
How to integrate intersectionality theory in quantitative health equity analysis? A rapid review and checklist of promising practices
Download the report (PDF)
(PDF format, 70 pages)
Organization: Public Health Agency of Canada
Published: 2022-06-13
For more information contact: health.inequalities-inegalites.en.sante@phac-aspc.gc.ca
Download the checklist (PDF)
(PDF format, 3 pages)
Download the checklist (Word)
(Docx format, 3 pages)
Organization: Public Health Agency of Canada
Published: 2022-06-13
For more information contact: health.inequalities-inegalites.en.sante@phac-aspc.gc.ca
Highlights
Highlights from the "How to integrate intersectionality theory in quantitative health equity analysis? A rapid review and checklist of promising practices" technical report.
On this page
Overview
The burden of diseases and health conditions isn't shared equally among all Canadians. Some people are more likely to get sick or die because of their social and economic conditions. We call these "health inequalities".
There are many ways to measure health inequalities. One main approach is to compare groups of people, based on one single factor. For example, we can calculate health inequalities by gender. To do so, we could compare the health of men compared to women.
Yet, this type of analysis is not perfect. When we only look at one factor, two things can happen. One, we can miss other important personal characteristics, like age or ethnicity. These other factors can also influence health. Two, when we only focus on one factor, we can miss out on understanding how it relates to other factors.
In the 1970s and 1980s, Black feminist scholars in the US explored this topic. One of these scholars was Kimberlé Crenshaw. She wrote about the experiences of Black women. Black women experience the world in a different way than Black men or white women. This is because Black women face discrimination based on their gender and their race.
Crenshaw coined the term "intersectionality". Intersectionality refers to how sources of discrimination overlap and reinforce each other. It also refers to the reality that we all have many identities that intersect to make us who we are.
In public health, we can apply intersectionality theory to better understand health inequalities. The Public Health Agency of Canada (PHAC) is eager to do this. But first, PHAC needed to develop a road map of how to do so. This information is crucial for future reporting by the Pan-Canadian Health Inequalities Reporting Initiative or "HIRI". HIRI aims to track and report on health inequalities in Canada. It does so to inform health and social policy, to ensure health and well-being for all.
This report helps fill the gap in evidence. It summarizes a literature review. This review explored how to apply intersectionality in data analyses of health inequalities.
Method
PHAC performed a rapid literature review. We looked at 34 studies that explored health inequalities. Each of these studies aimed to integrate intersectionality theory.
Reading these articles, we analyzed how they applied the theory. To do so, we used an existing framework. We used the Intersectionality-Based Policy Analysis (IBPA) framework. This framework identified the eight guiding principles of intersectionality theory:
- Intersecting categories
- Multi-level analysis
- Power
- Equity
- Social justice
- Time and space
- Diverse knowledges
- Reflexivity
We looked at out each of the studies to see how they integrated the eight principles. Then, we synthesized our findings.
Key findings
We identified over 35 promising practices of ways to integrate intersectionality theory. These practices include steps to take when designing an analysis. For example, it is important to:
- Engage with the communities that experience the inequalities that are being studied
- Review both qualitative and quantitative background evidence.
The promising practices also include steps to take at the data analysis phase:
- Exploring inequalities across time
- Analyzing determinants that could be addressed through interventions.
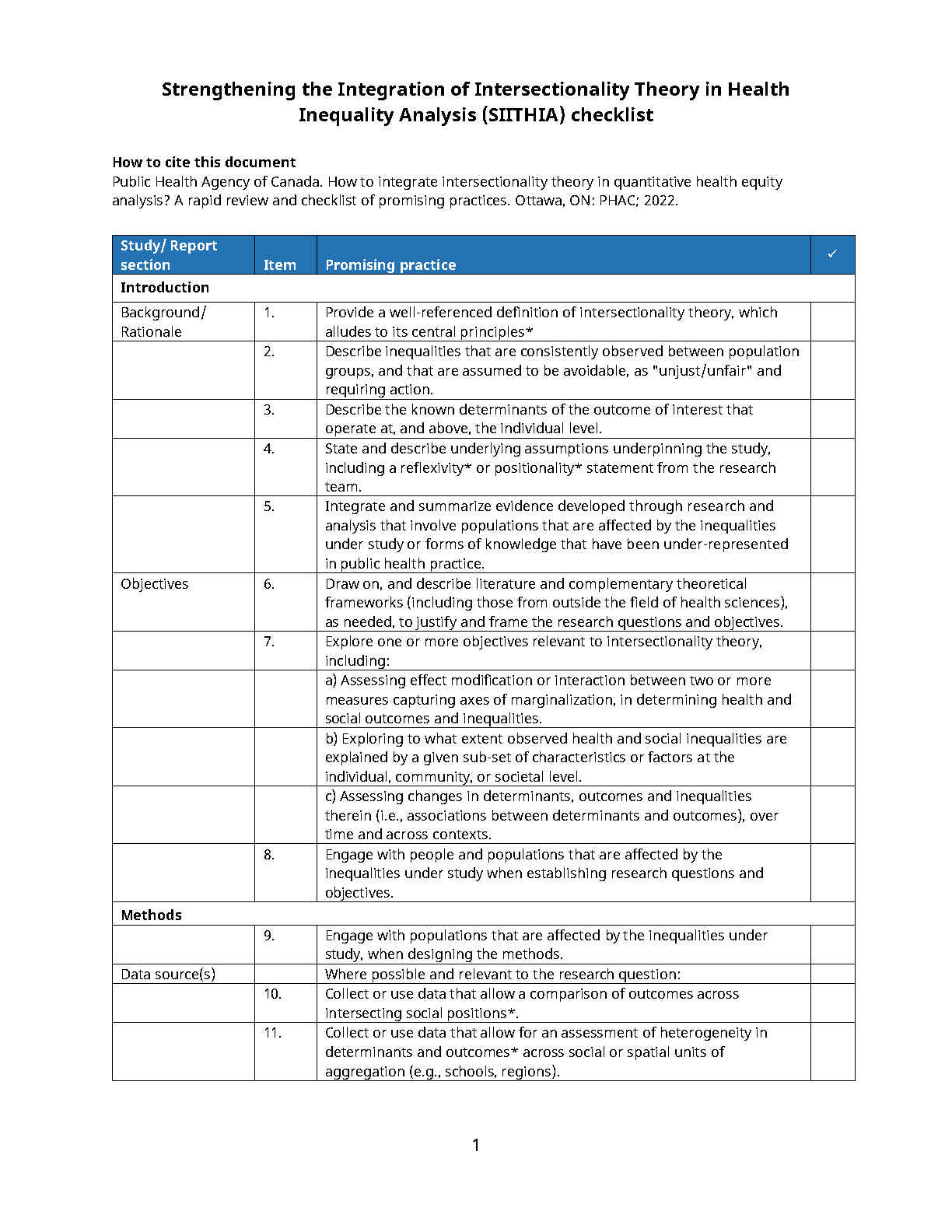
These are but a few examples. We present the full list of promising practices using a checklist format. We call this new checklist the "Strengthening the Integration of Intersectionality Theory in Health Inequality Analysis" (SIITHIA) checklist. The checklist is in Section 3.5 of the report.
Conclusion
Integrating intersectionality theory will be helpful for public health. It will help us study how sources of discrimination overlap and reinforce each other. In turn, this can help us better understand how health inequalities come to be.
The SIITHIA checklist is a tool to help guide the Pan-Canadian Health Inequalities Reporting Initiative. It is also a tool for health researchers and surveillance initiatives. The checklist should empower future studies to meaningfully integrate intersectionality theory into practice.
Table of contents
- Index of figures
- Index of tables
- Executive Summary
- 1.0 Introduction
- 2.0 Methods
- 3.0 Results
- 4.0 Discussion
- 5.0 Conclusion
- Recommended reading
- Glossary
- 6.0 References
- 7.0 Supplementary material
- 8.0 Acknowledgements and Authors
Index of figures
- Figure 1: Flowchart of study screening and selection
- Figure 2: Social stratification (exposure) measures used across the 34 reviewed studies
- Figure 3: Outcome (dependent) measures used across the 34 reviewed studies
- Figure 4: Integration of intersectionality principles, by study sub-sections (n=34 studies)
Index of tables
- Table 1: Rapid literature search terms
- Table 2: Data elements extracted from retained articles
- Table 3: Intersectionality principle definitions and deductive analysis employed
- Table 4: Promising practices for integrating intersectionality theory in the rationale for quantitative health equity analysis
- Table 5: Promising practices for integrating intersectionality theory in the analytic design of quantitative health equity analysis
- Table 6: Promising practices for integrating intersectionality theory in the interpretation phase of quantitative health equity analysis
- Table 7: Strengthening the Integration of Intersectionality Theory in Health Inequality Analysis (SIITHIA) checklist
Executive Summary
Background
Emerging from Black feminist scholarship in the late 1980s, intersectionality theory can be applied as an analytic framework to better understand, describe and respond to health inequalities in a way that addresses fundamental determinants of health, and promotes social justice and health equity. As such, integrating intersectionality theory into health inequalities surveillance activities has been identified as one of many priority topics, theories and methods for the Pan-Canadian Health Inequalities Reporting Initiative and Canadian health inequality surveillance more broadly. However, a summary of promising practices to operationalize this theory into practice, particularly in its integration at all stages of quantitative analysis, from problem identification, to methodological design and findings interpretation, is currently missing from the literature. This rapid literature review aimed to fill this knowledge gap.
Objective
The overall aim of this review was to identify promising practices to meaningfully integrate intersectionality theory in quantitative analyses of health inequalities between population sub-groups. Specifically, we aimed to identify how studies that have applied this theoretical framework integrated its central principles into each step of the analyses, from problem identification and rationale setting, to methodological design and the interpretation of results. Herein, we do not posit that the identified attempts at incorporating intersectionality theory’s principles can or should be defined as standard or "best" practices. Rather, they represent promising directions that could continue to be explored, in tandem, in future analyses that aim to meaningfully integrate intersectionality theory in health inequality analysis.
Purpose and intended audience
The primary purpose of this technical report is to guide future enhanced intersectionality-informed quantitative data analysis of health inequalities between population sub-groups, for the Pan-Canadian Health Inequalities Reporting (HIR) Initiative. This report is therefore intended for a technical audience of public health professionals and other health system actors with epidemiology and biostatistics training, who have completed initial readings on, and have a basic familiarity with intersectionality theory. A reading list and Glossary section are provided to define key tenets of intersectionality theory and relevant terminology. Readers who are less familiar with intersectionality theory are recommended to complete these readings and a review of this report’s glossary section before reading the rest of this report.
Methods
We performed a rapid literature review of works that were explicitly designed to integrate intersectionality theory in their quantitative analysis of health inequalities. Articles were identified through a search of Scopus and Medline databases. To guide our review’s assessment of how intersectionality theory was integrated throughout these studies, we drew on the Intersectionality-Based Policy Analysis (IBPA) framework’s eight "guiding principles" of intersectionality theory. Defined in detail in the text, these include intersecting categories, multi-level analysis, power, equity, social justice, time and space, diverse knowledges and reflexivity (see Glossary for definitions). Information from relevant publications was extracted. We performed a narrative synthesis of how each of the eight principles could be integrated when monitoring health inequalities using quantitative data sources.
Results
We identified over 35 promising practices of ways to integrate the core principles of intersectionality theory in quantitative analyses of health inequalities, at every step of research or surveillance design, from conceptualization to reporting. The application of stratified or interaction-based analyses is not sufficient to meaningfully integrate this theory into practice. A summary of the promising practices to more meaningfully integrate intersectionality theory is presented using a checklist format. The "Strengthening the Integration of Intersectionality Theory in Health Inequality Analysis" (SIITHIA) checklist prototype is proposed (Results Section 3.5). This tool can guide future Pan-Canadian Health Inequalities Reporting Initiative analyses, as well as research, evaluation and surveillance methodologies, so that they may overcome previously identified limitations in quantitative intersectionality-informed analyses of health inequalities.
1. Introduction
In 2018, the Pan-Canadian Health Inequalities Reporting (HIR) Initiative published its Key Health Inequalities in Canada: A National Portrait report Footnote 1, which provided a comprehensive baseline description of the state of health inequalities in Canada. The report describes the various population sub-groups that bear a disproportionate burden of adverse health and social outcomes in Canada. Drawing on the Social Determinants of Health Framework Footnote 2, the report highlights how these health inequalities are determined by systems and structures that represent "fundamental" determinants of health Footnote 3 and how these systems or structures are often intersecting. Indeed, scholars have described health determining "systems of domination" such as racism, sexism, and colonialism as "co-constitutive" (i.e., essential to each other’s existence) and mutually reinforcing Footnote 4, Footnote 5, for the ways in which they intersect or "interlock" to mutually reinforce inequitable distributions of health promoting resources and power within societies. However, the 2018 HIR Initiative report Footnote 1 acknowledged that it:
"did not attempt to disentangle the multiple intersections between and among different social positions and/or different determinants of health, although it is acknowledged that health inequalities are driven by a complex system of social factors (i.e. structural and intermediary determinants of health) that remain to be fully explored and understood."
Several theoretical traditions have explored the connectedness of structural determinants of health. Among them is the domain of intersectionality theory. As such, intersectionality theory was identified as one of many priority topics, theories and methods to explore in future HIR Initiative reporting.
1.1 What is intersectionality theory?
Broadly, intersectionality theory is an analytic framework and research paradigm that stresses a need to consider the ways in which connected systems and structures of power operate across time, place, and societal levels, to construct intersecting social locations and identities (e.g., along axes such as race, gender, class, and sexual orientation, among others) (see Box 1 through processes of privilege and oppression Footnote 6, Footnote 7. Intersectional feminist theorizing can be traced back to the unique challenges faced by African American women in the United States (US) who face systems of oppression that operate at different levels and are frequently interlocking Footnote 4. Intersectionality theory was developed as a theoretical paradigm to move beyond analyzing individual categories of difference Footnote 8, Footnote 9. Early formulations of intersectionality theory in the late 1970s, led by the Combahee River Collective—a collective of Black lesbian feminists committed to "struggling against racial, sexual, heterosexual, and class oppression"— Footnote 10, responded to how various forms of discrimination, including racism, classism and heterosexism shaped Black women’s lives simultaneously, contributing to multiple social inequalities Footnote 9, Footnote 11. Critical race theorist and legal scholar Kimberlé Crenshaw and sociologist Patricia Hill-Collins are credited as pioneering more contemporary understandings of this theoretical perspective, and have articulated how multiple forms of oppression interlock and result in patterns and processes distinct from singular forms of discrimination. Importantly, these scholars emphasized how embedded systems of power and oppression, result in patterns of domination, privilege and continued inequality Footnote 12–Footnote 14. Intersectionality theory seeks to address the convergence of these systems of power whereby multiple marginalization (effected along axes such as race, sex, gender, class, sexual orientation, dis/ability), at individual and structural levels, require analysis and policy solutions that can address how intersections of these categories create and maintain inequality Footnote 11, Footnote 15.
Box 1: Key intersectionality-related terms and concepts
The Glossary section of this report provides definitions of several key terms and concepts that pertain to the topic of intersectionality theory.
Throughout the text, the term "identity" will be used to refer to markers of the sub-groups defined along categories of difference. For example, Black identity is a sub-group marker the constructed category of difference of race Footnote 5.
Below, this report gives a brief overview of key historical references, theorists, concepts, and applications of intersectionality theory. Important theoretical conversations are on-going on how best to apply this theory across scientific domains and contexts. It was beyond the scope of this report to provide an in-depth history of this theoretical framework and these debates. These have been published elsewhere (e.g. see: Hancock, AM. Intersectionality. An Intellectual History. Oxford University Press, 2016).
1.2 How has intersectionality theory been applied in health research?
Intersectionality theory has been applied across a wide range of disciplines, including, more recently, in quantitative public health and epidemiologic research. Within the Federal Government of Canada, it forms the theoretical underpinning of the "Plus" of Gender Based Analysis PLUS (GBA PLUS) Footnote 16.
A recent systematic review of the application of intersectionality theory in quantitative research studies Footnote 17 found that a majority of published studies integrating this theory use what Leslie McCall Footnote 18 and others have described as an "inter-categorical" analysis approach. This approach presumes that complex relationships of inequality exist among social groups within and across identities, and seeks to focus analysis on these relationships Footnote 18. Operationally, inter-categorical analysis makes use of multiple categorical measures (or so-called "categories of difference"; see Glossary for definition) to study the experience of groups, defined according to multiple axes of identity Footnote 18, Footnote 19. For example, an inter-categorical analysis may seek to explore the prevalence of certain health condition (e.g. diabetes) across income quintiles and gender, to explore how the relationship between income and diabetes risk differs for men and women.
Inter-categorical analyses are often defined in contrast to two other approaches. More common in qualitative research methodologies such as ethnographic research, one is an "anti-categorical" approach, which rejects the notion that categories of difference are immutable (i.e, unchanging across time, place, or context) Footnote 18. An anti-categorical analysis is interested in questioning boundaries of constructed categories (e.g., studies that interrogate the "completeness" of binary gender categories such as "men" and "women"). The other type is an "intra-categorical" approach, which explores the experiences of a single sub-population/group (e.g., Arab people in the US) and explores within-group differences along one or more intersectional locations (e.g., class, gender, sexual orientation), such as the study of outcomes among "Arab American, middleclass, heterosexual [women]" Footnote 18). Both of the latter two approaches are common in qualitative research studies Footnote 17, and can be used in quantitative analyses as well.
In the domain of quantitative intersectionality-informed health inequality research, common types of statistical analyses include stratified descriptive or regression-based analysis, as well as regression-based effect measure modification or interaction analysis, multi-level modeling, structural equation modeling, as well as decision or classification tree, mediation, decomposition, latent class and cluster analysis, and multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) analysis (see Glossary for definition) Footnote 17.
However, the application of intersectionality theory in quantitative health inequality analyses has faced criticism. First, scholars have critiqued extant studies’ limited engagement with the central principles of intersectionality theory Footnote 17, Footnote 20, Footnote 21. Some studies omit a definition of the theory altogether Footnote 17, or focus primarily on differences in outcomes across multiple social identities, without a more in-depth analysis of structural discrimination through policies and institutional practices Footnote 22 or a focus on social justice Footnote 21 that are core to the theory’s understanding of power and oppression Footnote 12–Footnote 14, Footnote 21. Meaningful engagement with the theory has been identified as "essential in order to maintain the critical and transformative edge of intersectionality" Footnote 19.
Second, the focus of inter-categorical analyses on differences between groups can obscure within-group heterogeneity and reproduce binary constructs that negate the fluid and dynamic nature of group membership and intersections Footnote 23. Third, many studies describe inequalities without exploring the mechanisms that explain the observed differences and that could be addressed through health or social policy intervention. Methods such as mediation or decomposition analyses can help fill these knowledge gaps Footnote 23. Bauer et al. distinguish these as "descriptive" and "analytic" intersectionality approaches, respectively Footnote 17, Footnote 24, and note that many studies lack a clear central research question to guide their analytic approach. Fourth, many studies explore differences in outcomes across sex/gender, race/ethnicity and socioeconomic status (SES) measures, without considering other intersectional categories Footnote 23. Fifth, studies of health inequality often examine inequalities on either or both an absolute/additive and relative/multiplicative scale (e.g., prevalence differences and ratios, respectively) Footnote 25. Not all studies measuring inequalities on a multiplicative scale, however, explore the differences in the effects of social positions across intersecting identities (e.g., interaction or effect measure modification) on an additive scale. The additive scale has been identified as most relevant for public health application Footnote 17, since departure from additivity highlights instances when disease burden depends on the extent to which two or more factors occur together in the same individuals (see Box 2) Footnote 26.
Box 2: The importance of additive-scale effect modification for public health
Additive interaction (or departure from additivity) is present when the attributable risk of any given outcome or disease in those exposed to a risk factor, A, varies as a function of another risk factor, B. For example, if a risk factor A is tobacco smoking, and a risk factor B is diabetes, if the attributable risk of a disease such as lung cancer is higher among those who smoke and have diabetes, e.g. 20 cases/100,000 population, and lower among those who smoke but do not have diabetes, e.g. 5 cases/100,000 population, this information is important to guide public health interventions. Namely, it may be that targeting a tobacco cessation program to those who have diabetes could lead to a greater reduction in the number of incident cases of lung cancer. Further details on additive interaction or effect modification have been published Footnote 27.
1.3 Aims and purpose of this report
In sum, interest in this theory is growing, but guidance on the ways to integrate the theory systematically and rigorously into quantitative public health and epidemiologic study, is limited. Indeed, in their recent systematic review of intersectionality-informed quantitative studies, Bauer et al. Footnote 17 highlight the overall need for reporting guidelines and recommendations for future intersectionality-informed research.
Aiming to help fill this gap in the literature, the objective of this review was to identify promising practices to integrate intersectionality theory in quantitative analyses of health inequalities between population sub-groups. Specifically, we aimed to identify how studies that have applied this theoretical framework integrated its central tenets and principles into each step of the analysis, from problem identification and rationale setting, to methodological design, and the interpretation of results. To do so, we performed a rapid literature review of works that were designed explicitly to integrate intersectionality theory in their analysis of health inequalities between population sub-groups. To guide our review’s assessment of how intersectionality theory was integrated throughout these studies, we drew on the eight guiding principles underpinning Intersectionality-Based Policy Analysis (IBPA) framework Footnote 16. The IBPA framework provides a summary of the eight guiding principles of intersectionality theory. Defined in detail below, these include intersecting categories, multi-level analysis, power, reflexivity, time and space, diverse knowledges, social justice, and equity (see Glossary and Methods section 2.6b for definitions). We assessed how each of the eight principles could be integrated into quantitative analyses of health inequalities.
2. Methods
2.1 Positionality statement
In the field of intersectionality-informed research, it is customary for researchers to provide a written reflection on the social positions and operating contexts of the authorship team, its location within systems or structures of power, as well as their underlying scholarly or analytic assumptions, before launching into the details of their work. These details are referred to as "positionality statements" or "reflexivity statements" Footnote 28. This reflexive exercise can help practitioners acknowledge and deconstruct underlying assumptions or practices that, often unintentionally, reinforce structures of power or oppression Footnote 16. To ensure that this report is aligned with the fundamental principles of intersectionality theory, namely the principle of reflexivity, we (the authors) will begin by stating a few words about the positionality of our team and the broader context in which this work was conducted:
We (the authors) are working within Canada’s national public health agency (the Public Health Agency of Canada), as analytic leads for the Pan-Canadian Health Inequalities Reporting (HIR) Initiative. We come from diverse disciplinary backgrounds (epidemiology, public health, sociology, psychiatry, occupational health, environmental science). We also come from diverse economic, racial, ethnic, gender and sexual orientation backgrounds. However, none of our team members identify as Indigenous. We respectfully acknowledge that each of us contributed to this report from traditional, unceded First Nation territories. Specifically, this report was developed in Montreal, on the traditional and unceded territory of the Mohawk (Kanien’kehá:ka) Nation; and in Toronto, on the traditional territory of the Wendat, the Anishnaabeg, Haudenosaunee, Métis, and the Mississaugas of the New Credit First Nation; and in Ottawa, on the traditional and unceded territory of the Algonquin Anishnaabe people.
The HIR Initiative’s mandate is to monitor and report on health inequalities in Canada in order to guide health equity-informed health and social policy Footnote 1 . The Initiative is motivated by an understanding that health inequalities cannot be addressed without intervention on the broad social, economic, and political factors that generate and reinforce societal hierarchies and inform the social and material conditions in which individuals are born, grow, live, work and age Footnote 1 . This understanding of the fundamental determinants of health is aligned with several of the key principles of Intersectionality theory, namely of equity and social justice.
The HIR Initiative is informed by an empirical positivist tradition of quantitative epidemiologic surveillance Footnote 29 and social epidemiological understandings of population health Footnote 30 and the Social Determinants of Health framework Footnote 2. The methodology of this review was informed by those paradigms. Namely, since this review was designed to inform future analyses led by the HIR Initiative, we aimed to identify promising practices of applying intersectionality theory within quantitative, epidemiological analyses of health inequalities between population sub-groups. Although the application of purely qualitative methods has been outside the scope of past HIR Initiative data analyses, we acknowledge the importance of qualitative and mixed methods analyses for population and public health research and practice.
Further, as employees of Canada’s federal government, we are aware of our position within an institution of power and privilege that, due to the ways that systemic racism is "at the core of many institutions" Footnote 31 has and continues to perpetuate harms towards several groups and communities, in ways that hamper health equity goals Footnote 32–Footnote 36. Given our position within this institution, we wanted to ensure that the methods we employed in this review do not contribute to the previously-documented co-optation of intersectionality theory Footnote 37—a radical, anti-oppressive, grassroots-born theoretical paradigm—for further oppression or domination. Our work is aligned with the Federal Anti-Racism Strategy’s guiding values of justice, equity, human rights, diversity, inclusion, decolonization, integrity, anti-oppression and reconciliation Footnote 38. As such, we designed the review’s analysis and data extraction methods so as to be as thorough as possible in our identification of meaningful promising practices that could be employed at every step of study design, including those occurring before and after the step of data analysis.
This review was designed and conducted within a broader social and political moment in Canadian history. Namely, it was conducted in 2021, in the second year of the global COVID-19 pandemic, and following the murder of George Floyd and the resulting worldwide recognition of ongoing police brutality perpetuated against Black populations in the United States and other countries, including Canada. It was also a year that brought into focus the enduring legacy of colonialism and systemic racism in Canada Footnote 39, namely through the death of Joyce Echaquan Footnote 40 and the discovery of mass graves at the Kamloops Indian Residential School in the Tk’emlúps te Secwépemc Nation territory Footnote 41, and at other residential schools across the country. These deaths brought attention to the violence and on-going trauma of colonialism and Canada’s residential school system, as previously detailed in the Truth and Reconciliation Commission Reports Footnote 42. In Canadian society, including the federal public service, there has been an increasing recognition of ongoing violence, systemic racism, and discrimination against racialized and Indigenous populations and more established evidence of the unequal health and socioeconomic effects of the COVID-19 pandemic. This present report follows several reports developed by Canada’s Chief Public Health Officer, Dr. Theresa Tam, which focused on stigma and health equity during the COVID-19 pandemic Footnote 43, Footnote 44. These reports emphasize the importance social justice and equity for health promotion, and the need for transformative action to address structures of power—all of which is aligned with the central tenets of intersectionality theory.
This context has highlighted the need, within public health institutions such as PHAC, to draw on theoretical frameworks, such as intersectionality theory, that openly engage with topics such as racism, colonialism and other systems of oppression. This review is therefore shaped and informed by this broader historical and contemporary context.
Lastly, given that this report was produced in the second year of the global COVID-19 pandemic and our team faced several concurrent priorities, we did not have the time nor the human resources to conduct a full systematic review. A rapid review design was therefore employed.
2.2 Design
A rapid review design was selected to achieve this study’s objectives. Rapid reviews are increasingly recognized as a useful design for literature synthesis, particularly to inform and guide policy action in governmental contexts Footnote 45. While following similar rigorous methodological steps to a systematic review, a rapid review focuses on a non-systematic approach to finding evidence, which allows for the review to be completed in a shorter timeframe. Using a non-systematic study identification approach, rapid reviews risk overlooking relevant studies Footnote 46. However, evidence suggests that overall, general conclusions and take-home messages tend to be similar between rapid reviews and systematic reviews that are completed within three to six months Footnote 47.
2.3 Eligibility criteria
This rapid review aimed to identify studies with the following characteristics: 1) they were explicitly guided by intersectionality theory, and 2) applied a quantitative design or a mixed-methods design with a quantitative analysis element. Further, since this review was designed to identify promising practices to integrate intersectionality theory in quantitative analyses of health inequalities between population sub-groups, studies of interest were required to 3) have conducted an analysis of a health-related outcome—the outcome topic area was kept intentionally broad to capture a larger body of relevant studies—at the intersections of 4) two or more exposure measures, that capture "categories of difference" (see Glossary for definitions) (e.g., age, race, gender, etc.), i.e. applying a so-called "inter-categorical intersectional analysis" approach that compared outcomes between groups (the exclusion of intra- or anti-categorical analyses is discussed below). Further, 5) their target population and sampling design were sufficiently broad to allow for findings that could be generalizable to a large population and therefore meaningful for population health. They could come from any country, setting, or time frame, but 6) were required to be written in English or French due to the linguistic abilities of the authors of this report.
As such, studies were excluded if they 1) did not explicitly integrate intersectionality theory in any element of study design. More specifically, papers describing the importance of intersectionality theory without a practical application or integration of the theory in study design were excluded. Studies that introduced the concept of intersectionality and utilized the theory to develop their study objectives and design, despite providing no fulsome definition of the theory were not excluded since we assumed that certain journal audiences may be familiar with the theory and not to require a definition. Studies were excluded if they 2) did not explore health-related inequalities between two or more groups (i.e., that they used a so-called "inter-categorical" approach; see Glossary for definitions). We used this practical criterion rather excluding studies based on labels of "anti-" or "intra-categorical" analysis, insofar as previous reviews have identified challenges at applying McCall’s Footnote 18 typologies in quantitative analyses Footnote 17. For example, depending on its objectives and scope, an analysis of the intersections between race and sexual orientation within a sub-sample of women could be considered as an intra- or inter-categorical approach. Since we aimed to identify promising practices to integrate intersectionality when studying health inequalities between groups, we excluded studies that did not include any form of inequality estimation. We also excluded studies that 3) focused solely on outcomes pertaining to clinical practice; or 4) were purely qualitative in design. Lastly, we excluded (5) commentaries, editorials, conference abstracts and registered research protocols, as these did not present sufficient information to assess how intersectionality theory was integrated from methods design, to analysis, and results interpretation.
2.4 Search strategy
Studies were identified using Scopus and Medline databases (via Pubmed, Ovid Medline, and Global Health Ebsco). Search strings were constructed based on three themes: (1) intersectionality-related constructs or concepts; (2) public health and health equity; and (3) quantitative or mixed-methods analysis, as depicted in Table 1 (detailed search strings are described in Supplemental File Section 7.1 Search strategy). According to the rapid review framework’s Footnote 48 intention of rapidly identifying the most relevant set of articles to answer the study question Footnote 48, we applied a restrictive search strategy, such that articles were required to mention the terms "intersectionality" or "intersectional" in their title or abstract (Table 1). Lastly, a snowball search approach was also used to identify applied studies of intersectionality integration in quantitative analysis that were referenced in other papers but that were not found using the initial search strategy.
| Theme | Search terms |
|---|---|
| 1) Intersectionality-related constructs and concepts | Intersectionality, intersectional |
| 2) Public health & Health Equity | Health status disparities, health status indicators, health determinants, social determinants of health, minority health, underserved, public health, population health, health equity, health inequalities, health inequities, epidemiology, social determinants of health, marginalization, marginalized, marginalisation, marginalised, oppressed, discrimination, stigmatized, stigmatization, stigmatisation, stigmatised, social identit*, social position*, vulnerability, vulnerable, race, racialized, race-based, ethnicity, ethnocultural group*, ethnocultural concentration, LGBTQ2, LGBT, LGBTQ, sexual orientation, sexual minority, gender-based, socioeconomic status, indigenous people*, indigeneity, rural, urban, immigrant*, abilit*, disabilit*, age |
| 3) Quantitative or mixed-methods analysis | Quantitative, mixed, empirical research, evaluation studies, statistic, |
| * Indicates "truncation" or "wildcard" search term | |
2.5 Study identification
Initial title and abstract screening was conducted using Rayyan software Footnote 49. First, one reviewer (AES) screened all titles and abstracts of studies identified through the search strategy. A second independent reviewer (DC) screened 20% of identified studies to verify compatibility with AES’s review. There was 92% agreement between the two independent reviewers for this subset of articles. The two reviewers met to discuss any disagreements and reach consensus. The retained studies were kept for full-text review. A similar review process was completed for the full-text review stage. One reviewer (AES) screened all full texts. As second independent reviewer (DC) screened the full texts of 20% of retained articles. There was 86% agreement between the two independent reviewers for this subset of articles. The two reviewers met to discuss any disagreements and reach consensus. At this penultimate stage, a third reviewer (AB) reviewed the full texts of all (100%) retained eligible articles to validate whether all studies identified met inclusion criteria. All disagreements were discussed with the primary reviewer (AES) to reach consensus on the final set of articles included in the review.
2.6 Data extraction and analysis
a) Data elements
Data elements extracted from the articles included in the review fell into three themes: (1) general information about the study rationale, questions, and theory; (2) data on study design and methods; and (3) data on concrete examples of the integration of intersectionality theory principles in the rationale, analytic design, and interpretation sections of the studies, respectively (Table 2).
| Theme | Data element |
|---|---|
| Study rationale, objectives and theory |
|
| Study design and methods |
|
| Integration of intersectionality theory principles throughout the study |
|
b) Analysis of the integration of intersectionality theory
In a recent systematic review Footnote 17, researchers explored how intersectionality theory was applied in quantitative data analyses by assessing whether papers 1) included a definition of the theory, 2) cited its foundational authors, 3) cited seminal "quantitative intersectionality methods papers" (based on a pre-specified list), and whether 4) measures of "social position" or categories of difference (see Glossary for definitions) that were used in the studies were tied back to the concept of social power, and 5) outcomes were estimated and reported for all social position intersections under study. In their discussion of their findings, the authors of the latter review Footnote 17 highlighted gaps in existing studies, and identified the need for guidance on the ways to integrate the theory more systematically and rigorously into quantitative public health and epidemiologic analysis.
Thus, to build on the latter review, this rapid review took a different methodological approach. Namely, to be able to guide a more systematic application of the theory into future analyses, this review sought to explore how intersectionality-informed studies integrated 1) every major tenet of intersectionality theory, 2) at each step of analysis (from problem identification and rationale setting to methodological design, and the interpretation of results).
To do so, we first needed to select a conceptual framework that enabled the identification of each of the major central tenets of intersectionality theory. For this, we drew on the eight "Guiding Principles" of the Intersectionality-Based Policy Analysis (IBPA) framework. The IBPA framework was designed as a tool to "illuminate how policy constructs individuals’ and groups’ relative power and privileges vis-à-vis their socio-economic-political status, health and well-being" Footnote 50. The IBPA framework has two components: 1) a compendium of guiding principles, and 2) a list of overarching questions to guide analysis. Importantly for the purposes of this review, the IBPA framework’s set of eight guiding principles of intersectionality-based policy analysis are designed to "advance the central tenets of intersectionality" Footnote 16. Discussed in detail below, the eight principles are:
- Intersecting categories
- Multi-level analysis
- Power
- Reflexivity
- Time and space
- Diverse knowledges
- Social justice
- Equity
To assess how intersectionality theory was integrated throughout the selected studies in this review, we used the eight guiding principles of the IBPA framework as an analytic lens to ensure that we captured each of the central tenets of intersectionality theory. Specifically, we used a deductive thematic analysis approach Footnote 51, Footnote 52, wherein each study was analyzed to identify how they engaged with each of the eight pre-specified principles in their rationale, analytic design, and interpretations. As noted in previous reviews Footnote 21, applied alone, the identified practices and methods below should not be interpreted as inherently "intersectionality-informed" or sufficient for a study to be described as "intersectional". Rather, the objective of this review’s analysis was to identify promising practices that, when applied in tandem, could enable analysts to more meaningfully integrate each of the key tenets of intersectionality theory into to their work.
Table 3 summarizes the definitions of eight intersectionality principles that were examined, as well as how thematic analyses were performed to assess the integration of each principle in each study. Information on whether the principle was integrated (yes/no) and how it was integrated, was extracted. A complementary quantitative analysis was performed, wherein per study section, a score of 1 was attributed if the principle was integrated, and 0 if it was not. Scores ranged from 0 to 8 per study section (rationale, analytic design, interpretation). It should be noted that since the goal of this review was to identify promising practices to integrate intersectionality theory, overall, the categorization of methods across guiding principle categories was not done conservatively; some approaches or methods were attributed to more than one principle (e.g. both "space and time" and "multi-level analysis"). Due to time limitations, no quality assessment was performed on the reviewed works.
| Intersectionality principle | Meaning | Deductive analysis strategy |
|---|---|---|
| Intersecting categories | Refers to how "intersectionality conceptualizes social categoriesFootnote * as interacting with and co-constituting one another to create unique social locationsFootnote * that vary according to time and place. It is these intersections and their effects that are of concern in an intersectionality analysis" (p.35 in Footnote 16). |
Integration of this principle was assessed by exploring how studies operationalized multiple social stratification measures (i.e. "categories of difference" or "social categories"), such as race, Indigeneity, gender, etc., and considered their potential intersection or interaction. Note: we did not explicitly assess whether or how authors explored the co-constitution of social categories. |
| Multi-level analysis | Refers to the importance of "understanding the effects between and across various levels in society, including macro (global and national-level institutions and policies), meso or intermediate (provincial and regional-level institutions and policies) and micro levels (community-level, grassroots institutions and policies as well as the individual or ‘self’)" (p.35 in Footnote 16). |
We assessed the integration of this principle by identifying whether and how studies considered conceptually and analytically, multi-level determinants of health, including social processes, power structures, and policy, and their associations from the individual- to structural- or systems-levels. |
| Power | Captures the notions that "subject positions and categories (e.g.,, ‘race’) are constructed and shaped by processes and systems of power (e.g., racialization and racism); […] these processes operate together to shape experiences of privilege and penalty between and among groups" (p.35 in Footnote 16). |
Integration of this principle was assessed by seeking to identify whether and how studies considered, conceptually or analytically, how systems of powerFootnote * operate, intersect, are reproduced, or how they can be resisted. Particular attention was paid to identifying how studies move beyond an additive conceptualization of oppression or marginalization (e.g., to simply identify the most vulnerable groups), towards an analysis of the fundamental systems or structures that create and enable inequalities. |
| Reflexivity | Reflexivity refers to "practices that bring critical self-awareness, role-awareness, interrogation of power and privilege, and the questioning of assumptions and ‘truths’" (p.36 in Footnote 16). |
We explored whether and how studies demonstrated reflexive practices, namely if and how researchers acknowledged their own positions, their experiences of privilege, their underlying methodological assumptions or theoretical perspectives, and how the latter may be shaped by broader systems of power and social position experiences. |
| Time and space | Refers to the notion that "experiences and understandings of time and space are highly dependent upon when and where people live and interact in addition to their epistemological framesFootnote *, or ways of knowing, and the cultural frames of meaning they use to make sense of the world. […] Privileges and disadvantages, including intersecting identities and the processes that determine their value, change over time and place" (p.36 in Footnote 16). |
We assessed whether or how studies integrated, conceptually and analytically, notions of temporal or spatial variation of socio-political contexts, experiences, risks, or outcomes. |
| Diverse knowledges | Refers to intersectionality’s concern "with epistemologiesFootnote * (theories of knowledge) and power, and in particular, with the relationship between power and knowledge production. Including the perspectives and worldviews of people who are typically marginalized or excluded in the production of knowledge can work towards disrupting forces of power that are activated through the production of knowledge" (p. 37 in Footnote 16) |
The integration of the principle implies the acknowledgement and consideration of perspectives of diverse voices and communities. We assessed the integration of this principle by exploring whether works acknowledged knowledge produced through qualitative and quantitative research designs, whether populations who were affected by the inequalities under study were engaged in any component of the study design. |
| Social justice | Refers to the intersectionality’s concern for addressing inequities at their source, specifically by "transforming the way resources and relationships are produced and distributed so that all can live dignified lives in a way that is ecologically sustainable" (p. 38 in Footnote 16) |
We assessed whether and how studies integrated concepts of fairness, justice, advocacy, and the need for policy or systems change. |
| Equity | Refers to the preoccupation with fairness: "inequities exist where differences are unfair or unjust" (p.38 in Footnote 16). |
We assessed if and how studies conceptualized, measured, and described unjust and avoidable inequalities ("inequities" or "disparities") between population groups at the intersection of multiple positions and systems of power. |
|
||
We intentionally analyzed potential integration of the theory’s principles in each article section separately, rather than considering the application of the theory in the article as a whole. This was done for two reasons. First, we hypothesized that some studies might integrate principles of intersectionality theory in their rationale or interpretation sections, while failing to integrate those same principles in the analytic design (or vice versa) Footnote 23. Second, we hypothesized that within a study, the ways in which principles are integrated in each phase of the study may vary, and therefore provide insight into concrete ways to operationalize intersectionality principles from study conceptualization to completion. Applying such knowledge in future research and surveillance endeavors could be beneficial to avoid making the same mistakes and oversights as previous studies that have been criticized by scholars as failing to meaningfully incorporate all of the dimensions of intersectionality theory Footnote 19, Footnote 21, Footnote 24. Superficial applications of the theory can be appropriative if they neglect to acknowledge how transformative social change is required to address the intersecting systems of oppression that shape social and health inequalities Footnote 19, Footnote 21, Footnote 24.
3. Results
3.1 Description of studies
A total of 230 articles were identified using the search strategy described above. Of these, 34 met all inclusion criteria (Figure 1) (extracted results can be found in the Supplemental Material’s Section 7.2 Results: Data extraction). The main reasons for exclusion were: use of purely qualitative study design, use of one social stratifying measure rather than multiple, and a brief mention of intersectionality theory without an explicit aim of integrating the theory in the study.
a) Design and setting
Most studies (24 out of 34, 71%) used data from and were performed in the United States (US). Three studies were based in Canada (8%), including one study Footnote 53 that used data from both Canada and the US. Six papers (18%) used data gathered in Europe, including three in Sweden, one in Germany, one in Norway, and one that studied outcomes across 27 European countries. Only two of the included studies originated outside of Europe and North America. These used data gathered in India and Brazil, respectively.
Several studies explored outcomes in specific settings and contexts, namely schools (n=4, 12%) and health-related environments (n=3, 9%) such as long-term care facilities, maternity clinics, or sexual health centers. Almost half of the studies (n=14, 41%) studied outcomes in population sub-groups, such as individuals who inject drugs, pregnant individuals, mothers, students, sexual minority groups, individuals living with HIV or who consume alcohol). The other studies either explored outcomes in the general population as a whole, or age-specific general population sub-groups (youth, the elderly).
Out of 34 reviewed studies, a majority (n=31, 91%) used a cross-sectional observational design, while 3 (9%) used a longitudinal design. Of the latter, two studies used a mixed-methods design, integrating both qualitative and quantitative sources of dataFootnote 41,Footnote 42.
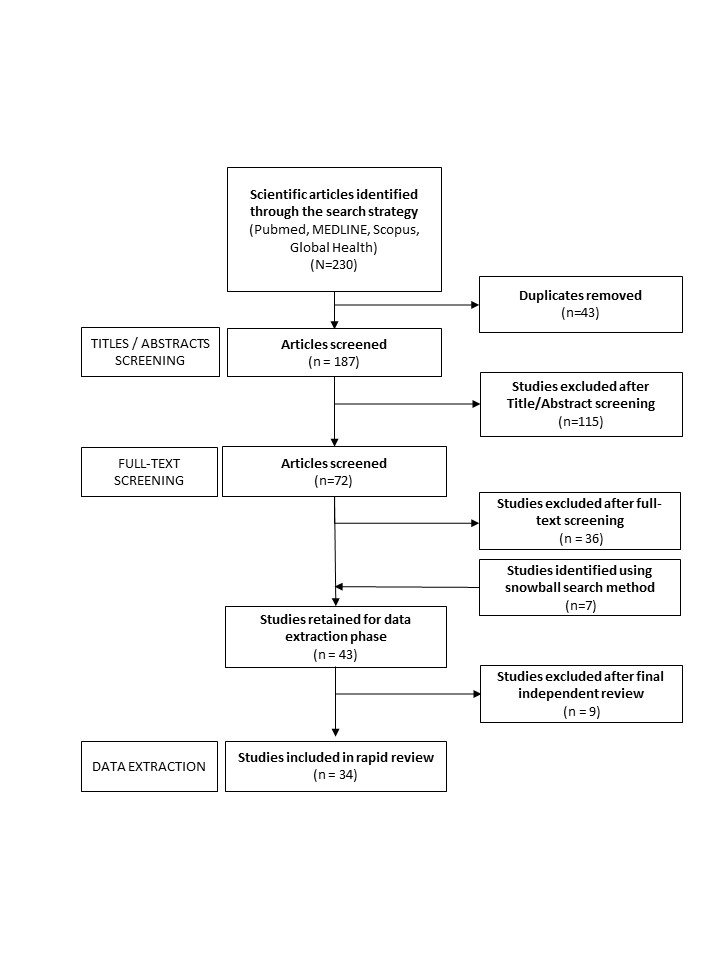
Figure 1 - Text description
Description: First, 230 articles were identified through PubMed, MEDLINE, Scopus and Global Health databases. Of these, 43 were duplicates. The titles and abstracts of the remaining 187 articles were screened for relevance. Of these 115 did not meet the review’s eligibility criteria, and therefore 72 articles remained. We reviewed the full text of these 72 articles to perform a more complete eligibility verification. Of these 72 studies, 36 articles were excluded. Reviewing the references of the studies, 7 additional relevant articles were identified. This provided 43 articles for final verification by an independent reviewer. At this stage, 9 studies were removed, because they did not meet the eligibility criteria. Thus, a final 34 studies were included in the review.
b) Conceptual framing and definitions
All studies provide some theoretical background of intersectionality. However, six studies (18%) do not explicitly articulate a definition of intersectionality theory. These were nonetheless included in the review, as they utilized the theory to develop their study objectives and design.
Of the 28 (82%) studies that did provide an explicit definition, five (15%)Footnote 41-Footnote 45 define the concept of "intersectionality" as referring to intersecting or interacting social identities or positions, which need to be analyzed concurrently rather than independently to capture the experiences of marginalized populations. The latter studies do not mention how intersecting social identities and experiences are related to or shaped by interlocking systems of power, oppression and privilege and/or by macro-, institutional or structural level factors. The remaining 23 studies (68% of all articles reviewed) provide a definition of intersectionality theory that integrates notions of interlocking systems of oppression, and how individual experiences are shaped by multi-level factors.
Almost all studies (n=33, 97%) reference key authors and seminal works of intersectionality theory, such as Kimberly W. Crenshaw—who first coined the term intersectionality in 1989 Footnote 12—Patricia H. Collins Footnote 13, Footnote 14, the Combahee River Collective Footnote 10 and Deborah K. King Footnote 56. Only one study did not reference any of the latter authors Footnote 57, but referenced instead other important contributors to intersectionality theory, such as Lisa Bowleg Footnote 6, Footnote 58 and Olena Hankivsky Footnote 16, Footnote 59–Footnote 61.
In addition to intersectionality theory, 18 of the reviewed studies (53%) introduced an additional framework or theory in their rationale, in combination with intersectionality theory. Several studies referenced health-specific theories related to systematic inequalities: four studies referenced Nancy Krieger’s Ecosocial theory Footnote 62; and two made reference to Link and Phelan’s Fundamental cause theory Footnote 63. Other frameworks or theories were referenced, many of which emerged from fields outside of health science research. Each appeared in only one of the studies, respectively. These included Chavis and Lee’s (1987) environmental justice theory and approach Footnote 64, Marmot and Bell (2012)’s proportionate universalism theory Footnote 65, the Identity Pathology framework Footnote 66, Feminist theory Footnote 67, Structural vulnerability theory Footnote 68, Syndemic theory Footnote 69, Discrimination theory Footnote 70, the Minority Stress Model Footnote 71, the Social Determinants of Health framework Footnote 2, and the Social Ecological model Footnote 72. Emerging out of fields of health research, including social epidemiology, many of the latter theories were utilized as a complement to intersectionality theory and its key principles, namely to provide additional theoretical background on the particular associations between the exposures and health outcomes under study.
c) Exposure and outcome measures
All studies included a minimum of two exposure measures, with the average study including 4 exposure measures. The most common social stratification measures used were those for race/ethnicity (79% of articles), followed by sex/gender (74%), educational attainment (38%), measures of sexual orientation and sexuality (29%), income (26%), immigration or citizenship status (18%), area of residence (urban/rural settings) (15%) and age (15%) (Figure 2). The three Canadian studies explored exposure measures of race/ethnicityFootnote 40,Footnote 60,Footnote 61, sexual or gender minority status Footnote 53, sexual orientation, partnership (marital) status, age, education, income, area of residence (urban, rural, suburban) Footnote 73, gender, and immigrant status Footnote 74.
The outcome (dependent) measures studied were varied. They included mental and physical health outcomes, health-related behaviours, as well as social conditions or experiences such as experience of discrimination, violence, incarceration, income level, or employment status or satisfaction. The most common outcome measures used were those pertaining to affective or mental health (29% of articles), self-reported health (15%) and smoking (12%) (Figure 3). The outcomes of interest in the three Canadian studies were: prevalence of hypertension, diabetes, and asthma, as well as self-rated health Footnote 74; condom-less sex, substance use, suicidality, anxiety, and depression Footnote 73; and psychological distress Footnote 24.
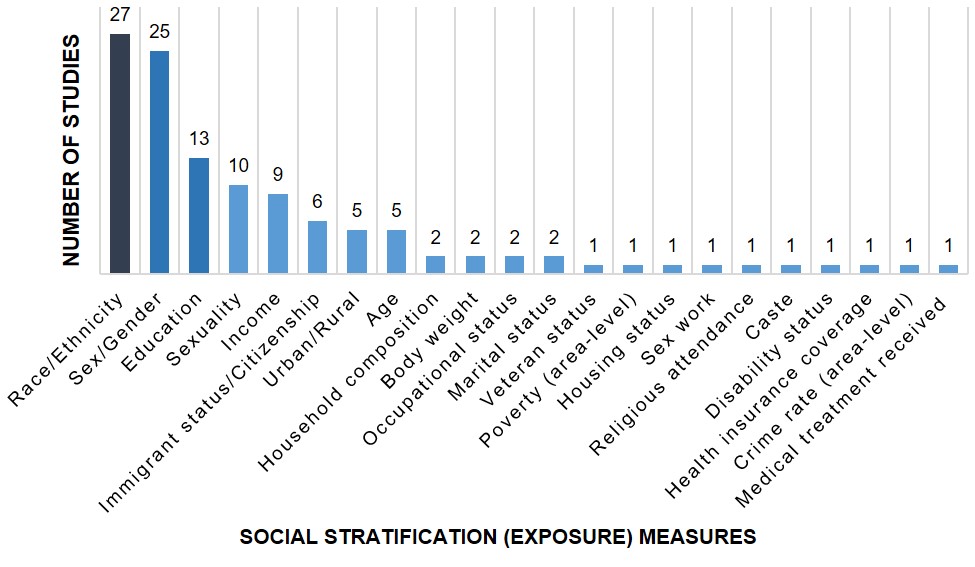
Figure 2 - Text description
Description: This figure presents the social stratification or "exposure" measures that were used in the 34 studies. The horizontal axis describes the exposure measures, while the vertical axis describes the number of studies (n). Overall, 27 studies used exposure measures of race or ethnicity; 25 used measures of sex or gender; 13 studies used measures of educational attainment; 10 studies used measures of sexuality or sexual orientation; 9 studies used measures of income; 6 studies used measures of immigration status or citizenship. Five studies used, respectively, measures of urban residence and age. Two studies used, respectively, measures of household composition, body weight, occupational status, and marital status. Lastly, only one study used, respectively, measures of veteran status, poverty, housing status, sex worker status, caste, disability, health insurance coverage, area-level crime rate, and use of medical treatment.
| Social stratification (exposure) measure | Number of studies (N) | Percent (%) |
|---|---|---|
| Race/Ethnicity | 27 | 79 |
| Sex/Gender | 25 | 74 |
| Education | 13 | 38 |
| Sexuality | 10 | 29 |
| Income | 9 | 26 |
| Immigrant status/Citizenship | 6 | 18 |
| Urban/Rural | 5 | 15 |
| Age | 5 | 15 |
| Household composition | 2 | 6 |
| Body weight | 2 | 6 |
| Occupational status | 2 | 6 |
| Marital status | 2 | 6 |
| Veteran status | 1 | 3 |
| Poverty (area-level) | 1 | 3 |
| Housing status | 1 | 3 |
| Sex work | 1 | 3 |
| Religious attendance | 1 | 3 |
| Caste | 1 | 3 |
| Disability status | 1 | 3 |
| Health insurance coverage | 1 | 3 |
| Crime rate (area-level) | 1 | 3 |
| Medical treatment received | 1 | 3 |
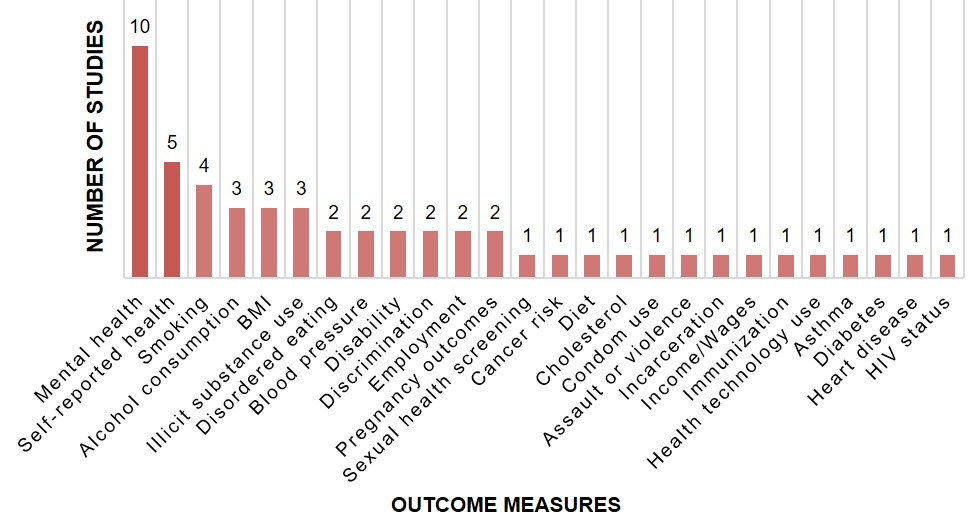
Figure 3 - Text description
Description: This figure presents the dependent or "outcome" measures that were used in the 34 studies. The horizontal axis describes the outcome measures, while the vertical axis describes the number of studies (n). Overall, 10 studies used measures of mental health; 5 studies used measures of self-reported health; 4 studies used measures of smoking. Three studies used, respectively, measures of alcohol consumption, body mass index (BMI), or illicit substance use. Two studies used, respectively, measures of disordered eating, blood pressure, disability, discrimination, employment status, or pregnancy outcomes. Lastly, one study used, respectively, measures of cancer risk, diet, cholesterol levels, condom use, experiences of assault or violence, incarceration, income or wages, immunization status, health technology use, asthma, diabetes, heart disease or human immunodeficiency virus or "HIV" infection status.
| Dependent (Outcome) measures | Number of studies (N) | Percent (%) |
|---|---|---|
| Mental health | 10 | 29 |
| Self-reported health | 5 | 15 |
| Smoking | 4 | 12 |
| Alcohol consumption | 3 | 9 |
| Body Mass Index (BMI) | 3 | 9 |
| Illicit substance use | 3 | 9 |
| Disordered eating | 2 | 6 |
| Blood pressure | 2 | 6 |
| Disability | 2 | 6 |
| Discrimination | 2 | 6 |
| Employment | 2 | 6 |
| Pregnancy outcomes | 2 | 6 |
| Sexual health screening | 1 | 3 |
| Cancer risk | 1 | 3 |
| Diet | 1 | 3 |
| Cholesterol | 1 | 3 |
| Condom use | 1 | 3 |
| Assault or violence | 1 | 3 |
| Incarceration | 1 | 3 |
| Income/Wages | 1 | 3 |
| Immunization | 1 | 3 |
| Health technology use | 1 | 3 |
| Asthma | 1 | 3 |
| Diabetes | 1 | 3 |
| Heart disease | 1 | 3 |
| Human immunodeficiency virus (HIV) status | 1 | 3 |
d) Scope of policy recommendations
Twenty two of the articles (64%) discussed the implications of their research for policy, and made policy recommendations. The most commonly recommended policy interventions were to improve access to culturally-safe and appropriate health care Footnote 54, Footnote 55, Footnote 75–Footnote 79 and to implement anti-discrimination policies, programs or interventions Footnote 24, Footnote 53, Footnote 73–Footnote 75.Additional policy directions included the implementation of anti-stigma initiatives Footnote 24, Footnote 75, Footnote 80, Footnote 81, namely through educational activities. Four studies recommended that existing public health programs be culturally adapted and targeted towards specific sub-populations that faced higher disease or outcome burdenFootnote 42,Footnote 67-Footnote 69. This is aligned with the two works that recommended a Proportional Universalism approach for public health intervention Footnote 80, Footnote 83. Other studies broadly recommended Intersectoral collaboration Footnote 84 and structural-level interventions Footnote 85, Footnote 86. Lastly, five studies made specific recommendations to address inequalities in social determinants of health, including improving financial security Footnote 84, working conditionsFootnote 44,Footnote 72, child care support Footnote 85, and pollution regulation Footnote 87. All studies also made recommendations regarding the direction of future analyses and research pertaining to the subject of study.
3.2 Integration of intersectionality in study rationale
Herein, the "rationale" section of articles refers to their Introduction or Background sections, including content on: background literature review (including the introduction of conceptual framework and theories) and research objectives and hypotheses.
On average, five of the eight principles were integrated in the rationale sections of the studies reviewed. Studies typically included between three to seven principles, with no study integrating all eight. One study Footnote 87 incorporated seven principles, while most incorporated 5 principles (mode=5).
The two most commonly integrated principles in the rationale of the 34 articles reviewed were principles of "intersecting categories" (100% of articles) and of "equity" (100% of articles) (Figure 4). This elevated coverage is likely due to the eligibility criteria applied for this review, which necessitated that included articles explore "joint or intersecting measures of social position or process" and "inequalities between two or more groups". In descending order, the other most commonly integrated principles in this section of the articles were elements of "multi-level analyses" (82% of articles), "power" (79% of articles), "social justice" (62% of articles), "time and space" (18% of articles), and "reflexivity" (12 % of articles). Two articles (<10%) integrated principles of "diverse knowledges" ( Figure 4).
A narrative summary of how these principles were integrated in the rationale sections is presented here, with a review of promising practices summarized in Table 4 below.
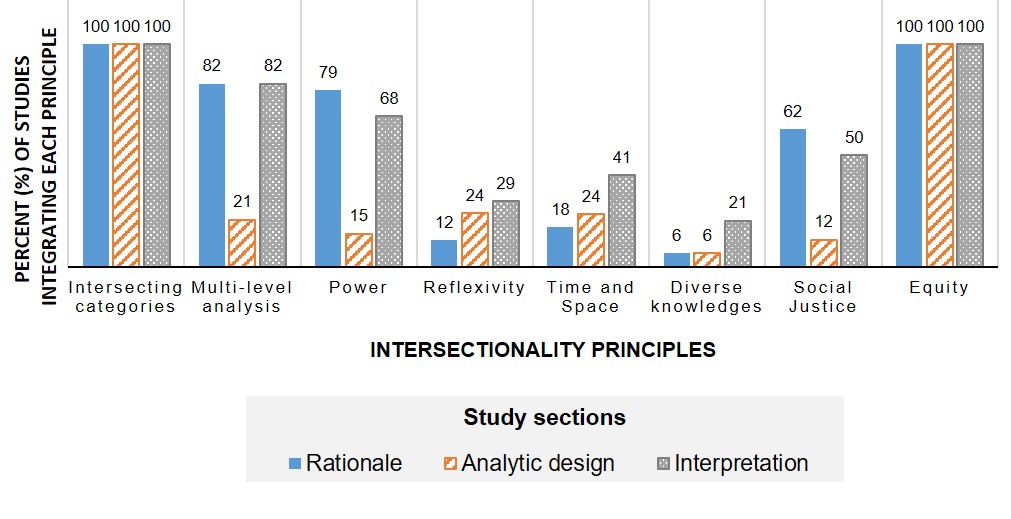
Figure 4 - Text description
Description: This figure presents the level of integration of each of the 8 principles of intersectionality theory in the three main sections of the 34 articles. The three main sections of the articles were the rationale, analytic design, and interpretation sections. The horizontal axis describes the 8 principles of intersectionality. These were: intersecting categories, multi-level analysis, power, reflexivity, time and space, diverse knowledges, social justice, and equity. The vertical axis describes the proportion of studies that integrated each principle.
For the principle of intersecting categories, 100% of studies integrated it in their rationale, analytic design, and interpretation sections, respectively. For the principle of multi-level analysis, 82 of studies integrated it in their rationale and interpretation sections, respectively, while 21% integrated in their analytic design. For the principle of power, 79% of studies integrated it in their rationale, 15% integrated it in their analytic design, 68% integrated it in their interpretation sections. For the principle of reflexivity, 12% of studies integrated it in their rationale, 24% integrated it in their analytic design, 29% integrated it in their interpretation sections. For the principle of time and space, 18% of studies integrated it in their rationale, 24% integrated it in their analytic design, 41% integrated it in their interpretation sections. For the principle of diverse knowledges, 6% of studies integrated it in their rationale and analytic design, respectively, and 21% integrated it in their interpretation sections. For the principle of social justice, 62% of studies integrated it in their rationale, 12% integrated it in their analytic design, and 50% integrated it in their interpretation sections. For the equity, 100% of studies integrated it in their rationale, analytic design, and interpretation sections, respectively.
| Key principles of intersectionality | ||||||||
|---|---|---|---|---|---|---|---|---|
| Intersecting Categories | Multi-level Analysis | Power | Reflexivity | Time and Space | Diverse Knowledges | Social Justice | Equity | |
| Article sections | Percent (%) of studies integrating each principle | |||||||
| Rationale | 100 | 82 | 79 | 12 | 18 | 6 | 62 | 100 |
| Analytic design | 100 | 21 | 15 | 24 | 24 | 6 | 12 | 100 |
| Intepretation | 100 | 82 | 68 | 29 | 41 | 21 | 50 | 100 |
a) Intersecting categories
Background literature review
In their background literature review, two studies Footnote 53, Footnote 88 described the differences between intra- and inter-categorical intersectionality analysis. They refer to these concepts to explain the importance of the use of multiple categorical measures to study the experience of groups at each of the intersections of various social positions, thereby integrating the principle of intersecting categories.
Objectives
A majority of studies (n=25, 74%), integrated this principle in their study questions and objectives. Though formulations varied, the objectives were generally to explore differences in experiences between groups or explore effect measure modification between two or more social stratification measures. For example, studies aimed to:
- Assess outcomes across groups, as defined by two or more social identities or positions;
- Assess how two or more social identities jointly influence a health or social outcome;
- Assess the potential effect modification of a certain social identity or position, on the association between another social stratification measure and an outcome.
The epidemiologic concept of effect measure modification was particularly common across the reviewed studies, although it was not always described using that terminology. For example, three studiesFootnote 44,Footnote 62,Footnote 74 framed their objectives using alternative wording such as:
- To explore whether the combined effect of social identities and positions is different (larger, smaller) than the sum of the individual effects of each identity on the outcome of interest;
- To explore how social positions or identities interact to influence inequalities in outcomes across sub-groups.
b) Multi-level analysis
Background literature review
The 28 studies that integrated the principle of multi-level analysis in the literature summary of their rationale, did so by referring to the multi-level factors (e.g., from the individual, to community and society level) that shape health and health inequalities (e.g., Footnote 79) and by introducing the notion of structures and systems of power that operate above the individual-level, to shape individual-level experiences, identities, and positions when defining intersectionality theory (e.g., Footnote 80). As mentioned above, five studies also integrated complementary theoretical frameworks (e.g., Footnote 89), such as Ecosocial theory or social-ecological models, which posit that individual-level experiences are shaped by multi-level determinants.
Objectives
In five studies (14%), objectives were framed as aiming to achieve a better understanding of how individual-level experiences are shaped by contextual- or structural-level determinants, thus integrating the principle of multi-level analysis. For instance, one study Footnote 90 considered individual-level social position makers such as race, class, and gender, as well as context characteristics of schools (e.g., school poverty status, measured in relation to the incomes of students’ household) and neighborhoods (e.g., neighbourhood poverty status), in determining the outcome of adolescent cigarette use. The objective was framed as follows:
- To examine how individual-level social positions and identities interact with contextual characteristics to produce variation in an outcome across a population
Two studies Footnote 87, Footnote 91 aimed to study the characteristics of neighborhoods and their independent relationships with health outcomes. Formulations of study objectives included:
-
A. To assess potential interaction between area (neighbourhood) level characteristics and their association with population health and health inequalities; and
B. To identify areas that are particularly vulnerable to experiencing the health outcome;
- To assess the extent to which contextual measures explain differences in outcomes across groups above and beyond individual-level measures.
c) Power
Background literature review
The seven studies that did not integrate the principle of power in their rationale section were those that introduced intersectionality theory solely by presenting how individual experiences are shaped by the intersections of various social identities or positions without reference to interlocking systems of power, oppression or privilege shaping those individual-level experiences. The remaining studies referred to the role that systems of power, oppression and privilege play in shaping health or social outcomes.
Objectives
At least two studies integrated the principle of power when introducing their study objectives Footnote 77, Footnote 84. For example, one study Footnote 84 aimed to:
- Examine health inequalities across social stratification measures that capture groups’ relative affluence, social standing and power (e.g., gender, income level);
- Better understand the health inequalities between groups with relatively more power (dominant groups) and those with relatively less power (subordinate groups), by performing a decomposition analysis that determines the relative contribution of various social and economic measures to the observed inequality.
d) Reflexivity
Background literature review
As mentioned in Section 3.1b, all of the studies acknowledged the underlying intersectional theoretical framing of their study, and provide some theoretical background on intersectionality. In addition to this, one study integrated the principle of reflexivity in their background literature review by acknowledging how all analyses are underpinned by underlying assumptions and values, even if these are not made visible Footnote 86. The study noted the importance of the reflexive practice of referencing underlying theories to note underlying assumptions Footnote 86. In another study, authors’ described their theoretical positionality at the outset of the work. They note how their proposed research is "position[ed] within intersectionality, environmental justice and the social determinants of health" literatures Footnote 87. The incorporation of critical theoretical frameworks, that emerged from multidisciplinary backgrounds, including but not limited to intersectionality theory, has been identified as an important future direction for quantitative health research Footnote 8.
Objectives
Two studies were identified as having integrated the principle of reflexivity when they described their research questions and hypotheses. In one study, authors specified that they aimed to identify subpopulations that face the highest disease burden Footnote 73. Referring to Hankivsky’s theorizing Footnote 61, the authors note that "intersectionality suggests that the significance of any given factor, or set of factors should not be predetermined but rather inductively revealed through the research process (Hankivsky, 2012)" (p.510-511 in Footnote 61). Guided by this underlying assumption, the authors explain that they did not aim to test a specific hypothesis as to which particular sub-group studied may experience greatest outcome burden, according to "multiple axes of sexual identity, relationship status, age, education, income, ethnicity, and living environment" (p.510 in Footnote 60).
Similarly, in another study Footnote 82, authors acknowledged how standard epidemiologic analyses of health inequalities based on comparisons between sub-groups and a standard reference category may "reinforce notions of a default, or standard, identity". They give the example of comparing non-white groups to white populations, and how this can "reinforce the culturally-laden value judgments such as the idea that White (or other privileged groups) are the norm to whom others should be compared" (p.2619 in Footnote 64) (see Box 3). Reflecting on these underlying methodological assumptions, the authors specified that their objective was to compare sub-group populations’ outcomes to a sample average.
Box 3: The use of reference groups in past HIRI reporting
Past HIRI data analysis and reporting Footnote 1 has been mindful of the potential risks of centering white or dominant group experiences by using these groups as reference groups for health inequality analyses. However, driven by a similar principle of reflexivity, HIRI chose to use reference groups (rather than population averages, for example). Chosen reference categories were based on understandings and assumptions of which groups tend to experience greater access to health promoting social and economic resources. Comparisons in relation to these dominant groups were interpreted as indications of unfair and potentially avoidable gaps in health promotion and prevention across populations.
e) Space and time
Background literature review
Five studies were identified as having integrated the principle of space and time in their background literature reviews. These studies summarized existing literature’s understanding of the determinants of spatial and temporal changes in health outcomes and health inequalities. Integrating notions that privileges or disadvantages can change over time Footnote 16, two studies discussed how experiences and determinants of health can vary or accumulate throughout the lifecourse, to shape health risks Footnote 76, Footnote 83. The lifecourse perspective requires a consideration of temporal concepts such as calendar time, birth cohorts, and age. Another study highlighted the role of historical and spatial secular shifts in exposures (e.g., levels of immunization), and how these variations in contexts shape population health and health inequalities Footnote 77.
Touching on the concept of space, one study described how systems of oppression can operate differently across local contexts Footnote 92. Another study described the role of neighbourhood-level exposures in shaping individual-level health risks Footnote 87.
Objectives
Three studies were identified as having integrated the principles of space and time when setting their research objectivesFootnote 41,Footnote 63,Footnote 64. These studies aimed to investigate spatial and/or temporal variations in health outcomes and health inequalities through time. For example, objectives specified in these studies, included:
- To assess trends in the prevalence or distribution of social identities or outcomes across space and time;
- To assess changes in the association between identified social identities and outcomes over time and across areas;
- To assess whether or how determinants interact to change outcomes over time.
f) Diverse knowledges
Objectives
Two studies (6% of articles reviewed) were identified as having integrated the principle of diverse knowledges when setting their study’s objectives. Both of these studies aimed to apply a mixed-methods design to explore the first-person perspectives and perceived experiences of specific populations, namely people who inject drugs Footnote 81 and pregnant Latina individuals Footnote 54, based on their other social positions, identities or contexts. For example, Morris et al. Footnote 54 aimed to explore the birth experiences of women, across categories of ethnicity and the region of giving birth. However, neither study indicated whether vulnerable populations were engaged in the definition of the research questions, study design, development of data collection instruments, analysis, interpretation of data, and knowledge mobilization.
g) Social justice
Background literature review
Three studies were identified as having integrated the principle of social justice in their background literature reviews by introducing concepts of fairness and justice. For example studies described the observed systematic and avoidable inequalities as "unjust", "unfair" or "discriminatory" and in need of redress Footnote 84, Footnote 93, Footnote 94.
One study referred to the importance addressing social or environmental injustice, in particular Footnote 84, Footnote 93, Footnote 94. Several studies also indicated the "need" or "importance" of studying and addressing avoidable inequalities. At least four studies acknowledge the need to provide information that could guide public health practitioners or decision-makers in implementing relevant policies to address inequalitiesFootnote 44,Footnote 70,Footnote 79,Footnote 81.
h) Equity
Background literature review
All of the studies were identified as integrating the principle of equity in their review of extant literature, namely by summarizing and describing systematic and avoidable inequalities as "inequitable" or "inequities" or "disparities". Many studies referred to Paula Braveman’s conceptualization and definitions of disparities and health equity Footnote 96. Braveman quotes the US’ Healthy People 2020 initiative’s definition of "health disparity" as: "a particular type of health difference that is closely linked with economic, social, or environmental disadvantage" Footnote 96.
Braveman (2014) highlights how the principle of equity is intertwined with the principles of nondiscrimination and equality, and how health inequities tend to affect groups that have historically faced discrimination Footnote 96. At least four studies described populations that experience "disadvantage" or "marginalization" (e.g.,Footnote 74,Footnote 79,Footnote 80,Footnote 83).
Objectives
As mentioned above, a majority of study objectives aimed to explore and better understand differences in experiences between groups or explore effect measure modification between two or more social stratification measures, which shape inequalities between groups.
Many of the studies used objective types described in the Results’ Section 3.2a: Intersecting categories. In addition, two studies explored the role of discrimination Footnote 88, Footnote 93 in shaping population-level differences in health or social outcomes. Objectives were framed as follows:
- To explore how lived experiences of discrimination impact the
associations between social stratification measures and health or
social outcomes
Three studies proposed objectives that sought to better understand drivers or determinants of avoidable inequalities Footnote 53, Footnote 84, Footnote 94, namely through mediation and decomposition analyses. In these instances, objectives were framed as follows:
- To assess whether and how social stratification measures or experiences are responsible for observed health inequities.
Table 4: Promising practices for integrating intersectionality theory in the rationale for quantitative health equity analysis
| RATIONALE | Intersecting categories | Multi-level analysis | Power | Reflexivity | Time and Space | Diverse knowledge | Social Justice | Equity |
|---|---|---|---|---|---|---|---|---|
Literature review |
Describe the scope of the problem or analysis, and if relevant, the study’s use of an inter-categorical analysis approach. |
|
|
|
|
|
|
Summarize observed inequalities between groups, and whether inequalities are systematic and avoidable. |
Objectives |
Aim to: (Q1) Assess outcomes across groups, as defined by two or more social identities or positions; (Q2) Assess the effect measure modification of a certain social stratification measure, on the association between other social stratification measures and an outcome. |
Aim to: (Q2) Assess how individual-level social positions are modified by contextual measures (and vice versa) in shaping health inequalities (Q3) Identify geographic areas or populations that may be particularly vulnerable to health outcomes (Q4) Assess to what extent contextual measures explain inequalities. |
Aim to: (Q5) Examine health inequalities using measures that capture groups’ relative affluence, social standing and power (e.g., gender, income level) (Q4) Assess to what extent experiences, or social or economic positions explain health inequalities (as a decomposition or mediation question). |
|
Aim to: (Q5) Assess trends in the prevalence or distribution of social identities or outcomes across space and time; (Q6) Assess changes in the association between identified social identities and outcomes over time and across areas; (Q7) Assess if and how determinants interact to change outcomes over time. |
|
Aim to: (Q4) Assess to what extent experiences, or social or economic positions explain avoidable health inequalities (as a decomposition or mediation question) (Q8) Explore how experiences of discrimination impact the associations between social stratification measures and health or social outcomes. |
|
|
||||||||
3.3 Integration of intersectionality in analytic design
Herein, the "analytic design" section of articles refers to the Methods section of texts, including content on data source(s), study measures, and analyses.
On average, three of the eight principles were integrated in the analytic design section of the studies. Studies included between two and six principles in this section, with no study integrating all eight. Most articles incorporated 3 principles (mode=3).
Similar to the rationale section, the two most commonly integrated principles in the analytic design section of the 34 articles reviewed were principles of "intersecting categories" (100% of articles) and of "equity" (100% of articles). However, compared to their use in the rationale sections of the reviewed articles, the remaining six principles were not as commonly integrated at the analytic design stage. In descending order, the other most commonly integrated principles were elements of "time and space" and "reflexivity" (24% of articles, each respectively), "multi-level analyses" (21% of articles), "power" (15% of articles), and "social justice" (12% of articles). Less than 3 articles (<10%) integrated principles of "diverse knowledges." Overall, the studies that integrated a larger number of principles in their analytic design tended to also integrate a higher number of principles in the other two sections reviewed (rationale and interpretation sections). A narrative summary of how these principles were integrated is presented here, with a summary in Table 5.
a) Intersecting categories
Measures
Many studies constructed joint stratification measures to capture the intersection of identities or social positions. Joint stratification measures were categorical variables, which allowed outcome description for two or more independent "exposure" measures (e.g., gender and caste Footnote 77, or gender, race, and sexual behaviour Footnote 82). These constructed "social strata" variables identify all the possible strata combinations of two more of measures. For example, a categorical joint stratification measure capturing intersections between race (3 categories: Black, Latino, White) and sex/gender (2 categories: men, women) could include the following six categories: Black women, Black men, White women, White men, Latina women, Latino men.
Six studies combined a higher level of social locations (i.e., more than three intersecting variables) Footnote 80, Footnote 87, and operationalized measures to manage this higher order level of variables. For example, one study Footnote 87 created a 5-digit code, in which each digit captures the value of five distinct exposure measures (an illustration is provided in the Supplementary File, Section 5.2). These types of higher-order joint stratification measures were typically used in MAIHDA Footnote 90, Footnote 95, Footnote 97, Footnote 98, or MAIHDA-like analyses (e.g., the "Eco-intersectional Multilevel Model" Footnote 87.
Analysis
In fifteen of the studies, the integration of the principle of intersecting categories within statistical analyses was done by including an interaction (product) term between two or more measures in regression-based analyses Footnote 55, Footnote 57, Footnote 99–Footnote 102, Footnote 74, Footnote 75, Footnote 77, Footnote 78, Footnote 83, Footnote 91, Footnote 94, Footnote 95. Alternatively, as mentioned above, at least six studies directly included joint stratification measures that captured every strata combination between two or more measures in their models Footnote 87, Footnote 90, Footnote 95, Footnote 97, Footnote 98.
Interaction terms were included in models to assess for effect measure modification. However, as it is understood in statistical theory, these analyses are scale dependent. Logistic, log-binomial, and proportional hazards models were used in several studies, and can help identify statistical interaction on a multiplicative scale. When these types of models were applied, some studies applied additional analyses to also estimate effect measure modification on the additive scale, using metrics such as Relative excess risk due to interaction (RERI) Footnote 55, Footnote 78, Footnote 79, Footnote 88, Footnote 94.
Two studies assessed inter-categorical experiences and identities using a causal mediation analysis approach Footnote 53, Footnote 91. These studies applied analyses that were informed by Baron and Kenny’s mediation analysis framework Footnote 103, and that have been designed to improve validity Footnote 104. Using information on the outcomes across joint stratification measures, as defined by the exposure and mediator measures, mediation analysis can be used to estimate direct and indirect effects of a main "exposure" measure (see Glossary for definitions) (e.g., a social position measure such as race) and the role of a potential mediating pathways or mediator (e.g., experiences of discrimination) to determine population health outcomes.
One study applied a decomposition analysis, to explore the potential determinants of inequalities between two groups, based on a measure of income Footnote 84. This method allowed for the exploration of outcomes across joint stratification measures, as defined by the hypothesized determinants and the measure of income.
Six studies explored outcomes across joint stratification measures using stratified analyses Footnote 54, Footnote 73, Footnote 74, Footnote 92, Footnote 101, Footnote 105, which can help detect differences in associations or outcome patterns across sub-groups. These types of analyses were more feasible when a smaller number of stratification measures were used, and when sample sizes allowed for such disaggregation.
Lastly, six studies applied other methods such as multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) analyses Footnote 90, Footnote 95, Footnote 97, Footnote 98, or MAIHDA-style analyses (e.g., "Eco-intersectional Multilevel Model" Footnote 87, as well as Classification and Regression Tree (CART) analyses Footnote 85. These types of analyses help detect population sub-groups, marked by certain joint positions or characteristics, who may experience a higher or lower disease burden. MAIHDA analyses do not require the use of interaction terms. Rather, in these analyses, joint stratification measures which capture every possible combination of social stratification measures are used (as described above). The modeling technique is used to assess variance and random effects across identified sub-groups.
In the next section, we discuss in greater detail how studies incorporated measures or analyses of measures that capture characteristics, and how multi-level MAIHDA analyses operationalize multi-level dimensions.
b) Multi-level analysis
Measures
The principle of multi-level analysis was integrated in the studies’ operationalized measures in two ways. First, some studies included measures that captured units of population aggregation or "clustering", within which there was potential interdependence of outcomes across the target populations measured. These included, for example, province, state, or region of residence Footnote 77, Footnote 99, Census tract of residence Footnote 87, schools Footnote 95, or specific health care clinics at which patients received services Footnote 82.
Second, other studies used individual- and area-level measures as proxies for contextual- and structural-level factors, respectively. For example, self-reported experiences of trauma were used to capture living contexts, and area-level density of poverty and lower educational attainment were used as measures of structural economic inequality Footnote 91.
Similarly, in studies that applied MAIHDA analyses, social locations are understood as outcomes of systems. As Merlo (2018) explains, MAIHDA analyses can be applied when characteristics such individual-level income, education, or race are considered as "contexts shaped by societal systems of oppression and privilege, where social processes and social determinants condition the experiences of individuals within the different intersectional strata" Footnote 106. As noted above in Results Section 3.3b, these studies constructed joint strata measures to capture these intersectional strata. Though MAIHDA can be applied to variables that capture both individual-level exposures (e.g., race, income, etc.) and environmental exposures (e.g., neighbourhood-level crime level), it can also be applied to a series of individual-level characteristics (e.g., income, education, race/ethnicity). A description of how these are operationalized in multi-level analyses is summarized below.
Analysis
The principle of multi-level analysis was integrated in statistical design in several ways. First, some studies performed analyses stratified by unit of aggregation (e.g., by province or region) Footnote 77. Secondly, several studies used regression-based analyses which accounted for potential clustering of individuals within the sample. These included generalized linear mixed effect models Footnote 82, Footnote 99, and random intercept models Footnote 95. Lastly, several studies used MAIHDA analyses (see Glossary for definitions). MAIHDA is described as a form of "multi-level analysis" insofar as it is designed to enable the decomposition of variance within and between intersectional strata to evaluate the contribution of each joint strata on individual heterogeneity in the health outcome Footnote 106. As Evans et al. explain, "multi-level models partition the residual variation in a model into within-group (level 1) and between-group (level 2) variation" Footnote 95. Individual- or area-level measures can be used in these analyses. As mentioned above, reviewed studies interpret individual- and area-level measures as proxies for contextual and structural determinants Footnote 91.
c) Power
In this section, we discuss how studies integrated the principle of sociopolitical power (rather than statistical power) in their analytic design:
Measures
Six studies integrated the principle of power in their analytic design sections, namely by selecting measures, and framing them, as proxies for potential power structures Footnote 84, Footnote 85, Footnote 87, Footnote 90, Footnote 95. Most of the measures that were used as such proxies were area-based measures, to capture contexts of power structures Footnote 90. For example, one study used an area-level measure of educational attainment (percentage of residence with some college education), over and above an area-based measure of income (median household income), as a proxy for area-level social capital and power. Communities with higher social capital and power were described as more likely to be protected against environmental health hazards at the local level Footnote 87. Inversely, this same study used an area-based measure of concentration of female-headed households as a proxy of potential deprivation, and lower power or privilege Footnote 87.
Using individual-level data, study used measures such as individual-level income and gender as markers of relative social power, and used these measures to identify and explain health differences between "dominant" and non-dominant or "subordinate" groups Footnote 84. This was not done with the intention to identify the "most" dominant (or non-dominant) groups in society. Rather, the authors described their variable operationalization approach as one that was used to capture groups that "have an [assumed] structural advantage along one axis" (e.g. here, along income or gender) Footnote 84.
Another study utilized measures such as household composition, household wage earner status, and perceived social support Footnote 85 to capture the potentially modifiable processes that create unequal power relations between sex/gender groups.
Analysis
One study that used environmental measures as proxies of structures and contexts of power applied a MAIHDA analysis Footnote 90. In this study, individuals were considered to be nested within joint strata of context types (e.g., based on the proportion of students receiving public assistance within each school studied; based on neighborhood disadvantage). In this analysis, the effects of these contexts of power were allowed to vary across individual-level measures of social identity and position. This method was used to assess the ways that intersecting social processes influence health inequalities Footnote 90.
d) Reflexivity
To assess how the principle of reflexivity was integrated in study design, we explored whether and how studies demonstrated reflexive practices, namely if and how researchers acknowledged their own positions, their experiences of privilege, their underlying methodological assumptions or theoretical perspectives, and how the latter may be shaped by broader systems of power and social position experiences.
Overall, none of the reviewed studies included an explicit statement of positionality or reflexivity (see Glossary for definitions) about the research team or their practices. Reflection on the relative diversity of research teams, in terms of personal, professional, substantive backgrounds has been recommended as an important direction for future intersectionality-informed population health research Footnote 8.
Measures
As noted above, five studies were explicit about how measures were chosen and what they were assumed to represent, in terms of proxies for broader systems of power Footnote 84, Footnote 85, Footnote 87, Footnote 90, Footnote 95. One study also offered reflection of the choice and meaning of identified reference categories Footnote 82.
Analysis
Two studies presented directed acyclic graphs (DAGs) (see Glossary for definitions) to describe the assumed direction of associations (i.e. causal ordering) of study measures Footnote 53, Footnote 79. DAGs were developed a priori, based on extant literature, to guide variable selection and inform the choice of covariates for statistical adjustment. Authors used the DAGs to identify a set of adjustment factors that captured confounding measures, rather than potential mediating pathways. Another reflexive practice applied at the statistical analysis stage was to state the potential analytic assumptions and limitations, and test the potential impacts of these assumptions and limitations using sensitivity analyses. This was done in a limited handful of studies Footnote 53, Footnote 82. For example, one study applied Bonferroni corrections when testing multiple associations between various study measures Footnote 92. Lastly, one study chose to compare population sub-group outcomes to that of the full population’s average, in order to avoid having to select a static reference group Footnote 82.
e) Space and time
Data sources
The principle of time was integrated in the five studies that applied a longitudinal Footnote 57, Footnote 76, Footnote 83, Footnote 98 or repeat cross sectional design Footnote 77. These types of design utilized data sources that captured individuals’ or communities’ experiences across several calendar time points, thus enabling an analysis of temporal variation in experiences and outcomes.
Measures
The latter studies used measures to capture changes in experiences or outcomes overall and across groups, between two or more calendar time points Footnote 77, Footnote 83, Footnote 98.
As noted above, the principle of space was integrated in the study design by using measures that captured spatial units of population aggregation (or spatial "clustering"). These included, for example, the use of measures to capture province, state, or region of residence Footnote 77, Footnote 78, Footnote 99, Census tract of residence Footnote 87, schools Footnote 95, specific health care clinics at which patients received services Footnote 82, or geographic areas within a country such as border towns Footnote 54.
Analysis
At the analytic stage, several practices were used to assess spatial and temporal variations of experiences and outcomes. As noted above, several studies performed analyses stratified by unit of aggregation (e.g., by province or regionFootnote 76, or by applying regression-based analyses which accounted for potential spatial clustering of individuals. These included generalized linear mixed effect models Footnote 82, Footnote 99 and random intercept models Footnote 95.
Similarly, two of the studies performed stratified analyses by time period and tested for changes in outcomes between time periods using regression-based modeling Footnote 77, Footnote 98.
f) Diverse knowledges
The intersectionality theory principle of diverse knowledge refers to the integration of data and information from a wide range of actors and experts, including individuals and groups who may not traditionally be included in scientific or policy decision-making processes. Only two studies reviewed were identified as having integrated the diverse knowledge principle in their analytic design.
Data source
Exploring how studies acknowledged or engaged with typically marginalized communities or integrated diverse voices or forms of knowledge, two studies were identified as having integrated the principle of "diverse knowledges" in their selection of data sources. Both studies utilized mixed-methods design Footnote 54, Footnote 81. One study conducted open-ended interviews with key informants to collect qualitative data Footnote 81, in addition to performing a survey. The survey was administered to individuals who inject drugs, while interviews were conducted with those offering health or harm reduction services to people who use drugs, in California Footnote 81. The other study included open-ended questions in their survey design, which allowed for a collection of more detailed, qualitative data Footnote 54. The survey was administered to individuals who had given birth, near versus farther away from the US border with Mexico Footnote 54. The use of mixed-methods research approaches has been identified as an important future direction for the integration of intersectionality in quantitative health research Footnote 8.
Analysis
Both of the studies described above performed qualitative thematic analyses of these open-ended responses, and used this additional source of information to complement their analysis and interpretation of quantitative survey-based data Footnote 54, Footnote 81. However, none of the latter studies indicated whether or how targeted populations—given their unique knowledges of historical contexts, social determinants, and community needs—were engaged in the designing the analyses. These details were absent from the studies.
g) Social justice
Measures
One of the ways that studies were identified as integrating the principle of social justice, was through their selection of exposure and outcome measures. Two studies utilized exposure measures that were assumed to be modifiable, and were named and used as such, for their potential as targets for policy intervention Footnote 53, Footnote 85. That is, the authors explicitly chose to study measures that, they believed, could be amenable to policy intervention. As such, this methodological design choice was interpreted to be aligned with the principle of social justice. This approach is aligned with calls for intersectionality-informed population health research to determine how their analyses will guide policies and interventions to improve health equity and social justice Footnote 8.
More specifically, it is aligned with the notion of needing to orient research towards informing policies that can address injustices and inequalities. One study utilized measures to capture the assumed modifiable processes that create unequal power relations between sex/gender groups Footnote 85. These included measures such as household wage earner status and perceived social support Footnote 85. Another study focused on a mediator measure of discrimination, which was also assumed to be modifiable Footnote 53. Another study integrated the principle of social justice through its choice of outcome (dependent) measure Footnote 87. This study explored the outcome of estimated cancer risk from air pollutants, and explicitly selected this measure (and the assessment of inequalities in its distribution) as a metric of environmental injustice. Here, environmental injustice refers to systematic, avoidable inequalities in exposure to environmental hazards across communities, based on income, race and other markers of social position Footnote 87. The study frames the cancer risk measure as a target for social and environmental justice advocacy and action.
Analysis
At the analytic stage, one study applied a causal mediation analysis approach Footnote 53, using a mediating factor that was assumed to be modifiable through policy intervention. This was one done explicitly to be able to inform strategies and potential areas of intervention to reduce inequalities.
h) Equity
Measures
All of the studies reviewed employed exposure (independent) measures to identify sub-populations (i.e. population strata) that could be compared to compute health inequality estimates. As mentioned above, joint stratification measures were often constructed using these measures Footnote 77, Footnote 80, Footnote 82, Footnote 87. Use of these measures enabled the identification of avoidable inequalities (inequities) in outcomes across groups.
Analysis
In the reviewed papers, both descriptive statistics and regression-based modeling approaches were utilized to measure the scope of avoidable inequalities (i.e., inequities) between groups. These included estimation of prevalence or rate ratios Footnote 55, Footnote 78–Footnote 80, Footnote 83, Footnote 88, hazard ratios Footnote 57, odds ratios (e.g., Footnote 75, Footnote 91, Footnote 95, Footnote 98, Footnote 100), prevalence or risk differences Footnote 53, Footnote 76, Footnote 98, Footnote 100, Footnote 84, Footnote 87, Footnote 89, Footnote 91, Footnote 93–Footnote 95, Footnote 97.
One study used concentrative curve, concentration index, and GINI coefficient measures Footnote 77. These measures capture the cumulative proportion of the population against the cumulative proportion of those with the identified outcome. It the outcome is equally distributed, these two proportions should coincide.
Table 5: Promising practices for integrating intersectionality theory in the analytic design of quantitative health equity analysis
| ANALYTIC DESIGN | Intersecting categories | Multi-level analysis | Power | Reflexivity | Time and Space | Diverse knowledge | Social Justice | Equity |
|---|---|---|---|---|---|---|---|---|
Data source(s) |
Collect or use data that allows comparison across intersecting characteristics |
Collect or use data that identifies potential units of aggregation (schools, cities, provinces) |
Utilize repeat cross-sectional or longitudinal data to capture changes through time |
Include qualitative data (interviews, open survey questionnaire items) |
Collect or use data that allows comparison between multiple groups |
|||
Measures |
Use joint strata measures that capture potential combination of two or more exposures (identities, social stratifying measures, experiences, etc.) |
Measure units of aggregation (schools, cities, provinces) |
Explore stratifying measures that represent proxies of social capital or power (e.g., area-level education, area-level % female-headed households) |
|
|
|
Use social stratification measures to capture outcomes across sub-groups |
|
Analysis |
|
|
Apply statistical analyses that can accommodate area-based measures that are used as proxies for structures of power |
|
|
|
Apply statistical analyses to identify the fundamental drivers of observed inequalities (e.g., regression-based analyses decomposition analyses), or the potential mediating pathways of health inequalities that could be modified through policy intervention (e.g., causal mediation analysis) |
Describe and statistically test absolute (i.e., on the additive scale) and relative inequalities differences between groups |
3.4 Integration of intersectionality in interpretation
Herein, the "interpretation" section of articles refers to the Results and Discussion sections of texts, including content on the presentation and interpretation of results, and the discussion of study implications and limitations.
Studies included between two and eight principles in this section, with only one study integrating all eight. Most articles incorporated 5 principles (mode=5).
Similar to the rationale section, the two most commonly integrated principles in the interpretation section of the 34 articles reviewed were principles of "intersecting categories" (100% of articles) and of "equity" (100% of articles). In descending order, the other most commonly integrated principles in this section of the articles were elements of "multi-level analyses" (82% of articles), "power" (68%), "social justice" (50%), "time and space" (41%), "reflexivity" (21%) and "diverse knowledges" (21%) (Figure 4). A narrative summary of how these principles were integrated is presented here, with a summary in Table 6.
a) Intersecting categories
Presentation and interpretation of results
As mentioned above, all studies explored two or more social stratification measures, with some constructing joint stratification measures to capture intersecting measures of identity or social position. Aligned with the principle of intersecting categories, the studies reviewed presented outcome values (e.g., prevalence, incidence rates) as well as inequality measures (e.g., odds or rate ratios, or rate differences, etc.) stratified by identified subgroups (e.g., Footnote 53). Articles that produced effect measure modification or interaction analysis presented and discussed the results of these analyses Footnote 79, Footnote 100. Authors clarified interpretations based on whether additive or multiplicative interaction was observed (e.g., Footnote 91).
Discussion of implications
Aligned with the principle of intersecting categories, studies recommended de-prioritizing the analysis and reporting of health inequalities along one single axis (e.g., gender), and instead prioritizing analysis along two or more axes of social identity, and to study effect modification Footnote 97, Footnote 98. However, authors such as Evans et al. Footnote 98 do note, that though the experiences of sub-groups may be distinct, statistical differences (e.g., statistically significant interaction) at a population health level may not always be identifiable. This is of particular relevance when samples are small, and statistical power is not sufficient to identify small effect sizes. Careful presentation and interpretation of null findings is needed to explain that an absence of statistically significant findings does not mean that there is a true absence of experienced differences.
Discussing the policy implications of their findings, seven studies highlighted the importance of policy and program intervention that addresses multiple concurrent forms of interpersonal and institutional discrimination or disadvantage Footnote 8, Footnote 53, Footnote 55, Footnote 76, Footnote 81, Footnote 84, Footnote 88.
b) Multi-level analysis
Presentation and interpretation of results
As mentioned above, many studies utilized measures of spatial aggregation, such as province or region of residence. Aligned with the principle of multi-level analysis, when describing results, studies presented outcome values (e.g., prevalence, incidence rates) as well as inequality measures (e.g., odds or rate ratios, or rate differences) stratified by spatial sub-groups (e.g., Footnote 77) Similarly, articles that applied multi-level regression-based analyses presented and discussed the results of these analyses (e.g., Footnote 87).
Overall, studies tended to refer back to their guiding theoretical frameworks to interpret inequalities (intersectionality and others) Footnote 54, Footnote 55, Footnote 57, Footnote 82, Footnote 88, Footnote 91, Footnote 92, Footnote 102, Footnote 105. For example, studies discussed how observed inequalities across multiple sub-groups are likely shaped by factors that operate above the individual-level, such as labour market forces, or immigration or health care policies (e.g., Footnote 57, Footnote 92). This acknowledgement of multi-level determinants of health is aligned with the principle of multi-level analysis.
Discussion of implications
Studies highlighted the importance of policy and program intervention that would target area- or structural-level factors, rather than individual-level factors alone Footnote 76, Footnote 80, Footnote 81, Footnote 86, Footnote 87. For example, one study of environmental determinants of cancer risk highlighted the importance of implementing pollution regulation policies and policy enforcement strategies to reduce inequalities in residential exposures to harmful emissions (e.g., Footnote 87). Another study highlighted the importance of interventions to reduce structural discrimination (e.g., strategies to improve marginalized groups’ access to health care), above and beyond strategies to reduce interpersonal discrimination Footnote 76.
c) Power
Presentation and interpretation of results
Echoing the definitions of intersectionality presented in the rationale section of articles, eleven studies interpreted their observed findings of effect modification and interaction between various social positions in relation to intersectionality theory’s understanding of interlocking systems of power.Footnote 57, Footnote 76, Footnote 102, Footnote 77, Footnote 85, Footnote 86, Footnote 89, Footnote 92, Footnote 94, Footnote 97, Footnote 101
Similarly, the study that applied statistical decomposition methods to assess the determinants of observed inequalities (e.g., Footnote 84) interpreted findings using an intersectionality theory lens, by highlighting the role of systems of power and privilege in shaping health and social differences in risk (e.g., Footnote 84). The latter study emphasized the importance of considering groups all along a power hierarchy or spectrum, not just those at the highest or lowest rung Footnote 84.
Discussion of implications
As mentioned above, several studies highlighted the importance of policy and program intervention that would target structural-level factors to address power inequalities (e.g.,Footnote 41,Footnote 62,Footnote 63,Footnote 76).
Among the studies that used MAIHDA analysis, one study recommended that this type of analysis could be used to identify populations that may be most disadvantaged by interlocking systems of power Footnote 90.
Discussing the policy implications of their findings, five studies highlighted the importance of policy and program intervention to address mediating determinants of power inequalities Footnote 8, Footnote 53, Footnote 79, Footnote 84 that is, of promoting interventions to empower disadvantaged groups, and reducing any barriers they may face in achieving health or social well-being. In the case of one study, for example, finding that health care-related factors mediated the intersecting effects of race/ethnicity and sexual orientation on Pap test screening for cervical cancer, the authors discussed the relevance of promoting access to health insurance to reduce observed inequalities Footnote 75. Studies using a mediation analysis approach recommended this analytic design specifically for its ability to identify sources of power differentials that could be the targets of policy intervention Footnote 53.
d) Reflexivity
Discussion of limitations
All studies acknowledged the limitations of their data sources and analyses. This section of articles’ discussions represents a valuable opportunity for reflexivity. Some important limitations noted by articles, which were aligned with intersectionality theory’s principle of reflexivity in relation to power and privilege, included the following: First, a recognition of the absence of diverse voices or perspectives integrated throughout the study process to better understand drivers of inequalities Footnote 57, Footnote 78, Footnote 80, Footnote 91. Engagement with the communities and stakeholders that are implicated in the research topic, throughout the study process, has been identified as a key direction for future intersectionality-informed quantitative health research Footnote 8.
Second, studies acknowledge a lack of data that could capture variation across space Footnote 94, Footnote 95 or time Footnote 53, Footnote 78, Footnote 100 or structural-level determinants Footnote 78. Third, studies also noted a recognition of the potential limitations of the categories used when operationalizing study measures Footnote 97.
At least one study acknowledged that they did not fully integrate all central tenets of intersectionality theory, as they were not able to make policy recommendations, nor did they explore multi-level determinants of health or social outcomes Footnote 101.
e) Space and time
Presentation and interpretation of results
As mentioned above, some studies used measures of space or time to explore spatial and temporal variation in outcomes or inequalities. Aligned with the principle of space and time, one study presented outcome values (e.g., prevalence, incidence rates) as well as inequality measures (e.g., odds or rate ratios, or rate differences, etc.) stratified by space and time measures Footnote 77. Another study included a summary of relative or absolute changes in outcomes through time Footnote 98. Information on changes in all three components (outcome values overall, absolute and relative inequalities) provide key pieces of information to interpret whether and how inequalities have changed over time.
Discussion of limitations
Discussing the implications of their findings for future research, three studies highlighted the importance of considering space and setting (be it rural versus urban, across provinces/countries, across occupational sectors, etc.) when seeking to explore and better understand health inequalities Footnote 76, Footnote 81, Footnote 90. One study also noted how findings may not be generalizable across all spatial contexts or units of aggregation Footnote 92.
f) Diverse knowledges
Presentation and interpretation of results
In the two mixed-methods studies, excerpts of first-person narratives were presented in the results section Footnote 54, Footnote 81. For example, in one of the studies, these were direct quotes from key informants who were either individuals who offered harm reduction services to people who inject drugs, or individuals who reported injection drug use in the past year Footnote 81. These two studies interpreted their quantitative analysis findings in relation to the themes that emerged from qualitative analyses Footnote 54, Footnote 81.
Discussion of implications
As mentioned in Results Section 3.1d, four studies recommended that public health programs be culturally adapted and targeted towards diverse sub-populations that faced higher disease or outcome burden Footnote 55, Footnote 82, Footnote 83, Footnote 102. Similarly, six studies recommended to improve culturally-safe and appropriate health care Footnote 54, Footnote 55, Footnote 75–Footnote 77, Footnote 79. In one study for example, finding inequalities in Pap test screening uptake for cervical cancer, authors discussed the importance of targeted public health programs that could help address fears or myths regarding HPV and Pap screening within racial or sexual minority sub-groups Footnote 75. Another study highlighted the need for culturally-adapted interventions to address problematic alcohol use, suggesting that programs be targeted in culturally-safe and relevant spaces Footnote 83. These recommendations were interpreted as examples of result interpretation that acknowledge diverse perspectives, particularly of vulnerable or marginalized populations. However, none of the latter studies indicated whether or how targeted populations—given their unique knowledges of historical contexts, social determinants, and community needs—could or should be engaged in the design, implementation, or evaluation of these interventions. These details were absent from the studies.
Discussion of limitations
As mentioned previously, at least four studies acknowledged the limitations of their data sources and analyses, and highlighted the need to integrate research methods that actively involve members of marginalized groups throughout the research process Footnote 80, including the use of qualitative research methodologies Footnote 57, Footnote 78, Footnote 80, Footnote 91.
g) Social justice
Discussion of implications
When discussing the policy implications of their findings, eleven studies highlighted the need to address the fundamental social determinants of population health outcomes, in order to improve both population-level health and reduce health inequalities Footnote 54, Footnote 57, Footnote 105, Footnote 77, Footnote 79, Footnote 80, Footnote 84, Footnote 86, Footnote 91, Footnote 101, Footnote 102. As mentioned previously, several studies highlighted the importance of policy and program intervention that would target structural-level factors to address power inequalities (e.g., Footnote 76, Footnote 80, Footnote 81. These types of policy recommendations are aligned with the principle of social justice. Specifically, the need to transform social structures and systems of power that create inequalities Footnote 16.
Three studies noted how the integration of intersectionality theory as a guiding theoretical framework is in itself a step towards integrating the principle of social justice in research practice Footnote 73, Footnote 85, Footnote 105.
h) Equity
Presentation and interpretation of results
As mentioned above, all studies explored inequalities in outcomes between groups. Aligned with the principle of equity, articles presented inequality measures (e.g., odds or rate ratios, or rate differences, etc.), in table or graphical format (e.g., bar or forest plots, e.g., Footnote 84). Examples of data visualization techniques used are presented in the Supplementary Material 7.4 Results: Data visualizations. Similarly, articles that conducted effect measure modification or interaction analysis, or mediation or decomposition analysis, or MAIHDA-style analyses presented and discussed the results of these analyses (e.g., Footnote 79, Footnote 84, Footnote 100). Among those conducting effect modification analysis, some clarified interpretations based on whether additive or multiplicative interaction was observed (e.g., Footnote 91).
Discussion of implications
Discussing the policy implications of their findings, studies highlighted the importance of designing policy specifically targeted to reduce observed health inequalities while still improving overall population-level health (e.g., Footnote 75, Footnote 80, Footnote 102). Many of these proposed actions involved combining universal policies with targeted interventions for the most disadvantaged Footnote 75, Footnote 77, Footnote 80. For example, this could include making policy changes to improve overall access to health insurance and care, while promoting local public programs targeted specifically to disadvantaged communities (e.g., Footnote 75). This is aligned with the proportionate universalism approach to reduce health inequities Footnote 65.
As mentioned above, several studies also highlighted the importance of policy and program intervention that would target structural-level factors to address power inequalities (e.g., Footnote 76, Footnote 80, Footnote 81). These types of policy recommendations are aligned with the principle of equity. Specifically, they acknowledge that inequalities are avoidable and require intervention Footnote 16.
Table 6: Promising practices for integrating intersectionality theory in the interpretation phase of quantitative health equity analysis
| INTERPRE-TATION | Intersecting categories | Multi-level analysis | Power | Reflexivity | Time and Space | Diverse knowledges | Social Justice | Equity |
|---|---|---|---|---|---|---|---|---|
| Presentation and interpretation of results | Present and interpret:
|
|
Refer to principles of intersectionality theory to interpret the results: discuss interlocking systems of power |
Present outcome burden and inequalities, stratified by units of time and space |
Present and interpret:
|
|
||
Discussion of implications |
Discuss relevance of studying inequalities according to multiple axes of social position |
Propose implications for policy from the individual- to structural-level |
Discuss:
|
|
Propose potential policy implications, with a focus on structural determinants of power and fundamental determinants of health |
|
||
Discussion of limitations |
Acknowledge:
|
Acknowledge if multi-level measures or analyses were not used, and the potential implications of this gap |
Acknowledge:
|
Acknowledge if measures of time or space were not considered, and the potential implications of this gap |
Acknowledge if diverse voices were not considered or included, and the potential implications of this gap |
3.5 Summary of promising practices: SIITHIA checklist
A synthesis of the observed promising practices summarized in Sections 3.1 to 3.4, including in tables 4-5, is presented below. Findings are summarized using a checklist format, modeled after checklists such as the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist Footnote 107 (see Section 7.5 STROBE checklistfor details). Here, the Strengthening the Integration of Intersectionality Theory in Health Inequality Analysis (SIITHIA) checklist is proposed. Reviewed by only a small set of experts (N=10), and informed by a limited set of studies (N=34) this checklist should be interpreted as a prototype that can and should evolve over time, based on, as the STROBE initiative notes "comments, critique and new evidence" Footnote 107. We do not posit that the identified procedures and methods should be defined as an exhaustive list of standard or "best" practices. Rather, they represent directions that could continue to be explored, in tandem, in future analyses that aim to meaningfully integrate intersectionality theory in analyses of health inequalities between population sub-groups. Ideally, the SIITHIA checklist would be used in combination with other checklists such as STROBE Footnote 107, which are focused on ensuring methodological rigour and transparency, to guide the planning and reporting of health inequality analyses. Lastly, it should be noted that due to this review’s focus on studies that explored inequalities between sub-populations to guide future HIRI analyses, the proposed checklist will likely be most useful for so-called "inter-categorical" data analyses (see Glossary for definitions) Footnote 18. Future expansion of the checklist, for application in other types of analyses will likely be warranted.
| Study/ Report section | Item | Promising practice | Section of reference in this report |
|---|---|---|---|
| Introduction | |||
| Background/ Rationale |
1. | Provide a well-referenced definition of intersectionality theory, which alludes to its central principlesFootnote *. | 3.1b 3.2c |
| 2. | Describe inequalities that are consistently observed between population groups, and that are assumed to be avoidable, as "unjust/unfair" and requiring action. | 3.2g 3.2h |
|
| 3. | Describe the known determinants of the outcome of interest that operate at, and above, the individual level. | 3.2b | |
| 4. | State and describe underlying assumptions underpinning the study, including a reflexivityFootnote * or positionalityFootnote * statement from the research team. | 3.2d 3.3d |
|
| 5. | Integrate and summarize evidence developed through research and analysis that involve populations that are affected by the inequalities under study or forms of knowledge that have been under-represented in public health practice. | 3.1b 3.4f |
|
| Objectives | 6. | Draw on, and describe literature and complementary theoretical frameworks (including those from outside the field of health sciences), as needed, to justify and frame the research questions and objectives. | 3.1b 3.2d |
| 7. | Explore one or more objectives relevant to intersectionality theory, including: | ||
| a) Assessing effect modification or interaction between two or more measures capturing axes of marginalization, in determining health and social outcomes and inequalities. | 3.2a | ||
| b) Exploring to what extent observed health and social inequalities are explained by a given sub-set of characteristics or factors at the individual, community, or societal level. | 3.2b 3.2d 3.2h |
||
| c) Assessing changes in determinants, outcomes and inequalities therein (i.e., associations between determinants and outcomes), over time and across contexts. | 3.2e | ||
| 8. | Engage with people and populations that are affected by the inequalities under study when establishing research questions and objectives. | 3.2f 3.4d |
|
| Methods | |||
| 9. | Engage with populations that are affected by the inequalities under study, when designing the methods. | 3.3f | |
| Data source(s) | Where possible and relevant to the research question: | ||
| 10. | Collect or use data that allow a comparison of outcomes across intersecting social positionsFootnote *. | 3.3a | |
| 11. | Collect or use data that allow for an assessment of heterogeneity in determinants and outcomes Footnote * across social or spatial units of aggregation (e.g., schools, regions). | 3.3b 3.3e |
|
| 12. | Collect or use data that allow for an assessment of heterogeneity in outcomes across time (including temporal contexts based on calendar time, and inter-generational and lifecourse perspectives). | 3.3e | |
| 13. | Collect or use data that allows for an assessment of independent measures that are hypothetically modifiable, and therefore amenable to intervention. | 3.3g | |
| 14. | Collect or use qualitative data (e.g., using interviews, focus groups, open-ended survey questions, program evaluations, etc.) to complement quantitative data sources, in a mixed-methods research design approach. | 3.3f | |
| Measures | Where relevant to the research question, operationalize independent measures that enable an assessment of outcomes across: | ||
| 15. | Two or more axes of marginalization; | 3.3a | |
| 16. | Units of social or spatial aggregation or clustering; | 3.3b 3.3e |
|
| 17. | Temporal contexts (including contexts based on calendar time, and inter-generational and lifecourse perspectives). | 3.3e | |
| 18. | Operationalize and utilize independent measures that are hypothetically modifiable, and therefore amenable to intervention. | 3.3g | |
| 19. | Describe assumptions about the relationship between study measures, including the assumed direction and temporal ordering of associations, using a causal map or Directed Acyclic Graph Footnote *. | 3.3d | |
| 20. | Describe assumptions about the broader social phenomena that measures are assumed to capture or represent. | 3.3c | |
| 21. | Describe and justify selected reference categories. | 3.3d | |
| Analysis | |||
| 22. | Select/design analyses according to study objectives. For example: | ||
| a) For objective 7a (assessing effect modification between two or more measures) potential analyses could include i) stratified analyses, ii) regression-based analyses with interaction terms, iii) or multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) analyses | 3.2a 3.3a |
||
| b) For objective 7b (exploring determinants of inequalities), potential analyses could include i) causal mediation or ii) decomposition analyses | 3.2h 3.3a |
||
| c) For objective 7c (assessing changes across time and place), potential analyses could include i) stratified descriptive analyses based on social, temporal, and/or geographic contexts, ii) multivariate mixed-effects regression analyses | 3.3b 3.3e |
||
| 23. | Assess both absolute and relative inequalities between groups. | 3.3a | |
| 24. | In regression-based analyses, use a parsimonious set of adjustment variables based on the causal map described (Item #19). | 3.3d | |
| 25. | State and test underlying analytic assumptions using sensitivity analyses. | 3.3d | |
| 26. | Where relevant to the research question, analyze qualitative data, using methods most appropriate for the study’s objectives. | 3.3f | |
| Results | |||
| 27. | Present and discuss determinants, outcomes, and inequalities therein, stratified by i) relevant sub-groups, ii) units of space, iii) units of time. | 3.4a 3.4b 3.4e |
|
| 28. | Present and interpret effect modification results, distinguishing between additive and multiplicative interaction. | 3.4a | |
| 29. | If available and relevant for the research question, present the results of the mixed-methods or qualitative analyses that were performed (Item #26), including key illustrative quotations. | 3.4f | |
| Discussion | |||
| 30. | Engage with populations that are affected by the inequalities under study, for the review and interpretation of findings. | 3.4g | |
| Findings | |||
| 31. | Refer to principles of intersectionality theory when interpreting the plausible mechanisms explaining results. | 3.4c | |
| Implications | |||
| 32. | Describe the implications of the study for public health practice, as well as policy and systems change. | 3.1d 3.4g |
|
| 33. | Describe the implications of the study for the potential population targets of intervention (e.g., universal policy, targeted/proportional universalist policy). | 3.4h | |
| Limitations | |||
| 34. | Describe how key/core principles of intersectionality were or were not integrated in the study. | 3.4d 3.4f 3.4g |
|
| 35. | Describe any limitations of data sources (including statistical power), measures and analyses, and their implications. | 3.4d 3.4f 3.4g |
|
| 36. | Include reflexivity about the power invested in (and reproduced by) the methods used. | 3.4d | |
|
|||
4. Discussion
Intersectionality theory offers a useful theoretical lens to better understand the etiology of, and potential areas of intervention against, avoidable and systematic health and social inequalities. However, its application and use across substantive fields of scholarship such as public health and epidemiology are hampered by a lack of clear guidance on how to operationalize and integrate each of the theory’s principles Footnote 17, Footnote 21, particularly across every methodological step, from background research, to objective setting, to methodological design, and results interpretation. The objectives of this review were to identify promising practices of ways to integrate each of the principles of intersectionality theory in quantitative analyses of health inequalities between population sub-groups.
Applying a rapid review design, and using the IBPA framework’s eight principles Footnote 16 to guide our analysis, we identified a subset (N=34) of studies that aimed to integrate intersectionality theory in their analysis of health or health-related inequalities. Within these 34 studies, we identified over 35 practices that represent promising directions for the integration of intersectionality theory in quantitative analyses of health inequalities. These practices were implemented across steps of research and surveillance design, from conceptualization to reporting. We summarize these practices in a checklist format, in the Results’ Section 3.5 of this report, in the proposed "Strengthening the Integration of Internationality Theory in Health Inequality Analysis (SIITHIA)" checklist. We do not posit that the identified procedures and methods should be defined as standard or "best" practices. Rather, they represent directions that could continue to be explored, in tandem, in future analyses that aim to meaningfully integrate intersectionality theory in health inequality analysis.
Several of the identified practices are aligned with those proposed in previous studies and reviews, to overcome existing gaps in intersectionality-informed quantitative analysis Footnote 17, Footnote 20. Namely, identified promising practices aim to ensure meaningful engagement with the principles of intersectionality theory Footnote 17, Footnote 20, including the acknowledgement of structural forms of discrimination through policies and institutional practices Footnote 22. The identified practices also invite reflection on the construction of study measures Footnote 23, and integrate both descriptive and analytic objectives and methods Footnote 17, Footnote 24.
4.1 Implications for the HIR Initiative
The primary purpose of this technical report was to guide future enhanced quantitative data analysis for the Pan-Canadian Health Inequalities Reporting (HIR) Initiative. Past and current HIR Initiative analyses have aimed to assess the presence and magnitude of health inequalities in Canada across key health and social indicators, using a predefined set of health inequality metrics (see Box 4). To meet these objectives, the Initiative has employed a mostly bivariate analysis design strategy (exceptions include age-standardized rate estimation), with analysis stratification by sex, and by province and territory of residence. Based on the findings of this review, a recommended next step for future enhanced HIR Initiative analysis planning, will be to attempt to implement the promising practices summarized in the Results’ Section 3.5’s SIITHIA checklist, for a small subset of research questions and key health indicators. Whereas the HIRI’s web-based Health Inequalities Data Tool (see Box 4) presents bivariate or stratified bivariate data visualization using histograms (bar charts), the data visualization output for these potential multivariate pilot analyses could resemble those presented in the Supplement’s Section 7.4 Results: Data visualizations.
These pilot analyses will be useful to assess the feasibility of applying the proposed practices, using Canadian data sources, within the context of a national, multi-stakeholder and –jurisdictional health inequalities reporting initiative. Though the checklist and the language and references used in this report represent important resources that can be leveraged for future reporting, additional insights will likely be gleaned through the process of applying the identified practices. This additional nuance can be used to iteratively adapt the SIITHIA checklist and its recommended promising practices for the HIR initiative and beyond.
Box 4: HIRI’s Health Inequalities Data Tool
HIRI’s web-based Health Inequalities Data Tool describes health and social inequalities between population sub-groups using several metrics. These include: rate ratios, rate differences, attributable fractions, population attributable rates, population attributable fractions, and population impact numbers.
The Health Inequalities Data Tool is available online: https://health-infobase.canada.ca/health-inequalities/inequality-measures
4.2 Implications for health inequalities reporting
Overall, integration of the principles of intersectionality theory in health inequalities analysis and reporting in Canada and beyond can be expected to have several important impacts for improving population health and health equity. First, intersectionality theory urges a reflexive consideration of underpinning philosophies and theories, methods, and constructed concepts implied in analytic design Footnote 8. Stronger consideration and questioning of underpinning assumptions can help problematize long-standing traditions that may unintentionally perpetuate harms and oppression Footnote 17. Second, integrating intersectionality theory can enable analyses to take into consideration how systems of oppression and social categories are co-constitutive and mutually-reinforcing. Instead of examining one system or category of difference at a time, this approach encourages the consideration of how systems co-occur Footnote 18, Footnote 19, for example – how income inequalities are gendered or racialized, etc. Thus, this approach will align future analyses with population health’s understanding that health inequalities are determined by intersecting systems and structures that represent "fundamental" determinants of health Footnote 3. Third, intersectionality theory acknowledges how health determinants and outcomes can vary across time and contexts. Integrating these considerations in analytical design can help guide targeted interventions Footnote 21. Lastly, intersectionality theory centers the importance of policy and systems change that can help reduce and eliminate inequities. Designing analyses and interpreting findings through this action-oriented lens can help ensure the consequentialism of health inequality analyses, to seek to improve population health and health equity.
4.3 Limitations
The findings of this review should be interpreted within the context of certain limitations. First, the search strategy was non-exhaustive and therefore likely missed other examples of studies of health inequalities that applied intersectionality theory. It is possible that other promising practices could be identified, to build on the findings of the present review. For example, none of the reviewed studies herein applied latent class analysis or principle component analysis, which have been discussed in previous reviews Footnote 21, Footnote 108. As these methods do not provide a clear reference or comparison group, Footnote 21 they are less relevant for analyses such as those performed by HIRI, of health inequalities between population sub-groups. Nonetheless, they can play an important role for hypothesis generation Footnote 21. As the number of epidemiologic studies that integrate intersectionality theory increases, updated review of statistical methods will likely be warranted. Guan et al. (2022)’s systematic review of statistical methods for assessing intersectionality Footnote 21 is a rich resource for readers to explore in concert with the checklist described in this report’s Section 3.5.
Second, due to the limitations of the review’s scope, certain areas of analysis were not explored. For example, in our analyses of studies’ integration of the principle of "intersecting categories", we did not assess whether or how authors explored the co-constitution of social categories. This represents an important topic for future analysis. Similarly, due to the intended purpose of this review to guide future HIRI analyses on inequalities between two or more sub-groups, this review focused exclusively on studies that explored so-called inter-categorical analyses. It did not explore how studies operationalize and explore intra-categorical measures such as "gendered racism" Footnote 24, Footnote 109. This topic is therefore lacking in the present review and the SIITHIA checklist, and represents an important area to consider in future reviews and analyses.
Third, none of the studies reviewed indicated whether populations who experienced the studied inequalities were engaged in the definition of the research questions, study design, development of data collection instruments, analysis, interpretation of data, and knowledge mobilization. This has been identified as a promising practice for the integration of intersectionality theory Footnote 8, particularly of the guiding principle of diverse knowledges. However, its application was not observed in the reviewed works. Future reviews, as well as applications of the SIITHIA checklist in practice settings, will require a consideration of how community engagement is performed in a way that does not reinforce existing power structures. Extant literature on community-based research Footnote 8 will provide a key resource for these future endeavors.
Fourth, this rapid review did not include a quality assessment of the research design of the included studies. Any plans to replicate the identified studies, without consideration of ways to improve the quality and rigour of the methods used should be avoided. Nonetheless, aligned with its primary objective, this review did include a quality assessment of the integration of intersectionality theory principles throughout the studies’ designs. This information is novel and intended to provide a more fulsome roadmap for the integration of intersectionality theory in future health inequality research and surveillance initiatives.
5. Conclusion
Meaningful engagement with intersectionality theory has been identified as "essential in order to maintain the critical and transformative edge of intersectionality" Footnote 19, to ensure that our analyses contribute to tackling structures and processes of oppression. This review identified ways that extant studies have attempted to integrate intersectionality theory at each step of research or surveillance design, from conceptualization to reporting. Together, these approaches can guide future research, evaluation and surveillance methodologies, and help strengthen quantitative intersectionality-informed analyses of health inequalities.
Recommended reading
Introductory texts on intersectionality to guide potential readers of this report:
- Hankivsky, O. (2014). Intersectionality 101. Vancouver: The Institute for Intersectionality Research and Policy, Simon Fraser University. https://bccampus.ca/wp-content/uploads/2020/07/Hankivsky-Intersectionality101-2014.pdf
- Morrison, V. (2014). Health inequalities and intersectionality. Montréal, QC: National Collaborating Centre for Healthy Public Policy. http://www.ncchpp.ca/docs/2015_Ineg_Ineq_Intersectionnalite_En.pdf
- Hankivsky, O., Grace, D., Hunting, G., Ferlatte, O., Clark, N., Fridkin, A., Giesbrecht, M., Rudrum, S., & Laviolette, T. (2012). Intersectionality-Based Policy Analysis. Vancouver: the Institute for Intersectionality Research and Policy, Simon Fraser University. https://data2.unhcr.org/en/documents/download/46176
- Hankivsky, O., Doyal, L., Einstein, G., Kelly, U., Shim, J., Weber, L., Repta, R. (2017) The odd couple: using biomedical and intersectional approaches to address health inequities. Glob Health Action. Jan-Dec 2017;10(sup2):1326686. doi: 10.1080/16549716.2017.1326686.
Glossary
Definitions of key intersectionality and inequality analysis terminology (in alphabetical order):
- Anticategorical analysis:
- Defined in McCall (2005), this analytic approach is interested in the deconstruction of analytical categories. It is based on the premise that social life is deemed too irreducibly complex to make fixed categories anything but simplifying social fictions that produce inequalities in the process of producing differences Footnote 18. See McCall (2005) for additional details and examples Footnote 18.
- Categories of difference:
- Defined in Dhamoon (2010), these are measures, factors, or concepts that capture constructs of difference between groups in society. Examples could include gender or race Footnote 5. In epidemiology, these could be utilized as "exposure" or "risk factor" measures.
- Continuum of disadvantage:
- This concepts refers to inequalities that can occur between social groups all along categories of difference that are typically continuous in nature, such as income level, in relation to a dominant group (e.g., those in a highest income decile). In health sciences, this is referred to as "gradient" Footnote 110. For example, scholars refer to the gradient in life expectancy across income levels, wherein life expectancy increases with every higher step in the income distribution, rather than across a threshold of income (e.g., below versus above a specific income value) Footnote 110.
- Cultural safety:
- This concept originated in New Zealand from the field of nursing education. It is a framework of practice that does not simply focus on "understanding indigenous culture" (p. 30 in Footnote 111). Instead this framework "considers the social and historical contexts of health and health care inequities" (p. 30 in Footnote 111). In this framework, practitioners apply self-reflexive practice to consider their role and position of power in relation to clients or patients Footnote 111. Safety is "defined by those who receive service not those who provide it" (p. 30 in Footnote 111).
- Directed Acyclic Graph:
- Directed Acyclic Graphs are graphical representations of the assumed direction of associations between various measures. Developed a priori before epidemiologic analyses, they are used to inform variable selection for statistical conditioningFootnote 112.
- Diverse knowledges:
- Based on one of Critical Race Theory’s key principles of centering the voices and perspectives of under-represented groups, the Intersectionality Based Policy Analysis concept of "diverse knowledges" refers to the importance of including the perspectives and worldviews of people who are typically excluded in the production of knowledge. Doing so can help to disrupt dominant discourses and help redistribute power Footnote 16.
- Effect modification:
- Also referred to as "effect measure modification" or "heterogeneity" Footnote 113, it is a phenomenon in epidemiology which "two or more risk factors modify the effect of each other with regard to the occurrence or level of a given outcome" (p. 185 in Footnote 27). Depending on the context, it can also be described as "association modification" Footnote 27 or "risk-difference modification" or "risk-ratio modification" Footnote 113. However, "effect modification" is used widely in the literature to describe both "causal and noncausal interactions" (p.185 in Footnote 27).
- Epistemological frames or framing:
- See epistemology.
- Epistemology:
- It is "the philosophical theory of knowledge—of how we know what we know" Footnote 114. Epistemology is the investigation of the "origin of knowledge; the place of experience in generating knowledge, and the place of reason in doing so; the relationship between knowledge and certainty, and between knowledge and the impossibility of error; the possibility of universal scepticism; and the changing forms of knowledge that arise from new conceptualizations of the world" Footnote 115.
- Exposure:
- In epidemiology, the term "exposure" is used to refer to any factor that may be associated with an outcome of interest (see Outcome, definition below) that is under study Footnote 116. In the context of intersectionality-informed analyses, "categories of difference" or "social locations" could be treated as "exposures" in statistical analyses.
- Identity or identities:
- Markers of the sub-groups defined along categories of difference (See: Categories of difference, above). Examples could include: Black, woman, queer identities Footnote 5.
- Interaction:
- Generally, interaction refers to a situation where two or more things or factors have an effect on each other Footnote 115. In epidemiology, interaction occurs when the risk of an outcome (disease, condition, etc.) in the presence of two or more risk factors (i.e. exposures), differs from the risk that would be expected to result from the individual effects of each risk factor. Statistical interaction refers to the "interdependence between the effects of two or more factors within the confines of a given model of risk" (p. 74 in Footnote 117) (also called effect modificationFootnote 113, see above). Biologic interaction refers to "the interdependent operation of two or more causes to produce disease" (p.74 in Footnote 117).
- Inter–categorical analysis:
- Defined in McCall (2005), this analytic approach is interested in the relationships of inequality between social groups, defined along multiple axes of identity or social position. It uses categories to better understand these relationships Footnote 18.
- Interlocking oppression(s):
- This term refers to the co-constitutive and mutually reinforcing systems of oppression that create social positions, and hierarchies of domination and subordination Footnote 118.
- Interlocking systems:
- See "interlocking oppressions". This term refers to systems that are interdependent, that "need one another" (p.2 in Footnote 5) to function and persist.
- Intersectionality theory :
- Originating from Black feminist theorizing Footnote 10, Footnote 12, Footnote 13, intersectionality theory is a theoretical framework of the ways in which interlocking, co-constitutive systems of power and oppression operate across time, place, and societal levels, to construct (and be enabled by) multiple social locations along axes such as race, gender, class, and sexual orientation. It is an analytic approach that stresses a need to consider the multiple, intertwined dimensions of social position and their structural determinants.
- Intracategorical analysis:
- Defined in McCall (2005), this analytic approach is interested in studying particular social groups that exist at neglected points of intersection, to reveal the complexity of lived experience within such groups. This approach interrogates the boundary-making and boundary-defining process of creating and defining social groups and categories of difference (see above). It acknowledges the stable and even durable relationships that social categories represent at any given point in time, though it also maintains a critical stance toward categories Footnote 18.
- Joint stratification (measure):
- This term refers to variables that are operationalized to capture intersection of identities or social positions. These constructed variables identify all the possible strata combinations of two more of measures. For example, a joint stratification measure capturing intersections between a measure of race with two operational categories (Black, white) and a measure of sex/gender with two operational categories (men, women), would include the following four categories: Black women, Black men, white women, white men.
- MAIHDA:
- An acronym for "multilevel analysis of individual heterogeneity and discriminatory accuracy". This type of analysis is designed to enable the decomposition of variance within and between intersectional strata to evaluate the contribution of each joint strata on individual heterogeneity in the health outcome Footnote 106. The approach is described by Guan et al. (2022) as follows: "The first step of the MAIHDA approach involves creating a "social strata" variable that corresponds to every social position of interest. Example, if interested in gender (male/female) and race (White, Black, Latino), the MAIHDA analysis would create a social strata variable with six unique categories. The multilevel MAIHDA model nests individuals (level 1) within their social strata (level 2). There are several MAIHDA models with corresponding interpretations. In a null model, the total variation between social strata is represented by the between-stratum variance parameter. In a MAIHDA model adjusting for main effects, the stratum specific residual can be interpreted as the remaining total "interaction effect" that remains unexplained by the main effects" Footnote 21. The latter can be described as the effect attributable to the intersection of gender and race.
- "Oppression Olympics" :
- Coined by Martinez (1993), this phenomenon occurs when "groups compete for the title of ‘most oppressed’ in order to gain political support, economic resources, and recognition. Intersectionality thus rejects an additive model of oppression that leaves the systems that create power differentials unchanged" (p.36 in Footnote 16).
- Outcome:
- In epidemiology, the term "outcome" is used to refer to any factor that is under consideration as a dependent variable in statistical analyses Footnote 116. A study may explore a health outcome (e.g., diabetes). However, social determinants could also be studied as "outcome" variables, as done commonly in other substantive domains (social sciences, economics, demography, etc.). For example, a study could explore the association between gender and the "outcome" of educational attainment.
- Positionality:
- Positionality refers to "the power inherent in [peoples’] immediate respective social positions, [which] greatly influences the differences in what individuals have access to in society" (p. 26 in Footnote 28). A "positionality statement" often refers to a written statement in which researchers reflect on their social positions or locations within systems of power, as well as their underlying assumptions. See also: "Reflexivity".
- Power:
- In this report and intersectionality literature, the term power typically refers to sociopolitical power as described and theorized by scholars such as Michel Foucault Footnote 119. Power refers to the arrangements that govern relationships between individuals. Systems of power (see also "Systems of domination") shape socials positions such as race (see "Categories of difference"), as well as "experiences of privilege and penalty between and among groups" (p. 35 in Footnote 16). In the context of population health, systems of power shape distributions of agency and access to health promoting resources across populations, as well as which types of knowledge and experiences are included or excluded in research or decision-making Footnote 16.
- Processes of differentiation :
- Defined in Dhamoon (2010), this refers to the sum of processes through which categories of difference (see above) are constructed and populations are differentiated Footnote 5. Examples include processes of racialization, gendering, sexualisation Footnote 5.
- Proportionate universalism:
- Defined by Marmot and Bell (2012), a proportionate universalist policy making approach involves considering "both the people at the bottom of the health gradient and the gradient as a whole, ensuring that their impact [of policy] is proportionately greater at the bottom end of the gradient" (p.S10) where the need is greatest Footnote 65.
- Reflexivity:
- This principle of intersectionality refers to the importance of recognizing power (see "Power") at the level of the self and our relationships with others, as well as at higher levels of society. In the context of research and policy analysis, reflexivity refers to the need for practitioners to acknowledge and deconstruct underlying assumptions and structures of oppression Footnote 16.
- Relative excess risk due to interaction (RERI):
- When studying two binary risk factors, e.g., A and B, and having measured the relative risk of exposure B on an outcome Y in the presence of A (RRB,A=1) and in the absence of A (RRB,A=0), as well as the relative risk of exposure A on Y in the absence of B (RRA.B=0), the RERI metric captures the "departure from additivity of effects [between A and B on Y] on a relative risk scale" (p.1 in Footnote 120). It is applied as follows: RERI = RRB=1,A=1 - RRB=1,A=0 - RRA=1.B=0 + 1.
- Social categories:
- See "categories of difference". Social categories are constructs of difference between groups in society, such as gender, race, ethnicity, class, sexuality, ability Footnote 5. In the context of intersectionality theory, these categories are acknowledged to be socially constructed, and can vary across time and contexts Footnote 16. In epidemiology, these could be considered as "exposure" or "risk factor" measures.
- Social justice:
- This refers to the objective of achieving equity in society, namely by challenging the sources or causes of inequities, including relationships, structures, or policies Footnote 16.
- Social location:
- This refers to an "externally imposed situation arising from the patterned attribution of positive and negative qualities to perceived social identities" (p.48 in Footnote 118) It is the result of how identity categories "interaction in terms of privileges and disadvantages and functions at more of a practical or everyday level" (p.45 in Footnote 118).
- Social position:
- See "categories of difference".
- Social stratification measure(s):
- See "categories of difference". These are measures that capture constructs of difference between groups in society, e.g., gender, race. In epidemiology, these might be described as "exposure" or "risk factor" measures.
- Systems of domination:
- Defined in Dhamoon (2010), these refer to "historically constituted structures of domination" (p.5 in Footnote 5). That is, structures that enable the subjugation of certain people or populations, to the benefit of others. Examples of these systems include racism, colonialism, sexism, patriarchy, heterosexism Footnote 5.
- Systems of oppression:
- See "systems of domination".
- Systems of power:
- See "systems of domination".
7. Supplementary material
7.1 Search strategy
PubMed
Query: (((Intersectionality[Title/Abstract] OR intersectional [Title/Abstract])) AND (public health OR population health OR health equity OR health inequalities OR health inequities OR epidemiology OR social determinants of health OR marginalization OR marginalized OR marginalisation OR marginalised OR oppressed OR discrimination OR stigmatized OR stigmatization OR stigmatisation OR stigmatised OR social identity* OR social position* OR vulnerability OR vulnerable OR race OR racialized OR race-based OR ethnicity OR ethnocultural group* OR ethnocultural concentration OR LGBTQ2+ OR LGBT OR LGBTQ OR sexual orientation OR sexual minority OR gender-based OR socioeconomic status OR indigenous people* OR indigeneity OR rural OR urban OR immigrant* OR ability* OR disability* OR age)) AND (quantitative OR mixed)
Search performed: July 7, 2021
Total: 166 results
Medline
Database(s): Ovid MEDLINE(R) ALL 1946 to June 28, 2021
Search Strategy:
| # | Searches | Results |
|---|---|---|
1 |
health status disparities/ or health services accessibility/ or health status indicators/ or health equity/ or social determinants of health/ or minority health/ |
122865 |
2 |
(inequalit* or equalit* or equit* or inequit* or in-equit* or disparit* or underserved or marginali#ed or discriminat* or vulnerab*).tw,kw,kf. |
552170 |
3 |
1 or 2 |
643789 |
4 |
empirical research/ or evaluation studies as topic/ |
125923 |
5 |
(quantitative* or mixed or statistic*).ti,kf. or (quantitative* or mixed or statistic*).ab. /freq=2 |
690956 |
6 |
4 or 5 |
811910 |
7 |
intersectional*.tw,kf. |
2206 |
8 |
3 and 6 and 7 |
54 |
Global Health (Ebsco)
Database(s): Global Health 1973 to 2021 Week 25
Search Strategy:
| # | Searches | Results |
|---|---|---|
1 |
health inequalities/ or exp health indicators/ or health determinants/ |
9430 |
2 |
(inequalit* or equalit* or equit* or inequit* or in-equit* or disparit* or underserved or marginali#ed or discriminat* or vulnerab*).tw,id. |
112482 |
3 |
1 or 2 |
113661 |
4 |
(quantitative* or mixed or statistic*).ti,id. or (quantitative* or mixed or statistic*).ab. /freq=2 |
110676 |
5 |
intersectional*.tw,id. |
549 |
6 |
3 and 4 and 5 |
22 |
Scopus
(TITLE ( inequalit* OR equalit* OR equit* OR inequit* OR "in-equit*" OR disparit* OR underserved OR marginali?ed OR discriminat* OR vulnerab* ) OR AUTHKEY ( inequalit* OR equalit* OR equit* OR inequit* OR "in-equit*" OR disparit* OR underserved OR marginali?ed OR discriminat* OR vulnerab* ) ) AND ( TITLE ( quantitative* OR mixed OR statistic* ) OR AUTHKEY ( quantitative* OR mixed OR statistic* ) ) AND ( TITLE ( intersectional* ) OR AUTHKEY ( intersectional* ) ) 21 Results
7.2 Results: Data extraction
A copy of the study’s data extraction table (Excel file) is available upon request from:
phac.health.inequalities-inegalites.en.sante.aspc@canada.ca
7.3 Results: Measure illustrations
For MAIHDA-style analyses, studies can created a multi-digit independent measure code, in which each digit captures the value of five distinct exposure measures. Here is an illustration of what such a code can represent:
| Multi-digit code value | Group meaning |
|---|---|
"23110" |
2= Black (vs. White=0, Latinx=1) 3=Income tercile 3 (vs. terciles 1,2) 1=Education tercile 1 (vs. terciles 2,3) 1=Urban (vs. Rural=0) 0=Female-headed household (vs Male=1) |
"03110" |
0= White (vs. Latinx=1, Black=2) 3=Income tercile 3 (vs. terciles 1,2) 1=Education tercile 1 (vs. terciles 2,3) 1=Urban (vs. Rural=0) 0=Female-headed household (vs Male=1) |
7.4 Results: Data visualizations
This section presents examples of data visualization tools presented in reviewed studies (n=34) to display the findings of their intersectionality-informed analyses.
a) Heat maps
Example: Friedman J, Syvertsen JL, Bourgois P, Bui A, Beletsky L, Pollini R. Intersectional structural vulnerability to abusive policing among people who inject drugs: A mixed methods assessment in California’s central valley. Int J Drug Policy. 2021;87. https://doi.org/10.1016/j.drugpo.2020.102981
- An example of a heat map can be found in Figure 1 of this article, entitled "Figure 1. Multivariate Associations between Vulnerability Factors and Police Interaction Outcomes." It depicts a table, with 6 rows of independent "vulnerability factor" measures, six columns of "policy interaction outcomes" dependent measures. Cells present the covariate-adjusted odds ratio (with 95% confidence intervals in parentheses) between each set of variables. Darker cells indicate stronger associations, while lighter cells indicate weaker associations. The color scale indicates the direction of the association, where green is protective, and purple indicates heightened risk.
b) Bar graphs (histograms)
Example 1: Albright DL, McDaniel J, Suntai Z, Horan H, York M. Pregnancy and Binge Drinking: An Intersectionality Theory Perspective Using Veteran Status and Racial/Ethnic Identity. Matern Child Health J. 2021;25(8). https://doi.org/10.1007/s10995-021-03171-x
- An example of a stratified bar graph can be found in Figure 1 of this article, entitled "Figure 1. Prevalence of binge drinking among pregnant women by veteran status and race/ethnicity, 2016-2018". The horizontal axis depicts veteran status (yes or no), the vertical axis depicts the prevalence of binge drinking (%). There are two bars per veteran status group: one bar for racial or ethnic minority respondents, another for white respondents. Prevalence values are presented for each group: racial/ethnic minority veterans, white veterans, racial/ethnic minority non-veterans, white non-veterans.
Example 2: Bauer GR, Scheim AI. Methods for analytic intercategorical intersectionality in quantitative research: Discrimination as a mediator of health inequalities. Soc Sci Med. 2019;226. https://doi.org/10.1016/j.socscimed.2018.12.015
- An example of a horizontal bar graph can be found in Figure 4 of this article, entitled "Figure 4. Intersectional components of effects on psychological distress, mediated by past-year day-to-day discrimination". This figure has 3 vertical panels. For each panel, the horizontal axis depicts effect sizes (here, in relation to differences in self-reported psychological distress scores), and the vertical axis identifies respondent sub-groups (here, by race/ethnicity identity). In the first panel, the horizontal bars depict the direct effect, indirect effect, and mediated interaction effect of discrimination for each of the race/ethnicity sub-groups. These effects are the results of causal mediation analyses.
Example 3: Beccia AL, Baek J, Jesdale WM, Austin SB, Forrester S, Curtin C, et al. Risk of disordered eating at the intersection of gender and racial/ethnic identity among U.S. high school students. Eat Behav. 2019;34. https://doi.org/10.1016/j.eatbeh.2019.05.002
- An example of a cumulative bar graph can be found in Figure 1 of this article, entitled "Figure 1. Ade-adjusted relative excess risk of disordered eating due to additive interaction (RERI) between girl gender and Hispanic/Latino ethnic identity, using White boys as the reference group". This figure has 4 vertical panels. For each panel, the vertical axis depicts the risk ratios (on a log scale), and the horizontal axis depicts three distinct respondent sub-groups: Hispanic/Latino Boys, White Girls, and Hispanic/Latina Girls. Each panel presents results for a distinct measure of disordered eating. In each panel, the vertical, cumulative bars depict the risk associated with marginalized ethnic identity, marginalized gender identity, and the relative excess risk due to interaction, respectively. Additionally, a text box is added to each figure to describe the value of the relative excess risk due to interaction (RERI).
c) Scatter and forest plots
Example 1: Axelsson Fisk S, Lindström M, Perez-Vicente R, Merlo J. Understanding the complexity of socioeconomic disparities in smoking prevalence in sweden: A cross-sectional study applying intersectionality theory. BMJ Open. 2021;11(2). https://doi.org/10.1136/bmjopen-2020-042323
- An example of a stratified, vertical scatter plot can be found in Figure 2 of this article, entitled "Figure 2: Absolute risk (ie, prevalence) and 95% Cis of smoking in different intersectional strata according the National health survey in Sweden between 2004 and 2018". The vertical axis of the figure presents prevalence rates of smoking. The horizontal axis depicts stratified sub-groups, by immigration status, living arrangement, sex, age, and income. The data points in the graph depict the prevalence estimates for each sub-group, with 95% confidence interval "whiskers" or error bars.
Example 2: Friedman J, Syvertsen JL, Bourgois P, Bui A, Beletsky L, Pollini R. Intersectional structural vulnerability to abusive policing among people who inject drugs: A mixed methods assessment in California’s central valley. Int J Drug Policy. 2021;87. https://doi.org/10.1016/j.drugpo.2020.102981
- An example of a vertical scatter plot can be found in Figure 4 of this article, entitled "Figure 4. Risk of Police Interaction Outcomes with Increasing Numbers of Vulnerability Factors". This figure represents one manner of visualizing the intersectional risk to police outcomes associated with increasing numbers of personal vulnerability factors. This figure has six panels. One panel is shown for each outcome. For each panel, the vertical axis depicts outcome prevalence, the horizontal axis depicts distinct respondent sub-groups: the overall population, males, males in rural areas, males in rural areas who are homeless, males in rural areas who are homeless and have a low education. Each panel presents results for a distinct measure of police interaction. In each panel, the scatter points depict the outcome prevalence in each sub-group. The baseline group, which has zero vulnerability factors, is represented on the far left. Vulnerability factors are introduced in a stepwise fashion according to the magnitude of positive association observed in adjusted odds ratios.
Example 3: Evans CR, Erickson N. Intersectionality and depression in adolescence and early adulthood: A MAIHDA analysis of the national longitudinal study of adolescent to adult health, 1995–2008. Soc Sci Med. 2019;220. https://doi.org/10.1016/j.socscimed.2018.10.019
- An example of a stratified, vertical scatter plot can be found in Figure 1 of this article, entitled "Predicted Values of CESD by Stratum in Wave 1". The vertical axis of the figure presents the predicted prevalence values of depression scores. The horizontal axis depicts stratified sub-groups, by sex, race/ethnicity, and income group. The data points in the graph depict the depression score values for each sub-group, with 95% credible interval "whiskers" or error bars for each point. Estimates are adjusted for age.
Example 4: Alvarez CH, Evans CR. Intersectional environmental justice and population health inequalities: A novel approach. Soc Sci Med. 2021;269. https://doi.org/10.1016/j.socscimed.2020.113559
- An example of a vertical forest plot can be found in Figure 2 of this article, entitled "Figure 2. Predicted Cancer Risk by Stratum, ranked from low to high". The figure has two panels, presenting results with and without outlier observations. For each panel, the vertical axis of the figure presents predicted cancer risk. The horizontal axis depicts the rank of social group strata (based on the size of predicted risk, ranked from low [rank 1] to high [rank 2016]). A scatter plot point is presented for each social group strata, with 95% credible interval "whiskers" or error bars for each point.
d) Decision trees
Example: Mena E, Bolte G. CART-analysis embedded in social theory: A case study comparing quantitative data analysis strategies for intersectionality-based public health monitoring within and beyond the binaries. SSM - Popul Heal. 2021;13. https://doi.org/10.1016/j.ssmph.2020.100722
- An example of a decision-tree plot can be found in Figure 1 of this article, entitled "Figure 1. Splitting variables, proportion of study population and prevalence of FMD within subgroups (nodes) detected by CART-analysis based on binary sex/gender variable and intersectional variables of the full sample (Model1)". "FMD" refers to frequent mental distress. This figures depicts a flowchart-like structure, that begins with a central text box. From this initial point, nodes emerge, each connecting to a subsequent text box, and so forth, such that a network of nodes and boxes are presented. In this figure, each text box presents information of the prevalence of mental distress, for a distinct population sub-group, based on sex, marital status, and disability status.
e) Concentration curves
Example: Joe W. Intersectional inequalities in immunization in India, 1992-93 to 2005-06: A progress assessment. Health Policy Plan. 2015;30(4). https://doi.org/10.1093/heapol/czu023
- An example of a concentration curve plot can be found in Figure 1 of this article, entitled "Figure 1. Concentration curves for immunization in India, 1992-93 and 2005-06". The figure has three panels. For each panel, the vertical axis of the figure presents the proportion of the burden in the population (0% to 100%). The horizontal axis depicts the proportion of the population (0% to 100%). A line of "equality" runs at 45 degrees across each panel, to indicate a true state of equality. Two curves are depicted on the figures, indicating the distribution of burden of non-immunization for two periods, respectively.
7.5 STROBE checklist
STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist of items that should be included in reports of observational studies:
| Item No | Recommendation | |
|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | ||
| Introduction | ||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported |
| Objectives | 3 | State specific objectives, including any pre-specified hypotheses |
| Methods | ||
| Study design | 4 | Present key elements of study design early in the paper |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection |
| Participants | 6 | (a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up Case-control study —Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls Cross-sectional study —Give the eligibility criteria, and the sources and methods of selection of participants |
| (b)Cohort study—For matched studies, give matching criteria and number of exposed and unexposed Case-control study —For matched studies, give matching criteria and the number of controls per case | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable |
| Data sources/ measurement | 8Footnote * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group |
| Bias | 9 | Describe any efforts to address potential sources of bias |
| Study size | 10 | Explain how the study size was arrived at |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding |
| (b) Describe any methods used to examine subgroups and interactions | ||
| (c) Explain how missing data were addressed | ||
| (d) Cohort study—If applicable, explain how loss to follow-up was addressed Case-control study —If applicable, explain how matching of cases and controls was addressed Cross-sectional study —If applicable, describe analytical methods taking account of sampling strategy | ||
| (e) Describe any sensitivity analyses | ||
| Results | ||
| Participants | 13Footnote * | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed |
| (b) Give reasons for non-participation at each stage | ||
| (c) Consider use of a flow diagram | ||
| Descriptive data | 14Footnote * | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders |
| (b) Indicate number of participants with missing data for each variable of interest | ||
| (c) Cohort study—Summarise follow-up time (e.g., average and total amount) | ||
| Outcome data | 15Footnote * | Cohort study —Report numbers of outcome events or summary measures over time |
| Case-control study— Report numbers in each exposure category, or summary measures of exposure | ||
| Cross-sectional study— Report numbers of outcome events or summary measures | ||
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included |
| (b) Report category boundaries when continuous variables were categorized | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses |
| Discussion | ||
| Key results | 18 | Summarise key results with reference to study objectives |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results |
| Other information | ||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based |
Note: The STROBE checklist is available from
https://www.strobe-statement.org/
|
||
8. Acknowledgements and Authors
This report is a product to guide the Pan-Canadian Health Inequalities Reporting (HIR) Initiative. The HIR Initiative is a collaborative effort of the Public Health Agency of Canada (PHAC), Statistics Canada, the Canadian Institute for Health Information (CIHI), and the Pan-Canadian Public Health Network (PHN). The PHN is a coordinating body of federal, provincial and territorial public health departments.
We would like to thank Katherine Merucci from the Health Canada Library for her assistance with the literature review search, as well as Radhika Sultania for her support with the report’s references and bibliography. We would also like to thank Natalie Osorio for her work on the preparation of this report for web-based publication. Lastly, we would like to thank the Canadian Institutes of Health Research (CIHR) for their support in facilitating the peer-review of this report.
We would also like to thank the generous contributions of reviewers who provided critical feedback on this report and the proposed Strengthening the Integration of Intersectionality Theory in Health Inequality Analysis (SIITHIA) checklist: Dr. Greta Bauer, Dr. Carla Hilario, Aganeta Enns (PHAC), Geoff Hynes (CIHI), Mayuri Mahendran (CIHI), Christina Catley (CIHI), Julie Stratton (CIHI), Brian Schnarch (CIHI), Nicole Aitken (Centre for Population Health Data, Statistics Canada), and Lawson Greenberg (Centre for Population Health Data, Statistics Canada). The analyses and conclusions in this report do not necessarily reflect those of the reviewers or their affiliated organizations.
Authors
At PHAC, this report was prepared by a core team within the Social Determinants of Health Division’s Equity Analysis and Policy Research team: Dr. Alexandra Blair, Ali El-Samra, MScPH, Dr. Dolon Chakravartty, Colin Steensma, MSc, Dr. Madeleine Bird, Dr. Beth Jackson.