
Recommendations on Screening for Chlamydia trachomatis and Neisseria gonorrhoeae in Pregnancy
An Advisory Committee Statement (ACS)
National Advisory Committee on Sexually Transmitted and Blood-Borne Infections (NAC-STBBI)
Recommendations on Screening for Chlamydia trachomatis and Neisseria gonorrhoeae in Pregnancy
Table of Contents
- Preamble
- Purpose and scope
- Introduction
- Summary of recommendations
- Methods
- Recommendations
- Justification
- Summary of the evidence
- Implementation
- Monitoring and evaluation
- Limitations
- Research gaps
- List of abbreviations
- Acknowledgements
- Suggested citation
- Correspondence
- Appendices
- Appendix A. Flow diagram of study selection for original and update searches on acceptability, feasibility, equity and resource use for prenatal screening for Chlamydia trachomatis and Neisseria gonorrhoeae
- Appendix B. Study characteristics and findings on acceptability, feasibility, equity and resource use for prenatal screening for Chlamydia trachomatis and Neisseria gonorrhoeae
- Appendix C. Interpretation of strong and conditional recommendations
- Appendix D. Grading of Recommendations, Assessment, Development and Evaluation Evidence to Decision Framework
- Appendix E. Estimated outcomes, cost and cost-effectiveness of different strategies to screen for Chlamydia trachomatis and Neisseria gonorrhoeae in pregnant women/pregnant individuals in Canada
Preamble
The National Advisory Committee on Sexually Transmitted and Blood-Borne Infections (NAC-STBBI) is an External Advisory Body that provides the Public Health Agency of Canada (PHAC) with ongoing scientific and public health advice and recommendations for the development of sexually transmitted and blood-borne infections (STBBI) guidance, in support of its mandate to prevent and control infectious diseases in Canada.
PHAC acknowledges that the advice and recommendations in this statement are based upon the best available scientific knowledge at the time of writing, and is disseminating this document for information purposes to primary care providers and public health professionals. The NAC-STBBI Statement may also assist policy makers or serve as the basis for adaptation by other guideline developers. NAC-STBBI members and liaison members conduct themselves within the context of PHAC’s Policy on Conflict of Interest, including yearly declaration of interests and affiliations.
The recommendations in this statement do not supersede any provincial/territorial legislative, regulatory, policy and practice requirements or professional guidelines that govern the practice of health professionals in their respective jurisdictions, whose recommendations may differ due to local epidemiology or context. The recommendations in this statement may not reflect all the situations that may arise in professional practice, and are not intended as a substitute for clinical judgment in consideration of individual circumstances and available resources.
Purpose and scope
For the purpose of these recommendations, screening is defined as testing asymptomatic individuals. The following recommendations apply to screening of asymptomatic pregnant women/pregnant individuals (PWPI). These recommendations do not replace recommendations to test and treat PWPI who have symptoms compatible with NG or CT infection or after sexual contact with a person known to have a NG or CT.
We suggest screening all PWPI for NG and CT during the first trimester or at the first antenatal visit, and again in the third trimester (conditional recommendation; low certainty evidence).
We suggest screening PWPI at the time of labour for NG and CT in any of the following situations (conditional recommendation; low certainty evidence):
- No prenatal screening has occurred (no valid results available at the time of labour).
- Third trimester screening has not occurred.
- A positive test result was obtained for NG or CT during pregnancy without appropriate follow-up, including treatment and a test-of-cure.
Introduction
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) are the most common of the reported sexually transmitted infections (STI) in Canada. Between 2010 and 2019, rates of reported cases of CT increased 33.1% and NG increased 181.7%.Footnote 1 In 2019, 139,386 cases of CT and 35,443 cases of NG were reported in Canada, corresponding to rates of 370.8 and 94.3 per 100,000 population, respectively.Footnote 1Footnote 2
In 2019, the highest rates of CT were among people from the Canadian territories (Yukon, Northwest Territories and Nunavut with 757.0, 1,901.0 and 3,876.8 cases per 100,000 population, respectively.Footnote 1 Since 2010 the highest rates of NG were among people from Nunavut and the Northwest Territories with rates above 1,000 cases per 100,000 population in 2019.Footnote 1
Among females, CT rates have been consistently highest in those between the ages of 15 and 24 since 2010.Footnote 1 In 2019, the highest NG rates among females were in those between the ages of 15 and 29.Footnote 1 In 2019, among all females (pregnant or not) with confirmed CT, 62.8% were aged 15-24 years; the corresponding proportion for NG was 42.8%.Footnote 2
In females, CT and NG infections are often asymptomatic. In PWPI, undetected and untreated infections could lead to pregnancy-related complications, sexual transmission, and transmission to neonates in the perinatal period.Footnote 3 If left untreated, CT in the birthing parent carries a 30-50% risk of ophthalmia neonatorum and 10-20% risk of CT pneumonia.Footnote 3 NG infection in the birthing parent carries a 30% risk of the neonate developing ophthalmia neonatorum.Footnote 4Footnote 5 Potential consequences of ophthalmia neonatorum include permanent visual impairment.
In 2010, PHAC recommended that all pregnant women should be evaluated for STI risk factors prior to and during pregnancy. Any woman with ongoing risk factors for STI acquisition during pregnancy should be considered for rescreening each trimester.Footnote 6 In 2010, PHAC also recommended to screen for C. trachomatis early in pregnancy. Repeat screening should be performed in the third trimester for women at continuing risk for STI acquisition.Footnote 6Footnote 7
In 2016 (reaffirmed in 2021), the Canadian Paediatric Society stated “Neonatal ocular prophylaxis with erythromycin, the only agent currently available in Canada for this purpose, may no longer be useful and, therefore, should not be routinely recommended. More effective means of preventing ophthalmia neonatorum include screening all pregnant women for gonorrhea and chlamydia infection, and treatment and follow-up of those found to be infected. Mothers who were not screened should be tested at delivery”.Footnote 8 Despite national prenatal screening recommendations, recent studies show suboptimal rates of prenatal screening for CT and NG in Canada with approximately 15-22% of PWPI not being screened for these infections.Footnote 9Footnote 10Footnote 11
Given the increasing rates of reported cases of CT and NG in the general population and suboptimal rates of prenatal screening for CT and NG in Canada,Footnote 9Footnote 10Footnote 11 the National Advisory Committee on Sexually Transmitted and Blood-Borne Infections (NAC-STBBI) reviewed and updated the PHAC’s recommendations on prenatal screening for CT and NG.
Summary of recommendations
The goal of the recommendations is to optimize the prevention of ophthalmia neonatorum and neonatal pneumonia, as well as adverse pregnancy outcomes. The recommendations address when to screen PWPI for CT and NG. It applies to all PWPI who do not have symptoms of an STI for whom testing is indicated. The target audience for these recommendations is national, provincial and local programmes, and health care professional teams who care for PWPI, including family physicians, midwives, and obstetrics and gynecology specialists.
Methods
NAC-STBBI provides PHAC with ongoing scientific and public health advice and recommendations for the development of sexually transmitted and blood-borne infections (STBBI) guidance, in support of its mandate to prevent and control infectious diseases in Canada. A Working Group composed of experts from NAC-STBBI was formed to develop the recommendations on prenatal screening for CT and NG to optimize the prevention of adverse pregnancy outcomes, as well as ophthalmia neonatorum and neonatal pneumonia. The Working Group received methodological and technical support from PHAC. The recommendations were developed by a Working Group of four NAC-STBBI members (ACL, JB, GO, and MY) with Secretariat (PHAC) support and in consultation with an external methodology expert (NS).
The Working Group developed the policy and research questions for a clinical review, an economic analysis and a review of patients’ perspectives and experiences. A protocol was drafted in consultation with the Working Group.
The Canadian Agency for Drugs and Technologies in Health (CADTH) conducted a health technology assessment (HTA)Footnote 12 to support the development of the NAC-STBBI recommendations. CADTH engaged members of the NAC-STBBI (formerly known as the Expert Working Group for the Canadian Guidelines on Sexually Transmitted Infections) and peer-reviewers (ACL and TH) to review the protocol and HTA. In 2018, members of the Working Group and a patient group were also engaged to rate the list of outcomes important to making the recommendations using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. After publication of the CADTH HTA in November 2018, the Working Group added ophthalmia neonatorum and neonatal pneumonia as critical outcomes and then narrowed down the list to six outcomes as listed below.
- Number and percent of positive NG and/or CT infections detected at screening (includes new or repeat infections)
- Surrogate outcome: number of females treated for infection
- Surrogate outcomes: true positives and false negatives and false positives and true negatives
- Adverse obstetric outcomes (pre-term and still births)
- Number of females declining screening
- Anxiety/fears
- Number and percent of ophthalmia neonatorum
- Number and percent of neonatal pneumonia
An updated search for the clinical review, economic analysis and patients’ perspectives and experiences was undertaken by CADTH in July 2020.Footnote 13 In the original HTA report and the updated search, there was no evidence for the two neonatal outcomes. In the absence of published literature evidence, the Working Group considered other types of evidence including surveillance and epidemiology information and a decision-analytic model to support the development of the recommendations.
CADTH constructed a decision-analytic model of prenatal screening for NG and/or CT infections to predict the outcomes for PWPI and their newborns in Canada. The model evaluated the impact of strategies for screening all or only high-risk PWPI at first, second and/or third trimesters and at labour over approximately one year. The structure and inputs were informed by literature and clinical experts in obstetrics and gynecology, as well as in adult and paediatric infectious diseases. Given uncertainties of some model parameters and assumptions in the base-case analysis, sensitivity analyses were performed, assuming a lifetime horizon, higher prevalence of infections in PWPI, higher rates of transmission to newborns, lower costs of tests, and greater risks of poor outcomes in PWPI with NG or CT. Outcomes included neonatal infections, adverse outcomes to PWPI, preterm births, quality-adjusted life-years (QALY) and costs.
A systematic review on acceptability, feasibility, equity and resource use of prenatal screening for NG and CT was undertaken by PHAC.Footnote 14 Information sources including MEDLINE® All, Embase, and Cochrane CENTRAL (January 2003 - January 2021) electronic databases were searched for studies that assessed acceptability, feasibility, equity or resource use of screening for NG and/or CT in PWPI aged 12 years and older. No study design or language limits were applied. Titles, abstracts, and selected full-text articles were screened based on pre-defined inclusion criteria and data were extracted by reviewers. Appendix A shows the flow diagram of study selection. The Risk of Bias Assessment tool for Non-randomized Studies was used for quality assessment and a narrative synthesis was prepared. Appendix B shows the characteristics and findings of the included studies on acceptability, feasibility, equity and resource use.
The GRADE approach was used to determine the certainty of the evidence and strength of the recommendations. Appendix C provides the interpretation of strong and conditional recommendations based on the GRADE approach. The GRADE Evidence to Decision framework was drafted by PHAC to help the Working Group use evidence in a structured and transparent way to develop the recommendations. Appendix D provides the Evidence to Decision framework that the Working Group used to assess the balance between benefits and harms, patient values and preferences, resource use, feasibility, acceptability, and equity in order to develop the recommendations. The Working Group drafted the recommendations using the GRADE wording for direction and strength. The entire NAC-STBBI reviewed this statement and voted on the recommendations. Peer-reviewers with expertise in obstetrics and gynecology, as well as in adult and paediatric infectious diseases were identified and engaged prior to the publication of the recommendations.
Management of competing interests
The NAC-STBBI is supported by PHAC. All NAC-STBBI members are required to disclose financial and nonfinancial conflicts of interest.
Recommendations
For the purpose of these recommendations, screening is defined as testing asymptomatic individuals. The following recommendations apply to screening of asymptomatic pregnant women/pregnant individuals (PWPI). These recommendations do not replace recommendations to test and treat PWPI who have symptoms compatible with NG or CT infection or after sexual contact with a person known to have a NG or CT.
We suggest screening all PWPI for NG and CT during the first trimester or at the first antenatal visit, and again in the third trimester (conditional recommendation; low certainty evidence).
We suggest screening PWPI at the time of labour for NG and CT in any of the following situations (conditional recommendation; low certainty evidence):
- No prenatal screening has occurred (no valid results available at the time of labour).
- Third trimester screening has not occurred.
- A positive test result was obtained for NG or CT during pregnancy without appropriate follow-up, including treatment and a test-of-cure.
Justification
Systematic reviews of the literature and a decision-analytic model were used to determine the effects of different screening strategies for NG or CT to prevent ophthalmia neonatorum, neonatal pneumonia and adverse pregnancy outcomes. As presented in Table 1, the evidence showed that there may be greater benefits and lower resource use and costs when screening for NG or CT is offered to all PWPI at first and third trimesters - and at labour when screening is not performed during pregnancy or follow-up has not occurred after a prior positive test result during pregnancy - compared with other screening strategies over the short-term (1 year) and long-term (lifetime) (low certainty evidence). There is evidence showing greatest benefit when third trimester screening is provided. Screening all PWPI at first and third trimesters is likely more acceptable than targeting high-risk PWPI because it may reduce stigma associated with screening for STI. In addition, the Working Group agreed that it may be more practical and therefore more likely to be done than inquiring about risk factors during busy prenatal visits and accessing partner risk factors. A recommendation about the sampling method for screening was not made since the preference and capacity may vary according to the patient, health care provider, and the health care system.
Summary of the evidence
Systematic reviews of the benefits, harms, feasibility, acceptability, resource use and the impact on equity of different screening strategies for NG or CT in PWPI were conducted. While there are several studies comparing different strategies to no screening, there are no studies directly comparing different strategies. Therefore, a decision-analytic model specific to the Canadian setting was used to inform the recommendations.Footnote 12
Table 1 presents a summary of the evidence for the effect of select strategies on important outcomes to PWPI and their newborns, but additional strategies were considered during the recommendation development process (see Appendix E).
The inputs into the model represent the best available evidence about current screening rates, follow-up after screening, prevalence of NG or CT in PWPI, probability of transmission to newborns, and consequences of infection to PWPI and newborns.
The costs from 2018 were used in the model and included medical, pharmacy and laboratory costs. Costs for births (including preterm, extremely preterm and still births), such as direct medical costs (including nursing and laboratory), pharmacy costs, and administration costs, informed the analysis. Costs for laboratory services for tests also informed the analysis. Further, management of infections for both PWPI and infants were included and covered costs of drugs and visits, outpatient and inpatient care (including per diem costs in hospital, diagnostic and test and test-of-cure visits, specialist consultation, and drug and pharmacy costs).
The Working Group agreed that the following key assumptions in the model are applicable to the Canadian setting:
- Even when screening is planned for all PWPI at a predefined visit, only 80% are tested; at labour, approximately 50% of women who were not previously screened or had previously tested positive receive testing.
- Screening at labour and delivery does not occur in extremely preterm births and preterm births.
- If a PWPI tests positive, treatment is provided and 100% effective; a test-of-cure and rescreening at the next trimester is provided.
- A positive test at labour for gonorrhoeae means that a newborn receives prophylactic treatment. For CT, newborns do not receive prophylactic treatment, but are monitored for symptoms. Otherwise, prophylactic treatment is not provided.
The prevalence of CT, NG and of both CT and NG infections in the whole population were respectively 1.9%, 0.2%, and 0.1%. The group with high risks of NG and CT infection was modeled as a group <25 years old with associated risks. The probability of CT infection in the high risk group was 2.15%; and otherwise was 0.63%. The probability of GC infection in the high risk group was 0.16%; and otherwise was 0.14%. The probability of CT or GC reinfection in the high risk group was 1.12 times greater than reinfection in the non-high risk group.
Inputs for higher prevalence and risk for NG/CT in the overall population used in the model for cost-effectiveness sensitivity analysis were 14.69% for CT-only infection, 0.47% for GC-only infection and 0.47% for coinfections;Footnote 15 and, for higher reinfection were the upper limit of the 95% confidence interval in the non-high risk model (CT infection: 2.25% annually in high risk group, 1.06% otherwise; GC infection: 0.18% annually in the high risk group, 0.21% otherwise; CT and GC reinfections: 2.79% annually in the high risk group, 2.49% otherwise).
Results of decision-analytic model for different screening strategies
Each strategy is shown in Table 1 by the screening provided during first (1), second (2), and third (3) trimester. Screening can be performed in all (referred to as all), in high-risk individuals (referred to as only high risk), in nobody (referred to as none) or at labour (if not previously screened or screened positive during pregnancy).
For example, if you consider strategy #2 (see the top row) and follow the column down, strategy #2 indicates that all PWPI are screened at first trimester (T1), none are screened at second trimester (T2), and all are screened at T3. In addition, if a PWPI is not screened during pregnancy, the PWPI is screened at labour. When using strategy #2 in a population of 400,000 PWPI, there will be 440 cases of ophthalmia neonatorum; 160 cases of CT pneumonia; and 34,056 cases of preterm, extremely preterm and still births over 1 year. These cases are fewer than or similar to the cases for strategies #3 to #7. In addition, 4.14% will be falsely identified as having NG or CT (and consequently unnecessarily treated) and 0.9% will be missed and not treated. When calculating the benefits and harms and the associated costs, the model found that in a setting where the risks of NG or CT are not high the additional cost of one quality adjusted life year (QALY) was $65 million more than another strategy (strategy #3 where instead of all screened at T1 only high risk are screened) over 1 year. Over a lifetime it was $11 million more. In a setting where the risk of NG and CT is higher, it was $7 million more than a strategy where only all are screened at T3. Although there is a cost for more benefits, most other strategies cost more but had fewer benefits (referred to as “More costly, less effective than other strategies”). Notably, strategy #5 (screening all PWPI in T1, only high risk in T1 and T2), which is currently used in some settings, is more costly and less effective than other strategies that were considered.
| Screening Strategies: Pregnant women/pregnant individuals (PWPI) screened (or not) at each trimester (T) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 New recommendation |
3 | 4 | 5 Strategy in some settings |
6 | 7 | 8 | ||
| Effects of Strategies | T1: All T2: Only HRTable 1 note a T3: All LabourTable 1 note b |
T1: All T2: NoneTable 1 note c T3: All Labour |
T1: Only HR T2: None T3: All Labour |
T1: None T2: None T3: All Labour |
T1: All T2: Only HR T3: Only HR Labour |
T1: All T2: None T3: Only HR Labour |
T1: All T2: None T3: None Labour |
T1: None T2: None T3: None Labour |
|
| Adverse infant & obstetric outcomes over 1 year | |||||||||
| Ophthalmia neonatorum | Cases per 100,000 PWPI | 110Table 1 note e | 110 | 124 | 128 | 148 | 149 | 170 | 357 |
| Cases per 400,000 PWPITable 1 note d | 440Table 1 note e | 440 | 496 | 512 | 592 | 596 | 680 | 1428 | |
| CT pneumonia | Cases per 100,000 PWPI | 40Table 1 note e | 40 | 46 | 48 | 53 | 53 | 62 | 132 |
| Cases per 400,000 PWPITable 1 note d | 160Table 1 note e | 160 | 184 | 192 | 212 | 212 | 248 | 528 | |
| Preterm, extremely preterm and still birthsTable 1 note f | Cases per 100,000 PWPI | 8,514Table 1 note e | 8,514 | 8,521 | 8,522 | 8,519 | 8,519 | 8,521 | 8,567 |
| Cases per 400,000 PWPITable 1 note d | 34,056Table 1 note e | 34,056 | 34,084 | 34,088 | 34,076 | 34,076 | 34,084 | 34,268 | |
| False results obtained (%) | |||||||||
| False positives leading to unnecessary treatment | Not Available | 4.14% | 4.11% | 4.10% | 4.13% | Not Available | Not Available | 4.01% | |
| False negatives leading to missed infections | Not Available | 0.09% | 0.14% | 0.16% | 0.12% | Not Available | Not Available | 0.18% | |
| Total cost per 100,000 PWPI over 1 year | $565,722,366 | $565,220,444 | $563,302,330 | $562,780,969 | $563,823,557 | $563,321,635 | $562,812,279 | $561,633,682 | |
| Cost-effectiveness per 100,000 PWPI | |||||||||
| Over 1 year (Baseline risk for NG/CT in the overall population) | $214M/QALY more than Strategy 2 | $65M/QALY more than Strategy 3 | $63M/QALY more than Strategy 4 | $3M/QALY more than screening only HR | More costly, less effective than other strategies | More costly, less effective than other strategies | Less costly, less effective than other strategies | Reference | |
| Over 1 year (Higher prevalence and risk for NG/CT in the overall population) | Likely more costly, less effective than less screening | $7M/QALY more than only screening all at T3 | More costly, less effective than other strategies | $481K/QALY more than Strategy 7 | More costly, less effective than other strategies | More costly, less effective than other strategies | $66K/QALY more than Strategy 8 | Reference | |
| Over lifetime (Baseline risk for NG/CT in the overall population) | Likely more costly, less effective than less screening | $11K/QALY more than Strategy 3 | $10K/QALY more than Strategy 4 | Reference | More costly, less effective than other strategies | More costly, less effective than other strategies | More costly, less effective than other strategies | More costly, less effective than other strategies | |
PHAC: Public Health Agency of Canada, PWPI: pregnant women/pregnant individuals, HR: high risk (PWPI less than 25 years old), T: trimester, T1: first trimester, T2: second trimester, T3: third trimester, QALY: quality-adjusted life-year. Table 1 Notes
In the table, starting from strategy #8 and moving towards strategy #1 shows that, as screening is added to each trimester, whether screening all individuals or high-risk groups (i.e., less than 25 years), there is a reduction in number of infants with ophthalmia neonatorum and CT pneumonia. |
|||||||||
In summary, evidence suggests that as screening is added to each trimester (whether screening all individuals or high-risk groups, (i.e., less than 25 years), there are fewer number of newborns with infection. However, providing screening at the third trimester (in particular for all) may reduce the numbers the most.
Although the sensitivity and specificity of the tests for NG and CT are high, there is still a risk of false negative (resulting in a missed infection at that trimester) and false positive (resulting in treatment of individuals who do not have an infection) results. However, the evidence from the model suggests that there are little to no differences in those numbers between the different strategies.
While the absolute cost differences are small, there are differences in quality-adjusted life-year (QALY; i.e., the cost per additional benefit of a strategy compared to another strategy) with high-risk screening. When reviewing most strategies across the analyses, the evidence suggests that adding screening at more trimesters and screening all at a trimester was more costly and provided fewer benefits. However, strategy #2 (screening all at first and third trimester) and #3 (screening high-risk individuals at first trimester and all at third trimester) may be cost-effective (more health benefit at a lower cost) regardless of the different assumptions in non-high risk and high risk settings. Although, the costs per additional benefit were lower when screening all only in the third trimester (strategy #4), there were more infections. Data for strategy #1, where all PWPI are screened at first and third trimesters and high-risk individuals are screened at second trimester may still be cost-effective but the cost per additional benefit was remarkably greater than the other strategies. Adding screening to the second trimester (e.g., strategy #6 versus #5), did not reduce newborn infections, and was still costly.
There is some evidence available about the feasibility and acceptability of screening for NG and CT in PWPI. Evidence from Canada suggests that not all PWPI receive prenatal care at each trimester.Footnote 17 Overall, testing in pregnancy may be acceptable to PWPI,Footnote 18 but there may be some feelings of stigma when they are offered testing and it is perceived to be targeted.Footnote 19 This could be reduced by offering universal testing.Footnote 18
There is some evidence in the literature that approximately 80% of PWPI are being screenedFootnote 9Footnote 10Footnote 20 under PHAC’s recommendations for “universal screening”, but it is unclear whether the lack of screening for some individuals is related to low uptake by PWPI or lower rates of screening offer or prescription by health care providers. Screening rates appear to be similar between different health care providers (e.g., family physicians, midwives and obstetrics and gynecology specialists).Footnote 10Footnote 20
Implementation
These recommendations are particularly important in settings where neonatal ocular prophylaxis for the prevention of ophthalmia neonatorum has stopped or is planned to be stopped. These recommendations do not replace recommendations to test and treat PWPI who have symptoms compatible with NG or CT infection or after sexual contact with a person known to have NG or CT.
Evidence suggests that screening all individuals could remove the fear of stigmatization and discrimination and normalize the testing practice.Footnote 18 In addition, the Working Group agreed that screening all PWPI may be more practical than clinicians’ efforts to gather risk factors from PWPI and partners. Further, co-infection rates for NG and CT are high and combined testing for these STI could contribute to the acceptability and feasibility of screening.
In settings where there are limited laboratory capacities, priority could be given to screening PWPI with higher risk of those infections during the first trimester (or at the first antenatal visit) and screening all PWPI in the latter part of the third trimester. When identifying PWPI at high risk for NG and CT infection, risks similar to individuals <25 years old could be used. For positive test results, healthcare providers could continue explaining to PWPI the risk of false positive tests.
Monitoring and evaluation
Metrics will be used to monitor and evaluate prospectively the evidence related to the recommendations for potential updating or reaffirming the recommendation(s) if new evidence becomes available that could influence the direction and strength.
Limitations
Mechanisms were not in place to have stakeholder engagement including patient representation within the Working Group. Although a patient group was engaged by CADTH to rate the relative importance of outcomes, the list of outcomes did not include ophthalmia neonatorum and neonatal pneumonia.
Research gaps
For the CADTH HTA, there was lack of published evidence on the impact of prenatal screening strategies for NG or CT on preventing ophthalmia neonatorum and neonatal pneumonia. For the systematic review on acceptability, feasibility, equity and resource use, limitations included the search not capturing eligible literature on acceptability, feasibility and equity of timing of repeating universal screening (e.g., third trimester or at delivery). In addition, it did not identify eligible literature on acceptability of prenatal screening for NG among partners of PWPI.
Addressing several research gaps could help inform whether to update or reaffirm these recommendations in the future. There is a need for studies assessing the impact of prenatal screening strategies for NG and CT on preventing ophthalmia neonatorum and neonatal pneumonia. In addition, comparative studies on the number and rates (or proportions) of PWPI who received screening, treatment, test-of-cure, and rescreening at the local and provincial/territorial levels could help inform future recommendations. Further, more studies are needed to monitor the impact and consequences of false positive tests. Also, primary studies on the acceptability, feasibility and equity of timing of repeating universal screening are required. Incidence and prevalence information on NG and CT in PWPI, ophthalmia neonatorum and neonatal pneumonia at the national level and more studies on adverse pregnancy outcomes of NG and CT are also required.
List of abbreviations
- ACS
- Advisory Committee Statement
- AOR
- Adjusted odds ratio
- CADTH
- Canadian Agency for Drugs and Technologies in Health
- CI
- Confidence interval
- CON
- Chlamydial ophthalmia neonatorum
- CPSP
- Canadian Paediatric Surveillance Program
- CT
- Chlamydia trachomatis
- GON
- Gonococcal ophthalmia neonatorum
- HTA
- Health Technology Assessment
- ISSTDR
- International Society for Sexually Transmitted Diseases Research
- IUSTI
- International Union against Sexually Transmitted Infections
- NAC-STBBI
- National Advisory Committee on Sexually Transmitted and Blood-Borne Infections
- NG
- Neisseria gonorrhoeae
- ON
- Ophthalmia neonatorum
- OR
- Odds ratio
- PHAC
- Public Health Agency of Canada
- PWPI
- Pregnant women/pregnant individuals
- QALY
- Quality-adjusted life-year
- SD
- Standard deviation
- STBBI
- Sexually Transmitted and Blood-Borne Infections
- STI
- Sexually Transmitted Infections
- TOC
- Test of Cure
- USD
- United States Dollar
Acknowledgements
This statement was prepared by Shamila Shanmugasegaram/PHAC and the Prenatal Screening for Neisseria gonorrhoeae and Chlamydia trachomatis Working Group with support from Nancy Santesso, on behalf of the NAC-STBBI. It was approved by the NAC-STBBI in October 2022.
NAC-STBBI Prenatal Screening for Neisseria gonorrhoeae and Chlamydia trachomatis Working Group
Members: Annie-Claude Labbé (Chair), Jared Bullard, Gina Ogilvie and Mark H. Yudin
NAC-STBBI
Other members (voting): Ian M. Gemmill (Chair), Troy Grennan (Vice Chair), William A. Fisher, Jennifer Gratrix, Todd F. Hatchette, Tim T. Y. Lau, Ed Lee, Petra Smyczek and Marc Steben
Former NAC-STBBI members (non-voting): Max Chernesky, Ron Read, Joan Robinson and Ameeta Singh
Ex-officio representatives (non-voting): Ibrahim Khan, Irene Martin and Tom Wong
Public Health Agency of Canada (Secretariat)
Shamila Shanmugasegaram, Ulrick Auguste, Stacy Sabourin and Margaret Gale-Rowe
External Contributors
Canadian Agency for Drugs and Technologies in Health
Nancy Santesso (McMaster University)
External Peer-reviewers
Dr. Julie van Schalkwyk
Dr. Romain Mandel
Suggested citation
National Advisory Committee on Sexually Transmitted and Blood-Borne Infections. An Advisory Committee Statement (ACS) National Advisory Committee on Sexually Transmitted and Blood-Borne Infections (NAC-STBBI). Recommendations on Screening for Neisseria Gonorrhoeae and Chlamydia Trachomatis in Pregnancy, March 2023. Retrieved from: https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/national-advisory-committee-stbbi/statements/recommendations-screening-chlamydia-trachomatis-neisseria-gonorrhoeae-pregnancy.html
Correspondence
NAC-STBBI Secretariat: sti.secretariat-its@phac-aspc.gc.ca
Appendices
Appendix A. Flow diagram of study selection for original and update searches on acceptability, feasibility, equity and resource use for prenatal screening for Chlamydia trachomatis and Neisseria gonorrhoeae
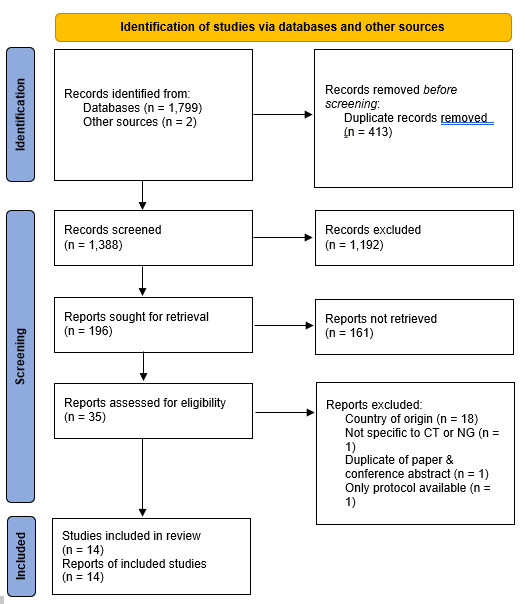
Figure 1 - Text description
The figure is a flow diagram outlining the steps for study selection. The diagram begins with the identification phase where 1,799 records from databases and 2 records from other sources were identified and 413 duplicate records were removed. It is followed by the screening phase where 1,388 records were screened, 1,192 records were excluded, 196 reports were sought for retrieval, 161 reports were not retrieved, 35 reports were assessed for eligibility, and 21 reports were excluded. The diagram concludes with the included phase where 14 studies and reports were included in the review.
Appendix B. Study characteristics and findings on acceptability, feasibility, equity and resource use for prenatal screening for Chlamydia trachomatis and Neisseria gonorrhoeae
| Author, Publication Year, Country; Infection(s) | Study Design, Time Frame | Setting | Participants (size and mean age ± SD/age range) | Outcome/Domain | Prevalence of CT and/or NG/ Screening Rates | Findings |
|---|---|---|---|---|---|---|
| Bilardi; 2010;Footnote 18 Australia; CT |
Cross-sectional; between December 2006 and July 2007 |
Four major antenatal services across Melbourne | 100 pregnant persons; age range (16-25 years) | Acceptability | Not reported (part of a larger study on prevalence by Chen et al. 2009).Footnote 21 | All pregnant persons supported testing for CT as part of their routine antenatal care. The main motivating factor in the acceptability of screening was concern for the health of the baby. Individuals felt the benefits of screening for themselves and their babies far outweighed any potential concerns about testing. Individuals’ main concern about testing for CT was whether testing and treatment could potentially harm the baby. |
| Chen; 2009;Footnote 21 Australia; CT |
Cross-sectional; between October 2006 and July 2007 |
Four major antenatal services across Melbourne | 987 pregnant persons; age range (16-25 years) | Feasibility and Equity | 32 tested positive for CT with a prevalence of 3.2% (95% CI 1.8 to 5.9) | More than one sexual partner in the past year (AOR 11.5, 95% CI 7.1-18.5) was associated with CT infection. Screening restricted to pregnant persons who report this factor would have detected 44% of infections in those aged 16-25 years and would have required only 7% of pregnant persons to be screened. The addition of individuals aged ≤20 years would have required 27% to be screened and detection of 72% of infections. |
| Ditkowsky; 2017;Footnote 22 United States; CT |
Cost-benefit; 12-month time horizon |
Third-party payer perspective in a high burden setting | Pregnant persons; aged 15-24 years | Resource use | 8% pre-screening era, 6.7% current prevalence and 16.9% threshold prevalence (screening costs equal to a “no screening” scenario). | Screening was proven to offer net cost savings when prevalence estimates were above 16.9%. At the prevalence estimate of 6.7%, there was an estimated net increase in expenditure of 142,666,014 million USD (22.14 USD/individual) with 204,630 cases of treated CT. |
| Leichliter; 2020;Footnote 23 United States; CT |
Cross-sectional; (national survey); 2011-2015 |
2011-2015 National Survey of Family Growth | 1,155 individuals who reported a pregnancy in the past 12 months or who were pregnant at time of interview; age range (15-44 years) | Feasibility and Equity | 48% of participants who were pregnant in the past 12 months reported that they received a CT test in the past 12 months. | Significantly more likely predicted receipt of a CT test:
Significantly less likely predicted receipt of a CT test:
|
| Logan; 2005;Footnote 24 Scotland, United Kingdom; CT |
Cross-sectional; between September and December 2001 |
Early pregnancy assessment unit at a hospital | 207 individuals, miscarriage population, 29.3±5.9 | Acceptability | 8/207 individuals were confirmed positive for CT. The overall prevalence was 3.9%, 95% CI 2.0%-7.4%. All positive individuals were less than 30. |
Majority accepted screening. Non-invasive sampling was more acceptable, but more likely to require repeat testing. Preferred method for screening were urine (144/207; 70%), self-administered vulval (61/207; 30%) and endocervical (4/140; 3%). Urine was significantly preferred compared to vulval (p<.0001) and endocervical (p<.0001). Vulval was significantly preferred compared to endocervical (p<.0001). |
| Miller; 2003;Footnote 25 United States; NG |
Retrospective chart review; between January 1998 and May 2000 |
Community-based prenatal program | 751 pregnant persons | Feasibility and Equity | 38 (5.1%) were positive in the initial testing, including one whose second test was positive. 19 (2.5%) were positive only in the later testing. Among individuals who initially screened negative, 2.7% were found to have NG at a subsequent evaluation. Overall, the prevalence of NG during pregnancy was 7.6%. |
23/318 (7.2%) of pregnant persons aged ≤19 years were positive in the initial testing and 11 (3.5%) were positive only in the later testing. 15/433 (3.5%) of individuals aged ≥20 years were positive in the initial testing and 8 (1.8%) were positive only in the later testing. Younger individuals were at higher risk than older persons for NG, both on initial and subsequent testing. |
| Miller; 2005;Footnote 26 United States; CT |
Retrospective cohort study (chart review); between January 1998 and May 2000 |
Community-based prenatal program | 752 pregnant persons | Feasibility and Equity | 105 (14.0%) had an initial positive test result. Retesting identified 29 (3.9%) with CT after an initial negative test result. Overall prevalence was 134/752 (17.8%). Of the 105 individuals who had positive initial tests, 14 (13.3%) had a second positive test after treatment representing those who either failed treatment or were reinfected. |
Of pregnant persons aged ≤19 years, 62/319 (19.4%) versus 43/433 (9.9%) for older patients were found to have CT at the time of initial testing, p<.001, OR 2.19 (95% CI 1.44-3.23). The follow-up screen at 34 weeks identified CT after the initial test was negative in 21/257 (8.2%) of patients aged ≤19 years versus 8/390 (2.1%) for older patients, p<.001, OR 4.24 (95% CI 1.85-9.74). Had repeat testing not been done, 29/134 (21.6%) infections identified would have been missed. Patients aged ≤19 years had a prevalence of 26.0%. However, even among older persons, the overall prevalence of 11.8% warranted testing. If repeat testing had been limited only to individuals aged ≤19 years, eight infections would have been missed. |
| Ong; 2016;Footnote 27 Australia; CT |
Cost-effectiveness based on a decision model; 12-month time horizon |
Third-party payer perspective | Pregnant persons; age range (16-25 years) | Resource use | 3% (current estimated CT prevalence in pregnant persons in Australia) | Screening all pregnant persons aged 16-25 years would have cost savings compared to no screening when CT prevalence was above 11%. Screening all pregnant persons aged 16-25 years was cost-effective compared to selective screening when CT prevalence was above 5%. |
| Pereboom; 2014;Footnote 19 The Netherlands; CT |
Cross-sectional; Between May 2012 and December 2013 |
22 primary midwifery care practices | 383 pregnant persons, age range (18-30 years) and 282 partners, age range (18-49 years) | Acceptability | 7 (1.9%) pregnant persons and 7 (2.6%) partners tested positive for CT. | 347 (54.2%) pregnant persons and partners reported that all pregnant individuals should routinely be tested for CT in antenatal care. 85 (13.3%) reported that only individuals at increased risk should be tested. 160 (25.0%) reported that pregnant persons should only be tested if they want to be tested. One person reported that testing pregnant persons for CT was not necessary. 47 (7.3%) reported that they had no opinion about whether or not pregnant persons should be tested for CT in antenatal care. 59.2% of pregnant persons and 56.2% of partners felt satisfied with the test offer for CT. For 70.5% of pregnant persons and 69.7% of partners, it had no emotional impact. 3.7% of pregnant persons and 1.8% of partners felt stigmatized by having a CT test offered 2.7% of the pregnant persons and 1.1% of the partners felt ashamed by having a test offered. |
| Perkins; 2003;Footnote 28 United Kingdom; CT |
Cross-sectional; 1999 | General practices and other healthcare settings including family planning clinics, antenatal clinics and genito-urinary medicine services | Pregnant persons (16-24 years) | Acceptability and Feasibility | Over 2000 positive cases detected. | While there was a general belief that it was appropriate to target young women, many professionals thought that the age range should have been extended to include women up to the age of 30 years. |
| Pimenta; 2003;Footnote 29 United Kingdom; CT |
Cross-sectional; September 1999 to August 2000 | General practice, family planning, genitourinary medicine, adolescent sexual health, termination of pregnancy clinics and women’s services in hospitals (antenatal, colposcopy, gynaecology and infertility clinics) | Sexually active women (16–24 years) | Acceptability | Not available | In one health authority, 66% (15,781/24,000) of the eligible female population were offered screening, of whom 76% (11,999/15,781) accepted testing. In the other health authority, 45% (5861/12,900) of the female population were offered screening with 84% (4931/5861) accepting a test. In both health authorities, rates were highest in genitourinary medicine clinics (97% and 92%) and lowest in family planning clinics (54% and 68%) and termination of pregnancy clinics (55% and 38%). The authors noted that both the opportunistic offer of screening and the method of screening were universally acceptable. Major factors influencing a decision to accept screening were the non-invasive nature of testing and treatment, desire to protect future fertility, and the experimental nature of the screening programme. |
| Rours; 2016;Footnote 30 The Netherlands; CT |
Cost-effectiveness; unclear (beyond 1- year) | Societal perspective | All pregnant persons | Resource use | 3.9% (157/4055) Age-specific: 21-25 years: 794 (6.7%) 26-30 years: 1,235 (3.3%) >30 years: 1,775 (1.6%) |
In sensitivity analysis, the net cost savings remained with test costs up to €22 (test price €19) for a range of underlying assumptions. In scenario and probabilistic analyses, the cost savings increased with targeted screening of individuals aged ≤30 years or with first pregnancies only. |
| Tyker; 2021;Footnote 31 Canada; CT and NG |
Retrospective chart review; between October 2016 and June 2020 | Adolescent obstetrics practice | 102 pregnant adolescents, age range (13 to 19 years at presentation to care) | Feasibility and Resource use | 100 (98.0%) pregnancies were screened at presentation to care (3-30 weeks gestation). In the third trimester, 89 (87.3%) pregnancies underwent routine screening. At presentation to care, 9 of 100 screened pregnancies (9.0%) were positive for CT. No cases of NG were detected. |
Used urine nucleic acid amplification test (NAAT) for 88 of 89 (98.9%) patients screened in the third trimester. Decision to use urine samples instead of endocervical swabs in the third trimester was based on feasibility and ease of collecting samples. Performing a speculum examination, which is required to obtain an endocervical swab, in the third trimester is more resource intensive and invasive for the patient. Midstream samples may be adequate when first-void samples are not feasible. Pregnant adolescents who were screened for CT and NG did not benefit from re-screening in the third trimester without any other indication or risk factor. |
| Vainder; 2019;Footnote 10 Canada; CT and NG |
Retrospective cohort study (electronic medical record); between November 1, 2015 and April 30, 2016 | An urban tertiary care centre | 1,220 pregnant persons; age of screened (32.3 ± 5.0) and age of not screened (33.0 ± 4.8) | Acceptability | 186 (15.3%) were not tested for NG and CT during pregnancy. Of 1,036 pregnant persons who were tested, there were 11 (1.1%) cases of CT and no cases of NG. |
Overall, there were no patient characteristics that affected the likelihood of being tested. Method of testing was recorded for 733 of the participants, with 92.0% tested by urine and 8.0% tested by cervical swab. Rates of testing among providers: Midwives (93.8%), family physicians (91.4%) and generalist obstetricians (88.5%). Maternal fetal medicine specialists had a significantly lower rate of testing at 64.8% (p<.0001). |
Abbreviations: SD, standard deviation; CT, Chlamydia trachomatis; NG, Neisseria gonorrhoeae; OR, odds ratio; AOR, adjusted odds ratio; CI, confidence interval; USD, United States Dollar |
||||||
Appendix C. Interpretation of strong and conditional recommendations
The recommendations are labeled as “strong” or “conditional” according to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. The words “the guideline panel recommends” are used for strong recommendations, and “the guideline panel suggests” for conditional recommendations. The table below provides GRADE’s interpretation of strong and conditional recommendations by patients, clinicians, health care policy makers, and researchers.
| Implications for: | Strong recommendation | Conditional recommendation |
|---|---|---|
| Patients | Most individuals in this situation would want the recommended course of action, and only a small proportion would not. | The majority of individuals in this situation would want the suggested course of action, but many would not. Decision aids may be useful in helping patients to make decisions consistent with their individual risks, values, and preferences. |
| Clinicians | Most individuals should follow the recommended course of action. Formal decision aids are not likely to be needed to help individual patients make decisions consistent with their values and preferences. | Different choices will be appropriate for individual patients; clinicians must help each patient arrive at a management decision consistent with his or her values and preferences. Decision aids may be useful in helping individuals to make decisions consistent with their individual risks, values, and preferences. |
| Policy makers | The recommendation can be adopted as policy in most situations. Adherence to this recommendation according to the guideline could be used as a quality criterion or performance indicator. | Policy-making will require substantial debate and involvement of various stakeholders. Performance measures should assess if decision-making is appropriate. |
| Researchers | The recommendation is supported by credible research or other convincing judgments that make additional research unlikely to alter the recommendation. On occasion, a strong recommendation is based on low or very low certainty of the evidence. In such instances, further research may provide important information that alters the recommendations. | The recommendation is likely to be strengthened (for future updates or adaptation) by additional research. An evaluation of the conditions and criteria (and the related judgments, research evidence, and additional considerations) that determined the conditional (rather than strong) recommendation will help identify possible research gaps. |
Appendix D. Grading of Recommendations, Assessment, Development and Evaluation Evidence to Decision Framework
Question
What screening strategy should we recommend for pregnant women/pregnant individuals to prevent adverse outcomes related to Chlamydia trachomatis (CT) and Neisseria Gonorrhoeae (NG) infections?
Problem: Optimal screening strategy for CT/NG during pregnancy
Option: An alternative screening strategy
Comparison: A different screening strategy.
- In 2010, PHAC recommended
- All pregnant women should be evaluated for STI risk factors prior to and during pregnancy. Any woman with ongoing risk factors for STI acquisition during pregnancy should be considered for rescreening each trimester.
- National recommendations are to screen for C. trachomatis early in pregnancy. Repeat screening should be performed in the third trimester for women at continuing risk for STI acquisition.
Main outcomes:
- Number/percent of positive CT and/or NG infections detected at screening (includes new or repeat infections)
Surrogate outcome: number of females treated for infection
Surrogate outcomes: true positives/false negatives and false positives/true negatives - Obstetric outcomes (pre-term and still births)
- Number of females declining screening
- Anxiety/fears
- Number/percent of ophthalmia neonatorum
- Number/percent of neonatal pneumonia
Setting: Prenatal and obstetric care in Canada
Perspective: Public health
Background: In Canada, CT and NG are the most commonly reported sexually transmitted infections (STI). Between 2010 and 2019, rates of reported cases of CT and NG have increased by 33.1% and 181.7%, respectively.Footnote 1 In 2019, 139,386 cases of CT and 35,443 cases of NG were reported in Canada, corresponding to rates of 370.8 and 94.3 per 100,000 population, respectively.Footnote 1Footnote 2
In females, CT and NG infections are often asymptomatic, but early detection and treatment could prevent potential complications, sexual transmission, and transmission to neonates in the perinatal period.Footnote 3
In 2010, PHAC recommended that all pregnant women should be evaluated for STI risk factors prior to and during pregnancy. Any woman with ongoing risk factors for STI acquisition during pregnancy should be considered for rescreening each trimester.Footnote 6 In 2010, PHAC also recommended to screen for C. trachomatis early in pregnancy. Repeat screening should be performed in the third trimester for women at continuing risk for STI acquisition.Footnote 6Footnote 7
Given the increasing rates of reported cases of CT and NG in the general population and suboptimal rates of prenatal screening for CT and NG in Canada,Footnote 9Footnote 10Footnote 20 the National Advisory Committee on Sexually Transmitted and Blood-Borne Infections (NAC-STBBI) reviewed the PHAC’s recommendation on prenatal screening for CT and NG.
Conflict of interests: None.
Assessment
Problem: Is the problem a priority?
Research evidence
In Canada, CT and NG are the most commonly reported STI. Between 2010 and 2019, rates of reported cases of CT increased 33.1% and NG increased 181.7%.Footnote 1 In 2019, 139,386 cases of CT and 35,443 cases of NG were reported in Canada, corresponding to rates of 370.8 and 94.3 per 100,000 population, respectively.Footnote 1Footnote 2
In 2019, the highest rates of CT were among people from the Canadian territories (Yukon, Northwest Territories and Nunavut with 757.0, 1,901.0 and 3,876.8 cases per 100,000 population, respectively).Footnote 1
Since 2010 the highest rates of NG were among people from Nunavut and the Northwest Territories with rates above 1,000 cases per 100,000 population in 2019.Footnote 1 In 2019, Manitoba had the third highest rate of NG, with 272.5 cases per 100,000 population.Footnote 1
Among females, CT rates have been consistently highest in those between the ages of 15 and 24 since 2010 in Canada. In 2019, the highest NG rates among females were in those between the ages of 15 and 29.Footnote 1 In Canada, there were 372,038 live births in 2019.Footnote 16 As shown in Table 1, among all females (pregnant or not) with confirmed CT infection in 2019, 62.8% were aged 15-24 years; the corresponding proportion for NG infection was 42.8%.Footnote 2 Among all females who delivered a live birth in 2019, 11.8% were aged 15-24 years.Footnote 16
| CT | NG | Live births | ||||||
|---|---|---|---|---|---|---|---|---|
| Age | n | Distribution | Rate (per 100,000) | n | Distribution | Rate (per 100,000) | n | Distribution |
| <15 | Not Available | Not Available | 64 | 0,02% | ||||
| 15-19 | 20 630 | 25,8% | 2000.36 | 1 935 | 16,2% | 187.62 | 6 385 | 1,7% |
| 20-24 | 29 664 | 37,0% | 2507.93 | 3 181 | 26,6% | 268.94 | 37 574 | 10,1% |
| 25-29 | 14 838 | 18,5% | 1166.36 | 2 710 | 22,6% | 213.02 | 102 823 | 27,6% |
| 30-39 | 11 045 | 13,8% | 428.38 | 2 947 | 24,6% | 114.30 | 209 058 | 56,2% |
| 40-59 | 3 932 | 4,9% | 77.54 | 1 195 | 10,0% | 23.56 | 16 062 | 4,3% |
| Unknown | 72 | 0,02% | ||||||
| Total | 80 109 | 100% | 11 968 | 100% | 372 038 | 100% | ||
Surveillance data on CT and NG infections in pregnant females is not available at the national level in Canada. In 2019, for infants less than 1 year, 29 cases of CT and 8 cases of NG were reported to the Canadian Notifiable Disease Surveillance System, corresponding to rates of 7.8 and 2.2 per 100,000 population, respectively.Footnote 2
In females, CT and NG infections are often asymptomatic, but early detection and treatment of these STI could prevent potential complications, sexual transmission, and transmission to neonates in the perinatal period. Ophthalmia neonatorum (ON) refers to conjunctivitis occurring within the first four weeks of lifeFootnote 34 and may lead to visual impairment. In the United States, gonococcal ophthalmia neonatorum (GON) accounts for less than 1% of reported cases of ON and chlamydial ophthalmia neonatorum (CON) accounts from 2% to 40%.Footnote 35 During delivery, untreated NG could lead to 30% risk of developing GONFootnote 4Footnote 5 and untreated CT could lead to 30% to 50% risk of developing CON and 10% to 20% risk of developing chlamydia pneumonia.Footnote 36 In Canada, national surveillance of ON was discontinued in 2000. There is lack of information in the Canadian Notifiable Disease Surveillance System on GON, CON and neonatal pneumonia cases.
Adherence to screening guidelines:
In 2010, PHAC recommended that all pregnant women should be evaluated for STI risk factors prior to and during pregnancy. Any woman with ongoing risk factors for STI acquisition during pregnancy should be considered for rescreening each trimester.Footnote 6 In 2010, PHAC also recommended to screen for C. trachomatis early in pregnancy. Repeat screening should be performed in the third trimester for women at continuing risk for STI acquisition.Footnote 6Footnote 7 In the recommendations, the groups at increased risk included individuals <25 years. Canadian studies show that prenatal screening rates for CT and NG are suboptimal with approximately 15% to 22% of pregnant persons not being screened at least once for these infections.Footnote 9Footnote 10Footnote 20 Given the increasing rates of reported cases of CT and NG in the general population and suboptimal rates of prenatal screening for CT and NG in Canada, the NAC-STBBI reviewed the PHAC’s recommendation on prenatal screening for CT and NG.
Judgement
- No
- Probably no
- Probably yes
- Yes
- Varies
- Don't know
Desirable effects
How substantial are the desirable anticipated effects?
Research evidence
The Canadian Agency for Drugs and Technologies in Health’s Health Technology Assessment (CADTH HTA, 2018; search updated in 2020) report did not identify any studies that met the selection criteria for the effects of prenatal screening for NG and CT on ON or neonatal pneumonia. After Working Group discussion, the list of included studies (total=10) in the HTA was checked for information on infant morbidity outcomes (i.e., ON and pneumonia). No evidence was identified.
Additional evidence in the literature
A few Canadian studies were identified from the literature. The studies by Boisvert et al. (2021)Footnote 37 and Ivensky et al. (2021)Footnote 20 were identified through a targeted search, and the study by Vainder et al. (2019)Footnote 10 was captured through a systematic review conducted on acceptability, feasibility, equity and resource use/cost-effectiveness for prenatal screening for CT and NG to support the development of the recommendations. These articles were published after the CADTH HTA report was released in November 2018. In summer 2020, CADTH updated the search for the clinical review, economic analysis, and patient experiences and perspectives parts of the HTA report and reported no new relevant literature evidence. The studies by Boisvert et al. (2021)Footnote 37 and Vainder et al. (2019)Footnote 10 may have been excluded by CADTH as they were not comparative studies.
Cases of ON:
Boisvert et al. (2021)Footnote 37 conducted a monthly survey of over 2,700 paediatricians and paediatric subspecialists through the Canadian Paediatric Surveillance Program (CPSP) and assessed proportion of GON and CON in infants of mothers who were screened and treated during pregnancy and infants who received ocular prophylaxis. Findings included 12 cases of ON from November 2018 to October 2020. Limitations of the data include under-representation of the infections in the population, as paediatricians and paediatric subspecialists participate in the CPSP on a voluntary basis, and there was limited representation from Québec. Further, the assumptions of the CPS recommendation were that adherence to screening and treatment of infected women were perfect, which is currently not the case.Footnote 9Footnote 10Footnote 20
Screening and prevalence of infections in pregnancy:
| Study | Population | Study year | Number Screened | Prevalence of Infections in Pregnancy |
|---|---|---|---|---|
| Poliquin et al. (2016)Footnote 9 | Live births in Manitoba | 2011 to 2014 | 78% (45,601/58,488) had at least one prenatal test for CT and NG. | 5.5% (n=2,489) of all births had a positive test for either CT or NG during pregnancy. |
| Vainder et al. (2019)Footnote 10 | Tertiary care hospital in Toronto | Six-month period in 2015-2016 | 85% (1,034/1,220) were screened at least once during pregnancy. | Of 1,036 pregnant persons who were tested, there were 11 (1.1%) cases of CT and no cases of NG. |
| Ivensky et al. (2021)Footnote 20 | Newborns of at least 19 weeks’ gestation; tertiary care hospital in Montréal | April 2015 to March 2016 | 82% (2,206/2,688) were screened at least once before the day of delivery. | Infection was detected in 46/2,206 (2.1%) of screened women (42 had CT infection, two had NG infection and two were co-infected). Women <25 years were more likely to have CT infection (29/296; 9.8%; 95% CI: 6.7%-13.8%) than those aged ≥25 years (15/1,910; 0.8%; 95% CI: 0.4%-1.3%; p<0.001). Prevalence of NG infection was also significantly higher in younger women (1.0% vs 0.05%; p<0.001). |
Test of cure and rescreening:
| Study | Number of infections | Documented treatment | Test of cure (TOC) | Rescreening |
|---|---|---|---|---|
| Poliquin et al. (2016)Footnote 20 | 2489 | N/A | 71.4% had a TOC (defined as a documented negative CT/NG test 30 or more days after positive test) | 25% (623/2489) of all persons who tested positive during pregnancy had repeat screening performed during the third trimester. |
| Ivensky et al. (2019)Footnote 11Table 1 note * | CT: 43 NG: 4 |
CT: 39 (91%) NG: 4 |
Among CT-infected females, 31 (72%) had a TOC, which was positive in 4 (13%) women. All NG-positive women were treated and had a negative TOC. | Rescreening rates amongst the 45 positive women (3-6 months after treatment): 16 (36%) were rescreened before delivery; 3 (7%) were rescreened after delivery, of which 2 were positive for CT (and had a negative TOC 4-5 months earlier). |
Table 3 Notes
|
||||
Ivensky et al. (2021)Footnote 20: Of those with an initial negative test result, 35/267 (13.1%; 95% CI 9.3%-17.8%) of women <25 years and 122/1,863 (6.6%; 95% CI 5.5%-7.8%; p<.001) of women ≥25 years were retested. Subsequent infection was detected in 4/35 (11%) women, all <25 years.
With a screening rate of 82% and prevalence estimates of 2.0% for CT and 0.2% for NG, the researchers extrapolated, for the whole province of Québec, 300 CT and 30 NG infections would be missed each year. With rates of vertical transmission to the eye of 30% for CT and 40% for NG, without universal ocular prophylaxis at delivery, 102 neonates would be expected to have CON and GON in Québec each year.Footnote 4
Modelling:
Modelling was performed to show the consequences of screening versus not screening on the prenatal and neonatal outcomes of interest. The findings included greatest benefits with screening all pregnant individuals at first and third trimester.
Judgement
- Trivial
- Small
- Moderate
- Large
- Varies
- Don't know
Undesirable effects
How substantial are the undesirable anticipated effects?
Research evidence
The CADTH HTA reported no research evidence on anxiety/fear from undergoing screening by any method or strategy. After Working Group discussion, the list of included studies (total=10) in the HTA was checked for information on false positives and false negatives. No evidence was identified.
Modelling was performed to show the consequences of screening versus not screening on the prenatal and neonatal outcomes of interest. Trivial harms were found with strategies with screening during pregnancy.
Judgement
- Large
- Moderate
- Small
- Trivial
- Varies
- Don't know
Certainty of evidence
What is the overall certainty of the evidence of effects?
Research evidence
The evidence from the modelling was assessed as low certainty. The Working Group agreed that the assumptions and inputs for the primary analysis are based on best available evidence about prevalence, infection rates, uptake and treatment outcomes.
Judgement
- Very low
- Low
- Moderate
- High
- No included studies
Values
Is there important uncertainty about or variability in how much people value the main outcomes?
Research evidence
| Outcome | Relative Importance |
|---|---|
Number/percent of positive CT and/or NG infections detected at screening
Surrogate outcome: number of females treated for infection Surrogate outcomes: true positives/false negatives and false positives/true negatives |
Important |
| Obstetric outcomes (pre-term and still births) | Important |
| Number of females declining screening | Important |
| Anxiety/fears | Important |
| Number/percent of ophthalmia neonatorum | Critical |
| Number/percent of neonatal pneumonia | Critical |
Judgement
- Important uncertainty or variability
- Possibly important uncertainty or variability
- Probably no important uncertainty or variability
- No important uncertainty or variability
Balance of effects
Does the balance between desirable and undesirable effects favor the intervention or the comparison?
Research evidence
The Working Group agreed that screening at first and third trimester probably provides greater benefits than harms.
Judgement
- Favors the comparison
- Probably favors the comparison
- Does not favor either the intervention or the comparison
- Probably favors the intervention
- Favors the intervention
- Varies
- Don't know
Cost effectiveness
Does the cost-effectiveness of the intervention favor the intervention or the comparison?
Research evidence
Evidence on cost-effectiveness models in the literature
The CADTH HTA did not include a systematic review specifically on resource use for prenatal screening for CT or NG. The Secretariat conducted a systematic review on resource use combining the GRADE search strategy specific to this domain with the clinical review search strategy used in the CADTH HTA. Information sources including MEDLINE® All, Embase, and Cochrane CENTRAL (January 2003 - January 2021) electronic databases were searched for studies that assessed resource use of any strategy to screen for CT and/or NG in pregnant persons ≥12 years. Of the 1,388 records identified, three economic evaluations on resource use/costs met the inclusion criteria.
Findings:
In general, screening all pregnant persons for CT has net cost savings compared to no screening.
In Australia, Ong et al. (2016)Footnote 27 assessed the cost-effectiveness of screening all pregnant persons 16-25 years for CT compared with selective screening or no screening using a 12-month time horizon and from a third-party payer perspective. With a CT prevalence estimate of 3%, screening all pregnant persons 16-25 years during their first antenatal visit compared to no screening was cost-effective as it would cost the health system 1,641 Australian Dollar (AUD) per CT case detected and treated, and 34,931 AUD per quality-adjusted life year (QALY) gained. Screening all pregnant persons 16-25 years compared to no screening would have cost savings when CT prevalence was above 11%. With a CT prevalence estimate of 3%, screening all pregnant persons 16-25 years compared to selective screening would cost the health system 5,448 AUD per CT case detected and treated, and 116,213 AUD per QALY gained. Screening all pregnant persons 16-25 years was cost-effective compared to selective screening when CT prevalence was above 5%.
In the Netherlands, Rours et al. (2016)Footnote 30 analyzed the cost-effectiveness of antenatal screening of all pregnant persons for CT from a societal perspective (inclusion of non-medical [indirect] costs due to production losses). In the base-case analysis, they estimated €527,900 to detect and treat CT for 1,000 pregnant persons and their partners and averted medical costs were estimated at €626,800. In sensitivity analysis, the net cost savings remained with test costs up to €22 (test price €19) for a range of underlying assumptions. In scenario and probabilistic analyses, the cost savings increased with targeted screening of individuals ≤30 years or with first pregnancies only.
In the United States, Ditkowsky et al. (2017)Footnote 22 assessed the cost-benefit of screening all pregnant persons 15-24 years for CT compared with no screening using a 12-month time horizon and from a third-party payer perspective in a high burden setting. Screening was proven to offer net cost savings when prevalence estimates were above 16.9%. At the prevalence estimate of 6.7%, there was an estimated net increase in expenditure of 142,666,014 million United States Dollar (USD) (22.14 USD/individual) with 204,630 cases of treated CT.
The studies that met the inclusion criteria for the systematic review were only on prenatal screening for CT and they were published in countries outside of Canada. Cost-effectiveness of screening versus no screening seemed to be influenced by prevalence – better cost-effectiveness with increasing prevalence. From the comprehensive search of the literature, there does not seem to be information from these studies about intensifying screening that met the inclusion criteria.
Modelling was performed to show the consequences of screening at different trimesters versus not screening on the prenatal and neonatal outcomes of interest. Please refer to Table 1 in the NAC-STBBI Statement for the modelling results. The Committee agreed that the costs per QALY for screening all at first and third trimester or targeted screening at first trimester instead were relatively acceptable and for most modelled analyses are cost-effective.
Judgement
- Favors the comparison
- Probably favors the comparison
- Does not favor either the intervention or the comparison
- Probably favors the intervention
- Favors the intervention
- Varies
- No included studies
Equity
What would be the impact on health equity?
Research evidence
The CADTH HTA did not include a systematic review specifically on equity of prenatal screening for CT or NG. The Secretariat conducted a systematic review on equity combining the GRADE search strategy specific to this domain with the clinical review search strategy used in the CADTH HTA and including quantitative and qualitative studies. Information sources including MEDLINE® All, Embase, and Cochrane CENTRAL (January 2003 - January 2021) electronic databases were searched for studies that assessed equity (e.g., age, education level, income level, socioeconomic status, health insurance coverage, race/ethnicity, religion, and geographical location) of any strategy to screen for CT and/or NG in pregnant persons ≥12 years. The following definition of equity by the World Health Organization (WHO) was used for this systematic review: “the absence of avoidable, unfair, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically or by other means of stratification. Health equity or equity in health implies that ideally everyone should have a fair opportunity to attain their full health potential and that no one should be disadvantaged from achieving this potential."Footnote 39 Of the 1,388 records identified in the systematic review, four articles reported on feasibility/accessibility and equity for prenatal screening for CT and/or NG.
Findings:
Repeating universal screening in a population with a high prevalence of CT/NG could improve detection yield compared to targeted screening. Miller et al. (2003)Footnote 25 examined NG in 751 pregnant persons attending a community-based prenatal program in an underserved area in Louisiana, United States. Among pregnant persons ≤19 years, 23 (7.2%) were positive in the initial testing and 11 (3.5%) were positive only in the later testing. Among those ≥20 years, 15 (3.5%) were positive in the initial testing and 8 (1.8%) were positive only in the later testing.Footnote 25 In another study, Miller et al. (2005)Footnote 26 assessed CT in 752 pregnant persons attending a community-based prenatal program in an underserved area in the United States. Pregnant persons ≤19 years had significantly higher rates of CT compared to those ≥20 years (odds ratio [OR] 2.19, 95% CI 1.44-3.23; p<.001) at the time of initial testing. Among those with an initial negative test, pregnant persons ≤19 years had significantly higher rates of CT compared to those ≥20 years at 34-week follow-up testing (OR 4.24, 95% CI 1.85-9.74; p<.001). The researchers noted that eight infections would have been missed if repeat testing had been limited to those ≤19 years.Footnote 26
Targeted screening based on more than one criterion could improve yield. Chen et al. (2009)Footnote 21 examined CT in 987 pregnant persons 16-25 years at four major antenatal services in Australia and found that having more than one sexual partner in the past year (adjusted OR 11.5, 95% CI 7.1-18.5) was associated with CT infection. The researchers noted that screening restricted to pregnant persons who reported more than one sexual partner in the past year would have detected 44% of CT in those 16-25 years and would have required only 7% of individuals to be screened. The addition of pregnant persons ≤20 years would have required 27% to be screened and detection of 72% of CT.Footnote 21
Pregnant persons receiving prenatal care may be more likely to receive CT screening. In a study of CT in 1,155 people who were pregnant in the past 12 months or at time of interview in the United States, those who reported receiving prenatal care (adjusted OR 2.10, 95% CI 1.35-3.28) were significantly more likely to receive CT testing than individuals who had not received prenatal care. People who were born outside of the United States (adjusted OR 0.35, 95% CI 0.19-0.64) were significantly less likely to receive CT testing than those who were born in the United States.Footnote 23 In Canada, findings from the Maternity Experience Survey in mothers aged ≥15 years showed that the prevalence of inadequate prenatal care was 18.9%, with the highest estimates in Nunavut (28.8%) and the Northern Territories (24.9%). In addition, mothers who were immigrants were more likely to receive inadequate prenatal care compared to people born in Canada (OR 1.40, 95% CI 1.13-1.74; 29).Footnote 17
The Committee agreed that in some populations screening may be lower than the general population, and therefore it would be important to communicate clearly to provide screening to all at first and third trimester.
Judgement
- Reduced
- Probably reduced
- Probably no impact
- Probably increased
- Increased
- Varies
- Don't know
Acceptability
Is the intervention acceptable to key stakeholders?
Research evidence
The CADTH HTA did not include a systematic review specifically on acceptability for prenatal screening for CT or NG. In addition, the patients’ preferences and experiences part of the CADTH HTA consisted of only qualitative studies. The Secretariat conducted a systematic review on acceptability combining the GRADE search strategy specific to this domain with the clinical review search strategy used in the CADTH HTA and including quantitative and qualitative studies. Information sources including MEDLINE® All, Embase, and Cochrane CENTRAL (January 2003 - January 2021) electronic databases were searched for studies that assessed acceptability of any strategy to screen for CT and/or NG in pregnant persons ≥12 years. Of the 1,388 records identified, five studies reported on acceptability of prenatal screening for CT and/or NG.
Findings:
Pregnant persons:
In general, pregnant persons accepted screening and preferred non-invasive sampling methods for CT. Pimenta et al. (2003)Footnote 29 assessed the acceptability of opportunistic screening for CT (regardless of the purpose of the visit) using urine samples in females 16-24 years in a variety of health care settings at two health authorities in the United Kingdom. In one health authority, 66% (15,781/24,000) of the eligible female population were offered screening, of whom 76% (11,999/15,781) accepted testing. In the other health authority, 45% (5861/12,900) of the female population were offered screening with 84% (4931/5861) accepting a test. In both health authorities, rates were highest in genitourinary medicine clinics (97% and 92%) and lowest in family planning clinics (54% and 68%) and termination of pregnancy clinics (55% and 38%). The authors noted that both the opportunistic offer of screening and the method of screening were universally acceptable. Major factors influencing a decision to accept screening were the non-invasive nature of testing and treatment, desire to protect future fertility, and the experimental nature of the screening programme.
In a study of 209 miscarriage individuals at a hospital in Scotland, United Kingdom, majority accepted screening for CT. When asked to state their preferred method for screening, 4/140 (3%), 61/207 (30%) and 144/207 (70%) individuals chose the endocervical, vulval and urine method, respectively. Urine was significantly preferred compared to vulval (p<.0001) and endocervical (p<.0001). Vulval was significantly preferred compared to endocervical (p<.0001).Footnote 24 In a study of 100 pregnant persons 16-25 years attending four major antenatal services across Melbourne, Australia, all individuals supported testing for CT as part of their routine antenatal care.Footnote 18
Pregnant persons and partners:
In general, pregnant persons and partners supported universal testing for CT. In a study of 383 pregnant persons and 282 partners at 22 primary midwifery care practices in the Netherlands, 347 (54.2%) of pregnant individuals and partners reported that all pregnant people should routinely be tested for CT in antenatal care and 85 (13.3%) reported that only pregnant people at increased risk should be tested. Some pregnant persons (3.7%) and partners (1.8%) felt stigmatized and 2.7% of pregnant individuals and 1.1% of partners felt ashamed by having a CT test offered.Footnote 19 Evidence suggests that routine universal screening could remove the fear of stigmatization and discrimination and normalize the testing practice.Footnote 18
Healthcare providers:
In general, healthcare providers accepted screening of pregnant persons. In a study of 1,220 pregnant persons who attended an urban tertiary care centre in Toronto, there was no statistically significant difference in the testing rates amongst midwives (93.8%), family physicians (91.4%) and obstetricians (88.5%). Maternal-fetal medicine specialists had a significantly lower rate of testing compared to the other three provider groups (64.8%; p<.0001).Footnote 10 The findings are generally similar to a more recently published study from Montréal showing that prenatal screening rates were identical for general practitioners (894/1,062; 84.2%; 95% CI 81.8%-86.3%) and obstetricians (1,308/1,571; 83.3%; 95% CI 83.1%-85.1%;).Footnote 20
Perkins et al. (2003)Footnote 28 assessed the acceptability of screening for CT (regardless of the purpose of the visit) in women 16-24 years attending general practices and other healthcare settings including family planning clinics, antenatal clinics and genito-urinary medicine services. The findings included while there was a general belief that it was appropriate to target young women, many professionals thought that the age range should have been extended to include women up to the age of 30 years.
Judgement
- No
- Probably no
- Probably yes
- Yes
- Varies
- Don't know
Feasibility
Is the intervention feasible to implement?
Research evidence
The CADTH HTA did not include a systematic review specifically on feasibility of prenatal screening for CT or NG. The Secretariat conducted a systematic review on feasibility combining the GRADE search strategy specific to this domain with the clinical review search strategy used in the CADTH HTA and including quantitative and qualitative studies. Information sources including MEDLINE® All, Embase, and Cochrane CENTRAL (January 2003 - January 2021) electronic databases were searched for studies that assessed feasibility of any strategy to screen for CT and/or NG in pregnant persons ≥12 years. Of the 1,388 records identified, two studies addressed feasibility of prenatal screening for CT and/or NG.
Findings:
A consideration for feasibility of prenatal screening for CT and/or NG is access to prenatal care. In a study of CT in 1,155 people who were pregnant in the past 12 months or at time of interview in the United States, those who reported receiving prenatal care (adjusted OR 2.10, 95% CI 1.35-3.28) were significantly more likely to receive CT testing than individuals who had not received prenatal care. People who were born outside of the United States (adjusted OR 0.35, 95% CI 0.19-0.64) were significantly less likely to receive CT testing than those who were born in the United States.Footnote 23 In Canada, findings from the Maternity Experience Survey in mothers aged ≥15 years showed that the prevalence of inadequate prenatal care was 18.9%, with the highest estimates in Nunavut (28.8%) and the Northern Territories (24.9%). In addition, mothers who were immigrants were more likely to receive inadequate prenatal care compared to people born in Canada (OR 1.40, 95% CI 1.13-1.74; 29).Footnote 17
Perkins et al. (2003)Footnote 28 assessed the feasibility of screening for CT (regardless of the purpose of the visit) in women 16-24 years attending general practices and other healthcare settings including family planning clinics, antenatal clinics and genito-urinary medicine services. While there was a general belief that it was appropriate to target young women, many professionals thought that the age range should be extended to include women up to the age of 30 years.
Another consideration for feasibility of prenatal screening for CT and/or NG is non-invasive sampling methods. Tyker et al. (2021)Footnote 31 examined screening for CT and NG in 102 pregnant persons 13-19 years at an adolescent obstetrics practice in Ontario, Canada. Urine NAAT was used for 88 of 89 (98.9%) patients screened in the third trimester. The researchers (from the perspective of healthcare providers) noted that the decision to use urine samples was based on feasibility and ease of collecting samples, whereas using an endocervical swab in the third trimester is more resource intensive and invasive.
Additional evidence on feasibility
Recommendations of provinces and territories:
Most provinces and territories in Canada recommend universal first trimester screening with repeat screening later in pregnancy for those who test positive or at increased risk of infection.
Impact of COVID-19 on health service providers:
For STBBI prevention, testing and treatment services providers, findings from a PHAC survey on the impact of COVID-19 showed that almost half (44%) experienced a decrease in their ability to deliver their services and 66% experienced a decrease in demand for their services.Footnote 40
Judgement
- No
- Probably no
- Probably yes
- Yes
- Varies
- Don't know
Summary of judgements
| Domain | Judgement |
|---|---|
| Problem | Yes |
| Desirable Effects | Moderate |
| Undesirable Effects | Trivial |
| Certainty of evidence | Very low |
| Values | Possibly important uncertainty or variability |
| Balance of effects | Probably favors the intervention |
| Resources required | Moderate costs |
| Certainty of evidence of required resources | Low |
| Cost effectiveness | Probably favors the intervention |
| Equity | Probably increased |
| Acceptability | Probably yes |
| Feasibility | Probably yes |
Type of recommendation
Strong recommendation against the option
Conditional recommendation against the option
Conditional recommendation for either the option or the comparison
Conditional recommendation for the option
Strong recommendation for the option
Conclusions
Recommendation
We suggest screening all PWPI for NG and CT during the first trimester or at the first antenatal visit, and again in the third trimester (conditional recommendation; low certainty evidence).
We suggest screening PWPI at the time of labour for NG and CT in any of the following situations (conditional recommendation; low certainty evidence):
- No prenatal screening has occurred (no valid results available at the time of labour).
- Third trimester screening has not occurred.
- A positive test result was obtained for NG or CT during pregnancy without appropriate follow-up, including treatment and a test-of-cure.
Justification
Systematic reviews of the literature and a decision-analytic model were used to determine the effects of different screening strategies for NG or CT to prevent ophthalmia neonatorum, neonatal pneumonia and adverse pregnancy outcomes. As presented in Table 1, the evidence showed that there may be greater benefits and lower resource use and costs when screening for NG or CT is offered to all PWPI at first and third trimesters - and at labour when screening is not performed during pregnancy or follow-up has not occurred after a prior positive test result during pregnancy - compared with other screening strategies over the short-term (1 year) and long-term (lifetime) (low certainty evidence). There is evidence showing greatest benefit when third trimester screening is provided. Screening all PWPI at first and third trimesters is likely more acceptable than targeting high-risk PWPI because it may reduce stigma associated with screening for STI. In addition, the Working Group agreed that it may be more practical and therefore more likely to be done than inquiring about risk factors during busy prenatal visits and accessing partner risk factors. A recommendation about the sampling method for screening was not made since the preference and capacity may vary according to the patient, health care provider, and the health care system.
Subgroup considerations
In settings where there are limited laboratory capacities, priority could be given to screening PWPI with higher risk of those infections during the first trimester (or at the first antenatal visit) and screening all PWPI in the latter part of the third trimester. When identifying PWPI at high risk for NG and CT infection, risks similar to individuals <25 years old could be used. For positive test results, healthcare providers could continue explaining to PWPI the risk of false positive tests.
Implementation considerations
These recommendations are particularly important in settings where neonatal ocular prophylaxis for the prevention of ophthalmia neonatorum has stopped or is planned to be stopped. These recommendations do not replace recommendations to test and treat PWPI who have symptoms compatible with NG or CT infection or after sexual contact with a person known to have NG or CT.
Evidence suggests that screening all individuals could remove the fear of stigmatization and discrimination and normalize the testing practice.Footnote 18 In addition, the Working Group agreed that screening all PWPI may be more practical than clinicians’ efforts to gather risk factors from PWPI and partners. Further, co-infection rates for NG and CT are high and combined testing for these STI could contribute to the acceptability and feasibility of screening.
In settings where there are limited laboratory capacities, priority could be given to screening PWPI with higher risk of those infections during the first trimester (or at the first antenatal visit), and screening all PWPI in the latter part of the third trimester. When identifying PWPI at high risk for NG and CT infection, risks similar to individuals <25 years old could be used. For positive test results, healthcare providers could continue explaining to PWPI the risk of false positive tests
Monitoring and evaluation
Metrics will be used to monitor and evaluate prospectively the evidence related to the recommendations for potential updating or reaffirming the recommendation(s) if new evidence becomes available that could influence the direction and strength.
Research priorities
Addressing several research gaps could help inform whether to update or reaffirm these recommendations in the future. There is a need for studies assessing the impact of prenatal screening strategies for NG and CT on preventing ophthalmia neonatorum and neonatal pneumonia. In addition, comparative studies on the number and rates (or proportions) of PWPI who received screening, treatment, test-of-cure, and rescreening at the local and provincial/territorial levels could help inform future recommendations. Further, more studies are needed to monitor the impact and consequences of false positive tests. Also, primary studies on the acceptability, feasibility and equity of timing of repeating universal screening are required. Incidence and prevalence information on NG and CT in PWPI, ophthalmia neonatorum and neonatal pneumonia at the national level and more studies on adverse pregnancy outcomes of NG and CT are also required.
Appendix E. Estimated outcomes, cost and cost-effectiveness of different strategies to screen for Chlamydia trachomatis and Neisseria gonorrhoeae in pregnant women/pregnant individuals in Canada
Note. Data for Table 1 was extracted from information provided in this table.
| Screening Strategies: Pregnant women/pregnant individuals (PWPI) screened (or not) at each trimester (T) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 New recommendation |
3 | 4 | 5 Strategy in some settings |
6 | 7 | 7A | 8 | ||
| Effects of Strategies | T1: All T2: Only HRTable note a T3: All LabourTable note b |
T1: All T2: NoneTable note c T3: All Labour |
T1: Only HR T2: None T3: All Labour |
T1: None T2: None T3: All Labour |
T1: All T2: Only HR T3: Only HR Labour |
T1: All T2: None T3: Only HR Labour |
T1: All T2: None T3: None Labour |
T1: None T2: None T3: Only HR Labour |
T1: None T2: None T3: None Labour |
|
| Adverse infant & obstetric outcomes over 1 year | ||||||||||
| Ophthalmia neonatorum | Cases per 100,000 PWPI | 110Table note e | 110 | 124 | 128 | 148 | 149 | 170 | 303 | 357 |
| Cases per 400,000 PWPITable note d | 440Table note e | 440 | 496 | 512 | 592 | 596 | 680 | 1212 | 1428 | |
| CT pneumonia | Cases per 100,000 PWPI | 40Table note e | 40 | 46 | 48 | 53 | 53 | 62 | 111 | 132 |
| Cases per 400,000 PWPITable note d | 160Table note e | 160 | 184 | 192 | 212 | 212 | 248 | 444 | 528 | |
| Preterm, extremely preterm and still birthsTable note f | Cases per 100,000 PWPI | 8,514Table note e | 8,514 | 8,521 | 8,522 | 8,519 | 8,519 | 8,521 | 8,557 | 8,567 |
| Cases per 400,000 PWPITable note d | 34,056Table note e | 34,056 | 34,084 | 34,088 | 34,076 | 34,076 | 34,084 | 34,228 | 34,268 | |
| False results obtained (%) | ||||||||||
| False positives leading to unnecessary treatment | Not Available | 4.14% | 4.11% | 4.10% | 4.13% | Not Available | Not Available | 4.04% | 4.01% | |
| False negatives leading to missed infections | Not Available | 0.09% | 0.14% | 0.16% | 0.12% | Not Available | Not Available | 0.18% | 0.18% | |
| Total cost per 100,000 PWPI over 1 year | $565,722,366 | $565,220,444 | $563,302,330 | $562,780,969 | $563,823,557 | $563,321,635 | $562,812,279 | $561,899,189 | $561,633,682 | |
| Cost-effectiveness per 100,000 PWPI | ||||||||||
| Over 1 year (Baseline risk for NG/CT in the overall population) | $214M/QALY more than Strategy 2 | $65M/QALY more than Strategy 3 | $63M/QALY more than Strategy 4 | $3M/QALY more than screening only HR | More costly, less effective than other strategies | More costly, less effective than other strategies | Less costly, less effective than other strategies | $2M/QALY more than Strategy 8 | Reference | |
| Over 1 year (Higher prevalence and risk for NG/CT in the overall population) | Likely more costly, less effective than less screening | $7M/QALY more than only screening all at T3 | More costly, less effective than other strategies | $481K/QALY more than Strategy 7 | More costly, less effective than other strategies | More costly, less effective than other strategies | $66K/QALY more than Strategy 8 | More costly, less effective than other strategies | Reference | |
| Over lifetime (Baseline risk for NG/CT in the overall population) | Likely more costly, less effective than less screening | $11K/QALY more than Strategy 3 | $10K/QALY more than Strategy 4 | Reference | More costly, less effective than other strategies | More costly, less effective than other strategies | More costly, less effective than other strategies | More costly, less effective than other strategies | More costly, less effective than other strategies | |
PHAC: Public Health Agency of Canada, PWPI: pregnant women/pregnant individuals, HR: high risk (PWPI less than 25 years old), T: trimester, T1: first trimester, T2: second trimester, T3: third trimester, QALY: quality-adjusted life-year. Table Notes
In the table, starting from strategy #8 and moving towards strategy #1 shows that, as screening is added to each trimester, whether screening all individuals or high-risk groups (i.e., less than 25 years), there is a reduction in number of infants with ophthalmia neonatorum and CT pneumonia. |
||||||||||
References
- Footnote 1
-
Public Health Agency of Canada. Report on Sexually Transmitted Infection Surveillance in Canada, 2019. . 2021; Available at: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/report-sexually-transmitted-infection-surveillance-canada-2019/pub1-eng.pdf. Accessed 12/27, 2022.
- Footnote 2
-
Public Health Agency of Canada. Notifiable Diseases Online. 2021; Available at: https://diseases.canada.ca/notifiable/. Accessed 02/01, 2022.
- Footnote 3
-
Hammerschlag MR. Conjunctivitis and pneumonia in newborns. In: Kliegman RM, St Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, editors. Nelson Textbook of Pediatrics. 21st ed.: Elsevier; 2020.
- Footnote 4
-
Laga M, Plummer FA, Nzanze H, Namaara W, Brunham RC, Ndinya-Achola JO, et al. Epidemiology of ophthalmia neonatorum in Kenya. Lancet 1986;2(8516):1145-1149.
- Footnote 5
-
Galega FP, Heymann DL, Nasah BT. Gonococcal ophthalmia neonatorum: the case for prophylaxis in tropical Africa. Bull World Health Organ 1984;62(1):95-98.
- Footnote 6
-
Public Health Agency of Canada. Canadian guidelines on Sexually Transmitted Infections. Revised version of the Canadian STI Guidelines –Pregnancy Chapter 2010. 2010; Available at: https://publications.gc.ca/collections/collection_2011/aspc-phac/HP40-1-2010-eng.pdf. Accessed 12/26, 2022.
- Footnote 7
-
Public Health Agency of Canada. Canadian guidelines on Sexually Transmitted Infections. Revised version of the Canadian STI Guidelines –- Chlamydial infections Chapter 2010. 2010; Available at: https://publications.gc.ca/collections/collection_2011/aspc-phac/HP40-1-2010-eng.pdf. Accessed 12/23, 2022.
- Footnote 8
-
Moore DL, MacDonald NE, Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Preventing ophthalmia neonatorum. Paediatr Child Health 2015;20(2):93-96.
- Footnote 9
-
Poliquin V, Wylie J, Cole R, Yudin MH, Van Caesseele P. Preparedness for Implementing Change in Neonatal Ocular Prophylaxis Policies [published correction appears in J Obstet Gynaecol Can. 2019 Jun;41(6):897]. J Obstet Gynaecol Can. 2016;38(1):7-8.
- Footnote 10
-
Vainder M, Kives S, Yudin MH. Screening for Gonorrhea and Chlamydia in Pregnancy: Room for Improvement. J Obstet Gynaecol Can 2019;41(9):1289-1294.
- Footnote 11
-
Ivensky V, Mandel R, Boulay AC, Lavallée C, Benoit J, Labbé AC. P470 Screening rates and follow-up of Chlamydia trachomatis and Neisseria gonorrhoeae infections during pregnancy. Sex Transm Infect 2019;95: A219.
- Footnote 12
-
Canadian Agency for Drugs and Technologies in Health. Screening for Chlamydia trachomatis and Neisseria gonorrhoeae during pregnancy: a health technology assessment. 2018; Available at: https://cadth.ca/ sites/default/files/pdf/ht0023_STIs_during-pregnancy.pdf. Accessed 02/01, 2022.
- Footnote 13
-
Canadian Agency for Drugs and Technologies in Health. Screening Strategies for the Detection of Chlamydia Trachomatis and/or Neisseria Gonorrhoeae during Pregnancy: Clinical Utility, Safety, and Cost Effectiveness. 2020 June 2020(CADTH rapid response report: reference list).
- Footnote 14
-
Shanmugasegaram S, Auguste U, Sabourin SG. Systematic review on acceptability, feasibility, equity and resource use for prenatal screening for chlamydia and gonorrhea. To be Submitted.
- Footnote 15
-
Aggarwal A, Spitzer RF, Caccia N, Stephens D, Johnstone J, Allen L. Repeat screening for sexually transmitted infection in adolescent obstetric patients. J Obstet Gynaecol Can. 2010;32(10):956-961.
- Footnote 16
-
Statistics Canada. Live births, by age of mother. 2020; Available at: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310041601&pickMembers%5B0%5D=3.1&cubeTimeFrame.startYear=2019&cubeTimeFrame.endYear=2019&referencePeriods=20190101%2C20190101. Accessed 09/03, 2021.
- Footnote 17
-
Debessai Y, Costanian C, Roy M, El-Sayed M, Tamim H. Inadequate prenatal care use among Canadian mothers: findings from the Maternity Experiences Survey. J Perinatol 2016;36(6):420-426.
- Footnote 18
-
Bilardi JE, De Guingand DL, Temple-Smith MJ, Garland S, Fairley CK, Grover S, et al. Young pregnant women's views on the acceptability of screening for chlamydia as part of routine antenatal care. BMC Public Health 2010; 10:505.
- Footnote 19
-
Pereboom M, Spelten E, Manniën J, Rours G, Morré S, Schellevis F, et al. Knowledge and acceptability of Chlamydia trachomatis screening among pregnant women and their partners; a cross-sectional study. BMC Public Health 2014(14):704.
- Footnote 20
-
Ivensky V, Mandel R, Boulay AC, Lavallée C, Benoît J, Labbé AC. Suboptimal prenatal screening of Chlamydia trachomatis and Neisseria gonorrhoeae infections in a Montréal birthing and tertiary care centre: A retrospective cohort study. Can Commun Dis Rep 2021;47(4):209-215.
- Footnote 21
-
Chen MY, Fairley CK, De Guingand D, Hocking J, Tabrizi S, Wallace EM, et al. Screening pregnant women for chlamydia: What are the predictors of infection? Sex Transm Infect 2009;85(1):31-35.
- Footnote 22
-
Ditkowsky J, Shah KH, Hammerschlag MR, Kohlhoff S, Smith-Norowitz TA. Cost-benefit analysis of Chlamydia trachomatis screening in pregnant women in a high burden setting in the United States. BMC Infect Dis 2017;17(1):155.
- Footnote 23
-
Leichliter JS, Haderxhanaj LT, Gift TL, Dittus PJ. Sexually transmissible infection testing among pregnant women in the US, 2011-15. Sex Health 2020;17(1):1-8.
- Footnote 24
-
Logan S, Browne J, McKenzie H, Templeton A, Bhattacharya S. Evaluation of endocervical, first-void urine and self-administered vulval swabs for the detection of Chlamydia trachomatis in a miscarriage population [published correction appears in BJOG. 2005 Apr;112(4):528]. BJOG. 2005;112(1):103-106.
- Footnote 25
-
Miller JM Jr, Maupin RT, Mestad RE, Nsuami M. Initial and repeated screening for gonorrhea during pregnancy. Sex Transm Dis. 2003;30(9):728-730.
- Footnote 26
-
Miller JM, Maupin RT, Nsuami M. Initial and repeat testing for chlamydia during pregnancy. J Matern Fetal Neonatal Med. 2005;18(4):231-235.
- Footnote 27
-
Ong JJ, Chen M, Hocking J, Fairley CK, Carter R, Bulfone L, et al. Chlamydia screening for pregnant women aged 16-25 years attending an antenatal service: a cost-effectiveness study. BJOG 2016;123(7):1194-1202.
- Footnote 28
-
Perkins E, Carlisle C, Jackson N. Opportunistic screening for Chlamydia in general practice: the experience of health professionals. Health Soc Care Community. 2003;11(4):314-320.
- Footnote 29
-
Pimenta JM, Catchpole M, Rogers PA, Perkins E, Jackson N, Carlisle C, et al. 1. Opportunistic screening for genital chlamydial infection. I: Acceptability of urine testing in primary and secondary health care settings. Sex transm infect. 2003; 79:16-21.
- Footnote 30
-
Rours GI, Smith-Norowitz TA, Ditkowsky J, Hammerschlag MR, Verkooyen RP, et al. Cost-effectiveness analysis of Chlamydia trachomatis screening in Dutch pregnant women. Pathog Glob Health 2016;110(7-8):292-302.
- Footnote 31
-
Tyker A., Pudwell J., Schneiderman M., Hundal P., Thorne J., Jamieson M.A. Prevalence of Chlamydia Trachomatis and Neisseria Gonorrhea Among a Pregnant Adolescent Population Screened in the Third Trimester using a Urine PCR Test: A Retrospective Chart Review. Poster Presentation Abstracts. J Pediatr Adolesc Gynecol 2020;33(2):217-218.
- Footnote 32
-
Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Updated 2013.
- Footnote 33
-
Nieuwlaat R, Wiercioch W, Brozek J, Santesso N, Kunkle R, Alonso-Coello P, et al. How to write a guideline: a proposal for a manuscript template that supports the creation of trustworthy guidelines. Blood Adv 2021;5(22):4721-4726.
- Footnote 34
-
Fredrick DR. Conjunctivitis in the neonatal period (ophthalmia neonatorum). In: Long SS, Prober CG, Fischer M, editors. Principles of practice of pediatric infectious diseases. 5th ed.: Elsevier; 2018. p. 497.
- Footnote 35
-
American Academy of Pediatrics. Neonatal Ophthalmia. In: Kimberlin DW, Barnett ED, Lynfield R, Sawyer MH, editors. Red book: 2021-2024 report of the Committee on Infectious Diseases. 32nd ed. Itasca, Illinois: American Academy of Pediatrics; 2021. p. 1023-1024.
- Footnote 36
-
Hammerschlag MR. Chlamydial and gonococcal infections in infants and children. Clin Infect Dis 2011;53(Suppl 3): S99-S102.
- Footnote 37
-
Canadian Paediatric Surveillance Program, Canadian Paediatric Society. CPSP 2020 Results. Ottawa 2021; Available at: https://cpsp.cps.ca/uploads/publications/CPSPResults2020-.pdf. Accessed 02/01, 2022.
- Footnote 38
-
STI & HIV 2019 World Congress: Joint meeting of the 23rd International Society for STD Research (ISSTDR) & 20th International Union against Sexually Transmitted Infections (IUSTI) in Vancouver, British Columbia, Canada in 2019.
- Footnote 39
-
World Health Organization. WHO Handbook for Guideline Development, 2nd ed. 2014; Available at: https://apps.who.int/iris/handle/10665/145714. Accessed 05/07, 2021.
- Footnote 40
-
Public Health Agency of Canada. Survey of the impact of COVID-19 on the ability to provide STBBI prevention, testing and treatment including harm reduction services in Canada. 2021; Available at: https://health-infobase.canada.ca/datalab/covid-19-impact-stbbi-services.html, 2022.