
At-a-glance – Population coverage of the Canadian Chronic Disease Surveillance System: a survey of the contents of health insurance registries across Canada

HPCDP Journal Home
Published by: The Public Health Agency of Canada
Date published: August 2021
ISSN: 2368-738X
Submit a manuscript
About HPCDP
Browse
Previous | Table of Contents | Next
Naomi C. Hamm, MScAuthor reference footnote 1; Cynthia Robitaille, MScAuthor reference footnote 2; Joellyn Ellison, MPHAuthor reference footnote 2; Siobhan O’Donnell, MScAuthor reference footnote 2; Louise McRae, BScAuthor reference footnote 2; Kimberley Hutchings, MScAuthor reference footnote 2; Louis Rochette, MScAuthor reference footnote 3; Karen A.M. Phillips, DVMAuthor reference footnote 4; Mahmoud Azimaee, BScAuthor reference footnote 5; MaryRose Stang, PhDAuthor reference footnote 6; Rolf Puchtinger, MAAuthor reference footnote 6; Megan McCallum, MPHAuthor reference footnote 7; Aijun Yang, MScAuthor reference footnote 8; Josh Squires, BScAuthor reference footnote 9; Yue Liu, MSEAuthor reference footnote 10; Lawrence W. Svenson, PhDAuthor reference footnote 11Author reference footnote 12Author reference footnote 13; Faisal Shibley, BScAuthor reference footnote 14; Aakash Amatya, MScAuthor reference footnote 14; Bin Zhang, PhDAuthor reference footnote 15; James Ayles, BScAuthor reference footnote 15; Lisa M. Lix, PhDAuthor reference footnote 1
https://doi.org/10.24095/hpcdp.41.7/8.04
This article has been peer reviewed.
Author references
Correspondence
Lisa M. Lix, Department of Community Health Sciences, University of Manitoba, S113-750 Bannatyne Avenue, Winnipeg, MB R3E 0W3; Tel: 204-789-3573; Fax: 204-789-3905; Email: lisa.lix@umanitoba.ca
Suggested citation
Hamm NC, Robitaille C, Ellison J, O’Donnell S, McRae L, Hutchings K, Rochette L, Phillips KAM, Azimaee M, Stang MR, Puchtinger R, McCallum M, Yang A, Squires J, Liu Y, Svenson LW, Shibley F, Amatya A, Zhang B, Ayles J, Lix LM. Population coverage of the Canadian Chronic Disease Surveillance System: a survey of the contents of health insurance registries across Canada. Health Promot Chronic Dis Prev Can. 2021;41(7/8):230-41. https://doi.org/10.24095/hpcdp.41.7/8.04
Abstract
Introduction: Health insurance registries, which capture insurance coverage and demographic information for entire populations, are a critical component of population health surveillance and research when using administrative data. Lack of standardization of registry information across Canada’s provinces and territories could affect the comparability of surveillance measures. We assessed the contents of health insurance registries across Canada to describe the populations covered and document registry similarities and differences.
Methods: A survey about the data and population identifiers in health insurance registries was developed by the study team and representatives from the Public Health Agency of Canada. The survey was completed by key informants from most provinces and territories and then descriptively analyzed.
Results: Responses were received from all provinces; partial responses were received from the Northwest Territories. Demographic information in health insurance registries, such as primary address, date of birth and sex, were captured in all jurisdictions. Data captured on familial relationships, ethnicity and socioeconomic status varied among jurisdictions, as did start and end dates of coverage and frequency of registry updates. Identifiers for specific populations, such as First Nations individuals, were captured in some, but not all jurisdictions.
Conclusion: Health insurance registries are a rich source of information about the insured populations of the provinces and territories. However, data heterogeneity may affect who is included and excluded in population surveillance estimates produced using administrative health data. Development of a harmonized data framework could support timely and comparable population health research and surveillance results from multi-jurisdiction studies.
Keywords: health insurance registries, administrative health data, population identifiers
Highlights
- All reporting Canadian health insurance registries contain data going back to at least 1996. The earliest year of available data was 1968, in Saskatchewan.
- Some features of registry data, such as change in coverage, primary address, date of birth and sex, were consistent across all reporting jurisdictions. Other features, such as family unit identifiers, socioeconomic status and population identifiers, varied across reporting jurisdictions.
- Differences in Canadian health insurance registries present opportunities for studies that compare the populations covered by provincial/territorial health insurance plans. Creation of a harmonized data framework would benefit national surveillance initiatives and multi-jurisdiction studies.
Introduction
Administrative health data are data originally collected for purposes of managing and monitoring the health care system. However, these data are also commonly used to measure and describe population health within Canada,Footnote 1Footnote 2Footnote 3Footnote 4Footnote 5Footnote 6Footnote 7 because they are routinely collected, inexpensive to use and have nearly complete population coverage. Administrative health data include physician billing claims, hospital discharge abstracts, prescription medication dispensations and health insurance registries.Footnote 8 Health insurance registries are a critical component of population-based surveillance and research studies in Canada, because they contain information about members of provincial or territorial populations who are eligible to receive publicly funded health services.Footnote 9 Understanding the populations captured in health insurance registries and the data that are collected about these populations is essential for comparing health measures between jurisdictions and over time, as well as determining generalizability of these comparisons.
Health care coverage in Canada primarily falls under provincial or territorial jurisdiction.Footnote 10 There is no standard for how data in health insurance registries are collected and coded, or for how different populations, such as those covered by federal health insurance, are identified in registry files. Differences in health insurance registries across Canada can present challenges to the comparability of surveillance and research studies.
The Canadian Chronic Disease Surveillance System (CCDSS) is a network supported by the Public Health Agency of Canada (PHAC) that aims to further the use of Canadian administrative health data for chronic disease surveillance and supports health care planning and health policies and programs.Footnote 8 Through the CCDSS, the provinces and territories provide PHAC with aggregate data derived from administrative health data that are then used to generate national estimates and trends over time for over twenty chronic diseases and conditions. Heterogeneity in the data contained within health insurance registries can affect who is included in or excluded from the CCDSS estimates. It also impacts which jurisdictions can conduct health research and surveillance on specific subpopulations (e.g. First Nations individuals).
There has been limited research on the data contained in Canadian provincial and territorial health insurance registries. The few studies that do exist primarily focus on health insurance registries from a single jurisdiction.Footnote 5Footnote 9Footnote 11 Two studies focus on the Manitoba health insurance registry,Footnote 9Footnote 11 and one provides a brief description of the Quebec registry as part of that province’s Integrated Chronic Disease Surveillance System.Footnote 5 Studies that include multiple jurisdictions are limited to reviews; no direct comparisons across jurisdictions have been made.Footnote 12Footnote 13 Detailed information about identifiable populations and those individuals who are included in or excluded from population-based health insurance registries could (1) improve our understanding of surveillance estimates produced from CCDSS data, and (2) inform the potential uses of registry data to describe specific subpopulations.
The purpose of this study was to assess the data contained within health insurance registries across Canadian provinces and territories. The objectives were to describe the populations covered and document registry similarities and differences.
Methods
Data were collected using a survey developed by the project team with input from content experts and advisors at PHAC. As well, the project team received input from research staff at the Manitoba Centre for Health Policy with experience working with population health insurance registry data. The survey included five sections: (1) general information (i.e. indication of province or territory); (2) temporal data coverage; (3) start and end dates of coverage for residents of the province or territory; (4) population characteristics captured in registry data; and (5) population identification. The final draft of the survey was approved by PHAC before distribution. A copy of the survey is available upon request.
A list of key informants from each of the provinces and territories was identified by the project team with input from PHAC. Informants were primarily identified from members of the CCDSS Science Committee and Data Quality Working Group. Informants who held positions that involved working with administrative data were contacted, as they were most likely to be knowledgeable about the registry data in their jurisdiction. In cases where two contacts were available with similar expertise, both were contacted.
In April 2019, the project team emailed the survey to the key respondents, who were given one week to complete it; extensions were provided as needed. Key informants were free to consult other experts in their jurisdiction to complete the survey if needed. If key informants were unable to complete the survey, they were asked to recommend an alternative informant. Phone and email follow-ups were conducted by the project team to clarify responses when needed.
This study was conducted out of the University of Manitoba. Research ethics approval was not required as data were collected on health insurance registry contents, not human participants.Footnote 14
Results
Thirteen key informants from the 10 provinces responded to the survey (two from Saskatchewan, Manitoba and New Brunswick), and one key informant from the Northwest Territories provided limited information. Where two key informants were consulted, informants worked together to fill out a single survey, which was returned to study researchers. No survey response was received from Yukon or Nunavut, as no one with sufficient expertise (i.e. knowledge of registry data) to address the questions was identified. Key informants included individuals employed by provincial ministries of health and experts associated with population-based research data repositories, such as ICES. Both Saskatchewan and Prince Edward Island indicated that registry staff were consulted when completing the survey.
Temporal data coverage
Information about temporal coverage of the health insurance registries is provided in Figure 1. The earliest available year of data was reported by Saskatchewan (1968). While Manitoba’s key informant reported that the earliest available year of data was from 1984, other published sources indicate this province’s health insurance registry data extends back to 1970.Footnote 9Footnote 15 However, data from these early years may not be consistently available to all data users and may be difficult to use when generating surveillance and research reports. All provinces reported that “snapshots” (i.e. a file to preserve the registry data at that point in time) of their registries are regularly saved and stored.
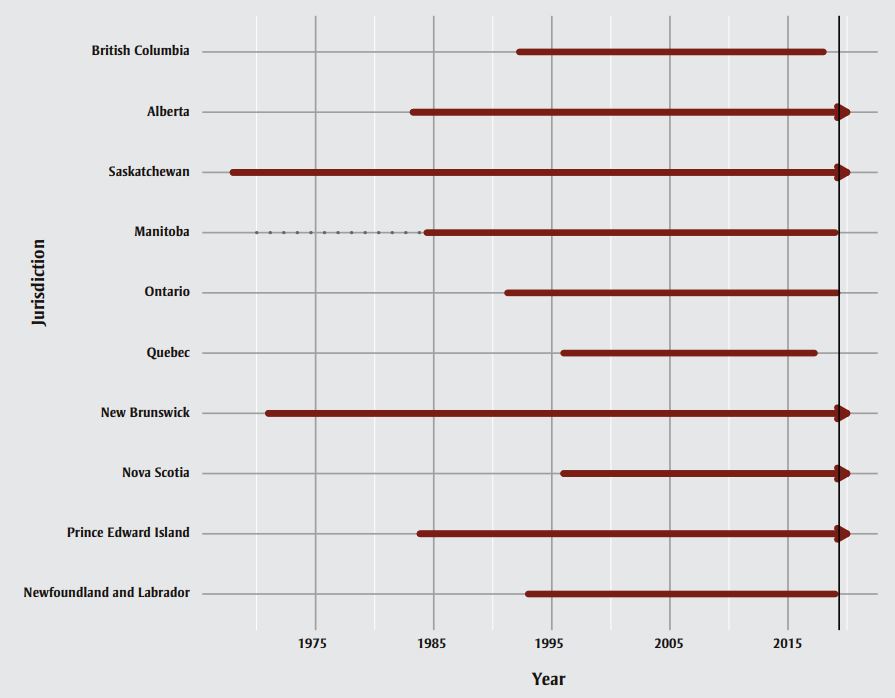
Figure 1 - Text description
| Jurisdiction | Start | Availability | End |
|---|---|---|---|
| British Columbia | 1992-04-01 | Full | 2018-01-01 |
| Alberta | 1983-04-01 | Full | 2020-01-01 |
| Saskatchewan | 1968-01-01 | Full | 2020-01-01 |
| Manitoba | 1970-01-01 | Variable | 1984-06-01 |
| Manitoba | 1984-06-01 | Full | 2018-12-31 |
| Ontario | 1991-04-01 | Full | 2019-02-28 |
| Quebec | 1996-01-01 | Full | 2017-03-31 |
| New Brunswick | 1971-01-01 | Full | 2020-01-01 |
| Nova Scotia | 1996-01-01 | Full | 2020-01-01 |
| Prince Edward Island | 1983-11-01 | Full | 2020-01-01 |
| Newfoundland and Labrador | 1993-01-01 | Full | 2018-12-31 |
Notes: Arrows indicate registry data are continually updated daily or weekly and data are available as of the last update. Dotted gray line indicates data availability may be limited. Vertical black line indicates date of survey administration (i.e. April 2019). Dates of data availability are current as of survey response date (May 2019); updates may be available after this date.
Start and end of coverage
Table 1 summarizes the responses provided around start and end dates of health insurance coverage for individuals. There was heterogeneity across the reporting jurisdictions on the capture of information about mobility of health-insured residents (i.e. where an individual moved to when leaving the jurisdiction and where they moved from when entering the jurisdiction). For most jurisdictions, individuals were added to the registry three months after moving into the jurisdiction and flagged for end of coverage three months after moving out of the jurisdiction. The timeline for being added to the registry and being flagged for end of coverage in cases of birth and death were variable across jurisdictions. There was substantial diversity in the end-of-coverage cancellation codes (e.g. deceased, left country, duplicate record) provided by the key informants; only Ontario indicated no end-of-coverage codes were available. While data quality checks for start and end of coverage were implemented in a number of jurisdictions (i.e. British Columbia, Alberta, Saskatchewan, Ontario, Quebec, Nova Scotia and Newfoundland and Labrador), key informants did not always have information about data quality assessment processes or did not report that data quality assessments were undertaken.
| Start and end of coverage | British Columbia | Alberta | Saskatchewan | Manitoba | Ontario | Quebec | New Brunswick | Nova Scotia | Prince Edward Island | Newfoundland and Labrador | Northwest Territories |
|---|---|---|---|---|---|---|---|---|---|---|---|
| For residents moving into jurisdiction: | |||||||||||
| Where the individual moved from | No | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes, if within Canada | NR |
| Length of time after moving that newcomers (from within Canada) are added to registryFootnote a | 3 months | Added immediately but must live in AB for 3 months before eligible | 3 months (i.e. first of the third month after arrival) | Added once applied for but must live in MB for 3 months (i.e. first day of full third month) before eligibleFootnote b | 3 months | 3 months | 90 days | 3 months | 3 months | 3 months | NR |
| Length of time after moving until immigrants are added to registry | 3 months | Varies | Varies | Unsure | 3 months | 3 months | 90 daysFootnote c | Date of arrival | First day of arrival or first day granted permanent residence, whichever is later | Date of arrival | NR |
| For residents moving out of jurisdiction: | |||||||||||
| Where the individual moved to | No | Yes | Yes, if within Canada | Yes | No | No | Yes, if within Canada | Yes | Yes, if within Canada | No | NR |
| Length of time after moving that residents are flagged for end of coverageFootnote a | Until residents submit request of cancellation | When coverage begins in the new province, OR the day they leave the country | 3 months (i.e. covered for remainder of month of departure plus 2 more months) | 3 months (i.e. covered for remainder of month of departure plus 2 more months) for Canadian citizens and permanent residents. Day of permanent move for work and study permit holders | Unclear from the data | 3 months | When coverage begins in the new province OR when NB Medicare is notified they left the country | 3 months | The day before coverage begins in the new province | 3 months | NR |
| For births and deaths: | |||||||||||
| Length of time after birth before added to registry | Before 2008: varies After 2008: immediately |
Within 24 hours | Immediately as of 1998 | Unsure | 3 months | 2–5 months | Until parent submits completed registration form | Typically within 10 business days | 24–48 hours | Until parent submits completed registration form | NR |
| Length of time after death before flagged in registry | Unsure | Varies | Varies | Unsure | Up to 3 months | Unsure | New deaths are flagged daily, but will be confirmed through Vital Statistics bi-weekly report | Varies | 24–48 hours | Typically a day after death | NR |
| End-of-coverage descriptions in registry data, as provided by the informant | Deceased Group cancel coverage Expired temporary permit Left the province |
Deceased Armed Forces Federal penitentiary Opted out of AHCIP Duplicate registration Left AB—normal extended coverage Left AB—circumstances unknown Left AB—notified by other provincial health office Left Canada Left Canada—maximum three months Left Canada—coverage extended 1 month Other |
Deceased Canadian Armed Forces Incarcerated in federal institution Mail return and current address unknown Left the province |
Deceased Registered in error Duplicate PHIN Temporary resident/non-Canadian Adopted Left province —unknown location Left province—NL Left province—ON Left province—SK Left province—AB Left province—BC Left province—YT Left province—NWT Left province—NU Left province—USA Left province—other country |
No reason for end of coverage givenFootnote d | End of eligibility Cancellation of health insurance |
Deceased Noncompliance Adopted Left the province Left the country To be determined |
Deceased, confirmed through Vital Statistics Terminated eligibility Left NS (new province notify) |
Deceased Federal government Left the province |
Deceased Not eligible for coverage, or Armed Forces Neonatal coverage terminated Work permit expired Student visa expired Visitor’s permit expired Minister’s permit expired Immigration documents expired Refugee documents expired Child of immigrant parents Out of province coverage InactiveFootnote e Left the province and under social services |
Transferred to Armed Forces Employed by RCMP Division of NWT/ creation of Nunavut, April 1999 Visa expired Duplicate registration NWT inmate released Coverage suspended Address box closed |
Abbreviations: AB, Alberta; AHCIP, Alberta Health Care Insurance Plan; BC, British Columbia; HCP, health care plan; NB, New Brunswick; NL, Newfoundland and Labrador; NR, no response; NS, Nova Scotia; NU, Nunavut; NWT, Northwest Territories; ON, Ontario; PEI, Prince Edward Island; PHIN, personal health information number; QC, Quebec; RCMP, Royal Canadian Mounted Police; SK, Saskatchewan; YT, Yukon Territory; USA, United States of America.
|
|||||||||||
Population characteristics and attributes captured
All jurisdictions reported that their registries contained a primary address, birth date and sex for health-insured residents (Table 2).
| Population characteristics | British ColumbiaFootnote a | Alberta | Saskatchewan | Manitoba | OntarioFootnote b | Quebec | New BrunswickFootnote c | Nova Scotia | Prince Edward Island | Newfoundland and Labrador | Northwest Territories |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Residence | |||||||||||
| Primary address | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Previous address available? | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Date of birth | |||||||||||
| Date of birth | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sex | |||||||||||
| Sex | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| New classifications implementedFootnote d | No | No | No | No | No | No | Yes | Yes | No | Yes | NR |
| Familial relationships | |||||||||||
| Family unit identifier | No, but can link to other databases to determine | Yes | Yes | Yes | No | No | Yes | No | YesFootnote e | No | Yes |
| Relationships available | N/A | Family unit | Head of family (max 2 per family) and dependents | Family unit containing registrant, and if applicable, spouse and dependents | N/A | N/A | Head of household identifier | N/A | NR | N/A | NR |
| Relationship coding | N/A | Family units are grouped together under a single account number Specific relationships codes: |
All members have the same family number and individuals are listed as either head of family or dependent | All family members residing in MB are assigned the same MB health registration number Specific relationships are indicated by number (from 0–8) for the following: |
N/A | N/A | There is a “Head of Household” ID that can be linked to all family members | N/A | N/A | N/A | NR |
| Ethnicity | |||||||||||
| Ethnicity | No | No | No | No | Yes | No | No | No | No | No | No |
| Identifiable ethnicities | N/A | N/A | N/A | N/A | GeneralFootnote f, Chinese, South Asian | N/A | N/A | N/A | N/A | N/A | N/A |
| Socioeconomic status | |||||||||||
| SES available | No, but can link for a subset to determine | No | No | No | Yes | Yes | No | No | No | No | No |
| Information used to define SES | N/A | N/A | N/A | N/A | Income | OtherFootnote g | N/A | N/A | N/A | N/A | N/A |
| SES coding | N/A | N/A | N/A | N/A | 1,2,3,4,5 (quintiles) | Deprivation index | N/A | N/A | N/A | N/A | N/A |
| Place of birth | |||||||||||
| Place of birth | No | Yes | No | No | No | No | No | No; can link to other databases/sources to determine if born in NS | Yes | No; can link to other databases/sources to determine if born in NL | NR |
| Coding | N/A | Structured text field | N/A | N/A | N/A | N/A | N/A | N/A | Country/province | N/A | NR |
Abbreviations: BC, British Columbia; MB, Manitoba; N/A, not applicable; NL, Newfoundland and Labrador; NR, no response; NS, Nova Scotia; RCMP, Royal Canadian Mounted Police; SES, socioeconomic status.
|
|||||||||||
A family unit identifier, that is, a code to indicate familial relationships, was reported for Alberta, Saskatchewan, Manitoba, New Brunswick and the Northwest Territories. Prince Edward Island reported having a household identifier, but noted limitations in its use (e.g. individuals in a group home have the same household identifier). British Columbia indicated that familial relationships among residents could be ascertained from other administrative data sources. Family relationship codes (i.e. indication of relationships among residents, such as parent, offspring, spouse or sibling) were available in Alberta, Saskatchewan, Manitoba and New Brunswick.
Only Ontario reported having information about ethnicity in its health insurance registry. Identifiable categories for ethnicity were general, Chinese and South Asian. These categories are derived from an algorithm applied to the data and not directly collected.
Measures of socioeconomic status (e.g. income quintile) were available in the health insurance registries of Ontario and Quebec; Ontario’s measure was algorithm-driven. British Columbia indicated socioeconomic status could be determined for a subset of individuals by linking to a supplementary database.
Lastly, place of birth was available in Alberta and Prince Edward Island, although other jurisdictions did note that linkage of registry data with other sources could aid in identifying this information.
Population identification
Table 3 provides information about the populations identifiable in health insurance registries. All jurisdictions indicated they could identify at least some of the populations in question, except for Quebec. Quality of population identifiers was heterogeneous. For example, the First Nations identifier in Manitoba’s health insurance registry may result in misclassification of individuals, because it is based on self-report. This means that a First Nations individual would only be flagged as such if that individual disclosed this information to insurance registry staff. In Alberta, the federal government had previously verified First Nations status, but stopped when Alberta eliminated health insurance premiums in 2009. To aid in preserving data quality, Alberta has maintained the flag for those present prior to the change, and any offspring are conferred unofficial status for reporting purposes. However, misclassification may still occur.
| Population identification | British ColumbiaFootnote a | Alberta | Saskatchewan | Manitoba | OntarioFootnote j | Quebec | New BrunswickFootnote k | Nova Scotia | Prince Edward Island | Newfoundland and Labrador | Northwest Territories |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Population | |||||||||||
| Full-time members of the Canadian Armed Forces | NR | Yes | YesFootnote d | YesFootnote g | No | No | YesFootnote l | NoFootnote o | No | No | NR |
| Part-time members of the Canadian Armed Forces | NR | No | YesFootnote d | YesFootnote g | No | No | No | No | No | No | NR |
| Veterans | No | Yes | No | NR | No | No | No | NoFootnote o | No | No | NR |
| Royal Canadian Mounted Police | No | Yes | No | Yes | No | No | Yes | NoFootnote o | No | No | NR |
| Federal penitentiary inmates | NR | Yes | YesFootnote e | YesFootnote h | No | No | No | No | Yes | No | NR |
| Provincial penitentiary inmates | Yes | YesFootnote b | Yes | NR | No | No | Yes | No | No | No | NR |
| First Nations on reserve | NR | YesFootnote b | YesFootnote f | YesFootnote i | Yes | No | NoFootnote m | No | No | No | Yes |
| First Nations off reserve | NR | YesFootnote b | YesFootnote f | YesFootnote i | Yes | No | NoFootnote m | No | No | No | Yes |
| Inuit | No | YesFootnote b | No | NR | Yes | No | No | No | No | No | Yes |
| Métis | No | NoFootnote c | No | NR | Yes | No | No | No | No | No | Yes |
| Nonpermanent residents | |||||||||||
| Refugee claimants | Yes | Yes | Yes | NR | Yes | No | No | No | Yes | Yes, upon termination of coverage | NR |
| Persons with a study permit | No | Yes | Yes | NR | No | No | Yes | Yes | Yes | Yes, upon termination of coverage | NR |
| Persons with a work permit | No | Yes | Yes | NR | No | No | No | Yes | Yes | Yes, upon termination of coverage | NR |
| Immigrants | |||||||||||
| Landed immigrants | NR | Yes | Yes | NR | Yes | No | YesFootnote n | Yes | Yes | Yes, upon termination of coverage | NR |
| Permanent residents | |||||||||||
| Economic immigrants | No | No | No | NR | Yes | No | No | No | Yes | No | NR |
| Family members of permanent residents | NR | Yes | No | NR | No | No | No | No | Yes | No | NR |
Abbreviations: BC, British Columbia; FN, First Nations; MB, Manitoba; NB, New Brunswick; NR, no response; RCMP, Royal Canadian Mounted Police; SK, Saskatchewan.
|
|||||||||||
Discussion
The results of this survey provide important insights about the data contained within health insurance registries across Canada (i.e. 10 provinces and the Northwest Territories). Health insurance registry data go back as far as 1968 (in the case of Saskatchewan). All reporting jurisdictions had data going back to at least 1996. Individuals moving in or out of the jurisdiction are generally added or flagged for end of coverage three months after moving; timelines are more variable for beginning or ending of coverage due to births and deaths. Events recorded for end of coverage differ among jurisdictions. All jurisdictions record a primary address, date of birth and sex. Family identifiers, ethnicity, socioeconomic status and place of birth are recorded in select jurisdictions. Ability to identify members of certain populations, such as First Nations, the Canadian Armed Forces and inmates of federal penitentiaries, is variable across jurisdictions.
Previous research has compared data contained in physician services databases across Canada.Footnote 16 However, there has been limited research on provincial and territorial health insurance registry data and its quality. Publications on registry data have reported on Manitoba’s and British Columbia’s health insurance registries.Footnote 9Footnote 11Footnote 17 However, the most recent Manitoban publication was in 1999,Footnote 9 and British Columbia’s paper focussed on the development of a research registry to which the provincial health insurance registry contributed.Footnote 17 Tang et al.Footnote 18 reported on ethnic classifications available in Canadian health insurance registries and found that flags only existed on First Nations people in the registries. In contrast, we found that Ontario had flags derived from an algorithm for subpopulations of South Asian and Chinese descent. A systematic review conducted by Hinds et al.Footnote 13 did not identify any studies that had investigated the quality of health insurance registry information.
Capture of population characteristics and attributes allows for surveillance measures to be stratified by potential risk factors (e.g. social determinants of health such as socioeconomic status, immigration status and ethnicity). Results reported here help summarize the jurisdictions that are suitable for these analyses. However, heterogeneity among jurisdictions in population identification also has implications for who is included in the CCDSS estimates, and suggests that inclusions and exclusions may not be consistent across jurisdictions.
A major value of the health insurance registry comes from preserving snapshots, or timestamped records, of registry data.Footnote 9 Our study results indicate that over 20 years of registry data are available in all reporting jurisdictions, with snapshots available to capture changes in the registry. There are challenges associated with using health insurance registries for longitudinal studies: health insurance registries are not static, registry data and data quality change over time, and older data are not always linkable. Nonetheless, the benefits of being able to use these data to conduct longitudinal cohort and intergenerational studies with minimal cost and data collection far outweigh the challenges.
Strengths and limitations
This study is unique in providing insights about the data contained within health insurance registries across Canada using a standardized survey with near complete coverage of the provinces and territories. Surveys were completed by individuals with in-depth knowledge of the registry data and access to other informants to provide additional information if needed.
However, there are some limitations. Our study did not employ a validated survey for information capture, as no such survey exists. This hinders international comparisons. As well, health insurance registries are complex databases, and it is not possible to capture all nuances of their features in a survey conducted at a single point in time. Not all elements collected during the registration process will be available to potential data users. Many of these elements are administrative in nature. Many systems are dynamic, being continually updated, so extracts or snapshots are created with a methodology to provide the most accurate and consistent view of the population.
Future research
Future studies could be undertaken to validate key population characteristics included in health insurance registry data, including dates of birth and death, coverage cancellation codes, location of residence and identifiers for specific populations. Another research opportunity lies in assessing the timeliness of characteristic updates. However, a key challenge with such studies is identifying and accessing appropriate population-based validation data sources that can be linked to health insurance registration data. While vital statistics data could be used to assess the accuracy of dates of birth and death, validation data sources for other key population characteristics may not be readily available in all jurisdictions.
Previous studies have compared aggregate population counts obtained from health insurance registries to counts from Statistics Canada census data.Footnote 19Footnote 20 However, potential sources of inaccuracies were not determined. Therefore, future research could look at potential sources of discrepancy between population counts in registry and census data, and estimate the impact of these discrepancies on health measures.
Exploring changes in health insurance registration coverage over time is another potential area of future research. Registries are not static; exclusions may not be consistent over time. Comprehensive information about changes in the data can help ensure accuracy of health trend estimates.
Future research should investigate the feasibility of a common data framework, such as the Generalized Data Model proposed by Danese et al.Footnote 21 to facilitate the systematic and standardized capture of information in health insurance registries. However, access to some registry data elements may be subject to privacy legislation, and data are primarily collected for administrative, not research, purposes. This could lead to challenges in implementing a common data framework.
Finally, there is a potential role for a national organization to facilitate the harmonization or standardization of data in health insurance registries. Examples of such organizations include the Canadian Institute for Health Information, which has recently proposed standards for collecting data on patient ethnicity,Footnote 22 and Health Data Research Network Canada, which aims to support multi-jurisdiction studies by connecting and establishing research data infrastructure.Footnote 23
Acknowledgements
This work was made possible through collaboration between PHAC and the respective provincial and territorial governments of British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec, New Brunswick, Nova Scotia, Prince Edward Island, Newfoundland and Labrador and Yukon. No endorsement by the provinces and territories is intended or should be inferred.
Conflicts of interest
The authors have no conflicts of interest to declare.
Authors’ contributions and statement
NCH and LML drafted the manuscript and all authors contributed to its revisions. LML, CR, JE, SO, LM and KH defined the scope of the survey. NCH, LML, CR, JE, SO, LM and KH developed the survey. LML and NCH contacted key informants and collected completed surveys. LR, KAMP, MA, MS, RP, MM, AY, JS, YL, LWS, FS, AA, BZ and JA reviewed the manuscript for accuracy and ensured appropriate interpretation of health registry data.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.