
Neonatal abstinence syndrome in Canada: a descriptive analysis of hospitalization data
Canada is currently experiencing an overdose crisis. In addition to ongoing surveillance, the Public Health Agency of Canada (PHAC) releases targeted analytical reports on specific topics related to substance-related harms to help fill gaps identified by stakeholders.
Neonatal abstinence syndrome is a set of withdrawal symptoms experienced when a newborn is exposed to certain substances in the womb before birthReference 1. Neonatal abstinence syndrome most commonly occurs when an infant is exposed to opioids, but can also occur from a pregnant person's use of antidepressants, benzodiazepines, nicotine, caffeine, alcohol, methamphetamine and inhalantsReference 2 Reference 3. Overall, there is some evidence to suggest that the rates of neonatal abstinence syndrome have been increasing in Canada; however, there are limited data available examining rates of neonatal abstinence syndrome in Canada over a longer period of time as well as more recent estimatesReference 1 Reference 3 Reference 4.
The objective of this analysis is to describe the trend of hospitalizations for newborns with neonatal abstinence syndrome in Canada (excluding Québec), between 2010 and 2020. The results of this analysis can be used to inform future promotion, prevention and harm reduction strategies in Canada.
Definitions included in this report
Neonatal abstinence syndrome: For the data included in this report, neonatal abstinence syndrome hospitalizations refer to hospitalizations of neonates who were born in hospital and received a significant diagnosis of neonatal abstinence syndrome before discharge, or those of neonates born outside of hospital who were admitted within 28 days of birth and received a significant diagnosis of neonatal abstinence syndrome. Neonatal abstinence syndrome was captured in hospitals using the ICD-10-CAFootnote a code "P96.1" for neonates defined as the first 28 days of life. In practice, the term neonatal abstinence syndrome is sometimes used interchangeably with neonatal withdrawal symptoms.
For more information on these definitions, please refer to the technical notes and appendices.
Key findings
Trends by year
Across Canada (excluding Québec) between 2010 and 2020, there were 16,920 total neonatal abstinence syndrome hospitalizations. In 2020, there were 1,755 hospitalizations for neonatal abstinence syndrome, which represents a 73% increase in the number of hospitalizations from 2010 (n=1,013) and a 5% increase in the number of hospitalizations from 2019 (n=1,665).
Data were available to calculate rates of hospitalizations for neonatal abstinence syndrome between 2010 and 2020Footnote b . In 2010, the rate of hospitalizations for neonatal abstinence syndrome was 3.5 per 1,000 live births which increased by 80% to a peak of 6.3 per 1,000 live births in 2020 (Figure 1).
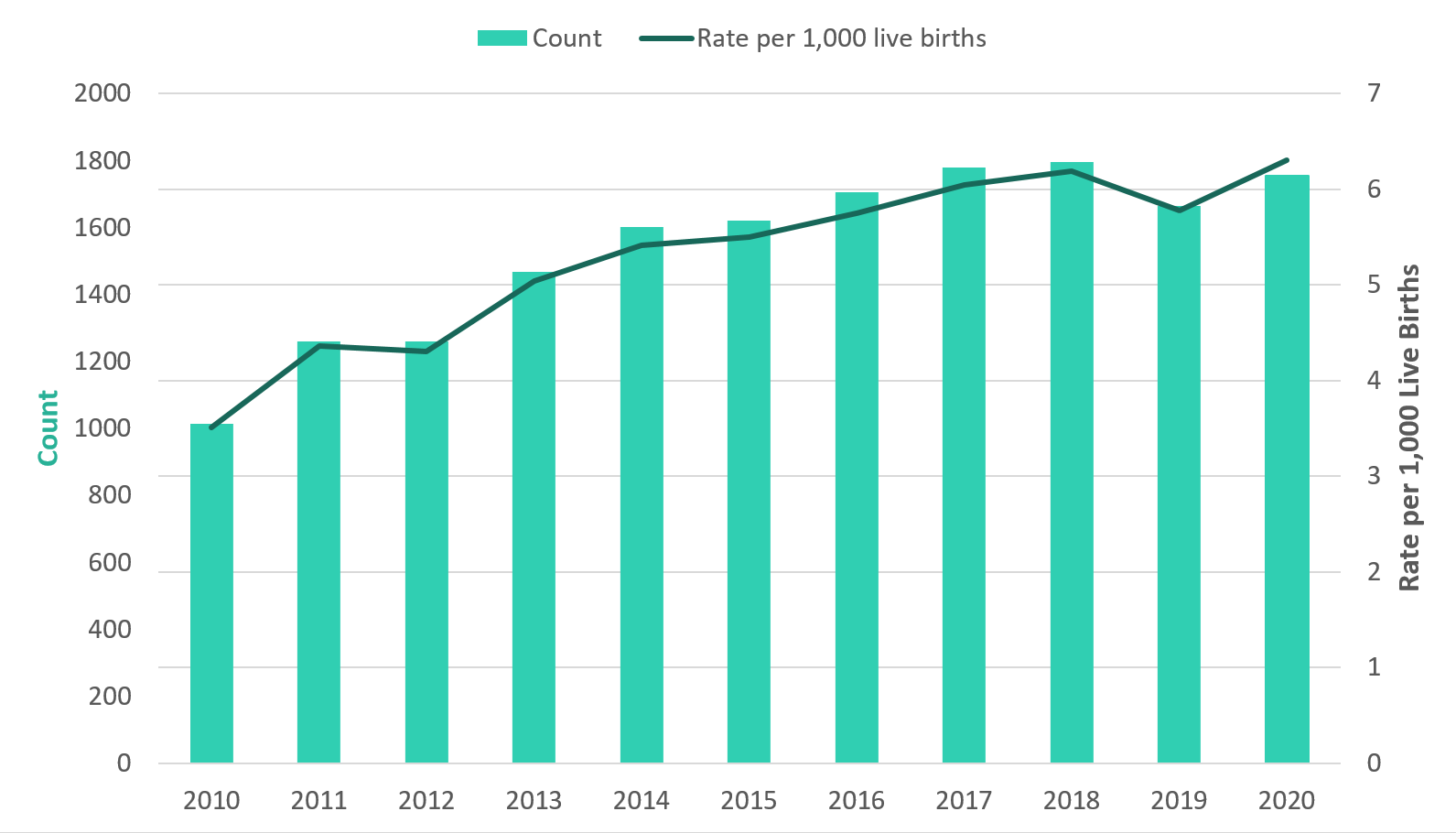
Figure 1 - Text description
| Hospitalizations for neonatal abstinence syndrome | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Crude rate per 1,000 live births | 3.5 | 4.4 | 4.3 | 5.0 | 5.4 | 5.5 | 5.7 | 6.0 | 6.2 | 5.8 | 6.3 |
| Count | 1,013 | 1,259 | 1,260 | 1,467 | 1,601 | 1,621 | 1,704 | 1,780 | 1,795 | 1,665 | 1,755 |
Note(s) Excludes data from Québec. Yukon is included for counts, but excluded from crude rates due to unavailability of consistent live birth data in this territory. |
|||||||||||
Data sources Discharge Abstract Database (DAD), fiscal years 2010/2011 to 2020/2021, Canadian Institute for Health Information (CIHI). Live births, by place of residence of mother (Table: 13-10-0414-01), 2010-2020, Statistics Canada. |
|||||||||||
Hospitalization characteristics and outcomes
Length of stay
The total length of stay in hospital is calculated by adding the number of days a patient was in acute inpatient care and alternate level of careReference 5. Overall, the mean length of stay in acute inpatient care each year among infants hospitalized for neonatal abstinence syndrome, varied between 14.6 and 16.4 days (Figure 2). In comparison, the mean total length of stay for all newborns across Canada was 2.09 days between 2008 and 2019Reference 6. The mean length of stay in alternate level of care decreased, on average, over the same period. Longer hospital stays may be due to increasing severity of neonatal abstinence syndrome, variability in management practices or better detection of the syndrome among high-risk groups (e.g., premature newborns) where the newborn may have lower severity of neonatal abstinence syndrome, but longer stays due to other comorbiditiesReference 3. Of note, the length of stay in hospital for 2020 should be interpreted with caution due to the potential impact of the COVID-19 pandemic.
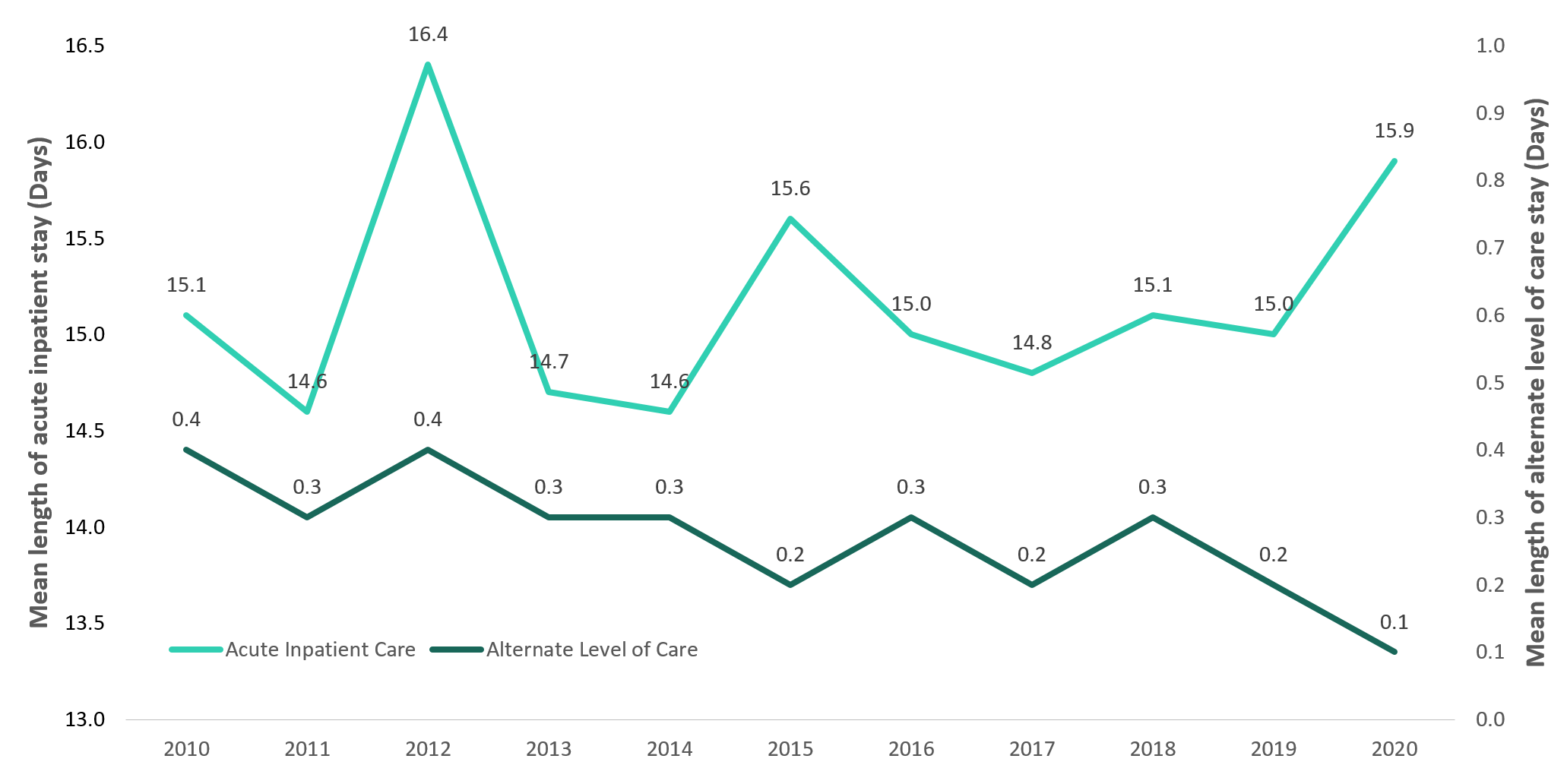
Figure 2 - Text description
| Hospitalizations for neonatal abstinence syndrome | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean length of stay in acute inpatient care (days) | 15.1 | 14.6 | 16.4 | 14.7 | 14.6 | 15.6 | 15.0 | 14.8 | 15.1 | 15.0 | 15.9 |
| Mean length of stay in alternate level of care (days) | 0.4 | 0.3 | 0.4 | 0.3 | 0.3 | 0.2 | 0.3 | 0.2 | 0.3 | 0.2 | 0.1 |
| Mean total length of stay (days) | 15.5 | 14.9 | 16.8 | 15.0 | 14.9 | 15.8 | 15.3 | 15.0 | 15.4 | 15.2 | 15.9 |
Note(s) Excludes data from Québec. |
|||||||||||
Data sources Discharge Abstract Database (DAD), fiscal years 2010/2011 to 2020/2021, Canadian Institute for Health Information (CIHI). |
|||||||||||
Special Care Unit (Intensive care)
The Special Care Unit (SCU) is an organized system which provides specialized medical care to critically ill patients and allows for enhanced life support and monitoringReference 7. Using the most recent data year (April 1st, 2020 - March 31st, 2021), the majority (71%) of neonatal abstinence syndrome hospitalizations were admitted to the SCU to receive additional care. In comparison, roughly 12% of all hospitalizations for newborns are admitted to the SCU in a given yearReference 6.
Discharge disposition
Discharge disposition describes where a patient was discharged to or the status of the patient upon discharge. The most recent data yearFootnote c, indicated the majority (70%) of neonatal abstinence syndrome hospitalizations were discharged home without additional support, while 16% were discharged home with additional supports. A smaller percentage (13%) of neonatal abstinence syndrome hospitalizations resulted in the patient being transferred.
Deaths in hospital for neonatal abstinence syndrome were not common. In the most recent data yearFootnote c, less than five neonatal abstinence syndrome hospitalizations indicated that the newborn died. An analysis of fiscal year 2019-2020 showed very similar results for both Special Care Unit admissions and discharge disposition.
In summary
Canada is facing a national overdose crisis and furthering our understanding for all substance-related harms, including those affecting newborns can help inform comprehensive clinical and public health actions.
There were almost 17,000 neonatal abstinence syndrome hospitalizations between 2010 and 2020 across Canada (excluding Québec). These data show that both the number and rates of neonatal abstinence syndrome hospitalizations have been generally increasing from 2010 to 2020. Infants born with neonatal abstinence syndrome often require high healthcare resource utilization, as evidenced by their lengthy hospital stays and high proportion of Special Care Unit admissions. These findings highlight the need for prevention of substance-related harms among people who are pregnant and their neonates through additional harm reduction strategies.
More specific diagnostic ICD-10-CA codes are needed to identify substance-specific cases for neonatal abstinence syndrome, in order to help determine appropriate interventions. Additional research is needed to better understand the long-term impacts of neonatal abstinence syndrome, how rates of neonatal abstinence syndrome were affected by the COVID-19 pandemic and what support is needed for those affected. The Government of Canada will continue to work with partners to explore opportunities to improve data and analysis to inform strategies and interventions that may help to reduce substance-related harms across Canada.
Acknowledgements
We would like to acknowledge the Canadian Institute for Health Information (CIHI) for collecting and providing the data used in this report.
Disclaimer
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of the Canadian Institute for Health Information (CIHI).
Suggested citation
Neonatal abstinence syndrome in Canada: a descriptive analysis of hospitalization data. Ottawa: Public Health Agency of Canada; December 2021. www.canada.ca/en/health-canada/services/opioids/data-surveillance-research/neonatal-abstinence-syndrome-descriptive-analysis-hospitalization.html
Technical notes
Methodology
Data from the Canadian Institute for Health Information's (CIHI) Discharge Abstract Database (DAD) for the period of January 2010 to March 2021 were analyzed for this descriptive report. Closed year data from the DAD (i.e., final data) were used to report trends of hospitalizations for neonatal abstinence syndrome between 2010 and 2020.
This analysis was limited to acute inpatient hospital discharges, which are nationally representative across Canada, except for Québec. This analysis presents the number of acute inpatient hospital discharges for neonates diagnosed with neonatal abstinence syndrome; it does not account for transfers, which may have occurred between acute inpatient care facilities.
Identifying hospitalizations for Neonatal Abstinence Syndrome
The methodology for identifying hospitalizations for neonatal abstinence syndrome was adapted from CIHI's Opioid-related Harms in Canada report. The scope of this analysis was to examine diagnoses of neonatal abstinence syndrome among neonates, defined as infants 28 days or younger at the time of admission.
The International Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) is used in the DAD to capture diagnoses from the patient's hospitalization. It is the national standard for reporting morbidity statistics. More information on the DAD and ICD-10-CA coding can be found on CIHI's website.
The ICD-10-CA diagnosis code of P96.1 "Neonatal withdrawal symptoms from maternal use of drugs of addiction, includes neonatal abstinence syndrome" was used to identify hospitalizations for neonatal abstinence syndrome. Of note, the ICD-10-CA diagnosis code of P96.1 code excludes reactions and intoxications from maternal opiates and tranquillizers administered during labour and delivery.
Analyses were restricted to the following significant diagnosis types:
- Most responsible diagnosis ("M")
- Pre-admit comorbidity ("1")
- Post-admit comorbidity ("2")
- Service transfer diagnosis ("W", "X", and "Y")
These significant diagnosis types capture hospitalizations in which neonatal abstinence syndrome was considered influential to the time spent and treatment received by the neonate in hospital. A diagnosis prefix of "Q", indicating unconfirmed diagnoses or query diagnoses recorded by the physician, were excluded from these analyses as the scope of the analysis was concerned with confirmed cases of neonatal abstinence syndrome only. Hospitalization records for stillbirths were excluded to align with the live birth data reported by Statistics Canada, which were used to produce the rate of hospitalizations for neonatal abstinence syndrome per 1,000 live births.
Calculating crude rates
Crude rates were calculated for each year by dividing the total number of hospitalizations for neonatal abstinence syndrome (numerator), by the total number of live births (denominator), multiplied by 1,000. Table "13-10-0414-01, live births by place of residence of mother" was downloaded as a CSV file from Statistics Canada's website on September 28, 2021 and was used to calculate the number of live births by year. To produce comparable denominators, live birth data for Québec were excluded to match the coverage of available hospitalization data from the DAD. In addition, as live birth data for Yukon were not consistently available for all data years, Yukon was excluded from reporting of crude rates, but included when presenting counts.
Limitations
- The data in this report is likely an underestimate as some cases of neonatal abstinence syndrome may go undiagnosed. Possible reasons for missed diagnosis can include milder symptoms not readily recognized, delayed onset of symptoms post delivery, and undisclosed use of substances by the pregnant parent.
- This analysis focuses on the number of hospitalizations for neonatal abstinence syndrome rather than the number of newborns with neonatal abstinence syndrome and therefore does not represent the overall prevalence of neonatal abstinence syndrome.
- Neonates with neonatal abstinence syndrome who were not birthed in or admitted to hospital are not included in this analysis.
- Due to availability of data, for crude rates calculations, the numerator (i.e., number of hospitalizations) was based on place of occurrence, whereas the denominator (i.e., live births) was based on the place of mother's residence.
- Data released by provinces and territories may differ from the data provided in this report due to the availability of updated data, differences in the type of data reported, the use of alternate case definitions, differences in time periods presented and/or population estimates used for calculations, etc.
Data suppression
Values representing less than five hospitalizations are suppressed according to CIHI's privacy guidelines.
References
- Reference 1
-
Opioid-Related Harms in Canada [Internet]. Ottawa, ON: Canadian Institute for Health Information; 2018 [cited 2021June21]. Available from: https://secure.cihi.ca/free_products/opioid-related-harms-report-2018-en-web.pdf
- Reference 2
-
Filteau J, Coo H, Dow K. Trends in incidence of neonatal abstinence syndrome in Canada and associated healthcare resource utilization. Drug and alcohol dependence. 2018 Apr 1;185:313-21.
- Reference 3
-
Haas A. Identification of neonatal abstinence syndrome in the community: Infants born into Canada's opioid crisis. Paediatrics & child health. 2019 Apr 13;24(2):81-4.
- Reference 4
-
Lacaze-Masmonteil T, O'Flaherty P. Managing infants born to mothers who have used opioids during pregnancy. Paediatrics & child health. 2018 May 11;23(3):220-6.
- Reference 5
-
Acute Care [Internet]. Ottawa, ON: Canadian Institute for Health Information [cited 2021June21]. Available from: https://www.cihi.ca/en/acute-care
- Reference 6
-
Data provided by the Canadian Perinatal Surveillance System, Public Health Agency of Canada, 2021
- Reference 7
-
Marshall JC, Bosco L, Adhikari NK, Connolly B, Diaz JV, Dorman T, Fowler RA, Meyfroidt G, Nakagawa S, Pelosi P, Vincent JL. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care. 2017 Feb 1;37:270-6.
Footnotes
- Footnote a
-
International Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA).
- Footnote b
-
Yukon was excluded from rate calculations due to unavailability of consistent live birth data in this territory.
- Footnote c
-
Fiscal year 2020-2021