
ARCHIVED - Chronic Diseases and Injuries in Canada
Volume 31, no. 4, September 2011
Chronic Diseases and Injuries in Canada
Online resources to enhance decision-making in public health – Cross-Canada Forum
D. Finkle-Perazzo, MA (1); N. Jetha, MPH (in progress) (2)
https://doi.org/10.24095/hpcdp.31.4.06
- Wordsmith Writing and Editing Services, Ottawa, Ontario, Canada
- Public Health Agency of Canada - Evidence and Risk Assessment Division, Ottawa, Ontario, Canada
Correspondence: Nina Jetha, Manager, Canadian Best Practices Initiative, Public Health Agency of Canada, 7th Floor, 785 Carling Avenue, AL 6807B, Ottawa ON K1A 0K9; Tel.: (613) 952-7608; Email: nina_i_jetha@phac-aspc.gc.ca
This article has been peer reviewed.
Introduction
A virtual front door, the Canadian Best Practices Portal for Health Promotion and Chronic Disease Prevention (“the Portal”) provides access to evaluated community and population health interventions relevant to chronic disease prevention and health promotion.(1) Designed to help Canadian public health practitioners and decision makers identify suitable interventions that they can adapt and replicate to meet their needs, the Portal is a highly accessible, easy to use and dynamic.(1) It has a flexible search function and is supported by an extensive array of resources to inform policy and practice.(1)
Launched in 2006, the Portal forms a central pillar of the Canadian Best Practices Initiative, which was established by the Public Health Agency of Canada (PHAC) to improve policy and program decision-making by enabling access to the best available evidence on chronic disease prevention and health promotion practices.(1) Throughout each phase of the Portal’s development, more and more current public health topics and new decision-making tools have been added. As of February 2011, the Portal provides information on about 357 interventions and access to 58 resources.
In this article, we aim to demonstrate the unique role of the Portal within the broader context of other available online resources. We use the concept of a “pyramid of evidence”(2) to compare the Portal with one specific resource, Health-evidence.ca, to illustrate how public health practitioners and decision makers can use these resources together to make better, more evidence-informed decisions.
Evidence-informed decision-making within the public health sector in Canada
A key recommendation of the final report of the National Forum on Health, Canada Health Action: Building on the Legacy, was to develop an evidence-informed health care system where high quality research influences policies and clinical decisions.(3) Since then, there has been a significant effort to promote evidence-informed health practices and to establish resources for knowledge transfer in both the clinical and the health promotion settings.
Nevertheless, the public health sector in Canada still faces significant barriers to making evidence-informed decisions.(4) Obstacles include individual barriers, such as lack of time and skill; organizational barriers, such as a lack of human resources; no clearly communicated values for evidence-informed decision-making (EIDM); lack of input from all levels of the organization; lack of leadership and champions; and inadequate resources and infrastructure to promote and support EIDM.(4)Decision makers also have an ongoing need for better access to systematic reviews so that their decisions are relevant and applicable to the “real world” practice setting.(5)
Improving the process of evidence-informed decision-making
The process of EIDM involves translating the best available evidence from a “systematically collected, appraised, and analyzed body of knowledge”(6) in a four-step process described by Robeson et al. as follows:
“1) clearly articulating a practice-based issue; 2) searching for and accessing relevant evidence; 3) appraising methodological rigour and choosing the most synthesized evidence of the highest quality and relevance to the practice issue and setting that is available; and 4) extracting, interpreting, and translating knowledge, in light of the local context and resources, into practice, program and policy decisions.”(4)
While the need to address the individual and organizational barriers to advancing and sustaining EIDM remains,(4) a recent proliferation of online resources provides decision makers with a range of high quality research. For example, PHAC also launched the Canadian Taskforce on Preventive Health Care to develop clinical practice guidelines that support primary care providers in delivering the best possible preventive health care.(7)Other Canadian sites include Health-Evidence.ca , which is partly funded by PHAC, as well as the Public Health Plus website[*] from the National Collaborating Centre for Methods and Tools .(8)Other sites include the Guide to Community Preventive Services website[†] from the Centers for Disease Control and Prevention, Cancer Control P.L.A.N.E.T. [‡] and The Cochrane Library .[§] Each of these offers different categorizations and levels of evidence on effective public health practice, with various focal points. Several are searchable databases that provide a wide range of information and often require training in search techniques. As a result, they can be daunting to those with limited time and expertise.
Dicenso et al. proposed a pyramid of pre-processed research evidence that can reduce the time spent finding synthesized research evidence to inform policy and practice.(2) The shape encourages the search for evidence to begin at the top of the pyramid. This holds the most synthesized evidence whereas the bottom holds evidence in its most raw form. Many users generally start their search the other way around, with the most raw information, which can be very overwhelming. In many cases, they stumble upon more highly synthesized evidence only by chance.(4)
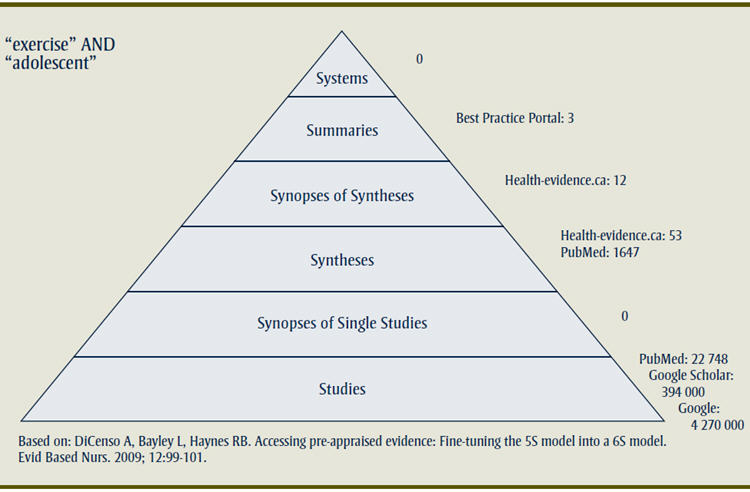
Figure 1 shows DiCenso’s pyramid of evidence using the example of a search focused on the issue of exercise and adolescents.
Figure 1
A pyramid of pre-processed research evidence focused on the issue of exercise and adolescents
Text Equivalent of Figure 1
Figure 1 shows DiCenso’s pyramid of evidence using the example of a search focused on the issue of exercise and adolescents. DiCenso’s pyramid of evidence identifies resources at six levels of evidence. In general, resources provided by the Portal fall within the category of “syntheses” or “studies”.
- [*] http://www.nccmt.ca/tools/public_health_plus-eng.html
- [†] http://www.thecommunityguide.org/index.html
- [‡] http://cancercontrolplanet.cancer.gov/
- [§] http://www.thecochranelibrary.com/view/0/index.html
The Canadian Best Practices Portal
The Canadian Best Practices Initiative(1) was the outcome of five years of Health Canada-funded work by Michael Goodstadt and Barbara Kahan at the University of Toronto. Their work led to the development of the Interactive Domain Model (IDM) Best Practices[**] and, ultimately, the Canadian Best Practice System for Chronic Disease Prevention and Control.(9)
The Canadian Best Practices Portal was born of these initiatives. Its key purpose is, quite simply, to help public health decision-makers make better decisions. The Portal is built upon the population-health approach, which recognizes that health is a capacity or resource rather than a state, a definition that corresponds more to the notion of being able to pursue one's goals, to acquire skills and education, and to grow. This broader notion of health recognizes the range of social, economic and physical environmental factors that contribute to health. The best articulation of this concept of health is “the capacity of people to adapt to, respond to, or control life's challenges and changes.”(10)
Over the years, the Portal has steadily grown to include more current public health topics and new decision-making tools. Its search function is designed to help public health decision-makers identify interventions that meet their particular needs.
- [**] http://www.idmbestpractices.ca/idm.php
Key features of the Canadian Best Practices Portal
The Portal includes a searchable database of evaluated community and population health interventions that can be replicated and adapted for use in similar fields. This can be a real time-saver for program and policy development and evaluation. Acting as a single point of access to evidence-informed best practices, the Portal makes public health planning easier and more efficient. Interventions are categorized by chronic disease/condition, health promotion topics, behaviour-related risk, strategy, population, determinants of health, country of origin and language. Searches can combine any of these categories and can be further narrowed by setting or by keywords. The information on interventions is well organized and easy to use. In the case where two or more interventions could be applicable, definitions described in a hierarchy of evidence(11) help users assess both qualitative and quantitative research evidence.
The interventions included in the Portal have all been consistently and rigorously screened through a comprehensive set of selection criteria that consists of six key steps:
- Literature and collection search by priority topic;
- Assessment of quality of evaluation or study design;
- Search for additional information on selected individual interventions;
- Expert review using inclusion criteria;
- Prioritization of selected interventions for annotation; and
- Selection of resources.
This intensive screening process ensures that Portal content is made up of best practices (supported by systematic reviews and experimental designs) and promising practices (supported by quasi-experimental design and/or observational studies). However, it is important to note that the scientific quality of evidence in the Portal varies due to differences in the evaluation approaches used by the interventions.(12) (More information on the selection and screening process is available elsewhere.(13))
The Portal also includes a selection of resources that help practitioners reach their public health planning, chronic disease prevention and health promotion goals. The resources—websites, documents, systematic reviews, databases, manuals and online tutorials—have been selected based on their specific ability to assist Portal users in making evidence-informed decisions. They are organized according to the National Collaborating Centre for Methods and Tools’ seven steps of evidence-informed public health.(14)
Health-evidence.ca
Dr. Maureen Dobbins at McMaster University established the Health-evidence.ca project to promote ongoing collaboration between the research community and the decision-making and practice setting. This initial goal evolved over the years to include an emphasis on facilitating the adoption and implementation of effective policies/programs/interventions at the local and regional public health decision-making levels across Canada.(15)
Health-evidence.ca is provided at no cost to users; despite that, it exists without any permanent funding and has received funding from a variety of agencies.(15) It offers a searchable online registry of systematic reviews about the effectiveness of public health and health promotion interventions. The registry is one part of a much larger and more comprehensive knowledge transfer and exchange site that will support users in accessing and interpreting research evidence. This approach connects users across Canada (and internationally) who work in similar areas or have similar interests.(15)
Key features of Health-evidence.ca
Users of Health-evidence.ca are able to manage and tailor the information they receive to their particular areas of interest. Usability is also enhanced by a searchable registry that recognizes commonly used public health and health promotion terms and categories (e.g. focus of the intervention, intervention strategy, intervention location, and target population).(15)
The reviews provided by Health-evidence.ca have been assessed using a rigorous process that includes an examination of methodological quality and ratings by two independent reviewers. Users are able to sort search results by the level of review quality (e.g. strong, moderate or weak). Built-in feedback links also request input on how to improve the site.(15)
What is the difference between the Portal and Health-evidence.ca?
The key difference between the Portal and Health-evidence.ca is that the former provides more information about actual interventions and resources while the latter focuses on the effectiveness of interventions and presents only pre-appraised and pre-synthesized information via systematic reviews.
DiCenso’s pyramid of evidence identifies resources at six levels of evidence. In general, resources provided by the Portal fall within the category of “syntheses” or “studies.”(2)(see Figure 1). In contrast, Health-evidence.ca’s resources can be categorized as “syntheses” that combine (using explicit and rigorous methods) the results of multiple single studies to provide a single set of findings, with some “synopses of syntheses.”(2)
Resources from the Portal are pre-screened to meet certain inclusion criteria, and resources from Health-evidence.ca are both pre-screened and pre-appraised (filtered to include only those studies of the best quality). Both these sources are also updated regularly so that the evidence is current.
The services and information provided through Health-evidence.ca overlap with those of the Portal, in that both focus on health promotion. However, Health-evidence.ca also addresses broader public health issues, such as immunization and emergency preparedness.(16)
How decision-makers can make the most of the Portal and other online resources such as Health-evidence.ca
By partnering with Health-evidence.ca, Portal searches are now supported by published systematic reviews that evaluate the effectiveness of public health interventions. Systematic reviews synthesize all the research that exists about an intervention and provide a much better understanding of the effectiveness of an intervention than do single studies.
Consider the example of a busy local public health planner who is charged with developing an exercise program for adolescents. An initial step would be to seek other, relevant programs that might be adapted, thereby saving valuable time and resources. Most planners would probably begin looking for information by conducting a web search. However, the terms “exercise” and “adolescent,” for example, would generate 4 270 000 hits using the Google search engine, 394 000 hits using the Google Scholar search engine and 22 748 hits using the PubMed database. It is quite likely that this amount of information would be both overwhelming and extremely discouraging.
In contrast, using Health-evidence.ca as a starting point, the same terms (“exercise” and “adolescent”) lead to 102 articles that can be sorted according to their date of publication or strength of evidence. Alternatively, consulting the Portal produces the list of programs/intervention shown in Figure 2.
Figure 2: Results of a Canadian Best Practices Portal search on exercise programs for adolescents| Title | Intervention Characteristics | Evaluation Methodology/Design |
|---|---|---|
| Jump Into Action | |
Quantitative |
| The Fourth R: Skills for Youth Relationships |
|
Quantitative |
| Youth Fit for Life (RTIPS) | |
Quantitative |
Let’s say that the planner decides to investigate “Jump into Action.” Clicking on the intervention title opens a page that provides a description of the program, a link to the intervention site, additional web links, and other details such as country of origin, evaluation design, language and the primary source document. Following this process, the planner efficiently finds 15 high quality resources that increase the potential of developing a better quality, more targeted intervention.
Conclusion
There are many important contextual factors to consider when planning programs for health promotion and chronic disease prevention, such as the breadth of research support, the applicability of the evidence in a variety of settings, political and economic factors, and the general feasibility of the intervention.(11) However, above all, front-line health practitioners and decision makers working in public health need efficient and easy access to good quality information to make better, more informed decisions about the services and programs they offer.
Although planners appreciate the importance of evidence, many are daunted by the process of analyzing and reviewing evidence to ensure that the programs they study are effective. Fortunately, Canadian planners can use a variety of resources that offer access to public health reviews and interventions. By using a hierarchical pyramid-of-evidence approach, planners can quickly access the high quality evidence needed to build the best possible programs.
Acknowledgements
The authors would like to acknowledge with thanks, the invaluable advice provided by Dr. Donna Ciliska, professor at McMaster University and Scientific Director at the National Collaborating Centre for Methods and Tools.
References:
- About the Canadian Best Practices Portal [Internet]. Ottawa (ON): Public Health Agency of Canada; [cited 2011 Apr 26]. Available from: http://cbpp-pcpe.phac-aspc.gc.ca/about/portal-eng.html
- DiCenso A, Bayley L, Haynes RB. Accessing pre-appraised evidence: Fine-tuning the 5S model into a 6S model. Evid Based Nurs. 2009;12:99-101.
- National Forum on Health. Canada health action: building on the legacy – Volume 1 – The final report [Internet]. Ottawa (ON): Health Canada; 1997 [cited 2011 Apr 26]. Available from: http://www.hc-sc.gc.ca/hcs-sss/pubs/renewal-renouv/1997-nfoh-fnss-v1/index-eng.php
- Robeson P, Dobbins M, DeCorby K, Tirilis D. Facilitating access to pre-processed research evidence in public health [Internet]. BMC Public Health. 2010 [cited 2011 Apr 26];10:95. Available from: http://www.biomedcentral.com/content/pdf/1471-2458-10-95.pdf
- Dobbins M, Jack S, Thomas H, Kothari A. Public health decision-makers’ informational needs and preferences for receiving research evidence [Internet]. Worldviews Evid Based Nurs. 2007 [cited 2011 Apr 26];4(3):156-63. Available from: http://health-evidence.ca/downloads/Dobbins2007Public_Health_Decision-Makers_Informational_Needs.pdf
- Brownson RC, Fielding JE, Maylahn CM. Evidence-based public health: a fundamental concept for public health practice. Annu Rev Public Health. 2009;30:175-201.
- Canadian Task Force on Preventive Health Care. [Internet]. Ottawa (ON): Public Health Agency of Canada; 2011 [cited 2011 Apr 26]. Available from: http://www.canadiantaskforce.ca/index.html
- Welcome to National Collaborating Centre for Methods and Tools [Internet]. Hamilton (ON): National Collaborating Centre for Methods and Tools; [cited 2011 Apr 26]. Available from: http://www.nccmt.ca/index-eng.html
- Public Health Agency of Canada. Population health in Canada: a working paper [Internet]. Ottawa (ON): PHAC; 2001 [cited 2011 Apr 26]. Available from: http://www.phac-aspc.gc.ca/ph-sp/docs/social-sociale/define-eng.php
- Frankish CJ, Green LW, Ratner P A, Chomik T, Larsen C. Health impact assessment as a tool for health promotion and population health. (1996) Report for Health Canada: Ottawa.
- Jackson SF, Fazal N, Giesbrecht N. A hierarchy of evidence: which intervention has the strongest evidence of effectiveness? [Internet]. Ottawa (ON): Public Health Agency of Canada; 2008 [cited 2011 Apr 26]. Available from: http://cbpp-pcpe.phac-aspc.gc.ca/pubs/hierachy_of_evidence.pdf
- Dubois N, Jetha N, Robinson K, Szuto I, Wan G, Wilkerson T. Canadian Best Practices Initiative methodology background paper [Internet]. Ottawa (ON): Public Health Agency of Canada; 2008 [cited 2011 Apr 26]. Available from: http://cbpp-pcpe.phac-aspc.gc.ca/pubs/CBPI-methodology.pdf
- X3 Understanding how interventions are chosen: summary of search, selection and inclusion process and criteria. [Internet]. Ontario (ON): Public Health Agency of Canada; [cited 2011 Apr 26]. Available from: http://cbpp-pcpe.phac-aspc.gc.ca/selection-eng.html
- National Collaborating Centre for Methods and Tools. Evidence-informed public health: [Internet]. Hamilton (ON): National Collaborating Centre for Methods and Tools; 2009 [cited 2011 Apr 26]. Available from: http://www.nccmt.ca/eiph/index-eng.html
- Health-evidence.ca. About Us. [Internet]. Hamilton (ON): McMaster University; c2003 [cited 2011 Apr 26]. Available from: http://health-evidence.ca/html/AboutUs
- Daghofer D. The value-added investment of the Canadian Best Practices Portal to the Public Health Agency of Canada. Ottawa (ON): Public Health Agency of Canada; 2008.