
Archived - NACI Summary on subunit and split virus influenza vaccine

 Download this article as a PDF
Download this article as a PDF Published by: The Public Health Agency of Canada
Issue: Volume 44-6 : Vaccine update
Date published: June 7, 2018
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 44-6, June 7, 2018: Vaccine update
Review
Summary of the NACI literature review on the comparative effectiveness of subunit and split virus inactivated influenza vaccines in older adults
I Gemmill1,2, K Young3 on behalf of the National Advisory Committee on Immunization (NACI)*
Affiliations
1 NACI Influenza Working Group Chair, Kingston, ON
2 Kingston, Frontenac and Lennox & Addington Public Health, Kingston, ON
3 Centre for Immunization and Respiratory Infectious Diseases, Public Health Agency of Canada, Ottawa, ON
Correspondence
Suggested citation
Gemmill I, Young K on behalf of the National Advisory Committee on Immunization (NACI). Summary of the NACI literature review on the comparative effectiveness of subunit and split virus inactivated influenza vaccines in older adults. Can Commun Dis Rep 2018;44(6):129-33. https://doi.org/10.14745/ccdr.v44i06a02
Keywords: National Advisory Committee on Immunization, influenza vaccine, subunit vaccine, split virus vaccine
Abstract
Background: Subunit and split virus inactivated influenza vaccines (IIV) are two commonly used types of seasonal influenza vaccines in Canada. The comparative effectiveness of these two formulations is particularly relevant for older adults, as older adults have reduced influenza vaccine effectiveness and experience more severe influenza than younger adults.
Objective: To compare the vaccine effectiveness and immunogenicity of unadjuvanted, standard-dose subunit IIVs versus unadjuvanted, standard-dose split virus IIVs in adults 65 years of age and older.
Methods: An a priori written protocol based on rapid review methods was developed that included studies published in 2007 or later in the EMBASE, MEDLINE and ClinicalTrials.gov databases with terms used in the objective. Due to the small number of records returned, hand searches of reference lists were completed, the publication date limit was removed, three additional databases (the Cochrane Central Register of Controlled Trials, Scopus and Web of Science) were searched, and studies including adults 60 years of age and older were included. Data from included studies were extracted into evidence tables and quality assessments were completed. The results were synthesized narratively.
Results: Eight eligible studies were identified. In the three studies that assessed vaccine effectiveness of subunit and split virus IIVs, there were no statistically significant differences in vaccine effectiveness in adults 65 years of age and older against laboratory-confirmed infection with any influenza virus strain, or against laboratory-confirmed infection with influenza A(H1N1), A(H3N2) or B virus, specifically. In the five studies that assessed immunogenicity, the findings were not consistent and the overall quality of immunogenicity evidence was weak.
Conclusion: The National Advisory Committee on Immunization (NACI) concludes that there is insufficient evidence to determine significant differences in the vaccine effectiveness or immunogenicity of unadjuvanted, standard-dose subunit and split virus IIVs in adults 65 years of age and older (Grade I evidence).
Introduction
Many different technologies are currently used in the formulation of influenza vaccines. Split virus and subunit inactivated influenza vaccines, both consisting of disrupted virus particles, were some of the first technologies developed following early inactivated whole virus vaccines, which were developed in the 1940sFootnote 1. Split virus vaccines contain whole inactivated viruses that have been split with detergent, ether or both, while subunit vaccines are made of purified hemagglutinin (HA) and neuraminidase.
Newer technologies and formulations for influenza vaccines have since been introduced, such as higher doses of antigen or combining the antigen with adjuvants; however, standard-dose subunit and split virus inactivated influenza vaccines (IIVs) are still the most commonly used seasonal influenza vaccines, as these vaccines have well-established safety profiles and are less expensive than newer formulations. A large number of the seasonal influenza vaccines available for use in Canada are standard-dose subunit or split virus IIVsFootnote 2.
The National Advisory Committee on Immunization (NACI) has not previously critically appraised the evidence on the comparative vaccine effectiveness and immunogenicity of subunit versus split virus IIV in any age group. If one of the vaccine types was more effective, it would be important to know, particularly for older Canadian adults (65 years of age and older), who are at highest risk of influenza-related hospitalizationsFootnote 3 and deathsFootnote 4. Older adults may also experience reduced vaccine effectiveness against influenza infection compared with younger age groupsFootnote 5.
The primary objective of this literature review was to compare the vaccine effectiveness and immunogenicity of unadjuvanted, standard-dose subunit IIV versus unadjuvanted, standard-dose split virus IIV in adults 65 years of age and older. A full report is available onlineFootnote 6.
Methods
A rapid review methodology was used that was based on methods developed by Tricco et al.Footnote 7. The research question addressed in this review is as follows: Does the vaccine effectiveness, immunogenicity, or both of unadjuvanted, standard-dose subunit IIV differ from unadjuvanted, standard-dose split virus IIV among adults 65 years of age and older?
A priori search strategy
A search strategy was developed in consultation with a federal Reference Librarian, and included search terms for subunit influenza vaccine, split virus influenza vaccine, vaccine effectiveness and immunogenicity. The search was restricted to studies published in English or French, in EMBASE, MEDLINE and ClinicalTrials.gov databases published in 2007 or later.
Inclusion and exclusion criteria
Studies were included if they met the following criteria:
- the study directly or indirectly compares the vaccine effectiveness or immunogenicity of an unadjuvanted, standard-dose subunit IIV to an unadjuvanted, standard-dose split virus IIV;
- the study population is within the age range of interest (65 years of age and older).
Studies were excluded if they met one or more of the following criteria:
- the study does not present vaccine effectiveness or immunogenicity for both vaccine types of interest;
- the study is in a language other than English or French;
- the study is a non-human, in vivo or in vitro study;
- the article is an editorial, opinion or news report;
- the study presents only secondary research.
Screening and eligibility assessments were completed by a single reviewer.
Data extraction, synthesis and quality assessment
Data from included studies were extracted into evidence tables, defined a priori. The quality (internal validity) of included studies was assessed using criteria outlined by Harris et al.Footnote 8. Data extraction and quality assessment were completed by one reviewer and verified by a second reviewer. Results from included studies were synthesized narratively.
Post-hoc modifications
Due to the small number of records retrieved from the initial database search, search criteria were modified. The publication date restriction was removed, three additional databases were added (the Cochrane Central Register of Controlled Trials, Scopus and Web of Science) and, since a number of studies defined older adults as individuals 60 years of age and older but were otherwise eligible, the eligibility criteria were modified to include adults 60 years of age and older.
Results
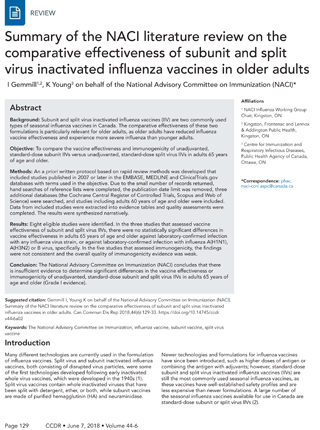
The initial database search retrieved 30 records; only three of these studies met inclusion criteria. After post-hoc modifications, 41 unique studies were identified through the search and eight met the revised inclusion criteria (Figure 1). Three of the included studies reported on vaccine effectiveness, and five of the studies reported on immunogenicity. None of the identified studies compared quadrivalent with trivalent vaccine formulations of subunit or split virus IIVs. The study characteristics of the included studies are shown in Table 1 below.
Figure 1: Flow diagram for comparative effectiveness and immunogenicity of subunit and split virus IIVs in older adults: October 2017 Figure 1 footnote a
Text description: Figure 1
Figure 1: Flow diagram for comparative effectiveness and immunogenicity of subunit and split virus IIVs in older adults: October 2017 Figure 1 footnote a
The initial search was performed on October 13, 2017 and re-run with modifications on October 16, 2017.
The attrition flow diagram describes the process by which articles were selected for the literature review. The process is broken down into four stages: Identification, Screening, Eligibility and Included.
Stage 1: Identification
105 records were identified through database searching. 5 additional records were identified through other sources.
41 records remained after duplicates were removed from the 110 records.
Stage 2: Screening
41 records were screened.
Of these 41 records, 25 records were excluded.
Stage 3: Eligibility
16 full-text articles were assessed for eligibility.
Of these 16 full-text articles, 8 full-text articles were excluded. The exclusion breakdown is as follows:
- n=5: Compared vaccine effectiveness for subunit and split virus inactivated influenza vaccine in different seasons
- n=1: No outcome of interest
- n=2: Secondary research
Stage 4: Included
Of the 16 full-text articles assessed for eligibility, 8 studies were included in the qualitative synthesis.
The initial search was performed on October 13, 2017 and re-run with modifications on October 16, 2017.
The attrition flow diagram describes the process by which articles were selected for the literature review. The process is broken down into four stages: Identification, Screening, Eligibility and Included.
Stage 1: Identification
105 records were identified through database searching. 5 additional records were identified through other sources.
41 records remained after duplicates were removed from the 110 records.
Stage 2: Screening
41 records were screened.
Of these 41 records, 25 records were excluded.
Stage 3: Eligibility
16 full-text articles were assessed for eligibility.
Of these 16 full-text articles, 8 full-text articles were excluded. The exclusion breakdown is as follows:
- n=5: Compared vaccine effectiveness for subunit and split virus inactivated influenza vaccine in different seasons
- n=1: No outcome of interest
- n=2: Secondary research
Stage 4: Included
Of the 16 full-text articles assessed for eligibility, 8 studies were included in the qualitative synthesis.
| Study | Location | Season | Design | Population | Outcome |
|---|---|---|---|---|---|
| Camilloni, 2016Footnote 9 | Italy | 1988–1989 to 2014–2015 |
Cohort | 60 years of age and older | Immunogenicity |
| Del Giudice, 2006Footnote 10 | Not stated | 2003–2004 | Not stated | 60 years of age and older | Immunogenicity |
| Kissling, 2014Footnote 11 | Seven European countries | 2012–2013 | Test-negative case-control | 60 years of age and older | Vaccine effectiveness |
| Morales, 2003Footnote 12 | Colombia | 1999–2000 | RCT | 60 years of age and older | Immunogenicity |
| Rondy, 2017Footnote 13 | 11 European countries | 2015–2016 | Test-negative case-control | 65 years of age and older | Vaccine effectiveness |
| Skowronski, 2012Footnote 14 | Canada | 2011–2012 | RCT | 65 years of age and older | Immunogenicity |
| Talbot, 2015Footnote 15 | United States | 2008–2009, 2010–2011, and 2011–2012 |
Test-negative case-control | 50 years of age and older (subpopulation: 65 years of age and older) | Vaccine effectiveness |
| Zei, 1991Footnote 16 | Italy | 1989–1990 | CCT | 60 years of age and older | Immunogenicity |
| Abbreviations: CCT, clinical controlled trial; RCT, randomized controlled trial | |||||
Vaccine effectiveness
Three of the included studies reported on the vaccine effectiveness of unadjuvanted, standard-dose subunit and split virus IIVsFootnote 11Footnote 13Footnote 15 with only one study reporting a direct estimate for the difference in vaccine effectiveness between the two types of influenza vaccinesFootnote 15. All three studies used test-negative case-control designs and all three were rated as “fair” according to criteria outlined by Harris et al.Footnote 8. None of the studies reported a significant difference in vaccine effectiveness between subunit IIV and split virus IIV against any laboratory-confirmed influenza virus strain Footnote 11Footnote 15 against influenza A(H1N1), A(H3N2) or B virus specificallyFootnote 11Footnote 15 or against hospitalization due to influenzaFootnote 13.
Immunogenicity
Five studies were identified that reported on the immunogenicity of subunit and split virus trivalent influenza vaccines (TIVs)Footnote 9Footnote 10Footnote 12Footnote 14Footnote 16. Of these studies, only two reported a direct comparison between the two types of vaccinesFootnote 9Footnote 16. Three of the five studies were evaluable by Harris et al. criteriaFootnote 9Footnote 12Footnote 16 of which one received a “fair” ratingFootnote 12 and two received “poor” ratingsFootnote 9Footnote 16. The two other studies did not report study methodology in sufficient detail to assess study qualityFootnote 10Footnote 14. The immunogenicity outcomes assessed by the identified studies included geometric mean fold rise in HA titres (i.e., ratio of post- to pre-vaccination geometric mean titre), seroprotection rate (i.e., proportion of participants with HA titres of at least 40 post-vaccination) and seroconversion rate (i.e., proportion of participants with at least a four-fold increase in HA titres post-vaccination, HA titre increase from less than 10 pre-vaccination to at least 40 post-vaccination, or both). Four studies assessed protection against the influenza virus strains contained within the vaccines. Two studies reported direct comparisons of immunogenicity measuresFootnote 9Footnote 16 and two reported indirect comparisonsFootnote 10Footnote 12. Overall, the studies showed no consistent significant differences in geometric mean fold rise, seroprotection rate or seroconversion rate between split virus IIVs and subunit IIVs against influenza A(H1N1), A(H3N2) or B. In addition, two studies indirectly assessed cross-protection against variant influenza strainsFootnote 10Footnote 14. Neither of these studies found a significant difference in geometric mean fold rise, seroprotection rate or seroconversion rate between split virus IIVs and subunit IIVs.
Discussion
The overall quality of vaccine effectiveness evidence was fair, with one study reporting a direct vaccine effectiveness estimate and two studies reporting an indirect vaccine effectiveness estimate. The reported vaccine effectiveness estimates for split virus IIVs and subunit IIVs all had widely overlapping confidence intervals; however, without a direct comparison, it is difficult to draw firm conclusions on the comparative vaccine effectiveness of the two vaccines types. The authors of one of these studies also noted that there were likely important differences between study sites that were not controlled for, and that any comparisons between vaccine effectiveness of subunit IIV and split virus IIV should be interpreted with cautionFootnote 13.
Findings from the studies that reported on immunogenicity were not consistent, and the overall quality of immunogenicity evidence was weak. All studies had at least one serious concern, the most common being the comparability between intervention groups. Two studies did not provide enough information to evaluate their qualityFootnote 10Footnote 14. Also, all included studies assessed immunogenicity by hemagglutination inhibition assay. These assays assess antibody as opposed to cell-mediated response, but the latter has been shown to be a more robust correlation of protection in older adultsFootnote 17. In addition, the amount of HA antigen in unadjuvanted, standard-dose subunit IIVs and split virus IIVs is standardized; therefore, HA antibody titres may not be an appropriate measure of immunogenicity to answer this research question.
Limitations
Due to the small number of records returned by the initial database search, post-hoc protocol modifications were made that were more consistent with a traditional systematic review than the initial rapid review protocol; however, screening was still conducted by a single reviewer. A study by Edwards et al. found that study selection involving only one reviewer missed an average of 8% of eligible studies compared with study selection involving two reviewersFootnote 18; therefore, some studies may have been erroneously excluded. The impact that this factor would have on the conclusions drawn from a rapid review are still unclear. In addition, it is possible that the database search strategy missed some studies that examined vaccine effectiveness or immunogenicity by vaccine type in sub-analyses or as a secondary outcome; however, hand searching reference lists would help mitigate the number of eligible articles of this type that may have been excluded by the search criteria. Another important limitation of this review is that many of the included studies defined older adults as participants who were 60 years of age and older. The inclusion of adults 60 to 64 years of age may lead to greater healthy vaccine bias, as adults in this age range on average may be healthier than adults 65 years of age and older; therefore, estimates from these studies should be interpreted with caution in the Canadian context, where older individuals are commonly defined as adults 65 years of age and older.
Conclusion
The NACI concludes that there is insufficient evidence to determine significant differences in the vaccine effectiveness or immunogenicity of unadjuvanted, standard-dose subunit and split virus IIVs in adults 65 years of age and older (Grade I evidence). The evidence is inconsistent and is not of sufficient quantity or quality to make specific recommendations on the differential use of unadjuvanted, standard-dose subunit and split virus IIVs in older adults.
Authors’ statement
IG – Writing – original draft, writing – review and editing
KY – Writing – original draft, writing – review and editing
The NACI Literature Review on the Comparative Effectiveness and Immunogenicity of Subunit and Split Virus Inactivated Influenza Vaccines in Adults 65 Years of Age and Older was prepared by K Young, L Zhao, R Stirling and MK Doll and approved by NACI.
Conflict of interest
None.
Acknowledgements
Influenza Working Group Members: I Gemmill (Chair), C Bancej, L Cochrane, N Dayneka, L Grohskopf, G Jayaraman, D Kumar, J Langley, M Lavoie, J McElhaney, A McGeer, D Moore, B Warshawsky and J Xiong
NACI Members: C Quach (Chair), W Vaudry (Vice-Chair), N Dayneka, S Deeks, P DeWals, V Dubey, R Harrison, M Lavoie, C Rotstein, M Salvadori, B Sander, N Sicard and R Warrington
Liaison Representatives: J Brophy (Canadian Association for Immunization Research and Evaluation), E Castillo (Society of Obstetricians and Gynaecologist of Canada), A Cohn (Centres for Disease Control and Prevention, United States), T Cole (Canadian Immunization Committee), J Emili (College of Family Physicians of Canada), K Klein (Council of Chief Medical Officers of Health), C Mah (Canadian Public Health Association), D Moore (Canadian Paediatric Society) and A Pham-Huy (Association of Medical Microbiology and Infectious Disease Canada)
Ex-Officio Representatives: K Barnes (National Defence and the Canadian Armed Forces), G Charos (Centre for Immunization and Respiratory Infectious Diseases [CIRID], Public Health Agency of Canada [PHAC]), G Coleman (Biologics and Genetic Therapies Directorate, Health Canada [HC]), J Gallivan (Marketed Health Products Directorate, HC), G Poliquin (National Microbiology Laboratory, PHAC), J Pennock (CIRID, PHAC) and T Wong (First Nations and Inuit Health Branch, HC)
The NACI gratefully acknowledges the contribution of L Glandon, A House, M Laplante, K Moncion and T Museau to the literature review.
Funding
The National Advisory Committee on Immunization work is supported by the Public Health Agency of Canada.