
Dementia and ischemic heart disease comorbidity among Canadians aged 65 years and older
Download in PDF format
(209 KB, 9 pages)
Organization: Public Health Agency of Canada
Date published: 2021-10-13
Highlights from the Canadian Chronic Disease Surveillance System
The Public Health Agency of Canada (PHAC) uses the Canadian Chronic Disease Surveillance System (CCDSS) to conduct national surveillance of 20 chronic conditions, including diagnosed dementia ("all types of dementia" when not specifically mentioned) and diagnosed ischemic heart disease (IHD) (Box 1). This publication provides the first estimates on dementia and IHD comorbidity among Canadians aged 65 years and older using data from the CCDSS. With the aging of the population, comorbidity is an area of growing interest that is being explored to better inform chronic disease policies and programs. Those with comorbid conditions tend to have worse health outcomes and more frequent use of health services.Footnote 1 Therefore, this publication is mainly intended for members of the research community, health professionals and policy/decision makers.
Dementia refers to a set of symptoms and signs associated with a progressive deterioration of cognitive functions that affect daily activities.Footnote 2 It is caused by multiple diseases, including cerebrovascular disease and injuries to the brain. Alzheimer disease represents the most common cause of dementia, while vascular dementia is the second most common cause. However, evidence suggests that mixed dementia, involving any combination of causes but often these two, is also common.Footnote 3Footnote 4
Ischemic heart disease (IHD), also known as coronary artery disease or coronary heart disease, is the most common type of heart disease. Plaque, composed of fat, cholesterol and other substances, builds on the inner wall of coronary arteries over time and leads to narrowed arteries. As a result, blood flow to the heart or other parts of the body may be blocked or reduced, which can cause a heart attack or stroke.Footnote 5
Comorbidity, defined as the co-occurrence of two or more conditions, is associated with poorer health outcomes and can make their management more challenging.Footnote 1 People living with any chronic condition are more likely to live with more than one condition.Footnote 6 Conservative estimates from self-reported data suggest that approximately 37% of Canadians aged 65 years and older have at least two of ten common chronic conditions.Footnote 7 A recent meta-analysis conducted in high-income countries reported that 66% of individuals ages 65 years and older had two or more chronic conditions, with the number of conditions considered ranging between 5 and 263.Footnote 8
The relationship between dementia and heart disease is complex. There are several factors, including lifestyle and socio-economic ones, associated with the development and progression of dementia and heart disease individually. Further, these two conditions share common risk factors such as hypertension, diabetes, obesity, physical inactivity, high blood cholesterol, smoking, and increasing age.Footnote 9Footnote 10 However, evidence also suggests that IHD is an independent risk factor for dementia, specifically vascular dementia. Indeed, the risk of dementia was found to be 45% higher in individuals with IHD.Footnote 9
Validated case definitions for diagnosed dementiaFootnote 11 and diagnosed IHD,Footnote 12 were applied to CCDSS longitudinal data (i.e., April 1, 1996 to March 31, 2018). Among individuals aged 65 years and older in 2017–2018, coexisting dementia and IHD cases (regardless of the order of occurrence) were identified as prevalent comorbid cases.
Box 1: What's in the data?
The data used in this publication are from the Canadian Chronic Disease Surveillance System (CCDSS), a collaborative network of provincial and territorial chronic disease surveillance systems, led by the Public Health Agency of Canada (PHAC).
The CCDSS identifies chronic disease cases from provincial and territorial administrative health databases, including physician billing claims, hospital discharge abstract records, and drug prescription records linked to provincial and territorial health insurance registry records using a unique personal identifier. Data on all residents eligible for provincial or territorial health insurance are captured in the health insurance registries.
The CCDSS identifies those individuals who interact with the health care system (either by physician visit, hospital separation or drug claim), and thus does not identify those who have not yet been diagnosed by a physician as having dementia or IHD.
Definition of diagnosed dementia, including Alzheimer disease, in the CCDSS
Canadians aged 65 years and older were identified as having diagnosed dementia, including Alzheimer disease, if they had: at least one hospitalization record or at least three physician claims in a two-year period (with at least 30 days between each claim) with an International Classification of Diseases (ICD)-9 or ICD-10-CA code for dementia, including Alzheimer disease; or at least one anti-dementia prescription drug record.
Definition of diagnosed ischemic heart disease in the CCDSS
Canadians aged 20 years and older were identified as having diagnosed IHD if they had: at least one hospitalization or procedure code, or at least two physician claims within one year with an ICD-9 or ICD-10-CA code for IHD. Data presented in this publication are limited to individuals aged 65 years and older.
For more information on CCDSS disease case definitions, please visit the CCDSS Data Tool.
How many Canadians aged 65 years and older have dementia and IHD (prevalence)?
Looking at the two conditions separately using 2017–2018 fiscal year data from the CCDSS, 6.7% (or 452,000) of individuals aged 65 years and older (N=6,714,000) were living with dementia, and 26.4% (or 1,775,000) were living with IHD.
Overall, in the population aged 65 years and older:
- The crude prevalence of dementia was higher in women than men (7.8% vs. 5.4%);
- Conversely, the crude prevalence of IHD was lower in women than men (21.7% vs. 32.0%).
Looking at the overlap between these two conditions, about 2.8% (or 186,000) of individuals aged 65 years and older were living with comorbid dementia and IHD, while 4.0% (or 266,000) were living with dementia, without IHD, and 23.7% (or 1,589,000) were living with IHD, without dementia (Figure 1).
Although a higher number of women aged 65 years and older had comorbid dementia and IHD than men (106,000 vs. 81,000), the age-standardizedNote de bas de page i prevalence was lower in women than men (2.5% vs. 2.9%), given the differences in age distribution.
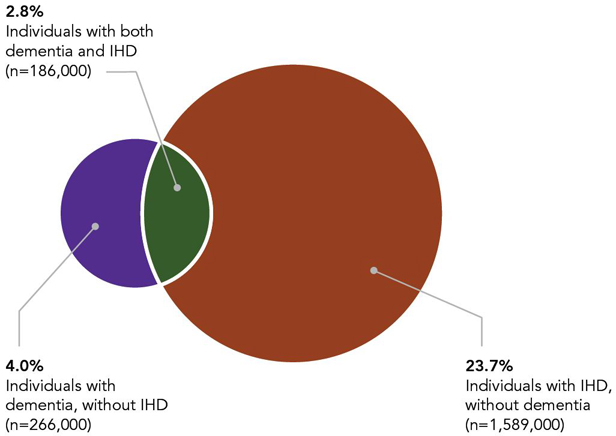
Table 1 footnotes
- Table 1 footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote *
-
Data from Nunavut and Northwest Territories were not available.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 1 - Text description
| Population | Count | Crude prevalence, % |
|---|---|---|
| Individuals with both dementia and IHD | 186,000 | 2.8 |
| Individuals with dementia, without IHD | 266,000 | 4.0 |
| Individuals with IHD, without dementia | 1,589,000 | 23.7 |
The prevalence of dementia (without IHD) increased with age and was greater in women than in men in all age groups (Figure 2a). The prevalence of IHD (without dementia) increased with age until 89 years and was smaller in women than in men in all age groups (Figure 2b).
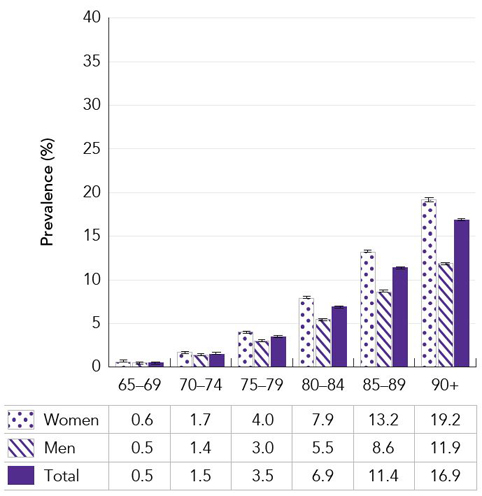
Table 2a footnotes
- Table 2a footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 2a *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 2a - Text description
| Age group (years) | Prevalence, % (95% Confidence Interval) | ||
|---|---|---|---|
| Women | Men | Total | |
| 65-69 | 0.6 (0.6-0.6) | 0.5 (0.5-0.5) | 0.5 (0.5-0.6) |
| 70-74 | 1.7 (1.6-1.7) | 1.4 (1.3-1.4) | 1.5 (1.5-1.5) |
| 75-79 | 4.0 (3.9-4.0) | 3.0 (2.9-3.0) | 3.5 (3.5-3.5) |
| 80-84 | 7.9 (7.9-8.0) | 5.5 (5.4-5.6) | 6.9 (6.8-6.9) |
| 85-89 | 13.2 (13.1-13.4) | 8.6 (8.5-8.8) | 11.4 (11.3-11.5) |
| 90+ | 19.2 (19.0-19.3) | 11.9 (11.7-12.0) | 16.9 (16.7-17.0) |
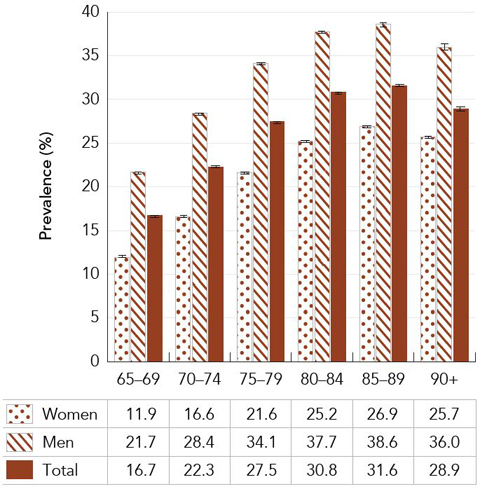
Table 2b footnotes
- Table 2b footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 2b *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 2b - Text description
| Age group (years) | Prevalence, % (95% Confidence Interval) | ||
|---|---|---|---|
| Women | Men | Total | |
| 65-69 | 11.9 (11.8-12.0) | 21.7 (21.6-21.8) | 16.7 (16.6-16.7) |
| 70-74 | 16.6 (16.6-16.7) | 28.4 (28.3-28.6) | 22.3 (22.3-22.4) |
| 75-79 | 21.6 (21.5-21.8) | 34.1 (34.0-34.3) | 27.5 (27.4-27.6) |
| 80-84 | 25.2 (25.1-25.4) | 37.7 (37.5-37.9) | 30.8 (30.7-30.9) |
| 85-89 | 26.9 (26.7-27.0) | 38.6 (38.4-38.9) | 31.6 (31.5-31.8) |
| 90+ | 25.7 (25.5-25.9) | 36.0 (35.7-36.3) | 28.9 (28.7-29.1) |
The prevalence of comorbid dementia and IHD markedly increased from 0.2% in individuals aged 65 to 69 years old, to 14.2% in those aged 90 years and older (Figure 3). The prevalence of comorbid dementia and IHD was smaller in women than in men until 90 years of age, where the prevalence did not differ significantly between sexes (the sex difference in the younger age group is not displayed due to rounding).
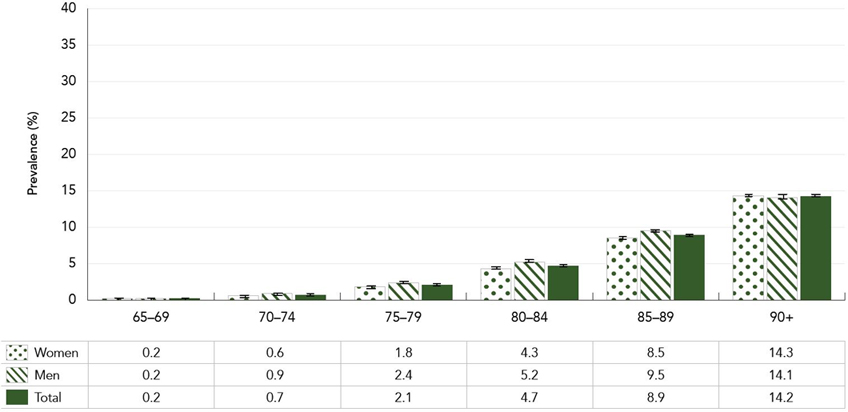
Table 3 footnotes
- Table 3 footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 3 *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 3 - Text description
| Age group (years) | Prevalence, % (95% Confidence Interval) | ||
|---|---|---|---|
| Women | Men | Total | |
| 65-69 | 0.2 (0.2-0.2) | 0.2 (0.2-0.3) | 0.2 (0.2-0.2) |
| 70-74 | 0.6 (0.6-0.6) | 0.9 (0.8-0.9) | 0.7 (0.7-0.7) |
| 75-79 | 1.8 (1.8-1.8) | 2.4 (2.3-2.4) | 2.1 (2.0-2.1) |
| 80-84 | 4.3 (4.3-4.4) | 5.2 (5.2-5.3) | 4.7 (4.7-4.8) |
| 85-89 | 8.5 (8.4-8.6) | 9.5 (9.4-9.6) | 8.9 (8.8-9.0) |
| 90+ | 14.3 (14.2-14.5) | 14.1 (13.9-14.3) | 14.2 (14.1-14.4) |
What are the mortality rates (due to any cause of death) among Canadians aged 65 years and older with dementia and IHD?
As people age, they are more likely to die of any cause, regardless of their dementia and IHD status. Therefore, while the all-cause mortality rates increased with age, the rate ratios (RRs) generally decreased with age.
When compared to individuals aged 65 years and older not living with either dementia or IHD (all-cause mortality rate: 18.2 per 1,000), age-standardized all-cause mortality rates and RRs were higher in individuals of the same age with at least one of the conditions:
- With IHD (without dementia): 40.8 per 1,000 and RR = 2.2;
- With dementia (without IHD): 94.8 per 1,000 and RR = 5.2; and
- With both dementia and IHD: 138.4 per 1,000 and RR = 7.6.
As observed in the general Canadian population, all-cause mortality rates by age group were generally smaller in women than men for all combinations of conditions, but the sex pattern was less consistent when looking at the RRs.
Specifically, in individuals living with dementia (without IHD) (Figure 4a), across all the age groups, there were no significant differences in RRs between sexes. In individuals living with IHD (without dementia) (Figure 4b) and those living with comorbid dementia and IHD (Figure 4c), RRs were generally higher in women than men with the sex differential decreasing across the age groups (i.e. not significantly different in some older age groups).
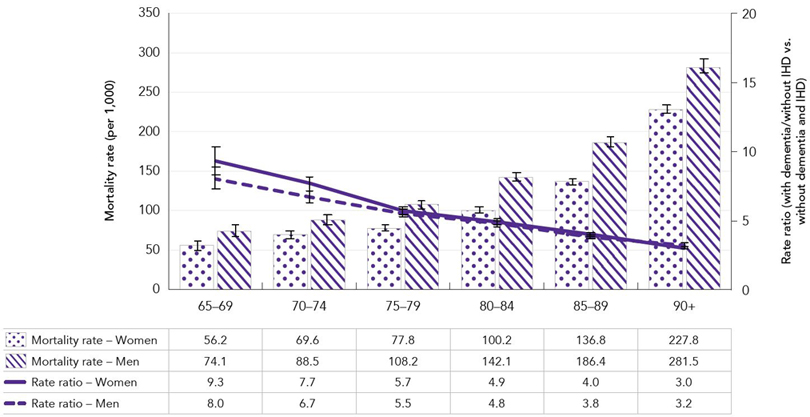
Table 4a footnotes
- Table 4a footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 4a *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 4a - Text description
| Age group (years) | Mortality rate per 1,000 (95% Confidence Interval) | Rate ratio: with dementia/without IHD vs. without dementia and IHD (95% Confidence Interval) | ||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| 65-69 | 56.2 (50.4-62.4) | 74.1 (67.0-81.9) | 9.3 (8.3-10.3) | 8.0 (7.2-8.9) |
| 70-74 | 69.6 (65.3-74.0) | 88.5 (83.1-94.2) | 7.7 (7.2-8.2) | 6.7 (6.2-7.1) |
| 75-79 | 77.8 (74.3-81.4) | 108.2 (103.2-113.4) | 5.7 (5.4-6.0) | 5.5 (5.2-5.8) |
| 80-84 | 100.2 (97.0-103.5) | 142.1 (137.0-147.5) | 4.9 (4.7-5.1) | 4.8 (4.6-5.0) |
| 85-89 | 136.8 (133.4-140.3) | 186.4 (180.4-192.5) | 4.0 (3.8-4.1) | 3.8 (3.6-3.9) |
| 90+ | 227.8 (223.7-231.9) | 281.5 (273.0-290.1) | 3.0 (2.9-3.1) | 3.2 (3.1-3.3) |
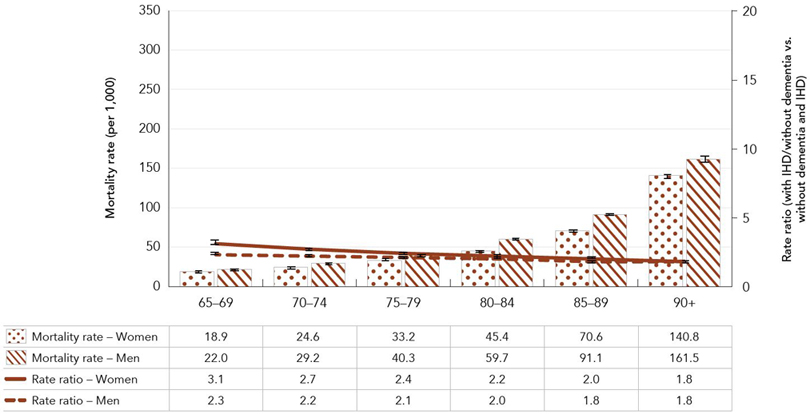
Table 4b footnotes
- Table 4b footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 4b *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 4b - Text description
| Age group (years) | Mortality rate per 1,000 (95% Confidence Interval) | Rate ratio: with IHD/without dementia vs. without dementia and IHD (95% Confidence Interval) | ||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| 65-69 | 18.9 (18.1-19.6) | 22.0 (21.4-22.6) | 3.1 (3.0-3.3) | 2.3 (2.2-2.4) |
| 70-74 | 24.6 (23.8-25.5) | 29.2 (28.5-29.9) | 2.7 (2.6-2.8) | 2.2 (2.1-2.3) |
| 75-79 | 33.2 (32.2-34.1) | 40.3 (39.4-41.2) | 2.4 (2.3-2.5) | 2.1 (2.0-2.1) |
| 80-84 | 45.4 (44.2-46.6) | 59.7 (58.4-61.0) | 2.2 (2.1-2.3) | 2.0 (1.9-2.1) |
| 85-89 | 70.6 (68.9-72.4) | 91.1 (89.1-93.1) | 2.0 (2.0-2.1) | 1.8 (1.8-1.9) |
| 90+ | 140.8 (138.1-143.6) | 161.5 (157.9-165.3) | 1.8 (1.8-1.9) | 1.8 (1.8-1.9) |
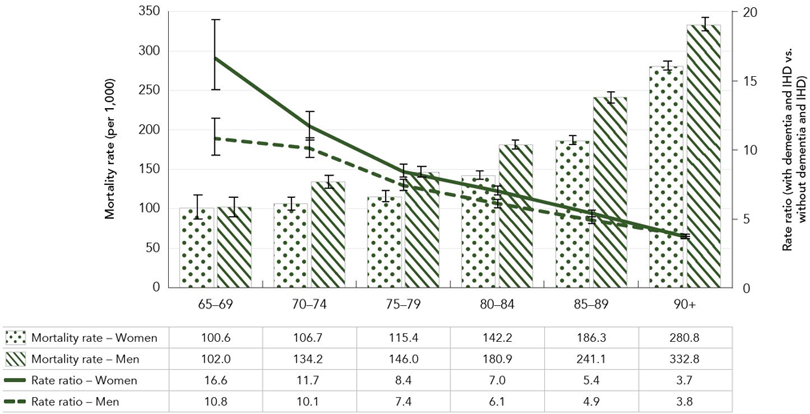
Table 4c footnotes
- Table 4c footnote †
-
To protect data confidentiality and avoid residual disclosure in the original data source, crude prevalence estimates are calculated using randomly rounded counts to an adjacent multiple of 10.
- Footnote 4c *
-
Data from Nunavut and Northwest Territories were not available.
Note: The 95% confidence interval shows an estimated range of values that is likely to include the true prevalence 19 times out of 20.
Source: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed by provinces and territories, February 2021.
Figure 4c - Text description
| Age group (years) | Mortality rate per 1,000 (95% Confidence Interval) | Rate ratio: with dementia and IHD vs. without dementia and IHD (95% Confidence Interval) | ||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| 65-69 | 100.6 (86.0-116.9) | 102.0 (89.9-115.1) | 16.6 (14.2-19.3) | 10.8 (9.5-12.2) |
| 70-74 | 106.7 (98.2-115.9) | 134.2 (125.7-143.1) | 11.7 (10.7-12.7) | 10.1 (9.4-10.8) |
| 75-79 | 115.4 (109.2-121.9) | 146.0 (139.4-152.7) | 8.4 (7.9-9.0) | 7.4 (7.1-7.8) |
| 80-84 | 142.2 (137.0-147.6) | 180.9 (174.9-187.0) | 7.0 (6.6-7.3) | 6.1 (5.8-6.4) |
| 85-89 | 186.3 (181.3-191.4) | 241.1 (234.6-247.7) | 5.4 (5.2-5.6) | 4.9 (4.7-5.1) |
| 90+ | 280.8 (275.6-286.1) | 332.8 (324.3-341.4) | 3.7 (3.6-3.8) | 3.8 (3.6-3.9) |
Conclusion
In 2017–2018, for Canadians aged 65 years and older, 2.8% (or 186,000) were living with both dementia and IHD. In addition, all-cause mortality rates were 7.6 times greater in those with dementia and IHD comorbidity compared to those without the two conditions. The prevalence of dementia and IHD comorbidity increased with age, from 0.2% in those aged 65 to 69 years to 14.2% in those aged 90 years and older.
As Canada's population of adults aged 65 years and older continues to grow rapidly, and since the risk of living with multiple chronic conditions increases with age, comorbidity is an important area of interest for public health. Comorbidity of chronic conditions, like dementia and IHD, can be associated with worse health outcomes, and requires more complex health care management. Ongoing comorbidity surveillance, such as the new data presented in this publication and that of a previous publication on dementia and stroke,Footnote 13 may help to better understand the co-occurrence of conditions and further support related program and services development and planning.
How to learn more about dementia and IHD
- Visit:
- Get data:
- More:
A dementia strategy for Canada: Together we aspire
The national dementia strategy has three objectives: prevent dementia; advance therapies and find a cure; and improve the quality of life of people living with dementia and caregivers.
Surveillance and data is one of the five pillars supporting these objectives. Advancing surveillance of dementia and its comorbidities will offer a more accurate picture of their impact in Canada.
To learn more about the strategy, visit: A dementia strategy for Canada: Together we aspire.
Acknowledgements
This work was made possible through collaboration between PHAC and all Canadian provincial and territorial governments and expert contributions from the CCDSS Neurological Conditions Working Group and the CCDSS Heart Disease Working Group. Results and interpretations reported are those of PHAC. No endorsement by the provinces and territories is intended.
Note
- Note i
-
Estimates were age-standardized to the 2011 Canadian population using five-year age groups. Age-standardized rates are based on non-rounded counts.
References
- Footnote 1
-
Valderas JM, Starfield B, Sibbald B, et al. Defining Comorbidity: Implications for Understanding Health and Health Services. Ann Fam Med. 2009;7(4):357-63. doi: 10.1370/afm.983.
- Footnote 2
-
Public Health Agency of Canada. Dementia in Canada, including Alzheimer's disease [Internet]. Ottawa (ON): Public Health Agency of Canada; [2017 Sept 21; cited 2021 Jan 12]. Available from: www.canada.ca/en/public-health/services/publications/diseases-conditions/dementia-highlights-canadian-chronic-disease-surveillance.
- Footnote 3
-
Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673-734. doi: 10.1016/S0140-6736(17)31363-6.
- Footnote 4
-
Vargas-González J-C, Hachinski V. Insidious Cerebrovascular Disease, The Uncool Iceberg. JAMA neurology. 2020;77(2):155-6. doi:10.1001/jamaneurol.2019.3933.
- Footnote 5
-
Public Health Agency in Canada. Report from the Canadian Chronic Disease Surveillance System: Heart Disease in Canada, 2018 [Internet]. Ottawa (ON): Public Health Agency of Canada; [2018 May 24; cited 2021 Jan 12]. Available from: www.canada.ca/en/public-health/services/publications/diseases-conditions/report-heart-disease-Canada-2018.html.
- Footnote 6
-
Violan C, Foguet-Boreu Q, Flores-Mateo G, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS One. 2014 Jul 21;9(7):e102149. doi: 10.1371/journal.pone.0102149.
- Footnote 7
-
Public Health Agency of Canada. Aging and chronic diseases: A profile of Canadians Seniors [Internet]. Ottawa (ON): Public Health Agency of Canada; [2020 Dec 16; cited 2021 Mar 2]. Available from: www.canada.ca/en/public-health/services/publications/diseases-conditions/aging-chronic-diseases-profile-canadian-seniors-report.html.
- Footnote 8
-
Ofori-Asenso R, Chin KL, Curtis AJ, et al. Recent patterns of multimorbidity among older adults in high-income countries. Popul Health Manag. 2019;22(2):127-137. doi: 10.1089/pop.2018.0069.
- Footnote 9
-
Deckers S, Shievink SH, Rodriquez MM, et al. Coronary heart disease and risk for cognitive impairment or dementia: Systematic review and meta-analysis. PloS one. 2017;12(9):e0184244. doi: 10.1371/journal.pone.0184244.
- Footnote 10
-
Santos CY, Snyder PJ, Wu WC, et al. Pathophysiologic relationship between Alzheimer's disease, cerebrovascular disease, and cardiovascular risk: A review and synthesis. Alzheimers Dement (Amst). 2017;7:69-87. doi: 10.1016/j.dadm.2017.01.005.
- Footnote 11
-
Jaakkimainen R, Bronskill S, Tierney M, et al. Identification of physician-diagnosed Alzheimer's disease and related dementias in population-based administrative data: A validation study using family physicians' electronic medical records. J Alzheimers Dis. 2016;54(1):337-349. doi: 10.3233/JAD-160105.
- Footnote 12
-
Tu K, Mitiku T, Lee DS, et al. Validation of physician billing and hospitalization data to identify patients with ischemic heart disease using data from the Electronic Medical Record Administrative data Linked Database (EMRALD). Can J Cardiol. 2010;26(7):e225-e228. doi: 10.1016/ s0828-282x(10)70412-8.
- Footnote 13
-
Public Health Agency of Canada. Dementia and stroke comorbidity among Canadians aged 65 years and older [Internet]. Ottawa (ON): Public Health Agency of Canada; [2020 Sept 18; cited 2020 Dec 23]. Available from: www.canada.ca/en/services/health/publications/diseases-conditions/dementia-stroke-comorbidity.html.