
Environmental factors associated with autism spectrum disorder: a scoping review for the years 2003-2013 - HPCDP: Volume 37-1, January 2017
Health Promotion and Chronic Disease Prevention in Canada
Navigate This Article
Volume 37 · Number 1 · January 2017
Environmental factors associated with autism spectrum disorder: a scoping review for the years 2003-2013
Michelle Ng, MPHFootnote 1. ,Footnote 2. ; Joanne G. de Montigny, MHAFootnote 3. ; Marianna Ofner, PhDFootnote 1. ,Footnote 2. ; Minh T. Do, PhDFootnote 1. ,Footnote 2.
https://doi.org/10.24095/hpcdp.37.1.01
This article has been peer reviewed.
Author references:
Correspondence: Minh T. Do, Surveillance and Epidemiology Division, Public Health Agency of Canada, 785 Carling Ave., Ottawa, ON K1A 0K9; Tel: 613-946-6958; Email: Minh.T.Do@phac-aspc.gc.ca
Abstract
Introduction: The number of children diagnosed with autism spectrum disorder (ASD) has been rapidly rising in the past decade. The etiology of this disorder, however, is largely unknown, although the environmental relative to the genetic contribution is substantial. We conducted a scoping review to comprehensively assess the current state of knowledge of the environmental factors present from preconception to early life associated with ASD, and to identify research gaps.
Methods: We searched electronic databases MEDLINE, PsycINFO and ERIC for articles on potential risk factors or protective factors from the physical and social environments associated with ASD and its subclassifications published between 1 January, 2003, and 12 July, 2013. We categorized articles into broad themes: chemical, physiological, nutritional and social factors, based on environmental exposure.
Results: We identified over 50 000 publications, but after ineligible studies were screened out, 315 articles remained. Most of these studies examined physiological factors, followed closely by chemical factors, and to a much lesser extent, nutritional and social factors, associated with ASD. Despite a vast literature and many heterogeneous studies, several risk factors emerged consistently: chemical factors such as traffic-related air pollutants; physiological factors including advanced parental age, preterm birth, low birth weight, hyperbilirubinemia and clustering of pregnancy complications; and maternal immigrant status. Despite extensive research on vaccines, findings overwhelmingly demonstrate no support for an association with ASD.
Conclusion: The lack of consistency, temporality and specificity of associations between environmental factors and ASD remains the largest barrier to establishing causal relationships. More robust research is required to resolve inconsistencies in the literature. Future research should explore underlying mechanisms of associations between the risk factors that we identified and ASD.
Keywords: ASD, autism spectrum disorder, autism, environmental exposure, etiology
Highlights
- The environmental factors most commonly studied in association with ASD were physiological and chemical factors. Research on nutritional and social factors is limited.
- Older parental age, low birth weight, premature birth, neonatal jaundice and clustering of pregnancy complications were consistently reported to be associated with ASD.
- Evidence for the association between traffic-related air pollutants and ASD has been emerging.
- Maternal immigrant status was consistently associated with ASD.
- The lack of consistency, temporality and specificity of associations between environmental factors and ASD remains the largest barrier to establishing causal relationships.
Introduction
Autism spectrum disorder (ASD) is a group of neurodevelopmental disorders with varying levels of severity in impairment in social communication and interaction, and restricted repetitive behaviours, interests and activities.Footnote 1 The number of children with ASD has been rapidly rising in the past decade.Footnote 2 In the US, the number of cases increased by 123% from 2002 to 2010, with an estimated prevalence of 1 in 68 children aged 8 years.Footnote 3 In Canada, from 2003 to 2010, increases of 70% and 95% were reported in Prince Edward Island and Southeastern Ontario, respectively, with corresponding prevalence of 1 in 106 and 1 in 63 children aged 6 to 9 years in 2010.Footnote 4 Greater ASD awareness and changes in diagnostic criteria may be contributing factors,Footnote 5 but explain only a portion of the increased prevalence.Footnote 6Footnote 7 Although the genetic contribution to the etiology of ASD is known,Footnote 8 the rapid increase in ASD prevalence cannot be fully attributed to genetics alone.
A twin concordance study has shown that shared environmental factors account for 58% of the variance in liability for ASD.Footnote 8 Furthermore, prenatal and early infancy periods are known to be critical periods of growth during which children are particularly vulnerable to harmful effects of environmental hazards that can result in childhood diseases.Footnote 9 However, the role of environmental factors in the onset of ASD is still largely unknown. Of the reviews that have explored possible risk factors of ASD to date,Footnote 10Footnote 11Footnote 12Footnote 13Footnote 14Footnote 15Footnote 16 none have comprehensively examined the entire scope of the environmental contribution to ASD.
The purpose of this scoping review is to comprehensively assess the current state of knowledge of environmental factors associated with ASD incidence and to identify research gaps. Specifically, we aim to identify any environmental exposures, including chemical, physiological, nutritional and social factors, from preconception to early-life periods associated with ASD.
Methods
This review followed Arksey and O'Malley's scoping framework.Footnote 17 We searched the electronic databases MEDLINE, PsycINFO and ERIC for primary studies or reviews on potential modifiable risk factors or protective factors from the physical or social environment associated with ASD. We developed a comprehensive list of medical subject headings and keywords with the help of a librarian at the University of Ottawa. Search terms were centred on two main concepts: (1) ASD and its subclassifications, including pervasive development disorder not otherwise specified (PDD-NOS), autism and Asperger syndrome; and (2) environmental exposures or risk factors, maternal condition before or during pregnancy, and paternal preconception condition. The search strategy was adapted appropriately to the other databases, PsycINFO and ERIC, using their corresponding subject heading terms. Searches were limited to articles with an abstract published in the English language with a publication date between 1 January, 2003, and 12 July, 2013, to focus on current literature. We excluded articles if the epidemiological associations they described included comorbidities, the result of living with ASD or biochemical pathways not directly related to etiology; we also excluded studies that used animal models, cell studies and strictly genetic studies. Commentaries, editorials, letters, news articles and articles that did not primarily focus on ASD etiology were also filtered out.
We categorized journal articles into broad themes: chemical, physiological, nutritional, social and other, based on the nature of the environmental exposure examined. Within each broad theme, we identified recurring subthemes. We abstracted publication year, study design, study population, exposure, confounders, case definition and main findings from each full-text article. The review process resulted in 315 articles for final analysis (Figure 1). Our review focussed mainly on primary studies and systematic reviews.
Figure 1
Process for searching and screening research on autism spectrum disorders found in three electronic databases, published between 2003 and 2013

Text Equivalent - Figure 1
This figure depicts the process for searching and screening research on autism spectrum disorders found in three electronic databases (MEDLINE, PsycINFO and ERIC), published between 2003 and 2013.
In this figure, journal articles were categorized into broad themes: chemical, physiological, nutritional, social and other, based on the nature of the environmental exposure examined. Within each broad them, we identified recurring subthemes. We abstracted publication year, study design, study population, exposure, confounders, case definition and main findings from each full-text article.
Search filters were applied to screen for eligibility. Subsequently, duplicates were removed, and various levels of screening were conducted in order to exclude articles that were out of scope or did not correspond to the eligibility criteria.
The review process resulted in 315 articles for final analysis. Our review focussed mainly on primary studies and systematic reviews.
Results
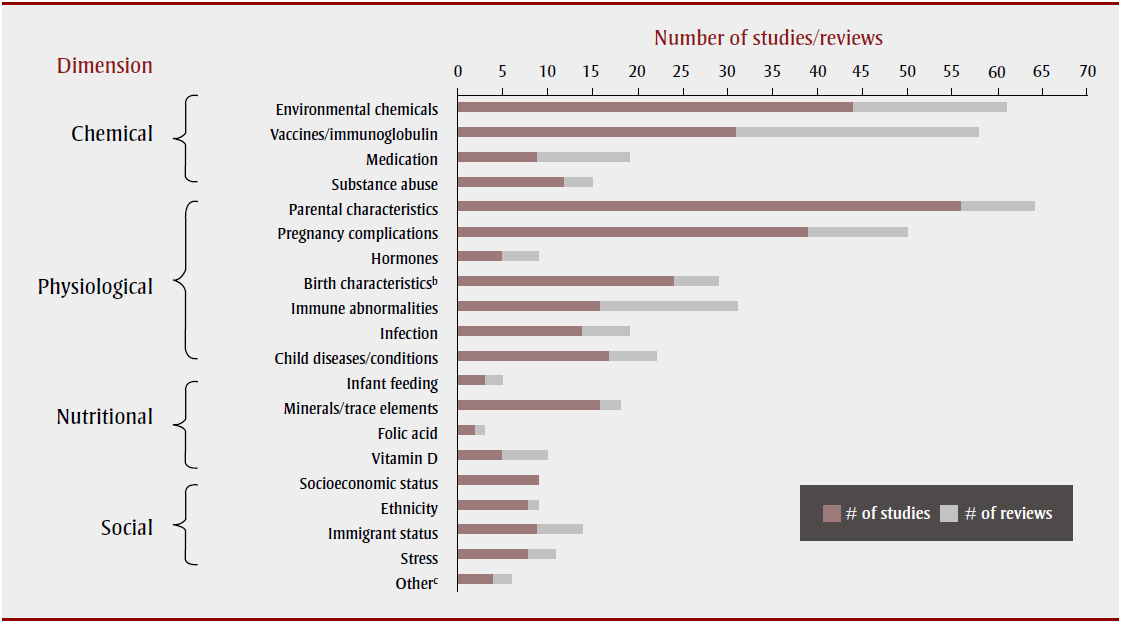
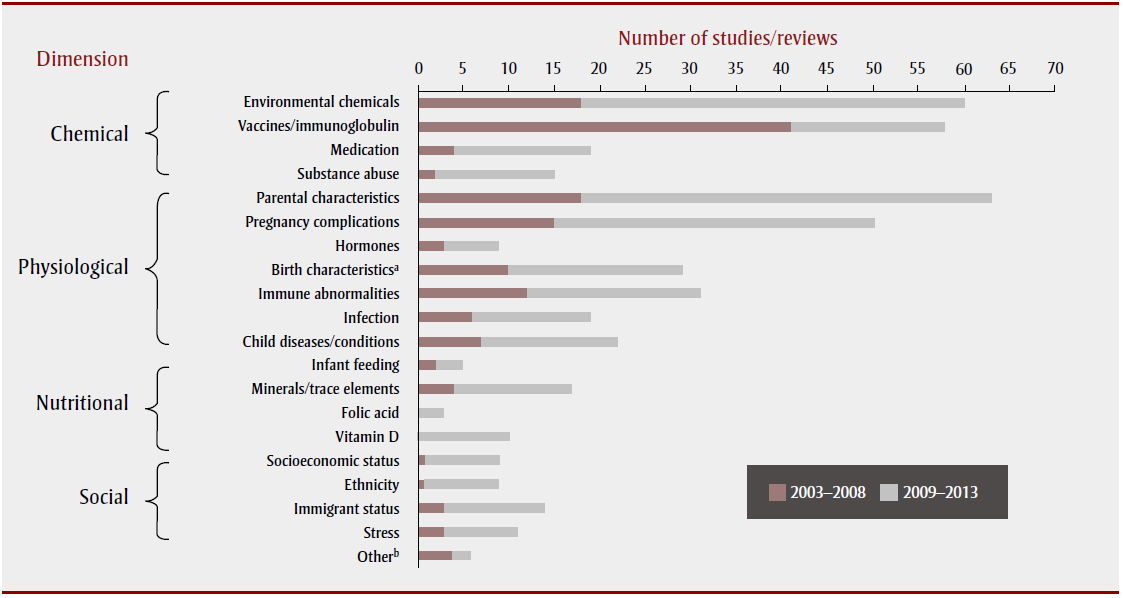
The literature encompassed a wide scope of research investigating potential environmental risk factors associated with ASD. Research has been conducted worldwide; many studies were concentrated in the Nordic countries, the United States, the United Kingdom, Australia and Japan. Most studies examined physiological factors, followed closely by chemical factors, and then nutritional and social factors associated with ASD (Table 1; Figure 2). There was some overlap between these areas as several studies examined a combination of factors; about 14% of the articles (44/315) explored more than one theme. The largest proportion of these examined chemical and nutritional factors (heavy metal exposures and mineral deficiencies). Figure 3 shows the frequency of articles published, by research area and publication period. Most articles were published between 2009 and 2013, with the exception of articles on vaccines, most of which were published between 2003 and 2008.
| Dimension | # of studies | # of reviews |
|---|---|---|
| Chemical | 94 | 44 |
| Physiological | 125Footnote 1.1 | 36 |
| Nutritional | 23 | 10 |
| Social | 25 | 7 |
| Other | 4 | 2 |
Note: Some studies/reviews explored more than one theme, and some studies also had a meta-analysis component—totals do not add up to 315.
Figure 2
Final selection of articlesFigure 2 - Note a on associations between environmental factors and autism spectrum disorder, by subject and article type
{kind=link}

Text Equivalent - Figure 2
The chemical factors investigated in association with ASD included environmental chemicals, vaccines, medication and substance abuse. Articles on exposure to environmental chemicals and vaccines (both primarily concerning postnatal exposure) each accounted for approximately 40% of the chemical dimension.
Figure 3
Final selection of articles on associations between environmental factors and autism spectrum disorder, by subject and time period, 2003-2008 and 2009-2013
{kind=link}

Text Equivalent - Figure 3
Figure 3 shows the final selection of articles published, by research area and publication period, on associations between environmental factors and autism spectrum disorder, by subject and time period. Most articles were published between 2009 and 2013, with the exception of articles on vaccines, most of which were published between 2003 and 2008.
Chemical dimension
The chemical factors we investigated in association with ASD included environmental chemicals, vaccines, medication and substance abuse. Articles on exposure to environmental chemicals and vaccines (both primarily concerning postnatal exposure) each accounted for approximately 40% of the chemical dimension (Figure 2).
Environmental chemicals
The environmental chemicals we examined in association with ASD were predominantly heavy metals, found in biological samples from children, followed by air pollutants; both mainly investigated in case-control studies (Table 2). A small number of the studies and/or reviews explored associations with prenatal or perinatal exposure to occupational chemicalsFootnote 18 ,Footnote 19 and pesticides.Footnote 20 ,Footnote 21
| Subtheme | # of studies | # of reviews |
|---|---|---|
| Environmental chemicals | 1Footnote 2.1 | |
| Heavy metals | ||
| Mercury | 31Footnote 2.2 | 13Footnote 2.3 |
| Other heavy metals | 15 | 6 |
| Pollutants | ||
| Air | 5 | 1 |
| Water | 2 | 0 |
| Occupational chemicals | 2 | 0 |
| Pesticides | 2 | 3 |
| Vaccines/medication | ||
| MMR vaccine | 13Footnote 2.4 | 19 |
| Thimerosal-containing vaccines/Ig | 17Footnote 2.5 | 16 |
| Other vaccine-relatedFootnote 2.6 | 2 | 0 |
| Valproate | 1 | 4 |
| Antibiotics | 3 | 1 |
| Acetaminophen | 2 | 4 |
| Terbutaline | 1 | 0 |
| Antidepressants | 2 | 2 |
| Substance abuse | ||
| Alcohol | 3 | 0 |
| Tobacco smoke | 10 | 3 |
Abbreviations: ASD, autism spectrum disorder; MMR, measles, mumps, rubella; Ig, immune globulin.
Note: Some research articles may have multiple study designs and some studies may have examined multiple exposures; there may be overlap between subthemes.
Heavy metals
Many studies examined biomarkers of postnatal exposure to heavy metals, particularly mercury, in children with ASD or autism compared to children without ASD. Assessing baby teeth, particularly tooth enamel, which begins to form in utero and continues up to one year after birth,Footnote 22 can also help determine prenatal exposure. The five most commonly studied heavy metals were mercury, lead, cadmium, aluminum and arsenic.
Mercury: biomarkers and sources of exposure
Mercury has received considerable attention because of the similarities in the symptoms of mercury poisoning and autism.Footnote 23 Biomarkers of mercury exposure in children with autism were primarily examined by measuring levels in hair (14 studies), blood (4), urine (4), teeth (2) and nails (1). However, findings were largely inconsistent (Table 3). Urinary porphyrins, intermediates in heme biosynthesis, have also been studied as potential biomarkers for mercury exposure in people with autism, as increased porphyrins have been associated with prolonged mercury exposure.Footnote 24 Elevated porphyrins have been found in children with autism compared to children without autism,Footnote 25Footnote 26Footnote 27Footnote 28Footnote 29 and may increase with severity of autistic symptoms.Footnote 30Footnote 31 Although nearly all studies attributed these findings to mercury exposure, none actually measured mercury exposure except for one study, which found no association with ASD despite finding a correlation between elevated porphyrins and ASD.Footnote 27
| Metals | Number of associations | Comments | ||
|---|---|---|---|---|
| Positive | Negative | NS | ||
| Mercury | 11
Ref.:
|
4
Ref.:
|
11
Ref.:
|
Findings: Trending toward positive or null findings. General information on mercury Sources of exposureFootnote 3.1 :
|
| Lead | 9
Ref.:
|
2
Ref.:
|
8
Ref.:
|
Findings: Trending toward either positive or null findings. General information on lead Sources of exposureFootnote 3.1 :
Overall assessment:
|
| Cadmium | 5
Ref.:
|
2
Ref.:
|
7
Ref.:
|
Findings: Trending toward either positive or null findings. General information on cadmium Sources of exposureFootnote 3.1 :
|
| Aluminum | 3
Ref.:
|
0 |
8
Ref.:
|
Findings: No significant association with aluminum in most studies. General information on aluminum Sources of exposureFootnote 3.1 :
|
| Arsenic | 5
Ref.:
|
1
Ref.:
|
3
Ref.:
|
Findings: Most study samples found positive association although inconsistencies exist. General information on arsenic Sources of exposureFootnote 3.5 :
|
Abbreviations: NS, not significant; Ref., references.
Note: Studies may examine associations with different heavy metals and/or specimens.
Few of the studies in this review investigated mercury exposure from sources other than thimerosal in vaccines and Rh immune globulins. Ecological studies have demonstrated an association between environmentally released mercury emissions and significant increases in autism rates,Footnote 32 which may be related to residential distance from mercury pollution sources such as industrial or power plant facilities.Footnote 33 Other studies have examined other prenatal and postnatal mercury exposure sources in relation to ASD, such as maternal dental amalgam fillingsFootnote 27Footnote 34Footnote 35 and maternal or child consumption of seafood,Footnote 27Footnote 36Footnote 37 with inconsistent findings.
A 2012 systematic review concluded that, due to methodological issues such as small sample size and inconsistent case ascertainment, the relationship between mercury exposure and ASD remains unclear.Footnote 38 Furthermore, according to a meta-analysis, hair mercury analysis may not be reliable.Footnote 39 The use of blood or hair mercury levels as accurate measures of prenatal and early-life exposure is questionableFootnote 38 considering mercury's relatively short half-life.Footnote 40Footnote 41
Other heavy metals
Sixteen studies examined the association between exposure to other heavy metals and ASD or autism by measuring levels mainly in hair samples. Lead, cadmium, aluminum and arsenic were the most-studied heavy metals in children with ASD or autism, but there were conflicting findings (Table 3). Most studies found no significant association between aluminum and ASD. None of these studies investigated possible exposure sources.
Pollutants
Only a few studies investigated the relationship between drinking water content and autism.Footnote 42Footnote 43 However, five population-based case-control studies, mostly in California, investigated air pollutant exposure while controlling for sociodemographic factors. Relatively consistent evidence for an association between prenatal, perinatal and/or early-life traffic-related air pollutant exposures and ASD or autism was foundFootnote 44Footnote 45Footnote 46Footnote 47Footnote 48 (Table 4). Exposure to traffic-related air pollution can result in respiratory and cardiovascular disease and certain neurological outcomes by triggering inflammation and oxidative stress,Footnote 49Footnote 50Footnote 51 which are common physiological abnormalities observed in children with ASD. Maternal residence in areas with higher levels of exposure to nitrogen dioxide,Footnote 44Footnote 47 exposure to particulate matter less than 2.5 µmFootnote 44Footnote 47 and exposure to nitric oxideFootnote 44 during gestation and/or the early life of the child were associated with having a child with autism. Also, residing near a freeway during pregnancy, especially during the third trimester, was associated with having children with autism.Footnote 46 Findings for prenatal exposure to other pollutants including ozone and particulate matter less than 10 µmFootnote 44Footnote 47 or prenatal and/or perinatal exposure to specific chlorinated solvents and metalsFootnote 45Footnote 48 in relation to autism or ASD have been inconsistent so far.
| Author (year) |
Sample size Characteristics |
Exposure | Outcome | Associations | |
|---|---|---|---|---|---|
| Positive | NS | ||||
| Becerra et al. (2013)Footnote 44 |
7603 cases 10 controls/case Age 3-5 years LA, California |
Prenatal exposure to traffic pollutants: CO, NO2, NO, O3, PM10, PM2.5 in mother's residence |
Autism | O3 PM2.5 NO NO2 |
PM10 CO |
| Kalkbrenner et al. (2010)Footnote 45 |
383 cases 2829 controls (speech/language impaired) Age 8 years North Carolina West Virginia |
Perinatal exposure to ambient metal, particulate and volatile organic air pollutants in census tract of child's birth residence |
ASD | Quinolone Styrene |
PAH Vinyl chloride Trichloroethylene Methylene chloride Perchloroethylene Mercury Cadmium Nickel Arsenic Lead Toluene Diesel particulate matter |
| Volk et al. (2011)Footnote 46 |
304 cases 259 controls (frequency matched by sex, age, geographic area) Age 2-5 years California |
Distance to nearest freeway and distance to nearest major road |
Autism | Living near freeway (≤ 309 m) during whole pregnancy and third trimester |
- |
| Volk et al. (2013)Footnote 47 |
279 cases 245 controls (frequency matched by sex, age, geographic area) Age 2-5 years California |
Prenatal and 1st year of life exposure to traffic air pollutants: PM2.5, PM10, O3, NO2 |
Autism | High quartile exposure to pollutants: NO2, PM2.5, PM10 during gestation and 1st year |
O3 |
| Windham et al. (2006)Footnote 48 |
284 cases 657 controls (matched 2:1 by sex and birth month) 1994 birth cohort San Francisco Bay Area |
Prenatal and early life exposures to hazardous air pollutants |
ASD | Metals (highest contribution from mercury, cadmium, nickel) Chlorinated solvents (contributed by trichloroethylene, vinyl chloride) Diesel particulate matter |
Methylene chloride Perchloroethylene Arsenic Lead Manganese Chromium Aromatic solvents |
Abbreviations: ASD, autism spectrum disorder; CO, carbon monoxide; NS, not significant; O3, ozone; NO, nitric oxide; NO2, nitrogen dioxide; PAH, polycyclic aromatic hydrocarbon; PM2.5, particulate matter < 2.5µm; PM10, particulate matter <10 µm.
Vaccines and medication
Vaccines
Measles Mumps Rubella (MMR) vaccination
Since the publication of the Wakefield case series study,Footnote 52 which found an increased prevalence of a new variant of autism characterized by gastrointestinal disorders and developmental regression, the safety of MMR vaccine has been questioned, although this paper was later retracted due to false data. Nine case-control and two time-series studiesFootnote 53Footnote 54Footnote 55Footnote 56Footnote 57Footnote 58Footnote 59Footnote 60Footnote 61Footnote 62Footnote 63 and two systematic reviewsFootnote 64Footnote 65 found no significant association between MMR vaccine and ASD or autism, although another time-series study did.Footnote 66 A systematic review found that studies with the lowest bias based on study quality criteria did not support a causal association.Footnote 64 Evidence for an association between the new variant form of ASDFootnote 58Footnote 59Footnote 65 and MMR vaccine, and between measles infection and autism,Footnote 61Footnote 67 was also lacking.
Thimerosal-containing vaccines and immune globulins
Thimerosal, a preservative that contains 50% ethylmercury and is used for multi-vial vaccines such as the diptheria-tetanus-pertussis vaccine, has been widely researched because of concerns about mercury overexposure stemming from the expansion of childhood vaccination schedules in the past several decades. Thimerosal in Rh immune globulins given to pregnant women with Rh incompatibility issues has also been investigated as a source of prenatal mercury exposure.
Postnatal thimerosal exposure: early childhood vaccines
Seven studies demonstrated no significant association between thimerosal-containing childhood vaccines and ASD,Footnote 68Footnote 69Footnote 70Footnote 71Footnote 72Footnote 73Footnote 74 while four studies did.Footnote 66Footnote 75Footnote 76Footnote 77 However, most of the studies that supported an association, which all came from the same authors, did not control for potential confounders such as the child's age and sex, in contrast to most studies that found a null association. Both cohort studies that found significant positive associations used the Vaccine Adverse Events Reporting System database, which has been criticized as potentially biased and unreliable because anyone can report an adverse event after vaccination and diagnoses are not medically validated.Footnote 78 Furthermore, no association has been found between autoimmune markers and autism in children given thimerosal-containing vaccines.Footnote 79Footnote 80
Prenatal thimerosal exposure: Rh anti-D immune globulin
Some studies, mostly larger case-control studies, refuted the association between maternal prenatal exposure to thimerosal-containing Rh immune globulin and ASD, adjusting for maternal and/or birth characteristics,Footnote 37Footnote 69Footnote 81Footnote 82 while others found significant associations without adjusting for potential confounders.Footnote 83Footnote 84
Medication
The increasing use of antidepressants, antibioticsFootnote 85 and acetaminophenFootnote 86 has sparked hypotheses of possible links with the use of these medications and synchronous rising ASD prevalence in the 1980s.
Research on selective serotonin reuptake inhibitors (SSRIs; a class of antidepressants) in relation to ASD has emerged recently, with reviews indicating biologically plausible evidence of an association from animal and preclinical studies.Footnote 87 ,Footnote 88 Two case-control studies found a moderate association between prenatal use of SSRIs and ASD.Footnote 89 Footnote 90 However, if the relationship was causal, prenatal antidepressant use would account for fewer than 1% of ASD cases.Footnote 90
Three reviews cited several clinical studies that provided evidence for increased ASD prevalence among children exposed to valproic acid (or valproate), a teratogenic broad spectrum antiepileptic drug and mood stabilizer, in early pregnancy compared to unexposed children.Footnote 91Footnote 92Footnote 93 Additionally, a large prospective cohort study showed that prenatal valproate exposure was associated with an absolute risk of ASD of 4.42% over a 14-year period among those exposed.Footnote 94
Some studies suggested a possible link between prenatal or early-life antibiotic use and autism.Footnote 85Footnote 95Footnote 96 Studies found ecological associations with prenatal use of acetaminophenFootnote 97 and circumcision rate (a proxy for acetaminophen, which was widely used following circumcision),Footnote 97 and an association with acetaminophen use following MMR vaccination.Footnote 98 Biologically plausible mechanisms related to the endocannabinoid system affecting central nervous system (CNS) developmentFootnote 98Footnote 99 or impaired detoxification ability upon overdoseFootnote 86 have been suggested.
Substance use
Tobacco smoke
A meta-analysis has indicated no significant association between smoking during pregnancy and ASD.Footnote 100 Likewise, no association was found in later studies.Footnote 101Footnote 102Footnote 103Footnote 104Footnote 105 However, an association between maternal smoking during pregnancy and subclassifications of ASD, including Asperger syndrome and/or PDD-NOS, has been demonstrated.Footnote 106Footnote 107Footnote 108 Maternal second-hand tobacco exposure may be associated with ASD or autism in children based on two small case-control studies.Footnote 37Footnote 109
Alcohol
Two studies, including a prospective cohort study, found no association between prenatal alcohol consumption and ASD or autism,Footnote 106Footnote 110 whereas a significant association with heavy prenatal consumption was evident in a small clinic sample.Footnote 111
Physiological dimension
The physiological dimension encompasses many recurring themes related to the physiology of the parents and the child with ASD. Parental characteristics, particularly parental age, and pregnancy complications, especially low birth weight and prematurity, have been the most-studied risk factors for ASD (Table 5).
| Subtheme | # of studies | # of reviews |
|---|---|---|
| Parental characteristics | ||
| Parental age | 39 | 7 |
| Assisted conception | 8 | 1 |
| Maternal chronic conditions: | 16 | 2 |
|
Aggregate
|
3 | 0 |
|
Diabetes
Table 5 - Note a
|
10 | 2 |
|
Weight/pregnancy weight gain
|
4 | 0 |
| Pregnancy complications | ||
| Low birth weight | 16 | 6 |
| Low gestational age | 19 | 6 |
| Post-term birth | 2 | 1 |
| SGA or LGA | 6 | 2 |
| Fetal growthTable 5 - Note b | 2 | 0 |
| Clustering of complications | 12 | 6 |
| All complications | 39 | 11 |
| Hormones | ||
| Testosterone | 2 | 1 |
| Thyroid | 3 | 3 |
| Birth characteristics | ||
| Birth order/spacing | 15 | 4 |
| Multiple births | 3 | 1 |
| Birth seasonality | 7 | 2 |
| Immune abnormalities | 1Table 5 - Note c | |
| Autoimmune disease | 10 | 8 |
| Brain inflammation | 5 | 10 |
| Other | 1 | 0 |
| Infection | 14 | 5 |
| Associated child diseases/conditions | ||
| Neonatal jaundice | 6 | 3 |
| Epileptic disorders | 5 | 2 |
| Oxidative stress | 6 | 2 |
Abbreviations: GA, gestational age; LGA, large for gestational age; SGA, small for gestational age.
Note: There is some overlap of subthemes across different studies/reviews.
Parental characteristics
Parental age
Five systematic reviews supported the association between advanced parental age and ASD.Footnote 13Footnote 100Footnote 112Footnote 113Footnote 114 A 2011 meta-analysis found a pooled odds ratio (OR) for autism of 1.78 (95% confidence interval [CI]: 1.52-2.07) for fathers 40 to 49 years of age compared with fathers aged 29 years or younger.Footnote 113 Since the latest systematic review,Footnote 13 four studies have found a significant association with ASD or autism,Footnote 115Footnote 116Footnote 117Footnote 118 whereas one did not.Footnote 119 De novo mutations and genomic copy number variations burden have been implicated as possible underlying mechanisms, because they increase with paternal age.Footnote 120Footnote 121 No association has been found between men with autistic-like traits and delayed parenting.Footnote 122Footnote 123
A 2012 meta-analysis found the relative risk (RR) of ASD for mothers aged 35 years or over compared to those aged 25 to 29 years to be 1.31 (95% CI: 1.19-1.45).Footnote 114 Since the most recent systematic review,Footnote 114 four studies have found significant associations between advanced maternal age and ASDFootnote 117Footnote 118Footnote 124Footnote 125 and one did not.Footnote 106
Some studies have found paternal and maternal ages to be independent risk factors for ASD after adjusting for spousal age,Footnote 126Footnote 127Footnote 128 and no evidence for a synergistic effect.Footnote 117 Other studies have accounted for multicollinearity of maternal and paternal ages and found that advanced maternal age was the primary independent contributor of the parental age effect.Footnote 118Footnote 129Footnote 130
Assisted conception
Assisted conception and ASD share risk factors such as high parental age, high rate of prematurity and low birth weight.Footnote 131 A systematic review cited methodological limitations as the source of inconsistent findings for the association between assisted conception and ASD.Footnote 132 Since then, two studies have found a positive association between assisted reproductive technology use and ASD,Footnote 133Footnote 134 whereas five studies have found none.Footnote 131Footnote 135Footnote 136Footnote 137Footnote 138 However, significant positive associations were found among subgroups such as women over age Footnote 34Footnote 136 multiple birthsFootnote 137 and those exposed to specific assisted conception methods.Footnote 131Footnote 135
Maternal chronic diseases and conditions
Some evidence exists for associations between maternal chronic conditions such as weight gain, obesity and diabetes and ASD in children. TwoFootnote 109Footnote 139 of four studies found a positive association between maternal chronic conditions (aggregate measure) and ASD or autism.Footnote 106Footnote 109Footnote 139Footnote 140 TwoFootnote 141Footnote 142 of three cohort studiesFootnote 141Footnote 142Footnote 143 found a significant association between either prepregnancy weight, pregnancy weight gain or early-life obesity and ASD. A 2009 meta-analysis found a positive association between maternal gestational diabetes and ASD.Footnote 100 Since then, there have been conflicting findings,Footnote 102Footnote 124Footnote 139Footnote 141Footnote 144Footnote 145 although some of these studies did not differentiate between prepregnancy and gestational diabetes.
Hormones
Prenatal testosterone
An association between elevated prenatal testosterone levels and ASD or autism has been implicated in a review of three meta-analysesFootnote 146 and a case-control study.Footnote 147 However, no significant correlation was found with neonatal testosterone levels in a cohort study.Footnote 148
Thyroid hormone
Thyroid dysfunction, whether due to prenatal or early-life exposure to the antithyroid effects of heavy metals, to endocrine-disrupting chemicals or to dietary deficiencies, may affect neurodevelopment.Footnote 149Footnote 150Footnote 151 However, evidence for the association between neonatal or maternal levels of thyroid hormone and ASD is limited and inconsistent.Footnote 152Footnote 153Footnote 154
Pregnancy complications
A 2012 systematic review found perinatal and neonatal pregnancy complications to be significantly associated with ASD.Footnote 13 However, findings were inconclusive for eclampsia and/or pregnancy-induced hypertension. Findings were also inconsistent among several other studies.Footnote 102Footnote 103Footnote 124Footnote 125Footnote 145Footnote 155Footnote 156
Birth weight and gestational age
Two systematic reviewsFootnote 112 Footnote 157 found low birth weight to be a significant risk factor for ASD; one of them, a meta-analysis, found a risk ratio (RR) of 1.63 (95% CI: 1.19-2.33).Footnote 157 However, a more recent systematic reviewFootnote 13 indicated mixed findings. Since then, threeFootnote 158 Footnote 159 Footnote 160 of five studiesFootnote 106 Footnote 109 Footnote 158 Footnote 159 Footnote 160 have found a significant association between low birth weight and ASD. In most studies, the low birth weight threshold was 2500 g.
TwoFootnote 13Footnote 112 of three systematic reviewsFootnote 13Footnote 112Footnote 157 supported the association between low gestational age and ASD. Since the 2012 systematic review,Footnote 13 most studies have provided more evidence for this associationFootnote 145Footnote 159Footnote 161Footnote 162Footnote 163 although two studies did not.Footnote 106Footnote 125 Based on the positive studies and the systematic review,Footnote 13 the effect estimates for ASD or autism ranged from 1.4 to 4.7. The 37-week cut-off to define "preterm" births and the 32-week cut-off to define "extremely preterm" births were used in many studies.
Systematic reviewsFootnote 13Footnote 157 along with subsequent studiesFootnote 159Footnote 164 have also found a significant association between small for gestational age and ASD. Other studies have suggested that a deviance in fetal growthFootnote 165 and physical developmentFootnote 140 may be associated with ASD onset.
Clustering of pregnancy complications
Eleven studies, including four cohort studies, found clustering of pregnancy complications to be significantly associated with ASD,Footnote 102Footnote 104Footnote 106Footnote 109Footnote 124Footnote 141Footnote 143Footnote 166Footnote 167Footnote 168Footnote 169 and only one case-control study did not.Footnote 140 Four systematic reviews also supported this association,Footnote 13Footnote 100Footnote 112Footnote 157 with a general consensus that the presence of multiple factors is associated with ASD. However, the types of pregnancy complications examined vary by study. Many studies have explored the association between optimality scores (composite measures of compromised prenatal, perinatal and neonatal health overall) and ASD. Systematic reviewsFootnote 100Footnote 157 have found that reduced prenatal and neonatal optimality is more evident than perinatal suboptimality in ASD cases. However, since those reviews, a prospective cohort study has found that having at least four obstetric suboptimality factors (mainly prenatal and perinatal) in the first birth were significantly correlated with ASD.Footnote 124 Three other studies have found that suboptimal birth conditionsFootnote 101Footnote 105Footnote 141 and/or prenatal pregnancy complicationsFootnote 102Footnote 106Footnote 141 were more common in children with ASD than in children without ASD.
Systematic reviewsFootnote 112Footnote 157 have implicated fetal hypoxia (intrauterine deprivation of oxygen) in ASD etiology, based on several perinatal factors that may serve as markers of hypoxia, including low Apgar score, caesarean section and growth retardation. However, fetal hypoxia has been weakly associated with ASD according to a population-based cohort study.Footnote 170
Birth characteristics
Birth order and spacing
Systematic reviews agree that first-born children are more likely to be diagnosed with ASD than children born third or later;Footnote 13 Footnote 100 the meta-analysis found a 61% increased risk of autism for first-born children compared to children born third or later.Footnote 100 This is also consistent with more recent studies,Footnote 106 Footnote 140Footnote 171 Footnote 172 one of which investigated only Asperger patients.Footnote 171 Suboptimal parity (giving birth more than two times) has been associated with ASD.Footnote 124 Earlier birth order and greater parity appear to be conflicting risk factors, because first-born children in sibship sizes of two, and later-born children in families with larger sibship sizes, are more likely to have ASD.Footnote 100 In addition, some studies have indicated that ASD symptom severity may be related to birth order, although these studies did not agree on which place in the birth order was more associated with severe symptoms,Footnote 173Footnote 174 possibly because interpregnancy intervals may also be a factor.Footnote 174 Interpregnancy intervals of less than 18 monthsFootnote 141 or less than a year have also been associated with autism in the second-born child.Footnote 175
Other birth characteristics
Multiple births have been associated with ASD according to a meta-analysisFootnote 157 as well as a cohort study,Footnote 176 whereas an ecological study did not find an association.Footnote 177 A meta-analysis also found a significant association between summer births and ASD.Footnote 157 However, conflicting findings are evident in several studies.Footnote 144Footnote 178Footnote 179Footnote 180Footnote 181
Immune abnormalities
According to a review of research trends, immune dysregulation has been widely studied and possesses the strongest evidence base of the physiological abnormalities in ASD.Footnote 12 Early evidence found a potential link between ASD and two main types of immune dysfunction: autoimmunity and brain inflammation.Footnote 182 In addition, significantly reduced neonatal blood immunoglobulin G has been observed in archived specimens from newborns subsequently diagnosed with ASD relative to newborns not subsequently diagnosed with ASD.Footnote 183
Autoimmune diseases
Several studies have examined the role of autoimmunity in ASD. Three case-control studies have consistently demonstrated that antibody reactivity to human fetal brain protein is more prevalent in mothers of children with ASD or specifically autism than in mothers of children who do not have ASD or specifically autism.Footnote 184Footnote 185Footnote 186 Additionally, there may be increased serum folate receptor autoantibodies in children with low-functioning autism with or without neurological deficits relative to control subjects without autism.Footnote 187 This suggests that folate transfer to the fetus during pregnancy may be blocked, which may increase risk of neural tube defects.Footnote 188 Because these elevated autoantibodies were also present in at least one parent of children with autism, parental antibodies may contribute to autism etiology.Footnote 189
Two cohort studies and a case-control study found an association between maternal or family history of autoimmune diseases and ASDFootnote 124Footnote 190 or autistic regression,Footnote 191 whereas another case-control study found no association.Footnote 192 However, the specific autoimmune diseases associated with ASD varied by study. Reviews have discussed growing evidence for the role of autoimmunity in ASD, stemming mostly from animal models and human clinical studies, but have indicated a need to identify the functions of the autoantibodies that might be affecting neurodevelopment.Footnote 193Footnote 194Footnote 195Footnote 196
Brain inflammation
Brain inflammation has also been implicated in the etiology of ASD. According to the reviews based mainly on animal and human clinical studies, early-life immune insults such as toxic substances, food additives or stress may result in a cascade of excitotoxicity in the brain,Footnote 197Footnote 198Footnote 199 and may be related to dysregulation of glutamate neurotransmission.Footnote 199Footnote 200 This cascade may trigger production of proinflammatory cytokines, resulting in chronic inflammation affecting neurodevelopment.
Emerging evidence, mostly from case-control studies, has shown that increased proinflammatory cytokine production is found in the serum or cerebrospinal fluid of ASD children or the amniotic fluid of their mothers,Footnote 201Footnote 202Footnote 203 although a decreased neonatal level of cytokines has also been observed.Footnote 204 Significantly altered adaptive cellular immune function in children with ASD may reflect defective immune activation, which may in turn be associated with ASD impairment.Footnote 203 Also, no significant differences have been reported for levels of certain chemokines in neonatal blood and amniotic fluid,Footnote 201Footnote 205 except in a subgroup with an ASD diagnosis based on the most recent diagnostic criteria.Footnote 201
Infection
Infections may trigger the chronic inflammation of the CNS, affecting brain development and maturation, which has been implicated in ASD etiology.Footnote 198 However, according to a meta-analysisFootnote 100 and 2012 literature review,Footnote 206 there was no significant association between maternal infection and ASD. A 2012 systematic review indicated that more research is required to explore this association.Footnote 13 Since then, only one case-control study found a significant association,Footnote 106 whereas one cohort and three case-control studies did not.Footnote 96 Footnote 125 Footnote 140 Footnote 207 The definition of maternal infection varies across studies; it may encompass any infection during pregnancy, or only specific infections such as influenza.Footnote 207 Some studies have suggested maternal fever during pregnancyFootnote 207 or extended febrile episodesFootnote 96 are associated with ASD, although findings are mixed.Footnote 145 Footnote 208
Associated child diseases
Neonatal jaundice
Neonatal jaundice, a result of elevated serum bilirubin levels (hyperbilirubinemia), has been a concern because unconjugated bilirubin can be toxic to the developing CNS. Five studiesFootnote 125Footnote 144Footnote 209Footnote 210Footnote 211 and two systematic reviewsFootnote 13Footnote 157 investigated this risk factor. According to the systematic reviews, hyperbilirubinemia was associated with an increased risk of autismFootnote 13Footnote 157 with a summary effect estimate of 1.87 (95% CI: 1.01-3.47), according to the meta-analysis.Footnote 157
Epileptic disorders
While a meta-analysis indicated no significant relationship between neonatal seizures and ASD,Footnote 157 four small studies have provided some evidence for a possible association.Footnote 125Footnote 212Footnote 213Footnote 214
Oxidative stress
According to a review of research trends, oxidative stress was one of the most-studied physiological abnormalities in ASD, with one of the strongest evidence bases, mainly consisting of clinical and animal studies.Footnote 12 Six case-control studies indicated a role for oxidative stress in ASD patientsFootnote 29Footnote 30Footnote 215Footnote 216Footnote 217Footnote 218 based on different biomarkers of oxidative stress and impaired antioxidant systems. Biomarkers included altered levels of oxidative stress defence systems, including metallothioneins and antioxidant enzymes.Footnote 215 Other markers of oxidative stress, associated heavy metal toxicity and/or low detoxification capacity included abnormal markers of thiol metabolism,Footnote 216 transsulfuration abnormalities,Footnote 30 urinary organic acids,Footnote 29 and increased lead and potassium ions, ATPase activity and lipid peroxidation products.Footnote 217
Nutritional dimension
Deficiencies in minerals and levels of trace elements were the most-studied of the nutritional factors in association with ASD, followed by vitamin D deficiency (Table 6).
| Subtheme | # of studies | # of reviews |
|---|---|---|
| Minerals/trace elements | 16 | 2 |
| Vitamin D | 5 | 5 |
| Infant feeding | 3 | 2 |
| Folic acid | 2 | 1 |
Note: There is some overlap of subthemes across different studies/reviews.
Minerals and trace elements
Evidence for mineral deficiencies and levels of trace elements in children with ASD or specifically, autism, comes mainly from case-control studies examining hair samples and remains inconclusive. Studies looking at associations between levels of zinc,Footnote 37Footnote 95Footnote 215Footnote 219Footnote 220Footnote 221Footnote 222Footnote 223 iron,Footnote 37Footnote 215Footnote 216Footnote 219Footnote 222Footnote 223Footnote 224 magnesium,Footnote 37Footnote 219Footnote 220Footnote 222Footnote 223 copper,Footnote 37Footnote 215Footnote 216Footnote 219Footnote 220Footnote 222Footnote 223Footnote 225Footnote 226 molybdenum,Footnote 37Footnote 219Footnote 222Footnote 223Footnote 225 nickel,Footnote 215Footnote 219Footnote 222Footnote 223Footnote 225 and seleniumFootnote 37Footnote 219Footnote 220Footnote 223Footnote 225 and ASD have had conflicting results. Calcium deficiencies have also been documented in association with ASD or autism in children,Footnote 219Footnote 222Footnote 223Footnote 227 with some inconsistencies.Footnote 37Footnote 215 Despite inconsistencies, differences in the levels of cobalt,Footnote 37Footnote 215Footnote 222Footnote 223Footnote 225Footnote 226 chromiumFootnote 37Footnote 215Footnote 222Footnote 223Footnote 225Footnote 228 and manganeseFootnote 37Footnote 215Footnote 219Footnote 223Footnote 225Footnote 226Footnote 229 in children with and without ASD or autism were mostly nonsignificant.
Vitamin D
Vitamin D plays a crucial role in various functions, such as neurodevelopment, the anti-inflammatory response and the detoxification pathway.Footnote 230Footnote 231 However, evidence for an association between vitamin D deficiency and ASD is limited and indirect. Two ecological studiesFootnote 63Footnote 232 and a case-control studyFootnote 227 have indicated an association between vitamin D deficiency in mothers and/or their children with autism, and the onset of autism. It has been suggested that migration may play a role in the etiology of ASD, because of increased autism prevalence rates among immigrants in northern European countries, and because immigrants with dark skin are more prone to vitamin D deficiency due to their skin pigmentation.Footnote 233 However, both a small case-control studyFootnote 234 and a recent Australian prospective cohort studyFootnote 235 found no significant association between maternal serum vitamin D levels and ASD or a majority of autistic-like traits in their offspring. Furthermore, a systematic review concluded that there was inadequate support for an association, and that more population-based longitudinal studies are needed, given the plausible biological evidence.Footnote 230
Infant feeding
We found few studies on infant feeding methods in relation to ASD, although two case-control studies found that the absence or late initiation of breastfeeding was significantly associated with ASD or autism,Footnote 236Footnote 237 in contrast to findings of an ecological study.Footnote 63
Folic acid
Evidence supporting an association between folic acid intake and ASD is very sparse, although a recent prospective cohort study found maternal folic acid intake to be protective against ASD,Footnote 238 in contrast to an ecological study that found positive correlations between the percentages of prescription prenatal vitamins and pediatric vitamins containing folic acid and ASD incidence.Footnote 239
Social dimension
Socioeconomic status (SES), ethnicity, immigrant status and stress were recurring social factors examined in association with ASD (Table 7).
| Subtheme | # of studies | # of reviews |
|---|---|---|
| Socioeconomic status | 9 | 0 |
| Ethnicity | 8 | 1 |
| Immigrant status | 9 | 5 |
| Stress | 8 | 3 |
Note: There is some overlap of subthemes across different studies/reviews.
Socioeconomic status
The importance of SES emerged as a predictor of ASD risk in nine studies,Footnote 102Footnote 119Footnote 172Footnote 240Footnote 241Footnote 242Footnote 243Footnote 244Footnote 245 but findings were mixed. Mainly in American studies, a higher SES, using proxies such as maternal income, occupation and education, was associated with ASD.Footnote 172Footnote 240Footnote 241Footnote 242 However, when researchers in one of these studies conducted a subanalysis by case ascertainment, no association with SES was found using case ascertainment only from school sources.Footnote 242 In an Australian study,Footnote 172 maternal residence in remote areas was negatively correlated with cases of ASD without intellectual disability (ID). However, other studies had different results.Footnote 102Footnote 119Footnote 243Footnote 244 In countries with universal health care programs, such as Sweden and Canada, lower family or maternal income was associated with ASD, which suggests that the associations between high SES and ASD found mainly in the US studies may reflect inequalities in access to health care services (e.g. under-diagnosis of ASD in families with lower SES).Footnote 102Footnote 244 Furthermore, spatial analysis of autism incidence in regions of California indicated a higher incidence that was independently characterized by higher levels of parental education.Footnote 245
Ethnicity
Most studies that examined the relationship between maternal ethnicity and ASD found a significant association,Footnote 102Footnote 119Footnote 172Footnote 242Footnote 243Footnote 246 with the exception of one study in the United Kingdom.Footnote 247 In particular, maternal minority ethnic status, such as Aboriginal status, was associated with reduced ASD diagnosis in offspringFootnote 102Footnote 119Footnote 172Footnote 243 with an OR ranging from 0.33 to 0.83 for certain non-White ethnic groups compared to White, non-Hispanic people. Furthermore, children who were Black, Hispanic or "other" race/ethnicity were less likely than White children to have ASD, which was more pronounced in children with ID for some ethnic groups, according to an American study.Footnote 246 The finding that minority groups would be less likely to be diagnosed with ASD may be due to ascertainment bias. Differential assessment of children's intellectual and developmental problems may account for these ethnic disparities. In contrast, another American study found that Black race was associated with increased odds of ASD, particularly with ID, but case ascertainment was more likely from school sources.Footnote 242 These studies suggest possible racial or ethnic disparities in ASD diagnosis such that for some groups, comorbid ID may affect its detection.
Immigrant status
Maternal immigrant status is another social factor that emerged in eight studiesFootnote 104Footnote 208Footnote 243Footnote 247Footnote 248Footnote 249Footnote 250Footnote 251 and two systematic reviewsFootnote 13Footnote 100 supporting an association with ASD or ASD subtype. Migrant mothers had a higher prevalence of offspring with ASD in studies from Sweden, the United Kingdom and Australia. The meta-analysis found a marginal association between maternal immigrant status and autism (summary effect estimate = 1.28; p = .06).Footnote 100 However, among Nordic countries, the association was statistically significant, with a 58% increased risk among children whose mothers were born abroad.Footnote 100 According to a Swedish study, migrant parents from countries with a low ranking on a human development index may be at increased risk of having children with ASD and comorbid ID compared with Swedish-born parents, particularly when migration occurred around time of pregnancy, suggesting a possible link with maternal stress.Footnote 249 However, migrant parents from developing countries may have a decreased risk of having children with PDD-NOS or Asperger.Footnote 250 Sociopolitical context such as changes in immigration policy has also been shown to influence trends in autism diagnosis rates. For example, a decline in autism rates among Hispanic children in the United States was attributed to undocumented immigrant parents' reluctance to seek diagnostic services due to fears of being reported to the authorities and having to face deportation when threatened by anti-immigrant policy enforcement.Footnote 251
Maternal stress
Prenatal exposure to environmental stressors, including stress-related immunological and neuroinflammatory abnormalities and placental dysfunction that can affect fetal neurodevelopment, may play a role in ASD etiology.Footnote 252Footnote 253 A 2012 systematic review indicated this association requires more study to provide conclusive evidence.Footnote 13 Since then, one cohort study and a case-control study have shown that maternal stress during pregnancy is associated with conceiving a child with ASD,Footnote 106Footnote 254 whereas three other case-control studies did not find an association.Footnote 140Footnote 145Footnote 255 In many of these studies, "stressors" may be defined broadly as any type of stressful event,106, Footnote 140Footnote 145Footnote 255 or specifically as certain stressful events such as early-life childhood abuse.Footnote 254
Other
In addition to the chemical, physiological, nutritional and social dimensions, several other factors emerged that were investigated for association with ASD. Two studies showed that autism births occur in geographical clusters, which could indicate that local factors are involved in the prevalence.Footnote 247Footnote 256 Another study found that while electromagnetic radiation has been hypothesized to be a risk factor due to biological plausibility, no epidemiological evidence is yet available.Footnote 257 Other studies have found no significant association between prenatal exposure to ultrasound and ASD. Footnote 256Footnote 258
Discussion
Most of the research on the environmental contribution to ASD etiology focussed on physiological or chemical risk factors, and less on social and nutritional factors. Within these dimensions, however, the vast literature is riddled with inconsistent findings. Heterogeneity is evident in study populations, exposure and outcome assessment, changing diagnostic criteria and/or ASD phenotypes, all of which vary between studies and may affect the validity of findings.
Biomarkers of heavy metal exposure, particularly mercury, from levels measured in biological specimens such as hair, blood and urine have been studied intensely, but its association with ASD remains uncertain due to conflicting findings. Because most of these studies only measure biomarkers of heavy metal, and do not ascertain actual exposure sources, temporality of association is unknown. Furthermore, many of the biomarker studies had small sample sizes. These findings are consistent with a recent systematic review by Rossignol and colleaguesFootnote 11 (published in 2014, after the completion of our review), who examined the association between environmental toxicant exposure and ASD.
In contrast, emerging evidence for the association between traffic-related air pollutants and ASD or autism has been relatively consistent, although further research is required to establish specificity of association and improve external validity beyond the American landscape. These findings are also consistent with Rossignol's review, which found that air pollution is the chemical risk factor with the strongest evidence of an association with ASD, although the association with pesticides was also relatively strong.
Despite numerous studies exploring the relationship between MMR or thimerosal-containing vaccines and ASD, there is a lack of convincing support for this association. Additionally, evidence of an association between fetal or childhood exposure to various medications and ASD is limited to a few studies. A lack of association between tobacco smoke exposure and ASD is also apparent, although some studies have indicated a possible link with PDD-NOS, warranting further study on ASD subgroups separately if causal relationships are to be elucidated. Moreover, studies on exposure to occupational chemicals, pesticides and alcohol were limited.
The most widely and consistently implicated physiological factors in ASD onset include advanced parental age, low birth weight, prematurity and clustering of pregnancy complications. A consistent association between hyperbilirubinemia and ASD has been demonstrated as well. More research is warranted on the effects of advanced grandparental age on ASD, based on preliminary findings.Footnote 115Footnote 259 Furthermore, studies are needed to understand the mechanisms for associations between these physiological factors and ASD. Emerging epidemiological evidence for immune abnormalities related to autoimmunity and brain inflammation have also been reported in children with ASD or their mothers. However, further work is required to establish temporality of association and to elucidate their possible role in ASD etiology.
More research is also needed to understand other physiological factors such as birth characteristics, maternal chronic conditions, hormones and child conditions in relation to ASD. Studies have indicated a potential relationship between chronic conditions such as pregnancy weight gain or maternal diabetes and ASD. However, due to heterogeneity and lack of specificity of exposures, further research is warranted. Evidence for a link between earlier birth order, greater parity and short interpregnancy intervals and ASD exists, although the etiological contribution is not clear. The association between oxidative stress and ASD has been demonstrated by a limited number of small epidemiological studies.
The relationship between nutritional factors and ASD has not been well studied compared to that with chemical and physiological factors. Although several studies investigated associations with mineral and/or trace element deficiencies and vitamin D deficiency, evidence is inconsistent and indirect. For example, maternal foreign birthplace and/or ethnicity were used as proxies for vitamin D concentration, based on the possibly inaccurate assumption that women in these categories would have darker skin pigmentation, affecting their vitamin D concentrations.Footnote 233 More direct evidence for an association between vitamin D and ASD by direct exposure measurements is required.
The current literature suggests that associations between social factors such as SES and ethnicity and ASD may vary across countries, depending on possible case ascertainment biases. However, maternal immigrant status has been consistently correlated with ASD. Whether this may relate to SES, adaptation to a new environment, stress or changes in vitamin D exposure as suggested by some studies requires further investigation.
Overall, the lack of consistency, temporality and specificity of the associations observed in many studies precludes the establishment of causality. Longitudinal studies may be helpful in establishing temporality to identify possible causal relationships. Consistent methods of measuring exposure and case ascertainment and consideration for potential confounders could reduce heterogeneity. Underlying mechanisms of some of these associations need to be investigated through further biological research.
Strengths and limitations
Of the reviews that have explored possible risk factors of ASD to date, none have examined the entire scope of the environmental contribution to ASD. We conducted a comprehensive, systematic search of the literature. Although all relevant articles may not have been retrieved in this review, a large number of potentially contributing factors were identified that can provide an adequate picture of the breadth of environmental contribution to ASD etiology.
Although the search strategy to retrieve relevant ASD articles aimed for comprehensiveness, key scientific journals were not hand-searched and no searches were performed on citations referenced in included studies and grey literature. Furthermore, more information on environmental factors may have been missed if articles covering them also dealt with animal models or genetic studies, which were excluded. This is evident for research in immune abnormalities and oxidative stress, because articles retrieved were fewer in number although reviews have indicated a vast amount of research, likely from clinical and animal studies. Because the aim of this scoping review was to assess the current state of knowledge of environmental risk factors of ASD, quality assessment of these studies was not performed to assess the strength of evidence.
Conclusion
Our scoping review examined research conducted between 2003 and 2013 on environmental factors potentially associated with ASD, grouped into four categories: chemical, physiological, nutritional and social. We found that physiological factors including advanced parental age, low birth weight, prematurity, hyperbilirubinemia and clustering of pregnancy complications have been consistently reported as risk factors for ASD. While evidence for an association with traffic-related air pollutants is emerging, research on nutritional factors associated with ASD is limited. Of the factors in the social dimension, immigrant status has been consistently associated with ASD, which warrants further research. Other associations with social factors such as SES and ethnicity may reflect disparities in ASD diagnosis. Large prospective studies, adjusting for sociodemographic confounders, are needed to resolve inconsistencies, especially in the area of heavy metal exposure, where evidence for an association with ASD is still inconclusive.
Because there are a variety of associations with ASD, the etiology is likely multifactorial. Future studies should continue exploring how these different factors may be interrelated. Overall, the lack of consistency, temporality and specificity of associations between environmental factors and ASD remains the largest barrier to establishing causal relationships.