
Economic Burden of Illness in Canada, 2010
Download the alternative format
(PDF format, 402 KB, 65 pages)
Organization:
Public Health Agency of Canada
Date published: February 2018
Reference as: 2018. The Public Health Agency of Canada. The Economic Burden of Illness in Canada, 2010.
Table of Contents
- Foreword
- Acknowledgements
- Introduction
- Cost-of-Illness
- Methods and Data Sources
- Results
- Limitations
- References
- Appendix: EBIC Diagnostic Categories
List of Figures
- Figure 1: Components of Cost-of-Illness
- Figure 2: Allocating Expenditures using a Top-Down Approach
- Figure 3: Current Health Expenditures by Use of Funds, Canada 2010 ($000,000)
- Figure 4: Costliest ICD chapters by health function, hospital expenditures only, Canada 2010
- Figure 5: Percentage of hospital expenditures and population by age group, Canada 2010
- Figure 6: Percentage of hospital expenditures by age group and health function, Canada 2010
- Figure 7: Inpatient hospital expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 8: Percentage of inpatient hospital expenditures by age group, selected ICD chapters, Canada 2010
- Figure 9: Day surgery hospital expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 10: Percentage of day surgery hospital expenditures by age group, selected ICD chapters, Canada 2010
- Figure 11: Emergency department hospital expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 12: Percentage of emergency department hospital expenditures by age group, selected ICD chapters, Canada 2010
- Figure 13: Drug expenditures by sex, selected ICD chapter, Canada 2010 ($000,000)
- Figure 14: Percentage of drug expenditures and population by age group, Canada 2010
- Figure 15: Percentage of drug expenditures by age group, selected ICD chapters, Canada 2010
- Figure 16: Physician expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 17: Percentage of physician expenditures and population by age group, Canada 2010
- Figure 18: Percentage of physician expenditures by age group, selected ICD chapters, Canada 2010
- Figure 19: Morbidity costs by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 20: Percentage of morbidity costs and population by age group, Canada 2010
- Figure 21: Percentage of morbidity costs by age group, selected ICD chapters, Canada 2010
- Figure 22: Premature mortality costs by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 23: Percentage of premature mortality costs and population by age group, Canada 2010
- Figure 24: Percentage of premature mortality costs by age group, selected ICD chapters, Canada 2010
- Figure 25: Caregiving costs by type, selected ICD chapters, Canada 2010 ($000,000)
- Figure 26: Total caregiving costs by sex, selected ICD chapters, Canada 2010 ($000,000)
- Figure 27: Percentage of total caregiving costs and population by age group, Canada 2010
- Figure 28: Percentage of total caregiving costs by age group, selected ICD chapters, Canada 2010
- Figure 29: Percentage of Direct and Indirect Costs comapred to Total Costs, Canada, 2010
List of Tables
- Table 1: NHEX Current Expenditures, Canada, 2010 ($000,000)
- Table 2: Data sources employed
- Table 3: SHA and NHEX totals by health function
- Table 4: Estimated expenditures as percentage of actual expenditures ($000,000)
- Table 5: Direct Costs by ICD chapter, Canada 2010
- Table 6: Hospital expenditures by ICD chapter and health function, Canada, 2010
- Table 7: Indirect Costs by ICD Chapter, Canada, 2010
- Table 8: Total EBIC Costs, Canada, 2010
Foreword
The first version of the Economic Burden of Illness in Canada was released, by Health Canada, in 1991 Reference 1. Several versions have been produced since that date, with the responsibility shifting to the Public Health Agency in Canada in 2004. Reference 2 Reference 3 Reference 4 The Economic Burden of Illness in Canada, 2010 contains the most recent comparable data on the economic burden of illness and injury in Canada broken down by disease, age, and sex. The first part of the report reviews the methods employed in the production of EBIC while the second half presents a summary of the results. Users who require EBIC data at the level of diagnostic category are directed towards the EBIC Online Tool. The online tool provides data on the direct costs and premature mortality costs available by diagnostic category, age, sex, and province.
The first version of EBIC closely followed the methodology set out in one the most significant cost-of-illness (COI) studies, by Rice (1967). Reference 5 Recent years have seen important methodological refinements to COI methods and to ensure that EBIC continues to produce valid and reliable policy-relevant data, these changes have been incorporated, as appropriate. Some of the most noteworthy revisions allow for increased international comparability of EBIC results. This includes a change in diagnostic categories which are now based on the International Short List of Hospital Morbidity Tabulation (ISHMT) and International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) chapters, as well as a closer alignment with the System of Health Accounts (SHA). Reference 6
Cost-of-illness studies such as EBIC, which cover the entire classification of diseases (enabling mutual comparison of disease costs in terms of resources used and foregone opportunities), provide valuable information for policy and planning purposes. Such information can help us understand changes in patterns of practice with respect to resource utilization and help to clarify the most important cost components of treating specific diseases. The data collected for EBIC can also be combined with data on outcomes and inform economic evaluations of health and health-care policies. EBIC costing data can also be utilized in modeling of future health costs.Footnote a
Acknowledgements
The Economic Burden of Illness in Canada, 2010 was prepared by the Public Health Agency of Canada's Population Health Economics team: Alan Diener, Jacqueline Dugas, Ken Eng, Sameer Rajbhandary, and Igor Zverev.
Acknowledgement is also due to the organisations that supplied the data: the Canadian Institute for Health Information, Statistics Canada, provincial ministries of health, and IMS Brogan. The analyses, conclusions and opinions expressed herein are solely those of the Public Health Agency of Canada, and not necessarily those of the data providers.
Introduction
The Economic Burden of Illness in Canada (EBIC) is a comprehensive cost-of-illness (COI) study that provides estimates of the cost-of-illness and injury by disease, age, and sex. The primary goal of EBIC is to supply objective and comparable information on the magnitude of the economic burden, or cost-of-illness and injury, in Canada based on standard reporting units and methods. EBIC is the only comprehensive Canadian COI study that provides comparable costing information for all major health conditions. EBIC includes information on the following direct and indirect cost components:
Direct costs
- Hospital care expenditures
- Physician care expenditures
- Prescription drug expenditures
- Dental services and vision care services
- Formal caregiving
Indirect Costs
- Lost production due to morbidity
- Lost production due to premature mortality
- Informal caregiving
Supplementing other health indicators, EBIC provides reliable evidence to support public health policy and program planning. Expenditure data (direct costs) can provide information on changes in patterns of practice and resource trends over time or across sectors. Thus, it can inform future allocation decisions within the healthcare sector. Also, when combined with data on outcomes, these data can be an important input for economic evaluations of policies and programmes and other analyses, with the ultimate goal of increasing the efficient use of resources.
One of the most important uses of aggregate economic statistics in health care involves their international comparison. Efforts have been made to follow the Organisation for Economic Cooperation and Development’s (OECD) guidelines on producing expenditure-by-disease estimates under the System of Health Accounts Framework, in order to derive internationally comparable estimates using standard, agreed-upon definitions. Reference 7 As such, the data are allocated according to International Statistical Classification of Diseases and Related Health Problems (ICD) Chapter and, when possible, to one of 185 EBIC diagnostic categories based on the International Short List for Hospital Morbidity Tabulation (ISHMT).Footnote b Reference 8 While these categories do not directly correspond to the categories used in previous versions of EBIC, they are more useful from a policy perspective and the goal is to continue to report on these categories in future versions of EBIC.
The inclusion of indirect costs is an important contribution of EBIC, and provides a better understanding of societal costs associated with illness, which is a key consideration in undertaking policy analysis. The relative size of indirect costs to direct costs varies considerably by type of illness, and thus their inclusion can result in different conclusions. The value of lost production can be considered to be the decrease in economic production, or Gross Domestic Product (GDP), as a result of illness or injury.
EBIC follows a prevalence-based approach. A prevalence-based COI study estimates the annual costs of all cases of illness existing in a given time period, and can provide a snapshot at any given point in time (e.g. year).
Two notable changes to the current version of EBIC include a further elaboration of hospital expenditures by health function and the inclusion of caregiving costs. Hospital expenditures are broken down by inpatient care, outpatient care, day surgery, and emergency department visits. The estimation of caregiving costs was possible as the 2012 General Social Survey included a module on Caregiving and Care Receiving, which provided the necessary data. Caregiving can either be provided formally with a direct payment made, or it may be provided by a relative or friend with no payment made. As the latter still involves the use of resources which cannot be otherwise employed, they are considered to be an indirect cost. EBIC includes both forms of caregiving costs. Having information on these costs can provide insight into another aspect of health policy.
Cost-of-Illness
The Economic Burden of Illness in Canada does not address the total costs of illness; rather it focuses on the direct and indirect costs – that is, those costs which have direct resource implications.
The direct costs focus on the consumption of resources in the treatment of illness and injury and, generally, refer to those items for which some form of payment has been made, including medical care expenses such as hospitalization, outpatient and physician visits, long-term care, drugs, medical care, formal caregiving, equipment, etc.
The indirect costs focus on those resources which are foregone due to the illness or injury and thus cannot be used for other purposes but involve no direct payment to service providers. These include labour supply effects such as the value of lost production due to absenteeism or presenteeism (working but not at full productivity) resulting from disability or premature mortality, or any type of caregiving without a formal payment.
Together these costs give us information on the magnitude of the resource use related to the illness or injury. While this information is an important consideration for planning purposes, it does not present the entire burden associated with illness.
Illness and injury not only create societal costs in the form of resources used, but also in the form of health impacts and loss of life. While outcomes such as emotional distress, pain, loss of life, and other forms of suffering as a result of illness and injury can be considered a cost of illness, they are usually not included in COI studies due to methodological challenges. These outcomes can, however, be expressed in utility terms such as quality-adjusted life years (QALYs) and disability-adjusted life years (DALYs), or in monetary terms using values obtained from stated preference studies and/or value of a statistical life (VSL) studies. These approaches are often employed in economic evaluation analyses and regulatory policy evaluations. As these adverse outcomes are not included in EBIC, the results can be considered as an under-estimation of the total magnitude.
Figure 1 provides a breakdown of the different components that can be included in COI studies.
The System of Health Accounts
The OECD’s recent guidelines on estimating expenditures by disease, age and sex, provide a systematic approach for estimating the direct costs of illness under the System of Health Accounts (SHA) framework. Reference f Reference g Reference 9 This allows for the estimation of internationally comparable cost of illness estimates. As the SHA provides a single global framework for producing health expenditure accounts it provides a useful starting point and common set of definitions related to the production and consumption of the health care services included in EBIC.
The SHA is founded on a tri-axial relationship tracking the flow of all health care goods and services according to their consumption, provision and financing. With respect to consumption, the SHA tracks expenditures by health functions focusing on the purpose of the goods and services being consumed. Health care providers encompass organizations that deliver health care goods and services as their primary activity, as well as those for which health care provision is only one among a number of activities. The financing component focuses on the source of funds. EBIC focuses only on the provider and consumption classifications as these are the most relevant from a policy and planning perspective.
While the SHA provides a systematic framework for allocating all health care expenditures according to all of the classification types (provider, function, financing), the level of detail is dependent on availability of data in a particular country. In Canada, data sources are generally linked to, or available by, the type of health provider with limited information on the health function. More details are provided in the Methods and Data Sources section.
| Direct | Transfer paymentsFigure 1 note b | Indirect | Health Outcomes |
|---|---|---|---|
|
|
|
|
|
|||
Methods and Data Sources
Direct Costs
EBIC employs a top-down approach where total health expenditures are allocated across diagnostic categories (based on ICD-10 and ISHMT), age, sex, and province/territory. In a top-down approach, actual health expenditures, often taken from national health accounting data, are used as the starting point, and expenditures are allocated across disease groups, using an allocation or utilization key (see Figure 2). One of the benefits of this approach is that expenditures can only be allocated once, avoiding instances of double counting.
Figure 2: Allocating Expenditures using a Top-Down Approach
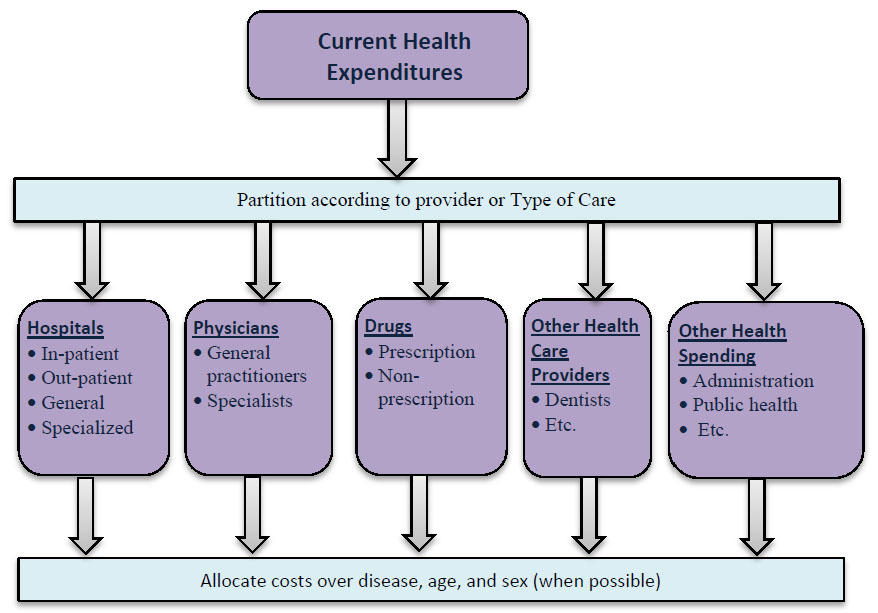
Figure 2 – Text description
Current health expenditures can be broken into several categories according to provider type or type of care provided. These categories include:
- Hospitals, including in-patient, out-patient, general, and specialized care
- Physicians, including general practitioners and specialists
- Drugs, including prescription and non-prescription
- Other health care providers, including dentists etc.
- Other health spending, including administration, public health, etc.
As previously noted, direct costs include all transactions for which some form of payment was made. The National Health Expenditure Database (NHEX) contains summary expenditure data from public and private sources broken down by the following categories: hospitals and other institutions, physicians and other professionals, drugs, public health, and other health spending. Reference 10 Note that while NHEX also reports expenditures on capital formation, EBIC only focuses on current expenditures in order to be consistent with the OECD and SHA guidelines. Table 1 shows current health expenditures for Canada in 2010 by use of funds.
| Health Function | Expenditures |
|---|---|
| HospitalsTable 1 note a | $56,734 |
| Other institutions | $19,991 |
| PhysiciansTable 1 note a | $27,445 |
| Other Professionals | $18,853 |
| Dental ServicesTable 1 note b | $11,885 |
| Vision Care ServicesTable 1 note b | $3,913 |
| Other | $3,055 |
| Drugs | $32,407 |
| Prescribed DrugsTable 1 note a | $27,565 |
| Non-Prescribed Drugs | $4,842 |
| Public health | $9,847 |
| Administration | $5,817 |
| Other Health Spending | $11,966 |
| Health Research | $3,409 |
| $8,557 | |
| Grand Total | $183,059 |
Source: NHEX 2015
|
|
In Canada, total current health expenditures, in 2010, were $183.1 billion. For EBIC, it was possible to allocate $127.6 billion (70%) at the ICD chapter level; this accounted for expenditures on hospitals, physicians, dental services, vision care services, and prescription drugs. It was not possible to allocate dental and vision care services beyond the ICD chapter level. At the EBIC diagnostic category level, it was only possible to allocate hospital, physician, and prescription drug expenditures, accounting for 61%, or $111.8 billion, of all health expenditures.
In order to allocate the expenditures to diagnostic categories it is necessary to have some form of allocation key. Several administrative databases were employed for this purpose. As this data was generally provided according to provider type, the specific methods are presented by provider type. In general, patient-level data was employed, which in a top-down framework increases the usefulness of the results as they more accurately represent the actual resource implications attributed to different diseases.
Hospital Care Expenditures
Hospital expenditures include all costs associated with operating and maintaining both public and private hospitals in Canada: drugs dispensed in hospitals, medical supplies, therapeutic and diagnostic outpatient costs, administrative costs, some research costs, accommodation and meals for patients, maintenance of hospital facilities, and gross salaries and wages for all hospital staff (such as physicians on hospital payroll, nurses, technicians and medical students). Reference j
The following databases were used to allocate costs by disease:
Discharge Abstract Database (DAD): The DAD contains information on hospital separations (discharges, deaths, sign-outs and transfers) from most hospitals in Canada, excluding Quebec. This includes data related to all acute inpatient stays, day surgery data for most provinces/territories and some data on chronic, rehabilitation and psychiatric hospital separations. Reference 11 Reference 12 The DAD contains approximately 75% of all inpatient hospital separations. This accounts for most of the inpatient expenditures outside of Quebec.
Hospital Morbidity Database (HMDB): The HMDB is a national database that contains information on all acute inpatient hospital separations. However, the HMDB holds information on Quebec acute inpatient separations and excludes all day surgery records. Reference 13 Reference 14
National Ambulatory Care Reporting System (NACRS): The NACRS contains records of all Ontario ambulatory care separations (day surgery, emergency department, clinics and other ambulatory care), as well as some ambulatory care separations for several other provinces/territories. Reference 15 Reference 16
Day surgery abstracts are submitted to both the DAD and NACRS (depending on the province/territory), with approximately 64% sent to NACRS and 36% sent to the DAD.Footnote c
Hospital Mental Health Database (HMHDB): The HMHDB contains information on all Ontario psychiatric hospital separations and on all separations from designated adult psychiatric beds in Ontario general hospitals. The information is partial for other provinces/territories. Reference 17 Reference 18 The HMHDB also holds information obtained from the DAD and the HMDB on all general hospital separations with a primary diagnosis of mental illness. Thus, the HMHDB holds all available data on mental health separations.
Estimating Costs
The databases contain up to twenty-five possible diagnoses for each separation recorded as an ICD-10, ICD-9, or a DSM-IV code, usually at the five-digit level. Each record notes the most responsible diagnosis, which is defined as “the diagnosis or condition that can be described as being most responsible for the patient’s stay in hospital. If there is more than one such condition, the one held most responsible for the greatest portion of the length of stay or greatest use of resources is selected.” Reference 19
Cost data was provided for each hospital separation in the DAD, the NACRS, and the HMHDB, making it possible to allocate hospital expenditures by disease, age, and sex. There are generally two methods for deriving costs using discharge-level data: the per diem method or employing resource intensity weights. Under the per diem method, the hospital length of stay is multiplied by the average daily hospital cost, which can be calculated at the individual hospital or regional level. While the number of hospital days may be a good indicator for part of the hospital care, using only data on length of stay would not take into account the type of care received. For example, there is a large cost differential between a day spent in a general ward versus a day spent in intensive care. In addition, certain diseases require more expensive and resource-intensive treatment. For these reasons the per diem method may not provide an accurate cost estimate.
In order to derive costs based on actual resource intensity, CIHI provided a resource intensity weight (RIW) and a cost per weighted case (CPWC) for each separation in two of their data sets, the DAD and the NACRS. RIWs provide a measure of the intensity with which hospital resources were used by each patient. Several factors were considered in CIHI’s calculation of RIW values: case mix group, age, comorbidity, a number of flagged interventions, intervention event(s), out-of-hospital intervention and possible interactions. Reference 20 Thus, using RIWs allows for a more reliable method of allocating expenditures by disease as it takes into account that patients utilize various intensities of resources due to patient characteristics, primary diagnoses and treatments. The RIWs were multiplied by the CPWC to obtain the record-level cost. As there was no information as to how much each of the recorded diagnoses may have added to the expenditures associated with that separation, all costs were attributed to the health condition defined as the most responsible for the hospital stay.
In order to estimate expenditures associated with separations contained in the other databases, average costs by diagnostic category, age-group, and sex were derived using the DAD and applied to the data from the HMDB and the HMHDB. Once costs were derived for each hospital separation, these costs were then aggregated over diagnostic categories and ICD chapters by sex, age group, and province/territory. (Note that the per-diem costing information and the RIW use different methodologies and include different costing components, making the total costs using each method different. Thus, while the HMHDB contained per-diem costing info, the aforementioned methodology was employed for consistency purposes.)
Table 2 contains information on the coverage of the data sets employed in the estimation of hospital expenditures by disease.
| Database | Geographical coverage | Health function coverage | Diagnostic categories covered | Resource intensity weight (RIW) or per diem |
|---|---|---|---|---|
| Discharge Abstract Database (DAD) | All of Canada, excluding Quebec |
|
All | RIW |
| Hospital Morbidity Database (HMDB) | All of Canada, including Quebec | Inpatient | All | N/A |
| National Ambulatory Care Reporting System (NACRS) |
|
|
All | RIW |
| Hospital Mental Health Database (HMHDB) | All of Canada, excluding Quebec. (Includes psychiatric facilities and mental health diagnoses in other hospitals) | Inpatient | AllTable 2 note a | Per diem |
|
||||
While NHEX provides data by use of funds, the categories employed focus more on the provider type than the health function related to the type of care. For example, hospitals provide several different types of care including inpatient, and various types of day and outpatient services. These services should be examined separately as they vary substantially in how care is provided, the resources used and the types of health conditions treated. Following the System of Health Accounts (SHA), hospital expenditures were further broken down by the following functions: inpatient care, day surgery, outpatient-clinic, emergency department visits, and other (includes home-based care, long-term care, preventive care, and ancillary services).Footnote d Note that these categories do not exactly match the SHA functional categories, which first distinguish between curative (HC.1) and rehabilitative care (HC.2), as the Canadian data combines these two categories.
Although both the SHA and the NHEX are both health accounting frameworks, and cover the same sets of expenditures, due to differences in definitions employed, the expenditure totals under each framework are slightly different. For example, hospital expenditures in the SHA do not include certain expenditures on such items as research, training of health workers, pastoral care, or social work. In 2010 these items accounted for $2.8 billion; the NHEX hospital expenditure total (and the one used in EBIC) was $56.7 billion whereas the SHA hospital expenditure total was $53.9 billionFootnote e.
Table 3 shows the SHA totals for all hospitals (HP.1) broken down by function. In order to allocate the NHEX hospital expenditure total across functions, the SHA distribution was employed. For example, 52% of the SHA expenditures were allocated towards inpatient care. Applying this percentage results in an estimate of $29.5 billion for inpatient care, according to the NHEX (and EBIC) total for the hospital category. The expenditure values for the rest of the functions were estimated in the same way.
| SHA Function | Type of Care | SHA expenditures ($000,000) |
Percentage of total hospital expenditures (using SHA) | NHEX expenditures ($000,000) |
|---|---|---|---|---|
| HC.1.1 & HC.2.1 | Inpatient Curative and Rehabilitative Care | 28,000 | 52.0% | 29,500 |
| HC.1.2 & HC.2.2 | Day Curative and Rehabilitative Care | 7,300 | 13.6% | 7,700 |
| HC.1.3 & HC.2.3 | Outpatient Curative and Rehabilitative Care | 14,100 | 26.2% | 14,900 |
| HC.1.4 & HC.2.4 | Home-based Curative and Rehabilitative Care | 200 | 0.4% | 0,200 |
| HC.3 | Long-term Care | 3,600 | 6.7% | 3,800 |
| HC.4 | Ancillary Services (not-specified by function) | 300 | 0.6% | 300 |
| HC.5 | Medical Goods (not-specified by function) | 0 | 0% | 0 |
| HC.6 | Preventive Care | 300 | 0.6% | 300 |
| HC.7 | Governance | 0 | 0% | 0 |
| All hospitals (HP.1) | 53,900 | 100% | 56,700 | |
| Source: OECD (2017) Reference 21 and CIHI (2015) Reference j | ||||
While the above databases contain administrative data, completion is not mandatory for all types of functions in all jurisdictions. Hence, the total estimated value of all expenditures accounted for in these databases was just over $33.1 billion, or 58% of the total value of hospital expenditures according to NHEX ($56.7 billion). Table 4 shows the total value of expenditures derived from the administrative data (i.e. separations), compared to the NHEX data, broken down by health function.
Note that outpatient care has been further broken down into emergency department (ED) visits and clinic visits. Outpatient care is comprised of those services delivered to a patient who is not formally admitted to a facility and does not stay overnight. This covers emergency department (ED) visits as well as other services that can be broadly defined as clinic-type visits. The SHA does not provide any information on a further breakdown of this category. However, according to CIHI the DAD and NACRS contain 50% of all ED expenditures. Thus, the total value of ED visits was estimated by doubling the value obtained in those two datasets. The “other” category includes home-based care, long-term care, ancillary services, and preventive care. Due to data limitations, it was not possible to provide results at a more granular level.
It is evident that the percentage of expenditures accounted for varied by function. For example, it was possible to account for 90% of inpatient expenditures, but only 16% of outpatient clinic expenditures using the separation data from the aforementioned databases. In order to estimate the difference, the average costs by diagnostic category were applied adjusting for age-group and sex. To ensure that the expenditures across provinces remained correct, this was repeated for each province and function.
| Health Function | NHEX expenditures total broken down by SHA allocation ($000,000) |
Estimated expenditures from separations data ($000,000) |
% of expenditures accounted for |
|---|---|---|---|
| Inpatient (HC.1.1 & HC.2.1) | $29,482.4 | $26,559.5 | 90% |
| Day surgery (HC.1.2 & HC.2.2) | $7,723.7 | $2,284.8 | 30% |
| Outpatient-Emergency dept.Table 4 note a | $4,075.2 | $2,035.2 | 50% |
| Outpatient-ClinicTable 4 note a | $10,782.8 | $1,746.9 | 16% |
| OtherTable 4 note b | $4,669.8 | $539.0 | 12% |
| Total | $56,733.9 | $33,165.5 | 58% |
|
|||
Drug Expenditures
Drug expenditure estimates comprise public and private costs associated with prescription drugs purchased in retail stores. Estimates represent the final costs to consumers, including dispensing fees, markups and appropriate taxes. Drugs dispensed in hospitals and other institutions are excluded as they are captured under the hospital care expenditures cost component of EBIC. Only prescription drug expenditures could be allocated by disease, age, and sex.
Data were obtained from two IMS Brogan datasets: CompuScript (CS) and the Canadian Disease and Therapeutic Index (CDTI). Reference 22 Reference 23 The CS contains information on total prescription drug costs for nearly 70% of all pharmacies across Canada, including retail price and dispensing fees, and total volume of prescriptions sold in retail pharmacies across Canada, excluding the territories.
The CDTI is a survey that provides information on the drug prescribing patterns of a panel of office-based physicians across Canada Reference v. It collects patient demographic characteristics (e.g. sex and age), diagnosis (coded using ICD-9) and drugs prescribed, thereby providing a mapping from drug names to diagnoses, according to patient characteristics. As such it serves the purpose of a utilization key in the allocation of drug expenditures to diagnostic category, age, and sex.
The CDTI uses the Uniform Classification System (USC), a categorization system developed by IMS Brogan, to standardize and categorize all drugs according to product type and therapeutic class. The USC is used by IMS Brogan in North America and classifies drugs based on therapeutic category, the drug’s pharmacology, chemical structure, and indications. It is somewhat similar to the Anatomical Therapeutic Classification (ATC) system developed by the World Health Organization.
The CDTI data for the Prairies (Manitoba, Saskatchewan, and Alberta) and Maritimes (Newfoundland and Labrador, Nova Scotia, Prince Edward Island, New Brunswick) are grouped as regions instead of by individual province. Thus, each province within a region was assumed to have a similar distribution of drug expenditures across age, sex, and diagnostic category. The CDTI does not include data for the territories.
Physician Care Expenditures
Physician care expenditures include all fee-for-service (FFS) payments made by provincial/territorial medical care insurance plans to physicians in private practice as well as payments made through alternative payment plans (APP), such as salaries, sessional fees, and capitation. Physician expenditures do not include expenditures for non-traditional practitioners and other health care professionals, which were included under the NHEX category Additional Direct Health Care Expenditures, nor did they include hospital-based physician care expenditures which were included in the Hospital Care Expenditures category. Reference j
Currently, only physician FFS data contains the necessary information to allocate the expenditures by diagnostic category, age and sex. As physician FFS data were only available for Ontario, Saskatchewan, Alberta, and British Columbia, they were employed to derive the physician care expenditures for the other provinces and territories using age-adjusted average values. This approach assumes that these four provinces are representative of the whole Canadian population. While including less than one-half of all Canadian jurisdictions, these provinces account for about 65% of the total population.
Provincial/territorial FFS physician billing information was used to distribute the amount billed across diagnostic categories, age group and sex. Average expenditures for diagnostic category adjusted for age-group and sex were derived and this information was used to estimate the difference between the expenditure totals from the FFS data and the totals included in NHEX.Footnote f
Indirect Costs
Value of Lost Production
Illness and injury may result in production losses to society as a whole, either as a result of morbidity or premature mortality. This can include losses related to both paid and unpaid labour. The two main impacts on paid labour are: (i) absenteeism, where as the result of illness, or premature death, a worker may miss time from paid work; and (ii) presenteeism, where an ill worker may still show up to work but operate at a less than optimal level.Footnote g Examples of presenteeism could include a mild illness, or the recovery period after an absence. Unpaid labour includes caregiving, volunteer work, household activities, or any other activity that is outside of the standard labour market. Due to insufficient data on presenteeism and unpaid labour, EBIC 2010 includes only estimates of production losses due to absenteeism as a result of morbidity and premature mortality.
When estimating the value of lost production, it is necessary to first measure the amount of time from work missed, and then to value this estimate using a proxy for the value of that production. There are two generally-accepted approaches used to estimate the period of lost production – the human capital method (HCM), and the friction cost method (FCM).
The HCM, used by earlier COI studies, estimates the production losses due to permanent disability or mortality for a given year as the value of an individual’s potential future earnings accrued to the expected age of retirement. Reference e This method is based on the assumption of zero involuntary unemployment or, in other words, it implicitly assumes that when a person dies he or she cannot be replaced. This assumption is likely to be untrue in today’s labour market, as evidenced by an unemployment rate that has not fallen below 6% since the 1970s (other than a brief period in late 2007 and early 2008). Thus, the HCM is likely to overestimate the true value of lost production.
More recently, researchers from Erasmus University developed the FCM. Reference 24 Reference 25 Reference 26 This method allows for non-zero involuntary unemployment, and assumes that after a person leaves a job due to morbidity, or premature mortality, they will be replaced by a worker who was previously unemployed. The time it takes for the new worker to find the job and be properly trained is referred to as the friction period. Specifically, the friction period is considered to start when the individual leaves his or her job, due to illness or injury, and to end when the job vacancy or chain of vacancies are filled.
In the FCM, lost productivity due to morbidity or premature mortality should not extend beyond the friction period. For short-term absences from work, the individual’s lost production may be partly restored by the individual when he or she returns to work, or by the company’s internal labour resources. When the time lost from paid work is short, the estimates from the two methods may not be different. For longer periods, the FCM will result in a lower cost estimate compared with the HCM. The FCM is consistent with the societal method and has been recommended by the Canadian Agency for Drugs and Technologies in Health (CADTH) in their guidelines for the Economic Evaluation of Health Technologies. Reference 27 Reference 28
It is important to note that the HCM, with its strong assumptions, generates what could be considered as the upper bound of the value of lost production due to mortality, whereas the FCM can be considered as the lower bound, and thus a more conservative estimate of the value of lost production due to mortality.
Vacancy duration data was employed by Koopmanschap and van Ineveld (1992) and Koopmanschap et al. (1995) to estimate the friction period for the Netherlands. Reference y Reference z As similar data was not available for Canada, provincial average unemployment duration was used as a proxy for the friction period. Unemployment duration data were not available for the territories, and so the national average unemployment duration was used as a proxy. The unemployment duration used in the analysis ranged from 13.6 weeks to 22 weeks. This is consistent with friction periods employed in the literature. Reference 29 Reference 30
The FCM was first employed by EBIC in the 2005-2008 version. Given the differences between the HCM and the FCM, estimates from these EBIC Reports should not be compared with estimates from previous EBIC versions. Koopmanschap et al. estimated 1988 mortality costs for the Netherlands using both methods and found that mortality costs were 53 times higher using the HCM. Reference y
The value of lost production was estimated for the working-age population using the appropriate age-sex-province-specific earnings. Reference 31 As earnings data for the territories were not available, corresponding national averages were used. In order to take into account those not in the labour force, the results were multiplied by the appropriate sex-age-province-specific employment rate. Reference 32
As a result of increased absences and decreased productivity, illness can affect an individual’s employment prospects and earnings. Those with chronic disease are likely to have recurrent sick leave, long-term absences from work, and often face an early retirement from the labour force. Recent research has focused on estimating these more precise labour market impacts and while these are important considerations they are currently beyond the purview of EBIC. Reference 33
Value of Lost Production due to Morbidity
Statistics Canada’s 2010 Canadian Community Health Survey (CCHS) Loss of Productivity (LOP) module was used to estimate missed work days due to illness and injury. Reference 34 The CCHS is a cross-sectional survey that collects information related to health status, health determinants and health care utilization for the Canadian population. Reference 35
For EBIC 2010 morbidity cost estimates, the period of lost production included missed work days due to chronic and acute conditions. Specifically, CCHS respondents were asked about missed work days due to illness or injury within the 3 month period prior to the survey. In the CCHS LOP module, chronic conditions are defined as a long-term physical or mental condition diagnosed by a health professional that has lasted or is expected to last 6 months or more. For the purpose of EBIC 2010 analyses, respondents who participated in the 2010 CCHS LOP module were grouped into the following three categories according to their responses to particular survey questions: missed less than 90 days of work due to illness or injury in the past 3 months; missed 90 consecutive days of work due to illness or injury in the past 3 months but had worked in the past 12 months; and excluded from analysis.Footnote h
For respondents who reported missing less than 90 days due to illness or injury in the past 3 months, the exact number of days missed multiplied by four (to reflect the entire year) was used as the period of lost production. For respondents who reported missing 90 consecutive days of work due to illness or injury in the past three months but had worked in the past 12 months, the estimated friction period (the unemployment duration) was employed. As these respondents indicated that they had worked in the past 12 months, it was assumed that their friction period fell within the year and that they were replaced after the duration of the friction period. All respondents who indicated that they had not worked in the past 12 months were excluded from the analysis, as the friction period and lost production for these individuals would have fallen in another year.
Estimated missed work days from the CCHS were allocated to EBIC diagnostic categories according to the physical and mental health conditions identified by respondents. Given that individuals were only asked about broad groups of illness or injury in the CCHS, EBIC 2010 estimates for the value of lost production are only available at the ICD chapter level. In addition, Statistics Canada guidelines restrict the release of data based on small cell counts which also affected the ways in which the data could be grouped. Therefore, morbidity cost estimates are only available by larger age-groups (15-34 years, 35-54 years, and 55-75 years).Footnote i It was possible to allocate 73% of the morbidity costs to an ICD chapter; the remainder was labelled as unallocated.
Note that methods used to produce these estimates are the exact same methods used to estimate the value of lost production due to morbidity in EBIC 2005-2008. The only difference is that information (in the form of ICD codes) for the CCHS 2010 LOP_050 “Other Specify” question on health condition was obtained from Statistics Canada. This allowed the unallocated portion of morbidity costs to be reduced by $2.0 billion.
Value of Lost Production due to Premature Mortality
In order to be consistent with a prevalence-based COI approach, all lost production that would have occurred in 2010, if it were not for the existence of the illness, or injury, should be included. This would entail going back to the final months of 2009 to determine which of those premature deaths contributed to lost production in 2010. The length of time to go back is dependent on the appropriate friction period. For 2010, the duration of unemployment ranged from 13.6 weeks (3.1 months) to 22 weeks (5.1 months).
Data from Statistics Canada's Vital Statistics Death Database (2010) were employed to estimate the value of lost production due to premature mortality. This database contains information on all deaths that occurred in Canada, including date of death, cause of death (coded using ICD-10), age, sex, and province/territory of residence. The value of lost production in 2010 was estimated by multiplying the number of deaths by the friction period, the labour force participation rate, and average monthly earnings (using age-sex-province-specific rates). The costs were then allocated to EBIC diagnostic categories based on the ICD-10 coded cause of death. The value of lost production was estimated for the working age population comprising individuals aged 15-64 years, broken down by the following age groups: 15-34 years, 35-54 years, and 55-64 years.Footnote j The results excluded mortality cost estimates for residents of other provinces/territories who died in Quebec.
Caregiving Costs
Caregiving can be classified as either a direct cost or an indirect cost depending on whether a formal, or direct, payment was made. Caregiving costs were estimated for 2010 using data from the General Social Survey (GSS) Cycle 26: Caregiving and Care Receiving. Reference 36 The survey included questions about any care received by the respondent for a health condition or aging, in the previous twelve months, and the main condition for which the respondent sought help. Caregiving was separated into two general groups: caregiving provided by family, friends and neighbours, and caregiving provided by paid workers and organizations. For the purpose of EBIC 2010, the former has been classified as informal caregiving (indirect costs) and the latter as formal caregiving (direct cost).
Cycle 26 of the GSS contains data for the year 2012, so adjustments were made for population differences. The target population for Cycle 26 of the GSS included all persons 15 years of age and older in Canada, excluding residents of the Yukon, Northwest Territories, and Nunavut, as well as full-time residents of institutions.
Caregiving time was valued using the caregiver’s characteristics and attributed to the respondent’s (person receiving the care) characteristics. Respondents were asked about the total number of hours of care received per week. The total caregiving hours were multiplied by the appropriate earnings for the caretaker based on province, age, and sex.Footnote k,Footnote l,Footnote m Annual average 2010 province-sex-age specific earnings were obtained from CANSIM.Footnote n Reference 37 Data on the caregiver’s age and sex were not available for formal caregiving, thus provincial specific earnings were employed. These costs were then allocated to the respondent’s sex and age group, and main condition (ICD chapter) for which they sought help. In some cases, the main health condition was not stated or unknown; costs associated with these records were included under the ‘Unallocated’ diagnostic category. Based on the survey format, if a respondent noted that they had received both formal and informal care, it was not possible to distinguish if the care was for different conditions. In such cases it was assumed that the main health condition identified applied to both types of caregiving. Results for the caregiving costs are available only at the ICD chapter level.
Results
Direct Costs
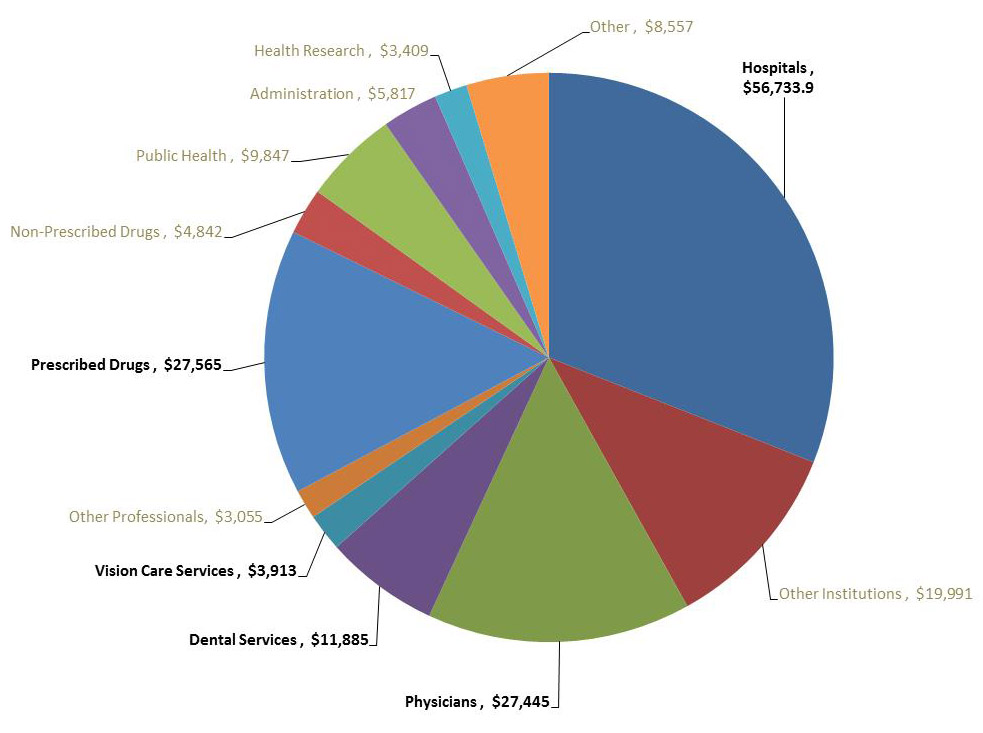
As previously noted, total current health expenditures in Canada in 2010 were $183.1 billion. It was possible to allocate $127.5 billion at the ICD chapter level, including expenditures associated with hospitals, prescribed drugs, physicians, as well as dental services and vision care services (see Figure 3). Excluding dental services and vision care, it was possible to allocate $111.7 billion, or 61%, of all direct health expenditures at the EBIC diagnostic category level.
Figure 3: Current Health Expenditures by Use of Funds, Canada 2010 ($000,000)
Source: Canadian Institute for Health Information (CIHI), 2015
Figure 3 – Text description
| Category | Amount | Percent |
|---|---|---|
| Hospitals | $56,734 | 31% |
| Other institutions | $19,991 | 11% |
| Physicians | $27,445 | 15% |
| Dental services | $11,885 | 6% |
| Vision care services | $3,913 | 2% |
| Other professionals | $3,055 | 2% |
| Prescribed drugs | $27,565 | 15% |
| Non-prescribed drugs | $4.842 | 3% |
| Public health | $9,847 | 5% |
| Administration | $5,817 | 3% |
| Health research | $3,409 | 2% |
| Other | $8,557 | 5% |
Dental services and vision care services could not be allocated beyond the ICD chapter level as there was no data available allowing for the allocation of these expenditures to a specific diagnostic category. Dental service expenditures were allocated entirely to ICD Chapter XI, Diseases of the Digestive System, as this chapter covers all dental related services. Vision care services were allocated to ICD Chapter VII, Eye and Related care.
Table 5 shows the breakdown of the direct costs by ICD chapter. In addition to the values from the current health expenditure data, formal caregiving costs have been included. The costliest ICD chapter was Chapter XI, Diseases of the Digestive System with $19.2 billion (17%) in total health expenditures; dental services accounted for the greatest amount of these expenditures. The next costliest ICD chapters were injuries (13.5 billion, 12%), diseases of the circulatory system ($13.1 billion, 12%), mental disorders ($10.5 billion, 9%) and musculoskeletal diseases ($6.8 billion, 6%).Footnote o Note that each ICD chapter employs a different mix of resources in the treatment of their respective diseases or conditions. For example, Chapter IV (Expenditures on endocrine and related conditions) and Chapter V, Mental Disorders employ a larger proportion of drug expenditures compared to many of the other conditions. Chapter XXI, Other Factors, is largely skewed towards hospital expenditures, but as will be discussed this is mainly focused on outpatient procedures.
| Hospital | Physician | Drugs | Dental Services | Vision Care Services | Formal Caregiving | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I: Infectious diseases | $1,080.4 | 1.9% | $380.8 | 1.4% | $792.5 | 2.9% | 0 | 0 | 0 | 0 | $2,253.8 | 2.0% |
| II: Neoplasms | $3,522.1 | 6.2% | $1,029.5 | 3.8% | $804.4 | 2.9% | 0 | 0 | $3.6 | 9.1% | $5,359.5 | 4.8% |
| III: Diseases of the blood | $329.0 | 0.6% | $156.8 | 0.6% | $109.4 | 0.4% | 0 | 0 | 0 | 0 | $595.2 | 0.5% |
| IV: Endocrine and related | $995.4 | 1.8% | $894.8 | 3.3% | $3,575.9 | 13.0% | 0 | 0 | $0.5 | 1.2% | $5,466.6 | 4.9% |
| V: Mental disorders | $4,137.2 | 7.3% | $2,404.5 | 8.8% | $3,889.4 | 14.1% | 0 | 0 | $8.9 | 22.8% | $10,440.0 | 9.4% |
| VI: Nervous system | $1,474.4 | 2.6% | $323.2 | 1.2% | $922.9 | 3.3% | 0 | 0 | $9.6 | 24.5% | $2,730.0 | 2.4% |
| VII: Eye and related | $894.5 | 1.6% | $1,241.3 | 4.5% | $398.8 | 1.4% | 0 | $3,913.1 | $1.0 | 2.5% | $6,448.7 | 5.8% |
| VIII: Ear and related | $315.9 | 0.6% | $236.2 | 0.9% | $158.7 | 0.6% | 0 | 0 | 0 | 0.0% | $710.8 | 0.6% |
| IX: Circulatory system | $6,128.0 | 10.8% | $1,909.6 | 7.0% | $4,957.3 | 18.0% | 0 | 0 | $5.1 | 13.2% | $13,000.0 | 11.7% |
| X: Respiratory system | $3,142.7 | 5.5% | $1,273.3 | 4.6% | $2,097.3 | 7.6% | 0 | 0 | $0.7 | 1.7% | $6,514.0 | 5.9% |
| XI: Digestive system | $4,399.1 | 7.8% | $984.6 | 3.6% | $1,915.3 | 6.9% | $11,884.8 | 0 | $0.6 | 1.6% | $19,184.4 | 17.2% |
| XII: Skin and related | $535.4 | 0.9% | $582.4 | 2.1% | $952.9 | 3.5% | 0 | 0 | 0 | 0 | $2,070.7 | 1.9% |
| XIII: Musculoskeletal | $2,686.4 | 4.7% | $1,382.8 | 5.0% | $2,641.6 | 9.6% | 0 | 0 | $5.5 | 14.2% | $6,716.3 | 6.0% |
| XIV: Genitourinary | $2,499.7 | 4.4% | $1,312.7 | 4.8% | $933.8 | 3.4% | 0 | 0 | $0.6 | 1.6% | $4,746.8 | 4.3% |
| XV: Pregnancy and childbirth | $1,831.7 | 3.2% | $560.8 | 2.0% | $76.7 | 0.3% | 0 | 0 | 0 | 0 | $2,469.2 | 2.2% |
| XVI: Perinatal conditions | $967.4 | 1.7% | $97.4 | 0.4% | $6.9 | 0.0% | 0 | 0 | 0 | 0 | $1,071.7 | 1.0% |
| XVII: Congenital malformations | $652.4 | 1.1% | $69.8 | 0.3% | $51.7 | 0.2% | 0 | 0 | 0 | 0 | $773.9 | 0.7% |
| XVIII: Symptoms, etc. | $2,588.4 | 4.6% | $2,444.9 | 8.9% | $1,985.4 | 7.2% | 0 | 0 | 0 | 0 | $7,018.6 | 6.3% |
| XIX and XX: Injuries | $4,038.7 | 7.1% | $9,412.6 | 34.3% | $416.5 | 1.5% | 0 | 0 | $3.0 | 7.6% | $13,870.7 | 12.1% |
| XXI: Other factors | $14,515.1 | 25.6% | $747.0 | 2.7% | $877.2 | 3.2% | 0 | 0 | 0 | 0 | $16,139.3 | 14.3% |
| Unallocated | --- | --- | --- | --- | --- | --- | 0 | 0 | $10.3 | 0 | $10.3 | 0 |
| Total | $56,733.9 | 100.0% | $27,445.0 | 100.0% | $27,564.6 | 100.0% | 0 | 0 | $49.2 | 100.0% | $127,590.7 | 100.0% |
| Source: EBIC 2010 | ||||||||||||
Hospital Care Expenditures
Total hospital costs in 2010 were $56.7 billion with inpatient treatment accounting for $29.5 billion (52%). Emergency department visits accounted for $10.7 billion of expenditures. Overall, ICD Chapter XXI (Factors influencing health status and contact with health services) accounted for over 26% of all hospital-related expenditures, but only 9% of inpatient expenditures. This category includes circumstances where the treatment was for a reason other than a disease, injury or external cause, including regular medical check-ups. Therefore, as expected this chapter accounted for the majority of outpatient clinic visits (71%). Table 6 shows hospital expenditures by ICD chapter and health function.
The costliest ICD chapters (other than Chapter XXI) were Chapter IX, Circulatory System Diseases ($6.1 billion, 11%), Chapter XI, Digestive System Diseases ($4.4 billion, 8%), Chapter V, Mental Disorders ($4.1 billion, 7%), Chapters XIX and XX, Injuries ($4 billion, 7%), and Chapter II, Neoplasms (cancer) ($3.5 billion, 6%).
Figure 4 shows the breakdown for these ICD chapters by health function. Injuries account for the largest portion of emergency department visits in comparison to the other conditions. Circulatory system diseases employ the greatest portion of clinic resources according to the EBIC data.
Figure 4: Costliest ICD chapters by health function, hospital expenditures only, Canada 2010
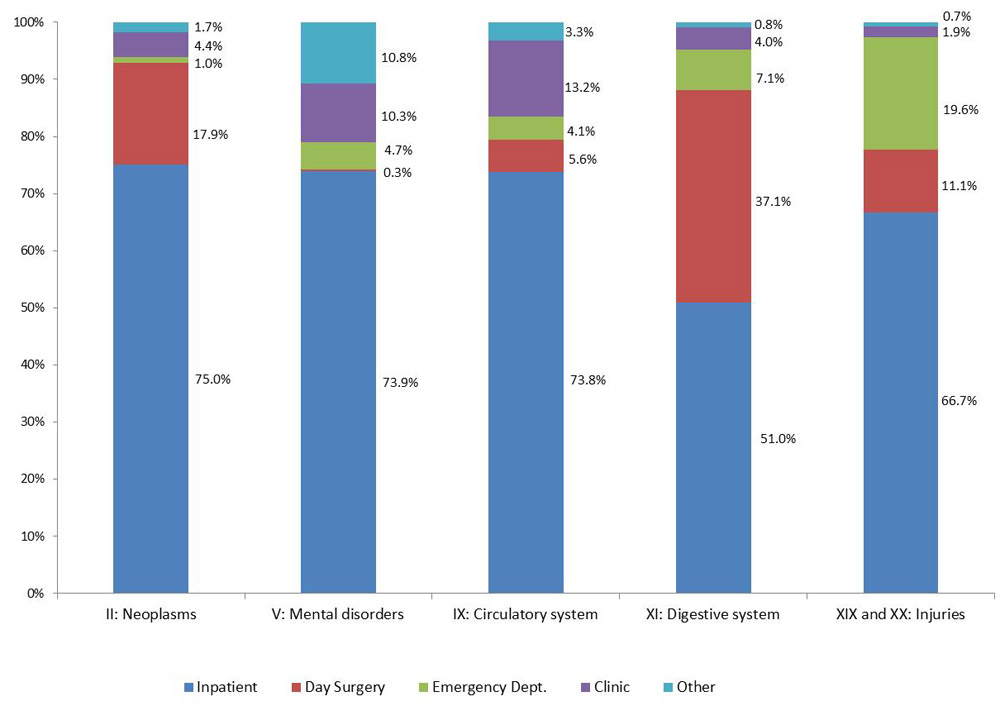
Figure 4 – Text description
| ICD Chapter | Inpatient | Day Surgery | Emergency Department | Clinic | Other | Total |
|---|---|---|---|---|---|---|
| Neoplasms | 2,642.9 | 629.2 | 36.5 | 153.9 | 59.7 | 3,522.1 |
| Mental disorders | 3,056.3 | 12.8 | 196.4 | 424.9 | 446.9 | 4,137.2 |
| Circulatory system | 4,521.7 | 344.9 | 250.4 | 810.9 | 200.3 | 6,128.0 |
| Digestive system | 2,242.3 | 1,632.4 | 311.9 | 175.4 | 37.2 | 4,399.1 |
| Injuries | 2,692.0 | 447.8 | 790.2 | 78.6 | 30.1 | 4,038.7 |
| Inpatient | Day Surgery | Outpatient - Emergency Dept. |
Outpatient - Clinic |
Other | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I: Infectious diseases | $847 | 2.90% | $44 | 0.60% | $152 | 3.70% | $30 | 0.30% | $8 | 0.20% | $1,080 | 1.90% |
| II: Neoplasms | $2,643 | 9.00% | $629 | 8.10% | $37 | 0.90% | $154 | 1.40% | $60 | 1.30% | $3,522 | 6.20% |
| III: Diseases of the blood | $215 | 0.70% | $28 | 0.40% | $27 | 0.70% | $57 | 0.50% | $2 | 0.00% | $329 | 0.60% |
| IV: Endocrine and related | $711 | 2.40% | $33 | 0.40% | $66 | 1.60% | $145 | 1.30% | $40 | 0.90% | $995 | 1.80% |
| V: Mental disorders | $3,056 | 10.40% | $13 | 0.20% | $196 | 4.80% | $425 | 3.90% | $447 | 9.60% | $4,137 | 7.30% |
| VI: Nervous system | $916 | 3.10% | $82 | 1.10% | $72 | 1.80% | $121 | 1.10% | $284 | 6.10% | $1,474 | 2.60% |
| VII: Eye and related | $31 | 0.10% | $738 | 9.60% | $34 | 0.80% | $85 | 0.80% | $6 | 0.10% | $895 | 1.60% |
| VIII: Ear and related | $55 | 0.20% | $188 | 2.40% | $54 | 1.30% | $14 | 0.10% | $4 | 0.10% | $316 | 0.60% |
| IX: Circulatory system | $4,522 | 15.30% | $345 | 4.50% | $250 | 6.10% | $811 | 7.50% | $200 | 4.30% | $6,128 | 10.80% |
| X: Respiratory system | $2,277 | 7.70% | $372 | 4.80% | $386 | 9.50% | $80 | 0.70% | $29 | 0.60% | $3,143 | 5.50% |
| XI: Digestive system | $2,242 | 7.60% | $1,632 | 21.10% | $312 | 7.70% | $175 | 1.60% | $37 | 0.80% | $4,399 | 7.80% |
| XII: Skin and related | $291 | 1.00% | $87 | 1.10% | $97 | 2.40% | $43 | 0.40% | $18 | 0.40% | $535 | 0.90% |
| XIII: Musculoskeletal | $1,566 | 5.30% | $808 | 10.50% | $197 | 4.80% | $82 | 0.80% | $33 | 0.70% | $2,686 | 4.70% |
| XIV: Genitourinary | $1,058 | 3.60% | $872 | 11.30% | $243 | 6.00% | $276 | 2.60% | $51 | 1.10% | $2,500 | 4.40% |
| XV: Pregnancy and childbirth | $1,498 | 5.10% | $86 | 1.10% | $77 | 1.90% | $168 | 1.60% | $3 | 0.10% | $1,832 | 3.20% |
| XVI: Perinatal conditions | $952 | 3.20% | $2 | 0.00% | $7 | 0.20% | $6 | 0.10% | $2 | 0.00% | $967 | 1.70% |
| XVII: Congenital malformations | $376 | 1.30% | $145 | 1.90% | $2 | 0.10% | $118 | 1.10% | $11 | 0.20% | $652 | 1.10% |
| XVIII: Symptoms, etc. | $1,037 | 3.50% | $283 | 3.70% | $875 | 21.50% | $290 | 2.70% | $104 | 2.20% | $2,588 | 4.60% |
| XIX and XX: Injuries | $2,692 | 9.10% | $448 | 5.80% | $790 | 19.40% | $79 | 0.70% | $30 | 0.60% | $4,039 | 7.10% |
| XXI: Factors influencing health | $2,496 | 8.50% | $889 | 11.50% | $204 | 5.00% | $7,626 | 70.70% | $3,301 | 70.70% | $14,515 | 25.60% |
| Total | $29,482 | 100.00% | $7,724 | 100.00% | $4,076 | 100.00% | $10,783 | 100.00% | $4,670 | 100.00% | $56,734 | 100.00% |
| Source: EBIC 2010 | ||||||||||||
Hospital Expenditures by Age
Figure 5 shows the percentage of hospital expenditures across each of the six age groups as well as the percentage of the overall population. Not surprisingly, those in the older age groups utilize a much larger proportion of hospital expenditures in comparison to their respective size of the population. For example, those aged 75 plus accounted for 20 percent of hospital expenditures, yet only account for 7% of the population. Conversely, those in the 15-34 age group accounted for 27% of the population yet only 16% of health expenditures.
Figure 6 shows the distribution of all hospital expenditures by health function for each age group. It can be seen that inpatient care comprises a greater proportion of hospital expenditures as the age groups increase. Day surgery peaks at 20% of hospital expenditures for those aged 15-34 years, while only accounting for 6% of hospital expenditures in those aged 75 plus.
Figure 5: Percentage of hospital expenditures and population by age group, Canada 2010
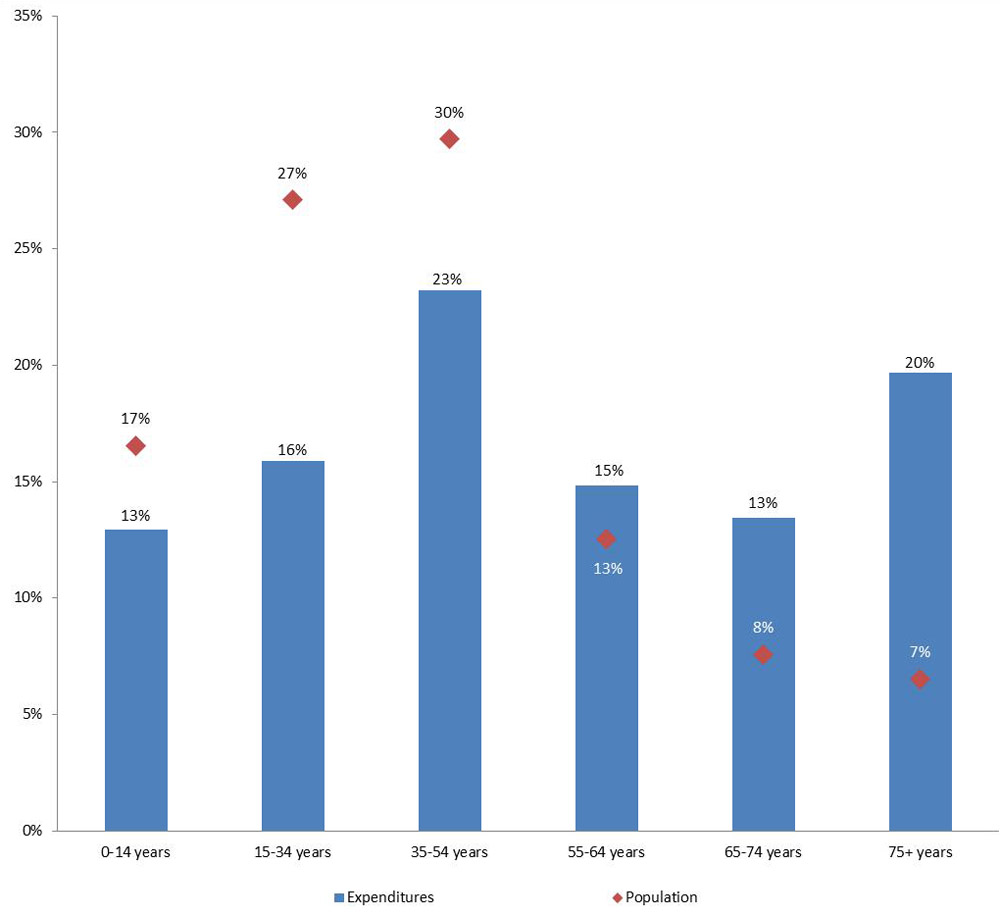
Figure 5 – Text description
| Age group | Share of total expenditures | Proportion of population |
|---|---|---|
| 0-14 years | 13% | 17% |
| 15-34 years | 16% | 27% |
| 35-54 years | 23% | 30% |
| 55-64 years | 15% | 13% |
| 65-74 years | 13% | 8% |
| 75 plus | 20% | 7% |
Figure 6: Percentage of hospital expenditures by age group and health function, Canada 2010
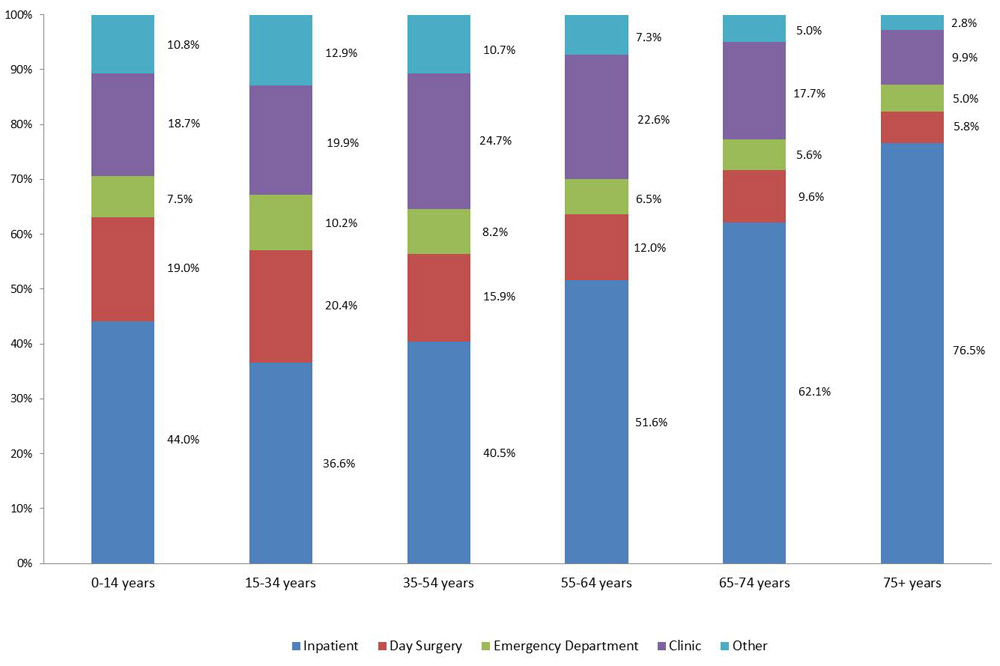
Figure 6 – Text description
| Health function | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Inpatient | 44.0% | 36.6% | 40.5% | 51.6% | 62.1% | 76.5% |
| Day surgery | 19.0% | 20.4% | 15.9% | 12.0% | 9.6% | 5.8% |
| Emergency | 7.5% | 10.2% | 8.2% | 6.5% | 5.6% | 5.0% |
| Clinic | 18.7% | 19.9% | 24.7% | 22.6% | 17.7% | 9.9% |
| Other | 10.8% | 12.9% | 10.7% | 7.3% | 5.0% | 2.8% |
Inpatient Hospital Expenditures
The six conditions with the largest inpatient hospital expenditures in 2010 were diseases of the circulatory system ($4.5 billion, 15%), mental disorders ($3.1 billion, 10%), injuries ($2.5 billion, 9%), neoplasms ($2.6 billion, 8.9%), diseases of the respiratory system ($2.3 billion, 8%) and diseases of the digestive system ($2.2 billion, 8%). Together these conditions represent almost 60% of all inpatient hospital expenditures. Figure 7 shows the breakdown for the six costliest ICD chapters by sex. Males accounted for a greater amount of expenditures, other than for digestive system diseases.
Figure 8 shows the breakdown of the costliest ICD chapters by age group. Expenditures for diseases of the circulatory system increase with age, becoming the costliest condition for those ages 75 plus. Diseases of the respiratory system were the costliest condition for those aged 0-14 years, while mental disorders accounted for the greatest amount of expenditures in the 15-34 age group.
Figure 7: Inpatient hospital expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
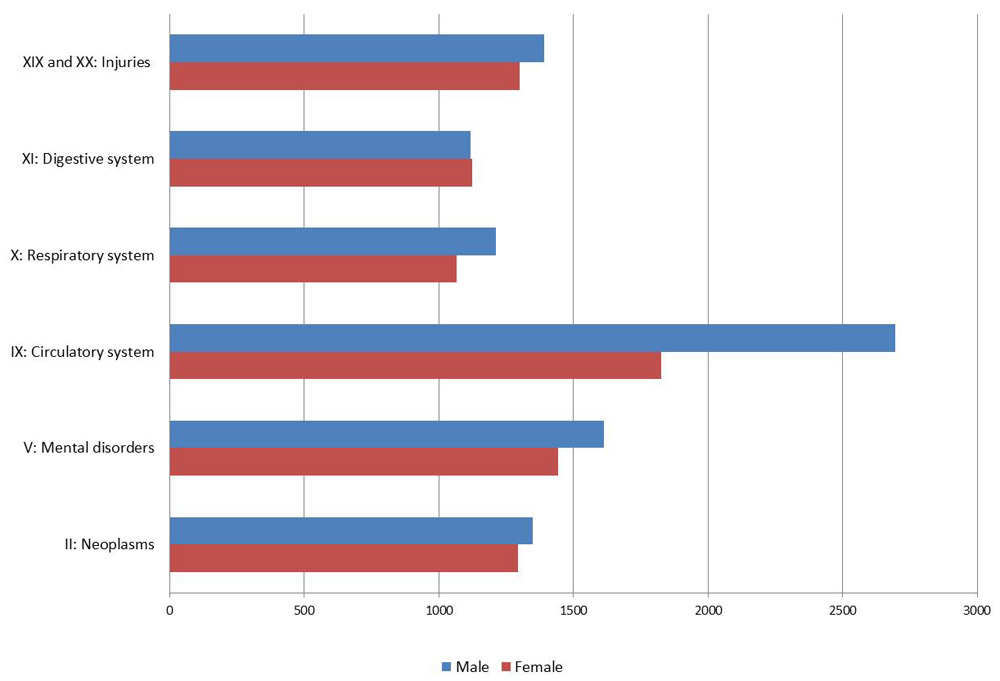
Figure 7 – Text description
| ICD Chapter | Expenditures on Neoplasms | Expenditures on Mental and behavioural disorders | Expenditures Diseases of the circulatory system | Expenditures on Diseases of the respiratory system | Expenditures on Diseases of the digestive system | Expenditures on Injury, poisoning and certain other consequences of external causes |
|---|---|---|---|---|---|---|
| Females | 1,295 | 1,442 | 1,825 | 1,066 | 1,123 | 1,301 |
| Males | 1,348 | 1,614 | 2,697 | 1,211 | 1,119 | 1,391 |
Figure 8: Percentage of inpatient hospital expenditures by age group, selected ICD chapters, Canada 2010
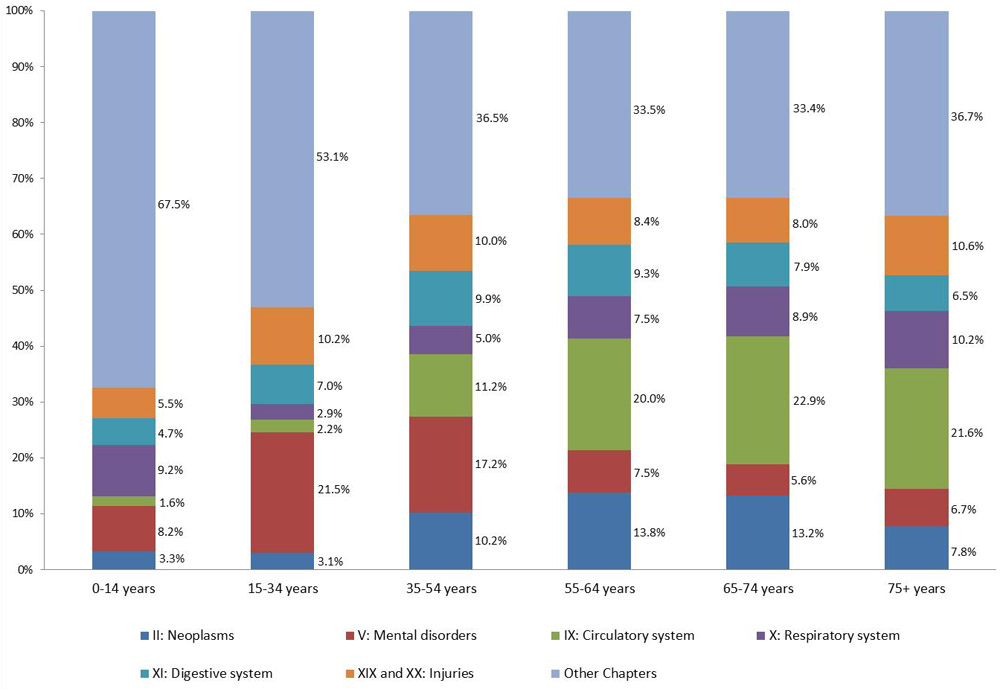
Figure 8 – Text description
| ICD Chapter | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Neoplasms | 3.3% | 3.1% | 10.2% | 13.8% | 13.2% | 7.8% |
| Mental disorders | 8.2% | 21.5% | 17.2% | 7.5% | 5.6% | 6.7% |
| Circulatory system | 1.6% | 2.2% | 11.2% | 20.0% | 22.9% | 21.6% |
| Respiratory system | 9.2% | 2.9% | 5.0% | 7.5% | 8.9% | 10.2% |
| Digestive system | 4.7% | 7.0% | 9.9% | 9.3% | 7.9% | 6.5% |
| Injuries | 5.5% | 10.2% | 10.0% | 8.4% | 8.0% | 10.6% |
| Other | 67.5% | 53.1% | 36.5% | 33.5% | 33.4% | 36.7% |
Day Surgery Expenditures
The health conditions with the largest day surgery expenditures in 2010 were digestive system diseases ($1.6 billion, 21%), genitourinary diseases ($872 million, 11%) musculoskeletal diseases ($808 million, 11%), eye and related diseases ($748 million, 10%), neoplasms (629 million, 8%), injuries ($448 million 6%); together with factors that influence health ($889 million, 12%), these accounted for almost 80% of all day surgery expenditures. Note that females accounted for a greater amount of expenditures in each of these instances, other than injuries (Figure 9).
Examining the breakdown of the costliest conditions, by age group, it is evident that eye and related conditions represent the greatest expenditures related to day surgery for those aged 75 years and over (37%). Digestive system diseases are the costliest condition for those in the youngest age group.
Figure 9: Day surgery expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
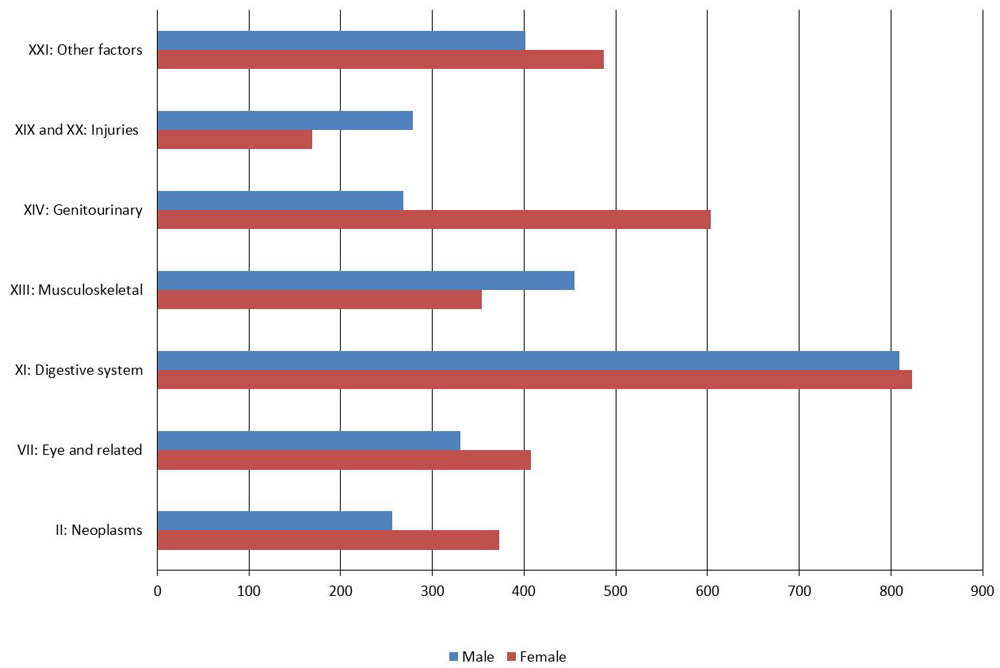
Figure 9 – Text description
| ICD Chapter | Female | Male | Total |
|---|---|---|---|
| Neoplasms | 372.7 | 256.5 | 629.2 |
| Eye and related | 407.2 | 330.5 | 737.7 |
| Digestive system | 823.3 | 809.1 | 1,632.4 |
| Musculoskeletal | 353.8 | 454.6 | 808.4 |
| Genitourinary | 603.7 | 268.2 | 871.8 |
| Injuries | 169.4 | 278.4 | 447.8 |
| Other factors | 487.3 | 401.5 | 888.9 |
Figure 10: Percentage of day surgery hospital expenditures by age group, selected ICD chapters, Canada 2010
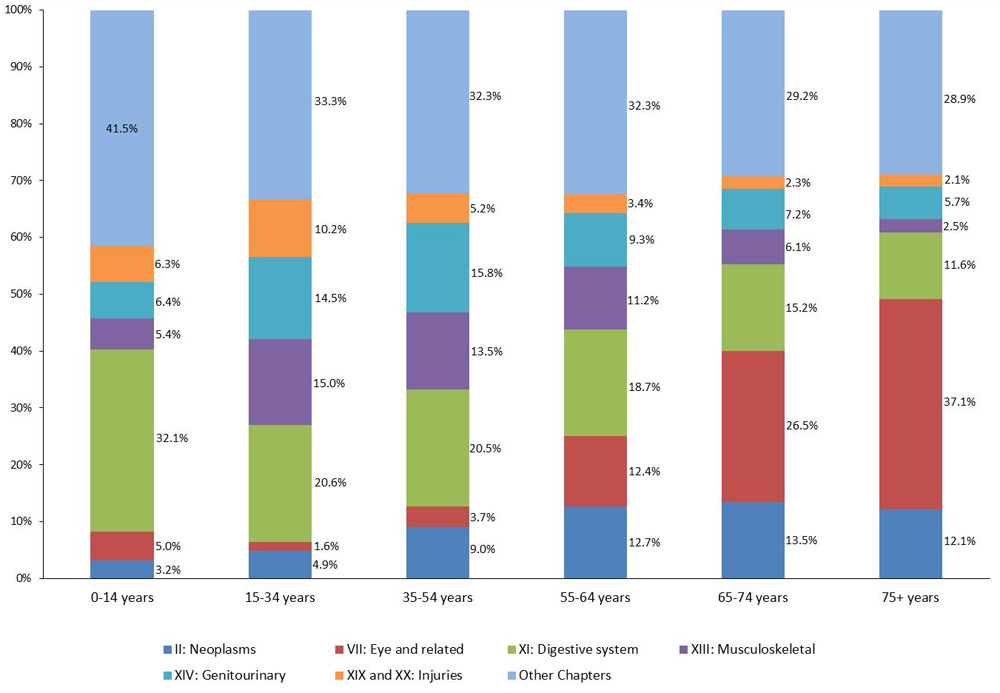
Figure 10 – Text description
| ICD Chapter | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Neoplasms | 3.2% | 4.9% | 9.0% | 12.7% | 13.5% | 12.1% |
| Eye and related | 5.0% | 1.6% | 3.7% | 12.4% | 26.5% | 37.1% |
| Digestive system | 32.1% | 20.6% | 20.5% | 18.7% | 15.2% | 11.6% |
| Musculoskeletal | 5.4% | 15.0% | 13.5% | 11.2% | 6.1% | 2.5% |
| Genitourinary | 6.4% | 14.5% | 15.8% | 9.3% | 7.2% | 5.7% |
| Injuries | 6.3% | 10.2% | 5.2% | 3.4% | 2.3% | 2.1% |
| Other | 41.5% | 33.3% | 32.3% | 32.3% | 29.2% | 28.9% |
Emergency Department Expenditures
Emergency department (ED) expenditures were dominated by two conditions – symptoms ($875 million, 22%), and injuries ($790 million, 19%) which were responsible for over 40% of all ED expenditures. The other top conditions were: respiratory system diseases ($386 million, 9.4%), digestive system diseases ($312 million, 7.6%), diseases of the circulatory system ($250 million, 6.1%), genitourinary diseases ($243 million, 5.9%), musculoskeletal diseases ($197 million, 4.8%), and mental disorders ($196 million, 4.8%). Together these conditions accounted for 83% of all ED expenditures.
Figure 11 shows the expenditures for the top conditions by sex. Females accounted for a slightly greater percentage of all ED expenditures (52% versus 48%). This observation is consistent for each of the conditions with the exception of injuries and circulatory system diseases.
Figure 12 shows the percentage of expenditures by age group. The percentage of expenditures allocated to symptoms was relatively constant across age groups. Circulatory system diseases were responsible for a growing percentage of expenditures as age increased, while expenditures on injuries fell as age increased.
Figure 11: Emergency department expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
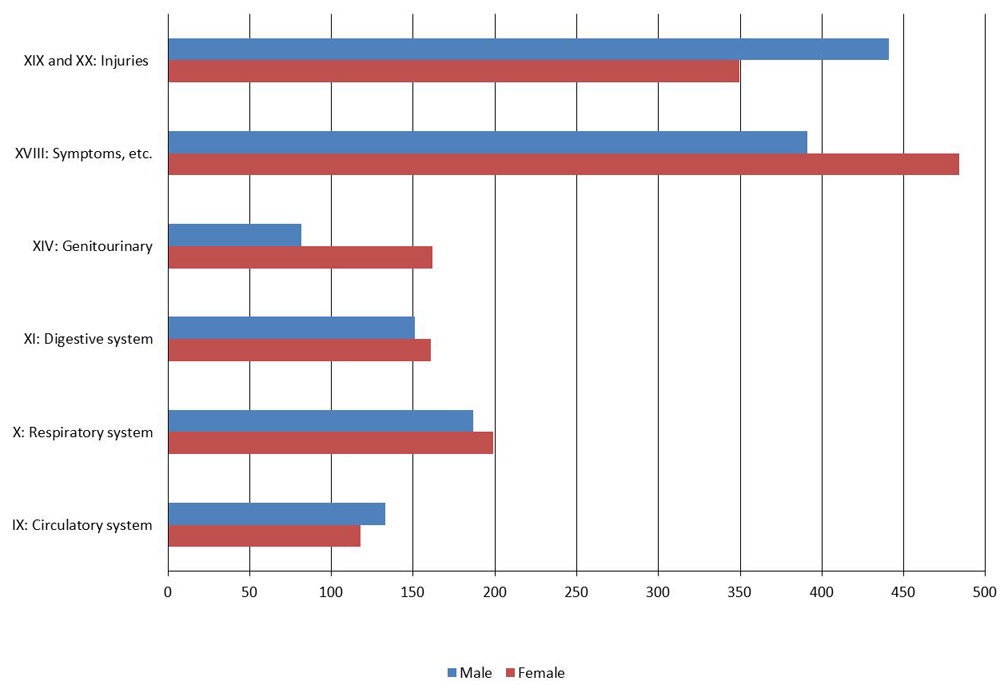
Figure 11 – Text description
| ICD Chapter | Female | Male | Total |
|---|---|---|---|
| Circulatory system | 117.7 | 132.7 | 250.4 |
| Respiratory system | 198.9 | 186.7 | 385.6 |
| Digestive system | 160.8 | 151.1 | 311.9 |
| Genitourinary | 161.8 | 81.3 | 243.1 |
| Symptoms, etc. | 483.8 | 391.2 | 874.9 |
| Injuries | 349.4 | 440.8 | 790.2 |
| Other | 659.1 | 560.5 | 1,219.6 |
Figure 12: Percentage of emergency department expenditures by age group, selected ICD chapters, Canada 2010
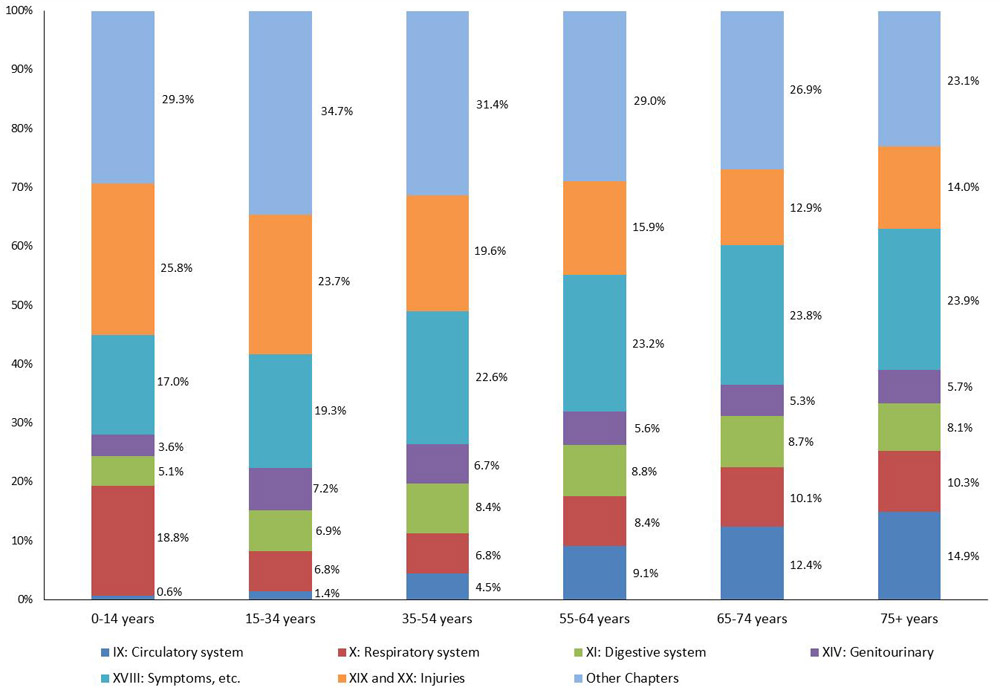
Figure 12 – Text description
| ICD Chapter | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Circulatory system | 0.6% | 1.4% | 4.5% | 9.1% | 12.4% | 14.9% |
| Respiratory system | 18.8% | 6.8% | 6.8% | 8.4% | 10.1% | 10.3% |
| Digestive system | 5.1% | 6.9% | 8.4% | 8.8% | 8.7% | 8.1% |
| Genitourinary | 3.6% | 7.2% | 6.7% | 5.6% | 5.3% | 5.7% |
| Symptoms, etc. | 17.0% | 19.3% | 22.6% | 23.2% | 23.8% | 23.9% |
| Injuries | 25.8% | 23.7% | 19.6% | 15.9% | 12.9% | 14.0% |
| Other Chapters | 29.3% | 34.7% | 31.4% | 29.0% | 26.9% | 23.1% |
Drug Expenditures
In 2010, prescription drug expenditures in Canada were $27.6 billion, all of which were allocated by EBIC diagnostic category, age, and sex. This amount represents 85% of all drug sales in Canada, with the remainder including over-the-counter drugs.
Figure 13 provides an overview of drug expenditures for the costliest conditions by sex; (endocrine and related, mental disorders, circulatory system, respiratory system, digestive system, musculoskeletal, and symptoms), accounting for over 76% of all prescription drug expenditures. The conditions with the greatest drug expenditures for females were circulatory diseases, mental disorders, and musculoskeletal. The top three conditions for males were circulatory diseases, endocrine and related diseases, and mental disorders. The greatest cost difference by sex was for musculoskeletal diseases where female expenditures were almost double that of male expenditures, $1.8 billion and $0.9 billion respectively.
Figure 13: Drug expenditures by sex, selected ICD chapter, Canada 2010 ($000,000)
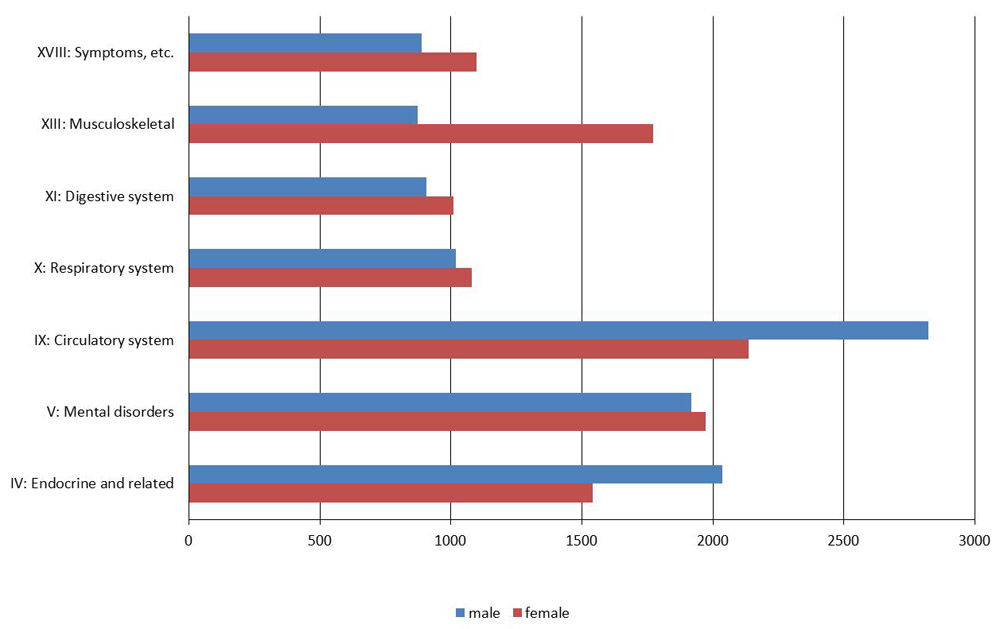
Figure 13 – Text description
| ICD Chapter | Expenditures on females | Expenditures on males |
|---|---|---|
| Endocrine and related | 2,035 | 1,541 |
| Mental disorders | 1,918 | 1,972 |
| Circulatory system | 2,823 | 2,134 |
| Respiratory system | 1,018 | 1,079 |
| Digestive system | 906 | 1,010 |
| Musculoskeletal | 871 | 1,771 |
| Symptoms, etc. | 888 | 1,098 |
Figure 14 shows the percentage of drug expenditures and population by age group. Individuals aged 0-14 years incurred the lowest percentage of drug expenditures (5%). As with the hospital expenditures, those in the older age groups utilize a much larger proportion of drug expenditures in comparison to their respective size of the population. Individuals aged 55 years and older accounted for approximately 52% of total drug expenditures, even though they accounted for only 28% of the total population.
Figure 15 shows the percentage distribution of drug expenditures by age group for the costliest conditions. The distribution of drug expenditures across ICD chapters varied considerably by age group. For example, while respiratory system diseases accounted for 32% of drug expenditures for those aged 0-14 years, they accounted for 10%, or less, of expenditures for all of the other age groups. Mental disorders make up a more significant portion of the drug expenditures for those in the younger age groups in comparison to the older age groups, while circulatory diseases represent the greatest percentage of drug expenditures in the older age groups.
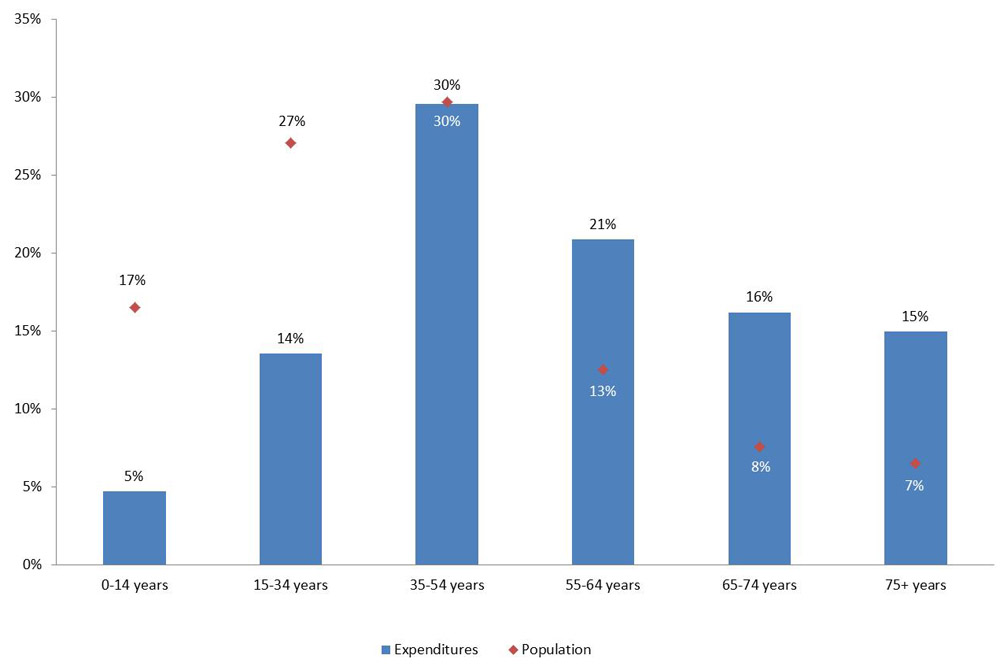
Figure 14 – Text description
| Age group | Proportion of population | Share of expenditures |
|---|---|---|
| 0-14 years | 17% | 5% |
| 15-34 years | 27% | 14% |
| 35-65 years | 30% | 30% |
| 55-64 years | 13% | 21% |
| 65-74 years | 8% | 16% |
| 75 plus | 7% | 15% |
Figure 15: Percentage of drug expenditures by age group, selected ICD chapters, Canada 2010
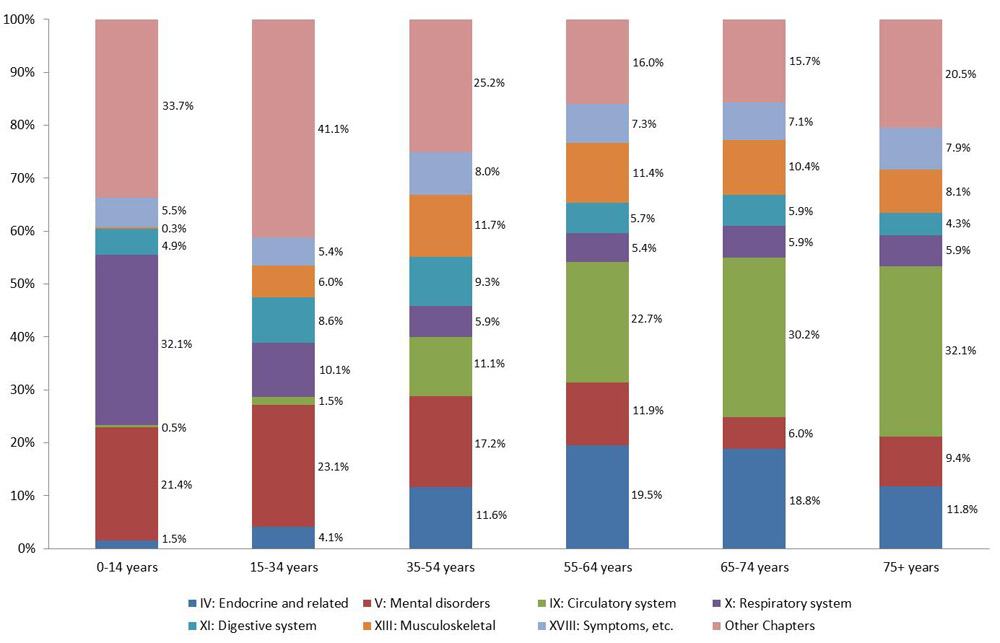
Figure 15 – Text description
| ICD Chapter | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Endocrine and related | 1.5% | 4.1% | 11.6% | 19.5% | 18.8% | 11.8% |
| Mental disorders | 21.4% | 23.1% | 17.2% | 11.9% | 6.0% | 9.4% |
| Circulatory system | 0.5% | 1.5% | 11.1% | 22.7% | 30.2% | 32.1% |
| Respiratory system | 32.1% | 10.1% | 5.9% | 5.4% | 5.9% | 5.9% |
| Digestive system | 4.9% | 8.6% | 9.3% | 5.7% | 5.9% | 4.3% |
| Musculoskeletal | 0.3% | 6.0% | 11.7% | 11.4% | 10.4% | 8.1% |
| Symptoms, etc. | 5.5% | 5.4% | 8.0% | 7.3% | 7.1% | 7.9% |
| Other Chapters | 33.7% | 41.1% | 25.2% | 16.0% | 15.7% | 20.5% |
Physician Care Expenditures
In 2010, physician expenditures totalled $27.4 billion, representing 14% of all health expenditures. Injuries accounted for the highest level of physician expenditures, representing 33% of all physician expenditures. The top eight conditions with the greatest physician expenditures (Mental disorders, eye and related conditions, circulatory system, respiratory system, musculoskeletal, genitourinary, symptoms, and injuries) accounted for approximately 78% of total physician expenditures.
Figure 16 shows the physician expenditures for costliest conditions broken down by sex. Given that females accounted for 57% of physician expenditures, the finding that female expenditures for most conditions were greater than male expenditures is not surprising. Note, however, that male expenditures related to circulatory system diseases were greater than female expenditures.
Figure 16: Physician expenditures by sex, selected ICD chapters, Canada 2010 ($000,000)
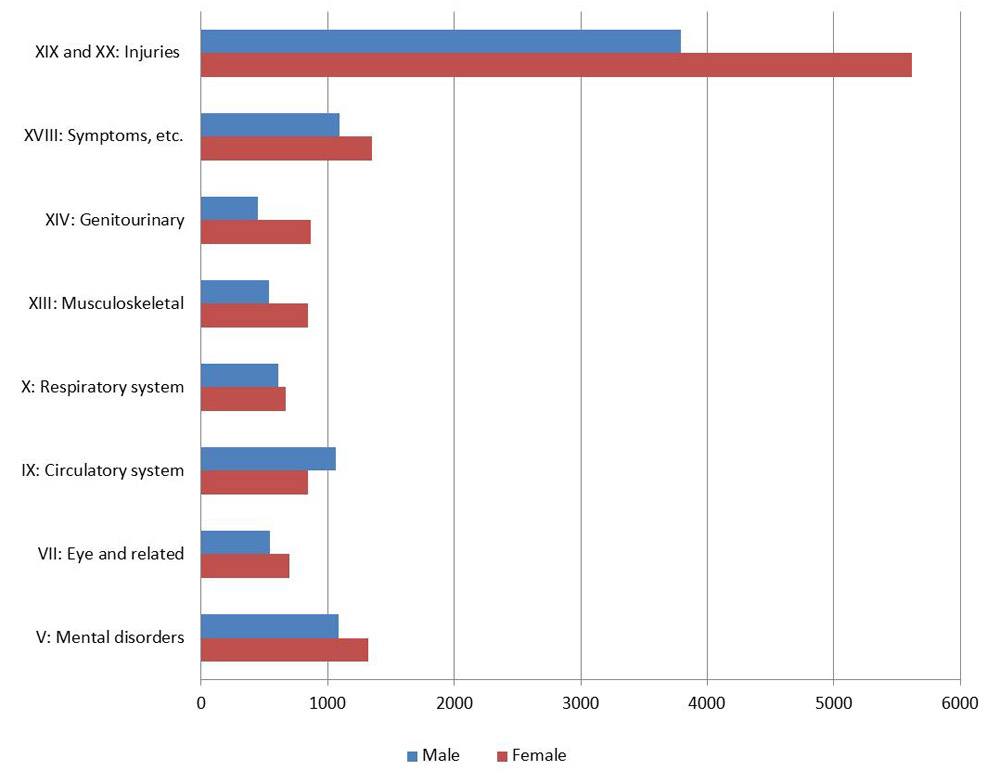
Figure 16 – Text description
| ICD Chapter | Physician expenditures on males | Physician expenditures on females |
|---|---|---|
| Mental disorders | 1,083.4 | 1,321.1 |
| Eye and related | 545.0 | 696.4 |
| Circulatory system | 1,064.2 | 845.4 |
| Respiratory system | 608.1 | 665.2 |
| Musculoskeletal | 535.5 | 847.3 |
| Genitourinary | 446.7 | 866.0 |
| Symptoms, etc. | 1,091.9 | 1,353.0 |
| Injuries | 3,793.2 | 5,619.4 |
Figure 17 shows the percentage of physician expenditures and population by age group. Those aged 55 years and over consumed a larger proportion of expenditures (49%) in comparison to their proportion of the population (28%). Examining physician expenditures by ICD chapter and age group (Figure 18), the overall cost distribution does not change significantly, other than an increase with age in the percentage of physician expenditures related to circulatory diseases.
Figure 17: Percentage of physician expenditures and population by age group, Canada 2010
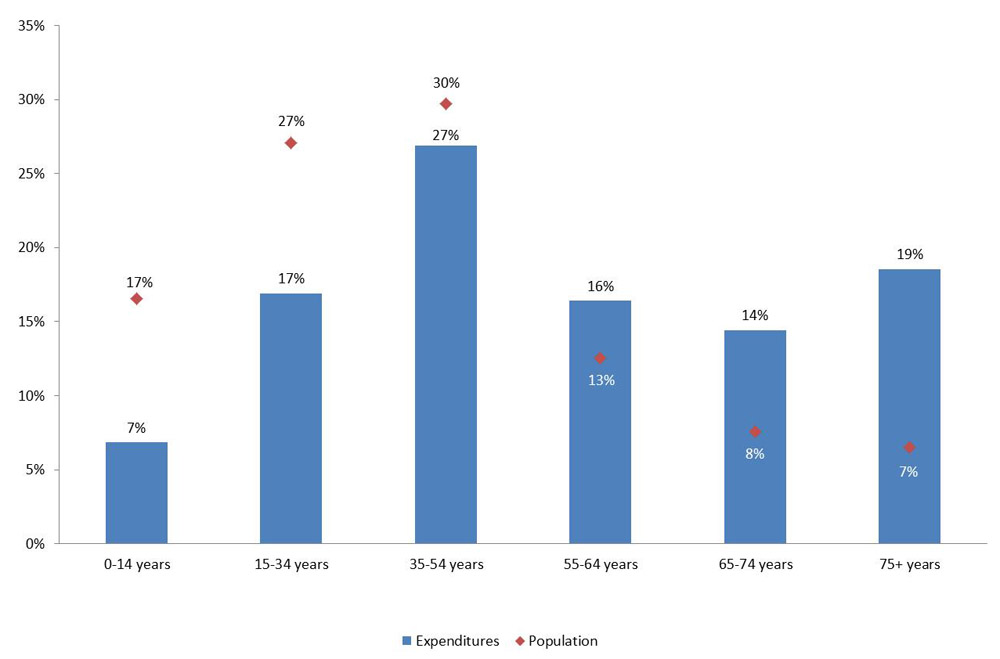
Figure 17 – Text description
| Age group | Proportion of population by age group | Share of total expenditures by age group |
|---|---|---|
| 0-14 years | 17% | 7% |
| 15-34 years | 27% | 17% |
| 35-65 years | 30% | 27% |
| 55-64 years | 13% | 17% |
| 65-74 years | 8% | 15% |
| 75 plus | 7% | 19% |
Figure 18: Percentage of physician expenditures by age group, selected ICD chapters, Canada 2010
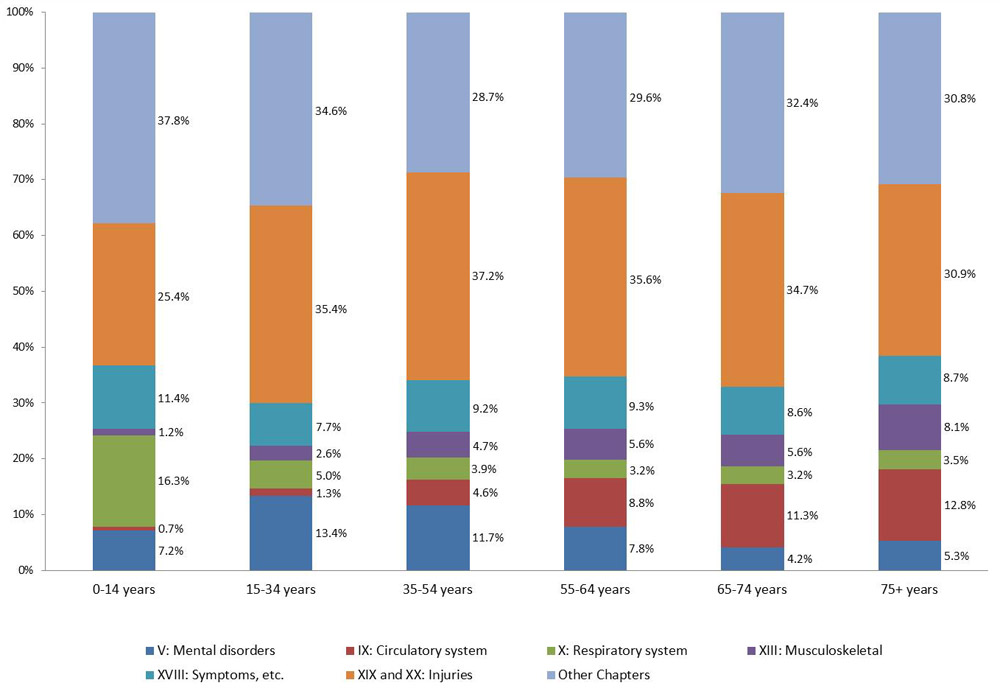
Figure 18 – Text description
| ICD Chapter | 0-14 years | 15-34 years | 35-54 years | 55-64 years | 65-74 years | 75 plus |
|---|---|---|---|---|---|---|
| Mental disorders | 7.2% | 13.4% | 11.7% | 7.8% | 4.2% | 5.3% |
| Circulatory system | 0.7% | 1.3% | 4.6% | 8.8% | 11.3% | 12.8% |
| Respiratory system | 16.3% | 5.0% | 3.9% | 3.2% | 3.2% | 3.5% |
| Musculoskeletal | 1.2% | 2.6% | 4.7% | 5.6% | 5.6% | 8.1% |
| Symptoms, etc. | 11.4% | 7.7% | 9.2% | 9.3% | 8.6% | 8.7% |
| Injuries | 25.4% | 35.4% | 37.2% | 35.6% | 34.7% | 30.9% |
| Other | 37.8% | 34.6% | 28.7% | 29.6% | 32.4% | 30.8% |
Indirect Costs
The total value of indirect costs in 2010 included in EBIC was $18.9 billion. This includes the value of lost production due to morbidity and premature mortality as well as the value of informal caregiving. Note that the value of lost production due to morbidity, which was estimated at $18.2 billion, accounted for the majority of the indirect costs. Table 7 shows the indirect costs by ICD chapter. The top two conditions, injuries ($3.8 billion, 27%) and diseases of the respiratory system ($3.1 billion, 22%) accounted for over half of the allocated indirect costs.Footnote p
| ICD chapter | Mortality | Morbidity | Informal Caregiving | Total | ||||
|---|---|---|---|---|---|---|---|---|
| $ (000,000s) |
% | $ (000,000s) |
% of allocated |
$ (000,000s) |
% of allocated |
$ (000,000s) |
% of allocated |
|
| I: Infectious diseases | 16.9 | 2.6 | 907.9 | 6.8 | 0 | 0 | 924.8 | 6.6 |
| II: Neoplasms | 237.8 | 36.4 | 540.0 | 4.1 | 12.3 | 9.3 | 790.2 | 5.6 |
| III: Diseases of the blood | 2.1 | 0.3 | 11.1 | 0.1 | 0 | 0 | 13.2 | 0.1 |
| IV: Endocrine and related | 24.7 | 3.8 | 184.9 | 1.4 | 5.3 | 4.0 | 214.9 | 1.5 |
| V: Mental disorders | 9.9 | 1.5 | 1,171.5 | 8.8 | 31.4 | 23.5 | 1,212.8 | 8.6 |
| VI: Nervous system | 19.3 | 3.0 | 388.1 | 2.9 | 21.7 | 16.3 | 429.2 | 3.1 |
| VII: Eye and related | 0.0 | 0.0 | 45.6 | 0.3 | 0.9 | 0.7 | 46.4 | 0.3 |
| VIII: Ear and related | 0.0 | 0.0 | 22.2 | 0.2 | 0 | 0 | 22.2 | 0.2 |
| IX: Circulatory system | 130.9 | 20.1 | 499.4 | 3.8 | 13.9 | 10.4 | 644.2 | 4.6 |
| X: Respiratory system | 23.4 | 3.6 | 3,067.4 | 23.1 | 2.7 | 2.0 | 3,093.5 | 22.0 |
| XI: Digestive system | 34.7 | 5.3 | 323.0 | 2.4 | 3.4 | 2.6 | 361.1 | 2.6 |
| XII: Skin and related | 0.6 | 0.1 | 20.8 | 0.2 | 0 | 0 | 21.4 | 0.2 |
| XIII: Musculoskeletal | 3.4 | 0.5 | 1,959.0 | 14.8 | 22.3 | 16.7 | 1,984.6 | 14.1 |
| XIV: Genitourinary | 5.8 | 0.9 | 336.3 | 2.5 | 1.6 | 1.2 | 343.7 | 2.4 |
| XV: Pregnancy and childbirth | 0.2 | 0.0 | 25.0 | 0.2 | 0 | 0 | 25.2 | 0.2 |
| XVI: Perinatal conditions | 0.0 | 0.0 | 0 | 0.0 | 0 | 0 | 0.0 | 0.0 |
| XVII: Congenital malformations | 4.4 | 0.7 | 14.0 | 0.1 | 0 | 0 | 18.3 | 0.1 |
| XVIII: Symptoms, etc. | 9.0 | 1.4 | 86.0 | 0.6 | 0 | 0 | 95.0 | 0.7 |
| XIX and XX: Injuries | 129.6 | 19.8 | 3,658.8 | 27.6 | 17.7 | 13.3 | 3,806.0 | 27.1 |
| XXI: Other factors | 0 | 0 | 8.6 | 0.1 | 0 | 0 | 8.6 | 0.1 |
| Unallocated | 0 | 0 | 4,894.5 | 0 | 23.9 | 0 | 4,918.4 | 0 |
| Total | 652.9 | 100.0 | 18,164.1 | 100.0 | 157.1 | 100.0 | 18,974.0 | 100.0 |
| Source: EBIC 2010 | ||||||||
Value of Lost Production due to Morbidity
The value of lost production due to morbidity was estimated at $18.2 billion, of which it was possible to allocate $13.3 billion, or 73%, by ICD chapter. The five most expensive conditions were injuries ($3.7 billion, 28%), diseases of the respiratory system ($3.1 billion, 23%), diseases of the musculoskeletal system ($2 billion, 15%), mental disorders ($1.2 billion, 9%), and infectious diseases ($908 million, 7%). Together, these conditions were responsible for 81% of allocated morbidity costs.Footnote q
Total morbidity costs were higher for males ($9.8 billion, 53.7%) than for females ($8.4 billion, 46.3%). Figure 19 illustrates the cost estimates of the value of lost production due to morbidity by sex for the five costliest conditions. The proportion of costs attributable to males and females varies considerably by condition. For example, morbidity costs due to injuries were more than double for males compared to females ($2.5 billion versus $1.1 billion).
Figure 19: Morbidity costs by sex, selected ICD chapters, Canada 2010 ($000,000)
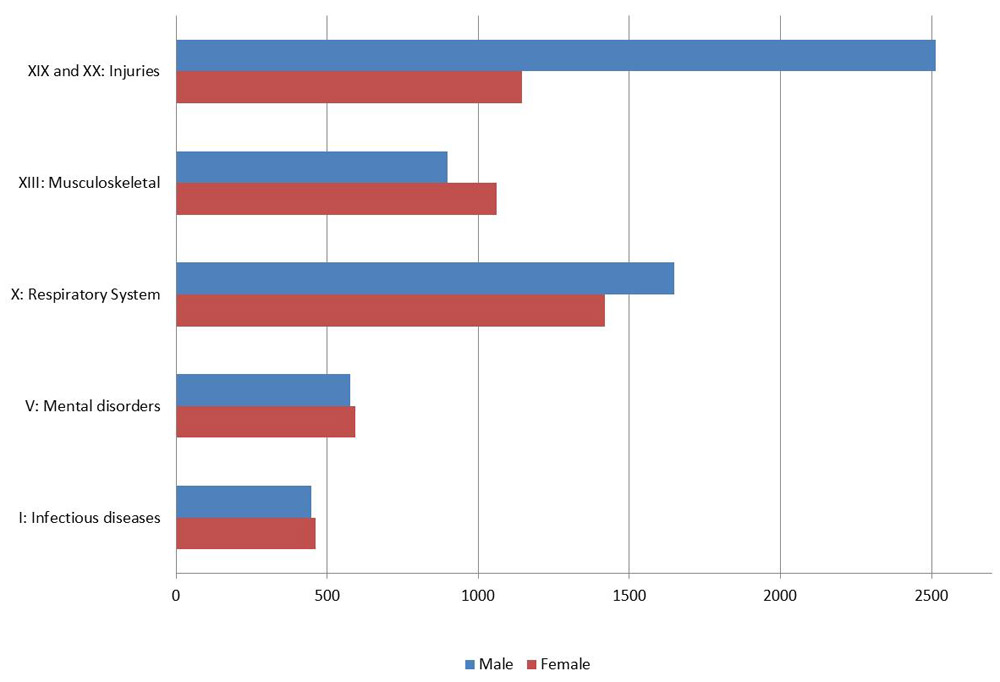
Figure 19 – Text description
| ICD Chapter | Morbidity costs for Females, millions of dollars | Morbidity costs for Males, millions of dollars |
|---|---|---|
| Infectious diseases | 460.34 | 447.60 |
| Mental disorders | 594.58 | 576.92 |
| Respiratory | 1,420.01 | 1,647.43 |
| Musculoskeletal | 1,060.27 | 898.76 |
| Injuries | 1,144.53 | 2,514.23 |
Figure 20 illustrates the percentage of the value of lost production due to morbidity and the percentage of population by age group. Those in the 35-54 age group had the highest share of expenditures compared to their share of the overall population. Individuals aged 35-54 years incurred the highest percentage of morbidity costs ($10.7 billion, 59.0%). This is a result of this group being the most likely to be employed and with the highest earnings (used to value lost production), with a higher prevalence of disability.
Figure 21 illustrates the percentage of the value of lost production due to morbidity by age group for the six costliest ICD chapters. The ICD chapters with the highest percentage of morbidity costs were diseases of the respiratory system for those aged 15-34 years and injuries for the two other age groups.
Figure 20: Percentage of morbidity costs and population by age group, Canada 2010
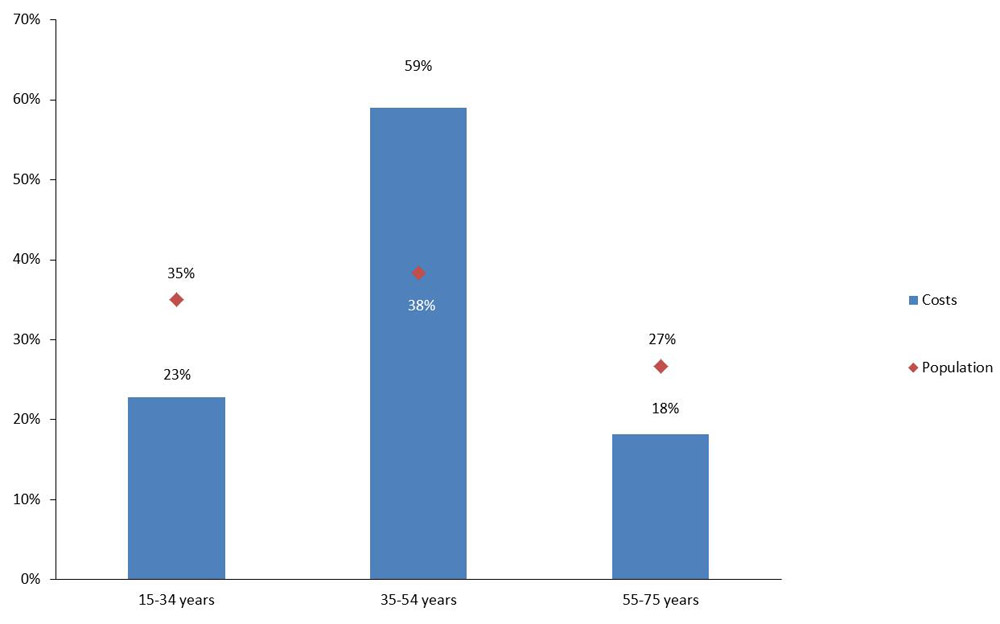
Figure 20 – Text description
| Age group | Proportion of population | Proportion of expenditures |
|---|---|---|
| 15-34 | 35% | 23% |
| 35-54 | 38% | 59% |
| 55-64 | 27% | 18% |
Figure 21: Percentage of morbidity costs by age group, selected ICD chapters, Canada 2010
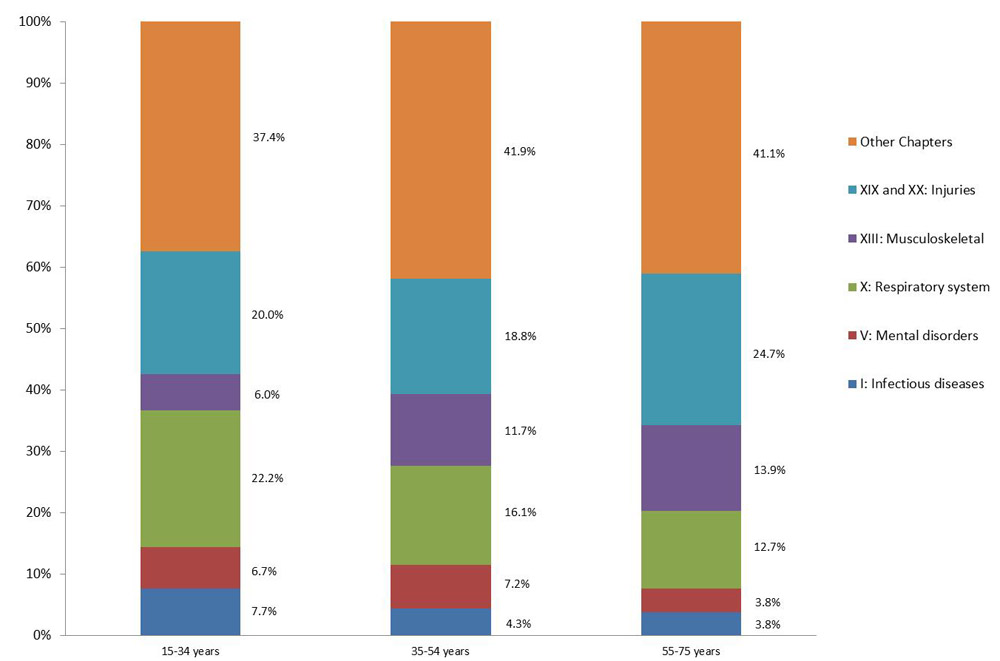
Figure 21 – Text description
| ICD Chapter | 15-34 years | 35-54 years | 55-74 years |
|---|---|---|---|
| Infectious diseases | 7.7% | 4.3% | 3.8% |
| Mental disorders | 6.7% | 7.2% | 3.8% |
| Respiratory system | 22.2% | 16.1% | 12.7% |
| Musculoskeletal | 6.0% | 11.7% | 13.9% |
| Injuries | 20.0% | 18.8% | 24.7% |
| Other Chapters | 37.4% | 41.9% | 41.1% |
Value of Lost Production due to Premature Mortality
In 2010, the value of lost production due to premature mortality was estimated at $653 million. The costliest conditions were: neoplasms ($238 million, 36%), diseases of the circulatory system ($131 million, 20%), injuries ($130 million, 20%), digestive system diseases ($35 million, 5%), endocrine and related diseases ($25 million, 4%), and diseases of respiratory system ($23 million, 4%). These six conditions accounted for 90% of the total value of lost production due to mortality, with the top three conditions accounting for over three-quarters of the costs. Total mortality costs were higher for males ($480.6 million, 73.6%) than for females ($172.3 million, 26.4%). Figure 22 illustrates the value of lost production due to premature mortality, by sex, for the six costliest conditions.
Figure 22: Premature mortality costs by sex, selected ICD chapters, Canada 2010 ($000,000)
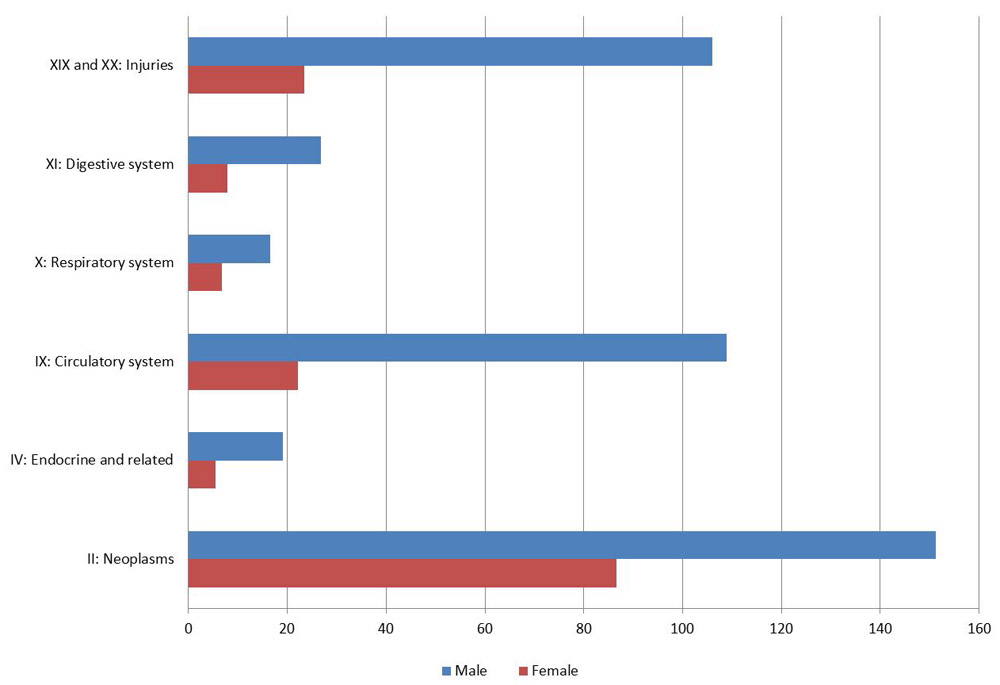
Figure 22 – Text description
| ICD Chapter | Mortality costs for Females, millions of dollars | Mortality costs for Males, millions of dollars |
|---|---|---|
| Neoplasms | 86.68 | 151.15 |
| Endocrine and related | 5.55 | 19.14 |
| Diseases of the circulatory system | 22.12 | 108.82 |
| Respiratory system | 6.81 | 16.55 |
| Digestive system | 7.83 | 26.88 |
| Injuries | 23.52 | 106.05 |
Figure 23 illustrates the percentage value of lost production due to premature mortality and population by age group. Individuals aged 35-54 years incurred the highest percentage of mortality costs (51%, $333.7 million) and individuals aged 15-34 years incurred the lowest percentage of mortality costs (7%, $44.2 million) even though they accounted for almost 39% of the population.
Figure 24 illustrates the percentage value of lost production due to mortality by age group for the six costliest ICD chapters. For individuals aged 15-34 years, the highest percentage of mortality costs were for injuries (62%) and lowest for diseases of the respiratory system (1%). In the oldest age group (55-64 years) the percentage of mortality costs attributable to neoplasms and diseases of the circulatory system accounted for the greatest percentage of expenditures at 45% and 24%, respectively.
Figure 23: Percentage of premature mortality costs and population by age group, Canada 2010
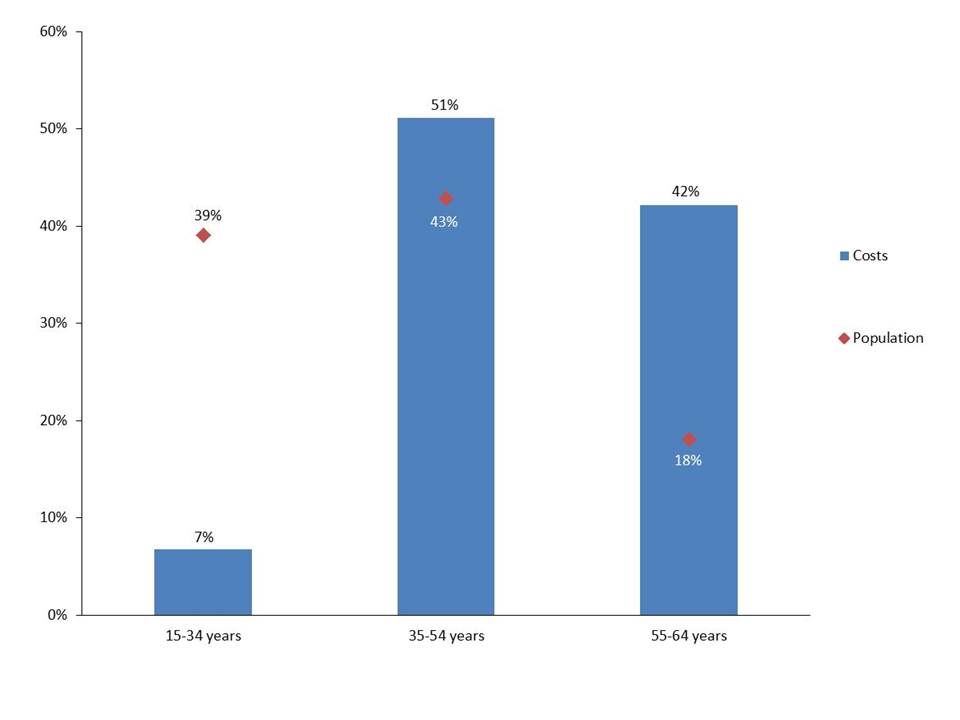
Figure 23 – Text description
| Age group | Proportion of population | Proportion of expenditures |
|---|---|---|
| 15-34 | 39% | 7% |
| 35-54 | 43% | 51% |
| 55-64 | 18% | 42% |
Figure 24: Percentage of premature mortality costs by age group, selected ICD chapters, Canada 2010
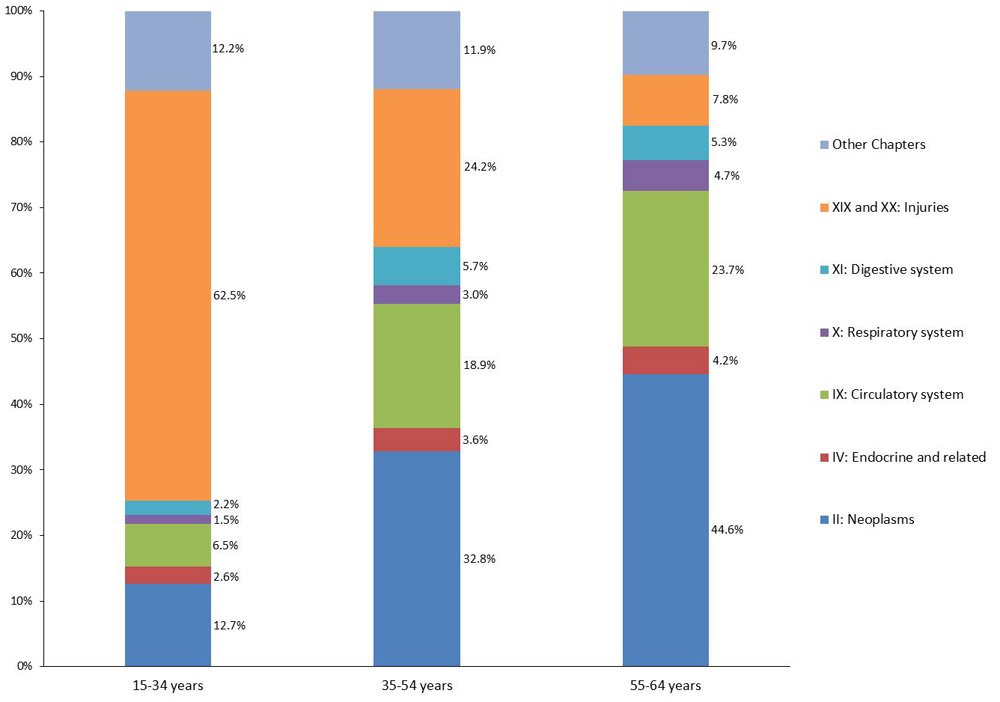
Figure 24 – Text description
| ICD Chapter | Proportion of total cost for the 15-34 year olds | Proportion of total cost for the 35-54 year olds | Proportion of total cost for the 55-64 year olds |
|---|---|---|---|
| Neoplasms | 12.7% | 32.8% | 44.6% |
| Endocrine and related | 2.6% | 3.6% | 4.2% |
| Circulatory system | 6.5% | 18.9% | 23.7% |
| Respiratory system | 1.5% | 3.0% | 4.7% |
| Digestive system | 2.2% | 5.7% | 5.3% |
| Injuries | 62.5% | 24.2% | 7.8% |
| Other Chapters | 12.2% | 11.9% | 9.7% |
Caregiving Costs
In 2010, the total value of caregiving was $206 million; formal caregiving was valued at $49 million, while informal caregiving was valued at $157 million. The former was included as a direct cost (as direct payments were made for the services), while the latter was included as an indirect cost. In this section, the results from both types of caregiving are presented.
Mental disorders were responsible for the greatest value of caregiving costs at $40 million. The next costliest conditions were nervous system disorders, musculoskeletal diseases, injuries, diseases of the circulatory system, and neoplasms. Figure 25 illustrates the caregiving costs by type, for the six costliest conditions, which were responsible for 90% of the allocated costs associated with caregiving.
Figure 25: Caregiving costs by type, selected ICD chapters, Canada 2010 ($000,000)
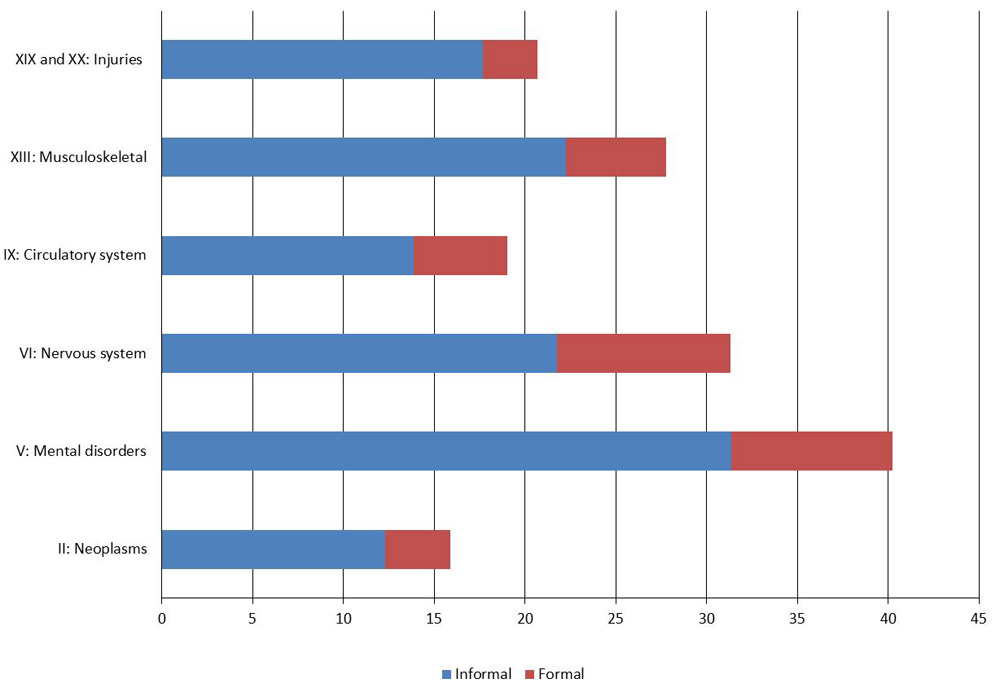
Figure 25 – Text description
| ICD Chapter | Informal | Formal | Total |
|---|---|---|---|
| Neoplasms | 12.3 | 3.6 | 15.9 |
| Mental disorders | 31.4 | 8.9 | 40.2 |
| Nervous system | 21.7 | 9.6 | 31.3 |
| Circulatory system | 13.9 | 5.1 | 19.0 |
| Musculoskeletal | 22.3 | 5.5 | 27.8 |
| Injuries | 17.7 | 3.0 | 20.7 |
Total caregiving costs were higher for females ($125.9 million, 61.0%) than for males ($80.4 million, 39.0%). Figure 26 shows the total caregiving costs by sex for the six costliest ICD chapters. Men only have higher costs, compared to females, for injuries and mental disorders.
Figure 26: Total caregiving costs by sex, selected ICD chapters, Canada 2010 ($000,000)
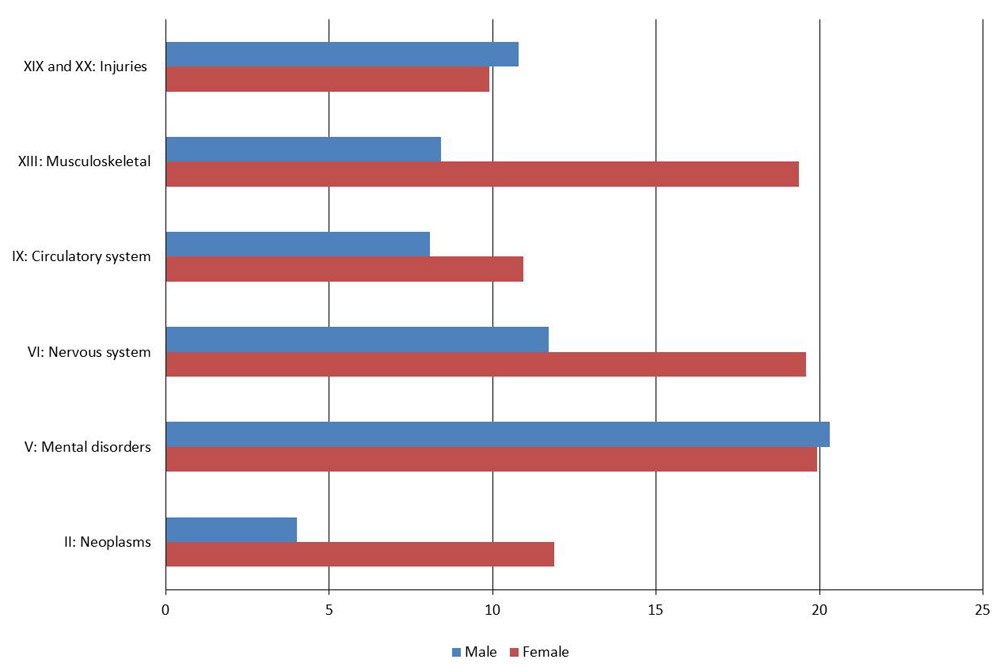
Figure 26 – Text description
| ICD Chapter | Male | Female | Total |
|---|---|---|---|
| Neoplasms | 4 | 12 | 16 |
| Mental disorders | 20 | 20 | 40 |
| Nervous system | 12 | 20 | 31 |
| Circulatory system | 8 | 11 | 19 |
| Musculoskeletal | 8 | 19 | 28 |
| Injuries | 11 | 10 | 21 |
Figure 27 illustrates the percentage of total caregiving costs and the percentage of the population by age group. Individuals aged 75 years and more incurred the highest percentage of caregiving costs (29%, $59 million), however those aged 15-54 accounted for almost half of the caregiving costs. Of note, is that for the two oldest age groups the percentage of costs is greater than their proportion of the population. For example, those aged 75 years and more account for only 8% of the population while incurring 29% of the total caregiving costs.
Figure 28 illustrates the percentage of total caregiving costs by age group for the five conditions with the highest cost.Footnote r For individuals aged 15-34 years, the highest percentage of the caregiving costs were for mental and behavioural disorders (57%). Injuries represented the greatest percentage of caregiving costs for those aged 35-54 years (23%), while nervous system disorders (19%) were the greatest contributor to caregiving costs for those aged 55 and greater.
Figure 27: Percentage of total caregiving costs and population by age group, Canada 2010
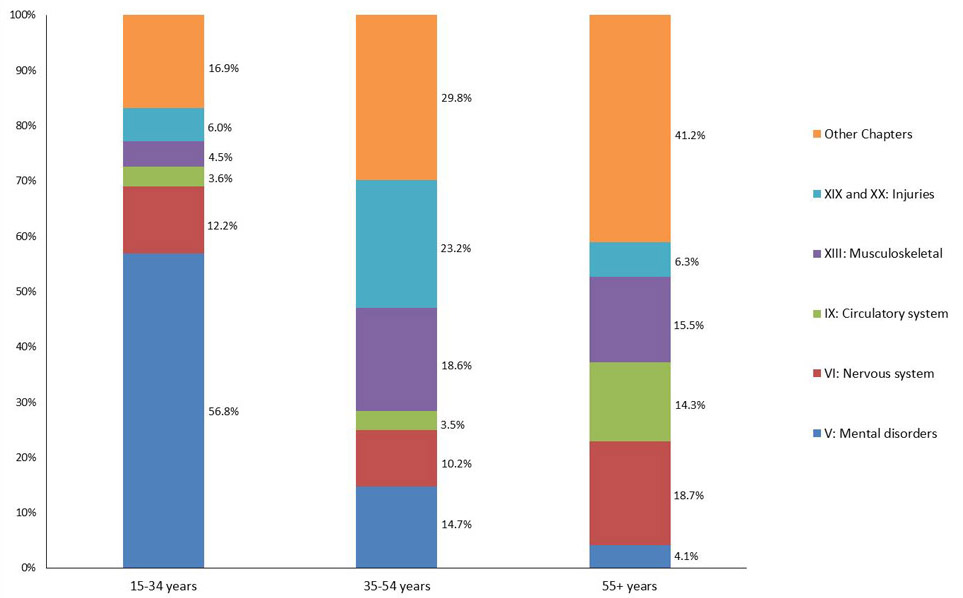
Figure 27 – Text description
| Age group | Expenditures | Population |
|---|---|---|
| 15-34 years | 24.64% | 39.07% |
| 35-54 years | 22.63% | 42.84% |
| 55-74 years | 52.73% | 18.10% |
Figure 28: Percentage of total caregiving costs by age group, selected ICD chapters, Canada 2010
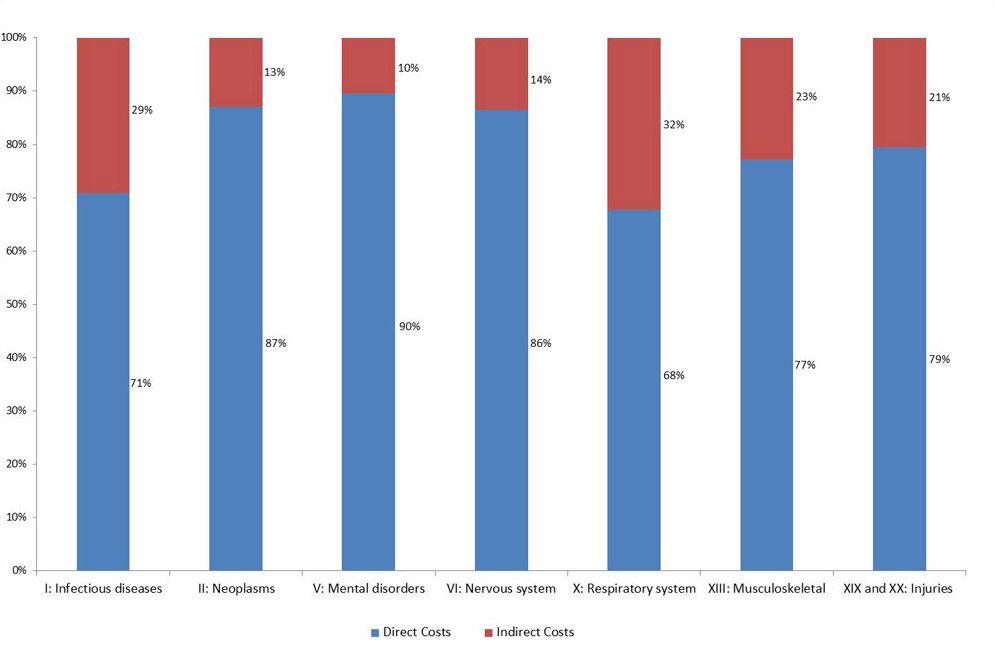
Figure 28 – Text description
| ICD Chapter | 15-34 years | 35-54 years | 55-74 years |
|---|---|---|---|
| Mental disorders | 56.80% | 14.74% | 4.13% |
| Nervous system | 12.20% | 10.18% | 18.70% |
| Circulatory system | 3.62% | 3.49% | 14.30% |
| Musculoskeletal | 4.50% | 18.61% | 15.46% |
| Injuries | 6.02% | 23.17% | 6.25% |
| Other Chapters | 16.87% | 29.82% | 41.16% |
Total Costs
Table 8 shows the total costs by ICD chapter and cost component, including dental care and vision care. The inclusion of dental services results in Ch. XI, Diseases of the Digestive System being the costliest ICD chapter accounting for 15% ($19.6 billion) of the total costs derived in EBIC. The next six costliest ICD chapters were: Ch. XXI, Injuries ($18.6 billion, 14%), Ch. XXI, Factors Influencing Health Status and Contact with Health Services ($15.3 billion, 12%), Ch. IX, Diseases of the Circulatory System ($13.6 billion, 10%), Ch. X, Diseases of the Respiratory System ($9.6 billion, 7%), and Ch. XIII, Musculoskeletal Diseases ($8.7 billion 7%).
| ICD chapter | Direct | Indirect | Total | |||
|---|---|---|---|---|---|---|
| I: Infectious diseases | $2,254 | 2.00% | $925 | 4.90% | $3,179 | 2.40% |
| II: Neoplasms | $5,360 | 4.80% | $790 | 4.20% | $6,150 | 4.70% |
| III: Diseases of the blood | $595 | 0.50% | $13 | 0.10% | $608 | 0.50% |
| IV: Endocrine and related | $5,467 | 4.90% | $215 | 1.10% | $5,682 | 4.30% |
| V: Mental disorders | $10,440 | 9.30% | $1,213 | 6.40% | $11,653 | 8.90% |
| VI: Nervous system | $2,730 | 2.40% | $429 | 2.30% | $3,159 | 2.40% |
| VII: Eye and related | $6,449 | 5.80% | $46 | 0.20% | $6,495 | 5.00% |
| VIII: Ear and related | $711 | 0.60% | $22 | 0.10% | $733 | 0.60% |
| IX: Circulatory system | $13,000 | 11.60% | $644 | 3.40% | $13,644 | 10.40% |
| X: Respiratory system | $6,514 | 5.80% | $3,094 | 16.30% | $9,608 | 7.30% |
| XI: Digestive system | $19,185 | 17.20% | $361 | 1.90% | $19,546 | 14.90% |
| XII: Skin and related | $2,071 | 1.90% | $21 | 0.10% | $2,092 | 1.60% |
| XIII: Musculoskeletal | $6,716 | 6.00% | $1,985 | 10.50% | $8,701 | 6.70% |
| XIV: Genitourinary | $4,747 | 4.20% | $344 | 1.80% | $5,091 | 3.90% |
| XV: Pregnancy and childbirth | $2,469 | 2.20% | $25 | 0.10% | $2,494 | 1.90% |
| XVI: Perinatal conditions | $1,072 | 1.00% | $0 | 0.00% | $1,072 | 0.80% |
| XVII: Congenital malformations | $774 | 0.70% | $18 | 0.10% | $792 | 0.60% |
| XVIII: Symptoms, etc. | $7,019 | 6.30% | $95 | 0.50% | $7,114 | 5.40% |
| XIX and XX: Injuries | $14,748 | 13.20% | $3,806 | 20.10% | $18,554 | 14.20% |
| XXI: Other factors | $15,262 | 13.70% | $9 | 0.00% | $15,271 | 11.70% |
| Unallocated | $10 | 0.00% | $4,918 | 25.90% | $4,929 | 3.80% |
| Total | $111,793 | 100.00% | $18,974 | 100.00% | $130,767 | 100.00% |
| Source: EBIC 2010 | ||||||
Figure 29 shows the percentage of direct and indirect costs in relation to the total costs for the ICD chapters with the greatest percentage of indirect costs. Indirect costs are most significant for respiratory system diseases (32%) and infectious diseases (29%). Given that the degree to which the indirect costs vary across the ICD chapters, it is important that they are considered when examining cost-of-illness and particularly in economic evaluations to ensure that the full societal burden is considered in decision making. The methodology employed (i.e. using the friction cost method) and not being able to consider the full extent of possible indirect costs, also assures that the estimates produced are conservative ones. In addition, EBIC does not include any health outcomes, or the costs associated with pain, suffering, and life. Thus, while EBIC does provide data that brings us closer to the full societal costs associated with disease and injury, it does not yet provide the whole picture.
Figure 29: Percentage of direct and indirect costs compared to total costs, Canada, 2010
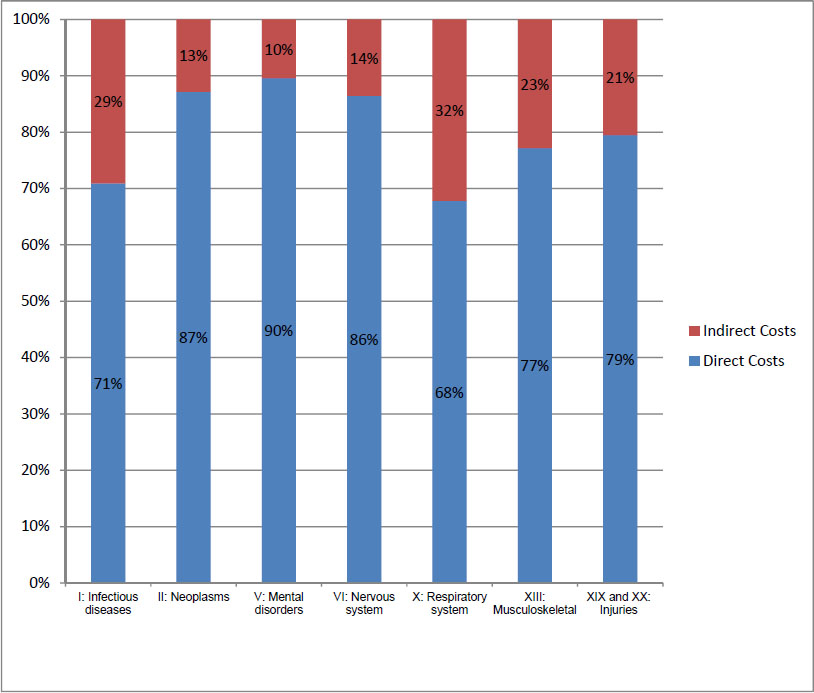
Figure 29 – Text description
| ICD Chapter | Direct Costs | Indirect Costs |
|---|---|---|
| Infectious diseases | 71% | 29% |
| Neoplasms | 87% | 13% |
| Mental disorders | 90% | 10% |
| Nervous system | 86% | 14% |
| Respiratory system | 68% | 32% |
| Musculoskeletal | 77% | 23% |
| Injuries | 79% | 21% |
Limitations
Since first being published in 1991, EBIC has seen changes to data sources and methods either in response to developments in COI methodology or in response to user and/or stakeholder needs.
The most obvious change over the different editions of EBIC relates to the diagnostic categories employed. EBIC 2010 allocates expenditures by ICD chapter and 185 diagnostic categories which are based upon the ISHMT. This change will ensure that available data is grouped in ways that are meaningful to the Canadian audience. It is also in accordance with recent guidelines produced by the OECD, and will help ensure international comparability. However, the change in diagnostic categories affects the ability to draw comparisons across the different versions of EBIC. While attempts have been made to make diagnostic categories as comparable as possible, users are cautioned against comparing results across years and to note that some differences may be attributable to the changes in categories, or methods, rather than any changes in actual resource utilization.
It is also important to note that the costs attributed to any disease or diagnostic category does not reflect the total economic burden associated with that disease. As not all expenditures could be allocated to a specific diagnostic category, it may be more appropriate to examine the percentage of allocated expenditures assigned to each diagnostic category. This, however, assumes that the distribution of non-allocated expenditures would be similar to that of the allocated expenditures.
EBIC 2010 estimates are based on a wide array of data sources, including different levels of information. Data was not always available for all provinces and in many cases had to be estimated based on distributions from other regions or jurisdictions. Data sources also included administrative data as well as survey data affecting the precision of the results. Most of the direct costs were based on actual expenditure data, however, the direct caregiving costs were based on survey data, resulting in different levels of quality. We have endeavoured, however, to allocate the data to the appropriate cost category based on the overall definitions. Also note that physician data was not available for all provinces/territories, and given significant demographic differences across jurisdictions caution should also be employed in analyzing these results.
One of the benefits of using a top-down approach to allocate health expenditures by disease, age and sex is that all expenditures are allocated to different disease groups in a mutually exclusive manner, thus avoiding any issues of double counting. However, a result of this approach may also be the under-estimation of the costs associated with certain diseases which may be associated with other co-morbid conditions or may be risk factors for other conditions. For example, diabetes, which has a unique ICD-10 code, is known to contribute to other diseases such as cardiovascular disease. Thus, when estimating the full costs, or impact, of such disease, one should also consider the associated co-morbid conditions. This can be achieved by employing population attributable fractions (e.g. Conference Board, 2017) Reference 38.
As previously noted, the labour effects associated with illness and injury including decreased productivity, lower wages, decreased working years, and other macroeconomic effects have not been fully modelled in EBIC. In addition, the use of the friction cost method in the valuation of mortality costs also presents a conservative estimate. Therefore, EBIC should be considered as a lower bound of the cost associated with illness and injury.
References
- Reference 1
-
Wigle, D.T., Y. Mao, T. Wong and R. Lane, Economic Burden of Illness in Canada, 1986, Chronic Dis Can, vol. 12, no. Suppl 3, pp. 1-37, 1991.
- Reference 2
-
Public Health Agency of Canada, Economic Burden of Illness in Canada, 2005-2008. PHAC, Ottawa, 2014.
- Reference 3
-
Moore, R.,Y. Mao, J. Zhang and K. Clarke, Economic Burden of Illness in Canada, 1993. Health Canada, Ottawa, 1997.
- Reference 4
-
Health Canada, Economic Burden of Illness in Canada, 1998. Health Canada, Ottawa, 2002.
- Reference 5
-
Rice, D. Estimating the Cost of Illness. American Journal of Public Health, vol. 57, no. 3, pp. 424-440, 1967.
- Reference 6
-
Organization for Economic Cooperation and Development (OECD), Eurostat, WHO, A System of Health Accounts, 2011 Edition. OECD Publishing, Paris, 2011.
- Reference 7
-
Organisation for Economic Cooperation and Development (OECD), Extension of work on expenditure by disease, age and gender. OECD, Health Division, Directorate for Employment, Labour and Social Affairs, Paris, 2013.
- Reference 8
-
Eurostat/OECD/WHO, International shortlist for hospital morbidity tabulation (ISHMT) Version 2008-11-10. Accessed August 2, 2017.
- Reference 9
-
Organisation for Economic Cooperation and Development (OECD), A System of Health Accounts. OECD, Paris, 2000.
- Reference 10
-
Canadian Institute for Health Information (CIHI), National Health Expenditure Trends, 1975 to 2015. CIHI, Ottawa, 2015.
- Reference 11
-
Canadian Institute for Health Information (CIHI), Data Quality Documentation: Discharge Abstract Database, 2010‐2011 (Executive Summary). CIHI, Ottawa, 2011.
- Reference 12
-
Canadian Institute for Health Information (CIHI), Discharge Abstract Database (DAD), 2010-2011. CIHI, Ottawa, 2011.
- Reference 13
-
Canadian Institute for Health Information (CIHI), Hospital Morbidity Database (HMDB), 2010. CIHI, Ottawa, 2011.
- Reference 14
-
Canadian Institute for Health Information (CIHI), Data Quality Documentation: Hospital Morbidity Database (HMDB), 2010-2011.
- Reference 15
-
Canadian Institute for Health Information (CIHI), National Ambulatory Care Reporting System (NACRS), 2010. CIHI, Ottawa, 2011.
- Reference 16
-
Canadian Institute for Health Information (CIHI), Data Quality Documentation for External Users: National Ambulatory Care Reporting System,2010–2011. CIHI, Ottawa, 2011.
- Reference 17
-
Canadian Institute for Health Information (CIHI), Hospital Mental Health Database, 2010–2011: User Documentation. CIHI, Ottawa, 2011.
- Reference 18
-
Canadian Institute for Health Information (CIHI), Hospital Mental Health Database, 2010–2011. CIHI, Ottawa, 2011.
- Reference 19
-
Canadian Institute for Health Information, Canadian Coding Standards for Version 2012 ICD-10-CA and CCI. CIHI, Ottawa, 2012.
- Reference 20
-
Canadian Institute for Health Information (CIHI), DAD Resource Intensity Weights and Expected Length of Stay for CMG+ 2008. CIHI, Ottawa, 2008.
- Reference 21
-
Organization for Economic Cooperation and Development, Health expenditures: OECD.Stat. Data extracted on September 6, 2017.
- Reference 22
-
IMS Brogan, Canadian Drug and Therapeutic Index (CDTI), 2010. IMS Health, Ottawa, 2010.
- Reference 23
-
IMS Brogan, CompuScript, 2010. IMS Health, Ottawa, 2010.
- Reference 24
-
Koopmanschap, M.A., and F. Rutten, A practical guide for calculating indirect costs of disease. Pharmacoeconomics, vol. 10, no. 5, pp. 460-466, 1996.
- Reference 25
-
Koopmanschap, M.A., F. Rutten, B. van Ineveld and L. van Roijen, The friction cost method for measuring indirect costs of disease. Journal of Health Economics, vol. 14, pp. 171-189, 1995.
- Reference 26
-
Koopmanschap, M.A., and B. van Ineveld, Towards a new approach for estimating indirect costs of disease. Soc. Sci. Med, vol. 34, no. 9, pp. 1005-1010, 1992.
- Reference 27
-
Nyman, J.A. Productivity costs revisited: Towards a new US policy. Health Economics, vol. 21, pp. 1387-1401, 2012.
- Reference 28
-
Canadian Agency for Drugs and Technologies in Health, Guidelines for the economic evaluation of health technologies: Canada [3rd Edition]. Ottawa, 2006.
- Reference 29
-
Goeree, R., B. J. O’Brien, G. Blackhouse, K. Agro and P. Goering. The valuation of productivity costs due to premature mortality: A comparison of the Human-Capital and Friction-Cost Methods for Schizophrenia. Can J Psychiatry 1999, vol. 44, pp. 455-463, 1999.
- Reference 30
-
Hopkins, R., Goeree, R and C. Longo. Estimating the national wage loss from cancer in Canada. Current Oncology, vol. 17, no. 2, pp. 40-49, 2010.
- Reference 31
-
Statistics Canada, Table 202-0407 - Income of individuals by sex, age group and income source.
- Reference 32
-
Statistics Canada, Table 282-0002: Labour Force survey (LFS) estimates, duration of unemployment by sex and age group, annual.
- Reference 33
-
Devaux, M., and F. Sassi. The Labour Market Impacts of Obesity, Smoking, Alcohol Use, and other Related Chronic Diseases. OECD Publishing, Paris, 2015.
- Reference 34
-
Statistics Canada. Canadian Community Health Survey‐Annual Component: 12 Month Share File, 2010. Statistics Canada, Ottawa, 2011.
- Reference 35
-
Statistics Canada, Canadian Community Health Survey: Annual Component-2010 Questionnaire.
- Reference 36
-
Statistics Canada, General Social Survey: Caregiving and Care Receiving, Public Use Microdata File: "2012 (Cycle 26). 2012.
- Reference 37
-
Statistics Canada. Table 202–0407—Income of individuals, by sex, age group and income source, 2010 constant dollars, annual, CANSIM (database).
- Reference 38
-
Conference Board of Canada, The Costs of Tobacco Use in Canada. Ottawa, 2017.
- Reference 39
-
Statistics Canada, Table 326–0021 - Consumer Price Index (CPI), 2009 basket, annual.
- Reference 40
-
Organization for Economic Cooperation and Development, Making Mental Health Count: The Social and Economic Costs of Neglecting Mental Health Care. OECD Publishing, Paris, 2014.
Appendix: EBIC Diagnostic Categories
| ICD Chapter | EBIC Code | ISHMT code | EBIC Diagnostic Category | ICD‑10 Code |
|---|---|---|---|---|
| I | 100 | 100 | Certain infectious and parasitic diseases | A00‑B99 |
| I | 101 | 101 | Clostridium difficile | A04.7 |
| I | 102 | 101 | Intestinal infectious diseases except diarrhoea (and C. difficile) | A00‑A08 (except A04.7) |
| I | 103 | 102 | Diarrhoea and gastroenteritis of presumed infectious origin | A09 |
| I | 104 | 103 | Tuberculosis | A15‑A19, B90 |
| I | 105 | 104 | Septicaemia | A40‑A41 |
| I | 106 | 105 | Human immunodeficiency virus [HIV] disease | B20‑B24 |
| I | 107 | 106 | Sexually Transmitted Diseases | A50‑A64 |
| I | 108 | 106 | Other infectious and parasitic diseases | remainder of A00‑B99 |
| II | 200 | 200 | Neoplasms | C00‑D48 |
| II | 201 | 209 | Malignant neoplasms of lip, oral cavity and pharynx | C00‑C14 |
| II | 202 | 209 | Malignant neoplasm of esophagus | C15 |
| II | 203 | 209 | Malignant neoplasm of stomach | C16 |
| II | 204 | 201 | Malignant neoplasm of colon, rectum and anus | C18‑C21 |
| II | 205 | 209 | Malignant neoplasm of liver | C22.0, C22.2‑C22.7 |
| II | 206 | 209 | Malignant neoplasm of pancreas | C25 |
| II | 207 | 209 | Malignant neoplasm of larynx | C32 |
| II | 208 | 202 | Malignant neoplasms of trachea, bronchus and lung | C33‑C34 |
| II | 209 | 203 | Malignant neoplasms of skin ‑ Melanoma | C43 |
| II | 210 | 203 | Malignant neoplasms of skin ‑ Other | C44 |
| II | 211 | 204 | Malignant neoplasm of breast | C50 |
| II | 212 | 205 | Malignant neoplasm of uterus ‑ Cervix uteri | C53 |
| II | 213 | 205 | Malignant neoplasm of uterus ‑ Other | C54‑C55 |
| II | 214 | 206 | Malignant neoplasm of ovary | C56 |
| II | 215 | 207 | Malignant neoplasm of prostate | C61 |
| II | 216 | 209 | Malignant neoplasm of testis | C62 |
| II | 217 | 209 | Malignant neoplasm of kidney | C64‑C65 |
| II | 218 | 208 | Malignant neoplasm of bladder | C67 |
| II | 219 | 209 | Malignant neoplasm of brain | C70‑C72 |
| II | 220 | 209 | Malignant neoplasm of thyroid | C73 |
| II | 221 | 209 | Hodgkin lymphoma | C81 |
| II | 222 | 209 | Non‑Hodgkin lymphoma | C82‑C85, C96.3 |
| II | 223 | 209 | Multiple myeloma | C90.0, C90.2 |
| II | 224 | 209 | Leukaemia | C90.1, C91‑C95 |
| II | 225 | 209 | Other malignant neoplasms | remainder of C00‑C97 |
| II | 226 | 210 | Carcinoma in situ | D00‑D09 |
| II | 227 | 211 | Benign neoplasm of colon, rectum and anus | D12 |
| II | 228 | 212 | Leiomyoma of uterus | D25 |
| II | 229 | 213 | Other benign neoplasms and neoplasms of uncertain or unknown behaviour | remainder of D00‑D48 |
| III | 300 | 300 | Diseases of the blood and blood forming organs and certain disorders involving the immune mechanism | D50‑D89 |
| III | 301 | 301 | Anaemias ‑ Iron‑deficiency anaemia | D50 |
| III | 302 | 301 | Anaemias ‑ Other | D51‑D64 |
| III | 303 | 302 | Other diseases of the blood and blood forming organs and certain disorders involving the immune mechanism | D65‑D89 |
| IV | 400 | 400 | Endocrine, nutritional and metabolic diseases | E00‑E90 |
| IV | 401 | 401 | Diabetes mellitus | E10‑E14 |
| IV | 402 | 402 | Other endocrine, nutritional and metabolic diseases | remainder of E00‑E90 |
| V | 500 | 500 | Mental and behavioural disorders | F00‑F99 |
| V | 501 | 501 | Dementia | F00‑F03 |
| V | 502 | 502 | Mental and behavioural disorders due to alcohol | F10 |
| V | 503 | 503 | Mental and behavioural disorders due to use of other psychoactive subst. | F11‑F19 |
| V | 504 | 504 | Schizophrenia, schizotypal and delusional disorders | F20‑F29 |
| V | 505 | 505 | Mood [affective] disorders | F30‑F39 |
| V | 506 | 506 | Other mental and behavioural disorders | remainder of F00‑F99 |
| VI | 600 | 600 | Diseases of the nervous system | G00‑G99 |
| VI | 601 | 601 | Alzheimer's disease | G30 |
| VI | 602 | 602 | Multiple sclerosis | G35 |
| VI | 603 | 603 | Epilepsy | G40‑G41 |
| VI | 604 | 604 | Transient cerebral ischaemic attacks and related syndromes | G45 |
| VI | 605 | 605 | Bacterial meningitis | G00 |
| VI | 606 | 605 | Meningitis due to other organisms or of unspecified cause | G03 |
| VI | 607 | 605 | Parkinson disease and secondary parkinsonism | G20‑G21 |
| VI | 608 | 605 | Migraine | G43 |
| VI | 609 | 605 | Other diseases of the nervous system | remainder of G00‑G99 |
| VII | 700 | 700 | Diseases of the eye and adnexa | H00‑H59 |
| VII | 701 | 701 | Cataract | H25‑H26, H28 |
| VII | 702 | 702 | Other diseases of the eye and adnexa | remainder of H00‑H59 |
| VIII | 800 | 800 | Diseases of the ear and mastoid process | H60‑H95 |
| VIII | 801 | 800 | Otitis media | H65‑H66 |
| VIII | 802 | 800 | Hearing loss | H90‑H91 |
| VIII | 803 | 800 | Other diseases of the ear and mastoid process | remainder of H60‑H95 |
| IX | 900 | 900 | Diseases of the circulatory system | I00‑I99 |
| IX | 901 | 901 | Essential hypertension | I10 |
| IX | 902 | 901 | Other hypertensive diseases | I11‑I13, I15 |
| IX | 903 | 902 | Angina pectoris | I20 |
| IX | 904 | 903 | Acute myocardial infarction | I21‑I22 |
| IX | 905 | 904 | Other ischaemic heart diseases | I23‑I25 |
| IX | 906 | 905 | Pulmonary heart disease & diseases of pulmonary circulation | I26‑I28 |
| IX | 907 | 906 | Conduction disorders and cardiac arrhythmias | I44‑I49 |
| IX | 908 | 907 | Heart failure | I50 |
| IX | 909 | 908 | Cerebral infarction | I63 |
| IX | 910 | 908 | Subarachnoid haemorrhage | I60 |
| IX | 911 | 908 | Intracerebral haemorrhage | I61 |
| IX | 912 | 908 | Acute but ill‑defined stroke | I64 |
| IX | 913 | 908 | Other cerebrovascular diseases | I62, I65‑I69 |
| IX | 914 | 909 | Atherosclerosis | I70 |
| IX | 915 | 910 | Varicose veins of lower extremities | I83 |
| IX | 916 | 911 | Other diseases of the circulatory system | remainder of I00‑I99 |
| X | 1000 | 1000 | Diseases of the respiratory system | J00‑J99 |
| X | 1001 | 1001 | Influenza | J09‑J11 |
| X | 1002 | 1001 | Other acute upper respiratory infections | J00‑J06 |
| X | 1003 | 1002 | Pneumonia | J12‑J18 |
| X | 1004 | 1003 | Other acute lower respiratory infections | J20‑J22 |
| X | 1005 | 1004 | Chronic diseases of tonsils and adenoids | J35 |
| X | 1006 | 1005 | Other diseases of upper respiratory tract | J30‑J34, J36‑J39 |
| X | 1007 | 1006 | Chronic obstructive pulmonary disease | J40‑J44 |
| X | 1008 | 1006 | Bronchiectasis | J47 |
| X | 1009 | 1007 | Asthma | J45‑J46 |
| X | 1010 | 1008 | Other diseases of the respiratory system | J60‑J99 |
| XI | 1100 | 1100 | Diseases of the digestive system | K00‑K93 |
| XI | 1101 | 1101 | Diseases of the teeth and supporting structures | K00‑K08 |
| XI | 1102 | 1102 | Other diseases of oral cavity, salivary glands and jaws | K09‑K14 |
| XI | 1103 | 1103 | Diseases of oesophagus | K20‑K23 |
| XI | 1104 | 1104 | Peptic ulcer | K25‑K28 |
| XI | 1105 | 1105 | Dyspepsia and other diseases of stomach and duodenum | K29‑K31 |
| XI | 1106 | 1106 | Diseases of appendix | K35‑K38 |
| XI | 1107 | 1107 | Inguinal hernia | K40 |
| XI | 1108 | 1108 | Other abdominal hernia | K41‑K46 |
| XI | 1109 | 1109 | Crohn's disease and ulcerative colitis | K50‑K51 |
| XI | 1110 | 1110 | Other noninfective gastroenteritis and colitis | K52 |
| XI | 1111 | 1111 | Paralytic ileus and intestinal obstruction without hernia | K56 |
| XI | 1112 | 1112 | Diverticular disease of intestine | K57 |
| XI | 1113 | 1113 | Diseases of anus and rectum | K60‑K62 |
| XI | 1114 | 1114 | Other diseases of intestine | K55, K58‑K59, K63 |
| XI | 1115 | 1115 | Alcoholic liver disease | K70 |
| XI | 1116 | 1116 | Fibrosis and cirrhosis of liver | K74 |
| XI | 1117 | 1117 | Other diseases of liver | K71‑K73, K75‑K77 |
| XI | 1118 | 1118 | Cholelithiasis | K80 |
| XI | 1119 | 1119 | Other diseases of gall bladder and biliary tract | K81‑K83 |
| XI | 1120 | 1120 | Diseases of pancreas | K85‑K87 |
| XI | 1121 | 1121 | Other diseases of the digestive system | remainder of K00‑K93 |
| XII | 1200 | 1200 | Diseases of the skin and subcutaneous tissue | L00‑L99 |
| XII | 1201 | 1201 | Infections of the skin and subcutaneous tissue | L00‑L08 |
| XII | 1202 | 1202 | Dermatitis, eczema and papulosquamous disorders | L20‑L45 |
| XII | 1203 | 1203 | Other diseases of the skin and subcutaneous tissue | remainder of L00‑L99 |
| XIII | 1300 | 1300 | Diseases of the musculoskeletal system and connective tissue | M00‑M99 |
| XIII | 1301 | 1301 | Coxarthrosis [arthrosis of hip] | M16 |
| XIII | 1302 | 1302 | Gonarthrosis [arthrosis of knee] | M17 |
| XIII | 1303 | 1303 | Internal derangement of knee | M23 |
| XIII | 1304 | 1304 | Other arthrosis | M15, M18‑M19 |
| XIII | 1305 | 1304 | Rheumatoid arthritis | M05‑M06 |
| XIII | 1306 | 1304 | Gout | M10 |
| XIII | 1307 | 1304 | Other arthropathies | M00‑M03, M07‑M09, M11‑M14, M20‑M22, M24‑M25 |
| XIII | 1308 | 1305 | Systemic connective tissue disorders | M30‑M36 |
| XIII | 1309 | 1306 | Deforming dorsopathies and spondylopathies | M40‑M49 |
| XIII | 1310 | 1307 | Intervertebral disc disorders | M50‑M51 |
| XIII | 1311 | 1308 | Dorsalgia | M54 |
| XIII | 1312 | 1309 | Soft tissue disorders | M60‑M79 |
| XIII | 1313 | 1310 | Osteoporosis | M80, M81 |
| XIII | 1314 | 1310 | Other disorders of the musculoskeletal system and connective tissue | M53, M80‑M99 |
| XIV | 1400 | 1400 | Diseases of the genitourinary system | N00‑N99 |
| XIV | 1401 | 1401 | Glomerular and renal tubulo‑interstitial diseases | N00‑N16 |
| XIV | 1402 | 1402 | Acute renal failure | N17 |
| XIV | 1403 | 1402 | Chronic renal failure | N18 |
| XIV | 1404 | 1402 | Unspecified renal failure | N19 |
| XIV | 1405 | 1403 | Urolithiasis | N20‑N23 |
| XIV | 1406 | 1404 | Other diseases of the urinary system | N25‑N39 |
| XIV | 1407 | 1405 | Hyperplasia of prostate | N40 |
| XIV | 1408 | 1406 | Other diseases of male genital organs | N41‑N51 |
| XIV | 1409 | 1407 | Disorders of breast | N60‑N64 |
| XIV | 1410 | 1408 | Inflammatory diseases of female pelvic organs | N70‑N77 |
| XIV | 1411 | 1409 | Menstrual, menopausal and other female genital conditions | N91‑N95 |
| XIV | 1412 | 1410 | Other disorders of the genitourinary system | remainder of N00‑N99 |
| XV | 1500 | 1500 | Pregnancy, childbirth and the puerperium | O00‑O99 |
| XV | 1501 | 1501 | Medical abortion | O04 |
| XV | 1502 | 1502 | Other pregnancy with abortive outcome | O00‑O03, O05‑O08 |
| XV | 1503 | 1503 | Oedema, proteinuria and hypertensive disorders in pregnancy, childbirth and the puerperium | O10‑O16 |
| XV | 1504 | 1503 | Other complications of pregnancy predominantly in the antenatal period | O20‑O48 |
| XV | 1505 | 1504 | Obstructed labour (Dystocia) | O64‑O66 |
| XV | 1506 | 1504 | Other complications of pregnancy predominantly during labour and delivery | O67‑O75 |
| XV | 1507 | 1505 | Single spontaneous delivery | O80 |
| XV | 1508 | 1506 | Other delivery | O81‑O84 |
| XV | 1509 | 1507 | Maternal Sepsis | O85‑O86 |
| XV | 1510 | 1507 | Other complications predominantly related to the puerperium | O87‑O92 |
| XV | 1511 | 1508 | Other obstetric conditions | O94, O95‑O99 |
| XVI | 1600 | 1600 | Certain conditions originating in the perinatal period | P00‑P96 |
| XVI | 1601 | 1601 | Disorders related to short gestation and low birth weight | P07 |
| XVI | 1602 | 1602 | Slow fetal growth and fetal malnutrition | P05 |
| XVI | 1603 | 1602 | Birth asphyxia and birth trauma | P03, P10‑P15, P20‑P29 |
| XVI | 1604 | 1602 | Other conditions originating in the perinatal period | remainder of P00‑P96 |
| XVII | 1700 | 1700 | Congenital malformations, deformations and chromosomal abnormalities | Q00‑Q99 |
| XVII | 1701 | 1700 | Congenital heart anomalies | Q20‑Q28 |
| XVII | 1702 | 1700 | Other congenital malformations, deformations and chromosomal abnormalities | remainder of Q00‑Q99 |
| XVIII | 1800 | 1800 | Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified | R00‑R99 |
| XVIII | 1801 | 1801 | Pain in throat and chest | R07 |
| XVIII | 1802 | 1802 | Abdominal and pelvic pain | R10 |
| XVIII | 1803 | 1803 | Unknown and unspecified causes of morbidity (incl. those without a diagnosis) | R69 |
| XVIII | 1804 | 1804 | Other symptoms, signs and abnormal clinical and laboratory findings | remainder of R00‑R99 |
| XIX | 1900 | 1900 | Injury, poisoning and certain other consequences of external causes (Injury coding type 1)Appendix note a | S00‑T98 |
| XIX | 1901 | 1901 | Intracranial injury | S06 |
| XIX | 1902 | 1902 | Other injuries to the head | S00‑S05, S07‑S09 |
| XIX | 1903 | 1903 | Fracture of forearm | S52 |
| XIX | 1904 | 1904 | Fracture of femur | S72 |
| XIX | 1905 | 1905 | Fracture of lower leg, including ankle | S82 |
| XIX | 1906 | 1906 | Other injuries | S10‑S51, S53‑S71, S73‑S81, S83‑T14, T79 |
| XIX | 1907 | 1907 | Burns and corrosions | T20‑T32 |
| XIX | 1908 | 1908 | Poisonings by drugs, medicaments and biological substances and toxic effects of substances chiefly nonmedicinal as to source | T36‑T65 |
| XIX | 1909 | 1909 | Complications of surgical and medical care, not elsewhere classified | T80‑T88 |
| XIX | 1910 | 1910 | Sequelae of injuries, of poisoning and of other consequences of external causes | T90‑T98 |
| XIX | 1911 | 1911 | Other and unspecified effects of external causes | remainder of S00‑T98 |
| XX | 2000 | n/a | External causes of morbidity and mortality (Injury coding type 2)Appendix note a | V01‑Y98 |
| XX | 2001 | n/a | Road traffic accidents | V01‑V06 fourth digits 1‑9 (example V01.1, V01.2, V01.3 etc.); V09.2; V09.3; V10, V11, V15‑V18 & V29‑V79 fourth digits 4‑9; V12‑V14 & V20‑V28 fourth digits 3‑9; V19.4‑V19.6; V80.3‑V80.5; V81.1; V82.1; V83‑V86 fourth digits 0‑3; V87.0‑V87.8, V89.2; V89.9; V99; Y85.0 |
| XX | 2002 | n/a | Poisonings | X40‑X49 |
| XX | 2003 | n/a | Falls | W00‑W19 |
| XX | 2004 | n/a | Fires | X00‑X09 |
| XX | 2005 | n/a | Drowning | W65‑W74 |
| XX | 2006 | n/a | Other unintentional injuries | Rest of V, W20‑W64, W75‑W99, X10‑X39, X50‑X59, Y40‑Y86 (minus Y85.0), Y88, Y89 (minus Y89.9) |
| XX | 2007 | n/a | Self‑inflicted injuries | X60‑X84, Y87.0 |
| XX | 2008 | n/a | Violence | X85‑Y09, Y87.1 |
| XX | 2009 | n/a | Other intentional injuries | Y35, Y36 |
| XX | 2010 | n/a | Injuries of undetermined intent | Y10‑Y34, Y87.2, Y89.9 |
| XXI | 2100 | 2100 | Factors influencing health status and contact with health services | Z00‑Z99 |
| XXI | 2101 | 2101 | Medical observation and evaluation for suspected diseases and conditions | Z03 |
| XXI | 2102 | 2102 | Contraceptive management | Z30 |
| XXI | 2103 | 2103 | Live born infants according to place of birth ("healthy newborn babies") | Z38 |
| XXI | 2104 | 2104 | Other medical care (including radiotherapy and chemotherapy sessions) | Z51 |
| XXI | 2105 | 2105 | Other factors influencing health status and contact with health services | remainder of Z00‑Z99 |
- Appendix note a
-
Note that the originating data for the direct costs (hospital, drug, and physician) classified injuries according to ICD Chapter XIX, Injury, poisoning and certain other consequences of external causes (Injury coding type 1). Mortality costs, associated with injuries, are based on Vital Statistics data and were coded only to ICD Chapter XX, External causes of morbidity and mortality (Injury coding type 2). When estimating the total costs associated with injuries it is necessary to include both ICD chapters.
Footnotes
- Footnote 1
-
Recent examples of EBIC or similar data being employed include Conference Board of Canada Reference al and OECD (2014) Reference 40.
- Footnote 2
-
Dental Services, Vision Care Services, Formal Caregiving and Morbidity Costs were only allocated at the ICD chapter level.
- Footnote 3
-
Day surgery records for Ontario and Alberta were captured in NACRS, while day surgery records for Nova Scotia are contained in both the DAD and NACRS. Quebec does not report day surgery records to the DAD or NACRS.
- Footnote 4
-
These categories correspond to the SHA categories HC.1.1 & HC.2.1 (inpatient curative and rehabilitative care), HC.1.2 & HC.2.2 (day curative and rehabilitative care), and HC.1.3 & HC.2.3 (outpatient curative and rehabilitative care). The “other category includes HC1.4 & HC.2.4 (Home-based curative and rehabilitative care), Long-term care (HC.3), Ancillary Services (HC.4) and Preventive care (HC.6)
- Footnote 5
-
This corresponds to SHA category HP.1 Hospitals
- Footnote 6
-
Which also include APP expenditures, as wells as spending by Municipal Governments, Social Security Funds and the Federal Government for physician expenditures.
- Footnote 7
-
The types of production losses are slightly more nuanced and may also include compensation mechanisms and multiplier effects. See Krol et al (2013) for further details on valuing production costs.
- Footnote 8
-
Individuals who indicated missed work days due to illness and injury but had not worked in the past 12 months were excluded from analysis.
- Footnote 9
-
Individuals less than 15 years and more than 75 years of age were excluded from participation in the CCHS LOP module, as these individuals were considered unlikely to be working and thus would have no lost production from labour market activities.
- Footnote 10
-
Note that mortality costs end at the age of 64. The data employed to estimate the value of lost production due to morbidity included individuals up to age of 75. Hence the age groups employed do not exactly match.
- Footnote 11
-
If the provider’s sex was unknown, province-age specific earnings were used. If age was unknown, province-sex specific earnings were used. If sex and age were unknown provincial specific earnings were used.
- Footnote 12
-
For informal caregiving, if the care provider was identified as 19 years or younger, they were assigned the earnings for the age group ‘less than 20 years’ (15-19 years).
- Footnote 13
-
For both formal and informal caregiving, it was assumed that the province of the respondent (caregiving receiver) was the same as the caregiving provider since the provider’s province was not asked.
- Footnote 14
-
Earnings include wages, salaries, commissions and self-employment income.
- Footnote 15
-
This excludes Chapter XXI, Factors influencing health status and contact with health services as these ICD codes refer to the reason for which the encounter occurred rather than the actual disease, or diagnosis itself.
- Footnote 16
-
As has been noted, not all of the indirect costs could be allocated. Note that the percentage values noted in this section refer to the percentage of allocated costs as these results are more meaningful.
- Footnote 17
-
These figures refer to the percentage of allocated costs, rather than the percentage of all costs.
- Footnote 18
-
Age groups have been combined due to small cell sizes that occur when the data is broken down by ICD chapter.