
Hepatitis C estimates in Canada, 2019

 Download this article as a PDF
Download this article as a PDFPublished by: The Public Health Agency of Canada
Issue: Volume 48-11/12, November/December 2022: Antimicrobial Use and Stewardship
Date published: November/December 2022
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 48-11/12, November/December 2022: Antimicrobial Use and Stewardship
Overview
National Hepatitis C estimates: Incidence, prevalence, undiagnosed proportion and treatment, Canada, 2019
Nashira Popovic1, Anson Williams1, Simone Périnet1, Laurence Campeau1, Qiuying Yang1, Fan Zhang1, Ping Yan1, Jordan Feld2, Naveed Janjua3, Marina Klein4, Mel Krajden3, William Wong5, Joseph Cox1
Affiliations
1 Centre for Communicable Diseases and Infection Control, Public Health Agency of Canada, Ottawa, ON
2 Toronto Centre for Liver Disease, Toronto General Hospital, University Health Network, Toronto, ON
3 British Columbia Centre for Disease Control, Vancouver, BC
4 Department of Medicine, McGill University Health Center, Montréal, QC
5 School of Pharmacy, University of Waterloo, Kitchener, ON
Correspondence
Suggested citation
Popovic N, Williams A, Périnet S, Campeau L, Yang Q, Zhang F, Yan P, Feld JJ, Janjua NZ, Klein MB, Krajden M, Wong W, Cox J. National Hepatitis C estimates: Incidence, prevalence, undiagnosed proportion and treatment, Canada, 2019. Can Commun Dis Rep 2022;48(11/12):540–9. https://doi.org/10.14745/ccdr.v48i1112a07
Keywords: Hepatitis C, prevalence, incidence, epidemiology, Canada
Abstract
Background: Estimates of the number of hepatitis C virus (HCV) infections are important for monitoring efforts aimed at preventing disease transmission, especially following the introduction of a highly effective treatment. This report provides updated estimates of HCV incidence, prevalence, undiagnosed proportion and treatment in Canada.
Methods: A combination of back calculation modelling and a modified version of the workbook method were used to estimate the incidence and prevalence of anti-HCV positive persons, the prevalence of chronic HCV infection and the undiagnosed proportion. The number of people treated for chronic HCV was estimated using administrative pharmaceutical data.
Results: An estimated 9,470 new infections occurred in 2019, corresponding to an incidence rate of 25 per 100,000 population, a 7.7% decrease since 2015. The estimated prevalence of anti-HCV antibodies in the Canadian population was 1.03% (plausible range: 0.83%–1.38%), and the estimated prevalence of chronic HCV was 0.54% (plausible range: 0.40%–0.79%). The overall proportion of anti-HCV positive persons who were undiagnosed was estimated at 24% of all infections, with individuals born between 1945 and 1975 being the priority population the most likely to be undiagnosed. An estimated 74,500 people with chronic HCV have been treated since the introduction of direct-acting antivirals in 2014.
Conclusion: Estimates of HCV incidence and prevalence are key metrics to guide interventions and resource allocation. While our estimates show that HCV incidence has decreased in Canada in recent years and treatment of chronic HCV has continued to increase, ongoing efforts are required to reduce the burden of HCV in Canada.
Introduction
Globally, an estimated 58 million people have chronic hepatitis C virus (HCV) infection, with about 1.5 million new infections occurring per year Note de bas de page 1. The number of people living with HCV has continued to increase, even though an effective cure exists Note de bas de page 2. Canada has developed a pan-Canadian framework for action Note de bas de page 3 as well as an accompanying Government of Canada five-year action plan Note de bas de page 4 to help guide Canada's efforts towards reducing the health impacts of sexually transmitted and blood-borne infections (STBBIs) in Canada by 2030.
The Global Health Sector Strategies on human immunodeficiency virus (HIV), viral hepatitis and sexually transmitted infections introduced targets for viral hepatitis control and elimination by 2030 Note de bas de page 2. These include targets for the following: reduction of the annual number of new infections overall and among people who inject drugs; the reduction of the number of deaths from HCV; and an increase in the proportion of people living with HCV who have been diagnosed and cured. While the Government of Canada endorses these global targets, the first priority of the pan-Canadian STBBI action plan Note de bas de page 4 is to develop domestic indicators and targets that will allow for the monitoring of Canada's progress.
This report provides an update for 2019 on Canada's estimates of HCV incidence, prevalence, proportion of undiagnosed and treated cases, which supports the Government of Canada's commitment to monitor and report on progress towards hepatitis C elimination.
Methods
A combination of back-calculation statistical modelling Note de bas de page 5 and a modified version of the workbook method Note de bas de page 6 were used to estimate new anti-HCV seropositivity (incidence), prevalence of anti-HCV positive persons (i.e. persons who have ever been infected with HCV), the prevalence of ribonucleic acid (RNA)-positive persons (i.e., persons with active infection, as a proxy for chronic HCV infection) and the undiagnosed/unaware proportion of the population. This methodology was developed and refined through a series of consultations that took place between 2019 and 2022. Experts from a variety of backgrounds were consulted, including hepatologists, research epidemiologists, laboratory specialists and mathematical modellers.
Back calculation modelling
Back calculation is a widely used computational method to infer disease infections—which are not observable—from consequential results such as reported diagnostic cases. The method was initially designed to estimate the HIV/acquired immunodeficiency syndrome incidence Note de bas de page 5 and was later adopted to estimate Canadian HCV incidence and prevalence for 2011 Note de bas de page 7. Following the same approach, back calculation modelling was conducted using HCV routine surveillance data from the Canadian Notifiable Diseases Surveillance System, extracted on October 22, 2021. All reported cases (acute, chronic and unspecified) from 1991 to 2019 from five large Canadian provinces (British Columbia, Alberta, Saskatchewan, Ontario and Québec) were used. These provinces, which represented 90% of the Canadian population in 2019 Note de bas de page 8, are the only ones who provide record-level HCV surveillance data. Modelled results were then extrapolated to the entire country. More information on the modelling can be found in Appendix A.
Modified workbook method
The workbook method is an established approach previously used to produce estimate of HIV prevalence in low level and concentrated HIV epidemics Note de bas de page 6. A modified version of this method was used to estimate the number of anti-HCV positive persons as well as their diagnosis status, and the number of HCV RNA-positive persons in Canada. We divided the Canadian population into subgroups that are known to be at higher risk of infection, and synthesized published and unpublished data to estimate prevalence within each subgroup. Each anti-HCV seroprevalence measure was classified as an "underestimate", "overestimate" or "appropriate estimate" based on a review of the methodology of each study. The under and over-estimates were used as plausible ranges of the appropriate estimates.
Estimates of the population size of each subgroup in Canada were based on data from Statistics Canada Note de bas de page 8 Note de bas de page 9 Note de bas de page 10, as well as unpublished data obtained through personal communications, as detailed in the systematic review section. Point estimates of HCV prevalence were produced along with their upper and lower bounds by multiplying the HCV prevalence by the corresponding population size estimate.
The workbook subgroup populations were based on the following priority populations, as outlined in the Blueprint to inform hepatitis C elimination efforts in Canada Note de bas de page 11:
- People who inject drugs (PWID)
- Adults in the 1945–1975 birth cohort
- Immigrant populations
- Indigenous peoples (First Nations, Inuit and Métis)
- Gay, bisexual and other men who have sex with men (gbMSM)
- People who are incarcerated (PWAI) in federal and provincial prisons
Due to the extensive overlap between these priority populations, they were not considered to be mutually exclusive.
Systematic review
A health librarian at the Public Health Agency of Canada conducted a series of literature searches to obtain data on 1) HCV incidence and prevalence in Canada from January 1, 2019, to October 1, 2021, and 2) the unaware/undiagnosed proportion of HCV infection in Canada from January 1, 2016, to October 1, 2021. The literature searches yielded an initial 1,187 records, with an additional 31 records found outside of the librarian search. Using the systematic review protocol for prevalence and incidence studies developed by Joanna Briggs Institute Note de bas de page 12, two independent reviewers screened all studies for inclusion. Discrepancies between reviewers were resolved through discussion. A total of 43 records were included after the final review and considered for use in the workbook method. Details about this process can be found in Appendix B.
In addition to the sources identified through the systematic review, unpublished data were requested from organizations and researchers. These sources included Canadian Blood Services (unpublished data from Hepatitis C Surveillance, Canadian Blood Services, 2015–2019) and Héma-Québec (unpublished data on first-time donors, Héma-Québec, 2015–2019), Correctional Services Canada (unpublished data from Correctional Services Canada, 2015–2021), Tracks bio-behavioural survey data (unpublished data from Tracks survey of people who inject drugs in Canada, Phase 4 Public Health Agency of Canada, 2017–2019), and the Engage cohort study (unpublished data from Engage Cohort Study, 2017–2019).
Chronic hepatitis C prevalence and undiagnosed proportion estimates
The overall seroprevalence estimate derived from the workbook method was used as the starting point to estimate the overall chronic hepatitis C prevalence in Canada (Figure 1). First, we subtracted the estimated number of individuals who had spontaneously cleared the virus, using a 30% clearance estimate based on a range of clearance proportions measured in Canadian studies Note de bas de page 13 Note de bas de page 14 Note de bas de page 15 Note de bas de page 16 Note de bas de page 17. We then subtracted the estimated number of cured individuals, which was calculated using Canadian treatment estimates from the British Columbia Centre for Disease Control (unpublished data on HCV Treatment Initiation in Canada, British Columbia Centre For Disease Control, 2012–2016) and IQVIA (unpublished data from Provincial Patient Summary report, IQVIA, 2017–2019), using a cure rate of 48% for 2012–2014, and of 90% for 2015–2019. This calculation yielded a remaining number of HCV RNA-positive individuals in Canada, which was used as a proxy for chronic HCV infection.
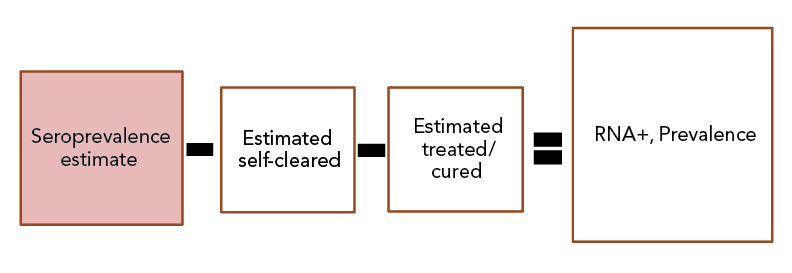
Figure 1 - Text description
The overall seroprevalence estimate derived from the workbook method was used as the starting point to estimate the overall chronic hepatitis C prevalence in Canada. From this number, we subtracted the estimated number of individuals who had spontaneously cleared the virus. We then subtracted the estimated number of cured individuals. This calculation yielded the remaining number of hepatitis C virus RNA positive individuals in Canada.
Lastly, the estimate of the undiagnosed/unaware proportion of anti-HCV infection in Canada was determined by taking the midpoint between the back calculation modelling estimate and the modified workbook estimate. This approach was chosen to minimize the uncertainty that is inherent to estimates, which are partly based on assumptions due to the incompleteness of available data. Although uncertainty can never be completely eliminated, the true number likely lies between those two estimates.
Results
Hepatitis C virus incidence
According to back calculation modelling, an estimated 9,470 new HCV antibody-positive infections occurred in 2019, corresponding to an annual incidence rate of 25 per 100,000 population. When modelled by birth cohort, the highest annual incidence was estimated among persons born after 1974 at 5,115 new infections, followed by persons born between 1945 and 1974 at 4,354 new infections. There were no new HCV infections estimated among persons born before 1945 (Figure 2).
Figure 2 - Text description
| Year | All | Before 1945 | 1945–1974 | 1975+ |
|---|---|---|---|---|
| 1980 | 3,702 | 1725 | 1,977 | 0 |
| 1981 | 5,155 | 1543 | 3,612 | 0 |
| 1982 | 7,321 | 1336 | 5,985 | 0 |
| 1983 | 10,069 | 1120 | 8,947 | 2 |
| 1984 | 13,021 | 904 | 12,112 | 6 |
| 1985 | 15,749 | 703 | 15,028 | 17 |
| 1986 | 17,945 | 530 | 17,369 | 45 |
| 1987 | 19,438 | 382 | 18,937 | 119 |
| 1988 | 20,062 | 267 | 19,542 | 253 |
| 1989 | 19,631 | 178 | 18,970 | 484 |
| 1990 | 18,142 | 115 | 17,230 | 796 |
| 1991 | 15,918 | 71 | 14,709 | 1,138 |
| 1992 | 13,577 | 41 | 12,014 | 1,522 |
| 1993 | 11,383 | 24 | 9,666 | 1,693 |
| 1994 | 9,705 | 14 | 7,924 | 1,768 |
| 1995 | 8,659 | 7 | 6,811 | 1,841 |
| 1996 | 8,142 | 3 | 6,204 | 1,934 |
| 1997 | 8,194 | 2 | 5,949 | 2,243 |
| 1998 | 8,197 | 1 | 5,898 | 2,298 |
| 1999 | 8,274 | 0 | 5,926 | 2,348 |
| 2000 | 8,425 | 0 | 5,947 | 2,478 |
| 2001 | 8,513 | 0 | 5,910 | 2,602 |
| 2002 | 8,682 | 0 | 5,811 | 2,872 |
| 2003 | 8,552 | 0 | 5,672 | 2,881 |
| 2004 | 8,394 | 0 | 5,524 | 2,870 |
| 2005 | 8,368 | 0 | 5,387 | 2,981 |
| 2006 | 8,508 | 0 | 5,267 | 3,241 |
| 2007 | 8,829 | 0 | 5,153 | 3,677 |
| 2008 | 9,257 | 0 | 5,012 | 4,245 |
| 2009 | 9,681 | 0 | 4,827 | 4,854 |
| 2010 | 10,000 | 0 | 4,596 | 5,404 |
| 2011 | 10,167 | 0 | 4,347 | 5,820 |
| 2012 | 10,173 | 0 | 4,133 | 6,040 |
| 2013 | 10,034 | 0 | 3,988 | 6,046 |
| 2014 | 9,836 | 0 | 3,955 | 5,881 |
| 2015 | 9,708 | 0 | 4,056 | 5,653 |
| 2016 | 9,736 | 0 | 4,264 | 5,473 |
| 2017 | 9,828 | 0 | 4,487 | 5,342 |
| 2018 | 9,670 | 0 | 4,471 | 5,199 |
| 2019 | 9,470 | 0 | 4,354 | 5,115 |
Hepatitis C virus treatment
We estimate that since the introduction of direct-acting antivirals in Canada in 2014, approximately 74,500 people living with chronic HCV were treated, with 65.9% of those treatments having occurred between 2017 and 2019. Figure 3 shows the yearly number of individuals treated, contrasted with the estimated number of new HCV infections.

Figure 3 - Text description
| Year | Estimated new antibody-positive infections | Treated individuals |
|---|---|---|
| 2012 | 10,173 | 1,424 |
| 2013 | 10,034 | 1,788 |
| 2014 | 9,836 | 3,760 |
| 2015 | 9,708 | 11,138 |
| 2016 | 9,736 | 10,496 |
| 2017 | 9,828 | 14,887 |
| 2018 | 9,670 | 17,878 |
| 2019 | 9,470 | 16,347 |
Hepatitis C virus prevalence
Using the modified workbook method, the estimated prevalence of anti-HCV in Canada in 2019 was 1.03% (plausible range: 0.83%–1.38%) or 387,000 (plausible range: 312,000–519,000) persons. Among priority populations, the highest prevalence of anti-HCV was among PWID (past 6–12 months) at 46.1% (plausible range: 28.0%–64.2%), followed by those with a lifetime history of infection drug use at 44.9% (plausible range: 25.6%–64.2%). Anti-HCV prevalence was also significantly higher among PWAI and Indigenous peoples than among the general population, at 10.7% (plausible range: 8.19%–13.2%) and 7.4% (plausible range: 3.49%–11.2%), respectively (Table 1).
| Population | Population size | Anti-HCV positive prevalence (%) | Number of anti-HCV positive persons | References | ||||
|---|---|---|---|---|---|---|---|---|
| Point estimate | Lower bound | Upper bound | Point estimate | Lower bound | Upper bound | |||
| General population | 37,601,230 | 1.03% | 0.83% | 1.38% | 387,000 | 312,000 | 519,000 | Note de bas de page 8 Note de bas de page 18 Note de bas de page 19 Note de bas de page 20 Note de bas de page 21 Unpublished data from Hepatitis C Surveillance, Canadian Blood Services, 2015–2019 Unpublished data on first-time donors, Héma-Québec, 2015–2019 |
| PWID—Current (PWID in the past 6–12 months) |
133,651 | 46.1% | 28.0% | 64.2% | 61,600 | 37,400 | 85,800 | Note de bas de page 18 Note de bas de page 22 Note de bas de page 23 Personal communication, Williams A. Sorge J., 2022 |
PWID—History (People who have a lifetime history of injection drug use) |
389,574 | 44.9% | 25.6% | 64.2% | 175,000 | 99,800 | 250,000 |
Personal communication, Williams A. Sorge J., 2022 |
| Adults in the 1945–1975 birth cohort | 13,975,919 | 1.74% | 1.27% | 2.20% | 242,000 | 177,000 | 307,000 | Note de bas de page 8 Note de bas de page 18 Note de bas de page 19 Note de bas de page 20 Note de bas de page 24 Note de bas de page 25 Note de bas de page 26 Note de bas de page 27 |
| Immigrant population | 11,778,177 | 1.51% | 0.70% | 2.32% | 178,000 | 82,500 | 273,000 | Note de bas de page 18 Note de bas de page 20 Note de bas de page 28 |
| Indigenous peoples (First Nations, Inuit, Métis) |
1,826,356 | 7.35% | 3.49% | 11.2% | 134,000 | 63,700 | 205,000 | Note de bas de page 18 Note de bas de page 29 |
| gbMSM | 640,785 | 3.70% | 1.70% | 5.10% | 23,400 | 10,900 | 32,700 | Note de bas de page 30 Note de bas de page 31 Note de bas de page 32 Unpublished data from Engage Cohort Study, 2017–2019 |
| People who are incarcerated—Federal and provincial | 37,932 | 10.7% | 8.19% | 13.2% | 4,050 | 3,110 | 5,000 | Note de bas de page 9 Note de bas de page 33 Note de bas de page 34 Note de bas de page 35 Unpublished data from Correctional Services Canada, 2015–2021 |
|
||||||||
Of the estimated number of persons ever infected with HCV (anti-HCV positive), an adjustment of 30% or 116,188 persons was made to account for individuals who spontaneously cleared HCV infection. A second adjustment of 67,018 persons was made to account for individuals who were cured of HCV infection through treatment. After adjusting for HCV clearance and treatment, the estimate of chronic HCV prevalence was 0.54% (plausible range: 0.40%–0.79%) or 204,000 persons (plausible range: 151,000–296,000).
Among priority populations, the highest prevalence rate of chronic HCV infection was among current PWID at 36.9% (plausible range: 12.6%–55.1%). The lowest prevalence rate among priority populations was found among adults in the 1945–1975 birth cohort at 0.9% (plausible range: 0.4%–1.3%) (Table 2).
| Population | Population size | Chronic hepatitis C prevalence (%) | Number of persons living with chronic hepatitis C | References | ||||
|---|---|---|---|---|---|---|---|---|
| Point estimate | Lower bound | Upper bound | Point estimate | Lower bound | Upper bound | |||
| PWID—Current (PWID in the past 6–12 months) |
133,651 | 36.9% | 12.6% | 55.1% | 49,300 | 16,800 | 73,600 | Note de bas de page 18 Note de bas de page 22 Unpublished data from Tracks survey of people who inject drugs in Canada, Phase 4 - Public Health Agency of Canada, 2017–2019 Personal, Williams A. Sorge J., 2022 |
| PWID—History (People who have a lifetime history of injection drug use) |
389,574 | 29.6% | 22.3% | 36.9% | 115,000 | 87,000 | 144,000 | Note de bas de page 18 Note de bas de page 22 Note de bas de page 24 |
| Adults in the 1945–1975 birth cohort | 13,975,919 | 0.87% | 0.44% | 1.30% | 122,000 | 61,500 | 182,000 | Note de bas de page 8 Note de bas de page 18 Note de bas de page 20 |
| Immigrant population | 11,778,177 | Insufficient data | N/A | |||||
| Indigenous peoples (First Nations, Inuit, Métis) |
1,826,356 | 3.5% | 2.0% | 5.0% | 63,900 | 36,500 | 91,300 | Note de bas de page 18 Note de bas de page 29 Note de bas de page 36 |
| gbMSM | 640,785 | 1.1% | 0.4% | 1.7% | 7,050 | 2,560 | 10,900 |
Unpublished data from Engage Cohort Study, 2017–2019 |
| People who are incarcerated—Federal and provincial | 37,932 | 3.7% | 2.3% | 5.1% | 1,400 | 870 | 1,940 |
Unpublished data from Correctional Services Canada, 2015–2021 |
|
||||||||
Undiagnosed proportion
The overall proportion of anti-HCV positive persons in Canada who were undiagnosed or unaware of their HCV status was estimated at 24% or 79,500 persons (data not shown). This was calculated by taking the midpoint between the modelling estimate (n=60,200, 19.2%) and the modified workbook estimate (n=98,800, 25.5%). Among priority populations, the highest proportion of undiagnosed/unaware HCV infection was estimated among adults in the 1945–1975 birth cohort at 34.4% (plausible range: 18.8%–50.0%), followed by 22% among current PWID (plausible range: 18.5%–25.4%) and 22% among PWAI (plausible range: 12.3%–31.6%). The lowest proportion of undiagnosed/unaware was among the gbMSM population at 8.8% (plausible range: 6.7%–22.2%) (Table 3). The proportion of undiagnosed individuals could not be measured for people with a lifetime history of injection drug use, Indigenous peoples, and immigrant populations due to insufficient data.
| Population | Anti-HCV positive estimate | Undiagnosed/unaware (%) | Number of anti-HCV positive persons who were unaware/undiagnosed | References | ||||
|---|---|---|---|---|---|---|---|---|
| Point estimate | Lower bound | Upper bound | Point estimate | Lower bound | Upper bound | |||
| PWID—Current (PWID in the past 6–12 months) |
61,600 | 22.0% | 18.5% | 25.4% | 12,400 | 10,500 | 14,300 | Unpublished data from Tracks survey of people who inject drugs in Canada, Phase 4 - Public Health Agency of Canada, 2017–2019 |
| PWID—History (People who have a lifetime history of injection drug use) |
175,000 | Insufficient data |
N/A | |||||
| Adults in the 1945–1975 birth cohort | 242,000 | 34.4% | 18.8% | 50.0% | 83,400 | 45,600 | 121,000 | Note de bas de page 27 Note de bas de page 37 Note de bas de page 38 Note de bas de page 39 Note de bas de page 40 |
| Immigrant population | 178,000 | Insufficient data |
N/A | |||||
| Indigenous peoples (First Nations, Inuit, Métis) |
134,000 | Insufficient data |
N/A | |||||
| gbMSM | 23,400 | 8.8% | 6.7% | 22.2% | 2,060 | 1,570 | 5,200 | Unpublished data from Engage Cohort Study, 2017–2019 |
| People who are incarcerated—Federal and provincial | 4,050 | 22.0% | 12.3% | 31.6% | 890 | 499 | 1,280 |
Unpublished data from Correctional Services Canada, 2015–2021 |
|
||||||||
Discussion
The national hepatitis C estimates for 2019 provided updated insights into the hepatitis trends in Canada. These estimates will be used to support the pan-Canada five-year action plan on STBBI, with the goal of reducing the health impacts of STBBI in Canada by 2030. Based on our modelling, an estimated 9,470 new hepatitis C infections (25 per 100,000 population) occurred in 2019 in Canada, which corresponds to a reduction of 7.7% in incidence compared to 2015 (Figure 3). However, this reduction rate is insufficient to meet the 90% reduction in new chronic infections outlined in the World Health Organization 2030 elimination goals, thus confirming the need for continued efforts to curb HCV transmission and improve access to treatment for all HCV-infected individuals. We estimated that in 2019, approximately 1% of the Canadian population, or roughly 387,000 persons, were anti-HCV positive, meaning they were infected by the virus at some point in time (i.e., past or current infection). Of these individuals, an estimated 76% were diagnosed as anti-HCV-positive, leaving an estimated 24% who were unaware of their anti-HCV positive status. While this figure is encouraging, more progress needs to be made to reach the goal of 90% of people living with HCV being diagnosed by 2030. Of the different priority groups, baby boomers (e.g., adults born between 1945 and 1975) were the most likely to be undiagnosed.
Additionally, an estimated 204,000 persons, or approximately half of those who were estimated to be anti-HCV positive, were HCV RNA-positive in 2019, suggesting an active infection. Direct-acting antivirals are a cornerstone in treatment to reduce the risk of complications among those individuals and avert further transmission. Since this highly effective treatment was introduced in Canada in 2014, an estimated 74,500 people with chronic hepatitis C were treated. Encouragingly, our data also shows that between 2017 and 2019, the yearly number of treated individuals largely exceeded the number of new infections. As suggested elsewhere Note de bas de page 41, maintaining high treatment uptake in the upcoming years will be essential to achieve HCV elimination in Canada by 2030.
Although our 2019 estimates confirmed that the burden of hepatitis C on the overall population is relatively low, certain populations and communities are disproportionately impacted. This is especially true for people who use injection drugs, who may face concomitant social, financial and health challenges and, therefore, require a more comprehensive approach to prevention, diagnosis and treatment. Other priority populations, including people who are incarcerated, Indigenous peoples and gbMSM, are also disproportionately affected. Targeted approaches, such as peer-supported and culturally competent outreach interventions, could be considered to reduce the burden of HCV among these groups.
Strengths and limitations
Key strengths of our approach include the use of Canadian Notifiable Diseases Surveillance System data, a comprehensive database that encompasses all laboratory-confirmed cases of HCV in Canada. The combination of back-calculation and workbook methods also provides an opportunity to improve the overall estimates and increase accuracy. Our modified workbook approach allowed us to produce the first national HCV estimates specific to the priority populations based on the Blueprint to inform hepatitis C elimination efforts in Canada Note de bas de page 11, thus making these data more actionable for policy-makers and service providers working with these groups.
Our analysis also has several limitations. First, estimates of HCV incidence were based on data on all reported cases (acute and chronic); therefore, the estimated incidence represents all individuals who developed anti-HCV antibodies. Separate estimates for the undiagnosed proportion among persons with acute and chronic infections could not be produced. Second, data by priority population were not available through routine national surveillance; therefore, national incidence estimates by priority population were not produced. As a result of these limitations, reporting on a full set of indicators against global targets was not possible at this time. Third, since individuals may identify as being members of more than one priority population, these categories are not mutually exclusive. However, unlike the workbook method used in previous national estimates, the modified workbook method does not use addition or subtraction between priority groups to yield an overall estimate for the general population. Instead, representative data for the general Canadian population were collected and a prevalence estimate was calculated independently of the other priority populations. Fourth, it was not possible to distinguish reinfections from initial infections; therefore, it is possible that individuals infected twice within the same year were counted twice in the yearly incidence estimates. Finally, treatment estimates were based on administrative pharmaceutical records of HCV treatment initiation; therefore, individuals who received HCV treatment through clinical trials or compassionate access may not be captured.
Conclusion
Estimates of HCV incidence and prevalence can be used to guide health interventions and resource allocation to link chronically infected persons to screening, care, treatment and ultimately cure. While our estimates show that overall HCV incidence has been decreasing in Canada since 2010, continued efforts are required to eliminate chronic HCV as a public health threat by 2030. Significant progress towards HCV elimination will require targeted interventions to prevent new infections, especially among priority populations, innovative testing approaches to find undiagnosed persons and strategies to ensure linkage to care and prompt treatment. The Public Health Agency of Canada will continue to work closely with provinces and territories and other partners to enhance methods and data sources to improve the ability to measure and assess progress against elimination targets.
Authors' statement
NP — Designed the study methodology, interpreted the results, drafted the manuscript
AW — Designed the study methodology, analyzed the data, interpreted the results, drafted the manuscript
SP — Designed the study methodology, analyzed the data, interpreted the results
LC — Interpreted the results, drafted the manuscript
QY — Designed the study methodology, interpreted the results
FZ — Designed the study methodology, analyzed the data
PY — Designed the study methodology
JJF — Designed the study methodology, reviewed the results
NZJ — Designed the study methodology, reviewed the results
MBK — Designed the study methodology, reviewed the results
MK — Designed the study methodology, reviewed the results
WWLW — Designed the study methodology, reviewed the results
JC — Designed the study methodology, reviewed the results
All authors approved the final version of the manuscript.
Competing interests
MBK reports grants for investigator-initiated studies from ViiV Healthcare, AbbVie, and Gilead, and consulting fees from ViiV Healthcare, AbbVie, and Gilead, all outside the submitted work. MBK is supported by a Tier I Canada Research Chair. NZJ has participated in advisory work for AbbVie and has received speaking fees from AbbVie and Gilead, not related to the submitted work. No other competing interests were declared.
Acknowledgements
The authors would like to thank the Canadian Blood Services, Héma-Québec, Correctional Services Canada and the Tracks survey team at the Public Health Agency of Canada for their ongoing collaboration and for sharing unpublished data.
Funding
This work was supported by the Public Health Agency of Canada.
References
- Footnote 1
-
World Health Organization. Hepatitis C. Geneva (CH): WHO; 2022; (accessed 2022-08-15). https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
- Footnote 2
-
World Health Organization. Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030. Geneva (CH): WHO; 2022; (accessed 2022-11-01). https://www.who.int/publications-detail-redirect/9789240053779
- Footnote 3
-
Public Health Agency of Canada. Reducing the health impact of sexually transmitted and blood-borne infections in Canada by 2030: A pan-Canadian STBBI framework for action. Ottawa, ON: PHAC; 2018; (accessed 2022-08-15). https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/reports-publications/sexually-transmitted-blood-borne-infections-action-framework.html
- Footnote 4
-
Public Health Agency of Canada. Accelerating our response: Government of Canada five-year action plan on sexually transmitted and blood-borne infections. Ottawa, ON: PHAC; 2020; (accessed 2022-08-15). https://www.canada.ca/en/public-health/services/reports-publications/accelerating-our-response-five-year-action-plan-sexually-transmitted-blood-borne-infections.html
- Footnote 5
-
Brookmeyer R, Gail MH. A Method for Obtaining Short-Term Projections and Lower Bounds on the Size of the AIDS Epidemic. J Am Stat Assoc 1988;83(402):301–8. https://doi.org/10.1080/01621459.1988.10478599
- Footnote 6
-
Lyerla R, Gouws E, García-Calleja JM, Zaniewski E. The 2005 Workbook: an improved tool for estimating HIV prevalence in countries with low level and concentrated epidemics. Sex Transm Infect 2006;82 Suppl 3:iii41–4. https://doi.org/10.1136/sti.2006.020198
- Footnote 7
-
Trubnikov M, Yan P, Archibald C. Estimated prevalence of Hepatitis C Virus infection in Canada, 2011. Can Commun Dis Rep 2014;40(19):429–36. https://doi.org/10.14745/ccdr.v40i19a02
- Footnote 8
-
Statistics Canada. Population estimates, quarterly. Ottawa, ON: StatCan; 2022; (accessed 2022-08-15). https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000901
- Footnote 9
-
Statistics Canada. Malakieh J. Canadian Centre for Justice and Community Safety Statistics. Adult and youth correctional statistics in Canada, 2018/2019. Ottawa, ON: StatCan; 2020. https://www150.statcan.gc.ca/n1/pub/85-002-x/2020001/article/00016-eng.html
- Footnote 10
-
Statistics Canada. Data products, 2016 Census. Ottawa, ON: StatCan; (modified 2021; accessed 2022-10-12). https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/index-eng.cfm
- Footnote 11
-
Canadian Network on Hepatitis C. Blueprint to inform hepatitis C elimination efforts in Canada. Montreal, QC: CanHepC; 2019; (accessed 2022-08-15). https://www.canhepc.ca/en/blueprint/publication
- Footnote 12
-
Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Chapter 5: Systematic reviews of prevalence and incidence. JBI Manual for Evidence Synthesis. Adelaide, AU: JBI; 2020; (accessed 2022-08-15). https://doi.org/10.46658/JBIMES-20-06
- Footnote 13
-
Krajden M, Cook DA, Wong S, Yu A, Butt ZA, Rossi C, Darvishian M, Alvarez M, Buxton JA, Tyndall M, Janjua NZ. What is killing people with hepatitis C virus infection? Analysis of a population-based cohort in Canada. Int J Drug Policy 2019;72:114–22. https://doi.org/10.1016/j.drugpo.2019.06.003
- Footnote 14
-
Adu PA, Rossi C, Binka M, Wong S, Wilton J, Wong J, Butt ZA, Bartlett S, Jeong D, Pearce M, Darvishian M, Yu A, Alvarez M, Velásquez García HA, Krajden M, Janjua NZ. HCV reinfection rates after cure or spontaneous clearance among HIV-infected and uninfected men who have sex with men. Liver Int 2021;41(3):482–93. https://doi.org/10.1111/liv.14762
- Footnote 15
-
Aisyah DN, Shallcross L, Hully AJ, O'Brien A, Hayward A. Assessing hepatitis C spontaneous clearance and understanding associated factors-A systematic review and meta-analysis. J Viral Hepat 2018;25(6):680–98. https://doi.org/10.1111/jvh.12866
- Footnote 16
-
Darvishian M, Janjua NZ, Chong M, Cook D, Samji H, Butt ZA, Yu A, Alvarez M, Yoshida E, Ramji A, Wong J, Woods R, Tyndall M, Krajden M. Estimating the impact of early hepatitis C virus clearance on hepatocellular carcinoma risk. J Viral Hepat 2018;25(12):1481–92. https://doi.org/10.1111/jvh.12977
- Footnote 17
-
Micallef JM, Kaldor JM, Dore GJ. Spontaneous viral clearance following acute hepatitis C infection: a systematic review of longitudinal studies. J Viral Hepat 2006;13(1):34–41. https://doi.org/10.1111/j.1365-2893.2005.00651.x
- Footnote 18
-
Statistics Canada. Data from the Canadian Health Measures Survey -, Cycle 4, 2014-2015 – Privacy impact assessment summary. Ottawa, ON: StatCan; (modified 2020-02-21). https://www.statcan.gc.ca/en/about/pia/chmsc4
- Footnote 19
-
Bartlett SR, Yu A, Chapinal N, Rossi C, Butt Z, Wong S, Darvishian M, Gilbert M, Wong J, Binka M, Alvarez M, Tyndall M, Krajden M, Janjua NZ. The population level care cascade for hepatitis C in British Columbia, Canada as of 2018: impact of direct acting antivirals. Liver Int 2019;39(12):2261–72. https://doi.org/10.1111/liv.14227
- Footnote 20
-
Yasseen AS 3rd, Kwong JC, Feld JJ, Janjua NZ, Greenaway C, Lapointe-Shaw L, Sherman M, Mazzulli T, Kustra R, MacDonald L, Sander B, Crowcroft NS. Viral hepatitis C cascade of care: A population-level comparison of immigrant and long-term residents. Liver Int 2021;41(8):1775–88. https://doi.org/10.1111/liv.14840
- Footnote 21
-
Biondi M, McDonald R, Marchand-Austin A, Goneau L, Mazulli T, Minion J, Feld J, Wong A. Comparison of hepatitis C prenatal screening approaches between provinces: seroprevalence and infection rates in universal vs risk-based screening. Can Liver J 2020;3(1):70–1. https://doi.org/10.3138/canlivj.3.1.abst
- Footnote 22
-
Tarasuk J, Zhang J, Lemyre A, Cholette F, Bryson M, Paquette D. National findings from the Tracks survey of people who inject drugs in Canada, Phase 4, 2017-2019. Can Commun Dis Rep 2020;46(5):138–48. https://doi.org/10.14745/ccdr.v46i05a07
- Footnote 23
-
Zietara F, Crotty P, Houghton M, Tyrrell L, Coffin CS, Macphail G. Sociodemographic risk factors for hepatitis C virus infection in a prospective cohort study of 257 persons in Canada who inject drugs. Can Liver J 2020;3(3):276–85. https://doi.org/10.3138/canlivj.2019-0023
- Footnote 24
-
Bolotin S, Feld JJ, Garber G, Wong WW, Guerra FM, Mazzulli T. Population-based estimate of hepatitis C virus prevalence in Ontario, Canada. PLoS One 2018;13(1):e0191184. https://doi.org/10.1371/journal.pone.0191184
- Footnote 25
-
Biondi MJ, Hirode G, Capraru C, Vanderhoff A, Karkada J, Wolfson-Stofko B, Smookler D, Friedman SM, Bates K, Mazzulli T, Juan JV, Shah H, Hansen BE, Feld JJ, Janssen H. Birth cohort hepatitis C antibody prevalence in real-world screening settings in Ontario. Can Liver J 2022;5(3):362–71. https://doi.org/10.3138/canlivj-2021-0036
- Footnote 26
-
Janjua NZ, Yu A, Kuo M, Alvarez M, Cook D, Wong J, Tyndall MW, Krajden M. Twin epidemics of new and prevalent hepatitis C infections in Canada: BC Hepatitis Testers Cohort. BMC Infect Dis 2016;16:334. https://doi.org/10.1186/s12879-016-1683-z
- Footnote 27
-
Martel-Laferriere V, Baril JG, Alarie I, Leblanc J, Côté J, Jourdenais E, Horth D, Lambert G, Tremblay C. Opt-out universal HCV and HIV screening in a Canadian emergency room: a cross-sectional study. BMJ Open 2022;12(1):e048748. https://doi.org/10.1136/bmjopen-2021-048748
- Footnote 28
-
Augustin B, Greenwald Z, Pruvost M, Merisilian L, Palayew A, Narasiah L, Klein M, Greenaway C. Mapping the Immigrant population and cultural and community organizations to inform community outreach and HCV microelimination efforts in Montreal. Can Liver J 2020;3(1):39–40. https://doi.org/10.3138/canlivj.3.1.abst
- Footnote 29
-
Lydon-Hassen K, Jonah L, Mayotte L, Hrabowy A, Graham B, Missens B, Nelson A, Andkhoie M, Nahachewsky D, Yalamanchili DT, Gupta S, Ndubuka N, Khan I, Yacoub W, Bryson M, Paquette D. Summary findings from Tracks surveys implemented by First Nations in Saskatchewan and Alberta, Canada, 2018-2020. Can Commun Dis Rep 2022;48(4):146–56. https://doi.org/10.14745/ccdr.v48i04a05
- Footnote 30
-
Wong J, Moore D, Kanters S, Buxton J, Robert W, Gustafson R, Hogg R, Ogunnaike-Cooke S, Wong T, Gilbert M; ManCount Study Team. Seroprevalence of hepatitis C and correlates of seropositivity among men who have sex with men in Vancouver, Canada: a cross-sectional survey. Sex Transm Infect 2015;91(6):430–3. https://doi.org/10.1136/sextrans-2014-051928
- Footnote 31
-
Salway T, Butt ZA, Wong S, Abdia Y, Balshaw R, Rich AJ, Ablona A, Wong J, Grennan T, Yu A, Alvarez M, Rossi C, Gilbert M, Krajden M, Janjua NZ. A Computable Phenotype Model for Classification of Men Who Have Sex With Men Within a Large Linked Database of Laboratory, Surveillance, and Administrative Healthcare Records. Front Digit Health 2020;2:547324. https://doi.org/10.3389/fdgth.2020.547324
- Footnote 32
-
Sorge J, Colyer S, Cox J, Kroch A, Lachowsky N, Popovic N Yang Q. (2022, July 29-August 2). Estimation of the Population Size of Gay, Bisexual and Other Men Who Have Sex with Men in Canada, 2020. [Poster presentation] p. 541. International AIDS Conference, Montreal, Canada. Montreal, QC; 2022. https://aids2022.org/wp-content/uploads/2022/08/AIDS2022_abstract_book.pdf
- Footnote 33
-
Gratrix J, Smyczek P, Bertholet L, Lee MC, Pyne D, Woods D, Courtney K, Ahmed R. A cross-sectional evaluation of opt-in testing for sexually transmitted and blood-borne infections in three Canadian provincial correctional facilities: a missed opportunity for public health? Int J Prison Health 2019;15(3):273–81. https://doi.org/10.1108/IJPH-07-2018-0043
- Footnote 34
-
Courtemanche Y, Poulin C, Serhir B, Alary M. HIV and hepatitis C virus infections in Québec's provincial detention centres: comparing prevalence and related risky behaviours between 2003 and 2014-2015. Can J Public Health 2018;109(3):353–61. https://doi.org/10.17269/s41997-018-0047-4
- Footnote 35
-
Kronfli N, Dussault C, Klein MB, Lebouché B, Sebastiani G, Cox J. The hepatitis C virus cascade of care in a Québec provincial prison: a retrospective cohort study. CMAJ Open 2019;7(4):E674–9. https://doi.org/10.9778/cmajo.20190068
- Footnote 36
-
Mendlowitz A, Bremner KE, Walker JD, Wong WW, Feld JJ, Sander B, Jones L, Isaranuwatchai W, Krahn M. Hepatitis C virus infection in First Nations populations in Ontario from 2006 to 2014: a population-based retrospective cohort analysis. CMAJ Open 2021;9(3):E886–96. https://doi.org/10.9778/cmajo.20200164
- Footnote 37
-
Hamadeh A, Feng Z, Krahn M, Wong WW. A model-based framework for chronic hepatitis C prevalence estimation. PLoS One 2019;14(11):e0225366. https://doi.org/10.1371/journal.pone.0225366
- Footnote 38
-
Wong WW, Hamadeh A, Haines A, Feng Z, Krahn M. MO3 - Towards a More Accurate Budget Impact Analysis: Population-Level Screening for Hepatitis C Virus (HCV) in Ontario, Canada. Value Health 2018;21 Suppl 2:S8. https://doi.org/10.1016/j.jval.2018.07.056
- Footnote 39
-
Hamadeh A, Haines A, Feng Z, Thein HH, Janjua NZ, Krahn M, Wong WW. Estimating chronic hepatitis C prevalence in British Columbia and Ontario, Canada, using population-based cohort studies. J Viral Hepat 2020;27(12):1419–29. https://doi.org/10.1111/jvh.13373
- Footnote 40
-
Wong WW, Haines A, Farhang Zangneh H, Shah H. Can we afford not to screen and treat hepatitis C virus infection in Canada? Can Liver J 2018;1(2):51–65. https://doi.org/10.3138/canlivj.1.2.005
- Footnote 41
-
Binka M, Janjua NZ, Grebely J, Estes C, Schanzer D, Kwon JA, Shoukry NH, Kwong JC, Razavi H, Feld JJ, Krajden M. Assessment of Treatment Strategies to Achieve Hepatitis C Elimination in Canada Using a Validated Model. JAMA Netw Open 2020;3(5):e204192. https://doi.org/10.1001/jamanetworkopen.2020.4192
Appendix
Appendix A: Methodology for back calculation modelling
Appendix B: Literature search
Appendix A: Methodology for back calculation modelling
We use the same back calculation modelling approach as in the previous work for Canadian hepatitis C virus (HCV) estimation Footnote 7. In the back calculation modelling method, the time from HCV infection to diagnosis is considered a random variable that follows a certain probabilistic distribution. Once the transition probabilities P are known, the back calculation method calculates the expected number of infections I (as the estimated HCV incidence) through minimizing the gap between the reported HCV cases and the expected diagnosed HCV cases which is P x I. In the computation process, other modelling outcomes, such as expected HCV infections diagnosed in the same year, the expected HCV-related mortality and not-yet diagnosed HCV cases, are also produced.
The probabilities P are not known in advance, however, and it is assumed to follow a commonly used family of distribution called log-logistic distribution with a shape parameter and a scale parameter. As in the previous work Footnote 7, these parameters are determined from a wide range through iteratively searching the optimal fitting of the reported diagnosed cases, and HCV-related mortality data. In addition, the reported acute cases are also used to further calibrate the parameters by minimizing the gap between the acute cases and the expected HCV infections diagnosed in the same year. The calibration uses the standard BFGS-method available in R.
Using this method, HCV incidence was estimated by five-year birth cohort plus an extra open cohort (born after the year 2000). Five-year birth cohorts were then grouped into larger birth cohorts: before 1945, 1945–1974, and after 1975.
Appendix B: Literature search
A health librarian at the Public Health Agency of Canada conducted a series of literature reviews based on the specific objectives of obtaining data on Footnote 1 HCV incidence and prevalence in Canada from January 1, 2019, to October 1, 2021, and Footnote 2 the unaware/undiagnosed proportion of HCV infection in Canada from January 1, 2016, to October 1, 2021. The following databases were searched by the Health Librarian for relevant publications: Ovid MEDLINE(R) ALL, Embase and Scopus. Additional grey literature searches were conducted using the Google search engine. In total, both literature searches yielded an initial 1,187 records, with an additional 31 records found outside of the librarian search.
Using the systematic review protocol for prevalence and incidence studies developed by Joanna Briggs Institute (JBI), two independent reviewers screened all studies for inclusion. For the initial screening, reviewers independently read either the abstract or the full text and made assessments based on the following inclusion criteria:
- Condition: HCV infection (past [seroprevalence] or present [active or chronic])
- Outcome:
- Literature search 1: Reporting data on proportion with HCV infection, prevalence or incidence
- Literature search 2: Reporting data on awareness of HCV infection, and/or undiagnosed proportion of people with HCV
- Context: In Canada
- Population: All populations used for the workbook method
After the initial screening, 66 records were included for final assessment. In the final assessment, both reviewers independently read and evaluated each paper using the JBI Critical Appraisal Checklist for Studies Reporting Prevalence Data to determine whether the paper should be included. Data from cross-sectional and cohort studies with a testing component were prioritized, but studies using administrative data and modelling studies were also included, when appropriate. Discrepancies between reviewers were resolved through discussion. After the final review, 43 records were included and considered for use in the workbook method (Tables 1, 2 and 3). Due to a limited number of records on the incidence and prevalence of HCV among gay, bisexual and other men who have sex with men (gbMSM) and baby boomers, a subsequent literature review with an extended date range of January 1, 2016, to December 31, 2018, was conducted for those two subgroups. This allowed us to find an additional seven records for inclusion in the workbook method.
