2012). It is the Canadian Paediatric Society's position that all children under the age of 16 should not use ATVs and require the use of helmets, mandatory safety training, licensing and registration, and restricting the number of passengers to what the vehicle was designed for (Yanchar, Warda, & Fuselli, 2012). To date, not one jurisdiction has implemented all of the above recommendations (Yanchar, Warda, & Fuselli, 2012).
Summary and Implications
Despite many public health efforts, some types of injuries do not appear to have decreased in Canadian youth. Boys in all grades more frequently miss significant time from school and other usual activities due to injuries than their female classmates. Grade 8 and Grade 10 boys were most likely to report experiencing injuries requiring medical treatment. Injuries that require medical treatment and time missed from school or other activities are an important issue due to their severity and impact and, therefore, require continued surveillance and intervention research.
One consistent trend is that reports of injuries are consistently lowest among Grade 6 students regardless of gender. Moreover, across survey cycles, the proportion of injuries that occur in the home tends to decrease with age, while the proportion or injuries occurring at sports facilities or fields increases.
Possible reasons for higher rates of injury among older students may include increased reports of risk-taking behaviours. Older children are less likely to wear helmets while riding bicycles or other vehicles (e.g., snowmobile, ATV, dirt bike) and are more likely to use alcohol or other drugs than Grade 6 students (Elgar & Pickett, 2012). On the other hand, injuries occurring at home or in the yard are more common proportionally for younger grades. This result may be attributable to their size and developmental abilities or because they simply may spend more time in the home or in the yard relative to time at a sports facility.
National organizations, such as Parachute, continue to advocate for policy and legislation initiatives to mitigate the risk of injury in youth, although there remains substantial work to be done. Improved collaboration and coordination of injury prevention efforts across jurisdictions, coupled with the enforcement of existing policies and legislation, may help reduce the incidence of injuries (Yanchar, Warda, & Fuselli, 2012). The recent federal program Active and Safe may help to facilitate and coordinate collaborative efforts to help implement strategy to this end (Public Health Agency of Canada, 2012). Injury prevention remains a national public health priority and with continued commitment to injury prevention efforts, one can hope for a decline in the occurrence and severity of injury and an improvement in the health and safety of Canadian youth.
References
- All-Terrain Vehicle Legislation Chart - Canada (2012). Retrieved from: parachutecanada.org
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control (2012). National Action Plan for Child Injury Prevention. Atlanta, GA.
- Elgar, F., Pickett, W. (2011). Substance use and risky behavior. In J.G. Freeman, M. King, W. Pickett (Eds.), The health of Canada's young people: A mental health focus (pp. 145-166). Ottawa, ON: Public Health Agency of Canada.
- Gropp, K., Janssen, I., Pickett, W. (2013). Active transportation to school in Canadian youth: should injury be a concern? Injury Prevention, 19, 64-67.
- Harel, R., Overpeck, M.D., Jones, D.H., et al. (1994). The effects of recall on estimating annual nonfatal injury rates for children and adolescents. American Journal of Public Health, 84, 599-605.
- Howard, A.W., MacArthur, C., Willan, A., et al. (2005). The effect of safer play equipment on playground injury rates among school children. Canadian Medical Association Journal, 172, 1443-1446.
- Hyman, J.E., Jewetz, S.T., Matsumoto, H., et al. (2007). Risk factors for school absence after acute orthopaedic injury in New York City. Journal of Pediatric Orthopedics, 27, 415-420.
- Kukaswadia, A., Warsh J., Mihalik, J.P., Pickett, W. (2010). Effects of changing body-checking rules on rates of injury in minor hockey. Pediatrics, 125, 735-741.
- Leitch, K. (2007). Reaching for the top: A report by the advisor on healthy children and youth. Ottawa, ON: Ministry of Health Canada.
- Macpherson, A.K., To, T.M., Macarthur, C., Chipman., M.L., Wright, J.G., Parking, P.C. (2002). Impact of mandatory helmet legislation on bicycle-related head injuries in children: A population-based study. Pediatrics, 110(5), e60.
- Parachute: Preventing Injuries Saving Lives (2013). Product safety. Retrieved from: http://www.parachutecanada.org/policy/item/283
- Pickett, W. (2011). Injury. In J.G. Freeman, M. King, W. Pickett (Eds.), The health of Canada's young people: A mental health focus (pp. 103-118). Ottawa, ON: Public Health Agency of Canada.
- Pickett, W., Brison, R., Berg, R., et al. (2005). Pediatric farm injuries involving non-working children injured by a farm work hazard: Five priorities for primary prevention. Injury Prevention, 11, 6-11.
- Public Health Agency of Canada [PHAC] (2012). Fact sheet - Funding to prevent injuries in the after-school time period. Retrieved from: http://www.phac-aspc.gc.ca/inj-bles/2012_0322-fs-fi-eng.php
- Safe Kids Canada (2006). Child & youth unintentional injury: 1994-2003; 10 years in review. National report 2006. Retrieved from: www.mhp.gov.on.ca/en/prevention/injury-prevention/skc_injuries.pdf
- Safe Kids Canada (2011). Child safety good practice guide: Good investments in unintentional child injury prevention and safety promotion - Canadian Edition. Retrieved from: http://www.safekidscanada.ca/Professionals/Tools-and-Resources/Guide/Good-Practice-Guide.aspx
- SMARTRISK (2005). Ending Canada's invisible epidemic: A strategy for injury prevention. Retrieved from: http://www.smartrisk.ca/index.php/publications/item/ending_canadas_invisible_epidemic_a_strategy_for_injury_prevention
- SMARTRISK online (n.d.). Our history and philosophy. Retrieved from: http://www.smartrisk.ca/index.php/aboutSR/C9
- Warda, L.J., Yanchar, N.L. (2012). Skiing and snowboarding injury prevention. Paediatrics & Child Health, 17(9), 35-36.
- Yanchar, N. (2012). Preventing injuries from all-terrain vehicles. Paediatrics & Child Health, 17(9), 513.
- Yanchar, N.L., Warda, L.J., Fuselli, P. (2012). Child and youth injury prevention: A public health approach. Position statement, Canadian Paediatric Society. Paediatric Child Health, 17, 511.
Chapter 7: Healthy Living
By Katelan Steward
Why are Healthy Living Behaviours Important?
Healthy living encompasses a broad range of behaviours that improve or maintain an individual's health. Adolescents' increased independence and opportunities for decision-making regarding free time activities and eating habits dramatically influence their healthy living. Encouraging adolescents to make healthy choices early on is crucial as the healthy living behaviours that young people select often stay with them through adulthood (Astrom, 2004; Friedman et al., 2008; Lien, Lytle, & Klepp, 2001). Therefore, promoting and encouraging young people towards healthy living behaviours can result in current and lifelong advantages.
Participating in at least 60 minutes of daily physical activity provides children and youth with health benefits of increased physical fitness and bone development, as well as decreased risks of high blood pressure, high cholesterol, and obesity (Janssen & LeBlanc, 2010). Additional psychological advantages of physical activity include reduced depression, anger, and stress, and an increase in life satisfaction (Hassmen, Koivula, & Uutela, 2000; Valois, Zullig, Huebner, & Drane, 2004). Although routine physical activity produces numerous health benefits, adolescents tend to be more influenced by enjoyment and social benefits when selecting free-time activities (Stuntz & Weiss, 2010).
Instead, adolescents may choose to take part in sedentary behaviours, defined as activities that require little energy expenditure or bodily movement and provide no health benefits (Canadian Society for Exercise Physiology, 2012). Common sedentary behaviours practiced by youth include inactive video game playing, extended computer time, and television viewing. Looking exclusively at the latter, excessive television viewing is believed to foster violence and irresponsible sexual behaviour, and have adverse effects on youth learning and academic performance (Canadian Pediatric Society, 2003).
Healthy foods, such as fruits and vegetables, provide individuals with necessary vitamins, minerals, and other nutrients reduce the risk of heart disease, type 2 diabetes, obesity, and certain types of cancer. Benefits from nutritious eating can also include a healthy body weight, increased energy, stronger bones and muscles, and positive psychological well-being. Conversely, foods that are high in fat, sugar, salt, and calories, such as potato chips, sweets, and soft drinks, should be limited (Health Canada, 2011). Unfortunately, it is often taste preferences and availability that determine food choices in youth (Brug et al., 2008) and not nutritional benefits.
Differing priorities and a lack of understanding of the benefits from certain healthy habits can lead to adolescents eliminating important tasks out of their daily routine. The morning habit of eating breakfast can contribute to a healthy body weight, enhanced cognitive functioning, academic success, and overall well-being in individuals (Niemeier et al., 2006; Rampersaud, et al., 2005). Likewise, routine teeth brushing can provide health benefits of a decreased risk of cavities, respiratory illness, and gum disease that can lead to serious infections (Health Canada, 2009c).
Based on the magnitude of benefits that individuals can gain from a lifestyle of physical activity, decreased sedentary behaviour, healthy eating habits, and oral health, these behaviours must be encouraged in Canadian youth. To effectively promote healthy living in adolescents, trends of these four behaviours should be identified and examined in relation to healthy living policies and initiatives.
What are We Examining in this Chapter?
In this chapter, we study trends related to healthy living behaviours in Canadian adolescents. These trends are divided into four major sections: 1) physical activity; 2) sedentary behaviours; 3) healthy eating habits; and 4) oral health. Policy initiatives and legislation related to these four groupings are presented. The HBSC surveyed boys and girls in Grade 6, Grade 8, and Grade 10 on all four categories of healthy living.
Students were asked to report the frequency of being physically active for at least 60 minutes for both a typical week and in the last seven days (possible responses ranged from 0 to 7 days). To ensure this item measured "moderate-to-vigorous physical activity," the questions were prefaced with the description of "any activity that increases your heart rate and makes you get out of breath some of the time" followed by specific examples. In alignment with the Canadian Physical Activity Guidelines (Canadian Society for Exercise Physiology, 2012), young people amassing at least 60 minutes of physical activity seven days a week were considered active.
To measure sedentary behaviours, adolescents were asked how many hours a week they watched television in their free time, including videos and DVDs. Possible responses ranged from 0 to 7 hours a day. Aligning with the Canadian Sedentary Behaviours Guidelines (Canadian Society for Exercise Physiology, 2012), two or more hours of recreational screen-time, in this case television viewing, was considered excessive.
Two components were measured for healthy eating; 1) food frequency and 2) eating behaviours. In measuring food frequency, students were asked to report how often they ate certain nutritious foods (e.g., fruits and vegetables) and non-nutritious foods (e.g., potato chips, sweets, and soft drinks). Possible responses ranged from 'never' to 'more than once a day' with the latter response demonstrating high consumption. Eating behaviours included questions of how often students ate breakfast on weekdays and weekends.
Oral health was measured by asking students to report how often they brushed their teeth, with more than once a day considered practicing good oral health according to Health Canada's Healthy Teeth, Healthy Body Guidelines (2009a).
Physical Activity
The percentage of young people reporting to be physically active every day for at least 60 minutes in a typical week has remained relatively stable since 2002, with minor fluctuations (Figures 7.1 and 7.2). In the 2006 survey, daily physical activity increased for Grade 8 and Grade 6 students but remained relatively stable for Grade 10 students. In the 2010 survey, 26% of Grade 6 boys and 20% of Grade 6 girls reported obtaining at least one hour of physical activity daily. Even fewer older students reported being physically active on a daily basis at rates of 20% and 11% for Grade 10 boys and girls, respectively. Adolescents' reporting of daily physical activity in the most recent cycle mirrored that of the 2002 survey. The increase in physical activity in the 2006 survey thus may be related to the time of administration predominantly during the spring (rather than winter) months. Overall, Grade 6 boys consistently reported the greatest prevalence of obtaining at least 60 minutes of daily physical activity.
Figure 7.1: Boys who were physically active daily during a typical week for at least 60 minutes a day (%)
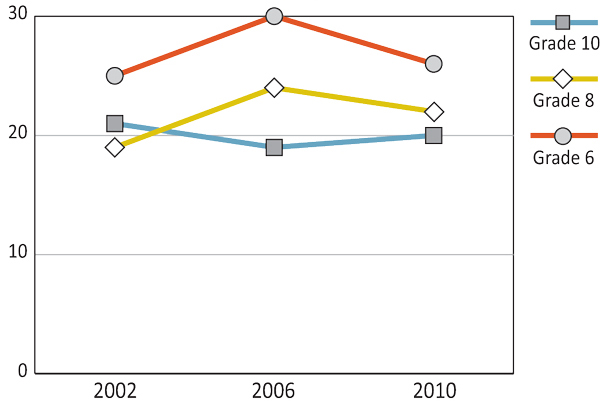
Text Equivalent - Figure 7.1
Figure 7.1 is a line graph that shows the percentage of boys who were physically active daily during a typical week for at least 60 minutes a day by grade and year of survey. The graph shows that among Grade 6 boys, 25% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 30% in 2006 and 26% in 2010. Among Grade 8 boys, 19% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 24% in 2006, and 22% in 2010. Among Grade 10 boys, 21% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 19% in 2006, and 20% in 2010.
Figure 7.2: Girls who were physically active daily during a typical week for at least 60 minutes a day (%)

Text Equivalent - Figure 7.2
Figure 7.2 is a line graph that shows the percentage of girls who were physically active daily during a typical week for at least 60 minutes a day by grade and year of survey. The graph shows that among Grade 6 girls, 20% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 21% in 2006 and 20% in 2010. Among Grade 8 girls, 12% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 16% in 2006, and 12% in 2010. Among Grade 10 girls, 12% were physically active daily during a typical week for at least 60 minutes a day in 2002, compared to 8% in 2006, and 11% in 2010.
Young people were asked to recall daily physical activity of at least 60 minutes in the last 7 days. As shown in Figures 7.3 and 7.4, their responses reflect similar trends to those found in physical activity recall on a typical week. The 2006 survey cycle demonstrated the highest percentage of younger students participating in daily physical activity: Grade 6 boys - 36%; Grade 6 girls - 26%; Grade 8 boys - 27%; and Grade 8 girls - 17%. In the most recent cycle, the prevalence of physically active youth returned to the 2002 levels for Grade 6 and 8 students. Overall, boys reported participating in more physical activity than girls with younger students being the most physically active.
Figure 7.3: Boys who were physically active daily over the past seven days for at least 60 minutes a day (%)
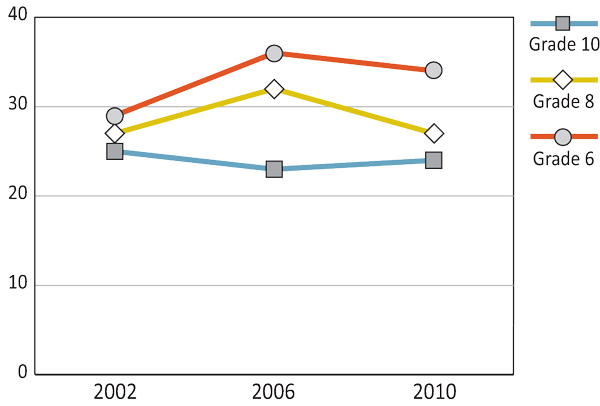
Text Equivalent - Figure 7.3
Figure 7.3 is a line graph that shows the percentage of boys who were physically active daily over the past seven days for at least 60 minutes a day by grade and year of survey. The graph shows that among Grade 6 boys, 29% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 36% in 2006 and 34% in 2010. Among Grade 8 boys, 27% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 32% in 2006, and 27% in 2010. Among Grade 10 boys, 25% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 23% in 2006, and 24% in 2010.
Figure 7.4: Girls who were physically active daily over the past seven days for at least 60 minutes a day (%)
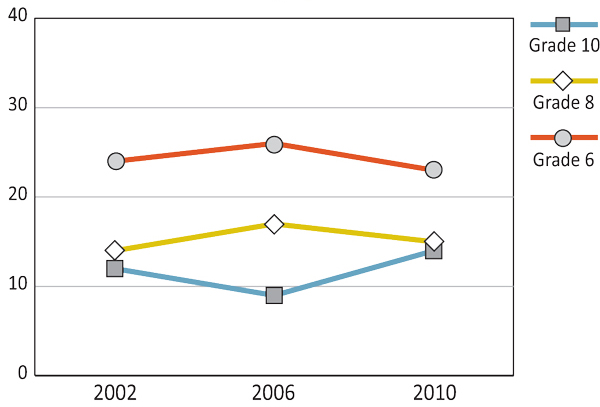
Text Equivalent - Figure 7.4
Figure 7.4 is a line graph that shows the percentage of girls who were physically active daily over the past seven days for at least 60 minutes a day by grade and year of survey. The graph shows that among Grade 6 girls, 20% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 21% in 2006 and 20% in 2010. Among Grade 8 girls, 12% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 16% in 2006, and 12% in 2010. Among Grade 10 girls, 12% were physically active daily over the past seven days for at least 60 minutes a day in 2002, compared to 8% in 2006, and 11% in 2010.
Sedentary Behaviour
The percentage of students who report watching two or more hours of television a day has declined since 2002, as illustrated in Figures 7.5 and 7.6. For example, between the 2006 and 2010 surveys, the number of Grade 8 students viewing two or more hours of television decreased from 70% to 62% for boys and 66% to 59% for girls. Overall, slightly more boys than girls watch more than two hours of television daily. However, irrespective of grade or gender, the majority of young people report watching two or more hours of television a day.
Figure 7.5: Boys who watch two or more hours of television daily (%)
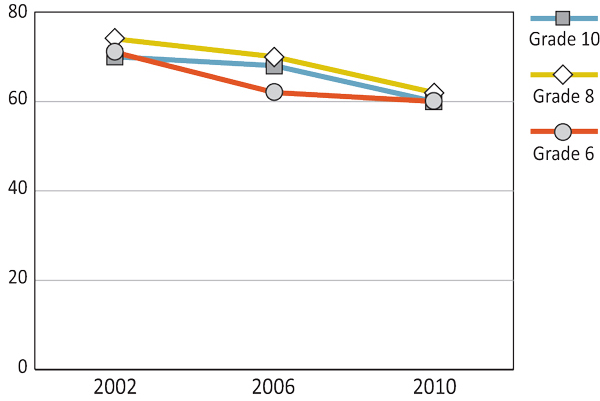
Text Equivalent - Figure 7.5
Figure 7.5 is a line graph that shows the percentage of boys who watch two or more hours of television daily by grade and year of survey. The graph shows that among Grade 6 boys, 71% who watch two or more hours of television daily in 2002, compared to 62% in 2006 and 60% in 2010. Among Grade 8 boys, 14% who watch two or more hours of television daily in 2002, compared to 17% in 2006, and 15% in 2010. Among Grade 10 boys, 12% who watch two or more hours of television daily in 2002, compared to 9% in 2006, and 14% in 2010.
Figure 7.6: Girls who watch two or more hours of television daily (%)
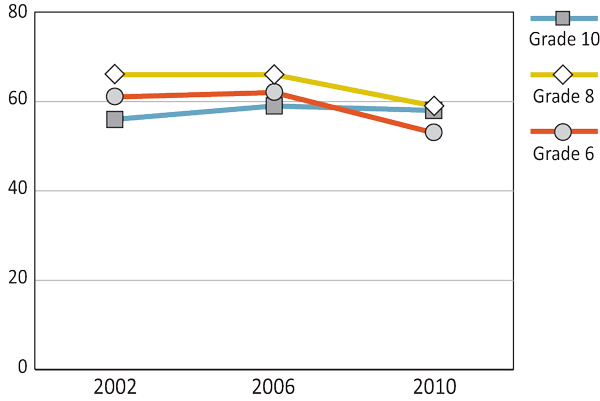
Text Equivalent - Figure 7.6
Figure 7.6 is a line graph that shows the percentage of girls who watch two or more hours of television daily by grade and year of survey. The graph shows that among Grade 6 girls, 24% who watch two or more hours of television daily in 2002, compared to 26% in 2006 and 23% in 2010. Among Grade 8 girls, 14% who watch two or more hours of television daily in 2002, compared to 17% in 2006, and 15% in 2010. Among Grade 10 girls, 12% who watch two or more hours of television daily in 2002, compared to 9% in 2006, and 14% in 2010.
The Canadian Sport Policy was created by Sport Canada in 2002. This inter-governmental policy for sport, the first of its kind, led the way for the creation of the Physical Activity and Sport Act.
The most recent 2012 version of the Canadian Sport Policy continues to build on the previous model, recognizing the benefits of sport on individuals, the community, and society, thereby encouraging participation at all levels. The Policy strives to increase the number and diversity of Canadians participating in sport over the next 20 years.
(Canadian Heritage, 2012; Physical Activity and Sport Act, 2003)
The federal Physical Activity and Sport Act, passed in 2003, aims:
- to promote physical activity as a fundamental element of health and well-being;
- to encourage all Canadians to improve their health by integrating physical activity into their daily lives;
- to assist in reducing barriers faced by all Canadians that prevent them from being active;
- to increase participation in the practice of sport and support the pursuit of excellence in sport; and
- to build capacity in the Canadian sport system.
This federal act replaces the 1985 Fitness and Amateur Sport Act and has led to additional physical activity and sport policy: Sport Canada's Policy on Aboriginal Peoples' Participation in Sport, 2005; Policy on Sport for Persons with a Disability, 2006; and Actively Engaged: A Policy on Sport for Women and Girls, 2009.
(Canadian Heritage, 2005; 2006; 2009; Physical Activity and Sport Act, 2003)
With the overall goal of improving the health of all Canadians, the 2005 Integrated Pan-Canadian Healthy Living Strategy focuses on two goals: 1) improve overall health outcomes and 2) reduce health disparities.
The strategy's first area of emphasis is to increase the number of Canadians who are physically active, eat healthy, and are at a healthy body weight by 20% for 2015.
(Public Health Agency of Canada, 2005)
In 2007, the Public Health Agency of Canada began the Children and Physical Activity Scenarios Project. The project is expected to continue over the next 50 years, exploring and analyzing physical activity participation of children 5-12 years of age, with the goal of identifying opportunities and challenges for organizations promoting physical activity.
(Public Health Agency of Canada, 2011a)
The Intersectoral Action on Children and Youth Physical Activity: Joint Policy Statement was signed by all Sport and Recreation Ministers (SPAR) in 2009 (except Québec who did not sign but endorsed it) and Health and Healthy Living Ministers in 2010. This policy statement recognizes the need for collaborative action by federal, provincial, and territorial governments across sectors to increase physical activity in children and youth. In 2011, Ministries of Education also agreed to work with SPAR Ministers to address the issue of youth inactivity and signed the statement.
(Health Canada, 2012b; Public Health Agency of Canada, 2013)
At the school level, the Pan-Canadian Joint Consortium for School Health is partnering with the Canadian federal, provincial, and territorial governments to support comprehensive school health, including healthy school policy.
Over time, all provincial and territorial governments have developed and enacted strategies to increase the physical activity in youth. Some examples include: Kino-Québec in 1978; Yukon Active Living Strategy in 2000; Saskatchewan in Motion in 2003; Manitoba in Motion in 2005; Active, Healthy Newfoundland and Labrador in 2007; go!PEI in 2010; Active Alberta in 2011; and Nova Scotia's Childhood Obesity Prevention Strategy in 2012.
In addition, many provincial and territorial governments have implemented specific after-school initiatives and policies to support physical activity in adolescents: Northwest Territories' Active After School in 2009; Nunavut Afterschool Physical Activity Funding in 2010; British Columbia's After School Sport Initiative in 2011; New Brunswick After School Hours Program Guidelines in 2011; and the Ontario After School Strategy 2011.
Furthermore, in the last decade, certain provincial and territorial education Ministries, have begun to mandate daily physical activity (DPA) in schools.
(Public Health Agency of Canada, 2005)
Healthy Eating Habits
The number of students who report eating fruit daily has significantly decreased since the 1990 survey (Figures 7.7 and 7.8). Regardless of grade or gender, the steepest decline in young people's fruit consumption came between the 1998 and 2002 survey cycles. This trend, most pronounced in Grade 10 students, demonstrated a fruit consumption decline of 36% for boys and 32% for girls. Since 2002, aside from stable rates for Grade 6 boys and a further decline for Grade 8 boys in the 2006 survey, the number of young people eating fruit has increased but has remained below the figures from the three surveys in the 1990s. The most recent survey found 44% of boys and 53% of girls in Grade 6 reported eating fruit daily. Across survey cycles, Grade 6 girls have maintained the highest level of daily fruit intake. Other than Grade 6 girls, the majority of adolescents report not eating fruit on a daily basis.
Figure 7.7: Boys who eat fruit daily (%)
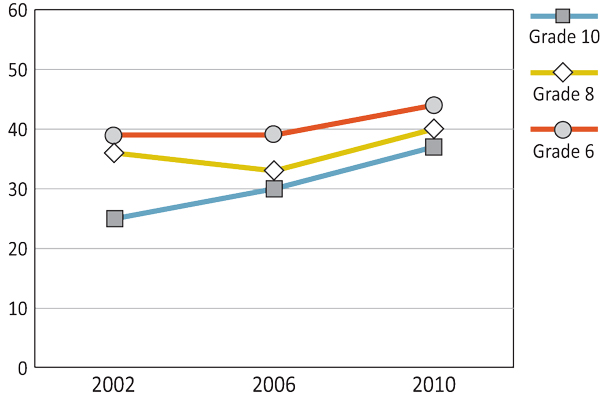
Text Equivalent - Figure 7.7
Figure 7.7 is a line graph that shows the percentage of boys who eat fruit daily by grade and year of survey. The graph shows that among Grade 6 boys, 39% eat fruit daily in 2002, 39% in 2006 and 44% in 2010. Among Grade 8 boys, 36% eat fruit daily in 2002, 33% in 2006 and 40% in 2010. Among Grade 10 boys, 25% eat fruit daily in 2002, 30% in 2006 and 37% in 2010.
Figure 7.8: Girls who eat fruit daily (%)
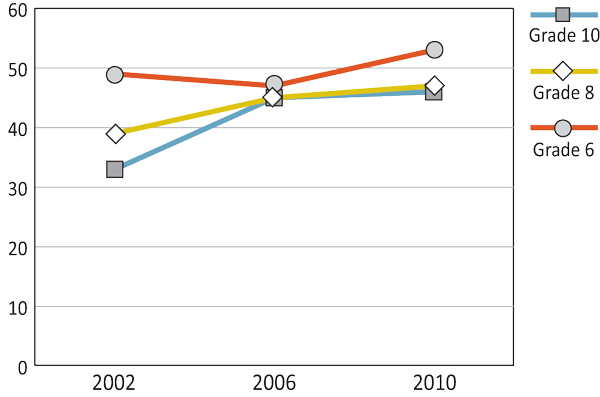
Text Equivalent - Figure 7.8
Figure 7.8 is a line graph that shows the percentage of girls who eat fruit daily by grade and year of survey. The graph shows that among Grade 6 girls, 49% eat fruit daily in 2002, 47% in 2006 and 53% in 2010. Among Grade 8 girls, 39% eat fruit daily in 2002, 45% in 2006 and 47% in 2010. Among Grade 10 girls, 33% eat fruit daily in 2002, 45% in 2006 and 46% in 2010.
In general, less than half of students report eating vegetables daily. The percentages of young people eating vegetables daily have varied little across the survey cycles (Figures 7.9 and 7.10), although Grade 10 students demonstrated an increase in eating vegetables daily of 9% for both boys and girls. Girls tend to report eating vegetables daily more often than boys.
Figure 7.9: Boys who eat vegetables daily (%)
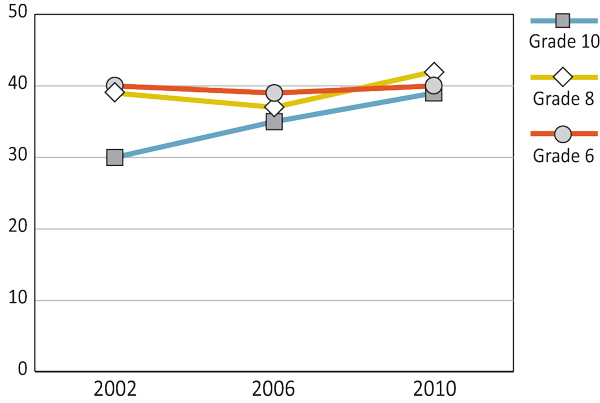
Text Equivalent - Figure 7.9
Figure 7.9 is a line graph that shows the percentage of boys who eat vegetables daily by grade and year of survey. The graph shows that among Grade 6 boys, 40% eat vegetables daily in 2002, compared to 39% in 2006 and 40% in 2010. Among Grade 8 boys, 39% eat vegetables daily in 2002, compared to 37% in 2006, and 42% in 2010. Among Grade 10 boys, 30% eat vegetables daily in 2002, compared to 35% in 2006, and 39% in 2010.
Figure 7.10: Girls who eat vegetables daily (%)
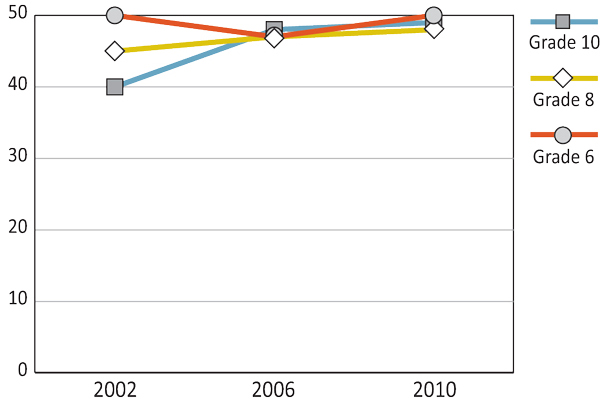
Text Equivalent - Figure 7.10
Figure 7.10 is a line graph that shows the percentage of girls who eat vegetables daily by grade and year of survey. The graph shows that among Grade 6 girls, 50% eat vegetables daily in 2002, compared to 47% in 2006 and 50% in 2010. Among Grade 8 girls, 45% eat vegetables daily in 2002, compared to 47% in 2006, and 48% in 2010. Among Grade 10 girls, 40% eat vegetables daily in 2002, compared to 48% in 2006, and 49% in 2010.
Figures 7.11 and 7.12 illustrate that the highest prevalence of adolescents reporting eating potato chips daily was found in the 1990 and 1994 surveys, with declining rates in subsequent survey cycles. For nearly all the grades, the lowest level of potato chip consumption was found in 2010 at rates of 4% to 6% for boys and girls. As was shown in the fruit and vegetable trends, girls report healthier eating habits than their male counterparts, herein shown by lower levels of potato chip consumption. In contrast to fruit and vegetable consumption and with the exception of the most recent survey, older girls eat potato chips less frequently than younger girls. This same relationship is not evident in boys.
Figure 7.11: Boys who eat potato chips daily (%)
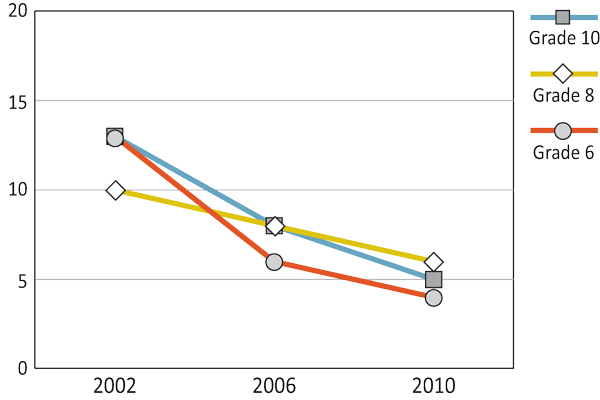
Text Equivalent - Figure 7.11
Figure 7.11 is a line graph that shows the percentage of boys who eat potato chips daily by grade and year of survey. The graph shows that among Grade 6 boys, 13% eat potato chips daily in 2002, 6% in 2006 and 4% in 2010. Among Grade 8 boys, 10% eat potato chips daily in 2002, 8% in 2006 and 6% in 2010. Among Grade 10 boys, 13% eat potato chips daily in 2002, 8% in 2006 and 5% in 2010.
Figure 7.12: Girls who eat potato chips daily (%)
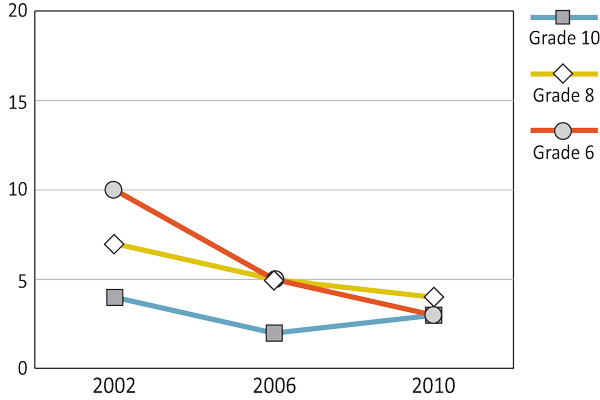
Text Equivalent - Figure 7.12
Figure 7.12 is a line graph that shows the percentage of girls who eat potato chips daily by grade and year of survey. The graph shows that among Grade 6 girls, 10% eat potato chips daily in 2002, 5% in 2006 and 3% in 2010. Among Grade 8 girls, 7% eat potato chips daily in 2002, 5% in 2006 and 4% in 2010. Among Grade 10 girls, 4% eat potato chips daily in 2002, 2% in 2006 and 3% in 2010.
Young people who reported eating sweets (candy or chocolate) daily has decreased over time, with slight fluctuations between certain survey cycles (Figures 7.13 and 7.14). The 1994 survey cycle demonstrates the biggest spike of sweets consumption with at least one quarter of students, irrespective of grade or gender, eating sweets daily. The greatest increase, found in 1994, was that of Grade 8 boys and Grade 8 girls, where levels rose to 34% and 28%, respectively. Subsequent cycles show lowered percentages of young people eating sweets daily. Aside from Grade 6 boys and Grade 10 girls, the lowest percentages of students eating sweets daily occurred in the 2010 survey at levels of 20% or lower. Overall, girls typically report eating sweets less often than boys. However, no clear relationship between age and sweets consumption is found.
Figure 7.13: Boys who eat sweets daily (%)
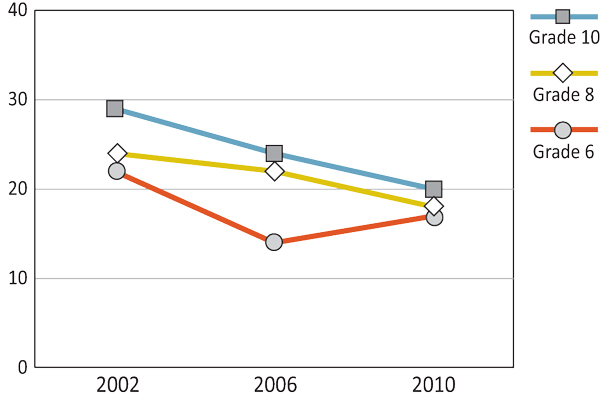
Text Equivalent - Figure 7.13
Figure 7.13 is a line graph that shows the percentage of boys who eat sweets daily by grade and year of survey. The graph shows that among Grade 6 boys, 22% eat sweets daily in 2002, 14% in 2006 and 17% in 2010. Among Grade 8 boys, 24% eat sweets daily in 2002, 22% in 2006 and 18% in 2010. Among Grade 10 boys, 29% eat sweets daily in 2002, 24% in 2006 and 20% in 2010.
Figure 7.14: Girls who eat sweets daily (%)
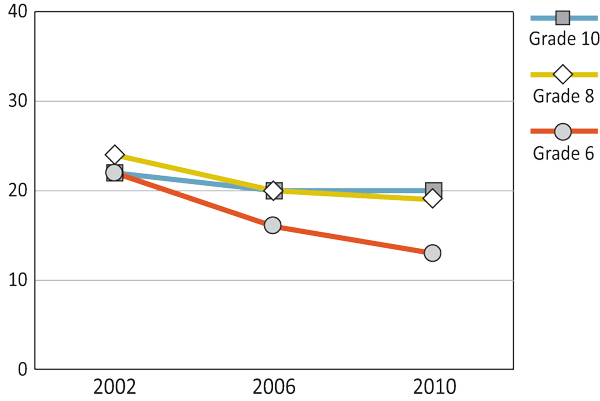
Text Equivalent - Figure 7.14
Figure 7.14 is a line graph that shows the percentage of girls who eat sweets daily by grade and year of survey. The graph shows that among Grade 6 girls, 22% eat sweets daily in 2002, 16% in 2006 and 13% in 2010. Among Grade 8 girls, 24% eat sweets daily in 2002, 20% in 2006 and 19% in 2010. Among Grade 10 girls, 22% eat sweets daily in 2002, 20% in 2006 and 20% in 2010.
As indicated in Figures 7.15 and 7.16, the percentage of students who report consuming non-diet soft drinks on a daily basis has declined substantially since 2002. Between the 2002 and 2006 surveys, the rate of student soft drink daily consumption decreased 16% for boys and 7% for girls in the tenth grade. With the exception of Grade 10 girls, this trend of decline continued from 2006 to 2010, where the lowest reports of daily soft drink consumption was found: Grade 6 boys - 10%; Grade 6 girls - 6%; Grade 8 boys - 16%; Grade 8 girls - 10%; and Grade 10 boys - 17%. Regardless of survey cycle, older boys report the highest prevalence of soft drink consumption with boys overall drinking more soft drinks than girls.
Figure 7.15: Boys who drink non-diet soft drinks daily or more (%)
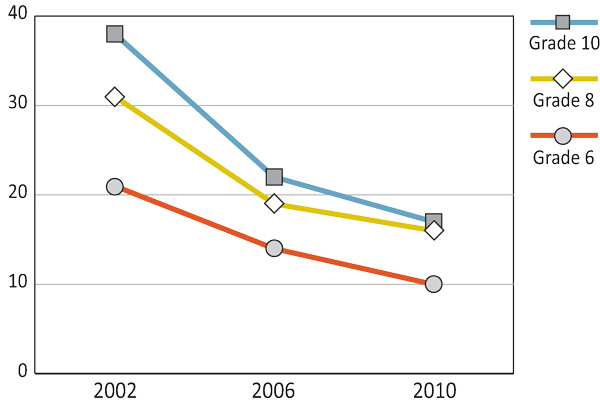
Text Equivalent - Figure 7.15
Figure 7.15 is a line graph that shows the percentage of boys who drink non-diet soft drinks daily or more by grade and year of survey. The graph shows that among Grade 6 boys, 21% drink non-diet soft drinks daily or more in 2002, compared to 14% in 2006 and 10% in 2010. Among Grade 8 boys, 31% drink non-diet soft drinks daily or more in 2002, compared to 19% in 2006, and 16% in 2010. Among Grade 10 boys, 38% drink non-diet soft drinks daily or more in 2002, compared to 22% in 2006, and 17% in 2010.
Figure 7.16: Girls who drink non-diet soft drinks daily or more (%)
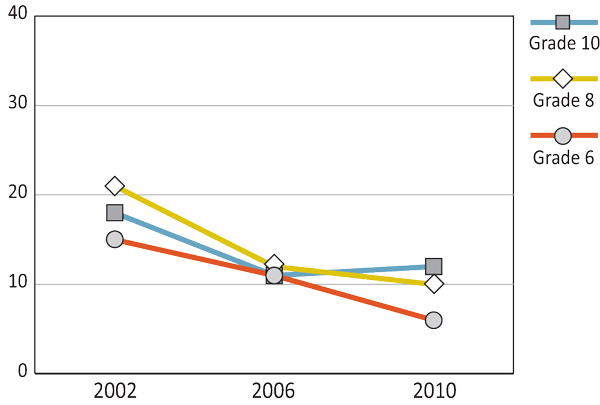
Text Equivalent - Figure 7.16
Figure 7.16 is a line graph that shows the percentage of girls who drink non-diet soft drinks daily or more by grade and year of survey. The graph shows that among Grade 6 girls, 15% drink non-diet soft drinks daily or more in 2002, compared to 11% in 2006 and 6% in 2010. Among Grade 8 girls, 21% drink non-diet soft drinks daily or more in 2002, compared to 12% in 2006, and 10% in 2010. Among Grade 10 girls, 18% drink non-diet soft drinks daily or more in 2002, compared to 11% in 2006, and 12% in 2010.
The number of young people who report eating breakfast every weekday morning (Figures 7.17 and 7.18) has remained relatively stable from the 2002 to 2010 survey cycles. A slight fluctuation in this breakfast trend occurred in 2006, where percentages peaked for Grade 10 boys and Grade 10 girl at rates of 56% and 50%, respectively. Weekday breakfast eating for Grade 10 boys remained at 56% into the 2010 survey cycle. Overall, the highest percentages of weekday breakfast consumption were found in Grade 6 students at 74% (boys) and 69% (girls) in the 2010 survey. Slightly more boys than girls report that they eat weekday breakfast.
Figure 7.17: Boys who usually eat breakfast all five days a week (%)
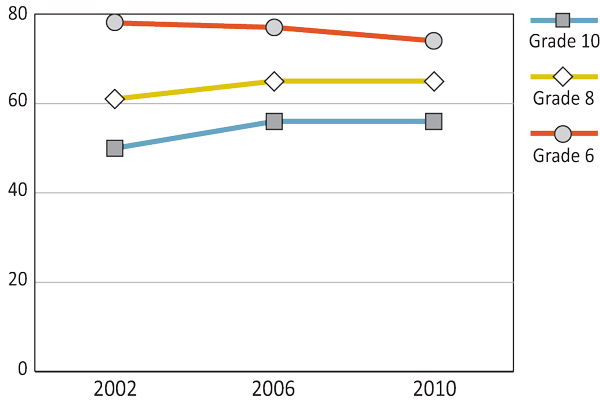
Text Equivalent - Figure 7.17
Figure 7.17 is a line graph that shows the percentage of boys who usually eat breakfast all five days a week by grade and year of survey. The graph shows that among Grade 6 boys, 78% usually eat breakfast all five days a week in 2002, compared to 77% in 2006 and 74% in 2010. Among Grade 8 boys, 61% usually eat breakfast all five days a week in 2002, compared to 65% in 2006, and 65% in 2010. Among Grade 10 boys, 50% usually eat breakfast all five days a week in 2002, compared to 56% in 2006, and 56% in 2010.
Figure 7.18: Girls who usually eat breakfast all five days a week (%)
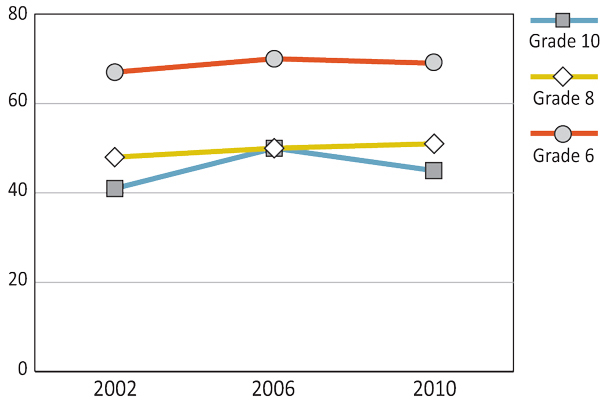
Text Equivalent - Figure 7.18
Figure 7.18 is a line graph that shows the percentage of girls who usually eat breakfast all five days a week by grade and year of survey. The graph shows that among Grade 6 girls, 67% usually eat breakfast all five days a week in 2002, compared to 70% in 2006 and 69% in 2010. Among Grade 8 girls, 48% usually eat breakfast all five days a week in 2002, compared to 50% in 2006, and 51% in 2010. Among Grade 10 girls, 41% usually eat breakfast all five days a week in 2002, compared to 50% in 2006, and 45% in 2010.
The percentage of young people who report eating breakfast on weekends has remained relatively constant over time. As shown in Figures 7.19 and 7.20, slight increases in the percentage of students eating weekend breakfast have occurred, with the most notable being in Grade 10 girls whose levels rose 10% between the 2002 and 2010 surveys. Younger students report eating weekend breakfast more often than older students. However, no differences exist between genders.
Figure 7.19: Boys who usually eat breakfast both Saturday and Sunday (%)
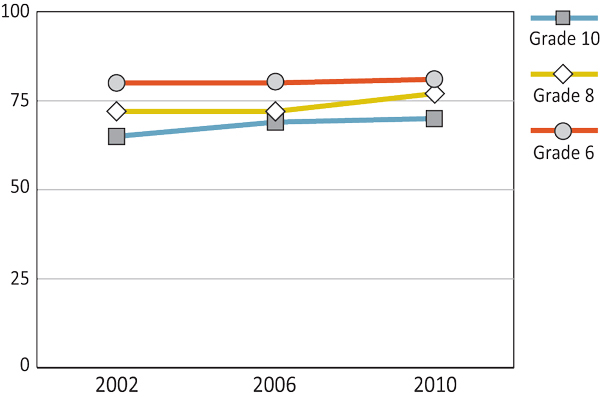
Text Equivalent - Figure 7.19
Figure 7.19 is a line graph that shows the percentage of boys who usually eat breakfast both Saturday and Sunday by grade and year of survey. The graph shows that among Grade 6 boys, 80% usually eat breakfast both Saturday and Sunday in 2002, compared to 80% in 2006 and 81% in 2010. Among Grade 8 boys, 72% usually eat breakfast both Saturday and Sunday in 2002, compared to 72% in 2006, and 77% in 2010. Among Grade 10 boys, 65% usually eat breakfast both Saturday and Sunday in 2002, compared to 69% in 2006, and 70% in 2010.
Figure 7.20: Girls who usually eat breakfast both Saturday and Sunday (%)
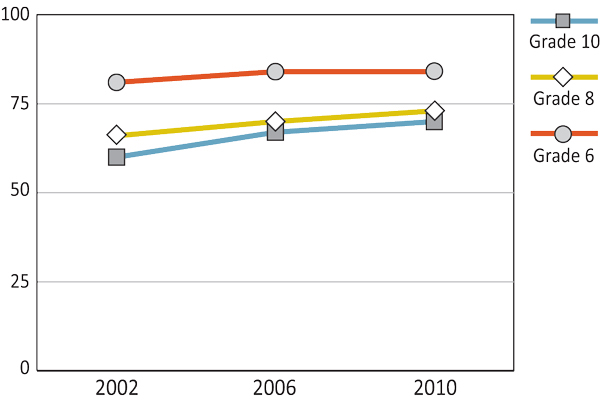
Text Equivalent - Figure 7.20
Figure 7.20 is a line graph that shows the percentage of girls who usually eat breakfast both Saturday and Sunday by grade and year of survey. The graph shows that among Grade 6 girls, 81% usually eat breakfast both Saturday and Sunday in 2002, compared to 84% in 2006 and 84% in 2010. Among Grade 8 girls, 66% usually eat breakfast both Saturday and Sunday in 2002, compared to 70% in 2006, and 73% in 2010. Among Grade 10 girls, 60% usually eat breakfast both Saturday and Sunday in 2002, compared to 67% in 2006, and 70% in 2010.
Canada's food guide, first released in 1942, outlines a pattern of eating that promotes health, meets nutrient needs, and minimizes the risk of chronic diseases. The current version, Eating Well with Canada's Food Guide, was released in 2007.
(Health Canada, 2007)
In 2007 the Advertising Standards of Canada (ASC), along with Concerned Children's Advertisers (CCA), and Food & Consumer Products of Canada (FCPC) began a three-pronged approach to promote health behaviours in children under 12 years of age:
- the Canadian Children's Food and Beverage Advertising Initiative, a voluntary alliance where participating companies agree to only present messages of healthy dietary and lifestyle choices to youth;
- Long Live Kids, a social marketing, educational, and media literacy program and;
- new, health-focused interpretations of the 1963 Canadian Code of Advertising Standards and the 1993 Broadcast Code of Advertising to Children.
In Quebec, the Consumer Protection Act has prohibited advertising directed at children less than 13 years of age since 1980.
(Advertising Standards Canada, 2007; Advertising Standards Canada, 2010; Advertising Standards Canada, 2012; Office de la protection du consommateur, 2013)
Provincial and territorial school nutrition guidelines and policies have been created to maximize students' access to healthy foods and beverages and minimize or eliminate the sale of unhealthy foods and beverages. Examples include: Province of Manitoba's School Nutrition Handbook implemented in 2006; Guidelines for Food and Beverage Sales in BC Schools implemented in 2009; and Ontario's School Food and Beverage Policy implemented in 2010.
(Dieticians of Canada, 2012)
In 2012, the Healthy Eating After School - Integrating healthy eating into after-school physical activity initiatives report was released. This synthesis of literature and expertise from key informants provides governments and stakeholders with guidance on how to integrate healthy eating and food skills into after-school physical activity initiatives. Two promising provincial examples of after-school health initiatives, both implemented in the last four years, are presented as models: Newfoundland and Labrador's Eat Great and Participate; and the Ontario After-School Program.
(Health Canada, 2012b)
Oral Health
The level of students who report brushing their teeth at least twice a day has remained relatively stable throughout the survey years. Slight increases in teeth brushing have occurred over time, with the most notable being in 2002 where levels rose 6% for Grade 6 boys and 9% for Grade 8 boys. Older girls demonstrate the highest prevalence of teeth brushing at 79% in the latest survey cycle. Overall, as shown in Figures 7.21 and 7.22, the large majority of young people report practicing good oral hygiene behaviours.
Figure 7.21: Boys who brush their teeth twice a day or more (%)
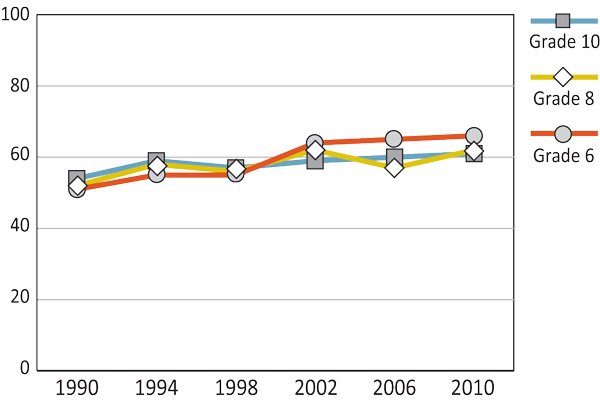
Text Equivalent - Figure 7.21
Figure 7.21 is a line graph that shows the percentage of boys who brush their teeth twice a day or more by grade and year of survey. The graph shows that among Grade 6 boys, 51% brush their teeth twice a day or more in 1990, compared to 55% in 1994, 55% in 1998, 64% in 2002, 65% in 2006 and 66% in 2010. Among Grade 8 boys, 52% brush their teeth twice a day or more in 1990, compared to 58% in 1994, 56% in 1998, 62% in 2002, 57% in 2006 and 62% in 2010. Among Grade 10 boys, 54% brush their teeth twice a day or more in 1990, compared to 59% in 1994, 57% in 1998, 59% in 2002, 60% in 2006 and 61% in 2010.
Figure 7.22: Girls who brush their teeth twice a day or more (%)
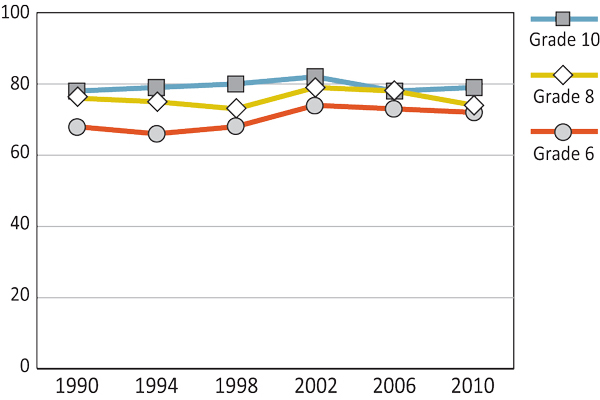
Text Equivalent - Figure 7.22
Figure 7.22 is a line graph that shows the percentage of girls who brush their teeth twice a day or more by grade and year of survey. The graph shows that among Grade 6 girls, 68% brush their teeth twice a day or more in 1990, compared to 66% in 1994, 68% in 1998, 74% in 2002, 73% in 2006 and 72% in 2010. Among Grade 8 girls, 76% brush their teeth twice a day or more in 1990, compared to 75% in 1994, 73% in 1998, 79% in 2002, 78% in 2006 and 74% in 2010. Among Grade 10 girls, 78% brush their teeth twice a day or more in 1990, compared to 79% in 1994, 80% in 1998, 82% in 2002, 78% in 2006 and 79% in 2010.
In 2004, the Office of the Chief Dental Officer (OCDO) was created to increase Canadians' awareness and practice of proper dental hygiene. The OCDO works to provide information, evidence, and advice on oral health at the federal, provincial, and community levels.
(Health Canada, 2009b)
The First Nations and Inuit Health Branch's (FNIHB) Dental Division developed the Children's Oral Health Initiative (COHI) in 2004. The COHI is focused on resolving the disparity between the oral health of the mainstream Canadian population and First Nations and Inuit. The initial initiative was directed at three groups: 1) pregnant women and primary caregivers; 2) pre-school children, 0-4 years of age; and 3) school children 5-7 years of age, with plans to expand over time.
(Health Canada, 2012a)
Summary and Implications
In 2004, recognizing the need to promote healthy living behaviours, the World Health Organization (WHO) created The Global Strategy on Diet, Physical Activity and Health (World Health Organization, 2004). Canada has followed suit and enacted a variety of policies and initiatives to encourage healthy living behaviours. Trends from the HBSC survey suggest that Canadian policies and initiatives are having moderate success in certain areas.
The 2002 Canadian Sport Policy and the 2003 Physical Activity and Sport Act have aimed to increase physical activity and sport in Canadians over the past decade. The 2005 Integrated Pan-Canadian Healthy Living Strategy further highlighted the importance of promoting active behaviours, with numerous policies and initiatives created and enacted since. At the school level, territorial and provincial governments have implemented a variety of policies and initiatives to increase physical activity.
Financial assistance through the Children Fitness Tax Credit (Canadian Revenue Agency; 2013) and a variety of funding programs, such as The Healthy Living Fund (Public Health Agency of Canada, 2011b) and the Gas Tax Fund (Active Healthy Kids Canada, 2012), also work to increase the accessibility of physical activity and sport to Canadians. Nonetheless, since 2002, fewer than 36% of adolescent boys and 26% of adolescent girls report obtaining the daily recommended 60-minutes of physical activity. Somewhat more encouraging is the slight decline in young people reporting more than two hours of daily television viewing. Still, almost twice as many students are watching two or more hours of television daily than being physically active for at least one hour.
Increasing active behaviours in youth remains important. Initiatives like the long-term Children and Physical Activity Scenarios Project and Active Canada 20/20 (Tremblay, 2012) acknowledge the need for conversations with Canadians to develop a national physical activity action plan. The 2011 release of the newly revised Canadian Physical Activity Guidelines and, for the first time ever, the Canadian Sedentary Behaviours Guidelines for Children and Youth continue to inform the Canadian public of the need to be active (Canadian Society of Exercise Physiology, 2013).
In contrast to physical activity behaviours, certain healthy eating habits of Canadian youth have shown noticeable change over time. From 1990 to 2002, adolescents' reporting of fruit consumption declined substantially, leveling off in the last survey cycle. Young people's daily intake of potato chips, sweets, and soft drinks has also declined over time, with students in the latest survey cycle reporting some of the lowest consumption rates. The healthy habit of eating breakfast on weekdays and weekends has remained relatively stable over time with the majority of youth reporting to take part in this behaviour in the 2010 survey.
The promotion of healthy eating has being approached from a variety of angles: 1) education through Eating Well with Canada's Food Guide (2007), the 2007 Canadian Children's Food and Beverage Advertising Initiative, and the Comprehensive School Health framework (Public Health Agency of Canada, 2008); 2) mandatory nutrition labelling through the 2002 Food and Drug Regulations; and 3) accessibility to healthy foods through the 2011 Nutrition North Canada Program (Government of Canada, 2013), Health Canada's 2007 Trans Fat Task Force (Health Canada, 2009d), and provincial and territorial nutrition policies. Nonetheless, as only 53% of Canadian youth report consuming one or more serving of fruits or vegetables a day, progress still needs to be made in this area of healthy living.
Adolescents' reports of daily teeth brushing have remained relatively stable since the 1990s with a slight increase for boys in the last few survey cycles. The 2004 creation of the Office of the Chief Dental Office and The Children's Oral Health Initiative may explain this latest improvement in oral health. The majority of Canadian youth, 61% of boys and 72% of girls, reported practicing good oral health behaviours in the 2010 survey.
Recent media campaigns use print, website, and television advertising to promote healthy living behaviours in youth, such as the Government of Canada's Healthy Eating and Awareness and Education Initiative, the federally-funded ParticipACTION 2011 Think Again Campaign and Bring Back Play Campaign, and the Canadian Broadcasting Corporation's 2011 Live Right Now Campaign (Health Canada, 2010; Tremblay, 2012). Considering that the healthy living behaviours of Canadian youth have not been worsening and, in some cases, improving, we can be hopeful that these new initiatives will foster change for future improvement.
References
- Active Healthy Kids Canada (2010). Active Healthy Kids Canada report card on physical activity for children and youth. Retrieved from http://dvqdas9jty7g6.cloudfront.net/reportcards2012/AHKC%202012%20-%20Report%20Card%20Long%20Form%20-%20FINAL.pdf
- Active Healthy Kids Canada (2012). Active Healthy Kids Canada report card on physical activity for children and youth. Retrieved from http://www.activehealthykids.ca/ReportCard/PhysicalActivity.aspx
- Advertising Standards Canada (2007). Canada's food and beverage industry unveils integrated children-focused initiatives. Retrieved from http://adstandards.com/en/MediaAndEvents/childrensInitiativePressRelease.aspx
- Advertising Standards Canada (2010). Canadian children's food and beverage advertising initiative. Retrieved from http://www.adstandards.com/en/childrensinitiative/CCFBAI_EN.pdf
- Advertising Standards Canada (2012). Broadcast code for advertising to children. Retrieved from http://www.adstandards.com/en/clearance/childrens/broadcastCodeForAdvertisingToChildren.aspx
- Astrom, A.N. (2004). Stability of oral health-related behaviour in a Norwegian cohort between the ages of 15 and 23 years. Community Dentistry and Oral Epidemiology, 32, 354-362.
- Brug, J., Tak, N.A., te Velde S.J., Bere, E., Bourdeaudhuij, I. (2008). Taste preferences, liking and other factors related to fruit and vegetable intakes among schoolchildren: Results from observational studies. British Journal of Nutrition, 99, S7-S14.
- Canadian Heritage (2005). Sport Canada's policy on Aboriginal peoples' participation in sport (Minister of Public Works and Government Services Canada No. CH24-10/2005). Retrieved from http://www.pch.gc.ca/pgm/sc/pol/aborigin/index-eng.cfm
- Canadian Heritage (2006). Policy on sport for persons with a disability (Her Majesty the Queen in Right of Canada No. CH24-14/2006). Retrieved from http://pch.gc.ca/pgm/sc/pol/spt/pwad-eng.pdf
- Canadian Heritage (2009). Actively engaged: A policy on sport for women and girls (Her Majesty the Queen in Right of Canada No. CH24-27/2009). Retrieved from http://www.pch.gc.ca/pgm/sc/pol/fewom/101-eng.cfm
- Canadian Heritage (2012). The Canadian sport policy 2013. Retrieved from http://www.canadianheritage.gc.ca/pgm/sc/pol/pcs-csp/index-eng.cfm
- Canadian Pediatric Society (2003). Impact of media use on children and youth. Pediatrics & Child Health, 8, 301-306.
- Canadian Revenue Agency (2013). Line 365 - Children's fitness amount. Retrieved from http://www.cra-arc.gc.ca/fitness/
- Canadian Society for Exercise Physiology (2012). Canadian physical activity, and sedentary behaviours guidelines. Retrieved from http://www.csep.ca/CMFiles/Guidelines/CSEP_Guidelines_Handbook.pdf
- Canadian Society for Exercise Physiology (2013). Canadian physical activity guidelines-Background information. Retrieved from http://www.csep.ca/english/view.asp?x=587
- Dieticians of Canada (2012). School nutrition policy. Retrieved from http://www.dietitians.ca/Dietitians-Views/Children-and-Teens/School-Nutrition-Policy.aspx
- Friedman, H.S., Martin, L.R., Tucker, J.S., Criqui, M.H., Kern, M.L., Reynolds, C.A. (2008). Stability of physical activity across the lifespan. Journal of Health Psychology, 13, 1092-1104.
- Gouvernement du Québec (2013). Physical Activity. Retrieved from http://www.msss.gouv.qc.ca/en/sujets/santepub/physical_activity.php
- Government of Canada (2013). Nutrition North Canada. Retrieved from http://www.nutritionnorthcanada.ca/index-eng.asp
- Hassmen, P., Koivula, N., Uutela, A. (2000). Physical exercise and psychological well-being: A population study in Finland. Preventative Medicine, 30, 17-25.
- Health Canada (2007). Canada's food guides from 1942 to 1992. Retrieved from http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/context/fg_history-histoire_ga-eng.php#a1992
- Health Canada (2009a). Smile: Healthy teeth, healthy body. Retrieved from http://www.hc-sc.gc.ca/hl-vs/alt_formats/pdf/pubs/oral-bucco/2009-smile-sourire/2009-smile-sourire-eng.pdf
- Health Canada (2009b). Office of the Chief Dental Officer. Retrieved from http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/fnihb-dgspni/ocdo-bdc/index-eng.php
- Health Canada (2009c). The effects of oral health on overall health. Retrieved from http://www.hc-sc.gc.ca/hl-vs/alt_formats/pacrb-dgapcr/pdf/iyh-vsv/life-vie/dent-eng.pdf
- Health Canada (2009d). Trans fat. Retrieved from http://www.hc-sc.gc.ca/fn-an/nutrition/gras-trans-fats/index-eng.php
- Health Canada (2010). Nutrition facts education campaign. Retrieved from http://www.hc-sc.gc.ca/ahc-asc/media/nr-cp/_2010/2010_180b-eng.php
- Health Canada (2011). Canada's food guide (Health Canada Publication No. 4651). Retrieved from http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/view_eatwell_vue_bienmang-eng.pdf
- Health Canada (2012a). First Nations and Inuit health. Retrieved from http://www.hc-sc.gc.ca/ahc-asc/activit/strateg/fnih-spni-eng.php
- Health Canada (2012b). Healthy eating after school: Integrating healthy eating after-school physical activity initiatives. Retrieved from http://www.hc-sc.gc.ca/fn-an/alt_formats/pdf/pubs/nutrition/heas-saae/heas-saae-eng.pdf
- Janssen, I., LeBlanc, A.G. (2010). Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. International Journal of Behavioral Nutrition & Physical Activity, 7, 1-16.
- Joint Consortium for School Health (2013). Comprehensive school health framework. Retrieved from: http://www.jcsh-cces.ca/index.php/school-health
- Lien, N., Lytle A.L., Klepp, K. (2001). Stability in consumption of fruit, vegetables, and sugary foods in a cohort from age 14 to age 21. Preventive Medicine, 33, 217-226.
- Niemeier, H.M., Raynor, H.A., Lloyd-Richardson, E.E., Rogers, M.L., Wing, R.R. (2006). Fast food consumption and breakfast skipping: Predictors of weight gain from adolescence to adulthood in a nationally representative sample. Journal of Adolescent Health, 39, 842-849.
- Office de la protection du consommateur (2013). Consumer Protection Act. Retrieved from http://www2.publicationsduquebec.gouv.qc.ca/dynamicSearch/telecharge.php?type=2&file=/P_40_1/P40_1_A.html
- Public Health Agency of Canada [PHAC] (2005). The integrated pan-Canadian healthy living strategy (Her Majesty the Queen in Right of Canada No. HP10-1/2005). Retrieved from http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/ipchls-spimmvs/pdf/ipchls-spimmvs-eng.pdf
- Public Health Agency of Canada [PHAC] (2008). Comprehensive school health. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/dca-dea/prog-ini/school-scolaire/csh-agss-eng.php
- Public Health Agency of Canada [PHAC] (2011a). Children and physical activity scenarios project. Retrieved from http://www.phac-aspc.gc.ca/publicat/cpasp-pseap/index-eng.php
- Public Health Agency of Canada [PHAC] (2011b). Healthy Living Unit. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/hlu-umvs/hlfund-fondspmvs-eng.php
- Public Health Agency of Canada [PHAC] (2013). Curbing childhood obesity: A federal, provincial and territorial framework for action to promote healthy weights. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/framework-cadre/pdf/ccofw-eng.pdf
- Physical Activity and Sport Act (2003). Physical Activity and Sport Act (S.C. 2003, c. 2). Retrieved from http://laws-lois.justice.gc.ca/eng/acts/P-13.4/page-1.html#h-1
- Rampersaud, G.C., Pereira, M.A., Girard, B.L., Adams, J., Metzl, J.D. (2005). Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. Journal of the American Dietetic Association, 105, 743-760.
- Stuntz, C.P., Weiss, M.R. (2010). Motivating children and adolescents to sustain a physically active lifestyle. American Journal of Lifestyle Medicine, 4, 433-444.
- Tremblay, M.S. (2012). Major initiatives related to childhood obesity and physical inactivity in Canada: The year in review. Canadian Journal of Public Health, 103, 164-169.
- Valois, R.F., Zullig, K.J., Huebner, E.S., Drane, W.J. (2004). Physical activity behaviours and perceived life satisfaction among public high school adolescents. Journal of School Health, 74, 59-65.
- World Health Organization [WHO] (2004). Global strategy on diet, physical activity and health. Retrieved from http://www.who.int/dietphysicalactivity/strategy/eb11344/strategy_english_web.pdf
Chapter 8: Healthy Weights
By Katelan Steward
Why are Healthy Weights Important?
Adolescence is a time of change with increased independence and peer influence affecting an individual's healthy weight, both directly and indirectly (Fletcher, Bonell, & Sorhaindo, 2011; Macdonald-Wallis, Jago, & Sterne, 2012). Unhealthy weight and negative body image can lead to a variety of negative physical and psychological consequences. Weight biases also exist with unequal treatment of overweight and obese individuals occurring in employment, health care, and educational settings (Puhl & Heur, 2009). As the discrimination and stigma associated with being overweight or obese can lead to an impaired quality of life (Puhl & Heur), adolescents should be encouraged towards healthy weights.
Excessive body weight, classified as either overweight or obese, has a variety of undesired health consequences including high blood pressure, high cholesterol, type 2 diabetes, and asthma. Additional psychological problems include depression, poor school performance, anxiety, emotional eating patterns, and poor self-esteem leading to decreased participation in social activities (Hassink, 2003). These adverse health and psychological consequences can negatively affect an individual throughout his or her life and shorten life expectancy (Leitch, 2007; Singh et al., 2008).
Body dissatisfaction, especially a fixation on being or becoming overweight or obese can lead to low self-esteem, depression, and eating problems and disorders (Stice & Shaw, 2002). Although healthy weight loss habits may be beneficial for some individuals, specifically those with excessive weights (Plourde, 2006), these behaviours can negatively impact others. For example, young people focused on weight loss can be at greater risk for physical and mental issues, substance abuse, sexual risk taking, and being physically and sexually abusive (Lock, Reisel, & Steiner, 2001).
What are We Examining in this Chapter?
In this chapter, we examine trends related to healthy weights in Grade 6, Grade 8, and Grade 10 students. Healthy weight topics are divided into two sections: 1) overweight and obesity and 2) body image and weight loss practices. Policy and initiatives related to healthy weights are provided.
To measure the proportion of young people classified as overweight or obese, students were asked to report their height and weight. This information was then used to calculate respondents' body mass index (BMI). BMIs are calculated by dividing a student's body weight, measured in kilograms, by the square of her or his height, measured in metres. BMIs are then compared to international gender- and age-specific standards to determine if an individual is overweight or obese (Cole et al., 2000). Due to the self-report approach of the HBSC in measuring BMI, the percentage of overweight and obese adolescents presented in this report may be lower than if physical measurements were taken (Elgar & Stewart, 2008).
Body image perceptions were measured by asking students how they perceived their body, with five possible responses: 1) much too fat; 2) a bit too fat; 3) about the right size; 4) a bit too thin; and 5) much too thin. Students who perceived their body to be about the right size were considered to have a positive body image. Adolescents were also asked to report if they were presently on a diet or attempting to lose weight.
Overweight and Obesity
The percentage of students classified as overweight or obese, based on self-reports of height and weight has remained relatively stable over time, with slight fluctuations (Figures 8.1 and 8.2). For Grade 10 boys, Grade 10 girls, and Grade 8 girls, overweight and obesity levels have remained nearly constant from 2002 to 2010. In contrast, the highest reported rates of overweight or obese adolescents were found in 2006 at 29% for Grade 8 boys and 22% for Grade 6 girls. Overall, higher percentages of boys are overweight or obese based on self-reported BMI. No clear relationship exists between age and higher BMI.
Figure 8.1: Boys classified as overweight or obese on BMI (%)
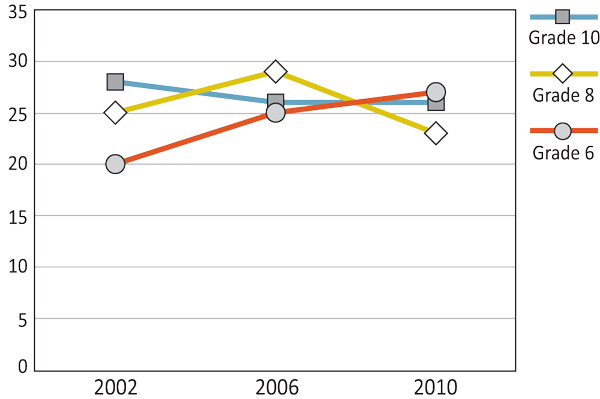
Text Equivalent - Figure 8.1
Figure 8.1 is a line graph that shows the percentage of boys who classified as overweight or obese on body mass index by grade and year of survey. The graph shows that among Grade 6 boys, 20% classified as overweight or obese on body mass index in 2002, compared to 25% in 2006 and 27% in 2010. Among Grade 8 boys, 25% classified as overweight or obese on body mass index in 2002, compared to 29% in 2006, and 23% in 2010. Among Grade 10 boys, 28% who classified as overweight or obese on body mass index in 2002, compared to 26% in 2006, and 26% in 2010.
Figure 8.2: Girls classified as overweight or obese on BMI (%)
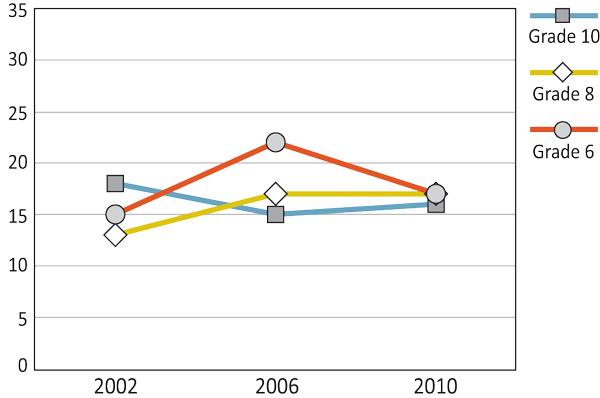
Text Equivalent - Figure 8.2
Figure 8.2 is a line graph that shows the percentage of girls who classified as overweight or obese on body mass index by grade and year of survey. The graph shows that among Grade 6 girls, 15% who classified as overweight or obese on body mass index in 2002, compared to 22% in 2006 and 17% in 2010. Among Grade 8 girls, 13% who classified as overweight or obese on body mass index in 2002, compared to 17% in 2006, and 17% in 2010. Among Grade 10 girls, 18% who classified as overweight or obese on body mass index in 2002, compared to 15% in 2006, and 16% in 2010.
In 2010 the Curbing Childhood Obesity: An Overview of the Federal, Provincial and Territorial Framework for Action to Promote Healthy Weights initiative was created and endorsed by Canadian Federal, Provincial, and Territorial Ministers of Health Promotion/Healthy Living. This initiative aims to decrease the prevalence of childhood obesity by making the issue a collective priority for action, focusing on three key policy priorities:
- making environments where children live, learn, and play more supportive of physical activity and healthy eating;
- identifying the risk of obesity in children and addressing it early; and
- increasing the availability and accessibility of nutritious foods and decreasing the marketing to children of food and beverages that are high in fat, sugar, or sodium.
One of the first projects of this initiative was Our Health Our Future - A National Dialogue on Healthy Weights in 2011, which set out to: 1) inform Canadians of the seriousness of the problem; 2) raise awareness of the factors that can contribute to excess weight in youth; 3) stimulate discussion on the topic; and 4) encourage commitment to take steps to foster healthy weights in youth.
(Public Health Agency of Canada, 2013a; Public Health Agency of Canada, 2013b)
At the provincial and territorial level, governments have also created and implemented their own strategies and initiatives aimed at preventing and reducing childhood obesity including Nova Scotia's 2012 Childhood Obesity Prevention Strategy and Ontario's 2010 Obesity Strategy.
(Active Healthy Kids Canada, 2012)
Body Images and Weight-loss Practices
As shown in Figures 8.3 and 8.4, young people's perception of their body being the right size has remained nearly constant (within 3%) from the 2002 to 2010 surveys. Boys consistently report slightly higher levels of body satisfaction than girls. The majority of young people are satisfied with the size of their body.
Figure 8.3: Boys who think their body is about the right size (%)
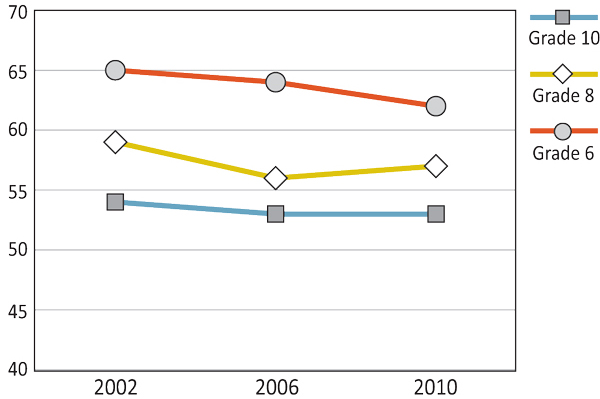
Text Equivalent - Figure 8.3
Figure 8.3 is a line graph that shows the percentage of boys who think their body is about right by grade and year of survey. The graph shows that among Grade 6 boys, 65% think their body is about right in 2002, compared to 64% in 2006 and 62% in 2010. Among Grade 8 boys, 59% think their body is about right in 2002, compared to 56% in 2006, and 57% in 2010. Among Grade 10 boys, 54% think their body is about right in 2002, compared to 53% in 2006, and 53% in 2010.
Figure 8.4: Girls who think their body is about the right size (%)
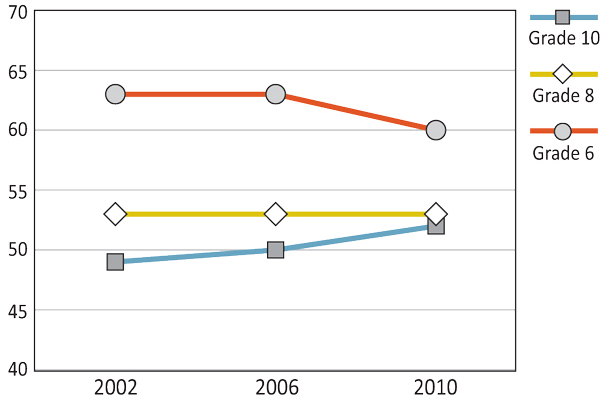
Text Equivalent - Figure 8.4
Figure 8.4 is a line graph that shows the percentage of girls who think their body is about right by grade and year of survey. The graph shows that among Grade 6 girls, 63% think their body is about right in 2002, compared to 63% in 2006 and 60% in 2010. Among Grade 8 girls, 53% think their body is about right in 2002, compared to 53% in 2006, and 53% in 2010. Among Grade 10 girls, 49% think their body is about right in 2002, compared to 50% in 2006, and 52% in 2010.
Similar to the trends in overweight and obesity (Figures 8.5 and 8.6), there are some cases of stability and others of slight fluctuations over the survey years with regards to students trying to lose weight. Between 2002 and 2010, the rates of Grade 8 boys, Grade 10 boys, and Grade 6 girls who reported dieting or doing something to lose weight remained relatively stable (within 2%). For Grade 6 boys and Grade 8 girls, a peak in weight loss efforts occurred in the 2006 survey, at 13% and 22%, respectively. Although the percentage of Grade 10 girls trying to lose weight has decreased 8% since 2002, this group still reported the highest levels in the 2010 survey. Whereas weight loss endeavours remain stable across age for boys, this behaviour increases with age for girls. For example, the 2010 survey demonstrated a difference of 10% between Grade 6 girls' and Grade 10 girls' weight loss efforts.
Figure 8.5: Boys on a diet or doing something to lose weight (%)
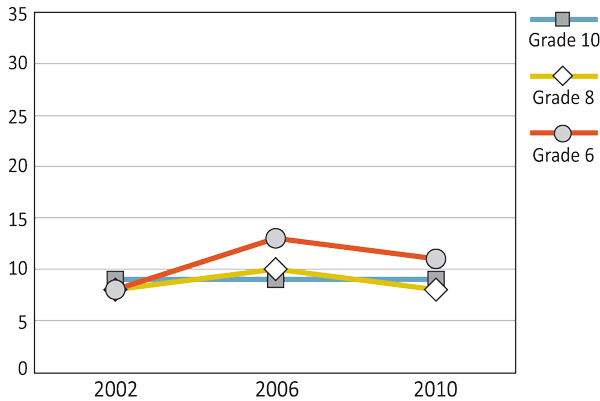
Text Equivalent - Figure 8.5
Figure 8.5 is a line graph that shows the percentage of boys on a diet or doing something to lose weight by grade and year of survey. The graph shows that among Grade 6 boys, 8% are on a diet or doing something to lose weight in 2002, compared to 13% in 2006 and 11% in 2010. Among Grade 8 boys, 8% are on a diet or doing something to lose weight in 2002, compared to 10% in 2006, and 8% in 2010. Among Grade 10 boys, 9% are on a diet or doing something to lose weight in 2002, compared to 9% in 2006, and 9% in 2010.
Figure 8.6: Girls on a diet or doing something to lose weight (%)
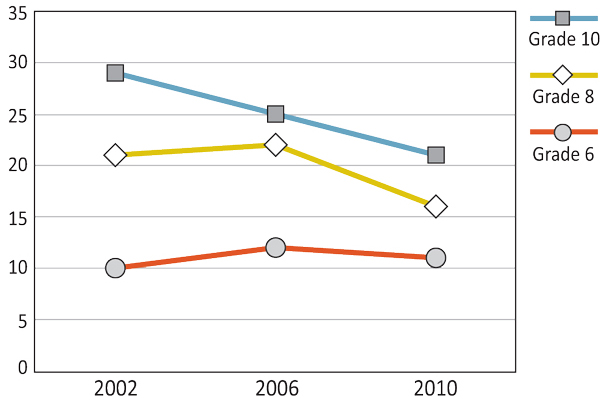
Text Equivalent - Figure 8.6
Figure 8.6 is a line graph that shows the percentage of girls on a diet or doing something to lose weight by grade and year of survey. The graph shows that among Grade 6 girls, 10% are on a diet or doing something to lose weight in 2002, compared to 12% in 2006 and 11% in 2010. Among Grade 8 girls, 21% are on a diet or doing something to lose weight in 2002, compared to 22% in 2006, and 16% in 2010. Among Grade 10 girls, 29% are on a diet or doing something to lose weight in 2002, compared to 25% in 2006, and 21% in 2010.
In 2007, the Mental Health Commission of Canada was established and made responsible for making mental health recommendations to the Canadian government over 10 years. Demonstrated in the 2012 Changing Directions, Changing Lives: The Mental Health Strategy for Canada, the Commission recognizes the necessity of acknowledging child and youth mental health issues, including eating disorders.
(Leitch, 2007; Mental Health Commission of Canada, 2012)
Summary and Implications
The healthy weights of young people have been recognized as a global problem, demonstrated in the World Health Organization's (WHO) 2009 Forum and Technical Meeting on Population-based Prevention Strategies for Childhood Obesity (World Health Organization, 2010). The most recent HBSC survey found one in four boys and one in six girls to be overweight or obese, according to their BMI, levels that have remained stable since the 2002 survey. Policies and initiatives created to encourage physical activity and healthy eating, as well as decrease sedentary behaviours (Walters, Holloman, Blomquist, & Bollier, 2003), have been in place over this time period. However, there has been recent recognition for the need to establish obesity-specific policies and initiatives.
The 2010 Curbing Childhood Obesity, a federal, provincial and territorial initiative, focuses on making excess weight in youth a collective priority and to continually measure and report on the effectiveness of its three key strategies. Additionally, federal funding, through the 2011 Achieving Healthier Weights in Canada's Communities and Managing Obesity Across the Lifecycle: An Interventions Approach, provides communities with financial assistance to help carry out these strategies (Public Health Agency of Canada, 2010). These homegrown action plans may lead to notable improvements in healthy weights as they are community-specific and recognize the diversity of particular populations. Similarly, insight into individuals' specific needs and potential solutions addressing obesity from Our Health Our Future - A National Dialogue on Healthy Weights Dialogue Report 2011 may improve the effectiveness of future healthy weights strategies. The latest HBSC survey results suggest that the prevalence of overweight and obese youth may have stabilized. In this respect, armed with recent policies and initiatives, we may begin to see a shift towards healthier weights.
Body image and weight loss practices have also remained relatively stable over time, with slight fluctuations in the latter. Overall, the majority of Canadian students report body satisfaction. Older girls demonstrate the highest prevalence of trying to lose weight at percentages more than double that of boys at the same grade level. This second finding is noteworthy as more boys than girls are classified as being overweight or obese. Currently, there are no federal policies or initiatives that focus specifically on positive body image. Nevertheless, the policies that are put in place to promote healthy weight behaviours emphasize health and not weight control or appearance. The latter elements are believed to foster a negative body image (Canadian Institute for Health Information [CIHI], 2003). Additionally, the Mental Health Commission of Canada acknowledges the importance of youth mental illness, including negative body images, that can possibly lead to other health problems including anxiety and eating disorders (Leitch, 2007).
References
- Active Healthy Kids Canada (2012). Active Healthy Kids Canada report card on physical activity for children and youth. Retrieved from http://www.activehealthykids.ca/ReportCard/PhysicalActivity.aspx
- Canadian Institute for Health Information [CIHI] (2003). Women's health surveillance report: A multi-dimensional look at the health of Canadian women. Ottawa, ON: Canadian Institution for Health Information.
- Elgar, F.J., Stewart J.M. (2008). Validity of screening for overweight and obesity using self-report data: Evidence from the Canadian Community Health Survey. Canadian Public Health Journal, 361, 423-427.
- Fletcher, A., Bonell, C., Sorhaindo, A. (2011). You are what your friends eat: Systematic review of social network analyses of young people's eating behaviours and bodyweight. Journal Epidemiology & Community Health, 65, 548-555.
- Hassink, S. (2003). Problems in childhood obesity. Primary Care Clinics Office Practice, 30, 357-374.
- Leitch, K.K. (2007). Reaching for the top: A report by the advisor on healthy children and youth. (HC Publication No. 4552). Retrieved from http://www.hc-sc.gc.ca/hl-vs/alt_formats/hpb-dgps/pdf/child-enfant/2007-advisor-conseillere/advisor-conseillere-eng.pdf
- Lock, J., Reisel, B., Steiner, H. (2001). Associated health risks of adolescents with disordered eating: How different are they from their peers? Results from a high school survey. Child Psychiatry and Human Development, 31, 249-265.
- Macdonald-Wallis, K., Jago, R., Sterne, J.A.C. (2012). Social network analysis of childhood and youth physical activity. American Journal of Preventative Medicine, 43, 636-642.
- Mental Health Commission of Canada [MHCC] (2012). Changing directions, changing lives: The mental health strategy for Canada. Retrieved from http://strategy.mentalhealthcommission.ca/pdf/strategy-images-en.pdf
- Plourde, G. (2006). Preventing and managing pediatric obesity: Recommendations for family physicians. Canadian Family Physician, 52, 322-328.
- Public Health Agency of Canada [PHAC] (2010). Solicitation: Achieving healthier weights in Canada's communities. Retrieved from http://www.phac-aspc.gc.ca/ph-sp/fund-fonds/ahwcc-apscc-eng.php
- Public Health Agency of Canada [PHAC] (2013a). Curbing childhood obesity: A federal, provincial and territorial framework for action to promote healthy weights. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/framework-cadre/pdf/ccofw-eng.pdf
- Public Health Agency of Canada [PHAC] (2013b). Our health our future - A National dialogue on healthy weights dialogue report. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/ohof-nsna/assets/pdf/ohof-nsna-eng.pdf
- Puhl, R.M., Heur, C.A. (2009). The stigma of obesity: A review and update. Obesity, 17, 941-964.
- Singh, A.S., Mulder, C., Twisk, J.W.R., van Mechelen, W., Chinapaw, M.J. (2008). Tracking of childhood overweight into adulthood: A systematic review of the literature. Obesity Reviews, 9, 474-488.
- Stice, E., Shaw, H.E. (2002). Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. Journal of Psychosomatic Research, 53, 985-993.
- Walters, P.H., Holloman, A., Blomquist, L., Bollier, M. (2003). Childhood obesity: Causes and treatment. American College of Sports Medicine Health and Fitness Journal, 7, 17-22.
- World Health Organization [WHO] (2012). Obesity and overweight. Retrieved from http://www.who.int/mediacentre/factsheets/fs311/en/
- World Health Organization [WHO] (2010). Population-based prevention strategies for childhood obesity. Geneva, Switzerland: World Health Organization.
Chapter 9: Substance Use and Related Risk Behaviours
By Heather Coe
Why are Health Risk Behaviours Important?
The adolescent years are a critical time for the development of healthy behaviours and lifelong health-related habits. For many youth, adolescence is also a period of exploration and discovery (Harris, Duncan, & Boisjoly, 2002). With an increase in autonomy, peer pressure, and the desire to push the boundaries of parental authority, many adolescents experiment with smoking, alcohol, drugs, and other risky behaviours (Chassin, Pitts, & Prost, 2002; Harris et al., 2002; Health Canada, 2010). Although some youth engage in these actions simply to test or try them out, others use substances as a way of coping with stress, or managing health symptoms of chronic physical and mental health conditions (Saewyc, 2007). Young people may go on to occasional or even frequent use, which can pose significant threat to their health and well-being. For example, substance abuse may lead to health-related problems, such as obesity and high blood pressure (Oesterle et al., 2004) and may increase the likelihood of further abuse in adulthood (D'Amico et al., 2005). Additionally, these adolescents may be exposed to negative consequences associated with decisions made while under the influence, such as injuries sustained from impaired driving (Chassin et al., 2002).
For some adolescents, the engagement in risky substance use tends to occur alongside other health difficulties, such as social and emotional problems (Elgar, Knight, Worrall, & Sherman, 2003), cognitive and psychomotor impairment (Squeglia, Jacobus, & Tapert, 2009), and academic difficulties (Suhrcke & de Paz Nieves, 2011). In addition, risk factors--such as exposure to violence and abuse, the quality of parenting and family support, peer behaviours, academic problems and negative perceptions of school, social norms that support heavy substance use, and even the availability of drugs and alcohol--are part of the social environment that influence substance use and other risk behaviours among youth (Saewyc, 2007; Simons-Morton & Chen, 2006).
To help minimize the negative impacts of substance use and related risk behaviours, prevention strategies must reflect the needs of the adolescent population. In this sense, it is important to examine trends related to these behaviours over time, as well as observe the current rates of engagement among youth, to best develop and adapt substance use prevention strategies.
What are We Examining in this Chapter?
In this chapter, we examine trends related to substance use and risky behaviour among Canadian youth. These trends are divided into three major categories: 1) smoking tobacco; 2) alcohol use; and 3) cannabis use. Policy initiatives and legislation related to smoking, alcohol, and drug use are also explored.
In the HBSC surveys, reports on Grade 6, Grade 8, and Grade 10 student daily tobacco use and weekly alcohol consumption were obtained. In particular, these reports focused on beer, wine, and liquor consumption among youth. In addition, rates of perceived drunkenness (having been "really drunk") were acquired. Older students (Grades 9 and 10) provided information about whether or not they had ever used cannabis.
Smoking Tobacco
Daily smoking has decreased in Canada since the 1990s among Grade 8 and Grade 10 students, while remaining at a low level for Grade 6 students across the years (Figures 9.1 and 9.2). For Grade 8 students, the steepest decline in daily smoking occurred between the 1998 and 2002 surveys with continuing small decreases since 2002. That trend is repeated for Grade 10 girls. The decrease for Grade 10 boys came between the 2002 and 2006 surveys with a slight increase between 2006 and 2010.
Figure 9.1: Boys who report daily smoking (%)
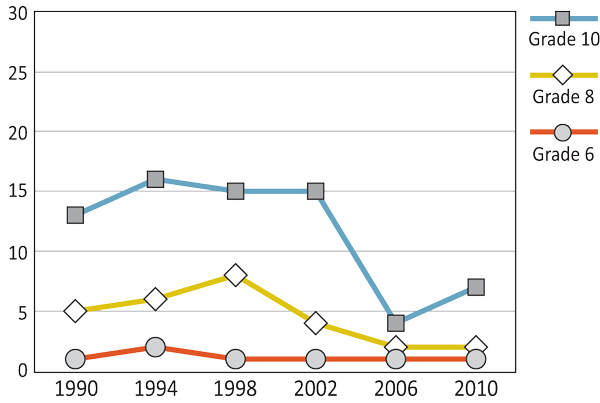
Text Equivalent - Figure 9.1
Figure 9.1 is a line graph that shows the percentage of boys who report daily smoking, by grade, gender and year of survey. The graph shows that 1% of Grade 6 boys who report daily smoking in 1990, compared to 2% in 1994, 1% in 1998, 1% in 2002, 1% in 2006, and 1% in 2010. Among Grade 8 boys, 5% who report daily smoking in 1990, compared to 6% in 1994, 8% in 1998, 4% in 2002, 2% in 2006, and 2% in 2010. Among Grade 10 boys, 13% who report daily smoking in 1990, compared to 16% in 1994, 15% in 1998, 15% in 2002, 4% in 2006, and 7% in 2010.
Figure 9.2: Girls who report daily smoking (%)
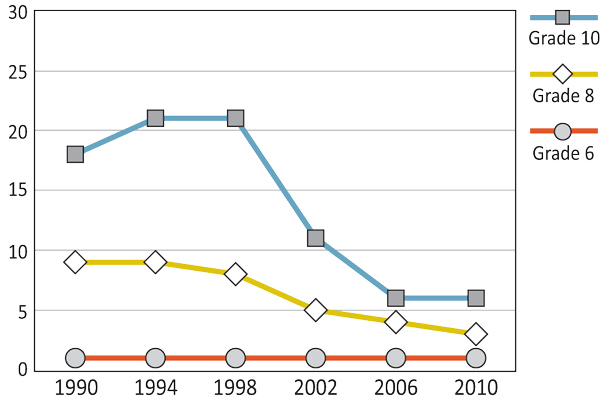
Text Equivalent - Figure 9.2
Figure 9.2 is a line graph that shows the percentage of girls who report daily smoking, by grade, gender and year of survey. The graph shows that 1% of Grade 6 girls who report daily smoking in 1990, compared to 1% in 1994, 1% in 1998, 1% in 2002, 1% in 2006, and 1% in 2010. Among Grade 8 girls, 9% who report daily smoking in 1990, compared to 9% in 1994, 8% in 1998, 5% in 2002, 4% in 2006, and 3% in 2010. Among Grade 10 girls, 18% who report daily smoking in 1990, compared to 21% in 1994, 21% in 1998, 11% in 2002, 6% in 2006, and 6% in 2010.
The federal Tobacco Act, passed in 1997, aims:
- to protect the health of Canadians in light of conclusive evidence implicating tobacco use in the incidence of numerous debilitating and fatal diseases;
- to protect young persons and others from inducements to use tobacco products and the consequent dependence on them;
- to protect the health of young persons by restricting access to tobacco products;
- to enhance public awareness of the health hazards of using tobacco products.
This federal act regulates the manufacture, sale, labelling, and promotion of tobacco within Canada. At the provincial and territorial level, the implementation of laws related to tobacco use, in particular the ban of smoking in public places, aspires to not only improve the overall health of Canadians but also reduce smoking behaviour and change social norms regarding smoking.
In 1999, the New Directions for Tobacco Control in Canada - A National Strategy was adopted at the federal, provincial, and territorial level. Providing a framework for action, this national tobacco control strategy outlines five strategic directions (policy and legislation; public education; industry accountability and product control; research; building and supporting capacity for action) and encourages collaborative action across governments and non-governmental organizations. Under the guidance of the Tobacco Control Liaison Committee, this strategy aims to accomplish four goals: 1) Prevention (preventing tobacco use among youth); 2) Cessation (encouraging and helping smokers to stop using tobacco products); 3) Protection (protecting Canadians from exposure to second-hand smoke); and 4) Denormalization (educating Canadians about industry marketing strategies and the health effects of tobacco products).
Recently implemented in 2011, the Tobacco Products Labelling Regulations (Cigarettes and Little Cigars) (TPLR-CLC)--part of the national strategy to reduce smoking rates--stipulates the requirements for health-related labels on all cigarette and little cigar packages sold. The TPLR-CLC requires that these packages must display:
- health warning messages covering 75% of the front and back of the packages;
- health information messages on the inside of the packages;
- toxic emissions statements on the side of the packages.
(Health Canada, 2007a; 2007b; 2011; Tobacco Act, 1997)
Alcohol Use
Overall, as shown in Figures 9.3 and 9.4, beer consumption rates among youth have consistently differed by age and gender, regardless of survey year. Grade 6 girls have maintained the lowest rates over time, while Grade 10 boys have continuously exhibited the highest prevalence of weekly beer consumption. Although Grade 10 girls have reliably displayed the second highest rates of beer consumption, these levels have remained relatively low compared to Grade 10 boys.
Figure 9.3: Boys who report drinking beer at least once a week (%)
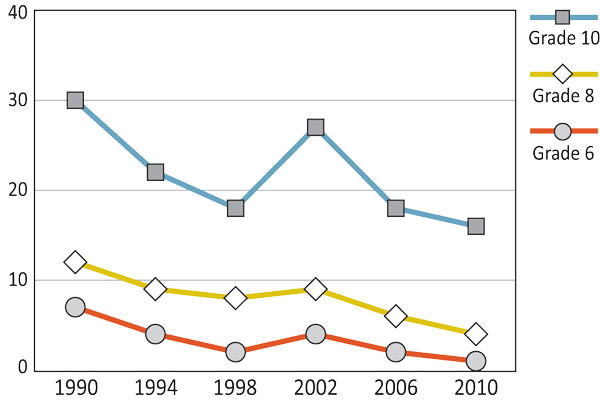
Text Equivalent - Figure 9.3
Figure 9.3 is a line graph that shows the percentage of boys who report drinking beer at least once a week, by grade, gender and year of survey. The graph shows that 7% of Grade 6 boys reported drinking beer at least once a week in 1990, compared to 4% in 1994, 2% in 1998, 4% in 2002, 2% in 2006, and 1% in 2010. Among Grade 8 boys, 12% reported drinking beer at least once a week in 1990, compared to 9% in 1994, 8% in 1998, 9% in 2002, 6% in 2006, and 4% in 2010. Among Grade 10 boys, 30% reported drinking beer at least once a week in 1990, compared to 22% in 1994, 18% in 1998, 27% in 2002, 18% in 2006, and 16% in 2010.
Figure 9.4: Girls who report drinking beer at least once a week (%)
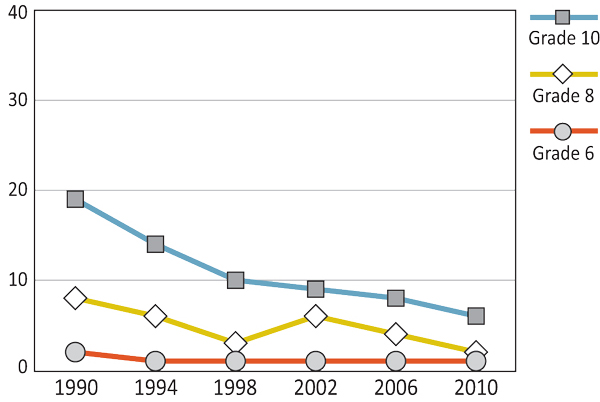
Text Equivalent - Figure 9.4
Figure 9.4 is a line graph that shows the percentage of girls who report drinking beer at least once a week, by grade, gender and year of survey. The graph shows that 2% of Grade 6 girls reported drinking beer at least once a week in 1990, compared to 1% in 1994, 1% in 1998, 1% in 2002, 1% in 2006, and 1% in 2010. Among Grade 8 girls, 8% reported drinking beer at least once a week in 1990, compared to 6% in 1994, 3% in 1998, 6% in 2002, 4% in 2006, and 2% in 2010. Among Grade 10 girls, 19% reported drinking beer at least once a week in 1990, compared to 14% in 1994, 10% in 1998, 9% in 2002, 8% in 2006, and 6% in 2010.
The percentage of students who report drinking beer at least once a week has declined from 1990 to 2010. One noticeable disruption to this pattern occurred in 2002, where Grade 10 boys' weekly beer consumption spiked, perhaps due to the timing of that survey during the spring months. This increase (also evident to a lesser degree in Grade 6 and Grade 8 boys, as well as Grade 8 girls) is uncharacteristic of the otherwise decreasing trend observed throughout the survey years. In fact, the 2010 survey displayed the lowest levels of reported beer consumption for all grade levels and genders: Grade 6 boys - 1%; Grade 6 girls - 1%; Grade 8 boys - 4%; Grade 8 girls - 2%; Grade 10 boys - 16%; and Grade 10 girls - 6%.
The level of wine consumption among youth has remained low across the survey years, with Grade 10 boys consistently displaying the highest levels of consumption (Figures 9.5 and 9.6). Comparable to that of beer consumption, student reports of drinking wine at least once a week declined between 1990 and 2010, with a small increase in rates for boys of all ages and Grade 8 girls in 2002. Similar to beer consumption, the 2010 survey results also yielded the lowest levels of wine consumption for all grade levels and genders: Grade 6 boys - 1%; Grade 6 girls - 1%; Grade 8 boys - 2%; Grade 8 girls - 1%; Grade 10 boys - 3%; and Grade 10 girls - 1%.
Figure 9.5: Boys who report drinking wine at least once a week (%)
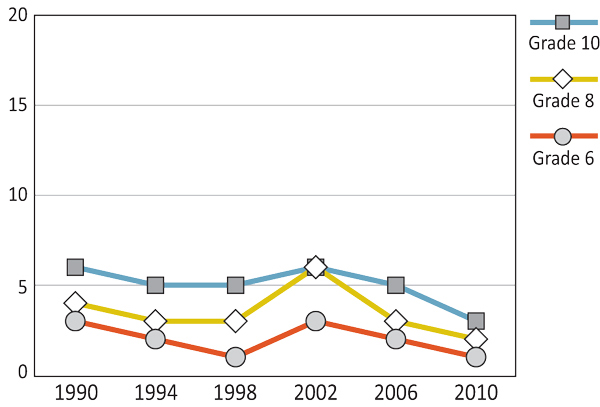
Text Equivalent - Figure 9.5
Figure 9.5 is a line graph that shows the percentage of boys who report drinking wine at least once a week, by grade, gender and year of survey. The graph shows that 3% of Grade 6 boys reported drinking wine at least once a week in 1990, compared to 2% in 1994, 1% in 1998, 3% in 2002, 2% in 2006, and 1% in 2010. Among Grade 8 boys, 4% reported drinking wine at least once a week in 1990, compared to 3% in 1994, 3% in 1998, 6% in 2002, 3% in 2006, and 2% in 2010. Among Grade 10 boys, 6% reported drinking wine at least once a week in 1990, compared to 5% in 1994, 5% in 1998, 6% in 2002, 5% in 2006, and 3% in 2010.
Figure 9.6: Girls who report drinking wine at least once a week (%)
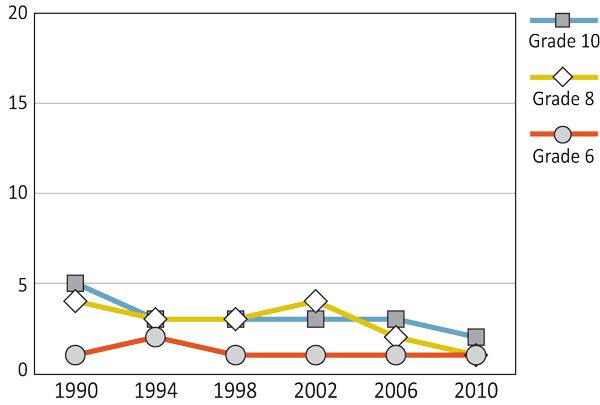
Text Equivalent - Figure 9.6
Figure 9.6 is a line graph that shows the percentage of girls who report drinking wine at least once a week, by grade, gender and year of survey. The graph shows that 1% of Grade 6 girls reported drinking wine at least once a week in 1990, compared to 2% in 1994, 1% in 1998, 1% in 2002, 1% in 2006, and 1% in 2010. Among Grade 8 girls, 4% reported drinking wine at least once a week in 1990, compared to 3% in 1994, 3% in 1998, 4% in 2002, 2% in 2006, and 1% in 2010. Among Grade 10 girls, 5% reported drinking wine at least once a week in 1990, compared to 3% in 1994, 3% in 1998, 3% in 2002, 3% in 2006, 2% in 2010.
Whereas Grade 6 students' liquor consumption has remained low throughout the survey years (Figures 9.7 and 9.8), the percentage of Grade 8 and Grade 10 students who reported drinking liquor at least once a week has fluctuated. In general, Grade 8 and Grade 10 student liquor consumption declined from 1990 to 2010, with a noticeable spike in 2002, similar to the trend found in beer and wine consumption. Despite these variations, the latest survey results indicated that 10% of both Grade 10 boys and Grade 10 girls drank liquor at least once a week. When compared to the declining rates of beer and wine consumption, Grade 10 liquor consumption shows minimal change for boys and no change for girls. In 2010, liquor rated as the most consumed form of alcohol for Grade 10 girls and the second most consumed form of alcohol for Grade 10 boys.
Figure 9.7: Boys who report drinking liquor at least once a week (%)
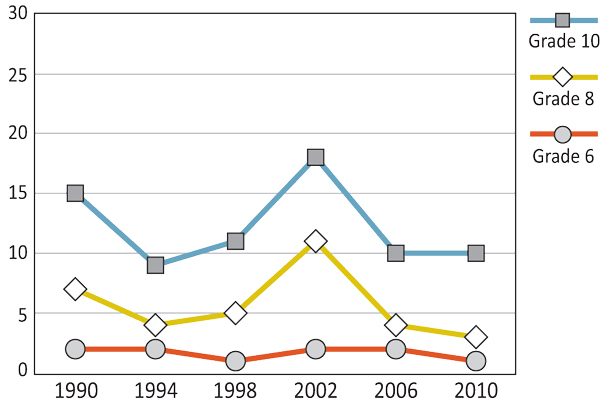
Text Equivalent - Figure 9.7
Figure 9.7 is a line graph that shows the percentage of boys who report drinking liquor at least once a week, by grade, gender and year of survey. The graph shows that 2% of Grade 6 boys reported drinking liquor at least once a week in 1990, compared to 2% in 1994, 1% in 1998, 2% in 2002, 2% in 2006, and 1% in 2010. Among Grade 8 boys, 7% reported drinking liquor at least once a week in 1990, compared to 4% in 1994, 5% in 1998, 11% in 2002, 4% in 2006, and 3% in 2010. Among Grade 10 boys, 15% reported drinking liquor at least once a week in 1990, compared to 9% in 1994, 11% in 1998, 18% in 2002, 10% in 2006, and 10% in 2010.
Figure 9.8: Girls who report drinking liquor at least once a week (%)
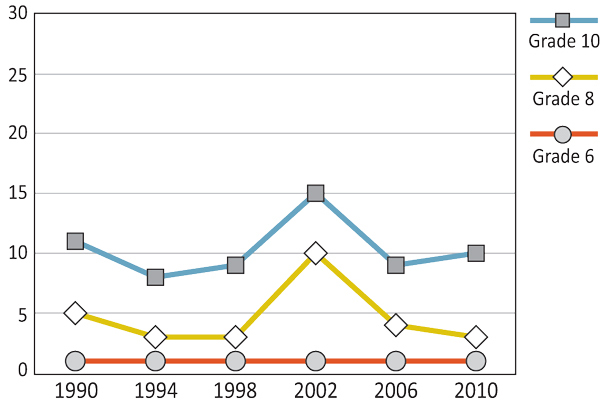
Text Equivalent - Figure 9.8
Figure 9.8 is a line graph that shows the percentage of students who report drinking liquor at least once a week, by grade, gender and year of survey. The graph shows that 1% of Grade 6 girls reported drinking liquor at least once a week in 1990, compared to 1% in 1994, 1% in 1998, 1% in 2002, 1% in 2006, and 1% in 2010. Among Grade 8 girls, 5% reported drinking liquor at least once a week in 1990, compared to 3% in 1994, 3% in 1998, 10% in 2002, 4% in 2006, and 3% in 2010. Among Grade 10girls, 11% reported drinking liquor at least once a week in 1990, compared to 8% in 1994, 9% in 1998, 15% in 2002, 9% in 2006, and 10% in 2010.
| Grade 10 Boys | Grade 10 Girls | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1990 | 1994 | 1998 | 2002 | 2006 | 2010 | 1990 | 1994 | 1998 | 2002 | 2006 | 2010 | |
| Beer | 30 | 22 | 18 | 27 | 18 | 16 | 19 | 14 | 10 | 9 | 8 | 6 |
| Wine | 6 | 5 | 5 | 6 | 5 | 3 | 5 | 3 | 3 | 3 | 3 | 2 |
| Liquor | 15 | 9 | 11 | 18 | 10 | 10 | 11 | 8 | 9 | 15 | 9 | 10 |
Text Equivalent - Table 9.1
Table 9.1 shows the percentage of Grade 10 students who drank beer, wine, liquor once a week or more by year of survey and gender. The table shows that in 1990, 30% of boys and 19% of girls drank beer once a week or more compared to 22% of boys and 14% of girls in 1994, 18% of boys and 10% of girls in 1998, 27% of boys and 9% of girls in 2002, 18% boys and 8% of girls in 2006 and 16% of boys and 6% of girls in 2010. On the same question, the table shows 6% of boys and 5% of girls drank wine once a week or more in 1990 compared to 5% of boys and 3% of girls in 1994, 5% of boys and 3% of girls in 1998, 6% of boys and 3% of girls in 2002, 5% boys and 3% of girls in 2006 and 3% of boys and 2% of girls in 2010. On the same question, the table shows 15% of boys and 11% of girls drank liquor once a week or more in 1990 compared to 9% of boys and 8% of girls in 1994, 11% of boys and 9% of girls in 1998, 18% of boys and 15% of girls in 2002, 10% boys and 9% of girls in 2006 and 10% of boys and 10% of girls in 2010.
Between 1990 and 2010, the percentage of students reporting to have been "really drunk" at least twice in their life has declined slightly. As illustrated in Figures 9.9 and 9.10, rates for boys and girls mirror each other from 1990-2010, being at equivalent levels within the same grade. While Grade 6 students have consistently reported the lowest levels of perceived "drunkenness," Grade 10 students have reliably displayed the highest levels throughout the survey years. Most recently in 2010, 41% of Grade 10 boys and 39% of Grade 10 girls reported to have been "really drunk" at least twice. These Grade 10 rates more than double those of the Grade 8 students, where 13% of boys and 14% of girls reported drunkenness.
Figure 9.9: Boys who report having been "really drunk" at least twice (%)

Text Equivalent - Figure 9.9
Figure 9.9 is a line graph that shows the percentage of boys who report having been “really drunk� at least twice, by grade, gender and year of survey. The graph shows that 7% of Grade 6 boys reported having been really drunk at least twice in 1990, compared to 4% in 1994, 3% in 1998, 4% in 2002, 3% in 2006, and 2% in 2010. Among Grade 8 boys, 23% reported having been really drunk at least twice in 1990, compared to 15% in 1994, 18% in 1998, 17% in 2002, 15% in 2006, and 13% in 2010. Among Grade 10 boys, 48% reported having been really drunk at least twice in 1990, compared to 39% in 1994, 43% in 1998, 46% in 2002, 39% in 2006, and 41% in 2010.
Figure 9.10: Girls who report having been "really drunk" at least twice (%)
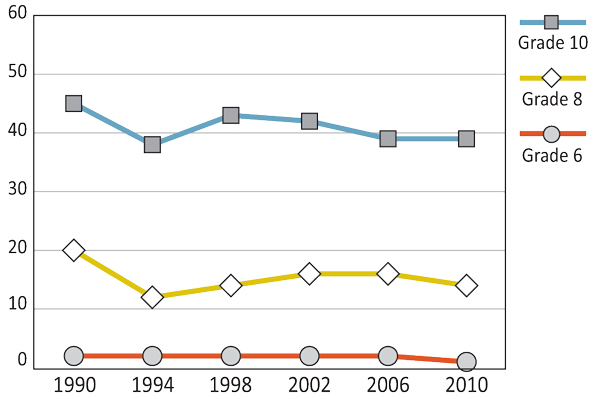
Text Equivalent - Figure 9.10
Figure 9.10 is a line graph that shows the percentage of girls who report having been “really drunk� at least twice, by grade, gender and year of survey. The graph shows that 2% of Grade 6 girls reported having been really drunk at least twice in 1990, compared to 2% in 1994, 2% in 1998, 2% in 2002, 2% in 2006, and 1% in 2010. Among Grade 8 girls, 20% reported having been really drunk at least twice in 1990, compared to 15% in 1994, 14% in 1998, 16% in 2002, 16% in 2006, and 14% in 2010. Among Grade 10 girls, 45% reported having been really drunk at least twice in 1990, compared to 38% in 1994, 43% in 1998, 42% in 2002, 39% in 2006, and 39% in 2010.
Implemented in 1996, the Canadian Radio-Television Telecommunications Commission (CRTC) Code for Broadcast Advertising of Alcoholic Beverages prohibits advertisers from targeting underage drinkers in their commercial messages.
(CRTC, 1996)
In the document, Reducing Alcohol-Related Harm in Canada: Toward a Culture of Moderation (2007), the National Alcohol Strategy Working Group outlines 41 recommendations to reduce alcohol-related harm and to encourage the development of a culture of moderate alcohol use within Canada. In 2008, the National Alcohol Strategy Advisory Committee--working under the umbrella of the Canadian Centre on Substance Abuse--was organized to implement, monitor, and evaluate these recommendations.
Recommendations for a National Alcohol Strategy are divided into four strategic areas for action: 1) health promotion, prevention, and education; 2) health impacts and treatment; 3) availability of alcohol; and 4) safer communities. Within this report, underage drinking is identified as one of 12 "risky drinking practices" (p. 8). As a result, a need for health promotion, prevention, and education programs for youth is identified as an important component within the Strategy.
(Canadian Centre on Substance Abuse, 2013; National Alcohol Strategy Working Group, 2007)
Cannabis Use
Between 1990 and 2010, the number of Grade 10 students who reported having ever tried cannabis has increased over time (Figures 9.11 and 9.12). In 2010, 40% of boys and 37% of girls reported having tried cannabis. When comparing these rates to those of the 1990 survey, a rise of 14% for boys and 13% for girls can be observed. For Grade 10 boys, cannabis use peaked in 2002 at a rate of 50%. For Grade 10 girls, peak levels of cannabis use were observed in 1998 and 2002, with rates of 41% and 40%, respectively.1
Because of the need to examine trends over time, some substances that have only recently been included in the HBSC survey, such as heroin and prescription drugs to get high, are not described in the current report.
Figure 9.11: Boys who report having ever tried cannabis (%)
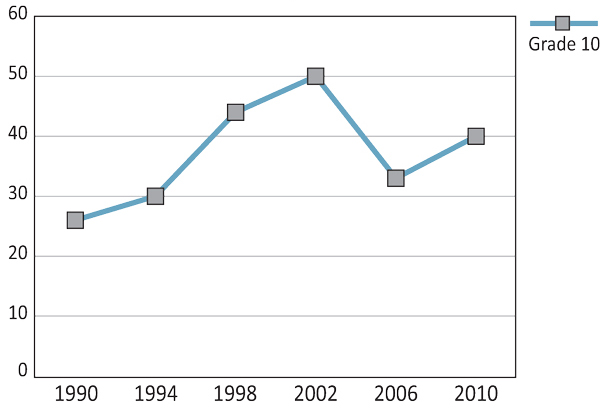
Text Equivalent - Figure 9.11
Figure 9.11 is a line graph that shows the percentage of Grade 10 boys who have ever tried cannabis, by gender and year of survey. The graph shows that 26% of Grade 10 boys had tried cannabis in 1990, compared to 30% in 1994, 44% in 1998, 50% in 2002, 33% in 2006, and 40% in 2010.
Figure 9.12: Girls who report having ever tried cannabis (%)
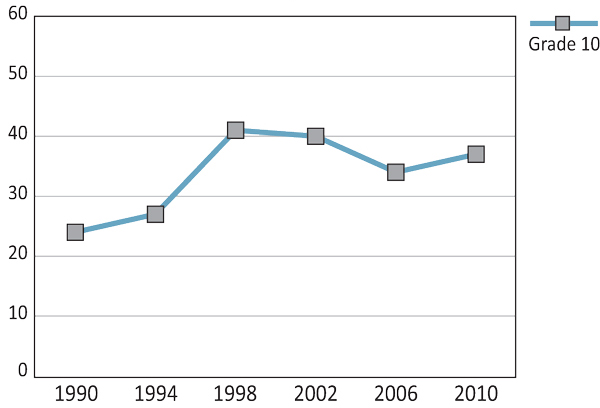
Text Equivalent - Figure 9.12
Figure 9.12 is a line graph that shows the percentage of Grade 10 girls who have ever tried cannabis, by gender and year of survey. The graph shows that 24% of Grade 10 girls had tried cannabis in 1990, compared to 27% in 1994, 41% in 1998, 40% in 2002, 34% in 2006, and 37% in 2010.
With the overall goal to contribute to safer and healthier communities, the National Anti-Drug Strategy (NADS) is a federal initiative aimed to prevent use, treat dependency, and reduce production and distribution of illicit drugs. Launched in 2007, this initiative places a particular emphasis on youth and incorporates three action plans: 1) prevention (to prevent youth from using illicit drugs through increasing awareness and understanding of harmful effects); 2) treatment (to support treatment and rehabilitation systems and services); and 3) enforcement (to disrupt illicit drug operations).
As part of NADS, A Drug Prevention Strategy for Canada's Youth--a national initiative directed by the Canadian Centre on Substance Abuse (CCSA)--aims to reduce illicit drug use among youth. This strategy is composed of three components: 1) standards for youth substance abuse prevention; 2) a media/youth consortium; and 3) sustainable partnerships.
(CCSA, 2012; Government of Canada, 2010; Treasury Board of Canada Secretariat, 2012)
Summary and Implications
Beginning in the late 1990s, there has been a decline in the prevalence of smoking among Canadian adolescents. This positive finding may reflect changes in social norms and attitudes among youth surrounding the use of tobacco products. The implementation of the Tobacco Act in 1997 and associated policy initiatives (such as the ban of smoking in public places) may mark the beginning of this trend. Similarly, the New Directions for Tobacco Control in Canada - A National Strategy framework may have further influenced the reduced rates of smoking among youth. With the ongoing collective efforts of federal, provincial, territorial, and municipal governments, as well as non-governmental organizations, the collaborative nature of this national tobacco control strategy may be key to the success of the initiative and its ability to accomplish the four overarching goals originally outlined within the framework (prevention, cessation, protection, and denormalization).
Whereas the overall rates of alcohol consumption have declined over the survey years, Grade 10 students have consistently displayed the highest levels of beer, wine, and liquor consumption. While the general decline in alcohol consumption may be reflective of health promotion efforts, the elevated levels of self-reported drunkenness among Grade 10 students within the 2010 survey, in conjunction with the relatively stable rates of liquor consumption, indicate the need for additional work in this area. Introduced in 2007, Reducing Alcohol-Related Harm in Canada: Toward a Culture of Moderation recognizes the need for health promotion, prevention, and education programs for youth as an important component when developing a culture of moderate alcohol use (National Alcohol Strategy Working Group, 2007).
While HBSC survey results indicate declining trends in smoking and alcohol consumption, cannabis use increased substantially between 1990 and 1998 among Canadian adolescents with minimal change since. The latest survey results indicated that 40% of Grade 10 boys and 37% of Grade 10 girls reported they had tried cannabis within their lifetime. The high level of cannabis use can be viewed as troubling and indicates the need for additional policy and drug prevention initiatives. While no initiatives focus solely on cannabis use, there are federal, provincial or territorial programs to support drug prevention efforts beyond alcohol and tobacco. The Canadian Centre of Substance Abuse's Drug Prevention Strategy introduced a number of Canadian Standards and Guidelines (2010a, 2010b and 2011) aiming to reduce drug use and influence future cannabis use among youth including delaying age of first use. In addition to CCSA's efforts there are also provincial and territorial programs that support drug prevention efforts including the Alberta Health Services Community Action on Drugs Use Prevention (2010).
References
- Alberta Health Services (2010). Community Action on Drugs Use Prevention. Retrieved from: http://www.albertahealthservices.ca/AddictionsSubstanceAbuse/if-com-community-action-manual.pdf
- Canadian Centre of Substance Abuse [CCSA] (2010a). Building on our strengths: Canadian standards for school-based youth substance abuse prevention. Ottawa, ON: Canadian Centre on Substance Abuse.
- Canadian Centre of Substance Abuse [CCSA] (2010b). Stronger Together: Canadian Standards for Community-based Youth Substance Abuse Prevention. Ottawa, ON: Canadian Centre on Substance Abuse.
- Canadian Centre of Substance Abuse [CCSA] (2011). Strengthening Our Skills: Canadian Guidelines for Youth Substance Abuse Prevention Family Skills Programs. Ottawa, ON: Canadian Centre on Substance Abuse.
- Canadian Centre on Substance Abuse [CCSA] (2012). Youth Drug Prevention. Retrieved from: http://www.ccsa.ca/Eng/Priorities/YouthPrevention/Pages/default.aspx
- Canadian Centre on Substance Abuse [CCSA] (2013). National alcohol strategy: Reducing alcohol-related harm in Canada. Retrieved from: http://www.ccsa.ca/Eng/Priorities/Alcohol/Pages/default.aspx
- Canadian Radio-television and Telecommunications Commission [CRTC] (1996). Code for broadcast advertising of alcoholic beverages. Retrieved from: http://www.crtc.gc.ca/eng/general/codes/alcohol.htm
- Government of Canada (2010). The national anti-drug strategy. Retrieved from: http://www.nationalantidrugstrategy.gc.ca/nads-sna.html
- Chassin, L., Pitts, S.C., Prost, J. (2002). Binge drinking trajectories from adolescence to emerging adulthood in high-risk sample: predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology, 70, 17-78. Doi: 10.1037//0022-006X.70.1.67
- D'Amico, E.J., Ellickson, P.L., Collins, R.L., Martino, S., Klein, D.J. (2005). Processes linking adolescent problems to substance-use problems in late young adulthood. Journal of Studies on Alcohol and Drugs, 6, 766-775.
- Elgar, F.J., Knight, J., Worrall, G.J., Sherman, G. (2003). Behavioural and substance use problems in rural and urban delinquent males. Canadian Journal of Psychiatry, 48, 633-636.
- Harris, K.M., Duncan, G.J., Boisjoly, J. (2002). Evaluating the role of "nothing to lose" attitudes on risky behavior in adolescence. Social Forces, 80, 1005-1039.
- Health Canada (2007a). A national strategy. Retrieved from: http://www.hc-sc.gc.ca/hc-ps/pubs/tobac-tabac/ns-sn/index-eng.php
- Health Canada (2007b). Public smoking bans by province and territory. Retrieved from: http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/res/news-nouvelles/ban-interdiction-public-eng.php
- Health Canada (2010). Keeping your kids smoke free. Retrieved from: http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/quit-cesser/kids-enfants/index-eng.php
- Health Canada (2011). Tobacco Act. Retrieved from: http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/legislation/federal/tobac-tabac-eng.php
- National Alcohol Strategy Working Group (2007). Reducing alcohol-related harm in Canada: Toward a culture of moderation. Ottawa, ON: Health Canada.
- Oesterle, S., Hill, K.G., Hawkins, J.D., Guo, J., Catalano, R.F., Abbott, R.D. (2004). Adolescent heavy episodic drinking trajectories and health in young adulthood. Journal of Studies on Alcohol and Drugs, 65, 204-212.
- Saewyc, E.M. (2007). Chapter 2. Substance abuse among non-mainstream youth. In Substance Abuse in Canada: Focus on Youth. Ottawa, ON: Canadian Centre on Substance Abuse.
- Simons-Morton, B., Chen, R.S. (2006). Over time relationships between early adolescent and peer substance use. Addictive Behaviors, 31, 1211-1223.
- Squeglia, L.M., Jacobus, J., Tapert, S.F. (2009). The influence of substance use on adolescent brain development. Clinical EEG and Neuroscience, 40, 31-38.
- Suhrcke, M., e Pas Nieves, C. (2011). The impact of health and health behaviours on educational outcomes in high-income countries: A review of the evidence. Copenhagen, Denmark: WHO Regional Office for Europe.
- Tobacco Act (1997). Tobacco Act (S.C. 1997, c. 13). Retrieved from: http://laws-lois.justice.gc.ca/eng/acts/T-11.5/page-1.html
- Treasury Board of Canada Secretariat (2012). National anti-drug strategy. Retrieved from: http://www.tbs-sct.gc.ca/hidb-bdih/initiative-eng.aspx?Hi=28
Chapter 10: Sexual Health
By Mary-Anne Reid
Why are Sexual Health Behaviours Among Youth Important?
Adolescence is an important time to set a foundation for life-long healthy behaviours, including sexual health behaviours. It is during this stage of life when psychosocial development is prominent and the number of youth engaging in sexual activities begins to increase (MacDonald et al., 2011). Sexual Education is necessary for this age group, as there are high consequences for engaging in risky sexual activity. These consequences could include HIV and other sexually transmitted infections (STIs), as well as teen pregnancies and resultant reproductive difficulties. Some of the highest rates of STIs in Canada are found in young people, highlighting the importance of educating this group so they are able to make informed decisions (Public Health Agency of Canada [PHAC], 2007).
In addition, risky sexual health behaviours are often linked with other risk-taking behaviours, harmful social relationships, and negative mental health in youth (Biglan et al., 1990; Boislard, Poulin, Kiesner, & Dishion, 2009; Elkington, Bauermeister, & Zimmerman, 2010). For example, not using condoms has been associated with antisocial behaviour, cigarette smoking, and illicit drug and alcohol use (Biglan et al., 1990). The social context also plays an important role in determining youth engagement in risky sexual activities. Youth problem behaviours (e.g., substance use) and risky sexual activity (e.g., not using a condom) have been found to be positively associated with delinquent peer groups and lack of positive parental practices (e.g., monitoring social behaviour; Boislard et al., 2009).
Education regarding the negative consequences of engaging in risky sexual activity may help to reduce the harm to public health (Kirby, Laris, & Rolleri, 2007). Youth who are in higher risk situations (e.g., homeless youth; Marshall et al., 2009; and aboriginal youth; Aboriginal Health Initiatives Sub-Committee, & Society of Obstetricians and Gynaecologists of Canada, 2011) may be more at risk of contracting STIs and HIV for a variety of reasons, including socioeconomic constraints, a lack of condom use, and sexual vulnerability. Providing resources and education for adolescents, including those in high-risk situations, may help to delay sexual activity and increase safer sex practices (Kirby, Laris, & Rolleri, 2007).
It is important to observe the trends associated with youth sexual activity to monitor the progression that sexual education and other initiatives are having on the reported number of individuals engaging in healthy sexual activity practices, such as abstinence and condom use. With a better understanding of youth's needs, as well as understanding of factors that may contribute to an increased chance of risk-taking behaviours, programs, strategies, and policies can be focused to best aid youth during this learning-centered time of life.
What are We Examining in this Chapter?
In this chapter, we are looking at trends related to sexual activity for Grade 9 and 10 students, divided by gender. Schools were given the option of including or excluding sexual health questions. If schools included the questions, students were asked about whether or not they had ever had sexual intercourse and if they had used a condom the last time they had sexual intercourse. Policy and government initiatives are included in this chapter regarding youth sexual health.
Since 2002, the number of Grade 9 and Grade 10 students who have reported having had sexual intercourse has increased (Figures 10.1 and 10.2). The biggest increase for reported sexual activity occurred between the 2006 and 2010 surveys, where levels rose 5% for Grade 9 boys, 6% for Grade 10 boys, and 4% for Grade 10 girls. This pattern, however, is not consistent for Grade 9 girls, whose levels of reported sexual activity have remained consistent throughout the survey years.
Figure 10.1: Boys in Grade 9 and Grade 10 who report having had sexual intercourse (%)
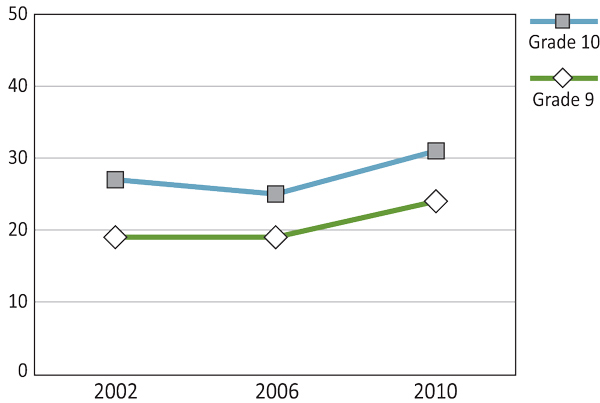
Text Equivalent - Figure 10.1
Figure 10.1 is a line graph that shows the percentage of Grade 9 and 10 boys who report having had sexual intercourse, by gender, in 2002, 2006, and 2010. The graph shows that 19% of Grade 9 boys reported having had sexual intercourse in 2002, compared to 19% in 2006, and 24% in 2010. Among Grade 10 boys, 27% reported having had sexual intercourse in 2002, compared to 25% in 2006, and 31% in 2010.
Figure 10.2: Girls in Grade 9 and Grade 10 who report having had sexual intercourse (%)

Text Equivalent - Figure 10.2
Figure 10.2 is a line graph that shows the percentage of Grade 9 and 10 girls who report having had sexual intercourse, by gender, in 2002, 2006, and 2010. The graph shows that 17% of Grade 9 girls reported having had sexual intercourse in 2002, compared to 18% in 2006, and 18% in 2010. Among Grade 10 girls, 25% reported having had sexual intercourse in 2002, compared to 27% in 2006, and 31% in 2010.
Canadian Federation for Sexual Health (CFSH; formerly Planned Parenthood Federation of Canada) is a national organization that aims to improve access to sexual and reproductive health services, education, abortion, and contraception with a focus on youth services. CSFH accomplishes this goal through:
- awareness campaigns;
- providing resources for sexual health educators;
- providing scholarships and awards to individuals researching sexual health;
- working on international, rights-based projects to improve sexual and reproductive health for youth in developing countries;
- writing positional statements regarding reproductive health and rights;
- providing policy advice to key decision-makers, based on nation-wide research.
Providing youth with these services increases the opportunity for awareness and education, decreasing some of the risks associated with sexual activity. By disseminating this knowledge in an easy-to-access manner, CSFH provides the nation with important resources for teens.
(CFSH, 2012)
The Canadian Guidelines for Sexual Health Education, originally created by Health Canada in 1994 and revised in 2008 by the Public Health Agency of Canada, aim to provide information to the nation through five guiding principles:
- Accessible sexual education for all Canadians;
- Creating comprehensive sexual education resources;
- Looking at the effectiveness of various methods and strategies employed to teach sexual health to youth;
- Training and administrative support for educators;
- How to appropriately implement sexual health education (via program planning, evaluation, and social development).
Providing a set of principles helps create a more unified approach for health professionals in the field of sexual health, as well as providing Canadians with similar goals and direction.
(Public Health Agency of Canada [PHAC], 2008)
The use of condoms in sexual intercourse reported by young people does not follow a clear trend across genders. For boys, safer sex practices peaked in 2006, followed by a steep decline in the 2010 survey to rates lower than those of the initial 2002 survey cycle (Figure 10.3). For Grade 9 girls, safer sex practices increased between the 2002 and 2006 survey years and have remained at this 75% level onwards to 2010 (Figure 10.4). Grade 10 girls do not demonstrate any change in their condom use during sexual intercourse and have remained at a lower constant 69% rate since the 2002 survey. In the last survey cycle, about one-quarter of adolescents surveyed had not used a condom during their last sexual intercourse.
Figure 10.3: Boys in Grade 9 and Grade 10 who report that they used a condom last time they had sexual intercourse (%)
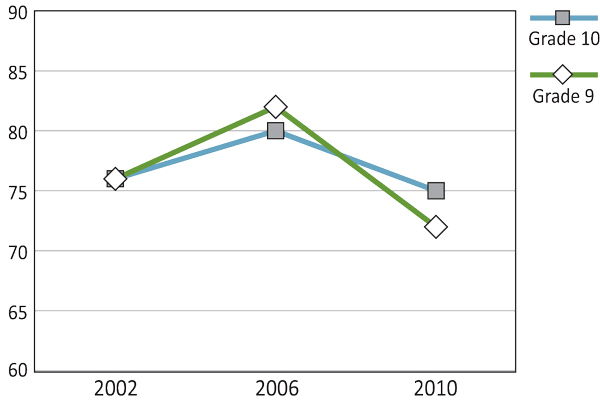
Text Equivalent - Figure 10.3
Figure 10.3 is a line graph that shows the percentage of Grade 9 and 10 boys who report having that they used a condom last time they used a condom last time they had sexual intercourse, by gender, in 2002, 2006, and 2010. The graph shows that 76% of Grade 9 boys who report having that they used a condom last time they used a condom last time they had sexual intercourse in 2002, compared to 82% in 2006, and 72% in 2010. Among Grade 10 boys, 76% who report having that they used a condom last time they used a condom last time they had sexual intercourse in 2002, compared to 80% in 2006, and 75% in 2010.
Figure 10.4: Girls in Grade 9 and Grade 10 who report that they used a condom last time they had sexual intercourse (%)
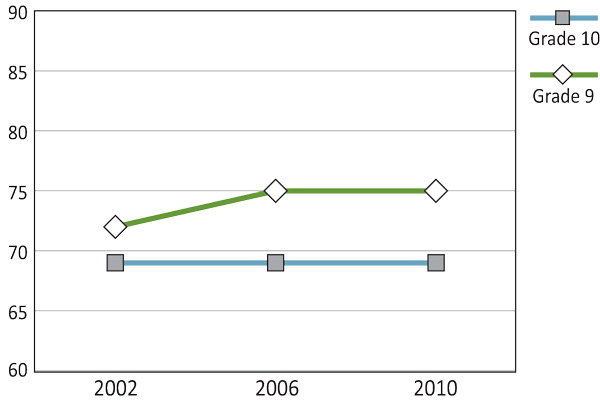
Text Equivalent - Figure 10.4
Figure 10.4 is a line graph that shows the percentage of Grade 9 and 10 girls who report having that they used a condom last time they used a condom last time they had sexual intercourse, by gender, in 2002, 2006, and 2010. The graph shows that 72% of Grade 9 girls who report having that they used a condom last time they used a condom last time they had sexual intercourse in 2002, compared to 75% in 2006, and 75% in 2010. Among Grade 10 girls, 69% who report having that they used a condom last time they used a condom last time they had sexual intercourse in 2002, compared to 69% in 2006, and 69% in 2010.
As youth are just beginning to learn about themselves sexually during the teenage years, there have been focused efforts within various provinces to create positive and informative sexual health resources for youth. One example is, Sex?--A Healthy Sexuality Resource, which was developed by the Nova Scotia Department of Health Promotion and Protection. This resource aims:
- to provide information in an easy-to-read format for youth;
- to provide resources with a focus on decision making, sexual assault, STIs, pregnancy prevention, and healthy sexuality.
(Healthy Sexuality Working Group, 2013)
Summary and Implications
As more teens are engaging in sexual activity behaviours (as indicated in the HBSC data trends), the importance of sexual health education continues to increase. By educating our youth and providing access to goods and services associated with healthy sexual activity (e.g., access to contraceptives, information, and counselling services), especially for those youth in higher risk situations (e.g., Aboriginal youth and youth living on the street), we can work to decrease the rates of STIs, as well as other negative impacts of risky sexual activity. By providing education, we also increase knowledge of sexual health for our youth, which can help guide them to make informed decisions when it comes to sexual intercourse. National organizations that have a strong focus on positive sexual health for youth, such as the Canadian Federation for Sexual Health, should be promoted to the age group with the highest rate of STIs.
Comprehensive frameworks, such as the Canadian Guidelines for Sexual Health Education (2008), may be able to help professionals in the field by providing a supportive network where young people can feel comfortable and safe discussing issues regarding sexual health. Both CFSH and Canadian Guidelines for Sexual Health Education are working towards increasing knowledge and awareness for positive sexual health, as well as providing resources for professionals in the field. It is hoped these nation-wide initiatives will lead to a decrease in the number of youth engaging in risky sexual activity behaviours.
The number of individuals who use (or whose partners use) condoms decreases for females between Grade 9 and Grade 10. In providing access to contraceptives and information, we walk a fine line between what may appear to be encouraging sexual activity versus providing support that effectively decreases the risks associated with sexual activity. Education about the implications of risky sexual activities is important for teens so that they are most informed about the problems that may arise, while still being given the rights to make their own decisions.
Provincial initiatives directed at professionals working in the field of youth sexual health, such as Sex--A Healthy Sexuality Resource (Healthy Sexuality Working Group, 2013), can help promote sexual well-being for young people. Safer sex practices should be promoted nation-wide to help decrease the problems associated with risky sexual activity. The documents and organizations mentioned in this chapter represent some of the most recent Canadian initiatives that promote healthy sexuality for youth.
References
- Biglan, A., Metzler, C.W., Wirt, R., Ary, D., Noell, J., Ochs, L., French, C., Hood, D. (1990). Social and behavioral factors associated with high-risk sexual behaviour among adolescents. Journal of Behavioral Medicine, 13, 245-261.
- Boislard, M., Poulin, F., Kiesner, J., Dishion, T.J. (2009). A longitudinal examination of risky sexual behaviors among Canadian and Italian adolescents: Considering individual, parental, and friend characteristics. International Journal of Behavioral Development, 33, 265-276. doi:10.1177/0165025408098036
- Canadian Federation for Sexual Health (2012). Retrieved from http://www.cfsh.ca/
- Elkington, K.S., Bauermeister, J.A., Zimmerman, M.A. (2010). Pyschological distress, substance use, and HIV/STI risk behaviors among youth. Journal of Youth and Adolescence, 39, 514-527. doi:10.1007/s10964-010-9524-7
- Healthy Sexuality Working Group (2013). Sex?--A healthy sexuality resource. Halifax, NS: Nova Scotia Department of Health and Wellness.
- Kirby, D., Laris, B., Rolleri, L. (2007). Sex and HIV education programs: Their impact on sexual behaviours of young people throughout the world. Journal of Adolescent Health, 40, 206-217.
- MacDonald, J., Gagnon, A.J., Mitchell, C., Di Meglio, G., Rennick, J.E., Cox, J. (2011). Asking to listen: Towards a youth perspective on sexual health education and needs. Sex Education, 11, 443-457.
- Marshall, B.D., Kerr, T., Shoveller, J.A., Montaner, J.S.G., Wood, E. (2009). Structural factors associated with an increased risk of HIV and sexually transmitted infection transmission among street involved youth. BMC Public Health, 9(1), 1-9. doi:10.1186/147-2458-9-7
- Public Health Agency of Canada [PHAC] (2007). Sexually Transmitted Infections. Retrieved from http://www.phac-aspc.gc.ca/publicat/std-mts/pdf/sti_pamph_e.pdf
- Public Health Agency of Canada [PHAC] (2008). Revised Canadian Guidelines for Sexual Health Education. Ottawa, ON: Authority of the Minister of Health.
Chapter 11: Bullying and Fighting Behaviour
By Jeffrey MacCormack
Why are Bullying Behaviours Important?
Bullying is a relationship problem. It is a pattern of behaviour that exploits an imbalance of power, whether real or perceived. The bullying behaviour can include face-to-face interactions (physical, teasing) or indirect interactions (cyberbullying, exclusion; Public Safety Canada, 2008).
Why is Understanding Bullying Important?
Bullying can have profoundly negative effects on the children and youth being victimized. Those who are bullied are more likely to experience depression, anxiety, low self-esteem, and increased aggression than those who are not. Compared to their peers, children who are bullied tend to experience more stomach aches and headaches, increased school truancy, greater incidents of self-injury, and more frequent suicide (Olweus, 1993). Regretfully, those adverse effects do not stop when the bullying stops. Those consequences can be experienced long into adulthood (Farrington & Ttofi, 2011).
There are also adverse effects for those who bully others. Children who bully at a young age are more likely to participate in antisocial behaviour, such as involvement in gangs, sexual harassment, and delinquency later in life (Farrington & Ttofi, 2011; Pepler, Jiang, Craig, & Connolly, 2008). There are strong connections between bullying as a child and criminal activity as an adult (Olweus, 1993).
Those who are victimized by bullying and who also bully others have the most problems. The adverse effects of being victimized are amplified if the individual engages in bullying behaviour. They are less likely to report emotional well-being and more likely to engage in antisocial behaviour later in life compared to their peers (Public Safety Canada, 2008).
What are We Examining in this Chapter?
In this chapter, we examine trends relating to bullying and fighting behaviour among Canadian youth. These trends describe the patterns for 1) those who bully others; 2) those who are bullied by others; 3) those who are bullied and who bully others. Provincial and territorial policies surrounding bullying and safe schools are also explored.
In HBSC surveys, school-aged children in Grade 6, Grade 8, and Grade 10 were asked questions about the incidence of being bullied and bullying others. Although we try to avoid the stigma around words like "victim" and "bully," clearly written questions are important when it comes to surveys.
There is some controversy over an appropriate threshold for bullying. For the purposes of this trend report, a behaviour frequency of "two or three times over the last few months" constitutes the minimum threshold for bullying. Regardless of the specific cut-off chosen, the effects of bullying tend to increase with increased frequency (Solberg & Olweus, 2003).
Victimization and Bullying
Despite gender differences that exist between types of bullying behaviours (such as physical bullying) over survey years, boys and girls have reported similar levels of victimization (Figures 11.1 and 11.2). For both genders and in all three surveys, the percentage of children who reported being victimized was highest in Grade 6. For boys and girls in Grade 6, self-reported victimization was the highest in 2006. For boys and girls in Grades 8 and Grade 10, self-reported victimization was the lowest in 2006.
Figure 11.1: Boys who were victimized by bullying more than once or twice in the past couple of months (%)

Text Equivalent - Figure 11.1
Figure 11.1 is a line graph that shows the percentage of boys who were victimized by bullying more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 30% of Grade 6 boys were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 40% in 2006 and 34% in 2010. Among Grade 8 boys, 33% were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 29% in 2006 and 30% in 2010. Among Grade 10 boys, 28% were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 20% in 2006 and 24% in 2010.
Figure 11.2: Girls who were victimized by bullying more than once or twice in the past couple of months (%)
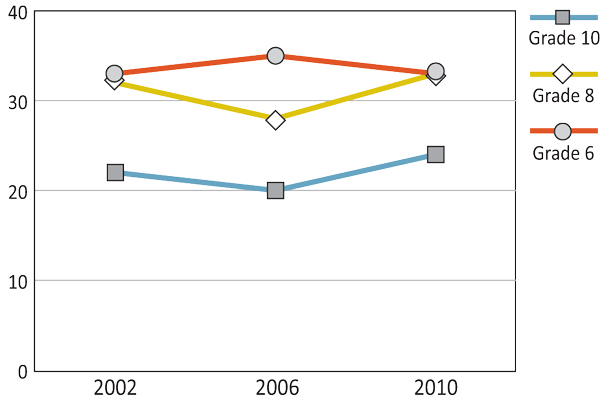
Text Equivalent - Figure 11.2
Figure 11.2 is a line graph that shows the percentage of girls who were victimized by bullying more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 33% of Grade 6 girls were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 35% in 2006 and 33% in 2010. Among Grade 8 girls, 32% were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 28% in 2006 and 33% in 2010. Among Grade 10 girls, 22% were victimized by bullying more than once or twice in the past couple of months in 2002, compared to 20% in 2006 and 24% in 2010.
As shown in Figures 11.3 and 11.4, boys consistently reported more bullying behaviour than girls across the survey cycles. The greatest gender discrepancy occurs in Grade 10.
Figure 11.3: Boys who bullied others more than once or twice in the past couple of months (%)
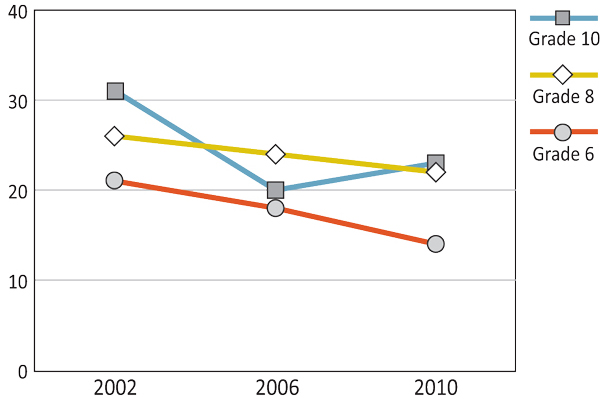
Text Equivalent - Figure 11.3
Figure 11.3 is a line graph that shows the percentage of boys who bullied others more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 21% of Grade 6 boys bullied others more than once or twice in the past couple of months in 2002, compared to 18% in 2006, and 14% in 2010. Among Grade 8 boys, 26% bullied others more than once or twice in the past couple of months in 2002, compared to 24% in 2006 and 22% in 2010. Among Grade 10 boys, 31% bullied others more than once or twice in the past couple of months in 2002, compared to 20% in 2006 and 23% in 2010.
Figure 11.4: Girls who bullied others more than once or twice in the past couple of months (%)

Text Equivalent - Figure 11.4
Figure 11.4 is a line graph that shows the percentage of girls who bullied others more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 13% of Grade 6 girls bullied others more than once or twice in the past couple of months in 2002, compared to 9% in 2006, and 10% in 2010. Among Grade 8 girls, 19% bullied others more than once or twice in the past couple of months in 2002, compared to 17% in 2006 and 17% in 2010. Among Grade 10 girls, 12% bullied others more than once or twice in the past couple of months in 2002, compared to 11% in 2006 and 13% in 2010.
The prevalence of bullying behaviour has declined for boys between the 2002 and 2010 survey years. The most dramatic decline has been in Grade 6 (7% decline). For girls, the rates have remained consistent over the survey years.
Overall, Grade 6 boys and Grade 6 girls self-reported bullying behaviour less than the older grades. The prevalence of bullying behaviour of boys was nearly the same for Grades 8 and 10, but the prevalence of bullying behaviour for girls in Grade 8 was higher than that for girls in Grade 10.
Figures 11.5 and 11.6 represent the percentage of boys and girls who self-reported bullying others and being bullied themselves at least two to three times over a few months. Bullying others and being bullied is largely unrelated to gender, grade, or survey year.
Figure 11.5: Boys who were victimized by bullying and bullied others more than once or twice in the past couple of months (%)
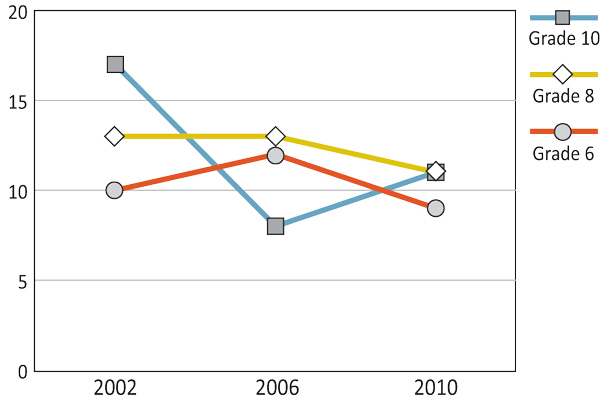
Text Equivalent - Figure 11.5
Figure 11.5 is a line graph that shows the percentage of boys who were victimized by bullying and bullied others more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 10% of Grade 6 boys were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 12% in 2006 and 9% in 2010. Among Grade 8 boys, 13% were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 13% in 2006 and 11% in 2010. Among Grade 10 boys, 17% were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 8% in 2006 and 11% in 2010.
Figure 11.6: Girls who were victimized by bullying and bullied others more than once or twice in the past couple of months (%)
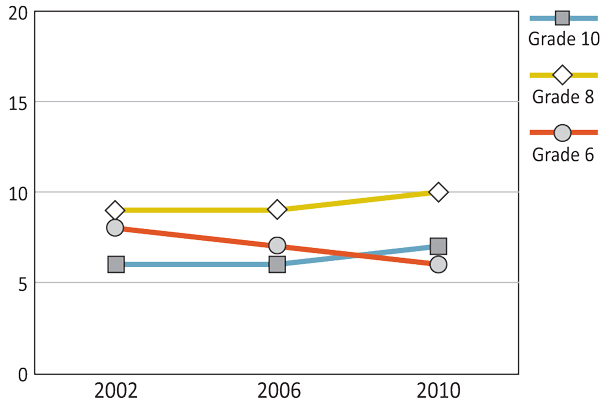
Text Equivalent - Figure 11.6
Figure 11.6 is a line graph that shows the percentage of girls who were victimized by bullying and bullied others more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 8% of Grade 6 girls were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 7% in 2006 and 6% in 2010. Among Grade 8 boys, 9% were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 9% in 2006 and 10% in 2010. Among Grade 10 girls, 6% were victimized by bullying and bullied others more than once or twice in the past couple of months in 2002, compared to 6% in 2006 and 7% in 2010.
Types of Bullying
Hurtful teasing is one of the most common forms of bullying and, unlike other forms of bullying it is experienced at nearly equal levels by both genders (Figures 11.7 and 11.8). Teasing bullying is experienced most often in Grade 6 and least often by Grade 10 with the greatest decline between Grades 8 and 10.
Figure 11.7: Boys who were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months (%)
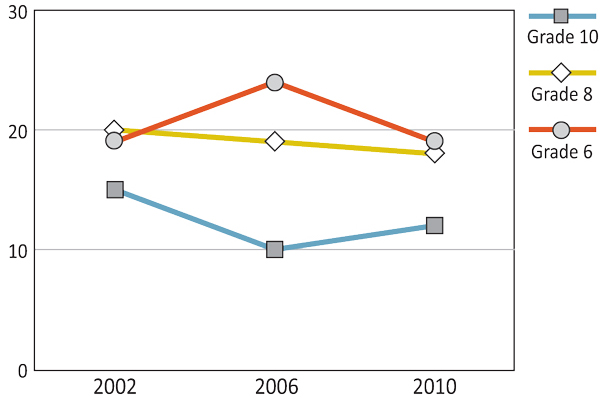
Text Equivalent - Figure 11.7
Figure 11.7 is a line graph that shows the percentage of boys who were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 19% of Grade 6 boys were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 24% in 2006 and 19% in 2010. Among Grade 8 boys, 20% were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 19% in 2006 and 18% in 2010. Among Grade 10 boys, 15%were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 10% in 2006 and 12% in 2010.
Figure 11.8: Girls who were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months (%)
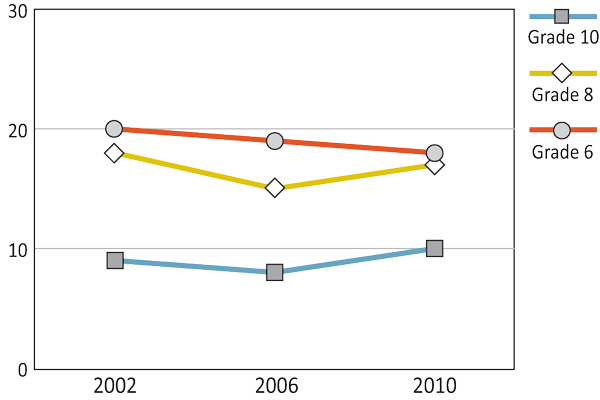
Text Equivalent - Figure 11.8
Figure 11.8 is a line graph that shows the percentage of girls who were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 20% of Grade 6 girls were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 19% in 2006 and 18% in 2010. Among Grade 8 girls, 18% were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 15% in 2006 and 17% in 2010. Among Grade 10 girls, 9%were called mean names, were made fun of, or teased in a hurtful way more than once or twice in the past couple of months in 2002, compared to 8% in 2006 and 10% in 2010.
As shown in Figures 11.9 and 11.10, more boys than girls reported being physically bullied by others. In 2010, for example, 11% of Grade 6 boys reported being physically bullied compared to 6% of Grade 7 girls. By Grade 10, out 7% of boys reported physical bullying, more than three times the prevalence for girls (2%). Similar to the other types of bullying, the prevalence of physical bullying is highest in Grade 6 and gradually declines over the grades.
Figure 11.9: Boys who were physically bullied more than once or twice in the past couple of months (%)
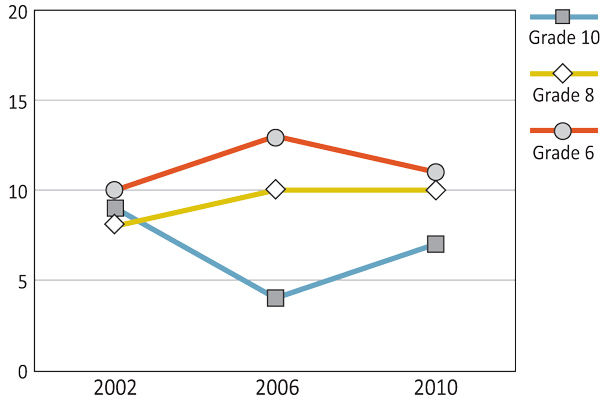
Text Equivalent - Figure 11.9
Figure 11.9 is a line graph that shows the percentage of boys who were physically bullied more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 10% of Grade 6 boys were physically bullied more than once or twice in the past couple of months in 2002, compared to 13% in 2006 and 11% in 2010. Among Grade 8 boys, 8% were physically bullied more than once or twice in the past couple of months in 2002, compared to 10% in 2006 and 11% in 2010. Among Grade 10 boys, 9% were physically bullied more than once or twice in the past couple of months in 2002, compared to 4% in 2006 and 7% in 2010.
Figure 11.10: Girls who were physically bullied more than once or twice in the past couple of months (%)
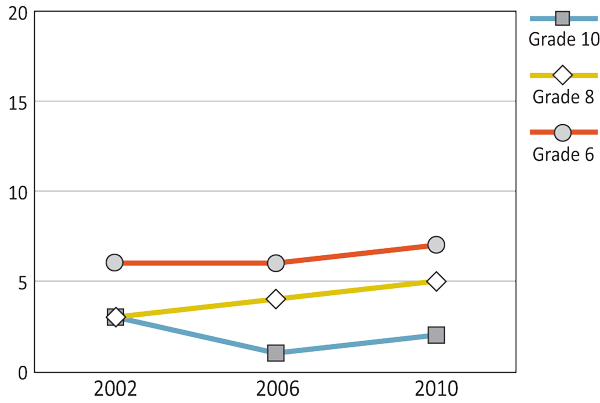
Text Equivalent - Figure 11.10
Figure 11.10 is a line graph that shows the percentage of girls who were physically bullied more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 6% of Grade 6 girls were physically bullied more than once or twice in the past couple of months in 2002, compared to 6% in 2006 and 7% in 2010. Among Grade 8 girls, 3% were physically bullied more than once or twice in the past couple of months in 2002, compared to 4% in 2006 and 5% in 2010. Among Grade 10 girls, 3% were physically bullied more than once or twice in the past couple of months in 2002, compared to 1% in 2006 and 2% in 2010.
The prevalence of bullying with sexual content remained fairly constant over the three cycles (Figures 11.11 and 11.12). Rates of bullying of a sexual nature for Grade 6 boys are higher than those for Grade 6 girls, while the reverse is true for Grade 10 students (except in 2002).
Figure 11.11: Boys who were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months (%)
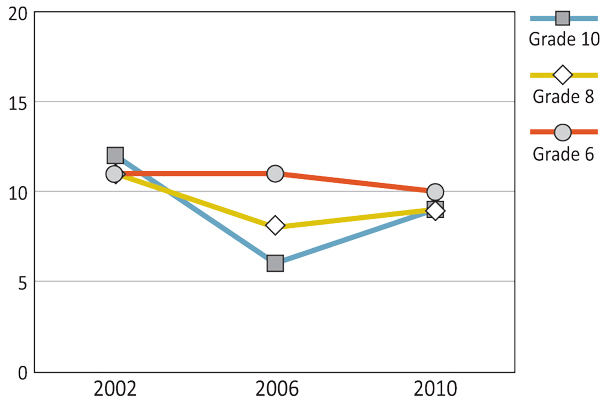
Text Equivalent - Figure 11.11
Figure 11.11 is a line graph that shows the percentage of boys who were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 11% of Grade 6 boys were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 11% in 2006 and 10% in 2010. Among Grade 8 boys, 11% were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 8% in 2006 and 9% in 2010. Among Grade 10 boys, 12% were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 6% in 2006 and 9% in 2010.
Figure 11.12: Girls who were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months (%)

Text Equivalent - Figure 11.12
Figure 11.12 is a line graph that shows the percentage of girls who were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 7% of Grade 6 girls were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 5% in 2006 and 7% in 2010. Among Grade 8 girls, 11% were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 9% in 2006 and 12% in 2010. Among Grade 10 girls, 9% were victimized by other students making sexual jokes, comments, or gestures to them more than once or twice in the past couple of months in 2002, compared to 9% in 2006 and 12% in 2010.
Indirect bullying includes both intentional exclusion from groups or activities by others and having lies or false rumours spread by others. As shown in Figures 11.13 and 11.14, there are minimal differences between the rates of indirect bullying between the genders, as well as minimal variation across the years. The prevalence for this type of bullying is highest in Grade 6 and decline by Grades 8 and Grade 10. For example, in 2010, 19% of Grade 6 boys and 21% of Grade 6 girls reported being bullied indirectly compared to 11% of Grade 10 boys and 13% of Grade 10 girls.
Figure 11.13: Boys who were victimized by indirect bullying more than once or twice in the past couple of months (%)
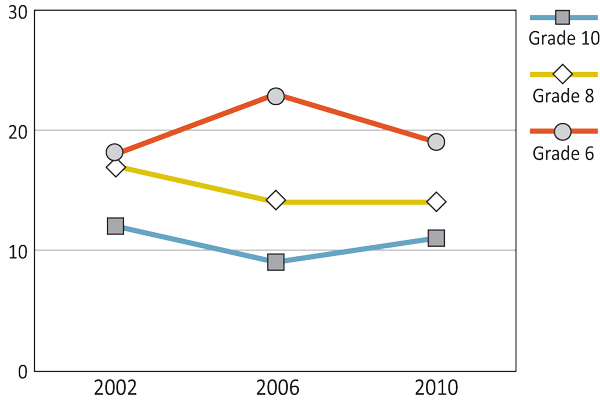
Text Equivalent - Figure 11.13
Figure 11.13 is a line graph that shows the percentage of boys who were victimized by indirect bullying more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 18% of Grade 6 boys were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to 23% in 2006 and 19% in 2010. Among Grade 8 boys, 17% were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to 14% in 2006 and 14% in 2010. Among Grade 10 boys, 12% were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to9% in 2006 and 11% in 2010.
Figure 11.14: Girls who were victimized by indirect bullying more than once or twice in the past couple of months (%)
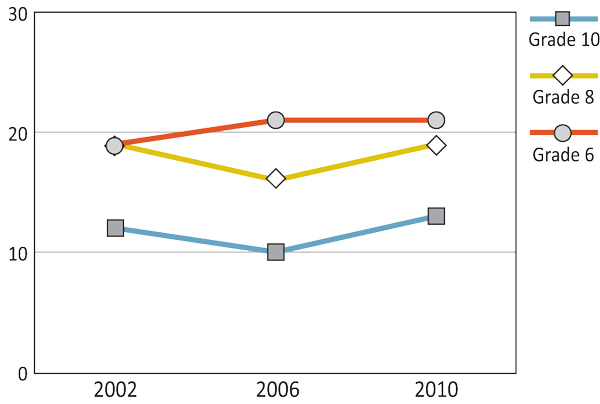
Text Equivalent - Figure 11.14
Figure 11.14 is a line graph that shows the percentage of girls who were victimized by indirect bullying more than once or twice in the past couple of months, by grade, gender and year of survey. The graph shows that 19% of Grade 6 girls were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to 21% in 2006 and 21% in 2010. Among Grade 8 girls, 19% were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to 16% in 2006 and 19% in 2010. Among Grade 10 girls, 12% were victimized by indirect bullying more than once or twice in the past couple of months in 2002, compared to 10% in 2006 and 13% in 2010.
Fighting
As illustrated in Figures 11.15 and 11.16, the prevalence of fighting for Grade 6 and 8 students peaked in 2006, especially for girls. The prevalence of fighting tends to be highest in Grade 6 and to decrease in the older grades. Boys tend to report fighting about twice as often as girls.
Figure 11.15: Boys who have been in a physical fight in the last 12 months (%)
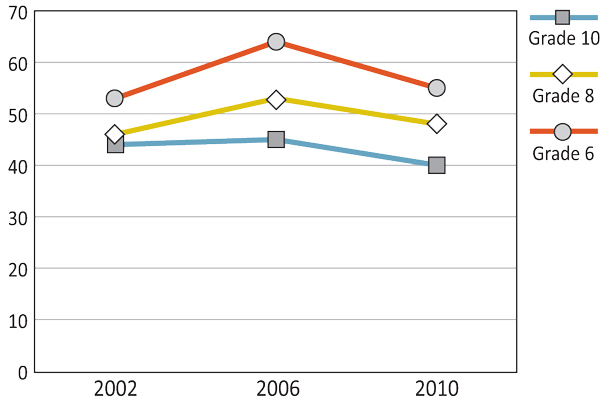
Text Equivalent - Figure 11.15
Figure 11.15 is a line graph that shows the percentage of boys who have been in a physical fight in the last 12 months, by grade, gender and year of survey. The graph shows that 53% of Grade 6 boys have been in a physical fight in the last 12 months in 2002, compared to 64% in 2006 and 55% in 2010. Among Grade 8 boys, 46% have been in a physical fight in the last 12 months in 2002, compared to 53% in 2006 and 48% in 2010. Among Grade 10 boys, 44% have been in a physical fight in the last 12 months in 2002, compared to 45% in 2006 and 40% in 2010.
Figure 11.16: Girls who have been in a physical fight in the last 12 months (%)
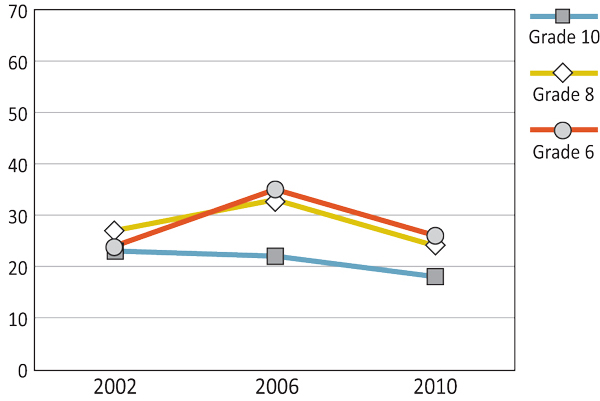
Text Equivalent - Figure 11.16
Figure 11.16 is a line graph that shows the percentage of girls who have been in a physical fight in the last 12 months, by grade, gender and year of survey. The graph shows that 24% of Grade 6 girls have been in a physical fight in the last 12 months in 2002, compared to 35% in 2006 and 26% in 2010. Among Grade 8 girls, 27% have been in a physical fight in the last 12 months in 2002, compared to 33% in 2006 and 24% in 2010. Among Grade 10 girls, 23% have been in a physical fight in the last 12 months in 2002, compared to 22% in 2006 and 18% in 2010.
National Agenda
The National Crime Prevention Strategy was established by the Government of Canada to reduce criminal activity and victimization using social development initiatives (Public Safety Canada, 2008). This strategy listed school-based anti-bullying programs as a priority focus for its 2002/03-2005/06 plans. As part of the initiative, the National Crime Prevention Strategy aimed to bring evidence-based best practice to the stakeholders who need it. The executive report recommended the 'whole school approach' (Olweus, 1993), which includes needs assessment, the involvement of multiple stakeholders, and formal introduction and evaluation.
Provincial and Territorial Initiatives
Because education and health care are not federal jurisdictions, legislation and policy on bullying have been created by provincial and territorial governments. Quebec passed An Act to prevent and stop bullying and violence in schools (Bill n°56), which amends the Education Act to include obligations of stakeholders and the inclusion of cyberbullying. The Accepting Schools Act (Bill 13) became law in Ontario in June of 2012. The Accepting Schools Act called on schools to create school-based anti-bullying programs, which include preventative measures, tougher consequences for bullies, and programs to promote respect. Alberta's new Education Act was passed in December 2012 with some controversy around whether or not schools have the authority to suspend bystanders to bullying. The differences across these responses to bullying create the need for a national conversation such as that undertaken through PREVNet.
PREVNet
The Canadian Guidelines for Sexual Health Education, originally created by Health Canada in 1994 and revised in 2008 by the Public Health Agency of Canada, aim to provide information to the nation through five guiding principles:
- Accessible sexual education for all Canadians;
- Creating comprehensive sexual education resources;
- Looking at the effectiveness of various methods and strategies employed to teach sexual health to youth;
- Training and administrative support for educators;
- How to appropriately implement sexual health education (via program planning, evaluation, and social development).
Providing a set of principles helps create a more unified approach for health professionals in the field of sexual health, as well as providing Canadians with similar goals and direction.
Summary and Implications
Potentially due to the increasing presence of bullying prevention programs across the country, the overall trends of bullying have shown declines since 2002 for boys. However, the prevalence of girls who engaged in bullying behaviour has remained fairly consistent across the survey years.
The rates of victimization have not declined between the 2002 and 2010 survey years. Other than pockets of progress, such as the Grade 6 boys for whom the rates of self-reported bullying have shown a decline (7%), nationwide rates of victimization are not showing significant reductions. For example, rates of victimization in Grade 8 and 10 increased slightly or stayed the same. The differences between the types and prevalence of bullying behaviour have not altered over time. Boys engage in physical bullying and fighting behaviour more often than girls. Girls engage in indirect bullying slightly more than the boys. However, both genders report similar levels of victimization of indirect teasing. These results support the findings of other researchers that bullying programs should be designed with gender-based tools (Public Safety Canada, 2008).
Even though Grade 8 and Grade 10 rates of bullying are typically lower than Grade 6, they have not been reduced since the 2002 survey. Between the years 2002 and 2010, the changes that have happened in Grades 8 and Grade 10 have been slight increases or no change at all.
Bullying prevention has been tackled with a three-pronged approach. A national agenda has been created that seeks to bring evidence-based strategies to practitioners. Provinces and territories have enacted legislation to reduce incidents of bullying, of which three are illustrated here. Finally, research, policy, and practice have been brought together through the PREVNet initiative. These combined efforts should create a national context whereby we see reductions in the bullying numbers in future surveys.
References
- Alberta Education (2012). Education Act 2012. Retrieved from: http://www.education.alberta.ca/department/policy/education-act.aspx
- Assemblée Nationale Quebec (2012). Bill Numéro 56: An act to prevent and stop bullying and violence in schools. Retrieved from: http://www.assnat.qc.ca/en/travaux-parlementaires/projets-loi/projet-loi-56-39-2.html.
- Farrington, D., Ttofi, M. (2011). Bullying as a predictor of offending, violence and later life outcomes. Criminal Behavior and Mental Health, 31, 90-98.
- Legislative Assembly of Ontario (2012). Bill 14: Anti-bullying Act. Retrieved from: http://www.ontla.on.ca/web/bills/bills_detail.do?locale=en&BillID=2550&isCurrent=&BillStagePrintId=&btnSubmit=go.
- Olweus, D. (1993). Bullying at school: What we know and what we can do. Oxford, UK: Blackwell.
- Pepler, D., Jiang, D., Craig, W., Connolly, J. (2008). Developmental trajectories of bullying and associated factors. Child Development, 79, 325-338
- PREVNet (2012). Frequently Asked Questions. In Promoting PREVNet: Relationships and Eliminating Violence. Retrieved March 18, 2013, from http://prevnet.ca/about
- Public Safety Canada (2008). Bullying prevention in schools: Executive summary. Retrieved from: http://www.publicsafety.gc.ca/res/cp/res/bully-eng.aspx
- Solberg, M., Olweus, D. (2003). Prevalence estimation of school bullying with the Olweus bully/victim questionnaire. Aggressive Behavior, 29, 239-268.
Chapter 12: International Trends
By John Freeman
The Importance of Studying International Trends
The previous chapters provide information about how Canadian adolescents describe their contexts, their health outcomes, and their health behaviours. However, one of the strengths of the HBSC study is the opportunity it provides to compare across countries. By doing so, we can see not only how Canadian adolescents have experienced their contexts and their health over an extended time period but also how they fare in comparison to countries in Europe, the United States, and Israel.
What are We Reporting in this Chapter?
This chapter uses previously published data from HBSC international reports to examine how Canada has been doing relative to other HBSC countries. For each survey year, we place Canadian adolescents into one of four quartiles from the 1st (top) quartile to the 4th bottom) quartile. In that we are relying on published reports, we can only describe a limited array of mandatory HBSC items. Also, some items are not reported in all the international reports so trends begin at different times and occasionally have gaps (most commonly with the 1998 survey cycle). We divide the chapter into four sections: (i) mental health, (ii) contexts for health, (iii) health behaviours, and (iv) causes for celebration and causes for concern.
Mental Health
Congruent with the results with respect to life satisfaction on the national level (Figures 2.9 and 2.10), the life satisfaction of Canadian adolescents reported in the HBSC survey has been worsening relative to their peers in other countries. While the numbers from the 2002 survey in Canada may have been somewhat of an anomaly in that they were obtained later in the school year, the differences between 2006 and 2010 cannot be attributed to survey timing. The worsening international comparison is especially evident for girls, who dropped from the third to the bottom quartile for ages 11 and 13 between 2006 and 2010, and from the top to the third quartile for age 15 (Figure 12.1).
Figure 12.1: Canadian students who report high life satisfaction
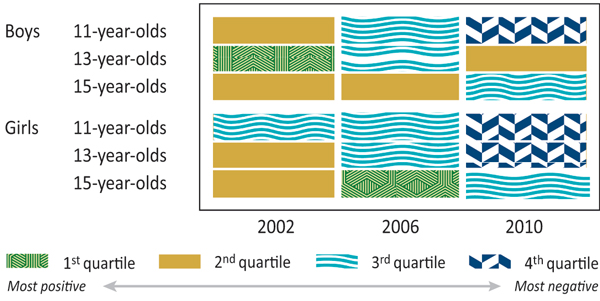
Text Equivalent - Figure 12.1
Figure 12.1 is a table that shows the international ranking of Canadian students who report high life satisfaction by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 2002, 11-year-old boys ranked in the second quartile, they ranked in the third quartile in 2006 and in the fourth quartile in 2010. In 2002, 13-year-old boys ranked in the first quartile, they ranked in the third quartile in 2006 and in the second quartile in 2010. In 2002 and 2006, 15-year-old boys ranked in the second quartile, and in the third quartile in 2010. In 2002 and 2006, 11-year-old girls ranked in the third quartile, and in the fourth quartile in 2010. In 2002, 13-year-old girls ranked in the second quartile, they ranked in the third quartile in 2006 and in the fourth quartile in 2010. In 2002, 15-year-old boys ranked in the second quartile, they ranked in the first quartile in 2006 and in the third quartile in 2010.
Contexts for Health
Although, since 1990, Canadian students in all age groups have shown an overall increase in ease of communication with their mothers and fathers (Figures 3.5 through 3.8), they continue to be lower relatively to same-aged adolescents in other HBSC countries, almost always ranking in the third or bottom quartile (Figures 12.2 and 12.3). Indeed, for all four survey cycles reported (figures for 1998 are unavailable), Canadian students aged 13 (boys and girls) were in the bottom quartile in ease of communication with their mothers, while 11-year-old Canadian girls were consistently in the bottom quartile in ease of communication with their fathers.
Figure 12.2: Canadian students who find it easy to talk to their mothers
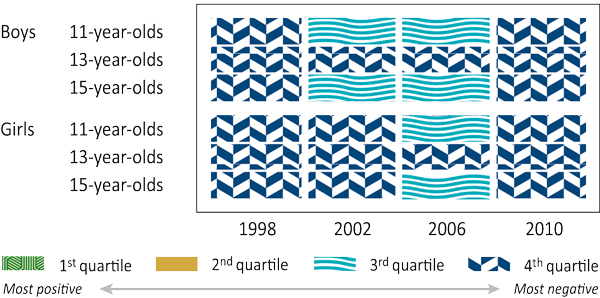
Text Equivalent - Figure 12.2
Figure 12.2 is a table that shows the international ranking of Canadian students who find it easy to talk to their mothers by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 1998, 11-year-old boys ranked in the fourth quartile, in the third quartile in 2002 and 2006 and in the fourth quartile in 2010. In 1998, 2002, 2006 and 2010, 13-year-old boys ranked in the fourth quartile. In 1998, 15-year-old boys ranked in the fourth quartile, in the third quartile in 2002 and 2006 and in the fourth quartile in 2010. In 1998 and 2002 11-year-old girls ranked in the fourth quartile, in the third quartile in 2006 and in the fourth quartile in 2010. In 1998, 2002, 2006 and 2010, 13-year-old girls ranked in the fourth quartile. In 1998 and 2002 11-year-old girls ranked in the fourth quartile, in the third quartile in 2006 and in the fourth quartile in 2010.
Figure 12.3: Canadian students who find it easy to talk to their fathers
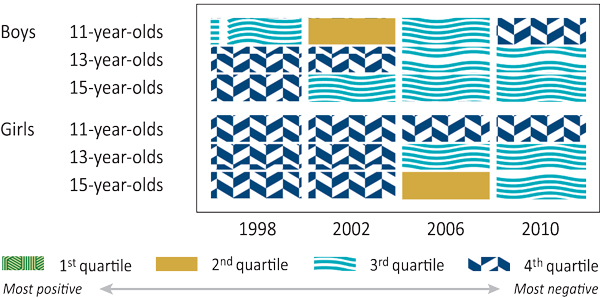
Text Equivalent - Figure 12.3
Figure 12.3 is a table that shows the international ranking of Canadian students who find it easy to talk to their fathers by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 1998, 11-year-old boys ranked in the third quartile, in the second quartile in 2002, in the third quartile in 2006 and the fourth quartile in 2010. In 1998 and 2002, 13-year-old boys ranked in the fourth quartile and in the third quartile in 2006 and 2010. In 1998, 15-year-old boys ranked in the fourth quartile and in the third quartile in 2002, 2006 and 2010. In 1998, 2002, 2006 and 2010, 11-year-old girls ranked in the fourth quartile. In 1998 and 2002, 13-year-old girls ranked in the fourth quartile and in the third quartile in 2006 and 2010. In 1998 and 2002, 15-year-old girls ranked in the fourth quartile, in the second quartile in 2006 and in the third quartile in 2010.
Figures 4.1 and 4.2 indicate that, across survey years, most Canadian adolescents have reported that their teachers thought their school performance was good or very good. Similarly, as seen in Figure 12.4, Canadian boys, regardless of age or survey year, have ranked in the second quartile internationally with respect to how they believed their teachers viewed their academic work. The relative international rankings for Canadian girls are even higher, especially so for 15-year-old Canadian girls, who have been continuously in the top quartile.
Figure 12.4: Canadian students who report good or very good perceived school performance
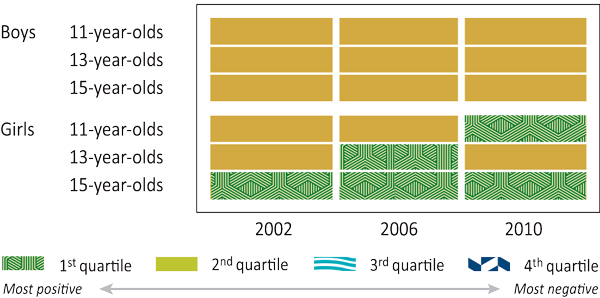
Text Equivalent - Figure 12.4
Figure 12.4 is a table that shows the international ranking of Canadian students who report good or very good perceived school performance by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 2002, 2006 and 2010, 11-year-old boys ranked in the second quartile. In 2002, 2006 and 2010, 13-year-old boys ranked in the second quartile. In 2002, 2006 and 2010, 15-year-old boys ranked in the second quartile. In 2002 and 2006, 11-year-old girls ranked in the second quartile and in the first quartile in 2010. In 2002, 13-year-old girls ranked in the second quartile, in the first quartile in 2006 and in the second quartile in 2010. In 2002, 2006 and 2010, 15-year-old girls ranked in the first quartile.
Even though across survey years, less than half of surveyed Canadian adolescents reported liking school a lot (Figures 4.3 and 4.4), Canadian adolescents tend to like school relatively more than adolescents in other countries (Figure 12.5). In particular, 15-year-old Canadian boys and girls consistently rank in the second quartile (or better). Students in the other groups tend to be in the 2nd or 3rd quartile and never in the bottom quartile.
Figure 12.5: Canadian students who like school a lot
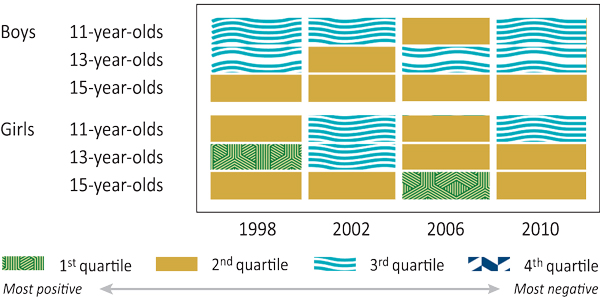
Text Equivalent - Figure 12.5
Figure 12.5 is a table that shows the international ranking of Canadian students who like school a lot by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 1998 and 2002, 11-year-old boys ranked in the third quartile, in the second quartile in 2006 and in the third quartile in 2010. In 1998, 13-year-old boys ranked in the third quartile, in the second quartile in 2002 and in the third quartile in 2006 and 2010. In 1998, 2002, 2006 and 2010, 13-year-old boys ranked in the second quartile. In 1998, 11-year-old girls ranked in the second quartile, in the third quartile in 2002, in the second quartile in 2006 and in the third quartile in 2010. In 1998, 13-year-old girls ranked in the first quartile, in the third quartile in 2002 and in the second quartile in 2006 and 2010. In 1998 and 2002, 15-year-old girls ranked in the second quartile, in the first quartile in 2006 and in the second quartile in 2010.
Figure 12.6 shows that Canadian boys and girls consistently report relatively high school pressure (compared to boys and girls in other HBSC countries) with an equal split between 1st quartile and 2nd quartile. The ranking for Canadian students is unaffected by age, gender, or survey year. Similarly, Canadian students have shown little change across survey years or gender, although younger Canadian students report lower levels of school pressure than older students (Figures 4.5 and 4.6).
Figure 12.6: Canadian students who feel pressured by schoolwork
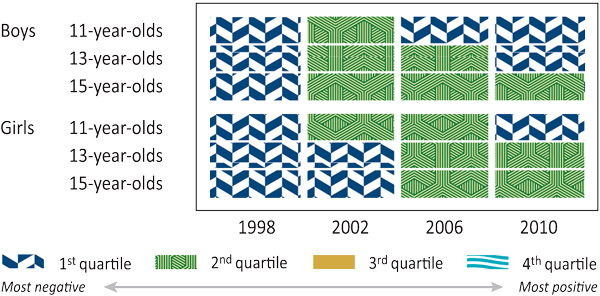
Text Equivalent - Figure 12.6
Figure 12.6 is a table that shows the international ranking of Canadian students who feel pressured by schoolwork by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 1998, 11-year-old boys ranked in the first quartile, in the second quartile in 2002 and in the first quartile in 2006 and 2010. In 1998, 13-year-old boys ranked in the first quartile, in the second quartile in 2002 and 2006 and in the first quartile in 2010. In 1998, 15-year-old boys ranked in the first quartile and in the second quartile in 2002, 2006 and 2010. In 1998, 11-year-old girls ranked in the first quartile, in the second quartile in 2002 and 2006 and in the first quartile in 2010. In 1998 and 2002, 13-year-old girls ranked in the first quartile and in the second quartile in 2006 and 2010. In 1998 and 2002, 15-year-old girls ranked in the first quartile and in the second quartile in 2006 and 2010.
While Canadian adolescents generally like school more than their international counterparts and see their teachers as thinking more highly of their school performance, they are relatively less likely to agree that their classmates are kind and helpful than their peers in other countries (Figure 12.7). In particular, in both 1998 and 2010, Canadian students ranked in the bottom quartile for five of the six age-gender combinations. Nationally, however, over the course of the three most recent HBSC surveys, a majority of Canadian students reported they felt that most of the students in their class(es) were kind and helpful with these proportions declining slightly during the time period for Grades 8 and 10 students (figure not shown).
Figure 12.7: Canadian students who agree that their classmates are kind and helpful
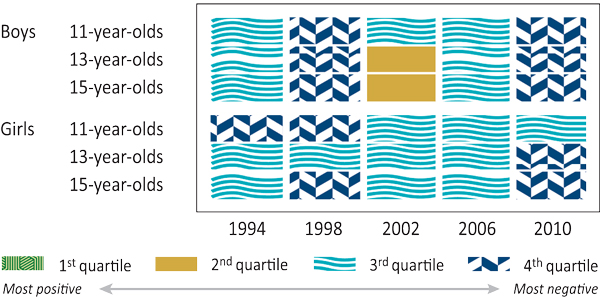
Text Equivalent - Figure 12.7
Figure 12.7 is a table that shows the international ranking of Canadian students who agree that their classmates are kind and helpful by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most positive and the fourth quartile being the most negative. In 1994, 11-year-old boys ranked in the third quartile, in the fourth quartile in 1998, in the third quartile in 2002 and 2006 and in the fourth quartile in 2010. In 1994, 13-year-old boys ranked in the third quartile, in the fourth quartile in 1998, in the second quartile in 2002, in the third quartile in 2006 and in the fourth quartile in 2010. In 1994, 15-year-old boys ranked in the third quartile, in the fourth quartile in 1998, in the second quartile in 2002, in the third quartile in 2006 and in the fourth quartile in 2010. In 1994 and 1998, 11-year-old girls ranked in the fourth quartile and in the third quartile in 2002, 2006 and 2010. In 1994, 1998, 2002 and 2006, 13-year-old girls ranked in the third quartile and in the fourth quartile in 2010. In 1994, 15-year-old girls ranked in the third quartile, in the fourth quartile in 1998, in the third quartile in 2002 and 2006 and in the fourth quartile in 2010.
Health Behaviours
Although higher percentages of Canadian adolescents reported a medically treated injury in 2010 versus 1994 (Figures 6.1 and 6.2), their relative ranking internationally improved over that time (Figure 12.8). While all three age groups of girls and 13-15-year-old boys were in the top quartile in 1994 and again in 2002 (1998 data are not available), that is, reported among the highest proportion of medically treated injuries internationally, they all ranked in the 2nd and 3rd quartile in 2010.
Figure 12.8: Canadian students who report at least one medically attended injury in the last 12 months
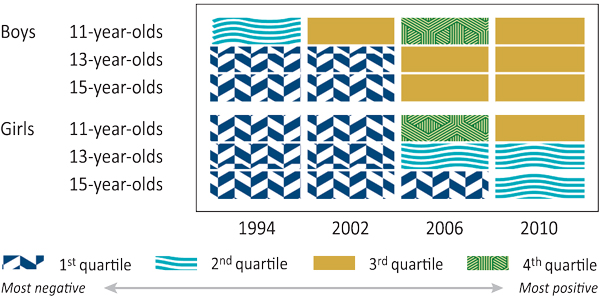
Text Equivalent - Figure 12.8
Figure 12.8 is a table that shows the international ranking of Canadian students who report at least one medically attended injury in the last 12 months by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 1994, 11-year-old boys ranked in the second quartile, in the third quartile in 2002, in the fourth quartile in 2006 and in the third quartile in 2010. In 1994 and 2002, 13-year-old boys ranked in the first quartile and in the third quartile in 2006 and 2010. In 1994 and 2002, 15-year-old boys ranked in the first quartile and in the third quartile in 2006 and 2010. In 1994 and 2002, 11-year-old girls ranked in the first quartile, in the fourth quartile in 2006 and in the third quartile in 2010. In 1994 and 2002, 13-year-old girls ranked in the first quartile and in the second quartile in 2006 and 2010. In 1994, 2002 and 2006, 15-year-old girls ranked in the first quartile and in the second quartile in 2010.
As indicated in Figures 7.15 and 7.16, the percentage of students who report consuming non-diet soft drinks on a daily basis has declined substantially since 2002. The international data mirror the declining Canadian pattern of daily soft drink consumption (Figure 12.9). Canadian youth are beginning to report some of the lowest levels of soft drink consumption internationally with all age-gender groups in the bottom quartile for 2006 and 2010. In comparison, five of six age-gender groups were in the 2nd quartile for soft drink consumption in 1998.
Figure 12.9: Canadian students who drink soft drinks daily
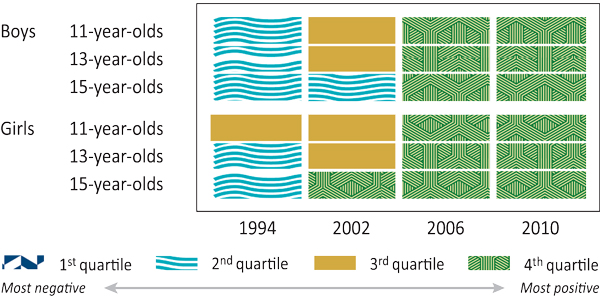
Text Equivalent - Figure 12.9
Figure 12.9 is a table that shows the international ranking of Canadian students who drink soft drinks daily by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 1994, 11-year-old boys ranked in the second quartile, in the third quartile in 2002 and in the fourth quartile in 2006 and 2010. In 1994, 13-year-old boys ranked in the second quartile, in the third quartile in 2002 and in the fourth quartile in 2006 and 2010. In 1994 and 2002, 15-year-old boys ranked in the second quartile and in the fourth quartile in 2006 and 2010. In 1994 and 2002, 11-year-old girls ranked in the third quartile and in the fourth quartile in 2006 and 2010. In 1994, 13-year-old girls ranked in the second quartile, in the third quartile in 2002 and in the fourth quartile in 2006 and 2010. In 1994, 15-year-old girls ranked in the second quartile and in the fourth quartile in 2002, 2006 and 2010.
Internationally, Canadian adolescents have consistently been in the top quartile for being overweight or obese (only 13 and 15 year old results are reported internationally; Figure 12.10). At the time of the most recent survey (2010), Canada ranked second of 39 HBSC countries in the prevalence of overweight and obese 15-year-old boys and girls. For overweight and obese 13-year-old boys and girls, Canada ranked fourth and third, respectively (figures not shown). As the international position of Canada has remained steady, so too has the percentage of Canadian students classified as overweight or obese, based on self-reports of height and weight, remained relatively stable over time (Figures 8.1 and 8.2).
Figure 12.10: Canadian students who report that they are overweight or obese according to BMI
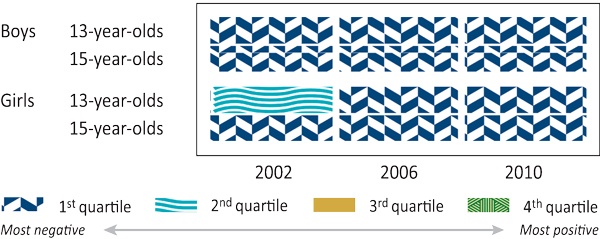
Text Equivalent - Figure 12.10
Figure 12.10 is a table that shows the international ranking of Canadian students who report that they are overweight or obese according to body mass index by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 2002, 2006 and 2010, 13-year-old boys ranked in the first quartile. In 2002, 15-year-old boys ranked in the first quartile. In 2002, 13-year-old girls ranked in the second quartile and in the first quartile in 2006 and 2010. In 2002, 2006 and 2010, 15-year-old girls ranked in the first quartile.
Daily smoking has decreased in Canada since the 1990s among Grade 8 and Grade 10 students (Figures 9.1 and 9.2).These patterns of decreased smoking among Canadian adolescents are mirrored in the international data. In 1994, Canadian 13-year-old boys and girls and 15-year-old girls ranked in the top quartile of countries, meaning they had among the highest rates of smoking at least once a week internationally, while Canadian 15-year-old boys were in the 3rd quartile. At the time of the latest survey, Canadian boys had the lowest weekly smoking rates among the HBSC countries surveyed (both 13-year-olds and 15-year-olds), while Canadian female adolescents were in the 3rd quartile for 13-year-olds and bottom quartile for 15-year-olds (Figure 12.11).
Figure 12.11: Canadian students who smoke at least once a week
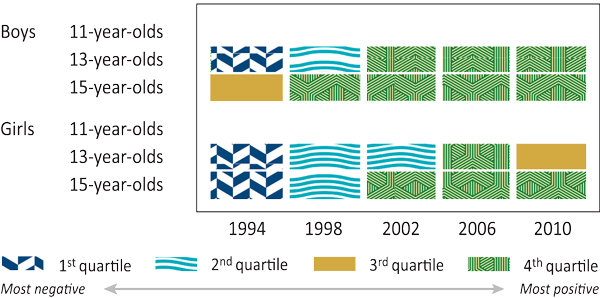
Text Equivalent - Figure 12.11
Figure 12.11 is a table that shows the international ranking of Canadian students who smoke at least once a week by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 1994, 13-year-old boys ranked in the first quartile, in the second quartile in 1998 and in the fourth quartile in 2002, 2006 and 2010. In 1994, 15-year-old boys ranked in the third quartile and in the fourth quartile in 1998, 2002, 2006 and 2010. In 1994, 13-year-old girls ranked in the first quartile, in the second quartile in 1998 and 2002, in the fourth quartile in 2006 and in the third quartile in 2010. In 1994, 15-year-old girls ranked in the first quartile, in the second quartile in 1998 and in the fourth quartile in 2002, 2006 and 2010.
Between 1990 and 2010, the percentage of Canadian students reporting to have been "really drunk" at least twice in their life has declined slightly (Figures 9.9 and 9.10). Similarly, as illustrated in Figure 12.12, little has changed over time in comparing Canadian adolescents to those from other HBSC countries. For example, in 1994, 1998, and 2010, all age groups of Canadian girls were in the 2nd quartile for having been "really drunk." Boys over those three survey cycles were consistently in the 2nd or 3rd quartile.
Figure 12.12: Canadian students who have been drunk at least twice
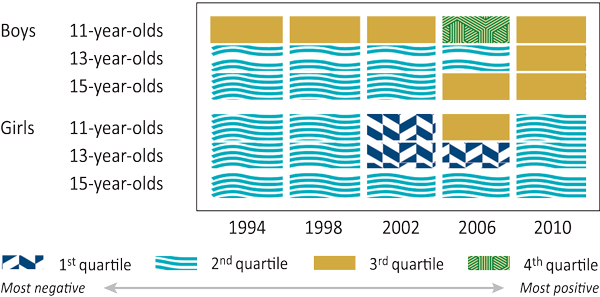
Text Equivalent - Figure 12.12
Figure 12.12 is a table that shows the international ranking of Canadian students who have been drunk at least twice by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 1994, 1998 and 2002, 11-year-old boys ranked in the third quartile, in the second quartile in 2006 and in the fourth quartile in 2010. In 1994, 1998, 2002 and 2006, 13-year-old boys ranked in the second quartile and in the third quartile in 2010. In 1994, 1998 and 2002, 15-year-old boys ranked in the second quartile and in the third quartile in 2006 and 2010. In 1994 and 1998, 11-year-old girls ranked in the second quartile, in the first quartile in 2002, in the third quartile in 2006 and in the second quartile in 2010. In 1994 and 1998, 13-year-old girls ranked in the second quartile, in the first quartile in 2002 and 2006 and in the second quartile in 2010. In 1994, 1998, 2002, 2006 and 2010, 15-year-old girls ranked in the second quartile.
International data indicate that Canadian adolescents have consistently been among the highest levels of cannabis users who have used it at least once in their life time (Figure 12.13; data collected only for 15-year-olds). Canadian 15-year-old girls ranked first among HBSC countries for cannabis use in 2006 and 2010 and second in 2002, while Canadian 15-year-old boys ranked second in all three survey years (figures not shown). Furthermore, the number of Grade 10 Canadian students who reported having ever tried cannabis has increased over time (Figures 9.11 and 9.12). For example, in 2010, 40% of Canadian boys and 37% of Canadian girls reported having tried cannabis.
Figure 12.13: Canadian students who have ever used cannabis
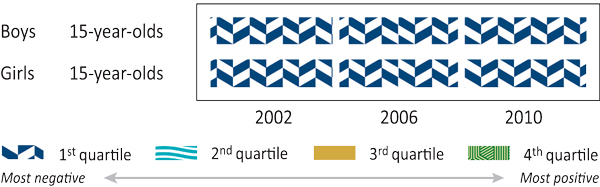
Text Equivalent - Figure 12.13
Figure 12.13 is a table that shows the international ranking Canadian students who have ever used cannabis by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and in the fourth quartile being the most positive. In 2002, 2006 and 2010, 15-year-old boys ranked in the first quartile. In 2002, 2006 and 2010, 15-year-old girls ranked in the first quartile.
Since 2002, the number of Grade 9 and Grade 10 students who have reported having had sexual intercourse has increased (Figures 10.1 and 10.2). However, during this same time span, Canada's international placement for reported sexual activity has remained relatively stable at the 3rd or 4th quartile for 15-year-old boys and the 2nd quartile for 15-year-old girls (Figure 12.14; data collected only for this age group).
Figure 12.14: Canadian students who have had sexual intercourse
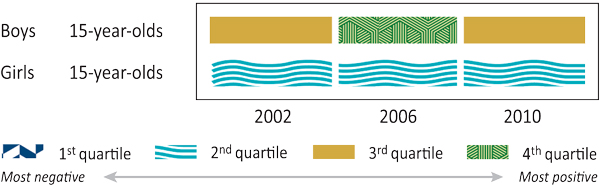
Text Equivalent - Figure 12.14
Figure 12.14 is a table that shows the international ranking Canadian students who have had sexual intercourse by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 2002, 15-year-old boys ranked in the third quartile, in the fourth quartile in 2006 and in the third quartile in 2010. In 2002, 2006 and 2010, 15-year-old girls ranked in the second quartile.
As illustrated in Figures 11.15 and 11.16, the prevalence of fighting for Grade 6 and 8 students peaked in 2006, especially for girls. These data are somewhat reflected in the 2006 international statistics in that Canadian girls ranked in the top quartile across all three age groups (Figure 12.15).
Figure 12.15: Canadian students who have been involved in a physical fight at least three times in the last 12 months
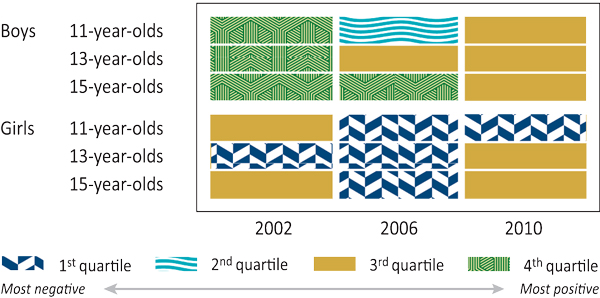
Text Equivalent - Figure 12.15
Figure 12.15 is a table that shows the international ranking Canadian students who have been involved in a physical fight at least three times in the last 12 months by age, year and gender. The table ranks students in either of four quartiles with the first quartile being the most negative and the fourth quartile being the most positive. In 2002, 11-year-old boys ranked in the fourth quartile, in the second in 2006 and in the third quartile in 2010. In 2002, 13-year-old boys ranked in the fourth quartile and in the third in 2006 and 2010. In 2002 and 2006, 15-year-old boys ranked in the fourth quartile and in the third in 2010. In 2002, 11-year-old girls ranked in the third quartile and in the first quartile in 2006 and 2010. In 2002 and 2006, 13-year-old girls ranked in the first quartile and in the third in 2010. In 2002, 15-year-old girls ranked in the third quartile, in the first quartile in 2006 and in the third quartile in 2010.
Causes for Celebration and Causes for Concern
Table 12.1 summaries the results from this chapter with corresponding international figures given in parentheses. Three areas are clearly ones where Canadians have cause for celebration (academic self-perceptions, soft drink consumption, cigarette smoking), while three areas are certainly cause for concern (life satisfaction, overweight/obesity, cannabis use). The remaining 10 areas cannot easily be classified as either a cause for celebration or a cause for concern. Implications of these international trends, in conjunction with the results from Chapters 2-11, are discussed in Chapter 13.
| Causes for Celebration | Causes for Concern | Cause for Celebration or Cause for Concern? |
|---|---|---|
| Academic self-perceptions (Figure 12.4) | Life satisfaction (Figure 12.1) | Communication with mother (Figure 12.2) |
| Soft drink consumption (Figure 12.9) | Overweight/obesity (Figure 12.10) | Communication with father (Figure 12.2) |
| Cigarette smoking (Figure 12.11) | Cannabis use (Figure 12.13) | Liking school (Figure 12.5) |
| School pressure (Figure 12.6) | ||
| Classmates helpful (Figure 12.7) | ||
| Injuries (Figure 12.8) | ||
| Drunkenness (Figure 12.12) | ||
| Sexual intercourse (Figure 12.14) | ||
| Fighting (Figure 12.15) |
Causes for Celebration
- Academic self-perceptions: Canadian students across the survey years have consistently felt that their teachers judged their academic performance as good or very good. They have also remained high internationally on this question, especially so for 15-year-old girls.
- Soft drink consumption: Daily non-diet soft drink consumption on a daily basis has declined substantially since 2002 for Canadian adolescents. Canadian youth are beginning to report some of the lowest levels of soft drink consumption internationally with all age-gender groups in the bottom quartile for 2006 and 2010.
- Cigarette smoking: Daily smoking has decreased in Canada since the 1990s among Grade 8 and Grade 10 students. At the time of the latest survey, Canadian boys had the lowest weekly smoking rates among the HBSC countries surveyed (both 13-year-olds and 15-year-olds), while Canadian female adolescents were in the 3rd quartile for 13-year-olds and bottom quartile for 15-year-olds.
Causes for Concern
- Life satisfaction: Although Canadian adolescents have strong academic self-perceptions, they do not have correspondingly high life satisfaction. Congruent with the results with respect to life satisfaction on the national level, the life satisfaction of Canadian adolescents reported in the HBSC survey has been worsening relative to their peers in other countries. The worsening international comparison is especially evident for girls, who dropped from the third to the bottom quartile for ages 11 and 13 between 2006 and 2010, and from the top to the third quartile for age 15.
- Overweight/obesity: Although Canadian adolescents are consuming fewer soft drinks than in the past, which might indicate a positive change in eating patterns, this shift has not been accompanied by a change in overweight/obesity. Internationally, Canadian adolescents have consistently been in the top quartile for being overweight or obese. At the time of the most recent survey (2010), Canada ranked second of 39 HBSC countries in the prevalence of overweight and obese 15-year-old boys and girls. For overweight and obese 13-year-old boys and girls, Canada ranked fourth and third, respectively. These figures reflect the Canadian results, which have changed little over time.
- Cannabis use: While the decrease in cigarette smoking among Canadian youth is, without a doubt, the largest cause for celebration in the Canadian HBSC data over the survey years, cannabis use has become a definite cause for concern. Canadian adolescents have consistently shown among the highest levels of cannabis use internationally. Canadian 15-year-old girls ranked first among HBSC countries for cannabis use in 2006 and 2010 and second in 2002, while Canadian 15-year-old boys ranked second in all three survey years. In the most recent survey (2010), 40% of Grade 10 Canadian boys and 37% of Grade 10 Canadian girls reported having ever tried cannabis.
Cause for Celebration or Cause for Concern?
- Communication with parents: On the one hand, communication with mothers and fathers might be considered a cause for celebration in that a large proportion of Canadian adolescents find it easy or very easy to communicate with their mothers and their fathers. This proportion has increased over time. However, Canada still ranks relatively low internationally with respect to this variable, a cause for concern.
- Liking school and helpful classmates: The majority of Canadian adolescents report not liking school with this percentage largely unaffected by survey year. Still, internationally, Canadians have relatively high scores for school liking. In contrast, the majority of Canadian adolescents report their classmates are kind and helpful, again with minimal differences across surveys, yet internationally Canadians have relatively low scores for classmate helpfulness.
- School pressure: It is difficult to classify school pressure as a celebration or concern because of the nature of the question. It is unclear what would be the optimum amount of school pressure for either academic or health outcomes, so Canadian adolescents' relatively high scores internationally on school pressure may be beneficial or hurtful for these outcomes, and possibly differentially so.
- Drunkenness, sexual intercourse, and fighting: So little has changed across these variables over the survey years, both nationally and internationally, that it is difficult to see the results for these three areas as either a cause for celebration or a cause for concern.
Chapter 13: Summary Observations
By John Freeman
This chapter synthesizes findings from the Health Behaviour in School-aged Children (HBSC) surveys discussed across the previous 12 chapters to provide five summary observations. These observations may prove useful for all individuals interested in improving the health and well-being of Canadian adolescents. The five observations are:
- The comprehensive approach that helped reduce smoking rates among Canadian adolescents provides an excellent example for how other health issues might be tackled.
- Overweight/obesity should remain a major focus for continuing adolescent public health efforts in Canada.
- Continuing efforts to reduce substance use, with particular attention to cannabis, should be supported.
- Mental health remains at the forefront of Canadian public health efforts.
- Youth voices should be heard on research, policy, and programming that affect their health.
Observation # 1: The comprehensive approach that helped reduce the smoking rates of Canadian adolescents should be adopted in tackling other health issues.
Cigarette smoking is the one public health concern that has shown the greatest improvement for Canadian adolescents over the past 20 years. Daily smoking has decreased in Canada since the 1990s for all grade-gender groups. In 1994, Canadian 13-year-old boys and girls and 15-year-old girls ranked in the top quartile of countries, meaning they had among the highest rates of smoking at least once a week internationally, while Canadian 15-year-old boys were in the 3rd quartile. At the time of the latest HBSC survey, Canadian boys had the lowest weekly smoking rates among the HBSC countries surveyed (both 13-year-olds and 15-year-olds), while Canadian female adolescents dropped to the 3rd quartile for 13-year-olds and to the bottom quartile for 15-year-olds.
The largest decreases in smoking rates in Canada came shortly after the passage of the federal Tobacco Act in 1997 and the adoption of New Directions for Tobacco Control in Canada-A National Strategy framework in 1999. Accompanying these efforts have been municipal and provincial/territorial bans on smoking in public places, increased regulation of cigarette selling practices, and ongoing vigilance in prohibiting adolescents from buying cigarettes. With the ongoing collective efforts of governments and non-governmental organizations, the collaborative nature of this national approach to cigarette smoking has allowed Canada to move closer to the goals outlined within the 1999 strategy framework: prevention, cessation, protection, and denormalization. This is a model approach that can be used with some public health concerns to have similar impacts, recognizing the differences in risk and protective factors across issues.
Observation # 2: Overweight/obesity should remain a major focus for continuing adolescent public health efforts in Canada.
Overweight/obesity is an ongoing concern for Canadian students in Grades 6-10. Internationally, Canadian adolescents have consistently been in the top quartile for being overweight or obese. At the time of the most recent survey (2010), Canada ranked second of 39 HBSC countries in the prevalence of overweight and obese 15-year-old boys and girls. For overweight and obese 13-year-old boys and girls, Canada ranked fourth and third, respectively. The figures for Canada have changed little over time.
Collaborative efforts are now underway to reduce the proportion of Canadian adolescents who are classified as overweight or obese. The 2010 Curbing Childhood Obesity, a federal, provincial and territorial initiative, focuses on making excess weight in youth a collective priority and on continually measuring and reporting on the effectiveness of its three key strategies (Public Health Agency of Canada [PHAC], 2013a). Federal funding, through the 2011 Achieving Healthier Weights in Canada's Communities and Managing Obesity Across the Lifecycle: An Interventions Approach, provides communities with financial assistance to help carry out these strategies (PHAC, 2010). Similarly, insight into individuals' specific needs and potential solutions addressing obesity from Our Health Our Future- A National Dialogue on Healthy Weights Dialogue Report 2011 may improve the effectiveness of future healthy weights strategies (PHAC, 2013b).
Observation # 3: Efforts to reduce substance use, with particular attention to cannabis, should be supported.
The HBSC survey has historically measured cannabis as an indicator of substance use. Canadian adolescents have consistently shown among the highest levels of cannabis use internationally. Canadian 15-year-old girls ranked first among HBSC countries for cannabis use in 2006 and 2010 and second in 2002, while Canadian 15-year-old boys ranked second in all three survey years. In the most recent survey (2010), 40% of Grade 10 Canadian boys and 37% of Grade 10 Canadian girls reported having ever tried cannabis.
While no initiatives focus solely on cannabis use, there are programs to support drug prevention efforts beyond alcohol and tobacco. Introduced as part of the Canadian Centre of Substance Abuse's strategy to reduce drug use among Canadian youth, Building On Our Strengths: Canadian Standards for School-based Youth Substance Abuse Prevention (2010a), Strengthening Our Skills: Canadian Guidelines for Youth Substance Abuse Prevention Family Skills Programs (2011), and Stronger Together: Canadian Standards for Community-based Youth Substance Abuse Prevention (2010b) aim to support new and existing efforts towards substance abuse prevention, including delaying age of first use. The effects of these types of programs should be reflected in the next HBSC survey cycle.
Observation # 4: Mental health remains at the forefront of Canadian public health efforts.
The prevalence of reported well-being for Canadian young people in the HBSC survey has been decreasing since the beginning of the survey cycles with other indices of mental health remaining relatively stable.
For example, congruent with the results with respect to life satisfaction on the national level, the life satisfaction of Canadian adolescents reported in the HBSC survey has been worsening relative to their peers in other countries. While the numbers from the 2002 survey in Canada may have been somewhat of an anomaly in that they were obtained later in the school year, the differences between 2006 and 2010 cannot be attributed to survey timing. The worsening international comparison is especially evident for girls, who dropped from the third to the bottom quartile for ages 11 and 13 between 2006 and 2010, and from the top to the third quartile for age 15.
In 2008, the growing awareness of and concern for mental health in Canada prompted the Standing Senate Committee on Social Affairs, Science and Technology to create the Mental Health Commission of Canada (MHCC). Among other initiatives, the MHCC set forward in 2010 to develop a Mental Health Strategy for Canada that includes a framework, Evergreen, specifically for child and youth mental health (Kutcher & McLuckie, 2010). In addition, this past year, the Economic Action Plan 2012 for Canada proposed $5.2 million for 2012 to 2013 to support the Canadian Depression Research and Intervention Network (Government of Canada, 2012). The goal was to have research focus on more effective diagnostic and treatment tools, as well as on improving the lives of individuals lacking mental well-being. Similarly, in 2009, when discussing the topic for the next national HBSC report, researchers, policymakers, and practitioners agreed that the focus should be on mental health as this topic was of prime concern to all stakeholders (Freeman, King, & Pickett, 2011).
However, in that the promotion of positive mental health is still in its early stages, the influence of such approaches on the mental health of students in Grades 6-10 is expected in the coming years.
Observation # 5: Youth voices should be heard on research, policy, and programming that affect their health.
In examining the trends over the years, it became apparent that the HBSC data provided an abundance of information about how youth experienced their contexts, their health, and engage in health behaviours in Canada. While this information is invaluable, it should be supplemented with an opportunity for youth to provide context by recognizing that young people can tell us a great deal about why they do what they do, insofar as we are ready to listen.
This view is congruent with the United Nations Convention on the Rights of the Child (UNCRC), Article 12, which states: When adults are making decisions that affect children, children have the right to say what they think should happen and have their opinions taken into account. ... This Convention encourages adults to listen to the opinions of children and involve them in decision-making-not give children authority over adults. This Convention is crucial to understanding the high value placed on youth engagement in public health issues as set out in the 2011 Canadian Public Health Officer's (CPHO) Report on the State of Public Health in Canada.
Recognizing not only the rights of the child but the benefits to adults that accrue by so doing, in disseminating the most recent national HBSC report, the HBSC Canada researchers and the Public Health Agency of Canada (PHAC) partners worked with the Students Commission of Canada, a nationally renowned organization dedicated to youth engagement, to ensure that young people's voices would be represented in the final report. Similarly, in March 2011, PHAC collaborated with the Students Commission to include a component on the 2011 CPHO Report on Young & Young Adults: Life in Transition at "Unite and Ignite," a youth conference in Ottawa with over 400 participants ages 12-29. These Canadian examples of collaboration have moved forward the international HBSC network so far as to including a youth engagement forum at the June 2013 international HBSC meeting in Scotland.
References
- Canadian Centre of Substance Abuse [CCSA] (2010a). Building on our strengths: Canadian standards for school-based youth substance abuse prevention. Ottawa, ON: Canadian Centre on Substance Abuse.
- Canadian Centre of Substance Abuse [CCSA] (2010b). Stronger Together: Canadian Standards for Community-based Youth Substance Abuse Prevention. Ottawa, ON: Canadian Centre on Substance Abuse.
- Canadian Centre of Substance Abuse [CCSA] (2011). Strengthening Our Skills: Canadian Guidelines for Youth Substance Abuse Prevention Family Skills Programs. Ottawa, ON: Canadian Centre on Substance Abuse.
- Freeman, J.G., King, M., Pickett, W., Eds. (2011). The health of Canada's young people: A mental health focus. Ottawa, ON: Public Health Agency of Canada.
- Government of Canada (2012). Budget plan 2012. Retrieved from
- Kutcher, S., McLuckie, A. For the Child and Youth Advisory Committee, Mental Health Commission of Canada (2010). Evergreen: A child and youth mental health framework for Canada. Calgary, AB: Mental Health Commission of Canada.
- McCart, S., Khanna, N. for the Students Commission of Canada (2011). Theoretical Toolkit: A Model for Engaging Youth in Evidence-Informed Policy and Program Development.
- Public Health Agency of Canada [PHAC] (2010). Solicitation: Achieving healthier weights in Canada's communities.
- Public Health Agency of Canada [PHAC] (2012). The Chief Public Health Officer's Report on the State of Public Health in Canada 2011.
- Public Health Agency of Canada [PHAC] (2013a). Curbing childhood obesity: A federal, provincial and territorial framework for action to promote healthy weights.
- Public Health Agency of Canada [PHAC] (2013b). Our health our future - A National dialogue on healthy weights dialogue report.
- Public Health Agency of Canada [PHAC] (2013b). Our health our future - A National dialogue on healthy weights dialogue report.
- Unicef (2005). FACT SHEET: A summary of the rights under the Convention on the Rights of the Child.