
Canada-Manitoba Emergency Treatment Fund Bilateral Agreement
BETWEEN:
HER MAJESTY THE QUEEN IN RIGHT OF CANADA (hereinafter referred to as “Canada” or “Government of Canada”) as represented by the Minister of Health (herein referred to as “the federal Minister”)
- and -
HER MAJESTY THE QUEEN IN RIGHT OF MANITOBA (hereinafter referred to as "Manitoba" or "Government of Manitoba") as represented by the Minister of Health, Seniors and Active Living herein referred to as "the Manitoba Minister")
REFERRED to collectively as the “Parties”
PREAMBLE
WHEREAS, Canada and Manitoba agree that Canada is in the midst of an opioid crisis that has had a significant effect on many communities, that has claimed the lives of thousands of Canadians from all walks of life, that has had a devastating impact on many Canadian families, and the Emergency Treatment Fund is designed to augment treatment services through one-time funding in response to the opioid crisis;
WHEREAS, Canada and Manitoba agree that immediate action and collaboration is needed among governments to help reduce harms and deaths associated with problematic substance use, including opioids;
WHEREAS, the governments of Canada and Manitoba have committed to work together to further address the opioid crisis, in full respect of their respective jurisdictional responsibilities, and recognizing that the Government of Manitoba has the primary responsibility for the design and delivery of substance use disorder treatment and response services in Manitoba, the one-time Emergency Treatment Fund is intended to augment services and Manitoba will be required to sustain any ongoing initiatives, as determined by Manitoba;
WHEREAS, Canada has established a transfer payment program called the Emergency Treatment Fund to provide one-time funding to the provincial and territorial governments for the development and delivery of treatment services for problematic substance use, including opioids;
WHEREAS, Canada authorizes the federal Minister to enter into agreements with the provinces and territories, for the purpose of promptly and effectively responding to the opioid crisis and problematic substance use through the Emergency Treatment Fund;
WHEREAS, the Manitoba Minister has received authorization under The Executive Government Organization Act to enter into this Agreement with the Government of Canada under which the Government of Manitoba undertakes to use the funding provided by Canada under the Emergency Treatment Fund for the provision of treatment services for problematic substance use, including opioids;
AND WHEREAS, Manitoba is responsible for the provision of treatment services including to Indigenous populations accessing treatment services off-reserve.
NOW THEREFORE, Canada and Manitoba agree as follows:
1.0 Purpose
1.1 The Parties are committed to protecting the health and safety of all Canadians through a compassionate and collaborative approach to addressing problematic substance use. The objective is to support single or multi-year projects that will improve access to evidence-based treatment services.
1.2 The purpose of this Agreement is to provide financial support from Canada to Manitoba to target treatment services for problematic substance use, including opioids. This funding will support single or multi-year projects that will build on and enhance existing initiatives, capacity, and priorities.
2.0 Emergency Treatment Services
2.1 Objectives
2.1.1 Canada and Manitoba agree that over the period of this Agreement, with financial support from Canada, Manitoba will address local, regional, and system priorities with an aim to reduce problematic substance use-related harms and deaths by further building on and enhancing Manitoba treatment services and programs to improve the availability and accessibility of treatment for problematic substance use towards achieving the objectives of:
- To increase access to flexible-length withdrawal management services in Winnipeg and Brandon that are appropriate for people who use methamphetamines.
- To increase the number of people who receive flexible-length withdrawal management services for methamphetamine use disorder.
- To increase the number of people who enter into longer-term treatment after receiving flexible-length withdrawal management services for methamphetamine use disorder.
- To reduce the number of methamphetamine-related deaths.
- To reduce the number of methamphetamine-related emergency department visits and hospitalizations.
Manitoba's approach to achieving these objectives is set out in its Action Plan attached as Annex 1.
2.2 Eligible Areas of Investment
2.2.1 Manitoba agrees to allocate funds provided by Canada under this Agreement in one or more of the following eligible areas of investment:
- support initiatives that will establish, build on, or enhance existing treatment approaches;
- encourage further implementation of innovative treatment solutions;
- recognize the importance of broader strategies to support access to treatment services by enhancing health care providers' knowledge of best practices.
2.2.2 The types of initiatives for which Manitoba agrees to use the funding may include: enhancements or expansion of existing treatment approaches such as opioid agonist treatments (e.g., methadone, buprenorphine/naloxone), withdrawal management products (e.g., opioid agonist taper and alpha2-adrenergic agonists), oral Naltrexone, psychosocial treatment interventions, and counseling services; innovative treatment solutions such as wrap-around care and injectable agonist therapies; and, implementation strategies to enhance health care providers' knowledge of best practices (alcohol, cannabis, and tobacco are excluded).
2.2.3 Treatment services specifically to address alcohol, cannabis, and tobacco are excluded from this funding.
2.2.4 Types of eligible expenditures may include:
- Operating costs;
- Capital costs;
- Training, professional development and related investments;
- Information technology and related investments; and,
- Other costs that in the opinion of the Parties are essential for the completion of the project and achievement of results.
3.0 Period of Agreement
3.1 This Agreement shall come into effect upon the last signature being affixed and will remain in effect until March 31, 2023, unless terminated in writing by Canada or Manitoba, in accordance with the terms and conditions set out in section 11. Funding provided under this Agreement, in accordance with section 4, will cover the period from April 1, 2018 to March 31, 2023.
3.2 Canada and Manitoba concur that the purpose of this time-limited, one-time Agreement is to help Manitoba more rapidly ramp up or otherwise augment treatment initiatives in light of the opioid crisis, and that ongoing funding for enhanced initiatives established under this Agreement are to be sustained by Manitoba, as determined by Manitoba.
4.0 Financial Provisions
4.1 The funding provided under this Agreement is in addition to, and not in lieu of, that which Canada currently provides to Manitoba through the Canada Health Transfer in order to support health care services within Manitoba. Furthermore, this funding is in addition to and not in lieu of those funds that Canada has already provided or may provide to address problematic substance use and the opioid crisis.
4.2 Allocation to Manitoba
4.2.1 Canada has designated the following maximum one-time amount of funding to be transferred in total to all provinces and territories under this Agreement: $150,000,000 for the period starting on April 1, 2018 and ending on March 31, 2023.
4.2.2 The final total amount to be paid to Manitoba will be calculated using the following formula:
(F –G x 500,000) x (0.33K/[N-P] + 0.33L/Q + 0.33M/R), where:
F is the total one-time funding amount available under this initiative;
G is the number of provinces and territories receiving only the minimum baseline funding (i.e., provinces and territories for which this funding allocation formula results in an allocation of less than $500,000);
K is the total population of Manitoba as determined using the 2017 population estimates from Statistics Canada;
L is the number of apparent opioid-related deaths in Manitoba as determined using 2016 data from the Public Health Agency of Canada’s National Report on apparent Opioid-Related Deaths in Canada (based on P/T reporting);
M is the number of opioid poisoning hospitalizations in Manitoba as determined using 2016-17 data from the Canadian Institute for Health Information’s Annual Report on Opioid-Related Harms (based on P/T reporting);
N is the total population of Canada as determined using the 2017 population estimate from Statistics Canada;
P is the total population of province and territories receiving only the minimum baseline funding, as determined using the 2017 population estimate from Statistics Canada;
Q is the total number of apparent opioid-related deaths in Canada, as determined using 2016 data from the Public Health Agency of Canada’s National Report on Apparent Opioid-Related Deaths in Canada; and,
R is the total number of opioid poisoning hospitalizations in Canada as determined using 2016-17 data from the Canadian Institute for Health Information’s Annual Report on Opioid-Related Harms (based on P/T reporting).
4.2.3 Manitoba agrees to match Canada's contribution at a 1:1 ratio, with the exception of the first $250,000 in federal funding, for which no cost-sharing is required. Manitoba's matching contribution shall be the equivalent to Canada's contribution less $250,000 and, as outlined in Annex A, can include eligible expenditures made specifically for treatment related to problematic substance use as of January 1, 2016. Manitoba agrees to make reasonable efforts to ensure that previous and ongoing funding from Canada under, pursuant to, or through other programs or agreements shall not be used to match Canada's contribution under this Agreement.
4.2.4 Based on the formula described in section 4.2.2, Manitoba's estimated share of the amounts identified in section 4.2.1 will be:
| Fiscal Year | Amount to be paid to Manitoba in Fiscal Year 2018-2019 | Amount that has been paid between January 1, 2016 and May 1, 2018 by Manitoba (section 4.2.3) |
|---|---|---|
| 2018-2019 | $ 4,187,161.00 | $ 5,052,463.00 |
4.3 In this Agreement, “Fiscal Year” means the period commencing on April 1 of any calendar year and terminating on March 31 of the immediately following calendar year.
4.4 Payment
4.4.1 Canada's contribution under this Agreement as set out in 4.2.4 will be paid in full to Manitoba within approximately 30 business days of both Parties' signatures being affixed to this Agreement and within Fiscal Year 2018-2019. Manitoba will defer the contribution received under this Agreement in Fiscal Year 2018-2019 and will bring such portions of the contribution into income in each subsequent Fiscal Year as needed to implement the expenditure plan in the Action Plan attached as Annex 1.
4.4.2 Manitoba must spend the entire amount of Canada's contribution by no later than March 31, 2023.
4.4.3 Manitoba must spend the entire amount of Manitoba's matching contribution by no later than March 31, 2023.
4.4.4 Payment of Canada's contribution under this Agreement is subject to an annual appropriation by the Parliament of Canada for this purpose.
4.5 Repayment of Overpayment
4.5.1 Canada and Manitoba agree that every effort will be made to ensure that the calculation of Canada's contribution installment to Manitoba will be accurate.
4.5.2 In the event payment made to Manitoba exceeds the amount to which Manitoba is entitled under this Agreement, the amount of the excess is a debt due to Canada and Manitoba shall repay the amount to Canada within 90 calendar days of written notice from Canada.
4.6 Repayment of Unmatched Funds
4.6.1 In the event that Manitoba does not clearly demonstrate that funds have been cost-matched to the federal funding on a 1:1 ratio less $250,000 by March 21, 2023 in accordance with section 4.2.3, including funding announced as of January 1, 2016, Manitoba agrees to repay the unmatched funds to Canada within 90 calendar days of written notice from Canada.
4.7 Use of Funds
4.7.1 Canada and Manitoba agree that funds provided under this Agreement will only be used by Manitoba in accordance with the areas for investment outlined in section 2.0 of this Agreement and detailed in Annex 1.
5.0 Accountability and Reporting
5.1 Action Plan
5.1.1 Manitoba has completed and shared its Action Plan for the years 2018-19 to 2022-23 of federal funding with Canada, as set out in Annex 1. Manitoba will publicly release its Action Plan which:
- Provides an overview of the significant increase in methamphetamine use in Manitoba and the need for increased access to appropriate supports and services to respond to this crisis;
- Identifies specific priority areas for investment and objectives, which builds upon the progress to date in delivering treatment services;
- Highlights those investments Manitoba has made in a cost-shared manner equivalent to the federal contribution less $250,000 including initiatives implemented as of January 1, 2016;
- Outlines the indicators and specific targets that Manitoba will use to track progress and report on annually according to their planned investments.
Manitoba agrees to publicly release its Action Plan (Annex 1) within thirty (30) business days after all tendered contracts under the Action Plan have been executed. Manitoba will advise Canada in writing when all such contracts have been executed.
5.1.2 The Action Plan may be amended by Manitoba with mutual consent from Canada in a manner consistent with the spirit and intent of this Agreement if deemed necessary by Manitoba to reflect shifts in approach necessitated by changing circumstances or priorities. Such amendments will be done in accordance with section 9.1 and will be made publicly available in accordance with section 7.2.
5.2 Reporting
5.2.1 Within 90 days of both Parties signing this Agreement, Manitoba agrees to:
- Provide all available baseline data on the agreed-to indicators; and
- Describe any initiatives being undertaken in Fiscal Year 2018-2019 as outlined in the Action Plan.
5.2.2 Beginning in Fiscal year 2019-20 and by no later than October 1 of the subsequent Fiscal Year during the Period of this Agreement, Manitoba agrees to:
- Report to the people of Manitoba and to Canada annually on the results and expenditures of the Emergency Treatment Fund allocation until March 31, 2023. The report shall show separately the results attributable to the funding provided by Canada under this Agreement and results attributable to funding provided by Manitoba.
- Provide to Canada an annual financial statement of revenues received from Canada under this Agreement during the preceding Fiscal Year
- The revenue section of the statement shall show the amount received from Canada under this Agreement during the Fiscal Year.
- The total amount of funding used for programs and services under section 2.2.
- If applicable, the amount of any amount carried forward by Manitoba under section 4.4.
- If applicable, the amount of any surplus funds that are to be repaid to Canada under section 4.5 and 4.6.
The annual financial statement shall be prepared in accordance with Canadian Generally Accepted Accounting Principles with attestation from the Department of Health, Seniors and Active Living's Chief Financial Officer.
5.2.3 Canada, with prior agreement from Manitoba may incorporate all or any part or parts of the said report into any public report that Canada may prepare for its own purposes, including any reports to the Parliament of Canada or reports that may be made public.
5.3 Expenditure Information
5.3.1 Manitoba will ensure that expenditure information presented in the annual report is, in accordance with Manitoba standard accounting practices, complete and accurate.
5.4 Evaluation
5.4.1 As per established policies and processes with respect to program effectiveness, Manitoba may evaluate programs and services receiving funds provided under this Agreement and make public the results of any such evaluations.
5.5 Data
5.5.1 It is agreed that all data shared or provided under this Agreement or included in any reports prepared under this Agreement shall be aggregate and non-identifying.
6.0 Long-Term Collaboration
6.1 Canada and Manitoba agree to share and release data as available, and to share knowledge, research and information on effective and innovative practices in treatment programs, to further support the development of and reporting on outcomes.
7.0 Communications
7.1 Canada and Manitoba agree on the importance of communicating with citizens about the objectives of this Agreement in an open, transparent, effective and proactive manner through appropriate public information activities.
7.2 Canada will make publicly available up-to-date Emergency Treatment Fund bilateral agreements entered into with all provinces and territories, including any amendments, on a Government of Canada website. Manitoba's Action Plan (Annex 1) will be publically released by Manitoba in accordance with section 5.1.1.
7.3 Each government will receive the appropriate credit and visibility when investments financed through funds granted under this Agreement are announced to the public.
7.4 Canada reserves the right to conduct public communications, announcements, events, outreach and promotional activities with respect to this Agreement. Canada agrees to give Manitoba 10 days advance notice and advance copies of public communications related to this Agreement and results of the investments of this Agreement.
7.5 Manitoba reserves the right to conduct public communications, announcements, events, outreach and promotional activities with respect to this Agreement. Manitoba agrees to give Canada 10 days advance notice and advance copies of public communications related to this Agreement and results of the investments of this Agreement.
8.0 Dispute Resolution
8.1 Canada and Manitoba are committed to working together and avoiding disputes through government-to-government information exchange, advance notice, early consultation, and discussion, clarification, and resolution of issues, as they arise.
8.2 If at any time either Canada or Manitoba is of the opinion that the other Party has failed to comply with any of its obligations or undertakings under this Agreement or is in breach of any term or condition of the Agreement, Canada or Manitoba as the case may be, may notify the other party in writing of the failure or breach. Upon such notice, Canada and Manitoba will endeavor to resolve the issue in dispute bilaterally through their designated officials at the Assistant Deputy Minister level (hereinafter “Designated Officials”).
8.3 If a dispute cannot be resolved by Designated Officials, then the dispute will be referred to the Deputy Ministers of Health for Canada and Manitoba, and if it cannot be resolved by them, then the federal Minister and Manitoba Minister shall endeavor to resolve the dispute.
9.0 Amendments to the Agreement
9.1 This Agreement, including the attached annex, may be amended at any time by mutual consent of the Parties. To be valid, any amendments shall be in writing and signed, in the case of Canada, by the federal Minister, and in the case of Manitoba, by the Manitoba Minister.
10.0 Equality of Treatment
10.1 During the term of this Agreement, if another province or territory, except the province of Quebec, negotiates and enters into an Emergency Treatment Fund agreement with Canada, or negotiates and enters into an amendment to such an agreement and if, in the reasonable opinion of Manitoba, any provision of that agreement or amended agreement is more favorable to that province or territory than the terms set forth in this Agreement, Canada agrees to amend this Agreement in order to afford similar treatment to Manitoba, if requested by Manitoba. This includes any provision of the bilateral agreement except for the Financial Provisions set out under section 4.0. This amendment shall be retroactive to the date on which the Emergency Treatment Fund Agreement or the amendment to such an agreement with the other province or territory, as the case may be, comes into force.
11.0 Termination
11.1 Canada may terminate this Agreement at any time if the terms of this Agreement are not respected by Manitoba by giving at least 12 months written notice of its intention to terminate. Manitoba may terminate this Agreement at any time if the terms of this Agreement are not respected by Canada by giving at least 12 months written notice of its intention to terminate.
11.2 As of the effective date of termination of this Agreement under section 11.1, Canada shall have no obligation to make any further payments to Manitoba after the date of effective termination.
11.3 As of the effective date of termination of this Agreement under section 11.1, Manitoba will repay, on a pro-rated basis, the amounts of federal funds not expended on initiatives set out in Annex A in accordance with the agreed schedule of expenditures, as of the effective date of termination.
11.4 As of the effective date of termination of this Agreement under section 11.1 Manitoba agrees to return any federal funding not cost-matched by Manitoba consistent with section 4.2.3 and section 4.7.1.
12.0 Notice
12.1 Any notice, information or document provided for under this Agreement will be effectively given if delivered or sent by letter, postage or other charges prepaid. Any notice that is delivered will have been received in delivery; and, except in periods of postal disruption, any notice mailed will be deemed to have been received eight calendar days after being mailed.
The address for notice or communication to Canada shall be:
70 Colombine Drive
Ottawa, Ontario, K1A 0K9
The address for notice or communication to Manitoba shall be:
Manitoba Health, Seniors and Active Living
300 Carlton St.
Winnipeg, Manitoba
R3B 3M9
Attention: Marcia Thomson
Email: Marcia.Thomson@gov.mb.ca
13.0 General
13.1 This Agreement, including Annex 1, comprise the entire agreement entered into by the Parties with respect to the subject matter hereof.
13.2 This Agreement shall be interpreted according to the laws of Canada and Manitoba.
13.3 No member of the House of Commons or of the Senate of Canada or of the Legislature of Manitoba shall be admitted to any share or part of this Agreement, or to any benefit arising therefrom that is not otherwise available to the general public.
13.4 If for any reason a provision of this Agreement that is not a fundamental term is found by a court of competent jurisdiction to be or to have become invalid or unenforceable, in whole or in part, it will be deemed to be severable and will be deleted from this Agreement, but all the other provisions of this Agreement will continue to be valid and enforceable.
13.5 This Agreement is drafted in English at the request of the Parties. Les parties ont convenu que le présent Accord soit rédigé en anglais.
SIGNED on behalf of Canada by the Minister of Health at Ottawa, Ontario this 6th day of December, 2018.
The Honourable Ginette Petitpas Taylor, Minister of Health
SIGNED on behalf of Manitoba by the Minister of Health, Seniors and Active Living at Winnipeg, Manitoba this 7th day of December, 2018.
The Honourable Cameron Friesen, Minister of Health, Seniors and Active Living
Annex 1 to the Agreement
Manitoba Action Plan
Introduction
Methamphetamine (also known as meth or crystal meth) is an illegal synthetic drug that is highly addictive and very dangerous to a user's health. The marked increase of meth use in Manitoba, particularly in the Winnipeg and Brandon areas, is of significant concern to stakeholders and has resulted in a number of negative impacts for individuals, families and communities, as well as legal, health and social services.
Meth use often leads to other chronic health and social problems. A recent survey (November 2016 to March 2017) indicates that more than half of injection drug users are injecting meth, putting them at increased risk of contracting or transmitting HIV or Hepatitis.
The increase in meth use has led to an increase in individuals coming to emergency departments and crisis response services in meth psychosis. Increasingly, health care and allied service providers are identifying a limited capacity to appropriately support and respond to individuals affected by meth, including a need for flexible length withdrawal management services (WMS).
Meth use is much more challenging to address than the use of many other substances including opioids as it is an illegal substance and there are no replacement drug therapies. Withdrawal management (also known as detox) from meth takes longer, and requires more support, than withdrawal from other substances (up to 30 days). Once withdrawal has occurred, people who use meth generally require longer stays at residential addictions treatment facilities (up to 1 year).
Overview
In Winnipeg, there are currently 11 medical WMS beds at the Health Sciences Centre Addiction Program, which provide clinical involvement and intervention, and 47 non-medical WMS beds (25 for males, 22 for females). In Thompson, there are currently six non-medical WMS beds. All of these are traditional, 7 to 10 day, WMS beds. While the numbers of people using meth have been increasing dramatically, there are no longer-term (up to 30 days) WMS in Manitoba that are appropriate for people who use meth. Existing WMS are not adequate to respond to the needs of individuals who use meth and new resources are indicated in Winnipeg and Brandon to address the critical gaps in those regions. Manitobans needing WMS for meth are currently using the non-medical WMS beds in Winnipeg and Thompson; however, this does not provide an appropriate length of withdrawal management, and is causing a backlog for others who need to access services. Currently, it can take up to seven days for individuals to access traditional 7 to 10 day WMS in Winnipeg.
In their 2017 Year in Review, Winnipeg Police Services indicated that charges of possession of meth under the Controlled Drugs and Substances Act have increased by 890% since 2012.
The Addictions Foundation of Manitoba (AFM) indicates that individuals self-reporting at intake with amphetamine use (including meth) as the primary presenting issue have more than doubled from 3.8% in 2014/15 to 8.5% of individuals in 2016/17. Other addictions treatment programs funded by Manitoba Health, Seniors and Active Living have also reported a significant increase in the self-reporting of meth use by individuals entering treatment:
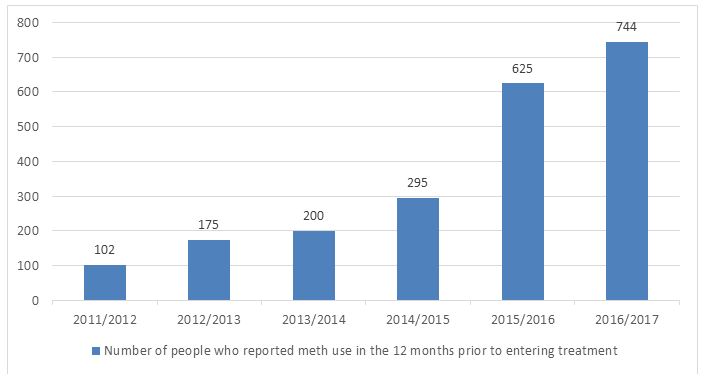
Figure 1 - Text Equivalent
| Year | Number of people who reported meth use in the 12 months prior to entering treatment |
|---|---|
| 2011/2012 | 102 |
| 2012/2013 | 175 |
| 2013/2014 | 200 |
| 2014/2015 | 295 |
| 2015/2016 | 625 |
| 2016/2017 | 744 |
Between January 2013 and December 2017, Emergency Department (ED) visits in Winnipeg by individuals under the influence of meth increased by approximately 1,700%. In response to this, in January 2018, the Winnipeg Regional Health Authority (WRHA) opened six new beds at the Health Sciences Centre to better support these individuals while they are in active psychosis, this does not, however, provide WMS.
In April 2017, Manitoba contracted with VIRGO Planning and Evaluation Consultants Inc. to develop a provincial Mental Health and Addictions (MHA) strategy in order to improve access to and coordination of mental health and addictions services.
During a year-long process, VIRGO engaged an extensive number and variety of stakeholders, including those with lived experience and their family members, Indigenous leaders, new Canadians, other departments and service providers. Information was gathered from over 350 in-person consultations; more than 3,800 online surveys; over 600 individuals engaged in a series of validation events to receive feedback on what was heard as well as the report's initial recommendations; and an extensive data and document review, including analyses of more than 275 documents from stakeholders and population, health and service data.
On May 14, 2018, VIRGO's report, Improving Access and Coordination of Mental Health and Addiction Services: A Provincial Strategy for all Manitobans was made available to the public. The VIRGO report identified several major challenges to the current state, including long waits to access services and limited availability of services in rural and northern communities.
The VIRGO report noted, "On top of the already concerning and often tragic opioid overdose crisis in the province, the rapidly growing use of, and complex consequences associated with, crystal methamphetamine has swamped EDs and crisis response services."
With the goal of transforming MHA services in the province, Manitoba is currently developing a plan to guide the implementation of recommendations in VIRGO's report.
In May 2018, Manitoba announced it would establish five Rapid Access to Addictions Medicine (RAAM) clinics across the province to treat individuals seeking help for substance-related addictions, including people struggling with opiate, methamphetamine and alcohol addiction. The RAAM clinics provide assessment, counselling, the prescription of appropriate medication, and connect patients to WMS, community treatment programs and primary care physicians. The RAAM clinical team will provide ongoing support to primary care providers including mentoring, re-assessment and referral of clients. Individuals who attend RAAM clinics, including those who use meth, are currently being referred to traditional 7 to 10 day WMS, however, there is a recognition that this restricted length of WMS is not best practice for people who use meth.
Priority Areas for Investment
Withdrawal Management Services (WMS)
Manitoba currently does not have adequate capacity to provide WMS for all people who need these services. Moreover, the province does not have any capacity to provide appropriate length of WMS for individuals who use meth.
With the Emergency Treatment Fund (ETF) funding, Manitoba will increase access to treatment by enhancing WMS services in both Winnipeg and Brandon. Beginning in 2019-20, to respond to the needs of those who use substances, particularly meth, a minimum of 11 new WMS spaces will be available in the province. It is expected that the additional services will increase access to flexible-length WMS appropriate for people who use meth for a minimum of 132 individuals per year.
The enhanced WMS in Winnipeg and Brandon will provide for flexible lengths of stays in order to respond to the needs of individuals who use meth and other substances. The WMS services will accept referrals from a variety of sources, including RAAM clinics, primary care providers, treatment programs and self-referrals. Individuals will be housed in single rooms to allow space during the acute phase of withdrawal and to provide a calm environment.
Participants will have access to medical practitioners who can offer medications, and psycho-social supports to facilitate assessment and treatment. Depending on the proposals received, these supports may be provided through RAAM clinics, Regional Health Authorities, the Addictions Foundation of Manitoba or other sources.
Individuals receiving flexible-length WMS would be assessed for intensity of substance use, evidence of co-occurring mental health disorders, and would develop a treatment plan and goals. Individuals would also be provided with education regarding the effects of meth, and what they can expect during withdrawal and stabilization. Services will provide referrals for ongoing treatment, whether it may be longer-term residential treatment or community based day treatment
Expected Outcomes
The proposed use of ETF funds will provide capacity for evidence-based, flexible length, and appropriate WMS for people in Manitoba who use meth. Individuals who participate will also be linked with primary care providers who will follow them over the long-term. By adding these services, and linking people with the RAAM clinics, Manitoba will be providing better navigation, and a continuity of service that is currently lacking in the MHA treatment system. This will help to fill a significant gap in Manitoba's current MHA treatment continuum, particularly for those individuals requiring WMS for meth.
By implementing these services, these individuals will be able to receive flexible-length WMS, and will be referred to longer-term treatment more seamlessly. By ensuring that more Manitobans will be able to access WMS services when they need them, it will reduce barriers and encourage more people to follow through with withdrawal and longer-term stabilization and treatment.
With access to appropriate WMS, treatment and follow up for people who use meth, it is anticipated that there will be a reduction in medical complications, ED visits and hospitalizations, and reduced societal costs, including criminal activity, homelessness, domestic violence, child neglect or abuse, and most importantly, it would allow users to withdraw and begin their journey of recovery.
Monitoring and Evaluation
Manitoba Health, Seniors and Active Living (MHSAL) will continue with on-going meth-use surveillance and will provide measuring and reporting to evaluate the success of this model in addressing the current gaps in services in Manitoba. These measurements will also assist in determining future service adjustments and recommendations for enhancements.
Success can be measured by improvements in indicators such as:
- Number of meth-related deaths
- Number of meth-related emergency department visits
- Number of meth-related hospital admissions
- Number of meth-related crisis response centre visits
- Number of WMS spaces available
- Number of people receiving WMS for meth use disorder
- Percentage of people who receive services within # days of referral
- Average number of days people receive WMS
- Number of people who enter into longer-term treatment after receiving WMS services
As meth is an illegal substance, it is difficult to estimate the number of people in the province who use it, and are in need of WMS. Based on the increasing numbers of people entering residential treatment to address their use of meth, it is essential that Manitoba address the growing need for appropriate WMS services.
Budget and Financial Requirements
Manitoba will receive $4,187,161 from the Emergency Treatment Fund (ETF) in 2018/19. These funds are required to be used by 2022/23.
While the ETF will be flowed to the province in 2018/19, in consideration of the time required to enter into a request for proposal process, it is anticipated that the funds will start to be used in 2019/20. As such, the funds will be budgeted equally over four years, which comes to $1,046,790 per year from 2019/20 to 2022/23
Funding Sources
Manitoba's allocation of one-time funding is $4,187,161. As a condition of funding, provinces/territories are required to match funds at a 1:1 ratio beyond the first $250,000 and expenditures allocated specifically for treatment in the context of the opioid crisis between January 2016 and May 2018 may be used to match federal funding.
| Eligible Treatment Service: | Provincial Expenditures from January 2016 to May 2018 |
|---|---|
Grant funding to Behavioural Health Foundation In 2016/17 the total funding was $3,362,550 and 45% of the clients entered the program for treatment of stimulants (including meth), opioids and benzodiazepines ($3,362,550 X 0.45 = $1,513,148) In 2017/18 the total funding was $3,093,300 and 55% of the clients entered the program for treatment of stimulants (including meth), opioids and benzodiazepines ($3,093,300 X 0.55 = $1,701,315) Total $1,513,148 + $1,701,315 = $3,214,463 |
$3,214,463 |
Grant funding to Main Street Project Women's Detox Unit:
|
$1,838,000 |
| Total Eligible Provincial Expenditures: | $5,052,463 |
Performance Measurement
| Name of Initiative | Description | Expected Results | Performance Measurement | Expenditure Plan | ||||
|---|---|---|---|---|---|---|---|---|
| Total ETF Funding from 2018/19 to 2022/23 is $4,187,161 - funding will be flowed to Manitoba in 2018/19, and will be used from 2019/20 to 2022/23 - A total of $1,046,790 per year. | ||||||||
| 2018-19 | 2019-20 | 2020-21 | 2021-22 | 2022-23 | ||||
| WMS services for meth | Manitoba will enter into a request for proposal process for the provision of enhanced WMS services in Winnipeg and Brandon | Increased capacity to provide WMS in Manitoba Quicker access to WMS Reduction of wait lists for WMS Increase of people who completed WMS accessing longer-term treatment |
# of WMS spots in Manitoba # of referrals for WMS Average wait times for WMS after referral # of people on the wait list for WMS # of people accessing WMS # of people who completed WMS accessing longer-term treatment |
$0 | $1,046,790 | $1,046,790 | $1,046,790 | $1,046,790 |