
Evaluation of the Emergency Preparedness and Response Program (2019-2020 to 2023-2024)

Download in PDF format
(1.01 MB, 71 pages)
Organization: Public Health Agency of Canada
Date published: 2025-06-18
Cat.: HP5-262/2025E-PDF
ISBN: 978-0-660-77316-2
Pub.: 250055
October 2024
Prepared by the Office of Audit and Evaluation
Public Health Agency of Canada
Table of contents
- List of acronyms
- Executive summary
- Overview and program description
- Evaluation scope and approach
- Findings
- Detection and reporting
- Emergency response and mobilization
- Collaboration, coordination and governance
- Sustained EPR system in Canada
- Conclusions and recommendations
- Management Response and Action Plan
- Appendix A: Financial information
- Appendix B: Evaluation description
- Appendix C: Exercises by activation centre
- Appendix D: Emergency management maturity model
- Appendix E: The emergency management cycle
- Appendix F: Program performance measurement
- Endnotes
List of acronyms
- AERO
- All-Events Response Operations
- AARs
- After Action Reviews
- CEP
- Centre for Emergency Preparedness
- CER
- Centre for Emergency Response
- CFEP
- Canadian Field Epidemiologist Program
- CMP
- Comprehensive Management Plan
- CPHS
- Canadian Public Health Service
- DG
- Director General
- DUA
- Detect, Understand, Act
- EM
- emergency management
- EMEC
- Emergency Management Executive Committee
- EPR
- Emergency Preparedness and Response
- F/P/T
- federal, provincial, and territorial
- GOARN
- Global Outbreak Alert and Response Network
- GOC
- Government Operations Centre
- GPHIN
- Global Public Health Intelligence Network
- HC
- Health Canada
- HECO
- Health Emergency Coordination Office
- HP
- Health Portfolio
- HP EPC
- Health Portfolio Emergency Preparedness Committee
- HP ERP
- Health Portfolio Emergency Response Plan
- HPOC
- Health Portfolio Operation Centre
- IHR
- International Health Regulations
- IMS
- Incident Management System
- LAC
- Logistics Advisory Committee
- NESS
- National Emergency Strategic Stockpile
- NMLB
- National Microbiology Laboratory Branch
- NMLB-EOC
- National Microbiology Laboratory Branch's Emergency Operations Centre
- OAG
- Office of Auditor General
- OFMAR
- Operational Framework for Mutual Aid Requests
- OGD
- other government department
- PHAC
- Public Health Agency of Canada
- PHEM
- Public Health Emergency Management
- PHEM-WG
- Public Health Emergency Management Working Group
- PHN
- Pan-Canadian Public Health Network
- P/T
- provincial and territorial
- P/Ts
- provinces and territories
- RECC
- Regional Emergency Coordination Centres
- RFA
- Requests for Assistance
- ROEMB
- Regulatory, Operations and Emergency Management Branch
- RSTA
- Response Support and Technical Assistance
- SAC
- Special Advisory Committee
- SGBA+
- Sex- and Gender-Based Analysis Plus
- SIIRA
- Surveillance, Integrated Insights and Risk Assessment
- SOPs
- Standard Operating Procedures
- SPAR
- State Parties Self-Assessment
- VP
- Vice-President
- WHO
- World Health Organization
Executive summary
Program description
The Public Health Agency of Canada's (PHAC) Emergency Preparedness and Response (EPR) program is responsible for strengthening Canada's capacity to prevent, mitigate, prepare for, and respond to public health events and emergencies, as well as mass gatherings and high-profile events.
The Regulatory, Operations and Emergency Management Branch (ROEMB) is PHAC's centre of expertise for emergency management functions, providing response coordination for unplanned or intentional emergency events, as well as planned mass gatherings and high-visibility events for PHAC and Health Canada (HC), referred to as the Health Portfolio (HP) in this report. ROEMB provides the HP with shared services in emergency management governance, emergency management plans, operations centres, field mobilizations, as well as continuous improvement through training, exercises, and identification of lessons learned. Not within of the shared services partnership, ROEMB also maintains programming key to event detection and information sharing through the Global Public Health Intelligence Network (GPHIN) and the International Health Regulations (IHR) as the national focal point for Canada. It also manage the National Emergency Strategic Stockpile (NESS) which provides medical assets to provinces and territories when requested. ROEMB is also responsible for the Regional Emergency Preparedness and Response Units, which are coordinating response to an event in a particular region.
The National Microbiology Laboratory Branch (NMLB) also contributes to PHAC's emergency preparedness and response activities by maintaining an Emergency Operations Centre (EOC). The NMLB-EOC is PHAC's scientific point of coordination for emergency response and day-to-day communications on infectious diseases from a laboratory perspective. The NMLB-EOC works with the Canadian Public Health Laboratory Network to coordinate the national public health laboratory response. The NMLB also provides scientific and mobile laboratory support for field investigations aimed at controlling outbreaks and potential threats domestically and in support of international partners.
Evaluation scope
This evaluation assessed the EPR program's activities from 2019-2020 to 2023-2024. It examined the achievement of intended results, and the efficiency of the program. The evaluation focused on PHAC's EPR program activities, which are led by ROEMB. It also assessed NMLB-EOC activities.
Many other centres with technical expertise across PHAC and HC also have activities that relate to EPR. However, the technical expertise provided by these centres in support of EPR is not covered by this evaluation. Given the supporting roles of these partners, this evaluation focused on ROEMB's engagement, collaboration, and how it coordinates activities with these partners, rather than on specific partner activities.
Findings
The evaluation found that PHAC is better prepared to respond to public health events than it was five years ago. Plans and procedures have been updated, exercises have taken place, and PHAC-wide Public Health Emergency Management (PHEM) training was implemented, including one mandatory course. Time-limited funding has also improved public health intelligence capacity by enhancing the GPHIN and improving event detection through the widespread distribution of GPHIN Daily Reports. Lessons learned from the COVID-19 pandemic have also been integrated into PHAC's future pandemic preparedness, and many past audit and review recommendations have been implemented.
Collaboration and external governance with federal, provincial, and territorial (F/P/T) partners is also strong with respect to emergency response, though there could be more opportunities to engage in preparedness activities. At the same time, while emergency management (EM) governance at PHAC has improved, there are still challenges with information sharing across the HP at all levels, both during and outside of a response. This issue should be addressed in order to strengthen internal EM activity coordination, engage with the appropriate HP program areas, minimize duplication, cultivate an EM culture, and support business continuity. Collaboration with international partners was also strengthened during the evaluation period; however, challenges were reported with respect to the clarity of internal branch roles on international EM-related files.
Over the last five years, PHAC responded to many requests for supports and mobilized several Incident Management Systems (IMS) to coordinate the response to multiple public health events. However, given the length and breadth of the COVID-19 IMS, mobilizing staff for concurrent mobilizations and maintaining the surge capacity over time was challenging. Since the creation of HC's Health Emergency Coordination Office (HECO) in the fall of 2023, ROEMB has been working with it on a HP framework to help mobilize adequate personnel and sustain effective responses to more frequent and intense emergencies. This framework is essential to readiness and response, and its success hinges on PHAC's adoption of an EM culture highlighted by readiness, resilience, and commitment to collective response.
Funding associated with the COVID-19 response allowed the NESS to procure a substantial volume of medical assets, which has temporarily enhanced their capacity to deploy assets during public health emergencies or events so long as the assets remain within their usable life and do not expire. In a post-COVID-19 context, reviewing the NESS' mandate and its strategic priorities will also help prepare an efficient response in the future and improve alignment with F/P/T needs and holdings. Timely implementation of the NESS Comprehensive Management Plan, approved in May 2024, will be important in tracking that action items continue to address key findings and recommendations from past audits and evaluations.
As PHAC is moving towards stabilization of its resources through renewal, a prioritization of key areas in EM will have to occur to support continuous system improvement and sustainability, and align resources accordingly. The implementation of a cyclical approach to EM, which would include risk and capability assessments, training, regular exercises, a strong mobilization framework and recovery strategy, regular plan updates, and timely integration of lessons learned, is needed to support system sustainability.
Recommendations
The findings from this evaluation have resulted in the three recommendations listed below. There is no recommendation directed at the NESS given, that a comprehensive management plan was approved in May 2024, and is being implemented to address outstanding challenges, as recommended by the Office of the Auditor General (OAG)Footnote 1.
Recommendation 1: Implement the mobilization framework and improve the rostering system.
The over-reliance on the same individuals to be mobilized was identified as a significant challenge for mobilization and overall staff retention. Since March 2024, joint work has been underway with HC's HECO to update the mobilization framework, which has been a long-standing challenge identified in previous reviews. Given that the All-Events Response Operations (AERO) system is sunsetting, ROEMB should evaluate what data management and rostering IT tools are needed to be more efficient and effective.
Recommendation 2: Promote a mobilization culture and EM training within the Agency.
Mobilization culture, policies, and processes within the Agency are not sufficiently developed. Supporting emergency response mobilization is critical for the success of the mobilization framework, including providing time for training as well as a recovery period following mobilization. Also, while a Public Health Emergency Management course is now mandatory for all staff at PHAC, continuing education and training is also key to maintaining skills and an emergency management culture.
Recommendation 3: Ensure continued sustainability of the EM system by prioritizing and formalizing a cyclical approach to EM.
Significant investments have allowed the program to build an EM system that is stronger and more stable. It will be important to prioritize continued sustainability of this system through the full implementation of a cyclical approach to EM. Over the last five years, the flow of this cyclical approach to EM was slow moving, and at times stalled, due in part to an emphasis on emergency response activities. Going forward, the Agency should strive to implement all of the elements of the EM cycle, while ensuring these elements work together efficiently and coherently.
More specifically, ROEMB should work collaboratively with the various PHAC and HC centres of expertise towards sustaining emergency preparedness activities through the implementation of a robust risk and capability assessment program that would support exercise prioritization and decision making related to an all-hazards approach. Such a system should leverage existing risk assessment expertise across the HP and provide concrete direction on necessary revisions to EM plans, which, once implemented, could be re-tested via subsequent exercises and validated through lessons identified in event response After Action Reviews to address gaps. Since the winter of 2024, HECO has been engaging HC programs to support the risk and capability assessment work led by ROEMB.
Overview and program description
This report presents the results of the Evaluation of the Public Health Agency of Canada's (PHAC) Emergency Preparedness and Response (EPR) Activities.
Program profile
Preparing for and responding to emergencies is a shared responsibility among all three levels of government (federal, provincial and territorial, municipal), with contributions from non-governmental public health partners. The Emergency Preparedness and Response (EPR) program within PHAC is responsible for strengthening Canada's capacity to prevent, mitigate, prepare for, and respond to public health events and emergencies, as well as mass gatherings and high-profile events.
The Regulatory, Operations and Emergency Management Branch (ROEMB) is PHAC's centre of expertise for emergency management functions, providing response coordination for unplanned or intentional emergency events, as well as planned mass gatherings and high-visibility events for PHAC and Health Canada (HC), referred to as the Health Portfolio (HP) in this report. ROEMB provides the HP with shared services in emergency management governance, emergency management plans, operations centres, field mobilizations, as well as continuous improvement through training, exercises, and identification of lessons learned. In assuming its role, ROEMB works in collaboration with other PHAC and HC programs that have their own EPR responsibilities and activities, including HC's Health Emergency Coordination Office (HECO), which was established in the fall 2023.
ROEMB also fulfils Canada's domestic and international obligations to detect, prepare for, and respond to public health events, such as infectious and communicable disease outbreaks, pandemics, and bioterrorism, and coordinates responses to address the public health implications of natural hazards or human-caused disasters.
The National Microbiology Laboratory Branch (NMLB) contributes to PHAC's emergency preparedness and response activities by maintaining an Emergency Operations Centre (EOC). NMLB-EOC acts as the scientific point of coordination for emergency response and day-to-day communications in infectious diseases from a laboratory perspective.
Below is a description of activities undertaken by ROEMB and NMLB as part of this program.
Within ROEMB
- The Centre for Emergency Preparedness (CEP) applies an all-hazards, risk-based approach, in collaboration with HP partner programs, to establish resilient and adaptable emergency preparedness capabilities that aim to detect, mitigate, prepare for, and recover from domestic and global public health threats to protect the health and safety of Canadians.
- The Centre for Emergency Response (CER) is the HP lead for public health emergency response efforts. This includes providing a 24/7 single window for the HP, with an operations centre offering centralized reception and triage, and reporting and distribution of health information. CER is the HP link to emergency management (EM) partners, supports domestic and international mobilizations, and mobilizes the Incident Management System (IMS) to coordinate responses to specific public health emergencies.
- The Regional Emergency Preparedness and Response (EPR) Units are responsible for coordinating the HP response to an event in a particular region. This includes the following:
- providing situational awareness to the Health Portfolio Operations Centre (HPOC), program leads, and regional stakeholders;
- supporting HP programs in their regional response activities;
- tracking and supporting the needs of any HP resources that are deployed to the region; and
- briefing regional HP executives.
- When additional capacity is required to support the HP emergency response in the region, the Regional EPR Units use their respective Regional Emergency Coordination Centre(s) (RECCs), scaled to event needs, to respond as required.
- The National Emergency Strategic Stockpile (NESS) program facilitates access to a range of medical countermeasures (MCMs), including life-saving drugs, medical supplies and equipment, and emergency social service supplies. It is intended to be leveraged as surge capacity to support provincial and territorial (P/T) responses to public health events and emergencies when their supplies are exhausted or not immediately available. It is also the sole provider of niche medical countermeasures required for rare public health emergencies, such as bioterrorism.
Within NMLB
- The NMLB-EOC works with the Canadian Public Health Laboratory Network to coordinate the national public health laboratory response. The NMLB also provides scientific and mobile laboratory support for field investigations aimed at controlling outbreaks and potential threats domestically and in support of international partners.
Internal HP partners
While ROEMB is the centre of expertise for the HP's emergency management function, ROEMB will work with a range of HP centres of expertise, depending on the nature of the activities:
- Within PHAC, this includes the Infectious Diseases and Vaccination Programs Branch (IDVPB), the Data, Science and Foresight Branch (DSFB), and the Centre for Border and Travel Health and the Centre for Biosecurity within ROEMB.
- Within HC, this includes HECO and other programs within the Healthy Environments and Consumer Safety Branch (HECSB), and the Health Products and Food Branch (HPFB).
- Within the shared services partnership this includes the Communications and Public Affairs Branch (CPAB), the Corporate Services Branch (CSB) and this Office of International Affairs (OIA).
Did you know? HECO was created in September 2023, within HC's Healthy Environments and Consumer Safety Branch. HECO provides a departmental focal point, as well as strategic advice and coordination, for horizontal health emergency management policy, planning, integration, and governance across HC for all health emergency preparedness, response, and recovery activities. HECO works with HC programs, and with PHAC as the lead for emergency management for the HP, in order to fulfill its mandate.
This evaluation does not assess the activities performed by these various HP centres of expertise as they related to EPR activities. However, it does examine how ROEMB engages, collaborates, and coordinates activities with them.
Intended results
The EPR program plays an important role in PHAC's core responsibility of preparing for and responding to public health events and emergencies. In support of this responsibility, the EPR program aims to achieve the following:
Immediate outcomes
- Public health emergency preparedness is sustained;
- Public health events and emergencies are detected and reported on a timely basis; and
- Public health emergencies are responded to on a timely basis.
Intermediate outcome
- Public health emergency preparedness and response capacity is improved.
Ultimate outcome
- A sustained public health emergency preparedness and response system for Canada is in place.
Financial resources
Table 1 presents the program's planned funding from 2019-20 to 2023-24. As the last quarter of 2019-20 marked the beginning of the COVID-19 pandemic, the EPR program received time-limited COVID-19 funding, which is also identified in the table. Actual spending data is presented in Appendix A.
| Year | Planned funding for regular activities | Planned funding for COVID-19 response | Total |
|---|---|---|---|
| 2019-2020 | $22,362,755 | n/a | $22,362,755 |
| 2020-2021 | $28,597,439 | $1,394,405,131 | $1,423,002,570 |
| 2021-2022 | $87,064,497 | $1,817,810,976 | $1,904,875,473 |
| 2022-2023 | $95,698,883 | $274,728,807 | $370,427,690 |
| 2023-2024 | $103,091,156 | $170,214,925 | $273,306,081 |
| Total | $336,814,030 | $3,657,159,839 | $3,993,974,869 |
|
Notes:
|
|||
Evaluation scope and approach
The purpose of this evaluation was to examine the EPR program's achievement of intended results, and the efficiency of its activities from 2019-2020 to 2023-2024.
Activities in scope
For ROEMB, the evaluation scope includes activities of the Centre for Emergency Preparedness (CEP), the Centre for Emergency Response (CER), the National Emergency Strategic Stockpile (NESS) and the Regional Emergency Preparedness and Response Units, as described in the previous section.
For NMLB, the scope includes activities of the Emergency Operations Centre (EOC), also as described in the previous section
Activities out of scope
Many other centres with technical expertise across HC and PHAC (and even within ROEMB, such as the Centre for Border and Travel Health and the Centre for Biosecurity), also have EPR activities that relate to public health. However, the technical expertise provided by these centres in support of the EPR program is not covered by this evaluation. The activities of these expert centres have been and will continue to be covered in separate evaluations.
Methodology
Data collection methods included a review of financial data, performance data and documents, as well as a comparative analysis, case studies, and key informant interviews with PHAC, other government departments (OGDs) and provincial and territorial (P/T) representatives. For more information on the evaluation methodology, including limitations, see Appendix B.
Findings
Evaluation findings are presented using the following themes: Emergency preparedness, Detection and reporting, Emergency response and mobilization, Sustained EPR system in Canada, and Collaboration, coordination, and governance.
Emergency preparedness
Key takeaways: Over the past five years, the EPR program has maintained and improved emergency preparedness within PHAC. Plans and procedures have been updated, exercises have taken place, and training has been enhanced and is easily accessible for all staff. Findings indicate that training and exercises need to remain a priority to support staff skills and overall readiness.
Plans and processes
PHAC relies on a series of emergency plans to guide roles, responsibilities and processes as they relate to emergency response. Recent emergencies such as COVID-19 underlined the need for clear roles and responsibilities, as well as regularly planned updates and exercises of these plans. Considerable progress has been made over the past three years on addressing recommendations from external and internal reviews, including those referenced in various Office of the Auditor General (OAG) reports. Most OAG recommendations related to PHAC's emergency response function have been substantially or fully implemented.
For example, ROEMB has updated and conducted exercises of the Health Portfolio Emergency Response Plan (HP ERP), is on track to meeting its commitment to update the Health Portfolio Strategic Emergency Management Plan, and has engaged with provinces and territories (P/Ts) on updating the Federal/Provincial/Territorial Public Health Response Plan for Biological Events.
Highlight: The updated HP ERP was implemented in September 2023. Key revisions to the Plan included enhanced process flexibility, integrating health equity considerations, clarifying roles and responsibilities as well as escalation and de-escalation criteria and steps. Updated criteria were applied successfully to support the de-escalation and deactivation decision for the 2023 Wildfires Activation. Other HP ERP updates were tested via several exercises. The next step is to develop a regular planning cycle to test and update plans on a continuous basis.
The updated HP ERP now provides a framework for applying health equity considerations before, during, and after an event response. Key elements of the framework include:
- enhancing health equity competencies for operational staff through training;
- considering population inequities in risk assessment and operational planning;
- advocating for event partners to assess and mitigate health equity impacts;
- integrating health equity considerations and principles as part of decision-making;
- embedding health equity perspectives in response processes; and
- incorporating health equity assessment in after action reports and recommendations.
As highlighted in a lessons learned review conducted by PHAC's Office of Audit and Evaluation, "(t)he COVID-19 pandemic and response illuminated and amplified existing social, economic, and health inequities in Canada and globally. Many of the lessons learned during the pandemic reflect the need to integrate equity considerations within future public health emergency planning and decision making to avoid unintended harm and consequences to populations already experiencing inequities and to support equitable outcomes for all people".Footnote 2 The updated HP ERP and integration of a health equity lens are expected to create more equitable outcomes and better support Canadians to sustain their wellness during the spectrum of public health emergencies in the years ahead, from infectious diseases to climate-related events.Footnote 3 Moreover, other HP ERP revisions, such as enhancing the flexibility given to activation levels, were also impactful on EPR performance following the implementation of the Plan.
Progress was also made on updating key operational documents in 2023-2024, including the CER's Concept of Operations and updated IMS job action sheets. CER also has an experienced Response Readiness team, with dedicated resources to continue updating the tools and operational guidance provided to staff that are mobilized during a response. Additional guidance may be needed on the steps and processes for those working in an IMS, including process maps, templates, critical paths, and SOPs as well as making continuous improvements an integral part of any activations.
Moreover, following best practices, each RECC has created a regional Annex to the HP ERP and customized the activation levels and regional response structures to reflect their appropriate P/T stakeholders and relationships. Revised activation levels provide clearer roles and responsibilities, as well as more flexibility and efficiency to address large scale or fast moving events, and better alignment with the HPOC, P/Ts, and the Government Operations Centre (GOC) activation levels and emergency management functions. New SOPs will also be prepared in line with the new HP ERP activation levels and processes. RECCs are also working on updating their Concept of Operations to include a hybrid response model comprised of physical and virtual presence. Lastly, the NMLB-EOC has updated eight of its SOPs since 2019, including the update to their operations centre SOP in January 2024, which provides clear mechanisms on how the NMLB-EOC functions, as well as updated response levels to align with HPOC and GOC.
Training
A lack of public health EM training was seen as an important gap in the early COVID-19 response at all levels of the Agency, including senior management. There have since been significant improvements in this area. For example, foundational Public Health Emergency Management (PHEM) training was mandated Agency-wide in 2022 and an Executive Committee Orientation on EM was implemented. A PHEM Portal was also launched in November 2023, which includes a full suite of more advanced EM training and resources. As of July 2024, nearly half (48.4%) of the target audience for the foundational emergency management and public health course had completed it, which is similar to the median completion rate for other PHAC mandatory courses. Targeted training sessions were also delivered to Directors General (DGs) and Vice-Presidents (VPs) to increase senior management knowledge and skills in EM principles.
As events and emergencies often require coordination between PHAC and HC centres of expertise, it would be a good practice to expand EM mandatory training to HC staff. This was a key area for consideration in the 2023 Wildfires Activation Case Study, as many of HC's staff had no prior experience or IMS training. While one EM course is mandatory at PHAC, none are mandatory at HC. However, in the winter of 2024, HECO developed a HC Emergency Management Training Strategy and has successfully promoted the training among HC employees.
Recognizing the progress to date, many internal interviewees identified training as an ongoing priority area for the EPR program, with some noting that continued regular training is needed to maintain skills, including practical training through mentoring, job shadowing, and participating in exercises. Moreover, EM training could be extended to the wider EM community, such as P/T partners, and the full set of training included on the PHEM portal could be better promoted to HP staff.
In addition to Agency-wide PHEM training, documents indicate that EM training for regional staff is ongoing, with many offices developing formal training plans and exercise calendars to build regional surge capacity. Documents shared by NMLB also showed ongoing commitments to train staff by combining practical and online training. Specifically, NMLB-EOC offers a 6-week practical training after the basic online training, including three 2-week rotations with shadowing, allowing for a more thorough experience and better preparedness for an efficient response.
Exercises
While the Agency participated in a broad range of partner-led exercises, given the COVID-19 context, CER and CEP were not in a position to lead regularly planned exercises and drive a strategic HP exercise agenda based on risk and capability assessments and lessons learned from previous activations over the last five years. As shown in Appendix C, throughout the evaluation scope period, CER and CEP were a part of five exercises, four of which were conducted in the last two years, including a tabletop exercise internal to PHAC related to H5N1, in collaboration with IDVPB. Interviews and documents indicate that there is a need to test plans and processes on a more regular basis in order to exercise different scenarios, as well as provide more opportunities to focus on the training of staff and senior management as part of the exercise cycle. In 2023-24, CEP developed an annual exercise calendar, as well as a service delivery model, that includes tools and templates to assist program areas with the development of exercises. Communication and promotion of this calendar will be imperative to raising awareness about upcoming exercises and opportunities to participate. The development and sharing of best practices for emergency preparedness, as well as more frequent exercises could also help to spread the responsibility for preparedness across the HP in a more coordinated way.
As shown in Appendix C, during the scope period, regional EPR units participated in 31 exercises with their respective external partners, including other government departments in the regions, P/Ts, and municipalities. NMLB also facilitated and participated in numerous internal and external training exercises to enhance outbreak preparedness. For example, Emergency Preparedness and Response Officers ran an internal and an external exercise in 2022-23, as well as 10 Incident Command System training sessions for 211 NMLB staff members. In total, NMLB-EOC participated in 12 internal and external exercises during the evaluation scope period, including a PHAC-led Canadian Polio Outbreak Simulation Exercise alongside federal, provincial, and territorial (F/P/T) partners to simulate a response to a laboratory-acquired polio infection in Canada.
Detection and reporting
Key takeaways: With investments over the last three years, detection has improved within the HP public health emergency preparedness and response system. Modernization of the GPHIN has enabled stronger collaboration with PHAC surveillance programs and external partners, strengthening and broadening GPHIN's reporting on potential public health threats. However, the establishment of the State-of-the-Art GPHIN Platform and Analytical System has been delayed.
Detection and risk assessment improvements
Various reviews conducted during the COVID-19 response identified weaknesses in terms of event detection. In response to the recommendations of OAG's 2021 Report 8 - Pandemic Preparedness, Surveillance, and Border Control Measures, the Agency committed to making further improvements to the GPHIN Program and its processes for issuing GPHIN alerts, now referred to as early-warning notifications, taking into account both the OAG recommendation as well as the final recommendations of the independent review of GPHIN.Footnote 4Footnote 5
Did you know? Established in 1997, GPHIN is an early-warning public health event-based surveillance (EBS) system, which relies on publicly available information sources and specialized staff with scientific and technical expertise. GPHIN provides increased situational awareness for all-hazards potential public health threats worldwide: including chemical, biological, radiological, nuclear and infectious diseases and outbreaks.
A Management Response and Action Plan (MRAP) was developed to address the recommendations from the GPHIN Independent Review. These recommendations informed the work underway at PHAC to review its processes, to identify improvements, and to clarify and streamline the decision-making process for the issuance of GPHIN products, including alerts. The Detect, Understand, and Act (DUA) Framework complemented the GPHIN review's MRAP and supported broader efforts to optimize the Agency's ability to detect public health threats, understand the risks, and act as needed to prevent and mitigate those risks. Specifically, DUA funding supported the creation of the Public Health Security Intelligence Division, which houses both GPHIN and the Agency's classified intelligence teams, GPHIN Program modernization, and enhancement of PHAC's security and intelligence capabilities. DUA funding also allowed ROEMB to expand and enhance its surveillance and reporting activities, including for classified information, establish new ways of working with internal and external partners to support the sharing of information about public health threats, and increase its capacity to track events in 10 languages, taking into account cultural and contextual considerations. Key GPHIN achievements include:
- expanding networks by doubling the GPHIN user base to over 1,700, including international stakeholders and all P/T public health organizations across Canada;
- establishing the GPHIN Flags and Tags Initiative to effectively share GPHIN signals with other surveillance programs and risk assessment functions;
- improving the Agency's capabilities for global and domestic all-hazards event-based surveillance;
- introducing the GPHIN Emerging Issue Report to provide early situational awareness of potential public health threats to Canadian and international stakeholders; and
- increasing access to classified intelligence to enhance the situational awareness of public health decision makers.
With support from DUA funding, GPHIN also established new processes and products. Internal interviews indicate that there is appreciation of the GPHIN daily reports and the new GPHIN emerging issues report. Some interviewees identified that the usefulness of these products could be enhanced through timelier distribution and better integration with program needs and priorities.
As shown in Appendix F, for 2023-2024, ROEMB provided 100% of GPHIN notifications and alerts to stakeholders within the defined timelines, a 10% increase from 2022-23. For the same period, they also completed 80% of requests for information (RFIs) to support the specific information needs of internal and external partners and stakeholders, which is under their target of 100%. RFIs are specific information requests made by partners and stakeholders, whereas GPHIN notification alerts are proactively developed and communicated to partners and stakeholders.
| Year | Planned | Actual | Total variance | % of budget spent |
|---|---|---|---|---|
| 2022-23 | $1,792,709.00 | $1,318,007.17 | $474,701.83 | 74% |
| 2023-24 | $11,010,468.00 | $5,554,296.00 | $5,456,172.00 | 50% |
| Total | $12,803,177.00 | $6,872,303.17 | $5,930,873.83 | 54% |
Although several improvements to GPHIN have been made, 7 out of the 25 GPHIN deliverables under the DUA Framework were moderately off track as of April 2024. Progress on achievement of deliverables advanced shortly after; however, this was after the evaluation's scope period. The variance analysis presented in Table 2 also shows important underspending for GPHIN-DUA funding in the last two fiscal years, and a projected large surplus for 2024-2025, which is the last year of DUA funding. Reviewed documents indicate that most of the delays appear to be attributed to organizational and human resource challenges. For example, they experienced challenges with hiring staff with the needed skillset due to only being able to offer term positions, given the temporary nature of the funding. Moreover, lengthy HR recruitment processes meant a shorter time frame for staff to be at strength, while the funding was still available. This includes the significant time of approximately six months involved in obtaining a Top-Secret level security clearance, which is a requirement for many members of the classified intelligence team. In addition to HR challenges, expanded classified activities are new to the Agency and it required significant time to establish intelligence processes and build relationships with security and intelligence partners.
Moreover, the establishment of an updated GPHIN Platform and Analytical System to increase analytical capabilities could not be completed within the original planned timelines. This project was known as the GPHIN Next Generation Project and faced delays due to its complexity and the necessary careful planning and due diligence needed for an IT initiative of this nature. At the time this report was written, the project team was exploring options to determine the best approach going forward, in collaboration with project partners.
DUA funding also supported improvements to integrated threats and risk assessment with the establishment of the Centre for Surveillance, Integrated Insights and Risk Assessment (SIIRA) within the Data, Science and Foresight Branch (DSFB). SIIRA coordinates and oversees integrated threat and risk assessment in PHAC to anticipate, detect and assess public health risks. Although SIIRA operates outside of ROEMB, and its specific activities are out of scope for this evaluation, the coordination role it plays in risk and threat assessments is an important part of the EPR program, as per its inclusion in the Health Portfolio Emergency Response Plan (HP ERP).Footnote 6
Within SIIRA's threat assessment process, signals are detected and verified by PHAC's various centres of expertise. If a signal poses a potential public health risk, the responsible PHAC centre of expertise initiates a threat assessment. They enter key information and their initial threat assessment, using a standardized methodology, into the Integrated Threat Assessment Platform (ITAP). On a weekly basis, SIIRA compiles the ITAP submissions from the various PHAC centres of expertise into a draft Threat Report that is used to inform and support decision making. These reports support situational awareness of threats, their assessment status by the various PHAC program areas, the actions taken to address them, as well as next steps. Between SIIRA's inception in April 2022 until the end of March 2024, 93 weekly threat reports had been produced and 14 risk assessments had been completed.
SIIRA's risk assessments and threat reports are important lines of evidence to support decisions on EPR measures. PHAC's various centres of expertise are at the core of SIIRA's threat and risk assessment process; however, this did not originally include the integration of HC's expertise on risks and threats in its authorities. In an effort to integrate HC's input, HECO was added in September 2024 to SIIRA's threat assessment process. HECO now receives SIIRA's signal requests, attends the weekly meeting, and is looping in HC programs as needed.
Emergency response and mobilization
Key takeaways: Over the last five years, PHAC has successfully responded to multiple requests for support and mobilized the IMS when needed to coordinate responses to public health events. However, given the length and breadth of the COVID-19 IMS mobilization, the main challenge encountered by the program was related to rapidly mobilizing staff for concurrent IMS mobilizations and maintaining a surge capacity over time.
Health Portfolio activations
Activation levels during the evaluation period from April 2019 to September 2023 were described as follows in the 2013 HP ERP:
- Level 1 – Surveillance, detection and alerting: This level corresponds to normal operations. All-hazard information is monitored and recorded by HPOC.
- Level 2 – Increased vigilance and readiness: This level is adopted when an event or emergency occurs or may occur that impacts the responsibilities of HP program areas beyond their capacity, requiring increased coordination and planning.
- Level 3 – Partial escalation: This level is reached when the impact, or potential impact, of an event or emergency requires the greater use of HP assets and resources to adequately respond.
- Level 4 – Full escalation: This level is adopted when the impact, or potential impact, of an event and emergency requires the greatest use of HP assets and resources to adequately respond.
With the update of the HP ERP approved in September 2023, routine operations now correspond to Level 0, Level 1 is enhanced reporting and planning, Level 2 is mobilized response, and Level 3 is full-scale activation.Footnote 7
The initial decision on the appropriate activation level begins with an assessment of the risk level associated with an event and considers a variety of factors. These include the complexity, severity, speed, duration, and extent of the resources needed to respond to the event, as well as the processes needed to support them, both for HP support requirements and to address requests for assistance (RFAs) from external partners. These activation levels are generally sequential, though some events may require an immediate Level 2 or 3 response. Table 3 summarizes the number of activations by level for HPOC, RECCs and NMLB-EOC. The only Level 3 activation corresponds to the COVID-19 response.
| Level | HPOC | RECCs | NMLB-EOC |
|---|---|---|---|
| Level 1 | 2 events; 60 days | 4 events; 142 days | 1 event; 90 days |
| Level 2 | 5 events; 806 days | 2 events; 38 days | 6 events; 626 days |
| Level 3 | 1 event; 1,080 days | 1 event; 1,080 days | 1 event; 987 days |
| Level 4 | 0 event; 0 days | 0 event; 0 days | 0 event; 0 days |
IMS mobilization
The IMS is a response tool that may be mobilized to support an event and then demobilized following the response. HP activations over the evaluation period have led to six IMS mobilizations, as identified in Figure 1.
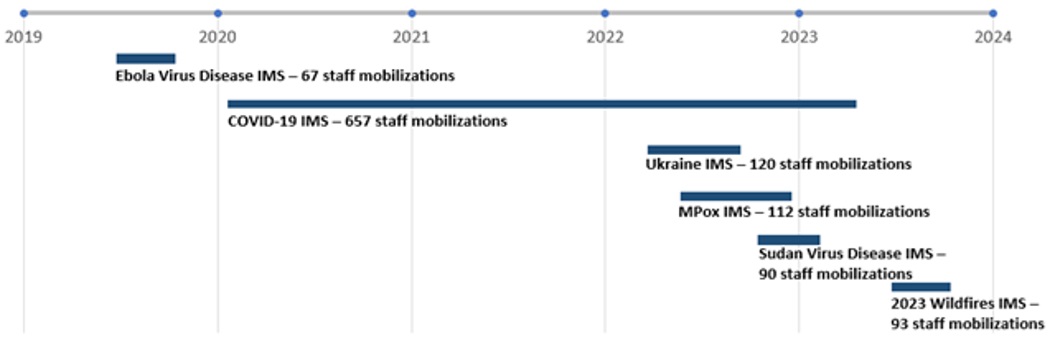
Figure 1: Text description
Figure 1 is a timeline showing the IMS mobilizations between fiscal years 2019-20 to 2023-24. The events are depicted by a bar to show the length and number of individuals mobilized for each event. From 2019 to 2023, the events shown are as follows:
- A small bar towards the end of 2019 for the Ebola Virus Disease, resulting in 67 mobilizations;
- A long bar spanning from 2020 to early 2023 for the COVID-19 IMS, resulting in 657 mobilizations;
- A medium bar mid-2022 for the Russian Invasion of Ukraine IMS which resulted in 120 mobilizations;
- A medium bar mid to end of 2022 for the Mpox IMS which resulted in 112 mobilizations;
- A small bar at the end of 2022 and beginning of 2023 for the Sudan Virus Disease IMS which resulted in 90 mobilizations; and
- A small bar mid-2023 for the 2023 Wildfires IMS which resulted on 91 mobilizations.
These six IMS led to a total of 1,139 staff mobilizations, with COVID-19 representing close to 60% of those mobilized in the past five years. While these are unique staff mobilizations, some individuals were most likely counted twice if they participated in more than one IMS. As can be seen in Figure 1, four IMS mobilizations overlapped, adding to the challenge faced by the Program in maintaining continuous surge capacity to mobilize staff within these IMS.
IMS mobilizations were overall successful at addressing the goal of responding to all hazard public health events. As shown in Appendix F, for the last two fiscal years (2022-23 and 2023-24) 90% of response objectives were met, as captured in the Incident Action Plans during an activation, slightly below their target of 100%. Still, some challenges were encountered:
- At the beginning of a response, it was not always clear which centres of expertise should lead the response process.
- At the end of a response, in some cases, it was not always clear who should continue to address the public health event after de-escalation, as part of regular or mandated responsibilities.
- Mobilized staff were unclear about their roles and responsibilities as outdated documents, like job action sheets, did not provide a clear sense of requirements.
These questions should be addressed early in an activation to engage the appropriate centres of expertise, minimize duplication, and support business continuity. In some cases, the nature of the public health event and its impacts were complex, as they overlapped with other areas of expertise or were not always clear. For example, at the beginning of the 2023 Wildfires Activation, it was unclear who the response lead should be and which plan should be used, including associated processes and governance, as wildfires are considered both natural and chemical events, due to smoke. According to emergency plans, PHAC is the lead for natural events while HC is the lead for chemical events. Early and ongoing engagement with HP programs in a response will be important for improved activity coordination going forward, in order to clarify who should be the lead of an event, as well as how programs will support the response or not.
In early 2024, processes were changed to include a CEP emergency plan expert in the HP Situational Assessment Team (HP SAT) meetings. This should help ensure that activations are informed by the appropriate plans, including associated processes and governance. In addition, since September 2024, the increased collaboration with HECO is expected to better support the identification of which program should be included as part of a response when an event's potential health impacts may fall within HC's authority.
Moreover, mobilized staff joining the IMS should be offered a systematic orientation program beyond the mandatory training in order to set them up for success. As previously noted, many documents provided to mobilized staff were out of date, such as job action sheets, leading to challenges. For example, the lack of formalized processes and standardized onboarding and handover policies and practices led to inconsistencies within the Mpox IMS, and created additional obstacles for response personnel already working in a stressful environment. Key operational documents such as IMS job action sheets were updated in 2023-24 and are expected to improve the efficiency of IMS onboarding.
Staff mobilizations within PHAC
Given the length and breadth of the COVID-19 IMS mobilization, maintaining surge capacity within the Agency has been an important challenge for the program over the last five years. Mobilization challenges experienced over this time highlight the need to re-prioritize a mobilization framework to support various types of events, including large and prolonged responses. More specifically, the COVID-19 lessons learned exercise conducted by the Office of Audit and Evaluation identified that PHAC needs a robust mobilization framework that can support the quick deployment of a surge capacity and the appropriate support to sustain this capacity in the longer term. The lessons learned also identified that this strategy should provide a foundation to:
- Ensure that the HP has the right blend of operational capacity and science-based expertise built in and ready to address future challenges.
- Allow for the quick mobilization of additional capacity and expertise within the HP and the rest of the federal government that could include having an inventory of expertise in core areas.
- Support the well-being of mobilized employees throughout the response.
- Build the foundation to quickly ramp up support functions, including staffing, financial management, procurement, and IT systems.
The various IMS mobilizations that occurred during the scope period of this evaluation allowed the Agency to collect a wide range of real-time mobilization data. This data and the respective staffing challenges experienced in each IMS mobilization should help inform the development and implementation of the mobilization strategy. The importance of considering such data was also identified in the Evaluation of Emergency Preparedness and Response Activities 2012-13 to 2016-17.
There are still shortcomings with current processes and policies that support mobilization within the HP. For example, there are no agreements in place for the release of staff to the IMS, and mobilization tools such as the All-Events Response Operations (AERO), as well as other rostering processes, are outdated. CER, in collaboration with partners including the Human Resources Services Directorate and HC's HECO, since winter 2024, has been working towards implementing a mobilization framework, that will include references to internal staffing, including program support, the Emergency Response Cell and IMS, and rostering, among others. In the meantime, pre-identified staff are ready to respond in key roles. While an IMS readiness roster of pre-identified individuals available for key roles is being piloted, some internal interviewees indicated that this approach to call upon the same targeted individuals is not sustainable and is leading to mobilization fatigue. There is also evidence that managers are still reluctant to release staff for mobilizations due to competing workloads or the inability to backfill positions. Also, for those who are mobilized, recovery periods are not always possible, and they must catch up on work that accumulated during their absence. To address this issue, participation in the decompression program following mobilization should be encouraged as a way to support recovery, coupled with feasible rotations to avoid burnout, and backfilling positions when required.
The mobilization framework should also take a coordinated approach with program areas and consider, as much as possible, their resource planning. This would further support an emergency management culture across the HP. Mobilization best practices from other government departments could be considered as part of the framework. Consultations and workshops on the development of the approach to mobilization identified the following key areas to be addressed as part of the mobilization framework:
- Creating a response mobilization culture and an ability to prioritize work to free up resources to be mobilized as part of a response;
- Providing a clear and measurable definition of response readiness and the requirement for preparedness activities, including training, to be tied to those personnel on response rosters;
- Providing increased predictability to staff and management as to when mobilizations will take place and for how long;
- Building more streamlined and uniformed mobilization processes and improving process transparency;
- Streamlining predictable HR processes and plans regarding mobilization to support rapid response; and
- Developing clear financial processes for event response, including for costs associated with preparedness activities and cost recovery.
Each RECC has built their own regional surge capacity by training and exercising regional staff. Regional EPR staff also provide surge capacity to each others' regions, as needed. For short-term responses, RECCs indicated that existing mobilization process could be leveraged. However, for more significant events or longer-term activations, RECCs would continue to require long-term surge capacity. At the time of writing this report, a framework for a new hybrid reservist model for border operations was being developed to improve surge readiness to carry out functions under the Quarantine Act.
Domestic surge support within Canada
Staff mobilization
CER's Response Support and Technical Assistance (RSTA) team is responsible for receiving, assessing and triaging RFAs received from both domestic and international partners. Evidence shows that processes to mobilize staff to support partners' surge needs are in place and are used regularly. For example, 100% of P/T RFAs for deployment of Agency staff to P/T partners were responded to within negotiated timelines each year during the evaluation period, highlighting the Agency's response capacity.
The Canadian Field Epidemiologist Program (CFEP) and the Canadian Public Health Service (CPHS) are the Agency's field service programs. The CFEP builds Canada's public health capacity by training public health professionals in applied epidemiology with the specialized techniques and competencies required to respond to diverse public health issues in real-life settings. As of fiscal year 2024-25, the size of the CFEP cohort went from five participants to seven, which increases the total number of deployable staff.
The CFEP also mobilizes field epidemiologists anywhere they are needed within Canada or around the world, supporting public health organizations as they respond to urgent public health events. Specifically, the CFEP has a highly trained and competent workforce ready to be mobilized for three-to-four-week durations to support surge requests for epidemiological assistance. Between January 1, 2019, and December 31, 2023, CFEP reported 78 domestic RFAs with a total of 93 epidemiologists mobilized within Canada.
CFEP mobilization can also occur within PHAC. For example, epidemiologists were mobilized to support PHAC program areas at the early stage of the COVID-19 pandemic, as well as the repatriation quarantine sites operations in Trenton and Cornwall. However, CFEP stopped tracking these mobilizations in 2023, thus data on these internal mobilizations cannot be reported.
The CPHS also recruits and places field staff at partner organizations across Canada to augment local capacity around priority public health needs, such as substance-related harms surveillance. Their work plans can be rapidly pivoted and new teams of public health officers can be scaled up to respond to emerging issues or public health emergencies, like the Opioids crisis in 2018 and COVID-19 in 2020. However, there remains a need to identify mechanisms to engage other professional categories beyond epidemiologists in surge response, such as nurses, and health informatics supports, as well as to build surge capacity for epidemiologists for longer than the traditional three-to-four-week period provided for by the CFEP program.
Other field services programs at the agency include laboratory field support led by NMLB, as well as Field Surveillance Officers in the Centre for Communicable Diseases and Infection Control. These may also provide rapid surge capacity, but their deployment processes and training are not coordinated by ROEMB. Documents indicate that CEP plans to coordinate activities with other field services groups within the Agency.
External mobilizations within Canada are also facilitated through the Operational Framework for Mutual Aid Requests (OFMAR), a non-binding mechanism that can be activated by P/Ts to identify and share health care professionals and health assets across jurisdictions during events. Although originally created for physicians and nurses, the tool is flexible and can be expanded to identify other health care professionals.Footnote 8 As shown in Appendix F, 100% of provincial and territorial RFAs through OFMAR were responded to within negotiated timelines throughout the evaluation period.
Asset surge support
In terms of the National Emergency Strategic Stockpile (NESS) surge capacity readiness, RFA processes are in place and PHAC's capacity to deploy assets is strong. During the evaluation scope period, 100% of P/T RFAs for supply provision were addressed within negotiated timelines, including during the COVID-19 pandemic. The NESS also maintains a comprehensive suite of SOPs that govern its key materiel management activities. Ongoing development and use of the NESS warehouse management system is expected to continue improving inventory tracking and management.
Did you know? P/Ts are primarily responsible for the provision of medical equipment and supplies and other goods necessary to support health care and reasonable preparedness for most common emergencies. However, consistent with the principles of the Emergency Management Act and various federal and F/P/T emergency management plans, the federal government, through the NESS, plays a critical surge capacity role in supporting public health emergency management by facilitating access to critical goods when PT capacities are exhausted or not immediately available.
In response to unprecedented global demand for medical equipment and supplies at the onset of the COVID-19 pandemic, and in order to address observed gaps in supply, the NESS made significant investments to adapt its approach and transform its capabilities. It also provided increased F/P/T surge support to respond to an unprecedented volume of RFAs and entered into bulk procurement on behalf of F/P/T partners.
NESS evolution
The NESS pre-COVID (2019):
- 31 employees
- 8 warehouses comprising 178K square feet
- Approximately 3 to 5 RFAs per year
- Priority focus on niche medical countermeasures (MCMs) for chemical, biological, radiological, and nuclear (CBRN) threats
- Limited holdings of routine MCMs
The NESS in 2023:
- 150 employees
- 20 warehouses comprising 1.7M square feet
- 600 RFAs from April 2020 to March 2023
- Capability to respond to multiple concurrent events with a wide range of MCMs
- Expanded focus on routine MCMs necessary to support pandemic response
Quick facts from March 2020 to December 2023:
- Over 300 contracts issued
- Over 4 billion units of medical supplies and equipment procured
- Over 2 billion units received, validated and deployed for emergency use
- Over 600 requests for assistance
- Over 14M units of medical supplies and equipment donated
- Scaled to approximately 3M square feet of warehousing space
NESS investments prior to the pandemic were supported by limited ongoing funding and time-limited investments for specific events. This resulted in prioritization of niche drug MCMs for high consequence and lower probability threats over PPE and other routine medical assets that were thought to be more readily available through the market.Footnote 9
According to the findings of the 2021 OAG Audit Report 10 – Securing Personal Protective Equipment and Medical Devices, PHAC, HC, and Public Services and Procurement Canada (PSPC) helped to meet the needs of P/Ts for medical devices during the pandemic, but PHAC was not as prepared as it could have been to respond to P/T requests as a result of long-standing funding gaps and unaddressed problems with the system and practices in place to manage the NESS. Therefore, the OAG recommended that PHAC "should develop and implement a comprehensive NESS management plan with clear timelines that responds to relevant federal stockpile recommendations made in previous internal audits and lessons learned from the COVID-19 pandemic".Footnote 10 In response, PHAC committed to developing and implementing a NESS Comprehensive Management Plan (CMP) to address the various recommendations made throughout the years. The CMP was approved in May 2024 and provides a roadmap for the systematic and scalable transformation of the NESS, with the aim of building upon gains already made with temporary funding to improve the management of the NESS and maintain an appropriate readiness posture in the face of an ever-evolving threat and risk landscape.
As outlined in the CMP, there is a need to establish national targets and clarify respective F/P/T expectations with regards to coverage of these targets for key commodities. As part of the CMP, the NESS intends to develop a data strategy that outlines requirements, sources, and mechanisms needed to support NESS decision making, including the development of national targets. This work is expected to leverage improved F/P/T information sharing on asset holdings, science assessments, risk assessments, modelling, and scenario planning to inform national targets for key MCMs. The NESS is collaborating across the Health Portfolio and with security and intelligence partners to identify and assess threats and potential supply chain issues, as well as to leverage their expertise in scenario planning and modelling to develop interim supply targets. Key partners and stakeholders are aware of health emergency material capabilities available in an emergency and how to access them; however, some gaps exist with respect to awareness of specialized assets such as pharmaceutical medical countermeasures, but these are being addressed.
Highlight: NESS has developed the CMP, which features a foundational analysis of key documents, including relevant findings from past audits, evaluations, and lessons learned. It also outlines a number of key action items that will help the NESS meet the strategic goals identified within the Plan. Some of these action items include clarifying F/P/T roles and responsibilities for medical supply readiness, securing additional policy and legal authorities, and strengthening NESS' capabilities for risk and capability assessments to better define medical supply targets.
While the CMP is expected to address many of the challenges raised in the context of past audits, evaluations and lessons learned, it will be important to prioritize timely implementation of the Plan. Given that many strategic goals are dependent on collaboration with P/Ts, OGDs, PHAC programs, and external partners and stakeholders, the CMP recognizes that early engagement to validate timelines and scope is required to implement the actions and to confirm the capacity of all partners involved to complete the work.
International mobilizations
PHAC's epidemiological and laboratory expertise is also required to support short-term, international responses. International efforts are undertaken to support outbreak investigations at the request of international organizations like the Global Outbreak Alert and Response Network (GOARN). Moreover, current processes allow the Agency to assess RFAs, identify qualified individuals, mobilize them internationally and bring them back to Canada safely. At the time of this report, the RSTA team was working on updating the 2012 policy on the mobilization of PHAC staff outside of Canadian borders. International RFAs have led to 19 mobilizations between 2019 to 2023.
Equity and official language considerations
The Mpox and 2023 Wildfires mobilizations were identified as recent examples where equity, diversity, and inclusion considerations were brought forward as key priorities during responses. Specifically, communications targeted to those who were disproportionately affected by the event, and the integration of differential risks for particular groups in risk assessments were highlighted as areas that have improved as a result of experience acquired during the COVID-19 response. Targeted engagement with stakeholders to reach key populations is another example. During the 2023 Wildfires response, in collaboration with P/Ts, NESS proactively distributed surplus N95 respirators to priority populations. In addition to PTs and OGD partners, NESS targeted alternative delivery channels, such as Indigenous Services Canada, northern and remote Indigenous networks, community organizations, and non-governmental organizations to distribute N95 respirators. NESS also leveraged the GCDonate platform to provide surplus N95 respirators to registered parties, including registered charities, non-profit organizations, and other levels of government.
Other challenges raised with respect to equity, diversity and inclusion during responses were related to balancing the need for urgent public health communications with accessibility requirements. In an emergency response, it is essential to provide information to the public as soon as possible. In some cases, for online content, this leads to publication delays and lower-quality translations. Interviews indicate that this is mainly due to quick reviews and fewer resources having the ability to work in both official languages.
Another challenge with respect to inclusive public health communication is presenting the information to the public in plain language. Often, CPAB receives content that is too technical and over the recommended reading level for the general public. CPAB must then work with subject matter experts to revise content into plain language, which takes time. Highly technical or jargon-heavy text can also be misinterpreted during translation, leading to errors or poorer quality. Interviewees identified a need for human resources that are proficient in both official languages, with the appropriate subject matter and public communications expertise to prioritize the quality and timeliness of products shared in both official languages.
Collaboration, coordination and governance
Key takeaways: Overall, the COVID-19 response strengthened PHAC's internal and external collaboration and coordination of activities. In addition, recent improvements have been made within the emergency management governance structure that already support and facilitate a more coordinated HP emergency preparedness and response system. However, improvements could be made with respect to information sharing across branches, as well as within ROEMB.
HP collaboration and governance
The HP emergency management governance structure has evolved over the course of the evaluation period. As a result of the COVID-19 response, key preparedness governance committees were put on hold as efforts were focused on response activities. As such, the HP governance structure for conducting strategic emergency management planning, known as the Health Portfolio Emergency Preparedness Committee (HP EPC), was halted, including the Risk and Capability Assessment Task Group, a HP EPC key working groups.
In 2022, the HP EPC was officially replaced by the VP Emergency Management Executive Committee (EMEC) and the DG EMEC. However, there was no replacement or reactivation of the Risk and Capability Assessment Task Group.
The Risk and Capability Assessment Task Group was responsible for leading the development of comprehensive risk and capability assessments for the HP. Before the COVID-19 pandemic, the HP EPC would use the assessments generated by this Task Group to assess the provision and level of emergency management services and their state of readiness. CEP is currently working on building a new risk and capability assessment program, which is discussed in more detail in the "Sustained EPR system in Canada" section of this report.
Following the implementation of the VP and DG EMEC in 2022, the evaluation found that executive decision-making governance was back in place to oversee departmental emergency management functions. The VP EMEC was setting the strategic direction on emergency management functions across the HP and making decisions on the emergency management function, while the DG EMEC implemented the directions set by the VP EMEC.
The VP EMEC and DG EMEC included both PHAC and HC representation. Having consistent representation of both PHAC and HC at governance tables has helped to maintain situational awareness across the HP, while providing an opportunity to represent respective mandates and interests. Specifically, the evaluation found that collaboration with HC has improved with the establishment of HC's Health Emergency Coordination Office (HECO), in fall 2023. HECO was highlighted as a key function in facilitating effective governance and coordination of activities between both organizations.
The roles and functions of the VP and DG EMECs as planning and preparedness governance committees were well understood; however, several interviewees indicated that the governance transition from preparedness to response was not always clear. More specifically, when an IMS response governance structure is implemented, it is not always clear who should be the lead, who should sit on the Health Portfolio Executive Group (HPEG), which is the executive-level forum that provides strategic decision making during a response, and how the approval processes should proceed when associated health challenges touch several areas of expertise within the HP. While the IMS governance structure is clearly defined in the updated HP ERP and its various annexes, there is a lack of awareness of these defined structures that can create challenges with approvals and coordination with partners.
Aside from the difficulties that can be observed during responses, internal collaboration and coordination for the EPR program work well overall. Information sharing occurs at the senior management level, and CER and HPOC have networks for sharing information to branch single windows and working contacts, such as HPOC Daily and Flash Reports. However, internal interviews indicate that some information is not always flowing across branches, which can lead to missed opportunities for early collaboration and duplication. As previously noted, ongoing and early engagement with programs and partners are important for coordination, both during and outside of a response, including effective integration with the regions and NMLB.
Despite improvements noted by the evaluation to the preparedness governance structure, the VP EMEC was discontinued in August 2024. This was the result of an Agency-wide governance review where the need to streamline the governance at the VP level was identified. This resulted in the creation of a new VP table responsible not only for EM, but also for other corporate subjects. The potential impact of no longer having a dedicated EM VP governance table on HP coordination of EM is unknown. As this new governance model is being implemented, considerations should be given to maintaining an engagement with HC when EM questions are being presented to this new committee. ROEMB and HECO are working together to address potential governance gaps resulting from the discontinuation of the VP EMEC.
F/P/T collaboration and governance
The Pan-Canadian Public Health Network (PHN) is a formal governing body of F/P/T governments across Canada, working together to strengthen and enhance public health. The PHN supports horizontal linkages across public health policy issues through close collaboration with senior government decision makers and other key players in the public health system. As part of this network, PHAC engages and collaborates with F/P/T partners on cross-cutting emergency management issues through the Public Health Emergency Management Working Group (PHEM-WG), previously called the PHEM Task Group.
The PHEM-WG did not meet in the early part of the COVID-19 pandemic due to the emphasis on response; however, committees were formed to support the Special Advisory Committee (SAC) within the F/P/T COVID-19 governance structure. These committees included the Technical Advisory Committee, the Logistics Advisory Committee (LAC), PHN Communications Working Group, and the Public Health Working Group on Remote and Isolated Communities.
Did you know? The PHEM-WG updated its reporting structure in January 2024. Prior to the COVID-19 pandemic, the PHEM WG reported through the Public Health Infrastructure Steering Committee (PHI-SC) whereas now it reports directly to the Public Health Network Council. The PHEM WG will support discussion on cross-cutting emergency management issues from a pan-Canadian perspective and help identify urgent and emerging issues.
A survey of LAC members showed that the LAC was useful and effective for F/P/T collaboration in the response to managing COVID-19; however, a need was identified to clarify the reporting relationship between LAC and other committees, including SAC, LAC Task Groups, and other ad-hoc committees, as well as the need to streamline all of the various information tools and resources into one place. Other suggestions included determining a set of guidelines on when the LAC could be activated on an ad-hoc basis to address other outbreaks, and a review of the LAC mandate to define appropriate membership and establish a clear distinction between the LAC and the PHEM-WG.
Coordination and collaboration between ROEMB and P/Ts were also strengthened during the COVID-19 pandemic period. F/P/T public health emergency management governance structures, primarily through the PHN, continue to work well. Internal documents and interviews indicate that clear structures, processes, and tools are in place to streamline information sharing, thus facilitating and supporting effective governance. However, external interviewees noted that they were less aware of PHAC's preparedness activities and welcomed the opportunity to engage more on the broader scope of preparedness activities.
Regional coordination and collaboration between Regional EPR Units, OGDs, and P/Ts were also highlighted by interviewees as very strong. Strong relationships are also observed between NMLB-EOC and its partners. HPOC has also developed strong relationships within the emergency operations community, including with the regions and F/P/T partners. Within CER, HPOC functions as a 24/7 all-hazard single window that triages public health events that require immediate attention, informs decision makers, and delivers regular and timely reporting to inform event-related situational awareness and decision making.
International collaboration and governance
International Health Regulations
The International Health Regulations (IHR) function as an international treaty requiring the World Health Organization (WHO) and signatory countries to build their capacity to detect, assess, report, and respond to public health events. As a signatory to the IHR, Canada is committed to help strengthen global health security and build capacities to detect, assess, report, and respond to public health events in Canada and abroad to minimize their spread or impact across borders.
IHR activities are a shared responsibility with OGDs and P/T governments. PHAC is the IHR National Focal Point (NFP) for Canada and acts as the single window for rapid communication between Canadian public health authorities, the WHO, the Pan-American Health Organization, and health authorities in other countries. The HPOC Watch Office serves as the operational arm of Canada's IHR NFP office by supporting 24/7 communications between Canada, the WHO and member states, as well as disseminating information with stakeholders.Footnote 11 Also within PHAC, the Office of International Affairs (OIA) leads the negotiations with other member states as part of the WHO process, while domestic implementation and guidance for negotiations resides with relevant HP and OGD programs, including ROEMB as the lead for Canada's NFP office. Despite some internal challenges, PHAC provided 100% of IHR-related communications to stakeholders within defined timelines for the last two fiscal years since this indicator was created (2022-23 and 2023-24).
Given the absence of dedicated governance tables at PHAC for EM related international issues, there are coordination challenges between both branches. As a result, key actions identified in internal documents included the need to define and distinguish ROEMB and OIA roles on EM-related international files, including how they work, and who leads what, as well as the need to clearly define governance and decision making on international files.
Collaboration with North American partners
Engagement between ROEMB and the U.S. Department of Health and Human Services' Administration for Strategic Preparedness and Response (ASPR) was formalized in 2018 with the establishment of a liaison program. As a result, collaboration has strengthened over the last five years with more frequent communication, including monthly calls between ROEMB and ASPR. There are two levels of regular liaison with ASPR, one is through the director or working level group and the second is through the HPOC and the ASPR's equivalent.
Canada is also committed to working with the US and Mexico to strengthen preparedness for animal and pandemic influenza through the North American Preparedness for Animal and Human Pandemics Initiative (NAPAHPI) and has been actively engaged in this partnership. The NAPAHPI recently expanded its scope to include a broader range of pathogens, such as COVID-19. Interviews indicate that the revised NAPAHPI has clearer expectations with respect to governance that will improve the trilateral communication between the three countries moving forward during emergencies.
Sustained EPR system in Canada
Key takeaways: Important investments in PHAC's EPR system allowed the program to build a system that is now stronger and more stable. However, some components of the EM cycle that support sustainability have been slower to progress. The implementation of a cyclical approach to EM, which would include risk and capability assessments, training, regular exercises, a strong mobilization framework and recovery strategy, regular plan updates, and timely integration of lessons learned, is needed to support system sustainability.
The public health emergency management cycle presented in Appendix E illustrates the ongoing process by which emergency organizations prevent, mitigate, prepare for, respond to, and take steps to recover after events. This cycle supports the sustainability of the system as it allows for continuous improvement.
Over the last five years, the program has improved activities related to detection, coordination, planning, training, and deployment of assets. The COVID-19 experience, and other recent activations have also allowed the program to build strong collaboration with its partners. While these improvements make for a stronger EPR program, the system has not yet reached a steady and sustainable state. In 2023, ROEMB implemented a maturity model that captures what the system requires to become sustainable and to monitor progress on those elements. As shown in Appendix D, while there is progress towards the goal of sustaining a public health emergency preparedness system, most elements of the framework are still emerging, including updates to plans, mobilization, continuous improvements, and risk and capability assessments.
In addition to the maturity model, the program uses some results from the WHO's IHR State Parties Self-Assessment (SPAR) as performance measurement data to track internal program progress. As shown in Appendix F, of the five indicators used by the program for performance reporting, three have consistently been maintained at 100%, with two years of data missing for all indicators due to the COVID-19 pandemic. The three indicators demonstrate Canada's capacity to deploy assets during a public health event, its capacity for timely reporting of a potential public health emergency of international concern and unusual or unexpected public health events, and its capacity to activate emergency response operations during a public health emergency. Canada's level of preparedness to respond to public health events and emergencies, as assessed against the WHO criteria, has also improved from 90% to 95% during the evaluation period. Canada's overall emergency preparedness and response score, as determined by the WHO's IHR Monitoring and Evaluation Framework and SPAR Tool, has remained consistently at 96%.
Canada's performance on the SPAR is excellent, at 96% overall, and ranks within the top results for all included countries, though this result should be interpreted with the caveat that it is based on self-assessment.Footnote 12 Canada's lowest score on the SPAR is related to gender equity in health emergencies. Since the data for each indicator is gathered across many levels of government and jurisdictions across the country, there are challenges in consolidating timely updates. In response, the EPR Program has taken steps within their scope to include Sex and Gender-Based Analysis Plus (SGBA+) considerations in the review and creation of their plans.
Recognizing that the Agency has been in a reactive state over the last five years, preparedness capacity has been limited by the unprecedented volume of response activities which were prioritized during that time. Specifically, there has been a gap in risk capability assessments since 2019, with most of the team dispersed for the COVID-19 response, as well as a gap in continuous improvement and implementation of lessons learned from AARs. For example, the last risk and capability assessment cycle took place in 2018 and most of the AARs conducted during the COVID-19 IMS period were delayed due to competing priorities. At the time of this report, ROEMB was updating methods to support risk and capability assessments and advancing work to ensure that they are completed on an annual cycle; however, broader endorsement and championing of capability-based planning for PHEM would be required across the HP to raise awareness of the risk and capability assessment process and products, and to ensure that specific program expertise across PHAC and HC for those who have responsibilities in risk preparedness and mitigation are involved in the risk and capability assessments. Implementing and maintaining an all-hazards risk and capability assessment process was a recommendation from the Evaluation of Emergency Preparedness and Response Activities 2012-13 to 2016-17.Footnote 13
Did you know? The risk and capability assessment process entails a formal, systematic process for estimating the risk level in terms of likelihood and consequences for the purpose of informing planning and decision-making. The results of the risk and capability assessment process should inform the HP's emergency management planning and capability enhancement cycle whereby successive iterations of risk assessment, training, exercises, response to and recovery from public health events, After Action Reviews (AARs), and lessons learned improve emergency planning and readiness.
Sound emergency management practices include the rapid identification and timely corrective actions for challenges experienced during an activation. Although the final reports for AARs stalled at times between 2018 and 2023, CEP conducted more than 30 hotwashes, which are discussions immediately following an exercise or event, and resulted in more than 800 observations in records of discussion. Nearly all the records of discussion included preliminary recommendations that were shared with hotwash participants. Additionally, PHAC's Office of Audit and Evaluation also conducted a series of lessons learned exercises throughout the COVID-19 pandemic, including a real-time audit and a case study on the 2023 Wildfires Activation. Recognizing that there have been an increasing number of concurrent events which have added to the workload, AARs are an integral part of continuous improvement and should be prioritized accordingly to facilitate their timely execution and use. Despite these delays, CEP is reviewing processes for follow up on lessons identified through AARs. It is working on implementing a recommendation tracker and identifying the appropriate processes for soliciting feedback on actions taken and determining the appropriate governance to maintain oversight and accountability for progress. CER also created and staffed a team responsible for collating, reviewing, and implementing continuous improvement recommendations pertaining to CER and IMS.
Financial analysis
On April 1, 2024, the Emergency Management Branch (EMB) and the Health Security and Regional Operations Branch (HSROB) merged into one branch, the ROEMB. During most of the evaluation period, EMB and HSROB were split and therefore reported separately on their expenditures. As a result, the financial analysis reports on EMB (CEP, CER, VPO, and NESS) and the regional EPR units separately. Variance analysis of NMLB-EOC was not possible as NMLB was not reporting its budget down to the cost centre level. Information on NMLB-EOC actual spending is captured in Appendix A.
The evaluation's financial analysis separates data for regular EPR activities from temporary financial investments provided to support the COVID-19 response by the Government of Canada during the pandemic. As shown in Table 4, budget and actual spending for regular EMB EPR activities increased nearly four-fold by 2023-24.
| Year | Start of year budget | Year-end budget | Actual spending | Total variance | % of budget spent |
|---|---|---|---|---|---|
| 2019-20 | $21,012,303 | $21,453,380 | $19,551,423 | $1,901,957 | 91% |
| 2020-21 | $27,246,286 | $46,911,813 | $32,355,041 | $14,556,772 | 69% |
| 2021-22 | $85,714,045 | $95,667,953 | $84,401,483 | $11,266,470 | 88% |
| 2022-23 | $94,290,001 | $216,168,747 | $202,535,893 | $13,632,854 | 94% |
| 2023-24 | $101,682,586 | $161,835,136 | $149,157,240 | $12,677,896 | 92% |
| Total | $329,945,221 | $542,037,029 | $488,001,080 | $54,035,949 | 90% |
|
Note: EMB received additional funding as part of its regular activities that is not captured in the start of year budget. As a result, the difference for the variance in spending and percentage of budget spent is calculated using budget at year end. |
|||||
There is also a significant variance between the budget at the start of the year and year-end, particularly for the last two fiscal years of the evaluation scope period. This variance is due to additional funding allocated to ROEMB later in the fiscal year. Specifically, in 2022-23, EMB received $94.4M for the Mpox response, in addition to DUA funding. As a result, this nearly doubled the planned spending by the end of 2022-23. ROEMB also received PHAC renewal funding later in fiscal year 2023-24, which was not originally captured in the initial budget.
Overall, when comparing actual spending to the budget at year-end, there is minimal variance in spending throughout the five year evaluation period, with the exception of fiscal year 2020-21 where only 69% of the year-end budget was spent. This also marked the first full year of the COVID-19 pandemic, as well as the year with the highest spending on the COVID-19 response (see Figure 2). Of note, temporary COVID-19 funding accounted for 92% of ROEMB's total actual spending during the evaluation period, excluding the regional EPR units. When broken down by directorate, overall data shows a surplus for NESS COVID-19 activities as a result of contingency planning. See Appendix A.
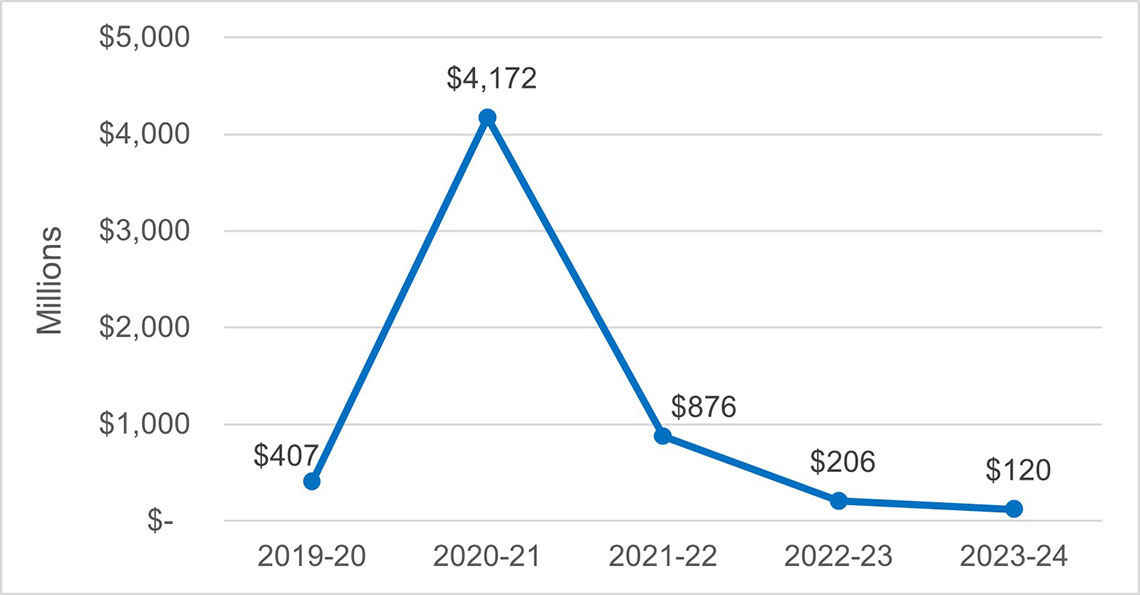
Figure 2: Text description
Figure 2 is a line chart that shows ROEMB actual spending on COVID-19 activities in millions, excluding the Regional EPR Units. The line chart starts with fiscal year 2019-20 and ends with 2023-24. The chart includes data points with the actual spending for each year as follows:
- 2019-20: $406,737,273
- 2020-21: $4,171,876,708
- 2021-22: $876,140,433
- 2022-23: $205,607,809
- 2023-24: $119,579,083
The NESS capitalized on significant investments made during the COVID-19 pandemic. Moving forward, the NESS will strive to sustain improvements implemented with supplemental funding, however, the scope and scale of the NESS program will be influenced by future funding received. Still, investments will continue to prioritize facilitating access to surge supports where the federal role is most critical and in the national interest in the face of an increasingly complex risk and threat environment.Footnote 14 At the time this report was written, ROEMB was developing cost estimates of what an appropriate A-base funding level would look like in the longer term.
As shown in Table 5, regular funding for regional EPR units remained relatively stable with a moderate surplus year after year. There were also minimal variances between the start of year and end of year budgets.
| Year | Start of year budget | Year-end budget | Actual spending | Total variance | % of budget spent |
|---|---|---|---|---|---|
| 2019-20 | $1,350,452 | $1,344,567 | $1,256,607 | $87,960 | 93% |
| 2020-21 | $1,350,452 | $1,351,153 | $1,354,046 | -$2,893 | 100% |
| 2021-22 | $1,350,452 | $1,531,347 | $1,320,404 | $210,943 | 86% |
| 2022-23 | $1,408,882 | $1,408,882 | $1,224,699 | $184,183 | 87% |
| 2023-24 | $1,408,570 | $1,870,620 | $1,645,989 | $224,631 | 88% |
| Total | $6,868,808 | $7,506,569 | $6,801,744 | $704,825 | 91% |
|
Note: The difference for the variance in spending and percentage of budget spent is calculated using the budget at year-end. |
|||||
Conclusions and recommendations
Conclusions
Overall, PHAC is better prepared to respond to public health events than it was five years ago. Plans and procedures have been updated, exercises have taken place, and PHAC-wide Public Health Emergency Management (PHEM) training was implemented, including one mandatory course. Time-limited funding has also improved public health intelligence capacity by enhancing the Global Public Health Intelligence Network (GPHIN) and improving event detection through the widespread distribution of GPHIN Daily Reports. However, the establishment of the state-of-the-art GPHIN platform and analytical system has been delayed. Lessons learned from the COVID-19 pandemic have also been integrated into PHAC's future pandemic preparedness and many audit and review recommendations have been implemented.
Collaboration and external governance with federal, provincial, and territorial partners is also strong with respect to emergency response, though there could be more opportunities to engage on preparedness activities. In parallel, while emergency management (EM) governance at PHAC has improved, there are still challenges with information sharing across the HP at all levels, both during and outside of a response. This issue should be addressed to strengthen internal EM activity coordination, to engage the appropriate HP program areas, to minimize duplication, to cultivate an EM culture, and to support business continuity. Collaboration with international partners also strengthened during the evaluation period; however, challenges were reported with respect to the clarity of internal branch roles on international EM-related files.
Moreover, while the Agency participated in a broad range of partner-led exercises, given the COVID-19 context, the Centre for Emergency Preparedness (CEP) was not in a position to lead regularly planned exercises and drive a strategic HP exercise agenda based on risk and capability assessments and lessons learned from previous activations. Recognizing the unprecedented nature of the COVID-19 pandemic and the human resources required for mobilization, much of the focus over the last five years has been on response activities.
During this time, PHAC responded to many requests for support and activated the IMS to coordinate responses to multiple public health events. However, given the length and breadth of the COVID-19 IMS, mobilizing staff for concurrent IMS mobilizations and maintaining surge capacity over time was a challenge. Since the creation of HC's Health Emergency Coordination Office (HECO) in the fall of 2023, ROEMB has been working with it on a HP framework to help mobilize adequate personnel and sustain effective responses to more frequent and intense emergencies. This framework is essential to readiness and response, and its success hinges on PHAC's adoption of an EM culture highlighted by readiness, resilience, and commitment to collective response.
Funding associated with the COVID-19 response also allowed the National Emergency Strategic Stockpile (NESS) to procure a substantial volume of medical countermeasures (MCMs), which has temporarily enhanced their capacity to deploy assets during public health emergencies or events, so long as the assets remain within their usable life, as in they are used prior to expiry. In a post COVID-19 context, reviewing the NESS mandate and its strategic priorities will also help prepare for an efficient response in the future and improve alignment with F/P/T needs and holdings. Timely implementation of the NESS Comprehensive Management Plan (CMP) will be important for tracking those action items that continue to address key findings and recommendations from past audits and evaluations.
As PHAC is moving towards resources stabilization through renewal, a prioritization of key areas in EM needs to occur to support continuous system improvement and sustainability, and align resources accordingly. The implementation of a cyclical approach to EM, which would include risk and capability assessments, training, regular exercises, a strong mobilization framework and recovery strategy, regular plan updates, and timely integration of lessons learned, is needed to support system sustainability.
Recommendations
The findings from this evaluation have resulted in the three recommendations listed below. There is no recommendation directed to NESS given that a CMP was approved in May 2024, and is being implemented to address outstanding challenges, as recommended by the OAG. Implementing this plan, in alignment with available funding profiles, will be instrumental to alleviating confusion and the potential for duplication of efforts, and to enhancing governance and collaborative planning in support of overall pan-Canadian preparedness. Given that many of the strategic goals are dependent on collaboration with provinces and territories (PTs), other government departments (OGDs), HP partners and programs, as well as external partners and stakeholders, the CMP recognizes that early engagement to validate its timelines and scope is required to implement the various action items.
Recommendation 1: Implement the mobilization framework and improve the rostering system.
The over-reliance on the same individuals to be mobilized was identified as a significant challenge for mobilization and overall staff retention. Since March 2024, joint work has been underway with HC's HECO to update the mobilization framework, which has been a long-standing challenge identified in previous reviews. Given that the All-Events Response Operations (AERO) system is sunsetting, ROEMB should evaluate what data management and rostering IT tools are needed to be more efficient and effective.
Recommendation 2: Promote a mobilization culture and EM training within the Agency.
Mobilization culture, policies, and processes within the Agency are not sufficiently developed. Supporting emergency response mobilization is critical for the success of the mobilization framework, including providing time for training as well as a recovery period following mobilization. Also, while a Public Health Emergency Management course is now mandatory for all staff at PHAC, continuing education and training is also key to maintaining skills and an emergency management culture.
Recommendation 3: Ensure continued sustainability of the EM system by prioritizing and formalizing a cyclical approach to EM.
Significant investments have allowed the program to build an EM system that is stronger and more stable. It will be important to prioritize continued sustainability of this system through the full implementation of a cyclical approach to EM. Over the last five years, the flow of this cyclical approach to EM was slow moving, and at times stalled, due in part to an emphasis on emergency response activities. Going forward, the Agency should strive to implement all of the elements of the EM cycle, while ensuring these elements work together efficiently and coherently.
More specifically, ROEMB should work collaboratively with the various PHAC and HC centres of expertise towards sustaining emergency preparedness activities through the implementation of a robust risk and capability assessment program that would support exercise prioritization and decision making related to an all-hazards approach. Such a system should leverage existing risk assessment expertise across the HP and provide concrete direction on necessary revisions to EM plans, which, once implemented, could be re-tested via subsequent exercises and validated through lessons identified in event response After Action Reviews to address gaps. Since the winter of 2024, HECO has been engaging HC programs to support the risk and capability assessment work led by ROEMB.
Management Response and Action Plan
The scope of this evaluation focused on the Emergency Preparedness and Response (EPR) activities as they relate to the Public Health Agency of Canada. However, per the Shared Services Partnership Agreement, many EPR activities are delivered on behalf of both Health Canada and the Agency. Given that the MRAP for this evaluation may have an impact on both organizations, the Agency will work with Health Canada's Health Emergency Coordination Office to consider impacts for the broader Health Portfolio and expand the scope of action plans and deliverables to Health Canada, where mutually beneficial.
Recommendation 1
Implement the mobilization framework and improve the rostering system.
Management response
Management agrees with this recommendation.
| Action plan | Deliverables | Expected completion date | Accountability | Resources |
|---|---|---|---|---|
| 1. Update the Mobilization Framework that outlines procedures, responsibilities, and protocols for mobilizing staff internally for public health emergency response activations (e.g., Incident Management System) domestically and internationally in response to Requests for Assistance (RFAs). | 1.1 Update the Mobilization Framework | April 2025 | Director General – Regional Operations (DG-RO); Vice President – Regulatory, Operations and Emergency Management Branch (VP-ROEMB) | Existing temporary resources in Emergency Response |
| 2. Improve rostering system. | 2.1 Develop business requirements, leveraging (as relevant) the All Events Response Operations (AERO) business requirements, for a rostering information management system that may include requirements for RFAs and mobilization. | 2.1 April 2025 | Director General – Regional Operations (DG-RO); Vice President – Regulatory, Operations and Emergency Management Branch (VP-ROEMB) | 2.1 Existing temporary and risk-managed resources in Emergency Response |
| 2.2 Build an enhanced rostering system for IMS and domestic and international mobilizations. | 2.2 September 2025 | 2.2 Existing temporary resources in Emergency Response for development phase | ||
| 2.3 Implement enhanced rostering system for IMS and domestic and international mobilizations | 2.3 October 2025 | 2.3 Existing risk-managed resources in Emergency Response for implementation |
Recommendation 2
Promote a mobilization culture and emergency management (EM) training within the Agency.
Management response
Management agrees with this recommendation.
| Action plan | Deliverables | Expected completion date | Accountability | Resources |
|---|---|---|---|---|
| 1. Promote an Agency-wide mobilization culture to build and sustain a collective commitment, at all levels, to mobilize the right people at the right time in response to public health events and emergencies. | 1.1 Work with ADM CSB to embed commitment to support Agency EM activities into Human Resources processes (e.g., Executive and employee letters of offer, Performance Management Agreement objectives). | November 2025 | DG-RO; VP-ROEMB | Existing temporary and risk-managed resources in Emergency Response |
| 2. Invest in emergency preparedness and response training and related activities, including continuing education through practical activities and exercises and deployments. | 2.1 Expand the public health emergency management (PH EM) training pathway and applied exercises for Agency staff, including a pathway for ongoing staff development and skill maintenance, with a focus on building depth and breadth of roster capacity. | November 2025 | DG-Centre for Emergency Preparedness (CEP); VP-ROEMB | Existing risk-managed resources in CEP |
| 3. Monitor, evaluate and promote staff participation (at all levels) in public health emergency management training, exercises, rostering and mobilizations | 3.1 Integrate PH EM training, rostering and exercises
|
November 2025 | DG-CEP; DG-RO; VP-ROEMB | Existing risk-managed resources in CEP |
Recommendation 3
Ensure continued sustainability of the EM system by prioritizing and formalizing a cyclical approach to EM.
Management response
Management agrees with this recommendation.
| Action plan | Deliverables | Expected completion date | Accountability | Resources |
|---|---|---|---|---|
| 1. Continue to build and strengthen the public health EM system at PHAC by strengthening the various components of the EM cycle, aligning activities under each component, and better integrating the various activities with each other. | 1.1 Launch an interactive tool to make lessons learned from past events available to a broader audience in a timely manner. | 1.1 November 2024 | DG CEP; VP ROEMB | 1.1 Existing resources |
| 1.2 Track the response to approved recommendations from after action reviews in a way that enables more seamless integration with exercise design and keystone plan updates. | 1.2 May 2025 | 1.2 Existing resources | ||
| 1.3 Re-launch risk and capability assessment process and complete first cycle helping to identify gaps in preparedness for future health emergencies and actively link to preparedness activities, including training and exercises. | 1.3 June 2025 | 1.3 Existing resources | ||
| 1.4 Create an evaluation framework and implement a systematic approach to enable continuous improvement of GPHIN products and services. | 1.4 April 2025 and ongoing | 1.4 Existing resources and PHAC Renewal Phase 2 | ||
1.5 Develop and maintain policies and standard operating procedures to support public health intelligence activities. For example:
|
1.5 April 2025 and ongoing | 1.5 Existing resources and PHAC Renewal Phase 2 |
Appendix A: Financial information
| Centre or activity | Year-end budget | Actual spending | Total variance | % of budget spent |
|---|---|---|---|---|
| CEP | $95,035,978 | $77,480,852 | $17,555,126 | 82% |
| Regular Activities | $77,808,155 | $62,239,358 | $15,568,797 | 80% |
| COVID Activities | $17,227,823 | $15,241,494 | $1,986,329 | 88% |
| CER | $33,252,204 | $31,788,470 | $1,463,734 | 96% |
| Regular Activities | $12,098,610 | $10,236,343 | $1,862,267 | 85% |
| COVID Activities | $21,153,594 | $21,552,127 | -$398,533 | 102% |
| NESS | $8,912,869,422 | $5,729,158,491 | $3,183,710,931 | 64% |
| Regular Activities | $430,559,712 | $394,642,753 | $35,916,959 | 92% |
| COVID Activities | $8,482,309,710 | $5,334,515,738 | $3,147,793,972 | 63% |
| EMB VPO | $1,434,384 | $3,225,877 | -$1,791,493 | 225% |
| Regular Activities | $117,172 | $1,331,203 | -$1,214,031 | 1136% |
| COVID Activities | $1,317,212 | $1,894,674 | -$577,462 | 144% |
|
Notes:
|
||||
| Region | Year-end budget | Actual spending | Total variance | % of budget spent |
|---|---|---|---|---|
| Atlantic | $1,084,629 | $893,431 | $191,198 | 82% |
| Quebec | $1,170,586 | $1,249,095 | -$78,509 | 107% |
| Ontario | $1,127,454 | $1,189,103 | -$61,649 | 105% |
| Manitoba and Saskatchewan | $1,450,662 | $1,311,546 | $139,116 | 90% |
| Western | $1,430,144 | $1,100,057 | $330,087 | 77% |
| Northern | $1,243,094 | $1,058,513 | $184,581 | 85% |
| Total | $7,506,569 | $6,801,744 | $704,825 | 91% |
|
Notes:
|
||||
| Year | Regular | COVID | Total spending |
|---|---|---|---|
| 2019-20 | $554,803.63 | $18,073.88 | $572,877.51 |
| 2020-21 | $933,089.88 | $106,602.63 | $1,039,692.51 |
| 2021-22 | $452,665.20 | $833,113.81 | $1,285,779.01 |
| 2022-23 | $660,691.98 | $1,200,402.37 | $1,861,094.35 |
| 2023-24 | $2,187,965.47 | $0.00 | $2,187,965.47 |
| Grand total | $4,789,216.16 | $2,158,192.69 | $6,947,408.85 |
Appendix B: Evaluation description
This evaluation focused on achievement of the Emergency Preparedness and Response (EPR) Program's outcomes, and efficiency of PHAC emergency management from 2019-20 to 2023-24. The analysis covered primary data collection through key informant interviews, financial data, document review, and case studies. Most of the review was conducted from January to June 2024. Therefore, the report does not account for studies published after that period.
Evaluation questions
The following questions were developed based on program considerations and used to guide the evaluation process in measuring achievement of program outcomes:
- How effective and reliable is our public health emergency preparedness and response system?
- There are 3 questions that were developed:
- Are public health events and emergencies prepared for, detected, and responded to in a timely basis?
- Are elements in place (such as governance, roles and responsibilities, plans, processes, coordination mechanisms, equity and official languages considerations) supporting effective execution of all hazards response and operations?
- Is the NESS mandate clear and understood? Are holdings reflective of that mandate?
- How efficient are the current approaches to mobilize the Agency response to an event?
- There are 2 questions that were developed:
- Have emergency management activities (surge capacity, NESS, activations, training) improved over time? Have we reached a steady and sustainable state? Are there tools missing (such as IM/IT).
- What progress has been made on the various recommendations made over the past few years?
Methods
The evaluation collected and analyzed multiple lines of evidence provided by the program areas as well as external sources, as described in this section. These lines of evidence were triangulated to improve the reliability and credibility of evaluation findings and conclusions. The evaluation team collected data using various sources and methods, including:
Document and file review: Evaluators reviewed approximately 450 files, including both internal and public documents submitted by ROEMB and the regions. These documents included annual reports, work plans, examples of deliverables, administrative files, guiding policies, briefing materials, and summary reports.
Interviews: Interviews were conducted with 79 representatives from the following groups:
- Internal PHAC EPR Program: EMB: 32; Regional EPR: 7; NMLB: 2;
- Internal Partners: IDVPB: 9; CPAB: 6; CSB: 2;
- External Stakeholders/Partners: OGD: 11; P/T: 6
Case studies: Evaluators conducted a focused review of program documents and interviews for the 2023 Wildfire Response and the Mpox case study. For the wildfire case study, evaluators conducted interviews within PHAC (14) and HC (10) to access all key functions. They also reviewed approximately 115 documents associated with the 2023 wildfire activation. For the Mpox case study, the evaluators reviewed a few key documents and conducted four interviews with PHAC staff that were mobilized as part of the response.
Comparative analysis: Evaluators conducted a comparative analysis with other international jurisdictions. Various aspects of emergency preparedness and response programs were compared from mandates to program plans and governance models.
Performance measurement data: Performance indicators were reviewed across multiple sources including, PIPs, the WHO's IHR SPAR, and PHAC's Emergency Management Maturity Model. The data was then analyzed for key trends and results against established targets, when possible. See Appendix F for a summary of the program's performance results.
Financial analysis: Planned versus actual expenditures for EPR activities were reviewed and analyzed for CER, CEP, and NESS. The funding data was also broken down to analyze spending variances and key trends for each region.
Limitations and mitigation strategies
Despite triangulation across various lines of evidence, most evaluations still face constraints that may affect the validity and reliability of findings and conclusions. Table 9 outlines the limitations encountered during the current evaluation, as well as mitigation strategies put in place to ensure evaluation findings were sufficiently robust.
| Limitations | Potential impact | Mitigation strategies |
|---|---|---|
| The COVID-19 pandemic affected many departments and agencies across the Government of Canada, requiring mobilization of priorities and resources. | A shift in resources and focus on COVID-19 response had an impact on planned deliverables, as well as availability of certain performance data. | Administrative data and evidence from other sources, such as interviews, were used to fill any gaps and to estimate the impact of COVID-19 on planned deliverables and expected results. When possible, financial data for regular activities and COVID-19 activities were analyzed separately. |
| There were several gaps in the performance measurement data collected by the program during the COVID-19 response and the revisions made during the scope of the evaluation. | Trend analysis for most of the performance indicators was not possible. | In 2023, the EPR program implemented a maturity model framework to regularly track progress on the five key emergency management (EM) components of the model: 1) governance and structure 2) surveillance and risk assessment 3) plans and procedures 4) sustainment and continuous improvement and 5) EM financing. This data was used to inform the evaluation and triangulated with other lines of evidence, including the World Health Organization International Health Regulations State Party Self-Assessment Report (limited due to self-report). |
| Key informant interviews are retrospective in nature, providing only a recent perspective on past events. | This could influence the validity of respondents' assessment of activities or results that may have changed over time. | The other lines of evidence were triangulated with the data received from interviews to substantiate or provide further information. Document review also provided corporate knowledge. |
| Most of the interviews were conducted with PHAC EPR program areas and internal partners. Given the timing of the evaluation coinciding with the start of the 2024 Wildfires season, as well as recent consultations taking place as part of other reviews, only a few external interviews were conducted. | Some perspectives may not have been captured, and those shared may not always be representative of all external partners. | To facilitate the evaluation and support the assessment of how the program works with its PT partners, the Office of Audit and Evaluation requested any PHN, SAC, or LAC "What We Heard Reports" or lessons learned related to emergency preparedness and response activities implicating PHAC. Recent survey results of LAC members were shared, analyzed and triangulated with other lines of evidence to capture additional external perspectives on collaboration and governance. |
| Financial data broken down by centre for 2019-20 was not available. Moreover, planned spending data was not available by centre for 2020-21, which limited the variance analysis at the centre level for the full five-year evaluation period. | The evaluation was unable to assess the financial data by centre for the full five-year evaluation scope. | Variance analysis at the centre-level was undertaken with available data for the last three years of the evaluation scope period to get a sense of the spending across each area. Additionally, financial data combining all centres was available for all years of the evaluation period and was used to get a broader sense of planned and actual spending. See Appendix A. |
| Key deliverables such as the mobilization framework, SGBA+ plan and NESS CMP were either in development or approvals during the evaluation. | The evaluation was unable to review finalized products, their implementation as well as the results or impacts of these. | Recent draft documents and briefing decks were reviewed as much as possible when they became available. |
Evaluation lenses
The evaluation applied an SGBA+ lens in its assessment of the EPR activities, including consideration of the importance of responsiveness to the needs of priority populations and the integration of health equity considerations in emergency preparedness and response. Official language considerations were also examined in the context of emergency response activities.
Additionally, in support of the United Nations' 2030 Agenda for Sustainable Development and the UN Sustainable Development Goals (SDG), PHAC's EPR activities contribute to SD3: "Good Health and Well-Being", in particular indicator 3.D, related to strengthening the capacity of all countries for early warning, risk reduction, and management of national and global health risks. For example, the Health Portfolio Operations Centre (HPOC) provided countries with technical assistance and tools to meet commitments under the International Health Regulations (IHR). Moreover, the National Emergency Strategic Stockpile's (NESS) lifecycle management practices is mindful of waste reduction and recycling and contributes to advancing SDG 12: "Responsible Consumption and Production" by protecting assets from degradation through sustainable consumption and production.
Appendix C: Exercises by activation centre
| Exercises by fiscal year | NMLB-EOC | HPOC | RECCs |
|---|---|---|---|
| 2019-2020 | |||
| BCP Exercise - Live Exercise (Pacific Led) | Yes | No | Yes |
| Train Derailment Full Scale Live Regional Exercise | No | No | Yes |
| Ex Firedrake | Yes | No | No |
| FESTI | Yes | No | No |
| Exercise Nexus Vitalis - led by Public Safety SK | No | No | Yes |
| North Dakota/Manitoba US/Canada - Measles at the Canadian Border Table Top Exercise (TTX) - CDC led - July 12, 2019 | No | No | Yes |
| Gathering for Health and Cultural Safety During Evacuations Exercise - Led by ISC and Indigenous organizations in Manitoba - March 20 & 21, 2019 | No | No | Yes |
| Flood Season Scenario Led Discussion Exercise - Manitoba - March 26, 2019 | No | No | Yes |
| Intentional Threat Discussion Exercise Saskatchewan - June 19, 2019 | No | No | Yes |
| Operation Nanook Tatigiit | No | No | Yes |
| 2020-2021 | |||
| Opération Cannetons | No | No | Yes |
| 2021-2022 | |||
| COVID-19 Potential Scenarios TTX | No | Yes | No |
| Regional Exercise: Microbiological Emergency Response Team (MERT) - led by RCMP | Yes | No | No |
| MB FNIHB Wildfire TTX - PHAC facilitated - August 26, 2021 | No | No | Yes |
| Exercise Huron Endeavour WOG | No | No | Yes |
| Cleared for Landing TTX Quarantine Exercise with Winnipeg Airport - PHAC led -August 31, 2021 | No | No | Yes |
| Broken Arrow Exercise - Regina Airport TTX - Led by PS Canada - September 27, 2022 | No | No | Yes |
| Pandemic Preparedness Exercise - 4th Wave TTX - led by Regional PS Canada- November 2021 | No | No | Yes |
| Return of International Travelers to Saskatchewan Airport Tabletop Exercise - Regina and Saskatoon - PHAC Led - Nov 29 & 30, 2021 | No | No | Yes |
| EX SYNERGY CHALLENGE | No | No | Yes |
| EPR officer participated as an extra for a Mass Casualties at YUL airport | No | No | Yes |
| Operation Nanook Tatigiit | No | No | Yes |
| 2022-2023 | |||
| QUAD Ex CAPEX17 - Sarum Solstice | Yes | No | No |
| "Exercise Broken Arrow" Full Scale Crash Live Exercise Regina Airport - Airport/PS Canada led - Sept 27, 2022 | No | No | Yes |
| Regional Exercise: Microbiological Emergency Response Team (MERT) - led by RCMP | Yes | No | No |
| Exercise Door Crasher | No | No | Yes |
| COP15 TTX | No | Yes | No |
| R U The Key Master | Yes | No | No |
| Arctic Thaw TTX | No | Yes | No |
| H5N1 TTX | No | Yes | No |
| CANPOSE | Yes | No | No |
| MB FNIHB Overland Flood TTX - PHAC facilitated - Apr 26 & May 19, 2022 | No | No | Yes |
| Operation Nanook Tatigiit | No | No | Yes |
| 2023-2024 | |||
| Regional Exercise: Microbiological Emergency Response Team (MERT) - led by RCMP | Yes | No | No |
| Exercise Fire and Lightning TTX | No | Yes | No |
| MB FNIHB Wildfire TTX - PHAC facilitated - May 4 & 11, 2023 | No | No | Yes |
| Rise of the Drones - Regina Airport TTX - Led by Regina Airport/PS Canada - Oct 11, 2023 | No | No | Yes |
| Rail/Chemical Disaster Exercise Large TTX - Led by City of Winnipeg - November 16 & 17, 2023 | No | No | Yes |
| CAF TTX Exercise Juno - CAF Led - March 8, 2024 | No | No | Yes |
| Coastal Response 2023 | No | No | Yes |
| Exercise Tail Spin | No | No | Yes |
| Winnipeg Airport Crash Scenario Live exercise - Oct 10, 2023 | No | No | Yes |
| EX CLOUDY SKIES | No | No | Yes |
| Operation Nanook Tatigiit | No | No | Yes |
| GOARN RRML IFX (Berlin, Germany) | Yes | No | No |
| GOARN RRML IFX.01 (Istanbul Türkiye) | Yes | No | No |
| GOARN RRML IFX.02 (Kachreti, Georgia) | Yes | No | No |
| Total | 12 | 5 | 31 |
Appendix D: Emergency management maturity model
The aim of the maturity model is to assist PHAC with the identification, development, tracking and continuous improvement of the components and elements that make up the Agency's Emergency Management Program. For ease of implementation, the model is divided into five key emergency management program components: plans, procedures and programs; sustainment and continuous improvement; governance and structure; emergency management finance; and surveillance and risk assessment.
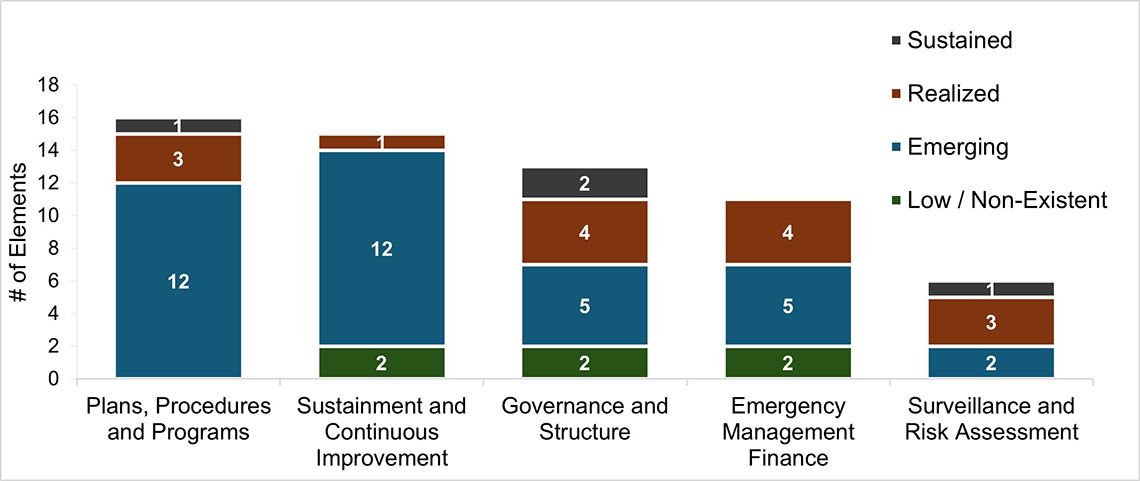
Figure 3: Text description
Figure 3 is a vertical stacked bar chart that shows the number of Emergency Management Maturity Model active elements by ranking and component, as of Spring 2024. Each column represents one of the Model's five components. Each segment within the columns represents the number of elements by ranking. In the figure, each ranking has its own shade of teal. Starting from the left side of the chart, the columns are presented as follows, from the component with the most elements to the least:
- Column 1: Plans, Procedures and Programs
- Emerging: 12
- Realized: 3
- Sustained: 1
- Column 2: Sustainment and Continuous Improvement
- Low/Non Existent: 2
- Emerging: 12
- Realized: 1
- Column 3: Governance and Structure
- Low/Non Existent: 2
- Emerging: 5
- Realized: 4
- Sustained: 2
- Column 4: Emergency Management Finance
- Low/Non Existent: 2
- Emerging: 5
- Realized: 4
- Column 5: Surveillance and Risk Assessment
- Emerging: 2
- Realized: 3
- Sustained: 1
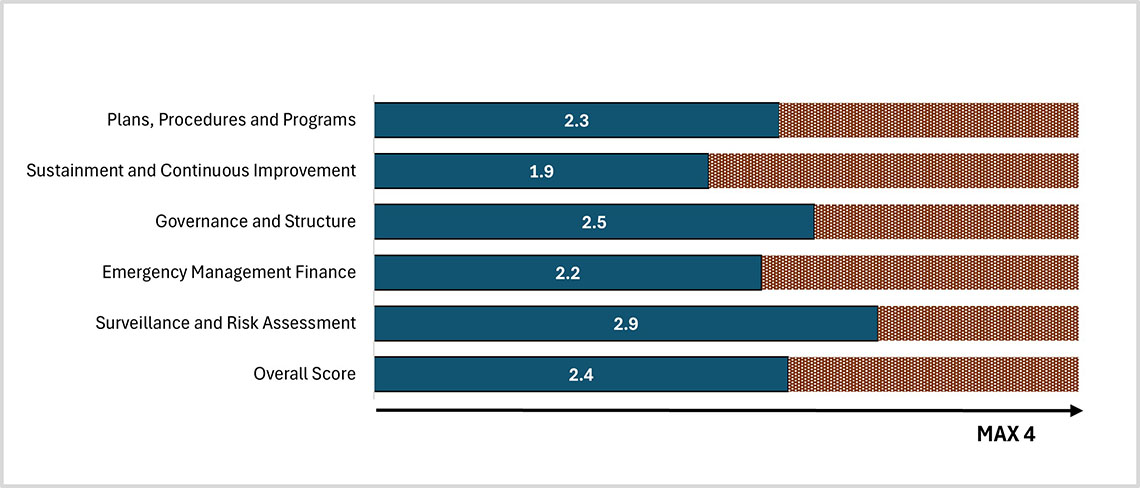
Figure 4: Text description
Figure 4 is a horizontal bar chart showing the average maturity ranking by component as of Spring 2024. Each bar represents a component and shows the average score against the maximum score of 4. Starting from the top and going down, each horizontal bar is summarized as follows:
- Plans, Procedures and Program: 2.3 out of 4
- Sustainment and Continuous Improvement: 1.9 out of 4
- Governance and Structure: 2.5 out of 4
- Emergency Management Finance: 2.2 out of 4
- Surveillance and Risk Assessment: 2.9 out of 4
- Overall Score: 2.4 out of 4
Appendix E: The emergency management cycle
Figure 5: Text description
Figure 5 is a diagram titled "Public Health Emergency Management Cycle". It is divided into four interconnected quadrants, each representing a distinct phase of the cycle with various activities as follows, starting from the top left:
- Prevent and Mitigate : Eliminate or reduce the public health impacts of events
- Security and Intelligence Analysis
- Public Health Emergency Management Capacity
- Early Warning System
- Prepare: Be ready to respond to an event and manage its public health consequences
- FPT Engagement
- Maintain Stockpile
- Threat and Capability Assessment
- Training and Exercises
- Emergency Management Plans
- Respond: Act during an event to manage its public health consequences
- Governance (Federal, National)
- Field Services (FPT Supports)
- Supplies and Equipment (FPT Surge Supports)
- Health Portfolio 24/7 Operations Hub
- Recover: Restore conditions after an event
- De-escalation
- Replenish Stockpile
- After Action Review
- Lessons Learned
Appendix F: Program performance measurement
Performance data for most indicators were not collected during the COVID-19 pandemic. As a result, many of the indicators for the first three years of the evaluation scope are not applicable (N/A). Some indicators were also revised or added in fiscal year 2022-2023. These are identified in the table notes.
| Output indicators | 2019-2020 | 2020-2021 | 2021-2022 | 2022-2023 | 2023-2024 |
|---|---|---|---|---|---|
| Percentage of exercise participants that self-identify as better prepared to perform their response role as a result of participating in a Health Portfolio exercise | 85% | N/A | N/A | 85% | 85% |
| Percentage of EMB risk and capability assessments completed for risks identified as priorities in a fiscal year Note: Indicator revised in 2023, hence the change in value. |
20% | N/A | N/A | 100% | 100% |
| Percentage of HP-led plans and guidelines updated within established review cycle timelines Note: Indicator revised in 2023, hence the change in value |
95% | N/A | N/A | 50% | 33% |
| Percentage of emergency management exercise objectives met, as set out in the exercise development plan | 90% | N/A | N/A | 90% | 100% |
| Percentage of IHR-related communications provided to stakeholders within defined timelines Note: New indicator added in 2023. Previous results data not available. |
N/A | N/A | N/A | 100% | 100% |
| Percentage of GPHIN notifications and alerts provided to stakeholders within defined timelines Note: New indicator added in 2023. Previous results data not available. |
N/A | N/A | N/A | 90% | 100% |
| Percentage Request for Information (RFI) completed by Public Health Security and Intelligence Division to support specific information needs of internal and external partners and stakeholders Note: New indicator added in 2023. Previous results data not available. |
N/A | N/A | N/A | 80% | 80% |
| Percentage of applicable recommendations implemented, related to activations, that are identified post-event through the recovery process Note: Revised indicator in 2023. Previous results data not available. |
N/A | N/A | N/A | 90% | 90% |
| Percentage of Field Epidemiologists that meet CFEP competencies profile at graduation Note: New indicator added in 2023. Previous results data not available. |
N/A | N/A | N/A | 100% | 100% |
| Percentage of Public Health Officer (PHO) placement sites self-reporting improved ability to deliver core public health functions as a result of PHO support in the last year Note: New indicator added in 2023. Previous results data not available. This indicator is being piloted with the Substance-Related Harms stream of the Canadian Field Services Program (CPHS) with the aim to expand the methodology to remaining streams next year. |
N/A | N/A | N/A | 85% | 64% |
| Capacity to deploy assets during a public health event | 100% | N/A | N/A | 100% | 100% |
| Immediate outcome: Public health emergency preparedness is sustained | |||||
| Level of Canada's preparedness to respond to public health events and emergencies as assessed by World Health Organization criteria Note: Data from 2019-20 to 2022-23 has been taken from DRRs. New data source for 2023-24, hence the change in value. New data source is the WHO IHR Monitoring and Evaluation Framework mandatory State Party Annual Self-Assessment Report (SPAR) C7.1 |
90% | 90% | 90% | 90% | 95% |
| Percentage of online trainings developed in the last year that are bilingual and have undergone accessibility and health equity reviews Note: New indicator added in 2022-23. Previous results data not available |
N/A | N/A | N/A | 100% | 100% |
| Immediate outcome: Public health events and emergencies are detected and reported on a timely basis | |||||
| Capacity for timely reporting of a potential public health emergency of international concern and an unusual or unexpected public health event Note: Indicator slightly revised in 2023. |
100% | N/A | N/A | 100% | 100% |
| Capacity to activate emergency response operations during a public health emergency | 100% | N/A | N/A | 100% | 100% |
| Intermediate outcome: Public health emergency preparedness and response capacity is improved | |||||
| Percentage of provincial and territorial requests for assistance (for deployment of Agency staff) responded to within negotiated timelines Note: This is a Departmental Results Framework indicator. Data from 2019-20 to 2022-23 has been taken from the Departmental Results Reports. |
100% | 100% | 100% | 100% | 100% |
| Percentage of provincial and territorial requests for assistance (for the provision of supplies) responded to within negotiated timelines Note: This is a Departmental Results Framework indicator. Data from 2019-20 to 2022-23 has been taken from the Departmental Results Reports. |
100% | 100% | 100% | 100% | 100% |
| Percentage of provincial and territorial requests for assistance (for inter-jurisdictional mutual aid for health care professionals, i.e., OFMAR) responded to within negotiated timelines Note: This is a Departmental Results Framework indicator. Data from 2019-20 to 2022-23 has been taken from the Departmental Results Reports. |
100% | 100% | 100% | 100% | 100% |
| Intermediate outcome: Public health emergency preparedness is sustained | |||||
| Percentage of response objectives met, as captured in Incident Action Plans (IAPs), during an activation Note: Indicator revised in 2023. Earlier data not available. |
N/A | N/A | N/A | 90% | 90% |
| Percentage of After-Action Reviews completed following a Health Portfolio response or exercise Note: New indicator added in 2023. Previous results data not available. Indicator has been revised for 2023: % of After-Action Reviews initiated within 6 months of an IMS de-escalation date. Change results in 100%. |
N/A | N/A | N/A | 90% | 100% |
| Ultimate outcome: A sustainable public health emergency preparedness and response system for Canada | |||||
| Canada's overall emergency preparedness and response score as determined by the WHO IHR Monitoring and Evaluation Framework/State Party Annual Self-Assessment Report (SPAR) Tool Note: New data source, hence the change in value. The indicator revised slightly in 2023. |
92% | N/A | N/A | 96% | 96% |
Endnotes
- Footnote 1
-
Public Health Agency of Canada. (2024). NESS Comprehensive Management Framework. Retrieved from: National Emergency Strategic Stockpile Comprehensive Management Plan - Canada.ca
- Footnote 2
-
Public Health Agency of Canada. (2023). Public Health Agency of Canada's COVID-19 Response: Lessons Learned prepared by the Office of Audit and Evaluation. Retrieved from: https://www.canada.ca/en/public-health/corporate/transparency/corporate-management-reporting/evaluation/covid-19-response-lessons-learned-summary.html
- Footnote 3
-
Public Health Agency of Canada. (2023). Health Portfolio Emergency Response Plan. Retrieved from: https://www.canada.ca/en/public-health/services/publications/health-risks-safety/health-portfolio-emergency-response-plan.html
- Footnote 4
-
Office of the Auditor General. (2021). Report 8 – Pandemic Preparedness, Surveillance, and Border Control Measures. Retrieved from: https://www.oag-bvg.gc.ca/internet/English/parl_oag_202103_03_e_43785.html
- Footnote 5
-
Public Health Agency of Canada. (2021). PHAC Management Response and Action Plan: In response to the recommendations of the Report 8 - Pandemic Preparedness, Surveillance, and Border Control Measures of the Auditor General of Canada to the Parliament of Canada. Retrieved from: https://www.ourcommons.ca/content/Committee/432/PACP/WebDoc/WD10867510/Action_Plans/PublicHealthAgencyOfCanada-2-e.pdf
- Footnote 6
-
In the Health Portfolio Emergency Response Plan (HP ERP), the role of the Centre for Surveillance, Integrated Insights and Risk Assessment (SIIRA) is discussed under the Centre former name, which was the Centre for Integrated Risk Assessment (CIRA).
- Footnote 7
-
Public Health Agency of Canada. (2023). Health Portfolio Emergency Response Plan. Retrieved from: https://www.canada.ca/en/public-health/services/publications/health-risks-safety/health-portfolio-emergency-response-plan.html
- Footnote 8
-
Public Health Agency of Canada. (2018). Operational framework for mutual aid requests (OFMAR). Retrieved from: https://publications.gc.ca/site/eng/9.828157/publication.html
- Footnote 9
-
Public Health Agency of Canada. (2024). NESS Comprehensive Management Framework. Retrieved from: https://www.canada.ca/en/public-health/services/emergency-preparedness-response/national-emergency-strategic-stockpile/comprehensive-management-plan.html
- Footnote 10
-
Office of the Auditor General of Canada. (2021). OAG Audit Report 10 – Securing Personal Protective Equipment and Medical Devices. Retrieved from: https://www.oag-bvg.gc.ca/internet/English/att__e_43841.html
- Footnote 11
-
Public Health Agency of Canada. (2023). Health Portfolio Emergency Response Plan. Retrieved from: https://www.canada.ca/en/public-health/services/publications/health-risks-safety/health-portfolio-emergency-response-plan.html
- Footnote 12
-
World Health Organization. (2024). IHR Score per capacity. Retrieved from: https://extranet.who.int/e-spar/Home/CapacityScoreDetails
- Footnote 13
-
Public Health Agency of Canada. (2018). Evaluation of Emergency Preparedness and Response Activities 2012-13 to 2016-17. Retrieved from: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/transparency/corporate-management-reporting/evaluation/2012-2013-2016-2017-evaluation-report-emergency-preparedness-response-activities/pub1-eng.pdf
- Footnote 14
-
Public Health Agency of Canada. (2024). NESS Comprehensive Management Framework. Retrieved from: https://www.canada.ca/en/public-health/services/emergency-preparedness-response/national-emergency-strategic-stockpile/comprehensive-management-plan.html