
COVID-19 and the need for sex-disaggregated mortality data

 Download this article as a PDF
Download this article as a PDFPublished by: The Public Health Agency of Canada
Issue: Volume 46–7/8: Mandatory childhood immunization programs
Date published: July 2, 2020
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 46–7/8, July 2, 2020: Mandatory childhood immunization programs
Rapid communication
COVID-19 and the increasing need for sex-disaggregated mortality data in Canada and worldwide
Amanda Lien1, Rojiemiahd Edjoc1, Nicole Atchessi1, Christine Abalos1, Imran Gabrani-Juma1, Marianne Heisz1
Affiliation
1 Centre for Biosecurity, Public Health Agency of Canada, Ottawa, ON
Correspondence
Suggested citation
Lien A, Edjoc R, Atchessi N, Abalos C, Gabrani-Juma I, Heisz M. COVID-19 and the increasing need for sex-disaggregated mortality data in Canada and worldwide. Can Commun Dis Rep 2020;46(7/8):231–5. https://doi.org/10.14745/ccdr.v46i78a03
Keywords: COVID-19, coronavirus, sex, gender, infectious disease
Abstract
In countries most impacted by coronavirus disease (COVID-19), such as Italy and China, surveillance reveals that the number of deaths differ by sex. Preliminary data suggest that while the distributions of cases vary by sex, men represent the larger proportion of deaths in these countries. Analyses of deaths can indicate differential disease progression between men and women more robustly than analyses of cases, as the former are less susceptible to biases of underreporting and bottlenecks in testing. Canada has an enormous opportunity to apply its sex-specific mortality data to conduct comprehensive health and medical research that captures sex-based differences in manifestation of the disease to improve outcomes and prevention methods. During the ongoing pandemic, it is difficult for complete and wholly accurate data of all COVID-19 deaths to be obtained when healthcare and public health personnel are operating at full capacity. However, it is crucial that efforts continue to be made to capture this information and make it accessible, as it can also be applied to inform implementation of more effective and equitable public health and clinical strategies, such as the dissemination of targeted health communication materials and therapy.
Introduction
Many countries, including Canada, have implemented substantial control measures such as physical distancing and travel restrictions to reduce the spread of coronavirus disease (COVID-19), a novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease that is highly transmissible through droplets and direct contactFootnote 1Footnote 2Footnote 3. On March 11, 2020, the World Health Organization declared the coronavirus outbreak a pandemicFootnote 4. As of June 10, there were approximately 7.27 million cases of COVID-19 worldwide and 412,013 deathsFootnote 5. In Canada, there were 96,653 confirmed cases and 7,897 deaths had occurred as of June 9, 2020Footnote 6.
During the 2002–2003 outbreak of severe acute respiratory syndrome (SARS), a disease also caused by a type of coronavirus, sex-based mortality data indicated that men had a higher case fatality rate than womenFootnote 7Footnote 8. Other studies have also established that sex is linked with response to infectious diseasesFootnote 9Footnote 10. Based on studies of SARS and other epidemic-prone infectious diseasesFootnote 11, the World Health Organization has encouraged the implementation of sex-based health communication, promotion and primary care strategies.
Early sex-based mortality data from the ongoing COVID-19 pandemic indicates that males account for more COVID-19 related deaths than do females in nearly every country for which such data are availableFootnote 12. Despite the preliminary observations suggesting that sex plays a role in disease outcome and severity, few countries collect complete sex-disaggregated data on deaths.
Data on COVID-19 cases can be subject to possible biases in symptom reporting and selection bias towards more severe manifestations of the illness due to bottlenecks in testingFootnote 13. In contrast, data on COVID-19 deaths are more robust. For instance, in April 2020 the Ontario Ministry of Health guidelines stated that high-risk individuals such as health care workers and persons living and working in congregate living institutions and their close contacts should be tested if displaying symptomsFootnote 14. With testing resource availability a likely barrier and women more likely to report bodily symptoms than menFootnote 15Footnote 16Footnote 17Footnote 18, there may be a sex-based bias that can result in more men failing to seek or receive adequate care.
Gathering sex-disaggregated mortality data is crucial to providing a better understanding of sex-based disparities in COVID-19 outcome severity and mortality riskFootnote 19. Knowing these risks, in turn, can inform more comprehensive research and equitable and effective public health interventions such as targeted health communication and clinical care. Focusing on capturing these data is a feasible start to creating a national dataset that contains disaggregated sex and gender data. This review focuses on the need to gather sex-based data, which can provide insight into the role that biological differences may play in mortality risk. However, gathering gender-based data is also necessary to determine the role of gender-based inequities, norms, and behaviours in mortality risk. Gathering sex-disaggregated mortality data could begin to provide even greater insight into differential disease progression that is associated with behaviours linked with gender normsFootnote 12Footnote 20.
Current situation
The role of sex in COVID-19 mortality risk
Women form a large proportion of the health workforce and are at greater risk of exposure to SARS-CoV-2Footnote 21. This is reflected in their greater representation among confirmed COVID-19 cases in CanadaFootnote 6. Unlike in most other countries, women also represent a larger proportion of deaths among confirmed cases. On the global scale, early studies suggested sex-based immunological differences as a possible partial explanation for the greater number of male deaths related to COVID-19Footnote 22Footnote 23. Various studies based on populations in China found that the presence of certain medical conditions, such as those for which smoking is a risk factor, which disproportionately affect menFootnote 24, may increase the risk of severe COVID-19 illness and outcomesFootnote 25Footnote 26. Studies in populations with different ethnic and genetic backgrounds are needed to better understand sex-based differences in the expression of angiotensin-converting enzyme 2 (ACE2)—which has increased expression with smoking and is the receptor of SARS-CoV-2—and how this relates to COVID-19 mortality riskFootnote 27. The observation that Canada’s mortality data does not follow the global trend of men having greater mortality risk may be attributable to other factors specific to Canada. For instance, although sex may play a role, other demographic variables such as age and other genetic factors may also contribute to mortality risk. The interplay between these factors in affecting COVID-19 mortality risk is unknown. In terms of responses to COVID-19, some studies using sex-based case data found major public health interventions such as travel restrictions and social distancing to be associated with equally improved control of the outbreak among both sexesFootnote 28Footnote 29. However, the effects of public health interventions and policy on mortality risk by sex is unknown.
Trends in sex-disaggregated mortality data
As of June 10, 2020, sex-disaggregated data for COVID-19-related deaths were available for various countriesFootnote 20. While the male-to-female ratio of confirmed cases varied by country, males represented a larger proportion of deaths among confirmed cases in all but two of these countries (Figure 1). Meanwhile, there were several highly affected countries for which the ratio of male-to-female deaths among confirmed COVID-19 cases could not be confirmed, including the United States and France.
Figure 1: Male-to-female ratio of deaths among confirmed cases of COVID-19 in the thirty countries with the most deaths outside of Canada, where the data were available, June 10, 2020
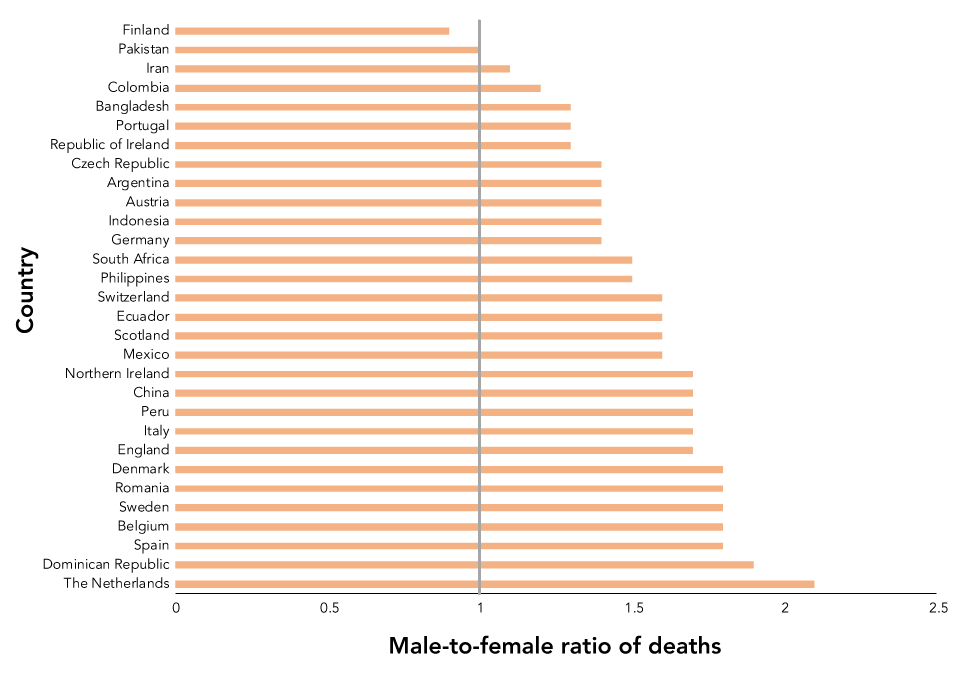
Text description: Figure 1
Figure 1: Male-to-female ratio of deaths among confirmed cases of COVID-19 in the thirty countries with the most deaths outside of Canada, where the data were available, June 10, 2020
| Country | Deaths in confirmed cases (Male-to-female ratio) |
|---|---|
| The Netherlands | 2.1 |
| Dominican Republic | 1.9 |
| Spain | 1.8 |
| Belgium | 1.8 |
| Sweden | 1.8 |
| Romania | 1.8 |
| Denmark | 1.8 |
| England | 1.7 |
| Italy | 1.7 |
| Peru | 1.7 |
| China | 1.7 |
| Northern Ireland | 1.7 |
| Mexico | 1.6 |
| Scotland | 1.6 |
| Ecuador | 1.6 |
| Switzerland | 1.6 |
| Philippines | 1.5 |
| South Africa | 1.5 |
| Germany | 1.4 |
| Indonesia | 1.4 |
| Austria | 1.4 |
| Argentina | 1.4 |
| Czech Republic | 1.4 |
| Republic of Ireland | 1.3 |
| Portugal | 1.3 |
| Bangladesh | 1.3 |
| Colombia | 1.2 |
| Iran | 1.1 |
| Pakistan | 1.0 |
| Finland | 0.9 |
Because sex-disaggregated mortality data on the global scale is somewhat incomplete, establishing the role that sex may play in COVID-19 mortality risk is challenging. The Government of Canada’s data suggest that Canada’s distribution of deaths by sex does not follow the trend that has been observed in other highly affected countriesFootnote 6. Among the deaths reported as of June 9, 2020, the male-to-female ratio of deaths among confirmed cases was 0.85. This observation may be attributable to factors such as sex-based age distribution, long-term care facility resident distribution, and frontline health workforce distributionFootnote 30Footnote 31. It also warrants exploration of possible sex-based disparities in the Canadian context pertaining to areas such as public health interventions, healthcare access, and disease progression.
The Public Health Agency of Canada houses a dataset that includes sex information of COVID-19 deaths; this dataset is made available publicly in an aggregated formatFootnote 6. The disaggregated line list is obtained from the provinces and territories but may be missing or lagging information due not only to challenges in data collection as the result of the pandemic but also to already existing data collection issues exacerbated by the pandemic. This obstacle may prevent complete and up-to-date information from being recorded and passed on to the federal government for timely dissemination. Nevertheless, it is important that this information continue to be captured as best as possible as it can inform research and the public health response. Furthermore, COVID-19 cases admitted to the intensive care unit (ICU) experienced longer durations between symptom onset to hospitalization than non-ICU casesFootnote 32. Therefore, health promotion efforts that encourage men to use health services earlier and more effectively may be a practical intervention to implement.
Recommendations
Despite local, provincial and national-level institutions operating at full capacity and the challenges that might come with resource and personnel availability in some regions during a pandemic, it is recommended that efforts continue to be made to capture sex-disaggregated COVID-19 mortality data in Canada and worldwide. An effective collaboration between provinces and government would also be a catalyst for the achievement of this goal in Canada. We acknowledge the efforts being made by Statistics Canada, the Public Health Agency of Canada, Health Canada and other federal partners, working closely with provinces, territories and coroners to provide more comprehensive and timely death statistics. Sex-disaggregated data would allow for sex-based analyses to be incorporated into research pertaining to the health behaviours and outcomes surrounding COVID-19Footnote 33 that serve to inform clinical care and health communication and to reveal how public health interventions differentially affect men and women. In terms of clinical care, improved outcomes such as reduced mortality could be seen with sex-based medical interventions if disease progression differs between men and women. In terms of public health interventions, implementing strategies such as sex-based, targeted health communication messages could be more effective in instilling prevention principles among male and female audiences. In order to gain a more comprehensive and clearer understanding of how sex and COVID-19 mortality are related, it is recommended that all countries strive to collect sex-disaggregated mortality data and make these data accessible. While we describe the rationale and advocate for the capture of comprehensive sex-disaggregated data, we have not explored the issue of gender. It is also important that gender-disaggregated data be captured as it can reveal the role of gender-based inequities, norms, and behaviours in COVID-19 mortality risk.
Conclusion
Early data from the COVID-19 pandemic suggest that men represent the larger proportion of COVID-19 deaths in most countries. Currently, Canadian response to the COVID-19 pandemic has included policies and public health efforts that consider various aspects of SARS-CoV-2, such as its infectivity and routes of transmission. However, there is an opportunity to curb the number COVID-19-related deaths and severe outcomes by incorporating the role of sex in mortality risk into more comprehensive and relevant research and to develop a more effective response that can include targeted health communication and clinical care. It is therefore essential that these data continue to be collected, made accessible and applied in Canada and other affected countries in a timely manner during the ongoing COVID-19 pandemic.
Authors’ statement
- AL — Methodology, investigation, writing – original draft
- RE — Conceptualization, writing – review and editing, supervision
- NA — Writing – review and editing
- CA — Writing – review and editing
- IGJ — Writing – review and editing
- MH — Writing – review and editing
Competing interests
None.
