
Pertussis in Canada: 2012


Download this article as a PDF (256 KB - 10 pages)
Published by: The Public Health Agency of Canada
Issue: Volume 40-3: Pertussis
Date published: February 7, 2014
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 40-3, February 7, 2014: Pertussis
Surveillance
Pertussis Surveillance in Canada: Trends to 2012
Smith T1*, Rotondo J1, Desai S1, Deehan H1
Affiliation
1 Public Health Agency of Canada, Center for Immunization and Respiratory Infectious Diseases, Ottawa, ON
Correspondence
DOI
https://doi.org/10.14745/ccdr.v40i03a01
Abstract
Objective: The purpose of this report is to provide a summary of the pertussis activity in Canada.
Methods: A descriptive analysis of pertussis incidence by year, age group, gender and province/territory was conducted using national surveillance data, clinical administrative data and vital statistics data.
Results: Pertussis is an endemic cyclical disease in Canada with peaks in activity occurring every 2 to 5 years. Canada has experienced a decline in pertussis activity following the introduction of routine pertussis immunization programs. The incidence of pertussis is highest in infants and children. Hospitalization and mortality are more common among infants, particularly those less than three months of age. Trends in pertussis vary by province and territory. Canada experienced a notable increase in incidence in 2012. Reasons for this increase are unknown.
Conclusion: Our understanding of the epidemiology of pertussis in Canada could be enhanced by improved approaches for monitoring the disease. Although the peak in activity observed in 2012 could be an isolated event, further work to support outbreak response in provinces and territories, including rapid research tools and resources, should be considered.
Introduction
In Canada, pertussis has been under national surveillance since 1924 and a target of childhood immunization programs since 1943. Infant, child, adolescent, and adult routine immunization programs exist across Canada, with notable differences in the vaccine product used and schedule of immunization, depending on the province/territoryFootnote 1. The introduction of childhood immunization programs contributed to a significant reduction in disease; however, pertussis remains one of the most commonly reported vaccine preventable diseases in Canada. In early 2012, the Public Health Agency of Canada (the Agency) received reports of increased pertussis activity in multiple jurisdictions which prompted a review of Canadian pertussis data. The purpose of this report is to provide a summary of pertussis activity in Canada since it became notifiable with an emphasis on more recent activity.
Methods
Data Sources
National Case Reports
Nationally reported confirmed cases of pertussis from 1924 to 2011 were extracted from the Canadian Notifiable Diseases Surveillance System (CNDSS) database in March 2013Footnote 2. National pertussis case definitions were published in 1991Footnote 3, 2000Footnote 4 and 2009Footnote 5. Prior to 2000, a confirmed case of pertussis required isolation of Bordetella pertussis and presence of clinically compatible symptoms. Between 2000 and 2008 the case definition required laboratory confirmation (via culture from an appropriate clinical specimen or detection of DNA) or an epidemiological link to a laboratory confirmed cases and one of a list of clinical symptoms. In 2009, the case definition was further refined to require those cases in which B. pertussis DNA was detected to also have clinically compatible symptoms. Confirmed pertussis cases for 2012 were obtained directly from the provinces and territories in March 2013 by the Agency's Centre for Immunization and Respiratory Infectious Diseases, and are preliminary.
Hospitalizations
Pertussis cases reported through the Canadian Immunization Monitoring Program Active (IMPACT) from 1991 to 2012 were extracted from the IMPACT database in April 2013Footnote 6. Data for 2012 are preliminary. IMPACT has provided enhanced data on paediatric pertussis cases treated at tertiary care centres in Canada to the Agency since 1991, initially from 5 centers and then expanded to 10 centers in 1993, 11 centers in 1995 and 12 centers in 1999.
Data on pertussis-related acute care hospitalizations from 1995 to 2010 were extracted from the Canadian Institute for Health Information's (CIHI) Hospital Morbidity Database (HMD) in June 2013. These dates were selected as the data sets were complete for each year. Pertussis hospitalizations were defined as those with the International Classification of Diseases (ICD) version 9 or 10 discharge diagnoses (all diagnosis levels) corresponding to pertussis (0330, 0339, 4843, A370 or A379). Exclusion criteria included hospital transfers and readmissions, with readmissions defined as hospitalizations which occurred <1 year apart.
Vital Statistics
Mortality data were obtained from the Death Database, a national mortality database which includes demographic and medical (underlying cause of death) information collected annually from all provincial and territorial vital statistics registries on all deaths in CanadaFootnote 7. Deaths with an underlying cause of pertussis were identified using the same ICD codes listed above.
Analysis
A descriptive analysis of pertussis incidence by year, age group, gender and province/territory was conducted. Population data for the calculation of rates was obtained from Statistics CanadaFootnote 8. Data sent to CNDSS are aggregated by age group, therefore the calculation of age-specific rates were limited to the following age groups in years <1, 1-4, 5-9, 10-14, 15-19, 20-24, 25-29, 30-39, 40-59, and 60 and over. Confirmed case rates are given per 100,000 population. Provinces/territories that were not able to report case counts were removed from the denominator for the corresponding year. Annual percent change was used to describe changes in reporting rates over time. Incidence rate ratios were calculated to examine gender differences.
Results
Annual Incidence
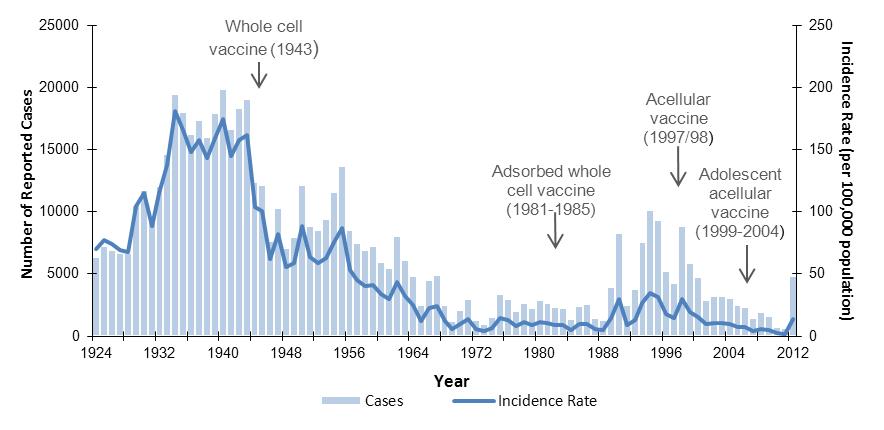
In the five years prior to vaccine introduction, the average incidence of pertussis was 156 cases per 100,000 population. After vaccine introduction, the incidence decreased to a mean annual low of 7 cases per 100,000 population from 1984 to 1988 (Figure 1). A resurgence of pertussis was observed beginning in 1989/90 which peaked at 34.9 cases per 100,000 in 1994. After 1998, incidence declined to the lowest incidence recorded in Canada at 2 cases per 100 000 in 2011. A seven-fold increase in national incidence to 13.9 per 100,000 was observed in 2012. Observing trends over time, peaks in activity occurred every 2 to 5 years. These peaks have become less obvious as incidence of disease has decreased.
Figure 1. Reported cases and incidence rate (per 100,000 population) of pertussis in Canada by year, 1924 to 2012Figure 1 Footnote *
Text Equivalent
This is a combined bar and line graph showing the number of pertussis cases, in bars, and the incidence rate of pertussis per 100,000 population, using a line, in Canada over time. The primary y axis is the number of cases and ranges from 0 to 25,000. The secondary y axis is the incidence rate per 100,000 population and ranges from 0 to 250 cases per 100,000. The x axis is year and ranges from 1924 to 2012. The years in which immunization programs were introduced are also depicted as follows:
- 1943 = whole cell vaccine
- 1981 to 1985 = adsorbed whole cell vaccine
- 1997 to 1998 = acellular vaccine
- 1999 to 2004 = adolescent acellular vaccine
The overall trend of the graph can be broken down into six sections
- An increase between 1924 and 1934, with cases increasing from 6,377 to 19,484 and incidence rate increasing from 68 to 181 cases per 100,000.
- Stable between 1935 and 1943, with the number of cases ranging between 16,003 and 19,878 and the incidence rate ranging between 144 and 175 cases per 100,000.
- A decrease from 1943 to 1975 and stable until 1989, at which point cases ranged between 1301 and 3387 and incidence rates between 5 and 13 cases per 100,000.
- A re-emergence in the 1990s with major peaks in activity occurring in 1990 (cases= 8,330; incidence rate= 30 cases per 100,000), 1994 (cases=10,117; incidence rate= 35 cases per 100,000) and 1998 (cases=8,896 incidence rate= 30 cases per 100,000).
- A decrease from 1998 to 2011, with cases and incidence rate declining steadily to 697 cases and an incidence rate of 2 cases per 100,000.
- A sharp increase in 2012 to 4,845 cases and an incidence rate of 13.9 per 100,000.
Within each overarching trend described above, peaks in activity are observed every 2 to 5 years.
- Figure 1 Footnote 1
-
Case data from 1924 to 2011 were obtained from the Canadian Notifiable Diseases Surveillance System. Case data for 2012 were obtained directly from provinces and territories by CIRID and are preliminary. PEI did not report 1924-1928; Newfoundland did not report until 1949; Yukon did not report 1924-1955; Northwest Territories did not report 1924-1958; Nunavut data for 1999 are only partial, for 2007 & 2009 are missing, and for 2008, 2010-2011 are preliminary. Population data (July 1st annual estimates) were obtained from Statistics Canada.
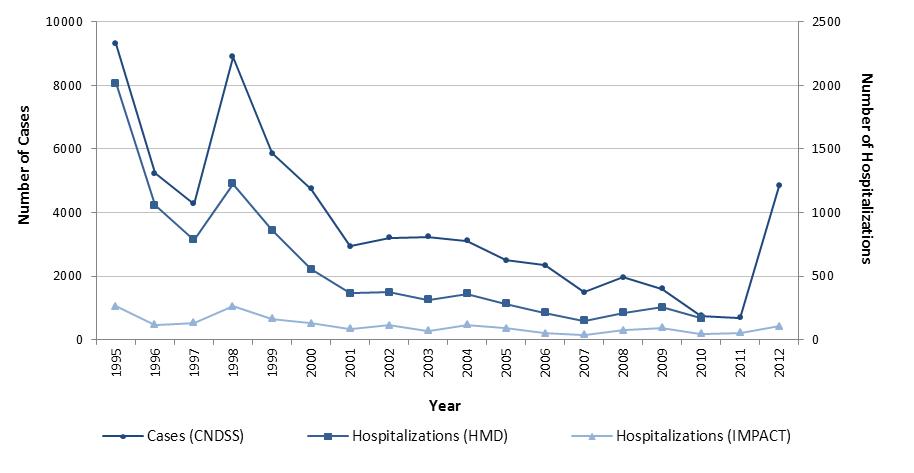
In general, trends in pertussis hospitalization data were similar to those observed in notifiable disease reports (Figure 2). National case reports and acute care hospitalizations decreased by 92% from 1995 to 2010; case reports from 9308 (31.8 per 100,000) in 1995 to 748 (2.2 per 100,000) in 2010, and HMD hospitalizations from 2,016 (6.8 per 100,000) in 1995 to 168 (0.5 per 100,000) in 2010. In this same time frame, IMPACT hospitalizations decreased by 82% from 264 in 1995 to 48 in 2010. Peaks in activity in 1998 and minor increases in 2002 and 2008 were observed across all data sources. However, minor increases in hospital admissions were also observed in 2004 (HMD: 16%; IMPACT: 65%) and 2009 (HMD: 20%; IMPACT: 26%) while case reports declined in these years from the preceding year by 4% and 18% respectively. As with national case reports, cases reported through IMPACT hospitals increased in 2012, but not as dramatically as the national incidence rate of disease (2-fold increase).
Figure 2. Number of reported cases and hospitalizations for pertussis in Canada by year, 1995 to 2012 Figure 2 Footnote *
Text Equivalent
This is a line graph that shows the number of pertussis cases and hospitalizations in Canada over time. The primary y axis is number of cases and ranges from 0 to 10,000. The secondary y axis is number of hospitalizations and ranges from 0 to 2,500. The x axis is year and ranges from 1995 to 2012. There are three lines; one for the number of nationally reported cases of pertussis via the Canadian Notifiable Diseases Surveillance System (CNDSS), one for the number of pertussis hospital admission recorded by the Canadian Immunization Monitoring Program Active (IMPACT) and one for the number of pertussis hospitalizations recorded in the national Hospital Morbidity Database (HMD). The HMD line only goes to 2010. All three lines show similar trends which can be broken down into 4 main sections:
- A decrease between 1995 and 1997: CNDSS from 9308 to 4281 cases, IMPACT from 264 to 135 hospitalizations and HMD from 2016 to 787 hospitalizations.
- A sharp increase in 1998: CNDSS to 8896 cases, IMPACT to 261 hospitalizations and HMD to 1225 hospitalizations
- A steady decrease from 1998 to 2010: CNDSS to 748 cases, IMPACT to 48 hospitalizations and HMD to 168 hospitalizations
- An increase in 2012: CNDSS to 4845 cases and IMPACT to 104 hospitalizations.
- Figure 2 Footnote 1
-
Case data from 1995 to 2011 were obtained from the Canadian Notifiable Diseases Surveillance System. Case data for 2012 were obtained directly from provinces and territories by CIRID and are preliminary. Nunavut data for 1999 are only partial, for 2007 & 2009 are missing, and for 2008, 2010-2011 are preliminary; IMPACT data for 2012 are preliminary.
Age Distribution
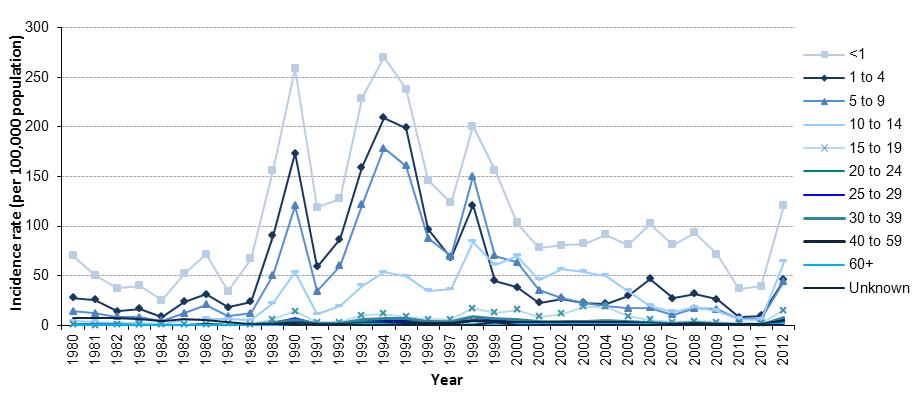
The incidence of pertussis is highest in infants and children, and decreases sharply in those older than 14 years (Figure 3). The highest mean incidence rates from 2005 to 2011 were 72.2 cases per 100,000 population among infants less than 1 year of age (mean: 261 cases per year), 25.6 cases per 100,000 population among 1 to 4 year olds (mean: 362 cases per year), and 16.0 cases per 100,000 population among 10 to 14 year olds (mean: 328 cases per year). Comparatively, the mean incidence of pertussis among all individuals 15 years and greater from 2005 to 2011 was 1.6 cases per 100,000 population (mean: 428 cases per year).
Between 2005 and 2011, the incidence of pertussis decreased in all age groups, most notably among those aged 10 to 14 years (84% decrease) and those aged 15 to 19 years of age (81% decrease). In 2012, increases in incidence were observed across all age groups nationally with the highest incidence rates in those less than one year (120.8 per 100,000; n=460) and those 10-14 years of age (64.1 per 100,000; n=1203). The highest incidence rates in the majority of provinces/territories were within age groups below 15 years of age.
Figure 3. Incidence rate (per 100,000 population) of pertussis reports in Canada by age group (in years) and year, 1980 to 2012Figure 3 Footnote *.
Text Equivalent
This is a line graph that shows the incidence rate of pertussis per 100,000 population by age group in years in Canada over time. The y axis is the incidence rate per 100,000 population and ranges from 0 to 300. The x axis is year and ranges from 1980 to 2012. In the graph there is a line for each of 11 age groups (<1, 1 to 4, 5 to 9, 10 to 14, 15 to 19, 20 to 24, 25 to 29, 30 to 39, 40 to 59, >60, and unknown); however, the incidence rates of cases over 15 years of age and of those with unknown age are so low compared to the younger age groups the values are not discernible.
The less than one year age group has the highest incidence each year. The second highest incidence rate is the 1 to 4 year age group from 1980 to 1996, the 5 to 9 age group from 1997 to 1999, the 10 to 14 age group from 2000 to 2005, the 1 to 4 age group from 2006 to 2011 and the 10 to 14 age group in 2012. The less than one group had its lowest incidence in 1984 with 25 cases per 100,000 and highest incidence in 1994 with 270 cases per 100,000. In 2012, the less than one group had 121 cases per 100,000.
- Figure 3 Footnote 1
-
Case data from 1980 to 2011 were obtained from the Canadian Notifiable Diseases Surveillance System. Case data for 2012 were obtained directly from provinces and territories by CIRID and are preliminary. Nunavut data for 1999 are only partial, for 2007 & 2009 are missing, and for 2008, 2010-2011 are preliminary. Population data (July 1st annual estimates) was obtained from Statistics Canada and uses.
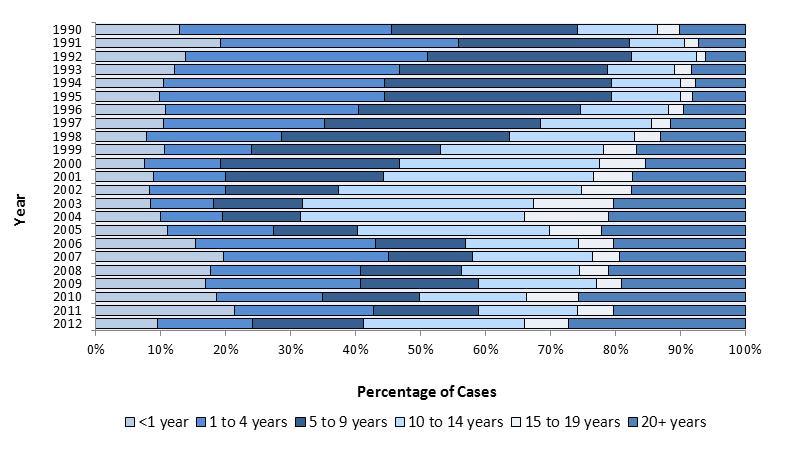
Fluctuations in the proportion of pertussis cases by age group have occurred in the last twenty years, particularly among children aged 1 to 9 years and adolescents aged 10 to 19 years (Figure 4). During the 1990s, the highest proportion of cases occurred in the 1 to 9 year age groups (mean: 62% per year). Between 2000 and 2005, the proportion of cases in adolescent age groups (i.e. 10 to 19 years) increased and was on average 42% of cases per year, while the proportion of cases among those 1 to 9 decreased to an average of 30% per year. Between 2006 and 2011, cases 10 to 19 years of age decreased (mean: 23% per year), while the number of cases 1 to 9 years increased marginally (mean: 38% per year). As these larger shifts occurred, minor increases occurred in infants (<1 year) and adults (20 years and older) from respective annual means of 12% and 10% of cases in the 1990s, to 18% and 21% of cases between 2006 and 2011. In 2012, 10% of cases were less than one, 32% were between 1 to 9 years, 31% were between 10 and 19 years and 27% were 20 years or older.
In contrast, the age distribution of acute care hospitalized cases has not varied considerably over time with the proportion of hospitalizations consistently highest among children less than one. Between 1995 and 2010, on average each year, a total of 69% of pertussis-related admissions were among those less than 1 (range: 59 to 78%). Of those less than one, the majority of admissions occurred in young infants with an annual mean of 62% cases under the age of 3 months (range: 49 to 71%).
Figure 4. Age distribution of pertussis cases in Canada, 1990 to 2012Figure 4 Footnote *.
Text Equivalent
This is a 100 percent stacked bar graph showing the percentage of cases by age group in years in Canada over time. The y axis is year ranging from 1990 to 2012. The x axis is percentage ranging from 0 to 100%. The following age groups are represented each year: less than 1 year, 1 to 4 years, 5 to 9 years, 10 to 14 years, 15 to 19 years and 20 years and over.
The trend depicted is one of shifting age distribution over time with three distinct time periods. From 1990 to 1999 the 1 to 4 and 5 to 9 age groups have the greatest percentage of cases. From 2000 to 2005 the percentage of cases in the 10 to 14 and 15 to 19 year age groups increase over time to the predominant age groups. From 2007 to 2012 cases are more evenly distributed among these groups.
- Figure 4 Footnote 1
-
Case data from 1990 to 2011 were obtained from the Canadian Notifiable Diseases Surveillance System. Case data for 2012 were obtained directly from provinces and territories by CIRID and are preliminary. Nunavut data for 1999 are only partial, for 2007 & 2009 are missing, and for 2008, 2010-2011 are preliminary
Gender Distribution
From 1990 to 2012, the number of nationally reported pertussis cases and incidence rate has been consistently higher among females in all age groups. During this time period, the annual median male to female ratio in incidence rate was 0.87:1 (range: 0.81:1 to 0.96:1). Females made up on average 54.0% of cases, males 45.8% of cases, and 0.2% had an unknown gender each year. Similarly, between 1995 and 2010, the median male to female ratio in the incidence rate of hospitalization was 0.89:1 (range: 0.73:1 to 1.05:1) and on average, each year, females made up 53.5% of cases.
Geographic Distribution
Asynchrony in the timing and geographic focus of 2-5 year cyclical pertussis peaks is expected. Although Canada experienced an overall decline in pertussis incidence from the late 1990s to 2011, the timing, magnitude and overall trend in decreased activity varied across the provinces and territories (Figure 5). From 1995 to 2011, peaks in laboratory-confirmed pertussis notifications were observed, with the highest incidence by province across this period variously occurring in 1995 (Manitoba, Ontario, New Brunswick and Nova Scotia), 1996 (Alberta), 1997 (Prince Edward Island), 1998 (Quebec), 1999 (Saskatchewan, Newfoundland, Northwest Territories and Nunavut) or 2000 (British Columbia and Yukon). The absolute difference between the highest and lowest incidence rates within a province/territory during this time, ranged from 18 cases per 100,000 to a much larger difference of 489 cases per 100,000, with large fluctuations more common in jurisdictions with smaller populations. From provincial-/territorial-specific peaks to 2011, each province and territory experienced a decline of more than 75% in incidence with the vast majority seeing decreases exceeding 90%.
National increases in incidence are typically the result of peaks observed in multiple jurisdictions. The national increase observed in 1998 was due to increased activity experienced in Manitoba, Ontario, Quebec and New Brunswick. This was also the case in 2012, when increases in incidence relative to 2011 were observed in 9 of the 13 provinces and territories. At the provincial/territorial level, these increases ranged from a negligible 0.7 cases per 100,000 to a more substantial 152 cases per 100,000. Within jurisdictions that experienced substantial increases, causes varied from province-wide outbreaks, to regional outbreaks, to localized outbreaks. The most notable increase in activity was observed in New Brunswick, due to a province-wide outbreak that accounted for approximately one-third of the national case count in 2012.
Figure 5. Trends in annual incidence of pertussis (per 100,000 population) by province/territory, 1995 to 2012Figure 5 Footnote *.
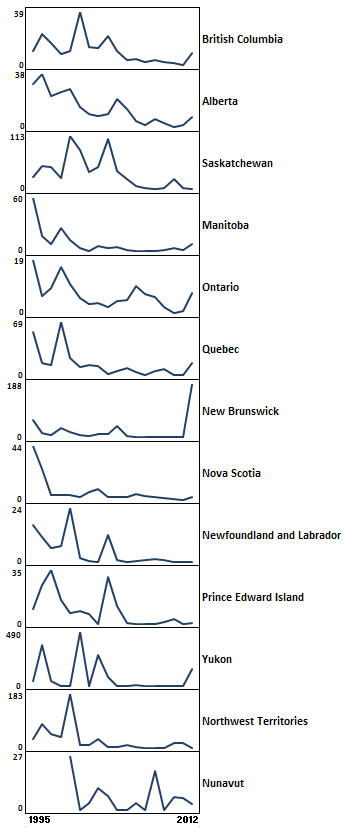
Text Equivalent
This figure contains 13 line graphs that are stacked vertically and illustrate the incidence rate of pertussis for each province and territory in Canada over time. There is a y axis for each graph for incidence rate per 100,000 with ranges in value varying by province and territory. The x axis depicts year and ranges from 1995 to 2012. The incidence rate values for each year are not discernible. Instead, the graph illustrates the variation in incidence rate trends by province and territory. All provinces and territories experienced a decline in incidence rate from 1995 to 2011 but there is asynchrony in the pattern of decline in terms of timing of 2-5 year peaks and magnitude of these peaks. The ranges in incidence rate by province and territory are provided as follows:
- British Columbia – 0 to 39 cases per 100,000
- Alberta – 0 to 38 cases per 100,000
- Saskatchewan – 0 to 113 cases per 100,000
- Manitoba – 0 to 60 cases per 100,000
- Ontario – 0 to 19 cases per 100,000
- Quebec – 0 to 69 cases per 100,000
- New Brunswick – 0 to 188 cases per 100,000
- Nova Scotia – 0 to 44 cases per 100,000
- Newfoundland and Labrador – 0 to 24 cases per 100,000
- Prince Edward Island – 0 to 35 cases per 100,000
- Yukon – 0 to 490 cases per 100,000
- Northwest Territories – 0 to 183 cases per 100,000
- Nunavut – 0 to 27 cases per 100,000
- Figure 5 Footnote 1
-
Case data from 1995 to 2011 were obtained from the Canadian Notifiable Diseases Surveillance System. Case data for 2012 were obtained directly from provinces and territories by CIRID and are preliminary. Nunavut data for 1999 are only partial, for 2007 & 2009 are missing, and for 2008, 2010-2011 are preliminary; Population data (July 1st annual estimates) were obtained from Statistics Canada.
Mortality
From 2000 to 2009, Statistics Canada reported a total of six deaths with pertussis listed as the underlying cause of death. Between zero and two deaths occurred each year and all deaths were reported in infants less than one year of age. However, this is likely an underestimation of the total deaths associated with pertussis in Canada. According to data from IMPACT, from 2000 to 2009, 11 of the 858 reported pertussis cases identified through IMPACT died (1.2%). From 1991 to 2012, 30 deaths have been reported through IMPACT, with the number ranging from zero to four per year (Figure 6). The majority of deaths occurred in infants less than 2 month of age (78%). All deaths, except for one, occurred in infants with no previous pertussis immunizations and 78% of deaths were in children considered previously healthy. Causes of death included respiratory distress/failure, pneumonia, hypoxia, pulmonary hypertension, pulmonary hemorrhage, fulminant septic shock, cardiovascular failure, and acute arrhythmia.
Figure 6. The number of pertussis cases and deaths, IMPACT, 1991 to 2012Figure 6 Footnote *.
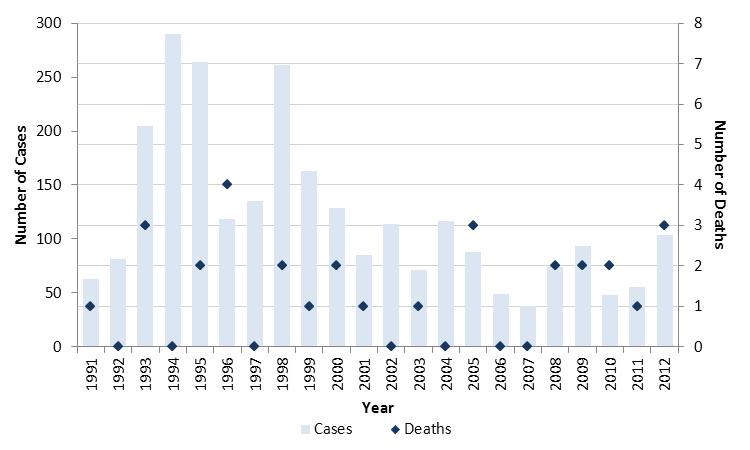
Text Equivalent
This is a combined bar and symbol graph showing the number of pertussis hospital admissions in bars and the number of those cases that died using a diamond symbol that were identified in the Canadian Immunization Monitoring Program Active (IMPACT) surveillance system over time. The primary y axis is the number of IMPACT cases and ranges from 0 to 300. The secondary y axis is the number of deaths and ranges from 0 to 8. The x axis is year and ranges from 1991 to 2012. Peaks in cases occur every 2 to 5 years are visible. A decline in cases from the 1990s to 2012 is depicted. After peaks of over 250 cases in 1994 and 1998 the case count declines and stays below 100 cases from 2005 to 2011. In 2012 there were 101 cases and 3 deaths. The number of deaths ranges from 0 to 4 and are sporadic with no clear trend.
- Figure 6 Footnote 1
-
Data for 2012 are preliminary
Discussion
Pertussis is an endemic cyclical disease in Canada with peaks in activity occurring every 2 to 5 years. Although resurgence was observed in the 1990s, overall, Canada has experienced a decline in pertussis activity following the introduction of routine pertussis immunization programs. This was first observed with the introduction of the whole–cell vaccine in 1943, followed by the introduction of the acellular vaccine in 1997/98 and lastly, between 2005 and 2011 after the introduction of adolescent immunization programs across the countryFootnote 9. As previously noted, the resurgence observed in the 1990s was likely due to a combination of factors, including the low efficacy of the wholecell vaccine introduced between 1981 and 1985, as well as increased physician awareness and improved diagnostics and reporting of pertussis infectionFootnote 10. From a geographic perspective, all provinces and territories experienced a decline in the incidence in pertussis in the seven years prior to 2012; however, trends in disease were unique to each jurisdiction in terms of timing and magnitude of cyclical peaks.
The incidence of pertussis is consistently highest among infants, as are hospitalization and death, particularly among those 3 months of age or less. This group is of particular interest as they are too young to benefit directly from immunizations. Different approaches have been tried which include cocooning and immunization of pregnant women to allow for passive immunity to the infantFootnote 11Footnote 12Footnote 13. Canada's National Advisory Committee on Immunization has recommended immunization in pregnancy if there is a regional outbreak of pertussisFootnote 14.
The increase in incidence observed in 2012 was due to outbreaks in several jurisdictions across the country. Increases in incidence were observed across all age groups nationally with the highest incidence rates in those less than one. However, age groups most affected varied by province/territory. As with national case reports, cases reported through IMPACT hospitals increased in 2012, but not as dramatically which could suggest that the increase in cases was not associated with increasing severity.
Increases in pertussis activity have also recently occurred in other countries with several reasons for increases proposed in the literature, including waning immunityFootnote 15, reduced natural immune boostingFootnote 16, higher rates of detectionFootnote 17, genetic changes in the bacteriaFootnote 18, as well as clustering of unvaccinated individualsFootnote 19. Based on nationally available data, it's difficult to determine the contributing factors for the increases observed in Canada in 2012. At present, data collected at the national level is minimal, often in an aggregate format that does not include the immunization history of cases. The National Microbiology Laboratory does not currently conduct routine surveillance of circulating pertussis strains. According to the validated results of the 2009 childhood National Immunization Coverage Surveys, immunization coverage is high; 98% for four or more doses in two year olds and 89% for five or more doses among seven year oldsFootnote 20. However, evaluations of specific immunization programs and coverage within populations and sub-populations in Canada have yet to be done in a systematic way.
Limitations
Due to the passive nature of CNDSS, reported cases are expected to be underestimates of the true burden of disease, particularly among adolescents and adults. It is likely that the incidence of pertussis is actually higher among adults than reported, as symptoms are generally milder, and testing for B. pertussis among adults with persistent cough is infrequent. In addition, the pertussis-related hospitalizations identified in the HMD are coded based on the physician's diagnosis as it appears in the medical chart and do not necessarily match the national case definition (e.g. may not be based on laboratory results). As a result, the number of pertussis-related acute care hospitalizations featured in this report could be an overestimate of the actual burden.
Conclusion
In conclusion, our understanding of the epidemiology of pertussis in Canada could be enhanced by improved approaches for monitoring the disease. National pertussis surveillance that also captures vaccine history, microbiological characteristics and indication of outbreaks, may yield answers that can inform public health action. Although the peak in activity observed in 2012 could be an isolated event, further work to support outbreak response in provinces and territories, including rapid research tools and resources, should be considered.
Reference
- Footnote 1
-
Public Health Agency of Canada. Publicly funded Immunization Programs in Canada - Routine Schedule for Infants and Children including special programs and catch-up programs (as of March 2013).
- Footnote 2
-
Public Health Agency of Canada. National Notifiable Diseases.
http://www.phac-aspc.gc.ca/aids-sida/about/dis-eng.php - Footnote 3
-
Health and Welfare Canada. Canadian Communicable Disease Surveillance System: disease-specific case definitions and surveillance methods. Can Dis Wkly Rep 1991;17(S3).
- Footnote 4
-
Health Canada. Case definitions for diseases under national surveillance. CCDR. 2000;26(S3).
- Footnote 5
-
Public Health Agency of Canada. Case definitions for communicable diseases under national surveillance. CCDR. 2009; 35(S2).
- Footnote 6
-
Canadian Paediatric Society. Canadian Immunization Monitoring Program Active.
http://www.cps.ca/en/impact. - Footnote 7
-
Canadian Vital Statistics - Death Database, Statistics Canada, Health Statistics Division, [2000 to 2009]. Accessed 2013 July 15.
- Footnote 8
-
Canadian Vital Statistics – July Provincial Population Estimates, Statistics Canada, Health Statistics Division, [1924-2005 (final intercensal estimates); 2006-09 (final postcensal estimates); 2010-11 (updated postcensal estimates); 2012 (preliminary postcensal estimates)]. Accessed 2013 July 15.
- Footnote 9
-
National Advisory Committee on Immunization. Prevention of pertussis in adolescents and adults. CCDR. 2003; 29(ACS5).
- Footnote 10
-
Health Canada. National Consensus Conference on Pertussis. CCDR. 2003; 29(S3):1-33.
- Footnote 11
-
Wiley KE, Zuo Y, Macartney KK, McIntyre PB. Sources of pertussis infection in young infants: a review of key evidence informing targeting of the cocoon strategy. Vaccine. 2013;31(4):618-25.
- Footnote 12
-
Healy CM, Rench MA, Baker CJ. Importance of timing of maternal combined tetanus, diphtheria, and acellular pertussis (Tdap) immunization and protection of young infants. Clin Infect Dis. 2013;56(4):539-44.
- Footnote 13
-
Hardy-Fairbanks AJ, Pan SJ, Decker MD, Johnson DR, Greenberg DP, Kirkland KB, et al. Immune responses in infants whose mothers received tdap vaccine during pregnancy. Pediatr Infect Dis J. 2013;32(11):1257-60.
- Footnote 14
-
Canadian Immunization Guide [web page]. Pertussis Vaccine.
http://www.phac-aspc.gc.ca/publicat/cig-gci/p04-pert-coqu-eng.php. - Footnote 15
-
Klein NP, Bartlett J, Rowhani-Rahbar A, Fireman B, Baxter R. Waning protection after fifth dose of acellular pertussis vaccine in children. N Engl J Med. 2012;367 (11):1012–1019.
- Footnote 16
-
Lavine JS, King AA, Bjørnstad ON. Natural immune boosting in pertussis dynamics and the potential for long-term vaccine failure. Proc Natl Acad Sci U S A. 2011;108(17):7259-64.
- Footnote 17
-
Cherry JD. Epidemic pertussis in 2012 - the resurgence of a vaccine-preventable disease. N Engl J Med. 2012;367(9):785–787.
- Footnote 18
-
Mooi FR, VAN DER Maas NA, De Melker HE. Pertussis resurgence: waning immunity and pathogen adaptation - two sides of the same coin. Epidemiol Infect. 2013 Feb 13:1-10.
- Footnote 19
-
Atwell JE, Van Otterloo J, Zipprich J, Winter K, Harriman K, Salmon DA et al. Nonmedical vaccine exemptions and pertussis in California, 2010. paediatrics. 2013;132(4):624-30.
- Footnote 20
-
Laroche J, Gendron MP, Abdel-Motagally M. Impact of validating respondent responses on national immunization coverage estimates [poster]. Canadian Immunization Conference. 2012 Dec.
Notes and Acknowledgements
Vital statistics data were provided to the Agency by Statistics Canada with the knowledge and consent of the Provincial and Territorial Vital Statistics Registrars whose cooperation is gratefully acknowledged. Although parts of this report are based on data provided by CIHI, the analyses, conclusions, opinions and statements expressed herein are those of the Agency, and not necessarily those of CIHI. Provincial/territorial estimates produced by the Agency may differ from those published by provinces/territories due to variations in data used at the time of analysis. We gratefully acknowledge the participation of health care providers, public health officials and laboratories across the country in the routine reporting of pertussis. We would also like to thank all who participated in the development of the report, including: Vicky Springman (PHAC), Monique St-Laurent (PHAC), John Spika (PHAC), Julie Bettinger (IMPACT), Scott Halperin (IMPACT), Danuta Skowronski (British Columbia), Monika Naus (British Columbia), Theresa St. Jean (Alberta), Kimberley Simmonds (Alberta), Helen Bangura (Saskatchewan), Valerie Mann (Saskatchewan), Patricia Caetano (Manitoba), Shelley Deeks (Ontario), Jastej Dhaliwal (New Brunswick), Carolyn Sanford (Prince Edward Island), Anne Neatby (Prince Edward Island), Cathy O'Keefe (Newfoundland and Labrador), Gillian Butler (Newfoundland and Labrador), Beverly A. Billard (Nova Scotia), Lori Strudwick (Yukon), Karolina Machalek (PHAC/Yukon), Heather Hannah (Northwest Territories), Bryany Denning (Northwest Territories), Carolina Palacios (Nunavut), and Angie Mullen (Nunavut).
Conflict of interest statement
There are no conflicts of interest to declare.
Funding
This work was supported by the Public Health Agency of Canada.
Page details
- Date modified: