
Section 1: Report on Sexually Transmitted Infections in Canada: 2012 – Chlamydia (Chlamydia trachomatis)
1. Chlamydia (Chlamydia trachomatis)
Chlamydia, an infection caused by the bacterium Chlamydia trachomatis, has been nationally notifiable since 1991. It is the most commonly reported sexually transmitted infection (STI) in Canada. Infections are often asymptomatic in both males and females. In the absence of screening, these infections remain undiagnosed and contribute to the spread of chlamydia in sexually active individualsFootnote 1.
A common complication associated with untreated and recurring chlamydia in females is pelvic inflammatory disease, which can lead to chronic pelvic pain, ectopic pregnancy, and infertility. In males, complications are rarer but include epididymo-orchitis and infertility. Untreated chlamydia in pregnant women can be transmitted to their newborns, causing neonatal conjunctivitis or pneumonia. As with other STIs, chlamydia increases infection with and transmission of the human immunodeficiency virus (HIV). It recruits target cells for HIV to the genital tract and increases the shedding of HIV-infected cellsFootnote 2,Footnote 3.
1.1 National Trends
Trends over Time
Between 1991 and 1997, the rate of reported cases of chlamydia decreased steadily among both males and females, after which rates began to rise and continued to do so (Figure 1). In 2012, 103,716 cases of chlamydia were reported, corresponding to a rate of 298.7 per 100,000. The 2012 rate was a 57.6% increase from the rate of 189.6 per 100,000 in 2003. Among males, rates increased by 74.8%, from 121.3 to 212.0 per 100,000; among females, they increased by 49.5%, from 256.5 to 383.5 per 100,000.
Trends by Age Group and Sex
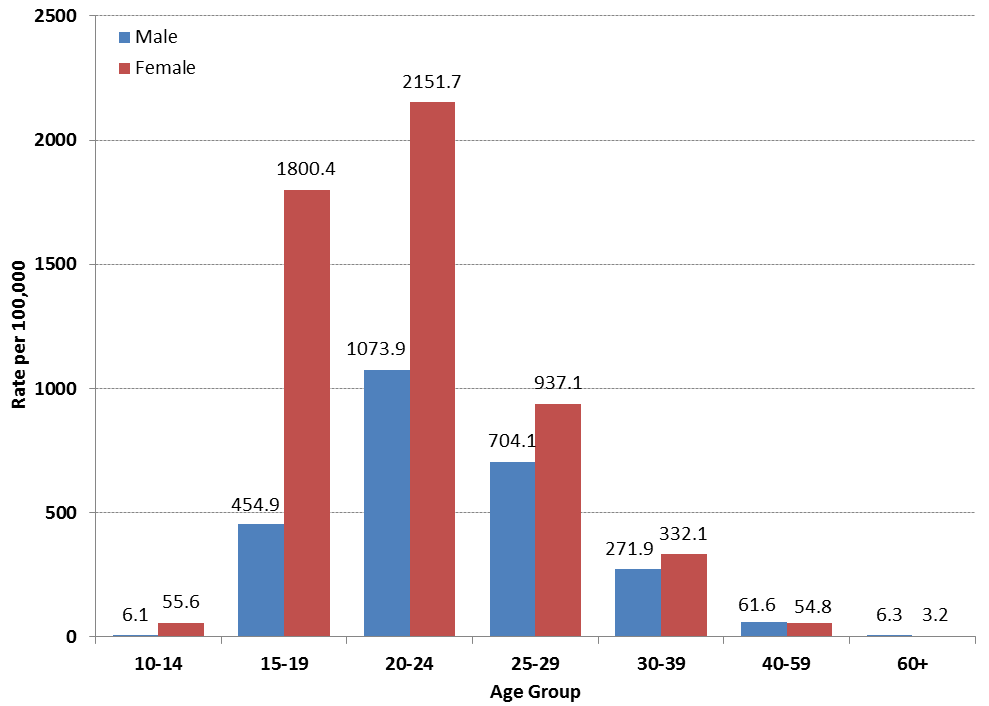
Historically, rates of reported cases of chlamydia in females have been substantially higher than corresponding rates in males (Figure 1). In 2012, rates were almost twice as high among females as compared to males and the majority (80.2%) of reported chlamydia infections occurred in persons under 30 years. In 2012, the highest rates were reported among females aged 20 to 24, followed by females aged 15 to 19. Among males, the highest rates were also observed in the 20 to 24 age group, though rates in females were more than double the rates in males of this age (2151.7 per 100,000 vs. 1073.9 per 100,000, respectively). Among older age groups, the gap between sexes was less pronounced and even reversed; in 2012, the rates of reported cases were higher among men than women in those aged 40 to 59 and 60 and older (Figure 2).
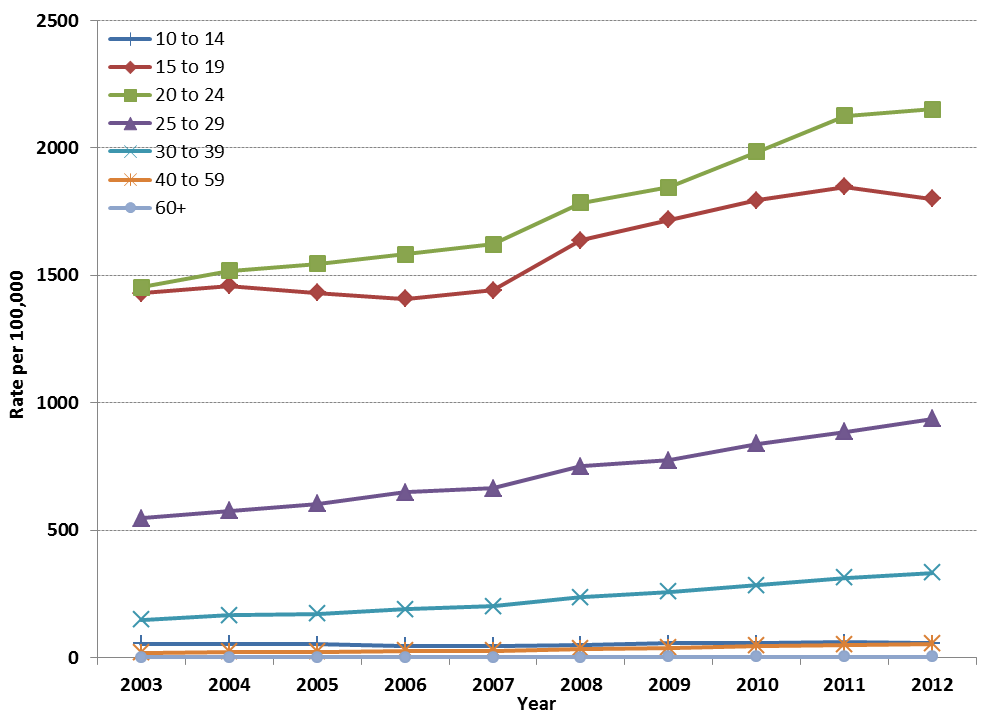
Between 2003 and 2012, rates of reported cases of chlamydia increased steadily among both males and females aged 10 and above. Between 2003 and 2012, in males, the highest relative rate increase occurred among those aged 10 to 14 (167.0%) (Figure 3), while the highest relative rate increase in females occurred among those aged 60 and over (266.8%), followed by those aged 40 to 59 (190.9%) (Figure 4).
Trends by Province/Territory
In 2012, as in the previous year, the highest rate of reported cases of chlamydia was observed in the Northwest Territories (2193.9 per 100,000). Chlamydia rates above the national average of 298.7 per 100,000 were also observed in Manitoba, Saskatchewan, Yukon, and Alberta (527.1, 526.0, 485.6, and 398.8 per 100,000). Between 2003 and 2012, all provinces and territories experienced a relative increase in the rate of reported cases of chlamydia, with the exception of Yukon which experienced a relative rate decrease of 16.5%. The greatest relative rate increase was observed in Ontario (74.7%), followed by the Northwest Territories (71.0%) (Table 1).
1.2 Lymphogranuloma Venereum
Lymphogranuloma venereum (LGV) is an STI caused by Chlamydia trachomatis serovars L1, L2, L2b and L3. Infections caused by these serovars preferentially invade lymph tissue and tend to be more invasive than those caused by non-LGV chlamydia. Untreated LGV infection can result in severe complications including destruction of rectal and genital tissue; in some cases, though uncommon, meningoencephalitis, hepatitis, and death can also occur.
Though LGV is endemic in parts of Africa, Asia, South America, and the Caribbean region, it was relatively uncommon in Canada until 2003Footnote 4. At that time, outbreaks of LGV serovar L2b began occurring among men who have sex with men (MSM) in urban centres in CanadaFootnote 5. Outbreaks among MSM have also been reported in European countries and the United StatesFootnote 6-Footnote 9. Recent data suggest that the infection has become endemic in the MSM population in some countriesFootnote 10.
In response to the emergence of LGV in Europe, Canada initiated enhanced surveillance of this STI in 2005. Confirmatory testing for suspected LGV cases is performed by the National Microbiology Laboratory (NML). Where possible, provincial/territorial health authorities use a standardized national case report form to collect enhanced epidemiological data on each case and submit the data to the Agency.
As of December 2012, 170 cases were reported to the Agency by provincial health authorities via case report forms (including 104 confirmed and 66 probable cases). Confirmed cases were reported from Quebec, Ontario, British Columbia and Alberta; probable cases were reported from these provinces as well as one from Nova Scotia. The NML has records for 128 confirmed cases, from 2004 to 2005 and from 2010 to 2012 (NML records from 2006 to 2009 were unavailable) (Table 2). All confirmed cases were male, and predominantly MSM.
1.3 Summary
Increases in the rates of reported cases of chlamydia have been observed in Canada despite numerous public health interventions designed to prevent, diagnose, and treat infection. However, some theories suggest that the increased rates may be only partially explained by a true increase in incidence and that the observed increases may also be reflective of improved case finding.
The introduction of more sensitive nucleic acid amplification testing (NAAT) in the mid-1990s undoubtedly led to an increase in the number of chlamydia cases detected. In fact, this change in diagnostic practice coincided with the beginning of the rise in rates of reported cases of chlamydia. NAAT allows urine specimens to be used rather than swabs, which are easier to collect and more acceptable to patients. As a result, in addition to increased sensitivity, the number of people, particularly males, who go for testing has likely increased as well. More effective screening and contact tracing may have a similar effectFootnote 11,Footnote 12. A recent estimation of chlamydia disease burden in Canada found that observed increases in chlamydia prevalence could be explained by effective case finding and expansion of screening programsFootnote 13.
Over time, the rate of reported cases of chlamydia has consistently been approximately twice as high in females as in males; however, this disparity is much more pronounced in younger age groups and among those aged 40 years and older, rates are higher among men. Younger women are biologically more susceptible to chlamydial infection due to a higher prevalence of cervical ectopyFootnote 14,Footnote 15. In addition, women are more likely to be screened for STIsFootnote 16,Footnote 17, while research has found that men have a tendency to delay seeking health care for any cause when neededFootnote 18.
Differences in STI screening behaviours across provinces and territories may also help explain some of the variation in rates by geographical location. For example, there is some evidence that chlamydia screening rates may be higher in Yukon than in some other Canadian jurisdictions, which may contribute to the high rate of reported cases of chlamydia infection observed in the territoryFootnote 17.
The arrested immunity hypothesis, which posits that early diagnosis and treatment of chlamydial infections may actually impede the development of an effective immune response, may also partly explain rising rates of chlamydia. According to this hypothesis, in the absence of any change in behaviour, treated individuals that have not developed an immune response are susceptible to re-infection upon returning to their sexual networksFootnote 19. Evidence supporting this theory has been observed in British Columbia, where the relative risk of re-infection with chlamydia was shown to increase between 1989 and 2003Footnote 20, and in Finland, where reported rates of chlamydia have increased despite a decrease in seroprevalenceFootnote 21.
High and continually increasing chlamydia rates have been observed worldwide. As in Canada, chlamydia was the most commonly reported bacterial STI in 2012 in the United StatesFootnote 22,Footnote 23, AustraliaFootnote 24 and in EnglandFootnote 25, countries that have similar socio-economic status and ethno-cultural makeup to Canada. Additionally, patterns in chlamydial infection (such as significantly higher rates in females than males) were similar across the four countries. However, there were some notable differences between countries, particularly in the magnitude of rates of reported cases. Compared to Canada's overall rate of 298.7 per 100,000, rates in Australia, England and the United States were significantly higher (355.1, 389.6, and 456.7 per 100,000, respectively). Differences in reported rates should be interpreted with caution due to inter-country differences in case definitions, reporting sources, screening programs and screening rates, age groupings, and other factors.
In Canada, cycle 2 of the Canadian Health Measures Survey (CHMS)Footnote 26 estimated the prevalence of chlamydia in the general population using urine specimens collected from a sample of respondents aged 14 to 59 at mobile examination centres. The resulting prevalence was 0.7% (95% confidence interval 0.4% to 1.3%), a weighted estimate of 158,000 individualsFootnote 27. Repeated measures of chlamydia prevalence in future cycles of the CHMS will facilitate interpretation of data received through routine surveillance and may help explain the drivers behind the continuing increase in reported cases.
Trends in LGV infection in Canada are difficult to interpret. Early surveillance efforts were intensive, followed by a period of time (2007-2009) when few cases were reported by provincial health authorities; this decrease may have been influenced by underreporting or underdiagnosis by health care providers rather than a true decrease in incidence. The more recent increase in cases beginning in 2010 and continuing into 2012 was driven largely by improved case finding and reporting in British ColumbiaFootnote 28.
In all, it is difficult to identify what factors are most responsible for the observed increase in chlamydia rates in Canada. A combination of factors is likely involved, and the possibility of a true increase in incidence cannot be ruled out. Continued monitoring of chlamydia rates and research into the reasons for observed changes will help in evaluating the public health response to STIs. National guidelines for the prevention and management of chlamydial infections are updated as new information becomes available, to provide users with the most up-to-date information for the management of STIs in CanadaFootnote 2,Footnote 29.
Figure 1: Overall and sex-specific rates of reported chlamydia cases, 1991 to 2012, Canada

Text Equivalent - Figure 1
| Year | Male rate per 100,000 | Female rate per 100,000 | Total rate per 100,000 |
|---|---|---|---|
| 1991 | 63.6 | 190.4 | 164.0 |
| 1992 | 76.9 | 247.1 | 163.4 |
| 1993 | 74.7 | 230.5 | 153.4 |
| 1994 | 69.6 | 212.8 | 142.0 |
| 1995 | 62.6 | 192.2 | 128.2 |
| 1996 | 56.6 | 174.0 | 115.9 |
| 1997 | 58.7 | 167.8 | 113.9 |
| 1998 | 73.7 | 183.1 | 129.0 |
| 1999 | 81.4 | 193.6 | 138.2 |
| 2000 | 88.9 | 211.6 | 150.9 |
| 2001 | 99.2 | 221.9 | 161.4 |
| 2002 | 112.3 | 245.1 | 179.5 |
| 2003 | 121.3 | 256.5 | 189.6 |
| 2004 | 131.8 | 267.7 | 200.5 |
| 2005 | 140.2 | 270.8 | 206.2 |
| 2006 | 145.8 | 278.1 | 212.7 |
| 2007 | 151.7 | 285.5 | 221.0 |
| 2008 | 165.5 | 321.2 | 244.2 |
| 2009 | 173.0 | 336.0 | 255.4 |
| 2010 | 186.9 | 358.8 | 273.7 |
| 2011 | 201.1 | 379.8 | 291.6 |
| 2012 | 212.0 | 383.5 | 298.7 |
{kind=link}
Figure 2: Rates of reported chlamydia cases by sex and age group, 2012, Canada

Text Equivalent - Figure 2
| Sex | 10-14 | 15-19 | 20-24 | 25-29 | 30-39 | 40-59 | 60+ |
|---|---|---|---|---|---|---|---|
| Male | 6.1 | 454.9 | 1073.9 | 704.1 | 271.9 | 61.6 | 6.3 |
| Female | 55.6 | 1800.4 | 2151.7 | 937.1 | 332.1 | 54.8 | 3.2 |
{kind=link}
Figure 3: Rates of reported chlamydia in Males by Age Group, 2003 to 2012, Canada

Text Equivalent - Figure 3
| Year | 10-14 | 15-19 | 20-24 | 25-29 | 30-39 | 40-59 | 60+ |
|---|---|---|---|---|---|---|---|
| 2003 | 2.3 | 265.9 | 656.5 | 385.5 | 138.7 | 27.1 | 2.9 |
| 2004 | 2.1 | 284.8 | 717.0 | 423.4 | 145.8 | 32.2 | 3.8 |
| 2005 | 2.2 | 287.1 | 742.1 | 457.6 | 168.0 | 36.1 | 4.0 |
| 2006 | 2.5 | 298.8 | 761.8 | 464.6 | 182.6 | 39.1 | 4.7 |
| 2007 | 3.5 | 311.9 | 792.6 | 492.0 | 185.3 | 40.9 | 5.0 |
| 2008 | 4.9 | 356.6 | 867.1 | 525.3 | 200.7 | 44.6 | 4.0 |
| 2009 | 5.5 | 394.7 | 890.5 | 548.6 | 205.7 | 46.4 | 4.9 |
| 2010 | 5.3 | 415.9 | 951.5 | 588.7 | 232.7 | 50.0 | 6.3 |
| 2011 | 5.0 | 437.2 | 1066.3 | 645.7 | 249.4 | 55.2 | 6.1 |
| 2012 | 6.1 | 454.9 | 1073.9 | 704.1 | 271.9 | 61.6 | 6.3 |
{kind=link}
Figure 4: Rates of reported chlamydia in Females by Age Group, 2003 to 2012, Canada

Text Equivalent - Figure 4
| Year | 10-14 | 15-19 | 20-24 | 25-29 | 30-39 | 40-59 | 60+ |
|---|---|---|---|---|---|---|---|
| 2003 | 54.6 | 1429.6 | 1453.3 | 546.8 | 148.5 | 18.8 | 0.9 |
| 2004 | 53.5 | 1458.0 | 1518.3 | 574.9 | 166.0 | 22.5 | 1.5 |
| 2005 | 51.9 | 1431.3 | 1545.0 | 602.6 | 171.3 | 23.5 | 1.4 |
| 2006 | 45.2 | 1407.2 | 1582.8 | 649.3 | 189.5 | 26.4 | 1.7 |
| 2007 | 46.7 | 1440.8 | 1622.3 | 664.3 | 200.4 | 27.2 | 1.8 |
| 2008 | 50.3 | 1636.6 | 1783.9 | 750.2 | 236.1 | 33.4 | 1.4 |
| 2009 | 55.0 | 1718.4 | 1845.0 | 773.8 | 257.3 | 39.2 | 2.2 |
| 2010 | 55.9 | 1794.1 | 1983.9 | 838.8 | 283.0 | 46.4 | 2.3 |
| 2011 | 60.8 | 1847.8 | 2126.1 | 886.2 | 313.9 | 50.0 | 3.0 |
| 2012 | 55.6 | 1800.4 | 2151.7 | 937.1 | 332.1 | 54.8 | 3.2 |
{kind=link}
Page details
- Date modified: