
Evidence synthesis – Practices for collecting, analyzing and disseminating data on health and its social determinants among Black populations in Quebec: a scoping review

HPCDP Journal Home
 Download in PDF format (735 kB, 25 pages)
Download in PDF format (735 kB, 25 pages)Published by: The Public Health Agency of Canada
Date published: April 2025
ISSN: 2368-738X
Submit a manuscript
About HPCDP
Browse
Previous | Table of Contents | Next
Nina Mombo, PhDAuthor reference footnote 1; Kim Ngan Le Nguyen, MScAuthor reference footnote 2
https://doi.org/10.24095/hpcdp.45.4.03
This article has been peer reviewed.

Recommended Attribution
Evidence synthesis by Mombo N et al. in the HPCDP Journal licensed under a Creative Commons Attribution 4.0 International License
Author references
Correspondence
Nina Mombo, Eval-Expert Santé, 5200 Boulevard des Laurentides, Laval, QC H7K 2J8; Tel: 450-628-3467; Email: evalexpertsante@gmail.com
Suggested citation
Mombo N, Le Nguyen KN. Practices for collecting, analyzing and disseminating data on health and its social determinants among Black populations in Quebec: a scoping review. Health Promot Chronic Dis Prev Can. 2025;45(4):165-89. https://doi.org/10.24095/hpcdp.45.4.03
Abstract
Introduction: The COVID-19 pandemic highlighted the deficiencies in healthcare systems both within and outside of Canada, affecting racialized populations, particularly Black communities, who face an increased risk of infection and mortality from the disease. Although Black populations in Quebec make up more than 25% of the Black population in Canada, detailed data on the impact of COVID-19 on these communities are only available at the national level. This scoping review documents the methods and issues related to the collection, analysis and dissemination of data on the health of Black populations in Quebec, and its social determinants.
Methods: We conducted a review of studies published in English and French from January 2010 to June 2024 by consulting six databases. This review exclusively comprised studies involving data collection from racialized populations, including Black populations in Quebec, and excluded Canada-wide studies involving only a subsample of Black populations in Quebec. The main keywords used were: “data on race”, “ethnic data collection”, “race data collection”, “culturally appropriate”, “health”, “survey”, “questionnaire”, “racial groups”, “racialized groups”, “Black and minority ethnic people”, “people of colour”, “migrants”, “Quebec”, “collecte de données”, “minorité”, “noir” and “ethnicité”.
Results: We selected 43 studies covering four sectors: health, social services, education and employment. We identified the main issues, methods and strategies used to recruit members of Black communities and to collect and analyze data according to ethnoracial categories while minimizing bias to better understand the sociocultural and socioeconomic context of the target populations.
Conclusion: Our review highlights the importance of collecting data on racialized groups, particularly Black communities in Quebec, to support public policies aimed at promoting health equity.
Keywords: racialized populations, ethnoracial data, health of Black populations, collection methods
Highlights
- Although Black populations in Quebec make up more than 25% of the Black population in Canada, detailed health data for these populations in Quebec are lacking.
- We analyzed 43 studies published since 2010 that focussed on research conducted among Black populations in Quebec.
- We identified key issues, methods and strategies used to recruit members of Black communities in Quebec, and to collect and analyze data according to ethnoracial categories, while limiting bias to better understand the realities of these populations.
- The results of this scoping review could support public policies focussed on these populations to promote health equity.
Introduction
Collecting ethnoracial data on health and its social determinants raises complex ethical issues.Footnote 1 The concept of “race” has no basis in biology (which is why we have chosen to set it in quotation marks throughout this paper), but has long been used as an excuse for discrimination. This fact in turn has led to hesitation in or misperceptions about collecting ethnoracial data in Canada, particularly in Quebec.Footnote 2Footnote 3Footnote 4 However, these data are crucial for measuring health inequalities and establishing informed public health policies.
For example, Statistics Canada data show that Black Canadians had the highest number of deaths due to COVID-19.Footnote 5 In Quebec, the COVID-19 mortality rate was three and a half times higher in neighbourhoods with at least 25% racialized populations.Footnote 5 Although the Black population in Quebec makes up more than 25% of the Black population in Canada, accurate data on the impact of COVID-19 on Black communities at the provincial level are lacking, and available only at the national level.Footnote 5Footnote 6 A report by the Direction régionale de santé publique de Montréal (the public health authority in Montréal) provides information on the COVID-19 situation in Montréal, but lacks data analysis by ethnic origin, despite the concentration of cases in the region, which has the largest Black population in the province of Quebec.Footnote 7 In contrast, Quebec researchers emphasize the importance of collecting health data based on ethnoracial background.Footnote 8
Compared with the United States and the United Kingdom, Canada has limited experience with the systematic collection of ethnoracial health data within provincial health systems.Footnote 9 However, early initiatives have been rolled out in Eastern Canada, OntarioFootnote 10 and Nova Scotia,Footnote 11 though their implementation remains difficult and raises significant issues.Footnote 2Footnote 3
Despite existing efforts, there is no consensus in Canada or the United States on the standards for collecting ethnoracial and sociodemographic data.Footnote 12Footnote 13 How to define the identity of racialized populations, particularly Black populations, is still under debate.Footnote 14Footnote 15Footnote 16Footnote 17 Additionally, the most relevant social determinants of health for understanding health equity issues of Black populations in Canada, and particularly in Quebec, are not clearly defined, nor is the method for obtaining these data.Footnote 18Footnote 19
Throughout the COVID-19 pandemic, the Institut national de santé publique du Québec (INSPQ) and the regional public health authorities (particularly in Montréal) collected data by age, gender and territory or borough of residence.Footnote 7Footnote 20 These data indirectly indicate a higher number of COVID-19 cases in areas of Montréal with a greater proportion of visible minorities.Footnote 7Footnote 21 However, Quebec still lacks systematically collected health data based on ethnoracial background. The purpose of this article is to document the methods and issues involved in collecting, analyzing and disseminating data on the health of Black populations in Quebec, and its social determinants.
We conducted a scoping review to identify studies dealing exclusively with Black populations or racialized groups, including Black populations in Quebec, to analyze the methods and issues faced by researchers.
Methods
Scoping reviews “aim to map rapidly the key concepts underpinning a research area and the main sources and types of evidence available, and can be undertaken as stand-alone projects in their own right, especially where an area is complex or has not been reviewed comprehensively before.”Footnote 22,p.194Footnote 23 This review was exploratory and non-exhaustive, providing an overview of the extent of research in the field of health and its social determinants as they pertain to Black populations in Quebec.Footnote 24 We applied the PRISMA-ScR approach (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) used by Tricco et al.Footnote 25
Review of studies
The review of studies was carried out in two stages: an initial review in September 2022 and an update in June 2024. We conducted an initial literature search on studies published in English and French between January 2010 and September 2022 by consulting the PubMed, Embase, Social Care Online, Érudit, CAIRN and CINAHL databases. The main keywords used were: “data on race”, “ethnic data collection”, “race data collection”, “culturally appropriate”, “health”, “survey”, “questionnaire”, “racial groups”, “racialized groups”, “Black and minority ethnic people” (which includes “African Caribbean people” and “African people”), “people of colour”, “migrants”, “Quebec”, “collecte de données”, “minorité”, “noir”, and “ethnicité” (Table 1). The update was carried out on 3 June 2024 on Google Scholar using the keywords “race-based data collection,” “Black” and “Quebec”. We consulted the first 20 pages of results. Despite the subjectiveness inherent in this search engine, past scoping reviews and systematic reviews have used it and justified its use.Footnote 26Footnote 27Footnote 28
| Database | Search terms |
|---|---|
| PubMed | (health[Title/Abstract] OR healthcare[Title/Abstract] OR hospital*[Title/Abstract]) AND ("Ethnicity"[Majr] OR "Racial Groups"[Majr:NoExp] "Black*" OR "African*" OR "Caribbean*" OR "Afro*" OR "Person of colo?r*" OR "People of colo?r*" OR "colo?red*" OR "African*"dark-skin*” OR "ethnic minorit*") AND ("Data Collection/methods"[Majr:NoExp] OR "Data Collection/organization and administration"[Majr:NoExp] OR "Data Collection/standards"[Majr:NoExp] OR "Data Collection/statistics and numerical data"[Majr:NoExp] OR "Focus Groups"[Majr] OR "Records/methods"[Majr] OR "Records/organization and administration"[Majr] OR "Records/statistics and numerical data"[Majr] OR "Records/supply and distribution"[Majr] OR "Surveys and Questionnaires/methods"[Majr:NoExp] OR "Surveys and Questionnaires/organization and administration"[Majr:NoExp] OR "Surveys and Questionnaires/standards"[Majr:NoExp] OR "Surveys and Questionnaires/statistics and numerical data"[Majr:NoExp] OR "culturally tailored"[Majr] OR "cultural competent"[Majr] OR "culturally targeting"[Majr] OR "culturally appropriate"[Majr]) Filters: from 2010–2022 (("ethnicity data"[Title/Abstract] OR "race data"[Title/Abstract] OR "data on race"[Title/Abstract] OR "ethnic data"[Title/Abstract]) AND (collect[Title/Abstract] OR collection[Title/Abstract] OR collecting[Title/Abstract] OR gather*[Title/Abstract] OR monitor*[Title/Abstract] OR questionnaire*[Title/Abstract] OR survey*[Title/Abstract]) AND (health[Title/Abstract] OR healthcare[Title/Abstract] OR hospital*[Title/Abstract]) AND (Quebec)[Title/Abstract] OR (Québec)[Title/Abstract])) Filters: from 2010–2022 |
| CAIRN | "collecte de données" W/5 ethnique; limite=10 ans; "ethnic data" W/5 monitor*; limite=10 ans "collectes de données" W/5 ethnique; limite=10 ans; "ethnic data" W/5 survey*; limite =10 ans "collecte de données" W/5 race; limite=10 ans; "ethnic data" W/5 questionnaire*; limite=10 ans "collectes de données" W/5 race; limite=10 ans; "ethnicity data" W/5 collect*; limite=10 ans "collecte de données" W/5 minorité*; limite=10 ans; "ethnicity data" W/5 gather*; limite=10 ans "collecte de données" W/5 ethnicité; limite=10 ans; "ethnicity data" W/5 monitor*; limite=10 ans "collectes de données" W/5 ethnicité; limite=10 ans; "ethnicity data" W/5 captur*; limite=10 ans "collecte de données" W/5 noir*; limite=10 ans; "ethnicity data" W/5 captur*; limite=10 ans "collectes de données" W/5 noir*; limite=10 ans; "ethnicity data" W/5 survey*; limite=10 ans "collecte de données" W/5 haitien*; limite=10 ans; "ethnicity data" W/5 questionnaire*; limite=10 ans questionnaire* W/5 ethnique; limite=10 ans; "race data" W/5 collect*; limite=10 ans questionnaire* W/5 race; limite=10 ans; "race data" W/5 gather*; limite=10 ans questionnaire* W/5 minorite; limite=10 ans; "race data" W/5 survey*; limite=10 ans questionnaire* W/5 ethnicité; limite=10 ans; "race data" W/5 questionnaire*; limite=10 ans sondage* W/5 ethnique; limite=10 ans; "data on race" W/5 collect*; limite=10 ans sondage* W/5 race; limite=10 ans; "data on race" W/5 gather*; limite=10 ans sondage* W/5 minorite; limite=10 ans; "data on race" W/5 captur*; limite=10 ans sondage* W/5 ethnicite; limite=10 ans; "data on race" W/5 monitor*; limite=10 ans "ethnic data" W/5 collect; limite=10 ans; ethnic W/5 data W/5 monitor*; limite-10 ans "ethnic data" W/5 gather*; limite=10 ans; ethnicity W/5 data W/5 collec; limite-10 ans "ethnic data" W/5 captur*; limite=10 ans; race W/5 data W/5 collect*; limite-10 ans race W/5 data W/5 captur*; limite-10 ans race W/5 data W/5 survey*; limite-10 ans |
Selection of studies
The two authors (NM and KNLN) independently selected the studies using the Population, Concept and Context (PCC) methodFootnote 29 based on the following criteria:
- Population: people from Black (skin colour) communities of all ages living in Quebec, regardless of whether they are Anglophone, Francophone or allophone;
- Concept: primary studies focussing exclusively on Black populations in Quebec, or on other racialized groups in Quebec including Black populations in Quebec, in the field of health and its social determinants (employment, education and access to social services); and
- Context: studies conducted between 2010 and 2024 in various settings in Quebec (schools, nonprofit organizations, hospitals, etc.) and published in English or French.
The exclusion criteria were as follows:
- studies involving Black populations in various Canadian provinces in which Black populations in Quebec formed only a subsample;
- studies including “race” or ethnicity as variables that did not involve analysis or reporting of data according to these variables;
- qualitative studies with fewer than five Black participants;
- studies dealing with Black populations in relation to feminism, racial profiling, the criminal justice system or the sociology of racism;
- studies that focussed specifically on the study of sexual diversity in Black populations; and
- reviews, opinion pieces, editorials and organization reports (grey literature).
Once the selection of studies had been completed, the two authors (NM and KNLN) met to review the list based on the previously established inclusion and exclusion criteria. Any discrepancies in the selection were resolved by consensus between the two authors. Additionally, the bibliography of the selected studies was reviewed by both authors to improve the literature search.
Data extraction
Two data extraction tables were developed and used. The following information was recorded for quantitative studies: first author, year, title, location, population, period (or study duration), purpose of study, data collection methods and study design, recruitment methods, variables collected, primary and secondary endpoints, types of analysis, main results, key findings and sources of funding (Table 2). The following information was added for qualitative and mixed studies: theoretical framework applied to data analysis, main topics addressed in the interviews and consent process. The data extracted from the studies have been verified by the two authors (NM and KNLN). Given the exploratory nature of this scoping review, the quality of the selected studies was not assessed.Footnote 22
| Authors (year) |
Purpose of the study | Population and period | Method and funding | Main results | Findings/implications |
|---|---|---|---|---|---|
| Adeponle et al. (2012)Footnote 70 | Assess the impact of using the DSM‑IV‑TR cultural formulation to diagnose psychotic disorders among patients of ethnic minorityFootnote a and immigrant backgrounds |
|
|
A total of 34/70 cases with a referral diagnosis of a psychotic disorder were rediagnosed as nonpsychotic, while 12/253 cases identified as nonpsychotic received a new diagnosis of a psychotic disorder. Receiving a new diagnosis of a psychotic disorder was significantly associated with being a recent immigrant (OR = 6.05), being non-Black (OR = 3.72) and having been referred by professionals other than physicians (OR = 3.23). | While the results highlight the clinical utility of the cultural formulation to improve diagnostic accuracy, the specific aspects of the cultural consultation that contribute to this outcome remain unknown. |
| Arcand et al. (2016)Footnote 68 |
Explore the academic perseverance of permanent resident students in Montréal |
|
|
Among the respondents, 40% found it difficult to establish interactions among ethnic groups. Students had difficulty establishing ties with the majority group. Most focus group participants felt that their isolation was mainly due to their difficulties in French. Some were thinking of moving to another province to find a job that matched their training. | Given the apparent inequalities in terms of intergroup relations, returning to university might be detrimental to their stated goal of rapid and successful integration into the host society, particularly the labour market. Returning to university in a migratory context might have a demoralizing effect, since the experience foreshadows the systemic barriers that these students may encounter in their efforts to enter the labour market. |
| Auger et al. (2012)Footnote 30 | Measure perinatal health outcomes among Haitian women and assess modifying factors in terms of severity |
|
|
Compared with Canadian‑born mothers, the risk for Haitian‑born mothers was 4 times higher for extreme preterm birth, 2 times higher for very preterm birth and 25% higher for moderate preterm birth. | Haitians in Quebec may be a particularly vulnerable group, as they are exposed to poor health outcomes. Additional efforts are needed to assess the health status of the Haitian community and of other minority communities to determine whether other health disparities exist. |
| Beauregard (2020)Footnote 64 | Analyze ethnic relations between Quebeckers in majority and minority situations in terms of access to employment |
|
|
While female gender decreases discrimination, the analysis reveals an ethnic‑gender hierarchy and significant variations among minorities. Racialized women are invited to interviews more often than their male peers. | While the ratio for the Latin American female candidate suggests a lack of discrimination against her, the indicators observed for the Arab and Black male candidates suggest that the latter experience more unequal treatment in Québec City than in Montréal. |
| Boatswain-Kyte et al. (2020)Footnote 58 | Examine racial inequalities related to services from the DPJ in Quebec |
|
|
Black children’s records were reviewed, corroborated, and brought to court 5 times more often than the records of White children. Black children were also 5 times more likely than White children to be placed in foster care. The protection reports of children from other visible minoritiesFootnote a were screened in twice as often as those of White children. The inequality rate has gradually decreased over 10 years for other visible minoritiesFootnote a but has continued to rise for Black children. | By partnering with communities, child protection services can help support the infrastructure needed to build capacity, improve service coordination and strengthen the community resilience needed to improve outcomes for Black children. |
| Boatswain-Kyte et al. (2022)Footnote 59 | Examine the results of reunifications of Black children following placement in out-of-home care |
|
|
Black children spend longer periods of time in out-of-home placement and are less likely to experience family reunification compared with other children. Poorer reunification outcomes for Black children are associated with placement instability, the age of the child and reasons for child welfare involvement. | Racial disparities in reunification vary depending on a combination of factors that are unique to the child, their family and the DPJ, as well as the family’s external factors. When younger children are reported, being Black significantly reduces the likelihood of reunification. Thus, being Black only leads to inequalities in the presence of other factors. |
| Boudarbat et al. (2010)Footnote 65 | Establish the professional profile of immigrants to Quebec |
|
|
There is a strong correlation between country of origin and the extent to which employment matches expectations for both men and women. Men from Eastern Europe, Africa (including the Maghreb region) and Western Asia are the least likely to be satisfied with their jobs. Among African women, there is a very strong tendency to occupy positions that fall short of their expectations. | The public policy implications of these results relate to the following: (1) the issue of resources dedicated to recruiting and providing information to immigrants in their country of origin; (2) the efforts that the host community must make to help them enter the job market; (3) the need to adjust the selection grid to increase the chances of success of newcomers. |
| Brousseau et al. (2021)Footnote 69 | Explore factors associated with SARS‑CoV-2 seroprevalence in healthcare workers during the first wave of the pandemic |
|
|
Of the 2056 healthcare workers, 11.7% were seropositive for SARS-CoV-2. The incidence of seropositivity was significantly higher among Black individuals and Latin Americans than White individuals, with an increased risk of 41%. The most exposed workers (support staff) had an increased risk of at least 30%. | The healthcare workers who were the most directly and most frequently in contact with patients were the most affected by COVID-19. Being Black or Latin American was associated with seropositivity. The high risk of SARS‑CoV-2 infection among healthcare workers requires making vaccination among this category of workers a priority. |
| Carazo et al. (2022)Footnote 54 | Measure the prevalence of psychological distress among Quebec healthcare workers, whether or not they were infected with SARS‑CoV-2 |
|
|
The prevalence of high work-related psychological distress was 42%. It was associated with risk factors such as work-life balance, value conflicts and high psychological demands but not associated with SARS-CoV-2 infection. COVID patients were more often men, older, identified as Black, and worked more often as patient healthcare assistants and in long-term care facilities. | Primary prevention measures targeting psychosocial risk factors are needed to reduce mental health risks for healthcare workers. |
| Collins et al. (2018)Footnote 39 | Study the postsecondary pathways of Montréal youth of Haitian origin |
|
|
The students’ pathways were marked by various financial, institutional and social barriers. They had negative experiences with guidance counsellors during the transition to postsecondary education level. Perceived racism and discrimination emerged as themes in the young people’s discourses. | The study provides complex insights on some aspects that may be hidden in studies that traditionally group Haitians into broader categories, such as “Caribbean,” “Black” or “immigrant.” |
| Dagher et al. (2024)Footnote 66 | Describe the experience of access to care and access to interpreters during admission to four Montréal hospitals |
|
|
There were 36% of immigrants with a language barrier who did not have access to an interpreter during hospitalization. Prior to admission, 14/41 of allophone immigrants had difficulty accessing COVID-19 information in their first language. Among non‑White allophone immigrants, 9/27 had difficulty accessing COVID-19 services. | A large proportion of patients had difficulty accessing COVID-19 information and services, which may have increased exposure to SARS‑CoV‑2 and hospitalizations. After hospitalization, a large proportion of them did not have access to interpreters. Providing information and care in the first language of these communities is important for promoting health equity. |
| Darwish et al. (2022)Footnote 56 | Describe the characteristics of healthcare workers admitted to hospital with COVID-19 and associated risk factors for ICU admission and death |
|
|
Migrants made up 68% of hospitalized workers, with sociodemographic characteristics that were similar to those of Canadian-born workers. Immigrants were more likely to be personal support workers than their Canadian‑born colleagues and more likely to be Black. Over 1/3 of workers had not received COVID-19-specific infection control training and over 50% did not always have access to personal protective equipment. | The results of this study are similar to those of a survey conducted by the INSPQ between May 2020 and May 2021, in which personal support workers and foreign‑born or Black healthcare workers were 2.2 times, 1.3 times and 2.5 times more likely, respectively, to test positive for SARS-CoV-2 than other healthcare workers. These health disparities are unexplained. |
| Debrosse et al. (2024)Footnote 49 | Explore the links between neighbourhood experiences, the ethnic/ideal alignment of identities and well‑being in youths |
|
|
Youths’ neighbourhoods predict the extent to which they perceive that opportunities are accessible to them. Youths who reported more opportunities for people similar to them in their neighbourhood tended to report higher alignment between their racial/ethnic and ideal future identities and higher flourishing. | The findings highlight the connection between neighbourhood factors—such as cues about whether similar people are welcomed, valued and have access to opportunities—and the identities and well‑being of Black and Indigenous youths and youths of other racialized groups. |
| Dufour et al. (2015)Footnote 60 | Study the relationships between neighbourhood characteristics and rates of immigrant children reported to child protective services |
|
|
Black children living in Montréal neighbourhoods where there are low education levels, a higher rate of lone-parent families, low population density and a small number of Black children are more likely to be reported to the DPJ. | Analyzing the distribution of reporting rates without considering ethnocultural background underestimates important observable differences. This shows that services need to be adapted to the realities specific to each neighbourhood and ethnocultural group. |
| Fang et al. (2023)Footnote 31 | Study the relationship between discrimination and disparities in healthcare accessibility |
|
|
Black Anglophone participants experienced more discrimination, had fewer healthcare providers, had less access to COVID-19 information during the pandemic and were more dissatisfied with the healthcare system than their Francophone peers. | Discrimination based on racialized identity and language is pervasive in healthcare, reinforcing greater dissatisfaction in this regard, which establishes the intersecting effects of multiple forms of discrimination as unique stressors with detrimental impacts on health. |
| Frounfelker et al. (2022)Footnote 50 | Study the link between social distancing due to COVID-19 and mental health |
|
|
Five classes of individuals were identified based on the perceived aspects of social distancing related to COVID-19: “Low Impact,” “Freedom/Flexibility,” “Safety,” “Family/Home” and “Hardships.” People in the “Hardships” class (more often from racialized groups and unemployed) were more likely to report a significant impact of COVID-19 on their mental health (OR = 2.09). | The analysis identified a subgroup of individuals (the “Hardships” class) who presented a higher risk of mental health problems than the rest of the population and who could be prioritized for awareness and intervention efforts. The “Low Impact” class suggests that, for healthcare workers, normalizing an abnormal crisis can be a successful coping strategy. |
| Gomez Cardona (2012)Footnote 32 | Explore the testimonies of children affected by gastrointestinal disorders and those of their mothers |
|
|
Six therapeutic dynamics were highlighted: (1) multiple care (illness of unknown origin); (2) nutrition and the mother’s central role (gas-related illnesses); (3) contagion and withdrawal into the family (illnesses of microbial origin); (4) social suffering; (5) medical/religious approach (prayers and maintaining ties with the community); (6) no medical consultation. | The results confirm that Haitian families’ low attendance at the gastroenterology clinic could be due to the following: (1) their ability to treat their children’s stomach aches using means other than biomedicine; and (2) the fact that stomach aches are seen as a problem that does not require a medical opinion. Mistrust of healthcare services is due to negative experiences. |
| Kamanzi et al. (2018)Footnote 62 | Study the postsecondary pathways of Quebec youth from immigrant backgrounds |
|
|
The rate of access to postsecondary education is higher among youth from East Asia (80%), the Maghreb region and the Middle East (74%), but lower among those from Latin America and the Caribbean (58%). Their access pathway is generally linear. | Despite significant differences in postsecondary education access, pathway morphology tends to be similar between immigrants when educational background in high school is accounted for: the commonality is a linear pathway to university specifically. |
| Kamanzi (2021)Footnote 61 | Explore the factors for academic resilience among young people of African and Caribbean origin |
|
|
Students of African and Caribbean origin attend college at a rate that is comparable to that of their peers of European-Canadian origin. Black students enrolled in college are less likely to graduate by age 22. In addition, university is less accessible to them. | Some Black Quebec students manage to overcome barriers despite the fact that they are more exposed to precarious living conditions. The author calls on public authorities to place greater emphasis on improving learning conditions and supporting success. |
| Kanouté et al. (2014)Footnote 45 | Explore academic issues and the use of community resources by Haitian families |
|
|
The data intersects the views of students, parents and school/community stakeholders on students’ resilience factors and the specific family realities that need to be considered to better support families. Parents and workers highlighted the effects of the migration journey on parenting and the intertwined relationship between the family’s migration journey and the child’s academic plans. | A better understanding of the links between the family’s migration journey and the student’s academic plans would better support students from an immigration background and anticipate various pitfalls likely to hinder the school/family relationship and the parents’ involvement with the school. Schools would benefit from working with community groups that have expertise in supporting immigrants. |
| Kanouté et al. (2016)Footnote 71 | Explore the academic experience of students from immigrant backgrounds |
|
|
The students shared their views on the variations in their identity, their relationship with learning, their academic plans and their use of spaces and resources in their neighbourhood. | An intercultural perspective at school should include the student’s social/educational experience, acknowledge the student in their identities and achievements, instill a certain heterocentric approach in the interpretation of the program, support living in harmony, manage daily school life in an inclusive way and develop a partnership with families and the community. |
| Kanouté et al. (2020)Footnote 46 | Examine the educational persistence of permanent resident students |
|
|
Students are worried about building a comfortable home in a new society. This comfort is tied to the financial resources available and the caregivers’ responsibility for their children. Students found it difficult to create the optimal conditions to support their family needs and balance family, studies and work. | It would be important to document the challenges relating to the transition to the workplace, social integration, balancing family/studies/work, decoding university culture and practices, and the perception of discriminatory practices. |
| Lafortune et al. (2020)Footnote 40 | Examine Haitian students’ relationship with their college‑level studies in Montréal |
|
|
The college experience: [translation] “We were abandoned in the wilderness, it was a cold plunge, I hit a wall, I was fed up” (p. 23). Participants were unanimous in emphasizing the individual factors in college success (motivation, vocational choice, work habits). The student experience was affected by immigration status and minority status. | The authors reiterate the importance of shared values, such as the principle of nondiscrimination. They suggest continuing to raise awareness among stakeholders about the impact of systemic factors that contribute to the marginalization and exclusion of certain minority groups. CEGEPs share responsibility for ensuring equality of opportunity and the inclusion of all students. |
| Lafortune et al. (2024)Footnote 48 | Examine the practices and activities that promote French language proficiency among immigrant youth in Montréal |
|
|
Young people and guardians reported improvements in language skills (vocabulary, oral fluency, improved reading skills, etc.). The camp gave young people with limited social networks an opportunity to expand their circle of friends. | The educational camp experience highlighted the levers for efficient community/family/school collaboration. It consolidated school/community collaboration, which allowed the partnership to be maintained for future camps and for the creation of new joint projects. |
| Leduc et al. (2021)Footnote 57 | Study barriers faced by Black students in entering medical school in Quebec |
|
|
The proportion of Black students in the applicant pool for medical school in 2020 is estimated to be 4.5%. It is estimated that Black students represented 1.8% of applicants invited to admission interviews and 1.2% of admitted students in Quebec in 2019. Although no direct comparisons can be made, it seems that Black applicants are disproportionately rejected compared with non‑Black students. | Two barriers are noted: (1) a significant proportion of students from Black communities in Quebec may not consider medicine as a career and do not apply to medical school; and (2) when Black students apply to medical school, their applications seem to be disproportionately rejected before the interview compared with non-Black students. A longitudinal study is needed to monitor progress and determine the factors that contribute to this progress. |
| Livingstone et al. (2014)Footnote 41 | Identify actions to reduce the dropout rate among Black students |
|
|
According to the students, their academic success was influenced by multiple and interrelated factors, including family, peers, school and neighbourhood. In their view, schools should offer more support to Black students by fostering a better school climate and introducing multicultural curricula and innovative pedagogies. | The authors recommended that participatory action research with youth be introduced in schools as a tool for enhancing school success in the long term. Young people’s insight and idealism shows that dropping out of school is not as an unsolvable issue as it might seem. |
| Magnan et al. (2017)Footnote 43 |
Explore immigrant children’s relationship to education and their postsecondary choices |
|
|
Young people from the Caribbean, sub‑Saharan Africa and Latin America are more likely to follow the paths that coincide with the following approaches: [translation] “elitist/laissez-faire, laissez-faire/laissez-faire and cocoon/laissez-faire.” | Two issues deserve more attention: How can the school system’s resources be used to facilitate young people’s freedom of choice and how can they be better equipped? How can we better support families in their understanding of the school system and the job market? |
| Magnan et al. (2017)Footnote 42 | Understand the experience of immigrant youth in their choice of CEGEP program |
|
|
An analysis of testimonies from immigrant youth shows that the family plays a determining role in the choice of postsecondary programs. Compared with youth from other countries, youth from sub-Saharan Africa, the Caribbean and Latin America perceived facing more constraints (familial, economic and academic) when choosing their programs. | Youth from Asia, Eastern Europe, the Maghreb region and the Middle East are more likely to follow an academic path in line with the [translation] “elitist/supportive approach.” Youth from the Caribbean, sub-Saharan Africa and Latin America are more likely to follow a path in line with the [translation] “elitist/laissez-faire approach.” This can be explained in part by the fact that Black families are more likely to belong to low or middle social classes. |
| Magnan et al. (2023)Footnote 72 | Study the factors that shape the academic pathways of Black students in Quebec |
|
|
Most students first enroll in a program other than their desired one to ensure their financial security or to improve their grades for a limited-enrollment program. Medicine and pharmacy studies remain a dream for most of the participants. | Students face a seemingly unfair admissions system for highly selective programs (medicine and health sciences). These results shed light on possible changes to admissions policies for certain programs. |
| Ménard et al. (2020)Footnote 63 | Measure the rate of pregnancy complications in a multicultural group of women |
|
|
The risk of anemia was higher in Black women than in White women (aOR = 1.74). Black women were at higher risk of preterm birth (aOR = 1.79). Immigrant women had an increased risk of anemia compared to Canadian-born women (aOR = 1.85). | Nutritional interventions need to be targeted toward prevention of adverse pregnancy outcomes, prioritization of higher-risk groups and adaptation of the community organization’s program to a multiethnic, low-income population. |
| Miconi et al. (2021)Footnote 51 | Investigate the association between risk of exposure to SARS-CoV-2 and mental health in ethnocultural groups |
|
|
Exposure to the virus, COVID-19-related discrimination and stigma were associated with poorer mental health. Black participants who were exposed and discriminated against reported greater mental distress. | Interventions that take into account race and culture and that consider factors such as discrimination and historical and racial trauma are needed. |
| Miconi et al. (2021)Footnote 52 | Examine the extent of experiences of discrimination related to COVID-19 |
|
|
COVID-19-related discrimination was reported by 16.6% of participants. Non‑White participants, younger participants and healthcare workers were more likely to experience discrimination. Participants of East Asian descent and essential workers were more likely to report discrimination because of their ethnicity and occupation. | Health communication actions informed by a social pedagogy approach should target public beliefs related to the association of COVID-19 with ethnicity, age and occupation to minimize pandemic-related discrimination. |
| Noubicier et al. (2013)Footnote 33 | Study the meaning of aging among older Black women living in Montréal |
|
|
For these women, aging is inevitable. They see this period of their lives as a privilege, placing great importance on intergenerational relationships, faith and social involvement. | Social policies should take gender and ethnicity into account. |
| Nweze et al. (2023)Footnote 34 | Analyze the impact of racial and linguistic discrimination on mental health |
|
|
English-speaking participants experienced more discrimination and reported more barriers to accessing mental health care. They also had poorer mental health than their French-speaking counterparts. | The study justifies a mechanism by which language affects mental health by exposing Black Quebeckers to more discrimination and thus higher barriers to care. |
| Paquette et al. (2019)Footnote 35 | Study the impact of ASD on the quality of life of mothers of Haitian origin living in Montréal |
|
|
Mothers anchored their strategies for controlling ASD in their religious faith. Their quality of life was considered to be average and their coping strategies were primarily focussed on problem-solving or seeking social support. They did not confide in strangers or professionals. | Family members are the first people consulted when a physical or mental illness appears. This is why it is so important that interventions consider the subjects’ culture and choices. It is vital to develop expertise in intervening with families who have a child with ASD and on using an ethnopsychiatric approach. |
| Passos-Castilho et al. (2022)Footnote 67 | Identify factors associated with ICU admission and hospital mortality among COVID-19 patients |
|
|
Immigrants are more likely to be admitted to intensive care. This risk is higher among Caribbean Black individuals than White individuals. The risk of hospital mortality is higher among Canadian‑born individuals than among immigrants, and higher among Caribbean Black individuals (but not Africans) than White individuals. | The data highlight the disproportionate impact of COVID-19 on foreign-born communities, the significant heterogeneity of COVID-19-related outcomes within ethnic groups and between countries, and the significant gaps in understanding the individual impacts of the social determinants of health and their interactions. |
| Salamanca (2018)Footnote 44 | Examine the role of temporary employment agencies in Montréal in exploiting immigrant labour |
|
|
Nurses and attendants with valid immigration status who work through an agency are underpaid compared with workers with similar degrees and levels of education. Agency workers in the health sector, the majority of whom are Black, believe they are underpaid. | Workers with precarious immigration status experience long-term hardship, making them a vulnerable labour pool when they work for poorly regulated employment agencies. As a result, the likelihood of experiencing the effects of systemic racism is greater. |
| Sherry et al. (2013)Footnote 36 | Understand the attitudes and beliefs of the Haitian adult population regarding organ donation |
|
|
Participants recommended that Haitian health professionals and leaders use community media to spread messages about organ donation and to spark debate within families. People over 45 were more reluctant. Some of them had never heard about this issue and showed an interest in it. | The use of bilingual French/Creole Haitian moderators facilitated discussions during the study. Some of the reluctance to participate was overcome by addressing participants’ questions and concerns. The authors plan to share the study’s results with Haitian community groups, ethnocultural consultants and the Haitian media. |
| Spence et al. (2014)Footnote 55 | Study the effect of age at time of circumcision and race on prostate cancer risk |
|
|
Circumcision proved protective among men who were circumcised at age 36 and over (OR = 0.55). The strongest protective effect of circumcision was recorded in Black men (OR = 0.40; p = 0.02). | There is an inverse relationship between prostate cancer risk and circumcision performed at age 36 y and over. The protective effect appears only among Black men, the group most at risk of prostate cancer. |
| St-Louis et al. (2014)Footnote 37 | Study antigens in red blood cells from Black donors living in Quebec |
|
|
Genotyping results predicted the presence of rare phenotypes. | Black donors, with or without a rare phenotype, are precious to the patient cohort depending on blood transfusions and to Héma-Québec. |
| Tran et al. (2013)Footnote 38 | Examine the factors leading to increased blood donation in Montréal’s Black communities |
|
|
The participation of groups interested in bettering the lives of those affected by sickle cell anemia combined with the fact that leaders felt more comfortable donating to someone close to the community suggests that promoting blood donation from this angle would be well received. | Pointing out that phenotyped blood can be set aside for patients with sickle cell anemia is an argument for encouraging members of the Black community to donate blood. Since 2010, donors have been able to specify their ethnoracial background. |
| van der Ven et al. (2012)Footnote 53 | Study first-episode psychotic symptoms by ethnic background |
|
|
Compared with the reference group (Euro‑Canadians), the African/Afro‑Caribbean group had a higher level of negative symptoms and general psychopathology scores. Ethnic groups did not differ on positive symptom scores. | Particular attention should be paid to targeting negative symptoms and improving cooperation and engagement among certain patients from racialized groups during the initial phase of psychosis. |
| Weiler et al. (2022)Footnote 47 | Assess vitamin D levels and modifiable factors |
|
|
Thirty-five percent of mothers gave their consent. Most newborns had adequate vitamin D levels. However, non-White groups, particularly Black newborns, had a higher risk of deficiency (5.5 times higher). | Most newborns had adequate vitamin D levels, but 1/5 were vitamin D deficient, with differences between population groups. |
Data analysis
We analyzed the data using a thematic approach and following the main steps involved in carrying out a research project: (1) devising participant recruitment strategies; (2) determining variables of interest to the researchers; (3) deciding on data collection and analysis methods; and (4) determining the limitations and biases inherent in studies dealing with ethnoracial background (Table 3).
| Characteristic | Number of studies n (%) |
|---|---|
| Sector | |
| Health | 23 (53.5) |
| Education | 14 (32.5) |
| Social services | 3 (7.0) |
| Employment | 3 (7.0) |
| Year of publication | |
| 2010–2019 | 22 (51.0) |
| 2020–2024 | 21 (49.0) |
| Methods | |
| Quantitative | 26 (60.5) |
| Qualitative | 14 (32.5) |
| Mixed | 3 (7.0) |
| Study focussed exclusively on Black populations | |
| Health | 9 (21) |
| Education | 3 (7) |
| Social services | 0 (0) |
| Employment | 0 (0) |
Results
Selection of studies
The initial literature search identified 259 articles from the six databases listed earlier. Once duplicates had been eliminated, 189 articles remained for the two authors to review (titles, abstracts) according to the process described in the PRISMA flow diagram (Figure 1). This resulted in 21 articles being selected and read in full by the authors (NM and KNLN). Eight studies were excluded on the basis that they had not been carried out in Quebec, or involved groups that fell within the exclusion criteria. Following a review of the bibliographic references of the selected articles, an additional six studies were selected. An update carried out in 2024 resulted in the selection of 24 additional articles, bringing the total to 43 studies (Figure 1).
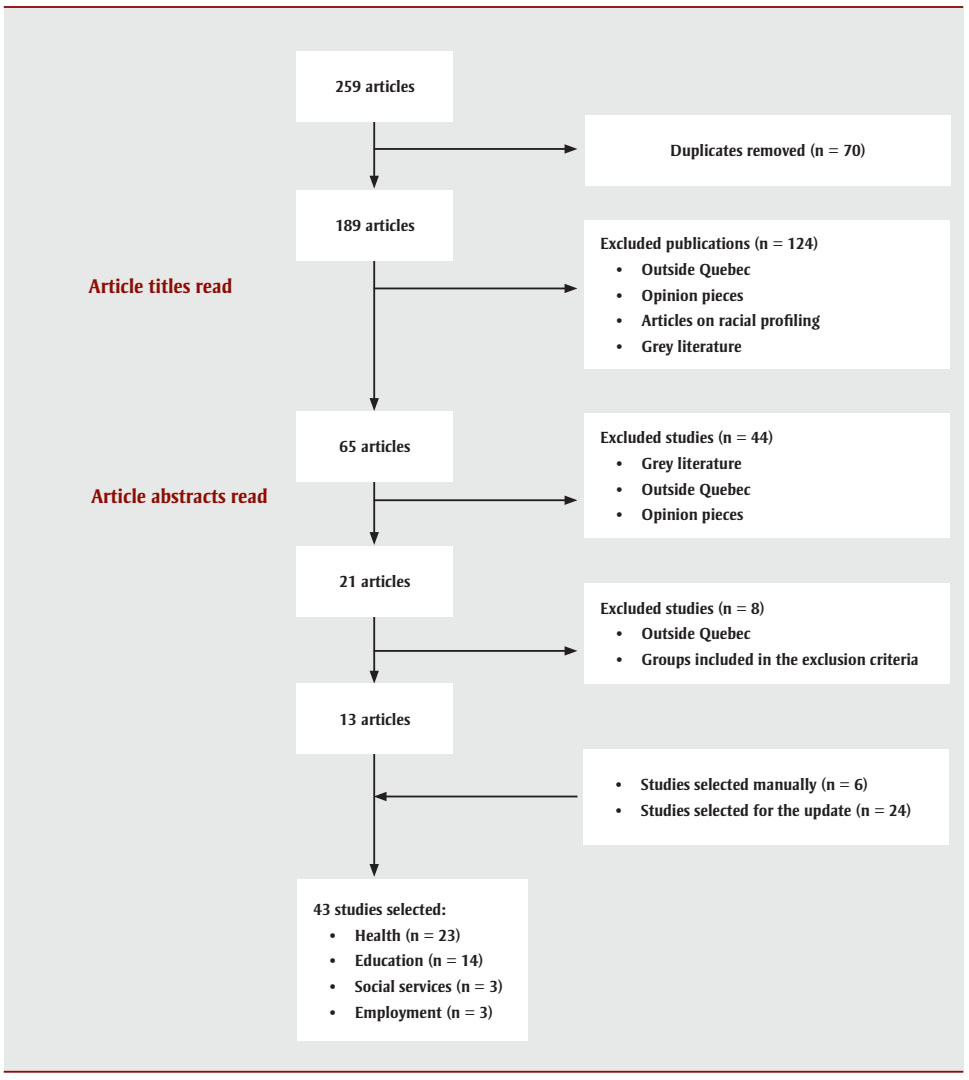
Figure 1 : Descriptive text
- Step 1: 259 articles
- Duplicates removed (n = 70)
- Step 2: 189 articles
- Article titles read
- Excluded publications (n = 124)
- Outside Quebec
- Opinion pieces
- Articles on racial profiling
- Grey literature
- Excluded publications (n = 124)
- Article titles read
- Step 3: 65 articles
- Article abstracts read
- Excluded studies (n = 44)
- Grey literature
- Outside Quebec
- Opinion pieces
- Excluded studies (n = 44)
- Article abstracts read
- Step 4: 21 articles
- Excluded studies (n = 8)
- Outside Quebec
- Groups included in the exclusion criteria
- Excluded studies (n = 8)
- Step 5: 13 articles
- Included studies (n = 30)
- Added:
- Studies selected manually (n = 6)
- Studies selected for the update (n = 24)
- Step 6: 43 studies selected:
- Health (n = 23)
- Education (n = 14)
- Social services (n = 3)
- Employment (n = 3)
Study characteristics
The studies selected relate to four sectors: health (n = 23), education (n = 14), social services (n = 3) and employment (n = 3), providing a cross-sectoral perspective on ethnoracial data collection on health and its social determinants (Table 2). Descriptive, empirical or experimental studies using qualitative, quantitative or mixed methodologies were selected, with the majority being quantitative (60%). Note that 12 of the selected studies focussed exclusively on Black populations in Quebec—9 on healthFootnote 30Footnote 31Footnote 32Footnote 33Footnote 34Footnote 35Footnote 36Footnote 37Footnote 38 and 3 on educationFootnote 39Footnote 40Footnote 41 (Table 3). The remaining studies relating to health, social services, education and employment were based on various ethnic groups living in Quebec, including Black communities (Table 3). Only 7 studies dealt with COVID-19.Footnote 50Footnote 51Footnote 52Footnote 56Footnote 66Footnote 67Footnote 69
Recruitment strategies
Common recruitment methods included posters, social media, community media and participation in local events.Footnote 31Footnote 33Footnote 34Footnote 36Footnote 42Footnote 43Footnote 44 However, recruiting individuals from specific populations with distinct characteristics (racialized populations with precarious migratory status) is more challenging owing to the difficulty in identifying them.Footnote 44 Some authors preferred direct recruitment strategies designed to build purposeful relationships with the people contacted, such as word-of-mouth,Footnote 33 referrals from key informants within the target communities or professionals who speak the language of the people involved.Footnote 36Footnote 45Footnote 46Footnote 47
Another approach involved working with community groups or students through a participatory research partnership (four studies),Footnote 31Footnote 41Footnote 44Footnote 48 or leveraging the expertise of local stakeholders (representatives of community groups, religious leaders).Footnote 35Footnote 36Footnote 38Footnote 40 These stakeholders’ input was especially useful in identifying Black community members as potential study participants from a database that contained no ethnoracial information.Footnote 38
Only a few studies (n = 7) provided details on the incentives used to boost participation or retention rates.Footnote 38Footnote 41Footnote 44Footnote 49Footnote 50Footnote 51Footnote 52 Incentives ranged from $0.50 to $20 for participation in a survey, and up to $50 for participation in an interview.Footnote 44Footnote 49Footnote 50Footnote 51Footnote 52 One study reported no financial compensation for participants after taking part in a two-hour interview.Footnote 38 In another, despite offering $50 per interview, recruiting and retaining participants proved challenging.Footnote 44 In a participatory research study in which 20 high school students were actively involved in data collection and analysis, financial compensation reached up to $500.Footnote 41 Nevertheless, 20% of the students withdrew from this study for lack of motivation or to take on other responsibilities.Footnote 41 The main reasons for students’ participation in the study were: wanting to make a difference in their school, and to take on the researcher’s role rather than that of the subject being observed.Footnote 41
Participant consent
The process of obtaining consent was documented in 17 studies, with consent typically obtained before the study began, either in writingFootnote 31Footnote 34Footnote 35Footnote 38Footnote 39Footnote 42Footnote 43Footnote 47Footnote 50Footnote 52Footnote 53Footnote 54Footnote 55 or verbally.Footnote 37Footnote 40Footnote 49Footnote 54Footnote 56 In one instance, consent was implied, as individuals were asked to complete a questionnaire on a voluntary basis.Footnote 57 In another study on Haitians’ beliefs about organ donation, researchers encountered difficulties with some participants, who were reluctant to sign the consent form.Footnote 36 Fearing that this would be used as consent to organ donation, these participants offered to sign a joint form involving all members of the focus group to avoid individual responsibility.Footnote 36 After the researchers clarified that the consent was limited to the study and addressed participants’ concerns, the participants ultimately signed individual consent forms after the focus group.Footnote 36 In other studies, individual consent was not required, as the research involved secondary data.Footnote 58Footnote 59Footnote 60Footnote 61Footnote 62Footnote 63
In one study examining the links between exposure to SARS-CoV-2, COVID-19-related discrimination and mental health in ethnocultural groups, researchers did not disclose the true purpose of their study, given its sensitive nature. Consequently, participants’ consent was voluntary but uninformed, as the study was presented as research on COVID-19 and social distancing.Footnote 51 In another study, researchers used a testing method that involved sending fictional resumés in order to document ethnoracial discrimination in hiring.Footnote 64
Variables of interest to researchers
The variables related to ethnicity, “race” and other social determinants of health collected in the selected studies are presented in Table 4. Ethnoracial background and immigration data encompass a range of variables and categories (Table 4). Ethnicity, whether assigned or self‑reported, is defined by researchers based on biological (skin colour),Footnote 31Footnote 34Footnote 37Footnote 41Footnote 47Footnote 49Footnote 50Footnote 51Footnote 52Footnote 53Footnote 54Footnote 56Footnote 57Footnote 58Footnote 59Footnote 63Footnote 64Footnote 66Footnote 67Footnote 69Footnote 70 geographical (country of birth or origin)Footnote 30Footnote 31Footnote 33Footnote 35Footnote 36Footnote 38Footnote 39Footnote 40Footnote 42Footnote 43Footnote 44Footnote 45Footnote 46Footnote 47Footnote 48Footnote 50Footnote 51Footnote 52Footnote 53Footnote 56Footnote 61Footnote 62Footnote 64Footnote 66Footnote 67Footnote 68Footnote 69Footnote 71Footnote 72 or cultural (mother tongue, home language, religion)Footnote 30Footnote 31Footnote 34Footnote 39Footnote 46Footnote 51Footnote 61markers (Table 4).
| Author (sample size) |
Age, gender, sex | Ethnoracial background |
Immigration | Socioeconomic status | Additional information |
|---|---|---|---|---|---|
| Health | |||||
| Adeponle et al. (2012)Footnote 70 (N = 323) |
Age Sex |
“Race” or ethnicity (White, Black, Asian, other) | Migration status Length of stay |
n/a | Mental health clinical data |
| Auger et al. (2012)Footnote 30 (N = 31 868) |
Age Female |
Haitian community Country of birth (Haiti, other Caribbean islands, other countries, Canada)Footnote a Mother tongue and language spoken at home (English, French, Creole) |
n/a | n/a | Perinatal health data |
| Brousseau et al. (2021)Footnote 69 (N = 2056) |
Age Sex |
“Race” or ethnicity (White, Black, HispanicFootnote b) | n/a | n/a | COVID-19 clinical data |
| Carazo et al. (2022)Footnote 54 (N = 8220) |
Age Sex |
“Race” or ethnicity (White, Black, other) | n/a | Type of employment | COVID-19 clinical data and psychological distress |
| Dagher et al. (2024)Footnote 66 (N = 1104) |
Age Sex |
Country of birth Ethnicity (White, Black, Asian, Latino,Footnote b Middle Eastern/North African, mixed, other) |
Migration status | Material and Social Deprivation Index | Language skills (English, French) Availability of interpreters Comorbidity score |
| Darwish et al. (2022)Footnote 56 (N = 150) |
Age Sex |
Country of origin Ethnicity (White, Black, Asian, Latino,Footnote b Middle Eastern/North African, mixed, other) |
Migration status | n/a | Intensive care admission, in-hospital mortality Length of hospital stay |
| Debrosse et al. (2024)Footnote 49 (N = 179) |
Age Sex |
“Race” (Black, non-Black people of colourFootnote b) Ethnicity (Afro, African descent, Caribbean; Latino,Footnote b Hispanic,Footnote b Peruvian or Maya; Arab, Lebanese or Middle Eastern; Algerian, Kabyle, Maghrebin; Indigenous) |
n/a | Median family income Unemployment rate |
Neighbourhood characteristics Social identity Future aspirations Well-being (having basic needs met) |
| Fang et al. (2023)Footnote 31 (N = 531) |
Age Gender |
Black communities in Quebec Language spoken Country of birth (participants, parents) |
Generational status | Employment status Family income |
Mental and physical health Access to healthcare Experiences of discrimination |
| Frounfelker et al. (2022)Footnote 50 (N = 3183) |
Age Gender |
“Race” or ethnicity (White, East Asian, South Asian, Southeast Asian, Black, Arab, other) | n/a | Family status Income Type of employment |
Mental health data Positive and negative effects of social distancing |
| Gomez Cardona (2012)Footnote 32 (N = 5) |
Age Female |
Haitian community | Migration status Generational status Length of stay |
Socioeconomic status Family status |
Strategies for coping with stomach aches |
| Ménard et al. (2020)Footnote 63 (N = 1387) |
Age Female |
“Race” (White, Black, Asian) | Migration status Country of origin Length of stay |
Level of education Family status Income |
Clinical data (pregnancy, nutritional intake) |
| Miconi et al. (2021)Footnote 51 (N = 3273) |
Age Gender |
“Race” or ethnicity (White, East Asian, South Asian, Southeast Asian, Black, Arab, other) Mother tongue, religion |
Generational status | Level of education Income Employment status |
COVID-19 and mental health clinical data |
| Miconi et al. (2021)Footnote 52 (N = 3273) |
Age Gender |
“Race” or ethnicity (White, East Asian, South Asian, Southeast Asian, Black, Arab, other) | Generational status | Level of education Employment status |
Exposure to COVID-19 Perceived discrimination related to COVID-19 |
| Noubicier et al. (2013)Footnote 33 (N = 7) |
Age Female |
Ethnicity (sub-Saharan African) | Migration path | Socioeconomic status | Perceptions of successful aging |
| Nweze et al. (2023)Footnote 34 (N = 531) |
Age Gender |
Black Spoken language |
Generational status | Employment status Family income |
Mental and physical health Experiences of discrimination Access to mental health care |
| Paquette et al. (2019)Footnote 35 (N = 12) |
Female Age of child |
Haitian community | Migration status Generational status |
n/a | Quality of life and ASD |
| Passos-Castilho et al. (2022)Footnote 67 (N = 1104) |
Age of mother Sex of child |
“Race” or ethnicity (White, Black [Caribbean, sub-Saharan African], Asian, LatinoFootnote b, North African/Middle Eastern, mixed, other) Country of birth |
n/a | Material and Social Deprivation Index | COVID-19 clinical data Perceived discrimination |
| Sherry et al. (2013)Footnote 36 (N = 24) |
Age | Haitian community | n/a | Level of education | Social role or position Past experiences Beliefs about organ donation |
| Spence et al. (2014)Footnote 55 (N = 3208) |
Age Male |
“Race” (White, Black, Asian, other) | n/a | Level of education | Clinical data (circumcision, prostate cancer screening) |
| St-Louis et al. (2014)Footnote 37 (N = 1476) |
n/a | Black | n/a | n/a | Genotypes |
| Tran et al. (2013)Footnote 38 (N = 33) |
Age Sex |
Ethnicity (African, Haitian, other Caribbean) | n/a | n/a | Beliefs and attitudes about blood donation |
| van der Ven et al. (2012)Footnote 53 (N = 301) |
Age of mother | Statistics Canada categories (2006)Footnote a Country of birth |
Migration status Generational status Migration path (previous countries of residence) |
Level of education | Mental health clinical data |
| Weiler et al. (2022)Footnote 47 (N = 1035 pairs) |
Age Female |
Ethnicity according to CIHI (White, Black, East Asian, South Asian, Southeast Asian, Latino/a,Footnote b Middle Eastern, other/mixed) Country of birth |
n/a | Level of education Income | Lifestyle habits Vitamin D levels |
| Social services | |||||
| Boatswain-Kyte et al. (2020)Footnote 58 (N = 15 875) |
Age (child, mother) | White, Black, other visible minorities,Footnote b unidentified | Migration status | Level of education Income Employment status Family status |
Reporting, placement, legal decision Rate of inequality |
| Boatswain-Kyte et al. (2022)Footnote 59 (N = 1395) |
Age at placement Sex |
White, Black, other visible minorities,Footnote b unidentified | n/a | Socioeconomic Disadvantage Index | Type of abuse Type of placement Number of breakdowns resulting from out-of-home placement |
| Dufour et al. (2015)Footnote 60 (N = 8263) |
Age | “Race” or ethnicity (Black, other visible minorities,Footnote b visible nonminoritiesFootnote b) | n/a | Level of education Income Family status Family size |
Relocation Population density |
| Education | |||||
| Arcand et al. (2016)Footnote 68 (N = 426) |
Age | Country of origin | Migration status Length of stay |
Employment status | Network and involvement with associations Perceived degree of loneliness and exclusion |
| Collins et al. (2018)Footnote 39 (N = 11) |
Age Sex |
Haitian (parents) Born in Quebec (students) Mother tongue |
n/a | n/a | Family experiences Elementary and high school experiences CEGEP experiences Linguistic, cultural and geographic identity Postsecondary endeavours Employment |
| Kamanzi et al. (2018)Footnote 62 (N = 20 387) |
Gender | Region of birth (parents) | Generational status | Level of education (parents) Family income |
Postsecondary education pathways |
| Kamanzi (2021)Footnote 61 (N = 8415) |
Gender | African/Caribbean, Euro‑Canadian Mother tongue |
Generational status | Income | Type of school Educational delay |
| Kanouté et al. (2014)Footnote 45 (N = 48) |
Age Sex |
Country of origin (parents) | Migration path | Economic profile (disadvantaged) | Day-to-day schooling Parental supervision Use of neighbourhood resources Social integration of families |
| Kanouté et al. (2016)Footnote 71 (N = 32 parent-child pairs) |
Age Sex |
Country of origin (parents) | Migration status Generational status |
Economic profile (disadvantaged) | Ethnocultural identity Relationship with school Follow-up and school project Neighbourhood life |
| Kanouté et al. (2020)Footnote 46 (N = 1077) |
Age Gender |
Region of birth Mother tongue |
Migration status Length of stay Premigration context |
Family situation Employment status Financial resources |
Institutional life experience Learning and training experience General living conditions in Quebec |
| Lafortune et al. (2020)Footnote 40 (N = 53) |
Age Sex |
Haitian community | Migration status | n/a | Social and family support Academic achievement |
| Lafortune et al. (2024)Footnote 48 (N = 27) |
Age Sex |
Country of origin | Migration status Length of stay |
n/a | Sociocultural integration Progress in French Commitment and interest |
| Leduc et al. (2021)Footnote 57 (N = 4283) |
n/a | “Race” (White, Black) | n/a | n/a | Admission to medical school |
| Livingstone et al. (2014)Footnote 41 (N = 20) |
Age | “Race” (Black) | n/a | n/a | Equity/diversity School climate Curriculum Academic support Extracurricular activities |
| Magnan et al. (2017)Footnote 43 (N = 60) |
Age Sex |
Region of origin (parents) | Generational status | Financial support from parents School capital (parents) |
Education pathways (four types defined) |
| Magnan et al. (2017)Footnote 42 (N = 60) |
Age | Region of origin (parents) | Generational status | Financial support from parents School capital (parents) |
Choice of postsecondary studies Family constraints Academic constraints |
| Magnan et al. (2023)Footnote 72 (N = 12) |
Age Gender |
Ethnicity: country of origin (father, mother) | Generational status | Level of education (father, mother) | Education pathway |
| Employment | |||||
| Beauregard (2020)Footnote 64 (N = 1569) |
Sex | “Race” or ethnicity (Arab, Latin American, Black) Majority/minority status |
n/a | n/a | Invitation for an interview |
| Boudarbat et al. (2010)Footnote 65 (N = 1875) |
Age Sex |
Region of origin | Generational status Migration status |
Level of education Employment status Salary |
Job matching aspirations |
| Salamanca (2018)Footnote 44 (N = 42) |
Gender Age |
Country of origin | Migration status Work permit |
Employment sector | Violations of labour legislation Interethnic relations in the workplace |
Various ethnoracial classification systems were used, including those from Statistics CanadaFootnote 53 and the Canadian Institute for Health Information,Footnote 47 with some systems adapted to the specific characteristics of the studies in which they were used.Footnote 38Footnote 42Footnote 43Footnote 46Footnote 49Footnote 51Footnote 52Footnote 56Footnote 58Footnote 59Footnote 62Footnote 64Footnote 65Footnote 66Footnote 67
Immigration data were self-reported in 60% (26/43) of the studies (Table 4),Footnote 31Footnote 32Footnote 33Footnote 34Footnote 35Footnote 40Footnote 42Footnote 43Footnote 44Footnote 45Footnote 46Footnote 48Footnote 49Footnote 51Footnote 52Footnote 53Footnote 56Footnote 58Footnote 60Footnote 61Footnote 62Footnote 63Footnote 65Footnote 66Footnote 68Footnote 70 with migratory status and generation status (first, second generation, etc.) being the most commonly used variables (24 studies). Socioeconomic status was generally defined in a consistent manner, with level of education, income and employment status being the most frequently used variables (Table 4),Footnote 31Footnote 32Footnote 33Footnote 34Footnote 36Footnote 42Footnote 43Footnote 45Footnote 46Footnote 47Footnote 49Footnote 50Footnote 51Footnote 52Footnote 53Footnote 54Footnote 55Footnote 58Footnote 59Footnote 61Footnote 62Footnote 63Footnote 66Footnote 67Footnote 68Footnote 69Footnote 71Footnote 72 alongside the Material and Social Deprivation Index.Footnote 59Footnote 66Footnote 67
Quantitative data collection
Primary data collection was carried out using questionnaires either distributed onlineFootnote 31Footnote 34Footnote 46Footnote 48Footnote 50Footnote 51Footnote 52Footnote 54Footnote 68Footnote 69 or given in person,Footnote 35Footnote 37Footnote 47Footnote 70 as well as by consulting medical recordsFootnote 51Footnote 52Footnote 53Footnote 55Footnote 56Footnote 66Footnote 67 and supplementing demographic information with telephone or in-person interviews.Footnote 46Footnote 55Footnote 56Footnote 66Footnote 67Footnote 68 In other studies, ethnicity was assigned by a third party based on the language spoken and the country of birth of the individual and their mother or both parents.Footnote 30Footnote 53Footnote 59
Data of interest were also extracted from various centralized databases, including those maintained by Statistics Canada,Footnote 58Footnote 59Footnote 60Footnote 61 the Quebec Register of Civil StatusFootnote 30 and other Quebec public agencies (departments, youth centres, etc.),Footnote 59Footnote 60Footnote 61Footnote 62Footnote 65Footnote 67 with cross-referencing of multiple datasets allowing for the inclusion of missing information on ethnoracial background or socioeconomic status.Footnote 58Footnote 59Footnote 60Footnote 61
Qualitative data collection
Data were primarily collected through individual interviews,Footnote 32Footnote 33Footnote 38Footnote 39Footnote 40Footnote 44Footnote 45Footnote 46Footnote 71Footnote 72 with occasional use of focus groups.Footnote 36Footnote 41Footnote 46Footnote 48Footnote 68 Some interviews were conducted in familiar environments (home, school, community centres) to ensure that participants felt comfortable sharing their experiences.Footnote 35Footnote 38Footnote 39Footnote 40Footnote 71 In one study, culturally appropriate food was offered during focus groups as a sign of respect.Footnote 36 In this study, the participants, all from the Haitian community, were grouped by age to facilitate discussion and avoid any shyness that younger participants might feel in relation to their elders because of cultural codes.Footnote 36 Another researcher facilitated informative workshops during which participants could share their experiences of discrimination, creating a safe space for open dialogue and knowledge-sharing.Footnote 44
To build trust between researchers and participants, other strategies included collecting data through professionals from the same community, with an immigrant background, who spoke the same language, or in the presence of a cultural mediator.Footnote 33Footnote 36Footnote 38Footnote 40Footnote 42Footnote 43Footnote 70 Some authors found that cultural proximity enhanced engagement, as it sparked participants’ interest in the subject matter.Footnote 36 However, some participants were hesitant to have their interviews recorded,Footnote 40 and researchers in some studies faced challenges in maintaining appropriate professional distance with participants, as cultural proximity sometimes blurred the boundaries of the study’s objectives.Footnote 33
Quantitative analysis methods
In some studies, researchers used descriptive statistics to document discrimination or coping strategies in response to health issues.Footnote 35Footnote 54Footnote 57Footnote 64Footnote 68 Many other researchers carried out quantitative analyses using a contextualized, intersectional approach. Multivariate or regression analyses were used to compare results with a reference group, controlling for as many variables as possible.Footnote 30Footnote 47Footnote 50Footnote 53Footnote 55Footnote 56Footnote 58Footnote 60Footnote 61Footnote 63Footnote 67Footnote 69Footnote 70 These analyses also measured the influence of ethnicity on different variables, calculated proportional risk over time (Cox analysis) and examined the geographic distribution of variables in relation to ethnicity.Footnote 30Footnote 51Footnote 59Footnote 60 Note that the reference group varied across studies, and participants could be designated as “White Canadians” or “Euro‑Canadians,”Footnote 30Footnote 47Footnote 51Footnote 53Footnote 56Footnote 61Footnote 67Footnote 69 “Whites,”Footnote 50Footnote 55Footnote 58Footnote 63 “Canadian-born”Footnote 56Footnote 63Footnote 67 or “Blacks.”Footnote 60Footnote 70
One study used the Latent Class Analysis statistical method to identify nonapparent homogeneous subgroups within a heterogeneous population.Footnote 50 Longitudinal surveys were used to track changes in variables or phenomena over time,Footnote 30Footnote 61Footnote 64 allowing for the identification of trends reflecting the impact of multiple waves of immigration from populations with varying sociodemographic profiles.Footnote 30
Qualitative analysis methods
In three studies, an intersectional approach was used to address complex notions such as the inequalities experienced by Haitian studentsFootnote 40 and Black African older adult women,Footnote 33 or the discrimination and racism experienced by temporary migrants.Footnote 44 These issues were analyzed from an intersectional perspective, taking into account identity markers such as skin colour, ethnic origin (minority/majority status), social origin (migratory and socioeconomic status) and gender.Footnote 33Footnote 40Footnote 44
An anthropological approach was used in another study on the experience of Haitian mothers in dealing with their children’s illness.Footnote 32 Life stories were also used to illustrate individual educational trajectories.Footnote 42Footnote 43Footnote 72 Four studies used inductive thematic analysis to examine the data.Footnote 35Footnote 36Footnote 38Footnote 46
Discussion
The purpose of this scoping review was to analyze the methods used to collect, analyze and disseminate health, education, social services and employment data regarding Black populations in Quebec. This review enabled us to present a comprehensive corpus of data illustrating the fields of interests of Quebec researchers, the challenges in recruiting and retaining participants from Black communities in Quebec, and the quantitative and qualitative methods of analysis used.
Few studies have examined disaggregated health data based on ethnoracial background in Quebec. Most studies included in this scoping review are cross-sectional in nature, with the exception of a few longitudinal surveysFootnote 30Footnote 58Footnote 59Footnote 61 conducted on secondary datasets. These longitudinal surveys allow for analyses on large samples covering the entire population targeted by the research, thereby reducing selection bias.
Several factors can influence the accuracy and relevance of conclusions drawn from studies on health issues affecting Black populations in Quebec. Biases may be introduced at various stages, from data collection to dissemination of results, posing significant methodological challenges.
Recruiting members of Black communities remains a significant challenge in qualitative studies, whereas quantitative studies rarely report this issue. However, this does not imply that researchers have not encountered such a challenge. Soliciting participation from members of Black communities requires a greater investment of time compared with other ethnocultural groups, particularly White people of European descent.Footnote 36
The reluctance of Black communities to participate in research is rooted in historical events in which members were exploited under the guise of science. Notable examples include the Tuskegee Syphilis Experiment in the United States (1932–1972) and the illegal blood trade in Haiti during the 1970s. Additionally, in the 1980s, the Haitian community was improperly associated with HIV by the Canadian Red Cross.Footnote 73Footnote 74
These historical precedents have fostered distrust of public and health authorities among Black populations in Quebec and Canada.Footnote 74Footnote 75Footnote 76 To address this, it is crucial to keep participants well informed about research objectives and results. However, the true purpose of a study can sometimes be difficult to disclose due to its nature.Footnote 51Footnote 64 These cases, though exceptions, are governed by the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (articles 3.7A and 10.3).Footnote 77 More attention must be paid to research dissemination practices in Quebec. Only a few studies have identified effective knowledge transfer strategies.Footnote 36Footnote 41Footnote 48 Providing feedback to participants and the broader community can help mitigate feelings of exploitation and encourage greater participation in future research projects.Footnote 36
Recruitment challenges can lead to selection bias, which is difficult to correct. For instance, an online survey with a low response rate (37%)Footnote 51Footnote 52 and a sample predominantly composed of college- or university-educated participants may not be representative of the broader population. Therefore, the results of the study are not applicable to populations with a lower level of education.Footnote 51Footnote 52 Similar logic can be applied to the language spoken, since the studies were conducted solely in English or French, which excludes allophones. Additionally, attrition bias, which involves certain participants dropping out selectively, is a common issue in research.Footnote 36Footnote 41Footnote 44Footnote 47 This bias can be estimated by comparing the characteristics of participants who remained in the study with those who left.Footnote 47
The attribution of ethnicity is another significant issue. Analysis of the studies in this review indicates that self-identification is the standard practice, compared with third-party identification. However, this method is not exempt from potential biases (nonresponses, willingness to self‑identify with the majority group), which may be difficult to measure.Footnote 64
Missing information on ethnoracial background or socioeconomic status can be supplemented by cross-referencing the data from the census or the Quebec Register of Civil Status, which contain details such as the mother’s country of birth, language spoken at home or mother tongue.Footnote 30Footnote 58Footnote 61 Missing data can be inferred from individuals’ country of birth and language spoken.Footnote 56Footnote 67 However, according to our analysis, this imputation method is not error-free if the data are not cross‑referenced with migration status and generation status.
The characteristics that define ethnicity are not fixed; they are often poorly defined and depend on the classification systems used.Footnote 16Footnote 17 Ethnicity is a flexible concept. While it differs from “race,” nationality, religion and migratory status, it can include aspects of these concepts.Footnote 78Footnote 79
Some researchers have tried to account for this fluidity by differentiating, within the same ethnoracial group, between individuals who speak French or English at home and those who speak their mother tongue.Footnote 30 This enables a more detailed analysis, highlighting the complex realities that define a given group that is neither monolithic nor static. Moreover, at the individual level, there is sometimes a discrepancy between how a person is perceived by society and how they define themselves on an ethnocultural level, a meaning that can shift with time and life circumstances. Some researchers suggest defining “race” not as a biological phenotype, but as a complex social phenomenon, or classifying populations according to socioenvironmental variables rather than “race.”Footnote 26
Our study shows that researchers prefer one-on-one interviews over focus groups for collecting qualitative data. In focus groups, the size, composition and internal dynamics of the group, as well as the topics addressed, can greatly influence what participants say and disclose, compared with the more confidential atmosphere of one-on-one interviews.Footnote 80 Some studies show that people are more inclined to discuss sensitive topics in one-on-one interviews than in groups,Footnote 81Footnote 82Footnote 83 while others find the opposite.Footnote 80Footnote 84 This raises confidentiality concerns, as participants in focus groups get to know each other, increasing the risk of unintentional disclosure of sensitive information. The risk is particularly critical in small, tightly knit communities.
At the analytical level, descriptive analyses carried out using an intersectional approach enable the generation of hypotheses about the processes underlying observed phenomena. Correlation studies on relevant quantitative data can test these hypotheses and measure the interaction between several variables, requiring granular data on target populations. When such data are unavailable, researchers use the Material and Social Deprivation IndexFootnote 7Footnote 59Footnote 66Footnote 67 to identify trends. However, the ability to establish causal links remains limited.Footnote 26 The common practice of documenting ethnoracial differences in health without adequately explaining their basis presents a number of risks. It limits primary prevention initiatives and reinforces the idea of biological determinism linked to “race.”Footnote 26Footnote 85
Additionally, processing data on individuals of mixed ethnic origin poses challenges.Footnote 47Footnote 56Footnote 66Footnote 67 How can these data provide us with more information, and what further analysis can be carried out? Additionally, creating broad ethnoracial categories (Black, White, Asian, Latin American, etc.) for comparisons introduces significant heterogeneity.Footnote 47Footnote 51Footnote 52Footnote 53Footnote 56Footnote 57Footnote 60Footnote 67Footnote 69 Therefore, the results of these studies must be interpreted carefully. Analyses based on nonstandardized ethnoracial categorization risk leading to erroneous conclusions that overlook nuances that have gone unnoticed as a result of classification bias.Footnote 26Footnote 79 This could jeopardize the ability to provide culturally appropriate healthcare and services.Footnote 4Footnote 85
Strengths and limitations
This scoping review sheds light on cross-sectoral practices (health, social services, education, employment) in the collection, analysis and dissemination of ethnoracial data relating to health and its social determinants among Black populations in Quebec. To our knowledge, this is the first scoping review to be carried out on this topic in Quebec. It analyzes the experiences of these populations, considering the intersections of ethnoracial background, age, gender and language. It also reflects the interest of researchers, physicians and other health and community professionals in issues affecting racialized populations, including Black populations in Quebec.
However, this scoping review has several limitations. It does not take into account the grey literature in Quebec on the topic. This was explored in another component of our research, which, in addition to the scoping review, included the analysis of case studies describing best practices in Quebec for culturally adapted approaches, as well as a qualitative study on the experiences and needs of researchers whose work focusses on Black populations in Quebec. Furthermore, since our review only includes studies conducted in Quebec, the results are not generally applicable to all Black populations in Canada, particularly due to Quebec’s migratory history.
Additionally, our literature search strategy focussed on specific fields (health, education, employment and social services), which means other potentially relevant studies may have been omitted. While there may be other methods of collecting, analyzing and disseminating health data based on ethnoracial background, their omission from this study does not invalidate the scope of our work. This study is intended to be exploratory. It provides an overview of the diversity of theoretical and methodological approaches used in Quebec to collect, analyze and disseminate ethnoracial data on health and its social determinants, and associated issues.
Future directions
Systematic health data collection initiatives among Black populations are still uncommon in Quebec. However, the COVID-19 pandemic has sparked growing interest among health authorities and researchers in health data based on ethnoracial background. The number of studies recorded since the start of the pandemic (in 2020) is equivalent to the number recorded between 2010 and 2019 (Table 3). A reflection on best practices governing the collection, protection and use of health data concerning Black populations is necessary in Quebec, in order to better equip researchers. Additionally, a qualitative study of these populations would provide a more in-depth understanding of their needs and the challenges they face.
The COVID-19 pandemic highlighted the glaring health inequities affecting Black populations in Quebec. The lack of data on the health of these populations hinders the development and implementation of public health policies. Initiatives to collect health data from Black populations in Ontario,Footnote 10 Nova ScotiaFootnote 11 and, more recently, Manitoba,Footnote 86 are a step in the right direction. These efforts are fostering a dynamic that could revive the political debate on this issue in Quebec.
Finally, note that 58% (25/43) of the studies presented in this scoping review were funded in part by the researchers’ respective institutions, or reported no funding at all (Table 2). Promoting research on the health of Black populations should be a priority in order to better address the challenges of inequity faced by these communities. To achieve this, increased funding is needed for this field of research.
Conclusion
The purpose of this scoping review was to document the methods and issues involved in collecting data on health and its social determinants for Black populations in Quebec. This review has enabled us to analyze current practices in Quebec using a cross-sectoral approach, with studies covering health, social services, education and employment. It also highlights the importance of collecting granular data on racialized groups, particularly on Black populations in Quebec, to support public policies designed for these populations and to promote health equity.
Acknowledgements
This scoping review was made possible by a grant from the Public Health Agency of Canada for the project entitled Approches culturellement adaptées et accessibles pour définir, mesurer, analyser et rendre compte des résultats de santé et de ses déterminants sociaux dans les communautés noires du Québec [Culturally adapted and accessible approaches to define, measure, analyze and report on health outcomes and social determinants in Black communities in Quebec].
Conflicts of interest
The authors declare that there are no conflicts of interest in relation to this work.
Authors’ contributions and statement
- NM, KNLN: conceptualization, data curation, formal analysis.
- NM: writing—original draft.
- NM, KNLN: writing—review and editing.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.