
Epidemiological summary report: 2022-2023 mpox outbreak in Canada
Download the alternative format
(PDF format, 579 KB, 14 pages)
Organization: Public Health Agency of Canada
Published: April 2024
On this page
- Background
- Highlights
- Progression of the outbreak over time and place
- Populations impacted by the outbreak
- Frequently reported symptoms
- Vaccination
- Summary
- Additional Resources
- Technical Notes
- Acknowledgements
- References
Background
Mpox (formerly monkeypox) is a viral infectious disease caused by the monkeypox virus (MPXV), and closely related to the virus that causes smallpox. Canada was among the countries affected by the global 2022-23 mpox outbreak caused by clade IIb MPXV, with cases primarily among gay, bisexual, and other men who have sex with men (GBMSM). Prior to the global mpox outbreak, MPXV was endemic in certain central and western African countries, with only occasional cases associated with travel and imported animals reported in other countries.Footnote 1
This report was developed by the Public Health Agency of Canada (PHAC), in collaboration with local, provincial and territorial public health partners, to summarize the outbreak of human cases of mpox in Canada, based on cases reported to PHAC between May 19, 2022 and December 31, 2023. Prior to this report, PHAC published routine updates through a dashboard to communicate the latest data on mpox in Canada. However, as the number of new mpox cases in Canada has continued to decline since reaching a peak around the end of June 2022, this report will replace the currently inactive dashboard with an updated and detailed snapshot of mpox in Canada, including a summary of important findings.
As the federal government's public health lead, PHAC played a cross-cutting role in facilitating interjurisdictional knowledge-sharing and collaboration, as well as supporting response activities, including the procurement and distribution of medical countermeasures, implementation of border measures and diagnostic testing.
Although this report includes data up to December 31, 2023, mpox continues to be detected and reported sporadically across Canada. PHAC will continue to work with stakeholders to maintain surveillance and assess emerging evidence to inform the timely implementation of public health interventions.
Note about terminology
On November 28 2022, the World Health Organization recommended the new preferred term "mpox" over the previous terminology "monkeypox" to refer to the disease caused by the monkeypox virus. This change in terminology was adapted to address growing reports of racism and stigma in the wake of the 2022-23 global mpox outbreak. While the name of the disease changed to mpox, the virus responsible for the disease continues to be referred to as "monkeypox virus" or MPXV. The term gay, bisexual and other men who have sex with men (GBMSM) is meant to include people who self-identify as cisgender or transgender men whose sexual partners are cisgender and/or transgender men, regardless of their sex assigned at birth. However, there is a lack of consistency across studies and surveillance programs in how gender identity, sex and sexual orientation variables are defined. This poses challenges when interpretating and comparing data from various sources.
Highlights
Text description
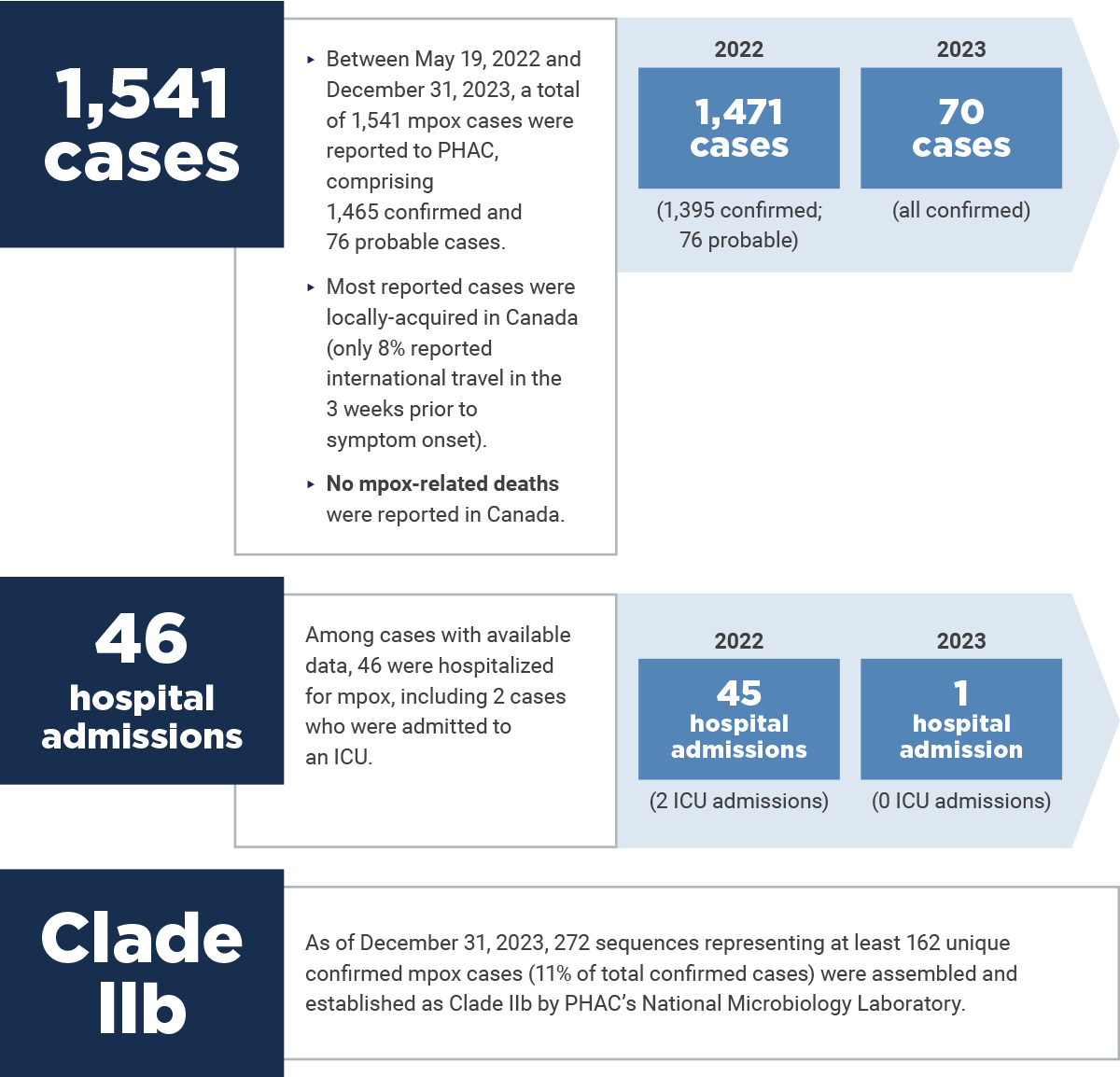
Between May 19, 2022 and December 31, 2023, a total of 1,541 mpox cases were reported to PHAC, comprising 1,465 confirmed and 76 probable cases. Most reported cases were locally-acquired in Canada (only 8% reported international travel in the 3 weeks prior to symptom onset). No mpox-related deaths were reported in Canada. Among cases with available data, 46 were hospitalized for mpox, including 2 cases who were admitted to an ICU. By year, a total of 1,471 cases (1,395 confirmed; 76 probable) were reported to PHAC in 2022, of whom 45 were hospitalized (including 2 cases who were admitted to an ICU). In 2023, a total of 70 confirmed mpox cases were reported to PHAC and 1 case was hospitalized (did not require ICU admission). As of December 31, 2023, 272 sequences representing at least 162 unique confirmed mpox cases (11% of total confirmed cases) were assembled and established as Clade IIb by PHAC's National Microbiology Laboratory.
Progression of the outbreak over time and place
Epidemic curve
The 2022-23 mpox outbreak in Canada peaked around the end of June 2022 and was followed by a steady decrease in cases (see Figure 1). While the first case was reported to PHAC on May 19, 2022, the earliest estimated date of symptom onset in Canada was later confirmed to be April 28, 2022.
Sporadic cases of mpox continue to be reported in Canada.

Text description
| Epidemiological Week | Number of confirmed cases | 7-day moving average |
|---|---|---|
| 2022-04-24 – 2022-04-30 | 2 | 0.29 |
| 2022-05-01 – 2022-05-07 | 6 | 0.86 |
| 2022-05-08 – 2022-05-14 | 13 | 1.86 |
| 2022-05-15 – 2022-05-21 | 24 | 3.43 |
| 2022-05-22 – 2022-05-28 | 45 | 6.43 |
| 2022-05-29 – 2022-06-04 | 62 | 8.86 |
| 2022-06-05 – 2022-06-11 | 60 | 8.57 |
| 2022-06-12 – 2022-06-18 | 63 | 9.00 |
| 2022-06-19 – 2022-06-25 | 104 | 14.86 |
| 2022-06-26 – 2022-07-02 | 138 | 19.71 |
| 2022-07-03 – 2022-07-09 | 121 | 17.29 |
| 2022-07-10 – 2022-07-16 | 131 | 18.71 |
| 2022-07-17 – 2022-07-23 | 134 | 19.14 |
| 2022-07-24 – 2022-07-30 | 87 | 12.43 |
| 2022-07-31 – 2022-08-06 | 89 | 12.71 |
| 2022-08-07 – 2022-08-13 | 103 | 14.71 |
| 2022-08-14 – 2022-08-20 | 67 | 9.57 |
| 2022-08-21 – 2022-08-27 | 34 | 4.86 |
| 2022-08-28 – 2022-09-03 | 28 | 4.00 |
| 2022-09-04 – 2022-09-10 | 17 | 2.43 |
| 2022-09-11 – 2022-09-17 | 17 | 2.43 |
| 2022-09-18 – 2022-09-24 | 12 | 1.71 |
| 2022-09-25 – 2022-10-01 | 16 | 2.29 |
| 2022-10-02 – 2022-10-08 | 5 | 0.71 |
| 2022-10-09 – 2022-10-15 | 3 | 0.43 |
| 2022-10-16 – 2022-10-22 | 2 | 0.29 |
| 2022-10-23 – 2022-10-29 | 4 | 0.57 |
| 2022-10-30 – 2022-11-05 | 3 | 0.43 |
| 2022-11-06 – 2022-11-12 | 4 | 0.57 |
| 2022-11-13 – 2022-11-19 | 2 | 0.29 |
| 2022-11-20 – 2022-11-26 | 0 | 0.00 |
| 2022-11-27 – 2022-12-03 | 1 | 0.14 |
| 2022-12-04 – 2022-12-10 | 1 | 0.14 |
| 2022-12-11 – 2022-12-17 | 3 | 0.43 |
| 2022-12-18 – 2022-12-24 | 0 | 0.00 |
| 2022-12-25 – 2022-12-31 | 0 | 0.00 |
| 2023-01-01 – 2023-01-07 | 0 | 0.00 |
| 2023-01-08 – 2023-01-14 | 1 | 0.14 |
| 2023-01-15 – 2023-01-21 | 3 | 0.43 |
| 2023-01-22 – 2023-01-28 | 1 | 0.14 |
| 2023-01-29 – 2023-02-04 | 3 | 0.43 |
| 2023-02-05 – 2023-02-11 | 2 | 0.29 |
| 2023-02-12 – 2023-02-18 | 3 | 0.43 |
| 2023-02-19 – 2023-02-25 | 1 | 0.14 |
| 2023-02-26 – 2023-03-04 | 4 | 0.57 |
| 2023-03-05 – 2023-03-11 | 3 | 0.43 |
| 2023-03-12 – 2023-03-18 | 1 | 0.14 |
| 2023-03-19 – 2023-03-25 | 1 | 0.14 |
| 2023-03-26 – 2023-04-01 | 0 | 0.00 |
| 2023-04-02 – 2023-04-08 | 0 | 0.00 |
| 2023-04-09 – 2023-04-15 | 1 | 0.14 |
| 2023-04-16 – 2023-04-22 | 3 | 0.43 |
| 2023-04-23 – 2023-04-29 | 3 | 0.43 |
| 2023-04-30 – 2023-05-06 | 2 | 0.29 |
| 2023-05-07 – 2023-05-13 | 1 | 0.14 |
| 2023-05-14 – 2023-05-20 | 2 | 0.29 |
| 2023-05-21 – 2023-05-27 | 2 | 0.29 |
| 2023-05-28 – 2023-06-03 | 2 | 0.29 |
| 2023-06-04 – 2023-06-10 | 2 | 0.29 |
| 2023-06-11 – 2023-06-17 | 0 | 0.00 |
| 2023-06-18 – 2023-06-24 | 0 | 0.00 |
| 2023-06-25 – 2023-07-01 | 2 | 0.29 |
| 2023-07-02 – 2023-07-08 | 2 | 0.29 |
| 2023-07-09 – 2023-07-15 | 0 | 0.00 |
| 2023-07-16 – 2023-07-22 | 1 | 0.14 |
| 2023-07-23 – 2023-07-29 | 0 | 0.00 |
| 2023-07-30 – 2023-08-05 | 0 | 0.00 |
| 2023-08-06 – 2023-08-12 | 4 | 0.57 |
| 2023-08-13 – 2023-08-19 | 0 | 0.00 |
| 2023-08-20 – 2023-08-26 | 0 | 0.00 |
| 2023-08-27 – 2023-09-02 | 0 | 0.00 |
| 2023-09-03 – 2023-09-09 | 1 | 0.14 |
| 2023-09-10 – 2023-09-16 | 2 | 0.29 |
| 2023-09-17 – 2023-09-23 | 2 | 0.29 |
| 2023-09-24 – 2023-09-30 | 1 | 0.14 |
| 2023-10-01 – 2023-10-07 | 0 | 0.00 |
| 2023-10-08 – 2023-10-14 | 1 | 0.14 |
| 2023-10-15 – 2023-10-21 | 2 | 0.29 |
| 2023-10-22 – 2023-10-28 | 0 | 0.00 |
| 2023-10-29 – 2023-11-04 | 0 | 0.00 |
| 2023-11-05 – 2023-11-11 | 1 | 0.14 |
| 2023-11-12 – 2023-11-18 | 2 | 0.29 |
| 2023-11-19 – 2023-11-25 | 1 | 0.14 |
| 2023-11-26 – 2023-12-02 | 1 | 0.14 |
| 2023-12-03 – 2023-12-09 | 0 | 0.00 |
| 2023-12-10 – 2023-12-16 | 0 | 0.00 |
| 2023-12-17 – 2023-12-23 | 0 | 0.00 |
| 2023-12-24 – 2023-12-30 | 0 | 0.00 |
| 2023-12-31 | 0 | 0.00 |
Geographic spread
Most mpox cases were reported in Ontario, Quebec and British Columbia (see Figure 2), accounting for 96% of all cases reported to PHAC between May 2022 and December 2023. Some Canadian provinces and territories reported a limited number of mpox cases, for which exposure likely occurred during travel. No mpox cases were reported in Prince Edward Island, Nunavut or Northwest Territories.
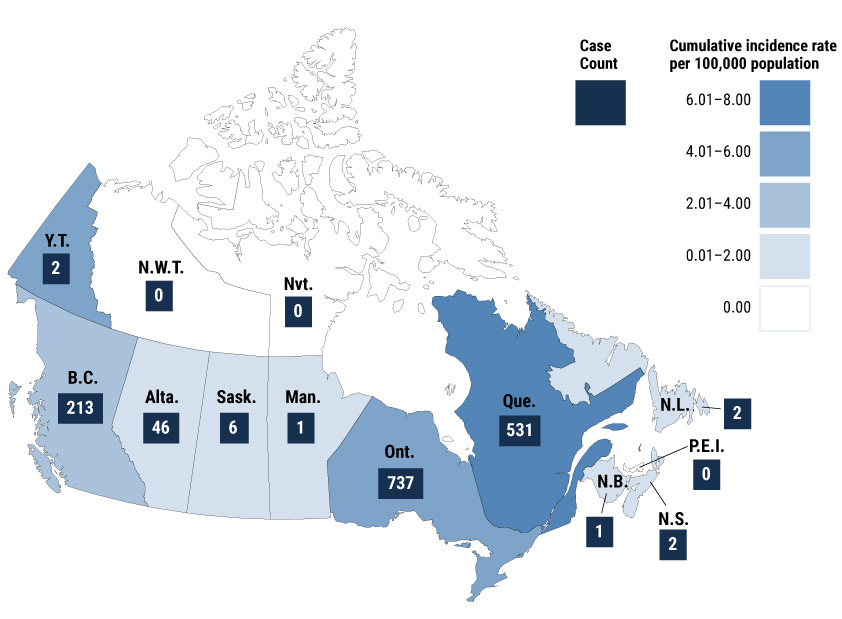
Note: Case counts include both confirmed and probable mpox cases reported to PHAC between May 19, 2022 and December 31, 2023.
Text description
| Province/Territory | Case count | Cumulative incidence rate per 100,000 population |
|---|---|---|
| British Columbia | 213 | 3.94 |
| Alberta | 46 | 1.01 |
| Saskatchewan | 6 | 0.51 |
| Manitoba | 1 | 0.07 |
| Ontario | 737 | 4.82 |
| Quebec | 531 | 6.08 |
| New Brunswick | 1 | 0.12 |
| Prince Edward Island | 0 | 0.00 |
| Nova Scotia | 2 | 0.19 |
| Newfoundland and Labrador | 2 | 0.37 |
| Nunavut | 0 | 0.00 |
| Yukon | 2 | 4.53 |
| Northwest Territories | 0 | 0.00 |
| Canada | 1,541 | 3.92 |
Populations impacted by the outbreak
General demographic information
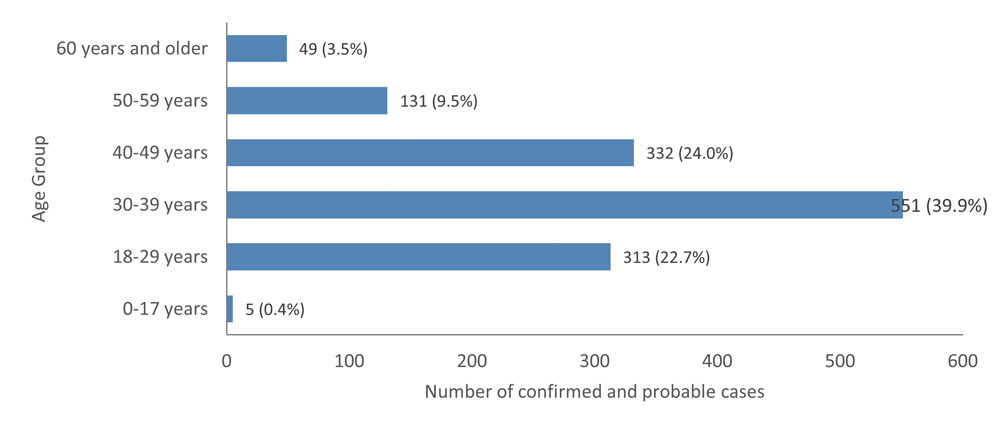
Among most cases, gender was reported as man, with the majority between the ages of 18 and 49 years (85%; see Table 1). Cases were most commonly reported among 30-39 year-olds (40%; see Figure 3).
| Age Group | Gender | Total | |
|---|---|---|---|
| Man | Other genders | ||
| 0-17 years | 4 (0.3%) | 1 (3.1%) | 5 (0.4%) |
| 18-29 years | 303 (22.5%) | 10 (31.2%) | 313 (22.7%) |
| 30-39 years | 536 (39.7%) | 15 (46.9%) | 551 (39.9%) |
| 40-49 years | 330 (24.5%) | 2 (6.2%) | 332 (24.0%) |
| 50-59 years | 128 (9.5%) | 3 (9.4%) | 131 (9.5%) |
| 60 years and older | 48 (3.6%) | 1 (3.1%) | 49 (3.5%) |
| Total | 1,349 | 32 | 1,381 |
| Notes: "Man" may include cisgender and transgender men. The "other genders" category includes the following values: woman (cisgender or transgender), non-binary person, and other gender identities. Other gender identities can also be reported using free text. Depending on reporting practices, transgender identity may have been captured as "man" or "woman" or using free text. Data on gender identity is based on self-reported information collected during public health case investigations. However, there are differences in data collection and data capture across provinces and territories in Canada, and the data presented here may not necessarily reflect gender identity. | |||
Text description
| Age Group | Number of confirmed and probable cases |
|---|---|
| 0-17 years | 5 (0.4%) |
| 18-29 years | 313 (22.7%) |
| 30-39 years | 551 (39.9%) |
| 40-49 years | 332 (24.0%) |
| 50-59 years | 131 (9.5%) |
| 60 years and older | 49 (3.5%) |
| Total | 1,381 |
Common case patterns
The 2022-23 mpox outbreak in Canada was primarily spread through sexual or close, intimate contact. Gay, bisexual and other men who have sex with men experienced a disproportionate burden of mpox in Canada (96% of all cases),Footnote 2Footnote 3 similar to other countries impacted by the global 2022-23 mpox outbreak. Among mpox cases with available information on likely source of exposure, 81% (650/803) reported a recent history of at least one of the following prior to symptom onset: having multiple and/or anonymous sexual partners; attending a sex-on-premise venue (e.g., bathhouse); attending a group sex event.
International evidence highlights the increased severity of mpox among people with immunosuppression and immunocompromising conditions, such as an advanced HIV infection (CD4 cell count < 200).Footnote 4 In Canada, 30% (265/884) of all mpox cases with available information reported living with HIV and 22% (183/848) reported either an ongoing or recent medical history of another sexually transmitted or blood-borne infection (STBBI). Among the 46 cases who were hospitalized for mpox, 59% (13/22) reported living with HIV and 55% (12/22) reported either an ongoing or recent medical history of another STBBI. Information about immunosuppression among cases living with HIV is incomplete, and limited conclusions can be drawn from these data.
Frequently reported symptoms
Similar to observations from the global 2022-23 mpox outbreak,Footnote 5 most confirmed mpox cases in Canada reported a rash or lesion, and more than half reported a fever, exhaustion and swollen lymph nodes (lymphadenopathy) (see Table 2).
| Symptom | Number of confirmed cases (%) | |
|---|---|---|
| 1 | Rash/Lesion | 1,305 (96.5%) |
| 2 | Fever | 732 (56.4%) |
| 3 | Fatigue/Exhaustion | 703 (54.3%) |
| 4 | Lymphadenopathy | 697 (52.9%) |
| 5 | Headache | 536 (41.8%) |
| 6 | Myalgia/Arthralgia | 509 (39.3%) |
| 7 | Sweating | 436 (58.1%) |
| 8 | Chills | 412 (44.1%) |
| 9 | Sore Throat | 374 (28.9%) |
| 10 | Back Pain | 259 (38.8%) |
| 11 | Cough | 112 (12.1%) |
| 12 | Vomiting/Nausea | 94 (7.4%) |
| 13 | Conjunctivitis | 17 (1.9%) |
Vaccination
Based on available information on vaccination history, 46% (328/715) of cases received at least one dose of an approved vaccine against mpox (Imvamune®), of whom 2% (5/328) received two doses. Approximately 2% of cases (12/715) reported historical vaccination against smallpox. Cases were primarily vaccinated through provincial/territorial immunization programs for mpox as either pre- or post-exposure prophylaxis in the summer of 2022. Eligible individuals continue to be offered mpox vaccines across Canada.
Summary
- Between May 19, 2022 and December 31, 2023, Canada experienced a large and first outbreak of mpox (total of 1,541 cases), which peaked around the end of June 2022.
- The outbreak disproportionately affected gay, bisexual men, and other men who have sex with men between the ages of 18 and 49 years.
- Nearly one-third (30%) of all mpox cases with available information reported living with HIV, and 59% of cases who were hospitalized for mpox with available information reported living with HIV.
- Most mpox cases in Canada were reported in Ontario, Quebec and British Columbia.
- While a small percentage of cases reported international travel (8%), public health investigations suggest that most cases acquired mpox locally through sexual or close, intimate contact with known or suspected mpox cases.
Additional Resources
Technical Notes
Methodology
PHAC receives detailed mpox case reports from provincial and territorial public health authorities through a secure data transfer. Data from case reports are anonymized, and each case is assigned a unique identifier. Data collection processes vary across Canadian provinces and territories, and often involve integration or compilation of different data inputs to better understand the epidemiology of mpox. Data for most variables are based on self-reported information from public health case investigations. Other data inputs include laboratory testing results, registries and administrative data. Microsoft Excel and R statistical software Footnote 6Footnote 7 were used to generate disaggregated case counts across variables of interest: case classification (confirmed/probable); epidemiological date; reporting province/territory; hospitalization status; ICU admission; gender; age; likely mode of disease acquisition; gender(s) of sexual partner(s); HIV status, concurrent or recent history of another STBBI.
The 7-day moving average was calculated by dividing the aggregate number of confirmed mpox cases for each week (based on epidemiological date) by 7. Incidence rates were estimated by dividing the total number of reported cases in a geographic area (province/territory/national) over the reporting period by the population count for that area. The proportion was then multiplied by 100,000 to permit population-based rate comparisons across different geographic areas. Statistics Canada's population estimates for 2022 (Q4) were used as rate denominators.Footnote 8
Caveats and limitations
- While mpox cases were reported by most jurisdictions in Canada, the occurrence, timing and scale of the outbreak varied across jurisdictions.
- The date of symptom onset was missing for 6.3% of cases. Therefore, epidemiological date was defined as the earliest reported date based on the following hierarchy: date of symptom onset, date of specimen collection for testing, and date reported to the local public health unit.
- For vaccination history, cases were assumed to have received the Imvamune® vaccine as either pre- or post-exposure prophylaxis within the context of the mpox outbreak in Canada, based on regional guidance and vaccination programs.
- Levels of missing data varied by reporting province/territory, variable and time. Some reported estimates may be over- or underestimated; readers are urged to use caution when interpreting and generalizing information included in this report.
- Information on age and gender was available for 99% and 90% of all cases, respectively.
- Sexual orientation was not self-reported during public health case investigations. For the purposes of this report, sexual orientation was derived based on available information from the following variables: sex, gender, sex/gender of sexual partner(s).
Abbreviations
- GBMSM
- Gay, bisexual and other men who have sex with men
- HIV
- Human Immunodeficiency Virus
- ICU
- Intensive Care Unit
- PHAC
- Public Health Agency of Canada
- Q4
- Fourth (Annual) Quarter: October-December
- STBBI
- Sexually Transmitted and Blood-Borne Infection
Acknowledgements
This report would not have been possible without the collaboration of local, provincial and territorial health and public health authorities and robust, regional surveillance systems that facilitated timely detection, investigation and reporting of mpox cases in Canada. We also acknowledge the work of federal leads, including PHAC's Mpox Incident Management System team for leading national surveillance, operations and communications and the National Microbiology Laboratory Branch for leading and expanding testing capacity for monkeypox virus.
References
- Footnote *
-
Epidemiological week is based on the earliest known date from the following: date of symptom onset, date of specimen collection or date reported
- Footnote 1
-
U.S. Centers for Disease Control and Prevention. Past U.S. Cases and Outbreaks; 2023 Aug 28 [cited 2024 Apr 03]. Available from: https://www.cdc.gov/poxvirus/mpox/outbreak/us-outbreaks.html
- Footnote 2
-
Harrison LB, Bergeron G, Cadieux G, Charest H, Fafard J, Levade I, Blais AC, Huchet E, Trottier B, Vlad D, Szabo J, Thomas R, Poulin S, Greenaway C, Zaharatos GJ, Oughton M, Chakravarti A, Pilarski R, Bui-Nguyen A, Benomar K, Libman MD, Vinh DC, Duggan AT, Graham M, Klein MB, Barkati S. Monkeypox in Montréal: Epidemiology, Phylogenomics, and Public Health Response to a Large North American Outbreak. Ann Intern Med. 2023 Jan;176(1):67-76. https://doi.org/10.7326/M22-2699
- Footnote 3
-
Ontario Agency for Health Protection and Promotion (Public Health Ontario). Enhanced epidemiological summary: Mpox in Ontario – May 1, 2022 to July 31, 2023. Toronto, ON: King's Printer for Ontario; 2023. Available from: https://www.publichealthontario.ca/-/media/Documents/M/2022/monkeypox-episummary.pdf?rev=ccdc118970104a4c9e634eb46e52839c&sc_lang=en
- Footnote 4
-
Mitjà O, Alemany A, Marks M, Lezama Mora JI, Rodríguez-Aldama JC, Torres Silva MS, Corral Herrera EA, Crabtree-Ramirez B, Blanco JL, Girometti N, Mazzotta V, Hazra A, Silva M, Montenegro-Idrogo JJ, Gebo K, Ghosn J, Peña Vázquez MF, Matos Prado E, Unigwe U, Villar-García J, Wald-Dickler N, Zucker J, Paredes R, Calmy A, Waters L, Galvan-Casas C, Walmsley S, Orkin CM; SHARE-NET writing group. Mpox in people with advanced HIV infection: a global case series. Lancet. 2023 Mar 18;401(10380):939-949. https://doi.org/10.1016/S0140-6736(23)00273-8
- Footnote 5
-
World Health Organization. Mpox Outbreak: Global Trends. Geneva: World Health Organization; 2023 [cited 2023 Dec 12]. Available from: https://worldhealthorg.shinyapps.io/mpx_global
- Footnote 6
-
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing 2022.
- Footnote 7
-
R Studio Team. RStudio: Integrated Development for R. 2022.
- Footnote 8
-
Statistics Canada. Table 17-10-0009-01 Population estimates, quarterly; 2023 Sep 27 [cited: 2023 Dec 14]. Available from: https://doi.org/10.25318/1710000901-eng