
Best practices for addressing vaccine hesitancy

 Download this article as a PDF
Download this article as a PDFPublished by: The Public Health Agency of Canada
Issue: Volume 46–2/3: Public Health Network
Date published: February 6, 2020
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 46–2/3, February 6, 2020: Public Health Network
Series
Optimizing communication material to address vaccine hesitancy
Eve Dubé1,2, Dominique Gagnon1, Maryline Vivion1
Affiliations
1 Institut national de santé publique du Québec, Québec, QC
2 Centre de recherche du CHU de Québec-Université Laval, Québec, QC
Correspondence
Suggested citation
Dubé E, Gagnon D, Vivion M. Optimizing communication material to address vaccine hesitancy. Can Commun Dis Rep 2020;46(2/3):48–52. https://doi.org/10.14745/ccdr.v46i23a05
Keywords: vaccine hesitancy, communication, vaccine uptake, information products, risk communication, vaccine acceptance, vaccine misinformation
Abstract
Vaccine hesitancy (the reluctance to accept recommended vaccines) is a complex issue that poses risk communication challenges for public health authorities and clinicians. Studies have shown that providing too much evidence on vaccine safety and efficacy to those who are vaccine-hesitant has done little to stem the growth of hesitancy-related beliefs and fears. The objective of this paper is to describe good practices in developing communication materials to address vaccine hesitancy.
An inventory of vaccination communication materials in Canada was assessed according to the Council of Canadian Academies Expert Panel on Health Product Risk Communication Evaluation (2015). Many of the current communication products could be improved to better align with evidence-based risk communication best practices. Five best practices were identified. First, identify target audience and establish trust. Second, provide both the risks and benefits of vaccination, as most people are looking for balanced information. Third, give the facts before addressing the myths. Fourth, use visual aids. Fifth, test communication material prior to launch.
Applying these best practices to current or future communication products will help vaccine providers (including physicians, nurse practitioners, pharmacists, public health professionals) to develop communication materials that are sensitive to the complex ways that people process and value information and thus more likely to optimize vaccine uptake in their communities.
Introduction
Studies have shown that providing evidence of vaccine safety and efficacy to those who are vaccine-hesitant has done little to stem the growth of hesitancy-related beliefs and fears. Previous research has shown that messaging that too strongly educates and advocates vaccination can be counterproductive for those who are already hesitantFootnote 1. Providing too much information can even generate hesitancyFootnote 2. To address this paradoxical effect of some communication material, research has been done on what communication techniques and strategies are most effective. Research evidence of what works (or not) in health risk communication has been compiled by Fischhoff and colleaguesFootnote 3 and endorsed as good practices by the Council of Canadian Academies Expert Panel on Health Product Risk Communication EvaluationFootnote 4. To explore how Canadian communication material reflects these best practices, we assessed an inventory of Canadian vaccination communication materials (websites, factsheets, posters, videos, etc.) using Fischhoff’s good practicesFootnote 3.
Although the communication of information is one of the primary tools at the disposal of vaccine providers, information alone is unlikely to dramatically change vaccine acceptance. Given the amount of financial and human resources invested in developing and diffusing communication materials about vaccination, it is critical to optimize these tools to ensure that they work as intended. The objective of this paper is to describe good practices in developing communication materials to address vaccine hesitancy. This is the second of a series of articles, produced by the Canadian Vaccination Evidence Resource and Exchange Centre (CANVax), which include both the identification of existing resources and the creation of new resources by this group of multidisciplinary professionalsFootnote 5Footnote 6.
General observations
Our analysis showed that existing communication materials in Canada could be improved to better align with established best practices in risk communication. We found that most communication material focused on risks of vaccine-preventable diseases, the risks of adverse events and “debunking common myths”. The approaches used to debunk myths generally focused on the myth itself rather than the correct information. We found the information about risk was mainly qualitative (e.g. “The risk of adverse events after immunization is small” and “The diseases we can prevent with vaccines can lead to pneumonia, deafness, brain damage, heart problems, blindness and paralysis in children who are not protected”). Few of the materials used probabilities to quantify risks. When probabilities appeared, they were unidirectional (e.g. presenting only risk of diseases or number of cases in an outbreak) rather than bidirectional (e.g. presenting risk of diseases and risk of adverse events after immunization). Only a minority of the materials used graphics or videos.
We then did a limited scan of international materials and found that some communication tools that have been developed do meet best practices and could be adapted for Canadian parents (e.g. http://talkingaboutimmunisation.org.au/).
Best practices
Addressing vaccine hesitancy requires tailored strategies that are tested, evidence-informed and take into account that vaccine hesitancy is complex and context specific, varying across time, place and vaccine typeFootnote 7.
1. Identify target audience and establish trust
“Understanding the perspectives of the people for whom immunization services are intended, and their engagement with the issue”, wrote Goldstein and colleagues, “is as important as the information that experts want to communicate”Footnote 8. The amount, content and type of information that is needed to move a vaccine-hesitant individual toward vaccine acceptance differs greatly from the basic information needed by a person who is already favourable to vaccination and intends to vaccinate. Research has shown that vaccine-hesitant individuals are “active information-seekers” that are looking for “balanced” information presenting both pros and cons of vaccination in order to make an informed decision about vaccinesFootnote 9Footnote 10. Their information needs are usually not fulfilled with typical information from public health authorities, as this information generally does not usually provide references to scientific studies and is often perceived as focusing on the benefits of vaccines and not discussing the potential risks of vaccinesFootnote 7. Addressing those who are strongly anti-vaccines merit specific strategies. This is not the subject of the current paper but will be addressed in a future CANVax Brief.
A key factor influencing vaccination decision-making is trust in the effectiveness and safety of vaccines, in the system that delivers them, including the reliability and competence of the health services and health professionals, and in the motivations of the policy-makers who decide which vaccines are needed when and whereFootnote 11. Many studies have shown that vaccine hesitancy was not due to being uninformed or misinformed, but reflected a general distrust of doctors, government sources and/or pharmaceutical companiesFootnote 12Footnote 13Footnote 14. In this context, the perceived credibility of the institutions delivering the vaccination information often matters more than the information itselfFootnote 15, highlighting the importance of transparency and honestyFootnote 16. Presenting both the potential benefits and potential harms of vaccines is also key. Studies in other countries have shown this to be a promising approach for increasing vaccine acceptanceFootnote 17Footnote 18Footnote 19.
Research has shown that individuals, when faced with information that contradicts their values, can feel threatened and react defensively. This creates resistance, resulting in a strengthening of their initial beliefs and reducing the likelihood of engaging in the desired behavior (i.e. vaccination acceptance)Footnote 20. However, messages can be framed in ways that addresses patients’ values and promotes trustFootnote 21. For example, when human papilloma virus vaccination was framed as a cancer-prevention vaccination, less resistance was generated than when it was framed as a means to prevent a sexually transmitted infectionFootnote 22.
2. Provide both the risks and benefits of vaccination
Providing information about the risk and benefits of vaccination is not as simple as it might seemFootnote 3. When developing communication material, healthcare workers must be sensitive to the complex ways by which people process and value information. Do not assume that “numbers will speak for themselves”. How the message is developed is as important as the contentFootnote 23: while the content of the tools should be based on available scientific evidence, the development should be based on risk communicationFootnote 24.
Best practices arising from this literature review include providing data on risks and benefits of vaccination and providing critical qualitative information:
- Providing numeric likelihood of risks and benefits of vaccination
Tools should clearly define both the risks and potential consequences of not being vaccinated (risks of vaccine-preventable diseases) and the risks of adverse events after vaccination. This should be done using not just words but also numbers. Keep denominators constant (e.g. one in 10,000; 25 in 10,000) and use whole numbers rather than fraction or decimalsFootnote 25Footnote 26.
- Providing critical qualitative information
Material should not only present quantitative numeric information on vaccination risks and benefits, but should also provide qualitative information to present the evidence supporting these estimates. Focus on the critical information and why it is critical that people understand this information in order to make their vaccination decision. For example, people might not realize that their individual vaccination decision has an impact on herd immunity, or parents may not understand that postponing vaccination is an option.
3. Give facts; then address myths
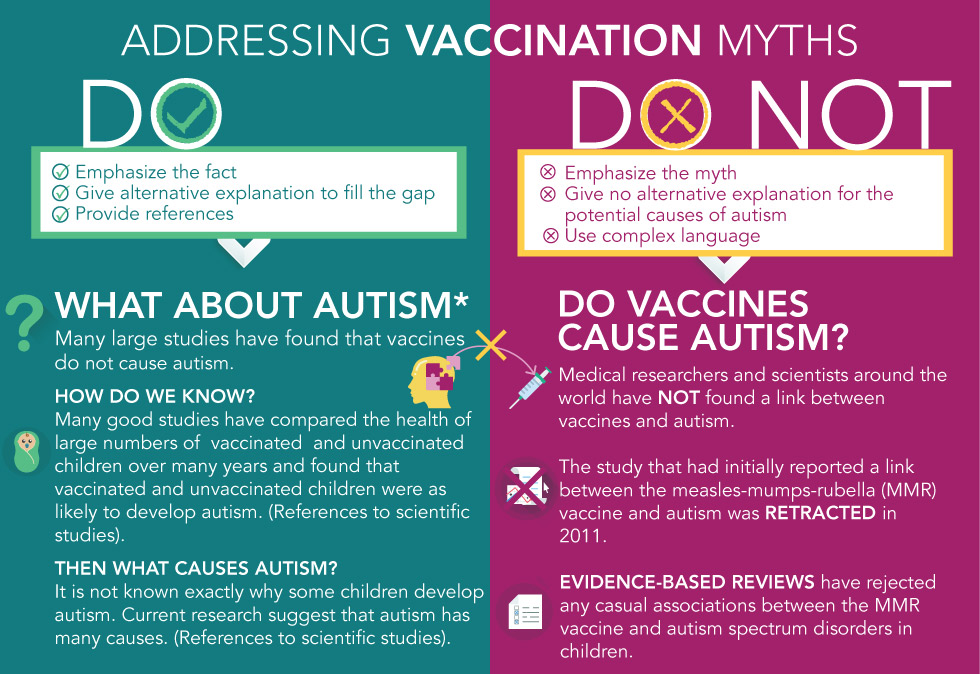
One of the main objectives of most communication material on vaccination is to “correct” misconceptions about vaccination. But communication material needs to be carefully designed, as attempts to debunk a myth could actually reinforce itFootnote 20. When developing communication material, put the emphasis on the facts, not the myths. The common technique of headlining the vaccination myth in big, bold letters is not the best strategy, as people will remember the myth, not the fact. Instead, communicate the core fact in the headline, and then follow-up with an alternative explanation. When a myth is debunked, a gap in the person’s mind is created. To be effective, the communication material must then fill that gap (Figure 1).
Figure 1: Addressing vaccination myths
Text description: Figure 1
Figure 1: Addressing vaccination myths
This figure notes the “Do’s” and “Dont’s” addressing vaccination myths. The image has two columns; the right column are the “Do’s” and on the left are the “Dont’s”. The “Do’s” column starts with three points:
- Emphasize the fact
- Give alternative explanation to fill the gap
- Provide references concerning vaccination
Immediately below these points are three questions and answers addressing a few vaccination myths:
Question: What about autism?
Answer: Many large studies have found that vaccines do not cause autism.
Question: How do we know?
Answer: Many good studies have compared the health of large numbers of vaccinated and unvaccinated children over many years and found that vaccinated and unvaccinated children were as likely to develop autism. (References to scientific studies).
Question: Then what causes autism?
Answer: It is not known exactly why some children develop autism. Current research suggest that autism has many causes. (References to scientific studies).
The “Dont’s” column has three points:
- Emphasize the myth
- Give no alternative explanation for the potential causes of autism
- Use complex language
Immediately below these points is a question and answer concerning a vaccination myth:
Question: Do vaccines cause autism?
Answer: Medical researchers and scientists around the world have NOT found a link between vaccines and autism.
The study that had initially reported a link between the measles-mumps-rubella (MMR) vaccine and autism was retracted in 2011.
Evidence-based reviews have rejected any casual associations between the MMR vaccine and autism spectrum disorders in children.
4. Use visual aids
Visual supports like infographics or video can enhance a person’s understanding of complex risk information. Studies have shown that visual aids may help people to understand health risks, especially for those with low numeracy skillsFootnote 27Footnote 28. Visual aids include videos, pictures, icons array (i.e. a picture using one shape that is repeated a specific number of times, usually 10, 100 or 1,000, with some of the shapes altered, usually in a different color, to represent a proportion) or infographics (i.e. a combination of images and text to quickly summarize a large amount of information). Graphs can make numeric information easier to understand and pictographs are the best strategy for communicating both gist (meaning) and verbatim (exact details) knowledge (Figure 2).
Figure 2: A short introduction on vaccine safety by Immunize Canada

Text description: Figure 2
Figure 2: A short introduction on vaccine safety by Immunize Canada
The figure is a snapshot that was taken from a short video on vaccine safety. This is a video that is currently on YouTube by Immunization Canada. The figure has multiple multicultural cartoon characters to the bottom right with the words above the characters noting “vaccination protects us from disease”.
5. Test communication prior to launching
It is important to test a communication material prior to launching to make sure it is working as intended for the target audience. The results might be surprising: a study showed that information given in frequency formats (e.g. one out of 10 infants will have a fever after a vaccination) were perceived as more risky than the same information conveyed in probabilistic terms (e.g. 10% of infants will have a fever after a vaccination)Footnote 27. Studies have also shown that as many as one out of two adults do not have the necessary skills to interpret probabilities and other mathematical conceptsFootnote 27Footnote 28.
- Use communication material that is clear and easy to understand
Use simple language, short sentences and subheadings. Avoid dramatic language and derogatory comments that alienate people. It is important that numbers used are easy to understandFootnote 28.
- Avoid the back-fire effect
For those who are strongly fixed in their views, being confronted with counter-arguments can cause their views to be strengthenedFootnote 29. Testing communication material is important, as even carefully crafted efforts to influence individuals holding factually incorrect beliefs can, in fact, reinforce these beliefsFootnote 29.
Conclusion
Risk messaging cannot be “one-size-fits-all”. Most people are seeking balanced information on vaccines when deciding whether to take them or not. People need to verify with their health care provider that there is misinformation on vaccines. People with strong antivaccination views may not change their minds, regardless of what the message is or how it is communicated, so short messaging may be all that is indicated. To address the spectrum of beliefs that contribute to vaccine hesitancy, communication materials need to be tailored and targeted to these different knowledge systems, and the unique information needs and preferences of particular communitiesFootnote 8Footnote 23. Updates on this issue will be published on the CANVax websiteFootnote 5.
Authors’ statement
- ED — Conceptualization, supervision, writing—original draft
- DG — Writing—review and editing
- MV — Data curation, formal analysis, writing—review and editing
Conflict of interest
Dr. Dubé reports grants from the Public Health Agency of Canada, the Quebec ministry of Health and Social services, le Fonds de recherche en Santé du Québec, the Canadian Institutes of Health Research, the Canadian Immunization Research Network, and the Social Sciences and Humanities Research Council of Canada. Dr. Vivion reports grants from Canadian Public Health Association and from Canadian Immunization Research Network during the conduct of the study.
Funding
The analysis of communication material was supported by the Canadian Immunization Research Network under Grant 385094. The development of the CANVax Briefs are supported by the Immunization Partnerships Funds of the Public Health Agency of Canada.
