
Archived - Canada’s biological response plan

 Download this article as a PDF
Download this article as a PDF Published by: The Public Health Agency of Canada
Issue: Volume 44-1: Emergency planning
Date published: January 4, 2018
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 44-1, January 4, 2018: Emergency planning
Implementation science
Federal, provincial and territorial public health response plan for biological events
R McNeill 1, J Topping 1* on behalf of the FPT Response Plan Task Group
Affiliation
1 Centre for Emergency Preparedness and Response, Public Health Agency of Canada, Ottawa, ON
Correspondence
Suggested citation
McNeill R, Topping J. Federal, provincial and territorial public health response plan for biological events. Can Commun Dis Rep. 2018;44(1):1-5. https://doi.org/10.14745/ccdr.v44i01a01
Abstract
The Federal/Provincial/Territorial (FPT) Public Health Response Plan for Biological Events was developed for the Public Health Network Council (PHNC). This plan outlines how the national response to public health events caused by biological agents will be conducted and coordinated, with a focus on *implementation of responses led by senior-level FPT public health decision-makers. The plan was developed by an expert task group and was approved by PHNC in October, 2017. The plan describes roles, responsibilities and authorities of FPT governments for public health and emergency management, a concept of operations outlining four scalable response levels and a governance structure that aims to facilitate an efficient, timely, evidence-informed and consistent approach across jurisdictions. Improving effective engagement amongst public health, health care delivery and health emergency management authorities is a key objective of the plan.
Introduction
Emerging infections, and other biological events, happen regularly in Canada and around the world, and require a coordinated health and public health response. Previous public health responses at a national level in Canada have addressed many hazards, ranging from epidemics of novel respiratory pathogens (e.g., SARS and H1N1 pandemics), to emerging infections, such as international and travel-related public health threats (e.g., Zika and Ebola), food-borne illness outbreaks, significant vaccine supply issues and the current opioid crisis.
Health planners have learned a great deal from previous experiences. The 2009 H1N1 pandemic revealed that coordination of decision-making and information sharing at the federal/provincial/territorial (FPT) level was often complex, challenging and time consuming; for example, multiple levels of government provided similar, but not identical, advice and recommendations regarding clinical guidelines for front-line health professionals and these differences led to confusion about whose advice to followFootnote 1.
Lessons learned have demonstrated the need for a nimble, flexible FPT governance structure that can be applied consistently, in whole or in part, to a range of public health scenarios. They also demonstrated the need to clarify roles and responsibilities, as well as decision-making and approval processes, at various levels of government within the health sector. To address these issues, FPT Deputy Ministers of Health agreed that improvements to the FPT governance structure developed during H1N1 should continue, with the understanding that they would need to be flexible enough to adapt to different types of urgent situations, while respecting various responsibilities and authorities.
Public health in Canada is a shared responsibility among municipal, provincial, territorial and federal governments. Significant public health events, including public health emergencies, require coordination between all levels of government and a consistent approach across jurisdictions. Consensus on response strategies at a national level is desirable, recognizing that some or all jurisdictions involved (e.g., local, FPT governments and others) may choose to implement actions dependent on the legislative frameworks and circumstances of the event. It was with this goal of facilitating collaboration and decision-making between multiple authorities and levels of government, that the FPT Public Health Response Plan for Biological Events was developed.
Legislation requires all jurisdictions in Canada have plans that set out the steps to be taken in the event of an emergency. These plans identify linkages and channels of communication to other ministries, programs and agencies of the government and contribute to a coordinated, system-wide approach to emergency management. In addition, the FPT health sector has in place well established hazard-specific tools that are routinely used to effectively plan and manage public health events. A feature of the FPT Public Health Response Plan for Biological Events is that it is intended to complement and, where appropriate, be used in conjunction with existing mechanisms. For example, the Canadian Pandemic Influenza Preparedness: Planning Guidance for the Health Sector (CPIP) provides pan-Canadian planning guidance for pandemic influenzaFootnote 2. In a pandemic, it is expected the CPIP will inform the technical aspects of the response while the FPT Public Health Response Plan for Biological Events will provide the overall governance structure that will support decision-making. The objective of this paper is to provide a high-level summary of the FPT Public Health Response Plan for Biological Events.
Key features of the plan
The plan is made up of a main body and various supporting appendices. The main body includes two key components: the concept of operations and the FPT governance structure. It also addresses health care sector engagement, describes how the governance structure will be supported and how it will interact with both federal and PT operations centres. The appendices include the guiding principles used in the development of the plan, a summary of key FPT roles and responsibilities for public health and emergency management and the Terms of Reference for the various groups within the governance structure.
Concept of operations
The concept of operations describes the steps that are taken from the initial notification of a public health event leading to the activation of the plan to the eventual de-escalation of the response. It describes how notification of public health events are made to the Public Health Agency of Canada (PHAC), and how response needs are assessed by technical experts and decision-makers. The concept of operations also describes four response levels to facilitate scaling of response activities as needed. Examples of scenarios where these response levels may be applied are given below.
- Routine: There is a need for information sharing regarding a public health event between an affected jurisdiction and other FPT or international authorities (e.g., outbreak of measles in a single jurisdiction).
- Heightened: There is a need for a routine public health response involving one or more jurisdictions (e.g., a food-borne outbreak occurring in multiple jurisdictions).
- Escalated: A coordinated response is required for a public health event that has potential implications for the Canadian health care system (e.g., outbreak due to a highly antibiotic-resistant bacterium).
- Emergency: A national response is required for an event in Canada causing significant illness and has the potential for rapid spread (e.g., a novel influenza virus is spreading efficiently between humans).
Governance structure
The governance structure is designed to streamline response processes, provide clarity on roles/responsibilities, facilitate a high degree of situational awareness and centralize risk management and task delegation. It is modelled on the 'day-to-day' governance structures of the Public Health Network Council and is made up of a Special Advisory Committee (SAC) and three main response streams (technical, logistical and communications) each led by advisory committees/working groups. The governance structure, through the SAC, reports to and is accountable to the FPT Conference of Deputy Ministers of Health (CDMH).
Special Advisory Committee
The SAC has a mandate to provide advice to the CDMH pertaining to the coordination, public health policy and technical content on matters related to the response to a significant public health event. As such, SAC is the main decision-making body of the governance and the main forum for approval of products developed by the governance such as recommendations, guidance documents, protocols and communication products. The SAC is composed of the members of the Pan-Canadian Public Health Network Council and the Council of Chief Medical Officers of Health (CCMOH).
Technical Advisory Committee
The Technical Advisory Committee (TAC) is largely focused on the characteristics of the public health event and what needs to be done from a technical, public health perspective to achieve the response objectives. Under TAC, task groups will be established to address public health response functions (e.g., surveillance, laboratory and medical countermeasures) and to provide technical input into products such as communications material aimed at informing media, health professionals and the public on the most current information available at the time. The TAC will develop products such as epidemiological reports, guidance on public health measures, and recommendations on the type of medical countermeasures (e.g., medications/antivirals or vaccines) to be used. The TAC will be co-chaired by the co-chairs of the Communicable and Infectious Disease Steering Committee (CID-SC).
Public Health Network Communications Group
The Public Health Network Communication Group (PHN CG) supports consistent and coordinated public communications by providing a mechanism by which FPT governments work together on common messaging. It provides a forum to share news releases and media material, conduct technical and media briefings, and direct Canadians on where to seek the most current information and guidance. Once the plan is activated, communication related response activities will be coordinated through the PHN CG, thus enabling FPT governments to align their communication strategies.
Logistics Advisory Committee
The Logistics Advisory Committee (LAC) will be largely focused on how the response activities will be implemented in order to achieve the response objectives. As with the TAC, under the LAC, task groups may be established to address specific logistical response issues. For example, LAC is responsible for engaging with the health care delivery sector and for establishing task groups as required to ensure this sector is represented in the governance. The LAC would develop products such as funding agreements, mutual aid agreements and recommendations regarding acquiring resources (e.g., vaccines or other medical countermeasures). The LAC is co-chaired by the co-chairs of the Public Health Infrastructure Steering Committee (PHI-SC).
Health care delivery engagement
Decisions of interest to health care clinicians are expected to be made at various fora in the governance structure. For example, the LAC may activate a Health Care Delivery Engagement Task Group to respond to requests by the SAC for products such as guidance documents. Task group members would include federal representatives and multidisciplinary experts, and provincial/territorial representatives that would also provide their perspective and expertise, including clinical expertise. The Task Group would engage non-governmental organizations, research communities and other stakeholders in the area of health care delivery. It would also coordinate with external expert organizations, such as the Association of Medical Microbiology and Infectious Disease (AMMI) Canada, to foster linkages between public health technical and response products and health care related products such as clinical care guidelines. The TAC would also establish task groups in this same fashion to help inform development of technical guidance and recommendations including those aimed at health professionals.
Health care delivery is further represented at a strategic level by SAC members who act as informal liaisons to the health care sector within their respective jurisidictions, and provide their unique jurisdictional views to SAC to ensure that the full continuum of the health sector is considered in response planning. Complementary to this, at the operational level, the health emergency management directors of provincial/territorial ministries of health may assume various roles within the governance structure and would act as liaisons to health care delivery within their jurisdiction as well.
Governance support
SAC Secretariat
The SAC Secretariat supports the SAC and the response streams by assuming multiple coordination functions. It is responsible for rapid centralized analysis of issues and response needs, prioritization and distribution of tasks. Specifically the SAC Secretariat, with direction from SAC co-chairs, will identify what type of product/action is required, task this to the appropriate groups (TAC, LAC or Communications) within the governance structure and monitor progress.
Another key activity of the SAC Secretariat is to consider the integration of analysis and evidence across the response streams, including policy implications on decisions related to a public health event. An example of when this would occur is if SAC requested a single product that includes technical recommendations, logistical issues and a communication response—such as a vaccine response strategy. In order to support effective decision-making by SAC, there is a need to ensure that all evidence is considered in a holistic manner, informed by the co-chairs of the relevant response streams.
Health Portfolio Operations Centre
Figure 1 outlines the FPT governance structure and illustrates the operational communications between the federal Health Portfolio Operations Centre (HPOC) and provincial/territorial Emergency Operations Centres (EOCs). The HPOC serves as the Health Portfolio focal point for the coordination of response activities to significant public health events of national interest within the Health Portfolio's mandate, and acts as the point of contact for operational communications with other government departments and internationally. When the plan is activated, the HPOC provides support to the governance structure and participates in its groups as required.
Figure 1: FPT governance structure and its relation to FPT operation centres
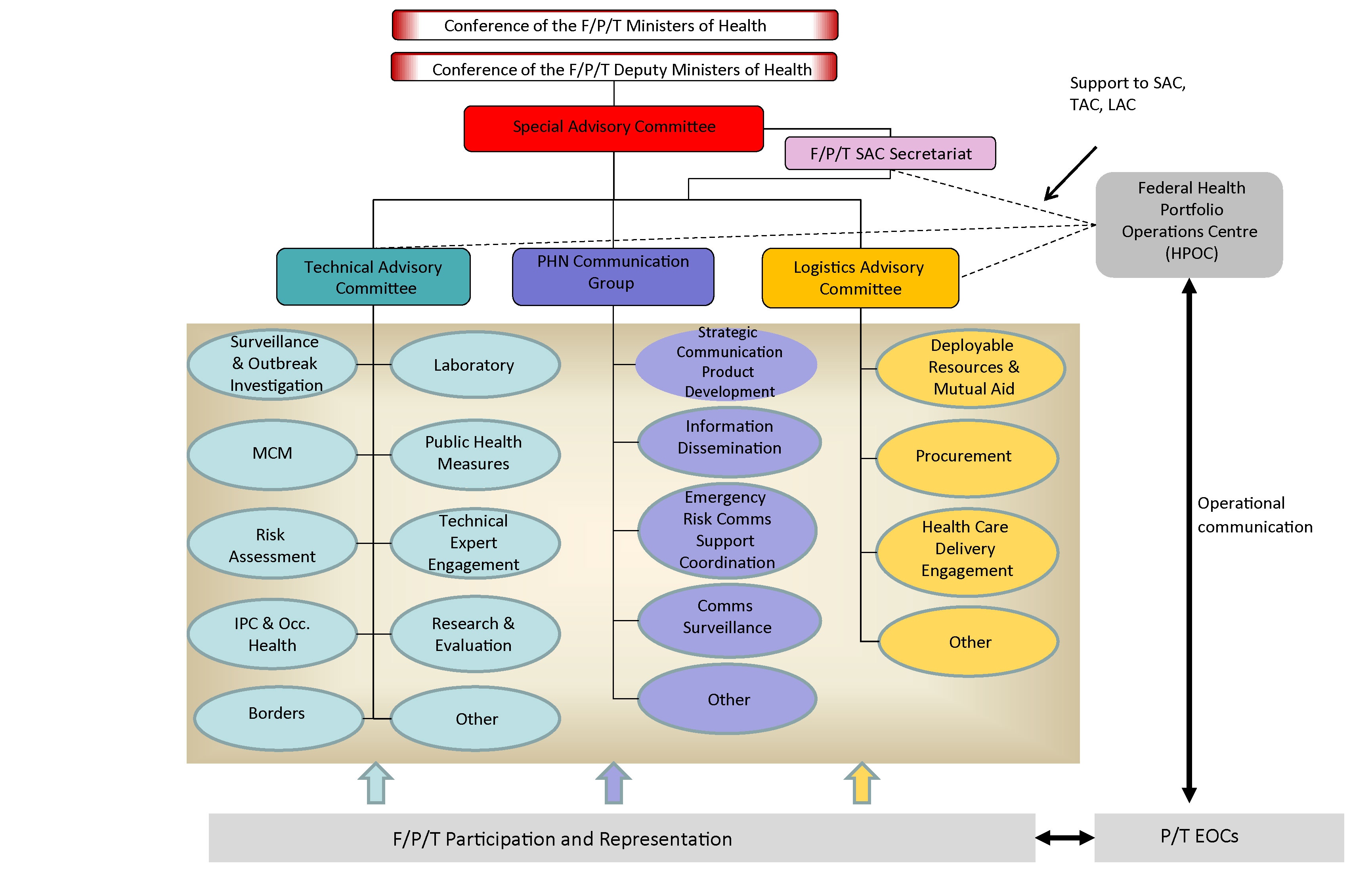
Figure 1 - Text Equivalent
The figure outlines the Federal/Provincial/Territories (FPT) governance structure and the operational communication between the federal Health Portfolio operations Center (HPOC) and provincial/territorial Emergency Operations Center (EOCs). The Conference of FPT Ministers of Health and the Conference of FPT Deputy Ministers of Health all connect through the Special Advisory Committee (F/P/T SAC). The HPOC supports the operational communication through three committees/groups that have full FPT participation and representation. Below lists the three groups and their representation:
1) Technical Advisory Committee consists of: Surveillance and Outbreak Investigation, Laboratory, Medical Counter-measures, Public Health measures, Risk Assessment, Technical Expert Engagement, Infection Prevention Control and Occupational Health, Research and Evaluation, Border and others.
2) Public Health Network Communication Group consists of: Strategic Communication and Product Development, Information Dissemination, Emergency Risk Communications Support and Coordination, Communications Surveillance, and other.
3) Logistic Advisory Committee consists of: Deployable Resources and Mutual Aid, Procurement, Health Care Delivery Engagement and other. The HPOC serves as the Health Portfolio's mandate, and acts as the point of contact for operation communication with other departments and internationally.
When the plan is activated, the HPOC provides support to the governance structure and participates in its groups as required.
Discussion
The FPT Public Health Response Plan for Biological Events, as all response plans, is an evergreen document. The need for revision will be guided by after action reviews following the response to a real or simulated event requiring implementation of the plan, in whole or in part. The revision of the plan may also include recommendations for the development of new event-specific Annexes as required, to further support implementation of the plan. Implementation will also be supported by training and exercises to familiarize various stakeholders with roles and responsibilities under the plan, and to identify areas for further improvement.
Conclusion
The FPT Public Health Response Plan for Biological Events is an important new tool that will help to support inter-jurisdictional collaboration, information-sharing and decision-making between and amongst various jurisdictions. It represents a continuing commitment on behalf of FPT governments to work collaboratively to ensure Canada is ready to respond to public health events and prepared to protect the health of Canadians.
Conflict of interest
None.
Acknowledgements
Special thanks to the Task Group who developed the plan (see Appendix A for membership) and to the Task Group co-chairs Dr. Howard Njoo of the Infection Prevention and Control Branch of PHAC and John Lavery of Health Emergency Management British Columbia—their leadership and commitment to this project has been instrumental in the completion of this significant piece of work. We also thank the following individuals for their valued contribution to the plan: J. Sciberras, L. Menard and JF. Duperré.Appendix A: Members of the FPT Response Plan Task Group
Thomas Appleyard
Manager: Training, Exercises & Awareness (A)
Emergency Management Branch
Population and Public Health Division
Ministry of Health and Long-Term Care
Toronto ON
Tamela Carroll
Senior Program Advisor
New Brunswick Department of Health
Office of the Chief Medical Officer of Health Communicable Disease Branch
Fredericton NB
Jean-François Duperré
A/Executive Director
Center for Emergency Preparedness and Response
Public Health Agency of Canada
Ottawa ON
Kelly Folz
Manager
Intergovernmental Affairs
Intergovernmental and Stakeholder Policy Division
Public Health Agency of Canada
Ottawa ON
Mélanie Goulette Nadon
Senior Communications Advisor
Public Health Strategic Communications Directorate
Communications and Public Affairs Branch
Health Canada
Ottawa ON
Dr. Karen Grimsrud
Chief Medical Officer of Health
Office of the Chief Medical Officer of Health
Edmonton AB
Steve Guercio
Executive Director
National Microbiology Laboratory
Infectious Disease Prevention and Control Branch
Public Health Agency of Canada
Winnipeg MB
Alternate
Dr. Cindi Corbett
Director, Bacterial Pathogens Division
National Microbiology Laboratory
Infectious Disease Prevention and Control Branch
Public Health Agency of Canada
Winnipeg MB
Erin Henry
Director
Communicable Disease Control Division
Office of Population and Public Health
Population Health and Primary Care Directorate
First Nations and Inuit Health Branch
Health Canada
Ottawa ON
Alternate
Fanie Lalonde
National Program Manager
Communicable Disease Emergencies/Infection Prevention & Control Program
Office of Population & Public Health
Population Health and Primary Care Directorate
First Nations and Inuit Health Branch
Health Canada
Ottawa ON
Althea House
Manager Seasonal and Pandemic Influenza
Centre for Immunization and Respiratory Infectious Diseases
Infectious Disease Prevention and Control Branch
Public Health Agency of Canada
Ottawa ON
John Lavery (Co-Chair)
Executive Director
Health Emergency Management British Columbia
2nd Floor-1770 West 7th Avenue
Vancouver BC
Alternate
Kathryn Forge
Director, Emergency Management Unit
Health Emergency Management British Columbia
Vancouver BC
Jason Letto
Manager
Health Emergency Management Program
Department of Health and Community Services
Government of Newfoundland and Labrador
St. John's NL
Garnet Matchett
Director of Operations
Health Emergency Management Unit
Saskatchewan Ministry of Health
Regina SK
Robin McNeill
Sr. Emergency Management Planner
Office of Situational Awareness and Operations
Centre for Emergency Preparedness and Response
Health Security and Infrastructure Branch
Public Health Agency of Canada
Ottawa ON
Dr. Howard Njoo (Co-Chair)
Deputy Chief Public Health Officer
Office of the Chief Public Health Officer
Public Health Agency of Canada
Ottawa ON
Gary O'Toole
Director, Public Health
Nova Scotia Health Authority, Northern Zone
Colchester East Hants Health Centre
Truro NS
Dr. Katarina Pintar
Manager, Policy Integration Division
Centre for Food-Borne, Environmental and Zoonotic Infectious Diseases
Infectious Disease Prevention and Control Branch
Public Health Agency of Canada
Ottawa ON
Dr. Barry N. Pakes
Deputy Chief Medical Officer of Health (acting)
Department of Health, Government of Nunavut
PO Box 1000, Station 1000
Iqaluit NU
Dr. Michel Savard
Médecin conseil
Direction générale de santé publique
Ministère de la Santé et des Services sociaux
Montréal QC
Jill Sciberras
Nursing Advisor
Centre for Emergency Preparedness and Response
Public Health Agency of Canada
Toronto ON
Dr. Saqib Shahab
Government of Saskatchewan
Chief Medical Health Officer
Ministry of Health, Population Health Branch
Regina SK
Mariyam Syed
Emergency Management Analyst
Public Health and Compliance Division
Health Protection Branch
Alberta Ministry of Health
Edmonton AB
John Topping
Director
Office of Situational Awareness and Operations
Centre for Emergency Preparedness and Response
Public Health Agency of Canada
Ottawa ON
Dr. Elise Weiss
Acting Chief Provincial Public Health Officer
Manitoba Health, Seniors and Active Living
Government of Manitoba
4004-300 Carlton Street
Winnipeg MB
Judith Wood Bayne
Regional Director – Atlantic Region
Health Promotion and Chronic Disease Prevention Branch
Public Health Agency of Canada
Halifax NS
Alternate
Lise Gauthier
Regional Coordinator Emergency Management Unit– Québec
Health Promotion and Chronic Disease Prevention Branch
Public Health Agency of Canada
Montreal QC