
Archived - Public health surveillance for the Pan/Parapan American Games

 Download this article as a PDF (1.2 MB - 8 pages)
Download this article as a PDF (1.2 MB - 8 pages) Published by: The Public Health Agency of Canada
Issue: Volume 43-7/8: Outbreak detection
Date published: July 6, 2017
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 43-7/8, July 6, 2017 (July/August Issue): Outbreak detection
Implementation science
Public health surveillance for the Toronto 2015 Pan/Parapan American Games
E Chan1*, K Hohenadel1, B Lee1, M Helferty2, JR Harris2, L Macdonald1,3, T Badiani1
Affiliations
1 Public Health Ontario, Toronto, ON
2 Population and Public Health Division, Ministry of Health and Long-Term Care, Toronto, ON
3 Dalla Lana School of Public Health, University of Toronto, Toronto, ON
Correspondence
Suggested citation
Chan E, Hohenadel K, Lee B, Helferty M, Harris JR, Macdonald L, Badiani T. Public health surveillance for the Toronto 2015 Pan/Parapan American Games. Can Commun Dis Rep. 2017;43(7/8):156-63. https://doi.org/10.14745/ccdr.v43i78a04
Abstract
Background: Public health surveillance for previous Olympic and Paralympic Games have been described in the literature, but surveillance for regional, multisport events on a smaller scale have rarely been explored.
Objective: To describe the public health surveillance planning, implementation, results, and lessons learned from the 2015 Pan/Parapan American Games in Toronto, Ontario, Canada.
Intervention: Public health surveillance planning for the Games began two years in advance and involved local, provincial and federal partners, primarily focusing on infectious disease. From June to August, 2015, enhanced public health surveillance was conducted to support situational awareness and to facilitate the detection of infectious diseases and outbreaks, environmental health hazards and impacts and other major health events.
Outcomes: No major public health incidents occurred that were associated with or a result of hosting the Games. There were two cases of reportable infectious diseases associated with the Games, and 18 public health investigations involving Games-accredited individuals (six related to vaccine-preventable diseases and 12 related to gastrointestinal illnesses or food/water safety violations). Enhanced communication mechanisms, rather than routine and syndromic surveillance systems, were the primary sources of initial notification to surveillance partners on investigations.
Conclusion: Working with its partners, Ontario created a robust public health surveillance system for the 2015 Pan/Parapan American Games. Lessons learned, as well as the relationships and capacity developed through this experience, will be applied towards public health surveillance planning for future events.
Introduction
In July and August 2015, Toronto and 15 neighbouring municipalities in Ontario, Canada hosted the Toronto 2015 Pan/Parapan American Games (referred to collectively as "the Games"), a regional multisport event involving approximately 10,000 athletes and officials representing 41 countries from the Americas. The combined event involved more athletes and competitions than any multisport event ever held in Canada, including the Vancouver 2010 Olympics and Paralympics. During the 2015 Games, which ran from July 10 to 26 for the Pan American Games and August 7 to 15 for the Parapan American Games, about 250,000 spectators and 20,000 volunteers participated in the sporting and associated cultural events Footnote 1Footnote 2.
Like other international multisport events, the Games are a type of planned mass gathering Footnote 3. The goals of the health-related planning for the Games were to mitigate their impact on the Ontario health care system and to protect the health of residents, event participants and visitors. This was a complex effort given the expansive geographic footprint of the Games across southern Ontario. One aspect of this process was public health surveillance planning, which required close collaboration between 15 surveillance partner organizations including the Toronto 2015 Pan/Parapan American Games Organizing Committee (TO2015), the Public Health Agency of Canada, provincial government agencies and ministries, a local public health informatics team, 10 local public health units and public health laboratories.
Many previous international multisport events have also involved significant advanced health planning. Potential public health-specific hazards that have been previously identified include trauma, injury and substance misuse; extreme weather events; chemical, radiological, biological and nuclear threats; and infectious diseases such as food- and waterborne disease, sexually transmitted infections and respiratory infections Footnote 4Footnote 5Footnote 6.
Despite a lack of clear evidence that international multisport events increase the risk of transmission of infectious diseases Footnote 4Footnote 7 these events may increase opportunities for disease transmission because:
- infectious diseases can be imported from visitors' countries of origin;
- susceptible visitors may be exposed to infectious diseases endemic to the host country;
- living arrangements are communal and events can be crowded;
- new, mobile or temporary food vendors and sanitation facilities are brought in; and
- the strain on the health care system may cause delayed responses Footnote 5Footnote 7Footnote 8Footnote 9.
During international multisport events, public health surveillance is intended to identify and quantify—or to reassure in the absence of—public health threats to allow for timely action, if necessary Footnote 5Footnote 8Footnote 10. Enhanced public health surveillance planning and response is not required for all mass gatherings; its usefulness depends on a number of factors: the type of event, geographic area, duration and number of international visitors. The need for enhanced surveillance is also influenced by the nature and comprehensiveness of the existing routine public health surveillance system Footnote 10.
Enhanced public health surveillance systems have been described for several previous Olympic Games Footnote 11Footnote 12Footnote 13Footnote 14; however, smaller-scale, regional, multisport events such as the Pan/Parapan American Games have rarely been explored.
This article describes the Toronto 2015 Pan/Parapan American Games public health surveillance planning, implementation, results, and lessons learned in order to help inform future planning for similar mass gathering events.
Intervention
The primary purpose of public health surveillance for the Pan/Parapan American Games was to support ongoing situational awareness leading up to, during, and immediately following the Games, facilitating the ability to quickly detect sporadic infectious disease activity, outbreak activity, environmental health hazards and impacts, and major health events.
Advance planning
From November 2013 to December 2014, an advance planning group of public health surveillance experts from multiple jurisdictions developed public health surveillance recommendations in Ontario using a consensus approach. The planning group was primarily focused on infectious disease; a separate group was responsible for ensuring food and water safety related to the Games. The group's work involved determining surveillance objectives for each phase (i.e., before/during/after the Games), identifying potential public health threats based on a review of literature and results from a Hazard Identification and Risk Assessment process; reviewing available sources of data and information; and identifying gaps in available sources. Sources were recommended based on an assessment of the threats to be monitored, population covered, timeliness, availability, status (i.e. whether established or needing development) and usage (pre, during or post event). Overarching themes considered in making the recommendations included how the information would meet surveillance objectives and inform public health action. The completed recommendations included strengthening reporting and analysis of established sources; adopting and using additional sources at local levels where available; and acquiring or developing new sources (Table 1).
| Surveillance type | Data or information source (surveillance partners responsible) | Games-specific/Enhanced/Routine surveillance activities |
|---|---|---|
| Event surveillance | Public health coordinator (provincial/Games): A public health professional who was embedded in the polyclinic in the athletes' village | Games-specific: The coordinator worked with the TO2015 medical team to gather and share information and provide support for public health-related issues |
| Surveillance teleconferences (all partners): Held on those days that public health surveillance reports for P/PAG were produced | Games-specific: Calls were used to share and assess situations of potential public health concern, and to help decide which situations would be listed as report highlights | |
| Reportable infectious diseases | iPHIS (provincial): Ontario's infectious disease surveillance and reporting system | Routine: Ran daily aberration-detection algorithms on select diseases Enhanced: Automated production of case counts of reportable diseases by week compared to historical averages; search for P/PAG-related exposures reported in a standardized format in accordance with a Games-specific enhanced surveillance directive |
| Laboratory | PHOL (provincial): Repository of all submissions to Public Health Ontario for laboratory testing and confirmation (excludes testing by hospitals and community laboratories) | Enhanced: Summarized notifications and submissions of Games-related specimens to PHOL for testing |
| Syndromic | Gold Medal System (provincial/Games): System included records of medical encounters with accredited individuals (including athletes, coaches, and officials) when they accessed medical services provided by TO2015 | Games-specific: TO2015 provided aggregate counts for provincial analysis of illness- and infection-related (determined by clinical assessment) medical encounters by day and overall, reporting on increases beyond two standard deviations above a three-day moving average |
| Telehealth Ontario (provincial): A free, confidential telephone service for Ontario's general public to seek health advice or information | Games-specific: Categorized calls across the province into five syndromesFootnote 2 during the Games and completed statistical analyses on these syndromes for potential geographic clusters that were greater than the expected number of calls for the time period and geographic area in question, using a three-year historical baseline; the number of callers with attendance at P/PAG events was available; also assessed call volume by syndrome | |
| ACES (local/provincial analysis by ACES team): System captures data on chief complaints from emergency department visits and all hospital admissions, covering 53 reporting hospitals across 10 local public health units in the Games geographical area Footnote 15 | Enhanced: Real-time analysis of 15 predefined syndromes of interest (e.g. heat-related illness, asthma and gastrointestinal issues). System-generated alerts or deviations over expected seasonal baseline levels were reported | |
| Situational | PHIMS (local/provincial analysis by the ACES team): Online platform displays real-time environmental data (e.g. air quality markers, storm events and temperature stress) along with ACES, demographic, and social deprivation indices on a geographical interface Footnote 16 | Enhanced: PHIMS platform data streams were monitored in the event that at-risk populations might need to be informed or evacuated due to a weather-related emergency or potential terrorist threat |
| International | GPHIN (provincial/federal): Program that uses an automated web-based system to scan newspapers and other communications worldwide for potential indicators of outbreaks. These are then analyzed and rapidly assessed by a multilingual, multidisciplinary team Footnote 17 | Enhanced: Assessed identified events for their potential risk and impact on the Games, with the most relevant or concerning events included in provincial surveillance report following subjective expert review |
Operational planning
A separate working group composed mainly of local and provincial epidemiologists implemented the recommendations. From December 2014 to June 2015, members collaborated to develop processes, schedules, templates and other reference documents for use when conducting surveillance for the Games. Concurrently, each surveillance partner also developed complementary surveillance plans and analyses for their organization, with the opportunity for sharing ideas through the working group. In spring 2015, the group completed three practice runs of the Games surveillance cycle and applied the lessons learned to finalizing the processes and materials.
Public health coordinator
In line with the surveillance recommendations, a Public Health Coordinator acted as a key link between TO2015 and the public health system. Before the Games, the coordinator met regularly with the TO2015 medical team to establish a strong relationship and to understand the processes and infrastructure associated with the Games. During the Games, the coordinator was embedded in the TO2015 medical team working from the polyclinic (a large multidisciplinary clinic) in the main athletes' village. The coordinator developed courses and arranged training on onsite infectious disease reporting and preventive measures; coordinated disease reporting, laboratory communications and requests for scientific/technical advice; participated in outbreak investigations; and extracted TO2015 clinic data for syndromic surveillance.
Surveillance cycle
The working group set the surveillance period for the Games to run from June 17 to August 27, 2015, that is, starting from approximately two weeks before the competitions began until approximately two weeks after the last one. As part of operational planning, the working group developed a schedule of 38 reporting dates within this surveillance period for holding surveillance teleconferences and producing the surveillance report. During the competitions, reporting took place Monday through Friday; whereas reporting was less frequent in the periods before and after competition days, as well as during the break between the Pan/Parapan American Games. The process, activities, responsibilities and timelines for the Games surveillance cycle on a reporting day are outlined in Figure 1.
Figure 1: Daily public health surveillance cycle for the Toronto 2015 Pan/Parapan American Games (June 17—August 27, 2015)
Text description: Figure 1
Figure 1: Daily public health surveillance cycle for the Toronto 2015 Pan/Parapan American Games (June 17—August 27, 2015)
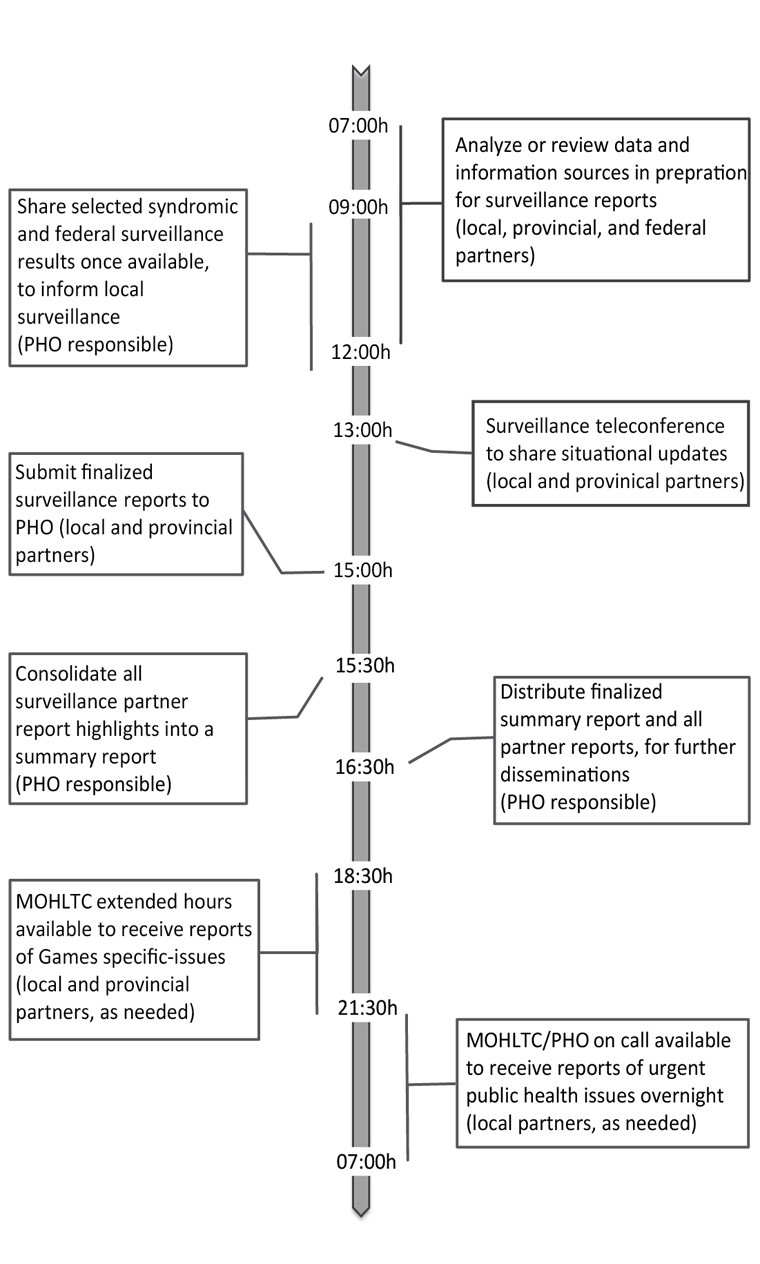
Figure 1 summarizes the daily public health surveillance cycle for the Toronto 2015 Pan/Parapan American Games (between June 17 and August 27, 2015). There are eight steps that occurred in a twenty four hour time span beginning at 07:00 AM.
- Step one occurred between the hours of 07:00 and 09:00; data and information sources were analyzed or reviewed in preparation for surveillance reports.
- Step two occurred between 9:00 and 12:00; once available, selected syndromic and federal surveillance results were shared to inform local surveillance (Public Health Ontario responsible).
- Step three occurred at 13:00; surveillance teleconference took place to share situational updates (Local and provincial partners).
- Step four occurred at 15:00 PM; finalized surveillance reports submitted to Public Health Ontario (local and provincial partners).
- Step five occurred at 15:30 PM; all surveillance partner report highlights consolidated into a summary report (Public Health Ontario responsible).
- Step six occurred at 16:30; finalized summary report and all partner reports distributed, for further dissemination (Public Health Ontario responsible).
- Step seven occurred between 18:30 and 21:30, the Ministry of Health and Long-Term Care provided extended hours to receive reports of Games specific-issues (Local and provincial partners, as needed).
- Step eight occurring between the hours of 21:30 and 07:00, the Ministry of Health and Long-Term Care and Public Health Ontario were on call to receive reports of urgent public health issues overnight (local partners, as needed).
The advanced planning group identified nine data and information sources that met the criteria for Games surveillance at the provincial level (Table 1). For each of the 38 reporting days, Public Health Ontario (an arms-length agency of the Ontario government) produced or distributed reports based on analyses of these sources. Generally, any increases above baseline or clusters/aberrations detected through statistical analysis were included in surveillance reports. Depending on when events were scheduled in their jurisdiction, each of the 10 public health units in the Games footprint produced reports based on surveillance data and information sources available at the local level (e.g. complaint hotlines, food establishment closures, water safety issues, weather alerts) and participated in surveillance teleconferences for a subset of these dates. All other surveillance partners participated throughout the entire surveillance period. The surveillance teleconferences that took place at 1 p.m. (13:00 hours) provided an opportunity for partners to share and assess situations of potential public health concern. A series of questions developed during operational planning (Text box) were used by partners as guiding principles to help determine which situations to include as highlights for their respective surveillance reports and for further dissemination. No rating scale or additional instructions were provided in applying the questions; surveillance partners were free to use the questions in any way that would be helpful for their assessment.
Criteria considered in selecting situations to highlight in surveillance reports for the 2015 Pan/Parapan Games
- Does the issue impact the Games or have the potential to impact the Games?
- Is the issue of public health significance (regardless of whether it is Games related)?
- Does the issue have the potential to have a high public health impact (e.g. pathogen with high potential to cause an epidemic)?
- Is the issue high profile (i.e., is receiving or has the potential to receive media attention)?
- Would other surveillance partners who receive the report benefit from being informed of the issue for their situational awareness?
- Will there be public health action as a result of the issue?
- Is the event usual or unexpected?
- Is there a significant risk of international spread?
After receiving surveillance partner reports, Public Health Ontario compiled local, provincial and national highlights into a summary report. The report was emailed, along with other surveillance reports, back to surveillance partners and was also sent to the Ontario Ministry of Health and Long-Term Care's Emergency Operations Centre for further dissemination.
Outside of this regular schedule, the Ministry Emergency Operations Centre and supporting on-call structures (Figure 1) provided after-hours support throughout the Games surveillance period so that partners could report any immediate, urgent public health incidents.
Disseminating surveillance findings
The Ministry Emergency Operations Centre was active throughout the surveillance period, coordinating situational awareness and response to the Games, including a daily health system communications cycle. This cycle included regularly scheduled calls with a variety of health system partners and culminated in daily situation reports that summarized each day's health system status, risks and actions.
Highlights of the summary surveillance reports were included in the daily situation reports. These situation reports were then shared across the Ontario health system within the geographical areas involved with the Games, including public health units, paramedic and ambulance services, hospitals and primary care. The reports were also disseminated to TO2015 and other non-health planning partners such as the central Provincial Emergency Operations Centre, which coordinates the Ontario government's overall response.
Outcomes
There were no major public health incidents associated with or as a result of hosting the Games. Surveillance partners highlighted 18 local public health investigations. Surveillance partners were initially notified of these investigations through the Public Health Coordinator, surveillance teleconferences and/or the extended hours and on-call processes (Figure 2); only two investigations involved confirmed cases of reportable infectious diseases: an athlete's case of chickenpox and a spectator's case of campylobacteriosis. Twelve of the investigations involved Games-accredited individuals (i.e. athletes, coaches and officials), including six investigations related to vaccine-preventable diseases and 12 related to gastrointestinal illnesses or food/water safety violations (three of these investigations are described in Appendix 1).
Figure 2: Highlighted public health investigations during the Toronto 2015 Pan/Parapan American Games public health surveillance period (June 17—August 27, 2015)

Text description: Figure 2
Figure 2: Highlighted public health investigations during the Toronto 2015 Pan/Parapan American Games public health surveillance period (June 17—August 27, 2015)
| Event (PHU) | Start date | Duration (in days) | Days from start of Games | End date | Number of cases |
Pan/Parapan American Games related? | Category |
|---|---|---|---|---|---|---|---|
| Mumps outbreak | 17-Jun-15 | 16 | 5 | 2-Jul-15 | N/A | no | VPD |
| Mumps investigation | 25-Jun-15 | 12 | 13 | 6-Jul-15 | 1 | no | VPD |
| E.coli cluster | 25-Jun-15 | 1 | 13 | 25-Jun-15 | 3 | no | Enterics |
| GI illness cluster | 30-Jun-15 | 7 | 18 | 6-Jul-15 | 5 | yes | Enterics |
| Varicella case | 8-Jul-15 | 6 | 26 | 13-Jul-15 | 1 | yes | VPD |
| Food safety violations | 9-Jul-15 | 8 | 27 | 16-Jul-15 | N/A | yes | Enterics |
| Boil water order | 13-Jul-15 | 3 | 31 | 15-Jul-15 | N/A | yes | Enterics |
| Norovirus outbreak | 14-Jul-15 | 1 | 32 | 14-Jul-15 | N/A | no | Enterics |
| Foodborne illness complaint | 14-Jul-15 | 2 | 32 | 15-Jul-15 | 1 | yes | Enterics |
| GI illness cluster | 20-Jul-15 | 4 | 38 | 23-Jul-15 | N/A | yes | Enterics |
| Mumps investigation | 21-Jul-15 | 3 | 39 | 23-Jul-15 | 1 | yes | VPD |
| GI illness cluster | 22-Jul-15 | 6 | 40 | 27-Jul-15 | N/A | yes | Enterics |
| Rubella investigation | 28-Jul-15 | 1 | 46 | 28-Jul-15 | 1 | no | VPD |
| Pertussis case | 28-Jul-15 | 3 | 46 | 30-Jul-15 | 1 | no | VPD |
| Campylobacteriosis cases | 30-Jul-15 | 1 | 48 | 30-Jul-15 | 2 | yes | Enterics |
| Foodborne illness complaint | 10-Aug-15 | 3 | 59 | 12-Aug-15 | 1 | yes | Enterics |
| GI illness cluster | 12-Aug-15 | 3 | 61 | 14-Aug-15 | 7 | yes | Enterics |
| Foodborne illness complaint | 17-Aug-15 | 2 | 66 | 18-Aug-15 | N/A | yes | Enterics |
The results of provincial-level surveillance activities by data and information source are summarized in Table 2. Syndromic surveillance systems did not identify any trends, clusters or other alerts that initiated or corresponded with any of the investigations reported by public health units. Although exposures and confirmed cases were reported through the reportable infectious disease information system, data entry occurred after the information had already been shared through the Games surveillance reporting process. In general, provincial-level surveillance was largely supportive in nature and provided situational awareness.
| Data/information source(s) | Surveillance results |
|---|---|
| Public health coordinator | Two individuals shared the role of providing rotating support over 44 days in the Athletes' Village Sixteen requests for public health support received |
| Surveillance teleconferences | A total of 38 surveillance teleconferences held with participation from up to 14 partner organizations, corresponding with each surveillance report production day |
| iPHIS | Four Games-related exposures reported in association with reportable disease investigations, resulting in two confirmed cases: a chickenpox case in a P/PAG athlete and a campylobacteriosis case in a spectator with foodborne exposure from an unknown food vendor |
| PHOL | Five notifications on incoming specimens to the P/PAG response phone number Nine Games-related specimens received for laboratory testing |
| Gold Medal System Footnote 1 | A total of 7,677 medical encounters were reported based on medical services provided by TO2015 to P/PAG-accredited individuals. Of these, 1,940 were illness-related (of these, 376 were infection-related) A total of 197 of infection-related medical encounters affected the respiratory system |
| Telehealth Ontario | A total of 75,547 calls from across Ontario during the surveillance period, with volumes highest for gastrointestinal syndrome (5,283 calls) and respiratory syndrome (4,195 calls) A total of 130 temporal-spatial clusters of public health interest detected across Ontario; the most common clusters of interest were for respiratory syndrome (46 clusters), followed by rash syndrome (34 clusters) and gastrointestinal syndrome (29 clusters) Eight callers from the detected clusters reported attending a P/PAG-related event |
| ACES and PHIMS | A total of 19 ACES syndromes and numerous PHIMS environmental indicators were monitored |
| GPHIN | A total of 237 events worldwide assessed with potential risk and impact to Games; 52 of these events further assessed as possibly having impact on the Games |
Discussion
Public health surveillance during the 2015 Pan/Parapan American Games in Toronto identified no major public health incidents that were associated with, or as a result of, hosting the Games. The lack of major incidents was not surprising given similar experiences from previous summer Olympic and Paralympic Games Footnote 11Footnote 12Footnote 13Footnote 14 Canada's well-established public health infrastructure, results from the Hazard Identification Risk Assessment, and the profile of visitors to the Pan/Parapan Games Footnote 18.
Performance of surveillance system
Syndromic surveillance systems are intended to provide rapid yet unspecific data as a complement to traditional surveillance systems, to enable early identification and intervention for potential public health threats Footnote 19. The provincial-level syndromic surveillance data sources used during the Games did not produce the initial notifications or alerts that triggered the highlighted public health investigations; nor were these alerts corroborated by the other data and information sources used for Games surveillance. Although alerting thresholds were developed as part of the planning process for the Games, limited prior experience in using these data sources and/or applying them for syndromic surveillance meant that these criteria were largely based on subjective expert input, and their usefulness had not been previously validated. When preparing new syndromic surveillance data sources or methods for future mass gathering events, sufficient time for training, practice and gathering of baseline data and trends should be allowed.
On the other hand, surveillance partners have had extensive experience with Ontario's routinely used reportable infectious disease information system, where reported cases must meet routine provincial case definitions. However, the time required to meet these criteria meant that initial notification of infectious disease case investigations during the Games arose through other sources. From our experience, a reportable disease surveillance system serves best as a historical record for details on Games-associated reportable disease cases and to understand baseline incidence.
The enhanced communication mechanisms (including the Public Health Coordinator, surveillance teleconferences, and extended hours/on-call process) implemented for Games were the primary sources of initial notification to surveillance partners on new investigations. Developing relationships, and new or enhanced communication mechanisms during planning phases, proved to be the most effective methods for providing timely and relevant updates to inform public health action. This experience further supports the importance of having processes and people in place to rapidly communicate potential public health threats and support public health action, a point often made in mass gatherings surveillance literature Footnote 7Footnote 10Footnote 13.
Lessons learned
The local public health units across the Games footprint had various levels of involvement with the Games, which led to planning challenges in balancing flexibility and consistency. Although efforts were made to accommodate variations in local systems, some public health units requested further provincial guidance and a standard surveillance report template. Another challenge was balancing a comprehensive approach with sustainability of activities. Planning and implementing the surveillance cycle throughout the Games had significant resource implications for all surveillance partners, with the commitment being particularly burdensome for public health units with few events.
The planning structure for the Games involved a separate planning process for food and water safety. Public health units and other health system partners were unsure of the appropriate forum for reporting food handling and water safety issues at venues, especially in the absence of any reported illness. As a result, such issues were inconsistently reported through various channels. The relationship between surveillance and other reporting structures could have benefited from more clarity and integration. During a mass gathering, an environmental health surveillance system that is integrated with the rest of the public health surveillance cycle could better facilitate timely public health interventions Footnote 20.
Over the course of the Games surveillance cycle, reaction to the disseminated public health surveillance information highlighted a knowledge gap between health partners and non-health partners (e.g. Games organizers; fire, police and intelligence services; other government ministries involved with the events such as transportation). Non-health partners who received surveillance reports often did not know what types of infectious diseases can be expected during the summer in Ontario; they occasionally needed to be reassured that the situations being reported were manageable through routine follow-up. In future, public health partners who disseminate surveillance information should be diligent in providing the necessary context and interpretation in reports and other pre-Games communications to help non-health partners understand the appropriate level of response for the reported situations.
Conclusion
Public health surveillance for the Toronto 2015 Pan/Parapan American Games provided situational awareness and reassured organizers, government partners and the media, thus fulfilling an important role. In carrying out these activities, we have learned that Ontario can provide efficient and sustainable support to future mass gathering events. Support for future events should involve continuing with Ontario's well-developed routine surveillance activities as well as ensuring that enhanced communication mechanisms are in place. Particular attention must be paid to integrating food and water safety into the communication channels and ensuring that non-health partners understand the context and implications of the updates presented. Moving forward, staff from all surveillance partner organizations can apply the relationships and capacity gained through their involvement with the Games to more efficiently support mass gathering events across the province, large and small. As technologies advance, new and evolving surveillance methods and sources such as crowd-sourced or participatory surveillance initiatives may be used for future events.
Authors' statements
- BL, TB, MH, JRH - advance planning group members (methodology)
- EC, KH, BL, TB, MH, JRH - operational planning and implementation of public health surveillance for the Games (methodology)
- BL, EC - software, validation, formal analysis
- EC, KH - data collection and curation, investigation
- BL, EC, KH - visualization
- EC, KH, BL, TB, MH, JRH - writing-original draft
- All authors - conceptualization, writing-review/editing
Conflict of interest
None.
Acknowledgements
We thank the following groups and individuals for their work in developing and carrying out the surveillance strategy for the Pan/Parapan Am Games: Surveillance Working Group; Surveillance Operationalization Working Group; Toronto 2015 medical team; at Public Health Ontario: Vicky Springmann, Ryan Walton, Morgan Barnes, Surveillance Services team, Communicable Diseases, Emergency Preparedness and Response department, Public Health Ontario Laboratory; at the Ministry of Health and Long-Term Care: Sarah Levitt and Marcilyn Cianfarani.
We would like to thank Dr Brian Schwartz for his review of this article, and Adam van Djik, Alex Marchand-Austin, Andrea Van Der Voort, Carole Craig, Gregory Kujbida, Dr Jessica Hopkins, Lise Trotz-Williams, Monali Varia, Philip Abdelmalik, Ruth Diaz-Chambers, Scott Cholewa, Shanna Hoetmer and Tony Camara for reviewing sections of this paper.
Funding
This work was supported by Public Health Ontario and the Ontario Ministry of Health and Long-Term Care as part of operational activities.