
Original qualitative research – Barriers and facilitators to improving health care for adults with intellectual and developmental disabilities: what do staff tell us?
Health Promotion and Chronic Disease Prevention in Canada
Avra Selick, MAAuthor reference 1; Janet Durbin, PhDAuthor reference 1Author reference 2; Ian Casson, MDAuthor reference 3; Jacques Lee, MDAuthor reference 4; Yona Lunsky, PhD C. Psych.Author reference 2Author reference 5
https://doi.org/10.24095/hpcdp.38.10.01
This article has been peer reviewed.
Author references:
- Author reference 1
-
Provincial System Support Program, Centre for Addiction and Mental Health, Toronto, Ontario, Canada
- Author reference 2
-
Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada
- Author reference 3
-
Department of Family Medicine, Queen's University, Kingston, Ontario, Canada
- Author reference 4
-
Sunnybrook Research Institute, Toronto, Ontario, Canada
- Author reference 5
-
Adult Neurodevelopmental Services, Centre for Addiction and Mental Health, Toronto, Ontario, Canada
Correspondence: Avra Selick, Provincial System Support Program, Centre for Addiction and Mental Health, 33 Russell Street, Toronto, ON M5S 2S1; Tel: 416-535-8501, ext. 30127; Email: avra.selick@camh.ca
Abstract
Introduction: Adults with intellectual and developmental disabilities (IDD) have high rates of morbidity and are less likely to receive preventive care. Emergency departments and primary care clinics are important entry points into the health care system. Improving care in these settings can lead to increased prevention activities, early disease identification, and ongoing management. We studied barriers and facilitators to improving the care of patients with IDD in three primary and three emergency care sites in Ontario.
Methods: Data sources included structured implementation logs at each site, focus groups (n=5) and interviews (n= 8). Barriers and facilitators were coded deductively based on the Consolidated Framework for Implementation Research (CFIR). Synthesis to higher level themes was achieved through review and discussion by the research team. Focus was given to differences between higher and lower implementing sites.
Results: All sites were challenged to prioritize care improvement for a small, complex population and varied levels of implementation were achieved. Having national guidelines, using local data to demonstrate need and sharing evidence on value were important engagement strategies. Factors present at higher implementing sites included strong champions, alignment with site mandate, and use of electronic prompts/reminders. Lower implementing sites showed more passive endorsement of the innovation and had lower capacity to implement.
Conclusion: Providing effective care for small, complex groups, such as adults with IDD, is critical to improving long-term health outcomes but is challenging to achieve. At a systemic level, funding incentives, access to expertise and improved electronic record systems may enhance capacity.
Keywords: intellectual disability, developmental disabilities, implementation, primary health care, emergency medical services, quality improvement, barriers and facilitators
Highlights
- We worked with three emergency departments and three primary care clinics across Ontario to implement evidence-based practices for high quality care of adults with intellectual and developmental disabilities.
- While some sites made considerable progress, others were challenged to make sustainable improvements.
- More successful implementation occurred when sites had strong champions, an interest in this patient group and used electronic prompts and automated point of care tools to embed new practices.
- Less successful sites were challenged by staff turnover, low morale and passive endorsement from leadership.
- Given these challenges, system level supports are important for wider spread of this intervention.
Introduction
Adults with intellectual and developmental disabilities (IDD) are an extremely vulnerable population with complex health needs. Compared to those without IDD, they are more likely to develop a range of chronic conditions including diabetes, congestive heart failure, chronic obstructive pulmonary disease, seizure disorders, gastrointestinal disorders and psychiatric disorders, and they are less likely to receive preventive care.Footnote 1Footnote 2Footnote 3Footnote 4
To improve health outcomes for adults with IDD, two important targets for improved practice are the emergency department (ED) and primary care (PC) settings. Both serve as main entry points into the health care system, playing a critical role in providing early and accurate diagnosis, early intervention, and linking individuals to needed community supports. Prior research has shown that although adults with IDD have similar rates of PC use and higher rates of ED visits than the general population,Footnote 1 care provided in these settings can be insufficient, or inappropriate.Footnote 5Footnote 6Footnote 7
The ED and PC are both generalist settings, in that they provide care to a wide variety of patients, and people with IDD are not their exclusive focus. Adults with IDD are more likely to have complex health profilesFootnote 3 and may additionally have difficulty communicating their health concerns.Footnote 8 Staff in these general health care settings often lack sufficient training in the specific health complexities of adults with IDD, and may lack the time and training to appropriately adapt communication and care processes.Footnote 9Footnote 10Footnote 11Footnote 12Footnote 13 Staff may also have difficulty recognizing which patients have IDD, making adapted or accommodated care impossible.Footnote 13Footnote 14 Finally, stigma and misconceptions regarding individuals with IDD still exist in wider society and health care professionals are not exempt.Footnote 15Footnote 16Footnote 17 Improving the quality of care in these settings can contribute to reduced hospital use, and improved long-term health outcomes.
An evidence base of strategies to improve quality of care for patients with IDD in these two settings is emerging,Footnote 9Footnote 18Footnote 19 yet, relatively little research has examined how to implement these strategies in practice. Practice change can be challengingFootnote 20 and interventions successful in research settings often fail to be implemented in practice.Footnote 21Footnote 22 Systematic efforts to improve care for adults with IDD face the additional challenge that they represent only about 1% of the populationFootnote 23 and thus may be viewed as having lower priority than other more frequently seen patient groups. A few studies in the UK and Australia have looked at barriers to PC improvement,Footnote 9 however, they were limited to physician feedback and, due to differences in health care systems, may not translate to the Canadian context. We only identified one previous study on barriers to implementation in the ED, conducted in the UK.Footnote 24 None of these studies reported a structured, staged approach to implementation, which was used in our study and has been shown to improve implementation success.Footnote 22
In our present study, we supported three hospital EDs and three PC clinics located across Ontario, Canada in a structured practice change process to improve care of adults with IDD. In each setting the improvement work addressed three common core components: (1) identification of patients with IDD; (2) provision of modified care (e.g. adapted communication, improved discharge planning, community linkages); and (3) staff training and support. The core components were identified based on input from patients, families, and clinicians, the literature and established guidelines, where available. The PC intervention (the periodic comprehensive health exam) was recommended in Canadian national clinical guidelines on the primary care of adults with IDDFootnote 18 whereas the ED intervention included evidence-based strategies, but these were not recommended in equivalent guidelines or standards. These common core components were adapted to fit within the specific context of each setting based on feedback from patients, families and clinicians; more detailed descriptions of intervention selection and development have been published elsewhere.Footnote 6Footnote 25Footnote 26Footnote 27
This paper reports staff perspectives on the extent of implementation achieved and barriers and facilitators encountered across the six study sites. Study findings can contribute knowledge about strategies to improve the quality of care for adults with IDD in these key settings and complement prior work from the service user perspective. Footnote 26Footnote 27Footnote 28Footnote 29Footnote 30Footnote 31
Methods
Implementation
A structured, staged implementation process was used at the six study sites following the four stages of the National Implementation Research Network (NIRN) model:Footnote 22
- Exploration: Generate staff awareness and engagement.
- Installation: Plan and implement required changes, tailored to the setting.
- Initial implementation: Begin intervention delivery, collect feedback to refine and improve the process.
- Full implementation: Fully incorporate intervention into ongoing routine practice.
Exploration was initiated in the first two sites (ED 1 and PC 1) in spring 2012, and in four additional sites in spring 2013. The study was completed in March 2015 and follow up data was collected from March to July 2015.
Implementation was supported through a partnership between the central research team and the local site implementation team, which minimally included a local lead (a senior physician or administrator), and a paid implementation facilitator. At some sites the local lead recruited additional staff (e.g. physicians, nurses, social workers, administrative staff) to participate on the implementation team. The central team provided content expertise, and together with appropriate experts depending on the tool (clinicians, patients, and families) helped to develop and adapt tools for each setting and provided overall project management support. The local site implementation team was responsible for the internal implementation of the practice change, including the logistics of incorporating new processes and resources, and engaging and training site staff.
Data sources
See Table 1 for an overview of data collection by site.
| Site | Focus groups, n | Interviews, n | Implementation logs, n |
|---|---|---|---|
| PC1 | 1 (7 participants) | 1 | 2 |
| PC2 | 1 (2 participants) | 0 | 2 |
| PC3 | 0 | 5 | 1 |
| ED1 | 1 (10 participants) | 1 | 2 |
| ED2 | 1 (5 participants) | 0 | 3 |
| ED3 | 1 (3 participants) | 1 | 3 |
| Abbreviations: ED, emergency department; PC, primary care. | |||
Implementation log
A structured template was used to record each site's progress through the implementation stages including: status, activities conducted to achieve progress and any helping or hindering factors. Each log was updated periodically during the study, minimally at the study mid-point and at study completion, by a central evaluator based on interviews with the site facilitator and other staff as needed. One site (PC3) left the study early and, therefore, only had one point of completion. The same evaluator conducted all interviews to maximize consistency and reliability. Multiple points of completion were critical to capture the evolving experience over time and to ensure no loss of data due to memory distortion or staff turnover.
Staff focus groups/ interviews
At study completion, focus groups, or individual interviews when focus group participation was not possible, were conducted with the site implementation teams using a semi-structured guide. Based on the implementation literatureFootnote 21Footnote 32Footnote 33Footnote 34 the guide addressed: barriers and facilitators to implementation, value of the facilitated implementation process, and strategies to support sustainability.
As indicated in Table 1, across the six sites, eight individual staff interviews and five focus groups with a total of 27 staff were conducted. Participation varied by site due to the range in size and composition of the site implementation teams. Focus group discussions lasted approximately one hour; individual interviews were generally 15-30 minutes. All were digitally recorded and transcribed.
While the research team supported both the implementation and the evaluation, the functions were separated and the evaluators on the team did not deliver implementation support.
Analysis
The stage of implementation achieved was determined based on the implementation logs and focus group feedback; final ratings were verified by the implementation leads.
Barriers and facilitators were identified though deductive analyses of all study data sources based on the Consolidated Framework for Implementation Research (CFIR),Footnote 21 while remaining open to newly emerging themes. CFIR was developed based on a synthesis of pre-existing implementation theories and offered an overarching typology of factors that influence implementation success from which researchers could select the constructs most relevant to their own research. Using CFIR allows for cross study comparisons and can help advance understanding of the critical components of successful implementation.Footnote 35
CFIR constructs are organized into five major domains. Four were applied to this study: characteristics of the intervention (e.g. evidence strength, complexity of target population); the outer setting (e.g. system policy, resources); inner setting (e.g. organizational culture, leadership, intervention compatibility with program mandate); and the implementation process (e.g. engagement of key stakeholders, implementation team). The fifth domain, characteristics of individuals involved (e.g. knowledge and attitudes), was not included as the study focused on organizational factors and data on individual staff characteristics were not collected.
All text was reviewed and coded according to CFIR. First level synthesis was conducted across data sources at site level. Themes were then synthesized across sites through review and discussion by three team members, focusing on differences between higher and lower implementing sites. Final results were reviewed by the site implementation leads for validation and accuracy. Quotations from focus groups and interviews are included to illustrate findings.
Research ethics board approval for the study was received from the home institution of the research team and the academic institutions of the participating sites.
Results
Stage of implementation achieved
The extent of implementation achieved at each site varied across the four NIRN stages (see Figure 1). Of the six sites: one reached full implementation (PC 1); four achieved some degree of implementation but were unable to fully incorporate the intervention into routine practice during the study period (ED 1, ED 2, ED 3, PC 2); one did not proceed past the exploration stage (PC 3).
Figure 1. Stage of implementation achieved by site
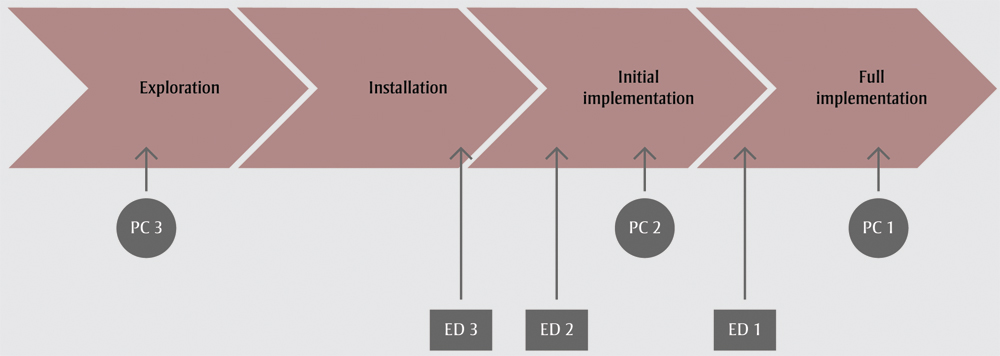
Abbreviations: ED, emergency department; PC, primary care.
Text Description
This figure depicts the stage of implementation achieved by each site. The implementation was composed of four stages: exploration, installation, initial implementation and full implementation. One site reached full implementation (primary care site 1); four achieved some degree of implementation but were unable to fully incorporate the intervention into routine practice during the study period (emergency department site 1, emergency department site 2, emergency department site 3, primary care site 2); one did not proceed past the exploration stage (primary care site 3).
Barriers and facilitators to implementation
Barriers and facilitators to implementation were organized according to CFIR. See Table 2 for an overview of themes identified.
| Domain | Themes (relevant CFIR construct) |
|---|---|
Intervention characteristics |
|
Outer setting |
|
Inner setting |
|
Process |
|
| Abbreviations: CFIR, Consolidated Framework for Implementation Research; EMR, electronic medical records; IDD, intellectual and developmental disabilities. | |
Intervention/population characteristics
A consistently noted barrier across sites was that adults with IDD represent only a very small portion of patients. They, furthermore, comprise a high need, time consuming and heterogeneous population that staff are often uncomfortable or unfamiliar with treating.
This is a complicated area of implementation. You have a high needs group that you don’t see every day. In a sense… and I have some experience with implementation, that’s why I’m so impressed with what we’ve achieved… that usually means zero uptake. That combination of – complicated but you have to remember the complexity and you don’t see them very often – that’s usually a full stop.(Site lead, ED 1)
This barrier was offset to some extent in the PC settings by the intervention’s grounding in national clinical guidelines, which informants felt provided legitimacy and some external pressure to implement. By contrast, there were no established guidelines to draw on for the ED intervention.
Outer setting
Less focus was given to the outer setting by informants. However, one issue raised in the PC sites, particularly the lowest implementing site (PC 3), was the absence of any financial incentives for this work. This is a complex, time-consuming population to care for and some felt that financial incentives for physicians would support implementation.
I’d like to say no. I don’t think any of us are rooting for money. However, on the other side when there are incentive payments for doing things, we do them more. Incentive payments I think would sadly make sure we follow up, make sure everybody gets seen. (Physician, PC 3)
Inner setting
Much of the feedback focused on issues related to the inner setting. Across all six sites a recurring challenge was lack of resources; staff were extremely busy, with a multitude of other projects competing for attention.
It’s the same that we face with all practice change where it’s competition for oxygen and bandwidth. There’s always a long list of potential quality improvement projects or other priorities. So, you’re always competing for people at the same time that we’re trying to reduce waiting times, and improve hand washing, and whatever the focus of the organization is. (Clerk, ED 1)
I think this piece gets buried under so many other problems. Sometimes, really, the DD thing isn’t on top of the list because there’s just so many other things there. (Site lead, PC 2)
Despite this common starting point, however, the presence of facilitators including alignment with site mandate, research or quality improvement experience, good timing, high perceived number of patients with IDD, strong leadership and available resources, allowed some sites to prioritize this work. These facilitators are described in more detail below.
All the higher performing sites emphasized the value of intervention alignment with their organizational cultures and mandates—i.e., collaboration (PC 1), improvement and innovation (ED 1, PC 2), patient centered care (ED 2) and marginalized populations (PC 2). Some sites also highlighted their experience with research and quality improvement as beneficial (PC 1, PC 2, ED 1, ED 2) and it helped that there was a small amount of funding attached to the project (ED 2).
Part of the reason we engaged in this was because of the supports, the frame, and then how it fits within what we envisioned was important. (Director, ED 2)
We like [projects] that allow us to take a quality improvement approach that can be collaborative, that can be interdisciplinary and so this aligned with all of those objectives, so it fit in nicely. (Clinical Program Coordinator, PC 1)
In contrast, the lower performing sites reported issues related to low staff morale, burnout and change fatigue (ED 3), or having a less collaborative, more business focused environment (PC 3). They emphasized that although providing high-quality care to adults with IDD was important, it was simply not their top priority, or it was something they felt they already provided (ED 3, PC 3).
I mean I think we recognize that these people need appropriate care and want to provide that but…I guess people haven’t really seen it as perhaps a bigger problem as some other things.(Physician, PC 3)
Several sites were also challenged by poor timing, with major structural changes or serious clinical interruptions that had to take precedence; for example: organizational restructuring (PC 2, ED 3), new electronic medical record (EMR) platform (ED 3, PC 3), moving physical locations (PC 3), community health crisis requiring ED response (ED 2).
Nurse managers changing over… clerical managers disappearing… people who were very good system implementers moving on to other positions. In that vacuum it is very hard to get traction on getting something going. (Site lead, PC 2)
Another important factor was whether there was a pre-existing focus on this population. PC 1 reported having a relatively high number of patients with IDD in comparison to other PC practices which facilitated buy-in.
We have a fairly large population of adults with IDD so … there’s a lot of people who were interested in the topic and again, it was a nice project for us. (Clinical care coordinator, PC 1)
Other sites initially felt they had very few patients with IDD and did not see the project’s relevance. For some, this perception was overcome through staff education, local data demonstrating high service use by adults with IDD, or, at one site, a sentinel event involving a patient with IDD. However, for others the perception prevailed.
A clear difference between the higher and lower performing sites was leadership. The higher performing sites (PC 1, PC 2, ED 1, ED 2) had strong clinical champions and support from senior leadership. Often champions who stepped forward had personal connections or significant clinical experiences with individuals with IDD.
I think the people that were on the team are leaders and were respected and credible champions […] I think the people that were brought in on this have a level of credibility and trust amongst their peers […] and that’s an important piece. (Implementation facilitator, ED 1)
At the lower performing sites (ED 3, PC 3), senior leadership only passively endorsed the project.
There was no support from administration, really it …just felt very… demoralizing. (Allied health worker, PC 3)
All sites faced competing demands on staff time; some, however, made the decision to prioritize and focus capacity on this project. There were also differences in the baseline resources available at each site. For example, ED 1 had full time social work coverage while ED 2 and ED 3 had very limited social work coverage. By necessity this led to differences, sometimes limitations, in how the intervention was implemented and the level of interprofessional involvement.
Process
An important part of the implementation process was staff engagement; however, this was challenging. It proved difficult for the implementation teams to set up meetings with site staff due to high clinical demands, even standing meetings were often cancelled (ED 1, PC 2, PC 3), and site leads lacked sufficient time for ongoing staff communication (PC 2). Some sites, however, offered examples of creative strategies to engage staff including continuous communication and ‘advertising’ the intervention, use of colourful posters, screen savers and email blasts.
I think just keeping it on the radar, it just can’t be a one-shot blitz of here’s [the intervention], here’s posters, here’s this, here’s that and then it just – that's it. I think it has to be revitalized on a regular basis. (Clinical educator, ED 1)
An important strategy at ED 2 was including frontline clinicians in designing the intervention, providing a sense of ownership. PC 1 emphasized the value of allowing participating staff to volunteer, rather than being assigned, to ensure the intervention is delivered by passionate and dedicated individuals.
…it wasn’t that it was dumped on someone, it was somebody who was actually interested in the topic. (Clinical program coordinator, PC 1)
Also important was engaging with stakeholders who were external to the setting. This was particularly true for the EDs who had to work closely with the community sector to implement communication tools. While one of the higher implementing sites (ED 2) reported developing an excellent relationship with the community, a lower implementing site (ED 3) described considerable barriers due to tensions between hospital and community perspectives.
I remember at the beginning of the project looking towards [community representatives] saying, ‘You are the experts. We are the experts in acute care, you are the expert in this area. Assume we know nothing. Teach us what we need to know.’ And I think that contributed to just valuing the expertise of others and not… we needed the expertise. I think that is the key point. (Director, ED 2)
I think that the agencies have really good relationships with the emergency department here… but the language of social services and the language of health are so different, and so sometimes that is difficult. (Community facilitator, ED 3)
A strong inter-professional implementation team was also identified as an important facilitator (PC 1, ED 1, ED 2). Missing representation from any professional group inevitably resulted in challenges implementing aspects of the intervention relevant to that group. It was also important that team members worked well together, were passionate about the project, and had the right skillset for the job.
Well, just one of the learnings is that it takes a team. It’s definitely not a one or two-person thing. It’s having facilitators and having [the manager] and [the nurse educator], and a physician contact [...] It really was a team approach.(Implementation facilitator, ED 2)
Challenges arose in the lower implementing sites where team members lacked the necessary skills and interest in the project or did not have the authority or receive the necessary support to move the project forward (ED 3, PC 3).
I think the lack of enthusiasm and support [was the biggest barrier]... because it just felt like dragging your feet through the mud… so with all the other stuff going on it was really easy for it to get lost, you know? It was just really, really easy for it to go ‘oh well nobody cares, what’s the point.’ (Allied health worker, PC 3)
The lower implementing sites (ED 3, PC 3) were also challenged by the turnover of key members of the implementation team mid-way through the project. These gaps in staffing considerably challenged implementation efforts.
Most sites emphasized that support from the central team, including tool development, content expertise and project management support, was critical to the success of the project and felt it was unlikely they would have proceeded with the project in the absence of the central team.
Because this population is seen infrequently, sites found one-time training to be insufficient. The higher implementing sites (ED 1, PC 1, PC 2) embedded automated prompts, flags, tools and reminders into their EMRs. Sites without flexible EMRs or who could not, or did not, work to modify their EMRs, faced greater challenges achieving sustainability (PC 3, ED 2, ED 3).
In some respects, the PC settings had an advantage because they are familiar with their patient population and can proactively identify and flag patients with IDD in their roster. In contrast, ED visits are not planned so most patients are new to the hospital, making identification challenging.
Finally, implementation is very time-consuming. ED 1 and PC 1 had the advantage of an extra year of exploration. Although they faced many setbacks and false starts, the extra time afforded them the opportunity to recover. When the remaining sites faced unexpected challenges, including difficulties achieving buy-in at the site and bureaucratic hurdles (e.g. contract delays, ethics approvals), they were left with less time to complete the installation and implementation of the intervention. The shift from project to sustainable practice was a hurdle that required time to achieve. If all the sites had equal time to implement, the results may have been different.
For me it really reinforced what I already knew, which is that this kind of stuff takes time and that it works best if you can build that enthusiasm and if you have a champion and that it can go wrong pretty, pretty easily. (Allied health worker, PC 3)
Discussion
This study explored barriers and facilitators to improving health care for adults with IDD, a group with high health complexity and high rates of health care utilization. Despite the acknowledged importance of improving care for this group and the structured implementation supports provided, all sites reported challenges and varied levels of implementation were achieved across sites.
An initial challenge was site buy in- i.e. achieving site agreement to proceed with the implementation. There are always a multitude of projects competing for attention and interventions that target a small number of patients can be perceived as having a smaller payoff. To address this, additional work was needed to demonstrate the value of this intervention and the presence of facilitators including alignment with site mandate, strong champions, a pre-existing focus on IDD and the existence of national guidelines, was important to allow the site to move forward. This aligns with previous research which found that a key barrier to uptake of primary care improvement for patients with IDD was low perceived value of the intervention.Footnote 9
Most of the study sites achieved initial implementation but, at study end, sustainability seemed uncertain at all but one of the sites. This occurred in part because, due to the nature of this population, staff received relatively low exposure to the intervention. Most clinicians see patients with IDD relatively infrequently, giving them few opportunities to ‘practice’ the intervention and incorporate it into their routine. We found that without some type of reminder mechanism, it was unlikely staff would remember to provide the intervention, and how to do so. Site feedback indicated the use of automated electronic reminders and clinical prompts to be immensely helpful in supporting intervention delivery; follow-up can determine how successful this strategy is in supporting long-term sustainability.
Beyond these challenges, many of the same barriers and facilitators generally identified in the implementation literature,Footnote 32Footnote 33Footnote 34 were also reported by the study sites. Higher implementing sites benefited from strong champions, alignment with site mandate, research or quality improvement capacity, and sufficient staff resources. Lower implementing sites were challenged by low morale, staff turnover, low staff engagement, passive endorsement from leadership, staff with insufficient skills or authority leading the project and insufficient time to implement. Previous studies on implementing practice change for patients with IDD identified some similar barriers including lack of resources, lack of leadership support, insufficient funding and low perceived value.Footnote 9Footnote 24
To support spread of this intervention, there are several system level strategies that can offset some of the challenges above, reduce the burden on individual organizations and facilitate wider implementation. Almost all study sites emphasized the critical role played by the central team, suggesting that spread would require ongoing implementation support to provide information, keep resources updated and help sustain momentum.
Implementation could also be supported by a central IDD patient registry, as has been established in other jurisdictions.Footnote 36 This would help ensure the often-invisible segments of the IDD population with more mild disabilities are identified. A registry could be linked to EMRs, facilitating identification in busy EDs where it is challenging and eliminating the need for labour intensive manual reviews of patient rosters in PCs, the method used by the study PC sites.
Another central support strategy is for EMR vendors to centrally incorporate IDD specific point-of-care tools and automated prompts, thereby reducing the need for each site to do so individually. At most study sites expanding EMR function required extensive time and sites without the resources to make these changes were uniformly less successful in their implementation efforts. This would be easier to accomplish in jurisdictions or sectors with a single common EMR platform.
Adults with IDD often require longer appointments, which can be a barrier for physicians reimbursed in fee-for-service models. Incentive payments are already used in Ontario for specific procedures (e.g. cancer screening) and may be a valuable strategy related to this population. Though studies from jurisdictions where financial incentives are available suggest that, while they can be beneficial, they alone are insufficient to achieve change.Footnote 12Footnote 37
This intervention could also be supported by improvements in medical, nursing and other clinical training programs which currently include relatively little content on IDD.Footnote 12Footnote 24Footnote 38Footnote 39 However, even with improved education, adults with IDD are a complex group and it may not always be possible for generalist teams to fully support them. Both ED and PC settings may benefit from working with clinicians who specialize in treating adults with IDD. One potential model to consider is the learning disability liaison nurse role used in the UK. The nurse liaison is a dedicated role that supports improved care for individuals with IDD in hospitals, either through direct care or by supporting the care team. Current research in this area is limited, but generally positive on the effectiveness of this model.Footnote 24Footnote 40Footnote 41 Primary care delivery could be supported by a referral or consultation model with IDD specialized PC practices.Footnote 12 The combination of improved education for all clinicians and access to support from IDD specialists could support widespread capacity for high quality care in generalist settings.
Strengths and limitations
Relatively few previous studies, and no Canadian studies, have examined barriers and facilitators to improving emergency and primary care for adults with IDD. To the best of our knowledge, this is the first study in any jurisdiction that has used a structured, staged implementation approach to improve care for this population, an approach that has been shown to improve implementation success. A strength of this study is that it included sites from three diverse localities across Ontario; however, each of these sites exists within a specific context and findings may not apply to other contexts. This effort was part of a grant which included commitment from sites to participate at the time of grant submission. It is likely that implementation success would be lower in a random sample.
This study focused on organizational and system level factors affecting implementation; we did not collect data on individual staff characteristics (the fifth CFIR domain) which may have identified additional barriers or facilitators to implementation. It was also not within the scope of this study to look at intervention outcomes. The next step in this ongoing work will be to engage with patients with IDD and their families, as well as providers, to discover if the new practices are effectively meeting patient needs and improving patient outcomes.
Conclusion
Providing effective and appropriate care to all is critical to improving population health outcomes but is challenging to achieve for small, complex groups, such as adults with IDD. Given the time-consuming, resource-intensive nature of implementation, and the importance of providing evidence-based care, it is critical we understand the factors associated with success. This study identifies some of the barriers and facilitators associated with successful practice improvement for adults with IDD in emergency and primary care settings. Particularly key for sites that made more progress were presence of strong champions, project alignment with site priorities, and use of electronic reminders. This study is an important addition to literature on implementing best practices for adults with IDD and may also have relevance for other low prevalence populations.
Acknowledgements
This study is part of the Health Care Access Research and Developmental Disabilities (H-CARDD) Program. We gratefully acknowledge the Province of Ontario for their support of this study through their research grants program. The opinions, results and conclusions in this paper are those of the authors and do not reflect that of the Province. We would also like to thank staff from all six sites for participating in the implementation and evaluation of this project.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Authors’ contributions and statement
YL conceived the project. JD, JL, IC and YL designed the study. AS led data collection, analysis and writing of the manuscript. JD and YL contributed to data synthesis. All authors discussed the results/interpretation, contributed to writing and approved the final manuscript.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
References
- Footnote 1
-
Lunsky Y, Klein-Geltink JE, Yates E. Atlas on the Primary Care of Adults with Developmental Disabilities in Ontario. Toronto, ON; 2013.
- Footnote 2
-
Ouellette-Kuntz H, Cobigo V, Balogh R, Wilton A, Lunsky Y. The uptake of secondary prevention by adults with intellectual and developmental disabilities. J Appl Res Intellect Disabil. 2015;28:43–54.
- Footnote 3
-
Ouellette-Kuntz H. Understanding health disparities and inequities faced by individuals with intellectual disabilities. J Appl Res Intellect Disabil. 2005;18:113–21.
- Footnote 4
-
van Schrojenstein Lantman-De Valk H, Metsemakers J, Haveman M, Crebolder H. Health problems in people with intellectual disability in general practice: a comparative study. Fam Pract. 2000;17(5):405–7.
- Footnote 5
-
Ombudsman Ontario. Nowhere to Turn. Investigation into the Ministry of Community and Social Services’ response to situations of crisis involving adults with developmental disabilities. Toronto, ON: Ombudsman Ontario; 2016.
- Footnote 6
-
Lunsky Y, Lake JK, Durbin J, et al. Understanding and improving care for individuals with intellectual and developmental disabilities in the emergency department. In: Hodapp RM, editor. International Review of Research in Developmental Disabilities, Vol 47. Burlington: Academic Press; 2014. p. 1–37.
- Footnote 7
-
Cooper S, Hughes-Mccormack L, Greenlaw N, et al. Management and prevalence of long-term conditions in primary health care for adults with intellectual disabilities compared with the general population: A population-based cohort study. J Appl Res Intellect Disabil. 2017:1–14.
- Footnote 8
-
Ziviani J, Lennox N, Allison H, Lyons M, Del Mar C. Meeting in the middle: improving communication in primary health care consultations with people with an intellectual disability. J Intellect Dev Disabil. 2004;29(3):211–25.
- Footnote 9
-
Robertson J, Hatton C, Emerson E, Baines S. The impact of health checks for people with intellectual disabilities: An updated systematic review of evidence. Res Dev Disabil. 2014;35(10):2450–62.
- Footnote 10
-
Sowney M, Barr OG. Caring for adults with intellectual disabilities: perceived challenges for nurses in accident and emergency units. J Adv Nurs. 2006;55(1):36–45.
- Footnote 11
-
Lunsky Y, Gracey C, Gelfand S. Emergency psychiatric services for individuals with intellectual disabilities: perspectives of hospital staff. Intellect Dev Disabil. 2008;46(6):446–55.
- Footnote 12
-
Walmsley J. An investigation into the implementation of annual health checks for people with intellectual disabilities. J Intellect Disabil. 2011;15(3):157–66.
- Footnote 13
-
Hemm C, Dagnan D, Meyer TD. Identifying training needs for mainstream healthcare professionals, to prepare them for working with individuals with intellectual disabilities: A systematic review. J Appl Res Intellect Disabil. 2015;28(2):98–110.
- Footnote 14
-
Bradley E. Learning disability in the accident and emergency department. Adv Psychiatr Treat. 2005;11(1):45–57.
- Footnote 15
-
While AE, Clark LL. Overcoming ignorance and stigma relating to intellectual disability in healthcare: A potential solution. J Nurs Manag. 2010;18(2):166–72.
- Footnote 16
-
Ouellette-Kuntz H. Attitudes of senior psychiatry residents toward persons with Intellectual Disabilities. Can J Psychiatry. 2003;48(8):538–45.
- Footnote 17
-
Lewis S, Stenfert-Kroese B. An investigation of nursing staff attitudes and emotional reactions towards patients with intellectual disability in a general hospital setting. J Appl Res Intellect Disabil. 2010;23(4):355–65.
- Footnote 18
-
Sullivan WF, Berg JM, Bradley E, et al. Primary care of adults with developmental disabilities: Canadian consensus guidelines. Can Fam Physician. 2011;57:541–53.
- Footnote 19
-
Lennox N, Bain C, Rey-conde T, Purdie D, Bush R. Effects of a comprehensive health assessment programme for Australian adults with intellectual disability: a cluster randomized trial. Int J Epidemiol. 2007;36:139–46.
- Footnote 20
-
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–65.
- Footnote 21
-
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(50):40–55.
- Footnote 22
-
Fixsen D, Blase K, Metz A, Van Dyke M. Statewide implementation of evidence-based programs. Except Child. 2013;79(2):213–30.
- Footnote 23
-
Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res Dev Disabil. 2011;32(2):419–36.
- Footnote 24
-
Tuffrey-Wijne I, Goulding L, Giatras N, et al. The barriers to and enablers of providing reasonably adjusted health services to people with intellectual disabilities in acute hospitals: evidence from a mixed-methods study. BMJ Open. 2014;4:1–11.
- Footnote 25
-
Durbin J, Selick A, Casson I, et al. Evaluating the implementation of health checks for adults with intellectual and developmental disabilities in primary care: The importance of organizational context. Intellect Dev Disabil. 2016;54(2):136–50.
- Footnote 26
-
Spassiani N, Abou Chacra M, Lunsky Y. “Why are you here? Can’t you cope at home?”: The psychiatric crisis of people with intellectual disabilities and the community’s response. J Ment Health Res Intellect Disabil. 2017;10(2):74–92.
- Footnote 27
-
Spassiani N, Sawyer A, Abou Chacra M, Koch K, Munoz Y, Lunsky Y. “Teaches people that I’m more than a disability:” Using nominal group technique in patient-oriented research for people with intellectual disabilities. Intellect Dev Disabil. 2016;54:112–22.
- Footnote 28
-
Iacono T, Davis R. The experiences of people with developmental disability in Emergency Departments and hospital wards. Res Dev Disabil. 2003;24(4):247–64.
- Footnote 29
-
Baumbusch J, Phinney A, Baumbusch S. Practising family medicine for adults with intellectual disabilities: Patient perspectives on helpful interactions. Can Fam Physician. 2014;60(7):356–61.
- Footnote 30
-
Lunsky Y, Gracey C. The reported experience of four women with intellectual disabilities receiving emergency psychiatric services in Canada: a qualitative study. J Intellect Disabil. 2009;13(2):87–98.
- Footnote 31
-
Michell B. Checking Up On Des: My Life My Choice’s research into annual health checks for people with learning disabilities in Oxfordshire. Br J Learn Disabil. 2012;40(2):152–61.
- Footnote 32
-
Stein BD, Celedonia KL, Kogan JN, Swartz HA, Frank E. Facilitators and barriers associated with implementation of evidence-based psychotherapy in community settings. Psychiatr Serv. 2013;64(12):1263–6.
- Footnote 33
-
Torrey WC, Bond GR, McHugo GJ, Swain K. Evidence-based practice implementation in community mental health settings: The relative importance of key domains of implementation activity. Adm Policy Ment Heal Ment Heal Serv Res. 2012;39(5):353–64.
- Footnote 34
-
Fixsen DL, Blase KA, Naoom SF, Wallace F. Core Implementation Components. Res Soc Work Pract. 2009;19(5):531–40.
- Footnote 35
-
Kirk MA, Kelley C, Yankey N, Birken SA, Abadie B, Damschroder L. A systematic review of the use of the Consolidated Framework for Implementation Research. Implement Sci. 2016;11(1):72.
- Footnote 36
-
Westerinen H, Kaski M, Virta L, Almqvist F, Iivanainen M. Prevalence of intellectual disability: a comprehensive study based on national registers. J Intellect Disabil Res. 2007;51(9):715–25.
- Footnote 37
-
McConkey R, Taggart L, Kane M. Optimizing the uptake of health checks for people with intellectual disabilities. J Intellect Disabil. 2015;19(3):205–14.
- Footnote 38
-
Burge P, Ouellette-Kuntz H, Isaacs B, Lunsky Y. Medical students’ views on training in intellectual disabilities. Can Fam Physician. 2008;54:568-9-5.
- Footnote 39
-
Burge P, Ouellette-Kuntz H, McCreary B, Bradley E, Leichner P. Senior residents in psychiatry: views on training in developmental disabilities. Can J Psychiatry. 2002;47(6):568–71.
- Footnote 40
-
Foster J. Learning disability liaison nurses in acute hospitals: Is there evidence to support the development of this role? Learn Disabil Pract. 2005;8(4):33–8.
- Footnote 41
-
Castles A, Bailey C, Gates B, Sooben R. Experiences of the implementation of a learning disability nursing liaison service within an acute hospital setting: A service evaluation. Br J Learn Disabil. 2014;42(4):272–81.