
Distinguishing female infectious syphilis in British Columbia

 Download this article as a PDF
Download this article as a PDF Published by: The Public Health Agency of Canada
Issue: Volume 48-2/3, February/March 2022: Syphilis Resurgence in Canada
Date published: February/March 2022
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 48-2/3, February/March 2022: Syphilis Resurgence in Canada
Surveillance
Characterizing female infectious syphilis cases in British Columbia to identify opportunities for optimization of care
Kaylie Willemsma1, Lindsay Barton2, Rochelle Stimpson2, Irene Pickell2, Venessa Ryan2, Amanda Yu2, Ann Pederson1,3, Gina Ogilvie1,2,3, Troy Grennan1,2, Jason Wong1,2
Affiliations
1 Faculty of Medicine, University of British Columbia, Vancouver, BC
2 BC Centre for Disease Control, Vancouver, BC
3 BC Women's Hospital, Vancouver, BC
Correspondence
Suggested citation
Willemsma K, Barton L, Stimpson R, Pickell I, Ryan V, Yu A, Pederson A, Ogilvie G, Grennan T, Wong J. Characterizing female infectious syphilis cases in British Columbia to identify opportunities for optimization of care. Can Commun Dis Rep 2022;48(2/3):68–75. https://doi.org/10.14745/ccdr.v48i23a03
Keywords: female infectious syphilis, sexually transmitted infections, syndemics, social determinants of health, substance use, housing instability, Canada
Abstract
Introduction: The rate of infectious syphilis continues to increase among females in British Columbia (BC) and Canada, raising concerns of increased incidence of congenital syphilis. We characterized syphilis cases among females in BC to identify opportunities to prevent syphilis and optimize its care.
Methods: All cases of infectious syphilis diagnosed in BC between March 13, 2018 and December 31, 2020 and reported as female gender were reviewed. Demographics, risk factors and concurrent conditions were collected from a provincial surveillance system. Subgroup analyses comparing cases with and without housing instability, substance use, mental illness and a recent sexually transmitted infection (STI) were conducted to understand differences between these subgroups. Statistical associations were calculated using chi–square or t-tests.
Results: There were 226 reported cases of female infectious syphilis in BC during this period: 38 (16.8%) in 2018; 74 (32.7%) in 2019; and 114 (50.4%) in 2020. Mean age was 32 years (range 15–75 years). Of those who reported concurrent conditions, most cases had experiences with housing instability (71.1%), substance use (68.2%) and mental illness (83.9%), while 42.9% had a recent STI. Cases who reported housing instability or substance use were significantly more likely to have experiences with a recent STI, street involvement, transactional sex, mental illness and income assistance (all p<0.01).
Conclusion: Our findings highlight the importance of fostering an enabling environment for syphilis care. Concurrent services to support individuals with syphilis as well as housing instability, substance use and mental illness, may help prevent syphilis and improve wellbeing.
Introduction
Rates of infectious syphilis have been increasing in British Columbia (BC) and across Canada. While infectious syphilis disproportionately affects gay, bisexual and other men who have sex with men (gbMSM), an increasing number of cases are being reported among the female and heterosexual populations, raising concern of increased incidence of congenital syphilis. From 2016 to 2020, the rates of female infectious syphilis increased by 740% in CanadaFootnote 1. Currently, one in three cases of infectious syphilis in Canada was among femalesFootnote 1. Concurrently, there has been an increase in congenital syphilis cases nationally, from four cases in 2016 to 50 cases in 2020Footnote 1.
In BC, the rate of infectious syphilis increased 138% among females from 2018 to 2020Footnote 2. The male-to-female ratio of cases of infectious syphilis in BC decreased from 15.9 in 2018 to 6.7 in 2020Footnote 2. Of note, the number of infectious syphilis cases reported in 2020 may be an underestimate due to reduced access to healthcare services and concerns related to coronavirus disease 2019 (COVID-19)Footnote 3. British Columbia reported three cases of early congenital syphilis in 2019; the first cases reported in six yearsFootnote 4. In response, the BC Centre for Disease Control (BCCDC) sought to update its provincial Syphilis Action PlanFootnote 5, with an added focus on the prevention of syphilis and related complications among females.
To inform the refresh of the Syphilis Action Plan, the BCCDC led consultations with stakeholders based on the pillars described in the Pan-Canadian Sexually Transmitted and Blood-Borne Infections (STBBI) Framework for ActionFootnote 6Footnote 7. The consultations emphasized the need for a syndemics approach to address syphilisFootnote 7Footnote 8. Syndemics theory postulates that health problems tend to co-occur, are synergistic, and combine to exacerbate the health burden among marginalized populationsFootnote 8. In particular, the consultations highlighted the need to address concurrent conditions, including housing instability, substance use and mental illness, as well as system factors such as relationship with a healthcare provider as part of the provincial syphilis responseFootnote 6Footnote 7. To better understand the prevalence of these concurrent conditions and risk factors and to identify opportunities to optimize care for females affected by syphilis, we reviewed all cases of infectious syphilis among females reported in BC.
Methods
Context
Clinicians at the BCCDC conducted and/or coordinated case and partner management with testing providers for all infectious syphilis cases diagnosed in BC to ensure appropriate testing, treatment, and follow-up. Since March 13, 2018, all case and partner information have been entered into the provincial Intrahealth Profile electronic medical record (EMR) systems.
Inclusion criteria
This descriptive study involved a retrospective chart review of all female cases of infectious syphilis (i.e. primary, secondary or early latent stage) diagnosed in BC from March 13, 2018 to December 31, 2020. Case definitions for the infectious stages of syphilis are available on the BCCDC websiteFootnote 9.
Data sources
Cases of female infectious syphilis were identified through the Intrahealth Profile EMR system. Details of the cases, including demographics, risk factors and concurrent conditions, were collected through both the EMR system and the CareConnect system. CareConnect is an integrated viewer of clinical information from across BC, including clinical encounters and laboratory informationFootnote 10.
Variables of interest
Geography was based on health authority boundaries in BCFootnote 11. Urbanity was defined as living in a metropolitan area with a population of more than 500,000.
The setting for syphilis testing was determined using the address of the ordering physician and classified as 1) community settings (including family practice, specialist and walk-in clinics), 2) hospital settings (including in-patient, out-patient and emergency departments) or 3) outreach settings (including clinics focused on caring for people living with human immunodeficiency virus [HIV], substance use, and/or mental illness).
The narrative notes were reviewed to understand the reason for testing that resulted in the syphilis diagnosis. Reason for testing was classified as 1) contact to a sexually transmitted infection (STI), 2) immigration medical examination, 3) incidental, 4) prenatal or at delivery, 5) routine screen or 6) symptomatic.
A recent STI was defined as a diagnosis of chlamydia, gonorrhea or syphilis in the five years prior to the syphilis diagnosis date.
Concurrent conditions (e.g. housing instability, street involvement, substance use and mental illness) were based on documentation of the condition in the clinical notes or as a diagnosis in the EMR with an International Classification of Diseases code. For simplicity, mental illness was categorized as yes/no. The types of substances used and housing status at the time of diagnosis were also collected when documented.
The number of partners included all those reported during the infectious period of syphilis. Partner notification was considered complete if syphilis clinicians were able to inform all partners or made all reasonable attempts to do so, or if the case indicated they would inform their partners themselves. Connection to a primary care provider was based on evidence of repeated visits and testing from the same provider.
Postal codes were used to estimate socioeconomic status using Statistics Canada's Canadian Index of Multiple Deprivation quintiles in four domains: 1) ethno-cultural composition; 2) situational vulnerability; 3) economic dependency; and 4) residential instabilityFootnote 12. If the client had no fixed address or an unknown postal code, the postal code of the ordering physician was used instead.
Statistical analyses
Descriptive analyses were conducted on the full cohort of female infectious syphilis cases, with further sub-analysis done on the maternal cases. Chi-square or t-tests were conducted on four subgroups: 1) housing instability; 2) substance use; 3) mental illness; and 4) a recent STI to explore associations between concurrent conditions. These subgroups were chosen because of their known association with syphilis and potentiality for prevention of syphilis, as described in the Pan-Canadian STBBI Framework and BC's Syphilis Action PlanFootnote 5Footnote 6Footnote 7. Statistical significance was defined as p<0.01.
Ethics
This study was undertaken to support syphilis surveillance and prevention efforts which are under BCCDC's public health mandate; thus, ethics approval was not required.
Results
In BC, there were 226 reported female cases of infectious syphilis between March 13, 2018 and December 31, 2020. The number of cases increased from 38 (16.8%) in 2018 to 74 (32.7%) in 2019 and 114 (50.4%) 2020. The mean number of cases per month was 4.0, 6.2 and 9.5 for 2018, 2019 and 2020, respectively. Mean age at diagnosis was 32 years (range 15–75 years). Cases were distributed across BC, with over half residing in BC's two most populated health authorities (i.e. Vancouver Coastal Health and Fraser Health Authority). Over two-thirds were diagnosed in the early latent stage of infection (Table 1).
| Variables | n | % |
|---|---|---|
| Age (years) (n=226) | ||
| Mean | 32.5 | N/A |
| Median | 30.9 | N/A |
| Min | 15.5 | N/A |
| Max | 75.4 | N/A |
| Age categories (n=226) | ||
| Younger than 20 years | 18 | 8.0% |
| 20–30 years | 81 | 35.8% |
| 30–40 years | 92 | 40.7% |
| 40–50 years | 16 | 7.1% |
| Older than 50 years | 19 | 8.4% |
| Year—total (n=226) | ||
| 2018Table 1 Footnote a | 38 | 16.8% |
| 2019 | 74 | 32.7% |
| 2020 | 114 | 50.4% |
| Year—mean cases per month (n=226) | ||
| 2018Table 1 Footnote a | 4.0 | N/A |
| 2019 | 6.2 | N/A |
| 2020 | 9.5 | N/A |
| Health Authority (n=223) | ||
| Northern | 9 | 4.0% |
| Interior | 24 | 10.8% |
| Vancouver Island | 59 | 26.5% |
| Fraser | 61 | 27.4% |
| Vancouver Coastal | 70 | 31.4% |
| Urbanity (n=213) | ||
| Metropolitan | 106 | 49.8% |
| Non-metropolitan | 107 | 50.2% |
| Ethnicity (n=92) | ||
| White | 31 | 33.7% |
| Non-white | 61 | 66.3% |
| Stage (n=226) | ||
| Primary | 22 | 9.7% |
| Secondary | 49 | 21.7% |
| Early latent | 155 | 68.6% |
| Pregnancy (n=116) | ||
| Yes | 24 | 20.7% |
| No | 92 | 79.3% |
| Diagnosis setting (n=148) | ||
| Community | 71 | 48.0% |
| Hospital | 28 | 18.9% |
| Outreach | 49 | 33.1% |
| Reason for testing (n=217) | ||
| Contact to STI | 34 | 15.7% |
| Immigration medical examination | 5 | 2.3% |
| Incidental | 22 | 10.1% |
| Prenatal or at delivery | 23 | 10.6% |
| Routine screen | 60 | 27.7% |
| Symptomatic | 73 | 33.6% |
| Recent STI (n=198) | ||
| Yes | 85 | 42.9% |
| No | 113 | 57.1% |
| HIV positive (n=198) | ||
| Yes | 8 | 4.0% |
| No | 190 | 96.0% |
| Housing (n=97) | ||
| Stable | 28 | 28.9% |
| Not stable | 69 | 71.1% |
| No fixed address | 43 | 44.3% |
| Single room occupancy/hotel | 15 | 15.5% |
| Modular/subsidized | 7 | 7.2% |
| Shelter | 4 | 4.1% |
| Street involved (n=89) | ||
| Yes | 64 | 71.9% |
| No | 25 | 28.1% |
| Transactional sex (n=42) | ||
| Yes | 26 | 61.9% |
| No | 16 | 38.1% |
| Substance use (n=157) | ||
| No | 50 | 31.9% |
| Yes | 107 | 68.2% |
| Alcohol | 10 | 6.4% |
| Stimulants | 17 | 10.8% |
| Opioids | 3 | 1.9% |
| Benzodiazepines | 1 | 0.6% |
| Polysubstance | 76 | 48.4% |
| Mental illness (n=87) | ||
| Yes | 73 | 83.9% |
| No | 14 | 16.1% |
| Income assistance (n=59) | ||
| Yes | 39 | 66.1% |
| No | 20 | 33.9% |
| History of incarceration (n=20) | ||
| Yes | 17 | 85.0% |
| No | 3 | 15.0% |
| Gender of partners (n=199) | ||
| Female only | 2 | 1.0% |
| Male only | 191 | 96.0% |
| Male and female | 6 | 3.0% |
| Number of partners (n=188) | ||
| Mean | 2.6 | N/A |
| 0 | 8 | 4.3% |
| 1 | 94 | 50.0% |
| 2–5 | 75 | 39.9% |
| 6 or more | 11 | 5.8% |
| Partner notification completion (n=217) | ||
| Yes | 146 | 67.3% |
| No | 71 | 32.7% |
| Connected to primary care provider (n=220) | ||
| Yes | 176 | 80.0% |
| No | 44 | 20.0% |
The most common setting of diagnosis was community (n=71/148, 48.0%) followed by outreach (n=49/148, 33.1%) and hospital (28/148, 18.9%). The most common reason for testing was the presentation of symptoms consistent with syphilis (n=73/217, 33.6%), followed by routine screening (n=60/217, 27.7%) and due to notification of exposure to an STI (n=34/217, 15.7%). Prenatal/at delivery screening for syphilis was the reason for diagnosis in about 10% of cases (n=23/217). Eight cases were co-infected with HIV, representing 4.0% of the 198 cases with known HIV status. On average, each case had 2.6 previous partners. Most cases completed the partner notification process (n=146/217, 67.3%) and were connected to a primary care provider (n=176/220, 80.0%) (Table 1).
Among cases where concurrent conditions were reported, 42.9% (n=85/198) had a recent STI and the majority had experiences with housing instability (n=69/97, 71.1%), street involvement (n=64/89, 71.9%), transactional sex (n=26/42, 61.9%), substance use (n=107/157, 68.2%), mental illness (n=73/87, 83.9%) and income assistance (n=39/59, 66.1%). Additionally, 17 cases reported a history of incarceration, which represented 85.0% (n=17/20) of those with known incarceration history, or 7.5% (n=17/226) of all cases (Table 1).
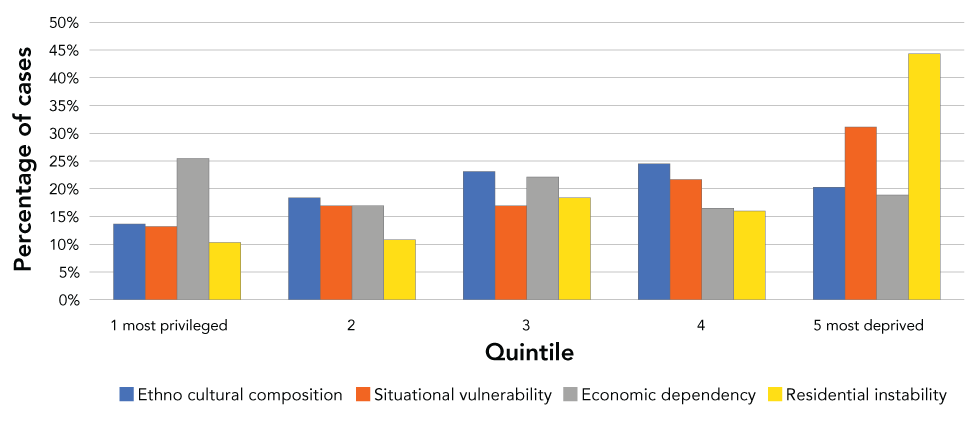
Over half the cases were in the two lowest quintiles for situational vulnerability and residential instability (52.8% and 60.3%, respectively), of Statistics Canada's Canadian Index of Multiple Deprivation Quintiles. The ethno-cultural and economic dependency composition quintiles were more evenly distributed (Figure 1).
Figure 1: Statistics Canada's Canadian Index of Multiple Deprivation Quintiles (n=212)Figure 1 Footnote a
Text description: Figure 1
| Quintile | Ethno-cultural composition | Situational vulnerability | Economic dependency | Residential instability | ||||
|---|---|---|---|---|---|---|---|---|
| 1 most privileged | 29 | 13.7% | 28 | 13.2% | 54 | 25.5% | 22 | 10.4% |
| 2 | 39 | 18.4% | 36 | 17.0% | 36 | 17.0% | 23 | 10.8% |
| 3 | 49 | 23.1% | 36 | 17.0% | 47 | 22.2% | 39 | 18.4% |
| 4 | 52 | 24.5% | 46 | 21.7% | 35 | 16.5% | 34 | 16.0% |
| 5 most deprived | 43 | 20.3% | 66 | 31.1% | 40 | 18.9% | 94 | 44.3% |
There were 24 cases of maternal infectious syphilis, representing 20.7% of the 116 cases of those with known pregnancy status. Mean age was 30 years (range 23–41 years). Nearly half (n=11/23, 47.8%) resided in a metropolitan area. Over 90% were diagnosed in the early latent stage of infection. With regard to concurrent conditions, many maternal cases of syphilis had a recent STI (n=8/21, 38.1%) and had experiences with housing instability (n=7/17, 41.2%), street involvement (n=7/12, 58.3%), substance use (n=10/17, 58.8%) and mental illness (n=6/9, 66.7%) (Annex Table A1).
Our analysis on the four subgroups found that cases with unstable housing were significantly more likely to have experiences with diagnosis of a recent STI, street involvement, transactional sex, substance use, mental illness, income assistance and to not complete partner notification (p<0.01 for all). Cases who used substances were significantly more likely to have experiences with diagnosis of a recent STI, unstable housing, street involvement, transactional sex, mental illness and income assistance (p<0.01 for all). Cases who were diagnosed with mental illness were significantly more likely to have experiences with housing instability, street involvement and substance use (p<0.01 for all). Lastly, cases who had a recent STI were significantly more likely to reside in a metropolitan area and to have experiences with unstable housing, street involvement and substance use (p<0.01 for all) (Table 2).
| Variables | Subgroups | ||||
|---|---|---|---|---|---|
| Housing instability (n=97) |
Substance use (n=157) |
Mental illness (n=87) |
Recent STI (n=198) |
||
| Urbanity | N/S | N/S | N/S | 0.0123 | |
| Recent STI | 0.0003 | 0.0025 | N/S | N/A | |
| Housing instability | N/A | <0.0001 | 0.0006 | 0.0003 | |
| Street involvement | <0.0001 | <0.0001 | 0.0005 | 0.0062 | |
| Transactional sex | <0.0001 | <0.0001 | N/S | N/S | |
| Substance use | <0.0001 | N/A | 0.0003 | 0.0025 | |
| Mental illness | 0.0006 | 0.0003 | N/A | N/S | |
| Income assistance | 0.0028 | 0.0003 | N/S | N/S | |
| Partner notification not completed | 0.0082 | N/S | N/S | N/S | |
Discussion
We described all female infectious syphilis cases diagnosed in BC between March 2018 to December 2021 to better understand the drivers of syphilis infection and opportunities to optimize care for females affected by syphilis. We found that a high proportion of the female cases of syphilis in BC reported housing instability, street involvement, substance use, mental illness and income assistance. Our analysis on each of the four subgroups found strong associations between these conditions.
There are few studies focused on female infectious syphilis globally. Recent studies from Manitoba, Canada have found a similarly high prevalence of concurrent conditionsFootnote 13Footnote 14. A descriptive study of female syphilis from 2003–2015 found that compared with male syphilis cases, female cases were more likely to report co-infection with chlamydia and alcohol useFootnote 13. Furthermore, the proportion of heterosexual cases of syphilis reporting co-infection with chlamydia, housing instability and substance use, were higher in 2015–2018 compared with 2011–2014, which coincided with a decrease in the ratio of male to female cases in ManitobaFootnote 14. The authors concluded there were two simultaneous epidemics of syphilis: one amongst gbMSM and a second amongst the heterosexual population, with the latter being more challenging to controlFootnote 14.
We also found a high proportion of maternal infectious syphilis cases had a recent STI; a finding similar to that reported in an American national case study from 2012–2016Footnote 15. Our analysis of maternal cases found a high proportion of street involvement, substance use, mental illness and income assistance, consistent with a recent review by the Public Health Agency of CanadaFootnote 16. These factors may also contribute to experiences of discrimination and impact access to prenatal care affecting the overall health and wellbeing of both the mother and babyFootnote 16.
The strong association between the socioeconomic determinants, concurrent conditions and syphilis infection support the need for a syndemics-based approach to respond to the current syphilis epidemicFootnote 6Footnote 7Footnote 17Footnote 18Footnote 19Footnote 20. This includes recognizing and deconstructing structural barriers such as those for affordable and stable housingFootnote 16. Our study found an overrepresentation of females with syphilis were in the most deprived residential instability quintiles, emphasizing the marginalization of female cases of syphilis in BC.
Incarceration is also a key factor that intersects and can exacerbate STBBI infection. Two recent Canadian reviews found that the incarcerated population was more mobile and had high rates of experiences with substance use, mental illness, transactional sex, and financial and housing instabilityFootnote 21Footnote 22. These concurrent conditions are mutually reinforcing, and complicate STBBI diagnosis and follow-up care, related to stigma and a lack of connection to a consistent care provider, ultimately contributing to worse health outcomesFootnote 21Footnote 22. Thus, partnerships with federal and provincial correctional institutions can help support people infected with syphilis. While most correctional institutions have STBBI screening programs, these programs vary greatly with regard to diseases screened, approach to testing (i.e. opt-in or opt-out) and whether individuals need to be symptomatic to be tested for STBBIsFootnote 23Footnote 24Footnote 25. Our study adds to existing literature supporting the implementation of universal client-centred STBBI screening in all correctional settingsFootnote 23Footnote 25.
Our study can offer insights into opportunities to improve syphilis care. We found almost half of diagnoses were in the community setting, which may be an area for investment to better address both syphilis and the other intersecting epidemics, such as housing instability, substance use and mental illness, through co-location of additional supports like social worker and counselling servicesFootnote 19. Moreover, engagement with emergency departments, urgent care centres and correctional institutions to develop standards and tailored resources for those settings may help identify cases of syphilis and improve linkage to care and public health outreach teams. While not the setting where the majority of cases in our study were diagnosed, emergency departments are frequently used by populations who do not have a primary care provider or who experience marginalization through financial instability, lack of housing and other support systemsFootnote 16.
Limitations
This study has several limitations. First, the chart review did not capture the full medical and social history of every case. As a result, presence or absence of risk factors and concurrent conditions was not known for all cases and certain variables had smaller sample sizes. For instance, there was limited and non-specific data documented in client's charts regarding the ethnicity of cases. Improved understanding of differential experiences by ethnic groups has previously been identified as a priority for further work in BCFootnote 26Footnote 27. Second, only cases of infectious syphilis that were diagnosed could be analyzed; thus, certain populations who lack access, awareness or agency to seek syphilis testing would have been under-represented in this study. Lastly, this study was descriptive in nature and does not demonstrate causality between the drivers of infection and the diagnosis of syphilis. However, our findings are consistent with the literature and strengthen the evidence for increased services to address socioeconomic and concurrent conditions in the response to the syphilis epidemic.
Conclusion
Overall, this study characterized all female cases of infectious syphilis diagnosed in BC over a nearly three-year period. We found that of the 226 female cases of infectious syphilis, a substantial proportion had concurrent conditions, including housing instability, substance use and mental illness. To our knowledge, this is the largest descriptive analysis of infectious syphilis among females in Canada. Additionally, the use of comprehensive, provincial clinical information systems allowed for a more in-depth understanding of the socioeconomic context of infectious syphilis cases. The findings from our study can help inform interventions to foster enabling environments to prevent and optimize the care for females affected by syphilis, such as integrating mental illness and substance use supports with STI care.
Authors' statement
KW — Conceptualization, methodology, investigation, data curation, writing–original draft, review and editing
LB — Conceptualization, methodology, investigation, review and editing
RS — Review and editing
IP — Investigation, review and editing
VR — Conceptualization, methodology, data curation, review and editing
AY — Data curation, review and editing
AP — Review and editing
GO — Review and editing
TG — Conceptualization, review and editing
JW — Conceptualization, methodology, writing–original draft, review and editing, project administration
The content and view expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
Competing interests
The authors have no conflicts of interest to declare.
Acknowledgements
The authors would like to thank E Wong for her contributions to this study. We would also like to recognize the BCCDC Public Health Laboratory and syphilis clinical team for their ongoing role in caring and advocating for those affected by syphilis.
Funding
No external funding was received for this project.
| Variables | n | % |
|---|---|---|
| Age (years) (n=24) | ||
| Mean | 30.6 | N/A |
| Median | 30.0 | N/A |
| Min | 23.3 | N/A |
| Max | 41.7 | N/A |
| Year—total (n=24) | ||
| 2018Table 1 Footnote a | 2 | 8.3% |
| 2019 | 7 | 29.2% |
| 2020 | 15 | 62.5% |
| Year—mean cases per month (n=24) | ||
| 2018Table 1 Footnote a | 0.2 | N/A |
| 2019 | 0.6 | N/A |
| 2020 | 1.3 | N/A |
| Health Authority (n=23) | ||
| Northern | 1 | 4.3% |
| Interior | 4 | 17.4% |
| Vancouver Island | 4 | 17.4% |
| Fraser | 7 | 30.4% |
| Vancouver Coastal | 7 | 30.4% |
| Urbanity (n=23) | ||
| Metropolitan | 11 | 47.8% |
| Non-metropolitan | 12 | 52.2% |
| Ethnicity (n=11) | ||
| White | 5 | 45.5% |
| Non-White | 6 | 54.5% |
| Stage (n=24) | ||
| Primary | 0 | 0% |
| Secondary | 1 | 4.2% |
| Early latent | 23 | 95.8% |
| Diagnosis setting (n=17) | ||
| Community | 13 | 76.5% |
| Hospital | 2 | 11.8% |
| Outreach | 2 | 11.8% |
| Reason for testing (n=24) | ||
| Contact to STI | 1 | 4.2% |
| Prenatal or at delivery | 21 | 87.5% |
| Routine screen | 2 | 8.3% |
| Symptomatic | 0 | 0% |
| Recent STI (n=21) | ||
| Yes | 8 | 38.1% |
| No | 13 | 61.9% |
| HIV positive (n=21) | ||
| Yes | 0 | 0% |
| No | 21 | 100% |
| Housing (n=17) | ||
| Stable | 10 | 58.8% |
| Not stable | 7 | 41.2% |
| No fixed address | 5 | 29.4% |
| Single room occupancy/hotel | 2 | 11.8% |
| Modular/subsidized | 0 | 0% |
| Shelter | 0 | 0% |
| Street involved (n=12) | ||
| Yes | 7 | 58.3% |
| No | 5 | 41.7% |
| Transactional sex (n=4) | ||
| Yes | 1 | 25.0% |
| No | 3 | 75.0% |
| Substance use (n=17) | ||
| No | 7 | 41.2% |
| Yes | 10 | 58.8% |
| Alcohol | 1 | 5.9% |
| Stimulants | 3 | 17.6% |
| Opioids | 0 | 0% |
| Benzodiazepines | 0 | 0% |
| Polysubstance | 6 | 35.3% |
| Mental illness (n=9) | ||
| Yes | 6 | 66.7% |
| No | 3 | 33.3% |
| Income assistance (n=4) | ||
| Yes | 3 | 75.0% |
| No | 1 | 25.0% |
| Incarceration (n=2) | ||
| Yes | 2 | 100% |
| No | 0 | 0% |
| Gender of partners (n=19) | ||
| Female | 0 | 0% |
| Male | 19 | 100% |
| Male and female | 0 | 0% |
| Number of partners (n=21) | ||
| Mean | 1.8 | N/A |
| 1 | 15 | 71.4% |
| 2–5 | 5 | 23.8% |
| 6 or more | 1 | 4.8% |
| Partner notification completion (n=23) | ||
| Yes | 17 | 73.9% |
| No | 6 | 26.1% |
| Connected to primary care provider (n=24) | ||
| Yes | 20 | 83.3% |
| No | 4 | 16.7% |
