
Statement on prevention of Japanese encephalitis
Last partial content update
September 2024: The Japanese Encephalitis (JE) statement was updated to include additional guidance on the timeframe of JE vaccine booster dose administration in the Non-GRADE recommendations. This update also includes changes to Appendix 2 and Appendix 3, which provide country-specific information on JE transmission and risk areas.
Table of content
- Preamble
- Key Points/Messages
- GRADE Recommendations
- Basis of GRADE Recommendation for Vaccine Use
- Interpretation of GRADE Recommendations
- Non-GRADE Recommendations
- Introduction
- Background
- Methods
- Results
- General
- GRADE questions
- PICO questions
- Figure 1. Japanese Encephalitis vaccine seroconversion rate (SCR) in adults (95% confidence interval)
- Contextual questions
- Figure 2. Cumulative proportion of Japanese Encephalitis cases among travellers by duration of travel in days.
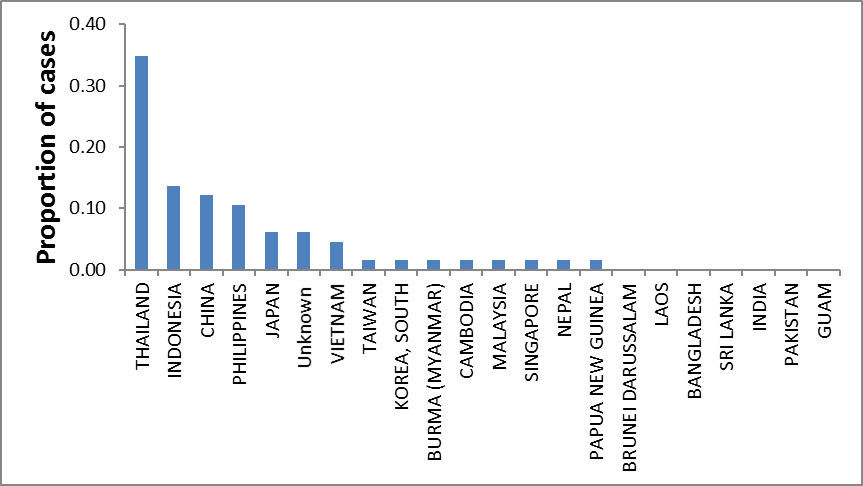
- Figure 3. Proportion of Japanese Encephalitis cases (N=66) among travellers by country of exposure
- Table 1: Estimated overall attack rate of clinical Japanese Encephalitis for 2006-2015. Based on Canadian travel statistics, the mean duration of travel to endemic areas was approximately 15 days.
- Table 2: Predicted JE event rates (clinical cases, long-term sequelae and deaths) with and without JEV if overall risk is 1 case/11.65 million trips. Expressed as attack rate per 10 million trips to endemic areas.
- Table 3: Number needed to vaccinate to prevent a case, long-term sequelae and death at our JEV recommendation threshold (1 case/100,000 trips) and at the estimated overall risk (1 case/11,650,000 trips) of JE for Canadian travellers1.
- Non-GRADE questions
- Conclusions and Research Needs
- Acknowledgements
- Conflict of Interest
- References
- Appendix 1. Summary of findings for comparison of JEV to placebo: Adverse events (AE)
- Appendix 2. Geographic distribution of Japanese encephalitis
- Appendix 3. Country-specific1 notes on Japanese encephalitis
- Appendix 4. Analytic framework for Japanese encephalitis vaccine (JEV)
- Appendix 5. Sample search strategy
- Appendix 6. Summary of findings for comparison of JEV and inactivated mouse-brain derived vaccine (MBV): Seroconversion rate (SCR) and adverse events (AE)
- Appendix 7. Summary of findings for comparison of conventional immunization schedule for JEV (0, 28 days) to accelerated schedule (0, 7 days): Seroconversion rate (SCR) and adverse events (AE)
- Appendix 8. Summary of Advisory Committee on Immunization Practice (ACIP) GRADE results
- Appendix 9. Quality assessment for risk of Japanese encephalitis in travellers from Canada, the United States and Europe
- Appendix 10. Factors to consider when evaluating a traveller's risk for Japanese encephalitis (JE) virus exposure
- Appendix 11. Study summaries considered for inclusion in GRADE analysis
Preamble
The Committee to Advise on Tropical Medicine and Travel (CATMAT) provides the Public Health Agency of Canada (PHAC) with ongoing and timely medical, scientific, and public health advice relating to tropical infectious disease and health risks associated with international travel. PHAC acknowledges that the advice and recommendations set out in this statement are based upon the best current available scientific knowledge and medical practices, and is disseminating this document for information purposes to both travellers and the medical community caring for travellers.
Persons administering or using drugs, vaccines, or other products should also be aware of the contents of the product monograph(s) or other similarly approved standards or instructions for use. Recommendations for use and other information set out herein may differ from that set out in the product monograph(s) or other similarly approved standards or instructions for use by the licensed manufacturer(s). Manufacturers have sought approval and provided evidence as to the safety and efficacy of their products only when used in accordance with the product monographs or other similarly approved standards or instructions for use.
Key Points/Messages
- Japanese encephalitis (JE) is a potentially fatal disease caused by a mosquito-transmitted virus. It is endemic through much of Asia and also occurs in parts of Oceania.
- Since 1973 there have been 66 cases of JE reported among Western travellers and expatriates including 2 cases among Canadian travellers. The overall risk of JE among travellers is estimated to be negligible, i.e. < 1 case/10,000,000 trips. Even allowing for 10-fold underreporting of JE cases, overall risk is estimated to be negligible, i.e. approximately 1 case/1,000,000 trips.
- The only JE vaccine (JEV) currently available in Canada is IXIARO®, an inactivated Vero cell culture-derived vaccine licenced for individuals aged 2 months of age and olderFootnote 1.
- Following a systematic review of the literature, recommendations for use of JEV were developed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology. Assessment focused on benefits and harms of JEV, use of an accelerated vaccination schedule, and use of JEV in children.
- No evidence on the values and preferences of travellers or health care providers related to use of JEV were found. However, there is evidence to indicate that some patients (including travellers) will choose and pay for vaccine-based protection against rare (e.g. a risk of 1/100,000), but serious diseases. Based partly on this evidence, CATMAT used a per trip risk for a case of JE of 1/100,000 as the threshold at which the majority of travellers would accept the harms, cost and inconvenience of JEV vaccination.
- Because the overall per trip JE risk estimate (< 1 case/10,000,000 or approximately 1 case/1,000,000 with 10-fold underreporting) is substantially less than this threshold, we suggest that JEV not be routinely used for travel to endemic areas.
- In some circumstances, based on factors that are thought to increase risk (e.g., rural exposure, repeated travel to risk areas, longer cumulative duration of travel (e.g., > 30 days), travel in areas suffering an outbreak), JEV will be of relatively greater absolute benefit and more travellers will likely choose to receive it.
GRADE Recommendations
When to use JEV
- CATMAT suggests that JEV (IXIARO®) not be routinely used for travel to endemic areas
(Conditional recommendation against [see Text Boxes 1 and 2 for what CATMAT suggests this means]; moderate confidence in estimate of effect)- For the large majority of travellers, the likelihood of developing clinical JE in endemic areas (see Table 1) is negligible (overall per trip attack rate estimated at approximately 1/10,000,000) as is the estimated absolute benefit of JEV (moderate confidence, intermediate risk of bias due to possibility of unreported clinical cases). Balanced against cost, inconvenience and the potential risk of adverse effects, most travellers would choose not to receive JEV in this situation.
- The relative likelihood of acquiring JE is likely elevated for some populations (e.g., long-term travel, exposure in rural areas, multiple trips to endemic areas and/or travel to an area suffering an outbreak) and more travellers would choose to receive vaccine in such circumstances (Risk factor evidence was not evaluated using GRADE, see below for explanation).
- Because this recommendation is conditional, there is a need for providers to discuss with the traveller the anticipated benefits and harms (including financial costs) associated with JEV to help the traveller reach a decision that is consistent with their own values and preferences. The discussion should include potential alternative and/or complementary strategies (e.g., use of personal protective methods against mosquito bites) to vaccination.
- See Text Box 3 for a list factors that influence decision-making related to JE vaccine.
- For more information on how CATMAT arrived at this recommendation, see "Basis of GRADE Recommendation for Vaccine Use".
Vaccine administration
The licensed primary adult schedule for JEV in Canada is 2 doses spaced 28 days apartFootnote 1.
- CATMAT suggests use of an accelerated (0 and 7 days) schedule for adults aged 18-65 if there is insufficient time to immunize travellers with the normal primary schedule (0 and 28 days)
(Conditional recommendation for; moderate confidence in estimate of effect)- This accelerated schedule has been approved for use in CanadaFootnote 1 and EuropeFootnote 2.
- The accelerated schedule elicited similar levels of seroconversion and adverse effects as the normal schedule.
- CATMAT suggests that JEV (normal schedule) can be used in children aged 2 months to <18 years
(Conditional recommendation for; moderate confidence in estimate of effect)- This normal schedule has been approved for use in children (2 months to <18 years) in CanadaFootnote 1 and is also approved in the United StatesFootnote 3.
- Seroconversion rates and rates of adverse effects were found to be similar in adults and children.
- Children aged 2 months to <3 years of age are recommended to receive a reduced dose of vaccine (0.25 ml) compared to older children and adults (0.5 ml)Footnote 1Footnote 4.
- While a normal schedule is preferred, an accelerated schedule can be considered (off-label) for children where there is not sufficient time to complete the normal schedule.
Basis of GRADE Recommendation for Vaccine Use
Quality of the Evidence
- Vaccine efficacy:
- moderate confidence in estimate of effect
- Vaccine harms:
- moderate to high confidence in estimate of effect
- Baseline risk of developing JE among travellers:
- moderate confidence in estimate of risk
- Risk factors for JE:
- insufficient evidence to assess with GRADE
- Values and Preference:
- insufficient evidence to assess with GRADE
Summary of Balance of Benefits and Harms
JEV (IXIARO®) is expected to provide a high level of protection (>95%) against JE (Figure 1). Further, it is a well-tolerated vaccine. In the pivotal safety trialFootnote 5, JEV had a similar AE profile to placebo, though minor AE, e.g., pain at injection site, are common (Appendix 1; moderate to high confidence in the estimates of effect). The exception was itching, which occurred less often (RR 0.52; 95% Confidence Interval [CI] 0.29 to 0.92) with JEV than compared to placebo.
However, as with other vaccines, rare but serious AE are possible. This last point becomes increasingly important with decreasing JE risk in that it increases the possibility that rare but serious AE will be more prevalent than JE cases averted through immunization.
There were 42 AE following JEV immunization reported to the US Vaccine Adverse Event Reporting System (VAERS) for the period of 2009-2012Footnote 6. The majority of these (25/42) were reported after a patient had received several immunizations including JEV. Using an estimated 275,848 doses of vaccine distributed, the overall AE rate was 15.2/100,000 doses; and the serious AE rate was 1.8/100,000 dosesFootnote 6. The most commonly reported serious AE were hypersensitivity reactions (0.7/100,000 doses). No cases of anaphylaxis or death were reported. Recently VAERS published an update on AE events reported during the period 2012-2016. There were 119 AE reported following JEV immunization. Using the estimated 802,229 doses of vaccine distributed, the overall AE rate during this time period was 14.8/100,000 doses. There were 9 serious AE reported for a rate of 1.1/100,000 doses. Serious AE included 1 report of anaphylaxis and 1 death (cardiac death due to ischemic heart disease)Footnote 7. Importantly, reports to VAERS do not necessarily imply causal relationships.
For most travellers to endemic areas, the likelihood of acquiring JE is negligible (estimated at approximately 1 clinical case/10 million trips) (Table 1) and the number needed to vaccinate (NNV) to prevent a case is correspondingly high, e.g., > 10,000,000 (see Tables 2 and 3). The median trip duration for travel to endemic areas was estimated to be approximately 2 weeks (see Figure 2).
At the estimated overall JE attack rate among Canadians traveling to endemic areas of 1 clinical case/11,650,000 (95% CI [1/2,056,512 to 1/65,996,483]) person trips (median trip duration estimated to be 15 days), the number needed to vaccinate (NNV) to prevent 1 clinical case of JE, 1 severe sequelae from JE or 1 JE related death is approximately 12 million, 33 million and 49 million, respectively (see Tables 2 and 3). At this same risk of disease, approximately 5 million mild AEs would be expected to occur.
We did not identify JEV-specific evidence on traveller values and preferences. However, there is evidence to indicate that some patients (including travellers) will choose and pay for vaccine-based protection against rare (e.g. a risk of 1/100,000), but serious diseasesFootnote 8Footnote 9.
The risk threshold should take into account patient values and preferences, risk of JE, the effectiveness and safety profile for JEV, and cost and inconvenience associated with the vaccineFootnote 10. In the absence of JEV-specific evidence on patient values and preferences, the committee judged that most travellers would be willing to accept the harms, cost (currently several hundred dollars) and inconvenience of vaccination if JEV risk was 1/100,000 or higher, but not at lower risks. This threshold for vaccine use is several orders of magnitude higher than the overall risk estimate for JE. Thus, we recommend against routine use of JEV for travel to endemic areas.
Certain populations, e.g., long term travellers (e.g., >30 days), travellers who make multiple trips to endemic areas, persons staying for extended periods in rural areas, persons visiting an area suffering a JE outbreak area, are likely at relatively higher risk for JE (see below section on risk factors). Due to the severity of potential consequences of JE, and the absence of specific treatments, it is plausible that individuals who are so affected would be more likely to choose to receive JEV.
Why is the recommendation a conditional recommendation?
The recommendation for use of JEV is conditional. This reflects, among other things, the poorly defined impact of risk factors such as destination, seasonality, travel itinerary and duration of stay on JE risk, and our belief that travellers could have divergent values and preferences (including willingness to pay) related to use of JEV. For a more detailed discussion of what a conditional recommendation means in the context of JE, see Text Box 2.
Interpretation of GRADE Recommendations
| Category of GRADE-based recommendation | Implication for practitioners |
|---|---|
StrongFootnote * recommendation for |
The balance of risks and benefits are such that most travellers would choose the intervention. |
Strong recommendation against |
The balance of risks and benefits are such that most travellers would not choose the intervention. |
ConditionalFootnote ** recommendation for |
With a conditional recommendation different travellers may make different choices. Practitioners should present the risks and benefits of the intervention and help each traveller make a decision consistent with his/her values and preferences. |
Conditional recommendation against |
With a conditional recommendation different travellers may make different choices. Practitioners should present the risks and benefits of the intervention and help each traveller make a decision consistent with his/her values and preferences. |
|
|
Text Box 2: What does a conditional recommendation mean in the context of JEV?
GRADE-based recommendations for JEV are "conditional". This means that the majority of well-informed travellers to endemic areas would choose the recommended course of action and not use JEV. However, it also means that some travellers would choose to receive JEV. Reasons for making recommendations conditional include the very low overall risk of travel-associated JE, the poorly defined impact of risk factors such as destination, seasonality, travel itinerary and duration of stay, and our belief that travellers could have divergent values and preferences related to use of JEV.
Applied to individual travellers, our recommendations could result in the following types of joint (traveller and clinician) decisions:
- Persons staying in urban areas of endemic countries for relatively short periods (e.g., < 1 month) are estimated to have an extremely low risk for developing JE. In this situation and given the cost and inconvenience of vaccination, very few travellers would choose to receive JEV.
- Persons staying for longer periods in urban areas of endemic countries and/or who have short-term (e.g., ≤ 1 week) exposure in rural areas are estimated to have a relatively higher, but still extremely low risk of developing JE. Very few travellers would choose to receive JEV in this situation.
- Persons staying for longer periods (e.g., > 30 days) in endemic areas with exposure in rural areas during the risk season are likely to have a relatively higher, but still very low risk of developing JE. However, there might be some individuals in this population for whom relative risk is substantially elevated, e.g., because they are staying in a highly endemic area for an extended period. In this situation, many more travellers would choose to receive JEV, but also that many, for example based on values and preferences, would choose not to receive the vaccine.
Text Box 3: Points to consider when discussing JE vaccine (adapted from referenceFootnote 11)
Reasons that might increase likelihood that traveller would choose to be vaccinated
- analytic uncertainty, i.e. overall risk might be underestimated due to non-reporting of cases
- seriousness of disease, high case fatality rate and many survivors with serious sequelae
- relatively lower risk tolerance for "exotic" diseases
- travelling to known epidemic area
- longer duration stays, e.g., > 30 days in endemic areas with rural exposure
- extensive overnight exposure in rural environments
- repeated travel to risk areas (cumulative time)
- established safety profile for vaccine
- high level of vaccine efficacy
Reasons that decrease likelihood that traveller would choose to be vaccinated
- very low overall risk for large majority of travellers
- relatively higher risk tolerance for "exotic" diseases
- relatively high cost of vaccine
- urban/short-term travel
- concern about adverse effects related to vaccination in general
- inconvenience of vaccination, including multiple doses
- availability of alternative interventions, e.g. bite prevention methods
Non-GRADE Recommendations
- For Canadians (adults and children) who remain at risk and desire vaccine-induced protection, CATMAT suggests that a single booster dose of JEV be administered 12-24 months after the primary series and that a second booster is not required for at least 10 years.
- After a primary series, 80-95% of fully immunized vaccine recipients maintained an adequate immune response after 6 months and 58-83% maintained it at 12-15 months.
- After receipt of a booster dose, there is evidence that an adequate immune response persists for an extended period among adultsFootnote 12Footnote 13. CATMAT therefore suggests that additional booster doses are not necessary for at least 10 years after the initial booster in the situation where protection against JE is desired.
- Among children, evidence of long term seroprotection is limited but does suggest that antibody responses are at least as persistent in children as in adultsFootnote 14. For this reason CATMAT suggests that it is reasonable to follow the same recommended second booster approach for children (off-label) as for adults.
- CATMAT acknowledges that no direct data are available on the response to a first booster dose administered >24 months after the primary series of JE-VC (manufactured as IXIARO in Canada), but as a general principle of vaccinology, an interrupted vaccination schedule does not need to be restarted. In situations where the interval between the primary series and booster dose is longer than 24 months, the schedule should be resumed, without needing to repeat the primary series.
- In adults 65 years or older CATMAT suggests that a single booster dose of JEV be considered earlier (before 12 months) following the primary series.
- JEV is generally well tolerated in older patients although seroconversion rates are lower than in younger adultsFootnote 15.
- Assessment of the precise timing of vaccine administration should be done on a case-by-case basis if the traveller remains at risk for JE and wishes to receive protection.
- CATMAT recommends that, if an adult traveller wishes to receive JEV and if there is insufficient time to provide a normal or accelerated schedule, then an additional dose of vaccine can be provided with the first dose (on day 0).
- This is based on evidence showing that this approach achieves a seroconversion rate of approximately 60% by 10 days post-vaccination, compared to approximately 30% following a single dose. If this double dose approach is used, subsequent doses (if protection is still required) should be as per the normal schedule.
- CATMAT recommends that all travellers use personal protective measures (PPM) such as topical repellents, treated bed nets and/or treated clothing to prevent mosquitoes from biting.
- Recommendations related to PPM are provided in the CATMAT statement on Personal Protective Measures to Prevent Arthropod BitesFootnote 16.
Introduction
Japanese encephalitis (JE) is caused by a flavivirus transmitted by Culex mosquitoes. It is one of the most important causes of viral encephalitis in Asia, with an estimated 70,000 cases and up to 20,000 deaths annuallyFootnote 17 Footnote 18. Appendix 2 shows areas where JE is endemic, and Appendix 3 provides country-specific information related to risk areas and seasonality. There is no specific treatment for JEFootnote 4 but a JE vaccine (IXIARO®) is licenced for adults in CanadaFootnote 1. Immunization and/or use of personal protective measures (PPMs) against mosquito bites will provide substantial protection against diseaseFootnote 4 Footnote 17 Footnote 19 Footnote 20.
Background
Clinical and Epidemiological features
The likelihood of developing clinical disease after infection with JE virus is low (approximately 1/250)Footnote 21. If clinical disease develops (after an incubation period of 5 to 15 days), the prognosis is poor. Approximately 20-30% of patients die and, among survivors, about 50% will develop long term neurological and/or psychological sequelaeFootnote 19 Footnote 21. In endemic areas without a vaccination program, disease often occurs in childrenFootnote 22; whereas older adults, perhaps because of immune senescence, seem to be at greatest risk for disease in countries/areas with robust and long-standing immunization programsFootnote 21.
JE virus is maintained in a zoonotic cycle involving Culex mosquitoes and wild birds with pigs sometimes acting as amplification hostsFootnote 21. Risk is primarily in rural areas, and transmission can be year round with rainy season peaks (subtropical/tropical areas), or constrained to warmer periods of the year when the mosquito vectors are active (temperate areas)Footnote 17 Footnote 23. Appendix 3 summarizes transmission patterns in JE-endemic countries.
JE vaccine programs, changes in animal husbandry practices and/or increased urbanization has led to a substantial reduction in human cases of JE in some countries like Japan and KoreaFootnote 17 Footnote 23. However, JE still presents a risk to non-immune persons (e.g., travellers) in these countries because zoonotic transmission persists.
Vaccine
The only JE vaccine currently available in Canada is IXIARO®, an inactivated Vero cell culture-derived vaccine marketed in Canada by Valneva Canada and licenced for individuals aged 2 months of age and older. It is important that the product monograph for IXIARO®Footnote 1 be read by those who prescribe and/or inoculate this vaccine. Information regarding important features of IXIARO®is also summarized in the Canadian Immunization GuideFootnote 24.
Methods
General
This statement was developed by a CATMAT working group (WG) of volunteers, none of whom declared a relevant conflict of interest. The WG, with support from the secretariat, was responsible for: literature retrieval, evidence synthesis and analysis; development of key questions and draft recommendations and writing of the statement. The final statement and recommendations were approved by CATMAT.
The GRADE process was used to formulate some of the recommendations in this statement. Other recommendations in this statement did not use GRADE, for example those related to boostering or use of personal protective measures to prevent mosquito bites. This did not reflect an absence of evidence on these topics, but rather a decision on the part of the WG and broader committee to focus resources on clinical questions that were judged most likely to benefit by a GRADE-based evidence appraisal. For non-GRADE recommendations, advice was based on a narrative review of the relevant literature evidence and expert opinion. For more information on the CATMAT approach to developing recommendations and guidelines, see the statement on Evidence Based process for developing travel and tropical medicine related guidelines and recommendationsFootnote 10.
The following summarizes the process used to develop this statement and recommendations:
GRADE Recommendations
- An analytic framework identifying clinical preventive actions (interventions) and risk factors for JE was developed (Appendix 4).
-
From the analytic framework, the working group framed key concepts in the form of a PICO question (Population of interest, Intervention, Comparison, and Outcome) in order to develop focused GRADE-based recommendations. Evidence on efficacy and harms of JEV was considered for each PICO question.
The following PICO questions were identified:
- Among adult Canadian travellers, does use of JEV (normal schedule) decrease the risk of acquiring JE compared to no vaccine (placebo)?
- Among adult Canadian travellers, does use of an accelerated (0, 7 days) JEV schedule achieve levels of protection similar to or greater than a normal JEV schedule (0, 28 days)?
- Among Canadian children, does use of JEV achieve levels of protection similar to that observed in adult travellers, and is use of JEV associated with similar harms to adults?
- Other concepts from the analytical framework were identified to support the GRADE assessment but were framed as non-PICO questions. The following contextual questions were identified:
- What is the risk of clinical JE among Canadian travellers?
- What are the important risk factors for JE among Canadian travellers (e.g., destination, duration of travel)?
- What are the values and preferences of Canadian travellers regarding the magnitude of risk reduction in JE that would make use of JEV worthwhile given associated costs and inconvenience?
- Evidence was retrieved by performing searches in electronic databases (Ovid MEDLINE, Embase, Global Health, and Scopus) and by manually searching in Google for grey literature. Time period for the search was from earliest available to June 2015. There were 2 literature searches: 1. JE vaccine (efficacy and harms) and travellers and 2. Baseline risk of and risk factors for developing JE among travellers. Details on search strategies and dates are provided in Appendix 5. The inclusion and exclusion criteria were applied by 2 WG members to the identified studies, based on an initial screening of titles and abstracts. Studies were excluded if they appeared to be irrelevant, were not published in English or French, or were duplicates.
- From these searches, relevant literature was identified. If evidence specific to Canadian travellers was not available, then evidence derived from other Western populations or from other populations, in that order of preference, was extracted.
- Quality assessments were performed for: vaccine efficacy and adverse events (AE); and, risk of developing JE among travellers. Results were collated into summary of findings tables (see Appendices 5-7 and 9). We decided that there was insufficient evidence to subject the other questions to the GRADE process.
- Recommendations were developed taking into considerationFootnote 10:
- CATMAT's confidence in the estimates of effect for efficacy and JEV-associated AE;
- the balance of harms and benefits; and,
- CATMAT's judgement on the likely values and preferences of travellers and health care providers related to use of JEV.
Non-GRADE Recommendations
- Additional questions were identified that were not selected for GRADE review by the working group. They were:
- What is the appropriate boostering interval for JEV?
- Among older (aged > 65 years) Canadian travellers, does use of JEV achieve levels of protection similar to adult travellers?
- Does an additional dose of vaccine on day 0 achieve a higher seroconversion rate than a single dose?
- Do personal protective measures provide protection against bites from the type(s) of mosquitoes that transmit JE?
- Evidence relevant to these questions was identified through the previously-described literature search, or was extracted from existing CATMAT statements. Recommendations are based on a narrative review of the evidence and expert opinion.
Results
General
The literature search on JE vaccine and travellers identified 423 studies of which 310 were excluded. The risk factors for JE search identified 131 studies of which 127 were excluded. The remaining 117 relevant articles addressed vaccine harms and/or benefits (N= 36), booster dose (N=10), accelerated schedule (N= 4), pediatric use (N=6) and risk factors (N=4). As well, 57 studies addressing burden of disease (incidence, morbidity, mortality, hospitalizations) among travellers, population-specific risk factors (e.g., age), itinerary-specific risk factors (e.g., destination, duration of travel), efficacy of preventive measures (e.g., personal protective measures), and/or disease treatment/management were retained. After the literature review was completed, an additional study on values and preferences was identified and includedFootnote 8. In addition, in 2018 an updated IXIARO®product monographFootnote 1 was released with expanded recommendations for use in Canada, and was used as a reference.
GRADE questions
PICO questions
Among adult Canadian travellers, does use of JEV (normal schedule) decrease the risk of acquiring JE as compared to no vaccine (placebo)?
We did not identify evidence showing JEV reduces the incidence of JE (and associated harms) among travellers to endemic areas. Rather, efficacy is inferred from studies using serological correlates of protection. Efficacy of JEV (IXIARO®) was initially established through a non-inferiority comparisonFootnote 25 to inactivated mouse brain-derived JE vaccine (MBV), trade name JEVAX, which is no longer licenced in Canada. Protection was defined using seroconversion rate (SCR) as an endpoint, i.e. a PRNT50 titre <10 at baseline and ≥10 post vaccination, or a 4-fold rise from a baseline titre of ≥10Footnote 17. The evidence from this trialFootnote 25, which included safety and immunogenicity outcomes, is summarized in Appendix 1 and 6. JEV and MBV performed similarly well in eliciting high SCR (> 95% of recipients) (moderate confidence in the estimates of effect, downgraded for indirectness given seroconversion is a surrogate of protection). The vaccines were associated with similar rates of systemic adverse effects; however, local reactions were more common with MBV (high confidence in estimate of effect).
Additional studies, without a comparator, have consistently shown that 2 doses of JEV (days 0, 28) achieve high SCRFootnote 15 Footnote 26 Footnote 27 Footnote 28 Footnote 29 Footnote 30 Footnote 31. Results from these studies are summarized in Figure 1.
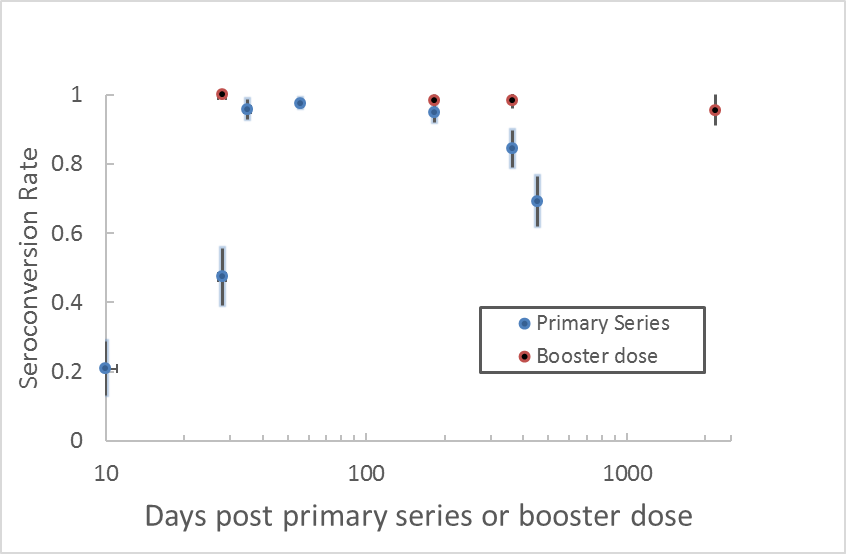
Data extracted from 9 studiesFootnote 12 Footnote 13 Footnote 15 Footnote 25 Footnote 26 Footnote 27 Footnote 28 Footnote 29 Footnote 30.
Among adult Canadian travellers, does use of an accelerated (0, 7 days) JEV schedule achieve levels of protection similar to or greater than a normal JEV schedule (0, 28 days)?
In adults, an accelerated JEV schedule (first dose on day 0 and second dose on day 7) yielded similar SCR to the normal schedule (1 dose on each of days 0 and 28) (moderate confidence in the estimate of effect) (Appendix 7). Compared at a similar time point (10-14 days) after the initial doseFootnote 26, the accelerated schedule was associated with a significantly higher SCR (RR 3.95; 95% CI 3.16 to 4.92) than the normal schedule (low confidence in the estimate of effect). Safety profiles (Appendix 7) for the accelerated and normal schedule were similar (moderate to high confidence in the estimates of effect). This accelerated schedule has recently been approved for use in Canada for adults aged 18-65 yearsFootnote 1.
Among Canadian children, does use of JEV achieve levels of protection similar to that observed in adult travellers and is JEV use associated with similar harms to adults?
Through the literature review, GRADE assessments published in 2013 by the United States Advisory Committee on Immunization Practices (ACIP)Footnote 32 were identified. This work specifically addressed the question "Should inactivated Vero cell culture-derived Japanese encephalitis vaccine (JE-VC) be recommended for use in children 2 months through 16 years of age at increased risk of travel-related exposure to Japanese encephalitis virus". Adults were included in the analyses as a comparator. We judged that the ACIP GRADE could be used to address our PICO question: "Among Canadian children, does use of JEV achieve levels of protection similar to that observed in adult travellers?" We did not identify additional and relevant evidence published since this review in our literature search.
The ACIP concluded that SCR (moderate confidence in the estimate of effect) and rates of serious (low confidence in the estimate of effect) or systemic (moderate confidence in estimate of effect) adverse effects were similar in adults and children (see Appendix 8). A complete explanation of the assessment of quality of evidence is available elsewhereFootnote 32. Briefly, downgrading of the quality of evidence was done because of indirectness (e.g., because efficacy was not directly measured and/or the evidence was primarily developed with adults) and potential sources of bias (e.g., lack of blinding). Use of JEV in children aged 2 months to <18 years has recently been approved in CanadaFootnote 1.
Evidence supporting the use of an accelerated schedule in children was not identified and use of an accelerated schedule in children is not approved in CanadaFootnote 1. Hence, the normal schedule for JEV should be used for children when possible. However, it appears reasonable to use an off-label accelerated schedule for children in the circumstance where time does not allow for the normal schedule to be used, especially in older children.
Contextual questions
What is the risk of clinical JE among Canadian travellers?
Likelihood estimates for travel-related clinical JE are shown in Table 1. For calculations, the numerator reflects the number of published cases over a 10 year period (2006-2015). We used cases identified in data from a previous reviewFootnote 33 published in 2010 and identified more recent reportsFootnote 34 Footnote 35 Footnote 36 Footnote 37 Footnote 38 Footnote 39 Footnote 40 Footnote 41 by applying the same search strategy as is described in the review. To be included, published cases must have been for a traveller returning to Canada, the United States (US) or Europe. For the denominator, we used outbound travel statistics for Canada, the United States and Europe Footnote 42 Footnote 43 Footnote 44.
We estimate the likelihood of clinical JE as approximately 1/10,000,000 trips (moderate confidence in the estimate of effect) for Canada, the United States and Europe (Table 1). The quality of the body of evidence was downgraded due to risk of bias (Appendix 9), i.e. not all cases in travellers may have been reported in the literature. In this respect, while we cannot be certain of the degree to which cases are under-reported, it has been suggestedFootnote 33 that the majority are identified in the literature. Moreover, even if it was assumed that only 1 in 10 cases of JE disease in travellers were reported, the overall risk of JE would remain very low, i.e. approximately 1 case/1,000,000 trips.
Previous estimates for US and European travellers Footnote 11 Footnote 45 have also suggested a very low overall risk for JE.
What are the important risk factors for JE among Canadian travellers (e.g., destination, duration of travel)?
For the period of 2006-2015, we identified 18 published reports of JE, of which 17 were in travellers returning to Canada (1 case), the United States (5 cases) or Europe (11 cases). Including reports published before 2006 increased the total to 67 cases. Only 1 case identified was not in a traveller from the Western hemisphere and hence was excluded from the analysis. Overall, the case fatality rate was 20% (12/60) (outcome was unknown in 6 cases); most cases were in males (59%); the average age of cases was 39 years; and the mean duration of travel was 35 days (Figure 2). The countries to which exposure was most often ascribed were: were ThailandFootnote 27, IndonesiaFootnote 46, ChinaFootnote 47 and the PhilippinesFootnote 48 (Figure 3).
We estimate that travel-associated JE is rare, consistent with previous estimatesFootnote 11. However, it also is widely accepted that certain subpopulations of travellers are at relatively higher risk for JE; examples include those travelling for an extended period and/or those spending substantial amounts of time in rural areas where vectors are more prevalent Footnote 33 Footnote 45 Footnote 49 Footnote 50 Footnote 51 Footnote 52 Footnote 53. We did not identify evidence (observational or randomized trials) that would allow robust estimates of the incremental impact of these factors on risk to be made, and for this reason did not assess this evidence with GRADE. Based on identified travel-related cases (N=66, see above) we nevertheless make the following observations:
- Among cases where age is available (N=57), there is not an obvious age associated trend, e.g., children aged 10 years or younger (5 cases) accounted for 9% of the total and adults aged 60 years or older (12 cases) accounted for 21% of the total.
- There is a trend towards increased likelihood of JE with longer duration travel. Specifically, median duration of travel for cases at 35 days (Figure 2) is approximately double the median duration (15 days) for all travel to endemic areasFootnote 43 Footnote 44. There is not, however, a clear cut-off for travel duration below which risk is absent (cases have been reported in short-term travellers) or for a travel duration at which disease likelihood crosses a "threshold" that would prompt use of JEV.
- Itineraries that include rural exposure are often reported in association with published casesFootnote 33. However, rural activity is not a universal risk factor nor, in the situation where time is spent in rural and urban areas, can the rural component of travel be definitively ascribed as the exposing activity. Hence, while there is consensus that activities in rural areas are "riskier", the absolute magnitude of the risk increase is unknown.
Appendix 10 describes how these and other factors might be used when undertaking a risk assessment for a person travelling to a JE risk area.

| Region of embarkation | Cases | Estimated travel volume (millions) 2006-2015 | Overall attack rate (cases/trips) for travellers (95% confidence interval) 2006-2015Footnote 6 |
|---|---|---|---|
| Canada | 1Footnote 1 | 11.65Footnote 3 | 1/11,650,000 (1/2,056,512 to 1/65,996,483) |
| United States | 5Footnote 2 | 55.4Footnote 4 | 1/11,078,000 (1/4,731859 to 1/25,935,276) |
| Europe | 11Footnote 2 | 150Footnote 5 | 1/13,636,363 (7,614,592 to 24,420,2750) |
| Group | Clinical JE (no vaccine) | Clinical JE (with vaccine) | JE sequelae (no vaccine) | JE sequelae (with vaccine) | Mortality (no vaccine) | Mortality (with vaccine) | |
|---|---|---|---|---|---|---|---|
| Attack rate (events/10,000,000 trips) | |||||||
| Canadian travellers to endemic areas | 0.858 | 0.043 | 0.322 | 0.016 | 0.215 | 0.011 | |
| Baseline risk (no vaccine) | Clinical JE | Severe sequelae | Death |
|---|---|---|---|
| 1/100,000 | 105,263 | 280,702 | 421,053 |
| 1/11,650,000 | 12,263,158 | 32,701,754 | 49,052,631 |
What are the values and preferences of travellers regarding the magnitude of risk reduction in JE that would make use of JEV worthwhile given associated costs and inconvenience?
Use of vaccines to prevent JE can be cost effective in endemic countriesFootnote 17 Footnote 54 Footnote 55 Footnote 56 Footnote 57 Footnote 58. However, these represent scenarios where the burden of disease is relatively elevated and the cost of the intervention relatively reduced compared to the typical travel context. Further, cost-effectiveness might be moot for travellers as they often pay for travel-related vaccines. We did not identify evidence specific to the values and preferences of travellers related to JEV, including their Willingness to Pay (WTP) for vaccine-based protection.
For other immunizations against low likelihood but high hazard diseases (like JE), there is evidence that patients are sometimes willing to pay a modest sum to receive protection. For example, a discrete choice experimentFootnote 9 indicated that patients, on average, were willing to pay approximately 250-300 Australian dollars for the protection afforded by a meningococcal B vaccine that was: 90% effective; required a single primary dose; provided protection that lasted for 10 years: and, was without adverse effects. However, WTP decreased substantially if vaccine characteristics did not meet these performance standards, e.g., if effectiveness was < 90%, duration of protection was shorter, there were associated adverse effects and/or more than 1 injection was required. Similarly, a discrete choice study of traveller willingness to pay for hypothetical travel vaccines identified disease risk, severity and intervention cost as having the most important impacts on decision makingFootnote 8. Moreover, the study respondents showed a significant bias towards not opting out of vaccination, up to a risk level of 1/100,000. Lower risk levels, e.g., as would typically be experienced for JE, were not evaluated in the study, nor were safety aspects of the hypothetical vaccines.
If WTP was influenced by similar factors for JEV, then some travellers might be willing to pay to receive immunization despite the low risk of disease. This would be tempered by vaccine characteristics perceived as suboptimal, which, in turn, would result in reduced WTP; for JEV, this would include the requirement for multiple doses and the relatively short duration of protection following primary vaccination.
Non-GRADE questions
What is the appropriate boostering interval for JEV?
In clinical trials to date, a primary series of JEV induced protective antibody levels that declined gradually over time, with 80-95% of fully immunized vaccine recipients maintaining adequate antibodies after 6 months and 58-83% maintaining adequate levels at 12-15 monthsFootnote 1 Footnote 13 Footnote 30 Footnote 60. At 24 months following primary series the evidence is less clear, with a study indicating that only 48% maintained seroprotection levelsFootnote 59 and another study showing that 82% maintained adequate SCRFootnote 1.
A phase 3 clinical study conducted with 198 subjects in Austria and Germany found that a booster provided at 15 months after the primary series increased SCR to 100% at 28 days and SCR remained at 99% 12 months after the booster doseFootnote 13. Longer term protection was demonstrated in an extension of the trial which followed a subset of the previous participants (N=67)Footnote 12. At month 76, 96% of participants had adequate SCRFootnote 12 (see Figure 1). Geometric mean titres (GMT) were examined stratified by age and sex and prior vaccinations. Differences were found by age, where participants older than 50 years (N=6) had statistically significantly lower GMT compared to participants less than 50 years of age, although the sample size was very smallFootnote 12.
Data on immunogenicity of a booster vaccine in children remains limited. Data from a small study of children (N=18) from non-JE endemic areas indicted that although antibodies titres declined over time, SCR was still high (89%) 36 months after vaccinationFootnote 14. A larger pediatric study of 149 children and adolescents from a JE-endemic area found similar results, with SCR over 80% in all age groups up to month 36Footnote 14. Though limited, the available evidence suggests that antibody responses are at least as persistent in children as in adults.
Early evidence from a mathematical model based on titres after primary immunization and 12 months after booster administration predicted that 50% of vaccine recipients would remain protected after 8 yearsFootnote 13. An updated modeling estimate based on data at 76 months indicates that a single booster may provide an even longer period of protection than previously estimatedFootnote 12. Additional information is required on length of protection, stratified by population subgroups of interest.
Based on the available human data, it seems reasonable to administer a single booster dose of JEV if the primary series was administered more than 1 year previously. In 2011 ACIP stated that a booster dose may be given if the primary series was administered more than a year previously, and there is potential for JE virus exposureFootnote 20. In 2018 the Canadian product monograph for IXIARO®was updatedFootnote 1 and now recommends that adults and children receive a booster dose 12-24 months after the primary series, prior to re-exposureFootnote 1.
A second booster dose is suggested by the Canadian product monograph for adults (aged 18-65), 10 years after the first boosterFootnote 1 and prior to any re-exposure. A similar approach has been approved by the European Medicine AgencyFootnote 2. Among children, evidence of long term seroprotection is limited but does suggest that antibody responses are at least as persistent in children as in adults. For this reason CATMAT suggests that it is reasonable to follow the same recommended second booster approach for children (off-label) as for adults.
Among older (aged >65 years) Canadian travellers, does use of JEV achieve levels of protection similar to adult travellers?
In general, older individuals are more likely to acquire infection and experience more severe disease, possibly due to immunosenescence, less robust physical barriers to infection, and medical comorbiditiesFootnote 60. It should be noted that only a tiny minority of the participants in the important JEV clinical trials that established safety and efficacy appear to have been over the age of 65Footnote 13 Footnote 15 Footnote 25 Footnote 30 Footnote 31 Footnote 61. Interestingly, 9.8% of travellers evaluated at Global TravEpiNet travel medicine clinics in the United States between 2009-2012 judged to be at risk for the acquisition of Japanese encephalitis were over the age of 65Footnote 62. This proportion may be increasing; from 2012 to 2015, the annual number of Canadian travellers aged 54 years and older visiting areas of JE risk has increased from approximately 600,000 to over 1 millionFootnote 43. Fortunately, none of the 42 AEs following immunization with JEV in the United States reported to the Vaccine Adverse Event Reporting System between 2009-2012 occurred in individuals older than 60 years of ageFootnote 6.
One open-label uncontrolled phase IV clinical trial of JEV was conducted in healthy adults aged > 65 years to evaluate safety and immunogenicity in this particular population Footnote 15. Of the 249 individuals screened at travel medicine clinics and clinical vaccine trial sites, 200 received the first dose, and 193 received a second dose 28 days later. Seroconversion was observed in 65% (95% CI 58 - 71%) at day 70; no significant differences were found in adults aged 65-74 and those over 75 years of age. These SCR appear to be substantially lower than those observed in previous trials enrolling younger adultsFootnote 25. The authors postulated that duration of protection may also be much shorter in elderly individuals and recommended consideration of booster immunizations before 1 year after the primary series, though they did not specify exactly what the optimal booster interval should be. Only a small minority (24 of 200, 12%) were older than 75 years of age. Overall, 61% percent of participants experienced any AE, with 47% of participants having had an AE thought to be related to vaccine; no differences were observed between the different age groups. These rates may have been higher than AE following immunization rates observed in previous clinical trials enrolling younger adultsFootnote 31. A third of participants reported local AEs within the first week after any dose of vaccine and 27% reported systemic AEs (72% of which were judged to be mild), most frequently headache and myalgia. There were no AEs found to be caused by the vaccine that were either serious or medically attended.
The new IXIARO® product monograph recommends that for adults 65 and older who remain at risk for re-exposure that an earlier booster dose may be considered, although the time period is not specifiedFootnote 1. CATMAT suggests that for adults aged > 65 a single booster dose of JEV be considered before 12 months following the primary series and assessment of the precise timing of vaccine administration should be done on a case-by-case basis.
Does an additional dose of vaccine on day 0 achieve a higher SCR than a single dose?
As noted previously, there are obvious advantages to abbreviating vaccination regimens. An initial dose-finding phase II study demonstrated that 22 of 23 (96%) healthy individuals recruited at the Walter Reed Army Institute of Research who received a double dose (12 μg) of JE-VC seroconverted at 1 month post-immunizationFootnote 28. Unfortunately, a follow-up multicentre phase III study was not able to duplicate these resultsFootnote 27. Of 490 individuals screened in Germany and Northern Ireland, 374 were enrolled and randomized 1:1:1 to a single 12 μg dose, two 6 μg doses (standard regimen), and a single 6 μg dose. Only 66% (95% CI 57-74%) of those randomized to the single 12 μg-dose arm seroconverted at 28 days, which further decreased to 41% (95% CI 32-50%) at 56 days. This was obviously inferior to the standard 2x6 μg dose regimen, which was associated with a 97% (95% CI 94-100%) seroconversion rate at 56 daysFootnote 27.
As a result, a single 12 μg-dose regimen cannot be routinely recommended. In certain specific scenarios, when the travel timeframe precludes administration of JEV using standard or accelerated schedules, vaccine providers may consider giving a 12 μg dose, as this would appear to elicit a superior immune response as compared to a single standard dose. These travellers should have their vaccine series completed when possible, should they remain at risk for JE acquisition in future.
Do personal protective measures provide protection against bites from the type(s) of mosquitoes that transmit JE?
Insect repellentsFootnote 63 Footnote 64, permethrin-treated bed netsFootnote 65 Footnote 66 and permethrin-treated clothingFootnote 67 have efficacy against the types of mosquitoes (Culex species) that transmit JE virus. Hence, these interventions should be used to reduce exposure to the mosquito vectors of JE. For more detail on these interventions as well as other approaches to prevent the bites of arthropods, readers are referred to the CATMAT statement on personal protective measures to prevent insect bitesFootnote 16.
Conclusions and Research Needs
Our recommendations are based on the supposition that likelihood of JE is negligible for the large majority of travellers (moderate confidence). However, we were unable to determine the magnitude of increased JE risk due to other factors, such as duration of travel, or rural exposure. Research to define the impact of such risk factors on the likelihood of developing travel-associated JE would allow for the development of more precise recommendations. Similarly, CATMAT's confidence in estimates of patient values and preferences, including WTP for JEV, was low. A greater focus on the development of evidence to define these parameters for JEV, as well as other travel-related interventions, would allow: guideline developers to elaborate more precise recommendations; and, practitioners to develop more targeted advice for individual patients.
Acknowledgements
This statement was developed by the Japanese Encephalitis Working Group: Schofield S (Lead), Brophy J, Pernica J and approved by CATMAT.
CATMAT would like to acknowledge the technical and administrative support from the Office of Border and Travel Health at the Public Health Agency of Canada for the development of this statement.
- CATMAT members:
- McCarthy A (Chair), Acharya A, Boggild A, Brophy J, Bui Y, Crockett M, Greenaway C, Libman M, Teitelbaum P and Vaughan S.
- Liaison members:
- Angelo K (United States Centers for Disease Control and Prevention), Audcent T (Canadian Paediatric Society) and Pernica J (Association of Medical Microbiology and Infectious Disease Canada).
- Ex officio members:
- Marion D (Canadian Forces Health Services Centre, Department of National Defence), McDonald P (Bureau of Medical Sciences, Health Canada), Rossi C (Medical Intelligence, Department of National Defence) and Schofield S (Pest Management Entomology, Department of National Defence).
Conflict of Interest
None declared.
References
- Footnote 1
-
Valneva Austria GmbH. IXIARO Product Monograph. 2018.
- Footnote 2
-
European Medicines Agency. Ixiaro - Japanese-encephalitis vaccine (inactivated, adsorbed). 2016; Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000963/human_med_000862.jsp&mid=WC0b01ac058001d124.
- Footnote 3
-
US Food and Drug Administration. Approval Letter - IXIARO. May 17, 2013; Available at: https://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm353334.htm. Accessed April 11, 2017.
- Footnote 4
-
Centers for Disease Control and Prevention. Use of Japanese encephalitis vaccine in children: Recommendations of the advisory committee on immunization practices, 2013. MMWR Morb Mortal Wkly Rep 2013;62(45):898-900.
- Footnote 5
-
Tauber E, Kollaritsch H, Von Sonnenburg F, Lademann M, Jilma B, Firbas C, et al. Randomized, double-blind, placebo-controlled phase 3 trial of the safety and tolerability of IC51, an inactivated Japanese encephalitis vaccine. J Infect Dis 2008 15 Aug 2008;198(4):493-499.
- Footnote 6
-
Rabe IB, Miller ER, Fischer M, Hills SL. Adverse events following vaccination with an inactivated, Vero cell culture-derived Japanese encephalitis vaccine in the United States, 2009-2012. Vaccine 2015 Jan 29;33(5):708-712.
- Footnote 7
-
Walker WL, Hills SL, Miller ER, Fischer M, Rabe IB. Adverse events following vaccination with an inactivated, Vero cell culture-derived Japanese encephalitis vaccine in the United States, 2012-2016. Vaccine 2018 Jul 5;36(29):4369-4374.
- Footnote 8
-
Poulos C, Curran D, Anastassopoulou A, De Moerlooze L. German travelers' preferences for travel vaccines assessed by a discrete choice experiment. Vaccine 2018 Feb 8;36(7):969-978.
- Footnote 9
-
Marshall HS, Chen G, Clarke M, Ratcliffe J. Adolescent, parent and societal preferences and willingness to pay for meningococcal B vaccine: A Discrete Choice Experiment. Vaccine 2016 1/27;34(5):671-677.
- Footnote 10
-
Committee to Advise on Tropical Medicine and Travel (CATMAT). Evidence Based Process for developing travel and tropical medicine related guidelines and recommendations. 2017; Available at: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/evidence-based-process-developing-travel-tropical-medicine-guidelines-recommendations.html. Accessed January 9 2018, 2018.
- Footnote 11
-
Hatz C, Werlein J, Mutsch M, Hufnagel M, Behrens RH. Japanese encephalitis: defining risk incidence for travelers to endemic countries and vaccine prescribing from the UK and Switzerland. Journal of Travel Medicine 2009;16(3):200-203.
- Footnote 12
-
Paulke-Korinek M, Kollaritsch H, Kundi M, Zwazl I, Seidl-Friedrich C, Jelinek T. Persistence of antibodies six years after booster vaccination with inactivated vaccine against Japanese encephalitis. Vaccine 2015;33(30):3600-3604.
- Footnote 13
-
Eder S, Dubischar-Kastner K, Firbas C, Jelinek T, Jilma B, Kaltenboeck A, et al. Long term immunity following a booster dose of the inactivated Japanese Encephalitis vaccine IXIARO(R), IC51. Vaccine 2011 Mar 21;29(14):2607-2612.
- Footnote 14
-
Valneva Austria GmbH. New Clinical Data for IXIARO®Japanese Encephalitis Vaccine, Inactivated, Adsorbed. 2016 February 24.
- Footnote 15
-
Cramer JP, Jelinek T, Paulke-Korinek M, Reisinger EC, Dieckmann S, Alberer M, et al. One-year immunogenicity kinetics and safety of a purified chick embryo cell rabies vaccine and an inactivated Vero cell-derived Japanese encephalitis vaccine administered concomitantly according to a new, 1-week, accelerated primary series. J Travel Med 2016 Mar 19;23(3):10.1093/jtm/taw011. Print 2016 Mar.
- Footnote 16
-
Committee to Advise on Tropical Medicine and Travel. Statement on personal protective measures to prevent arthropod bites. Can Commun Dis Rep 2012;38(ACS-3).
- Footnote 17
-
World Health Organization. Japanese Encephalitis Vaccines: WHO position paper - February 2015. Weekly Epidemiological Record 2015;9(90):69-88.
- Footnote 18
-
Campbell GL, Hills SL, Fischer M, Jacobson JA, Hoke CH, Hombach JM, et al. Estimated global incidence of Japanese encephalitis: a systematic review. Bull World Health Organ 2011;89(10):766-774.
- Footnote 19
-
Centers for Disease Control and Prevention. Japanese Encephalitis Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2010;59(RR01):1-27.
- Footnote 20
-
Centers for Disease Control and Prevention. Recommendations for use of a booster dose of inactivated vero cell culture-derived Japanese encephalitis vaccine: advisory committee on immunization practices, 2011. MMWR Morb Mortal Wkly Rep 2011;60(20):661-663.
- Footnote 21
-
Halstead SB, Jacobson J, Dubischar-Kastner K. Japanese encephaltis vaccines. In: Plotkin S, Orenstein WA, Offit P, editors. Vaccines. 6th ed. China: Elsevier Saunders; 2013. p. 312-351.
- Footnote 22
-
Solomon T, Nguyen MD, Kneen R, Gainsboroug M, Vaughn DW, Khanh VT. Japanese encephalitis. J Neurol Neurosurg Ps 2000;68:405-415.
- Footnote 23
-
Erlanger TE, Weiss S, Keiser J, Utzinger J, Wiedenmayer K. Past, Present, and Future of Japanese Encephalitis. Emerg Infect Dis 2009;15(1):1-7.
- Footnote 24
-
Public Health Agency of Canada. Canadian Immunization Guide: Part 4 - Active Vaccines. 2014; Available at: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-11-japanese-encephalitis-vaccine.html.
- Footnote 25
-
Tauber E, Kollaritsch H, Korinek M, Rendi-Wagner P, Jilma B, Firbas C, et al. Safety and immunogenicity of a Vero-cell-derived, inactivated Japanese encephalitis vaccine: a non-inferiority, phase III, randomised controlled trial. Lancet 2007;370(9602):1847-1853.
- Footnote 26
-
Jelinek T, Burchard GD, Dieckmann S, Bühler S, Paulke-Korinek M, Nothdurft HD, et al. Short-Term Immunogenicity and Safety of an Accelerated Pre-Exposure Prophylaxis Regimen With Japanese Encephalitis Vaccine in Combination With a Rabies Vaccine: A Phase III, Multicenter, Observer-Blind Study. Journal of Travel Medicine 2015.
- Footnote 27
-
Schuller E, Klade CS, Wölfl G, Kaltenböck A, Dewasthaly S, Tauber E. Comparison of a single, high-dose vaccination regimen to the standard regimen for the investigational Japanese encephalitis vaccine, IC51: A randomized, observer-blind, controlled Phase 3 study. Vaccine 2009;27(15):2188-2193.
- Footnote 28
-
Lyons A, Kanesa-thasan N, Kuschner RA, Eckels KH, Putnak R, Sun W, et al. A Phase 2 study of a purified, inactivated virus vaccine to prevent Japanese encephalitis. Vaccine 2007;25(17):3445-3453.
- Footnote 29
-
Kaltenböck A, Dubischar-Kastner K, Schuller E, Datla M, Klade CS, Kishore TSA. Immunogenicity and safety of IXIARO®(IC51) in a Phase II study in healthy Indian children between 1 and 3 years of age. Vaccine 2010;28(3):834-839.
- Footnote 30
-
Schuller E, Jilma B, Voicu V, Golor G, Kollaritsch H, Kaltenböck A, et al. Long-term immunogenicity of the new Vero cell-derived, inactivated Japanese encephalitis virus vaccine IC51. Six and 12 month results of a multicenter follow-up phase 3 study. Vaccine 2008;26(34):4382-4386.
- Footnote 31
-
Tauber E, Kollaritsch H, Von Sonnenburg F, Lademann M, Jilma B, Firbas C, et al. Randomized, double-blind, placebo-controlled phase 3 trial of the safety and tolerability of IC51, an inactivated Japanese encephalitis vaccine. J Infect Dis 2008;198(4):493-499.
- Footnote 32
-
Centers for Disease Control and Prevention. Grading of recommendations, assessment, development, and evaluation (GRADE) for use of inactivated Vero cell culture-derived Japanese encephalitis vaccine in children. 2014; Available at: http://www.cdc.gov/vaccines/acip/recs/grade/je-child.html. Accessed May 16, 2016.
- Footnote 33
-
Hills SL, Griggs AC, Fischer M. Japanese encephalitis in travelers from non-endemic countries, 1973-2008. Am J Trop Med Hyg 2010;82(5):930-936.
- Footnote 34
-
Hills S.L., Stoltey J., Martinez D., Kim P.Y., Sheriff H., Zangeneh A., et al. A case series of three US adults with Japanese encephalitis, 2010-2012. 2014;. Accessed 5, 21.
- Footnote 35
-
Lagarde S., Lagier J.-C., Charrel R., Querat G., Vanhomwegen J., Despres P., et al. Japanese encephalitis in a French traveler to Nepal. 2014;. Accessed 1, 20.
- Footnote 36
-
Chen L, Peek M, Stokich D, Todd R, Anderson M, Murphy FK, et al. Japanese encephalitis in two children-United States, 2010. Morb Mortal Weekly Rep 2011;60(9):276-278.
- Footnote 37
-
Langevin S, Libman M, Drebot MA, Laverdiere M. A case of Japanese encephalitis virus infection acquired during a trip in Thailand. Journal of Travel Medicine 2012 March-April 2012;19(2):127-129.
- Footnote 38
-
Werlinrud AM, Christiansen CB, Koch A. Japanese encephalitis in a Danish short-term traveler to Cambodia. Journal of Travel Medicine 2011;18(6):411-413. 10 ref.
- Footnote 39
-
Doti P, Castro P, Martinez MJ, Zboromyrska Y, Aldasoro E, Inciarte A, et al. A case of Japanese encephalitis in a 20 year-old Spanish sportsman, February 2013. Euro Surveill 2013 Aug 29;18(35):20573.
- Footnote 40
-
Tappe D, Nemecek A, Zipp F, Emmerich P, Gabriel M, Gunther S, et al. Two laboratory-confirmed cases of Japanese encephalitis imported to Germany by travelers returning from Southeast Asia. J Clin Virol 2012 Jul;54(3):282-285.
- Footnote 41
-
Jeurissen A, Strauven T. A case of aseptic meningitis due to Japanese encephalitis virus in a traveller returning from the Philippines. Acta Neurol Belg 2011 Jun;111(2):143-145.
- Footnote 42
-
Eurostat: Statistics Explained. File: Extra -EU-28 Transport of passengers in 2014. 2015; Available at: http://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Extra-EU-28_transport_of_passengers_in_2014.jpg&direction=prev&oldid=314881. Accessed April 11, 2017.
- Footnote 43
-
Statistics Canada. International Travel Survey. Custom extract. 2014.
- Footnote 44
-
U.S. Department of Commerce. National Travel and Tourism Office: 2014 U.S. Resident Travel to Asia. 2014; Available at: http://travel.trade.gov/outreachpages/download_data_table/2014-US-to-Asia.pdf.
- Footnote 45
-
Fischer M, Lindsey N, Staples JE, Hills S, Centers for Disease Control and Prevention (CDC). Japanese encephalitis vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity & Mortality Weekly Report.Recommendations & Reports 2010;59(RR-1):1-27.
- Footnote 46
-
Artsob H, Spence L. Imported arbovirus infections in Canada, 1974-89. Can J Infect Dis 1991;2(3):95-100.
- Footnote 47
-
Boggild AK, Castelli F, Gautret P, Torresi J, von Sonnenburg F, Barnett ED, et al. Vaccine preventable diseases in returned international travelers: Results from the GeoSentinel Surveillance Network. Vaccine 2010;28(46):7389-7395.
- Footnote 48
-
Freedman DO, Weld LH, Kozarsky PE, Fisk T, Robins R, Von Sonnenburg F, et al. Spectrum of disease and relation to place of exposure among ill returned travelers. New Engl J Med 2006;354(2):119-130.
- Footnote 49
-
World Health Organization. Japanese Encephalitis. International Travel and Health;2017.
- Footnote 50
-
World Health Organization. BACKGROUND PAPER ON JAPANESE ENCEPHALITIS VACCINES. International Health and Travel 2014.
- Footnote 51
-
Australian Government Department of Health. 4.8 Japanese encephalitis. THE AUSTRALIAN IMMUNISATION HANDBOOK 10TH EDITION; 2015. p. 261-270.
- Footnote 52
-
Direction générale de la Santé, Comité technique des vaccinations. Guide des vaccinations. Édition 2012. Saint-Denis : Inpes, France; 2012.
- Footnote 53
-
Institut de veille sanitaire: Bulletin epidemiologique hebdomadaire. Recommendations sanitaire pour les voyageurs 2014. 2014 3 juin;16-17.
- Footnote 54
-
Touch S, Suraratdecha C, Samnang C, Heng S, Gazley L, Huch C, et al. A cost-effectiveness analysis of Japanese encephalitis vaccine in Cambodia. Vaccine 2010 6/23;28(29):4593-4599.
- Footnote 55
-
Yin Z, Beeler Asay GR, Zhang L, Li Y, Zuo S, Hutin YJ, et al. An economic evaluation of the use of Japanese encephalitis vaccine in the expanded program of immunization of Guizhou province, China. Vaccine 2012 8/10;30(37):5569-5577.
- Footnote 56
-
Upreti SR, Janusz KB, Schluter WW, Bichha RP, Shakya G, Biggerstaff BJ, et al. Estimation of the impact of a Japanese encephalitis immunization program with live, attenuated SA 14-14-2 vaccine in Nepal. Am J Trop Med Hyg 2013 Mar;88(3):464-468.
- Footnote 57
-
GAVI Alliance. Japanese encephalitis vaccine. 2017; Available at: http://www.gavi.org/support/process/apply/.
- Footnote 58
-
Elias C, Okwo-Bele JM, Fischer M. A strategic plan for Japanese encephalitis control by 2015. Lancet Infect Dis 2009 Jan;9(1):7-3099(08)70290-1.
- Footnote 59
-
Dubischar-Kastner K, Eder S, Buerger V, Gartner-Woelfl G, Kaltenboeck A, Schuller E, et al. Long-term immunity and immune response to a booster dose following vaccination with the inactivated Japanese encephalitis vaccine IXIARO®, IC51. Vaccine 2010;28(32):5197-5202.
- Footnote 60
-
Liang SY. Sepsis and Other Infectious Disease Emergencies in the Elderly. Emerg Med Clin North Am 2016 8;34(3):501-522.
- Footnote 61
-
Erra EO, Askling HH, Yoksan S, Rombo L, Riutta J, Vene S, et al. Cross-protection elicited by primary and booster vaccinations against Japanese encephalitis: A two-year follow-up study. Vaccine 2013 12/17;32(1):119-123.
- Footnote 62
-
Deshpande BR, Rao SR, Jentes ES, Hills SL, Fischer M, Gershman MD, et al. Use of Japanese encephalitis vaccine in US travel medicine practices in Global TravEpiNet. Am J Trop Med Hyg 2014;91(4):694-698. 13 ref.
- Footnote 63
-
Croft AM. Malaria: prevention in travellers (non-drug interventions). Clinical Evidence 2014;2014.
- Footnote 64
-
Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 2011 Apr;64(4):401-406.
- Footnote 65
-
Moore SJ DM. History of insect repellents. In: Debboun M, Francis S, Strickman D, editor. Insect repellents: Principles, methods and uses: CRC Press; 2007. p. 3-29.
- Footnote 66
-
Pest Management Regulatory Agency. Homepage. 2011; Available at: http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/pmra-arla/index-eng.php.
- Footnote 67
-
United States Environmental Protection Agency. Office of Pesticide Programs. 2011; Available at: http://www.epa.gov/pesticides.
- Footnote 68
-
Centers for Disease Control and Prevention (CDC). CDC Yellow Book 2024: Health Information for International Travel. (New York, 2023).
- Footnote 69
-
Schuller E, Klingler A, DubischarKastner K, Dewasthaly S, Muller Z. Safety profile of the Vero cell-derived Japanese encephalitis virus (JEV) vaccine IXIAROReg.. Vaccine 2011;29(47):8669-8676. 39 ref.
- Footnote 70
-
Kaltenböck A, Dubischar-Kastner K, Eder G, Jilg W, Klade C, Kollaritsch H, et al. Safety and immunogenicity of concomitant vaccination with the cell-culture based Japanese Encephalitis vaccine IC51 and the hepatitis A vaccine HAVRIX®1440 in healthy subjects: A single-blind, randomized, controlled Phase 3 study. Vaccine 2009;27(33):4483-4489.
- Footnote 71
-
Yun KW, Lee HJ, Kang JH, Eun BW, Kim Y, Kim K, et al. Safety and immunogenicity of a freeze-dried, Vero cell culture-derived, inactivated Japanese encephalitis vaccine (KD-287, ENCEVAC®) versus a mouse brain-derived inactivated Japanese encephalitis vaccine in children: a phase III, multicenter, double-blinded, randomized trial. BMC infectious diseases 2015;15(1):1.
- Footnote 72
-
Eder S, DubischarKastner K, Firbas C, Jelinek T, Jilma B, Kaltenboeck A, et al. Long term immunity following a booster dose of the inactivated Japanese Encephalitis vaccine IXIAROReg., IC51. Vaccine 2011;29(14):2607-2612. 27 ref.
Appendix 1. Summary of findings for comparison of JEV to placebo: Adverse events (AE)
| Outcomes | Illustrative comparative risksFootnote * (95% CI) | Relative effect (95% CI) |
No of Participants (studies) |
Quality of the evidence (GRADE) Footnote ɫ |
Comments | |
|---|---|---|---|---|---|---|
| Assumed risk Placebo (AE) |
Corresponding risk JEV |
|||||
| Any SAEFI | Study population | RR 0.55 (0.2 to 1.51) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 9 per 1000 | 5 per 1000 (2 to 14) |
|||||
| Any AEFI | Study population | RR 1.04 (0.96 to 1.12) |
2650 (1 study) |
⊕⊕⊕⊕ high |
None | |
| 566 per 1000 | 589 per 1000 (544 to 634) |
|||||
| Gastrointestinal | Study population | RR 1.06 (0.81 to 1.39) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 94 per 1000 | 100 per 1000 (76 to 131) |
|||||
| Musculoskeletal | Study population | RR 0.99 (0.82 to 1.19) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 183 per 1000 | 181 per 1000 (150 to 217) |
|||||
| Headache | Study population | RR 1.07 (0.93 to 1.24) |
2656 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 261 per 1000 | 279 per 1000 (243 to 324) |
|||||
| Rash | Study population | RR 0.86 (0.42 to 1.77) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 15 per 1000 | 13 per 1000 (6 to 27) |
|||||
| Pain | Study population | RR 1.16 (1 to 1.35) |
2650 Footnote 1 |
⊕⊕⊕⊕ high |
None | |
| 250 per 1000 | 290 per 1000 (250 to 337) |
|||||
| Itching | Study population | RR 0.52 (0.29 to 0.92) |
2650 (1 study) |
⊕⊕⊕⊕ high |
None | |
| 29 per 1000 | 15 per 1000 (8 to 27) |
|||||
| Tenderness | Study population | RR 1.21 (1.06 to 1.38) |
2650 (1 study) |
⊕⊕⊕⊕ high |
None | |
| 294 per 1000 | 355 per 1000 (311 to 405) |
|||||
| Hardness | Study population | RR 0.95 (0.66 to 1.38) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 55 per 1000 | 52 per 1000 (36 to 76) |
|||||
| Swelling | Study population | RR 1.01 (0.59 to 1.73) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 26 per 1000 | 26 per 1000 (15 to 45) |
|||||
| Redness | Study population | RR 1.23 (0.85 to 1.79) |
2650 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 50 per 1000 | 62 per 1000 (43 to 90) |
|||||
Appendix 2. Geographic distribution of Japanese encephalitis
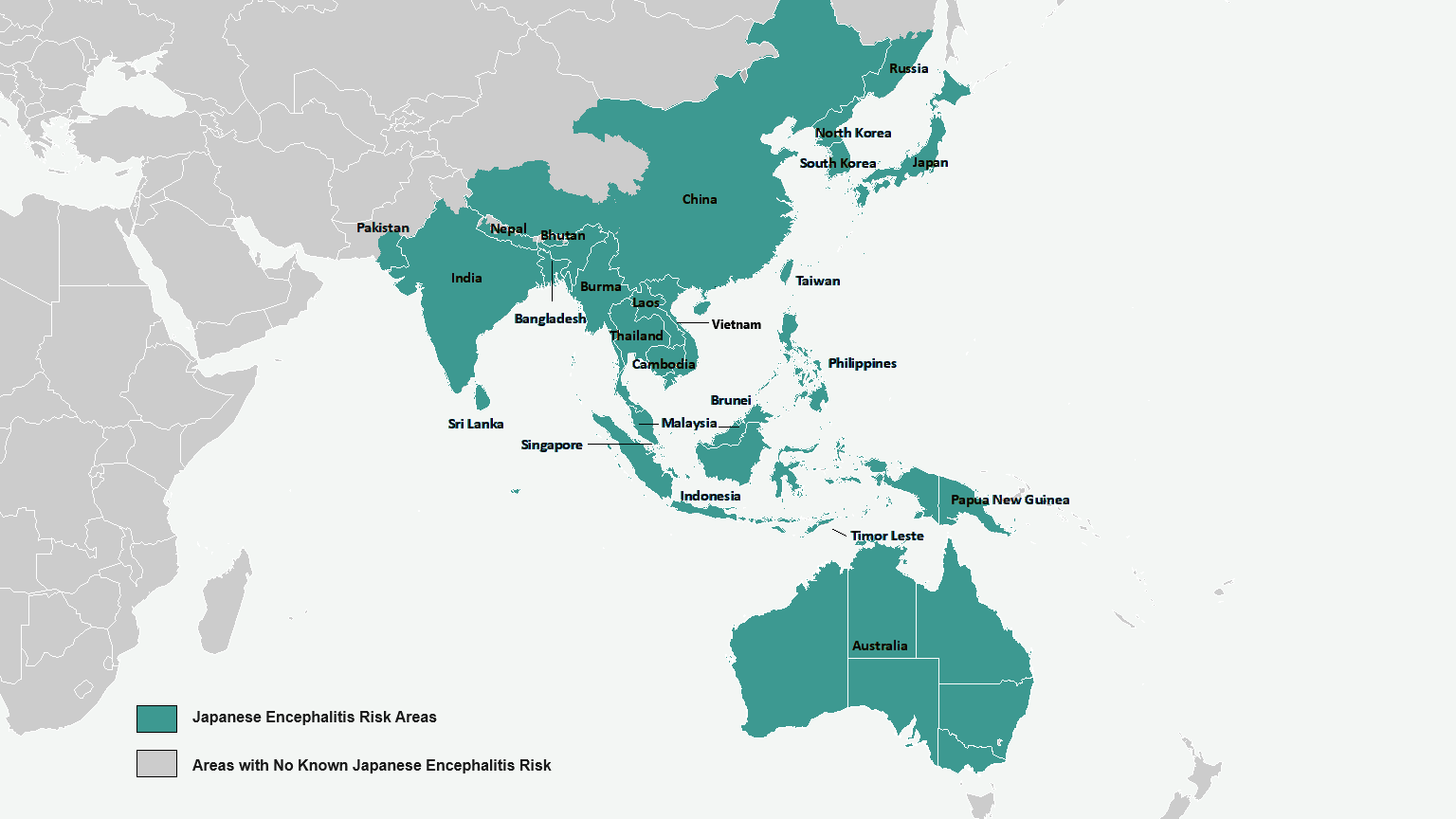
The countries which have areas with identified Japanese encephalitis virus risk are listed below with a description of the affected areas within each country. Other areas outside of these countries have no known Japanese encephalitis risk.
Text description
| Country | Japanese Encephalitis Risk Areas |
|---|---|
| Australia | In southeastern Australia (Victoria, New South Wales, southern Queensland, and South Australia), particularly in rural areas surrounding the Murray River, as well as the Outer Torres Strait Islands and the Tiwi Islands |
| Bangladesh | Widespread |
| Bhutan | Presumed widespread in non mountainous areas |
| Brunei Darussalam | Presumed widespread |
| Cambodia | Widespread |
| China | Human cases reported from all provinces except Xizang (Tibet), Xinjiang, and Qinghai; JE virus isolated from mosquitoes in Tibet |
| India | Human cases reported from all states except Dadra, Daman, Diu, Gujarat, Himachal Pradesh, Jammu and Kashmir, Lakshadweep, Meghalaya, Nagar Haveli, Punjab, Rajasthan, and Sikkim |
| Indonesia | Widespread |
| Japan | Rare sporadic human cases on all islands except Hokkaido; enzootic activity ongoing |
| Korea, North | Limited data; presumed widespread |
| Korea, South | Widespread |
| Laos | Widespread |
| Malaysia | Widespread |
| Myanmar (Burma) | Limited data; presumed widespread |
| Nepal | Endemic in southern lowlands (Terai); cases also reported from hill and mountain districts, including the Kathmandu valley |
| Pakistan | Limited data |
| Papua New Guinea | Widespread |
| Philippines | Widespread |
| Russia | Rare human cases reported from the Far Eastern maritime areas south of Khabarovsk |
| Singapore | Presumed in focal areas |
| Sri Lanka | Widespread, except in mountainous areas |
| Taiwan | Rare sporadic human cases island-wide |
| Thailand | Widespread; seasonal epidemics in the northern provinces |
| Timor-Leste (East Timor) | Presumed widespread |
| Vietnam | Widespread |
Appendix 3. Country-specificFootnote 1 notes on Japanese encephalitis
| COUNTRY | AFFECTED AREAS | TRANSMISSION SEASON | COMMENTS |
|---|---|---|---|
| Australia | In southeastern Australia (Victoria, New South Wales, southern Queensland, and South Australia), particularly in rural areas surrounding the Murray River, as well as the Outer Torres Strait Islands and the Tiwi Islands | Most cases reported November-April; all human cases reported February-April | From January 2021 to February 2023, 45 cases of JE were reported on mainland Australia, focused in rural areas surrounding the Murray River In November 2022, JE virus was detected in pigs in the Murray River region, confirming risk of infection in humans |
| Bangladesh | Widespread | Most human cases reported July-November | Sentinel surveillance has identified human cases in Chittagong, Dhaka, Khulna, Rajshahi, Ranjpur, and Sylhet Divisions; highest incidence reported from Rajshahi Division; outbreak reported from Tangail District, Dhaka Division, in 1977 |
| Bhutan | Presumed widespread in non mountainous areas | Unknown | Proximity to other endemic areas and presence of vectors suggests virus transmission is likely |
| Brunei Darussalam | Presumed widespread | Unknown; presumed year-round | Outbreak with laboratory confirmed cases occurred in October-December 2013 |
| Myanmar (Burma) | Limited data; presumed widespread | Unknown; most human cases reported May-October | Outbreaks of human disease documented in Shan and Rakhine States; antibodies documented in animals and humans in other areas |
| Cambodia | Widespread | Year-round with peak season May-October | Sentinel surveillance has identified human cases in at least 15 of 23 provinces, including Phnom Penh, Takeo, Kampong Cham, Battambang, Svay Rieng, and Siem Reap; 1 case reported in 2010 in a traveller who visited Phnom Penh and Angkor Wat/Siem Reap only |
| China | Human cases reported from all provinces except Xizang (Tibet), Xinjiang, and Qinghai; JE virus isolated from mosquitoes in Tibet | Most human cases reported June-October | Highest rates reported from Guizhou, Shaanxi, Sichuan, and Yunnan provinces, and Chongqing City; vaccine not routinely recommended for travel limited to Beijing, Shanghai, Hong Kong City/Kowloon, Macau, or other major cities |
| India | Human cases reported from all states except Dadra, Daman, Diu, Gujarat, Himachal Pradesh, Jammu and Kashmir, Lakshadweep, Meghalaya, Nagar Haveli, Punjab, Rajasthan, and Sikkim | Most human cases reported May-November, especially in northern India; the season may be extended or year-round in some areas, especially in southern India | Highest rates of human disease reported from the states of Andhra Pradesh, Assam, Bihar, Goa, Haryana, Karnataka, Kerala, Tamil Nadu, Uttar Pradesh, and West Bengal |
| Indonesia | Widespread | Year-round; peak season varies by island | Sentinel surveillance has identified human cases in Bali, Kalimantan, Java, Nusa Tenggara, Papua, and Sumatra; several traveller cases reported in recent years from Bali |
| JapanFootnote 2 | Rare sporadic human cases on all islands except Hokkaido; enzootic activity ongoing | Most human cases reported June-October | Large number of human cases reported until JE vaccination program introduced in late 1960s; most recent small outbreak reported from Chugoku district in 2002; enzootic transmission without human cases observed on Hokkaido; vaccine not routinely recommended for travel limited to Tokyo or other major cities |
| Korea, North | Limited data; presumed widespread | No data; proximity to South Korea suggests peak transmission is likely to be May-November | N/A |
| Korea, SouthFootnote 2 | Widespread | Most human cases reported May-October | Large number of human cases reported until routine JE vaccination program introduced in mid-1980s; last major outbreak reported in 1982; vaccine not routinely recommended for travel limited to Seoul or other major cities |
| Laos | Widespread | Year-round, with peak season June-September | Sentinel surveillance has identified human cases in north, central, and southern Laos |
| Malaysia | Widespread | Year-round; in Sarawak, peak season October-December | Most human cases from reported from Sarawak; vaccine not routinely recommended for travel limited to Kuala Lumpur or other major cities |
| Nepal | Endemic in southern lowlands (Terai); cases also reported from hill and mountain districts, including the Kathmandu valley | Most human cases reported June-October | Highest rates of human disease reported from southern lowlands Terai districts; vaccine not routinely recommended for those trekking in high altitude areas |
| Pakistan | Limited data | Unknown | Human cases reported from around Karachi |
| Papua New Guinea | Widespread | Unknown; presumed year-round | Sporadic human cases reported from Western Province; serologic evidence of disease from Gulf and Southern Highland Provinces; a case of JE was reported from near Port Moresby in 2004 |
| Philippines | Widespread | Year-round, with peak season April-August | Human, animal and mosquito studies have indicated transmission in 32 provinces located in all regions of the country Transmission likely on all islands |
| Russia | Rare human cases reported from the Far Eastern maritime areas south of Khabarovsk | Most human cases reported July-September | Vaccine not routinely recommended |
| Singapore | Presumed in focal areas | Year-round | Rare sporadic human cases reported Vaccine not routinely recommended |
| Sri Lanka | Widespread, except in mountainous areas | Year-round with variable peaks based on monsoon rains | Highest rates of human disease reported from Anuradhapura, Gampaha, Kurunegala, Polonnaruwa, and Puttalam districts |
| TaiwanFootnote 2 | Rare sporadic human cases island-wide | Most human cases reported May-October | Large number of human cases reported until routine JE vaccination introduced in 1968; vaccine not routinely recommended for travel limited to Taipei or other major cities |
| Thailand | Widespread; seasonal epidemics in the northern provinces | Year-round with peak season May-October, especially in the north | Highest rates of human disease reported from the Chiang Mai Valley; several cases reported recently in travellers who visited resort or coastal areas of southern Thailand. |
| Timor-Leste (East Timor) | Presumed widespread | No data; cases reported year-round in neighboring West Timor | N/A |
| Vietnam | Widespread | Year-round with peak season May-October, especially in northern Vietnam | Highest rates of disease in the northern provinces around Hanoi and northwestern and northeastern provinces bordering China |
| Western Pacific Islands | Outbreaks of human disease reported in Guam in 1947-1948 and Saipan in 1990 | Unknown; most human cases reported October-March | Outbreaks likely followed introduction of virus, with enzootic cycle not sustained; vaccine not recommended |
Adapted from U.S. Centers for Disease Control and Prevention (CDC) Yellow Book 2024, Section 5 - Travel-Associated Infections & Diseases: Japanese encephalitis (68).
Appendix 4. Analytic framework for Japanese encephalitis vaccine (JEV)
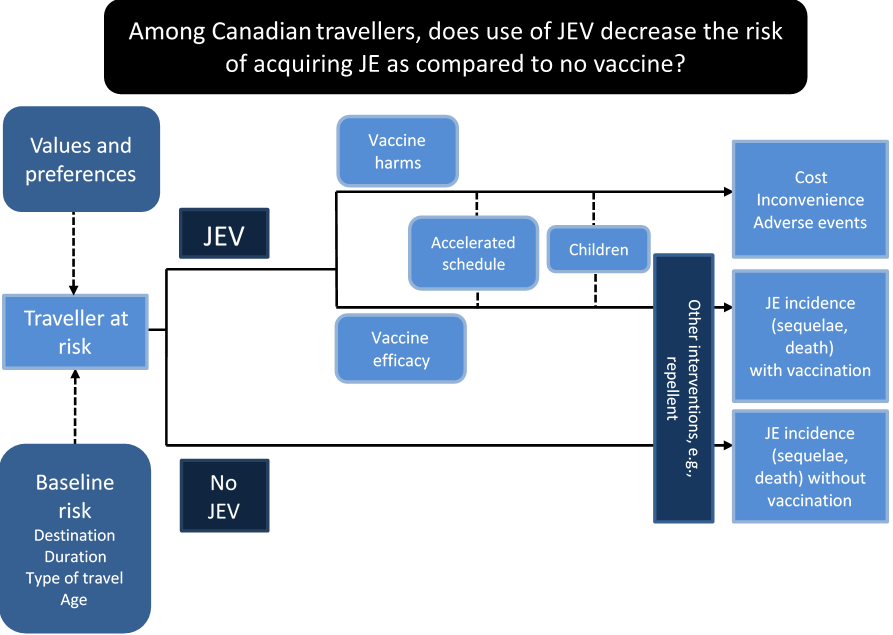
Appendix 5. Sample search strategy
Japanese encephalitis vaccination in travellers
Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE(R) and Ovid OLDMEDLINE(R) 1946 to June 22, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Encephalitis, Japanese/ep, mo, pc, px, sn, th | 1155 |
| 2 | Footnote *Encephalitis, Japanese/ | 1985 |
| 3 | Footnote *Encephalitis Virus, Japanese/ | 1417 |
| 4 | "Japanese encephalitis".tw,kw,kf. | 3739 |
| 5 | or/1-4 | 4188 |
| 6 | Japanese Encephalitis Vaccines/ad, ae, ct, im, st, tu, to [Administration & Dosage, Adverse Effects, Contraindications, Immunology, Standards, Therapeutic Use, Toxicity] | 334 |
| 7 | Footnote *Japanese Encephalitis Vaccines/ | 296 |
| 8 | Vaccination/ | 57681 |
| 9 | Immunization, Secondary/ or Immunization/ or Immunization Schedule/ | 56292 |
| 10 | (immunizFootnote * or immunisFootnote * or vaccinFootnote *).tw. | 306066 |
| 11 | or/6-10 | 333811 |
| 12 | ("IC51" or "IC-51" or "IC 51" or Ixiaro).mp. | 41 |
| 13 | Travel/ | 20053 |
| 14 | (touristFootnote * or travelFootnote *).tw. | 44184 |
| 15 | 13 or 14 | 53724 |
| 16 | 5 and 11 and (12 or 15) | 172 |
| 17 | exp Canada/ or (Canada or CanadianFootnote *).mp. | 162641 |
| 18 | (5 or 6 or 7) and 17 | 16 |
| 19 | 16 or 18 | 177 |
| 20 | animals/ not (humans/ and animals/) | 3968004 |
| 21 | letter/ or comment/ or editorial/ | 1418699 |
| 22 | 19 not (20 or 21) | 168 |
| 23 | remove duplicates from 22 | 165 |
Embase 1974 to June 22, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Japanese encephalitis/co, dt, ep, et, pc, th [Complication, Drug Therapy, Epidemiology, Etiology, Prevention, Therapy] | 430 |
| 2 | Footnote *Japanese encephalitis/ | 502 |
| 3 | Footnote *Japanese encephalitis virus/ | 1664 |
| 4 | "Japanese encephalitis".tw,kw. | 4291 |
| 5 | or/1-4 | 4601 |
| 6 | Japanese encephalitis vaccine/ae, ct, ad, it, dt, to [Adverse Drug Reaction, Clinical Trial, Drug Administration, Drug Interaction, Drug Therapy, Drug Toxicity] | 791 |
| 7 | Footnote *Japanese encephalitis vaccine/ | 478 |
| 8 | vaccination reaction/ or vaccination/ | 108357 |
| 9 | immunization/ | 82401 |
| 10 | (immunizFootnote * or immunisFootnote * or vaccinFootnote *).tw. | 351057 |
| 11 | or/6-10 | 389810 |
| 12 | ("IC51" or "IC-51" or "IC 51" or Ixiaro).mp. | 124 |
| 13 | travel/ | 28902 |
| 14 | (touristFootnote * or travelFootnote *).tw. | 54771 |
| 15 | or/13-14 | 65389 |
| 16 | 5 and 11 and (12 or 15) | 275 |
| 17 | exp Canada/ or (Canada or CanadianFootnote *).mp. | 213446 |
| 18 | 17 and (5 or 6 or 7) | 25 |
| 19 | 16 or 18 | 290 |
| 20 | animal/ not (human/ and animal/) | 1258280 |
| 21 | editorial/ or letter/ | 1363656 |
| 22 | 19 not (20 or 21) | 278 |
| 23 | remove duplicates from 22 | 276 |
Global Health 1973 to June 22, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Japanese encephalitis/ | 2266 |
| 2 | "Japanese encephalitis".tw,hw. | 4114 |
| 3 | Japanese encephalitis virus.od. | 3202 |
| 4 | or/1-3 | 4114 |
| 5 | vaccination/ | 46057 |
| 6 | immunization/ | 51546 |
| 7 | (immunizFootnote * or immunisFootnote * or vaccinFootnote *).tw. | 104918 |
| 8 | or/5-7 | 104918 |
| 9 | ("IC51" or "IC-51" or "IC 51" or Ixiaro).mp. | 22 |
| 10 | exp travel/ or exp travel associated diseases/ | 4246 |
| 11 | (touristFootnote * or travelFootnote *).tw. | 17930 |
| 12 | or/10-11 | 18052 |
| 13 | 4 and 8 and (9 or 12) | 162 |
| 14 | exp Canada/ or (Canada or CanadianFootnote *).mp. | 33670 |
| 15 | 14 and 4 | 14 |
| 16 | 13 or 15 | 171 |
| 17 | remove duplicates from 16 | 170 |
- Footnote 1
-
denotes truncation; a technique used in developing literature search strategies that broadens the search to include various endings to the search term.
SCOPUS to June 22, 2015
(((TITLE-ABS("Japanese encephalitis")) and (TITLE-ABS-KEY((immuniz* or immunis* or vaccin*)))) and ((TITLE-ABS-KEY(("IC51" or "IC-51" or "IC 51" or Ixiaro))) or (TITLE-ABS-KEY((tourist* or travel*))))) or ((TITLE-ABS((Canada or Canadian*))) and (TITLE-ABS("Japanese encephalitis"))) AND ( EXCLUDE(DOCTYPE,"le") OR EXCLUDE(DOCTYPE,"ch") OR EXCLUDE(DOCTYPE,"ed")) 214 Document results
Google Search, June 22, 2015
Centers for Disease Control and Prevention
CDC's Health Information for International Travel (Yellow Book)
http://wwwnc.cdc.gov/travel/yellowbook/2010/chapter-2/japanese-encephalitis.aspx
Use of Japanese Encephalitis Vaccine in Children: Recommendations of the Advisory Committee on Immunization Practices, 2013
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6245a3.htm
Novartis Product Monograph: https://www.ask.novartispharma.ca/download.htm?res=ixiaro_patient_e.pdf&resTitleId=462
Public Health Agency of Canada
https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines.html?page=11
U.S. Food and Drug Administration
http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm179132.htm
Japanese encephalitis: Risk factors for travellers
Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE(R) and Ovid OLDMEDLINE(R) 1946 to June 19, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Encephalitis, Japanese/ep, mo, pc, px, sn, th | 1155 |
| 2 | Footnote *Encephalitis, Japanese/ | 1985 |
| 3 | Footnote *Encephalitis Virus, Japanese/ | 1417 |
| 4 | (Japanese adj encephalitis).mp. | 3771 |
| 5 | or/1-4 | 4205 |
| 6 | Risk Factors/ | 603019 |
| 7 | ("risk factorFootnote *" or (riskFootnote * adj25 "japanese encephalitis")).tw. | 386859 |
| 8 | 6 or 7 | 792870 |
| 9 | Travel/ | 20052 |
| 10 | (travelFootnote * or touristFootnote *).tw. | 44149 |
| 11 | or/9-10 | 53689 |
| 12 | 5 and 8 and 11 | 61 |
| 13 | animals/ not (humans/ and animals/) | 3967673 |
| 14 | letter/ or comment/ or editorial/ | 1417918 |
| 15 | 12 not (13 or 14) | 59 |
| 16 | remove duplicates from 15 | 58 |
Embase 1974 to June 19, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Japanese encephalitis/ | 957 |
| 2 | Japanese encephalitis virus/ | 2887 |
| 3 | (Japanese adj encephalitis).mp. | 5454 |
| 4 | or/1-3 | 5454 |
| 5 | risk factor/ | 685974 |
| 6 | ("risk factorFootnote *" or (riskFootnote * adj25 "japanese encephalitis")).tw. | 531075 |
| 7 | or/5-6 | 876042 |
| 8 | travel/ | 28870 |
| 9 | travelFootnote *.tw. | 52460 |
| 10 | (travelFootnote * or touristFootnote *).tw. | 54731 |
| 11 | 8 or 10 | 65347 |
| 12 | 4 and 7 and 11 | 85 |
| 13 | animal/ not (human/ and animal/) | 1258280 |
| 14 | letter/ or editorial/ | 1363439 |
| 15 | 12 not (13 or 14) | 85 |
Global Health 1973 to June 19, 2015
| # | Searches | Results |
|---|---|---|
| 1 | Japanese encephalitis/ | 2266 |
| 2 | "Japanese encephalitis".tw,hw. | 4114 |
| 3 | Japanese encephalitis virus.od. | 3202 |
| 4 | or/1-3 | 4114 |
| 5 | risk factors/ | 134937 |
| 6 | ("risk factorFootnote *" or (riskFootnote * adj25 "japanese encephalitis")).tw. | 168829 |
| 7 | 5 or 6 | 168829 |
| 8 | exp travel/ | 4046 |
| 9 | (touristFootnote * or travelFootnote *).tw. | 17930 |
| 10 | 8 or 9 | 18052 |
| 11 | 4 and 7 and 10 | 43 |
- Footnote 1
-
denotes truncation; a technique used in developing literature search strategies that broadens the search to include various endings to the search term.
Scopus to June 19, 2015
(TITLE("Japanese encephalitis") AND TITLE-ABS-KEY(risk*)AND TITLE-ABS-KEY(travel*)) AND ( LIMIT-TO(DOCTYPE,"ar") OR LIMIT-TO(DOCTYPE,"re"))
Appendix 6. Summary of findings for comparison of JEV and inactivated mouse-brain derived vaccine (MBV): Seroconversion rate (SCR) and adverse events (AE)
| Outcomes | Illustrative comparative risksFootnote * (95% CI) | Relative effect (95% CI) |
No of Participants (studies) |
Quality of the evidence (GRADE) ɫ |
|
|---|---|---|---|---|---|
| Assumed risk MBV |
Corresponding risk JEV |
||||
| SCR | Study population | RR 1.03 (1.01 to 1.06) |
725 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
|
| 953 per 1000 | 982 per 1000 (963 to 1000) |
||||
|
|||||
| Outcomes | Illustrative comparative risksFootnote * (95% CI) | Relative effect (95% CI) |
No of Participants (studies) |
Quality of the evidence (GRADE) Footnote ɫ |
|
|---|---|---|---|---|---|
| Assumed risk MBV |
Corresponding risk JEV |
||||
| Headache | Study population | RR 0.92 (0.74 to 1.14) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 287 per 1000 | 264 per 1000 (213 to 328) |
||||
| ILI | Study population | RR 1 (0.7 to 1.42) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 126 per 1000 | 126 per 1000 (89 to 180) |
||||
| Myalgia | Study population | RR 1.3 (0.97 to 1.72) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 159 per 1000 | 206 per 1000 (154 to 273) |
||||
| Fatigue | Study population | RR 1.14 (0.79 to 1.65) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 110 per 1000 | 126 per 1000 (87 to 182) |
||||
| Redness | Study population | RR 0.09 (0.03 to 0.24) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 106 per 1000 | 10 per 1000 (3 to 25) |
||||
| Swelling | Study population | RR 0.13 (0.04 to 0.44) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 53 per 1000 | 7 per 1000 (2 to 23) |
||||
| Hardness | Study population | RR 0.16 (0.06 to 0.46) |
863 (1 study) |
⊕⊕⊕⊕ high |
|
| 57 per 1000 | 9 per 1000 (3 to 26) |
||||
|
|||||
Appendix 7. Summary of findings for comparison of conventional immunization schedule for JEV (0, 28 days) to accelerated schedule (0, 7 days): Seroconversion rate (SCR) and adverse events (AE)
| Outcomes | Illustrative comparative risksFootnote * (95% CI) | Relative effect (95% CI) |
No of Participants (studies) |
Quality of the evidence (GRADE)ɫ |
Comments | |
|---|---|---|---|---|---|---|
| Assumed risk Conventional |
Corresponding risk Accelerated |
|||||
| SCR day 10-14 | Study population | RR 3.95 (3.16 to 4.92) |
441 (1 study) |
⊕⊕⊝⊝ lowFootnote 1,Footnote 2 |
None | |
| 252 per 1000 | 996 per 1000 (797 to 1000) |
|||||
| SCR 35 | Study population | RR 0.99 (0.97 to 1.01) |
410 (1 study) |
⊕⊕⊕⊝ moderateFootnote 2 |
None | |
| 995 per 1000 | 985 per 1000 (965 to 1000) |
|||||
| Outcomes | Illustrative comparative risksFootnote * (95% CI) | Relative effect (95% CI) |
No of Participants (studies) |
Quality of the evidence (GRADE)Footnote ɫ |
Comments | |
|---|---|---|---|---|---|---|
| Assumed risk Control |
Corresponding risk IXIARO®accelerated AE |
|||||
| Any AE | Study population | RR 1 (0.91 to 1.09) |
383 (1 study) |
⊕⊕⊕⊕ high |
None | |
| 831 per 1000 | 831 per 1000 (757 to 906) |
|||||
| Local | Study population | RR 0.99 (0.88 to 1.11) |
383 (1 study) |
⊕⊕⊕⊕ high |
None | |
| 753 per 1000 | 745 per 1000 (663 to 836) |
|||||
| Systemic | Study population | OR 1.28 (0.84 to 1.94) |
383 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 602 per 1000 | 660 per 1000 (560 to 746) |
|||||
| Other | Study population | OR 1.01 (0.59 to 1.74) |
383 (1 study) |
⊕⊕⊕⊝ moderateFootnote 1 |
None | |
| 169 per 1000 | 170 per 1000 (107 to 261) |
|||||
Appendix 8. Summary of Advisory Committee on Immunization Practice (ACIP) GRADE results
Background:
- In 2009, ACIP at the Centers for Disease Control and Prevention (CDC) approved recommendations for use of inactivated Vero cell culture-derived Japanese encephalitis vaccine JEV for use in adults 17 years of age and olderFootnote 45.
- In 2013 the ACIP performed a GRADE review for the use of JE-VC in children (4,32). The question was: Should inactivated Vero cell culture-derived Japanese encephalitis vaccine be recommended for used in children 2 months through 16 years of age at increased risk of travel-related exposure to Japanese encephalitis virus?
- Population: children 2 months through 16 years
- Intervention: JEV administered as a 2-dose primary series
- Current option: No JEV recommended and available for use in children
- Benefits were seroprotection at 1 and 6 months after vaccination. Harms were systemic adverse effects (e.g. fever, rash, hypersensitivity or uticaria, neurologic and medically attended adverse effects) or serious adverse effects (Table A1).
Methods:
- Literature published from January 1 2006 to April 30 2013 was retrieved for review and inclusion/exclusion criteria are provided in the document (primary data, no case studies, FDA approved dose, human subjects, etc.).
- 67 studies identified and 51 excluded
- Evidence for critical outcomes was assessed using GRADE criteria (Table A2).
Findings:
- JEV is effective using seroprotection as the endpoint and safe in children aged 2 months through 16 years. The workgroup proposed to extend the previous ACIP recommendationsFootnote 45 for use of JEV in adults to include children ≥2 months of age; no other changes to the existing ACIP recommendations were proposed. Key factors considered in making the recommendation are summarized in Table A3.
| Outcome | Design (# studies)Footnote 1 |
Risk of bias | Inconsistency | Indirectness | Imprecision | OtherFootnote 2 | Evidence typeFootnote 3 |
|---|---|---|---|---|---|---|---|
| Benefits | |||||||
| Seroprotection at 1 month | RCTFootnote 4 | No serious | No serious | YesFootnote 4 | No serious | None | 2 |
| ObsFootnote 6 | No serious | No serious | No serious | No serious | None | 3 | |
| Seroprotection at 6 months | RCTFootnote 2 | No serious | No serious | YesFootnote 4 | No serious | None | 2 |
| ObsFootnote 3 | No serious | No serious | No serious | No serious | None | 3 | |
| Harms | |||||||
| Serious adverse events | RCTFootnote 8 | YesFootnote 5 | No serious | YesFootnote 6 | No serious | None | 3 |
| ObsFootnote 5 | No serious | No serious | YesFootnote 6 | No serious | None | 4 | |
| Systemic adverse events | RCTFootnote 5 | YesFootnote 5 | No serious | No serious | No serious | None | 2 |
| ObsFootnote 4 | No serious | No serious | No serious | No serious | None | 3 | |
| Outcome | Study design (# studies)Footnote 1 |
Finding | Evidence TypeFootnote 2,Footnote 3 |
Overall quality of evidence |
|---|---|---|---|---|
| Seroprotection at 1 month | RCTFootnote 4 | High (>95%) at 1 month | 2 | 2 |
| Seroprotection at 6 months | RCTFootnote 2 | Maintained (85-90%) at 6 months | 2 | |
| Serious adverse events | RCTFootnote 8 | Low incidence; similar to comparison vaccines | 3 | |
| Systemic adverse events | RCTFootnote 5 | Similar to comparison vaccines | 2 | |
|
||||
| Key factors | Comments |
|---|---|
Evidence type for benefits and harms |
|
Balance between benefits and harms |
|
Value |
|
Cost-effectiveness |
|
Appendix 9. Quality assessment for risk of Japanese encephalitis in travellers from Canada, the United States and Europe
| Jurisdiction | Risk of biasFootnote 1 | Inconsistency | Indirectness | Imprecision | Other considerations | Estimated attack rate | Confidence in baseline estimateFootnote ɫ |
|---|---|---|---|---|---|---|---|
| CanadaFootnote 2 | |||||||
| Case reports against travel denominator (2006-2015) |
intermediate | no serious | no serious | none | none | 1/11,650,000 (95% CI 1/65,996,483; 1/2,056,512) | ⊕⊕⊕⊝ MODERATE |
| United StatesFootnote 3 | |||||||
| Case reports against travel denominator (2006-2015) |
intermediate | no serious | no serious | none | none | 1/11,078,000 (95% CI 1/25,935,276; 1/4,731859) | ⊕⊕⊕⊝ MODERATE |
| EuropeFootnote 4 | |||||||
| Case reports against travel denominator (2006-2015) |
intermediate | no seriousFootnote i | no serious | none | none | 1/13,636,363 (95% CI 24,420,2750; 7,614,592) | ⊕⊕⊕⊝ MODERATE |
Appendix 10. Factors to consider when evaluating a traveller's risk for Japanese encephalitis (JE) virus exposure
- Destination
- JE occurs in areas throughout most of Asia and parts of the western Pacific. It is generally accepted that the likelihood of JE exposure is highest in rural agricultural areas.
- Duration of travel
- A longer duration of travel increases the likelihood that a traveller might be exposed to a JEV-infected mosquito.
- Season
- In most temperate areas of Asia, JEV transmission is seasonal, and human disease usually peaks in summer and fall. In the subtropics and tropics, JEV transmission patterns vary, and human disease can be sporadic or occur year-round. Appendix 2 provides country level information.
- Activities
-
The mosquitoes that transmit JEV feed on humans most often in the outdoors, with peak feeding times usually being during the hours of darkness.
Extensive outdoor activities (e.g., camping, hiking, trekking, biking, fishing, hunting, or farming), especially during the evening or night, increase the risk of being exposed to a JEV-infected mosquito.
Accommodations with no air conditioning, screens, or bed nets increase the risk of exposure to mosquitoes that transmit JEV and other vector-borne diseases (e.g., dengue and malaria).
- Use of Personal Protective Measures (PPM)
- Use of PPMs, e.g. bed net, repellent, clothing treatment, are expected to provide substantial protection against the bites of the mosquito that transmits JE. The level of personal compliance with PPMs can significantly alter the risk of exposure to JE.
Appendix 11. Study summaries considered for inclusion in GRADE analysis
| Reference | Topic | Study design | Vaccine/comparator dose and schedule | Population | Demographic | Objectives | Comments |
|---|---|---|---|---|---|---|---|
| Tauber 2008Footnote 31 | Safety | Randomized, double-blind, placebo-controlled, multicentre phase 3 trial. | JEV at 0, 28 days (6 μg of virus in 0.5 ml/dose) compared to PBS solution w/ aluminum hydroxide at 0,28 days (0.5 ml/dose). | 2,650 subjects. 1,993 received JEV and 657 received placebo. | Healthy male and female subjects aged 18 years and older and without history of JE vaccination. | Primary endpoint rate of SAEFI and MAEFI from first dose until 4 weeks after completion of vaccination. Secondary endpoint was local AEFI recoded in patient diary. | Included |
| Tauber 2007Footnote 25 | Immunogenicity and safety | Multicentre, observer-blinded, centrally randomised, controlled, non-inferiority phase 3 trial. | JEV at days 0, 28 (6 μg of virus in 0.5 ml/dose) and a placebo (0.5ml of aluminum hydroxide) at day 7 compared to JE-VAX at days 0, 7, 28 (1ml/dose). | 863 received study medication of 867 randomized. 428 received JEV and 435 received MBV. | Male and females aged 18 or older. No previous immunization for JE or YF. | Primary endpoint seroconversion, assessed on day 56. Secondary endpoint safety, assessed during visits and via patient diary. | Included |
| Schuller 2011Footnote 69 | Safety | Review article | 10 individual Phase 3 trials were examined | N/A | N/A | Reports on safety profiles derived from post marketing data and pooled analyses of clinical safety data | Excluded (review article) |
| Schuller 2009Footnote 27 | Safety and Immunogenicity | Randomized, controlled, observer-blind, parallel-group, multicentre phase 3 trial. | Single dose of JEV (6 μg/dose) at days 0, 28 compared to 2 doses of JEV (6 μg/dose) at day 0 compared to a single dose of JEV (6 μg/dose) at day 0. | 374 subjects. 124 received the single, high-dose (1x12 μg), 125 received the standard regimen (2x6 μg) and 125 received the single, standard dose (1x6 μg). | Healthy male and female subjects aged 18 years and older. No previous immunization for JE. | Primary endpoint seroconversion, assessed on days 10, 28, 35 and 56 after first vaccination. Secondary endpoint safety, assessed during visits and via patient diary. | Included |
| Kaltenböck 2009Footnote 70 | Safety and Immunogenicity | Multicentre, randomized, controlled, single-blind phase 3 trial. | JEV (6 μg/dose) at days 0,28 and placebo (0.5 ml) at day 0 compared to placebo (0.5 ml) at days 0,28 and HAV at day 0 compared to JEV (6 μg/dose) at days 0,28 and HAV at day 0 | 192 subjects. 65 received JEV + placebo, 65 received HAV + placebo and 62 received JEV + HAV. | Healthy male and female subjects 18 years of age or older. No previous immunization for JE, Yellow fever or hepatitis A. | Primary endpoint seroconversion for JEV (day 56). Secondary endpoint seroconversion compared JEV with concomitant JEV + HAV (day 56). Secondary endpoint safety, assessed during visits and via patient diary. | N/A |
| Dubischar-Kastner 2010Footnote 59 | Safety and Immunogenicity | Uncontrolled, multicentre, open-label, phase 3 follow-up study. Extension of previously described study (Schuller et al., 2009). |
Immunogenicity assessed in subjects from previous study at 6, 12 and 24 months after first vaccination. Subjects with a negative plaque reduction neutralization test (PRNT) result at 6 or 12 months received a booster dose of JEV (6 μg) at 11 or 23 months after. | 349 subjects. 206 received a booster at month 11, 43 received a booster at month 23 and 1 subject received a booster at months 11 and 23. | Healthy male and female subjects, 18 years and older, having previously participated in JEV study. | Primary endpoint seroconversion, assessed 24 months after first JEV vaccination. Safety, assessed during visits and via patient diary. |
Excluded (only related to booster) |
| Lyons 2007Footnote 28 | Safety and Immunogenicity | Randomized, open label, single center phase 2 trial. |
JEV (6 μg/dose) at days 0, 28 compared to JEV (6 μg/dose) at days 0, 14, 28 compared to JEV (12 μg/dose) at days 0, compared to JE-Vax on days 0, 7, 28. | 94 subjects. 24 received JEV (2x6 μg), 24 received JEV (3x6 μg), 25 received (2x12 μg) and 21 received JE-Vax (3 doses). | Military or civilian subjects aged between 18 and 49 years old. Exclusions included previous exposure to dengue, JE, YF or TBE. | Primary endpoint seroconversion, assessed on days 28 and 56. Optional follow up at 6, 12, 18 and 24 months. Secondary endpoint safety, assessed during visits and via patient diary. | Included |
| Kaltenböck 2010Footnote 29 | Safety and Immunogenicity | Randomized, open-label, single center phase 2 trial. | JEV (3 μg /dose) compared to JEV (6 μg /dose) compared to JenceVac (0.5 ml/dose) | 60 subjects. 24 received JEV 3 μg, 24 received JEV 6 μg and 12 received JenceVac. | Healthy children of either sex between 1-3 years old. No previous immunization for JE, Yellow fever or Dengue. | Primary endpoint seroconversion, assessed on days 28 and 56. Safety assessed during visits and via patient diary completed by proxy. |
Included |
| Yun 2015Footnote 71 | N/A | Multicentre, double-blind, centrally randomised study with ENCEVAC, not JEV. |
N/A | N/A | N/A | N/A | Excluded (JEV was not used). |
| Jelinek 2015Footnote 26 | Safety and Immunogenicity | Phase 3, randomized, observer-blind, multicentre trial. | JEV (0.5 ml/dose) at days 0, 28 + rabies at days 0, 7 compared to JEV (0.5 ml/dose) at days 0, 7 + rabies at days 0, 3 compared to JEV (0.5 ml/dose) alone at days 0, 28. |
440 subjects. 167 received the standard JE + rabies regimen, 217 received the accelerated JE + rabies regimen and 56 received the standard JE regimen. | N/A | 440 healthy adults aged 18-65. Persons previously receiving JE vaccination. Primary endpoint seroconversion, assessed 28 days after completion of series (day 35 or day 56). Secondary endpoint safety, assessed during visits and via patient diary. | N/A |
| Eder 2011Footnote 72 | Safety and Immunogenicity | Prospective, open-label, multi-center phase 3 extension study. Booster dose of JEV provided 15 months after the first dose of the primary series. | N/A | N/A | N/A | Healthy male and female subjects at least 18 YOA (198 subjects). Previously had completed JEV series. Primary endpoint seroconversion, assessed 1, 6 and 12 months after booster. Secondary endpoint safety, assessed during visits and via patient diary. | N/A |
| Paulke-Korinek 2015Footnote 12 |
Immunogenicity | Extension of previously described study (Eder et al 2011). | N/A | N/A | N/A | Blood draw at 76 months from 67 patients who participated in boostering study. Primary endpoint seroconversion. | N/A |
| Schuller 2008Footnote 30 | Immunogenicity | Multi-centre phase 3 uncontrolled follow-up study. JEV and MBV. | N/A | N/A | N/A | Of the 3258 subjects that completed previous phase 3 studies, 298 were enrolled. Primary endpoint seroconversion, assessed at 6 (298 subjects) and 12 months (180 subjects). | N/A |
| ACIP 2013Footnote 4 | Safety and Immunogenicity | GRADE analysis for use of JEV in children. | N/A | N/A | N/A | Multiple studies included, includes unpublished evidence. | Include |